Embed Size (px)
Citation preview

ACHA June 1, 2013
SHORT-TERM PREVENTION GROUPS FOR COLLEGE STUDENTS
ELIMINATING WAITING LISTS
PROGRAM AUTHORS – CAMPUS MENTAL HEALTH SERVICES
• Shane Owens, Ph.D., ABPP, Assistant Director• Andrew Berger, Ph.D., ABPP, Director• Jill Bandura, Ph.D., Staff Psychologist• Christopher Browne, Ph.D., Staff Psychologist• 2012-2013 Psychology Externs:• Meredith McWillams, MS• Kristin Lopez, MS• Jameela Youssef, MS
ACHA June 1, 2013
ACHA June 1, 2013
INTRODUCTION
CAMPUS MENTAL HEALTH SERVICES
• Four Full Time Staff• Three Licensed• One License-Eligible• Two Board Certified in Cognitive Behavioral Psychology
by ABPP
• Three Part-Time Psychology Externs• Master’s Level• In pursuit of Doctoral Degree
ACHA June 1, 2013
CAMPUS MENTAL HEALTH SERVICES
• All staff are on call 24 hours per day, 365 days per year• Services• Individual, couples, and group psychotherapy• Consultation and liaison services• Education and outreach
• Works on an outpatient treatment facility model• Multisymptomatic outpatient population
ACHA June 1, 2013
STATEMENT OF THE PROBLEM
• 29% of college counseling centers place limits on sessions• 48% promote themselves as short-term services• Average number of sessions is 6.2• 88% of directors report an increase in the number
of students on campus with severe psychological problems• 92% of directors report an increase in the number
of students seeking services
ACHA June 1, 2013Source: National Survey of College
Counseling, Gallagher, 2012
STATEMENT OF THE PROBLEM (CTD.)
• More than half of schools that responded place limits on number of sessions (as low as 5 sessions)• Survey respondents are seeing an average of 223
new cases per semester• Survey respondents indicated truncated hours
based on budget and placing services when most needed
ACHA June 1, 2013Source: Unpublished SUNY CCD survey results, Owens & Berger,
2012

STATEMENT OF THE PROBLEM (CTD.)
• At Farmingdale, we do not, nor have we in the last 30 years, had a waiting list• New patients are offered an appointment within
48 hours of calling or visiting the office• ALL crisis cases are seen immediately (some
after-hours cases are dealt with by phone with the assistance of University Police and Residence Life staff)• University police attend the State Police Academy• Not campus security• Well-trained (most are EMTs)
ACHA June 1, 2013Source: Internal Data from FSC
CMHS File Review
STATEMENT OF THE PROBLEM (CTD.)
• No session limits• Average number of sessions at CMHS: 5.95• Modal number of sessions at CMHS: 1• Median number of sessions at CMHS: 2 (heavy
positive skew)
ACHA June 1, 2013Source: Internal Data from FSC
CMHS File Review

ACHA June 1, 2013
PROGRAM DESCRIPTION
PROGRAM OVERVIEW
• 4 Sessions• Delivered in groups of 4 to 8 students• Content:• Psychoeducation• Training in specific cognitive-behavioral technique for
stress management• Highlighting other ways to manage stress
ACHA June 1, 2013
SESSION 1: ICEBREAKER AND INTRO TO GROUP WORK
• Set goals• Set rules for the group• Ice breaker• Initial measurement of symptoms
ACHA June 1, 2013
SESSION 2: INTRODUCTION OF STRESS MANAGEMENT TECHNIQUES
• Stress reaction• Symptoms of stress• Long-term effects of stress• Sources of stress• Some coping mechanisms• Discussion of rational and irrational thought
patterns• Assign REBT homework
ACHA June 1, 2013
REBT PRIMER“PEOPLE ARE NOT DISTURBED BY THINGS, BUT BY THE VIEW THEY TAKE OF THEM” –
EPICTETUS – GREEK STOIC PHILOSOPHER

REBT
• A form of CBT created and developed by Albert Ellis (1913-2007)• Both a system of psychotherapy and a philosophy• Largely based on the writings of Greek Stoic
philosophers
REBT
• Fundamental premise: we cause/increase emotional disturbance by the way in which we view events• Through the language we use, our beliefs, attitudes, and
the meaning we give to events, others, and ourselves, we create/increase emotional disturbance.
• Typically, people blame their emotional disturbance on events or on people ‘doing things’ to them (‘he/she makes me so angry!’) – REBT sees our beliefs, and specifically, the meaning we give those events, as the cause of those disturbances.
A-B-C MODEL OF EMOTIONAL DISTURBANCE
• A: Activating event – can be external or internal• B: Beliefs – include meanings, assumptions,
attributions, desires, demands, etc. • C: (emotional/behavioral) Consequence• To the extent that one’s beliefs are rigid, absolute, and
dogmatic, REBT predicts that individual will experience emotional and behavioral consequences that are frequently negative and self-defeating.
ELLIS: THREE CORE IRRATIONAL BELIEFS – THE ‘3 MUSTS’
• I must do well and win the approval of others or I’m no good• Other people must treat me fairly and well 100%
of the time, in exactly the way I want them to treat me, and if they don’t I’m no good and they deserve to be condemned• I must get exactly what I want, when I want it,
and I must never get what I don’t want. It’s terrible if I don’t’ get what I want, and I can’t stand it

