Embed Size (px)
Citation preview

Aksi hormon yang meregulasimetabolisme bahan bakar tubuh
Dr. Syazili Mustofa, M.BiomedLektor mata kuliah ilmu biomedik
Departemen Biokimia, Biologi Molekuler, danFisiologi
Fakultas Kedokteran Unila
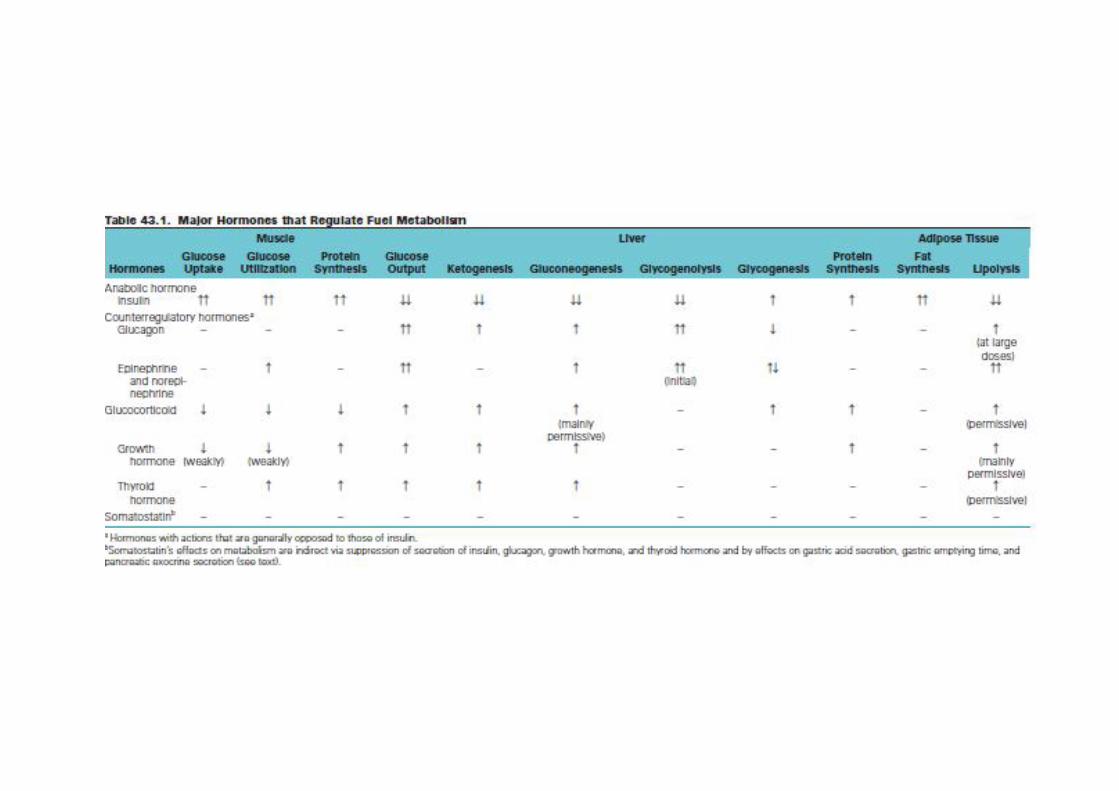
Hormon yang mempengaruhimetabolisme bahan bakar di tubuh
• Anabolik (Insulin) mempromosikanpenyimpanan nutrien ( glikogen di hati, Triasilgliserol di jarangan adiposa) danmenstimulasi sintesis protein di otot
• Lawan insulin (Counterregulatory Hormone)memobilisasi bahan bakar ( memicuglikogenolisis dan glukoneogenesis)– Glukagon , Epinephrine, norepinephrine, cortisol,
somatostatin, growth hormone– Thyroid hormone
• INSULIN
- disintesis oleh sel beta pankreas- mengandung dua rantai polipeptida
rantai A dihubungkan oleh 2 jembatansulfida antara A7 – B7 dan
A20 – B19 rantai B
pada rantai A terdapat jembatan sulfida A6 – A11
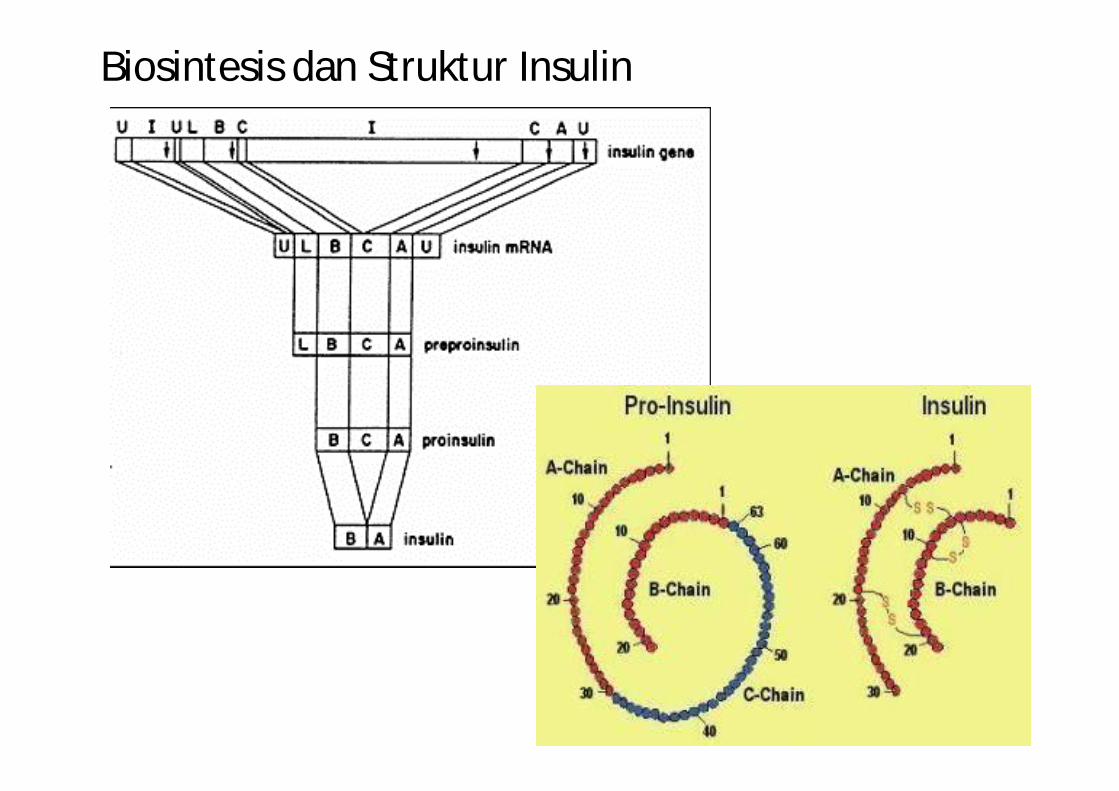
Biosintesis dan Struktur Insulin
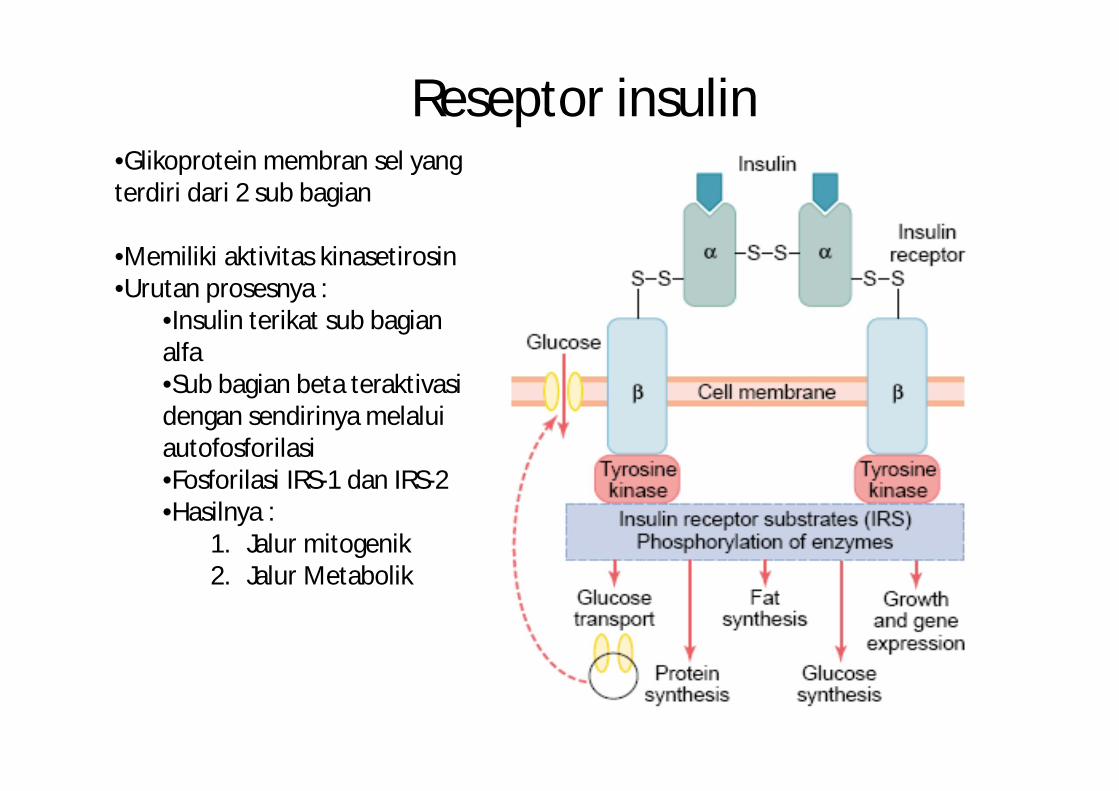
Reseptor insulin •Glikoprotein membran sel yang terdiri dari 2 sub bagian
•Memiliki aktivitas kinasetirosin•Urutan prosesnya :
•Insulin terikat sub bagianalfa•Sub bagian beta teraktivasidengan sendirinya melaluiautofosforilasi•Fosforilasi IRS-1 dan IRS-2•Hasilnya :
1. Jalur mitogenik2. Jalur Metabolik
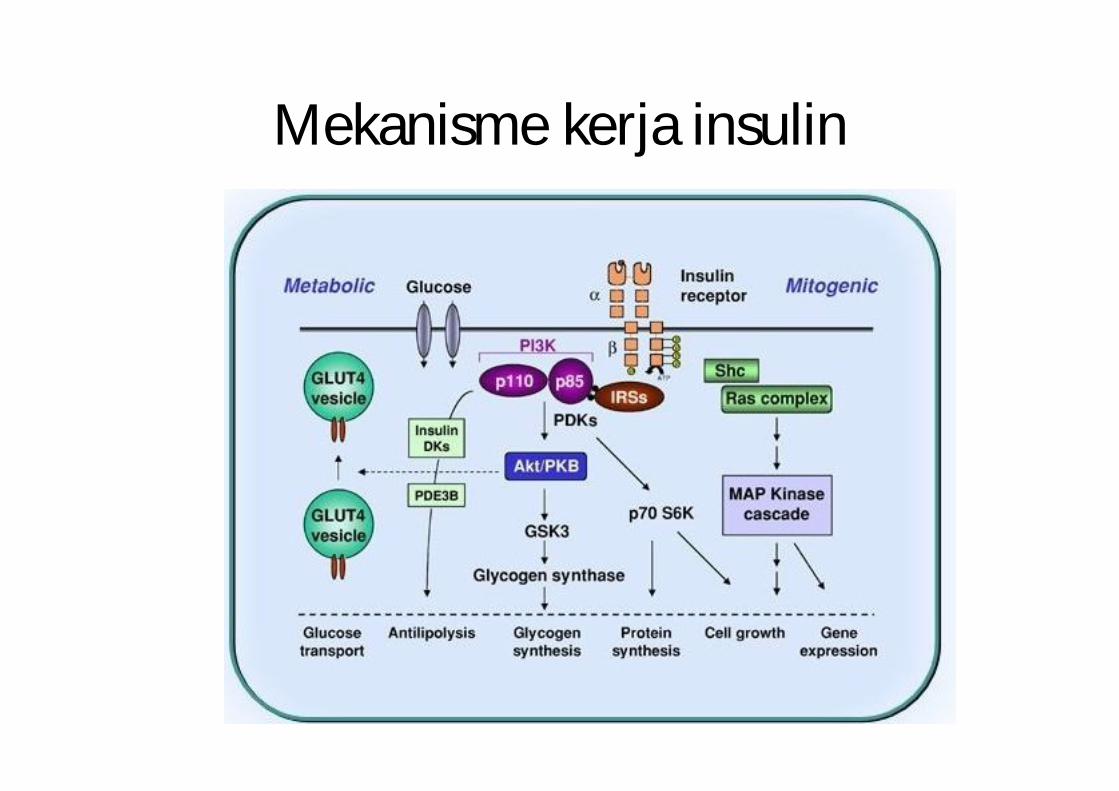
Mekanisme kerja insulin
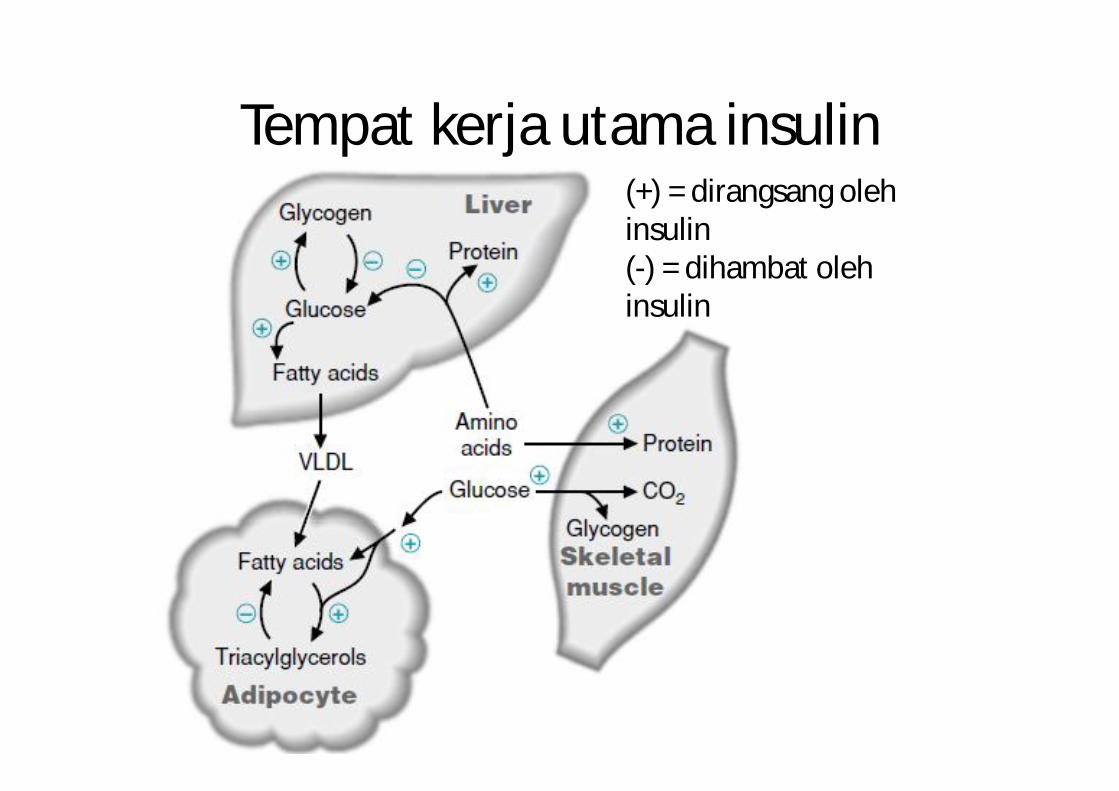
