Embed Size (px)
Citation preview
Clinical Radiology (2001) 00: 000±000doi:10.1053/crad.2000.0713, available online at http://www.idealibrary.com on
Case Report
Adrenal Histoplasmosis Manifested as Addison's Disease: Unusual CT
Features with Magnetic Resonance Imaging Correlation
ALLA M. ROZENBLIT, ANDREW KIM, JOSEPH TUVIA, BRUCE M. WENIG
Departments of Radiology and Pathology, Albert Einstein College of Medicine and Monte®ore Medical Center, New York,U.S.A.
Disseminated histoplasmosis is one of the rare causes ofadrenal insu�ciency. It is commonly associated withbilateral adrenal enlargement that has been reported oncomputed tomography (CT) [1±4]. We present a case ofadrenal histoplasmosis in a patient with Addison's disease,who underwent both CT and magnetic resonance imaging(MRI) of the abdomen. In this case, enhanced CT ®ndingswere unusual, showing homogeneous texture of the adrenallesions at presentation and interval enlargement withliquefaction developed during antibiotic therapy. MRI®ndings of adrenal histoplasmosis are not widely known.
CASE REPORT
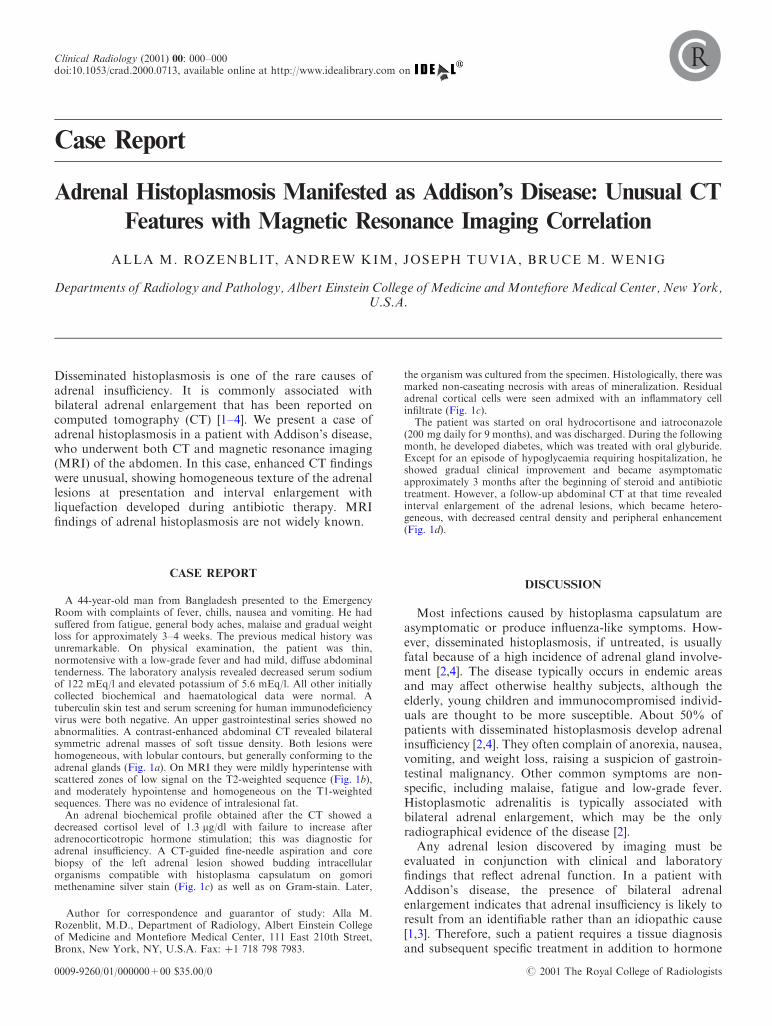
A 44-year-old man from Bangladesh presented to the EmergencyRoom with complaints of fever, chills, nausea and vomiting. He hadsu�ered from fatigue, general body aches, malaise and gradual weightloss for approximately 3±4 weeks. The previous medical history wasunremarkable. On physical examination, the patient was thin,normotensive with a low-grade fever and had mild, di�use abdominaltenderness. The laboratory analysis revealed decreased serum sodiumof 122 mEq/l and elevated potassium of 5.6 mEq/l. All other initiallycollected biochemical and haematological data were normal. Atuberculin skin test and serum screening for human immunode®ciencyvirus were both negative. An upper