SECONDARY IB’S
• Demands: musts/shoulds/oughts• Awfulizing/Catastrophizing: it’s awful, terrible,
horrible• Low Frustration Tolerance: I can’t stand it!• Self/Other/Life Ratings: I’m bad/worthless; life
is not worthwhile; he/she is bad/worthless
EXAMPLE INTERVENTION: IDENTIFYING IB’S, DISPUTING THEM,
AND SUBSTITUTING RB’S• A) Final exams, Final projects• B) ‘it’s unfair! This professor expects too
much from us’ - unrealistic demand
‘I can’t stand it! There’s no way I can do this’ - low frustration tolerance
‘I’m going to fail out of school!’ - catastrophizing
C) Emotional: Anxiety, anger, frustration; Self-defeating Behavior (procrastination,
avoidance)

SESSION 3: REINFORCING THOUGHT-CHANGING TECHNIQUES
• Review REBT homework• Extend awareness of IBs and RBs to working
toward change• Assign homework
ACHA June 1, 2013
SESSION 4: EXTENDING TECHNIQUES TO THE REST OF YOUR LIFE
• Review homework• Discuss any difficulty that participants had with
homework• Elicit future problems and strategies for dealing
with them utilizing REBT principles• Elicit feedback• Encourage future help-seeking• Administer post measures
ACHA June 1, 2013

ACHA June 1, 2013
RESULTS AND DISCUSSION

MEASURES USED
• Beck Depression Inventory-Second Edition (BDI-2)• Beck Anxiety Inventory (BAI)• Beck Hopelessness Scale (BHS)• Patient Health Questionnaire-9 (PHQ-9)
ACHA June 1, 2013
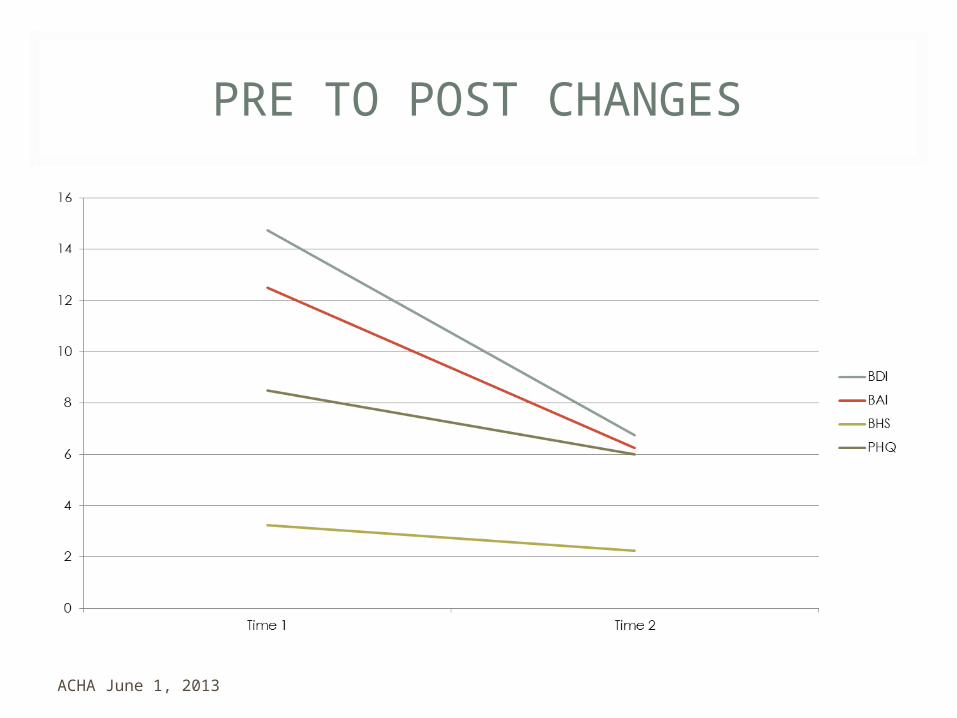
PRE TO POST CHANGES
ACHA June 1, 2013

PRE TO POST CHANGES
Measure PRE (N = 4) POST (N = 4) T (df = 3) D
M SD M SD
BDI2 14.75 3.10 6.75 1.89 3.36* 3.10**
BAI 12.50 8.10 6.25 3.30 2.20 1.01**
BHS 5.25 3.40 2.25 1.89 1.23 0.36
PHQ-9 8.50 2.08 6.00 1.83 3.87* 1.28**
ACHA June 1, 2013
DISCUSSION
• This was in 2, imagine if we’d been able to do 4.• Program is easy to administer and repeatable.• Program can be extended in length and altered to
fit specific diagnoses.• Program is efficient.• A more desirable alternative to waiting list or
referral to outside providers.• May be used in conjunction with traditional
approaches (e.g., individual therapy).• Not for those with serious psychopathology.
ACHA June 1, 2013

QUESTIONS
ACHA June 1, 2013