Embed Size (px)
Citation preview
Original Studies
Acute and Late Outcome After Use of 2.5-mmIntracoronary Stents in Small ( F 2.5 mm)
Coronary Arteries
Paul Huang, MD, Thomas Levin, MD, Ameer Kabour, MD, and Ted Feldman, * MD
We describe the high-pressure deployment of 2.5-mm stents in small ( F 2.5 mm) coronaryvessels. Forty-three lesions in 40 patients were treated. The mean reference vesseldiameter was 2.3 6 0.2 mm. The mean % luminal stenosis was 90 6 9. The mean lesionlength was 11.7 6 9.1 mm. Sixteen lesions were pretreated with rotational atherectomy,and the remainder with PTCA. The rate of successful stent deployment was 41/43(95%). The mean postintervention % stenosis was -1 6 10. There were no in-hospitaldeaths or procedure-related Q-wave MI. The patients were followed for a mean of18 months. Eight patients (or 21%) developed recurrent chest pain and/or angio-graphically proven restenosis. One patient (3%) developed intermediate restenosis.Twenty-nine patients (or 76%) either remain symptom-free or have patent target siteson repeat angiography. It appears that reasonable acute and long-term results canbe achieved with 2.5-mm stents in small coronary arteries using high-pressuredeployment techniques. Cathet. Cardiovasc. Intervent. 49:121–126, 2000.r 2000 Wiley-Liss, Inc.
Key words: angioplasty; atherectomy; restenosis
INTRODUCTION
The use of stents has revolutionized percutaneouscoronary revascularization. Stenting has proved invalu-able in the treatment of suboptimal or failed percutaneoustransluminal coronary angioplasty (PTCA), acute vesselclosure, restenotic lesions, and bypass graft lesions [1–8].While stents for vessels larger than 3.0 mm in diameter havelower angiographic and clinical recurrence ratescomparedwith balloon angioplasty, the technique is limited by muchhigher rates of in-stent restenosis in smaller arteries[9,10].Several factors appear most predictive of restenosis. Amongthem are reference vessel diameter (RVD), lesion length,whether a lesion is restenotic, and the presence of diabetesmellitus [11].
There are many reports of stent outcomes in vessels,3.0 mm. Some experience has been described for bailoutuse of 2.5-mm stents and for the use of 3.0-mm stents invessels with RVD, 3.0 mm [12,13]. However, relativelylittle has been reported on the use of 2.5-mm stents invessels with RVD, 2.5 mm. We describe our experiencein the deployment of 2.5-mm stents in such target vesselsusing high-pressure deployment.
MATERIALS AND METHODS
Between January of 1995 and October of 1997, 40consecutive patients with evidence of myocardial isch-emia or injury and diseased coronary vessels with RVD,2.5 mm were treated with one or more 2.5-mm Gianturco-Roubin (Cook, Bloomington, IN) intracoronary stents.Their clinical follow-up, both acute and long-term, isincluded in our report.
All angiographic measurements were determined byhand-held calipers using selected cine frames at end-diastole, which showed the worst view without overlapand with the least degree of foreshortening as previouslydescribed [14,15]. The centered contrast-filled guidingcatheter was used for calibration. Lesion morphology wasclassified according to the modified American College of
Hans Hecht Hemodynamics Laboratory, Pritzker School of Medi-cine, the University of Chicago Hospital, Chicago, Illinois
*Correspondence to: Dr. Ted Feldman, the University of ChicagoHospital, 5841 S. Maryland Avenue, MC 5076, Chicago, IL 60637.
Received 7 June 1999; Revision accepted 17 August 1999
Catheterization and Cardiovascular Interventions 49:121–126 (2000)
r 2000 Wiley-Liss, Inc.
Cardiology/American Heart Association (ACC/AHA)grading system [16].
All of the patients were followed longitudinally. Thedischarge summaries for all subsequent admissions wereobtained, as were reports of all follow-up stress tests. Allof the patients were interviewed by telephone. Data withregard to symptom recurrence, functional status, rehospi-talization, stress testing, and revascularization were col-lected.
