Embed Size (px)
DESCRIPTION
MRCS Questions
Citation preview

A 53 year old man undergoes a reversal of a loop colostomy. He recovers well and is discharged home. He is readmitted 10 days later with symptoms of vomiting and colicky abdominal pain. On examination he has a swelling of the loop colostomy site and it is tender. What is the most likely underlying diagnosis?
A. Haematoma
B. Intra abdominal adhesions
C. Anastomotic leak
D. Anastomotic stricture
E. Obstructed incisional hernia
Theme from September 2011 Exam
In this scenario the most likely diagnosis would be obstructed incisional hernia. The tender swelling coupled with symptoms of obstruction point to this diagnosis. Prompt surgical exploration is warranted. Loop colostomy reversals are at high risk of this complication as the operative site is at increased risk of the development of post operative wound infections.
Acute incisional hernia
Any surgical procedure involving entry into a cavity containing viscera may be complicated by post operative hernia
The abdomen is the commonest site The deep layer of the wound has usually broken down, allowing internal
viscera to protrude through Management is dictated by the patients clinical status and the timing of the
hernia in relation to recent surgery Bowel obstruction or tenderness at the hernia site both mandate early surgical
intervention to reduce the risk of bowel necrosis Mature incisional hernias with a wide neck and no symptoms may be either
left or listed for elective repair Risk factors for the development of post operative incisional hernias include
post operative wound infections, long term steroid use, obesity and chronic cough
Theme: Abdominal stomas
A. End ileostomyB. End colostomyC. Loop ileostomyD. Loop colostomyE. End jejunostomy

F. Loop jejunostomyG. Caecostomy
For each of the following scenarios, please select the most appropriate type of stoma to be constructed. Each option may be selected once, more than once or not at all.
2. A 56 year old man is undergoing a low anterior resection for carcinoma of the rectum. It is planned to restore intestinal continuity.
You answered End colostomy
The correct answer is Loop ileostomy
Colonic resections with an anastomosis below the peritoneal reflection may have an anastomotic leak rate (both clinical and radiological) of up to 15%. Therefore most surgeons will defunction such an anastomosis to reduce the clinical severity of an anastomotic leak. A loop ileostomy will achieve this end point and is relatively easy to reverse.
3. A 23 year old man with uncontrolled ulcerative colitis is undergoing an emergency sub total colectomy.
You answered Loop ileostomy
The correct answer is End ileostomy
Following a sub total colectomy the immediate surgical options include an end ileostomy or ileorectal anastomosis. In the emergency setting an ileorectal anastomosis would be unsafe.
4. A 63 year old women presents with large bowel obstruction. On examination she has a carcinoma 10cm from the anal verge.
You answered End colostomy
The correct answer is Loop colostomy
Large bowel obstruction resulting from carcinoma should be resected, stented or defunctioned. The first two options typically apply to tumours above the peritoneal reflection. Lower tumours should be defunctioned with a loop colostomy and then formal staging undertaken prior to definitive surgery. An emergency attempted rectal resection carries a high risk of involvement of the circumferential resection margin and is not recommended.

Abdominal stomas
Stomas may be sited during a range of abdominal procedures and involve bringing the lumen or visceral contents onto the skin. In most cases this applies to the bowel. However, other organs or their contents may be diverted in case of need.
With bowel stomas the type method of construction and to a lesser extent the site will be determined by the contents of the bowel. In practice, small bowel stomas should be spouted so that their irritant contents are not in contact with the skin. Colonic stomas do not need to be spouted as their contents are less irritant.
In the ideal situation the site of the stoma should be marked with the patient prior to surgery. Stoma siting is important as it will ultimately influence the ability of the patient to manage their stoma and also reduce the risk of leakage. Leakage of stoma contents and subsequent maceration of the surrounding skin can rapidly progress into a spiraling loss of control of stoma contents.
Types of stomasName of stoma Use Common sitesGastrostomy Gastric decompression or fixation
FeedingEpigastrium
Loop jejunostomy
Seldom used as very high output May be used following emergency
laparotomy with planned early closure
Any location according to need
Percutaneous jejunostomy
Usually performed for feeding purposes and site in the proximal bowel
Usually left upper quadrant
Loop ileostomy Defunctioning of colon e.g. following rectal cancer surgery
Does not decompress colon (if ileocaecal valve competent)
Usually right iliac fossa
End ilestomy Usually following complete excision of colon or where ileo-colic anastomosis is not planned
May be used to defunction colon, but reversal is more difficult
Usually right iliac fossa
End colostomy Where a colon is diverted or resected and anastomosis is not primarily achievable or desirable
Either left or right iliac fossa
Loop colostomy To defunction a distal segment of colon
May be located in any region of the abdomen, depending upon colonic

Since both lumens are present the distal lumen acts as a vent
segment used
Caecostomy Stoma of last resort where loop colostomy is not possible
Right iliac fossa
Mucous fistula To decompress a distal segment of bowel following colonic division or resection
Where closure of a distal resection margin is not safe or achievable
May be located in any region of the abdomen according to clinical need
Theme: Acute abdominal pain
A. Ruptured abdominal aortic aneurysmB. Perforated peptic ulcerC. Perforated appendicitisD. Mesenteric infarctionE. Small bowel obstructionF. Large bowel obstructionG. Pelvic inflammatory diseaseH. Mesenteric adenitisI. PancreatitisJ. None of the above
Please select the most likely cause of abdominal pain for the scenario given. Each option may be used once, more than once or not at all.
5. A 75 year old man is admitted with sudden onset severe generalised abdominal pain, vomiting and a single episode of bloody diarrhoea. On examination he looks unwell and is in uncontrolled atrial fibrillation. Although diffusely tender his abdomen is soft.
Mesenteric infarction
In mesenteric infarction there is sudden onset of pain together with vomiting and occasionally passage of bloody diarrhoea. The pain present is usually out of proportion to the physical signs.
6. A 19 year old lady is admitted with lower abdominal pain. On examination she is diffusely tender. A laparoscopy is performed and at operation multiple fine adhesions are noted between the liver and abdominal wall. Her appendix is normal.
You answered Small bowel obstruction

The correct answer is Pelvic inflammatory disease
This is Fitz Hugh Curtis syndrome in which pelvic inflammatory disease (usually Chlamydia) causes the formation of fine peri hepatic adhesions.
7. A 78 year old man is walking to the bus stop when he suddenly develops severe back pain and collapses. On examination he has a blood pressure of 90/40 and pulse rate of 110. His abdomen is distended and he is obese. Though tender his abdomen itself is soft.
Ruptured abdominal aortic aneurysm
This will be a retroperitoneal rupture (anterior ones generally don't survive to hospital). The debate regarding CT varies, it is the authors opinion that a systolic BP of <100mmHg at presentation mandates immediate laparotomy.
Acute mesenteric ischaemia- Pain out of proportion to the physical signs.Atrial fibrillation is often present.
Fitz Hugh Curtis = Fine Hepatic Connections
Acute abdominal pain-diagnoses
Conditions presenting with acute abdominal painCondition Features Investigations ManagementAppendicitis History of
migratory pain.Fever.Anorexia.Evidence of right iliac fossa tenderness.Mild pyrexia.
Differential white cell countPregnancy testC-Reactive proteinAmylaseUrine dipstick testing
Appendicectomy
Mesenteric adenitis
Usually recent upper respiratory tract infection.High fever.Generalised abdominal discomfort- true localised pain and signs are rare.
Full blood count- may show slightly raised white cell countUrine dipstick often normalAbdominal ultrasound scan - usually no free fluid
Conservative management- appendicectomy if diagnostic doubt

Mittelschmerz Only seen in females.Mid cycle pain.Usually occurs two weeks after last menstrual period.Pain is usually has a supra-pubic location.Usually subsides over a 24-48 hour period.
Full blood count- normalUrine dipstick- normalAbdominal and pelvic ultrasound- may show a trace of pelvic free fluid
Manage conservatively if doubt or symptoms fail to settle then laparoscopy
Fitz-Hugh Curtis syndrome
Disseminated infection with Chlamydia.Usually seen in females.Consists of evidence of pelvic inflammatory disease together with peri-hepatic inflammation and subsequent adhesion formation.
Abdominal ultrasound scan- may show free fluidHigh vaginal swabs - may show evidence of sexually transmitted infections
Usually medically managed- doxycycline or azithromycin
Abdominal aortic aneurysm (ruptured)
Sudden onset of abdominal pain radiating to the back in older adults (look for risk factors).Collapse.May be moribund on arrival in casualty, more stable if contained haematoma.Careful clinical assessment may reveal pulsatile mass.
Patients who are haemodynamically stable should have a CT scan
Unstable patients should undergo immediate surgery (unless it is not in their best interests).Those with evidence of contained leak on CT should undergo immediate surgeryIncreasing aneurysmal size is an indication for urgent surgical intervention (that can wait until the next working day)
Perforated peptic ulcer
Sudden onset of pain (usually epigastric).Often preceding history of upper abdominal pain.Soon develop generalised abdominal pain.
Erect CXR may show free air. A CT scan may be indicated where there is diagnostic doubt
Laparotomy (laparoscopic surgery for perforated peptic ulcers is both safe and feasible in experienced hands)

On examination may have clinical evidence of peritonitis.
Intestinal obstruction
Colicky abdominal pain and vomiting (the nature of which depends on the level of the obstruction).Abdominal distension and constipation (again depending upon site of obstruction).Features of peritonism may occur where local necrosis of bowel loops is occurring.
A plain abdominal film may help with making the diagnosis. A CT scan may be useful where diagnostic uncertainty exists
In those with a virgin abdomen and lower and earlier threshold for laparotomy should exist than in those who may have adhesional obstruction
Mesenteric infarction
Embolic events present with sudden pain and forceful evacuation.Acute on chronic events usually have a longer history and previous weight loss.On examination the pain is typically greater than the physical signs would suggest.
Arterial pH and lactateArterial phase CT scanning is the most sensitive test
Immediate laparotomy and resection of affected segments, in acute embolic events SMA embolectomy may be needed.
Theme: Gastrointestinal bleeding
A. HaemorroidsB. Meckels diverticulumC. AngiodysplasiaD. Colonic cancerE. Diverticular bleedF. Ulcerative colitisG. Ischaemic colitis
Please select the most likely cause of colonic bleeding for the scenario given. Each option may be used once, more than once or not at all

8. A 73 year old lady is admitted with a brisk rectal bleed. She is otherwise well and the bleed settles. On examination her abdomen is soft and non tender. Elective colonoscopy shows a small erythematous lesion in the right colon, but no other abnormality.
Angiodysplasia
Angiodysplasia can be difficult to identify and treat. The colonoscopic stigmata are easily missed by poor bowel preparation.
9. A 23 year old man complains of passing bright red blood rectally. It has been occurring over the past week and tends to occur post defecation. He also suffers from pruritus ani.
Haemorroids
Classical haemorroidal symptoms include bright red rectal bleeding, it typically occurs post defecation and is noticed on the toilet paper and in the toilet pan. It is usually painless, however, thrombosed external haemorroids may be very painful.
10. A 63 year old man presents with episodic rectal bleeding the blood tends to be dark in colour and may be mixed with stool. His bowel habit has been erratic since an abdominal aortic aneurysm repair 6 weeks previously.
Ischaemic colitis
The inferior mesenteric artery may have been ligated and being an arteriopath collateral flow through the marginal may be imperfect.
Gastrointestinal bleeding
Colonic bleedingThis typically presents as bright red or dark red blood per rectum. Colonic bleeding rarely presents as malaena type stool, this is because blood in the colon has a powerful laxative effect and is rarely retained long enough for transformation to occur and because the digestive enzymes present in the small bowel are not present in the colon. Up to 15% of patients presenting with haemochezia will have an upper gastrointestinal source of haemorrhage.
As a general rule right sided bleeds tend to present with darker coloured blood than left sided bleeds. Haemorrhoidal bleeding typically presents as bright red rectal bleeding that occurs post defecation either onto toilet paper or into the toilet pan. It is

very unusual for haemorrhoids alone to cause any degree of haemodynamic compromise.
CausesCause Presenting featuresColitis Bleeding may be brisk in advanced cases, diarrhoea is commonly
present. Abdominal x-ray may show featureless colon.Diverticular disease
Acute diverticulitis often is not complicated by major bleeding and diverticular bleeds often occur sporadically. 75% all will cease spontaneously within 24-48 hours. Bleeding is often dark and of large volume.
Cancer Colonic cancers often bleed and for many patients this may be the first sign of the disease. Major bleeding from early lesions is uncommon
Haemorrhoidal bleeding
Typically bright red bleeding occurring post defecation. Although patients may give graphic descriptions bleeding of sufficient volume to cause haemodynamic compromise is rare.
Angiodysplasia Apart from bleeding, which may be massive, these arteriovenous lesions cause little in the way of symptoms. The right side of the colon is more commonly affected.
Management
Prompt correction of any haemodynamic compromise is required. Unlike upper gastrointestinal bleeding the first line management is usually supportive. This is because in the acute setting endoscopy is rarely helpful.
When haemorrhoidal bleeding is suspected a proctosigmoidoscopy is reasonable as attempts at full colonoscopy are usually time consuming and often futile.
In the unstable patient the usual procedure would be an angiogram (either CT or percutaneous), when these are performed during a period of haemodynamic instability they may show a bleeding point and may be the only way of identifying a patch of angiodysplasia.
In others who are more stable the standard procedure would be a colonoscopy in the elective setting. In patients undergoing angiography attempts can be made to address the lesion in question such as coiling. Otherwise surgery will be necessary.
In patients with ulcerative colitis who have significant haemorrhage the standard approach would be a sub total colectomy, particularly if medical management has already been tried and is not effective.
Indications for surgeryPatients > 60 yearsContinued bleeding despite endoscopic intervention Recurrent bleeding Known cardiovascular disease with poor response to hypotension

SurgerySelective mesenteric embolisation if life threatening bleeding. This is most helpful if conducted during a period of relative haemodynamic instability. If all haemodynamic parameters are normal then the bleeding is most likely to have stopped and any angiography normal in appearance. In many units a CT angiogram will replace selective angiography but the same caveats will apply.
If source of colonic bleeding unclear perform a laparotomy, on table colonic lavage and following this attempt a resection. A blind sub total colectomy is most unwise, for example bleeding from an small bowel arterio-venous malformation will not be treated by this manoeuvre.
Summary of Acute Lower GI bleeding recommendationsConsider admission if:* Over 60 years* Haemodynamically unstable/profuse PR bleeding* On aspirin or NSAID* Significant co morbidity
Management
All patients should have a history and examination, PR and proctoscopy Colonoscopic haemostasis aimed for in post polypectomy or diverticular
bleeding
Referenceshttp://www.sign.ac.uk/guidelines/fulltext/105/index.htmlheme: Surgical signs
A. Rovsing's signB. Boas' signC. Psoas stretch signD. Cullen's signE. Grey-Turner's signF. Murphy's signG. None of the above
Please select the most appropriate eponymous abdominal sign for the scenario given. Each option may be used once, more than once or not at all.
11. Severe acute peri-umbilical bruising in the setting of acute pancreatitis.
Cullen's sign
Cullens sign occurs when there has been intraabdominal haemorrage. It is seen in cases of severe haemorrhagic pancreatitis and is associated with a poor

prognosis. It is also seen in other cases of intraabdominal haemorrhage (such as ruptured ectopic pregnancy).
12. In acute cholecystitis there is hyperaesthesia beneath the right scapula.
Boas' sign
Boas sign refers to this hyperaesthesia. It occurs because the abdominal wall innervation of this region is from the spinal roots that lie at this level.
13. In appendicitis palpation of the left iliac fossa causes pain in the right iliac fossa.
Rovsing's sign
Rovsings sign elicits tenderness because the deep palpation induces shift of the appendix (which is inflamed) against the peritoneal surface. This has somatic innervation and will therefore localise the pain. It is less reliable in pelvic appendicitis and when the appendix is truly retrocaecal
Abdominal signs
A number of eponymous abdominal signs are noted. These include:
Rovsings sign- appendicitis Boas sign -cholecystitis Murphys sign- cholecystitis Cullens sign- pancreatitis (other intraabdominal haemorrhage) Grey-Turners sign- pancreatitis (or other retroperitoneal haemorrhage)
In clinical practice haemorrhagic pancreatitis is thankfully rare. The signs are important and thus shown below:
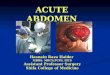
Cullen's sign

Image sourced from Wikipedia
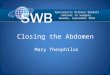
Grey Turner's sign
Image sourced from Wikipedia
Theme: Surgical access
A. GridironB. LanzC. McEvedyD. Midline abdominalE. Rutherford MorrisonF. Battle (abdominal)G. Lower midline
Please select the most appropriate incision for the procedure required. Each option may be used once, more than once or not at all.
14. A 78 year old lady is admitted with a tender lump in her right groin. It is within the femoral triangle and there is concern that there may be small bowel obstruction developing.

