Embed Size (px)
Citation preview

Clinical Research
Altered Coronal Tissue of the Human Dental Pulpin Chronic Hepatitis C Virus Infected PatientsMohammed EL-Awady Grawish, PhD,*† Rita Khounganian, PhD,* Magdy K. Hamam, PhD,*Ahmed Ragheb Zaher, PhD,† Doha Hegazy, PhD,‡ Salwa Abd El-Raof El-Negoly, PhD,§
Ghada Hassan, MSc,k and Manal Mohamed Zyada, PhD¶
Abstract
Introduction: Hepatitis C virus (HCV) infection is char-acterized by a high rate of chronicity and concerns 170million individuals worldwide. Extrahepatic manifesta-tions are frequently observed in patients with chronicviral hepatitis. Although extrahepatic manifestationsdo exist with all hepatitis viruses, they are morecommonly associated with chronic HCV infection. Thisstudy aimed to evaluate qualitatively and quantitativelythe effect of chronic HCV infection on the coronal tissueof the human dental pulp. Methods: Thirty soundimpacted teeth were obtained from healthy individualsas healthy controls. The patient group included another30 sound impacted teeth obtained from chronic HCV–in-fected patients. The coronal pulp tissues were carefullyremoved, fixed, and processed to be stained withhematoxylin-eosin, alcian blue (2.5)/periodic acid–Schiff, van Gieson, and fibronectin. Results: The tissuesections of chronic HCV patients revealed disorganizedpulp tissue, chronic inflammatory cell infiltrate, thick-ening, stenosis and occlusion of large-sized blood vesselarteriole, and collapsed venule and lymphatic system.The acidic, neutral, and mixed mucins were increased,whereas the amount of collagen was decreased, accom-panied with marked decrease in the distribution andquantity of fibronectin glycoprotein. Application ofKruskal-Wallis test showed that there were statisticallysignificant changes between the 2 groups (P # .05).Conclusions: The coronal tissue of the dental pulp,like any other body tissues, is affected by chronic HCVinfection, with an inappropriate cellularity, vasculature,and extracellular matrix proteins. The clinician should bealerted to these histologic changes and their subsequentimplications. (J Endod 2013;39:752–758)From the *Department of Oral Medicine and Diagnostic SciencFaculty of Dentistry, Mansoura University, Mansoura, Egypt; ‡Hepamouth, United Kingdom; §Department of Dental Biomaterials, FacuApplied Medical Science, King Saud University, Riyadh, Saudi Arabia
Address requests for reprints to Dr Ahmed Ragheb Zaher, Departaddress: [email protected]/$ - see front matter
Copyright ª 2013 American Association of Endodontists.http://dx.doi.org/10.1016/j.joen.2012.11.031
752 Grawish et al.
Key WordsCoronal tissue, hepatitis C virus infection, histochemical, human dental pulp, immuno-histochemical
To effectively treat endodontic infections, the clinician must recognize the cause andeffect of microbial invasion of the dental pulp and surrounding periradicular tissues
(1). Ferreira et al (2) concluded that papillomavirus and herpesviruses types 1–8,namely herpes simplex virus-1/2, varicella-zoster virus, Epstein-Barr virus, human cyto-megalovirus, human herpesvirus-6, human herpesvirus-7, and human herpesvirus-8were found in endodontic abscesses. They suggested a specific role of viruses in thepathogenesis of acute apical abscesses, but this role awaits further clarification. A puta-tive role of human cytomegalovirus and Epstein-Barr virus in the pathogenesis of symp-tomatic periapical pathosis was reported by Sabeti et al (3). These pathologic changeswere attributed to the release of tissue-destructive cytokines.
Nowadays, hepatitis C virus (HCV) infection has become a severe healthproblem worldwide. Infection with HCV may affect not only the liver but also variousnonhepatic tissues (4). A broad clinical spectrum of extrahepatic complications anddiseases associated with chronic HCV infection include mixed cryoglobulinemia,non-Hodgkin’s lymphoma, cutaneous vasculitis, glomerulonephritis, neuropathy,lymphoproliferative disorders, and porphyria cutanea tarda (5). There are 2 immu-nologic features of HCV infection that may predispose to extrahepatic disease mani-festations. The first feature is the avoidance of immune elimination by the virusleading. This feature leads to chronic infection, accumulation of circulating immunecomplexes, and autoimmune phenomena associated with chronic viral infections.The second feature is viral stimulation for the production of monoclonal rheumatoidfactors (6).
