Embed Size (px)
Citation preview

Antibodies for Infectious Diseases
Antibodies for Infectious Diseases
Edited by
James E Crowe JrVanderbilt University Medical CenterNashville Tennessee
Diana BoraschiNational Research CouncilNapoli Italy
AND
Rino RappuoliNovartis VaccinesSiena Italy
Washington DC
Copyright copy 2015 American Society for Microbiology All rights reserved No part of this publication may be reproduced or transmitted in whole or in part or reused in any form or by any means electronic or mechanical including photocopying and recording or by any information storage and retrieval system without permission in writing from the publisher
Disclaimer To the best of the publisherrsquos knowledge this publication provides information concerning the subject matter covered that is accurate as of the date of publication The publisher is not providing legal medical or other professional services Any reference herein to any specific commercial products procedures or services by trade name trademark manufacturer or otherwise does not constitute or imply endorsement recommendation or favored status by the American Society for Microbiology (ASM) The views and opinions of the author(s) expressed in this publication do not necessarily state or reflect those of ASM and they shall not be used to advertise or endorse any product
Library of Congress Cataloging-in-Publication Data
Antibodies for infectious diseases edited by James E Crowe Jr Vanderbilt University Medical Center Nashville Tennessee Diana Boraschi National Research Council Napoli Italy and Rino Rappuoli Novartis Vaccines Siena Italypages cmIncludes bibliographical references and indexISBN 978-1-55581-735-0 (alk paper)1 Immunoglobulins 2 Communicable diseases--Immunological aspects I Crowe James E Jr editor II Boraschi D (Diana) editor III Rappuoli Rino editor QR1867A534 201561607rsquo98--dc232015009356eISBN 978-1-55581-741-1doi101128978155581741110 9 8 7 6 5 4 3 2 1
All Rights ReservedPrinted in the United States of America
Address editorial correspondence to ASM Press 1752 N St NWWashington DC 20036-2904 USASend orders to ASM Press PO Box 605 Herndon VA 20172 USAPhone 800-546-2416 703-661-1593Fax 703-661-1501E-mail booksasmusaorgOnline httpestoreasmorg
Cover image Cancer cell with high details (source 123RF)
Contents
ContributorsemspixPrefaceemspxvii
IntroductIon
1 History and Practice Antibodies in Infectious Diseasesemsp3 Adam Hey
General Features oF ImmunoGlobulIns
2 Functions of Antibodiesemsp25 Donald N Forthal
3 Antibody Structureemsp49 Robyn L Stanfield and Ian A Wilson
4 The Role of Complement in Antibody Therapy for Infectious Diseasesemsp63 Peter P Wibroe Shen Y Helvig and S Moein Moghimi
5 Immunoglobulin E and Allergy Antibodies in Immune Inflammation and Treatmentemsp75
Sophia N Karagiannis Panagiotis Karagiannis Debra H Josephs Louise Saul Amy E Gilbert Nadine Upton and Hannah J Gould
antIbody dIscovery approaches
6 Phage and Yeast Displayemsp105 Jared Sheehan and Wayne A Marasco
7 Efficient Methods To Isolate Human Monoclonal Antibodies from Memory B Cells and Plasma Cellsemsp129
Davide Corti and Antonio Lanzavecchia
8 Use of Human Hybridoma Technology To Isolate Human Monoclonal Antibodiesemsp141 Scott A Smith and James E Crowe Jr
9 Humanized Mice for Studying Human Immune Responses and Generating Human Monoclonal Antibodiesemsp157
Ramesh Akkina
10 Antibodies Computer-Aided Prediction of Structure and Design of Functionemsp173 Alexander M Sevy and Jens Meiler
v
vi contents
pathoGen-specIFIc antIbodIes
11 Antibodies Targeting the Envelope of HIV-1emsp193 Luzia M Mayr and Susan Zolla-Pazner
12 Committing the Oldest Sins in the Newest Kind of WaysmdashAntibodies Targeting the Influenza Virus Type A Hemagglutinin Globular Heademsp209
Jens C Krause and James E Crowe Jr
13 Prevention of Respiratory Syncytial Virus Infection From Vaccine to Antibodyemsp221
Kelly Huang and Herren Wu
14 Human Metapneumovirusemsp237 Jennifer E Schuster and John V Williams
15 Dengue Antibody-Dependent Enhancement Knowns and Unknownsemsp249
Scott B Halstead
16 Immunotherapeutic Approaches To Prevent Cytomegalovirus-Mediated Diseaseemsp273
Edith Acquaye-Seedah Zachary P Frye and Jennifer A Maynard
17 Rotavirusemsp289 Manuel A Franco and Harry B Greenberg
18 Bacterial ToxinsmdashStaphylococcal Enterotoxin Bemsp303 Bettina C Fries and Avanish K Varshney
technIcal advances
19 Antibody Engineeringemsp321 Kin-Ming Lo Olivier Leger and Bjoumlrn Hock
20 High-Throughput DNA Sequencing Analysis of Antibody Repertoiresemsp345
Scott D Boyd and Shilpa A Joshi
21 Antibody Informatics IMGT the International ImMunoGeneTics Information Systememsp363
Marie-Paule Lefranc
22 Probing Antibody-Antigen Interactionsemsp381 Guocheng Yang Stefanie N Velgos Shanta P Boddapati
and Michael R Sierks
23 Radiolabeled Antibodies for Therapy of Infectious Diseasesemsp399 Ekaterina Dadachova and Arturo Casadevall
alternate systems For expressIon
24 Plant-Derived Monoclonal Antibodies for Prevention and Treatment of Infectious Diseaseemsp413
Andrew Hiatt Kevin J Whaley and Larry Zeitlin
25 Vector-Mediated In Vivo Antibody Expressionemsp427 Bruce C Schnepp and Philip R Johnson
Indexemsp441
contents vii
Contributors
Edith Acquaye-SeedahDepartment of BiochemistryUniversity of Texas at AustinAustin TX 78712
Ramesh AkkinaDepartment of Microbiology Immunology and PathologyColorado State University1619 Campus DeliveryFort Collins CO 80523
Shanta P BoddapatiDepartment of Biomedical EngineeringOregon Health and Science University3181 SW Sam Jackson Park RoadPortland OR 97239
Scott D BoydDepartment of PathologyStanford UniversityStanford CA 94305
Arturo CasadevallDepartments of Microbiology and Immunology and MedicineAlbert Einstein College of Medicine of Yeshiva University1695A Eastchester RoadBronx NY 10461
Davide CortiHumabs BioMed SAvia Mirasole 1Bellinzona 6500Switzerland
James E Crowe JrSchool of MedicineVanderbilt UniversityNashville TN 37232
ix
x contRIBUtoRs
Ekaterina (Kate) DadachovaDepartments of Radiology Microbiology and ImmunologyAlbert Einstein College of Medicine of Yeshiva University1695A Eastchester RoadBronx NY 10461
Donald N ForthalDepartment of Infectious Diseases3044 Hewitt HallUniversity of California IrvineIrvine CA 92617
Manuel A FrancoFacultad de Ciencias y MedicinaPontificia Universidad JaverianaOficina 306 Edificio 50Carrera 7 40-62BogotaacuteColombia
Bettina C FriesDepartment of MedicineInfectious Diseases and Department of Microbiology and ImmunologyAlbert Einstein College of MedicineBronx NY 10461
Zachary P FryeDepartment of Chemical EngineeringUniversity of Texas at AustinAustin TX 78712
Amy E GilbertCutaneous Medicine and Immunotherapy UnitSt Johnrsquos Institute of DermatologyDivision of Genetics and Molecular Medicine amp NIHR Biomedical Research Centre at Guyrsquos and St Thomasrsquos Hospitals and Kingrsquos College London School of MedicineGuyrsquos HospitalLondon SE1 9RTUnited Kingdom
Hannah J GouldRandall Division of Cell and Molecular BiophysicsDivision of Asthma Allergy and Lung BiologyMRC and Asthma UK Centre for Allergic Mechanisms of AsthmaKingrsquos College LondonNew Huntrsquos HouseGuyrsquos CampusLondon SE1 1ULUnited Kingdom
contRIBUtoRs xi
Harry B GreenbergDepartments of Medicine and Microbiology and ImmunologyStanford University School of Medicine and the VAPAHCSPalo Alto CA 94305
Scott B HalsteadDepartment of Preventive Medicine and BiometricsUniformed Services University of the Health SciencesBethesda MD 20814
Shen Y HelvigDepartment of PharmacyCenter for Pharmaceutical Nanotechnology and NanotoxicologyFaculty of Health and Medical SciencesUniversity of CopenhagenCopenhagen DK-2100Denmark
Adam HeyPreclinical Safety BiologicsNovartis AGBaselSwitzerland
Andrew HiattMapp Biopharmaceutical Inc6160 Lusk Blvd C105San Diego CA 92121
Bjoumlrn HockDepartment of Protein Engineering and Antibody TechnologiesMerck Serono Merck KgaAFrankfurter Str 250D-64293 DarmstadtGermany
Kelly HuangDepartment of Infectious DiseaseMedImmune LLCOne MedImmune WayGaithersburg MD 20878
Philip R JohnsonThe Childrenrsquos Hospital of PhiladelphiaAbramson Research CenterPhiladelphia PA 19104
Debra H JosephsCutaneous Medicine and Immunotherapy UnitSt Johnrsquos Institute of DermatologyDivision of Genetics and Molecular Medicine amp NIHR Biomedical Research Centre at Guyrsquos and St Thomasrsquos HospitalsKingrsquos College London School of MedicineGuyrsquos HospitalLondon SE1 9RTUnited Kingdom
Shilpa A JoshiDepartment of PathologyStanford UniversityStanford CA 94305
Sophia N KaragiannisCutaneous Medicine and Immunotherapy UnitSt Johnrsquos Institute of DermatologyDivision of Genetics and Molecular Medicine amp NIHR Biomedical Research Centre at Guyrsquos and St Thomasrsquos HospitalsKingrsquos College London School of MedicineGuyrsquos HospitalLondon SE1 9RTUnited Kingdom
Panagiotis KaragiannisCutaneous Medicine and Immunotherapy UnitSt Johnrsquos Institute of DermatologyDivision of Genetics and Molecular Medicine amp NIHR Biomedical Research Centre at Guyrsquos and St Thomasrsquos HospitalsKingrsquos College London School of MedicineGuyrsquos HospitalLondon SE1 9RTUnited Kingdom
Jens C KrauseChildrenrsquos HospitalUniversity of Freiburg Medical Center79106 FreibergGermany
Antonio LanzavecchiaInstitute for Research in Biomedicinevia Vincenzo Vela 6Bellinzona 6500Switzerland
xii contRIBUtoRs
Marie-Paule LefrancLaboratoire drsquoImmunoGeacuteneacutetique Moleacuteculaire LIGMIMGTreg the international ImMunoGeneTics information systemregInstitut de Geacuteneacutetique Humaine IGHUniversiteacute Montpellier 2UPR CNRS 1142Montpellier 34396 cedex 5 40202France
Olivier LegerDepartment of Protein Engineering and Antibody TechnologiesMerck Serono SA--Geneva9 chemin des Mines1202 GenevaSwitzerland
Kin-Ming LoDepartment of Protein Engineering and Antibody TechnologiesEMD Serono Research Institute45A Middlesex TurnpikeBillerica MA 01821
Wayne A MarascoDepartment of Cancer Immunology and AIDSDana-Farber Cancer InstituteHarvard Medical SchoolBoston MA 02215
Jennifer A MaynardDepartment of Chemical EngineeringUniversity of Texas at AustinAustin TX 78712
Luzia M MayrINSERM U1109Universiteacute de Strasbourg3 Rue Koeberleacute67000 StrasbourgFrance
Jens MeilerDepartment of Chemistry and Center for Structural BiologyVanderbilt UniversityNashville TN 37212
contRIBUtoRs xiii
S Moein MoghimiDepartment of PharmacyCenter for Pharmaceutical Nanotechnology and NanotoxicologyFaculty of Health and Medical SciencesUniversity of CopenhagenCopenhagen DK-2100Denmark
Susan Zolla-PaznerNew York University School of Medicine550 First AvenueNew York NY 10016
Louise SaulCutaneous Medicine and Immunotherapy UnitSt Johnrsquos Institute of DermatologyDivision of Genetics and Molecular Medicine amp NIHR Biomedical Research Centre at Guyrsquos and St Thomasrsquos HospitalsKingrsquos College London School of MedicineGuyrsquos HospitalLondon SE1 9RTUnited Kingdom
Bruce C SchneppThe Childrenrsquos Hospital of PhiladelphiaAbramson Research CenterPhiladelphia PA 19104
Jennifer E SchusterDepartment of PediatricsChildrenrsquos Mercy HospitalKansas City MO 64108-4619
Alexander M SevyDepartment of Chemistry and Center for Structural BiologyVanderbilt UniversityNashville TN 37212
Jared SheehanDepartment of Cancer Immunology and AIDSDana-Farber Cancer InstituteHarvard Medical SchoolBoston MA 02215
Michael R SierksDepartment of Chemical EngineeringArizona State UniversityTempe AZ 85287-6006
xiv contRIBUtoRs
Scott A SmithThe Vanderbilt Vaccine Center and the Department of MedicineVanderbilt University Medical CenterNashville TN 37232
Robyn L StanfieldDepartment of Molecular BiologyThe Scripps Research Institute10550 North Torrey Pines RoadLa Jolla CA 92037
Nadine UptonRandall Division of Cell and Molecular BiophysicsDivision of Asthma Allergy and Lung BiologyMRC and Asthma UK Centre for Allergic Mechanisms of AsthmaKingrsquos College LondonNew Huntrsquos HouseGuyrsquos CampusLondon SE1 1ULUnited Kingdom
Avanish K VarshneyDepartment of MedicineInfectious Diseases and Department of Microbiology and ImmunologyAlbert Einstein College of MedicineBronx NY 10461
Stefanie N VelgosMayo Clinic Arizona5777 East Mayo BoulevardPhoenix AZ 85054
Kevin J WhaleyMapp Biopharmaceutical Inc6160 Lusk Blvd C105San Diego CA 92121
Peter P WibroeCentre for Pharmaceutical Nanotechnology and NanotoxicologyDepartment of PharmacyFaculty of Health and Medical SciencesUniversity of CopenhagenCopenhagen DK-2100Denmark
John V WilliamsDepartment of PediatricsSchool of MedicineVanderbilt UniversityNashville TN 37232-2581
contRIBUtoRs xv
Ian A WilsonDepartment of Molecular Biology and Skaggs Institute for Chemical BiologyThe Scripps Research Institute10550 North Torrey Pines RoadLa Jolla CA 92037
Herren WuDepartment of Antibody Discovery and Protein EngineeringMedImmune LLCOne MedImmune WayGaithersburg MD 20879
Guocheng YangDepartment of Chemical EngineeringArizona State UniversityTempe AZ 85287-6006
Larry ZeitlinMapp Biopharmaceutical Inc6160 Lusk Blvd C105San Diego CA 92121
xvi contRIBUtoRs
Preface
Antibodies form the principal foundation for modern intervention against in-fectious diseases Emil Adolf von Behring was awarded the first Nobel Prize in Physiology or Medicine in 1901 ldquofor his work on serum therapy especially its appli-cation against diphtheria by which he has opened a new road in the domain of med-ical science and thereby placed in the hands of the physician a victorious weapon against illness and deathsrdquo Antibodies now provide the focus for understanding mechanisms of immunity to most infectious diseases and they play a central role in passive immunotherapy and active vaccination as mechanisms or correlates of immunity For most of the 20th century immunotherapy was based on passive transfer of polyclonal hyperimmune animal serum immune human serum or even hyperimmune human serum Georges JF Koumlhler and Ceacutesar Milstein re-ported the generation of monoclonal antibodies in 1979 for which they shared the 1984 Nobel Prize in Physiology or Medicine ldquofor the discovery of the princi-ple for production of monoclonal antibodiesrdquo Since that time entire fields related to antibodies for infectious diseases including antibody gene cloning engineer-ing and expression antibody libraries and high-throughput antibody gene rep-ertoire sequence analysis have extended our capabilities to explore the diversity of antibody specificity and function with unprecedented depth and breadth
This book provides a broad survey of many of the most important aspects of the field of antibodies for infectious diseases The book begins with a general introduction followed by chapters 2 through 5 on general features pertaining to structure function isotype and the role of complement in antibody function Chapters 6 through 10 review contemporary approaches for antibody discovery using phage and yeast display plasma cell and memory B cell cloning human hybridomas humanized mice and computational methods Chapters 11 through 18 review in depth the biology of antibodies specific for particular pathogens including viruses and bacterial toxins to illustrate the role of antibodies in anti- microbial immunity with specific targets These chapters reveal that attempts to raise effective antibody responses to each of these pathogens faces unique and pathogen-specific challenges Chapters 19 to 23 cover major technical advances pertaining to antibody engineering repertoire sequencing and analysis and new methods for study or therapeutic use of antibodies including radiotherapy Fi-nally chapters 24 and 25 cover new methods for expression of monoclonal anti-bodies in plants or by transfer of antibody genes for in vivo expression in treated subjects
Recent literature is exploding with new antibody-related techniques and re-ports of antimicrobial antibodies with unprecedented potency breadth of activ-
xvii
xviii PReface
ity and therapeutic potential We hope that this timely compilation of state-of-the-art reviews of major aspects of this field will be of interest to both antibody cognoscenti and those new to this exciting field We thank the authors for their dedication in producing definitive reviews of the topics at hand
James E Crowe JrDiana BoraschiRino Rappuoli
INTRODUCTION
History and PracticeAntibodies in Infectious Diseases 1ADAM HEY1
Antibodies in Infectious Diseases aims to inform update and inspire studentsteachers researchers pharmaceutical developers and health care professionalson the status of the development of antibody-based therapies for treatinginfectious diseases and the potential for these in times of growing antibioticresistance to provide alternative treatment solutions to the currently usedantibiotics and new treatments for infectious diseases where no propertreatments are available
This introductory article will provide a historical perspective on the useof antibody-based therapies followed by a high-level overview of whatmakes antibodies attractive tools for this purpose This will include the prosand cons of such therapies compared to the use of antibiotics and thepractical and strategic considerations involved in selecting the best formatand development path for new antibody-based therapies targeting specificinfectious agents Then examples of antibody-based therapies in thedevelopment of treatments for infectious diseases will be presented andfinally a look into the future will summarize the different aspects that willinfluence what the future might bring for this type of treatments forinfectious diseases
1Preclinical Safety Biologics Novartis AG Basel Switzerland
Antibodies for Infectious DiseasesEdited by James E Crowe Jr Diana Boraschi and Rino Rappuolicopy 2015 American Society for Microbiology Washington DCdoi101128microbiolspecAID-0026-2014
3
HISTORICAL PERSPECTIVE
Antibodies and the use of passive antibodytherapy in the treatment of infectious dis-eases is the story of a treatment conceptwhich dates back more than 120 years to thelate 19th century and which originally bythe use of serum from immunized animalsprovided the first effective treatment optionsagainst severe bacterial infections (1 2) Byimmunizing horses with bacterial toxinsfrom Clostridium tetani and Corynebacteri-um diphtheriae Emil A Von Behring andShibasaburo Kitasato (3) generated serumcontaining antibodies capable of neutraliz-ing the effects of the toxins produced bythese bacteria and successfully providedtreatment for these serious diseases wherethe pathogenesis is driven by the effects ofthe bacterial toxins For his work on provid-ing treatment for diphtheria Behring re-ceived the Nobel Prize in Physiology orMedicine in 1901 These radical treatmentresults quickly prompted development ofmultiple additional serum therapies for thetreatment of infectious diseases caused byeg Neisseria meningitidis Haemophilus in-fluenza and group A Streptococcus Sinceserum therapy involved administration oflarge amounts of crude mixtures of animalproteins including antibodies they wereassociated with side effects in the form ofhypersensitivity and serum sickness (2)
Due to the crude and unpurified nature ofthese products side effects were seen evenwhen administering human serum prepa-rations Side effects were observed in up to50 of patients and were considered to becaused by immune complex formations thatresulted in symptoms such as rash itchingjoint pain fever and in serious cases hypoten-sion and shock However due to the lack ofalternative options these treatments weredespite their side effects widely used Serumwas normally administered by intravenousinfusion in patients after a test for hypersensi-tivity where a small amount of serum wasinjected subcutaniously (1) As described
above serum therapy applied in these earlydays (late 19th century and early 20th century)involved preparations of serum from rabbitsand horses immunized with the infectiousagent or in live andor neutralized versions ortoxins from these (1) The costs of keeping theimmunized animals and the production andpotency testing of the materials made this arelatively expensive treatment In 1891 datafrom Klemperer (4) showed serum therapy toprotect rabbits from Streptococcus pneumoniaeinfection and paved the way for this type oftreatment and for development of similarserum-based treatments of streptococcal in-fections in humans When treating humansearly administration of serum could reducemortality significantly down to around 5compared to when administered 4 to 5 daysafter onset of symptoms when serum treat-ment was largely without effect This stronglyindicated the need for quick diagnosis andquick treatment to control the infection beforeit got out of control Consequently in theabsence of a specific diagnosis mixtures ofserum from immunizations with differentserotypes were used to circumvent this needfor early treatment without having a serotype-specific diagnosis The understanding thatdifferent serotypes existed for pneumococciand that efficient treatment relied on usingserotype-specific serum was being built upduring the 1920s and 1930s through experiencefrom extensive clinical trials
By the end of the 1930s serum therapywasthe standard of care for treatment of pneu-mococcal pneumonia At that time theefficacy and potency of the derived serawere assessed in mice in ldquothe mouse pro-tection testrdquo by testing survival after aconcomitant intraperitoneal injection of alethal dose of pneumococci and the serum tobe tested Due to the inherent variation inthis test efficacy and survival in two thirds ofthe animals was the acceptance criteria and10 times the lowest dose providing this wasused for defining a unit of the serum Thisallowed for large batch-to-batch variationand the use of different strains of bacteria for
4 HEY
immunization probably explains part of themissing responses observed (1) In the early20th century a pandemic of meningitis inEurope and the United States with mortalityrates up to 80 spurred the development ofserum therapy treatment options Althoughin the 1930s this became the recommendedtreatment in children assumed to be suffer-ing from meningitis failure to reduce mor-tality in several meningitis epidemics duringthat time raised doubts about the generalapplicability of serum treatment In thosedays serum therapy often involved quiteextensive procedures and infusion of largevolumes of serum The following exampleclearly illustrates this Data from Flexnerand Jobling (5) from treating meningitis inmonkeys resulted in the development of serafrom immunized horses for treatment inhumans The treatment protocol includedlumbar puncture and withdrawal of morethan 30 ml of spinal fluid representing anamount slightly larger than the expectedamount of horse serum to be injected subse-quently This treatment involved such dailyslow infusions of up to 30 ml of serum untilthe patientrsquos condition improved This treat-ment was used in outbreaks in New York in1905 and 1906 and did markedly decreasemortality
After the discovery of penicillin by Flemingin 1928 and the subsequent introduction ofantibiotics in the 1930s serum therapy waslargely abandoned over a period of 10 years dueto the availability of these new more broadlyeffective and cheaper treatment optionswhichalso had fewer side effects Although improve-ments in the purification of antibodies hadresulted in preparations with better safety andside effect profiles high manufacturing costsand narrow specificity resulted in antibodytherapy being mostly restricted to a smallernumber of selected treatments for snakevenoms bacterial toxins and some viral infec-tions (1 2) Currently antibody administrationis used for treatment and prevention ofhepatitis B virus rabies virus respiratorysyncytial virus (RSV) Clostridium tetani Clos-
tridium botulinum vaccinia virus echovirusand enterovirus For the most part thesetreatments consist of pooled immunoglobulinalso known as IVIG (intravenous immunoglob-ulin) from several postexposure donors Thisresults in both batch-to-batch variation in theneed for relatively large amounts of serum dueto low specificity and to restricted supplies dueto reliance on exposed donors
However several challengeshave resulted inthe need for new tools in the treatment andpreventionof infectiousdiseasesThebroadandgeneral use of antibiotics in human and veter-inary medicine for many years has resulted inthe development of multi-resistant strains ofbacteria with limited to no response to existingtreatments such as methicillin-resistant Staph-ylococcusaureus (MRSA) vancomycin-resistantS aureus and others This has resulted inpatients needing screening and treatment withseveral antibacterial agents and longer treat-ment time causing extra strain on patients andhealth care providers (6 httpwwwcdcgovdrugresistancethreat-report-2013indexhtml) According to the WHO and CDC morethan 25000 people in European Unioncountries and similar numbers in the UnitedStates die every year as a result of antibiotic-resistant infections This together with theemergence of new pathogens (eg severeacute respiratory syndrome Middle East respi-ratory syndrome) the re-emergenceepidemicsof oldknown pathogens (eg Ebola) and thedifficulties in treating infections in immune-deficient patients (eg HIV patients) has high-lighted the need for new solutions The 2014Ebola epidemic in West Africa (Liberia SierraLeone Guinea Nigeria and Senegal) has fur-ther highlighted this No treatment or prophy-lactic vaccine is available to treat or prevent thespread of Ebola infections which have anaveragemortality of gt50 Local health author-ities in the affected countries are struggling tocontain and handle the disease which isthreatening to go out of control and spreadmorewidelyVariousproductsmainly antibodycocktails from previously recovered patientsare being used despite a lack of clinical data on
CHAPTER 1 bull History and Practice Antibodies in Infectious Diseases 5
their safety and efficacy and those are the onlysporadically available treatment options andonly in small amounts and for a few patients
Ebola is an example of a disease whichnormally affects only a small number ofindividuals and which normally burns outwhen disease outbreaks are contained There-fore given the small number of potentialpatients affected by previous Ebola infectionsto date there was no incentive for big pharmacompanies to do research and development ofdrugs for EbolaWith the increasing number ofinfected (13567) andadeath toll of 4951 (7) andthe lack of the ability to contain the epidemic itwill be interesting to follow the aftermath ofthis outbreak and see whether there will berequests for new ways to ensure that vaccinesand treatment options are available for Ebolaand similar high-mortality and potential bio-warfare infections that have no availabletreatments or procedures to for mass-produc-tion upon the first signsreports of activeinfections Although both the CDC and theWHO have special programs focusing on thesetypes of infections the Ebola outbreak in 2014clearly shows that more financial support forresearch and development of new diagnosticsand treatments is needed This is one examplewhere antibody-based treatments would havethe potential to play a major role To put this inthe right perspective one should however notforget that other infectious diseases such astuberculosis influenza and malaria kill hun-dreds of thousands each year There is there-fore plenty of room for improvement indeveloping treatments for these diseases aswell but the high attention drawn to eg theEbola outbreak creates a special niche andopportunity where antibody treatments couldgain extraordinary development funding andsupport and prove their value and treatmentpotential
That antibody-based therapies could takethis role is supported by the revolution intechnologies for the development selectiongeneration and purification of fully humanantibodies described in more detail later in thesection ldquoMethodsandPlatforms forGenerating
Antibodiesrdquo Antibody-based programs cur-rently at different stages of developmentinclude investigations into the potential use ofsingle antibody preparations combinations ofantibodies (to avoid survival of escape mu-tants) fragments of antibodies and antibodiescarrying radioactive isotopesorcytotoxicdrugsor antibody-like frameworks (eg fibronectin)either alone as a first-line treatment or as anadjunct to existing treatments This multitudeof possible formats the ability to raise anti-bodies to almost any target and the ability toengineer both size effector functions and half-life are now considered by many to providevery valuable tools for designing specificantibody-based treatments toeradicate specifictargeted infectious agents However althoughseveral antibody-based therapies have beenapproved for oncology and anti-inflammatoryindications (see Table 1) only one monoclonalantibody (mAb) is approved against an infec-tious disease agentmdashSynagis (palivizumabMedImmune) for the prevention and treat-ment of respiratory syncytical virus (RSV) inhigh-risk children Economic obstacles such asthe high cost of mAb therapies and relativelysmall markets have resulted in less interestfrom pharmaceutical companies in developingthese Also highlighting the challenges indeveloping these types of antibody-basedtreatments are the difficulties encountered indeveloping a follow-up higher-affinity candi-date to Synagis Poor translatability of dataobtained in the available animal disease mod-els for RSV in cotton rats has resulted in non-approval due to inferiority relative to SynagisIn other viral diseases such as cytomegalovirus(CMV) the high species specificity of thestrains of CMV makes it impossible to testhuman antibody therapies in vivo Thereforeany real data on the efficacy of treatments forCMV will not be obtained until testing inclinical trials As described later in this articleseveral new antibody-based therapies for in-fectious diseases are in development andhopefully this will gradually open the fieldand result in better treatment options andoutcomes for patients
6 HEY
TABLE 1 Approved and pending antibody-based therapies
Name antibody Target antibody type Indication Company Approval date
OKT3a Muronomab-CD3 CD3 murine IgG2a Autoimmune Johnson ampJohnson
1986 (US)
ReoPro abciximab PIIbIIIa chimeric IgG1Fab
Homeostasis Johnson ampJohnson
1984 (US)
Rituxan rituximab CD20 chimeric IgG1 Cancer Genentech 1997 (US) 1998 (EU)Zenapaxa daclizumab CD25 humanized IgG1 Autoimmune Roche 1997 (US) 1999 (EU)Simulect basiliximab CD25 chimeric IgG1 Autoimmune Novartis 1998 (US EU)Synagis palivizumab RSV humanized IgG1 Infections MedImmune 1998 (US) 1999 (EU)Remicade infliximab TNFα chimeric IgG1 Autoimmune Johnson amp
Johnson1998 (US) 1999 (EU)
Herceptin trastuzumab HER2 humanized IgG1 Cancer GenentechRoche
1998 (US) 2000 (EU)
Mylotarga gemtuzumabozogamicin
CD33 humanized IgG4immunotoxin
Cancer WyethPfizer 2000 (US)
Campath alemtuzumab CD52 humanized IgG1 Cancer Genzyme 2001 (US) 2001 (EU)Zevalin ibritumomabtiuxetan
CD20 murine IgG1radiolabeled (yttrium 90)
Cancer Biogen Idec 2002 (US) 2004 (EU)
Humira adalimumab TNFα human IgG1 Autoimmune Abbott 2002 (US) 2003 (EU)Xolair omalizumab IgE humanized IgG1 Autoimmune Genentech
Roche2003 (US)
Bexxar tositumomab-I-131 CD20 murine IgG2aradiolabeled (iodine131)
Cancer CorixaGSK 2003 (US)
Raptivaa falizumab CD11a humanized IgG1 Autoimmune GenentechRoche
2003 (US) 2004 (EU)
Erbitux cetuximab EGFR chimeric IgG1 Cancer ImcloneLilly 2004 (US) 2004 (EU)Avastin bevacizumab VEGF humanized IgG1 Cancer Genentech
Roche2004 (US) 2005 (EU)
Tysabri natalizumab α4-Intergrin humanizedIgG4
Autoimmune Biogen Idec 2004 (US)
Actemra tocilizumab Anti-IL-6R humanizedIgG1
Autoimmune ChugaiRoche
2005 (Japan) 2010 (US)
Vectibix panitumumab EGFR human IgG2 Cancer Amgen 2006 (US)Lucentis ranibizumab VEGF humanized IgG1
FabMaculardegeneration
GenentechRoche
2006 (US)
Soliris eculizumab C5 humanized IgG24 Blood disorders Alexion 2007 (US)Cimzia certolizumab pegol TNFα humanized
pegylated FabAutoimmune UCB 2008 (US)
Simponi golimumab TNFα human IgG1 Autoimmune Johnson ampJohnson
2009 (US EU Canada)
Ilaris canakinumab IL1b human IgG1 Infalmmatory Novartis 2009 (US EU)Stelara ustekinumab IL-1223 human IgG1 Autoimmune Johnson amp
Johnson2008 (EU) 2009 (US)
Arzerra ofatumumab CD20 human IgG1 Cancer Genmab 2009 (EU)Prolia denosumab RANK ligand human
IgG2Bone loss Amgen 2010 (US)
Numax motavizumab RSV humanized IgG1 Anti-infective MedImmune PendingABthrax Raxibacumab B anthrasis PA human
IgG1Anti-infection GSK 2012 (US)
Benlysta belimumab BLyS human IgG1 Autoimmune HGS 2011 (US)Yervoy ipilimumab CTLA-4 human IgG1 Cancer BMS 2011 (US)Adcetris brentuximabvedotin
CD30 chimeric IgG1drug- conjugate
Cancer SeattleGenetics
2011 (US)
(Continued on next page)
CHAPTER 1 bull History and Practice Antibodies in Infectious Diseases 7
INTRODUCTION TO ANTIBODIES
Antibodies also called immunoglobulins basedon their combined structure and function inimmune responses are produced by B cells ofthe immune system They are part of theadaptive immune response and are speciallydesigned for neutralizing and eliminating theinfectious agents and toxins produced by theseAntibodies are present in blood plasma andextracellular fluids and since these fluids wereformerly known as humors they were said tobe part of the humoral immune responseAntibodies are Y-shaped structures consistingof two main parts the upper arms of the Ywhich contain two identical variable-regionantigen binding sites and the lower regioncalled the constant regionwhich is responsiblefor the initiation of effector functions that leadto the removal and destruction of the pathogenor cells harboring the pathogen (see Fig 1) Theantigen-binding sites on an antibody can bythemselves bind to and neutralize bacterialtoxins and viruses thereby preventing themfrom binding to their target cells or receptorscausing toxic effects or spread of the infection
Antibodies consist of two pairs of heavy andlight chainswhich as described above are heldtogether in a Y-shaped arrangement Each ofthe heavy and light chains in these pairs isseparated into constant and variable chainsThe upper armsof theY each contain a variableand a constant sectionof the light and theheavychain where the upper variable parts of theheavy and light chains contain the antigen-binding site and the constant parts areconnected via disulfide bonds The lower partof theYcalled theconstantpart consistsof twoor three constant segments (immunoglobulindomains) from each of the two heavy chainsinteracting and also linked via disulfide bondsThe sectionsof theheavy chains connecting theconstant part of the upper arms to the constantparts of the constant region contain specialhinge regions that provide flexibility to thedifferent sections of the antibody to bind toantigens and effector cells The constant re-gions of the heavy chain also contain attachedoligosaccharide moieties which provide func-tional specialization to the antibodies (8)
The variable domains of the heavy and lightchains form the antigen-binding sites and
TABLE 1 Approved and pending antibody-based therapies (Continued)
Name antibody Target antibody type Indication Company Approval date
Perjeta pertuzumab Her2 humanized IgG1 Cancer GenentechRoche
2012 (US)
Kadcyla ado-trastuzumabemtansine
Her2 humanized IgG1Drug-conjugate
Cancer GenentechRoche
2013 (US)
Raxibacumab Anti-B anthrasis PAhuman IgG1
Anthraxinfection
Notapproved
2012
Entyvio vedolizumab Integrin α4β7humanized IgG1
Crohnrsquos diseaseulcerative colitis
Takeda 2014 (US)
Cyramza ramuciruumab Anti-VEGFR2Human IgG1
Gastric cancer Lilly 2014 (US)
Gazyva obinutuzumab Anti-CD20 humanizedIgG1 glucoengineered
CancerCLLb GenentechRoche
2014 (US)
Sylvant situximab Anti IL-6 chimeric IgG1 Castlemandisease
Janssen 2014 (US) 2014 (EU)
Cosentyx sekukinumab Anti IL-17a human IgG1 Psoriasis Novartis 2015 (US) 2015 (EU)Nivolumab Anti PD-1 human IgG4 Melanoma BMS Not approvedKeytruda pembrolizuumab Anti-PD-1 humanized
IgG4Melanoma Merck 2014 (US)
aAntibodies approved but later withdrawnbCLL chronic lymphocytic leukemia
8 HEY
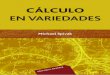
FIGURE 1 (Left panel) Model of antibody structure exemplified by IgG On top the antigen-binding sitesin orange each contain one variable light and variable heavy domain with the three complementaritydetermining regions (CDRs) that are responsible for the specific binding of the antibody to its target Foreach arm of the antibody an additional set of variable heavy and light domains together with the CDR-containing domains represent the two fragment antigen binding (Fab) regions The two Fabs are heldtogether via two disulfide bridges Below the Fabs is the Fc region which contains four constant heavydomains On the upper pair of these domains are binding sites for oligosaccharides which have majorimportance for the ability of the antibody Fc part to trigger effector functions when the Fc portion isbound to Fc gamma receptors on natural killer cells neutrophil granulocytes monocytesmacrophagesdendritic cells and B cells (Right panel) Examples of some of the antibody-derived alternative formatsused to exploit the specific features of the CDRs the Fabs and the Fc parts of the antibodies ScFv Thesingle chain fragment variable consists of the variable domains of the heavy and light chains heldtogether by a flexible linker This can also be used as a carrier of a cytotoxic drug in a so-called antibodydrug complex (ADC) where the specificity of the ScFv is used to target the cytotoxic drug to eg atumor Bite (bi-specific T cell engager) Fusion proteins consisting of two ScFvs one directed against thetarget on a tumor cell and the other against the T cell receptor (CD3) Diabody ScFv dimers where shortlinker peptides (five amino acids) ensure dimerization and not folding of the ScFvs Fab and F(ab)2fragments Single Fab fragments or fragments containing two Fabs linked via disulfide bridges This isused where effector functions related to the Fc part of the antibody are unwanted and where a smallersize is desired to obtain better tissue penetration in eg tumors Due to the lack of the FcRn binding viathe Fc part Fab and F(ab)2 fragments have much shorter half-lives (hours or days) than full-sizeantibodies (weeks) These can also be used as carriers of cytotoxic payloads or cytotoxic radioactiveisotopes and for the F(ab)2 fragments can be constructed as bi-specifics which can cross-link immunecells and target cells Fc fusion protein Fusion protein containing the Fc domain of an immunoglobulinbound to a peptide The peptide can be a ligand for a specific receptor on a target cell or a blockingpeptide for a soluble ligand The Fc part provides a longer half-life to the construct and the potential tobind to and engage effector functions in the killing of eg tumor cells or infected cells ADCsRIAs andbi-specifics Full-size IgG antibodies carrying either a cytotoxic chemical or radioactive payload whichmay also carry different CDRs enabling cross-linking of effector and target cells for increased killingdoi101128microbiolspecAID-0026-2014f1
CHAPTER 1 bull History and Practice Antibodies in Infectious Diseases 9
contain special hyper-variable segments calledcomplementarity-determining regions (CDRs)which allow the B cells via genetic recom-bination to generate antibodies to all thedifferent antigens specific to amino acid se-quences or three-dimensional structuralmotifs(polysaccharides DNA and RNA) found onpathogens
Based on the structure of their heavy chainconstant regions antibodies or immuno-globulins are separated into five classesmdashIgM IgG IgE IgD and IgA Differences inthe sequences of the constant regions providedistinct characteristics to these different clas-ses These characteristics include the numberof heavy chain constant segments the numberand location of interconnecting disulfidebridges the length of the hinge region andthe number and location of oligosaccharidemoieties For IgG four heavy chain versionsexist creating IgG1 2 3 and 4 isotypes eachwith different characteristics in their serumhalf-lives and ability to trigger different effec-tor functions Because of the combined ad-vantage from ability to trigger effectormechanisms long [21 days] half-life theirability to be transported over the placentaand their stability in the production processantibodies of the IgG class and of the IgG1isotype are preferred as the basis for newantibody-based therapies The effector func-tions are triggered by the Fc part of an antibodywhen the variable parts of the antibody arebound directly to an infectious agent or toproteins from an infectious agent expressed onan infected cell This binding leaves the Fc partfree to interactwithFc receptors onphagocyticcells and neutrophils eosinophils and naturalkiller cells capable of inducing phagocytosis orlysis of infectious agents or infected cellsThese effector functions include (i) the abilityto activate the complement system for lysis(complement-dependent cellular cytotoxicity)(ii) triggering of uptake and destruction byphagocytic cells such as macrophages andneutrophils via interaction with Fc receptorson these cells (iii) activation of macrophageseosinophils neutrophils and natural killer
cells to kill infected cells via binding to Fcreceptors on these cells and antibody-depen-dent cellular cytotoxicity and (iv) neutraliza-tion of bacterial toxins and blocking of bindingand uptake of bacteria or viruses to target cells(see Fig 2) (9)
The Fcpart of IgG antibodies also contains aregion that interacts with the neonatal Fcreceptor (FcRn) expressed on most immuno-competent cells and inmany other cells such asendothelial cells in kidney liver placenta lungand breast (10) which protects antibodies fromdegradation by phagocytoticexocytotic cy-cling into FcRn-expressing cells thereby pro-longing their half-life This results in half-livesof 20 to 21 days for most IgG1 2 and 4antibodies whereas half-lives are 10 6 and 2days respectively for IgM IgA and IgE Thehighly specific binding sites on the variableregions of the upper arms of the antibody allowfor several important features of antibodiesndashbinding to and neutralization of eg bacterialtoxins binding to pathogens and blocking theirbinding to or interaction with target cells (egcyncytia formation of CMV-infected cells) orblocking of binding and interactions of infec-tious agents with target cells via blockingreceptors on the target cells
METHODS AND PLATFORMS FORGENERATING ANTIBODIES
As described above the early use of passiveantibody transfer as a therapy in infectiousdiseases involved the use of immune serumfrom immunized sheep and horses These pre-parations were crude and contained a broadmixture of neutralizing and non-neutralizingantibodies and both the foreign nature of theantibodies and the numerous host serumproteins This resulted in less specific andthus less efficient therapies due to a highvariability in efficacy between batches derivedfrom different animals immunized with dif-ferent strains of bacteria in different labor-atories and resulted in multiple unwantedside effects related to hypersensitivity and
10 HEY
anaphylactic reactions to foreign proteinsThese days antibodies being developed fortreatment of diseases in humans are highlypurified and are mostly fully human mono-clonal antibodies The term monoclonal anti-body refers to that cell cultures used forgenerating these antibodies each originatesfrom a single cell and thus produces onlyone specific antibody Development of fullyhuman monoclonal antibodies happened instages over a time span of more than 15 yearsFirst stage in this process was generation ofmonoclonalmurine IgG antibodies (eg OKT3[muronomab-CD3 Johnson and Johnson] ap-proved in 1986) Next stage was generation ofso called chimeric antibodies consisting ofhuman heavy and light chain constant sec-tions but with murine variable sections (eg
Rituxan [rituximab Genentech]) Next stagewas then the humanized antibodies wherethe only remaining murine part of the anti-body is the antigen-binding CDR (eg Xolair[omalizumab NovartisGenentech]) Both thefirst chimeric and humanized antibodies wereapproved in the late 1990s Then finally 16years later the first fully human antibodyHumira (adalimumab Abbott) was approvedin 2002 Since the time of the crude and low-scale manufacturing of the original antibodyserum products much has changed andtherapeutic antibodies are now produced byfermentation in 5000 liter scale using highlycontrolled and documented yeast or mamma-lian cell lines that are genetically engineered toexpress a single specific antibody This hasresulted in a pure and highly specific antibody
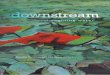
FIGURE 2 Effector functions of antibodies (a) Antibodies bind to pathogen-derived or endogenousantigens expressed on the surface of an infected cell which triggers binding to Fc receptors on naturalkiller cells and lysis of the infected cell by antibody-dependent cellular cytotoxicity (b) Antibodies bindto pathogen-derived or endogenous antigens expressed on the surface of infected cells which triggersactivation of complement through binding of complement factor C1q (c) Neutralization Top Bacterialtoxin neutralized by bound antigen Bottom Antibody bound to either receptor for the virus or to thevirus itself which blocks virus binding and entry into the cell (d) Antibody bound to viral surfaceproteins binds to Fc receptors on phagocytic cells eg macrophages and triggers endocytosis anddestruction of virus in endolysosome doi101128microbiolspecAID-0026-2014f2
CHAPTER 1 bull History and Practice Antibodies in Infectious Diseases 11

Antibodies for Infectious Diseases
Antibodies for Infectious Diseases
Edited by
James E Crowe JrVanderbilt University Medical CenterNashville Tennessee
Diana BoraschiNational Research CouncilNapoli Italy
AND
Rino RappuoliNovartis VaccinesSiena Italy
Washington DC
Copyright copy 2015 American Society for Microbiology All rights reserved No part of this publication may be reproduced or transmitted in whole or in part or reused in any form or by any means electronic or mechanical including photocopying and recording or by any information storage and retrieval system without permission in writing from the publisher
Disclaimer To the best of the publisherrsquos knowledge this publication provides information concerning the subject matter covered that is accurate as of the date of publication The publisher is not providing legal medical or other professional services Any reference herein to any specific commercial products procedures or services by trade name trademark manufacturer or otherwise does not constitute or imply endorsement recommendation or favored status by the American Society for Microbiology (ASM) The views and opinions of the author(s) expressed in this publication do not necessarily state or reflect those of ASM and they shall not be used to advertise or endorse any product
Library of Congress Cataloging-in-Publication Data
Antibodies for infectious diseases edited by James E Crowe Jr Vanderbilt University Medical Center Nashville Tennessee Diana Boraschi National Research Council Napoli Italy and Rino Rappuoli Novartis Vaccines Siena Italypages cmIncludes bibliographical references and indexISBN 978-1-55581-735-0 (alk paper)1 Immunoglobulins 2 Communicable diseases--Immunological aspects I Crowe James E Jr editor II Boraschi D (Diana) editor III Rappuoli Rino editor QR1867A534 201561607rsquo98--dc232015009356eISBN 978-1-55581-741-1doi101128978155581741110 9 8 7 6 5 4 3 2 1
All Rights ReservedPrinted in the United States of America
Address editorial correspondence to ASM Press 1752 N St NWWashington DC 20036-2904 USASend orders to ASM Press PO Box 605 Herndon VA 20172 USAPhone 800-546-2416 703-661-1593Fax 703-661-1501E-mail booksasmusaorgOnline httpestoreasmorg
Cover image Cancer cell with high details (source 123RF)
Contents
ContributorsemspixPrefaceemspxvii
IntroductIon
1 History and Practice Antibodies in Infectious Diseasesemsp3 Adam Hey
General Features oF ImmunoGlobulIns
2 Functions of Antibodiesemsp25 Donald N Forthal
3 Antibody Structureemsp49 Robyn L Stanfield and Ian A Wilson
4 The Role of Complement in Antibody Therapy for Infectious Diseasesemsp63 Peter P Wibroe Shen Y Helvig and S Moein Moghimi
5 Immunoglobulin E and Allergy Antibodies in Immune Inflammation and Treatmentemsp75
Sophia N Karagiannis Panagiotis Karagiannis Debra H Josephs Louise Saul Amy E Gilbert Nadine Upton and Hannah J Gould
antIbody dIscovery approaches
6 Phage and Yeast Displayemsp105 Jared Sheehan and Wayne A Marasco
7 Efficient Methods To Isolate Human Monoclonal Antibodies from Memory B Cells and Plasma Cellsemsp129
Davide Corti and Antonio Lanzavecchia
8 Use of Human Hybridoma Technology To Isolate Human Monoclonal Antibodiesemsp141 Scott A Smith and James E Crowe Jr
9 Humanized Mice for Studying Human Immune Responses and Generating Human Monoclonal Antibodiesemsp157
Ramesh Akkina
10 Antibodies Computer-Aided Prediction of Structure and Design of Functionemsp173 Alexander M Sevy and Jens Meiler
v
vi contents
pathoGen-specIFIc antIbodIes
11 Antibodies Targeting the Envelope of HIV-1emsp193 Luzia M Mayr and Susan Zolla-Pazner
12 Committing the Oldest Sins in the Newest Kind of WaysmdashAntibodies Targeting the Influenza Virus Type A Hemagglutinin Globular Heademsp209
Jens C Krause and James E Crowe Jr
13 Prevention of Respiratory Syncytial Virus Infection From Vaccine to Antibodyemsp221
Kelly Huang and Herren Wu
14 Human Metapneumovirusemsp237 Jennifer E Schuster and John V Williams
15 Dengue Antibody-Dependent Enhancement Knowns and Unknownsemsp249
Scott B Halstead
16 Immunotherapeutic Approaches To Prevent Cytomegalovirus-Mediated Diseaseemsp273
Edith Acquaye-Seedah Zachary P Frye and Jennifer A Maynard
17 Rotavirusemsp289 Manuel A Franco and Harry B Greenberg
18 Bacterial ToxinsmdashStaphylococcal Enterotoxin Bemsp303 Bettina C Fries and Avanish K Varshney
technIcal advances
19 Antibody Engineeringemsp321 Kin-Ming Lo Olivier Leger and Bjoumlrn Hock
20 High-Throughput DNA Sequencing Analysis of Antibody Repertoiresemsp345
Scott D Boyd and Shilpa A Joshi
21 Antibody Informatics IMGT the International ImMunoGeneTics Information Systememsp363
Marie-Paule Lefranc
22 Probing Antibody-Antigen Interactionsemsp381 Guocheng Yang Stefanie N Velgos Shanta P Boddapati
and Michael R Sierks
23 Radiolabeled Antibodies for Therapy of Infectious Diseasesemsp399 Ekaterina Dadachova and Arturo Casadevall
alternate systems For expressIon
24 Plant-Derived Monoclonal Antibodies for Prevention and Treatment of Infectious Diseaseemsp413
Andrew Hiatt Kevin J Whaley and Larry Zeitlin
25 Vector-Mediated In Vivo Antibody Expressionemsp427 Bruce C Schnepp and Philip R Johnson
Indexemsp441
contents vii
Contributors
Edith Acquaye-SeedahDepartment of BiochemistryUniversity of Texas at AustinAustin TX 78712
Ramesh AkkinaDepartment of Microbiology Immunology and PathologyColorado State University1619 Campus DeliveryFort Collins CO 80523
Shanta P BoddapatiDepartment of Biomedical EngineeringOregon Health and Science University3181 SW Sam Jackson Park RoadPortland OR 97239
Scott D BoydDepartment of PathologyStanford UniversityStanford CA 94305
Arturo CasadevallDepartments of Microbiology and Immunology and MedicineAlbert Einstein College of Medicine of Yeshiva University1695A Eastchester RoadBronx NY 10461
Davide CortiHumabs BioMed SAvia Mirasole 1Bellinzona 6500Switzerland
James E Crowe JrSchool of MedicineVanderbilt UniversityNashville TN 37232
ix
x contRIBUtoRs
Ekaterina (Kate) DadachovaDepartments of Radiology Microbiology and ImmunologyAlbert Einstein College of Medicine of Yeshiva University1695A Eastchester RoadBronx NY 10461
Donald N ForthalDepartment of Infectious Diseases3044 Hewitt HallUniversity of California IrvineIrvine CA 92617
Manuel A FrancoFacultad de Ciencias y MedicinaPontificia Universidad JaverianaOficina 306 Edificio 50Carrera 7 40-62BogotaacuteColombia
Bettina C FriesDepartment of MedicineInfectious Diseases and Department of Microbiology and ImmunologyAlbert Einstein College of MedicineBronx NY 10461
Zachary P FryeDepartment of Chemical EngineeringUniversity of Texas at AustinAustin TX 78712
Amy E GilbertCutaneous Medicine and Immunotherapy UnitSt Johnrsquos Institute of DermatologyDivision of Genetics and Molecular Medicine amp NIHR Biomedical Research Centre at Guyrsquos and St Thomasrsquos Hospitals and Kingrsquos College London School of MedicineGuyrsquos HospitalLondon SE1 9RTUnited Kingdom
Hannah J GouldRandall Division of Cell and Molecular BiophysicsDivision of Asthma Allergy and Lung BiologyMRC and Asthma UK Centre for Allergic Mechanisms of AsthmaKingrsquos College LondonNew Huntrsquos HouseGuyrsquos CampusLondon SE1 1ULUnited Kingdom
contRIBUtoRs xi
Harry B GreenbergDepartments of Medicine and Microbiology and ImmunologyStanford University School of Medicine and the VAPAHCSPalo Alto CA 94305
Scott B HalsteadDepartment of Preventive Medicine and BiometricsUniformed Services University of the Health SciencesBethesda MD 20814
Shen Y HelvigDepartment of PharmacyCenter for Pharmaceutical Nanotechnology and NanotoxicologyFaculty of Health and Medical SciencesUniversity of CopenhagenCopenhagen DK-2100Denmark
Adam HeyPreclinical Safety BiologicsNovartis AGBaselSwitzerland
Andrew HiattMapp Biopharmaceutical Inc6160 Lusk Blvd C105San Diego CA 92121
Bjoumlrn HockDepartment of Protein Engineering and Antibody TechnologiesMerck Serono Merck KgaAFrankfurter Str 250D-64293 DarmstadtGermany
Kelly HuangDepartment of Infectious DiseaseMedImmune LLCOne MedImmune WayGaithersburg MD 20878
Philip R JohnsonThe Childrenrsquos Hospital of PhiladelphiaAbramson Research CenterPhiladelphia PA 19104
Debra H JosephsCutaneous Medicine and Immunotherapy UnitSt Johnrsquos Institute of DermatologyDivision of Genetics and Molecular Medicine amp NIHR Biomedical Research Centre at Guyrsquos and St Thomasrsquos HospitalsKingrsquos College London School of MedicineGuyrsquos HospitalLondon SE1 9RTUnited Kingdom
Shilpa A JoshiDepartment of PathologyStanford UniversityStanford CA 94305
Sophia N KaragiannisCutaneous Medicine and Immunotherapy UnitSt Johnrsquos Institute of DermatologyDivision of Genetics and Molecular Medicine amp NIHR Biomedical Research Centre at Guyrsquos and St Thomasrsquos HospitalsKingrsquos College London School of MedicineGuyrsquos HospitalLondon SE1 9RTUnited Kingdom
Panagiotis KaragiannisCutaneous Medicine and Immunotherapy UnitSt Johnrsquos Institute of DermatologyDivision of Genetics and Molecular Medicine amp NIHR Biomedical Research Centre at Guyrsquos and St Thomasrsquos HospitalsKingrsquos College London School of MedicineGuyrsquos HospitalLondon SE1 9RTUnited Kingdom
Jens C KrauseChildrenrsquos HospitalUniversity of Freiburg Medical Center79106 FreibergGermany
Antonio LanzavecchiaInstitute for Research in Biomedicinevia Vincenzo Vela 6Bellinzona 6500Switzerland
xii contRIBUtoRs
Marie-Paule LefrancLaboratoire drsquoImmunoGeacuteneacutetique Moleacuteculaire LIGMIMGTreg the international ImMunoGeneTics information systemregInstitut de Geacuteneacutetique Humaine IGHUniversiteacute Montpellier 2UPR CNRS 1142Montpellier 34396 cedex 5 40202France
Olivier LegerDepartment of Protein Engineering and Antibody TechnologiesMerck Serono SA--Geneva9 chemin des Mines1202 GenevaSwitzerland
Kin-Ming LoDepartment of Protein Engineering and Antibody TechnologiesEMD Serono Research Institute45A Middlesex TurnpikeBillerica MA 01821
Wayne A MarascoDepartment of Cancer Immunology and AIDSDana-Farber Cancer InstituteHarvard Medical SchoolBoston MA 02215
Jennifer A MaynardDepartment of Chemical EngineeringUniversity of Texas at AustinAustin TX 78712
Luzia M MayrINSERM U1109Universiteacute de Strasbourg3 Rue Koeberleacute67000 StrasbourgFrance
Jens MeilerDepartment of Chemistry and Center for Structural BiologyVanderbilt UniversityNashville TN 37212
contRIBUtoRs xiii
S Moein MoghimiDepartment of PharmacyCenter for Pharmaceutical Nanotechnology and NanotoxicologyFaculty of Health and Medical SciencesUniversity of CopenhagenCopenhagen DK-2100Denmark
Susan Zolla-PaznerNew York University School of Medicine550 First AvenueNew York NY 10016
Louise SaulCutaneous Medicine and Immunotherapy UnitSt Johnrsquos Institute of DermatologyDivision of Genetics and Molecular Medicine amp NIHR Biomedical Research Centre at Guyrsquos and St Thomasrsquos HospitalsKingrsquos College London School of MedicineGuyrsquos HospitalLondon SE1 9RTUnited Kingdom
Bruce C SchneppThe Childrenrsquos Hospital of PhiladelphiaAbramson Research CenterPhiladelphia PA 19104
Jennifer E SchusterDepartment of PediatricsChildrenrsquos Mercy HospitalKansas City MO 64108-4619
Alexander M SevyDepartment of Chemistry and Center for Structural BiologyVanderbilt UniversityNashville TN 37212
Jared SheehanDepartment of Cancer Immunology and AIDSDana-Farber Cancer InstituteHarvard Medical SchoolBoston MA 02215
Michael R SierksDepartment of Chemical EngineeringArizona State UniversityTempe AZ 85287-6006
xiv contRIBUtoRs
Scott A SmithThe Vanderbilt Vaccine Center and the Department of MedicineVanderbilt University Medical CenterNashville TN 37232
Robyn L StanfieldDepartment of Molecular BiologyThe Scripps Research Institute10550 North Torrey Pines RoadLa Jolla CA 92037
Nadine UptonRandall Division of Cell and Molecular BiophysicsDivision of Asthma Allergy and Lung BiologyMRC and Asthma UK Centre for Allergic Mechanisms of AsthmaKingrsquos College LondonNew Huntrsquos HouseGuyrsquos CampusLondon SE1 1ULUnited Kingdom
Avanish K VarshneyDepartment of MedicineInfectious Diseases and Department of Microbiology and ImmunologyAlbert Einstein College of MedicineBronx NY 10461
Stefanie N VelgosMayo Clinic Arizona5777 East Mayo BoulevardPhoenix AZ 85054
Kevin J WhaleyMapp Biopharmaceutical Inc6160 Lusk Blvd C105San Diego CA 92121
Peter P WibroeCentre for Pharmaceutical Nanotechnology and NanotoxicologyDepartment of PharmacyFaculty of Health and Medical SciencesUniversity of CopenhagenCopenhagen DK-2100Denmark
John V WilliamsDepartment of PediatricsSchool of MedicineVanderbilt UniversityNashville TN 37232-2581
contRIBUtoRs xv
Ian A WilsonDepartment of Molecular Biology and Skaggs Institute for Chemical BiologyThe Scripps Research Institute10550 North Torrey Pines RoadLa Jolla CA 92037
Herren WuDepartment of Antibody Discovery and Protein EngineeringMedImmune LLCOne MedImmune WayGaithersburg MD 20879
Guocheng YangDepartment of Chemical EngineeringArizona State UniversityTempe AZ 85287-6006
Larry ZeitlinMapp Biopharmaceutical Inc6160 Lusk Blvd C105San Diego CA 92121
xvi contRIBUtoRs
Preface
Antibodies form the principal foundation for modern intervention against in-fectious diseases Emil Adolf von Behring was awarded the first Nobel Prize in Physiology or Medicine in 1901 ldquofor his work on serum therapy especially its appli-cation against diphtheria by which he has opened a new road in the domain of med-ical science and thereby placed in the hands of the physician a victorious weapon against illness and deathsrdquo Antibodies now provide the focus for understanding mechanisms of immunity to most infectious diseases and they play a central role in passive immunotherapy and active vaccination as mechanisms or correlates of immunity For most of the 20th century immunotherapy was based on passive transfer of polyclonal hyperimmune animal serum immune human serum or even hyperimmune human serum Georges JF Koumlhler and Ceacutesar Milstein re-ported the generation of monoclonal antibodies in 1979 for which they shared the 1984 Nobel Prize in Physiology or Medicine ldquofor the discovery of the princi-ple for production of monoclonal antibodiesrdquo Since that time entire fields related to antibodies for infectious diseases including antibody gene cloning engineer-ing and expression antibody libraries and high-throughput antibody gene rep-ertoire sequence analysis have extended our capabilities to explore the diversity of antibody specificity and function with unprecedented depth and breadth
This book provides a broad survey of many of the most important aspects of the field of antibodies for infectious diseases The book begins with a general introduction followed by chapters 2 through 5 on general features pertaining to structure function isotype and the role of complement in antibody function Chapters 6 through 10 review contemporary approaches for antibody discovery using phage and yeast display plasma cell and memory B cell cloning human hybridomas humanized mice and computational methods Chapters 11 through 18 review in depth the biology of antibodies specific for particular pathogens including viruses and bacterial toxins to illustrate the role of antibodies in anti- microbial immunity with specific targets These chapters reveal that attempts to raise effective antibody responses to each of these pathogens faces unique and pathogen-specific challenges Chapters 19 to 23 cover major technical advances pertaining to antibody engineering repertoire sequencing and analysis and new methods for study or therapeutic use of antibodies including radiotherapy Fi-nally chapters 24 and 25 cover new methods for expression of monoclonal anti-bodies in plants or by transfer of antibody genes for in vivo expression in treated subjects
Recent literature is exploding with new antibody-related techniques and re-ports of antimicrobial antibodies with unprecedented potency breadth of activ-
xvii
xviii PReface
ity and therapeutic potential We hope that this timely compilation of state-of-the-art reviews of major aspects of this field will be of interest to both antibody cognoscenti and those new to this exciting field We thank the authors for their dedication in producing definitive reviews of the topics at hand
James E Crowe JrDiana BoraschiRino Rappuoli
INTRODUCTION
History and PracticeAntibodies in Infectious Diseases 1ADAM HEY1
Antibodies in Infectious Diseases aims to inform update and inspire studentsteachers researchers pharmaceutical developers and health care professionalson the status of the development of antibody-based therapies for treatinginfectious diseases and the potential for these in times of growing antibioticresistance to provide alternative treatment solutions to the currently usedantibiotics and new treatments for infectious diseases where no propertreatments are available
This introductory article will provide a historical perspective on the useof antibody-based therapies followed by a high-level overview of whatmakes antibodies attractive tools for this purpose This will include the prosand cons of such therapies compared to the use of antibiotics and thepractical and strategic considerations involved in selecting the best formatand development path for new antibody-based therapies targeting specificinfectious agents Then examples of antibody-based therapies in thedevelopment of treatments for infectious diseases will be presented andfinally a look into the future will summarize the different aspects that willinfluence what the future might bring for this type of treatments forinfectious diseases
1Preclinical Safety Biologics Novartis AG Basel Switzerland
Antibodies for Infectious DiseasesEdited by James E Crowe Jr Diana Boraschi and Rino Rappuolicopy 2015 American Society for Microbiology Washington DCdoi101128microbiolspecAID-0026-2014
3
HISTORICAL PERSPECTIVE
Antibodies and the use of passive antibodytherapy in the treatment of infectious dis-eases is the story of a treatment conceptwhich dates back more than 120 years to thelate 19th century and which originally bythe use of serum from immunized animalsprovided the first effective treatment optionsagainst severe bacterial infections (1 2) Byimmunizing horses with bacterial toxinsfrom Clostridium tetani and Corynebacteri-um diphtheriae Emil A Von Behring andShibasaburo Kitasato (3) generated serumcontaining antibodies capable of neutraliz-ing the effects of the toxins produced bythese bacteria and successfully providedtreatment for these serious diseases wherethe pathogenesis is driven by the effects ofthe bacterial toxins For his work on provid-ing treatment for diphtheria Behring re-ceived the Nobel Prize in Physiology orMedicine in 1901 These radical treatmentresults quickly prompted development ofmultiple additional serum therapies for thetreatment of infectious diseases caused byeg Neisseria meningitidis Haemophilus in-fluenza and group A Streptococcus Sinceserum therapy involved administration oflarge amounts of crude mixtures of animalproteins including antibodies they wereassociated with side effects in the form ofhypersensitivity and serum sickness (2)
Due to the crude and unpurified nature ofthese products side effects were seen evenwhen administering human serum prepa-rations Side effects were observed in up to50 of patients and were considered to becaused by immune complex formations thatresulted in symptoms such as rash itchingjoint pain fever and in serious cases hypoten-sion and shock However due to the lack ofalternative options these treatments weredespite their side effects widely used Serumwas normally administered by intravenousinfusion in patients after a test for hypersensi-tivity where a small amount of serum wasinjected subcutaniously (1) As described
above serum therapy applied in these earlydays (late 19th century and early 20th century)involved preparations of serum from rabbitsand horses immunized with the infectiousagent or in live andor neutralized versions ortoxins from these (1) The costs of keeping theimmunized animals and the production andpotency testing of the materials made this arelatively expensive treatment In 1891 datafrom Klemperer (4) showed serum therapy toprotect rabbits from Streptococcus pneumoniaeinfection and paved the way for this type oftreatment and for development of similarserum-based treatments of streptococcal in-fections in humans When treating humansearly administration of serum could reducemortality significantly down to around 5compared to when administered 4 to 5 daysafter onset of symptoms when serum treat-ment was largely without effect This stronglyindicated the need for quick diagnosis andquick treatment to control the infection beforeit got out of control Consequently in theabsence of a specific diagnosis mixtures ofserum from immunizations with differentserotypes were used to circumvent this needfor early treatment without having a serotype-specific diagnosis The understanding thatdifferent serotypes existed for pneumococciand that efficient treatment relied on usingserotype-specific serum was being built upduring the 1920s and 1930s through experiencefrom extensive clinical trials
By the end of the 1930s serum therapywasthe standard of care for treatment of pneu-mococcal pneumonia At that time theefficacy and potency of the derived serawere assessed in mice in ldquothe mouse pro-tection testrdquo by testing survival after aconcomitant intraperitoneal injection of alethal dose of pneumococci and the serum tobe tested Due to the inherent variation inthis test efficacy and survival in two thirds ofthe animals was the acceptance criteria and10 times the lowest dose providing this wasused for defining a unit of the serum Thisallowed for large batch-to-batch variationand the use of different strains of bacteria for
4 HEY
immunization probably explains part of themissing responses observed (1) In the early20th century a pandemic of meningitis inEurope and the United States with mortalityrates up to 80 spurred the development ofserum therapy treatment options Althoughin the 1930s this became the recommendedtreatment in children assumed to be suffer-ing from meningitis failure to reduce mor-tality in several meningitis epidemics duringthat time raised doubts about the generalapplicability of serum treatment In thosedays serum therapy often involved quiteextensive procedures and infusion of largevolumes of serum The following exampleclearly illustrates this Data from Flexnerand Jobling (5) from treating meningitis inmonkeys resulted in the development of serafrom immunized horses for treatment inhumans The treatment protocol includedlumbar puncture and withdrawal of morethan 30 ml of spinal fluid representing anamount slightly larger than the expectedamount of horse serum to be injected subse-quently This treatment involved such dailyslow infusions of up to 30 ml of serum untilthe patientrsquos condition improved This treat-ment was used in outbreaks in New York in1905 and 1906 and did markedly decreasemortality
After the discovery of penicillin by Flemingin 1928 and the subsequent introduction ofantibiotics in the 1930s serum therapy waslargely abandoned over a period of 10 years dueto the availability of these new more broadlyeffective and cheaper treatment optionswhichalso had fewer side effects Although improve-ments in the purification of antibodies hadresulted in preparations with better safety andside effect profiles high manufacturing costsand narrow specificity resulted in antibodytherapy being mostly restricted to a smallernumber of selected treatments for snakevenoms bacterial toxins and some viral infec-tions (1 2) Currently antibody administrationis used for treatment and prevention ofhepatitis B virus rabies virus respiratorysyncytial virus (RSV) Clostridium tetani Clos-
tridium botulinum vaccinia virus echovirusand enterovirus For the most part thesetreatments consist of pooled immunoglobulinalso known as IVIG (intravenous immunoglob-ulin) from several postexposure donors Thisresults in both batch-to-batch variation in theneed for relatively large amounts of serum dueto low specificity and to restricted supplies dueto reliance on exposed donors
However several challengeshave resulted inthe need for new tools in the treatment andpreventionof infectiousdiseasesThebroadandgeneral use of antibiotics in human and veter-inary medicine for many years has resulted inthe development of multi-resistant strains ofbacteria with limited to no response to existingtreatments such as methicillin-resistant Staph-ylococcusaureus (MRSA) vancomycin-resistantS aureus and others This has resulted inpatients needing screening and treatment withseveral antibacterial agents and longer treat-ment time causing extra strain on patients andhealth care providers (6 httpwwwcdcgovdrugresistancethreat-report-2013indexhtml) According to the WHO and CDC morethan 25000 people in European Unioncountries and similar numbers in the UnitedStates die every year as a result of antibiotic-resistant infections This together with theemergence of new pathogens (eg severeacute respiratory syndrome Middle East respi-ratory syndrome) the re-emergenceepidemicsof oldknown pathogens (eg Ebola) and thedifficulties in treating infections in immune-deficient patients (eg HIV patients) has high-lighted the need for new solutions The 2014Ebola epidemic in West Africa (Liberia SierraLeone Guinea Nigeria and Senegal) has fur-ther highlighted this No treatment or prophy-lactic vaccine is available to treat or prevent thespread of Ebola infections which have anaveragemortality of gt50 Local health author-ities in the affected countries are struggling tocontain and handle the disease which isthreatening to go out of control and spreadmorewidelyVariousproductsmainly antibodycocktails from previously recovered patientsare being used despite a lack of clinical data on
CHAPTER 1 bull History and Practice Antibodies in Infectious Diseases 5
their safety and efficacy and those are the onlysporadically available treatment options andonly in small amounts and for a few patients
Ebola is an example of a disease whichnormally affects only a small number ofindividuals and which normally burns outwhen disease outbreaks are contained There-fore given the small number of potentialpatients affected by previous Ebola infectionsto date there was no incentive for big pharmacompanies to do research and development ofdrugs for EbolaWith the increasing number ofinfected (13567) andadeath toll of 4951 (7) andthe lack of the ability to contain the epidemic itwill be interesting to follow the aftermath ofthis outbreak and see whether there will berequests for new ways to ensure that vaccinesand treatment options are available for Ebolaand similar high-mortality and potential bio-warfare infections that have no availabletreatments or procedures to for mass-produc-tion upon the first signsreports of activeinfections Although both the CDC and theWHO have special programs focusing on thesetypes of infections the Ebola outbreak in 2014clearly shows that more financial support forresearch and development of new diagnosticsand treatments is needed This is one examplewhere antibody-based treatments would havethe potential to play a major role To put this inthe right perspective one should however notforget that other infectious diseases such astuberculosis influenza and malaria kill hun-dreds of thousands each year There is there-fore plenty of room for improvement indeveloping treatments for these diseases aswell but the high attention drawn to eg theEbola outbreak creates a special niche andopportunity where antibody treatments couldgain extraordinary development funding andsupport and prove their value and treatmentpotential
That antibody-based therapies could takethis role is supported by the revolution intechnologies for the development selectiongeneration and purification of fully humanantibodies described in more detail later in thesection ldquoMethodsandPlatforms forGenerating
Antibodiesrdquo Antibody-based programs cur-rently at different stages of developmentinclude investigations into the potential use ofsingle antibody preparations combinations ofantibodies (to avoid survival of escape mu-tants) fragments of antibodies and antibodiescarrying radioactive isotopesorcytotoxicdrugsor antibody-like frameworks (eg fibronectin)either alone as a first-line treatment or as anadjunct to existing treatments This multitudeof possible formats the ability to raise anti-bodies to almost any target and the ability toengineer both size effector functions and half-life are now considered by many to providevery valuable tools for designing specificantibody-based treatments toeradicate specifictargeted infectious agents However althoughseveral antibody-based therapies have beenapproved for oncology and anti-inflammatoryindications (see Table 1) only one monoclonalantibody (mAb) is approved against an infec-tious disease agentmdashSynagis (palivizumabMedImmune) for the prevention and treat-ment of respiratory syncytical virus (RSV) inhigh-risk children Economic obstacles such asthe high cost of mAb therapies and relativelysmall markets have resulted in less interestfrom pharmaceutical companies in developingthese Also highlighting the challenges indeveloping these types of antibody-basedtreatments are the difficulties encountered indeveloping a follow-up higher-affinity candi-date to Synagis Poor translatability of dataobtained in the available animal disease mod-els for RSV in cotton rats has resulted in non-approval due to inferiority relative to SynagisIn other viral diseases such as cytomegalovirus(CMV) the high species specificity of thestrains of CMV makes it impossible to testhuman antibody therapies in vivo Thereforeany real data on the efficacy of treatments forCMV will not be obtained until testing inclinical trials As described later in this articleseveral new antibody-based therapies for in-fectious diseases are in development andhopefully this will gradually open the fieldand result in better treatment options andoutcomes for patients
6 HEY
TABLE 1 Approved and pending antibody-based therapies
Name antibody Target antibody type Indication Company Approval date
OKT3a Muronomab-CD3 CD3 murine IgG2a Autoimmune Johnson ampJohnson
1986 (US)
ReoPro abciximab PIIbIIIa chimeric IgG1Fab
Homeostasis Johnson ampJohnson
1984 (US)
Rituxan rituximab CD20 chimeric IgG1 Cancer Genentech 1997 (US) 1998 (EU)Zenapaxa daclizumab CD25 humanized IgG1 Autoimmune Roche 1997 (US) 1999 (EU)Simulect basiliximab CD25 chimeric IgG1 Autoimmune Novartis 1998 (US EU)Synagis palivizumab RSV humanized IgG1 Infections MedImmune 1998 (US) 1999 (EU)Remicade infliximab TNFα chimeric IgG1 Autoimmune Johnson amp
Johnson1998 (US) 1999 (EU)
Herceptin trastuzumab HER2 humanized IgG1 Cancer GenentechRoche
1998 (US) 2000 (EU)
Mylotarga gemtuzumabozogamicin
CD33 humanized IgG4immunotoxin
Cancer WyethPfizer 2000 (US)
Campath alemtuzumab CD52 humanized IgG1 Cancer Genzyme 2001 (US) 2001 (EU)Zevalin ibritumomabtiuxetan
CD20 murine IgG1radiolabeled (yttrium 90)
Cancer Biogen Idec 2002 (US) 2004 (EU)
Humira adalimumab TNFα human IgG1 Autoimmune Abbott 2002 (US) 2003 (EU)Xolair omalizumab IgE humanized IgG1 Autoimmune Genentech
Roche2003 (US)
Bexxar tositumomab-I-131 CD20 murine IgG2aradiolabeled (iodine131)
Cancer CorixaGSK 2003 (US)
Raptivaa falizumab CD11a humanized IgG1 Autoimmune GenentechRoche
2003 (US) 2004 (EU)
Erbitux cetuximab EGFR chimeric IgG1 Cancer ImcloneLilly 2004 (US) 2004 (EU)Avastin bevacizumab VEGF humanized IgG1 Cancer Genentech
Roche2004 (US) 2005 (EU)
Tysabri natalizumab α4-Intergrin humanizedIgG4
Autoimmune Biogen Idec 2004 (US)
Actemra tocilizumab Anti-IL-6R humanizedIgG1
Autoimmune ChugaiRoche
2005 (Japan) 2010 (US)
Vectibix panitumumab EGFR human IgG2 Cancer Amgen 2006 (US)Lucentis ranibizumab VEGF humanized IgG1
FabMaculardegeneration
GenentechRoche
2006 (US)
Soliris eculizumab C5 humanized IgG24 Blood disorders Alexion 2007 (US)Cimzia certolizumab pegol TNFα humanized
pegylated FabAutoimmune UCB 2008 (US)
Simponi golimumab TNFα human IgG1 Autoimmune Johnson ampJohnson
2009 (US EU Canada)
Ilaris canakinumab IL1b human IgG1 Infalmmatory Novartis 2009 (US EU)Stelara ustekinumab IL-1223 human IgG1 Autoimmune Johnson amp
Johnson2008 (EU) 2009 (US)
Arzerra ofatumumab CD20 human IgG1 Cancer Genmab 2009 (EU)Prolia denosumab RANK ligand human
IgG2Bone loss Amgen 2010 (US)
Numax motavizumab RSV humanized IgG1 Anti-infective MedImmune PendingABthrax Raxibacumab B anthrasis PA human
IgG1Anti-infection GSK 2012 (US)
Benlysta belimumab BLyS human IgG1 Autoimmune HGS 2011 (US)Yervoy ipilimumab CTLA-4 human IgG1 Cancer BMS 2011 (US)Adcetris brentuximabvedotin
CD30 chimeric IgG1drug- conjugate
Cancer SeattleGenetics
2011 (US)
(Continued on next page)
CHAPTER 1 bull History and Practice Antibodies in Infectious Diseases 7
INTRODUCTION TO ANTIBODIES
Antibodies also called immunoglobulins basedon their combined structure and function inimmune responses are produced by B cells ofthe immune system They are part of theadaptive immune response and are speciallydesigned for neutralizing and eliminating theinfectious agents and toxins produced by theseAntibodies are present in blood plasma andextracellular fluids and since these fluids wereformerly known as humors they were said tobe part of the humoral immune responseAntibodies are Y-shaped structures consistingof two main parts the upper arms of the Ywhich contain two identical variable-regionantigen binding sites and the lower regioncalled the constant regionwhich is responsiblefor the initiation of effector functions that leadto the removal and destruction of the pathogenor cells harboring the pathogen (see Fig 1) Theantigen-binding sites on an antibody can bythemselves bind to and neutralize bacterialtoxins and viruses thereby preventing themfrom binding to their target cells or receptorscausing toxic effects or spread of the infection
Antibodies consist of two pairs of heavy andlight chainswhich as described above are heldtogether in a Y-shaped arrangement Each ofthe heavy and light chains in these pairs isseparated into constant and variable chainsThe upper armsof theY each contain a variableand a constant sectionof the light and theheavychain where the upper variable parts of theheavy and light chains contain the antigen-binding site and the constant parts areconnected via disulfide bonds The lower partof theYcalled theconstantpart consistsof twoor three constant segments (immunoglobulindomains) from each of the two heavy chainsinteracting and also linked via disulfide bondsThe sectionsof theheavy chains connecting theconstant part of the upper arms to the constantparts of the constant region contain specialhinge regions that provide flexibility to thedifferent sections of the antibody to bind toantigens and effector cells The constant re-gions of the heavy chain also contain attachedoligosaccharide moieties which provide func-tional specialization to the antibodies (8)
The variable domains of the heavy and lightchains form the antigen-binding sites and
TABLE 1 Approved and pending antibody-based therapies (Continued)
Name antibody Target antibody type Indication Company Approval date
Perjeta pertuzumab Her2 humanized IgG1 Cancer GenentechRoche
2012 (US)
Kadcyla ado-trastuzumabemtansine
Her2 humanized IgG1Drug-conjugate
Cancer GenentechRoche
2013 (US)
Raxibacumab Anti-B anthrasis PAhuman IgG1
Anthraxinfection
Notapproved
2012
Entyvio vedolizumab Integrin α4β7humanized IgG1
Crohnrsquos diseaseulcerative colitis
Takeda 2014 (US)
Cyramza ramuciruumab Anti-VEGFR2Human IgG1
Gastric cancer Lilly 2014 (US)
Gazyva obinutuzumab Anti-CD20 humanizedIgG1 glucoengineered
CancerCLLb GenentechRoche
2014 (US)
Sylvant situximab Anti IL-6 chimeric IgG1 Castlemandisease
Janssen 2014 (US) 2014 (EU)
Cosentyx sekukinumab Anti IL-17a human IgG1 Psoriasis Novartis 2015 (US) 2015 (EU)Nivolumab Anti PD-1 human IgG4 Melanoma BMS Not approvedKeytruda pembrolizuumab Anti-PD-1 humanized
IgG4Melanoma Merck 2014 (US)
aAntibodies approved but later withdrawnbCLL chronic lymphocytic leukemia
8 HEY
FIGURE 1 (Left panel) Model of antibody structure exemplified by IgG On top the antigen-binding sitesin orange each contain one variable light and variable heavy domain with the three complementaritydetermining regions (CDRs) that are responsible for the specific binding of the antibody to its target Foreach arm of the antibody an additional set of variable heavy and light domains together with the CDR-containing domains represent the two fragment antigen binding (Fab) regions The two Fabs are heldtogether via two disulfide bridges Below the Fabs is the Fc region which contains four constant heavydomains On the upper pair of these domains are binding sites for oligosaccharides which have majorimportance for the ability of the antibody Fc part to trigger effector functions when the Fc portion isbound to Fc gamma receptors on natural killer cells neutrophil granulocytes monocytesmacrophagesdendritic cells and B cells (Right panel) Examples of some of the antibody-derived alternative formatsused to exploit the specific features of the CDRs the Fabs and the Fc parts of the antibodies ScFv Thesingle chain fragment variable consists of the variable domains of the heavy and light chains heldtogether by a flexible linker This can also be used as a carrier of a cytotoxic drug in a so-called antibodydrug complex (ADC) where the specificity of the ScFv is used to target the cytotoxic drug to eg atumor Bite (bi-specific T cell engager) Fusion proteins consisting of two ScFvs one directed against thetarget on a tumor cell and the other against the T cell receptor (CD3) Diabody ScFv dimers where shortlinker peptides (five amino acids) ensure dimerization and not folding of the ScFvs Fab and F(ab)2fragments Single Fab fragments or fragments containing two Fabs linked via disulfide bridges This isused where effector functions related to the Fc part of the antibody are unwanted and where a smallersize is desired to obtain better tissue penetration in eg tumors Due to the lack of the FcRn binding viathe Fc part Fab and F(ab)2 fragments have much shorter half-lives (hours or days) than full-sizeantibodies (weeks) These can also be used as carriers of cytotoxic payloads or cytotoxic radioactiveisotopes and for the F(ab)2 fragments can be constructed as bi-specifics which can cross-link immunecells and target cells Fc fusion protein Fusion protein containing the Fc domain of an immunoglobulinbound to a peptide The peptide can be a ligand for a specific receptor on a target cell or a blockingpeptide for a soluble ligand The Fc part provides a longer half-life to the construct and the potential tobind to and engage effector functions in the killing of eg tumor cells or infected cells ADCsRIAs andbi-specifics Full-size IgG antibodies carrying either a cytotoxic chemical or radioactive payload whichmay also carry different CDRs enabling cross-linking of effector and target cells for increased killingdoi101128microbiolspecAID-0026-2014f1
CHAPTER 1 bull History and Practice Antibodies in Infectious Diseases 9
contain special hyper-variable segments calledcomplementarity-determining regions (CDRs)which allow the B cells via genetic recom-bination to generate antibodies to all thedifferent antigens specific to amino acid se-quences or three-dimensional structuralmotifs(polysaccharides DNA and RNA) found onpathogens
Based on the structure of their heavy chainconstant regions antibodies or immuno-globulins are separated into five classesmdashIgM IgG IgE IgD and IgA Differences inthe sequences of the constant regions providedistinct characteristics to these different clas-ses These characteristics include the numberof heavy chain constant segments the numberand location of interconnecting disulfidebridges the length of the hinge region andthe number and location of oligosaccharidemoieties For IgG four heavy chain versionsexist creating IgG1 2 3 and 4 isotypes eachwith different characteristics in their serumhalf-lives and ability to trigger different effec-tor functions Because of the combined ad-vantage from ability to trigger effectormechanisms long [21 days] half-life theirability to be transported over the placentaand their stability in the production processantibodies of the IgG class and of the IgG1isotype are preferred as the basis for newantibody-based therapies The effector func-tions are triggered by the Fc part of an antibodywhen the variable parts of the antibody arebound directly to an infectious agent or toproteins from an infectious agent expressed onan infected cell This binding leaves the Fc partfree to interactwithFc receptors onphagocyticcells and neutrophils eosinophils and naturalkiller cells capable of inducing phagocytosis orlysis of infectious agents or infected cellsThese effector functions include (i) the abilityto activate the complement system for lysis(complement-dependent cellular cytotoxicity)(ii) triggering of uptake and destruction byphagocytic cells such as macrophages andneutrophils via interaction with Fc receptorson these cells (iii) activation of macrophageseosinophils neutrophils and natural killer
cells to kill infected cells via binding to Fcreceptors on these cells and antibody-depen-dent cellular cytotoxicity and (iv) neutraliza-tion of bacterial toxins and blocking of bindingand uptake of bacteria or viruses to target cells(see Fig 2) (9)
The Fcpart of IgG antibodies also contains aregion that interacts with the neonatal Fcreceptor (FcRn) expressed on most immuno-competent cells and inmany other cells such asendothelial cells in kidney liver placenta lungand breast (10) which protects antibodies fromdegradation by phagocytoticexocytotic cy-cling into FcRn-expressing cells thereby pro-longing their half-life This results in half-livesof 20 to 21 days for most IgG1 2 and 4antibodies whereas half-lives are 10 6 and 2days respectively for IgM IgA and IgE Thehighly specific binding sites on the variableregions of the upper arms of the antibody allowfor several important features of antibodiesndashbinding to and neutralization of eg bacterialtoxins binding to pathogens and blocking theirbinding to or interaction with target cells (egcyncytia formation of CMV-infected cells) orblocking of binding and interactions of infec-tious agents with target cells via blockingreceptors on the target cells
METHODS AND PLATFORMS FORGENERATING ANTIBODIES
As described above the early use of passiveantibody transfer as a therapy in infectiousdiseases involved the use of immune serumfrom immunized sheep and horses These pre-parations were crude and contained a broadmixture of neutralizing and non-neutralizingantibodies and both the foreign nature of theantibodies and the numerous host serumproteins This resulted in less specific andthus less efficient therapies due to a highvariability in efficacy between batches derivedfrom different animals immunized with dif-ferent strains of bacteria in different labor-atories and resulted in multiple unwantedside effects related to hypersensitivity and
10 HEY
anaphylactic reactions to foreign proteinsThese days antibodies being developed fortreatment of diseases in humans are highlypurified and are mostly fully human mono-clonal antibodies The term monoclonal anti-body refers to that cell cultures used forgenerating these antibodies each originatesfrom a single cell and thus produces onlyone specific antibody Development of fullyhuman monoclonal antibodies happened instages over a time span of more than 15 yearsFirst stage in this process was generation ofmonoclonalmurine IgG antibodies (eg OKT3[muronomab-CD3 Johnson and Johnson] ap-proved in 1986) Next stage was generation ofso called chimeric antibodies consisting ofhuman heavy and light chain constant sec-tions but with murine variable sections (eg
Rituxan [rituximab Genentech]) Next stagewas then the humanized antibodies wherethe only remaining murine part of the anti-body is the antigen-binding CDR (eg Xolair[omalizumab NovartisGenentech]) Both thefirst chimeric and humanized antibodies wereapproved in the late 1990s Then finally 16years later the first fully human antibodyHumira (adalimumab Abbott) was approvedin 2002 Since the time of the crude and low-scale manufacturing of the original antibodyserum products much has changed andtherapeutic antibodies are now produced byfermentation in 5000 liter scale using highlycontrolled and documented yeast or mamma-lian cell lines that are genetically engineered toexpress a single specific antibody This hasresulted in a pure and highly specific antibody
FIGURE 2 Effector functions of antibodies (a) Antibodies bind to pathogen-derived or endogenousantigens expressed on the surface of an infected cell which triggers binding to Fc receptors on naturalkiller cells and lysis of the infected cell by antibody-dependent cellular cytotoxicity (b) Antibodies bindto pathogen-derived or endogenous antigens expressed on the surface of infected cells which triggersactivation of complement through binding of complement factor C1q (c) Neutralization Top Bacterialtoxin neutralized by bound antigen Bottom Antibody bound to either receptor for the virus or to thevirus itself which blocks virus binding and entry into the cell (d) Antibody bound to viral surfaceproteins binds to Fc receptors on phagocytic cells eg macrophages and triggers endocytosis anddestruction of virus in endolysosome doi101128microbiolspecAID-0026-2014f2
CHAPTER 1 bull History and Practice Antibodies in Infectious Diseases 11

