Embed Size (px)
Citation preview

All About the Prostate For Intelligent Internists
Part 1: Benign Prostatic Hyperplasia

Objectives
Part A: DiagnosisFormulate a differential diagnosis for LUTSPerform appropriate evaluation/ w/uUse the AUA symptom score to assess
severityPart B: Management
counsel on what to expect from medications
appropriately manage persistent symptoms

Diagnosis: MKSAP!• An 80-year-old man is evaluated for a 1-year history of progressive
urinary symptoms including weak stream, hesitancy, and nocturia four times nightly. He has coronary artery disease and chronic heart failure. His current medications are lisinopril, isosorbide dinitrate, aspirin, and metoprolol.
• On physical examination, vital signs are normal. He has mild suprapubic tenderness and a symmetrically enlarged prostate without nodules or tenderness. The remainder of the physical examination is normal.
• Which of the following is the most appropriate diagnostic test to perform next?
A. Postvoid residual urinary volume measurementB. Plasma glucose levelC. Prostate-specific antigen testingD. Transrectal ultrasoundE. Urinalysis

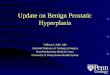
Anatomy of a large prostate• Prevalence: 25% of men in 40s, 80% in 70s • not all are symptomatic

LUTS!
More than half of men in their 60s have LUTS• LUTS ≠ BPH• Storage, Voiding, Postmicturition Sx
Differential Diagnosis• bladder irritants (e.g. caffeine, alcohol) or excess
fluid• Diuretics, anticholinergic, antihistaminic meds• UTI/prostatitis• Overactive Bladder• Neurogenic Bladder (e.g. parkinson’s, spinal cord)• Bladder, prostate Ca

Workup
• U/a generally indicated• (eval for UTI/hematuria)• *Consider* DRE/PSA to evaluate for
prostate ca after discussing risks/harms• Might also consider DRE to evaluate
prostate size as it pertains to management• PVR if sensation of incomplete emptying
(or renal insufficiency and suspect postrenal issue)

Diagnosis: MKSAP!• An 80-year-old man is evaluated for a 1-year history of progressive
urinary symptoms including weak stream, hesitancy, and nocturia four times nightly. He has coronary artery disease and chronic heart failure. His current medications are lisinopril, isosorbide dinitrate, aspirin, and metoprolol.
• On physical examination, vital signs are normal. He has mild suprapubic tenderness and a symmetrically enlarged prostate without nodules or tenderness. The remainder of the physical examination is normal.
• Which of the following is the most appropriate diagnostic test to perform next?
A. Postvoid residual urinary volume measurementB. Plasma glucose levelC. Prostate-specific antigen testingD. Transrectal ultrasoundE. Urinalysis

AUA Symptom Score/I-PSS
•Part of initial evaluation that can help confirm dx and guide management•35 point scale• In prism: .aua•Used to evaluate response to therapy • 3-4 point difference clinically
significant


Objectives
Part A: DiagnosisFormulate a differential diagnosis for LUTSPerform appropriate evaluation/ w/uUse the AUA symptom score to assess
severityPart B: Management
counsel on what to expect from medications
appropriately manage persistent symptoms

Management: MKSAP!• A 68-year-old man is evaluated for continuing urinary frequency and
nocturia. His symptoms have been slowly progressive over the past 1 to 2 years with a weak urinary stream and hesitancy. He was started on doxazosin 6 months ago, which he tolerates well and initially provided some improvement. However, his symptoms have continued and are beginning to interfere with his quality of life, particularly the urinary frequency and nocturia. His only other medical problem is hypertension, for which he takes lisinopril and metoprolol.
• On physical examination, he is afebrile, blood pressure is 140/85 mm Hg, pulse rate is 70/min, and respiration rate is 14/min. BMI is 25. He has a symmetric moderately enlarged prostate gland with no prostate nodules or areas of tenderness. A urinalysis is normal.
• Which of the following is most appropriate next step in treatment of this patient's benign prostatic hyperplasia?
A. Add finasterideB. Change doxazosin to finasterideC. Change doxazosin to tamsulosinD. Prescribe a fluoroquinolone antibiotic for 4 weeks

Management
• AUA < 8 -> watchful waiting usually appropriate• AUA >8 usually med mgmt• Keep it patient centered! depends on how
bothersome sx are. • Absolute indications for treatment?• Postrenal AKI• Urinary retention (PVR >250? 300?)• Bladder stones• Recurrent UTIs


Alpha-1 blockers• All equally effective in head to head studies• More efficacious than finasteride for reducing
symptoms• Selective have a better safety profile, but more $

5- reductase inhibitorsα
Finasteride/Dutasteride• Decreases size of prostate (part of inclusion criteria for
studies: prostates>30 g on US, PSA >1.5)• 5-year trial shown to decrease risk of urinary retention and
surgery• Takes ~6 months for improvement in AUA score
Side Effects• Decreased libido, ED, gynecomastia• Will decrease PSA by ~50% at 6 months• May reduce incidence of prostate cancer overall but
increase risk of high grade prostate ca

Combination therapy
• One-year trial 1996 showed combination therapy not superior to terazosin alone in reducing symptom scores and urinary flow rates• MTOPS trial 2003: • mean f/u 4.5 years• AUA score 8-30• Composite Primary Outcome: Clinical progression• increase in AUA score ≥4, acute urinary retention,
renal insufficiency, incontinence, recurrent UTI• Secondary outcomes: improvement in AUA score




MTOPS Take-Homes
Significant reduction in composite clinical progression with combination than either doxazosin or finasteride alone
not better than alpha blocker alone in preventing progression of AUA scores (although AUA more improved by year 5 with combo vs. doxazosin alone: -7 points vs. -6)
not better than finasteride alone in risk of urinary retention/invasive therapy
more AEs, more $Who might you choose combo tx for?
failure of alpha blocker tx alonelarge prostate size/higher PSA?higher AUA score? Urinary retention?

Other options
• Antimuscarinics (oxybutynin)• If predominantly storage sx (frequency, urgency)• In men with PVR <250, reduced symptoms when
added to α –blocker, did not increase risk of retention• PDE inhibitors (tadalafil 5 mg daily) • PDE present in prostatic tissue: PDE-I may enhance
smooth muscle relaxation, decrease proliferation of hyperplasia• Reduced AUA score 3.8 points at 12 weeks
• Saw Palmetto? Data does not show efficacy

When to Refer to Urology
• Refractory sx• Urinary retention• recurrent UTIs• Rising PSA if you choose to monitor (e.g. on 5-
alpha reductase inhibitor)

Management: MKSAP!• A 68-year-old man is evaluated for continuing urinary frequency and
nocturia. His symptoms have been slowly progressive over the past 1 to 2 years with a weak urinary stream and hesitancy. He was started on doxazosin 6 months ago, which he tolerates well and initially provided some improvement. However, his symptoms have continued and are beginning to interfere with his quality of life, particularly the urinary frequency and nocturia. His only other medical problem is hypertension, for which he takes lisinopril and metoprolol.
• On physical examination, he is afebrile, blood pressure is 140/85 mm Hg, pulse rate is 70/min, and respiration rate is 14/min. BMI is 25. He has a symmetric moderately enlarged prostate gland with no prostate nodules or areas of tenderness. A urinalysis is normal.
• Which of the following is most appropriate next step in treatment of this patient's benign prostatic hyperplasia?
A. Add finasterideB. Change doxazosin to finasterideC. Change doxazosin to tamsulosinD. Prescribe a fluoroquinolone antibiotic for 4 weeks