Embed Size (px)
Citation preview

Clinical Endocrinology (1998) 48, 251–255
Review
251q 1998 Blackwell Science Ltd
ACTH precursors: biological significance and clinicalrelevance
Anne White and Sarah GibsonEndocrine Sciences Research Group, Department ofMedicine and School of Biological Sciences, Universityof Manchester, Manchester, UK
(Received 16 September 1997; returned for revision 13 October1997; finally revised 8 December 1997; accepted 7 January1998)
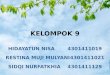
ACTH is synthesized as part of the precursor proopiomelano-cortin or POMC (Fig. 1). In the human pituitary POMC isenzymatically processed to pro-ACTH, which is then cleaved togive ACTH. Processing of POMC in the pituitary takes placewithin the regulated secretory pathway and is accomplished bythe protease PC1 located within mature dense core granules(Benjannetet al., 1991; Smeekenset al., 1991).
The presence of ACTH precursors in plasma was firstdemonstrated in normal subjects after stimulation withmetyrapone (Yalow & Berson, 1971) and was later observedafter insulin-induced hypoglycaemia (Haleet al., 1986).However, complex chromatographic techniques were requiredto separate ACTH precursors from ACTH. Clearly, thisapproach could not be used for large numbers of patientsamples and would not provide a quantitative assessment of theconcentrations of the ACTH precursors in plasma.
We have subsequently quantified the concentrations ofACTH precursors in the human circulation under basalconditions. Direct measurement of these peptides was madepossible by the development of a two-site immunoradiometricassay for the ACTH precursors, POMC and pro-ACTH (Crosbyet al., 1988). The assay is based on a labelled monoclonalantibody which binds within the ACTH region of POMCand a solid phase antibody which recognizes N-terminal POMC(N-POC, Fig. 1). As binding of both antibodies is required togenerate a signal, the assay does not detect ACTH. Using thisassay, the concentrations of ACTH precursors in normalsubjects were found to be 5-40 pmol/l which is equivalent toor greater than those of ACTH, N-POC,b-lipotrophin (b-LPH)andb-endorphin (Gibsonet al., 1994).
The levels of ACTH precursors and ACTH in the circulationat any given time are dependent on regulatory mechanismsinfluencing expression of the POMC gene. However, the
relative concentrations of ACTH precursors and ACTH willdepend on precursor processing and mechanisms of secretionfrom the corticotroph cells. Evidence from studies with themouse corticotroph adenoma cell line, AtT20, suggests that inthe absence of stimulation, corticotroph cells ‘leak’ newlysynthesized POMC (Kelly, 1985). Furthermore, results we haveobtained in normal subjects and from clinical studies indicatethat acute regulation of secretion of ACTH and ACTHprecursors differs (see below).
Clinical relevance
The development of sensitive immunoradiometric assays forACTH has improved the reliability of ACTH measurement.This is particularly important for the differentiation of ACTHdependent and independent Cushing’s syndrome. However,ACTH measurement rarely distinguishes between pituitary andectopic sources of ACTH in Cushing’s syndrome because of theconsiderable overlap in ACTH concentrations in these twopatient groups.
Approximately 15-20% of cases of ACTH-dependentCushing’s syndrome are traced to ectopic tumours and smallcell lung carcinoma (SCLC) is the most common cause. Thesetumours are almost always visible on plain chest X-ray but canalso be distinguished from pituitary tumours by the shorthistory, weight loss, severe myopathy, pigmentation andhypokalaemia (Wajchenberget al., 1994; Trainer & Grossman,1991). However, small ‘occult’ ectopic ACTH secretingtumours such as carcinoids frequently present a clinical pictureidentical to that seen with pituitary-dependent Cushing’sdisease and can be difficult to diagnose.
Chromatographic studies performed as early as 1971suggested that high molecular weight forms of ACTH werepresent in extracts from ectopic tumours (Yalow & Berson,1971). However, the relevance of this to circulating hormonelevels and their action on distant tissues was uncertain.Subsequently, Rees and colleagues demonstrated the presenceof POMC and pro-ACTH in plasma obtained from 7 patientswith the ectopic ACTH syndrome (Ratteret al., 1983; Haleet al., 1986).
