Embed Size (px)
Citation preview

Acute and Chronic Urticaria:Evaluation and TreatmentPAUL SCHAEFER, MD, PhD, University of Toledo College ofMedicine and Life Sciences, Toledo, Ohio
Urticaria commonly presents with intensely pruritic wheals, sometimes with edema ofthe subcutaneous or interstitialtissue. It has a lifetime prevalence of about 20%. Although often self-limited -and benign, it can cause significant dis-comfort, continue for months to years, and uncommonly represent a serious systemic disease or life-threatening aller-gic reaction. Urticaria is caused by immunoglobulin E- and non—immunoglobulin E-mediated release of histamineand other inflammatory mediators from mast cells and basophils. Diagnosis is made clinically; anaphylaxis mustbe ruled out. Chronic urticaria is idiopathic in 80% to 90% of cases. Only a limited nonspecific laboratory workupshould be considered unless elements of the history or physical examination suggest specific underlying conditions.The mainstay of treatment is avoidance of triggers, if identified. The first-line pharmacotherapy is second—generation
H, antihistamines, which can be titrated to greater than standard doses. First—generation H, antihistamines, H, anti-histamines, leukotriene receptor antagonists, high-potency antihistamines, and brief corticosteroid bursts may beused as adjunctive treatment. In refractory chronic urticaria, patients can be referred to subspecialists for additionaltreatments, such as omalizumab or cyclosporine. More than one-half of patients with chronic urticaria will have
resolution or improvement of symptoms within a year. (Am Fam Physician. 2017;95(ll):7l7-724. Copyright © 2017
American Academy of Family Physicians.)
This clinical contentconforms to AAFP criteriafor continuing medical
education (CME). See CME
Quiz on page 697. Authordisclosure: No relevantfinancial affiliations.
V Patient information:A handout on this topic,written by the author ofthis article, is availableat http://www.aafp.org/afp/2017/0601Ip717-S1.html.
Scan the QR code belowfor easy access to thepatient information hand-out on the AFP mobile site.
Iune 1, 2017 ‘ Volume 95, Number 11
rticaria is a common dermato-logic condition that typicallypresents with intensely pru-ritic, well-circumscribed, raised
wheals ranging from several millimeters toseveral centimeters or larger in size. Urticariacan occur with angioedema, which is local-ized nonpitting edema of the subcutaneousor interstitial tissue that may be painful andwarm. The intense pruritus can cause signif-icant impairment in daily functioning anddisrupt sleep.‘ Typically otherwise benignand self-limited, urticaria can be a symptomof life—threatening anaphylaxis or, rarely,indicate significant underlying disease.
Urticaria can appear on any part of theskin. The wheals can be pale to brightly ery-thematous in color, often with surroundingerythema. The lesions are round, polymor-phic, or serpiginous, and can rapidly growand coalesce (Figures 1 through 3). Angio-edema presents primarily in the face, lips,mouth, upper airway, genitalia, and extrem-ities. The onset of symptoms for urticariaor angioedema is rapid, usually occurringover minutes. Individual urticarial lesionstypically resolve in one to 24 hours withouttreatment, although additional wheals can
www.aafp.org/afp
erupt in new crops. Angioedema may takedays to resolve?
Urticaria, with or without angioedema,can be classified as acute or chronic. Urti-caria that recurs within a period of less thansix weeks is acute. Recurring chronic urti-caria lasts longer than six weeks. Urticariacan present in persons of any age, with a
lifetime prevalence of approximately 20%.Chronic urticaria has a lifetime prevalenceof approximately 0.5% to 5%.“
EtiologyUrticaria and angioedema have similar under-lying pathophysiologic mechanisms: hista-mine and other mediators released from mastcells and basophils. If the release occurs in thedermis, it results in urticaria, whereas if therelease occurs in the deeper dermis and sub-cutaneous tissues, it results in angioedema.Immunoglobulin E (IgE) often mediates thisrelease, but non—IgE and nonimmunologicmast cell activation also can occur. Prote-ases from aeroallergens and activation of thecomplement system have been proposed as
examples of non-lgE triggers.‘ There may be a
serologic autoimmune component in a subsetof patients with chronic urticaria, including
American Family Physician 717

Urticaria
Figure 1. Sharply demarcated annular urti-carial plaques.
Image used with permission from VisuaIDx.
©20
'1(.
~\/i
=su
alD
x
Figure 2. Coalescing urticarial papules.
