Embed Size (px)
Citation preview
Abstract of thesis entitled
“A Standardized Protocol to Increase Triage Accuracy for
Patients Presenting with Cardiac Symptoms in AED”
Submitted by
Choi Wing In
for the degree of Master of Nursing
at The University of Hong Kong
in August 2014
Cardiovascular disease is the disease involving the heart and the blood vessels. Clinical
manifestations included chest pain or chest discomfort, shortness of breath, palpitations,
dizziness etc. Cardiovascular diseases have significant mortality and morbidity. According to
the World Health Organization global burden of disease 2004 update, it is the leading cause
of death worldwide (WHO, 2008).
Chest pain is one of the typical signs of cardiovascular diseases, and it is also one of the
most commonly seen complaints among patients attending accident and emergency
departments (AED). The early identification of patients impending cardiovascular events is
particularly important, to allow prompt nursing actions and early interventions to be initiated.
However, in clinical practice, not all chest pain is related to myocardial ischemia. Chest
pain can be caused by many other conditions such as gastrointestinal, respiratory or
musculoskeletal problems, which are not cardiac in origin (Scher, 1995). It is important for
health care professionals in AED to differentiate life threatening cardiovascular events from
other conditions that require less urgent attentions. To ensure health resources are effectively
used and prioritize who are in need of immediate attentions, accurate triage decisions are
highly emphasized.
Currently there is no standardized assessment tool adopted for chest pain nursing triage in
accidents and emergency departments in Hong Kong, therefore a structured and standardized
guideline in performing assessments, applying interventions and triaging patients with chest
pain is needed.
In this dissertation, a translational research was conducted to aid developing a
standardized protocol to increase triage accuracy for patients presenting with cardiac
symptoms in accident and emergency department.
In the first chapter, the background and the need for a standardized protocol to aid chest
pain triage in AED will be introduced. In the second chapter, methods to search for relevant
evidence related to chest pain risk stratification in AED will be described. Critical appraisal
of the selected studies will be undertaken by using appraisal checklist of Scottish
Intercollegiate Guideline Network (SIGN). Several risk stratification tools have been
identified from the literature review, among those, the Front Door Score (FDS) was selected
to aid chest pain triage. In the third chapter, the implementation potential of the FDS will be
assessed, in terms of the target setting and audience, the transferability of the selected studies,
the feasibility to carry out the FDS and the cost & benefit ratio. The evidence based guideline
of using FDS in AED will also be discussed. In the fourth chapter, the implementation plan of
FDS will be discussed, including the communication plan, pilot study and evaluation plan of
the proposed guideline.
A Standardized Protocol to Increase Triage Accuracy for Patients
Presenting with Cardiac Symptoms in AED
by
Choi Wing In
BNurs. (Hon), HKU
A thesis submitted in partial fulfillment of the requirements for
the degree of Master of Nursing
at The University of Hong Kong
August 2014
i
Declaration
I declare that this thesis represents my own work, except where due acknowledgment is
made, and that it has not been previously included in a thesis, dissertation or report submitted
to this University or to any other institution for a degree, diploma or other qualifications.
Signed…………………………………………
CHOI Wing In
ii
Acknowledgments
I would like to express my gratitude to my dissertation supervisor, Ms. Idy Fu and Dr.
Elizabeth Hui, for their guidance and assistance with my dissertation throughout the process.
They have offered me inspirations and suggestions using their expert knowledge and research
experience.
I would also like to express my special thanks to Ms. Margaret Yuen, Nurse Specialist,
Accidents and Emergency Department, Pamela Youde Nethersole Eastern Hospital for
providing valuable data from the Accidents and Emergency Department.
iii
Contents
Declaration……………………………………………………………………………………………….i
Acknowledgments……………………………………………………………………………………….ii
Table of Contents…………………………………………………………………………………….iii-v
List of Appendices…………………………………………………………………………………..….vi
List of Abbreviations and Symbols…………………………………………………………………..vii
CHAPTER 1: INTRODUCTION
1.1 Background………………………………………………………………………….…...1
1.2 Significance …………………………………………………………………..………….2
1.3 Affirming the Need…………………………………………………………………….....3
1.4 Objectives………………………………………………………………………………...6
CHAPTER 2: CRITICAL APPRAISAL
2.1 Search Strategies
2.1.1 Keyword Search…………………………………………………………………......7
2.1.2 Inclusion and Exclusion Criteria…………………………………………………….8
2.2 Results………………………………………………………………………………........8
2.3 Appraisal Strategies……………………………………………………………............10
2.3.1 Relatively High level of evidence………………………………………………...10
2.3.2 Medium level of evidence……………………………………….……………….11
2.3.3 Low level of evidence …………………………………………………………..….12
2.4 Summary of Data
2.4.1 Purpose and objective………………………………………………………………13
2.4.2 Patient selection…………………………………………………………………….13
2.4.3 Risk stratification tools……………………………………………………………..13
iv
2.4.4 Outcome measures…………………………………………………………………14
2.4.5 Statistical Analysis…………………………………………………………………14
2.4.6 Findings…………………………………………………………………………….15
2.5 Synthesis of Data…………………………………………………………………….....16
2.5.1 GRACE score………………………………………………………………………17
2.5.2 TIMI risk score……………………………………………………………………..17
2.5.3 Front Door Score…………………………………………………………………...18
CHAPTER 3: TRANSLATION AND APPLICATION......................................................20
3.1 Transferability of the findings…………………………………………………………20
3.1.1 Target Setting……………………………………………………………………….20
3.1.2 Target Audience…………………………………………………………………….21
3.1.3 Philosophy of Care…………………………………………………………………22
3.1.4 Clients Benefitted from the Innovation…………………………………………….22
3.2 Feasibility of the Innovation
3.2.1 Freedom to Implement……………………………………………………………..23
3.2.2 Administrative Support……………………………………………………………..23
3.2.3 Staff Competence & Training………………………………………………………23
3.2.4 Staff Acceptability………………………………………………………………….24
3.2.5 Availability of Equipment, facilities & Resources…………………………………25
3.3 Cost-Benefit Ratio of the Innovation
3.3.1 Potential Benefits of the Innovation………………………………………………..25
3.3.2 Potential Risks of the Current Practice……………………………………………..26
3.3.3 Material Costs………………………………………………………………………26
3.3.4 Potential Non-material Costs and Benefits………………………………………...27
3.4 Evidence Based Practice Guideline ……………………………………………….29-31
v
CHAPTER 4: IMPLEMENTATION PLAN
4.1 Communication Plan
4.1.1 Identify Stakeholders……………………………………………………………….32
4.1.2 Potential Oppose……………………………………………………………………33
4.1.3 Process of Communicating the Plan………………………………………………..33
4.1.4 Setting Up a Communication Team………………………………………………..34
4.1.5 Staff Training……………………………………………………………………….35
4.2 Pilot Study
4.2.1 Objectives of the Pilot Study Plan……………………………………………….…36
4.2.2 Time Frame…………………………………………………………………………37
4.2.3 Patient Selection……………………………………………………………………37
4.2.4 Method……………………………………………………………………………...37
4.2.5 Evaluation of the Pilot Study……………………………………………………….38
4.3 Evaluation Plan
4.3.1 Identifying Outcomes………………………………………………………………39
4.3.2 When and How Often to take Measurement……………………………………….41
4.3.3 Data Analysis……………………………………………………………………….42
Conclusion………………………………………………………………………………..43
References……………………………………………………………………………44-46
Appendices…………………………………………………………………………..…47-63

vi
List of Appendices
Appendix 1: Search History…………………………………………………………………47
Appendix 2: Table of Evidence…………………………………………………………48-51
Appendix 3: SIGN Appraisal Checklists………………………………………………...52-59
Appendix 4: Level of Evidence and Grades of Recommendation by SIGN……………….60
Appendix 5: Costs of Implementation………………………………………………………61
Appendix 6: Front Door Score Data Entry Form………………………………….……62-63
vii
List of Abbreviations and Symbols
Abbreviations
ACS Acute coronary syndrome
AED Accidents and emergency department
AMI Acute myocardial infarction
CABG Coronary artery bypass graft
COS Chief of Service
CREC Clinical research ethics committee
DOM Department operating manager
ECG Electrocardiogram
FDS Front Door Score
GRACE the Global Registry of Acute Coronary Events
HCA Health care assistance
HFA/CS-ANZ the Heart Foundation of Australia and Cardiac Society of Australia and New
Zealand
NS Nurse Specialist
PCI Percutaneous coronary intervention
PURSUIT Platelet glycoprotein IIb/IIIa in Unstable angina: Receptor Suppression Using
Integrilin
ROC Receiver operating characteristic
STEMI ST-elevation myocardial infraction
TIMI Thrombolysis in myocardial infarction
WM Ward manager
Symbols
κ Kappa
1
CHAPTER 1
INTRODUCTION
1.1 BACKGROUND
Cardiovascular disease is the disease involving the heart and the blood vessels. Clinical
manifestations included chest pain or chest discomfort, shortness of breath, palpitations,
dizziness etc. Cardiovascular diseases have significant mortality and morbidity. According to
the World Health Organization global burden of disease 2004 update, it is the leading cause
of death worldwide (WHO, 2008).
Chest pain is one of the most common complaints among patients attending accident and
emergency departments (AED) (Ho et al., 2013). It can be a typical sign of coronary artery
disease. It is widely accepted that early interventions in these patients can reduce mortality
and morbidity (Speake et al., 2003). Therefore, it is important to stratify the risk of chest pain
accurately, provide prompt nursing actions and initiate early interventions for patients in AED,
with suspected coronary artery disease.
However, in clinical practice, not all chest pain is related to myocardial ischemia. Chest
pain can be caused by many other conditions such as gastrointestinal, respiratory or
musculoskeletal problems, which are not cardiac in origin (Scher, 1995). It is important for
health care professionals in AED to differentiate life threatening cardiovascular events from
other conditions. To ensure health resources are effectively used and prioritize who are in
2
need of immediate attentions, accurate triage decisions are highly emphasized. At present,
there are no standardized assessment tools to help nurses in accidents and emergency
departments in Hong Kong to stratifying the risk of chest pain in triage patients. Therefore
there is a need to implement a structured and standardized approach to aid nursing triage
decision making.
1.2 SIGNIFICANCE
According to the World Health Organization global burden of disease 2004 update,
cardiovascular diseases are the leading cause of death in the world, such diseases caused
almost 32% of all deaths in women and 27% in men in 2004 (WHO, 2008). The disease of
the heart is also the second leading cause of death in Hong Kong (Department of Health
annual report 2009/2010). Chest pain may be a signal of an impending life threatening
cardiac event, but it can also be caused by other non-cardiac conditions such as
gastrointestinal, respiratory or musculoskeletal problems, thus it is necessary to differentiate
the nature of chest pain, so as to identify who are in need of immediate treatment.
According to the American Heart Association (AHA), the door-to-first ECG time should
be less than ten minutes, and the door-to-balloon time should be within 90 minutes (AHA,
2013). That means every patient who attends AED presenting with chest pain should receive
first ECG within ten minutes, and for those who are having acute myocardial infarction
should receive percutaneous coronary intervention or thrombolytic treatment within 90
3
minutes. A revised concept of “first medical contact (FMC)-to-device time” is launched in
2013, representing both the recognition that the key issue is triaging and treating the patient
as soon as possible (AHA, 2013 STEMI guideline). Under AHA guidelines in managing
patients with chest pain, timely intervention is one of the major concerns. Accurate triage
decisions are crucial to allow prompt initial nursing actions and allow timely medical
interventions.
The purpose of triage is to assign patients’ urgency among all those who attend accidents
and emergency department. Decision making is a very crucial constituent in nursing triage.
Triage nurses are responsible to provide care for all patients who are pending medical
consultations. Also, triage nurses have a unique overview of the workload of the department,
and they play an important role in management of the patient flow through the department
(Chung, 2005).
1.3 AFFIRMING THE NEED
At present, patients attending accidents and emergency departments are firstly assessed
by triage nurses, assessments included medical history taking, interview on chief complaint
and vital signs taking. After triage assessments, patients are assigned with an acuity rating
based on a 5-level triage scale typically adopted by public hospitals in Hong Kong nowadays.
Patients are divided into 5 categories according to their medical conditions, category 1 to
category 5, which refer to critical, emergency, urgent, semi-urgent and non-urgent
4
respectively. For critical patients who are dying or in life-threatening condition, they are
accorded top priority and attended immediately by a team of medical and nursing staff
without waiting. According to the Triage Guideline published by Hospital Authority 2011
edition, for patients with suspected myocardial infarction or acute coronary syndrome with
ECG changes, category 1 (critical) is assigned. For patients with suspected unstable angina,
category 2 (emergency) is assigned. For patients with chest pain suspected to be of cardiac
origin with stable vital signs, category 3 (urgent) is assigned. For patients with suspected
non-cardiac chest pain, category 4 (semi-urgent) is assigned.
Triage decision is always a challenge to nurses as nurses are required to make quick
decisions when very limited understanding of patients’ problem and patient information are
available. Three possible outcomes on the acuity of triage decisions are: appropriate decision,
which means that the assigned triage category is optimal; under-triage, means the assigned
triage category is less acute than required; over-triage, which means the assigned triage
category is more acute than required. In the study of Goransson et al. (2005), there are
discrepancies between patient assessments made by physicians and nurses. It was found that
only 57.6% of the triage acuity ratings made by nurses were in line with that made by
physicians (Goransson et al., 2005).
Moreover, nurses tended to over-triage patients. The study of Chung (2005), had explored
the experiences of triage decision making of accidents and emergency nurses in Hong Kong.
5
She found that sometimes nurses were uncertain in triage decision making. Such uncertainties
have making them feel that triage decision makings were stressful and risky. Some of them
would choose to upgrade the triage category to prevent patient conditions from deteriorating.
Although triage guidelines are available, it can only be a reference for triage decision
makings. Many nurses reported that they followed the guideline loosely, as not all of the
situations related to patient conditions fitted well into the guideline categories (Chung, 2005).
In addition, some nurses may not be knowledgeable or experienced enough in performing
chest pain triage. As a result, under-triage, over-triage or discrepancy in triage decisions
among different nurses can occur, when nurses made triage decisions according to personal
clinical experiences or intuitions, but not based on standardized and valid assessment tools.
Inaccurate triage decisions can lead to inappropriate utilization of health resources and
adversed patient outcomes (Gerdtz & Bucknall, 1999). An incorrect triage category allocation
can lead to delay in treatment and death of a patient at worst. Such outcomes may have legal
consequences. An over-triage can induce inconsistency in triage decisions, and will invariably
lengthen the waiting time within the same triage category group. The trend to over-triage is
not a good practice in which the ultimate goal of triage cannot be achieved.
Furthermore, currently no standard guideline is specifically designed and adopted for
chest pain triage in accidents and emergency departments in Hong Kong. The American
Heart Association College of Cardiology had published guidelines on managing patients with
6
chest pain, but these guidelines are mainly focused on goals and algorithms in the
management of acute coronary syndrome or acute myocardial infarction, rather than on
nursing triage. A standardized approach for chest pain triage is currently not available.
1.4 OBJECTIVES
In view of the serious health consequences of coronary artery diseases which can be
presented initially by experiencing chest pain, and the importance of prompt actions in
managing these patients, accurate triage decision is crucial to ensure health resources are
effectively used in prioritized patients. Currently there is no standardized assessment tool
adopted for chest pain nursing triage in accidents and emergency departments in Hong Kong,
therefore a structured and standardized guideline in performing assessments, applying
interventions and triaging patients with chest pain is needed.
The objectives of this study are:
1. To identify a valid and reliable risk stratification tool from existing literatures to aid chest
pain triage in emergency department.
2. To develop a standardized protocol for chest pain triage in emergency department.
3. To assess the transferability and feasibility of the proposed chest pain triage protocol.
4. To design an implementation and evaluation plan for the chest pain triage protocol.
7
CHAPTER 2
CRITICAL APPRAISAL
In this chapter, method to search for relevant evidence related to chest pain risk
stratification in accidents and emergency departments will be described. Systematic search on
different database using keywords search will be demonstrated. Screening on the titles and
abstracts were done using inclusion and exclusion criteria to identify relevant research
evidence. Critical appraisal of evidence was done by using the appraisal checklist of Scottish
Intercollegiate Guidelines Network (SIGN). Research articles will be listed as high, medium
or low level of evidence. Summary and synthesis of data will also be provided.
2.1 SEARCH STRATEGIES
2.1.1 Keyword search
Electronic database including PubMed, Ovid MEDLINE, CINAHL were used for the
systematic search. The keywords search comprise of three parts, firstly keywords of: “chest
pain”, “acute coronary syndrome” and “angina” were searched individually and combined for
“OR” search. Secondly, “risk stratification” and “risk score” were input and also searched as
“OR”. Thirdly, “emergency department” was searched. Lastly, all the three advanced searches
were combined for “AND” search. Keywords of “computer tomography”, “computed
tomography” and “troponin” were added to the advanced search for “NOT” search. As a
result, there were 188 results from PubMed, 157 results from Ovid MEDLINE and 43 results
8
from CINAHL.
