Embed Size (px)
Citation preview

Urol Radiol 6:7-13 (1984) Urologic Radiology
© Springer-Verlag 1984
Adrenal Myelolipoma: CT and Ultrasound Findings
C. Whitley Vick, ~ Robert K. Zeman, 2 Eric Mannes, John J. Cronan, and James W. Walsh ~ Department of Radiology, Yale University School of Medicine, New Haven, Connecticut, USA
Abstract. The computed tomographic (CT) and ultrasound (US) appearances of 5 adrenal myeloli- pomas in 4 patients are reported. The component tissues o f a myelol ipoma determine its CT and US appearance. A myelol ipoma consisting primarily o f fat has a characteristic CT and US appearance. A myelol ipoma also containing macroscopic quan- tities of nonfatty material (blood, calcium, or mye- loid tissue) may have a nonspecific CT or US ap- pearance if fat is not identified in the lesion. In equivocal cases, needle biopsy may be used to es- tablish the diagnosis of myelolipoma.
Key words: Adrenal tumor -- Adrenal myeloli- poma.
Although computed tomography (CT) and ultra- sound (US) are capable of detecting the majority o f adrenal tumors, these techniques are often limited in their ability to suggest specific histologic diag- noses. The adrenal myelol ipoma represents an ap- parent exception to this limitation, because mye- lolipomas large enough to be imaged with CT or US often contain macroscopic fat. I f this fat can be dem- onstrated by CT or US, the diagnosis of myeloli- poma is highly likely. We report 5 myelol ipomas in 4 patients and discuss the CT and US appearances o f these lesions.
t Present address: Medical College of Virginia/Commonwealth University, MCV Station, Box 615, Richmond, VA 23298, USA Present address: Department of Radiology, Georgetown Uni- versity Hospital, Washington, D.C. 20007, USA
Address reprint requests to: C. Whitley Vick, M.D., Medical Col- lege of Virginia/Commonwealth University, MCV Station, Box 615, Richmond, VA 23298, USA
Materials and Methods
Records of 4 patients having a total of 5 adrenal myelolipomas were available from the files of 4 hospitals.* All 5 myelolipomas were studied with CT, and 4 were also evaluated with US. Each of the myelolipomas was pathologically proven, 4 after surgical removal and 1 following needle biopsy. The needle biopsy (pa- tient 4, Table l) was performed with CT guidance using both 14- gauge (Tru-cut) and 23-gauge (Chiba) needles. The pathologist reported that both needles yielded adequate tissue for diagnosis.
Commercially available CT and US scanners were used. The density of a myelolipoma on CT was determined by visual and/ or computer-generated numerical comparison with normal ab- dominal or subcutaneous fat. A drip infusion of urographic con- trast was administered in each case although precontrast scans were not routinely performed. Therefore, the possibility of en- hancement within the myelolipomas was not assessed. On US, the amplitude and distribution of echoes within a myelolipoma was compared with normal surrounding structures, including ad- jacent renal parenchyma and sinus, liver or spleen, and dia- phragm.
Results
Clinical, radiographic, and pathologic findings are summarized in Table 1. Three patients had unilat- eral myelolipomas, and 1 had bilateral lesions.
On CT, 3 of the 5 myelol ipomas contained focal or diffuse areas equivalent in density to normal ab- dominal and/or subcutaneous fat (Figs. 1-3). Den- sity in l myelol ipoma was slightly higher than nor- mal fat, but this lesion clearly contained fat (as opposed to water) density (Fig. 1). In the fifth mye- lolipoma, the areas o f lowest density measured be- tween water and fat ( - 3 0 HU in the lesion, - 9 6 H U in normal fat, and + 2 H U in water) (Fig. 4).