The following definitions were used in the study.Suboptimal results indicate a. 50% residual stenosisafter primary treatment (PTCA or rotational atherec-tomy). Acute vessel closure indicates complete occlusionof a previously treated arterial segment with Thromboly-sis in Myocardial Infarction (TIMI) grade 0 or 1 flowwithin 48 hr of the intervention. Threatened vesselclosure indicates the presence of a significant dissectionand/or recoil with. 50% residual stenosis and TIMI I/IIflow or clinical evidence of active ischemia, includingpersistent angina and ST segment changes on ECG.
RESULTS
Patient Characteristics
Of the 40 patients studied, there were 24 men (60%)and 16 women (40%; Table I). Twenty-six patients (65%)were white and 14 (35%) were black. The mean age was
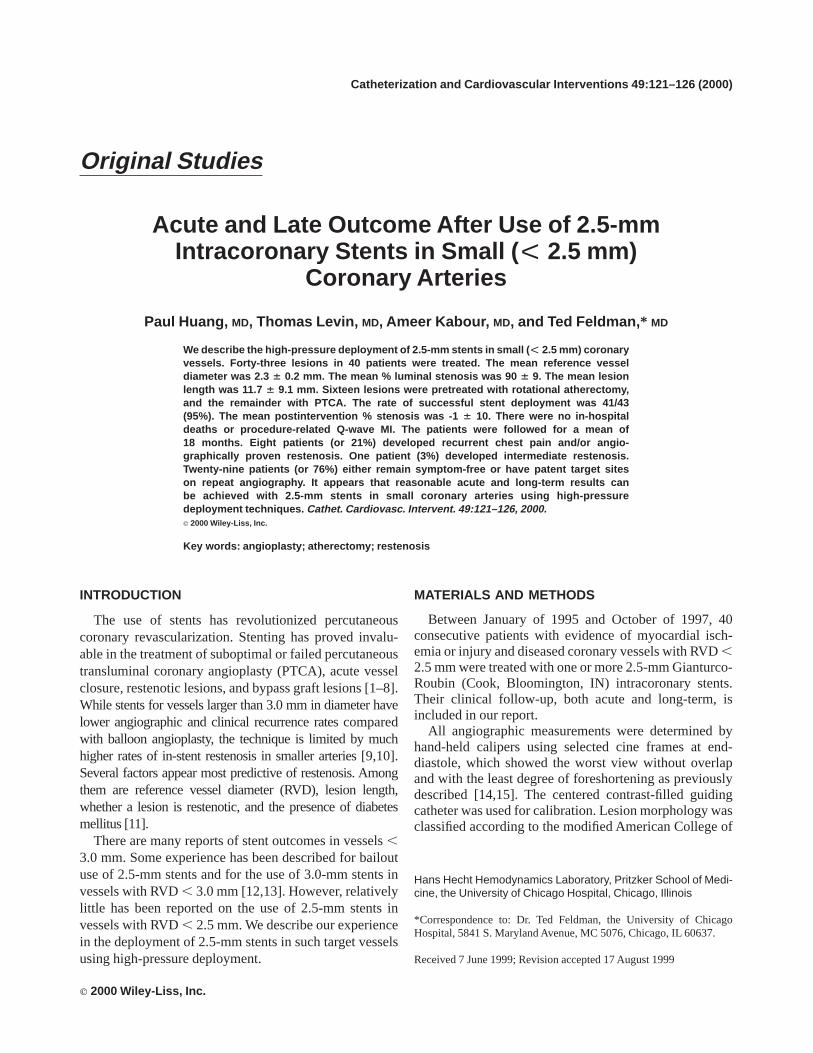
Fig. 1. An 83-year-old woman presented with a long LAD stenosis seen in the upper left portionof the figure (arrows). After rotational atherectomy, there was a smooth lumen with a modestcaliber. Three months later she was admitted with restenosis and underwent angioplasty andplacement of a 2.5-mm GR 1 stent. Restenosis occurred 5 months later and was treated withballoon angioplasty. On the right hand panel, after 2.5 years, the stented segment of the mid LADremains widely patent.