Image used with permission from visuaIDx.
antibodies to IgE and the high—affinity IgEreceptor. However, the clinical significanceof these autoantibodies is unclear.‘-5 Anti—IgE
antibodies can also be found in atopic derma-titis and several autoimmune diseases.
There are a number of identified causes
of urticaria (Table 1).“'7*‘ Common causes
include allergens (Figure 4), food pseudo-allergens (foods that contain histamine or
salicylates, or cause the release of histaminedirectly), insect envenomation, medications,and infections.“-7" Infections are the mostcommon cause of urticaria in children.‘°
Recommendation
' _’l"l'?';ACl1CE_SlN ALLEkéYANl53lMMUNOLOGlc MEDICINE": *
.,REceMMsupAnoNs—moM TH'E>_CHOOSlNG.‘\9IISELY’CA‘,MPAiGN
Sponsoring organization
Do not routinely do diagnostic testing in
patients with chronic urticaria.
Do not rely on antihistamines as first-linetreatment in severe allergic reactions.
American Academy of Allergy,Asthma, and Immunology
American Academy of Allergy,Asthma, and Immunology
tions/search. htm.
Source: For more information on the Choosing Wisely Campaign, see http://wvi/w.choosingwiseIy.org. For supporting citations and to search Choosing Wisely recom-
mendations relevant to primary care, see http://wwwaafp.org/afp/recommenda
718 American Family Physician www.aafp.org/afp
Figure 3. Serpiginous erythematous urticarialplaques.
Image used with permission from VisuaIDx.
The infectious agents commonly associ-ated with urticaria include various viruses(e.g., rhinovirus, rotavirus, Epstein—Barr,hepatitis A, hepatitis B, hepatitis C, herpessimplex, human immunodeficiency virus),bacteria (e.g., urinary tract infections,streptococcus, mycoplasma, Helicobacterpylori), and parasites. Medications, notablybeta—lactam antibiotics, typically cause urti-caria via allergic reactions, although some
medications (e.g., aspirin, nonsteroidalanti—inflammatory drugs [NSAIDS], van-
comycin, opiates) can also trigger urticariathrough direct mast cell degranulation.
In some patients, physical stimuli, includ-ing pressure, cold (Figure 5), heat, and theraising of the core body temperature (cho-linergic urticaria; Figure 6), cause urticariathat tends to be chronic." Systemic disease
is an uncommon cause of urticaria. Illnessesthat have been associated with urticaria or
angioedema include I-Iashimoto thyroiditis,mastocytosis, systemic lupus erythematosus,Sjogren syndrome, rheumatoid arthritis,vasculitis (Figures 7 and 8), celiac disease,
and lymphoma.” Causes of acute urticariaoften can be identified during the patient
Volume 95, Number 11 ° Iune I, 2017
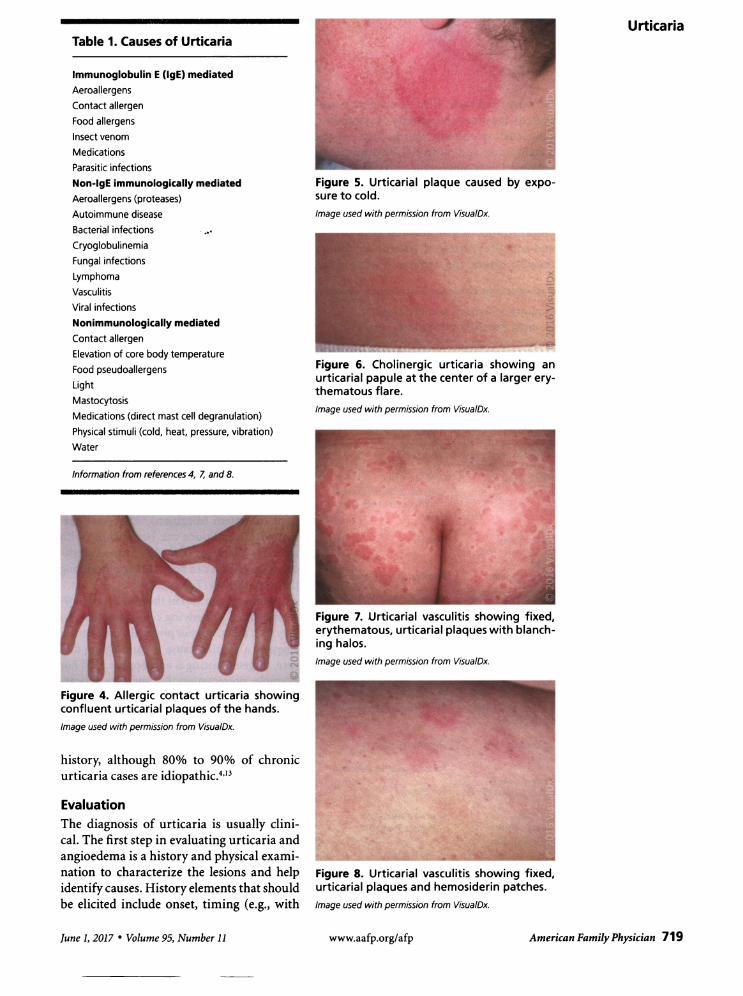
Table 1. Causes of Urticaria
Immunoglobulin E (IgE) mediatedAeroallergens
Contact allergen
Food allergens
Insect venom
Medications
Parasitic infections
Non-lgE immunologically mediatedAeroallergens (proteases)
Autoimmune disease
Bacterial infections ~
Cryoglobulinemia
Fungal infections
Lymphoma
Vasculitis
Viral infections
Nonimmunologically mediated
Contact allergen
Elevation of core body temperature
Food pseudoallergens
Light
Mastocytosis
Medications (direct mast cell degranulation)
Physical stimuli (cold, heat, pressure, vibration)
Water
Information from references 4, 7, and 8.