* Yale-New Haven Hospital, New Haven, Connecticut; Mas- sachusetts General Hospital, Boston, Massachusetts; St. Vin- cent's Hospital, Bridgeport, Connecticut; and Medical College of Virginia, Richmond, Virginia
8
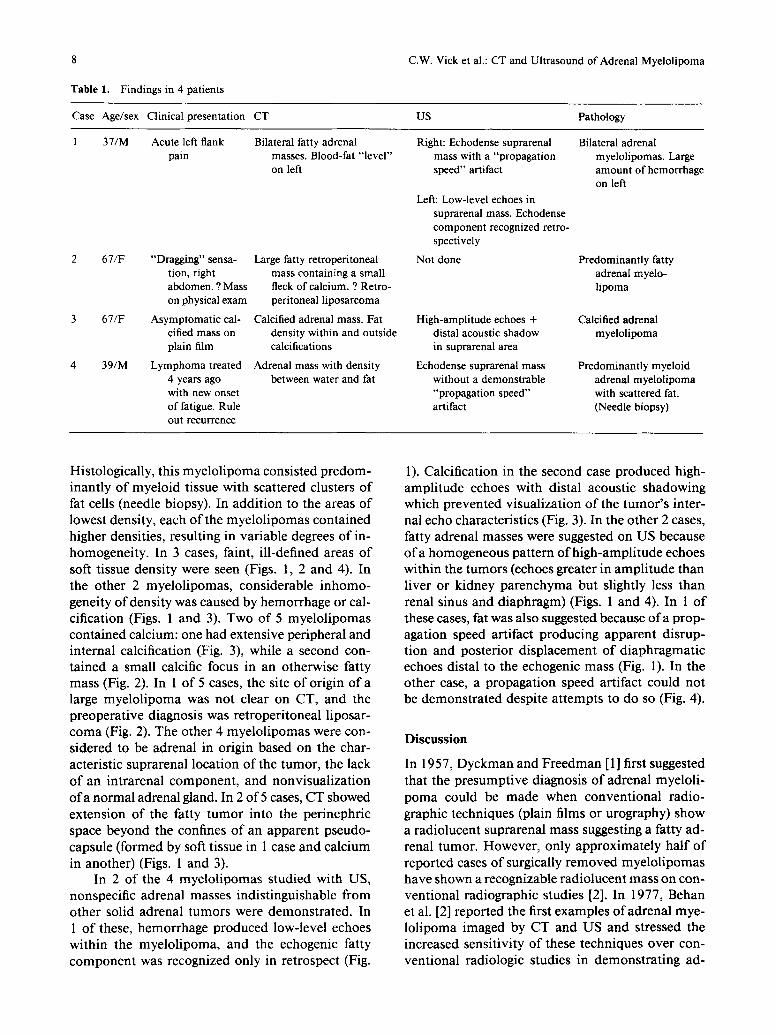
Table 1. Findings in 4 patients
C.W. Vick et al.: CT and Ultrasound of Adrenal Myelolipoma
Case Age/sex Clinical presentation CT US Pathology
1 37/M Acute left f lank Bilateral fatty adrenal Right: Echodense suprarenal Bilateral adrenal pain masses. Blood-fat "level" mass with a "propagation myelolipomas. Large
on left speed" artifact amount of hemorrhage on left
2 67/F "Dragging" sensa- Large fatty retroperitoneal tion, right mass containing a small abdomen. ? Mass fleck of calcium. ? Retro- on physical exam peritoneal liposarcoma
3 67/F Asymptomatic cal- Calcified adrenal mass. Fat cified mass on density within and outside plain f i l m calcifications
4 39/M Lymphoma treated Adrenal mass with density 4 years ago between water and fat with new onset of fatigue. Rule out recurrence
Left: Low-level echoes in suprarenal mass. Echodense component recognized retro- spectively
Not done
High-amplitude echoes + distal acoustic shadow in suprarenal area
Echodense suprarenal mass without a demonstrable "propagation speed" artifact
Predominantly fatty adrenal myelo- lipoma
Calcified adrenal myelolipoma
Predominantly myeloid adrenal myelolipoma with scattered fat. (Needle biopsy)
Histologically, this myelol ipoma consisted predom- inantly of myeloid tissue with scattered clusters o f fat cells (needle biopsy). In addit ion to the areas of lowest density, each o f the myelol ipomas contained higher densities, resulting in variable degrees of in- homogeneity. In 3 cases, faint, ill-defined areas o f soft tissue density were seen (Figs. 1, 2 and 4). In the other 2 myelolipomas, considerable inhomo- geneity o f density was caused by hemorrhage or cal- cification (Figs. 1 and 3). Two of 5 myelol ipomas contained calcium: one had extensive peripheral and internal calcification (Fig. 3), while a second con- tained a small calcific focus in an otherwise fatty mass (Fig. 2). In 1 of 5 cases, the site o f origin of a large myelol ipoma was not clear on CT, and the preoperative diagnosis was retroperi toneal liposar- coma (Fig. 2). The other 4 myelol ipomas were con- sidered to be adrenal in origin based on the char- acteristic suprarenal location of the tumor, the lack o f an intrarenal component , and nonvisualization o f a normal adrenal gland. In 2 of 5 cases, CT showed extension o f the fatty tumor into the perinephric space beyond the confines o f an apparent pseudo- capsule (formed by soft tissue in 1 case and calcium in another) (Figs. 1 and 3).
