Embed Size (px)
Citation preview
Acute Ischemic Stroke: Overcoming
Barriers by Improving Systems of Care
© 2015 Vindico Medical Education
Activity presentations are
considered intellectual property.
• These slides may not be published
or posted online without permission from
Vindico Medical Education
• Please be respectful of this request so
we may continue to provide you with
presentation materials.
Current Tools for the Diagnosis and
Treatment of Acute Ischemic Stroke
Andy Jagoda, MD, FACEP
Professor and Chair of Emergency Medicine
Mount Sinai School of Medicine
New York, NY
Objectives
• Discuss clinical evaluations and the use of
stroke scale tools in decision-making
• Discuss neuro-imaging tools in the
assessment of patients with TIA and acute
stroke
• Discuss care map / protocol tools in
facilitating quality stroke care
Acute Ischemic Stroke: Overcoming
Barriers by Improving Systems of Care
© 2015 Vindico Medical Education
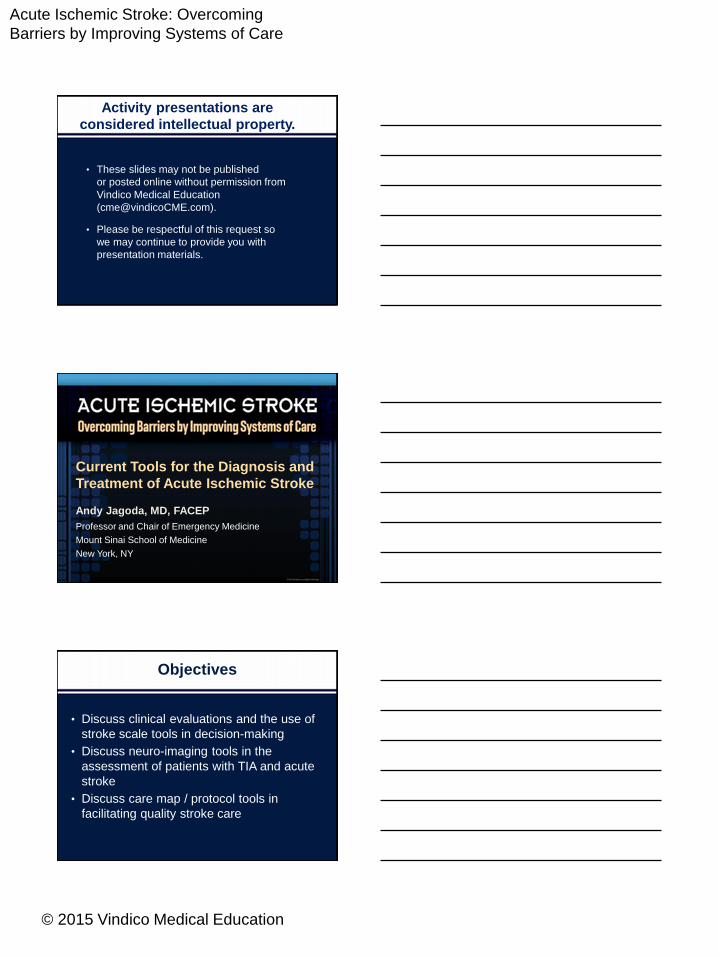
CT Insensitive for StrokeCT is often normal for gross signs of
infarction for the first 6-12 hours, though
subtle, early changes are seen in up to 67%Latchaw RE, et al. Stroke. 2009;40:3646-3678.
Clinical DiagnosisStroke Assessment Tools
Stroke Mimic in about 3% of
Patients Treated with tPAWinkler DT, et al. Stroke. 2009;40:1522-1525.
Scott PA, Silbergleit R. Ann Emerg Med. 2003;42:611-618.
Symptom onset: Date Time
GCS E= M= V
BP / BS: If BS < 60 treat urgently and reassess
Has there been loss of consciousness or syncope? Y (-1) □ N (0) □
Has there been seizure activity? Y (-1) □ N (0) □
Asymmetric facial weakness Y (+1) □ N (0) □
Asymmetric arm weakness Y (+1) □ N (0) □
Asymmetric leg weakness Y (+1) □ N (0) □
Speech disturbance Y (+1) □ N (0) □
Visual field defect Y (+1) □ N (0) □
Total Score _____ (-2 to +5)
Provisional diagnosis: □ Stroke □ Non-stroke (specify) ___________________
* Stroke is likely if total scores are > 0. Scores of ≤ 0 have a low possibility of stroke
but not completely excluded.
Nor AM, et al. Lancet Neurol. 2005;4:727-734.
ROSIER Scale: Stroke Recognition Tool
TIA: ABCD2 Assessment Tool
• 20% to 50% of strokes
preceded by a TIA
• 75% resolve in <15
minutes; 97% <3 hours
• New definition: event lasting
less than 1 hour and not
associated with changes on
neuroimaging
• ABCD2 for risk stratification
Predictor Points
Age > 60 y 1
Blood Pressure >140/90 mm Hg 1
Clinical features (maximum 2)
Unilateral weakness (2)
Speech difficulty without
weakness (1)
2
Duration (maximum 2)
>60 min (2)
10-59 min (1)
<10 min (0)
2
Diabetes 1
Maximum total score 7
Bhatt A, Jani V. ISRN Neurol. 2011; 2011: 518621.
Acute Ischemic Stroke: Overcoming
Barriers by Improving Systems of Care
© 2015 Vindico Medical Education
NIH Stroke Scale Score
• 11 Domains
– 1-5 minor
– 6-20 moderate
– >20 severe
• Stroke scales help quantify the deficit, facilitate
communication, identify location, provide prognosis, direct
testing
• Severe strokes are associated with increased risk of sICH
• “Minor” strokes are a relative contraindication for tPA
– Studies suggest that patients with minor or rapidly improving
deficits may benefit from treatment**
** Smith EE, et al. Stroke. 2005;36:2497-2499.
Posterior Circulation Strokes
• CT misses 60%-90% of acute ischemic strokes in the
brainstem or cerebellum
• MRI with diffusion-weighted imaging is more reliable than
CT, but is still misses 15%-20% of patients with posterior
circulation stroke in the early period
• HINTS is reported to be up to 99% sensitive when
performed by an experienced clinician
• www.emcrit/misc/posterior-stroke-video/
Newman-Toker DE, et al. Acad Emerg Med. 2013;20:986-996.
Kattah JC, et al. Stroke. 2009;40:3504-3510.
Non-Contrast CT
• Sensitive
• Available
• Fast
• Findings on CT
related to: – Size of infarct
– Severity of ischemia
– Time of onset
• Hypodensity or mass
effect associated with
8x increase risk of sICH
Miller DJ, et al. Neurohospitalist. 2011 Jul;1(3):138–147.
Acute Ischemic Stroke: Overcoming
Barriers by Improving Systems of Care
© 2015 Vindico Medical Education
Alberta Stroke Program Early CT
Score (ASPECTS)
• 10 points quantitative topographic
CT score
• Defined scan protocol
• Developed to provide a reliable
grading system
• Early ischemic change predict
outcome and risk• Focal parenchymal hypodensity
• Cortical swelling with sulcal effacement /
loss of gray white differentiation
• Hyperdense MCA sign
• Scoring is limited to MCA strokes
• www.aspectsinstroke.com
www.aspectsinstroke.com
MRI – DWI • 88%-100% sensitivity
• Better than CT (Level IA)
• Takes 6 minutes
• Visible minutes after infarct
• Better than CT for distinguishing acute vs chronic lesions
• Better than CT for small CVAs, posterior fossa
MRI – Gradient Echo
• Blood dependent on age
and pulsing sequences
used
• As accurate as CT for
acute hemorrhage
• Micro-hemorrhages
• Relevance?
Jauch EC, et al. Stroke. 2013;44:870-947.
Vascular Imaging
• Digital Subtraction Angiography Gold standard
Risks, time-consuming
• CT w/o contrast + CTA Equivalent to DSA (Level IB evidence)
• MRI (DWI, FLAIR, GRE/SWI +/- PWI) +/- MRA Equivalent to DSA (Level IB evidence)
American Society of Neuroradiology, the American College of Radiology, and the Society of
NeuroInterventional Surgery, 2013
Acute Ischemic Stroke: Overcoming
Barriers by Improving Systems of Care
© 2015 Vindico Medical Education
Imaging in Acute Ischemic Stroke
• P’s of acute stroke imaging:
Parenchyma (brain), Pipes (vasculature),
Perfusion (blood flow), and Penumbra
(at-risk tissue).
• Multimodal imaging
– Sequence studies: Image, angiography
perfusion, diffusion
– Enhances the sensitivity of
emergent neuroimaging for
acute ischemic processes
– Identifies patients who may
benefit from endovascular
interventions
Sa de Camargo EC, Koroshetz WJ. NeuroRx. 2005 Apr; 2(2): 265–276.
Does the Penumbra Matter?
Downloaded from http://radiologyassistant.nl/data/bin/w440/a50979784dd693_MR10.jpg
Indications/Contraindications
• Contraindications:
– Current intracranial
bleeding/SAH
– Active internal bleeding
– Head or spine surgery or
severe TBI within 3 months
– History of serious intracranial
conditions
i.e., AVM, neoplasm,
aneurysm
– Bleeding diathesis
– Current uncontrolled
hypertension
• Relative Contraindications:
– Minor or rapidly improving
symptoms
– Pregnancy
– Seizure at onset
– Major surgery or serious
trauma within previous 14 days
– Recent GI or urinary tract
hemorrhage within 21 days
– Recent AMI within previous 3
months
Alteplase [package insert]. Genentech. South San Francisco, CA. 2015.
Acute Ischemic Stroke: Overcoming
Barriers by Improving Systems of Care
© 2015 Vindico Medical Education
ACEP Clinical Policy – 2015
Is IV r-tPA safe and effective for patients with acute ischemic
stroke if given within 3 hours of symptom onset?
• Level A Recommendation – none
• Level B Recommendation – with a goal to improve functional
outcomes, IV r-tPA should be offered and may be given to selected
patients with AIS within 3 hours of symptom onset at institutions. where
systems are in place to safely administer the medication. The
increased risk of sICH should be considered when deciding whether to
administer IV r-tPA to patients with AIS.
• Level C Recommendation – when feasible, shared decision-making
between the patient (and/or their surrogate) and a member of the
health care team should include a discussion of potential benefits and
harms prior to the decision whether to administer IV r-tPA for AIS.
Ann Emerg Med. 2015. In Press.
ACEP Clinical Policy – 2015
Is IV r-tPA safe and effective for patients with acute ischemic
stroke treated between 3-4.5 hours of symptom onset?
• Level A Recommendation – none
• Level B Recommendation – despite the known risk of sICH and the
variability in the degree of benefit in functional outcomes, IV r-tPA may
be offered and may be given to carefully selected patients with AIS within
3-4.5 hours after symptom onset at institutions where systems are in
place to safely administer the medication
• Level C Recommendation – when feasible, shared decision-making
between the patient (and/or their surrogate) and a member of the health
care team should include a discussion of potential benefits and harms
prior to the decision whether to administer IV r-tPA for AIS.
Ann Emerg Med. 2015. In Press.
