Embed Size (px)
Citation preview

THIEME
80 Original Article
Antegonial Notch and Mandibular Symphysis as indicators of Growth PatternBeena Kar1 Isha Aggarwal1 Sanjay Mittal1 Mandeep Bhullar1 Divya Singla1 Abhishek Sharma1
1Department of Orthodontics and Dentofacial Orthopedics, Bhojia Dental College and Hospital, Baddi, Himachal Pradesh, India
received November 21, 2018accepted December 2, 2018published onlineJanuary 28, 2019
Address for correspondence Beena Kar, MDS, III year, Department of Orthodontics and Dentofacial Orthopedics, Bhojia Dental College and Hospital, Baddi 173205, Himachal Pradesh, India (e-mail: [email protected]).
Introduction The knowledge of the nature and magnitude of growth and develop-ment of human face is important for sound diagnosis and treatment of dentofacial disharmonies. The depth of antegonial notch and morphology of mandible are important indicators of growth pattern.Objective The purpose of this study was to evaluate the antegonial notch depth, mandibular symphysis morphology, and symphysis inclination in various facial types categorized into the normo-, hypo-, and hyperdivergent groups using various parameters.Materials and Methods Pretreatment lateral cephalograms of 45 adult patients with age group between 16 and 30 years were taken. The antegonial notch depth, symphysis height, symphysis depth, ratio (height of symphysis/depth of symphysis), angulation of symphysis, and inclination of symphysis to mandibular plane were analyzed statistically.Result It was found that the mandible with the hyperdivergent growth pattern was associated with an increased antegonial notch depth, increased symphysis height, reduced symphysis depth, large ratio, small symphysis angle, and large inclination angle of the symphysis.Conclusion The results for the antegonial notch depth, symphysis height, symphysis depth, and ratio of symphysis height to symphysis depth were statistically significant whereas the angulation of the symphysis and inclination of the symphysis did not show statistically significant results.
Abstract
Keywords ► hypodivergent ► hyperdivergent ► antegonial notch ►mandibular morphology
Dent J Adv Stud 2018;6:80–88
DOI https://doi.org/ 10.1055/s-0039-1677777 ISSN 2321-1482.
©2018 Bhojia Dental College and Hospital affiliated to Himachal Pradesh University
IntroductionGrowth of the mandible plays an important role in overall growth and development of the face. An accurate, valid, and reliable method to predict the mandibular growth of an individual would be an indispensable and key asset to ortho-dontists. The ability to predict the nature, magnitude, and direction of mandibular growth in early stages of life would help in better diagnosis and selection of the most appropriate treatment plan for a given individual. Björk,1 in his implant studies to determine the mandibular growth pattern, has confirmed that most of the growth in length of the mandible occurs at the condyles. There is apposition as well as resorp-tion especially in the lower border of the mandible, and
these processes result in shaping of the mandible, which characterizes the type of growth.
The term “facial divergence” was introduced by Schudy,2,3 and the two extremes of facial divergence are the hypo- and hyperdivergent facial types. As stated by Scott4,5 “certain types of faces may be associated with a tendency towards certain types of malocclusions.” In a hypodivergent pattern or short face, the anteroposterior growth exceeds vertical growth and the posterior facial height is more than the anterior facial height as compared with a hyperdivergent or a long face where anterior facial height is excessive in relation to the posterior facial height.3 Till date, a variety of methods have been used with varying success to predict the nature
Published online: 2019-01-28

81Antegonial Notch and Mandibular Symphysis Kar et al.
Dental Journal of Advance Studies Vol. 6 No. 2-3/2018
of growth, but as Björk1 said it correctly, not all the features would be found in a particular individual. Once the growth is complete, the growth pattern does not change.
Apposition beneath the gonial angle together with exces-sive resorption under the symphysis in mandibles with backward and downward rotation results in upward curving of the inferior border of the mandible anterior to the angular process (gonion) and is known as antegonial notching.6 Definite mandibular morphologic patterns are associated with deep and shallow antegonial notching. Various studies have shown that patients with deep antegonial notching have either a diminished mandibular growth potential or a disturbed condylar growth.7 Singer et al8 in 1987 stated that in adolescents with deep mandibular antegonial notch-es, the mandible was retrusive with a short corpus, ramus height was less, and the gonial angle was greater than the adolescents with shallow mandibular antegonial notches.
Mandibular symphysis (MS) morphology has an impact on diagnosis and treatment planning in orthodontic patients; it serves as a reference anatomical landmark for esthetics and beauty of the face in general and of the lower part in particular. MS morphology results from an interplay of various factors that can be genetic, nongenetic, or the adaptive factors. The MS shape during the growth period may indirectly be affected by the inclination of lower incisors, and dentoalve-olar compensation occurring during that period as a result of anteroposterior (AP) jaw discrepancy might be reflected in the morphology and dimension of the symphysis.9 Also, the variables such as the symphysis depth, symphysis height, symphysis ratio, symphysis angle, and symphysis inclination to the mandibular plane are associated with the growth pat-tern of an individual. Ricketts10 stated that in patients with anterior growth direction a thick symphysis can be seen. An important consideration in evaluation of a specific treatment plan for an individual is the MS size and shape. If the symphy-sis is large, it is esthetically acceptable to leave the incisors a bit proclined, and thus, we can opt for a nonextraction plan to compensate for tooth size arch length discrepancies, whereas in patients with small chin and the same arch length discrep-ancies, proclined incisors would be unaesthetic, and in these cases, we have to go for an extraction treatment plan.11
The inclination of symphysis is an important feature. As stated by Björk,1 in vertical growth pattern or hyperdivergent cases, the chin is prominent and the symphysis swings for-ward, whereas in cases of horizontal or hypodivergent cases, a receding chin is seen with the symphysis swung back.