In 2 o f the 4 myelol ipomas studied with US, nonspecific adrenal masses indistinguishable from other solid adrenal tumors were demonstrated. In 1 o f these, hemorrhage produced low-level echoes within the myelol ipoma, and the echogenic fatty component was recognized only in retrospect (Fig.
1). Calcification in the second case produced high- amplitude echoes with distal acoustic shadowing which prevented visualization o f the tumor ' s inter- nal echo characteristics (Fig. 3). In the other 2 cases, fatty adrenal masses were suggested on US because o f a homogeneous pattern o f high-amplitude echoes within the tumors (echoes greater in ampli tude than liver or kidney parenchyma but slightly less than renal sinus and diaphragm) (Figs. 1 and 4). In 1 o f these cases, fat was also suggested because o f a prop- agation speed artifact producing apparent disrup- tion and posterior displacement of diaphragmatic echoes distal to the echogenic mass (Fig. 1). In the other case, a propagation speed artifact could not be demonstra ted despite at tempts to do so (Fig. 4).
D i s c u s s i o n
In 1957, Dyckman and Freedman [1 ] first suggested that the presumptive diagnosis o f adrenal myeloli- poma could be made when conventional radio- graphic techniques (plain films or urography) show a radiolucent suprarenal mass suggesting a fatty ad- renal tumor. However, only approximately half of reported cases of surgically removed myelol ipomas have shown a recognizable radiolucent mass on con- ventional radiographic studies [2]. In 1977, Behan et al. [2] reported the first examples o f adrenal mye- lolipoma imaged by CT and US and stressed the increased sensitivity of these techniques over con- ventional radiologic studies in demonstrat ing ad-
C.W. Vick et al.: CT and Ultrasound of Adrenal Myelolipoma 9
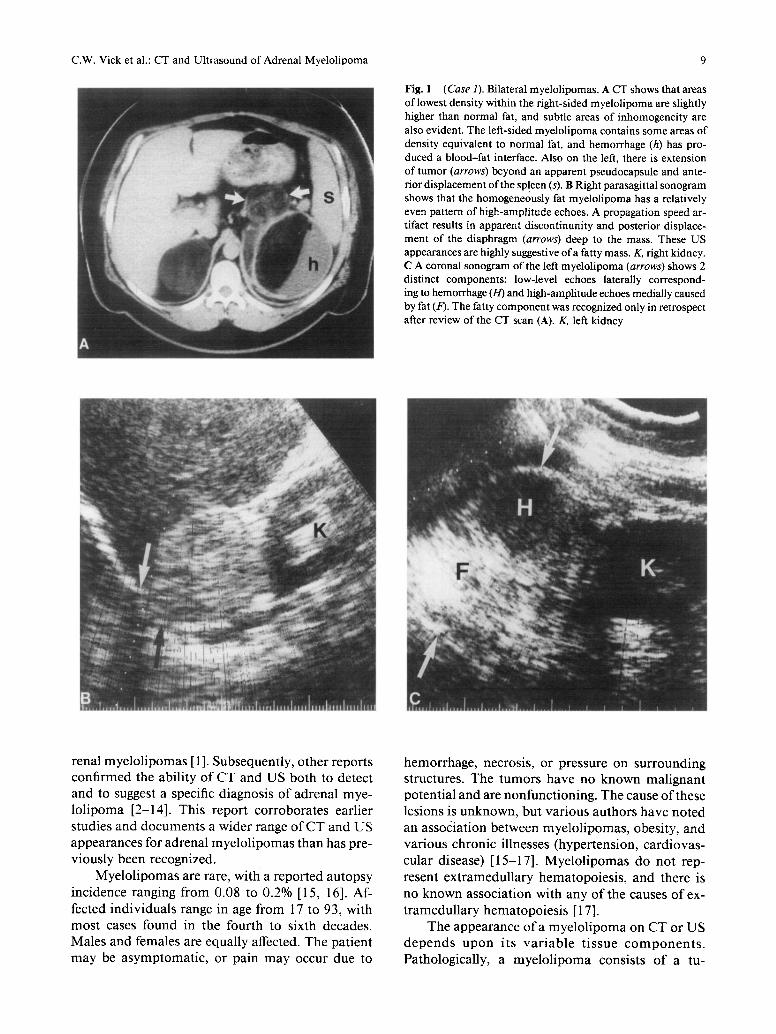
Fig. 1 (Case 1). Bilateral myelolipomas. ACT shows that areas of lowest density within the right-sided myelolipoma are slightly higher than normal fat, and subtle areas of inhomogeneity are also evident. The left-sided myelolipoma contains some areas of density equivalent to normal fat, and hemorrhage (h) has pro- duced a blood-fat interface. Also on the left, there is extension of tumor (arrows) beyond an apparent pseudocapsule and ante- rior displacement of the sp!een !s). B Right parasagittal sonogram shows that