Embed Size (px)
Citation preview
03
24
Surgical Treatment of Adrenal Myelolipoma
Original Article
Introduction
Adrenal myelolipomas are rare benign tumors com-
posed of maturated adipose tissue and hematopoietic
cells. In most cases they are small and asymptomatic.
Discovered incidentally by ultrasound or computed to-
mography examination, they are classified as “adrenal
incidentalomas” and follow the corresponding indica-
tions for surgical removal.
Materials and methods
We present 6 patients within a prospective study
who were performed retroperitoneal endoscopic
adrenalectomy (REA) between June 2007 and Janu-
ary 2010 at the Second Surgical Department of UM-
HAT ”Alexandrovska”, Sofia, on the occasion of adrenal
gland myelolipoma. Five of the patients had unilateral
pathology and one - bilateral. In the patient with bilat-
eral pathology we performed a two-stage procedure
– REA on the first stage and conventional contralateral
adrenalectomy on the second.
The demographic characteristic of patients is pre-
sented in Table 1.
SURGICAL TREATMENT OF ADRENAL MYELOLIPOMAG. Todorov1, Ts. Lukanova1, M. Georgiev2
1Second Surgical Department, Medical University, Sofia2Department of Urology, Medical University, Sofia
Key words: endoscopic adrenalectomy, adrenal tumors, myelolipomaContact details: G. Todorov, Second Surgical Department, Medical University, 1 Sv. Georgi Sofiiski Blvd. – 1431, e-mail: [email protected]
Abstract: Objective: To evaluate the potential of different surgical techniques in the treatment of rare tumors of the adrenal
glands.
Material and methods: We present 6 patients within a prospective study who underwent retroperitoneal endoscopic
adrenalectomy (REA) between June 2007 and January 2010 at the Second Surgical Department of UMHAT ”Alexandrovska”,
Sofia, on the occasion of adrenal gland myelolipoma.
Results: REA was carried out in 5 patients, while in one with bilateral myelolipomas - REA was performed followed by
a conventional contralateral adrenalectomy on the 2nd stage. The mean operative time for endoscopic surgery was 70 min
- (60’-90’), with an average intraoperative blood loss of 50 ml. There were no intraoperative and postoperative complica-
tions.
Conclusions: Myelolipomas are rare diseases of the adrenal glands, most often discovered incidentally in imaging diag-
nostics. The indications for their surgical treatment follow those of the incidentalomas. Mini-invasive techniques performed
by experienced endocrine and laparoscopic team are an effective and feasible way for their removal.
03
25
J Clin Med. 2010; 3(3):24-30
Patients went through
the following examinations:
- clinical (including BMI),
- paraclinical (including precise adrenal hormonal
status for exclusion of subclinical Cushing-syndrome
and “occult” pheochromocytoma)
- imaging (standard ultrasound examination of ab-
dominal organs and retroperitoneal areas and contrast
computed tomography, if necessary - MRI) in order to
confirm the diagnosis, assess the malignant potential
of the formation and implement appropriate preop-
erative preparation.
Within the prospective study, we evaluated and
analyzed age, sex, BMI, size and location of tumor,
operative time, intraoperative and postoperative com-
plications, and postoperative hospital stay. Clinical
symptoms and relapse of the disease were tracked
during the follow-up period.
Results
In four patients the “adrenal tumor formation” was
detected incidentally during examinations on other
occasions. In one patient, the diagnosis myelolipoma
was suspected in the CT scan. One of the women had
been operated in another clinic on occasion of “chron-
ic calculous cholecystitis” eight years earlier. The per-
formed conventional cholecystectomy simultaneously
had revealed a tumor formation in the right adrenal
gland (25/25 mm preoperative CT size, intraoperative
- 50/60 mm), so a biopsy had been carried out. There
had not been total extirpation of the gland because
of proximity to vena cava inferior, difficult access and
benign macroscopic feature of the formation. The his-
tological examination of the material had indicated
a presence of “adrenal myelolipoma”. The formation
had been monitored in dynamics by nuclear magnetic
resonance with a noticed increase in size while main-
taining structural characteristics and normal size and
structure of the left adrenal gland. Eight years later
that patient manifested also hormonal secretion with
elevated levels of aldosterone and rennin triple tested
in upright position and within normal potassium lev-
els. The functional activity and the size of the forma-
tion required surgical intervention. The identified for-
mations in the other two patients were between 8-10
cm in size and hormonally inactive.
The analysis focuses on the characteristics of the
tumor formations - their size and location (Table 2),
clinical symptoms and comorbidity and CT - features.
