Embed Size (px)
Citation preview
AdultBrainTumours:anapproachbasedonimaging
findingsRobertJSevick,MD,FRCPC,FACR
Professor,RadiologyandClinicalNeurosciencesCummingSchoolofMedicine
UniversityofCalgary
Learningobjectives:
• Learnimagingcharacteristicsofadultbraintumours• Formulatebasicdifferentialdiagnosesbasedontheseimagingfeatures
• “pearlsofwisdom”forimageinterpretationthatcanleadtospecificdiagnosis
Disclosures,acknowledgements
• Nodisclosures…• Manyacknowledgements!• Dr.WalterMontanera - St.Michael’sHospital,UniversityofToronto(http://www.radiologyassistant.nl/en/p47f86aa182b3a/brain-tumor-systematic-approach.html)
• Faculty/fellowsUCalgary Neuroradiology,(particularlyJamesScott)• UCSFNeuroradiology/Neuropathology
The Lancet 2012 379, 1984-1996DOI: (10.1016/S0140-6736(11)61346-9) Copyright © 2012 Elsevier Ltd Terms and Conditions
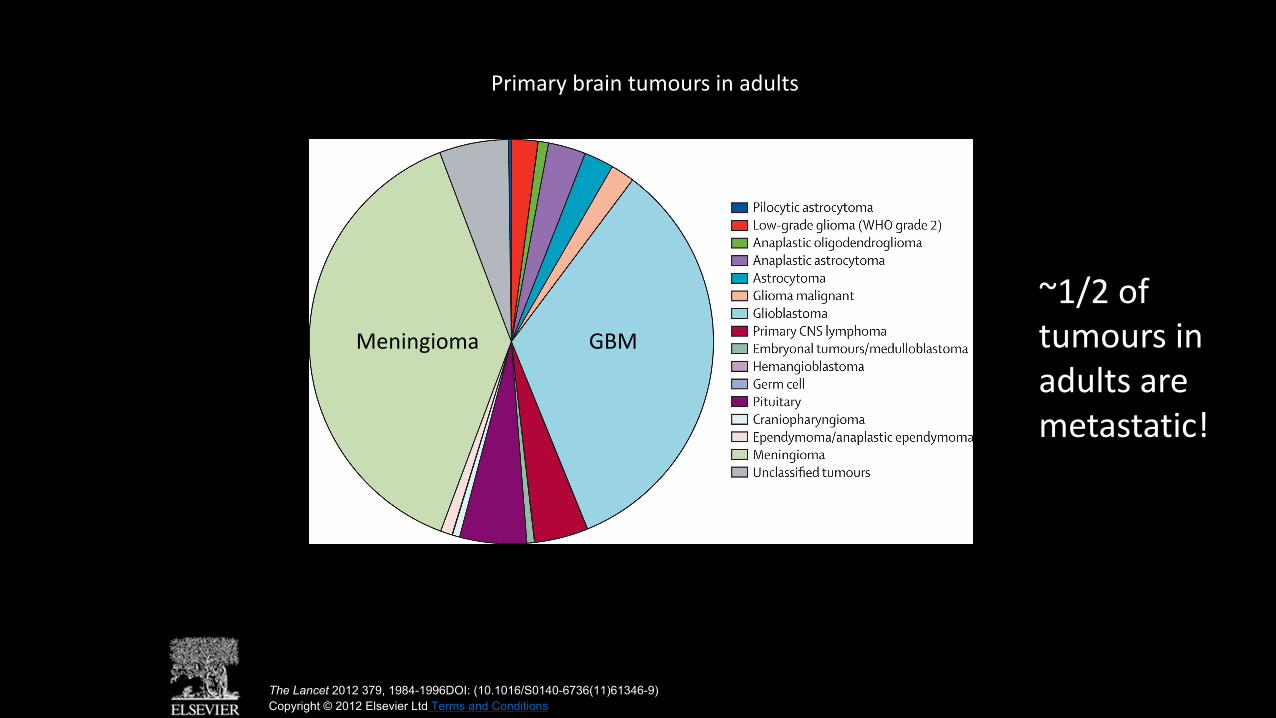
Primarybraintumours inadults
GBMMeningioma
~1/2oftumours inadultsaremetastatic!
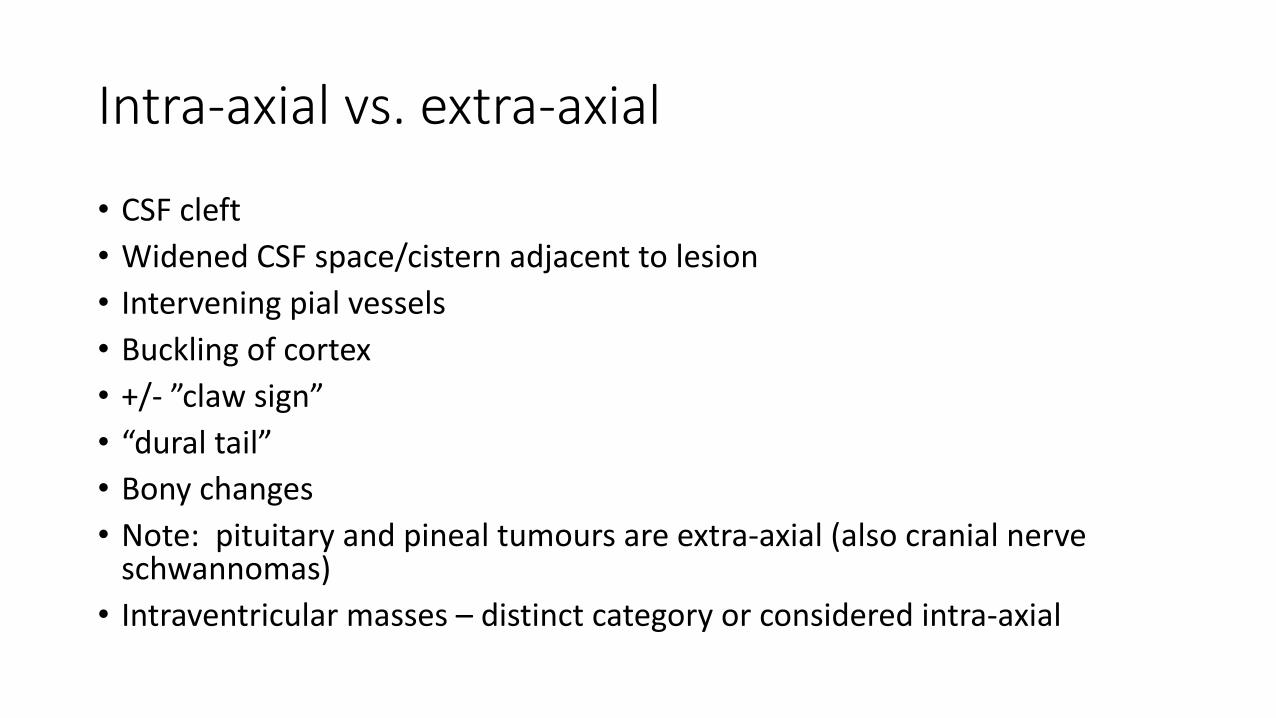
Intra-axialvs.extra-axial
• CSFcleft• WidenedCSFspace/cisternadjacenttolesion• Interveningpial vessels• Bucklingofcortex• +/- ”clawsign”• “dural tail”• Bonychanges• Note:pituitaryandpinealtumours areextra-axial(alsocranialnerveschwannomas)
• Intraventricularmasses– distinctcategoryorconsideredintra-axial
