Embed Size (px)
DESCRIPTION
Discussion about superficial venous aneurysms.
Citation preview
1
Aneurysms of the GSV, SSV, & AAGSV
Ron Bush, MD, FACS
2
Saphenous vein aneurysms were once thought to be rare. However, with the increased use of
ultrasound, more aneurysms are being found in those patients presenting for evaluation of venous
disease. Pascaralli et al., found 65 superficial aneurysms (43 patients), out of 366 evaluated over a
24-month period. This represents an incidence of 12%.
The classification in this study is as follows:
Type I - Located in the proximal third of the SFJ, not at the junction, but instead just distal to the sub-
terminal valve (52% of their series).
Type II – Located in the shaft of the saphenous vein in the distal thigh. In our experience, this is just
distal to the valve in the lower third of the thigh. (Region anatomically corresponding to Hunter’s
Canal)
Type III – Are the simultaneous occurrence of Type I and Type II.
Type IV – Involves the SSV, 6% both in Pascaralli and Gillespie series.
In the following discussion, I will demonstrate why the above classification system is
erroneous, revisions needed, and appropriate treatment criteria developed.
Very little has been written on the topic of venous aneurysms, excluding the popliteal vein.
Below is an abstract recently submitted detailing my experience and documenting those patients
seen in a two-year period.
3
Abstract:
Title: Diagnosis and Treatment of Saphenous Vein AneurysmsBACKGROUND:Superficial venous aneurysms of the greater saphenous vein (GSV), small saphenous vein (SSV), have been documented and classified as to anatomic presentation. This study documents aneurysms of the anterior accessory greater saphenous vein (AAGSV), posterior medial thigh circumflex branch, as well as variations of GSV aneurysms. Reclassification of saphenous aneurysms is proposed, as well as treatment protocols.METHODS:In a 2-year period, records of patients (330), presenting at our center for evaluation and treatment of symptomatic venous disease were examined. Aneurysm criteria included both dilatation of 2 times the size of the contiguous vein and 3 times the size of normal vein diameter. All aneurysms were documented as to location, size, and clinical presentation. Histological evaluation of resected specimens was performed.RESULTS:A total of 18 patients met the criteria for aneurysm, 4 males and 14 females. The mean age was 44, with a range from 16 to 75. Aneurysm location was GSV (9), AAGSV (6), SSV (2), and posterior medial thigh circumflex branch (1). Treatment was determined according to location, aneurysmal neck size, and presence of collateral inflow. Modalities of treatment included foam sclerotherapy, surgical procedures, and thermal ablation either done alone or in combination. Aneurysm size is related to the degree of internal elastic membrane disruption.CONCLUSION:Reclassification of aneurysms should include standardized size criteria and should include AAGSV pathology and GSV aneurysm classification as to terminal and sub-terminal valve involvement. Aneurysms of the AAGSV commonly present as acute thrombosis. Aneurysms involving the terminal valve, SSV aneurysms, and AAGSV aneurysms, with a communication >4mm at the saphenofemoral junction (SFJ) should be ligated to decrease the possibility of clot embolization. Histological evaluation of aneurysms reveal smooth muscle hypertrophy and disruption of the internal elastic membrane.
Reclassification is necessary:
Type I aneurysms (GSV) should be divided as follows:
Ia - Distal to terminal valve (involves branches at junction)
Ib - Distal to subterminal valve (Junction is of normal size or slightly dilated)
II. Involves only distal GSV (thigh or below knee)
III. Combination of Ia or Ib and II
IV. SSV aneurysm
IVa – involves SPJ
4
IVb – Involves distal SSV
V AAGSV
Va – Involves proximal AAGSV
Vb – Involves mid AAGSV
The etiology of aneurysms is usually in association with venous reflux and resultant superficial
venous hypertension. Since aneurysms are usually distal to a valve, turbulent flow just distal to the
valve has been postulated as a causative effect.