(Table 3)
All patients had accompanying diseases - obesity
class I-II and arterial hypertension. Dyslipidemia within
metabolic syndrome was found in one female patient,
in two there was thyroid gland pathology – struma
nodosa and Hashimoto’s thyroiditis. One of the men
had been operated in the past with brain cyst and
nephro-and ureterolithiasis in the left.
CT-scans were carried out in all patients, including
MRI for the woman with 8-year follow up of the my-
elolipoma. In that woman’s case the mass of the right
adrenal gland was described as hyperintense, with
inhomogeneous intralesional structure, originating
from the adrenal gland, with rounded shape, benign
macromorphological characteristics and dimensions
68.3/49.2 mm, visibly enlarged compared to previ-
ous MRI examinations. The formation was with highly
03
26
expansive cranial growth, and in its development it
pressed, without infiltrating v.c. inferioris, reduced the
pararenal space to the right, and pushed the right
kidney in the caudal direction. In STIR (sequence with
fat suppression), the lesion is presented with distinct
hyperintense signal characteristic, suggesting reduced
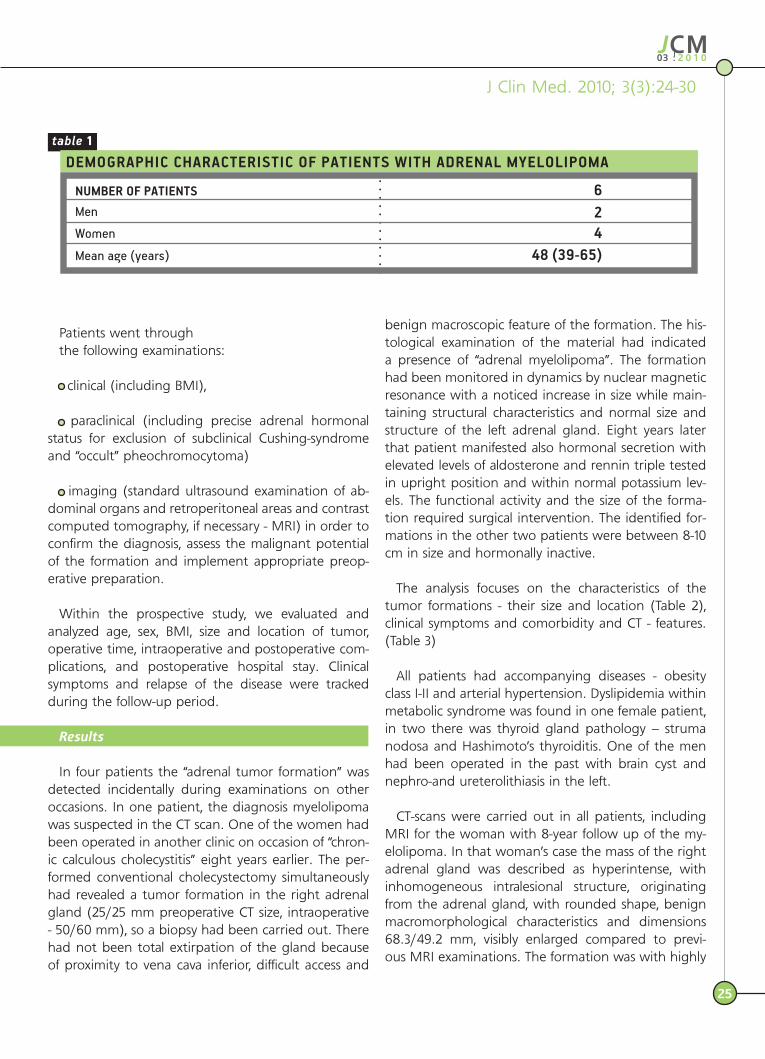
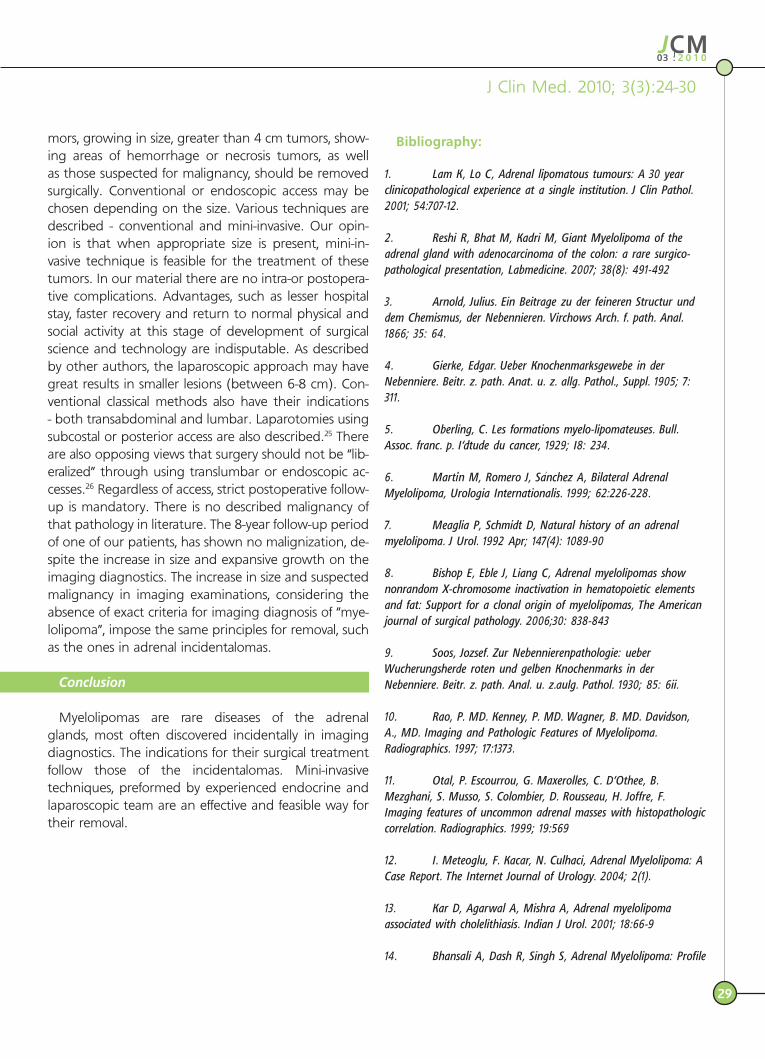
fat contents. The CT-characteristics of the myelolipo-
ma-like tumor formation are presented in Table 3,
while the CT image of the bilateral myelolipomas - in
Figure 1.
“Hand-assisted” retroperitoneal endoscopic adrena-
lectomy was carried out in two of the patients with
unilateral pathology. The patient with bilateral inci-
dentalomas underwent a two-stage procedure - the
first stage was total retroperitoneoscopic adrenalec-
tomy on the right, and the second - left lumbotomy
with adrenalectomy because of previous surgery in
the area – pyelolithotomy and ureterolithotomy, on
the occasion of nephrolithiasis, which considering the
10-cm size and the corresponding malignant poten-
tial, was evaluated as contraindication for mini-invasive
procedure.
