Embed Size (px)
Citation preview

1128 AJR:193, October 2009
Hormonal abnormalities related to the ad-renal gland include hypercortisolism (Cush-ing’s syndrome) and hyperaldosteronism (Conn’s syndrome). Hypercortisolism is ad-renocorticotropic hormone (ACTH)–depen-dent in 80–85% of cases: of pituitary origin or in Cushing’s disease in 80–85%, due to an ectopic ACTH-secreting tumor in 10–15% [2, 4]; ACTH-independent Cushing’s syndrome is due to either adrenal adenoma or carcino-ma in most cases [4]. The adrenal enlarge-ment is most commonly diffuse (Figs. 1 and 2) but can be nodular or mixed. In patients with ACTH-dependent hyperplasia, Sohaib et al. [2] showed that ectopic tumor ACTH produced adrenal hyperplasia in a higher per-centage of cases (90%) than pituitary ACTH hypersecretion. In those patients with hyper-plasia due to ectopic ACTH production, the adrenal gland morphology was lobular in 40% and either smooth or nodular in 30% each. In the setting of pituitary-induced hy-perplasia, 62% of adrenals were enlarged, most commonly smooth (55%), followed by lobular (28%) or nodular (17%) [2].
In the setting of hyperaldosteronism (Conn’s syndrome), the absence of an ade-noma traditionally suggested adrenal hyper-plasia as the cause. With improved CT res-olution, gland measurements have proven useful. Lingam et al. [5] revealed that the medial and lateral limbs were significantly larger in hyperplasia. A cutoff of 5 mm was 47% sensitive and 100% specific; using a 3-mm cutoff, sensitivity was 100% and spec-ificity, 54%. In comparison, the absence of
Adrenal Imaging with MDCT: Nonneoplastic Disease
Pamela T. Johnson1
Karen M. HortonElliot K. Fishman
Johnson PT, Horton KM, Fishman EK
1All authors: The Russell H. Morgan Department of Radiology and Radiologic Science, Johns Hopkins School of Medicine, 601 N Caroline St., Rm. 3140D, Baltimore, MD 21287. Address correspondence to P. T. Johnson ([email protected]).
Genitour inar y Imaging • Pictor ia l Essay
CMEThis article is available for CME credit.See www.arrs.org for more information.
AJR 2009; 193:1128–1135
0361–803X/09/1934–1128
© American Roentgen Ray Society
In addition to neoplastic disease, a range of disorders can alter the size or morphology of the adrenal gland. These include hyperplasia,
hemorrhage, infection, and cystic lesions. Al-though these abnormalities may not represent potential malignancy, identification is impor-tant nonetheless. Associated clinical manifes-tations that can be corrected are not insignif-icant (i.e., Cushing’s syndrome, Conn’s syndrome, refractory hypertension), second-ary adrenal insufficiency can be life-threaten-ing (i.e., hemorrhage), and findings may rep-resent systemic infection (i.e., granulomatous disease). In this article, the CT appearance of adrenal hyperplasia, hemorrhage, granuloma-tous infection, calcification, and pseudocyst are shown in conjunction with discussion of important correlative clinical findings.
HyperplasiaVincent et al. [1] reported, in a study per-
formed with 10-mm sections, that normal adrenal limbs should be ≤ 5 mm. Perform-ing CT with both 10- and 3- to 5-mm sec-tions, Sohaib et al. [2] showed that slightly, but significantly larger measurements were obtained using the thinner sections (mean limb width, ~ 15% greater). Normal adrenal shape varies, even in the same patient at dif-ferent levels, according to Wilms et al. [3]. The right side can be linear, an inverted V (with or without asymmetric limbs), hori-zontally linear, or K-shaped. The left adrenal gland has been described as an inverted V, an inverted Y, triangular, or linear [2, 3].
Keywords: adrenal gland, adrenal hyperplasia, hemorrhage, infection, MDCT, pseudocyst
DOI:10.2214/AJR.09.2551
Received February 9, 2009; accepted after revision March 19, 2009.