TABLE I. Patient Characteristics (Total 5 40)
VariablesNumber of
patients Percent
Male:female ratio 24:16 60:40Hypertension 23 58Diabetes mellitus 14 35Hyperlipidemia 20 50Smoking 20 50Previous CABG 7 18Three-vessel disease 11 27Two-vessel disease 12 30One-vessel disease 10 25LVEF .0.5 21 52More than one lesion treated 21 52
122 Huang et al.
62 years (range, 39–83 years). The incidence of hyperten-sion was 58% (23/40), diabetes mellitus 35% (14/40),hyperlipidemia 50% (20/40), tobacco smoking 50% (20/40). Seven patients (18%) had previous CABG, 11 (27%)had three-vessel disease, 12 (30%) had two-vessel dis-ease, and 10 (25%) had one-vessel disease. The leftventricular ejection fraction as determined by ventriculog-raphy was greater than 50% in 21 patients (52%) andbetween 30% and 50% in 19 patients (48%).
Lesion Characteristics
Twenty-one patients had more than one lesion treatedduring the index percutaneous coronary revascularization(Table II). In three of these patients, both lesions treatedhad RVD, 2.5 mm. A total of 43 lesions were treated.Forty-two lesions were in native vessels and one was in asaphenous vein graft. Stenting was elective in 21 lesions,for suboptimal primary treatment results in 11, and foracute or threatened vessel closure in 8. Three patientsreceived stents after primary percutaneous transluminalcoronary angioplasty (PTCA) for acute myocardial infarc-tion. In 10 patients, stents were deployed to treat lesionrestenosis.
Three of the lesions (7%) were type A by ACC/AHAclassification, 11 (25%) B1, 14 (33%) B2, and 15 (35%)C. TIMI 3 flow was present in 10 of the lesions (23%).Sixteen lesions (37%) had TIMI 2 flow, 7 lesions (17%)TIMI 1 flow, 10 lesions (23%) no flow. The mean RVDwas 2.2 6 0.2 mm (range, 1.7–2.4 mm). The meanbaseline minimal luminal diameter was 0.26 0.2 mm.The mean % luminal stenosis was 906 9. The meanlesion length was 11.76 9.1 mm (range, 1.7–40 mm).
Fourteen lesions (33%) were in the LAD, five (12%) inthe diagonal artery, one (2%) in the ramus intermediusartery, six (14%) in the circumflex artery, four (9%) in theobtuse marginal artery, nine (21%) in the RCA, three(7%) in the posterior descending artery, and one (2%) in asaphenous vein graft to the posterior ventricular branch.
Coronary Intervention
Sixteen lesions (37%) were pretreated with rotationalatherectomy, the remainder (63%) with PTCA. Twenty-three 12-mm-long stents and 26 20-mm-long stents wereplaced (44 GR 1 and 5 GR 2). Six lesions (14%) weretreated with deployment of two overlapping stents. Forpoststent dilatation, the mean balloon diameter used was2.6 mm (range, 2.5–3.0 mm). The mean maximumpressure was 156 2 atm (range, 10–20 atm). The ratio ofballoon to reference vessel diameter was 1.26 0.1(range, 1.0–1.6). Twenty-three patients received ticlopi-dine (250 mg b.i.d. for 2 weeks) after stent implantation.We did not rely on intravascular ultrasound guidance inthe deployment of any of the stents.
Acute Outcome
The procedural success rate was 95% (41 of 43 lesions;Table III). One 2.5/12-mm stent could not be delivered toa diagonal artery where PTCA was complicated by vesselperforation distally requiring protamine administrationand prolonged balloon inflation, which resulted in aflow-limiting dissection proximally. Urgent bypass sur-gery was performed in one patient in whom rotationalatherectomy of an ostial LAD lesion was complicated bya flow-limiting dissection that extended to the firstdiagonal artery and in whom bailout stenting with a2.5/12-mm stent failed to reestablish flow. Both patientsdid well subsequently.
In the remaining 41 lesions, the mean postinterventionminimal luminal diameter was 2.36 0.3 mm. The mean% luminal stenosis after coronary intervention was21 610 (range,219 to 32). In each case, coronary blood flowimproved after stent placement. TIMI 2 flow was presentin five of the vessels (12%) and TIMI 3 flow was presentin the remaining vessels (88%). There were no hospitaldeaths or Q-wave myocardial infarctions.
