Embed Size (px)
Citation preview
1973
SCHERING
SYMPOSIUM
Allergy Problems in School-Aged Children
ALLERGY PROBLEMS IN SCHOOL-AGED CHILDREN John P. McGovern, M.D., Moderator
ALLERGY IN THE SCHOOLS Howard G. Rapaport, M.D.
Shirley H. Flint, Ed.D.
HYMENOPTERA INSECT HYPERSENSITIVITY Orville C. Thomas, M.D. John P. McGovern, M.D.
RECOGNITION OF THE ALLERGIC CHILD AT SCHOOL: VISUAL AND AUDITORY SIGNS
Meyer B. Marks, M.D.
John P. McGovern, M.D., F.A.S.H.A.
Howard G. Rapaport, M.D., F.A.S.H.A.(Hon.)
258
Meyer B. Marks, M.D.
Orvil le C. Thomas, M.D.
MAY 1974 VOLUME XLlV NO. 5
The 1973 Schering Symposium
ALLERGY PROBLEMS IN
SCHOOL-AGED CHILDREN
Dear Reader,
The participants at the 47th Annual Convention of the American School Health Association were fortunate to have available for their professional growth a general session devoted to The 1973 Schering Symposium, "Allergy Problems in School-Aged Children." Four distinguished allergists-Doctors John P. McGovern, Meyer 8 . Marks, Howard G. Rapaport, and Orvi Ile C. Thomas-were brought together for this program as a professional service of the Schering Corporation, pharmaceutical manu fac tu re rs. Their remarks and selected q u esti on-a nd-answer segments of the program appear in this special section of THE JOURNAL OF SCHOOL HEALTH. The Association extends its appreciation to these prominent physicians for their significant contributions to school health and to the Schering Corporation for making the Symposium possible.
For those members who were unable to attend the Convention, and for those who did attend and desire a transcript of the Symposium, we are pleased to make available this published record of The 1973 Schering Symposium. We feel the information contained in this document wi l l be extremely valuable and useful to ASHA members and other readers of THE JOURNAL.
I n behalf of the membership of the American School Health Association, I am pleased to express sincere appreciation to Doctors McGovern. Marks, Rapaport, and Thomas for their presentations. To the Schering Corporation, I extend our deepest gratitude for once again contributing to the success of the Association's Annual Convention. I t is a personal and professional pleasure to present this special feature of THE JOURNAL, The 1973 Schering Symposium.
Sincerely,
Michael S. Haro, EdS. President
The Symposium articles were edited by Glenn R. Knotts, Ph.D., Professor, Department of Allied Health Sciences, Kent State University.
THE JOURNAL OF SCHOOL HEALTH 2 59
ALLERGY PROBLEMS IN SCHOOL-AGED CHILDREN
John P. McQovern, M.D., F.A.S.H.A., Is Professor and Chalrman, Department of the Hlstory of Medlclne and Professor of Allergy, The University of Texas Qraduate School of Biomedlcel Sclences; Cllnlcal Professor of Pediatrlcs (Allergy) and Adiunct Professor of Mlcroblology, Baylor College of Medlclne; Director, McQovern Allergy Clinic, Houston, Texas.
Why d id we choose for this Schering Symposium the subject matter and title, “Allergy Problems in School-Aged Children?” Why not just”A1lergy Problems in Human Beings?” Could there be a valid, well-defined rationale other than that this is the 47th annual meeting of the American School Health Association and therefore i t is requisite that we relate our subject to the child and, where appropriate, to some relationship within the school framework?
Indeed, there are sound reasons, for there is an urgent generic imperative within the very nature of our subject matter that demands a broad platform-at what more appropriate time and meeting than this? Thus, we are grateful for the opportunity to speak for a few moments upon the nature of this generic mandate, both from the quantitative and qualitative aspects.
The quantitative aspect of “Allergy Problems in School-Aged Children” can be dispensed with celerity in terms of incidence and the resultant m o r b i d i c h e a l t h ledger . C e r t a i n new perspectives of the qualitative etiological aspects wil l be dealt with briefly by me and at some length by our panelists, and is the primary raison d‘etre for this Symposium.
