Embed Size (px)
Citation preview

Leiomyomas are benign tumors and develop fromsmooth muscle cells. They can occur in any part ofthe body where smooth muscle layers exist, and theyoccur frequently in the uterus and gastrointestinaltract. Adrenal leiomyomas are rare. In a review of thefew reported cases, most patients underwent openadrenalectomy. Here, we report a case of left adrenalleiomyoma treated successfully with hand-assistedlaparoscopic adrenalectomy.
CASE PRESENTATION
A 53-year-old woman who had a history of non-insulin dependent diabetes mellitus was admitteddue to hyperglycemia with poor control. A mass wasincidentally discovered over the left adrenal fossa byabdominal ultrasonography. The tumor had hetero-
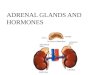
echogenicity on ultrasonogram and measured 5 cm insize. Precontrast enhancement computed tomography(CT) revealed a well-circumscribed soft tissue massat the left renal fossa measuring about 5.5×4.5×3.5cm.The mass showed low density (32 HU) on precontrastscan and heterogeneous enhancement with central lowdensity on postcontrast scan (Figure 1). Laboratoryexaminations showed that the mass was nonfunc-tional. The 24-hour urine vanillylmandelic acid level(6.45mg/day), aldosterone level, renin level, and bloodcortisol level were all within normal limits. Physicalexamination was unremarkable. Because of the tumorsize and radiographic findings, a nonfunctional adre-nal tumor with malignant potential was determined.
The patient underwent successful hand-assistedlaparoscopic adrenalectomy with en bloc removal ofthe surrounding fatty tissue. A midline incision, 7 cmin length, was made for the hand-assisted device. Thewhole procedure was performed by the transperi-toneal technique. The operation time was 135 minutesand blood loss was 70 mL. Recovery was uneventful,and the patient began oral intake the day after surgery.The patient did not request parenteral narcotics but only took oral analgesics postoperatively. The
Kaohsiung J Med Sci November 2006 • Vol 22 • No 11 575© 2006 Elsevier. All rights reserved.
Received: February 7, 2006 Accepted: June 6, 2006Address correspondence and reprint requests to: Dr Wen-JengWu, Department of Urology, Kaohsiung Medical University,100 Shih-Chuan 1st Road, Kaohsiung 807, Taiwan.E-mail: [email protected]
ADRENAL LEIOMYOMA TREATED BY
HAND-ASSISTED LAPAROSCOPIC
ADRENALECTOMY: A CASE REPORT
Tu-Hao Chang, Yung-Chin Lee, Chia-Chu Liu, Chun-Hsiung Huang,1 and Wen-Jeng Wu1
Department of Urology, Kaohsiung Medical University Hospital, and 1Department of Urology, Faculty of Medicine, Kaohsiung Medical University, Kaohsiung, Taiwan.
A left adrenal incidentaloma was found by abdominal ultrasound and computed tomography(CT) in a 53-year-old woman who had a history of non-insulin dependent diabetes mellitus.Abdominal CT showed a well-circumscribed adrenal mass (5.5 × 4.5 × 3.5 cm) with low density(32 HU) on precontrast scan and heterogeneous enhancement on postcontrast scan. Laboratoryexaminations revealed a nonfunctional adrenal tumor. As the malignant potential of the tumorcould not be ruled out, the patient underwent hand-assisted laparoscopic adrenalectomy. Post-operative recovery was uneventful, and pathologic examination revealed leiomyoma.
Key Words: adrenal, laparoscopic adrenalectomy, leiomyoma(Kaohsiung J Med Sci 2006;22:575–9)

Kaohsiung J Med Sci November 2006 • Vol 22 • No 11576
T.H. Chang, Y.C. Lee, C.C. Liu, et al
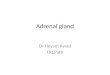
specimen measured 18×7.2×4cm in size, and patho-logic examination revealed a well-defined nodulecomposed of bland looking spindle cells arranged inwhirling bundles in the adipose tissue. A diagnosis ofleiomyoma was confirmed by immunohistochemicalstudies including smooth muscle actin(+), vimentin(+),CD34(–), and CD117(–) (Figure 2).
DISCUSSION
Adrenal masses are often found during the course ofinvestigation of an unrelated condition. A variety oftumors may arise within the adrenal gland. Adrenalleiomyoma is a rare entity. Nishida et al and Goldmanand Brody each have reported a case of symptomaticadrenal leiomyoma [1,2]. Evrad et al incidentally dis-covered one of these tumors in a girl with ataxia-telangiectasis [3]. In addition, two examples of adrenalleiomyosarcomas have been reported [4]. Most ofthese patients underwent open adrenalectomy and
diagnoses were subsequently confirmed by patho-logic examination.
There have been several reported cases of adrenalleiomyomas found in patients with acquired immu-nodeficiency syndrome (AIDS) [5–8]. Patients withAIDS are more inclined to develop certain types ofcancers, especially lymphomas and Kaposi’s sarcoma.The relationship between smooth muscle tumors andHIV infection remains unclear.
Leiomyoma or leiomyosarcoma occur in immuno-compromised patients at a greater frequency than the general population, and several cases have beenreported in patients with various types of organ trans-plants, congenital immunodeficiency, and AIDS. Theadrenal gland is also an exceptional site of localiza-tion of smooth muscle tumors [9]. Leiomyomas showa variety of imaging findings. No specific features are present, but CT or magnetic resonance imaging willshow a solid mass. The mass often has a smooth bor-der and peripheral enhancement on postcontrast scan.Leiomyomas are often hypervascular on angiography,
A B
C D
Figure 1. (A) Precontrast enhancement computed tomography (CT) shows a well-circumscribed soft tissue mass at the left adrenalfossa (5.5 × 4.5 × 3.5 cm) with low density (32 HU). (B) The mass is low density on precontrast CT and shows heterogeneous enhance-ment with central low density. (C, D) Postcontrast CT with image reconstruction (coronal view).

