Embed Size (px)
Citation preview
AASCIT Journal of Medicine
2015; 1(2): 10-13
Published online May 10, 2015 (http://www.aascit.org/journal/medicine)
Keywords Alobar Holoprosencephaly,
Craniosynostosis,
Microcephaly,
Frontonasal Encephalocele,
Cavernous Angioma
Received: April 4, 2015
Revised: April 28, 2015
Accepted: April 29, 2015
Alobar Holoprosencephaly, Craniosynostosis and Microcephaly: A Constellation of Abnormalities in a Neonate with Frontonasal Encephalocele
Obande Joseph O.1, Jimoh Abdullahi O.
2, Oluwole Peter
3,
Onyejekwe Kenneth1
1Division of Neurosurgery,Department of Surgery, University of Abuja Teaching Hospital,
Gwagwalada-Abuja, Nigeria 2Division of Neurosurgery, Department of Surgery, Ahmadu Bello University Teaching Hospital,
Zaria, Nigeria 3Department of Pathology, University of Abuja Teaching Hospital, Gwagwalada-Abuja, Nigeria
Email address [email protected] (Obande J. O.)
Citation Obande Joseph O., Jimoh Abdullahi O., Oluwole Peter, Onyejekwe Kenneth. Alobar
Holoprosencephaly, Craniosynostosis and Microcephaly: A Constellation of Abnormalities in a
Neonate with Frontonasal Encephalocele. AASCIT Journal of Medicine.
Vol. 1, No. 2, 2015, pp. 10-13.
Abstract A female neonate who was born with a frontonasal ulcerated protrusion. On examination,
she had a frontanasal ulcerated protrusion, microcephaly and pancraniosynostosis.
Computerized tomography scan revealed alobar holoprosencephaly. The combination of
craniosynostosis with frontonasal encephalocele is rarely described in the literature, and
more so is the combination with alobar holoprosencephaly. Problems in syndrome
diagnosis can arise when previously unreported findings are seen in usual conditions. We
describe our patient with an unusual constellation of conditions.
1. Introduction
Frontonasal encephalocele is an anterior neural tube defect and is rare, constituting
15% of all cases. It presents as a dysplastic mass of brain tissue at the root of the nose.
It is very unusual for the protruding mass to be described as cavernous angioma
histologically. Holoprosencephaly is the result of absent or incomplete cleavage of the
fetal prosencephalon. The alobar type of holoprosencephaly is even rarer as it is said to
be incompatible with life. The combination of frontonasal encephalocele and alobar
holoprosencephaly is hardly described in the literatures; the presence of microcephaly
and craniosynostosis completes this rare presentation. We describe our patient with this
unusual presentation and subsequent management.
2. Case Report
A term female neonate delivered to a 32 year-old healthy Nigerian mother, who was
gravida 3, para 0, from a non-consanguinous marriage. Gestation was complicated in
the 1st month with high grade fever managed only with paracetamol. There was
unremarkable family history. At birth, the neonate was noted to have ulcerated
frontonasal protrusion without cerebrospinal fluid (CSF) leak and a dysmorphic face
11 Obande Joseph O. et al.: Alobar Holoprosencephaly, Craniosynostosis and Microcephaly: A Constellation of Abnormalities in a
Neonate with Frontonasal Encephalocele
with associated microcephaly, and pancraniosynostosis.
There was hypertelorism and a shallow orbit but no
syndactyly. She weighed 2.0 Kg, and had an occipitofrontal
circumference (OFC) of 27cm. A cranial CT scan showed
features of alobar holoprosencephaly with a monoventricle,
absent basal ganglia and corpus callosum, a frontonasal
defect with an encephalocele. On the 5th
day of life she had
excision of the frontonasal encephalocele and repair of the
frontal defect, as well as performance of the
craniosynostosis� procedure and excision of the metopic
suture.
Histologically, the excised tissue was described as
cavernous angioma. Postoperatively, she did well with no
new neurological or feeding problems.
