Embed Size (px)
Citation preview
Access to Care and Health Disparities Among People with Epilepsy
December 7, 2013
David J. Thurman, MD, MPH
Emory University
American Epilepsy Society | Annual Meeting
Disclosure
UCB, Inc.
American Epilepsy Society | 2013 Annual Meeting
Grant funding
Learning Objectives
• Identify key literature on health care disparities
• Describe recent U.S. studies addressing health disparities in epilepsy
• Discuss implications
American Epilepsy Society | 2013 Annual Meeting
Brief Review of Literature
• Studies of health disparities—factors affecting occurrence and outcome:
• Demographic: Age, Sex, and Ethnicity
• Socioeconomic
• Access to health care
Systematic Reviews
Review Article
How common are the “common”
Neurologic disorders?
D. Hirtz, MD; D.J. Thurman, MD, MPH; K. Gwinn-Hardy, MD; M. Mohamed, MPH
A.R. Chaudhuri, PhD; and R. Zalutsky, PhD
NEUROLOGY 2007;68:326-337
Epilepsia, 50(10):2285–2295, 2009
SPECIAL REPORT
Disparities in epilepsy: Report of a systematic review by the North American Commission of the
International League Against Epilepsy *Jorge G. Burneo, †Nathalie Jette, ‡William Theodore, §Charles Begley,
¶Karen Parko, **David J. Thurman, and †Samuel Wiebe for the Task Force on Disparities in Epilepsy Care, on behalf of the North American Commission
of the International League Against Epilepsy
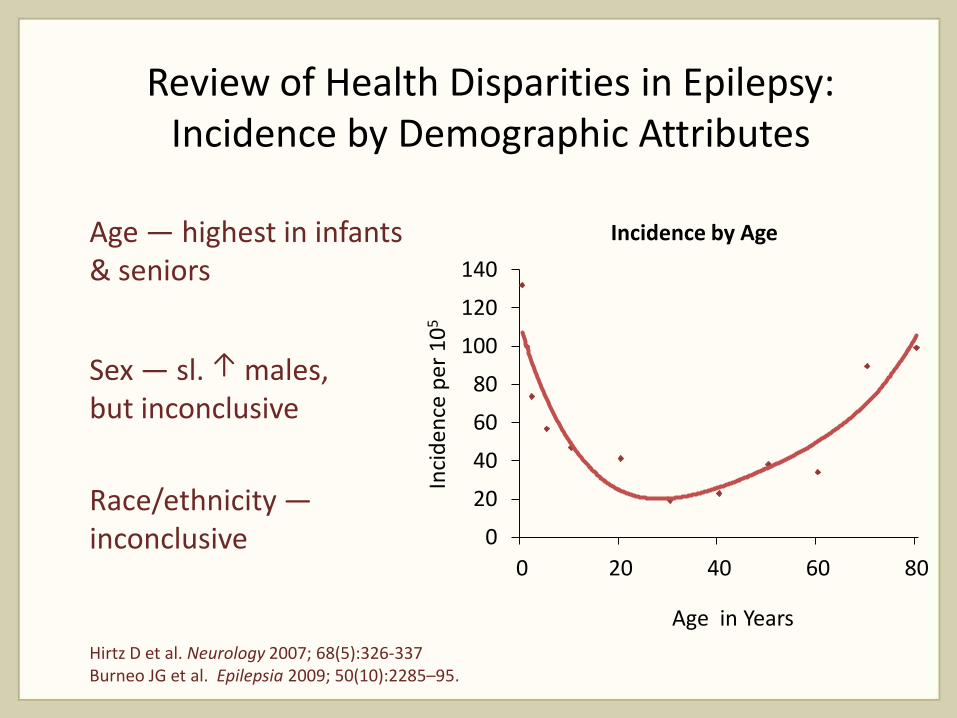
Review of Health Disparities in Epilepsy: Incidence by Demographic Attributes
Age — highest in infants & seniors
Sex — sl. ↑ males, but inconclusive
Race/ethnicity — inconclusive 0
20
40
60
80
100
120
140
0 20 40 60 80
Incidence by Age
Inci
de
nce
pe
r 1
05
Age in Years
Hirtz D et al. Neurology 2007; 68(5):326-337 Burneo JG et al. Epilepsia 2009; 50(10):2285–95.