Long-Term Follow-Up
The 38 patients in whom initial stent deployment weresuccessful were followed for 206 7 months (range,8–35). There were no deaths or Q-wave myocardialinfarctions. Thirteen patients (14 lesions or 34%) had atleast one follow-up coronary angiography because ofrecurrent angina. Repeat cardiac catheterization wasperformed, on average, 4 months after the initial interven-tion (range, 1–20 months). Eight patients (eight lesions or
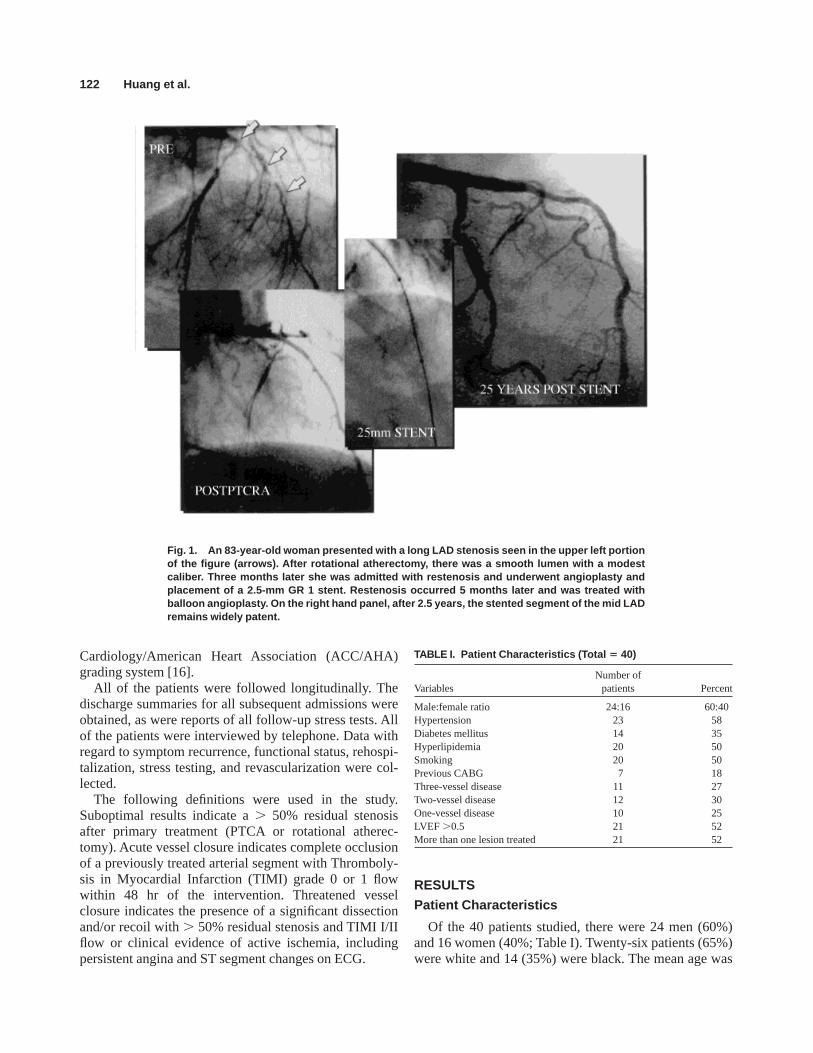
TABLE II. Lesions Characteristics (Total 43)
VariablesNumber of
lesions Percent
Native vessels 42 98Type A 3 7Type B1 11 25Type B2 14 33Type C 15 35Lesion length$15 mm 11 25LAD 14 33LCX 6 14RCA 9 21Restenotic lesions 10 23
TABLE III. Pr ocedural Outcome
Procedural success 41%/43%Mean RVD 2.26 0.2 mmMean MLD prestent 0.26 0.12 mmMean % stenosis prestent 906 9Mean maximal inflation pressure 156 2 atmBalloon diameter, RVD 1.26 0.1Mean MLD poststent 2.36 0.3 mmMean % stenosis poststent 21 6 10
Stents for Small Vessels 123
20%) had developed significant restenosis (mean, 92% –7%; range, 85%–100%). Four of these patients underwentCABG because of multivessel disease. Three patientsunderwent PTCA for treatment of in-stent restenosis andhave done well without recurrent angina. One patient(repeat angiography was performed at 20 months) haddeveloped extensive collateral flow and therefore did notundergo repeat intervention. One lesion had developed a49% restenosis. This patient also developed significantatherosclerotic lesions in other vessels as well andunderwent a three-vessel CABG after the repeat catheter-ization. In the remaining four patients (five lesions), nosignificant restenosis (, 10%) was noted on repeatcatheterization. In these patients, chest pain was eithernoncardiac (one patient) or due to lesions in other vessels(three patients).