Prediction of growth pattern by the morphology of the mandible has clinical implications in treatment planning for the patient as the extraction decision, type of anchorage preparation, mechanics, and retention period are influenced by the growth pattern of an individual. The purpose of this study is to evaluate the various variables of mandibular morphology in hyper-, normo-, and hypodivergent growth patterns.
ObjectivesThe objective of the article is to assess the depth of antego-nial notch in patients with different growth patterns and
assess the symphysis morphology in patients with different growth patterns.
Materials and MethodsPretreatment lateral cephalograms of 45 adult patients (15 males, 30 females) with age group between 16 and 30 years (mean age 20.59 years) were taken. All lateral cephalographs were taken by the same operator with the patients standing with Frankfort horizontal plane parallel to the floor, the sagittal plane perpendicu-lar to the X-ray beam, and the teeth in centric occlusion. All radiographs were taken using the cephalostat from ADVAPEX Panoramic Systems. The exposure data of the X-ray source was 65 kV and 16 mA for 1.2 seconds. The equipment had a fixed film to focus plane distance of 190 cm and a fixed film to midsagittal plane distance of 10 cm with a final enlargement of 10%. For all patients, 8- × 10-in (20.32- × 25.4-cm) films were used.
Inclusion Criteria
• No history of orthodontic treatment • All landmarks should be readily identifiable on lateral
cephalographs • Age group: 16 to 30 years • No temporomandibular joint (TMJ) disorders • No mandibular bony deformities
Exclusion Criteria
• Patients having primary dentition, supernumerary teeth, and congenitally missing teeth
• Facial asymmetry, trauma, and syndromes • TMJ or cervical spine disorders • Incomplete dentition (extracted or missing teeth)
All the cephalograms were traced by the same operator on an acetate sheet of 0.5 mm thickness. All the landmarks were identified and marked. The 45 patients were divided into three groups, that is, hyper-, normo-, and hypodivergent, of 15 patients each on the basis of their Frankfort- mandibular plane angle (FMA) angle, J ratio ( Jarabak’s ratio), y-axis, and Go-Gn-SN (Gonion-Gnathion–Sella- Nasion) angle (►Table 1).
Patients of these three groups were evaluated to study the antegonial notch depth and symphysis morphology.
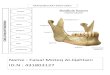
Calculation of Depth of Antegonial NotchAntegonial notch is a concavity on the inferior border of the mandible. Two points traced on the mandible were anterior convexity point (ACP) and inferior gonion (IGo), where ACP is the point of greatest convexity along the anterior-inferior border of the mandible and IGo is the point of greatest convexity along the posterior-inferior border of the mandible. A line was drawn joining these two reference points. Antegonial notch depth is the greatest point of convexity in antegonial notch area in the lower border of mandible (►Fig. 1).
82 Antegonial Notch and Mandibular Symphysis Kar et al.
Dental Journal of Advance Studies Vol. 6 No. 2-3/2018
Cephalometric Evaluation of SymphysisCalculation Symphysis DimensionsA line tangent to point B was taken as the long axis of the symphysis. A grid was formed with lines of grid parallel and perpendicular to constructed tangent line. Superior limit of symphysis was taken as point B with inferior, anterior, and posterior limits taken at most inferior, anterior, and posterior borders of symphyseal outline, respectively (►Fig. 1).
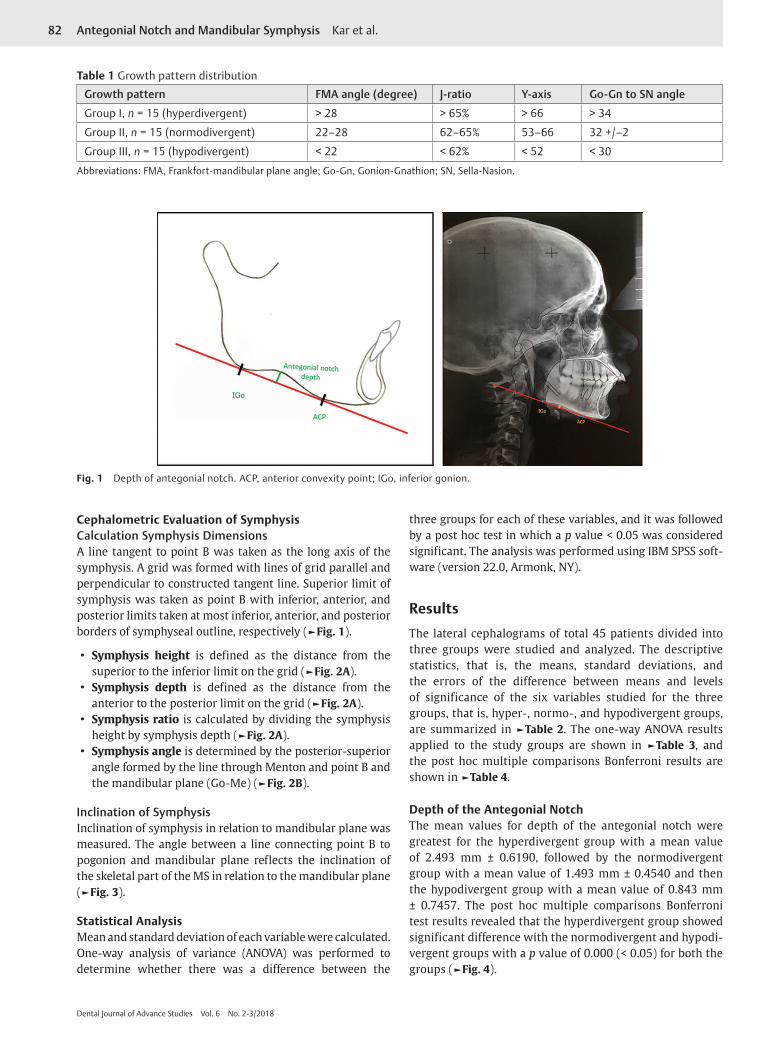
• Symphysis height is defined as the distance from the superior to the inferior limit on the grid (►Fig. 2A).
