Embed Size (px)
Citation preview
ABDOMINAL GAS: A ROENTGEN APPROACH
Benjamin Felson Department of Radiology, University of Cincinnati College of Medicine and
Medical Center, Cincinnati, Ohio
There is much to be learned about gastrointestinal (GI) gas from the roent- genogram. While one gas looks like another to the roentgenologist, its distribution within the intestinal canal and, for that matter, its occasional presence outside the lumen provide fundamental information that the basic scientist as well as the clinician cannot afford to ignore. My own approach to the problem of GI gas must be entirely clinical, simply because of my inability to interpret the physio- logical principles involved. I will therefore present certain clinical facts and leave it to others to interpret their deeper meaning.
Intestinal Gas Patterns in the Acute Abdomen From the clinician's standpoint, the value of the plain-film approach to the
diagnosis of the acute abdomen is well established and reliable. But this widely- held assumption requires critical revaluation. For reasons unknown, the roent- genologist, upon examining the flat and upright films of the abdomen, is expected to come up with an accurate diagnostic pronouncement, so that the surgeon can proceed with the appropriate therapy. But there is no dictum that states that the roentgenologist must be able to distinguish between small-bowel obstruction, large-bowel obstruction, and nonobstructive distension. As a matter of fact, he cannot consistently do it. Working from the films alone, he is as insecure as the surgeon who depends I dely on clinical acumen, and as often wrong.
There is no justificat,:n for this go-it-alone game. The surgeon and ro- entgenologist must work side by side-yes, even at 3 a.m. Neither functions alone as well as the two together. Though the surgeon may become pretty expert with the plain film, the stakes are too high for self-indulgence and egotism.
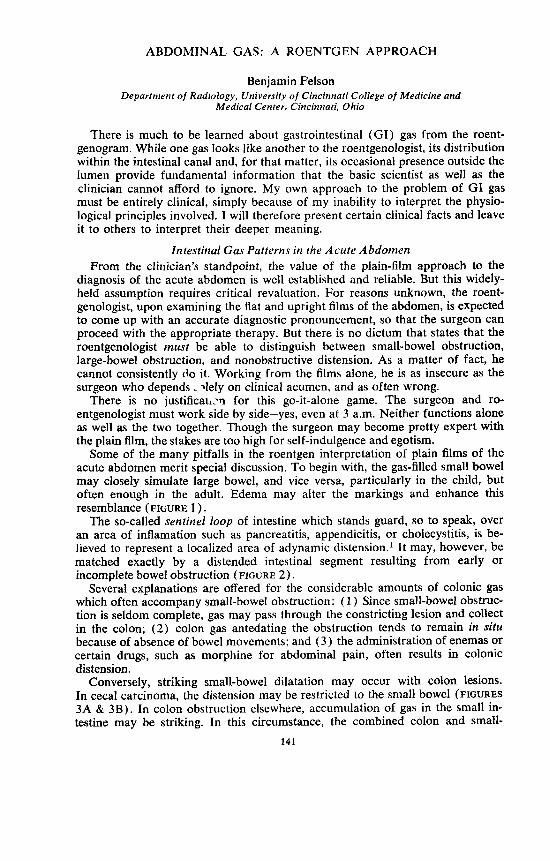
Some of the many pitfalls in the roentgen interpretation of plain films of the acute abdomen merit special discussion. To begin with, the gas-filled small bowel may closely simulate large bowel, and vice versa, particularly in the child, but often enough in the adult. Edema may alter the markings and enhance this resemblance (FIGURE 1 ) .
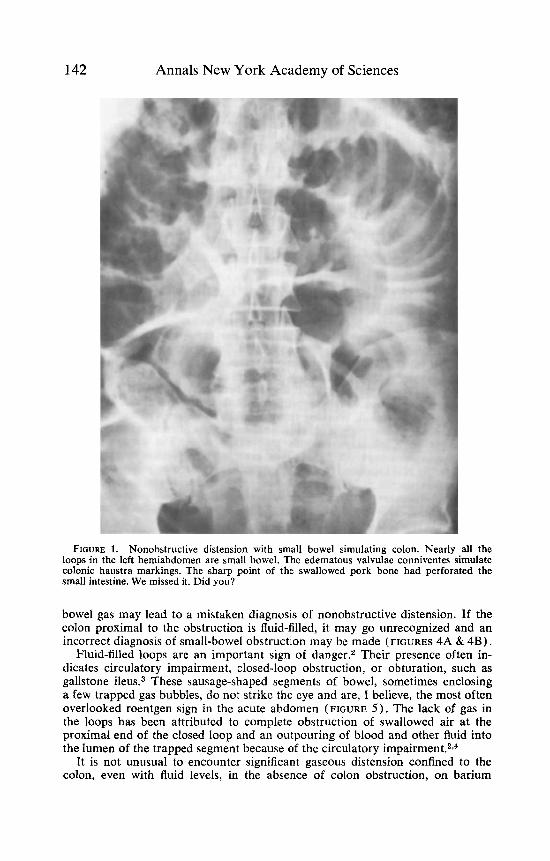
The so-called sentinel loop of intestine which stands guard, so to speak, over an area of inflamation such as pancreatitis, appendicitis, or cholecystitis, is be- lieved to represent a localized area of adynamic distension.' It may, however, be matched exactly by a distended intestinal segment resulting from early or incomplete bowel obstruction (FIGURE 2 ) .
Several explanations are offered for the considerable amounts of colonic gas which often accompany small-bowel obstruction: ( 1 ) Since small-bowel obstruc- tion is seldom complete, gas may pass through the constricting lesion and collect in the colon; ( 2 ) colon gas antedating the obstruction tends to remain in sifu because of absence of bowel movements; and (3) the administration of enemas or certain drugs, such as morphine for abdominal pain, often results in colonic distension.
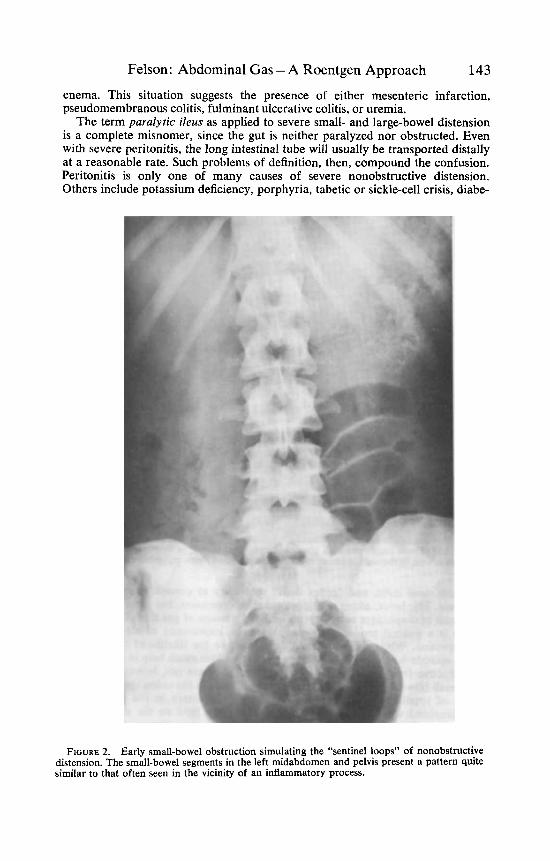
Conversely, striking small-bowel dilatation may occur with colon lesions. In cecal carcinoma, the distension may be restricted to the small bowel (FIGURES 3A & 3B). In colon obstruction elsewhere, accumulation of gas in the small in- testine may be striking. In this circumstance, the combined colon and small-
141
142 Annals New York Academy of Sciences
FIGURE 1. Nonobstructive distension with small bowel simulating colon. Nearly all the loops in the left hemiabdomen are small bowel. The edematous valvulae conniventes simulate colonic haustra markings. The sharp point of the swallowed pork bone had perforated the small intestine. We missed it. Did you?