38yfemalewithseverelyincreasedheadache,1-2x/dx1/12+caffeineuse(Pepsi- 2-3L/dx1yr).
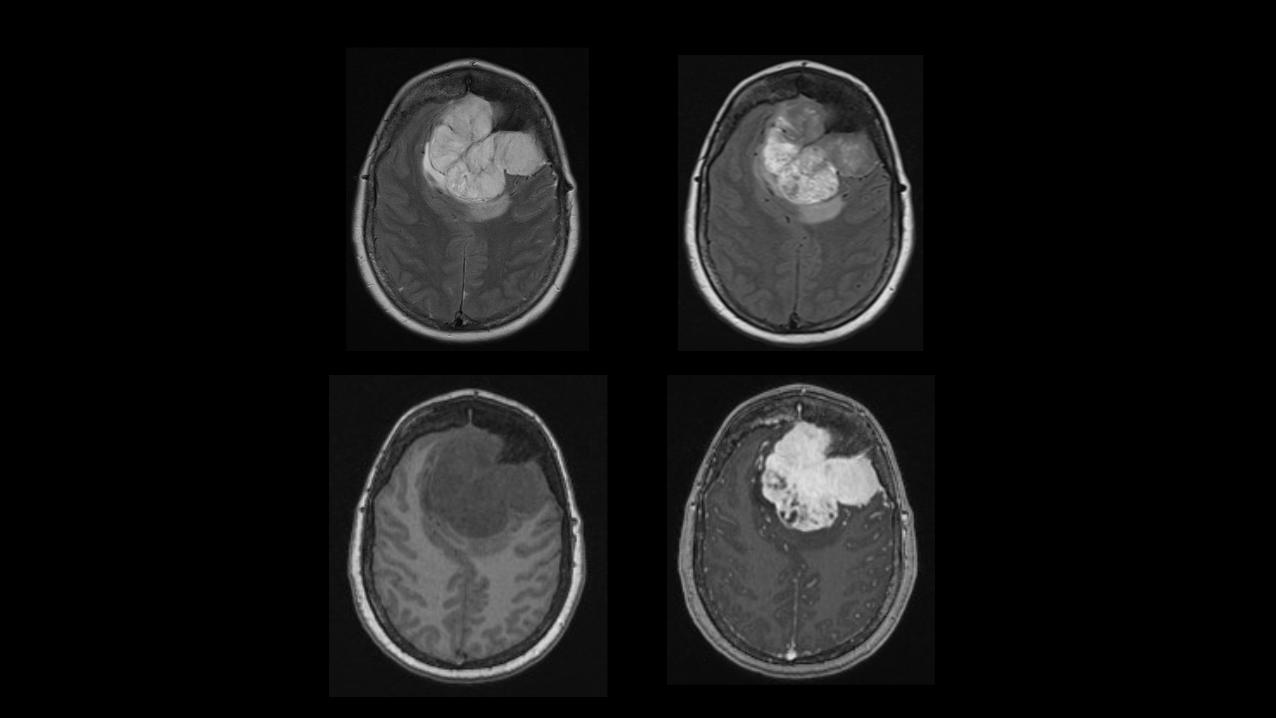
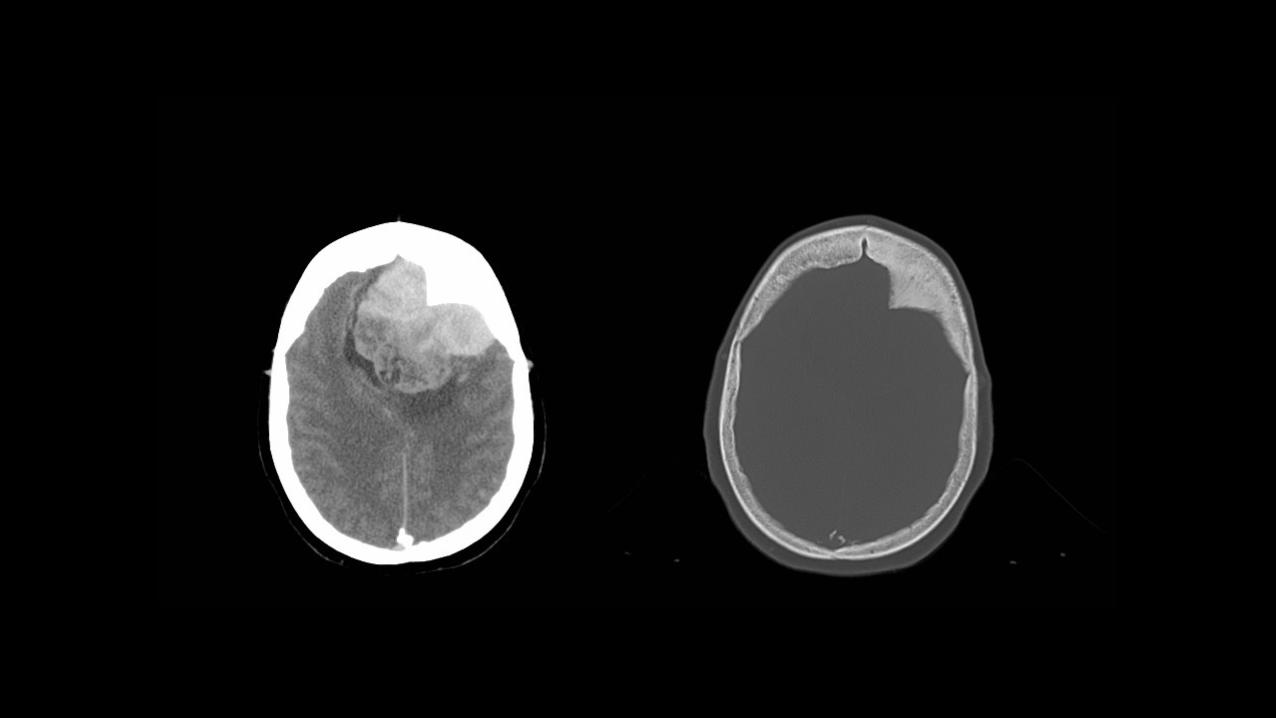
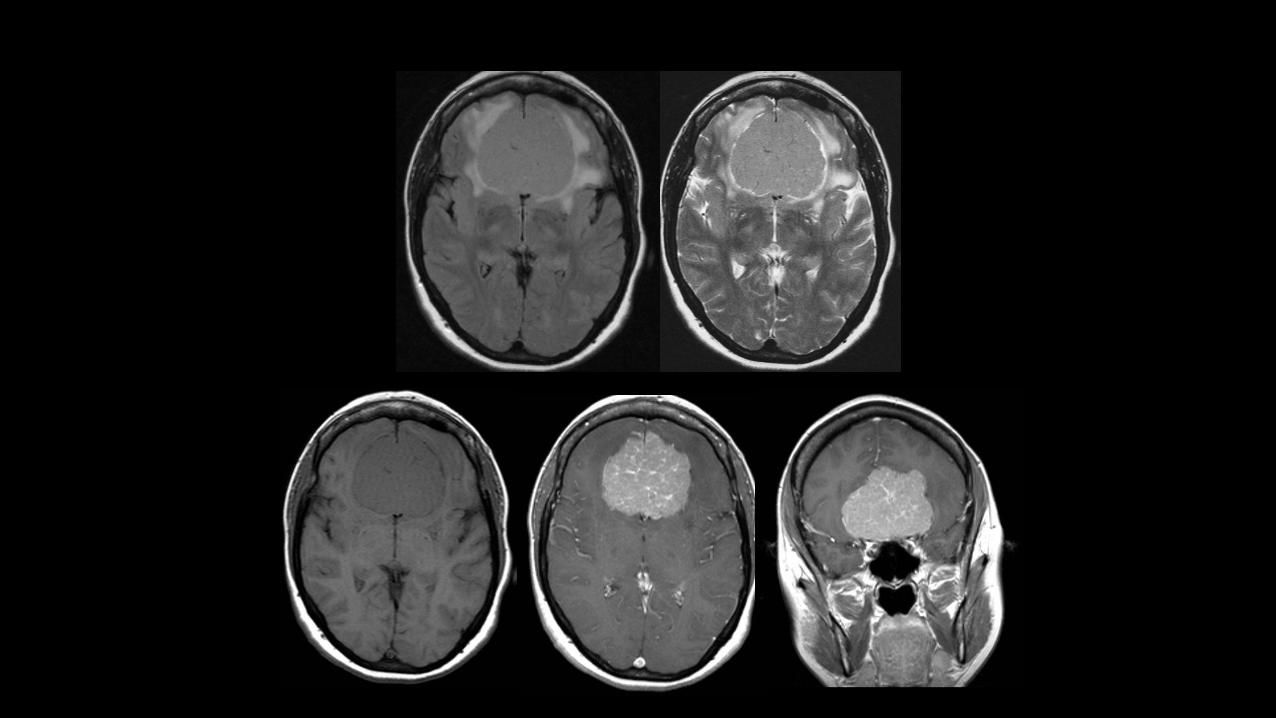
MR/CTimagingofmeningiomas
• T1Wiso-hypointense,T2Wiso-hyperintense (hyperintensity maycorrelatewithsoftertumor)
• Assessforbraininvasion,brainedema• Intenseenhancement• Duraltail– neoplasticinfiltrationvs.non-neoplasticmeningothelialproliferation,hyper-vascularity
• CTforbonechanges– infiltration,hyperostosis

Localtumour spread– inthebrain
• Astrocytoma• Infiltrative• Whitemattertracts• Donotrespectlobarboundaries
• Ependymoma• “plastic”spreadthroughventricularsystem
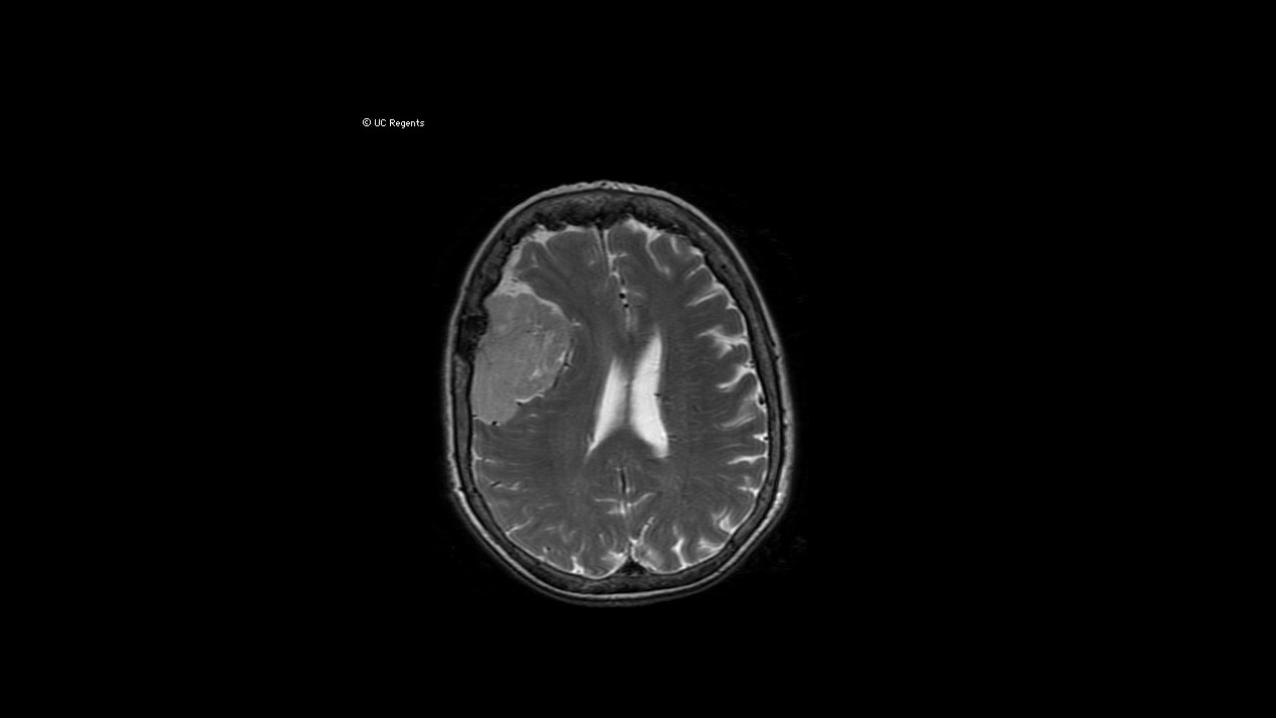
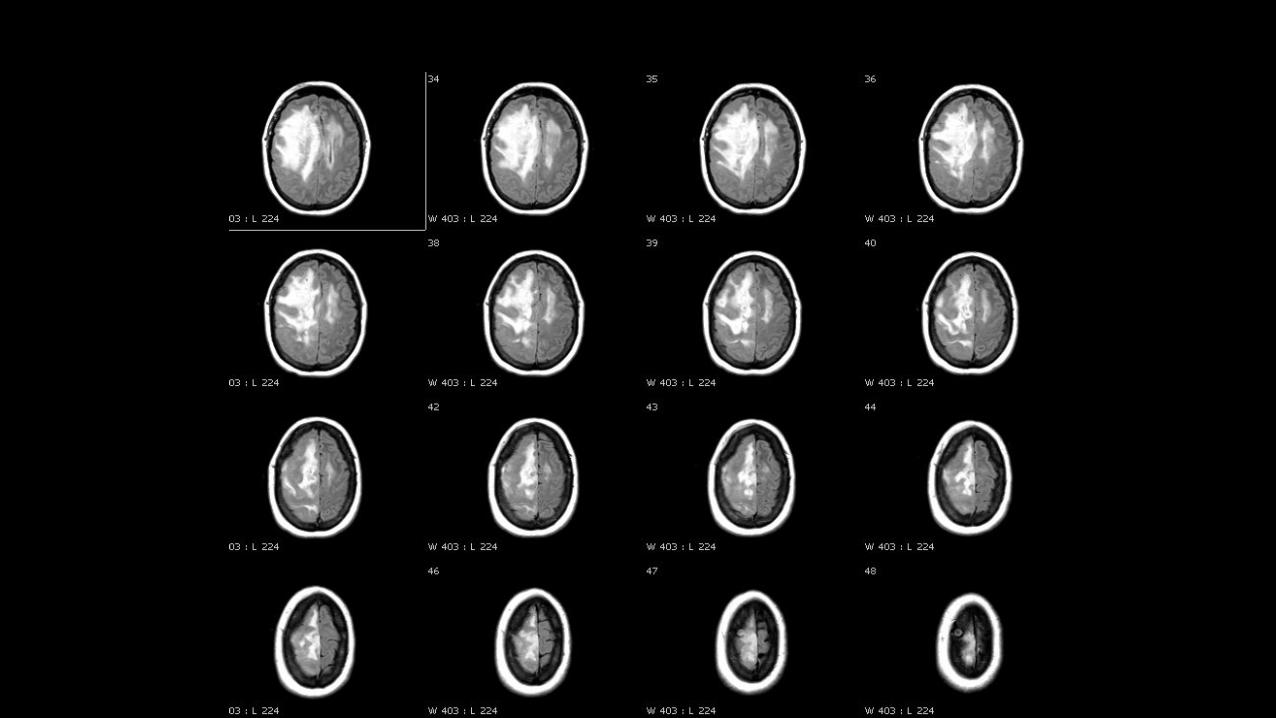
Hugetumour,littlemasseffect
• Lowgradeglioma/gliomatosis
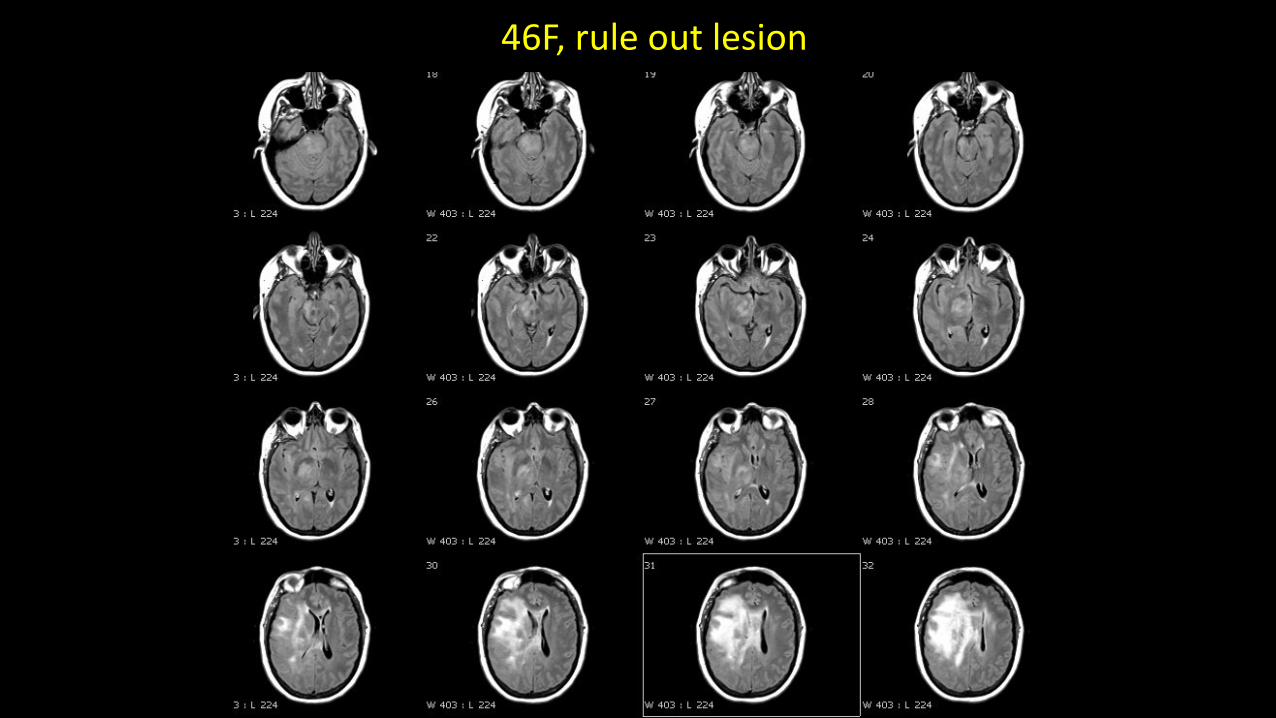
46F,ruleoutlesion
WHO2016
• Gliomatosis cerebri deletedasadistinctentity• Itisagrowthpattern,foundinmanydifferentgliomas• Growthpattern=threeormorecerebrallobes,frequentlybilateral,infratentorial extension
Smalltumour withlotsofmasseffect/edema
• Metastatic(butmakesureit’snotanabscess)
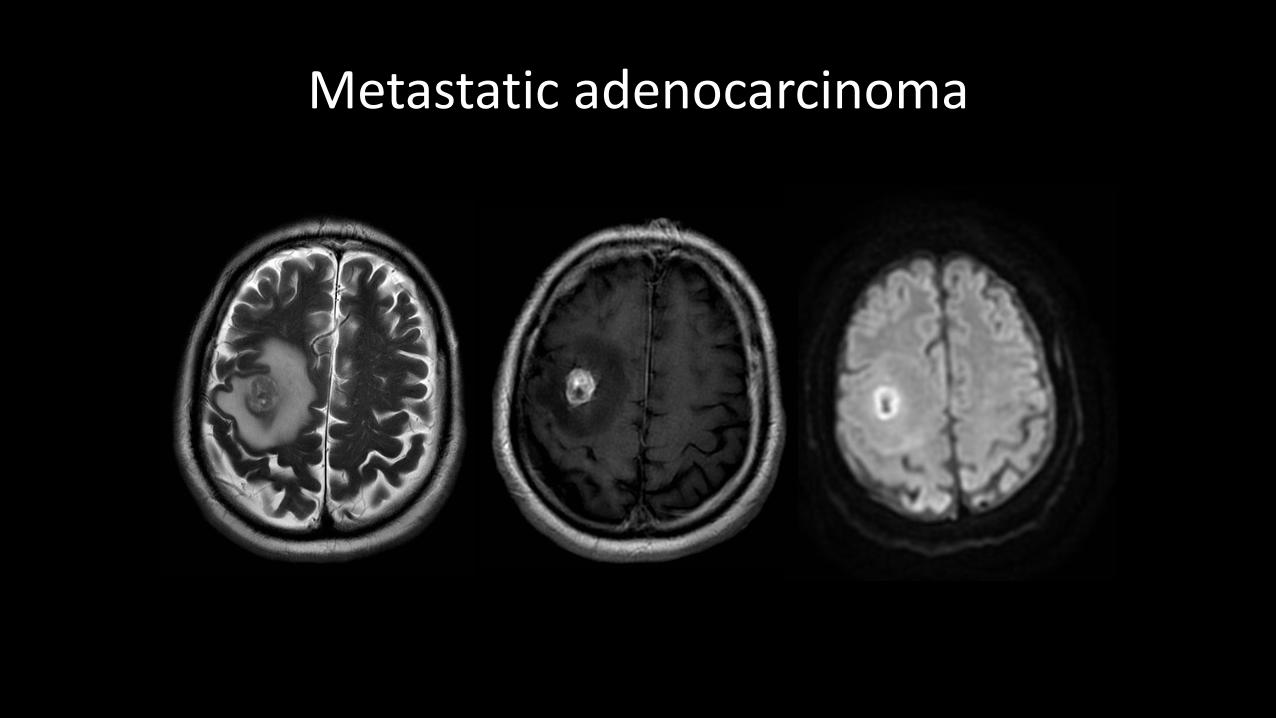
Metastaticadenocarcinoma
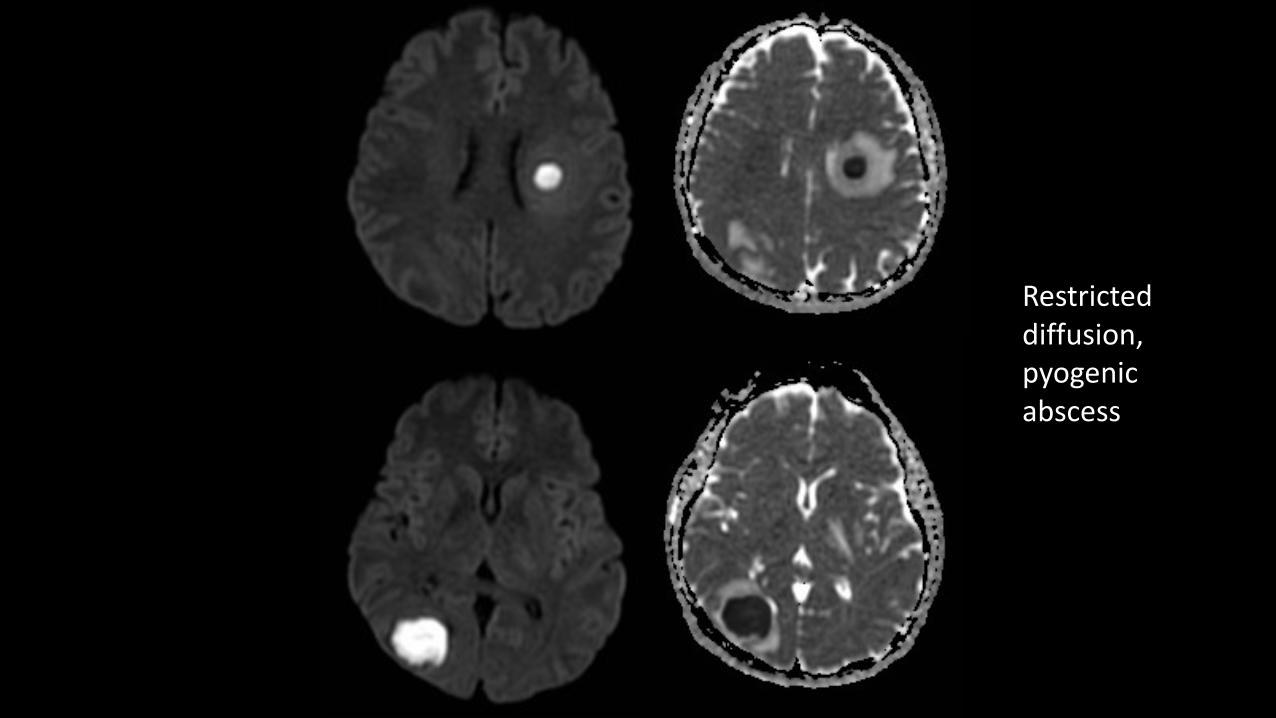
Restricteddiffusion,pyogenicabscess
Tumour spread
• Fullanatomicalextent• Perineural spreadofheadandnecktumours• Leptomeningealmetastases