The presentation of these aneurysms may be incidental, masses, (as in hernia presentation),
thrombosis, or pulmonary embolism.
5
The image below demonstrates a Type Ia aneurysm. Notice the branches empty into the aneurysm.
This aneurysm should be surgically resected to prevent thrombosis at the junction and possible
pulmonary embolization.
6
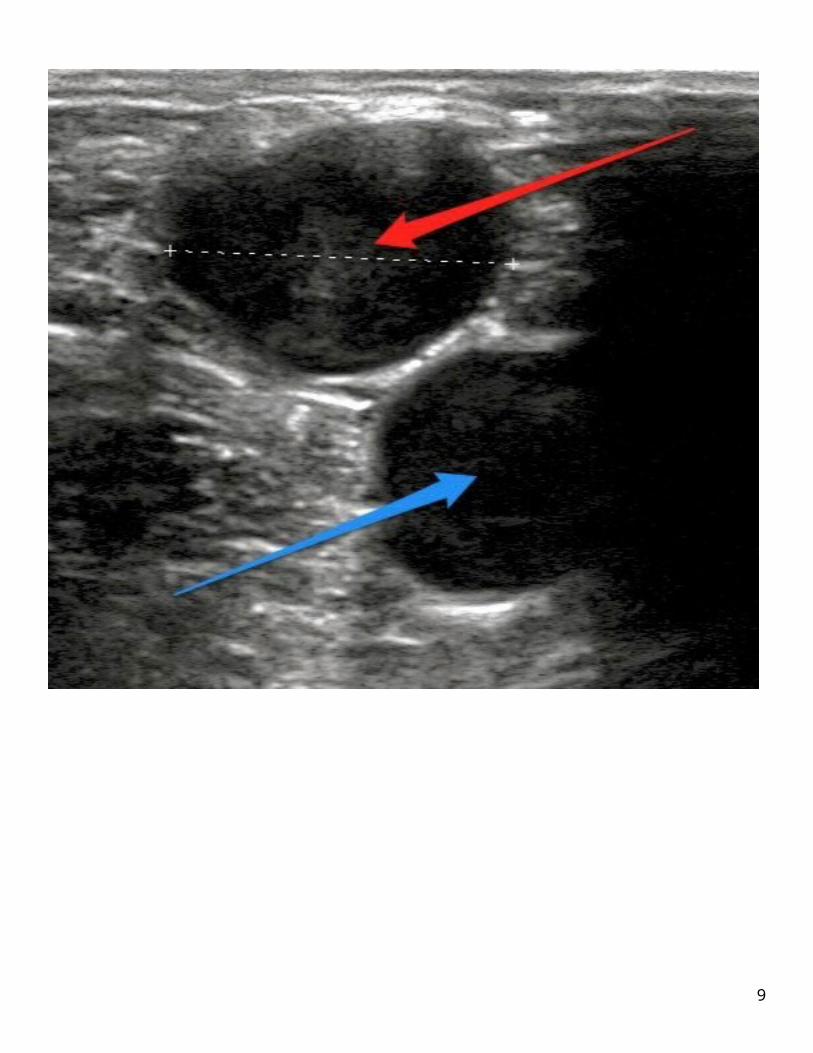
The red arrow points to the terminal valve.