The viral proteins are believed to be among the most important factors thatcontribute to HCV-mediated pathogenesis (7). Some of the most frequent predominantand exclusive extrahepatic manifestations of HCV infection involve the oral region. HCVinfection has been related to diseases with oral manifestations such as lichen planus,Sj€ogren syndrome, or chronic lymphocytic sialadenitis (8, 9). Most of these areimmune mediated, possibly as a result of virus-dependent proliferation of monoclonalor polyclonal lymphocytes (10).
The dental pulp is a loose connective tissue located within rigid dentinal walls. Thedental pulp is infiltrated by a network of blood vessels and nerve bundles emanatingfrom the apical region (11). The cells in the dental pulp, similar to other cells in the
e, College of Dentistry, King Saud University, Riyadh, Saudi Arabia; †Department of Oral Biology,tology Research Group, Peninsula College of Medicine and Dentistry, University of Plymouth, Ply-lty of Dentistry, Mansoura University, Mansoura, Egypt; kDepartment of Oral Biology, College of; and ¶Department of Oral Pathology, Faculty of Dentistry, Mansoura University, Mansoura, Egypt.ment of Oral Biology, Faculty of Dentistry, Mansoura University, Mansoura, Egypt, PB 35516. E-mail
JOE — Volume 39, Number 6, June 2013

TABLE1.
HistologicFeatures
andtheGrading
MethodUsedinthePresentStudytoEvaluatetheSamples
Location
Stain
Feature
Grading
III
III
Centralzo
ne
ofco
ronal
pulp
tissue
H&E
Quality
Well-organized(physiological
appearance
ofthepulp
tissue)
Moderately
disorganized
Disorganized
Fibroblastsandprogenitorcells
Highly
cellular
Moderately
cellular
Less
cellular
Inflammatory
cells
Slight(a
few
scatteredinflammatory
cells)
Moderate
Seve
re(presence
ofmassesof
inflammatory
cellsin
thepulp
tissue)
Term
inalarterioles
Density
Relative
lyuniform
density
Dim
inisheddensity
Low
density
Perimeter
Eve
nthickness
Moderately
thickened
Increasedthickness
Postcapillary
venules
Density
Relative
lyuniform
density
Dim
inisheddensity
Low
density
Lymphaticcapillaries
Density
Relative
lyuniform
density
Dim
inisheddensity
Low
density
Alcianblue/PAS
Muco
substances
Faint
Moderate
Abundant
Acidmucins
Neutralmucins
Mixture
vanGieson
Collagenbundlesandfibers
Less
fibrous
Moderately
fibrous
Highly
fibrous
FNECM
FNWeakbutvisible
stainingintensity
Moderate
stainingintensity
Strongstainingintensity
Clinical Research
body, largely depend on the blood plasma and interstitial fluidssurrounding the cells to perform the various metabolic activities forthe cells to remain vital and function normally (12).The extracellular components are interesting subjects for study,because they are largely responsible for the physiological propertiesof the pulp tissue (13). The main extracellular matrix (ECM) macro-molecules of the dental pulp are collagenous proteins especially typeI and III collagen, non-collagenous proteins such as fibronectin(FN), tenascin, osteonectin, and osteocalcin and glycosaminoglycansincluding hyaluronic acid, chondroitin sulfate, heparin sulfate, andphospholipids (14).
The ECM has a wide functional significance, forming a substratethat provides adequate conditions for growth and differentiation ofthe cells (15). The ground substance, including proteoglycans andglycoproteins, is thought to play multiple roles in organizing ECMcomponents such as collagen fibrils and regulating cell functions aswell as in the transport of nutrients and metabolites through theirprotein and carbohydrate components (16). The gelated ECM mayalso act as a barrier against the spread of microorganisms and toxicproducts (17). The present study was undertaken to evaluate qualita-tively and quantitatively the effect of chronic HCV infection on thecoronal tissue of the human dental pulp by using histochemical andimmunohistochemical staining methods.
Materials and MethodsStudy Design and Patient Selection
Sixty freshly surgically extracted human impacted teeth wereobtained from the clinic at the Faculty of Dentistry, King Saud Univer-sity. Informed consents were obtained from all study participantsunder a protocol approved by the College of Dentistry ResearchCenter, King Saud University. Thirty teeth were obtained from healthyindividuals and considered as healthy controls. The patient groupcomprised another 30 teeth obtained from chronic HCV–infectedpatients.