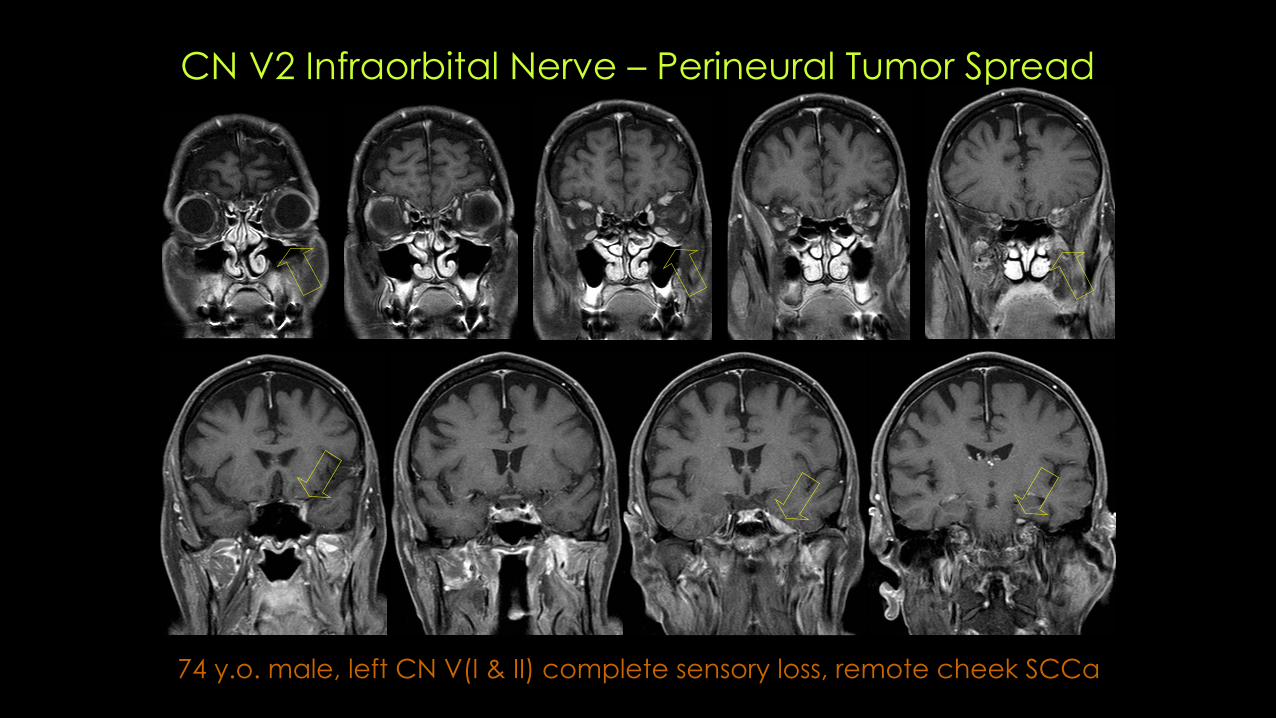
74 y.o. male, left CN V(I & II) complete sensory loss, remote cheek SCCa
CN V2 Infraorbital Nerve – Perineural Tumor Spread
Subarachnoidspreadoftumours
• Metastasesfromnon-CNSprimaries• GBM• Lymphoma• Ependymoma• Choroidplexustumours• PNET(medulloblastoma,pineoblastoma)
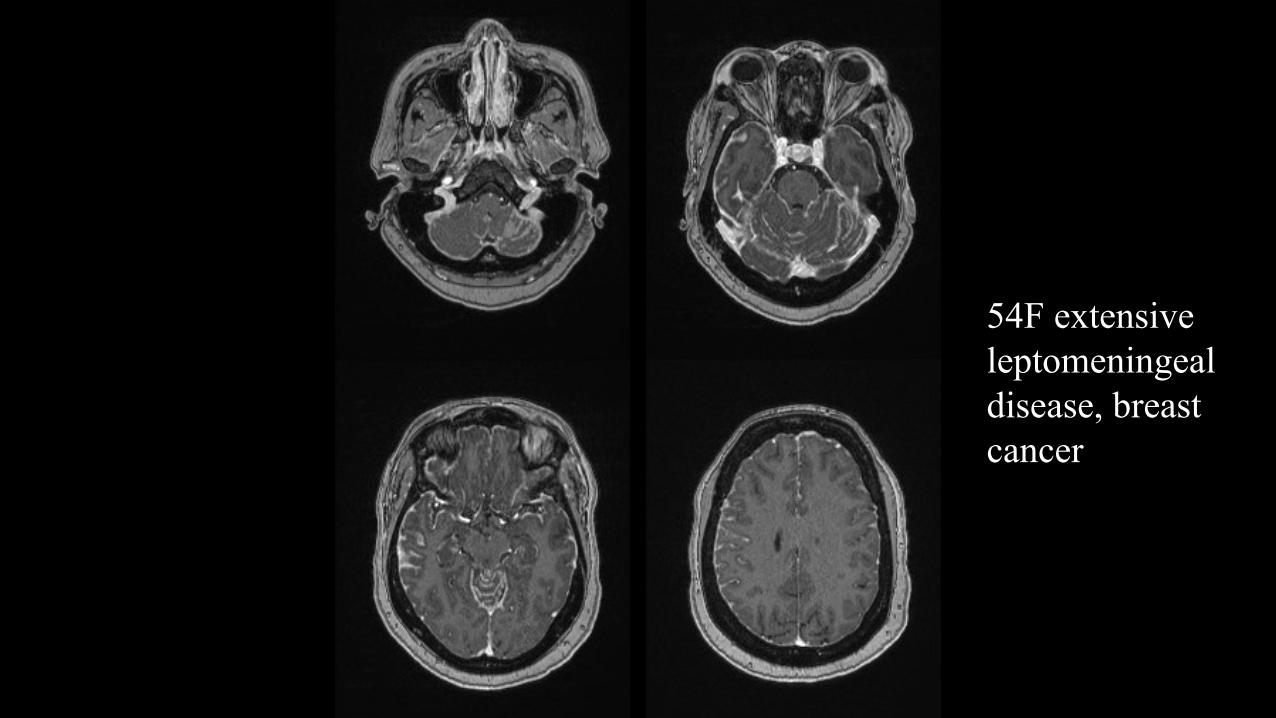
54F extensive leptomeningeal disease, breast cancer
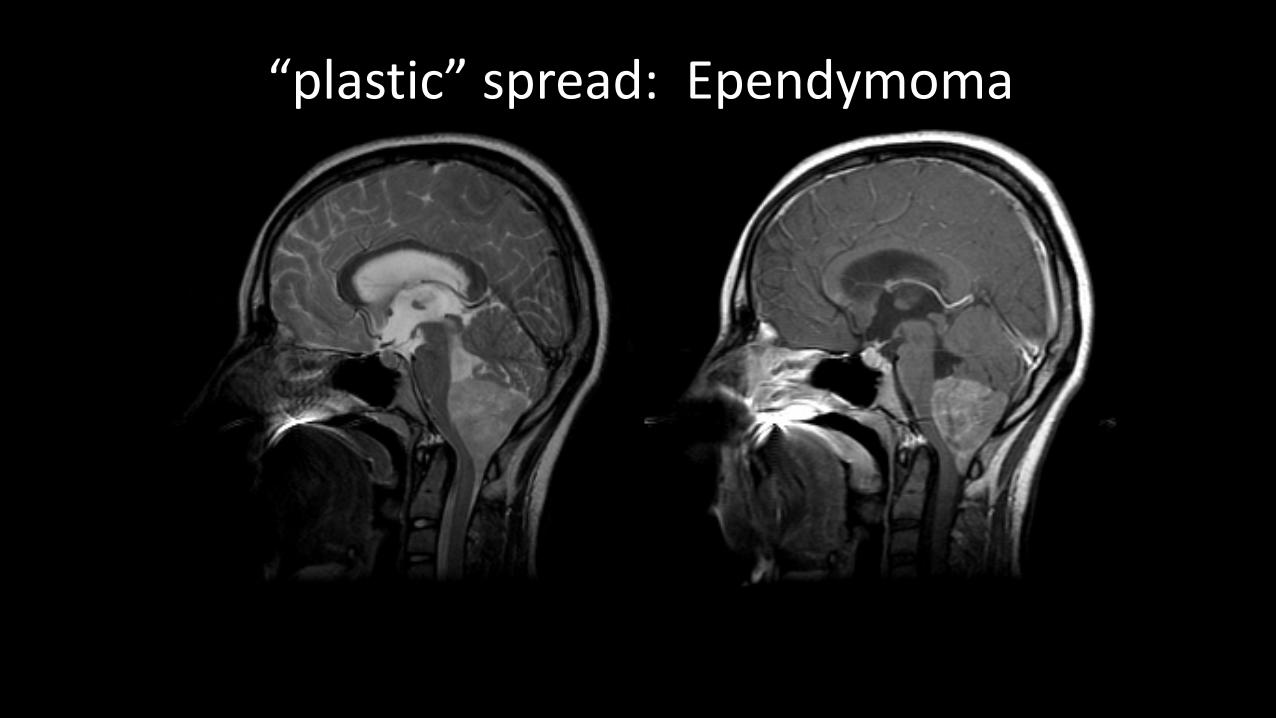
“plastic”spread:Ependymoma
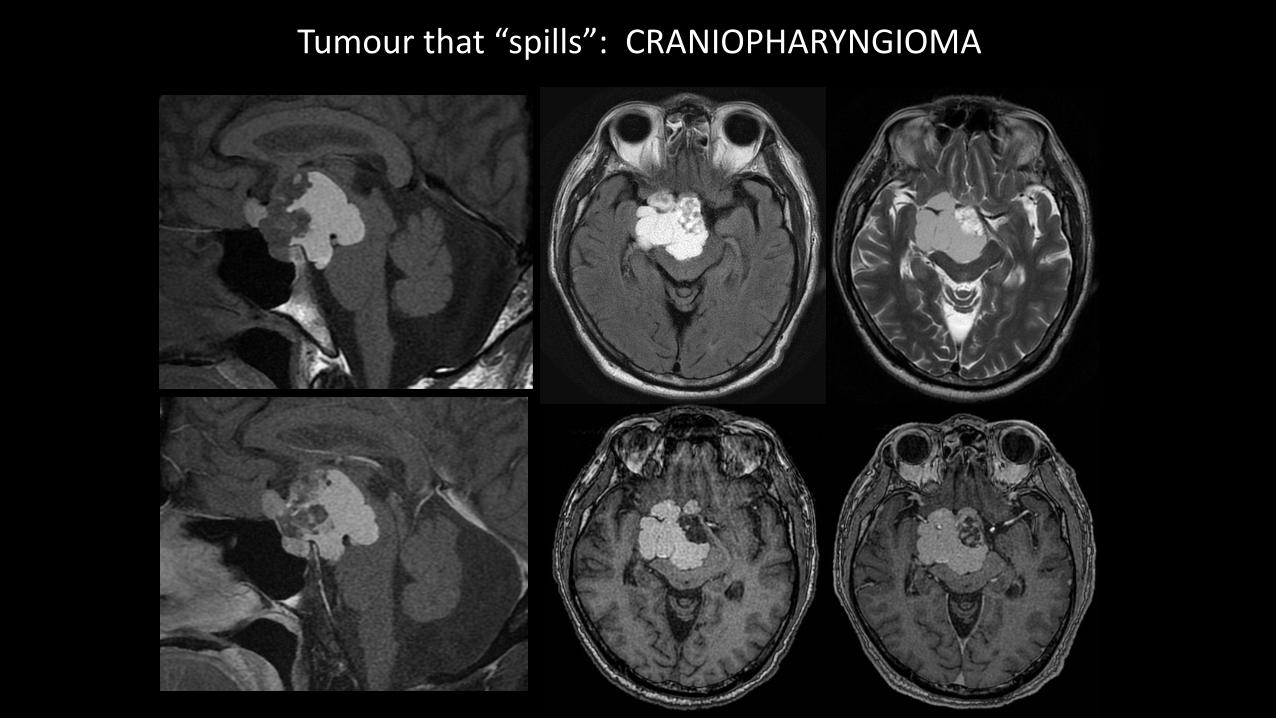
Tumourthat“spills”:CRANIOPHARYNGIOMA
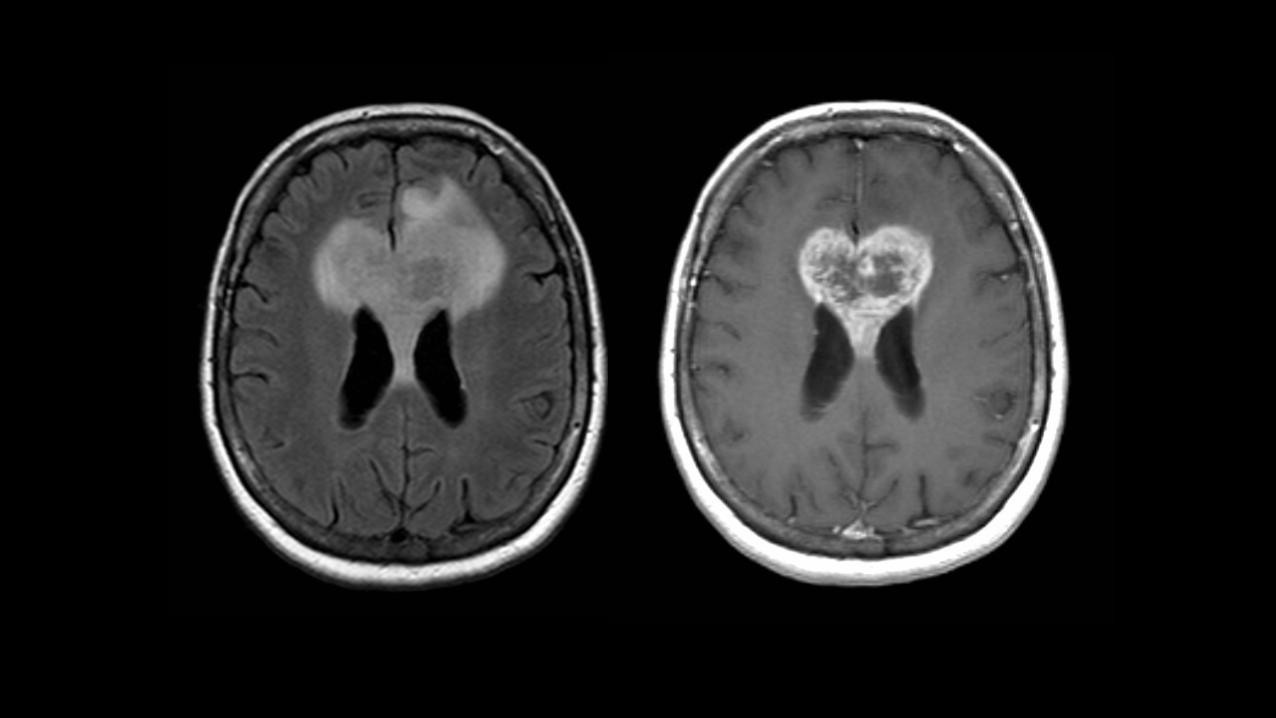
Tumours thatcrossthemidline
• Meningioma• GBM• (radiationnecrosis)• PrimaryCNSlymphoma• Epidermoidcyst• (tumefactive MS)
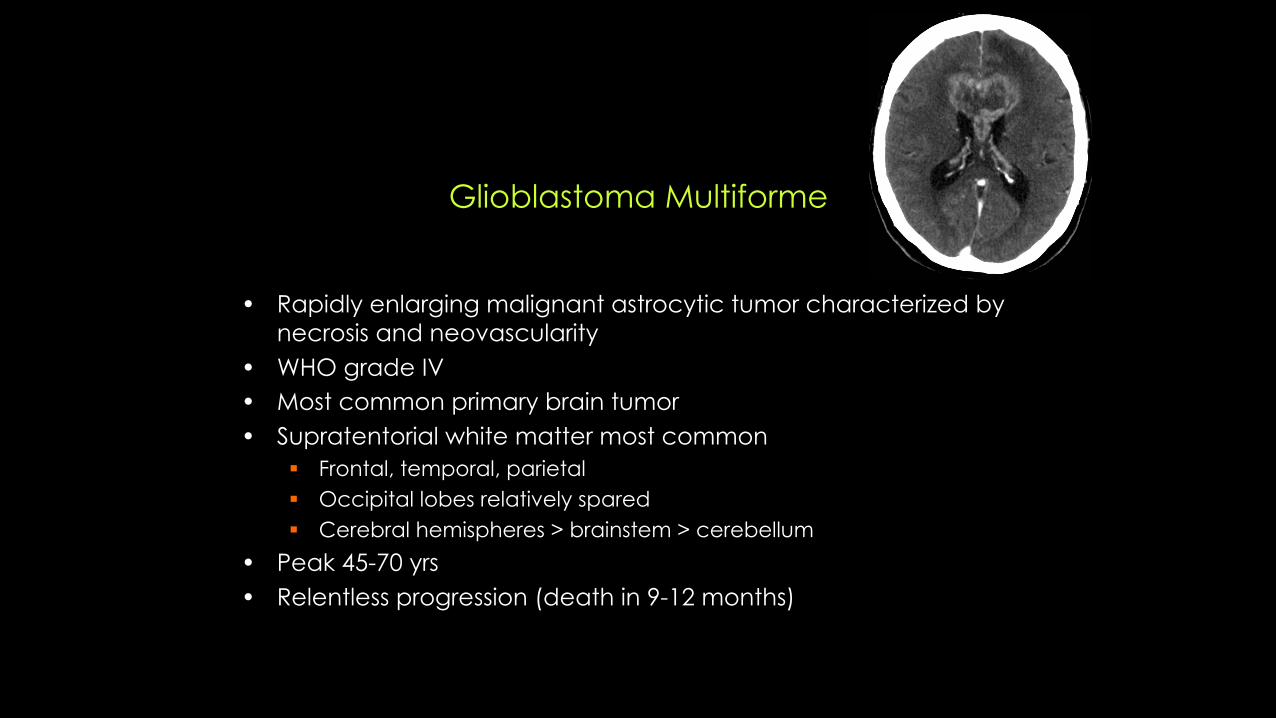
Glioblastoma Multiforme
• Rapidly enlarging malignant astrocytic tumor characterized by necrosis and neovascularity
• WHO grade IV• Most common primary brain tumor• Supratentorial white matter most common
§ Frontal, temporal, parietal§ Occipital lobes relatively spared§ Cerebral hemispheres > brainstem > cerebellum
• Peak 45-70 yrs• Relentless progression (death in 9-12 months)
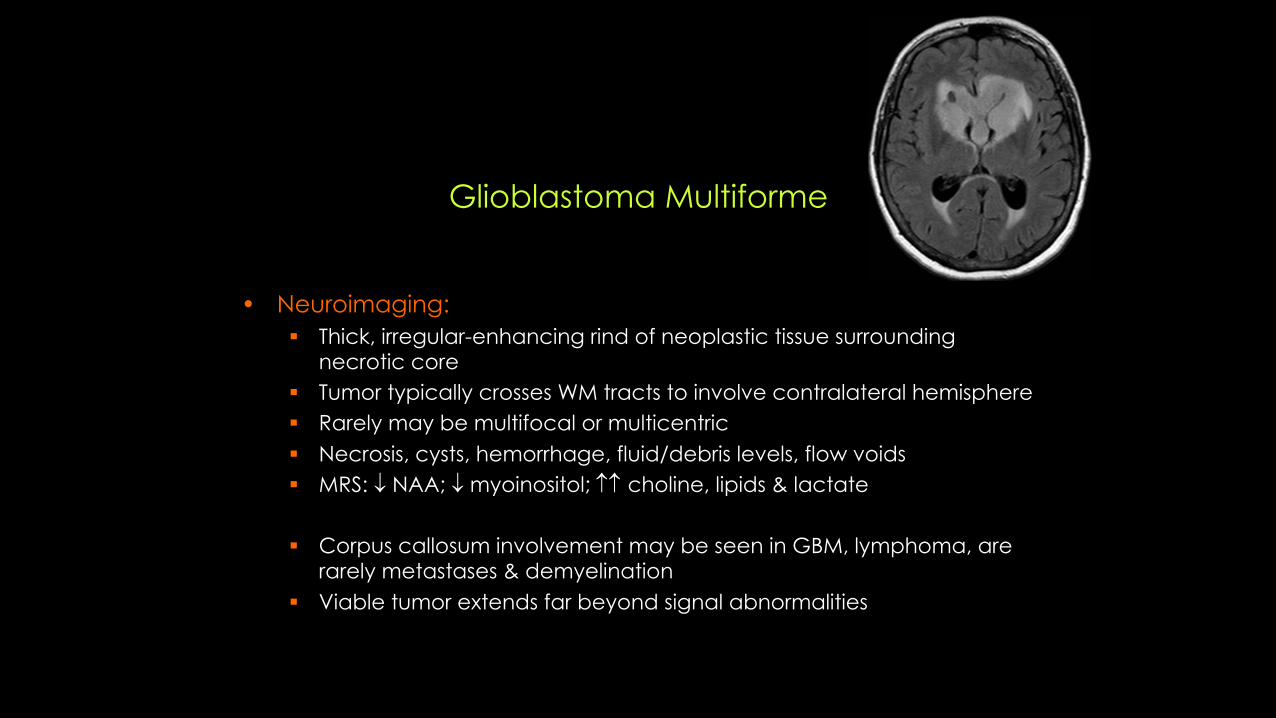
Glioblastoma Multiforme
• Neuroimaging:§ Thick, irregular-enhancing rind of neoplastic tissue surrounding