OBJECTIVE. The adrenal gland can enlarge or alter morphology in the presence of a range of nonneoplastic entities, including hyperplasia, hemorrhage, infection, or cystic mass. This article presents a description and representative CT images for each of these disorders.
CONCLUSION. Proper characterization is essential to ensure that life-threatening se-quelae from Addisonian crisis are averted in infection and hemorrhage, or to identify “leave-alone” lesions such as pseudocyst and chronic calcification.
Johnson et al.MDCT of Adrenal Disease
Genitourinary ImagingPictorial Essay

AJR:193, October 2009 1129
MDCT of Adrenal Disease
an adenoma at imaging was 93.3% sensitive and 84.6% specific.
HemorrhagePotential causes of unilateral or bilateral
hemorrhage [6–9] are listed in Table 1. Tumors that are known to hemorrhage include myelo-lipoma, hemangioma, pheochromocytoma, adenoma, adrenal cortical carcinoma, and metastases. Patients with antiphospholipid an-tibody syndrome (APLS) who develop adrenal hemorrhage (Fig. 3) usually have concomitant predisposing factors such as infection, antico-agulation, or a postoperative state. Provenzale et al. [10] reported on a series of four primary antiphospholipid antibody syndrome patients who had adrenal hemorrhage diagnosed with CT. In three of the four, the hemorrhage was bilateral, and two presented with “abrupt onset of adrenal insufficiency.”
Trauma typically produces unilateral hem-orrhage. In a study by Rana et al. [8] that in-cluded 54 adrenal hematomas, most were right-sided (Fig. 4), and adrenal hemorrhage was associated with injuries of higher sever-ity. Right-sided hemorrhage was associated with liver, spleen, bilateral renal injuries, and pneumothorax; when hemorrhage involved the left adrenal, splenic, left kidney, and pneu-mothoracic injuries were the most common accompanying injuries. In this series of 51 pa-tients, the hematomas appeared as a mass (2/3 ovoid, 1/3 round) with mean maximum diam-eter of 2.8 cm and mean attenuation of 52 ± 12 (SD) HU. Periadrenal stranding was identi-fied in most cases (89%) [8]. Sinelnikov et al. [9] reported their findings in 73 traumatic ad-renal injuries, 77% of which were right-sided. CT often revealed a focal hematoma (30%) or mass (11%), but injury was also reflected by an indistinct (27%) or enlarged (18%) gland. Most patients in this series also had periadre-nal stranding. Both investigations noted that active contrast extravasation was an infre-quent finding (1–6%) [8, 9].
InfectionAmong infectious disorders, both tuber-
culosis (TB) and histoplasmosis can involve the adrenal gland [11–15]. In addition to the morbidity associated with these systemic in-fections, if most (> 90%) of the gland is de-stroyed, patients develop Addison’s disease [11, 14].
The appearance of the gland at CT depends on the chronicity of the infection and whether it has been treated. Most patients have bilat-eral gland enlargement, masslike in 50–65%
and adreniform in 35–50% [11, 12, 14]. Un-enhanced CT shows attenuation to be more commonly homogeneous, but one third are heterogeneous [14]. After contrast infusion, the classic appearance of peripheral enhance-ment with central necrosis is seen in 40–50% of cases; alternatively, the glands may en-hance heterogeneously [11, 14]. Yang et al. [11] showed that peripheral enhancement with central necrosis is significantly more common in tuberculosis than tumor. Untreat-ed, TB causes adrenal calcification in 40–60% of patients [11, 14]. Atrophy and calcification both develop after treatment [12, 13].
CalcificationAdrenal calcification may reflect granu-
lomatous infection (Fig. 5), may evolve after previous hemorrhage (Fig. 6), or can be pres-ent in an adrenal mass (myelolipoma, adre-nocortical carcinoma [ACC], pheochromo-cytoma, cyst) [11–14].