The mean operative time of the endoscopic surger-
ies was 70 min - (60’-90’), with an average intraopera-
tive blood loss of 50 ml. In one case, we succeeded
to perform subtotal adrenalectomy with preservation
of apparently unchanged parenchyma of the adrenal
gland. The other required the removal of the entire
gland. Extirpation of the specimen was accomplished
by the use of “Endo-bag”, with skin excision expanded
whenever required by the size of the tumor. There
were no intraoperative and postoperative complica-
Surgical Treatment of Adrenal Myelolipoma
CT-image - a tumor formation in the right adrenal gland area, with transversal dimensions 54/74 mm; density is fat-equivalent - 60-90 HU; a capsule with irregular thickness; density does not change a�er application of contrast material
Postoperative view of the removed specimen and its macroscopic characteristics

03
27
J Clin Med. 2010; 3(3):24-30
tions. Conventional adrenalectomy was performed
through lumbotomy and resection of the XII rib, while
intraoperatively were revealed multiple adhesions of
the renal capsule to the peritoneum and lumbar mus-
cle. The adrenal tumor formation was also accreted to
the tail of the pancreas. Verticalization and oral intake
in retroperitoneoscopic operations began on the 6th
postoperative hour; the mean postoperative stay was
2 days. With the conventional access this stay was ex-
tended to 6 days.
The histological diagnosis in all patients was “adrenal
myelolipoma”.
The follow up of the patients includes clinical, ul-
trasound and hormonal examinations on the 1st, 6th
and 12th postoperative months. There are no records
of recurrence or changes in the contralateral gland in
patients with unilateral pathology on the 12th month
of the follow-up. In the female patient with renin
overproduction, there was no such problem on the
6th month of the follow-up within normal potassium
levels. The man with bilateral adrenalectomy was ad-
ministered hormone replacement therapy.