necrotic core§ Tumor typically crosses WM tracts to involve contralateral hemisphere§ Rarely may be multifocal or multicentric§ Necrosis, cysts, hemorrhage, fluid/debris levels, flow voids§ MRS: ¯ NAA; ¯ myoinositol; choline, lipids & lactate
§ Corpus callosum involvement may be seen in GBM, lymphoma, are rarely metastases & demyelination
§ Viable tumor extends far beyond signal abnormalities

Solitaryvs.multiplelesions
• Primarydistinguishingcharacteristicforprimaryvs.metastaticlesions• Primarybraintumours canbemulticentric (highgradeandlowgradegliomas)
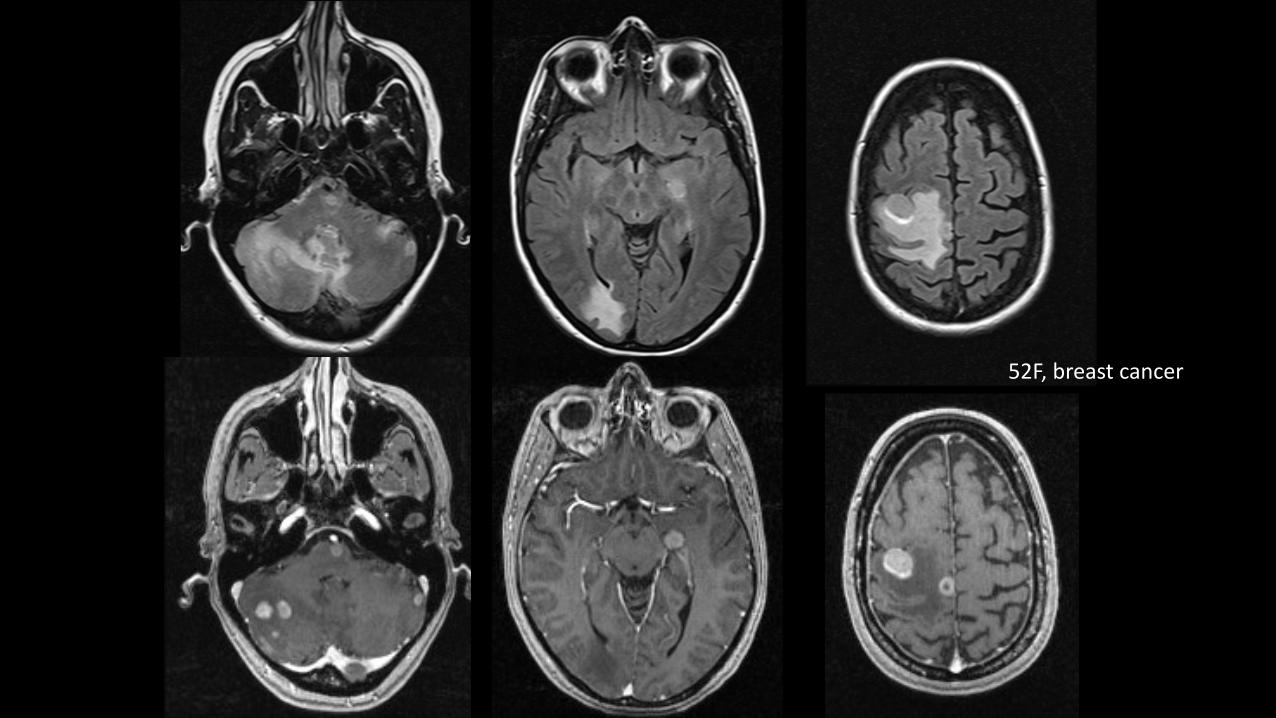
52F,breastcancer
Braintumours inthephakomatoses
• NFI– opticpathwaygliomas,astrocytoma• NFII– meningiomas,ependymomas,schwannomas• Tuberoussclerosis– SEGA• Von-HippelLindau– multiplehemangioblastomas
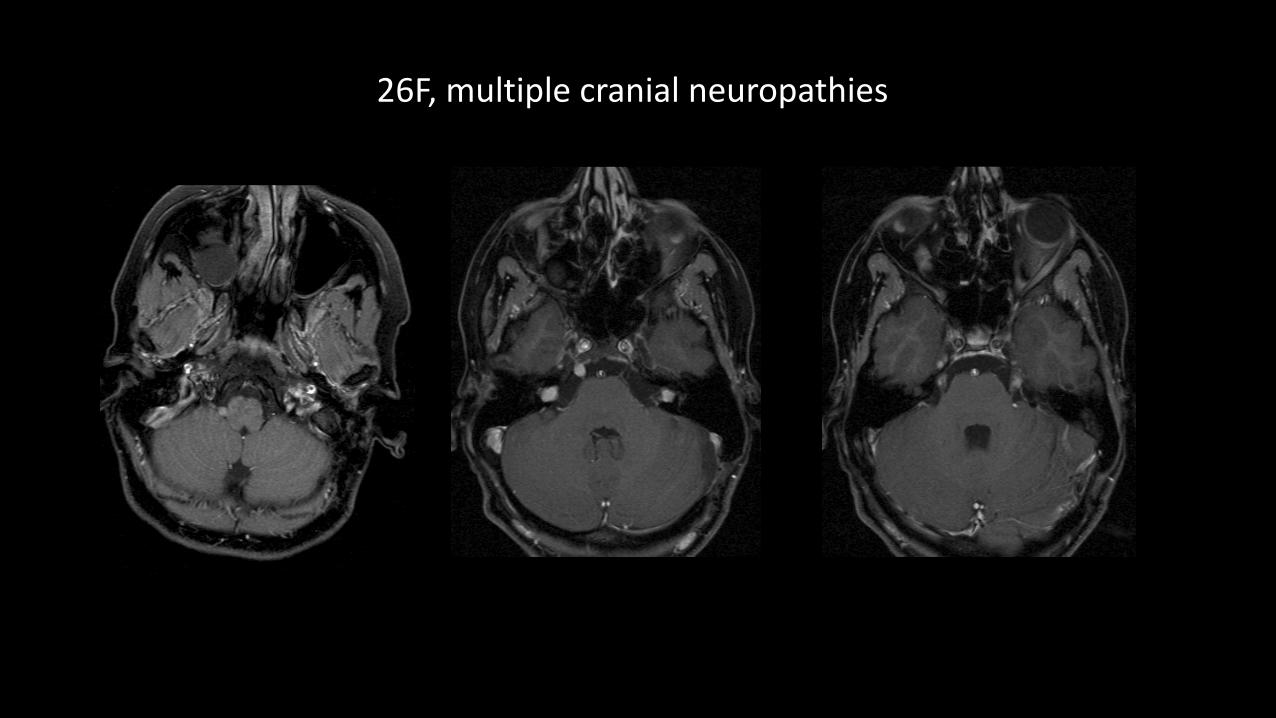
26F,multiplecranialneuropathies
NF2:IMAGING
• BilateralenhancingCPA-IACmasses– Ovoidwhensmall;"icecreamoncone"whenlargeenoughtofillIAC&CPA
• CNS– Calcifications:Choroidplexus,cerebellarhemispheres,&cerebralcortex– Othermeningiomas &schwannoma (CN3-12)– Ependymomas >>gliomas
• Spine– Meningiomas,schwannomas,&ependymomas
PATHOLOGY
• Autosomaldominantdisorder• MutationofNF2genechromosome22• 50% resultfromnew dominantgenemutation
Corticalbasedtumours
• Ganglioglioma• DNET• oligodendroglioma
