Embed Size (px)
Citation preview

A Systematic Approach to Teaching Social Skills to Children With AutismSpectrum Disorders: A Guide for Practitioners
Scott Bellini, Lauren Benner, AND Jessica Peters-Myszak, Indiana Resource Center for Autism, Indiana University, Bloomington
Social skills training (SST) is atopic of great importance in thefield of autism as social skill
deficits are a prominent feature ofautism spectrum disorders (ASD).Common social deficits include (a)difficulty with receptive andexpressive use of nonverbal cues suchas facial expressions, gestures, andbody language; (b) difficultyestablishing peer relationships andfriendships; (c) lack of sharedenjoyment and failure to consider theinterests of others; and (d) lack ofsocial and emotional reciprocity(American Psychiatric Association,2000). Deficits in social cognition arealso common, including difficultiestaking another person’s perspective,difficulties with social problemsolving, and lack of self-awareness(Bellini, 2006). Thus, improving and/or facilitating the acquisition andperformance of social skills acrossmultiple settings should be theprimary purpose of SST.Unfortunately, few children receiveSST as an integral part of theirtreatment and educationalprogramming (Hume, Bellini, &Pratt, 2005). To make matters worse,those youth who are receiving SSTmay not be benefitting from theprogramming.
Although SST can be viewed asan essential component of anytreatment or educational plan forchildren with ASD, the results ofnumerous meta-analytical studieshave questioned the effectiveness ofthis modality. In general, thesestudies have demonstrated thattraditional SST programs are onlyminimally effective in teaching socialskills to youth with learningdisabilities, emotional and behavioraldisorders, and ASD (Bellini, Peters,
Benner, & Hopf, 2007; Forness &Kavale, 1996; Gresham, Sugai, &Horner, 2001; Mathur, Kavale, Quinn,Forness, & Rutherford, 1998; Quinn,Kavale, Mathur, Rutherford, &Forness, 1999). Results of thesestudies indicate that traditional SST isparticularly ineffective in promotingthe transfer of skills across settingsand persons. In addition, whencompared with 12 other interventionmodalities, SST training ranked as theninth most effective strategy, wellbehind behavioral, language,academic, and psychopharmacologicalinterventions (Forness & Kavale,1996).
Bellini et al. (2007) conducted theonly meta-analysis of SST for youthwith ASD. The meta-analysisincluded 55 published researchstudies investigating school-basedSST for youth with ASD. Nearly halfof the reviewed studies produced lowtreatment effects, and a majority ofthe studies produced lowgeneralization effects across persons,settings, and play stimuli. Althoughthe collective outcomes of school-based SST for youth with ASD weredisappointing, the results do help toelucidate factors that lead to morebeneficial social outcomes for youthwith ASD. A synthesis of the Bellini etal. (2007) meta-analysis with othermeta-analytical reviews reveals thefollowing eight recommendations foreffective social skills programming(Bellini, 2009): (a) Increase the dosageof social skill interventions, (b)provide instruction within the child’snatural setting, (c) match theintervention strategy with the type ofskill deficit, (d) conduct a reliable andvalid social skill assessment, (e)develop clear and measureabletreatment objectives, (f) facilitate the
generalization of skills across settingsand persons, (g) ensure interventionfidelity, and (h) implementsystematic social skills programming.
The final recommendation (i.e.,implement systematic social skillsprogramming) is critical as itincorporates many of the otherrecommendations for programming.That is, SST cannot be systematicallydelivered without the inclusion ofreliable and valid social skillsassessment.
The present article will focus onthe eighth and final recommendationby outlining a program tosystematically deliver social skillsinstruction to children with ASD. Thearticle will discuss the structure,format, procedures, and methodsused at the Social Skills ResearchCenter (SSRC) to teach social skills andmeasure the social outcomes of youthwith ASD. The primary purpose of thearticle is to provide a model forpractitioners seeking to deliversystematic social skills programmingto children with ASD. The collectiveoutcomes of children participating inthe SSRC program over the course of a15-month period will be presented.The purpose of presenting these datais to provide an example of how to usedata to evaluate overall programeffectiveness and to makeprogramming modifications. Thearticle will conclude with a discussionof clinical observations gleaned fromthe analysis of these data.
What Is Systematic Programming?
Merriam-Webster dictionarydefines systematic as ‘‘methodical inplan and procedure, and marked bythoroughness and regularity;presented or formulated as a coherent
A SYSTEMATIC APPROACH TO TEACHING SOCIAL SKILLS
26 B E Y O N D B E H A V I O R

body of ideas or principles’’.Applying this definition, we can saythat much of the programming inschools is often deliveredsystematically. When dealing withproblem behaviors, schools oftenfollow a process that uses a functionalbehavior assessment (FBA). First,they determine the function of abehavior by identifying salientantecedent and consequent events.Next, educators develop a hypothesisas to why the behavior is occurringand then develop an individualbehavior plan that addresses the datacollected in the FBA. In addition tobehavioral programming, schoolsroutinely address academicfunctioning systematically. Foracademic skills, many schools areimplementing a response-to-intervention (RtI) approach toprogramming that emphasizes thecollection of systematic data. In thisapproach, teachers collectpreassessment data to ascertain thechild’s current level of functioning.They then provide instruction that issuited to the child’s individual level ofperformance. Performance is thenassessed on a continual basisthroughout the school year. The use ofFBA and RtI approaches in the schoolsis driven by federal special educationlaws that mandate their use.