gastrointestinal series showed noabnormalities. A contrast-enhanced abdominal CT revealed bilateralsymmetric adrenal masses of soft tissue density. Both lesions werehomogeneous, with lobular contours, but generally conforming to theadrenal glands (Fig. 1a). On MRI they were mildly hyperintense withscattered zones of low signal on the T2-weighted sequence (Fig. 1b),and moderately hypointense and homogeneous on the T1-weightedsequences. There was no evidence of intralesional fat.An adrenal biochemical pro®le obtained after the CT showed a
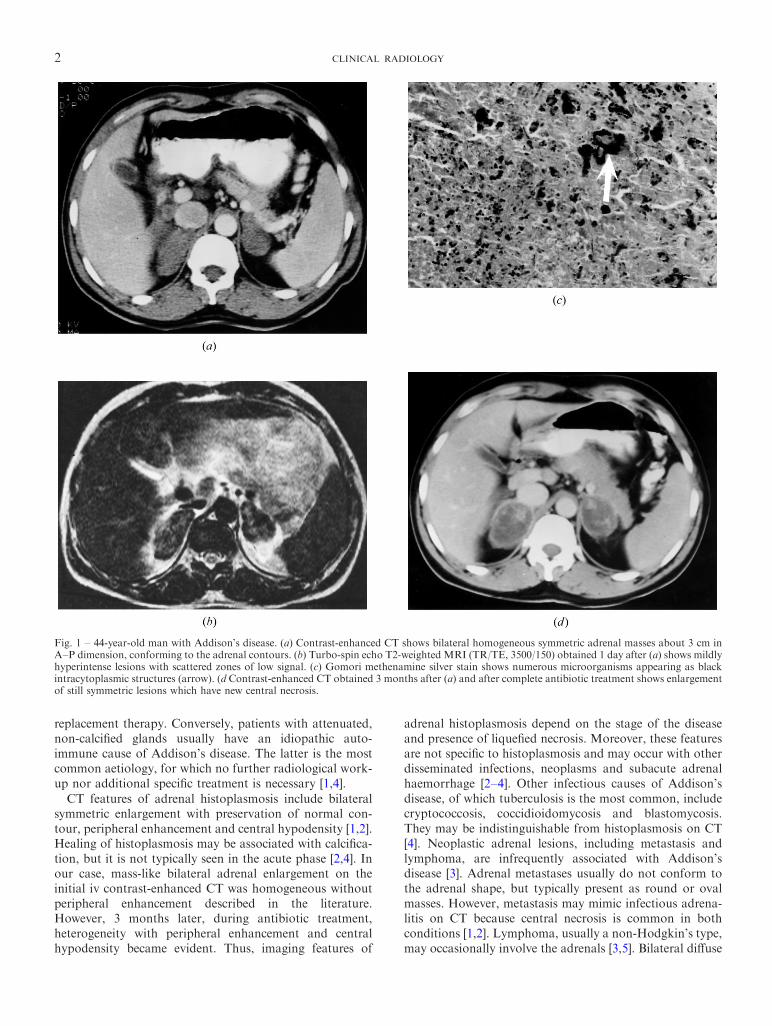
decreased cortisol level of 1.3 mg/dl with failure to increase afteradrenocorticotropic hormone stimulation; this was diagnostic foradrenal insu�ciency. A CT-guided ®ne-needle aspiration and corebiopsy of the left adrenal lesion showed budding intracellularorganisms compatible with histoplasma capsulatum on gomorimethenamine silver stain (Fig. 1c) as well as on Gram-stain. Later,
the organism was cultured from the specimen. Histologically, there wasmarked non-caseating necrosis with areas of mineralization. Residualadrenal cortical cells were seen admixed with an in¯ammatory cellin®ltrate (Fig. 1c).The patient was started on oral hydrocortisone and iatroconazole
(200 mg daily for 9 months), and was discharged. During the followingmonth, he developed diabetes, which was treated with oral glyburide.Except for an episode of hypoglycaemia requiring hospitalization, heshowed gradual clinical improvement and became asymptomaticapproximately 3 months after the beginning of steroid and antibiotictreatment. However, a follow-up abdominal CT at that time revealedinterval enlargement of the adrenal lesions, which became hetero-geneous, with decreased central density and peripheral enhancement(Fig. 1d).