In a study comparing patients with pituitary and ectopictumours causing Cushing’s syndrome, we quantified ACTHprecursor concentrations and compared the molar ratio ofACTH precursors to ACTH. This provided clear evidence thatACTH precursor concentrations were elevated in all of the 15patients with ectopic tumours when compared with patients
Correspondence: Dr A White, Endocrine Sciences Research Group,Department of Medicine and School of Biological Sciences,University of Manchester, Stopford Building, Manchester M13 9PT,UK. Fax: þ 44 (0)161 2755958, E-mail: [email protected]

with pituitary microadenomas. In comparison, ACTH levels inthe two patient groups did not discriminate because theyshowed significant overlap (Stewartet al., 1994). Themeasurement of ACTH precursors requires only a singlesample. This is in contrast to the extensive and costlyprocedures required for inferior petrosal sinus sampling, nowcommonly used to differentiate between pituitary and ectopiccauses of Cushing’s syndrome (Oldfieldet al, 1991).
In our study, the majority of patients with the ectopic ACTHsyndrome had clinically obvious small cell carcinoma of thelung. Clearly, the value of ACTH precursor measurementdepends on establishing the differential diagnosis betweenpatients with a small corticotroph adenoma and patients withsmall and slow-growing carcinoid tumours. The most commonof these are bronchial and thymic carcinoids which can bothgive misleading results in dynamic tests.
To date we have studied a group of 48 patients histologicallyproven to have the ectopic ACTH syndrome. Of these, 12patients had carcinoid tumours with ACTH precursor concen-trations of 151-1300 pmol/l (median, 544 pmol/l) and corre-sponding ACTH results of 7-44 pmol/l (median, 17·5 pmol/l)(Table 1). In the remaining 36 patients ACTH precursorsranged from 139-18000 pmol/l (median 1911 pmol/l) andACTH from 1-564 pmol/l (median 50 pmol/l). These resultssuggest that the levels of ACTH precursors and ACTH arelower in carcinoid tumours than in other ectopic tumours.However, ACTH precursor measurement still differentiatedbetween carcinoid tumours and pituitary microadenomas(Fig. 2).
A recent report indicated that bronchial carcinoids were noteasily identified by an assay which detects POMC but not pro-ACTH (Raffin-Sansonet al., 1996). In view of this, it is clearlyimportant to measure both POMC and pro-ACTH in clinicalsamples. Further support for this is given by the detection of theenzyme PC1 responsible for processing POMC to pro-ACTH inbronchial carcinoid tumours (n¼ 7) and in carcinoid tumours of
the GI tract (n¼ 26) (Scopsiet al., 1995). However, PC1 hasbeen shown to process pro-ACTH to ACTH. Therefore for pro-ACTH to be elevated this mechanism must be inefficient inthese tumours. In addition, expression of the processing enzymePC2 was noted in 76% of the carcinoid tumours studiedsuggesting that some carcinoid tumours may process POMC tothe smaller derivatives such as the C-terminal fragment ofACTH, corticotrophin-like intermediate lobe peptide (CLIP).Indeed, the presence of CLIP has been described in somecarcinoids, but in tumour extracts rather than in the circulation(Vieauet al., 1989).
Expression of PC1 and PC2 has been demonstrated in only aminority of SCLC tumours and in a study of 13 SCLC cell linesexpression of PC1 was restricted (Creemerset al, 1992). Thisdata complements our work with a panel of SCLC cell lineswhich secrete high levels of ACTH precursors but haveundetectable ACTH in chromatographic studies (Stewartet al., 1989; Crosbyet al., 1990).
While we and others have shown that patients with pituitarycorticotroph microadenomas have low levels of ACTHprecursors, patients with large invasive pituitary tumoursexhibit impaired processing resulting in high ACTH precursorlevels (Gibsonet al., 1996; Raffin-Sansonet al., 1996). In aseries of 13 such patients, ACTH precursor concentrations were138-5640 pmol/l (median, 1096 pmol/l) while ACTH levelswere 4-66 pmol/l (median, 20 pmol/l). In some cases the ACTHlevels could be explained by high levels of ACTH precursorswhich can cross-react up to 10% in the ACTH assay. We haveused this characteristic secretion of ACTH precursors tomonitor for tumour recurrence after surgery or treatment.