bowel gas may lead to a mistaken diagnosis of nonobstructive distension. If the colon proximal to the obstruction is fluid-filled, it may go unrecognized and an incorrect diagnosis of small-bowel obstruction may be made (FIGURES 4A & 4 B ) .
Fluid-filled loops are an important sign of danger.2 Their presence often in- dicates circulatory impairment, closed-loop obstruction, or obturation, such as gallstone i l e ~ s . ~ These sausage-shaped segments of bowel, sometimes enclosing a few trapped gas bubbles, do not strike the eye and are, I believe, the most often overlooked roentgen sign in the acute abdomen (FIGURE 5). The lack of gas in the loops has been attributed to complete obstruction of swallowed air at the proximal end of the closed loop and an outpouring of blood and other fluid into the lumen of the trapped segment because of the circulatory i m ~ a i r m e n t . ~ , ~
It is not unusual to encounter significant gaseous distension confined to the colon, even with fluid levels, in the absence of colon obstruction, on barium
Felson: Abdominal Gas - A Roentgen Approach 143
enema. This situation suggests the presence of either mesenteric infarction, pseudomembranous colitis, fulminant ulcerative colitis, or uremia.
The term paralytic ileus as applied to severe small- and large-bowel distension is a complete misnomer, since the gut is neither paralyzed nor obstructed. Even with severe peritonitis, the long intestinal tube will usually be transported distally at a reasonable rate. Such problems of definition, then, compound the confusion. Peritonitis is only one of many causes of severe nonobstructive distension. Others include potassium deficiency, porphyria, tabetic or sickle-cell crisis, diabe-
FIGURE 2. Early small-bowel obstruction simulating the “sentinel loops” of nonobstructive distension. The small-bowel segments in the left midabdomen and pelvis present a pattern quite similar to that often seen in the vicinity of an inflammatory process.
144 Annals New York Academy of Sciences
FIGURE 3A. Cecal carcinoma with gaseous distension confined to the small intestine. The tumor mass is seen in the right midabdomen. All the gas-filled loops represent small bowel.
tic acidosis, lead colic, and “reflex ileus” secondary to coronary thrombosis or pneumonia. The latter, along with postoperative distension, has been ascribed to impairment of diaphragm activity with lessened passage of gas from the r e ~ t u m . ~
There is a general tendency to exaggerate the importance of air-fluid levels in the intestine. While their presence does increase the likelihood that the ab- dominal episode is serious, fluid levels per se are seldom much help in distinguish- ing obstructive from nonobstructive distension. They are not, however, without value. Small-bowel fluid levels in the absence of levels in the colon speak strongly in favor of small-bowel obstruction. Also, the wall pattern in the gut is often better visualized when outlined by the gas above the fluid on the upright film.
Gaslessness is just as important a roentgen sign as gaseousness. Closed-loop obstruction may present with a relatively gas-free roentgenogram, and thus a patient may be sent home from the receiving department with a “bellyache,”

Felson : Abdominal Gas - A Roentgen Approach 145
only to return with necrotic sequelae. A gas-free abdominal film is also seen occasionally in pancreatitis and other conditions that are associated with severe vomiting. I suspect that these patients. in seeking relief from pain, find they are in less distress in the upright or right decubitus position. Thus, the air they swallow remains in the gastric fundus, to be vomited or eructed rather than propelled into the intestine.
In an occasional case of cardiospasm or other acquired obstruction of the esophagus, the abdomen is relatively free of gas because the swallowed air remains in the distended esophagus. Curiously, when a gas-forming beverage, such as a carbonated drink, is administered to a patient with cardiospasm, there is im- mediate and complete emptying of the esophagus. This is only momentary, how- ever, and with the next swallow the esophagus refills with fluid and remains filled.
Esophageal atresia of the newborn, in the absence of a fistula between the post- atretic segment and the trachea, is another cause of gasless abdomen, but in this case there is no gas at all. On the other hand, if the distal fistula is present, striking
FIGURE 3B. Barium enema reveals the carcinoma of the cecum. Since the obstruction is at the ileocecal valve, only small-bowel distension can occur.
146 Annals New York Academy of Sciences
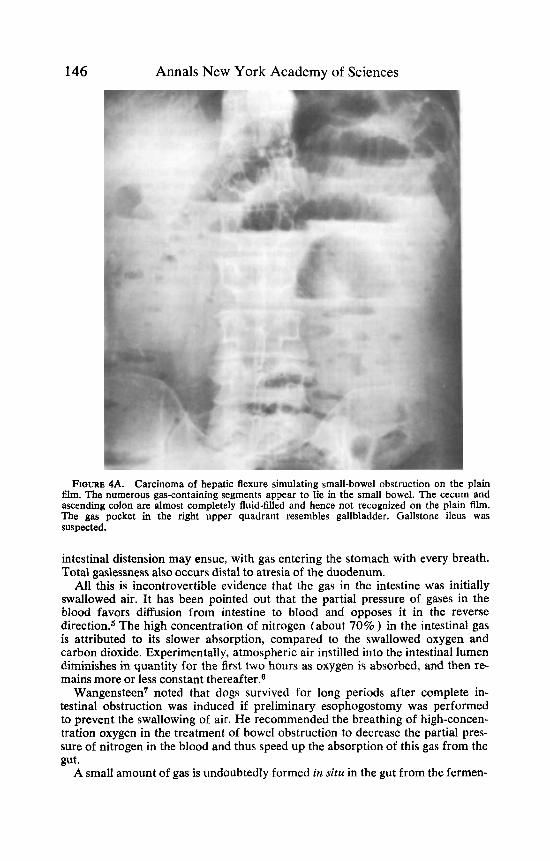
FIGURE 4A. Carcinoma of hepatic flexure simulating small-bowel obstruction on the plain 61m. The numerous gas-containing segments appear to lie in the small bowel. The cecum and ascending colon are almost completely fluid-filled and hence not recognized on the plain film. The gas pocket in the right upper quadrant resembles gallbladder. Gallstone ileus was suspected.
intestinal distension may ensue, with gas entering the stomach with every breath. Total gaslessness also occurs distal to atresia of the duodenum.