Tempat kerja utama insulin(+) = dirangsang olehinsulin(-) = dihambat olehinsulin
INSULIN
efek fisiologis nya :
* merangsang penyimpanan glikogen di hati danotot
* merangsang pembentukan asam lemak dantriasil gliserol serta penyimpanannya di adiposa
Physiological effect of insulin
* merangasng sintesis lebih dari 50 jenis protein sebagain berhubungan dengan pertumbuhanorganisme.
* punya efek parakrin, insulin menekan produksiglukagon pada sel alfa pankreas
GLUCAGON* synthesized as part of large precursor
protein (proglucagon).* Proglukcagon produced by
- α cell of the Langerhans islet of the pancreas
- Intestine L cells
* contain several peptides linked as tandem with :
- glisentin peptida linked to-glisentin (glycentin-related peptide)
- glucagon peptida linked to glukagon I(GLP-1)peptida linked to glukagon II(GLP-2)
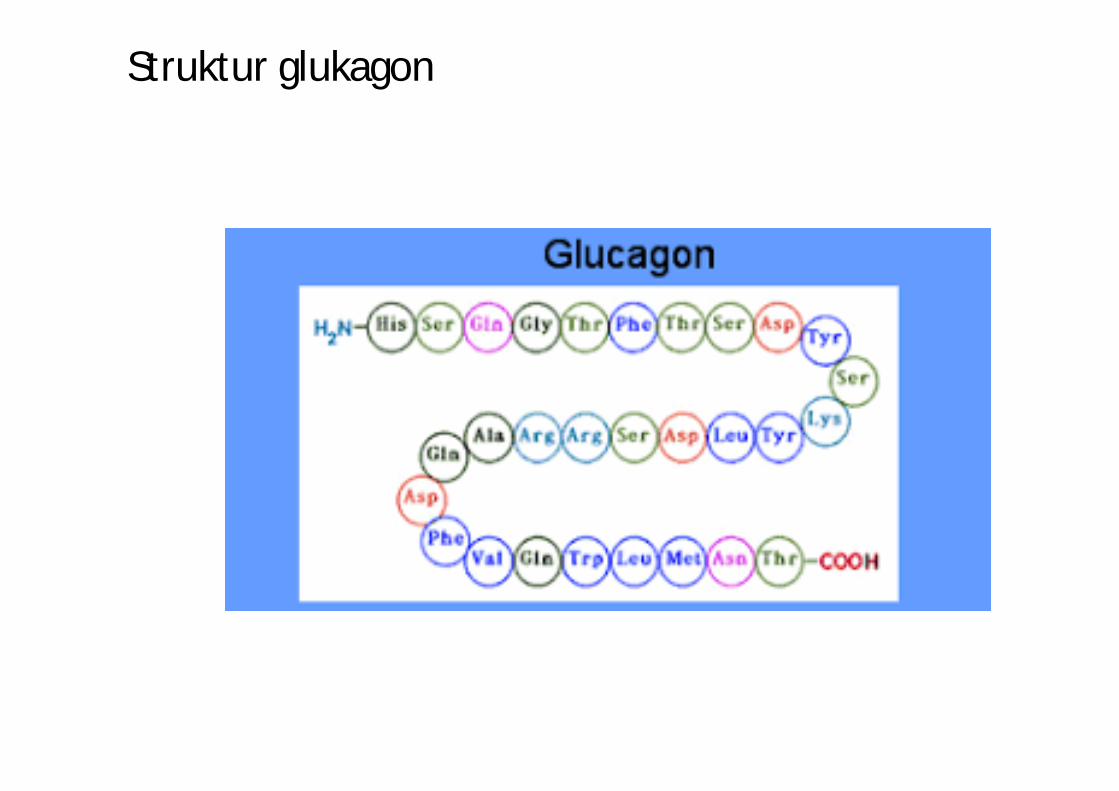
Struktur glukagon
• GLUCAGON* stimulate glycogenolisis, gluconeogenesis &
ketogenesis by stimulate synthesis cAMP in side the targeted cells.* Liver the main targeted organ* Stimulate the release of Insulin from β cell of the pancreas
Somatostatin (growth hormone-inhibiting hormone, somatotropin
release-inhibiting factor, GHIH, SRIF)) • hormon peptida• berpengaruh terhadap transmisi sinyal saraf dan
perkembangan sel tubuh. • GHIH mempunyai dua bentuk dari irisan sebuah
preproprotein, satu dengan 14 asam amino dan 28 asamamino.