the homogeneously fat myelolipoma has a relatively even pattern of high-amplitude echoes. A propagation speed ar- tifact results in apparent discontinunity and posterior displace- ment of the diaphragm (arrows) deep to the mass. These US appearances are highly suggestive of a fatty mass. K, right kidney. C A coronal sonogram of the left myelolipoma (arrows) shows 2 distinct components: low-level echoes laterally correspond- ing to hemorrhage (H) and high-amplitude echoes medially caused by fat (F). The fatty component was recognized only in retrospect after review of the CT scan (A). K, left kidney
rena l m y e l o l i p o m a s [ 1 ]. Subsequen t ly , o t h e r r epo r t s c o n f i r m e d the ab i l i t y o f C T a n d U S b o t h to de tec t a n d to suggest a specif ic d i agnos i s o f a d r e n a l m y e -
l o l i p o m a [2-14] . Th i s r e p o r t c o r r o b o r a t e s ea r l i e r s tud ies a n d d o c u m e n t s a w i d e r range o f C T a n d U S a p p e a r a n c e s for a d r e n a l m y e l o l i p o m a s t han has pre- v i o u s l y been recogn ized .
M y e l o l i p o m a s are rare , w i th a r e p o r t e d a u t o p s y
i n c i d e n c e rang ing f rom 0.08 to 0 .2% [15, 16]. Af-
fec ted i n d i v i d u a l s range in age f r o m 17 to 93, wi th m o s t cases f o u n d in the fou r th to s ix th decades . M a l e s a n d females a re equa l ly affected. T h e p a t i e n t
m a y be a s y m p t o m a t i c , o r p a i n m a y occur due to
h e m o r r h a g e , necros is , o r p re s su re on s u r r o u n d i n g s t ruc tures . T h e t u m o r s h a v e no k n o w n m a l i g n a n t p o t e n t i a l a n d are n o n f u n c t i o n i n g . T h e cause o f these les ions is u n k n o w n , b u t v a r i o u s a u t h o r s h a v e n o t e d an a s s o c i a t i o n be tween m y e l o l i p o m a s , obes i ty , a n d v a r i o u s c h r o n i c i l lnesses ( h y p e r t e n s i o n , c a r d i o v a s -
cu la r d i sease) [15-17] . M y e l o l i p o m a s d o n o t rep-
r esen t e x t r a m e d u l l a r y h e m a t o p o i e s i s , a n d the re is
no k n o w n a s s o c i a t i o n wi th any o f the causes o f ex-
t r a m e d u l l a r y h e m a t o p o i e s i s [ 17].
T h e a p p e a r a n c e o f a m y e l o l i p o m a on C T or U S d e p e n d s u p o n i t s v a r i a b l e t i s s u e c o m p o n e n t s .