All this is incontrovertible evidence that the gas in the intestine was initially swallowed air. It has been pointed out that the partial pressure of gases in the blood favors diffusion from intestine to blood and opposes it in the reverse direction.5 The high concentration of nitrogen (about 70% ) in the intestinal gas is attributed to its slower absorption, compared to the swallowed oxygen and carbon dioxide. Experimentally, atmospheric air instilled into the intestinal lumen diminishes in quantity for the first two hours as oxygen is absorbed, and then re- mains more or less constant thereafter.6
Wangensteen' noted that dogs survived for long periods after complete in- testinal obstruction was induced if preliminary esophogostomy was performed to prevent the swallowing of air. He recommended the breathing of high-concen- tration oxygen in the treatment of bowel obstruction to decrease the partial pres- sure of nitrogen in the blood and thus speed up the absorption of this gas from the gut.
A small amount of gas is undoubtedly formed in situ in the gut from the fermen-

Felson: Abdominal Gas - A Roentgen Approach 147
tation of carbon dioxide and the putrefaction of pro teh6 Frimann-Dahl noted a moderate-sized bubble of gas distal to the ligature in experimental strangulation ob~truction.~
To return to the clinical side of the coin, perhaps I have overemphasized the negative aspects of plain-film interpretation. Actually, there are frequent in- stances in which the roentgen signs specifically pinpoint the diagnosis-GI perforation, gallstone ileus, and ileocolic intussusception, to name a few.
It should be further noted that when the clinical and plain-film conclusions are consistent with each other, preoperative diagnostic accuracy is quite high. On the other hand, when the clinical and roentgen impressions do not coincide, the old clichi, “Ignore the laboratory,” is foolish, for certain roentgen signs, such as those of calculus appendicitis, are almost infallible.s When doubts occur with either approach, further studies are indicated. These should usually include the instillation of contrast medium by rectum or by mouth. Barium enema is, of course, a tremendous asset in identifying loops of gut and in establishing or excluding colon obstruction. Barium is also generally my preference for oral administration, although many surgeons are reluctant to utilize it and prefer the water-soluble media. The latter are very poor contrast agents when compared with barium, and have their own hazard^.^ I strongly urge their abandonment except under such special circumstances as suspected perforation. I must admit, however, that I have been unable to convince many of my own surgical colleagues of this.
FIGURE 4B. Carcinoma of hepatic flexure simulating small-bowel obstruction on the plain film. Barium enema reveals obstruction of the hepatic flexture by neoplasm. A decubitus film with the right side up almost certainly would have shown a long, shallow air-fluid level in the ascending colon.

148 Annals New York Academy of Sciences
FIGURE 5. Fluid-filled loops in small-bowel obstruction. The loops appear as multiple soft- tissue masses of water density (arrows) with occasional gas bubbles. The patient had a femoral hernia with circulatory impairment of the obstructed segment.
Postoperative Pneumoperitoneum Free peritoneal gas is a common finding following laparotomy. How then,
does one detect perforation or anastomotic disruption in a recently operated patient? In other words, how long does gas remain in the peritoneal sac following an uncomplicated operation? A variety of answers is obtainable from the literature. Harrison and coworkers14 found a higher incidence of post- operative pneumoperitoneum among asthenic individuals and in those with upper-abdominal incisions. They also noted that the duration of the pneum- operitoneum was directly proportionate to the original volume of gas and was unrelated to the presence of ileus, postoperative infection, or other factors.
A study of 200 consecutive patients who underwent laparotomy at the Cincin- nati General Hospital was made by Bryant and colleagues in 1963.15 Upright or
Felson: Abdominal Gas -A Roentgen Approach 149
decubitus films were made on the day of operation and every day or two there- after, until all the gas had disappeared. Postoperative pneumoperitoneurn was demonstrated in 58% of the cases. When sequential films were taken at intervals of 5 , 10, and 20 min after the patient was placed in either upright or decubitus position, there was a definite increase in the amount of free gas between the five-minute and ten-minute films, but not thereafter. The amount of gas appeared greater on the upright than on the decubitus film.
The time required for absorption of the pneumoperitoneum varied from one to 24 days and appeared to depend only on the volume originally trapped, as seen on the first film. Larger amounts of gas were found in the patients who underwent upper-abdominal and pelvic operations. In contradistinction, no free air at all was found following appendectomy (eight patients) or vaginal hysterec- tomy (three patients). The use of drains did not seem to affect the quantity of gas except for one patient, in whom air obviously had entered the peritoneum through a drain. Neither the type of incision nor the nature of the anesthesia appeared to be related to the presence or amount of pneumoperitoneum.
Surprisingly, peritonitis seemed to be without influence as far as the presence and rate of absorption of the gas were concerned. The body habitus of the patient, however, appeared to play a major role. Over 80% of the asthenic patients showed pneumoperitoneum, while only 25% of the obese showed it. The thin patients also showed larger amounts of gas, and consequently it persisted longer. In the obese patients, the gas was nearly always gone by the third postoperative day.
In another study at this center, Wiot and coworkers16 obtained early postopera- tive roentgenograms on about 100 infants and children from newborn to age six- teen. About 30% showed free air on the first postoperative day. Each day there- after, for the next three days, the number of cases decreased by about one half, so that at four days, free gas was still present in four patients. At six days, gas was
TABLE 1 ASSOCIATED CONDITIONS.
No. of Cased
Peptic ulcer I
Pulmonary tuberculosis 5
Pneumatosis cystoides intestinalis 4
Postpartum (1 to 5 weeks) 3
Postoperative 3
Jejunal diverticulosis 2
Lobar pneumonia 2
Pneumomediastinum 2
Carcinoma of stomach, regional enteritis, megacolon with volvulus,
Other (heart disease, stroke, uropathy, et cetera)
ankylostoma infestation, carcinoma of lung, pulmonary emphysema 1 each
I None 8
Some patients had more than one.

150 Annals New York Academy of Sciences
still seen in two, in one of whom it remained for 38 days. Essentially, all the find- ings in the first study were corroborated. I t was concluded that children were similar to obese adults in that they tended to trap less air initially and, therefore, to retain it only briefly.
In addition, they performed an experimental study on mice. In one group, a known amount of air was injected into the peritoneal cavity and a daily erect roentgenogram of the abdomen was obtained. In a second group, an identical method was used after dilute turpentine was administered intraperitoneally (i.p.) to produce a mild peritonitis. It was found that the peritonitis influenced neither the absorption rate of the gas nor the time required for its complete disappear- ance.la
To sum up, in the event of postoperative abdominal symptoms, the roentgen demonstration of free gas should not enter into decisions of diagnosis or manage- ment, with the important exception that in obese patients and children more than three days postoperative, free peritoneal gas suggests perforation. Increase in postoperative pneumoperitoneum has significance only if the films were made with the patient ifl the same position for the same length of time and in the absence of abdominal drains.