Review of Health Disparities in Epilepsy: Prevalence by Social Attributes
Epilepsy is associated with:
• Lower income
• Higher unemployment
• Lower completion of post-secondary education
Burneo JG et al. Epilepsia 2009; 50(10):2285–95.
Review of Health Disparities in Epilepsy: Populations with Reduced Medical Care
• ↓AED adherence
– Lower SES
– No Insurance or Medicaid
– Non-whites
• ↓Surgery
– African Americans
• ↓Mental health services
– Lower education, comorbidities
Burneo JG et al. Epilepsia 2009; 50(10):2285-2295.
Health Disparities: Populations at Risk
“Racial and ethnic minorities tend to receive a lower quality of healthcare than non-minorities, even when access-related factors, such as patients’ insurance status and income, are controlled.”
Institute of Medicine, 2003
Access to Health Care, Quality of Care, and
Specialty Care
Limits To The Safety Net:
Teaching Hospital Faculty
Report On Their Patients’
Access To Care Access to certain specialty services and to routine inpatient care is often severly limited, even for insured patients.
by Joel S Weissman, Ernest Moy, Eric G. Campbell, Manjusha Gokhale,
Recal Yucel, Nancyanne Causino, and David Blumenthal
Health Affairs 2003;27(6):156-165
Original Paper _________________________________________________________________
VISITS TO SPECIALISTS
UNDER MEDICARE:
SOCIOECONOMIC ADVANTAGE
AND ACCESS TO CARE
JAN BLUSTEIN, MD, PhD
LINDA J. WEISS, PhD
Journal of Health Care for the Poor and Underserved • Vol. 9, No. 2 • 1998
Special Article
Report of the AAN Task Force on access
to health care:
The effect of no personal health insurance on health care for people
with neurologic disorders
Michael P. Earnest, MD; Jill M. Norris, PhD; Mark S Eberhardt, PhD; George H. Sands, MD; and the Task
Force on Access to Health care of the American Academy of Neurology
NEUROLOGY 1996;46:1471-1480
Unmet Need for Routine and Specialty Care: Data From the National
Survey of Children With Special Health Care Needs
Michell L. Mayer, PhD, MPH, RN; Asheley Cockrell Skinner, BS;
and Rebecca T. Slifkin, PhD
Pediatrics 2004; 113(2):109-115
Access-to-Care Studies: Specialty Care
• Identify limitations on access to specialty care in the United States
• Even in populations with some insurance coverage
• Even in populations with conditions recognized as requiring such care
Epilepsia, 50(5):1040–1050, 2009
Sociodemographic disparities in epilepsy care: Results from the Houston/New York City health care use and
outcomes study. Charles E. Begley, Rituparna Basu , Thomas Reynolds, David R. Lairson, Stephanie Dubinsky, Michael Newmark, Forbes Barnwell, Allen Hauser,
Dale Hesdorffer, Nora Hernandez, Steven C. Karceski, and Tina Shih
The Houston/NYC Health Care Use and Outcomes Study
• Longitudinal survey of 560 epilepsy clinic attendees in 4 hospitals (NYC & Houston)
• Represents spectrum of SES, not pop’n-based
• Non-whites compared to whites:
• Non-specialist visits - odds ratio (OR) 5.3
• Specialist visits - OR 0.3
• ER visits - OR 3.1
• Hospitalization - OR 5.4
Begley CE, et al. Epilepsia 2009; 50(5):1040-1050.
The Houston/NYC Health Care Use and Outcomes Study (cont.)
• Differences related to clinic/hospital
• Worse in sites serving predominantly lower income populations
• Site of care more important than individual characteristics
Begley CE, et al. Epilepsia 2009; 50(5):1040-1050.
Recent CDC studies addressing health disparities in epilepsy
From the National Health Interview Survey—U.S. 2010
• Adult active epilepsy prevalence is 1%.
• Of these, only 53% have seen neurologist or epilepsy specialist in past year.
