Embed Size (px)
Citation preview
Management of Acute Ischemic Stroke
Anna Finley Caulfield, MD*,Christine A.C. Wijman, MD, PhD
Department of Neurology and Neurological Sciences, Neurocritical Care Program,
Stanford Stroke Center, Stanford University School of Medicine, 701 Welch Road,
B-325, Palo Alto, CA 94304, USA
Stroke is the third leading cause of death and the leading cause of dis-ability in the United States and is associated with a tremendous cost bur-den to society [1]. Most strokes are ischemic, but about 15% of strokesare caused by intracerebral or subarachnoid hemorrhage. Currently, thereis only one drug approved by the US Food and Drug Administration(FDA), intravenous tissue plasminogen activator (tPA), for the treatmentof acute ischemic stroke within 3 hours of symptom onset [2]. Many strokepatients do not receive intravenous tPA, however, most commonly becausethey present beyond the 3-hour therapeutic window. More recently devel-oped therapeutic strategies offer the hope of safe and effective treatmentbeyond the 3-hour time window in selected patients. This article is an up-date of a recent publication that reviewed established and novel treatmentsfor acute ischemic stroke and the management issues that may arise in thefirst hours to days after symptom onset [3]. Blood pressure management,management of intracranial hypertension, and temperature managementare discussed in greater detail elsewhere in this issue.
Neurol Clin 26 (2008) 345–371
Initial management
The initial management of acute ischemic stroke involves medical stabi-lization, including airway protection and ventilatory and hemodynamic
Material for this article is reprinted in part from the American Academy of Neurology
2006 meeting syllabus titled ‘‘Critical Care for Cerebrovascular Patients: What General
Neurologists Need to Know’’; with permission.
This is an updated version of an article that originally appeared in Critical Care Clinics,
volume 22, issue 4.
* Corresponding author.
E-mail address: [email protected] (A. Finley Caulfield).
0733-8619/08/$ - see front matter � 2008 Elsevier Inc. All rights reserved.
doi:10.1016/j.ncl.2008.03.016 neurologic.theclinics.com

346 FINLEY CAULFIELD & WIJMAN
support, followed by neurologic assessment, brain imaging, and evaluationof the appropriateness of thrombolytic therapy [4,5].
Airway and ventilatory support
Patients with acute stroke are at risk for respiratory failure from aspira-tion and pneumonia [6,7] often in the setting of difficulty protecting the air-way and clearing secretions because of facial or bulbar weakness or analtered level of consciousness [8]. Hypoxemia may worsen the injurious ef-fects of cerebral ischemia, and patients must be monitored closely witha goal to keep oxygen saturation greater than 95% [4]. If a patient requiresendotracheal intubation, short-acting sedatives should be used, and the he-modynamic changes associated with intubation should be minimized[5,9,10]. No prospective trials have been undertaken to establish the idealmode of ventilation in intubated stroke patients. A commonly used modefor patients who are awake but in need of airway protection is pressure sup-port ventilation, whereas synchronized intermittent mandatory ventilationor assist control ventilation is recommended for patients who have intracra-nial hypertension or are comatose [5]. Excessive positive end-expiratorypressures (ie, O10 cm H2O) may be deleterious in patients with elevatedintracranial pressure (ICP) [11,12].
Mechanically ventilated patients frequently require sedation; however,sedatives may cause hypotension and additional brain injury by lowering ce-rebral perfusion pressure [13–15]. Propofol, popular because of its short du-ration of action, has been associated with a ‘‘propofol infusion syndrome’’when used at high doses for prolonged periods. This syndrome originallywas described in pediatric patients, but it also can occur in adults. It presentswith metabolic acidosis, rhabdomyolysis, hypotension, bradyarrhythmias,and death [16]. Frequent discontinuation of sedatives is indicated to monitorcarefully for changes in the patient’s neurologic status.
Blood pressure and fluid management
Patients with acute ischemic stroke often have elevated blood pressures inthe first few days after symptom onset. Elevated blood pressure may occurfor a variety of reasons, including physiologic compensation for cerebral is-chemia, increased ICP, pain, or long-standing underlying hypertension [4].Theoretic advantages of treating hypertension in acute ischemic stroke in-clude concerns for hemorrhagic transformation of the ischemic infarctand worsening cerebral edema. Lowering blood pressure may compromisecerebral blood flow in the area surrounding the infarct, however, resultingin stroke extension.
In normotensive individuals, cerebral blood flow is maintained overa wide range of mean arterial pressures (50–150 mm Hg) [17,18]. Chronicallyhypertensive patients require a higher range of mean arterial pressures to
347MANAGEMENT OF ACUTE ISCHEMIC STROKE
maintain normal cerebral blood flow [19–21]. Because many stroke patientshave long-standing hypertension, blood pressure lowering may result in ce-rebral hypoperfusion and worsening ischemia. It is generally accepted thatelevated blood pressures should not be lowered, unless the patient has re-ceived thrombolytic treatment; has a hypertensive emergency (aortic dissec-tion, hypertensive encephalopathy, acute renal failure, acute pulmonaryedema, or acute myocardial infarction); or has another contraindicationto elevated blood pressure, such as recent surgery. In the absence of con-trolled clinical trials, the American Stroke Association guidelines recom-mend that antihypertensive agents should be withheld unless the systolicblood pressure is greater than 220 mm Hg or the diastolic blood pressureis greater than 120 mm Hg [20,22–25]. If patients have received thrombolytictherapy, the guidelines advocate maintaining systolic blood pressure lessthan or equal to 180 mm Hg and diastolic blood pressure less than or equalto 105 mm Hg [2,22–25]. If blood pressure lowering is indicated, it should beinstituted cautiously to avoid hypotension. A variety of intravenous agentsmay be used to lower blood pressures. a- and b-adrenergic blockers (labeta-lol), calcium channel blockers (nicardipine), and angiotensin-converting en-zyme inhibitors (enalaprilat) are preferred in patients with acute strokebecause these agents are less likely to cause cerebral vasodilation and ICPelevation, effects that might be anticipated with sodium nitroprusside orhydralazine [4,5,26–30].
Some patients with acute cerebral ischemia resulting from severe extra-cranial or intracranial vessel stenosis may benefit from induced hypertension[31]. Typically, mean arterial pressure is increased 20% to 25% from base-line using intravenous isotonic fluids, phenylephrine, dopamine, or norepi-nephrine, while the patient’s neurologic status and hemodynamic stabilityare monitored closely. The impact of this therapy on stroke outcome isbeing evaluated in ongoing clinical trials.
In patients with ischemic brain injury, a key therapeutic goal is to max-imize brain perfusion and collateral blood flow to the injured area. It isimportant to assess the patient’s volume status and correct any dehydra-tion. Because stroke patients may be dehydrated on admission, andmany of them cannot tolerate intake of oral fluids, normal saline infusionstypically are started immediately. Hypotonic fluids should be avoided be-cause these may contribute to worsening cerebral edema and increasedICP [32].
Neurologic examination
Assessing the patient for neurologic deficits may be accomplished in anefficient and reproducible manner by using the National Institutes of HealthStroke Scale (NIHSS) [25,33,34]. This is a series of neurologic tests designedto assess the patient’s level of alertness; comprehension; and motor, sensory,visual, and language function (Table 1) [2].

Table 1
The National Institutes of Health Stroke Scale
Tested item Title Responses and scores
1a Level of consciousness 0 ¼ Alert
1 ¼ Drowsy
2 ¼ Obtunded
3 ¼ Coma/unresponsive1b Orientation questions (two) 0 ¼ Answers both correctly
1 ¼ Answers one correctly
2 ¼ Answers neither correctly1c Response to commands (two) 0 ¼ Performs both tasks correctly
1 ¼ Performs one task correctly
2 ¼ Performs neither task2 Gaze 0 ¼ Normal horizontal movements
1 ¼ Partial gaze palsy
2 ¼ Complete gaze palsy3 Visual fields 0 ¼ No visual field defect
1 ¼ Partial hemianopsia
2 ¼ Complete hemianopsia
3 ¼ Bilateral hemianopsia
4 Facial movement 0 ¼ Normal
1 ¼ Minor facial weakness
2 ¼ Partial facial weakness
3 ¼ Complete unilateral paralysis5 Motor function arm 0 ¼ No drift
a. left 1 ¼ Drift before 10 seconds
b. right 2 ¼ Falls before 10 seconds
3 ¼ No effort against gravity
4 ¼ No movement
6 Motor function leg 0 ¼ No drift
a. left 1 ¼ Drift before 5 seconds
b. right 2 ¼ Falls before 5 seconds
3 ¼ No effort against gravity
4 ¼ No movement
7 Ataxia 0 ¼ Absent
1 ¼ Ataxia in one limb
2 ¼ Ataxia in two limbs
8 Sensory 0 ¼ Normal
1 ¼ Mild sensory loss
2 ¼ Severe sensory loss
9 Language 0 ¼ Normal
1 ¼ Mild aphasia
2 ¼ Severe aphasia
3 ¼ Mute or global aphasia
10 Articulation 0 ¼ Normal
1 ¼ Mild dysarthria
2 ¼ Severe dysarthria
11 Extinction or inattention 0 ¼ Normal
1 ¼ Mild (loss 1 sensory modality)
2 ¼ Severe (loss 2 modalities)
Adapted from the National Institutes of Neurological Disorders and Stroke (NINDS).
National Institute of Health Stroke Scale. Available at http://www.ninds.nih.gov/doctors/
index.htm.
348 FINLEY CAULFIELD & WIJMAN

349MANAGEMENT OF ACUTE ISCHEMIC STROKE
Diagnostic work-up
Brain imaging
CT and MRI can assess rapidly the type of stroke (hemorrhagic versusischemic) and the condition of the cerebral vasculature. Advances in CTand MRI techniques of cerebral perfusion hold the promise of identifyingpatients with salvageable brain tissue who could benefit from recanalizationtherapies beyond the 3-hour time window.