Antibodies for Infectious Diseases
Edited by
James E Crowe JrVanderbilt University Medical CenterNashville Tennessee
Diana BoraschiNational Research CouncilNapoli Italy
AND
Rino RappuoliNovartis VaccinesSiena Italy
Washington DC
Copyright copy 2015 American Society for Microbiology All rights reserved No part of this publication may be reproduced or transmitted in whole or in part or reused in any form or by any means electronic or mechanical including photocopying and recording or by any information storage and retrieval system without permission in writing from the publisher
Disclaimer To the best of the publisherrsquos knowledge this publication provides information concerning the subject matter covered that is accurate as of the date of publication The publisher is not providing legal medical or other professional services Any reference herein to any specific commercial products procedures or services by trade name trademark manufacturer or otherwise does not constitute or imply endorsement recommendation or favored status by the American Society for Microbiology (ASM) The views and opinions of the author(s) expressed in this publication do not necessarily state or reflect those of ASM and they shall not be used to advertise or endorse any product
Library of Congress Cataloging-in-Publication Data
Antibodies for infectious diseases edited by James E Crowe Jr Vanderbilt University Medical Center Nashville Tennessee Diana Boraschi National Research Council Napoli Italy and Rino Rappuoli Novartis Vaccines Siena Italypages cmIncludes bibliographical references and indexISBN 978-1-55581-735-0 (alk paper)1 Immunoglobulins 2 Communicable diseases--Immunological aspects I Crowe James E Jr editor II Boraschi D (Diana) editor III Rappuoli Rino editor QR1867A534 201561607rsquo98--dc232015009356eISBN 978-1-55581-741-1doi101128978155581741110 9 8 7 6 5 4 3 2 1
All Rights ReservedPrinted in the United States of America
Address editorial correspondence to ASM Press 1752 N St NWWashington DC 20036-2904 USASend orders to ASM Press PO Box 605 Herndon VA 20172 USAPhone 800-546-2416 703-661-1593Fax 703-661-1501E-mail booksasmusaorgOnline httpestoreasmorg
Cover image Cancer cell with high details (source 123RF)
Contents
ContributorsemspixPrefaceemspxvii
IntroductIon
1 History and Practice Antibodies in Infectious Diseasesemsp3 Adam Hey
General Features oF ImmunoGlobulIns
2 Functions of Antibodiesemsp25 Donald N Forthal
3 Antibody Structureemsp49 Robyn L Stanfield and Ian A Wilson
4 The Role of Complement in Antibody Therapy for Infectious Diseasesemsp63 Peter P Wibroe Shen Y Helvig and S Moein Moghimi
5 Immunoglobulin E and Allergy Antibodies in Immune Inflammation and Treatmentemsp75
Sophia N Karagiannis Panagiotis Karagiannis Debra H Josephs Louise Saul Amy E Gilbert Nadine Upton and Hannah J Gould
antIbody dIscovery approaches
6 Phage and Yeast Displayemsp105 Jared Sheehan and Wayne A Marasco
7 Efficient Methods To Isolate Human Monoclonal Antibodies from Memory B Cells and Plasma Cellsemsp129
Davide Corti and Antonio Lanzavecchia
8 Use of Human Hybridoma Technology To Isolate Human Monoclonal Antibodiesemsp141 Scott A Smith and James E Crowe Jr
9 Humanized Mice for Studying Human Immune Responses and Generating Human Monoclonal Antibodiesemsp157
Ramesh Akkina
10 Antibodies Computer-Aided Prediction of Structure and Design of Functionemsp173 Alexander M Sevy and Jens Meiler
v
vi contents
pathoGen-specIFIc antIbodIes
11 Antibodies Targeting the Envelope of HIV-1emsp193 Luzia M Mayr and Susan Zolla-Pazner
12 Committing the Oldest Sins in the Newest Kind of WaysmdashAntibodies Targeting the Influenza Virus Type A Hemagglutinin Globular Heademsp209
Jens C Krause and James E Crowe Jr
13 Prevention of Respiratory Syncytial Virus Infection From Vaccine to Antibodyemsp221
Kelly Huang and Herren Wu
14 Human Metapneumovirusemsp237 Jennifer E Schuster and John V Williams
15 Dengue Antibody-Dependent Enhancement Knowns and Unknownsemsp249
Scott B Halstead
16 Immunotherapeutic Approaches To Prevent Cytomegalovirus-Mediated Diseaseemsp273
Edith Acquaye-Seedah Zachary P Frye and Jennifer A Maynard
17 Rotavirusemsp289 Manuel A Franco and Harry B Greenberg
18 Bacterial ToxinsmdashStaphylococcal Enterotoxin Bemsp303 Bettina C Fries and Avanish K Varshney
technIcal advances
19 Antibody Engineeringemsp321 Kin-Ming Lo Olivier Leger and Bjoumlrn Hock
20 High-Throughput DNA Sequencing Analysis of Antibody Repertoiresemsp345
Scott D Boyd and Shilpa A Joshi
21 Antibody Informatics IMGT the International ImMunoGeneTics Information Systememsp363
Marie-Paule Lefranc
22 Probing Antibody-Antigen Interactionsemsp381 Guocheng Yang Stefanie N Velgos Shanta P Boddapati
and Michael R Sierks
23 Radiolabeled Antibodies for Therapy of Infectious Diseasesemsp399 Ekaterina Dadachova and Arturo Casadevall
alternate systems For expressIon
24 Plant-Derived Monoclonal Antibodies for Prevention and Treatment of Infectious Diseaseemsp413
Andrew Hiatt Kevin J Whaley and Larry Zeitlin
25 Vector-Mediated In Vivo Antibody Expressionemsp427 Bruce C Schnepp and Philip R Johnson
Indexemsp441
contents vii
Contributors
Edith Acquaye-SeedahDepartment of BiochemistryUniversity of Texas at AustinAustin TX 78712
Ramesh AkkinaDepartment of Microbiology Immunology and PathologyColorado State University1619 Campus DeliveryFort Collins CO 80523
Shanta P BoddapatiDepartment of Biomedical EngineeringOregon Health and Science University3181 SW Sam Jackson Park RoadPortland OR 97239
Scott D BoydDepartment of PathologyStanford UniversityStanford CA 94305
Arturo CasadevallDepartments of Microbiology and Immunology and MedicineAlbert Einstein College of Medicine of Yeshiva University1695A Eastchester RoadBronx NY 10461
Davide CortiHumabs BioMed SAvia Mirasole 1Bellinzona 6500Switzerland
James E Crowe JrSchool of MedicineVanderbilt UniversityNashville TN 37232
ix
x contRIBUtoRs
Ekaterina (Kate) DadachovaDepartments of Radiology Microbiology and ImmunologyAlbert Einstein College of Medicine of Yeshiva University1695A Eastchester RoadBronx NY 10461
Donald N ForthalDepartment of Infectious Diseases3044 Hewitt HallUniversity of California IrvineIrvine CA 92617
Manuel A FrancoFacultad de Ciencias y MedicinaPontificia Universidad JaverianaOficina 306 Edificio 50Carrera 7 40-62BogotaacuteColombia
Bettina C FriesDepartment of MedicineInfectious Diseases and Department of Microbiology and ImmunologyAlbert Einstein College of MedicineBronx NY 10461
Zachary P FryeDepartment of Chemical EngineeringUniversity of Texas at AustinAustin TX 78712
Amy E GilbertCutaneous Medicine and Immunotherapy UnitSt Johnrsquos Institute of DermatologyDivision of Genetics and Molecular Medicine amp NIHR Biomedical Research Centre at Guyrsquos and St Thomasrsquos Hospitals and Kingrsquos College London School of MedicineGuyrsquos HospitalLondon SE1 9RTUnited Kingdom
Hannah J GouldRandall Division of Cell and Molecular BiophysicsDivision of Asthma Allergy and Lung BiologyMRC and Asthma UK Centre for Allergic Mechanisms of AsthmaKingrsquos College LondonNew Huntrsquos HouseGuyrsquos CampusLondon SE1 1ULUnited Kingdom
contRIBUtoRs xi
Harry B GreenbergDepartments of Medicine and Microbiology and ImmunologyStanford University School of Medicine and the VAPAHCSPalo Alto CA 94305
Scott B HalsteadDepartment of Preventive Medicine and BiometricsUniformed Services University of the Health SciencesBethesda MD 20814
Shen Y HelvigDepartment of PharmacyCenter for Pharmaceutical Nanotechnology and NanotoxicologyFaculty of Health and Medical SciencesUniversity of CopenhagenCopenhagen DK-2100Denmark
Adam HeyPreclinical Safety BiologicsNovartis AGBaselSwitzerland
Andrew HiattMapp Biopharmaceutical Inc6160 Lusk Blvd C105San Diego CA 92121
Bjoumlrn HockDepartment of Protein Engineering and Antibody TechnologiesMerck Serono Merck KgaAFrankfurter Str 250D-64293 DarmstadtGermany
Kelly HuangDepartment of Infectious DiseaseMedImmune LLCOne MedImmune WayGaithersburg MD 20878
Philip R JohnsonThe Childrenrsquos Hospital of PhiladelphiaAbramson Research CenterPhiladelphia PA 19104
Debra H JosephsCutaneous Medicine and Immunotherapy UnitSt Johnrsquos Institute of DermatologyDivision of Genetics and Molecular Medicine amp NIHR Biomedical Research Centre at Guyrsquos and St Thomasrsquos HospitalsKingrsquos College London School of MedicineGuyrsquos HospitalLondon SE1 9RTUnited Kingdom
Shilpa A JoshiDepartment of PathologyStanford UniversityStanford CA 94305
Sophia N KaragiannisCutaneous Medicine and Immunotherapy UnitSt Johnrsquos Institute of DermatologyDivision of Genetics and Molecular Medicine amp NIHR Biomedical Research Centre at Guyrsquos and St Thomasrsquos HospitalsKingrsquos College London School of MedicineGuyrsquos HospitalLondon SE1 9RTUnited Kingdom
Panagiotis KaragiannisCutaneous Medicine and Immunotherapy UnitSt Johnrsquos Institute of DermatologyDivision of Genetics and Molecular Medicine amp NIHR Biomedical Research Centre at Guyrsquos and St Thomasrsquos HospitalsKingrsquos College London School of MedicineGuyrsquos HospitalLondon SE1 9RTUnited Kingdom
Jens C KrauseChildrenrsquos HospitalUniversity of Freiburg Medical Center79106 FreibergGermany
Antonio LanzavecchiaInstitute for Research in Biomedicinevia Vincenzo Vela 6Bellinzona 6500Switzerland
xii contRIBUtoRs
Marie-Paule LefrancLaboratoire drsquoImmunoGeacuteneacutetique Moleacuteculaire LIGMIMGTreg the international ImMunoGeneTics information systemregInstitut de Geacuteneacutetique Humaine IGHUniversiteacute Montpellier 2UPR CNRS 1142Montpellier 34396 cedex 5 40202France
Olivier LegerDepartment of Protein Engineering and Antibody TechnologiesMerck Serono SA--Geneva9 chemin des Mines1202 GenevaSwitzerland
Kin-Ming LoDepartment of Protein Engineering and Antibody TechnologiesEMD Serono Research Institute45A Middlesex TurnpikeBillerica MA 01821
Wayne A MarascoDepartment of Cancer Immunology and AIDSDana-Farber Cancer InstituteHarvard Medical SchoolBoston MA 02215
Jennifer A MaynardDepartment of Chemical EngineeringUniversity of Texas at AustinAustin TX 78712
Luzia M MayrINSERM U1109Universiteacute de Strasbourg3 Rue Koeberleacute67000 StrasbourgFrance
Jens MeilerDepartment of Chemistry and Center for Structural BiologyVanderbilt UniversityNashville TN 37212
contRIBUtoRs xiii
S Moein MoghimiDepartment of PharmacyCenter for Pharmaceutical Nanotechnology and NanotoxicologyFaculty of Health and Medical SciencesUniversity of CopenhagenCopenhagen DK-2100Denmark
Susan Zolla-PaznerNew York University School of Medicine550 First AvenueNew York NY 10016
Louise SaulCutaneous Medicine and Immunotherapy UnitSt Johnrsquos Institute of DermatologyDivision of Genetics and Molecular Medicine amp NIHR Biomedical Research Centre at Guyrsquos and St Thomasrsquos HospitalsKingrsquos College London School of MedicineGuyrsquos HospitalLondon SE1 9RTUnited Kingdom
Bruce C SchneppThe Childrenrsquos Hospital of PhiladelphiaAbramson Research CenterPhiladelphia PA 19104
Jennifer E SchusterDepartment of PediatricsChildrenrsquos Mercy HospitalKansas City MO 64108-4619
Alexander M SevyDepartment of Chemistry and Center for Structural BiologyVanderbilt UniversityNashville TN 37212
Jared SheehanDepartment of Cancer Immunology and AIDSDana-Farber Cancer InstituteHarvard Medical SchoolBoston MA 02215
Michael R SierksDepartment of Chemical EngineeringArizona State UniversityTempe AZ 85287-6006
xiv contRIBUtoRs
Scott A SmithThe Vanderbilt Vaccine Center and the Department of MedicineVanderbilt University Medical CenterNashville TN 37232
Robyn L StanfieldDepartment of Molecular BiologyThe Scripps Research Institute10550 North Torrey Pines RoadLa Jolla CA 92037
Nadine UptonRandall Division of Cell and Molecular BiophysicsDivision of Asthma Allergy and Lung BiologyMRC and Asthma UK Centre for Allergic Mechanisms of AsthmaKingrsquos College LondonNew Huntrsquos HouseGuyrsquos CampusLondon SE1 1ULUnited Kingdom
Avanish K VarshneyDepartment of MedicineInfectious Diseases and Department of Microbiology and ImmunologyAlbert Einstein College of MedicineBronx NY 10461
Stefanie N VelgosMayo Clinic Arizona5777 East Mayo BoulevardPhoenix AZ 85054
Kevin J WhaleyMapp Biopharmaceutical Inc6160 Lusk Blvd C105San Diego CA 92121
Peter P WibroeCentre for Pharmaceutical Nanotechnology and NanotoxicologyDepartment of PharmacyFaculty of Health and Medical SciencesUniversity of CopenhagenCopenhagen DK-2100Denmark
John V WilliamsDepartment of PediatricsSchool of MedicineVanderbilt UniversityNashville TN 37232-2581
contRIBUtoRs xv
Ian A WilsonDepartment of Molecular Biology and Skaggs Institute for Chemical BiologyThe Scripps Research Institute10550 North Torrey Pines RoadLa Jolla CA 92037
Herren WuDepartment of Antibody Discovery and Protein EngineeringMedImmune LLCOne MedImmune WayGaithersburg MD 20879
Guocheng YangDepartment of Chemical EngineeringArizona State UniversityTempe AZ 85287-6006
Larry ZeitlinMapp Biopharmaceutical Inc6160 Lusk Blvd C105San Diego CA 92121
xvi contRIBUtoRs
Preface
Antibodies form the principal foundation for modern intervention against in-fectious diseases Emil Adolf von Behring was awarded the first Nobel Prize in Physiology or Medicine in 1901 ldquofor his work on serum therapy especially its appli-cation against diphtheria by which he has opened a new road in the domain of med-ical science and thereby placed in the hands of the physician a victorious weapon against illness and deathsrdquo Antibodies now provide the focus for understanding mechanisms of immunity to most infectious diseases and they play a central role in passive immunotherapy and active vaccination as mechanisms or correlates of immunity For most of the 20th century immunotherapy was based on passive transfer of polyclonal hyperimmune animal serum immune human serum or even hyperimmune human serum Georges JF Koumlhler and Ceacutesar Milstein re-ported the generation of monoclonal antibodies in 1979 for which they shared the 1984 Nobel Prize in Physiology or Medicine ldquofor the discovery of the princi-ple for production of monoclonal antibodiesrdquo Since that time entire fields related to antibodies for infectious diseases including antibody gene cloning engineer-ing and expression antibody libraries and high-throughput antibody gene rep-ertoire sequence analysis have extended our capabilities to explore the diversity of antibody specificity and function with unprecedented depth and breadth
This book provides a broad survey of many of the most important aspects of the field of antibodies for infectious diseases The book begins with a general introduction followed by chapters 2 through 5 on general features pertaining to structure function isotype and the role of complement in antibody function Chapters 6 through 10 review contemporary approaches for antibody discovery using phage and yeast display plasma cell and memory B cell cloning human hybridomas humanized mice and computational methods Chapters 11 through 18 review in depth the biology of antibodies specific for particular pathogens including viruses and bacterial toxins to illustrate the role of antibodies in anti- microbial immunity with specific targets These chapters reveal that attempts to raise effective antibody responses to each of these pathogens faces unique and pathogen-specific challenges Chapters 19 to 23 cover major technical advances pertaining to antibody engineering repertoire sequencing and analysis and new methods for study or therapeutic use of antibodies including radiotherapy Fi-nally chapters 24 and 25 cover new methods for expression of monoclonal anti-bodies in plants or by transfer of antibody genes for in vivo expression in treated subjects
Recent literature is exploding with new antibody-related techniques and re-ports of antimicrobial antibodies with unprecedented potency breadth of activ-
xvii
xviii PReface
ity and therapeutic potential We hope that this timely compilation of state-of-the-art reviews of major aspects of this field will be of interest to both antibody cognoscenti and those new to this exciting field We thank the authors for their dedication in producing definitive reviews of the topics at hand
James E Crowe JrDiana BoraschiRino Rappuoli
INTRODUCTION
History and PracticeAntibodies in Infectious Diseases 1ADAM HEY1
Antibodies in Infectious Diseases aims to inform update and inspire studentsteachers researchers pharmaceutical developers and health care professionalson the status of the development of antibody-based therapies for treatinginfectious diseases and the potential for these in times of growing antibioticresistance to provide alternative treatment solutions to the currently usedantibiotics and new treatments for infectious diseases where no propertreatments are available
This introductory article will provide a historical perspective on the useof antibody-based therapies followed by a high-level overview of whatmakes antibodies attractive tools for this purpose This will include the prosand cons of such therapies compared to the use of antibiotics and thepractical and strategic considerations involved in selecting the best formatand development path for new antibody-based therapies targeting specificinfectious agents Then examples of antibody-based therapies in thedevelopment of treatments for infectious diseases will be presented andfinally a look into the future will summarize the different aspects that willinfluence what the future might bring for this type of treatments forinfectious diseases
1Preclinical Safety Biologics Novartis AG Basel Switzerland
Antibodies for Infectious DiseasesEdited by James E Crowe Jr Diana Boraschi and Rino Rappuolicopy 2015 American Society for Microbiology Washington DCdoi101128microbiolspecAID-0026-2014
3
HISTORICAL PERSPECTIVE
Antibodies and the use of passive antibodytherapy in the treatment of infectious dis-eases is the story of a treatment conceptwhich dates back more than 120 years to thelate 19th century and which originally bythe use of serum from immunized animalsprovided the first effective treatment optionsagainst severe bacterial infections (1 2) Byimmunizing horses with bacterial toxinsfrom Clostridium tetani and Corynebacteri-um diphtheriae Emil A Von Behring andShibasaburo Kitasato (3) generated serumcontaining antibodies capable of neutraliz-ing the effects of the toxins produced bythese bacteria and successfully providedtreatment for these serious diseases wherethe pathogenesis is driven by the effects ofthe bacterial toxins For his work on provid-ing treatment for diphtheria Behring re-ceived the Nobel Prize in Physiology orMedicine in 1901 These radical treatmentresults quickly prompted development ofmultiple additional serum therapies for thetreatment of infectious diseases caused byeg Neisseria meningitidis Haemophilus in-fluenza and group A Streptococcus Sinceserum therapy involved administration oflarge amounts of crude mixtures of animalproteins including antibodies they wereassociated with side effects in the form ofhypersensitivity and serum sickness (2)
Due to the crude and unpurified nature ofthese products side effects were seen evenwhen administering human serum prepa-rations Side effects were observed in up to50 of patients and were considered to becaused by immune complex formations thatresulted in symptoms such as rash itchingjoint pain fever and in serious cases hypoten-sion and shock However due to the lack ofalternative options these treatments weredespite their side effects widely used Serumwas normally administered by intravenousinfusion in patients after a test for hypersensi-tivity where a small amount of serum wasinjected subcutaniously (1) As described
above serum therapy applied in these earlydays (late 19th century and early 20th century)involved preparations of serum from rabbitsand horses immunized with the infectiousagent or in live andor neutralized versions ortoxins from these (1) The costs of keeping theimmunized animals and the production andpotency testing of the materials made this arelatively expensive treatment In 1891 datafrom Klemperer (4) showed serum therapy toprotect rabbits from Streptococcus pneumoniaeinfection and paved the way for this type oftreatment and for development of similarserum-based treatments of streptococcal in-fections in humans When treating humansearly administration of serum could reducemortality significantly down to around 5compared to when administered 4 to 5 daysafter onset of symptoms when serum treat-ment was largely without effect This stronglyindicated the need for quick diagnosis andquick treatment to control the infection beforeit got out of control Consequently in theabsence of a specific diagnosis mixtures ofserum from immunizations with differentserotypes were used to circumvent this needfor early treatment without having a serotype-specific diagnosis The understanding thatdifferent serotypes existed for pneumococciand that efficient treatment relied on usingserotype-specific serum was being built upduring the 1920s and 1930s through experiencefrom extensive clinical trials
By the end of the 1930s serum therapywasthe standard of care for treatment of pneu-mococcal pneumonia At that time theefficacy and potency of the derived serawere assessed in mice in ldquothe mouse pro-tection testrdquo by testing survival after aconcomitant intraperitoneal injection of alethal dose of pneumococci and the serum tobe tested Due to the inherent variation inthis test efficacy and survival in two thirds ofthe animals was the acceptance criteria and10 times the lowest dose providing this wasused for defining a unit of the serum Thisallowed for large batch-to-batch variationand the use of different strains of bacteria for
4 HEY
immunization probably explains part of themissing responses observed (1) In the early20th century a pandemic of meningitis inEurope and the United States with mortalityrates up to 80 spurred the development ofserum therapy treatment options Althoughin the 1930s this became the recommendedtreatment in children assumed to be suffer-ing from meningitis failure to reduce mor-tality in several meningitis epidemics duringthat time raised doubts about the generalapplicability of serum treatment In thosedays serum therapy often involved quiteextensive procedures and infusion of largevolumes of serum The following exampleclearly illustrates this Data from Flexnerand Jobling (5) from treating meningitis inmonkeys resulted in the development of serafrom immunized horses for treatment inhumans The treatment protocol includedlumbar puncture and withdrawal of morethan 30 ml of spinal fluid representing anamount slightly larger than the expectedamount of horse serum to be injected subse-quently This treatment involved such dailyslow infusions of up to 30 ml of serum untilthe patientrsquos condition improved This treat-ment was used in outbreaks in New York in1905 and 1906 and did markedly decreasemortality
After the discovery of penicillin by Flemingin 1928 and the subsequent introduction ofantibiotics in the 1930s serum therapy waslargely abandoned over a period of 10 years dueto the availability of these new more broadlyeffective and cheaper treatment optionswhichalso had fewer side effects Although improve-ments in the purification of antibodies hadresulted in preparations with better safety andside effect profiles high manufacturing costsand narrow specificity resulted in antibodytherapy being mostly restricted to a smallernumber of selected treatments for snakevenoms bacterial toxins and some viral infec-tions (1 2) Currently antibody administrationis used for treatment and prevention ofhepatitis B virus rabies virus respiratorysyncytial virus (RSV) Clostridium tetani Clos-
tridium botulinum vaccinia virus echovirusand enterovirus For the most part thesetreatments consist of pooled immunoglobulinalso known as IVIG (intravenous immunoglob-ulin) from several postexposure donors Thisresults in both batch-to-batch variation in theneed for relatively large amounts of serum dueto low specificity and to restricted supplies dueto reliance on exposed donors
However several challengeshave resulted inthe need for new tools in the treatment andpreventionof infectiousdiseasesThebroadandgeneral use of antibiotics in human and veter-inary medicine for many years has resulted inthe development of multi-resistant strains ofbacteria with limited to no response to existingtreatments such as methicillin-resistant Staph-ylococcusaureus (MRSA) vancomycin-resistantS aureus and others This has resulted inpatients needing screening and treatment withseveral antibacterial agents and longer treat-ment time causing extra strain on patients andhealth care providers (6 httpwwwcdcgovdrugresistancethreat-report-2013indexhtml) According to the WHO and CDC morethan 25000 people in European Unioncountries and similar numbers in the UnitedStates die every year as a result of antibiotic-resistant infections This together with theemergence of new pathogens (eg severeacute respiratory syndrome Middle East respi-ratory syndrome) the re-emergenceepidemicsof oldknown pathogens (eg Ebola) and thedifficulties in treating infections in immune-deficient patients (eg HIV patients) has high-lighted the need for new solutions The 2014Ebola epidemic in West Africa (Liberia SierraLeone Guinea Nigeria and Senegal) has fur-ther highlighted this No treatment or prophy-lactic vaccine is available to treat or prevent thespread of Ebola infections which have anaveragemortality of gt50 Local health author-ities in the affected countries are struggling tocontain and handle the disease which isthreatening to go out of control and spreadmorewidelyVariousproductsmainly antibodycocktails from previously recovered patientsare being used despite a lack of clinical data on
CHAPTER 1 bull History and Practice Antibodies in Infectious Diseases 5
their safety and efficacy and those are the onlysporadically available treatment options andonly in small amounts and for a few patients
Ebola is an example of a disease whichnormally affects only a small number ofindividuals and which normally burns outwhen disease outbreaks are contained There-fore given the small number of potentialpatients affected by previous Ebola infectionsto date there was no incentive for big pharmacompanies to do research and development ofdrugs for EbolaWith the increasing number ofinfected (13567) andadeath toll of 4951 (7) andthe lack of the ability to contain the epidemic itwill be interesting to follow the aftermath ofthis outbreak and see whether there will berequests for new ways to ensure that vaccinesand treatment options are available for Ebolaand similar high-mortality and potential bio-warfare infections that have no availabletreatments or procedures to for mass-produc-tion upon the first signsreports of activeinfections Although both the CDC and theWHO have special programs focusing on thesetypes of infections the Ebola outbreak in 2014clearly shows that more financial support forresearch and development of new diagnosticsand treatments is needed This is one examplewhere antibody-based treatments would havethe potential to play a major role To put this inthe right perspective one should however notforget that other infectious diseases such astuberculosis influenza and malaria kill hun-dreds of thousands each year There is there-fore plenty of room for improvement indeveloping treatments for these diseases aswell but the high attention drawn to eg theEbola outbreak creates a special niche andopportunity where antibody treatments couldgain extraordinary development funding andsupport and prove their value and treatmentpotential
That antibody-based therapies could takethis role is supported by the revolution intechnologies for the development selectiongeneration and purification of fully humanantibodies described in more detail later in thesection ldquoMethodsandPlatforms forGenerating
Antibodiesrdquo Antibody-based programs cur-rently at different stages of developmentinclude investigations into the potential use ofsingle antibody preparations combinations ofantibodies (to avoid survival of escape mu-tants) fragments of antibodies and antibodiescarrying radioactive isotopesorcytotoxicdrugsor antibody-like frameworks (eg fibronectin)either alone as a first-line treatment or as anadjunct to existing treatments This multitudeof possible formats the ability to raise anti-bodies to almost any target and the ability toengineer both size effector functions and half-life are now considered by many to providevery valuable tools for designing specificantibody-based treatments toeradicate specifictargeted infectious agents However althoughseveral antibody-based therapies have beenapproved for oncology and anti-inflammatoryindications (see Table 1) only one monoclonalantibody (mAb) is approved against an infec-tious disease agentmdashSynagis (palivizumabMedImmune) for the prevention and treat-ment of respiratory syncytical virus (RSV) inhigh-risk children Economic obstacles such asthe high cost of mAb therapies and relativelysmall markets have resulted in less interestfrom pharmaceutical companies in developingthese Also highlighting the challenges indeveloping these types of antibody-basedtreatments are the difficulties encountered indeveloping a follow-up higher-affinity candi-date to Synagis Poor translatability of dataobtained in the available animal disease mod-els for RSV in cotton rats has resulted in non-approval due to inferiority relative to SynagisIn other viral diseases such as cytomegalovirus(CMV) the high species specificity of thestrains of CMV makes it impossible to testhuman antibody therapies in vivo Thereforeany real data on the efficacy of treatments forCMV will not be obtained until testing inclinical trials As described later in this articleseveral new antibody-based therapies for in-fectious diseases are in development andhopefully this will gradually open the fieldand result in better treatment options andoutcomes for patients
6 HEY
TABLE 1 Approved and pending antibody-based therapies
Name antibody Target antibody type Indication Company Approval date
OKT3a Muronomab-CD3 CD3 murine IgG2a Autoimmune Johnson ampJohnson
1986 (US)
ReoPro abciximab PIIbIIIa chimeric IgG1Fab
Homeostasis Johnson ampJohnson
1984 (US)
Rituxan rituximab CD20 chimeric IgG1 Cancer Genentech 1997 (US) 1998 (EU)Zenapaxa daclizumab CD25 humanized IgG1 Autoimmune Roche 1997 (US) 1999 (EU)Simulect basiliximab CD25 chimeric IgG1 Autoimmune Novartis 1998 (US EU)Synagis palivizumab RSV humanized IgG1 Infections MedImmune 1998 (US) 1999 (EU)Remicade infliximab TNFα chimeric IgG1 Autoimmune Johnson amp
Johnson1998 (US) 1999 (EU)
Herceptin trastuzumab HER2 humanized IgG1 Cancer GenentechRoche
1998 (US) 2000 (EU)
Mylotarga gemtuzumabozogamicin
CD33 humanized IgG4immunotoxin
Cancer WyethPfizer 2000 (US)
Campath alemtuzumab CD52 humanized IgG1 Cancer Genzyme 2001 (US) 2001 (EU)Zevalin ibritumomabtiuxetan
CD20 murine IgG1radiolabeled (yttrium 90)
Cancer Biogen Idec 2002 (US) 2004 (EU)
Humira adalimumab TNFα human IgG1 Autoimmune Abbott 2002 (US) 2003 (EU)Xolair omalizumab IgE humanized IgG1 Autoimmune Genentech
Roche2003 (US)
Bexxar tositumomab-I-131 CD20 murine IgG2aradiolabeled (iodine131)
Cancer CorixaGSK 2003 (US)
Raptivaa falizumab CD11a humanized IgG1 Autoimmune GenentechRoche
2003 (US) 2004 (EU)
Erbitux cetuximab EGFR chimeric IgG1 Cancer ImcloneLilly 2004 (US) 2004 (EU)Avastin bevacizumab VEGF humanized IgG1 Cancer Genentech
Roche2004 (US) 2005 (EU)
Tysabri natalizumab α4-Intergrin humanizedIgG4
Autoimmune Biogen Idec 2004 (US)
Actemra tocilizumab Anti-IL-6R humanizedIgG1
Autoimmune ChugaiRoche
2005 (Japan) 2010 (US)
Vectibix panitumumab EGFR human IgG2 Cancer Amgen 2006 (US)Lucentis ranibizumab VEGF humanized IgG1
FabMaculardegeneration
GenentechRoche
2006 (US)
Soliris eculizumab C5 humanized IgG24 Blood disorders Alexion 2007 (US)Cimzia certolizumab pegol TNFα humanized
pegylated FabAutoimmune UCB 2008 (US)
Simponi golimumab TNFα human IgG1 Autoimmune Johnson ampJohnson
2009 (US EU Canada)
Ilaris canakinumab IL1b human IgG1 Infalmmatory Novartis 2009 (US EU)Stelara ustekinumab IL-1223 human IgG1 Autoimmune Johnson amp
Johnson2008 (EU) 2009 (US)
Arzerra ofatumumab CD20 human IgG1 Cancer Genmab 2009 (EU)Prolia denosumab RANK ligand human
IgG2Bone loss Amgen 2010 (US)
Numax motavizumab RSV humanized IgG1 Anti-infective MedImmune PendingABthrax Raxibacumab B anthrasis PA human
IgG1Anti-infection GSK 2012 (US)
Benlysta belimumab BLyS human IgG1 Autoimmune HGS 2011 (US)Yervoy ipilimumab CTLA-4 human IgG1 Cancer BMS 2011 (US)Adcetris brentuximabvedotin
CD30 chimeric IgG1drug- conjugate
Cancer SeattleGenetics
2011 (US)
(Continued on next page)
CHAPTER 1 bull History and Practice Antibodies in Infectious Diseases 7
INTRODUCTION TO ANTIBODIES
Antibodies also called immunoglobulins basedon their combined structure and function inimmune responses are produced by B cells ofthe immune system They are part of theadaptive immune response and are speciallydesigned for neutralizing and eliminating theinfectious agents and toxins produced by theseAntibodies are present in blood plasma andextracellular fluids and since these fluids wereformerly known as humors they were said tobe part of the humoral immune responseAntibodies are Y-shaped structures consistingof two main parts the upper arms of the Ywhich contain two identical variable-regionantigen binding sites and the lower regioncalled the constant regionwhich is responsiblefor the initiation of effector functions that leadto the removal and destruction of the pathogenor cells harboring the pathogen (see Fig 1) Theantigen-binding sites on an antibody can bythemselves bind to and neutralize bacterialtoxins and viruses thereby preventing themfrom binding to their target cells or receptorscausing toxic effects or spread of the infection
Antibodies consist of two pairs of heavy andlight chainswhich as described above are heldtogether in a Y-shaped arrangement Each ofthe heavy and light chains in these pairs isseparated into constant and variable chainsThe upper armsof theY each contain a variableand a constant sectionof the light and theheavychain where the upper variable parts of theheavy and light chains contain the antigen-binding site and the constant parts areconnected via disulfide bonds The lower partof theYcalled theconstantpart consistsof twoor three constant segments (immunoglobulindomains) from each of the two heavy chainsinteracting and also linked via disulfide bondsThe sectionsof theheavy chains connecting theconstant part of the upper arms to the constantparts of the constant region contain specialhinge regions that provide flexibility to thedifferent sections of the antibody to bind toantigens and effector cells The constant re-gions of the heavy chain also contain attachedoligosaccharide moieties which provide func-tional specialization to the antibodies (8)
The variable domains of the heavy and lightchains form the antigen-binding sites and
TABLE 1 Approved and pending antibody-based therapies (Continued)
Name antibody Target antibody type Indication Company Approval date
Perjeta pertuzumab Her2 humanized IgG1 Cancer GenentechRoche
2012 (US)
Kadcyla ado-trastuzumabemtansine
Her2 humanized IgG1Drug-conjugate
Cancer GenentechRoche
2013 (US)
Raxibacumab Anti-B anthrasis PAhuman IgG1
Anthraxinfection
Notapproved
2012
Entyvio vedolizumab Integrin α4β7humanized IgG1
Crohnrsquos diseaseulcerative colitis
Takeda 2014 (US)
Cyramza ramuciruumab Anti-VEGFR2Human IgG1
Gastric cancer Lilly 2014 (US)
Gazyva obinutuzumab Anti-CD20 humanizedIgG1 glucoengineered
CancerCLLb GenentechRoche
2014 (US)
Sylvant situximab Anti IL-6 chimeric IgG1 Castlemandisease
Janssen 2014 (US) 2014 (EU)
Cosentyx sekukinumab Anti IL-17a human IgG1 Psoriasis Novartis 2015 (US) 2015 (EU)Nivolumab Anti PD-1 human IgG4 Melanoma BMS Not approvedKeytruda pembrolizuumab Anti-PD-1 humanized
IgG4Melanoma Merck 2014 (US)
aAntibodies approved but later withdrawnbCLL chronic lymphocytic leukemia
8 HEY
FIGURE 1 (Left panel) Model of antibody structure exemplified by IgG On top the antigen-binding sitesin orange each contain one variable light and variable heavy domain with the three complementaritydetermining regions (CDRs) that are responsible for the specific binding of the antibody to its target Foreach arm of the antibody an additional set of variable heavy and light domains together with the CDR-containing domains represent the two fragment antigen binding (Fab) regions The two Fabs are heldtogether via two disulfide bridges Below the Fabs is the Fc region which contains four constant heavydomains On the upper pair of these domains are binding sites for oligosaccharides which have majorimportance for the ability of the antibody Fc part to trigger effector functions when the Fc portion isbound to Fc gamma receptors on natural killer cells neutrophil granulocytes monocytesmacrophagesdendritic cells and B cells (Right panel) Examples of some of the antibody-derived alternative formatsused to exploit the specific features of the CDRs the Fabs and the Fc parts of the antibodies ScFv Thesingle chain fragment variable consists of the variable domains of the heavy and light chains heldtogether by a flexible linker This can also be used as a carrier of a cytotoxic drug in a so-called antibodydrug complex (ADC) where the specificity of the ScFv is used to target the cytotoxic drug to eg atumor Bite (bi-specific T cell engager) Fusion proteins consisting of two ScFvs one directed against thetarget on a tumor cell and the other against the T cell receptor (CD3) Diabody ScFv dimers where shortlinker peptides (five amino acids) ensure dimerization and not folding of the ScFvs Fab and F(ab)2fragments Single Fab fragments or fragments containing two Fabs linked via disulfide bridges This isused where effector functions related to the Fc part of the antibody are unwanted and where a smallersize is desired to obtain better tissue penetration in eg tumors Due to the lack of the FcRn binding viathe Fc part Fab and F(ab)2 fragments have much shorter half-lives (hours or days) than full-sizeantibodies (weeks) These can also be used as carriers of cytotoxic payloads or cytotoxic radioactiveisotopes and for the F(ab)2 fragments can be constructed as bi-specifics which can cross-link immunecells and target cells Fc fusion protein Fusion protein containing the Fc domain of an immunoglobulinbound to a peptide The peptide can be a ligand for a specific receptor on a target cell or a blockingpeptide for a soluble ligand The Fc part provides a longer half-life to the construct and the potential tobind to and engage effector functions in the killing of eg tumor cells or infected cells ADCsRIAs andbi-specifics Full-size IgG antibodies carrying either a cytotoxic chemical or radioactive payload whichmay also carry different CDRs enabling cross-linking of effector and target cells for increased killingdoi101128microbiolspecAID-0026-2014f1
CHAPTER 1 bull History and Practice Antibodies in Infectious Diseases 9
contain special hyper-variable segments calledcomplementarity-determining regions (CDRs)which allow the B cells via genetic recom-bination to generate antibodies to all thedifferent antigens specific to amino acid se-quences or three-dimensional structuralmotifs(polysaccharides DNA and RNA) found onpathogens
Based on the structure of their heavy chainconstant regions antibodies or immuno-globulins are separated into five classesmdashIgM IgG IgE IgD and IgA Differences inthe sequences of the constant regions providedistinct characteristics to these different clas-ses These characteristics include the numberof heavy chain constant segments the numberand location of interconnecting disulfidebridges the length of the hinge region andthe number and location of oligosaccharidemoieties For IgG four heavy chain versionsexist creating IgG1 2 3 and 4 isotypes eachwith different characteristics in their serumhalf-lives and ability to trigger different effec-tor functions Because of the combined ad-vantage from ability to trigger effectormechanisms long [21 days] half-life theirability to be transported over the placentaand their stability in the production processantibodies of the IgG class and of the IgG1isotype are preferred as the basis for newantibody-based therapies The effector func-tions are triggered by the Fc part of an antibodywhen the variable parts of the antibody arebound directly to an infectious agent or toproteins from an infectious agent expressed onan infected cell This binding leaves the Fc partfree to interactwithFc receptors onphagocyticcells and neutrophils eosinophils and naturalkiller cells capable of inducing phagocytosis orlysis of infectious agents or infected cellsThese effector functions include (i) the abilityto activate the complement system for lysis(complement-dependent cellular cytotoxicity)(ii) triggering of uptake and destruction byphagocytic cells such as macrophages andneutrophils via interaction with Fc receptorson these cells (iii) activation of macrophageseosinophils neutrophils and natural killer
cells to kill infected cells via binding to Fcreceptors on these cells and antibody-depen-dent cellular cytotoxicity and (iv) neutraliza-tion of bacterial toxins and blocking of bindingand uptake of bacteria or viruses to target cells(see Fig 2) (9)
The Fcpart of IgG antibodies also contains aregion that interacts with the neonatal Fcreceptor (FcRn) expressed on most immuno-competent cells and inmany other cells such asendothelial cells in kidney liver placenta lungand breast (10) which protects antibodies fromdegradation by phagocytoticexocytotic cy-cling into FcRn-expressing cells thereby pro-longing their half-life This results in half-livesof 20 to 21 days for most IgG1 2 and 4antibodies whereas half-lives are 10 6 and 2days respectively for IgM IgA and IgE Thehighly specific binding sites on the variableregions of the upper arms of the antibody allowfor several important features of antibodiesndashbinding to and neutralization of eg bacterialtoxins binding to pathogens and blocking theirbinding to or interaction with target cells (egcyncytia formation of CMV-infected cells) orblocking of binding and interactions of infec-tious agents with target cells via blockingreceptors on the target cells
METHODS AND PLATFORMS FORGENERATING ANTIBODIES
As described above the early use of passiveantibody transfer as a therapy in infectiousdiseases involved the use of immune serumfrom immunized sheep and horses These pre-parations were crude and contained a broadmixture of neutralizing and non-neutralizingantibodies and both the foreign nature of theantibodies and the numerous host serumproteins This resulted in less specific andthus less efficient therapies due to a highvariability in efficacy between batches derivedfrom different animals immunized with dif-ferent strains of bacteria in different labor-atories and resulted in multiple unwantedside effects related to hypersensitivity and
10 HEY
anaphylactic reactions to foreign proteinsThese days antibodies being developed fortreatment of diseases in humans are highlypurified and are mostly fully human mono-clonal antibodies The term monoclonal anti-body refers to that cell cultures used forgenerating these antibodies each originatesfrom a single cell and thus produces onlyone specific antibody Development of fullyhuman monoclonal antibodies happened instages over a time span of more than 15 yearsFirst stage in this process was generation ofmonoclonalmurine IgG antibodies (eg OKT3[muronomab-CD3 Johnson and Johnson] ap-proved in 1986) Next stage was generation ofso called chimeric antibodies consisting ofhuman heavy and light chain constant sec-tions but with murine variable sections (eg
Rituxan [rituximab Genentech]) Next stagewas then the humanized antibodies wherethe only remaining murine part of the anti-body is the antigen-binding CDR (eg Xolair[omalizumab NovartisGenentech]) Both thefirst chimeric and humanized antibodies wereapproved in the late 1990s Then finally 16years later the first fully human antibodyHumira (adalimumab Abbott) was approvedin 2002 Since the time of the crude and low-scale manufacturing of the original antibodyserum products much has changed andtherapeutic antibodies are now produced byfermentation in 5000 liter scale using highlycontrolled and documented yeast or mamma-lian cell lines that are genetically engineered toexpress a single specific antibody This hasresulted in a pure and highly specific antibody
FIGURE 2 Effector functions of antibodies (a) Antibodies bind to pathogen-derived or endogenousantigens expressed on the surface of an infected cell which triggers binding to Fc receptors on naturalkiller cells and lysis of the infected cell by antibody-dependent cellular cytotoxicity (b) Antibodies bindto pathogen-derived or endogenous antigens expressed on the surface of infected cells which triggersactivation of complement through binding of complement factor C1q (c) Neutralization Top Bacterialtoxin neutralized by bound antigen Bottom Antibody bound to either receptor for the virus or to thevirus itself which blocks virus binding and entry into the cell (d) Antibody bound to viral surfaceproteins binds to Fc receptors on phagocytic cells eg macrophages and triggers endocytosis anddestruction of virus in endolysosome doi101128microbiolspecAID-0026-2014f2
CHAPTER 1 bull History and Practice Antibodies in Infectious Diseases 11

Copyright copy 2015 American Society for Microbiology All rights reserved No part of this publication may be reproduced or transmitted in whole or in part or reused in any form or by any means electronic or mechanical including photocopying and recording or by any information storage and retrieval system without permission in writing from the publisher
Disclaimer To the best of the publisherrsquos knowledge this publication provides information concerning the subject matter covered that is accurate as of the date of publication The publisher is not providing legal medical or other professional services Any reference herein to any specific commercial products procedures or services by trade name trademark manufacturer or otherwise does not constitute or imply endorsement recommendation or favored status by the American Society for Microbiology (ASM) The views and opinions of the author(s) expressed in this publication do not necessarily state or reflect those of ASM and they shall not be used to advertise or endorse any product
Library of Congress Cataloging-in-Publication Data
Antibodies for infectious diseases edited by James E Crowe Jr Vanderbilt University Medical Center Nashville Tennessee Diana Boraschi National Research Council Napoli Italy and Rino Rappuoli Novartis Vaccines Siena Italypages cmIncludes bibliographical references and indexISBN 978-1-55581-735-0 (alk paper)1 Immunoglobulins 2 Communicable diseases--Immunological aspects I Crowe James E Jr editor II Boraschi D (Diana) editor III Rappuoli Rino editor QR1867A534 201561607rsquo98--dc232015009356eISBN 978-1-55581-741-1doi101128978155581741110 9 8 7 6 5 4 3 2 1
All Rights ReservedPrinted in the United States of America
Address editorial correspondence to ASM Press 1752 N St NWWashington DC 20036-2904 USASend orders to ASM Press PO Box 605 Herndon VA 20172 USAPhone 800-546-2416 703-661-1593Fax 703-661-1501E-mail booksasmusaorgOnline httpestoreasmorg
Cover image Cancer cell with high details (source 123RF)
Contents
ContributorsemspixPrefaceemspxvii
IntroductIon
1 History and Practice Antibodies in Infectious Diseasesemsp3 Adam Hey
General Features oF ImmunoGlobulIns
2 Functions of Antibodiesemsp25 Donald N Forthal
3 Antibody Structureemsp49 Robyn L Stanfield and Ian A Wilson
4 The Role of Complement in Antibody Therapy for Infectious Diseasesemsp63 Peter P Wibroe Shen Y Helvig and S Moein Moghimi
5 Immunoglobulin E and Allergy Antibodies in Immune Inflammation and Treatmentemsp75
Sophia N Karagiannis Panagiotis Karagiannis Debra H Josephs Louise Saul Amy E Gilbert Nadine Upton and Hannah J Gould
antIbody dIscovery approaches
6 Phage and Yeast Displayemsp105 Jared Sheehan and Wayne A Marasco
7 Efficient Methods To Isolate Human Monoclonal Antibodies from Memory B Cells and Plasma Cellsemsp129
Davide Corti and Antonio Lanzavecchia
8 Use of Human Hybridoma Technology To Isolate Human Monoclonal Antibodiesemsp141 Scott A Smith and James E Crowe Jr
9 Humanized Mice for Studying Human Immune Responses and Generating Human Monoclonal Antibodiesemsp157
Ramesh Akkina
10 Antibodies Computer-Aided Prediction of Structure and Design of Functionemsp173 Alexander M Sevy and Jens Meiler
v
vi contents
pathoGen-specIFIc antIbodIes
11 Antibodies Targeting the Envelope of HIV-1emsp193 Luzia M Mayr and Susan Zolla-Pazner
12 Committing the Oldest Sins in the Newest Kind of WaysmdashAntibodies Targeting the Influenza Virus Type A Hemagglutinin Globular Heademsp209
Jens C Krause and James E Crowe Jr
13 Prevention of Respiratory Syncytial Virus Infection From Vaccine to Antibodyemsp221
Kelly Huang and Herren Wu
14 Human Metapneumovirusemsp237 Jennifer E Schuster and John V Williams
15 Dengue Antibody-Dependent Enhancement Knowns and Unknownsemsp249
Scott B Halstead
16 Immunotherapeutic Approaches To Prevent Cytomegalovirus-Mediated Diseaseemsp273
Edith Acquaye-Seedah Zachary P Frye and Jennifer A Maynard
17 Rotavirusemsp289 Manuel A Franco and Harry B Greenberg
18 Bacterial ToxinsmdashStaphylococcal Enterotoxin Bemsp303 Bettina C Fries and Avanish K Varshney
technIcal advances
19 Antibody Engineeringemsp321 Kin-Ming Lo Olivier Leger and Bjoumlrn Hock
20 High-Throughput DNA Sequencing Analysis of Antibody Repertoiresemsp345
Scott D Boyd and Shilpa A Joshi
21 Antibody Informatics IMGT the International ImMunoGeneTics Information Systememsp363
Marie-Paule Lefranc
22 Probing Antibody-Antigen Interactionsemsp381 Guocheng Yang Stefanie N Velgos Shanta P Boddapati
and Michael R Sierks
23 Radiolabeled Antibodies for Therapy of Infectious Diseasesemsp399 Ekaterina Dadachova and Arturo Casadevall
alternate systems For expressIon
24 Plant-Derived Monoclonal Antibodies for Prevention and Treatment of Infectious Diseaseemsp413
Andrew Hiatt Kevin J Whaley and Larry Zeitlin
25 Vector-Mediated In Vivo Antibody Expressionemsp427 Bruce C Schnepp and Philip R Johnson
Indexemsp441
contents vii
Contributors
Edith Acquaye-SeedahDepartment of BiochemistryUniversity of Texas at AustinAustin TX 78712
Ramesh AkkinaDepartment of Microbiology Immunology and PathologyColorado State University1619 Campus DeliveryFort Collins CO 80523
Shanta P BoddapatiDepartment of Biomedical EngineeringOregon Health and Science University3181 SW Sam Jackson Park RoadPortland OR 97239
Scott D BoydDepartment of PathologyStanford UniversityStanford CA 94305
Arturo CasadevallDepartments of Microbiology and Immunology and MedicineAlbert Einstein College of Medicine of Yeshiva University1695A Eastchester RoadBronx NY 10461
Davide CortiHumabs BioMed SAvia Mirasole 1Bellinzona 6500Switzerland
James E Crowe JrSchool of MedicineVanderbilt UniversityNashville TN 37232
ix
x contRIBUtoRs
Ekaterina (Kate) DadachovaDepartments of Radiology Microbiology and ImmunologyAlbert Einstein College of Medicine of Yeshiva University1695A Eastchester RoadBronx NY 10461
Donald N ForthalDepartment of Infectious Diseases3044 Hewitt HallUniversity of California IrvineIrvine CA 92617
Manuel A FrancoFacultad de Ciencias y MedicinaPontificia Universidad JaverianaOficina 306 Edificio 50Carrera 7 40-62BogotaacuteColombia
Bettina C FriesDepartment of MedicineInfectious Diseases and Department of Microbiology and ImmunologyAlbert Einstein College of MedicineBronx NY 10461
Zachary P FryeDepartment of Chemical EngineeringUniversity of Texas at AustinAustin TX 78712
Amy E GilbertCutaneous Medicine and Immunotherapy UnitSt Johnrsquos Institute of DermatologyDivision of Genetics and Molecular Medicine amp NIHR Biomedical Research Centre at Guyrsquos and St Thomasrsquos Hospitals and Kingrsquos College London School of MedicineGuyrsquos HospitalLondon SE1 9RTUnited Kingdom
Hannah J GouldRandall Division of Cell and Molecular BiophysicsDivision of Asthma Allergy and Lung BiologyMRC and Asthma UK Centre for Allergic Mechanisms of AsthmaKingrsquos College LondonNew Huntrsquos HouseGuyrsquos CampusLondon SE1 1ULUnited Kingdom
contRIBUtoRs xi
Harry B GreenbergDepartments of Medicine and Microbiology and ImmunologyStanford University School of Medicine and the VAPAHCSPalo Alto CA 94305
Scott B HalsteadDepartment of Preventive Medicine and BiometricsUniformed Services University of the Health SciencesBethesda MD 20814
Shen Y HelvigDepartment of PharmacyCenter for Pharmaceutical Nanotechnology and NanotoxicologyFaculty of Health and Medical SciencesUniversity of CopenhagenCopenhagen DK-2100Denmark
Adam HeyPreclinical Safety BiologicsNovartis AGBaselSwitzerland
Andrew HiattMapp Biopharmaceutical Inc6160 Lusk Blvd C105San Diego CA 92121
Bjoumlrn HockDepartment of Protein Engineering and Antibody TechnologiesMerck Serono Merck KgaAFrankfurter Str 250D-64293 DarmstadtGermany
Kelly HuangDepartment of Infectious DiseaseMedImmune LLCOne MedImmune WayGaithersburg MD 20878
Philip R JohnsonThe Childrenrsquos Hospital of PhiladelphiaAbramson Research CenterPhiladelphia PA 19104
Debra H JosephsCutaneous Medicine and Immunotherapy UnitSt Johnrsquos Institute of DermatologyDivision of Genetics and Molecular Medicine amp NIHR Biomedical Research Centre at Guyrsquos and St Thomasrsquos HospitalsKingrsquos College London School of MedicineGuyrsquos HospitalLondon SE1 9RTUnited Kingdom
Shilpa A JoshiDepartment of PathologyStanford UniversityStanford CA 94305
Sophia N KaragiannisCutaneous Medicine and Immunotherapy UnitSt Johnrsquos Institute of DermatologyDivision of Genetics and Molecular Medicine amp NIHR Biomedical Research Centre at Guyrsquos and St Thomasrsquos HospitalsKingrsquos College London School of MedicineGuyrsquos HospitalLondon SE1 9RTUnited Kingdom
Panagiotis KaragiannisCutaneous Medicine and Immunotherapy UnitSt Johnrsquos Institute of DermatologyDivision of Genetics and Molecular Medicine amp NIHR Biomedical Research Centre at Guyrsquos and St Thomasrsquos HospitalsKingrsquos College London School of MedicineGuyrsquos HospitalLondon SE1 9RTUnited Kingdom
Jens C KrauseChildrenrsquos HospitalUniversity of Freiburg Medical Center79106 FreibergGermany
Antonio LanzavecchiaInstitute for Research in Biomedicinevia Vincenzo Vela 6Bellinzona 6500Switzerland
xii contRIBUtoRs
Marie-Paule LefrancLaboratoire drsquoImmunoGeacuteneacutetique Moleacuteculaire LIGMIMGTreg the international ImMunoGeneTics information systemregInstitut de Geacuteneacutetique Humaine IGHUniversiteacute Montpellier 2UPR CNRS 1142Montpellier 34396 cedex 5 40202France
Olivier LegerDepartment of Protein Engineering and Antibody TechnologiesMerck Serono SA--Geneva9 chemin des Mines1202 GenevaSwitzerland
Kin-Ming LoDepartment of Protein Engineering and Antibody TechnologiesEMD Serono Research Institute45A Middlesex TurnpikeBillerica MA 01821
Wayne A MarascoDepartment of Cancer Immunology and AIDSDana-Farber Cancer InstituteHarvard Medical SchoolBoston MA 02215
Jennifer A MaynardDepartment of Chemical EngineeringUniversity of Texas at AustinAustin TX 78712
Luzia M MayrINSERM U1109Universiteacute de Strasbourg3 Rue Koeberleacute67000 StrasbourgFrance
Jens MeilerDepartment of Chemistry and Center for Structural BiologyVanderbilt UniversityNashville TN 37212
contRIBUtoRs xiii
S Moein MoghimiDepartment of PharmacyCenter for Pharmaceutical Nanotechnology and NanotoxicologyFaculty of Health and Medical SciencesUniversity of CopenhagenCopenhagen DK-2100Denmark
Susan Zolla-PaznerNew York University School of Medicine550 First AvenueNew York NY 10016
Louise SaulCutaneous Medicine and Immunotherapy UnitSt Johnrsquos Institute of DermatologyDivision of Genetics and Molecular Medicine amp NIHR Biomedical Research Centre at Guyrsquos and St Thomasrsquos HospitalsKingrsquos College London School of MedicineGuyrsquos HospitalLondon SE1 9RTUnited Kingdom
Bruce C SchneppThe Childrenrsquos Hospital of PhiladelphiaAbramson Research CenterPhiladelphia PA 19104
Jennifer E SchusterDepartment of PediatricsChildrenrsquos Mercy HospitalKansas City MO 64108-4619
Alexander M SevyDepartment of Chemistry and Center for Structural BiologyVanderbilt UniversityNashville TN 37212
Jared SheehanDepartment of Cancer Immunology and AIDSDana-Farber Cancer InstituteHarvard Medical SchoolBoston MA 02215
Michael R SierksDepartment of Chemical EngineeringArizona State UniversityTempe AZ 85287-6006
xiv contRIBUtoRs
Scott A SmithThe Vanderbilt Vaccine Center and the Department of MedicineVanderbilt University Medical CenterNashville TN 37232
Robyn L StanfieldDepartment of Molecular BiologyThe Scripps Research Institute10550 North Torrey Pines RoadLa Jolla CA 92037
Nadine UptonRandall Division of Cell and Molecular BiophysicsDivision of Asthma Allergy and Lung BiologyMRC and Asthma UK Centre for Allergic Mechanisms of AsthmaKingrsquos College LondonNew Huntrsquos HouseGuyrsquos CampusLondon SE1 1ULUnited Kingdom
Avanish K VarshneyDepartment of MedicineInfectious Diseases and Department of Microbiology and ImmunologyAlbert Einstein College of MedicineBronx NY 10461
Stefanie N VelgosMayo Clinic Arizona5777 East Mayo BoulevardPhoenix AZ 85054
Kevin J WhaleyMapp Biopharmaceutical Inc6160 Lusk Blvd C105San Diego CA 92121
Peter P WibroeCentre for Pharmaceutical Nanotechnology and NanotoxicologyDepartment of PharmacyFaculty of Health and Medical SciencesUniversity of CopenhagenCopenhagen DK-2100Denmark
John V WilliamsDepartment of PediatricsSchool of MedicineVanderbilt UniversityNashville TN 37232-2581
contRIBUtoRs xv
Ian A WilsonDepartment of Molecular Biology and Skaggs Institute for Chemical BiologyThe Scripps Research Institute10550 North Torrey Pines RoadLa Jolla CA 92037
Herren WuDepartment of Antibody Discovery and Protein EngineeringMedImmune LLCOne MedImmune WayGaithersburg MD 20879
Guocheng YangDepartment of Chemical EngineeringArizona State UniversityTempe AZ 85287-6006
Larry ZeitlinMapp Biopharmaceutical Inc6160 Lusk Blvd C105San Diego CA 92121
xvi contRIBUtoRs
Preface
Antibodies form the principal foundation for modern intervention against in-fectious diseases Emil Adolf von Behring was awarded the first Nobel Prize in Physiology or Medicine in 1901 ldquofor his work on serum therapy especially its appli-cation against diphtheria by which he has opened a new road in the domain of med-ical science and thereby placed in the hands of the physician a victorious weapon against illness and deathsrdquo Antibodies now provide the focus for understanding mechanisms of immunity to most infectious diseases and they play a central role in passive immunotherapy and active vaccination as mechanisms or correlates of immunity For most of the 20th century immunotherapy was based on passive transfer of polyclonal hyperimmune animal serum immune human serum or even hyperimmune human serum Georges JF Koumlhler and Ceacutesar Milstein re-ported the generation of monoclonal antibodies in 1979 for which they shared the 1984 Nobel Prize in Physiology or Medicine ldquofor the discovery of the princi-ple for production of monoclonal antibodiesrdquo Since that time entire fields related to antibodies for infectious diseases including antibody gene cloning engineer-ing and expression antibody libraries and high-throughput antibody gene rep-ertoire sequence analysis have extended our capabilities to explore the diversity of antibody specificity and function with unprecedented depth and breadth
This book provides a broad survey of many of the most important aspects of the field of antibodies for infectious diseases The book begins with a general introduction followed by chapters 2 through 5 on general features pertaining to structure function isotype and the role of complement in antibody function Chapters 6 through 10 review contemporary approaches for antibody discovery using phage and yeast display plasma cell and memory B cell cloning human hybridomas humanized mice and computational methods Chapters 11 through 18 review in depth the biology of antibodies specific for particular pathogens including viruses and bacterial toxins to illustrate the role of antibodies in anti- microbial immunity with specific targets These chapters reveal that attempts to raise effective antibody responses to each of these pathogens faces unique and pathogen-specific challenges Chapters 19 to 23 cover major technical advances pertaining to antibody engineering repertoire sequencing and analysis and new methods for study or therapeutic use of antibodies including radiotherapy Fi-nally chapters 24 and 25 cover new methods for expression of monoclonal anti-bodies in plants or by transfer of antibody genes for in vivo expression in treated subjects
Recent literature is exploding with new antibody-related techniques and re-ports of antimicrobial antibodies with unprecedented potency breadth of activ-
xvii
xviii PReface
ity and therapeutic potential We hope that this timely compilation of state-of-the-art reviews of major aspects of this field will be of interest to both antibody cognoscenti and those new to this exciting field We thank the authors for their dedication in producing definitive reviews of the topics at hand
James E Crowe JrDiana BoraschiRino Rappuoli
INTRODUCTION
History and PracticeAntibodies in Infectious Diseases 1ADAM HEY1
Antibodies in Infectious Diseases aims to inform update and inspire studentsteachers researchers pharmaceutical developers and health care professionalson the status of the development of antibody-based therapies for treatinginfectious diseases and the potential for these in times of growing antibioticresistance to provide alternative treatment solutions to the currently usedantibiotics and new treatments for infectious diseases where no propertreatments are available
This introductory article will provide a historical perspective on the useof antibody-based therapies followed by a high-level overview of whatmakes antibodies attractive tools for this purpose This will include the prosand cons of such therapies compared to the use of antibiotics and thepractical and strategic considerations involved in selecting the best formatand development path for new antibody-based therapies targeting specificinfectious agents Then examples of antibody-based therapies in thedevelopment of treatments for infectious diseases will be presented andfinally a look into the future will summarize the different aspects that willinfluence what the future might bring for this type of treatments forinfectious diseases
1Preclinical Safety Biologics Novartis AG Basel Switzerland
Antibodies for Infectious DiseasesEdited by James E Crowe Jr Diana Boraschi and Rino Rappuolicopy 2015 American Society for Microbiology Washington DCdoi101128microbiolspecAID-0026-2014
3
HISTORICAL PERSPECTIVE
Antibodies and the use of passive antibodytherapy in the treatment of infectious dis-eases is the story of a treatment conceptwhich dates back more than 120 years to thelate 19th century and which originally bythe use of serum from immunized animalsprovided the first effective treatment optionsagainst severe bacterial infections (1 2) Byimmunizing horses with bacterial toxinsfrom Clostridium tetani and Corynebacteri-um diphtheriae Emil A Von Behring andShibasaburo Kitasato (3) generated serumcontaining antibodies capable of neutraliz-ing the effects of the toxins produced bythese bacteria and successfully providedtreatment for these serious diseases wherethe pathogenesis is driven by the effects ofthe bacterial toxins For his work on provid-ing treatment for diphtheria Behring re-ceived the Nobel Prize in Physiology orMedicine in 1901 These radical treatmentresults quickly prompted development ofmultiple additional serum therapies for thetreatment of infectious diseases caused byeg Neisseria meningitidis Haemophilus in-fluenza and group A Streptococcus Sinceserum therapy involved administration oflarge amounts of crude mixtures of animalproteins including antibodies they wereassociated with side effects in the form ofhypersensitivity and serum sickness (2)
Due to the crude and unpurified nature ofthese products side effects were seen evenwhen administering human serum prepa-rations Side effects were observed in up to50 of patients and were considered to becaused by immune complex formations thatresulted in symptoms such as rash itchingjoint pain fever and in serious cases hypoten-sion and shock However due to the lack ofalternative options these treatments weredespite their side effects widely used Serumwas normally administered by intravenousinfusion in patients after a test for hypersensi-tivity where a small amount of serum wasinjected subcutaniously (1) As described
above serum therapy applied in these earlydays (late 19th century and early 20th century)involved preparations of serum from rabbitsand horses immunized with the infectiousagent or in live andor neutralized versions ortoxins from these (1) The costs of keeping theimmunized animals and the production andpotency testing of the materials made this arelatively expensive treatment In 1891 datafrom Klemperer (4) showed serum therapy toprotect rabbits from Streptococcus pneumoniaeinfection and paved the way for this type oftreatment and for development of similarserum-based treatments of streptococcal in-fections in humans When treating humansearly administration of serum could reducemortality significantly down to around 5compared to when administered 4 to 5 daysafter onset of symptoms when serum treat-ment was largely without effect This stronglyindicated the need for quick diagnosis andquick treatment to control the infection beforeit got out of control Consequently in theabsence of a specific diagnosis mixtures ofserum from immunizations with differentserotypes were used to circumvent this needfor early treatment without having a serotype-specific diagnosis The understanding thatdifferent serotypes existed for pneumococciand that efficient treatment relied on usingserotype-specific serum was being built upduring the 1920s and 1930s through experiencefrom extensive clinical trials
By the end of the 1930s serum therapywasthe standard of care for treatment of pneu-mococcal pneumonia At that time theefficacy and potency of the derived serawere assessed in mice in ldquothe mouse pro-tection testrdquo by testing survival after aconcomitant intraperitoneal injection of alethal dose of pneumococci and the serum tobe tested Due to the inherent variation inthis test efficacy and survival in two thirds ofthe animals was the acceptance criteria and10 times the lowest dose providing this wasused for defining a unit of the serum Thisallowed for large batch-to-batch variationand the use of different strains of bacteria for
4 HEY
immunization probably explains part of themissing responses observed (1) In the early20th century a pandemic of meningitis inEurope and the United States with mortalityrates up to 80 spurred the development ofserum therapy treatment options Althoughin the 1930s this became the recommendedtreatment in children assumed to be suffer-ing from meningitis failure to reduce mor-tality in several meningitis epidemics duringthat time raised doubts about the generalapplicability of serum treatment In thosedays serum therapy often involved quiteextensive procedures and infusion of largevolumes of serum The following exampleclearly illustrates this Data from Flexnerand Jobling (5) from treating meningitis inmonkeys resulted in the development of serafrom immunized horses for treatment inhumans The treatment protocol includedlumbar puncture and withdrawal of morethan 30 ml of spinal fluid representing anamount slightly larger than the expectedamount of horse serum to be injected subse-quently This treatment involved such dailyslow infusions of up to 30 ml of serum untilthe patientrsquos condition improved This treat-ment was used in outbreaks in New York in1905 and 1906 and did markedly decreasemortality
After the discovery of penicillin by Flemingin 1928 and the subsequent introduction ofantibiotics in the 1930s serum therapy waslargely abandoned over a period of 10 years dueto the availability of these new more broadlyeffective and cheaper treatment optionswhichalso had fewer side effects Although improve-ments in the purification of antibodies hadresulted in preparations with better safety andside effect profiles high manufacturing costsand narrow specificity resulted in antibodytherapy being mostly restricted to a smallernumber of selected treatments for snakevenoms bacterial toxins and some viral infec-tions (1 2) Currently antibody administrationis used for treatment and prevention ofhepatitis B virus rabies virus respiratorysyncytial virus (RSV) Clostridium tetani Clos-
tridium botulinum vaccinia virus echovirusand enterovirus For the most part thesetreatments consist of pooled immunoglobulinalso known as IVIG (intravenous immunoglob-ulin) from several postexposure donors Thisresults in both batch-to-batch variation in theneed for relatively large amounts of serum dueto low specificity and to restricted supplies dueto reliance on exposed donors
However several challengeshave resulted inthe need for new tools in the treatment andpreventionof infectiousdiseasesThebroadandgeneral use of antibiotics in human and veter-inary medicine for many years has resulted inthe development of multi-resistant strains ofbacteria with limited to no response to existingtreatments such as methicillin-resistant Staph-ylococcusaureus (MRSA) vancomycin-resistantS aureus and others This has resulted inpatients needing screening and treatment withseveral antibacterial agents and longer treat-ment time causing extra strain on patients andhealth care providers (6 httpwwwcdcgovdrugresistancethreat-report-2013indexhtml) According to the WHO and CDC morethan 25000 people in European Unioncountries and similar numbers in the UnitedStates die every year as a result of antibiotic-resistant infections This together with theemergence of new pathogens (eg severeacute respiratory syndrome Middle East respi-ratory syndrome) the re-emergenceepidemicsof oldknown pathogens (eg Ebola) and thedifficulties in treating infections in immune-deficient patients (eg HIV patients) has high-lighted the need for new solutions The 2014Ebola epidemic in West Africa (Liberia SierraLeone Guinea Nigeria and Senegal) has fur-ther highlighted this No treatment or prophy-lactic vaccine is available to treat or prevent thespread of Ebola infections which have anaveragemortality of gt50 Local health author-ities in the affected countries are struggling tocontain and handle the disease which isthreatening to go out of control and spreadmorewidelyVariousproductsmainly antibodycocktails from previously recovered patientsare being used despite a lack of clinical data on
CHAPTER 1 bull History and Practice Antibodies in Infectious Diseases 5
their safety and efficacy and those are the onlysporadically available treatment options andonly in small amounts and for a few patients
Ebola is an example of a disease whichnormally affects only a small number ofindividuals and which normally burns outwhen disease outbreaks are contained There-fore given the small number of potentialpatients affected by previous Ebola infectionsto date there was no incentive for big pharmacompanies to do research and development ofdrugs for EbolaWith the increasing number ofinfected (13567) andadeath toll of 4951 (7) andthe lack of the ability to contain the epidemic itwill be interesting to follow the aftermath ofthis outbreak and see whether there will berequests for new ways to ensure that vaccinesand treatment options are available for Ebolaand similar high-mortality and potential bio-warfare infections that have no availabletreatments or procedures to for mass-produc-tion upon the first signsreports of activeinfections Although both the CDC and theWHO have special programs focusing on thesetypes of infections the Ebola outbreak in 2014clearly shows that more financial support forresearch and development of new diagnosticsand treatments is needed This is one examplewhere antibody-based treatments would havethe potential to play a major role To put this inthe right perspective one should however notforget that other infectious diseases such astuberculosis influenza and malaria kill hun-dreds of thousands each year There is there-fore plenty of room for improvement indeveloping treatments for these diseases aswell but the high attention drawn to eg theEbola outbreak creates a special niche andopportunity where antibody treatments couldgain extraordinary development funding andsupport and prove their value and treatmentpotential
That antibody-based therapies could takethis role is supported by the revolution intechnologies for the development selectiongeneration and purification of fully humanantibodies described in more detail later in thesection ldquoMethodsandPlatforms forGenerating
Antibodiesrdquo Antibody-based programs cur-rently at different stages of developmentinclude investigations into the potential use ofsingle antibody preparations combinations ofantibodies (to avoid survival of escape mu-tants) fragments of antibodies and antibodiescarrying radioactive isotopesorcytotoxicdrugsor antibody-like frameworks (eg fibronectin)either alone as a first-line treatment or as anadjunct to existing treatments This multitudeof possible formats the ability to raise anti-bodies to almost any target and the ability toengineer both size effector functions and half-life are now considered by many to providevery valuable tools for designing specificantibody-based treatments toeradicate specifictargeted infectious agents However althoughseveral antibody-based therapies have beenapproved for oncology and anti-inflammatoryindications (see Table 1) only one monoclonalantibody (mAb) is approved against an infec-tious disease agentmdashSynagis (palivizumabMedImmune) for the prevention and treat-ment of respiratory syncytical virus (RSV) inhigh-risk children Economic obstacles such asthe high cost of mAb therapies and relativelysmall markets have resulted in less interestfrom pharmaceutical companies in developingthese Also highlighting the challenges indeveloping these types of antibody-basedtreatments are the difficulties encountered indeveloping a follow-up higher-affinity candi-date to Synagis Poor translatability of dataobtained in the available animal disease mod-els for RSV in cotton rats has resulted in non-approval due to inferiority relative to SynagisIn other viral diseases such as cytomegalovirus(CMV) the high species specificity of thestrains of CMV makes it impossible to testhuman antibody therapies in vivo Thereforeany real data on the efficacy of treatments forCMV will not be obtained until testing inclinical trials As described later in this articleseveral new antibody-based therapies for in-fectious diseases are in development andhopefully this will gradually open the fieldand result in better treatment options andoutcomes for patients
6 HEY
TABLE 1 Approved and pending antibody-based therapies
Name antibody Target antibody type Indication Company Approval date
OKT3a Muronomab-CD3 CD3 murine IgG2a Autoimmune Johnson ampJohnson
1986 (US)
ReoPro abciximab PIIbIIIa chimeric IgG1Fab
Homeostasis Johnson ampJohnson
1984 (US)
Rituxan rituximab CD20 chimeric IgG1 Cancer Genentech 1997 (US) 1998 (EU)Zenapaxa daclizumab CD25 humanized IgG1 Autoimmune Roche 1997 (US) 1999 (EU)Simulect basiliximab CD25 chimeric IgG1 Autoimmune Novartis 1998 (US EU)Synagis palivizumab RSV humanized IgG1 Infections MedImmune 1998 (US) 1999 (EU)Remicade infliximab TNFα chimeric IgG1 Autoimmune Johnson amp
Johnson1998 (US) 1999 (EU)
Herceptin trastuzumab HER2 humanized IgG1 Cancer GenentechRoche
1998 (US) 2000 (EU)
Mylotarga gemtuzumabozogamicin
CD33 humanized IgG4immunotoxin
Cancer WyethPfizer 2000 (US)
Campath alemtuzumab CD52 humanized IgG1 Cancer Genzyme 2001 (US) 2001 (EU)Zevalin ibritumomabtiuxetan
CD20 murine IgG1radiolabeled (yttrium 90)
Cancer Biogen Idec 2002 (US) 2004 (EU)
Humira adalimumab TNFα human IgG1 Autoimmune Abbott 2002 (US) 2003 (EU)Xolair omalizumab IgE humanized IgG1 Autoimmune Genentech
Roche2003 (US)
Bexxar tositumomab-I-131 CD20 murine IgG2aradiolabeled (iodine131)
Cancer CorixaGSK 2003 (US)
Raptivaa falizumab CD11a humanized IgG1 Autoimmune GenentechRoche
2003 (US) 2004 (EU)
Erbitux cetuximab EGFR chimeric IgG1 Cancer ImcloneLilly 2004 (US) 2004 (EU)Avastin bevacizumab VEGF humanized IgG1 Cancer Genentech
Roche2004 (US) 2005 (EU)
Tysabri natalizumab α4-Intergrin humanizedIgG4
Autoimmune Biogen Idec 2004 (US)
Actemra tocilizumab Anti-IL-6R humanizedIgG1
Autoimmune ChugaiRoche
2005 (Japan) 2010 (US)
Vectibix panitumumab EGFR human IgG2 Cancer Amgen 2006 (US)Lucentis ranibizumab VEGF humanized IgG1
FabMaculardegeneration
GenentechRoche
2006 (US)
Soliris eculizumab C5 humanized IgG24 Blood disorders Alexion 2007 (US)Cimzia certolizumab pegol TNFα humanized
pegylated FabAutoimmune UCB 2008 (US)
Simponi golimumab TNFα human IgG1 Autoimmune Johnson ampJohnson
2009 (US EU Canada)
Ilaris canakinumab IL1b human IgG1 Infalmmatory Novartis 2009 (US EU)Stelara ustekinumab IL-1223 human IgG1 Autoimmune Johnson amp
Johnson2008 (EU) 2009 (US)
Arzerra ofatumumab CD20 human IgG1 Cancer Genmab 2009 (EU)Prolia denosumab RANK ligand human
IgG2Bone loss Amgen 2010 (US)
Numax motavizumab RSV humanized IgG1 Anti-infective MedImmune PendingABthrax Raxibacumab B anthrasis PA human
IgG1Anti-infection GSK 2012 (US)
Benlysta belimumab BLyS human IgG1 Autoimmune HGS 2011 (US)Yervoy ipilimumab CTLA-4 human IgG1 Cancer BMS 2011 (US)Adcetris brentuximabvedotin
CD30 chimeric IgG1drug- conjugate
Cancer SeattleGenetics
2011 (US)
(Continued on next page)
CHAPTER 1 bull History and Practice Antibodies in Infectious Diseases 7
INTRODUCTION TO ANTIBODIES
Antibodies also called immunoglobulins basedon their combined structure and function inimmune responses are produced by B cells ofthe immune system They are part of theadaptive immune response and are speciallydesigned for neutralizing and eliminating theinfectious agents and toxins produced by theseAntibodies are present in blood plasma andextracellular fluids and since these fluids wereformerly known as humors they were said tobe part of the humoral immune responseAntibodies are Y-shaped structures consistingof two main parts the upper arms of the Ywhich contain two identical variable-regionantigen binding sites and the lower regioncalled the constant regionwhich is responsiblefor the initiation of effector functions that leadto the removal and destruction of the pathogenor cells harboring the pathogen (see Fig 1) Theantigen-binding sites on an antibody can bythemselves bind to and neutralize bacterialtoxins and viruses thereby preventing themfrom binding to their target cells or receptorscausing toxic effects or spread of the infection
Antibodies consist of two pairs of heavy andlight chainswhich as described above are heldtogether in a Y-shaped arrangement Each ofthe heavy and light chains in these pairs isseparated into constant and variable chainsThe upper armsof theY each contain a variableand a constant sectionof the light and theheavychain where the upper variable parts of theheavy and light chains contain the antigen-binding site and the constant parts areconnected via disulfide bonds The lower partof theYcalled theconstantpart consistsof twoor three constant segments (immunoglobulindomains) from each of the two heavy chainsinteracting and also linked via disulfide bondsThe sectionsof theheavy chains connecting theconstant part of the upper arms to the constantparts of the constant region contain specialhinge regions that provide flexibility to thedifferent sections of the antibody to bind toantigens and effector cells The constant re-gions of the heavy chain also contain attachedoligosaccharide moieties which provide func-tional specialization to the antibodies (8)
The variable domains of the heavy and lightchains form the antigen-binding sites and
TABLE 1 Approved and pending antibody-based therapies (Continued)
Name antibody Target antibody type Indication Company Approval date
Perjeta pertuzumab Her2 humanized IgG1 Cancer GenentechRoche
2012 (US)
Kadcyla ado-trastuzumabemtansine
Her2 humanized IgG1Drug-conjugate
Cancer GenentechRoche
2013 (US)
Raxibacumab Anti-B anthrasis PAhuman IgG1
Anthraxinfection
Notapproved
2012
Entyvio vedolizumab Integrin α4β7humanized IgG1
Crohnrsquos diseaseulcerative colitis
Takeda 2014 (US)
Cyramza ramuciruumab Anti-VEGFR2Human IgG1
Gastric cancer Lilly 2014 (US)
Gazyva obinutuzumab Anti-CD20 humanizedIgG1 glucoengineered
CancerCLLb GenentechRoche
2014 (US)
Sylvant situximab Anti IL-6 chimeric IgG1 Castlemandisease
Janssen 2014 (US) 2014 (EU)
Cosentyx sekukinumab Anti IL-17a human IgG1 Psoriasis Novartis 2015 (US) 2015 (EU)Nivolumab Anti PD-1 human IgG4 Melanoma BMS Not approvedKeytruda pembrolizuumab Anti-PD-1 humanized
IgG4Melanoma Merck 2014 (US)
aAntibodies approved but later withdrawnbCLL chronic lymphocytic leukemia
8 HEY
FIGURE 1 (Left panel) Model of antibody structure exemplified by IgG On top the antigen-binding sitesin orange each contain one variable light and variable heavy domain with the three complementaritydetermining regions (CDRs) that are responsible for the specific binding of the antibody to its target Foreach arm of the antibody an additional set of variable heavy and light domains together with the CDR-containing domains represent the two fragment antigen binding (Fab) regions The two Fabs are heldtogether via two disulfide bridges Below the Fabs is the Fc region which contains four constant heavydomains On the upper pair of these domains are binding sites for oligosaccharides which have majorimportance for the ability of the antibody Fc part to trigger effector functions when the Fc portion isbound to Fc gamma receptors on natural killer cells neutrophil granulocytes monocytesmacrophagesdendritic cells and B cells (Right panel) Examples of some of the antibody-derived alternative formatsused to exploit the specific features of the CDRs the Fabs and the Fc parts of the antibodies ScFv Thesingle chain fragment variable consists of the variable domains of the heavy and light chains heldtogether by a flexible linker This can also be used as a carrier of a cytotoxic drug in a so-called antibodydrug complex (ADC) where the specificity of the ScFv is used to target the cytotoxic drug to eg atumor Bite (bi-specific T cell engager) Fusion proteins consisting of two ScFvs one directed against thetarget on a tumor cell and the other against the T cell receptor (CD3) Diabody ScFv dimers where shortlinker peptides (five amino acids) ensure dimerization and not folding of the ScFvs Fab and F(ab)2fragments Single Fab fragments or fragments containing two Fabs linked via disulfide bridges This isused where effector functions related to the Fc part of the antibody are unwanted and where a smallersize is desired to obtain better tissue penetration in eg tumors Due to the lack of the FcRn binding viathe Fc part Fab and F(ab)2 fragments have much shorter half-lives (hours or days) than full-sizeantibodies (weeks) These can also be used as carriers of cytotoxic payloads or cytotoxic radioactiveisotopes and for the F(ab)2 fragments can be constructed as bi-specifics which can cross-link immunecells and target cells Fc fusion protein Fusion protein containing the Fc domain of an immunoglobulinbound to a peptide The peptide can be a ligand for a specific receptor on a target cell or a blockingpeptide for a soluble ligand The Fc part provides a longer half-life to the construct and the potential tobind to and engage effector functions in the killing of eg tumor cells or infected cells ADCsRIAs andbi-specifics Full-size IgG antibodies carrying either a cytotoxic chemical or radioactive payload whichmay also carry different CDRs enabling cross-linking of effector and target cells for increased killingdoi101128microbiolspecAID-0026-2014f1
CHAPTER 1 bull History and Practice Antibodies in Infectious Diseases 9
contain special hyper-variable segments calledcomplementarity-determining regions (CDRs)which allow the B cells via genetic recom-bination to generate antibodies to all thedifferent antigens specific to amino acid se-quences or three-dimensional structuralmotifs(polysaccharides DNA and RNA) found onpathogens
Based on the structure of their heavy chainconstant regions antibodies or immuno-globulins are separated into five classesmdashIgM IgG IgE IgD and IgA Differences inthe sequences of the constant regions providedistinct characteristics to these different clas-ses These characteristics include the numberof heavy chain constant segments the numberand location of interconnecting disulfidebridges the length of the hinge region andthe number and location of oligosaccharidemoieties For IgG four heavy chain versionsexist creating IgG1 2 3 and 4 isotypes eachwith different characteristics in their serumhalf-lives and ability to trigger different effec-tor functions Because of the combined ad-vantage from ability to trigger effectormechanisms long [21 days] half-life theirability to be transported over the placentaand their stability in the production processantibodies of the IgG class and of the IgG1isotype are preferred as the basis for newantibody-based therapies The effector func-tions are triggered by the Fc part of an antibodywhen the variable parts of the antibody arebound directly to an infectious agent or toproteins from an infectious agent expressed onan infected cell This binding leaves the Fc partfree to interactwithFc receptors onphagocyticcells and neutrophils eosinophils and naturalkiller cells capable of inducing phagocytosis orlysis of infectious agents or infected cellsThese effector functions include (i) the abilityto activate the complement system for lysis(complement-dependent cellular cytotoxicity)(ii) triggering of uptake and destruction byphagocytic cells such as macrophages andneutrophils via interaction with Fc receptorson these cells (iii) activation of macrophageseosinophils neutrophils and natural killer
cells to kill infected cells via binding to Fcreceptors on these cells and antibody-depen-dent cellular cytotoxicity and (iv) neutraliza-tion of bacterial toxins and blocking of bindingand uptake of bacteria or viruses to target cells(see Fig 2) (9)
The Fcpart of IgG antibodies also contains aregion that interacts with the neonatal Fcreceptor (FcRn) expressed on most immuno-competent cells and inmany other cells such asendothelial cells in kidney liver placenta lungand breast (10) which protects antibodies fromdegradation by phagocytoticexocytotic cy-cling into FcRn-expressing cells thereby pro-longing their half-life This results in half-livesof 20 to 21 days for most IgG1 2 and 4antibodies whereas half-lives are 10 6 and 2days respectively for IgM IgA and IgE Thehighly specific binding sites on the variableregions of the upper arms of the antibody allowfor several important features of antibodiesndashbinding to and neutralization of eg bacterialtoxins binding to pathogens and blocking theirbinding to or interaction with target cells (egcyncytia formation of CMV-infected cells) orblocking of binding and interactions of infec-tious agents with target cells via blockingreceptors on the target cells
METHODS AND PLATFORMS FORGENERATING ANTIBODIES
As described above the early use of passiveantibody transfer as a therapy in infectiousdiseases involved the use of immune serumfrom immunized sheep and horses These pre-parations were crude and contained a broadmixture of neutralizing and non-neutralizingantibodies and both the foreign nature of theantibodies and the numerous host serumproteins This resulted in less specific andthus less efficient therapies due to a highvariability in efficacy between batches derivedfrom different animals immunized with dif-ferent strains of bacteria in different labor-atories and resulted in multiple unwantedside effects related to hypersensitivity and
10 HEY
anaphylactic reactions to foreign proteinsThese days antibodies being developed fortreatment of diseases in humans are highlypurified and are mostly fully human mono-clonal antibodies The term monoclonal anti-body refers to that cell cultures used forgenerating these antibodies each originatesfrom a single cell and thus produces onlyone specific antibody Development of fullyhuman monoclonal antibodies happened instages over a time span of more than 15 yearsFirst stage in this process was generation ofmonoclonalmurine IgG antibodies (eg OKT3[muronomab-CD3 Johnson and Johnson] ap-proved in 1986) Next stage was generation ofso called chimeric antibodies consisting ofhuman heavy and light chain constant sec-tions but with murine variable sections (eg
Rituxan [rituximab Genentech]) Next stagewas then the humanized antibodies wherethe only remaining murine part of the anti-body is the antigen-binding CDR (eg Xolair[omalizumab NovartisGenentech]) Both thefirst chimeric and humanized antibodies wereapproved in the late 1990s Then finally 16years later the first fully human antibodyHumira (adalimumab Abbott) was approvedin 2002 Since the time of the crude and low-scale manufacturing of the original antibodyserum products much has changed andtherapeutic antibodies are now produced byfermentation in 5000 liter scale using highlycontrolled and documented yeast or mamma-lian cell lines that are genetically engineered toexpress a single specific antibody This hasresulted in a pure and highly specific antibody
FIGURE 2 Effector functions of antibodies (a) Antibodies bind to pathogen-derived or endogenousantigens expressed on the surface of an infected cell which triggers binding to Fc receptors on naturalkiller cells and lysis of the infected cell by antibody-dependent cellular cytotoxicity (b) Antibodies bindto pathogen-derived or endogenous antigens expressed on the surface of infected cells which triggersactivation of complement through binding of complement factor C1q (c) Neutralization Top Bacterialtoxin neutralized by bound antigen Bottom Antibody bound to either receptor for the virus or to thevirus itself which blocks virus binding and entry into the cell (d) Antibody bound to viral surfaceproteins binds to Fc receptors on phagocytic cells eg macrophages and triggers endocytosis anddestruction of virus in endolysosome doi101128microbiolspecAID-0026-2014f2
CHAPTER 1 bull History and Practice Antibodies in Infectious Diseases 11