2.1.2 Inclusion and Exclusion Criteria
The articles were selected if: (1) its target population are adult patients attending AED
with chest pain as their chief compliant, (2) the risk stratification method or assessment tool
was examined.
Articles were excluded if: (1) the studied population was limited to some special
population for examples: patients with renal disease or cocaine user, and (2) the risk
stratification method studied were not nursing related, for examples the study of
echocardiography or computer tomography.
2.2 RESULTS
Using the inclusion and exclusion criteria, the titles and abstracts of the total 388 articles
were screened. Articles were limited to English language and full text. Full text was also
screened for potential eligible articles. 43 articles were identified in CINAHL, 41 were
excluded and 2 were selected. 257 articles were identified in Ovid MEDLINE, 150 were
excluded and 7 were selected. 188 articles were identified in PubMed, 179 were excluded and
9 were selected. Duplicated and irrelevant studies were eliminated. The reference lists from
these selected articles were also screened to identify any relevant literatures.
Finally, eight studies were selected for the review, six studies were identified from
PubMed, one study was identified from CINAHL and one study was identified from Ovid
9
MEDLINE (see Appendix 1). The useful data from the studies was extracted and summarized
in the “Table of Evidence”. The columns in the Table of Evidence were listed according to
bibliographic citation, study type, sample size, patients’ characteristics, assessment tool,
comparison, outcome measures and conclusion (see Appendix 2). No RCTs were available in
the systematic search. In these eight articles, five were prospective observational cohort
studies (Chase et al., 2006; Pollack et al., 2006; Ramsay et al., 2007; Cullen et al., 2013; Lee
et al., 2011) and three were descriptive studies (Ho et al., 2013; Morris et al., 2006; Lyon et
al., 2007).
The descriptive study done by Ho et al. (2013) was conducted in Hong Kong. Three
studies were conducted in the United Kingdom (Morris et al., 2006; Ramsay et al., 2007;
Lyon et al., 2007). Three studies were conducted in the US (Chase et al., 2006; Pollack et al.,
2006; Lee et al., 2011), and one study was conducted in Australia (Cullen et al., 2013).
Among the eight studies included in this review, two of the observational cohort studies
aimed to validate the TIMI risk score (Chase et al.,2006; Pollack et al., 2006); two descriptive
studies aimed to evaluate the TIMI risk score and Front Door Score (Ho et al., 2013; Morris
et al., 2006); two studies compared the TIMI risk score and GRACE score on their ability to
risk stratifying chest pain patients in emergency departments (Ramsay et al., 2007; Lyon et al.,
2007); and finally two studies compared TIMI risk scores with GRACE score, PURSUIT
score and HFA/CS-ANZ guideline (Cullen et al., 2013; Lee et al., 2011).
10
2.3 APPRAISAL STRATEGIES
The critical appraisal checklist designed for diagnostic studies of Scottish Intercollegiate
Guidelines Network (SIGN, 2006) was used to assess the quality of the eight selected articles
(see Appendix 3). In the SIGN grading system, the level of evidence is ranked into four
categories, listed from level one to level four (see Appendix 4). Level one is the highest level
of evidence including high quality meta-analyses, systematic reviews of RCTs or RCTs.
Level two includes case control studies and cohort studies. Level three includes non-analytic
studies such as case reports or case series. Level four is expert opinions. Studies ranked level
one or two will be rated as “++” if it is of high quality with very low risk of confounding or
bias; rated as “+” if it is well-conducted with low risk of confounding of bias; rated as “-“ if it
is of a high risk of confounding or bias.
2.3.1 Relatively High level of evidence
The prospective observational cohort studies done by Chase et al. (2006), Cullen et al.
(2013) and Lee et al. (2011) attained high level of evidence, and were rated as “2++”,
according to the critical appraisal checklist of Scottish Intercollegiate Guidelines Network
(SIGN, 2006).
All three studies have clearly stated the study objectives and designs. The study of Chase
et al. (2006) aimed to validate the use of TIMI risk score in unselected chest pain patients in
emergency departments, with the diagnostic accuracy of TIMI risk score being examined; the
11
study of Cullen et al. (2013), compared the diagnostic accuracy of HFA/CS-ANZ guideline,
GRACE score and TIMI risk score on 30-day adverse cardiac outcomes; while the study of
Lee et al. (2011) compared the diagnostic accuracy of PURSUIT score, GRACE score and
TIMI risk score. All three studies had large sample size enrolled without inappropriate
exclusion criteria. Sample size ranged from 948 to 4743. Consecutive sequences of samples
were enrolled. Detailed descriptions and definitions of outcome measures including
diagnostic criteria for ACS, all-cause mortality, AMI, revascularization and unstable angina
were clearly stated and defined in all three studies. In the study of Chase et al. (2006), method
to blinding of researchers was mentioned, the investigators were unaware of the calculated
score, and this could minimize bias when evaluating the patients’ outcomes. Precise statistical
results for diagnostic accuracy statistics on sensitivity, specificity, and the relative risk of
outcomes for each score component were reported in all three studies, provide with
confidence intervals.
2.3.2 Medium level of evidence
Two descriptive studies (Ho et al., 2013; Morris et al., 2006) and two prospective
observation cohort study (Pollack et al., 2006; Ramsay et al., 2007) in this review attained
medium level of evidence, and were rated as “2+”.
Aims and objectives of the four studies were clearly stated. The study of Ho et al. (2013)
aimed to evaluate the ability of Front Door Score to enhance triage accuracy. Morris et al.
12
(2006) validated TIMI risk score and Front Door Score in undifferentiated chest pain
population in emergency departments. Pollack et al. (2006) and Ramsay et al. (2007)
examined TIMI risk score and GRACE score. The sample selection methods were
appropriate with consecutive eligible samples being enrolled. Outcome measures were clearly
stated in all four studies. Some bias and confounding factors was observed in the study design.
For examples, in the study of Ho et al. (2013), foreigners were excluded in the study due to
possible language barriers, there is possible selection bias. Besides, methods to minimize bias
of researchers in evaluating patient outcomes were not mentioned in these four studies, thus
bias may occur upon data collection and outcome evaluation process.
2.3.3 Low level of evidence
The descriptive study of Lyon et al. (2007) attained low level of evidence of “2-“,
according to the critical appraisal checklist of Scottish Intercollegiate Guidelines Network
(SIGN, 2006). Some limitations of the study design can be identified. Firstly, the method of
sample selection, the inclusion and exclusion criteria for sample selection was not mentioned.
Both GRACE and TIMI risk scores were calculated retrospectively, instead of prospectively.
Besides, definitions of outcomes measures were not clearly specified. Also, 24% of recruited
eligible sample were excluded due to incompleteness of data to calculate the score. Methods
of blinding of researchers were also not addressed.
13
2.4 SUMMARY OF DATA
2.4.1 Purpose and objective
All eight articles have clearly stated purpose and objectives. Seven of them aimed to
validate one or more risk stratification tools to risk stratify unselected patients attending AED
for chest pain (Morris et al., 2006; Chase et al., 2006; Pollack et al.,2006; Ramsay et al., 2007;
Lyon et al., 2007; Cullen et al., 2013; Lee et al.,2011). The diagnostic accuracy of the risk
stratification tools was compared. One aimed to examine the effectiveness of using the risk
stratification tools to increase triage accuracy (Ho et al., 2013).
2.4.2 Patient selection
All samples enrolled for the eight studies were adult patients attending emergency
departments with the chief compliant of chest pain. Those patients with clear signs of
non-cardiac chest pain, for example due to trauma or surgery, were excluded in these studies.
Sample size of these eight studies ranged from 200 to 4743.
2.4.3 Risk stratification tools
All of the eight studies examined risk stratification tools that are designed to risk stratify
chest pain patients. Their relationships with adverse cardiac outcomes were studied in seven
studies, and the relationship of TIMI risk score and Front door score with triage accuracy was
studied in one study. TIMI risk score was validated in two of the studies (Chase et al., 2006;
Pollack et al., 2006). In the studies of Ho et al. (2013) and Morris et al. (2006), both TIMI
14
risk score and Front Door Score were examined. TIMI risk score were evaluated and
compared with GRACE score in the studies of Ramsay et al. (2007) and Lyon et al. (2007).
The study of Cullen et al. (2013) compared the TIMI risk score with GRACE score and
HFA/CS-ANZ guideline, while that of Lee et al. (2011) compared TIMI risk score with
GRACE score and PURSUIT score.
2.4.4 Outcome measures
All eight studies have similar outcome measures. Outcome measures in four studies were
all-cause mortality, AMI, and revascularization by percutaneous coronary intervention or
coronary artery bypass surgery (Chase et al., 2006; Pollack et al., 2006; Ramsay et al., 2007;
Lee et al., 2011). Outcome measures in three studies included all-cause mortality, AMI,
revascularization by percutaneous coronary intervention or coronary artery bypass surgery
and acute coronary syndrome (Morris et al., 2006; Lyon et al., 2007; Cullen et al., 2013). In
Ho et al. (2013) study, the outcome measure was the triage reliability using TIMI risk score,
Front Door Score and 5-level triage scale when compared to the gold standard, which is the
final physician diagnoses.
2.4.5 Statistical Analysis
In the study of Chase et al. (2006) and Pollack et al. (2006), the reliability of TIMI risk
score were illustrated by its correlation with the incidence rate of AMI, death or
revascularization within 30-days in patients of each score group. The analyses were done by
15
using chi-square testing and Cochran-Armitage trend test. In another five studies (Morris et
al., 2006; Lyon et al., 2007; Cullen et al., 2013; Ramsay et al., 2007; Lee et al., 2011), the
reliability of the risk stratification tools including TIMI risk score, Front Door Score,
GRACE score, HFA/CS-ANZ guideline and PURSUIT score were illustrated by their
sensitivity and specificity. By using the sensitivity and specificity of each tool, Receiver
operating characteristic (ROC) curves were plotted. The diagnostic accuracy of different tools
were compared by the area under the ROC curves. In the study of Ho et al. (2013), the triage
reliability of nurses using TIMI risk score, Front Door Score and 5-level triage scale were
compared, by their agreement rates with the gold standard, analyzed by kappa statistics.
2.4.6 Findings
Among the eight articles included in this review, seven have shown that TIMI risk score
was correlated with adverse cardiac outcomes (Morris et al., 2006; Chase et al., 2006; Pollack
et al., 2006; Ramsay et al., 2007; Lyon et al., 2007; Cullen et al., 2013; Lee et al., 2011). Its
correlation to the likelihood of adverse outcomes was demonstrated by a p-value of < 0.001.
In two studies, Front Door Score was also found to be correlated with adverse cardiac
outcomes (Morris et al., 2006; Ho et al., 2013). Its diagnostic accuracy was shown to be
inferior when compared to TIMI risk score, but its clinical importance was addressed. Front
Door Score was also proved to be effective to enhance reliability of chest pain triage (Ho et
al., 2013).
16
Diagnostic accuracy was represented by area under the Receiver operating characteristic
(ROC) curves. By calculating the sensitivity and specificity of the tools, ROC curves can be
plotted and diagnostic accuracies can be obtained. For a diagnostic accuracy equals to one,
mean that the risk stratification tool is of 100% accuracy. The calculated diagnostic accuracy
of GRACE score ranged from 0.73(Lee et al., 2011) to 0.82(Ramsay et al., 2007); that for
TIMI risk score ranged from 0.74(Ramsay et al., 2007) to 0.79(Lyon et al., 2007); that for
Front Door Score was 0.70 (Morris et al., 2006). Among the four studies which compared the
risk stratification tools (Ramsay et al., 2007; Lyon et al., 2007; Cullen et al., 2013; Lee et al.,
2011), three of them (Ramsay et al., 2007; Lyon et al., 2007; Cullen et al., 2013) have shown
that GRACE score is slightly more superior to TIMI risk score. In the study of Lee et al.
(2011), results have shown that TIMI risk score performs better. To conclude, the diagnostic
accuracies of TIMI risk score, Front Door Score & GRACE score were all found to be
satisfactory (Ramsay et al., 2007; Lyon et al., 2007; Cullen et al., 2013; Lee et al., 2011).
2.5 SYNTHESIS OF DATA
Several risk stratification tools were developed for the use to risk stratify chest pain
patients in emergency departments. Among those, Global Registry of Acute Coronary Events
(GRACE) score and Thrombolysis in myocardial infarction (TIMI) risk score are the most
widely validated tools.
17
2.5.1 GRACE score
GRACE score consists of 8 variables: 1)age, 2)heart rate, 3) SBP, 4)Killip class,
5)Creatinine, 6) cardiac arrest at admission, 7)ST segment deviation, 8) elevated cardiac
enzyme. The calculation of GRACE score has been published as an online calculator
(http://www.outcomes-umassmed.org/Grace). By imputing patient data via the online
calculator, risk of death and risk of AMI at different time intervals will be calculated. Thus it
can be used as a reference to guide clinical management according to individual’s risk. It can
also be used in emergency departments which focus is on early and accurate identification of
ACS or AMI.
2.5.2 TIMI risk score
TIMI risk score consists of 7 predictors, each score one point. The predictors are: 1)
age>65, 2) known coronary heart disease, 3) at least 3 risk factors for coronary heart disease,
4) aspirin use in previous 7 days, 5) at least 2 angina episodes in last 24 hours, 6) ST segment
deviation of 0.5mm 7) elevated cardiac markers. TIMI risk score ranges from zero to seven.
Calculation of TIMI risk score of chest pain patients in emergency departments helps to
identify who are at higher risk for ACS or AMI. Patients with score of zero are considered
low risk. Patients score one to four are considered intermediate risk, and those who scored
five to seven are considered high risk. Such score can guide clinical decision making. Unlike
GRACE score, which is derived from ACS populations, TIMI risk score has been proved to
18
perform well in unselected chest pain population in emergency departments.
2.5.3 Front Door Score
Front Door Score (FDS) is a simplified version of TIMI risk score, with the exclusion of
cardiac markers component. Despite the sensitivity and specificity of FDS is not as good as
the full score, it retain its ability to risk stratify the chest pain population in emergency
departments.
The ability of GRACE score, TIMI risk score and Front Door Score to risk stratify chest
pain patients in accidents and emergency departments were validated in various studies. All
of them are of good diagnostic accuracy. However, the complexity of GRACE score has
limited its usage in accidents and emergency departments to stratify risk of adverse outcomes
in chest pain patients. For examples, an online calculator is needed to obtain the GRACE
score, which can be a time-consuming procedure. Also, some components to calculate
GRACE score are difficult to be obtained at triage level, making it not feasible for triage
nurse to use it to aid chest pain triage. For TIMI risk score, despite its ability to predict risk of
adverse cardiac outcomes in chest pain patients, its usage in nursing triage is also limited. It is
because cardiac marker component which is needed for calculation of TIMI risk score cannot
be initially obtained at the time of triage. For Front Door score, it is also of good diagnostic
accuracy, despite its exclusion of the cardiac marker component in its calculation. It is also
19
validated in various studies for its sensitivity & specificity. In contrast to GRACE score or
TIMI risk score, Front Door Score is easy to calculate, which consists of only six components
in its calculation. All six components can be easily obtained during history taking process at
triage level. It is practical and feasible for triage use where cardiac markers cannot be initially
obtained and thus can be used to inform triage decision making.
In view of no standardized assessment tool is adopted in Hong Kong to help nurses in
accidents and emergency departments to stratify the risk of chest pain in triage patients, Front
Door Score can be consider as a standard tool to enhance chest pain triage decisions.
To conclude, patients attending emergency departments for chest pain should be firstly
assessed by a trained triage nurse, using a standardized assessment protocol. The Front Door
Score is proposed to be adopted as the standardized guideline. Front Door Score has been
shown to be a reliable tool to enhance chest pain triage accuracy, predict the risk of
developing adverse cardiac outcomes and thus ensure effective use of health resources in
prioritized patients.
20
CHAPTER 3
TRANSLATION AND APPLICATION
CHAPTER SUMMARY
As discussed in the previous chapter, cardiovascular diseases have significant mortality
and morbidity. Chest pain is one of its typical signs, and it is also one of the most commonly
seen complaints among patients attending accident and emergency departments. The early
identification of patients impending cardiovascular events is particularly important, to allow
prompt nursing actions and early interventions to be initiated. Several risk stratification tools
have been identified from a literature review to risk stratify chest pain patients in accident
and emergency departments. The Front Door Score (FDS) was selected to aid chest pain
triage.
In this chapter, the implementation potential of the FDS will be assessed, in terms of the
target setting and audience, the transferability of the selected studies, the feasibility to carry
out the new innovation and the cost & benefit ratio. The evidence-based guideline of using
the FDS to aid chest pain triage in AED will also be discussed.
3.1 TRANSFERABILITY OF THE FINDINGS
3.1.1 Target Setting
The target setting for the implementation of FDS will be the accident and emergency
department (AED) in a public hospital of the Hong Kong East cluster. It is an acute hospital
21
with 1597 beds and 24-hour AED service.