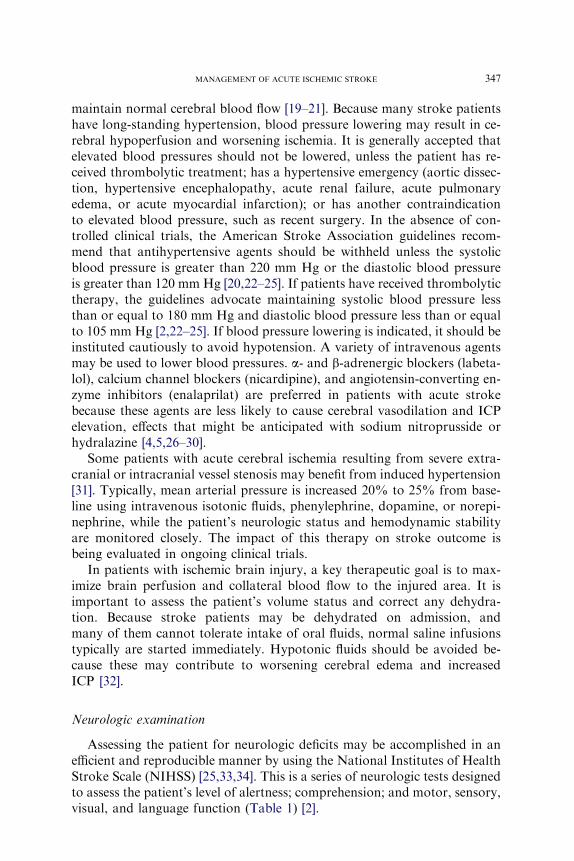
The most widely used and available brain imaging technology is CT. Anoncontrast head CT scan quickly excludes an intracranial hemorrhageand sometimes reveals an occluded artery that appears hyperdense becauseof fresh clot in the vessel lumen (Fig. 1A). The admission CT scan also mayshow early signs of infarction, including swelling of the brain parenchyma(sulcal effacement); hypoattenuation (hypodensity) of the brain paren-chyma; or loss of gray-white matter differentiation (Fig. 1B) [35–37]. Earlysigns of cerebral infarction in the 3-hour time window slightly increase therisk of hemorrhagic transformation after intravenous tPA, but are not con-sidered a contraindication for tPA treatment [38]. A large area of hypoden-sity on the admission CT scan obtained within the 3-hour time window isuncommon, however, and warrants verification of the accuracy of the re-ported time of symptom onset. Because a noncontrast head CT scan mayfail to detect subarachnoid hemorrhage in approximately 10% of cases,a lumbar puncture to assess for the presence of subarachnoid blood is man-datory in patients who present with a clinical history of a sudden severeheadache and a normal brain CT scan [39].
CT angiography of the head and neck may be used to assess the intracra-nial and cervical circulation for stenoses and occlusions [40]. CT angiogra-phy uses a helical scanner to map out a contrast bolus as it passes throughthe vessels. It requires adequate peripheral intravenous access for injectionof an iodine-based contrast bolus (150–170 mL). Although CT angiographyincreases the incidence of renal dysfunction, this risk is relatively small; inone series of patients undergoing cerebral CT angiography and CT perfu-sion, only 4 (0.37%) of 1075 subjects had an increase in creatinine equalto or greater than 0.5 mg/dL [41]. CT angiography may be particularly use-ful in patients who present just outside of the treatment window for intrave-nous thrombolysis, and who may be candidates for intra-arterial clot lysisbecause it can provide valuable information as to the location and extentof the clot. CT angiography also may be useful to assess the head andneck vessels in patients who cannot undergo MRI because of the presenceof pacemakers or other metal objects in the body, claustrophobia, or criticalillness precluding extended periods in a MRI scanner. Perfusion CT assessescerebral perfusion of the brain by tracking the first pass of an intravenouslyadministered bolus of contrast material using helical CT scanning [42]. Thistechnique is promising because of its ability to measure absolute cerebral
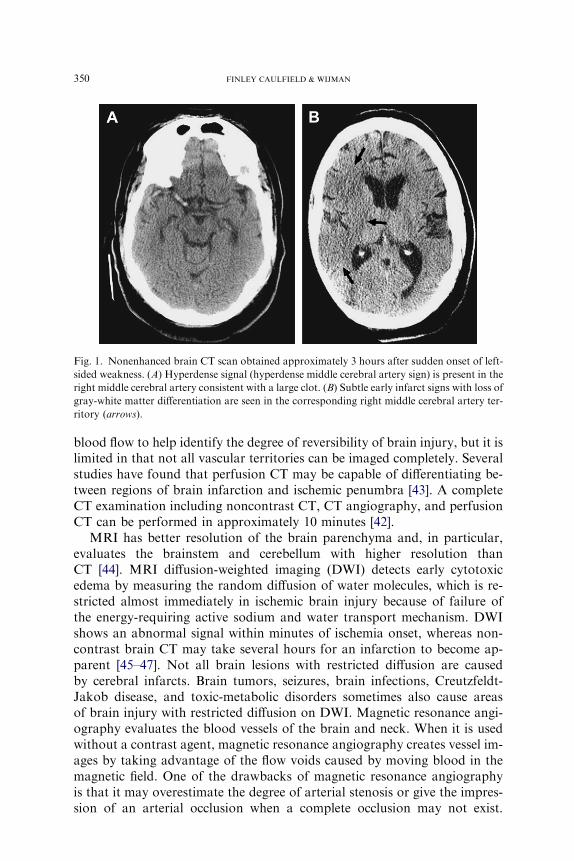
Fig. 1. Nonenhanced brain CT scan obtained approximately 3 hours after sudden onset of left-
sided weakness. (A) Hyperdense signal (hyperdense middle cerebral artery sign) is present in the
right middle cerebral artery consistent with a large clot. (B) Subtle early infarct signs with loss of
gray-white matter differentiation are seen in the corresponding right middle cerebral artery ter-
ritory (arrows).
350 FINLEY CAULFIELD & WIJMAN
blood flow to help identify the degree of reversibility of brain injury, but it islimited in that not all vascular territories can be imaged completely. Severalstudies have found that perfusion CT may be capable of differentiating be-tween regions of brain infarction and ischemic penumbra [43]. A completeCT examination including noncontrast CT, CT angiography, and perfusionCT can be performed in approximately 10 minutes [42].
MRI has better resolution of the brain parenchyma and, in particular,evaluates the brainstem and cerebellum with higher resolution thanCT [44]. MRI diffusion-weighted imaging (DWI) detects early cytotoxicedema by measuring the random diffusion of water molecules, which is re-stricted almost immediately in ischemic brain injury because of failure ofthe energy-requiring active sodium and water transport mechanism. DWIshows an abnormal signal within minutes of ischemia onset, whereas non-contrast brain CT may take several hours for an infarction to become ap-parent [45–47]. Not all brain lesions with restricted diffusion are causedby cerebral infarcts. Brain tumors, seizures, brain infections, Creutzfeldt-Jakob disease, and toxic-metabolic disorders sometimes also cause areasof brain injury with restricted diffusion on DWI. Magnetic resonance angi-ography evaluates the blood vessels of the brain and neck. When it is usedwithout a contrast agent, magnetic resonance angiography creates vessel im-ages by taking advantage of the flow voids caused by moving blood in themagnetic field. One of the drawbacks of magnetic resonance angiographyis that it may overestimate the degree of arterial stenosis or give the impres-sion of an arterial occlusion when a complete occlusion may not exist.
351MANAGEMENT OF ACUTE ISCHEMIC STROKE
Contrast-enhanced magnetic resonance angiography is thought to decreasethe likelihood of overestimation of the severity of luminal stenosis [48,49].
MRI perfusion-weighted imaging (PWI) was developed to measure rela-tive blood flow in the brain. A bolus injection of paramagnetic contrastagent is given and tracked on the first pass through the brain parenchyma.A variety of parameters may be measured from this injection and displayedon perfusion maps, including bolus arrival time, mean transit time, and rel-ative cerebral blood volume [42,46,50,51]. Perfusion maps may take 5 to40 minutes of postprocessing time. The use of PWI and DWI may identifypatients who would benefit from recanalization therapy outside the estab-lished 3-hour time window for intravenous tPA. An example of a patientin the 3- to 6-hour window with a mismatch between a large perfusion deficitand a small diffusion abnormality and a persistent corresponding vessel oc-clusion is presented in Fig. 2 [52]. The patient received intravenous tPA 3 to
Fig. 2. MRI of the brain with diffusion-weighted imaging (DWI) on the left, perfusion-
weighted imaging (PWI) in the middle, and magnetic resonance angiography on the right.
(Top row) MRI obtained approximately 5 hours after acute onset of aphasia and right-sided
weakness showing a small area of infarction (white) on DWI, a large area of decreased perfusion
of the left middle cerebral artery brain territory (white) at risk for infarction on PWI, and absent
flow in the left middle cerebral artery flow on magnetic resonance angiography. (Bottom row)
MRI obtained 4.5 hours later (after intravenous tissue plasminogen activator [tPA] administra-
tion) shows marked improvement in the PWI and reconstitution of flow in the left middle
cerebral artery. There is a marked improvement in neurologic function (National Institutes
of Health Stroke Scale [NIHSS] changed from 16 to 5) and no growth of the DWI lesion.
(Courtesy of Gregory W. Albers, MD, Palo Alto, CA.)

352 FINLEY CAULFIELD & WIJMAN
6 hours after symptom onset, which resulted in vessel recanalization and res-olution of the PWI deficit. The patient’s neurologic status improved sub-stantially (NIHSS improved from 16 to 5). If the vessel had remainedoccluded, the DWI lesion likely would have grown to the size of the corre-sponding PWI lesion, reducing the chances of clinical improvement.
Emergent laboratory evaluation and other tests
In addition to brain imaging, several laboratory tests must be performedexpeditiously to evaluate whether the patient is a candidate for tPA, includ-ing a complete blood count, coagulation parameters, and serum glucose(Box 1) [2,4,22,53]. An electrocardiogram is indicated in all patients withacute stroke to detect myocardial ischemia and cardiac arrhythmias, suchas atrial fibrillation. Blood urea nitrogen and creatinine levels should bechecked, in particular in patients who will be exposed to iodine-based con-trast agents. In selected patients, one should consider obtaining (1) arterialblood gas measurements; (2) cardiac biomarkers, including troponin andbrain natriuretic peptide; (3) liver function tests and ammonia level (forpatients with an unexplained altered level of consciousness); (4) chestradiograph (for patients with respiratory distress or hypoxia); (5) blood cul-tures (for patients with fever raising a concern for septic emboli); (6) urinetoxicology screen (for patients with possible substance abuse); (7) electroen-cephalogram (for suspected seizures); (8) lumbar puncture (for suspectedmeningitis or subarachnoid hemorrhage); and (9) CT of the cervical spineif neck trauma has occurred or is suspected [4].
Treatment of acute ischemic stroke
Antiplatelet therapy in acute ischemic stroke
For patients who are not eligible for tPA, aspirin is the only antiplateletdrug that has been evaluated in the acute treatment of stroke. The ChineseAcute Stroke Trial enrolled 21,106 patients to receive aspirin, 160 mg/d, orplacebo within 48 hours of stroke onset with continued therapy for 4 weeks[54]. The aspirin-treated group had a small but significant decrease in mor-tality (3.3% versus 3.9%; P ¼ .04) and recurrent ischemic stroke (1.6% ver-sus 2.1%; P ¼ .01). The International Stroke Trial enrolled 19,435 patientsfor randomized treatment with aspirin alone (300 mg/d), subcutaneous hep-arin alone, aspirin and heparin combined, or neither agent within 48 hoursof stroke onset [55]. In the aspirin-only group, there were significantly fewerrecurrent strokes within the first 2 weeks (2.8% versus 3.9%) and a trendtoward a reduction of death or dependence at 6 months (61.2% versus63.5%). Based on the results of these trials, most experts agree that patientsshould be treated within 48 hours of ischemic stroke with aspirin [25,53]. Inpatients who receive tPA, antiplatelet therapy should start 24 hours afterthrombolytic therapy [2,4,22,25,53].