• Symphysis depth is defined as the distance from the anterior to the posterior limit on the grid (►Fig. 2A).
• Symphysis ratio is calculated by dividing the symphysis height by symphysis depth (►Fig. 2A).
• Symphysis angle is determined by the posterior-superior angle formed by the line through Menton and point B and the mandibular plane (Go-Me) (►Fig. 2B).
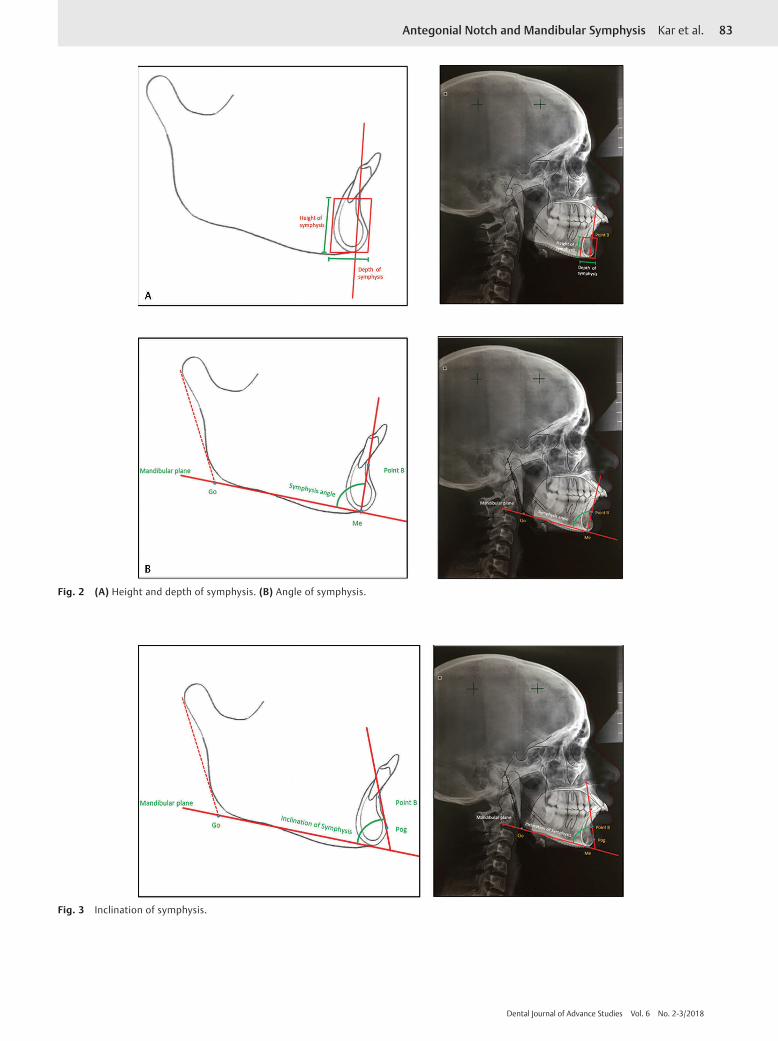
Inclination of SymphysisInclination of symphysis in relation to mandibular plane was measured. The angle between a line connecting point B to pogonion and mandibular plane reflects the inclination of the skeletal part of the MS in relation to the mandibular plane (►Fig. 3).
Statistical AnalysisMean and standard deviation of each variable were calculated. One-way analysis of variance (ANOVA) was performed to determine whether there was a difference between the
three groups for each of these variables, and it was followed by a post hoc test in which a p value < 0.05 was considered significant. The analysis was performed using IBM SPSS soft-ware (version 22.0, Armonk, NY).