The eight studies selected for the review were all conducted in AEDs. One study was
conducted in Hong Kong (Ho et al., 2013), three in United Kingdom (Morris et al., 2006;
Ramsay et al., 2007; Lyon et al., 2007), three in the US (Chase et al., 2006; Pollack et al.,
2006; Lee et al., 2011) and one in Australia (Cullen et al., 2013). All AEDs from different
countries in the selected studies are 24-hours operating, providing acute care to patients who
present without prior appointments. Patients presenting with chest pain symptoms with
possible acute coronary syndrome accounts for a significant proportion of the overall
attendance of the AEDs in the selected studies, this share similar conditions to the target
setting in this proposal.
3.1.2 Target Audience
The target audience for the new innovation is patients attending the AED, aged 18
year-old or above, with chest pain as chief compliant. Those patients who are below age of 18
years; mentally incapability for communicate e.g. post stroke; have clear signs of non-cardiac
chest pain, for example due to trauma or injury; critically ill or having hemodynamically
unstable vital sign on presentation and initial triage ECG already showed obvious ST
segment elevation myocardial infarction (STEMI) will be excluded.
All participants in the eight selected studies were aged 18 years-old or above, with chest
pain as their chief complaint. Although the ethnicity of the participants in the studies may not
22
be the same as the target audience, both groups are unselected populations in the AEDs, the
participants are still comparable to our proposed target audience.
3.1.3 Philosophy of Care
The target hospital was established in 1993, as a major acute hospital providing a full
range of specialist services to residents of the eastern district of Hong Kong Island. The
hospital has been upholding the philosophy of providing holistic people-centered quality care
through love, dedication and teamwork. The AED of the target hospital is committed to
deliver timely, quality emergency services to our patients.
As such philosophy is in-line with the aim of the proposed innovation. The aim of
adopting FDS is to risk stratify chest pain patients in AED, identify their risk of developing
significant cardiac events and inform triage decisions, thus optimize treatments and improve
patient outcomes. The innovation can ensure the high quality emergency services.
3.1.4 Clients Benefitted from the Innovation
All those patients presenting to the AED with undifferentiated chest pain will be
benefitted from the innovation. According to the statistical report of the target AED setting in
2012, the annual attendance of patients in 2012 was 146,000 (HA statistical report, 2012).
Among them, 10% were admitted with chest pain as their chief compliant. The proposed
innovation targeted this group of patients. By the calculation based on 2012 statistics, it is
estimated that 14,600 patients can benefit from the innovation annually.
23
3.2 FEASIBILITY OF THE INNOVATION
3.2.1 Freedom to Implement
The new innovation can be commenced with the approval from the administrative and
management team in the proposed setting. They will be involved and consulted for
implementation of the evidence-based guideline. Meanwhile, evaluation plans, cost & benefit
analysis of the innovation will also be presented to them before the commencement. The
guideline will also be proposed to the Clinical Research Ethics Committee (CREC) of the
corresponding cluster. With both approvals, the guideline can be formal launched.
3.2.2 Administrative Support
Evidence-based practice is highly emphasized in the proposed setting. There are existing
nurse development programs ongoing in the department, including sharing sessions for nurses
to share ideas and new research findings on emergency nursing care. Staffs are also
enthusiastic to update themselves with new knowledge, through attending various trainings
and workshops. These have shown that the organization climate is conducive to research
utilization. As both frontline and management staffs are very supportive to new innovations,
the new evidence-based guideline will be highly appreciated.
3.2.3 Staff Competence & Training
Our nurses are competent and adequately trained for triage skills and knowledge. All
nurses with two years or more AED working experience were sent for triage training
24
workshops. They are qualified to perform triage after passing the triage audit. Updated triage
guideline published by the Hospital Authority is also readily available for all nurses in the
department. Triage nurses are being regularly audited by senior nurses about their triage skills
and competence.
To implement the FDS as a new innovation in the department, introduction of the FDS to
all nursing and medical staff is needed. Therefore training sessions will be offered by the FDS
communication team to all staff to introduce the philosophy of care of the FDS, communicate
corresponding research evidence and discuss the new triage workflow. The target population
for applying FDS, its calculation, and the subsequent nursing actions for patients of each
score group will also be discussed.
3.2.4 Staff Acceptability
To incorporate FDS in current triage practice, extra efforts will need to be made by triage
nurses. Due to the heavy workload and fast working pace at triage station, nurses may find it
difficult to adopt the change.
In order to facilitate the usage of FDS, orientation of the FDS and the benefits of adopting
it must be addressed to management team, frontline nurses and the doctors in order to gain
their support. We need to emphasize on the possible positive outcomes bring out by FDS to
aid chest pain triage, such as increase nursing triage accuracy, improved patient outcomes,
improved nursing autonomy, improved staff satisfaction and reduced health costs etc.
25
During the implementation process, feedbacks and comments from staff will be taken into
account for the evaluation of FDS. Modification and fine-tuning of the FDS guideline can be
made.
3.2.5 Availability of Equipment, facilities & Resources
In the proposed setting, well-equipped meeting rooms are readily available for conducting
the training sessions. Necessary equipment like computers and projectors were installed and
ready to be used.
The FDS is an assessment tool to risk stratifies the risk of developing adverse cardiac
outcomes in chest pain population to aid chest pain triage. Neither license nor copyright
charge is needed, no extra equipment is needed for its usage in triage. To incorporate the FDS
into current triage practice, simple flow chart will be developed for nurses’ quick reference at
triage station.
3.3 COST-BENEFIT RATIO OF THE INNOVATION
3.3.1 Potential Benefits of the Innovation
The FDS is a simplified version of TIMI risk score, which was originally designed to risk
stratify chest pain population in AED. By calculating the FDS, patients can be identified as
high, intermediate or low risk in terms of their susceptibility in developing adverse cardiac
outcomes. Integrating FDS into current triage system allows a more accurate, systematic and
specific assessment for patients with undifferentiated chest pain. In short term, proper
26
allocation of resources can be made possible, early interventions can be initiated. In long term,
cost from mortality and morbidity in patients impending coronary heart diseases can be
reduced from prompt & timely intervention after more accurate triage.
3.3.2 Potential Risks of the Current Practice
Currently no standardized guideline is in use for chest pain triage in the proposed setting.
The American Heart Association (AHA) resuscitation guidelines 2010 guidelines mainly
focused on goals and algorithms in the management of ST-elevation myocardial infarction,
rather than on nursing triage. Although HA triage guideline is available, many nurses found
that it can only be a reference for triage decision making. The study of Chung (2005) has
found that many nurses were not confident in chest pain triage, tendencies to over-triage
patients often occurred, ultimate goal of triage was therefore not achieved. Besides, the study
of Ho (2013) demonstrated that the accuracies of chest pain triage of nurses using HA triage
guideline are far from satisfactory. Subsequently, such inaccurate triage decisions can lead to
inappropriate utilization of resources and adverse patient outcomes. Therefore, the accuracies
of chest pain triage in the proposed setting cannot be improved if the current practice is not
modified.
3.3.3 Material Costs
The material costs for implementing the FDS in the proposed setting includes the cost for
the printing of the reference FDS flow charts and FDS forms. For the meeting rooms and
27
necessary equipment like computers and projectors are readily available in the proposed
setting, therefore no extra expenditure in this area is needed.
Training sessions on FDS will be conducted during regular nursing training sessions held
weekly in the department, which will last for 1 hour per session. All nurses will be arranged
to attend. In the proposed AED setting, there are 68 nurses in total, the man-hour required
will be 68. The cost of implementation is summarized in Appendix 5.
3.3.4 Potential Non-material Costs and Benefits
The implementation of FDS into current triage practice may need extra effort make by
triage nurses. This may increase the workload and stress of our nurses. Nurses’ morale may
temporarily reduce due to the frustration arise from the innovation. A proper training and staff
support is therefore necessary. The appreciation of staff contributions to the usage of FDS
should be highlighted. Evaluation of the innovation is also crucial to fine-tune the guideline
and allow staff to express their concerns and difficulties being encountered, which could help
to reduce staff frustration.
The FDS can help to aid chest pain triage and increase triage accuracy, which can in turn
increase staff confidence and job satisfaction. In long term, improved patient outcomes are
also expected.
To conclude, the aim of the innovation is to maximize patients’ benefits and minimize
potential risks and costs. The FDS was reported to be effective in improving patient outcomes,
28
and the costs of implementation are minimal. The potential benefits of FDS have outweighed
the potential costs. The findings from the reviewed studies are considered transferrable and
the FDS is feasible to be implemented in the proposed setting.
29
3.4 EVIDENCE-BASED PRACTICE GUIDELINE
Title of Guideline
A standardized protocol to increase triage accuracy for patients presenting with cardiac
symptoms in AED
Purpose of the Guideline
The purpose of this guideline is to help nurses to identify the risk of developing adverse
cardiac outcomes in chest pain patients, and guide triage decision makings. This will in turn
result in improved chest pain triage accuracy.
Objectives of the Guideline
1) To provide a practical and systematic approach to perform chest pain triage
2) To stratify the risk in patients with undifferentiated chest pain and sort out those high risk
group for early assessment & intervention
3) To improve triage accuracy for patients presenting with undifferentiated chest pain in
AED
Target Audience
Inclusions:
Age of 18year-old or above
Present to AED with chest pain as chief compliant
Stable vital signs at presentation
30
Exclusions:
Age below 18 year-old
Mentally incapable of communication
Obvious non-cardiac origin account for the chest pain e.g. trauma or injury.
Critically ill or hemodynamically unstable at presentation
Initial triage ECG showed obvious STEMI
Recommendations
The guideline is developed based on the eight reviewed articles (see appendix 2). The
evidence of these reviewed articles are graded according to the Level of Evidence (SIGN,
2011), and the recommendations suggested are graded according to the Grade of
Recommendation (see appendix 4).
Recommendation 1.0 B
FDS should be used in AED for risk stratification as well as prediction of outcome.
(2+ Morris et al, 2006; 2++ Chase et al, 2006; 2+ Pollack et al, 2006; 2+ Ramsay et al, 2007;
2- Lyon et al, 2007; 2++ Cullen et al, 2013; 2++ Lee et al, 2011)
Evidence: FDS was found to be positively correlated with adverse cardiac outcomes, in terms
of higher score with higher risk (Morris et al., 2006; Chase et al., 2006; Pollack et al., 2006;
Ramsay et al., 2007; Lyon et al., 2007; Cullen et al., 2013; Lee et al., 2011). Its diagnostic
31
accuracy was also found to be satisfactory (Ramsay et al, 2007; Lyon et al, 2007; Cullen et al,
2013; Lee et al, 2011)
Recommendation 2.0 C
Triage nurses should integrate FDS with clinical judgment and current 5-level triage
scale when performing chest pain triage.
(2+ Ho et al, 2013)
Evidence: FDS can be used in combination with clinical judgment and be incorporated to
5-level triage scale. In which resulting in improvement in patient documentation, assessment,
and interventions, as well as alleviates the uncertainties in performing chest pain triage (Ho et
al, 2013).
Recommendation 3.0 B
Nurses should perform triage by obtaining the circumstantial information and vital
signs, and then perform FDS for eligible patients.
(2+ Ho et al, 2013; 2++ Chase et al, 2006; 2+ Pollack et al, 2006)
Evidence: FDS cannot be used in isolation (Chase et al, 2006; Pollack et al, 2006). The
likelihood of an adverse outcome in patients with a FDS score of zero is not zero, FDS should
therefore be used in conjunction with clinical judgment (Ho et al, 2013; Pollack et al, 2006).
32
CHAPTER 4
IMPLEMENTATION PLAN
CHAPTER SUMMARY
In the previous chapter, the implementation potential of Front Door Score (FDS) in terms
of target audience, target setting, transferability of the selected studies and feasibility of the
FDS has been assessed. Based on the translation and application of the evidence, an evidence
based guideline of integrating FDS into current triage practice has been developed. In this
chapter, the implementation plan of FDS will be discussed, including the communication plan,
pilot study and evaluation plan of the proposed guideline.
4.1 COMMUNICATION PLAN
4.1.1 Identify Stakeholders
To integrate FDS into current triage practice, one important step is to identify all the
stakeholders involved. Anyone who is affected by the FDS is considered the stakeholders.
The stakeholders of the proposed guideline include the Chief of Service (COS), Department
Operating Manager (DOM), ward managers (WM), Nurse Specialist (NS), all nursing staff,
doctors and health care assistances (HCA) within the proposed AED setting, as well as all
targeted subjects of the proposed guideline.
Nurses who are eligible to perform triage are primarily important as they are involved in
the assessment and calculation of FDS as well as divert patient for subsequent management
33
based on the risk stratification.
HCAs are involved in performing ECG, their availability and willingness to quickly
perform the ECG is crucial in order to shorten the door-to-ECG time.
The role of doctors in the implementation of FDS is to interpret the first triage ECG and
identify those with ST-segment elevation myocardial infract (STEMI) for immediate
interventions. Secondly the attending doctors help to manage the patients and make the
provisional diagnosis accordingly.
Lastly are the targeted subjects, they are the patients attending the AED with
undifferentiated chest pain.
4.1.2 Potential Oppose
The potential opposes for the proposed guideline will be the nursing staff, doctors as well
as the target subjects. However, the proposed guideline is incorporated into current triage
workflow except with the additional FDS calculation. It imposes minimal burden to current
triage system as well as minimal increase in workload of triage nurses, the opposition from
staff is expected to be limited. The proposed guideline also imposes minimal risk and delay to
target subjects and therefore the opposition from target subjects also expected to be small.
4.1.3 Process of Communicating the Plan
In order to obtain support and approval from the administrators, the NS will be the first
one to be consulted as she is experienced and she also has frequent communication with the
34
administrators. The details of the FDS guidelines will be discussed with her. Later on, the NS
will be invited to communicate with COS, DOM & WM. Further communication with the
administrators on the evidence of the proposed guideline will be arranged. The discussion
includes the evidence of the proposed guideline, its practical feasibility and logistic
arrangement. Support from these administrative staff is crucial to the implementation of the
new guideline.
After getting the support from the departmental administrative staff, the new guideline
should be proposed to the Clinical Research Ethics Committee (CREC) of the corresponding
cluster, before it can be launched. As mentioned in Chapter 2, the proposed guideline fulfilled
the criteria of patient safety, reasonable prospects of improving healthcare management,
favorable risk-benefit ratio, foreseeable minimal risks and adverse outcomes, therefore the
chance for success in obtaining approval from CREC is high.
4.1.4 Setting Up a Communication Team
After the approval for implementation is obtained from CREC and departmental
administrative staff, communication process to all staff will begin. The objective of the
communication plan is to ensure that all staff involved in the new guideline to understand and
follow the FDS workflow.
A communication team will be formed to facilitate the implementation of the guideline.
The communication will include the NS, three experienced nurses, one doctor and the
35
proposer. The communication team promotes the new guideline to all AED nurses and
doctors, shares the evidence regarding FDS, conducts staff training, monitors implementation
process and conducts evaluation.
4.1.5 Staff Training
AED staff including all doctors and nurses will be involved in the staff training. The
evidence based guideline of integrating FDS into current triage practice will be introduced.
The communication team will share the evidence from the literatures, regarding the benefits
of using FDS in chest pain triage, the limitations of current chest pain triage practice, and
possible changes that the proposed guideline might bring out. Besides, the practical feasibility
and logistics arrangement of FDS will also be discussed.
Based on the shift duty of AED nurses, the most appropriate time to disseminate
departmental message is during the daily meetings held every afternoon. The communication
team will make use of such time to introduce the protocol. Meanwhile, training sessions on
the implementation of FDS guideline will also be conducted during regular nursing training
sessions which are held weekly in the department. All nurses will be arranged to attend.
Compulsory departmental meetings are held monthly in AED for AED doctors, briefing
sessions of FDS can therefore be taken place in the meetings. By estimation, in three monthly
meetings, all AED doctors will be acknowledged about the new FDS guideline. Details of the
proposed guideline will also be announced via staff intranet emails.
36
The target time frame for the dissemination of the proposed guideline among AED staff is
within 3 months. Within the three months, all nurses are expected to have attended the
weekly nursing training sessions at least once, and all doctors are expected to be
acknowledged with the proposed guideline. Once the initial dissemination process finished,
then a guardian program lead by the communication team will proceed. At least one nurse of
the communication team will be arranged to work in the triage station in each shift, to guide
the triage nurses and ensure that they manage to follow the proposed guideline correctly. To
ease the use of FDS, a hard copy of the evidence based guideline and the new chest pain
triage workflow will be kept at triage station. A quick reference showing eligible subjects
criteria and FDS calculation will also be available.
4.2 PILOT STUDY
Before the formal launch of the FDS guideline, a pilot study will be conducted. The
purposes of the pilot study include evaluating the effectiveness of the FDS, testing out the
feasibility of the FDS guideline, and identifying necessary revisions of the guideline.
4.2.1 Objectives of the Pilot Study Plan
1. To measure the clinical benefits of the proposed guideline, in terms of triage reliability
2. To test out the feasibility of integrating FDS into current triage practice
3. To identify difficulties encountered when performing FDS
4. To collect staff opinions and feedbacks, and to determine necessary revision of the
37
guideline
4.2.2 Time Frame
The pilot study will take place in the proposed AED setting in a public hospital of the
Hong Kong East cluster. As mentioned in chapter 3, the total attendance of the AED in 2012
is 146,000. Among those patients, approximately 10% were admitted with chest pain as their
chief compliant. By calculation, there are 40 potential eligible cases per day. The target
number of subject recruitment is 100. The target duration of the pilot study plan is within 1
month, but depends on when the target number of subjects is achieved.