Box 1. Characteristics of patients with ischemic stroke whocould be treated with recombinant tissue plasminogen activator
Diagnosis of ischemic stroke causing measurable neurologicdeficit
Neurologic signs should not be clearing spontaneouslyNeurologic signs should not be minor and isolatedCaution should be exercised in treating a patient with major
deficitsSymptoms of stroke should not suggest subarachnoid
hemorrhageOnset of symptoms less than 3 hours before beginning treatmentNo head trauma or prior stroke in previous 3 monthsNo myocardial infarction in the previous 3 monthsNo gastrointestinal or urinary tract hemorrhage in previous
21 daysNo major surgery in the previous 14 daysNo arterial puncture at a noncompressible site in the previous
7 daysNo history of previous intracranial hemorrhageBlood pressure not elevated (systolic <185 mm Hg and diastolic
<110 mm Hg)No evidence of active bleeding or acute trauma (fracture) on
examinationNot taking an oral anticoagulant, or if anticoagulant being taken,
international normalized ratio is 1.7 or lessIf receiving heparin in previous 48 hours, activated partial
thromboplastin time must be in normal rangePlatelet count equal to or greater than 100,000 mm3
Blood glucose concentration equal to or greater than 50 mg/dL(‚2.7 mmol/L)
No seizure with postictal residual neurologic impairmentsCT does not show a multilobar infarction (hypodensity greater
than one third cerebral hemisphere)Patient or family members understand the potential risks and
benefits from treatment
From Adams H, Adams R, Del Zoppo G, et al. Guidelines for the early manage-ment of patients with ischemic stroke: 2005 guidelines updateda scientific state-ment from the Stroke Council of the American Heart Association/American StrokeAssociation. Stroke 2005;36:916–23; with permission.
353MANAGEMENT OF ACUTE ISCHEMIC STROKE
354 FINLEY CAULFIELD & WIJMAN
Intravenous thrombolytic therapy within the 3-hour time window
tPA is a fibrin-specific thrombolytic agent that activates plasminogen toform plasmin, a protease that cleaves fibrin. The National Institute of Neu-rologic Disorders and Stroke (NINDS) acute stroke study group enrolled624 patients presenting within 3 hours of symptom onset in a randomized,double-blind, placebo-controlled, two-part study evaluating the effect of in-travenous tPA (at 75% of the recommended dose for myocardial infarction)for all types of ischemic stroke [2]. The first part of the study measured earlyresponse to tPA and showed improvement in the NIHSS score by 4 or morepoints at 24 hours after treatment [2,53]. The 3-month functional outcomeevaluation also showed improved neurologic outcomes in the tPA group,which paved the way for verification of these results in the second part ofthe study. The primary end point for part two was a combined 3-month out-come assessment using several rating scales: the NIHSS, Barthel index, mod-ified Rankin scale, and Glasgow outcome scale. All outcome measuresshowed benefit in the tPA group with 11% to 13% absolute difference inneurologic scores in the tPA-treated patients [53]. The symptomatic intra-cranial hemorrhage rate was higher in the tPA group (6.4%) than in the pla-cebo group (0.6%) (P!.001) [2]. Mortality rates at 3 months were similar inboth groups, however, at 17% for the tPA group and 21% for the placebogroup (P ¼ .30) [2]. Based on these results, the FDA approved the use ofintravenous tPA within 3 hours from stroke onset at a dose of 0.9 mg/kg,with a maximum dose of 90 mg [2,53,56,57]. Box 1 lists the characteristicsof patients with ischemic stroke who are eligible for treatment with tPA [22].
Since the approval of intravenous tPA, two prospective, monitored,phase 4 studies have shown similar results [58,59]. These studies were de-signed to assess the safety profile and clinical efficacy of intravenous tPAtherapy for acute ischemic stroke in clinical practice. The Standard Treat-ment with Alteplase to Reverse Stroke study enrolled 389 patients andshowed that 43% of patients treated with intravenous tPA had independentfunctional outcomes (defined as a modified Rankin score of 0–2) at 1 monthpost treatment [58]. The percentage of symptomatic intracranial hemorrhagewas 3.3%, and mortality was 13% at 1 month. The Canadian Activase forStroke Effectiveness Study enrolled 1132 patients and found that 36% oftPA-treated patients had favorable outcomes at 3 months [59]. The rate ofsymptomatic intracranial hemorrhage was 4.6% and mortality was 21%at 3 months.
Intravenous thrombolytic therapy beyond the 3-hour time window
The European Cooperative Acute Stroke Study (ECASS) consisted oftwo trials evaluating the use of intravenous tPA within 6 hours of symptomonset in patients with a moderate-to-severe hemispheric stroke [60,61].ECASS I [60] used 85% of the dose for myocardial infarction (1.1 mg/kg,
355MANAGEMENT OF ACUTE ISCHEMIC STROKE
maximum dose 100 mg), and ECASS II [61] used 75% of the dose formyocardial infarction (0.9 mg/kg, maximum dose 90 mg). In ECASS I,620 patients were enrolled, but 17% had protocol violations mainly becauseof misinterpretations of the admission brain CT scans. After excluding thepatients with protocol violations, modified Rankin scores (asymptomaticor minimal disability) were significantly better in the tPA group comparedwith the placebo group. Among all patients enrolled in ECASS I, therewas a 20% symptomatic intracranial hemorrhage rate in the treatmentgroup compared with 7% in the placebo group (P!.001). This increasedrate of hemorrhage in ECASS I likely is related to the tPA dose (1.1 mg/kg,100 mg maximum), which was substantially higher than in the NINDStPA study. In ECASS II, 800 patients were enrolled with a primary end pointof 3-month favorable outcome defined as a modified Rankin score of 0 to1 (asymptomatic or no significant disability despite symptoms). The tPA-treated group faired slightly better at 3 months than the placebo groupwith a 3.7% higher percentage of patients with favorable outcomes[4,53,60,61].
The Alteplase Thrombolysis for Acute Noninterventional Therapy in Is-chemic Stroke trial was a randomized, placebo-controlled trial evaluatingthe use of 0.9 mg/kg of intravenous tPA in the 3- to 5-hour treatment win-dow [62]. The study was stopped early when interim analysis revealed a lowlikelihood of benefit in the treatment group. Several clinical trials evaluatedintravenous streptokinase for acute stroke in Europe and Australia. TheMulti-center Acute Stroke TrialdItaly and Multi-center Acute StrokeTrialdEurope used a 6-hour time window for intravenous treatment with1.5 million U of streptokinase (100% of myocardial infarction dosage)[63,64]. The Australia Streptokinase Trial used the same dose, but shortenedthe time window to 4 hours [65]. All three trials were stopped early becauseof an unacceptable high number of deaths and symptomatic intracranialhemorrhages in the treatment groups.
Newer thrombolytic and antiplatelet agents
Recent studies have evaluated alternative thrombolytic agents, such asancrod (Viprinex), a viper-derived enzyme that cleaves fibrinogen and pro-motes endogenous release of plasminogen activator from the vessel wall[4,66–68]. The phase III Ancrod Study compared intravenous Ancrodwith placebo within 6 hours of stroke symptom onset and found no differ-ence in 3-month functional success defined as survival with a Barthel indexof greater than or equal to 95 (or return to prestroke value) between thetreated group (42%) and the placebo group (42%) [69]. Desmoteplase, a pro-tease found in vampire bat saliva, is similar to human plasminogen activa-tor, but in laboratory models works faster and causes a more sustainedvessel recanalization compared with tPA. Based on promising phase II trialresults (DEDAS and DIAS trials), it was evaluated in the DIAS 2 trial in the
356 FINLEY CAULFIELD & WIJMAN
3- to 9-hour time window for acute stroke patients with a presumed penum-bra based on MRI or CT imaging results [70,71]. The preliminary results ofthis trial were presented at the 2007 European Stroke Conference and showno significant difference in 3-month clinical outcome between the desmote-plase-treated and the placebo groups [72].
Glycoprotein IIb/IIIa antagonists also are being evaluated alone(AbESST, SaTIS, SETIS) and in combination with low-dose intravenoustPA (the Clear Stroke Trial) [73–76]. The ReoPro Retavase Reperfusionof Stroke Safety StudydImaging Evaluation trial is assessing the use of ab-ciximab alone and in conjunction with escalating doses of reteplase. Prelim-inary results suggest promise for the combination therapy, but not forabciximab alone [77].
Although several novel pharmacologic agents hold promise for acute is-chemic stroke patients, current care of patients with acute ischemic strokestill emphasizes NINDS- and FDA-defined use of intravenous tPA dosedat 0.9 mg/kg with a maximum dose of 90 mg. The risk of symptomatic in-tracranial hemorrhage is approximately 6% when the NINDS- and FDA-approved guidelines are strictly adhered to (see Box 1).
Intra-arterial thrombolysis
Direct administration of intra-arterial thrombolytic agents into the clot,while passing the catheter through the clot and mechanically disrupting it,allows for a lower tPA dose and a decreased risk of systemic hemorrhagiccomplications. A disadvantage of intra-arterial thrombolytic therapy isthe time and expertise required for catheterization, restricting this therapeu-tic modality to medical centers that have interventional neuroradiologistsand critical care services available 24 hours a day.
Prolyse in Acute Cerebral Thromboembolism (PROACT) was a random-ized clinical trial evaluating the efficacy of intra-arterial prourokinase plusintravenous heparin compared with placebo plus intravenous heparin in pa-tients presenting with middle cerebral artery occlusions less than 6 hours old[78,79]. Mechanical disruption of the clot was not permitted. PROACT I[78] randomized 46 patients and showed that intra-arterial prourokinase in-fusion was associated with superior recanalization rates compared with pla-cebo. The symptomatic intracranial hemorrhage rate was 15.4% in theprourokinase group versus 7.1% in the placebo group. In PROACT II[79], there was a statistically significant benefit with 40% of prourokinase-treated patients having a good 3-month functional outcome (modifiedRankin score %2) compared with 25% of the control group. Symptomaticintracranial hemorrhage occurred in 10% of the prourokinase group and2% of the control group (P ¼ .063). Because prourokinase is not availablein the United States for clinical use, tPA and urokinase have been usedinstead for intra-arterial thrombolysis with favorable outcomes in selectedpatients [53,78,79].

357MANAGEMENT OF ACUTE ISCHEMIC STROKE
Intra-arterial thrombolytic therapy for acute stroke is not approved bythe FDA, but may be considered in patients with middle cerebral artery oc-clusions who can be treated within 3 to 6 hours after symptom onset andwho have no (or minimal) signs of infarction on their baseline CT scans[4,53]. Given the high mortality associated with basilar artery and internalcarotid artery bifurcation (carotid T) occlusions, patients with these lesionsalso may be considered for intra-arterial thrombolytic therapy on a case-by-case basis [4,53].