Pa tho log ica l ly , a m y e l o l i p o m a cons i s t s o f a tu-
10 C.W. Vick et al.: CT and Ultrasound of Adrenal Myelolipoma
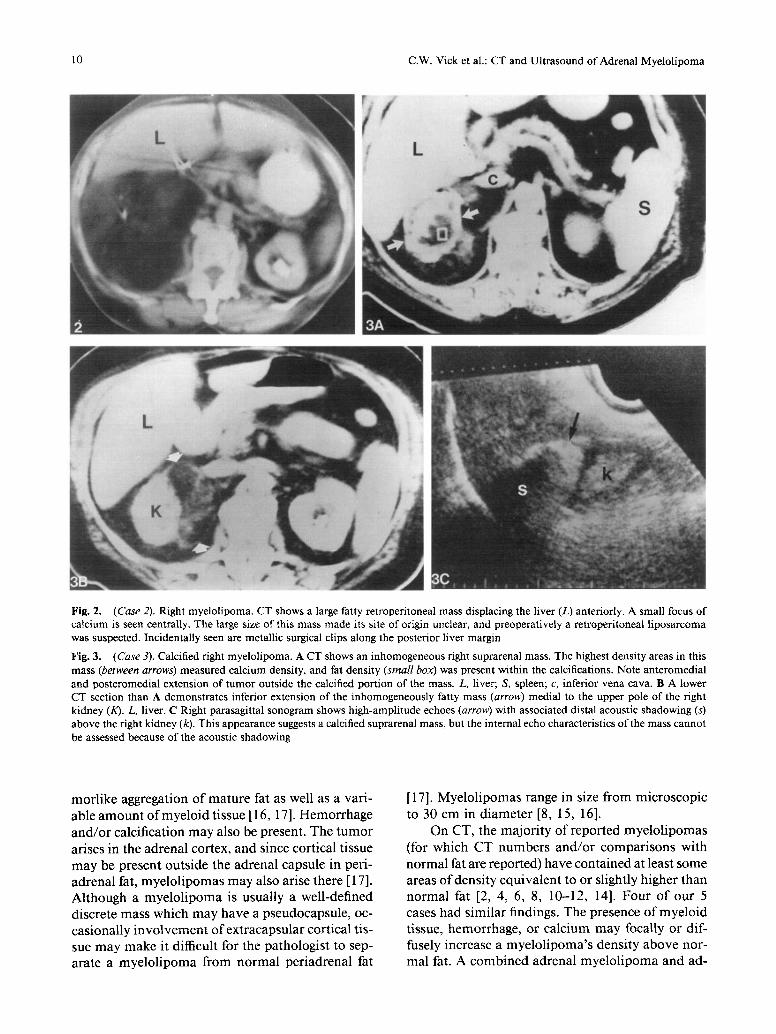
Fig. 2. (Case 2). Right myelolipoma. CT shows a large fatty retroperitoneal mass displacing the liver (L) anteriorly. A small focus of calcium is seen centrally. The large size of this mass made its site of origin unclear, and preoperatively a retroperitoneal liposarcoma was suspected. Incidentally seen are metallic surgical clips along the posterior liver margin
Fig. 3. (Case 3). Calcified right myelolipoma. A C T shows an inhomogeneous right suprarenal mass. The highest density areas in this mass (between arrows) measured calcium density, and fat density (small box) was present within the calcifications. Note anteromedial and posteromedial extension of tumor outside the calcified portion of the mass. L, liver; S, spleen; c, inferior vena cava. B A lower CT section than A demonstrates inferior extension of the inhomogeneously fatty mass (arrow) medial to the upper pole of the right kidney (K). L, liver. C Right parasagittal sonogram shows high-amplitude echoes (arrow) with associated distal acoustic shadowing (s) above the right kidney (k). This appearance suggests a calcified suprarenal mass, but the internal echo characteristics of the mass cannot be assessed because of the acoustic shadowing
morlike aggregation of mature fat as well as a vari- able amount ofmyeloid tissue [ 16, 17]. Hemorrhage and/or calcification may also be present. The tumor arises in the adrenal cortex, and since cortical tissue may be present outside the adrenal capsule in peri- adrenal fat, myelolipomas may also arise there [ 17]. Although a myelolipoma is usually a well-defined discrete mass which may have a pseudocapsule, oc- casionally involvement of extracapsular cortical tis- sue may make it difficult for the pathologist to sep- arate a myelolipoma from normal periadrenal fat
[17]. Myelolipomas range in size from microscopic to 30 cm in diameter [8, 15, 16].