Discussion
Adrenal myelolipomas are rare benign tumors com-
posed of fatty connective tissue and hematopoietic ele-
ments in different proportions. No malignant potential
of these lesions is reported in literature. Myelolipomas
are most often incidental findings (incidentalomas) of
imaging diagnostics, performed on another occasion.
They constitute about 3% of all primary adrenal tumors,
and their incidence in autopsies is 0.06% to 0.2%.1 Their
approximate share of the “incidentalomas” is 7-15%.15 My-
elolipomas are found among people aged 25-65 years,
most often affecting those aged 50-60 years2. The right
adrenal gland is more frequently involved than the left
(ratio 3:2.1) and the bilateral myelolipomas are rare.14
Our patients were in the age range 39-65 years and the
ratio right: left adrenal gland was respectively - 1.3:1. In
one case there was bilateral myelolipoma.
Far back in 1866, while exploring questions about the
biochemistry and cytology of the adrenal gland, Arnold3
reported the possibility that blood cells available from
ectopic tissue elements of bone marrow may develop
in the adrenal gland. For the first time, Gierke in 1905
represented a histological evidence of bone marrow in
the adrenal gland.4 Researchers of that time discussed
the presence of heterotopic bone tissue in the adre-
nal gland as a “pre-myeloma”. The name “myelolipoma”
was introduced in 1929 by Oberling to describe this ect-
opy.5 Etiopathogenesis of this disease remains unclear.
Experimental myeloid transformation in the adrenal
gland was induced by subcutaneous injection of extract
of anterior pituitary and metiltestosteron.19 Currently,
there are various theories about the origin and devel-
opment of the adrenal myelolipomas - development of
clusters of mesenchymal stem cells, bone marrow em-
boli, extramedullary hemopoiesis6, as the most widely
accepted is the theory of metaplasia of the reticuloen-
dothelial cells of capillaries as a result of stressful stimuli
- infection, ischemia, necrosis.7 Nonrandom inactivation
of the X-chromosome is established in these tumors,
suggesting their clonal origin and consequently the
presence of a single precursor for the fatty and myeloid
cell elements.8 Myelolipomas are morphologically dif-
ferent from normal bone marrow, showing differences
in cellular composition, cellularity and structure of the
stromal component.8
Myelolipomas originate in the adrenal cortex and
their surface is composed by pseudo-capsule of the
compressed zona glomerulosa and zona fasciculata.2
Yet in 1930, Soos9 classified the myelolipomas into two
categories:
Figure 1. CT image of bilateral myelolipomas

03
28
Type I - tumor formations with yellow-orange color
and predominance of fatty connective tissue, non-
abundant presence of myeloid elements, large quantity
of erythroblasts.
Type II - tumor formations dark red, red-brown in
color, with predominance of bone marrow compo-
nent in which myeloid prevail the erythroblastic ele-
ments.
Myelolipomas are most often incidental findings of
imaging diagnostics performed on other occasions and
are asymptomatic. .
In most cases, the ultrasonography examination shows
suprarenal lesion with a heterogeneous structure, con-
taining hyperechogenic and hypoechogenic loci, corre-
lating respectively with the fat and hematopoietic ele-
ments. Calcifications can also be identified. Abdominal
radiography or intravenous urography can demonstrate
in some cases x-rays negative tumor mass in the adrenal
zone, dislocating the kidney caudally.
On computed tomography scan the myelolipomas
present different percentage of fatty tissue scattered
among low-density hematopoietic elements (usually
with a density 20-30 HU), which are often referred to as
soft tissue elements. MRI is sometimes necessary to es-
tablish the origin of the tumor and to compare the sig-
nal intensity of the formation to that of the liver in order
to distinguish malignant from benign lesion.17
Bone marrow elements are often isointense with
spleen. According to some authors, the presence of fat
density in an adrenal tumor formation on a CT scan
is virtually pathognomonic for mielolipoma18 and there
is no need for further diagnostics.10,11 However, others
suggest the opposite – the presence of fat tissue in
the formation may not be pathognomonic for myelol-
ipoma for two reasons - first - other rare diseases, such
as lipomas and liposarcoma contain such tissue, and
second – there are described cases of adrenal lipomas
and adrenocortical carcinomas, containing small areas
of fat tissue.20,21 We observed histologically confirmed
adrenal lipoma and adenolipoma in our operative ma-
terial, which gives us no reason to suggest “myelolipo-
ma” diagnosis only by imaging examination.