Contents
ContributorsemspixPrefaceemspxvii
IntroductIon
1 History and Practice Antibodies in Infectious Diseasesemsp3 Adam Hey
General Features oF ImmunoGlobulIns
2 Functions of Antibodiesemsp25 Donald N Forthal
3 Antibody Structureemsp49 Robyn L Stanfield and Ian A Wilson
4 The Role of Complement in Antibody Therapy for Infectious Diseasesemsp63 Peter P Wibroe Shen Y Helvig and S Moein Moghimi
5 Immunoglobulin E and Allergy Antibodies in Immune Inflammation and Treatmentemsp75
Sophia N Karagiannis Panagiotis Karagiannis Debra H Josephs Louise Saul Amy E Gilbert Nadine Upton and Hannah J Gould
antIbody dIscovery approaches
6 Phage and Yeast Displayemsp105 Jared Sheehan and Wayne A Marasco
7 Efficient Methods To Isolate Human Monoclonal Antibodies from Memory B Cells and Plasma Cellsemsp129
Davide Corti and Antonio Lanzavecchia
8 Use of Human Hybridoma Technology To Isolate Human Monoclonal Antibodiesemsp141 Scott A Smith and James E Crowe Jr
9 Humanized Mice for Studying Human Immune Responses and Generating Human Monoclonal Antibodiesemsp157
Ramesh Akkina
10 Antibodies Computer-Aided Prediction of Structure and Design of Functionemsp173 Alexander M Sevy and Jens Meiler
v
vi contents
pathoGen-specIFIc antIbodIes
11 Antibodies Targeting the Envelope of HIV-1emsp193 Luzia M Mayr and Susan Zolla-Pazner
12 Committing the Oldest Sins in the Newest Kind of WaysmdashAntibodies Targeting the Influenza Virus Type A Hemagglutinin Globular Heademsp209
Jens C Krause and James E Crowe Jr
13 Prevention of Respiratory Syncytial Virus Infection From Vaccine to Antibodyemsp221
Kelly Huang and Herren Wu
14 Human Metapneumovirusemsp237 Jennifer E Schuster and John V Williams
15 Dengue Antibody-Dependent Enhancement Knowns and Unknownsemsp249
Scott B Halstead
16 Immunotherapeutic Approaches To Prevent Cytomegalovirus-Mediated Diseaseemsp273
Edith Acquaye-Seedah Zachary P Frye and Jennifer A Maynard
17 Rotavirusemsp289 Manuel A Franco and Harry B Greenberg
18 Bacterial ToxinsmdashStaphylococcal Enterotoxin Bemsp303 Bettina C Fries and Avanish K Varshney
technIcal advances
19 Antibody Engineeringemsp321 Kin-Ming Lo Olivier Leger and Bjoumlrn Hock
20 High-Throughput DNA Sequencing Analysis of Antibody Repertoiresemsp345
Scott D Boyd and Shilpa A Joshi
21 Antibody Informatics IMGT the International ImMunoGeneTics Information Systememsp363
Marie-Paule Lefranc
22 Probing Antibody-Antigen Interactionsemsp381 Guocheng Yang Stefanie N Velgos Shanta P Boddapati
and Michael R Sierks
23 Radiolabeled Antibodies for Therapy of Infectious Diseasesemsp399 Ekaterina Dadachova and Arturo Casadevall
alternate systems For expressIon
24 Plant-Derived Monoclonal Antibodies for Prevention and Treatment of Infectious Diseaseemsp413
Andrew Hiatt Kevin J Whaley and Larry Zeitlin
25 Vector-Mediated In Vivo Antibody Expressionemsp427 Bruce C Schnepp and Philip R Johnson
Indexemsp441
contents vii
Contributors
Edith Acquaye-SeedahDepartment of BiochemistryUniversity of Texas at AustinAustin TX 78712
Ramesh AkkinaDepartment of Microbiology Immunology and PathologyColorado State University1619 Campus DeliveryFort Collins CO 80523
Shanta P BoddapatiDepartment of Biomedical EngineeringOregon Health and Science University3181 SW Sam Jackson Park RoadPortland OR 97239
Scott D BoydDepartment of PathologyStanford UniversityStanford CA 94305
Arturo CasadevallDepartments of Microbiology and Immunology and MedicineAlbert Einstein College of Medicine of Yeshiva University1695A Eastchester RoadBronx NY 10461
Davide CortiHumabs BioMed SAvia Mirasole 1Bellinzona 6500Switzerland
James E Crowe JrSchool of MedicineVanderbilt UniversityNashville TN 37232
ix
x contRIBUtoRs
Ekaterina (Kate) DadachovaDepartments of Radiology Microbiology and ImmunologyAlbert Einstein College of Medicine of Yeshiva University1695A Eastchester RoadBronx NY 10461
Donald N ForthalDepartment of Infectious Diseases3044 Hewitt HallUniversity of California IrvineIrvine CA 92617
Manuel A FrancoFacultad de Ciencias y MedicinaPontificia Universidad JaverianaOficina 306 Edificio 50Carrera 7 40-62BogotaacuteColombia
Bettina C FriesDepartment of MedicineInfectious Diseases and Department of Microbiology and ImmunologyAlbert Einstein College of MedicineBronx NY 10461
Zachary P FryeDepartment of Chemical EngineeringUniversity of Texas at AustinAustin TX 78712
Amy E GilbertCutaneous Medicine and Immunotherapy UnitSt Johnrsquos Institute of DermatologyDivision of Genetics and Molecular Medicine amp NIHR Biomedical Research Centre at Guyrsquos and St Thomasrsquos Hospitals and Kingrsquos College London School of MedicineGuyrsquos HospitalLondon SE1 9RTUnited Kingdom
Hannah J GouldRandall Division of Cell and Molecular BiophysicsDivision of Asthma Allergy and Lung BiologyMRC and Asthma UK Centre for Allergic Mechanisms of AsthmaKingrsquos College LondonNew Huntrsquos HouseGuyrsquos CampusLondon SE1 1ULUnited Kingdom
contRIBUtoRs xi
Harry B GreenbergDepartments of Medicine and Microbiology and ImmunologyStanford University School of Medicine and the VAPAHCSPalo Alto CA 94305
Scott B HalsteadDepartment of Preventive Medicine and BiometricsUniformed Services University of the Health SciencesBethesda MD 20814
Shen Y HelvigDepartment of PharmacyCenter for Pharmaceutical Nanotechnology and NanotoxicologyFaculty of Health and Medical SciencesUniversity of CopenhagenCopenhagen DK-2100Denmark
Adam HeyPreclinical Safety BiologicsNovartis AGBaselSwitzerland
Andrew HiattMapp Biopharmaceutical Inc6160 Lusk Blvd C105San Diego CA 92121
Bjoumlrn HockDepartment of Protein Engineering and Antibody TechnologiesMerck Serono Merck KgaAFrankfurter Str 250D-64293 DarmstadtGermany
Kelly HuangDepartment of Infectious DiseaseMedImmune LLCOne MedImmune WayGaithersburg MD 20878
Philip R JohnsonThe Childrenrsquos Hospital of PhiladelphiaAbramson Research CenterPhiladelphia PA 19104
Debra H JosephsCutaneous Medicine and Immunotherapy UnitSt Johnrsquos Institute of DermatologyDivision of Genetics and Molecular Medicine amp NIHR Biomedical Research Centre at Guyrsquos and St Thomasrsquos HospitalsKingrsquos College London School of MedicineGuyrsquos HospitalLondon SE1 9RTUnited Kingdom
Shilpa A JoshiDepartment of PathologyStanford UniversityStanford CA 94305
Sophia N KaragiannisCutaneous Medicine and Immunotherapy UnitSt Johnrsquos Institute of DermatologyDivision of Genetics and Molecular Medicine amp NIHR Biomedical Research Centre at Guyrsquos and St Thomasrsquos HospitalsKingrsquos College London School of MedicineGuyrsquos HospitalLondon SE1 9RTUnited Kingdom
Panagiotis KaragiannisCutaneous Medicine and Immunotherapy UnitSt Johnrsquos Institute of DermatologyDivision of Genetics and Molecular Medicine amp NIHR Biomedical Research Centre at Guyrsquos and St Thomasrsquos HospitalsKingrsquos College London School of MedicineGuyrsquos HospitalLondon SE1 9RTUnited Kingdom
Jens C KrauseChildrenrsquos HospitalUniversity of Freiburg Medical Center79106 FreibergGermany
Antonio LanzavecchiaInstitute for Research in Biomedicinevia Vincenzo Vela 6Bellinzona 6500Switzerland
xii contRIBUtoRs
Marie-Paule LefrancLaboratoire drsquoImmunoGeacuteneacutetique Moleacuteculaire LIGMIMGTreg the international ImMunoGeneTics information systemregInstitut de Geacuteneacutetique Humaine IGHUniversiteacute Montpellier 2UPR CNRS 1142Montpellier 34396 cedex 5 40202France
Olivier LegerDepartment of Protein Engineering and Antibody TechnologiesMerck Serono SA--Geneva9 chemin des Mines1202 GenevaSwitzerland
Kin-Ming LoDepartment of Protein Engineering and Antibody TechnologiesEMD Serono Research Institute45A Middlesex TurnpikeBillerica MA 01821
Wayne A MarascoDepartment of Cancer Immunology and AIDSDana-Farber Cancer InstituteHarvard Medical SchoolBoston MA 02215
Jennifer A MaynardDepartment of Chemical EngineeringUniversity of Texas at AustinAustin TX 78712
Luzia M MayrINSERM U1109Universiteacute de Strasbourg3 Rue Koeberleacute67000 StrasbourgFrance
Jens MeilerDepartment of Chemistry and Center for Structural BiologyVanderbilt UniversityNashville TN 37212
contRIBUtoRs xiii
S Moein MoghimiDepartment of PharmacyCenter for Pharmaceutical Nanotechnology and NanotoxicologyFaculty of Health and Medical SciencesUniversity of CopenhagenCopenhagen DK-2100Denmark
Susan Zolla-PaznerNew York University School of Medicine550 First AvenueNew York NY 10016
Louise SaulCutaneous Medicine and Immunotherapy UnitSt Johnrsquos Institute of DermatologyDivision of Genetics and Molecular Medicine amp NIHR Biomedical Research Centre at Guyrsquos and St Thomasrsquos HospitalsKingrsquos College London School of MedicineGuyrsquos HospitalLondon SE1 9RTUnited Kingdom
Bruce C SchneppThe Childrenrsquos Hospital of PhiladelphiaAbramson Research CenterPhiladelphia PA 19104
Jennifer E SchusterDepartment of PediatricsChildrenrsquos Mercy HospitalKansas City MO 64108-4619
Alexander M SevyDepartment of Chemistry and Center for Structural BiologyVanderbilt UniversityNashville TN 37212
Jared SheehanDepartment of Cancer Immunology and AIDSDana-Farber Cancer InstituteHarvard Medical SchoolBoston MA 02215
Michael R SierksDepartment of Chemical EngineeringArizona State UniversityTempe AZ 85287-6006
xiv contRIBUtoRs
Scott A SmithThe Vanderbilt Vaccine Center and the Department of MedicineVanderbilt University Medical CenterNashville TN 37232
Robyn L StanfieldDepartment of Molecular BiologyThe Scripps Research Institute10550 North Torrey Pines RoadLa Jolla CA 92037
Nadine UptonRandall Division of Cell and Molecular BiophysicsDivision of Asthma Allergy and Lung BiologyMRC and Asthma UK Centre for Allergic Mechanisms of AsthmaKingrsquos College LondonNew Huntrsquos HouseGuyrsquos CampusLondon SE1 1ULUnited Kingdom
Avanish K VarshneyDepartment of MedicineInfectious Diseases and Department of Microbiology and ImmunologyAlbert Einstein College of MedicineBronx NY 10461
Stefanie N VelgosMayo Clinic Arizona5777 East Mayo BoulevardPhoenix AZ 85054
Kevin J WhaleyMapp Biopharmaceutical Inc6160 Lusk Blvd C105San Diego CA 92121
Peter P WibroeCentre for Pharmaceutical Nanotechnology and NanotoxicologyDepartment of PharmacyFaculty of Health and Medical SciencesUniversity of CopenhagenCopenhagen DK-2100Denmark
John V WilliamsDepartment of PediatricsSchool of MedicineVanderbilt UniversityNashville TN 37232-2581
contRIBUtoRs xv
Ian A WilsonDepartment of Molecular Biology and Skaggs Institute for Chemical BiologyThe Scripps Research Institute10550 North Torrey Pines RoadLa Jolla CA 92037
Herren WuDepartment of Antibody Discovery and Protein EngineeringMedImmune LLCOne MedImmune WayGaithersburg MD 20879
Guocheng YangDepartment of Chemical EngineeringArizona State UniversityTempe AZ 85287-6006
Larry ZeitlinMapp Biopharmaceutical Inc6160 Lusk Blvd C105San Diego CA 92121
xvi contRIBUtoRs
Preface
Antibodies form the principal foundation for modern intervention against in-fectious diseases Emil Adolf von Behring was awarded the first Nobel Prize in Physiology or Medicine in 1901 ldquofor his work on serum therapy especially its appli-cation against diphtheria by which he has opened a new road in the domain of med-ical science and thereby placed in the hands of the physician a victorious weapon against illness and deathsrdquo Antibodies now provide the focus for understanding mechanisms of immunity to most infectious diseases and they play a central role in passive immunotherapy and active vaccination as mechanisms or correlates of immunity For most of the 20th century immunotherapy was based on passive transfer of polyclonal hyperimmune animal serum immune human serum or even hyperimmune human serum Georges JF Koumlhler and Ceacutesar Milstein re-ported the generation of monoclonal antibodies in 1979 for which they shared the 1984 Nobel Prize in Physiology or Medicine ldquofor the discovery of the princi-ple for production of monoclonal antibodiesrdquo Since that time entire fields related to antibodies for infectious diseases including antibody gene cloning engineer-ing and expression antibody libraries and high-throughput antibody gene rep-ertoire sequence analysis have extended our capabilities to explore the diversity of antibody specificity and function with unprecedented depth and breadth
This book provides a broad survey of many of the most important aspects of the field of antibodies for infectious diseases The book begins with a general introduction followed by chapters 2 through 5 on general features pertaining to structure function isotype and the role of complement in antibody function Chapters 6 through 10 review contemporary approaches for antibody discovery using phage and yeast display plasma cell and memory B cell cloning human hybridomas humanized mice and computational methods Chapters 11 through 18 review in depth the biology of antibodies specific for particular pathogens including viruses and bacterial toxins to illustrate the role of antibodies in anti- microbial immunity with specific targets These chapters reveal that attempts to raise effective antibody responses to each of these pathogens faces unique and pathogen-specific challenges Chapters 19 to 23 cover major technical advances pertaining to antibody engineering repertoire sequencing and analysis and new methods for study or therapeutic use of antibodies including radiotherapy Fi-nally chapters 24 and 25 cover new methods for expression of monoclonal anti-bodies in plants or by transfer of antibody genes for in vivo expression in treated subjects
Recent literature is exploding with new antibody-related techniques and re-ports of antimicrobial antibodies with unprecedented potency breadth of activ-
xvii
xviii PReface
ity and therapeutic potential We hope that this timely compilation of state-of-the-art reviews of major aspects of this field will be of interest to both antibody cognoscenti and those new to this exciting field We thank the authors for their dedication in producing definitive reviews of the topics at hand
James E Crowe JrDiana BoraschiRino Rappuoli
INTRODUCTION
History and PracticeAntibodies in Infectious Diseases 1ADAM HEY1
Antibodies in Infectious Diseases aims to inform update and inspire studentsteachers researchers pharmaceutical developers and health care professionalson the status of the development of antibody-based therapies for treatinginfectious diseases and the potential for these in times of growing antibioticresistance to provide alternative treatment solutions to the currently usedantibiotics and new treatments for infectious diseases where no propertreatments are available
This introductory article will provide a historical perspective on the useof antibody-based therapies followed by a high-level overview of whatmakes antibodies attractive tools for this purpose This will include the prosand cons of such therapies compared to the use of antibiotics and thepractical and strategic considerations involved in selecting the best formatand development path for new antibody-based therapies targeting specificinfectious agents Then examples of antibody-based therapies in thedevelopment of treatments for infectious diseases will be presented andfinally a look into the future will summarize the different aspects that willinfluence what the future might bring for this type of treatments forinfectious diseases
1Preclinical Safety Biologics Novartis AG Basel Switzerland
Antibodies for Infectious DiseasesEdited by James E Crowe Jr Diana Boraschi and Rino Rappuolicopy 2015 American Society for Microbiology Washington DCdoi101128microbiolspecAID-0026-2014
3
HISTORICAL PERSPECTIVE
Antibodies and the use of passive antibodytherapy in the treatment of infectious dis-eases is the story of a treatment conceptwhich dates back more than 120 years to thelate 19th century and which originally bythe use of serum from immunized animalsprovided the first effective treatment optionsagainst severe bacterial infections (1 2) Byimmunizing horses with bacterial toxinsfrom Clostridium tetani and Corynebacteri-um diphtheriae Emil A Von Behring andShibasaburo Kitasato (3) generated serumcontaining antibodies capable of neutraliz-ing the effects of the toxins produced bythese bacteria and successfully providedtreatment for these serious diseases wherethe pathogenesis is driven by the effects ofthe bacterial toxins For his work on provid-ing treatment for diphtheria Behring re-ceived the Nobel Prize in Physiology orMedicine in 1901 These radical treatmentresults quickly prompted development ofmultiple additional serum therapies for thetreatment of infectious diseases caused byeg Neisseria meningitidis Haemophilus in-fluenza and group A Streptococcus Sinceserum therapy involved administration oflarge amounts of crude mixtures of animalproteins including antibodies they wereassociated with side effects in the form ofhypersensitivity and serum sickness (2)
Due to the crude and unpurified nature ofthese products side effects were seen evenwhen administering human serum prepa-rations Side effects were observed in up to50 of patients and were considered to becaused by immune complex formations thatresulted in symptoms such as rash itchingjoint pain fever and in serious cases hypoten-sion and shock However due to the lack ofalternative options these treatments weredespite their side effects widely used Serumwas normally administered by intravenousinfusion in patients after a test for hypersensi-tivity where a small amount of serum wasinjected subcutaniously (1) As described
above serum therapy applied in these earlydays (late 19th century and early 20th century)involved preparations of serum from rabbitsand horses immunized with the infectiousagent or in live andor neutralized versions ortoxins from these (1) The costs of keeping theimmunized animals and the production andpotency testing of the materials made this arelatively expensive treatment In 1891 datafrom Klemperer (4) showed serum therapy toprotect rabbits from Streptococcus pneumoniaeinfection and paved the way for this type oftreatment and for development of similarserum-based treatments of streptococcal in-fections in humans When treating humansearly administration of serum could reducemortality significantly down to around 5compared to when administered 4 to 5 daysafter onset of symptoms when serum treat-ment was largely without effect This stronglyindicated the need for quick diagnosis andquick treatment to control the infection beforeit got out of control Consequently in theabsence of a specific diagnosis mixtures ofserum from immunizations with differentserotypes were used to circumvent this needfor early treatment without having a serotype-specific diagnosis The understanding thatdifferent serotypes existed for pneumococciand that efficient treatment relied on usingserotype-specific serum was being built upduring the 1920s and 1930s through experiencefrom extensive clinical trials
By the end of the 1930s serum therapywasthe standard of care for treatment of pneu-mococcal pneumonia At that time theefficacy and potency of the derived serawere assessed in mice in ldquothe mouse pro-tection testrdquo by testing survival after aconcomitant intraperitoneal injection of alethal dose of pneumococci and the serum tobe tested Due to the inherent variation inthis test efficacy and survival in two thirds ofthe animals was the acceptance criteria and10 times the lowest dose providing this wasused for defining a unit of the serum Thisallowed for large batch-to-batch variationand the use of different strains of bacteria for
4 HEY
immunization probably explains part of themissing responses observed (1) In the early20th century a pandemic of meningitis inEurope and the United States with mortalityrates up to 80 spurred the development ofserum therapy treatment options Althoughin the 1930s this became the recommendedtreatment in children assumed to be suffer-ing from meningitis failure to reduce mor-tality in several meningitis epidemics duringthat time raised doubts about the generalapplicability of serum treatment In thosedays serum therapy often involved quiteextensive procedures and infusion of largevolumes of serum The following exampleclearly illustrates this Data from Flexnerand Jobling (5) from treating meningitis inmonkeys resulted in the development of serafrom immunized horses for treatment inhumans The treatment protocol includedlumbar puncture and withdrawal of morethan 30 ml of spinal fluid representing anamount slightly larger than the expectedamount of horse serum to be injected subse-quently This treatment involved such dailyslow infusions of up to 30 ml of serum untilthe patientrsquos condition improved This treat-ment was used in outbreaks in New York in1905 and 1906 and did markedly decreasemortality
After the discovery of penicillin by Flemingin 1928 and the subsequent introduction ofantibiotics in the 1930s serum therapy waslargely abandoned over a period of 10 years dueto the availability of these new more broadlyeffective and cheaper treatment optionswhichalso had fewer side effects Although improve-ments in the purification of antibodies hadresulted in preparations with better safety andside effect profiles high manufacturing costsand narrow specificity resulted in antibodytherapy being mostly restricted to a smallernumber of selected treatments for snakevenoms bacterial toxins and some viral infec-tions (1 2) Currently antibody administrationis used for treatment and prevention ofhepatitis B virus rabies virus respiratorysyncytial virus (RSV) Clostridium tetani Clos-
tridium botulinum vaccinia virus echovirusand enterovirus For the most part thesetreatments consist of pooled immunoglobulinalso known as IVIG (intravenous immunoglob-ulin) from several postexposure donors Thisresults in both batch-to-batch variation in theneed for relatively large amounts of serum dueto low specificity and to restricted supplies dueto reliance on exposed donors
However several challengeshave resulted inthe need for new tools in the treatment andpreventionof infectiousdiseasesThebroadandgeneral use of antibiotics in human and veter-inary medicine for many years has resulted inthe development of multi-resistant strains ofbacteria with limited to no response to existingtreatments such as methicillin-resistant Staph-ylococcusaureus (MRSA) vancomycin-resistantS aureus and others This has resulted inpatients needing screening and treatment withseveral antibacterial agents and longer treat-ment time causing extra strain on patients andhealth care providers (6 httpwwwcdcgovdrugresistancethreat-report-2013indexhtml) According to the WHO and CDC morethan 25000 people in European Unioncountries and similar numbers in the UnitedStates die every year as a result of antibiotic-resistant infections This together with theemergence of new pathogens (eg severeacute respiratory syndrome Middle East respi-ratory syndrome) the re-emergenceepidemicsof oldknown pathogens (eg Ebola) and thedifficulties in treating infections in immune-deficient patients (eg HIV patients) has high-lighted the need for new solutions The 2014Ebola epidemic in West Africa (Liberia SierraLeone Guinea Nigeria and Senegal) has fur-ther highlighted this No treatment or prophy-lactic vaccine is available to treat or prevent thespread of Ebola infections which have anaveragemortality of gt50 Local health author-ities in the affected countries are struggling tocontain and handle the disease which isthreatening to go out of control and spreadmorewidelyVariousproductsmainly antibodycocktails from previously recovered patientsare being used despite a lack of clinical data on
CHAPTER 1 bull History and Practice Antibodies in Infectious Diseases 5
their safety and efficacy and those are the onlysporadically available treatment options andonly in small amounts and for a few patients
Ebola is an example of a disease whichnormally affects only a small number ofindividuals and which normally burns outwhen disease outbreaks are contained There-fore given the small number of potentialpatients affected by previous Ebola infectionsto date there was no incentive for big pharmacompanies to do research and development ofdrugs for EbolaWith the increasing number ofinfected (13567) andadeath toll of 4951 (7) andthe lack of the ability to contain the epidemic itwill be interesting to follow the aftermath ofthis outbreak and see whether there will berequests for new ways to ensure that vaccinesand treatment options are available for Ebolaand similar high-mortality and potential bio-warfare infections that have no availabletreatments or procedures to for mass-produc-tion upon the first signsreports of activeinfections Although both the CDC and theWHO have special programs focusing on thesetypes of infections the Ebola outbreak in 2014clearly shows that more financial support forresearch and development of new diagnosticsand treatments is needed This is one examplewhere antibody-based treatments would havethe potential to play a major role To put this inthe right perspective one should however notforget that other infectious diseases such astuberculosis influenza and malaria kill hun-dreds of thousands each year There is there-fore plenty of room for improvement indeveloping treatments for these diseases aswell but the high attention drawn to eg theEbola outbreak creates a special niche andopportunity where antibody treatments couldgain extraordinary development funding andsupport and prove their value and treatmentpotential
That antibody-based therapies could takethis role is supported by the revolution intechnologies for the development selectiongeneration and purification of fully humanantibodies described in more detail later in thesection ldquoMethodsandPlatforms forGenerating
Antibodiesrdquo Antibody-based programs cur-rently at different stages of developmentinclude investigations into the potential use ofsingle antibody preparations combinations ofantibodies (to avoid survival of escape mu-tants) fragments of antibodies and antibodiescarrying radioactive isotopesorcytotoxicdrugsor antibody-like frameworks (eg fibronectin)either alone as a first-line treatment or as anadjunct to existing treatments This multitudeof possible formats the ability to raise anti-bodies to almost any target and the ability toengineer both size effector functions and half-life are now considered by many to providevery valuable tools for designing specificantibody-based treatments toeradicate specifictargeted infectious agents However althoughseveral antibody-based therapies have beenapproved for oncology and anti-inflammatoryindications (see Table 1) only one monoclonalantibody (mAb) is approved against an infec-tious disease agentmdashSynagis (palivizumabMedImmune) for the prevention and treat-ment of respiratory syncytical virus (RSV) inhigh-risk children Economic obstacles such asthe high cost of mAb therapies and relativelysmall markets have resulted in less interestfrom pharmaceutical companies in developingthese Also highlighting the challenges indeveloping these types of antibody-basedtreatments are the difficulties encountered indeveloping a follow-up higher-affinity candi-date to Synagis Poor translatability of dataobtained in the available animal disease mod-els for RSV in cotton rats has resulted in non-approval due to inferiority relative to SynagisIn other viral diseases such as cytomegalovirus(CMV) the high species specificity of thestrains of CMV makes it impossible to testhuman antibody therapies in vivo Thereforeany real data on the efficacy of treatments forCMV will not be obtained until testing inclinical trials As described later in this articleseveral new antibody-based therapies for in-fectious diseases are in development andhopefully this will gradually open the fieldand result in better treatment options andoutcomes for patients
6 HEY
TABLE 1 Approved and pending antibody-based therapies
Name antibody Target antibody type Indication Company Approval date
OKT3a Muronomab-CD3 CD3 murine IgG2a Autoimmune Johnson ampJohnson
1986 (US)
ReoPro abciximab PIIbIIIa chimeric IgG1Fab
Homeostasis Johnson ampJohnson
1984 (US)
Rituxan rituximab CD20 chimeric IgG1 Cancer Genentech 1997 (US) 1998 (EU)Zenapaxa daclizumab CD25 humanized IgG1 Autoimmune Roche 1997 (US) 1999 (EU)Simulect basiliximab CD25 chimeric IgG1 Autoimmune Novartis 1998 (US EU)Synagis palivizumab RSV humanized IgG1 Infections MedImmune 1998 (US) 1999 (EU)Remicade infliximab TNFα chimeric IgG1 Autoimmune Johnson amp
Johnson1998 (US) 1999 (EU)
Herceptin trastuzumab HER2 humanized IgG1 Cancer GenentechRoche
1998 (US) 2000 (EU)
Mylotarga gemtuzumabozogamicin
CD33 humanized IgG4immunotoxin
Cancer WyethPfizer 2000 (US)
Campath alemtuzumab CD52 humanized IgG1 Cancer Genzyme 2001 (US) 2001 (EU)Zevalin ibritumomabtiuxetan
CD20 murine IgG1radiolabeled (yttrium 90)
Cancer Biogen Idec 2002 (US) 2004 (EU)
Humira adalimumab TNFα human IgG1 Autoimmune Abbott 2002 (US) 2003 (EU)Xolair omalizumab IgE humanized IgG1 Autoimmune Genentech
Roche2003 (US)
Bexxar tositumomab-I-131 CD20 murine IgG2aradiolabeled (iodine131)
Cancer CorixaGSK 2003 (US)
Raptivaa falizumab CD11a humanized IgG1 Autoimmune GenentechRoche
2003 (US) 2004 (EU)
Erbitux cetuximab EGFR chimeric IgG1 Cancer ImcloneLilly 2004 (US) 2004 (EU)Avastin bevacizumab VEGF humanized IgG1 Cancer Genentech
Roche2004 (US) 2005 (EU)
Tysabri natalizumab α4-Intergrin humanizedIgG4
Autoimmune Biogen Idec 2004 (US)
Actemra tocilizumab Anti-IL-6R humanizedIgG1
Autoimmune ChugaiRoche
2005 (Japan) 2010 (US)
Vectibix panitumumab EGFR human IgG2 Cancer Amgen 2006 (US)Lucentis ranibizumab VEGF humanized IgG1
FabMaculardegeneration
GenentechRoche
2006 (US)
Soliris eculizumab C5 humanized IgG24 Blood disorders Alexion 2007 (US)Cimzia certolizumab pegol TNFα humanized
pegylated FabAutoimmune UCB 2008 (US)
Simponi golimumab TNFα human IgG1 Autoimmune Johnson ampJohnson
2009 (US EU Canada)
Ilaris canakinumab IL1b human IgG1 Infalmmatory Novartis 2009 (US EU)Stelara ustekinumab IL-1223 human IgG1 Autoimmune Johnson amp
Johnson2008 (EU) 2009 (US)
Arzerra ofatumumab CD20 human IgG1 Cancer Genmab 2009 (EU)Prolia denosumab RANK ligand human
IgG2Bone loss Amgen 2010 (US)
Numax motavizumab RSV humanized IgG1 Anti-infective MedImmune PendingABthrax Raxibacumab B anthrasis PA human
IgG1Anti-infection GSK 2012 (US)
Benlysta belimumab BLyS human IgG1 Autoimmune HGS 2011 (US)Yervoy ipilimumab CTLA-4 human IgG1 Cancer BMS 2011 (US)Adcetris brentuximabvedotin
CD30 chimeric IgG1drug- conjugate
Cancer SeattleGenetics
2011 (US)
(Continued on next page)
CHAPTER 1 bull History and Practice Antibodies in Infectious Diseases 7
INTRODUCTION TO ANTIBODIES
Antibodies also called immunoglobulins basedon their combined structure and function inimmune responses are produced by B cells ofthe immune system They are part of theadaptive immune response and are speciallydesigned for neutralizing and eliminating theinfectious agents and toxins produced by theseAntibodies are present in blood plasma andextracellular fluids and since these fluids wereformerly known as humors they were said tobe part of the humoral immune responseAntibodies are Y-shaped structures consistingof two main parts the upper arms of the Ywhich contain two identical variable-regionantigen binding sites and the lower regioncalled the constant regionwhich is responsiblefor the initiation of effector functions that leadto the removal and destruction of the pathogenor cells harboring the pathogen (see Fig 1) Theantigen-binding sites on an antibody can bythemselves bind to and neutralize bacterialtoxins and viruses thereby preventing themfrom binding to their target cells or receptorscausing toxic effects or spread of the infection
Antibodies consist of two pairs of heavy andlight chainswhich as described above are heldtogether in a Y-shaped arrangement Each ofthe heavy and light chains in these pairs isseparated into constant and variable chainsThe upper armsof theY each contain a variableand a constant sectionof the light and theheavychain where the upper variable parts of theheavy and light chains contain the antigen-binding site and the constant parts areconnected via disulfide bonds The lower partof theYcalled theconstantpart consistsof twoor three constant segments (immunoglobulindomains) from each of the two heavy chainsinteracting and also linked via disulfide bondsThe sectionsof theheavy chains connecting theconstant part of the upper arms to the constantparts of the constant region contain specialhinge regions that provide flexibility to thedifferent sections of the antibody to bind toantigens and effector cells The constant re-gions of the heavy chain also contain attachedoligosaccharide moieties which provide func-tional specialization to the antibodies (8)
The variable domains of the heavy and lightchains form the antigen-binding sites and
TABLE 1 Approved and pending antibody-based therapies (Continued)
Name antibody Target antibody type Indication Company Approval date
Perjeta pertuzumab Her2 humanized IgG1 Cancer GenentechRoche
2012 (US)
Kadcyla ado-trastuzumabemtansine
Her2 humanized IgG1Drug-conjugate
Cancer GenentechRoche
2013 (US)
Raxibacumab Anti-B anthrasis PAhuman IgG1
Anthraxinfection
Notapproved
2012
Entyvio vedolizumab Integrin α4β7humanized IgG1
Crohnrsquos diseaseulcerative colitis
Takeda 2014 (US)
Cyramza ramuciruumab Anti-VEGFR2Human IgG1
Gastric cancer Lilly 2014 (US)
Gazyva obinutuzumab Anti-CD20 humanizedIgG1 glucoengineered
CancerCLLb GenentechRoche
2014 (US)
Sylvant situximab Anti IL-6 chimeric IgG1 Castlemandisease
Janssen 2014 (US) 2014 (EU)
Cosentyx sekukinumab Anti IL-17a human IgG1 Psoriasis Novartis 2015 (US) 2015 (EU)Nivolumab Anti PD-1 human IgG4 Melanoma BMS Not approvedKeytruda pembrolizuumab Anti-PD-1 humanized
IgG4Melanoma Merck 2014 (US)
aAntibodies approved but later withdrawnbCLL chronic lymphocytic leukemia
8 HEY
FIGURE 1 (Left panel) Model of antibody structure exemplified by IgG On top the antigen-binding sitesin orange each contain one variable light and variable heavy domain with the three complementaritydetermining regions (CDRs) that are responsible for the specific binding of the antibody to its target Foreach arm of the antibody an additional set of variable heavy and light domains together with the CDR-containing domains represent the two fragment antigen binding (Fab) regions The two Fabs are heldtogether via two disulfide bridges Below the Fabs is the Fc region which contains four constant heavydomains On the upper pair of these domains are binding sites for oligosaccharides which have majorimportance for the ability of the antibody Fc part to trigger effector functions when the Fc portion isbound to Fc gamma receptors on natural killer cells neutrophil granulocytes monocytesmacrophagesdendritic cells and B cells (Right panel) Examples of some of the antibody-derived alternative formatsused to exploit the specific features of the CDRs the Fabs and the Fc parts of the antibodies ScFv Thesingle chain fragment variable consists of the variable domains of the heavy and light chains heldtogether by a flexible linker This can also be used as a carrier of a cytotoxic drug in a so-called antibodydrug complex (ADC) where the specificity of the ScFv is used to target the cytotoxic drug to eg atumor Bite (bi-specific T cell engager) Fusion proteins consisting of two ScFvs one directed against thetarget on a tumor cell and the other against the T cell receptor (CD3) Diabody ScFv dimers where shortlinker peptides (five amino acids) ensure dimerization and not folding of the ScFvs Fab and F(ab)2fragments Single Fab fragments or fragments containing two Fabs linked via disulfide bridges This isused where effector functions related to the Fc part of the antibody are unwanted and where a smallersize is desired to obtain better tissue penetration in eg tumors Due to the lack of the FcRn binding viathe Fc part Fab and F(ab)2 fragments have much shorter half-lives (hours or days) than full-sizeantibodies (weeks) These can also be used as carriers of cytotoxic payloads or cytotoxic radioactiveisotopes and for the F(ab)2 fragments can be constructed as bi-specifics which can cross-link immunecells and target cells Fc fusion protein Fusion protein containing the Fc domain of an immunoglobulinbound to a peptide The peptide can be a ligand for a specific receptor on a target cell or a blockingpeptide for a soluble ligand The Fc part provides a longer half-life to the construct and the potential tobind to and engage effector functions in the killing of eg tumor cells or infected cells ADCsRIAs andbi-specifics Full-size IgG antibodies carrying either a cytotoxic chemical or radioactive payload whichmay also carry different CDRs enabling cross-linking of effector and target cells for increased killingdoi101128microbiolspecAID-0026-2014f1
CHAPTER 1 bull History and Practice Antibodies in Infectious Diseases 9
contain special hyper-variable segments calledcomplementarity-determining regions (CDRs)which allow the B cells via genetic recom-bination to generate antibodies to all thedifferent antigens specific to amino acid se-quences or three-dimensional structuralmotifs(polysaccharides DNA and RNA) found onpathogens
Based on the structure of their heavy chainconstant regions antibodies or immuno-globulins are separated into five classesmdashIgM IgG IgE IgD and IgA Differences inthe sequences of the constant regions providedistinct characteristics to these different clas-ses These characteristics include the numberof heavy chain constant segments the numberand location of interconnecting disulfidebridges the length of the hinge region andthe number and location of oligosaccharidemoieties For IgG four heavy chain versionsexist creating IgG1 2 3 and 4 isotypes eachwith different characteristics in their serumhalf-lives and ability to trigger different effec-tor functions Because of the combined ad-vantage from ability to trigger effectormechanisms long [21 days] half-life theirability to be transported over the placentaand their stability in the production processantibodies of the IgG class and of the IgG1isotype are preferred as the basis for newantibody-based therapies The effector func-tions are triggered by the Fc part of an antibodywhen the variable parts of the antibody arebound directly to an infectious agent or toproteins from an infectious agent expressed onan infected cell This binding leaves the Fc partfree to interactwithFc receptors onphagocyticcells and neutrophils eosinophils and naturalkiller cells capable of inducing phagocytosis orlysis of infectious agents or infected cellsThese effector functions include (i) the abilityto activate the complement system for lysis(complement-dependent cellular cytotoxicity)(ii) triggering of uptake and destruction byphagocytic cells such as macrophages andneutrophils via interaction with Fc receptorson these cells (iii) activation of macrophageseosinophils neutrophils and natural killer
cells to kill infected cells via binding to Fcreceptors on these cells and antibody-depen-dent cellular cytotoxicity and (iv) neutraliza-tion of bacterial toxins and blocking of bindingand uptake of bacteria or viruses to target cells(see Fig 2) (9)
The Fcpart of IgG antibodies also contains aregion that interacts with the neonatal Fcreceptor (FcRn) expressed on most immuno-competent cells and inmany other cells such asendothelial cells in kidney liver placenta lungand breast (10) which protects antibodies fromdegradation by phagocytoticexocytotic cy-cling into FcRn-expressing cells thereby pro-longing their half-life This results in half-livesof 20 to 21 days for most IgG1 2 and 4antibodies whereas half-lives are 10 6 and 2days respectively for IgM IgA and IgE Thehighly specific binding sites on the variableregions of the upper arms of the antibody allowfor several important features of antibodiesndashbinding to and neutralization of eg bacterialtoxins binding to pathogens and blocking theirbinding to or interaction with target cells (egcyncytia formation of CMV-infected cells) orblocking of binding and interactions of infec-tious agents with target cells via blockingreceptors on the target cells
METHODS AND PLATFORMS FORGENERATING ANTIBODIES
As described above the early use of passiveantibody transfer as a therapy in infectiousdiseases involved the use of immune serumfrom immunized sheep and horses These pre-parations were crude and contained a broadmixture of neutralizing and non-neutralizingantibodies and both the foreign nature of theantibodies and the numerous host serumproteins This resulted in less specific andthus less efficient therapies due to a highvariability in efficacy between batches derivedfrom different animals immunized with dif-ferent strains of bacteria in different labor-atories and resulted in multiple unwantedside effects related to hypersensitivity and
10 HEY
anaphylactic reactions to foreign proteinsThese days antibodies being developed fortreatment of diseases in humans are highlypurified and are mostly fully human mono-clonal antibodies The term monoclonal anti-body refers to that cell cultures used forgenerating these antibodies each originatesfrom a single cell and thus produces onlyone specific antibody Development of fullyhuman monoclonal antibodies happened instages over a time span of more than 15 yearsFirst stage in this process was generation ofmonoclonalmurine IgG antibodies (eg OKT3[muronomab-CD3 Johnson and Johnson] ap-proved in 1986) Next stage was generation ofso called chimeric antibodies consisting ofhuman heavy and light chain constant sec-tions but with murine variable sections (eg
Rituxan [rituximab Genentech]) Next stagewas then the humanized antibodies wherethe only remaining murine part of the anti-body is the antigen-binding CDR (eg Xolair[omalizumab NovartisGenentech]) Both thefirst chimeric and humanized antibodies wereapproved in the late 1990s Then finally 16years later the first fully human antibodyHumira (adalimumab Abbott) was approvedin 2002 Since the time of the crude and low-scale manufacturing of the original antibodyserum products much has changed andtherapeutic antibodies are now produced byfermentation in 5000 liter scale using highlycontrolled and documented yeast or mamma-lian cell lines that are genetically engineered toexpress a single specific antibody This hasresulted in a pure and highly specific antibody
FIGURE 2 Effector functions of antibodies (a) Antibodies bind to pathogen-derived or endogenousantigens expressed on the surface of an infected cell which triggers binding to Fc receptors on naturalkiller cells and lysis of the infected cell by antibody-dependent cellular cytotoxicity (b) Antibodies bindto pathogen-derived or endogenous antigens expressed on the surface of infected cells which triggersactivation of complement through binding of complement factor C1q (c) Neutralization Top Bacterialtoxin neutralized by bound antigen Bottom Antibody bound to either receptor for the virus or to thevirus itself which blocks virus binding and entry into the cell (d) Antibody bound to viral surfaceproteins binds to Fc receptors on phagocytic cells eg macrophages and triggers endocytosis anddestruction of virus in endolysosome doi101128microbiolspecAID-0026-2014f2
CHAPTER 1 bull History and Practice Antibodies in Infectious Diseases 11

vi contents
pathoGen-specIFIc antIbodIes
11 Antibodies Targeting the Envelope of HIV-1emsp193 Luzia M Mayr and Susan Zolla-Pazner
12 Committing the Oldest Sins in the Newest Kind of WaysmdashAntibodies Targeting the Influenza Virus Type A Hemagglutinin Globular Heademsp209
Jens C Krause and James E Crowe Jr
13 Prevention of Respiratory Syncytial Virus Infection From Vaccine to Antibodyemsp221
Kelly Huang and Herren Wu
14 Human Metapneumovirusemsp237 Jennifer E Schuster and John V Williams
15 Dengue Antibody-Dependent Enhancement Knowns and Unknownsemsp249
Scott B Halstead
16 Immunotherapeutic Approaches To Prevent Cytomegalovirus-Mediated Diseaseemsp273
Edith Acquaye-Seedah Zachary P Frye and Jennifer A Maynard
17 Rotavirusemsp289 Manuel A Franco and Harry B Greenberg
18 Bacterial ToxinsmdashStaphylococcal Enterotoxin Bemsp303 Bettina C Fries and Avanish K Varshney
technIcal advances
19 Antibody Engineeringemsp321 Kin-Ming Lo Olivier Leger and Bjoumlrn Hock
20 High-Throughput DNA Sequencing Analysis of Antibody Repertoiresemsp345
Scott D Boyd and Shilpa A Joshi
21 Antibody Informatics IMGT the International ImMunoGeneTics Information Systememsp363
Marie-Paule Lefranc
22 Probing Antibody-Antigen Interactionsemsp381 Guocheng Yang Stefanie N Velgos Shanta P Boddapati
and Michael R Sierks
23 Radiolabeled Antibodies for Therapy of Infectious Diseasesemsp399 Ekaterina Dadachova and Arturo Casadevall
alternate systems For expressIon
24 Plant-Derived Monoclonal Antibodies for Prevention and Treatment of Infectious Diseaseemsp413
Andrew Hiatt Kevin J Whaley and Larry Zeitlin
25 Vector-Mediated In Vivo Antibody Expressionemsp427 Bruce C Schnepp and Philip R Johnson
Indexemsp441
contents vii
Contributors
Edith Acquaye-SeedahDepartment of BiochemistryUniversity of Texas at AustinAustin TX 78712
Ramesh AkkinaDepartment of Microbiology Immunology and PathologyColorado State University1619 Campus DeliveryFort Collins CO 80523
Shanta P BoddapatiDepartment of Biomedical EngineeringOregon Health and Science University3181 SW Sam Jackson Park RoadPortland OR 97239
Scott D BoydDepartment of PathologyStanford UniversityStanford CA 94305
Arturo CasadevallDepartments of Microbiology and Immunology and MedicineAlbert Einstein College of Medicine of Yeshiva University1695A Eastchester RoadBronx NY 10461
Davide CortiHumabs BioMed SAvia Mirasole 1Bellinzona 6500Switzerland
James E Crowe JrSchool of MedicineVanderbilt UniversityNashville TN 37232
ix
x contRIBUtoRs
Ekaterina (Kate) DadachovaDepartments of Radiology Microbiology and ImmunologyAlbert Einstein College of Medicine of Yeshiva University1695A Eastchester RoadBronx NY 10461
Donald N ForthalDepartment of Infectious Diseases3044 Hewitt HallUniversity of California IrvineIrvine CA 92617
Manuel A FrancoFacultad de Ciencias y MedicinaPontificia Universidad JaverianaOficina 306 Edificio 50Carrera 7 40-62BogotaacuteColombia
Bettina C FriesDepartment of MedicineInfectious Diseases and Department of Microbiology and ImmunologyAlbert Einstein College of MedicineBronx NY 10461
Zachary P FryeDepartment of Chemical EngineeringUniversity of Texas at AustinAustin TX 78712
Amy E GilbertCutaneous Medicine and Immunotherapy UnitSt Johnrsquos Institute of DermatologyDivision of Genetics and Molecular Medicine amp NIHR Biomedical Research Centre at Guyrsquos and St Thomasrsquos Hospitals and Kingrsquos College London School of MedicineGuyrsquos HospitalLondon SE1 9RTUnited Kingdom
Hannah J GouldRandall Division of Cell and Molecular BiophysicsDivision of Asthma Allergy and Lung BiologyMRC and Asthma UK Centre for Allergic Mechanisms of AsthmaKingrsquos College LondonNew Huntrsquos HouseGuyrsquos CampusLondon SE1 1ULUnited Kingdom
contRIBUtoRs xi
Harry B GreenbergDepartments of Medicine and Microbiology and ImmunologyStanford University School of Medicine and the VAPAHCSPalo Alto CA 94305
Scott B HalsteadDepartment of Preventive Medicine and BiometricsUniformed Services University of the Health SciencesBethesda MD 20814
Shen Y HelvigDepartment of PharmacyCenter for Pharmaceutical Nanotechnology and NanotoxicologyFaculty of Health and Medical SciencesUniversity of CopenhagenCopenhagen DK-2100Denmark
Adam HeyPreclinical Safety BiologicsNovartis AGBaselSwitzerland
Andrew HiattMapp Biopharmaceutical Inc6160 Lusk Blvd C105San Diego CA 92121
Bjoumlrn HockDepartment of Protein Engineering and Antibody TechnologiesMerck Serono Merck KgaAFrankfurter Str 250D-64293 DarmstadtGermany
Kelly HuangDepartment of Infectious DiseaseMedImmune LLCOne MedImmune WayGaithersburg MD 20878
Philip R JohnsonThe Childrenrsquos Hospital of PhiladelphiaAbramson Research CenterPhiladelphia PA 19104
Debra H JosephsCutaneous Medicine and Immunotherapy UnitSt Johnrsquos Institute of DermatologyDivision of Genetics and Molecular Medicine amp NIHR Biomedical Research Centre at Guyrsquos and St Thomasrsquos HospitalsKingrsquos College London School of MedicineGuyrsquos HospitalLondon SE1 9RTUnited Kingdom
Shilpa A JoshiDepartment of PathologyStanford UniversityStanford CA 94305
Sophia N KaragiannisCutaneous Medicine and Immunotherapy UnitSt Johnrsquos Institute of DermatologyDivision of Genetics and Molecular Medicine amp NIHR Biomedical Research Centre at Guyrsquos and St Thomasrsquos HospitalsKingrsquos College London School of MedicineGuyrsquos HospitalLondon SE1 9RTUnited Kingdom
Panagiotis KaragiannisCutaneous Medicine and Immunotherapy UnitSt Johnrsquos Institute of DermatologyDivision of Genetics and Molecular Medicine amp NIHR Biomedical Research Centre at Guyrsquos and St Thomasrsquos HospitalsKingrsquos College London School of MedicineGuyrsquos HospitalLondon SE1 9RTUnited Kingdom
Jens C KrauseChildrenrsquos HospitalUniversity of Freiburg Medical Center79106 FreibergGermany
Antonio LanzavecchiaInstitute for Research in Biomedicinevia Vincenzo Vela 6Bellinzona 6500Switzerland
xii contRIBUtoRs
Marie-Paule LefrancLaboratoire drsquoImmunoGeacuteneacutetique Moleacuteculaire LIGMIMGTreg the international ImMunoGeneTics information systemregInstitut de Geacuteneacutetique Humaine IGHUniversiteacute Montpellier 2UPR CNRS 1142Montpellier 34396 cedex 5 40202France
Olivier LegerDepartment of Protein Engineering and Antibody TechnologiesMerck Serono SA--Geneva9 chemin des Mines1202 GenevaSwitzerland
Kin-Ming LoDepartment of Protein Engineering and Antibody TechnologiesEMD Serono Research Institute45A Middlesex TurnpikeBillerica MA 01821
Wayne A MarascoDepartment of Cancer Immunology and AIDSDana-Farber Cancer InstituteHarvard Medical SchoolBoston MA 02215
Jennifer A MaynardDepartment of Chemical EngineeringUniversity of Texas at AustinAustin TX 78712
Luzia M MayrINSERM U1109Universiteacute de Strasbourg3 Rue Koeberleacute67000 StrasbourgFrance
Jens MeilerDepartment of Chemistry and Center for Structural BiologyVanderbilt UniversityNashville TN 37212
contRIBUtoRs xiii
S Moein MoghimiDepartment of PharmacyCenter for Pharmaceutical Nanotechnology and NanotoxicologyFaculty of Health and Medical SciencesUniversity of CopenhagenCopenhagen DK-2100Denmark
Susan Zolla-PaznerNew York University School of Medicine550 First AvenueNew York NY 10016
Louise SaulCutaneous Medicine and Immunotherapy UnitSt Johnrsquos Institute of DermatologyDivision of Genetics and Molecular Medicine amp NIHR Biomedical Research Centre at Guyrsquos and St Thomasrsquos HospitalsKingrsquos College London School of MedicineGuyrsquos HospitalLondon SE1 9RTUnited Kingdom
Bruce C SchneppThe Childrenrsquos Hospital of PhiladelphiaAbramson Research CenterPhiladelphia PA 19104
Jennifer E SchusterDepartment of PediatricsChildrenrsquos Mercy HospitalKansas City MO 64108-4619
Alexander M SevyDepartment of Chemistry and Center for Structural BiologyVanderbilt UniversityNashville TN 37212
Jared SheehanDepartment of Cancer Immunology and AIDSDana-Farber Cancer InstituteHarvard Medical SchoolBoston MA 02215
Michael R SierksDepartment of Chemical EngineeringArizona State UniversityTempe AZ 85287-6006
xiv contRIBUtoRs
Scott A SmithThe Vanderbilt Vaccine Center and the Department of MedicineVanderbilt University Medical CenterNashville TN 37232
Robyn L StanfieldDepartment of Molecular BiologyThe Scripps Research Institute10550 North Torrey Pines RoadLa Jolla CA 92037
Nadine UptonRandall Division of Cell and Molecular BiophysicsDivision of Asthma Allergy and Lung BiologyMRC and Asthma UK Centre for Allergic Mechanisms of AsthmaKingrsquos College LondonNew Huntrsquos HouseGuyrsquos CampusLondon SE1 1ULUnited Kingdom
Avanish K VarshneyDepartment of MedicineInfectious Diseases and Department of Microbiology and ImmunologyAlbert Einstein College of MedicineBronx NY 10461
Stefanie N VelgosMayo Clinic Arizona5777 East Mayo BoulevardPhoenix AZ 85054
Kevin J WhaleyMapp Biopharmaceutical Inc6160 Lusk Blvd C105San Diego CA 92121
Peter P WibroeCentre for Pharmaceutical Nanotechnology and NanotoxicologyDepartment of PharmacyFaculty of Health and Medical SciencesUniversity of CopenhagenCopenhagen DK-2100Denmark
John V WilliamsDepartment of PediatricsSchool of MedicineVanderbilt UniversityNashville TN 37232-2581
contRIBUtoRs xv
Ian A WilsonDepartment of Molecular Biology and Skaggs Institute for Chemical BiologyThe Scripps Research Institute10550 North Torrey Pines RoadLa Jolla CA 92037
Herren WuDepartment of Antibody Discovery and Protein EngineeringMedImmune LLCOne MedImmune WayGaithersburg MD 20879
Guocheng YangDepartment of Chemical EngineeringArizona State UniversityTempe AZ 85287-6006
Larry ZeitlinMapp Biopharmaceutical Inc6160 Lusk Blvd C105San Diego CA 92121
xvi contRIBUtoRs
Preface
Antibodies form the principal foundation for modern intervention against in-fectious diseases Emil Adolf von Behring was awarded the first Nobel Prize in Physiology or Medicine in 1901 ldquofor his work on serum therapy especially its appli-cation against diphtheria by which he has opened a new road in the domain of med-ical science and thereby placed in the hands of the physician a victorious weapon against illness and deathsrdquo Antibodies now provide the focus for understanding mechanisms of immunity to most infectious diseases and they play a central role in passive immunotherapy and active vaccination as mechanisms or correlates of immunity For most of the 20th century immunotherapy was based on passive transfer of polyclonal hyperimmune animal serum immune human serum or even hyperimmune human serum Georges JF Koumlhler and Ceacutesar Milstein re-ported the generation of monoclonal antibodies in 1979 for which they shared the 1984 Nobel Prize in Physiology or Medicine ldquofor the discovery of the princi-ple for production of monoclonal antibodiesrdquo Since that time entire fields related to antibodies for infectious diseases including antibody gene cloning engineer-ing and expression antibody libraries and high-throughput antibody gene rep-ertoire sequence analysis have extended our capabilities to explore the diversity of antibody specificity and function with unprecedented depth and breadth
This book provides a broad survey of many of the most important aspects of the field of antibodies for infectious diseases The book begins with a general introduction followed by chapters 2 through 5 on general features pertaining to structure function isotype and the role of complement in antibody function Chapters 6 through 10 review contemporary approaches for antibody discovery using phage and yeast display plasma cell and memory B cell cloning human hybridomas humanized mice and computational methods Chapters 11 through 18 review in depth the biology of antibodies specific for particular pathogens including viruses and bacterial toxins to illustrate the role of antibodies in anti- microbial immunity with specific targets These chapters reveal that attempts to raise effective antibody responses to each of these pathogens faces unique and pathogen-specific challenges Chapters 19 to 23 cover major technical advances pertaining to antibody engineering repertoire sequencing and analysis and new methods for study or therapeutic use of antibodies including radiotherapy Fi-nally chapters 24 and 25 cover new methods for expression of monoclonal anti-bodies in plants or by transfer of antibody genes for in vivo expression in treated subjects
Recent literature is exploding with new antibody-related techniques and re-ports of antimicrobial antibodies with unprecedented potency breadth of activ-
xvii
xviii PReface
ity and therapeutic potential We hope that this timely compilation of state-of-the-art reviews of major aspects of this field will be of interest to both antibody cognoscenti and those new to this exciting field We thank the authors for their dedication in producing definitive reviews of the topics at hand
James E Crowe JrDiana BoraschiRino Rappuoli
INTRODUCTION
History and PracticeAntibodies in Infectious Diseases 1ADAM HEY1
Antibodies in Infectious Diseases aims to inform update and inspire studentsteachers researchers pharmaceutical developers and health care professionalson the status of the development of antibody-based therapies for treatinginfectious diseases and the potential for these in times of growing antibioticresistance to provide alternative treatment solutions to the currently usedantibiotics and new treatments for infectious diseases where no propertreatments are available
This introductory article will provide a historical perspective on the useof antibody-based therapies followed by a high-level overview of whatmakes antibodies attractive tools for this purpose This will include the prosand cons of such therapies compared to the use of antibiotics and thepractical and strategic considerations involved in selecting the best formatand development path for new antibody-based therapies targeting specificinfectious agents Then examples of antibody-based therapies in thedevelopment of treatments for infectious diseases will be presented andfinally a look into the future will summarize the different aspects that willinfluence what the future might bring for this type of treatments forinfectious diseases
1Preclinical Safety Biologics Novartis AG Basel Switzerland
Antibodies for Infectious DiseasesEdited by James E Crowe Jr Diana Boraschi and Rino Rappuolicopy 2015 American Society for Microbiology Washington DCdoi101128microbiolspecAID-0026-2014
3
HISTORICAL PERSPECTIVE
Antibodies and the use of passive antibodytherapy in the treatment of infectious dis-eases is the story of a treatment conceptwhich dates back more than 120 years to thelate 19th century and which originally bythe use of serum from immunized animalsprovided the first effective treatment optionsagainst severe bacterial infections (1 2) Byimmunizing horses with bacterial toxinsfrom Clostridium tetani and Corynebacteri-um diphtheriae Emil A Von Behring andShibasaburo Kitasato (3) generated serumcontaining antibodies capable of neutraliz-ing the effects of the toxins produced bythese bacteria and successfully providedtreatment for these serious diseases wherethe pathogenesis is driven by the effects ofthe bacterial toxins For his work on provid-ing treatment for diphtheria Behring re-ceived the Nobel Prize in Physiology orMedicine in 1901 These radical treatmentresults quickly prompted development ofmultiple additional serum therapies for thetreatment of infectious diseases caused byeg Neisseria meningitidis Haemophilus in-fluenza and group A Streptococcus Sinceserum therapy involved administration oflarge amounts of crude mixtures of animalproteins including antibodies they wereassociated with side effects in the form ofhypersensitivity and serum sickness (2)
Due to the crude and unpurified nature ofthese products side effects were seen evenwhen administering human serum prepa-rations Side effects were observed in up to50 of patients and were considered to becaused by immune complex formations thatresulted in symptoms such as rash itchingjoint pain fever and in serious cases hypoten-sion and shock However due to the lack ofalternative options these treatments weredespite their side effects widely used Serumwas normally administered by intravenousinfusion in patients after a test for hypersensi-tivity where a small amount of serum wasinjected subcutaniously (1) As described
above serum therapy applied in these earlydays (late 19th century and early 20th century)involved preparations of serum from rabbitsand horses immunized with the infectiousagent or in live andor neutralized versions ortoxins from these (1) The costs of keeping theimmunized animals and the production andpotency testing of the materials made this arelatively expensive treatment In 1891 datafrom Klemperer (4) showed serum therapy toprotect rabbits from Streptococcus pneumoniaeinfection and paved the way for this type oftreatment and for development of similarserum-based treatments of streptococcal in-fections in humans When treating humansearly administration of serum could reducemortality significantly down to around 5compared to when administered 4 to 5 daysafter onset of symptoms when serum treat-ment was largely without effect This stronglyindicated the need for quick diagnosis andquick treatment to control the infection beforeit got out of control Consequently in theabsence of a specific diagnosis mixtures ofserum from immunizations with differentserotypes were used to circumvent this needfor early treatment without having a serotype-specific diagnosis The understanding thatdifferent serotypes existed for pneumococciand that efficient treatment relied on usingserotype-specific serum was being built upduring the 1920s and 1930s through experiencefrom extensive clinical trials
By the end of the 1930s serum therapywasthe standard of care for treatment of pneu-mococcal pneumonia At that time theefficacy and potency of the derived serawere assessed in mice in ldquothe mouse pro-tection testrdquo by testing survival after aconcomitant intraperitoneal injection of alethal dose of pneumococci and the serum tobe tested Due to the inherent variation inthis test efficacy and survival in two thirds ofthe animals was the acceptance criteria and10 times the lowest dose providing this wasused for defining a unit of the serum Thisallowed for large batch-to-batch variationand the use of different strains of bacteria for
4 HEY
immunization probably explains part of themissing responses observed (1) In the early20th century a pandemic of meningitis inEurope and the United States with mortalityrates up to 80 spurred the development ofserum therapy treatment options Althoughin the 1930s this became the recommendedtreatment in children assumed to be suffer-ing from meningitis failure to reduce mor-tality in several meningitis epidemics duringthat time raised doubts about the generalapplicability of serum treatment In thosedays serum therapy often involved quiteextensive procedures and infusion of largevolumes of serum The following exampleclearly illustrates this Data from Flexnerand Jobling (5) from treating meningitis inmonkeys resulted in the development of serafrom immunized horses for treatment inhumans The treatment protocol includedlumbar puncture and withdrawal of morethan 30 ml of spinal fluid representing anamount slightly larger than the expectedamount of horse serum to be injected subse-quently This treatment involved such dailyslow infusions of up to 30 ml of serum untilthe patientrsquos condition improved This treat-ment was used in outbreaks in New York in1905 and 1906 and did markedly decreasemortality
After the discovery of penicillin by Flemingin 1928 and the subsequent introduction ofantibiotics in the 1930s serum therapy waslargely abandoned over a period of 10 years dueto the availability of these new more broadlyeffective and cheaper treatment optionswhichalso had fewer side effects Although improve-ments in the purification of antibodies hadresulted in preparations with better safety andside effect profiles high manufacturing costsand narrow specificity resulted in antibodytherapy being mostly restricted to a smallernumber of selected treatments for snakevenoms bacterial toxins and some viral infec-tions (1 2) Currently antibody administrationis used for treatment and prevention ofhepatitis B virus rabies virus respiratorysyncytial virus (RSV) Clostridium tetani Clos-
tridium botulinum vaccinia virus echovirusand enterovirus For the most part thesetreatments consist of pooled immunoglobulinalso known as IVIG (intravenous immunoglob-ulin) from several postexposure donors Thisresults in both batch-to-batch variation in theneed for relatively large amounts of serum dueto low specificity and to restricted supplies dueto reliance on exposed donors
However several challengeshave resulted inthe need for new tools in the treatment andpreventionof infectiousdiseasesThebroadandgeneral use of antibiotics in human and veter-inary medicine for many years has resulted inthe development of multi-resistant strains ofbacteria with limited to no response to existingtreatments such as methicillin-resistant Staph-ylococcusaureus (MRSA) vancomycin-resistantS aureus and others This has resulted inpatients needing screening and treatment withseveral antibacterial agents and longer treat-ment time causing extra strain on patients andhealth care providers (6 httpwwwcdcgovdrugresistancethreat-report-2013indexhtml) According to the WHO and CDC morethan 25000 people in European Unioncountries and similar numbers in the UnitedStates die every year as a result of antibiotic-resistant infections This together with theemergence of new pathogens (eg severeacute respiratory syndrome Middle East respi-ratory syndrome) the re-emergenceepidemicsof oldknown pathogens (eg Ebola) and thedifficulties in treating infections in immune-deficient patients (eg HIV patients) has high-lighted the need for new solutions The 2014Ebola epidemic in West Africa (Liberia SierraLeone Guinea Nigeria and Senegal) has fur-ther highlighted this No treatment or prophy-lactic vaccine is available to treat or prevent thespread of Ebola infections which have anaveragemortality of gt50 Local health author-ities in the affected countries are struggling tocontain and handle the disease which isthreatening to go out of control and spreadmorewidelyVariousproductsmainly antibodycocktails from previously recovered patientsare being used despite a lack of clinical data on
CHAPTER 1 bull History and Practice Antibodies in Infectious Diseases 5
their safety and efficacy and those are the onlysporadically available treatment options andonly in small amounts and for a few patients
Ebola is an example of a disease whichnormally affects only a small number ofindividuals and which normally burns outwhen disease outbreaks are contained There-fore given the small number of potentialpatients affected by previous Ebola infectionsto date there was no incentive for big pharmacompanies to do research and development ofdrugs for EbolaWith the increasing number ofinfected (13567) andadeath toll of 4951 (7) andthe lack of the ability to contain the epidemic itwill be interesting to follow the aftermath ofthis outbreak and see whether there will berequests for new ways to ensure that vaccinesand treatment options are available for Ebolaand similar high-mortality and potential bio-warfare infections that have no availabletreatments or procedures to for mass-produc-tion upon the first signsreports of activeinfections Although both the CDC and theWHO have special programs focusing on thesetypes of infections the Ebola outbreak in 2014clearly shows that more financial support forresearch and development of new diagnosticsand treatments is needed This is one examplewhere antibody-based treatments would havethe potential to play a major role To put this inthe right perspective one should however notforget that other infectious diseases such astuberculosis influenza and malaria kill hun-dreds of thousands each year There is there-fore plenty of room for improvement indeveloping treatments for these diseases aswell but the high attention drawn to eg theEbola outbreak creates a special niche andopportunity where antibody treatments couldgain extraordinary development funding andsupport and prove their value and treatmentpotential
That antibody-based therapies could takethis role is supported by the revolution intechnologies for the development selectiongeneration and purification of fully humanantibodies described in more detail later in thesection ldquoMethodsandPlatforms forGenerating
Antibodiesrdquo Antibody-based programs cur-rently at different stages of developmentinclude investigations into the potential use ofsingle antibody preparations combinations ofantibodies (to avoid survival of escape mu-tants) fragments of antibodies and antibodiescarrying radioactive isotopesorcytotoxicdrugsor antibody-like frameworks (eg fibronectin)either alone as a first-line treatment or as anadjunct to existing treatments This multitudeof possible formats the ability to raise anti-bodies to almost any target and the ability toengineer both size effector functions and half-life are now considered by many to providevery valuable tools for designing specificantibody-based treatments toeradicate specifictargeted infectious agents However althoughseveral antibody-based therapies have beenapproved for oncology and anti-inflammatoryindications (see Table 1) only one monoclonalantibody (mAb) is approved against an infec-tious disease agentmdashSynagis (palivizumabMedImmune) for the prevention and treat-ment of respiratory syncytical virus (RSV) inhigh-risk children Economic obstacles such asthe high cost of mAb therapies and relativelysmall markets have resulted in less interestfrom pharmaceutical companies in developingthese Also highlighting the challenges indeveloping these types of antibody-basedtreatments are the difficulties encountered indeveloping a follow-up higher-affinity candi-date to Synagis Poor translatability of dataobtained in the available animal disease mod-els for RSV in cotton rats has resulted in non-approval due to inferiority relative to SynagisIn other viral diseases such as cytomegalovirus(CMV) the high species specificity of thestrains of CMV makes it impossible to testhuman antibody therapies in vivo Thereforeany real data on the efficacy of treatments forCMV will not be obtained until testing inclinical trials As described later in this articleseveral new antibody-based therapies for in-fectious diseases are in development andhopefully this will gradually open the fieldand result in better treatment options andoutcomes for patients
6 HEY
TABLE 1 Approved and pending antibody-based therapies
Name antibody Target antibody type Indication Company Approval date
OKT3a Muronomab-CD3 CD3 murine IgG2a Autoimmune Johnson ampJohnson
1986 (US)
ReoPro abciximab PIIbIIIa chimeric IgG1Fab
Homeostasis Johnson ampJohnson
1984 (US)
Rituxan rituximab CD20 chimeric IgG1 Cancer Genentech 1997 (US) 1998 (EU)Zenapaxa daclizumab CD25 humanized IgG1 Autoimmune Roche 1997 (US) 1999 (EU)Simulect basiliximab CD25 chimeric IgG1 Autoimmune Novartis 1998 (US EU)Synagis palivizumab RSV humanized IgG1 Infections MedImmune 1998 (US) 1999 (EU)Remicade infliximab TNFα chimeric IgG1 Autoimmune Johnson amp
Johnson1998 (US) 1999 (EU)
Herceptin trastuzumab HER2 humanized IgG1 Cancer GenentechRoche
1998 (US) 2000 (EU)
Mylotarga gemtuzumabozogamicin
CD33 humanized IgG4immunotoxin
Cancer WyethPfizer 2000 (US)
Campath alemtuzumab CD52 humanized IgG1 Cancer Genzyme 2001 (US) 2001 (EU)Zevalin ibritumomabtiuxetan
CD20 murine IgG1radiolabeled (yttrium 90)
Cancer Biogen Idec 2002 (US) 2004 (EU)
Humira adalimumab TNFα human IgG1 Autoimmune Abbott 2002 (US) 2003 (EU)Xolair omalizumab IgE humanized IgG1 Autoimmune Genentech
Roche2003 (US)
Bexxar tositumomab-I-131 CD20 murine IgG2aradiolabeled (iodine131)
Cancer CorixaGSK 2003 (US)
Raptivaa falizumab CD11a humanized IgG1 Autoimmune GenentechRoche
2003 (US) 2004 (EU)
Erbitux cetuximab EGFR chimeric IgG1 Cancer ImcloneLilly 2004 (US) 2004 (EU)Avastin bevacizumab VEGF humanized IgG1 Cancer Genentech
Roche2004 (US) 2005 (EU)
Tysabri natalizumab α4-Intergrin humanizedIgG4
Autoimmune Biogen Idec 2004 (US)
Actemra tocilizumab Anti-IL-6R humanizedIgG1
Autoimmune ChugaiRoche
2005 (Japan) 2010 (US)
Vectibix panitumumab EGFR human IgG2 Cancer Amgen 2006 (US)Lucentis ranibizumab VEGF humanized IgG1
FabMaculardegeneration
GenentechRoche
2006 (US)
Soliris eculizumab C5 humanized IgG24 Blood disorders Alexion 2007 (US)Cimzia certolizumab pegol TNFα humanized
pegylated FabAutoimmune UCB 2008 (US)
Simponi golimumab TNFα human IgG1 Autoimmune Johnson ampJohnson
2009 (US EU Canada)
Ilaris canakinumab IL1b human IgG1 Infalmmatory Novartis 2009 (US EU)Stelara ustekinumab IL-1223 human IgG1 Autoimmune Johnson amp
Johnson2008 (EU) 2009 (US)
Arzerra ofatumumab CD20 human IgG1 Cancer Genmab 2009 (EU)Prolia denosumab RANK ligand human
IgG2Bone loss Amgen 2010 (US)
Numax motavizumab RSV humanized IgG1 Anti-infective MedImmune PendingABthrax Raxibacumab B anthrasis PA human
IgG1Anti-infection GSK 2012 (US)
Benlysta belimumab BLyS human IgG1 Autoimmune HGS 2011 (US)Yervoy ipilimumab CTLA-4 human IgG1 Cancer BMS 2011 (US)Adcetris brentuximabvedotin
CD30 chimeric IgG1drug- conjugate
Cancer SeattleGenetics
2011 (US)
(Continued on next page)
CHAPTER 1 bull History and Practice Antibodies in Infectious Diseases 7
INTRODUCTION TO ANTIBODIES
Antibodies also called immunoglobulins basedon their combined structure and function inimmune responses are produced by B cells ofthe immune system They are part of theadaptive immune response and are speciallydesigned for neutralizing and eliminating theinfectious agents and toxins produced by theseAntibodies are present in blood plasma andextracellular fluids and since these fluids wereformerly known as humors they were said tobe part of the humoral immune responseAntibodies are Y-shaped structures consistingof two main parts the upper arms of the Ywhich contain two identical variable-regionantigen binding sites and the lower regioncalled the constant regionwhich is responsiblefor the initiation of effector functions that leadto the removal and destruction of the pathogenor cells harboring the pathogen (see Fig 1) Theantigen-binding sites on an antibody can bythemselves bind to and neutralize bacterialtoxins and viruses thereby preventing themfrom binding to their target cells or receptorscausing toxic effects or spread of the infection
Antibodies consist of two pairs of heavy andlight chainswhich as described above are heldtogether in a Y-shaped arrangement Each ofthe heavy and light chains in these pairs isseparated into constant and variable chainsThe upper armsof theY each contain a variableand a constant sectionof the light and theheavychain where the upper variable parts of theheavy and light chains contain the antigen-binding site and the constant parts areconnected via disulfide bonds The lower partof theYcalled theconstantpart consistsof twoor three constant segments (immunoglobulindomains) from each of the two heavy chainsinteracting and also linked via disulfide bondsThe sectionsof theheavy chains connecting theconstant part of the upper arms to the constantparts of the constant region contain specialhinge regions that provide flexibility to thedifferent sections of the antibody to bind toantigens and effector cells The constant re-gions of the heavy chain also contain attachedoligosaccharide moieties which provide func-tional specialization to the antibodies (8)
The variable domains of the heavy and lightchains form the antigen-binding sites and
TABLE 1 Approved and pending antibody-based therapies (Continued)
Name antibody Target antibody type Indication Company Approval date
Perjeta pertuzumab Her2 humanized IgG1 Cancer GenentechRoche
2012 (US)
Kadcyla ado-trastuzumabemtansine
Her2 humanized IgG1Drug-conjugate
Cancer GenentechRoche
2013 (US)
Raxibacumab Anti-B anthrasis PAhuman IgG1
Anthraxinfection
Notapproved
2012
Entyvio vedolizumab Integrin α4β7humanized IgG1
Crohnrsquos diseaseulcerative colitis
Takeda 2014 (US)
Cyramza ramuciruumab Anti-VEGFR2Human IgG1
Gastric cancer Lilly 2014 (US)
Gazyva obinutuzumab Anti-CD20 humanizedIgG1 glucoengineered
CancerCLLb GenentechRoche
2014 (US)
Sylvant situximab Anti IL-6 chimeric IgG1 Castlemandisease
Janssen 2014 (US) 2014 (EU)
Cosentyx sekukinumab Anti IL-17a human IgG1 Psoriasis Novartis 2015 (US) 2015 (EU)Nivolumab Anti PD-1 human IgG4 Melanoma BMS Not approvedKeytruda pembrolizuumab Anti-PD-1 humanized
IgG4Melanoma Merck 2014 (US)
aAntibodies approved but later withdrawnbCLL chronic lymphocytic leukemia
8 HEY
FIGURE 1 (Left panel) Model of antibody structure exemplified by IgG On top the antigen-binding sitesin orange each contain one variable light and variable heavy domain with the three complementaritydetermining regions (CDRs) that are responsible for the specific binding of the antibody to its target Foreach arm of the antibody an additional set of variable heavy and light domains together with the CDR-containing domains represent the two fragment antigen binding (Fab) regions The two Fabs are heldtogether via two disulfide bridges Below the Fabs is the Fc region which contains four constant heavydomains On the upper pair of these domains are binding sites for oligosaccharides which have majorimportance for the ability of the antibody Fc part to trigger effector functions when the Fc portion isbound to Fc gamma receptors on natural killer cells neutrophil granulocytes monocytesmacrophagesdendritic cells and B cells (Right panel) Examples of some of the antibody-derived alternative formatsused to exploit the specific features of the CDRs the Fabs and the Fc parts of the antibodies ScFv Thesingle chain fragment variable consists of the variable domains of the heavy and light chains heldtogether by a flexible linker This can also be used as a carrier of a cytotoxic drug in a so-called antibodydrug complex (ADC) where the specificity of the ScFv is used to target the cytotoxic drug to eg atumor Bite (bi-specific T cell engager) Fusion proteins consisting of two ScFvs one directed against thetarget on a tumor cell and the other against the T cell receptor (CD3) Diabody ScFv dimers where shortlinker peptides (five amino acids) ensure dimerization and not folding of the ScFvs Fab and F(ab)2fragments Single Fab fragments or fragments containing two Fabs linked via disulfide bridges This isused where effector functions related to the Fc part of the antibody are unwanted and where a smallersize is desired to obtain better tissue penetration in eg tumors Due to the lack of the FcRn binding viathe Fc part Fab and F(ab)2 fragments have much shorter half-lives (hours or days) than full-sizeantibodies (weeks) These can also be used as carriers of cytotoxic payloads or cytotoxic radioactiveisotopes and for the F(ab)2 fragments can be constructed as bi-specifics which can cross-link immunecells and target cells Fc fusion protein Fusion protein containing the Fc domain of an immunoglobulinbound to a peptide The peptide can be a ligand for a specific receptor on a target cell or a blockingpeptide for a soluble ligand The Fc part provides a longer half-life to the construct and the potential tobind to and engage effector functions in the killing of eg tumor cells or infected cells ADCsRIAs andbi-specifics Full-size IgG antibodies carrying either a cytotoxic chemical or radioactive payload whichmay also carry different CDRs enabling cross-linking of effector and target cells for increased killingdoi101128microbiolspecAID-0026-2014f1
CHAPTER 1 bull History and Practice Antibodies in Infectious Diseases 9
contain special hyper-variable segments calledcomplementarity-determining regions (CDRs)which allow the B cells via genetic recom-bination to generate antibodies to all thedifferent antigens specific to amino acid se-quences or three-dimensional structuralmotifs(polysaccharides DNA and RNA) found onpathogens
Based on the structure of their heavy chainconstant regions antibodies or immuno-globulins are separated into five classesmdashIgM IgG IgE IgD and IgA Differences inthe sequences of the constant regions providedistinct characteristics to these different clas-ses These characteristics include the numberof heavy chain constant segments the numberand location of interconnecting disulfidebridges the length of the hinge region andthe number and location of oligosaccharidemoieties For IgG four heavy chain versionsexist creating IgG1 2 3 and 4 isotypes eachwith different characteristics in their serumhalf-lives and ability to trigger different effec-tor functions Because of the combined ad-vantage from ability to trigger effectormechanisms long [21 days] half-life theirability to be transported over the placentaand their stability in the production processantibodies of the IgG class and of the IgG1isotype are preferred as the basis for newantibody-based therapies The effector func-tions are triggered by the Fc part of an antibodywhen the variable parts of the antibody arebound directly to an infectious agent or toproteins from an infectious agent expressed onan infected cell This binding leaves the Fc partfree to interactwithFc receptors onphagocyticcells and neutrophils eosinophils and naturalkiller cells capable of inducing phagocytosis orlysis of infectious agents or infected cellsThese effector functions include (i) the abilityto activate the complement system for lysis(complement-dependent cellular cytotoxicity)(ii) triggering of uptake and destruction byphagocytic cells such as macrophages andneutrophils via interaction with Fc receptorson these cells (iii) activation of macrophageseosinophils neutrophils and natural killer
cells to kill infected cells via binding to Fcreceptors on these cells and antibody-depen-dent cellular cytotoxicity and (iv) neutraliza-tion of bacterial toxins and blocking of bindingand uptake of bacteria or viruses to target cells(see Fig 2) (9)
The Fcpart of IgG antibodies also contains aregion that interacts with the neonatal Fcreceptor (FcRn) expressed on most immuno-competent cells and inmany other cells such asendothelial cells in kidney liver placenta lungand breast (10) which protects antibodies fromdegradation by phagocytoticexocytotic cy-cling into FcRn-expressing cells thereby pro-longing their half-life This results in half-livesof 20 to 21 days for most IgG1 2 and 4antibodies whereas half-lives are 10 6 and 2days respectively for IgM IgA and IgE Thehighly specific binding sites on the variableregions of the upper arms of the antibody allowfor several important features of antibodiesndashbinding to and neutralization of eg bacterialtoxins binding to pathogens and blocking theirbinding to or interaction with target cells (egcyncytia formation of CMV-infected cells) orblocking of binding and interactions of infec-tious agents with target cells via blockingreceptors on the target cells
METHODS AND PLATFORMS FORGENERATING ANTIBODIES
As described above the early use of passiveantibody transfer as a therapy in infectiousdiseases involved the use of immune serumfrom immunized sheep and horses These pre-parations were crude and contained a broadmixture of neutralizing and non-neutralizingantibodies and both the foreign nature of theantibodies and the numerous host serumproteins This resulted in less specific andthus less efficient therapies due to a highvariability in efficacy between batches derivedfrom different animals immunized with dif-ferent strains of bacteria in different labor-atories and resulted in multiple unwantedside effects related to hypersensitivity and
10 HEY
anaphylactic reactions to foreign proteinsThese days antibodies being developed fortreatment of diseases in humans are highlypurified and are mostly fully human mono-clonal antibodies The term monoclonal anti-body refers to that cell cultures used forgenerating these antibodies each originatesfrom a single cell and thus produces onlyone specific antibody Development of fullyhuman monoclonal antibodies happened instages over a time span of more than 15 yearsFirst stage in this process was generation ofmonoclonalmurine IgG antibodies (eg OKT3[muronomab-CD3 Johnson and Johnson] ap-proved in 1986) Next stage was generation ofso called chimeric antibodies consisting ofhuman heavy and light chain constant sec-tions but with murine variable sections (eg
Rituxan [rituximab Genentech]) Next stagewas then the humanized antibodies wherethe only remaining murine part of the anti-body is the antigen-binding CDR (eg Xolair[omalizumab NovartisGenentech]) Both thefirst chimeric and humanized antibodies wereapproved in the late 1990s Then finally 16years later the first fully human antibodyHumira (adalimumab Abbott) was approvedin 2002 Since the time of the crude and low-scale manufacturing of the original antibodyserum products much has changed andtherapeutic antibodies are now produced byfermentation in 5000 liter scale using highlycontrolled and documented yeast or mamma-lian cell lines that are genetically engineered toexpress a single specific antibody This hasresulted in a pure and highly specific antibody
FIGURE 2 Effector functions of antibodies (a) Antibodies bind to pathogen-derived or endogenousantigens expressed on the surface of an infected cell which triggers binding to Fc receptors on naturalkiller cells and lysis of the infected cell by antibody-dependent cellular cytotoxicity (b) Antibodies bindto pathogen-derived or endogenous antigens expressed on the surface of infected cells which triggersactivation of complement through binding of complement factor C1q (c) Neutralization Top Bacterialtoxin neutralized by bound antigen Bottom Antibody bound to either receptor for the virus or to thevirus itself which blocks virus binding and entry into the cell (d) Antibody bound to viral surfaceproteins binds to Fc receptors on phagocytic cells eg macrophages and triggers endocytosis anddestruction of virus in endolysosome doi101128microbiolspecAID-0026-2014f2
CHAPTER 1 bull History and Practice Antibodies in Infectious Diseases 11