Another interesting facet of GI gas is its spread beyond the lumen of the in t e s t ine4 the gut wall, in the peritoneum, in the biliary tree, in the portal vein branches. Each of these locations presents its own special problems of diagnosis and interpretation, many features of which must be omitted here. Nonetheless, it is worthwhile to examine certain aspects of the topic of extra- luminal gas.
Spontaneous Pneumoperitoneum without Peritonitis
Spontaneous pneumoperitoneum is generally considered pathognomonic of ruptured hollow viscus. However, occasional instances of free peritoneal gas without GI perforation have been reported. Although asymptomatic or only mildly ill, many of these patients have been subjected to immediate laparotomy, with puzzling results: no perforation, no peritonitis, and often no explanation at all for the presence of the peritoneal gas. This condition has been called idiopathic pneumoperitoneum,'7 but because an etiology is known or suspected for some of the cases, we prefer the term spontaneous pneumoperitoneum without acute peritonitis.
Although only 30 cases were found in a review of the literature, we have en- countered ten cases at the University of Cincinnati Medical Center in the past ten years.l8 Of these 40 cases, 2 were infants, 1 1 were in their twenties, 5 were in the thirties or forties, and 22 were over fifty. The oldest patient was eighty- one. The total sex distribution was about even, but all 11 of those in the third decade were women, a fact which may have some bearing on the etiology in this age group, as will be discussed later.
At the time the pneumoperitoneum was discovered, abdominal symptoms were present in 28 cases, absent in seven, and unstated in five. Few of the symptomatic patients appeared severely ill, and most were hardly sick at all. In the seven patients without acute symptoms, the free peritoneal air was usually discovered accidentally on films taken for other conditions. All but eight of the 40 cases had at least one associated condition, recent or current (TABLE 1 ) .
Spontaneous pneumoperitoneum without acute peritonitis was confirmed by operation or autopsy in 24 of the patients. In most, there was a gush of odorless gas on opening the peritoneum. In 14 of the 24 proven cases, the gross appearance
Felson: Abdominal Gas -A Roentgen Approach 151
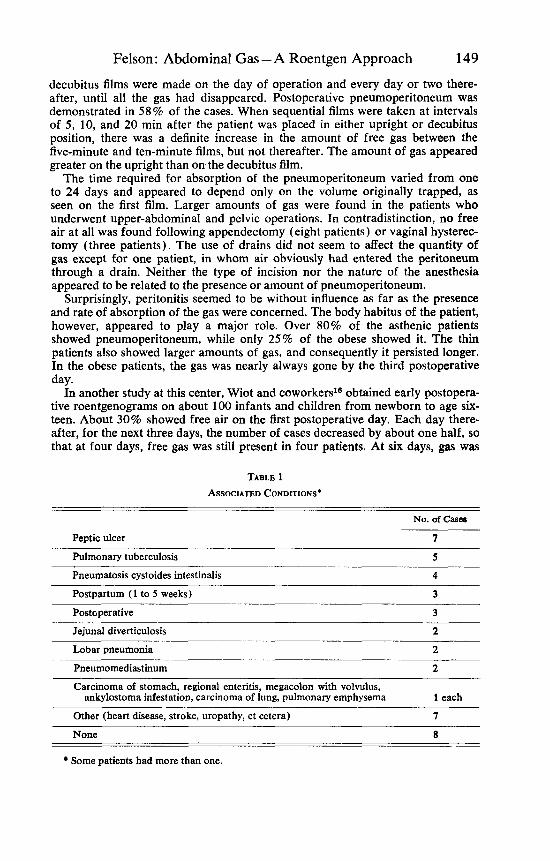
FIGURE 6. Spontaneous pneumoperitoneum without peritonitis. This 77-year-old woman was found unconscious with a stroke, her head on the floor and her body in bed. This upright Nm, made because marked abdominal distention was noted, shows an enormous amount of free peritoneal air surrounding the liver and gallbladder. At operation and at autopsy there was no evidence of perforation or peritonitis. It is surmised that the patient “aspirated” the gas through the uterus and tubes, as in the Rubin test.
of the peritoneum and viscera was entirely normal. The remaining verified cases showed a variety of G I lesions, including peptic ulcer, pneumatosis cystoides intestinalis, jejunal diverticulosis, and others, as listed in TABLE 1.
The peritoneal gas was analyzed in only three cases. In one, the percentages were: nitrogen, 93.9; carbon dioxide, 3.6; and oxygen, 2.519 In another, the corresponding figures were: nitrogen, 85.8; carbon dioxide, 6.4; oxygen, 3; and methane, 4.4. In the third, the percentage of nitrogen plus water vapor was 76; hydrogen, 11; carbon dioxide, 6.1; oxygen, 5.8; and methane, 1.1.20 The gas was generally odorless, although occasionally a fecal odor was noted.
In ten of the 16 unoperated patients, followup examinations were recorded. The pneumoperitoneum disappeared in less than 11 days in four, but persisted from two weeks to “many months” in six. Four of our own cases were included in the persistent group, the peritoneal gas remaining for two weeks, five weeks, two months, and eight months, respectively. At least nine of the total group of 40 cases had recurrent episodes of pneumoperitoneum.
152 Annals New York Academy of Sciences
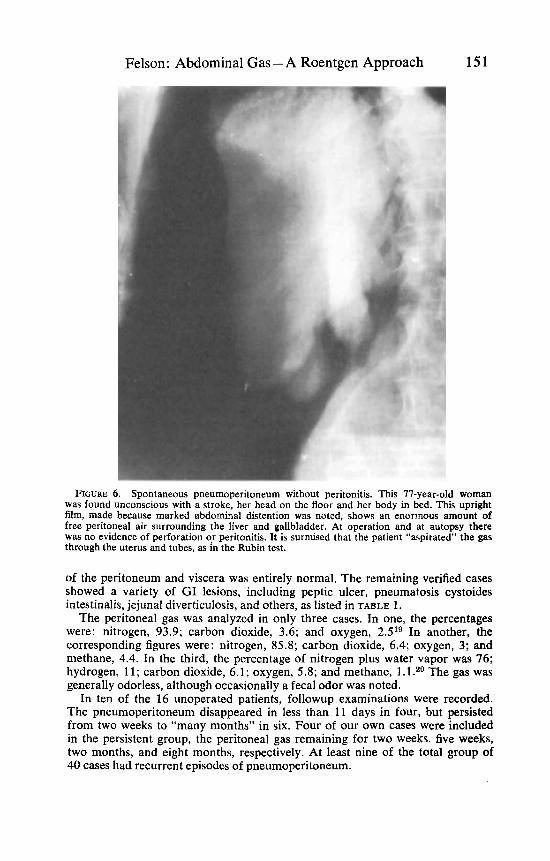
FIGURE 7A. Upright film of abdomen shows a small amount of free peritoneal gas in a man with moderate acute abdominal pain and no rigidity. There. was a history of gastric re- section for peptic ulcer. (FIGURES 7A, 7B, 7C, and 7D are shown through the courtesy Of Dr. Harold Margolin, Jewish Hospital of Cincinnati.)