McEvedy
This is one approach to an obstructed femoral hernia. It is possible to undertake a small bowel resection through this approach. Although recourse to laparotomy may be needed if access is difficult.
15. A 45 year old woman with end stage renal failure is due to undergo a cadaveric renal transplant. This will be her first transplant.
Rutherford Morrison
This is the incision of choice for the extraperitoneal approach to the iliac vessels which will be required for a renal transplant.
16. A slim 20 year old lady is suffering from appendicitis and requires an appendicectomy.
Lanz
Either a Lanz or Gridiron incision will give access for appendicectomy. However, in the case described a Lanz incision will give better cosmesis and can be extended should pelvic surgery be required eg for gynaecological disease.
Abdominal incisions
Theme in January 2012 exam
Midline incision Commonest approach to the abdomen Structures divided: linea alba, transversalis fascia,
extraperitoneal fat, peritoneum (avoid falciform ligament above the umbilicus)
Bladder can be accessed via an extraperitoneal approach through the space of Retzius
Paramedian incision
Parallel to the midline (about 3-4cm) Structures divided/retracted: anterior rectus sheath, rectus
(retracted), posterior rectus sheath, transversalis fascia, extraperitoneal fat, peritoneum
Incision is closed in layers
Battle Similar location to paramedian but rectus displaced medially

(and thus denervated) Now seldom used
Kocher's Incision under right subcostal margin e.g. Cholecystectomy (open)Lanz Incision in right iliac fossa e.g. AppendicectomyGridiron Oblique incision centered over McBurneys point- usually
appendicectomy (less cosmetically acceptable than LanzGable Rooftop incisionPfannenstiel's Transverse supra pubic, primarily used to access pelvic organsMcEvedy's Groin incision e.g. Emergency repair strangulated femoral herniaRutherford Morrison
Extraperitoneal approach to left or right lower quadrants. Gives excellent access to iliac vessels and is the approach of choice for first time renal transplantation.
Image sourced from Wikipedia
Theme: Hernias
A. Littres herniaB. Richters herniaC. Bochdalek herniaD. Morgagni herniaE. Spigelian herniaF. Lumbar herniaG. Obturator hernia
Please select the type of hernia that most closely matches the description given. Each option may be used once, more than once or not at all.
17. A 73 year old lady presents with peritonitis and tenderness of the left groin. At operation she has a left femoral hernia with perforation of the anti mesenteric border of ileum associated with the hernia.

Richters hernia
When part of the bowel wall is trapped in a hernia such as this it is termed a Richters hernia and may complicate any hernia although femoral and obturator hernias are most typically implicated.
18. A 22 year old man is operated on for a left inguinal hernia, at operation the sac is opened to reveal a large Meckels diverticulum.
Littres hernia
Hernia containing Meckels diverticulum is termed a Littres hernia.
19. A 45 year old man has recurrent colicky abdominal pain. As part of a series of investigations he undergoes a CT scan and this demonstrates a hernia lateral to the rectus muscle at the level of the arcuate line.
Spigelian hernia
This is the site for a spigelian hernia.
Theme: Groin masses
A. Femoral herniaB. LymphadenitisC. Inguinal herniaD. Psoas abscessE. Saphenous varixF. Femoral artery aneurysmG. Metastatic lymphadenopathyH. LymphangitisI. False femoral artery aneurysm
What is the likely diagnosis for groin mass described? Each option may be used once, more than once, or not at all.
20. A 52 year old obese lady reports a painless grape sized mass in her groin area. She has no medical conditions apart from some varicose veins. There is a cough impulse and the mass disappears on lying down.
Saphenous varix

The history of varicose veins should indicate a more likely diagnosis of a varix. The varix can enlarge during coughing/sneezing. A blue discolouration may be noted.
21. A 32 year old male is noted to have a tender mass in the right groin area. There are also red streaks on the thigh, extending from a small abrasion.
You answered Lymphangitis
The correct answer is Lymphadenitis
The red streaks are along the line of the lymphatics, indicating infection of the lymphatic vessels. Lymphadenitis is infection of the local lymph nodes.
22. A 23 year old male suffering from hepatitis C presents with right groin pain and swelling. On examination there is a large abscess in the groin. Adjacent to this is an expansile swelling. There is no cough impulse.
False femoral artery aneurysm
False aneurysms may occur following arterial trauma in IVDU. They may have associated blood borne virus infections and should undergo duplex scanning prior to surgery. False aneurysms do not contain all layers of the arterial wall.
Groin masses clinical
Groin masses are common and include:
Herniae Lipomas Lymph nodes Undescended testis Femoral aneurysm Saphena varix (more a swelling than a mass!)
In the history features relating to systemic illness and tempo of onset will often give a clue as to the most likely underlying diagnosis.
Groin lumps- some key questions

Is there a cough impulse Is it pulsatile AND is it expansile (to distinguish between false and true
aneurysm) Are both testes intra scrotal Any lesions in the legs such as malignancy or infections (?lymph nodes) Examine the ano rectum as anal cancer may metastasise to the groin Is the lump soft, small and very superficial (?lipoma)
Scrotal lumps - some key questions
Is the lump entirely intra scrotal Does it transilluminate (?hydrocele) Is there a cough impulse (?hernia)
In most cases a diagnosis can be made clinically. Where it is not clear an ultrasound scan is often the most convenient next investigation.heme: Right iliac fossa pain
A. Urinary tract infectionB. AppendicitisC. MittelschmerzD. Mesenteric adenitisE. Crohns diseaseF. Ulcerative colitisG. Meckels diverticulum
Please select the most likely cause for right iliac fossa pain for the scenario given. Each option may be used once, more than once or not at all.
23. A 17 year old male is admitted with lower abdominal discomfort. He has been suffering from intermittent right iliac fossa pain for the past few months. His past medical history includes a negative colonoscopy and gastroscopy for iron deficiency anaemia. The pain is worse after meals. Inflammatory markers are normal.
Meckels diverticulum
This scenario should raise suspicion for Meckels as these may contain ectopic gastric mucosa which may secrete acid with subsequent bleeding and ulceration.
24. A 14 year old female is admitted with sudden onset right iliac fossa pain. She is otherwise well and on examination has some right iliac fossa tenderness but no guarding. She is afebrile. Urinary dipstick is normal. Her previous

menstrual period two weeks ago was normal and pregnancy test is negative.
Mittelschmerz
Typical story and timing for mid cycle pain. Mid cycle pain typically occurs because a small amount of fluid is released at the time of ovulation. It will usually resolve over 24-48 hours.
25. A 21 year old male is admitted with a 3 month history of intermittent right iliac fossa pain. He suffers from episodic diarrhoea and has lost 2 kilos in weight. On examination he has some right iliac fossa tenderness and is febrile.
Crohns disease
Weight loss and chronic symptoms coupled with change in bowel habit should raise suspicion for Crohns. The presence of intermittent right iliac fossa pain is far more typical of terminal ileal Crohns disease. Both UC and Crohns may be associated with a low grade pyrexia. The main concern here would be locally perforated Crohns disease with a small associated abscess.
Right iliac fossa pain
Differential diagnosis
Appendicitis Pain radiating to right iliac fossa Anorexia Typically short history Diarrhoea and profuse vomiting rare
Crohn's disease Often long history Signs of malnutrition Change in bowel habit, especially diarrhoea
Mesenteric adenitis Mainly affects children Causes include Adenoviruses, Epstein Barr Virus,
beta-haemolytic Streptococcus, Staphylococcus spp., Escherichia coli, Streptococcus viridans and Yersinia spp.
Patients have a higher temperature than those with appendicitis
If laparotomy is performed, enlarged mesenteric lymph nodes will be present
Diverticulitis Both left and right sided disease may present with

right iliac fossa pain Clinical history may be similar, although some
change in bowel habit is usual When suspected a CT scan may help in refining the
diagnosis
Meckel's diverticulitis A Meckel's diverticulum is a congenital abnormality that is present in about 2% of the population
Typically 2 feet proximal to the ileocaecal valve May be lined by ectopic gastric mucosal tissue and
produce bleeding
Perforated peptic ulcer This usually produces upper quadrant pain but pain may be lower
Perforations typically have a sharp sudden onset of pain in the history
Incarcerated right inguinal or femoral hernia
Usually only right iliac fossa pain if right sided or bowel obstruction.
Bowel perforation secondary to caecal or colon carcinoma
Seldom localised to right iliac fossa, although complete large bowel obstruction with caecal distension may cause pain prior to perforation.
Gynaecological causes Pelvic inflammatory disease/salpingitis/pelvic abscess/Ectopic pregnancy/Ovarian torsion/Threatened or complete abortion/Mittelschmerz
Urological causes Ureteric colic/UTI/Testicular torsion
Other causes TB/Typhoid/Herpes Zoster/AAA/Situs inversus
A 78 year old lady presents with colicky abdominal pain and a tender mass in her groin. On examination there is a small firm mass below and lateral to the pubic tubercle. Which of the following is the most likely underlying diagnosis?
A. Incarcerated inguinal hernia
B. Thrombophlebitis of a saphena varix
C. Incarcerated femoral hernia
D. Incarcerated obturator hernia
E. Deep vein thrombosis
Femoral hernia = High risk of

strangulation (repair urgently)
Femoral herniae account for <10% of all groin hernias. In the scenario the combination of symptoms of intestinal compromise with a mass in the region of the femoral canal points to femoral hernia as the most likely cause.
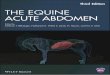
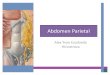
Femoral canal
The femoral canal lies at the medial aspect of the femoral sheath. The femoral sheath is a fascial tunnel containing both the femoral artery laterally and femoral vein medially. The canal lies medial to the vein.
Borders of the femoral canalLaterally Femoral veinMedially Lacunar ligamentAnteriorly Inguinal ligamentPosteriorly Pectineal ligament
Image showing dissection of femoral canal
Image sourced from Wikipedia
Contents

Lymphatic vessels Cloquet's lymph node
Physiological significanceAllows the femoral vein to expand to allow for increased venous return to the lower limbs.
Pathological significanceAs a potential space, it is the site of femoral hernias. The relatively tight neck places these at high risk of strangulation.hich of the following is not a typical feature of acute appendicitis?
A. Neutrophilia
B. Profuse vomiting
C. Anorexia
D. Low grade pyrexia
E. Small amounts of protein on urine analysis
Profuse vomiting and diarrhoea are rare in early appendicitis
Whilst patients may vomit once or twice, profuse vomiting is unusual, and would fit more with gastroenteritis or an ileus. A trace of protein is not an uncommon occurrence in acute appendicitis. A free lying pelvic appendix may result in localised bladder irritation, with inflammation occurring as a secondary phenomena. This latter feature may result in patients being incorrectly diagnosed as having a urinary tract infection. A urine dipstick test is useful in differentiating between the two conditions.
Appendicitis
History
Peri umbilical abdominal pain (visceral stretching of appendix lumen and appendix is mid gut structure) radiating to the right iliac fossa due to localised parietal peritoneal inflammation.
Vomit once or twice but marked and persistent vomiting is unusual. Diarrhoea is rare. However, pelvic appendicitis may cause localised rectal
irritation of some loose stools. A pelvic abscess may also cause diarrhoea. Mild pyrexia is common - temperature is usually 37.5 -38oC. Higher
temperatures are more typical of conditions like mesenteric adenitis. Anorexia is very common. It is very unusual for patients with appendicitis to
be hungry.

Examination
Generalised peritonitis if perforation has occurred or localised peritonism. Retrocaecal appendicitis may have relatively few signs. Digital rectal examination may reveal boggy sensation if pelvic abscess is
present, or even tenderness with a pelvic appendix.
Diagnosis
Typically raised inflammatory markers coupled with compatible history and examination findings should be enough to justify appendicectomy.
Urine analysis may show mild leucocytosis but no nitrites. Ultrasound is useful if females where pelvic organ pathology is suspected.
Although it is not always possible to visualise the appendix on ultrasound the presence of free fluid (always pathological in males) should raise suspicion.
Ultrasound examination may show evidence of lumenal obstruction and thickening of the appendiceal wall as shown below
Image sourced from Wikipedia
Treatment
Appendicectomy which can be performed via either an open or laparoscopic approach.
Administration of metronidazole reduces wound infection rates. Patients with perforated appendicitis require copious abdominal lavage.