alternate systems For expressIon
24 Plant-Derived Monoclonal Antibodies for Prevention and Treatment of Infectious Diseaseemsp413
Andrew Hiatt Kevin J Whaley and Larry Zeitlin
25 Vector-Mediated In Vivo Antibody Expressionemsp427 Bruce C Schnepp and Philip R Johnson
Indexemsp441
contents vii
Contributors
Edith Acquaye-SeedahDepartment of BiochemistryUniversity of Texas at AustinAustin TX 78712
Ramesh AkkinaDepartment of Microbiology Immunology and PathologyColorado State University1619 Campus DeliveryFort Collins CO 80523
Shanta P BoddapatiDepartment of Biomedical EngineeringOregon Health and Science University3181 SW Sam Jackson Park RoadPortland OR 97239
Scott D BoydDepartment of PathologyStanford UniversityStanford CA 94305
Arturo CasadevallDepartments of Microbiology and Immunology and MedicineAlbert Einstein College of Medicine of Yeshiva University1695A Eastchester RoadBronx NY 10461
Davide CortiHumabs BioMed SAvia Mirasole 1Bellinzona 6500Switzerland
James E Crowe JrSchool of MedicineVanderbilt UniversityNashville TN 37232
ix
x contRIBUtoRs
Ekaterina (Kate) DadachovaDepartments of Radiology Microbiology and ImmunologyAlbert Einstein College of Medicine of Yeshiva University1695A Eastchester RoadBronx NY 10461
Donald N ForthalDepartment of Infectious Diseases3044 Hewitt HallUniversity of California IrvineIrvine CA 92617
Manuel A FrancoFacultad de Ciencias y MedicinaPontificia Universidad JaverianaOficina 306 Edificio 50Carrera 7 40-62BogotaacuteColombia
Bettina C FriesDepartment of MedicineInfectious Diseases and Department of Microbiology and ImmunologyAlbert Einstein College of MedicineBronx NY 10461
Zachary P FryeDepartment of Chemical EngineeringUniversity of Texas at AustinAustin TX 78712
Amy E GilbertCutaneous Medicine and Immunotherapy UnitSt Johnrsquos Institute of DermatologyDivision of Genetics and Molecular Medicine amp NIHR Biomedical Research Centre at Guyrsquos and St Thomasrsquos Hospitals and Kingrsquos College London School of MedicineGuyrsquos HospitalLondon SE1 9RTUnited Kingdom
Hannah J GouldRandall Division of Cell and Molecular BiophysicsDivision of Asthma Allergy and Lung BiologyMRC and Asthma UK Centre for Allergic Mechanisms of AsthmaKingrsquos College LondonNew Huntrsquos HouseGuyrsquos CampusLondon SE1 1ULUnited Kingdom
contRIBUtoRs xi
Harry B GreenbergDepartments of Medicine and Microbiology and ImmunologyStanford University School of Medicine and the VAPAHCSPalo Alto CA 94305
Scott B HalsteadDepartment of Preventive Medicine and BiometricsUniformed Services University of the Health SciencesBethesda MD 20814
Shen Y HelvigDepartment of PharmacyCenter for Pharmaceutical Nanotechnology and NanotoxicologyFaculty of Health and Medical SciencesUniversity of CopenhagenCopenhagen DK-2100Denmark
Adam HeyPreclinical Safety BiologicsNovartis AGBaselSwitzerland
Andrew HiattMapp Biopharmaceutical Inc6160 Lusk Blvd C105San Diego CA 92121
Bjoumlrn HockDepartment of Protein Engineering and Antibody TechnologiesMerck Serono Merck KgaAFrankfurter Str 250D-64293 DarmstadtGermany
Kelly HuangDepartment of Infectious DiseaseMedImmune LLCOne MedImmune WayGaithersburg MD 20878
Philip R JohnsonThe Childrenrsquos Hospital of PhiladelphiaAbramson Research CenterPhiladelphia PA 19104
Debra H JosephsCutaneous Medicine and Immunotherapy UnitSt Johnrsquos Institute of DermatologyDivision of Genetics and Molecular Medicine amp NIHR Biomedical Research Centre at Guyrsquos and St Thomasrsquos HospitalsKingrsquos College London School of MedicineGuyrsquos HospitalLondon SE1 9RTUnited Kingdom
Shilpa A JoshiDepartment of PathologyStanford UniversityStanford CA 94305
Sophia N KaragiannisCutaneous Medicine and Immunotherapy UnitSt Johnrsquos Institute of DermatologyDivision of Genetics and Molecular Medicine amp NIHR Biomedical Research Centre at Guyrsquos and St Thomasrsquos HospitalsKingrsquos College London School of MedicineGuyrsquos HospitalLondon SE1 9RTUnited Kingdom
Panagiotis KaragiannisCutaneous Medicine and Immunotherapy UnitSt Johnrsquos Institute of DermatologyDivision of Genetics and Molecular Medicine amp NIHR Biomedical Research Centre at Guyrsquos and St Thomasrsquos HospitalsKingrsquos College London School of MedicineGuyrsquos HospitalLondon SE1 9RTUnited Kingdom
Jens C KrauseChildrenrsquos HospitalUniversity of Freiburg Medical Center79106 FreibergGermany
Antonio LanzavecchiaInstitute for Research in Biomedicinevia Vincenzo Vela 6Bellinzona 6500Switzerland
xii contRIBUtoRs
Marie-Paule LefrancLaboratoire drsquoImmunoGeacuteneacutetique Moleacuteculaire LIGMIMGTreg the international ImMunoGeneTics information systemregInstitut de Geacuteneacutetique Humaine IGHUniversiteacute Montpellier 2UPR CNRS 1142Montpellier 34396 cedex 5 40202France
Olivier LegerDepartment of Protein Engineering and Antibody TechnologiesMerck Serono SA--Geneva9 chemin des Mines1202 GenevaSwitzerland
Kin-Ming LoDepartment of Protein Engineering and Antibody TechnologiesEMD Serono Research Institute45A Middlesex TurnpikeBillerica MA 01821
Wayne A MarascoDepartment of Cancer Immunology and AIDSDana-Farber Cancer InstituteHarvard Medical SchoolBoston MA 02215
Jennifer A MaynardDepartment of Chemical EngineeringUniversity of Texas at AustinAustin TX 78712
Luzia M MayrINSERM U1109Universiteacute de Strasbourg3 Rue Koeberleacute67000 StrasbourgFrance
Jens MeilerDepartment of Chemistry and Center for Structural BiologyVanderbilt UniversityNashville TN 37212
contRIBUtoRs xiii
S Moein MoghimiDepartment of PharmacyCenter for Pharmaceutical Nanotechnology and NanotoxicologyFaculty of Health and Medical SciencesUniversity of CopenhagenCopenhagen DK-2100Denmark
Susan Zolla-PaznerNew York University School of Medicine550 First AvenueNew York NY 10016
Louise SaulCutaneous Medicine and Immunotherapy UnitSt Johnrsquos Institute of DermatologyDivision of Genetics and Molecular Medicine amp NIHR Biomedical Research Centre at Guyrsquos and St Thomasrsquos HospitalsKingrsquos College London School of MedicineGuyrsquos HospitalLondon SE1 9RTUnited Kingdom
Bruce C SchneppThe Childrenrsquos Hospital of PhiladelphiaAbramson Research CenterPhiladelphia PA 19104
Jennifer E SchusterDepartment of PediatricsChildrenrsquos Mercy HospitalKansas City MO 64108-4619
Alexander M SevyDepartment of Chemistry and Center for Structural BiologyVanderbilt UniversityNashville TN 37212
Jared SheehanDepartment of Cancer Immunology and AIDSDana-Farber Cancer InstituteHarvard Medical SchoolBoston MA 02215
Michael R SierksDepartment of Chemical EngineeringArizona State UniversityTempe AZ 85287-6006
xiv contRIBUtoRs
Scott A SmithThe Vanderbilt Vaccine Center and the Department of MedicineVanderbilt University Medical CenterNashville TN 37232
Robyn L StanfieldDepartment of Molecular BiologyThe Scripps Research Institute10550 North Torrey Pines RoadLa Jolla CA 92037
Nadine UptonRandall Division of Cell and Molecular BiophysicsDivision of Asthma Allergy and Lung BiologyMRC and Asthma UK Centre for Allergic Mechanisms of AsthmaKingrsquos College LondonNew Huntrsquos HouseGuyrsquos CampusLondon SE1 1ULUnited Kingdom
Avanish K VarshneyDepartment of MedicineInfectious Diseases and Department of Microbiology and ImmunologyAlbert Einstein College of MedicineBronx NY 10461
Stefanie N VelgosMayo Clinic Arizona5777 East Mayo BoulevardPhoenix AZ 85054
Kevin J WhaleyMapp Biopharmaceutical Inc6160 Lusk Blvd C105San Diego CA 92121
Peter P WibroeCentre for Pharmaceutical Nanotechnology and NanotoxicologyDepartment of PharmacyFaculty of Health and Medical SciencesUniversity of CopenhagenCopenhagen DK-2100Denmark
John V WilliamsDepartment of PediatricsSchool of MedicineVanderbilt UniversityNashville TN 37232-2581
contRIBUtoRs xv
Ian A WilsonDepartment of Molecular Biology and Skaggs Institute for Chemical BiologyThe Scripps Research Institute10550 North Torrey Pines RoadLa Jolla CA 92037
Herren WuDepartment of Antibody Discovery and Protein EngineeringMedImmune LLCOne MedImmune WayGaithersburg MD 20879
Guocheng YangDepartment of Chemical EngineeringArizona State UniversityTempe AZ 85287-6006
Larry ZeitlinMapp Biopharmaceutical Inc6160 Lusk Blvd C105San Diego CA 92121
xvi contRIBUtoRs
Preface
Antibodies form the principal foundation for modern intervention against in-fectious diseases Emil Adolf von Behring was awarded the first Nobel Prize in Physiology or Medicine in 1901 ldquofor his work on serum therapy especially its appli-cation against diphtheria by which he has opened a new road in the domain of med-ical science and thereby placed in the hands of the physician a victorious weapon against illness and deathsrdquo Antibodies now provide the focus for understanding mechanisms of immunity to most infectious diseases and they play a central role in passive immunotherapy and active vaccination as mechanisms or correlates of immunity For most of the 20th century immunotherapy was based on passive transfer of polyclonal hyperimmune animal serum immune human serum or even hyperimmune human serum Georges JF Koumlhler and Ceacutesar Milstein re-ported the generation of monoclonal antibodies in 1979 for which they shared the 1984 Nobel Prize in Physiology or Medicine ldquofor the discovery of the princi-ple for production of monoclonal antibodiesrdquo Since that time entire fields related to antibodies for infectious diseases including antibody gene cloning engineer-ing and expression antibody libraries and high-throughput antibody gene rep-ertoire sequence analysis have extended our capabilities to explore the diversity of antibody specificity and function with unprecedented depth and breadth
This book provides a broad survey of many of the most important aspects of the field of antibodies for infectious diseases The book begins with a general introduction followed by chapters 2 through 5 on general features pertaining to structure function isotype and the role of complement in antibody function Chapters 6 through 10 review contemporary approaches for antibody discovery using phage and yeast display plasma cell and memory B cell cloning human hybridomas humanized mice and computational methods Chapters 11 through 18 review in depth the biology of antibodies specific for particular pathogens including viruses and bacterial toxins to illustrate the role of antibodies in anti- microbial immunity with specific targets These chapters reveal that attempts to raise effective antibody responses to each of these pathogens faces unique and pathogen-specific challenges Chapters 19 to 23 cover major technical advances pertaining to antibody engineering repertoire sequencing and analysis and new methods for study or therapeutic use of antibodies including radiotherapy Fi-nally chapters 24 and 25 cover new methods for expression of monoclonal anti-bodies in plants or by transfer of antibody genes for in vivo expression in treated subjects
Recent literature is exploding with new antibody-related techniques and re-ports of antimicrobial antibodies with unprecedented potency breadth of activ-
xvii
xviii PReface
ity and therapeutic potential We hope that this timely compilation of state-of-the-art reviews of major aspects of this field will be of interest to both antibody cognoscenti and those new to this exciting field We thank the authors for their dedication in producing definitive reviews of the topics at hand
James E Crowe JrDiana BoraschiRino Rappuoli
INTRODUCTION
History and PracticeAntibodies in Infectious Diseases 1ADAM HEY1
Antibodies in Infectious Diseases aims to inform update and inspire studentsteachers researchers pharmaceutical developers and health care professionalson the status of the development of antibody-based therapies for treatinginfectious diseases and the potential for these in times of growing antibioticresistance to provide alternative treatment solutions to the currently usedantibiotics and new treatments for infectious diseases where no propertreatments are available
This introductory article will provide a historical perspective on the useof antibody-based therapies followed by a high-level overview of whatmakes antibodies attractive tools for this purpose This will include the prosand cons of such therapies compared to the use of antibiotics and thepractical and strategic considerations involved in selecting the best formatand development path for new antibody-based therapies targeting specificinfectious agents Then examples of antibody-based therapies in thedevelopment of treatments for infectious diseases will be presented andfinally a look into the future will summarize the different aspects that willinfluence what the future might bring for this type of treatments forinfectious diseases
1Preclinical Safety Biologics Novartis AG Basel Switzerland
Antibodies for Infectious DiseasesEdited by James E Crowe Jr Diana Boraschi and Rino Rappuolicopy 2015 American Society for Microbiology Washington DCdoi101128microbiolspecAID-0026-2014
3
HISTORICAL PERSPECTIVE
Antibodies and the use of passive antibodytherapy in the treatment of infectious dis-eases is the story of a treatment conceptwhich dates back more than 120 years to thelate 19th century and which originally bythe use of serum from immunized animalsprovided the first effective treatment optionsagainst severe bacterial infections (1 2) Byimmunizing horses with bacterial toxinsfrom Clostridium tetani and Corynebacteri-um diphtheriae Emil A Von Behring andShibasaburo Kitasato (3) generated serumcontaining antibodies capable of neutraliz-ing the effects of the toxins produced bythese bacteria and successfully providedtreatment for these serious diseases wherethe pathogenesis is driven by the effects ofthe bacterial toxins For his work on provid-ing treatment for diphtheria Behring re-ceived the Nobel Prize in Physiology orMedicine in 1901 These radical treatmentresults quickly prompted development ofmultiple additional serum therapies for thetreatment of infectious diseases caused byeg Neisseria meningitidis Haemophilus in-fluenza and group A Streptococcus Sinceserum therapy involved administration oflarge amounts of crude mixtures of animalproteins including antibodies they wereassociated with side effects in the form ofhypersensitivity and serum sickness (2)
Due to the crude and unpurified nature ofthese products side effects were seen evenwhen administering human serum prepa-rations Side effects were observed in up to50 of patients and were considered to becaused by immune complex formations thatresulted in symptoms such as rash itchingjoint pain fever and in serious cases hypoten-sion and shock However due to the lack ofalternative options these treatments weredespite their side effects widely used Serumwas normally administered by intravenousinfusion in patients after a test for hypersensi-tivity where a small amount of serum wasinjected subcutaniously (1) As described
above serum therapy applied in these earlydays (late 19th century and early 20th century)involved preparations of serum from rabbitsand horses immunized with the infectiousagent or in live andor neutralized versions ortoxins from these (1) The costs of keeping theimmunized animals and the production andpotency testing of the materials made this arelatively expensive treatment In 1891 datafrom Klemperer (4) showed serum therapy toprotect rabbits from Streptococcus pneumoniaeinfection and paved the way for this type oftreatment and for development of similarserum-based treatments of streptococcal in-fections in humans When treating humansearly administration of serum could reducemortality significantly down to around 5compared to when administered 4 to 5 daysafter onset of symptoms when serum treat-ment was largely without effect This stronglyindicated the need for quick diagnosis andquick treatment to control the infection beforeit got out of control Consequently in theabsence of a specific diagnosis mixtures ofserum from immunizations with differentserotypes were used to circumvent this needfor early treatment without having a serotype-specific diagnosis The understanding thatdifferent serotypes existed for pneumococciand that efficient treatment relied on usingserotype-specific serum was being built upduring the 1920s and 1930s through experiencefrom extensive clinical trials
By the end of the 1930s serum therapywasthe standard of care for treatment of pneu-mococcal pneumonia At that time theefficacy and potency of the derived serawere assessed in mice in ldquothe mouse pro-tection testrdquo by testing survival after aconcomitant intraperitoneal injection of alethal dose of pneumococci and the serum tobe tested Due to the inherent variation inthis test efficacy and survival in two thirds ofthe animals was the acceptance criteria and10 times the lowest dose providing this wasused for defining a unit of the serum Thisallowed for large batch-to-batch variationand the use of different strains of bacteria for
4 HEY
immunization probably explains part of themissing responses observed (1) In the early20th century a pandemic of meningitis inEurope and the United States with mortalityrates up to 80 spurred the development ofserum therapy treatment options Althoughin the 1930s this became the recommendedtreatment in children assumed to be suffer-ing from meningitis failure to reduce mor-tality in several meningitis epidemics duringthat time raised doubts about the generalapplicability of serum treatment In thosedays serum therapy often involved quiteextensive procedures and infusion of largevolumes of serum The following exampleclearly illustrates this Data from Flexnerand Jobling (5) from treating meningitis inmonkeys resulted in the development of serafrom immunized horses for treatment inhumans The treatment protocol includedlumbar puncture and withdrawal of morethan 30 ml of spinal fluid representing anamount slightly larger than the expectedamount of horse serum to be injected subse-quently This treatment involved such dailyslow infusions of up to 30 ml of serum untilthe patientrsquos condition improved This treat-ment was used in outbreaks in New York in1905 and 1906 and did markedly decreasemortality
After the discovery of penicillin by Flemingin 1928 and the subsequent introduction ofantibiotics in the 1930s serum therapy waslargely abandoned over a period of 10 years dueto the availability of these new more broadlyeffective and cheaper treatment optionswhichalso had fewer side effects Although improve-ments in the purification of antibodies hadresulted in preparations with better safety andside effect profiles high manufacturing costsand narrow specificity resulted in antibodytherapy being mostly restricted to a smallernumber of selected treatments for snakevenoms bacterial toxins and some viral infec-tions (1 2) Currently antibody administrationis used for treatment and prevention ofhepatitis B virus rabies virus respiratorysyncytial virus (RSV) Clostridium tetani Clos-
tridium botulinum vaccinia virus echovirusand enterovirus For the most part thesetreatments consist of pooled immunoglobulinalso known as IVIG (intravenous immunoglob-ulin) from several postexposure donors Thisresults in both batch-to-batch variation in theneed for relatively large amounts of serum dueto low specificity and to restricted supplies dueto reliance on exposed donors
However several challengeshave resulted inthe need for new tools in the treatment andpreventionof infectiousdiseasesThebroadandgeneral use of antibiotics in human and veter-inary medicine for many years has resulted inthe development of multi-resistant strains ofbacteria with limited to no response to existingtreatments such as methicillin-resistant Staph-ylococcusaureus (MRSA) vancomycin-resistantS aureus and others This has resulted inpatients needing screening and treatment withseveral antibacterial agents and longer treat-ment time causing extra strain on patients andhealth care providers (6 httpwwwcdcgovdrugresistancethreat-report-2013indexhtml) According to the WHO and CDC morethan 25000 people in European Unioncountries and similar numbers in the UnitedStates die every year as a result of antibiotic-resistant infections This together with theemergence of new pathogens (eg severeacute respiratory syndrome Middle East respi-ratory syndrome) the re-emergenceepidemicsof oldknown pathogens (eg Ebola) and thedifficulties in treating infections in immune-deficient patients (eg HIV patients) has high-lighted the need for new solutions The 2014Ebola epidemic in West Africa (Liberia SierraLeone Guinea Nigeria and Senegal) has fur-ther highlighted this No treatment or prophy-lactic vaccine is available to treat or prevent thespread of Ebola infections which have anaveragemortality of gt50 Local health author-ities in the affected countries are struggling tocontain and handle the disease which isthreatening to go out of control and spreadmorewidelyVariousproductsmainly antibodycocktails from previously recovered patientsare being used despite a lack of clinical data on
CHAPTER 1 bull History and Practice Antibodies in Infectious Diseases 5
their safety and efficacy and those are the onlysporadically available treatment options andonly in small amounts and for a few patients
Ebola is an example of a disease whichnormally affects only a small number ofindividuals and which normally burns outwhen disease outbreaks are contained There-fore given the small number of potentialpatients affected by previous Ebola infectionsto date there was no incentive for big pharmacompanies to do research and development ofdrugs for EbolaWith the increasing number ofinfected (13567) andadeath toll of 4951 (7) andthe lack of the ability to contain the epidemic itwill be interesting to follow the aftermath ofthis outbreak and see whether there will berequests for new ways to ensure that vaccinesand treatment options are available for Ebolaand similar high-mortality and potential bio-warfare infections that have no availabletreatments or procedures to for mass-produc-tion upon the first signsreports of activeinfections Although both the CDC and theWHO have special programs focusing on thesetypes of infections the Ebola outbreak in 2014clearly shows that more financial support forresearch and development of new diagnosticsand treatments is needed This is one examplewhere antibody-based treatments would havethe potential to play a major role To put this inthe right perspective one should however notforget that other infectious diseases such astuberculosis influenza and malaria kill hun-dreds of thousands each year There is there-fore plenty of room for improvement indeveloping treatments for these diseases aswell but the high attention drawn to eg theEbola outbreak creates a special niche andopportunity where antibody treatments couldgain extraordinary development funding andsupport and prove their value and treatmentpotential
That antibody-based therapies could takethis role is supported by the revolution intechnologies for the development selectiongeneration and purification of fully humanantibodies described in more detail later in thesection ldquoMethodsandPlatforms forGenerating
Antibodiesrdquo Antibody-based programs cur-rently at different stages of developmentinclude investigations into the potential use ofsingle antibody preparations combinations ofantibodies (to avoid survival of escape mu-tants) fragments of antibodies and antibodiescarrying radioactive isotopesorcytotoxicdrugsor antibody-like frameworks (eg fibronectin)either alone as a first-line treatment or as anadjunct to existing treatments This multitudeof possible formats the ability to raise anti-bodies to almost any target and the ability toengineer both size effector functions and half-life are now considered by many to providevery valuable tools for designing specificantibody-based treatments toeradicate specifictargeted infectious agents However althoughseveral antibody-based therapies have beenapproved for oncology and anti-inflammatoryindications (see Table 1) only one monoclonalantibody (mAb) is approved against an infec-tious disease agentmdashSynagis (palivizumabMedImmune) for the prevention and treat-ment of respiratory syncytical virus (RSV) inhigh-risk children Economic obstacles such asthe high cost of mAb therapies and relativelysmall markets have resulted in less interestfrom pharmaceutical companies in developingthese Also highlighting the challenges indeveloping these types of antibody-basedtreatments are the difficulties encountered indeveloping a follow-up higher-affinity candi-date to Synagis Poor translatability of dataobtained in the available animal disease mod-els for RSV in cotton rats has resulted in non-approval due to inferiority relative to SynagisIn other viral diseases such as cytomegalovirus(CMV) the high species specificity of thestrains of CMV makes it impossible to testhuman antibody therapies in vivo Thereforeany real data on the efficacy of treatments forCMV will not be obtained until testing inclinical trials As described later in this articleseveral new antibody-based therapies for in-fectious diseases are in development andhopefully this will gradually open the fieldand result in better treatment options andoutcomes for patients
6 HEY
TABLE 1 Approved and pending antibody-based therapies
Name antibody Target antibody type Indication Company Approval date
OKT3a Muronomab-CD3 CD3 murine IgG2a Autoimmune Johnson ampJohnson
1986 (US)
ReoPro abciximab PIIbIIIa chimeric IgG1Fab
Homeostasis Johnson ampJohnson
1984 (US)
Rituxan rituximab CD20 chimeric IgG1 Cancer Genentech 1997 (US) 1998 (EU)Zenapaxa daclizumab CD25 humanized IgG1 Autoimmune Roche 1997 (US) 1999 (EU)Simulect basiliximab CD25 chimeric IgG1 Autoimmune Novartis 1998 (US EU)Synagis palivizumab RSV humanized IgG1 Infections MedImmune 1998 (US) 1999 (EU)Remicade infliximab TNFα chimeric IgG1 Autoimmune Johnson amp
Johnson1998 (US) 1999 (EU)
Herceptin trastuzumab HER2 humanized IgG1 Cancer GenentechRoche
1998 (US) 2000 (EU)
Mylotarga gemtuzumabozogamicin
CD33 humanized IgG4immunotoxin
Cancer WyethPfizer 2000 (US)
Campath alemtuzumab CD52 humanized IgG1 Cancer Genzyme 2001 (US) 2001 (EU)Zevalin ibritumomabtiuxetan
CD20 murine IgG1radiolabeled (yttrium 90)
Cancer Biogen Idec 2002 (US) 2004 (EU)
Humira adalimumab TNFα human IgG1 Autoimmune Abbott 2002 (US) 2003 (EU)Xolair omalizumab IgE humanized IgG1 Autoimmune Genentech
Roche2003 (US)
Bexxar tositumomab-I-131 CD20 murine IgG2aradiolabeled (iodine131)
Cancer CorixaGSK 2003 (US)
Raptivaa falizumab CD11a humanized IgG1 Autoimmune GenentechRoche
2003 (US) 2004 (EU)
Erbitux cetuximab EGFR chimeric IgG1 Cancer ImcloneLilly 2004 (US) 2004 (EU)Avastin bevacizumab VEGF humanized IgG1 Cancer Genentech
Roche2004 (US) 2005 (EU)
Tysabri natalizumab α4-Intergrin humanizedIgG4
Autoimmune Biogen Idec 2004 (US)
Actemra tocilizumab Anti-IL-6R humanizedIgG1
Autoimmune ChugaiRoche
2005 (Japan) 2010 (US)
Vectibix panitumumab EGFR human IgG2 Cancer Amgen 2006 (US)Lucentis ranibizumab VEGF humanized IgG1
FabMaculardegeneration
GenentechRoche
2006 (US)
Soliris eculizumab C5 humanized IgG24 Blood disorders Alexion 2007 (US)Cimzia certolizumab pegol TNFα humanized
pegylated FabAutoimmune UCB 2008 (US)
Simponi golimumab TNFα human IgG1 Autoimmune Johnson ampJohnson
2009 (US EU Canada)
Ilaris canakinumab IL1b human IgG1 Infalmmatory Novartis 2009 (US EU)Stelara ustekinumab IL-1223 human IgG1 Autoimmune Johnson amp
Johnson2008 (EU) 2009 (US)
Arzerra ofatumumab CD20 human IgG1 Cancer Genmab 2009 (EU)Prolia denosumab RANK ligand human
IgG2Bone loss Amgen 2010 (US)
Numax motavizumab RSV humanized IgG1 Anti-infective MedImmune PendingABthrax Raxibacumab B anthrasis PA human
IgG1Anti-infection GSK 2012 (US)
Benlysta belimumab BLyS human IgG1 Autoimmune HGS 2011 (US)Yervoy ipilimumab CTLA-4 human IgG1 Cancer BMS 2011 (US)Adcetris brentuximabvedotin
CD30 chimeric IgG1drug- conjugate
Cancer SeattleGenetics
2011 (US)
(Continued on next page)
CHAPTER 1 bull History and Practice Antibodies in Infectious Diseases 7
INTRODUCTION TO ANTIBODIES
Antibodies also called immunoglobulins basedon their combined structure and function inimmune responses are produced by B cells ofthe immune system They are part of theadaptive immune response and are speciallydesigned for neutralizing and eliminating theinfectious agents and toxins produced by theseAntibodies are present in blood plasma andextracellular fluids and since these fluids wereformerly known as humors they were said tobe part of the humoral immune responseAntibodies are Y-shaped structures consistingof two main parts the upper arms of the Ywhich contain two identical variable-regionantigen binding sites and the lower regioncalled the constant regionwhich is responsiblefor the initiation of effector functions that leadto the removal and destruction of the pathogenor cells harboring the pathogen (see Fig 1) Theantigen-binding sites on an antibody can bythemselves bind to and neutralize bacterialtoxins and viruses thereby preventing themfrom binding to their target cells or receptorscausing toxic effects or spread of the infection
Antibodies consist of two pairs of heavy andlight chainswhich as described above are heldtogether in a Y-shaped arrangement Each ofthe heavy and light chains in these pairs isseparated into constant and variable chainsThe upper armsof theY each contain a variableand a constant sectionof the light and theheavychain where the upper variable parts of theheavy and light chains contain the antigen-binding site and the constant parts areconnected via disulfide bonds The lower partof theYcalled theconstantpart consistsof twoor three constant segments (immunoglobulindomains) from each of the two heavy chainsinteracting and also linked via disulfide bondsThe sectionsof theheavy chains connecting theconstant part of the upper arms to the constantparts of the constant region contain specialhinge regions that provide flexibility to thedifferent sections of the antibody to bind toantigens and effector cells The constant re-gions of the heavy chain also contain attachedoligosaccharide moieties which provide func-tional specialization to the antibodies (8)
The variable domains of the heavy and lightchains form the antigen-binding sites and
TABLE 1 Approved and pending antibody-based therapies (Continued)
Name antibody Target antibody type Indication Company Approval date
Perjeta pertuzumab Her2 humanized IgG1 Cancer GenentechRoche
2012 (US)
Kadcyla ado-trastuzumabemtansine
Her2 humanized IgG1Drug-conjugate
Cancer GenentechRoche
2013 (US)
Raxibacumab Anti-B anthrasis PAhuman IgG1
Anthraxinfection
Notapproved
2012
Entyvio vedolizumab Integrin α4β7humanized IgG1
Crohnrsquos diseaseulcerative colitis
Takeda 2014 (US)
Cyramza ramuciruumab Anti-VEGFR2Human IgG1
Gastric cancer Lilly 2014 (US)
Gazyva obinutuzumab Anti-CD20 humanizedIgG1 glucoengineered
CancerCLLb GenentechRoche
2014 (US)
Sylvant situximab Anti IL-6 chimeric IgG1 Castlemandisease
Janssen 2014 (US) 2014 (EU)
Cosentyx sekukinumab Anti IL-17a human IgG1 Psoriasis Novartis 2015 (US) 2015 (EU)Nivolumab Anti PD-1 human IgG4 Melanoma BMS Not approvedKeytruda pembrolizuumab Anti-PD-1 humanized
IgG4Melanoma Merck 2014 (US)
aAntibodies approved but later withdrawnbCLL chronic lymphocytic leukemia
8 HEY
FIGURE 1 (Left panel) Model of antibody structure exemplified by IgG On top the antigen-binding sitesin orange each contain one variable light and variable heavy domain with the three complementaritydetermining regions (CDRs) that are responsible for the specific binding of the antibody to its target Foreach arm of the antibody an additional set of variable heavy and light domains together with the CDR-containing domains represent the two fragment antigen binding (Fab) regions The two Fabs are heldtogether via two disulfide bridges Below the Fabs is the Fc region which contains four constant heavydomains On the upper pair of these domains are binding sites for oligosaccharides which have majorimportance for the ability of the antibody Fc part to trigger effector functions when the Fc portion isbound to Fc gamma receptors on natural killer cells neutrophil granulocytes monocytesmacrophagesdendritic cells and B cells (Right panel) Examples of some of the antibody-derived alternative formatsused to exploit the specific features of the CDRs the Fabs and the Fc parts of the antibodies ScFv Thesingle chain fragment variable consists of the variable domains of the heavy and light chains heldtogether by a flexible linker This can also be used as a carrier of a cytotoxic drug in a so-called antibodydrug complex (ADC) where the specificity of the ScFv is used to target the cytotoxic drug to eg atumor Bite (bi-specific T cell engager) Fusion proteins consisting of two ScFvs one directed against thetarget on a tumor cell and the other against the T cell receptor (CD3) Diabody ScFv dimers where shortlinker peptides (five amino acids) ensure dimerization and not folding of the ScFvs Fab and F(ab)2fragments Single Fab fragments or fragments containing two Fabs linked via disulfide bridges This isused where effector functions related to the Fc part of the antibody are unwanted and where a smallersize is desired to obtain better tissue penetration in eg tumors Due to the lack of the FcRn binding viathe Fc part Fab and F(ab)2 fragments have much shorter half-lives (hours or days) than full-sizeantibodies (weeks) These can also be used as carriers of cytotoxic payloads or cytotoxic radioactiveisotopes and for the F(ab)2 fragments can be constructed as bi-specifics which can cross-link immunecells and target cells Fc fusion protein Fusion protein containing the Fc domain of an immunoglobulinbound to a peptide The peptide can be a ligand for a specific receptor on a target cell or a blockingpeptide for a soluble ligand The Fc part provides a longer half-life to the construct and the potential tobind to and engage effector functions in the killing of eg tumor cells or infected cells ADCsRIAs andbi-specifics Full-size IgG antibodies carrying either a cytotoxic chemical or radioactive payload whichmay also carry different CDRs enabling cross-linking of effector and target cells for increased killingdoi101128microbiolspecAID-0026-2014f1
CHAPTER 1 bull History and Practice Antibodies in Infectious Diseases 9
contain special hyper-variable segments calledcomplementarity-determining regions (CDRs)which allow the B cells via genetic recom-bination to generate antibodies to all thedifferent antigens specific to amino acid se-quences or three-dimensional structuralmotifs(polysaccharides DNA and RNA) found onpathogens
Based on the structure of their heavy chainconstant regions antibodies or immuno-globulins are separated into five classesmdashIgM IgG IgE IgD and IgA Differences inthe sequences of the constant regions providedistinct characteristics to these different clas-ses These characteristics include the numberof heavy chain constant segments the numberand location of interconnecting disulfidebridges the length of the hinge region andthe number and location of oligosaccharidemoieties For IgG four heavy chain versionsexist creating IgG1 2 3 and 4 isotypes eachwith different characteristics in their serumhalf-lives and ability to trigger different effec-tor functions Because of the combined ad-vantage from ability to trigger effectormechanisms long [21 days] half-life theirability to be transported over the placentaand their stability in the production processantibodies of the IgG class and of the IgG1isotype are preferred as the basis for newantibody-based therapies The effector func-tions are triggered by the Fc part of an antibodywhen the variable parts of the antibody arebound directly to an infectious agent or toproteins from an infectious agent expressed onan infected cell This binding leaves the Fc partfree to interactwithFc receptors onphagocyticcells and neutrophils eosinophils and naturalkiller cells capable of inducing phagocytosis orlysis of infectious agents or infected cellsThese effector functions include (i) the abilityto activate the complement system for lysis(complement-dependent cellular cytotoxicity)(ii) triggering of uptake and destruction byphagocytic cells such as macrophages andneutrophils via interaction with Fc receptorson these cells (iii) activation of macrophageseosinophils neutrophils and natural killer
cells to kill infected cells via binding to Fcreceptors on these cells and antibody-depen-dent cellular cytotoxicity and (iv) neutraliza-tion of bacterial toxins and blocking of bindingand uptake of bacteria or viruses to target cells(see Fig 2) (9)
The Fcpart of IgG antibodies also contains aregion that interacts with the neonatal Fcreceptor (FcRn) expressed on most immuno-competent cells and inmany other cells such asendothelial cells in kidney liver placenta lungand breast (10) which protects antibodies fromdegradation by phagocytoticexocytotic cy-cling into FcRn-expressing cells thereby pro-longing their half-life This results in half-livesof 20 to 21 days for most IgG1 2 and 4antibodies whereas half-lives are 10 6 and 2days respectively for IgM IgA and IgE Thehighly specific binding sites on the variableregions of the upper arms of the antibody allowfor several important features of antibodiesndashbinding to and neutralization of eg bacterialtoxins binding to pathogens and blocking theirbinding to or interaction with target cells (egcyncytia formation of CMV-infected cells) orblocking of binding and interactions of infec-tious agents with target cells via blockingreceptors on the target cells
METHODS AND PLATFORMS FORGENERATING ANTIBODIES
As described above the early use of passiveantibody transfer as a therapy in infectiousdiseases involved the use of immune serumfrom immunized sheep and horses These pre-parations were crude and contained a broadmixture of neutralizing and non-neutralizingantibodies and both the foreign nature of theantibodies and the numerous host serumproteins This resulted in less specific andthus less efficient therapies due to a highvariability in efficacy between batches derivedfrom different animals immunized with dif-ferent strains of bacteria in different labor-atories and resulted in multiple unwantedside effects related to hypersensitivity and
10 HEY
anaphylactic reactions to foreign proteinsThese days antibodies being developed fortreatment of diseases in humans are highlypurified and are mostly fully human mono-clonal antibodies The term monoclonal anti-body refers to that cell cultures used forgenerating these antibodies each originatesfrom a single cell and thus produces onlyone specific antibody Development of fullyhuman monoclonal antibodies happened instages over a time span of more than 15 yearsFirst stage in this process was generation ofmonoclonalmurine IgG antibodies (eg OKT3[muronomab-CD3 Johnson and Johnson] ap-proved in 1986) Next stage was generation ofso called chimeric antibodies consisting ofhuman heavy and light chain constant sec-tions but with murine variable sections (eg
Rituxan [rituximab Genentech]) Next stagewas then the humanized antibodies wherethe only remaining murine part of the anti-body is the antigen-binding CDR (eg Xolair[omalizumab NovartisGenentech]) Both thefirst chimeric and humanized antibodies wereapproved in the late 1990s Then finally 16years later the first fully human antibodyHumira (adalimumab Abbott) was approvedin 2002 Since the time of the crude and low-scale manufacturing of the original antibodyserum products much has changed andtherapeutic antibodies are now produced byfermentation in 5000 liter scale using highlycontrolled and documented yeast or mamma-lian cell lines that are genetically engineered toexpress a single specific antibody This hasresulted in a pure and highly specific antibody
FIGURE 2 Effector functions of antibodies (a) Antibodies bind to pathogen-derived or endogenousantigens expressed on the surface of an infected cell which triggers binding to Fc receptors on naturalkiller cells and lysis of the infected cell by antibody-dependent cellular cytotoxicity (b) Antibodies bindto pathogen-derived or endogenous antigens expressed on the surface of infected cells which triggersactivation of complement through binding of complement factor C1q (c) Neutralization Top Bacterialtoxin neutralized by bound antigen Bottom Antibody bound to either receptor for the virus or to thevirus itself which blocks virus binding and entry into the cell (d) Antibody bound to viral surfaceproteins binds to Fc receptors on phagocytic cells eg macrophages and triggers endocytosis anddestruction of virus in endolysosome doi101128microbiolspecAID-0026-2014f2
CHAPTER 1 bull History and Practice Antibodies in Infectious Diseases 11

Contributors
Edith Acquaye-SeedahDepartment of BiochemistryUniversity of Texas at AustinAustin TX 78712
Ramesh AkkinaDepartment of Microbiology Immunology and PathologyColorado State University1619 Campus DeliveryFort Collins CO 80523
Shanta P BoddapatiDepartment of Biomedical EngineeringOregon Health and Science University3181 SW Sam Jackson Park RoadPortland OR 97239
Scott D BoydDepartment of PathologyStanford UniversityStanford CA 94305
Arturo CasadevallDepartments of Microbiology and Immunology and MedicineAlbert Einstein College of Medicine of Yeshiva University1695A Eastchester RoadBronx NY 10461
Davide CortiHumabs BioMed SAvia Mirasole 1Bellinzona 6500Switzerland
James E Crowe JrSchool of MedicineVanderbilt UniversityNashville TN 37232
ix
x contRIBUtoRs
Ekaterina (Kate) DadachovaDepartments of Radiology Microbiology and ImmunologyAlbert Einstein College of Medicine of Yeshiva University1695A Eastchester RoadBronx NY 10461
Donald N ForthalDepartment of Infectious Diseases3044 Hewitt HallUniversity of California IrvineIrvine CA 92617
Manuel A FrancoFacultad de Ciencias y MedicinaPontificia Universidad JaverianaOficina 306 Edificio 50Carrera 7 40-62BogotaacuteColombia
Bettina C FriesDepartment of MedicineInfectious Diseases and Department of Microbiology and ImmunologyAlbert Einstein College of MedicineBronx NY 10461
Zachary P FryeDepartment of Chemical EngineeringUniversity of Texas at AustinAustin TX 78712
Amy E GilbertCutaneous Medicine and Immunotherapy UnitSt Johnrsquos Institute of DermatologyDivision of Genetics and Molecular Medicine amp NIHR Biomedical Research Centre at Guyrsquos and St Thomasrsquos Hospitals and Kingrsquos College London School of MedicineGuyrsquos HospitalLondon SE1 9RTUnited Kingdom
Hannah J GouldRandall Division of Cell and Molecular BiophysicsDivision of Asthma Allergy and Lung BiologyMRC and Asthma UK Centre for Allergic Mechanisms of AsthmaKingrsquos College LondonNew Huntrsquos HouseGuyrsquos CampusLondon SE1 1ULUnited Kingdom
contRIBUtoRs xi
Harry B GreenbergDepartments of Medicine and Microbiology and ImmunologyStanford University School of Medicine and the VAPAHCSPalo Alto CA 94305
Scott B HalsteadDepartment of Preventive Medicine and BiometricsUniformed Services University of the Health SciencesBethesda MD 20814
Shen Y HelvigDepartment of PharmacyCenter for Pharmaceutical Nanotechnology and NanotoxicologyFaculty of Health and Medical SciencesUniversity of CopenhagenCopenhagen DK-2100Denmark
Adam HeyPreclinical Safety BiologicsNovartis AGBaselSwitzerland
Andrew HiattMapp Biopharmaceutical Inc6160 Lusk Blvd C105San Diego CA 92121
Bjoumlrn HockDepartment of Protein Engineering and Antibody TechnologiesMerck Serono Merck KgaAFrankfurter Str 250D-64293 DarmstadtGermany
Kelly HuangDepartment of Infectious DiseaseMedImmune LLCOne MedImmune WayGaithersburg MD 20878
Philip R JohnsonThe Childrenrsquos Hospital of PhiladelphiaAbramson Research CenterPhiladelphia PA 19104
Debra H JosephsCutaneous Medicine and Immunotherapy UnitSt Johnrsquos Institute of DermatologyDivision of Genetics and Molecular Medicine amp NIHR Biomedical Research Centre at Guyrsquos and St Thomasrsquos HospitalsKingrsquos College London School of MedicineGuyrsquos HospitalLondon SE1 9RTUnited Kingdom
Shilpa A JoshiDepartment of PathologyStanford UniversityStanford CA 94305
Sophia N KaragiannisCutaneous Medicine and Immunotherapy UnitSt Johnrsquos Institute of DermatologyDivision of Genetics and Molecular Medicine amp NIHR Biomedical Research Centre at Guyrsquos and St Thomasrsquos HospitalsKingrsquos College London School of MedicineGuyrsquos HospitalLondon SE1 9RTUnited Kingdom
Panagiotis KaragiannisCutaneous Medicine and Immunotherapy UnitSt Johnrsquos Institute of DermatologyDivision of Genetics and Molecular Medicine amp NIHR Biomedical Research Centre at Guyrsquos and St Thomasrsquos HospitalsKingrsquos College London School of MedicineGuyrsquos HospitalLondon SE1 9RTUnited Kingdom
Jens C KrauseChildrenrsquos HospitalUniversity of Freiburg Medical Center79106 FreibergGermany
Antonio LanzavecchiaInstitute for Research in Biomedicinevia Vincenzo Vela 6Bellinzona 6500Switzerland
xii contRIBUtoRs
Marie-Paule LefrancLaboratoire drsquoImmunoGeacuteneacutetique Moleacuteculaire LIGMIMGTreg the international ImMunoGeneTics information systemregInstitut de Geacuteneacutetique Humaine IGHUniversiteacute Montpellier 2UPR CNRS 1142Montpellier 34396 cedex 5 40202France
Olivier LegerDepartment of Protein Engineering and Antibody TechnologiesMerck Serono SA--Geneva9 chemin des Mines1202 GenevaSwitzerland
Kin-Ming LoDepartment of Protein Engineering and Antibody TechnologiesEMD Serono Research Institute45A Middlesex TurnpikeBillerica MA 01821
Wayne A MarascoDepartment of Cancer Immunology and AIDSDana-Farber Cancer InstituteHarvard Medical SchoolBoston MA 02215
Jennifer A MaynardDepartment of Chemical EngineeringUniversity of Texas at AustinAustin TX 78712
Luzia M MayrINSERM U1109Universiteacute de Strasbourg3 Rue Koeberleacute67000 StrasbourgFrance
Jens MeilerDepartment of Chemistry and Center for Structural BiologyVanderbilt UniversityNashville TN 37212
contRIBUtoRs xiii
S Moein MoghimiDepartment of PharmacyCenter for Pharmaceutical Nanotechnology and NanotoxicologyFaculty of Health and Medical SciencesUniversity of CopenhagenCopenhagen DK-2100Denmark
Susan Zolla-PaznerNew York University School of Medicine550 First AvenueNew York NY 10016
Louise SaulCutaneous Medicine and Immunotherapy UnitSt Johnrsquos Institute of DermatologyDivision of Genetics and Molecular Medicine amp NIHR Biomedical Research Centre at Guyrsquos and St Thomasrsquos HospitalsKingrsquos College London School of MedicineGuyrsquos HospitalLondon SE1 9RTUnited Kingdom
Bruce C SchneppThe Childrenrsquos Hospital of PhiladelphiaAbramson Research CenterPhiladelphia PA 19104
Jennifer E SchusterDepartment of PediatricsChildrenrsquos Mercy HospitalKansas City MO 64108-4619
Alexander M SevyDepartment of Chemistry and Center for Structural BiologyVanderbilt UniversityNashville TN 37212
Jared SheehanDepartment of Cancer Immunology and AIDSDana-Farber Cancer InstituteHarvard Medical SchoolBoston MA 02215
Michael R SierksDepartment of Chemical EngineeringArizona State UniversityTempe AZ 85287-6006
xiv contRIBUtoRs
Scott A SmithThe Vanderbilt Vaccine Center and the Department of MedicineVanderbilt University Medical CenterNashville TN 37232
Robyn L StanfieldDepartment of Molecular BiologyThe Scripps Research Institute10550 North Torrey Pines RoadLa Jolla CA 92037
Nadine UptonRandall Division of Cell and Molecular BiophysicsDivision of Asthma Allergy and Lung BiologyMRC and Asthma UK Centre for Allergic Mechanisms of AsthmaKingrsquos College LondonNew Huntrsquos HouseGuyrsquos CampusLondon SE1 1ULUnited Kingdom
Avanish K VarshneyDepartment of MedicineInfectious Diseases and Department of Microbiology and ImmunologyAlbert Einstein College of MedicineBronx NY 10461
Stefanie N VelgosMayo Clinic Arizona5777 East Mayo BoulevardPhoenix AZ 85054
Kevin J WhaleyMapp Biopharmaceutical Inc6160 Lusk Blvd C105San Diego CA 92121
Peter P WibroeCentre for Pharmaceutical Nanotechnology and NanotoxicologyDepartment of PharmacyFaculty of Health and Medical SciencesUniversity of CopenhagenCopenhagen DK-2100Denmark
John V WilliamsDepartment of PediatricsSchool of MedicineVanderbilt UniversityNashville TN 37232-2581
contRIBUtoRs xv
Ian A WilsonDepartment of Molecular Biology and Skaggs Institute for Chemical BiologyThe Scripps Research Institute10550 North Torrey Pines RoadLa Jolla CA 92037
Herren WuDepartment of Antibody Discovery and Protein EngineeringMedImmune LLCOne MedImmune WayGaithersburg MD 20879
Guocheng YangDepartment of Chemical EngineeringArizona State UniversityTempe AZ 85287-6006
Larry ZeitlinMapp Biopharmaceutical Inc6160 Lusk Blvd C105San Diego CA 92121
xvi contRIBUtoRs
Preface
Antibodies form the principal foundation for modern intervention against in-fectious diseases Emil Adolf von Behring was awarded the first Nobel Prize in Physiology or Medicine in 1901 ldquofor his work on serum therapy especially its appli-cation against diphtheria by which he has opened a new road in the domain of med-ical science and thereby placed in the hands of the physician a victorious weapon against illness and deathsrdquo Antibodies now provide the focus for understanding mechanisms of immunity to most infectious diseases and they play a central role in passive immunotherapy and active vaccination as mechanisms or correlates of immunity For most of the 20th century immunotherapy was based on passive transfer of polyclonal hyperimmune animal serum immune human serum or even hyperimmune human serum Georges JF Koumlhler and Ceacutesar Milstein re-ported the generation of monoclonal antibodies in 1979 for which they shared the 1984 Nobel Prize in Physiology or Medicine ldquofor the discovery of the princi-ple for production of monoclonal antibodiesrdquo Since that time entire fields related to antibodies for infectious diseases including antibody gene cloning engineer-ing and expression antibody libraries and high-throughput antibody gene rep-ertoire sequence analysis have extended our capabilities to explore the diversity of antibody specificity and function with unprecedented depth and breadth
This book provides a broad survey of many of the most important aspects of the field of antibodies for infectious diseases The book begins with a general introduction followed by chapters 2 through 5 on general features pertaining to structure function isotype and the role of complement in antibody function Chapters 6 through 10 review contemporary approaches for antibody discovery using phage and yeast display plasma cell and memory B cell cloning human hybridomas humanized mice and computational methods Chapters 11 through 18 review in depth the biology of antibodies specific for particular pathogens including viruses and bacterial toxins to illustrate the role of antibodies in anti- microbial immunity with specific targets These chapters reveal that attempts to raise effective antibody responses to each of these pathogens faces unique and pathogen-specific challenges Chapters 19 to 23 cover major technical advances pertaining to antibody engineering repertoire sequencing and analysis and new methods for study or therapeutic use of antibodies including radiotherapy Fi-nally chapters 24 and 25 cover new methods for expression of monoclonal anti-bodies in plants or by transfer of antibody genes for in vivo expression in treated subjects
Recent literature is exploding with new antibody-related techniques and re-ports of antimicrobial antibodies with unprecedented potency breadth of activ-
xvii
xviii PReface
ity and therapeutic potential We hope that this timely compilation of state-of-the-art reviews of major aspects of this field will be of interest to both antibody cognoscenti and those new to this exciting field We thank the authors for their dedication in producing definitive reviews of the topics at hand
James E Crowe JrDiana BoraschiRino Rappuoli
INTRODUCTION
History and PracticeAntibodies in Infectious Diseases 1ADAM HEY1
Antibodies in Infectious Diseases aims to inform update and inspire studentsteachers researchers pharmaceutical developers and health care professionalson the status of the development of antibody-based therapies for treatinginfectious diseases and the potential for these in times of growing antibioticresistance to provide alternative treatment solutions to the currently usedantibiotics and new treatments for infectious diseases where no propertreatments are available
This introductory article will provide a historical perspective on the useof antibody-based therapies followed by a high-level overview of whatmakes antibodies attractive tools for this purpose This will include the prosand cons of such therapies compared to the use of antibiotics and thepractical and strategic considerations involved in selecting the best formatand development path for new antibody-based therapies targeting specificinfectious agents Then examples of antibody-based therapies in thedevelopment of treatments for infectious diseases will be presented andfinally a look into the future will summarize the different aspects that willinfluence what the future might bring for this type of treatments forinfectious diseases
1Preclinical Safety Biologics Novartis AG Basel Switzerland
Antibodies for Infectious DiseasesEdited by James E Crowe Jr Diana Boraschi and Rino Rappuolicopy 2015 American Society for Microbiology Washington DCdoi101128microbiolspecAID-0026-2014
3
HISTORICAL PERSPECTIVE
Antibodies and the use of passive antibodytherapy in the treatment of infectious dis-eases is the story of a treatment conceptwhich dates back more than 120 years to thelate 19th century and which originally bythe use of serum from immunized animalsprovided the first effective treatment optionsagainst severe bacterial infections (1 2) Byimmunizing horses with bacterial toxinsfrom Clostridium tetani and Corynebacteri-um diphtheriae Emil A Von Behring andShibasaburo Kitasato (3) generated serumcontaining antibodies capable of neutraliz-ing the effects of the toxins produced bythese bacteria and successfully providedtreatment for these serious diseases wherethe pathogenesis is driven by the effects ofthe bacterial toxins For his work on provid-ing treatment for diphtheria Behring re-ceived the Nobel Prize in Physiology orMedicine in 1901 These radical treatmentresults quickly prompted development ofmultiple additional serum therapies for thetreatment of infectious diseases caused byeg Neisseria meningitidis Haemophilus in-fluenza and group A Streptococcus Sinceserum therapy involved administration oflarge amounts of crude mixtures of animalproteins including antibodies they wereassociated with side effects in the form ofhypersensitivity and serum sickness (2)
Due to the crude and unpurified nature ofthese products side effects were seen evenwhen administering human serum prepa-rations Side effects were observed in up to50 of patients and were considered to becaused by immune complex formations thatresulted in symptoms such as rash itchingjoint pain fever and in serious cases hypoten-sion and shock However due to the lack ofalternative options these treatments weredespite their side effects widely used Serumwas normally administered by intravenousinfusion in patients after a test for hypersensi-tivity where a small amount of serum wasinjected subcutaniously (1) As described
above serum therapy applied in these earlydays (late 19th century and early 20th century)involved preparations of serum from rabbitsand horses immunized with the infectiousagent or in live andor neutralized versions ortoxins from these (1) The costs of keeping theimmunized animals and the production andpotency testing of the materials made this arelatively expensive treatment In 1891 datafrom Klemperer (4) showed serum therapy toprotect rabbits from Streptococcus pneumoniaeinfection and paved the way for this type oftreatment and for development of similarserum-based treatments of streptococcal in-fections in humans When treating humansearly administration of serum could reducemortality significantly down to around 5compared to when administered 4 to 5 daysafter onset of symptoms when serum treat-ment was largely without effect This stronglyindicated the need for quick diagnosis andquick treatment to control the infection beforeit got out of control Consequently in theabsence of a specific diagnosis mixtures ofserum from immunizations with differentserotypes were used to circumvent this needfor early treatment without having a serotype-specific diagnosis The understanding thatdifferent serotypes existed for pneumococciand that efficient treatment relied on usingserotype-specific serum was being built upduring the 1920s and 1930s through experiencefrom extensive clinical trials
By the end of the 1930s serum therapywasthe standard of care for treatment of pneu-mococcal pneumonia At that time theefficacy and potency of the derived serawere assessed in mice in ldquothe mouse pro-tection testrdquo by testing survival after aconcomitant intraperitoneal injection of alethal dose of pneumococci and the serum tobe tested Due to the inherent variation inthis test efficacy and survival in two thirds ofthe animals was the acceptance criteria and10 times the lowest dose providing this wasused for defining a unit of the serum Thisallowed for large batch-to-batch variationand the use of different strains of bacteria for
4 HEY
immunization probably explains part of themissing responses observed (1) In the early20th century a pandemic of meningitis inEurope and the United States with mortalityrates up to 80 spurred the development ofserum therapy treatment options Althoughin the 1930s this became the recommendedtreatment in children assumed to be suffer-ing from meningitis failure to reduce mor-tality in several meningitis epidemics duringthat time raised doubts about the generalapplicability of serum treatment In thosedays serum therapy often involved quiteextensive procedures and infusion of largevolumes of serum The following exampleclearly illustrates this Data from Flexnerand Jobling (5) from treating meningitis inmonkeys resulted in the development of serafrom immunized horses for treatment inhumans The treatment protocol includedlumbar puncture and withdrawal of morethan 30 ml of spinal fluid representing anamount slightly larger than the expectedamount of horse serum to be injected subse-quently This treatment involved such dailyslow infusions of up to 30 ml of serum untilthe patientrsquos condition improved This treat-ment was used in outbreaks in New York in1905 and 1906 and did markedly decreasemortality
After the discovery of penicillin by Flemingin 1928 and the subsequent introduction ofantibiotics in the 1930s serum therapy waslargely abandoned over a period of 10 years dueto the availability of these new more broadlyeffective and cheaper treatment optionswhichalso had fewer side effects Although improve-ments in the purification of antibodies hadresulted in preparations with better safety andside effect profiles high manufacturing costsand narrow specificity resulted in antibodytherapy being mostly restricted to a smallernumber of selected treatments for snakevenoms bacterial toxins and some viral infec-tions (1 2) Currently antibody administrationis used for treatment and prevention ofhepatitis B virus rabies virus respiratorysyncytial virus (RSV) Clostridium tetani Clos-
tridium botulinum vaccinia virus echovirusand enterovirus For the most part thesetreatments consist of pooled immunoglobulinalso known as IVIG (intravenous immunoglob-ulin) from several postexposure donors Thisresults in both batch-to-batch variation in theneed for relatively large amounts of serum dueto low specificity and to restricted supplies dueto reliance on exposed donors
However several challengeshave resulted inthe need for new tools in the treatment andpreventionof infectiousdiseasesThebroadandgeneral use of antibiotics in human and veter-inary medicine for many years has resulted inthe development of multi-resistant strains ofbacteria with limited to no response to existingtreatments such as methicillin-resistant Staph-ylococcusaureus (MRSA) vancomycin-resistantS aureus and others This has resulted inpatients needing screening and treatment withseveral antibacterial agents and longer treat-ment time causing extra strain on patients andhealth care providers (6 httpwwwcdcgovdrugresistancethreat-report-2013indexhtml) According to the WHO and CDC morethan 25000 people in European Unioncountries and similar numbers in the UnitedStates die every year as a result of antibiotic-resistant infections This together with theemergence of new pathogens (eg severeacute respiratory syndrome Middle East respi-ratory syndrome) the re-emergenceepidemicsof oldknown pathogens (eg Ebola) and thedifficulties in treating infections in immune-deficient patients (eg HIV patients) has high-lighted the need for new solutions The 2014Ebola epidemic in West Africa (Liberia SierraLeone Guinea Nigeria and Senegal) has fur-ther highlighted this No treatment or prophy-lactic vaccine is available to treat or prevent thespread of Ebola infections which have anaveragemortality of gt50 Local health author-ities in the affected countries are struggling tocontain and handle the disease which isthreatening to go out of control and spreadmorewidelyVariousproductsmainly antibodycocktails from previously recovered patientsare being used despite a lack of clinical data on
CHAPTER 1 bull History and Practice Antibodies in Infectious Diseases 5
their safety and efficacy and those are the onlysporadically available treatment options andonly in small amounts and for a few patients
Ebola is an example of a disease whichnormally affects only a small number ofindividuals and which normally burns outwhen disease outbreaks are contained There-fore given the small number of potentialpatients affected by previous Ebola infectionsto date there was no incentive for big pharmacompanies to do research and development ofdrugs for EbolaWith the increasing number ofinfected (13567) andadeath toll of 4951 (7) andthe lack of the ability to contain the epidemic itwill be interesting to follow the aftermath ofthis outbreak and see whether there will berequests for new ways to ensure that vaccinesand treatment options are available for Ebolaand similar high-mortality and potential bio-warfare infections that have no availabletreatments or procedures to for mass-produc-tion upon the first signsreports of activeinfections Although both the CDC and theWHO have special programs focusing on thesetypes of infections the Ebola outbreak in 2014clearly shows that more financial support forresearch and development of new diagnosticsand treatments is needed This is one examplewhere antibody-based treatments would havethe potential to play a major role To put this inthe right perspective one should however notforget that other infectious diseases such astuberculosis influenza and malaria kill hun-dreds of thousands each year There is there-fore plenty of room for improvement indeveloping treatments for these diseases aswell but the high attention drawn to eg theEbola outbreak creates a special niche andopportunity where antibody treatments couldgain extraordinary development funding andsupport and prove their value and treatmentpotential
That antibody-based therapies could takethis role is supported by the revolution intechnologies for the development selectiongeneration and purification of fully humanantibodies described in more detail later in thesection ldquoMethodsandPlatforms forGenerating
Antibodiesrdquo Antibody-based programs cur-rently at different stages of developmentinclude investigations into the potential use ofsingle antibody preparations combinations ofantibodies (to avoid survival of escape mu-tants) fragments of antibodies and antibodiescarrying radioactive isotopesorcytotoxicdrugsor antibody-like frameworks (eg fibronectin)either alone as a first-line treatment or as anadjunct to existing treatments This multitudeof possible formats the ability to raise anti-bodies to almost any target and the ability toengineer both size effector functions and half-life are now considered by many to providevery valuable tools for designing specificantibody-based treatments toeradicate specifictargeted infectious agents However althoughseveral antibody-based therapies have beenapproved for oncology and anti-inflammatoryindications (see Table 1) only one monoclonalantibody (mAb) is approved against an infec-tious disease agentmdashSynagis (palivizumabMedImmune) for the prevention and treat-ment of respiratory syncytical virus (RSV) inhigh-risk children Economic obstacles such asthe high cost of mAb therapies and relativelysmall markets have resulted in less interestfrom pharmaceutical companies in developingthese Also highlighting the challenges indeveloping these types of antibody-basedtreatments are the difficulties encountered indeveloping a follow-up higher-affinity candi-date to Synagis Poor translatability of dataobtained in the available animal disease mod-els for RSV in cotton rats has resulted in non-approval due to inferiority relative to SynagisIn other viral diseases such as cytomegalovirus(CMV) the high species specificity of thestrains of CMV makes it impossible to testhuman antibody therapies in vivo Thereforeany real data on the efficacy of treatments forCMV will not be obtained until testing inclinical trials As described later in this articleseveral new antibody-based therapies for in-fectious diseases are in development andhopefully this will gradually open the fieldand result in better treatment options andoutcomes for patients
6 HEY
TABLE 1 Approved and pending antibody-based therapies
Name antibody Target antibody type Indication Company Approval date
OKT3a Muronomab-CD3 CD3 murine IgG2a Autoimmune Johnson ampJohnson
1986 (US)
ReoPro abciximab PIIbIIIa chimeric IgG1Fab
Homeostasis Johnson ampJohnson
1984 (US)
Rituxan rituximab CD20 chimeric IgG1 Cancer Genentech 1997 (US) 1998 (EU)Zenapaxa daclizumab CD25 humanized IgG1 Autoimmune Roche 1997 (US) 1999 (EU)Simulect basiliximab CD25 chimeric IgG1 Autoimmune Novartis 1998 (US EU)Synagis palivizumab RSV humanized IgG1 Infections MedImmune 1998 (US) 1999 (EU)Remicade infliximab TNFα chimeric IgG1 Autoimmune Johnson amp
Johnson1998 (US) 1999 (EU)
Herceptin trastuzumab HER2 humanized IgG1 Cancer GenentechRoche
1998 (US) 2000 (EU)
Mylotarga gemtuzumabozogamicin
CD33 humanized IgG4immunotoxin
Cancer WyethPfizer 2000 (US)
Campath alemtuzumab CD52 humanized IgG1 Cancer Genzyme 2001 (US) 2001 (EU)Zevalin ibritumomabtiuxetan
CD20 murine IgG1radiolabeled (yttrium 90)
Cancer Biogen Idec 2002 (US) 2004 (EU)
Humira adalimumab TNFα human IgG1 Autoimmune Abbott 2002 (US) 2003 (EU)Xolair omalizumab IgE humanized IgG1 Autoimmune Genentech
Roche2003 (US)
Bexxar tositumomab-I-131 CD20 murine IgG2aradiolabeled (iodine131)
Cancer CorixaGSK 2003 (US)
Raptivaa falizumab CD11a humanized IgG1 Autoimmune GenentechRoche
2003 (US) 2004 (EU)
Erbitux cetuximab EGFR chimeric IgG1 Cancer ImcloneLilly 2004 (US) 2004 (EU)Avastin bevacizumab VEGF humanized IgG1 Cancer Genentech
Roche2004 (US) 2005 (EU)
Tysabri natalizumab α4-Intergrin humanizedIgG4
Autoimmune Biogen Idec 2004 (US)
Actemra tocilizumab Anti-IL-6R humanizedIgG1
Autoimmune ChugaiRoche
2005 (Japan) 2010 (US)
Vectibix panitumumab EGFR human IgG2 Cancer Amgen 2006 (US)Lucentis ranibizumab VEGF humanized IgG1
FabMaculardegeneration
GenentechRoche
2006 (US)
Soliris eculizumab C5 humanized IgG24 Blood disorders Alexion 2007 (US)Cimzia certolizumab pegol TNFα humanized
pegylated FabAutoimmune UCB 2008 (US)
Simponi golimumab TNFα human IgG1 Autoimmune Johnson ampJohnson
2009 (US EU Canada)
Ilaris canakinumab IL1b human IgG1 Infalmmatory Novartis 2009 (US EU)Stelara ustekinumab IL-1223 human IgG1 Autoimmune Johnson amp
Johnson2008 (EU) 2009 (US)
Arzerra ofatumumab CD20 human IgG1 Cancer Genmab 2009 (EU)Prolia denosumab RANK ligand human
IgG2Bone loss Amgen 2010 (US)
Numax motavizumab RSV humanized IgG1 Anti-infective MedImmune PendingABthrax Raxibacumab B anthrasis PA human
IgG1Anti-infection GSK 2012 (US)
Benlysta belimumab BLyS human IgG1 Autoimmune HGS 2011 (US)Yervoy ipilimumab CTLA-4 human IgG1 Cancer BMS 2011 (US)Adcetris brentuximabvedotin
CD30 chimeric IgG1drug- conjugate
Cancer SeattleGenetics
2011 (US)
(Continued on next page)
CHAPTER 1 bull History and Practice Antibodies in Infectious Diseases 7
INTRODUCTION TO ANTIBODIES
Antibodies also called immunoglobulins basedon their combined structure and function inimmune responses are produced by B cells ofthe immune system They are part of theadaptive immune response and are speciallydesigned for neutralizing and eliminating theinfectious agents and toxins produced by theseAntibodies are present in blood plasma andextracellular fluids and since these fluids wereformerly known as humors they were said tobe part of the humoral immune responseAntibodies are Y-shaped structures consistingof two main parts the upper arms of the Ywhich contain two identical variable-regionantigen binding sites and the lower regioncalled the constant regionwhich is responsiblefor the initiation of effector functions that leadto the removal and destruction of the pathogenor cells harboring the pathogen (see Fig 1) Theantigen-binding sites on an antibody can bythemselves bind to and neutralize bacterialtoxins and viruses thereby preventing themfrom binding to their target cells or receptorscausing toxic effects or spread of the infection
Antibodies consist of two pairs of heavy andlight chainswhich as described above are heldtogether in a Y-shaped arrangement Each ofthe heavy and light chains in these pairs isseparated into constant and variable chainsThe upper armsof theY each contain a variableand a constant sectionof the light and theheavychain where the upper variable parts of theheavy and light chains contain the antigen-binding site and the constant parts areconnected via disulfide bonds The lower partof theYcalled theconstantpart consistsof twoor three constant segments (immunoglobulindomains) from each of the two heavy chainsinteracting and also linked via disulfide bondsThe sectionsof theheavy chains connecting theconstant part of the upper arms to the constantparts of the constant region contain specialhinge regions that provide flexibility to thedifferent sections of the antibody to bind toantigens and effector cells The constant re-gions of the heavy chain also contain attachedoligosaccharide moieties which provide func-tional specialization to the antibodies (8)
The variable domains of the heavy and lightchains form the antigen-binding sites and
TABLE 1 Approved and pending antibody-based therapies (Continued)
Name antibody Target antibody type Indication Company Approval date
Perjeta pertuzumab Her2 humanized IgG1 Cancer GenentechRoche
2012 (US)
Kadcyla ado-trastuzumabemtansine
Her2 humanized IgG1Drug-conjugate
Cancer GenentechRoche
2013 (US)
Raxibacumab Anti-B anthrasis PAhuman IgG1
Anthraxinfection
Notapproved
2012
Entyvio vedolizumab Integrin α4β7humanized IgG1
Crohnrsquos diseaseulcerative colitis
Takeda 2014 (US)
Cyramza ramuciruumab Anti-VEGFR2Human IgG1
Gastric cancer Lilly 2014 (US)
Gazyva obinutuzumab Anti-CD20 humanizedIgG1 glucoengineered
CancerCLLb GenentechRoche
2014 (US)
Sylvant situximab Anti IL-6 chimeric IgG1 Castlemandisease
Janssen 2014 (US) 2014 (EU)
Cosentyx sekukinumab Anti IL-17a human IgG1 Psoriasis Novartis 2015 (US) 2015 (EU)Nivolumab Anti PD-1 human IgG4 Melanoma BMS Not approvedKeytruda pembrolizuumab Anti-PD-1 humanized
IgG4Melanoma Merck 2014 (US)
aAntibodies approved but later withdrawnbCLL chronic lymphocytic leukemia
8 HEY
FIGURE 1 (Left panel) Model of antibody structure exemplified by IgG On top the antigen-binding sitesin orange each contain one variable light and variable heavy domain with the three complementaritydetermining regions (CDRs) that are responsible for the specific binding of the antibody to its target Foreach arm of the antibody an additional set of variable heavy and light domains together with the CDR-containing domains represent the two fragment antigen binding (Fab) regions The two Fabs are heldtogether via two disulfide bridges Below the Fabs is the Fc region which contains four constant heavydomains On the upper pair of these domains are binding sites for oligosaccharides which have majorimportance for the ability of the antibody Fc part to trigger effector functions when the Fc portion isbound to Fc gamma receptors on natural killer cells neutrophil granulocytes monocytesmacrophagesdendritic cells and B cells (Right panel) Examples of some of the antibody-derived alternative formatsused to exploit the specific features of the CDRs the Fabs and the Fc parts of the antibodies ScFv Thesingle chain fragment variable consists of the variable domains of the heavy and light chains heldtogether by a flexible linker This can also be used as a carrier of a cytotoxic drug in a so-called antibodydrug complex (ADC) where the specificity of the ScFv is used to target the cytotoxic drug to eg atumor Bite (bi-specific T cell engager) Fusion proteins consisting of two ScFvs one directed against thetarget on a tumor cell and the other against the T cell receptor (CD3) Diabody ScFv dimers where shortlinker peptides (five amino acids) ensure dimerization and not folding of the ScFvs Fab and F(ab)2fragments Single Fab fragments or fragments containing two Fabs linked via disulfide bridges This isused where effector functions related to the Fc part of the antibody are unwanted and where a smallersize is desired to obtain better tissue penetration in eg tumors Due to the lack of the FcRn binding viathe Fc part Fab and F(ab)2 fragments have much shorter half-lives (hours or days) than full-sizeantibodies (weeks) These can also be used as carriers of cytotoxic payloads or cytotoxic radioactiveisotopes and for the F(ab)2 fragments can be constructed as bi-specifics which can cross-link immunecells and target cells Fc fusion protein Fusion protein containing the Fc domain of an immunoglobulinbound to a peptide The peptide can be a ligand for a specific receptor on a target cell or a blockingpeptide for a soluble ligand The Fc part provides a longer half-life to the construct and the potential tobind to and engage effector functions in the killing of eg tumor cells or infected cells ADCsRIAs andbi-specifics Full-size IgG antibodies carrying either a cytotoxic chemical or radioactive payload whichmay also carry different CDRs enabling cross-linking of effector and target cells for increased killingdoi101128microbiolspecAID-0026-2014f1
CHAPTER 1 bull History and Practice Antibodies in Infectious Diseases 9
contain special hyper-variable segments calledcomplementarity-determining regions (CDRs)which allow the B cells via genetic recom-bination to generate antibodies to all thedifferent antigens specific to amino acid se-quences or three-dimensional structuralmotifs(polysaccharides DNA and RNA) found onpathogens
Based on the structure of their heavy chainconstant regions antibodies or immuno-globulins are separated into five classesmdashIgM IgG IgE IgD and IgA Differences inthe sequences of the constant regions providedistinct characteristics to these different clas-ses These characteristics include the numberof heavy chain constant segments the numberand location of interconnecting disulfidebridges the length of the hinge region andthe number and location of oligosaccharidemoieties For IgG four heavy chain versionsexist creating IgG1 2 3 and 4 isotypes eachwith different characteristics in their serumhalf-lives and ability to trigger different effec-tor functions Because of the combined ad-vantage from ability to trigger effectormechanisms long [21 days] half-life theirability to be transported over the placentaand their stability in the production processantibodies of the IgG class and of the IgG1isotype are preferred as the basis for newantibody-based therapies The effector func-tions are triggered by the Fc part of an antibodywhen the variable parts of the antibody arebound directly to an infectious agent or toproteins from an infectious agent expressed onan infected cell This binding leaves the Fc partfree to interactwithFc receptors onphagocyticcells and neutrophils eosinophils and naturalkiller cells capable of inducing phagocytosis orlysis of infectious agents or infected cellsThese effector functions include (i) the abilityto activate the complement system for lysis(complement-dependent cellular cytotoxicity)(ii) triggering of uptake and destruction byphagocytic cells such as macrophages andneutrophils via interaction with Fc receptorson these cells (iii) activation of macrophageseosinophils neutrophils and natural killer
cells to kill infected cells via binding to Fcreceptors on these cells and antibody-depen-dent cellular cytotoxicity and (iv) neutraliza-tion of bacterial toxins and blocking of bindingand uptake of bacteria or viruses to target cells(see Fig 2) (9)
The Fcpart of IgG antibodies also contains aregion that interacts with the neonatal Fcreceptor (FcRn) expressed on most immuno-competent cells and inmany other cells such asendothelial cells in kidney liver placenta lungand breast (10) which protects antibodies fromdegradation by phagocytoticexocytotic cy-cling into FcRn-expressing cells thereby pro-longing their half-life This results in half-livesof 20 to 21 days for most IgG1 2 and 4antibodies whereas half-lives are 10 6 and 2days respectively for IgM IgA and IgE Thehighly specific binding sites on the variableregions of the upper arms of the antibody allowfor several important features of antibodiesndashbinding to and neutralization of eg bacterialtoxins binding to pathogens and blocking theirbinding to or interaction with target cells (egcyncytia formation of CMV-infected cells) orblocking of binding and interactions of infec-tious agents with target cells via blockingreceptors on the target cells
METHODS AND PLATFORMS FORGENERATING ANTIBODIES
As described above the early use of passiveantibody transfer as a therapy in infectiousdiseases involved the use of immune serumfrom immunized sheep and horses These pre-parations were crude and contained a broadmixture of neutralizing and non-neutralizingantibodies and both the foreign nature of theantibodies and the numerous host serumproteins This resulted in less specific andthus less efficient therapies due to a highvariability in efficacy between batches derivedfrom different animals immunized with dif-ferent strains of bacteria in different labor-atories and resulted in multiple unwantedside effects related to hypersensitivity and
10 HEY
anaphylactic reactions to foreign proteinsThese days antibodies being developed fortreatment of diseases in humans are highlypurified and are mostly fully human mono-clonal antibodies The term monoclonal anti-body refers to that cell cultures used forgenerating these antibodies each originatesfrom a single cell and thus produces onlyone specific antibody Development of fullyhuman monoclonal antibodies happened instages over a time span of more than 15 yearsFirst stage in this process was generation ofmonoclonalmurine IgG antibodies (eg OKT3[muronomab-CD3 Johnson and Johnson] ap-proved in 1986) Next stage was generation ofso called chimeric antibodies consisting ofhuman heavy and light chain constant sec-tions but with murine variable sections (eg
Rituxan [rituximab Genentech]) Next stagewas then the humanized antibodies wherethe only remaining murine part of the anti-body is the antigen-binding CDR (eg Xolair[omalizumab NovartisGenentech]) Both thefirst chimeric and humanized antibodies wereapproved in the late 1990s Then finally 16years later the first fully human antibodyHumira (adalimumab Abbott) was approvedin 2002 Since the time of the crude and low-scale manufacturing of the original antibodyserum products much has changed andtherapeutic antibodies are now produced byfermentation in 5000 liter scale using highlycontrolled and documented yeast or mamma-lian cell lines that are genetically engineered toexpress a single specific antibody This hasresulted in a pure and highly specific antibody
FIGURE 2 Effector functions of antibodies (a) Antibodies bind to pathogen-derived or endogenousantigens expressed on the surface of an infected cell which triggers binding to Fc receptors on naturalkiller cells and lysis of the infected cell by antibody-dependent cellular cytotoxicity (b) Antibodies bindto pathogen-derived or endogenous antigens expressed on the surface of infected cells which triggersactivation of complement through binding of complement factor C1q (c) Neutralization Top Bacterialtoxin neutralized by bound antigen Bottom Antibody bound to either receptor for the virus or to thevirus itself which blocks virus binding and entry into the cell (d) Antibody bound to viral surfaceproteins binds to Fc receptors on phagocytic cells eg macrophages and triggers endocytosis anddestruction of virus in endolysosome doi101128microbiolspecAID-0026-2014f2
CHAPTER 1 bull History and Practice Antibodies in Infectious Diseases 11

x contRIBUtoRs
Ekaterina (Kate) DadachovaDepartments of Radiology Microbiology and ImmunologyAlbert Einstein College of Medicine of Yeshiva University1695A Eastchester RoadBronx NY 10461
Donald N ForthalDepartment of Infectious Diseases3044 Hewitt HallUniversity of California IrvineIrvine CA 92617
Manuel A FrancoFacultad de Ciencias y MedicinaPontificia Universidad JaverianaOficina 306 Edificio 50Carrera 7 40-62BogotaacuteColombia
Bettina C FriesDepartment of MedicineInfectious Diseases and Department of Microbiology and ImmunologyAlbert Einstein College of MedicineBronx NY 10461
Zachary P FryeDepartment of Chemical EngineeringUniversity of Texas at AustinAustin TX 78712
Amy E GilbertCutaneous Medicine and Immunotherapy UnitSt Johnrsquos Institute of DermatologyDivision of Genetics and Molecular Medicine amp NIHR Biomedical Research Centre at Guyrsquos and St Thomasrsquos Hospitals and Kingrsquos College London School of MedicineGuyrsquos HospitalLondon SE1 9RTUnited Kingdom
Hannah J GouldRandall Division of Cell and Molecular BiophysicsDivision of Asthma Allergy and Lung BiologyMRC and Asthma UK Centre for Allergic Mechanisms of AsthmaKingrsquos College LondonNew Huntrsquos HouseGuyrsquos CampusLondon SE1 1ULUnited Kingdom
contRIBUtoRs xi
Harry B GreenbergDepartments of Medicine and Microbiology and ImmunologyStanford University School of Medicine and the VAPAHCSPalo Alto CA 94305
Scott B HalsteadDepartment of Preventive Medicine and BiometricsUniformed Services University of the Health SciencesBethesda MD 20814
Shen Y HelvigDepartment of PharmacyCenter for Pharmaceutical Nanotechnology and NanotoxicologyFaculty of Health and Medical SciencesUniversity of CopenhagenCopenhagen DK-2100Denmark
Adam HeyPreclinical Safety BiologicsNovartis AGBaselSwitzerland
Andrew HiattMapp Biopharmaceutical Inc6160 Lusk Blvd C105San Diego CA 92121
Bjoumlrn HockDepartment of Protein Engineering and Antibody TechnologiesMerck Serono Merck KgaAFrankfurter Str 250D-64293 DarmstadtGermany
Kelly HuangDepartment of Infectious DiseaseMedImmune LLCOne MedImmune WayGaithersburg MD 20878
Philip R JohnsonThe Childrenrsquos Hospital of PhiladelphiaAbramson Research CenterPhiladelphia PA 19104
Debra H JosephsCutaneous Medicine and Immunotherapy UnitSt Johnrsquos Institute of DermatologyDivision of Genetics and Molecular Medicine amp NIHR Biomedical Research Centre at Guyrsquos and St Thomasrsquos HospitalsKingrsquos College London School of MedicineGuyrsquos HospitalLondon SE1 9RTUnited Kingdom
Shilpa A JoshiDepartment of PathologyStanford UniversityStanford CA 94305
Sophia N KaragiannisCutaneous Medicine and Immunotherapy UnitSt Johnrsquos Institute of DermatologyDivision of Genetics and Molecular Medicine amp NIHR Biomedical Research Centre at Guyrsquos and St Thomasrsquos HospitalsKingrsquos College London School of MedicineGuyrsquos HospitalLondon SE1 9RTUnited Kingdom
Panagiotis KaragiannisCutaneous Medicine and Immunotherapy UnitSt Johnrsquos Institute of DermatologyDivision of Genetics and Molecular Medicine amp NIHR Biomedical Research Centre at Guyrsquos and St Thomasrsquos HospitalsKingrsquos College London School of MedicineGuyrsquos HospitalLondon SE1 9RTUnited Kingdom
Jens C KrauseChildrenrsquos HospitalUniversity of Freiburg Medical Center79106 FreibergGermany
Antonio LanzavecchiaInstitute for Research in Biomedicinevia Vincenzo Vela 6Bellinzona 6500Switzerland
xii contRIBUtoRs
Marie-Paule LefrancLaboratoire drsquoImmunoGeacuteneacutetique Moleacuteculaire LIGMIMGTreg the international ImMunoGeneTics information systemregInstitut de Geacuteneacutetique Humaine IGHUniversiteacute Montpellier 2UPR CNRS 1142Montpellier 34396 cedex 5 40202France
Olivier LegerDepartment of Protein Engineering and Antibody TechnologiesMerck Serono SA--Geneva9 chemin des Mines1202 GenevaSwitzerland
Kin-Ming LoDepartment of Protein Engineering and Antibody TechnologiesEMD Serono Research Institute45A Middlesex TurnpikeBillerica MA 01821
Wayne A MarascoDepartment of Cancer Immunology and AIDSDana-Farber Cancer InstituteHarvard Medical SchoolBoston MA 02215
Jennifer A MaynardDepartment of Chemical EngineeringUniversity of Texas at AustinAustin TX 78712
Luzia M MayrINSERM U1109Universiteacute de Strasbourg3 Rue Koeberleacute67000 StrasbourgFrance
Jens MeilerDepartment of Chemistry and Center for Structural BiologyVanderbilt UniversityNashville TN 37212
contRIBUtoRs xiii
S Moein MoghimiDepartment of PharmacyCenter for Pharmaceutical Nanotechnology and NanotoxicologyFaculty of Health and Medical SciencesUniversity of CopenhagenCopenhagen DK-2100Denmark
Susan Zolla-PaznerNew York University School of Medicine550 First AvenueNew York NY 10016
Louise SaulCutaneous Medicine and Immunotherapy UnitSt Johnrsquos Institute of DermatologyDivision of Genetics and Molecular Medicine amp NIHR Biomedical Research Centre at Guyrsquos and St Thomasrsquos HospitalsKingrsquos College London School of MedicineGuyrsquos HospitalLondon SE1 9RTUnited Kingdom
Bruce C SchneppThe Childrenrsquos Hospital of PhiladelphiaAbramson Research CenterPhiladelphia PA 19104
Jennifer E SchusterDepartment of PediatricsChildrenrsquos Mercy HospitalKansas City MO 64108-4619
Alexander M SevyDepartment of Chemistry and Center for Structural BiologyVanderbilt UniversityNashville TN 37212
Jared SheehanDepartment of Cancer Immunology and AIDSDana-Farber Cancer InstituteHarvard Medical SchoolBoston MA 02215
Michael R SierksDepartment of Chemical EngineeringArizona State UniversityTempe AZ 85287-6006
xiv contRIBUtoRs
Scott A SmithThe Vanderbilt Vaccine Center and the Department of MedicineVanderbilt University Medical CenterNashville TN 37232
Robyn L StanfieldDepartment of Molecular BiologyThe Scripps Research Institute10550 North Torrey Pines RoadLa Jolla CA 92037
Nadine UptonRandall Division of Cell and Molecular BiophysicsDivision of Asthma Allergy and Lung BiologyMRC and Asthma UK Centre for Allergic Mechanisms of AsthmaKingrsquos College LondonNew Huntrsquos HouseGuyrsquos CampusLondon SE1 1ULUnited Kingdom
Avanish K VarshneyDepartment of MedicineInfectious Diseases and Department of Microbiology and ImmunologyAlbert Einstein College of MedicineBronx NY 10461
Stefanie N VelgosMayo Clinic Arizona5777 East Mayo BoulevardPhoenix AZ 85054
Kevin J WhaleyMapp Biopharmaceutical Inc6160 Lusk Blvd C105San Diego CA 92121
Peter P WibroeCentre for Pharmaceutical Nanotechnology and NanotoxicologyDepartment of PharmacyFaculty of Health and Medical SciencesUniversity of CopenhagenCopenhagen DK-2100Denmark
John V WilliamsDepartment of PediatricsSchool of MedicineVanderbilt UniversityNashville TN 37232-2581
contRIBUtoRs xv
Ian A WilsonDepartment of Molecular Biology and Skaggs Institute for Chemical BiologyThe Scripps Research Institute10550 North Torrey Pines RoadLa Jolla CA 92037
Herren WuDepartment of Antibody Discovery and Protein EngineeringMedImmune LLCOne MedImmune WayGaithersburg MD 20879
Guocheng YangDepartment of Chemical EngineeringArizona State UniversityTempe AZ 85287-6006
Larry ZeitlinMapp Biopharmaceutical Inc6160 Lusk Blvd C105San Diego CA 92121
xvi contRIBUtoRs
Preface
Antibodies form the principal foundation for modern intervention against in-fectious diseases Emil Adolf von Behring was awarded the first Nobel Prize in Physiology or Medicine in 1901 ldquofor his work on serum therapy especially its appli-cation against diphtheria by which he has opened a new road in the domain of med-ical science and thereby placed in the hands of the physician a victorious weapon against illness and deathsrdquo Antibodies now provide the focus for understanding mechanisms of immunity to most infectious diseases and they play a central role in passive immunotherapy and active vaccination as mechanisms or correlates of immunity For most of the 20th century immunotherapy was based on passive transfer of polyclonal hyperimmune animal serum immune human serum or even hyperimmune human serum Georges JF Koumlhler and Ceacutesar Milstein re-ported the generation of monoclonal antibodies in 1979 for which they shared the 1984 Nobel Prize in Physiology or Medicine ldquofor the discovery of the princi-ple for production of monoclonal antibodiesrdquo Since that time entire fields related to antibodies for infectious diseases including antibody gene cloning engineer-ing and expression antibody libraries and high-throughput antibody gene rep-ertoire sequence analysis have extended our capabilities to explore the diversity of antibody specificity and function with unprecedented depth and breadth
This book provides a broad survey of many of the most important aspects of the field of antibodies for infectious diseases The book begins with a general introduction followed by chapters 2 through 5 on general features pertaining to structure function isotype and the role of complement in antibody function Chapters 6 through 10 review contemporary approaches for antibody discovery using phage and yeast display plasma cell and memory B cell cloning human hybridomas humanized mice and computational methods Chapters 11 through 18 review in depth the biology of antibodies specific for particular pathogens including viruses and bacterial toxins to illustrate the role of antibodies in anti- microbial immunity with specific targets These chapters reveal that attempts to raise effective antibody responses to each of these pathogens faces unique and pathogen-specific challenges Chapters 19 to 23 cover major technical advances pertaining to antibody engineering repertoire sequencing and analysis and new methods for study or therapeutic use of antibodies including radiotherapy Fi-nally chapters 24 and 25 cover new methods for expression of monoclonal anti-bodies in plants or by transfer of antibody genes for in vivo expression in treated subjects
Recent literature is exploding with new antibody-related techniques and re-ports of antimicrobial antibodies with unprecedented potency breadth of activ-
xvii
xviii PReface
ity and therapeutic potential We hope that this timely compilation of state-of-the-art reviews of major aspects of this field will be of interest to both antibody cognoscenti and those new to this exciting field We thank the authors for their dedication in producing definitive reviews of the topics at hand
James E Crowe JrDiana BoraschiRino Rappuoli
INTRODUCTION
History and PracticeAntibodies in Infectious Diseases 1ADAM HEY1
Antibodies in Infectious Diseases aims to inform update and inspire studentsteachers researchers pharmaceutical developers and health care professionalson the status of the development of antibody-based therapies for treatinginfectious diseases and the potential for these in times of growing antibioticresistance to provide alternative treatment solutions to the currently usedantibiotics and new treatments for infectious diseases where no propertreatments are available
This introductory article will provide a historical perspective on the useof antibody-based therapies followed by a high-level overview of whatmakes antibodies attractive tools for this purpose This will include the prosand cons of such therapies compared to the use of antibiotics and thepractical and strategic considerations involved in selecting the best formatand development path for new antibody-based therapies targeting specificinfectious agents Then examples of antibody-based therapies in thedevelopment of treatments for infectious diseases will be presented andfinally a look into the future will summarize the different aspects that willinfluence what the future might bring for this type of treatments forinfectious diseases
1Preclinical Safety Biologics Novartis AG Basel Switzerland
Antibodies for Infectious DiseasesEdited by James E Crowe Jr Diana Boraschi and Rino Rappuolicopy 2015 American Society for Microbiology Washington DCdoi101128microbiolspecAID-0026-2014
3
HISTORICAL PERSPECTIVE
Antibodies and the use of passive antibodytherapy in the treatment of infectious dis-eases is the story of a treatment conceptwhich dates back more than 120 years to thelate 19th century and which originally bythe use of serum from immunized animalsprovided the first effective treatment optionsagainst severe bacterial infections (1 2) Byimmunizing horses with bacterial toxinsfrom Clostridium tetani and Corynebacteri-um diphtheriae Emil A Von Behring andShibasaburo Kitasato (3) generated serumcontaining antibodies capable of neutraliz-ing the effects of the toxins produced bythese bacteria and successfully providedtreatment for these serious diseases wherethe pathogenesis is driven by the effects ofthe bacterial toxins For his work on provid-ing treatment for diphtheria Behring re-ceived the Nobel Prize in Physiology orMedicine in 1901 These radical treatmentresults quickly prompted development ofmultiple additional serum therapies for thetreatment of infectious diseases caused byeg Neisseria meningitidis Haemophilus in-fluenza and group A Streptococcus Sinceserum therapy involved administration oflarge amounts of crude mixtures of animalproteins including antibodies they wereassociated with side effects in the form ofhypersensitivity and serum sickness (2)
Due to the crude and unpurified nature ofthese products side effects were seen evenwhen administering human serum prepa-rations Side effects were observed in up to50 of patients and were considered to becaused by immune complex formations thatresulted in symptoms such as rash itchingjoint pain fever and in serious cases hypoten-sion and shock However due to the lack ofalternative options these treatments weredespite their side effects widely used Serumwas normally administered by intravenousinfusion in patients after a test for hypersensi-tivity where a small amount of serum wasinjected subcutaniously (1) As described
above serum therapy applied in these earlydays (late 19th century and early 20th century)involved preparations of serum from rabbitsand horses immunized with the infectiousagent or in live andor neutralized versions ortoxins from these (1) The costs of keeping theimmunized animals and the production andpotency testing of the materials made this arelatively expensive treatment In 1891 datafrom Klemperer (4) showed serum therapy toprotect rabbits from Streptococcus pneumoniaeinfection and paved the way for this type oftreatment and for development of similarserum-based treatments of streptococcal in-fections in humans When treating humansearly administration of serum could reducemortality significantly down to around 5compared to when administered 4 to 5 daysafter onset of symptoms when serum treat-ment was largely without effect This stronglyindicated the need for quick diagnosis andquick treatment to control the infection beforeit got out of control Consequently in theabsence of a specific diagnosis mixtures ofserum from immunizations with differentserotypes were used to circumvent this needfor early treatment without having a serotype-specific diagnosis The understanding thatdifferent serotypes existed for pneumococciand that efficient treatment relied on usingserotype-specific serum was being built upduring the 1920s and 1930s through experiencefrom extensive clinical trials
By the end of the 1930s serum therapywasthe standard of care for treatment of pneu-mococcal pneumonia At that time theefficacy and potency of the derived serawere assessed in mice in ldquothe mouse pro-tection testrdquo by testing survival after aconcomitant intraperitoneal injection of alethal dose of pneumococci and the serum tobe tested Due to the inherent variation inthis test efficacy and survival in two thirds ofthe animals was the acceptance criteria and10 times the lowest dose providing this wasused for defining a unit of the serum Thisallowed for large batch-to-batch variationand the use of different strains of bacteria for
4 HEY
immunization probably explains part of themissing responses observed (1) In the early20th century a pandemic of meningitis inEurope and the United States with mortalityrates up to 80 spurred the development ofserum therapy treatment options Althoughin the 1930s this became the recommendedtreatment in children assumed to be suffer-ing from meningitis failure to reduce mor-tality in several meningitis epidemics duringthat time raised doubts about the generalapplicability of serum treatment In thosedays serum therapy often involved quiteextensive procedures and infusion of largevolumes of serum The following exampleclearly illustrates this Data from Flexnerand Jobling (5) from treating meningitis inmonkeys resulted in the development of serafrom immunized horses for treatment inhumans The treatment protocol includedlumbar puncture and withdrawal of morethan 30 ml of spinal fluid representing anamount slightly larger than the expectedamount of horse serum to be injected subse-quently This treatment involved such dailyslow infusions of up to 30 ml of serum untilthe patientrsquos condition improved This treat-ment was used in outbreaks in New York in1905 and 1906 and did markedly decreasemortality
After the discovery of penicillin by Flemingin 1928 and the subsequent introduction ofantibiotics in the 1930s serum therapy waslargely abandoned over a period of 10 years dueto the availability of these new more broadlyeffective and cheaper treatment optionswhichalso had fewer side effects Although improve-ments in the purification of antibodies hadresulted in preparations with better safety andside effect profiles high manufacturing costsand narrow specificity resulted in antibodytherapy being mostly restricted to a smallernumber of selected treatments for snakevenoms bacterial toxins and some viral infec-tions (1 2) Currently antibody administrationis used for treatment and prevention ofhepatitis B virus rabies virus respiratorysyncytial virus (RSV) Clostridium tetani Clos-
tridium botulinum vaccinia virus echovirusand enterovirus For the most part thesetreatments consist of pooled immunoglobulinalso known as IVIG (intravenous immunoglob-ulin) from several postexposure donors Thisresults in both batch-to-batch variation in theneed for relatively large amounts of serum dueto low specificity and to restricted supplies dueto reliance on exposed donors
However several challengeshave resulted inthe need for new tools in the treatment andpreventionof infectiousdiseasesThebroadandgeneral use of antibiotics in human and veter-inary medicine for many years has resulted inthe development of multi-resistant strains ofbacteria with limited to no response to existingtreatments such as methicillin-resistant Staph-ylococcusaureus (MRSA) vancomycin-resistantS aureus and others This has resulted inpatients needing screening and treatment withseveral antibacterial agents and longer treat-ment time causing extra strain on patients andhealth care providers (6 httpwwwcdcgovdrugresistancethreat-report-2013indexhtml) According to the WHO and CDC morethan 25000 people in European Unioncountries and similar numbers in the UnitedStates die every year as a result of antibiotic-resistant infections This together with theemergence of new pathogens (eg severeacute respiratory syndrome Middle East respi-ratory syndrome) the re-emergenceepidemicsof oldknown pathogens (eg Ebola) and thedifficulties in treating infections in immune-deficient patients (eg HIV patients) has high-lighted the need for new solutions The 2014Ebola epidemic in West Africa (Liberia SierraLeone Guinea Nigeria and Senegal) has fur-ther highlighted this No treatment or prophy-lactic vaccine is available to treat or prevent thespread of Ebola infections which have anaveragemortality of gt50 Local health author-ities in the affected countries are struggling tocontain and handle the disease which isthreatening to go out of control and spreadmorewidelyVariousproductsmainly antibodycocktails from previously recovered patientsare being used despite a lack of clinical data on
CHAPTER 1 bull History and Practice Antibodies in Infectious Diseases 5
their safety and efficacy and those are the onlysporadically available treatment options andonly in small amounts and for a few patients
Ebola is an example of a disease whichnormally affects only a small number ofindividuals and which normally burns outwhen disease outbreaks are contained There-fore given the small number of potentialpatients affected by previous Ebola infectionsto date there was no incentive for big pharmacompanies to do research and development ofdrugs for EbolaWith the increasing number ofinfected (13567) andadeath toll of 4951 (7) andthe lack of the ability to contain the epidemic itwill be interesting to follow the aftermath ofthis outbreak and see whether there will berequests for new ways to ensure that vaccinesand treatment options are available for Ebolaand similar high-mortality and potential bio-warfare infections that have no availabletreatments or procedures to for mass-produc-tion upon the first signsreports of activeinfections Although both the CDC and theWHO have special programs focusing on thesetypes of infections the Ebola outbreak in 2014clearly shows that more financial support forresearch and development of new diagnosticsand treatments is needed This is one examplewhere antibody-based treatments would havethe potential to play a major role To put this inthe right perspective one should however notforget that other infectious diseases such astuberculosis influenza and malaria kill hun-dreds of thousands each year There is there-fore plenty of room for improvement indeveloping treatments for these diseases aswell but the high attention drawn to eg theEbola outbreak creates a special niche andopportunity where antibody treatments couldgain extraordinary development funding andsupport and prove their value and treatmentpotential
That antibody-based therapies could takethis role is supported by the revolution intechnologies for the development selectiongeneration and purification of fully humanantibodies described in more detail later in thesection ldquoMethodsandPlatforms forGenerating
Antibodiesrdquo Antibody-based programs cur-rently at different stages of developmentinclude investigations into the potential use ofsingle antibody preparations combinations ofantibodies (to avoid survival of escape mu-tants) fragments of antibodies and antibodiescarrying radioactive isotopesorcytotoxicdrugsor antibody-like frameworks (eg fibronectin)either alone as a first-line treatment or as anadjunct to existing treatments This multitudeof possible formats the ability to raise anti-bodies to almost any target and the ability toengineer both size effector functions and half-life are now considered by many to providevery valuable tools for designing specificantibody-based treatments toeradicate specifictargeted infectious agents However althoughseveral antibody-based therapies have beenapproved for oncology and anti-inflammatoryindications (see Table 1) only one monoclonalantibody (mAb) is approved against an infec-tious disease agentmdashSynagis (palivizumabMedImmune) for the prevention and treat-ment of respiratory syncytical virus (RSV) inhigh-risk children Economic obstacles such asthe high cost of mAb therapies and relativelysmall markets have resulted in less interestfrom pharmaceutical companies in developingthese Also highlighting the challenges indeveloping these types of antibody-basedtreatments are the difficulties encountered indeveloping a follow-up higher-affinity candi-date to Synagis Poor translatability of dataobtained in the available animal disease mod-els for RSV in cotton rats has resulted in non-approval due to inferiority relative to SynagisIn other viral diseases such as cytomegalovirus(CMV) the high species specificity of thestrains of CMV makes it impossible to testhuman antibody therapies in vivo Thereforeany real data on the efficacy of treatments forCMV will not be obtained until testing inclinical trials As described later in this articleseveral new antibody-based therapies for in-fectious diseases are in development andhopefully this will gradually open the fieldand result in better treatment options andoutcomes for patients
6 HEY
TABLE 1 Approved and pending antibody-based therapies
Name antibody Target antibody type Indication Company Approval date
OKT3a Muronomab-CD3 CD3 murine IgG2a Autoimmune Johnson ampJohnson
1986 (US)
ReoPro abciximab PIIbIIIa chimeric IgG1Fab
Homeostasis Johnson ampJohnson
1984 (US)
Rituxan rituximab CD20 chimeric IgG1 Cancer Genentech 1997 (US) 1998 (EU)Zenapaxa daclizumab CD25 humanized IgG1 Autoimmune Roche 1997 (US) 1999 (EU)Simulect basiliximab CD25 chimeric IgG1 Autoimmune Novartis 1998 (US EU)Synagis palivizumab RSV humanized IgG1 Infections MedImmune 1998 (US) 1999 (EU)Remicade infliximab TNFα chimeric IgG1 Autoimmune Johnson amp
Johnson1998 (US) 1999 (EU)
Herceptin trastuzumab HER2 humanized IgG1 Cancer GenentechRoche
1998 (US) 2000 (EU)
Mylotarga gemtuzumabozogamicin
CD33 humanized IgG4immunotoxin
Cancer WyethPfizer 2000 (US)
Campath alemtuzumab CD52 humanized IgG1 Cancer Genzyme 2001 (US) 2001 (EU)Zevalin ibritumomabtiuxetan
CD20 murine IgG1radiolabeled (yttrium 90)
Cancer Biogen Idec 2002 (US) 2004 (EU)
Humira adalimumab TNFα human IgG1 Autoimmune Abbott 2002 (US) 2003 (EU)Xolair omalizumab IgE humanized IgG1 Autoimmune Genentech
Roche2003 (US)
Bexxar tositumomab-I-131 CD20 murine IgG2aradiolabeled (iodine131)
Cancer CorixaGSK 2003 (US)
Raptivaa falizumab CD11a humanized IgG1 Autoimmune GenentechRoche
2003 (US) 2004 (EU)
Erbitux cetuximab EGFR chimeric IgG1 Cancer ImcloneLilly 2004 (US) 2004 (EU)Avastin bevacizumab VEGF humanized IgG1 Cancer Genentech
Roche2004 (US) 2005 (EU)
Tysabri natalizumab α4-Intergrin humanizedIgG4
Autoimmune Biogen Idec 2004 (US)
Actemra tocilizumab Anti-IL-6R humanizedIgG1
Autoimmune ChugaiRoche
2005 (Japan) 2010 (US)
Vectibix panitumumab EGFR human IgG2 Cancer Amgen 2006 (US)Lucentis ranibizumab VEGF humanized IgG1
FabMaculardegeneration
GenentechRoche
2006 (US)
Soliris eculizumab C5 humanized IgG24 Blood disorders Alexion 2007 (US)Cimzia certolizumab pegol TNFα humanized
pegylated FabAutoimmune UCB 2008 (US)
Simponi golimumab TNFα human IgG1 Autoimmune Johnson ampJohnson
2009 (US EU Canada)
Ilaris canakinumab IL1b human IgG1 Infalmmatory Novartis 2009 (US EU)Stelara ustekinumab IL-1223 human IgG1 Autoimmune Johnson amp
Johnson2008 (EU) 2009 (US)
Arzerra ofatumumab CD20 human IgG1 Cancer Genmab 2009 (EU)Prolia denosumab RANK ligand human
IgG2Bone loss Amgen 2010 (US)
Numax motavizumab RSV humanized IgG1 Anti-infective MedImmune PendingABthrax Raxibacumab B anthrasis PA human
IgG1Anti-infection GSK 2012 (US)
Benlysta belimumab BLyS human IgG1 Autoimmune HGS 2011 (US)Yervoy ipilimumab CTLA-4 human IgG1 Cancer BMS 2011 (US)Adcetris brentuximabvedotin
CD30 chimeric IgG1drug- conjugate
Cancer SeattleGenetics
2011 (US)
(Continued on next page)
CHAPTER 1 bull History and Practice Antibodies in Infectious Diseases 7
INTRODUCTION TO ANTIBODIES
Antibodies also called immunoglobulins basedon their combined structure and function inimmune responses are produced by B cells ofthe immune system They are part of theadaptive immune response and are speciallydesigned for neutralizing and eliminating theinfectious agents and toxins produced by theseAntibodies are present in blood plasma andextracellular fluids and since these fluids wereformerly known as humors they were said tobe part of the humoral immune responseAntibodies are Y-shaped structures consistingof two main parts the upper arms of the Ywhich contain two identical variable-regionantigen binding sites and the lower regioncalled the constant regionwhich is responsiblefor the initiation of effector functions that leadto the removal and destruction of the pathogenor cells harboring the pathogen (see Fig 1) Theantigen-binding sites on an antibody can bythemselves bind to and neutralize bacterialtoxins and viruses thereby preventing themfrom binding to their target cells or receptorscausing toxic effects or spread of the infection
Antibodies consist of two pairs of heavy andlight chainswhich as described above are heldtogether in a Y-shaped arrangement Each ofthe heavy and light chains in these pairs isseparated into constant and variable chainsThe upper armsof theY each contain a variableand a constant sectionof the light and theheavychain where the upper variable parts of theheavy and light chains contain the antigen-binding site and the constant parts areconnected via disulfide bonds The lower partof theYcalled theconstantpart consistsof twoor three constant segments (immunoglobulindomains) from each of the two heavy chainsinteracting and also linked via disulfide bondsThe sectionsof theheavy chains connecting theconstant part of the upper arms to the constantparts of the constant region contain specialhinge regions that provide flexibility to thedifferent sections of the antibody to bind toantigens and effector cells The constant re-gions of the heavy chain also contain attachedoligosaccharide moieties which provide func-tional specialization to the antibodies (8)
The variable domains of the heavy and lightchains form the antigen-binding sites and
TABLE 1 Approved and pending antibody-based therapies (Continued)
Name antibody Target antibody type Indication Company Approval date
Perjeta pertuzumab Her2 humanized IgG1 Cancer GenentechRoche
2012 (US)
Kadcyla ado-trastuzumabemtansine
Her2 humanized IgG1Drug-conjugate
Cancer GenentechRoche
2013 (US)
Raxibacumab Anti-B anthrasis PAhuman IgG1
Anthraxinfection
Notapproved
2012
Entyvio vedolizumab Integrin α4β7humanized IgG1
Crohnrsquos diseaseulcerative colitis
Takeda 2014 (US)
Cyramza ramuciruumab Anti-VEGFR2Human IgG1
Gastric cancer Lilly 2014 (US)
Gazyva obinutuzumab Anti-CD20 humanizedIgG1 glucoengineered
CancerCLLb GenentechRoche
2014 (US)
Sylvant situximab Anti IL-6 chimeric IgG1 Castlemandisease
Janssen 2014 (US) 2014 (EU)
Cosentyx sekukinumab Anti IL-17a human IgG1 Psoriasis Novartis 2015 (US) 2015 (EU)Nivolumab Anti PD-1 human IgG4 Melanoma BMS Not approvedKeytruda pembrolizuumab Anti-PD-1 humanized
IgG4Melanoma Merck 2014 (US)
aAntibodies approved but later withdrawnbCLL chronic lymphocytic leukemia
8 HEY
FIGURE 1 (Left panel) Model of antibody structure exemplified by IgG On top the antigen-binding sitesin orange each contain one variable light and variable heavy domain with the three complementaritydetermining regions (CDRs) that are responsible for the specific binding of the antibody to its target Foreach arm of the antibody an additional set of variable heavy and light domains together with the CDR-containing domains represent the two fragment antigen binding (Fab) regions The two Fabs are heldtogether via two disulfide bridges Below the Fabs is the Fc region which contains four constant heavydomains On the upper pair of these domains are binding sites for oligosaccharides which have majorimportance for the ability of the antibody Fc part to trigger effector functions when the Fc portion isbound to Fc gamma receptors on natural killer cells neutrophil granulocytes monocytesmacrophagesdendritic cells and B cells (Right panel) Examples of some of the antibody-derived alternative formatsused to exploit the specific features of the CDRs the Fabs and the Fc parts of the antibodies ScFv Thesingle chain fragment variable consists of the variable domains of the heavy and light chains heldtogether by a flexible linker This can also be used as a carrier of a cytotoxic drug in a so-called antibodydrug complex (ADC) where the specificity of the ScFv is used to target the cytotoxic drug to eg atumor Bite (bi-specific T cell engager) Fusion proteins consisting of two ScFvs one directed against thetarget on a tumor cell and the other against the T cell receptor (CD3) Diabody ScFv dimers where shortlinker peptides (five amino acids) ensure dimerization and not folding of the ScFvs Fab and F(ab)2fragments Single Fab fragments or fragments containing two Fabs linked via disulfide bridges This isused where effector functions related to the Fc part of the antibody are unwanted and where a smallersize is desired to obtain better tissue penetration in eg tumors Due to the lack of the FcRn binding viathe Fc part Fab and F(ab)2 fragments have much shorter half-lives (hours or days) than full-sizeantibodies (weeks) These can also be used as carriers of cytotoxic payloads or cytotoxic radioactiveisotopes and for the F(ab)2 fragments can be constructed as bi-specifics which can cross-link immunecells and target cells Fc fusion protein Fusion protein containing the Fc domain of an immunoglobulinbound to a peptide The peptide can be a ligand for a specific receptor on a target cell or a blockingpeptide for a soluble ligand The Fc part provides a longer half-life to the construct and the potential tobind to and engage effector functions in the killing of eg tumor cells or infected cells ADCsRIAs andbi-specifics Full-size IgG antibodies carrying either a cytotoxic chemical or radioactive payload whichmay also carry different CDRs enabling cross-linking of effector and target cells for increased killingdoi101128microbiolspecAID-0026-2014f1
CHAPTER 1 bull History and Practice Antibodies in Infectious Diseases 9
contain special hyper-variable segments calledcomplementarity-determining regions (CDRs)which allow the B cells via genetic recom-bination to generate antibodies to all thedifferent antigens specific to amino acid se-quences or three-dimensional structuralmotifs(polysaccharides DNA and RNA) found onpathogens
Based on the structure of their heavy chainconstant regions antibodies or immuno-globulins are separated into five classesmdashIgM IgG IgE IgD and IgA Differences inthe sequences of the constant regions providedistinct characteristics to these different clas-ses These characteristics include the numberof heavy chain constant segments the numberand location of interconnecting disulfidebridges the length of the hinge region andthe number and location of oligosaccharidemoieties For IgG four heavy chain versionsexist creating IgG1 2 3 and 4 isotypes eachwith different characteristics in their serumhalf-lives and ability to trigger different effec-tor functions Because of the combined ad-vantage from ability to trigger effectormechanisms long [21 days] half-life theirability to be transported over the placentaand their stability in the production processantibodies of the IgG class and of the IgG1isotype are preferred as the basis for newantibody-based therapies The effector func-tions are triggered by the Fc part of an antibodywhen the variable parts of the antibody arebound directly to an infectious agent or toproteins from an infectious agent expressed onan infected cell This binding leaves the Fc partfree to interactwithFc receptors onphagocyticcells and neutrophils eosinophils and naturalkiller cells capable of inducing phagocytosis orlysis of infectious agents or infected cellsThese effector functions include (i) the abilityto activate the complement system for lysis(complement-dependent cellular cytotoxicity)(ii) triggering of uptake and destruction byphagocytic cells such as macrophages andneutrophils via interaction with Fc receptorson these cells (iii) activation of macrophageseosinophils neutrophils and natural killer
cells to kill infected cells via binding to Fcreceptors on these cells and antibody-depen-dent cellular cytotoxicity and (iv) neutraliza-tion of bacterial toxins and blocking of bindingand uptake of bacteria or viruses to target cells(see Fig 2) (9)
The Fcpart of IgG antibodies also contains aregion that interacts with the neonatal Fcreceptor (FcRn) expressed on most immuno-competent cells and inmany other cells such asendothelial cells in kidney liver placenta lungand breast (10) which protects antibodies fromdegradation by phagocytoticexocytotic cy-cling into FcRn-expressing cells thereby pro-longing their half-life This results in half-livesof 20 to 21 days for most IgG1 2 and 4antibodies whereas half-lives are 10 6 and 2days respectively for IgM IgA and IgE Thehighly specific binding sites on the variableregions of the upper arms of the antibody allowfor several important features of antibodiesndashbinding to and neutralization of eg bacterialtoxins binding to pathogens and blocking theirbinding to or interaction with target cells (egcyncytia formation of CMV-infected cells) orblocking of binding and interactions of infec-tious agents with target cells via blockingreceptors on the target cells
METHODS AND PLATFORMS FORGENERATING ANTIBODIES
As described above the early use of passiveantibody transfer as a therapy in infectiousdiseases involved the use of immune serumfrom immunized sheep and horses These pre-parations were crude and contained a broadmixture of neutralizing and non-neutralizingantibodies and both the foreign nature of theantibodies and the numerous host serumproteins This resulted in less specific andthus less efficient therapies due to a highvariability in efficacy between batches derivedfrom different animals immunized with dif-ferent strains of bacteria in different labor-atories and resulted in multiple unwantedside effects related to hypersensitivity and
10 HEY
anaphylactic reactions to foreign proteinsThese days antibodies being developed fortreatment of diseases in humans are highlypurified and are mostly fully human mono-clonal antibodies The term monoclonal anti-body refers to that cell cultures used forgenerating these antibodies each originatesfrom a single cell and thus produces onlyone specific antibody Development of fullyhuman monoclonal antibodies happened instages over a time span of more than 15 yearsFirst stage in this process was generation ofmonoclonalmurine IgG antibodies (eg OKT3[muronomab-CD3 Johnson and Johnson] ap-proved in 1986) Next stage was generation ofso called chimeric antibodies consisting ofhuman heavy and light chain constant sec-tions but with murine variable sections (eg
Rituxan [rituximab Genentech]) Next stagewas then the humanized antibodies wherethe only remaining murine part of the anti-body is the antigen-binding CDR (eg Xolair[omalizumab NovartisGenentech]) Both thefirst chimeric and humanized antibodies wereapproved in the late 1990s Then finally 16years later the first fully human antibodyHumira (adalimumab Abbott) was approvedin 2002 Since the time of the crude and low-scale manufacturing of the original antibodyserum products much has changed andtherapeutic antibodies are now produced byfermentation in 5000 liter scale using highlycontrolled and documented yeast or mamma-lian cell lines that are genetically engineered toexpress a single specific antibody This hasresulted in a pure and highly specific antibody
FIGURE 2 Effector functions of antibodies (a) Antibodies bind to pathogen-derived or endogenousantigens expressed on the surface of an infected cell which triggers binding to Fc receptors on naturalkiller cells and lysis of the infected cell by antibody-dependent cellular cytotoxicity (b) Antibodies bindto pathogen-derived or endogenous antigens expressed on the surface of infected cells which triggersactivation of complement through binding of complement factor C1q (c) Neutralization Top Bacterialtoxin neutralized by bound antigen Bottom Antibody bound to either receptor for the virus or to thevirus itself which blocks virus binding and entry into the cell (d) Antibody bound to viral surfaceproteins binds to Fc receptors on phagocytic cells eg macrophages and triggers endocytosis anddestruction of virus in endolysosome doi101128microbiolspecAID-0026-2014f2
CHAPTER 1 bull History and Practice Antibodies in Infectious Diseases 11