• GHIH disekresi oleh beberapa organ antara lain lambung, usus, sel delta pankreas,[dan neuron (sel saraf)dari nukleusperventrikular dari hipotalamus, kelenjar hipokampus danbatang otak pada bagian nucleus tractus solitarii.
• GHIH adalah sebuah hormon inhibitor yang antagonisterhadap GHRH dalam proses sekresi GH.
SOMATOSTATIN* Precursor – praprosomatostatin,
peptide that consist of 116 AA
* Two kind of prosomatostatin :- S-14 cyclic peptide, 14 aa, BM 1600
produced in hipothalamus, sel δof Langerhans islet, Central nervous system& in stomach & duodenum cells
- S-28 more potent 7-10 times inhibite the release of GH & insulin
• SOMATOSTATIN
* its secretion is stimulated by :- metabolites: glucose, arginine & leusin.- hormon adl : glucagon, vasoaktif intestine
peptide(VIP), Cholecystokinin (CCK)
SOMATOSTATIN
* Physiological effect :- supress the secretion of GH & TSH
(thyroid- stimulating hormone) from Hipofisis anterior
- supress the secretion of insulin & glucagon

Struktur Somatostatin
* Physiological effect
- decrease the absorption of nutrient from intestine for delay the time to emty the stomach by :
. Gastrin secretion & gastric acid
. Decrease the pancreatic exocrine(ie. digestive Enz, bicarbonate, & water
. Decrease blood flow in the splanknik area
CATECOLAMIN(Epinephrin, Norepinephrin, Dopamine)
* are product secreted by sympatoadrenal system
to adapt againts acute and chronic stress.

* Storaged in the form- Epinephrin (80-85%) synthesized in theadrenal medulla
- norepinephrin (15-20%) synthesis & storaged in
. adrenal medulla
. CNS
. The end of adrenergic nervous system
- Dopamine act mainly as aneurotransmiter
metabolic effect in fuels is small
• CATECOLAMIN* Synthesized from thyrosin (its precursor)* secretion of epinefrin & norepinefrin dirangsang
by severals stres including- pain- bleeding- exercise- hypoglicemia- hypoxia
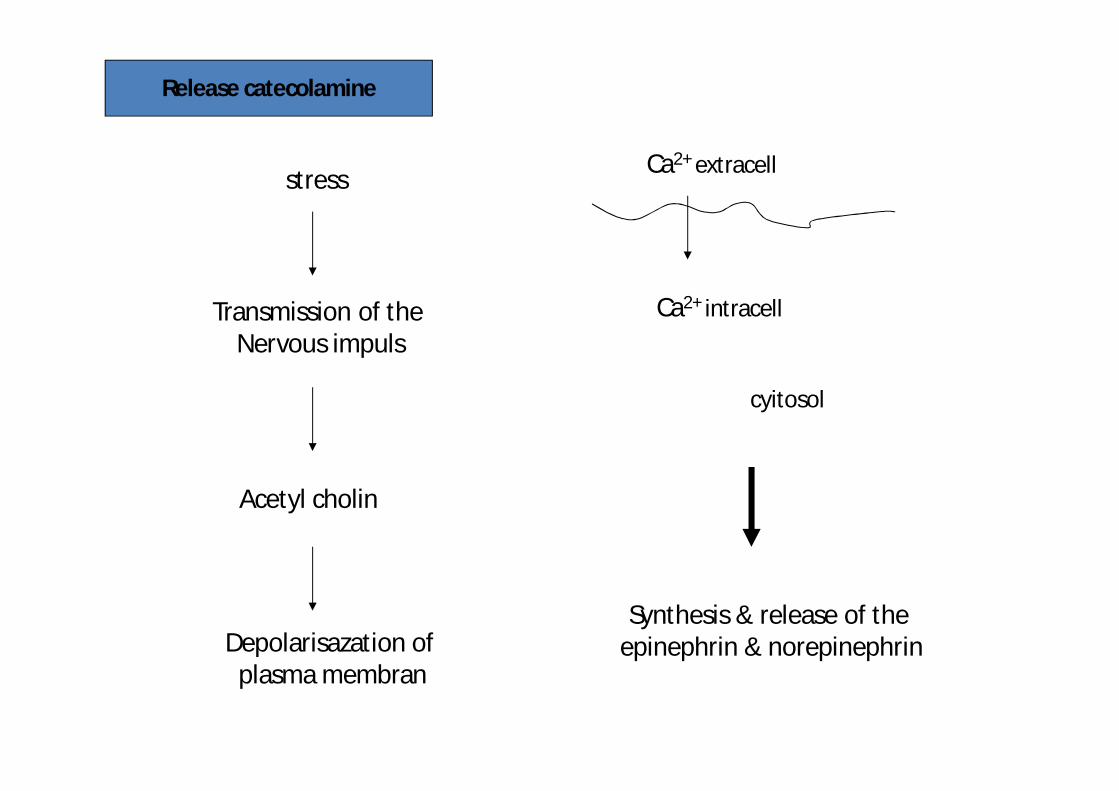
stress
Transmission of the Nervous impuls
Acetyl cholin
Depolarisazation of plasma membran
Ca2+ extracell
Ca2+ intracell
cyitosol
Synthesis & release of the epinephrin & norepinephrin
Release catecolamine
• PHYSIOLOGICAL EFFECT of CATECOLAMIN* act through 2 kind of main receptors in targeted cell ie :
- α-adrenergic receptor- β-adrenergic receptor
* action of epinephrin & norepinephrin in :- liver influence directly on fuels metab- adipocyte- sceletal muscle. - α & β pancreatic cells
CATECOLAMIN (Epinefrin & Norepinefrin)
* Hormone that act conversely/ againts Insulin action
* create metabolic effect toimmobilyzed the fuel to cell that need
energy when prone to acute and chronic stresses
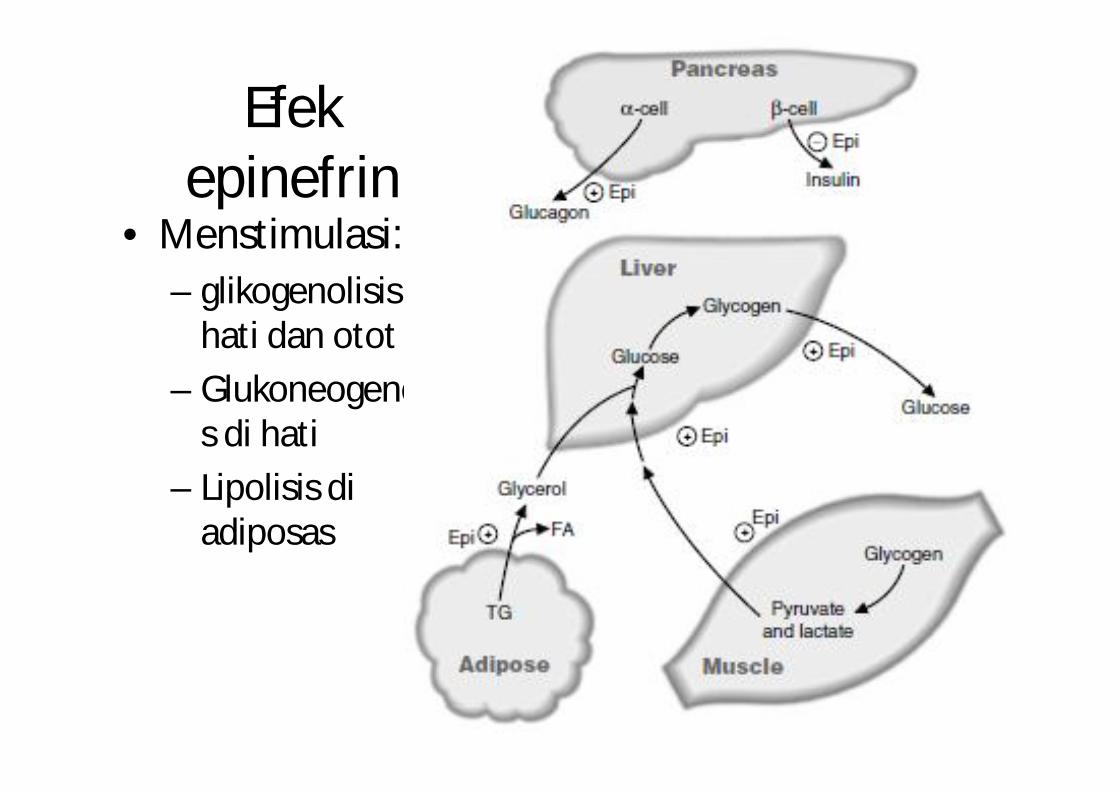
Efekepinefrin
• Menstimulasi:– glikogenolisis di
hati dan otot– Glukoneogenesi
s di hati– Lipolisis di
adiposas
* Both simultanly supress secretion of insulin make sure that fuel flow will continue to using do not storing during stimulation of stress
* effect in heart & vasculer increase blood flow & systemic blood pressure
CATECOLAMIN(Metabolism & inactivation)
* have affinity relatively low to theα & β receptors
after binding – quickly release (free katekolamin) duration of the biological response is
short.