Figure 4. Allergic contact urticaria showingconfluent urticarial plaques of the hands.
Image used with permission from VisuaIDx.
history, although 80% to 90% of chronicurticaria cases are idiopathic.”
EvaluationThe diagnosis of urticaria is usually clini-cal. The first step in evaluating urticaria andangioedema is a history and physical exami-nation to characterize the lesions and helpidentify causes. History elements that shouldbe elicited include onset, timing (e.g., with
lune 1, 2017 ' Volume 95, Number 11
Figure 5. Urticarial plaque caused by expo-sure to cold.
Image used with permission from VisuaIDx.
Figure 6. Cholinergic urticaria showing anurticarial papule at the center of a larger ery-thematous flare.Image used with permission from VisuaIDx.
Figure 7. Urticarial vasculitis showing fixed,erythematous, urticarial plaques with blanch-ing halos.
Image used with permission from Visua/Dx.
Figure 8. Urticarial vasculitis showing fixed,urticarial plaques and hemosiderin patches.
Image used with permission from VisualDx.
www.aafp.org/afp
Urticaria
American Family Physician 719

Urticaria
the menstrual cycle, if an association is sus-
pected), location, and severity of symptoms;associated symptoms, which may suggest
anaphylaxis; and potential environmentaltriggers. Other important parts of the his-tory include medication and supplement use,
(especially new or recently changed dosages),allergies, recent infections, travel history,family history of urticaria and angioedema,and complete review of systems to identifypossible causes and symptoms of systemic
Table 2. Urticaria—Associated History and PhysicalExamination Findings with Possible Etiologies
Clinical clue Possible etiology
Abdominal pain, dizziness, hypotension, largeerythematous patches, shortness of breath,stridor, tachycardia
Dermatographism, physical stimuli
Food ingestion temporally related to symptoms
High-risk sexual behavior or illicit druguse history
Infectious exposure, symptoms of upperrespiratory tract or urinary tract infections
Joint pain, uveitis, fever, systemic symptoms
Medication use or change
Pregnancy
Premenstrual flare—up
Smaller wheals (1 to 3 mm); burning or itching;brought on by heat, exercise, or stress
Thyromegaly, weight gain, cold intolerance
Travel
Weight loss (unintentional), fevers, night sweats
Wheals lasting longer than 24 hours,nonblanching papules, burning or otherdiscomfort, residual hyperpigmentation,fevers, arthralgias
Anaphylaxis
Physical urticaria
Food allergy
Hepatitis B or C
(cryoglobulinemia) virus,human immunodeficiencyvirus
Infection
Autoimmune disease
Medication allergy or directmast cell degranulation
Pruritic urticarial papulesand plaques of pregnancy
Autoimmune progesteronedermatitis
Cholinergic urticaria
Hypothyroidism
Parasitic or other infection
Lymphoma
Urticarial vasculitis(Figures 7 and 8)
information from references 4, 7, 8, 74, and 15.
720 American Family Physician www.aafp.orglafp
illnesses. Sexual history, illicit drug use his-tory, and transfusion history may provideimportant information about the risk ofinfectious causes, such as viral hepatitis andhuman immunodeficiency virus.