• 20yo female.Suspectedabsenceseizures. ?organicetiologyofepisodes.
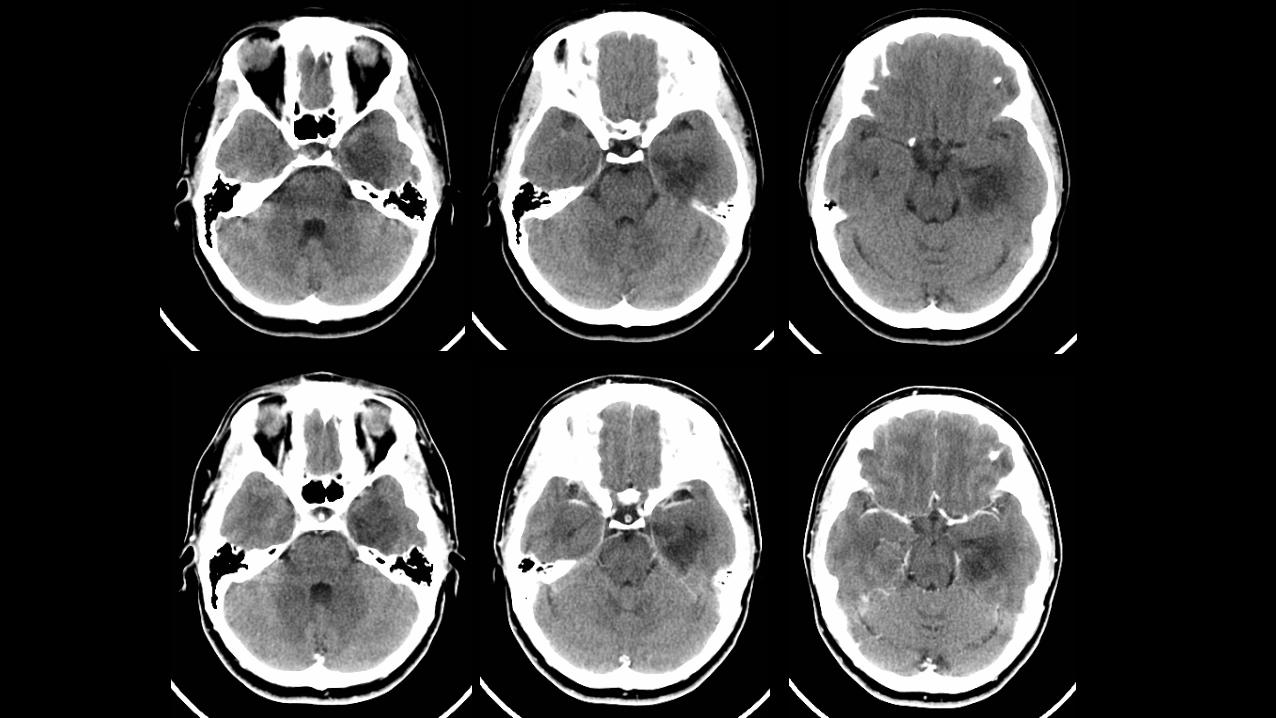
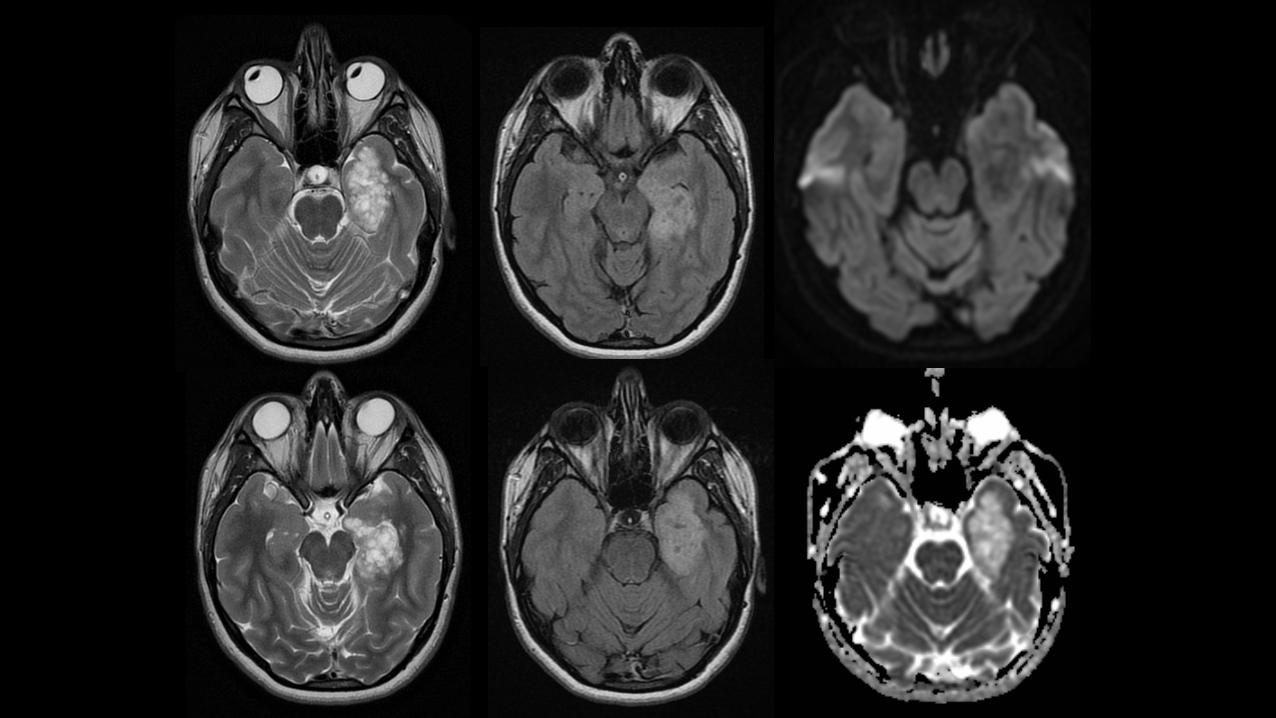
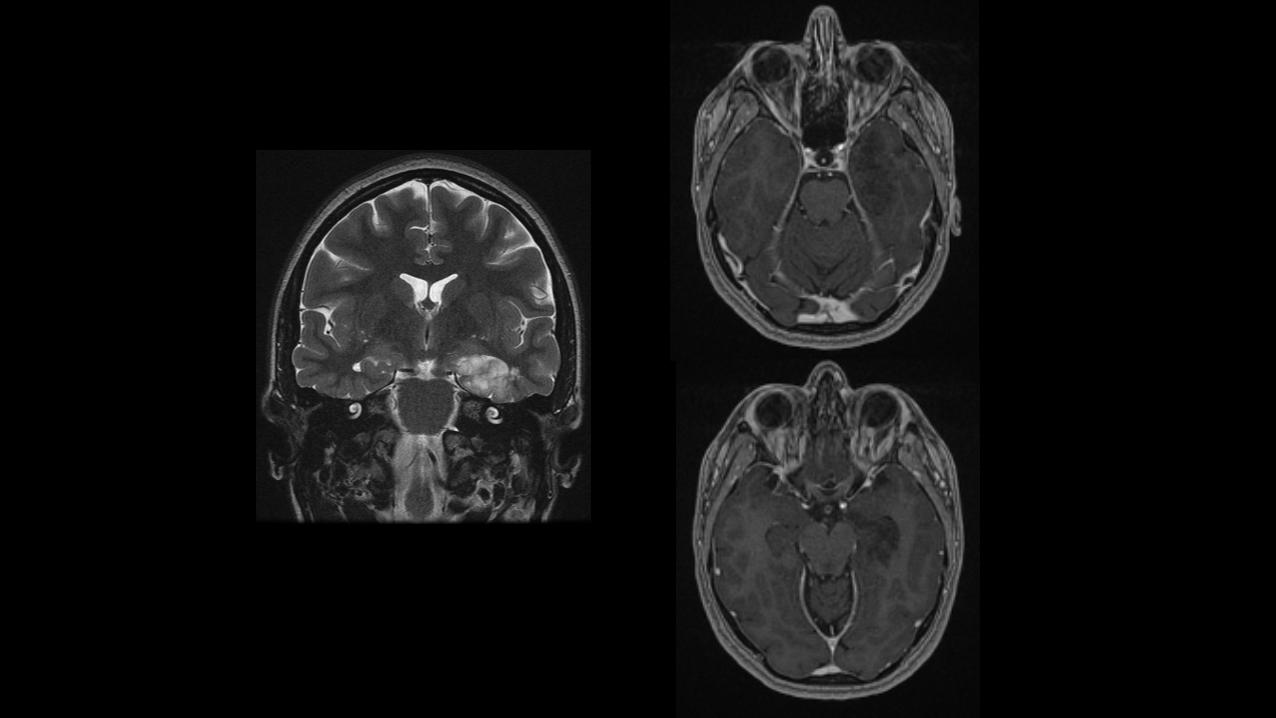
DNET• Dysembryoplastic neuroepithelial tumour• Hx – longstandingpartialcomplexseizuresinchild/youngadult• Benignmixedglial-neuronalneoplasm• Frequentassociationwithcorticaldysplasia• Wedgeshape,“point”towardventricle• Mesialtemporalmostcommonlocation• Welldemarcated,non-enhancing,littleornomasseffect/edema• Cystic,bubblyappearanceonT2W• Surgicalresectionusuallycurative
Fat,calcificationandcysts
• Fat=verylimitedddx• Lipoma• dermoid
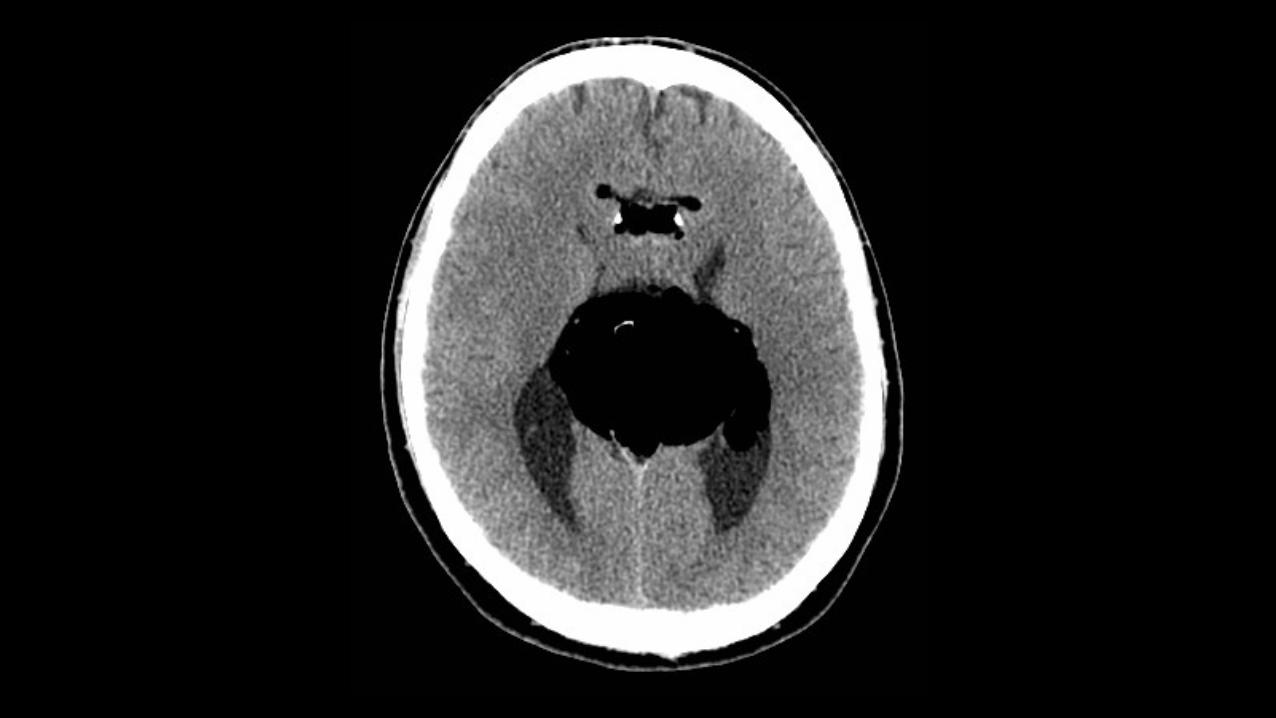
37yearoldmaleHistoryofseizures
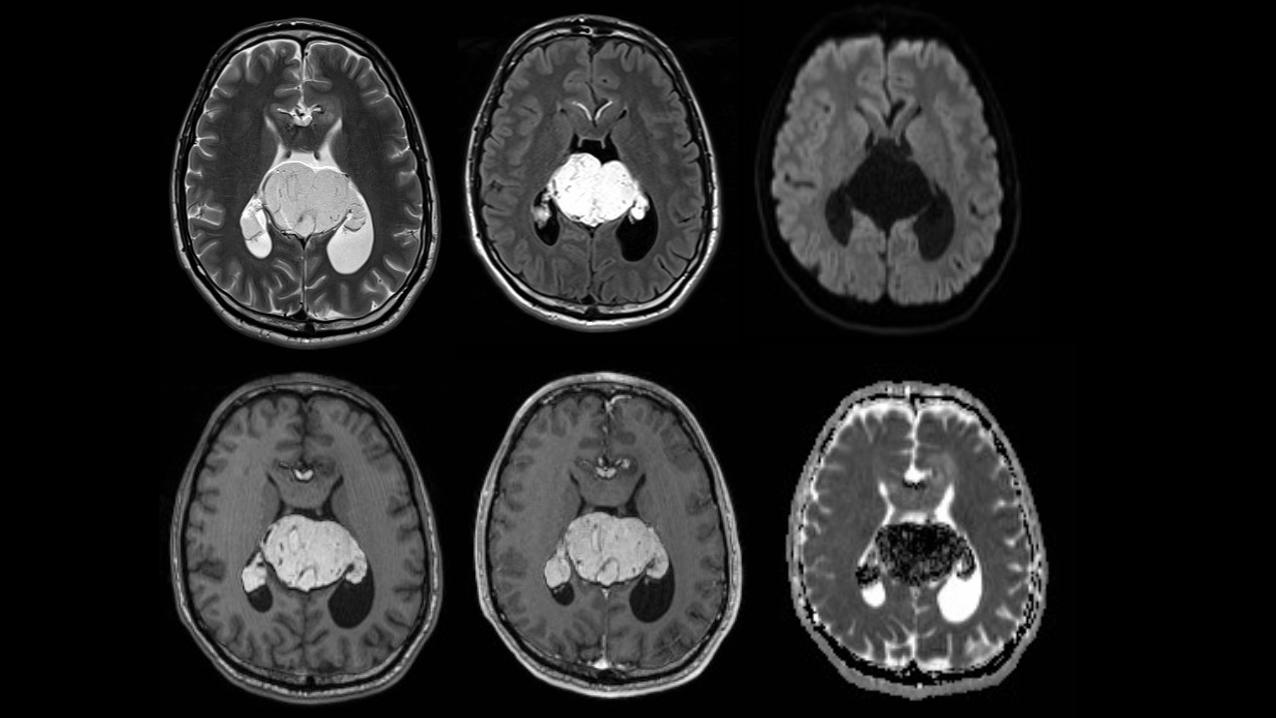
LIPOMA
• Massofmaturenon-neoplasticadiposetissue• Congenitalmalformation• Midlinelocationcommon,80%supratentorial• 40-50%interhemisphericfissure
– Twokindsofinterhemisphericlipoma• Curvilinear– curvesaroundCC,splenium• Tubulonodular– bulkymass,maycalcifyassociatedCCagensis/dysgenesis
• T1hyperintense• ChemicalshiftartefactonT2
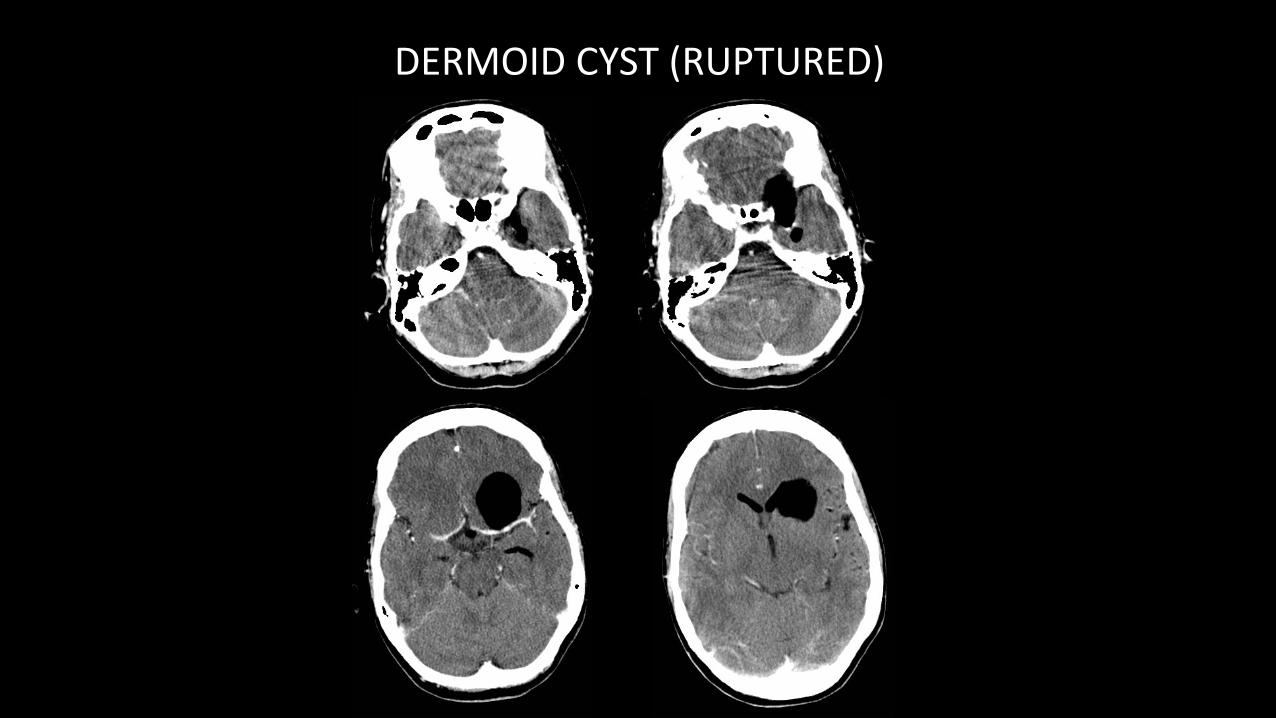
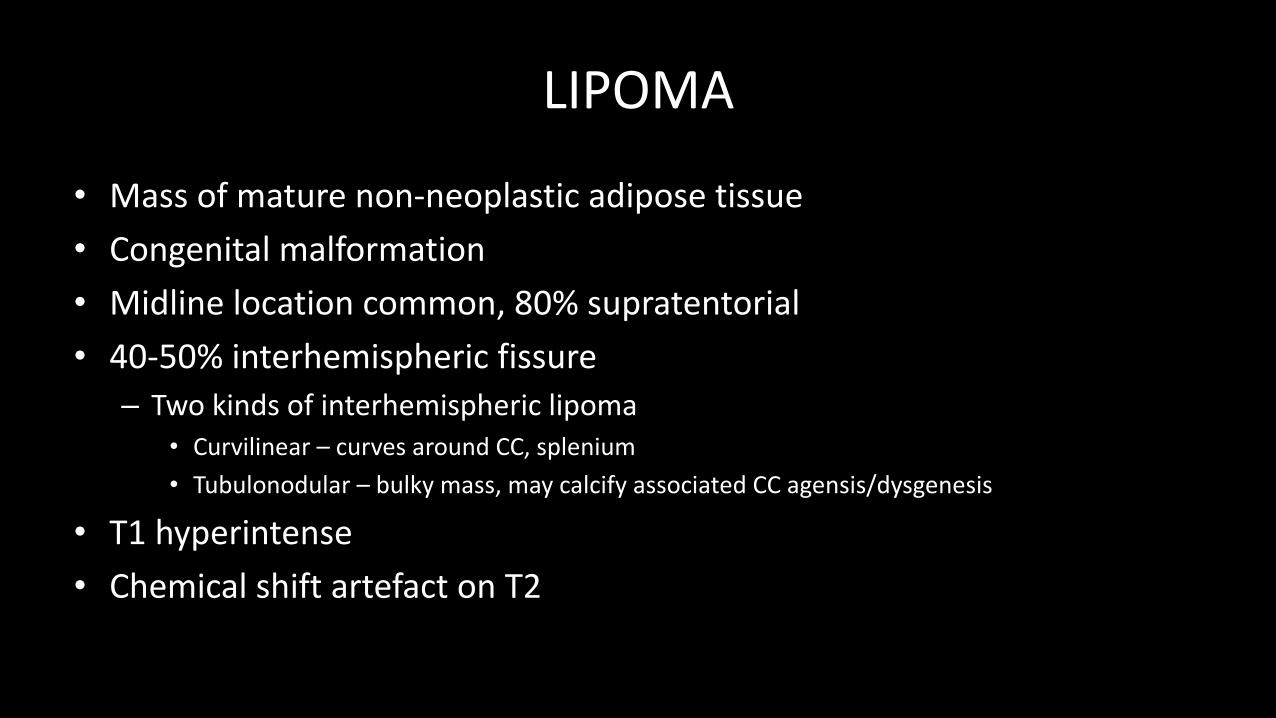
DERMOIDCYST(RUPTURED)
DERMOIDCYST(RUPTURED)
calcification
• Intra-axial:• Gliomas– “oldelephantsagegracefully”– oligodendroglioma (almostall),ependymoma,astrocytoma,GBM
• Other– metastases,choroidplexustumours,ganglioglioma