Tools: Guidelines / Protocols
• AHA/ASA Get With The Guidelines: Stroke program
registry of 58,353 tPA treated patients
• Faster onset to treatment time in 15 minute increments
led to:
– Reduced in-hospital mortality (OR=0.96; 95% CI: 0.95, 0.98*)
– Symptomatic intracranial bleeding (OR=0.96; 95% CI: 0.95, 0.98*)
– Increase of independent ambulation at discharge
(OR=1.04; 95% CI: 1.03, 1.05*)
– Discharge to home (OR=1.03; 95% CI: 1.02, 1.04*)
• Conclusion: Rapidity or treatment significantly
influences outcomes with IV t-PA in AIS
Schwamm LH, et al. Circ Cardiovasc Qual Outcomes. 2013;6:543-549.
Acute Ischemic Stroke: Overcoming
Barriers by Improving Systems of Care
© 2015 Vindico Medical Education
Conclusions
• Stroke scales are helpful in identifying stroke, determining
severity and prognosis
• The history and physical findings direct type of
neuroimaging
• CT, MRI equivalent for detecting hemorrhage
• Micro-hemorrhages seen on MRI may predict
hemorrhagic response to tPA
• MRI clearly superior for detecting acute stroke
• Multiple options for vascular imaging
• Unclear relevance of penumbra
• MRI findings in TIA may predict recurrence/CVA
• Protocols are useful tools for safety and efficiency
New Concepts for
Improving Time to Reperfusion
Edward C. Jauch, MD, MS, FAHA, FACEP
Professor and Director, Division of Emergency Medicine
Professor, Department of Neurosciences
Associate Vice Chair, Research, Department of Medicine
Medical University of South Carolina
Professor, Department of Bioengineering
Clemson University
Clemson, SC
Objectives
Attendees will be able to discuss:
• Mechanisms for coordinating stroke care to
improve door-to-needle/door-to-groin
• Experiences of individual hospital systems of
care
• Lessons from Get With The Guidelines (GWTG)
efforts and Target Stroke
Acute Ischemic Stroke: Overcoming
Barriers by Improving Systems of Care
© 2015 Vindico Medical Education
Lessons Learned Over 20 Years
• Reperfusion is critical
– Minimize delay to reperfusion
– Maximize penumbral salvageability by:
Collateral flow
Physiologic optimization
• Time to reperfusion – Predicts clinical outcomes
– Significant tolerance-heterogeneity in populations
– Should drive all system development
Stroke Care in 2015
Changing Landscape for
Acute Ischemic Stroke
• New guidelines and policies imminent– Guideline update July 2015
• Measured national goals– Door to Needle (DTN) Time < 60 min
(soon even lower?)
– Computed Tomography (CT) to Thrombectomy Time < 90 min*
– Treatment rates by percent eligible for intravenous (IV) and intra-arterial (IA)
• New US Food and Drug Administration (FDA) product label
Acute Ischemic Stroke: Overcoming
Barriers by Improving Systems of Care
© 2015 Vindico Medical Education
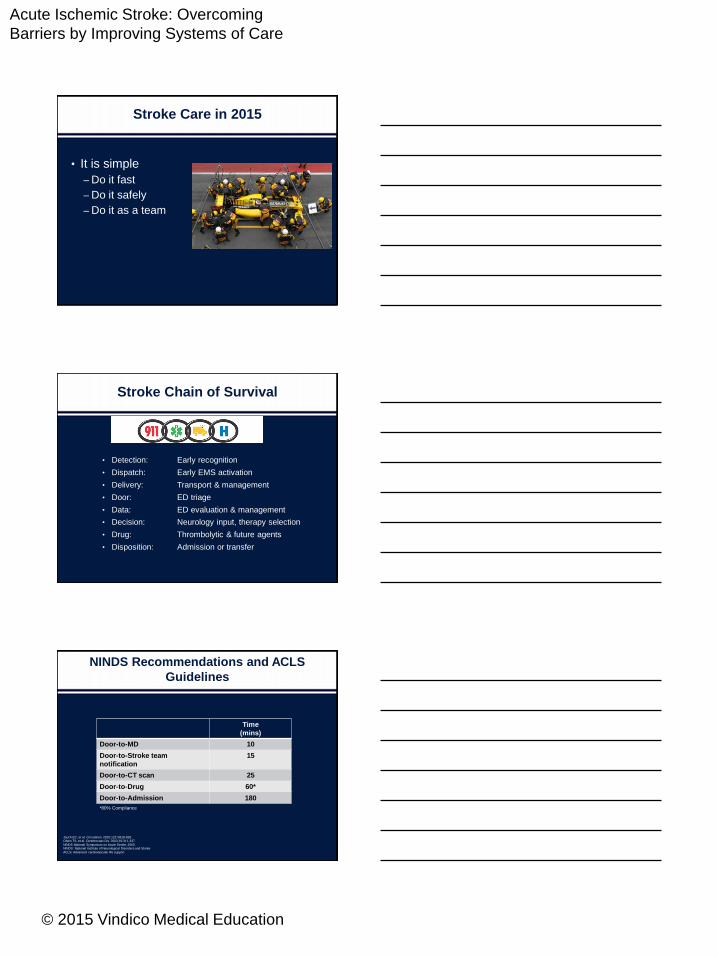
Stroke Care in 2015
• It is simple
– Do it fast
– Do it safely
– Do it as a team
• Detection: Early recognition
• Dispatch: Early EMS activation
• Delivery: Transport & management
• Door: ED triage
• Data: ED evaluation & management
• Decision: Neurology input, therapy selection
• Drug: Thrombolytic & future agents
• Disposition: Admission or transfer
Stroke Chain of Survival
NINDS Recommendations and ACLS
Guidelines
Jauch EC, et al. Circulation. 2010;122:S818-828.Olsen TS, et al. Cerebrovasc Dis. 2003;16:311-337.
NINDS National Symposium on Acute Stroke, 2003.NINDS: National Institute of Neurological Disorders and Stroke
ACLS: Advanced cardiovascular life support
Time
(mins)
Door-to-MD 10
Door-to-Stroke team
notification
15
Door-to-CT scan 25
Door-to-Drug 60*
Door-to-Admission 180
*80% Compliance
Acute Ischemic Stroke: Overcoming
Barriers by Improving Systems of Care
© 2015 Vindico Medical Education
NINDS Recommendations and ACLS Guidelines
Jauch EC, et al. Circulation. 2010;122:S818-828.
Olsen TS, et al. Cerebrovasc Dis. 2003;16:311-337.NINDS National Symposium on Acute Stroke, 2003.
NINDS: National Institute of Neurological Disorders and Stroke
ACLS: Advanced cardiovascular life support
†NIH Stroke Scale or Canadian Neurologic Scale
No Hemorrhage Hemorrhage
Immediate general assessment and stabilization
• Assess ABCs, vitals
• Provide O2 if hypoxicemic
• Obtain IV access and blood samples
• Check glucose, treat if indicated
• Perform neurologic screening assessment
• Activate stroke team
• Order emergent CT scan of brain
• Obtain 12-lead ECG
Critical EMS assessments and actions
• Support ABCs, give O2 if needed
• Perform prehospital stroke assessment
• Establish time when patient was last known
normal
• Note: Therapies may be available beyond
3 hrs from onset
• Transport; consider triage to a center with a
stroke unit, if appropriate: Consider bringing a
witness, family member, or caregiver
• Alert hospital
• Check glucose, if possible
Immediate neurologic assessment by stroke
team or designee
• Review patient history
• Establish symptom onset
• Perform neurologic examination†
Suspected
Stroke
Does CT scan show any hemorrhage?
Probable AIS, consider fibrinolytic
therapy
• Check for fibrinolytic exclusions
• Repeat neurologic exam: are deficits
rapidly improving to normal?
Consult neurologist or neurosurgeon;
consider transfer if not available
Patient remains candidate
for fibrinolytic therapy?
Yes
Review risks/benefits with patient
and family: If acceptable:
• Give tPA
• No anticoagulants or antiplatelet
treatment for 24 hours
No
Administer aspirin • Begin stroke pathway
• Admit to stroke unit, if available
• Monitor BP, treat if indicated
• Monitor neurologic status: emergent
CT if deterioration
• Monitor blood glucose: treat if needed
• Initiate supportive therapy: treat
comorbidities
10 mins from ED arrival
25 mins from arrival
45 mins from arrival
60 mins from arrival
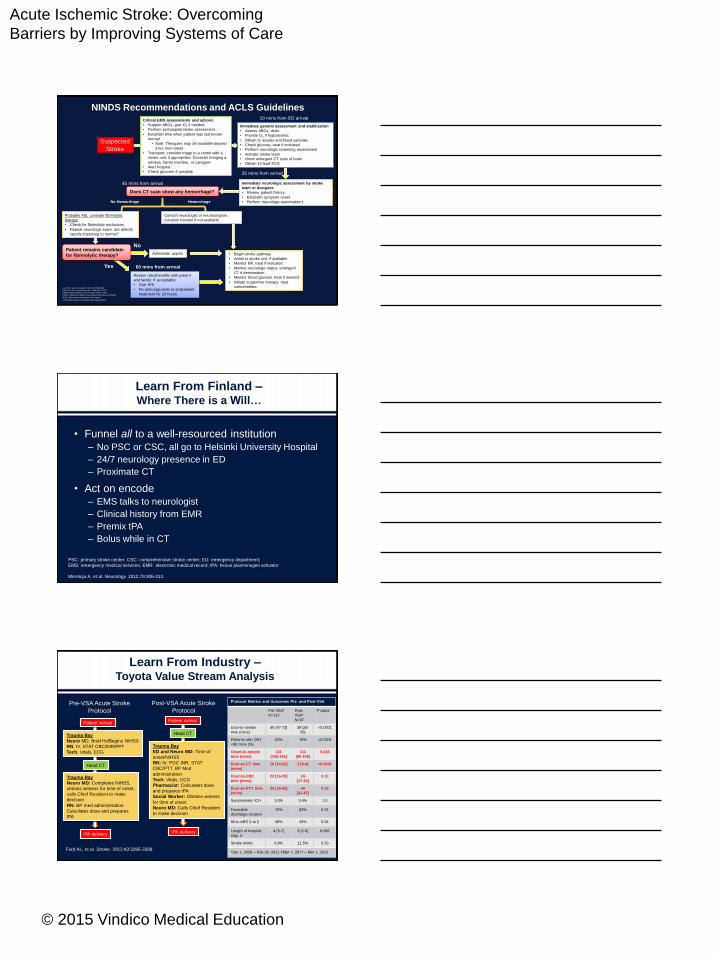
Learn From Finland –Where There is a Will…
PSC: primary stroke center; CSC: comprehensive stroke center; ED: emergency department;
EMS: emergency medical services; EMR: electronic medical record; tPA: tissue plasminogen activator
Meretoja A, et al. Neurology. 2012;79:306-313.
• Funnel all to a well-resourced institution– No PSC or CSC, all go to Helsinki University Hospital
– 24/7 neurology presence in ED
– Proximate CT
• Act on encode– EMS talks to neurologist
– Clinical history from EMR
– Premix tPA
– Bolus while in CT
Learn From Industry –Toyota Value Stream Analysis
Ford AL, et al. Stroke. 2012;43:3395-3398.