Combined intravenous and intra-arterial thrombolysis
The combination of intravenous and intra-arterial thrombolysis has beeninvestigated in several pilot studies and may be more effective than eithertherapy alone in patients with acute, very large vessel occlusions. The Na-tional Institutes of Health Interventional Management of Stroke trial I(IMS I) investigated the feasibility and safety of a combined intravenousand intra-arterial approach to recanalization in patients with ischemicstroke and a substantial neurologic deficit (NIHSS R10) [80]. The study en-rolled 80 patients, and their outcome was compared with historical intrave-nous tPA controls. The patients received 0.6 mg/kg of intravenous tPA over30 minutes within 3 hours from stroke symptom onset followed by intra-arterial tPA within 5 hours if a vessel occlusion was still present on angiog-raphy. The 3-month mortality rate and the symptomatic intracerebralhemorrhage rate in IMS patients were similar to intravenous tPA–treatedpatients in the NINDS tPA Stroke Trial. IMS subjects showed a nonsignif-icant trend toward better clinical outcomes than historical intravenous tPAcontrols (odds ratio 1.35; 95% confidence interval, 0.78–2.37). The results ofthis study and other pilot studies suggest that a combined intravenous plusintra-arterial approach to recanalization is feasible and safe. Further studiesassessing the efficacy of this combined approach to recanalization are pres-ently ongoing and have incorporated the use of endovascular mechanicaldevices.
Mechanical thrombolysis
Several endovascular devices have been developed in recent years to re-move clots from the cerebral circulation. These devices have been tested inpatients with acute stroke who are ineligible for or who failed intravenoustPA treatment [81–85]. The Mechanical Embolus Removal in Cerebral Is-chemia (MERCI) retrieval device has been studied most extensively andwas approved by the FDA for use in acute stroke patients who are inel-igible or fail intravenous tPA therapy [85]. The device is deployed just be-yond the clot with release of two nitinol helices and pulled back into theclot with the remainder of the helices deployed (Fig. 3). It is twisted threeto five times to capture the clot better. A balloon is inflated in the internal
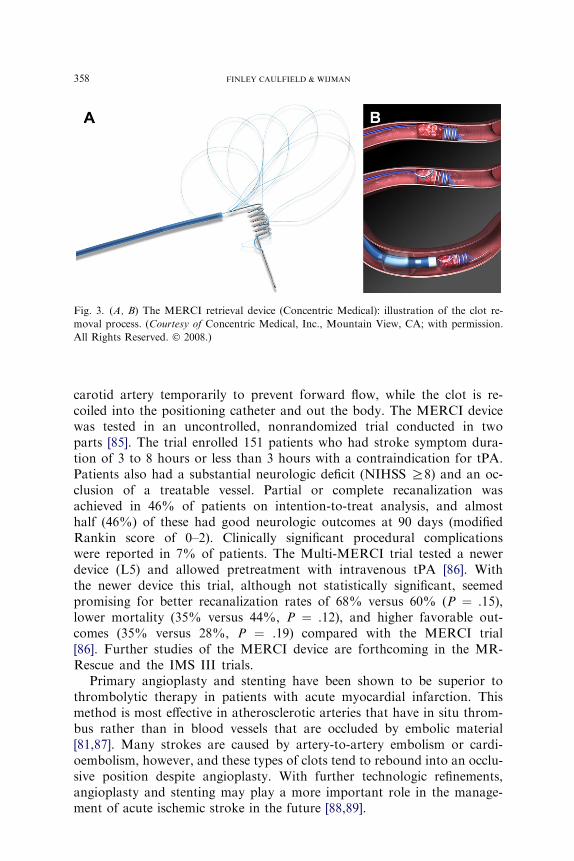
Fig. 3. (A, B) The MERCI retrieval device (Concentric Medical): illustration of the clot re-
moval process. (Courtesy of Concentric Medical, Inc., Mountain View, CA; with permission.
All Rights Reserved. � 2008.)
358 FINLEY CAULFIELD & WIJMAN
carotid artery temporarily to prevent forward flow, while the clot is re-coiled into the positioning catheter and out the body. The MERCI devicewas tested in an uncontrolled, nonrandomized trial conducted in twoparts [85]. The trial enrolled 151 patients who had stroke symptom dura-tion of 3 to 8 hours or less than 3 hours with a contraindication for tPA.Patients also had a substantial neurologic deficit (NIHSS R8) and an oc-clusion of a treatable vessel. Partial or complete recanalization wasachieved in 46% of patients on intention-to-treat analysis, and almosthalf (46%) of these had good neurologic outcomes at 90 days (modifiedRankin score of 0–2). Clinically significant procedural complicationswere reported in 7% of patients. The Multi-MERCI trial tested a newerdevice (L5) and allowed pretreatment with intravenous tPA [86]. Withthe newer device this trial, although not statistically significant, seemedpromising for better recanalization rates of 68% versus 60% (P ¼ .15),lower mortality (35% versus 44%, P ¼ .12), and higher favorable out-comes (35% versus 28%, P ¼ .19) compared with the MERCI trial[86]. Further studies of the MERCI device are forthcoming in the MR-Rescue and the IMS III trials.
Primary angioplasty and stenting have been shown to be superior tothrombolytic therapy in patients with acute myocardial infarction. Thismethod is most effective in atherosclerotic arteries that have in situ throm-bus rather than in blood vessels that are occluded by embolic material[81,87]. Many strokes are caused by artery-to-artery embolism or cardi-oembolism, however, and these types of clots tend to rebound into an occlu-sive position despite angioplasty. With further technologic refinements,angioplasty and stenting may play a more important role in the manage-ment of acute ischemic stroke in the future [88,89].
359MANAGEMENT OF ACUTE ISCHEMIC STROKE
Neuroprotective strategies
Many neuroprotective agents that were promising in laboratory modelsof focal ischemia have not shown benefit in clinical studies, partly becauseof limitations in trial design. Interest in neuroprotective agents for patientswith acute ischemic stroke remains, however, and several phase 3 studies arepresently ongoing. One of the most robust neuroprotective strategies in ex-perimental stroke models is mild-to-moderate hypothermia (2�C–5�C belownormal brain temperature) [90–92]. Hypothermia consistently has been as-sociated with a marked reduction in ischemic damage and improved behav-ioral outcomes in these models. The beneficial effects seem to be greatestwhen hypothermia is initiated early. The therapeutic window of mild hypo-thermia in patients with acute ischemic stroke is unknown, but likely to belimited to several hours after ischemia onset. The feasibility of hypothermiafor acute ischemic stroke patients has been tested in several clinical pilot tri-als. The Cooling for Acute Ischemic brain Damage study was a phase 2 ran-domized clinical trial using hypothermia in patients less than 12 hours fromstroke onset. There was no significant clinical benefit in 18 patients treatedwith hypothermia compared with 22 patients who received standard medicaltherapy. The study showed, however, that endovascular cooling at 33�C wasfeasible and tolerated by most patients [93]. The Intravascular Cooling forthe Treatment of StrokedLonger window trial is presently ongoing. Thisis a multicenter, controlled, randomized trial designed to investigate the fea-sibility and safety of a combination of therapeutic hypothermia with intra-venous tPA in the 0- to 6-hour window in awake stroke patients [94].
The Stroke-Acute Ischemic NXY-059 Treatment (SAINT) trials were de-signed to evaluate the therapeutic benefit of intravenous NXY-059, a nitroneradical trapping agent, administered within 6 hours of stroke onset [95,96].The SAINT I trial enrolled more than 1700 patients with acute ischemicstroke and showed a modest, but statistically significant (P ¼ .038) im-proved outcome in the treatment group as measured by the modified Rankinscale at 90 days; however, the definitive SAINT II trial, which enrolled morethan 3300 patients, did not confirm these results [95,96]. Ongoing phase IIItrials evaluating neuroprotective agents in acute ischemic stroke include theField Administration of Stroke TherapydMagnesium trial assessing thebenefit of intravenous magnesium within 2 hours from stroke onset andthe Albumin in Acute Stroke study, a trial of high-dose albumin within5 hours of symptom onset [97–99].
Anticoagulation in acute ischemic stroke
There is no evidence to support urgent anticoagulation to prevent strokerecurrence or extension in patients with acute stroke [25,53,100]. Intrave-nous heparin infused for 7 days was evaluated in a small randomized, con-trolled study with 225 patients with acute ischemic stroke [101]. No
360 FINLEY CAULFIELD & WIJMAN
significant difference in stroke progression or neurologic outcome was foundbetween the treatment and the control groups. Analysis of the combinedheparin groups from International Stroke Trial showed that a decreased re-current stroke risk at 14 days was offset by an increased risk of intracranialhemorrhage [55]. The low-dose heparin group (5000 U twice a day) had de-creased mortality with only a slight and nonsignificant increase in bleedingrisk. The low-dose heparin in combination with aspirin group had the lowestrate of stroke recurrence and no significant increase in bleeding risk com-pared with patients on only low-dose heparin. A subgroup analysis of pa-tients who presented with atrial fibrillation and acute ischemic strokeshowed a significant reduced risk of recurrent ischemic strokes (4.9% versus2.8%), but the increased risk of intracranial hemorrhage negated any poten-tial benefits (2.1% versus 0.4%) at 14 days [53,55].
Studies evaluating low-molecular-weight heparins in acute ischemicstroke failed to show a beneficial effect [102–105]. In a subgroup analysisof the TOAST trial, however, better outcomes were observed in patientswith stroke caused by large artery atherosclerosis [103,105,106]. In a recentstudy among Asian stroke patients with large artery occlusive disease (intra-cranial and extracranial), low-molecular-weight heparin (nadroparin) over-all did not support a significant benefit over aspirin in acute stroke patients[107]. Benefits observed in secondary outcome measures, however, may war-rant further study of low-molecular-weight heparins in acute stroke patientsattributed to large artery atherosclerosis.