The physical examination should includevital signs, identification and characteriza-tion of current lesions and their completeextent, testing for dermatographism (i.e.,urticaria that appears in the pattern oflocal-ized pressure elicited by stroking with theblunt end ofa pen or tongue blade), and car-
diopulmonary examination to help rule outanaphylaxis and infectious causes. Exami-nation of the eyes, ears, nose, throat, lymphnodes, abdomen, and musculoskeletal sys-
tem may help identify underlying causes.
Table 2 lists clinical clues from the historyand physical examination that suggest cer-
tain etiologies for urticaria.“'7'3"“5It is critical to rule out anaphylaxis, which
has findings or symptoms involving otherorgan systems beyond the skin, such as thepulmonary (wheezing, stridor), cardiovascu-lar (tachycardia, hypotension), gastrointesti-nal (diarrhea, vomiting, abdominal pain), or
nervous system (dizziness).2"'9 Several der-matologic conditions can be confused withurticaria. Elements of the history and physi-cal examination can help distinguish amongthese conditions (Table 3).“'7'“5
Laboratory workup in the absence of indi-cations of an underlying cause is not neces-
sary.“"‘ lfthe history or physical examinationsuggests a specific cause or underlying dis-ease, targeted testing is appropriate.2"‘*°"‘ Forexample, presentation that suggests urticar-ial vasculitis should prompt a skin biopsy,whereas if the history suggests an allergictrigger, allergy testing may be useful afterresolution of symptoms. With chronic urti-caria, or in acute cases if there are patientor parental concerns, a limited nonspecificworkup including a complete blood countwith differential, erythrocyte sedimentationrate and/or C-reactive protein testing, liverenzymes, and thyroid-stimulating hormonemeasurement can be considered to rule outunderlying causes. When the history sug-gests a physical urticaria, challenge test-ing with standardized physical stimuli can
Volume 95, Number 11 ' lune 1, 2017

confirm the diagnosis.""7 Allergy testing is
not recommended unless there is specificindication of an allergic cause.‘
General Principles of TreatmentMethods of treatment for urticaria are thesame for adults and children. The mainstayof treatment is avoidance of identified trig-gers. It is also recommended that patientsavoid using aspirin, alcohol, and NSAIDS, as
well as avoid wearing tight clothing, because
these may worsen symptoms. Iftrigger avoid-ance is impossible, no trigger is identified,or symptom relief is needed despite triggeravoidance, H,—antihistamines are first—line
pharmacotherapy. Second—generation H,antihistamines such as loratadine (Clari-tin), desloratadine (Clarinex), fexofenadine(Allegra), cetirizine (Zyrtec), and levoceti-rizine (Xyzal) are relatively nonsedating at
standard dosages and are dosed once per day.
First-generation H, antihistamines, such
as diphenhydramine (Benadryl), hydroxy-zine, chlorpheniramine, and cyprohepta-dine, are faster acting and, in some cases,
have parenteral forms. However, they requiremore frequent dosing and have more adverse
effects, including sedation, confusion, dizzi-ness, impaired concentration, and decreased
psychomotor performance. Because of anti-cholinergic adverse effects, first—generation
H, antihistamines should be used with cau-
tion in older patients. Individual responsesto a given antihistamine vary, and there is
no strong evidence that a particular antihis-tamine is superior. Potential adverse effectsshould be discussed with patients before ini-tiating therapy.
TREATMENT OF ACUTE URTICARIA ANDANGIOEDEMA
Second—generation H, antihistamines are
first—line medication for the treatment ofacute urticaria. In some cases, they may betitrated to two or even four times the nor-
mal dose to control symptoms.“-9 Withhigher doses, there is greater possibility ofadverse effects.