Those patients had HCV RNA serum level (Amphcor HCVMonitor; Roche Molecular System, Basel, Switzerland) 1.4 � 106
IU/mL as an average (range, 1.0 � 106 to 1.8 � 106 IU/mL). Liverenzyme tests showed an increase of alanine aminotransferase serumlevels (average, 72 IU/L; normal value, <45 IU/L) in the last 5 yearsfor each case. From the patient records, the patients were diagnosedas HCV-positive carriers for 6–8 years, and the diagnosis was asfollows: 5 cases were minimally active chronic hepatitis, 17 caseswere moderately active chronic hepatitis, and 8 were cases withsevere chronic active hepatitis. Patients were excluded if they had de-compensated cirrhosis; other causes of liver disease, seizure disor-ders, cardiovascular disease, thyroid disease, hemophilia, poorlycontrolled diabetes, autoimmune disease, or previous organ trans-plant.
The inclusion criteria for all the participants were male gender,25–30 years of age, with impacted teeth having complete root forma-tion, no relevant other medical problems that could affect pulphistology, and not under any medications. The exclusion criteriawere presence of caries, visible structural defects, pulpal symptoms,or radiographic periapical lesions.
Staining ProtocolsThe extracted teeth were sectioned vertically through the bucco-
lingual aspect by using a chisel and hammer. The coronal pulp tissueswere removed carefully with a blunt instrument, washed with a salinesolution, and immediately immersed in 4% paraformaldehyde in 0.1mol/L phosphate buffer solution (pH 7.2). The fixation lasted for 24
JOE — Volume 39, Number 6, June 2013 Dental Pulp of HCV Patients 753

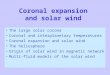
Figure 1. Photomicrograph (original magnification, �200) showing healthy human coronal tissues of the dental pulp at the central area stained with H&E (A)revealed spindle-shaped fibroblast stroma cells (F), thick-walled arteriole with muscular layer (A), thin-walled venule (V) and lymphatic (L). Heterogeneouscolloid of acidic mucins and other carboxylated or weakly sulfated acid mucosubstances (blue), basement membranes, glycogen, and neutral mucosubstances(magenta), and mixtures of neutral and acidic mucosubstances (purple) evidenced in alcian blue/PAS (B). In van Gieson (C) stained preparations, collagenstains (pink to deep red), the cytoplasm of the fibroblasts, the muscle fibers in the wall of the blood vessels, and fibrin (yellow), and the nuclei of the fibroblasts(brownish). The FN immunostain (D) revealed a rich extracellular network of FN (brown) in the ECM and around the blood vessels. The sections of chronic HCVpatients stained with H&E (E) revealed disorganized pulp tissue, chronic inflammatory cell infiltrate consisting of lymphocytes and cells that morphologically arefibroblast-like, thickening, stenosis, and occlusion of large-sized blood vessel arteriole (A), collapsed venule (V) and lymphatic system (L). The deposits of acidic,neutral, and mixed mucins increased as evidenced in alcian blue/PAS (F). The amount of collagen fibers decreased in van Gieson (G). The distribution and quantityof the ECM FN are markedly decreased in FN immunostain (H). Scale bars = 100 mm.
Clinical Research
hours, in accordance with standard protocols. The central region ofthe coronal pulp tissues was taken sagittally midway between thebuccal and lingual walls to display the mid-coronal pulp chamber.After paraffin embedding, serial sections of 4-mm thickness werecut with a Microslicer (VT1000S; Leica, Nussloch, Germany).Sections of each specimen were accordingly stained withhematoxylin-eosin (H&E) by using the conventional methods of vanGieson special stain for collagen detection, alcian blue (pH 2.5)/peri-odic acid–Schiff (PAS) histochemical stain to demonstrate the neutraland acidic mucosubstances, and FN immunostain expressing the FN
754 Grawish et al.
distribution in the ECM. The results were qualitatively and quantita-tively compared.
Immunohistochemical ProcedureThe slices were deparaffinized in xylene, rehydrated, and
washed in Tris-buffered saline (TBS). The sections were immersedin 0.3% hydrogen peroxide in TBS for 1 hour. The slides werethen incubated with monoclonal antibodies for FN (Santa CruzBiotechnology Inc, Santa Cruz, CA) for 60 minutes and rinsed
JOE — Volume 39, Number 6, June 2013

TABLE2.