CystThe most common adrenal cyst is report-
edly a pseudocyst (Figs. 7 and 8), believed to be the sequela of previous hemorrhage (or possibly infection). These can also arise sec-ondary to bleeding within a tumor, for exam-ple as occurs with melanoma [7]. Wang et al. [16] correlated CT appearance with pathol-ogy in seven pseudocysts. Only 43% (3/7) were predominantly cystic, with mixed or solid lesions reflecting organized hematoma; the predominantly cystic lesions contained liquefied hemorrhage (86%). Pseudocysts may be unilocular (Figs. 6–8) or multilocular (Fig. 9); calcification—mural, septal, or cen-tral—was identified in 43%. In six of the 32 pseudocysts analyzed by Erickson et al. [17], associated tumors were identified, including pheochromocytoma, adenoma, and ACC.
Other adrenal cysts include endothelial cysts, and less commonly, epithelial and par-asitic cysts (i.e., echinococcus) [18]. In a case series and literature review, Rozenblit et al. [19] reported that pseudocysts were more likely to be unilocular (81%) with calcifica-tion (74%); multilocularity and calcification were identified in 44% of endothelial cysts. Those authors also noted that the wall was generally imperceptible in benign cystic masses but measured 4 mm in a cystic pheo-chromocytoma and > 6 mm in a cystic ACC. Accordingly, although it may not be possible to definitively determine whether the under-lying mass is benign or malignant, the pres-ence of nodular wall thickening (Fig. 10) should prompt consideration of tumor. In ad-dition, the cyst fluid density was higher in tu-mors (22–25 HU) than in benign nonhemor-rhagic cysts (5–17 HU); two hemorrhagic cysts measured 67 and 75 HU [19].
ConclusionWith respect to adrenal imaging, the key
role of CT is to distinguish “leave-alone” le-sions from those requiring further evaluation or representing specific disease processes. Correct characterization of benign entities that do not require intervention (i.e., longstanding calcification or pseudocyst) is important to properly guide patient management. Identifi-cation of hyperplasia warrants additional clin-ical evaluation. In addition to these, nonneo-plastic pathologic processes that can involve the adrenal glands range from harbingers of serious systemic disease, as in tuberculosis, to complications of underlying medical condi-tions, such as hemorrhage in the setting of co-agulopathy. Because adrenal insufficiency is a potentially life-threatening sequela of bilateral infection or hemorrhage, findings must be rec-ognized as such and promptly communicated.
TABLE 1: Causes of Adrenal Hemorrhage
Unilateral Bilateral
Spontaneous (rule out tumor) Heparin-associated thrombocytopenia
Trauma Antiphospholipid antibody syndrome
Biopsy Use of steroids
Incidental Anticoagulation
Tumor Stress: surgery, burn, sepsis, hypotension
(Sepsis or stress) Waterhouse-Friderichsen syndrome: meningococcal sepsis
Spontaneous in setting of bilateral metastases
(Trauma)
(Incidental)
Note—Causes that are less frequent are indicated by parentheses.

1130 AJR:193, October 2009
Johnson et al.
References 1. Vincent JM, Morrison ID, Armstrong P, Reznek
RH. The size of normal adrenal glands on com-
puted tomography. Clin Radiol 1994; 49:453–455
2. Sohaib SA, Hanson JA, Newell-Price JD, et al. CT
appearance of the adrenal glands in adrenocorti-
cotrophic hormone-dependent Cushing’s syn-
drome. AJR 1999; 172:997–1002
3. Wilms G, Baert A, Marchal G, Goddeeris P. Com-
puted tomography of the normal adrenal glands:
correlative study with autopsy specimens. J Com-
put Assist Tomogr 1979; 3:467–469
4. Doppman JL, Chrousos GP, Papanicolaou DA,
Stratakis CA, Alexander HR, Nieman LK. Adre-
nocorticotropin-independent macronodular adre-
nal hyperplasia: an uncommon cause of primary
adrenal hypercortisolism. Radiology 2000; 216:
797–802
5. Lingam RK, Sohaib SA, Vlahos I, et al. CT of pri-
mary hyperaldosteronism (Conn’s syndrome): the
value of measuring the adrenal gland. AJR 2003;
181:843–849
6. Vella A, Nippoldt TB, Morris JC. Adrenal hemor-
rhage: a 25-year experience at the Mayo Clinic.