If symptoms are not sufficiently con-
trolled with second-generation H, antihista-mines, H, antihistamines such as cimetidine
June 1, 2017 ' Volume 95, Number 11
(Tagamet), famotidine (Pepcid), and raniti-dine (Zantac) may be added.” In severe
cases, corticosteroids such as prednisone or
prednisolone (0.5 to 1 mg per kg per day)may be added for three to 10 days to controlsymptoms.“-9""
If systemic symptoms are suggested, espe-
cially when an identified trigger is associatedwith anaphylaxis (e.g., insect envenomation,certain foods), it may be prudent to pre-scribe epinephrine autoinjectors in sufficientnumbers so that the patient will have one
for home, one for work or school, and one
for the car, as appropriate. Patients should
Urticaria
Table 3. Conditions That May Be Confused with Urticaria
Condition Distinguishing characteristics
Arthropod bites
Atopic dermatitis
Bullous pemphigoid
Contact dermatitis
Erythema multiforme
Fixed-drug reactions
Henoch-Schonleinpurpura
Mastocytoma
Mastocytosis, diffusecutaneous
Morbilliform drugreactions
Pityriasis rosea
Urticaria pigmentosa
Viral exanthem
Lesions lasting several days, insect exposure history
Maculopapular, scaling, characteristic distribution
Lesions lasting more than 24 hours, blistering, Nikolskysign (light friction causes erosion or vesicle)
Indistinct margins, papular, persistent lesions,
epidermal component present
Lesions lasting several days, iris-shaped papules, targetappearance, may have fever
Offending drug exposure, not pruritic, often bullous,hyperpigmentation
Lower extremity distribution, purpuric lesions, systemicsymptoms
Yellow to orange pigmentation, Darier sign (a wheeland flare-up reaction produced by stroking the lesion),flushing, bullae, occurs most commonly in children
Normal to ye||ow—brown skin color, diffuse thickening,bullae
Maculopapular, associated with medication use
Lesions lasting weeks, herald patch, Christmas treepattern, often not pruritic
Smaller lesions (1 to 3 mm), orange to brownpigmentation, Darier sign (a wheel and flare-upreaction produced by stroking the lesion)
Not pruritic, prodrome, fever, maculopapular lesions,individual lesions lasting days
Information from references 4, 7, 8, and 15.
www.aafp.org/afp American Family Physician 721
Urticaria
722 American Family Physician
follow up in two to six weeks to evaluatetreatment success and tolerance.
Treatment of acute angioedema is largelythe same as treatment for urticaria, althoughcorticosteroids may be more commonly rec-
ommended.” However, angioedema of thelarynx and massive angioedema ofthe tongueare medical emergencies because of therisk of airway obstruction, and they requireintramuscular epinephrine and airway man-
agement. Patients with angioedema that pre-viously threatened airway compromise shouldbe prescribed epinephrine autoinjectors.
TREATMENT OF CHRONIC URTICARIA
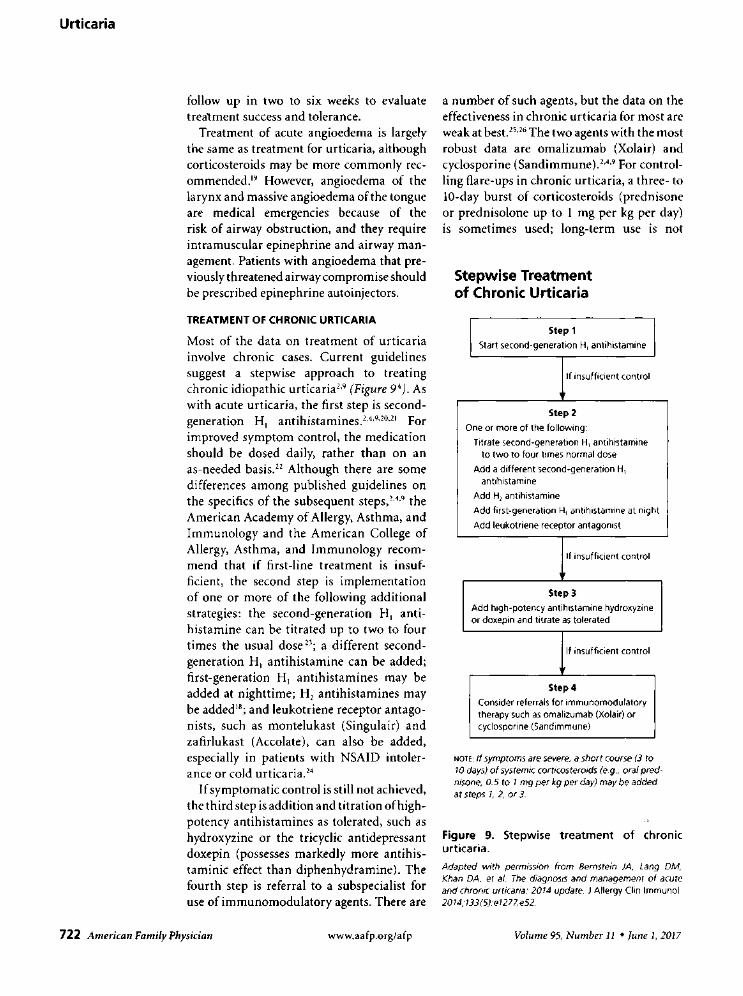
Most of the data on treatment of urticariainvolve chronic cases. Current guidelinessuggest a stepwise approach to treatingchronic idiopathic urticaria” (Figure 9‘). Aswith acute urticaria, the first step is second-generation H, antihistamines."‘*°"°"‘ Forimproved symptom control, the medicationshould be dosed daily, rather than on an
as—needed basis." Although there are some
differences among published guidelines on
the specifics of the subsequent steps,“" theAmerican Academy of Allergy, Asthma, andImmunology and the American College ofAllergy, Asthma, and Immunology recom-
mend that if first-line treatment is insuf-ficient, the second step is implementationof one or more of the following additionalstrategies: the second—generation H, anti-histamine can be titrated up to two to fourtimes the usual dose 2’; a different second-generation H, antihistamine can be added;first-generation H, antihistamines may be
added at nighttime; H, antihistamines maybe added”; and leukotriene receptor antago-nists, such as montelukast (Singulair) andzafirlukast (Accolate), can also be added,especially in patients with NSAID intoler-ance or cold urticaria."