* 2 kind of inactivation
1. Free catecolamin was reabsorp by end of adrenergic nervous can be reused/ resecreted then can be:
- deaminated by monoamin oksidase (MAO)
- or metilated by katekol O-metiltransferase (COMT) 3- metoxy-4-hidroximandelic acid (inside the end nervous) released to the circulation.
Liver and kidney could absorp catecolamin in the blood by enzymes: MAO & COMT
3-metoksi-4-hidroksimandelic acid (vanililmandelic acid / VMA)
Free catecolamin will be inactivated by conjugation process in pathological condition ( neoplasma
medula adrenal ) increase the release of Epinephrin & norepinephrin ( overexpress)
it can be measured: catecolamin or its metabolite (VMA)
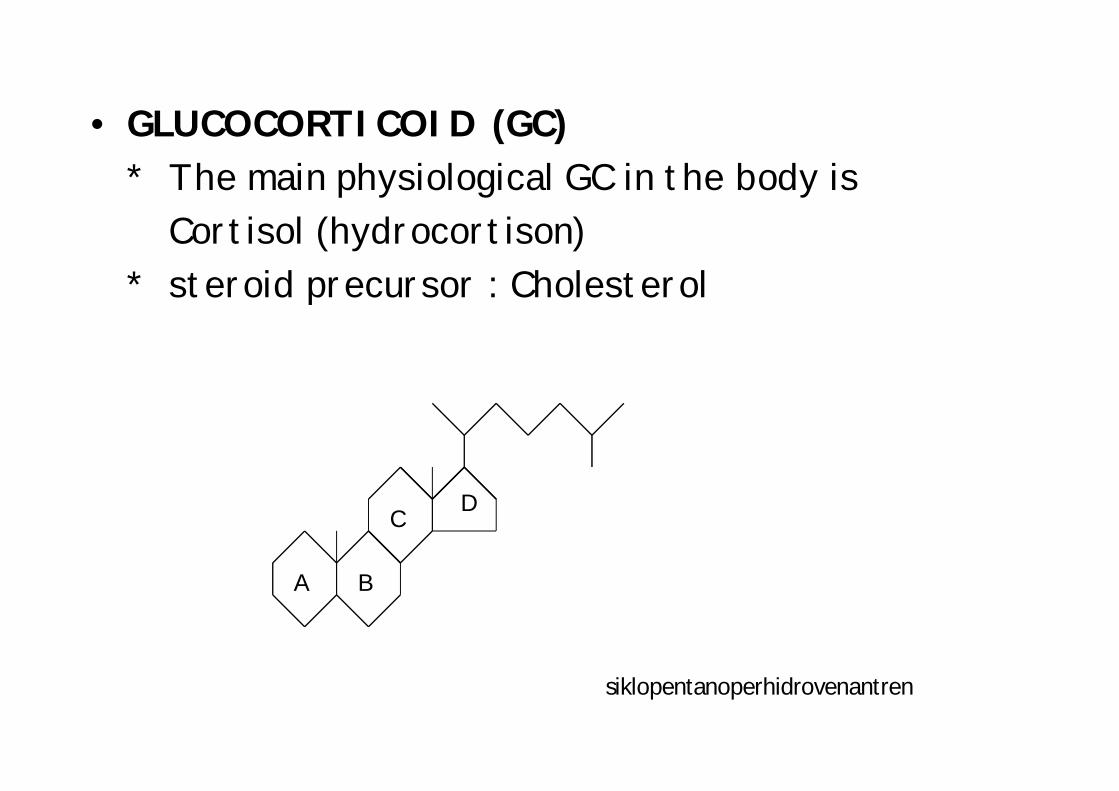
• GLUCOCORTICOID (GC)* The main physiological GC in the body is
Cortisol (hydrocortison)* steroid precursor : Cholesterol
A B
CD
siklopentanoperhidrovenantren
• GLUCOCORTICOID* synthesis & secretion are controlled by signal
cascade: nervous & endocrine that sequentially carried in cerebrocortex-hipothalamus-hipofisis-adrenocortex axis.
* Stress signal trigger the systhesis of monoamin (setil choline & serotonin) stimulate synthesis & release of CRH
(corticotropin-releasing hormone) enter the blood vessel of porta -
hipothalamus-hipofisis
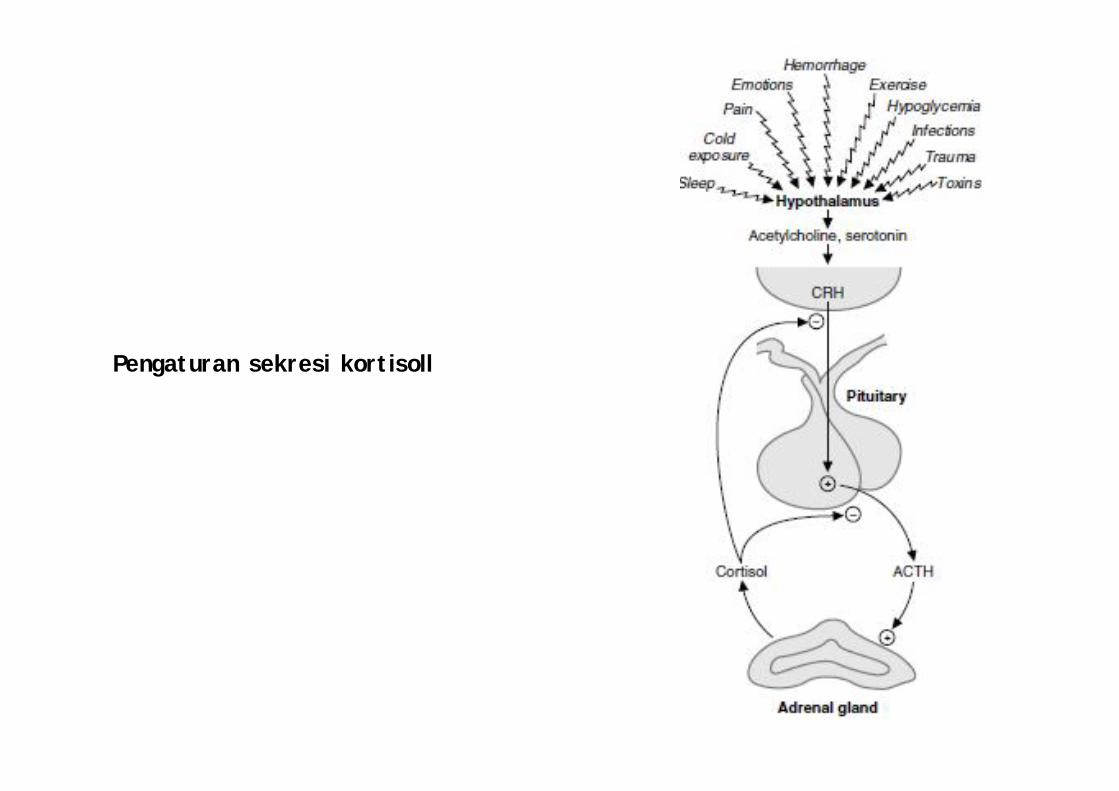
Adrenal gland
Pengaturan sekresi kortisoll
* CRH flow to specific receptor in ant hypophysis cell membrane