In two patients, exercise stress perfusion scintigraphywas performed for routine follow-up. In each case, nosignificant reversible ischemia was noted in the targetvessel distribution. In one other patient, a dobutaminestress echocardiography performed as part of preopera-tive evaluation revealed no regional wall motion abnor-mality suggestive of ischemia. In the remaining 22patients (24 lesions), clinical follow-up revealed noevidence of recurrent ischemia.
In summary, of the 41 lesions (38 patients) in whichinitial stent deployment had been successful, 32 lesions(78%) in 29 patients did not show any evidence ofclinically significant restenosis. Eight lesions (20%) ineight patients developed significant restenosis. One lesion(2%) in the remaining patient developed intermediaterestenosis.
Analysis of Lesion Restenoses
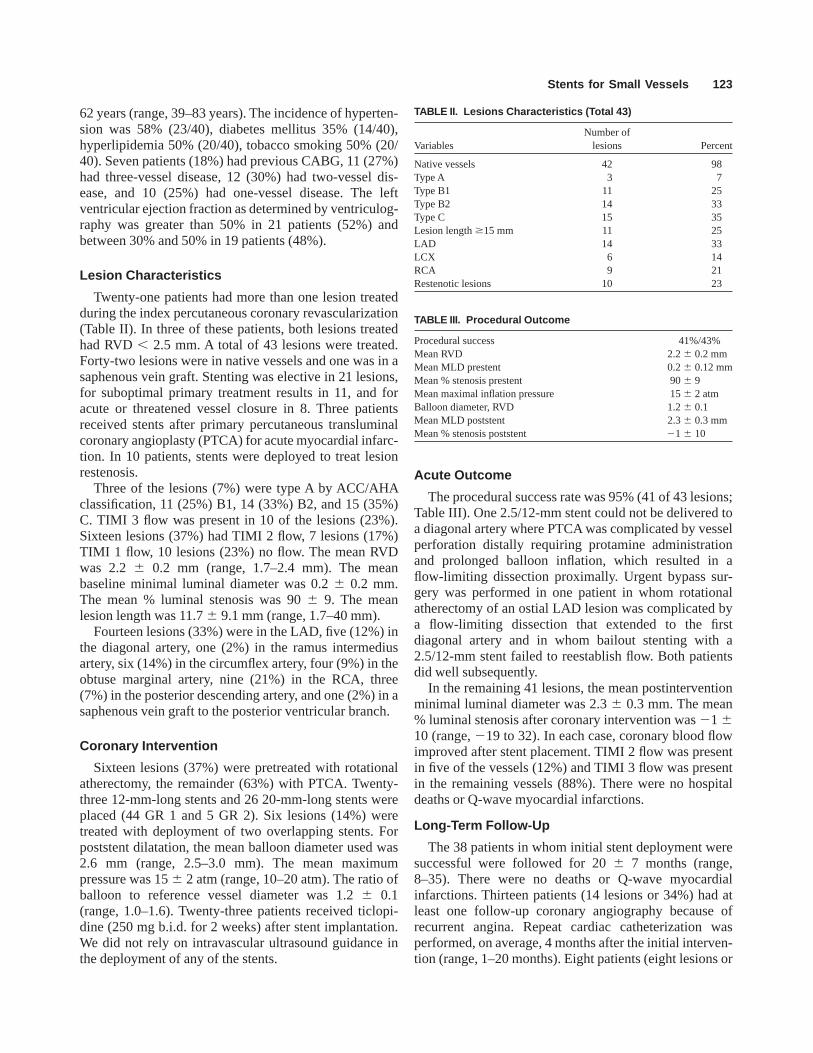
Table IV summarizes the patients whose coronarylesions developed significant angiographic restenosisafter deployment of 2.5-mm intracoronary stents . Amongthe eight patients who developed restenosis, seven werediabetic. Four patients had lesion length greater than
15 mm and two greater than 30 mm. Five of the lesionswere B2 or C. Three of the lesions were restenotic. Fiveof the lesions were pretreated with rotational atherec-tomy. Seven patients received GR 1 stents and onereceived a GR 2 stent.
In contrast, none of the four patients without angio-graphic restenosis were diabetic. All of the lesions wereshorter than 10 mm. None were restenotic. All fourpatients received GR 1 stents.