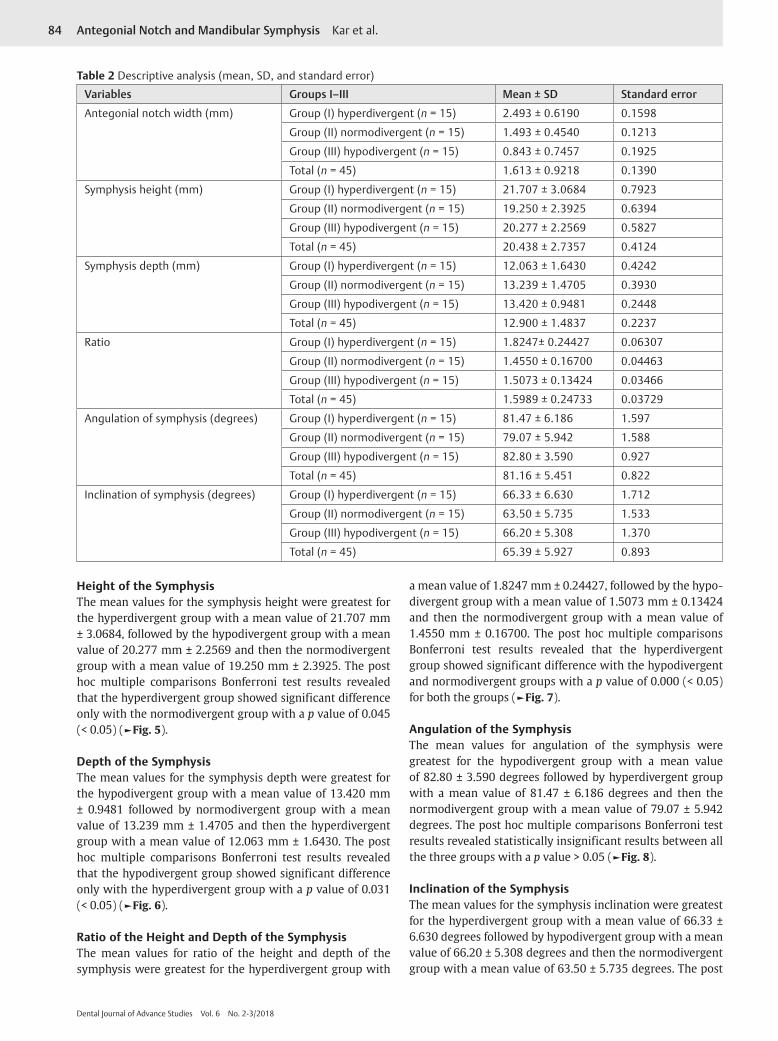
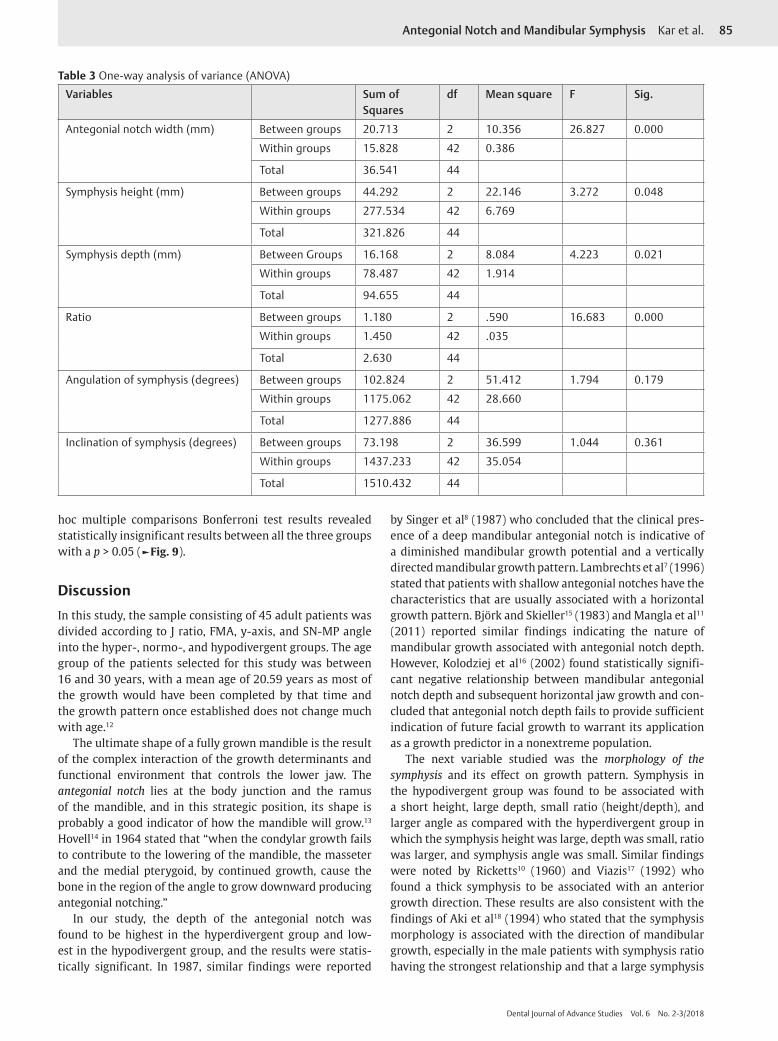
ResultsThe lateral cephalograms of total 45 patients divided into three groups were studied and analyzed. The descriptive statistics, that is, the means, standard deviations, and the errors of the difference between means and levels of significance of the six variables studied for the three groups, that is, hyper-, normo-, and hypodivergent groups, are summarized in ►Table 2. The one-way ANOVA results applied to the study groups are shown in ►Table 3, and the post hoc multiple comparisons Bonferroni results are shown in ►Table 4.
Depth of the Antegonial NotchThe mean values for depth of the antegonial notch were greatest for the hyperdivergent group with a mean value of 2.493 mm ± 0.6190, followed by the normodivergent group with a mean value of 1.493 mm ± 0.4540 and then the hypodivergent group with a mean value of 0.843 mm ± 0.7457. The post hoc multiple comparisons Bonferroni test results revealed that the hyperdivergent group showed significant difference with the normodivergent and hypodi-vergent groups with a p value of 0.000 (< 0.05) for both the groups (►Fig. 4).
