Embed Size (px)
Citation preview

Anatomy of the medial orbit and various approaches to access it
Osamu Akiyama, MD1,2; Akihide Kondo, MD1; Hajime Arai, MD1; Albert L. Rhoton, Jr., MD2†
1Juntendo university, Department of Neurosurgery, Japan2Department of Neurological Surgery, University of Florida
Osamu Akiyama MD, PhD.Juntendo University, Department of NeurosurgeryEmail:[email protected]
Contact1. Düz, B., Secer, H. I., & Gonul, E. (2009). Endoscopic approaches to the orbit: a cadaveric study. min-Minimally Invasive Neurosurgery, 52(03),
107-113.2. Wu, W., Selva, D., Jiang, F., Jing, W., Tu, Y., Chen, B., ... & Qu, J. (2013). Endoscopic transethmoidal approach with or without medial rectus
detachment for orbital apical cavernous hemangiomas. American journal of ophthalmology, 156(3), 593-599.3. Gönül, E., Erdogan, E., Düz, B., & Timurkaynak, E. (2003). Transmaxillary approach to the orbit: an anatomic study. Neurosurgery, 53(4), 935-
942.4. Moe, K. S. (2003). The precaruncular approach to the medial orbit. Archives of facial plastic surgery, 5(6), 483-487.5. Rhoton Jr, A. L. (2003) Cranial anatomy and surgical approaches. Neurosurgery, 53(2)331-362.6. Natori, Y., & Rhoton Jr, A. L. (1994). Transcranial approach to the orbit: microsurgical anatomy. Journal of neurosurgery, 81(1), 78-86.
References
The medial orbit can be the site of several pathological lesions such as cavernomas, neurinomas, and lymphomas. However, approaching the medial orbit remains a challenging task because of the narrow surgical corridors, surrounding critical neural structures, and complicated vascular relationships.
BackgroundThe surgical approaches to the medial orbit can be classified into three categories: (1) transcranial approach, (2) trans-sinus approaches: transethmoidal and transmaxillary approaches, and (3) transorbital approaches: precaruncular and medial orbital approaches. The transcranial approach exposes the superior and medial surfaces of the orbit and the optic apex widely. The trans-sinus approach exposes the medial and inferior surfaces of the orbit and optic nerve. The transorbital approach exposes the anterior and medial surfaces of the orbit, but the surgical corridor to the optic canal and apex in this approach is relatively narrower and deeper compared to that in the previous two approaches.
Ten adult cadaveric specimens were examined using magnifications ranging from 3X to 40X after perfusion of the arteries and veins with colored silicone. The microsurgical anatomy of the medial orbit and surgical approaches to it were examined. All approaches were performed using 0° rigid endoscopes or the surgical microscope.
Methods and Materials
The knowledge of the microsurgical anatomy of the medial orbit and surrounding critical structures and the selection of an appropriate surgical approach will make surgical procedures safe and precise.
Conclusions
ObjectiveTo examine the microsurgical anatomy of the medial orbit and compare the various surgical approaches1-6 to access it.
Results
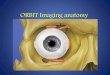
Microsurgical anatomy of the medial orbit
Transcranial approach
Trans-sinus approach
Illustrative case –Orbitofrontal approach-A Illustrative Case. A 37-year-old woman presented with right exophthalmos. The orbitofrontal approach was performed. The pathological finding was schwannoma.
A: Oblique anterior view B: Anterior view of the combined medial orbital and maxillary exposures. C: Inferior view of the anterior and middle cranial base. D: Enlarged inferior view of the orbit. E: Anterior view. F: Enlarged lateral view of the orbit. G: Medial view of the orbit.
Illustrative case –Medial approach-7-year-old girl presented with exophthalmos. MR imaging demonstrated aanteromedial tumor of the orbit. The medial approach was performed. The pathological finding was a lymphangioma.
Transmaxillary approach
A: Anterior view. B: Medial view. C: Anterior view D: Inferior view.
Transorbital approachOrbitofrontal approach Medial approach Precaruncular approach
V2
CN I
Front. Sinus
Eth. Sinus
Ant. Eth. A.
Sphen. Sinus
Sup. Troch. N.
Supraorb. N.
Lac. Gland Lev. M.
Sup. Rec. M.
Front. N. CN IILac. N.
Post. Eth. A.
Trochlea
Sup. Obl. M.
Infra. Temp. Fossa
Sup. Rec. M.(Reflected)
Lev. M. Reflected) V1
Ophth. A. Nasocil. N.
Car. A.
Bifrontal approach
Sphen.Sinus
Car. A.
Max. A.
Med. Obl. M.