From the BRFSS—U.S., 2005
Behavioral Risk Factor Surveillance System
Survey on Epilepsy
BRFSS* Design
• State-based, random-digit-dialed telephone survey
• Surveys civilian, noninstitutionalized population aged >18 years
• Core questions used in 50 states
• Epilepsy questions added in some states in 2005 • Screening question in 19 states
• 3 or 4 follow-up questions in 13 states
*Behavioral Risk Factor Surveillance System
BRFSS Epilepsy Questions
• Have you ever been told by a doctor that you have a seizure disorder or epilepsy?
• Are you currently taking any medicine to control your seizure disorder or epilepsy?
• How many seizures of any type have you had in the last three months?
• In the past year have you seen a neurologist or epilepsy specialist for your epilepsy or seizure disorder?
BRFSS Categories of Epilepsy
• Lifetime epilepsy
• Active epilepsy • ever told they had epilepsy AND
• currently taking AED or had seizure(s) in last 3 months
• Active epilepsy strata: • with recent seizures
• without recent seizures.
BRFSS Results:
Epilepsy Prevalence, 2005
• Active Epilepsy (n=892) - 8.4 / 1000*
• Those w/ active epilepsy report:
• Recent Seizure in 44%
• No recent Seizure in 56%
Source: Behavioral Risk Factor Surveillance System, 13 States, 2005 MMWR 2008; 57(SS-6)
Socioeconomic Comparisons: Active Epilepsy vs. No Epilepsy
People w/ epilepsy are more likely:
• Not employed (unemployed or disabled) Odds ratio (O.R.) = 6.2 (5.4 - 7.1)
• Household income <$25,000 O.R. = 3.0 (2.6 - 3.4)
• Education < HS O.R. = 1.5 (1.3 – 1.9))
BRFSS, 2005. See MMWR 2008; 57(SS-6)
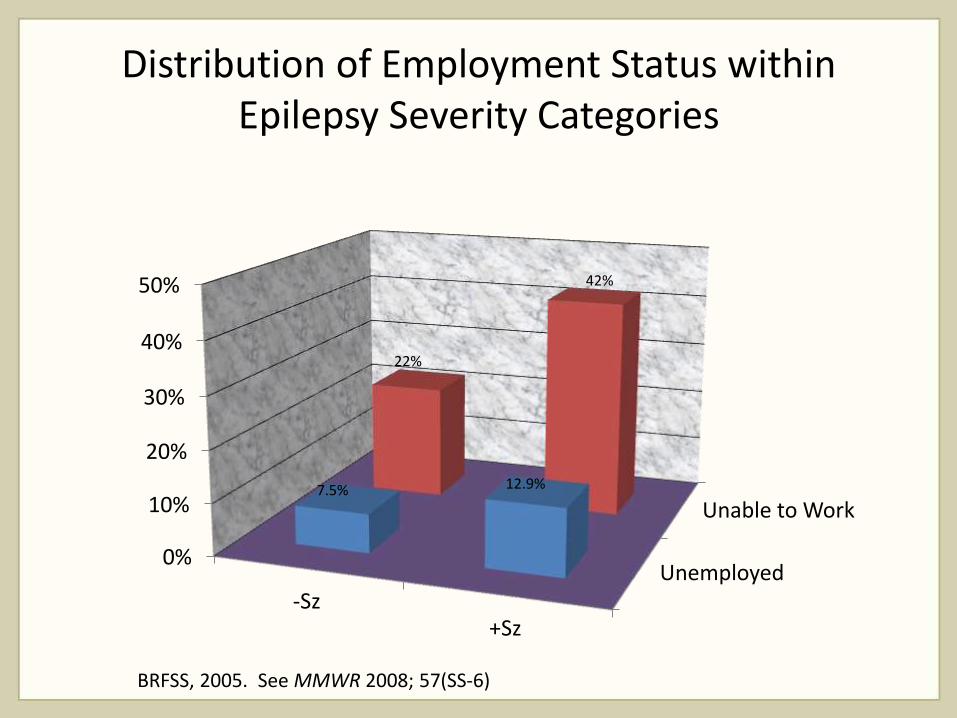
Distribution of Employment Status within Epilepsy Severity Categories