DISCUSSION
Most infections caused by histoplasma capsulatum areasymptomatic or produce in¯uenza-like symptoms. How-ever, disseminated histoplasmosis, if untreated, is usuallyfatal because of a high incidence of adrenal gland involve-ment [2,4]. The disease typically occurs in endemic areasand may a�ect otherwise healthy subjects, although theelderly, young children and immunocompromised individ-uals are thought to be more susceptible. About 50% ofpatients with disseminated histoplasmosis develop adrenalinsu�ciency [2,4]. They often complain of anorexia, nausea,vomiting, and weight loss, raising a suspicion of gastroin-testinal malignancy. Other common symptoms are non-speci®c, including malaise, fatigue and low-grade fever.Histoplasmotic adrenalitis is typically associated withbilateral adrenal enlargement, which may be the onlyradiographical evidence of the disease [2].
Any adrenal lesion discovered by imaging must beevaluated in conjunction with clinical and laboratory®ndings that re¯ect adrenal function. In a patient withAddison's disease, the presence of bilateral adrenalenlargement indicates that adrenal insu�ciency is likely toresult from an identi®able rather than an idiopathic cause[1,3]. Therefore, such a patient requires a tissue diagnosisand subsequent speci®c treatment in addition to hormone
0009-9260/01/000000+00 $35.00/0 # 2001 The Royal College of Radiologists
Author for correspondence and guarantor of study: Alla M.Rozenblit, M.D., Department of Radiology, Albert Einstein Collegeof Medicine and Monte®ore Medical Center, 111 East 210th Street,Bronx, New York, NY, U.S.A. Fax: �1 718 798 7983.
2 CLINICAL RADIOLOGY
replacement therapy. Conversely, patients with attenuated,non-calci®ed glands usually have an idiopathic auto-immune cause of Addison's disease. The latter is the mostcommon aetiology, for which no further radiological work-up nor additional speci®c treatment is necessary [1,4].CT features of adrenal histoplasmosis include bilateral
symmetric enlargement with preservation of normal con-tour, peripheral enhancement and central hypodensity [1,2].Healing of histoplasmosis may be associated with calci®ca-tion, but it is not typically seen in the acute phase [2,4]. Inour case, mass-like bilateral adrenal enlargement on theinitial iv contrast-enhanced CT was homogeneous withoutperipheral enhancement described in the literature.However, 3 months later, during antibiotic treatment,heterogeneity with peripheral enhancement and centralhypodensity became evident. Thus, imaging features of
adrenal histoplasmosis depend on the stage of the diseaseand presence of lique®ed necrosis. Moreover, these featuresare not speci®c to histoplasmosis and may occur with otherdisseminated infections, neoplasms and subacute adrenalhaemorrhage [2±4]. Other infectious causes of Addison'sdisease, of which tuberculosis is the most common, includecryptococcosis, coccidioidomycosis and blastomycosis.They may be indistinguishable from histoplasmosis on CT[4]. Neoplastic adrenal lesions, including metastasis andlymphoma, are infrequently associated with Addison'sdisease [3]. Adrenal metastases usually do not conform tothe adrenal shape, but typically present as round or ovalmasses. However, metastasis may mimic infectious adrena-litis on CT because central necrosis is common in bothconditions [1,2]. Lymphoma, usually a non-Hodgkin's type,may occasionally involve the adrenals [3,5]. Bilateral di�use
Fig. 1 ± 44-year-old man with Addison's disease. (a) Contrast-enhanced CT shows bilateral homogeneous symmetric adrenal masses about 3 cm inA±P dimension, conforming to the adrenal contours. (b) Turbo-spin echo T2-weighted MRI (TR/TE, 3500/150) obtained 1 day after (a) shows mildlyhyperintense lesions with scattered zones of low signal. (c) Gomori methenamine silver stain shows numerous microorganisms appearing as blackintracytoplasmic structures (arrow). (d Contrast-enhanced CT obtained 3 months after (a) and after complete antibiotic treatment shows enlargementof still symmetric lesions which have new central necrosis.