Many theories have been advanced to explain specific instances of spontaneous pneumoperitoneum without peritonitis. I believe that there are actually a number of mechanisms involved, each accounting for some of the cases.
There is much evidence to indicate that in women gas may enter the peritoneal cavity via the genital tract, as in the Rubin test. In several of the reported cases, the pneumoperitoneum followed a vaginal d o ~ c h e . ~ ~ - ~ ~ The sound of gas bubbling into the abdomen can sometimes be heard during pelvic examination, according to some of my gynecologist colleagues, but, as with pneumoperitoneum in fqnale water skiers, the evidence is, to my knowledge, undocumented roentgenographic- ally. It has even been conjectured that cough and dyspnea, by causing sudden alteration in i.p. pressure, promote uterotubal entry of air. Position may play a role (FIGURE 6). The occurrence of spontaneous pneumoperitoneum during the postpartum period (three cases), a time when douches and knee-chest exercises are commonly utilized, may be significant.Z4-26 The fact that all 11 of the patients in their twenties were women also lends support to this theory of genital “aspira- tion.” The amounts of pneumoperitoneum in these women were generally con- siderably smaller than those in the rest of the patients. In four of the five young women who were operated for pneumoperitoneum, no associated disease was found. Perhaps the best evidence favoring this portal of entry of the gas is that offered by the cases of FredriksonZ7 and of Wright.2s Each of these women had five bouts of pneumoperitoneum. Application of a well-fitted cervical diaphragm
Felson: Abdominal Gas - A Roentgen Approach 153
in one and bilateral salpingectomy in the other prevented further recurrences. Pneumoperitoneum complicating pneumatosis cystoides intestinalis is well
documented in the I i t e r a t ~ r e . ~ ~ There were four cases in the overall series in which the pneumoperitoneum was shown to be accompanied by intramural intestinal gas. In three, including two of our own cases, leakage of gas through the intact intestinal wall was actually observed at operation.20 In none of these was there evidence of acute inflammation at the site of the leakage. The gas seemed to well up, bubble-like, and dissipate through the intact gut wall. In the fourth case, typical pneumatosis cysts were visible in the colon wall on barium enema, and the pneumoperitoneum persisted for a month. Since intramural in- testinal gas is readily overlooked roentgenographically and even surgically, it is reasonable to suspect that other cases of unexplained chronic pneumoperiton- eum are the results of rupture of gas cysts.
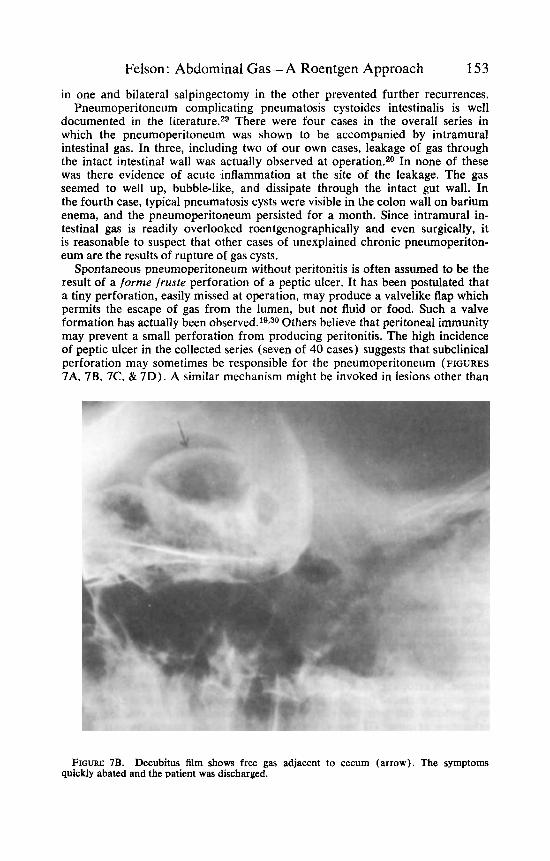
Spontaneous pneumoperitoneum without peritonitis is often assumed to be the result of a forme fruste perforation of a peptic ulcer. It has been postulated that a tiny perforation, easily missed at operation, may produce a valvelike flap which permits the escape of gas from the lumen, but not fluid or food. Such a valve formation bas actually been o b s e r ~ e d . ~ ~ . ~ ~ Others believe that peritoneal immunity may prevent a small perforation from producing peritonitis. The high incidence of peptic ulcer in the collected series (seven of 40 cases) suggests that subclinical perforation may sometimes be responsible for the pneumoperitoneum (FIGURES 7A, 7B, 7C. & 7D). A similar mechanism might be invoked in lesions other than
FIGURE 7B. Decubitus film shows free gas adjacent to cecum (arrow). The symptoms quickly abated and the patient was discharged.
154 Annals New York Academy of Sciences
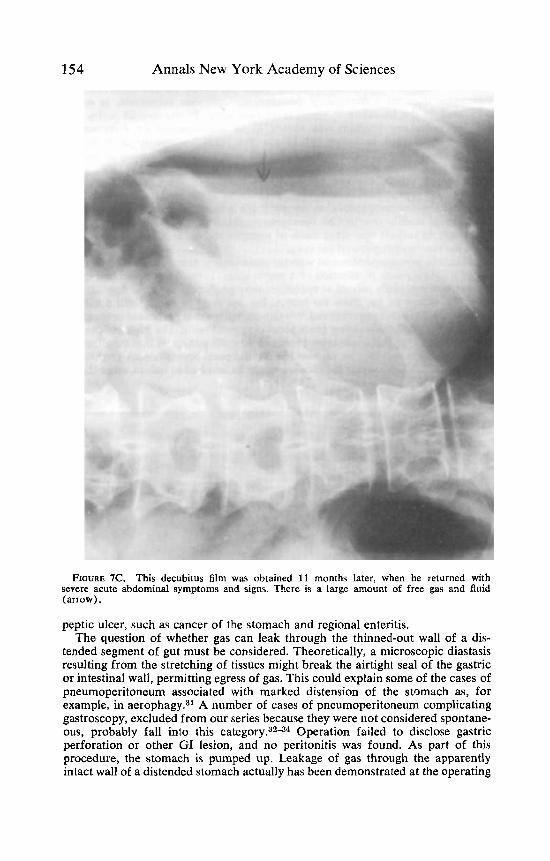
FIGURE 7C. This decubitus film was obtained 11 months later, when he returned with severe acute abdominal symptoms and signs. There is a large amount of free gas and fluid (arrow).