• Extra-axial:• Meningioma• Craniopharyngioma• Chordoma• Chondrosarcoma
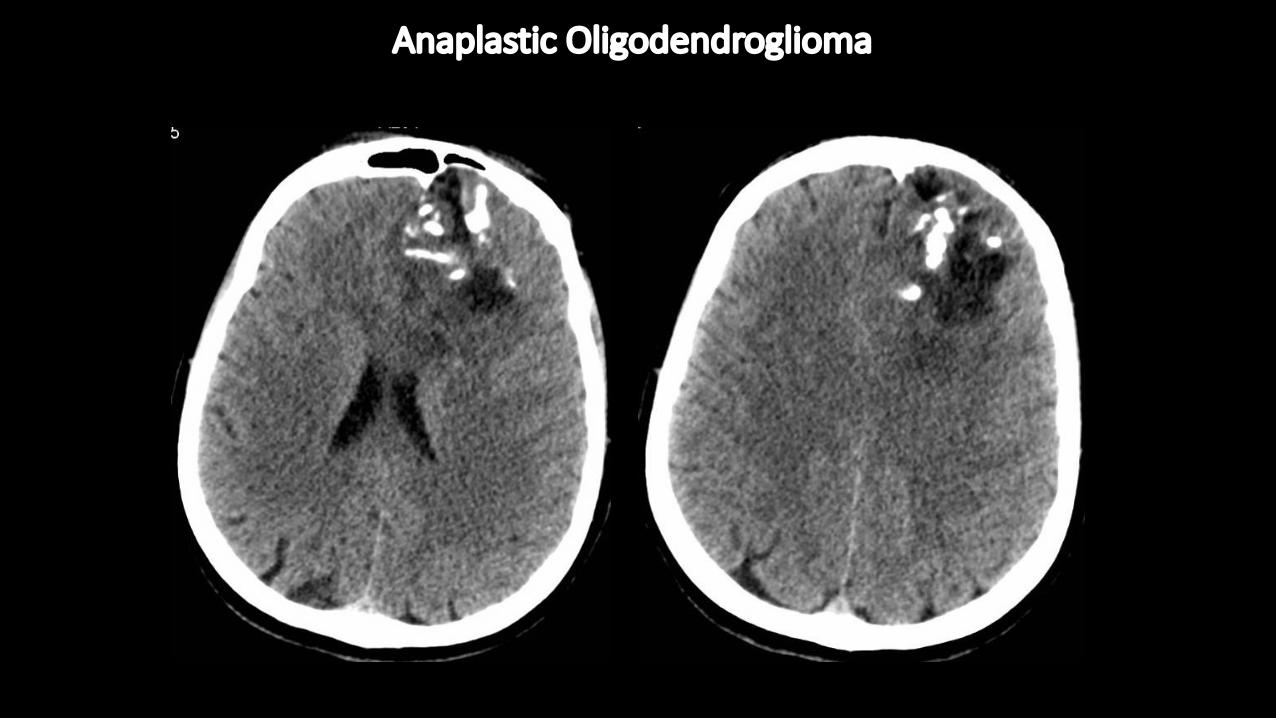
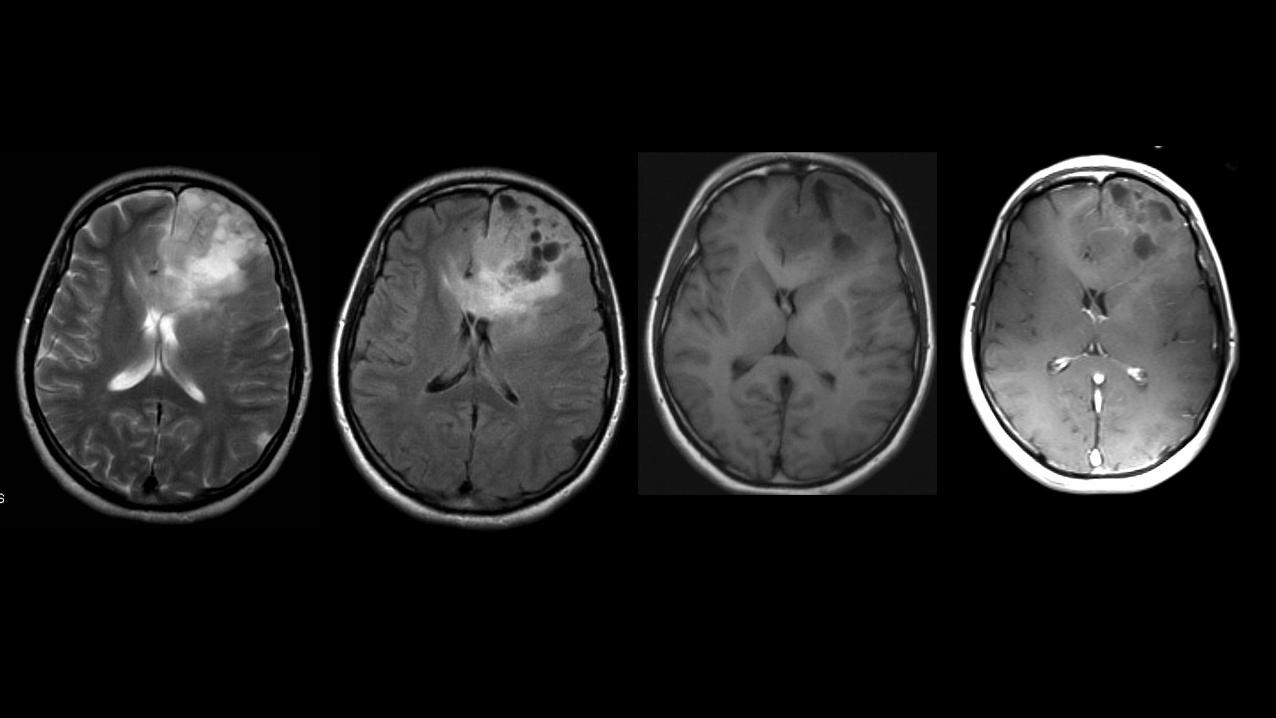
AnaplasticOligodendroglioma
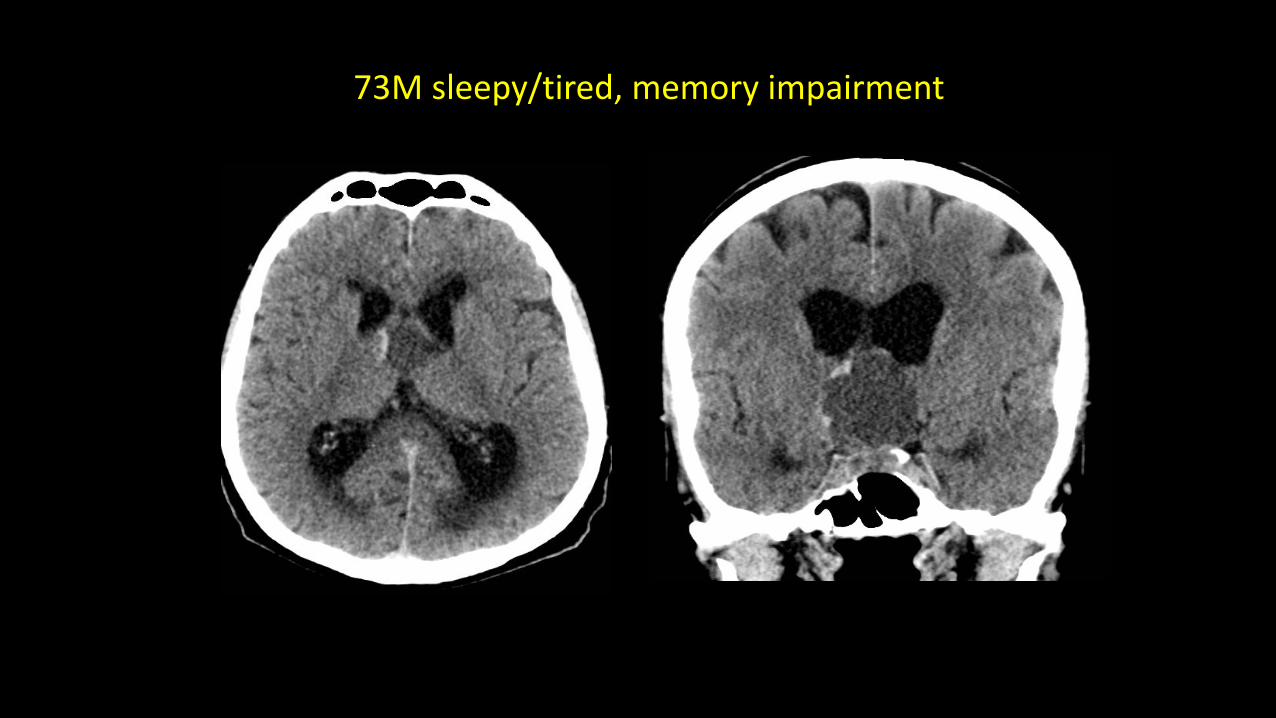
73Msleepy/tired,memoryimpairment
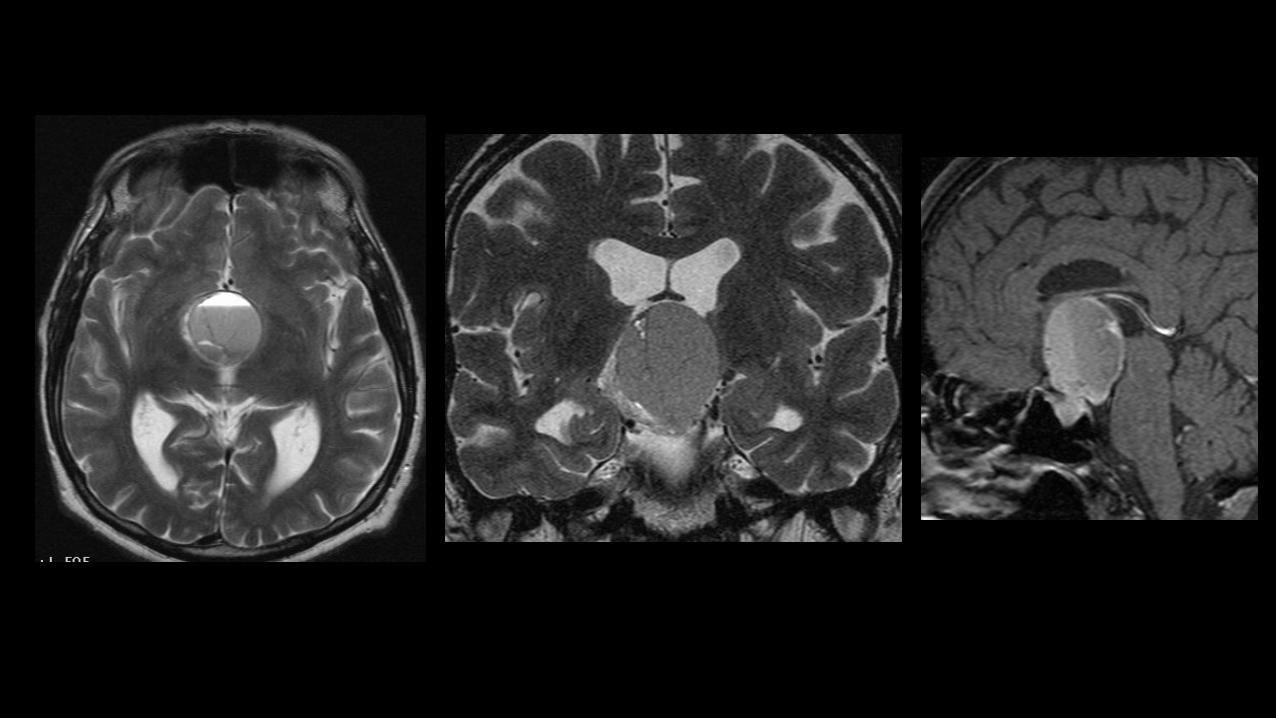
Craniopharyngioma
• ArisesfromremnantsofRathke’s pouch• Primarilysuprasellar,canbequitelargeand“spill”outofthesellar region– middleandanteriorfossa,prepontine
• Adamantinomatous mostcommon• Cystic/solidbutmostlycystic,“machineryoil”• Bimodal=5-10,50-60years• Visualsymptoms• Slowgrowingbuttendtorecur
Craniopharyngioma Imaging
• CT“ruleof90’s”– 90%cystic/solid,90%Ca++,90%enhance• MRappearancevariabledependingoncystcontents• Multiplecystscommonandmayhavedifferentsignal• Hypo-hyperintense onT1,hyperintense onT2• Noduleoftencalcifiedandhypointense onT2• Cystwallsandnodulesenhance
Relativelydense(CT)/hypointense T2tumours
• Correspondencewithreduceddiffusion• Lymphoma• PNET• SolidpartofGBM
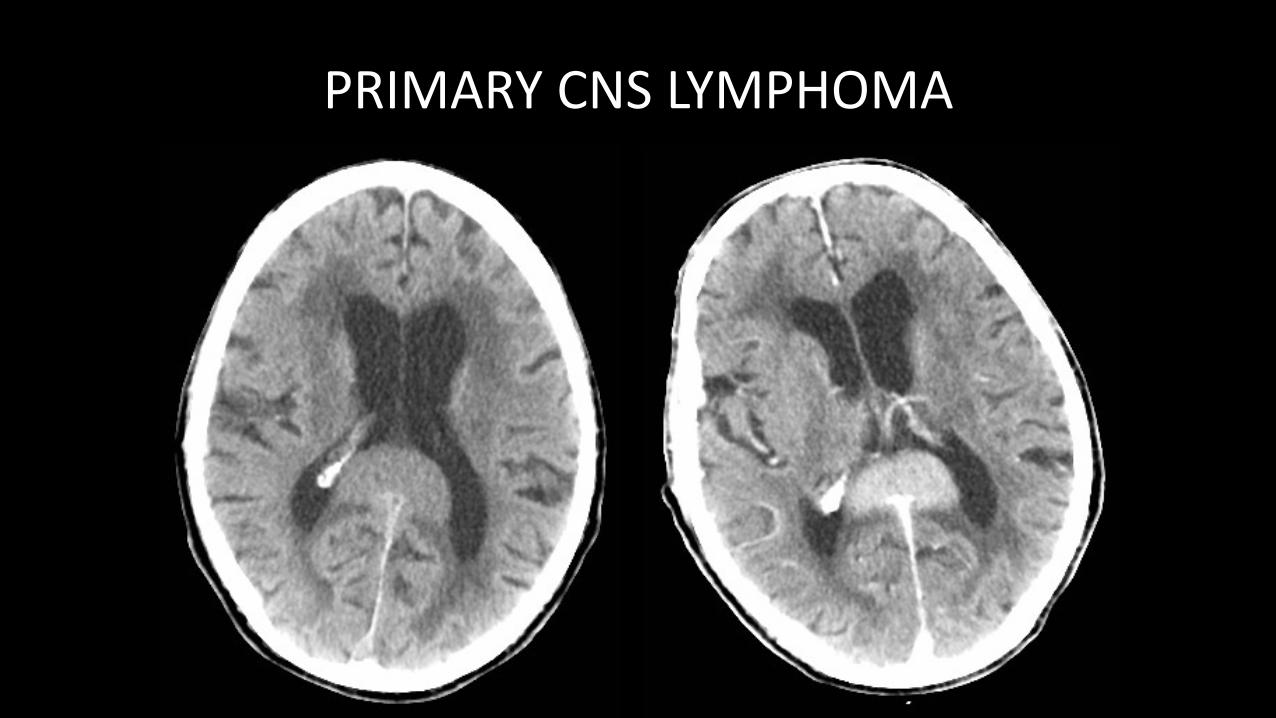
PRIMARYCNSLYMPHOMA
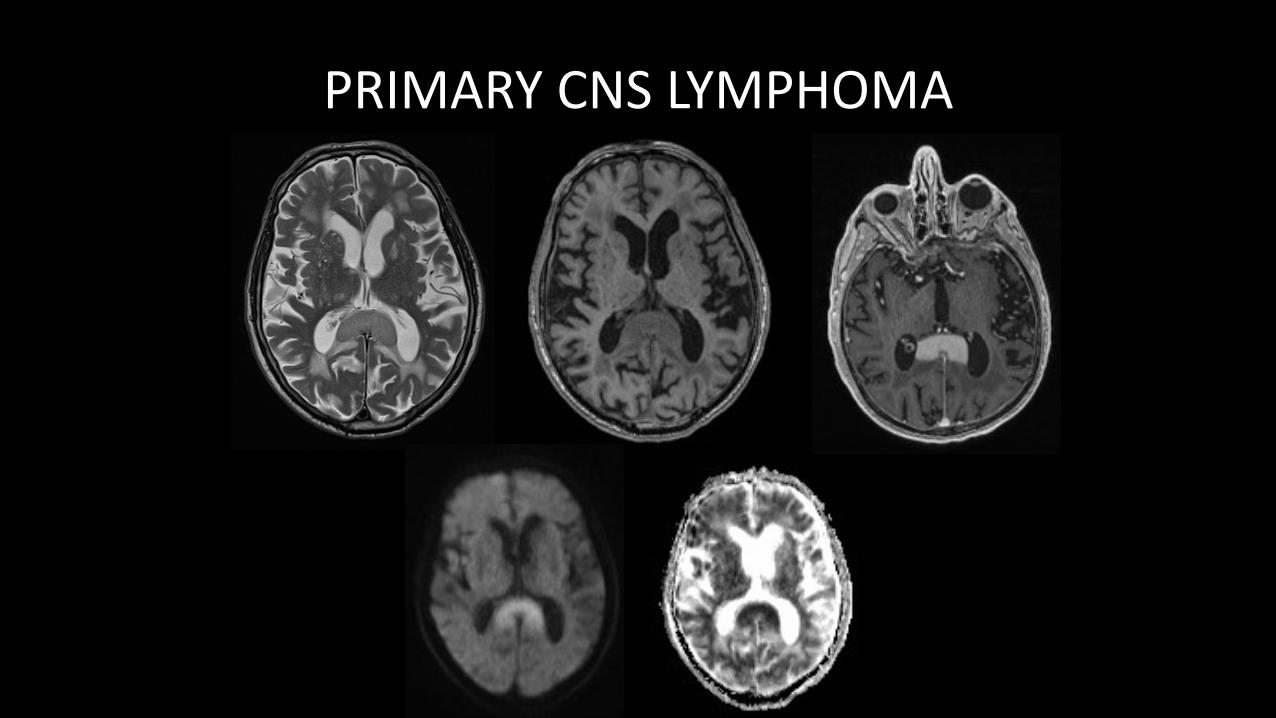
PRIMARYCNSLYMPHOMA
Tumours thatcharacteristicallyhavecysticcomponents• Intra-axial
• GBM• Hemangioblastoma• Ganglioglioma,DNET,PXA
• Extra-axial• Craniopharyngioma
• Non-neoplastic• Dermoid/epidermoid
• Bewareofmimics!