Patients without peritonitis who have an appendix mass should receive broad spectrum antibiotics and consideration given to performing an interval appendicectomy.
Be wary in the older patients who may have either an underlying caecal malignancy or perforated sigmoid diverticular disease.
Laparoscopic appendicectomy is becoming increasing popular as demonstrated below
Image sourced from Wikipedia
An 28 year old man presents with a direct inguinal hernia. A decision is made to perform an open inguinal hernia repair. Which of the following is the best option for abdominal wall reconstruction in this case?
A. Suture plication of the transversalis fascia using PDS only
B. Suture plication of the hernial defect with nylon and placement of prolene mesh anterior to external oblique
C. Suture plication of the hernia defect using nylon and re-enforcing with a sutured repair of the abdominal wall
D. Sutured repair of the hernial defect with prolene and placement of prolene mesh over the cord structures in the inguinal canal
E. Sutured repair of the hernial defect using nylon and placement of a prolene mesh posterior to the cord structures

Laparoscopic repair- bilateral and recurrent cases
During an inguinal hernia repair in males the cord structures will always lie anterior to the mesh. In the conventional open repairs the cord structures are mobilised and the mesh placed behind them, with a slit made to allow passage of the cord structures through the deep inguinal ring. Placement of the mesh over the cord structures results in chronic pain and usually a higher risk of recurrence.
Laparoscopic inguinal hernia repair is the procedure of choice for bilateral inguinal hernias.
Types of surgery include:
Onlay mesh repair (Litchenstein style) Inguinal herniorrhaphy Shouldice repair Darn repair Laparoscopic mesh repair
Open mesh repair and laparoscopic repair are the two main procedures in mainstream use. The Shouldice repair is a useful procedure in cases where a mesh repair would be associated with increased risk of infection, e.g. repair of case with strangulated bowel, as it avoids the use of mesh. It is, however, far more technically challenging to perform.
Inguinal hernia surgery
Inguinal hernias occur when the abdominal viscera protrude through the anterior abdominal wall into the inguinal canal. They may be classified as being either direct or indirect. The distinction between these two rests on their relation to Hesselbach's triangle.
Boundaries of Hesselbach's Triangle
Medial: Rectus abdominis Lateral: Inferior epigastric vessels Inferior: Inguinal ligament

Image sourced from Wikipedia
Hernias occurring within the triangle tend to be direct and those outside - indirect.
DiagnosisMost cases are diagnosed clinically, a reducible swelling may be located at the level of the inguinal canal. Large hernia may extend down into the male scrotum, these will not trans-illuminate and it is not possible to "get above" the swelling. Cases that are unclear on examination, but suspected from the history, may be further investigated using ultrasound or by performing a herniogram.
TreatmentHernias associated with few symptoms may be managed conservatively. Symptomatic hernias or those which are at risk of developing complications are usually treated surgically. First time hernias may be treated by performing an open inguinal hernia repair; the inguinal canal is opened, the hernia reduced and the defect repaired. A prosthetic mesh may be placed posterior to the cord structures to re-inforce the repair and reduce the risk of recurrence.Recurrent hernias and those which are bilateral are generally managed with a laparoscopic approach. This may be via an intra or extra peritoneal route. As in open surgery a mesh is deployed. However, it will typically lie posterior to the deep ring.
Inguinal hernia in childrenInguinal hernias in children are almost always of an indirect type and therefore are usually dealt with by herniotomy, rather than herniorraphy. Neonatal hernias especially in those children born prematurely are at highest risk of strangulation and should be repaired urgently. Other hernias may be repaired on an elective basis.

ReferencesThe UK Based National Institute of Clinical Excellence has published guidelines relating to the choice between open and laparoscopic inguinal hernia repair. Which users may find interesting:Theme: Abdominal closure methods
A. Looped 1/0 PDS (polydiaxone)B. Looped 1/0 silkC. 1/0 Vicryl (polyglactin)D. 1/0 Vicryl rapideE. 2/0 Prolene (Polypropylene)F. Re-inforced 1/0 NylonG. Re-inforced 1/0 SilkH. Application of VAC system without separation filmI. Application of VAC System with separation filmJ. Application of a 'Bogota Bag'
Please select the most appropriate wound closure method (for the deep layer) for the abdominal surgery described.
29. A 59 year old man with morbid obesity undergoes a laparotomy and Hartmans procedure for perforated sigmoid diverticular disease. At the conclusion of the procedure the abdomen cannot be primarily closed. The Vac system is not available for use.
Application of a 'Bogota Bag'
Application of a Bogota bag is safest as attempted closure will almost certainly fail. Repeat look at 48 hours to determine the best definitive option is needed.
30. A 73 year old lady undergoes a low anterior resection for carcinoma of the rectum.
Looped 1/0 PDS (polydiaxone)
Mass closure obeying Jenkins rule is required and this states that the suture must be 4 times the length of the wound with tissue bites 1cm deep and 1 cm apart.
31. A 67 year old is returned to theatre after developing a burst abdomen on the ward. She has originally undergone a right hemicolectomy and the SHO who closed the wound had failed to tie the midline suture correctly. The wound edges appear healthy.

You answered Re-inforced 1/0 Silk
The correct answer is Re-inforced 1/0 Nylon
Attempt at re-closing the wound is reasonable in which case 1/0 nylon (reinforced with drainage tubing) is often used.
Abdominal wound dehiscence
This is a significant problem facing all surgeons who undertake abdominal surgery on a regular basis. Traditionally it is said to occur when all layers of an abdominal mass closure fail and the viscera protrude externally (associated with 30% mortality).
It can be subdivided into superficial, in which the skin wound alone fails and complete, implying failure of all layers.
Factors which increase the risk are:* Malnutrition* Vitamin deficiencies * Jaundice * Steroid use * Major wound contamination (e.g. faecal peritonitis)* Poor surgical technique (Mass closure technique is the preferred method-Jenkins Rule)
When sudden full dehiscence occurs the management is as follows:* Analgesia* Intravenous fluids* Intravenous broad spectrum antibiotics* Coverage of the wound with saline impregnated gauze (on the ward)* Arrangements made for a return to theatre
Surgical strategy
Correct the underlying cause (eg TPN or NG feed if malnourished) Determine the most appropriate strategy for managing the wound
OptionsResuturing of the wound
This may be an option if the wound edges are healthy and there is enough tissue for sufficient coverage. Deep tension sutures are traditionally used for this purpose.
Application of a wound manager
This is a clear dressing with removable front. Particularly suitable when some granulation tissue is present over the viscera or where

there is a high output bowel fistula present in the dehisced wound.Application of a 'Bogota bag'
This is a clear plastic bag that is cut and sutured to the wound edges and is only a temporary measure to be adopted when the wound cannot be closed and will necessitate a return to theatre for definitive management.
Application of a VAC dressing system
These can be safely used BUT ONLY if the correct layer is interposed between the suction device and the bowel. Failure to adhere to this absolute rule will almost invariably result in the development of multiple bowel fistulae and create an extremely difficult management problem.
Theme: Hernias
A. Umbilical herniaB. Para umbilical herniaC. Morgagni herniaD. Littres herniaE. Bochdalek herniaF. Richters herniaG. Obturator hernia
Please select the hernia that most closely matches the description given. Each option may be used once, more than once or not at all.
32. A 1 day old infant is born with severe respiratory compromise. On examination he has a scaphoid abdomen and an absent apex beat.
Bochdalek hernia
Theme from 2011 examThe large hernia may displace the heart although true dextrocardia is not present. The associated pulmonary hypoplasia will compromise lung development.
33. A 2 month old infant is troubled by recurrent colicky abdominal pain and intermittent intestinal obstruction. On imaging the transverse colon is herniated into the thoracic cavity, through a mid line defect.
Morgagni hernia
Morgagni hernia may contain the transverse colon. Unless there is substantial herniation pulmonary hypoplasia is uncommon.
34. A 78 year old lady is admitted with small bowel obstruction, on examination she has a distended abdomen and the leg is held semi flexed. She has some

groin pain radiating to the ipsilateral knee.
Obturator hernia
The groin swelling in obturator hernia is subtle and hard to elicit clinically.
Hernia
Hernias occur when a viscus or part of it protrudes from within its normal anatomical cavity. Specific hernias are covered under their designated titles the remainder are addressed here.
Spigelian hernia
Interparietal hernia occurring at the level of the arcuate line. Rare. May lie beneath internal oblique muscle. Usually between internal and
external oblique. Equal sex distribution. Position is lateral to rectus abdominis. Both open and laparoscopic repair are possible, the former in cases of
strangulation.
Lumbar hernia
The lumbar triangle (through which these may occur) is bounded by:
Crest of ilium (inferiorly)External oblique (laterally)Latissimus dorsi (medially)
Primary lumbar herniae are rare and most are incisional hernias following renal surgery.
Direct anatomical repair with or without mesh re-enforcement is the procedure of choice.
Obturator hernia
Herniation through the obturator canal. Commoner in females. Usually lies behind pectineus muscle. Elective diagnosis is unusual most will present acutely with obstruction. When presenting acutely most cases with require laparotomy or laparoscopy
(and small bowel resection if indicated).

Richters hernia
Condition in which part of the wall of the small bowel (usually the anti mesenteric border) is strangulated within a hernia (of any type).
They do not present with typical features of intestinal obstruction as luminal patency is preserved.
Where vomiting is prominent it usually occurs as a result of paralytic ileus from peritonitis (as these hernias may perforate).
Incisional hernia
Occur through sites of surgical access into the abdominal cavity. Most common following surgical wound infection. To minimise following midline laparotomy Jenkins Rule should be followed
and this necessitates a suture length 4x length of incision with bites taken at 1cm intervals, 1 cm from the wound edge.
Repair may be performed either at open surgery or laparoscopically and a wide variety of techniques are described.
Bochdalek hernia
Typically congenital diaphragmatic hernia. 85% cases are located in the left hemi diaphragm. Associated with lung hypoplasia on the affected side. More common in males. Associated with other birth defects. May contain stomach. May be treated by direct anatomical apposition or placement of mesh. In
infants that have severe respiratory compromise mechanical ventilation may be needed and mortality rate is high.
Morgagni Hernia
Rare type of diaphragmatic hernia (approx 2% cases). Herniation through foramen of Morgagni. Usually located on the right and tend to be less symptomatic. More advanced cases may contain transverse colon. As defects are small pulmonary hypoplasia is less common. Direct anatomical repair is performed.
Umbilical hernia
Hernia through weak umbilicus. Usually presents in childhood. Often symptomatic.

Equal sex incidence. 95% will resolve by the age of 2 years. Thereafter surgical repair is warranted.
Paraumbilical hernia
Usually a condition of adulthood. Defect is in the linea alba. More common in females. Multiparity and obesity are risk factors. Traditionally repaired using Mayos technique - overlapping repair, mesh may
be used though not if small bowel resection is required owing to acute strangulation.
Littres hernia
Hernia containing Meckels diverticulum. Resection of the diverticulum is usually required and this will preclude a mesh
repair.
Theme: Right iliac fossa pain
A. Open AppendicectomyB. Laparoscopic appendicectomyC. LaparotomyD. CT ScanE. ColonoscopyF. Ultrasound scan abdomen/pelvisG. Active observation
For each scenario please select the most appropriate management option from the list. Each option may be used once, more than once or not at all.
35. A 21 year old women is admitted with a 48 hour history of worsening right iliac fossa pain. She has been nauseated and vomited twice. On examination she is markedly tender in the right iliac fossa with localised guarding. Vaginal examination is unremarkable. Urine dipstick is negative. Blood tests show a WCC of 13.5 and CRP 70.
You answered Open Appendicectomy
The correct answer is Laparoscopic appendicectomy
She is likely to have appendicitis. In women of this age there is always diagnostic uncertainty. With a normal vaginal exam laparoscopy would be preferred over USS.

36. An 8 year old boy presents with a 4 hour history of right iliac fossa pain with nausea and vomiting. He has been back at school for two days after being kept home with a flu like illness. On examination he is tender in the right iliac fossa, although his abdomen is soft. Temperature is 38.3oc. Blood tests show a CRP of 40 and a WCC of 8.1.
You answered CT Scan
The correct answer is Active observation
This is mesenteric adenitis. Note history of flu like illness and temp > 38o c.The decision as to how to manage this situation is based on the abdominal findings. Patients with localising signs such as guarding or peritonism should undergo surgery.
37. A 21 year old women presents with right iliac fossa pain. She reports some bloodstained vaginal discharge. She has a HR of 65 bpm.
Ultrasound scan abdomen/pelvis
This patient is suspected of having an ectopic pregnancy. She needs an urgent β HCG and USS of the pelvis. If she were haemodynamically unstable then laparotomy would be indicated.
Right iliac fossa pain
Differential diagnosis
Appendicitis Pain radiating to right iliac fossa Anorexia Typically short history Diarrhoea and profuse vomiting rare
Crohn's disease Often long history Signs of malnutrition Change in bowel habit, especially diarrhoea
Mesenteric adenitis Mainly affects children Causes include Adenoviruses, Epstein Barr Virus,
beta-haemolytic Streptococcus, Staphylococcus spp., Escherichia coli, Streptococcus viridans and Yersinia spp.
Patients have a higher temperature than those with appendicitis

If laparotomy is performed, enlarged mesenteric lymph nodes will be present
Diverticulitis Both left and right sided disease may present with right iliac fossa pain
Clinical history may be similar, although some change in bowel habit is usual
When suspected a CT scan may help in refining the diagnosis
Meckel's diverticulitis A Meckel's diverticulum is a congenital abnormality that is present in about 2% of the population
Typically 2 feet proximal to the ileocaecal valve May be lined by ectopic gastric mucosal tissue and
produce bleeding
Perforated peptic ulcer This usually produces upper quadrant pain but pain may be lower
Perforations typically have a sharp sudden onset of pain in the history
Incarcerated right inguinal or femoral hernia
Usually only right iliac fossa pain if right sided or bowel obstruction.
Bowel perforation secondary to caecal or colon carcinoma
Seldom localised to right iliac fossa, although complete large bowel obstruction with caecal distension may cause pain prior to perforation.
Gynaecological causes Pelvic inflammatory disease/salpingitis/pelvic abscess/Ectopic pregnancy/Ovarian torsion/Threatened or complete abortion/Mittelschmerz
Urological causes Ureteric colic/UTI/Testicular torsion
Other causes TB/Typhoid/Herpes Zoster/AAA/Situs inversus
Which of the following is not a typical feature of irritable bowel syndrome?
A. A change in the consistency of stools
B. Abdominal pain relieved with defecation
C. A change in frequency of defecation
D. Abdominal bloating

E. Pain at a single fixed site
The pain or discomfort of IBS is typically migratory and variable in intensity. Pain at a fixed site is suggestive of malignancy.Abdominal bloating is an extremely common feature.
Irritable bowel syndrome
The diagnosis of irritable bowel syndrome is made according to the ROME III diagnostic criteria which state:
Recurrent abdominal pain or discomfort at 3 days per month for the past 3 months associated with two or more of the following:
Improvement with defecation. Onset associated with a change in the frequency of stool. Onset associated with a change in the form of the stool.
Features such as lethargy, nausea, backache and bladder symptoms may also support the diagnosis
Red flag features should be inquired about:
Rectal bleeding Unexplained/unintentional weight loss Family history of bowel or ovarian cancer Onset after 60 years of age
Suggested investigations are:
Full blood count ESR/CRP Coeliac disease screen (tissue transglutaminase antibodies) Colonoscopy (if worrying symptoms, positive family history) Thyroid function tests Glucose (ensure not diabetic)
The NICE criteria state that blood tests alone will suffice in people fulfilling the diagnostic criteria. We would point out that luminal colonic studies should be considered early in patients with altered bowel habit referred to hospital and a diagnosis of IBS should still be largely one of exclusion.
Treatment
Usually reduce fibre intake. Tailored prescriptions of laxatives or loperamide according to clinical picture.