Mayo Clin Proc 2001; 76:161–168
7. Kawashima A, Sandler CM, Ernst RD, et al. Im-
aging of nontraumatic hemorrhage of the adrenal
gland. RadioGraphics 1999; 19:949–963
8. Rana AI, Kenney PJ, Lockhart ME, et al. Adrenal
gland hematomas in trauma patients. Radiology
2004; 230:669–675
9. Sinelnikov AO, Abujudeh HH, Chan D, Novelline
RA. CT manifestations of adrenal trauma: experi-
ence with 73 cases. Emerg Radiol 2007; 13:313–
318
10. Provenzale JM, Ortel TL, Nelson RC. Adrenal
hemorrhage in patients with primary antiphos-
pholipid syndrome: imaging findings. AJR 1995;
165:361–364
11. Yang ZG, Guo YK, Li Y, Min PQ, Yu JQ, Ma ES.
Differentiation between tuberculosis and primary
tumors in the adrenal gland: evaluation with con-
trast enhanced CT. Eur Radiol 2006; 16:2031–
2036
12. Liatsikos EN, Kalogeropoulou CP, Papathanas-
siou Z, et al. Primary adrenal tuberculosis: role of
computed tomography and CT-guided biopsy in
diagnosis. Urol Int 2006; 76:285–287
13. Guo YK, Yang ZG, Li Y, et al. Addison’s disease
due to adrenal tuberculosis: contrast-enhanced
CT features and clinical duration correlation. Eur
J Radiol 2007; 62:126–131
14. Ma ES, Yang ZG, Li Y, Guo YK, Deng YP, Zhang
XC. Tuberculous Addison’s disease: morphologi-
cal and quantitative evaluation with multidetector-
row CT. Eur J Radiol 2007; 62:352–358
15. Kumar N, Singh S, Govil S. Adrenal histoplasmo-
sis: clinical presentation and imaging features in
nine cases. Abdom Imaging 2003; 28:703–708
16. Wang LJ, Wong YC, Chen CJ, Chu SH. Imaging
spectrum of adrenal pseudocysts on CT. Eur Ra-
diol 2003; 13:531–535
17. Erickson LA, Lloyd RV, Hartman R, Thompson
G. Cystic adrenal neoplasms. Cancer 2004; 101:
1537–1544
18. Pradeep PV, Mishra AK, Aggarwal V, Bhargave
PRK, Gupta SK, Agarwal A. Adrenal cysts: an
institutional experience. World J Surg 2006; 30:
1817–1820
19. Rozenblit A, Morehouse HT, Amis ES. Cystic ad-
renal lesions: CT features. Radiology 1996; 201:
541–548
A
Fig. 1—79-year-old woman with adrenocorticotropic hormone (ACTH)–dependent Cushing’s disease. A and B, Axial arterial (A) and venous phase (B) images show that limbs of adrenal glands (arrows) are enlarged bilaterally, but shape is adreniform, compatible with hyperplasia. Precise source of Cushing’s disease could not be localized and symptoms were not controlled by medication, necessitating adrenalectomy. Pathology revealed nodular expansion of adrenal cortices bilaterally.
B
AJR:193, October 2009 1131
MDCT of Adrenal Disease
A
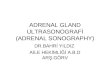
Fig. 2—27-year-old woman with history of Cushing’s disease. A and B, Axial unenhanced CT image (A) and coronal contrast-enhanced multiplanar reformation (B) show bilateral adrenal enlargement (arrows) and mild asymmetry of lateral limbs (arrowheads, B).
B
A
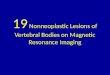
Fig. 3—51-year-old man with antiphospholipid antibody syndrome and clinical concern for pulmonary embolism underwent contrast-enhanced CT (not shown), which revealed high-density right adrenal mass with mild periadrenal stranding. A and B, Repeated MDCT scan 12 hours later (A) for delayed phase characterization confirmed persistent high density (arrow, A). In conjunction with previous study from 7 days prior (B) showing no adrenal mass, findings are compatible with adrenal hemorrhage. Subsequent studies over 4 months confirmed progressive decrease in size.