DISCUSSION
One of the most important predictors of in-stentrestenosis is reference vessel diameter. In a study byAgrawal et al. [9], in-stent restenosis occurred morefrequently in patients who received 2.0- or 2.5-mmGianturco-Roubin stents than those who received largerstents (13% vs. 2%;P 5 0.0002). George et al. [6]reported a 25% stent thrombosis rate in patients whoreceived 2.0-mm Gianturco-Roubin stents vs. 0% rate inthose who received 4.0-mm stents. Rozenman et al. [10]reported a higher incidence of in-stent restenosis insmaller (, 3.0 mm) vessels in a small series of patientsreceiving Palmaz-Schatz stents. Even though the use ofantiplatelet therapy such as glycoprotein IIb/IIIa recep-tors (abciximab, tirofiban, and integrellin) and ADPreceptor antagonists (ticlopidine and clopidogrel) mostlikely will decrease the risk of in-stent thrombosis,deployment of stents in small coronary vessels remains achallenging task. Many vessels with RVD, 3.0 mm, andespecially those with RVD, 2.5 mm, are not electivelystented. If stent deployment is desired in these vessels,3.0-mm stents are preferentially used, even with signifi-cant stent oversizing and adventitial stretching.
In this report, we have demonstrated that 2.5-mmintracoronary stents could be safely deployed with highpressure to treat lesions in vessels with RVD, 2.5 mm.All of the lesions studied had RVD, 2.5 mm. Deploy-
TABLE IV. Patients With In- Sent Restenosis
Patient 1 2 3 4 5 6 7 8
DM Y Y Y Y Y N Y YStented vessel Mid LAD Ostial RCA Proximal LAD Distal LAD Distal LCX Proximal Ramus Mid OM Distal RCAOther vessel None LAD None Mid LAD OM LAD None NoneLength (mm) 32 4.6 11.5 5 40 15.6 15.8 4.2Type C B2 B1 A C B1 C B2RVD (mm) 2.0 2.5 2.4 2.1 2.6 2.5 2.5 1.9Restenosis Yes No No Yes Yes No No NoPretreat PTCA PTCRA PTCRA PTCRA PTCRA PTCA PTCRA PTCAPre 100 79 92 86 100 92 100 79Post 210 0 3 219 7 5 0 216F/U catheterization (months) 5 3 20 3 1 3 1 5% restnosis 85 86 99 85 100 90 100 90
124 Huang et al.

ment of 3.0-mm stents in these vessels would have beentechnically difficult and possibly dangerous.
Our patient demographics also include several otherrisk factors for in-stent restenosis in addition to the smallRVD such as high-grade lesions (68% of the lesions beingtype B2 or C), lesion length (mean of 11.2 mm and 10lesions. 15 mm), poor flow (76% with less than TIMI 3flow), diabetes (35%), and restenotic lesions (23%).Seven of the patients (18%) had undergone prior CABGand 23 other patients (57%) had multivessel disease.Sixteen lesions (37%) were complex or long enough torequire debulking with rotational atherectomy.
Acute procedural success was 95%. The two failedcases involved bailout stent deployment. There were noin-hospital deaths or Q-wave myocardial infarctions,even when taking into account the two failed cases. Moreimportantly, long-term follow-up (8 months or more)revealed no deaths or Q-wave myocardial infarction.Only 8 of the 38 remaining patients (21%) developedclinically significant target lesion restenosis. Overlappingstents, a risk factor for restenosis, were used in two ofthese patients. Three were restenotic lesions at the time ofstent deployment. Seven of the patients were diabetic.Five of the lesions in diabetic patients required pretreat-ment with rotational atherectomy.
Our observation represents a small and nonrandomizedstudy. None of the patients received Gp IIb/IIIa antago-nist therapy, and not every patient received ticloipdineafter stent deployment. In addition, only Gianturco-Roubin stents were used. It should be pointed out that 22patients did not have repeat angiography or stress testwith imaging in their clinical follow-up. Ten of thesepatients had one or two other larger vessels revascular-ized at the time of 2.5-mm stent deployment. It may beargued that their symptoms on initial presentation weredue to lesions in the larger vessels and subsequentresolution of angina may not have resulted from treat-ment of lesions in the smaller vessels. Even so, theirexcellent long-term outcome does point to the safety, ifnot convincingly the efficacy, of our management of theirsmall-vessel disease. With the availability of newer-generation stents and more efficacious antiplatelet therapy,one would expect more promising results in the manage-ment of lesions in coronary vessel with RVD, 2.5 mm.