Without the support of explicitfederal mandates, experience tells usthat systematic programming of SSTis not taking place in schools. Usuallyschools have no organized plan forteaching social skills. Although socialobjectives are commonly developedfor students with ASD, they are rarelybased on a reliable and validassessment of social functioning.Furthermore, seldom does SSTproceed in a methodical or systematicfashion. Commonly, SST is relegatedto inferior status and implementedonly when teachers and other schoolpractitioners have the extra time toaddress it. Another commonoccurrence is for educators to delivera single intervention strategy underthe guise of social skillsprogramming. For instance, a
member of the school team might goto a workshop on the topic of SocialStories, become enthusiastic aboutwriting stories, and then proceed toimplement this strategy for numerousstudents on her caseload. Theproblem with this method is thatimplementing a single strategywithout conducting an assessment ordetermining how the strategy fits intothe child’s overall social skillsprogram is not systematicprogramming. Perhaps a student onthe educator’s caseload is havingdifficulties maintaining personalspace during interactions with peers,so the educator writes a Social Storyto address this. However, anintervention addressing this singlesocial behavior would probably missthe fact that the student’s difficultywith personal space is a result of hisor her inability to read nonverbalcues of others or his lack of self-awareness. Instead of a single SocialStory, the student would likelybenefit more from the Social Storyintervention in addition to instructionon reading nonverbal cues, a self-monitoring intervention, andbehavior rehearsal to practice theskills covered in the Social Story. Inthe example above, the educator’smistake was not the use of a SocialStory; it was the use of the SocialStory in isolation, without firstcollecting data on the nature of thechild’s social skill deficits. Herintervention, though well intended,was short-sighted, disjointed, and toonarrowly focused. Systematicprogramming follows a methodicaland orderly process that is thoroughand comprehensive.
Teaching Social Skills From aSystematic Framework
The SSRC is a university-basedclinic specializing in delivering andmeasuring the outcomes of social skillinterventions for children with ASD.The SSRC was established in the springof 2008 and is a collaborative effortbetween the Indiana Resource Centerfor Autism and the Indiana University
School Psychology Program. Servicesare delivered by school psychologygraduate students under thesupervision of the first author. Thesocial skills program at the SSRC followsthe Building Social Relationships model(Bellini, 2006), which incorporates thefollowing five steps:
1. Assess social functioning2. Distinguish between skill
acquisition and performancedeficits
3. Select intervention strategies4. Implement intervention5. Evaluate and monitor progress
A conceptual underpinning of theBuilding Social Relationships modelis that social interactions involvethree integrated components: socialcognitive processes (e.g., perspectivetaking, attention, self-awareness,declarative/procedural knowledge),emotional regulation (e.g., reducinganxious symptomatology), and theperformance of discrete socialbehaviors (e.g., joining in, respondingto initiations, asking questions). Assuch, social skills programming mustaddress each of these integratedcomponents. (See Bellini [2006] for athorough description of theconceptual foundation of the model.)The present article will focus on theimplementation of the Building SocialRelationships model at the SSRC.
Children receiving services at theSSRC range in age from 5 to 12 yearsand have been diagnosed withautism, Asperger syndrome, andpervasive developmental disordernot otherwise specified (PDD-NOS)as reported by parents at intake. Atleast one child in the program doesnot have a diagnosis of an autismspectrum disorder. His parentsreported that he has been diagnosedwith attention-deficit hyperactivitydisorder–combined type and hasexperienced significant difficultieswith peer relationships. Specificdiagnoses are not determined viaassessment as they have no impact onthe procedures used in the SSRCsocial skills program. The cognitivefunctioning of the children in theprogram ranges from mild cognitive
A SYSTEMATIC APPROACH TO TEACHING SOCIAL SKILLS
F A L L 2 0 0 9 2 7

impairment to above averageintelligence. Some children havelimited expressive language skills anduse only two- to three-word phrases,whereas others exhibit age-appropriateexpressive language. Although theprogram was designed specifically forchildren with ASD, we admit childrenirrespective of diagnosis, cognitivefunctioning, and language ability. TheSSRC social skills program targets skilldeficits that are identified during theassessment process. From apractitioner’s standpoint, confirmingthe child’s diagnosis is not nearly asuseful as determining the nature of thechild’s social skill difficulties andselecting strategies that directly targetthese difficulties.
Assess Social Functioning
Evaluation of social skills andsocial competence is a critical elementof SST (Bellini, 2006) and is thefirst step of the Building SocialRelationships model. The first stepof the model consists of conductinga thorough assessment of theindividual’s current level of socialskills functioning. The purpose of thesocial skills assessment is to identifyskill deficits that will be the directtarget of the intervention and toestablish a baseline for current socialfunctioning. The SSRC socialassessment involves the directassessment of social skills (viasystematic observation) and theevaluation of social competence (viainterview and rating scales).
Gresham (2002) divided socialskills assessment methods into threecategories that measure differentlevels of social functioning and socialvalidity. Type I measures includerating scales and interviewsdesigned to measure socialcompetence or perceptions of socialperformance. An advantage ofType I measures is that treatmentobjectives developed from thesemeasures are likely to be acceptedand viewed as socially acceptable bythe key stakeholders who providedthe behavior ratings. Another majoradvantage of Type I measures is
their ability to efficiently obtaininformation regarding socialbehavior from a variety of sourcesand across a variety of settings. TypeII measures involve the directassessment of the child’s social skillsor social behaviors. As such, thesemeasures are valuable to progressmonitoring and are used extensivelyin applied research studies involvingsingle-subject methodology. Type IImeasures are sensitive to smallchanges in behavior because they arelinked directly to the skills beingtaught. For instance, if the clinicianidentifies ‘‘joining-in activities withpeers’’ as a skill to teach, she wouldthen observe the child to measurewhether joining-in behavior hasincreased over the course of theintervention. Determination oftreatment effectiveness would bebased on changes in the targetbehavior. Type III measures are theleast valid assessment measures butstill have clinical utility. Type IIImeasures involve conducting role-play scenarios or asking questionsrelated to social cognition (e.g., socialproblem solving or perspectivetaking scenarios). For instance, if theclinician is teaching a child toeffectively respond to bullying, shecould set up a role-play scenario thatrequires the child to deal effectivelywith a bully. Or, if she is teachingperspective taking to a child, shecould set up a role-play that requiresthe child to infer the thoughts orfeelings of another person. Althoughthese are important areas to addressvia intervention and should bemeasured via assessment, researchhas demonstrated that thesemeasures are not related to measuresof social competence (Type Imeasures) or measures of socialskills (Type II measures). At thispoint in time, the SSRC does not useType III measures as outcomemeasures, but we do use them toperiodically probe improvements inperspective taking and other socialcognitive components.