Now, with respect to the quantitative aspect-the cold f igures-al lerg i c disease represents perhaps the most significant school health problem, since a minimum of ten per cent of the population suffers from major allergy, while an additional 40 to 50 per cent have experienced, or wi l l experience, some relativeb less severe, frequently evanescent, allergic manifestations, often insufficiently pronounced to requ i re med ica l consultat ion.’ More spec if ica I ly, hay fever, peren nia I a I lerg ic rh i ni tis, asthma and other allergies account for one third of all chronic conditions reported for children under 17.’
John P. McGovern, M.D., Moderator
In one national survey,”’ the total time lost from school because of chronic afflictions amounted to approximately 33 million days. Asthma accounted for more than 7.5 million days, and hay fever (usually with perennial allergic rhinitis) along with other allergies, for another 1.5 million days. Also, an allergic component probably exists in most cases of chronic sinusitis ’ and “chronic bronchitis” with cough,’t‘ along with a significant incidence in hearing impairment,’ recurrent headache:‘’ urinary tract problems ’ and tension-fatigue syndrome.’’ By comparison, in the same survey, school days lost each year because of heart disease and diseases of the genitourinary tract were 858,000 and 885,000 respectively.
In the United States an estimated 1,600,000 children through 16 years of age have asthma. In a 1961 survey, asthma accounted for 11.4 per cent of al l chronic conditions in children under the age of 17, and for 22.9 per cent of all days lost from school by children from age six through 16 because of chronic conditions.
According to Karpinos,” among every 10,000 youth medically rejected for military service, 557 were disqualified because of an allergic disorder as the primary cause, or 588 had an allergic dis- order of a disqualifying nature that was either the primary or secondary cause for disqualification. Thus, allergic disorders represented approx- imately six per cent of all medical disquali- fications. Of the 557 disqualified for rea- sons of allergy, 526 were rejected because of asthma and 11 because of hay fever. Since asthma accounts for more than 95 per cent of those who are rejected because of allergy, i t might be assumed that some examinees are taken into the service with known major allergies or that they are inadequately screened.
These all are shocking figures; however, incidence of an illness, days lost from school and the high cause for army rejection do not accurately reflect the total deleterious impact on the individuals tnvolved, or the cumulative loss to the nation in terms of the aberrations of physical, mental and emotional growth and development of our youth. This condition is a problem of compelling magnitude; one in which all primary physicians and other members of the
260 MAY 1974 VOLUME XLlV NO. 5
“health team” caring for children can and must play an increasingly more effective role.
Now, what about that aforementioned most im- portant second aspect, the qualitative or generic basic of “allergy problems in school-aged children?” For a real insight into a workable and effective understanding of this, certain new per- spectives of several basic principles of disease, especially al lergic disease, need to be considered.
When man, over the course of recorded history, has contemplated new perspectives in the nature of almost any disease process, he has vacillated between placing the blame on outside hostile forces and on himself. A hundred years ago the work of Pasteur seemed to settle the question decisively in favor of the outside forces. Yet even as Pasteur was inducted into the French Academy, his opponent, Pidoux, objected that “Disease is the common result of a variety of diverse external and internal causes that bring about the destruction of an organ by a number of roads which the hygienist and the physician must endeavor to close.””
Thus, within a context of newer perspectives, we shall develop the thesis that allergic disease is, in Pidoux’s words, “the common result of a variety of diverse external and internal causes.”
Shortly following the fundamental studies of Charles Richet in 1902, and his coining of the term, “anaphylaxis,” Clemens von Pirquet and Bela Schick published in 1905 their classic monograph, “Die Serum krank hei t.”“ The next year, 1906, primarily on the basis of these and other findings, von Pirquet coined the word “allergy.” Since then, there has been not only much understanding but also considerable con- fusion surrounding the full, concise meaning of this word and the clinical specialty which i t has come to signify. Schick, in 1959, wrote that von Pirquet’s first observations were made in 1902 on a patient who developed serum sickness after he had been given scarlet fever serum. In 1906, a reviewer commented that von Pirquet’s paper was not important and that i t was a superfluous publication introducing a new and useless term (a I lerg y) .I *
Originally and subsequently, von Pirquet implied by his term that he believed an antigen- antibody reaction occurs in the anaphylactic or a \krg ic response and thus he inferred that these phenomsna were to be p laced o n an immunologic basis. In spite of the tremendous advances in immunology labolratory techniques and the accretion of knowledge in this area,
during the intervening 67 years since von Pirquet’s findings, i t has more recently become increasingly evident that for a large group of “allergic diseases” immunologic mechanisms alone cannot adequately explain the clinical phenomena observed. Serum s ickness, anaphylactic shock from insect stings, poison ivy, penicillin hypersensitivity, organ transplant rejection, and o thers-t hese disease processes or reaction processes no doubt have a more clear-cut immunologic basis. For the much more common so-called allergic or atopic diseases such as asthma, hay fever, eczema, perennial allergic rhinitis, and other clinical forms of allergy with which allergists spend perhaps 97 per cent of their time in diagnosis and therapy, immunologic mechanisms alone have failed to explain the whole story. I t must be emphasized, however, that an immunologic mechanism most certainly is one contributing factor to allergic disease processes and is usually considered the most important one. However, i t has become evident that there are other quite significant determinant forces involved.