H-R complex stimulate the secretion of ACTH (adreno
corticothropic) into systemic circulation flow to spec. receptor in cortex adrenal
cell membran H-R complex stimulate Cortisol secretion
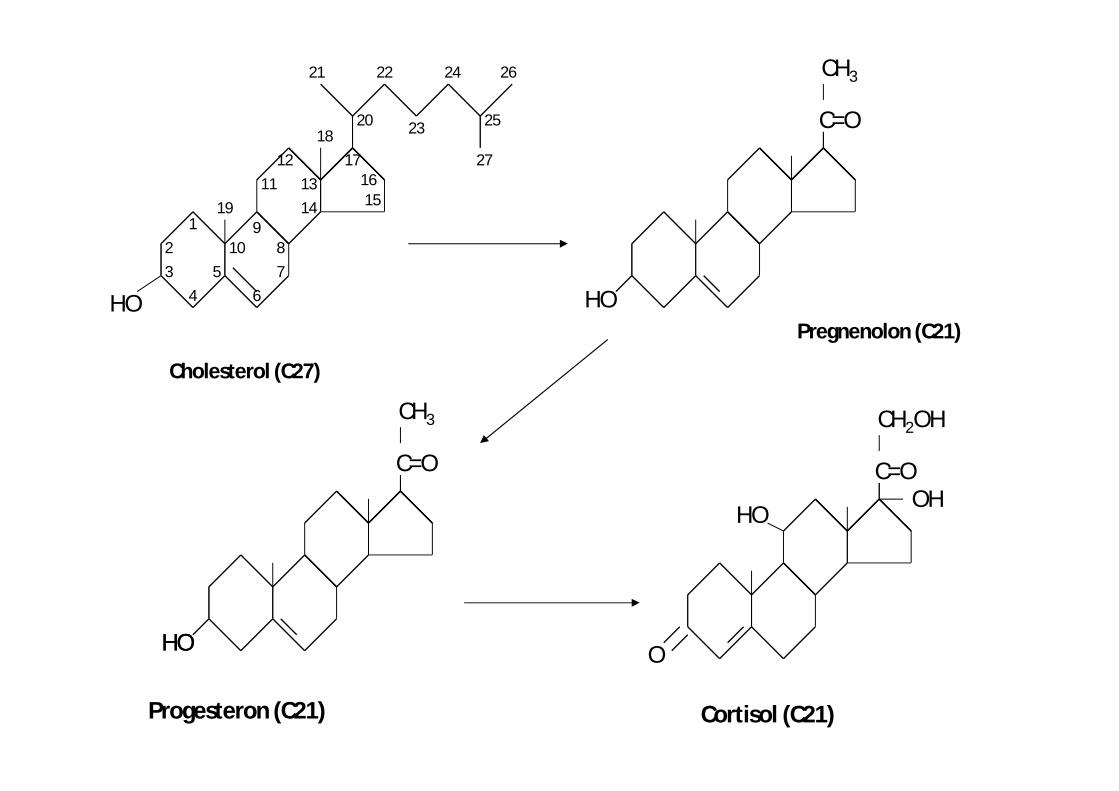
Cholesterol (C27)
HO5
432
1
678
910
141311
12
1516
17
19
25
21
2018
22
27
24
23
26
Pregnenolon (C21)
HO
C=O
CH3
HO
C=O
CH3
Progesteron (C21) Cortisol (C21)
HO O
C=O
CH2OH
HOOH
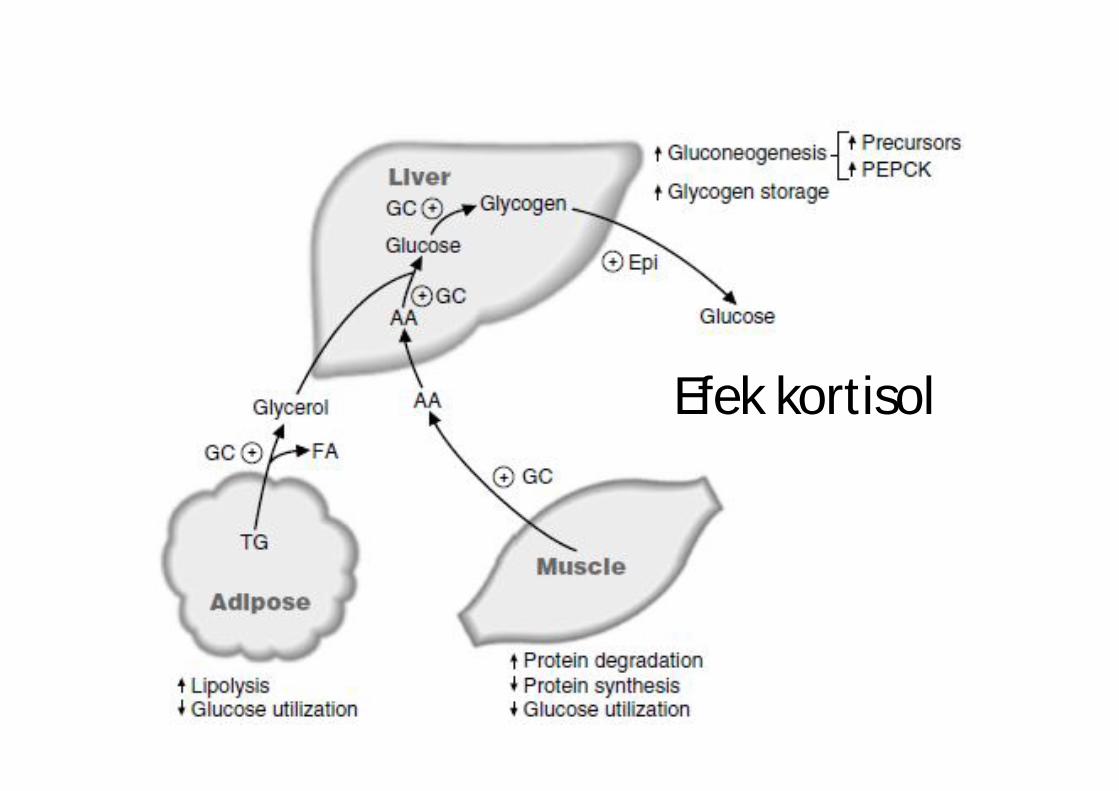
Efek kortisol
∑ free kortisol in the blood as negative feedback signal to secretion of CRH & ACTH cortisol - supress secretion of CRH &
ACTH cortisol - stimulate secretion CRH &
ACTH
PATHOLOGIC CONDITION- Cushing Syndrome
Secretion of kortisol excessive caused by ACTH secretion excessive.
. Hipercortisolemia caused by benign adenoma (tumor) producingACTH in the anterior hipofisis gland
. This tumor produce ACTH autonomically (do not influenced by normal cortisol negative feedback)
- Cushing Syndr. Tumor in the adrenal cortex
hipersecretion of cortisol kdr kortisol in the blood
. If level of kortisol & , the tumor may be in the anterior hipofisis.
• Physiological effect GC in tissues* inhibit synthesis of DNA, RNA & protein and
stimulate degradation those makromolekul.* act to make sure the energy fuel is available as
response to chronic stress-* Bila GC glucose absorption by cell in tissues
inhibited, cause:
- lypolisis in. adipocyte- proteolisis in skin, lymfoid cell &