The SSRC uses two measures ofsocial competence (or Type I
measures): the Social Skills RatingSystem (SSRS; Gresham & Elliot,1990) and the Autism Social SkillProfile (ASSP; Bellini & Hopf, 2007).The SSRS is a widely used measure ofsocial competence. This questionnaireprovides information on the socialcompetence of youth aged 3 to 18years. The SSRS has been used instudies examining the social skills ofindividuals with ASD (Bellini, 2004,2006; Koning & Magill-Evans, 2001;Ozonoff & Miller, 1995). The ASSP(Bellini & Hopf, 2007) is anassessment tool that provides acomprehensive measure of socialcompetence for youth with ASD. Theitems on the ASSP represent a broadrange of social behaviors typicallyexhibited by individuals with ASD,including initiation skills, socialreciprocity, perspective taking, andnonverbal communication skills. TheASSP was designed for use withyouth with ASD between the ages of6 and 17 years. A preliminaryanalysis of the psychometricproperties of the ASSP with 340 youthwith ASD indicated that theinstrument has strong validity andreliability for this age group (Bellini &Hopf, 2007). The items on the ASSPrepresent specific social behaviorsthat are commonly associated withASD. These items represent thebehaviors that become the directtarget of the subsequent intervention.We refer to these targeted skills ascomponent skills.
The SSRC also uses Type IImeasures to determine progress onour program objectives. We routinelymeasure three common socialobjectives for every child in theprogram (social initiation, socialresponding, and social engagement).The percentage of social engagementwith peers is used as the primarysocial skills outcome in the SSRC.Social engagement is defined asactive participation in an activity orplay sequence with a peer involvingshared toys, objects, and play items.For instance, if the child was seated ata table with other children andplayed with play dough, the activity
A SYSTEMATIC APPROACH TO TEACHING SOCIAL SKILLS
28 B E Y O N D B E H A V I O R

would not be counted as socialengagement unless there was areciprocal exchange of play dough(sharing) or unless the two childrenplayed jointly with the play dough(e.g., making a shape together), wereshowing their creations to oneanother or others, or telling eachother what they were doing. Negativebehaviors such as taking an objectfrom another child or pushinganother child are not counted associal engagement. Examples ofsocial engagement include pullinganother or being pulled in a wagon,taking turns during a board game,and playing jointly with paint, playdough, building blocks, cars, dolls,and so forth. Instances ofunprompted verbal and nonverbalsocial initiations and responses topeers are coded as social engagement(a complete description of behavioralcodes is available from the firstauthor on request). Bothopportunities to respond (i.e.,initiations made by others) andfrequency of responses are recordedto calculate a response ratio(frequency of responses divided byopportunities to respond).
When examining the collectiveoutcomes of the program, only socialengagement data are analyzed due tothe fact that we do not seek toincrease initiations for every childand due to the variability of ourresponse ratio data. For instance,some children initiate socialinteractions quite frequently(upwards of 10–15 times per 5-minobservation), but their totalpercentage of social engagement isless than 10%. For these children, weattempt to decrease the number ofinitiations by increasing their totalpercentage of engagement. It ispreferable to have a child initiate onetime and stay engaged for 5 minrather to have him initiate 10 timeswith only 30 s of engagement.Similarly, response ratios vary fromchild to child and are highlyinfluenced by the number ofopportunities to respond. Forinstance, in some early sessions, the
child might have only oneopportunity to respond (or noopportunities to respond because theother children have infrequentinitiations) during the free-playactivity. If the child failed to respondduring the data collection phase, hisresponse ratio would be zero,which may or may not reflect hisperformance on this variable. Inaddition, some children achieve anear 100% response ratio at baselinebecause they respond to the oneopportunity they have to respond.Again, these ratios skew the collectiveresults of the program. We use thesetwo variables to monitor individualstudent improvement and to makedecisions regarding skills to teachand which strategies to use, ratherthan to evaluate the collectiveoutcomes of the program. These othertwo variables are most useful whenexamined within the context of totalsocial engagement. For instance, ifa child has low levels of socialengagement, we can examine socialinitiation and response ratios todetermine where to focus theintervention. If both socialengagement and frequency ofinitiations are low, then we mustfocus our efforts on increasinginitiations. If initiations are high (butengagement is still low), then wemust focus our efforts on teaching thechild to maintain active engagementwith peers. If the child’s responseratio is low, then we must focus onimproving her social responding inan effort to increase totalengagement. However, if responseratios are high but the child has fewopportunities to respond, then weknow that we can increaseengagement simply by providingmore opportunities for the child torespond.
Although we use common socialobjectives across all children in theprogram, our assessment proceduresalso identify specific component skillsto target for each child. Componentskills are the skills necessary for thechild to successfully achieve thestated social objectives of the
program. For instance, to increasesocial engagement for Child A, wemay need to teach the child to join inactivities, read nonverbal cues,improve social problem solving,engage in reciprocal conversations,and take another person’sperspective. Although the objectivesbecome the focus of our assessmentefforts, it is the component skills thatbecome the primary target of ourintervention and teaching efforts.When selecting skills to teach, wemake a concentrated effort to selectskills that are commonly used, arepivotal to the performance of otherskills (e.g., joining in activities andreading nonverbal cues), and arewithin the child’s zone of proximaldevelopment (i.e., skills that a child iscapable of performing but only withsupport or guidance). Goals for theintervention are thus to teachchildren to perform the skills withoutthe need for guidance or support.Parents are provided an interventionplanning form toward the beginningof the 9-week session that outlinesthe intervention objectives, thecomponent skills that will be taught,and the evaluation measures that willbe used to monitor outcomes.