Dietary modification (caffeine avoidance, less carbonated drinks). Consider low dose tricyclic antidepressants if pain is a dominant symptom. Biofeedback may help.
Theme: Causes of abdominal pain
A. Acute on chronic mesenteric ischaemiaB. Ruptured aortic aneurysmC. Acute PancreatitisD. Acute mesenteric embolusE. Acute appendicitisF. Chronic pancreatitisG. Mesenteric vein thrombosis
Please select the most likely underlying diagnosis from the list above. Each option may be used once, more than once or not at all.
39. A 41 year old man is admitted with peritonitis secondary to a perforated appendix. He is treated with a laparoscopic appendicectomy but has a stormy post operative course. He in now developing increasing abdominal pain and has been vomiting. A laparotomy is performed and at operation a large amount of small bowel shows evidence of patchy areas of infarction.
Mesenteric vein thrombosis
Mesenteric vein thrombosis may complicate severe intra abdominal sepsis and when it progresses may impair bowel perfusion. The serosa is quite resistant to ischaemia so in this case the appearances are usually patchy.
40. A 68 year old man is admitted with abdominal pain and vomiting of 48 hours duration, the pain radiates to his back and he has required a considerable amount of volume replacement. Amylase is 741.
Acute Pancreatitis
Although back pain and abdominal pain coupled with haemodynamic compromise may suggest ruptured AAA the 48 hour history and amylase >3 times normal go against this diagnosis.
41. A 79 year old lady develops sudden onset of abdominal pain and collapses, she has passed a large amount of diarrhoea. In casualty her pH is 7.35 and WCC is 18.

You answered Acute on chronic mesenteric ischaemia
The correct answer is Acute mesenteric embolus
Although mesenteric infarct may raise the lactate the pH may be raised often secondary to vomiting.
Mesenteric vessel disease
Mesenteric ischaemia accounts for 1 in 1000 acute surgical admissions. It is primarily caused by arterial embolism resulting in infarction of the colon. It is more likely to occur in areas such as the splenic flexure that are located at the borders of the territory supplied by the superior and inferior mesenteric arteries.
TypesAcute mesenteric embolus (commonest 50%)
Sudden onset abdominal pain followed by profuse diarrhoea.
May be associated with vomiting. Rapid clinical deterioration. Serological tests: WCC, lactate, amylase may all be
abnormal particularly in established disease. These can be normal in the early phases.
Acute on chronic mesenteric ischaemia
Usually longer prodromal history. Post prandial abdominal discomfort and weight loss are
dominant features. Patients will usually present with an acute on chronic event, but otherwise will tend not to present until mesenteric flow is reduced by greater than 80%.
When acute thrombosis occurs presentation may be as above. In the chronic setting the symptoms will often be those of ischaemic colitis (mucosa is the most sensitive area to this insult).
Mesenteric vein thrombosis
Usually a history over weeks. Overt abdominal signs and symptoms will not occur until
venous thrombosis has reached a stage to compromise arterial inflow.
Thrombophilia accounts for 60% of cases.
Low flow mesenteric infarction
This occurs in patients with multiple co morbidities in whom mesenteric perfusion is significantly compromised by overuse of inotropes or background cardiovascular compromise.

The end result is that the bowel is not adequately perfused and infarcts occur from the mucosa outwards.
Diagnosis
Serological tests: WCC, lactate, CRP, amylase (can be normal in early disease).
Cornerstone for diagnosis of arterial AND venous mesenteric disease is CT angiography scanning in the arterial phase with thin slices (<5mm). Venous phase contrast is not helpful.
SMA duplex USS is useful in the evaluation of proximal SMA disease in patients with chronic mesenteric ischaemia.
MRI is of limited use due to gut peristalsis and movement artefact.
Management
Overt signs of peritonism: Laparotomy Mesenteric vein thrombosis: If no peritonism: Medical management with IV
heparin At operation limited resection of frankly necrotic bowel with view to relook
laparotomy at 24-48h. In the interim urgent bowel revascularisation via endovascular (preferred) or surgery.
PrognosisOverall poor. Best outlook is from an acute ischaemia from an embolic event where surgery occurs within 12h. Survival may be 50%. This falls to 30% with treatment delay. The other conditions carry worse survival figures.Theme: Groin masses
A. Femoral aneurysmB. LymphadenitisC. Saphena varixD. Femoral herniaE. Indirect inguinal herniaF. Direct inguinal herniaG. Psoas abscess
What is the likely diagnosis for the groin mass described? Each option may be used once, more than once or not at all.
42. A 3 year old boy is referred to the clinic with a scrotal swelling. On examination the mass does not transilluminate and it is impossible to palpate normal cord above it.

Indirect inguinal hernia
This is likely to be an indirect hernia. In children these arise from persistent processus vaginalis and require herniotomy.
43. A 52 year old obese lady reports a painless mass in the groin area. A mass is noted on coughing. It is below and lateral to the pubic tubercle.
Femoral hernia
A mass below and lateral to the pubic tubercle is indicative of a femoral hernia.
44. A 21 year old man is admitted with a tender mass in the right groin, fevers and sweats. He is on multiple medical therapy for HIV infection. On examination he has a swelling in his right groin, hip extension exacerbates the pain.
Psoas abscess
Psoas abscesses may be either primary or secondary. Primary cases often occur in the immunosuppressed and may occur as a result of haematogenous spread. Secondary cases may complicated intra abdominal diseases such as Crohns. Patients usually present with low back pain and if the abscess is extensive a mass that may be localised to the inguinal region or femoral triangle . Smaller collections may be percutaneously drained. If the collection is larger, or the percutaneous route fails, then surgery (via a retroperitoneal approach) should be performed.
Groin masses clinical
Groin masses are common and include:
Herniae Lipomas Lymph nodes Undescended testis Femoral aneurysm Saphena varix (more a swelling than a mass!)
In the history features relating to systemic illness and tempo of onset will often give a clue as to the most likely underlying diagnosis.

Groin lumps- some key questions
Is there a cough impulse Is it pulsatile AND is it expansile (to distinguish between false and true
aneurysm) Are both testes intra scrotal Any lesions in the legs such as malignancy or infections (?lymph nodes) Examine the ano rectum as anal cancer may metastasise to the groin Is the lump soft, small and very superficial (?lipoma)
Scrotal lumps - some key questions
Is the lump entirely intra scrotal Does it transilluminate (?hydrocele) Is there a cough impulse (?hernia)
In most cases a diagnosis can be made clinically. Where it is not clear an ultrasound scan is often the most convenient next investigation.A 56 year old lady is admitted with colicky abdominal pain. A plain x-ray is performed. Which of the following should not show fluid levels on a plain abdominal film?
A. Stomach
B. Jejunum
C. Ileum
D. Caecum
E. Descending colon
Fluid levels in the distal colon are nearly always pathological. In general contents of the left colon transit quickly and are seldom held in situ for long periods, the content is also more solid.
Abdominal radiology
Plain abdominal x-rays are often used as a first line investigation in patients with acute abdominal pain. A plain abdominal film may demonstrate free air, evidence of bowel obstruction and possibly other causes of pain (e.g. renal or gallbladder stones). Investigation of potential visceral perforation is usually best performed by obtaining an erect chest x-ray, as this is a more sensitive investigation for suspected visceral perforation.
Features which are usually abnormal

Large amounts of free air (colonic perforation), smaller volumes seen with more proximal perforations.
A positive Riglers sign (gas on both sides of the bowel wall). Caecal diameter of >8cm Fluid levels in the colon Ground glass appearance to film (usually due to large amounts of free fluid). Sentinel loop in patients with inflammation of other organs (e.g. pancreatitis).
Features which should be expected/ or occur without pathology
In Chialditis syndrome, a loop of bowel may be interposed between the liver and diaphragm, giving the mistaken impression that free air is present.
Following ERCP (and sphincterotomy) air may be identified in the biliary tree. Free intra abdominal air following laparoscopy / laparotomy, although usually
dissipates after 48-72 hours.
A 56 year old lady presents with a large bowel obstruction and abdominal distension. Which of the following confirmatory tests should be performed prior to surgery
A. Abdominal ultrasound scan
B. Barium enema
C. Rectal MRI Scan
D. Endoanal ultrasound scan
E. Gastrograffin enema
Patients with clinical evidence of large bowel obstruction, should have the presence or absence of an obstructing lesion confirmed prior to surgery. This is because colonic pseudo-obstruction may produce a similar radiological picture. A gastrograffin enema is the traditional test, as barium is too toxic if it spills into the abdominal cavity. An MRI scan will not provide the relevant information, unless the lesion is rectal and below the peritoneal reflection.
Abdominal radiology
Plain abdominal x-rays are often used as a first line investigation in patients with acute abdominal pain. A plain abdominal film may demonstrate free air, evidence of bowel obstruction and possibly other causes of pain (e.g. renal or gallbladder stones). Investigation of potential visceral perforation is usually best performed by obtaining an erect chest x-ray, as this is a more sensitive investigation for suspected visceral perforation.
Features which are usually abnormal

Large amounts of free air (colonic perforation), smaller volumes seen with more proximal perforations.
A positive Riglers sign (gas on both sides of the bowel wall). Caecal diameter of >8cm Fluid levels in the colon Ground glass appearance to film (usually due to large amounts of free fluid). Sentinel loop in patients with inflammation of other organs (e.g. pancreatitis).
Features which should be expected/ or occur without pathology
In Chialditis syndrome, a loop of bowel may be interposed between the liver and diaphragm, giving the mistaken impression that free air is present.
Following ERCP (and sphincterotomy) air may be identified in the biliary tree. Free intra abdominal air following laparoscopy / laparotomy, although usually
dissipates after 48-72 hours.
Theme: Management of splenic trauma
A. SplenectomyB. AngiographyC. CT ScanD. Admit for bed rest and observationE. Ultrasound scanF. Splenic conservationG. MRI of the abdomen
Please select the most appropriate intervention for the scenario given. Each option may be used once, more than once or not at all.
1. A 7 year old boy falls off a wall the distance is 7 feet. He lands on his left side and there is left flank bruising. There is no haematuria. He is otherwise stable and haemoglobin is within normal limits.
Ultrasound scan
This will demonstrate any overt splenic injury. A CT scan carries a significant dose of radiation. In the absence of haemodynamic instability or other major associated injuries the use of USS to exclude intraabdominal free fluid (blood) would seem safe when coupled with active observation. An USS will also show splenic haematomas.
2. A 42 year old motorcyclist is involved in a road traffic accident. A FAST scan in the emergency department shows free intrabdominal fluid and a laparotomy is performed. At operation there is evidence of small liver laceration that has stopped bleeding and a tear to the inferior pole of the spleen.

Splenic conservation
As minimum damage, attempt conservation.
3. An 18 year old man is involved in a road traffic accident. A CT scan shows disruption of the splenic hilum and a moderate sized perisplenic haematoma.
Splenectomy
Hilar injuries usually mandate splenectomy. The main risk with conservative management here is that he will rebleed and with hilar injuries this can be dramatic.
Splenic trauma
The spleen is one of the more commonly injured intra abdominal organs In most cases the spleen can be conserved. The management is dictated by the
associated injuries, haemodynamic status and extent of direct splenic injury.
Management of splenic traumaConservative Small subcapsular haematoma
Minimal intra abdominal bloodNo hilar disruption
Laparotomy with conservation Increased amounts of intraabdominal bloodModerate haemodynamic compromiseTears or lacerations affecting <50%
Resection Hilar injuriesMajor haemorrhageMajor associated injuries
SplenectomyTechniqueTrauma
GA Long midline incision If time permits insert a self retaining retractor (e.g. Balfour/ omnitract) Large amount of free blood is usually present. Pack all 4 quadrants of the
abdomen. Allow the anaesthetist to 'catch up' Remove the packs and assess the viability of the spleen. Hilar injuries and
extensive parenchymal lacerations will usually require splenectomy. Divide the short gastric vessels and ligate them.

Clamp the splenic artery and vein. Two clamps on the patient side are better and allow for double ligation and serve as a safety net if your assistant does not release the clamp smoothly.
Be careful not to damage the tail of the pancreas, if you do then this will need to be formally removed and the pancreatic duct closed.
Wash out the abdomen and place a tube drain to the splenic bed. Some surgeons implant a portion of spleen into the omentum, whether you
decide to do this is a matter of personal choice. Post operatively the patient will require prophylactic penicillin V and
pneumococcal vaccine.
ElectiveElective splenectomy is a very different operation from that performed in the emergency setting. The spleen is often large (sometimes massive). Most cases can be performed laparoscopically. The spleen will often be macerated inside a specimen bag to facilitate extraction.
Complications
Haemorrhage (may be early and either from short gastrics or splenic hilar vessels
Pancreatic fistula (from iatrogenic damage to pancreatic tail) Thrombocytosis: prophylactic aspirin Encapsulated bacteria infection e.g. Strep. pneumoniae, Haemophilus
influenzae and Neisseria meningitidis
Which of the following does not increase the risk of abdominal wound dehiscence following laparotomy?
A. Jaundice
B. Abdominal compartment syndrome
C. Poorly controlled diabetes mellitus
D. Administration of intravenous steroids
E. Use of Ketamine as an anaesthetic agent
Ketamine does not affect healing. All the other situations in the list carry a strong association with poor healing and risk of dehisence.
Abdominal wound dehiscence
This is a significant problem facing all surgeons who undertake abdominal surgery on a regular basis. Traditionally it is said to occur when all layers of

an abdominal mass closure fail and the viscera protrude externally (associated with 30% mortality).
It can be subdivided into superficial, in which the skin wound alone fails and complete, implying failure of all layers.
Factors which increase the risk are:* Malnutrition* Vitamin deficiencies * Jaundice * Steroid use * Major wound contamination (e.g. faecal peritonitis)* Poor surgical technique (Mass closure technique is the preferred method-Jenkins Rule)
When sudden full dehiscence occurs the management is as follows:* Analgesia* Intravenous fluids* Intravenous broad spectrum antibiotics* Coverage of the wound with saline impregnated gauze (on the ward)* Arrangements made for a return to theatre
Surgical strategy
Correct the underlying cause (eg TPN or NG feed if malnourished) Determine the most appropriate strategy for managing the wound
OptionsResuturing of the wound
This may be an option if the wound edges are healthy and there is enough tissue for sufficient coverage. Deep tension sutures are traditionally used for this purpose.
Application of a wound manager
This is a clear dressing with removable front. Particularly suitable when some granulation tissue is present over the viscera or where there is a high output bowel fistula present in the dehisced wound.
Application of a 'Bogota bag'
This is a clear plastic bag that is cut and sutured to the wound edges and is only a temporary measure to be adopted when the wound cannot be closed and will necessitate a return to theatre for definitive management.
Application of a VAC dressing system
These can be safely used BUT ONLY if the correct layer is interposed between the suction device and the bowel. Failure to adhere to this absolute rule will almost invariably result in the development of multiple bowel fistulae and create an extremely difficult management problem.
Theme: Causes of diarrhoea
A. Campylobacter jejuni infectionB. Salmonella gastroenteritis infectionC. Crohns disease