Complications of stroke
Hemorrhagic transformation
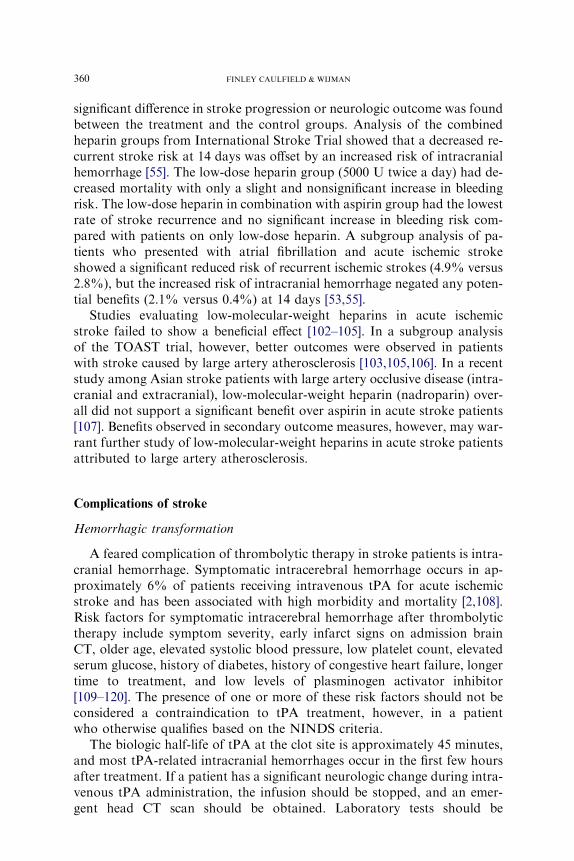
A feared complication of thrombolytic therapy in stroke patients is intra-cranial hemorrhage. Symptomatic intracerebral hemorrhage occurs in ap-proximately 6% of patients receiving intravenous tPA for acute ischemicstroke and has been associated with high morbidity and mortality [2,108].Risk factors for symptomatic intracerebral hemorrhage after thrombolytictherapy include symptom severity, early infarct signs on admission brainCT, older age, elevated systolic blood pressure, low platelet count, elevatedserum glucose, history of diabetes, history of congestive heart failure, longertime to treatment, and low levels of plasminogen activator inhibitor[109–120]. The presence of one or more of these risk factors should not beconsidered a contraindication to tPA treatment, however, in a patientwho otherwise qualifies based on the NINDS criteria.
The biologic half-life of tPA at the clot site is approximately 45 minutes,and most tPA-related intracranial hemorrhages occur in the first few hoursafter treatment. If a patient has a significant neurologic change during intra-venous tPA administration, the infusion should be stopped, and an emer-gent head CT scan should be obtained. Laboratory tests should be
361MANAGEMENT OF ACUTE ISCHEMIC STROKE
performed immediately, including coagulation parameters, fibrinogen, andcomplete blood count with platelets. If a symptomatic intracerebral hemor-rhage is diagnosed, emergent infusion of fresh frozen plasma (5–10 mL/kg)and cryoprecipitate (0.1 bag/kg) is recommended [121].
Cerebral edema
Patients with ischemic stroke with cerebral edema and mass effect are atrisk for brain herniation, brainstem compression, coma, and death. Exam-ples are patients with large hemispheric infarctions involving the middle ce-rebral artery territory and patients with large cerebellar infarctions. Masseffect caused by ischemic infarcts typically peaks 3 to 5 days after symptomonset. The clinical examination is more sensitive in detecting worsening ce-rebral edema, local tissue shifts, and impending uncal or transtentorial her-niation than continuous ICP monitoring because the clinical deteriorationcaused by regional tissue injury and compression precedes a global increasein ICP in most patients [5,122,123].
In patients with suspected elevated ICP, initial management should con-sider adequacy of airway, breathing, and circulatory function. The headshould be elevated 30 degrees to decrease ICP and optimize cerebral venousreturn [124,125]. Hyperosmolar therapy should be instituted using mannitol,hypertonic saline, or both [126–128]. Mannitol extracts intracellular andinterstitial water from the brain. This agent also is a free radical scavenger,inhibits programmed cell death, and lowers blood viscosity [129]. It is ad-ministered as a 0.5 to 1 g/kg loading dose and can be followed by bolusesof 0.25 g/kg every 6 hours. The main complications associated with manni-tol use are hypovolemia, hypotension, and electrolyte disturbances resultingfrom osmotic diuresis. Hypertonic saline has been proposed as an alterna-tive to mannitol and may be of particular advantage in hypovolemic pa-tients. Rebound edema may occur after abrupt cessation of mannitol orhypertonic saline [128]. Experimental and clinical studies suggest potentialbenefits of hypertonic saline over mannitol in the treatment of stroke-relatedbrain edema and increased ICP [130,131]. More details on the treatment ofincreased ICP and the use of hyperosmolar therapy can be found elsewherein this issue. Because of the concern of compromising cerebral blood flow,hyperventilation should be used only in emergency situations and as a tem-porizing measure until more definitive therapies can be initiated. Corticoste-roid therapy, although effective in decreasing cerebral edema in patientswith brain tumors and brain abscesses, does not improve cerebral edemaassociated with ischemic or hemorrhagic stroke and ought to be avoidedbecause corticosteroids are of no benefit and may worsen outcome [132].
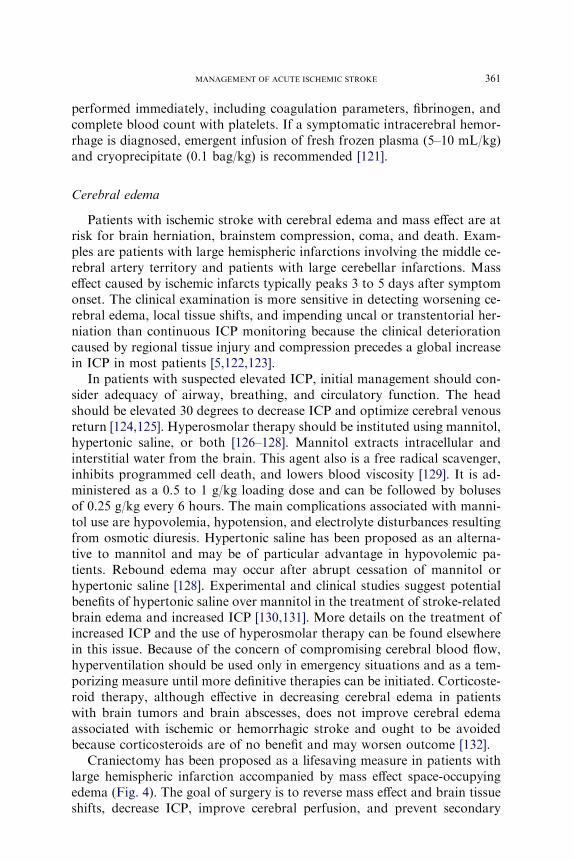
Craniectomy has been proposed as a lifesaving measure in patients withlarge hemispheric infarction accompanied by mass effect space-occupyingedema (Fig. 4). The goal of surgery is to reverse mass effect and brain tissueshifts, decrease ICP, improve cerebral perfusion, and prevent secondary
Fig. 4. Nonenhanced CT scan 3 days after a right middle cerebral artery territory infarction
that required a hemicraniectomy to decrease tissue shifts and prevent transtentorial herniation
and death.
362 FINLEY CAULFIELD & WIJMAN
injury. Several observational studies demonstrated a decrease in mortalityand improved neurologic outcome, in particular in young patients (age!60 years) with hemispheric infarctions who underwent decompressivehemicraniectomy when compared with historic controls [133–135]. Basedon these encouraging reports, three randomized controlled trials were un-dertaken in Europe to assess the beneficial effect of decompressive surgeryin patients with space-occupying hemispheric strokes. A meta-analysis com-bining data from the three studies was recently published and demonstratedthat decompressive hemicraniectomy reduced mortality and improvedfunctional outcome [136]. A substantial proportion of survivors (40%)had a 12-month modified Rankin scale score of 4, however, leading theauthors to conclude that ‘‘the decision to perform decompressive surgeryshould be made on an individual basis in every patient’’ [136]. Decompres-sive surgery also may benefit patients with large cerebellar infarctions, inparticular patients with hydrocephalus, brainstem compression, and neuro-logic deterioration.
Deep venous thrombosis
Deep venous thrombosis and pulmonary embolism are a cause of earlydeath in 5% of stroke patients [137]. Low-dose heparin or low-molecular-weight heparin may be used for prevention of deep venous thrombosis [53].In the PROTECT study, citraparin, a low-molecular-weight heparin, wasfound to be at least as effective as unfractionated heparin (5000 units

363MANAGEMENT OF ACUTE ISCHEMIC STROKE
subcutaneous three times a day) in preventing proximal deep venousthromboembolism, pulmonary embolism, and death related to venousthromboembolism in patients with acute ischemic stroke [138]. Majorbleeding events were similar between the citraparin (1.1%) and the unfrac-tionated heparin (1.8%) treated groups [138]. In the PREVAIL study,enoxaparin significantly reduced the risk of thromboembolism (relativerisk reduction 43%) compared with unfractionated heparin (5000 unitssubcutaneous twice a day) (P ¼ .0001) [139]. Symptomatic intracranialhemorrhage and extracranial major hemorrhages were similar betweenthe two groups [139]. Patients who have received thrombolytic therapyshould not receive anticoagulation therapy for deep venous thrombosisprophylaxis in the first 24 hours [2,4,22,25,53]. Sequential compressiondevices are indicated in nonambulatory stroke patients who are unableto receive heparin or low-molecular-weight heparin [53].
Hyperglycemia
Hyperglycemia has been associated with larger cerebral infarct volumesin animal models [140]. In humans, worsened outcomes have been reportedin patients with elevated admission glucose levels [141]. Hyperglycemia hasalso been associated with increased cerebral edema volumes and higher hem-orrhagic transformation rates with or without intravenous tPA administra-tion [113,142,143]. Stroke patients often have surges in their blood glucoselevels because of the sympathetic stress response in the acute phase [4].Based on these observations it is recommended to avoid dextrose-containingintravenous infusions and serially to check blood glucose and adequatelycorrect elevated blood sugars with short-acting insulin. Further studies areneeded to investigate the benefit of tight blood glucose control on strokeoutcome [144].
Fever
Hyperthermia adversely affects stroke outcome in animal models andin observational clinical studies [91,145–147]. Proposed mechanisms bywhich hyperthermia may worsen outcome include promotion of an in-flammatory response, an increase in release of excitotoxic amino acids,and an increase in cerebral metabolic demand in an already compromisedcerebral blood flow state [147–149]. Pneumonia and urinary tract infec-tions are common in stroke patients and must be worked-up aggressivelyin a febrile patient. Deep venous thrombosis also may cause fevers andshould be considered in patients with unexplained fevers. Further studiesare needed to evaluate the therapeutic impact of antipyretic agents andcooling therapies in acute stroke. A detailed discussion on temperaturemanagement in patients with neurologic injuries can be found elsewherein this issue.

364 FINLEY CAULFIELD & WIJMAN
Summary
Intravenous tPA should be administered to all patients with acute ische-mic stroke who present within 3 hours of stroke onset and meet the NINDSinclusion and exclusion criteria. The risk of symptomatic intracranial hem-orrhage with intravenous tPA is approximately 6%. Intra-arterial tPA andmechanical thrombectomy are alternative treatment strategies for acutestroke patients who are ineligible for or fail intravenous tPA treatment. Fur-ther studies are needed to assess the benefit of these treatments. Patientswith acute ischemic stroke should be maintained euglycemic, euvolemic,and normothermic. Permissive hypertension may be beneficial, but in pa-tients receiving tPA blood pressures should be maintained at or less than180/105 mm Hg. Patients with life-threatening cerebral edema from hemi-spheric infarctions require hyperosmolar therapy and may benefit fromearly surgical decompression. Novel management strategies under investiga-tion include the use of multimodal imaging to identify patients who mightbenefit from tPA beyond the 3-hour time window, new thrombolytic agents,and neuroprotective therapies.