These d e t e r m i n a n t f o rces , o r newer perspectives, may be divided or grouped into two separate yet intertwining categories. The first may be considered as a basic concept that clinical allergic disease is, in its essence, usually an immuno-physiologic entity; and that, secondly, there are many other quanta, both within and without the body, about several of which we are rapidly learning more, which affect the product or end result of the interaction in these two areas; namely, a specific allergic disease.
Perhaps this notion ’ * was most succinctly expressed by Beckman a few years ago, in a statement in an openiiig chapter of his classic textbook, Pharmacology in Clinical Practice. He said, “You w i l l probably observe, as I have, that allergists are an apprehensive group. This is not su rprisi ng s i nce their preferred i m mu no log ic approach is constantly being assailed by such brash fellows as psychiatrists, endocrinologists and pharmacologists.” He probably should have added physiologists, though perhaps they are a somewhat milder or less vocal group and thus escaped his attention.
Therefore, in order to clarify these general observations within the framework of “newer perspectives,” we need to visualize the simple concept of an antigen-antibody mechanism in operation in an allergic disease process and concurrently convert this into an interrelation-
THE JOURNAL OF SCHOOL HEALTH 201
#01)(yuCu -1
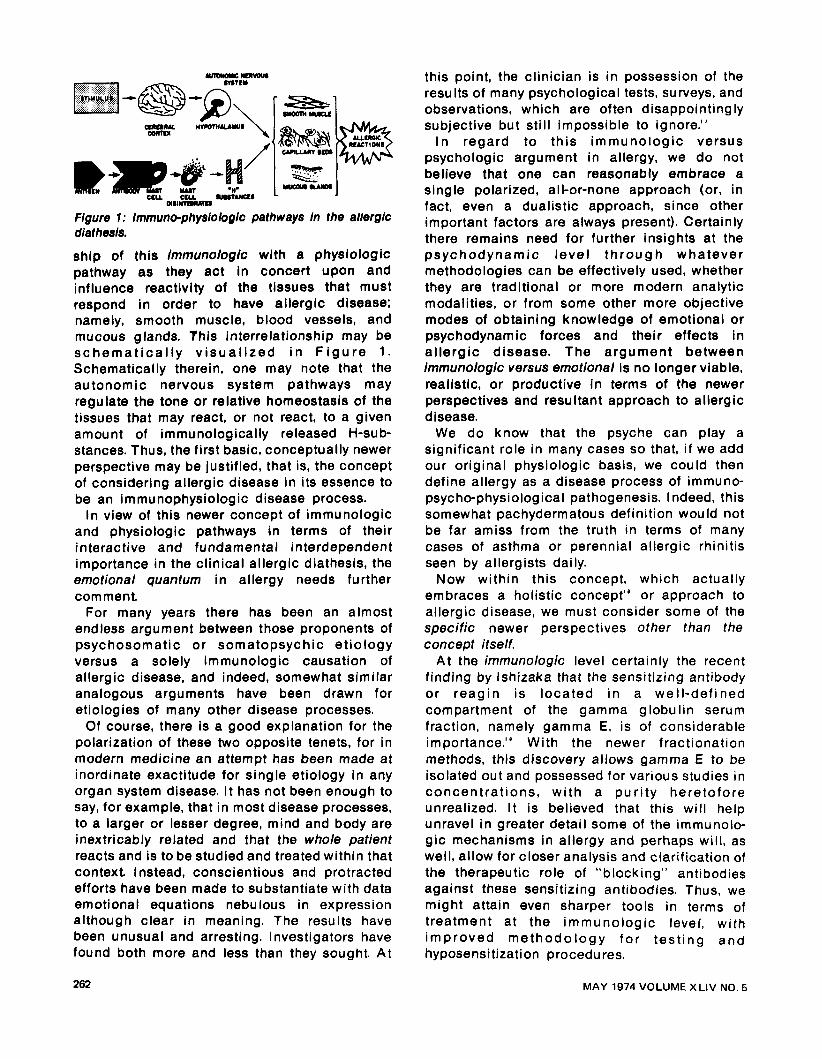
Figure 1: immuno-physiologic pathways in the allerglc diet hesis.