Distinguish Between SkillAcquisition and Performance Deficits
After the initial assessment iscomplete, the next step is to discernbetween skill acquisition deficits andperformance deficits. The informationcollected during the assessmentallows us to focus our interventionefforts on either skill development(skill acquisition deficit) orperformance enhancement(performance deficit). A performancedeficit refers to a skill or behavior thatis present but not demonstrated orperformed, whereas a skill acquisitiondeficit refers to the absence of aparticular skill or behavior. Greshamet al. (2001) asserted that a keycomponent of effective social skillsprogramming is the ability of theinterventionist to match theintervention strategy with the type ofskill deficit. This position is
A SYSTEMATIC APPROACH TO TEACHING SOCIAL SKILLS
F A L L 2 0 0 9 2 9

supported by Quinn et al. (1999), whoconcluded that the failure of manysocial skill interventions results froma mismatch between strategy andskill deficits. Of the 55 studiesincluded in the Bellini et al. (2007)meta-analysis, only 1 identified thetype of skill deficit exhibited by theparticipants. SSRC clinicianssystematically match the interventionstrategy to the type of skill deficitsexhibited by the child. For instance, ifthe child lacks the skills necessary tojoin in an interaction with peers (skillacquisition strategy), a strategy isselected that promotes skillacquisition. In contrast, if the childhas the skills to join in an activity butregularly fails to do so (performancedeficit), a strategy should be selectedthat enhances performance of theexisting skill.
To determine whether a deficit isthe result of a skill acquisition orperformance deficit, our cliniciansanswer the following questions: (a)Can the child perform the skill acrossmultiple settings and with peers? (b)Can the child perform the skillwithout support or assistance? (c)Does the child perform the skill ifreinforcement is provided? (d) Doesthe child perform the skill ifenvironmental modifications aremade? Answers of ‘‘yes’’ to any ofthese four questions would indicatethe presence of a performance deficit.That is, the child has the skill in his orher repertoire but is not performingthe skill on a consistent basis or at alevel commensurate with peers. It isimperative to determine whether thechild is performing the skills acrosssettings and with peers as opposed toadults. The skills required tomaintain an interaction with an adultdiffer from the skills required tomaintain an interaction with peers. Inthe SSRC social skills program, weare primarily concerned with thelatter. We also want to determinewhether the child is performing theskill without support or guidance.Often, parents report that a skill ispresent, but the evaluation revealsthat the child requires continual
prompting to perform the skill. Thethird question allows us to determinewhether motivational issues areprecluding the performance of thesocial skills. If a child is able to turn askill on when additionalreinforcement is provided, then wecould conclude that it is aperformance deficit. Finally, thefourth question allows us todetermine whether sensorysensitivities are precluding the childfrom performing skills already in herrepertoire.
The answers to these questionsalso elucidate the factors precludingthe performance of already learnedskills. For instance, if the child joins inactivities, but only in quietenvironments, then we can concludethat the child has a performancedeficit and the factor precludingperformance is sound sensitivities.The implication for practice is that wewould not need to teach this childhow to join in as she already has theskill. Instead, we would have toaddress the factor precludingperformance (sound sensitivity).Similarly, if the child is able toperform the skill when reinforcementis provided, then it is unnecessary toteach her the skill. Instead,performance enhancement strategiesshould be selected.
Select Intervention Strategies
Based on this information, theselection and implementation ofintervention strategies takes place. Tosuccessfully teach social skills,clinicians must have a large collectionof intervention strategies at theirdisposal. We have yet to find astrategy that works for all childrenand all behaviors. In addition,clinicians are required to select astrategy based on logic, rationale,and/or empirical evidence asopposed to selecting a strategysimply because it resonates with theirtheoretical orientation. Admittedly,the SSRC program draws heavily onbehavioral principles and techniques,but clinicians are continuallyencouraged to challenge their
assumptions to find strategies thatwork for their clients. This emphasison clinical judgment ensures thatstrategies are matched to the uniqueneeds of the child and to the nature ofthe skill deficits. There are a numberof strategy options to choose fromwhen teaching social skills. As such,making prudent and logicalselections is critical to programsuccess. We use the following criteriawhen selecting strategies: (a) Does theselected strategy have a functionalrelationship with the targeted skills?(b) Does the strategy match the typeof skill deficit (for each skill)? (c) Doesthe selected strategy match thedevelopmental level of child (i.e.,language and cognitive functioning)?(d) Is the strategy supported byresearch? If the strategy is notsupported by research, what is therationale/logic for using the strategy,and how will data be collected tosubstantiate its effectiveness?Furthermore, strategies must beselected that have a direct impact onthe targeted skills. A recurringquestion asked of clinicians is, ‘‘Howwill this strategy target the skill wewant to teach?’’ Will teaching kids torecognize emotional icons on picturecards teach them to recognize realhuman emotions? Or, will playing aboard game about appropriateclassroom behavior have a directimpact on the child’s classroombehavior?
Selecting strategies that match thetype of skill deficit is a criticalcomponent of successfulprogramming. We separate availablestrategies into two categories:strategies to teach skills and strategiesto enhance the performance ofexisting skills. A list of thesestrategies is presented in Table 1.Strategies should also be tailored tothe specific developmental level ofthe child. Many of the social cognitivestrategies that we use, such as socialproblem solving and conversationaltasks, are not appropriate for thechildren in our program who havelimited expressive communicationskills or who have comorbid
A SYSTEMATIC APPROACH TO TEACHING SOCIAL SKILLS
30 B E Y O N D B E H A V I O R

cognitive disabilities. Finally,although we favor strategies that areempirically based, such as videomodeling, prompting, socialnarratives, and peer-mediatedinstruction, we do not use onlyresearch-based strategies. In thesecases, our clinicians are required topresent a logical rationale for why thestrategy will be effective for that childand for that particular skill. Theinclusion of untested and newlydeveloped strategies is done topromote innovation and creativity onthe part of our clinicians. Weacknowledge the fact that today’sevidence-based practices wereyesterdays’ untested ideas.
Implement InterventionThe SSRC social skills program
consists of 9 weeks of social skillstraining in a group format. Theduration of the program (i.e., 9weeks) was chosen to match thelength of a school quarter. Groupsmeet once per week with sessionslasting 45 min. The four groupsconsist of two to four children withASD. Children are grouped based onage and gender. Some groups alsoinclude one peer mentor, althoughthe use of peers is dependent on
availability. We use numerousstrategies in the SSRC social skillsprogram, and a comprehensivereview of each strategy is beyond thescope of this article (see Bellini, 2006,for a more extensive description ofstrategy options). This section (Step 4)will provide a brief description of thethree most frequently used strategiesof the SSRC social skills program:Social Story with behavioralrehearsal, video modeling, andprompting. These three strategies areimplemented in nearly every socialskills session. These strategies havealso been identified as evidence-based practices by the recentlyreleased National Standards Report(National Autism Center, 2009).