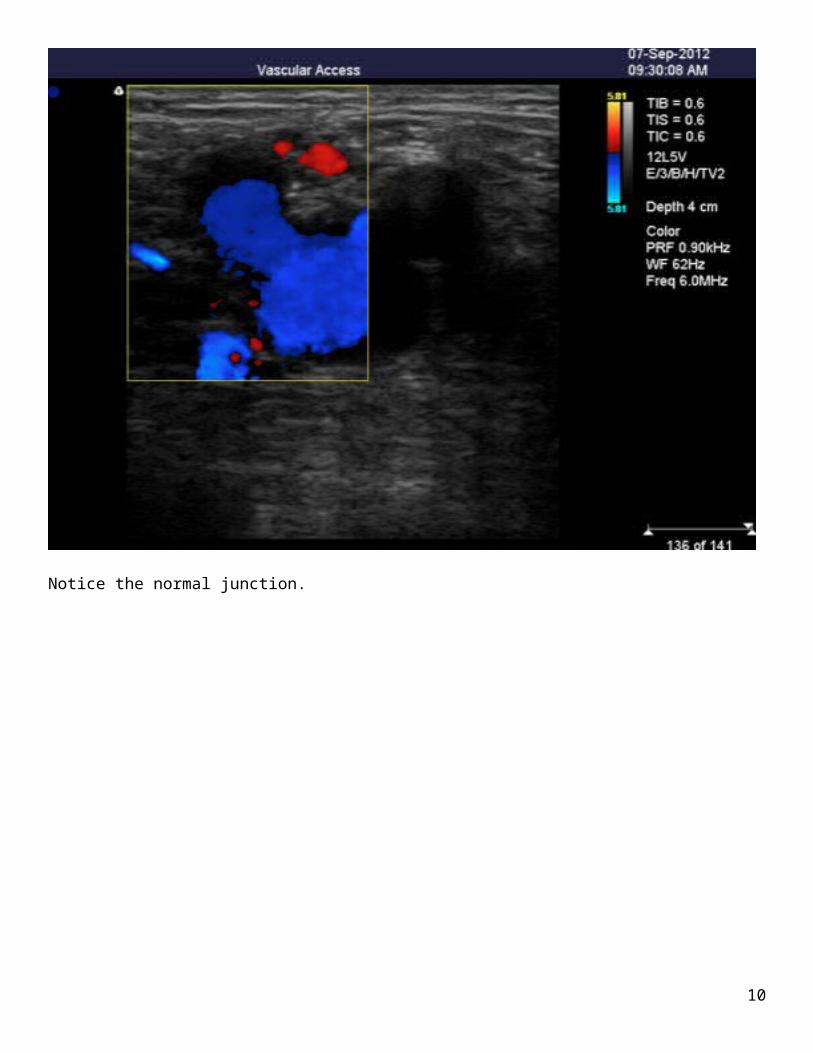
The following ultrasound (US) images demonstrate Type Ib aneurysm. As you will see, the junction is uninvolved. The branches empty into a normal sized SFJ.
7

Notice the normal junction.
8
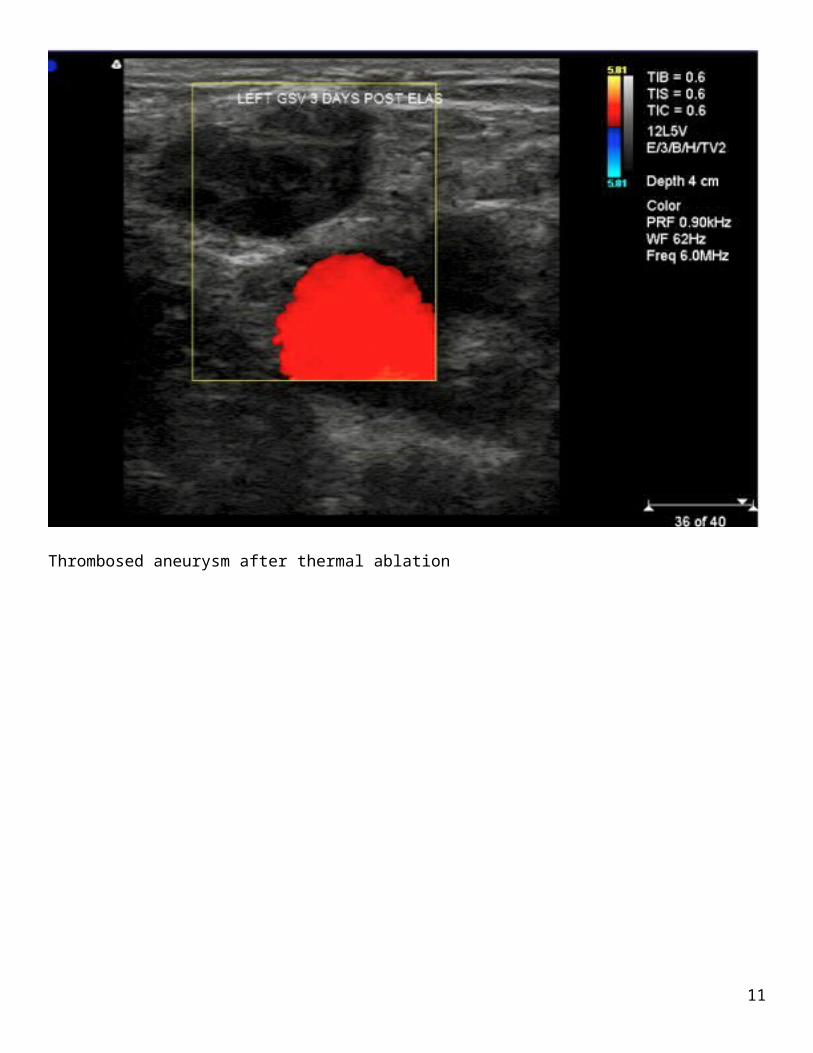