Temp. M.
Inf. Rec. M.
Inf. Orb. N. & A.
Pterygopal. A.
CN I
Clivus
Max. Sinus
CN II
Inf. Rec. M.
Lat. Rec. M.
CN IV
CN III to Inf. Rec. M.
Med. Rec. M.
Sphen. Sinus
Car. A.Pit.
Gland
Ophth. A.
Chiasm
Sup. Hyp. A.
V2Infraorb. N. & A.
Max. A.
Pterygopal. A.Zygo. N.
Ophth. V.
CN II
CN III Sup. Div.
to Lev. M.
CN III Inf. Div. to Inf. Obl. M.
Sup. Rec. M.
Front. N.
V 1
V 2
CN III
Cil. Gang.
Ophth. A
CN III Sup. Div.To Sup. Rec. M.
Periorbita(reflected)
Inf. Obl. M.
Short Cil. N.
Long. Cil. N.
Nasocil. N.
CN III Motor Root
Inf. Rec. M.CN III Inf. Div. to Inf. Rec. M.
CN III Inf. Div.
Med. Rec. M.
Inf. Obl. M.
Lat. Rec. M.
CN III Inf. Div.To Inf. Obl. M.
Inf. Ophth. V.
Short. Cil. N.
Cent. Ret. A.
Nasolac. Duct
Eth. Sinus
Nasal Septum
Ant. Eth. A.
Med. Canth. Lig.
Inf. Concha
Max. Sinus
Mid. Concha
Sup. Concha
Nasal Septum Max. Sinus
Font. Sinus Eth.
Sinus
Zygoma
Nasolac. Duct
Nasal Cavity
Oral Cavity
Inf. Orb. N.
Short. Cil. N.
Inf. Orb. N. & A.
Lat. Rec. M.
Nasal Cavity
Med. Rec. M.
Inf. Rec. M.
Inf. Orb. N. & A. Max. A.
Cav. Sinus v
Müllers’s M.
V2
OpticCanal
Inf. Rec. M.
Lat. Rec. M.
Med. Rec. M.
Sup. obl. M.
Sup. Ophth. V.
Ophth. A.
Max. A.
Orbit FloorInf. Orb. N. Nasal
Cavity
Max. Sinus
Nasal Septum
Cav. Sinus
Car. A.
Optic Canal
Eth. Sinus
Max. A.
CN II
Med. Rec. M.
Inf. Rec. M.
Sup. Rec. M.
Ophth. A
CN IIPit. Gland
Sphen. Sinus
Inf. Rec. M.
CN III Sup. Div.to Lev. M.
Pterygopal. A.
Max. A.
Inf. Orb. N. & A.
V2
Cav. Sinus
Front. Sinus
Sup. Opthal. V.
Trochlea
Lev. M. Lac. Gland
Ant. Eth. A.
Sup. Troch. N.
Supraorb. N.
Sup. Obl. M.
Front. N.
Lac. N. & A.
Optic. Canal
Lat. Rec. M.
Eth. Sinus
Sphen. Sinus
Post. Eth. A.
Long Cil. N.
Ophth. A.
Ant. Eth. N. & A.
Front. N.(reflected)
Lat. Rec. M.
Nasocil. N.
Sup. Rec. M.(Reflected)
CN VI
ShortCil. N.
Med. Rec. M.
Sphen. Sinus
Front. N.
Periorbita
Eth. Sinus
Front. LobeCN II
Front. Lobe
Orbit
Temp. M.Front. Sinus
Front. Bone
Transethmoidal approach
Front. Bone
Orbit Orbit
Nasal BoneTemp. M.
Orbit
Front. Lobe
Ant. Eth. Sinus
Post. Eth. Sinus
Nasal Cavity
Nasal Septum
Ant. Eth. A.Optic Canal
Post. Eth. A.
Periorbita
Med. Canth. Lig.
Med. Canth.
Lig.
Med. Rec. M.
Ant. Eth. A.
Periorbita CN II
Ophth. A
Inf. Obl. M.
Inf. Rec. M.
Sup. Ophth. V.
Periorbita
Med. Wall
Caruncle
Caruncle
Med. Canth.
Lig.
Preoperative MRI (T1 High Resolution Isotropic Volume Excitation: THRIVE) Postoperative MRI (THRIVE)
Periorbita
Tumor
Tumor
Orb. Oculi M.
Tumor
Preoperative MRI (T1WI) Postoperative MRI (T1WI)
Tumor
Sup. Orb. N.
Sup. Rec. M.
Intraoperative photograph
Intraoperative photograph
Globe
Globe
Medial Lateral Medial Lateral