Patient Arrival
Trauma Bay
Neuro MD: Brief Hx/Begins NIHSS
RN: IV, STAT CBC/INR/PPT
Tech: Vitals, ECG
Head CT
Trauma Bay
Neuro MD: Completes NIHSS,
obtains witness for time of onset,
calls Chief Resident to make
decision
RN: BP med administration.
Calculates dose and prepares
tPA
tPA delivery
Pre-VSA Acute Stroke
Protocol
Post-VSA Acute Stroke
Protocol
Patient Arrival
Head CT
Trauma Bay
ED and Neuro MD: Time of
onset/NIHSS
RN: IV, POC INR, STAT
CBC/PTT, BP Med
administration
Tech: Vitals, ECG
Pharmacist: Calculates dose
and prepares tPA
Social Worker: Obtains witness
for time of onset
Neuro MD: Calls Chief Resident
to make decision
tPA delivery
Protocol Metrics and Outcomes Pre- and Post-VSA
Pre-VSA*
N=132
Post-
VSA*
N=87
P-value
Door-to-needle
time (mins)
60 [47-73] 39 [28-
56]
<0.0001
Patients with DNT
<60 mins (%)
52% 78% <0.0001
Onset-to-needle
time (mins)
131
[105-165]
111
[80-158]
0.016
Door-to-CT time
(mins)
16 [10-22] 1 [0-4] <0.0001
Door-to-CBC
time (mins)
22 [16-29] 24
[17-34]
0.13
Door-to-PTT time
(mins)
34 [29-42] 40
[31-47]
0.14
Symptomatic ICH 3.0% 3.4% 1.0
Favorable
discharge location
76% 83% 0.24
90-d mRS 0 to 2 49% 43% 0.34
Length of hospital
stay, d
4 [3-7] 3 [2-6] 0.056
Stroke mimic 6.8% 11.5% 0.33
*Jan 1, 2009 – Feb 28, 2011 †Mar 1, 2011 – Mar 1, 2012
Acute Ischemic Stroke: Overcoming
Barriers by Improving Systems of Care
© 2015 Vindico Medical Education
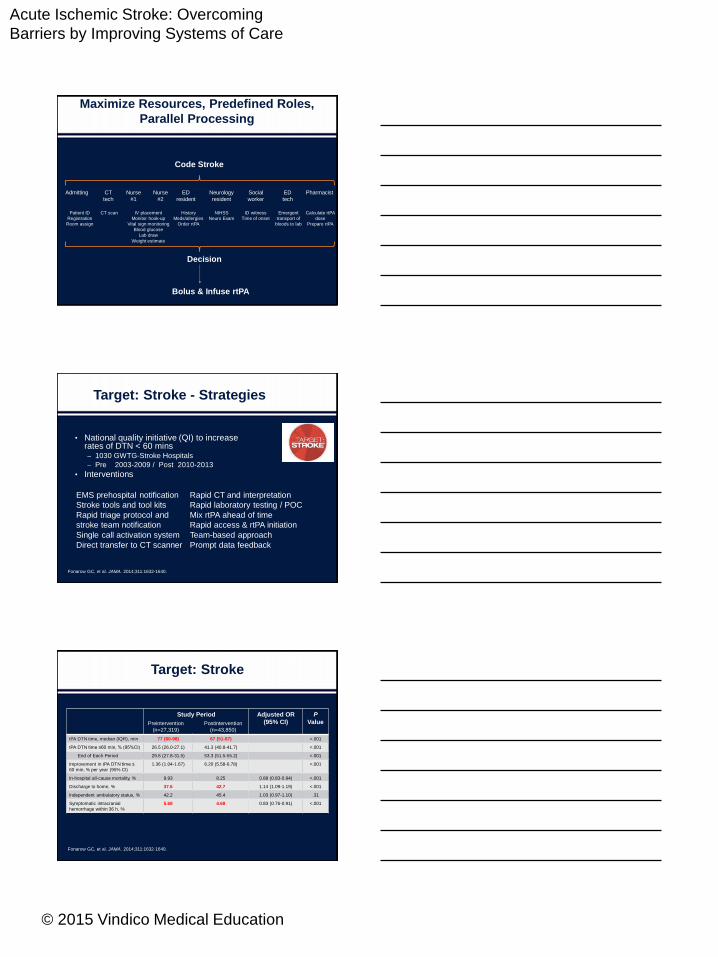
Maximize Resources, Predefined Roles,
Parallel Processing
Pharmacist
Calculate rtPA
dose
Prepare rtPA
Neurology
resident
ED
resident
Nurse
#1
Nurse
#2
CT
tech
Social
worker
ED
tech
Admitting
Code Stroke
Patient ID
Registration
Room assign
CT scan IV placement
Monitor hook-up
Vital sign monitoring
Blood glucose
Lab draw
Weight estimate
NIHSS
Neuro Exam
History
Meds/allergies
Order rtPA
ID witness
Time of onset
Emergent
transport of
bloods to lab
Decision
Bolus & Infuse rtPA
Target: Stroke - Strategies
• National quality initiative (QI) to increase rates of DTN < 60 mins – 1030 GWTG-Stroke Hospitals
– Pre 2003-2009 / Post 2010-2013
• Interventions
Fonarow GC, et al. JAMA. 2014;311:1632-1640.
EMS prehospital notification
Stroke tools and tool kits
Rapid triage protocol and
stroke team notification
Single call activation system
Direct transfer to CT scanner
Rapid CT and interpretation
Rapid laboratory testing / POC
Mix rtPA ahead of time
Rapid access & rtPA initiation
Team-based approach
Prompt data feedback
Target: Stroke
Study Period Adjusted OR
(95% CI)
P
Value
tPA DTN time, median (IQR), min 77 (60-98) 67 (51-87) <.001
tPA DTN time ≤60 min, % (95%CI) 26.5 (26.0-27.1) 41.3 (40.8-41.7) <.001
End of Each Period 29.6 (27.8-31.5) 53.3 (51.5-55.2) <.001
Improvement in tPA DTN time ≤
60 min, % per year (95% CI)
1.36 (1.04-1.67) 6.20 (5.58-6.78) <.001
In-hospital all-cause mortality, % 9.93 8.25 0.89 (0.83-0.94) <.001
Discharge to home, % 37.6 42.7 1.14 (1.09-1.19) <.001
Independent ambulatory status, % 42.2 45.4 1.03 (0.97-1.10) .31
Symptomatic intracranial
hemorrhage within 36 h, %
5.68 4.68 0.83 (0.76-0.91) <.001
Fonarow GC, et al. JAMA. 2014;311:1632-1640.
Postintervention
(n=43,850)
Preintervention
(n=27,319)
Acute Ischemic Stroke: Overcoming
Barriers by Improving Systems of Care
© 2015 Vindico Medical Education
What Are Other Patient-Centered
Outcome of These Systems?
• Triage to most appropriate hospital
– PSC more likely to have a plan and administer tPA
• Increased EMS prehospital activation
– Decreases Door to MD, CT, and Needle times
• Decreases Onset to Needle Time
– 30’ decrease increases relative favorable outcome 10%
• Decreases Onset to Reperfusion Time
– 30’ decrease increases absolute favorable outcome 10%
Monitoring Stroke Center Quality
• Comparison of Performance Achievement Award (PAA)
Recognition With Primary Stroke Center Certification for Acute
Ischemic Stroke Care
• 1356 hospitals in GWTG-Stroke from 2010 to 2012 reviewed
• After adjustment PSC and PAA improved measure adherence
“While both PSC certification and GWTG-Stroke PAA recognition
identified hospitals providing higher conformity with care measures
for patients hospitalized with acute ischemic stroke, PAA recognition
was a more robust identifier of hospitals with better performance.”
Fonarow GC, et al. J Am Heart Assoc. 2013 Oct 14;2(5):e000451.
In-patient Stroke
• Review of in-patient stroke cases from 2006 to
2012 in GWTG-Stroke
• After adjustment and in comparison to
community-onset ischemic stroke, inpatient
strokes were:
– Less likely discharged home (odds ratio [OR] 0.37)
– Less likely ambulatory at discharge (OR 0.42)
– In-hospital mortality also higher (OR 2.72)
Cumbler E, et al. Stroke. 2014 Jan;45(1):231-8. Epub 2013 Nov 19.
Acute Ischemic Stroke: Overcoming
Barriers by Improving Systems of Care
© 2015 Vindico Medical Education
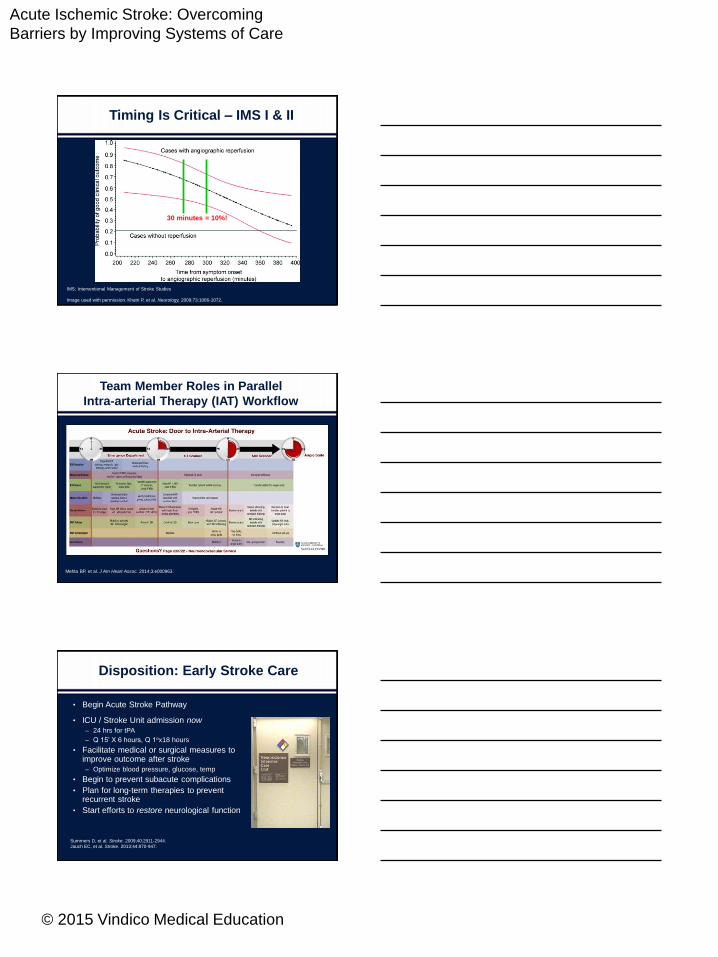
Timing Is Critical – IMS I & II
30 minutes = 10%!
IMS: Interventional Management of Stroke Studies
Image used with permission. Khatri P, et al. Neurology, 2009;73:1066-1072.
Team Member Roles in Parallel
Intra-arterial Therapy (IAT) Workflow
Mehta BP, et al. J Am Heart Assoc. 2014;3:e000963.