Table 1 Growth pattern distribution
Growth pattern FMA angle (degree) J-ratio Y-axis Go-Gn to SN angle
Group I, n = 15 (hyperdivergent) > 28 > 65% > 66 > 34
Group II, n = 15 (normodivergent) 22–28 62–65% 53–66 32 +/–2
Group III, n = 15 (hypodivergent) < 22 < 62% < 52 < 30
Abbreviations: FMA, Frankfort-mandibular plane angle; Go-Gn, Gonion-Gnathion; SN, Sella-Nasion.
Fig. 1 Depth of antegonial notch. ACP, anterior convexity point; IGo, inferior gonion.
83Antegonial Notch and Mandibular Symphysis Kar et al.
Dental Journal of Advance Studies Vol. 6 No. 2-3/2018
Fig. 2 (A) Height and depth of symphysis. (B) Angle of symphysis.
Fig. 3 Inclination of symphysis.
84 Antegonial Notch and Mandibular Symphysis Kar et al.
Dental Journal of Advance Studies Vol. 6 No. 2-3/2018
Height of the SymphysisThe mean values for the symphysis height were greatest for the hyperdivergent group with a mean value of 21.707 mm ± 3.0684, followed by the hypodivergent group with a mean value of 20.277 mm ± 2.2569 and then the normodivergent group with a mean value of 19.250 mm ± 2.3925. The post hoc multiple comparisons Bonferroni test results revealed that the hyperdivergent group showed significant difference only with the normodivergent group with a p value of 0.045 (< 0.05) (►Fig. 5).
Depth of the SymphysisThe mean values for the symphysis depth were greatest for the hypodivergent group with a mean value of 13.420 mm ± 0.9481 followed by normodivergent group with a mean value of 13.239 mm ± 1.4705 and then the hyperdivergent group with a mean value of 12.063 mm ± 1.6430. The post hoc multiple comparisons Bonferroni test results revealed that the hypodivergent group showed significant difference only with the hyperdivergent group with a p value of 0.031 (< 0.05) (►Fig. 6).
Ratio of the Height and Depth of the SymphysisThe mean values for ratio of the height and depth of the symphysis were greatest for the hyperdivergent group with
a mean value of 1.8247 mm ± 0.24427, followed by the hypo-divergent group with a mean value of 1.5073 mm ± 0.13424 and then the normodivergent group with a mean value of 1.4550 mm ± 0.16700. The post hoc multiple comparisons Bonferroni test results revealed that the hyperdivergent group showed significant difference with the hypodivergent and normodivergent groups with a p value of 0.000 (< 0.05) for both the groups (►Fig. 7).
Angulation of the SymphysisThe mean values for angulation of the symphysis were greatest for the hypodivergent group with a mean value of 82.80 ± 3.590 degrees followed by hyperdivergent group with a mean value of 81.47 ± 6.186 degrees and then the normodivergent group with a mean value of 79.07 ± 5.942 degrees. The post hoc multiple comparisons Bonferroni test results revealed statistically insignificant results between all the three groups with a p value > 0.05 (►Fig. 8).
Inclination of the SymphysisThe mean values for the symphysis inclination were greatest for the hyperdivergent group with a mean value of 66.33 ± 6.630 degrees followed by hypodivergent group with a mean value of 66.20 ± 5.308 degrees and then the normodivergent group with a mean value of 63.50 ± 5.735 degrees. The post
Table 2 Descriptive analysis (mean, SD, and standard error)
Variables Groups I–III Mean ± SD Standard error
Antegonial notch width (mm) Group (I) hyperdivergent (n = 15) 2.493 ± 0.6190 0.1598
Group (II) normodivergent (n = 15) 1.493 ± 0.4540 0.1213
Group (III) hypodivergent (n = 15) 0.843 ± 0.7457 0.1925
Total (n = 45) 1.613 ± 0.9218 0.1390
Symphysis height (mm) Group (I) hyperdivergent (n = 15) 21.707 ± 3.0684 0.7923
Group (II) normodivergent (n = 15) 19.250 ± 2.3925 0.6394
Group (III) hypodivergent (n = 15) 20.277 ± 2.2569 0.5827
Total (n = 45) 20.438 ± 2.7357 0.4124
Symphysis depth (mm) Group (I) hyperdivergent (n = 15) 12.063 ± 1.6430 0.4242
Group (II) normodivergent (n = 15) 13.239 ± 1.4705 0.3930
Group (III) hypodivergent (n = 15) 13.420 ± 0.9481 0.2448
Total (n = 45) 12.900 ± 1.4837 0.2237
Ratio Group (I) hyperdivergent (n = 15) 1.8247± 0.24427 0.06307
Group (II) normodivergent (n = 15) 1.4550 ± 0.16700 0.04463
Group (III) hypodivergent (n = 15) 1.5073 ± 0.13424 0.03466
Total (n = 45) 1.5989 ± 0.24733 0.03729
Angulation of symphysis (degrees) Group (I) hyperdivergent (n = 15) 81.47 ± 6.186 1.597
Group (II) normodivergent (n = 15) 79.07 ± 5.942 1.588
Group (III) hypodivergent (n = 15) 82.80 ± 3.590 0.927
Total (n = 45) 81.16 ± 5.451 0.822
Inclination of symphysis (degrees) Group (I) hyperdivergent (n = 15) 66.33 ± 6.630 1.712
Group (II) normodivergent (n = 15) 63.50 ± 5.735 1.533
Group (III) hypodivergent (n = 15) 66.20 ± 5.308 1.370
Total (n = 45) 65.39 ± 5.927 0.893
85Antegonial Notch and Mandibular Symphysis Kar et al.