References
[1] American Heart Association. Heart disease and stroke statistics: 2006dupdate. Dallas
(TX): American Heart Association; 2006.
[2] Tissue plasminogen activator for acute ischemic stroke. The National Institute of Neuro-
logical Disorders and Stroke rt-PA Stroke Study Group. N Engl J Med 1995;333:1581–7.
[3] Finley Caulfield A,Wijman CA. Critical care of acute ischemic stroke. Crit Care Clin 2006;
22(4):581–606.
[4] Kalafut MA, Saver JL. The acute stroke patient: the first six hours. In: Cohen SN, editor.
Management of ischemic stroke. New York: McGraw-Hill; 2000. p. 17–52.
[5] Becker K. Intensive care unit management of the stroke patient. Neurol Clin 2000;18:
439–54.
[6] Daniels SK, Brailey K, Priestly DH, et al. Aspiration in patients with acute stroke. Arch
Phys Med Rehabil 1998;79:14–9.
[7] Gujjar AR, Diebert E, Manno EM, et al. Mechanical ventilation for ischemic stroke and
intracerebral hemorrhage: indications, timing, and outcome. Neurology 1998;51:447–51.
[8] Wijdicks EF, Scott JP. Outcome in patients with acute basilar artery occlusion requiring
mechanical ventilation. Stroke 1996;27:1301–3.
[9] Mirski MA, Muffelman B, Ulatowski JA, et al. Sedation for the critically ill neurologic
patient. Crit Care Med 1995;23:2038–53.
[10] Shibutani T,HirotaY,NiwaH, et al. Cerebral arterial blood flow velocity during induction
of general anesthesia: rapid intravenous induction versus awake intubation. Anesth Prog
1993;40:122–6.
[11] Burchiel KJ, Steege TD,Wyler AR. Intracranial pressure changes in brain-injured patients
requiring positive end-expiratory pressure ventilation. Neurosurgery 1981;8:443–9.
[12] Cooper KR, Boswell PA, Choi SC. Safe use of PEEP in patients with severe head injury.
J Neurosurg 1985;63:552–5.
[13] Knudsen L, ColdGE,HoldgardHO, et al. The effects of midazolam on cerebral blood flow
and oxygen consumption: interactionwith nitrous oxide in patients undergoing craniotomy
for supratentorial tumors. Anaesthesia 1990;45:1016–9.
365MANAGEMENT OF ACUTE ISCHEMIC STROKE
[14] Papazian L, Albanese J, ThirionX, et al. Effect of bolus doses of midazolam on intracranial
pressure and cerebral perfusion pressure in patients with severe head injury. Br J Anaesth
1993;71:267–71.
[15] Albanese J, Viviand X, Potie F, et al. Sufentanil, fentanyl, and alfentanil in head trauma
patients: a study on cerebral hemodynamics. Crit Care Med 1999;27:262–3.
[16] KumarMA,UrrutiaVC, ThomasCE, et al. The syndrome of irreversible acidosis after pro-
longed propofol infusion. Neurocrit Care 2005;3:257–9.
[17] Paulson OB, Strandgaard S, Edvinsson L. Cerebral autoregulation. Cerebrovasc Brain
Metab Rev 1990;2:161–92.
[18] Sugimori H, Ibayashi S, Fujii K, et al. Brain infarction developed in hypertensive and nor-
motensive patients during hospitalization: hemodynamic factors. Angiology 1995;46:473–80.
[19] Strandgaard S. Autoregulation of cerebral blood flow in hypertensive patients: the modify-
ing influence of prolonged antihypertensive treatment on the tolerance to acute, drug-
induced hypotension. Circulation 1976;53:720–7.
[20] Powers WJ. Acute hypertension after stroke: the scientific basis for treatment decisions.
Neurology 1993;43(3 Pt 1):461–7.
[21] Meyer JS, ShimazuK, Fukuuchi Y, et al. Impaired neurogenic cerebrovascular control and
dysautoregulation after stroke. Stroke 1973;4:169–86.
[22] Adams H, Adams R, Del Zoppo G, et al. Guidelines for the early management of
patients with ischemic stroke: 2005 guidelines updateda scientific statement from the
Stroke Council of the American Heart Association/American Stroke Association. Stroke
2005;36:916–23.
[23] Brott T, LuM,Kothari R, et al. Hypertension and its treatment in theNINDS rt-PA stroke
trial. Stroke 1998;29:1504–9.
[24] The NINDS t-PA Stroke Study Group. Intracerebral hemorrhage after intravenous t-PA
therapy for acute ischemic stroke. Stroke 1997;28:2109–18.
[25] Adams HP, Robert J, Adams RJ, et al. Guidelines for the early management of patients
with ischemic stroke: a scientific statement from the Stroke Council of the American Stroke
Association. Stroke 2003;34:1056–83.
[26] Cottrell JE, Patel K, Turndorf H, et al. Intracranial pressure changes induced by sodium
nitroprusside in patients with intracranial mass lesions. J Neurosurg 1978;48:329–31.
[27] Schroeder T, Sillesen H. Dihydralazine induces marked cerebral vasodilation in man. Eur J
Clin Invest 1987;17:214–7.
[28] Skinhoj E, Overgaard J. Effect of dihydralazine on intracranial pressure in patients with
severe brain damage. Acta Med Scand 1983;678(Suppl):83–7.
[29] Nazir FS, Overell JR, Bolster A, et al. Effect of perindopril on cerebral and renal perfusion
on normotensives in mild early ischaemic stroke: a randomized controlled trial. Cerebro-
vasc Dis 2005;19:77–83.
[30] TohmoH,KarankoM. Enalaprilat controls postoperative hypertension while maintaining
cardiac function and systemic oxygenation after neurosurgery. Intensive Care Med 1995;
21:651–6.
[31] Hillis AE, Ulatowski JA, Barker PB, et al. A pilot randomized trial of induced blood pres-
sure elevation: effects on function and focal perfusion in acute and subacute stroke.
Cerebrovasc Dis 2003;16:236–46.
[32] White OB, Norris JW, Hachinski VC, et al. Death in early stroke: causes and mechanisms.
Stroke 1979;10:743.
[33] Adams HP Jr, Brott TG, Furlan AJ, et al. Guidelines for thrombolytic therapy for acute
stroke: a supplement to the guidelines for the management of patients with acute ischemic
strokeda statement for healthcare professionals from a Special Writing Group of the
Stroke Council, American Heart Association. Stroke 1996;27:1711–8.
[34] Practice advisory: thrombolytic therapy for acute ischemic strokedsummary statement.
Report of the Quality Standards Subcommittee of the American Academy of Neurology.
Neurology 1996;47:835–9.
366 FINLEY CAULFIELD & WIJMAN
[35] Johnston KC, Haley EC Jr. Emergency imaging of the acute stroke patient. J Neuroimag-
ing 1997;7:111–7.
[36] Truwit CL, Barkovich AJ, Gean-Marton A, et al. Loss of the insular ribbon: another early
CT sign of acute middle cerebral artery infarction. Radiology 1990;176:801–6.
[37] Moulin T, Cattin F, Crepin-Leblond T, et al. Early CT signs in acute middle cerebral artery
infarction: predictive value for subsequent infarct locations and outcome. Neurology 1996;
47:366–75.
[38] Patel SC, Levine SR, Tilley BC, et al. Lack of clinical significance of early ischemic changes
on computed tomography in acute stroke.National Institute ofNeurologicalDisorders and
Stroke rt-PA Stroke Study Group. JAMA 2001;286:2830–8.
[39] Morgenstern LB, Luna-Gonzales H, Huber JC Jr, et al. Worst headache and subarachnoid
hemorrhage: prospective, modern computed tomography and spinal fluid analysis. Ann
Emerg Med 1998;32(3 Pt 1):297–304.
[40] Hunter GJ, Hamberg LM, Ponzo JA, et al. Assessment of cerebral perfusion and arterial
anatomy in hyperacute stroke with three-dimensional functional CT: early clinical results.
AJNR Am J Neuroradiol 1998;19:29–37.
[41] Josephson SA, DillonWP, SmithWS. Incidence of contrast nephropathy from cerebral CT
angiography and CT perfusion imaging. Neurology 2005;64:1805–6.
[42] Kidwell CS, Hsia AW. Imaging of the brain and cerebral vasculature in patients with sus-
pected stroke: advantages and disadvantages of CT and MRI. Curr Neurol Neurosci Rep
2006;6:9–16.
[43] Wintermark M, Reichhart M, Thiran JP, et al. Prognostic accuracy of cerebral blood flow
measurement by perfusion computed tomography, at the time of emergency room admis-
sion, in acute stroke patients. Ann Neurol 2002;51:417–32.
[44] Shuaib A, Lee D, Pelz D, et al. The impact of magnetic resonance imaging on the manage-
ment of acute ischemic stroke. Neurology 1992;42:816–8.
[45] Lutsep HL, Albers GW, DeCrespigny A, et al. Clinical utility of diffusion-weighted mag-
netic resonance imaging in the assessment of ischemic stroke. Ann Neurol 1997;41:574–80.
[46] Tong DC, Yenari MA, Albers GW, et al. Correlation of perfusion- and diffusion-weighted
MRI with NIHSS score in acute (!6.5 hour) ischemic stroke. Neurology 1998;50:864–70.
[47] Warach S, Gaa J, Siewert B, et al. Acute human stroke studied by whole brain echo planar
diffusion-weighted magnetic resonance imaging. Ann Neurol 1995;37:231–41.
[48] Willig DS, Turski PA, Frayne R, et al. Contrast-enhanced 3DMR DSA of the carotid ar-
tery bifurcation: preliminary study of comparison with unenhanced 2D and 3D time-of-
flight MR angiography. Radiology 1998;208:447–51.
[49] Remonda L, Heid O, Schroth G. Carotid artery stenosis, occlusion, and pseudo-occlusion:
first-pass, gadolinium-enhanced, three-dimensional MR angiographydpreliminary study.
Radiology 1998;209:95–102.
[50] Siewert B, Schlaug G, Edelman RR, et al. Comparison of EPISTAR and T2*-weighted ga-
dolinium-enhanced perfusion imaging in patients with acute cerebral ischemia. Neurology
1997;48:673–9.
[51] Warach S, Dashe JF, Edelman RR. Clinical outcome in ischemic stroke predicted by early
diffusion-weighted and perfusion magnetic resonance imaging: a preliminary analysis.
J Cereb Blood Flow Metab 1996;16:53–9.
[52] Albers GW, Thijs VN, Wechsler L, et al. Results of the Diffusion-weighted imaging Eval-
uation For Understanding Stroke Evolution (DEFUSE) study. DEFUSE investigators.