On CT, the majority of reported myelolipomas (for which CT numbers and/or comparisons with normal fat are reported) have contained at least some areas of density equivalent to or slightly higher than normal fat [2, 4, 6, 8, 10-12, 14]. Four of our 5 cases had similar findings. The presence ofmyeloid tissue, hemorrhage, or calcium may focally or dif- fusely increase a myelolipoma's density above nor- mal fat. A combined adrenal myelolipoma and ad-
C.W. Vick et al.: CT and Ultrasound of Adrenal Myelolipoma 11
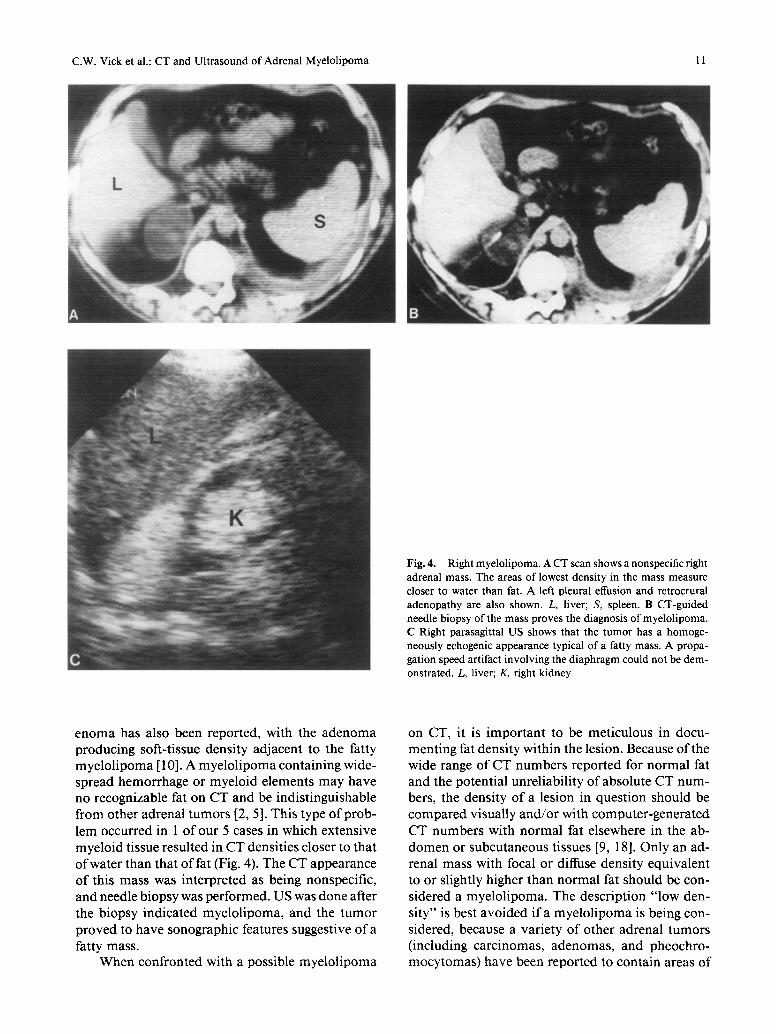
Fig. 4. Right myelolipoma. ACT scan shows a nonspecific right adrenal mass. The areas of lowest density in the mass measure closer to water than fat. A left pleural effusion and retrocrural adenopathy are also shown. L, liver; S, spleen. B CT-guided needle biopsy of the mass proves the diagnosis of myelolipoma. C Right parasagittal US shows that the tumor has a homoge- neously echogenic appearance typical of a fatty mass. A propa- gation speed artifact involving the diaphragm could not be dem- onstrated. L, liver; K, right kidney
e n o m a has also been reported, with the a d e n o m a producing soft-tissue density adjacent to the fatty mye lo l ipoma [ 10]. A mye lo l ipoma containing wide- spread hemorrhage or myeloid elements may have no recognizable fat on CT and be indistinguishable f rom other adrenal tumors [2, 5]. This type of prob- lem occurred in 1 of our 5 cases in which extensive myeloid tissue resulted in CT densities closer to that o f water than that o f fat (Fig. 4). The CT appearance o f this mass was interpreted as being nonspecific, and needle biopsy was performed. US was done after the biopsy indicated myelo l ipoma, and the t u m o r proved to have sonographic features suggestive of a fatty mass.
When confronted with a possible mye lo l ipoma
on CT, it is impor tan t to be meticulous in docu- ment ing fat density within the lesion. Because of the wide range of CT numbers repor ted for normal fat and the potential unreliabili ty o f absolute CT num- bers, the density of a lesion in question should be compa red visually and /o r with computer -genera ted CT numbers with normal fat elsewhere in the ab- d o m e n or subcutaneous tissues [9, 18]. Only an ad- renal mass with focal or diffuse density equivalent to or slightly higher than normal fat should be con- sidered a myelo l ipoma. The descript ion " low den- si ty" is best avoided if a mye lo l ipoma is being con- sidered, because a variety o f other adrenal tumors (including carcinomas, adenomas , and pheochro- mocy tomas) have been repor ted to contain areas o f
12 C.W. Vick et al.: CT and Ultrasound of Adrenal Myelolipoma
relative "low densi ty" due to hemorrhage, necrosis, or cellular lipid [4, 5, 6, 1 1, 13, 19]. However, al- though hemorrhage, necrosis, or cellular lipid may result in a CT density near or slightly less than water's, density equivalent to or slightly greater than normal fat's is not to be expected in these more c o m m o n adrenal tumors.