Dental Journal of Advance Studies Vol. 6 No. 2-3/2018
hoc multiple comparisons Bonferroni test results revealed statistically insignificant results between all the three groups with a p > 0.05 (►Fig. 9).
DiscussionIn this study, the sample consisting of 45 adult patients was divided according to J ratio, FMA, y-axis, and SN-MP angle into the hyper-, normo-, and hypodivergent groups. The age group of the patients selected for this study was between 16 and 30 years, with a mean age of 20.59 years as most of the growth would have been completed by that time and the growth pattern once established does not change much with age.12
The ultimate shape of a fully grown mandible is the result of the complex interaction of the growth determinants and functional environment that controls the lower jaw. The antegonial notch lies at the body junction and the ramus of the mandible, and in this strategic position, its shape is probably a good indicator of how the mandible will grow.13 Hovell14 in 1964 stated that “when the condylar growth fails to contribute to the lowering of the mandible, the masseter and the medial pterygoid, by continued growth, cause the bone in the region of the angle to grow downward producing antegonial notching.”
In our study, the depth of the antegonial notch was found to be highest in the hyperdivergent group and low-est in the hypodivergent group, and the results were statis-tically significant. In 1987, similar findings were reported
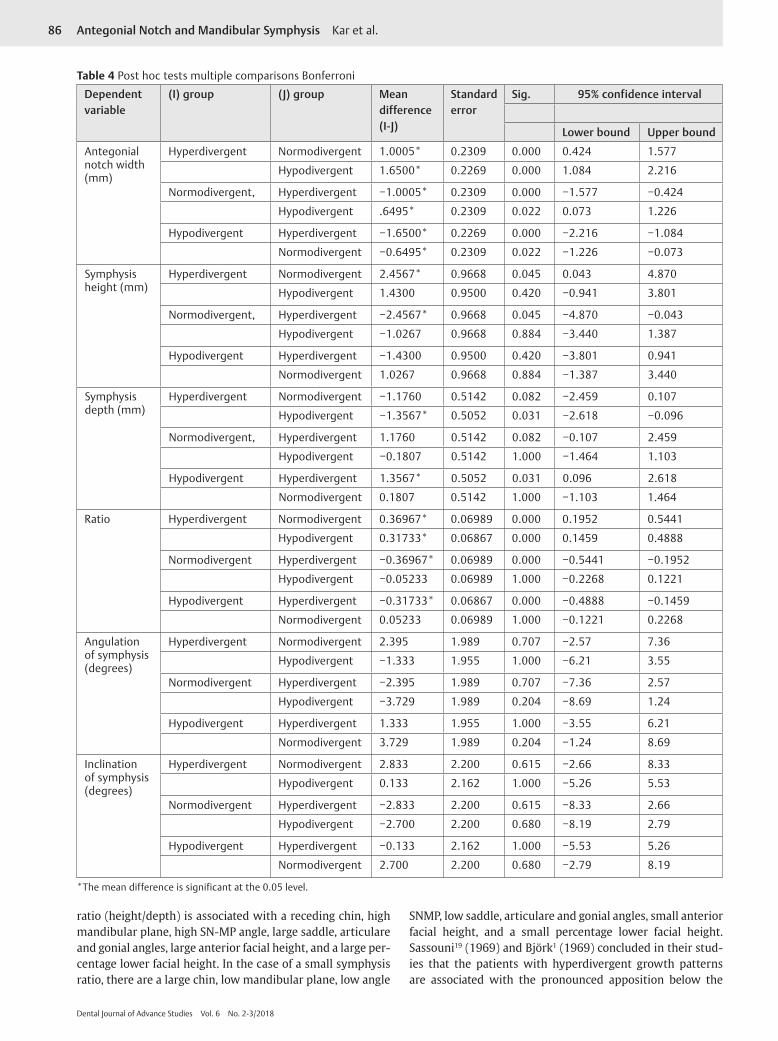
by Singer et al8 (1987) who concluded that the clinical pres-ence of a deep mandibular antegonial notch is indicative of a diminished mandibular growth potential and a vertically directed mandibular growth pattern. Lambrechts et al7 (1996) stated that patients with shallow antegonial notches have the characteristics that are usually associated with a horizontal growth pattern. Björk and Skieller15 (1983) and Mangla et al11 (2011) reported similar findings indicating the nature of mandibular growth associated with antegonial notch depth. However, Kolodziej et al16 (2002) found statistically signifi-cant negative relationship between mandibular antegonial notch depth and subsequent horizontal jaw growth and con-cluded that antegonial notch depth fails to provide sufficient indication of future facial growth to warrant its application as a growth predictor in a nonextreme population.
The next variable studied was the morphology of the symphysis and its effect on growth pattern. Symphysis in the hypodivergent group was found to be associated with a short height, large depth, small ratio (height/depth), and larger angle as compared with the hyperdivergent group in which the symphysis height was large, depth was small, ratio was larger, and symphysis angle was small. Similar findings were noted by Ricketts10 (1960) and Viazis17 (1992) who found a thick symphysis to be associated with an anterior growth direction. These results are also consistent with the findings of Aki et al18 (1994) who stated that the symphysis morphology is associated with the direction of mandibular growth, especially in the male patients with symphysis ratio having the strongest relationship and that a large symphysis
Table 3 One-way analysis of variance (ANOVA)
Variables Sum of Squares
df Mean square F Sig.