It is sometimes argued that clinical outcomes in smallervessels do not reflect angiographic restenosis becausethese vessels are more likely to occlude silently. Thisstudy includes 33% (14/43) LAD and 63% (27/43) trunkvessels. In addition, all patients had clinical evidence ofactive ischemia prior to intervention. While some branchvessels may indeed restenose or reocclude without symp-toms, this is not a major limitation for this population, asevidenced also by the clinical recurrence of ischemia inpatients needing revascularization.
It is unlikely that any mechanical approach in smallvessels will lead to the kind of low target lesion revascu-larization rate that stents have achieved in vessels largerthan 3-mm diameter [17]. This is especially true in longerlesions and in diabetic patients. At the same time, morethan half of the vessels in some reported populations areless than 3 mm in diameter by angiographic analysis [18].The release of third-generation, 2.5-mm-diameter stentshas resulted in an increase in small-vessel stenting. Sincethese stents have been approved in registries for abrupt orthreatened closure, no long-term follow-up data havecome from them. While the results of the stents in thesmaller vessels remain less than ideal, all of the availabledevices must be used in concert to achieve the bestpossible acute results. Until effective antirestenosis mo-lecular or radiation therapy is available, the best predictorof favorable long-term outcome remains a good acuteresult [19–21]. This has been demonstrated using transle-sional pressure gradients even early during the experiencewith PTCA, and more recently using pressure gradientsand Doppler flow reserve [19–21]. Stents as an adjunct totherapy and smaller vessels will remain useful for sometime.
REFERENCES
1. Sigwart U, Puel J, Mirkovitch V, Joffre F, Kappenberger L.Intravascular stents to prevent occlusion and restenosis aftertransluminal angioplasty. N Engl J Med 1987;316:701–706.
2. Hermann HC, Buchbinder M, Clemen MW, Fischman D, GoldbergS, Leon MB, Schatz RA, Teirstein P, Walker CM, Hirshfield JW.Emergent use of balloon-expandable coronary artery stenting forfailed percutaneous transluminal coronary angioplasty. Circulation1992;86:812–819.
3. Roubin GS, Cannon AD, Agrawal SK, Macander PJ, Dean LS,Baxley WA, Breland J. Intracoronary stenting for acute andthreatened closure complicating percutaneous transluminal coro-nary angioplasty. Circulation 1992;85:916–927.
4. Lincoff AM, Topol EJ, Chapejis AT, George BS, Candela RJ,Muller DW, Zimmermann CA, Ellis SG. Intracoronary stentingcompared with conventional therapy for abrupt vessel closurecomplicating coronary angioplasty: a matched case-control study.J Am Coll Cardiol 1993;21:886–875.
5. Colombo A, Goldberg SL, Almagor Y, Maiello L, Finci L. A novelstrategy for stent deployment in the treatment of acute or threat-ened closure complicating balloon coronary angioplasty. J AmColl Cardiol 1993;22:1887–1891.
6. George BS, Voorhees WD, Roubin GS, Fearnot NE, Pinkerton CA,Raizner AE, King SB, Holmes DR, Topol EJ, Kereiakes DJ,Hartzler GO. Multicenter investigation of coronary stenting totreat acute or threatened closure after percutaneous transluminalcoronary angioplasty: clinical and angiographic outcomes. J AmColl Cardiol 1993;22:135–143.
7. Serruys PW, de Jaegere P, Kiemeneij F, Macaya C, Rutsch W,Heyndrickx G, Emanuelsson H, Marco J, Legrand V, Materne P,Belardi J, Sigwart U, Colombo A, Goy JJ, van den Heuvel P,Delcan J, Morel MA, for the Benestent Study Group. A compari-son of balloon expandable-stent implantation with balloon angio-plasty in patients with coronary artery disease. N Engl J Med1994;331:489–495.
Stents for Small Vessels 125

8. Fischman DL, Leon MB, Baim DS, Schatz RA, Savage MP, PennI,Detre K, Veltri L, Ricci D, Nobuyoshi M, Cleman M, Heuser R,Almond D, Teirstein PS, Fish RD, Colombo A, Brinker J, Moses J,Shaknovich A, Hirshfeld J, Bailey S, Ellis S, Rake R, Goldberg S,for the Stent Restenosis Study Investigators. A randomized com-parison of coronary-stent placement and balloon angioplasty in thetreatment of coronary artery disease. N Engl J Med 1994;331:489–495.