Social Story with behavioralrehearsal. A Social StoryTM (Gray,2000) is a frequently used andempirically supported strategy toteach social skills to youth with ASD(Sansosti, Powell-Smith, & Kincaid,2004). A Social Story presents socialskills and rules to children in theform of a brief story. We use SocialStories to teach a number ofcomponent skills, such as initiatinginteractions, making transitions,playing a game, and speaking withappropriate volume and intonation.
A Social Story may also include apicture of the child performing thetask to provide the child with a visualcue. We have also incorporated asocial story into a video modelingintervention. In these interventions,the video depicts a person readingthe story and then an adult or childdemonstrating the skill. When aSocial Story is used, we pair it withbehavioral rehearsal. We use theSocial Story to introduce a skill orconcept and then follow the storywith behavioral rehearsal so that thechild can practice the skills. Weconceptualize the Social Story asaddressing social thinking (i.e.,declarative knowledge) and thebehavioral rehearsal as addressingthe social behavior.
Behavioral rehearsal is aneffective approach to teaching socialskills that allows for the positivepractice of skills (Gresham, 2002).Rehearsal involves acting outsituations or activities in a structuredenvironment to practice newlyacquired skills and strategies orpreviously learned skills that thechild is having difficultiesperforming. We use behavioralrehearsal to teach a variety ofinteraction skills, particularly thoseinvolving initiating, responding, andterminating interactions. In fact,every newly introduced or learnedskill is paired with behavioralrehearsal. In one scenario, the child isrequired to initiate a conversationwith another person, who is engagedin a separate task. Consequently, hewould have to ask to join in or ask theother person to join him in an activity.Rehearsal allows the child to executethe skill or behavior without thepressure and anxiety that sometimesare associated with real-lifesituations, and allows practice of themechanics of a movement throughmultiple behavioral repetitions.Rehearsal activities can be performedwith adults or with other children asparticipants. Repetition is a keyaspect of rehearsal, as is ending withan errorless (or at least a positive)performance. We aim for 3 repetitions
Table 1 SKILL ACQUISITION AND PERFORMANCE ENHANCEMENT STRATEGIES
Strategies That Promote SkillAcquisition
Strategies That Enhance SocialPerformance
Strategies to teach nonverbal recognitionand perspective taking
Reinforcement/contingency strategies
Reciprocal intervention strategies Gaming skills/play skillsConversation game Environmental modificationsBehavioral rehearsal Peer-mediated instructionSocial storiesa Increased social opportunities/live
practiceSocial problem solving and social rules Peer training strategiesSelf-monitoringa Priming social behaviorRelaxation techniques/emotional
regulationaPrompting strategiesa
Video modelinga Relaxation techniques/emotionalregulationa
Prompting strategiesa Self-monitoringa
Video modelinga
Social storiesa
a These strategies may be used to promote skill acquisition and to enhance performance.
A SYSTEMATIC APPROACH TO TEACHING SOCIAL SKILLS
F A L L 2 0 0 9 3 1

Figure 1 EXAMPLE OF SESSION STRUCTURE PLAN
A SYSTEMATIC APPROACH TO TEACHING SOCIAL SKILLS
32 B E Y O N D B E H A V I O R

for newly learned skills in the clinic.When the child is able to perform theskill in the clinic, we then leave theclinic to allow the child to apply skillsto real-life situations with peopleother than the clinicians. Promptingis provided to the child as necessaryto perform the skill successfully.
Video modeling interventions. Avideo modeling intervention typicallyinvolves an individual watching avideo demonstration of positivebehavior and then imitating thebehavior of the model. Video self-modeling (VSM) is a specificapplication of video modeling inwhich the individual learns by
watching her own behavior. Resultsof a meta-analytical study suggestthat video modeling and VSM arehighly effective interventionstrategies for addressing social-communication skills, behavioralfunctioning, and functional skills inyouth with ASD (Bellini & Akullian,2007). In the SSRC social skillsprogram, every session is videorecorded, and a VSM intervention isimplemented in nearly every sessionto teach a variety of social skills. TheSSRC program employs two types ofVSM interventions: positive self-review (PSR) and video feedforward(Dowrick, 1999). PSR refers to
individuals viewing themselvessuccessfully engaging in a behavioror activity that is currently in theirbehavioral repertoire. PSR can beused with low-frequency behaviors.In PSR interventions, the individual isrecorded while engaging in the low-frequency behavior (e.g., initiating aninteraction with peer) and thenshown a video of the behavior beingperformed. Video feedforwardinterventions are used when theindividual possesses a component ofthe target skill in her behavioralrepertoire or is performing the skill ata low level of mastery or autonomy.In feedforward interventions,
Figure 1 (Continued )
A SYSTEMATIC APPROACH TO TEACHING SOCIAL SKILLS
F A L L 2 0 0 9 3 3

individuals observe themselvessuccessfully, independentlyperforming skills that they arecurrently incapable of performing ontheir own. This is accomplished via ahidden support technique. Forinstance, the child is prompted by aclinician to ask a playmate to join herin an activity, or the child might beprompted to respond to theinitiations of another child. Theclinician’s prompt is then edited out(i.e., hidden) so that when the childviews the video segment, she seesherself as independently andsuccessfully performing the behavior.Hidden support interventions are themost common VSM intervention usedat the SSRC. See Bellini andMcConnell (in press) for moreinformation on how to record andedit videos.
Prompting procedures. Promptsare supports and assistance providedto the child to help him or her acquireskills and successfully performbehaviors (McConnell, 2002; Rogers,2000). Prompts can be used to teachnew social skills (in the case ofphysical and modeling prompts)and to enhance performance ofpreviously acquired skills. In theSSRC program, prompts aredelivered by either adult cliniciansor by the peer mentors. A limitationof prompting strategies is that thechild with ASD may limit socialinteractions to only instances inwhich prompting is provided. Assuch, whenever prompting is used, aprompt-fading plan is implementedto systematically fade prompts.