Thrombosed aneurysm after thermal ablation
9
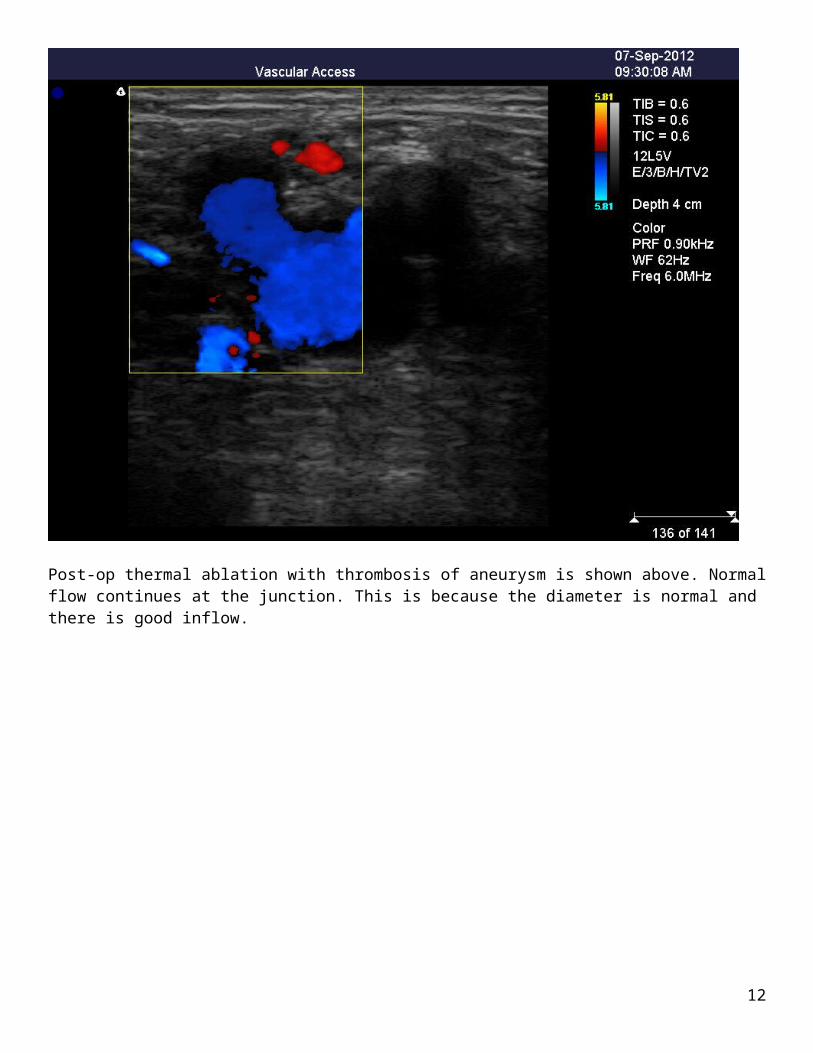
Post-op thermal ablation with thrombosis of aneurysm is shown above. Normal flow continues at the junction. This is because the diameter is normal and there is good inflow.