Regulation of ACTH precursor secretion
Given that concentrations of ACTH precursors in the circula-tion are at least as high as those of ACTH, it is important todetermine how they may be regulated. As indicated previously,
252 A. White & S. Gibson
q 1998 Blackwell Science Ltd,Clinical Endocrinology, 48, 251–255
N-POC JP ACTH γ-LPH β-EP
pro-ACTH β-LPH
POMC
Y Y
Y Y
Fig. 1 Peptides derived from POMC in thehuman pituitary gland.b-LPH, b-lipotrophin;N-POC, N-terminal proopiomelanocortin;JP, joining peptide;g-LPH, g-lipotrophin;b-EP,b-endorphin.Y: Binding sites ofmonoclonal antibodies used in the ACTHprecursor IRMA and the ACTH IRMA.

where regulation is at the level of the POMC gene the effectsshould be seen on both ACTH and ACTH precursors. However,in inferior petrosal sinus sampling (IPSS), CRH-stimulatedACTH concentrations are seen within 1-2 min, representingrelease of stored ACTH.
Our data on responsiveness of ACTH precursors to CRHcomes from patients with Cushing’s disease studied during IPSS.Concentrations of both ACTH precursors and ACTH wereincreased in the petrosal sinus after CRH administration.However, the magnitude of response was very different. Themedian increment (% increase above basal) in ACTH levels afterCRH was 459% compared to only 96% for ACTH precursors(Gibsonet al., 1994). These data emphasize the high degree ofprocessing to ACTH which occurs in secretory granules.
The regulation of ACTH and ACTH precursor secretion byglucocorticoids is rather more complicated. In normal subjects,ACTH concentrations were undetectable after an overnightdexamethasone suppression test while ACTH precursor levelsremained within the normal range (Gibsonet al., 1994). Thismay to some extent reflect differences in plasma half-lives ofthe ACTH precursors and ACTH. Following prolongedtreatment with glucocorticoids, we would expect ACTHprecursors to suppress due to down-regulation of the POMCgene. Our results in a patient with isolated ACTH deficiencywould seem to confirm this view. The patient’s initial ACTHprecursor levels were 129 pmol/l, but reduced to within thenormal range during hydrocortisone replacement (Nusseyet al.,1993).
ACTH precursors 253
q 1998 Blackwell Science Ltd,Clinical Endocrinology, 48, 251–255
Table 1 ACTH precursor secretion in carcinoid tumours
ACTHprecursors ACTH Precursor/ACTH
Patient Histology (pmol/l) (pmol/l) ratio
1 Bronchial carcinoid 690 18 382 Bronchial carcinoid 262 16 163 Bronchial carcinoid 151 17 94 Bronchial carcinoid 794 44 185 Bronchial carcinoid 567 17 336 Thymic carcinoid 437 19 237 Thymic carcinoid 520 11 478 Thymic carcinoid 1157 34 349 Metastatic carcinoid 273 7 39
10 Metastatic carcinoid 174 17 1011 Metastatic carcinoid 673 32 2112 Metastatic carcinoid 1300 43 3013-48 Other than carcinoid* 139–18000 1–564 4–401
* Other ectopic tumours: 25 small cell carcinoma of the lung, 3 pancreatic tumours, 3 medullary carcinoma of the thyroid, 2 thymomas, 2 squamous cellcarcinoma of the lung and 1 ovarian carcinoma.
AC
TH
pre
cu
rso
rs (
pm
ol/
l)
100 000
1000
100
10
Carcinoid
tumours
10 000
Other
ectopic
tumours
Cushing’s
disease
Fig. 2 Comparison of ACTH precursor levels in patients with theectopic ACTH syndrome and patients with Cushing’s disease(excluding those patients with macroadenomas).