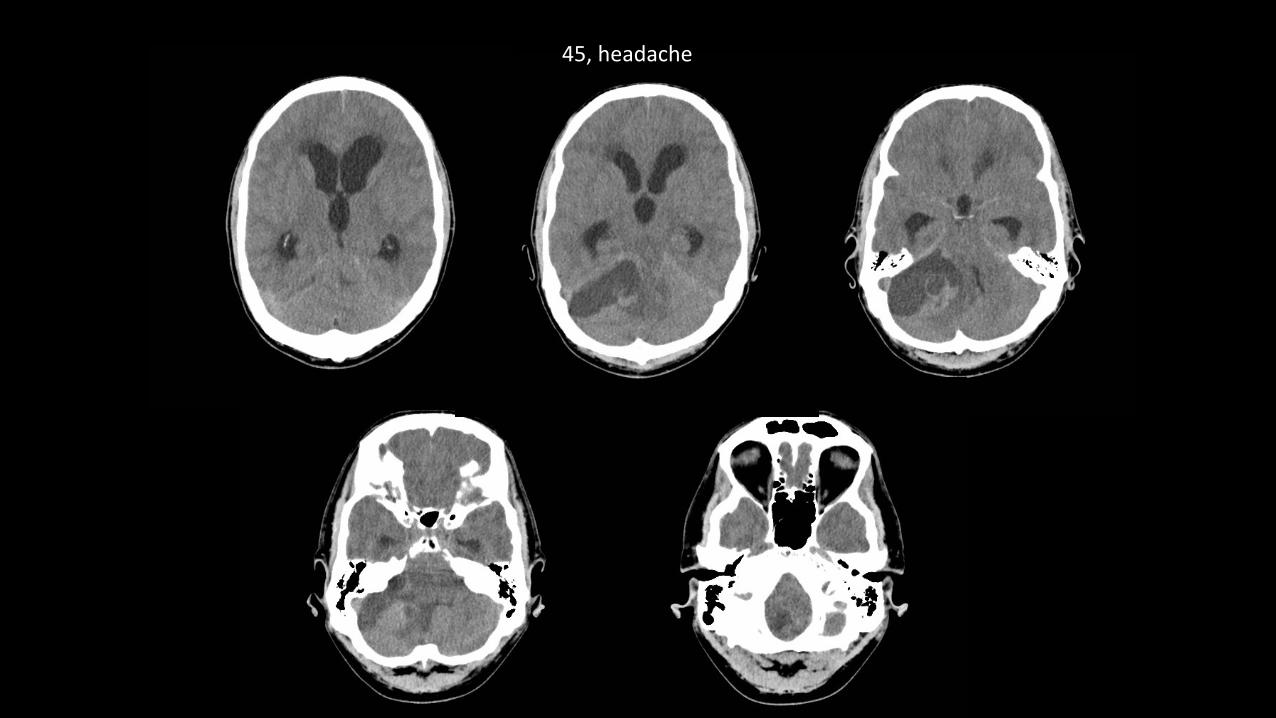
45,headache
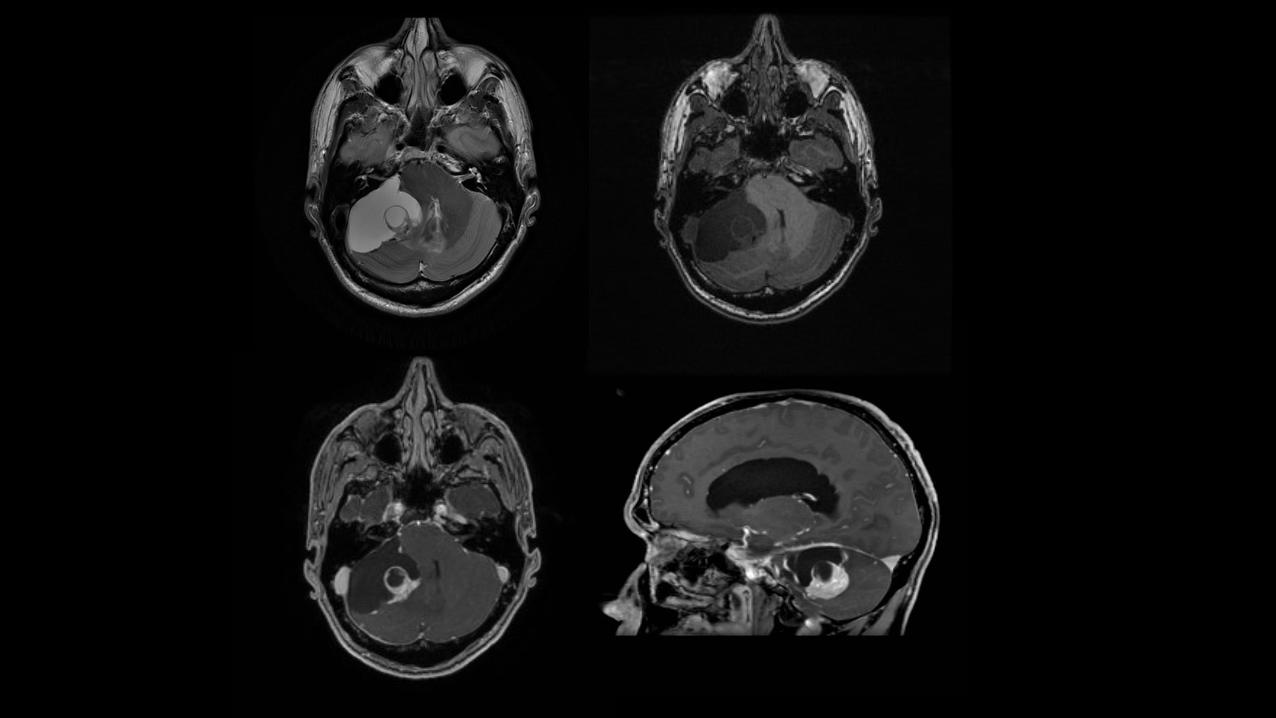
Hemangioblastoma
• Benignandslowgrowing• Sporadicormultiple(VHL)• MostinPF,noduletypicallyabutspial surface• Nodulewithperi-tumoral non-neoplasticcystmostcommon• Theycanbeentirelysolid• canalsohaveintratumoral neoplasticcyst• bothperitumoral non-neoplasticandintratumoral neoplasticcysts(asinthiscase)
Hyperintensity T1W(-contrast)
• Hemorrhage• Calcification• Proteinacious cyst• melanin
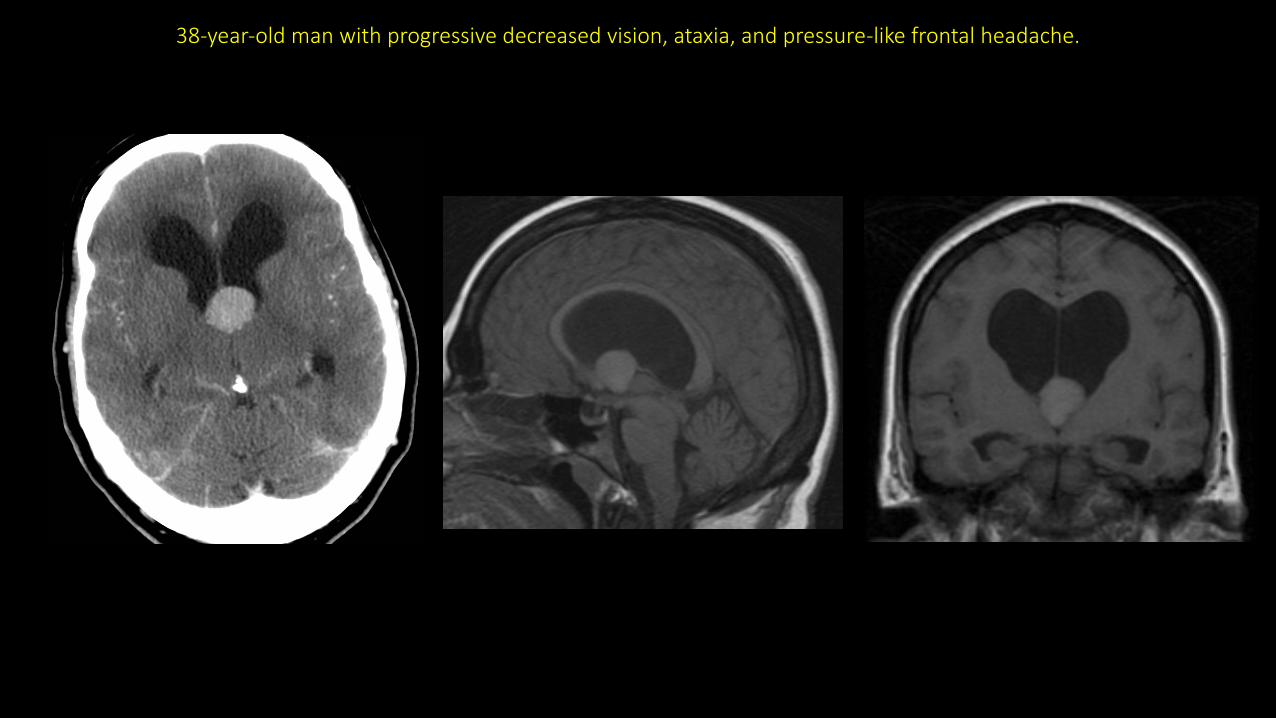
38-year-oldmanwithprogressivedecreasedvision,ataxia,andpressure-likefrontalheadache.
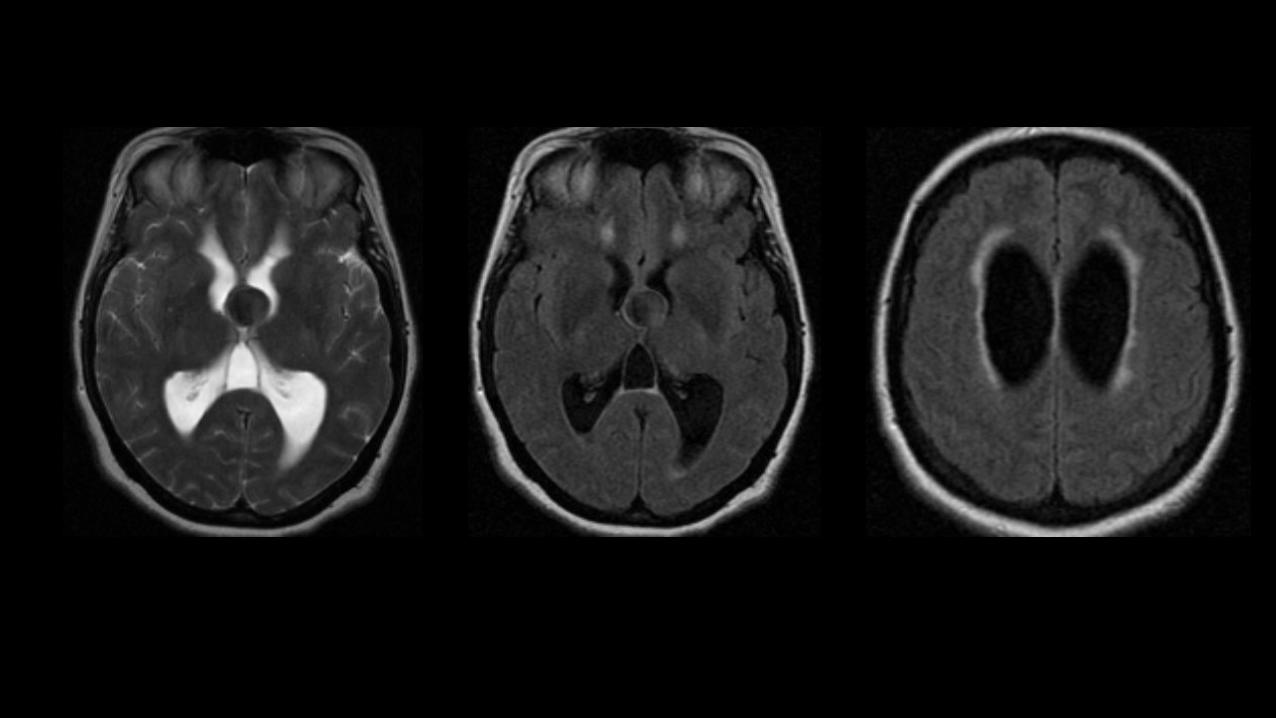
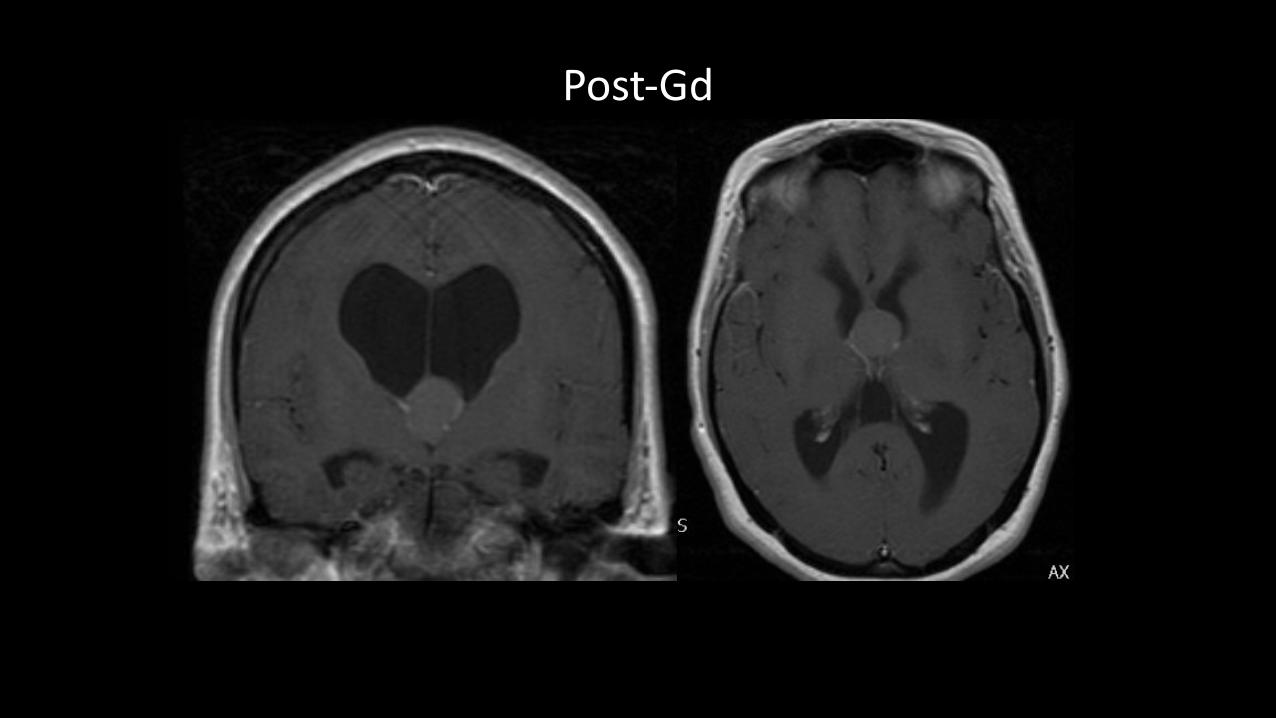
Post-Gd
COLLOIDCYST• Mucin containing3rd ventricularcyst• Hyperdense foramenofMonro massonunenhancedCT• <1%othersites(lateral&4th ventricles,extraaxial)• 1/3isointense onT1,2/3hyperintense onT1• VariableT2signal• NoDWIrestriction• Enhancementunusual• 90%stable,10%enlarge• Acuteobstructionmayleadtorapidonsethydrocephalus
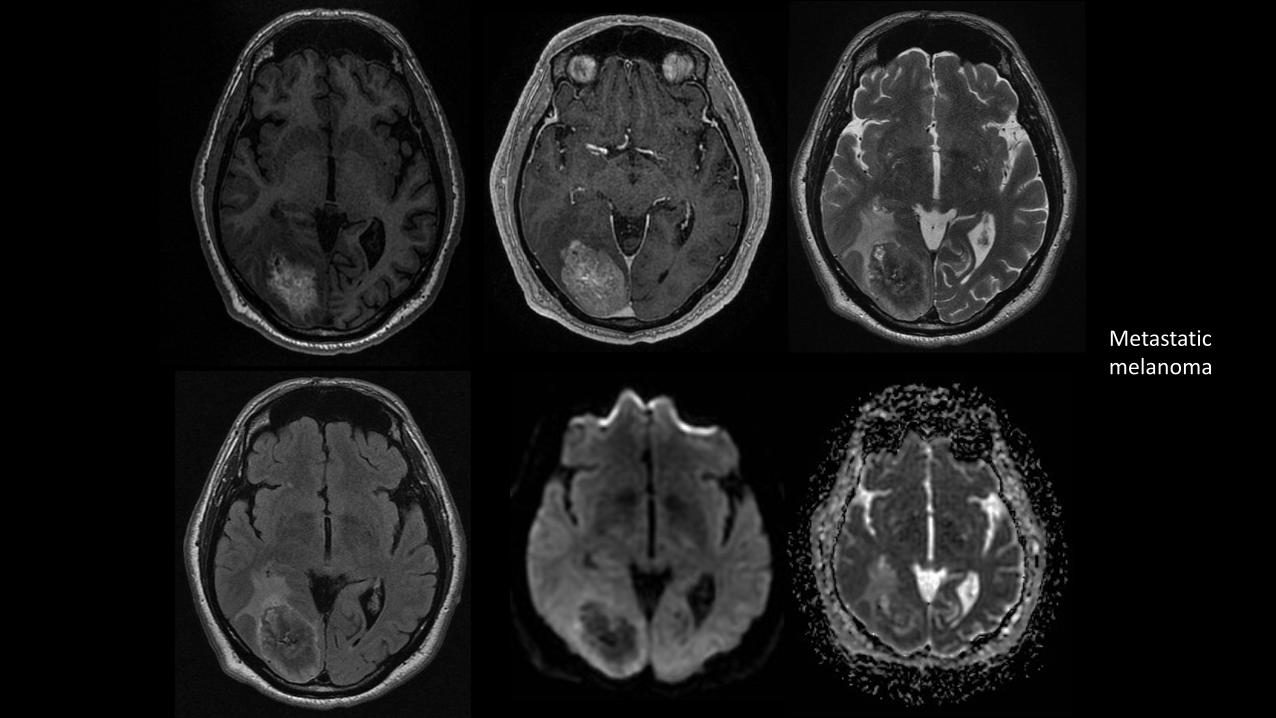
Metastaticmelanoma
Density/SignalintensitysimilartoCSF
• Epidermoidcyst• Neurocysticercosis
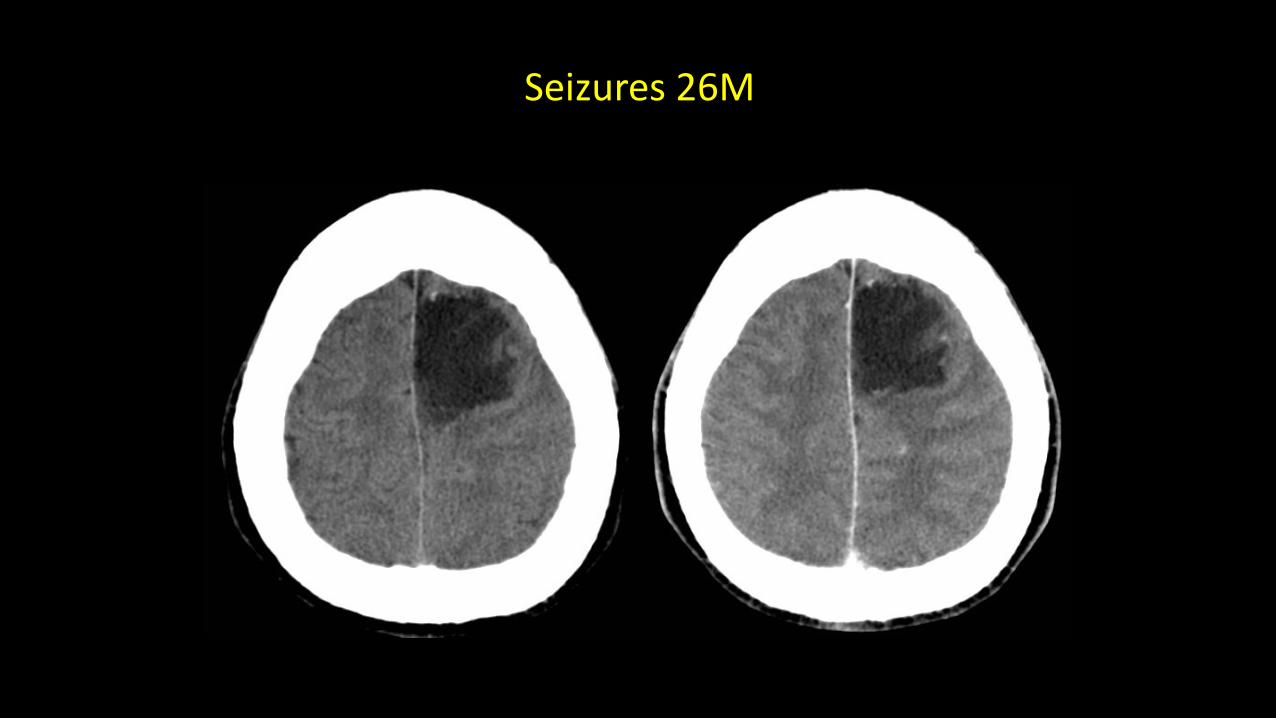