Stroke 2006;37:635.
[53] Albers GW, Amarenco P, Easton JD, et al. Antithrombotic and thrombolytic therapy for
ischemic stroke: the Seventh ACCP Conference on Antithrombotic and Thrombolytic
Therapy. Chest 2004;126(Suppl 3):483S–512S.
[54] CAST. Randomised placebo-controlled trial of early aspirin use in 20,000 patients with
acute ischaemic stroke. CAST (Chinese Acute Stroke Trial) Collaborative Group. Lancet
1997;349:1641–9.
367MANAGEMENT OF ACUTE ISCHEMIC STROKE
[55] The International Stroke Trial (IST). A randomized trial of aspirin, subcutaneous heparin,
both, or neither among 19435 patients with acute ischaemic stroke. International Stroke
Trial Collaborative Group. Lancet 1997;349:1569–81.
[56] The NINDS t-PA Stroke Study Group. Generalized efficacy of t-PA for acute stroke: sub-
group analysis of the NINDS t-PA Stroke Trial. Stroke 1997;28:2119–25.
[57] Haley EC Jr, Lewandowski C, Tilley BC. Myths regarding the NINDS rt-PA Stroke Trial:
setting the record straight. Ann Emerg Med 1997;30:676–82.
[58] Albers GW, Bates VE, ClarkWM, et al. Intravenous tissue-type plasminogen activator for
treatment of acute stroke: the Standard Treatment with Alteplase to Reverse Stroke
(STARS) study. JAMA 2000;283:1145–50.
[59] Hill MD, Buchan AM. Methodology for the Canadian Activase for Stroke Effectiveness
Study (CASES). CASES investigators. Can J Neurol Sci 2001;28:232–8.
[60] Hacke W, Kaste M, Fieschi C, et al. Intravenous thrombolysis with recombinant tissue
plasminogen activator for acute hemispheric stroke. The European Cooperative Acute
Stroke Study (ECASS). JAMA 1995;274:1017–25.
[61] Hacke W, Kaste M, Fieschi C, et al. Randomised double-blind placebo-controlled trial of
thrombolytic therapy with intravenous alteplase in acute ischaemic stroke (ECASS II). Sec-
ond European-Australasian Acute Stroke Study Investigators. Lancet 1998;352:1245–51.
[62] Clark WM, Albers GW, Madden KP, et al. The rtPA (alteplase) 0- to 6-hour acute stroke
trial, part A (A0276g): results of a double-blind, placebo-controlled, multicenter study.
Thrombolytic Therapy in Acute Ischemic Stroke Study Investigators. Stroke 2000;31:811–6.
[63] Randomized controlled trial of streptokinase, aspirin, and combination of both in treat-
ment of acute ischaemic stroke. Multicentre Acute Stroke Trial–Italy (MAST-I) Group.
Lancet 1995;346:1509–14.
[64] Thrombolytic therapy with streptokinase in acute ischemic stroke. The Multicenter Acute
Stroke TrialdEurope Study Group. N Engl J Med 1996;335:145–50.
[65] Donnan GA, Davis SM, Chambers BR, et al. Streptokinase for acute ischemic stroke with
relationship to time of administration. Australian Streptokinase (ASK) Trial StudyGroup.
JAMA 1996;276:961–6.
[66] Ancrod for the treatment of acute ischemic brain infarction. The Ancrod Stroke Study
investigators. Stroke 1994;25:1755–9.
[67] Levy DE. Ancrod in stroke program ASP I: ancrod (viprinex) for the treatment of acute,
ischemic stroke. American Stroke Association International Conference Ongoing Trials
Abstracts. Kissimmee, FL, February 16–18, 2006:CTP8.
[68] Sherman DG, Atkinson RP, Chippendale T, et al. Intravenous ancrod for treatment of
acute ischemic stroke: the STAT study: a randomized controlled trial. Stroke Treatment
with Ancrod Trial. JAMA 2000;283:2395–403.
[69] Hennerici MG, Kay R, Bogousslavsky J, et al. Intravenous ancrod for acute ischaemic
stroke in the European Stroke Treatment with Ancrod Trial: a randomized controlled trial.
Lancet 2006;368:1871–8.
[70] Furlan AJ, Eyding D, Albers GW, et al. Dose Escalation of Desmoteplase for Acute
Ischemic Stroke (DEDAS): evidence of safety and efficacy 3 to 9 hours after stroke onset.
Stroke 2006;37:1227–31.
[71] Hacke W, Albers G, Al-Rawi Y, et al. The Desmoteplase in Acute Ischemic Stroke Trial
(DIAS): a phase II MRI-based 9-hour window acute stroke thrombolysis trial with intra-
venous desmoteplase. Stroke 2005;36:66–73.
[72] Hacke W, et al. DIAS2 phase III study of desmoteplase in acute ischemic stroke. Oral pre-
sentation for European Stroke Conference. Glasgow, UK, May 29–June 1, 2007.
[73] Abciximab Emergent Stroke Treatment Trial (AbESTT) investigators. Emergency admin-
istration of abciximab for treatment of patients with acute ischemic stroke: results of a ran-
domized phase 2 trial. Stroke 2005;36:880–90.
[74] Ciccone A, Abraha I, Santilli I. Glycoprotein IIb-IIIa inhibitors for acute ischaemic stroke.
Cochrane Database Syst Rev 2006;(4):CD005208.
368 FINLEY CAULFIELD & WIJMAN
[75] Ciccone A, Abraha I, Santilli I. Glycoprotein IIb-IIIa inhibitors for acute ischemic stroke.
Stroke 2007;38:1113–4.
[76] Pancioli A. The combined approach to lysis utilizing eptifibatide and rtPA in acute ischemic
stroke (theCLEARStrokeTrial): blinded results tier I and II. American StrokeAssociation
International Conference Ongoing Trials Abstracts. Kissimmee, FL, February 16–18,
2006:CTP17.
[77] Warach S, Butman J, Davis L. Reopro Retavase reperfusion of stroke safety studydimag-
ing evaluation (ROSIE): interim safety and efficacy results. The ROSIE Investigators.
American StrokeAssociation InternationalConference late breaking science oral abstracts.
Kissimmee, FL, February 16–18, 2006.
[78] del Zoppo GJ, Higashida RT, Furlan AJ, et al. PROACT: a phase II randomized trial of
recombinant pro-urokinase by direct arterial delivery in acutemiddle cerebral artery stroke.
PROACT investigators. Prolyse in Acute Cerebral Thromboembolism. Stroke 1998;29:
4–11.
[79] Furlan A, Higashida R, Wechsler L, et al. Intra-arterial prourokinase for acute ischemic
stroke. The PROACT II study: a randomized controlled trial. Prolyse in Acute Cerebral
Thromboembolism. JAMA 1999;282:2003–11.
[80] The IMS study investigators. Combined intravenous and intra-arterial recanalization for
acute ischemic stroke: the Interventional Management of Stroke study (IMS). Stroke
2004;35:904–12.
[81] Molina CA, Saver JL. Extending reperfusion therapy for acute ischemic stroke: emerging
pharmacological, mechanical, and imaging strategies. Stroke 2005;36:2311–20.
[82] Berlis A, LutsepH, Barnwell S, et al.Mechanical thrombolysis in acute ischemic strokewith
endovascular photoacoustic recanalization. Stroke 2004;35:1112–6.
[83] WikholmG. Transarterial embolectomy in acute stroke. AJNRAmJNeuroradiol 2003;24:
892–4.
[84] Mayer TE,HamannGF, BrueckmannHJ. Treatment of basilar artery embolismwith ame-
chanical extraction device: necessity of flow reversal. Stroke 2002;33:2232–5.
[85] Smith WS, Sung G, Starkman S, et al. Safety and efficacy of mechanical embolectomy in
acute ischemic stroke: results of the MERCI trial. Stroke 2005;36:1432–8.
[86] Smith WS. Final results of the multi-MERCI trial. American Stroke Association Interna-
tional Conference Late Breaking Science Abstracts. San Francisco, CA, February 7–9,
2007:LB5.
[87] Ringer AJ, Qureshi AI, Fessler RD, et al. Angioplasty of intracranial occlusion resistant to
thrombolysis in acute ischemic stroke. Neurosurgery 2001;48:1282–8.
[88] LearyMC, Saver JL, Gobin YP, et al. Beyond tissue plasminogen activator: mechanical in-
tervention in acute stroke. Ann Emerg Med 2003;41:838–46.
[89] Nesbit GM, Luh G, Tien R, et al. New and future endovascular treatment strategies for
acute ischemic stroke. J Vasc Interv Radiol 2004;15(1 Pt 2):S103–10.
[90] Busto R, Dietrich WD, Globus MY, et al. Small differences in intraischemic brain temper-
ature critically determine the extent of ischemic neuronal injury. J CerebBloodFlowMetab
1987;7:729–38.
[91] GinsbergMD, BustoR. Combating hyperthermia in acute stroke: a significant clinical con-
cern. Stroke 1998;29:529–34.
[92] Ginsberg MD. Adventures in the pathophysiology of brain ischemia: penumbra, gene ex-
pression, neuroprotection: the 2002 Thomas Willis Lecture. Stroke 2003;34:214–23.
[93] DeGeorgiaMA,KriegerDW,Abou-CheblA, et al. Cooling forAcute Ischemic brainDam-
age (COOL AID): a feasibility trial of endovascular cooling. Neurology 2004;63:312–7.
[94] Guluma KZ, Hemmen TM, Olsen SE, et al. A trial of therapeutic hypothermia via endo-
vascular approach in awake patients with acute ischemic stroke:methodology. AcadEmerg
Med 2006;13(8):820–7.
[95] Lees KR, Zivin JA, Ashwood T, et al. NXY-059 for acute stroke. SAINT I investigators.
N Engl J Med 2006;354:588–600.

369MANAGEMENT OF ACUTE ISCHEMIC STROKE
[96] Shuaib A, Lees KR, Lyden P, et al. NXY-059 for the treatment of acute ischemic stroke.
SAINT II investigators. N Engl J Med 2007;357:562–71.
[97] Saver JL, Eckstein M, Stratton S, et al. The field administration of stroke therapy-magne-
sium (FAST-MAG) phase 3 clinical trial. FAST-MAG trial investigators. American Stroke
Association International Conference Ongoing Trials Abstracts. Kissimmee, FL, February
16–18, 2006:CTP 35.
[98] Ginsberg MD, Hill MD, Palesch YY, et al. The ALIAS Pilot Trial: a dose escalation and
safety study of albumin therapy for acute ischemic strokedI: physiologic responses and
safety results. Stroke 2006;37:2100–6.
[99] Palesch YY, Hill MD, Ryckborst KJ, et al. The ALIAS Pilot Trial: a dose escalation and
safety study of albumin therapy for acute ischemic strokedII: neurologic outcome and
efficacy analysis. Stroke 2006;37:2107–14.
[100] Gubitz G, Counsell C, Sandercock P, et al. Anticoagulants for acute ischaemic stroke.