StatisticalResultsforIntraexaminer
andInterexaminer
VariabilityAttributed
toSamples
ofHealthyControlsandChronicHCV
Patients
Features
Samplesofhea
lthypatients
SamplesofchronicHCVpatients
Intrae
xaminer
variab
ility
Interexaminer
variab
ility
Intraexaminer
variab
ility
Interexaminer
variab
ility
First
read
ing,
mea
n±SD
Second
read
ing,
mea
n±SD
Pvalue
First
exam
iner,
mea
n±SD
Second
exam
iner,
mea
n±SD
Pvalue
First
read
ing,
mea
n±SD
Second
read
ing,
mea
n±SD
Pvalue
First
exam
iner,
mea
n±SD
Second
exam
iner,
mea
n±SD
Pvalue
Quality
0.2
�0.4
0.1
�0.3
.542
0.2
�0.4
0.3
�0.5
.615
0.3
�0.5
0.3
�0.7
.726
0.3
�0.5
0.2
�0.4
.615
Fibroblastsand
progenitorcells
0.3
�0.4
0.4
�0.5
.648
0.3
�0.4
0.3
�0.7
.724
0.5
�0.5
0.6�
0.5
.661
0.5
�0.5
0.6�
0.5
.661
Inflammatory
cells
2.9
�1.0
2.7
�0.7
.600
2.9
�1.0
3.2
�1.1
.587
3.9
�0.9
3.0
�1.7
.101
3.9
�0.9
4.3
�0.5
.104
Term
inalarterioles,
postcapillary
venules,
lymphaticcapillaries
1.3
�0.8
1.4
�0.8
.935
1.3
�0.8
0.9
�0.7
.676
3.3
�1.3
3.5
�0.8
.681
3.3
�1.1
2.9
�1.3
.587
Muco
substances
1.7
�0.9
1.9
�0.8
.519
1.7
�0.9
1.6
�0.8
.557
3.0
�1.7
3.5
�0.9
.101
3.5
�3.7
2.7
�4.4
.293
Collagenbundlesand
fibers
0.3
�0.1
0.2
�0.1
.153
0.3
�0.1
0.3
�0.5
.716
0.8
�0.6
0.7
�0.5
.752
0.8
�0.6
0.9
�0.3
.582
ECM
FN0.7
�0.5
0.8
�0.6
.752
0.7
�0.5
0.8
�0.1
.224
0.9
�0.6
1.0
�0.8
.769
0.9
�0.7
1.1
�0.9
.676
SD,standard
deviation.
Clinical Research
JOE — Volume 39, Number 6, June 2013
with TBS for 3 minutes 3 times. The secondary biotinylated anti-body (Vector Laboratories, Burlingame, CA) was then applied tothe sections, which were incubated for 30 minutes and rinsedagain with TBS. The streptavidin-biotin-peroxidase complex wasthen applied to the slides and counterstained with Mayer hematox-ylin (18).
Statistical AnalysisTwo representative sections of each specimen for each stain were
randomly selected to be analyzed under light microscope (OlympusBX41, Tokyo, Japan). The analysis was performed individually ina blinded fashion by 2 calibrated examiners. Each examiner hadapproximately 15 years of experience in investigating the biopsy spec-imens under the light microscope in their practical laboratories. Thedensity (the number per field area) of arterioles and venules wasanalyzed on van Gieson stained slides at�200 magnification. Five fieldsfrom each slide were selected, 1 from the center and 4 at the corners(19).The arterioles were defined as vessels that had the thickest wallwith 2 layers of smooth muscle in its media. Meanwhile, the venuleshad a thinner wall and relatively larger lumen, which was filled witherythrocytes. The lymphatic capillaries had an attenuated wall linedby endothelium. The basement membrane was almost completelyabsent, and the endothelial cells were not tightly connected.
The histologic features and the gradingmethod used in the presentstudy to evaluate the samples are shown in Table 1. The data obtainedwere graded and coded to be analyzed with Kruskal-Wallis nonpara-metric test by using Statistical Package for Social Sciences (version16; SPSS Inc, Chicago, IL). Medians were considered statistically signif-icant when P < .05. In addition, statistical evaluation was performed toassess the intraexaminer and interexaminer accuracy of their submicro-scopic investigations. Specimens were read by one expert examiner.Two days later, the same examiner read all the specimens again to eval-uate the intraexaminer variability. Then the same specimens were readby the second examiner to assess the interexaminer variability. The t testwas used to analyze the hypothesis of no difference between and withinexaminers (20). Pearson correlation method (R) for multiple compar-isons was performed to assess the relationship between severity of HCVdisease and features of coronal dental pulp of chronic HCV–infectedpatients. The results were considered to be significant when the P valuewas less than .05, and R was more than �0.01.
ResultsDental Pulp Tissue Quality
The healthy specimens were pink, soft in consistency, and resil-ient, whereas those obtained from the chronic HCV–infected patientswere of low quality and were easily torn.