10
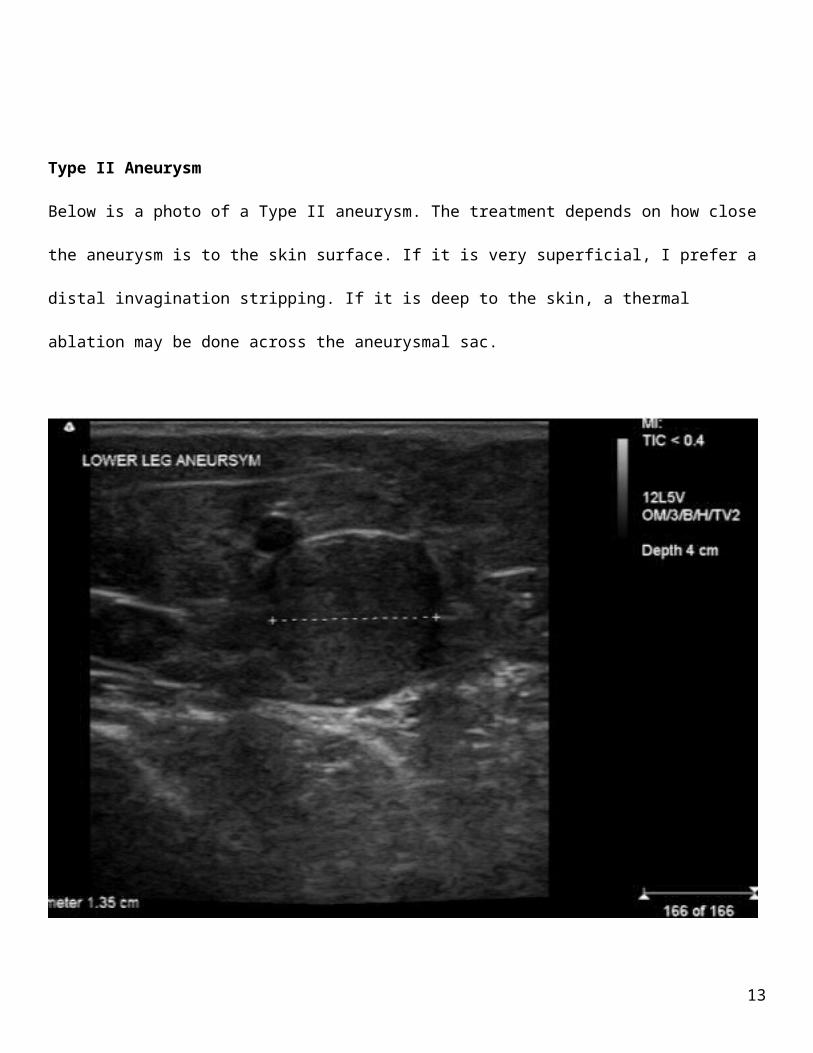
Type II Aneurysm
Below is a photo of a Type II aneurysm. The treatment depends on how close the aneurysm is to the
skin surface. If it is very superficial, I prefer a distal invagination stripping. If it is deep to the skin, a
thermal ablation may be done across the aneurysmal sac.
11
Type III Aneurysm
Treatment depends on the presentation at each site as described above.