9. Agrawal SK, Ho SW, Liu MW, Iyer S, Hearn JA, Cannon AD,Macander PJ, Dean LS, Baxley WA, Roubin GS. Predictors ofthrombotic complications after placement of the flexible coil stent.Am J Cardiol 1994;73:1216–1219.
10. Rozenman Y, Lotan C, Mosseri M, Gotsman MS. Relation ofthrombotic occlusion of coronary stents to the indication forstenting, stent size, and anticoagulation. Am J Cardiol 1995;75:84–85.
11. Hong MK, Mehran R, Mintz GS, Leon MB. Restenosis aftercoronary angioplasty. Curr Probl Cardiol 1997;22:33–35.
12. Chan CNS, Tan ATH, Koh TH, Koh P, Lau DW, Gunawan SA,Charkraborty B, Ng A. Intracoronary stenting in the treatment ofacute or threatened closure in angiographically small coronaryarteries (, 3.0 mm) complicating percutaneous transluminalcoronary angioplasty. Am J Cardiol 1995;75:23–25.
13. Lau KW, He Q, Ding ZP, Johan A. Safety and efficacy ofangiography-guided stent placement in small native coronaryarteries of, 3.0 mm in diameter. Clin Cardiol 1997;20:711–716.
14. Levin TN, Carroll JD, Feldman T. Bail-out stenting for flowlimiting dissections after rotational atherectomy in complex coro-nary lesions. Cathet Cardiovasc Diagn 1996;37:300–304.
15. Feldman T, Kabour A, Carroll JD, Levin TN. Improved techniquefor use of half-stents remounted on a stent delivery system. CathetCardiovasc Diagn 1996;39:17–20.
16. Ellis SG, Vandormael MG, Cowley MJ, Di Sciascio G, DeligonulU, Topol EJ, Bulle TM, Multivessel Angioplasty Prognosis StudyGroup. Coronary morphology and clinical determinants of proce-dural outcome with angioplasty for multivessel coronary disease.Circulation 1990;82:1193–1202.
17. Feldman T. Smaller isn’t bigger. Cathet Cardiovasc Diagn 1998;43:271–272.
18. Feldman T. Is bigger always better in arterial intervention: smallerisn’t bigger. J Invasive Cardiol 1998;10:521–525.
19. Anderson HV, Roubin GS, Leimbruger PP, Cox WR, Douglas JSJr, King SB III, Gruentzig R. Measurement of transstenoticpressure gradient during percutaneous transluminal coronary angio-plasty. Circulation 1986;73:1223–1230.
20. Martinez CA, Froidcoaur M, Mathus F, Tilman CS, Belgium L.Kubertus HE. Quantitative angiographic results after coronaryangioplasty can predict early and long-term outcome. Circulation1997;96(Suppl 1):136.
21. Serruys PW, di Mario C, Piek J, Schroeder E, Vrints C, Probst P, deBruyne B, Hanet C, Fleck E, Haude M, Verna E, Voudris V,Geschwind H, Emanuelsson H, Muhlberger V, Danzi G, Peels HO,Ford AJ, Boersma E, for the DEBATE study group. Prognosticvalue of intracoronary flow velocity and diameter stenosis inassessing the short and long term outcomes of coronary balloonangioplasty: the DEBATE study (Doppler Endpoints BalloonAngioplasty Trial in Europe). Circulation 1997;96:3369–3377.
126 Huang et al.














![Teknisk brochure - Krah Pipes€¦ · Rør dimension DN/ID [mm] s1, PE rør [mm] s1 PP rør [mm] 300 2.0 2.0 400 2.5 2.5 500 2.5 3.0 600 3.3 3.5 800 4.5 4.5 1000 5.0 5.0 > 1200 5.0](https://img.pdfslide.net/doc/110x75/5fd81ad8d972a95d261e3f35/teknisk-brochure-krah-rr-dimension-dnid-mm-s1-pe-rr-mm-s1-pp-rr-mm.jpg)