Histopathologic ResultsThe healthy coronal tissues of the dental pulp show homogeneity
in its blend of cells, intercellular substance, fiber elements, and vessels.The H&E staining revealed spindle-shaped fibroblast stroma cells,thick-walled arteriole with muscular layer, and thin-walled venuleand lymphatic capillaries. Heterogeneous colloid of acidic mucinsand mixtures of acidic and neutral mucosubstances were evident inthe alcian blue/PAS stained specimens. In the van Gieson sections,the collagen appeared pink to deep red in color, and the FN immuno-staining revealed a rich network of FN in the ECM of the dental pulptissue (Fig. 1).
The human coronal tissues of the dental pulp of chronic HCVpatients stained with H&E revealed disorganized pulp tissue, chronicinflammatory cell infiltrate consisting of lymphocytes and cells that
Dental Pulp of HCV Patients 755

TABLE 3. Number of Variables Attributed for Each Group, Percentage, and Their Statistical Analysis
Feature
Healthy coronal dental pulp(%)
Coronal dental pulp ofchronic HCV patients
Chi-square P valueI II III I II III
Quality 93.33 6.66 0 16.66 73.33 6.66 34.390 .000Fibroblasts and progenitor cells 6.66 90 3.33 0 10 90 43.642 .000Inflammatory cells 86.66 6.66 6.66 3.33 83.33 13.33 33.528 .000Terminal arteriolesDensity 96.66 3.33 0 6.66 40 53.33 44.748 .000Perimeter 90 6.66 3.33 10 60 30 33.984 .000
Postcapillary venulesDensity 90 3.33 6.66 13.33 50 36.66 29.530 .000
Lymphatic capillariesDensity 86.66 6.66 6.66 20 40 40 23.900 .000
MucosubstancesAcid mucins 13.33 73.33 13.33 0 33.33 66.66 18.113 .000Neutral mucins 10 76.66 13.33 3.33 43.33 53.33 10.344 .001Mixture 20 73.33 6.66 6.66 26.66 66.66 17.432 .000
Collagen bundles and fibers 0 86.66 13.33 60 40 0 26.282 .000ECM FN 6.66 16.66 76.66 46.66 40 13.33 8.949 .003
Clinical Research
morphologically resemble fibroblasts, thickening, stenosis, and occlu-sion of large-sized blood vessel arterioles, and collapsed venules andlymphatic system. The deposits of acidic, neutral, and mixed mucinswere obviously increased in alcian blue/PAS histochemical stainedsections. The nuclei of the lymphocytes and the fibroblast-like cellsstained brownish, whereas the scanty amount of collagen fibers stainedpink to deep red in the van Gieson special stained specimens. The distri-bution and quantity of FN in the ECM were markedly decreased in FNimmunostaining (Fig. 1).
Statistical ResultsThere were no statistically significant differences between the in-
traexaminer or interexaminer readings regarding the histologic featuresthat were measured (Table 2). Variables, grades, and the statisticalanalysis for healthy coronal tissues of the dental pulp versus those ofchronic HCV patients are shown in Table 3. In the healthy controls,most of the grades were I or II, whereas those of the other groupwere deviated to grade II or III. Application of Kruskal-Wallis testshowed that there were statistically significant differences in the qualityof the pulp tissues, fibroblast and inflammatory cell numbers, density ofarterioles, venules, and lymphatics, the thickness of the arterioles,quantity of acid, neutral, and mixed mucosubstances, amount ofcollagen, and FN distribution. The correlation between severity ofHCV disease and features of coronal dental pulp of chronic HCV–in-fected patients is summarized in Table 4. A highly significant correlationwas found between the 3 types of hepatitis depending on their severityand both quality and density of postcapillary venules and lymphaticcapillaries of coronal dental pulp (r = 0.853, P = .000; r = 0.560,P = .001; and r = 0.575, P = .001, respectively). Moreover, a tendencytoward an inverse correlation between FN reactivity in coronal dentalpulp and severity of HCV disease was observed. Statistically, there wasa significant correlation between FN reactivity and severity disease(r=�0.513, P= .004). However, no associations were noted betweenseverity of HCV disease and other features of coronal dental pulp ofchronic HCV–infected patients.