Cochrane Database Syst Rev 2000;(2):CD000024.
[101] DukeRJ, BlochRF,TurpieAG, et al. Intravenous heparin for the prevention of stroke pro-
gression in acute partial stable stroke. Ann Intern Med 1986;105:825–8.
[102] Bath PM, Lindenstrom E, Boysen G, et al. Tinzaparin in acute ischaemic stroke (TAIST):
a randomised aspirin-controlled trial. Lancet 2001;358:702–10.
[103] Low molecular weight heparinoid, ORG 10172 (danaparoid), and outcome after acute
ischemic stroke: a randomized controlled trial. The Publications Committee for the Trial
of ORG 10172 in Acute Stroke Treatment (TOAST) investigators. JAMA 1998;279:
1265–72.
[104] Kay R, Wong KS, Yu YL, et al. Low-molecular-weight heparin for the treatment of acute
ischemic stroke. N Engl J Med 1995;333:1588–93.
[105] HommelM.Fraxiparine in Ischaemic Stroke Study. FISS bis investigators group [abstract].
Cerebrovasc Dis 1998;8(suppl 4):S19.
[106] Wong LKS, Chen C, Ng PW, et al. Different effects of low-molecular weight heparin on
acute ischemic stroke patient with or without large artery occlusive disease. American
StrokeAssociation International StrokeConference Late-BreakingOral ScienceAbstracts.
Kissimmee, FL, February 16–18, 2006.
[107] WongKS, ChenC,Ng PW, et al. Low-molecular-weight heparin comparedwith aspirin for
the treatment of acute ischaemic stroke inAsian patients with large artery occlusive disease:
a randomized study. Lancet Neurol 2007;6:407–13.
[108] HackeW, DonnanG, Fieschi C, et al. Association of outcome with early stroke treatment:
pooled analysis of the ATLANTIS, ECASS, and NINDS rt-PA stroke trials. ATLANTIS
Trial Investigators; ECASS Trial Investigators; NINDS rt-PA Study Group Investigators.
Lancet 2004;363:768–74.
[109] Intracerebral hemorrhage after intravenous t-PA therapy for ischemic stroke. TheNational
Institute of Neurological Disorders and Stroke rt-PA Stroke StudyGroup. Stroke 1997;28:
2109–18.
[110] Hill MD, Buchan AM, , for the Canadian Alteplase for Stroke Effectiveness Study
(CASES) investigators. Thrombolysis for acute ischemic stroke: results of the Canadian
Alteplase for Stroke Effectiveness Study. Can Med Assoc J 2005;172:1307–12.
[111] Tanne D, Kasner SE, Demchuk AM, et al. Markers of increased risk of intracerebral hem-
orrhage after intravenous recombinant tissue plasminogen activator therapy for acute is-
chemic stroke in clinical practice: the Multicenter rt-PA Stroke Survey. Circulation 2002;
105:1679–85.
[112] Larrue V, vonKummer R, del Zoppo G, et al. Hemorrhagic transformation in acute ische-
mic stroke: potential contributing factors in the EuropeanCooperativeAcute Stroke Study.
Stroke 1997;28:957–60.
[113] Demchuk AM,Morgenstern LB, Krieger DW, et al. Serum glucose level and diabetes pre-
dict tissue plasminogen activator-related intracerebral hemorrhage in acute ischemic
stroke. Stroke 1999;30:34–9.

370 FINLEY CAULFIELD & WIJMAN
[114] Jaillard A, Cornu C, Durieux A, et al. Hemorrhagic transformation in acute ischemic
stroke. The MAST-E study. MAST-E Group. Stroke 1999;30:1326–32.
[115] Barber PA, Demchuk AM, Zhang J, et al. Validity and reliability of a quantitative com-
puted tomography score in predicting outcome of hyperacute stroke before thrombolytic
therapy. ASPECTS Study Group. Alberta Stroke Programme Early CT Score. Lancet
2000;355:1670–4.
[116] Dubey N, Bakshi R, Wasay M, et al. Early computed tomography hypodensity predicts
hemorrhage after intravenous tissue plasminogen activator in acute ischemic stroke. J Neu-
roimaging 2001;11:184–8.
[117] Kase CS, Furlan AJ, Wechsler LR, et al. Cerebral hemorrhage after intra-arterial throm-
bolysis for ischemic stroke: the PROACT II trial. Neurology 2001;57:1603–10.
[118] Larrue V, vonKummerR,Muller A, et al. Risk factors for severe hemorrhagic transforma-
tion in ischemic stroke patients treated with recombinant tissue plasminogen activator:
a secondary analysis of the European-AustralasianAcute Stroke Study (ECASS II). Stroke
2001;32:438–41.
[119] Gilligan AK, Markus R, Read S, et al. Baseline blood pressure but not early computed to-
mography changes predicts major hemorrhage after streptokinase in acute ischemic stroke.
Stroke 2002;33:2236–42.
[120] Ribo M, Montaner J, Molina CA, et al. Admission fibrinolytic profile is associated with
symptomatic hemorrhagic transformation in stroke patients treated with tissue plasmino-
gen activator. Stroke 2004;35:2123–7.
[121] Badjatia N, Rosand J. Intracerebral hemorrhage. Neurologist 2005;11:311–24.
[122] Frank JI. Large hemispheric infarction, deterioration, and intracranial pressure. Neurol-
ogy 1995;45:1286–90.
[123] Ropper AH. Syndrome of transtentorial herniation: is vertical displacement necessary?
J Neurol Neurosurg Psychiatry 1993;56:932–5.
[124] Schneider GH, von Helden GH, Franke R, et al. Influence of body position on jugular ve-
nous oxygen saturation, intracranial pressure and cerebral perfusion pressure. ActaNeuro-
chir Suppl (Wien) 1993;59:107–12.
[125] Wojner-Alexander AW, Garami Z, Chernyshev OY, et al. Heads down: flat positioning
improves blood flow velocity in acute ischemic stroke. Neurology 2005;64:1354–7.
[126] Qureshi AI, Suarez JI, Bhardwaj A, et al. Use of hypertonic (3%) saline/acetate infusion in
the treatment of cerebral edema: effect on intracranial pressure and lateral displacement of
the brain. Crit Care Med 1998;26:440–6.
[127] Paczynski RP, He YY, Diringer MN, et al. Multiple-dose mannitol reduces brain water
content in a rat model of cortical infarction. Stroke 1997;28:1437–43.
[128] Qureshi AI, Wilson DA, Traystman RJ. Treatment of elevated intracranial pressure in ex-
perimental intracerebral hemorrhage: comparison betweenmannitol and hypertonic saline.
Neurosurgery 1999;44:1055–63.
[129] Diringer MN, Zazulia AR. Osmotic therapy: fact and fiction. Neurocrit Care 2004;1:
219–33.
[130] Toung TJ, ChangY, Bhardwaj A. Increases in lung and brain water following experimental
stroke: effect of mannitol and hypertonic saline. Crit Care Med 2005;33:203–8.
[131] Battison C, Andrews PJ, Graham C, et al. Randomized, controlled trial on the effect of
a 20%mannitol solution and a 7.5% saline/6% dextran solution on increased intracranial
pressure after brain injury. Crit Care Med 2005;33:196–202.
[132] Norris JW, Hachinski VC. High dose steroid treatment in cerebral infarction. Br Med J
(Clin Res Ed) 1986;292:21–3.
[133] Wijman CAC. Can we predict massive space-occupying edema in large hemispheric infarc-
tion? Stroke 2003;34:1899–900.
[134] Rieke K, Schwab S, Krieger D, et al. Decompressive surgery in space-occupying hemi-
spheric infarction: results of an open, prospective trial. Crit Care Med 1995;23:1576–87.
371MANAGEMENT OF ACUTE ISCHEMIC STROKE
[135] Schwab S, Steiner T, Aschoff A, et al. Early hemicraniectomy in patients with complete
middle cerebral artery infarction. Stroke 1998;29:1888–93.
[136] Vahedi K, Hofmeijer J, Juettler E, et al. Early decompressive surgery in malignant infarc-
tion of the middle cerebral artery: a pooled analysis of three randomized controlled trials.
Lancet Neurol 2007;6:215–22.
[137] Collaborative overviewof randomised trials of antiplatelet therapy: III. reduction in venous
thrombosis and pulmonary embolism by antiplatelet prophylaxis among surgical and med-
ical patients. Antiplatelet Trialists’ Collaboration. BMJ 1994;308:235–46.
[138] Diener HC, Ringelstein EB, von Kummer R, et al. Prophylaxis of thrombotic and embolic
events in acute ischemic stroke with low-molecular-weight heparin certoparin: results of the
PROTECT trial. Stroke 2006;37:139–44.
[139] ShermanDG, Albers GW, Bladin C, et al. The efficacy and safety of enoxaparin versus un-
fractionated heparin for the prevention of venous thromboembolism after acute ischaemic
stroke (PREVAIL Study): an open-label randomized comparison. Lancet 2007;369:
1347–55.
[140] Pulsinelli WA, Waldman S, Rawlinson D, et al. Moderate hyperglycemia augments ische-
mic brain damage: a neuropathologic study in the rat. Neurology 1982;32:1239–46.
[141] BrunoA, Biller J, AdamsHP Jr, et al. Acute blood glucose level and outcome from ischemic
stroke. Trial of ORG 10172 in Acute Stroke Treatment (TOAST) investigators. Neurology
1999;52:280–4.
[142] Berger L, Hakim AM. The association of hyperglycemia with cerebral edema in stroke.
Stroke 1986;17:865–71.
[143] Broderick JP, Hagen T, Brott T, et al. Hyperglycemia and hemorrhagic transformation of
cerebral infarcts. Stroke 1995;26:484–7.
[144] Gray CS, Hildreth AJ, Sandercock PA, et al. Glucose-potassium-insulin infusions in the
management of post-stroke hyperglycaemia: the UK Glucose Insulin Stroke Trial
(GIST-UK). Lancet Neurol 2007;6:397–406.
[145] Busija DW, Leffler CW, Pourcyrous M. Hyperthermia increases cerebral metabolic rate
and blood flow in neonatal pigs. Am J Physiol 1988;255(2 Pt 2):H343–6.
[146] Reith J, Jorgensen HS, Pedersen PM, et al. Body temperature in acute stroke: relation to
stroke severity, infarct size, mortality, and outcome. Lancet 1996;347:422–5.
[147] Castillo J, Davalos A, Noya M. Progression of ischaemic stroke and excitotoxic aminoa-
cids. Lancet 1997;349:79–83.
[148] Castillo J, Davalos A, Marrugat J, et al. Timing for fever-related brain damage in acute
ischemic stroke. Stroke 1998;29:2455–60.
[149] Castillo J, Davalos A, Noya M. Aggravation of acute ischemic stroke by hyperthermia is
related to an excitotoxic mechanism. Cerebrovasc Dis 1999;9:22–7.