The existence of distinct constitutive and regulated pathwaysfor ACTH secretion in corticotrophs has been proposed basedon studies in the mouse corticotroph adenoma cell line AtT20and in rat anterior pituitary cells. In the constitutive pathway,unprocessed POMC would be continuously released withoutbecoming subject to regulatory events affecting secretoryvesicles. The apparent lack of responsiveness of ACTHprecursors to acute regulation by CRH and dexamethasonesuggests that precursors may be released in this manner.
Biological significance of ACTH precursors
The clinical significance of ACTH precursors is dependent ontheir biological activity. However, it has proved difficult to geta clear indication of precursor bioactivity because of problemsin obtaining pure preparations of the peptides and thelimitations of available bioassays.
POMC itself is thought to have little biological activity(Odell, 1991) while pro-ACTH was shown to be equipotentwith ACTH in a rat adrenal cell bioassay (A.C. Haleet al.,personal communication) or 8-33% as potent in a cytochemicalACTH bioassay (Ratteret al., 1983). Nothing is currentlyknown about the binding of POMC and pro-ACTH to theACTH receptor (MC2-R) and the MSH receptors (MC1-R,MC3-R, MC4-R, MC5-R) (see Coneet al, 1996). It will beimportant to examine the agonist/antagonist activity of theprecursors at the human receptors since precursors couldpreferentially bind MSH receptors in certain tissues, forexample MC1-R in the skin. In a study of 24 patients withpigmentation related to postadrenalectomy Cushing’s disease,concentrations of both ACTH and ACTH precursors correlatedwith pigmentation score (Rayet al., 1995). The interaction ofACTH precursor peptides with the recently cloned receptorMC4-R found exclusively in the brain may also be of interest aswe have demonstrated that concentrations of ACTH precursorsin CSF are 100-fold those of ACTH (4146 83 pmol/l vs3·26 0·6 pmol/l,n¼ 26) (Tsigoset al, 1993).
Some information regardingin vivo POMC bioactivity canbe gained from clinical studies. If patients with the ectopicACTH syndrome due to SCLC produce POMC alone (assuggested by the evidence above) then it must either havebiological activity when present at very high levels or becleaved to ACTH in the periphery. Our study in patients withinvasive pituitary macroadenomas indicates that ACTHprecursors are of lower biological activity than ACTH, as twopatients had normal cortisol levels in the presence of up to2000 pmol/l ACTH precursors. In a case of isolated congenitalACTH deficiency in which the patient had ACTH precursorlevels of 39-57 pmol/l, there was no authentic ACTH 1-39 andundetectable cortisol, inferring that these concentrations ofprecursors had no biological activity (Nusseyet al., 1993).
What do ACTH assays measure?
How well current ACTH assays recognize the ACTHprecursors is an important consideration for clinicians. Inrecent years there has been a shift towards the measurement ofACTH by two-site immunometric assays in preference to RIA.This change provides many benefits including speed, reprodu-cibility, sensitivity and parallel results. The high samplethroughput and wide working range of these assays makesthem ideal for measuring samples taken during inferior petrosalsinus sampling, a test which is fast becoming an importantcomponent in the diagnosis of pituitary tumours secretingACTH.
However, we must recognize that there are clinical situationsin which the use of an assay which is highly specific for ACTH1-39 may be insufficient or misleading. In one patient with theectopic ACTH syndrome shown by chromatography to beproducing high molecular weight ACTH precursors, the ACTHwas very low when measured by immunoradiometric assay(Raff & Findling, 1989). To ensure that patients with theectopic ACTH syndrome are flagged up by an ACTH assay, it isimportant that there is a high degree of cross-reactivity of theACTH precursors in the ACTH assay or that a separate specificassay for ACTH precursors is available.
Since the initial observations in the early 1970s of thepresence of ACTH precursors in the circulation, much has beenlearnt about their existence in a range of ACTH-relateddisorders. This review has considered situations whereprecursors are in marked excess of ACTH including ectopicACTH syndrome, pituitary macroadenomas, Nelson’s syn-drome, a case of isolated ACTH deficiency and in cerebro-spinal fluid.