DiscussionThe dental pulp is a unique tissue, and its importance in the long-
term prognosis of the tooth is often ignored by clinicians. Whilepursuing technical excellence in endodontics, it is important that clini-
756 Grawish et al.
cians also have an awareness and understanding of the physiologicaland pathologic features of the dental pulp as well as the biologicalconsequences of treatment interventions (17). Although some peopleinfected with hepatitis C spontaneously clear the virus, up to 85% ofthose exposed develop chronic hepatitis (21). Hepatitis C consists of6 genotypes. Response rates to treatment by pegylated interferon andribavirin combination are about 88% for genotype 2 and 3 and about48% for genotypes 1, 4, 5, and 6 (22).
The large number of treatment failures is attributed to factorsrelated to both the virus and the host response that induce antiviral stateby secreting cytokines and accruing immune cells in the microenviron-ments (23). Although extrahepatic manifestations do exist with all hepa-titis viruses, they are more commonly associated with chronic HCVinfection. The joints, muscle, and skin are the main locations of clinicalmanifestations in HCV-infected patients, whereas the presence of mixedcryoglobulins, antinuclear antibodies, and anti–smooth muscle anti-bodies are the most frequent immunologic abnormalities (24).
In a previous case report study (25), it was concluded that cryo-globulinemia associated with uncontrolled HCV infection in patientsendangers the dental pulp vasculature and alters its normal tissue archi-tecture. In the present study, the authors decided to demonstrate theeffect of chronic HCV infection on the coronal tissue of the dentalpulp qualitatively and quantitatively in a well-designed controlled studywithout randomization. The results of the present study demonstratedhomogeneity in the healthy coronal tissues of the dental pulp regardingits blend of cells, intercellular substance, fiber elements, and vessels.This is in compliance with Kim et al (26), who reported that the dentalpulp is a specialized loose connective tissue containing cells, fibers,ground substance, blood vessels, and nerve endings.
The histologic results related to the tissue sections of chronic HCVpatients in the present study might be attributed to the cryoglobulinsprecipitated inside the blood vessel walls of the arterial circulationthat keep them less permeable and might impair local blood flow tothe dental pulp tissue, which results in lack of oxygen and nutrient trans-portation. This ultimately leads to permanent tissue hypoxia and celldeath with the decrease in their synthetic ability. Also, occlusion ofthe venous circulation leads to blood stasis, which can cause numerousproblems in the form of an increase in the inflammatory cells with anincrease in the interstitial fluid.
Also, another possible reason for these alterations is the appear-ance of diabetes type 2, which is associated with high insulin
JOE — Volume 39, Number 6, June 2013

TABLE4.
SeverityofHepatitisCVirus(HCV)DiseaseandRelationshipbetweenThatSeverityandFeatureofCoronalDentalPulpofChronicHCV–infected
Patients
Feature/grading
(I,II,III)
No.ofcases
Typeofhep
atitis
Pea
rson
correlation(R)
Pvalue
Minim
ally
active
hep
atitis
Moderatelyactive
hep
atitis
Severelyactive
hep
atitis
Quality
5(16.7%
),21(70%
),4(13.3%
)5(100%
),0(0%),0(0%
)0(0%),17(80.99%
),0(0%)
0(0%),4(19.01%),4(100%)
0.853
.000
Fibroblastsand
progenitorcells
0(0%),3(10%
),27(90%
)0(0%),2(66.7%),3(11.1%
)0(0%),1(33.3%
),16(59.2%
)0(0%),0(0%),8(29.7%
)0.393
.032
Inflammatory
cells
1(3.3%
),25(83.3%
),4(13.4%
)1(100%
),3(12%
),1(25%
)0(0%),16(64%
),1(25%
)0(0%),6(24%
),2(50%
)0.220
.243
Term
inalarterioles
Density
2(6.7%
),12(40%
),16(53.3%
)2(100%
),3(25%
),0(0%)
0(0%),4(33.3%
),13(81.2%
)0(0%),5(41.3%
),3(18.6%
)0.298
.109
Perimeter
3(10%
),18(60%
),9(40%
)3(100%
),2(11.1%
),0(0%)
0(0%),10(55.6%
),7(77.8%
)0(0%),6(33.3%
),2(22.2%
)0.117
.538
Postcapillary
venules
Density
4(13.4%
),15(50%
),11(36.6%
)3(75%