Unemployed
Unable to Work
0%
10%
20%
30%
40%
50%
-Sz +Sz
7.5% 12.9%
22%
42%
BRFSS, 2005. See MMWR 2008; 57(SS-6)
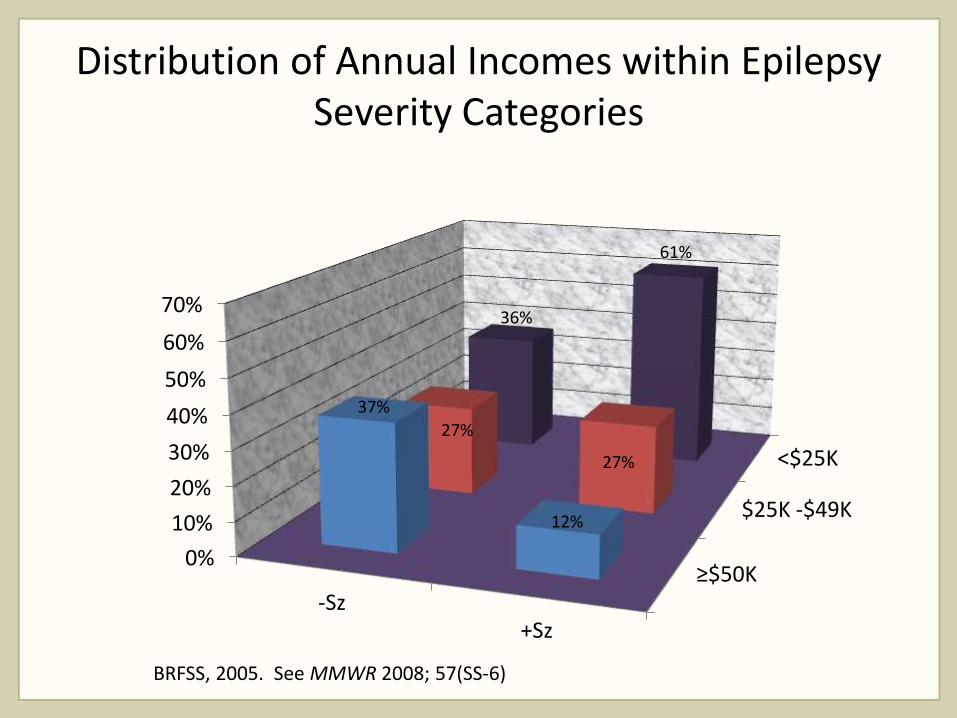
Distribution of Annual Incomes within Epilepsy Severity Categories
≥$50K
$25K -$49K
<$25K
0%
10%
20%
30%
40%
50%
60%
70%
-Sz +Sz
37%
12%
27%
27%
36%
61%
BRFSS, 2005. See MMWR 2008; 57(SS-6)
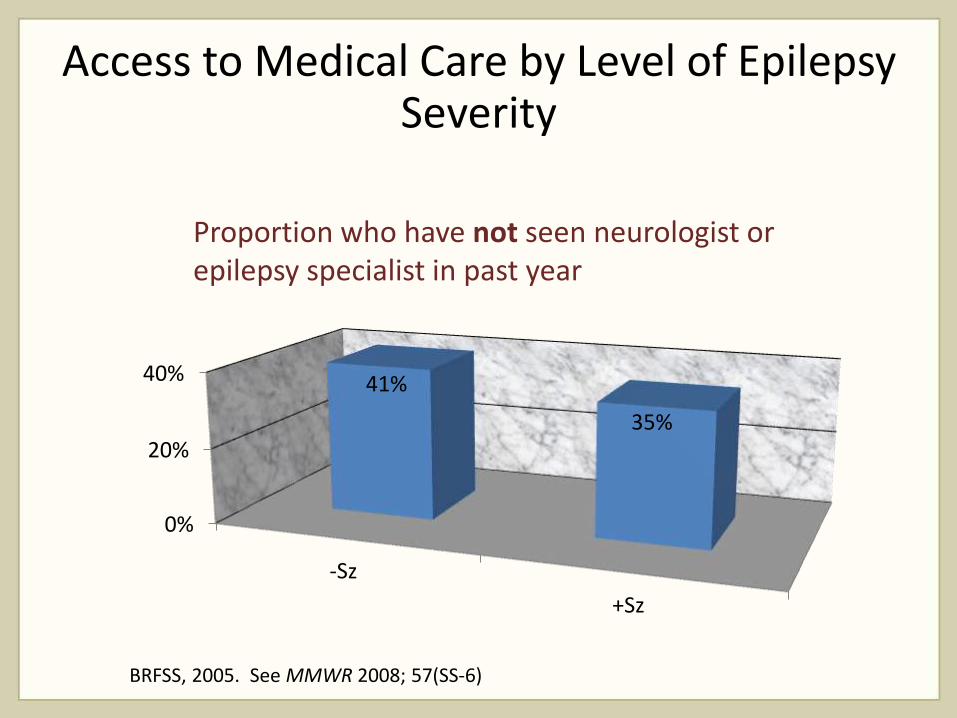
Access to Medical Care by Level of Epilepsy Severity
0%
20%
40%
-Sz
+Sz
41%
35%
Proportion who have not seen neurologist or epilepsy specialist in past year
BRFSS, 2005. See MMWR 2008; 57(SS-6)
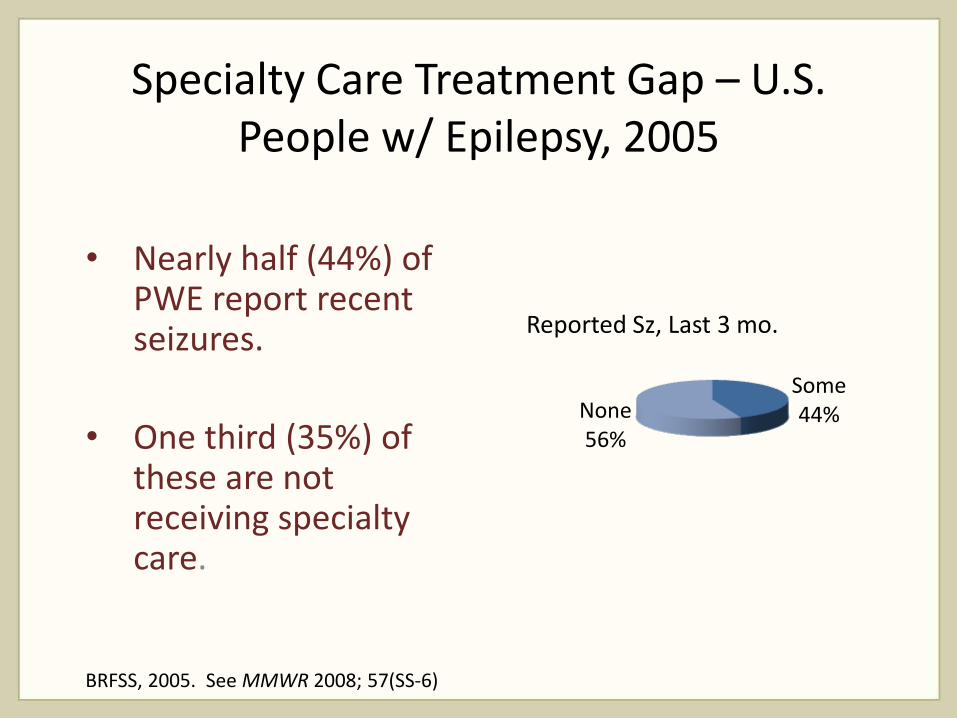
Specialty Care Treatment Gap – U.S. People w/ Epilepsy, 2005
• Nearly half (44%) of PWE report recent seizures.
• One third (35%) of these are not receiving specialty care.
Some 44% None
56%
Reported Sz, Last 3 mo.