Ifsymptomatic control is still not achieved,the third step is addition and titration ofhigh-potency antihistamines as tolerated, such as
hydroxyzine or the tricyclic antidepressantdoxepin (possesses markedly more antihis-taminic effect than diphenhydramine). Thefourth step is referral to a subspecialist foruse of immunomodulatory agents. There are
www.aafp.org/afp
a number of such agents, but the data on theeffectiveness in chronic urticaria for most are
weak at best.”*’‘ The two agents with the mostrobust data are omalizumab (Xolair) andcyclosporine (Sandimmune).’-"9 For control-ling flare-ups in chronic urticaria, a three- to10-day burst of corticosteroids (prednisoneor prednisolone up to 1 mg per kg per day)is sometimes used; long-term use is not
Stepwise Treatmentof Chronic Urticaria
Step 1
Start second—generation H, antihistamine
If insufficient control
Step 2
One or more of the following:
Titrate second-generation H, antihistamineto two to four times normal dose
Add a different second-generation H,
antihistamine
Add H, antihistamine
Add first-generation H, antihistamine at night
Add leukotriene receptor antagonist
If insufficient control
V
Step 3
Add high-potency antihistamine hydroxyzineor doxepin and titrate as tolerated
lf insufficient control
7
Step 4
Consider referrals for immunomodulatorytherapy such as omalizumab (Xolair) or
cyclosporine (Sandimmune)
NOTE: If symptoms are severe, a short course (3 to70 days) of systemic corticosteroids (e.g., oral pred-nisone, 0.5 to 1 mg per kg per day) may be addedat steps I, 2, or 3.
Figure 9. Stepwise treatment of chronicurticaria.Adapted with permission from Bernstein IA, Lang DM,Khan DA, et al. The diagnosis and management of acuteand chronic urticaria: 2014 update. 1 Allergy Clin lmmunol.20I4,‘733(5):e1277.e52.
Volume 95, Number 11 ' June I, 2017

Urticaria
H, antihistamines, H, antihistamines, andleukotriene receptor antagonists may be addedto control symptoms of chronic urticaria.
EvidenceClinical recommendation rating References Comments
It is important to rule out underlying anaphylaxis C 2,4,9 Evaluate vital signs and symptoms involving otherin patients presenting with urticaria. organ systems such as pulmonary, cardiovascular,
neurologic, or gastrointestinal.
An extensive laboratory workup for urticaria is C 2, 4, 9, 16 Complete blood count with differential, erythrocytenot generally recommended. Additional testing sedimentation rate or C-reactive protein, thyroid-can be performed if the presentation suggests stimulating hormone, urinalysis, and liver functionunderlying causes requiring confirmation. tests can be considered.
Second-generation H, antihistamines are safe A 2,4, 9, 19,20 Second-generation H, antihistamines are recommendedand effective symptomatic therapy for urticaria. over older antihistamines because of adverse effect
profiles. All H, antihistamines appear to be effective.
If needed to control symptoms of urticaria, C 2, 4, 9 A higher risk of adverse effects is present with highersecond-generation H, antihistamines can be doses. Limited effectiveness data are available.titrated to two to four times the normal dose.
A short course of systemic corticosteroids may C 2, 4, 9 Few clinical data support this recommendation, but ithelp control severe cases of urticaria. is widely practiced.
Other medications such as first-generation B 2, 4, 9 Several studies have produced varying results, butthese are generally safe medications with some
evidence of benefit.