CASE REPORT 3
or nodular enlargement of the glands without necrosis hasbeen described [6].Adrenal abnormalities suspicious of a neoplasm are often
evaluated with MRI in order to exclude a commonincidental lesion, non-hyperfunctioning adenoma. In ourpatient, the presence of adrenal hypofunction practicallyexcluded a benign adenoma and macronodular hyperplasiafrom the di�erential diagnosis. MRI was obtained in thiscase to exclude subacute adrenal haemorrhage and possiblyto direct a subsequent biopsy to the side or an area withmost pronounced signal abnormality. Acute bilateraladrenal haemorrhage or adrenal apoplexy was not aconsideration in our patient because radiographically,there was no high attenuation in the adrenal lesions onCT (typical for acute haemorrhage), and clinically, therewere no predisposing factors. The latter usually includesshock, sepsis, bleeding diathesis or anticoagulant therapy,which may lead to acute Addison's disease [4]. Chronic orsubacute adrenal haemorrhage may cause a subacute formof Addison's disease and present with soft-tissue-attenu-ation lesions on CT. Such haemorrhage may be associatedwith a coagulopathy. On MRI, subacute haematoma ishyperintense on both T1-weighted and T2-weighted images.In the chronic stage, this is associated with T1 and T2-hypointense rim of haemosiderin [7]. If MRI indicateshaemorrhage, an adrenal biopsy should be avoided [2]. Inour patient, the signal characteristics of the adrenal lesionswere inconsistent with haemorrhage, but compatible withsome solid tumours [7]. Reviewing the literature, we foundonly one MRI illustration of histoplasmosis with similar®ndings in a recent review article [8]. Somewhat unusual fora neoplasm in our case were scattered T2-hypointense zoneswithin the mildly hyperintense lesions. We speculate thatthese areas may be related to early mineralization that wasseen microscopically. They are less likely to representnormal residual adrenal tissue because only scatteredadrenal cortical cells were present in multiple biopsyspecimens. A mild degree of T2-hyperintensity can beexplained by the solid nature of non-caseating necroticdebris and cellular type of the associated in¯ammatoryreaction (Fig. 1c). Signal characteristics of adrenalhistoplasmosis will probably vary depending on the
combination of necrosis, in¯ammation, ®brosis and calci-®cation. With the development of liquefaction, a greaterdegree of T2-hyperintensity is expected, similar to theappearance of a necrotic metastasis. By analogy with CTand regardless of the probable variability of signalintensities, bilaterality and symmetry of adrenal lesionscombined with preservation of the adrenal shape shouldsuggest histoplasmosis, particularly in an endemic area [2].The role of MRI for patients with adrenal histoplasmosis islimited because MRI is less commonly employed for thedetection of adrenal lesions than CT. However, with theincreased use of abdominal MRI, it can be the ®rst cross-sectional technique to detect histoplasmotic adrenal invol-vement. This may occur when MRI is used as screening foroccult malignancies, typically in patients with non-speci®cclinical ®ndings and concomitant contraindications foriodinated iv contrast medium. In patients with documentedAddison's disease and adrenal enlargement, MRI may behelpful to exclude subacute or chronic haemorrhage beforebiopsy.
REFERENCES
1 Doppman JL, Gill JR Jr, Nienhuis AW, Earll JM, Long JA Jr. CT®ndings in Addison's disease. J Comput Assist Tomogr 1982;6:757±761.
2 Levine E. CT evaluation of active adrenal histoplasmosis. UrolRadiol 1991;3:103±106.
3 Efremidis SC, Harsoulis F, Douma S, Za®riadou E, Zamboulis C,Kouri A. Adrenal insu�ciency with enlarged adrenals. AbdomImaging 1996;21:168±171.
4 Kawashima A, Sandler CM, Fishman EK, et al. Spectrum of CT®ndings in nonmalignant disease of the adrenal gland. Radiographics1998;18:393±412.
5 Lee FT Jr, Thornbury JR, Grist TM, Kelcz F. MR imaging ofadrenal lymphoma. Abdom Imaging 1993;18:95±96.
6 Krebs TL, Wagner BJ. MR Imaging of the adrenal glands:radiologic-pathologic correlation. Radiographics 1998;18:1425±1440.
7 Kawashima A, Sandler CM, Ernst RD, et al. Imaging ofnontraumatic hemorrhage of the adrenal gland. Radiographics1999;19:949±963.
8 Kenney PJ, Lee JKT. The adrenal glands. In: Lee JKT, Sagel SS,Stanley RJ, Heiken JP, eds. Computed Body Tomography with MRICorrelation, 3rd edn. New York: Lippincott-Raven, 1998,1171±1208.





