muscle FA released will be oxydized by the liver to
produce energy
glycerol & AA – act as substrate to synthesis glucose glikogen & to be stored
acute signal of epinephrin stimulate degradation of glycogen
became glucose (for handling acute stress)
* Mecanism of action of GC : binding to intrasel Receptor kompleks steroid H-R interaksi kompleks steroid H-R dg elemen respons GC pd DNA gene transcription specifik protein
• GROWTH HORMON (GH)* A polipeptide that stimulate growth* the effect mediated by IGF (insulin like
growth factor) produced by cell as response to binding of GH to receptor in cell membrane
* GH has effect direct to metabolism of the fuels..
* produced by anterior hipofisis – as main thropic hormone: 5-15 mg/g – other tropik H ± µg/g.
* water soluble – half life 20-50 menit.
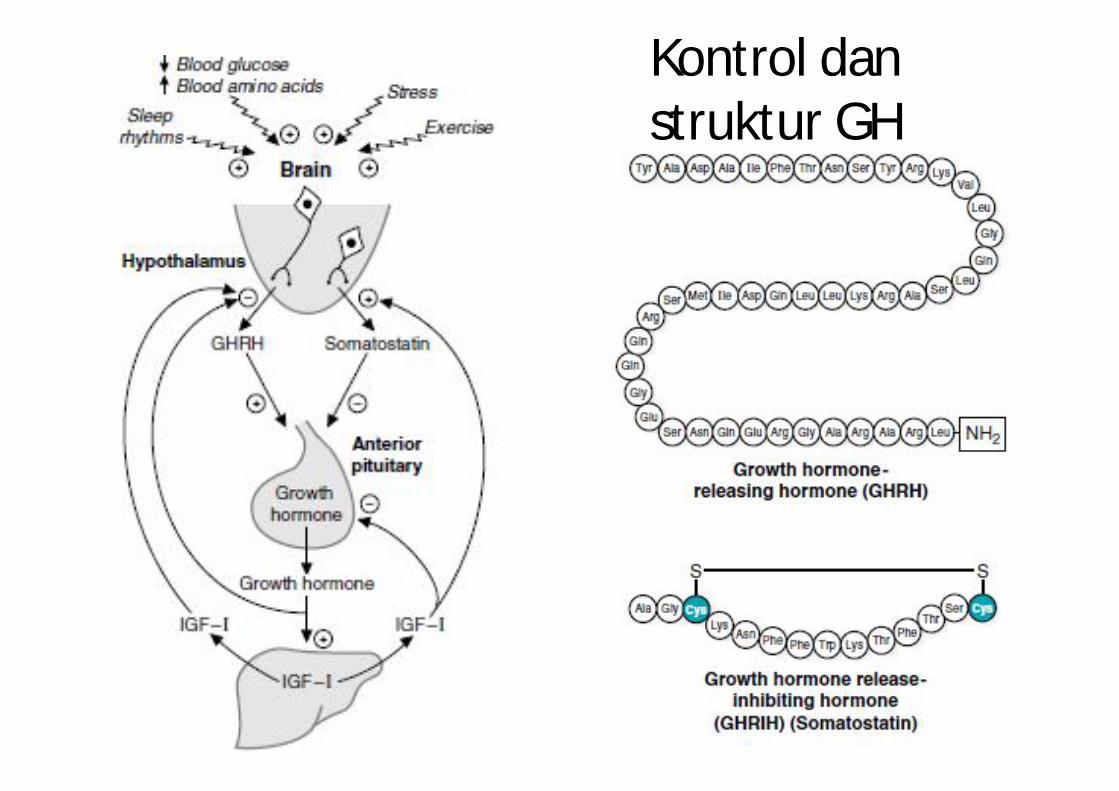
Kontrol danstruktur GH
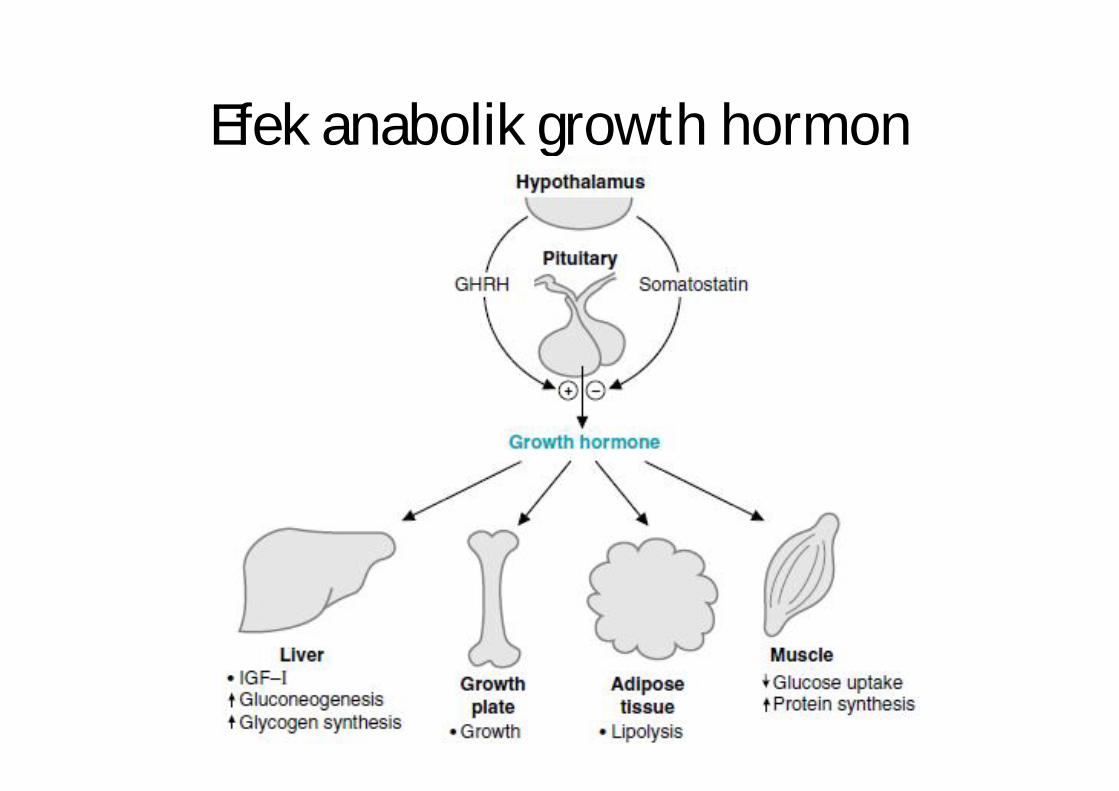
Efek anabolik growth hormon
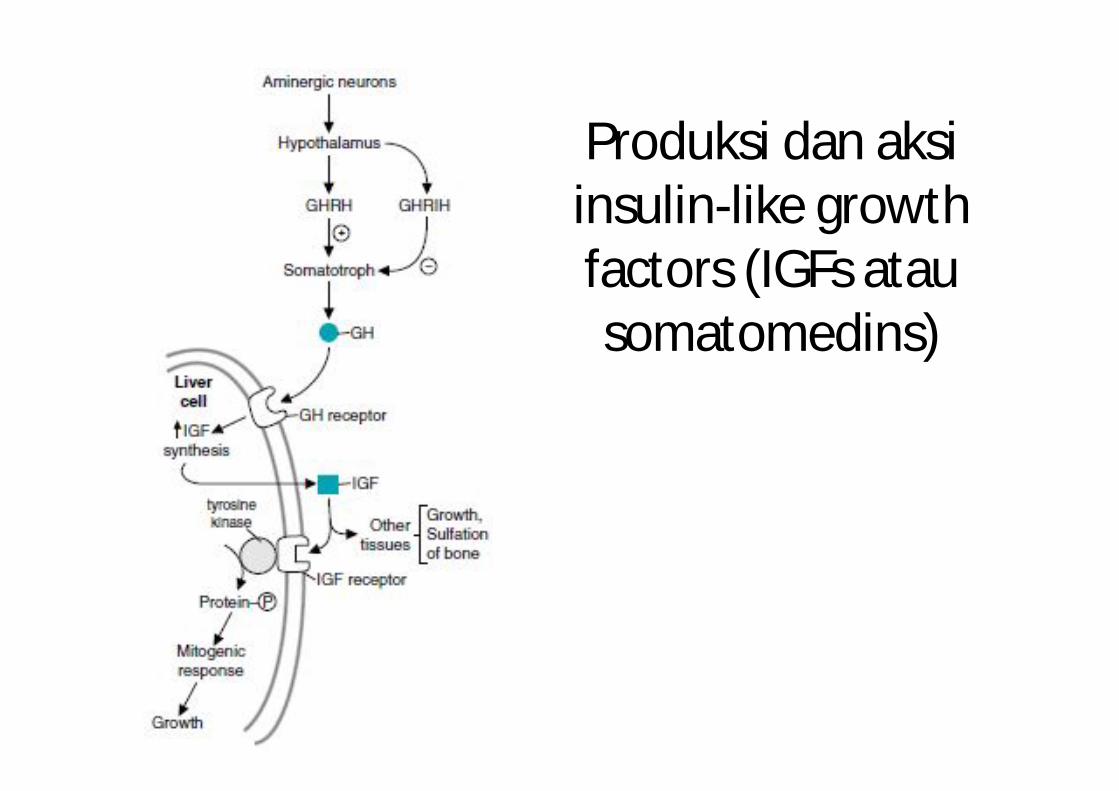
Produksi dan aksiinsulin-like growth factors (IGFs atausomatomedins)
• Regulation of secretion* stimulated by GHRH (growth hormone- releasing
hormone)* inhibited by GHRIH (growth hormone release-I nhibiting hormone), somatostatin.
* synth GHRH limited in the hipotalamussomatostatin synth by variuos nucleus
- in brain- δ Langerhans pankreas islet- mukosa intestin
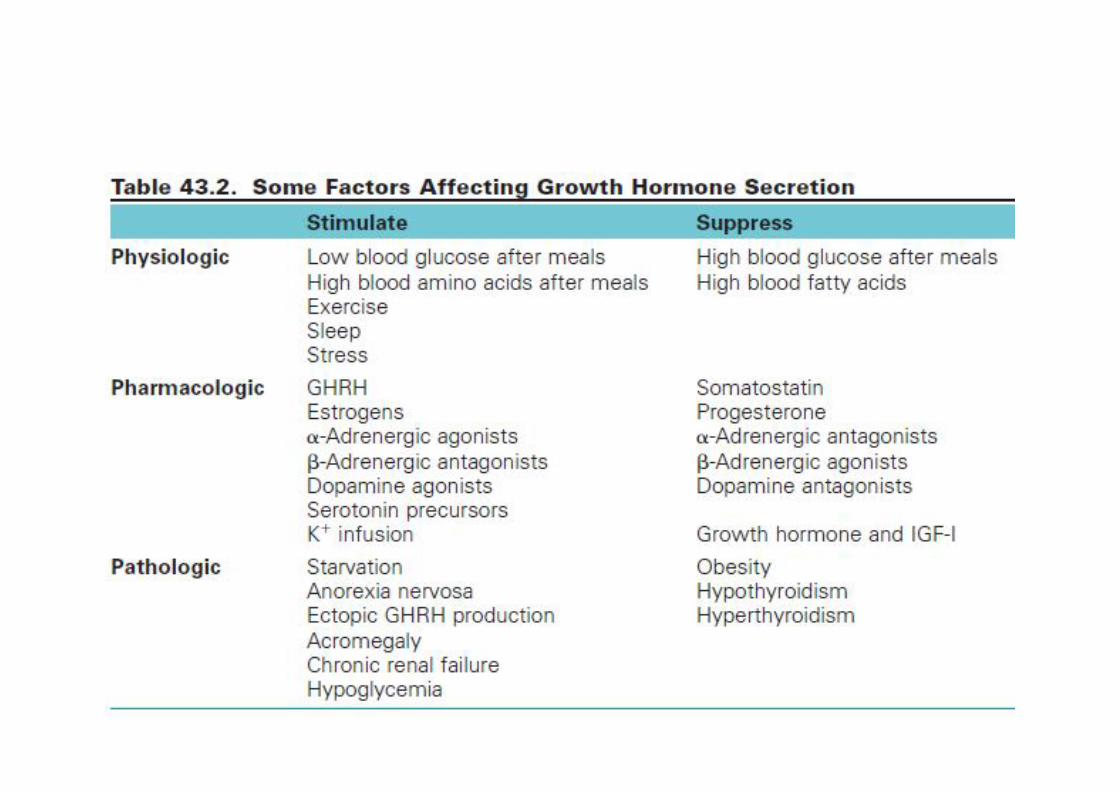
* secr GH modulated by fuel level metabolite prot, lipid , Carb.