contRIBUtoRs xi
Harry B GreenbergDepartments of Medicine and Microbiology and ImmunologyStanford University School of Medicine and the VAPAHCSPalo Alto CA 94305
Scott B HalsteadDepartment of Preventive Medicine and BiometricsUniformed Services University of the Health SciencesBethesda MD 20814
Shen Y HelvigDepartment of PharmacyCenter for Pharmaceutical Nanotechnology and NanotoxicologyFaculty of Health and Medical SciencesUniversity of CopenhagenCopenhagen DK-2100Denmark
Adam HeyPreclinical Safety BiologicsNovartis AGBaselSwitzerland
Andrew HiattMapp Biopharmaceutical Inc6160 Lusk Blvd C105San Diego CA 92121
Bjoumlrn HockDepartment of Protein Engineering and Antibody TechnologiesMerck Serono Merck KgaAFrankfurter Str 250D-64293 DarmstadtGermany
Kelly HuangDepartment of Infectious DiseaseMedImmune LLCOne MedImmune WayGaithersburg MD 20878
Philip R JohnsonThe Childrenrsquos Hospital of PhiladelphiaAbramson Research CenterPhiladelphia PA 19104
Debra H JosephsCutaneous Medicine and Immunotherapy UnitSt Johnrsquos Institute of DermatologyDivision of Genetics and Molecular Medicine amp NIHR Biomedical Research Centre at Guyrsquos and St Thomasrsquos HospitalsKingrsquos College London School of MedicineGuyrsquos HospitalLondon SE1 9RTUnited Kingdom
Shilpa A JoshiDepartment of PathologyStanford UniversityStanford CA 94305
Sophia N KaragiannisCutaneous Medicine and Immunotherapy UnitSt Johnrsquos Institute of DermatologyDivision of Genetics and Molecular Medicine amp NIHR Biomedical Research Centre at Guyrsquos and St Thomasrsquos HospitalsKingrsquos College London School of MedicineGuyrsquos HospitalLondon SE1 9RTUnited Kingdom
Panagiotis KaragiannisCutaneous Medicine and Immunotherapy UnitSt Johnrsquos Institute of DermatologyDivision of Genetics and Molecular Medicine amp NIHR Biomedical Research Centre at Guyrsquos and St Thomasrsquos HospitalsKingrsquos College London School of MedicineGuyrsquos HospitalLondon SE1 9RTUnited Kingdom
Jens C KrauseChildrenrsquos HospitalUniversity of Freiburg Medical Center79106 FreibergGermany
Antonio LanzavecchiaInstitute for Research in Biomedicinevia Vincenzo Vela 6Bellinzona 6500Switzerland
xii contRIBUtoRs
Marie-Paule LefrancLaboratoire drsquoImmunoGeacuteneacutetique Moleacuteculaire LIGMIMGTreg the international ImMunoGeneTics information systemregInstitut de Geacuteneacutetique Humaine IGHUniversiteacute Montpellier 2UPR CNRS 1142Montpellier 34396 cedex 5 40202France
Olivier LegerDepartment of Protein Engineering and Antibody TechnologiesMerck Serono SA--Geneva9 chemin des Mines1202 GenevaSwitzerland
Kin-Ming LoDepartment of Protein Engineering and Antibody TechnologiesEMD Serono Research Institute45A Middlesex TurnpikeBillerica MA 01821
Wayne A MarascoDepartment of Cancer Immunology and AIDSDana-Farber Cancer InstituteHarvard Medical SchoolBoston MA 02215
Jennifer A MaynardDepartment of Chemical EngineeringUniversity of Texas at AustinAustin TX 78712
Luzia M MayrINSERM U1109Universiteacute de Strasbourg3 Rue Koeberleacute67000 StrasbourgFrance
Jens MeilerDepartment of Chemistry and Center for Structural BiologyVanderbilt UniversityNashville TN 37212
contRIBUtoRs xiii
S Moein MoghimiDepartment of PharmacyCenter for Pharmaceutical Nanotechnology and NanotoxicologyFaculty of Health and Medical SciencesUniversity of CopenhagenCopenhagen DK-2100Denmark
Susan Zolla-PaznerNew York University School of Medicine550 First AvenueNew York NY 10016
Louise SaulCutaneous Medicine and Immunotherapy UnitSt Johnrsquos Institute of DermatologyDivision of Genetics and Molecular Medicine amp NIHR Biomedical Research Centre at Guyrsquos and St Thomasrsquos HospitalsKingrsquos College London School of MedicineGuyrsquos HospitalLondon SE1 9RTUnited Kingdom
Bruce C SchneppThe Childrenrsquos Hospital of PhiladelphiaAbramson Research CenterPhiladelphia PA 19104
Jennifer E SchusterDepartment of PediatricsChildrenrsquos Mercy HospitalKansas City MO 64108-4619
Alexander M SevyDepartment of Chemistry and Center for Structural BiologyVanderbilt UniversityNashville TN 37212
Jared SheehanDepartment of Cancer Immunology and AIDSDana-Farber Cancer InstituteHarvard Medical SchoolBoston MA 02215
Michael R SierksDepartment of Chemical EngineeringArizona State UniversityTempe AZ 85287-6006
xiv contRIBUtoRs
Scott A SmithThe Vanderbilt Vaccine Center and the Department of MedicineVanderbilt University Medical CenterNashville TN 37232
Robyn L StanfieldDepartment of Molecular BiologyThe Scripps Research Institute10550 North Torrey Pines RoadLa Jolla CA 92037
Nadine UptonRandall Division of Cell and Molecular BiophysicsDivision of Asthma Allergy and Lung BiologyMRC and Asthma UK Centre for Allergic Mechanisms of AsthmaKingrsquos College LondonNew Huntrsquos HouseGuyrsquos CampusLondon SE1 1ULUnited Kingdom
Avanish K VarshneyDepartment of MedicineInfectious Diseases and Department of Microbiology and ImmunologyAlbert Einstein College of MedicineBronx NY 10461
Stefanie N VelgosMayo Clinic Arizona5777 East Mayo BoulevardPhoenix AZ 85054
Kevin J WhaleyMapp Biopharmaceutical Inc6160 Lusk Blvd C105San Diego CA 92121
Peter P WibroeCentre for Pharmaceutical Nanotechnology and NanotoxicologyDepartment of PharmacyFaculty of Health and Medical SciencesUniversity of CopenhagenCopenhagen DK-2100Denmark
John V WilliamsDepartment of PediatricsSchool of MedicineVanderbilt UniversityNashville TN 37232-2581
contRIBUtoRs xv
Ian A WilsonDepartment of Molecular Biology and Skaggs Institute for Chemical BiologyThe Scripps Research Institute10550 North Torrey Pines RoadLa Jolla CA 92037
Herren WuDepartment of Antibody Discovery and Protein EngineeringMedImmune LLCOne MedImmune WayGaithersburg MD 20879
Guocheng YangDepartment of Chemical EngineeringArizona State UniversityTempe AZ 85287-6006
Larry ZeitlinMapp Biopharmaceutical Inc6160 Lusk Blvd C105San Diego CA 92121
xvi contRIBUtoRs
Preface
Antibodies form the principal foundation for modern intervention against in-fectious diseases Emil Adolf von Behring was awarded the first Nobel Prize in Physiology or Medicine in 1901 ldquofor his work on serum therapy especially its appli-cation against diphtheria by which he has opened a new road in the domain of med-ical science and thereby placed in the hands of the physician a victorious weapon against illness and deathsrdquo Antibodies now provide the focus for understanding mechanisms of immunity to most infectious diseases and they play a central role in passive immunotherapy and active vaccination as mechanisms or correlates of immunity For most of the 20th century immunotherapy was based on passive transfer of polyclonal hyperimmune animal serum immune human serum or even hyperimmune human serum Georges JF Koumlhler and Ceacutesar Milstein re-ported the generation of monoclonal antibodies in 1979 for which they shared the 1984 Nobel Prize in Physiology or Medicine ldquofor the discovery of the princi-ple for production of monoclonal antibodiesrdquo Since that time entire fields related to antibodies for infectious diseases including antibody gene cloning engineer-ing and expression antibody libraries and high-throughput antibody gene rep-ertoire sequence analysis have extended our capabilities to explore the diversity of antibody specificity and function with unprecedented depth and breadth
This book provides a broad survey of many of the most important aspects of the field of antibodies for infectious diseases The book begins with a general introduction followed by chapters 2 through 5 on general features pertaining to structure function isotype and the role of complement in antibody function Chapters 6 through 10 review contemporary approaches for antibody discovery using phage and yeast display plasma cell and memory B cell cloning human hybridomas humanized mice and computational methods Chapters 11 through 18 review in depth the biology of antibodies specific for particular pathogens including viruses and bacterial toxins to illustrate the role of antibodies in anti- microbial immunity with specific targets These chapters reveal that attempts to raise effective antibody responses to each of these pathogens faces unique and pathogen-specific challenges Chapters 19 to 23 cover major technical advances pertaining to antibody engineering repertoire sequencing and analysis and new methods for study or therapeutic use of antibodies including radiotherapy Fi-nally chapters 24 and 25 cover new methods for expression of monoclonal anti-bodies in plants or by transfer of antibody genes for in vivo expression in treated subjects
Recent literature is exploding with new antibody-related techniques and re-ports of antimicrobial antibodies with unprecedented potency breadth of activ-
xvii
xviii PReface
ity and therapeutic potential We hope that this timely compilation of state-of-the-art reviews of major aspects of this field will be of interest to both antibody cognoscenti and those new to this exciting field We thank the authors for their dedication in producing definitive reviews of the topics at hand
James E Crowe JrDiana BoraschiRino Rappuoli
INTRODUCTION
History and PracticeAntibodies in Infectious Diseases 1ADAM HEY1
Antibodies in Infectious Diseases aims to inform update and inspire studentsteachers researchers pharmaceutical developers and health care professionalson the status of the development of antibody-based therapies for treatinginfectious diseases and the potential for these in times of growing antibioticresistance to provide alternative treatment solutions to the currently usedantibiotics and new treatments for infectious diseases where no propertreatments are available
This introductory article will provide a historical perspective on the useof antibody-based therapies followed by a high-level overview of whatmakes antibodies attractive tools for this purpose This will include the prosand cons of such therapies compared to the use of antibiotics and thepractical and strategic considerations involved in selecting the best formatand development path for new antibody-based therapies targeting specificinfectious agents Then examples of antibody-based therapies in thedevelopment of treatments for infectious diseases will be presented andfinally a look into the future will summarize the different aspects that willinfluence what the future might bring for this type of treatments forinfectious diseases
1Preclinical Safety Biologics Novartis AG Basel Switzerland
Antibodies for Infectious DiseasesEdited by James E Crowe Jr Diana Boraschi and Rino Rappuolicopy 2015 American Society for Microbiology Washington DCdoi101128microbiolspecAID-0026-2014
3
HISTORICAL PERSPECTIVE
Antibodies and the use of passive antibodytherapy in the treatment of infectious dis-eases is the story of a treatment conceptwhich dates back more than 120 years to thelate 19th century and which originally bythe use of serum from immunized animalsprovided the first effective treatment optionsagainst severe bacterial infections (1 2) Byimmunizing horses with bacterial toxinsfrom Clostridium tetani and Corynebacteri-um diphtheriae Emil A Von Behring andShibasaburo Kitasato (3) generated serumcontaining antibodies capable of neutraliz-ing the effects of the toxins produced bythese bacteria and successfully providedtreatment for these serious diseases wherethe pathogenesis is driven by the effects ofthe bacterial toxins For his work on provid-ing treatment for diphtheria Behring re-ceived the Nobel Prize in Physiology orMedicine in 1901 These radical treatmentresults quickly prompted development ofmultiple additional serum therapies for thetreatment of infectious diseases caused byeg Neisseria meningitidis Haemophilus in-fluenza and group A Streptococcus Sinceserum therapy involved administration oflarge amounts of crude mixtures of animalproteins including antibodies they wereassociated with side effects in the form ofhypersensitivity and serum sickness (2)
Due to the crude and unpurified nature ofthese products side effects were seen evenwhen administering human serum prepa-rations Side effects were observed in up to50 of patients and were considered to becaused by immune complex formations thatresulted in symptoms such as rash itchingjoint pain fever and in serious cases hypoten-sion and shock However due to the lack ofalternative options these treatments weredespite their side effects widely used Serumwas normally administered by intravenousinfusion in patients after a test for hypersensi-tivity where a small amount of serum wasinjected subcutaniously (1) As described
above serum therapy applied in these earlydays (late 19th century and early 20th century)involved preparations of serum from rabbitsand horses immunized with the infectiousagent or in live andor neutralized versions ortoxins from these (1) The costs of keeping theimmunized animals and the production andpotency testing of the materials made this arelatively expensive treatment In 1891 datafrom Klemperer (4) showed serum therapy toprotect rabbits from Streptococcus pneumoniaeinfection and paved the way for this type oftreatment and for development of similarserum-based treatments of streptococcal in-fections in humans When treating humansearly administration of serum could reducemortality significantly down to around 5compared to when administered 4 to 5 daysafter onset of symptoms when serum treat-ment was largely without effect This stronglyindicated the need for quick diagnosis andquick treatment to control the infection beforeit got out of control Consequently in theabsence of a specific diagnosis mixtures ofserum from immunizations with differentserotypes were used to circumvent this needfor early treatment without having a serotype-specific diagnosis The understanding thatdifferent serotypes existed for pneumococciand that efficient treatment relied on usingserotype-specific serum was being built upduring the 1920s and 1930s through experiencefrom extensive clinical trials
By the end of the 1930s serum therapywasthe standard of care for treatment of pneu-mococcal pneumonia At that time theefficacy and potency of the derived serawere assessed in mice in ldquothe mouse pro-tection testrdquo by testing survival after aconcomitant intraperitoneal injection of alethal dose of pneumococci and the serum tobe tested Due to the inherent variation inthis test efficacy and survival in two thirds ofthe animals was the acceptance criteria and10 times the lowest dose providing this wasused for defining a unit of the serum Thisallowed for large batch-to-batch variationand the use of different strains of bacteria for
4 HEY
immunization probably explains part of themissing responses observed (1) In the early20th century a pandemic of meningitis inEurope and the United States with mortalityrates up to 80 spurred the development ofserum therapy treatment options Althoughin the 1930s this became the recommendedtreatment in children assumed to be suffer-ing from meningitis failure to reduce mor-tality in several meningitis epidemics duringthat time raised doubts about the generalapplicability of serum treatment In thosedays serum therapy often involved quiteextensive procedures and infusion of largevolumes of serum The following exampleclearly illustrates this Data from Flexnerand Jobling (5) from treating meningitis inmonkeys resulted in the development of serafrom immunized horses for treatment inhumans The treatment protocol includedlumbar puncture and withdrawal of morethan 30 ml of spinal fluid representing anamount slightly larger than the expectedamount of horse serum to be injected subse-quently This treatment involved such dailyslow infusions of up to 30 ml of serum untilthe patientrsquos condition improved This treat-ment was used in outbreaks in New York in1905 and 1906 and did markedly decreasemortality
After the discovery of penicillin by Flemingin 1928 and the subsequent introduction ofantibiotics in the 1930s serum therapy waslargely abandoned over a period of 10 years dueto the availability of these new more broadlyeffective and cheaper treatment optionswhichalso had fewer side effects Although improve-ments in the purification of antibodies hadresulted in preparations with better safety andside effect profiles high manufacturing costsand narrow specificity resulted in antibodytherapy being mostly restricted to a smallernumber of selected treatments for snakevenoms bacterial toxins and some viral infec-tions (1 2) Currently antibody administrationis used for treatment and prevention ofhepatitis B virus rabies virus respiratorysyncytial virus (RSV) Clostridium tetani Clos-
tridium botulinum vaccinia virus echovirusand enterovirus For the most part thesetreatments consist of pooled immunoglobulinalso known as IVIG (intravenous immunoglob-ulin) from several postexposure donors Thisresults in both batch-to-batch variation in theneed for relatively large amounts of serum dueto low specificity and to restricted supplies dueto reliance on exposed donors
However several challengeshave resulted inthe need for new tools in the treatment andpreventionof infectiousdiseasesThebroadandgeneral use of antibiotics in human and veter-inary medicine for many years has resulted inthe development of multi-resistant strains ofbacteria with limited to no response to existingtreatments such as methicillin-resistant Staph-ylococcusaureus (MRSA) vancomycin-resistantS aureus and others This has resulted inpatients needing screening and treatment withseveral antibacterial agents and longer treat-ment time causing extra strain on patients andhealth care providers (6 httpwwwcdcgovdrugresistancethreat-report-2013indexhtml) According to the WHO and CDC morethan 25000 people in European Unioncountries and similar numbers in the UnitedStates die every year as a result of antibiotic-resistant infections This together with theemergence of new pathogens (eg severeacute respiratory syndrome Middle East respi-ratory syndrome) the re-emergenceepidemicsof oldknown pathogens (eg Ebola) and thedifficulties in treating infections in immune-deficient patients (eg HIV patients) has high-lighted the need for new solutions The 2014Ebola epidemic in West Africa (Liberia SierraLeone Guinea Nigeria and Senegal) has fur-ther highlighted this No treatment or prophy-lactic vaccine is available to treat or prevent thespread of Ebola infections which have anaveragemortality of gt50 Local health author-ities in the affected countries are struggling tocontain and handle the disease which isthreatening to go out of control and spreadmorewidelyVariousproductsmainly antibodycocktails from previously recovered patientsare being used despite a lack of clinical data on
CHAPTER 1 bull History and Practice Antibodies in Infectious Diseases 5
their safety and efficacy and those are the onlysporadically available treatment options andonly in small amounts and for a few patients
Ebola is an example of a disease whichnormally affects only a small number ofindividuals and which normally burns outwhen disease outbreaks are contained There-fore given the small number of potentialpatients affected by previous Ebola infectionsto date there was no incentive for big pharmacompanies to do research and development ofdrugs for EbolaWith the increasing number ofinfected (13567) andadeath toll of 4951 (7) andthe lack of the ability to contain the epidemic itwill be interesting to follow the aftermath ofthis outbreak and see whether there will berequests for new ways to ensure that vaccinesand treatment options are available for Ebolaand similar high-mortality and potential bio-warfare infections that have no availabletreatments or procedures to for mass-produc-tion upon the first signsreports of activeinfections Although both the CDC and theWHO have special programs focusing on thesetypes of infections the Ebola outbreak in 2014clearly shows that more financial support forresearch and development of new diagnosticsand treatments is needed This is one examplewhere antibody-based treatments would havethe potential to play a major role To put this inthe right perspective one should however notforget that other infectious diseases such astuberculosis influenza and malaria kill hun-dreds of thousands each year There is there-fore plenty of room for improvement indeveloping treatments for these diseases aswell but the high attention drawn to eg theEbola outbreak creates a special niche andopportunity where antibody treatments couldgain extraordinary development funding andsupport and prove their value and treatmentpotential
That antibody-based therapies could takethis role is supported by the revolution intechnologies for the development selectiongeneration and purification of fully humanantibodies described in more detail later in thesection ldquoMethodsandPlatforms forGenerating
Antibodiesrdquo Antibody-based programs cur-rently at different stages of developmentinclude investigations into the potential use ofsingle antibody preparations combinations ofantibodies (to avoid survival of escape mu-tants) fragments of antibodies and antibodiescarrying radioactive isotopesorcytotoxicdrugsor antibody-like frameworks (eg fibronectin)either alone as a first-line treatment or as anadjunct to existing treatments This multitudeof possible formats the ability to raise anti-bodies to almost any target and the ability toengineer both size effector functions and half-life are now considered by many to providevery valuable tools for designing specificantibody-based treatments toeradicate specifictargeted infectious agents However althoughseveral antibody-based therapies have beenapproved for oncology and anti-inflammatoryindications (see Table 1) only one monoclonalantibody (mAb) is approved against an infec-tious disease agentmdashSynagis (palivizumabMedImmune) for the prevention and treat-ment of respiratory syncytical virus (RSV) inhigh-risk children Economic obstacles such asthe high cost of mAb therapies and relativelysmall markets have resulted in less interestfrom pharmaceutical companies in developingthese Also highlighting the challenges indeveloping these types of antibody-basedtreatments are the difficulties encountered indeveloping a follow-up higher-affinity candi-date to Synagis Poor translatability of dataobtained in the available animal disease mod-els for RSV in cotton rats has resulted in non-approval due to inferiority relative to SynagisIn other viral diseases such as cytomegalovirus(CMV) the high species specificity of thestrains of CMV makes it impossible to testhuman antibody therapies in vivo Thereforeany real data on the efficacy of treatments forCMV will not be obtained until testing inclinical trials As described later in this articleseveral new antibody-based therapies for in-fectious diseases are in development andhopefully this will gradually open the fieldand result in better treatment options andoutcomes for patients
6 HEY
TABLE 1 Approved and pending antibody-based therapies
Name antibody Target antibody type Indication Company Approval date
OKT3a Muronomab-CD3 CD3 murine IgG2a Autoimmune Johnson ampJohnson
1986 (US)
ReoPro abciximab PIIbIIIa chimeric IgG1Fab
Homeostasis Johnson ampJohnson
1984 (US)
Rituxan rituximab CD20 chimeric IgG1 Cancer Genentech 1997 (US) 1998 (EU)Zenapaxa daclizumab CD25 humanized IgG1 Autoimmune Roche 1997 (US) 1999 (EU)Simulect basiliximab CD25 chimeric IgG1 Autoimmune Novartis 1998 (US EU)Synagis palivizumab RSV humanized IgG1 Infections MedImmune 1998 (US) 1999 (EU)Remicade infliximab TNFα chimeric IgG1 Autoimmune Johnson amp
Johnson1998 (US) 1999 (EU)
Herceptin trastuzumab HER2 humanized IgG1 Cancer GenentechRoche
1998 (US) 2000 (EU)
Mylotarga gemtuzumabozogamicin
CD33 humanized IgG4immunotoxin
Cancer WyethPfizer 2000 (US)
Campath alemtuzumab CD52 humanized IgG1 Cancer Genzyme 2001 (US) 2001 (EU)Zevalin ibritumomabtiuxetan
CD20 murine IgG1radiolabeled (yttrium 90)
Cancer Biogen Idec 2002 (US) 2004 (EU)
Humira adalimumab TNFα human IgG1 Autoimmune Abbott 2002 (US) 2003 (EU)Xolair omalizumab IgE humanized IgG1 Autoimmune Genentech
Roche2003 (US)
Bexxar tositumomab-I-131 CD20 murine IgG2aradiolabeled (iodine131)
Cancer CorixaGSK 2003 (US)
Raptivaa falizumab CD11a humanized IgG1 Autoimmune GenentechRoche
2003 (US) 2004 (EU)
Erbitux cetuximab EGFR chimeric IgG1 Cancer ImcloneLilly 2004 (US) 2004 (EU)Avastin bevacizumab VEGF humanized IgG1 Cancer Genentech
Roche2004 (US) 2005 (EU)
Tysabri natalizumab α4-Intergrin humanizedIgG4
Autoimmune Biogen Idec 2004 (US)
Actemra tocilizumab Anti-IL-6R humanizedIgG1
Autoimmune ChugaiRoche
2005 (Japan) 2010 (US)
Vectibix panitumumab EGFR human IgG2 Cancer Amgen 2006 (US)Lucentis ranibizumab VEGF humanized IgG1
FabMaculardegeneration
GenentechRoche
2006 (US)
Soliris eculizumab C5 humanized IgG24 Blood disorders Alexion 2007 (US)Cimzia certolizumab pegol TNFα humanized
pegylated FabAutoimmune UCB 2008 (US)
Simponi golimumab TNFα human IgG1 Autoimmune Johnson ampJohnson
2009 (US EU Canada)
Ilaris canakinumab IL1b human IgG1 Infalmmatory Novartis 2009 (US EU)Stelara ustekinumab IL-1223 human IgG1 Autoimmune Johnson amp
Johnson2008 (EU) 2009 (US)
Arzerra ofatumumab CD20 human IgG1 Cancer Genmab 2009 (EU)Prolia denosumab RANK ligand human
IgG2Bone loss Amgen 2010 (US)
Numax motavizumab RSV humanized IgG1 Anti-infective MedImmune PendingABthrax Raxibacumab B anthrasis PA human
IgG1Anti-infection GSK 2012 (US)
Benlysta belimumab BLyS human IgG1 Autoimmune HGS 2011 (US)Yervoy ipilimumab CTLA-4 human IgG1 Cancer BMS 2011 (US)Adcetris brentuximabvedotin
CD30 chimeric IgG1drug- conjugate
Cancer SeattleGenetics
2011 (US)
(Continued on next page)
CHAPTER 1 bull History and Practice Antibodies in Infectious Diseases 7
INTRODUCTION TO ANTIBODIES
Antibodies also called immunoglobulins basedon their combined structure and function inimmune responses are produced by B cells ofthe immune system They are part of theadaptive immune response and are speciallydesigned for neutralizing and eliminating theinfectious agents and toxins produced by theseAntibodies are present in blood plasma andextracellular fluids and since these fluids wereformerly known as humors they were said tobe part of the humoral immune responseAntibodies are Y-shaped structures consistingof two main parts the upper arms of the Ywhich contain two identical variable-regionantigen binding sites and the lower regioncalled the constant regionwhich is responsiblefor the initiation of effector functions that leadto the removal and destruction of the pathogenor cells harboring the pathogen (see Fig 1) Theantigen-binding sites on an antibody can bythemselves bind to and neutralize bacterialtoxins and viruses thereby preventing themfrom binding to their target cells or receptorscausing toxic effects or spread of the infection
Antibodies consist of two pairs of heavy andlight chainswhich as described above are heldtogether in a Y-shaped arrangement Each ofthe heavy and light chains in these pairs isseparated into constant and variable chainsThe upper armsof theY each contain a variableand a constant sectionof the light and theheavychain where the upper variable parts of theheavy and light chains contain the antigen-binding site and the constant parts areconnected via disulfide bonds The lower partof theYcalled theconstantpart consistsof twoor three constant segments (immunoglobulindomains) from each of the two heavy chainsinteracting and also linked via disulfide bondsThe sectionsof theheavy chains connecting theconstant part of the upper arms to the constantparts of the constant region contain specialhinge regions that provide flexibility to thedifferent sections of the antibody to bind toantigens and effector cells The constant re-gions of the heavy chain also contain attachedoligosaccharide moieties which provide func-tional specialization to the antibodies (8)
The variable domains of the heavy and lightchains form the antigen-binding sites and
TABLE 1 Approved and pending antibody-based therapies (Continued)
Name antibody Target antibody type Indication Company Approval date
Perjeta pertuzumab Her2 humanized IgG1 Cancer GenentechRoche
2012 (US)
Kadcyla ado-trastuzumabemtansine
Her2 humanized IgG1Drug-conjugate
Cancer GenentechRoche
2013 (US)
Raxibacumab Anti-B anthrasis PAhuman IgG1
Anthraxinfection
Notapproved
2012
Entyvio vedolizumab Integrin α4β7humanized IgG1
Crohnrsquos diseaseulcerative colitis
Takeda 2014 (US)
Cyramza ramuciruumab Anti-VEGFR2Human IgG1
Gastric cancer Lilly 2014 (US)
Gazyva obinutuzumab Anti-CD20 humanizedIgG1 glucoengineered
CancerCLLb GenentechRoche
2014 (US)
Sylvant situximab Anti IL-6 chimeric IgG1 Castlemandisease
Janssen 2014 (US) 2014 (EU)
Cosentyx sekukinumab Anti IL-17a human IgG1 Psoriasis Novartis 2015 (US) 2015 (EU)Nivolumab Anti PD-1 human IgG4 Melanoma BMS Not approvedKeytruda pembrolizuumab Anti-PD-1 humanized
IgG4Melanoma Merck 2014 (US)
aAntibodies approved but later withdrawnbCLL chronic lymphocytic leukemia
8 HEY
FIGURE 1 (Left panel) Model of antibody structure exemplified by IgG On top the antigen-binding sitesin orange each contain one variable light and variable heavy domain with the three complementaritydetermining regions (CDRs) that are responsible for the specific binding of the antibody to its target Foreach arm of the antibody an additional set of variable heavy and light domains together with the CDR-containing domains represent the two fragment antigen binding (Fab) regions The two Fabs are heldtogether via two disulfide bridges Below the Fabs is the Fc region which contains four constant heavydomains On the upper pair of these domains are binding sites for oligosaccharides which have majorimportance for the ability of the antibody Fc part to trigger effector functions when the Fc portion isbound to Fc gamma receptors on natural killer cells neutrophil granulocytes monocytesmacrophagesdendritic cells and B cells (Right panel) Examples of some of the antibody-derived alternative formatsused to exploit the specific features of the CDRs the Fabs and the Fc parts of the antibodies ScFv Thesingle chain fragment variable consists of the variable domains of the heavy and light chains heldtogether by a flexible linker This can also be used as a carrier of a cytotoxic drug in a so-called antibodydrug complex (ADC) where the specificity of the ScFv is used to target the cytotoxic drug to eg atumor Bite (bi-specific T cell engager) Fusion proteins consisting of two ScFvs one directed against thetarget on a tumor cell and the other against the T cell receptor (CD3) Diabody ScFv dimers where shortlinker peptides (five amino acids) ensure dimerization and not folding of the ScFvs Fab and F(ab)2fragments Single Fab fragments or fragments containing two Fabs linked via disulfide bridges This isused where effector functions related to the Fc part of the antibody are unwanted and where a smallersize is desired to obtain better tissue penetration in eg tumors Due to the lack of the FcRn binding viathe Fc part Fab and F(ab)2 fragments have much shorter half-lives (hours or days) than full-sizeantibodies (weeks) These can also be used as carriers of cytotoxic payloads or cytotoxic radioactiveisotopes and for the F(ab)2 fragments can be constructed as bi-specifics which can cross-link immunecells and target cells Fc fusion protein Fusion protein containing the Fc domain of an immunoglobulinbound to a peptide The peptide can be a ligand for a specific receptor on a target cell or a blockingpeptide for a soluble ligand The Fc part provides a longer half-life to the construct and the potential tobind to and engage effector functions in the killing of eg tumor cells or infected cells ADCsRIAs andbi-specifics Full-size IgG antibodies carrying either a cytotoxic chemical or radioactive payload whichmay also carry different CDRs enabling cross-linking of effector and target cells for increased killingdoi101128microbiolspecAID-0026-2014f1
CHAPTER 1 bull History and Practice Antibodies in Infectious Diseases 9
contain special hyper-variable segments calledcomplementarity-determining regions (CDRs)which allow the B cells via genetic recom-bination to generate antibodies to all thedifferent antigens specific to amino acid se-quences or three-dimensional structuralmotifs(polysaccharides DNA and RNA) found onpathogens
Based on the structure of their heavy chainconstant regions antibodies or immuno-globulins are separated into five classesmdashIgM IgG IgE IgD and IgA Differences inthe sequences of the constant regions providedistinct characteristics to these different clas-ses These characteristics include the numberof heavy chain constant segments the numberand location of interconnecting disulfidebridges the length of the hinge region andthe number and location of oligosaccharidemoieties For IgG four heavy chain versionsexist creating IgG1 2 3 and 4 isotypes eachwith different characteristics in their serumhalf-lives and ability to trigger different effec-tor functions Because of the combined ad-vantage from ability to trigger effectormechanisms long [21 days] half-life theirability to be transported over the placentaand their stability in the production processantibodies of the IgG class and of the IgG1isotype are preferred as the basis for newantibody-based therapies The effector func-tions are triggered by the Fc part of an antibodywhen the variable parts of the antibody arebound directly to an infectious agent or toproteins from an infectious agent expressed onan infected cell This binding leaves the Fc partfree to interactwithFc receptors onphagocyticcells and neutrophils eosinophils and naturalkiller cells capable of inducing phagocytosis orlysis of infectious agents or infected cellsThese effector functions include (i) the abilityto activate the complement system for lysis(complement-dependent cellular cytotoxicity)(ii) triggering of uptake and destruction byphagocytic cells such as macrophages andneutrophils via interaction with Fc receptorson these cells (iii) activation of macrophageseosinophils neutrophils and natural killer
cells to kill infected cells via binding to Fcreceptors on these cells and antibody-depen-dent cellular cytotoxicity and (iv) neutraliza-tion of bacterial toxins and blocking of bindingand uptake of bacteria or viruses to target cells(see Fig 2) (9)
The Fcpart of IgG antibodies also contains aregion that interacts with the neonatal Fcreceptor (FcRn) expressed on most immuno-competent cells and inmany other cells such asendothelial cells in kidney liver placenta lungand breast (10) which protects antibodies fromdegradation by phagocytoticexocytotic cy-cling into FcRn-expressing cells thereby pro-longing their half-life This results in half-livesof 20 to 21 days for most IgG1 2 and 4antibodies whereas half-lives are 10 6 and 2days respectively for IgM IgA and IgE Thehighly specific binding sites on the variableregions of the upper arms of the antibody allowfor several important features of antibodiesndashbinding to and neutralization of eg bacterialtoxins binding to pathogens and blocking theirbinding to or interaction with target cells (egcyncytia formation of CMV-infected cells) orblocking of binding and interactions of infec-tious agents with target cells via blockingreceptors on the target cells
METHODS AND PLATFORMS FORGENERATING ANTIBODIES
As described above the early use of passiveantibody transfer as a therapy in infectiousdiseases involved the use of immune serumfrom immunized sheep and horses These pre-parations were crude and contained a broadmixture of neutralizing and non-neutralizingantibodies and both the foreign nature of theantibodies and the numerous host serumproteins This resulted in less specific andthus less efficient therapies due to a highvariability in efficacy between batches derivedfrom different animals immunized with dif-ferent strains of bacteria in different labor-atories and resulted in multiple unwantedside effects related to hypersensitivity and
10 HEY
anaphylactic reactions to foreign proteinsThese days antibodies being developed fortreatment of diseases in humans are highlypurified and are mostly fully human mono-clonal antibodies The term monoclonal anti-body refers to that cell cultures used forgenerating these antibodies each originatesfrom a single cell and thus produces onlyone specific antibody Development of fullyhuman monoclonal antibodies happened instages over a time span of more than 15 yearsFirst stage in this process was generation ofmonoclonalmurine IgG antibodies (eg OKT3[muronomab-CD3 Johnson and Johnson] ap-proved in 1986) Next stage was generation ofso called chimeric antibodies consisting ofhuman heavy and light chain constant sec-tions but with murine variable sections (eg
Rituxan [rituximab Genentech]) Next stagewas then the humanized antibodies wherethe only remaining murine part of the anti-body is the antigen-binding CDR (eg Xolair[omalizumab NovartisGenentech]) Both thefirst chimeric and humanized antibodies wereapproved in the late 1990s Then finally 16years later the first fully human antibodyHumira (adalimumab Abbott) was approvedin 2002 Since the time of the crude and low-scale manufacturing of the original antibodyserum products much has changed andtherapeutic antibodies are now produced byfermentation in 5000 liter scale using highlycontrolled and documented yeast or mamma-lian cell lines that are genetically engineered toexpress a single specific antibody This hasresulted in a pure and highly specific antibody
FIGURE 2 Effector functions of antibodies (a) Antibodies bind to pathogen-derived or endogenousantigens expressed on the surface of an infected cell which triggers binding to Fc receptors on naturalkiller cells and lysis of the infected cell by antibody-dependent cellular cytotoxicity (b) Antibodies bindto pathogen-derived or endogenous antigens expressed on the surface of infected cells which triggersactivation of complement through binding of complement factor C1q (c) Neutralization Top Bacterialtoxin neutralized by bound antigen Bottom Antibody bound to either receptor for the virus or to thevirus itself which blocks virus binding and entry into the cell (d) Antibody bound to viral surfaceproteins binds to Fc receptors on phagocytic cells eg macrophages and triggers endocytosis anddestruction of virus in endolysosome doi101128microbiolspecAID-0026-2014f2
CHAPTER 1 bull History and Practice Antibodies in Infectious Diseases 11

Debra H JosephsCutaneous Medicine and Immunotherapy UnitSt Johnrsquos Institute of DermatologyDivision of Genetics and Molecular Medicine amp NIHR Biomedical Research Centre at Guyrsquos and St Thomasrsquos HospitalsKingrsquos College London School of MedicineGuyrsquos HospitalLondon SE1 9RTUnited Kingdom
Shilpa A JoshiDepartment of PathologyStanford UniversityStanford CA 94305
Sophia N KaragiannisCutaneous Medicine and Immunotherapy UnitSt Johnrsquos Institute of DermatologyDivision of Genetics and Molecular Medicine amp NIHR Biomedical Research Centre at Guyrsquos and St Thomasrsquos HospitalsKingrsquos College London School of MedicineGuyrsquos HospitalLondon SE1 9RTUnited Kingdom
Panagiotis KaragiannisCutaneous Medicine and Immunotherapy UnitSt Johnrsquos Institute of DermatologyDivision of Genetics and Molecular Medicine amp NIHR Biomedical Research Centre at Guyrsquos and St Thomasrsquos HospitalsKingrsquos College London School of MedicineGuyrsquos HospitalLondon SE1 9RTUnited Kingdom
Jens C KrauseChildrenrsquos HospitalUniversity of Freiburg Medical Center79106 FreibergGermany
Antonio LanzavecchiaInstitute for Research in Biomedicinevia Vincenzo Vela 6Bellinzona 6500Switzerland
xii contRIBUtoRs
Marie-Paule LefrancLaboratoire drsquoImmunoGeacuteneacutetique Moleacuteculaire LIGMIMGTreg the international ImMunoGeneTics information systemregInstitut de Geacuteneacutetique Humaine IGHUniversiteacute Montpellier 2UPR CNRS 1142Montpellier 34396 cedex 5 40202France
Olivier LegerDepartment of Protein Engineering and Antibody TechnologiesMerck Serono SA--Geneva9 chemin des Mines1202 GenevaSwitzerland
Kin-Ming LoDepartment of Protein Engineering and Antibody TechnologiesEMD Serono Research Institute45A Middlesex TurnpikeBillerica MA 01821
Wayne A MarascoDepartment of Cancer Immunology and AIDSDana-Farber Cancer InstituteHarvard Medical SchoolBoston MA 02215
Jennifer A MaynardDepartment of Chemical EngineeringUniversity of Texas at AustinAustin TX 78712
Luzia M MayrINSERM U1109Universiteacute de Strasbourg3 Rue Koeberleacute67000 StrasbourgFrance
Jens MeilerDepartment of Chemistry and Center for Structural BiologyVanderbilt UniversityNashville TN 37212
contRIBUtoRs xiii
S Moein MoghimiDepartment of PharmacyCenter for Pharmaceutical Nanotechnology and NanotoxicologyFaculty of Health and Medical SciencesUniversity of CopenhagenCopenhagen DK-2100Denmark
Susan Zolla-PaznerNew York University School of Medicine550 First AvenueNew York NY 10016
Louise SaulCutaneous Medicine and Immunotherapy UnitSt Johnrsquos Institute of DermatologyDivision of Genetics and Molecular Medicine amp NIHR Biomedical Research Centre at Guyrsquos and St Thomasrsquos HospitalsKingrsquos College London School of MedicineGuyrsquos HospitalLondon SE1 9RTUnited Kingdom
Bruce C SchneppThe Childrenrsquos Hospital of PhiladelphiaAbramson Research CenterPhiladelphia PA 19104
Jennifer E SchusterDepartment of PediatricsChildrenrsquos Mercy HospitalKansas City MO 64108-4619
Alexander M SevyDepartment of Chemistry and Center for Structural BiologyVanderbilt UniversityNashville TN 37212
Jared SheehanDepartment of Cancer Immunology and AIDSDana-Farber Cancer InstituteHarvard Medical SchoolBoston MA 02215
Michael R SierksDepartment of Chemical EngineeringArizona State UniversityTempe AZ 85287-6006
xiv contRIBUtoRs
Scott A SmithThe Vanderbilt Vaccine Center and the Department of MedicineVanderbilt University Medical CenterNashville TN 37232
Robyn L StanfieldDepartment of Molecular BiologyThe Scripps Research Institute10550 North Torrey Pines RoadLa Jolla CA 92037
Nadine UptonRandall Division of Cell and Molecular BiophysicsDivision of Asthma Allergy and Lung BiologyMRC and Asthma UK Centre for Allergic Mechanisms of AsthmaKingrsquos College LondonNew Huntrsquos HouseGuyrsquos CampusLondon SE1 1ULUnited Kingdom
Avanish K VarshneyDepartment of MedicineInfectious Diseases and Department of Microbiology and ImmunologyAlbert Einstein College of MedicineBronx NY 10461
Stefanie N VelgosMayo Clinic Arizona5777 East Mayo BoulevardPhoenix AZ 85054
Kevin J WhaleyMapp Biopharmaceutical Inc6160 Lusk Blvd C105San Diego CA 92121
Peter P WibroeCentre for Pharmaceutical Nanotechnology and NanotoxicologyDepartment of PharmacyFaculty of Health and Medical SciencesUniversity of CopenhagenCopenhagen DK-2100Denmark
John V WilliamsDepartment of PediatricsSchool of MedicineVanderbilt UniversityNashville TN 37232-2581
contRIBUtoRs xv
Ian A WilsonDepartment of Molecular Biology and Skaggs Institute for Chemical BiologyThe Scripps Research Institute10550 North Torrey Pines RoadLa Jolla CA 92037
Herren WuDepartment of Antibody Discovery and Protein EngineeringMedImmune LLCOne MedImmune WayGaithersburg MD 20879
Guocheng YangDepartment of Chemical EngineeringArizona State UniversityTempe AZ 85287-6006
Larry ZeitlinMapp Biopharmaceutical Inc6160 Lusk Blvd C105San Diego CA 92121
xvi contRIBUtoRs
Preface
Antibodies form the principal foundation for modern intervention against in-fectious diseases Emil Adolf von Behring was awarded the first Nobel Prize in Physiology or Medicine in 1901 ldquofor his work on serum therapy especially its appli-cation against diphtheria by which he has opened a new road in the domain of med-ical science and thereby placed in the hands of the physician a victorious weapon against illness and deathsrdquo Antibodies now provide the focus for understanding mechanisms of immunity to most infectious diseases and they play a central role in passive immunotherapy and active vaccination as mechanisms or correlates of immunity For most of the 20th century immunotherapy was based on passive transfer of polyclonal hyperimmune animal serum immune human serum or even hyperimmune human serum Georges JF Koumlhler and Ceacutesar Milstein re-ported the generation of monoclonal antibodies in 1979 for which they shared the 1984 Nobel Prize in Physiology or Medicine ldquofor the discovery of the princi-ple for production of monoclonal antibodiesrdquo Since that time entire fields related to antibodies for infectious diseases including antibody gene cloning engineer-ing and expression antibody libraries and high-throughput antibody gene rep-ertoire sequence analysis have extended our capabilities to explore the diversity of antibody specificity and function with unprecedented depth and breadth
This book provides a broad survey of many of the most important aspects of the field of antibodies for infectious diseases The book begins with a general introduction followed by chapters 2 through 5 on general features pertaining to structure function isotype and the role of complement in antibody function Chapters 6 through 10 review contemporary approaches for antibody discovery using phage and yeast display plasma cell and memory B cell cloning human hybridomas humanized mice and computational methods Chapters 11 through 18 review in depth the biology of antibodies specific for particular pathogens including viruses and bacterial toxins to illustrate the role of antibodies in anti- microbial immunity with specific targets These chapters reveal that attempts to raise effective antibody responses to each of these pathogens faces unique and pathogen-specific challenges Chapters 19 to 23 cover major technical advances pertaining to antibody engineering repertoire sequencing and analysis and new methods for study or therapeutic use of antibodies including radiotherapy Fi-nally chapters 24 and 25 cover new methods for expression of monoclonal anti-bodies in plants or by transfer of antibody genes for in vivo expression in treated subjects
Recent literature is exploding with new antibody-related techniques and re-ports of antimicrobial antibodies with unprecedented potency breadth of activ-
xvii
xviii PReface
ity and therapeutic potential We hope that this timely compilation of state-of-the-art reviews of major aspects of this field will be of interest to both antibody cognoscenti and those new to this exciting field We thank the authors for their dedication in producing definitive reviews of the topics at hand
James E Crowe JrDiana BoraschiRino Rappuoli
INTRODUCTION
History and PracticeAntibodies in Infectious Diseases 1ADAM HEY1
Antibodies in Infectious Diseases aims to inform update and inspire studentsteachers researchers pharmaceutical developers and health care professionalson the status of the development of antibody-based therapies for treatinginfectious diseases and the potential for these in times of growing antibioticresistance to provide alternative treatment solutions to the currently usedantibiotics and new treatments for infectious diseases where no propertreatments are available
This introductory article will provide a historical perspective on the useof antibody-based therapies followed by a high-level overview of whatmakes antibodies attractive tools for this purpose This will include the prosand cons of such therapies compared to the use of antibiotics and thepractical and strategic considerations involved in selecting the best formatand development path for new antibody-based therapies targeting specificinfectious agents Then examples of antibody-based therapies in thedevelopment of treatments for infectious diseases will be presented andfinally a look into the future will summarize the different aspects that willinfluence what the future might bring for this type of treatments forinfectious diseases
1Preclinical Safety Biologics Novartis AG Basel Switzerland
Antibodies for Infectious DiseasesEdited by James E Crowe Jr Diana Boraschi and Rino Rappuolicopy 2015 American Society for Microbiology Washington DCdoi101128microbiolspecAID-0026-2014
3
HISTORICAL PERSPECTIVE
Antibodies and the use of passive antibodytherapy in the treatment of infectious dis-eases is the story of a treatment conceptwhich dates back more than 120 years to thelate 19th century and which originally bythe use of serum from immunized animalsprovided the first effective treatment optionsagainst severe bacterial infections (1 2) Byimmunizing horses with bacterial toxinsfrom Clostridium tetani and Corynebacteri-um diphtheriae Emil A Von Behring andShibasaburo Kitasato (3) generated serumcontaining antibodies capable of neutraliz-ing the effects of the toxins produced bythese bacteria and successfully providedtreatment for these serious diseases wherethe pathogenesis is driven by the effects ofthe bacterial toxins For his work on provid-ing treatment for diphtheria Behring re-ceived the Nobel Prize in Physiology orMedicine in 1901 These radical treatmentresults quickly prompted development ofmultiple additional serum therapies for thetreatment of infectious diseases caused byeg Neisseria meningitidis Haemophilus in-fluenza and group A Streptococcus Sinceserum therapy involved administration oflarge amounts of crude mixtures of animalproteins including antibodies they wereassociated with side effects in the form ofhypersensitivity and serum sickness (2)
Due to the crude and unpurified nature ofthese products side effects were seen evenwhen administering human serum prepa-rations Side effects were observed in up to50 of patients and were considered to becaused by immune complex formations thatresulted in symptoms such as rash itchingjoint pain fever and in serious cases hypoten-sion and shock However due to the lack ofalternative options these treatments weredespite their side effects widely used Serumwas normally administered by intravenousinfusion in patients after a test for hypersensi-tivity where a small amount of serum wasinjected subcutaniously (1) As described
above serum therapy applied in these earlydays (late 19th century and early 20th century)involved preparations of serum from rabbitsand horses immunized with the infectiousagent or in live andor neutralized versions ortoxins from these (1) The costs of keeping theimmunized animals and the production andpotency testing of the materials made this arelatively expensive treatment In 1891 datafrom Klemperer (4) showed serum therapy toprotect rabbits from Streptococcus pneumoniaeinfection and paved the way for this type oftreatment and for development of similarserum-based treatments of streptococcal in-fections in humans When treating humansearly administration of serum could reducemortality significantly down to around 5compared to when administered 4 to 5 daysafter onset of symptoms when serum treat-ment was largely without effect This stronglyindicated the need for quick diagnosis andquick treatment to control the infection beforeit got out of control Consequently in theabsence of a specific diagnosis mixtures ofserum from immunizations with differentserotypes were used to circumvent this needfor early treatment without having a serotype-specific diagnosis The understanding thatdifferent serotypes existed for pneumococciand that efficient treatment relied on usingserotype-specific serum was being built upduring the 1920s and 1930s through experiencefrom extensive clinical trials
By the end of the 1930s serum therapywasthe standard of care for treatment of pneu-mococcal pneumonia At that time theefficacy and potency of the derived serawere assessed in mice in ldquothe mouse pro-tection testrdquo by testing survival after aconcomitant intraperitoneal injection of alethal dose of pneumococci and the serum tobe tested Due to the inherent variation inthis test efficacy and survival in two thirds ofthe animals was the acceptance criteria and10 times the lowest dose providing this wasused for defining a unit of the serum Thisallowed for large batch-to-batch variationand the use of different strains of bacteria for
4 HEY
immunization probably explains part of themissing responses observed (1) In the early20th century a pandemic of meningitis inEurope and the United States with mortalityrates up to 80 spurred the development ofserum therapy treatment options Althoughin the 1930s this became the recommendedtreatment in children assumed to be suffer-ing from meningitis failure to reduce mor-tality in several meningitis epidemics duringthat time raised doubts about the generalapplicability of serum treatment In thosedays serum therapy often involved quiteextensive procedures and infusion of largevolumes of serum The following exampleclearly illustrates this Data from Flexnerand Jobling (5) from treating meningitis inmonkeys resulted in the development of serafrom immunized horses for treatment inhumans The treatment protocol includedlumbar puncture and withdrawal of morethan 30 ml of spinal fluid representing anamount slightly larger than the expectedamount of horse serum to be injected subse-quently This treatment involved such dailyslow infusions of up to 30 ml of serum untilthe patientrsquos condition improved This treat-ment was used in outbreaks in New York in1905 and 1906 and did markedly decreasemortality
After the discovery of penicillin by Flemingin 1928 and the subsequent introduction ofantibiotics in the 1930s serum therapy waslargely abandoned over a period of 10 years dueto the availability of these new more broadlyeffective and cheaper treatment optionswhichalso had fewer side effects Although improve-ments in the purification of antibodies hadresulted in preparations with better safety andside effect profiles high manufacturing costsand narrow specificity resulted in antibodytherapy being mostly restricted to a smallernumber of selected treatments for snakevenoms bacterial toxins and some viral infec-tions (1 2) Currently antibody administrationis used for treatment and prevention ofhepatitis B virus rabies virus respiratorysyncytial virus (RSV) Clostridium tetani Clos-
tridium botulinum vaccinia virus echovirusand enterovirus For the most part thesetreatments consist of pooled immunoglobulinalso known as IVIG (intravenous immunoglob-ulin) from several postexposure donors Thisresults in both batch-to-batch variation in theneed for relatively large amounts of serum dueto low specificity and to restricted supplies dueto reliance on exposed donors
However several challengeshave resulted inthe need for new tools in the treatment andpreventionof infectiousdiseasesThebroadandgeneral use of antibiotics in human and veter-inary medicine for many years has resulted inthe development of multi-resistant strains ofbacteria with limited to no response to existingtreatments such as methicillin-resistant Staph-ylococcusaureus (MRSA) vancomycin-resistantS aureus and others This has resulted inpatients needing screening and treatment withseveral antibacterial agents and longer treat-ment time causing extra strain on patients andhealth care providers (6 httpwwwcdcgovdrugresistancethreat-report-2013indexhtml) According to the WHO and CDC morethan 25000 people in European Unioncountries and similar numbers in the UnitedStates die every year as a result of antibiotic-resistant infections This together with theemergence of new pathogens (eg severeacute respiratory syndrome Middle East respi-ratory syndrome) the re-emergenceepidemicsof oldknown pathogens (eg Ebola) and thedifficulties in treating infections in immune-deficient patients (eg HIV patients) has high-lighted the need for new solutions The 2014Ebola epidemic in West Africa (Liberia SierraLeone Guinea Nigeria and Senegal) has fur-ther highlighted this No treatment or prophy-lactic vaccine is available to treat or prevent thespread of Ebola infections which have anaveragemortality of gt50 Local health author-ities in the affected countries are struggling tocontain and handle the disease which isthreatening to go out of control and spreadmorewidelyVariousproductsmainly antibodycocktails from previously recovered patientsare being used despite a lack of clinical data on
CHAPTER 1 bull History and Practice Antibodies in Infectious Diseases 5
their safety and efficacy and those are the onlysporadically available treatment options andonly in small amounts and for a few patients
Ebola is an example of a disease whichnormally affects only a small number ofindividuals and which normally burns outwhen disease outbreaks are contained There-fore given the small number of potentialpatients affected by previous Ebola infectionsto date there was no incentive for big pharmacompanies to do research and development ofdrugs for EbolaWith the increasing number ofinfected (13567) andadeath toll of 4951 (7) andthe lack of the ability to contain the epidemic itwill be interesting to follow the aftermath ofthis outbreak and see whether there will berequests for new ways to ensure that vaccinesand treatment options are available for Ebolaand similar high-mortality and potential bio-warfare infections that have no availabletreatments or procedures to for mass-produc-tion upon the first signsreports of activeinfections Although both the CDC and theWHO have special programs focusing on thesetypes of infections the Ebola outbreak in 2014clearly shows that more financial support forresearch and development of new diagnosticsand treatments is needed This is one examplewhere antibody-based treatments would havethe potential to play a major role To put this inthe right perspective one should however notforget that other infectious diseases such astuberculosis influenza and malaria kill hun-dreds of thousands each year There is there-fore plenty of room for improvement indeveloping treatments for these diseases aswell but the high attention drawn to eg theEbola outbreak creates a special niche andopportunity where antibody treatments couldgain extraordinary development funding andsupport and prove their value and treatmentpotential
That antibody-based therapies could takethis role is supported by the revolution intechnologies for the development selectiongeneration and purification of fully humanantibodies described in more detail later in thesection ldquoMethodsandPlatforms forGenerating
Antibodiesrdquo Antibody-based programs cur-rently at different stages of developmentinclude investigations into the potential use ofsingle antibody preparations combinations ofantibodies (to avoid survival of escape mu-tants) fragments of antibodies and antibodiescarrying radioactive isotopesorcytotoxicdrugsor antibody-like frameworks (eg fibronectin)either alone as a first-line treatment or as anadjunct to existing treatments This multitudeof possible formats the ability to raise anti-bodies to almost any target and the ability toengineer both size effector functions and half-life are now considered by many to providevery valuable tools for designing specificantibody-based treatments toeradicate specifictargeted infectious agents However althoughseveral antibody-based therapies have beenapproved for oncology and anti-inflammatoryindications (see Table 1) only one monoclonalantibody (mAb) is approved against an infec-tious disease agentmdashSynagis (palivizumabMedImmune) for the prevention and treat-ment of respiratory syncytical virus (RSV) inhigh-risk children Economic obstacles such asthe high cost of mAb therapies and relativelysmall markets have resulted in less interestfrom pharmaceutical companies in developingthese Also highlighting the challenges indeveloping these types of antibody-basedtreatments are the difficulties encountered indeveloping a follow-up higher-affinity candi-date to Synagis Poor translatability of dataobtained in the available animal disease mod-els for RSV in cotton rats has resulted in non-approval due to inferiority relative to SynagisIn other viral diseases such as cytomegalovirus(CMV) the high species specificity of thestrains of CMV makes it impossible to testhuman antibody therapies in vivo Thereforeany real data on the efficacy of treatments forCMV will not be obtained until testing inclinical trials As described later in this articleseveral new antibody-based therapies for in-fectious diseases are in development andhopefully this will gradually open the fieldand result in better treatment options andoutcomes for patients
6 HEY
TABLE 1 Approved and pending antibody-based therapies
Name antibody Target antibody type Indication Company Approval date
OKT3a Muronomab-CD3 CD3 murine IgG2a Autoimmune Johnson ampJohnson
1986 (US)
ReoPro abciximab PIIbIIIa chimeric IgG1Fab
Homeostasis Johnson ampJohnson
1984 (US)
Rituxan rituximab CD20 chimeric IgG1 Cancer Genentech 1997 (US) 1998 (EU)Zenapaxa daclizumab CD25 humanized IgG1 Autoimmune Roche 1997 (US) 1999 (EU)Simulect basiliximab CD25 chimeric IgG1 Autoimmune Novartis 1998 (US EU)Synagis palivizumab RSV humanized IgG1 Infections MedImmune 1998 (US) 1999 (EU)Remicade infliximab TNFα chimeric IgG1 Autoimmune Johnson amp
Johnson1998 (US) 1999 (EU)
Herceptin trastuzumab HER2 humanized IgG1 Cancer GenentechRoche
1998 (US) 2000 (EU)
Mylotarga gemtuzumabozogamicin
CD33 humanized IgG4immunotoxin
Cancer WyethPfizer 2000 (US)
Campath alemtuzumab CD52 humanized IgG1 Cancer Genzyme 2001 (US) 2001 (EU)Zevalin ibritumomabtiuxetan
CD20 murine IgG1radiolabeled (yttrium 90)
Cancer Biogen Idec 2002 (US) 2004 (EU)
Humira adalimumab TNFα human IgG1 Autoimmune Abbott 2002 (US) 2003 (EU)Xolair omalizumab IgE humanized IgG1 Autoimmune Genentech
Roche2003 (US)
Bexxar tositumomab-I-131 CD20 murine IgG2aradiolabeled (iodine131)
Cancer CorixaGSK 2003 (US)
Raptivaa falizumab CD11a humanized IgG1 Autoimmune GenentechRoche
2003 (US) 2004 (EU)
Erbitux cetuximab EGFR chimeric IgG1 Cancer ImcloneLilly 2004 (US) 2004 (EU)Avastin bevacizumab VEGF humanized IgG1 Cancer Genentech
Roche2004 (US) 2005 (EU)
Tysabri natalizumab α4-Intergrin humanizedIgG4
Autoimmune Biogen Idec 2004 (US)
Actemra tocilizumab Anti-IL-6R humanizedIgG1
Autoimmune ChugaiRoche
2005 (Japan) 2010 (US)
Vectibix panitumumab EGFR human IgG2 Cancer Amgen 2006 (US)Lucentis ranibizumab VEGF humanized IgG1
FabMaculardegeneration
GenentechRoche
2006 (US)
Soliris eculizumab C5 humanized IgG24 Blood disorders Alexion 2007 (US)Cimzia certolizumab pegol TNFα humanized
pegylated FabAutoimmune UCB 2008 (US)
Simponi golimumab TNFα human IgG1 Autoimmune Johnson ampJohnson
2009 (US EU Canada)
Ilaris canakinumab IL1b human IgG1 Infalmmatory Novartis 2009 (US EU)Stelara ustekinumab IL-1223 human IgG1 Autoimmune Johnson amp
Johnson2008 (EU) 2009 (US)
Arzerra ofatumumab CD20 human IgG1 Cancer Genmab 2009 (EU)Prolia denosumab RANK ligand human
IgG2Bone loss Amgen 2010 (US)
Numax motavizumab RSV humanized IgG1 Anti-infective MedImmune PendingABthrax Raxibacumab B anthrasis PA human
IgG1Anti-infection GSK 2012 (US)
Benlysta belimumab BLyS human IgG1 Autoimmune HGS 2011 (US)Yervoy ipilimumab CTLA-4 human IgG1 Cancer BMS 2011 (US)Adcetris brentuximabvedotin
CD30 chimeric IgG1drug- conjugate
Cancer SeattleGenetics
2011 (US)
(Continued on next page)
CHAPTER 1 bull History and Practice Antibodies in Infectious Diseases 7
INTRODUCTION TO ANTIBODIES
Antibodies also called immunoglobulins basedon their combined structure and function inimmune responses are produced by B cells ofthe immune system They are part of theadaptive immune response and are speciallydesigned for neutralizing and eliminating theinfectious agents and toxins produced by theseAntibodies are present in blood plasma andextracellular fluids and since these fluids wereformerly known as humors they were said tobe part of the humoral immune responseAntibodies are Y-shaped structures consistingof two main parts the upper arms of the Ywhich contain two identical variable-regionantigen binding sites and the lower regioncalled the constant regionwhich is responsiblefor the initiation of effector functions that leadto the removal and destruction of the pathogenor cells harboring the pathogen (see Fig 1) Theantigen-binding sites on an antibody can bythemselves bind to and neutralize bacterialtoxins and viruses thereby preventing themfrom binding to their target cells or receptorscausing toxic effects or spread of the infection
Antibodies consist of two pairs of heavy andlight chainswhich as described above are heldtogether in a Y-shaped arrangement Each ofthe heavy and light chains in these pairs isseparated into constant and variable chainsThe upper armsof theY each contain a variableand a constant sectionof the light and theheavychain where the upper variable parts of theheavy and light chains contain the antigen-binding site and the constant parts areconnected via disulfide bonds The lower partof theYcalled theconstantpart consistsof twoor three constant segments (immunoglobulindomains) from each of the two heavy chainsinteracting and also linked via disulfide bondsThe sectionsof theheavy chains connecting theconstant part of the upper arms to the constantparts of the constant region contain specialhinge regions that provide flexibility to thedifferent sections of the antibody to bind toantigens and effector cells The constant re-gions of the heavy chain also contain attachedoligosaccharide moieties which provide func-tional specialization to the antibodies (8)
The variable domains of the heavy and lightchains form the antigen-binding sites and
TABLE 1 Approved and pending antibody-based therapies (Continued)
Name antibody Target antibody type Indication Company Approval date
Perjeta pertuzumab Her2 humanized IgG1 Cancer GenentechRoche
2012 (US)
Kadcyla ado-trastuzumabemtansine
Her2 humanized IgG1Drug-conjugate
Cancer GenentechRoche
2013 (US)
Raxibacumab Anti-B anthrasis PAhuman IgG1
Anthraxinfection
Notapproved
2012
Entyvio vedolizumab Integrin α4β7humanized IgG1
Crohnrsquos diseaseulcerative colitis
Takeda 2014 (US)
Cyramza ramuciruumab Anti-VEGFR2Human IgG1
Gastric cancer Lilly 2014 (US)
Gazyva obinutuzumab Anti-CD20 humanizedIgG1 glucoengineered
CancerCLLb GenentechRoche
2014 (US)
Sylvant situximab Anti IL-6 chimeric IgG1 Castlemandisease
Janssen 2014 (US) 2014 (EU)
Cosentyx sekukinumab Anti IL-17a human IgG1 Psoriasis Novartis 2015 (US) 2015 (EU)Nivolumab Anti PD-1 human IgG4 Melanoma BMS Not approvedKeytruda pembrolizuumab Anti-PD-1 humanized
IgG4Melanoma Merck 2014 (US)
aAntibodies approved but later withdrawnbCLL chronic lymphocytic leukemia
8 HEY
FIGURE 1 (Left panel) Model of antibody structure exemplified by IgG On top the antigen-binding sitesin orange each contain one variable light and variable heavy domain with the three complementaritydetermining regions (CDRs) that are responsible for the specific binding of the antibody to its target Foreach arm of the antibody an additional set of variable heavy and light domains together with the CDR-containing domains represent the two fragment antigen binding (Fab) regions The two Fabs are heldtogether via two disulfide bridges Below the Fabs is the Fc region which contains four constant heavydomains On the upper pair of these domains are binding sites for oligosaccharides which have majorimportance for the ability of the antibody Fc part to trigger effector functions when the Fc portion isbound to Fc gamma receptors on natural killer cells neutrophil granulocytes monocytesmacrophagesdendritic cells and B cells (Right panel) Examples of some of the antibody-derived alternative formatsused to exploit the specific features of the CDRs the Fabs and the Fc parts of the antibodies ScFv Thesingle chain fragment variable consists of the variable domains of the heavy and light chains heldtogether by a flexible linker This can also be used as a carrier of a cytotoxic drug in a so-called antibodydrug complex (ADC) where the specificity of the ScFv is used to target the cytotoxic drug to eg atumor Bite (bi-specific T cell engager) Fusion proteins consisting of two ScFvs one directed against thetarget on a tumor cell and the other against the T cell receptor (CD3) Diabody ScFv dimers where shortlinker peptides (five amino acids) ensure dimerization and not folding of the ScFvs Fab and F(ab)2fragments Single Fab fragments or fragments containing two Fabs linked via disulfide bridges This isused where effector functions related to the Fc part of the antibody are unwanted and where a smallersize is desired to obtain better tissue penetration in eg tumors Due to the lack of the FcRn binding viathe Fc part Fab and F(ab)2 fragments have much shorter half-lives (hours or days) than full-sizeantibodies (weeks) These can also be used as carriers of cytotoxic payloads or cytotoxic radioactiveisotopes and for the F(ab)2 fragments can be constructed as bi-specifics which can cross-link immunecells and target cells Fc fusion protein Fusion protein containing the Fc domain of an immunoglobulinbound to a peptide The peptide can be a ligand for a specific receptor on a target cell or a blockingpeptide for a soluble ligand The Fc part provides a longer half-life to the construct and the potential tobind to and engage effector functions in the killing of eg tumor cells or infected cells ADCsRIAs andbi-specifics Full-size IgG antibodies carrying either a cytotoxic chemical or radioactive payload whichmay also carry different CDRs enabling cross-linking of effector and target cells for increased killingdoi101128microbiolspecAID-0026-2014f1
CHAPTER 1 bull History and Practice Antibodies in Infectious Diseases 9
contain special hyper-variable segments calledcomplementarity-determining regions (CDRs)which allow the B cells via genetic recom-bination to generate antibodies to all thedifferent antigens specific to amino acid se-quences or three-dimensional structuralmotifs(polysaccharides DNA and RNA) found onpathogens
Based on the structure of their heavy chainconstant regions antibodies or immuno-globulins are separated into five classesmdashIgM IgG IgE IgD and IgA Differences inthe sequences of the constant regions providedistinct characteristics to these different clas-ses These characteristics include the numberof heavy chain constant segments the numberand location of interconnecting disulfidebridges the length of the hinge region andthe number and location of oligosaccharidemoieties For IgG four heavy chain versionsexist creating IgG1 2 3 and 4 isotypes eachwith different characteristics in their serumhalf-lives and ability to trigger different effec-tor functions Because of the combined ad-vantage from ability to trigger effectormechanisms long [21 days] half-life theirability to be transported over the placentaand their stability in the production processantibodies of the IgG class and of the IgG1isotype are preferred as the basis for newantibody-based therapies The effector func-tions are triggered by the Fc part of an antibodywhen the variable parts of the antibody arebound directly to an infectious agent or toproteins from an infectious agent expressed onan infected cell This binding leaves the Fc partfree to interactwithFc receptors onphagocyticcells and neutrophils eosinophils and naturalkiller cells capable of inducing phagocytosis orlysis of infectious agents or infected cellsThese effector functions include (i) the abilityto activate the complement system for lysis(complement-dependent cellular cytotoxicity)(ii) triggering of uptake and destruction byphagocytic cells such as macrophages andneutrophils via interaction with Fc receptorson these cells (iii) activation of macrophageseosinophils neutrophils and natural killer
cells to kill infected cells via binding to Fcreceptors on these cells and antibody-depen-dent cellular cytotoxicity and (iv) neutraliza-tion of bacterial toxins and blocking of bindingand uptake of bacteria or viruses to target cells(see Fig 2) (9)
The Fcpart of IgG antibodies also contains aregion that interacts with the neonatal Fcreceptor (FcRn) expressed on most immuno-competent cells and inmany other cells such asendothelial cells in kidney liver placenta lungand breast (10) which protects antibodies fromdegradation by phagocytoticexocytotic cy-cling into FcRn-expressing cells thereby pro-longing their half-life This results in half-livesof 20 to 21 days for most IgG1 2 and 4antibodies whereas half-lives are 10 6 and 2days respectively for IgM IgA and IgE Thehighly specific binding sites on the variableregions of the upper arms of the antibody allowfor several important features of antibodiesndashbinding to and neutralization of eg bacterialtoxins binding to pathogens and blocking theirbinding to or interaction with target cells (egcyncytia formation of CMV-infected cells) orblocking of binding and interactions of infec-tious agents with target cells via blockingreceptors on the target cells
METHODS AND PLATFORMS FORGENERATING ANTIBODIES
As described above the early use of passiveantibody transfer as a therapy in infectiousdiseases involved the use of immune serumfrom immunized sheep and horses These pre-parations were crude and contained a broadmixture of neutralizing and non-neutralizingantibodies and both the foreign nature of theantibodies and the numerous host serumproteins This resulted in less specific andthus less efficient therapies due to a highvariability in efficacy between batches derivedfrom different animals immunized with dif-ferent strains of bacteria in different labor-atories and resulted in multiple unwantedside effects related to hypersensitivity and
10 HEY
anaphylactic reactions to foreign proteinsThese days antibodies being developed fortreatment of diseases in humans are highlypurified and are mostly fully human mono-clonal antibodies The term monoclonal anti-body refers to that cell cultures used forgenerating these antibodies each originatesfrom a single cell and thus produces onlyone specific antibody Development of fullyhuman monoclonal antibodies happened instages over a time span of more than 15 yearsFirst stage in this process was generation ofmonoclonalmurine IgG antibodies (eg OKT3[muronomab-CD3 Johnson and Johnson] ap-proved in 1986) Next stage was generation ofso called chimeric antibodies consisting ofhuman heavy and light chain constant sec-tions but with murine variable sections (eg
Rituxan [rituximab Genentech]) Next stagewas then the humanized antibodies wherethe only remaining murine part of the anti-body is the antigen-binding CDR (eg Xolair[omalizumab NovartisGenentech]) Both thefirst chimeric and humanized antibodies wereapproved in the late 1990s Then finally 16years later the first fully human antibodyHumira (adalimumab Abbott) was approvedin 2002 Since the time of the crude and low-scale manufacturing of the original antibodyserum products much has changed andtherapeutic antibodies are now produced byfermentation in 5000 liter scale using highlycontrolled and documented yeast or mamma-lian cell lines that are genetically engineered toexpress a single specific antibody This hasresulted in a pure and highly specific antibody
FIGURE 2 Effector functions of antibodies (a) Antibodies bind to pathogen-derived or endogenousantigens expressed on the surface of an infected cell which triggers binding to Fc receptors on naturalkiller cells and lysis of the infected cell by antibody-dependent cellular cytotoxicity (b) Antibodies bindto pathogen-derived or endogenous antigens expressed on the surface of infected cells which triggersactivation of complement through binding of complement factor C1q (c) Neutralization Top Bacterialtoxin neutralized by bound antigen Bottom Antibody bound to either receptor for the virus or to thevirus itself which blocks virus binding and entry into the cell (d) Antibody bound to viral surfaceproteins binds to Fc receptors on phagocytic cells eg macrophages and triggers endocytosis anddestruction of virus in endolysosome doi101128microbiolspecAID-0026-2014f2
CHAPTER 1 bull History and Practice Antibodies in Infectious Diseases 11

Marie-Paule LefrancLaboratoire drsquoImmunoGeacuteneacutetique Moleacuteculaire LIGMIMGTreg the international ImMunoGeneTics information systemregInstitut de Geacuteneacutetique Humaine IGHUniversiteacute Montpellier 2UPR CNRS 1142Montpellier 34396 cedex 5 40202France
Olivier LegerDepartment of Protein Engineering and Antibody TechnologiesMerck Serono SA--Geneva9 chemin des Mines1202 GenevaSwitzerland
Kin-Ming LoDepartment of Protein Engineering and Antibody TechnologiesEMD Serono Research Institute45A Middlesex TurnpikeBillerica MA 01821
Wayne A MarascoDepartment of Cancer Immunology and AIDSDana-Farber Cancer InstituteHarvard Medical SchoolBoston MA 02215
Jennifer A MaynardDepartment of Chemical EngineeringUniversity of Texas at AustinAustin TX 78712
Luzia M MayrINSERM U1109Universiteacute de Strasbourg3 Rue Koeberleacute67000 StrasbourgFrance
Jens MeilerDepartment of Chemistry and Center for Structural BiologyVanderbilt UniversityNashville TN 37212
contRIBUtoRs xiii
S Moein MoghimiDepartment of PharmacyCenter for Pharmaceutical Nanotechnology and NanotoxicologyFaculty of Health and Medical SciencesUniversity of CopenhagenCopenhagen DK-2100Denmark
Susan Zolla-PaznerNew York University School of Medicine550 First AvenueNew York NY 10016
Louise SaulCutaneous Medicine and Immunotherapy UnitSt Johnrsquos Institute of DermatologyDivision of Genetics and Molecular Medicine amp NIHR Biomedical Research Centre at Guyrsquos and St Thomasrsquos HospitalsKingrsquos College London School of MedicineGuyrsquos HospitalLondon SE1 9RTUnited Kingdom
Bruce C SchneppThe Childrenrsquos Hospital of PhiladelphiaAbramson Research CenterPhiladelphia PA 19104
Jennifer E SchusterDepartment of PediatricsChildrenrsquos Mercy HospitalKansas City MO 64108-4619
Alexander M SevyDepartment of Chemistry and Center for Structural BiologyVanderbilt UniversityNashville TN 37212
Jared SheehanDepartment of Cancer Immunology and AIDSDana-Farber Cancer InstituteHarvard Medical SchoolBoston MA 02215
Michael R SierksDepartment of Chemical EngineeringArizona State UniversityTempe AZ 85287-6006
xiv contRIBUtoRs
Scott A SmithThe Vanderbilt Vaccine Center and the Department of MedicineVanderbilt University Medical CenterNashville TN 37232
Robyn L StanfieldDepartment of Molecular BiologyThe Scripps Research Institute10550 North Torrey Pines RoadLa Jolla CA 92037
Nadine UptonRandall Division of Cell and Molecular BiophysicsDivision of Asthma Allergy and Lung BiologyMRC and Asthma UK Centre for Allergic Mechanisms of AsthmaKingrsquos College LondonNew Huntrsquos HouseGuyrsquos CampusLondon SE1 1ULUnited Kingdom
Avanish K VarshneyDepartment of MedicineInfectious Diseases and Department of Microbiology and ImmunologyAlbert Einstein College of MedicineBronx NY 10461
Stefanie N VelgosMayo Clinic Arizona5777 East Mayo BoulevardPhoenix AZ 85054
Kevin J WhaleyMapp Biopharmaceutical Inc6160 Lusk Blvd C105San Diego CA 92121
Peter P WibroeCentre for Pharmaceutical Nanotechnology and NanotoxicologyDepartment of PharmacyFaculty of Health and Medical SciencesUniversity of CopenhagenCopenhagen DK-2100Denmark
John V WilliamsDepartment of PediatricsSchool of MedicineVanderbilt UniversityNashville TN 37232-2581
contRIBUtoRs xv
Ian A WilsonDepartment of Molecular Biology and Skaggs Institute for Chemical BiologyThe Scripps Research Institute10550 North Torrey Pines RoadLa Jolla CA 92037
Herren WuDepartment of Antibody Discovery and Protein EngineeringMedImmune LLCOne MedImmune WayGaithersburg MD 20879
Guocheng YangDepartment of Chemical EngineeringArizona State UniversityTempe AZ 85287-6006
Larry ZeitlinMapp Biopharmaceutical Inc6160 Lusk Blvd C105San Diego CA 92121
xvi contRIBUtoRs
Preface
Antibodies form the principal foundation for modern intervention against in-fectious diseases Emil Adolf von Behring was awarded the first Nobel Prize in Physiology or Medicine in 1901 ldquofor his work on serum therapy especially its appli-cation against diphtheria by which he has opened a new road in the domain of med-ical science and thereby placed in the hands of the physician a victorious weapon against illness and deathsrdquo Antibodies now provide the focus for understanding mechanisms of immunity to most infectious diseases and they play a central role in passive immunotherapy and active vaccination as mechanisms or correlates of immunity For most of the 20th century immunotherapy was based on passive transfer of polyclonal hyperimmune animal serum immune human serum or even hyperimmune human serum Georges JF Koumlhler and Ceacutesar Milstein re-ported the generation of monoclonal antibodies in 1979 for which they shared the 1984 Nobel Prize in Physiology or Medicine ldquofor the discovery of the princi-ple for production of monoclonal antibodiesrdquo Since that time entire fields related to antibodies for infectious diseases including antibody gene cloning engineer-ing and expression antibody libraries and high-throughput antibody gene rep-ertoire sequence analysis have extended our capabilities to explore the diversity of antibody specificity and function with unprecedented depth and breadth
This book provides a broad survey of many of the most important aspects of the field of antibodies for infectious diseases The book begins with a general introduction followed by chapters 2 through 5 on general features pertaining to structure function isotype and the role of complement in antibody function Chapters 6 through 10 review contemporary approaches for antibody discovery using phage and yeast display plasma cell and memory B cell cloning human hybridomas humanized mice and computational methods Chapters 11 through 18 review in depth the biology of antibodies specific for particular pathogens including viruses and bacterial toxins to illustrate the role of antibodies in anti- microbial immunity with specific targets These chapters reveal that attempts to raise effective antibody responses to each of these pathogens faces unique and pathogen-specific challenges Chapters 19 to 23 cover major technical advances pertaining to antibody engineering repertoire sequencing and analysis and new methods for study or therapeutic use of antibodies including radiotherapy Fi-nally chapters 24 and 25 cover new methods for expression of monoclonal anti-bodies in plants or by transfer of antibody genes for in vivo expression in treated subjects
Recent literature is exploding with new antibody-related techniques and re-ports of antimicrobial antibodies with unprecedented potency breadth of activ-
xvii
xviii PReface
ity and therapeutic potential We hope that this timely compilation of state-of-the-art reviews of major aspects of this field will be of interest to both antibody cognoscenti and those new to this exciting field We thank the authors for their dedication in producing definitive reviews of the topics at hand
James E Crowe JrDiana BoraschiRino Rappuoli
INTRODUCTION
History and PracticeAntibodies in Infectious Diseases 1ADAM HEY1
Antibodies in Infectious Diseases aims to inform update and inspire studentsteachers researchers pharmaceutical developers and health care professionalson the status of the development of antibody-based therapies for treatinginfectious diseases and the potential for these in times of growing antibioticresistance to provide alternative treatment solutions to the currently usedantibiotics and new treatments for infectious diseases where no propertreatments are available
This introductory article will provide a historical perspective on the useof antibody-based therapies followed by a high-level overview of whatmakes antibodies attractive tools for this purpose This will include the prosand cons of such therapies compared to the use of antibiotics and thepractical and strategic considerations involved in selecting the best formatand development path for new antibody-based therapies targeting specificinfectious agents Then examples of antibody-based therapies in thedevelopment of treatments for infectious diseases will be presented andfinally a look into the future will summarize the different aspects that willinfluence what the future might bring for this type of treatments forinfectious diseases
1Preclinical Safety Biologics Novartis AG Basel Switzerland
Antibodies for Infectious DiseasesEdited by James E Crowe Jr Diana Boraschi and Rino Rappuolicopy 2015 American Society for Microbiology Washington DCdoi101128microbiolspecAID-0026-2014
3
HISTORICAL PERSPECTIVE
Antibodies and the use of passive antibodytherapy in the treatment of infectious dis-eases is the story of a treatment conceptwhich dates back more than 120 years to thelate 19th century and which originally bythe use of serum from immunized animalsprovided the first effective treatment optionsagainst severe bacterial infections (1 2) Byimmunizing horses with bacterial toxinsfrom Clostridium tetani and Corynebacteri-um diphtheriae Emil A Von Behring andShibasaburo Kitasato (3) generated serumcontaining antibodies capable of neutraliz-ing the effects of the toxins produced bythese bacteria and successfully providedtreatment for these serious diseases wherethe pathogenesis is driven by the effects ofthe bacterial toxins For his work on provid-ing treatment for diphtheria Behring re-ceived the Nobel Prize in Physiology orMedicine in 1901 These radical treatmentresults quickly prompted development ofmultiple additional serum therapies for thetreatment of infectious diseases caused byeg Neisseria meningitidis Haemophilus in-fluenza and group A Streptococcus Sinceserum therapy involved administration oflarge amounts of crude mixtures of animalproteins including antibodies they wereassociated with side effects in the form ofhypersensitivity and serum sickness (2)
Due to the crude and unpurified nature ofthese products side effects were seen evenwhen administering human serum prepa-rations Side effects were observed in up to50 of patients and were considered to becaused by immune complex formations thatresulted in symptoms such as rash itchingjoint pain fever and in serious cases hypoten-sion and shock However due to the lack ofalternative options these treatments weredespite their side effects widely used Serumwas normally administered by intravenousinfusion in patients after a test for hypersensi-tivity where a small amount of serum wasinjected subcutaniously (1) As described
above serum therapy applied in these earlydays (late 19th century and early 20th century)involved preparations of serum from rabbitsand horses immunized with the infectiousagent or in live andor neutralized versions ortoxins from these (1) The costs of keeping theimmunized animals and the production andpotency testing of the materials made this arelatively expensive treatment In 1891 datafrom Klemperer (4) showed serum therapy toprotect rabbits from Streptococcus pneumoniaeinfection and paved the way for this type oftreatment and for development of similarserum-based treatments of streptococcal in-fections in humans When treating humansearly administration of serum could reducemortality significantly down to around 5compared to when administered 4 to 5 daysafter onset of symptoms when serum treat-ment was largely without effect This stronglyindicated the need for quick diagnosis andquick treatment to control the infection beforeit got out of control Consequently in theabsence of a specific diagnosis mixtures ofserum from immunizations with differentserotypes were used to circumvent this needfor early treatment without having a serotype-specific diagnosis The understanding thatdifferent serotypes existed for pneumococciand that efficient treatment relied on usingserotype-specific serum was being built upduring the 1920s and 1930s through experiencefrom extensive clinical trials
By the end of the 1930s serum therapywasthe standard of care for treatment of pneu-mococcal pneumonia At that time theefficacy and potency of the derived serawere assessed in mice in ldquothe mouse pro-tection testrdquo by testing survival after aconcomitant intraperitoneal injection of alethal dose of pneumococci and the serum tobe tested Due to the inherent variation inthis test efficacy and survival in two thirds ofthe animals was the acceptance criteria and10 times the lowest dose providing this wasused for defining a unit of the serum Thisallowed for large batch-to-batch variationand the use of different strains of bacteria for
4 HEY
immunization probably explains part of themissing responses observed (1) In the early20th century a pandemic of meningitis inEurope and the United States with mortalityrates up to 80 spurred the development ofserum therapy treatment options Althoughin the 1930s this became the recommendedtreatment in children assumed to be suffer-ing from meningitis failure to reduce mor-tality in several meningitis epidemics duringthat time raised doubts about the generalapplicability of serum treatment In thosedays serum therapy often involved quiteextensive procedures and infusion of largevolumes of serum The following exampleclearly illustrates this Data from Flexnerand Jobling (5) from treating meningitis inmonkeys resulted in the development of serafrom immunized horses for treatment inhumans The treatment protocol includedlumbar puncture and withdrawal of morethan 30 ml of spinal fluid representing anamount slightly larger than the expectedamount of horse serum to be injected subse-quently This treatment involved such dailyslow infusions of up to 30 ml of serum untilthe patientrsquos condition improved This treat-ment was used in outbreaks in New York in1905 and 1906 and did markedly decreasemortality
After the discovery of penicillin by Flemingin 1928 and the subsequent introduction ofantibiotics in the 1930s serum therapy waslargely abandoned over a period of 10 years dueto the availability of these new more broadlyeffective and cheaper treatment optionswhichalso had fewer side effects Although improve-ments in the purification of antibodies hadresulted in preparations with better safety andside effect profiles high manufacturing costsand narrow specificity resulted in antibodytherapy being mostly restricted to a smallernumber of selected treatments for snakevenoms bacterial toxins and some viral infec-tions (1 2) Currently antibody administrationis used for treatment and prevention ofhepatitis B virus rabies virus respiratorysyncytial virus (RSV) Clostridium tetani Clos-
tridium botulinum vaccinia virus echovirusand enterovirus For the most part thesetreatments consist of pooled immunoglobulinalso known as IVIG (intravenous immunoglob-ulin) from several postexposure donors Thisresults in both batch-to-batch variation in theneed for relatively large amounts of serum dueto low specificity and to restricted supplies dueto reliance on exposed donors
However several challengeshave resulted inthe need for new tools in the treatment andpreventionof infectiousdiseasesThebroadandgeneral use of antibiotics in human and veter-inary medicine for many years has resulted inthe development of multi-resistant strains ofbacteria with limited to no response to existingtreatments such as methicillin-resistant Staph-ylococcusaureus (MRSA) vancomycin-resistantS aureus and others This has resulted inpatients needing screening and treatment withseveral antibacterial agents and longer treat-ment time causing extra strain on patients andhealth care providers (6 httpwwwcdcgovdrugresistancethreat-report-2013indexhtml) According to the WHO and CDC morethan 25000 people in European Unioncountries and similar numbers in the UnitedStates die every year as a result of antibiotic-resistant infections This together with theemergence of new pathogens (eg severeacute respiratory syndrome Middle East respi-ratory syndrome) the re-emergenceepidemicsof oldknown pathogens (eg Ebola) and thedifficulties in treating infections in immune-deficient patients (eg HIV patients) has high-lighted the need for new solutions The 2014Ebola epidemic in West Africa (Liberia SierraLeone Guinea Nigeria and Senegal) has fur-ther highlighted this No treatment or prophy-lactic vaccine is available to treat or prevent thespread of Ebola infections which have anaveragemortality of gt50 Local health author-ities in the affected countries are struggling tocontain and handle the disease which isthreatening to go out of control and spreadmorewidelyVariousproductsmainly antibodycocktails from previously recovered patientsare being used despite a lack of clinical data on
CHAPTER 1 bull History and Practice Antibodies in Infectious Diseases 5
their safety and efficacy and those are the onlysporadically available treatment options andonly in small amounts and for a few patients
Ebola is an example of a disease whichnormally affects only a small number ofindividuals and which normally burns outwhen disease outbreaks are contained There-fore given the small number of potentialpatients affected by previous Ebola infectionsto date there was no incentive for big pharmacompanies to do research and development ofdrugs for EbolaWith the increasing number ofinfected (13567) andadeath toll of 4951 (7) andthe lack of the ability to contain the epidemic itwill be interesting to follow the aftermath ofthis outbreak and see whether there will berequests for new ways to ensure that vaccinesand treatment options are available for Ebolaand similar high-mortality and potential bio-warfare infections that have no availabletreatments or procedures to for mass-produc-tion upon the first signsreports of activeinfections Although both the CDC and theWHO have special programs focusing on thesetypes of infections the Ebola outbreak in 2014clearly shows that more financial support forresearch and development of new diagnosticsand treatments is needed This is one examplewhere antibody-based treatments would havethe potential to play a major role To put this inthe right perspective one should however notforget that other infectious diseases such astuberculosis influenza and malaria kill hun-dreds of thousands each year There is there-fore plenty of room for improvement indeveloping treatments for these diseases aswell but the high attention drawn to eg theEbola outbreak creates a special niche andopportunity where antibody treatments couldgain extraordinary development funding andsupport and prove their value and treatmentpotential
That antibody-based therapies could takethis role is supported by the revolution intechnologies for the development selectiongeneration and purification of fully humanantibodies described in more detail later in thesection ldquoMethodsandPlatforms forGenerating
Antibodiesrdquo Antibody-based programs cur-rently at different stages of developmentinclude investigations into the potential use ofsingle antibody preparations combinations ofantibodies (to avoid survival of escape mu-tants) fragments of antibodies and antibodiescarrying radioactive isotopesorcytotoxicdrugsor antibody-like frameworks (eg fibronectin)either alone as a first-line treatment or as anadjunct to existing treatments This multitudeof possible formats the ability to raise anti-bodies to almost any target and the ability toengineer both size effector functions and half-life are now considered by many to providevery valuable tools for designing specificantibody-based treatments toeradicate specifictargeted infectious agents However althoughseveral antibody-based therapies have beenapproved for oncology and anti-inflammatoryindications (see Table 1) only one monoclonalantibody (mAb) is approved against an infec-tious disease agentmdashSynagis (palivizumabMedImmune) for the prevention and treat-ment of respiratory syncytical virus (RSV) inhigh-risk children Economic obstacles such asthe high cost of mAb therapies and relativelysmall markets have resulted in less interestfrom pharmaceutical companies in developingthese Also highlighting the challenges indeveloping these types of antibody-basedtreatments are the difficulties encountered indeveloping a follow-up higher-affinity candi-date to Synagis Poor translatability of dataobtained in the available animal disease mod-els for RSV in cotton rats has resulted in non-approval due to inferiority relative to SynagisIn other viral diseases such as cytomegalovirus(CMV) the high species specificity of thestrains of CMV makes it impossible to testhuman antibody therapies in vivo Thereforeany real data on the efficacy of treatments forCMV will not be obtained until testing inclinical trials As described later in this articleseveral new antibody-based therapies for in-fectious diseases are in development andhopefully this will gradually open the fieldand result in better treatment options andoutcomes for patients
6 HEY
TABLE 1 Approved and pending antibody-based therapies
Name antibody Target antibody type Indication Company Approval date
OKT3a Muronomab-CD3 CD3 murine IgG2a Autoimmune Johnson ampJohnson
1986 (US)
ReoPro abciximab PIIbIIIa chimeric IgG1Fab
Homeostasis Johnson ampJohnson
1984 (US)
Rituxan rituximab CD20 chimeric IgG1 Cancer Genentech 1997 (US) 1998 (EU)Zenapaxa daclizumab CD25 humanized IgG1 Autoimmune Roche 1997 (US) 1999 (EU)Simulect basiliximab CD25 chimeric IgG1 Autoimmune Novartis 1998 (US EU)Synagis palivizumab RSV humanized IgG1 Infections MedImmune 1998 (US) 1999 (EU)Remicade infliximab TNFα chimeric IgG1 Autoimmune Johnson amp
Johnson1998 (US) 1999 (EU)
Herceptin trastuzumab HER2 humanized IgG1 Cancer GenentechRoche
1998 (US) 2000 (EU)
Mylotarga gemtuzumabozogamicin
CD33 humanized IgG4immunotoxin
Cancer WyethPfizer 2000 (US)
Campath alemtuzumab CD52 humanized IgG1 Cancer Genzyme 2001 (US) 2001 (EU)Zevalin ibritumomabtiuxetan
CD20 murine IgG1radiolabeled (yttrium 90)
Cancer Biogen Idec 2002 (US) 2004 (EU)
Humira adalimumab TNFα human IgG1 Autoimmune Abbott 2002 (US) 2003 (EU)Xolair omalizumab IgE humanized IgG1 Autoimmune Genentech
Roche2003 (US)
Bexxar tositumomab-I-131 CD20 murine IgG2aradiolabeled (iodine131)
Cancer CorixaGSK 2003 (US)
Raptivaa falizumab CD11a humanized IgG1 Autoimmune GenentechRoche
2003 (US) 2004 (EU)
Erbitux cetuximab EGFR chimeric IgG1 Cancer ImcloneLilly 2004 (US) 2004 (EU)Avastin bevacizumab VEGF humanized IgG1 Cancer Genentech
Roche2004 (US) 2005 (EU)
Tysabri natalizumab α4-Intergrin humanizedIgG4
Autoimmune Biogen Idec 2004 (US)
Actemra tocilizumab Anti-IL-6R humanizedIgG1
Autoimmune ChugaiRoche
2005 (Japan) 2010 (US)
Vectibix panitumumab EGFR human IgG2 Cancer Amgen 2006 (US)Lucentis ranibizumab VEGF humanized IgG1
FabMaculardegeneration
GenentechRoche
2006 (US)
Soliris eculizumab C5 humanized IgG24 Blood disorders Alexion 2007 (US)Cimzia certolizumab pegol TNFα humanized
pegylated FabAutoimmune UCB 2008 (US)
Simponi golimumab TNFα human IgG1 Autoimmune Johnson ampJohnson
2009 (US EU Canada)
Ilaris canakinumab IL1b human IgG1 Infalmmatory Novartis 2009 (US EU)Stelara ustekinumab IL-1223 human IgG1 Autoimmune Johnson amp
Johnson2008 (EU) 2009 (US)
Arzerra ofatumumab CD20 human IgG1 Cancer Genmab 2009 (EU)Prolia denosumab RANK ligand human
IgG2Bone loss Amgen 2010 (US)
Numax motavizumab RSV humanized IgG1 Anti-infective MedImmune PendingABthrax Raxibacumab B anthrasis PA human
IgG1Anti-infection GSK 2012 (US)
Benlysta belimumab BLyS human IgG1 Autoimmune HGS 2011 (US)Yervoy ipilimumab CTLA-4 human IgG1 Cancer BMS 2011 (US)Adcetris brentuximabvedotin
CD30 chimeric IgG1drug- conjugate
Cancer SeattleGenetics
2011 (US)
(Continued on next page)
CHAPTER 1 bull History and Practice Antibodies in Infectious Diseases 7
INTRODUCTION TO ANTIBODIES
Antibodies also called immunoglobulins basedon their combined structure and function inimmune responses are produced by B cells ofthe immune system They are part of theadaptive immune response and are speciallydesigned for neutralizing and eliminating theinfectious agents and toxins produced by theseAntibodies are present in blood plasma andextracellular fluids and since these fluids wereformerly known as humors they were said tobe part of the humoral immune responseAntibodies are Y-shaped structures consistingof two main parts the upper arms of the Ywhich contain two identical variable-regionantigen binding sites and the lower regioncalled the constant regionwhich is responsiblefor the initiation of effector functions that leadto the removal and destruction of the pathogenor cells harboring the pathogen (see Fig 1) Theantigen-binding sites on an antibody can bythemselves bind to and neutralize bacterialtoxins and viruses thereby preventing themfrom binding to their target cells or receptorscausing toxic effects or spread of the infection
Antibodies consist of two pairs of heavy andlight chainswhich as described above are heldtogether in a Y-shaped arrangement Each ofthe heavy and light chains in these pairs isseparated into constant and variable chainsThe upper armsof theY each contain a variableand a constant sectionof the light and theheavychain where the upper variable parts of theheavy and light chains contain the antigen-binding site and the constant parts areconnected via disulfide bonds The lower partof theYcalled theconstantpart consistsof twoor three constant segments (immunoglobulindomains) from each of the two heavy chainsinteracting and also linked via disulfide bondsThe sectionsof theheavy chains connecting theconstant part of the upper arms to the constantparts of the constant region contain specialhinge regions that provide flexibility to thedifferent sections of the antibody to bind toantigens and effector cells The constant re-gions of the heavy chain also contain attachedoligosaccharide moieties which provide func-tional specialization to the antibodies (8)
The variable domains of the heavy and lightchains form the antigen-binding sites and
TABLE 1 Approved and pending antibody-based therapies (Continued)
Name antibody Target antibody type Indication Company Approval date
Perjeta pertuzumab Her2 humanized IgG1 Cancer GenentechRoche
2012 (US)
Kadcyla ado-trastuzumabemtansine
Her2 humanized IgG1Drug-conjugate
Cancer GenentechRoche
2013 (US)
Raxibacumab Anti-B anthrasis PAhuman IgG1
Anthraxinfection
Notapproved
2012
Entyvio vedolizumab Integrin α4β7humanized IgG1
Crohnrsquos diseaseulcerative colitis
Takeda 2014 (US)
Cyramza ramuciruumab Anti-VEGFR2Human IgG1
Gastric cancer Lilly 2014 (US)
Gazyva obinutuzumab Anti-CD20 humanizedIgG1 glucoengineered
CancerCLLb GenentechRoche
2014 (US)
Sylvant situximab Anti IL-6 chimeric IgG1 Castlemandisease
Janssen 2014 (US) 2014 (EU)
Cosentyx sekukinumab Anti IL-17a human IgG1 Psoriasis Novartis 2015 (US) 2015 (EU)Nivolumab Anti PD-1 human IgG4 Melanoma BMS Not approvedKeytruda pembrolizuumab Anti-PD-1 humanized
IgG4Melanoma Merck 2014 (US)
aAntibodies approved but later withdrawnbCLL chronic lymphocytic leukemia
8 HEY
FIGURE 1 (Left panel) Model of antibody structure exemplified by IgG On top the antigen-binding sitesin orange each contain one variable light and variable heavy domain with the three complementaritydetermining regions (CDRs) that are responsible for the specific binding of the antibody to its target Foreach arm of the antibody an additional set of variable heavy and light domains together with the CDR-containing domains represent the two fragment antigen binding (Fab) regions The two Fabs are heldtogether via two disulfide bridges Below the Fabs is the Fc region which contains four constant heavydomains On the upper pair of these domains are binding sites for oligosaccharides which have majorimportance for the ability of the antibody Fc part to trigger effector functions when the Fc portion isbound to Fc gamma receptors on natural killer cells neutrophil granulocytes monocytesmacrophagesdendritic cells and B cells (Right panel) Examples of some of the antibody-derived alternative formatsused to exploit the specific features of the CDRs the Fabs and the Fc parts of the antibodies ScFv Thesingle chain fragment variable consists of the variable domains of the heavy and light chains heldtogether by a flexible linker This can also be used as a carrier of a cytotoxic drug in a so-called antibodydrug complex (ADC) where the specificity of the ScFv is used to target the cytotoxic drug to eg atumor Bite (bi-specific T cell engager) Fusion proteins consisting of two ScFvs one directed against thetarget on a tumor cell and the other against the T cell receptor (CD3) Diabody ScFv dimers where shortlinker peptides (five amino acids) ensure dimerization and not folding of the ScFvs Fab and F(ab)2fragments Single Fab fragments or fragments containing two Fabs linked via disulfide bridges This isused where effector functions related to the Fc part of the antibody are unwanted and where a smallersize is desired to obtain better tissue penetration in eg tumors Due to the lack of the FcRn binding viathe Fc part Fab and F(ab)2 fragments have much shorter half-lives (hours or days) than full-sizeantibodies (weeks) These can also be used as carriers of cytotoxic payloads or cytotoxic radioactiveisotopes and for the F(ab)2 fragments can be constructed as bi-specifics which can cross-link immunecells and target cells Fc fusion protein Fusion protein containing the Fc domain of an immunoglobulinbound to a peptide The peptide can be a ligand for a specific receptor on a target cell or a blockingpeptide for a soluble ligand The Fc part provides a longer half-life to the construct and the potential tobind to and engage effector functions in the killing of eg tumor cells or infected cells ADCsRIAs andbi-specifics Full-size IgG antibodies carrying either a cytotoxic chemical or radioactive payload whichmay also carry different CDRs enabling cross-linking of effector and target cells for increased killingdoi101128microbiolspecAID-0026-2014f1
CHAPTER 1 bull History and Practice Antibodies in Infectious Diseases 9
contain special hyper-variable segments calledcomplementarity-determining regions (CDRs)which allow the B cells via genetic recom-bination to generate antibodies to all thedifferent antigens specific to amino acid se-quences or three-dimensional structuralmotifs(polysaccharides DNA and RNA) found onpathogens
Based on the structure of their heavy chainconstant regions antibodies or immuno-globulins are separated into five classesmdashIgM IgG IgE IgD and IgA Differences inthe sequences of the constant regions providedistinct characteristics to these different clas-ses These characteristics include the numberof heavy chain constant segments the numberand location of interconnecting disulfidebridges the length of the hinge region andthe number and location of oligosaccharidemoieties For IgG four heavy chain versionsexist creating IgG1 2 3 and 4 isotypes eachwith different characteristics in their serumhalf-lives and ability to trigger different effec-tor functions Because of the combined ad-vantage from ability to trigger effectormechanisms long [21 days] half-life theirability to be transported over the placentaand their stability in the production processantibodies of the IgG class and of the IgG1isotype are preferred as the basis for newantibody-based therapies The effector func-tions are triggered by the Fc part of an antibodywhen the variable parts of the antibody arebound directly to an infectious agent or toproteins from an infectious agent expressed onan infected cell This binding leaves the Fc partfree to interactwithFc receptors onphagocyticcells and neutrophils eosinophils and naturalkiller cells capable of inducing phagocytosis orlysis of infectious agents or infected cellsThese effector functions include (i) the abilityto activate the complement system for lysis(complement-dependent cellular cytotoxicity)(ii) triggering of uptake and destruction byphagocytic cells such as macrophages andneutrophils via interaction with Fc receptorson these cells (iii) activation of macrophageseosinophils neutrophils and natural killer
cells to kill infected cells via binding to Fcreceptors on these cells and antibody-depen-dent cellular cytotoxicity and (iv) neutraliza-tion of bacterial toxins and blocking of bindingand uptake of bacteria or viruses to target cells(see Fig 2) (9)
The Fcpart of IgG antibodies also contains aregion that interacts with the neonatal Fcreceptor (FcRn) expressed on most immuno-competent cells and inmany other cells such asendothelial cells in kidney liver placenta lungand breast (10) which protects antibodies fromdegradation by phagocytoticexocytotic cy-cling into FcRn-expressing cells thereby pro-longing their half-life This results in half-livesof 20 to 21 days for most IgG1 2 and 4antibodies whereas half-lives are 10 6 and 2days respectively for IgM IgA and IgE Thehighly specific binding sites on the variableregions of the upper arms of the antibody allowfor several important features of antibodiesndashbinding to and neutralization of eg bacterialtoxins binding to pathogens and blocking theirbinding to or interaction with target cells (egcyncytia formation of CMV-infected cells) orblocking of binding and interactions of infec-tious agents with target cells via blockingreceptors on the target cells
METHODS AND PLATFORMS FORGENERATING ANTIBODIES
As described above the early use of passiveantibody transfer as a therapy in infectiousdiseases involved the use of immune serumfrom immunized sheep and horses These pre-parations were crude and contained a broadmixture of neutralizing and non-neutralizingantibodies and both the foreign nature of theantibodies and the numerous host serumproteins This resulted in less specific andthus less efficient therapies due to a highvariability in efficacy between batches derivedfrom different animals immunized with dif-ferent strains of bacteria in different labor-atories and resulted in multiple unwantedside effects related to hypersensitivity and
10 HEY
anaphylactic reactions to foreign proteinsThese days antibodies being developed fortreatment of diseases in humans are highlypurified and are mostly fully human mono-clonal antibodies The term monoclonal anti-body refers to that cell cultures used forgenerating these antibodies each originatesfrom a single cell and thus produces onlyone specific antibody Development of fullyhuman monoclonal antibodies happened instages over a time span of more than 15 yearsFirst stage in this process was generation ofmonoclonalmurine IgG antibodies (eg OKT3[muronomab-CD3 Johnson and Johnson] ap-proved in 1986) Next stage was generation ofso called chimeric antibodies consisting ofhuman heavy and light chain constant sec-tions but with murine variable sections (eg
Rituxan [rituximab Genentech]) Next stagewas then the humanized antibodies wherethe only remaining murine part of the anti-body is the antigen-binding CDR (eg Xolair[omalizumab NovartisGenentech]) Both thefirst chimeric and humanized antibodies wereapproved in the late 1990s Then finally 16years later the first fully human antibodyHumira (adalimumab Abbott) was approvedin 2002 Since the time of the crude and low-scale manufacturing of the original antibodyserum products much has changed andtherapeutic antibodies are now produced byfermentation in 5000 liter scale using highlycontrolled and documented yeast or mamma-lian cell lines that are genetically engineered toexpress a single specific antibody This hasresulted in a pure and highly specific antibody
FIGURE 2 Effector functions of antibodies (a) Antibodies bind to pathogen-derived or endogenousantigens expressed on the surface of an infected cell which triggers binding to Fc receptors on naturalkiller cells and lysis of the infected cell by antibody-dependent cellular cytotoxicity (b) Antibodies bindto pathogen-derived or endogenous antigens expressed on the surface of infected cells which triggersactivation of complement through binding of complement factor C1q (c) Neutralization Top Bacterialtoxin neutralized by bound antigen Bottom Antibody bound to either receptor for the virus or to thevirus itself which blocks virus binding and entry into the cell (d) Antibody bound to viral surfaceproteins binds to Fc receptors on phagocytic cells eg macrophages and triggers endocytosis anddestruction of virus in endolysosome doi101128microbiolspecAID-0026-2014f2
CHAPTER 1 bull History and Practice Antibodies in Infectious Diseases 11