peptic ulcer, such as cancer of the stomach and regional enteritis. The question of whether gas can leak through the thinned-out wall of a dis-
tended segment of gut must be considered. Theoretically, a microscopic diastasis resulting from the stretching of tissues might break the airtight seal of the gastric or intestinal wall, permitting egress of gas. This could explain some of the cases of pneumoperitoneum associated with marked distension of the stomach as, for example, in aer~phagy.~' A number of cases of pneumoperitoneum complicating gastroscopy, excluded from our series because they were not considered spontane- ous, probably fall into this category.3234 Operation failed to disclose gastric perforation or other GI lesion, and no peritonitis was found. As part of this procedure, the stomach is pumped up. Leakage of gas through the apparently intact wall of a distended stomach actually has been demonstrated at the operating
Felson: Abdominal Gas -A Roentgen Approach 155
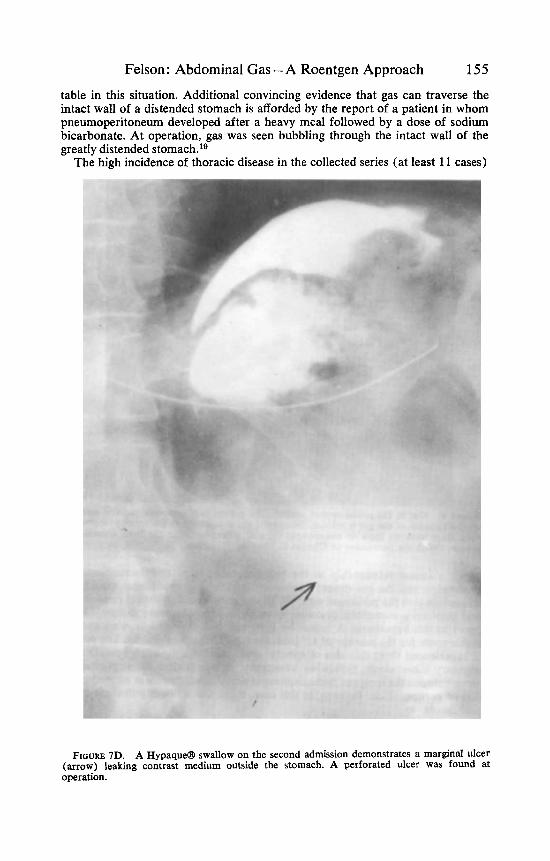
table in this situation. Additional convincing evidence that gas can traverse the intact wall of a distended stomach is afforded by the report of a patient in whom pneumoperitoneum developed after a heavy meal followed by a dose of sodium bicarbonate. At operation, gas was seen bubbling through the intact wall of the greatly distended stomach.lg
The high incidence of thoracic disease in the collected series (at least 11 cases)
FIGURE 7D. A Hypaqua swallow on the second admission demonstrates a marginal ulcer (arrow) leaking contrast medium outside the stomach. A perforated ulcer was found at operation.

156 Annals New York Academy of Sciences
FIGURE 8. Gas in the portal venous system. The patient was in severe diabetic acidosis. Marked distension of the gut is evident. The portal gas is confined to the small branches. At autopsy there were no gross or microscopic signs of inflammation in the liver, intestine, or elsewhere. (With the permission of Charles C Thomas, Springfield, Ill.3g)
suggests a causal relationship to the pneumoperitoneum. Pneumomediastinum may develop and the gas dissect downward into the extraperitoneal tissues and then rupture into the peritoneal ~ a c . 3 5 . ~ ~ The recently noted statistical relationship found between pneumatosis cystoides intestinalis and pulmonary disease37 lends support to this hypothesis. A report by Britt and colleagues38 brings up another possible route for the passage of air from the lung to the peritoneum. The patient had experienced three episodes of spontaneous pneurnoperitoneum complicating pulmonary tuberculosis. Following lobectomy, at which time dense pleural ad- hesions between the lung and hemidiaphragm were found, there was no reaccumu- lation of peritoneal air. Perhaps, in this case, there was a direct pulmonary-peri- toned fistula.
We believe that each of the mechanisms described above probably accounts for some of the cases of pneumoperitoneum without peritonitis. In young females, the genital system appears to be the commonest site of entry. In other groups, i.p.
Felson: Abdominal Gas -A Roentgen Approach 157
rupture of an intestinal gas cyst is probably a fairly common cause, and pneumo- mediastinum an occasional one. The high incidence of peptic ulcer and other G I diseases, especially those associated with distension of the stomach or intestine, cannot be ignored, although the actual route of entry of gas into the peritoneum is speculative.
It is important that the surgeon and the roentgenologist realize that pneumo- peritoneum does not invariably mean GI perforation and therefore does not always require operation. Spontaneous pneumoperitoneum without peritonitis can be recognized by the trivial or absent clinical and laboratory signs. Obviously, patients on steroid therapy and those in whom the level of consciousness is im- paired may have frank perforation of the gut with few symptoms and signs. Thus, prudent judgment and meticulous observation are, of course, always required.
Gas in the Portal Venous System Gas in the portal vein branches is a fascinating condition accompanied by a
dramatic roentgen picture. The source of the gas is as yet uncertain, although it probably arises in some manner from the intestinal lumen.
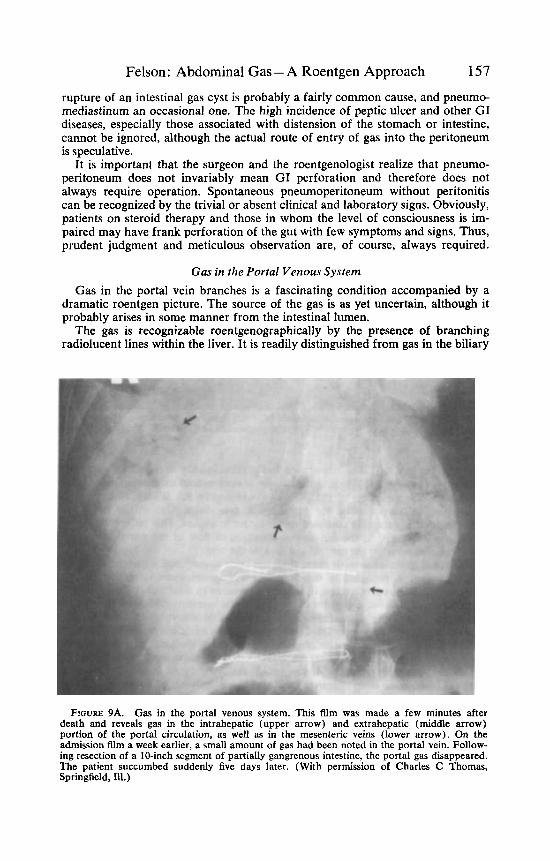
The gas is recognizable roentgenographically by the presence of branching radiolucent lines within the liver. It is readily distinguished from gas in the biliary
FIGURE 9A. Gas in the portal venous system. This film was made a few minutes after death and reveals gas in the intrahepatic (upper arrow) and extrahepatic (middle arrow) portion of the portal circulation, as well as in the mesenteric veins (lower arrow). On the admission film a week earlier, a small amount of gas had been noted in the portal vein. Follow- ing resection of a 10-inch segment of partially gangrenous intestine, the portal gas disappeared. The patient succumbed suddenly five days later. (With permission of Charles C Thomas, Springfield, Ill.)