B

1132 AJR:193, October 2009
Johnson et al.
A
Fig. 4—69-year-old man with history of lymphoma and motor vehicle accident 2 months earlier, who presented with right-sided flank pain. A, Axial unenhanced CT scan shows 6.4-cm mildly heterogeneous mass (arrows) in right adrenal gland with some regions of high attenuation (47 HU), compatible with resolving hematoma. MRI confirmed presence of hemorrhage, and PET/CT from several weeks earlier (not shown) revealed no hypermetabolic activity below diaphragm. B, Follow-up CT image 10 months later shows decrease in size and liquefaction (18 HU) of mass (arrows), consistent with interval resolution of hemorrhage.
B
A
Fig. 5—54-year-old man with pancreatic mass (not shown). A and B, Axial (A) and coronal (B) volume-rendered images from contrast-enhanced CT show dense calcification of both adrenal glands (arrows), compatible with prior granulomatous disease.
B

AJR:193, October 2009 1133
MDCT of Adrenal Disease
A
Fig. 6—58-year-old woman with incidentally discovered adrenal mass. A–D, Unenhanced axial image (A), unenhanced coronal multiplanar reformation (B), delayed contrast-enhanced coronal volume-rendered image (C), and coronal volume-rendered image with parameters modified to show calcification (D) show nonenhancing, low-density right adrenal mass (arrows, A–C) with dense peripheral calcification, compatible with pseudocyst or old hematoma. Attenuation in center of lesion ranged from 23 HU on unenhanced, to 21 HU at 1 minute and 18 HU on delayed acquisition, reflecting lack of enhancement.
B
C D

1134 AJR:193, October 2009
Johnson et al.
A
Fig. 7—55-year-old woman with abdominal pain. A and B, Coronal arterial (A) and delayed phase (B) volume-rendered images from IV contrast-enhanced MDCT show 4 × 3 cm cystic mass (arrows) with dense calcifications superiorly and inferiorly (arrowheads), most compatible with pseudocyst caused by old adrenal hematoma.
B
A
Fig. 8—55-year-old man with stable cystic mass in right adrenal gland. A–D, Axial unenhanced (A), axial contrast-enhanced (B), and contrast-enhanced coronal volume-rendered (C and D) images show cyst (arrows) with peripheral calcification. Fluid measured 13 HU. Findings are most compatible with pseudocyst caused by old hematoma.
B
C D

AJR:193, October 2009 1135
MDCT of Adrenal Disease
A
Fig. 9—48-year-old woman with history of pancreatitis secondary to pancreas divisum and hypertriglyceridemia. A and B, Coronal (A) and sagittal (B) multiplanar reformations from contrast-enhanced CT show bilobed cyst (arrows) and mural calcification in region of adrenal gland. C, Varices in the gastric fundus (arrowheads) reflect splenic vein occlusion. Biopsy of suprarenal mass confirmed pseudocyst.
B
C
A
Fig. 10—47-year-old woman with abdominal pain and history of neurofibromas. A and B, Bilateral pheochromocytomas are present in adrenal glands, depicted on contrast-enhanced axial section (A) and coronal multiplanar reformation (B). Left-sided mass is predominantly cystic and right is solid with cystic components. Note thickened, irregular wall (arrowheads), a finding associated with neoplasms as opposed to pseudocyst.
B
F O R Y O U R I N F O R M A T I O N
This article is available for CME credit. See www.arrs.org for more information.





![Adrenal Imaging - University of Floridaxray.ufl.edu/files/2010/02/Adrenal-Imaging.pdfadrenal glands [3], and a metastasis might ... CT, adrenal imaging, adrenal lymphoma imaging, adrenal](https://img.pdfslide.net/doc/110x75/5b26814c7f8b9a8c0f8b4820/adrenal-imaging-university-of-glands-3-and-a-metastasis-might-ct-adrenal.jpg)