D. Ulcerative colitisE. Irritable bowel syndromeF. Ischaemic colitisG. Laxative abuseH. Clostridium difficile infection
Please select the most likely cause of diarrhoea for each scenario given. Each option may be used once, more than once or not at all.
5. A 23 year old lady has suffered from diarrhoea for 8 months, she has also lost 2 Kg in weight. At colonoscopy appearances of melanosis coli are identified and confirmed on biopsy
You answered Ulcerative colitis
The correct answer is Laxative abuse
This may occur as a result of laxative abuse and consists of lipofuschin laden marcophages that appear brown.
6. A 68 year old lady has recently undergone an abdominal aortic aneurysm repair. The operation was performed electively and was uncomplicated. Since surgery she has had repeated episodes of diarrhoea.
Ischaemic colitis
The IMA is commonly ligated during and AAA repair and this may then render the left colon relatively ischaemic, thereby causing mesenteric colitis. Treatment is supportive and most cases will settle with conservative management.
7. A 23 year old man is admitted to hospital with diarrhoea and severe abdominal pain. He was previously well and his illness has lasted 18 hours.
You answered Irritable bowel syndrome
The correct answer is Campylobacter jejuni infection
Severe abdominal pain tends to favour Campylobacter infection.
Diarrhoea
World Health Organisation definitions

Diarrhoea: > 3 loose or watery stool per dayAcute diarrhoea < 14 daysChronic diarrhoea > 14 days
Acute DiarrhoeaGastroenteritis May be accompanied by abdominal pain or
nausea/vomitingDiverticulitis Classically causes left lower quadrant pain, diarrhoea
and feverAntibiotic therapy More common with broad spectrum antibiotics
Clostridium difficile is also seen with antibiotic useConstipation causing overflow
A history of alternating diarrhoea and constipation may be givenMay lead to faecal incontinence in the elderly
Chronic Diarrhoea Irritable bowel syndrome
Extremely common. The most consistent features are abdominal pain, bloating and change in bowel habit. Patients may be divided into those with diarrhoea predominant IBS and those with constipation predominant IBS.Features such as lethargy, nausea, backache and bladder symptoms may also be present
Ulcerative colitis
Bloody diarrhoea may be seen. Crampy abdominal pain and weight loss are also common. Faecal urgency and tenesmus may occur
Crohn's disease
Crampy abdominal pains and diarrhoea. Bloody diarrhoea less common than in ulcerative colitis. Other features include malabsorption, mouth ulcers perianal disease and intestinal obstruction
Colorectal cancer
Symptoms depend on the site of the lesion but include diarrhoea, rectal bleeding, anaemia and constitutional symptoms e.g. Weight loss and anorexia
Coeliac disease
In children may present with failure to thrive, diarrhoea and abdominal distension
In adults lethargy, anaemia, diarrhoea and weight loss are seen. Other autoimmune conditions may coexist
Other conditions associated with diarrhoea include:
Thyrotoxicosis Laxative abuse Appendicitis with pelvic abscess or pelvic appendix Radiation enteritis
DiagnosisStool cultureAbdominal and digital rectal examinationConsider colonoscopy (radiological studies unhelpful)Thyroid function tests, serum calcium, anti endomysial antibodies, glucose

A 6 year old child presents with colicky abdominal pain, vomiting and the passage of red current jelly stool per rectum. On examination the child has a tender abdomen and a palpable mass in the right upper quadrant. Imaging shows an intussusception. Which of the conditions below is least recognised as a precipitant
A. Inflammation of Payers patches
B. Cystic fibrosis
C. Meckels diverticulum
D. Mesenteric cyst
E. Mucosal polyps
Mesenteric cysts may be associated with intra abdominal catastrophes where these occur they are typically either intestinal volvulus or intestinal infarction. They seldom cause intussusception. Cystic fibrosis may lead to the formation of meconium ileus equivalent and plugs may occasionally serve as the lead points for an intussusception.
Intussusception- Paediatric
Intussusception typcially presents with colicky abdominal pain and vomiting. The telescoping of the bowel produces mucosal ischaemia and bleeding may occur resulting in the passage of "red current jelly" stools. Recognised causes include lumenal pathologies such as polyps, lymphadenopathy and diseases such as cystic fibrosis. Idiopathic intussceception of the ileocaecal valve and terminal ileum is the most common variant and typically affects young children and toddlers. The diagnosis is usually made by abdominal ultrasound investigation. The decision as to the optimal treatment is dictated by the patients physiological status and abdominal signs. In general children who are unstable with localising peritoneal signs should undergo laparotomy as should those in whom attempted radiological reduction has failed. In relatively well children without localising signs attempted hydrostatic reduction under fluroscopic guidance is the usual treatment.Which one of the following is least likely to cause malabsorption?
A. Primary biliary cirrhosis
B. Ileo-colic bypass
C. Chronic pancreatitis
D. Whipples disease
E. Hartmans procedure

In a Hartmans procedure the sigmoid colon is removed and an end colostomy is fashioned. The bowel remains in continuity and no absorptive ability is lost.An ileo-colic bypass leaves a redundant loop of small bowel in continuity, where the contents will stagnate and bacterial overgrowth will occur. Therefore this is recognised cause of malabsorption.
Malabsorption
Malabsorption is characterised by diarrhoea, steatorrhoea and weight loss. Causes may be broadly divided into intestinal (e.g. villous atrophy), pancreatic (deficiency of pancreatic enzyme production or secretion) and biliary (deficiency of bile-salts needed for emulsification of fats)
Intestinal causes of malabsorption
coeliac disease Crohn's disease tropical sprue Whipple's disease Giardiasis brush border enzyme deficiencies (e.g. lactase insufficiency)
Pancreatic causes of malabsorption
chronic pancreatitis cystic fibrosis pancreatic cancer
Biliary causes of malabsorption
biliary obstruction primary biliary cirrhosis
Other causes
bacterial overgrowth (e.g. systemic sclerosis, diverticulae, blind loop) short bowel syndrome lymphoma
Theme: Intra abdominal malignancies
A. Metastatic adenocarcinoma of the pancreasB. Metastatic appendiceal carcinoidC. Metastatic colonic cancerD. Pseudomyxoma peritonei

E. MALT lymphomaF. Retroperitoneal liposarcomaG. Retroperitoneal fibrosis
For the disease given please give the most likely primary disease process. Each option may be used once, more than once or not at all.
10. A 32 year old man is admitted with a distended tense abdomen. He previously underwent a difficult appendicectomy 1 year previously and was discharged. At laparotomy the abdomen is filled with a gelatinous substance.
You answered Metastatic appendiceal carcinoid
The correct answer is Pseudomyxoma peritonei
Pseudomyxoma is classically associated with mucin production and the appendix is the commonest source.
11. A 62 year old man is admitted with dull lower back pain and abdominal discomfort. On examination he is hypertensive and a lower abdominal fullness is elicited on examination. An abdominal ultrasound demonstrates hydronephrosis and intravenous urography demonstrated medially displaced ureters. A CT scan shows a periaortic mass.
You answered Metastatic colonic cancer
The correct answer is Retroperitoneal fibrosis
Retroperitoneal fibrosis is an uncommon condition and its aetiology is poorly understood. In a significant proportion the ureters are displaced medially. In most retroperitoneal malignancies they are displaced laterally. Hypertension is another common finding. A CT scan will often show a para-aortic mass
12. A 48 year old lady is admitted with abdominal distension. On examination she is cachectic and has ascites. Her CA19-9 returns highly elevated.
Metastatic adenocarcinoma of the pancreas
Although not specific CA 19-9 in the context of this history is highly suggestive of pancreatic cancer over the other scenarios.
Pseudomyxoma peritoneii- Curative treatment is peritonectomy (Sugarbaker procedure) and heated intra peritoneal

chemotherapy.
Pseudomyxoma Peritonei
Rare mucinous tumour Most commonly arising from the appendix (other abdominal viscera are also
recognised as primary sites) Incidence of 1-2/1,000,000 per year The disease is characterised by the accumulation of large amounts of
mucinous material in the abdominal cavity
TreatmentIs usually surgical and consists of cytoreductive surgery (and often peritonectomy c.f Sugarbaker procedure) combined with intra peritoneal chemotherapy with mitomycin C.
Survival is related to the quality of primary treatment and in Sugarbakers own centre 5 year survival rates of 75% have been quoted. Patients with disseminated intraperitoneal malignancy from another source fare far worse.In selected patients a second look laparotomy is advocated and some practice this routinely.Theme: Abdominal pain
A. Acute mesenteric embolusB. Acute on chronic mesenteric ischaemiaC. Mesenteric vein thrombosisD. Ruptured abdominal aortic aneurysmE. PancreatitisF. AppendicitisG. Acute cholecystitis
Please select the most likely underlying diagnosis from the list above. Each option may be used once, more than once or not at all.
13. A 72 year old man collapses with sudden onset abdominal pain. He has been suffering from back pain recently and has been taking ibuprofen.
Ruptured abdominal aortic aneurysm
Back pain is a common feature with expanding aneurysms and may be miss classified as being of musculoskeletal origin.

14. A 73 year old women collapses with sudden onset of abdominal pain and the passes a large amount of diarrhoea. On admission she is vomiting repeatedly. She has recently been discharged from hospital following a myocardial infarct but recovered well.
You answered Mesenteric vein thrombosis
The correct answer is Acute mesenteric embolus
Sudden onset of abdominal pain and forceful bowel evacuation are features of acute mesenteric infarct.
15. A 66 year old man has been suffering from weight loss and develops severe abdominal pain. He is admitted to hospital and undergoes a laparotomy. At operation the entire small bowel is infarcted and only the left colon is viable.
You answered Mesenteric vein thrombosis
The correct answer is Acute on chronic mesenteric ischaemia
This man is likely to have underlying chronic mesenteric vascular disease. Only 15% of emboli will occlude SMA orifice leading to entire small bowel infarct. The background history of weight loss also favours an acute on chronic event.
Mesenteric vessel disease
Mesenteric ischaemia accounts for 1 in 1000 acute surgical admissions. It is primarily caused by arterial embolism resulting in infarction of the colon. It is more likely to occur in areas such as the splenic flexure that are located at the borders of the territory supplied by the superior and inferior mesenteric arteries.
TypesAcute mesenteric embolus (commonest 50%)
Sudden onset abdominal pain followed by profuse diarrhoea.
May be associated with vomiting. Rapid clinical deterioration. Serological tests: WCC, lactate, amylase may all be
abnormal particularly in established disease. These can be normal in the early phases.
Acute on chronic mesenteric ischaemia
Usually longer prodromal history. Post prandial abdominal discomfort and weight loss are
dominant features. Patients will usually present with an

acute on chronic event, but otherwise will tend not to present until mesenteric flow is reduced by greater than 80%.
When acute thrombosis occurs presentation may be as above. In the chronic setting the symptoms will often be those of ischaemic colitis (mucosa is the most sensitive area to this insult).
Mesenteric vein thrombosis
Usually a history over weeks. Overt abdominal signs and symptoms will not occur until
venous thrombosis has reached a stage to compromise arterial inflow.
Thrombophilia accounts for 60% of cases.
Low flow mesenteric infarction
This occurs in patients with multiple co morbidities in whom mesenteric perfusion is significantly compromised by overuse of inotropes or background cardiovascular compromise.
The end result is that the bowel is not adequately perfused and infarcts occur from the mucosa outwards.
Diagnosis
Serological tests: WCC, lactate, CRP, amylase (can be normal in early disease).
Cornerstone for diagnosis of arterial AND venous mesenteric disease is CT angiography scanning in the arterial phase with thin slices (<5mm). Venous phase contrast is not helpful.
SMA duplex USS is useful in the evaluation of proximal SMA disease in patients with chronic mesenteric ischaemia.
MRI is of limited use due to gut peristalsis and movement artefact.
Management
Overt signs of peritonism: Laparotomy Mesenteric vein thrombosis: If no peritonism: Medical management with IV
heparin At operation limited resection of frankly necrotic bowel with view to relook
laparotomy at 24-48h. In the interim urgent bowel revascularisation via endovascular (preferred) or surgery.
PrognosisOverall poor. Best outlook is from an acute ischaemia from an embolic event where surgery occurs within 12h. Survival may be 50%. This falls to 30% with treatment delay. The other conditions carry worse survival figures.Theme: Surgical incisions

A. Lanz incision
B. Gridiron incision
C. Kochers incision
D. Rutherford Morrison
E. Rooftop incision
F. McEvedy Incision
G. Lothissen Incision
Please select the most appropriate incision for the procedure described. Each option may be used once, more than once or not at all.
16. A 78 year old lady is admitted with an incarcerated femoral hernia. Abdominal signs are absent and there are no symptoms of obstruction. AXR is normal.
McEvedy Incision
From the list the McEvedy approach is the most appropriate. The Lothissen incision may compromise the posterior wall of the inguinal canal and is best avoided. The author prefers a limited pfannenstial type incision for this procedure, as it gives better control of the hernia, but this is not on the list.
17. A 15 year old girl presents with right iliac fossa pain and guarding, pregnancy test is negative and WCC is 16.
Lanz incision
She requires an appendicectomy although there is an increasing vogue for performing this procedure laparoscopically an open procedure is entirely suitable. However, although both a Gridiron and Lanz incision are suitable for appendicectomy a Lanz will give a superior cosmetic result and would be the preferred option for most young females.
18. A 45 year old man is due to undergo a live donor renal transplant. This will be his first procedure.

Rutherford Morrison
The Rutherford Morrison incision will typically give access to the iliac vessels and bladder for the procedure
Abdominal incisions
Theme in January 2012 exam
Midline incision Commonest approach to the abdomen Structures divided: linea alba, transversalis fascia, extraperitoneal
fat, peritoneum (avoid falciform ligament above the umbilicus) Bladder can be accessed via an extraperitoneal approach through
the space of Retzius
Paramedian incision
Parallel to the midline (about 3-4cm) Structures divided/retracted: anterior rectus sheath, rectus
(retracted), posterior rectus sheath, transversalis fascia, extraperitoneal fat, peritoneum
Incision is closed in layers
Battle Similar location to paramedian but rectus displaced medially (and thus denervated)
Now seldom used
Kocher's Incision under right subcostal margin e.g. Cholecystectomy (open)
Lanz Incision in right iliac fossa e.g. Appendicectomy
Gridiron Oblique incision centered over McBurneys point- usually appendicectomy (less cosmetically acceptable than Lanz
Gable Rooftop incision
Pfannenstiel's Transverse supra pubic, primarily used to access pelvic organs
McEvedy's Groin incision e.g. Emergency repair strangulated femoral hernia
Rutherford Morrison
Extraperitoneal approach to left or right lower quadrants. Gives excellent access to iliac vessels and is the approach of choice for first time renal transplantation.