The SSRC uses five primary typesof prompts to facilitate socialbehavior: physical, modeling, verbal,gestural, and natural (arranged frommost to least supportive). The mostsupportive prompts require thegreatest amount of adult support andthe least amount of independence onthe part of the child, whereas the leastsupportive prompts require moreindependence on the part of the childand less adult assistance. The goal isto use the prompt that provides justenough support—or the least
supportive prompt necessary for thechild to successfully complete a task.The order of prompts will have greatimportance for the eventual fading ofprompts.
Prompts are used each sessionduring the 15 min of structured playactivities and during otherinstructional strategies such asbehavioral rehearsal. The goal of thestructured activities is to maintainactive engagement between thechildren in the group. We do this byproviding as much prompting asnecessary to promote interaction andthen systematically fading thesesupports while the level ofengagement is maintained. SSRCclinicians are provided with aprompting cheat sheet as a trainingtool to promote consistency acrosstherapists. We fade the prompts asquickly as feasible from most to leastsupportive, or via a time delayprocedure. Prompts typically need tobe faded gradually. If a child requiresa modeling prompt, first fade to a lesssupportive modeling prompt (e.g.,from modeling the whole behavior tomodeling a part of the behavior).From there you will fade to a verbalprompt (which is less supportive thanthe modeling prompt). If you arefading verbal prompts, fade theprompt from specific to general (e.g.,from ‘‘Tommy, hand the ball toAddison’’ to ‘‘Tommy, play withAddison’’ to ‘‘Tommy, time to play,’’and so on). Prompt fading isaccomplished by providing the lesssupportive prompt just before, orsimultaneously with, the moresupportive prompt; for instance,providing a verbal directive prior tomodeling the behavior or providing agestural prompt prior to providing averbal directive. The more supportiveprompt would then be withdrawnduring subsequent performances ofthe skill or behavior. For instance,you would no longer use the verbalprompt after the delivery of thegestural prompt.
Session structure plans. Cliniciansgenerate session structure plans foreach of the 9 weekly sessions. The
session structure plans detail everyminute of the 45-min sessions byexplicitly outlining what skills will betaught and the strategies used toteach the skill. These plans provide adescription of the procedures thatwill be used with each child duringthe session and also indicateprompting responsibilities for theclinicians. The session structure plansare reviewed and approved by thefirst author prior to each session. Allthe session structure plansincorporate a 10- to 15-min structuredplay activity in which the primaryinstructional strategy involvesprompting the children to maintainengagement. The plans also allow5 min at the end of each session fordata collection. An example of asession structure plan is provided inFigure 1.
Facilitate the generalization of skills.A critical aspect of all social skillsprogramming is to develop a plan forgeneralization, or transfer of skillsacross settings, persons, situations,and time. Gresham et al. (2001)concluded that a persistent weaknessin social skills training research is itsfailure to demonstrate adequategeneralization effects. This isprimarily a result of interventionsthat fail to plan for generalization.The ultimate goal of social skillstraining is to teach the child tointeract successfully with multiplepersons and in multiple naturalenvironments. From a behavioralperspective, the inability togeneralize a skill or behavior is aresult of too much stimulus control.That is, the child performs the skill orbehavior only in the presence of aspecific stimulus (person, prompt,directives, etc.). Generalization isparticularly important for childrenwith ASD who often havepronounced difficulties transferringskills across persons and settings.The SSRC uses the followingtechniques to facilitategeneralization: (a) Train withmultiple persons and in multiplesettings, (b) ensure the presence anddelivery of natural reinforcers for the
A SYSTEMATIC APPROACH TO TEACHING SOCIAL SKILLS
34 B E Y O N D B E H A V I O R

performance of social skills, (c)practice the skill in the naturalenvironment, (d) fade prompts asquickly as feasible, (e) providemultiple exemplars for social rulesand concepts, (f) train skills loosely(i.e., vary the instruction, directives,strategies, and prompts used duringskill instruction), and (g) teach self-monitoring strategies.
Evaluate and Monitor Progress
The purpose of the evaluation atStep 5 is to monitor the outcomes ofthe social skills program for eachchild. The procedures used at thisstage mirror the procedures usedduring Step 1. Social competencemeasures (i.e., rating forms) areadministered at the beginning andend of the 9-week program.Observations of social skills areconducted each week during groupsessions. Week 1 serves as a baselineperiod, and no instruction isdelivered. Data are collected duringthe first and last 5 min of Session 1and during the first 5 min of Session2, giving us three baseline data pointsfor each child. Data on socialbehaviors are then collected at theend of each group session throughoutthe 9 weeks of the program. To
measure generalization of skillsacross settings, data on socialengagement with peers is collectedvia observation at the children’sschool. School observations areconducted at the beginning and endof the 9-week program (note that theschool observations are conductedonly for students living within a 20-mile radius of our clinic).
At the end of the program,parents are given a summary reportthat lists the social objectives,component skills, and a detaileddescription of the strategies used toteach the component skills. Parentsare encouraged to share the reportwith the child’s educational team toencourage consistency of instructionacross settings. The summary reportalso provides a graphicalpresentation of the child’s socialoutcomes, including socialcompetence (parent and teacherSSRS reports and ASSP parentreports) and data on socialengagement at the clinic and atschool.
Collective Outcomes of the Program
To date, the SSRC has conductedthree 9-week sessions of socials skills
programming. Groups were run inthe spring and fall of 2008 and thespring of 2009. This section willsummarize and discuss the collectiveoutcomes of the 8 childrenparticipating in all three of thesesessions. The process of collectingand analyzing data over the course of15 months has been extremely usefulin evaluating the collective outcomesof our program and has revealed anumber of patterns and phenomenathat would not have been revealedhad we not aggregated the data orhad we examined the outcomes ofeach 9-week session only in isolation.