158 Annals New York Academy of Sciences
FIGURE 9B. Roentgenogram of the liver following injection of barium in the portal veins confirms the location of the gas. (With the permission of Charles C Thomas, Springfield, 1u .39
tract by the fact that it nearly always lies predominantly in the small intrahepatic branches (FIGURE 8). When, occasionally, it does extend extrahepatically, it takes the transverse direction of the portal vein (FIGURES 9A & 9B) , rather than the more vertical direction of the extrahepatic bile ducts. Gas in the intrahepatic biliary ducts is generally confined to the larger branches. This difference in distri- bution is attributed to the centripetal direction of flow of the portal blood in the liver, as compared to the centrifugal flow of the bile.
Personal experience with more than ten such cases39 and a review of about 20 additional cases reported in the l i terat~re~O-4~ reveal some interesting features. The condition is encountered in infants as well as in adults and is nearly always accompanied by severe gaseous distension of the intestines. Mesenteric infarction or other necrotizing diseases, such as severe acute enterocolitis or strangulated hernia, are commonly associated, but by no means invariably so. Mucosal ulcera- tion or destruction need not be present, and several of the cases reported, including some of our own, have shown an intact GI tract at autopsy. Gas-forming or- ganisms, such as Aerobacter aerogenes, E. coli, and other normal inhabitants of the GI tract, have been cultured from the blood in some of the cases. In one of our cases, analysis of the gas collected from the portal vein at autopsy showed a high COz content, similar to that produced by Aerobacter aerogenes, which was cultured from the blood antemortern and postmortem. Only two of the reported cases ~ u r v i v e d ; ~ ~ . ~ ~ most died within a day or two of the discovery of the portal gas.
In searching among these cases for a common denominator, certain factors
Felson: Abdominal Gas -A Roentgen Approach 159
come to light. In the first place, the cases with positive blood culture raise the possibility of sepsis, at least in the portal circulation, caused by gas-forming organisms. The well-known association of diabetes and gas infections is under- scored by several cases in the series and lends further support to an infectious etiology of the intravascular gas.
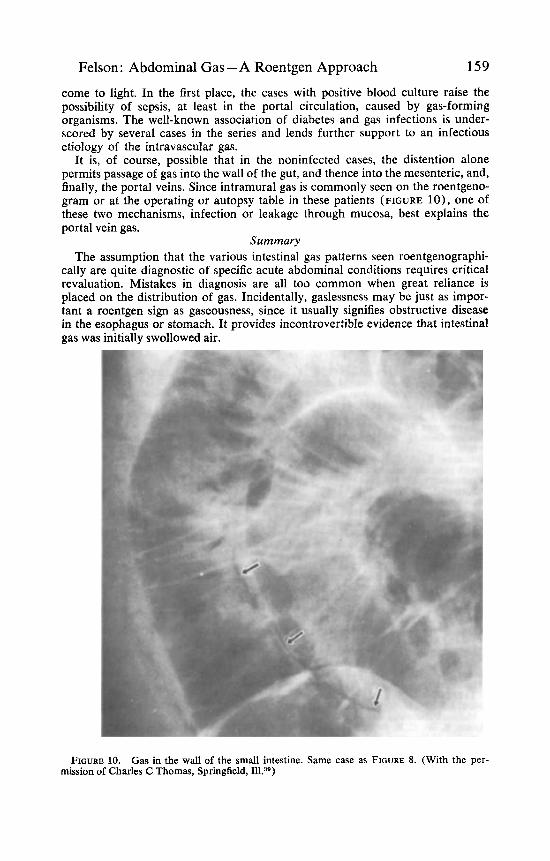
It is, of course, possible that in the noninfected cases, the distention alone permits passage of gas into the wall of the gut, and thence into the mesenteric, and, finally, the portal veins. Since intramural gas is commonly seen on the roentgeno- gram or at the operating or autopsy table in these patients (FIGURE lo), one of these two mechanisms, infection or leakage through mucosa, best explains the portal vein gas.
Summary The assumption that the various intestinal gas patterns seen roentgenographi-
cally are quite diagnostic of specific acute abdominal conditions requires critical revaluation. Mistakes in diagnosis are all too common when great reliance is placed on the distribution of gas. Incidentally, gaslessness may be just as impor- tant a roentgen sign as gaseousness, since it usually signifies obstructive disease in the esophagus or stomach. It provides incontrovertible evidence that intestinal gas was initially swollowed air.
FIGURE 10. Gas in the wall of the small intestine. Same case as FIGURE 8. (With the per- mission of Charles C Thomas, Springfield, Ill.38)
160 Annals New York Academy of Sciences
The rate of disappearance of gas from the peritoneal cavity following an opera- tion is an important consideration in the detection of postoperative complications. False assumptions have been made on the basis of normal persistence of post- operative pneumoperitoneum. Daily postoperative roentgenograms were made in a sizable series of adults and children, as well as in experimental animals, with some interesting results.
The normal intestine is probably not always gas-tight, especially when dis- tended. Spontaneous pneumoperitoneum without peritonitis is a surprisingly common finding, and on occasion the gas undoubtedly traverses the “intact” in- testinal wall. Furthermore, intestinal gas may enter the portal venous system during life through an apparently normal gut wall. Portal-vein gas is readily recog- nizable on the roentgenogram. The condition is nearly always fatal.
Acknowledgments
I wish to express my deep appreciation to Drs. Jerome F. Wiot, Lester R. Bryant, R. J. Kloecker, William H. McAlister, and Corning Benton for permitting me to examine their material on postoperative pneumoperitoneum. Drs. John E. Albers and William A. Altemeier worked with me on spontaneous pneumoperi- toneum.
1.
2.
3.
4.
5.
6.
7.
8. 9.
10.
11 .
12.
13.
14.
15.
16.
17.
18.
References GROLLMAN, A. I., S. GOODMAN & A. FINE. 1950, Localized paralytic ileus: an early
roentgen sign in acute pancreatitis. Sur., Gynec., Obstet. 91: 65. MELLINS, H. 2. & L. G. RIGLER. 1954. The roentgen findings in strangulating obstruc-
tions of the small intestine. Amer. J. Roentgen. 71: 404. EISENMAN, J. I., E. J. FINCK & B. J. O’LOUGHLIN. 1966. Gallstone ileus-a new radio-
graphic sign. To be published. FRIMANN-DAHL, J. 1960. Acute abdominal diseases. 2nd edit. Charles C Thomas. Spring-
field, Ill. ANDERSEN, K. & A. RINGSTED. 1943. Clinical and experimental investigations in ileus
with particular reference to genesis of intestinal gas. Ada. Chir. Scand. 88: 475. WANGENSTEEN, 0. H. 1955. Intestinal obstructions. 3rd edit. : 22. Charles C Thomas.