ship of this immunologic with a physiologic pathway as they act in concert upon and influence reactivity of the tissues that must respond in order to have allergic disease; namely, smooth muscle, blood vessels, and mucous glands. This interrelationship may be schemat i ca l l y v i sua l i zed i n F i g u r e 1. Schematically therein, one may note that the autonomic nervous system pathways may regulate the tone or relative homeostasis of the tissues that may react, or not react, to a given amount of immunologically released H-sub- stances. Thus, the first basic, conceptually newer perspective may be justified, that is, the concept of considering allergic disease in its essence to be an immunophysiologic disease process.
In view of this newer concept of immunologic and physiologic pathways in terms of their interactive and fundamental interdependent importance in the clinical allergic diathesis, the emotional quantum in allergy needs further com ment.
For many years there has been an almost endless argument between those proponents of psychosomatic or somatopsychic etiology versus a solely immunologic causation of allergic disease, and indeed, somewhat similar analogous arguments have been drawn for etiologies of many other disease processes.
Of course, there is a good explanation for the polarization of these two opposite tenets, for in modern medicine an attempt has been made at inordinate exactitude for single etiology in any organ system disease. I t has not been enough to say, for example, that in most disease processes, to a larger or lesser degree, mind and body are inextricably related and that the whole patient reacts and is to be studied and treated within that context. Instead, conscientious and protracted efforts have been made to substantiate with data emotional equations nebulous in expression although clear in meaning. The results have been unusual and arresting. Investigators have found both more and less than they sought. At
this point, the clinician is i n possession of the results of many psychological tests, surveys, and observations, which are often disappointingly subjective but still impossible to ignore.“
I n regard to this immunologic versus psychologic argument in allergy, we do not believe that one can reasonably embrace a single polarized, all-or-none approach (or, in fact, even a dualistic approach, since other important factors are always present). Certainly there remains need for further insights at the psychodynamic leve l th rough whatever methodologies can be effectively used, whether they are traditional or more modern analytic modalities, or from some other more objective modes of obtaining knowledge of emotional or psychodynamic forces and their effects in al lergic disease. The argument between immunologic versus emotional is no longer viable, realistic, or productive i n terms of the newer perspectives and resultant approach to allergic disease.
We do know that the psyche can play a significant role in many cases so that, i f we add our original physiologic basis, we could then define allergy as a disease process of immuno- psycho-physiological pathogenesis. Indeed, this somewhat pachydermatous definition would not be far amiss from the truth in terms of many cases of asthma or perennial allergic rhinitis seen by allergists daily.
Now within this concept, which actually embraces a holistic concept” or approach to allergic disease, we must consider some of the specific newer perspectives other than the concept itself.
A t the immunologic level certainly the recent finding by lshizaka that the sensitizing antibody or reagin is located i n a well-defined compartment of the gamma globulin serum fraction, namely gamma E, is of considerable importance.” With the newer fractionation methods, this discovery allows gamma E to be isolated out and possessed for various studies in concentrat ions, with a pur i ty heretofore unrealized. I t is believed that this w i l l help unravel in greater detail some of the immunolo- gic mechanisms in allergy and perhaps wil l , as well, allow for closer analysis and clarification of the therapeutic role of “blocking” antibodies against these sensitizing antibodies. Thus, we might attain even sharper tools in terms of treatment at the immunologic level, w i t h improved methodo logy fo r test ing and hyposensitization procedures.
262 MAY 1974 VOLUME XLlV NO. 5
To return to the physiologic front, perhaps the most important recent findings are those relating to the beta adrenergic receptor sites and how drug manipulation at a physiologic level might likely modify allergic asthma.Ja This particular or related work promises to have considerable clinical application for the future.