Antegonial notch width (mm) Between groups 20.713 2 10.356 26.827 0.000
Within groups 15.828 42 0.386
Total 36.541 44
Symphysis height (mm) Between groups 44.292 2 22.146 3.272 0.048
Within groups 277.534 42 6.769
Total 321.826 44
Symphysis depth (mm) Between Groups 16.168 2 8.084 4.223 0.021
Within groups 78.487 42 1.914
Total 94.655 44
Ratio Between groups 1.180 2 .590 16.683 0.000
Within groups 1.450 42 .035
Total 2.630 44
Angulation of symphysis (degrees) Between groups 102.824 2 51.412 1.794 0.179
Within groups 1175.062 42 28.660
Total 1277.886 44
Inclination of symphysis (degrees) Between groups 73.198 2 36.599 1.044 0.361
Within groups 1437.233 42 35.054
Total 1510.432 44
86 Antegonial Notch and Mandibular Symphysis Kar et al.
Dental Journal of Advance Studies Vol. 6 No. 2-3/2018
ratio (height/depth) is associated with a receding chin, high mandibular plane, high SN-MP angle, large saddle, articulare and gonial angles, large anterior facial height, and a large per-centage lower facial height. In the case of a small symphysis ratio, there are a large chin, low mandibular plane, low angle
SNMP, low saddle, articulare and gonial angles, small anterior facial height, and a small percentage lower facial height. Sassouni19 (1969) and Björk1 (1969) concluded in their stud-ies that the patients with hyperdivergent growth patterns are associated with the pronounced apposition below the
Table 4 Post hoc tests multiple comparisons Bonferroni
Dependent variable
(I) group (J) group Mean difference (I-J)
Standard error
Sig. 95% confidence interval
Lower bound Upper bound
Antegonial notch width (mm)
Hyperdivergent Normodivergent 1.0005* 0.2309 0.000 0.424 1.577
Hypodivergent 1.6500* 0.2269 0.000 1.084 2.216
Normodivergent, Hyperdivergent −1.0005* 0.2309 0.000 −1.577 −0.424
Hypodivergent .6495* 0.2309 0.022 0.073 1.226
Hypodivergent Hyperdivergent −1.6500* 0.2269 0.000 −2.216 −1.084
Normodivergent −0.6495* 0.2309 0.022 −1.226 −0.073
Symphysis height (mm)
Hyperdivergent Normodivergent 2.4567* 0.9668 0.045 0.043 4.870
Hypodivergent 1.4300 0.9500 0.420 −0.941 3.801
Normodivergent, Hyperdivergent −2.4567* 0.9668 0.045 −4.870 −0.043
Hypodivergent −1.0267 0.9668 0.884 −3.440 1.387
Hypodivergent Hyperdivergent −1.4300 0.9500 0.420 −3.801 0.941
Normodivergent 1.0267 0.9668 0.884 −1.387 3.440
Symphysis depth (mm)
Hyperdivergent Normodivergent −1.1760 0.5142 0.082 −2.459 0.107
Hypodivergent −1.3567* 0.5052 0.031 −2.618 −0.096
Normodivergent, Hyperdivergent 1.1760 0.5142 0.082 −0.107 2.459
Hypodivergent −0.1807 0.5142 1.000 −1.464 1.103
Hypodivergent Hyperdivergent 1.3567* 0.5052 0.031 0.096 2.618
Normodivergent 0.1807 0.5142 1.000 −1.103 1.464
Ratio Hyperdivergent Normodivergent 0.36967* 0.06989 0.000 0.1952 0.5441
Hypodivergent 0.31733* 0.06867 0.000 0.1459 0.4888
Normodivergent Hyperdivergent −0.36967* 0.06989 0.000 −0.5441 −0.1952
Hypodivergent −0.05233 0.06989 1.000 −0.2268 0.1221
Hypodivergent Hyperdivergent −0.31733* 0.06867 0.000 −0.4888 −0.1459
Normodivergent 0.05233 0.06989 1.000 −0.1221 0.2268
Angulation of symphysis (degrees)
Hyperdivergent Normodivergent 2.395 1.989 0.707 −2.57 7.36
Hypodivergent −1.333 1.955 1.000 −6.21 3.55
Normodivergent Hyperdivergent −2.395 1.989 0.707 −7.36 2.57
Hypodivergent −3.729 1.989 0.204 −8.69 1.24
Hypodivergent Hyperdivergent 1.333 1.955 1.000 −3.55 6.21
Normodivergent 3.729 1.989 0.204 −1.24 8.69
Inclination of symphysis (degrees)
Hyperdivergent Normodivergent 2.833 2.200 0.615 −2.66 8.33
Hypodivergent 0.133 2.162 1.000 −5.26 5.53
Normodivergent Hyperdivergent −2.833 2.200 0.615 −8.33 2.66
Hypodivergent −2.700 2.200 0.680 −8.19 2.79
Hypodivergent Hyperdivergent −0.133 2.162 1.000 −5.53 5.26
Normodivergent 2.700 2.200 0.680 −2.79 8.19
*The mean difference is significant at the 0.05 level.

87Antegonial Notch and Mandibular Symphysis Kar et al.
Dental Journal of Advance Studies Vol. 6 No. 2-3/2018
symphysis with more overall concavity of the lower mandib-ular border. Based on various studies stated and this study results, the antegonial notch can be used as a good indicator for prediction of growth.