Disposition: Early Stroke Care
• Begin Acute Stroke Pathway
• ICU / Stroke Unit admission now
– 24 hrs for tPA
– Q 15’ X 6 hours, Q 1ox18 hours
• Facilitate medical or surgical measures to improve outcome after stroke
– Optimize blood pressure, glucose, temp
• Begin to prevent subacute complications
• Plan for long-term therapies to prevent recurrent stroke
• Start efforts to restore neurological function
Summers D, et al. Stroke. 2009;40:2911-2944.
Jauch EC, et al. Stroke. 2013;44:870-947.
Acute Ischemic Stroke: Overcoming
Barriers by Improving Systems of Care
© 2015 Vindico Medical Education
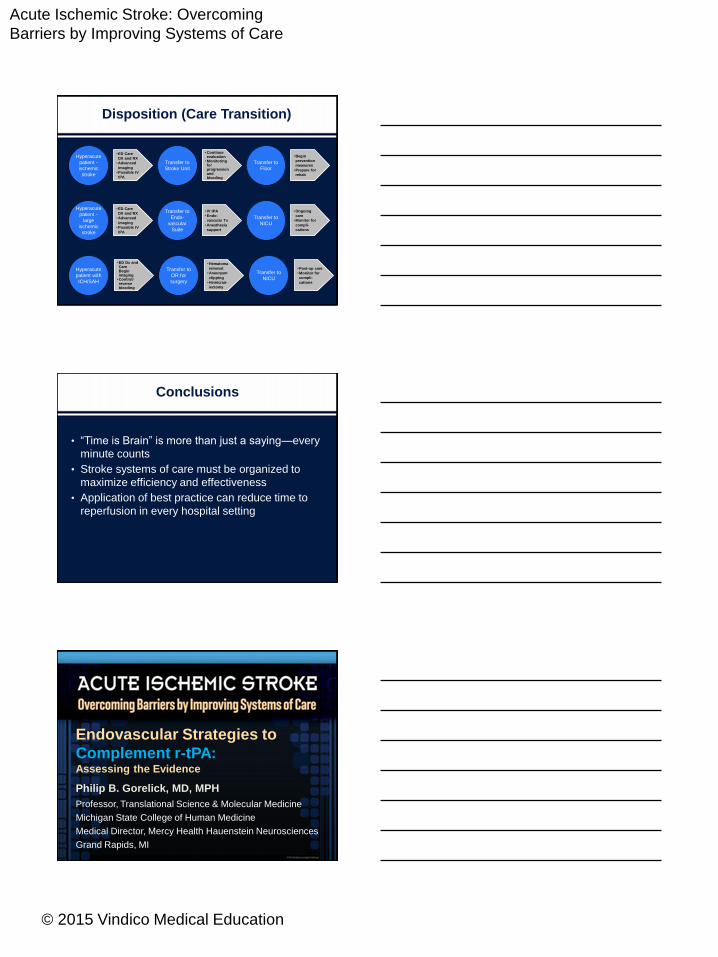
Disposition (Care Transition)
Hyperacute
patient -
ischemic
stroke
Transfer to
Stroke Unit
Transfer to
Floor
Hyperacute
patient -
large
ischemic
stroke
Transfer to
Endo-
vascular
Suite
Transfer to
NICU
Transfer to
NICU
Transfer to
OR for
surgery
Hyperacute
patient with
ICH/SAH
•ED Care
DX and RX
•Advanced
imaging
•Possible IV
tPA
•Continue evaluation
•Monitoring for progression and bleeding
•Begin
prevention
measures
•Prepare for
rehab
•ED Care
DX and RX
•Advanced
imaging
•Possible IV
tPA
• IV tPA
•Endo-
vascular Tx
•Anesthesia
support
•Ongoing
care
•Monitor for
compli-
cations
•ED Dx and CareBegin imaging
•Control/ reverse bleeding
•Post-op care
•Monitor for
compli-
cations
•Hematoma
removal
•Aneurysm
clipping
•Hemicran-
iectomy
Conclusions
• “Time is Brain” is more than just a saying—every
minute counts
• Stroke systems of care must be organized to
maximize efficiency and effectiveness
• Application of best practice can reduce time to
reperfusion in every hospital setting
Endovascular Strategies to
Complement r-tPA: Assessing the Evidence
Philip B. Gorelick, MD, MPH
Professor, Translational Science & Molecular Medicine
Michigan State College of Human Medicine
Medical Director, Mercy Health Hauenstein Neurosciences
Grand Rapids, MI
Acute Ischemic Stroke: Overcoming
Barriers by Improving Systems of Care
© 2015 Vindico Medical Education
Objectives
• In relation to endovascular strategies to complement tPA,
learners will be able to discuss:
1. Set-up time (work processes) for tPA versus endovascular
intervention
2. MR CLEAN, ESCAPE, SWIFT PRIME, EXTEND-IA,
& REVASCAT
3. Prior endovascular trial data SYNTHESIS, SYNTHESIS
Expansion, IMS III, & MR RESCUE
4. The next steps for intravenous (IV) & intra-arterial (IA)
reperfusion
Process Time for IV tPA &
Endovascular Therapy
Need to Eliminate Redundancies and Need
for Speed to Groin Puncture and
Reperfusion
More Efficient (“LEAN”) Systems
Hospital Strategies & Door-to-Needle Time
• 304 AHA Get with the Guideline-Stroke Hospitals
• 5460 patients receiving tPA within 3 hours
• Median door-to-needle time: 72 minutes
• Rapid triage: 8.1 minutes
• Single-call activation system: 4.3 minutes
• Tissue plasminogen activator (tPA) stored in ED:
3.5 minutes
• Each strategy shortened door-to-needle time by 1.3
minutes (adjusted mean difference)
• Total minutes saved if all strategies used: – 14 minutes
Xian Y, et al. Stroke. 2014;45:1387-1395.
Acute Ischemic Stroke: Overcoming
Barriers by Improving Systems of Care
© 2015 Vindico Medical Education
Process Touch Points/Times of Interest in
Acute Ischemic Stroke (AIS) Therapy
Stroke onset to:
1. Study randomization
2. CT head study
3. Start of IV alteplase therapy
4. Groin puncture
5. CT head study to 1st reperfusion
6. 1st reperfusion
Goyal M, et al. N Engl J Med. 2015;372:1019-1030.
What the New Trials Accomplished: Reduction in Median
Time from Stroke Onset to Reperfusion
• IMS III: Mean time from onset to IA end/reperfusion: 325 (5 hours, 25 minutes): range: 180-418
• MR CLEAN: (stroke onset to groin puncture: 260 minutes)
• SWIFT PRIME: (stroke onset to first stent deployment: 252 minutes)
• ESCAPE: 241 minutes
• EXTEND-IA: 248 minutes
• REVASCAT: 355 minutes
Berkhemer OA, et al. N Engl J Med. 2015;372:11-20. Campbell BC, et al. N Engl J Med. 2015;372:1009-1018.
Goyal M, et al. N Engl J Med. 2015;372:1019-1030. Jovin TG, et al. N Engl J Med. 2015;372:2296-2306.
Saver JL, et al. N Engl J Med. 2015;372:2285-2295.
Approaches to Set-up
Scenario #1:
A. Treat acute ischemic stroke with IV tPA in field in mobile stroke
unit to soften or dissolve clot & pre-notification by EMS to ED
B. Transfer from ED door to CT/CTA machine or MRI/MRA next to or
in angiography suite
C. If appropriate, ICA or MCA thrombosis neuro-thrombectomy
procedure
Scenario #2:
A. Pre-notification by EMS ED door to CT/CTA machine
& mix tPA
B. If appropriate findings, give tPA in CT room
C. Transfer next door to angiography suite & start angiography
procedure if appropriate lesion neuro-thrombectomy
procedure
Acute Ischemic Stroke: Overcoming
Barriers by Improving Systems of Care
© 2015 Vindico Medical Education
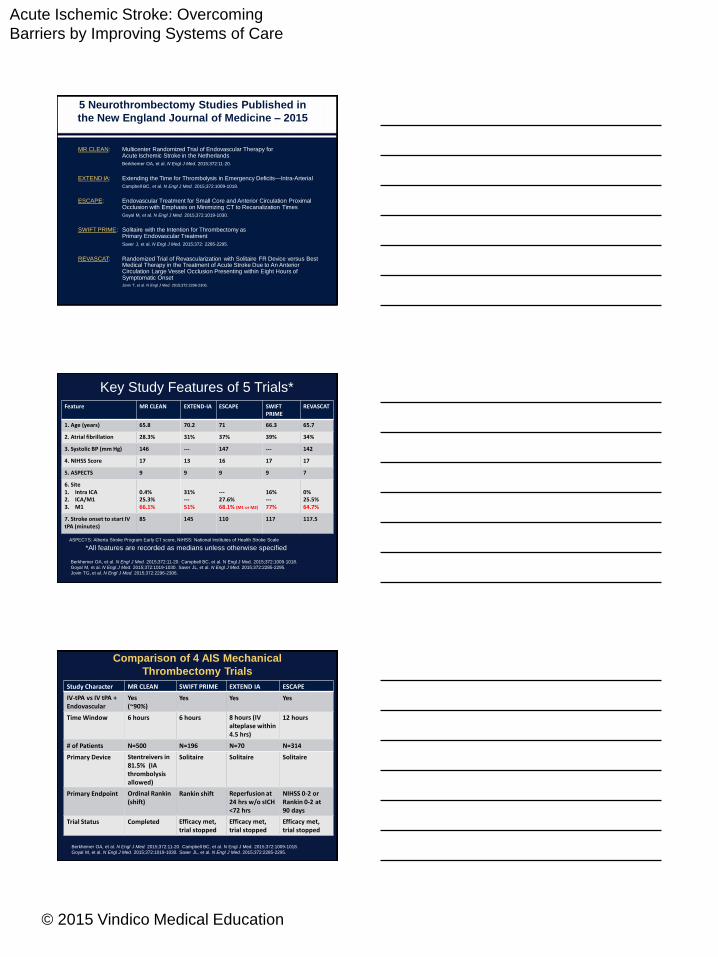
5 Neurothrombectomy Studies Published in
the New England Journal of Medicine – 2015
MR CLEAN: Multicenter Randomized Trial of Endovascular Therapy for Acute Ischemic Stroke in the Netherlands
Berkhemer OA, et al. N Engl J Med. 2015;372:11-20.
EXTEND IA: Extending the Time for Thrombolysis in Emergency Deficits—Intra-Arterial
Campbell BC, et al. N Engl J Med. 2015;372:1009-1018.
ESCAPE: Endovascular Treatment for Small Core and Anterior Circulation Proximal Occlusion with Emphasis on Minimizing CT to Recanalization Times
Goyal M, et al. N Engl J Med. 2015;372:1019-1030.
SWIFT PRIME: Solitaire with the Intention for Thrombectomy as Primary Endovascular Treatment
Saver J, et al. N Engl J Med. 2015;372: 2285-2295.
REVASCAT: Randomized Trial of Revascularization with Solitaire FR Device versus Best Medical Therapy in the Treatment of Acute Stroke Due to An Anterior Circulation Large Vessel Occlusion Presenting within Eight Hours of Symptomatic Onset Jovin T, et al. N Engl J Med. 2015;372:2296-2306.