The anomalies are as illustrated below;
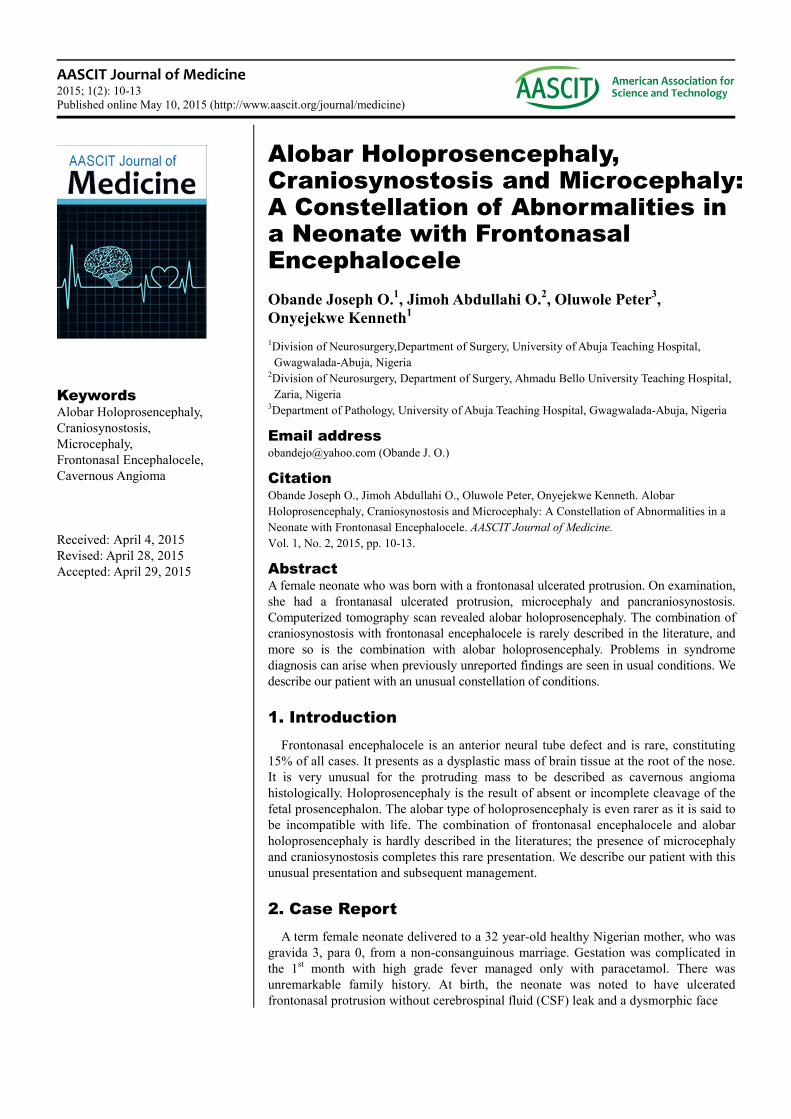
Figure 1. Patient showing the frontonasal protrusion on the 1st day of life.