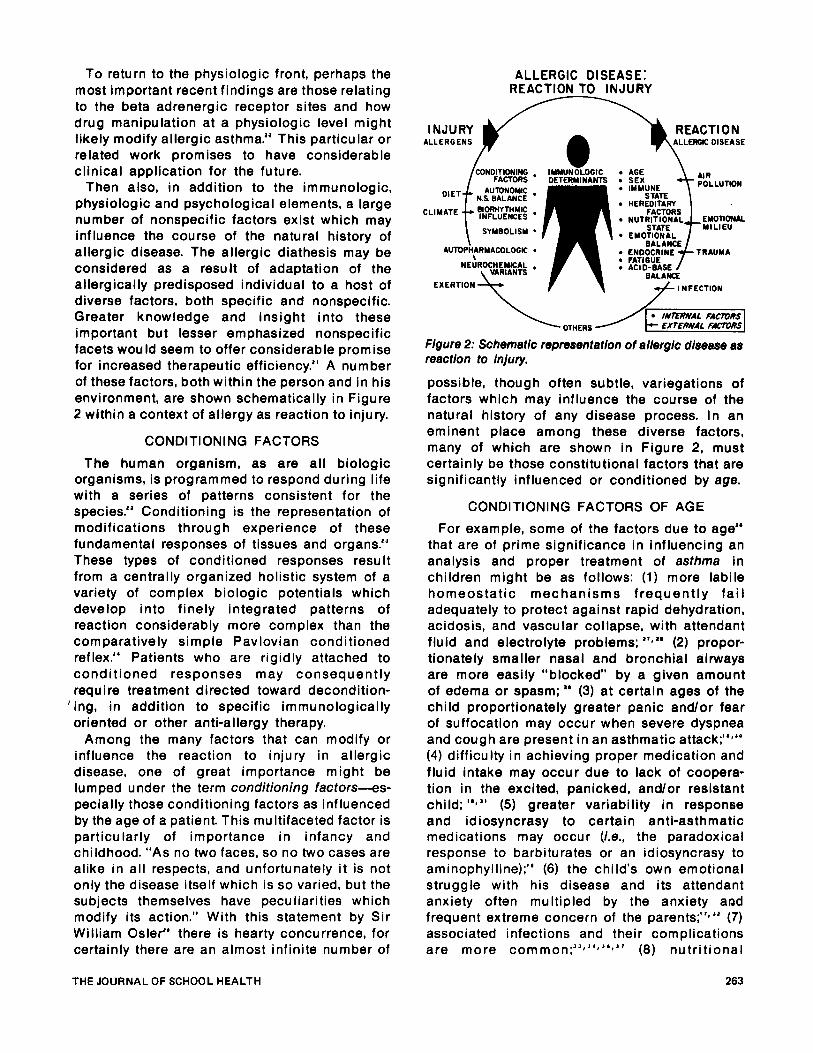
Then also, in addition to the immunologic, physiologic and psychological elements, a large number of nonspecific factors exist which may influence the course of the natural history of allergic disease. The allergic diathesis may be considered as a result of adaptation of the allergically predisposed individual to a host of diverse factors, both specific and nonspecific. Greater knowledge and insight into these important but lesser emphasized nonspecific facets would seem to offer considerable promise for increased therapeutic efficiency." A number of these factors, both within the person and in his environment, are shown schematically in Figure 2 within a context of allergy as reaction to injury.
CONDITIONING FACTORS
The human organism, as are al l biologic organisms, is programmed to respond during life with a series of patterns consistent for the species." Conditioning is the representation of modifications through experience of these fundamental responses of tissues and organs." These types of conditioned responses result from a centrally organized holistic system of a variety of complex biologic potentials which develop into finely integrated patterns of reaction considerably more complex than the com para t ive I y si m p le P av lovi an con d i t ioned reflex." Patients who are rigidly attached to conditioned responses may consequently require treatment directed toward decondition- ing, in addition to specific immunologically oriented or other anti-allergy therapy.