Key Study Features of 5 Trials*
*All features are recorded as medians unless otherwise specified
Feature MR CLEAN EXTEND-IA ESCAPE SWIFT PRIME
REVASCAT
1. Age (years) 65.8 70.2 71 66.3 65.7
2. Atrial fibrillation 28.3% 31% 37% 39% 34%
3. Systolic BP (mm Hg) 146 --- 147 --- 142
4. NIHSS Score 17 13 16 17 17
5. ASPECTS 9 9 9 9 7
6. Site1. Intra ICA2. ICA/M13. M1
0.4%25.3%66.1%
31%---51%
---27.6%68.1% (M1 or M2)
16%---77%
0%25.5%64.7%
7. Stroke onset to start IV tPA (minutes)
85 145 110 117 117.5
Berkhemer OA, et al. N Engl J Med. 2015;372:11-20. Campbell BC, et al. N Engl J Med. 2015;372:1009-1018.
Goyal M, et al. N Engl J Med. 2015;372:1019-1030. Saver JL, et al. N Engl J Med. 2015;372:2285-2295.
Jovin TG, et al. N Engl J Med. 2015;372:2296-2306.
ASPECTS: Alberta Stroke Program Early CT score, NIHSS: National Institutes of Health Stroke Scale
Comparison of 4 AIS Mechanical
Thrombectomy Trials
Study Character MR CLEAN SWIFT PRIME EXTEND IA ESCAPE
IV-tPA vs IV tPA + Endovascular
Yes (~90%)
Yes Yes Yes
Time Window 6 hours 6 hours 8 hours (IV alteplase within 4.5 hrs)
12 hours
# of Patients N=500 N=196 N=70 N=314
Primary Device Stentreivers in 81.5% (IA thrombolysis allowed)
Solitaire Solitaire Solitaire
Primary Endpoint Ordinal Rankin(shift)
Rankin shift Reperfusion at 24 hrs w/o sICH <72 hrs
NIHSS 0-2 orRankin 0-2 at 90 days
Trial Status Completed Efficacy met, trial stopped
Efficacy met, trial stopped
Efficacy met, trial stopped
Berkhemer OA, et al. N Engl J Med. 2015;372:11-20. Campbell BC, et al. N Engl J Med. 2015;372:1009-1018.
Goyal M, et al. N Engl J Med. 2015;372:1019-1030. Saver JL, et al. N Engl J Med. 2015;372:2285-2295.
Acute Ischemic Stroke: Overcoming
Barriers by Improving Systems of Care
© 2015 Vindico Medical Education
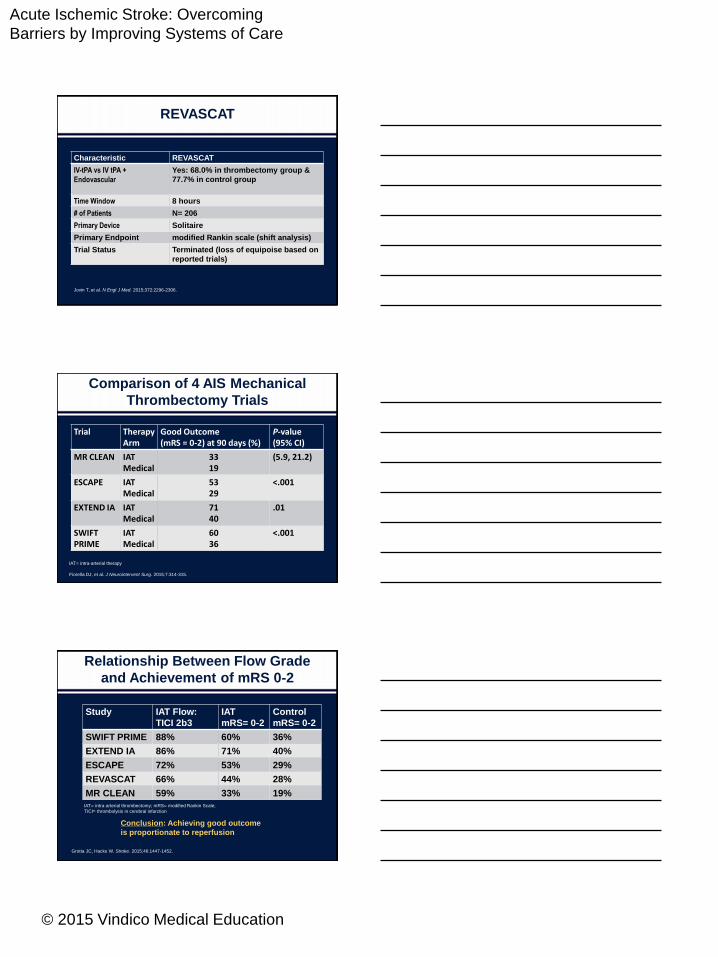
REVASCAT
Characteristic REVASCAT
IV-tPA vs IV tPA +
Endovascular
Yes: 68.0% in thrombectomy group &
77.7% in control group
Time Window 8 hours
# of Patients N= 206
Primary Device Solitaire
Primary Endpoint modified Rankin scale (shift analysis)
Trial Status Terminated (loss of equipoise based on
reported trials)
Jovin T, et al. N Engl J Med. 2015;372:2296-2306.
Comparison of 4 AIS Mechanical
Thrombectomy Trials
IAT= intra-arterial therapy
Fiorella DJ, et al. J Neurointervent Surg. 2015;7:314-315.
Trial TherapyArm
Good Outcome (mRS = 0-2) at 90 days (%)
P-value (95% CI)
MR CLEAN IATMedical
3319
(5.9, 21.2)
ESCAPE IAT Medical
5329
<.001
EXTEND IA IATMedical
7140
.01
SWIFTPRIME
IATMedical
6036
<.001
Relationship Between Flow Grade
and Achievement of mRS 0-2
Study IAT Flow:
TICI 2b3
IAT
mRS= 0-2
Control
mRS= 0-2
SWIFT PRIME 88% 60% 36%
EXTEND IA 86% 71% 40%
ESCAPE 72% 53% 29%
REVASCAT 66% 44% 28%
MR CLEAN 59% 33% 19%IAT= intra-arterial thrombectomy; mRS= modified Rankin Scale;
TICI= thrombolysis in cerebral infarction
Conclusion: Achieving good outcome
is proportionate to reperfusion
Grotta JC, Hacke W. Stroke. 2015;46:1447-1452.
Acute Ischemic Stroke: Overcoming
Barriers by Improving Systems of Care
© 2015 Vindico Medical Education
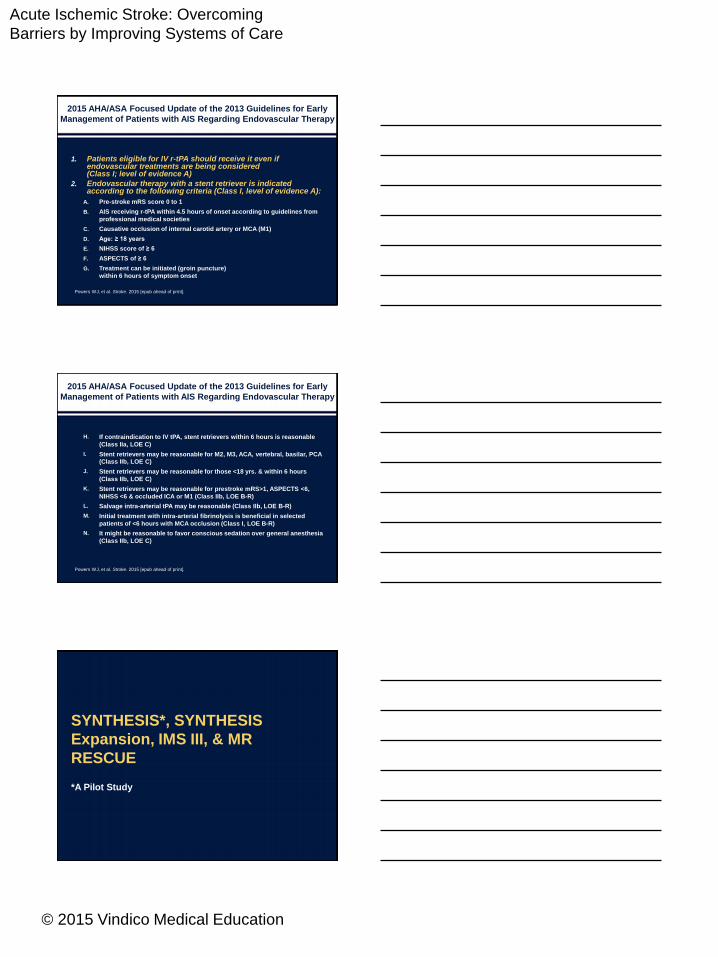
2015 AHA/ASA Focused Update of the 2013 Guidelines for Early
Management of Patients with AIS Regarding Endovascular Therapy
1. Patients eligible for IV r-tPA should receive it even if endovascular treatments are being considered (Class I; level of evidence A)
2. Endovascular therapy with a stent retriever is indicated according to the following criteria (Class I, level of evidence A):
A. Pre-stroke mRS score 0 to 1
B. AIS receiving r-tPA within 4.5 hours of onset according to guidelines from
professional medical societies
C. Causative occlusion of internal carotid artery or MCA (M1)
D. Age: ≥ 18 years
E. NIHSS score of ≥ 6
F. ASPECTS of ≥ 6
G. Treatment can be initiated (groin puncture)
within 6 hours of symptom onset
Powers WJ, et al. Stroke. 2015 [epub ahead of print].
H. If contraindication to IV tPA, stent retrievers within 6 hours is reasonable
(Class IIa, LOE C)
I. Stent retrievers may be reasonable for M2, M3, ACA, vertebral, basilar, PCA
(Class IIb, LOE C)
J. Stent retrievers may be reasonable for those <18 yrs. & within 6 hours
(Class IIb, LOE C)
K. Stent retrievers may be reasonable for prestroke mRS>1, ASPECTS <6,
NIHSS <6 & occluded ICA or M1 (Class IIb, LOE B-R)
L. Salvage intra-arterial tPA may be reasonable (Class IIb, LOE B-R)
M. Initial treatment with intra-arterial fibrinolysis is beneficial in selected
patients of <6 hours with MCA occlusion (Class I, LOE B-R)
N. It might be reasonable to favor conscious sedation over general anesthesia
(Class IIb, LOE C)
Powers WJ, et al. Stroke. 2015 [epub ahead of print].