4.2.3 Patient Selection
The inclusion and exclusion criteria of the subjects in the pilot study will be identical to
that of the proposed FDS guideline. All recruited subjects should be of aged 18 or above,
presenting to the AED with undifferentiated chest pain as their major complaint. Those with
chest pain of non-cardiac origins such as trauma or surgery, and those with obvious
ST-elevation in first ECG will be excluded.
4.2.4 Method
A well written guideline of FDS flow chart is available at triage station for reference. The
triage nurses will recruit eligible participants according to the guideline. A verbal consent
from the participants will be obtained. The triage nurses will perform triage, order ECG to the
participants, calculate FDS, and categorize participants according to the risk stratification and
38
other clinical data. All demographic data, vital signs, corresponding FDS score, triage
category, the provisional and final diagnosis of the study subjects and their final disposal will
be recorded in AED notes. For patients who are admitted to the hospital, their discharge
records, information on any cardiac procedures done and other patients outcomes can be
retrieved from hospital electronic patient record (ePR) and can be used for subsequent
analysis.
4.2.5 Evaluation of the Pilot Study
After implementation of the 1-month pilot study, the evaluation of the pilot study will be
performed. The aim of doing the evaluation is to determine whether the objectives of the pilot
study have been achieved. The communication team will review the data collected during the
pilot study. The team will review all the data of the recruited subjects by retrospectively
retrieve patient data from electronic patient record (ePR). The team will analyze data
regarding the recruitment of participants, FDS score calculated, assignment of triage category
based on FDS risk stratification, subsequent patient management, triage reliability, any
adverse outcomes of patient that possible attributed by the study or any other unforeseen
outcomes happened both for patient or for staff involved.
Furthermore, the team will arrange meetings to meet frontline nursing staff, so as to
gather feedbacks from them. Staff will be encouraged to express their feelings and concerns
about the pilot study, share their opinions, and point out the obstacles that they encountered
39
during the pilot study.
Based on the staff feedbacks, and the data analysis on the FDS effectiveness and patient
outcomes, the communication team will identify necessary revisions of the FDS guideline. A
written report of the pilot study will be handover to CREC as well as to AED administrative
staff for assessment. Formal launch of the FDS protocol will proceed after approvals have
been obtained from CREC & administrative staff.
4.3 EVALUATION PLAN
4.3.1 Identifying Outcomes
The implementation of FDS guideline is expected to increase the triage accuracy for
patients present to AED with undifferentiated chest pain. It is expected to have the
subsequent potential in improvement for the followings: (1) Early identification of chest pain
patient that result from Acute Coronary Syndrome (ACS) or Angina, (2) Improve triage
accuracy and sort out high risk patients, (3) Allow those high risk patients to achieve earlier
assessments & interventions, (4) Improve patient outcomes in term of morbidity and
mortality.
Patient Outcomes
The primary outcome variable for the study is the accuracy of triage category based on
FDS assessment. It is partly reflected by the provisional diagnosis in AED note or hospital
discharge diagnosis, which can be retrieved from ePR. High risk group patients (FDS score
40
5-6) are expected to have high chance of chest pain that are likely due to cardiac in origin, if
the provisional diagnosis from AED is ACS/Angina/Non-ST segment Elevation Myocardial
Infarction (NSTEMI), it show a positive correlation with urgent triage category and
intervention. In addition, the needs for those high risk group patients to receive thrombolytic
therapy, refer for urgent Percutaneous Coronary Intervention (PCI) or admit to Critical
Cardiac Unit (CCU) / Intensive Care Unit (ICU) also reflect the triage accuracy &
appropriateness of FDS guideline.
Comparison between the triage accuracy among patients of low risk group (FDS 0-2),
intermediate risk group (FDS 3-4) and high risk group (FDS 5-6) will also be done. The
accuracy can be reflected from the hospital discharge diagnosis or provisional diagnosis from
AED, as well as the need for urgent interventions like PCI or thrombolytic treatments. It
reflects the sensitivity and specificity for the risk stratification of FDS. For example if low
risk group patient is discharged from AED with provisional diagnosis of chest pain or
atypical chest pain and no immediate intervention is need, this reflects that the low risk group
is associated with low chance of adverse cardiac outcomes.
Healthcare Provider Outcomes
Healthcare provider outcomes can be reflected by the staff satisfaction regarding the
utilization of FDS guideline and their perceived skills, knowledge and confidence on
performing chest pain triage. As described in chapter one, many AED nurses in Hong Kong
41
are feeling uncertain in triage decision making, resulting in increased stress among them. As
FDS guideline is expected to aid chest pain triage decision making, the effectiveness of using
FDS guideline to increase staff morale, especially for triage nurses is one of our major
concerns.
System Outcomes
Inaccurate triage decisions can lead to inappropriate utilization of health resources and
adverse patient outcomes (Gerdtz & Bucknall, 1999). An incorrect triage category allocation
can lead to delay in treatment and death of a patient at worst. Such outcomes may have legal
consequences. FDS guideline is expected to minimize such adverse consequences.
Furthermore, FDS guideline is expected to identify high risk patients to achieve earlier
assessments and interventions, which in turn improve patients outcomes in terms of mortality
and morbidity, healthcare costs are expected to be reduced in long term.
4.3.2 When and How Often to take Measurement
The target subjects are patients present to AED with undifferentiated chest pain as chief
complaint. The recruitment of subjects will be done by triage nurses in all shifts. The triage
nurses calculate FDS, assign triage category according to FDS calculation and fill up the FDS
data entry form part 1 (see Appendix 6).
The data entry forms will be collected by working group. The outcome data will be
recorded by investigator in part 2 of the FDS data entry form (see Appendix 6). The
42
investigator will retrieve the corresponding AED diagnosis from Accident & Emergency
Information System (AEIS) and hospital discharge diagnosis from electronic patient record
(ePR) and record the data for subsequent analysis. The analysis will start after the target
number of subjects is achieved in the pilot study.
4.3.3 Data Analysis
The primary outcome variable for the study is the accuracy of triage based on FDS
assessment. It is reflected by the correlation of FDS risk grouping to hospital discharge
diagnosis or provisional diagnosis from AED e.g. ACS/Angina/Non-ST segment Elevation
Myocardial Infarction (NSTEMI). In addition, the correlation with the need for urgent
interventions like PCI or thrombolytic therapy also reflects the correlation agreement.
The triage reliability and accuracy of using FDS is our main evaluation objectives, which
can be analyzed by using Kappa (κ) statistics. Kappa (κ) statistic is used as a quantitative
measure of the magnitude of agreement between FDS risk grouping, triage categories and
final diagnosis of patient. The calculation is based on the difference between "observed"
agreement compare to "expected" agreement. The following guideline will be used for the
interpretation of κ statistic: κ of <0, less than chance agreement; κ of 0.01-0.20, slight
agreement; κ of 0.21 – 0.40, fair agreement; κ of 0.41-0.60, moderate agreement; κ of
0.61-0.80, substantial agreement; κ of 0.81-0.99, almost perfect agreement. The FDS is
considered successful if the agreement rate is of substantial or above, i.e. κ > 0.61.
43
The target subjects of the FDS protocol will be the consecutive eligible patients
presenting to the AED with undifferentiated chest pain as their chief compliant. Evaluation of
the FDS protocol will be performed after the implementation of the pilot study, subsequent
evaluations will be done annually after the formal launch of the protocol.
CONCLUSION
The objectives of the FDS guideline are to provide a practical and systematic approach to
perform chest pain triage; to stratify the risk in patients with undifferentiated chest pain; sort
out those high risk patients for early assessments & interventions and to improve triage
accuracy for patients presenting with undifferentiated chest pain in AED. When considering
the effectiveness of the guideline, triage reliability is assessed. The FDS guideline is
considered effective if the patient outcomes (diagnosis of ACS, Angina, Non STEMI and
need for urgent intervention like thrombolytic or PCI) show a statistically significant
correlation with high FDS scoring. The agreement rates between FDS scoring, triage category
with the final provisional diagnosis is also suggestive of the success of the FDS guideline as a
standard tool to enhance chest pain triage accuracy in AED.
44
References
American Heart Association. (2013). ACC/AHA guidelines for the management of patients
with ST-elevation myocardial infarction. American Heart Association: Dallas.
Chase, M., Robey, J. L., Zogby, K. E., Sease, K. L., Shofer, F. S., & Hollander, J. E. (2006).
Prospective validation of the thrombolysis in myocardial infraction risk score in the
emergency department chest pain population. Annuals of Emergency Medicine, 48(3),
252-259.
Chung, Y. M. (2005). An exploration of accident and emergency nurse experiences of triage
decision making in Hong Kong. Accident and Emergency Nursing, 13(4), 206-213.
Cullen, L., Greenslade, J., Hammett, C. J., Brown, A., Chew, D., Bilesky, J., Than, M.,
Lamanna, A. L., Kimderley, R., Chu, K., & Parsonage, W. A. (2013). Comparison of three
risk stratification rules for predicting patients with acute coronary syndrome presenting to
an Australian emergency department. Heart, Lung and Circulation, In Press, Corrected
Proof, 1-8.
Department of Health Hong Kong. (2010). Annual report 2009/2010. Retrieved August, 2014,
from http://www.dh.gov.hk/english/pub_rec/pub_rec_ar/pub_rec_arpis_0910_html.html
Gerdtz, M.F., & Bucknall, T.K. (1999). Why we do the things we do: applying clinical
decision-making framework to triage practice. Accident and Emergency Nursing, 7 (1),
50-57.
45
Goransson, K., Ehrenberg, A., Marklund, B., & Ehnfors, M. (2005). Accuracy and
concordance of nurses in emergency department triage. Scandinavian Journal of Caring
Sciences, 19(4), 432-438.
Ho, K. M., & Suen, K. P. (2013). Effectiveness of using the front door score to enhance the
chest pain triage accuracy of emergency nurse triage decisions. Journal of Cardiovascular
Nursing, 28(1), 1-10.
Hospital Authority (2011). Triage guideline (2011 edition). Hospital Authority: Hong Kong.
Hospital Authority (2012). HA Statistical Report 2011-2012. Retrieved August 2014, from
http://www.ha.org.hk/gallery/ha_publications.asp?Library_ID=15
Lee, B. S., Chang, A. M., Matsuura, A. C., Marcoon, S., & Hollander, M. D. (2011).
Comparison of cardiac risk scores in ED patients with potential acute coronary syndrome.
Critical Pathways in Cardiology, 10(2), 64-68.
Lyon, R., Morris, A. C., Caesar, D., Gray, S., & Gray, A. (2007). Chest pain to the emergency
department-to stratify risk with GRACE or TIMI? Resuscitation, 74, 90-93.
Morris, A. C., Caesar, D., Gray S. & Gray, A. (2006). TIMI risk score accurately risk
stratifies patients with undifferentiated chest pain presenting to an emergency department.
British Heart Journal, 92(9), 1333-1334.
Pollack, C. V., Sites, F. D., Shofer, F. S., Sease, K. L., & Hollander, J. E. (2006). Application
of the TIMI risk score for unstable angina and non-ST elevation acute coronary syndrome
46
to an unselected emergency department chest pain population. Academic Emergency
Medicine, 13, 13-18.
Ramsay, G., Podogrodzka, M., McClure, C., & Fox, K. A. A. (2007). Risk prediction in
patients presenting with suspected cardiac pain: the GRACE and TIMI risk scores versus
clinical evaluation. The Quarterly Journal of Medicine, 100(1), 11-18.
Scher, H. E. (1995). Chest pain: rapid assessment skills. Journal of Orthopedic Nursing,
14(3), 30-34.
Speake, D. (2003). Detecting high-risk patients with chest pain. Journal of Emergency Nurse,
11(5), 19-21.
World Health Organization (2008). The global burden of disease: 2004 update. Retrieved August,
2014 from http://www.who.int/healthinfo/global_burden_disease/2004_report_update/en/
47
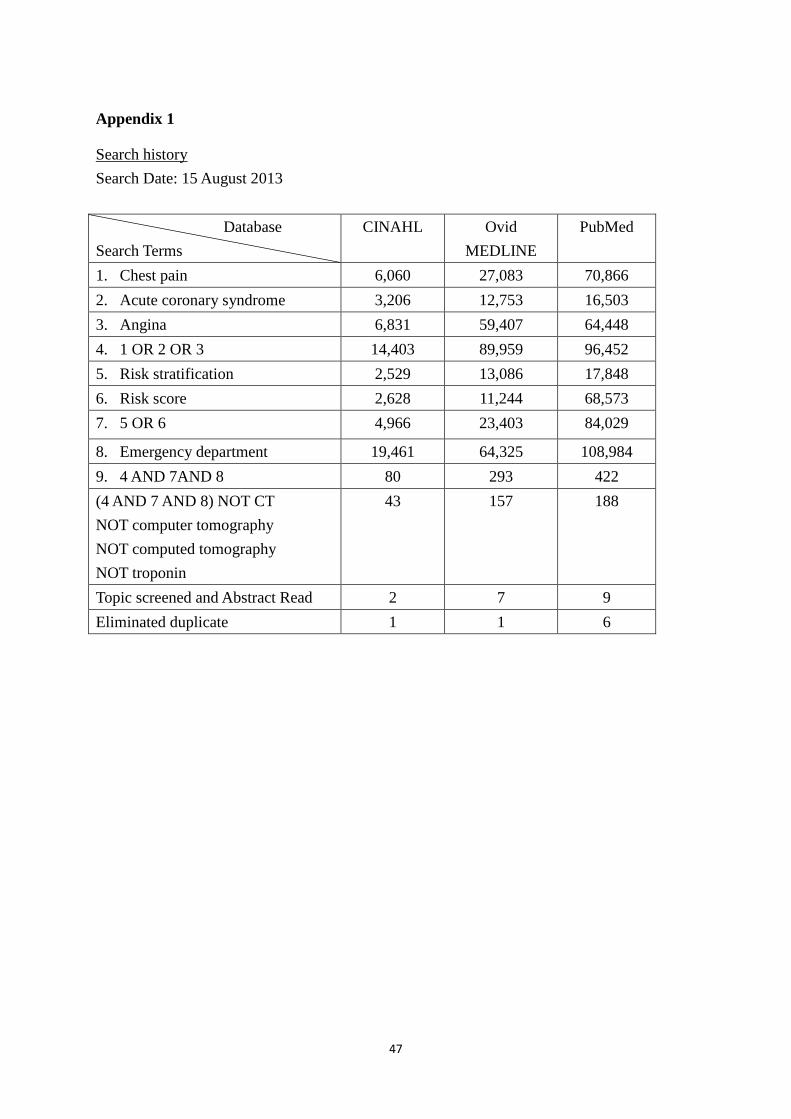
Appendix 1
Search history
Search Date: 15 August 2013
Database
Search Terms
CINAHL Ovid
MEDLINE
PubMed
1. Chest pain 6,060 27,083 70,866
2. Acute coronary syndrome 3,206 12,753 16,503
3. Angina 6,831 59,407 64,448
4. 1 OR 2 OR 3 14,403 89,959 96,452
5. Risk stratification 2,529 13,086 17,848
6. Risk score 2,628 11,244 68,573
7. 5 OR 6 4,966 23,403 84,029
8. Emergency department 19,461 64,325 108,984
9. 4 AND 7AND 8 80 293 422
(4 AND 7 AND 8) NOT CT
NOT computer tomography
NOT computed tomography
NOT troponin
43 157 188
Topic screened and Abstract Read 2 7 9
Eliminated duplicate 1 1 6
48
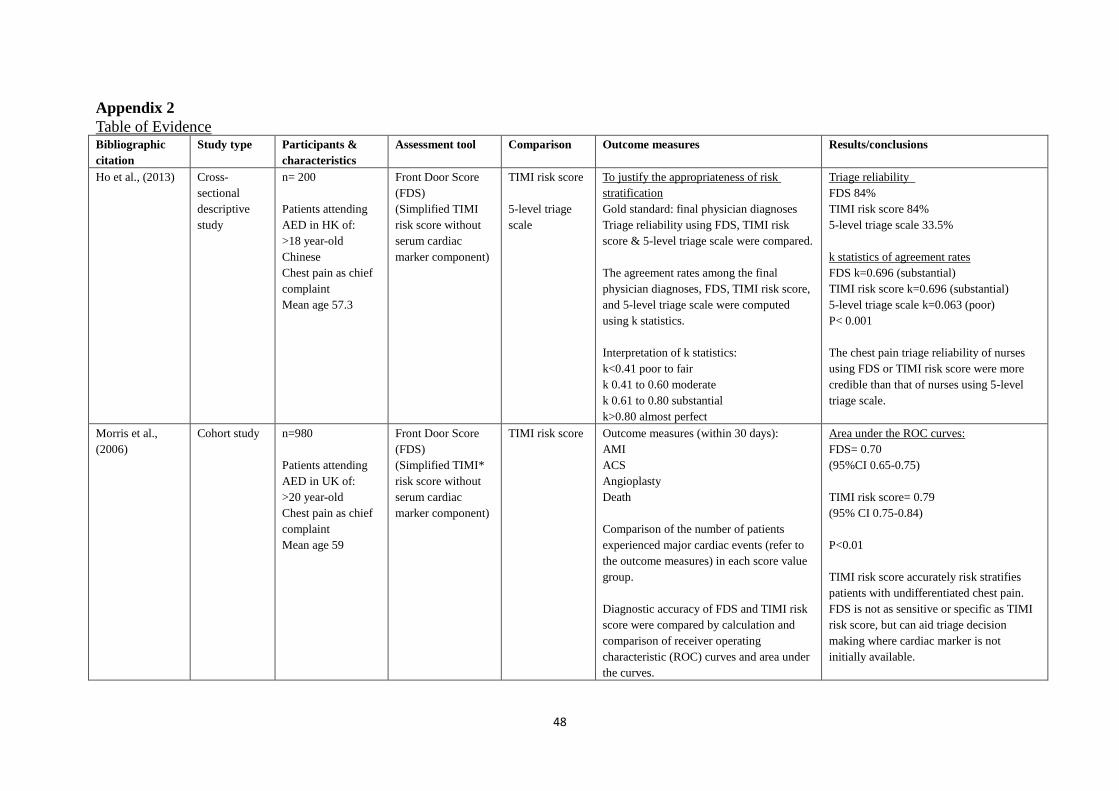
Appendix 2
Table of Evidence Bibliographic
citation
Study type Participants &
characteristics
Assessment tool Comparison Outcome measures
Results/conclusions
Ho et al., (2013) Cross-
sectional
descriptive
study
n= 200
Patients attending
AED in HK of:
>18 year-old
Chinese
Chest pain as chief
complaint
Mean age 57.3
Front Door Score
(FDS)
(Simplified TIMI
risk score without
serum cardiac
marker component)
TIMI risk score
5-level triage
scale
To justify the appropriateness of risk
stratification
Gold standard: final physician diagnoses
Triage reliability using FDS, TIMI risk
score & 5-level triage scale were compared.