Among the many factors that can modify or influence the reaction to injury in allergic disease, one of great importance might be lumped under the term conditioning factors-es- pecially those conditioning factors as influenced by the age of a patient. This multifaceted factor is particularly of importance in infancy and childhood. "As no two faces, so no two cases are alike in all respects, and unfortunately i t is not only the disease itself which is so varied, but the subjects themselves have peculiarities which modify its action." With this statement by Sir William Osler" there is hearty concurrence, for certainly there are an almost infinite number of
ALLERGIC DISEASE: REACTION TO INJURY
REACT1 0 N INJURY ALLERGENS
CL
CONDITIONING FACTORS
AUTDNOMIC 'IET N.S BALANCE
JMATE BIORHYTHMIC INFLUENCES t SYMBOLISM
AUTOPMARMACOLOGIC \
NEUROCtiEYEAL VARIANTS
EXERTION
IMMUNEOGIC DETERMINANTS
AGE
IMMUNE
HEREDITARY FACTORS
NUTRITIONAL STATE
EMOTIONAL BALANCE
ENDOCRINE FATIGUE ACI 0-BASE
BALANQ
AIR POLLUTION
TRAUMA
INFECTION
Figure 2: Schematic representation of allergic disease as reaction to injury.
possible, though often subtle, variegations of factors which may influence the course of the natural history of any disease process. In an eminent place among these diverse factors, many of which are shown in Figure 2, must certainly be those constitutional factors that are significantly influenced or conditioned by age.
CONDITIONING FACTORS OF AGE
For example, some of the factors due to age" that are of prime significance in influencing an analysis and proper treatment of asthma in children might be as follows: (1) more labile homeostatic mechanisms frequently fa i l adequately to protect against rapid dehydration, acidosis, and vascular collapse, with attendant fluid and electrolyte problems; " t a ' (2) propor- tionately smaller nasal and bronchial airways are more easily "blocked' by a given amount of edema or spasm; " (3) at certain ages of the child proportionately greater panic and/or fear of suffocation may occur when severe dyspnea and cough are present in an asthmatic attack;"+' (4) difficulty in achieving proper medication and fluid intake may occur due to lack of coopera- tion in the excited, panicked, and/or resistant child; '')" (5) greater variability in response and idiosyncrasy to certain anti-asthmatic medications may occur (Le., the paradoxical response to barbiturates or an idiosyncrasy to aminophylline);" (6) the child's own emotional struggle with his disease and its attendant anxiety often multipled by the anxiety and frequent extreme concern of the parent^;"^" (7) associated infections and their complications are more common;JJ~"~"~" (8) nutrit ional
THE JOURNAL OF SCHOOL HEALTH 263
problems more frequently are superimposed;" (9) there exists a greater potential hazard in the use of steroids (La, the occurrence of varicella while a chi ld is on steroid therapy, or the more frequent accident rate in children);" (10) v a r i a b i l i t y o f i m m u n o l o g i c h o m e o s t a t i s mechanisms."t" These perhaps are but a few of the conditioning factors in one allergic disease problem in children-asthma.
With this fundamental knowledge of the quantitative and qualitative aspects of allergy i n ch i ldhood one should better be able to understand both the need for and the directions of appropriate care of "allergy problems in sc hool-aged chi Idren."
REFERENCES 1. Barkln GD, McGovern JP: Allergy statistics. Ann
Allerg 24:602 (Nov) 1966. 2. Schiffer CG, Hunt EP: Illness Among Children.
Chlldren'e Bureau Publlcatlon No. 405, washington DC, US Govt Printing Office, 1963.
3. McGovern JP, Thomas OC, Haywood TJ et al: Respiratory allergy In Infants and Children: data from 5,000 consecutive cases. Med Rec Ann60:444 (Nov) 1887.
4. Murray JA, Alexander SR, Travis BT et al: Allergic cough syndrome. Sou Med J 63:1159 (Oct) 1970.
5. McGovern JP, Haywood TJ, Fernandez AA: Allergy and secretory otitis media; an analysis of 512 cases. JAMA 200:124 (Apr 10) 1967.
6. McGovern JP, Haywood TJ: Headache of multiple etlologles and Its holistic management. Headache 3(2):78, 1963.
7. McGovern JP: On etiologic mechanisms and a new classification of allergic headaches. Headache 4(2):205 (Jul) 1963.
8. McGovern JP, Haywood TJ: Allergic headache. Allergy of the Nervous System. Springfield, Illinois, Charles C. Thomas, 1970.