Image sourced from Wikipedia
Theme: Acute abdominal pain
A. AppendicitisB. Henoch Schonlein purpuraC. Diabetes mellitusD. IntussusceptionE. MittelschmerzF. PneumoniaG. Sickle cell crisisH. Spontaneous bacterial peritonitisI. Rupure of follicular cyst
Please select the most likely cause of abdominal pain for the scenario given. Each option may be used once, more than once or not at all.
19. An 11 month-old girl develops sudden onset abdominal pain. She has a high pitched scream and draws up her legs. Her BP is 90/40 mm/Hg, her pulse 118/min and abdominal examination is normal.
Intussusception
Intussusception should be considered in toddlers and infants presenting with screaming attacks. The child often has a history of being unwell for one to three days prior to presentation. The child may pass bloody mucus stool, which is a late sign. Examination of the abdomen is often normal as the sausage mass in the right upper quadrant is difficult to feel.
20. An 8 year-old West Indian boy presents with periumbilical abdominal pain. He

has vomited twice and is refusing fluids. His temperature is 38.1oC and blood tests are as follows: Haemoglobin 8 g/dl, WCC 13 x 109/l, with a neutrophilia.
Sickle cell crisis
Sickle cell anaemia is characterised by severe chronic haemolytic anaemia resulting from poorly formed erythrocytes. Painful crises result from vaso-occlusive episodes, which may occur spontaneously or may be precipitated by infection. Consider this diagnosis in all children of appropriate ethnic background.
21. A 15-month-old girl presents with a three day history of periorbital oedema. She is brought to hospital. On examination she has facial oedema and a tender distended abdomen. Her temperature is 39oC and her blood pressure is 90/45 mmHg. There is clinical evidence of poor peripheral perfusion.
Spontaneous bacterial peritonitis
The 15-month-old girl is a patient with nephrotic syndrome. Patients with this condition are at risk of septicaemia and peritonitis from Streptococcus pneumoniae, due to the loss of immunoglobulins and opsonins in the urine.
Acute abdominal pain-diagnoses
Conditions presenting with acute abdominal painCondition Features Investigations ManagementAppendicitis History of
migratory pain.Fever.Anorexia.Evidence of right iliac fossa tenderness.Mild pyrexia.
Differential white cell countPregnancy testC-Reactive proteinAmylaseUrine dipstick testing
Appendicectomy
Mesenteric adenitis
Usually recent upper respiratory tract infection.High fever.Generalised abdominal discomfort- true localised pain and signs are rare.
Full blood count- may show slightly raised white cell countUrine dipstick often normalAbdominal ultrasound scan - usually no free fluid
Conservative management- appendicectomy if diagnostic doubt
Mittelschmerz Only seen in Full blood count- normal Manage conservatively

females.Mid cycle pain.Usually occurs two weeks after last menstrual period.Pain is usually has a supra-pubic location.Usually subsides over a 24-48 hour period.
Urine dipstick- normalAbdominal and pelvic ultrasound- may show a trace of pelvic free fluid
if doubt or symptoms fail to settle then laparoscopy
Fitz-Hugh Curtis syndrome
Disseminated infection with Chlamydia.Usually seen in females.Consists of evidence of pelvic inflammatory disease together with peri-hepatic inflammation and subsequent adhesion formation.
Abdominal ultrasound scan- may show free fluidHigh vaginal swabs - may show evidence of sexually transmitted infections
Usually medically managed- doxycycline or azithromycin
Abdominal aortic aneurysm (ruptured)
Sudden onset of abdominal pain radiating to the back in older adults (look for risk factors).Collapse.May be moribund on arrival in casualty, more stable if contained haematoma.Careful clinical assessment may reveal pulsatile mass.
Patients who are haemodynamically stable should have a CT scan
Unstable patients should undergo immediate surgery (unless it is not in their best interests).Those with evidence of contained leak on CT should undergo immediate surgeryIncreasing aneurysmal size is an indication for urgent surgical intervention (that can wait until the next working day)
Perforated peptic ulcer
Sudden onset of pain (usually epigastric).Often preceding history of upper abdominal pain.Soon develop generalised abdominal pain.On examination
Erect CXR may show free air. A CT scan may be indicated where there is diagnostic doubt
Laparotomy (laparoscopic surgery for perforated peptic ulcers is both safe and feasible in experienced hands)

may have clinical evidence of peritonitis.
Intestinal obstruction
Colicky abdominal pain and vomiting (the nature of which depends on the level of the obstruction).Abdominal distension and constipation (again depending upon site of obstruction).Features of peritonism may occur where local necrosis of bowel loops is occurring.
A plain abdominal film may help with making the diagnosis. A CT scan may be useful where diagnostic uncertainty exists
In those with a virgin abdomen and lower and earlier threshold for laparotomy should exist than in those who may have adhesional obstruction
Mesenteric infarction
Embolic events present with sudden pain and forceful evacuation.Acute on chronic events usually have a longer history and previous weight loss.On examination the pain is typically greater than the physical signs would suggest.
Arterial pH and lactateArterial phase CT scanning is the most sensitive test
Immediate laparotomy and resection of affected segments, in acute embolic events SMA embolectomy may be needed.
How to reduce post operative adhesions :
A. Peritoneal lavage with cetrimide following elective right hemicolectomy
B. Use of a laparoscopic approach over open surgery
C. Use of talc to coat surgical gloves
D. Performing a Nobles plication of the small bowel
E. Using stapled rather than a hand sewn anastamosis

Laparoscopy results in fewer adhesions. When talc was used to coat surgical gloves it was a major cause of adhesion formation and withdrawn for that reason. A Nobles plication is an old fashioned operation which has no place in the prevention of adhesion formation. Use of an anastamotic stapling device will not influence the development of adhesions per se although clearly an anastamotic leak will result in more adhesion formation
Surgical complications
Complications occur in all branches of surgery and require vigilance in their detection. In many cases anticipating the likely complications and appropriate avoidance will minimise their occurrence. For the purposes of the MRCS the important principles to appreciate are:
The anatomical principles that underpin complications The physiological and biochemical derangements that occur The most appropriate diagnostic modalities to utilise The principles which underpin their management
This is clearly a very broad area and impossible to cover comprehensively. There is considerable overlap with other topic areas within the website.
Avoiding complications
Some points to hopefully avert complications:
World Health Organisation checklist- now mandatory prior to all operations Prophylactic antibiotics - right dose, right drug, right time. Assess DVT/ PE risk and ensure adequate prophylaxis MARK site of surgery Use tourniquets with caution and with respect for underlying structures Remember the danger of end arteries and in situations where they occur avoid
using adrenaline containing solutions and monopolar diathermy. Handle tissues with care- devitalised tissue serves as a nidus for infection Be very wary of the potential for coupling injuries when using diathermy
during laparoscopic surgery The inferior epigastric artery is a favourite target for laparoscopic ports and
surgical drains!
Anatomical principles
Understanding the anatomy of a surgical field will allow appreciation of local and systemic complications that may occur. For example nerve injuries may occur following surgery in specific regions the table below lists some of the more important nerves to consider and mechanisms of injury

Nerve MechanismAccessory Posterior triangle lymph node biopsySciatic Posterior approach to hipCommon peroneal Legs in Lloyd Davies positionLong thoracic Axillary node clearancePelvic autonomic nerves Pelvic cancer surgeryRecurrent laryngeal nerves During thyroid surgeryHypoglossal nerve During carotid endarterectomyUlnar and median nerves During upper limb fracture repairs
These are just a few. The detailed functional sequelae are particularly important and will often be tested. In addition to nerve injuries certain procedures carry risks of visceral or structural injury. Again some particular favourites are given below:
Structure MechanismThoracic duct During thoracic surgery e.g. Pneumonectomy, oesphagectomyParathyroid glands
During difficult thyroid surgery
Ureters During colonic resections/ gynaecological surgeryBowel perforation Use of Verres Needle to establish pneumoperitoneumBile duct injury Failure to delineate Calots triangle carefully and careless use of
diathermyFacial nerve Always at risk during ParotidectomyTail of pancreas When ligating splenic hilumTesticular vessels During re-do open hernia surgeryHepatic veins During liver mobilisation
Again many could be predicted from the anatomy of the procedure.
Physiological derangements
A very common complication is bleeding and this is covered under the section of haemorrhagic shock. Another variant is infection either superficial or deep seated. The organisms are covered under microbiology and the features of sepsis covered under shock. Do not forget that immunocompromised and elderly patients may present will atypical physiological parameters.
Selected physiological and biochemical issues are given below:
Complication Physiological/ Biochemical ProblemArrhythmias following cardiac surgery
Susceptibility to hypokalaemia (K+ <4.0 in cardiac patients)
Neurosurgical electrolyte disturbance
SIADH following cranial surgery causing hyponatraemia
Ileus following gastrointestinal surgery
Fluid sequestration and loss of electrolytes

Pulmonary oedema following pneumonectomy
Loss of lung volume makes these patients very sensitive to fluid overload
Anastamotic leak Generalised sepsis causing mediastinitis or peritonitis depending on site of leak
Myocardial infarct May follow any type of surgery and in addition to direct cardiac effects the decreased cardiac output may well compromise grafts etc.
Try making a short list of problems and causes specific to your own clinical area.
Diagnostic modalities
Depends largely on the suspected complication. In the acutely unwell surgical patient the following baseline investigations are often helpful:
Full blood count, urea and electrolytes, C- reactive protein (trend rather than absolute value), serum calcium, liver function tests, clotting (don't forget to repeat if on-going bleeding)
Arterial blood gases ECG (+cardiac enzymes if MI suspected) Chest x-ray to identify collapse/ consolidation Urine analysis for UTI
These will often identify the most common complications.
Special tests
CT scanning for identification of intra-abdominal abscesses, air and if luminal contrast is used an anastamotic leak
Gatrograffin enema- for rectal anastamotic leaks Doppler USS of leg veins- for identification of DVT CTPA for PE Sending peritoneal fluid for U+E (if ureteric injury suspected) or amylase (if
pancreatic injury suspected) Echocardiogram if pericardial effusion suspected post cardiac surgery and no
pleural window made.
Management of complications
The guiding principal should be safe and timely intervention. Patients should be stabilised and if an operation needs to occur in tandem with resuscitation then generally this should be of a damage limitation type procedure rather than definitive surgery (which can be more safely undertaken in a stable patient the following day).
Remember that recent surgery is a contra indication to thrombolysis and that in some patients IV heparin may be preferable to a low molecular weight heparin (easier to reverse).

As a general rule laparotomies for bleeding should follow the core principle of quadrant packing and then subsequent pack removal rather than plunging large clamps into pools of blood. The latter approach invariable worsens the situation is often accompanied by significant visceral injury particularly when done by the inexperienced. If packing controls a situation it is entirely acceptable practice to leak packs in situ and return the patient to ITU for pack removal the subsequent day.Theme: Abdominal pain
A. AppendicitisB. Threatened miscarriageC. Ectopic pregnancyD. Irritable bowel syndromeE. MittelschmerzF. Pelvic inflammatory diseaseG. Adnexial torsionH. EndometriosisI. Degenerating fibroid
Please select the most likely cause of abdominal pain for the clinical scenario given. Each option may be used once, more than once or not at all.
23. An 18 year-old girl presents to the Emergency Department with sudden onset sharp, tearing pelvic pain associated with a small amount of vaginal bleeding. She also complains of shoulder tip pain. On examination she is hypotensive, tachycardic and has marked cervical excitation.
Ectopic pregnancy
The history of tearing pain and haemodynamic compromise in a women of child bearing years should prompt a diagnosis of ectopic pregnancy.
24. A 25 year-old lady presents to her GP complaining of a two day history of right upper quadrant pain, fever and a white vaginal discharge. She has seen the GP twice in 12 weeks complaining of pelvic pain and dyspareunia.
Pelvic inflammatory disease
The most likely diagnosis is pelvic inflammatory disease. Right upper quadrant pain occurs as part of the Fitz Hugh Curtis syndrome in which peri hepatic inflammation occurs.
25. A 16 year old female presents to the emergency department with a 12 hour history of pelvic discomfort. She is otherwise well and her last normal

menstrual period was 2 weeks ago. On examination she has a soft abdomen with some mild supra pubic discomfort.
Mittelschmerz
Mid cycle pain is very common and is due to the small amount of fluid released during ovulation. Inflammatory markers are usually normal and the pain typically subsides over the next 24-48 hours.
Gynaecological causes of abdominal pain
A number of women will present with abdominal pain and subsequently be diagnosed with a gynaecological disorder. In addition to routine diagnostic work up of abdominal pain, all female patients should also undergo a bimanual vaginal examination, urine pregnancy test and consideration given to abdominal and pelvic ultrasound scanning. When diagnostic doubt persists a laparoscopy provides a reliable method of assessing suspected tubulo-ovarian pathology.
Differential diagnoses of abdominal pain in femalesDiagnosis Features Investigation TreatmentMittelschmerz Usually mid cycle
pain.Often sharp onset.Little systemic disturbance.May have recurrent episodes.Usually settles over 24-48 hours.
Full blood count- usually normalUltrasound- may show small quantity of free fluid
Conservative
Endometriosis 25% asymptomatic, in a further 25% associated with other pelvic organ pathology. Remaining 50% may have menstrual irregularity, infertility, pain and deep dyspareurina.Complex disease may result in pelvic adhesional formation with episodes of intermittent small
Ultrasound- may show free fluidLaparoscopy will usually show lesions
Usually managed medically, complex disease will often require surgery and some patients will even require formal colonic and rectal resections if these areas are involved

bowel obstruction.Intra-abdominal bleeding may produce localised peritoneal inflammation.Recurrent episodes are common.
Ovarian torsion Usually sudden onset of deep seated colicky abdominal pain.Associated with vomiting and distress.Vaginal examination may reveal adnexial tenderness.
Ultrasound may show free fluidLaparoscopy is usually both diagnostic and therapeutic
Laparoscopy
Ectopic gestation
Symptoms of pregnancy without evidence of intra uterine gestation.Present as an emergency with evidence of rupture or impending rupture.Open tubular ruptures may have sudden onset of abdominal pain and circulatory collapse, in other the symptoms may be more prolonged and less marked.Small amount of vaginal discharge is common.There is usually adnexial tenderness.
Ultrasound showing no intra uterine pregnancy and beta HCG that is elevatedMay show intra abdominal free fluid
Laparoscopy or laparotomy is haemodynamically unstable. A salphingectomy is usually performed.
Pelvic inflammatory disease
Bilateral lower abdominal pain associated with vaginal discharge.Dysuria may also be present.Peri-hepatic inflammation secondary to Chlamydia (Fitz Hugh Curtis Syndrome) may produce right upper quadrant discomfort.Fever >38o
Full blood count- LeucocytosisPregnancy test negative (Although infection and pregnancy may co-exist)Amylase - usually normal or slightly raisedHigh vaginal and urethral swabs
Usually medical management