Another variable was the inclination of the symphysis to the mandibular plane. In our study, the values for this variable were highest for the hyperdivergent group, but the results were not statistically significant. Oz and Rubenduz20 (2013)
reported similar findings and stated that the internal inclina-tion of the symphysis was more obtuse in the hyperdivergent group, whereas patients in the hypodivergent had the smallest value. It has been reported that a greater inclination of the symphysis is associated with an anterior growth direction and that a smaller inclination is often consistent with hyperdiver-gent patterns. However, Arruda et al21 (2012) stated that facial type has no correlation with the symphysis inclination.
Fig. 4 The depth of antegonial notch in hyper-, normo-, and hypo-divergent groups.
Fig. 5 The height of the symphysis in hyper-, normo-, and hypodi-vergent groups.
Fig. 6 The depth of symphysis in hyper-, normo-, and hypodiver-gent groups.
Fig. 7 The ratio of height of symphysis to the depth of symphysis in hyper-, normo-, and hypodivergent groups.
Fig. 8 The angulation of symphysis in hyper-, normo-, and hypodi-vergent groups.
Fig. 9 The inclination of symphysis in hyper-, normo-, and hypodi-vergent groups.

88 Antegonial Notch and Mandibular Symphysis Kar et al.
Dental Journal of Advance Studies Vol. 6 No. 2-3/2018
ConclusionsAntegonial notch depth values were greater in the hyperdi-vergent group as compared with the normodivergent and hypodivergent groups, and the results were statistically significant.
In patients with hypodivergent growth pattern, the sym-physis height was short, the depth was large, and the ratio was small as compared with the hyperdivergent group, and the results were statistically significant.
The symphysis angulation, on an average, was larger in the hypodivergent group. Conversely, the symphysis inclina-tion was more in the hyperdivergent group, but the results for both the angular measurements were not statistically significant.
Conf lict of InterestNone declared.
References
1 Björk A. Prediction of mandibular growth rotation. Am J Orthod 1969;55(6):585–599
2 Schudy FF. The rotation of mandible resulting from growth: its implications in orthodontic treatment. Angle Orthod 1965;35(1):36–50
3 Schudy FF. Vertical growth versus anteroposterior growth as related to function and treatment. Angle Orthod 1964;34(2):75–93
4 Scott JH. The analysis of facial growth: I. The anteroposterior and vertical dimensions. Am J Orthod 1958;44(7):507–512
5 Scott JH. The analysis of facial growth: II. The horizontal and vertical dimensions. Am J Orthod 1958;44(8):585–589
6 Singh S, Kumar S, Pandey R, Passi D, Mehrotra D, Mohammad S. Dimensional differences in mandibular antegonial notches in temporomandibular joint ankylosis. J Oral Biol Craniofac Res 2011;1(1):7–11
7 Lambrechts AH, Harris AM, Rossouw PE, Stander I. Dimen-sional differences in the craniofacial morphologies of groups with deep and shallow mandibular antegonial notching. Angle Orthod 1996;66(4):265–272
8 Singer CP, Mamandras AH, Hunter WS. The depth of the mandibular antegonial notch as an indicator of mandibular growth potential. Am J Orthod Dentofacial Orthop 1987; 91(2):117–124
9 Al-Khateeb SN, Al Maaitah EF, Abu Alhaija ES, Badran SA. Mandibular symphysis morphology and dimensions in dif-ferent anteroposterior jaw relationships. Angle Orthod 2014;84(2):304–309
10 Ricketts RM. Cephalometric synthesis: an exercise in stating objectives and planning treatment with tracings of the head roentgenogram. Am J Orthod 1960;46(9):647–673
11 Mangla R, Singh N, Dua V, Padmanabhan P, Khanna M. Evaluation of mandibular morphology in different facial types. Contemp Clin Dent 2011;2(3):200–206
12 Creekmore TD. Inhibition or stimulation of the vertical growth of the facial complex, its significance to treatment. Angle Orthod 1967;37(4):285–297
13 Salem OH, Al-Sehaibany F, Preston CB. Aspects of mandibular morphology, with specific reference to the antegonial notch and the curve of Spee. J Clin Pediatr Dent 2003;27(3):261–265
14 Hovell JH. Variations in mandibular form: Charles Tomes lec-ture delivered at the Royal College of Surgeons of England on 17th July 1964. Ann R Coll Surg Engl 1965;37(1):1–18
15 Björk A, Skieller V. Normal and abnormal growth of the mandible. A synthesis of longitudinal cephalometric implant studies over a period of 25 years. Eur J Orthod 1983;5(1):1–46
16 Kolodziej RP, Southard TE, Southard KA, Casko JS, Jakobsen JR. Evaluation of antegonial notch depth for growth prediction. Am J Orthod Dentofacial Orthop 2002;121(4):357–363
17 Viazis AD. Cephalometric evaluation of skeletal open- and deep-bite tendencies. J Clin Orthod 1992;26(6):338–343
18 Aki T, Nanda RS, Currier GF, Nanda SK. Assessment of symphysis morphology as a predictor of the direction of mandibular growth. Am J Orthod Dentofacial Orthop 1994;106(1):60–69
19 Sassouni V. A classification of skeletal facial types. Am J Orthod 1969;55(2):109–123
20 Oz U, Rubenduz M. Craniofacial differences between skeletal class II and skeletal class I malocclusions according to vertical classification. Int J Stomatol Occlusion Med 2011;4(3):105–111
21 Arruda KE, Valladares Neto J, Almeida GD. Assessment of the mandibular symphysis of Caucasian Brazilian adults with well-balanced faces and normal occlusion: the influence of gender and facial type. Dental Press J Orthod 2012;17(3):40–50