The agreement rates among the final
physician diagnoses, FDS, TIMI risk score,
and 5-level triage scale were computed
using k statistics.
Interpretation of k statistics:
k<0.41 poor to fair
k 0.41 to 0.60 moderate
k 0.61 to 0.80 substantial
k>0.80 almost perfect
Triage reliability
FDS 84%
TIMI risk score 84%
5-level triage scale 33.5%
k statistics of agreement rates
FDS k=0.696 (substantial)
TIMI risk score k=0.696 (substantial)
5-level triage scale k=0.063 (poor)
P< 0.001
The chest pain triage reliability of nurses
using FDS or TIMI risk score were more
credible than that of nurses using 5-level
triage scale.
Morris et al.,
(2006)
Cohort study n=980
Patients attending
AED in UK of:
>20 year-old
Chest pain as chief
complaint
Mean age 59
Front Door Score
(FDS)
(Simplified TIMI*
risk score without
serum cardiac
marker component)
TIMI risk score Outcome measures (within 30 days):
AMI
ACS
Angioplasty
Death
Comparison of the number of patients
experienced major cardiac events (refer to
the outcome measures) in each score value
group.
Diagnostic accuracy of FDS and TIMI risk
score were compared by calculation and
comparison of receiver operating
characteristic (ROC) curves and area under
the curves.
Area under the ROC curves:
FDS= 0.70
(95%CI 0.65-0.75)
TIMI risk score= 0.79
(95% CI 0.75-0.84)
P<0.01
TIMI risk score accurately risk stratifies
patients with undifferentiated chest pain.
FDS is not as sensitive or specific as TIMI
risk score, but can aid triage decision
making where cardiac marker is not
initially available.
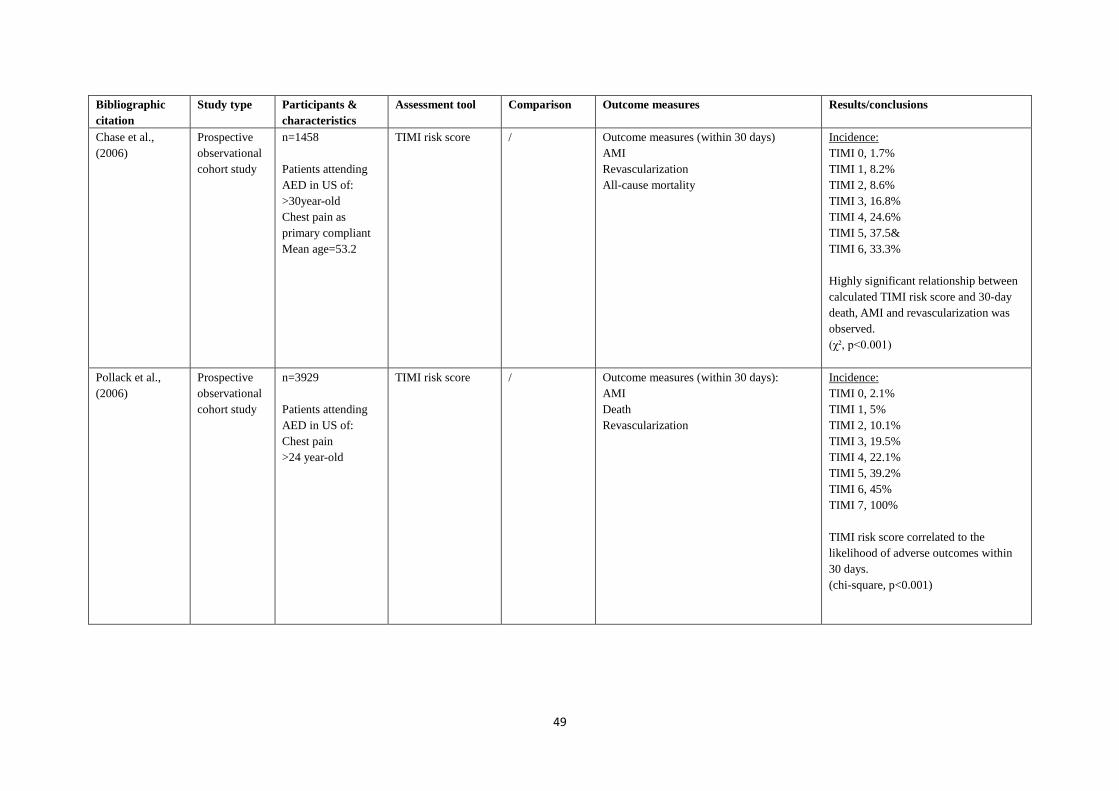
49
Bibliographic
citation
Study type Participants &
characteristics
Assessment tool Comparison Outcome measures
Results/conclusions
Chase et al.,
(2006)
Prospective
observational
cohort study
n=1458
Patients attending
AED in US of:
>30year-old
Chest pain as
primary compliant
Mean age=53.2
TIMI risk score / Outcome measures (within 30 days)
AMI
Revascularization
All-cause mortality
Incidence:
TIMI 0, 1.7%
TIMI 1, 8.2%
TIMI 2, 8.6%
TIMI 3, 16.8%
TIMI 4, 24.6%
TIMI 5, 37.5&
TIMI 6, 33.3%
Highly significant relationship between
calculated TIMI risk score and 30-day
death, AMI and revascularization was
observed.
(χ², p<0.001)
Pollack et al.,
(2006)
Prospective
observational
cohort study
n=3929
Patients attending
AED in US of:
Chest pain
>24 year-old
TIMI risk score / Outcome measures (within 30 days):
AMI
Death
Revascularization
Incidence:
TIMI 0, 2.1%
TIMI 1, 5%
TIMI 2, 10.1%
TIMI 3, 19.5%
TIMI 4, 22.1%
TIMI 5, 39.2%
TIMI 6, 45%
TIMI 7, 100%
TIMI risk score correlated to the
likelihood of adverse outcomes within
30 days.
(chi-square, p<0.001)
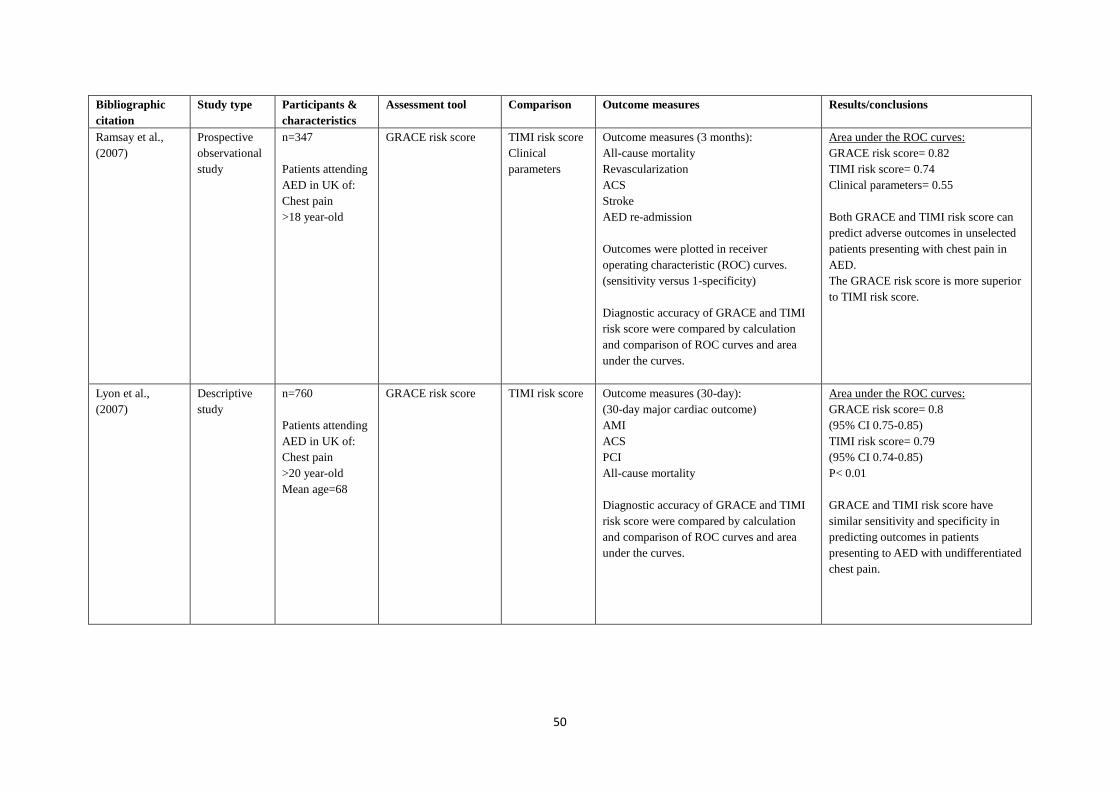
50
Bibliographic
citation
Study type Participants &
characteristics
Assessment tool Comparison Outcome measures
Results/conclusions
Ramsay et al.,
(2007)
Prospective
observational
study
n=347
Patients attending
AED in UK of:
Chest pain
>18 year-old
GRACE risk score TIMI risk score
Clinical
parameters
Outcome measures (3 months):
All-cause mortality
Revascularization
ACS
Stroke
AED re-admission
Outcomes were plotted in receiver
operating characteristic (ROC) curves.
(sensitivity versus 1-specificity)
Diagnostic accuracy of GRACE and TIMI
risk score were compared by calculation
and comparison of ROC curves and area
under the curves.
Area under the ROC curves:
GRACE risk score= 0.82
TIMI risk score= 0.74
Clinical parameters= 0.55
Both GRACE and TIMI risk score can
predict adverse outcomes in unselected
patients presenting with chest pain in
AED.
The GRACE risk score is more superior
to TIMI risk score.
Lyon et al.,
(2007)
Descriptive
study
n=760
Patients attending
AED in UK of:
Chest pain
>20 year-old
Mean age=68
GRACE risk score TIMI risk score Outcome measures (30-day):
(30-day major cardiac outcome)
AMI
ACS
PCI
All-cause mortality
Diagnostic accuracy of GRACE and TIMI
risk score were compared by calculation
and comparison of ROC curves and area
under the curves.
Area under the ROC curves:
GRACE risk score= 0.8
(95% CI 0.75-0.85)
TIMI risk score= 0.79
(95% CI 0.74-0.85)
P< 0.01
GRACE and TIMI risk score have
similar sensitivity and specificity in
predicting outcomes in patients
presenting to AED with undifferentiated
chest pain.
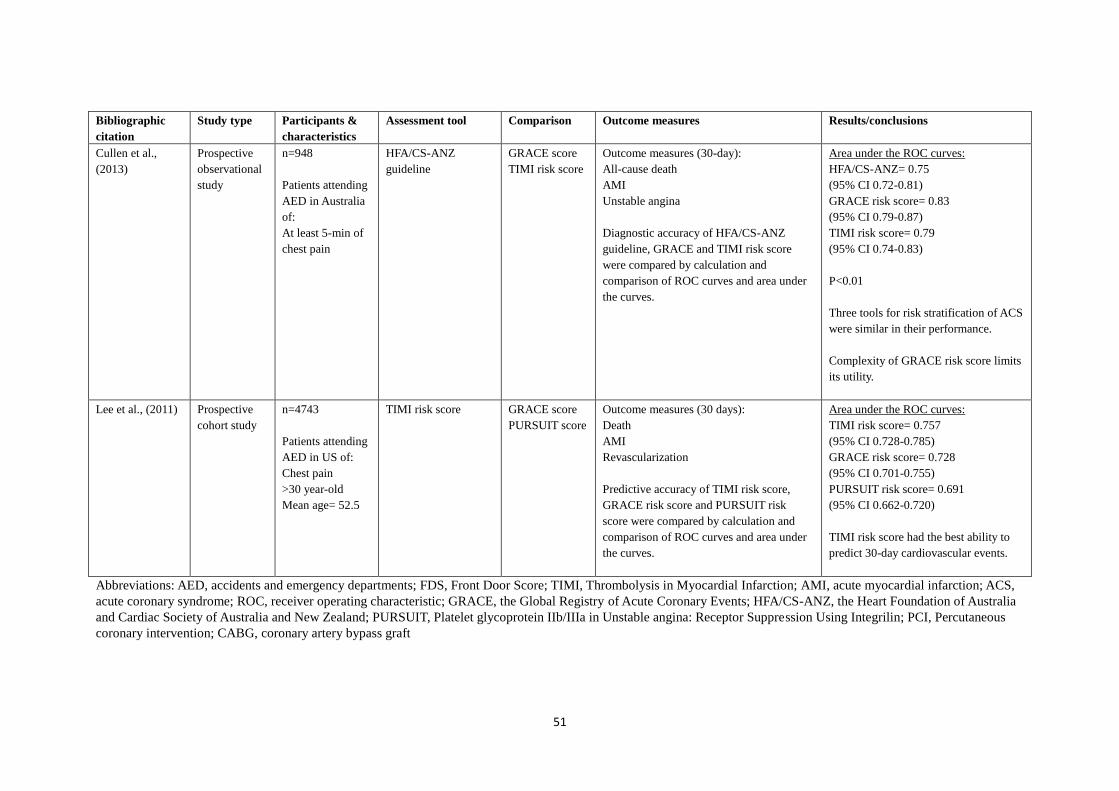
51
Bibliographic
citation
Study type Participants &
characteristics
Assessment tool Comparison Outcome measures
Results/conclusions
Cullen et al.,
(2013)
Prospective
observational
study
n=948
Patients attending
AED in Australia
of:
At least 5-min of
chest pain
HFA/CS-ANZ
guideline
GRACE score
TIMI risk score
Outcome measures (30-day):
All-cause death
AMI
Unstable angina
Diagnostic accuracy of HFA/CS-ANZ
guideline, GRACE and TIMI risk score
were compared by calculation and
comparison of ROC curves and area under
the curves.
Area under the ROC curves:
HFA/CS-ANZ= 0.75
(95% CI 0.72-0.81)
GRACE risk score= 0.83
(95% CI 0.79-0.87)
TIMI risk score= 0.79
(95% CI 0.74-0.83)
P<0.01
Three tools for risk stratification of ACS
were similar in their performance.
Complexity of GRACE risk score limits
its utility.
Lee et al., (2011)
Prospective
cohort study
n=4743
Patients attending
AED in US of:
Chest pain
>30 year-old
Mean age= 52.5
TIMI risk score GRACE score
PURSUIT score
Outcome measures (30 days):
Death
AMI
Revascularization
Predictive accuracy of TIMI risk score,
GRACE risk score and PURSUIT risk
score were compared by calculation and
comparison of ROC curves and area under
the curves.
Area under the ROC curves:
TIMI risk score= 0.757
(95% CI 0.728-0.785)
GRACE risk score= 0.728
(95% CI 0.701-0.755)
PURSUIT risk score= 0.691
(95% CI 0.662-0.720)
TIMI risk score had the best ability to
predict 30-day cardiovascular events.