BRFSS, 2005. See MMWR 2008; 57(SS-6)
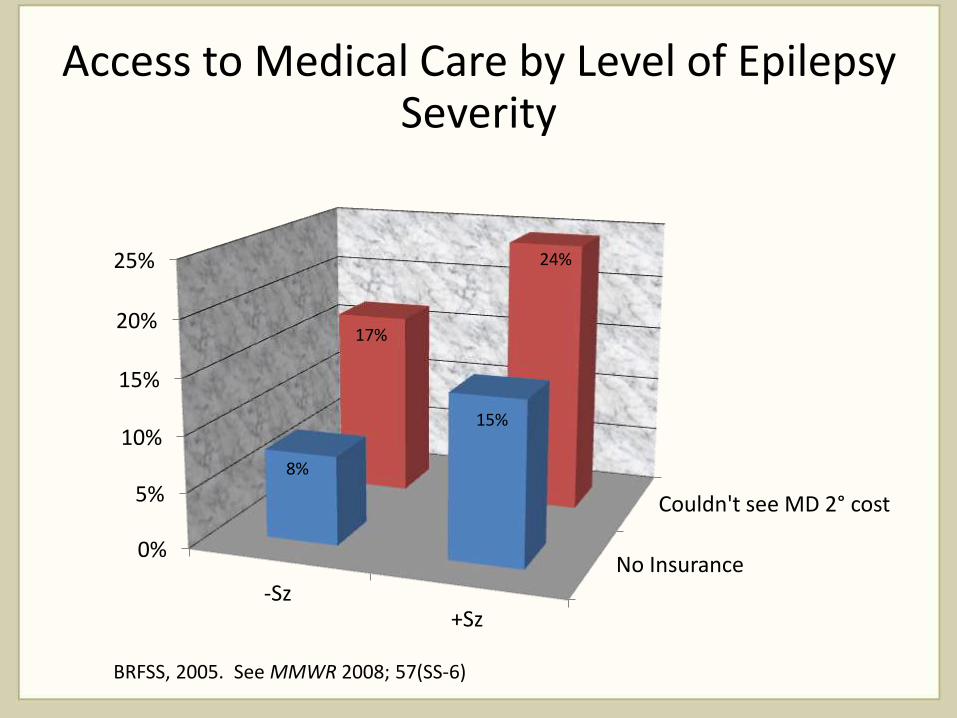
Access to Medical Care by Level of Epilepsy Severity
No Insurance
Couldn't see MD 2° cost
0%
5%
10%
15%
20%
25%
-Sz +Sz
8%
15%
17%
24%
BRFSS, 2005. See MMWR 2008; 57(SS-6)
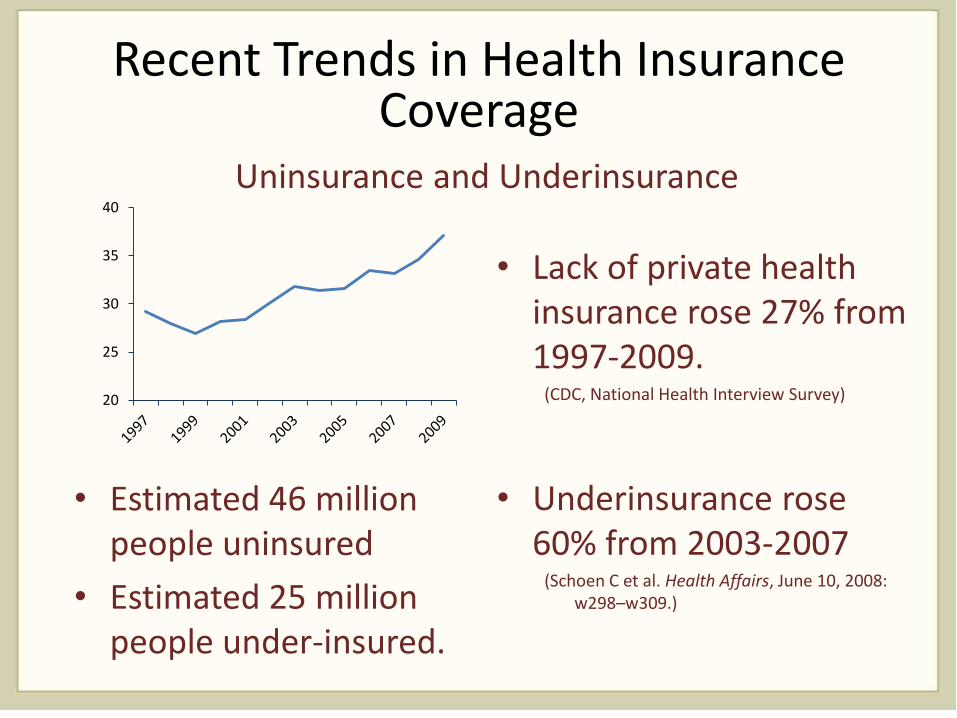
Recent Trends in Health Insurance Coverage
• Estimated 46 million people uninsured
• Estimated 25 million people under-insured.
