Embed Size (px)
Citation preview

ABC of Colorectal Diseases
PAEDIATRIC PROBLEMS- IICaroline M Doig
Rectal bleeding
£r -
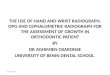
Contrast barium enema radiograph showingstalked polyp (arrowed) and more sessilepolyp opposite.
!.
Meckel's diverticulum which has beeninvolved in an intussusception.
PolypsPainless bleeding suggests a solitary rectal polyp. These are almost alwaysnot adenomatous. The bleeding, separate from the stool and of moderatequantity, necessitates sigmoidoscopy and snaring of the polyp. Such polypsshould be sent for histological examination to check that they are notpremalignant. Multiple polyps elsewhere in the colon may require eitherflexible sigmoidoscopy or colonoscopy to make the diagnosis, to take abiopsy specimen, and for treatment. Contrast barium enema examinationcan help to pin point the area. If the polyps are adenomatous follow up withrepeated endoscopy is necessary. Polyposis coli can occur in children underthe age of 15 years, so follow up and treatment, even colectomy, may benecessary early.
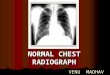
IntussusceptionIntussusception occurs most commonly in
infants 7-12 months old. In older children thereis usually an associated polyp, diverticulum, ortumour. Although classically the diagnosis ismade on the basis of colicky abdominal pain, asausage shaped mass, and dark red blood throughthe rectum, 10% present with diarrhoea andvomiting suggestive of gastroenteritis. Bleedingthrough the rectum indicates that the bowel iscompromised and occurs in about a half ofpatients.
If the child is not in shock, which is often thecase, barium or air enema examination may notonly confirm the diagnosis but also treat theintussusception as the hydrostatic pressure canreduce the bowel. More often surgery may haveto be performed after resuscitation. If resection ofthe bowel is necessary the ileocaecal valve andterminal ileum may be lost.
Meckel's diverticulum may present withbleeding because of an intussusception orbecause of the presence of gastric mucosa.
Duplication cyst
Any part of the gastrointestinal tract may beduplicated; the colon is the part least commonlyduplicated. The diagnosis is made by usingultrasonography and radiography to showdisplacement of the bowel. Spinalabnormalities -for example, hemivertebrae canbe associated, though not necessarily at the levelof the abnormality. When a duplication cystoccurs in a short portion ofbowel it is usuallypossible to excise both the cyst and the segment ofbowel affected, with reanastomosis of the colon.
.~~~~~~~~
Barium enema radiographshowing intussusception inright transverse colon.
Duplication cyst of small bowel withflattened bowel.
BMJ VOLUME 305 29 AUGUST 1992
Bright red bleeding through theanus usually indicates one of thefollowing:* Anal fissure* Rectal polyp* Dysentery* Inflammatory bowel disease
511
on 4 Septem
ber 2020 by guest. Protected by copyright.
http://ww
w.bm
j.com/
BM
J: first published as 10.1136/bmj.305.6852.511 on 29 A
ugust 1992. Dow
nloaded from

Inflammatory bowel disease,.
*:~~~~~~~'0s'~ , f5. 'e F s
Age at diagnosis of Crohn's'disease and ulcerative colitis.1
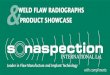
Small bowel barium enemaradiograph in a child with Crohn'sdisease showing narrowed ileum justproximal to ileocaecal valve.
Inflammatory bowel disease does occur inchildhood. The number ofchildren under the ageof 12 years with Crohn's disease is increasing.
The presentation, diagnosis, and treatment of
ulcerative colitis and Crohn's disease in children
are similar to those in adults. Children m'aypresent with extragastrointestinal problems,such as arthritis, skin rashes, and uveitis, manymonths or years before abdominal pain, weight
loss, and mouth ulcers make the diagnosis of
Crohn's disease obvious. In addition to
endoscopy and biopsy diagnosis has been
improvedbytheuseofsmall bwelenemasandsucralphate scans to pin point active areas.
Iren in
Surgery for Crohn's disease in children, when
)wel performed early because of stunting of growthand failure of sexual development, has tended to
44 give fewer immediate postoperative problems
305 than in adults and may lead to a growth spurt,
iry though the risk of recurrence is high.
Anorectal anomalies
Anorectal anomalies are congenitalabnormalities of either the anus or rectum, or
both. The anus can be absent, abnormal, or
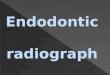
ectopic. There are many different types ofanomally, which may or may not involve fistulousconnections to skin, vagina, or urethra. The maindistinction, however, is whether the bowel endsabove or below the levator ani muscle. Isolatedcolonic atresia may also occur.
Common anorectal anomalies (a) in boys and (b) in girls showing relation inhigh and low anorectal abnormalities between bowel, levator ani muscle, skin,urethra, and vagina.
BMJ VOLUME 305 29 AUGUST 1992
Number of childBritain withinflammatory bcdisease'* Crohn's disease* Ulcerative colitis* Other inflammato
bowel disease 34
T, -P,f"141%,.. i.
in.:-', ., ;:," z
L-M.
..': ., --n
512
on 4 Septem
ber 2020 by guest. Protected by copyright.
http://ww
w.bm
j.com/
BM
J: first published as 10.1136/bmj.305.6852.511 on 29 A
ugust 1992. Dow
nloaded from