Type IV Aneurysm
Type IVa involves the SP junction. All of these aneurysms must be resected. These should be
considered equivalent to popliteal aneurysms.
12
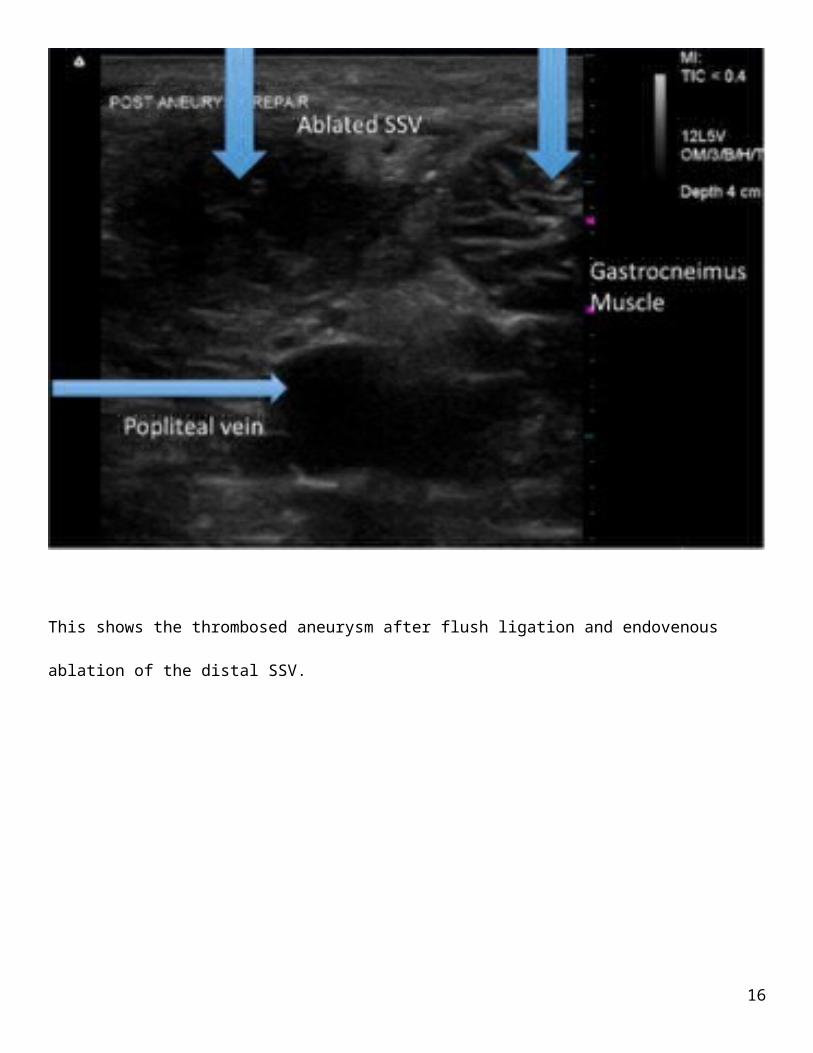
This shows the thrombosed aneurysm after flush ligation and endovenous ablation of the distal SSV.