S Moein MoghimiDepartment of PharmacyCenter for Pharmaceutical Nanotechnology and NanotoxicologyFaculty of Health and Medical SciencesUniversity of CopenhagenCopenhagen DK-2100Denmark
Susan Zolla-PaznerNew York University School of Medicine550 First AvenueNew York NY 10016
Louise SaulCutaneous Medicine and Immunotherapy UnitSt Johnrsquos Institute of DermatologyDivision of Genetics and Molecular Medicine amp NIHR Biomedical Research Centre at Guyrsquos and St Thomasrsquos HospitalsKingrsquos College London School of MedicineGuyrsquos HospitalLondon SE1 9RTUnited Kingdom
Bruce C SchneppThe Childrenrsquos Hospital of PhiladelphiaAbramson Research CenterPhiladelphia PA 19104
Jennifer E SchusterDepartment of PediatricsChildrenrsquos Mercy HospitalKansas City MO 64108-4619
Alexander M SevyDepartment of Chemistry and Center for Structural BiologyVanderbilt UniversityNashville TN 37212
Jared SheehanDepartment of Cancer Immunology and AIDSDana-Farber Cancer InstituteHarvard Medical SchoolBoston MA 02215
Michael R SierksDepartment of Chemical EngineeringArizona State UniversityTempe AZ 85287-6006
xiv contRIBUtoRs
Scott A SmithThe Vanderbilt Vaccine Center and the Department of MedicineVanderbilt University Medical CenterNashville TN 37232
Robyn L StanfieldDepartment of Molecular BiologyThe Scripps Research Institute10550 North Torrey Pines RoadLa Jolla CA 92037
Nadine UptonRandall Division of Cell and Molecular BiophysicsDivision of Asthma Allergy and Lung BiologyMRC and Asthma UK Centre for Allergic Mechanisms of AsthmaKingrsquos College LondonNew Huntrsquos HouseGuyrsquos CampusLondon SE1 1ULUnited Kingdom
Avanish K VarshneyDepartment of MedicineInfectious Diseases and Department of Microbiology and ImmunologyAlbert Einstein College of MedicineBronx NY 10461
Stefanie N VelgosMayo Clinic Arizona5777 East Mayo BoulevardPhoenix AZ 85054
Kevin J WhaleyMapp Biopharmaceutical Inc6160 Lusk Blvd C105San Diego CA 92121
Peter P WibroeCentre for Pharmaceutical Nanotechnology and NanotoxicologyDepartment of PharmacyFaculty of Health and Medical SciencesUniversity of CopenhagenCopenhagen DK-2100Denmark
John V WilliamsDepartment of PediatricsSchool of MedicineVanderbilt UniversityNashville TN 37232-2581
contRIBUtoRs xv
Ian A WilsonDepartment of Molecular Biology and Skaggs Institute for Chemical BiologyThe Scripps Research Institute10550 North Torrey Pines RoadLa Jolla CA 92037
Herren WuDepartment of Antibody Discovery and Protein EngineeringMedImmune LLCOne MedImmune WayGaithersburg MD 20879
Guocheng YangDepartment of Chemical EngineeringArizona State UniversityTempe AZ 85287-6006
Larry ZeitlinMapp Biopharmaceutical Inc6160 Lusk Blvd C105San Diego CA 92121
xvi contRIBUtoRs
Preface
Antibodies form the principal foundation for modern intervention against in-fectious diseases Emil Adolf von Behring was awarded the first Nobel Prize in Physiology or Medicine in 1901 ldquofor his work on serum therapy especially its appli-cation against diphtheria by which he has opened a new road in the domain of med-ical science and thereby placed in the hands of the physician a victorious weapon against illness and deathsrdquo Antibodies now provide the focus for understanding mechanisms of immunity to most infectious diseases and they play a central role in passive immunotherapy and active vaccination as mechanisms or correlates of immunity For most of the 20th century immunotherapy was based on passive transfer of polyclonal hyperimmune animal serum immune human serum or even hyperimmune human serum Georges JF Koumlhler and Ceacutesar Milstein re-ported the generation of monoclonal antibodies in 1979 for which they shared the 1984 Nobel Prize in Physiology or Medicine ldquofor the discovery of the princi-ple for production of monoclonal antibodiesrdquo Since that time entire fields related to antibodies for infectious diseases including antibody gene cloning engineer-ing and expression antibody libraries and high-throughput antibody gene rep-ertoire sequence analysis have extended our capabilities to explore the diversity of antibody specificity and function with unprecedented depth and breadth
This book provides a broad survey of many of the most important aspects of the field of antibodies for infectious diseases The book begins with a general introduction followed by chapters 2 through 5 on general features pertaining to structure function isotype and the role of complement in antibody function Chapters 6 through 10 review contemporary approaches for antibody discovery using phage and yeast display plasma cell and memory B cell cloning human hybridomas humanized mice and computational methods Chapters 11 through 18 review in depth the biology of antibodies specific for particular pathogens including viruses and bacterial toxins to illustrate the role of antibodies in anti- microbial immunity with specific targets These chapters reveal that attempts to raise effective antibody responses to each of these pathogens faces unique and pathogen-specific challenges Chapters 19 to 23 cover major technical advances pertaining to antibody engineering repertoire sequencing and analysis and new methods for study or therapeutic use of antibodies including radiotherapy Fi-nally chapters 24 and 25 cover new methods for expression of monoclonal anti-bodies in plants or by transfer of antibody genes for in vivo expression in treated subjects
Recent literature is exploding with new antibody-related techniques and re-ports of antimicrobial antibodies with unprecedented potency breadth of activ-
xvii
xviii PReface
ity and therapeutic potential We hope that this timely compilation of state-of-the-art reviews of major aspects of this field will be of interest to both antibody cognoscenti and those new to this exciting field We thank the authors for their dedication in producing definitive reviews of the topics at hand
James E Crowe JrDiana BoraschiRino Rappuoli
INTRODUCTION
History and PracticeAntibodies in Infectious Diseases 1ADAM HEY1
Antibodies in Infectious Diseases aims to inform update and inspire studentsteachers researchers pharmaceutical developers and health care professionalson the status of the development of antibody-based therapies for treatinginfectious diseases and the potential for these in times of growing antibioticresistance to provide alternative treatment solutions to the currently usedantibiotics and new treatments for infectious diseases where no propertreatments are available
This introductory article will provide a historical perspective on the useof antibody-based therapies followed by a high-level overview of whatmakes antibodies attractive tools for this purpose This will include the prosand cons of such therapies compared to the use of antibiotics and thepractical and strategic considerations involved in selecting the best formatand development path for new antibody-based therapies targeting specificinfectious agents Then examples of antibody-based therapies in thedevelopment of treatments for infectious diseases will be presented andfinally a look into the future will summarize the different aspects that willinfluence what the future might bring for this type of treatments forinfectious diseases
1Preclinical Safety Biologics Novartis AG Basel Switzerland
Antibodies for Infectious DiseasesEdited by James E Crowe Jr Diana Boraschi and Rino Rappuolicopy 2015 American Society for Microbiology Washington DCdoi101128microbiolspecAID-0026-2014
3
HISTORICAL PERSPECTIVE
Antibodies and the use of passive antibodytherapy in the treatment of infectious dis-eases is the story of a treatment conceptwhich dates back more than 120 years to thelate 19th century and which originally bythe use of serum from immunized animalsprovided the first effective treatment optionsagainst severe bacterial infections (1 2) Byimmunizing horses with bacterial toxinsfrom Clostridium tetani and Corynebacteri-um diphtheriae Emil A Von Behring andShibasaburo Kitasato (3) generated serumcontaining antibodies capable of neutraliz-ing the effects of the toxins produced bythese bacteria and successfully providedtreatment for these serious diseases wherethe pathogenesis is driven by the effects ofthe bacterial toxins For his work on provid-ing treatment for diphtheria Behring re-ceived the Nobel Prize in Physiology orMedicine in 1901 These radical treatmentresults quickly prompted development ofmultiple additional serum therapies for thetreatment of infectious diseases caused byeg Neisseria meningitidis Haemophilus in-fluenza and group A Streptococcus Sinceserum therapy involved administration oflarge amounts of crude mixtures of animalproteins including antibodies they wereassociated with side effects in the form ofhypersensitivity and serum sickness (2)
Due to the crude and unpurified nature ofthese products side effects were seen evenwhen administering human serum prepa-rations Side effects were observed in up to50 of patients and were considered to becaused by immune complex formations thatresulted in symptoms such as rash itchingjoint pain fever and in serious cases hypoten-sion and shock However due to the lack ofalternative options these treatments weredespite their side effects widely used Serumwas normally administered by intravenousinfusion in patients after a test for hypersensi-tivity where a small amount of serum wasinjected subcutaniously (1) As described
above serum therapy applied in these earlydays (late 19th century and early 20th century)involved preparations of serum from rabbitsand horses immunized with the infectiousagent or in live andor neutralized versions ortoxins from these (1) The costs of keeping theimmunized animals and the production andpotency testing of the materials made this arelatively expensive treatment In 1891 datafrom Klemperer (4) showed serum therapy toprotect rabbits from Streptococcus pneumoniaeinfection and paved the way for this type oftreatment and for development of similarserum-based treatments of streptococcal in-fections in humans When treating humansearly administration of serum could reducemortality significantly down to around 5compared to when administered 4 to 5 daysafter onset of symptoms when serum treat-ment was largely without effect This stronglyindicated the need for quick diagnosis andquick treatment to control the infection beforeit got out of control Consequently in theabsence of a specific diagnosis mixtures ofserum from immunizations with differentserotypes were used to circumvent this needfor early treatment without having a serotype-specific diagnosis The understanding thatdifferent serotypes existed for pneumococciand that efficient treatment relied on usingserotype-specific serum was being built upduring the 1920s and 1930s through experiencefrom extensive clinical trials
By the end of the 1930s serum therapywasthe standard of care for treatment of pneu-mococcal pneumonia At that time theefficacy and potency of the derived serawere assessed in mice in ldquothe mouse pro-tection testrdquo by testing survival after aconcomitant intraperitoneal injection of alethal dose of pneumococci and the serum tobe tested Due to the inherent variation inthis test efficacy and survival in two thirds ofthe animals was the acceptance criteria and10 times the lowest dose providing this wasused for defining a unit of the serum Thisallowed for large batch-to-batch variationand the use of different strains of bacteria for
4 HEY
immunization probably explains part of themissing responses observed (1) In the early20th century a pandemic of meningitis inEurope and the United States with mortalityrates up to 80 spurred the development ofserum therapy treatment options Althoughin the 1930s this became the recommendedtreatment in children assumed to be suffer-ing from meningitis failure to reduce mor-tality in several meningitis epidemics duringthat time raised doubts about the generalapplicability of serum treatment In thosedays serum therapy often involved quiteextensive procedures and infusion of largevolumes of serum The following exampleclearly illustrates this Data from Flexnerand Jobling (5) from treating meningitis inmonkeys resulted in the development of serafrom immunized horses for treatment inhumans The treatment protocol includedlumbar puncture and withdrawal of morethan 30 ml of spinal fluid representing anamount slightly larger than the expectedamount of horse serum to be injected subse-quently This treatment involved such dailyslow infusions of up to 30 ml of serum untilthe patientrsquos condition improved This treat-ment was used in outbreaks in New York in1905 and 1906 and did markedly decreasemortality
After the discovery of penicillin by Flemingin 1928 and the subsequent introduction ofantibiotics in the 1930s serum therapy waslargely abandoned over a period of 10 years dueto the availability of these new more broadlyeffective and cheaper treatment optionswhichalso had fewer side effects Although improve-ments in the purification of antibodies hadresulted in preparations with better safety andside effect profiles high manufacturing costsand narrow specificity resulted in antibodytherapy being mostly restricted to a smallernumber of selected treatments for snakevenoms bacterial toxins and some viral infec-tions (1 2) Currently antibody administrationis used for treatment and prevention ofhepatitis B virus rabies virus respiratorysyncytial virus (RSV) Clostridium tetani Clos-
tridium botulinum vaccinia virus echovirusand enterovirus For the most part thesetreatments consist of pooled immunoglobulinalso known as IVIG (intravenous immunoglob-ulin) from several postexposure donors Thisresults in both batch-to-batch variation in theneed for relatively large amounts of serum dueto low specificity and to restricted supplies dueto reliance on exposed donors
However several challengeshave resulted inthe need for new tools in the treatment andpreventionof infectiousdiseasesThebroadandgeneral use of antibiotics in human and veter-inary medicine for many years has resulted inthe development of multi-resistant strains ofbacteria with limited to no response to existingtreatments such as methicillin-resistant Staph-ylococcusaureus (MRSA) vancomycin-resistantS aureus and others This has resulted inpatients needing screening and treatment withseveral antibacterial agents and longer treat-ment time causing extra strain on patients andhealth care providers (6 httpwwwcdcgovdrugresistancethreat-report-2013indexhtml) According to the WHO and CDC morethan 25000 people in European Unioncountries and similar numbers in the UnitedStates die every year as a result of antibiotic-resistant infections This together with theemergence of new pathogens (eg severeacute respiratory syndrome Middle East respi-ratory syndrome) the re-emergenceepidemicsof oldknown pathogens (eg Ebola) and thedifficulties in treating infections in immune-deficient patients (eg HIV patients) has high-lighted the need for new solutions The 2014Ebola epidemic in West Africa (Liberia SierraLeone Guinea Nigeria and Senegal) has fur-ther highlighted this No treatment or prophy-lactic vaccine is available to treat or prevent thespread of Ebola infections which have anaveragemortality of gt50 Local health author-ities in the affected countries are struggling tocontain and handle the disease which isthreatening to go out of control and spreadmorewidelyVariousproductsmainly antibodycocktails from previously recovered patientsare being used despite a lack of clinical data on
CHAPTER 1 bull History and Practice Antibodies in Infectious Diseases 5
their safety and efficacy and those are the onlysporadically available treatment options andonly in small amounts and for a few patients
Ebola is an example of a disease whichnormally affects only a small number ofindividuals and which normally burns outwhen disease outbreaks are contained There-fore given the small number of potentialpatients affected by previous Ebola infectionsto date there was no incentive for big pharmacompanies to do research and development ofdrugs for EbolaWith the increasing number ofinfected (13567) andadeath toll of 4951 (7) andthe lack of the ability to contain the epidemic itwill be interesting to follow the aftermath ofthis outbreak and see whether there will berequests for new ways to ensure that vaccinesand treatment options are available for Ebolaand similar high-mortality and potential bio-warfare infections that have no availabletreatments or procedures to for mass-produc-tion upon the first signsreports of activeinfections Although both the CDC and theWHO have special programs focusing on thesetypes of infections the Ebola outbreak in 2014clearly shows that more financial support forresearch and development of new diagnosticsand treatments is needed This is one examplewhere antibody-based treatments would havethe potential to play a major role To put this inthe right perspective one should however notforget that other infectious diseases such astuberculosis influenza and malaria kill hun-dreds of thousands each year There is there-fore plenty of room for improvement indeveloping treatments for these diseases aswell but the high attention drawn to eg theEbola outbreak creates a special niche andopportunity where antibody treatments couldgain extraordinary development funding andsupport and prove their value and treatmentpotential
That antibody-based therapies could takethis role is supported by the revolution intechnologies for the development selectiongeneration and purification of fully humanantibodies described in more detail later in thesection ldquoMethodsandPlatforms forGenerating
Antibodiesrdquo Antibody-based programs cur-rently at different stages of developmentinclude investigations into the potential use ofsingle antibody preparations combinations ofantibodies (to avoid survival of escape mu-tants) fragments of antibodies and antibodiescarrying radioactive isotopesorcytotoxicdrugsor antibody-like frameworks (eg fibronectin)either alone as a first-line treatment or as anadjunct to existing treatments This multitudeof possible formats the ability to raise anti-bodies to almost any target and the ability toengineer both size effector functions and half-life are now considered by many to providevery valuable tools for designing specificantibody-based treatments toeradicate specifictargeted infectious agents However althoughseveral antibody-based therapies have beenapproved for oncology and anti-inflammatoryindications (see Table 1) only one monoclonalantibody (mAb) is approved against an infec-tious disease agentmdashSynagis (palivizumabMedImmune) for the prevention and treat-ment of respiratory syncytical virus (RSV) inhigh-risk children Economic obstacles such asthe high cost of mAb therapies and relativelysmall markets have resulted in less interestfrom pharmaceutical companies in developingthese Also highlighting the challenges indeveloping these types of antibody-basedtreatments are the difficulties encountered indeveloping a follow-up higher-affinity candi-date to Synagis Poor translatability of dataobtained in the available animal disease mod-els for RSV in cotton rats has resulted in non-approval due to inferiority relative to SynagisIn other viral diseases such as cytomegalovirus(CMV) the high species specificity of thestrains of CMV makes it impossible to testhuman antibody therapies in vivo Thereforeany real data on the efficacy of treatments forCMV will not be obtained until testing inclinical trials As described later in this articleseveral new antibody-based therapies for in-fectious diseases are in development andhopefully this will gradually open the fieldand result in better treatment options andoutcomes for patients
6 HEY
TABLE 1 Approved and pending antibody-based therapies
Name antibody Target antibody type Indication Company Approval date
OKT3a Muronomab-CD3 CD3 murine IgG2a Autoimmune Johnson ampJohnson
1986 (US)
ReoPro abciximab PIIbIIIa chimeric IgG1Fab
Homeostasis Johnson ampJohnson
1984 (US)
Rituxan rituximab CD20 chimeric IgG1 Cancer Genentech 1997 (US) 1998 (EU)Zenapaxa daclizumab CD25 humanized IgG1 Autoimmune Roche 1997 (US) 1999 (EU)Simulect basiliximab CD25 chimeric IgG1 Autoimmune Novartis 1998 (US EU)Synagis palivizumab RSV humanized IgG1 Infections MedImmune 1998 (US) 1999 (EU)Remicade infliximab TNFα chimeric IgG1 Autoimmune Johnson amp
Johnson1998 (US) 1999 (EU)
Herceptin trastuzumab HER2 humanized IgG1 Cancer GenentechRoche
1998 (US) 2000 (EU)
Mylotarga gemtuzumabozogamicin
CD33 humanized IgG4immunotoxin
Cancer WyethPfizer 2000 (US)
Campath alemtuzumab CD52 humanized IgG1 Cancer Genzyme 2001 (US) 2001 (EU)Zevalin ibritumomabtiuxetan
CD20 murine IgG1radiolabeled (yttrium 90)
Cancer Biogen Idec 2002 (US) 2004 (EU)
Humira adalimumab TNFα human IgG1 Autoimmune Abbott 2002 (US) 2003 (EU)Xolair omalizumab IgE humanized IgG1 Autoimmune Genentech
Roche2003 (US)
Bexxar tositumomab-I-131 CD20 murine IgG2aradiolabeled (iodine131)
Cancer CorixaGSK 2003 (US)
Raptivaa falizumab CD11a humanized IgG1 Autoimmune GenentechRoche
2003 (US) 2004 (EU)
Erbitux cetuximab EGFR chimeric IgG1 Cancer ImcloneLilly 2004 (US) 2004 (EU)Avastin bevacizumab VEGF humanized IgG1 Cancer Genentech
Roche2004 (US) 2005 (EU)
Tysabri natalizumab α4-Intergrin humanizedIgG4
Autoimmune Biogen Idec 2004 (US)
Actemra tocilizumab Anti-IL-6R humanizedIgG1
Autoimmune ChugaiRoche
2005 (Japan) 2010 (US)
Vectibix panitumumab EGFR human IgG2 Cancer Amgen 2006 (US)Lucentis ranibizumab VEGF humanized IgG1
FabMaculardegeneration
GenentechRoche
2006 (US)
Soliris eculizumab C5 humanized IgG24 Blood disorders Alexion 2007 (US)Cimzia certolizumab pegol TNFα humanized
pegylated FabAutoimmune UCB 2008 (US)
Simponi golimumab TNFα human IgG1 Autoimmune Johnson ampJohnson
2009 (US EU Canada)
Ilaris canakinumab IL1b human IgG1 Infalmmatory Novartis 2009 (US EU)Stelara ustekinumab IL-1223 human IgG1 Autoimmune Johnson amp
Johnson2008 (EU) 2009 (US)
Arzerra ofatumumab CD20 human IgG1 Cancer Genmab 2009 (EU)Prolia denosumab RANK ligand human
IgG2Bone loss Amgen 2010 (US)
Numax motavizumab RSV humanized IgG1 Anti-infective MedImmune PendingABthrax Raxibacumab B anthrasis PA human
IgG1Anti-infection GSK 2012 (US)
Benlysta belimumab BLyS human IgG1 Autoimmune HGS 2011 (US)Yervoy ipilimumab CTLA-4 human IgG1 Cancer BMS 2011 (US)Adcetris brentuximabvedotin
CD30 chimeric IgG1drug- conjugate
Cancer SeattleGenetics
2011 (US)
(Continued on next page)
CHAPTER 1 bull History and Practice Antibodies in Infectious Diseases 7
INTRODUCTION TO ANTIBODIES
Antibodies also called immunoglobulins basedon their combined structure and function inimmune responses are produced by B cells ofthe immune system They are part of theadaptive immune response and are speciallydesigned for neutralizing and eliminating theinfectious agents and toxins produced by theseAntibodies are present in blood plasma andextracellular fluids and since these fluids wereformerly known as humors they were said tobe part of the humoral immune responseAntibodies are Y-shaped structures consistingof two main parts the upper arms of the Ywhich contain two identical variable-regionantigen binding sites and the lower regioncalled the constant regionwhich is responsiblefor the initiation of effector functions that leadto the removal and destruction of the pathogenor cells harboring the pathogen (see Fig 1) Theantigen-binding sites on an antibody can bythemselves bind to and neutralize bacterialtoxins and viruses thereby preventing themfrom binding to their target cells or receptorscausing toxic effects or spread of the infection
Antibodies consist of two pairs of heavy andlight chainswhich as described above are heldtogether in a Y-shaped arrangement Each ofthe heavy and light chains in these pairs isseparated into constant and variable chainsThe upper armsof theY each contain a variableand a constant sectionof the light and theheavychain where the upper variable parts of theheavy and light chains contain the antigen-binding site and the constant parts areconnected via disulfide bonds The lower partof theYcalled theconstantpart consistsof twoor three constant segments (immunoglobulindomains) from each of the two heavy chainsinteracting and also linked via disulfide bondsThe sectionsof theheavy chains connecting theconstant part of the upper arms to the constantparts of the constant region contain specialhinge regions that provide flexibility to thedifferent sections of the antibody to bind toantigens and effector cells The constant re-gions of the heavy chain also contain attachedoligosaccharide moieties which provide func-tional specialization to the antibodies (8)
The variable domains of the heavy and lightchains form the antigen-binding sites and
TABLE 1 Approved and pending antibody-based therapies (Continued)
Name antibody Target antibody type Indication Company Approval date
Perjeta pertuzumab Her2 humanized IgG1 Cancer GenentechRoche
2012 (US)
Kadcyla ado-trastuzumabemtansine
Her2 humanized IgG1Drug-conjugate
Cancer GenentechRoche
2013 (US)
Raxibacumab Anti-B anthrasis PAhuman IgG1
Anthraxinfection
Notapproved
2012
Entyvio vedolizumab Integrin α4β7humanized IgG1
Crohnrsquos diseaseulcerative colitis
Takeda 2014 (US)
Cyramza ramuciruumab Anti-VEGFR2Human IgG1
Gastric cancer Lilly 2014 (US)
Gazyva obinutuzumab Anti-CD20 humanizedIgG1 glucoengineered
CancerCLLb GenentechRoche
2014 (US)
Sylvant situximab Anti IL-6 chimeric IgG1 Castlemandisease
Janssen 2014 (US) 2014 (EU)
Cosentyx sekukinumab Anti IL-17a human IgG1 Psoriasis Novartis 2015 (US) 2015 (EU)Nivolumab Anti PD-1 human IgG4 Melanoma BMS Not approvedKeytruda pembrolizuumab Anti-PD-1 humanized
IgG4Melanoma Merck 2014 (US)
aAntibodies approved but later withdrawnbCLL chronic lymphocytic leukemia
8 HEY
FIGURE 1 (Left panel) Model of antibody structure exemplified by IgG On top the antigen-binding sitesin orange each contain one variable light and variable heavy domain with the three complementaritydetermining regions (CDRs) that are responsible for the specific binding of the antibody to its target Foreach arm of the antibody an additional set of variable heavy and light domains together with the CDR-containing domains represent the two fragment antigen binding (Fab) regions The two Fabs are heldtogether via two disulfide bridges Below the Fabs is the Fc region which contains four constant heavydomains On the upper pair of these domains are binding sites for oligosaccharides which have majorimportance for the ability of the antibody Fc part to trigger effector functions when the Fc portion isbound to Fc gamma receptors on natural killer cells neutrophil granulocytes monocytesmacrophagesdendritic cells and B cells (Right panel) Examples of some of the antibody-derived alternative formatsused to exploit the specific features of the CDRs the Fabs and the Fc parts of the antibodies ScFv Thesingle chain fragment variable consists of the variable domains of the heavy and light chains heldtogether by a flexible linker This can also be used as a carrier of a cytotoxic drug in a so-called antibodydrug complex (ADC) where the specificity of the ScFv is used to target the cytotoxic drug to eg atumor Bite (bi-specific T cell engager) Fusion proteins consisting of two ScFvs one directed against thetarget on a tumor cell and the other against the T cell receptor (CD3) Diabody ScFv dimers where shortlinker peptides (five amino acids) ensure dimerization and not folding of the ScFvs Fab and F(ab)2fragments Single Fab fragments or fragments containing two Fabs linked via disulfide bridges This isused where effector functions related to the Fc part of the antibody are unwanted and where a smallersize is desired to obtain better tissue penetration in eg tumors Due to the lack of the FcRn binding viathe Fc part Fab and F(ab)2 fragments have much shorter half-lives (hours or days) than full-sizeantibodies (weeks) These can also be used as carriers of cytotoxic payloads or cytotoxic radioactiveisotopes and for the F(ab)2 fragments can be constructed as bi-specifics which can cross-link immunecells and target cells Fc fusion protein Fusion protein containing the Fc domain of an immunoglobulinbound to a peptide The peptide can be a ligand for a specific receptor on a target cell or a blockingpeptide for a soluble ligand The Fc part provides a longer half-life to the construct and the potential tobind to and engage effector functions in the killing of eg tumor cells or infected cells ADCsRIAs andbi-specifics Full-size IgG antibodies carrying either a cytotoxic chemical or radioactive payload whichmay also carry different CDRs enabling cross-linking of effector and target cells for increased killingdoi101128microbiolspecAID-0026-2014f1
CHAPTER 1 bull History and Practice Antibodies in Infectious Diseases 9
contain special hyper-variable segments calledcomplementarity-determining regions (CDRs)which allow the B cells via genetic recom-bination to generate antibodies to all thedifferent antigens specific to amino acid se-quences or three-dimensional structuralmotifs(polysaccharides DNA and RNA) found onpathogens
Based on the structure of their heavy chainconstant regions antibodies or immuno-globulins are separated into five classesmdashIgM IgG IgE IgD and IgA Differences inthe sequences of the constant regions providedistinct characteristics to these different clas-ses These characteristics include the numberof heavy chain constant segments the numberand location of interconnecting disulfidebridges the length of the hinge region andthe number and location of oligosaccharidemoieties For IgG four heavy chain versionsexist creating IgG1 2 3 and 4 isotypes eachwith different characteristics in their serumhalf-lives and ability to trigger different effec-tor functions Because of the combined ad-vantage from ability to trigger effectormechanisms long [21 days] half-life theirability to be transported over the placentaand their stability in the production processantibodies of the IgG class and of the IgG1isotype are preferred as the basis for newantibody-based therapies The effector func-tions are triggered by the Fc part of an antibodywhen the variable parts of the antibody arebound directly to an infectious agent or toproteins from an infectious agent expressed onan infected cell This binding leaves the Fc partfree to interactwithFc receptors onphagocyticcells and neutrophils eosinophils and naturalkiller cells capable of inducing phagocytosis orlysis of infectious agents or infected cellsThese effector functions include (i) the abilityto activate the complement system for lysis(complement-dependent cellular cytotoxicity)(ii) triggering of uptake and destruction byphagocytic cells such as macrophages andneutrophils via interaction with Fc receptorson these cells (iii) activation of macrophageseosinophils neutrophils and natural killer
cells to kill infected cells via binding to Fcreceptors on these cells and antibody-depen-dent cellular cytotoxicity and (iv) neutraliza-tion of bacterial toxins and blocking of bindingand uptake of bacteria or viruses to target cells(see Fig 2) (9)
The Fcpart of IgG antibodies also contains aregion that interacts with the neonatal Fcreceptor (FcRn) expressed on most immuno-competent cells and inmany other cells such asendothelial cells in kidney liver placenta lungand breast (10) which protects antibodies fromdegradation by phagocytoticexocytotic cy-cling into FcRn-expressing cells thereby pro-longing their half-life This results in half-livesof 20 to 21 days for most IgG1 2 and 4antibodies whereas half-lives are 10 6 and 2days respectively for IgM IgA and IgE Thehighly specific binding sites on the variableregions of the upper arms of the antibody allowfor several important features of antibodiesndashbinding to and neutralization of eg bacterialtoxins binding to pathogens and blocking theirbinding to or interaction with target cells (egcyncytia formation of CMV-infected cells) orblocking of binding and interactions of infec-tious agents with target cells via blockingreceptors on the target cells
METHODS AND PLATFORMS FORGENERATING ANTIBODIES
As described above the early use of passiveantibody transfer as a therapy in infectiousdiseases involved the use of immune serumfrom immunized sheep and horses These pre-parations were crude and contained a broadmixture of neutralizing and non-neutralizingantibodies and both the foreign nature of theantibodies and the numerous host serumproteins This resulted in less specific andthus less efficient therapies due to a highvariability in efficacy between batches derivedfrom different animals immunized with dif-ferent strains of bacteria in different labor-atories and resulted in multiple unwantedside effects related to hypersensitivity and
10 HEY
anaphylactic reactions to foreign proteinsThese days antibodies being developed fortreatment of diseases in humans are highlypurified and are mostly fully human mono-clonal antibodies The term monoclonal anti-body refers to that cell cultures used forgenerating these antibodies each originatesfrom a single cell and thus produces onlyone specific antibody Development of fullyhuman monoclonal antibodies happened instages over a time span of more than 15 yearsFirst stage in this process was generation ofmonoclonalmurine IgG antibodies (eg OKT3[muronomab-CD3 Johnson and Johnson] ap-proved in 1986) Next stage was generation ofso called chimeric antibodies consisting ofhuman heavy and light chain constant sec-tions but with murine variable sections (eg
Rituxan [rituximab Genentech]) Next stagewas then the humanized antibodies wherethe only remaining murine part of the anti-body is the antigen-binding CDR (eg Xolair[omalizumab NovartisGenentech]) Both thefirst chimeric and humanized antibodies wereapproved in the late 1990s Then finally 16years later the first fully human antibodyHumira (adalimumab Abbott) was approvedin 2002 Since the time of the crude and low-scale manufacturing of the original antibodyserum products much has changed andtherapeutic antibodies are now produced byfermentation in 5000 liter scale using highlycontrolled and documented yeast or mamma-lian cell lines that are genetically engineered toexpress a single specific antibody This hasresulted in a pure and highly specific antibody
FIGURE 2 Effector functions of antibodies (a) Antibodies bind to pathogen-derived or endogenousantigens expressed on the surface of an infected cell which triggers binding to Fc receptors on naturalkiller cells and lysis of the infected cell by antibody-dependent cellular cytotoxicity (b) Antibodies bindto pathogen-derived or endogenous antigens expressed on the surface of infected cells which triggersactivation of complement through binding of complement factor C1q (c) Neutralization Top Bacterialtoxin neutralized by bound antigen Bottom Antibody bound to either receptor for the virus or to thevirus itself which blocks virus binding and entry into the cell (d) Antibody bound to viral surfaceproteins binds to Fc receptors on phagocytic cells eg macrophages and triggers endocytosis anddestruction of virus in endolysosome doi101128microbiolspecAID-0026-2014f2
CHAPTER 1 bull History and Practice Antibodies in Infectious Diseases 11

Scott A SmithThe Vanderbilt Vaccine Center and the Department of MedicineVanderbilt University Medical CenterNashville TN 37232
Robyn L StanfieldDepartment of Molecular BiologyThe Scripps Research Institute10550 North Torrey Pines RoadLa Jolla CA 92037
Nadine UptonRandall Division of Cell and Molecular BiophysicsDivision of Asthma Allergy and Lung BiologyMRC and Asthma UK Centre for Allergic Mechanisms of AsthmaKingrsquos College LondonNew Huntrsquos HouseGuyrsquos CampusLondon SE1 1ULUnited Kingdom
Avanish K VarshneyDepartment of MedicineInfectious Diseases and Department of Microbiology and ImmunologyAlbert Einstein College of MedicineBronx NY 10461
Stefanie N VelgosMayo Clinic Arizona5777 East Mayo BoulevardPhoenix AZ 85054
Kevin J WhaleyMapp Biopharmaceutical Inc6160 Lusk Blvd C105San Diego CA 92121
Peter P WibroeCentre for Pharmaceutical Nanotechnology and NanotoxicologyDepartment of PharmacyFaculty of Health and Medical SciencesUniversity of CopenhagenCopenhagen DK-2100Denmark
John V WilliamsDepartment of PediatricsSchool of MedicineVanderbilt UniversityNashville TN 37232-2581
contRIBUtoRs xv
Ian A WilsonDepartment of Molecular Biology and Skaggs Institute for Chemical BiologyThe Scripps Research Institute10550 North Torrey Pines RoadLa Jolla CA 92037
Herren WuDepartment of Antibody Discovery and Protein EngineeringMedImmune LLCOne MedImmune WayGaithersburg MD 20879
Guocheng YangDepartment of Chemical EngineeringArizona State UniversityTempe AZ 85287-6006
Larry ZeitlinMapp Biopharmaceutical Inc6160 Lusk Blvd C105San Diego CA 92121
xvi contRIBUtoRs
Preface
Antibodies form the principal foundation for modern intervention against in-fectious diseases Emil Adolf von Behring was awarded the first Nobel Prize in Physiology or Medicine in 1901 ldquofor his work on serum therapy especially its appli-cation against diphtheria by which he has opened a new road in the domain of med-ical science and thereby placed in the hands of the physician a victorious weapon against illness and deathsrdquo Antibodies now provide the focus for understanding mechanisms of immunity to most infectious diseases and they play a central role in passive immunotherapy and active vaccination as mechanisms or correlates of immunity For most of the 20th century immunotherapy was based on passive transfer of polyclonal hyperimmune animal serum immune human serum or even hyperimmune human serum Georges JF Koumlhler and Ceacutesar Milstein re-ported the generation of monoclonal antibodies in 1979 for which they shared the 1984 Nobel Prize in Physiology or Medicine ldquofor the discovery of the princi-ple for production of monoclonal antibodiesrdquo Since that time entire fields related to antibodies for infectious diseases including antibody gene cloning engineer-ing and expression antibody libraries and high-throughput antibody gene rep-ertoire sequence analysis have extended our capabilities to explore the diversity of antibody specificity and function with unprecedented depth and breadth
This book provides a broad survey of many of the most important aspects of the field of antibodies for infectious diseases The book begins with a general introduction followed by chapters 2 through 5 on general features pertaining to structure function isotype and the role of complement in antibody function Chapters 6 through 10 review contemporary approaches for antibody discovery using phage and yeast display plasma cell and memory B cell cloning human hybridomas humanized mice and computational methods Chapters 11 through 18 review in depth the biology of antibodies specific for particular pathogens including viruses and bacterial toxins to illustrate the role of antibodies in anti- microbial immunity with specific targets These chapters reveal that attempts to raise effective antibody responses to each of these pathogens faces unique and pathogen-specific challenges Chapters 19 to 23 cover major technical advances pertaining to antibody engineering repertoire sequencing and analysis and new methods for study or therapeutic use of antibodies including radiotherapy Fi-nally chapters 24 and 25 cover new methods for expression of monoclonal anti-bodies in plants or by transfer of antibody genes for in vivo expression in treated subjects
Recent literature is exploding with new antibody-related techniques and re-ports of antimicrobial antibodies with unprecedented potency breadth of activ-
xvii
xviii PReface
ity and therapeutic potential We hope that this timely compilation of state-of-the-art reviews of major aspects of this field will be of interest to both antibody cognoscenti and those new to this exciting field We thank the authors for their dedication in producing definitive reviews of the topics at hand
James E Crowe JrDiana BoraschiRino Rappuoli
INTRODUCTION
History and PracticeAntibodies in Infectious Diseases 1ADAM HEY1
Antibodies in Infectious Diseases aims to inform update and inspire studentsteachers researchers pharmaceutical developers and health care professionalson the status of the development of antibody-based therapies for treatinginfectious diseases and the potential for these in times of growing antibioticresistance to provide alternative treatment solutions to the currently usedantibiotics and new treatments for infectious diseases where no propertreatments are available
This introductory article will provide a historical perspective on the useof antibody-based therapies followed by a high-level overview of whatmakes antibodies attractive tools for this purpose This will include the prosand cons of such therapies compared to the use of antibiotics and thepractical and strategic considerations involved in selecting the best formatand development path for new antibody-based therapies targeting specificinfectious agents Then examples of antibody-based therapies in thedevelopment of treatments for infectious diseases will be presented andfinally a look into the future will summarize the different aspects that willinfluence what the future might bring for this type of treatments forinfectious diseases
1Preclinical Safety Biologics Novartis AG Basel Switzerland
Antibodies for Infectious DiseasesEdited by James E Crowe Jr Diana Boraschi and Rino Rappuolicopy 2015 American Society for Microbiology Washington DCdoi101128microbiolspecAID-0026-2014
3
HISTORICAL PERSPECTIVE
Antibodies and the use of passive antibodytherapy in the treatment of infectious dis-eases is the story of a treatment conceptwhich dates back more than 120 years to thelate 19th century and which originally bythe use of serum from immunized animalsprovided the first effective treatment optionsagainst severe bacterial infections (1 2) Byimmunizing horses with bacterial toxinsfrom Clostridium tetani and Corynebacteri-um diphtheriae Emil A Von Behring andShibasaburo Kitasato (3) generated serumcontaining antibodies capable of neutraliz-ing the effects of the toxins produced bythese bacteria and successfully providedtreatment for these serious diseases wherethe pathogenesis is driven by the effects ofthe bacterial toxins For his work on provid-ing treatment for diphtheria Behring re-ceived the Nobel Prize in Physiology orMedicine in 1901 These radical treatmentresults quickly prompted development ofmultiple additional serum therapies for thetreatment of infectious diseases caused byeg Neisseria meningitidis Haemophilus in-fluenza and group A Streptococcus Sinceserum therapy involved administration oflarge amounts of crude mixtures of animalproteins including antibodies they wereassociated with side effects in the form ofhypersensitivity and serum sickness (2)
Due to the crude and unpurified nature ofthese products side effects were seen evenwhen administering human serum prepa-rations Side effects were observed in up to50 of patients and were considered to becaused by immune complex formations thatresulted in symptoms such as rash itchingjoint pain fever and in serious cases hypoten-sion and shock However due to the lack ofalternative options these treatments weredespite their side effects widely used Serumwas normally administered by intravenousinfusion in patients after a test for hypersensi-tivity where a small amount of serum wasinjected subcutaniously (1) As described
above serum therapy applied in these earlydays (late 19th century and early 20th century)involved preparations of serum from rabbitsand horses immunized with the infectiousagent or in live andor neutralized versions ortoxins from these (1) The costs of keeping theimmunized animals and the production andpotency testing of the materials made this arelatively expensive treatment In 1891 datafrom Klemperer (4) showed serum therapy toprotect rabbits from Streptococcus pneumoniaeinfection and paved the way for this type oftreatment and for development of similarserum-based treatments of streptococcal in-fections in humans When treating humansearly administration of serum could reducemortality significantly down to around 5compared to when administered 4 to 5 daysafter onset of symptoms when serum treat-ment was largely without effect This stronglyindicated the need for quick diagnosis andquick treatment to control the infection beforeit got out of control Consequently in theabsence of a specific diagnosis mixtures ofserum from immunizations with differentserotypes were used to circumvent this needfor early treatment without having a serotype-specific diagnosis The understanding thatdifferent serotypes existed for pneumococciand that efficient treatment relied on usingserotype-specific serum was being built upduring the 1920s and 1930s through experiencefrom extensive clinical trials
By the end of the 1930s serum therapywasthe standard of care for treatment of pneu-mococcal pneumonia At that time theefficacy and potency of the derived serawere assessed in mice in ldquothe mouse pro-tection testrdquo by testing survival after aconcomitant intraperitoneal injection of alethal dose of pneumococci and the serum tobe tested Due to the inherent variation inthis test efficacy and survival in two thirds ofthe animals was the acceptance criteria and10 times the lowest dose providing this wasused for defining a unit of the serum Thisallowed for large batch-to-batch variationand the use of different strains of bacteria for
4 HEY
immunization probably explains part of themissing responses observed (1) In the early20th century a pandemic of meningitis inEurope and the United States with mortalityrates up to 80 spurred the development ofserum therapy treatment options Althoughin the 1930s this became the recommendedtreatment in children assumed to be suffer-ing from meningitis failure to reduce mor-tality in several meningitis epidemics duringthat time raised doubts about the generalapplicability of serum treatment In thosedays serum therapy often involved quiteextensive procedures and infusion of largevolumes of serum The following exampleclearly illustrates this Data from Flexnerand Jobling (5) from treating meningitis inmonkeys resulted in the development of serafrom immunized horses for treatment inhumans The treatment protocol includedlumbar puncture and withdrawal of morethan 30 ml of spinal fluid representing anamount slightly larger than the expectedamount of horse serum to be injected subse-quently This treatment involved such dailyslow infusions of up to 30 ml of serum untilthe patientrsquos condition improved This treat-ment was used in outbreaks in New York in1905 and 1906 and did markedly decreasemortality
After the discovery of penicillin by Flemingin 1928 and the subsequent introduction ofantibiotics in the 1930s serum therapy waslargely abandoned over a period of 10 years dueto the availability of these new more broadlyeffective and cheaper treatment optionswhichalso had fewer side effects Although improve-ments in the purification of antibodies hadresulted in preparations with better safety andside effect profiles high manufacturing costsand narrow specificity resulted in antibodytherapy being mostly restricted to a smallernumber of selected treatments for snakevenoms bacterial toxins and some viral infec-tions (1 2) Currently antibody administrationis used for treatment and prevention ofhepatitis B virus rabies virus respiratorysyncytial virus (RSV) Clostridium tetani Clos-
tridium botulinum vaccinia virus echovirusand enterovirus For the most part thesetreatments consist of pooled immunoglobulinalso known as IVIG (intravenous immunoglob-ulin) from several postexposure donors Thisresults in both batch-to-batch variation in theneed for relatively large amounts of serum dueto low specificity and to restricted supplies dueto reliance on exposed donors
However several challengeshave resulted inthe need for new tools in the treatment andpreventionof infectiousdiseasesThebroadandgeneral use of antibiotics in human and veter-inary medicine for many years has resulted inthe development of multi-resistant strains ofbacteria with limited to no response to existingtreatments such as methicillin-resistant Staph-ylococcusaureus (MRSA) vancomycin-resistantS aureus and others This has resulted inpatients needing screening and treatment withseveral antibacterial agents and longer treat-ment time causing extra strain on patients andhealth care providers (6 httpwwwcdcgovdrugresistancethreat-report-2013indexhtml) According to the WHO and CDC morethan 25000 people in European Unioncountries and similar numbers in the UnitedStates die every year as a result of antibiotic-resistant infections This together with theemergence of new pathogens (eg severeacute respiratory syndrome Middle East respi-ratory syndrome) the re-emergenceepidemicsof oldknown pathogens (eg Ebola) and thedifficulties in treating infections in immune-deficient patients (eg HIV patients) has high-lighted the need for new solutions The 2014Ebola epidemic in West Africa (Liberia SierraLeone Guinea Nigeria and Senegal) has fur-ther highlighted this No treatment or prophy-lactic vaccine is available to treat or prevent thespread of Ebola infections which have anaveragemortality of gt50 Local health author-ities in the affected countries are struggling tocontain and handle the disease which isthreatening to go out of control and spreadmorewidelyVariousproductsmainly antibodycocktails from previously recovered patientsare being used despite a lack of clinical data on
CHAPTER 1 bull History and Practice Antibodies in Infectious Diseases 5
their safety and efficacy and those are the onlysporadically available treatment options andonly in small amounts and for a few patients
Ebola is an example of a disease whichnormally affects only a small number ofindividuals and which normally burns outwhen disease outbreaks are contained There-fore given the small number of potentialpatients affected by previous Ebola infectionsto date there was no incentive for big pharmacompanies to do research and development ofdrugs for EbolaWith the increasing number ofinfected (13567) andadeath toll of 4951 (7) andthe lack of the ability to contain the epidemic itwill be interesting to follow the aftermath ofthis outbreak and see whether there will berequests for new ways to ensure that vaccinesand treatment options are available for Ebolaand similar high-mortality and potential bio-warfare infections that have no availabletreatments or procedures to for mass-produc-tion upon the first signsreports of activeinfections Although both the CDC and theWHO have special programs focusing on thesetypes of infections the Ebola outbreak in 2014clearly shows that more financial support forresearch and development of new diagnosticsand treatments is needed This is one examplewhere antibody-based treatments would havethe potential to play a major role To put this inthe right perspective one should however notforget that other infectious diseases such astuberculosis influenza and malaria kill hun-dreds of thousands each year There is there-fore plenty of room for improvement indeveloping treatments for these diseases aswell but the high attention drawn to eg theEbola outbreak creates a special niche andopportunity where antibody treatments couldgain extraordinary development funding andsupport and prove their value and treatmentpotential
That antibody-based therapies could takethis role is supported by the revolution intechnologies for the development selectiongeneration and purification of fully humanantibodies described in more detail later in thesection ldquoMethodsandPlatforms forGenerating
Antibodiesrdquo Antibody-based programs cur-rently at different stages of developmentinclude investigations into the potential use ofsingle antibody preparations combinations ofantibodies (to avoid survival of escape mu-tants) fragments of antibodies and antibodiescarrying radioactive isotopesorcytotoxicdrugsor antibody-like frameworks (eg fibronectin)either alone as a first-line treatment or as anadjunct to existing treatments This multitudeof possible formats the ability to raise anti-bodies to almost any target and the ability toengineer both size effector functions and half-life are now considered by many to providevery valuable tools for designing specificantibody-based treatments toeradicate specifictargeted infectious agents However althoughseveral antibody-based therapies have beenapproved for oncology and anti-inflammatoryindications (see Table 1) only one monoclonalantibody (mAb) is approved against an infec-tious disease agentmdashSynagis (palivizumabMedImmune) for the prevention and treat-ment of respiratory syncytical virus (RSV) inhigh-risk children Economic obstacles such asthe high cost of mAb therapies and relativelysmall markets have resulted in less interestfrom pharmaceutical companies in developingthese Also highlighting the challenges indeveloping these types of antibody-basedtreatments are the difficulties encountered indeveloping a follow-up higher-affinity candi-date to Synagis Poor translatability of dataobtained in the available animal disease mod-els for RSV in cotton rats has resulted in non-approval due to inferiority relative to SynagisIn other viral diseases such as cytomegalovirus(CMV) the high species specificity of thestrains of CMV makes it impossible to testhuman antibody therapies in vivo Thereforeany real data on the efficacy of treatments forCMV will not be obtained until testing inclinical trials As described later in this articleseveral new antibody-based therapies for in-fectious diseases are in development andhopefully this will gradually open the fieldand result in better treatment options andoutcomes for patients
6 HEY
TABLE 1 Approved and pending antibody-based therapies
Name antibody Target antibody type Indication Company Approval date
OKT3a Muronomab-CD3 CD3 murine IgG2a Autoimmune Johnson ampJohnson
1986 (US)
ReoPro abciximab PIIbIIIa chimeric IgG1Fab
Homeostasis Johnson ampJohnson
1984 (US)
Rituxan rituximab CD20 chimeric IgG1 Cancer Genentech 1997 (US) 1998 (EU)Zenapaxa daclizumab CD25 humanized IgG1 Autoimmune Roche 1997 (US) 1999 (EU)Simulect basiliximab CD25 chimeric IgG1 Autoimmune Novartis 1998 (US EU)Synagis palivizumab RSV humanized IgG1 Infections MedImmune 1998 (US) 1999 (EU)Remicade infliximab TNFα chimeric IgG1 Autoimmune Johnson amp
Johnson1998 (US) 1999 (EU)
Herceptin trastuzumab HER2 humanized IgG1 Cancer GenentechRoche
1998 (US) 2000 (EU)
Mylotarga gemtuzumabozogamicin
CD33 humanized IgG4immunotoxin
Cancer WyethPfizer 2000 (US)
Campath alemtuzumab CD52 humanized IgG1 Cancer Genzyme 2001 (US) 2001 (EU)Zevalin ibritumomabtiuxetan
CD20 murine IgG1radiolabeled (yttrium 90)
Cancer Biogen Idec 2002 (US) 2004 (EU)
Humira adalimumab TNFα human IgG1 Autoimmune Abbott 2002 (US) 2003 (EU)Xolair omalizumab IgE humanized IgG1 Autoimmune Genentech
Roche2003 (US)
Bexxar tositumomab-I-131 CD20 murine IgG2aradiolabeled (iodine131)
Cancer CorixaGSK 2003 (US)
Raptivaa falizumab CD11a humanized IgG1 Autoimmune GenentechRoche
2003 (US) 2004 (EU)
Erbitux cetuximab EGFR chimeric IgG1 Cancer ImcloneLilly 2004 (US) 2004 (EU)Avastin bevacizumab VEGF humanized IgG1 Cancer Genentech
Roche2004 (US) 2005 (EU)
Tysabri natalizumab α4-Intergrin humanizedIgG4
Autoimmune Biogen Idec 2004 (US)
Actemra tocilizumab Anti-IL-6R humanizedIgG1
Autoimmune ChugaiRoche
2005 (Japan) 2010 (US)
Vectibix panitumumab EGFR human IgG2 Cancer Amgen 2006 (US)Lucentis ranibizumab VEGF humanized IgG1
FabMaculardegeneration
GenentechRoche
2006 (US)
Soliris eculizumab C5 humanized IgG24 Blood disorders Alexion 2007 (US)Cimzia certolizumab pegol TNFα humanized
pegylated FabAutoimmune UCB 2008 (US)
Simponi golimumab TNFα human IgG1 Autoimmune Johnson ampJohnson
2009 (US EU Canada)
Ilaris canakinumab IL1b human IgG1 Infalmmatory Novartis 2009 (US EU)Stelara ustekinumab IL-1223 human IgG1 Autoimmune Johnson amp
Johnson2008 (EU) 2009 (US)
Arzerra ofatumumab CD20 human IgG1 Cancer Genmab 2009 (EU)Prolia denosumab RANK ligand human
IgG2Bone loss Amgen 2010 (US)
Numax motavizumab RSV humanized IgG1 Anti-infective MedImmune PendingABthrax Raxibacumab B anthrasis PA human
IgG1Anti-infection GSK 2012 (US)
Benlysta belimumab BLyS human IgG1 Autoimmune HGS 2011 (US)Yervoy ipilimumab CTLA-4 human IgG1 Cancer BMS 2011 (US)Adcetris brentuximabvedotin
CD30 chimeric IgG1drug- conjugate
Cancer SeattleGenetics
2011 (US)
(Continued on next page)
CHAPTER 1 bull History and Practice Antibodies in Infectious Diseases 7
INTRODUCTION TO ANTIBODIES
Antibodies also called immunoglobulins basedon their combined structure and function inimmune responses are produced by B cells ofthe immune system They are part of theadaptive immune response and are speciallydesigned for neutralizing and eliminating theinfectious agents and toxins produced by theseAntibodies are present in blood plasma andextracellular fluids and since these fluids wereformerly known as humors they were said tobe part of the humoral immune responseAntibodies are Y-shaped structures consistingof two main parts the upper arms of the Ywhich contain two identical variable-regionantigen binding sites and the lower regioncalled the constant regionwhich is responsiblefor the initiation of effector functions that leadto the removal and destruction of the pathogenor cells harboring the pathogen (see Fig 1) Theantigen-binding sites on an antibody can bythemselves bind to and neutralize bacterialtoxins and viruses thereby preventing themfrom binding to their target cells or receptorscausing toxic effects or spread of the infection
Antibodies consist of two pairs of heavy andlight chainswhich as described above are heldtogether in a Y-shaped arrangement Each ofthe heavy and light chains in these pairs isseparated into constant and variable chainsThe upper armsof theY each contain a variableand a constant sectionof the light and theheavychain where the upper variable parts of theheavy and light chains contain the antigen-binding site and the constant parts areconnected via disulfide bonds The lower partof theYcalled theconstantpart consistsof twoor three constant segments (immunoglobulindomains) from each of the two heavy chainsinteracting and also linked via disulfide bondsThe sectionsof theheavy chains connecting theconstant part of the upper arms to the constantparts of the constant region contain specialhinge regions that provide flexibility to thedifferent sections of the antibody to bind toantigens and effector cells The constant re-gions of the heavy chain also contain attachedoligosaccharide moieties which provide func-tional specialization to the antibodies (8)
The variable domains of the heavy and lightchains form the antigen-binding sites and
TABLE 1 Approved and pending antibody-based therapies (Continued)
Name antibody Target antibody type Indication Company Approval date
Perjeta pertuzumab Her2 humanized IgG1 Cancer GenentechRoche
2012 (US)
Kadcyla ado-trastuzumabemtansine
Her2 humanized IgG1Drug-conjugate
Cancer GenentechRoche
2013 (US)
Raxibacumab Anti-B anthrasis PAhuman IgG1
Anthraxinfection
Notapproved
2012
Entyvio vedolizumab Integrin α4β7humanized IgG1
Crohnrsquos diseaseulcerative colitis
Takeda 2014 (US)
Cyramza ramuciruumab Anti-VEGFR2Human IgG1
Gastric cancer Lilly 2014 (US)
Gazyva obinutuzumab Anti-CD20 humanizedIgG1 glucoengineered
CancerCLLb GenentechRoche
2014 (US)
Sylvant situximab Anti IL-6 chimeric IgG1 Castlemandisease
Janssen 2014 (US) 2014 (EU)
Cosentyx sekukinumab Anti IL-17a human IgG1 Psoriasis Novartis 2015 (US) 2015 (EU)Nivolumab Anti PD-1 human IgG4 Melanoma BMS Not approvedKeytruda pembrolizuumab Anti-PD-1 humanized
IgG4Melanoma Merck 2014 (US)
aAntibodies approved but later withdrawnbCLL chronic lymphocytic leukemia
8 HEY
FIGURE 1 (Left panel) Model of antibody structure exemplified by IgG On top the antigen-binding sitesin orange each contain one variable light and variable heavy domain with the three complementaritydetermining regions (CDRs) that are responsible for the specific binding of the antibody to its target Foreach arm of the antibody an additional set of variable heavy and light domains together with the CDR-containing domains represent the two fragment antigen binding (Fab) regions The two Fabs are heldtogether via two disulfide bridges Below the Fabs is the Fc region which contains four constant heavydomains On the upper pair of these domains are binding sites for oligosaccharides which have majorimportance for the ability of the antibody Fc part to trigger effector functions when the Fc portion isbound to Fc gamma receptors on natural killer cells neutrophil granulocytes monocytesmacrophagesdendritic cells and B cells (Right panel) Examples of some of the antibody-derived alternative formatsused to exploit the specific features of the CDRs the Fabs and the Fc parts of the antibodies ScFv Thesingle chain fragment variable consists of the variable domains of the heavy and light chains heldtogether by a flexible linker This can also be used as a carrier of a cytotoxic drug in a so-called antibodydrug complex (ADC) where the specificity of the ScFv is used to target the cytotoxic drug to eg atumor Bite (bi-specific T cell engager) Fusion proteins consisting of two ScFvs one directed against thetarget on a tumor cell and the other against the T cell receptor (CD3) Diabody ScFv dimers where shortlinker peptides (five amino acids) ensure dimerization and not folding of the ScFvs Fab and F(ab)2fragments Single Fab fragments or fragments containing two Fabs linked via disulfide bridges This isused where effector functions related to the Fc part of the antibody are unwanted and where a smallersize is desired to obtain better tissue penetration in eg tumors Due to the lack of the FcRn binding viathe Fc part Fab and F(ab)2 fragments have much shorter half-lives (hours or days) than full-sizeantibodies (weeks) These can also be used as carriers of cytotoxic payloads or cytotoxic radioactiveisotopes and for the F(ab)2 fragments can be constructed as bi-specifics which can cross-link immunecells and target cells Fc fusion protein Fusion protein containing the Fc domain of an immunoglobulinbound to a peptide The peptide can be a ligand for a specific receptor on a target cell or a blockingpeptide for a soluble ligand The Fc part provides a longer half-life to the construct and the potential tobind to and engage effector functions in the killing of eg tumor cells or infected cells ADCsRIAs andbi-specifics Full-size IgG antibodies carrying either a cytotoxic chemical or radioactive payload whichmay also carry different CDRs enabling cross-linking of effector and target cells for increased killingdoi101128microbiolspecAID-0026-2014f1
CHAPTER 1 bull History and Practice Antibodies in Infectious Diseases 9
contain special hyper-variable segments calledcomplementarity-determining regions (CDRs)which allow the B cells via genetic recom-bination to generate antibodies to all thedifferent antigens specific to amino acid se-quences or three-dimensional structuralmotifs(polysaccharides DNA and RNA) found onpathogens
Based on the structure of their heavy chainconstant regions antibodies or immuno-globulins are separated into five classesmdashIgM IgG IgE IgD and IgA Differences inthe sequences of the constant regions providedistinct characteristics to these different clas-ses These characteristics include the numberof heavy chain constant segments the numberand location of interconnecting disulfidebridges the length of the hinge region andthe number and location of oligosaccharidemoieties For IgG four heavy chain versionsexist creating IgG1 2 3 and 4 isotypes eachwith different characteristics in their serumhalf-lives and ability to trigger different effec-tor functions Because of the combined ad-vantage from ability to trigger effectormechanisms long [21 days] half-life theirability to be transported over the placentaand their stability in the production processantibodies of the IgG class and of the IgG1isotype are preferred as the basis for newantibody-based therapies The effector func-tions are triggered by the Fc part of an antibodywhen the variable parts of the antibody arebound directly to an infectious agent or toproteins from an infectious agent expressed onan infected cell This binding leaves the Fc partfree to interactwithFc receptors onphagocyticcells and neutrophils eosinophils and naturalkiller cells capable of inducing phagocytosis orlysis of infectious agents or infected cellsThese effector functions include (i) the abilityto activate the complement system for lysis(complement-dependent cellular cytotoxicity)(ii) triggering of uptake and destruction byphagocytic cells such as macrophages andneutrophils via interaction with Fc receptorson these cells (iii) activation of macrophageseosinophils neutrophils and natural killer
cells to kill infected cells via binding to Fcreceptors on these cells and antibody-depen-dent cellular cytotoxicity and (iv) neutraliza-tion of bacterial toxins and blocking of bindingand uptake of bacteria or viruses to target cells(see Fig 2) (9)
The Fcpart of IgG antibodies also contains aregion that interacts with the neonatal Fcreceptor (FcRn) expressed on most immuno-competent cells and inmany other cells such asendothelial cells in kidney liver placenta lungand breast (10) which protects antibodies fromdegradation by phagocytoticexocytotic cy-cling into FcRn-expressing cells thereby pro-longing their half-life This results in half-livesof 20 to 21 days for most IgG1 2 and 4antibodies whereas half-lives are 10 6 and 2days respectively for IgM IgA and IgE Thehighly specific binding sites on the variableregions of the upper arms of the antibody allowfor several important features of antibodiesndashbinding to and neutralization of eg bacterialtoxins binding to pathogens and blocking theirbinding to or interaction with target cells (egcyncytia formation of CMV-infected cells) orblocking of binding and interactions of infec-tious agents with target cells via blockingreceptors on the target cells
METHODS AND PLATFORMS FORGENERATING ANTIBODIES
As described above the early use of passiveantibody transfer as a therapy in infectiousdiseases involved the use of immune serumfrom immunized sheep and horses These pre-parations were crude and contained a broadmixture of neutralizing and non-neutralizingantibodies and both the foreign nature of theantibodies and the numerous host serumproteins This resulted in less specific andthus less efficient therapies due to a highvariability in efficacy between batches derivedfrom different animals immunized with dif-ferent strains of bacteria in different labor-atories and resulted in multiple unwantedside effects related to hypersensitivity and
10 HEY
anaphylactic reactions to foreign proteinsThese days antibodies being developed fortreatment of diseases in humans are highlypurified and are mostly fully human mono-clonal antibodies The term monoclonal anti-body refers to that cell cultures used forgenerating these antibodies each originatesfrom a single cell and thus produces onlyone specific antibody Development of fullyhuman monoclonal antibodies happened instages over a time span of more than 15 yearsFirst stage in this process was generation ofmonoclonalmurine IgG antibodies (eg OKT3[muronomab-CD3 Johnson and Johnson] ap-proved in 1986) Next stage was generation ofso called chimeric antibodies consisting ofhuman heavy and light chain constant sec-tions but with murine variable sections (eg
Rituxan [rituximab Genentech]) Next stagewas then the humanized antibodies wherethe only remaining murine part of the anti-body is the antigen-binding CDR (eg Xolair[omalizumab NovartisGenentech]) Both thefirst chimeric and humanized antibodies wereapproved in the late 1990s Then finally 16years later the first fully human antibodyHumira (adalimumab Abbott) was approvedin 2002 Since the time of the crude and low-scale manufacturing of the original antibodyserum products much has changed andtherapeutic antibodies are now produced byfermentation in 5000 liter scale using highlycontrolled and documented yeast or mamma-lian cell lines that are genetically engineered toexpress a single specific antibody This hasresulted in a pure and highly specific antibody
FIGURE 2 Effector functions of antibodies (a) Antibodies bind to pathogen-derived or endogenousantigens expressed on the surface of an infected cell which triggers binding to Fc receptors on naturalkiller cells and lysis of the infected cell by antibody-dependent cellular cytotoxicity (b) Antibodies bindto pathogen-derived or endogenous antigens expressed on the surface of infected cells which triggersactivation of complement through binding of complement factor C1q (c) Neutralization Top Bacterialtoxin neutralized by bound antigen Bottom Antibody bound to either receptor for the virus or to thevirus itself which blocks virus binding and entry into the cell (d) Antibody bound to viral surfaceproteins binds to Fc receptors on phagocytic cells eg macrophages and triggers endocytosis anddestruction of virus in endolysosome doi101128microbiolspecAID-0026-2014f2
CHAPTER 1 bull History and Practice Antibodies in Infectious Diseases 11