Abbreviations: AED, accidents and emergency departments; FDS, Front Door Score; TIMI, Thrombolysis in Myocardial Infarction; AMI, acute myocardial infarction; ACS,
acute coronary syndrome; ROC, receiver operating characteristic; GRACE, the Global Registry of Acute Coronary Events; HFA/CS-ANZ, the Heart Foundation of Australia
and Cardiac Society of Australia and New Zealand; PURSUIT, Platelet glycoprotein IIb/IIIa in Unstable angina: Receptor Suppression Using Integrilin; PCI, Percutaneous
coronary intervention; CABG, coronary artery bypass graft
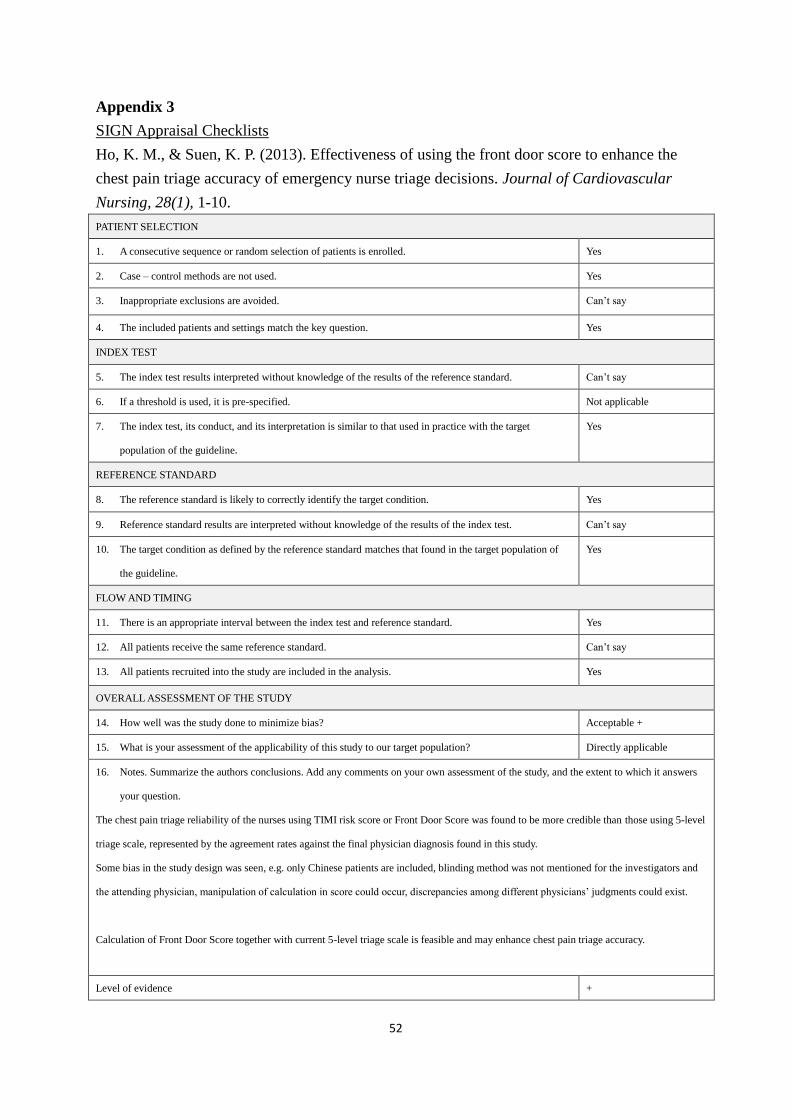
52
Appendix 3
SIGN Appraisal Checklists
Ho, K. M., & Suen, K. P. (2013). Effectiveness of using the front door score to enhance the
chest pain triage accuracy of emergency nurse triage decisions. Journal of Cardiovascular
Nursing, 28(1), 1-10.
PATIENT SELECTION
1. A consecutive sequence or random selection of patients is enrolled. Yes
2. Case – control methods are not used. Yes
3. Inappropriate exclusions are avoided. Can’t say
4. The included patients and settings match the key question. Yes
INDEX TEST
5. The index test results interpreted without knowledge of the results of the reference standard. Can’t say
6. If a threshold is used, it is pre-specified. Not applicable
7. The index test, its conduct, and its interpretation is similar to that used in practice with the target
population of the guideline.
Yes
REFERENCE STANDARD
8. The reference standard is likely to correctly identify the target condition. Yes
9. Reference standard results are interpreted without knowledge of the results of the index test. Can’t say
10. The target condition as defined by the reference standard matches that found in the target population of
the guideline.
Yes
FLOW AND TIMING
11. There is an appropriate interval between the index test and reference standard. Yes
12. All patients receive the same reference standard. Can’t say
13. All patients recruited into the study are included in the analysis. Yes
OVERALL ASSESSMENT OF THE STUDY
14. How well was the study done to minimize bias? Acceptable +
15. What is your assessment of the applicability of this study to our target population? Directly applicable
16. Notes. Summarize the authors conclusions. Add any comments on your own assessment of the study, and the extent to which it answers
your question.
The chest pain triage reliability of the nurses using TIMI risk score or Front Door Score was found to be more credible than those using 5-level
triage scale, represented by the agreement rates against the final physician diagnosis found in this study.
Some bias in the study design was seen, e.g. only Chinese patients are included, blinding method was not mentioned for the investigators and
the attending physician, manipulation of calculation in score could occur, discrepancies among different physicians’ judgments could exist.
Calculation of Front Door Score together with current 5-level triage scale is feasible and may enhance chest pain triage accuracy.
Level of evidence +
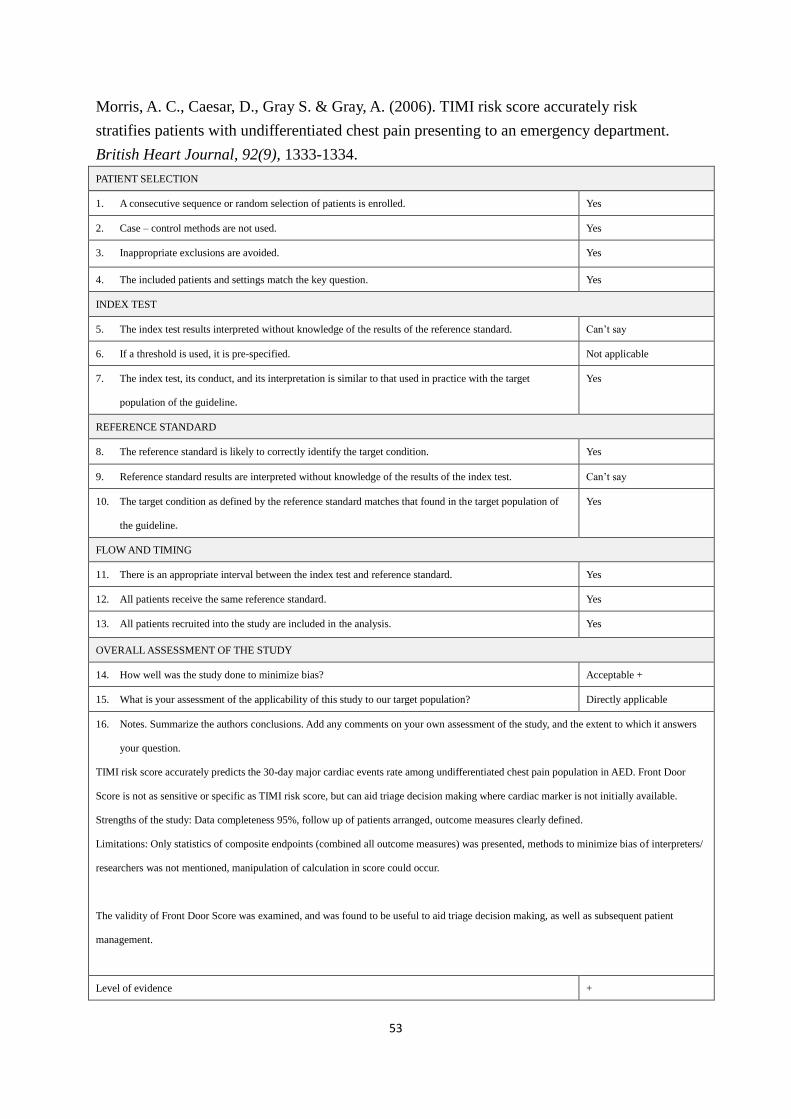
53
Morris, A. C., Caesar, D., Gray S. & Gray, A. (2006). TIMI risk score accurately risk
stratifies patients with undifferentiated chest pain presenting to an emergency department.
British Heart Journal, 92(9), 1333-1334.
PATIENT SELECTION
1. A consecutive sequence or random selection of patients is enrolled. Yes
2. Case – control methods are not used. Yes
3. Inappropriate exclusions are avoided. Yes
4. The included patients and settings match the key question. Yes
INDEX TEST
5. The index test results interpreted without knowledge of the results of the reference standard. Can’t say
6. If a threshold is used, it is pre-specified. Not applicable
7. The index test, its conduct, and its interpretation is similar to that used in practice with the target
population of the guideline.
Yes
REFERENCE STANDARD
8. The reference standard is likely to correctly identify the target condition. Yes
9. Reference standard results are interpreted without knowledge of the results of the index test. Can’t say
10. The target condition as defined by the reference standard matches that found in the target population of
the guideline.
Yes
FLOW AND TIMING
11. There is an appropriate interval between the index test and reference standard. Yes
12. All patients receive the same reference standard. Yes
13. All patients recruited into the study are included in the analysis. Yes
OVERALL ASSESSMENT OF THE STUDY
14. How well was the study done to minimize bias? Acceptable +
15. What is your assessment of the applicability of this study to our target population? Directly applicable
16. Notes. Summarize the authors conclusions. Add any comments on your own assessment of the study, and the extent to which it answers
your question.
TIMI risk score accurately predicts the 30-day major cardiac events rate among undifferentiated chest pain population in AED. Front Door
Score is not as sensitive or specific as TIMI risk score, but can aid triage decision making where cardiac marker is not initially available.
Strengths of the study: Data completeness 95%, follow up of patients arranged, outcome measures clearly defined.
Limitations: Only statistics of composite endpoints (combined all outcome measures) was presented, methods to minimize bias of interpreters/
researchers was not mentioned, manipulation of calculation in score could occur.
The validity of Front Door Score was examined, and was found to be useful to aid triage decision making, as well as subsequent patient
management.
Level of evidence +
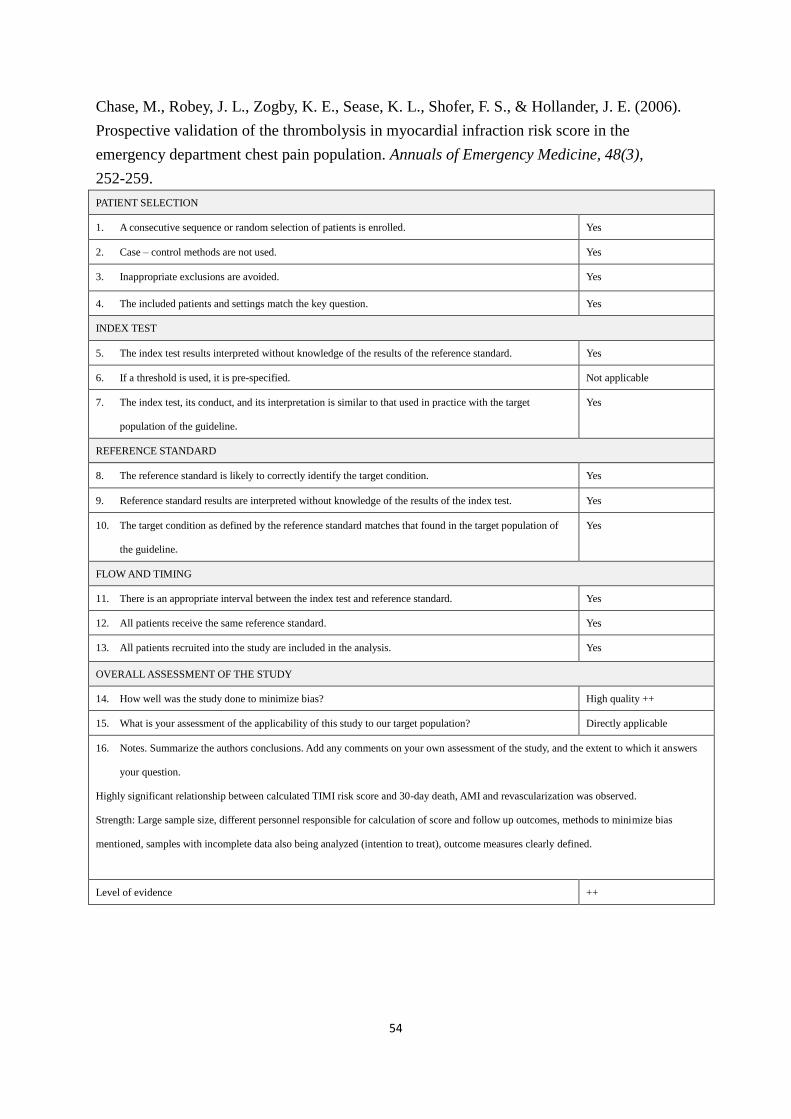
54
Chase, M., Robey, J. L., Zogby, K. E., Sease, K. L., Shofer, F. S., & Hollander, J. E. (2006).
Prospective validation of the thrombolysis in myocardial infraction risk score in the
emergency department chest pain population. Annuals of Emergency Medicine, 48(3),
252-259.
PATIENT SELECTION
1. A consecutive sequence or random selection of patients is enrolled. Yes
2. Case – control methods are not used. Yes
3. Inappropriate exclusions are avoided. Yes
4. The included patients and settings match the key question. Yes
INDEX TEST
5. The index test results interpreted without knowledge of the results of the reference standard. Yes
6. If a threshold is used, it is pre-specified. Not applicable
7. The index test, its conduct, and its interpretation is similar to that used in practice with the target
population of the guideline.
Yes
REFERENCE STANDARD
8. The reference standard is likely to correctly identify the target condition. Yes
9. Reference standard results are interpreted without knowledge of the results of the index test. Yes
10. The target condition as defined by the reference standard matches that found in the target population of
the guideline.
Yes
FLOW AND TIMING
11. There is an appropriate interval between the index test and reference standard. Yes
12. All patients receive the same reference standard. Yes
13. All patients recruited into the study are included in the analysis. Yes
OVERALL ASSESSMENT OF THE STUDY
14. How well was the study done to minimize bias? High quality ++
15. What is your assessment of the applicability of this study to our target population? Directly applicable
16. Notes. Summarize the authors conclusions. Add any comments on your own assessment of the study, and the extent to which it answers
your question.
Highly significant relationship between calculated TIMI risk score and 30-day death, AMI and revascularization was observed.
Strength: Large sample size, different personnel responsible for calculation of score and follow up outcomes, methods to minimize bias
mentioned, samples with incomplete data also being analyzed (intention to treat), outcome measures clearly defined.
Level of evidence ++
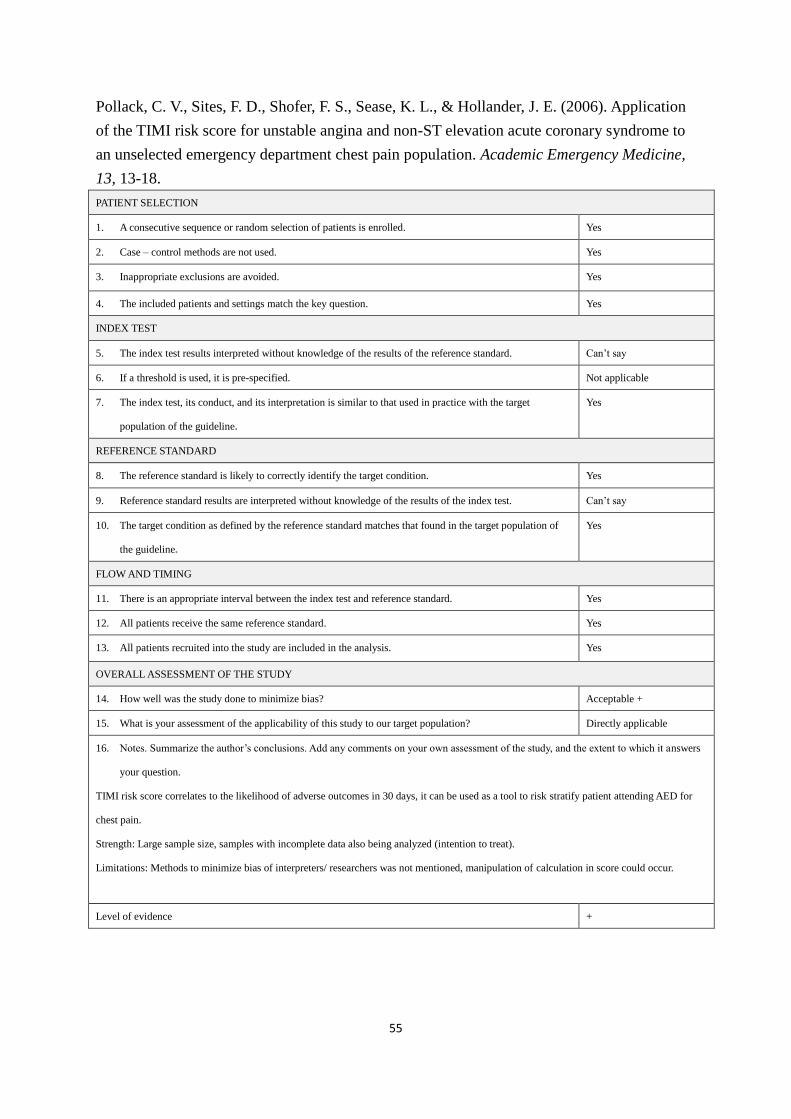
55
Pollack, C. V., Sites, F. D., Shofer, F. S., Sease, K. L., & Hollander, J. E. (2006). Application
of the TIMI risk score for unstable angina and non-ST elevation acute coronary syndrome to
an unselected emergency department chest pain population. Academic Emergency Medicine,
13, 13-18.