2015 AHA/ASA Focused Update of the 2013 Guidelines for Early
Management of Patients with AIS Regarding Endovascular Therapy
SYNTHESIS*, SYNTHESIS
Expansion, IMS III, & MR
RESCUE
*A Pilot Study
Acute Ischemic Stroke: Overcoming
Barriers by Improving Systems of Care
© 2015 Vindico Medical Education
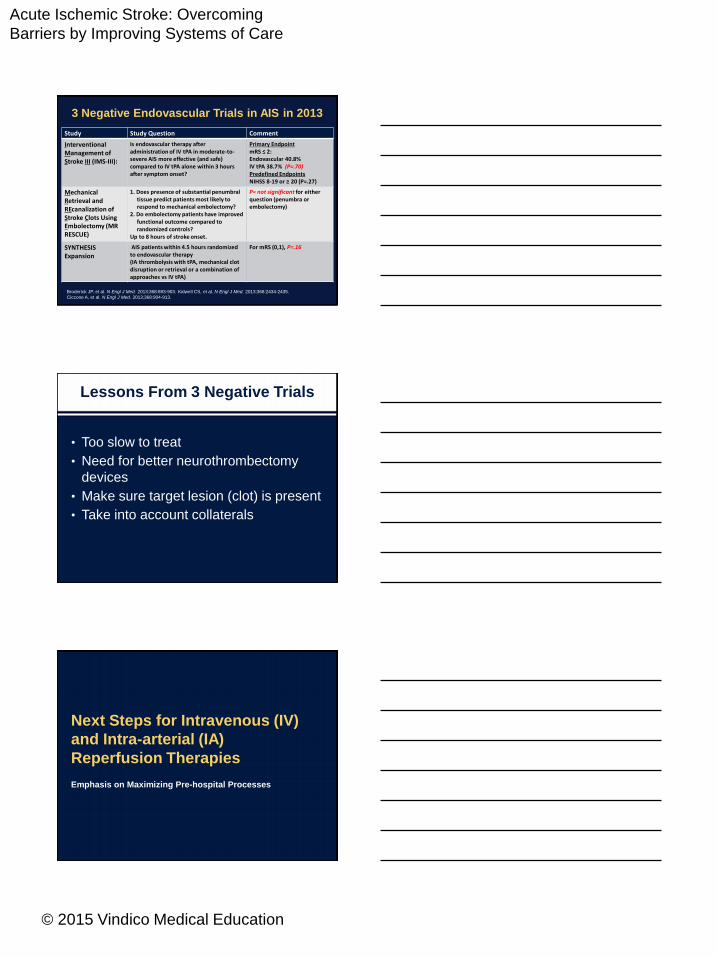
3 Negative Endovascular Trials in AIS in 2013
Broderick JP, et al. N Engl J Med. 2013;368:893-903. Kidwell CS, et al. N Engl J Med. 2013;368:2434-2435.
Ciccone A, et al. N Engl J Med. 2013;368:904-913.
Study Study Question Comment
Interventional Management of Stroke III (IMS-III):
Is endovascular therapy after administration of IV tPA in moderate-to-severe AIS more effective (and safe) compared to IV tPA alone within 3 hours after symptom onset?
Primary EndpointmRS ≤ 2:Endovascular 40.8%IV tPA 38.7% (P=.70)Predefined EndpointsNIHSS 8-19 or ≥ 20 (P=.27)
Mechanical Retrieval and REcanalization of Stroke Clots Using Embolectomy (MR RESCUE)
1. Does presence of substantial penumbral tissue predict patients most likely to respond to mechanical embolectomy?
2. Do embolectomy patients have improved functional outcome compared to randomized controls?
Up to 8 hours of stroke onset.
P= not significant for either question (penumbra or embolectomy)
SYNTHESIS Expansion
AIS patients within 4.5 hours randomized to endovascular therapy (IA thrombolysis with tPA, mechanical clot disruption or retrieval or a combination of approaches vs IV tPA)
For mRS (0,1), P=.16
Lessons From 3 Negative Trials
• Too slow to treat
• Need for better neurothrombectomy
devices
• Make sure target lesion (clot) is present
• Take into account collaterals
Next Steps for Intravenous (IV)
and Intra-arterial (IA)
Reperfusion Therapies
Emphasis on Maximizing Pre-hospital Processes
Acute Ischemic Stroke: Overcoming
Barriers by Improving Systems of Care
© 2015 Vindico Medical Education
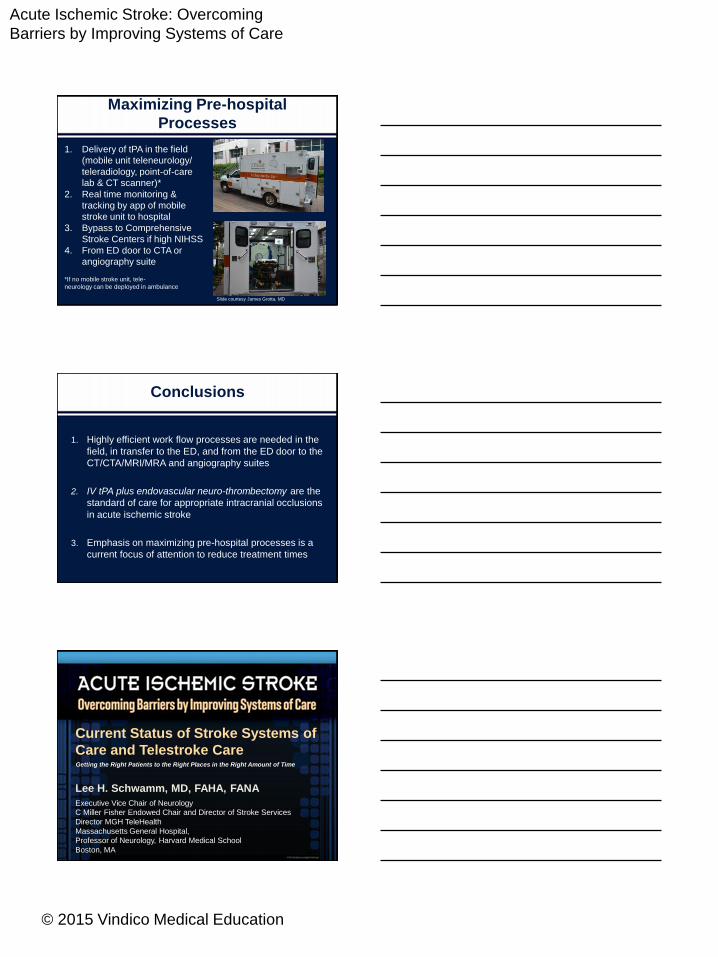
Maximizing Pre-hospital
Processes
1. Delivery of tPA in the field
(mobile unit teleneurology/
teleradiology, point-of-care
lab & CT scanner)*
2. Real time monitoring &
tracking by app of mobile
stroke unit to hospital
3. Bypass to Comprehensive
Stroke Centers if high NIHSS
4. From ED door to CTA or
angiography suite
*If no mobile stroke unit, tele-
neurology can be deployed in ambulance
Slide courtesy James Grotta, MD
Conclusions
1. Highly efficient work flow processes are needed in the
field, in transfer to the ED, and from the ED door to the
CT/CTA/MRI/MRA and angiography suites
2. IV tPA plus endovascular neuro-thrombectomy are the
standard of care for appropriate intracranial occlusions
in acute ischemic stroke
3. Emphasis on maximizing pre-hospital processes is a
current focus of attention to reduce treatment times
Current Status of Stroke Systems of
Care and Telestroke Care
Lee H. Schwamm, MD, FAHA, FANA
Executive Vice Chair of Neurology
C Miller Fisher Endowed Chair and Director of Stroke Services
Director MGH TeleHealth
Massachusetts General Hospital,
Professor of Neurology, Harvard Medical School
Boston, MA
Getting the Right Patients to the Right Places in the Right Amount of Time
Acute Ischemic Stroke: Overcoming
Barriers by Improving Systems of Care
© 2015 Vindico Medical Education
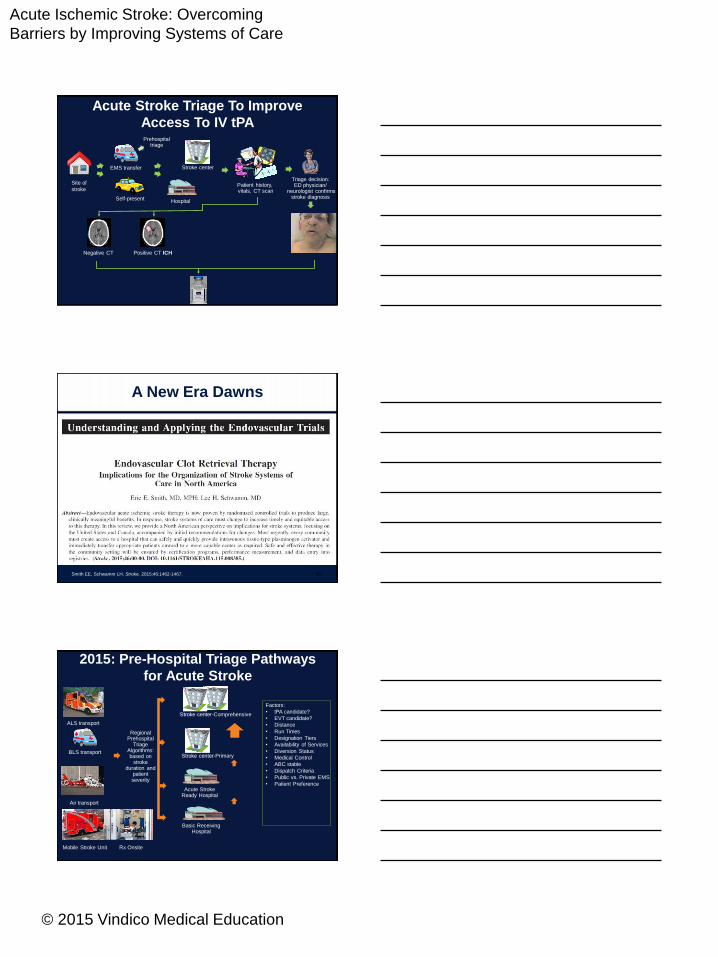
Site of
strokePatient history, vitals, CT scan
Triage decision:ED physician/
neurologist confirmsstroke diagnosis
Negative CT Positive CT ICH
EMS transfer
Prehospitaltriage
Self-present
Stroke center
Hospital
Acute Stroke Triage To Improve
Access To IV tPA
A New Era Dawns
65Smith EE, Schwamm LH. Stroke. 2015;46:1462-1467.
Acute Stroke Ready Hospital
BLS transport
ALS transport
Air transport
Mobile Stroke Unit Rx Onsite
Basic Receiving Hospital
Stroke center-Primary
Stroke center-Comprehensive
Factors:
• tPA candidate?
• EVT candidate?