* Normal : - hiperglicemia supress GH- hipoglicemia increase GH
* AA arginin (blood) sekresi GH
* kdr blood FA blunt respons ofGH to the increase arginin & p’ mendadak
glukosa.* proloong fasting mobilization FA to save the protein p’ sekresi GH
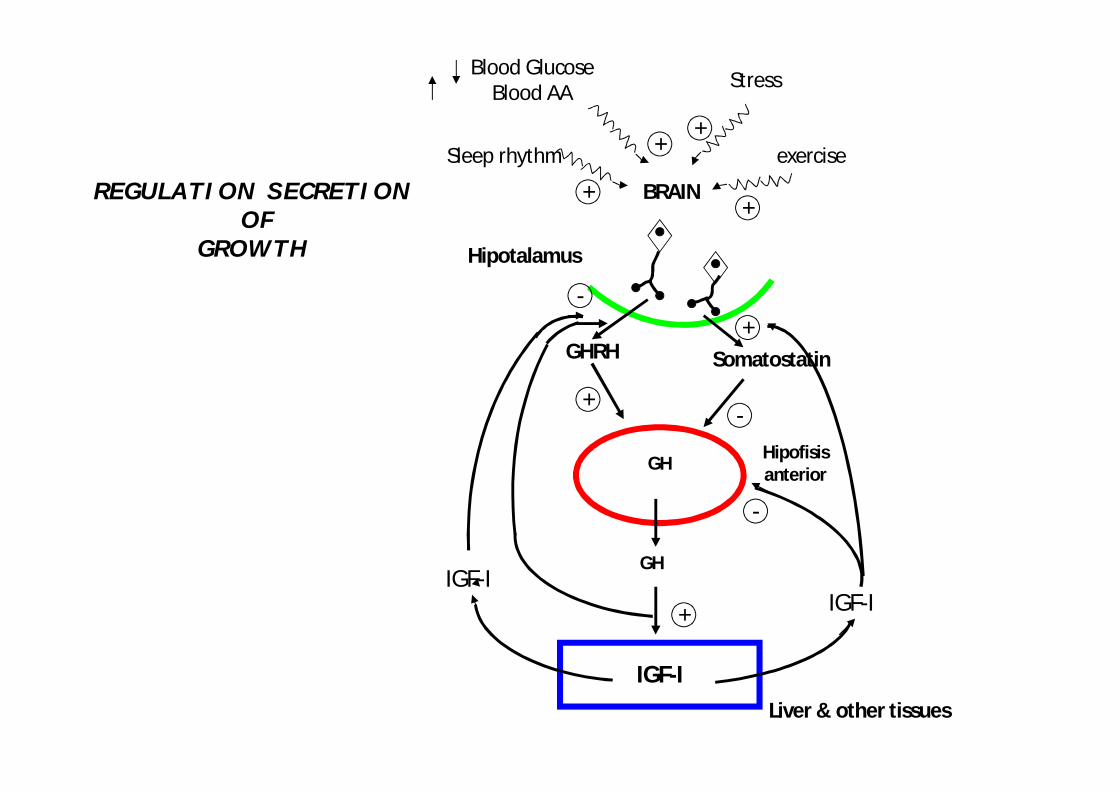
BRAIN
Stress
exercise
+
+
+
+-
+
++Sleep rhythm
GH
IGF-ILiver & other tissues
Blood GlucoseBlood AA
GH
SomatostatinGHRH
Hipotalamus
Hipofisisanterior
IGF-IIGF-I
-
-
REGULATION SECRETIONOF
GROWTH
• EFFECT of GH* on Energi metab :
- absorp & oksid of the fuel in adipocyte, muscle, liver
availability FA beta oidation energy save the glucose & protein (directly oxydation of glucosa & AA

* In adipocyte (GH)- sensitivity of adipocyte againts lipolitic
effect of katekolamin
& to lipogenic effect of insulin release FA & glicerol
into the blood liver metabolism
- esterification of FA to betriasilgliserol in adipocyte decreased
• In MUSCLE :* Effect lipolitic of GH to FFA in the blood that flow to muscles
FA tend to be used as fuels
therefore indirectly suppress absorption of glucose by the muscles (the rate of glycolisis decrease proportionally)
• In Muscle :* to transport of AA into muscle cells
generate substrate for protein synthesis.
* to synthesis of DNA & RNA
* Positive effect on nitrogen balance because of lypolisis effect of GH create protein saving and the FFA provide altenative energy
sourch for the muscle.

• GH in LIVER:* When fasting plasma insulin level (puasa) :- GH will FA oxidation asetil KoA- will ketogenesis- will lypolisis gliserol level (be the gluconeogenesis substrate).
* Stimulate synthesis of glicogen in the liver because the glukoneogenesis is on it suppress glucose metabolism
* The main effect are to stimulate synthesis and excretion of IGF
• THYROID HORMONE* from single AA: thyrosin* secreted by acinus cells of the thyroid ie :
- T3 – triiodothyronin- T4 – tetraiodothyronin
* Half life in the plasm :- T4 ± 7 days- T3 = 1 – 1,5 day long period of half life cause by the binding
ofT4 & T3 to their specific transport protein(ie. globulin : thyroid binding globulin – TBG)
OO OHOH CH2-CH-COOHI NH2
I I
I I
OHOOHOH
I
I I
CH2-CH-COOHI NH2
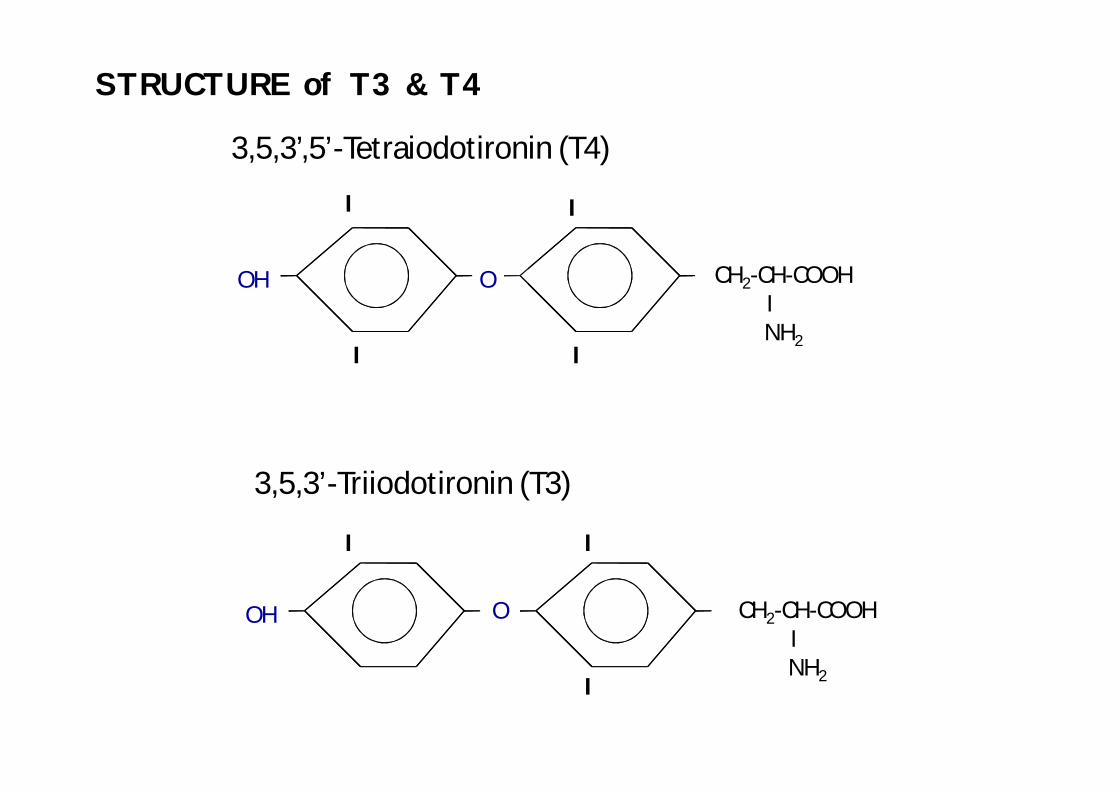
3,5,3’,5’-Tetraiodotironin (T4)
3,5,3’-Triiodotironin (T3)
STRUCTURE of T3 & T4
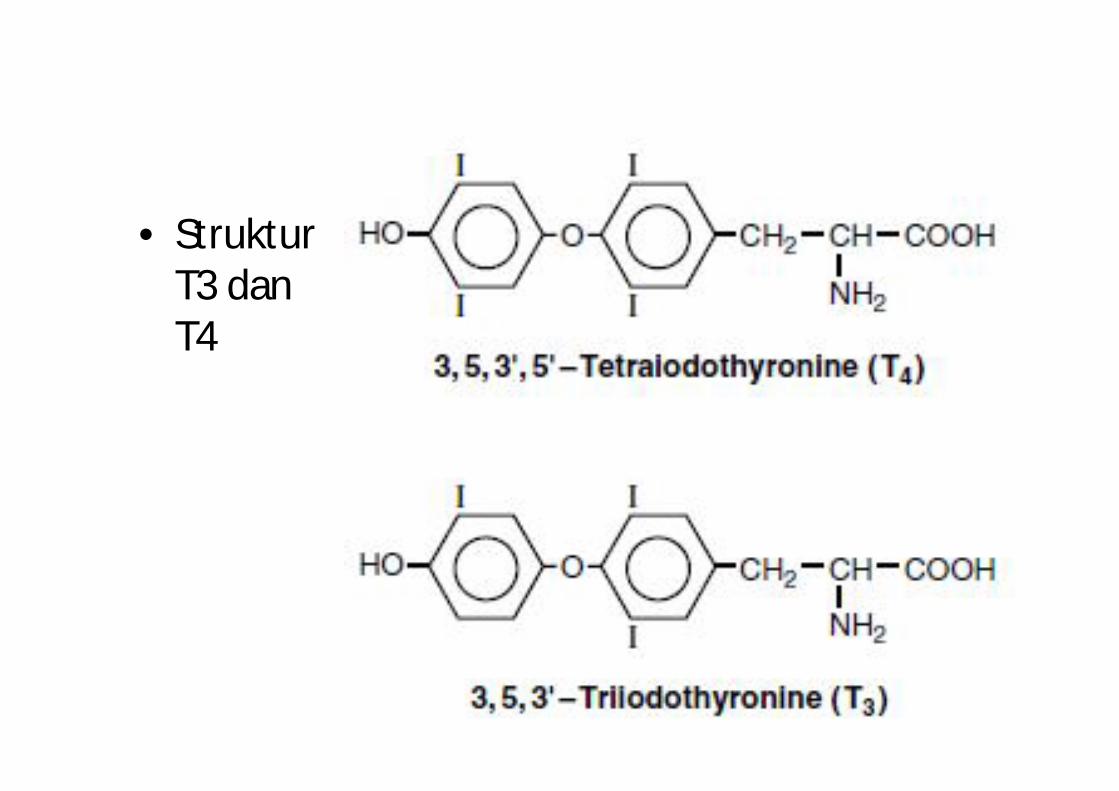
• StrukturT3 danT4
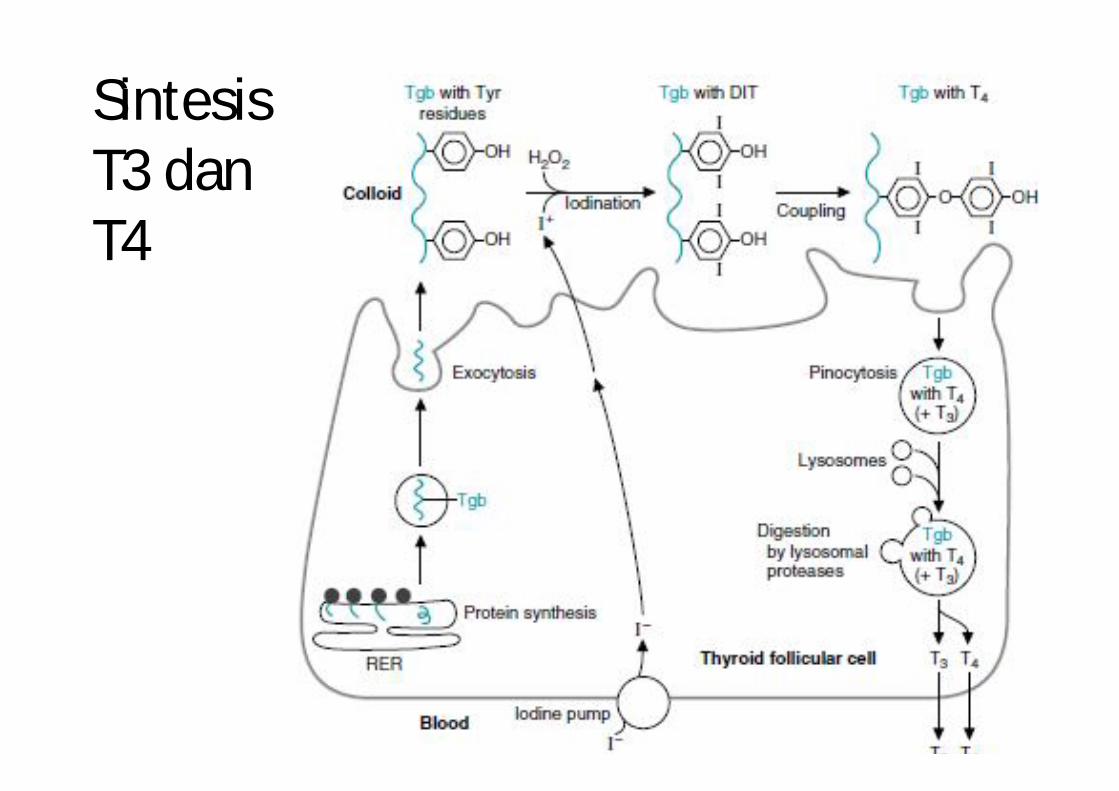
SintesisT3 danT4
* Synthesis of T3 & T4 stimulated by TSH