• Lack of private health insurance rose 27% from 1997-2009.
(CDC, National Health Interview Survey)
• Underinsurance rose 60% from 2003-2007
(Schoen C et al. Health Affairs, June 10, 2008: w298–w309.)
20
25
30
35
40
Uninsurance and Underinsurance
Conclusions
• Major health disparities exist for PWE compared to the general population
• PWE, especially those w/o seizure remission, are more likely to have: • ↓income, ↑ unemployment, & ↓education
• ↓ access to & utilization of health care svcs.
• ↓ access to care greater for minority populations
Conclusions (cont.)
• There is a substantial “treatment gap” for PWE involving access to specialty care
• Insurance coverage may not guarantee adequate access to specialty care
• Epilepsy is an example whose lessons apply to other chronic neurologic disorders.
Future Research Needs
• Distinguish access to epilepsy subspecialty care
• Health disparities and access to care among children with epilepsy
• Trends under the Affordable Care Act
“While research has documented disparities in receiving equitable and timely epilepsy care, the reasons for these inequities . . . and their magnitude . . . have to be better understood in order to improve access to care.”
— Institute of Medicine, 2012
“Medicine, as a social science, as the science of human beings, has the obligation to point out problems and to attempt their theoretical solution: the politician, the practical anthropologist, must find the means for their actual solution….”
— Rudolf Virchow (1821-1902)
Impact on Clinical Care and Practice
• Identify and address access-to-care barriers in patients
• Advocacy
References 1. Begley CE, Basu R, Reynolds T, et al. Sociodemographic disparities in epilepsy care: results from the
Houston/New York City health care use and outcomes study. Epilepsia 2009; 50(5):1040–1050. 2. Burneo JG, Jette N, Theodore W, et al. Disparities in epilepsy: Report of a systematic review by the North
American Commission of the International League Against Epilepsy. Epilepsia, 50(10):2285–2295, 2009 3. Centers for Disease Control and Prevention (Kobau R et al.). Epilepsy in adults and access to care—United
States, 2010. MMWR 2012; 61(45):909-913. 4. Centers for Disease Control and Prevention (Kobau R et al.). Epilepsy surveillance among adults—19 states:
Behavioral Risk Factor Surveillance System, 2005. MMWR 2008; 57(SS-6). 5. Earnest MP, Norris JM, Eberhardt MS, et al. Report of the AAN Task Force on Access to Health Care: The
effect of no personal health insurance on health care for people with neurologic disorders. Neurology 1996;46:1471-1480.
6. Hirtz D, Thurman DJ, Gwinn-Hardy K, et al. How common are the “common” neurologic disorders? Neurology 2007;68:326-337
7. Institute of Medicine. Smedley BD, Stith AY, and Nelson AR, Editors. Unequal Treatment: Confronting Racial and Ethnic Disparities in Health Care. Washington, D.C., The National Academies Press, 2003.
8. Institute of Medicine Committee on the Public Health Dimensions of the Epilepsies. Epilepsy across the Spectrum: Promoting Health and Understanding. Washington, D.C.; The National Academies Press, 2012.
9. Mayer ML, Skinner AC, Slifkin RT. Unmet Need for Routine and Specialty Care: Data From the National Survey of Children With Special Health Care Needs. Pediatrics 2004; 113(2):109-115.
10. National Center for Health Statistics. Early Release of Selected Estimates Based on Data From the 2009 National Health Interview Survey. Hyattsville, MD: 2007. (http://www.cdc.gov/nchs/nhis/released201006.htm#1)
11. Schoen C, Collins SR, Kriss JL, Doty MM. How Many Are Underinsured? Trends Among U.S. Adults, 2003 and 2007, Health Affairs Web Exclusive, June 10, 2008:w298–w309. (http://www.commonwealthfund.org/Content/Publications/In-the-Literature/2008/Jun/How-Many-Are-Underinsured--Trends-Among-U-S--Adults--2003-and-2007.aspx.)





