but can also be hypovascular. The varying vascularitymight be related to the presence of different subtypes.
Surgical excision should be strongly considered forall patients with functional adrenal incidentalomas.Beyond this, the indication for surgery is suspicion ofmalignancy based on the size criteria, radiographicfindings, or interval growth. The most useful param-eter for assessing risk of malignancy for adrenal inci-dentalomas is tumor size with a 5–6 cm cut-off pointmost commonly used [10].
In 1992, the laparoscopic approach to resection ofthe adrenal gland was first reported [11]. Since its intro-duction, laparoscopic adrenalectomy has become thestandard method for removal of most adrenal tumors.Laparoscopic adrenalectomy offers the general bene-fits of minimally invasive surgery such as significantlydecreased morbidity, shorter length of hospitalization,more rapid convalescence, decreased postoperativepain, and improved cosmesis compared with openresection. With improved technologic advances in thefield and growing technical experience, surgeonshave successfully expanded the indications for laparo-scopic adrenalectomy to large, nonfunctioning tumorswith malignant potential and to metastatic lesions.While local tumors are large (> 5–6 cm) or potentially
malignant, curative en bloc resection is difficult throughpure laparoscopic adrenalectomy. The hand-assistedlaparoscopic procedure may be an alternative [12].
In conclusion, adrenal leiomyoma is a rare adrenaltumor. Hand-assisted laparoscopic adrenalectomycan safely and efficiently treat large, nonfunctioning,but potentially malignant tumors, which need en blocresection and are difficult to manage by a pure laparo-scopic procedure. Hand-assisted laparoscopic adrena-lectomy has most of the benefits of laparoscopicsurgery compared to open techniques.
REFERENCES
1. Nishida S, Tanimura A, Takasaki S, et al. Surgicallyresected adrenal leiomyoma: report of a case. Surg Today1995;25:455–7.
2. Goldman RL, Brody PA. Symptomatic leiomyoma ofthe adrenal. Clin Imaging 1994;18:277–8.
3. Evrad P, Vermyle C, Scheift JM, et al. Leiomyoma of thesuprarenal gland in a child with ataxia-telangiectascia.Pediatr Hematol Oncol 1991;8:235–41.
4. Lack EE, Graham CW, Azumi N, et al. Primary leio-myosarcoma of adrenal gland: case report with immuno-histochemical and ultrastructural study. Am J SurgPathol 1991;15:899.
Adrenal leiomyoma treated by laparoscopic adrenalectomy
Kaohsiung J Med Sci November 2006 • Vol 22 • No 11 577
SMA(+)
H&E stain 10�H&E stain 4�
CD34(–)
CD117(–)
Vimentin(+)
Figure 2. Microscopically, the sections show a well-defined nodule composed of bland looking spindle cells arranged in whirling bundlesin the adipose tissue. The tumor cells have vesicular nuclei, clumping chromatin, inconspicuous nuclei, and pink cytoplasm. Immuno-histochemical study showed smooth muscle actin(+), vimentin(+), CD117(–) and CD34(–).

5. Parola P, Petit N, Azzedine A, et al. Symptomatic leiomy-oma of the adrenal gland in a women with AIDS. AIDS1996;10:340–1.
6. Jimenez-Heffernan JA, Hardisson D, Palacious J, et al.Adrenal gland leiomyoma in a child with AIDS. PediatrPathol Lab Med 1995;15:923–9.
7. Dahan H, Beges C, Weiss L, et al. Leiomyoma of theadrenal gland in a patient with AIDS. Abdom Imaging1994;19:259–61.
8. Radin DR, Kiyabu M. Multiple smooth muscle tumorsof the colon and the adrenal gland in adult with AIDS.AJNR 1992;159:545–6.
9. Rogatsch H, Bonatti H, Menet A, et al. Epstein–Barrvirus-associated multicentric leiomyoma in an adultpatient after heart transplantation: case report andreview of the literature. Am J Surg Pathol 2000;245:614–21.
10. Brunt LM, Moley JF. Adrenal incidentaloma. World JSurg 2001;25:905.
11. Gagner M, Lacroix A, Botle E. Laparoscopic adrenalec-tomy in Cushing’s syndrome and pheochromocytoma.N Engl J Med 1992;327:1033.
12. Cobb WS, Kercher KW, Sing RF, et al. Laparoscopicadrenalectomy for malignancy. Am J Surg 2005;189:405–11.
Kaohsiung J Med Sci November 2006 • Vol 22 • No 11578
T.H. Chang, Y.C. Lee, C.C. Liu, et al

Kaohsiung J Med Sci November 2006 • Vol 22 • No 11 579
�� !"VR=�=O=�=T=�
�� !"VR=�=S=�=S=�
�� !"#$%&'
�� !"!#$ %&'(
�� UMT�� !"#$NMM�
�� !"#$%&'()*+,
�� !"#$%&=�=�� !��
N= =��
N= =��
N= =��
O= =��
O
N�� !"!#$ %= =��
O�� !"!= =�� ��!= =�� !
�� !"#$%&'()*+',-.'/$012345612789:;<=
�� !"#$%&'()*+,=RKR=�=QKR=�=PKR=�� !"#$%&'()
�� !"#$%&'()�!"*+,-#./0123456789:;<(#
�� !"#$%&�'()*+,-./012345678
�� ��� !"#$�� %&'(!)*+,
E�� !=OMMSXOOWRTR�VF