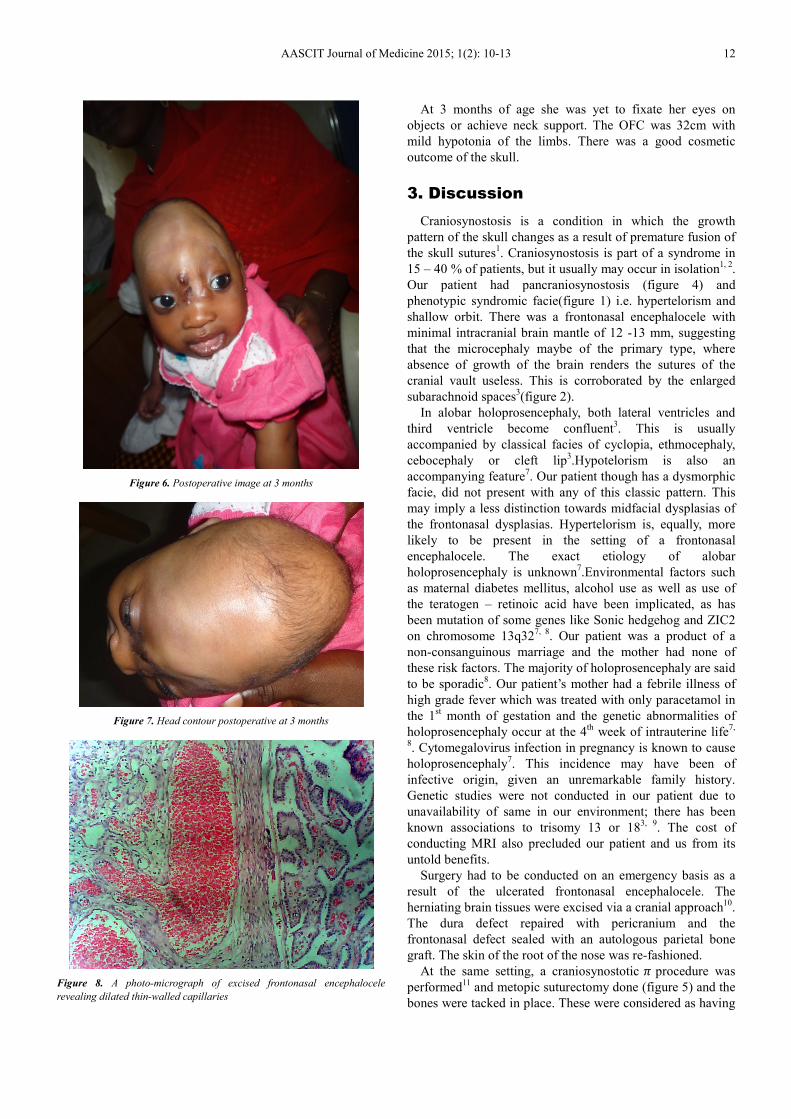
Figure 2. Cranial CT scan showing the single ventricle and the frontonasal
protrusion and obvious subarachnoid spaces
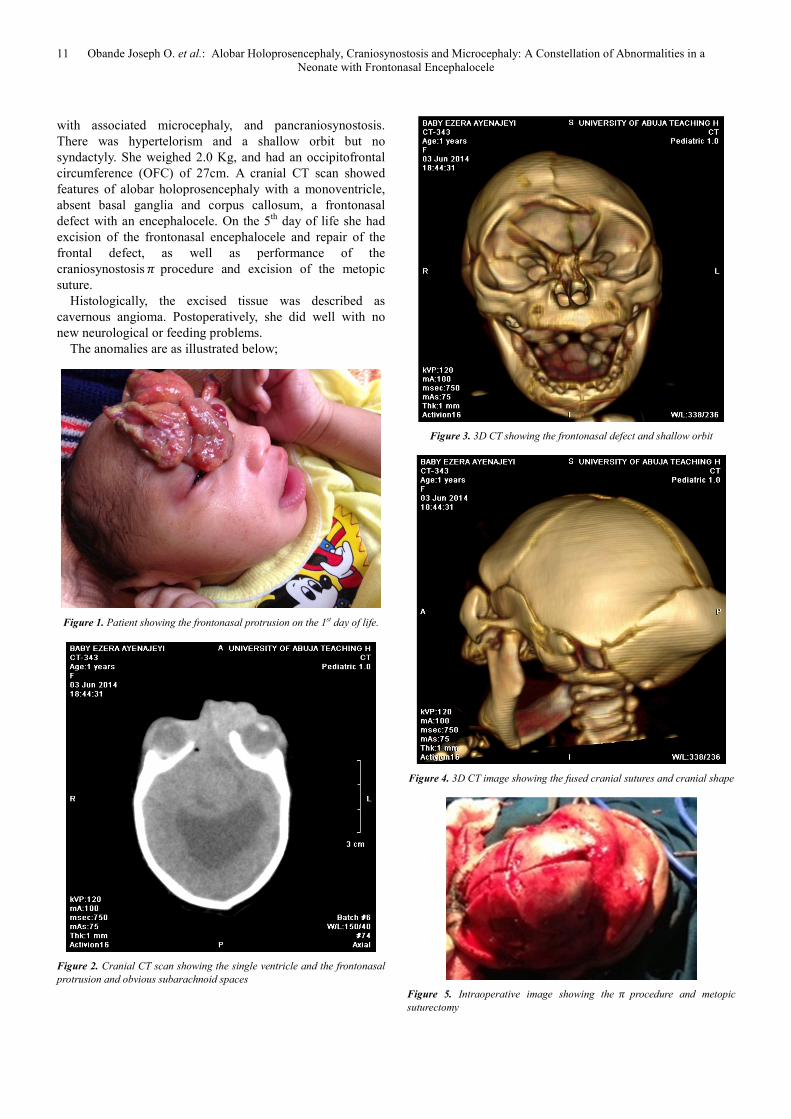
Figure 3. 3D CT showing the frontonasal defect and shallow orbit
Figure 4. 3D CT image showing the fused cranial sutures and cranial shape
Figure 5. Intraoperative image showing the � procedure and metopic
suturectomy
AASCIT Journal of Medicine 2015; 1(2): 10-13 12