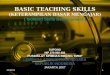
Mean social engagement withpeers increased during each 9-weeksession (see Fig 2 Fig 3 Fig 4).Although baseline levels of meansocial engagement increased fromsession to session, the averagepercentage of engagement reachedduring the treatment phases wasrather consistent (50%, 55.4%, and55.9%). All 8 children showedincreases in the mean percentage ofsocial engagement in the clinic duringthe spring 2008 and fall 2008 sessions,whereas only 1 child showed declines(28% to 24%) during the spring 2009session. Data on social engagement atschool were collected and analyzed
Figure 2 MEAN PERCENTAGE OF UNPROMPTED SOCIAL ENGAGEMENT WITHIN THE CLINIC FOR BASELINE AND TREATMENT (N 5 8) PHASES IN SOCIAL
SKILLS GROUPS, SPRING SEMESTER 2008
A SYSTEMATIC APPROACH TO TEACHING SOCIAL SKILLS
F A L L 2 0 0 9 3 5

for one school semester (spring 2008)and over the course of 1 school year(fall 2008 and spring 2009). Becauseall of the children changed gradesand some of the students changedschools between the spring 2008session and fall 2009 session, we didnot make comparisons between thesetwo sessions because variables withinthe school settings were notconsistent (different students,different teachers, different settings,etc.). We did, however, compare peerengagement across the fall 2008 and
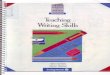
spring 2009 sessions because allchildren remained in the same schooland classroom throughout the schoolyear. School data were collected forthe 5 children who lived within a20-mile radius of our clinic. Thechildren’s social engagement withpeers at school improvedsubstantially after the first 9 weeks ofsocial skills training (see Fig 5). Acomparison of the spring 2008treatment phase and fall 2009baseline phase indicates thatengagement was maintained over the
summer (between the spring and fallsessions). During this school year, all5 children demonstrated increases inpeer engagement at school. Moderateimprovements were also observedduring the 2008–2009 school year (seeFig 6), although 2 of the 5 childrenshowed decreases in percentage ofengagement with peers. Mean scoreson the teacher version of the SSRSimproved from 85 (SD 5 7.7) to 91.1(SD 5 8.8), whereas mean scores onthe parent version of the SSRSincreased from 83.9 (SD 5 11.6) to
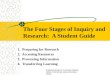
Figure 4 MEAN PERCENTAGE OF UNPROMPTED SOCIAL ENGAGEMENT WITHIN THE CLINIC FOR BASELINE AND TREATMENT (N 5 8) PHASES IN SOCIAL
SKILLS GROUPS, SPRING SEMESTER 2009
Figure 3 MEAN PERCENTAGE OF UNPROMPTED SOCIAL ENGAGEMENT WITHIN THE CLINIC FOR BASELINE AND TREATMENT (N 5 8) PHASES IN SOCIAL
SKILLS GROUPS, FALL SEMESTER 2008
A SYSTEMATIC APPROACH TO TEACHING SOCIAL SKILLS
36 B E Y O N D B E H A V I O R

91.4 (SD 5 9.4). Mean scores on theASSP increased from 110.6 (SD 5
11.7) to 121(SD 5 10.3). Increaseswere observed for 6 of the 8 childrenon all three measures of socialcompetence.
There are a number of benefits toexamining the collective outcomes ofthree 9-week sessions rather than justone session. It allowed us todetermine whether skills weremaintained from one 9-week session
to the next. Collectively, baseline orpretest scores increased from onesession to the next on all measures.For returning children, we no longerview the baseline measures as apretest for the current session butrather as a maintenance measure forthe prior session. The collection ofdata across 15 months also revealedvarious patterns with regard to thescores of our various assessmentmeasures. For instance, we have
found that the SSRS is sometimes notsensitive to change, at least duringthe first 9 weeks of the program.Often, scores on the SSRS are the lastof our outcome metrics to change. It isnot uncommon for us to seeimprovements on the ASSP and in thesocial engagement data during thefirst 9-week session but not on theSSRS. A child with ASD might bemaking steady improvements insocial behavior, but her standard
Figure 6 MEAN PERCENTAGE OF UNPROMPTED SOCIAL ENGAGEMENT WITH PEERS DURING SCHOOL OBSERVATIONS PRETREATMENT AND
POSTTREATMENT FOR SCHOOL YEAR 2 (n 5 5)
Figure 5 MEAN PERCENTAGE OF UNPROMPTED SOCIAL ENGAGEMENT WITH PEERS DURING SCHOOL OBSERVATIONS PRETREATMENT AND
POSTTREATMENT FOR SCHOOL YEAR 1 (n 5 5)
A SYSTEMATIC APPROACH TO TEACHING SOCIAL SKILLS
F A L L 2 0 0 9 3 7

score on the SSRS may remainunchanged after 9 weeks ofprogramming. On many occasions,scores on the SSRS improved duringthe second 9-week session. The lackof change on the SSRS measure maybe due to the fact that the SSRS wasnot intended to detect changes insuch a short period of time. Or, it maybe due to the fact that the items on theSSRS do not precisely match thesocial characteristics of children withASD. Thus, the skills typicallytargeted by our social skill programare not directly measured by theSSRS. Instead, the SSRS may bemeasuring a more globalrepresentation of social functioning.
We have also noted a plateaueffect for our children on the SSRSmeasures. Scores would routinely risefrom the below-average range to theaverage range (i.e., scores wouldincrease from 80 to 99), but rarely didthey continue to rise past the mean of100. This would indicate that theseparticular children are functioningwithin the average range of socialcompetence when compared with thegeneral population of children.Perhaps it is unrealistic to expectchildren with ASD to exceed theaverage social competence level ofother children. Indeed, if scores farexceeded the mean on the SSRS, itwould call into question the validityof the parent and teacher ratingforms. The implication of thisphenomenon is that educators andpractitioners may not detect changeson the SSRS measure when workingwith some children with ASD,especially those already scoringwithin the average range of socialcompetence at the onset of theprogram. It would also be imprudentto discontinue social skillsprogramming for a child with ASDwho scores within the average rangeof social functioning. Children withASD will likely need programming tomaintain a level commensurate withpeers. Thus, success of the socialskills program in these cases shouldbe judged by whether the child staysat this average level of functioning.