9. Powell NR, Bogge PB, McGovern JP: Allergy of the lower urinary tract. Ann Allerg 28:252, 1963.
10. McGovern JP, Haywood TJ: Allergic tension- fatigue syndrome with headache. Headache 2(4):230, 1963.
11. Barkln GD, McGovern JP: What the classroom
12.
13.
14.
15.
16.
17.
264
teacher can do for the asthmatic child. NEA J (Nov) 1967. Karpinoe BD: Qualifications of American Youths for Military Service. Medical Statlstlce Division, Office of the Surgeon General, Dept of the Army, Washington DC, US Govt Printing Office, 1962. Wolf S: A new view of disease. JAMA 184:129-130, 1963. von Plrquet C, Schick B: Die serumkrankhelt. Lelpzlg, Franz Deuticke, 1905. Wolf IJ: Aphorlsms and Fscetiae of Bela Schick. Orange, New Jersey, Knoll Pharmaceutical Co, 1965. McGovern JP: On Doctor Beckman's observation. Ann Allerg 23:340 (Jul) 1965. McQovern JP, Knight JA: Allergy and Human
Emotions. Springfield, I Ilinois, Charles C. Thomas, 1967.
18. McGovern JP, Haywood TJ: Holistic approach to management of bronchial asthma. Ped Clin N Amer 10:109, Philadelphia, WB Saunders Co, 1963.
19. lshizaka K , lshizaka T, Hornbrook MM: Physicochemical properties of reaginic antibody. V. Correlation of reaginic activity with gamma-E- globulin antibody. J lmmunol 97:840, 1966.
20. Szentivanyi A: The beta adrenergic theory of the atopic abnormality in bronchial asthma. J Allerg 42:203, 1966.
2f. Haywood TJ, McGovern JP: Conditioning factors in allergic disease. Sou Med J 60:301, 1967.
22. Wolberg LR: Psychotherapy and the Behavioral Sciences. New York, Grune and Stratton, 1966.
23. Wolpe J, Salter A, Reyna LJ: The Conditioning Therapies. New York, Holt, Rinehart and Winston, Inc, 1964.
24. Franks CM: Conditioning Techniques In Clinical Practice and Research. New York, Spring Pub Co, 1964.
25. Osier W: Teaching and thinking: the two functions of a medical school. Montreal Med J 23:561, 1894- 1895.
26. McGovern JP: On conditioning factors of age in allergic disease. Ann Alerg 23:577, 1965.
27. McGovern JP, Dauschner CW Jr: The role of fluid and electrolytes in the management of severe asthma. Sou Med J 51:1197, 1958.
28. Haywood TJ, McGovern JP: Prevention and treatment of fluid and electrolyte problems in asthma. Ann Allerg 22:33, 1964.
29. McGovern JP: Management of allergy i n childhood. Texas Med 54:290, 1958.
30. McGovern JP: How to control allergy. Parents Mag (Jul) 1964.
31. McGovern JP: Respiratory allergy in childhood. In Conn HF (ed): Current Therapy. Philadelphia, WB Saunders Co, 1959.
32. McGovern JP, Fernandez AA: On the role of emotional factors in allergy. J Asth Res 1:213, 1964.
33. Buffman WP: Asthma in infancy. Rhode Island Med J 41:134, 1958.
34. Felngold BF: Influence of acute infection upon course of allergy In children: some clinical observations. J Ped 34:545, 1949.
35. McGovern JP, Haywood TJ: Allergic eczema. In Speer F (ed): The Allergic Child. New York, Heober-Harper, 1963.
36. Fernandez AA, McGovern JP: Secretory otitis media in allergic infants and children. Sou Med J 58581, 1965.
37. McGovern JP, Haywood TJ: Nasal allergy due to inhalant factors. In Conn HF (ed): Current Therapy. Philadelphia, WB Saunders Co, 1965.
38. McGovern JP, Zuckerman JI: Nutrition In pediatric allergy. Borden Rev Nutr Res 27:27-46, 1956.
39. McGovern JP: Therapy of acute attacks of asthma In infants and children. JAMA 169:20, 1959.
40. Thomas OC, McGovern JP: The gamma globulins with special reference to the controversy concerning their use for asthmatic children. Sou Med J 57:498, 1964.
MAY 1974 VOLUME XLlV NO. 5