A = consistent, good—quality patient—or/ented evidence,’ B = inconsistent or limited—qua/ity patient-oriented evidence; C = consensus, disease—oriented
evidence, usual practice, expert opinion, or case series. For information about the SORT evidence rating system, go to http://www.aat’p.org/afpsort.
recommended because of adverse effects.Potent topical corticosteroids may have a ben-efit in localized delayed-pressure urticaria."
Once symptoms are adequately controlled,physicians should consider stepping downtreatment sequentially. Empiric eliminationdiets are not recommended. Ifan underlyingcause of chronic urticaria is identified, thecondition should be treated or the patientreferred to an appropriate subspecialist.
PrognosisAcute urticaria is typically self—limited andresolves with proper avoidance of triggers.With chronic urticaria, a prospective cohortstudy found that 35% of patients are symp-tom free within one year, with another 29%having some reduction ofsymptoms. Sponta-neous remission occurred within three years
in 48% of the cases of idiopathic chronicurticaria, but only 16% of the cases of physi-cal urticaria.” Another prospective studyin children found remission rates at one,three, and five years to be 18%, 54%, and68%, respectively.” Patients may experiencerepeated episodes throughout their lives.
lune I, 2017 ’ Volume 95, Number 11
This article updates previous articles on this topic by
Schaefer‘ and Muller.”
Data Sources: A search was conducted in PubMedClinical Queries using urticaria with each category and
systematic review. Also searched were the Agency forHealthcare Research and Quality Evidence Reports,
Cochrane Database of Systematic Reviews (completereviews), Dynamed, Essential Evidence Plus, Institute forClinical Systems Improvement, National Guideline Clear-
inghouse, and UpToDate. Search dates: February to May2016, and January 2017.
The AuthorPAUL SCHAEFER, MD, PhD, is vice chair and associate pro-fessor in the Department of Family Medicine and assistantdean for student affairs at the University of Toledo (Ohio)College of Medicine and Life Sciences.
Address correspondence to Paul Schaefer, MD, PhD, Uni-versity of Toledo Health Sciences Campus, MS 1179, 2240Dowling Hall, 3000 Arlington Ave., Toledo, OH 43614(e—mail: [email protected]). Reprints are notavailable from the author.
REFERENCES
1. Hay RJ, Johns NE, Williams HC, et al. The global burdenof skin disease in 2010: an analysis of the prevalenceand impact of skin conditions. J Invest Dermatol. 2014;134(6):1527-1534.
2. Powell RJ, Leech SC, Till S, et al. BSACI guideline for the
www.aafp.org/afp American Family Physician 723

Urticaria
10.
724 American Family Physician
management of chronic urticaria and angioedema. ClinExp Allergy. 2015;45(3):547—565.
. Hellgren L. The prevalence of urticaria in the total popu-lation. Acta Allergol. 1972;27(3):236-240.
. Bernstein JA, Lang DM, Khan DA, et al. The diagnosisand management of acute and chronic urticaria: 2014update. .IAIlergy Clin Immunol. 2014;133(5):1270-1277.
. Sokol CL, Barton GM, Farr AG, Medzhitov R. A mecha-nism for the initiation of allergen-induced T helper type2 responses. Nat Immunol. 2008;9(3):310-318.
. Konstantinou GN, Asero R, Ferrer M, et al. EAACI task-force position paper: evidence for autoimmune urticariaand proposal for defining diagnostic criteria. Allergy.2013;68(1):27-36.
. UpToDate. New-onset urticaria. http://www.uptodate.com/contents/new-onset-urticariarequired]. Accessed February 1, 2016.
[subscription
. Schaefer P. Urticaria: evaluation and treatment. Am Fam
Physician. 2011;83(9):‘l078-1084.
. Zuberbier T, Aberer W, Asero R, et al.; European Acad-emy of Allergy and Clinical immunology; Global Allergyand Asthma European Network; European Dermatol-ogy Forum; World Allergy Organization. The EAACl/GA(2) LEN/EDF/WAO Guideline for the definition, clas-
sification, diagnosis, and management of urticaria: the2013 revision and update. Allergy. 2014;69(7):868-887.
Sackesen C, Sekerel BE, Orhan F, Kocabas CN, Tuncer A,Adalioglu G. The etiology of different forms of urticariain childhood. Pediatr Dermatol. 2004;21(2):102-108.
. Magerl M, Altrichter S, Borzova E, et al. The defini-tion, diagnostic testing, and management of chronicinducible urticarias - The EAACI/GA(2) LEN/EDF/UNEV
consensus recommendations 2016 update and revision.Allergy. 2016;71(6):780-802.