In addition, occasionally scoresdid not improve during one of the9-week sessions. This was due to anumber of variables from medical orbehavior issues or due to the fact thatour program was ineffectual duringthat particular 9-week session. Thecollection of data across threesessions allowed us to view thechild’s short-term progress (or lackthereof) within the context of longerterm change. We were able todetermine if the current session wasan anomaly or whether dramaticchanges needed to be made in thechild’s programming. Beyondindividual child progress, whichsometimes varied, the examination ofcollective outcomes allowed us todetermine whether we were on theright track as a program. Aspractitioners, we sometimes getcaught up in our single success storyor dramatic failure, but by looking atcollective outcomes of the childrenwe serve, we are better able tomake decisions regarding ourprogrammatic effectiveness. Successor failure of individual cases is bestunderstood within the context ofthese collective outcomes.
Summary
The purpose of this article wasnot to demonstrate the relativeeffectiveness of the SSRC social skillsprogram compared with otheravailable programs. Instead, our goalwas to provide an example topractitioners wishing to design andimplement systematic social skillsinstruction. Teaching social skillssystematically allows practitioners topractice with purpose in the deliveryof social skills programming.Evaluating outcomes and selectingstrategies based on a combination oflogic and data does not ensureprogram success but certainlyincreases the probability of success.We were not always successful inimproving the social skills and socialcompetence of the children withwhom we worked, but because weengaged in systematic programming,
we knew precisely when and whythose failures occurred. It alsoallowed us to assess our ownmethods and become betterpractitioners and thus deliver moreeffective social skills programming tochildren with ASD.
REFERENCES
American Psychiatric Association. (2000).
Diagnostic and statistical manual of
mental disorders (4th ed.).
Washington, DC: Author.
Bellini, S. (2004). Social Skills and Anxiety
in Higher Functioning Adolescents
with Autism Spectrum Disorders.
Focus on Autism and Other
Developmental Disabilities, 19(3),
78–86.
Bellini, S. (2006). Building social
relationships: A systematic approach to
teaching social interaction skills to
children and adolescents with autism
spectrum disorders and other social
difficulties. Shawnee Mission, KS:
Autism Asperger Publishing.
Bellini, S. The ingredients of effective social
skill interventions for youth with autism
spectrum disorders: A synthesis of meta-
analytical research and clinical
experience. Manuscript in preparation.
Bellini, S., & Akullian, J. (2007). A meta-
analysis of video modeling and video
self-modeling interventions for
children and adolescents with autism
spectrum disorders. Exceptional
Children, 73, 261–284.
Bellini, S., & Hopf, A. (2007). Assessing
the psychometric properties of the
Autism Social Skills Profile. Focus on
Autism and Other Developmental
Disabilities, 22, 80–87.
Bellini, S., & McConnell, L. (in press).
Strength based educational
programming for students with
autism spectrum disorders: A case
for video self-modeling. Preventing
School Failure.
Bellini, S., Peters, J., Benner, L., & Hopf, A.
(2007). A meta-analysis of school-
based social skill interventions for
children with autism spectrum
disorders. Remedial and Special
Education, 28, 153–162.
A SYSTEMATIC APPROACH TO TEACHING SOCIAL SKILLS
38 B E Y O N D B E H A V I O R

Dowrick, P. (1999). A review of self-
modeling and related interventions.
Applied and Preventive Psychology, 8,
23–39.
Forness, S. R., & Kavale, K. A. (1996).
Treating social skills deficits in
children with learning disabilities: A
meta-analysis of the research.
Learning Disabilities Quarterly, 19,
2–13.
Gray, C. (2000). The new social story book:
Illustrated edition. Arlington, TX:
Future Horizons.
Gresham, F. M. (2002). Best practices in
social skills training. In A. Thomas &
J. Grimes (Eds.), Best practices in school
psychology (4th ed.). Bethesda, MD:
NASP.
Gresham, F. M., & Elliot, S. N. (1990).
Social Skills Rating System manual.
Circle Pines, MN: American
Guidance Service.
Gresham, F. M., Sugai, G., & Horner, R. H.
(2001). Interpreting outcomes of
social skills training for students with
high-incidence disabilities. Teaching
Exceptional Children, 67, 331–344.
Hume, K., Bellini, S., & Pratt, C. (2005).
The usage and perceived outcomes of
early intervention and early
childhood programs for young
children with autism spectrum
disorder. Topics in Early Childhood
Special Education, 25, 195–207.
Koning, C., & Magill-Evans, J. (2001).
Social and language skills in
adolescent boys with Asperger
syndrome. Autism, 5, 23–36.
Mathur, S. R., Kavale, K. A., Quinn, M.
M., Forness, S. R., & Rutherford, R. B.
(1998). Social skills interventions with
students with emotional and
behavioral problems: A quantitative
synthesis of single subject
research. Behavioral Disorders, 23,
193–201.
McConnell, S. R. (2002). Interventions to
facilitate social interaction for young
children with autism: Review of
available research and recommendations
for educational intervention and future
research. Journal of Autism and
Developmental Disorders, 32, 351–372.
National Autism Center. (2009). National
standards report. National Autism
Center. Retrieved November 6, 2009
from http://www.
nationalautismcenter.org/affiliates/
Ozonoff, S., & Miller, J. N. (1995).
Teaching theory of mind: A new
approach for social skills training for
individuals with autism. Journal of
Autism and Developmental Disorders,
25, 415–433.
Quinn, M. M., Kavale, K. A., Mathur, S.
R., Rutherford, R. B. Jr, & Forness, S.
R. (1999). A meta-analysis of social
skills interventions for students with
emotional and behavioral disorders.
Journal of Emotional and Behavioral
Disorders, 7, 54–64.
Rogers, S. (2000). Interventions that
facilitate socialization in children
with autism. Journal of Autism and
Developmental Disorders, 30, 399–409.
Sansosti, F. J., Powell-Smith, K. A., &
Kincaid, D. (2004). A research
synthesis of social story interventions
for children with autism spectrum
disorders. Focus on Autism and Other
Developmental Disabilities, 19, 194–
204.
Systematic. 2008. In Merriam-Webster
Online Dictionary. Retrieved
September 29, 2009 from http://
www.merriam-webster.com/
dictionary/systematic
A SYSTEMATIC APPROACH TO TEACHING SOCIAL SKILLS
F A L L 2 0 0 9 3 9