PATIENT SELECTION
1. A consecutive sequence or random selection of patients is enrolled. Yes
2. Case – control methods are not used. Yes
3. Inappropriate exclusions are avoided. Yes
4. The included patients and settings match the key question. Yes
INDEX TEST
5. The index test results interpreted without knowledge of the results of the reference standard. Can’t say
6. If a threshold is used, it is pre-specified. Not applicable
7. The index test, its conduct, and its interpretation is similar to that used in practice with the target
population of the guideline.
Yes
REFERENCE STANDARD
8. The reference standard is likely to correctly identify the target condition. Yes
9. Reference standard results are interpreted without knowledge of the results of the index test. Can’t say
10. The target condition as defined by the reference standard matches that found in the target population of
the guideline.
Yes
FLOW AND TIMING
11. There is an appropriate interval between the index test and reference standard. Yes
12. All patients receive the same reference standard. Yes
13. All patients recruited into the study are included in the analysis. Yes
OVERALL ASSESSMENT OF THE STUDY
14. How well was the study done to minimize bias? Acceptable +
15. What is your assessment of the applicability of this study to our target population? Directly applicable
16. Notes. Summarize the author’s conclusions. Add any comments on your own assessment of the study, and the extent to which it answers
your question.
TIMI risk score correlates to the likelihood of adverse outcomes in 30 days, it can be used as a tool to risk stratify patient attending AED for
chest pain.
Strength: Large sample size, samples with incomplete data also being analyzed (intention to treat).
Limitations: Methods to minimize bias of interpreters/ researchers was not mentioned, manipulation of calculation in score could occur.
Level of evidence +
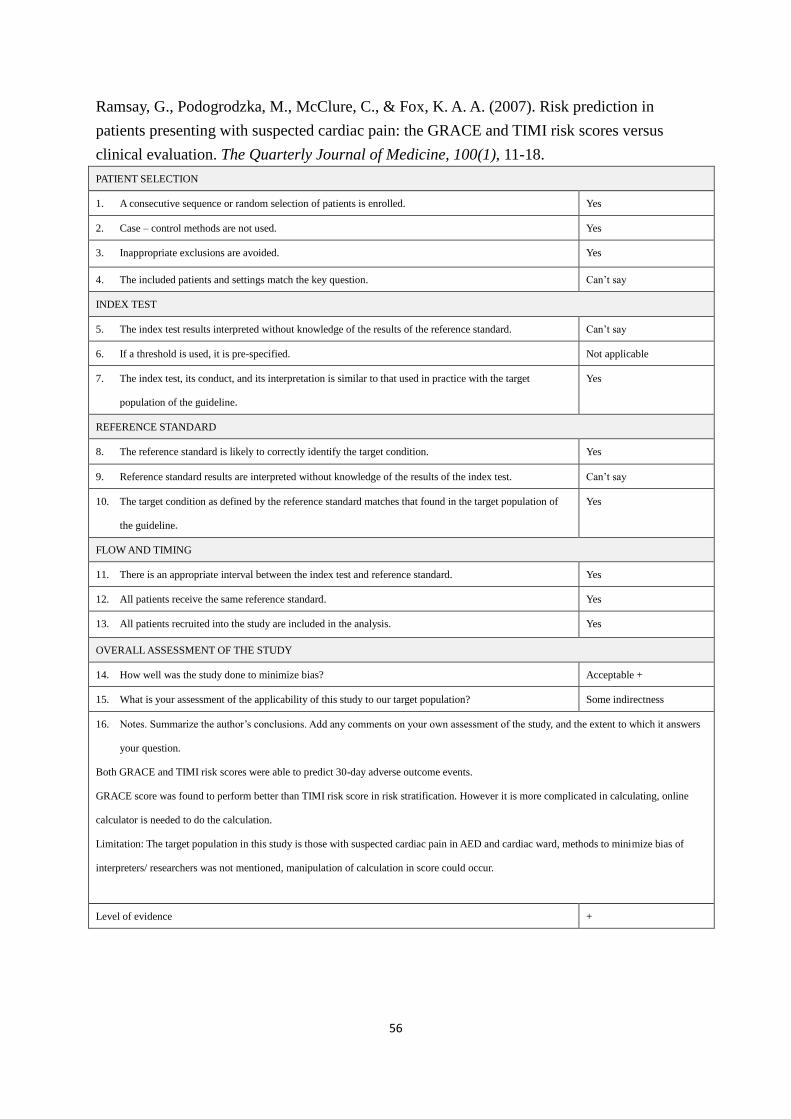
56
Ramsay, G., Podogrodzka, M., McClure, C., & Fox, K. A. A. (2007). Risk prediction in
patients presenting with suspected cardiac pain: the GRACE and TIMI risk scores versus
clinical evaluation. The Quarterly Journal of Medicine, 100(1), 11-18.
PATIENT SELECTION
1. A consecutive sequence or random selection of patients is enrolled. Yes
2. Case – control methods are not used. Yes
3. Inappropriate exclusions are avoided. Yes
4. The included patients and settings match the key question. Can’t say
INDEX TEST
5. The index test results interpreted without knowledge of the results of the reference standard. Can’t say
6. If a threshold is used, it is pre-specified. Not applicable
7. The index test, its conduct, and its interpretation is similar to that used in practice with the target
population of the guideline.
Yes
REFERENCE STANDARD
8. The reference standard is likely to correctly identify the target condition. Yes
9. Reference standard results are interpreted without knowledge of the results of the index test. Can’t say
10. The target condition as defined by the reference standard matches that found in the target population of
the guideline.
Yes
FLOW AND TIMING
11. There is an appropriate interval between the index test and reference standard. Yes
12. All patients receive the same reference standard. Yes
13. All patients recruited into the study are included in the analysis. Yes
OVERALL ASSESSMENT OF THE STUDY
14. How well was the study done to minimize bias? Acceptable +
15. What is your assessment of the applicability of this study to our target population? Some indirectness
16. Notes. Summarize the author’s conclusions. Add any comments on your own assessment of the study, and the extent to which it answers
your question.
Both GRACE and TIMI risk scores were able to predict 30-day adverse outcome events.
GRACE score was found to perform better than TIMI risk score in risk stratification. However it is more complicated in calculating, online
calculator is needed to do the calculation.
Limitation: The target population in this study is those with suspected cardiac pain in AED and cardiac ward, methods to minimize bias of
interpreters/ researchers was not mentioned, manipulation of calculation in score could occur.
Level of evidence +
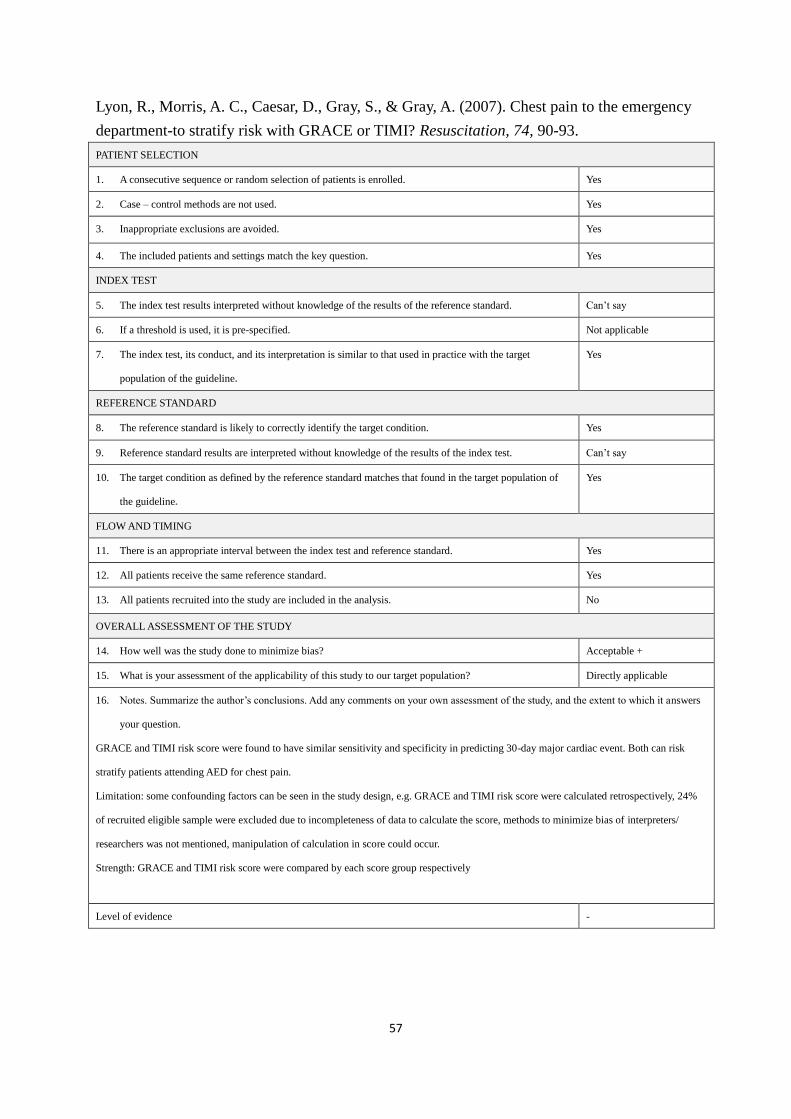
57
Lyon, R., Morris, A. C., Caesar, D., Gray, S., & Gray, A. (2007). Chest pain to the emergency
department-to stratify risk with GRACE or TIMI? Resuscitation, 74, 90-93.
PATIENT SELECTION
1. A consecutive sequence or random selection of patients is enrolled. Yes
2. Case – control methods are not used. Yes
3. Inappropriate exclusions are avoided. Yes
4. The included patients and settings match the key question. Yes
INDEX TEST
5. The index test results interpreted without knowledge of the results of the reference standard. Can’t say
6. If a threshold is used, it is pre-specified. Not applicable
7. The index test, its conduct, and its interpretation is similar to that used in practice with the target
population of the guideline.
Yes
REFERENCE STANDARD
8. The reference standard is likely to correctly identify the target condition. Yes
9. Reference standard results are interpreted without knowledge of the results of the index test. Can’t say
10. The target condition as defined by the reference standard matches that found in the target population of
the guideline.
Yes
FLOW AND TIMING
11. There is an appropriate interval between the index test and reference standard. Yes
12. All patients receive the same reference standard. Yes
13. All patients recruited into the study are included in the analysis. No
OVERALL ASSESSMENT OF THE STUDY
14. How well was the study done to minimize bias? Acceptable +
15. What is your assessment of the applicability of this study to our target population? Directly applicable
16. Notes. Summarize the author’s conclusions. Add any comments on your own assessment of the study, and the extent to which it answers
your question.
GRACE and TIMI risk score were found to have similar sensitivity and specificity in predicting 30-day major cardiac event. Both can risk
stratify patients attending AED for chest pain.
Limitation: some confounding factors can be seen in the study design, e.g. GRACE and TIMI risk score were calculated retrospectively, 24%
of recruited eligible sample were excluded due to incompleteness of data to calculate the score, methods to minimize bias of interpreters/
researchers was not mentioned, manipulation of calculation in score could occur.
Strength: GRACE and TIMI risk score were compared by each score group respectively
Level of evidence -
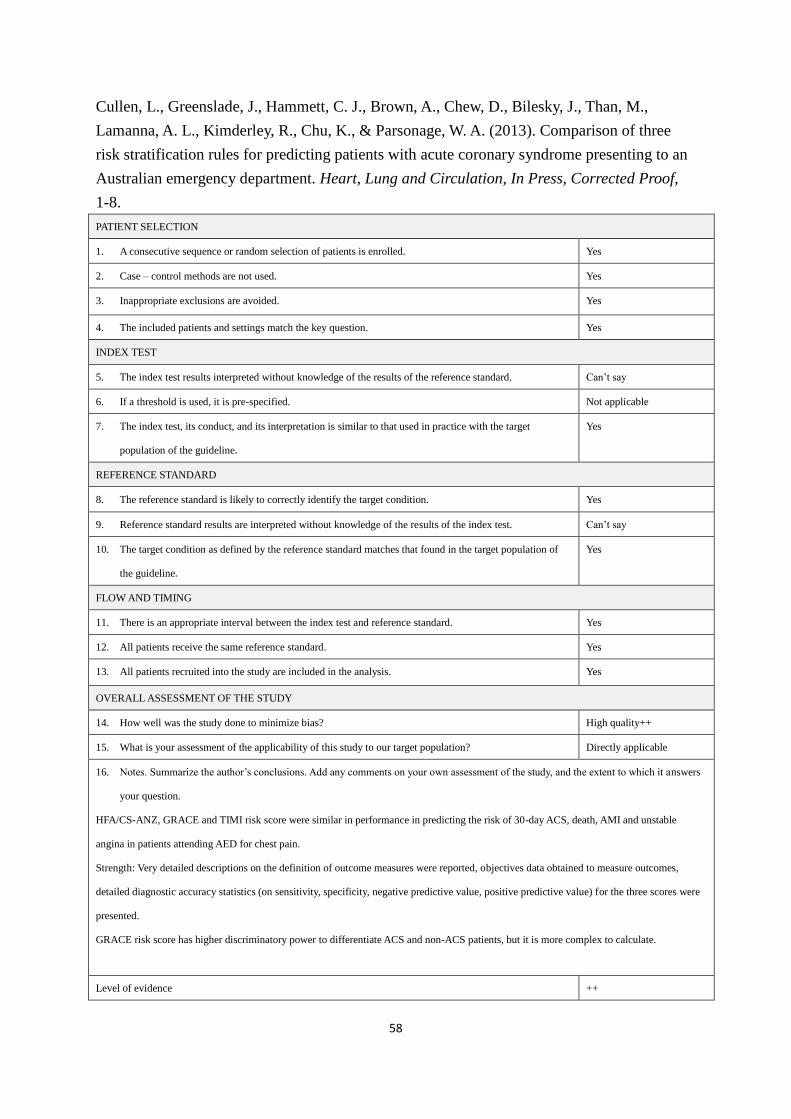
58
Cullen, L., Greenslade, J., Hammett, C. J., Brown, A., Chew, D., Bilesky, J., Than, M.,
Lamanna, A. L., Kimderley, R., Chu, K., & Parsonage, W. A. (2013). Comparison of three
risk stratification rules for predicting patients with acute coronary syndrome presenting to an
Australian emergency department. Heart, Lung and Circulation, In Press, Corrected Proof,
1-8.
PATIENT SELECTION
1. A consecutive sequence or random selection of patients is enrolled. Yes
2. Case – control methods are not used. Yes
3. Inappropriate exclusions are avoided. Yes
4. The included patients and settings match the key question. Yes
INDEX TEST
5. The index test results interpreted without knowledge of the results of the reference standard. Can’t say
6. If a threshold is used, it is pre-specified. Not applicable
7. The index test, its conduct, and its interpretation is similar to that used in practice with the target
population of the guideline.
Yes
REFERENCE STANDARD
8. The reference standard is likely to correctly identify the target condition. Yes
9. Reference standard results are interpreted without knowledge of the results of the index test. Can’t say
10. The target condition as defined by the reference standard matches that found in the target population of
the guideline.
Yes
FLOW AND TIMING
11. There is an appropriate interval between the index test and reference standard. Yes
12. All patients receive the same reference standard. Yes
13. All patients recruited into the study are included in the analysis. Yes
OVERALL ASSESSMENT OF THE STUDY
14. How well was the study done to minimize bias? High quality++
15. What is your assessment of the applicability of this study to our target population? Directly applicable
16. Notes. Summarize the author’s conclusions. Add any comments on your own assessment of the study, and the extent to which it answers
your question.
HFA/CS-ANZ, GRACE and TIMI risk score were similar in performance in predicting the risk of 30-day ACS, death, AMI and unstable
angina in patients attending AED for chest pain.
Strength: Very detailed descriptions on the definition of outcome measures were reported, objectives data obtained to measure outcomes,
detailed diagnostic accuracy statistics (on sensitivity, specificity, negative predictive value, positive predictive value) for the three scores were
presented.
GRACE risk score has higher discriminatory power to differentiate ACS and non-ACS patients, but it is more complex to calculate.