),2(13.3%
),0(0%
)1(25%
),10(66.7%
),6(54.6%
)0(0%),3(20%
),5(45.4%
)0.560
.001
Lymphaticcapillaries
Density
6(20%
),12(40%
),12(40%
)4(66.7%
),1(8.3%),0(0%)
2(33.3%
),8(66.7%
),7(58.3%
)0(0%),3(25%
),5(41.7%
)0.575
.001
Muco
substances
Acidmucins
0(0%),10(33.3%
),20(66.7%
)0(0%),5(50%
),0(0%)
0(0%),4(40%
),13(65%
)0(0%),1(10%
),7(35%
)0.543
.002
Neutralmucins
1(1.3%
),13(43.3%
),16(53.3%
)1(100%
),2(15.4%
),2(12.5%
)0(0%),9(69.2%
),8(50%
)0(0%),2(15.4%
),6(37.5%
)0.319
.086
Mixture
2(6.7%
),8(26.7%
),20(66.6%
)2(100%
),2(25%
),1(5%)
0(0%),5(62.5%
),12(60%
)0(0%),1(12.5%
),7(35%
)0.161
.395
Collagenbundles
andfibers
18(60%
),12(40%
),0(0%)
2(11.1%
),3(25%
),0(0%
)10(55.6%
),7(58.3%
),0(0%)
6(33.3%
),2(16.7%
),0(0%)
0.230
.221
ECM
FN14(46.7%
),12(40%
),4(13.3%
)0(0%),2(16.7%
),3(75%
)9(64.4%
),7(58.3%
),1(25%
)5(36.6%
),3(25%
),0(0%
)0.513
.004
Total
30(100%
)5(16.7%
)17(56.7%
)8(26.6)
Clinical Research
JOE — Volume 39, Number 6, June 2013
resistance and was considered a part of a complex virus-induced dys-metabolic syndrome including both hepatic (steatosis) and extrahe-patic manifestations (27). High levels of proinflammatory cytokineshave been found in HCV-infected patients; therefore, they could beinvolved in the pathogenesis of insulin resistance associated withHCV infection (28).
Radkowski et al (29) suggested that HCV may infect B cells oraffect B-cell functions in natural infection. Negative-strand HCV RNAhas been detected by reverse transcriptase polymerase chain reactionin the peripheral lymphocytes, bone marrow, lymph nodes, and centralnervous system of some HCV-infected patients. The endotoxemia seemsto be multifactorial, likely depending on impaired phagocytic functionsand reduced T-cell mediated antibacterial activity (30). The presentstudy clarified that there is an alteration of the coronal tissue of thedental pulp in chronically HCV-infected patients. Demonstration ofleveling of pulpal HCV and determining the actual cause for these pulpalchanges need further research.
ConclusionLike any other tissue in the body, the coronal tissues of the dental
pulp are affected by chronic HCV infection. There is a decrease in thenumber of fibroblasts and an increase in the number of inflammatorycells. There is an increase in the amount of mucosubstances, with thedecrease in the amount of collagen fibers and FN glycoprotein. Theclinician should be alerted to these histologic changes and their subse-quent implications.
AcknowledgmentsThe authors deny any conflicts of interest related to this study.
References1. Rosaline H, Satish ES, Kandaswamy D. Detection of presence or absence of herpes
simplex virus, Epstein Barr virus and human cytomegalovirus in infected pulp usinga polymerase chain reaction. Aust Endod J 2009;35:9–12.
2. Ferreira DC, Paiva SS, Carmo FL, et al. Identification of herpesviruses types 1 to 8and human papillomavirus in acute apical abscesses. J Endod 2011;37:10–6.
3. Sabeti M, Kermani V, Sabeti S, Simon JH. Significance of human cytomegalovirus andEpstein-Barr virus in inducing cytokine expression in periapical lesions. J Endod2012;38:47–50.
4. Hadziyannis SJ. The spectrum of extrahepatic manifestations in hepatitis C virusinfection. J Viral Hepat 1997;4:9–28.
5. Blackard JT, Kemmer N, Sherman KE. Extrahepatic replication of HCV: insights intoclinical manifestations and biological consequences. Hepatology 2006;44:15–22.
6. Agnello V, De Rosa FG. Extrahepatic disease manifestations of HCV infection: somecurrent issues. J Hepatol 2004;40:341–52.
7. Li B, Li X, Li Y, et al. The effects of hepatitis C virus non-structural protein 3 on cellgrowth mediated by extracellular signal-related kinase cascades in human hepato-cytes in vitro. Int J Mol Med 2010;26:273–9.
8. Aceti A, Taliani G, Sorice M, Amendolea MA. HCV and Sj€ogren’s syndrome. Lancet1992;339:1425–6.
9. Imhof M, Popal H, Lee JH, et al. Prevalence of hepatitis C virus antibodies and eval-uation of hepatitis C virus genotypes in patients with lichen planus. Dermatology1997;195:1–5.