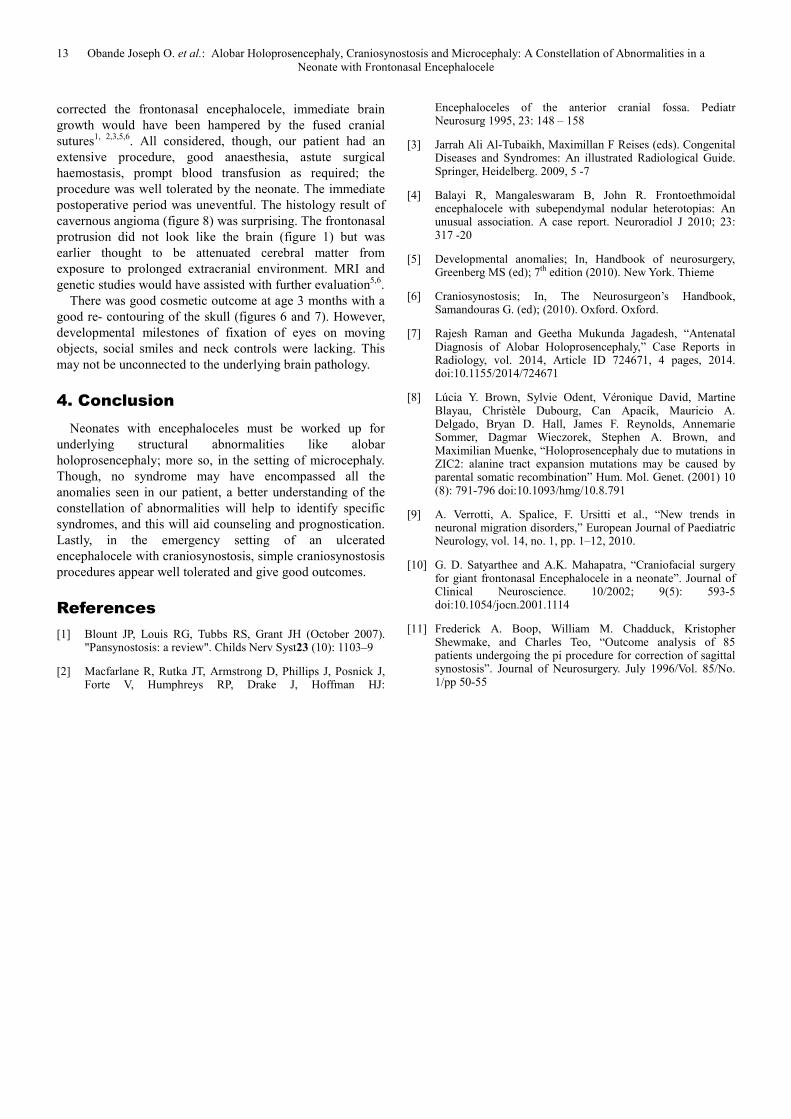
Figure 6. Postoperative image at 3 months
Figure 7. Head contour postoperative at 3 months
Figure 8. A photo-micrograph of excised frontonasal encephalocele
revealing dilated thin-walled capillaries
At 3 months of age she was yet to fixate her eyes on
objects or achieve neck support. The OFC was 32cm with
mild hypotonia of the limbs. There was a good cosmetic
outcome of the skull.