Important questions remain to be answered not least of whichis how POMC and pro-ACTH bind to and activate the recentlycloned ACTH and MSH receptors. Does the folding of POMCspecify whether it binds through its ACTH,bMSH or gMSHsequences? Could POMC have biological activity distinct fromits role as a precursor of ACTH by binding through itsbMSH orgMSH sequences? Thein vivoevidence of the relative biologicalactivity of ACTH precursors and ACTH is sparse and limited tocortisol levels. Clearly further studies are required on the roleand regulation of ACTH precursors before we fully understandtheir biological significance and clinical relevance.
References
Benjannet, S., Rondeau, N., Day, R., Chretien, M. & Seidah, N.G.(1991) PC1 and PC2 are proprotein convertases capable of cleavingproopiomelanocortin at distinct pairs of basic residues.Proceedingsof the National Academy of Sciences of the United States of America,88, 3564–3568.
Cone, R.D., Ly, D., Koppula, S., Vage, D.I., Klungland, H., Boston, B.,
254 A. White & S. Gibson
q 1998 Blackwell Science Ltd,Clinical Endocrinology, 48, 251–255

Chen, W., Orth, D.N., Poulton, C. & Kesterton, R.A. (1996) Themelanocortin receptors: agonists, antagonists, and the hormonalcontrol of pigmentation.Recent Progress in Hormone Research(United States), 51, 287–317.
Creemers, J.W.M., Van Roebroek, A.J.M. & de Ven, W.J.M. (1992)Expression in human lung tumor cells of the proprotein processingenzyme PC1/PC3 Cloning and primary sequence of a 5kb cDNA.FEBS Letters, 300,82–88.
Crosby, S.R., Stewart, M.F., Farrell, W.E., Gibson, S. & White, A.(1990) Comparison of ACTH and ACTH precursor peptides secretedby human pituitary and lung tumour cellsin vitro. Journal ofEndocrinology, 125,147–152.
Crosby, S.R., Stewart, M.F., Ratcliffe, J.G. & White, A. (1988) Directmeasurement of the precursors of adrenocorticotrophin in humanplasma by two-site immunoradiometric assay.Journal of ClinicalEndocrinology and Metabolism, 67, 1271–1277.
Gibson, S., Crosby, S.R., Stewart, M.F., Jennings, A.M., McCall, E. &White, A. (1994) Differential release of proopiomelanocortin-derived peptides from the human pituitary: evidence from apanel of two-site immunoradiometric assays.Journal of ClinicalEndocrinology and Metabolism, 78, 835–841.
Gibson, S., Ray, D.W., Crosby, S.R., Dornan, T.L., Jennings, A.M.,Bevan, J.S., Davis, J.R.E. & White, A. (1996) Impaired processing ofproopiomelanocortin in corticotroph macroadenomas.Journal ofClinical Endocrinology and Metabolism, 81, 497–502.
Hale, A.C., Besser, G.M. & Rees, L.H. (1986) Characterisation of pro-opiomelanocortin-derived peptides in pituitary and ectopic adreno-corticotrophin-secreting tumours.Journal of Endocrinology, 108,49–56.
Kelly, R.B. (1985) Pathways of protein secretion in eukaryotes.Science, 230,25–32.
Nussey, S.S., Soo, S.-C., Gibson, S., Gout, I., White, A., Bain, M. &Johnstone, A.P. (1993) Isolated congenital ACTH deficiency: acleavage enzyme defect?Clinical Endocrinology, 39, 381–385.
Odell, W.D. (1991) Ectopic ACTH syndrome: a misnomer.Endocrin-ology and Metabolism Clinics of North America, 20, 371–379.
Oldfield, E.H., Doppman, J.L., Nieman, L.K., Chrousos, G.P., Miller,D.L., Katz, D.A., Cutler, G.B. & Loriaux, D.L. (1991) Petrosal sinussampling with and without corticotrophin-releasing hormone for thedifferential diagnosis of Cushing’s syndrome.The New EnglandJournal of Medicine, 325,897–905.
Raff, H. & Findling, J.W. (1989) A new immunoradiometric assay forcorticotrophin evaluated in normal subjects and patients withCushing’s syndrome.Clinical Chemistry, 35, 596–600.