Ian A WilsonDepartment of Molecular Biology and Skaggs Institute for Chemical BiologyThe Scripps Research Institute10550 North Torrey Pines RoadLa Jolla CA 92037
Herren WuDepartment of Antibody Discovery and Protein EngineeringMedImmune LLCOne MedImmune WayGaithersburg MD 20879
Guocheng YangDepartment of Chemical EngineeringArizona State UniversityTempe AZ 85287-6006
Larry ZeitlinMapp Biopharmaceutical Inc6160 Lusk Blvd C105San Diego CA 92121
xvi contRIBUtoRs
Preface
Antibodies form the principal foundation for modern intervention against in-fectious diseases Emil Adolf von Behring was awarded the first Nobel Prize in Physiology or Medicine in 1901 ldquofor his work on serum therapy especially its appli-cation against diphtheria by which he has opened a new road in the domain of med-ical science and thereby placed in the hands of the physician a victorious weapon against illness and deathsrdquo Antibodies now provide the focus for understanding mechanisms of immunity to most infectious diseases and they play a central role in passive immunotherapy and active vaccination as mechanisms or correlates of immunity For most of the 20th century immunotherapy was based on passive transfer of polyclonal hyperimmune animal serum immune human serum or even hyperimmune human serum Georges JF Koumlhler and Ceacutesar Milstein re-ported the generation of monoclonal antibodies in 1979 for which they shared the 1984 Nobel Prize in Physiology or Medicine ldquofor the discovery of the princi-ple for production of monoclonal antibodiesrdquo Since that time entire fields related to antibodies for infectious diseases including antibody gene cloning engineer-ing and expression antibody libraries and high-throughput antibody gene rep-ertoire sequence analysis have extended our capabilities to explore the diversity of antibody specificity and function with unprecedented depth and breadth
This book provides a broad survey of many of the most important aspects of the field of antibodies for infectious diseases The book begins with a general introduction followed by chapters 2 through 5 on general features pertaining to structure function isotype and the role of complement in antibody function Chapters 6 through 10 review contemporary approaches for antibody discovery using phage and yeast display plasma cell and memory B cell cloning human hybridomas humanized mice and computational methods Chapters 11 through 18 review in depth the biology of antibodies specific for particular pathogens including viruses and bacterial toxins to illustrate the role of antibodies in anti- microbial immunity with specific targets These chapters reveal that attempts to raise effective antibody responses to each of these pathogens faces unique and pathogen-specific challenges Chapters 19 to 23 cover major technical advances pertaining to antibody engineering repertoire sequencing and analysis and new methods for study or therapeutic use of antibodies including radiotherapy Fi-nally chapters 24 and 25 cover new methods for expression of monoclonal anti-bodies in plants or by transfer of antibody genes for in vivo expression in treated subjects
Recent literature is exploding with new antibody-related techniques and re-ports of antimicrobial antibodies with unprecedented potency breadth of activ-
xvii
xviii PReface
ity and therapeutic potential We hope that this timely compilation of state-of-the-art reviews of major aspects of this field will be of interest to both antibody cognoscenti and those new to this exciting field We thank the authors for their dedication in producing definitive reviews of the topics at hand
James E Crowe JrDiana BoraschiRino Rappuoli
INTRODUCTION
History and PracticeAntibodies in Infectious Diseases 1ADAM HEY1
Antibodies in Infectious Diseases aims to inform update and inspire studentsteachers researchers pharmaceutical developers and health care professionalson the status of the development of antibody-based therapies for treatinginfectious diseases and the potential for these in times of growing antibioticresistance to provide alternative treatment solutions to the currently usedantibiotics and new treatments for infectious diseases where no propertreatments are available
This introductory article will provide a historical perspective on the useof antibody-based therapies followed by a high-level overview of whatmakes antibodies attractive tools for this purpose This will include the prosand cons of such therapies compared to the use of antibiotics and thepractical and strategic considerations involved in selecting the best formatand development path for new antibody-based therapies targeting specificinfectious agents Then examples of antibody-based therapies in thedevelopment of treatments for infectious diseases will be presented andfinally a look into the future will summarize the different aspects that willinfluence what the future might bring for this type of treatments forinfectious diseases
1Preclinical Safety Biologics Novartis AG Basel Switzerland
Antibodies for Infectious DiseasesEdited by James E Crowe Jr Diana Boraschi and Rino Rappuolicopy 2015 American Society for Microbiology Washington DCdoi101128microbiolspecAID-0026-2014
3
HISTORICAL PERSPECTIVE
Antibodies and the use of passive antibodytherapy in the treatment of infectious dis-eases is the story of a treatment conceptwhich dates back more than 120 years to thelate 19th century and which originally bythe use of serum from immunized animalsprovided the first effective treatment optionsagainst severe bacterial infections (1 2) Byimmunizing horses with bacterial toxinsfrom Clostridium tetani and Corynebacteri-um diphtheriae Emil A Von Behring andShibasaburo Kitasato (3) generated serumcontaining antibodies capable of neutraliz-ing the effects of the toxins produced bythese bacteria and successfully providedtreatment for these serious diseases wherethe pathogenesis is driven by the effects ofthe bacterial toxins For his work on provid-ing treatment for diphtheria Behring re-ceived the Nobel Prize in Physiology orMedicine in 1901 These radical treatmentresults quickly prompted development ofmultiple additional serum therapies for thetreatment of infectious diseases caused byeg Neisseria meningitidis Haemophilus in-fluenza and group A Streptococcus Sinceserum therapy involved administration oflarge amounts of crude mixtures of animalproteins including antibodies they wereassociated with side effects in the form ofhypersensitivity and serum sickness (2)
Due to the crude and unpurified nature ofthese products side effects were seen evenwhen administering human serum prepa-rations Side effects were observed in up to50 of patients and were considered to becaused by immune complex formations thatresulted in symptoms such as rash itchingjoint pain fever and in serious cases hypoten-sion and shock However due to the lack ofalternative options these treatments weredespite their side effects widely used Serumwas normally administered by intravenousinfusion in patients after a test for hypersensi-tivity where a small amount of serum wasinjected subcutaniously (1) As described
above serum therapy applied in these earlydays (late 19th century and early 20th century)involved preparations of serum from rabbitsand horses immunized with the infectiousagent or in live andor neutralized versions ortoxins from these (1) The costs of keeping theimmunized animals and the production andpotency testing of the materials made this arelatively expensive treatment In 1891 datafrom Klemperer (4) showed serum therapy toprotect rabbits from Streptococcus pneumoniaeinfection and paved the way for this type oftreatment and for development of similarserum-based treatments of streptococcal in-fections in humans When treating humansearly administration of serum could reducemortality significantly down to around 5compared to when administered 4 to 5 daysafter onset of symptoms when serum treat-ment was largely without effect This stronglyindicated the need for quick diagnosis andquick treatment to control the infection beforeit got out of control Consequently in theabsence of a specific diagnosis mixtures ofserum from immunizations with differentserotypes were used to circumvent this needfor early treatment without having a serotype-specific diagnosis The understanding thatdifferent serotypes existed for pneumococciand that efficient treatment relied on usingserotype-specific serum was being built upduring the 1920s and 1930s through experiencefrom extensive clinical trials
By the end of the 1930s serum therapywasthe standard of care for treatment of pneu-mococcal pneumonia At that time theefficacy and potency of the derived serawere assessed in mice in ldquothe mouse pro-tection testrdquo by testing survival after aconcomitant intraperitoneal injection of alethal dose of pneumococci and the serum tobe tested Due to the inherent variation inthis test efficacy and survival in two thirds ofthe animals was the acceptance criteria and10 times the lowest dose providing this wasused for defining a unit of the serum Thisallowed for large batch-to-batch variationand the use of different strains of bacteria for
4 HEY
immunization probably explains part of themissing responses observed (1) In the early20th century a pandemic of meningitis inEurope and the United States with mortalityrates up to 80 spurred the development ofserum therapy treatment options Althoughin the 1930s this became the recommendedtreatment in children assumed to be suffer-ing from meningitis failure to reduce mor-tality in several meningitis epidemics duringthat time raised doubts about the generalapplicability of serum treatment In thosedays serum therapy often involved quiteextensive procedures and infusion of largevolumes of serum The following exampleclearly illustrates this Data from Flexnerand Jobling (5) from treating meningitis inmonkeys resulted in the development of serafrom immunized horses for treatment inhumans The treatment protocol includedlumbar puncture and withdrawal of morethan 30 ml of spinal fluid representing anamount slightly larger than the expectedamount of horse serum to be injected subse-quently This treatment involved such dailyslow infusions of up to 30 ml of serum untilthe patientrsquos condition improved This treat-ment was used in outbreaks in New York in1905 and 1906 and did markedly decreasemortality
After the discovery of penicillin by Flemingin 1928 and the subsequent introduction ofantibiotics in the 1930s serum therapy waslargely abandoned over a period of 10 years dueto the availability of these new more broadlyeffective and cheaper treatment optionswhichalso had fewer side effects Although improve-ments in the purification of antibodies hadresulted in preparations with better safety andside effect profiles high manufacturing costsand narrow specificity resulted in antibodytherapy being mostly restricted to a smallernumber of selected treatments for snakevenoms bacterial toxins and some viral infec-tions (1 2) Currently antibody administrationis used for treatment and prevention ofhepatitis B virus rabies virus respiratorysyncytial virus (RSV) Clostridium tetani Clos-
tridium botulinum vaccinia virus echovirusand enterovirus For the most part thesetreatments consist of pooled immunoglobulinalso known as IVIG (intravenous immunoglob-ulin) from several postexposure donors Thisresults in both batch-to-batch variation in theneed for relatively large amounts of serum dueto low specificity and to restricted supplies dueto reliance on exposed donors
However several challengeshave resulted inthe need for new tools in the treatment andpreventionof infectiousdiseasesThebroadandgeneral use of antibiotics in human and veter-inary medicine for many years has resulted inthe development of multi-resistant strains ofbacteria with limited to no response to existingtreatments such as methicillin-resistant Staph-ylococcusaureus (MRSA) vancomycin-resistantS aureus and others This has resulted inpatients needing screening and treatment withseveral antibacterial agents and longer treat-ment time causing extra strain on patients andhealth care providers (6 httpwwwcdcgovdrugresistancethreat-report-2013indexhtml) According to the WHO and CDC morethan 25000 people in European Unioncountries and similar numbers in the UnitedStates die every year as a result of antibiotic-resistant infections This together with theemergence of new pathogens (eg severeacute respiratory syndrome Middle East respi-ratory syndrome) the re-emergenceepidemicsof oldknown pathogens (eg Ebola) and thedifficulties in treating infections in immune-deficient patients (eg HIV patients) has high-lighted the need for new solutions The 2014Ebola epidemic in West Africa (Liberia SierraLeone Guinea Nigeria and Senegal) has fur-ther highlighted this No treatment or prophy-lactic vaccine is available to treat or prevent thespread of Ebola infections which have anaveragemortality of gt50 Local health author-ities in the affected countries are struggling tocontain and handle the disease which isthreatening to go out of control and spreadmorewidelyVariousproductsmainly antibodycocktails from previously recovered patientsare being used despite a lack of clinical data on
CHAPTER 1 bull History and Practice Antibodies in Infectious Diseases 5
their safety and efficacy and those are the onlysporadically available treatment options andonly in small amounts and for a few patients
Ebola is an example of a disease whichnormally affects only a small number ofindividuals and which normally burns outwhen disease outbreaks are contained There-fore given the small number of potentialpatients affected by previous Ebola infectionsto date there was no incentive for big pharmacompanies to do research and development ofdrugs for EbolaWith the increasing number ofinfected (13567) andadeath toll of 4951 (7) andthe lack of the ability to contain the epidemic itwill be interesting to follow the aftermath ofthis outbreak and see whether there will berequests for new ways to ensure that vaccinesand treatment options are available for Ebolaand similar high-mortality and potential bio-warfare infections that have no availabletreatments or procedures to for mass-produc-tion upon the first signsreports of activeinfections Although both the CDC and theWHO have special programs focusing on thesetypes of infections the Ebola outbreak in 2014clearly shows that more financial support forresearch and development of new diagnosticsand treatments is needed This is one examplewhere antibody-based treatments would havethe potential to play a major role To put this inthe right perspective one should however notforget that other infectious diseases such astuberculosis influenza and malaria kill hun-dreds of thousands each year There is there-fore plenty of room for improvement indeveloping treatments for these diseases aswell but the high attention drawn to eg theEbola outbreak creates a special niche andopportunity where antibody treatments couldgain extraordinary development funding andsupport and prove their value and treatmentpotential
That antibody-based therapies could takethis role is supported by the revolution intechnologies for the development selectiongeneration and purification of fully humanantibodies described in more detail later in thesection ldquoMethodsandPlatforms forGenerating
Antibodiesrdquo Antibody-based programs cur-rently at different stages of developmentinclude investigations into the potential use ofsingle antibody preparations combinations ofantibodies (to avoid survival of escape mu-tants) fragments of antibodies and antibodiescarrying radioactive isotopesorcytotoxicdrugsor antibody-like frameworks (eg fibronectin)either alone as a first-line treatment or as anadjunct to existing treatments This multitudeof possible formats the ability to raise anti-bodies to almost any target and the ability toengineer both size effector functions and half-life are now considered by many to providevery valuable tools for designing specificantibody-based treatments toeradicate specifictargeted infectious agents However althoughseveral antibody-based therapies have beenapproved for oncology and anti-inflammatoryindications (see Table 1) only one monoclonalantibody (mAb) is approved against an infec-tious disease agentmdashSynagis (palivizumabMedImmune) for the prevention and treat-ment of respiratory syncytical virus (RSV) inhigh-risk children Economic obstacles such asthe high cost of mAb therapies and relativelysmall markets have resulted in less interestfrom pharmaceutical companies in developingthese Also highlighting the challenges indeveloping these types of antibody-basedtreatments are the difficulties encountered indeveloping a follow-up higher-affinity candi-date to Synagis Poor translatability of dataobtained in the available animal disease mod-els for RSV in cotton rats has resulted in non-approval due to inferiority relative to SynagisIn other viral diseases such as cytomegalovirus(CMV) the high species specificity of thestrains of CMV makes it impossible to testhuman antibody therapies in vivo Thereforeany real data on the efficacy of treatments forCMV will not be obtained until testing inclinical trials As described later in this articleseveral new antibody-based therapies for in-fectious diseases are in development andhopefully this will gradually open the fieldand result in better treatment options andoutcomes for patients
6 HEY
TABLE 1 Approved and pending antibody-based therapies
Name antibody Target antibody type Indication Company Approval date
OKT3a Muronomab-CD3 CD3 murine IgG2a Autoimmune Johnson ampJohnson
1986 (US)
ReoPro abciximab PIIbIIIa chimeric IgG1Fab
Homeostasis Johnson ampJohnson
1984 (US)
Rituxan rituximab CD20 chimeric IgG1 Cancer Genentech 1997 (US) 1998 (EU)Zenapaxa daclizumab CD25 humanized IgG1 Autoimmune Roche 1997 (US) 1999 (EU)Simulect basiliximab CD25 chimeric IgG1 Autoimmune Novartis 1998 (US EU)Synagis palivizumab RSV humanized IgG1 Infections MedImmune 1998 (US) 1999 (EU)Remicade infliximab TNFα chimeric IgG1 Autoimmune Johnson amp
Johnson1998 (US) 1999 (EU)
Herceptin trastuzumab HER2 humanized IgG1 Cancer GenentechRoche
1998 (US) 2000 (EU)
Mylotarga gemtuzumabozogamicin
CD33 humanized IgG4immunotoxin
Cancer WyethPfizer 2000 (US)
Campath alemtuzumab CD52 humanized IgG1 Cancer Genzyme 2001 (US) 2001 (EU)Zevalin ibritumomabtiuxetan
CD20 murine IgG1radiolabeled (yttrium 90)
Cancer Biogen Idec 2002 (US) 2004 (EU)
Humira adalimumab TNFα human IgG1 Autoimmune Abbott 2002 (US) 2003 (EU)Xolair omalizumab IgE humanized IgG1 Autoimmune Genentech
Roche2003 (US)
Bexxar tositumomab-I-131 CD20 murine IgG2aradiolabeled (iodine131)
Cancer CorixaGSK 2003 (US)
Raptivaa falizumab CD11a humanized IgG1 Autoimmune GenentechRoche
2003 (US) 2004 (EU)
Erbitux cetuximab EGFR chimeric IgG1 Cancer ImcloneLilly 2004 (US) 2004 (EU)Avastin bevacizumab VEGF humanized IgG1 Cancer Genentech
Roche2004 (US) 2005 (EU)
Tysabri natalizumab α4-Intergrin humanizedIgG4
Autoimmune Biogen Idec 2004 (US)
Actemra tocilizumab Anti-IL-6R humanizedIgG1
Autoimmune ChugaiRoche
2005 (Japan) 2010 (US)
Vectibix panitumumab EGFR human IgG2 Cancer Amgen 2006 (US)Lucentis ranibizumab VEGF humanized IgG1
FabMaculardegeneration
GenentechRoche
2006 (US)
Soliris eculizumab C5 humanized IgG24 Blood disorders Alexion 2007 (US)Cimzia certolizumab pegol TNFα humanized
pegylated FabAutoimmune UCB 2008 (US)
Simponi golimumab TNFα human IgG1 Autoimmune Johnson ampJohnson
2009 (US EU Canada)
Ilaris canakinumab IL1b human IgG1 Infalmmatory Novartis 2009 (US EU)Stelara ustekinumab IL-1223 human IgG1 Autoimmune Johnson amp
Johnson2008 (EU) 2009 (US)
Arzerra ofatumumab CD20 human IgG1 Cancer Genmab 2009 (EU)Prolia denosumab RANK ligand human
IgG2Bone loss Amgen 2010 (US)
Numax motavizumab RSV humanized IgG1 Anti-infective MedImmune PendingABthrax Raxibacumab B anthrasis PA human
IgG1Anti-infection GSK 2012 (US)
Benlysta belimumab BLyS human IgG1 Autoimmune HGS 2011 (US)Yervoy ipilimumab CTLA-4 human IgG1 Cancer BMS 2011 (US)Adcetris brentuximabvedotin
CD30 chimeric IgG1drug- conjugate
Cancer SeattleGenetics
2011 (US)
(Continued on next page)
CHAPTER 1 bull History and Practice Antibodies in Infectious Diseases 7
INTRODUCTION TO ANTIBODIES
Antibodies also called immunoglobulins basedon their combined structure and function inimmune responses are produced by B cells ofthe immune system They are part of theadaptive immune response and are speciallydesigned for neutralizing and eliminating theinfectious agents and toxins produced by theseAntibodies are present in blood plasma andextracellular fluids and since these fluids wereformerly known as humors they were said tobe part of the humoral immune responseAntibodies are Y-shaped structures consistingof two main parts the upper arms of the Ywhich contain two identical variable-regionantigen binding sites and the lower regioncalled the constant regionwhich is responsiblefor the initiation of effector functions that leadto the removal and destruction of the pathogenor cells harboring the pathogen (see Fig 1) Theantigen-binding sites on an antibody can bythemselves bind to and neutralize bacterialtoxins and viruses thereby preventing themfrom binding to their target cells or receptorscausing toxic effects or spread of the infection
Antibodies consist of two pairs of heavy andlight chainswhich as described above are heldtogether in a Y-shaped arrangement Each ofthe heavy and light chains in these pairs isseparated into constant and variable chainsThe upper armsof theY each contain a variableand a constant sectionof the light and theheavychain where the upper variable parts of theheavy and light chains contain the antigen-binding site and the constant parts areconnected via disulfide bonds The lower partof theYcalled theconstantpart consistsof twoor three constant segments (immunoglobulindomains) from each of the two heavy chainsinteracting and also linked via disulfide bondsThe sectionsof theheavy chains connecting theconstant part of the upper arms to the constantparts of the constant region contain specialhinge regions that provide flexibility to thedifferent sections of the antibody to bind toantigens and effector cells The constant re-gions of the heavy chain also contain attachedoligosaccharide moieties which provide func-tional specialization to the antibodies (8)
The variable domains of the heavy and lightchains form the antigen-binding sites and
TABLE 1 Approved and pending antibody-based therapies (Continued)
Name antibody Target antibody type Indication Company Approval date
Perjeta pertuzumab Her2 humanized IgG1 Cancer GenentechRoche
2012 (US)
Kadcyla ado-trastuzumabemtansine
Her2 humanized IgG1Drug-conjugate
Cancer GenentechRoche
2013 (US)
Raxibacumab Anti-B anthrasis PAhuman IgG1
Anthraxinfection
Notapproved
2012
Entyvio vedolizumab Integrin α4β7humanized IgG1
Crohnrsquos diseaseulcerative colitis
Takeda 2014 (US)
Cyramza ramuciruumab Anti-VEGFR2Human IgG1
Gastric cancer Lilly 2014 (US)
Gazyva obinutuzumab Anti-CD20 humanizedIgG1 glucoengineered
CancerCLLb GenentechRoche
2014 (US)
Sylvant situximab Anti IL-6 chimeric IgG1 Castlemandisease
Janssen 2014 (US) 2014 (EU)
Cosentyx sekukinumab Anti IL-17a human IgG1 Psoriasis Novartis 2015 (US) 2015 (EU)Nivolumab Anti PD-1 human IgG4 Melanoma BMS Not approvedKeytruda pembrolizuumab Anti-PD-1 humanized
IgG4Melanoma Merck 2014 (US)
aAntibodies approved but later withdrawnbCLL chronic lymphocytic leukemia
8 HEY
FIGURE 1 (Left panel) Model of antibody structure exemplified by IgG On top the antigen-binding sitesin orange each contain one variable light and variable heavy domain with the three complementaritydetermining regions (CDRs) that are responsible for the specific binding of the antibody to its target Foreach arm of the antibody an additional set of variable heavy and light domains together with the CDR-containing domains represent the two fragment antigen binding (Fab) regions The two Fabs are heldtogether via two disulfide bridges Below the Fabs is the Fc region which contains four constant heavydomains On the upper pair of these domains are binding sites for oligosaccharides which have majorimportance for the ability of the antibody Fc part to trigger effector functions when the Fc portion isbound to Fc gamma receptors on natural killer cells neutrophil granulocytes monocytesmacrophagesdendritic cells and B cells (Right panel) Examples of some of the antibody-derived alternative formatsused to exploit the specific features of the CDRs the Fabs and the Fc parts of the antibodies ScFv Thesingle chain fragment variable consists of the variable domains of the heavy and light chains heldtogether by a flexible linker This can also be used as a carrier of a cytotoxic drug in a so-called antibodydrug complex (ADC) where the specificity of the ScFv is used to target the cytotoxic drug to eg atumor Bite (bi-specific T cell engager) Fusion proteins consisting of two ScFvs one directed against thetarget on a tumor cell and the other against the T cell receptor (CD3) Diabody ScFv dimers where shortlinker peptides (five amino acids) ensure dimerization and not folding of the ScFvs Fab and F(ab)2fragments Single Fab fragments or fragments containing two Fabs linked via disulfide bridges This isused where effector functions related to the Fc part of the antibody are unwanted and where a smallersize is desired to obtain better tissue penetration in eg tumors Due to the lack of the FcRn binding viathe Fc part Fab and F(ab)2 fragments have much shorter half-lives (hours or days) than full-sizeantibodies (weeks) These can also be used as carriers of cytotoxic payloads or cytotoxic radioactiveisotopes and for the F(ab)2 fragments can be constructed as bi-specifics which can cross-link immunecells and target cells Fc fusion protein Fusion protein containing the Fc domain of an immunoglobulinbound to a peptide The peptide can be a ligand for a specific receptor on a target cell or a blockingpeptide for a soluble ligand The Fc part provides a longer half-life to the construct and the potential tobind to and engage effector functions in the killing of eg tumor cells or infected cells ADCsRIAs andbi-specifics Full-size IgG antibodies carrying either a cytotoxic chemical or radioactive payload whichmay also carry different CDRs enabling cross-linking of effector and target cells for increased killingdoi101128microbiolspecAID-0026-2014f1
CHAPTER 1 bull History and Practice Antibodies in Infectious Diseases 9
contain special hyper-variable segments calledcomplementarity-determining regions (CDRs)which allow the B cells via genetic recom-bination to generate antibodies to all thedifferent antigens specific to amino acid se-quences or three-dimensional structuralmotifs(polysaccharides DNA and RNA) found onpathogens
Based on the structure of their heavy chainconstant regions antibodies or immuno-globulins are separated into five classesmdashIgM IgG IgE IgD and IgA Differences inthe sequences of the constant regions providedistinct characteristics to these different clas-ses These characteristics include the numberof heavy chain constant segments the numberand location of interconnecting disulfidebridges the length of the hinge region andthe number and location of oligosaccharidemoieties For IgG four heavy chain versionsexist creating IgG1 2 3 and 4 isotypes eachwith different characteristics in their serumhalf-lives and ability to trigger different effec-tor functions Because of the combined ad-vantage from ability to trigger effectormechanisms long [21 days] half-life theirability to be transported over the placentaand their stability in the production processantibodies of the IgG class and of the IgG1isotype are preferred as the basis for newantibody-based therapies The effector func-tions are triggered by the Fc part of an antibodywhen the variable parts of the antibody arebound directly to an infectious agent or toproteins from an infectious agent expressed onan infected cell This binding leaves the Fc partfree to interactwithFc receptors onphagocyticcells and neutrophils eosinophils and naturalkiller cells capable of inducing phagocytosis orlysis of infectious agents or infected cellsThese effector functions include (i) the abilityto activate the complement system for lysis(complement-dependent cellular cytotoxicity)(ii) triggering of uptake and destruction byphagocytic cells such as macrophages andneutrophils via interaction with Fc receptorson these cells (iii) activation of macrophageseosinophils neutrophils and natural killer
cells to kill infected cells via binding to Fcreceptors on these cells and antibody-depen-dent cellular cytotoxicity and (iv) neutraliza-tion of bacterial toxins and blocking of bindingand uptake of bacteria or viruses to target cells(see Fig 2) (9)
The Fcpart of IgG antibodies also contains aregion that interacts with the neonatal Fcreceptor (FcRn) expressed on most immuno-competent cells and inmany other cells such asendothelial cells in kidney liver placenta lungand breast (10) which protects antibodies fromdegradation by phagocytoticexocytotic cy-cling into FcRn-expressing cells thereby pro-longing their half-life This results in half-livesof 20 to 21 days for most IgG1 2 and 4antibodies whereas half-lives are 10 6 and 2days respectively for IgM IgA and IgE Thehighly specific binding sites on the variableregions of the upper arms of the antibody allowfor several important features of antibodiesndashbinding to and neutralization of eg bacterialtoxins binding to pathogens and blocking theirbinding to or interaction with target cells (egcyncytia formation of CMV-infected cells) orblocking of binding and interactions of infec-tious agents with target cells via blockingreceptors on the target cells
METHODS AND PLATFORMS FORGENERATING ANTIBODIES
As described above the early use of passiveantibody transfer as a therapy in infectiousdiseases involved the use of immune serumfrom immunized sheep and horses These pre-parations were crude and contained a broadmixture of neutralizing and non-neutralizingantibodies and both the foreign nature of theantibodies and the numerous host serumproteins This resulted in less specific andthus less efficient therapies due to a highvariability in efficacy between batches derivedfrom different animals immunized with dif-ferent strains of bacteria in different labor-atories and resulted in multiple unwantedside effects related to hypersensitivity and
10 HEY
anaphylactic reactions to foreign proteinsThese days antibodies being developed fortreatment of diseases in humans are highlypurified and are mostly fully human mono-clonal antibodies The term monoclonal anti-body refers to that cell cultures used forgenerating these antibodies each originatesfrom a single cell and thus produces onlyone specific antibody Development of fullyhuman monoclonal antibodies happened instages over a time span of more than 15 yearsFirst stage in this process was generation ofmonoclonalmurine IgG antibodies (eg OKT3[muronomab-CD3 Johnson and Johnson] ap-proved in 1986) Next stage was generation ofso called chimeric antibodies consisting ofhuman heavy and light chain constant sec-tions but with murine variable sections (eg
Rituxan [rituximab Genentech]) Next stagewas then the humanized antibodies wherethe only remaining murine part of the anti-body is the antigen-binding CDR (eg Xolair[omalizumab NovartisGenentech]) Both thefirst chimeric and humanized antibodies wereapproved in the late 1990s Then finally 16years later the first fully human antibodyHumira (adalimumab Abbott) was approvedin 2002 Since the time of the crude and low-scale manufacturing of the original antibodyserum products much has changed andtherapeutic antibodies are now produced byfermentation in 5000 liter scale using highlycontrolled and documented yeast or mamma-lian cell lines that are genetically engineered toexpress a single specific antibody This hasresulted in a pure and highly specific antibody
FIGURE 2 Effector functions of antibodies (a) Antibodies bind to pathogen-derived or endogenousantigens expressed on the surface of an infected cell which triggers binding to Fc receptors on naturalkiller cells and lysis of the infected cell by antibody-dependent cellular cytotoxicity (b) Antibodies bindto pathogen-derived or endogenous antigens expressed on the surface of infected cells which triggersactivation of complement through binding of complement factor C1q (c) Neutralization Top Bacterialtoxin neutralized by bound antigen Bottom Antibody bound to either receptor for the virus or to thevirus itself which blocks virus binding and entry into the cell (d) Antibody bound to viral surfaceproteins binds to Fc receptors on phagocytic cells eg macrophages and triggers endocytosis anddestruction of virus in endolysosome doi101128microbiolspecAID-0026-2014f2
CHAPTER 1 bull History and Practice Antibodies in Infectious Diseases 11

Preface
Antibodies form the principal foundation for modern intervention against in-fectious diseases Emil Adolf von Behring was awarded the first Nobel Prize in Physiology or Medicine in 1901 ldquofor his work on serum therapy especially its appli-cation against diphtheria by which he has opened a new road in the domain of med-ical science and thereby placed in the hands of the physician a victorious weapon against illness and deathsrdquo Antibodies now provide the focus for understanding mechanisms of immunity to most infectious diseases and they play a central role in passive immunotherapy and active vaccination as mechanisms or correlates of immunity For most of the 20th century immunotherapy was based on passive transfer of polyclonal hyperimmune animal serum immune human serum or even hyperimmune human serum Georges JF Koumlhler and Ceacutesar Milstein re-ported the generation of monoclonal antibodies in 1979 for which they shared the 1984 Nobel Prize in Physiology or Medicine ldquofor the discovery of the princi-ple for production of monoclonal antibodiesrdquo Since that time entire fields related to antibodies for infectious diseases including antibody gene cloning engineer-ing and expression antibody libraries and high-throughput antibody gene rep-ertoire sequence analysis have extended our capabilities to explore the diversity of antibody specificity and function with unprecedented depth and breadth
This book provides a broad survey of many of the most important aspects of the field of antibodies for infectious diseases The book begins with a general introduction followed by chapters 2 through 5 on general features pertaining to structure function isotype and the role of complement in antibody function Chapters 6 through 10 review contemporary approaches for antibody discovery using phage and yeast display plasma cell and memory B cell cloning human hybridomas humanized mice and computational methods Chapters 11 through 18 review in depth the biology of antibodies specific for particular pathogens including viruses and bacterial toxins to illustrate the role of antibodies in anti- microbial immunity with specific targets These chapters reveal that attempts to raise effective antibody responses to each of these pathogens faces unique and pathogen-specific challenges Chapters 19 to 23 cover major technical advances pertaining to antibody engineering repertoire sequencing and analysis and new methods for study or therapeutic use of antibodies including radiotherapy Fi-nally chapters 24 and 25 cover new methods for expression of monoclonal anti-bodies in plants or by transfer of antibody genes for in vivo expression in treated subjects
Recent literature is exploding with new antibody-related techniques and re-ports of antimicrobial antibodies with unprecedented potency breadth of activ-
xvii
xviii PReface
ity and therapeutic potential We hope that this timely compilation of state-of-the-art reviews of major aspects of this field will be of interest to both antibody cognoscenti and those new to this exciting field We thank the authors for their dedication in producing definitive reviews of the topics at hand
James E Crowe JrDiana BoraschiRino Rappuoli
INTRODUCTION
History and PracticeAntibodies in Infectious Diseases 1ADAM HEY1
Antibodies in Infectious Diseases aims to inform update and inspire studentsteachers researchers pharmaceutical developers and health care professionalson the status of the development of antibody-based therapies for treatinginfectious diseases and the potential for these in times of growing antibioticresistance to provide alternative treatment solutions to the currently usedantibiotics and new treatments for infectious diseases where no propertreatments are available
This introductory article will provide a historical perspective on the useof antibody-based therapies followed by a high-level overview of whatmakes antibodies attractive tools for this purpose This will include the prosand cons of such therapies compared to the use of antibiotics and thepractical and strategic considerations involved in selecting the best formatand development path for new antibody-based therapies targeting specificinfectious agents Then examples of antibody-based therapies in thedevelopment of treatments for infectious diseases will be presented andfinally a look into the future will summarize the different aspects that willinfluence what the future might bring for this type of treatments forinfectious diseases
1Preclinical Safety Biologics Novartis AG Basel Switzerland
Antibodies for Infectious DiseasesEdited by James E Crowe Jr Diana Boraschi and Rino Rappuolicopy 2015 American Society for Microbiology Washington DCdoi101128microbiolspecAID-0026-2014
3
HISTORICAL PERSPECTIVE
Antibodies and the use of passive antibodytherapy in the treatment of infectious dis-eases is the story of a treatment conceptwhich dates back more than 120 years to thelate 19th century and which originally bythe use of serum from immunized animalsprovided the first effective treatment optionsagainst severe bacterial infections (1 2) Byimmunizing horses with bacterial toxinsfrom Clostridium tetani and Corynebacteri-um diphtheriae Emil A Von Behring andShibasaburo Kitasato (3) generated serumcontaining antibodies capable of neutraliz-ing the effects of the toxins produced bythese bacteria and successfully providedtreatment for these serious diseases wherethe pathogenesis is driven by the effects ofthe bacterial toxins For his work on provid-ing treatment for diphtheria Behring re-ceived the Nobel Prize in Physiology orMedicine in 1901 These radical treatmentresults quickly prompted development ofmultiple additional serum therapies for thetreatment of infectious diseases caused byeg Neisseria meningitidis Haemophilus in-fluenza and group A Streptococcus Sinceserum therapy involved administration oflarge amounts of crude mixtures of animalproteins including antibodies they wereassociated with side effects in the form ofhypersensitivity and serum sickness (2)
Due to the crude and unpurified nature ofthese products side effects were seen evenwhen administering human serum prepa-rations Side effects were observed in up to50 of patients and were considered to becaused by immune complex formations thatresulted in symptoms such as rash itchingjoint pain fever and in serious cases hypoten-sion and shock However due to the lack ofalternative options these treatments weredespite their side effects widely used Serumwas normally administered by intravenousinfusion in patients after a test for hypersensi-tivity where a small amount of serum wasinjected subcutaniously (1) As described
above serum therapy applied in these earlydays (late 19th century and early 20th century)involved preparations of serum from rabbitsand horses immunized with the infectiousagent or in live andor neutralized versions ortoxins from these (1) The costs of keeping theimmunized animals and the production andpotency testing of the materials made this arelatively expensive treatment In 1891 datafrom Klemperer (4) showed serum therapy toprotect rabbits from Streptococcus pneumoniaeinfection and paved the way for this type oftreatment and for development of similarserum-based treatments of streptococcal in-fections in humans When treating humansearly administration of serum could reducemortality significantly down to around 5compared to when administered 4 to 5 daysafter onset of symptoms when serum treat-ment was largely without effect This stronglyindicated the need for quick diagnosis andquick treatment to control the infection beforeit got out of control Consequently in theabsence of a specific diagnosis mixtures ofserum from immunizations with differentserotypes were used to circumvent this needfor early treatment without having a serotype-specific diagnosis The understanding thatdifferent serotypes existed for pneumococciand that efficient treatment relied on usingserotype-specific serum was being built upduring the 1920s and 1930s through experiencefrom extensive clinical trials
By the end of the 1930s serum therapywasthe standard of care for treatment of pneu-mococcal pneumonia At that time theefficacy and potency of the derived serawere assessed in mice in ldquothe mouse pro-tection testrdquo by testing survival after aconcomitant intraperitoneal injection of alethal dose of pneumococci and the serum tobe tested Due to the inherent variation inthis test efficacy and survival in two thirds ofthe animals was the acceptance criteria and10 times the lowest dose providing this wasused for defining a unit of the serum Thisallowed for large batch-to-batch variationand the use of different strains of bacteria for
4 HEY
immunization probably explains part of themissing responses observed (1) In the early20th century a pandemic of meningitis inEurope and the United States with mortalityrates up to 80 spurred the development ofserum therapy treatment options Althoughin the 1930s this became the recommendedtreatment in children assumed to be suffer-ing from meningitis failure to reduce mor-tality in several meningitis epidemics duringthat time raised doubts about the generalapplicability of serum treatment In thosedays serum therapy often involved quiteextensive procedures and infusion of largevolumes of serum The following exampleclearly illustrates this Data from Flexnerand Jobling (5) from treating meningitis inmonkeys resulted in the development of serafrom immunized horses for treatment inhumans The treatment protocol includedlumbar puncture and withdrawal of morethan 30 ml of spinal fluid representing anamount slightly larger than the expectedamount of horse serum to be injected subse-quently This treatment involved such dailyslow infusions of up to 30 ml of serum untilthe patientrsquos condition improved This treat-ment was used in outbreaks in New York in1905 and 1906 and did markedly decreasemortality
After the discovery of penicillin by Flemingin 1928 and the subsequent introduction ofantibiotics in the 1930s serum therapy waslargely abandoned over a period of 10 years dueto the availability of these new more broadlyeffective and cheaper treatment optionswhichalso had fewer side effects Although improve-ments in the purification of antibodies hadresulted in preparations with better safety andside effect profiles high manufacturing costsand narrow specificity resulted in antibodytherapy being mostly restricted to a smallernumber of selected treatments for snakevenoms bacterial toxins and some viral infec-tions (1 2) Currently antibody administrationis used for treatment and prevention ofhepatitis B virus rabies virus respiratorysyncytial virus (RSV) Clostridium tetani Clos-
tridium botulinum vaccinia virus echovirusand enterovirus For the most part thesetreatments consist of pooled immunoglobulinalso known as IVIG (intravenous immunoglob-ulin) from several postexposure donors Thisresults in both batch-to-batch variation in theneed for relatively large amounts of serum dueto low specificity and to restricted supplies dueto reliance on exposed donors
However several challengeshave resulted inthe need for new tools in the treatment andpreventionof infectiousdiseasesThebroadandgeneral use of antibiotics in human and veter-inary medicine for many years has resulted inthe development of multi-resistant strains ofbacteria with limited to no response to existingtreatments such as methicillin-resistant Staph-ylococcusaureus (MRSA) vancomycin-resistantS aureus and others This has resulted inpatients needing screening and treatment withseveral antibacterial agents and longer treat-ment time causing extra strain on patients andhealth care providers (6 httpwwwcdcgovdrugresistancethreat-report-2013indexhtml) According to the WHO and CDC morethan 25000 people in European Unioncountries and similar numbers in the UnitedStates die every year as a result of antibiotic-resistant infections This together with theemergence of new pathogens (eg severeacute respiratory syndrome Middle East respi-ratory syndrome) the re-emergenceepidemicsof oldknown pathogens (eg Ebola) and thedifficulties in treating infections in immune-deficient patients (eg HIV patients) has high-lighted the need for new solutions The 2014Ebola epidemic in West Africa (Liberia SierraLeone Guinea Nigeria and Senegal) has fur-ther highlighted this No treatment or prophy-lactic vaccine is available to treat or prevent thespread of Ebola infections which have anaveragemortality of gt50 Local health author-ities in the affected countries are struggling tocontain and handle the disease which isthreatening to go out of control and spreadmorewidelyVariousproductsmainly antibodycocktails from previously recovered patientsare being used despite a lack of clinical data on
CHAPTER 1 bull History and Practice Antibodies in Infectious Diseases 5
their safety and efficacy and those are the onlysporadically available treatment options andonly in small amounts and for a few patients
Ebola is an example of a disease whichnormally affects only a small number ofindividuals and which normally burns outwhen disease outbreaks are contained There-fore given the small number of potentialpatients affected by previous Ebola infectionsto date there was no incentive for big pharmacompanies to do research and development ofdrugs for EbolaWith the increasing number ofinfected (13567) andadeath toll of 4951 (7) andthe lack of the ability to contain the epidemic itwill be interesting to follow the aftermath ofthis outbreak and see whether there will berequests for new ways to ensure that vaccinesand treatment options are available for Ebolaand similar high-mortality and potential bio-warfare infections that have no availabletreatments or procedures to for mass-produc-tion upon the first signsreports of activeinfections Although both the CDC and theWHO have special programs focusing on thesetypes of infections the Ebola outbreak in 2014clearly shows that more financial support forresearch and development of new diagnosticsand treatments is needed This is one examplewhere antibody-based treatments would havethe potential to play a major role To put this inthe right perspective one should however notforget that other infectious diseases such astuberculosis influenza and malaria kill hun-dreds of thousands each year There is there-fore plenty of room for improvement indeveloping treatments for these diseases aswell but the high attention drawn to eg theEbola outbreak creates a special niche andopportunity where antibody treatments couldgain extraordinary development funding andsupport and prove their value and treatmentpotential
That antibody-based therapies could takethis role is supported by the revolution intechnologies for the development selectiongeneration and purification of fully humanantibodies described in more detail later in thesection ldquoMethodsandPlatforms forGenerating
Antibodiesrdquo Antibody-based programs cur-rently at different stages of developmentinclude investigations into the potential use ofsingle antibody preparations combinations ofantibodies (to avoid survival of escape mu-tants) fragments of antibodies and antibodiescarrying radioactive isotopesorcytotoxicdrugsor antibody-like frameworks (eg fibronectin)either alone as a first-line treatment or as anadjunct to existing treatments This multitudeof possible formats the ability to raise anti-bodies to almost any target and the ability toengineer both size effector functions and half-life are now considered by many to providevery valuable tools for designing specificantibody-based treatments toeradicate specifictargeted infectious agents However althoughseveral antibody-based therapies have beenapproved for oncology and anti-inflammatoryindications (see Table 1) only one monoclonalantibody (mAb) is approved against an infec-tious disease agentmdashSynagis (palivizumabMedImmune) for the prevention and treat-ment of respiratory syncytical virus (RSV) inhigh-risk children Economic obstacles such asthe high cost of mAb therapies and relativelysmall markets have resulted in less interestfrom pharmaceutical companies in developingthese Also highlighting the challenges indeveloping these types of antibody-basedtreatments are the difficulties encountered indeveloping a follow-up higher-affinity candi-date to Synagis Poor translatability of dataobtained in the available animal disease mod-els for RSV in cotton rats has resulted in non-approval due to inferiority relative to SynagisIn other viral diseases such as cytomegalovirus(CMV) the high species specificity of thestrains of CMV makes it impossible to testhuman antibody therapies in vivo Thereforeany real data on the efficacy of treatments forCMV will not be obtained until testing inclinical trials As described later in this articleseveral new antibody-based therapies for in-fectious diseases are in development andhopefully this will gradually open the fieldand result in better treatment options andoutcomes for patients
6 HEY
TABLE 1 Approved and pending antibody-based therapies
Name antibody Target antibody type Indication Company Approval date
OKT3a Muronomab-CD3 CD3 murine IgG2a Autoimmune Johnson ampJohnson
1986 (US)
ReoPro abciximab PIIbIIIa chimeric IgG1Fab
Homeostasis Johnson ampJohnson
1984 (US)
Rituxan rituximab CD20 chimeric IgG1 Cancer Genentech 1997 (US) 1998 (EU)Zenapaxa daclizumab CD25 humanized IgG1 Autoimmune Roche 1997 (US) 1999 (EU)Simulect basiliximab CD25 chimeric IgG1 Autoimmune Novartis 1998 (US EU)Synagis palivizumab RSV humanized IgG1 Infections MedImmune 1998 (US) 1999 (EU)Remicade infliximab TNFα chimeric IgG1 Autoimmune Johnson amp
Johnson1998 (US) 1999 (EU)
Herceptin trastuzumab HER2 humanized IgG1 Cancer GenentechRoche
1998 (US) 2000 (EU)
Mylotarga gemtuzumabozogamicin
CD33 humanized IgG4immunotoxin
Cancer WyethPfizer 2000 (US)
Campath alemtuzumab CD52 humanized IgG1 Cancer Genzyme 2001 (US) 2001 (EU)Zevalin ibritumomabtiuxetan
CD20 murine IgG1radiolabeled (yttrium 90)
Cancer Biogen Idec 2002 (US) 2004 (EU)
Humira adalimumab TNFα human IgG1 Autoimmune Abbott 2002 (US) 2003 (EU)Xolair omalizumab IgE humanized IgG1 Autoimmune Genentech
Roche2003 (US)
Bexxar tositumomab-I-131 CD20 murine IgG2aradiolabeled (iodine131)
Cancer CorixaGSK 2003 (US)
Raptivaa falizumab CD11a humanized IgG1 Autoimmune GenentechRoche
2003 (US) 2004 (EU)
Erbitux cetuximab EGFR chimeric IgG1 Cancer ImcloneLilly 2004 (US) 2004 (EU)Avastin bevacizumab VEGF humanized IgG1 Cancer Genentech
Roche2004 (US) 2005 (EU)
Tysabri natalizumab α4-Intergrin humanizedIgG4
Autoimmune Biogen Idec 2004 (US)
Actemra tocilizumab Anti-IL-6R humanizedIgG1
Autoimmune ChugaiRoche
2005 (Japan) 2010 (US)
Vectibix panitumumab EGFR human IgG2 Cancer Amgen 2006 (US)Lucentis ranibizumab VEGF humanized IgG1
FabMaculardegeneration
GenentechRoche
2006 (US)
Soliris eculizumab C5 humanized IgG24 Blood disorders Alexion 2007 (US)Cimzia certolizumab pegol TNFα humanized
pegylated FabAutoimmune UCB 2008 (US)
Simponi golimumab TNFα human IgG1 Autoimmune Johnson ampJohnson
2009 (US EU Canada)
Ilaris canakinumab IL1b human IgG1 Infalmmatory Novartis 2009 (US EU)Stelara ustekinumab IL-1223 human IgG1 Autoimmune Johnson amp
Johnson2008 (EU) 2009 (US)
Arzerra ofatumumab CD20 human IgG1 Cancer Genmab 2009 (EU)Prolia denosumab RANK ligand human
IgG2Bone loss Amgen 2010 (US)
Numax motavizumab RSV humanized IgG1 Anti-infective MedImmune PendingABthrax Raxibacumab B anthrasis PA human
IgG1Anti-infection GSK 2012 (US)
Benlysta belimumab BLyS human IgG1 Autoimmune HGS 2011 (US)Yervoy ipilimumab CTLA-4 human IgG1 Cancer BMS 2011 (US)Adcetris brentuximabvedotin
CD30 chimeric IgG1drug- conjugate
Cancer SeattleGenetics
2011 (US)
(Continued on next page)
CHAPTER 1 bull History and Practice Antibodies in Infectious Diseases 7
INTRODUCTION TO ANTIBODIES
Antibodies also called immunoglobulins basedon their combined structure and function inimmune responses are produced by B cells ofthe immune system They are part of theadaptive immune response and are speciallydesigned for neutralizing and eliminating theinfectious agents and toxins produced by theseAntibodies are present in blood plasma andextracellular fluids and since these fluids wereformerly known as humors they were said tobe part of the humoral immune responseAntibodies are Y-shaped structures consistingof two main parts the upper arms of the Ywhich contain two identical variable-regionantigen binding sites and the lower regioncalled the constant regionwhich is responsiblefor the initiation of effector functions that leadto the removal and destruction of the pathogenor cells harboring the pathogen (see Fig 1) Theantigen-binding sites on an antibody can bythemselves bind to and neutralize bacterialtoxins and viruses thereby preventing themfrom binding to their target cells or receptorscausing toxic effects or spread of the infection
Antibodies consist of two pairs of heavy andlight chainswhich as described above are heldtogether in a Y-shaped arrangement Each ofthe heavy and light chains in these pairs isseparated into constant and variable chainsThe upper armsof theY each contain a variableand a constant sectionof the light and theheavychain where the upper variable parts of theheavy and light chains contain the antigen-binding site and the constant parts areconnected via disulfide bonds The lower partof theYcalled theconstantpart consistsof twoor three constant segments (immunoglobulindomains) from each of the two heavy chainsinteracting and also linked via disulfide bondsThe sectionsof theheavy chains connecting theconstant part of the upper arms to the constantparts of the constant region contain specialhinge regions that provide flexibility to thedifferent sections of the antibody to bind toantigens and effector cells The constant re-gions of the heavy chain also contain attachedoligosaccharide moieties which provide func-tional specialization to the antibodies (8)
The variable domains of the heavy and lightchains form the antigen-binding sites and
TABLE 1 Approved and pending antibody-based therapies (Continued)
Name antibody Target antibody type Indication Company Approval date
Perjeta pertuzumab Her2 humanized IgG1 Cancer GenentechRoche
2012 (US)
Kadcyla ado-trastuzumabemtansine
Her2 humanized IgG1Drug-conjugate
Cancer GenentechRoche
2013 (US)
Raxibacumab Anti-B anthrasis PAhuman IgG1
Anthraxinfection
Notapproved
2012
Entyvio vedolizumab Integrin α4β7humanized IgG1
Crohnrsquos diseaseulcerative colitis
Takeda 2014 (US)
Cyramza ramuciruumab Anti-VEGFR2Human IgG1
Gastric cancer Lilly 2014 (US)
Gazyva obinutuzumab Anti-CD20 humanizedIgG1 glucoengineered
CancerCLLb GenentechRoche
2014 (US)
Sylvant situximab Anti IL-6 chimeric IgG1 Castlemandisease
Janssen 2014 (US) 2014 (EU)
Cosentyx sekukinumab Anti IL-17a human IgG1 Psoriasis Novartis 2015 (US) 2015 (EU)Nivolumab Anti PD-1 human IgG4 Melanoma BMS Not approvedKeytruda pembrolizuumab Anti-PD-1 humanized
IgG4Melanoma Merck 2014 (US)
aAntibodies approved but later withdrawnbCLL chronic lymphocytic leukemia
8 HEY
FIGURE 1 (Left panel) Model of antibody structure exemplified by IgG On top the antigen-binding sitesin orange each contain one variable light and variable heavy domain with the three complementaritydetermining regions (CDRs) that are responsible for the specific binding of the antibody to its target Foreach arm of the antibody an additional set of variable heavy and light domains together with the CDR-containing domains represent the two fragment antigen binding (Fab) regions The two Fabs are heldtogether via two disulfide bridges Below the Fabs is the Fc region which contains four constant heavydomains On the upper pair of these domains are binding sites for oligosaccharides which have majorimportance for the ability of the antibody Fc part to trigger effector functions when the Fc portion isbound to Fc gamma receptors on natural killer cells neutrophil granulocytes monocytesmacrophagesdendritic cells and B cells (Right panel) Examples of some of the antibody-derived alternative formatsused to exploit the specific features of the CDRs the Fabs and the Fc parts of the antibodies ScFv Thesingle chain fragment variable consists of the variable domains of the heavy and light chains heldtogether by a flexible linker This can also be used as a carrier of a cytotoxic drug in a so-called antibodydrug complex (ADC) where the specificity of the ScFv is used to target the cytotoxic drug to eg atumor Bite (bi-specific T cell engager) Fusion proteins consisting of two ScFvs one directed against thetarget on a tumor cell and the other against the T cell receptor (CD3) Diabody ScFv dimers where shortlinker peptides (five amino acids) ensure dimerization and not folding of the ScFvs Fab and F(ab)2fragments Single Fab fragments or fragments containing two Fabs linked via disulfide bridges This isused where effector functions related to the Fc part of the antibody are unwanted and where a smallersize is desired to obtain better tissue penetration in eg tumors Due to the lack of the FcRn binding viathe Fc part Fab and F(ab)2 fragments have much shorter half-lives (hours or days) than full-sizeantibodies (weeks) These can also be used as carriers of cytotoxic payloads or cytotoxic radioactiveisotopes and for the F(ab)2 fragments can be constructed as bi-specifics which can cross-link immunecells and target cells Fc fusion protein Fusion protein containing the Fc domain of an immunoglobulinbound to a peptide The peptide can be a ligand for a specific receptor on a target cell or a blockingpeptide for a soluble ligand The Fc part provides a longer half-life to the construct and the potential tobind to and engage effector functions in the killing of eg tumor cells or infected cells ADCsRIAs andbi-specifics Full-size IgG antibodies carrying either a cytotoxic chemical or radioactive payload whichmay also carry different CDRs enabling cross-linking of effector and target cells for increased killingdoi101128microbiolspecAID-0026-2014f1
CHAPTER 1 bull History and Practice Antibodies in Infectious Diseases 9
contain special hyper-variable segments calledcomplementarity-determining regions (CDRs)which allow the B cells via genetic recom-bination to generate antibodies to all thedifferent antigens specific to amino acid se-quences or three-dimensional structuralmotifs(polysaccharides DNA and RNA) found onpathogens
Based on the structure of their heavy chainconstant regions antibodies or immuno-globulins are separated into five classesmdashIgM IgG IgE IgD and IgA Differences inthe sequences of the constant regions providedistinct characteristics to these different clas-ses These characteristics include the numberof heavy chain constant segments the numberand location of interconnecting disulfidebridges the length of the hinge region andthe number and location of oligosaccharidemoieties For IgG four heavy chain versionsexist creating IgG1 2 3 and 4 isotypes eachwith different characteristics in their serumhalf-lives and ability to trigger different effec-tor functions Because of the combined ad-vantage from ability to trigger effectormechanisms long [21 days] half-life theirability to be transported over the placentaand their stability in the production processantibodies of the IgG class and of the IgG1isotype are preferred as the basis for newantibody-based therapies The effector func-tions are triggered by the Fc part of an antibodywhen the variable parts of the antibody arebound directly to an infectious agent or toproteins from an infectious agent expressed onan infected cell This binding leaves the Fc partfree to interactwithFc receptors onphagocyticcells and neutrophils eosinophils and naturalkiller cells capable of inducing phagocytosis orlysis of infectious agents or infected cellsThese effector functions include (i) the abilityto activate the complement system for lysis(complement-dependent cellular cytotoxicity)(ii) triggering of uptake and destruction byphagocytic cells such as macrophages andneutrophils via interaction with Fc receptorson these cells (iii) activation of macrophageseosinophils neutrophils and natural killer
cells to kill infected cells via binding to Fcreceptors on these cells and antibody-depen-dent cellular cytotoxicity and (iv) neutraliza-tion of bacterial toxins and blocking of bindingand uptake of bacteria or viruses to target cells(see Fig 2) (9)
The Fcpart of IgG antibodies also contains aregion that interacts with the neonatal Fcreceptor (FcRn) expressed on most immuno-competent cells and inmany other cells such asendothelial cells in kidney liver placenta lungand breast (10) which protects antibodies fromdegradation by phagocytoticexocytotic cy-cling into FcRn-expressing cells thereby pro-longing their half-life This results in half-livesof 20 to 21 days for most IgG1 2 and 4antibodies whereas half-lives are 10 6 and 2days respectively for IgM IgA and IgE Thehighly specific binding sites on the variableregions of the upper arms of the antibody allowfor several important features of antibodiesndashbinding to and neutralization of eg bacterialtoxins binding to pathogens and blocking theirbinding to or interaction with target cells (egcyncytia formation of CMV-infected cells) orblocking of binding and interactions of infec-tious agents with target cells via blockingreceptors on the target cells
METHODS AND PLATFORMS FORGENERATING ANTIBODIES
As described above the early use of passiveantibody transfer as a therapy in infectiousdiseases involved the use of immune serumfrom immunized sheep and horses These pre-parations were crude and contained a broadmixture of neutralizing and non-neutralizingantibodies and both the foreign nature of theantibodies and the numerous host serumproteins This resulted in less specific andthus less efficient therapies due to a highvariability in efficacy between batches derivedfrom different animals immunized with dif-ferent strains of bacteria in different labor-atories and resulted in multiple unwantedside effects related to hypersensitivity and
10 HEY
anaphylactic reactions to foreign proteinsThese days antibodies being developed fortreatment of diseases in humans are highlypurified and are mostly fully human mono-clonal antibodies The term monoclonal anti-body refers to that cell cultures used forgenerating these antibodies each originatesfrom a single cell and thus produces onlyone specific antibody Development of fullyhuman monoclonal antibodies happened instages over a time span of more than 15 yearsFirst stage in this process was generation ofmonoclonalmurine IgG antibodies (eg OKT3[muronomab-CD3 Johnson and Johnson] ap-proved in 1986) Next stage was generation ofso called chimeric antibodies consisting ofhuman heavy and light chain constant sec-tions but with murine variable sections (eg
Rituxan [rituximab Genentech]) Next stagewas then the humanized antibodies wherethe only remaining murine part of the anti-body is the antigen-binding CDR (eg Xolair[omalizumab NovartisGenentech]) Both thefirst chimeric and humanized antibodies wereapproved in the late 1990s Then finally 16years later the first fully human antibodyHumira (adalimumab Abbott) was approvedin 2002 Since the time of the crude and low-scale manufacturing of the original antibodyserum products much has changed andtherapeutic antibodies are now produced byfermentation in 5000 liter scale using highlycontrolled and documented yeast or mamma-lian cell lines that are genetically engineered toexpress a single specific antibody This hasresulted in a pure and highly specific antibody
FIGURE 2 Effector functions of antibodies (a) Antibodies bind to pathogen-derived or endogenousantigens expressed on the surface of an infected cell which triggers binding to Fc receptors on naturalkiller cells and lysis of the infected cell by antibody-dependent cellular cytotoxicity (b) Antibodies bindto pathogen-derived or endogenous antigens expressed on the surface of infected cells which triggersactivation of complement through binding of complement factor C1q (c) Neutralization Top Bacterialtoxin neutralized by bound antigen Bottom Antibody bound to either receptor for the virus or to thevirus itself which blocks virus binding and entry into the cell (d) Antibody bound to viral surfaceproteins binds to Fc receptors on phagocytic cells eg macrophages and triggers endocytosis anddestruction of virus in endolysosome doi101128microbiolspecAID-0026-2014f2
CHAPTER 1 bull History and Practice Antibodies in Infectious Diseases 11

xviii PReface
ity and therapeutic potential We hope that this timely compilation of state-of-the-art reviews of major aspects of this field will be of interest to both antibody cognoscenti and those new to this exciting field We thank the authors for their dedication in producing definitive reviews of the topics at hand
James E Crowe JrDiana BoraschiRino Rappuoli
INTRODUCTION
History and PracticeAntibodies in Infectious Diseases 1ADAM HEY1
Antibodies in Infectious Diseases aims to inform update and inspire studentsteachers researchers pharmaceutical developers and health care professionalson the status of the development of antibody-based therapies for treatinginfectious diseases and the potential for these in times of growing antibioticresistance to provide alternative treatment solutions to the currently usedantibiotics and new treatments for infectious diseases where no propertreatments are available
This introductory article will provide a historical perspective on the useof antibody-based therapies followed by a high-level overview of whatmakes antibodies attractive tools for this purpose This will include the prosand cons of such therapies compared to the use of antibiotics and thepractical and strategic considerations involved in selecting the best formatand development path for new antibody-based therapies targeting specificinfectious agents Then examples of antibody-based therapies in thedevelopment of treatments for infectious diseases will be presented andfinally a look into the future will summarize the different aspects that willinfluence what the future might bring for this type of treatments forinfectious diseases
1Preclinical Safety Biologics Novartis AG Basel Switzerland
Antibodies for Infectious DiseasesEdited by James E Crowe Jr Diana Boraschi and Rino Rappuolicopy 2015 American Society for Microbiology Washington DCdoi101128microbiolspecAID-0026-2014
3
HISTORICAL PERSPECTIVE
Antibodies and the use of passive antibodytherapy in the treatment of infectious dis-eases is the story of a treatment conceptwhich dates back more than 120 years to thelate 19th century and which originally bythe use of serum from immunized animalsprovided the first effective treatment optionsagainst severe bacterial infections (1 2) Byimmunizing horses with bacterial toxinsfrom Clostridium tetani and Corynebacteri-um diphtheriae Emil A Von Behring andShibasaburo Kitasato (3) generated serumcontaining antibodies capable of neutraliz-ing the effects of the toxins produced bythese bacteria and successfully providedtreatment for these serious diseases wherethe pathogenesis is driven by the effects ofthe bacterial toxins For his work on provid-ing treatment for diphtheria Behring re-ceived the Nobel Prize in Physiology orMedicine in 1901 These radical treatmentresults quickly prompted development ofmultiple additional serum therapies for thetreatment of infectious diseases caused byeg Neisseria meningitidis Haemophilus in-fluenza and group A Streptococcus Sinceserum therapy involved administration oflarge amounts of crude mixtures of animalproteins including antibodies they wereassociated with side effects in the form ofhypersensitivity and serum sickness (2)
Due to the crude and unpurified nature ofthese products side effects were seen evenwhen administering human serum prepa-rations Side effects were observed in up to50 of patients and were considered to becaused by immune complex formations thatresulted in symptoms such as rash itchingjoint pain fever and in serious cases hypoten-sion and shock However due to the lack ofalternative options these treatments weredespite their side effects widely used Serumwas normally administered by intravenousinfusion in patients after a test for hypersensi-tivity where a small amount of serum wasinjected subcutaniously (1) As described
above serum therapy applied in these earlydays (late 19th century and early 20th century)involved preparations of serum from rabbitsand horses immunized with the infectiousagent or in live andor neutralized versions ortoxins from these (1) The costs of keeping theimmunized animals and the production andpotency testing of the materials made this arelatively expensive treatment In 1891 datafrom Klemperer (4) showed serum therapy toprotect rabbits from Streptococcus pneumoniaeinfection and paved the way for this type oftreatment and for development of similarserum-based treatments of streptococcal in-fections in humans When treating humansearly administration of serum could reducemortality significantly down to around 5compared to when administered 4 to 5 daysafter onset of symptoms when serum treat-ment was largely without effect This stronglyindicated the need for quick diagnosis andquick treatment to control the infection beforeit got out of control Consequently in theabsence of a specific diagnosis mixtures ofserum from immunizations with differentserotypes were used to circumvent this needfor early treatment without having a serotype-specific diagnosis The understanding thatdifferent serotypes existed for pneumococciand that efficient treatment relied on usingserotype-specific serum was being built upduring the 1920s and 1930s through experiencefrom extensive clinical trials
By the end of the 1930s serum therapywasthe standard of care for treatment of pneu-mococcal pneumonia At that time theefficacy and potency of the derived serawere assessed in mice in ldquothe mouse pro-tection testrdquo by testing survival after aconcomitant intraperitoneal injection of alethal dose of pneumococci and the serum tobe tested Due to the inherent variation inthis test efficacy and survival in two thirds ofthe animals was the acceptance criteria and10 times the lowest dose providing this wasused for defining a unit of the serum Thisallowed for large batch-to-batch variationand the use of different strains of bacteria for
4 HEY
immunization probably explains part of themissing responses observed (1) In the early20th century a pandemic of meningitis inEurope and the United States with mortalityrates up to 80 spurred the development ofserum therapy treatment options Althoughin the 1930s this became the recommendedtreatment in children assumed to be suffer-ing from meningitis failure to reduce mor-tality in several meningitis epidemics duringthat time raised doubts about the generalapplicability of serum treatment In thosedays serum therapy often involved quiteextensive procedures and infusion of largevolumes of serum The following exampleclearly illustrates this Data from Flexnerand Jobling (5) from treating meningitis inmonkeys resulted in the development of serafrom immunized horses for treatment inhumans The treatment protocol includedlumbar puncture and withdrawal of morethan 30 ml of spinal fluid representing anamount slightly larger than the expectedamount of horse serum to be injected subse-quently This treatment involved such dailyslow infusions of up to 30 ml of serum untilthe patientrsquos condition improved This treat-ment was used in outbreaks in New York in1905 and 1906 and did markedly decreasemortality
After the discovery of penicillin by Flemingin 1928 and the subsequent introduction ofantibiotics in the 1930s serum therapy waslargely abandoned over a period of 10 years dueto the availability of these new more broadlyeffective and cheaper treatment optionswhichalso had fewer side effects Although improve-ments in the purification of antibodies hadresulted in preparations with better safety andside effect profiles high manufacturing costsand narrow specificity resulted in antibodytherapy being mostly restricted to a smallernumber of selected treatments for snakevenoms bacterial toxins and some viral infec-tions (1 2) Currently antibody administrationis used for treatment and prevention ofhepatitis B virus rabies virus respiratorysyncytial virus (RSV) Clostridium tetani Clos-
tridium botulinum vaccinia virus echovirusand enterovirus For the most part thesetreatments consist of pooled immunoglobulinalso known as IVIG (intravenous immunoglob-ulin) from several postexposure donors Thisresults in both batch-to-batch variation in theneed for relatively large amounts of serum dueto low specificity and to restricted supplies dueto reliance on exposed donors
However several challengeshave resulted inthe need for new tools in the treatment andpreventionof infectiousdiseasesThebroadandgeneral use of antibiotics in human and veter-inary medicine for many years has resulted inthe development of multi-resistant strains ofbacteria with limited to no response to existingtreatments such as methicillin-resistant Staph-ylococcusaureus (MRSA) vancomycin-resistantS aureus and others This has resulted inpatients needing screening and treatment withseveral antibacterial agents and longer treat-ment time causing extra strain on patients andhealth care providers (6 httpwwwcdcgovdrugresistancethreat-report-2013indexhtml) According to the WHO and CDC morethan 25000 people in European Unioncountries and similar numbers in the UnitedStates die every year as a result of antibiotic-resistant infections This together with theemergence of new pathogens (eg severeacute respiratory syndrome Middle East respi-ratory syndrome) the re-emergenceepidemicsof oldknown pathogens (eg Ebola) and thedifficulties in treating infections in immune-deficient patients (eg HIV patients) has high-lighted the need for new solutions The 2014Ebola epidemic in West Africa (Liberia SierraLeone Guinea Nigeria and Senegal) has fur-ther highlighted this No treatment or prophy-lactic vaccine is available to treat or prevent thespread of Ebola infections which have anaveragemortality of gt50 Local health author-ities in the affected countries are struggling tocontain and handle the disease which isthreatening to go out of control and spreadmorewidelyVariousproductsmainly antibodycocktails from previously recovered patientsare being used despite a lack of clinical data on
CHAPTER 1 bull History and Practice Antibodies in Infectious Diseases 5
their safety and efficacy and those are the onlysporadically available treatment options andonly in small amounts and for a few patients
Ebola is an example of a disease whichnormally affects only a small number ofindividuals and which normally burns outwhen disease outbreaks are contained There-fore given the small number of potentialpatients affected by previous Ebola infectionsto date there was no incentive for big pharmacompanies to do research and development ofdrugs for EbolaWith the increasing number ofinfected (13567) andadeath toll of 4951 (7) andthe lack of the ability to contain the epidemic itwill be interesting to follow the aftermath ofthis outbreak and see whether there will berequests for new ways to ensure that vaccinesand treatment options are available for Ebolaand similar high-mortality and potential bio-warfare infections that have no availabletreatments or procedures to for mass-produc-tion upon the first signsreports of activeinfections Although both the CDC and theWHO have special programs focusing on thesetypes of infections the Ebola outbreak in 2014clearly shows that more financial support forresearch and development of new diagnosticsand treatments is needed This is one examplewhere antibody-based treatments would havethe potential to play a major role To put this inthe right perspective one should however notforget that other infectious diseases such astuberculosis influenza and malaria kill hun-dreds of thousands each year There is there-fore plenty of room for improvement indeveloping treatments for these diseases aswell but the high attention drawn to eg theEbola outbreak creates a special niche andopportunity where antibody treatments couldgain extraordinary development funding andsupport and prove their value and treatmentpotential
That antibody-based therapies could takethis role is supported by the revolution intechnologies for the development selectiongeneration and purification of fully humanantibodies described in more detail later in thesection ldquoMethodsandPlatforms forGenerating
Antibodiesrdquo Antibody-based programs cur-rently at different stages of developmentinclude investigations into the potential use ofsingle antibody preparations combinations ofantibodies (to avoid survival of escape mu-tants) fragments of antibodies and antibodiescarrying radioactive isotopesorcytotoxicdrugsor antibody-like frameworks (eg fibronectin)either alone as a first-line treatment or as anadjunct to existing treatments This multitudeof possible formats the ability to raise anti-bodies to almost any target and the ability toengineer both size effector functions and half-life are now considered by many to providevery valuable tools for designing specificantibody-based treatments toeradicate specifictargeted infectious agents However althoughseveral antibody-based therapies have beenapproved for oncology and anti-inflammatoryindications (see Table 1) only one monoclonalantibody (mAb) is approved against an infec-tious disease agentmdashSynagis (palivizumabMedImmune) for the prevention and treat-ment of respiratory syncytical virus (RSV) inhigh-risk children Economic obstacles such asthe high cost of mAb therapies and relativelysmall markets have resulted in less interestfrom pharmaceutical companies in developingthese Also highlighting the challenges indeveloping these types of antibody-basedtreatments are the difficulties encountered indeveloping a follow-up higher-affinity candi-date to Synagis Poor translatability of dataobtained in the available animal disease mod-els for RSV in cotton rats has resulted in non-approval due to inferiority relative to SynagisIn other viral diseases such as cytomegalovirus(CMV) the high species specificity of thestrains of CMV makes it impossible to testhuman antibody therapies in vivo Thereforeany real data on the efficacy of treatments forCMV will not be obtained until testing inclinical trials As described later in this articleseveral new antibody-based therapies for in-fectious diseases are in development andhopefully this will gradually open the fieldand result in better treatment options andoutcomes for patients
6 HEY
TABLE 1 Approved and pending antibody-based therapies
Name antibody Target antibody type Indication Company Approval date
OKT3a Muronomab-CD3 CD3 murine IgG2a Autoimmune Johnson ampJohnson
1986 (US)
ReoPro abciximab PIIbIIIa chimeric IgG1Fab
Homeostasis Johnson ampJohnson
1984 (US)
Rituxan rituximab CD20 chimeric IgG1 Cancer Genentech 1997 (US) 1998 (EU)Zenapaxa daclizumab CD25 humanized IgG1 Autoimmune Roche 1997 (US) 1999 (EU)Simulect basiliximab CD25 chimeric IgG1 Autoimmune Novartis 1998 (US EU)Synagis palivizumab RSV humanized IgG1 Infections MedImmune 1998 (US) 1999 (EU)Remicade infliximab TNFα chimeric IgG1 Autoimmune Johnson amp
Johnson1998 (US) 1999 (EU)
Herceptin trastuzumab HER2 humanized IgG1 Cancer GenentechRoche
1998 (US) 2000 (EU)
Mylotarga gemtuzumabozogamicin
CD33 humanized IgG4immunotoxin
Cancer WyethPfizer 2000 (US)
Campath alemtuzumab CD52 humanized IgG1 Cancer Genzyme 2001 (US) 2001 (EU)Zevalin ibritumomabtiuxetan
CD20 murine IgG1radiolabeled (yttrium 90)
Cancer Biogen Idec 2002 (US) 2004 (EU)
Humira adalimumab TNFα human IgG1 Autoimmune Abbott 2002 (US) 2003 (EU)Xolair omalizumab IgE humanized IgG1 Autoimmune Genentech
Roche2003 (US)
Bexxar tositumomab-I-131 CD20 murine IgG2aradiolabeled (iodine131)
Cancer CorixaGSK 2003 (US)
Raptivaa falizumab CD11a humanized IgG1 Autoimmune GenentechRoche
2003 (US) 2004 (EU)
Erbitux cetuximab EGFR chimeric IgG1 Cancer ImcloneLilly 2004 (US) 2004 (EU)Avastin bevacizumab VEGF humanized IgG1 Cancer Genentech
Roche2004 (US) 2005 (EU)
Tysabri natalizumab α4-Intergrin humanizedIgG4
Autoimmune Biogen Idec 2004 (US)
Actemra tocilizumab Anti-IL-6R humanizedIgG1
Autoimmune ChugaiRoche
2005 (Japan) 2010 (US)
Vectibix panitumumab EGFR human IgG2 Cancer Amgen 2006 (US)Lucentis ranibizumab VEGF humanized IgG1
FabMaculardegeneration
GenentechRoche
2006 (US)
Soliris eculizumab C5 humanized IgG24 Blood disorders Alexion 2007 (US)Cimzia certolizumab pegol TNFα humanized
pegylated FabAutoimmune UCB 2008 (US)
Simponi golimumab TNFα human IgG1 Autoimmune Johnson ampJohnson
2009 (US EU Canada)
Ilaris canakinumab IL1b human IgG1 Infalmmatory Novartis 2009 (US EU)Stelara ustekinumab IL-1223 human IgG1 Autoimmune Johnson amp
Johnson2008 (EU) 2009 (US)
Arzerra ofatumumab CD20 human IgG1 Cancer Genmab 2009 (EU)Prolia denosumab RANK ligand human
IgG2Bone loss Amgen 2010 (US)
Numax motavizumab RSV humanized IgG1 Anti-infective MedImmune PendingABthrax Raxibacumab B anthrasis PA human
IgG1Anti-infection GSK 2012 (US)
Benlysta belimumab BLyS human IgG1 Autoimmune HGS 2011 (US)Yervoy ipilimumab CTLA-4 human IgG1 Cancer BMS 2011 (US)Adcetris brentuximabvedotin
CD30 chimeric IgG1drug- conjugate
Cancer SeattleGenetics
2011 (US)
(Continued on next page)
CHAPTER 1 bull History and Practice Antibodies in Infectious Diseases 7
INTRODUCTION TO ANTIBODIES
Antibodies also called immunoglobulins basedon their combined structure and function inimmune responses are produced by B cells ofthe immune system They are part of theadaptive immune response and are speciallydesigned for neutralizing and eliminating theinfectious agents and toxins produced by theseAntibodies are present in blood plasma andextracellular fluids and since these fluids wereformerly known as humors they were said tobe part of the humoral immune responseAntibodies are Y-shaped structures consistingof two main parts the upper arms of the Ywhich contain two identical variable-regionantigen binding sites and the lower regioncalled the constant regionwhich is responsiblefor the initiation of effector functions that leadto the removal and destruction of the pathogenor cells harboring the pathogen (see Fig 1) Theantigen-binding sites on an antibody can bythemselves bind to and neutralize bacterialtoxins and viruses thereby preventing themfrom binding to their target cells or receptorscausing toxic effects or spread of the infection
Antibodies consist of two pairs of heavy andlight chainswhich as described above are heldtogether in a Y-shaped arrangement Each ofthe heavy and light chains in these pairs isseparated into constant and variable chainsThe upper armsof theY each contain a variableand a constant sectionof the light and theheavychain where the upper variable parts of theheavy and light chains contain the antigen-binding site and the constant parts areconnected via disulfide bonds The lower partof theYcalled theconstantpart consistsof twoor three constant segments (immunoglobulindomains) from each of the two heavy chainsinteracting and also linked via disulfide bondsThe sectionsof theheavy chains connecting theconstant part of the upper arms to the constantparts of the constant region contain specialhinge regions that provide flexibility to thedifferent sections of the antibody to bind toantigens and effector cells The constant re-gions of the heavy chain also contain attachedoligosaccharide moieties which provide func-tional specialization to the antibodies (8)
The variable domains of the heavy and lightchains form the antigen-binding sites and
TABLE 1 Approved and pending antibody-based therapies (Continued)
Name antibody Target antibody type Indication Company Approval date
Perjeta pertuzumab Her2 humanized IgG1 Cancer GenentechRoche
2012 (US)
Kadcyla ado-trastuzumabemtansine
Her2 humanized IgG1Drug-conjugate
Cancer GenentechRoche
2013 (US)
Raxibacumab Anti-B anthrasis PAhuman IgG1
Anthraxinfection
Notapproved
2012
Entyvio vedolizumab Integrin α4β7humanized IgG1
Crohnrsquos diseaseulcerative colitis
Takeda 2014 (US)
Cyramza ramuciruumab Anti-VEGFR2Human IgG1
Gastric cancer Lilly 2014 (US)
Gazyva obinutuzumab Anti-CD20 humanizedIgG1 glucoengineered
CancerCLLb GenentechRoche
2014 (US)
Sylvant situximab Anti IL-6 chimeric IgG1 Castlemandisease
Janssen 2014 (US) 2014 (EU)
Cosentyx sekukinumab Anti IL-17a human IgG1 Psoriasis Novartis 2015 (US) 2015 (EU)Nivolumab Anti PD-1 human IgG4 Melanoma BMS Not approvedKeytruda pembrolizuumab Anti-PD-1 humanized
IgG4Melanoma Merck 2014 (US)
aAntibodies approved but later withdrawnbCLL chronic lymphocytic leukemia
8 HEY
FIGURE 1 (Left panel) Model of antibody structure exemplified by IgG On top the antigen-binding sitesin orange each contain one variable light and variable heavy domain with the three complementaritydetermining regions (CDRs) that are responsible for the specific binding of the antibody to its target Foreach arm of the antibody an additional set of variable heavy and light domains together with the CDR-containing domains represent the two fragment antigen binding (Fab) regions The two Fabs are heldtogether via two disulfide bridges Below the Fabs is the Fc region which contains four constant heavydomains On the upper pair of these domains are binding sites for oligosaccharides which have majorimportance for the ability of the antibody Fc part to trigger effector functions when the Fc portion isbound to Fc gamma receptors on natural killer cells neutrophil granulocytes monocytesmacrophagesdendritic cells and B cells (Right panel) Examples of some of the antibody-derived alternative formatsused to exploit the specific features of the CDRs the Fabs and the Fc parts of the antibodies ScFv Thesingle chain fragment variable consists of the variable domains of the heavy and light chains heldtogether by a flexible linker This can also be used as a carrier of a cytotoxic drug in a so-called antibodydrug complex (ADC) where the specificity of the ScFv is used to target the cytotoxic drug to eg atumor Bite (bi-specific T cell engager) Fusion proteins consisting of two ScFvs one directed against thetarget on a tumor cell and the other against the T cell receptor (CD3) Diabody ScFv dimers where shortlinker peptides (five amino acids) ensure dimerization and not folding of the ScFvs Fab and F(ab)2fragments Single Fab fragments or fragments containing two Fabs linked via disulfide bridges This isused where effector functions related to the Fc part of the antibody are unwanted and where a smallersize is desired to obtain better tissue penetration in eg tumors Due to the lack of the FcRn binding viathe Fc part Fab and F(ab)2 fragments have much shorter half-lives (hours or days) than full-sizeantibodies (weeks) These can also be used as carriers of cytotoxic payloads or cytotoxic radioactiveisotopes and for the F(ab)2 fragments can be constructed as bi-specifics which can cross-link immunecells and target cells Fc fusion protein Fusion protein containing the Fc domain of an immunoglobulinbound to a peptide The peptide can be a ligand for a specific receptor on a target cell or a blockingpeptide for a soluble ligand The Fc part provides a longer half-life to the construct and the potential tobind to and engage effector functions in the killing of eg tumor cells or infected cells ADCsRIAs andbi-specifics Full-size IgG antibodies carrying either a cytotoxic chemical or radioactive payload whichmay also carry different CDRs enabling cross-linking of effector and target cells for increased killingdoi101128microbiolspecAID-0026-2014f1
CHAPTER 1 bull History and Practice Antibodies in Infectious Diseases 9
contain special hyper-variable segments calledcomplementarity-determining regions (CDRs)which allow the B cells via genetic recom-bination to generate antibodies to all thedifferent antigens specific to amino acid se-quences or three-dimensional structuralmotifs(polysaccharides DNA and RNA) found onpathogens
Based on the structure of their heavy chainconstant regions antibodies or immuno-globulins are separated into five classesmdashIgM IgG IgE IgD and IgA Differences inthe sequences of the constant regions providedistinct characteristics to these different clas-ses These characteristics include the numberof heavy chain constant segments the numberand location of interconnecting disulfidebridges the length of the hinge region andthe number and location of oligosaccharidemoieties For IgG four heavy chain versionsexist creating IgG1 2 3 and 4 isotypes eachwith different characteristics in their serumhalf-lives and ability to trigger different effec-tor functions Because of the combined ad-vantage from ability to trigger effectormechanisms long [21 days] half-life theirability to be transported over the placentaand their stability in the production processantibodies of the IgG class and of the IgG1isotype are preferred as the basis for newantibody-based therapies The effector func-tions are triggered by the Fc part of an antibodywhen the variable parts of the antibody arebound directly to an infectious agent or toproteins from an infectious agent expressed onan infected cell This binding leaves the Fc partfree to interactwithFc receptors onphagocyticcells and neutrophils eosinophils and naturalkiller cells capable of inducing phagocytosis orlysis of infectious agents or infected cellsThese effector functions include (i) the abilityto activate the complement system for lysis(complement-dependent cellular cytotoxicity)(ii) triggering of uptake and destruction byphagocytic cells such as macrophages andneutrophils via interaction with Fc receptorson these cells (iii) activation of macrophageseosinophils neutrophils and natural killer
cells to kill infected cells via binding to Fcreceptors on these cells and antibody-depen-dent cellular cytotoxicity and (iv) neutraliza-tion of bacterial toxins and blocking of bindingand uptake of bacteria or viruses to target cells(see Fig 2) (9)
The Fcpart of IgG antibodies also contains aregion that interacts with the neonatal Fcreceptor (FcRn) expressed on most immuno-competent cells and inmany other cells such asendothelial cells in kidney liver placenta lungand breast (10) which protects antibodies fromdegradation by phagocytoticexocytotic cy-cling into FcRn-expressing cells thereby pro-longing their half-life This results in half-livesof 20 to 21 days for most IgG1 2 and 4antibodies whereas half-lives are 10 6 and 2days respectively for IgM IgA and IgE Thehighly specific binding sites on the variableregions of the upper arms of the antibody allowfor several important features of antibodiesndashbinding to and neutralization of eg bacterialtoxins binding to pathogens and blocking theirbinding to or interaction with target cells (egcyncytia formation of CMV-infected cells) orblocking of binding and interactions of infec-tious agents with target cells via blockingreceptors on the target cells
METHODS AND PLATFORMS FORGENERATING ANTIBODIES
As described above the early use of passiveantibody transfer as a therapy in infectiousdiseases involved the use of immune serumfrom immunized sheep and horses These pre-parations were crude and contained a broadmixture of neutralizing and non-neutralizingantibodies and both the foreign nature of theantibodies and the numerous host serumproteins This resulted in less specific andthus less efficient therapies due to a highvariability in efficacy between batches derivedfrom different animals immunized with dif-ferent strains of bacteria in different labor-atories and resulted in multiple unwantedside effects related to hypersensitivity and
10 HEY
anaphylactic reactions to foreign proteinsThese days antibodies being developed fortreatment of diseases in humans are highlypurified and are mostly fully human mono-clonal antibodies The term monoclonal anti-body refers to that cell cultures used forgenerating these antibodies each originatesfrom a single cell and thus produces onlyone specific antibody Development of fullyhuman monoclonal antibodies happened instages over a time span of more than 15 yearsFirst stage in this process was generation ofmonoclonalmurine IgG antibodies (eg OKT3[muronomab-CD3 Johnson and Johnson] ap-proved in 1986) Next stage was generation ofso called chimeric antibodies consisting ofhuman heavy and light chain constant sec-tions but with murine variable sections (eg
Rituxan [rituximab Genentech]) Next stagewas then the humanized antibodies wherethe only remaining murine part of the anti-body is the antigen-binding CDR (eg Xolair[omalizumab NovartisGenentech]) Both thefirst chimeric and humanized antibodies wereapproved in the late 1990s Then finally 16years later the first fully human antibodyHumira (adalimumab Abbott) was approvedin 2002 Since the time of the crude and low-scale manufacturing of the original antibodyserum products much has changed andtherapeutic antibodies are now produced byfermentation in 5000 liter scale using highlycontrolled and documented yeast or mamma-lian cell lines that are genetically engineered toexpress a single specific antibody This hasresulted in a pure and highly specific antibody
FIGURE 2 Effector functions of antibodies (a) Antibodies bind to pathogen-derived or endogenousantigens expressed on the surface of an infected cell which triggers binding to Fc receptors on naturalkiller cells and lysis of the infected cell by antibody-dependent cellular cytotoxicity (b) Antibodies bindto pathogen-derived or endogenous antigens expressed on the surface of infected cells which triggersactivation of complement through binding of complement factor C1q (c) Neutralization Top Bacterialtoxin neutralized by bound antigen Bottom Antibody bound to either receptor for the virus or to thevirus itself which blocks virus binding and entry into the cell (d) Antibody bound to viral surfaceproteins binds to Fc receptors on phagocytic cells eg macrophages and triggers endocytosis anddestruction of virus in endolysosome doi101128microbiolspecAID-0026-2014f2
CHAPTER 1 bull History and Practice Antibodies in Infectious Diseases 11

INTRODUCTION
History and PracticeAntibodies in Infectious Diseases 1ADAM HEY1
Antibodies in Infectious Diseases aims to inform update and inspire studentsteachers researchers pharmaceutical developers and health care professionalson the status of the development of antibody-based therapies for treatinginfectious diseases and the potential for these in times of growing antibioticresistance to provide alternative treatment solutions to the currently usedantibiotics and new treatments for infectious diseases where no propertreatments are available
This introductory article will provide a historical perspective on the useof antibody-based therapies followed by a high-level overview of whatmakes antibodies attractive tools for this purpose This will include the prosand cons of such therapies compared to the use of antibiotics and thepractical and strategic considerations involved in selecting the best formatand development path for new antibody-based therapies targeting specificinfectious agents Then examples of antibody-based therapies in thedevelopment of treatments for infectious diseases will be presented andfinally a look into the future will summarize the different aspects that willinfluence what the future might bring for this type of treatments forinfectious diseases
1Preclinical Safety Biologics Novartis AG Basel Switzerland
Antibodies for Infectious DiseasesEdited by James E Crowe Jr Diana Boraschi and Rino Rappuolicopy 2015 American Society for Microbiology Washington DCdoi101128microbiolspecAID-0026-2014
3
HISTORICAL PERSPECTIVE
Antibodies and the use of passive antibodytherapy in the treatment of infectious dis-eases is the story of a treatment conceptwhich dates back more than 120 years to thelate 19th century and which originally bythe use of serum from immunized animalsprovided the first effective treatment optionsagainst severe bacterial infections (1 2) Byimmunizing horses with bacterial toxinsfrom Clostridium tetani and Corynebacteri-um diphtheriae Emil A Von Behring andShibasaburo Kitasato (3) generated serumcontaining antibodies capable of neutraliz-ing the effects of the toxins produced bythese bacteria and successfully providedtreatment for these serious diseases wherethe pathogenesis is driven by the effects ofthe bacterial toxins For his work on provid-ing treatment for diphtheria Behring re-ceived the Nobel Prize in Physiology orMedicine in 1901 These radical treatmentresults quickly prompted development ofmultiple additional serum therapies for thetreatment of infectious diseases caused byeg Neisseria meningitidis Haemophilus in-fluenza and group A Streptococcus Sinceserum therapy involved administration oflarge amounts of crude mixtures of animalproteins including antibodies they wereassociated with side effects in the form ofhypersensitivity and serum sickness (2)
Due to the crude and unpurified nature ofthese products side effects were seen evenwhen administering human serum prepa-rations Side effects were observed in up to50 of patients and were considered to becaused by immune complex formations thatresulted in symptoms such as rash itchingjoint pain fever and in serious cases hypoten-sion and shock However due to the lack ofalternative options these treatments weredespite their side effects widely used Serumwas normally administered by intravenousinfusion in patients after a test for hypersensi-tivity where a small amount of serum wasinjected subcutaniously (1) As described
above serum therapy applied in these earlydays (late 19th century and early 20th century)involved preparations of serum from rabbitsand horses immunized with the infectiousagent or in live andor neutralized versions ortoxins from these (1) The costs of keeping theimmunized animals and the production andpotency testing of the materials made this arelatively expensive treatment In 1891 datafrom Klemperer (4) showed serum therapy toprotect rabbits from Streptococcus pneumoniaeinfection and paved the way for this type oftreatment and for development of similarserum-based treatments of streptococcal in-fections in humans When treating humansearly administration of serum could reducemortality significantly down to around 5compared to when administered 4 to 5 daysafter onset of symptoms when serum treat-ment was largely without effect This stronglyindicated the need for quick diagnosis andquick treatment to control the infection beforeit got out of control Consequently in theabsence of a specific diagnosis mixtures ofserum from immunizations with differentserotypes were used to circumvent this needfor early treatment without having a serotype-specific diagnosis The understanding thatdifferent serotypes existed for pneumococciand that efficient treatment relied on usingserotype-specific serum was being built upduring the 1920s and 1930s through experiencefrom extensive clinical trials
By the end of the 1930s serum therapywasthe standard of care for treatment of pneu-mococcal pneumonia At that time theefficacy and potency of the derived serawere assessed in mice in ldquothe mouse pro-tection testrdquo by testing survival after aconcomitant intraperitoneal injection of alethal dose of pneumococci and the serum tobe tested Due to the inherent variation inthis test efficacy and survival in two thirds ofthe animals was the acceptance criteria and10 times the lowest dose providing this wasused for defining a unit of the serum Thisallowed for large batch-to-batch variationand the use of different strains of bacteria for
4 HEY
immunization probably explains part of themissing responses observed (1) In the early20th century a pandemic of meningitis inEurope and the United States with mortalityrates up to 80 spurred the development ofserum therapy treatment options Althoughin the 1930s this became the recommendedtreatment in children assumed to be suffer-ing from meningitis failure to reduce mor-tality in several meningitis epidemics duringthat time raised doubts about the generalapplicability of serum treatment In thosedays serum therapy often involved quiteextensive procedures and infusion of largevolumes of serum The following exampleclearly illustrates this Data from Flexnerand Jobling (5) from treating meningitis inmonkeys resulted in the development of serafrom immunized horses for treatment inhumans The treatment protocol includedlumbar puncture and withdrawal of morethan 30 ml of spinal fluid representing anamount slightly larger than the expectedamount of horse serum to be injected subse-quently This treatment involved such dailyslow infusions of up to 30 ml of serum untilthe patientrsquos condition improved This treat-ment was used in outbreaks in New York in1905 and 1906 and did markedly decreasemortality
After the discovery of penicillin by Flemingin 1928 and the subsequent introduction ofantibiotics in the 1930s serum therapy waslargely abandoned over a period of 10 years dueto the availability of these new more broadlyeffective and cheaper treatment optionswhichalso had fewer side effects Although improve-ments in the purification of antibodies hadresulted in preparations with better safety andside effect profiles high manufacturing costsand narrow specificity resulted in antibodytherapy being mostly restricted to a smallernumber of selected treatments for snakevenoms bacterial toxins and some viral infec-tions (1 2) Currently antibody administrationis used for treatment and prevention ofhepatitis B virus rabies virus respiratorysyncytial virus (RSV) Clostridium tetani Clos-
tridium botulinum vaccinia virus echovirusand enterovirus For the most part thesetreatments consist of pooled immunoglobulinalso known as IVIG (intravenous immunoglob-ulin) from several postexposure donors Thisresults in both batch-to-batch variation in theneed for relatively large amounts of serum dueto low specificity and to restricted supplies dueto reliance on exposed donors
However several challengeshave resulted inthe need for new tools in the treatment andpreventionof infectiousdiseasesThebroadandgeneral use of antibiotics in human and veter-inary medicine for many years has resulted inthe development of multi-resistant strains ofbacteria with limited to no response to existingtreatments such as methicillin-resistant Staph-ylococcusaureus (MRSA) vancomycin-resistantS aureus and others This has resulted inpatients needing screening and treatment withseveral antibacterial agents and longer treat-ment time causing extra strain on patients andhealth care providers (6 httpwwwcdcgovdrugresistancethreat-report-2013indexhtml) According to the WHO and CDC morethan 25000 people in European Unioncountries and similar numbers in the UnitedStates die every year as a result of antibiotic-resistant infections This together with theemergence of new pathogens (eg severeacute respiratory syndrome Middle East respi-ratory syndrome) the re-emergenceepidemicsof oldknown pathogens (eg Ebola) and thedifficulties in treating infections in immune-deficient patients (eg HIV patients) has high-lighted the need for new solutions The 2014Ebola epidemic in West Africa (Liberia SierraLeone Guinea Nigeria and Senegal) has fur-ther highlighted this No treatment or prophy-lactic vaccine is available to treat or prevent thespread of Ebola infections which have anaveragemortality of gt50 Local health author-ities in the affected countries are struggling tocontain and handle the disease which isthreatening to go out of control and spreadmorewidelyVariousproductsmainly antibodycocktails from previously recovered patientsare being used despite a lack of clinical data on
CHAPTER 1 bull History and Practice Antibodies in Infectious Diseases 5
their safety and efficacy and those are the onlysporadically available treatment options andonly in small amounts and for a few patients
Ebola is an example of a disease whichnormally affects only a small number ofindividuals and which normally burns outwhen disease outbreaks are contained There-fore given the small number of potentialpatients affected by previous Ebola infectionsto date there was no incentive for big pharmacompanies to do research and development ofdrugs for EbolaWith the increasing number ofinfected (13567) andadeath toll of 4951 (7) andthe lack of the ability to contain the epidemic itwill be interesting to follow the aftermath ofthis outbreak and see whether there will berequests for new ways to ensure that vaccinesand treatment options are available for Ebolaand similar high-mortality and potential bio-warfare infections that have no availabletreatments or procedures to for mass-produc-tion upon the first signsreports of activeinfections Although both the CDC and theWHO have special programs focusing on thesetypes of infections the Ebola outbreak in 2014clearly shows that more financial support forresearch and development of new diagnosticsand treatments is needed This is one examplewhere antibody-based treatments would havethe potential to play a major role To put this inthe right perspective one should however notforget that other infectious diseases such astuberculosis influenza and malaria kill hun-dreds of thousands each year There is there-fore plenty of room for improvement indeveloping treatments for these diseases aswell but the high attention drawn to eg theEbola outbreak creates a special niche andopportunity where antibody treatments couldgain extraordinary development funding andsupport and prove their value and treatmentpotential
That antibody-based therapies could takethis role is supported by the revolution intechnologies for the development selectiongeneration and purification of fully humanantibodies described in more detail later in thesection ldquoMethodsandPlatforms forGenerating
Antibodiesrdquo Antibody-based programs cur-rently at different stages of developmentinclude investigations into the potential use ofsingle antibody preparations combinations ofantibodies (to avoid survival of escape mu-tants) fragments of antibodies and antibodiescarrying radioactive isotopesorcytotoxicdrugsor antibody-like frameworks (eg fibronectin)either alone as a first-line treatment or as anadjunct to existing treatments This multitudeof possible formats the ability to raise anti-bodies to almost any target and the ability toengineer both size effector functions and half-life are now considered by many to providevery valuable tools for designing specificantibody-based treatments toeradicate specifictargeted infectious agents However althoughseveral antibody-based therapies have beenapproved for oncology and anti-inflammatoryindications (see Table 1) only one monoclonalantibody (mAb) is approved against an infec-tious disease agentmdashSynagis (palivizumabMedImmune) for the prevention and treat-ment of respiratory syncytical virus (RSV) inhigh-risk children Economic obstacles such asthe high cost of mAb therapies and relativelysmall markets have resulted in less interestfrom pharmaceutical companies in developingthese Also highlighting the challenges indeveloping these types of antibody-basedtreatments are the difficulties encountered indeveloping a follow-up higher-affinity candi-date to Synagis Poor translatability of dataobtained in the available animal disease mod-els for RSV in cotton rats has resulted in non-approval due to inferiority relative to SynagisIn other viral diseases such as cytomegalovirus(CMV) the high species specificity of thestrains of CMV makes it impossible to testhuman antibody therapies in vivo Thereforeany real data on the efficacy of treatments forCMV will not be obtained until testing inclinical trials As described later in this articleseveral new antibody-based therapies for in-fectious diseases are in development andhopefully this will gradually open the fieldand result in better treatment options andoutcomes for patients
6 HEY
TABLE 1 Approved and pending antibody-based therapies
Name antibody Target antibody type Indication Company Approval date
OKT3a Muronomab-CD3 CD3 murine IgG2a Autoimmune Johnson ampJohnson
1986 (US)
ReoPro abciximab PIIbIIIa chimeric IgG1Fab
Homeostasis Johnson ampJohnson
1984 (US)
Rituxan rituximab CD20 chimeric IgG1 Cancer Genentech 1997 (US) 1998 (EU)Zenapaxa daclizumab CD25 humanized IgG1 Autoimmune Roche 1997 (US) 1999 (EU)Simulect basiliximab CD25 chimeric IgG1 Autoimmune Novartis 1998 (US EU)Synagis palivizumab RSV humanized IgG1 Infections MedImmune 1998 (US) 1999 (EU)Remicade infliximab TNFα chimeric IgG1 Autoimmune Johnson amp
Johnson1998 (US) 1999 (EU)
Herceptin trastuzumab HER2 humanized IgG1 Cancer GenentechRoche
1998 (US) 2000 (EU)
Mylotarga gemtuzumabozogamicin
CD33 humanized IgG4immunotoxin
Cancer WyethPfizer 2000 (US)
Campath alemtuzumab CD52 humanized IgG1 Cancer Genzyme 2001 (US) 2001 (EU)Zevalin ibritumomabtiuxetan
CD20 murine IgG1radiolabeled (yttrium 90)
Cancer Biogen Idec 2002 (US) 2004 (EU)
Humira adalimumab TNFα human IgG1 Autoimmune Abbott 2002 (US) 2003 (EU)Xolair omalizumab IgE humanized IgG1 Autoimmune Genentech
Roche2003 (US)
Bexxar tositumomab-I-131 CD20 murine IgG2aradiolabeled (iodine131)
Cancer CorixaGSK 2003 (US)
Raptivaa falizumab CD11a humanized IgG1 Autoimmune GenentechRoche
2003 (US) 2004 (EU)
Erbitux cetuximab EGFR chimeric IgG1 Cancer ImcloneLilly 2004 (US) 2004 (EU)Avastin bevacizumab VEGF humanized IgG1 Cancer Genentech
Roche2004 (US) 2005 (EU)
Tysabri natalizumab α4-Intergrin humanizedIgG4
Autoimmune Biogen Idec 2004 (US)
Actemra tocilizumab Anti-IL-6R humanizedIgG1
Autoimmune ChugaiRoche
2005 (Japan) 2010 (US)
Vectibix panitumumab EGFR human IgG2 Cancer Amgen 2006 (US)Lucentis ranibizumab VEGF humanized IgG1
FabMaculardegeneration
GenentechRoche
2006 (US)
Soliris eculizumab C5 humanized IgG24 Blood disorders Alexion 2007 (US)Cimzia certolizumab pegol TNFα humanized
pegylated FabAutoimmune UCB 2008 (US)
Simponi golimumab TNFα human IgG1 Autoimmune Johnson ampJohnson
2009 (US EU Canada)
Ilaris canakinumab IL1b human IgG1 Infalmmatory Novartis 2009 (US EU)Stelara ustekinumab IL-1223 human IgG1 Autoimmune Johnson amp
Johnson2008 (EU) 2009 (US)
Arzerra ofatumumab CD20 human IgG1 Cancer Genmab 2009 (EU)Prolia denosumab RANK ligand human
IgG2Bone loss Amgen 2010 (US)
Numax motavizumab RSV humanized IgG1 Anti-infective MedImmune PendingABthrax Raxibacumab B anthrasis PA human
IgG1Anti-infection GSK 2012 (US)
Benlysta belimumab BLyS human IgG1 Autoimmune HGS 2011 (US)Yervoy ipilimumab CTLA-4 human IgG1 Cancer BMS 2011 (US)Adcetris brentuximabvedotin
CD30 chimeric IgG1drug- conjugate
Cancer SeattleGenetics
2011 (US)
(Continued on next page)
CHAPTER 1 bull History and Practice Antibodies in Infectious Diseases 7
INTRODUCTION TO ANTIBODIES
Antibodies also called immunoglobulins basedon their combined structure and function inimmune responses are produced by B cells ofthe immune system They are part of theadaptive immune response and are speciallydesigned for neutralizing and eliminating theinfectious agents and toxins produced by theseAntibodies are present in blood plasma andextracellular fluids and since these fluids wereformerly known as humors they were said tobe part of the humoral immune responseAntibodies are Y-shaped structures consistingof two main parts the upper arms of the Ywhich contain two identical variable-regionantigen binding sites and the lower regioncalled the constant regionwhich is responsiblefor the initiation of effector functions that leadto the removal and destruction of the pathogenor cells harboring the pathogen (see Fig 1) Theantigen-binding sites on an antibody can bythemselves bind to and neutralize bacterialtoxins and viruses thereby preventing themfrom binding to their target cells or receptorscausing toxic effects or spread of the infection
Antibodies consist of two pairs of heavy andlight chainswhich as described above are heldtogether in a Y-shaped arrangement Each ofthe heavy and light chains in these pairs isseparated into constant and variable chainsThe upper armsof theY each contain a variableand a constant sectionof the light and theheavychain where the upper variable parts of theheavy and light chains contain the antigen-binding site and the constant parts areconnected via disulfide bonds The lower partof theYcalled theconstantpart consistsof twoor three constant segments (immunoglobulindomains) from each of the two heavy chainsinteracting and also linked via disulfide bondsThe sectionsof theheavy chains connecting theconstant part of the upper arms to the constantparts of the constant region contain specialhinge regions that provide flexibility to thedifferent sections of the antibody to bind toantigens and effector cells The constant re-gions of the heavy chain also contain attachedoligosaccharide moieties which provide func-tional specialization to the antibodies (8)
The variable domains of the heavy and lightchains form the antigen-binding sites and
TABLE 1 Approved and pending antibody-based therapies (Continued)
Name antibody Target antibody type Indication Company Approval date
Perjeta pertuzumab Her2 humanized IgG1 Cancer GenentechRoche
2012 (US)
Kadcyla ado-trastuzumabemtansine
Her2 humanized IgG1Drug-conjugate
Cancer GenentechRoche
2013 (US)
Raxibacumab Anti-B anthrasis PAhuman IgG1
Anthraxinfection
Notapproved
2012
Entyvio vedolizumab Integrin α4β7humanized IgG1
Crohnrsquos diseaseulcerative colitis
Takeda 2014 (US)
Cyramza ramuciruumab Anti-VEGFR2Human IgG1
Gastric cancer Lilly 2014 (US)
Gazyva obinutuzumab Anti-CD20 humanizedIgG1 glucoengineered
CancerCLLb GenentechRoche
2014 (US)
Sylvant situximab Anti IL-6 chimeric IgG1 Castlemandisease
Janssen 2014 (US) 2014 (EU)
Cosentyx sekukinumab Anti IL-17a human IgG1 Psoriasis Novartis 2015 (US) 2015 (EU)Nivolumab Anti PD-1 human IgG4 Melanoma BMS Not approvedKeytruda pembrolizuumab Anti-PD-1 humanized
IgG4Melanoma Merck 2014 (US)
aAntibodies approved but later withdrawnbCLL chronic lymphocytic leukemia
8 HEY
FIGURE 1 (Left panel) Model of antibody structure exemplified by IgG On top the antigen-binding sitesin orange each contain one variable light and variable heavy domain with the three complementaritydetermining regions (CDRs) that are responsible for the specific binding of the antibody to its target Foreach arm of the antibody an additional set of variable heavy and light domains together with the CDR-containing domains represent the two fragment antigen binding (Fab) regions The two Fabs are heldtogether via two disulfide bridges Below the Fabs is the Fc region which contains four constant heavydomains On the upper pair of these domains are binding sites for oligosaccharides which have majorimportance for the ability of the antibody Fc part to trigger effector functions when the Fc portion isbound to Fc gamma receptors on natural killer cells neutrophil granulocytes monocytesmacrophagesdendritic cells and B cells (Right panel) Examples of some of the antibody-derived alternative formatsused to exploit the specific features of the CDRs the Fabs and the Fc parts of the antibodies ScFv Thesingle chain fragment variable consists of the variable domains of the heavy and light chains heldtogether by a flexible linker This can also be used as a carrier of a cytotoxic drug in a so-called antibodydrug complex (ADC) where the specificity of the ScFv is used to target the cytotoxic drug to eg atumor Bite (bi-specific T cell engager) Fusion proteins consisting of two ScFvs one directed against thetarget on a tumor cell and the other against the T cell receptor (CD3) Diabody ScFv dimers where shortlinker peptides (five amino acids) ensure dimerization and not folding of the ScFvs Fab and F(ab)2fragments Single Fab fragments or fragments containing two Fabs linked via disulfide bridges This isused where effector functions related to the Fc part of the antibody are unwanted and where a smallersize is desired to obtain better tissue penetration in eg tumors Due to the lack of the FcRn binding viathe Fc part Fab and F(ab)2 fragments have much shorter half-lives (hours or days) than full-sizeantibodies (weeks) These can also be used as carriers of cytotoxic payloads or cytotoxic radioactiveisotopes and for the F(ab)2 fragments can be constructed as bi-specifics which can cross-link immunecells and target cells Fc fusion protein Fusion protein containing the Fc domain of an immunoglobulinbound to a peptide The peptide can be a ligand for a specific receptor on a target cell or a blockingpeptide for a soluble ligand The Fc part provides a longer half-life to the construct and the potential tobind to and engage effector functions in the killing of eg tumor cells or infected cells ADCsRIAs andbi-specifics Full-size IgG antibodies carrying either a cytotoxic chemical or radioactive payload whichmay also carry different CDRs enabling cross-linking of effector and target cells for increased killingdoi101128microbiolspecAID-0026-2014f1
CHAPTER 1 bull History and Practice Antibodies in Infectious Diseases 9
contain special hyper-variable segments calledcomplementarity-determining regions (CDRs)which allow the B cells via genetic recom-bination to generate antibodies to all thedifferent antigens specific to amino acid se-quences or three-dimensional structuralmotifs(polysaccharides DNA and RNA) found onpathogens
Based on the structure of their heavy chainconstant regions antibodies or immuno-globulins are separated into five classesmdashIgM IgG IgE IgD and IgA Differences inthe sequences of the constant regions providedistinct characteristics to these different clas-ses These characteristics include the numberof heavy chain constant segments the numberand location of interconnecting disulfidebridges the length of the hinge region andthe number and location of oligosaccharidemoieties For IgG four heavy chain versionsexist creating IgG1 2 3 and 4 isotypes eachwith different characteristics in their serumhalf-lives and ability to trigger different effec-tor functions Because of the combined ad-vantage from ability to trigger effectormechanisms long [21 days] half-life theirability to be transported over the placentaand their stability in the production processantibodies of the IgG class and of the IgG1isotype are preferred as the basis for newantibody-based therapies The effector func-tions are triggered by the Fc part of an antibodywhen the variable parts of the antibody arebound directly to an infectious agent or toproteins from an infectious agent expressed onan infected cell This binding leaves the Fc partfree to interactwithFc receptors onphagocyticcells and neutrophils eosinophils and naturalkiller cells capable of inducing phagocytosis orlysis of infectious agents or infected cellsThese effector functions include (i) the abilityto activate the complement system for lysis(complement-dependent cellular cytotoxicity)(ii) triggering of uptake and destruction byphagocytic cells such as macrophages andneutrophils via interaction with Fc receptorson these cells (iii) activation of macrophageseosinophils neutrophils and natural killer
cells to kill infected cells via binding to Fcreceptors on these cells and antibody-depen-dent cellular cytotoxicity and (iv) neutraliza-tion of bacterial toxins and blocking of bindingand uptake of bacteria or viruses to target cells(see Fig 2) (9)
The Fcpart of IgG antibodies also contains aregion that interacts with the neonatal Fcreceptor (FcRn) expressed on most immuno-competent cells and inmany other cells such asendothelial cells in kidney liver placenta lungand breast (10) which protects antibodies fromdegradation by phagocytoticexocytotic cy-cling into FcRn-expressing cells thereby pro-longing their half-life This results in half-livesof 20 to 21 days for most IgG1 2 and 4antibodies whereas half-lives are 10 6 and 2days respectively for IgM IgA and IgE Thehighly specific binding sites on the variableregions of the upper arms of the antibody allowfor several important features of antibodiesndashbinding to and neutralization of eg bacterialtoxins binding to pathogens and blocking theirbinding to or interaction with target cells (egcyncytia formation of CMV-infected cells) orblocking of binding and interactions of infec-tious agents with target cells via blockingreceptors on the target cells
METHODS AND PLATFORMS FORGENERATING ANTIBODIES
As described above the early use of passiveantibody transfer as a therapy in infectiousdiseases involved the use of immune serumfrom immunized sheep and horses These pre-parations were crude and contained a broadmixture of neutralizing and non-neutralizingantibodies and both the foreign nature of theantibodies and the numerous host serumproteins This resulted in less specific andthus less efficient therapies due to a highvariability in efficacy between batches derivedfrom different animals immunized with dif-ferent strains of bacteria in different labor-atories and resulted in multiple unwantedside effects related to hypersensitivity and
10 HEY
anaphylactic reactions to foreign proteinsThese days antibodies being developed fortreatment of diseases in humans are highlypurified and are mostly fully human mono-clonal antibodies The term monoclonal anti-body refers to that cell cultures used forgenerating these antibodies each originatesfrom a single cell and thus produces onlyone specific antibody Development of fullyhuman monoclonal antibodies happened instages over a time span of more than 15 yearsFirst stage in this process was generation ofmonoclonalmurine IgG antibodies (eg OKT3[muronomab-CD3 Johnson and Johnson] ap-proved in 1986) Next stage was generation ofso called chimeric antibodies consisting ofhuman heavy and light chain constant sec-tions but with murine variable sections (eg
Rituxan [rituximab Genentech]) Next stagewas then the humanized antibodies wherethe only remaining murine part of the anti-body is the antigen-binding CDR (eg Xolair[omalizumab NovartisGenentech]) Both thefirst chimeric and humanized antibodies wereapproved in the late 1990s Then finally 16years later the first fully human antibodyHumira (adalimumab Abbott) was approvedin 2002 Since the time of the crude and low-scale manufacturing of the original antibodyserum products much has changed andtherapeutic antibodies are now produced byfermentation in 5000 liter scale using highlycontrolled and documented yeast or mamma-lian cell lines that are genetically engineered toexpress a single specific antibody This hasresulted in a pure and highly specific antibody
FIGURE 2 Effector functions of antibodies (a) Antibodies bind to pathogen-derived or endogenousantigens expressed on the surface of an infected cell which triggers binding to Fc receptors on naturalkiller cells and lysis of the infected cell by antibody-dependent cellular cytotoxicity (b) Antibodies bindto pathogen-derived or endogenous antigens expressed on the surface of infected cells which triggersactivation of complement through binding of complement factor C1q (c) Neutralization Top Bacterialtoxin neutralized by bound antigen Bottom Antibody bound to either receptor for the virus or to thevirus itself which blocks virus binding and entry into the cell (d) Antibody bound to viral surfaceproteins binds to Fc receptors on phagocytic cells eg macrophages and triggers endocytosis anddestruction of virus in endolysosome doi101128microbiolspecAID-0026-2014f2
CHAPTER 1 bull History and Practice Antibodies in Infectious Diseases 11