Which of the following statements relating to a burst abdomen is false?
A. Is seen in 1-2% of modern laparotomies
B. Is more common in faecal peritonitis
C. Is less common when a 'mass closure' technique is used
D. When it does occur is most common at 15 days
E. Is similar in incidence regardless of whether 1/0 polydiaxone or 1/0 polypropylene are used
When it does occur a burst abdomen is most common at 6 days and is usually the result of technical error when Jenkins rule is not followed and sutures are placed in the zone of collagenolysis. The choice of materials given above does not influence dehisence rates.
Abdominal wound dehiscence
This is a significant problem facing all surgeons who undertake abdominal surgery on a regular basis. Traditionally it is said to occur when all layers of an abdominal mass closure fail and the viscera protrude externally (associated with 30% mortality).
It can be subdivided into superficial, in which the skin wound alone fails and complete, implying failure of all layers.
Factors which increase the risk are:* Malnutrition* Vitamin deficiencies * Jaundice * Steroid use * Major wound contamination (e.g. faecal peritonitis)* Poor surgical technique (Mass closure technique is the preferred method-Jenkins Rule)
When sudden full dehiscence occurs the management is as follows:* Analgesia* Intravenous fluids* Intravenous broad spectrum antibiotics* Coverage of the wound with saline impregnated gauze (on the ward)* Arrangements made for a return to theatre
Surgical strategy
Correct the underlying cause (eg TPN or NG feed if malnourished) Determine the most appropriate strategy for managing the wound

OptionsResuturing of the wound
This may be an option if the wound edges are healthy and there is enough tissue for sufficient coverage. Deep tension sutures are traditionally used for this purpose.
Application of a wound manager
This is a clear dressing with removable front. Particularly suitable when some granulation tissue is present over the viscera or where there is a high output bowel fistula present in the dehisced wound.
Application of a 'Bogota bag'
This is a clear plastic bag that is cut and sutured to the wound edges and is only a temporary measure to be adopted when the wound cannot be closed and will necessitate a return to theatre for definitive management.
Application of a VAC dressing system
These can be safely used BUT ONLY if the correct layer is interposed between the suction device and the bowel. Failure to adhere to this absolute rule will almost invariably result in the development of multiple bowel fistulae and create an extremely difficult management problem.
Which of the following statements about diarrhoea is false?
A. Nocturnal diarrhoea is uncommon in irritable bowel syndrome
B. World Health Organisation definition of diarrhoea is greater than 3 episodes of loose or watery stool a day
C. Pancreatic disease causes osmotic diarrhoea
D. Vitamin C deficiency causes diarrhoea
E. The World Health Organisation definition of chronic diarrhoea is greater than 14 days of diarrhoea
Vitamin C toxicity causes osmotic diarrhoea.
Diarrhoea
World Health Organisation definitionsDiarrhoea: > 3 loose or watery stool per dayAcute diarrhoea < 14 daysChronic diarrhoea > 14 days
Acute DiarrhoeaGastroenteritis May be accompanied by abdominal pain or
nausea/vomitingDiverticulitis Classically causes left lower quadrant pain, diarrhoea
and feverAntibiotic therapy More common with broad spectrum antibiotics
Clostridium difficile is also seen with antibiotic useConstipation causing A history of alternating diarrhoea and constipation may

overflow be givenMay lead to faecal incontinence in the elderly
Chronic Diarrhoea Irritable bowel syndrome
Extremely common. The most consistent features are abdominal pain, bloating and change in bowel habit. Patients may be divided into those with diarrhoea predominant IBS and those with constipation predominant IBS.Features such as lethargy, nausea, backache and bladder symptoms may also be present
Ulcerative colitis
Bloody diarrhoea may be seen. Crampy abdominal pain and weight loss are also common. Faecal urgency and tenesmus may occur
Crohn's disease
Crampy abdominal pains and diarrhoea. Bloody diarrhoea less common than in ulcerative colitis. Other features include malabsorption, mouth ulcers perianal disease and intestinal obstruction
Colorectal cancer
Symptoms depend on the site of the lesion but include diarrhoea, rectal bleeding, anaemia and constitutional symptoms e.g. Weight loss and anorexia
Coeliac disease
In children may present with failure to thrive, diarrhoea and abdominal distension
In adults lethargy, anaemia, diarrhoea and weight loss are seen. Other autoimmune conditions may coexist
Other conditions associated with diarrhoea include:
Thyrotoxicosis Laxative abuse Appendicitis with pelvic abscess or pelvic appendix Radiation enteritis
DiagnosisStool cultureAbdominal and digital rectal examinationConsider colonoscopy (radiological studies unhelpful)Thyroid function tests, serum calcium, anti endomysial antibodies, glucoseA 40 year old man presents with a long standing inguinal hernia. On examination he has a small, direct inguinal hernia. He inquires as to the risk of strangulation over the next twelve months should he decide not to undergo surgery. Which of the following most closely matches the likely risk of strangulation over the next 12 months?
A. 50%
B. 40%

C. 25%
D. 15%
E. <5%
The annual probability of strangulation is up to 3% and is more common in indirect hernias. Elective repair poses few risks. However, emergency repair is associated with increased mortality, particularly in the elderly.
Inguinal hernia surgery
Inguinal hernias occur when the abdominal viscera protrude through the anterior abdominal wall into the inguinal canal. They may be classified as being either direct or indirect. The distinction between these two rests on their relation to Hesselbach's triangle.
Boundaries of Hesselbach's Triangle
Medial: Rectus abdominis Lateral: Inferior epigastric vessels Inferior: Inguinal ligament

Image sourced from Wikipedia
Hernias occurring within the triangle tend to be direct and those outside - indirect.
DiagnosisMost cases are diagnosed clinically, a reducible swelling may be located at the level of the inguinal canal. Large hernia may extend down into the male scrotum, these will not trans-illuminate and it is not possible to "get above" the swelling. Cases that are unclear on examination, but suspected from the history, may be further investigated using ultrasound or by performing a herniogram.
TreatmentHernias associated with few symptoms may be managed conservatively. Symptomatic hernias or those which are at risk of developing complications are usually treated surgically. First time hernias may be treated by performing an open inguinal hernia repair; the inguinal canal is opened, the hernia reduced and the defect repaired. A prosthetic mesh may be placed posterior to the cord structures to re-inforce the repair and reduce the risk of recurrence.Recurrent hernias and those which are bilateral are generally managed with a laparoscopic approach. This may be via an intra or extra peritoneal route. As in open surgery a mesh is deployed. However, it will typically lie posterior to the deep ring.
Inguinal hernia in childrenInguinal hernias in children are almost always of an indirect type and therefore are usually dealt with by herniotomy, rather than herniorraphy. Neonatal hernias especially in those children born prematurely are at highest risk of strangulation and should be repaired urgently. Other hernias may be repaired on an elective basis.
ReferencesThe UK Based National Institute of Clinical Excellence has published guidelines relating to the choice between open and laparoscopic inguinal hernia repair. Which users may find interesting:
http://guidance.nice.org.uk/TA83/Guidance/pdf/English
A 60 year old women has fully recovered from an attack of pancreatitis. Over the following 12 months she develops episodic epigastric discomfort. Un upper GI endoscopy shows gastric varices only. An abdominal CT scan demonstrates a splenic vein thrombosis. What is the treatment of choice?
A. Splenectomy
B. Insertion of transjugular porto-systemic shunt

C. Surgical bypass of the splenic vein
D. Gastrectomy
E. Stapling of the gastro-oesophgeal junction
Splenic vein thrombosis
Thrombosis of the splenic vein may complicate pancreatitis, pancreatic carcinoma, iatrogenic trauma and hypercoagulable diseases. The condition may predispose to the development of gastric varices, oesophageal varices are uncommon in splenic vein thrombosis alone.Diagnosis is made by CT angiography.Treatment is with splenectomy.heme: Surgical signs
A. Rovsing's sign
B. Boas' sign
C. Psoas stretch sign
D. Cullen's sign
E. Grey-Turner's sign
F. Murphy's sign
G. None of the above
Please match the clinical sign to the clinical scenario described. Each option may be used once, more than once or not at all.
30. Acute retrocaecal appendicitis is indicated when the right thigh is passively extended with the patient lying on their side with their knees extended.
Psoas stretch sign
31. In acute pancreatitis there is bruising in the flanks.

Grey-Turner's sign
Grey-Turners sign occurs in patients with severe haemorrhagic pancreatitis. In this situation the major vessels surrounding the pancreas bleed. The pancreatitis process also results in local fat destruction, this results in blood tracking in the tissue planes of the retroperitoneum and appearing as flank bruising.
32. In cholecystitis there is pain/catch of breath elicited on palpation of the right hypochondrium during inspiration.
Murphy's sign
Invariably present when patients are assessed in the emergency department! This sign occurs because the inflamed gallbladder irritates the parietal peritoneum in this manoeuvre.
Abdominal signs
A number of eponymous abdominal signs are noted. These include:
Rovsings sign- appendicitis Boas sign -cholecystitis Murphys sign- cholecystitis Cullens sign- pancreatitis (other intraabdominal haemorrhage) Grey-Turners sign- pancreatitis (or other retroperitoneal haemorrhage)
In clinical practice haemorrhagic pancreatitis is thankfully rare. The signs are important and thus shown below:
Cullen's sign

Image sourced from Wikipedia
Grey Turner's sign
Image sourced from Wikipedia
Which of the following is commonest cause of acute abdominal pain in acute unselected surgical 'take'?
A. Non specific abdominal pain
B. Biliary colic
C. Acute appendicitis
D. Ureteric colic
E. Pancreatitis
Non specific abdominal pain is a commonly recorded diagnosis for patients

presenting with acute abdominal pain. Following careful diagnostic work up a proportion of patients may be identified with disorders such as coeliac disease and the diagnosis of non specific abdominal pain should be used lightly.
Acute abdominal pain
Acute abdominal pain is a common cause of admission to hospital. The relative proportions of conditions presenting with abdominal pain is given below:
Non specific abdominal pain (35%) Appendicitis (17%) Intestinal obstruction (15%) Urological disease (6%) Gallstone disease (5%) Colonic diverticular disease (4%) Abdominal trauma (3%) Perforated peptic ulcer (3%) Pancreatitis (2%)
(Data derived from Irvin T Br. J. Surg 1989 76:1121-1125)
Non specific abdominal pain should really be a diagnosis of exclusion and if care is taken in excluding organic disease the proportion of cases labeled such should decline. It should also be appreciated that a proportion of patients may have an underlying medical cause for their symptoms such as pneumonia or diabetic ketoacidosis.
Key points in management
Early administration of adequate analgesia (including opiates). Abdominal ultrasound is safe, non invasive and cheap and yields significantly
more information than plain radiology. However, plain radiology is still the main test for suspected perforated viscus, especially out of hours.
In up to 50% cases with perforated peptic ulcer, the plain x-rays may show no evidence of free air. If clinical signs suggest otherwise, then a CT scan may be a more accurate investigation, if plain films are normal.
Plain film radiology usually cannot detect <1mm free air, and is 33% sensitive for detection of 1-13mm pockets of free air (Stoker et al. Radiology 2009 253: 31-46).
Think of strangulated intestine when there is fever, raised white cell count, tachycardia and peritonism.
In suspected large bowel obstruction a key investigation is either a water soluble contrast enema or CT scan.
Where need for surgery is difficult to define and imaging is inconclusive the use of laparoscopy as a definitive diagnostic test is both safe and sensible.
A 72 year old obese man undergoes and emergency repair of a ruptured abdominal aortic aneurysm. The wound is closed with an onlay prolene mesh to augment the closure. Post operatively he is taken to the intensive care unit. Over the following

twenty four hours his nasogastric aspirates increase, his urine output falls and he has a metabolic acidosis. What is the most likely underlying cause?
A. Colonic ischaemia
B. Abdominal compartment syndrome
C. Peritonitis
D. Reactionary haemorrhage
E. Aorto-duodenal fistula
Obese patients with ileus following major abdominal surgery are at increased risk of intra abdominal compartment syndrome.The risk is increased by the use of prosthetic meshes, which some surgeons favor following a major vascular case as they may reduce the incidence of incisional hernia. They prevent abdominal distension and may increase the risk of intra abdominal hypertension in the short term. Although colonic ischaemia may occur following major aortic surgery it would not typically present in this way.
Abdominal compartment syndrome
BackgroundIntra-abdominal pressure is the steady state pressure concealed within the abdominal cavity.
In critically ill adults the normal intra abdominal pressure = 5-7mmHg Intra abdominal hypertension has pressures of 12-25mmHg Changes >15mmHg are associated with microvascular hypoperfusion Abdominal compartment syndrome is defined as sustained intra abdominal
pressure >20mmHg coupled with new organ dysfunction / failure It may occur either primarily without previous surgical intervention e.g.
Following intestinal ischaemia or secondarily following a surgical procedure Diagnosis is typically made by transvesical pressure measurements coupled
with an index of clinical suspicion.
ManagementOnce the diagnosis is made non operative measures should be instituted including:
Gastric decompression Improve abdominal wall compliance e.g. muscle relaxants/ sedation Drain abdominal fluid collections. Consider fluid restriction/ diuretics if clinically indicated.
In those whom non operative treatment is failing; the correct treatment is laparotomy and laparostomy. Options for laparostomy are many although the Bogota bag or VAC

techniques are the most widely practised. Re-look laparotomy and attempts at delayed closure will follow in due course.Theme: Surgical drains
A. Redivac suction drainB. Corrugated drainC. Wallace Robinson drainD. Penrose tubingE. Latex T Tube drainF. Silastic T Tube drain
Please select the most appropriate surgical drainage system for the indication given. Each option may be used once, more than once or not at all.
35. A 56 year old lady undergoes and open cholecystectomy and exploration of common bile duct. The bile duct is closed over a drain.
Latex T Tube drain
Latex is used for this indication as it will encourage track formation.
36. A 48 year old lady undergoes a mastectomy and axillary node clearance for an invasive ductal cancer of the breast with lymph node metastasis.
Redivac suction drain
Suction drains are commonly used following mastectomy and axillary surgery to prevent haematoma formation. Not all surgeons routinely drain the axilla.
37. A 75 year old man undergoes a hartmans procedure for sigmoid diverticular disease with pericolic abscess and colovesical fistula.
Wallace Robinson drain
These tube drains are often used in abdominal surgery to drain abscess cavities. Debate might occur around the use of low pressure vs no suction in this setting so this option is deliberately omitted.
Surgical drains
Drains are inserted in many surgical procedures and are of many types.