- start with iodide active transport from the blood into the cells of thyroid acinus (across the gradient)
- oxidation of the iodide spesies iodinating- iodination of the thyrosil reside in the
thyroglobulin protein create an iodothyrosin- condensation monoiodothyrosin reside &
diiodothyrosin in the thyroglobulin becameT3 & T4 resides- Cleavage of thyroglobulin by proteolytic enzyme
produce free T3 & T4
* Transport of TH in the blood by prottransthyretin (in prealbumin fraction)
* transport from blood acinus thyroidby iodide trap need energy
* transport rate of iodide influenced by: absolut concentration of iodide in the thyroid
* There is an internal autoregulation to transport of iodida into cell if intracellular iodide level more than certain treshold & transport if iodide level intracell is low
* Free hormone fraction has high biologically affinity (T3) because this form can across the membrane of targeted cell.
* transport prot act as hormon reservoir at any time can release TH when it needed
* Thyroid degraded in the- liver, - kidney , - muscle & other tissues
• Secretion of Thyroid* released from prot : tiroglobulin (T3 & T4 peptida bond)
* release is depend on TSH (thyroid-Stimulating Hormone)
* TSH stimulate endocytosis of Thyroglobulininto acinus thyroid enzim lysosom cleavage T3 & T4 from tiroglobulin T3 & T4 release into blood
* Feedback control if blood T3 inhibit secretion of TSH till free T3 in the blood this
mechanism make sure the availability offree T3 that biologically active.
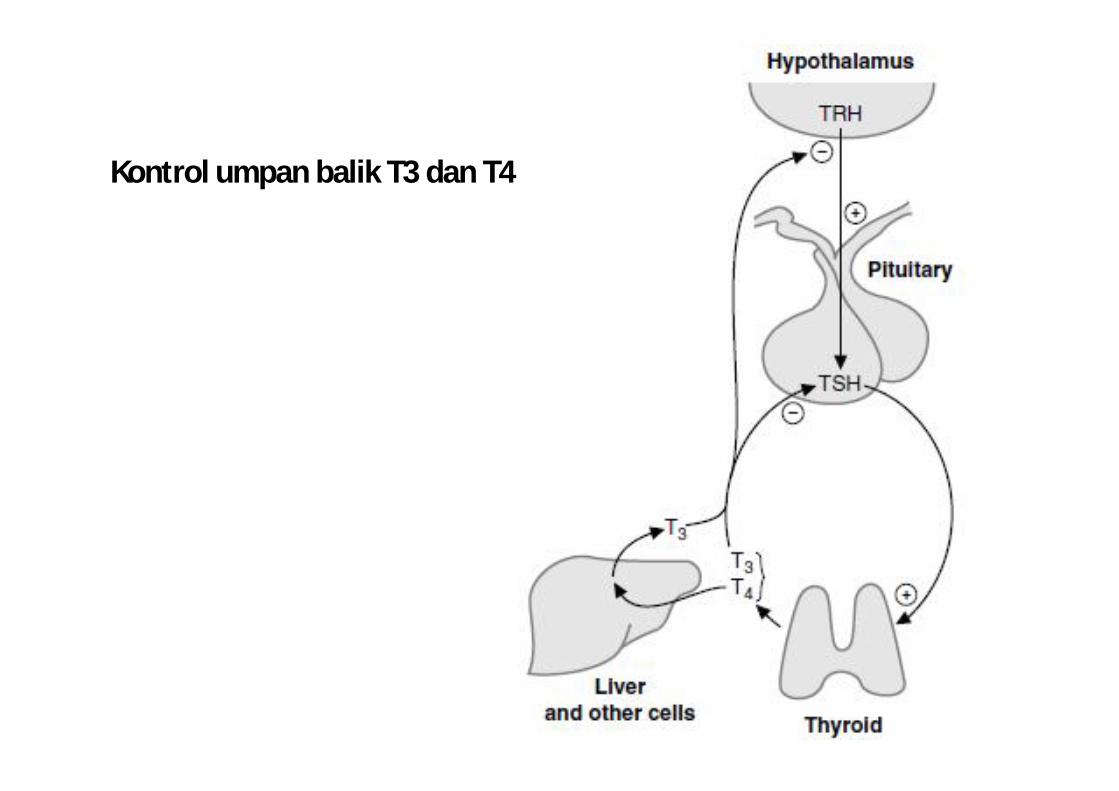
Kontrol umpan balik T3 dan T4
• Effek of Thyroid ;
* (Physiological effect TH tiroid that influence metabolism)
* Effect in the LIVER :- influence Carb. & lipid metabolism- glicolysis & synthesis cholesterol- change of cholesterol bile salt - sensitifity of hepaticyte to :
- gluconeogenic & - glicogenolitic to epinefrin
T3 indirectly increase liver glucose
- sensitivity adipocyte to the action of epinefrin lipolytic T3 to flow of FA to liver TAGliver
- flow of glycerol to liver ( lipolysis) gluconeogenesis in liver
* Effek in Adipocyte :- availability of glucose for adipocytes as precursor f/ FA synthesis
& glicerol 3-fosfat
* Effect in muscle :- level physiologic absorption of glucose by muscle- stimulate synthesis protein,
muscle growth m’ .- muscle glicolysis .
* Effect in pancreas- sensitivity of B cell of pancreas to
stimulation optimal secretion of insulin