3. Discussion
Craniosynostosis is a condition in which the growth
pattern of the skull changes as a result of premature fusion of
the skull sutures1. Craniosynostosis is part of a syndrome in
15 – 40 % of patients, but it usually may occur in isolation1, 2
.
Our patient had pancraniosynostosis (figure 4) and
phenotypic syndromic facie(figure 1) i.e. hypertelorism and
shallow orbit. There was a frontonasal encephalocele with
minimal intracranial brain mantle of 12 -13 mm, suggesting
that the microcephaly maybe of the primary type, where
absence of growth of the brain renders the sutures of the
cranial vault useless. This is corroborated by the enlarged
subarachnoid spaces3(figure 2).
In alobar holoprosencephaly, both lateral ventricles and
third ventricle become confluent3. This is usually
accompanied by classical facies of cyclopia, ethmocephaly,
cebocephaly or cleft lip3.Hypotelorism is also an
accompanying feature7. Our patient though has a dysmorphic
facie, did not present with any of this classic pattern. This
may imply a less distinction towards midfacial dysplasias of
the frontonasal dysplasias. Hypertelorism is, equally, more
likely to be present in the setting of a frontonasal
encephalocele. The exact etiology of alobar
holoprosencephaly is unknown7.Environmental factors such
as maternal diabetes mellitus, alcohol use as well as use of
the teratogen – retinoic acid have been implicated, as has
been mutation of some genes like Sonic hedgehog and ZIC2
on chromosome 13q327, 8
. Our patient was a product of a
non-consanguinous marriage and the mother had none of
these risk factors. The majority of holoprosencephaly are said
to be sporadic8. Our patient’s mother had a febrile illness of
high grade fever which was treated with only paracetamol in
the 1st month of gestation and the genetic abnormalities of
holoprosencephaly occur at the 4th
week of intrauterine life7,
8. Cytomegalovirus infection in pregnancy is known to cause
holoprosencephaly7. This incidence may have been of
infective origin, given an unremarkable family history.
Genetic studies were not conducted in our patient due to
unavailability of same in our environment; there has been
known associations to trisomy 13 or 183, 9
. The cost of
conducting MRI also precluded our patient and us from its
untold benefits.
Surgery had to be conducted on an emergency basis as a
result of the ulcerated frontonasal encephalocele. The
herniating brain tissues were excised via a cranial approach10
.
The dura defect repaired with pericranium and the
frontonasal defect sealed with an autologous parietal bone
graft. The skin of the root of the nose was re-fashioned.
At the same setting, a craniosynostotic � procedure was
performed11
and metopic suturectomy done (figure 5) and the
bones were tacked in place. These were considered as having
13 Obande Joseph O. et al.: Alobar Holoprosencephaly, Craniosynostosis and Microcephaly: A Constellation of Abnormalities in a
Neonate with Frontonasal Encephalocele
corrected the frontonasal encephalocele, immediate brain
growth would have been hampered by the fused cranial
sutures1, 2,3,5,6
. All considered, though, our patient had an
extensive procedure, good anaesthesia, astute surgical
haemostasis, prompt blood transfusion as required; the
procedure was well tolerated by the neonate. The immediate
postoperative period was uneventful. The histology result of
cavernous angioma (figure 8) was surprising. The frontonasal
protrusion did not look like the brain (figure 1) but was
earlier thought to be attenuated cerebral matter from
exposure to prolonged extracranial environment. MRI and
genetic studies would have assisted with further evaluation5,6
.