As a broad rule they can be divided into those using suction and those which do not.
The diameter of the drain will depend upon the substance being drained, for example smaller lumen drain for pneumothoraces vs haemothorax.
Drains can be associated with complications and these begin with insertion when there may be iatrogenic damage. When in situ they serve as a route for infections. In some specific situations they may cause other complications, for example suction drains left in contact with bowel for long periods may carry a risk of inducing fistulation.
Drains should be inserted for a defined purpose and removed once the need has passed.
A brief overview of types of drain and sites is given below
CNS
Low suction drain or free drainage systems may be used for situations such as drainage of sub dural haematomas.
CVS
Following cardiothoracic procedures of thoracic trauma underwater seal drains are often placed. These should be carefully secured. When an air leak is present they may be placed on suction whilst the air leak settles
Orthopaedics and trauma
In this setting drains are usually used to prevent haematoma formation (with associated risk of infection). Some orthopaedic drains may also be specially adapted to allow the drained blood to be auto transfused.
Gastro-intestinal surgery
Surgeons often place abdominal drains either to prevent or drain abscesses, or to turn an anticipated complication into one that can be easily controlled such as a bile leak following cholecystectomy. The type of drain used will depend upon the indication.
Drain typesType of drain FeaturesRedivac Suction type of drain
Closed drainage system High pressure vacuum system
Low pressure Consist of small systems such as the lantern style drain that

drainage systems may be used for short term drainage of small wounds and cavities
Larger systems are sometimes used following abdominal surgery, they have a lower pressure than the redivac system, which decreases the risks of fistulation
May be emptied and re-pressurised
Latex tube drains May be shaped (e.g. T Tube) or straight Usually used in non pressurised systems and act as sump
drains Most often used when it is desirable to generate fibrosis
along the drain trach (e.g. following exploration of the CBD)
Chest drains May be large or small diameter (depending on the indication)
Connected to underwater seal system to ensure one way flow of air
Corrugated drain Thin, wide sheet of plastic, usually soft Contains corrugations, along which fluids can track
Theme: Right iliac fossa pathology
A. AppendicitisB. Mesenteric adenitisC. Inflammatory bowel diseaseD. Irritable bowel syndromeE. Mesenteric cystF. Campylobacter infectionG. Appendix abscess
Please select the most likely diagnosis for the scenario given. Each option may be used once, more than once or not at all.
38. An 8 year old boy is examined by his doctor as part of a routine clinical examination. The doctor notices a smooth swelling in the right iliac fossa. It is mobile and the patient is otherwise well.
Mesenteric cyst
Theme from April 2012 ExamMesenteric cysts are often smooth. Imaging with ultrasound and CT is usually sufficient. Although rare, they most often occur in young children (up to 30% present before the age of 15). Many are asymptomatic and discovered incidentally. Acute presentations are recognised and may occur following cyst torsion, infarction or rupture. Most cysts will be surgically resected.

39. An 8 year old boy presents with abdominal pain,a twelve hour history of vomiting, a fever of 38.3 oC and four day history of diarrhoea. His abdominal pain has been present for the past week.
Appendix abscess
The high fever and diarrhoea together with vomiting all point to a pelvic abscess. The presence of pelvic pus is highly irritant to the rectum, and many patients in this situation will complain of diarrhoea.
40. A 7 year old boy presents with a three day history of right iliac fossa pain and fever. On examination he has a temperature of 39.9o C. His abdomen is soft and mildly tender in the right iliac fossa.
You answered Campylobacter infection
The correct answer is Mesenteric adenitis
High fever and mild abdominal signs in a younger child should raise suspicion for mesenteric adenitis. The condition may mimic appendicitis and many may require surgery.
Right iliac fossa pain
Differential diagnosis
Appendicitis Pain radiating to right iliac fossa Anorexia Typically short history Diarrhoea and profuse vomiting rare
Crohn's disease Often long history Signs of malnutrition Change in bowel habit, especially diarrhoea
Mesenteric adenitis Mainly affects children Causes include Adenoviruses, Epstein Barr Virus,
beta-haemolytic Streptococcus, Staphylococcus spp., Escherichia coli, Streptococcus viridans and Yersinia spp.
Patients have a higher temperature than those with appendicitis
If laparotomy is performed, enlarged mesenteric

lymph nodes will be present
Diverticulitis Both left and right sided disease may present with right iliac fossa pain
Clinical history may be similar, although some change in bowel habit is usual
When suspected a CT scan may help in refining the diagnosis
Meckel's diverticulitis A Meckel's diverticulum is a congenital abnormality that is present in about 2% of the population
Typically 2 feet proximal to the ileocaecal valve May be lined by ectopic gastric mucosal tissue and
produce bleeding
Perforated peptic ulcer This usually produces upper quadrant pain but pain may be lower
Perforations typically have a sharp sudden onset of pain in the history
Incarcerated right inguinal or femoral hernia
Usually only right iliac fossa pain if right sided or bowel obstruction.
Bowel perforation secondary to caecal or colon carcinoma
Seldom localised to right iliac fossa, although complete large bowel obstruction with caecal distension may cause pain prior to perforation.
Gynaecological causes Pelvic inflammatory disease/salpingitis/pelvic abscess/Ectopic pregnancy/Ovarian torsion/Threatened or complete abortion/Mittelschmerz
Urological causes Ureteric colic/UTI/Testicular torsion
Other causes TB/Typhoid/Herpes Zoster/AAA/Situs inversus
A 56 year old man undergoes a difficult splenectomy and is left with a pancreatic fistula. There are ongoing problems with very high fistula output. Which of the following agents may be administered to reduce the fistula output?
A. Metoclopramide
B. Erthyromycin
C. Octreotide
D. Loperamide

E. Omeprazole
Octreotide is a useful agent in reducing the output from pancreatic fistulae. Prokinetic agents will increase fistula output and should be avoided.
Fistulas
A fistula is defined as an abnormal connection between two epithelial surfaces.
There are many types ranging from Branchial fistulae in the neck to entero-cutaneous fistulae abdominally.
In general surgical practice the abdominal cavity generates the majority and most of these arise from diverticular disease and Crohn's.
As a general rule all fistulae will resolve spontaneously as long as there is no distal obstruction. This is particularly true of intestinal fistulae.
The four types of fistulae are:
EnterocutaneousThese link the intestine to the skin. They may be high (>1L) or low output (<1L) depending upon source. Duodenal /jejunal fistulae will tend to produce high volume, electrolyte rich secretions which can lead to severe excoriation of the skin. Colo-cutaneous fistulae will tend to leak faeculent material. Both fistulae may result from the spontaneous rupture of an abscess cavity onto the skin (such as following perianal abscess drainage) or may occur as a result of iatrogenic input. In some cases it may even be surgically desirable e.g. mucous fistula following sub total colectomy for colitis.
Suspect if there is excess fluid in the drain.
Enteroenteric or EnterocolicThis is a fistula that involves the large or small intestine. They may originate in a similar manner to enterocutaneous fistulae. A particular problem with this fistula type is that bacterial overgrowth may precipitate malabsorption syndromes. This may be particularly serious in inflammatory bowel disease.
EnterovaginalAetiology as above.
EnterovesicularThis type of fistula goes to the bladder. These fistulas may result in frequent urinary tract infections, or the passage of gas from the urethra during urination.
ManagementSome rules relating to fistula management:

They will heal provided there is no underlying inflammatory bowel disease and no distal obstruction, so conservative measures may be the best option
Where there is skin involvement, protect the overlying skin, often using a well fitted stoma bag- skin damage is difficult to treat
A high output fistula may be rendered more easily managed by the use of octreotide, this will tend to reduce the volume of pancreatic secretions.
Nutritional complications are common especially with high fistula (e.g. high jejunal or duodenal) these may necessitate the use of TPN to provide nutritional support together with the concomitant use of octreotide to reduce volume and protect skin.
When managing perianal fistulae surgeons should avoid probing the fistula where acute inflammation is present, this almost always worsens outcomes.
When perianal fistulae occur secondary to Crohn's disease the best management option is often to drain acute sepsis and maintain that drainage through the judicious use of setons whilst medical management is implemented.
Always attempt to delineate the fistula anatomy, for abscesses and fistulae that have an intra abdominal source the use of barium and CT studies should show a track. For perianal fistulae surgeons should recall Goodsall's rule in relation to internal and external openings.
heme: Inguinal hernia management
A. Bassini repair
B. Inguinal herniotomy
C. Lichtenstein repair
D. Laparoscopic hernia repair
E. Shouldice repair
F. McVey repair
For the herniae described please select the most appropriate procedure from the list. Each option may be used once, more than once or not at all.
42. A 11 month old child presents with intermittent groin swelling, it has a cough impulse and is easily reducible.
Inguinal herniotomy
Infants usually suffer from a patent processus vaginalis (a congential problem). As a result a simple herniotomy is all that is required. A mesh is not required as there is

not specific muscle weakness.
43. A 25 year old builder presents with a reducible swelling in the right groin, it is becoming larger and has not been operated on previously.
Lichtenstein repair
An open Lichtenstein repair using mesh is appropriate. There is a 0.77% recurrence rate with this technique. A Shouldice repair is an acceptable alternative if the surgeon is experienced
44. A 28 year old man presents with a recurrent inguinal hernia on the left side of his abdomen and a newly diagnosed inguinal hernia on the right side.
Laparoscopic hernia repair
Laparoscopic hernia repairs are specifically indicated where there are bilateral hernias or recurrence of a previous open repair.
Inguinal hernia surgery
Inguinal hernias occur when the abdominal viscera protrude through the anterior abdominal wall into the inguinal canal. They may be classified as being either direct or indirect. The distinction between these two rests on their relation to Hesselbach's triangle.
Boundaries of Hesselbach's Triangle
Medial: Rectus abdominis Lateral: Inferior epigastric vessels Inferior: Inguinal ligament

Image sourced from Wikipedia
Hernias occurring within the triangle tend to be direct and those outside - indirect.
DiagnosisMost cases are diagnosed clinically, a reducible swelling may be located at the level of the inguinal canal. Large hernia may extend down into the male scrotum, these will not trans-illuminate and it is not possible to "get above" the swelling. Cases that are unclear on examination, but suspected from the history, may be further investigated using ultrasound or by performing a herniogram.
TreatmentHernias associated with few symptoms may be managed conservatively. Symptomatic hernias or those which are at risk of developing complications are usually treated surgically. First time hernias may be treated by performing an open inguinal hernia repair; the inguinal canal is opened, the hernia reduced and the defect repaired. A prosthetic mesh may be placed posterior to the cord structures to re-inforce the repair and reduce the risk of recurrence.Recurrent hernias and those which are bilateral are generally managed with a laparoscopic approach. This may be via an intra or extra peritoneal route. As in open surgery a mesh is deployed. However, it will typically lie posterior to the deep ring.
Inguinal hernia in childrenInguinal hernias in children are almost always of an indirect type and therefore are usually

dealt with by herniotomy, rather than herniorraphy. Neonatal hernias especially in those children born prematurely are at highest risk of strangulation and should be repaired urgently. Other hernias may be repaired on an elective basis.
ReferencesThe UK Based National Institute of Clinical Excellence has published guidelines relating to the choice between open and laparoscopic inguinal hernia repair. Which users may find interesting:
http://guidance.nice.org.uk/TA83/Guidance/pdf/English
Theme: Surgical access
A. Kocher's
B. Lanz
C. Rooftop
D. Pfannenstiel's
E. Midline
F. Paramedian incision
G. Mcevedy
Please select the most appropriate incision for the procedure described. Each option may be used once, more than once or not at all.
45. A 19 year old girl who is 39 weeks pregnant goes into labour. The labour is prolonged and she is found to have an undiagnosed breech baby.
Pfannenstiel's
This patient needs an emergency cesarean section.
46. A 49 year old woman presents with jaundice and abdominal pain. She is haemodynamically unstable. An USS shows a dilated common bile duct and gallstones in the gallbladder.

Kocher's
This lady needs a cholecystectomy and bile duct exploration.
47. A 42 year old man with history of alcohol abuse is diagnosed with pancreatic cancer and requires a Whipples resection.
You answered Midline
The correct answer is Rooftop
A pancreatectomy is usually performed through a roof top incision. This provides excellent access to the upper abdomen.
Abdominal incisions
Theme in January 2012 exam
Midline incision Commonest approach to the abdomen Structures divided: linea alba, transversalis fascia, extraperitoneal
fat, peritoneum (avoid falciform ligament above the umbilicus) Bladder can be accessed via an extraperitoneal approach through
the space of Retzius
Paramedian incision
Parallel to the midline (about 3-4cm) Structures divided/retracted: anterior rectus sheath, rectus
(retracted), posterior rectus sheath, transversalis fascia, extraperitoneal fat, peritoneum
Incision is closed in layers
Battle Similar location to paramedian but rectus displaced medially (and thus denervated)
Now seldom used
Kocher's Incision under right subcostal margin e.g. Cholecystectomy (open)
Lanz Incision in right iliac fossa e.g. Appendicectomy
Gridiron Oblique incision centered over McBurneys point- usually appendicectomy (less cosmetically acceptable than Lanz

Gable Rooftop incision
Pfannenstiel's Transverse supra pubic, primarily used to access pelvic organs
McEvedy's Groin incision e.g. Emergency repair strangulated femoral hernia
Rutherford Morrison
Extraperitoneal approach to left or right lower quadrants. Gives excellent access to iliac vessels and is the approach of choice for first time renal transplantation.
Image sourced from Wikipedia
Theme: Surgical access
A. Kocher's
B. Lanz
C. Rooftop
D. Pfannenstiel's
E. Midline
F. Paramedian incision
G. Mcevedy
Please select the most appropriate incision for the procedure described. Each option may be used once, more than once or not at all.

45. A 19 year old girl who is 39 weeks pregnant goes into labour. The labour is prolonged and she is found to have an undiagnosed breech baby.
Pfannenstiel's
This patient needs an emergency cesarean section.
46. A 49 year old woman presents with jaundice and abdominal pain. She is haemodynamically unstable. An USS shows a dilated common bile duct and gallstones in the gallbladder.
Kocher's
This lady needs a cholecystectomy and bile duct exploration.
47. A 42 year old man with history of alcohol abuse is diagnosed with pancreatic cancer and requires a Whipples resection.
You answered Midline
The correct answer is Rooftop
A pancreatectomy is usually performed through a roof top incision. This provides excellent access to the upper abdomen.
Abdominal incisions
Theme in January 2012 exam
Midline incision Commonest approach to the abdomen Structures divided: linea alba, transversalis fascia, extraperitoneal
fat, peritoneum (avoid falciform ligament above the umbilicus) Bladder can be accessed via an extraperitoneal approach through
the space of Retzius
Paramedian incision
Parallel to the midline (about 3-4cm) Structures divided/retracted: anterior rectus sheath, rectus

(retracted), posterior rectus sheath, transversalis fascia, extraperitoneal fat, peritoneum
Incision is closed in layers
Battle Similar location to paramedian but rectus displaced medially (and thus denervated)
Now seldom used
Kocher's Incision under right subcostal margin e.g. Cholecystectomy (open)
Lanz Incision in right iliac fossa e.g. Appendicectomy
Gridiron Oblique incision centered over McBurneys point- usually appendicectomy (less cosmetically acceptable than Lanz
Gable Rooftop incision
Pfannenstiel's Transverse supra pubic, primarily used to access pelvic organs
McEvedy's Groin incision e.g. Emergency repair strangulated femoral hernia
Rutherford Morrison
Extraperitoneal approach to left or right lower quadrants. Gives excellent access to iliac vessels and is the approach of choice for first time renal transplantation.
Image sourced from Wikipedia