Differential diagnosis includes adrenal liposarcoma,
renal angiomyelolipoma, retroperitoneal lipomas and
others. With the significant predominance of myeloid
tissue, calcifications and hemorrhagic areas, the fatty
component may remain unrecognized. Although most
myelolipomas are presented as isolated adrenal masses,
myelolipoma fields have been described in association
with other pathological changes in the adrenal gland
as adrenocortical hyperplasia, adrenocortical adeno-
mas, adrenocortical carcinomas and endocrinological
dysfunctions, including Addison’s Disease, Conn’s syn-
drome, 21-hydroxylase deficiency, 17-hydroxylase defi-
ciency and ectopic corticotropic production.12 In one of
our cases, there was a hormonal hypersecretion featur-
ing elevated levels of aldosterone and renin in triple
upright position testing, which was normalized on the
sixth month after the operation within normal potas-
sium levels and persistent hypertension. We considered
this abnormal hormonal production as part of the pre-
sented pathology, as the contralateral gland showed no
imaging changes in the follow-up.
The clinical manifestation of myelolipomas may be
acute abdominal pain and hemorrhagic shock due to
rupture and hemorrhage from the formation, or ab-
dominal discomfort as a result of their large size. Spon-
taneous hemorrhage is more typical for tumors with
predominantly myeloid components.16
Comorbidity of myelolipomas with obesity and hyper-
tension are often reported, as in some cases the sug-
gested reason for the hypertension is the compression
of the renal artery.22,23 In our study, one of the female
patients had had a 5-year history of hypertension, and
on the postoperative follow-up the dosage of the ACE-
inhibitor taken as systemic therapy, was reduced, and
the diuretic therapy - stopped. Association with chole-
lithiasis, however, is rare, as the most probable discussed
cause is an accidental coincidence.13 In our case, the
conventional cholecystectomy is the reason for diagnos-
ing myelolipoma in one of the patients. Associated ma-
lignant pathology, such as renal cell cancer23, colon can-
cer2 etc. and simultaneous adrenal and extra-adrenal
myelolipomas have been described.24
Surgical treatment is the main therapeutic approach in
symptomatic and complicated lesions. Symptomatic tu-
Surgical Treatment of Adrenal Myelolipoma
03
29
J Clin Med. 2010; 3(3):24-30
mors, growing in size, greater than 4 cm tumors, show-
ing areas of hemorrhage or necrosis tumors, as well
as those suspected for malignancy, should be removed
surgically. Conventional or endoscopic access may be
chosen depending on the size. Various techniques are
described - conventional and mini-invasive. Our opin-
ion is that when appropriate size is present, mini-in-
vasive technique is feasible for the treatment of these
tumors. In our material there are no intra-or postopera-
tive complications. Advantages, such as lesser hospital
stay, faster recovery and return to normal physical and
social activity at this stage of development of surgical
science and technology are indisputable. As described
by other authors, the laparoscopic approach may have
great results in smaller lesions (between 6-8 cm). Con-
ventional classical methods also have their indications
- both transabdominal and lumbar. Laparotomies using
subcostal or posterior access are also described.25 There
are also opposing views that surgery should not be “lib-
eralized” through using translumbar or endoscopic ac-
cesses.26 Regardless of access, strict postoperative follow-
up is mandatory. There is no described malignancy of
that pathology in literature. The 8-year follow-up period
of one of our patients, has shown no malignization, de-
spite the increase in size and expansive growth on the
imaging diagnostics. The increase in size and suspected
malignancy in imaging examinations, considering the
absence of exact criteria for imaging diagnosis of “mye-
lolipoma”, impose the same principles for removal, such
as the ones in adrenal incidentalomas.
Conclusion
Myelolipomas are rare diseases of the adrenal
glands, most often discovered incidentally in imaging
diagnostics. The indications for their surgical treatment
follow those of the incidentalomas. Mini-invasive
techniques, preformed by experienced endocrine and
laparoscopic team are an effective and feasible way for
their removal.
Bibliography:
1. Lam K, Lo C, Adrenal lipomatous tumours: A 30 year clinicopathological experience at a single institution. J Clin Pathol. 2001; 54:707-12.
2. Reshi R, Bhat M, Kadri M, Giant Myelolipoma of the adrenal gland with adenocarcinoma of the colon: a rare surgico-pathological presentation, Labmedicine. 2007; 38(8): 491-492
3. Arnold, Julius. Ein Beitrage zu der feineren Structur und dem Chemismus, der Nebennieren. Virchows Arch. f. path. Anal. 1866; 35: 64.