• Distance
• Run Times
• Designation Tiers
• Availability of Services
• Diversion Status
• Medical Control
• ABC stable
• Dispatch Criteria
• Public vs. Private EMS
• Patient Preference
Regional Prehospital
TriageAlgorithms:based on
stroke duration and
patient severity
2015: Pre-Hospital Triage Pathways
for Acute Stroke
Acute Ischemic Stroke: Overcoming
Barriers by Improving Systems of Care
© 2015 Vindico Medical Education
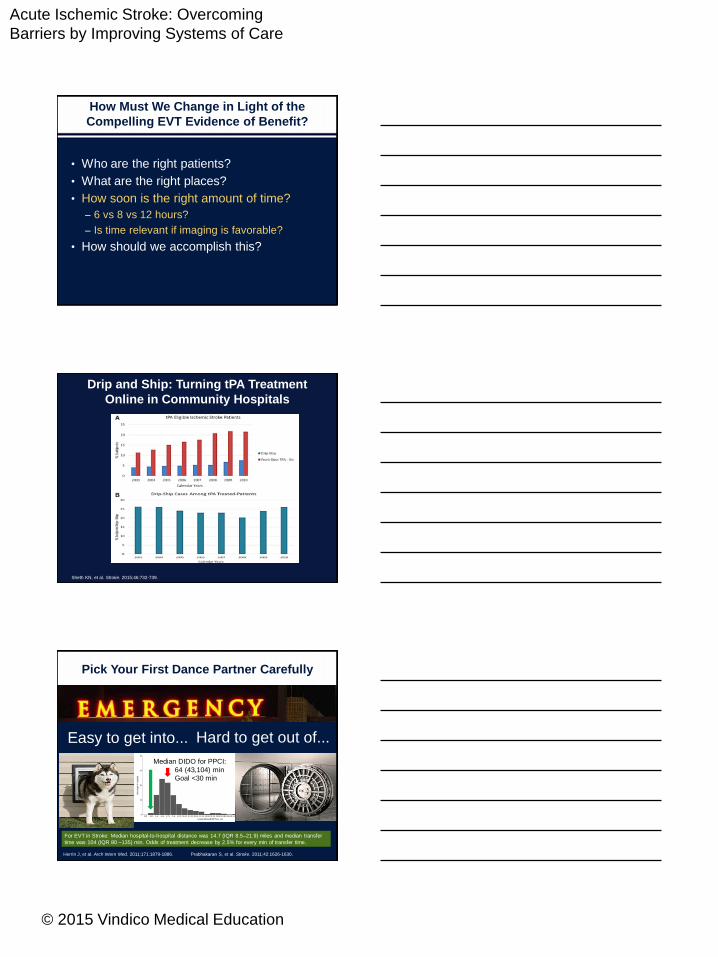
How Must We Change in Light of the
Compelling EVT Evidence of Benefit?
• Who are the right patients?
– How can we detect them reliably?
• What are the right places?
• How soon is the right amount of time?
• How should we accomplish this?
"Sy says — When having a stroke, get to
the hospital as soon as possible — within
the first 6 hours. Ask for a T.P.A”
http://www.theatlantic.com/health/archive/2009/12/about-my-father/32221/
Most Patients Don’t Come with a Note Pinned to
their Chest that says “Get me a thrombectomy!”
Penumbra(at risk)
Core(irreversibly
damaged)
Major Strokes:
How to Define?
Acute Ischemic Stroke: Overcoming
Barriers by Improving Systems of Care
© 2015 Vindico Medical Education
By Imaging Criteria? Preserved Parenchyma &
Good Collaterals if CTA Available and Reliable
70
Collaterals: From Rags ………………………………………………………to Riches
for
undergoo MRI-DWI
o CT
o Vessel Imaging
o Perfusion Imaging
o Removing Shoes
Clinical Criteria: Basically, It’s a Bad Stroke
• NIHSS: PPV 86.4% for NIHSS ≥9; 84.4% for NIHSS ≥71
• sNIHSS is a valid short form for prehospital use
• The Los Angeles Motor Scale (LAMS) for LVO, 5 versus
2 points, had sensitivity 81%, specificity 89%
• Cincinnati Prehospital Stroke Severity Scale to identify
stroke patients with NIHSS ≥15 (sensitivity 92%) or with
LVO (sensitivity 83%)2
• Rapid Arterial oCclusion Evaluation (RACE) scale to
detect LVO had sensitivity 85%, specificity 68%, PPV
42%, NPV 94%
1. Heldner MR, et al. Stroke. 2013 Apr;44(4):1153-7.
2. Katz BS, et al. Stroke. 2015 Jun;46(6):1508-12.
Acute Ischemic Stroke: Overcoming
Barriers by Improving Systems of Care
© 2015 Vindico Medical Education
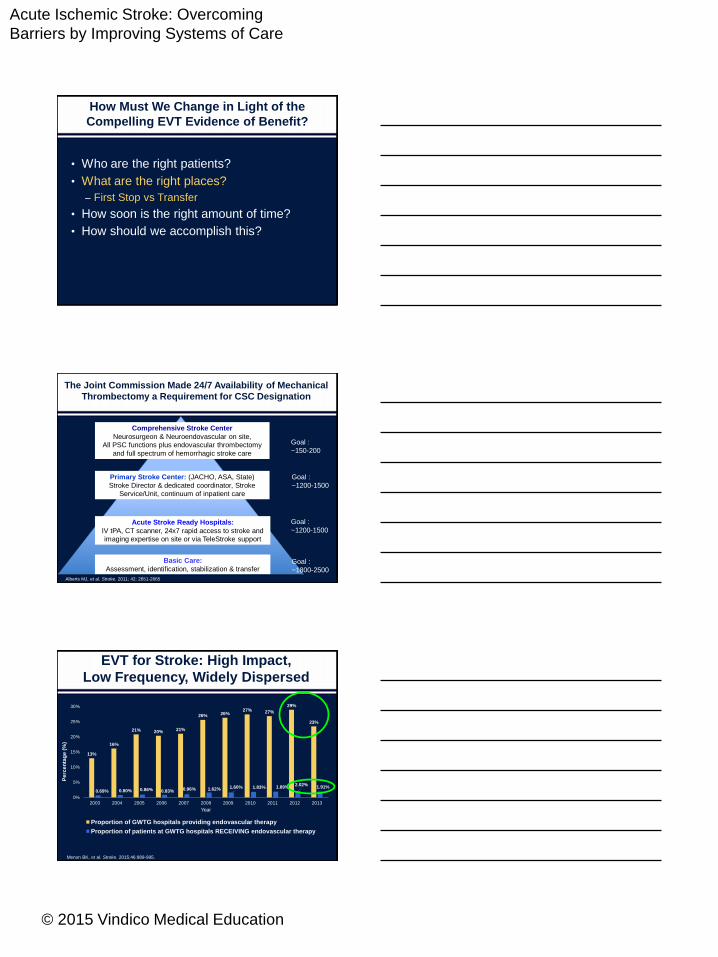
• Who are the right patients?
• What are the right places?
– First Stop vs Transfer
• How soon is the right amount of time?
• How should we accomplish this?
How Must We Change in Light of the
Compelling EVT Evidence of Benefit?
The Joint Commission Made 24/7 Availability of Mechanical
Thrombectomy a Requirement for CSC Designation
Basic Care:
Assessment, identification, stabilization & transfer
Acute Stroke Ready Hospitals:
IV tPA, CT scanner, 24x7 rapid access to stroke and
imaging expertise on site or via TeleStroke support
Primary Stroke Center: (JACHO, ASA, State)
Stroke Director & dedicated coordinator, Stroke
Service/Unit, continuum of inpatient care
Comprehensive Stroke Center
Neurosurgeon & Neuroendovascular on site,
All PSC functions plus endovascular thrombectomy
and full spectrum of hemorrhagic stroke care
Goal :
~150-200
Goal :
~1200-1500
Goal :
~1200-1500
Goal :
~1800-2500Alberts MJ, et al. Stroke. 2011; 42: 2651-2665
EVT for Stroke: High Impact,
Low Frequency, Widely Dispersed
Menon BK, et al. Stroke. 2015;46:989-995.
13%
16%
21% 20% 21%
26% 26%27% 27%
29%
23%
0.69% 0.80% 0.86% 0.83% 0.96% 1.62% 1.60% 1.83% 1.89%2.02%
1.91%
0%
5%
10%
15%
20%
25%
30%
2003 2004 2005 2006 2007 2008 2009 2010 2011 2012 2013
Year
Proportion of GWTG hospitals providing endovascular therapy
Proportion of patients at GWTG hospitals RECEIVING endovascular therapy
Pe
rce
nta
ge
(%
)
Acute Ischemic Stroke: Overcoming
Barriers by Improving Systems of Care
© 2015 Vindico Medical Education
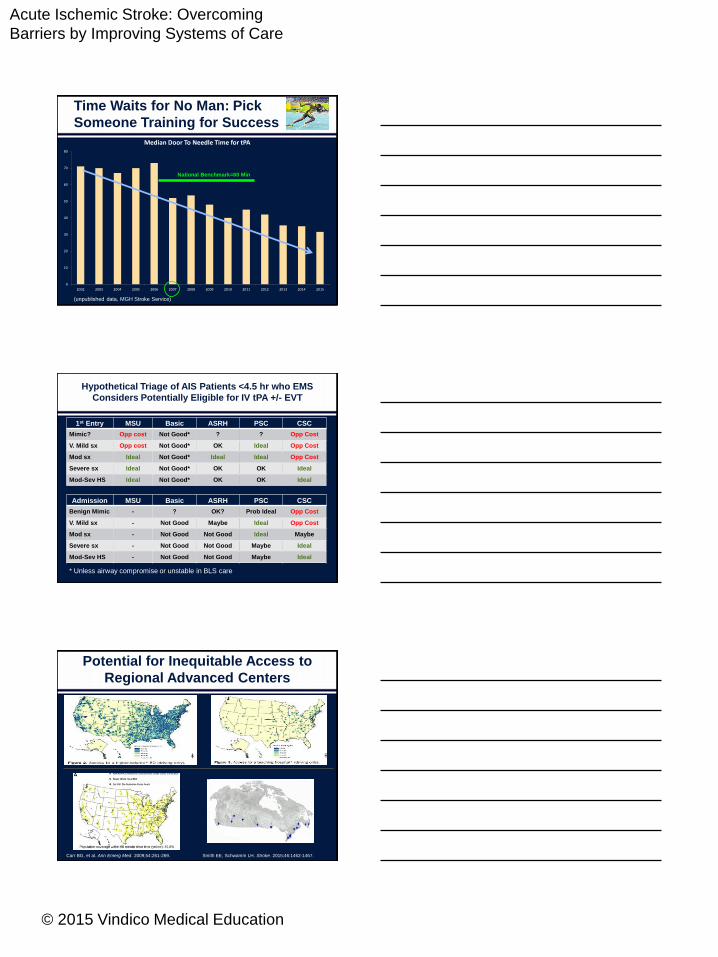
Time Waits for No Man: Pick
Someone Training for Success
0
10
20
30
40
50
60
70
80
2002 2003 2004 2005 2006 2007 2008 2009 2010 2011 2012 2013 2014 2015
Median Door To Needle Time for tPA
National Benchmark=60 Min
(unpublished data, MGH Stroke Service)
Hypothetical Triage of AIS Patients <4.5 hr who EMS
Considers Potentially Eligible for IV tPA +/- EVT
1st Entry MSU Basic ASRH PSC CSC
Mimic? Opp cost Not Good* ? ? Opp Cost
V. Mild sx Opp cost Not Good* OK Ideal Opp Cost
Mod sx Ideal Not Good* Ideal Ideal Opp Cost
Severe sx Ideal Not Good* OK OK Ideal
Mod-Sev HS Ideal Not Good* OK OK Ideal
Admission MSU Basic ASRH PSC CSC
Benign Mimic - ? OK? Prob Ideal Opp Cost
V. Mild sx - Not Good Maybe Ideal Opp Cost
Mod sx - Not Good Not Good Ideal Maybe
Severe sx - Not Good Not Good Maybe Ideal
Mod-Sev HS - Not Good Not Good Maybe Ideal
* Unless airway compromise or unstable in BLS care
Potential for Inequitable Access to
Regional Advanced Centers
Carr BG, et al. Ann Emerg Med. 2009;54:261-269. Smith EE, Schwamm LH. Stroke. 2015;46:1462-1467.