Raffin-Sanson, M.-L., Massias, J.-F., Dumont, C., Raux-Demay, M.-C.,Proeschel, M.F., Luton, J.-P. & Bertagna, X. (1996) High plasmaproopiomelanocortin in aggressive adrenocorticotropin-secreting
tumours.Journal of Clinical Endocrinology and Metabolism, 81,4272–4277.
Ratter, S.J., Gillies, G., Hope, J., Hale, A.C., Grossman, A., Gillard, R.,Cook, D., Edwards, C.R.W. & Rees, L.H. (1983) Pro-opiomelanocortinrelated peptides in human pituitary and ectopic ACTH secretingtumours.Clinical Endocrinology, 18, 211–218.
Ray, D.W., Gibson, S., Crosby, S.R., Davies, D., Davis, J.R.E. &White, A. (1995) Elevated levels of adrenocorticotropin (ACTH)precursors in post-adrenalectomy Cushing’s disease and theirregulation by glucocorticoids.Journal of Clinical Endocrinologyand Metabolism, 80, 2430–2436.
Scopsi, L., Gullo, M., Rilke, F., Martin, S. & Steiner, D.F. (1995)Proprotein convertases (PC1/PC3 and PC2) in normal and neoplastichuman tissues: their use as markers of neuroendocrine differentia-tion. Journal of Clinical Endocrinology and Metabolism, 80, 294–301.
Smeekens, S.P., Avruch, A.S., LaMendola, J., Chan, S.J. & Steiner, D.F.(1991) Identification of a cDNA encoding a second putativeprohormone convertase related to PC2 in AtT20 cells and islets ofLangerhans.Proceedings of the National Academy of Sciences of theUnited States of America, 88, 340–344.
Stewart, M.F., Crosby, S.R., Gibson, S., Twentyman, P.R. & White, A.(1989) Small cell lung cancer cell lines secrete predominantlyACTH precursor peptides not ACTH.British Journal of Cancer, 60,20–24.
Stewart, P.M., Gibson, S., Crosby, S.R., Penn, R., Holder, R., Ferry, D.,Thatcher, N., Phillips, P., London, D.R. & White, A. (1994) ACTHprecursors characterize the ectopic ACTH syndrome.ClinicalEndocrinology, 40, 199–204.
Trainer, P.J. & Grossman, A. (1991) The diagnosis and differentialdiagnosis of Cushing’s syndrome.Clinical Endocrinology, 34,314–330.
Tsigos, C., Crosby, S.R., Gibson, S., Young, R.J. & White, A. (1993)Proopiomelanocortin is the predominant adrenocorticotropin-relatedpeptide in human cerebrospinal fluid.Journal of Clinical Endocrin-ology and Metabolism, 76, 620–624.
Vieau, D., Massias, J.-F., Girard, F., Luton, J.-P. & Bertagna, X. (1989)Corticotrophin-like intermediary lobe peptide as a marker ofalternate pro-opiomelanocortin processing in ACTH-producingnon-pituitary tumours.Clinical Endocrinology, 31, 691–700.
Wajchenberg, B.L., Mendonca, B.B., Liberman, B., AlbergariaPereira, M.A., Carneiro, P.C., Wakamatsu, A. & Kirschner, M.A.(1994) Ectopic adrenocorticotrophin hormone syndrome.EndocrineReviews, 15, 752–787.
Yalow, R.S. & Berson, S.A. (1971) Size heterogeneity of immuno-reactive human ACTH in plasma and in extracts of pituitary glandsand ACTH-producing thymomas.Biochemical and BiophysicalResearch Communications, 44, 439–445.
ACTH precursors 255
q 1998 Blackwell Science Ltd,Clinical Endocrinology, 48, 251–255






![Case Report An Ectopic ACTH Secreting Metastatic Parotid ...downloads.hindawi.com/journals/crie/2016/4852907.pdf · True CS can either be ACTH dependent or ACTH inde-pendent []. ACTH](https://img.pdfslide.net/doc/110x75/6081617cd3269750d158a9a3/case-report-an-ectopic-acth-secreting-metastatic-parotid-true-cs-can-either.jpg)