4. Gierke, Edgar. Ueber Knochenmarksgewebe in der Nebenniere. Beitr. z. path. Anat. u. z. allg. Pathol., Suppl. 1905; 7: 311.
5. Oberling, C. Les formations myelo-lipomateuses. Bull. Assoc. franc. p. I‘dtude du cancer, 1929; I8: 234.
6. Marti‘n М, Romero J, Sa‘nchez A, Bilateral Adrenal Myelolipoma, Urologia Internationalis. 1999; 62:226-228.
7. Meaglia P, Schmidt D, Natural history of an adrenal myelolipoma. J Urol. 1992 Apr; 147(4): 1089-90
8. Bishop E, Eble J, Liang C, Adrenal myelolipomas show nonrandom X-chromosome inactivation in hematopoietic elements and fat: Support for a clonal origin of myelolipomas, The American journal of surgical pathology. 2006;30: 838-843
9. Soоs, Jozsef. Zur Nebennierenpathologie: ueber Wucherungsherde roten und gelben Knochenmarks in der Nebenniere. Beitr. z. path. Anal. u. z.aulg. Pathol. 1930; 85: 6ii.
10. Rao, P. MD. Kenney, P. MD. Wagner, B. MD. Davidson, A., MD. Imaging and Pathologic Features of Myelolipoma. Radiographics. 1997; 17:1373.
11. Otal, P. Escourrou, G. Maxerolles, C. D’Othee, B. Mezghani, S. Musso, S. Colombier, D. Rousseau, H. Joffre, F. Imaging features of uncommon adrenal masses with histopathologic correlation. Radiographics. 1999; 19:569
12. I. Meteoglu, F. Kacar, N. Culhaci, Adrenal Myelolipoma: A Case Report. The Internet Journal of Urology. 2004; 2(1).
13. Kar D, Agarwal A, Mishra A, Adrenal myelolipoma associated with cholelithiasis. Indian J Urol. 2001; 18:66-9
14. Bhansali A, Dash R, Singh S, Adrenal Myelolipoma: Profile
03
30
Surgical Treatment of Adrenal Myelolipoma
of Six Patients With a Brief Review of Literature, Int J Endocrinol Metab. 2003; 1:33-40
15. Kloss RT, Gross MD, Francis IR, Korobkin M, Shapiro B. Incidentally discovered adrenal masses. Endocrine Reviews. 1995; 16: 460-84.
16. Sanders R, Bissada N, Curry N, Gordon B. Clinical spectrum of adrenal myelolipoma: Analysis of 8 tumors in 7 patients. J Urol. 1995; 153: 1791-3.
17. Francis IR, Gross MP, Shapiro B, Koropkin M, Quint LE. Integrated imaging of adrenal disease. Radiology. 1992; 184: 1-13.
18. Кenney PJ, Wagner BJ, Rao P, Heffess CS. Myelolipoma: CT and pathologic features. Radiology. 1998; 208: 87-95
19. Selye H: Stone H: Hormonally-induced transformation of adrenal into myeloid tissue. Am J Pathol. 1950; 26: 211-233
20. Ferrozzi F: Bova D: CT and MR demonstration of fat within an adrenal cortical carcinoma. Abdom Imaging. 1995; 20: 272-274
21. Sato N: Watanabe Y, Saga T, Mitsudo K, Dohke M, Minami K: Adrenocortical adenoma containing fat component: CT and MR image evaluation. Abdom Imaging. 1995; 20: 489-490
22. Del Gaudio A: Solidoro G: Myelolipoma of the adrenal gland, report of two cases with review of the literature. Surgery. 1986; 99: 293-301
23. Hofmockel G, Dammrich J, Manzanilla Garia H, Frohmuller H. Myelolipoma of the adrenal gland associated with contralateral renal cell carcinoma. Case report and review of literature. J Urol. 1995; 153: 129-132
24. Zieker D, Ko..nigsrainer I, Miller S Simultaneous adrenal
and extra-adrenal myelolipoma – an uncommon incident: case report and review of the literature. World Journal of Surgical Oncology. 2008; 6:72
25. Al. Mondrago‘n-Sa‘nchez, R. Mondrago‘n–Sa‘nchez, S. Shuchleib-Chaba, Symptomatic adrenal myelolipoma. Indications and results of surgical excision. Clinical and Translational Oncology. 2002; 4(1): 33-36.
26. Meyer A, Behrend M, Presentation and therapy of myelolipoma. International Journal of Urology. 2005; 12(3): 239-243