Level of evidence ++
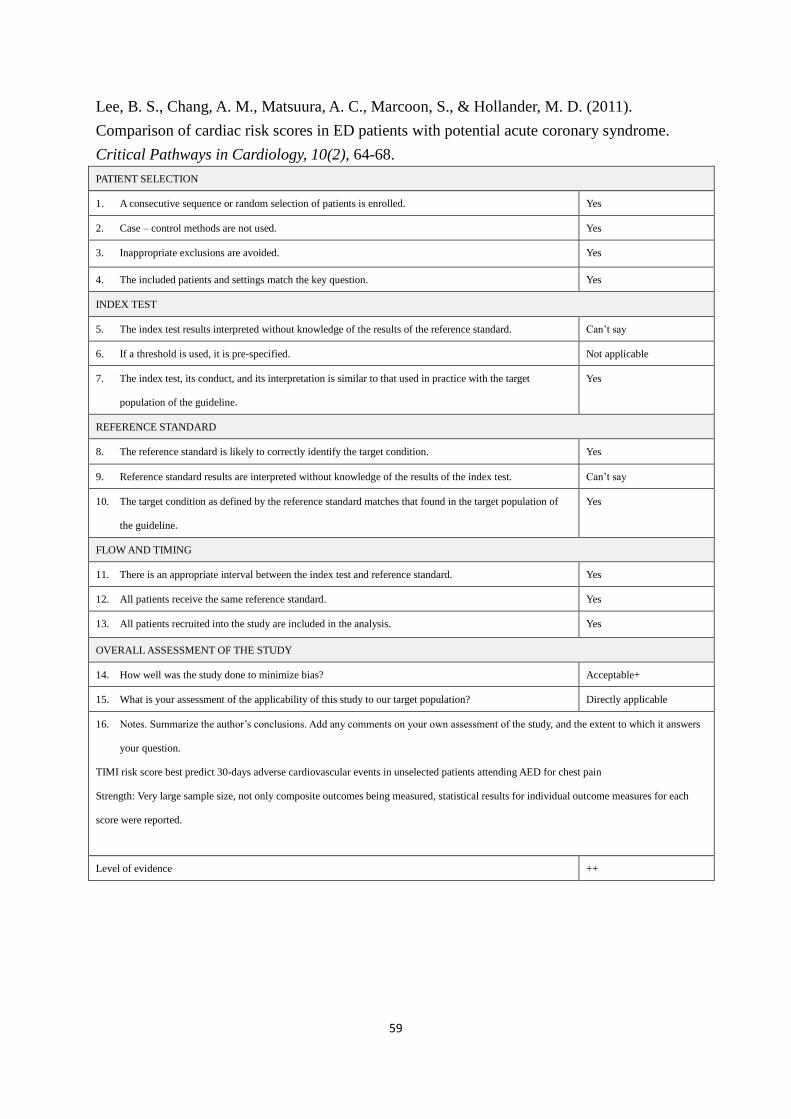
59
Lee, B. S., Chang, A. M., Matsuura, A. C., Marcoon, S., & Hollander, M. D. (2011).
Comparison of cardiac risk scores in ED patients with potential acute coronary syndrome.
Critical Pathways in Cardiology, 10(2), 64-68.
PATIENT SELECTION
1. A consecutive sequence or random selection of patients is enrolled. Yes
2. Case – control methods are not used. Yes
3. Inappropriate exclusions are avoided. Yes
4. The included patients and settings match the key question. Yes
INDEX TEST
5. The index test results interpreted without knowledge of the results of the reference standard. Can’t say
6. If a threshold is used, it is pre-specified. Not applicable
7. The index test, its conduct, and its interpretation is similar to that used in practice with the target
population of the guideline.
Yes
REFERENCE STANDARD
8. The reference standard is likely to correctly identify the target condition. Yes
9. Reference standard results are interpreted without knowledge of the results of the index test. Can’t say
10. The target condition as defined by the reference standard matches that found in the target population of
the guideline.
Yes
FLOW AND TIMING
11. There is an appropriate interval between the index test and reference standard. Yes
12. All patients receive the same reference standard. Yes
13. All patients recruited into the study are included in the analysis. Yes
OVERALL ASSESSMENT OF THE STUDY
14. How well was the study done to minimize bias? Acceptable+
15. What is your assessment of the applicability of this study to our target population? Directly applicable
16. Notes. Summarize the author’s conclusions. Add any comments on your own assessment of the study, and the extent to which it answers
your question.
TIMI risk score best predict 30-days adverse cardiovascular events in unselected patients attending AED for chest pain
Strength: Very large sample size, not only composite outcomes being measured, statistical results for individual outcome measures for each
score were reported.
Level of evidence ++

60
Appendix 4
Scottish Intercollegiate Guidelines Network SIGN
SIGN GRADING SYSTEM 1999 – 2012
LEVELS OF EVIDENCE
1++ High quality meta-analyses, systematic reviews of RCTs, or RCTs with a very low risk of bias
1+ Well-conducted meta-analyses, systematic reviews, or RCTs with a low risk of bias
1- Meta-analyses, systematic reviews, or RCTs with a high risk of bias
2++ High quality systematic reviews of case control or cohort or studies
High quality case control or cohort studies with a very low risk of confounding or bias and a high
probability that the relationship is causal
2+ Well-conducted case control or cohort studies with a low risk of confounding or bias and a moderate
probability that the relationship is causal
2- Case control or cohort studies with a high risk of confounding or bias and a significant risk that the
relationship is not causal
3 Non-analytic studies, e.g. case reports, case series
4 Expert opinion
GRADES OF RECOMMENDATIONS
A At least one meta-analysis, systematic review, or RCT rated as 1++, and directly applicable to the target
population; or
A body of evidence consisting principally of studies rated as 1+, directly applicable to the target
population, and demonstrating overall consistency of results
B A body of evidence including studies rated as 2++, directly applicable to the target population, and
demonstrating overall consistency of results; or
Extrapolated evidence from studies rated as 1++ or 1+
C A body of evidence including studies rated as 2+, directly applicable to the target population and
demonstrating overall consistency of results; or
Extrapolated evidence from studies rated as 2++
D Evidence level 3 or 4; or
Extrapolated evidence from studies rated as 2+
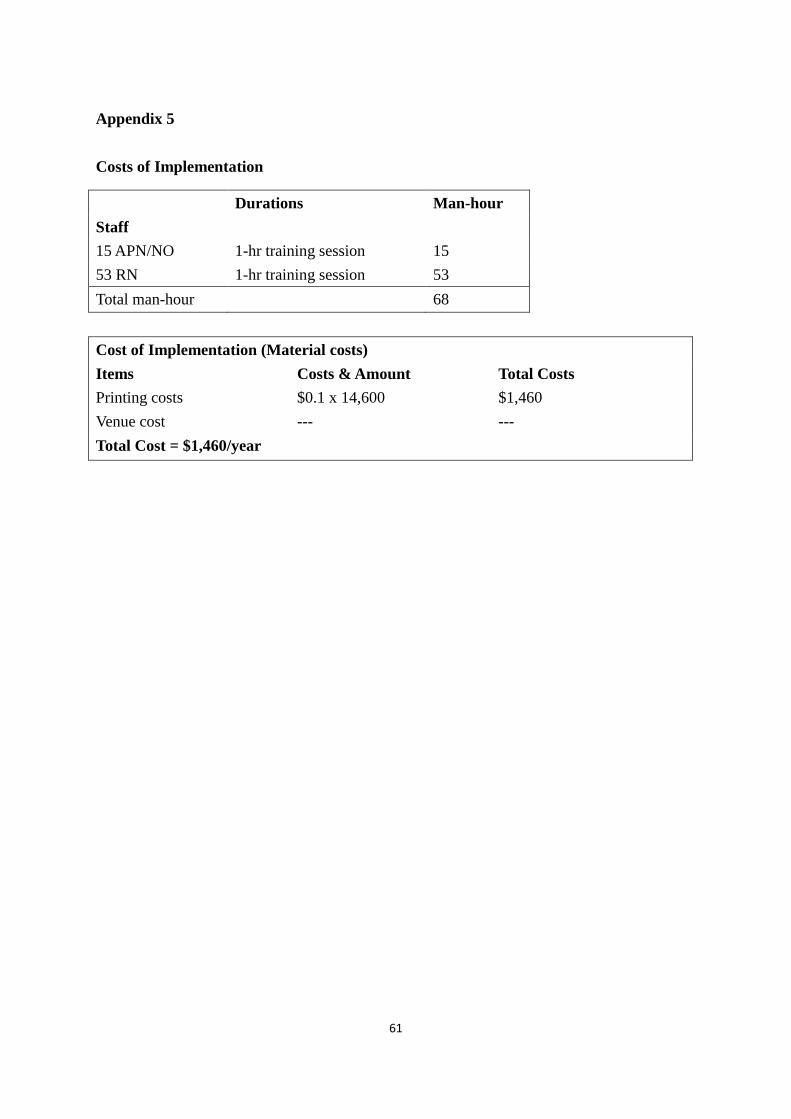
61
Appendix 5
Costs of Implementation
Durations Man-hour
Staff
15 APN/NO 1-hr training session 15
53 RN 1-hr training session 53
Total man-hour 68
Cost of Implementation (Material costs)
Items Costs & Amount Total Costs
Printing costs $0.1 x 14,600 $1,460
Venue cost --- ---
Total Cost = $1,460/year
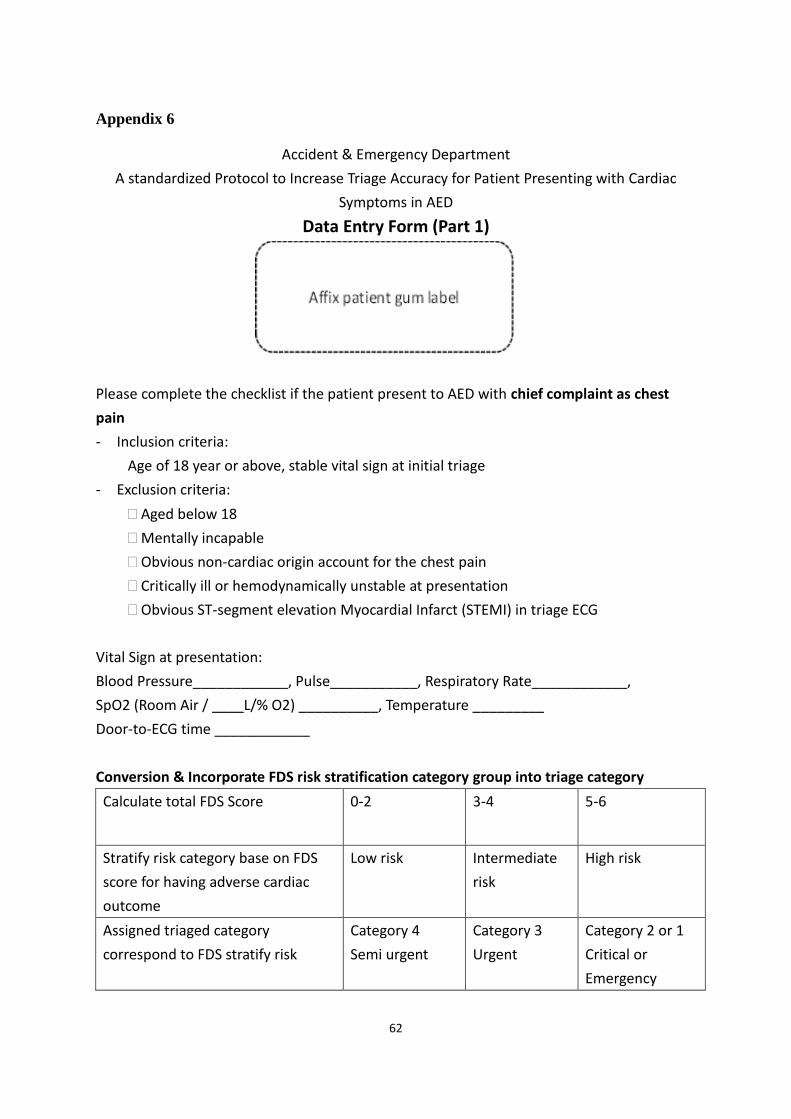
62
Appendix 6
Accident & Emergency Department
A standardized Protocol to Increase Triage Accuracy for Patient Presenting with Cardiac
Symptoms in AED
Data Entry Form (Part 1)
Please complete the checklist if the patient present to AED with chief complaint as chest
pain
- Inclusion criteria:
Age of 18 year or above, stable vital sign at initial triage
- Exclusion criteria:
Aged below 18
Mentally incapable
Obvious non-cardiac origin account for the chest pain
Critically ill or hemodynamically unstable at presentation
Obvious ST-segment elevation Myocardial Infarct (STEMI) in triage ECG
Vital Sign at presentation:
Blood Pressure____________, Pulse___________, Respiratory Rate____________,
SpO2 (Room Air / ____L/% O2) __________, Temperature _________
Door-to-ECG time ____________
Conversion & Incorporate FDS risk stratification category group into triage category
Calculate total FDS Score 0-2 3-4 5-6
Stratify risk category base on FDS
score for having adverse cardiac
outcome
Low risk Intermediate
risk
High risk
Assigned triaged category
correspond to FDS stratify risk
Category 4
Semi urgent
Category 3
Urgent
Category 2 or 1
Critical or
Emergency
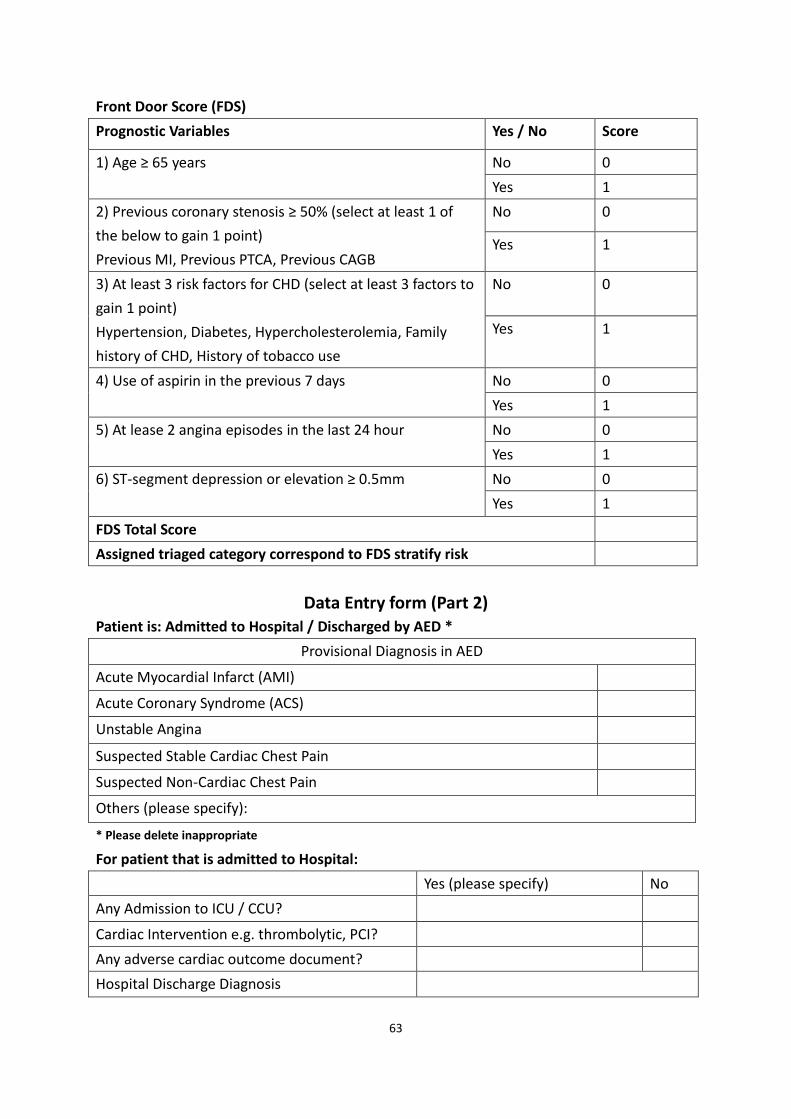
63
Front Door Score (FDS)
Prognostic Variables Yes / No Score
1) Age ≥ 65 years No 0
Yes 1
2) Previous coronary stenosis ≥ 50% (select at least 1 of
the below to gain 1 point)
Previous MI, Previous PTCA, Previous CAGB
No 0
Yes 1
3) At least 3 risk factors for CHD (select at least 3 factors to
gain 1 point)
Hypertension, Diabetes, Hypercholesterolemia, Family
history of CHD, History of tobacco use
No 0
Yes 1
4) Use of aspirin in the previous 7 days No 0
Yes 1
5) At lease 2 angina episodes in the last 24 hour No 0
Yes 1
6) ST-segment depression or elevation ≥ 0.5mm No 0
Yes 1
FDS Total Score
Assigned triaged category correspond to FDS stratify risk
Data Entry form (Part 2) Patient is: Admitted to Hospital / Discharged by AED *
Provisional Diagnosis in AED
Acute Myocardial Infarct (AMI)
Acute Coronary Syndrome (ACS)
Unstable Angina
Suspected Stable Cardiac Chest Pain
Suspected Non-Cardiac Chest Pain
Others (please specify):
* Please delete inappropriate
For patient that is admitted to Hospital:
Yes (please specify) No
Any Admission to ICU / CCU?
Cardiac Intervention e.g. thrombolytic, PCI?
Any adverse cardiac outcome document?
Hospital Discharge Diagnosis

64