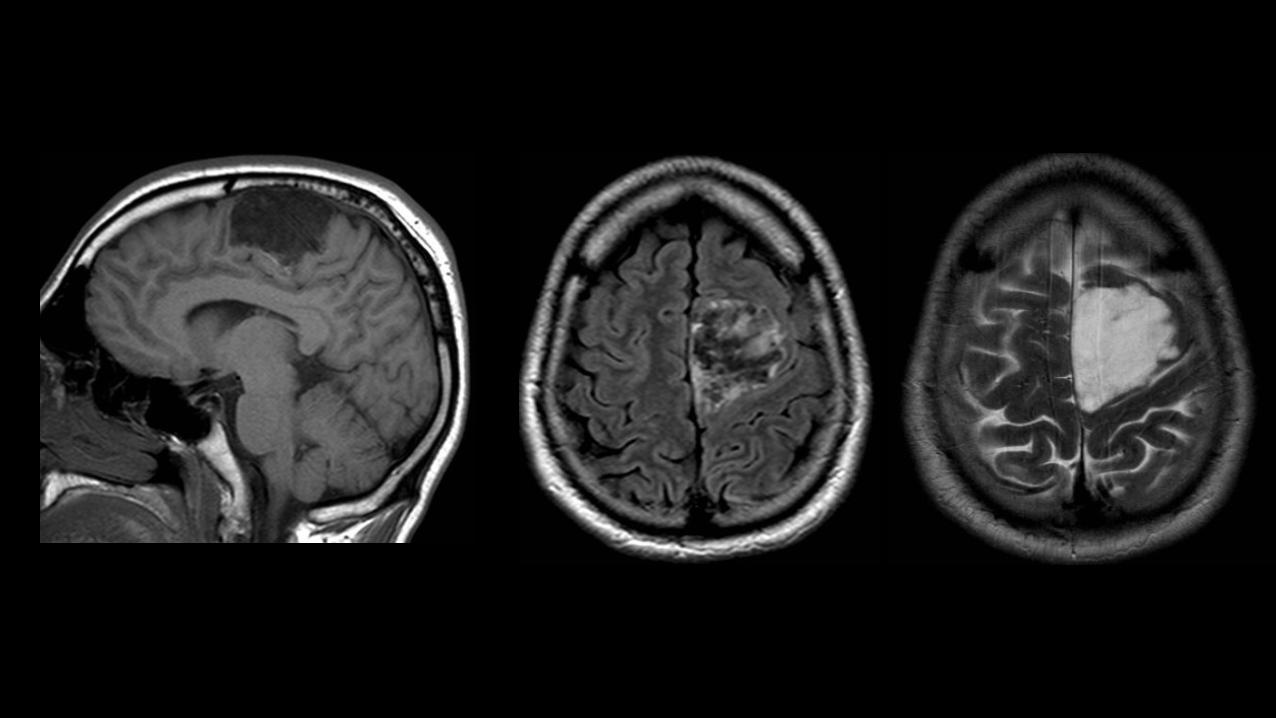
Seizures26M
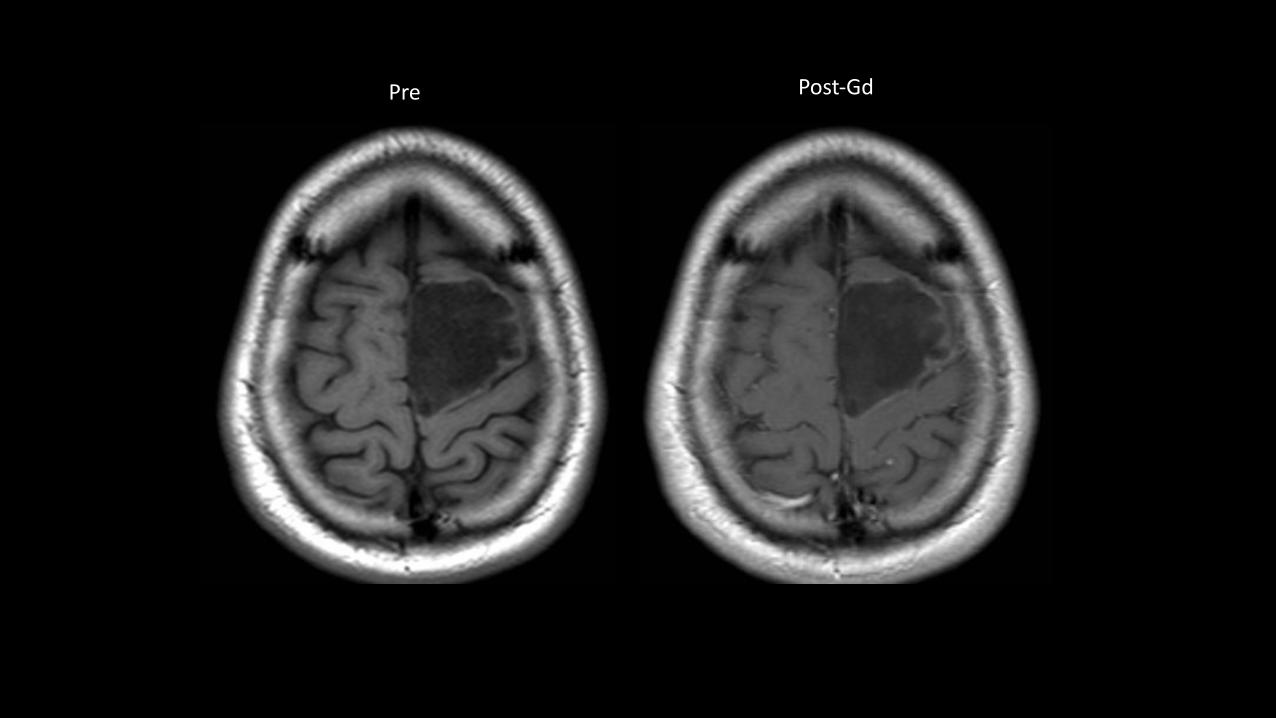
Pre Post-Gd
Epidermoid tumours
• Stratifiedsquamousepithelium,containskeratinaceous debrisandcholesterol
• CPAmostcommon,middlefossa,parasellar• Cerebralconvexitieslesscommon• CThypodense,Ca++in25%• Iso-slightlyhyperintense relativetoCSFonT1andT2,slightlyheterogeneous
• DonotsuppressonFLAIR,restrictonDWI• Insinuatein/aroundstructures,burrowintobrain
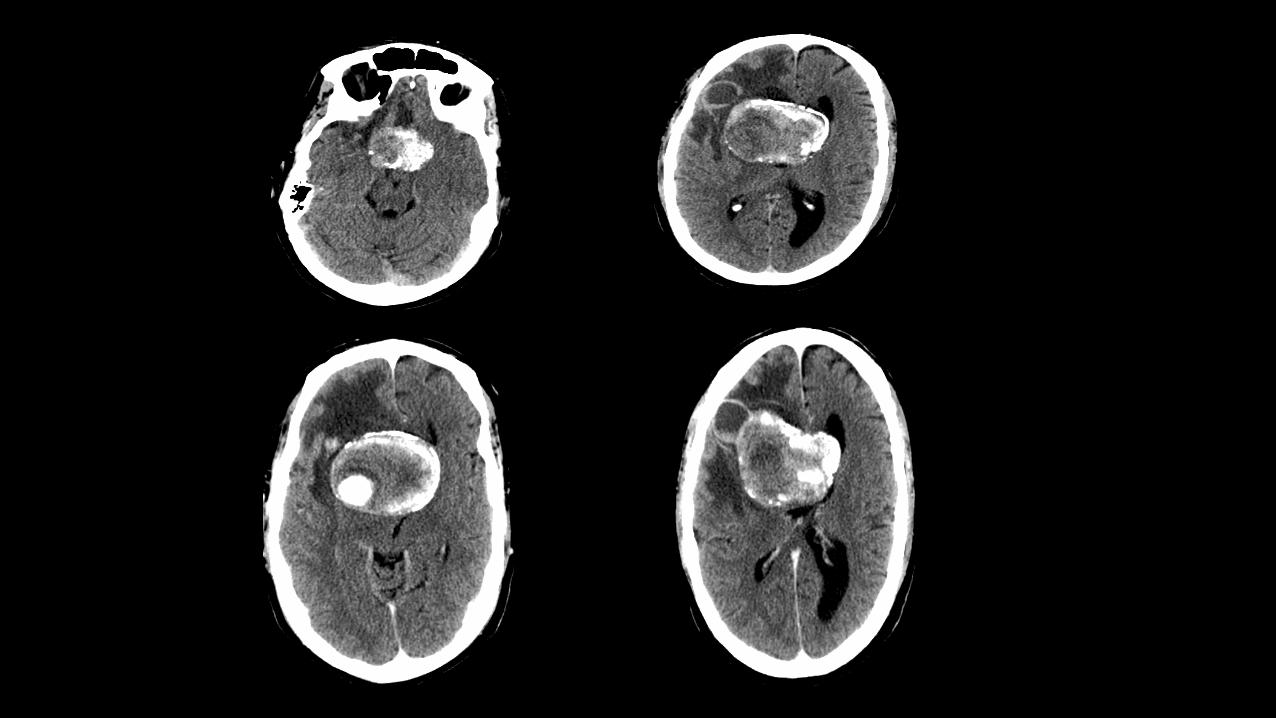
Testyourskills!
• 45yr/Mwithh/oIncreasingbehaviouralchangesx3yrs
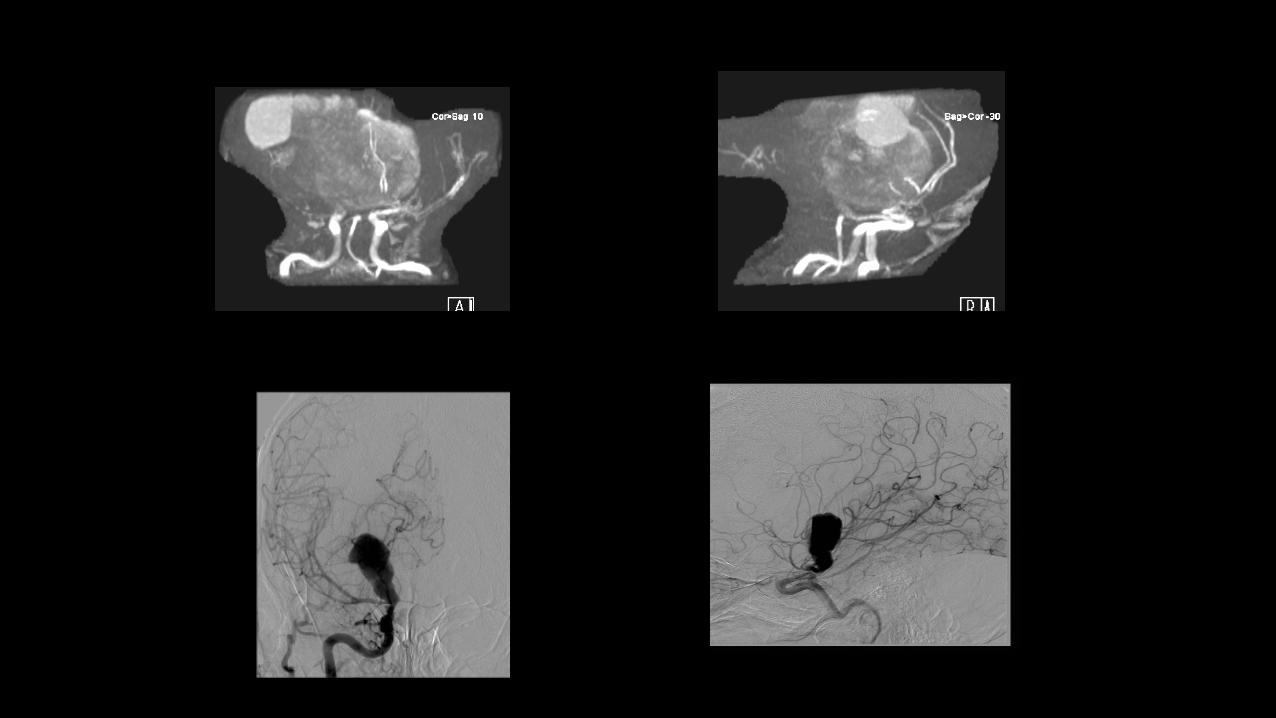
MRA
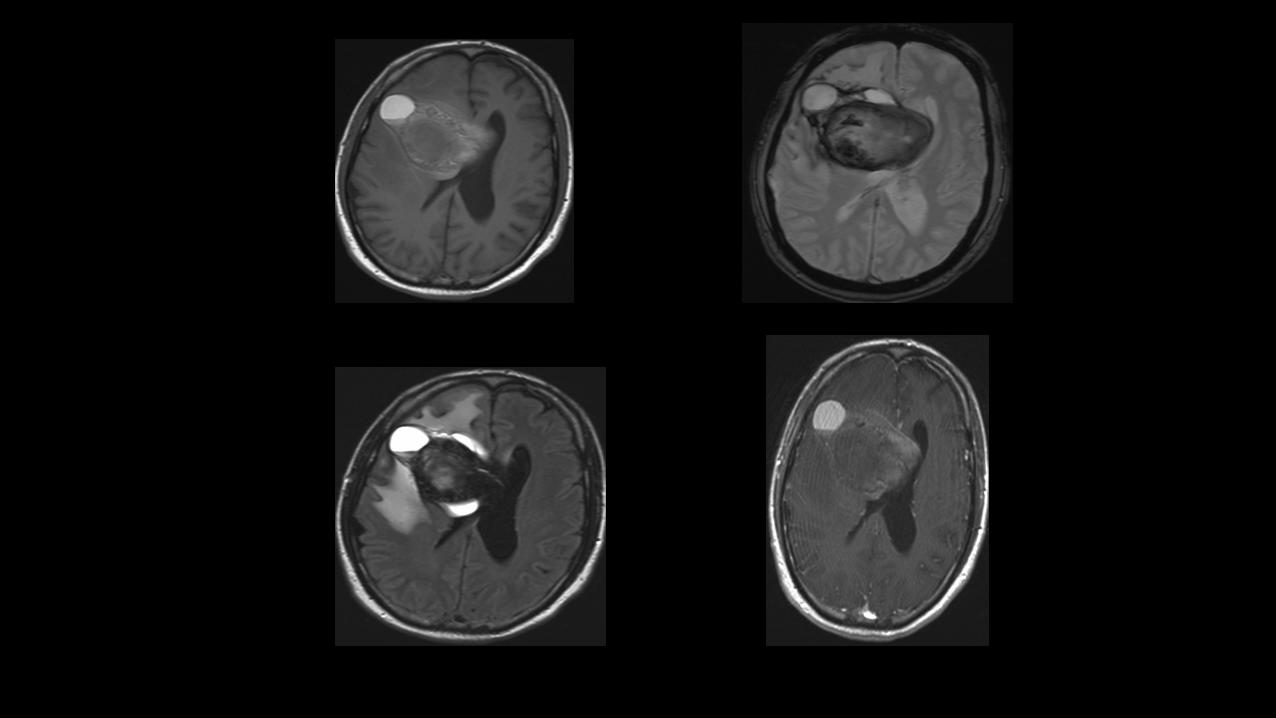
ANSWER:IT’SNOTATUMOUR!
a. Centralneurocytomab. Meningiomac. CNSlymphomad. IT’SNOTATUMOUR!!
Giantintracranialaneurysms.Def.:>2.5cm..Types:Saccular
fusiform..Epidemiologyandnaturalhistory
- Comprise3-5%ofintracranialaneurysms- peakageofpresentation30-60yr- F:M,3:1- 2/3rd Antcirculation1/3rd Postcirculation
§Slowgrowingwithrepeatedinternalhemorrhage
§Laminatedthrombusofvaryingages
§Symptomscommonlyrelatedtomasseffect,lowerrateofrupture
§Imaging:CT–hyperdense masswithcalcification.MRI-Mixedsignalintensitymasswiththrombusofvariousstages,Perianeurysmhematomaandedema