US may suggest a fatty mass if the lesion con- tains a relatively uniform pattern of high-amplitude echoes [2, 3]. Two of our 4 myelol ipomas studied with US showed this pattern (Figs. 1 and 4). An additional finding suggesting fat is apparent discon- t inuity and posterior displacement o f an acoustic interface (e.g., the diaphragm) distal to the fatty le- sion (Fig. 1). This "propagat ion speed" or "tissue veloci ty" artifact is thought to be produced by the relatively slow speed of sound in fat compared with the speed assumed in ultrasound signal processing [20, 21]. Although these findings are highly sugges- tive of a fatty mass, CT confirmation is recom- mended because o f the small number o f reported cases studied with US and the possibility that other adrenal tumors might look similar [2]. When there is extensive hemorrhage or calcification in a myelo- l ipoma, the tumor ' s fatty component may not be identified on US, and a nonspecific adrenal mass will be suggested (Figs. 1 and 3).
CT and US may occasionally provide comple- mentary informat ion in the evaluation o f a mye- lolipoma. In 2 o f our cases, US findings were non- specific because of extensive blood or calcium within the tumors, but CT was diagnostic by showing focal areas o f fat in the lesions (Figs. 1 and 3). On the other hand, in 1 myelol ipoma, the CT findings were nondiagnostic because of widespread myeloid tissue in the tumor, while the US appearance was char- acteristic for a fatty mass (Fig. 4).
The differential diagnosis of a fatty mass in the suprarenal area includes lipoma, lymphangioma, myelol ipoma, angiomyolipoma, increased intraab- dominal fat deposition, retroperitoneal teratoma, and l iposarcoma [2, 8, 9]. Renal angiomyolipomas extending into the perinephric space usually contain a recognizable intrarenal component [22], and an- giography can be used for localization and differ- entiation of a myelol ipoma (avascular) from an an- g iomyol ipoma (usually vascular) in difficult cases [2, 8]. An extraadrenal or adrenal l ipoma may be difficult or impossible to distinguish from a mye- lolipoma, although this distinction is not clinically significant. Of more importance is differentiating a well-differentiated l iposarcoma arising in the peri- nephric space from a myelolipoma. Retroperi toneal
l iposa rcomas , l ike m y e l o l i p o m a s , ma y con ta in varying proport ions of soft tissue and fat density on CT [9]. I f the fatty tumor can be confidently local- ized to the adrenal, a myelol ipoma should be sus- pected [9]. However, absolute radiologic differen- tiation between a l iposarcoma and a myelol ipoma may be impossible, particularly in the case of a large fatty retroperitoneal tumor which distorts ana tomy and makes the site of origin difficult to determine (as in patient 2) [8, 23].
If CT and US findings are equivocal for mye- lolipoma, needle biopsy may be used to make the diagnosis as in patient 4 (Fig. 4). To our knowledge, this is the first reported case of a myelol ipoma di- agnosed by needle biopsy. The presence o f mature fat cells, and myeloid precursors in the biopsy spec- imen is characteristic for myelol ipoma.
In summary, the documenta t ion of fat within an adrenal tumor represents the key to the nonin- vasive diagnosis of adrenal myelolipoma.
Acknowledgement. We thank Pauline E. Friedman for skillful preparation of the manuscript.