10. Bonkovsky HL, Mehta S. Hepatitis C: a review and update. J Am Acad Dermatol 2001;44:159–82.
11. Nakashima M, Akamine A. The application of tissue engineering to regeneration ofpulp and dentin in endodontics. J Endod 2005;31:711–8.
12. Heyeraas KJ, Berggreen E. Interstitial fluid pressure in normal and inflamed pulp.Crit Rev Oral Biol Med 1999;10:328–36.
13. Linde A. The extracellular matrix of the dental pulp and dentin. J Dent Res 1985;64:523–9.
14. Zago M, Teti G, Mazzotti G, et al. Expression of procollagen alpha1 type I and tenas-cin proteins induced by HEMA in human pulp fibroblasts. Toxicol In Vitro 2008;22:1153–9.
15. Martinez EF, Machado de Souza SO, Corr̂ea L, Cavalcanti de Ara�ujo V. Immunohis-tochemical localization of tenascin, fibronectin, and type III collagen in humandental pulp. J Endod 2000;26:708–11.
Dental Pulp of HCV Patients 757

Clinical Research
16. Yamauchi S, Cheng H, Neame P, et al. Identification, partial characterization, anddistribution of versican and link protein in bovine dental pulp. J Dent Res 1997;76:1730–6.
17. Yu C, Abbott PV. An overview of the dental pulp: its functions and responses toinjury. Aust Dent J 2007;52:S4–16.
18. Fernandes AM, Silva GA, Lopes N Jr, et al. Direct capping of human pulps witha dentin bonding system and calcium hydroxide: an immunohistochemicalanalysis. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2008;105:385–90.
19. Jiang CY, Gui C, He AN, et al. Optimal time for mesenchymal stem cell transplantationin rats with myocardial infarction. J Zhejiang Univ Sci B 2008;9:630–7.
20. Palioto DB, Sato S, Ritman G, et al. Computer assisted image analysis methods forevaluation of periodontal wound healing. Braz Dent J 2001;12:167–72.
21. Leblebicioglu H, Bayirli D, Esen S, et al. Treatment of acute hepatitis C virus infectionwith interferon-alpha 2b and ribavirin: case report and review of the literature. AnnClin Microbiol Antimicrob 2002;14:1–3.
22. Poynard T, Yuen MF, Ratziu V, Lai CL. Viral hepatitis C. Lancet 2003;362:2095–100.23. Dammacco F, Tucci FA, Lauletta G, et al. Pegylated interferon-alpha, ribavirin, and
rituximab combined therapy of hepatitis C virus-related mixed cryoglobulinemia:a long-term study. Blood 2010;116:343–53.
758 Grawish et al.
24. Cacoub P, Poynard T, Ghillani P, et al. Extrahepatic manifestations of chronic hepa-titis C: MULTIVIRC Group. Multidepartment Virus C. Arthritis Rheum 1999;42:2204–12.
25. Grawish Mel-A, Zaher AR, Elsabaa HM, Hegazy D. Vasculitis of dental pulp associatedwith cryoglobulinemia in hepatitis C virus patients: case report. J Endod 2011;37:1593–5.
26. Kim S, Liu M, Simchon S, Dorscher-Kim JE. Effects of selected inflammatory medi-ators on blood flow and vascular permeability in the dental pulp. Proc Finn Dent Soc1992;88:387–92.
27. Crax�ı A, Laffi G, Zignego AL. Hepatitis C virus (HCV) infection: a systemic disease.Mol Aspects Med 2008;29:85–95.
28. Elsammak M, Refai W, Elsawaf A, et al. Elevated serum tumor necrosis alpha andferritin may contribute to the insulin resistance found in HCV positive Egyptianpatients. Curr Med Res Opin 2005;21:527–34.
29. Radkowski M, Wilkinson J, Nowicki M, et al. Search for hepatitis C virus negative-strand RNA sequences and analysis of viral sequences in the central nervous system:evidence of replication. J Virol 2002;76:600–8.
30. Caradonna L, Mastronardi ML, Magrone T, et al. Biological and clinical significanceof endotoxemia in the course of hepatitis C virus infection. Curr Pharm Des 2002;8:995–1005.
JOE — Volume 39, Number 6, June 2013
![MSK CT PROTOCOL[2] - jefferson.edu · AC joint. SHOULDER Coronal Imaging Plane Coronal Imaging Plane •Prescribe coronal plane off of axial images parallel to supraspinatus muscle](https://img.pdfslide.net/doc/110x75/5d645f8588c9930e728b6075/msk-ct-protocol2-ac-joint-shoulder-coronal-imaging-plane-coronal-imaging.jpg)