.Confino-Cohen R, Chodick G, Shalev V, Leshno M,Kimhi O, Goldberg A. Chronic urticaria and autoim-munlty: associations found in a large population study.JAI/ergy Clin Immunol. 2012;129(5):1307-1313.
. Kulthanan K, Jiamton S, Thumpimukvatana N, Pinkaew5. Chronic idiopathic urticaria: prevalence and clinicalcourse. J Dermatol. 2007;34(5):294-301.
. Peroni A, Colato C, Zanoni G, Girolomoni G. Urticariallesions: if not urticaria, what else? The differential diag-nosis of urticaria: part II. Systemic diseases. J Am AcadDermatol. 2010;62(4):5S7-S70.
. Peroni A, Colato C, Schena D, Girolomoni G. Urticariallesions: if not urticaria, what else? The differential diag-nosis of urticaria: part I. Cutaneous diseases. J Am AcadDermatol. 2010;62(4):541-555.
. Kozel MM, Bossuyt PM, Mekkes JR, Bos JD. Laboratorytests and identified diagnoses in patients with physicaland chronic urticaria and angioedema: a systematicreview. J Am Acad Dermatol. 2003;48(3):409-416.
www.aafp.org/afp
18.
19.
20.
21.
22.
23.
24.
25.
26.
27.
28.
30.
. Trevisonno J, Balram B, Netchiporouk E, Ben-ShoshanM. Physical urticaria: review on classification, triggersand management with special focus on prevalenceincluding a meta-analysis. Postgrad Med. 2015;127(6):565-S70.
Fedorowicz Z, van Zuuren EJ, Hu N. HistamineH2-receptor antagonists for urticaria. Cochrane Data-base Syst Rev. 2012;(3):CD008596.
Pollack CV Jr, Romano Tl. Outpatient management ofacute urticaria: the role of prednisone. Ann Emerg Med.1995;26(5):547-S51.
Sharma M, Bennett C, Carter 8, Cohen SN.
H1-antihistamines for chronic spontaneous urticaria:an abridged Cochrane Systematic Review. J Am AcadDermatol. 2015;73(4):710-716.e4.
Kavosh ER, Khan DA. Second-generationH1-antihistamines in chronic urticaria: an evidence-based review. Am J Clin Dermatol. 2011;12(6):361-376.
Grob JJ, Auquier P, Dreyfus I, Ortonne JP. How to pre-scribe antihistamines for chronic idiopathic urticaria:desloratadine daily vs PRN and quality of life. Allergy.2009;64(4):605-612.
Guillén-Aguinaga S, Jauregui Presa I, Aguinaga-OntosoE, Guillén-Grima F, Ferrer M. Updosing nonsedatingantihistamines in patients with chronic spontaneousurticaria: a systematic review and meta-analysis. Br J
Dermatol. 2016;17S(6):1153-1165.
de Silva NL, Damayanthi H, Rajapakse AC, RodrigoC, Rajapakse S. Leukotriene receptor antagonists forchronic urticaria: a systematic review. Allergy AsthmaClin Immunol. 20l4;10(l):24.Morgan M, Khan DA. Therapeutic alternatives forchronic urticaria: an evidence-based review, part 2. AnnAllergy Asthma Immunol. 2008;100(6):51 7-S26.
Mitchell 5, Balp MM, Samuel M, McBride D, Maurer M.Systematic review of treatments for chronic spontane-ous urticaria with inadequate response to licensed first-line treatments. Int} Dermatol. 2015;54(9):1088-1104.
Vena GA, Cassano N, D'Argento V, Milani M. C|obeta-sol propionate 005% in a novel loam formulationis safe and effective in the short-term treatment ofpatients with delayed pressure urticaria: a randomized,double-blind, placebo-controlled trial. Br J Dermatol.2006;154(2):353-356.
Kozel MM, Mekkes JR, Bossuyt PM, Bos JD. Naturalcourse of physical and chronic urticaria and angio-edema in 220 patients. I Am Acad Dermatol. 2001;45(3):387-391.
. Chansakulporn S, Pongpreuksa S, Sangacharoenkit P, etal. The natural history of chronic urticaria in childhood:a prospective study. J Am Acad Dermatol. 2014;71(4):663-668.
Muller BA. Urticaria and angioedema: a practicalapproach. Am Fam Physician. 2004;69(5):1123-1128.
Volume 95, Number 11 ° lune 1, 2017