Acute Ischemic Stroke: Overcoming
Barriers by Improving Systems of Care
© 2015 Vindico Medical Education
• Who are the right patients?
• What are the right places?
• How soon is the right amount of time?
– 6 vs 8 vs 12 hours?
– Is time relevant if imaging is favorable?
• How should we accomplish this?
How Must We Change in Light of the
Compelling EVT Evidence of Benefit?
Drip and Ship: Turning tPA Treatment
Online in Community Hospitals
Sheth KN, et al. Stroke. 2015;46:732-739.
Pick Your First Dance Partner Carefully
Hard to get out of...
Herrin J, et al. Arch Intern Med. 2011;171:1879-1886. Prabhakaran S, et al. Stroke. 2011;42:1626-1630.
Median DIDO for PPCI:
64 (43,104) min
Goal <30 min
For EVT in Stroke: Median hospital-to-hospital distance was 14.7 (IQR 8.5–21.9) miles and median transfer
time was 104 (IQR 80 –135) min. Odds of treatment decrease by 2.5% for every min of transfer time.
Easy to get into...
Acute Ischemic Stroke: Overcoming
Barriers by Improving Systems of Care
© 2015 Vindico Medical Education
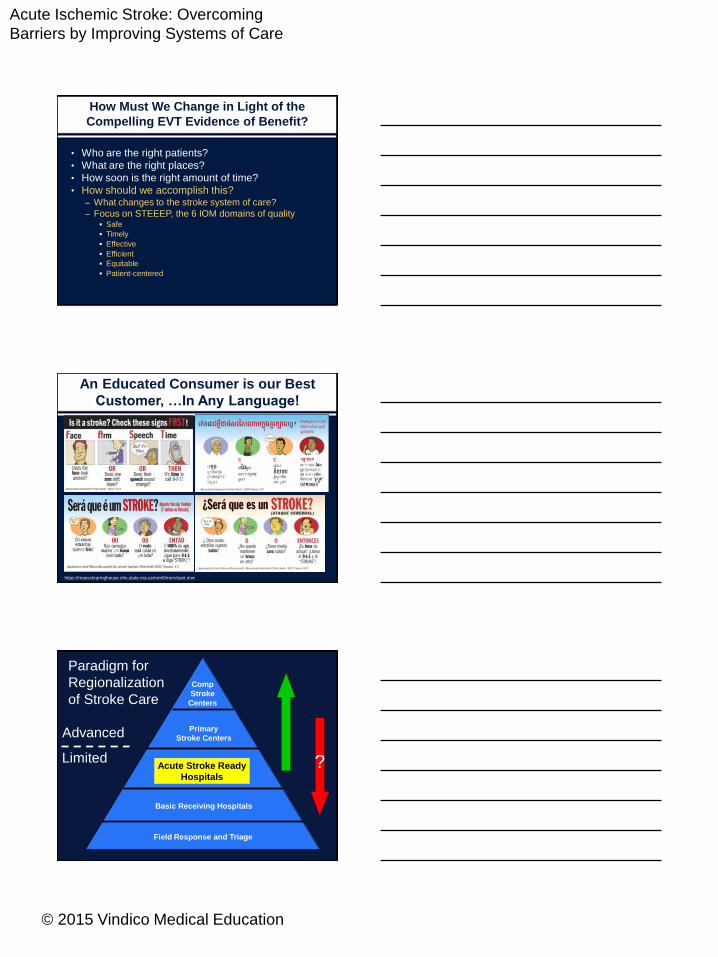
How Must We Change in Light of the
Compelling EVT Evidence of Benefit?
• Who are the right patients?
• What are the right places?
• How soon is the right amount of time?
• How should we accomplish this?– What changes to the stroke system of care?
– Focus on STEEEP, the 6 IOM domains of quality Safe
Timely
Effective
Efficient
Equitable
Patient-centered
An Educated Consumer is our Best
Customer, …In Any Language!
https://massclearinghouse.ehs.state.ma.us/mm5/merchant.mvc
Primary
Stroke Centers
Comp
Stroke
Centers
Acute Stroke Ready
Hospitals
Basic Receiving Hospitals
Field Response and Triage
Paradigm for
Regionalization
of Stroke Care
Limited ?
Advanced
Acute Ischemic Stroke: Overcoming
Barriers by Improving Systems of Care
© 2015 Vindico Medical Education
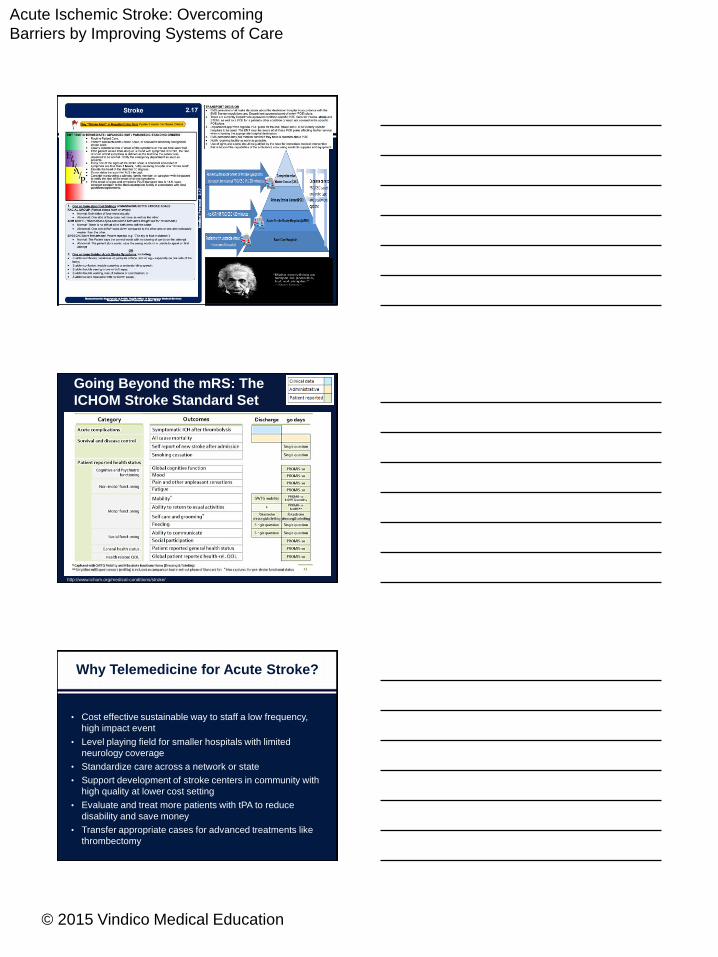
Going Beyond the mRS: The
ICHOM Stroke Standard Set
http://www.ichom.org/medical-conditions/stroke/
Why Telemedicine for Acute Stroke?
• Cost effective sustainable way to staff a low frequency,
high impact event
• Level playing field for smaller hospitals with limited
neurology coverage
• Standardize care across a network or state
• Support development of stroke centers in community with
high quality at lower cost setting
• Evaluate and treat more patients with tPA to reduce
disability and save money
• Transfer appropriate cases for advanced treatments like
thrombectomy
Acute Ischemic Stroke: Overcoming
Barriers by Improving Systems of Care
© 2015 Vindico Medical Education
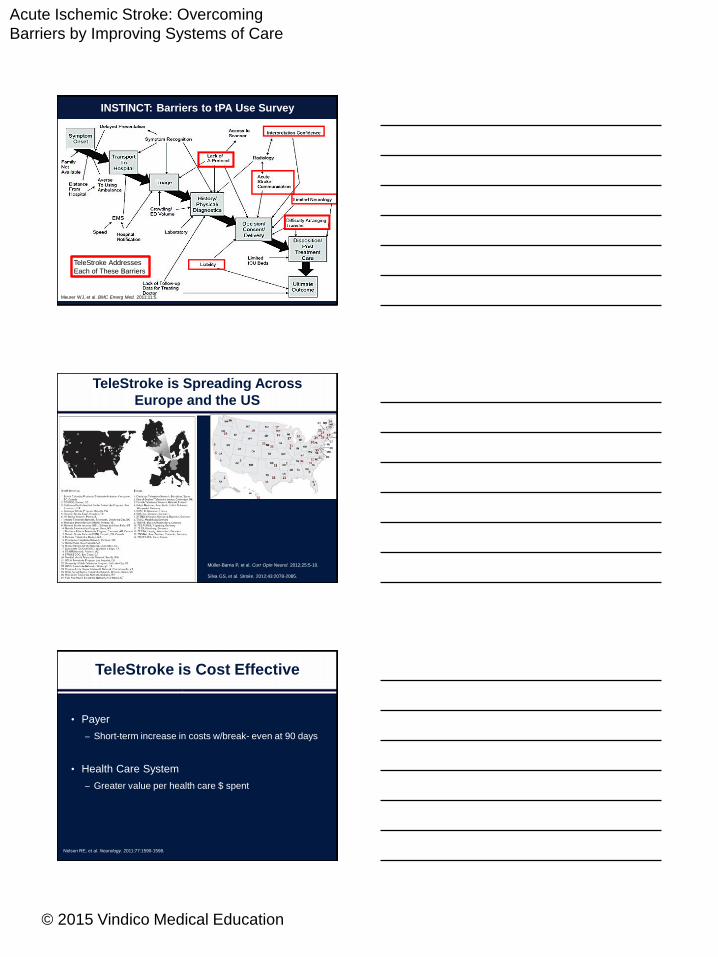
INSTINCT: Barriers to tPA Use Survey
TeleStroke Addresses
Each of These Barriers
Meurer WJ, et al. BMC Emerg Med. 2011;11:5.
TeleStroke is Spreading Across
Europe and the US
Müller-Barna P, et al. Curr Opin Neurol. 2012;25:5-10.
Silva GS, et al. Stroke. 2012;43:2078-2085.
TeleStroke is Cost Effective
• Payer
– Short-term increase in costs w/break- even at 90 days
• Health Care System
– Greater value per health care $ spent
Nelson RE, et al. Neurology. 2011;77:1590-1598.
1

Acute Ischemic Stroke: Overcoming
Barriers by Improving Systems of Care
© 2015 Vindico Medical Education
Caring for the Region: A 4 to 1 Multiplier
0
50
100
150
200
250
2005 2006 2007 2008 2009 2010 2011 2012 2013
MGH Thrombolysis Volume Trends over Time (n=1357)
IV tPA @MGH
IV tPA via TS
IAT@ MGH
Total
(unpublished data, MGH Stroke Service)
MGH
TeleStroke
Program
(unpublished data, MGH Stroke Service)
Calendar Year 2013 Snapshot:
Efficient, Effective Stroke Care
93(unpublished data, MGH Stroke Service)
Acute Ischemic Stroke: Overcoming
Barriers by Improving Systems of Care
© 2015 Vindico Medical Education
Scorecard
Specificity Delay, Risk
Smith EE, Schwamm LH. Stroke. 2015;46:1462-1467.
Really Radical Redesign?
Volunteers Giving IV tPA at the Minute Clinic!