Male infant perineum with pin holeanus showing excoriation due topassage of "toothpaste stools" as aresult of delayed diagnosis.
Female perineum showing anteriorplaced anus just inside the forchette.
L' .. 'i;"'.'.,......
Perineum with no anus or fistula -probable hightype anomaly.
l ...
Inverted lateral radiograph showing intestinal gasjust at level of coccyx-pubis line (high typeanomaly).
Anomalies associated withcolorectal problems in children* Congenital heartdisease 12-20%* Skeletal problems 15-20%* Tetralogy of fallot and atresia 5-10%* Other intestinal problems 5%* Urological problems 30-50%
The low type of anomaly includes those inwhich the bowel passes through a normallevator ani muscle to end blindly a fewcentimetres from the anus (imperforate anus) orenters the perineum in an abnormal position. Thediagnosis is made by careful inspection of theperineum for a fistulous connection to skin on thepenile shaft or median raphe of the scrotum in aboy or just within the vestibule in a girl.Treatment usually involves the deroofing of sucha fistula by cutting back to a normal anus. Longterm continence is ensured if the sphinctermuscles are normal. Occasionally an anoplasty toplace an ectopic anus in a normal position may benecessary. Early inspection of the perineum inbabies to pick up an ectopic or stenotic analopening improves long term outlook.
It is important that the high type of anorectal anomaly is notmisdiagnosed as a low imperforate anus. In these children the bowel endsabove the levator ani, which is often poorly developed. The distinction canbe made by inspection and lateral inverted radiography performed 24 hoursafter birth to find out where the intestinal gas ends. Should gas appear not toreach the pubococcygeal line, a high type of anomaly is probable andperineal exploration should not be done.
Treatment entails performing a colostomy with subsequent "pullthrough" of the colon through the pelvic muscles and involving thesphincter muscles present to the perineum. It has been suggested that theearlier such reconstruction surgery is carried out the more likely the childwill develop normal continence. Various operations have been developedthat use abdominal, sacral, and perineal approaches to reconstitute theanatomy. The most recent, a posterior approach dividing the muscles andtapering the colon before bringing it on to the perineum, has had promisingearly results.
As a result of poor or absent musculature children with high anomaliesmay be slow to gain continence, but by strenuous training to use suchmuscles as are present, tightening the muscles later by levatorplasty, givingadvice about diet, and keeping the "neorectum" empty, improvement mayoccur. More than a half of children with any type of anorectal anomaly willhave at least one other abnormality. In view of the high incidence of renalproblems all ofthese children should have their urinary tract examined at anearly age.
The photographs were prepared by the medical illustration department, North ManchesterGeneral Hospital.
Miss CarolineM Doig is senior lecturer in paediatric surgery, Booth Hall Children'sHospital, University of Manchester.
The ABC of Colorectal Diseases has been edited by Mr D J Jones, lecturer and honorarysenior registrar, and Professor M H Irving, department of general surgery, Hope Hospital,Salford.
1 Ferguson A, Rifkind E, Doig CM. Prevalence of chronic inflammatory bowel disease in Britishchildren. In: Frontiers ofgastrointestinal research. Vol 11. Basle: Karger, 1986:68-72.
BMJ VOLUME 305 29 AUGUST 1992 513
on 4 Septem
ber 2020 by guest. Protected by copyright.
http://ww
w.bm
j.com/
BM
J: first published as 10.1136/bmj.305.6852.511 on 29 A
ugust 1992. Dow
nloaded from