There was good cosmetic outcome at age 3 months with a
good re- contouring of the skull (figures 6 and 7). However,
developmental milestones of fixation of eyes on moving
objects, social smiles and neck controls were lacking. This
may not be unconnected to the underlying brain pathology.
4. Conclusion
Neonates with encephaloceles must be worked up for
underlying structural abnormalities like alobar
holoprosencephaly; more so, in the setting of microcephaly.
Though, no syndrome may have encompassed all the
anomalies seen in our patient, a better understanding of the
constellation of abnormalities will help to identify specific
syndromes, and this will aid counseling and prognostication.
Lastly, in the emergency setting of an ulcerated
encephalocele with craniosynostosis, simple craniosynostosis
procedures appear well tolerated and give good outcomes.
References
[1] Blount JP, Louis RG, Tubbs RS, Grant JH (October 2007). "Pansynostosis: a review". Childs Nerv Syst23 (10): 1103–9
[2] Macfarlane R, Rutka JT, Armstrong D, Phillips J, Posnick J, Forte V, Humphreys RP, Drake J, Hoffman HJ:
Encephaloceles of the anterior cranial fossa. Pediatr Neurosurg 1995, 23: 148 – 158
[3] Jarrah Ali Al-Tubaikh, Maximillan F Reises (eds). Congenital Diseases and Syndromes: An illustrated Radiological Guide. Springer, Heidelberg. 2009, 5 -7
[4] Balayi R, Mangaleswaram B, John R. Frontoethmoidal encephalocele with subependymal nodular heterotopias: An unusual association. A case report. Neuroradiol J 2010; 23: 317 -20
[5] Developmental anomalies; In, Handbook of neurosurgery, Greenberg MS (ed); 7th edition (2010). New York. Thieme
[6] Craniosynostosis; In, The Neurosurgeon’s Handbook, Samandouras G. (ed); (2010). Oxford. Oxford.
[7] Rajesh Raman and Geetha Mukunda Jagadesh, “Antenatal Diagnosis of Alobar Holoprosencephaly,” Case Reports in Radiology, vol. 2014, Article ID 724671, 4 pages, 2014. doi:10.1155/2014/724671
[8] Lúcia Y. Brown, Sylvie Odent, Véronique David, Martine Blayau, Christèle Dubourg, Can Apacik, Mauricio A. Delgado, Bryan D. Hall, James F. Reynolds, Annemarie Sommer, Dagmar Wieczorek, Stephen A. Brown, and Maximilian Muenke, “Holoprosencephaly due to mutations in ZIC2: alanine tract expansion mutations may be caused by parental somatic recombination” Hum. Mol. Genet. (2001) 10 (8): 791-796 doi:10.1093/hmg/10.8.791
[9] A. Verrotti, A. Spalice, F. Ursitti et al., “New trends in neuronal migration disorders,” European Journal of Paediatric Neurology, vol. 14, no. 1, pp. 1–12, 2010.
[10] G. D. Satyarthee and A.K. Mahapatra, “Craniofacial surgery for giant frontonasal Encephalocele in a neonate”. Journal of Clinical Neuroscience. 10/2002; 9(5): 593-5 doi:10.1054/jocn.2001.1114
[11] Frederick A. Boop, William M. Chadduck, Kristopher Shewmake, and Charles Teo, “Outcome analysis of 85 patients undergoing the pi procedure for correction of sagittal synostosis”. Journal of Neurosurgery. July 1996/Vol. 85/No. 1/pp 50-55





