Springfield, Ill.. WANGENSIEEN, 0. H. 1940. The value of diagnostic criteria for the choice of therapeutic
procedure in the management of acute intestinal obstruction: experimental and clinical observations. Radiology 35: 680.
FELSON, B. 1949. Appendical calculi: incidence and clinical significance. Surgery 25: 734. HARRIS, P. D., E. B. D. NEUH~JSER & R. GERTH. 1964. The osmotic effect of water
soluble contrast media on circulating plasma volume. Amer. J. Roentgen. 91: 694. SERGIRVSKIY, S . A. 1947. Postoperative pneumoperitoneum and its influence on the
development of pulmonary complications. Vest. Khir. Grekov. 67: 23. VON KEISER, D. & K. LEMMERTZ. 1947. Uber die dauer des postoperativen pneumoperi-
toneums. Chirurg. 17-18: 260. BEVAN, P. G. 1961. Incidence of postoperative pneumoperitoneum and its significance.
Brit. Med. J. 2: 605. BEVAN, P. G. 1961. Postoperative pneumoperitoneum and pulmonary collapse. Brit.
Med. J. 2: 609. HARRISON, I., H. LITMER & W. GERWIG, JR. 1957. Studies on the incidence and the dura-
tion of postoperative pneumoperitoneum. Ann. Surg. 145: 591. BRYANT, L. R., J. F. WIOT & R. J. KLOECKER. 1963. A study of the factors affecting the
incidence and duration of postoperative pneumoperitoneum. Surg., Gynec., Obstet. 117: 145.
WIOT, J. F., W. H. MCALISTER & C. BENTON. 1967. Postoperative pneumoperitoneum in children. Radiology 89: 285.
AYRES, R. W., C. R. BRESON & J. B. SCRUGGS, JR. 1950. Idiopathic pneumoperitoneum: review of literature and report of a case. Amer. J. Dig. Dis. 17: 345.
ALBERS, J. E., W. A. ALTEMEIER & B. FELSON. Spontaneous pneumoperitoneum without acute peritonitis. To be published.
Felson: Abdominal Gas -A Roentgen Approach 161 19. NORPOTR, H. 1950. Beitrag zur Frage spontanen pneumoperitoneums. Zbl. Chir. 75: 450. 20. NANSON, E. M. & G. E. DRAGAN. 1956. Spontaneous pneumoperitoneum due to jejunal
diverticulosis. Ann. Surg. 143: 112. 21. STENSTROM, B. 1937. Discussion of etiology of spontaneous pneumoperitoneum found
during roentgen examination. Acta Radiologica (Stockholm) 18: 625. 22. MOBERG, G. 1937. Two cases of pneumoperitoneum without any signs of perforation
of alimentary canal or abdominaI wall. Acta Radiologica (Stockholm) 18: 798. 23. WALKER, M. A. 1942. Pneumoperitoneurn following douche. J. Kansas Med. SOC. 43: 55. 24. BEAN, L. L. & R. I. GARRETT. 1954. Spontaneous pneumoperitoneum (from exercise
25. CONN, H. 0. & W. F. LA Fou. 1956. Recurrent spontaneous pneumoperitoneum. Amer.
26. LOZMAN, H. & A. J. NEWMAN. 1956. Spontaneous pneumoperitoneum occurring during
27. FREDRIKSON, H. 1956. A case of pneumoperitoneum. Acta Obstet. Gynec. Scand. 35: 568. 28. WRIGHT, A. R. 1959. Spontaneous pneumoperitoneum. Arch. Surg. (Chicago) 78: 500. 29. BILGER, M. 1956. Pneumatosis cystoides intestinalis in children: report of a case com-
30. SINGER, H. A. 1932. Valvular pneumoperitoneum. JAMA 99: 2177. 31. PAPP, J. P. & B. H. SULLIVAN, JR. 1965. Spontaneous pneumoperitoneum without peri-
tonitis. Report of a case. Cleveland Clin. Quart. 32: 149. 32. SCHIFF, L., R. J. STEVENS & S. GOODMAN. 1941. Pneumoperitoneum following use of
flexible gastroscope. Ann. Intern. Med. 14: 1283. 33. BERK, J. E. 1946. Pneumoperitoneum following gastroscopy without evidence of per-
foration at laparotomy 14 hours later. Gastroenterology 6: 218. 34. FIERST, S. M., H. M. ROBINSON & L. LASAGNA. 1951. Interstitial gastric emphysema
following gastroscopy; its relation to the syndrome of pneumoperitoneum and general- ized emphysema with no evident perforation. Ann. Intern. Med. 34: 1202.
35. CONOLE, F. D. & A. A. DANCELO. 1952. Resection of pharyngeal diverticulum with spontaneous development of tension pneumoper:lfoneum. Amer. J. Surg. 83: 580.
36. WOLF, H. G. 1958. Beitrage zur Diagnose und Atiologie des spontanen Pneumoperito- neums beim Neugebornen. Radio]. Clin. Base1 27: 193.
37. KEYTING, W. S., R. R. MCCARVER, J. L. KOVARIK & A. L. DAYWITT. 1961. Pneumatosis intestinalis: a new concept. Radiology 76: 733.
38. BRITT, C. I., A. J. CHRISTOFORIDIS & N. E. ANDREWS. 1961. Asymptomatic spontaneous pneumoperitoneum. Amer. J. Surg. 101: 232.
39. W~OT, J. F. & B. FELSON. 1961. Gas in the portal venous system. Amer. J. Roentgen. 86: 920.
40. WOLFE, J. N. & W. A. EVANS. 1955. Gas in portal veins of liver in infants; roentgeno- graphic demonstration with postmortem anatomical correlation. Amer. J. Roentgen.
41. SUSMAN, N. & H. R. SENTURIA. 1960. Gas embolization of portal venous system. Amer. J.
42. SCHORR, S. 1963. Small intestinal intramural air. Radiology 81: 285. 43. RIGLER, L. G. & W. L. POGUE. 1965. Roentgen signs of intestinal necrosis. Amer. J.
44. LAZAR, H. P. 1965. Survival following portal venous air embolization. Amer. J. Dig. Dis.
45. SEAMAN, W. B., R. J. FLEMING & D. H. BAKER. 1966. Pneumatosis intestinalis of the small
during puerperium). U.S. Armed Forces M. J. 5 : 375.
J. Obstet. Gynec. 71: 1342.
post-partum exercises in the knee chest position. Amer. J. Obstet. Gynec. 72: 903.
plicated with fatal pneumoperitoneum. J. Pediat. 49: 445.
74: 486.
Roentgen. 83: 847.
Roentgen. 94: 402.
10: 259.
bowel. Seminars in Roentg. 1: 234.






![SanPIN2[1].6.1.1192_2003 Roentgen](https://img.pdfslide.net/doc/110x75/54f7b87c4a7959303c8b47a0/sanpin216111922003-roentgen.jpg)





