References
1. Dyckman J, Freedman D: Myelolipoma of the adrenal with clinical features and surgical excision. J Mt Sinai Hosp NY 24:793-796, 1957
2. Behan M, Martin EC, Muecke EC, Kazam E: Myelolipoma of the adrenal: two cases with ultrasound and CT findings. A JR 129:993-996, 1977
3. Scheible W, Ellenbogen PH, Leopold GR, Siao NT: Lipom- atous tumors of the kidney and adrenal: apparent echograph- ic specificity. Radiology 129:153-156, 1978
4. Karstaedt N, Sagel SS, Stanley R J, Melson GL, Levitt RG: Computed tomography of the adrenal gland. Radiology. 129: 723-730, 1978
5. Fink DW, Wurtzebach LR: Symptomatic myelolipoma of the adrenal. Radiology 134:451-452, 1980
6. Egharari ME, McLoughlin M J, Rosen IE, St Louis EL, Wil- son SR, Wise D J, Yeung HPH: The role of computed tomog- raphy in assessment of tumoral pathology of the adrenal glands. J Comput Assist Tomogr 4:71-77, 1980
7. Ayyat F, Fosslin E, Kent R, Hudson HC: Myelolipoma of adrenal gland. Urology 16:415-418, 1980
8. Liebman R, Strikantaswamy S: Adrenal myelolipoma dem- onstrated by computed tomography. J Comput Assist Tom- ogr 5:262-263, 1981
9. Friedman AC, Hartman DS, Sherman J, Lautin EM, Gold- man N: Computed tomography of abdominal fatty masses .
Radiology 139:415-429, 1981 10. Weiner SN, Bernstein RG, Lowy S, Karp H: Combined ad-
renal adenoma and myelolipoma. J Comput Assist Tomogr 5:440-442, 1981
11. Hattery RR, Sheedy PF, Stephens DH, Van Heerden JA: Computed tomography of the adrenal gland. Semin Roent- genol 16:290-300, 1981
C.W. Vick et al.: CT and Ultrasound of Adrenal Myelolipoma
12. Ishikawa H, Tachibana M, Hata M, Tazaki H, Akatsuka S, Iri H: Myelolipoma of the adrenal gland. J Urol 126:777- 779, 1981
13. Noble M J, Montague DK, Levin HS: Myelolipoma: an un- usual surgical lesion of the adrenal gland. Cancer 49:952- 958, 1981
14. Lamki N, Raval B, Carey LS, Wyatt JK: CT appearance of adrenal myelolipoma. J Comput Assist Tomogr 6:30--31, 1982
15. Olsson CA, Krane RJ, Klugo RC, Selikowitz SM: Adrenal myetolipoma. Surgery 73:665-670, 1973
16. McDonnell WY: Myelolipoma of adrenal. Arch Pathol 61: 416-419, 1956
17. Plaut A: Myelolipoma in the adrenal cortex. Am J Pathol 34:487-507, 1958
18. Levi C, Gray JE, McCullough EC, Hattery RR: The unre- liability of CT numbers as absolute values. A JR 139:443- 447, 1982
13
19. Schaner EG, Dunnick NR, Doppman JL, Strott CA, Gill JR, Javadpour N: Adrenal cortical tumors with low attenuation coefficients: a pitfall in computed tomography diagnosis. J Comput Assist Tomogr 2:11-15, 1978
20. Pierce G, Golding RH, Cooperberg PL: The effects of tissue velocity changes on acoustical interfaces. J Ultrasound Med 1:185-187, 1982
21. Richman TS, Taylor KJW, Kremkau FW: Propagation speed artifact in a fatty tumor (myelolipoma): significance for tissue differential diagnosis. J Ultrasound Med 2:45-47, 1983
22. Sherman JL, Hartman DS, Friedman AC, Madewell JE, Da- vis CJ, Goldman SM: Angiomyelolipoma: computed tomo- graphic-pathologic correlation of 17 cases. A JR 137:1221- 1226, 1981
23. Tsukaguchi I, Sato K, Ohara S, Kadowaki T, Shin T, Kotoh K: Adrenal myelolipoma: report of a case with CT and an- giographic evaluation. Urol Radiol 5:47-49, 1983

![Myelolipoma: A Rare Adrenal Incidentaloma · insufficiency, and pheochromocytoma [23-28]. The extensive use of abdominal CT-scan and magnetic resonance imaging has led to a dramatic](https://img.pdfslide.net/doc/110x75/5f0e41897e708231d43e5c5c/myelolipoma-a-rare-adrenal-incidentaloma-insufficiency-and-pheochromocytoma-23-28.jpg)




![Adrenal Imaging - University of Floridaxray.ufl.edu/files/2010/02/Adrenal-Imaging.pdfadrenal glands [3], and a metastasis might ... CT, adrenal imaging, adrenal lymphoma imaging, adrenal](https://img.pdfslide.net/doc/110x75/5b26814c7f8b9a8c0f8b4820/adrenal-imaging-university-of-glands-3-and-a-metastasis-might-ct-adrenal.jpg)