13
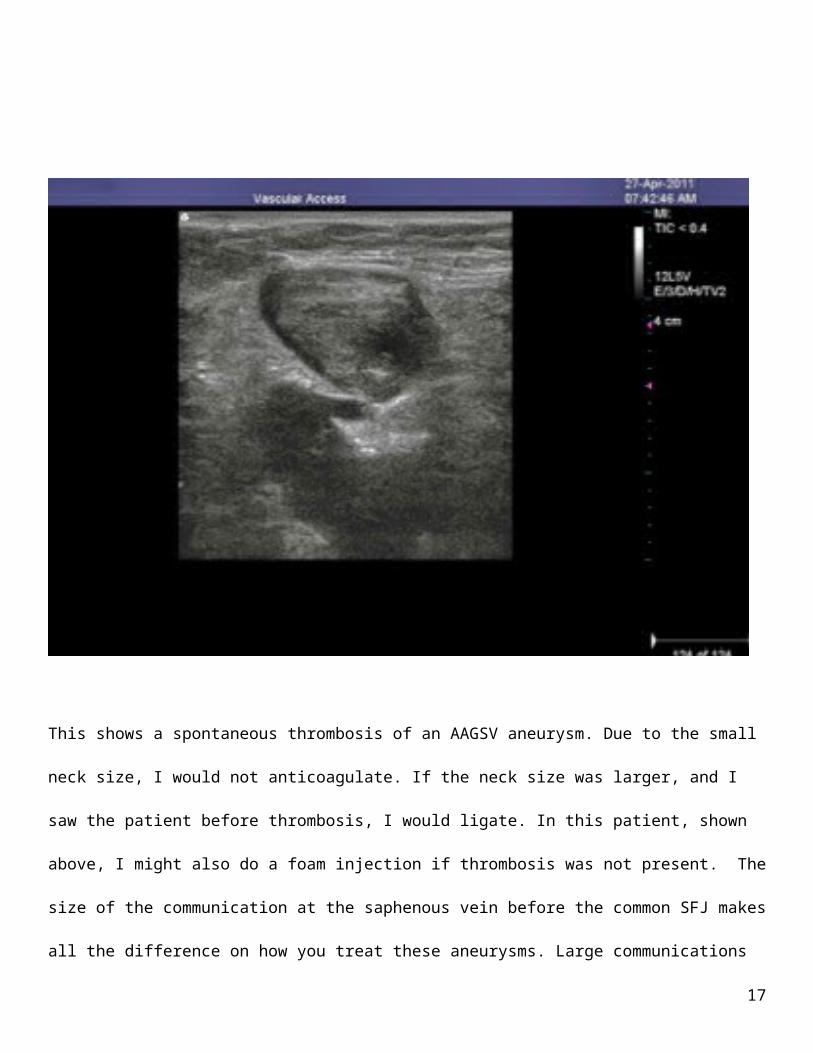
This shows a spontaneous thrombosis of an AAGSV aneurysm. Due to the small neck size, I would
not anticoagulate. If the neck size was larger, and I saw the patient before thrombosis, I would ligate.
In this patient, shown above, I might also do a foam injection if thrombosis was not present. The size
of the communication at the saphenous vein before the common SFJ makes all the difference on how
you treat these aneurysms. Large communications >4 mm, ligate. Small communications, you may do
thermal ablations of the distal AAGSV and spontaneous thrombosis of the aneurysm will occur.
Alternatively, you can foam the aneurysm safely if a small communication is present.
14
11/1/12
AAGSV Aneurysmal Dilation and Treatment
48-year old female presents with aneurysmal dilatation just distal to the takeoff of the AAGSV from the saphenous vein. (Figure 1 video)
She has multiple varicosities on the anterior leg that go laterally. 7 years ago she had endovenous ablation of the GSV, which remains closed.
This patient can safely be treated with foam sclerotherapy. The aneurysm was approx 22 mm in diameter and 3cc of Stotradecol 1% foam was injected using ultrasound guidance. (Figure 2)
15
16
The reason this can be safely treated is because the patient has good collateral flow into the SFJ as shown by the red arrow. (Figure 3)
17
As can be seen in (Figure 4) tumescent compression was done after injection.
18




























![GSV Publications requiring copyright permission Publications requiring copyright permission: 4 GSV Library 929.2 CANE CAN 67. Canty, Wendy. All the shades of Gray. [Photocopy] GSV](https://img.pdfslide.net/doc/110x75/5aa7f75b7f8b9a54748cb5e9/gsv-publications-requiring-copyright-permission-publications-requiring-copyright.jpg)