History and PracticeAntibodies in Infectious Diseases 1ADAM HEY1
Antibodies in Infectious Diseases aims to inform update and inspire studentsteachers researchers pharmaceutical developers and health care professionalson the status of the development of antibody-based therapies for treatinginfectious diseases and the potential for these in times of growing antibioticresistance to provide alternative treatment solutions to the currently usedantibiotics and new treatments for infectious diseases where no propertreatments are available
This introductory article will provide a historical perspective on the useof antibody-based therapies followed by a high-level overview of whatmakes antibodies attractive tools for this purpose This will include the prosand cons of such therapies compared to the use of antibiotics and thepractical and strategic considerations involved in selecting the best formatand development path for new antibody-based therapies targeting specificinfectious agents Then examples of antibody-based therapies in thedevelopment of treatments for infectious diseases will be presented andfinally a look into the future will summarize the different aspects that willinfluence what the future might bring for this type of treatments forinfectious diseases
1Preclinical Safety Biologics Novartis AG Basel Switzerland
Antibodies for Infectious DiseasesEdited by James E Crowe Jr Diana Boraschi and Rino Rappuolicopy 2015 American Society for Microbiology Washington DCdoi101128microbiolspecAID-0026-2014
3
HISTORICAL PERSPECTIVE
Antibodies and the use of passive antibodytherapy in the treatment of infectious dis-eases is the story of a treatment conceptwhich dates back more than 120 years to thelate 19th century and which originally bythe use of serum from immunized animalsprovided the first effective treatment optionsagainst severe bacterial infections (1 2) Byimmunizing horses with bacterial toxinsfrom Clostridium tetani and Corynebacteri-um diphtheriae Emil A Von Behring andShibasaburo Kitasato (3) generated serumcontaining antibodies capable of neutraliz-ing the effects of the toxins produced bythese bacteria and successfully providedtreatment for these serious diseases wherethe pathogenesis is driven by the effects ofthe bacterial toxins For his work on provid-ing treatment for diphtheria Behring re-ceived the Nobel Prize in Physiology orMedicine in 1901 These radical treatmentresults quickly prompted development ofmultiple additional serum therapies for thetreatment of infectious diseases caused byeg Neisseria meningitidis Haemophilus in-fluenza and group A Streptococcus Sinceserum therapy involved administration oflarge amounts of crude mixtures of animalproteins including antibodies they wereassociated with side effects in the form ofhypersensitivity and serum sickness (2)
Due to the crude and unpurified nature ofthese products side effects were seen evenwhen administering human serum prepa-rations Side effects were observed in up to50 of patients and were considered to becaused by immune complex formations thatresulted in symptoms such as rash itchingjoint pain fever and in serious cases hypoten-sion and shock However due to the lack ofalternative options these treatments weredespite their side effects widely used Serumwas normally administered by intravenousinfusion in patients after a test for hypersensi-tivity where a small amount of serum wasinjected subcutaniously (1) As described
above serum therapy applied in these earlydays (late 19th century and early 20th century)involved preparations of serum from rabbitsand horses immunized with the infectiousagent or in live andor neutralized versions ortoxins from these (1) The costs of keeping theimmunized animals and the production andpotency testing of the materials made this arelatively expensive treatment In 1891 datafrom Klemperer (4) showed serum therapy toprotect rabbits from Streptococcus pneumoniaeinfection and paved the way for this type oftreatment and for development of similarserum-based treatments of streptococcal in-fections in humans When treating humansearly administration of serum could reducemortality significantly down to around 5compared to when administered 4 to 5 daysafter onset of symptoms when serum treat-ment was largely without effect This stronglyindicated the need for quick diagnosis andquick treatment to control the infection beforeit got out of control Consequently in theabsence of a specific diagnosis mixtures ofserum from immunizations with differentserotypes were used to circumvent this needfor early treatment without having a serotype-specific diagnosis The understanding thatdifferent serotypes existed for pneumococciand that efficient treatment relied on usingserotype-specific serum was being built upduring the 1920s and 1930s through experiencefrom extensive clinical trials
By the end of the 1930s serum therapywasthe standard of care for treatment of pneu-mococcal pneumonia At that time theefficacy and potency of the derived serawere assessed in mice in ldquothe mouse pro-tection testrdquo by testing survival after aconcomitant intraperitoneal injection of alethal dose of pneumococci and the serum tobe tested Due to the inherent variation inthis test efficacy and survival in two thirds ofthe animals was the acceptance criteria and10 times the lowest dose providing this wasused for defining a unit of the serum Thisallowed for large batch-to-batch variationand the use of different strains of bacteria for
4 HEY
immunization probably explains part of themissing responses observed (1) In the early20th century a pandemic of meningitis inEurope and the United States with mortalityrates up to 80 spurred the development ofserum therapy treatment options Althoughin the 1930s this became the recommendedtreatment in children assumed to be suffer-ing from meningitis failure to reduce mor-tality in several meningitis epidemics duringthat time raised doubts about the generalapplicability of serum treatment In thosedays serum therapy often involved quiteextensive procedures and infusion of largevolumes of serum The following exampleclearly illustrates this Data from Flexnerand Jobling (5) from treating meningitis inmonkeys resulted in the development of serafrom immunized horses for treatment inhumans The treatment protocol includedlumbar puncture and withdrawal of morethan 30 ml of spinal fluid representing anamount slightly larger than the expectedamount of horse serum to be injected subse-quently This treatment involved such dailyslow infusions of up to 30 ml of serum untilthe patientrsquos condition improved This treat-ment was used in outbreaks in New York in1905 and 1906 and did markedly decreasemortality
After the discovery of penicillin by Flemingin 1928 and the subsequent introduction ofantibiotics in the 1930s serum therapy waslargely abandoned over a period of 10 years dueto the availability of these new more broadlyeffective and cheaper treatment optionswhichalso had fewer side effects Although improve-ments in the purification of antibodies hadresulted in preparations with better safety andside effect profiles high manufacturing costsand narrow specificity resulted in antibodytherapy being mostly restricted to a smallernumber of selected treatments for snakevenoms bacterial toxins and some viral infec-tions (1 2) Currently antibody administrationis used for treatment and prevention ofhepatitis B virus rabies virus respiratorysyncytial virus (RSV) Clostridium tetani Clos-
tridium botulinum vaccinia virus echovirusand enterovirus For the most part thesetreatments consist of pooled immunoglobulinalso known as IVIG (intravenous immunoglob-ulin) from several postexposure donors Thisresults in both batch-to-batch variation in theneed for relatively large amounts of serum dueto low specificity and to restricted supplies dueto reliance on exposed donors
However several challengeshave resulted inthe need for new tools in the treatment andpreventionof infectiousdiseasesThebroadandgeneral use of antibiotics in human and veter-inary medicine for many years has resulted inthe development of multi-resistant strains ofbacteria with limited to no response to existingtreatments such as methicillin-resistant Staph-ylococcusaureus (MRSA) vancomycin-resistantS aureus and others This has resulted inpatients needing screening and treatment withseveral antibacterial agents and longer treat-ment time causing extra strain on patients andhealth care providers (6 httpwwwcdcgovdrugresistancethreat-report-2013indexhtml) According to the WHO and CDC morethan 25000 people in European Unioncountries and similar numbers in the UnitedStates die every year as a result of antibiotic-resistant infections This together with theemergence of new pathogens (eg severeacute respiratory syndrome Middle East respi-ratory syndrome) the re-emergenceepidemicsof oldknown pathogens (eg Ebola) and thedifficulties in treating infections in immune-deficient patients (eg HIV patients) has high-lighted the need for new solutions The 2014Ebola epidemic in West Africa (Liberia SierraLeone Guinea Nigeria and Senegal) has fur-ther highlighted this No treatment or prophy-lactic vaccine is available to treat or prevent thespread of Ebola infections which have anaveragemortality of gt50 Local health author-ities in the affected countries are struggling tocontain and handle the disease which isthreatening to go out of control and spreadmorewidelyVariousproductsmainly antibodycocktails from previously recovered patientsare being used despite a lack of clinical data on
CHAPTER 1 bull History and Practice Antibodies in Infectious Diseases 5
their safety and efficacy and those are the onlysporadically available treatment options andonly in small amounts and for a few patients
Ebola is an example of a disease whichnormally affects only a small number ofindividuals and which normally burns outwhen disease outbreaks are contained There-fore given the small number of potentialpatients affected by previous Ebola infectionsto date there was no incentive for big pharmacompanies to do research and development ofdrugs for EbolaWith the increasing number ofinfected (13567) andadeath toll of 4951 (7) andthe lack of the ability to contain the epidemic itwill be interesting to follow the aftermath ofthis outbreak and see whether there will berequests for new ways to ensure that vaccinesand treatment options are available for Ebolaand similar high-mortality and potential bio-warfare infections that have no availabletreatments or procedures to for mass-produc-tion upon the first signsreports of activeinfections Although both the CDC and theWHO have special programs focusing on thesetypes of infections the Ebola outbreak in 2014clearly shows that more financial support forresearch and development of new diagnosticsand treatments is needed This is one examplewhere antibody-based treatments would havethe potential to play a major role To put this inthe right perspective one should however notforget that other infectious diseases such astuberculosis influenza and malaria kill hun-dreds of thousands each year There is there-fore plenty of room for improvement indeveloping treatments for these diseases aswell but the high attention drawn to eg theEbola outbreak creates a special niche andopportunity where antibody treatments couldgain extraordinary development funding andsupport and prove their value and treatmentpotential
That antibody-based therapies could takethis role is supported by the revolution intechnologies for the development selectiongeneration and purification of fully humanantibodies described in more detail later in thesection ldquoMethodsandPlatforms forGenerating
Antibodiesrdquo Antibody-based programs cur-rently at different stages of developmentinclude investigations into the potential use ofsingle antibody preparations combinations ofantibodies (to avoid survival of escape mu-tants) fragments of antibodies and antibodiescarrying radioactive isotopesorcytotoxicdrugsor antibody-like frameworks (eg fibronectin)either alone as a first-line treatment or as anadjunct to existing treatments This multitudeof possible formats the ability to raise anti-bodies to almost any target and the ability toengineer both size effector functions and half-life are now considered by many to providevery valuable tools for designing specificantibody-based treatments toeradicate specifictargeted infectious agents However althoughseveral antibody-based therapies have beenapproved for oncology and anti-inflammatoryindications (see Table 1) only one monoclonalantibody (mAb) is approved against an infec-tious disease agentmdashSynagis (palivizumabMedImmune) for the prevention and treat-ment of respiratory syncytical virus (RSV) inhigh-risk children Economic obstacles such asthe high cost of mAb therapies and relativelysmall markets have resulted in less interestfrom pharmaceutical companies in developingthese Also highlighting the challenges indeveloping these types of antibody-basedtreatments are the difficulties encountered indeveloping a follow-up higher-affinity candi-date to Synagis Poor translatability of dataobtained in the available animal disease mod-els for RSV in cotton rats has resulted in non-approval due to inferiority relative to SynagisIn other viral diseases such as cytomegalovirus(CMV) the high species specificity of thestrains of CMV makes it impossible to testhuman antibody therapies in vivo Thereforeany real data on the efficacy of treatments forCMV will not be obtained until testing inclinical trials As described later in this articleseveral new antibody-based therapies for in-fectious diseases are in development andhopefully this will gradually open the fieldand result in better treatment options andoutcomes for patients
6 HEY
TABLE 1 Approved and pending antibody-based therapies
Name antibody Target antibody type Indication Company Approval date
OKT3a Muronomab-CD3 CD3 murine IgG2a Autoimmune Johnson ampJohnson
1986 (US)
ReoPro abciximab PIIbIIIa chimeric IgG1Fab
Homeostasis Johnson ampJohnson
1984 (US)
Rituxan rituximab CD20 chimeric IgG1 Cancer Genentech 1997 (US) 1998 (EU)Zenapaxa daclizumab CD25 humanized IgG1 Autoimmune Roche 1997 (US) 1999 (EU)Simulect basiliximab CD25 chimeric IgG1 Autoimmune Novartis 1998 (US EU)Synagis palivizumab RSV humanized IgG1 Infections MedImmune 1998 (US) 1999 (EU)Remicade infliximab TNFα chimeric IgG1 Autoimmune Johnson amp
Johnson1998 (US) 1999 (EU)
Herceptin trastuzumab HER2 humanized IgG1 Cancer GenentechRoche
1998 (US) 2000 (EU)
Mylotarga gemtuzumabozogamicin
CD33 humanized IgG4immunotoxin
Cancer WyethPfizer 2000 (US)
Campath alemtuzumab CD52 humanized IgG1 Cancer Genzyme 2001 (US) 2001 (EU)Zevalin ibritumomabtiuxetan
CD20 murine IgG1radiolabeled (yttrium 90)
Cancer Biogen Idec 2002 (US) 2004 (EU)
Humira adalimumab TNFα human IgG1 Autoimmune Abbott 2002 (US) 2003 (EU)Xolair omalizumab IgE humanized IgG1 Autoimmune Genentech
Roche2003 (US)
Bexxar tositumomab-I-131 CD20 murine IgG2aradiolabeled (iodine131)
Cancer CorixaGSK 2003 (US)
Raptivaa falizumab CD11a humanized IgG1 Autoimmune GenentechRoche
2003 (US) 2004 (EU)
Erbitux cetuximab EGFR chimeric IgG1 Cancer ImcloneLilly 2004 (US) 2004 (EU)Avastin bevacizumab VEGF humanized IgG1 Cancer Genentech
Roche2004 (US) 2005 (EU)
Tysabri natalizumab α4-Intergrin humanizedIgG4
Autoimmune Biogen Idec 2004 (US)
Actemra tocilizumab Anti-IL-6R humanizedIgG1
Autoimmune ChugaiRoche
2005 (Japan) 2010 (US)
Vectibix panitumumab EGFR human IgG2 Cancer Amgen 2006 (US)Lucentis ranibizumab VEGF humanized IgG1
FabMaculardegeneration
GenentechRoche
2006 (US)
Soliris eculizumab C5 humanized IgG24 Blood disorders Alexion 2007 (US)Cimzia certolizumab pegol TNFα humanized
pegylated FabAutoimmune UCB 2008 (US)
Simponi golimumab TNFα human IgG1 Autoimmune Johnson ampJohnson
2009 (US EU Canada)
Ilaris canakinumab IL1b human IgG1 Infalmmatory Novartis 2009 (US EU)Stelara ustekinumab IL-1223 human IgG1 Autoimmune Johnson amp
Johnson2008 (EU) 2009 (US)
Arzerra ofatumumab CD20 human IgG1 Cancer Genmab 2009 (EU)Prolia denosumab RANK ligand human
IgG2Bone loss Amgen 2010 (US)
Numax motavizumab RSV humanized IgG1 Anti-infective MedImmune PendingABthrax Raxibacumab B anthrasis PA human
IgG1Anti-infection GSK 2012 (US)
Benlysta belimumab BLyS human IgG1 Autoimmune HGS 2011 (US)Yervoy ipilimumab CTLA-4 human IgG1 Cancer BMS 2011 (US)Adcetris brentuximabvedotin
CD30 chimeric IgG1drug- conjugate
Cancer SeattleGenetics
2011 (US)
(Continued on next page)
CHAPTER 1 bull History and Practice Antibodies in Infectious Diseases 7
INTRODUCTION TO ANTIBODIES
Antibodies also called immunoglobulins basedon their combined structure and function inimmune responses are produced by B cells ofthe immune system They are part of theadaptive immune response and are speciallydesigned for neutralizing and eliminating theinfectious agents and toxins produced by theseAntibodies are present in blood plasma andextracellular fluids and since these fluids wereformerly known as humors they were said tobe part of the humoral immune responseAntibodies are Y-shaped structures consistingof two main parts the upper arms of the Ywhich contain two identical variable-regionantigen binding sites and the lower regioncalled the constant regionwhich is responsiblefor the initiation of effector functions that leadto the removal and destruction of the pathogenor cells harboring the pathogen (see Fig 1) Theantigen-binding sites on an antibody can bythemselves bind to and neutralize bacterialtoxins and viruses thereby preventing themfrom binding to their target cells or receptorscausing toxic effects or spread of the infection
Antibodies consist of two pairs of heavy andlight chainswhich as described above are heldtogether in a Y-shaped arrangement Each ofthe heavy and light chains in these pairs isseparated into constant and variable chainsThe upper armsof theY each contain a variableand a constant sectionof the light and theheavychain where the upper variable parts of theheavy and light chains contain the antigen-binding site and the constant parts areconnected via disulfide bonds The lower partof theYcalled theconstantpart consistsof twoor three constant segments (immunoglobulindomains) from each of the two heavy chainsinteracting and also linked via disulfide bondsThe sectionsof theheavy chains connecting theconstant part of the upper arms to the constantparts of the constant region contain specialhinge regions that provide flexibility to thedifferent sections of the antibody to bind toantigens and effector cells The constant re-gions of the heavy chain also contain attachedoligosaccharide moieties which provide func-tional specialization to the antibodies (8)
The variable domains of the heavy and lightchains form the antigen-binding sites and
TABLE 1 Approved and pending antibody-based therapies (Continued)
Name antibody Target antibody type Indication Company Approval date
Perjeta pertuzumab Her2 humanized IgG1 Cancer GenentechRoche
2012 (US)
Kadcyla ado-trastuzumabemtansine
Her2 humanized IgG1Drug-conjugate
Cancer GenentechRoche
2013 (US)
Raxibacumab Anti-B anthrasis PAhuman IgG1
Anthraxinfection
Notapproved
2012
Entyvio vedolizumab Integrin α4β7humanized IgG1
Crohnrsquos diseaseulcerative colitis
Takeda 2014 (US)
Cyramza ramuciruumab Anti-VEGFR2Human IgG1
Gastric cancer Lilly 2014 (US)
Gazyva obinutuzumab Anti-CD20 humanizedIgG1 glucoengineered
CancerCLLb GenentechRoche
2014 (US)
Sylvant situximab Anti IL-6 chimeric IgG1 Castlemandisease
Janssen 2014 (US) 2014 (EU)
Cosentyx sekukinumab Anti IL-17a human IgG1 Psoriasis Novartis 2015 (US) 2015 (EU)Nivolumab Anti PD-1 human IgG4 Melanoma BMS Not approvedKeytruda pembrolizuumab Anti-PD-1 humanized
IgG4Melanoma Merck 2014 (US)
aAntibodies approved but later withdrawnbCLL chronic lymphocytic leukemia
8 HEY
FIGURE 1 (Left panel) Model of antibody structure exemplified by IgG On top the antigen-binding sitesin orange each contain one variable light and variable heavy domain with the three complementaritydetermining regions (CDRs) that are responsible for the specific binding of the antibody to its target Foreach arm of the antibody an additional set of variable heavy and light domains together with the CDR-containing domains represent the two fragment antigen binding (Fab) regions The two Fabs are heldtogether via two disulfide bridges Below the Fabs is the Fc region which contains four constant heavydomains On the upper pair of these domains are binding sites for oligosaccharides which have majorimportance for the ability of the antibody Fc part to trigger effector functions when the Fc portion isbound to Fc gamma receptors on natural killer cells neutrophil granulocytes monocytesmacrophagesdendritic cells and B cells (Right panel) Examples of some of the antibody-derived alternative formatsused to exploit the specific features of the CDRs the Fabs and the Fc parts of the antibodies ScFv Thesingle chain fragment variable consists of the variable domains of the heavy and light chains heldtogether by a flexible linker This can also be used as a carrier of a cytotoxic drug in a so-called antibodydrug complex (ADC) where the specificity of the ScFv is used to target the cytotoxic drug to eg atumor Bite (bi-specific T cell engager) Fusion proteins consisting of two ScFvs one directed against thetarget on a tumor cell and the other against the T cell receptor (CD3) Diabody ScFv dimers where shortlinker peptides (five amino acids) ensure dimerization and not folding of the ScFvs Fab and F(ab)2fragments Single Fab fragments or fragments containing two Fabs linked via disulfide bridges This isused where effector functions related to the Fc part of the antibody are unwanted and where a smallersize is desired to obtain better tissue penetration in eg tumors Due to the lack of the FcRn binding viathe Fc part Fab and F(ab)2 fragments have much shorter half-lives (hours or days) than full-sizeantibodies (weeks) These can also be used as carriers of cytotoxic payloads or cytotoxic radioactiveisotopes and for the F(ab)2 fragments can be constructed as bi-specifics which can cross-link immunecells and target cells Fc fusion protein Fusion protein containing the Fc domain of an immunoglobulinbound to a peptide The peptide can be a ligand for a specific receptor on a target cell or a blockingpeptide for a soluble ligand The Fc part provides a longer half-life to the construct and the potential tobind to and engage effector functions in the killing of eg tumor cells or infected cells ADCsRIAs andbi-specifics Full-size IgG antibodies carrying either a cytotoxic chemical or radioactive payload whichmay also carry different CDRs enabling cross-linking of effector and target cells for increased killingdoi101128microbiolspecAID-0026-2014f1
CHAPTER 1 bull History and Practice Antibodies in Infectious Diseases 9
contain special hyper-variable segments calledcomplementarity-determining regions (CDRs)which allow the B cells via genetic recom-bination to generate antibodies to all thedifferent antigens specific to amino acid se-quences or three-dimensional structuralmotifs(polysaccharides DNA and RNA) found onpathogens
Based on the structure of their heavy chainconstant regions antibodies or immuno-globulins are separated into five classesmdashIgM IgG IgE IgD and IgA Differences inthe sequences of the constant regions providedistinct characteristics to these different clas-ses These characteristics include the numberof heavy chain constant segments the numberand location of interconnecting disulfidebridges the length of the hinge region andthe number and location of oligosaccharidemoieties For IgG four heavy chain versionsexist creating IgG1 2 3 and 4 isotypes eachwith different characteristics in their serumhalf-lives and ability to trigger different effec-tor functions Because of the combined ad-vantage from ability to trigger effectormechanisms long [21 days] half-life theirability to be transported over the placentaand their stability in the production processantibodies of the IgG class and of the IgG1isotype are preferred as the basis for newantibody-based therapies The effector func-tions are triggered by the Fc part of an antibodywhen the variable parts of the antibody arebound directly to an infectious agent or toproteins from an infectious agent expressed onan infected cell This binding leaves the Fc partfree to interactwithFc receptors onphagocyticcells and neutrophils eosinophils and naturalkiller cells capable of inducing phagocytosis orlysis of infectious agents or infected cellsThese effector functions include (i) the abilityto activate the complement system for lysis(complement-dependent cellular cytotoxicity)(ii) triggering of uptake and destruction byphagocytic cells such as macrophages andneutrophils via interaction with Fc receptorson these cells (iii) activation of macrophageseosinophils neutrophils and natural killer
cells to kill infected cells via binding to Fcreceptors on these cells and antibody-depen-dent cellular cytotoxicity and (iv) neutraliza-tion of bacterial toxins and blocking of bindingand uptake of bacteria or viruses to target cells(see Fig 2) (9)
The Fcpart of IgG antibodies also contains aregion that interacts with the neonatal Fcreceptor (FcRn) expressed on most immuno-competent cells and inmany other cells such asendothelial cells in kidney liver placenta lungand breast (10) which protects antibodies fromdegradation by phagocytoticexocytotic cy-cling into FcRn-expressing cells thereby pro-longing their half-life This results in half-livesof 20 to 21 days for most IgG1 2 and 4antibodies whereas half-lives are 10 6 and 2days respectively for IgM IgA and IgE Thehighly specific binding sites on the variableregions of the upper arms of the antibody allowfor several important features of antibodiesndashbinding to and neutralization of eg bacterialtoxins binding to pathogens and blocking theirbinding to or interaction with target cells (egcyncytia formation of CMV-infected cells) orblocking of binding and interactions of infec-tious agents with target cells via blockingreceptors on the target cells
METHODS AND PLATFORMS FORGENERATING ANTIBODIES
As described above the early use of passiveantibody transfer as a therapy in infectiousdiseases involved the use of immune serumfrom immunized sheep and horses These pre-parations were crude and contained a broadmixture of neutralizing and non-neutralizingantibodies and both the foreign nature of theantibodies and the numerous host serumproteins This resulted in less specific andthus less efficient therapies due to a highvariability in efficacy between batches derivedfrom different animals immunized with dif-ferent strains of bacteria in different labor-atories and resulted in multiple unwantedside effects related to hypersensitivity and
10 HEY
anaphylactic reactions to foreign proteinsThese days antibodies being developed fortreatment of diseases in humans are highlypurified and are mostly fully human mono-clonal antibodies The term monoclonal anti-body refers to that cell cultures used forgenerating these antibodies each originatesfrom a single cell and thus produces onlyone specific antibody Development of fullyhuman monoclonal antibodies happened instages over a time span of more than 15 yearsFirst stage in this process was generation ofmonoclonalmurine IgG antibodies (eg OKT3[muronomab-CD3 Johnson and Johnson] ap-proved in 1986) Next stage was generation ofso called chimeric antibodies consisting ofhuman heavy and light chain constant sec-tions but with murine variable sections (eg
Rituxan [rituximab Genentech]) Next stagewas then the humanized antibodies wherethe only remaining murine part of the anti-body is the antigen-binding CDR (eg Xolair[omalizumab NovartisGenentech]) Both thefirst chimeric and humanized antibodies wereapproved in the late 1990s Then finally 16years later the first fully human antibodyHumira (adalimumab Abbott) was approvedin 2002 Since the time of the crude and low-scale manufacturing of the original antibodyserum products much has changed andtherapeutic antibodies are now produced byfermentation in 5000 liter scale using highlycontrolled and documented yeast or mamma-lian cell lines that are genetically engineered toexpress a single specific antibody This hasresulted in a pure and highly specific antibody
FIGURE 2 Effector functions of antibodies (a) Antibodies bind to pathogen-derived or endogenousantigens expressed on the surface of an infected cell which triggers binding to Fc receptors on naturalkiller cells and lysis of the infected cell by antibody-dependent cellular cytotoxicity (b) Antibodies bindto pathogen-derived or endogenous antigens expressed on the surface of infected cells which triggersactivation of complement through binding of complement factor C1q (c) Neutralization Top Bacterialtoxin neutralized by bound antigen Bottom Antibody bound to either receptor for the virus or to thevirus itself which blocks virus binding and entry into the cell (d) Antibody bound to viral surfaceproteins binds to Fc receptors on phagocytic cells eg macrophages and triggers endocytosis anddestruction of virus in endolysosome doi101128microbiolspecAID-0026-2014f2
CHAPTER 1 bull History and Practice Antibodies in Infectious Diseases 11

HISTORICAL PERSPECTIVE
Antibodies and the use of passive antibodytherapy in the treatment of infectious dis-eases is the story of a treatment conceptwhich dates back more than 120 years to thelate 19th century and which originally bythe use of serum from immunized animalsprovided the first effective treatment optionsagainst severe bacterial infections (1 2) Byimmunizing horses with bacterial toxinsfrom Clostridium tetani and Corynebacteri-um diphtheriae Emil A Von Behring andShibasaburo Kitasato (3) generated serumcontaining antibodies capable of neutraliz-ing the effects of the toxins produced bythese bacteria and successfully providedtreatment for these serious diseases wherethe pathogenesis is driven by the effects ofthe bacterial toxins For his work on provid-ing treatment for diphtheria Behring re-ceived the Nobel Prize in Physiology orMedicine in 1901 These radical treatmentresults quickly prompted development ofmultiple additional serum therapies for thetreatment of infectious diseases caused byeg Neisseria meningitidis Haemophilus in-fluenza and group A Streptococcus Sinceserum therapy involved administration oflarge amounts of crude mixtures of animalproteins including antibodies they wereassociated with side effects in the form ofhypersensitivity and serum sickness (2)
Due to the crude and unpurified nature ofthese products side effects were seen evenwhen administering human serum prepa-rations Side effects were observed in up to50 of patients and were considered to becaused by immune complex formations thatresulted in symptoms such as rash itchingjoint pain fever and in serious cases hypoten-sion and shock However due to the lack ofalternative options these treatments weredespite their side effects widely used Serumwas normally administered by intravenousinfusion in patients after a test for hypersensi-tivity where a small amount of serum wasinjected subcutaniously (1) As described
above serum therapy applied in these earlydays (late 19th century and early 20th century)involved preparations of serum from rabbitsand horses immunized with the infectiousagent or in live andor neutralized versions ortoxins from these (1) The costs of keeping theimmunized animals and the production andpotency testing of the materials made this arelatively expensive treatment In 1891 datafrom Klemperer (4) showed serum therapy toprotect rabbits from Streptococcus pneumoniaeinfection and paved the way for this type oftreatment and for development of similarserum-based treatments of streptococcal in-fections in humans When treating humansearly administration of serum could reducemortality significantly down to around 5compared to when administered 4 to 5 daysafter onset of symptoms when serum treat-ment was largely without effect This stronglyindicated the need for quick diagnosis andquick treatment to control the infection beforeit got out of control Consequently in theabsence of a specific diagnosis mixtures ofserum from immunizations with differentserotypes were used to circumvent this needfor early treatment without having a serotype-specific diagnosis The understanding thatdifferent serotypes existed for pneumococciand that efficient treatment relied on usingserotype-specific serum was being built upduring the 1920s and 1930s through experiencefrom extensive clinical trials
By the end of the 1930s serum therapywasthe standard of care for treatment of pneu-mococcal pneumonia At that time theefficacy and potency of the derived serawere assessed in mice in ldquothe mouse pro-tection testrdquo by testing survival after aconcomitant intraperitoneal injection of alethal dose of pneumococci and the serum tobe tested Due to the inherent variation inthis test efficacy and survival in two thirds ofthe animals was the acceptance criteria and10 times the lowest dose providing this wasused for defining a unit of the serum Thisallowed for large batch-to-batch variationand the use of different strains of bacteria for
4 HEY
immunization probably explains part of themissing responses observed (1) In the early20th century a pandemic of meningitis inEurope and the United States with mortalityrates up to 80 spurred the development ofserum therapy treatment options Althoughin the 1930s this became the recommendedtreatment in children assumed to be suffer-ing from meningitis failure to reduce mor-tality in several meningitis epidemics duringthat time raised doubts about the generalapplicability of serum treatment In thosedays serum therapy often involved quiteextensive procedures and infusion of largevolumes of serum The following exampleclearly illustrates this Data from Flexnerand Jobling (5) from treating meningitis inmonkeys resulted in the development of serafrom immunized horses for treatment inhumans The treatment protocol includedlumbar puncture and withdrawal of morethan 30 ml of spinal fluid representing anamount slightly larger than the expectedamount of horse serum to be injected subse-quently This treatment involved such dailyslow infusions of up to 30 ml of serum untilthe patientrsquos condition improved This treat-ment was used in outbreaks in New York in1905 and 1906 and did markedly decreasemortality
After the discovery of penicillin by Flemingin 1928 and the subsequent introduction ofantibiotics in the 1930s serum therapy waslargely abandoned over a period of 10 years dueto the availability of these new more broadlyeffective and cheaper treatment optionswhichalso had fewer side effects Although improve-ments in the purification of antibodies hadresulted in preparations with better safety andside effect profiles high manufacturing costsand narrow specificity resulted in antibodytherapy being mostly restricted to a smallernumber of selected treatments for snakevenoms bacterial toxins and some viral infec-tions (1 2) Currently antibody administrationis used for treatment and prevention ofhepatitis B virus rabies virus respiratorysyncytial virus (RSV) Clostridium tetani Clos-
tridium botulinum vaccinia virus echovirusand enterovirus For the most part thesetreatments consist of pooled immunoglobulinalso known as IVIG (intravenous immunoglob-ulin) from several postexposure donors Thisresults in both batch-to-batch variation in theneed for relatively large amounts of serum dueto low specificity and to restricted supplies dueto reliance on exposed donors
However several challengeshave resulted inthe need for new tools in the treatment andpreventionof infectiousdiseasesThebroadandgeneral use of antibiotics in human and veter-inary medicine for many years has resulted inthe development of multi-resistant strains ofbacteria with limited to no response to existingtreatments such as methicillin-resistant Staph-ylococcusaureus (MRSA) vancomycin-resistantS aureus and others This has resulted inpatients needing screening and treatment withseveral antibacterial agents and longer treat-ment time causing extra strain on patients andhealth care providers (6 httpwwwcdcgovdrugresistancethreat-report-2013indexhtml) According to the WHO and CDC morethan 25000 people in European Unioncountries and similar numbers in the UnitedStates die every year as a result of antibiotic-resistant infections This together with theemergence of new pathogens (eg severeacute respiratory syndrome Middle East respi-ratory syndrome) the re-emergenceepidemicsof oldknown pathogens (eg Ebola) and thedifficulties in treating infections in immune-deficient patients (eg HIV patients) has high-lighted the need for new solutions The 2014Ebola epidemic in West Africa (Liberia SierraLeone Guinea Nigeria and Senegal) has fur-ther highlighted this No treatment or prophy-lactic vaccine is available to treat or prevent thespread of Ebola infections which have anaveragemortality of gt50 Local health author-ities in the affected countries are struggling tocontain and handle the disease which isthreatening to go out of control and spreadmorewidelyVariousproductsmainly antibodycocktails from previously recovered patientsare being used despite a lack of clinical data on
CHAPTER 1 bull History and Practice Antibodies in Infectious Diseases 5
their safety and efficacy and those are the onlysporadically available treatment options andonly in small amounts and for a few patients
Ebola is an example of a disease whichnormally affects only a small number ofindividuals and which normally burns outwhen disease outbreaks are contained There-fore given the small number of potentialpatients affected by previous Ebola infectionsto date there was no incentive for big pharmacompanies to do research and development ofdrugs for EbolaWith the increasing number ofinfected (13567) andadeath toll of 4951 (7) andthe lack of the ability to contain the epidemic itwill be interesting to follow the aftermath ofthis outbreak and see whether there will berequests for new ways to ensure that vaccinesand treatment options are available for Ebolaand similar high-mortality and potential bio-warfare infections that have no availabletreatments or procedures to for mass-produc-tion upon the first signsreports of activeinfections Although both the CDC and theWHO have special programs focusing on thesetypes of infections the Ebola outbreak in 2014clearly shows that more financial support forresearch and development of new diagnosticsand treatments is needed This is one examplewhere antibody-based treatments would havethe potential to play a major role To put this inthe right perspective one should however notforget that other infectious diseases such astuberculosis influenza and malaria kill hun-dreds of thousands each year There is there-fore plenty of room for improvement indeveloping treatments for these diseases aswell but the high attention drawn to eg theEbola outbreak creates a special niche andopportunity where antibody treatments couldgain extraordinary development funding andsupport and prove their value and treatmentpotential
That antibody-based therapies could takethis role is supported by the revolution intechnologies for the development selectiongeneration and purification of fully humanantibodies described in more detail later in thesection ldquoMethodsandPlatforms forGenerating
Antibodiesrdquo Antibody-based programs cur-rently at different stages of developmentinclude investigations into the potential use ofsingle antibody preparations combinations ofantibodies (to avoid survival of escape mu-tants) fragments of antibodies and antibodiescarrying radioactive isotopesorcytotoxicdrugsor antibody-like frameworks (eg fibronectin)either alone as a first-line treatment or as anadjunct to existing treatments This multitudeof possible formats the ability to raise anti-bodies to almost any target and the ability toengineer both size effector functions and half-life are now considered by many to providevery valuable tools for designing specificantibody-based treatments toeradicate specifictargeted infectious agents However althoughseveral antibody-based therapies have beenapproved for oncology and anti-inflammatoryindications (see Table 1) only one monoclonalantibody (mAb) is approved against an infec-tious disease agentmdashSynagis (palivizumabMedImmune) for the prevention and treat-ment of respiratory syncytical virus (RSV) inhigh-risk children Economic obstacles such asthe high cost of mAb therapies and relativelysmall markets have resulted in less interestfrom pharmaceutical companies in developingthese Also highlighting the challenges indeveloping these types of antibody-basedtreatments are the difficulties encountered indeveloping a follow-up higher-affinity candi-date to Synagis Poor translatability of dataobtained in the available animal disease mod-els for RSV in cotton rats has resulted in non-approval due to inferiority relative to SynagisIn other viral diseases such as cytomegalovirus(CMV) the high species specificity of thestrains of CMV makes it impossible to testhuman antibody therapies in vivo Thereforeany real data on the efficacy of treatments forCMV will not be obtained until testing inclinical trials As described later in this articleseveral new antibody-based therapies for in-fectious diseases are in development andhopefully this will gradually open the fieldand result in better treatment options andoutcomes for patients
6 HEY
TABLE 1 Approved and pending antibody-based therapies
Name antibody Target antibody type Indication Company Approval date
OKT3a Muronomab-CD3 CD3 murine IgG2a Autoimmune Johnson ampJohnson
1986 (US)
ReoPro abciximab PIIbIIIa chimeric IgG1Fab
Homeostasis Johnson ampJohnson
1984 (US)
Rituxan rituximab CD20 chimeric IgG1 Cancer Genentech 1997 (US) 1998 (EU)Zenapaxa daclizumab CD25 humanized IgG1 Autoimmune Roche 1997 (US) 1999 (EU)Simulect basiliximab CD25 chimeric IgG1 Autoimmune Novartis 1998 (US EU)Synagis palivizumab RSV humanized IgG1 Infections MedImmune 1998 (US) 1999 (EU)Remicade infliximab TNFα chimeric IgG1 Autoimmune Johnson amp
Johnson1998 (US) 1999 (EU)
Herceptin trastuzumab HER2 humanized IgG1 Cancer GenentechRoche
1998 (US) 2000 (EU)
Mylotarga gemtuzumabozogamicin
CD33 humanized IgG4immunotoxin
Cancer WyethPfizer 2000 (US)
Campath alemtuzumab CD52 humanized IgG1 Cancer Genzyme 2001 (US) 2001 (EU)Zevalin ibritumomabtiuxetan
CD20 murine IgG1radiolabeled (yttrium 90)
Cancer Biogen Idec 2002 (US) 2004 (EU)
Humira adalimumab TNFα human IgG1 Autoimmune Abbott 2002 (US) 2003 (EU)Xolair omalizumab IgE humanized IgG1 Autoimmune Genentech
Roche2003 (US)
Bexxar tositumomab-I-131 CD20 murine IgG2aradiolabeled (iodine131)
Cancer CorixaGSK 2003 (US)
Raptivaa falizumab CD11a humanized IgG1 Autoimmune GenentechRoche
2003 (US) 2004 (EU)
Erbitux cetuximab EGFR chimeric IgG1 Cancer ImcloneLilly 2004 (US) 2004 (EU)Avastin bevacizumab VEGF humanized IgG1 Cancer Genentech
Roche2004 (US) 2005 (EU)
Tysabri natalizumab α4-Intergrin humanizedIgG4
Autoimmune Biogen Idec 2004 (US)
Actemra tocilizumab Anti-IL-6R humanizedIgG1
Autoimmune ChugaiRoche
2005 (Japan) 2010 (US)
Vectibix panitumumab EGFR human IgG2 Cancer Amgen 2006 (US)Lucentis ranibizumab VEGF humanized IgG1
FabMaculardegeneration
GenentechRoche
2006 (US)
Soliris eculizumab C5 humanized IgG24 Blood disorders Alexion 2007 (US)Cimzia certolizumab pegol TNFα humanized
pegylated FabAutoimmune UCB 2008 (US)
Simponi golimumab TNFα human IgG1 Autoimmune Johnson ampJohnson
2009 (US EU Canada)
Ilaris canakinumab IL1b human IgG1 Infalmmatory Novartis 2009 (US EU)Stelara ustekinumab IL-1223 human IgG1 Autoimmune Johnson amp
Johnson2008 (EU) 2009 (US)
Arzerra ofatumumab CD20 human IgG1 Cancer Genmab 2009 (EU)Prolia denosumab RANK ligand human
IgG2Bone loss Amgen 2010 (US)
Numax motavizumab RSV humanized IgG1 Anti-infective MedImmune PendingABthrax Raxibacumab B anthrasis PA human
IgG1Anti-infection GSK 2012 (US)
Benlysta belimumab BLyS human IgG1 Autoimmune HGS 2011 (US)Yervoy ipilimumab CTLA-4 human IgG1 Cancer BMS 2011 (US)Adcetris brentuximabvedotin
CD30 chimeric IgG1drug- conjugate
Cancer SeattleGenetics
2011 (US)
(Continued on next page)
CHAPTER 1 bull History and Practice Antibodies in Infectious Diseases 7
INTRODUCTION TO ANTIBODIES
Antibodies also called immunoglobulins basedon their combined structure and function inimmune responses are produced by B cells ofthe immune system They are part of theadaptive immune response and are speciallydesigned for neutralizing and eliminating theinfectious agents and toxins produced by theseAntibodies are present in blood plasma andextracellular fluids and since these fluids wereformerly known as humors they were said tobe part of the humoral immune responseAntibodies are Y-shaped structures consistingof two main parts the upper arms of the Ywhich contain two identical variable-regionantigen binding sites and the lower regioncalled the constant regionwhich is responsiblefor the initiation of effector functions that leadto the removal and destruction of the pathogenor cells harboring the pathogen (see Fig 1) Theantigen-binding sites on an antibody can bythemselves bind to and neutralize bacterialtoxins and viruses thereby preventing themfrom binding to their target cells or receptorscausing toxic effects or spread of the infection
Antibodies consist of two pairs of heavy andlight chainswhich as described above are heldtogether in a Y-shaped arrangement Each ofthe heavy and light chains in these pairs isseparated into constant and variable chainsThe upper armsof theY each contain a variableand a constant sectionof the light and theheavychain where the upper variable parts of theheavy and light chains contain the antigen-binding site and the constant parts areconnected via disulfide bonds The lower partof theYcalled theconstantpart consistsof twoor three constant segments (immunoglobulindomains) from each of the two heavy chainsinteracting and also linked via disulfide bondsThe sectionsof theheavy chains connecting theconstant part of the upper arms to the constantparts of the constant region contain specialhinge regions that provide flexibility to thedifferent sections of the antibody to bind toantigens and effector cells The constant re-gions of the heavy chain also contain attachedoligosaccharide moieties which provide func-tional specialization to the antibodies (8)
The variable domains of the heavy and lightchains form the antigen-binding sites and
TABLE 1 Approved and pending antibody-based therapies (Continued)
Name antibody Target antibody type Indication Company Approval date
Perjeta pertuzumab Her2 humanized IgG1 Cancer GenentechRoche
2012 (US)
Kadcyla ado-trastuzumabemtansine
Her2 humanized IgG1Drug-conjugate
Cancer GenentechRoche
2013 (US)
Raxibacumab Anti-B anthrasis PAhuman IgG1
Anthraxinfection
Notapproved
2012
Entyvio vedolizumab Integrin α4β7humanized IgG1
Crohnrsquos diseaseulcerative colitis
Takeda 2014 (US)
Cyramza ramuciruumab Anti-VEGFR2Human IgG1
Gastric cancer Lilly 2014 (US)
Gazyva obinutuzumab Anti-CD20 humanizedIgG1 glucoengineered
CancerCLLb GenentechRoche
2014 (US)
Sylvant situximab Anti IL-6 chimeric IgG1 Castlemandisease
Janssen 2014 (US) 2014 (EU)
Cosentyx sekukinumab Anti IL-17a human IgG1 Psoriasis Novartis 2015 (US) 2015 (EU)Nivolumab Anti PD-1 human IgG4 Melanoma BMS Not approvedKeytruda pembrolizuumab Anti-PD-1 humanized
IgG4Melanoma Merck 2014 (US)
aAntibodies approved but later withdrawnbCLL chronic lymphocytic leukemia
8 HEY
FIGURE 1 (Left panel) Model of antibody structure exemplified by IgG On top the antigen-binding sitesin orange each contain one variable light and variable heavy domain with the three complementaritydetermining regions (CDRs) that are responsible for the specific binding of the antibody to its target Foreach arm of the antibody an additional set of variable heavy and light domains together with the CDR-containing domains represent the two fragment antigen binding (Fab) regions The two Fabs are heldtogether via two disulfide bridges Below the Fabs is the Fc region which contains four constant heavydomains On the upper pair of these domains are binding sites for oligosaccharides which have majorimportance for the ability of the antibody Fc part to trigger effector functions when the Fc portion isbound to Fc gamma receptors on natural killer cells neutrophil granulocytes monocytesmacrophagesdendritic cells and B cells (Right panel) Examples of some of the antibody-derived alternative formatsused to exploit the specific features of the CDRs the Fabs and the Fc parts of the antibodies ScFv Thesingle chain fragment variable consists of the variable domains of the heavy and light chains heldtogether by a flexible linker This can also be used as a carrier of a cytotoxic drug in a so-called antibodydrug complex (ADC) where the specificity of the ScFv is used to target the cytotoxic drug to eg atumor Bite (bi-specific T cell engager) Fusion proteins consisting of two ScFvs one directed against thetarget on a tumor cell and the other against the T cell receptor (CD3) Diabody ScFv dimers where shortlinker peptides (five amino acids) ensure dimerization and not folding of the ScFvs Fab and F(ab)2fragments Single Fab fragments or fragments containing two Fabs linked via disulfide bridges This isused where effector functions related to the Fc part of the antibody are unwanted and where a smallersize is desired to obtain better tissue penetration in eg tumors Due to the lack of the FcRn binding viathe Fc part Fab and F(ab)2 fragments have much shorter half-lives (hours or days) than full-sizeantibodies (weeks) These can also be used as carriers of cytotoxic payloads or cytotoxic radioactiveisotopes and for the F(ab)2 fragments can be constructed as bi-specifics which can cross-link immunecells and target cells Fc fusion protein Fusion protein containing the Fc domain of an immunoglobulinbound to a peptide The peptide can be a ligand for a specific receptor on a target cell or a blockingpeptide for a soluble ligand The Fc part provides a longer half-life to the construct and the potential tobind to and engage effector functions in the killing of eg tumor cells or infected cells ADCsRIAs andbi-specifics Full-size IgG antibodies carrying either a cytotoxic chemical or radioactive payload whichmay also carry different CDRs enabling cross-linking of effector and target cells for increased killingdoi101128microbiolspecAID-0026-2014f1
CHAPTER 1 bull History and Practice Antibodies in Infectious Diseases 9
contain special hyper-variable segments calledcomplementarity-determining regions (CDRs)which allow the B cells via genetic recom-bination to generate antibodies to all thedifferent antigens specific to amino acid se-quences or three-dimensional structuralmotifs(polysaccharides DNA and RNA) found onpathogens
Based on the structure of their heavy chainconstant regions antibodies or immuno-globulins are separated into five classesmdashIgM IgG IgE IgD and IgA Differences inthe sequences of the constant regions providedistinct characteristics to these different clas-ses These characteristics include the numberof heavy chain constant segments the numberand location of interconnecting disulfidebridges the length of the hinge region andthe number and location of oligosaccharidemoieties For IgG four heavy chain versionsexist creating IgG1 2 3 and 4 isotypes eachwith different characteristics in their serumhalf-lives and ability to trigger different effec-tor functions Because of the combined ad-vantage from ability to trigger effectormechanisms long [21 days] half-life theirability to be transported over the placentaand their stability in the production processantibodies of the IgG class and of the IgG1isotype are preferred as the basis for newantibody-based therapies The effector func-tions are triggered by the Fc part of an antibodywhen the variable parts of the antibody arebound directly to an infectious agent or toproteins from an infectious agent expressed onan infected cell This binding leaves the Fc partfree to interactwithFc receptors onphagocyticcells and neutrophils eosinophils and naturalkiller cells capable of inducing phagocytosis orlysis of infectious agents or infected cellsThese effector functions include (i) the abilityto activate the complement system for lysis(complement-dependent cellular cytotoxicity)(ii) triggering of uptake and destruction byphagocytic cells such as macrophages andneutrophils via interaction with Fc receptorson these cells (iii) activation of macrophageseosinophils neutrophils and natural killer
cells to kill infected cells via binding to Fcreceptors on these cells and antibody-depen-dent cellular cytotoxicity and (iv) neutraliza-tion of bacterial toxins and blocking of bindingand uptake of bacteria or viruses to target cells(see Fig 2) (9)
The Fcpart of IgG antibodies also contains aregion that interacts with the neonatal Fcreceptor (FcRn) expressed on most immuno-competent cells and inmany other cells such asendothelial cells in kidney liver placenta lungand breast (10) which protects antibodies fromdegradation by phagocytoticexocytotic cy-cling into FcRn-expressing cells thereby pro-longing their half-life This results in half-livesof 20 to 21 days for most IgG1 2 and 4antibodies whereas half-lives are 10 6 and 2days respectively for IgM IgA and IgE Thehighly specific binding sites on the variableregions of the upper arms of the antibody allowfor several important features of antibodiesndashbinding to and neutralization of eg bacterialtoxins binding to pathogens and blocking theirbinding to or interaction with target cells (egcyncytia formation of CMV-infected cells) orblocking of binding and interactions of infec-tious agents with target cells via blockingreceptors on the target cells
METHODS AND PLATFORMS FORGENERATING ANTIBODIES
As described above the early use of passiveantibody transfer as a therapy in infectiousdiseases involved the use of immune serumfrom immunized sheep and horses These pre-parations were crude and contained a broadmixture of neutralizing and non-neutralizingantibodies and both the foreign nature of theantibodies and the numerous host serumproteins This resulted in less specific andthus less efficient therapies due to a highvariability in efficacy between batches derivedfrom different animals immunized with dif-ferent strains of bacteria in different labor-atories and resulted in multiple unwantedside effects related to hypersensitivity and
10 HEY
anaphylactic reactions to foreign proteinsThese days antibodies being developed fortreatment of diseases in humans are highlypurified and are mostly fully human mono-clonal antibodies The term monoclonal anti-body refers to that cell cultures used forgenerating these antibodies each originatesfrom a single cell and thus produces onlyone specific antibody Development of fullyhuman monoclonal antibodies happened instages over a time span of more than 15 yearsFirst stage in this process was generation ofmonoclonalmurine IgG antibodies (eg OKT3[muronomab-CD3 Johnson and Johnson] ap-proved in 1986) Next stage was generation ofso called chimeric antibodies consisting ofhuman heavy and light chain constant sec-tions but with murine variable sections (eg
Rituxan [rituximab Genentech]) Next stagewas then the humanized antibodies wherethe only remaining murine part of the anti-body is the antigen-binding CDR (eg Xolair[omalizumab NovartisGenentech]) Both thefirst chimeric and humanized antibodies wereapproved in the late 1990s Then finally 16years later the first fully human antibodyHumira (adalimumab Abbott) was approvedin 2002 Since the time of the crude and low-scale manufacturing of the original antibodyserum products much has changed andtherapeutic antibodies are now produced byfermentation in 5000 liter scale using highlycontrolled and documented yeast or mamma-lian cell lines that are genetically engineered toexpress a single specific antibody This hasresulted in a pure and highly specific antibody
FIGURE 2 Effector functions of antibodies (a) Antibodies bind to pathogen-derived or endogenousantigens expressed on the surface of an infected cell which triggers binding to Fc receptors on naturalkiller cells and lysis of the infected cell by antibody-dependent cellular cytotoxicity (b) Antibodies bindto pathogen-derived or endogenous antigens expressed on the surface of infected cells which triggersactivation of complement through binding of complement factor C1q (c) Neutralization Top Bacterialtoxin neutralized by bound antigen Bottom Antibody bound to either receptor for the virus or to thevirus itself which blocks virus binding and entry into the cell (d) Antibody bound to viral surfaceproteins binds to Fc receptors on phagocytic cells eg macrophages and triggers endocytosis anddestruction of virus in endolysosome doi101128microbiolspecAID-0026-2014f2
CHAPTER 1 bull History and Practice Antibodies in Infectious Diseases 11

immunization probably explains part of themissing responses observed (1) In the early20th century a pandemic of meningitis inEurope and the United States with mortalityrates up to 80 spurred the development ofserum therapy treatment options Althoughin the 1930s this became the recommendedtreatment in children assumed to be suffer-ing from meningitis failure to reduce mor-tality in several meningitis epidemics duringthat time raised doubts about the generalapplicability of serum treatment In thosedays serum therapy often involved quiteextensive procedures and infusion of largevolumes of serum The following exampleclearly illustrates this Data from Flexnerand Jobling (5) from treating meningitis inmonkeys resulted in the development of serafrom immunized horses for treatment inhumans The treatment protocol includedlumbar puncture and withdrawal of morethan 30 ml of spinal fluid representing anamount slightly larger than the expectedamount of horse serum to be injected subse-quently This treatment involved such dailyslow infusions of up to 30 ml of serum untilthe patientrsquos condition improved This treat-ment was used in outbreaks in New York in1905 and 1906 and did markedly decreasemortality
After the discovery of penicillin by Flemingin 1928 and the subsequent introduction ofantibiotics in the 1930s serum therapy waslargely abandoned over a period of 10 years dueto the availability of these new more broadlyeffective and cheaper treatment optionswhichalso had fewer side effects Although improve-ments in the purification of antibodies hadresulted in preparations with better safety andside effect profiles high manufacturing costsand narrow specificity resulted in antibodytherapy being mostly restricted to a smallernumber of selected treatments for snakevenoms bacterial toxins and some viral infec-tions (1 2) Currently antibody administrationis used for treatment and prevention ofhepatitis B virus rabies virus respiratorysyncytial virus (RSV) Clostridium tetani Clos-
tridium botulinum vaccinia virus echovirusand enterovirus For the most part thesetreatments consist of pooled immunoglobulinalso known as IVIG (intravenous immunoglob-ulin) from several postexposure donors Thisresults in both batch-to-batch variation in theneed for relatively large amounts of serum dueto low specificity and to restricted supplies dueto reliance on exposed donors
However several challengeshave resulted inthe need for new tools in the treatment andpreventionof infectiousdiseasesThebroadandgeneral use of antibiotics in human and veter-inary medicine for many years has resulted inthe development of multi-resistant strains ofbacteria with limited to no response to existingtreatments such as methicillin-resistant Staph-ylococcusaureus (MRSA) vancomycin-resistantS aureus and others This has resulted inpatients needing screening and treatment withseveral antibacterial agents and longer treat-ment time causing extra strain on patients andhealth care providers (6 httpwwwcdcgovdrugresistancethreat-report-2013indexhtml) According to the WHO and CDC morethan 25000 people in European Unioncountries and similar numbers in the UnitedStates die every year as a result of antibiotic-resistant infections This together with theemergence of new pathogens (eg severeacute respiratory syndrome Middle East respi-ratory syndrome) the re-emergenceepidemicsof oldknown pathogens (eg Ebola) and thedifficulties in treating infections in immune-deficient patients (eg HIV patients) has high-lighted the need for new solutions The 2014Ebola epidemic in West Africa (Liberia SierraLeone Guinea Nigeria and Senegal) has fur-ther highlighted this No treatment or prophy-lactic vaccine is available to treat or prevent thespread of Ebola infections which have anaveragemortality of gt50 Local health author-ities in the affected countries are struggling tocontain and handle the disease which isthreatening to go out of control and spreadmorewidelyVariousproductsmainly antibodycocktails from previously recovered patientsare being used despite a lack of clinical data on
CHAPTER 1 bull History and Practice Antibodies in Infectious Diseases 5
their safety and efficacy and those are the onlysporadically available treatment options andonly in small amounts and for a few patients
Ebola is an example of a disease whichnormally affects only a small number ofindividuals and which normally burns outwhen disease outbreaks are contained There-fore given the small number of potentialpatients affected by previous Ebola infectionsto date there was no incentive for big pharmacompanies to do research and development ofdrugs for EbolaWith the increasing number ofinfected (13567) andadeath toll of 4951 (7) andthe lack of the ability to contain the epidemic itwill be interesting to follow the aftermath ofthis outbreak and see whether there will berequests for new ways to ensure that vaccinesand treatment options are available for Ebolaand similar high-mortality and potential bio-warfare infections that have no availabletreatments or procedures to for mass-produc-tion upon the first signsreports of activeinfections Although both the CDC and theWHO have special programs focusing on thesetypes of infections the Ebola outbreak in 2014clearly shows that more financial support forresearch and development of new diagnosticsand treatments is needed This is one examplewhere antibody-based treatments would havethe potential to play a major role To put this inthe right perspective one should however notforget that other infectious diseases such astuberculosis influenza and malaria kill hun-dreds of thousands each year There is there-fore plenty of room for improvement indeveloping treatments for these diseases aswell but the high attention drawn to eg theEbola outbreak creates a special niche andopportunity where antibody treatments couldgain extraordinary development funding andsupport and prove their value and treatmentpotential
That antibody-based therapies could takethis role is supported by the revolution intechnologies for the development selectiongeneration and purification of fully humanantibodies described in more detail later in thesection ldquoMethodsandPlatforms forGenerating
Antibodiesrdquo Antibody-based programs cur-rently at different stages of developmentinclude investigations into the potential use ofsingle antibody preparations combinations ofantibodies (to avoid survival of escape mu-tants) fragments of antibodies and antibodiescarrying radioactive isotopesorcytotoxicdrugsor antibody-like frameworks (eg fibronectin)either alone as a first-line treatment or as anadjunct to existing treatments This multitudeof possible formats the ability to raise anti-bodies to almost any target and the ability toengineer both size effector functions and half-life are now considered by many to providevery valuable tools for designing specificantibody-based treatments toeradicate specifictargeted infectious agents However althoughseveral antibody-based therapies have beenapproved for oncology and anti-inflammatoryindications (see Table 1) only one monoclonalantibody (mAb) is approved against an infec-tious disease agentmdashSynagis (palivizumabMedImmune) for the prevention and treat-ment of respiratory syncytical virus (RSV) inhigh-risk children Economic obstacles such asthe high cost of mAb therapies and relativelysmall markets have resulted in less interestfrom pharmaceutical companies in developingthese Also highlighting the challenges indeveloping these types of antibody-basedtreatments are the difficulties encountered indeveloping a follow-up higher-affinity candi-date to Synagis Poor translatability of dataobtained in the available animal disease mod-els for RSV in cotton rats has resulted in non-approval due to inferiority relative to SynagisIn other viral diseases such as cytomegalovirus(CMV) the high species specificity of thestrains of CMV makes it impossible to testhuman antibody therapies in vivo Thereforeany real data on the efficacy of treatments forCMV will not be obtained until testing inclinical trials As described later in this articleseveral new antibody-based therapies for in-fectious diseases are in development andhopefully this will gradually open the fieldand result in better treatment options andoutcomes for patients
6 HEY
TABLE 1 Approved and pending antibody-based therapies
Name antibody Target antibody type Indication Company Approval date
OKT3a Muronomab-CD3 CD3 murine IgG2a Autoimmune Johnson ampJohnson
1986 (US)
ReoPro abciximab PIIbIIIa chimeric IgG1Fab
Homeostasis Johnson ampJohnson
1984 (US)
Rituxan rituximab CD20 chimeric IgG1 Cancer Genentech 1997 (US) 1998 (EU)Zenapaxa daclizumab CD25 humanized IgG1 Autoimmune Roche 1997 (US) 1999 (EU)Simulect basiliximab CD25 chimeric IgG1 Autoimmune Novartis 1998 (US EU)Synagis palivizumab RSV humanized IgG1 Infections MedImmune 1998 (US) 1999 (EU)Remicade infliximab TNFα chimeric IgG1 Autoimmune Johnson amp
Johnson1998 (US) 1999 (EU)
Herceptin trastuzumab HER2 humanized IgG1 Cancer GenentechRoche
1998 (US) 2000 (EU)
Mylotarga gemtuzumabozogamicin
CD33 humanized IgG4immunotoxin
Cancer WyethPfizer 2000 (US)
Campath alemtuzumab CD52 humanized IgG1 Cancer Genzyme 2001 (US) 2001 (EU)Zevalin ibritumomabtiuxetan
CD20 murine IgG1radiolabeled (yttrium 90)
Cancer Biogen Idec 2002 (US) 2004 (EU)
Humira adalimumab TNFα human IgG1 Autoimmune Abbott 2002 (US) 2003 (EU)Xolair omalizumab IgE humanized IgG1 Autoimmune Genentech
Roche2003 (US)
Bexxar tositumomab-I-131 CD20 murine IgG2aradiolabeled (iodine131)
Cancer CorixaGSK 2003 (US)
Raptivaa falizumab CD11a humanized IgG1 Autoimmune GenentechRoche
2003 (US) 2004 (EU)
Erbitux cetuximab EGFR chimeric IgG1 Cancer ImcloneLilly 2004 (US) 2004 (EU)Avastin bevacizumab VEGF humanized IgG1 Cancer Genentech
Roche2004 (US) 2005 (EU)
Tysabri natalizumab α4-Intergrin humanizedIgG4
Autoimmune Biogen Idec 2004 (US)
Actemra tocilizumab Anti-IL-6R humanizedIgG1
Autoimmune ChugaiRoche
2005 (Japan) 2010 (US)
Vectibix panitumumab EGFR human IgG2 Cancer Amgen 2006 (US)Lucentis ranibizumab VEGF humanized IgG1
FabMaculardegeneration
GenentechRoche
2006 (US)
Soliris eculizumab C5 humanized IgG24 Blood disorders Alexion 2007 (US)Cimzia certolizumab pegol TNFα humanized
pegylated FabAutoimmune UCB 2008 (US)
Simponi golimumab TNFα human IgG1 Autoimmune Johnson ampJohnson
2009 (US EU Canada)
Ilaris canakinumab IL1b human IgG1 Infalmmatory Novartis 2009 (US EU)Stelara ustekinumab IL-1223 human IgG1 Autoimmune Johnson amp
Johnson2008 (EU) 2009 (US)
Arzerra ofatumumab CD20 human IgG1 Cancer Genmab 2009 (EU)Prolia denosumab RANK ligand human
IgG2Bone loss Amgen 2010 (US)
Numax motavizumab RSV humanized IgG1 Anti-infective MedImmune PendingABthrax Raxibacumab B anthrasis PA human
IgG1Anti-infection GSK 2012 (US)
Benlysta belimumab BLyS human IgG1 Autoimmune HGS 2011 (US)Yervoy ipilimumab CTLA-4 human IgG1 Cancer BMS 2011 (US)Adcetris brentuximabvedotin
CD30 chimeric IgG1drug- conjugate
Cancer SeattleGenetics
2011 (US)
(Continued on next page)
CHAPTER 1 bull History and Practice Antibodies in Infectious Diseases 7
INTRODUCTION TO ANTIBODIES
Antibodies also called immunoglobulins basedon their combined structure and function inimmune responses are produced by B cells ofthe immune system They are part of theadaptive immune response and are speciallydesigned for neutralizing and eliminating theinfectious agents and toxins produced by theseAntibodies are present in blood plasma andextracellular fluids and since these fluids wereformerly known as humors they were said tobe part of the humoral immune responseAntibodies are Y-shaped structures consistingof two main parts the upper arms of the Ywhich contain two identical variable-regionantigen binding sites and the lower regioncalled the constant regionwhich is responsiblefor the initiation of effector functions that leadto the removal and destruction of the pathogenor cells harboring the pathogen (see Fig 1) Theantigen-binding sites on an antibody can bythemselves bind to and neutralize bacterialtoxins and viruses thereby preventing themfrom binding to their target cells or receptorscausing toxic effects or spread of the infection
Antibodies consist of two pairs of heavy andlight chainswhich as described above are heldtogether in a Y-shaped arrangement Each ofthe heavy and light chains in these pairs isseparated into constant and variable chainsThe upper armsof theY each contain a variableand a constant sectionof the light and theheavychain where the upper variable parts of theheavy and light chains contain the antigen-binding site and the constant parts areconnected via disulfide bonds The lower partof theYcalled theconstantpart consistsof twoor three constant segments (immunoglobulindomains) from each of the two heavy chainsinteracting and also linked via disulfide bondsThe sectionsof theheavy chains connecting theconstant part of the upper arms to the constantparts of the constant region contain specialhinge regions that provide flexibility to thedifferent sections of the antibody to bind toantigens and effector cells The constant re-gions of the heavy chain also contain attachedoligosaccharide moieties which provide func-tional specialization to the antibodies (8)
The variable domains of the heavy and lightchains form the antigen-binding sites and
TABLE 1 Approved and pending antibody-based therapies (Continued)
Name antibody Target antibody type Indication Company Approval date
Perjeta pertuzumab Her2 humanized IgG1 Cancer GenentechRoche
2012 (US)
Kadcyla ado-trastuzumabemtansine
Her2 humanized IgG1Drug-conjugate
Cancer GenentechRoche
2013 (US)
Raxibacumab Anti-B anthrasis PAhuman IgG1
Anthraxinfection
Notapproved
2012
Entyvio vedolizumab Integrin α4β7humanized IgG1
Crohnrsquos diseaseulcerative colitis
Takeda 2014 (US)
Cyramza ramuciruumab Anti-VEGFR2Human IgG1
Gastric cancer Lilly 2014 (US)
Gazyva obinutuzumab Anti-CD20 humanizedIgG1 glucoengineered
CancerCLLb GenentechRoche
2014 (US)
Sylvant situximab Anti IL-6 chimeric IgG1 Castlemandisease
Janssen 2014 (US) 2014 (EU)
Cosentyx sekukinumab Anti IL-17a human IgG1 Psoriasis Novartis 2015 (US) 2015 (EU)Nivolumab Anti PD-1 human IgG4 Melanoma BMS Not approvedKeytruda pembrolizuumab Anti-PD-1 humanized
IgG4Melanoma Merck 2014 (US)
aAntibodies approved but later withdrawnbCLL chronic lymphocytic leukemia
8 HEY
FIGURE 1 (Left panel) Model of antibody structure exemplified by IgG On top the antigen-binding sitesin orange each contain one variable light and variable heavy domain with the three complementaritydetermining regions (CDRs) that are responsible for the specific binding of the antibody to its target Foreach arm of the antibody an additional set of variable heavy and light domains together with the CDR-containing domains represent the two fragment antigen binding (Fab) regions The two Fabs are heldtogether via two disulfide bridges Below the Fabs is the Fc region which contains four constant heavydomains On the upper pair of these domains are binding sites for oligosaccharides which have majorimportance for the ability of the antibody Fc part to trigger effector functions when the Fc portion isbound to Fc gamma receptors on natural killer cells neutrophil granulocytes monocytesmacrophagesdendritic cells and B cells (Right panel) Examples of some of the antibody-derived alternative formatsused to exploit the specific features of the CDRs the Fabs and the Fc parts of the antibodies ScFv Thesingle chain fragment variable consists of the variable domains of the heavy and light chains heldtogether by a flexible linker This can also be used as a carrier of a cytotoxic drug in a so-called antibodydrug complex (ADC) where the specificity of the ScFv is used to target the cytotoxic drug to eg atumor Bite (bi-specific T cell engager) Fusion proteins consisting of two ScFvs one directed against thetarget on a tumor cell and the other against the T cell receptor (CD3) Diabody ScFv dimers where shortlinker peptides (five amino acids) ensure dimerization and not folding of the ScFvs Fab and F(ab)2fragments Single Fab fragments or fragments containing two Fabs linked via disulfide bridges This isused where effector functions related to the Fc part of the antibody are unwanted and where a smallersize is desired to obtain better tissue penetration in eg tumors Due to the lack of the FcRn binding viathe Fc part Fab and F(ab)2 fragments have much shorter half-lives (hours or days) than full-sizeantibodies (weeks) These can also be used as carriers of cytotoxic payloads or cytotoxic radioactiveisotopes and for the F(ab)2 fragments can be constructed as bi-specifics which can cross-link immunecells and target cells Fc fusion protein Fusion protein containing the Fc domain of an immunoglobulinbound to a peptide The peptide can be a ligand for a specific receptor on a target cell or a blockingpeptide for a soluble ligand The Fc part provides a longer half-life to the construct and the potential tobind to and engage effector functions in the killing of eg tumor cells or infected cells ADCsRIAs andbi-specifics Full-size IgG antibodies carrying either a cytotoxic chemical or radioactive payload whichmay also carry different CDRs enabling cross-linking of effector and target cells for increased killingdoi101128microbiolspecAID-0026-2014f1
CHAPTER 1 bull History and Practice Antibodies in Infectious Diseases 9
contain special hyper-variable segments calledcomplementarity-determining regions (CDRs)which allow the B cells via genetic recom-bination to generate antibodies to all thedifferent antigens specific to amino acid se-quences or three-dimensional structuralmotifs(polysaccharides DNA and RNA) found onpathogens
Based on the structure of their heavy chainconstant regions antibodies or immuno-globulins are separated into five classesmdashIgM IgG IgE IgD and IgA Differences inthe sequences of the constant regions providedistinct characteristics to these different clas-ses These characteristics include the numberof heavy chain constant segments the numberand location of interconnecting disulfidebridges the length of the hinge region andthe number and location of oligosaccharidemoieties For IgG four heavy chain versionsexist creating IgG1 2 3 and 4 isotypes eachwith different characteristics in their serumhalf-lives and ability to trigger different effec-tor functions Because of the combined ad-vantage from ability to trigger effectormechanisms long [21 days] half-life theirability to be transported over the placentaand their stability in the production processantibodies of the IgG class and of the IgG1isotype are preferred as the basis for newantibody-based therapies The effector func-tions are triggered by the Fc part of an antibodywhen the variable parts of the antibody arebound directly to an infectious agent or toproteins from an infectious agent expressed onan infected cell This binding leaves the Fc partfree to interactwithFc receptors onphagocyticcells and neutrophils eosinophils and naturalkiller cells capable of inducing phagocytosis orlysis of infectious agents or infected cellsThese effector functions include (i) the abilityto activate the complement system for lysis(complement-dependent cellular cytotoxicity)(ii) triggering of uptake and destruction byphagocytic cells such as macrophages andneutrophils via interaction with Fc receptorson these cells (iii) activation of macrophageseosinophils neutrophils and natural killer
cells to kill infected cells via binding to Fcreceptors on these cells and antibody-depen-dent cellular cytotoxicity and (iv) neutraliza-tion of bacterial toxins and blocking of bindingand uptake of bacteria or viruses to target cells(see Fig 2) (9)
The Fcpart of IgG antibodies also contains aregion that interacts with the neonatal Fcreceptor (FcRn) expressed on most immuno-competent cells and inmany other cells such asendothelial cells in kidney liver placenta lungand breast (10) which protects antibodies fromdegradation by phagocytoticexocytotic cy-cling into FcRn-expressing cells thereby pro-longing their half-life This results in half-livesof 20 to 21 days for most IgG1 2 and 4antibodies whereas half-lives are 10 6 and 2days respectively for IgM IgA and IgE Thehighly specific binding sites on the variableregions of the upper arms of the antibody allowfor several important features of antibodiesndashbinding to and neutralization of eg bacterialtoxins binding to pathogens and blocking theirbinding to or interaction with target cells (egcyncytia formation of CMV-infected cells) orblocking of binding and interactions of infec-tious agents with target cells via blockingreceptors on the target cells
METHODS AND PLATFORMS FORGENERATING ANTIBODIES
As described above the early use of passiveantibody transfer as a therapy in infectiousdiseases involved the use of immune serumfrom immunized sheep and horses These pre-parations were crude and contained a broadmixture of neutralizing and non-neutralizingantibodies and both the foreign nature of theantibodies and the numerous host serumproteins This resulted in less specific andthus less efficient therapies due to a highvariability in efficacy between batches derivedfrom different animals immunized with dif-ferent strains of bacteria in different labor-atories and resulted in multiple unwantedside effects related to hypersensitivity and
10 HEY
anaphylactic reactions to foreign proteinsThese days antibodies being developed fortreatment of diseases in humans are highlypurified and are mostly fully human mono-clonal antibodies The term monoclonal anti-body refers to that cell cultures used forgenerating these antibodies each originatesfrom a single cell and thus produces onlyone specific antibody Development of fullyhuman monoclonal antibodies happened instages over a time span of more than 15 yearsFirst stage in this process was generation ofmonoclonalmurine IgG antibodies (eg OKT3[muronomab-CD3 Johnson and Johnson] ap-proved in 1986) Next stage was generation ofso called chimeric antibodies consisting ofhuman heavy and light chain constant sec-tions but with murine variable sections (eg
Rituxan [rituximab Genentech]) Next stagewas then the humanized antibodies wherethe only remaining murine part of the anti-body is the antigen-binding CDR (eg Xolair[omalizumab NovartisGenentech]) Both thefirst chimeric and humanized antibodies wereapproved in the late 1990s Then finally 16years later the first fully human antibodyHumira (adalimumab Abbott) was approvedin 2002 Since the time of the crude and low-scale manufacturing of the original antibodyserum products much has changed andtherapeutic antibodies are now produced byfermentation in 5000 liter scale using highlycontrolled and documented yeast or mamma-lian cell lines that are genetically engineered toexpress a single specific antibody This hasresulted in a pure and highly specific antibody
FIGURE 2 Effector functions of antibodies (a) Antibodies bind to pathogen-derived or endogenousantigens expressed on the surface of an infected cell which triggers binding to Fc receptors on naturalkiller cells and lysis of the infected cell by antibody-dependent cellular cytotoxicity (b) Antibodies bindto pathogen-derived or endogenous antigens expressed on the surface of infected cells which triggersactivation of complement through binding of complement factor C1q (c) Neutralization Top Bacterialtoxin neutralized by bound antigen Bottom Antibody bound to either receptor for the virus or to thevirus itself which blocks virus binding and entry into the cell (d) Antibody bound to viral surfaceproteins binds to Fc receptors on phagocytic cells eg macrophages and triggers endocytosis anddestruction of virus in endolysosome doi101128microbiolspecAID-0026-2014f2
CHAPTER 1 bull History and Practice Antibodies in Infectious Diseases 11

their safety and efficacy and those are the onlysporadically available treatment options andonly in small amounts and for a few patients
Ebola is an example of a disease whichnormally affects only a small number ofindividuals and which normally burns outwhen disease outbreaks are contained There-fore given the small number of potentialpatients affected by previous Ebola infectionsto date there was no incentive for big pharmacompanies to do research and development ofdrugs for EbolaWith the increasing number ofinfected (13567) andadeath toll of 4951 (7) andthe lack of the ability to contain the epidemic itwill be interesting to follow the aftermath ofthis outbreak and see whether there will berequests for new ways to ensure that vaccinesand treatment options are available for Ebolaand similar high-mortality and potential bio-warfare infections that have no availabletreatments or procedures to for mass-produc-tion upon the first signsreports of activeinfections Although both the CDC and theWHO have special programs focusing on thesetypes of infections the Ebola outbreak in 2014clearly shows that more financial support forresearch and development of new diagnosticsand treatments is needed This is one examplewhere antibody-based treatments would havethe potential to play a major role To put this inthe right perspective one should however notforget that other infectious diseases such astuberculosis influenza and malaria kill hun-dreds of thousands each year There is there-fore plenty of room for improvement indeveloping treatments for these diseases aswell but the high attention drawn to eg theEbola outbreak creates a special niche andopportunity where antibody treatments couldgain extraordinary development funding andsupport and prove their value and treatmentpotential
That antibody-based therapies could takethis role is supported by the revolution intechnologies for the development selectiongeneration and purification of fully humanantibodies described in more detail later in thesection ldquoMethodsandPlatforms forGenerating
Antibodiesrdquo Antibody-based programs cur-rently at different stages of developmentinclude investigations into the potential use ofsingle antibody preparations combinations ofantibodies (to avoid survival of escape mu-tants) fragments of antibodies and antibodiescarrying radioactive isotopesorcytotoxicdrugsor antibody-like frameworks (eg fibronectin)either alone as a first-line treatment or as anadjunct to existing treatments This multitudeof possible formats the ability to raise anti-bodies to almost any target and the ability toengineer both size effector functions and half-life are now considered by many to providevery valuable tools for designing specificantibody-based treatments toeradicate specifictargeted infectious agents However althoughseveral antibody-based therapies have beenapproved for oncology and anti-inflammatoryindications (see Table 1) only one monoclonalantibody (mAb) is approved against an infec-tious disease agentmdashSynagis (palivizumabMedImmune) for the prevention and treat-ment of respiratory syncytical virus (RSV) inhigh-risk children Economic obstacles such asthe high cost of mAb therapies and relativelysmall markets have resulted in less interestfrom pharmaceutical companies in developingthese Also highlighting the challenges indeveloping these types of antibody-basedtreatments are the difficulties encountered indeveloping a follow-up higher-affinity candi-date to Synagis Poor translatability of dataobtained in the available animal disease mod-els for RSV in cotton rats has resulted in non-approval due to inferiority relative to SynagisIn other viral diseases such as cytomegalovirus(CMV) the high species specificity of thestrains of CMV makes it impossible to testhuman antibody therapies in vivo Thereforeany real data on the efficacy of treatments forCMV will not be obtained until testing inclinical trials As described later in this articleseveral new antibody-based therapies for in-fectious diseases are in development andhopefully this will gradually open the fieldand result in better treatment options andoutcomes for patients
6 HEY
TABLE 1 Approved and pending antibody-based therapies
Name antibody Target antibody type Indication Company Approval date
OKT3a Muronomab-CD3 CD3 murine IgG2a Autoimmune Johnson ampJohnson
1986 (US)
ReoPro abciximab PIIbIIIa chimeric IgG1Fab
Homeostasis Johnson ampJohnson
1984 (US)
Rituxan rituximab CD20 chimeric IgG1 Cancer Genentech 1997 (US) 1998 (EU)Zenapaxa daclizumab CD25 humanized IgG1 Autoimmune Roche 1997 (US) 1999 (EU)Simulect basiliximab CD25 chimeric IgG1 Autoimmune Novartis 1998 (US EU)Synagis palivizumab RSV humanized IgG1 Infections MedImmune 1998 (US) 1999 (EU)Remicade infliximab TNFα chimeric IgG1 Autoimmune Johnson amp
Johnson1998 (US) 1999 (EU)
Herceptin trastuzumab HER2 humanized IgG1 Cancer GenentechRoche
1998 (US) 2000 (EU)
Mylotarga gemtuzumabozogamicin
CD33 humanized IgG4immunotoxin
Cancer WyethPfizer 2000 (US)
Campath alemtuzumab CD52 humanized IgG1 Cancer Genzyme 2001 (US) 2001 (EU)Zevalin ibritumomabtiuxetan
CD20 murine IgG1radiolabeled (yttrium 90)
Cancer Biogen Idec 2002 (US) 2004 (EU)
Humira adalimumab TNFα human IgG1 Autoimmune Abbott 2002 (US) 2003 (EU)Xolair omalizumab IgE humanized IgG1 Autoimmune Genentech
Roche2003 (US)
Bexxar tositumomab-I-131 CD20 murine IgG2aradiolabeled (iodine131)
Cancer CorixaGSK 2003 (US)
Raptivaa falizumab CD11a humanized IgG1 Autoimmune GenentechRoche
2003 (US) 2004 (EU)
Erbitux cetuximab EGFR chimeric IgG1 Cancer ImcloneLilly 2004 (US) 2004 (EU)Avastin bevacizumab VEGF humanized IgG1 Cancer Genentech
Roche2004 (US) 2005 (EU)
Tysabri natalizumab α4-Intergrin humanizedIgG4
Autoimmune Biogen Idec 2004 (US)
Actemra tocilizumab Anti-IL-6R humanizedIgG1
Autoimmune ChugaiRoche
2005 (Japan) 2010 (US)
Vectibix panitumumab EGFR human IgG2 Cancer Amgen 2006 (US)Lucentis ranibizumab VEGF humanized IgG1
FabMaculardegeneration
GenentechRoche
2006 (US)
Soliris eculizumab C5 humanized IgG24 Blood disorders Alexion 2007 (US)Cimzia certolizumab pegol TNFα humanized
pegylated FabAutoimmune UCB 2008 (US)
Simponi golimumab TNFα human IgG1 Autoimmune Johnson ampJohnson
2009 (US EU Canada)
Ilaris canakinumab IL1b human IgG1 Infalmmatory Novartis 2009 (US EU)Stelara ustekinumab IL-1223 human IgG1 Autoimmune Johnson amp
Johnson2008 (EU) 2009 (US)
Arzerra ofatumumab CD20 human IgG1 Cancer Genmab 2009 (EU)Prolia denosumab RANK ligand human
IgG2Bone loss Amgen 2010 (US)
Numax motavizumab RSV humanized IgG1 Anti-infective MedImmune PendingABthrax Raxibacumab B anthrasis PA human
IgG1Anti-infection GSK 2012 (US)
Benlysta belimumab BLyS human IgG1 Autoimmune HGS 2011 (US)Yervoy ipilimumab CTLA-4 human IgG1 Cancer BMS 2011 (US)Adcetris brentuximabvedotin
CD30 chimeric IgG1drug- conjugate
Cancer SeattleGenetics
2011 (US)
(Continued on next page)
CHAPTER 1 bull History and Practice Antibodies in Infectious Diseases 7
INTRODUCTION TO ANTIBODIES
Antibodies also called immunoglobulins basedon their combined structure and function inimmune responses are produced by B cells ofthe immune system They are part of theadaptive immune response and are speciallydesigned for neutralizing and eliminating theinfectious agents and toxins produced by theseAntibodies are present in blood plasma andextracellular fluids and since these fluids wereformerly known as humors they were said tobe part of the humoral immune responseAntibodies are Y-shaped structures consistingof two main parts the upper arms of the Ywhich contain two identical variable-regionantigen binding sites and the lower regioncalled the constant regionwhich is responsiblefor the initiation of effector functions that leadto the removal and destruction of the pathogenor cells harboring the pathogen (see Fig 1) Theantigen-binding sites on an antibody can bythemselves bind to and neutralize bacterialtoxins and viruses thereby preventing themfrom binding to their target cells or receptorscausing toxic effects or spread of the infection
Antibodies consist of two pairs of heavy andlight chainswhich as described above are heldtogether in a Y-shaped arrangement Each ofthe heavy and light chains in these pairs isseparated into constant and variable chainsThe upper armsof theY each contain a variableand a constant sectionof the light and theheavychain where the upper variable parts of theheavy and light chains contain the antigen-binding site and the constant parts areconnected via disulfide bonds The lower partof theYcalled theconstantpart consistsof twoor three constant segments (immunoglobulindomains) from each of the two heavy chainsinteracting and also linked via disulfide bondsThe sectionsof theheavy chains connecting theconstant part of the upper arms to the constantparts of the constant region contain specialhinge regions that provide flexibility to thedifferent sections of the antibody to bind toantigens and effector cells The constant re-gions of the heavy chain also contain attachedoligosaccharide moieties which provide func-tional specialization to the antibodies (8)
The variable domains of the heavy and lightchains form the antigen-binding sites and
TABLE 1 Approved and pending antibody-based therapies (Continued)
Name antibody Target antibody type Indication Company Approval date
Perjeta pertuzumab Her2 humanized IgG1 Cancer GenentechRoche
2012 (US)
Kadcyla ado-trastuzumabemtansine
Her2 humanized IgG1Drug-conjugate
Cancer GenentechRoche
2013 (US)
Raxibacumab Anti-B anthrasis PAhuman IgG1
Anthraxinfection
Notapproved
2012
Entyvio vedolizumab Integrin α4β7humanized IgG1
Crohnrsquos diseaseulcerative colitis
Takeda 2014 (US)
Cyramza ramuciruumab Anti-VEGFR2Human IgG1
Gastric cancer Lilly 2014 (US)
Gazyva obinutuzumab Anti-CD20 humanizedIgG1 glucoengineered
CancerCLLb GenentechRoche
2014 (US)
Sylvant situximab Anti IL-6 chimeric IgG1 Castlemandisease
Janssen 2014 (US) 2014 (EU)
Cosentyx sekukinumab Anti IL-17a human IgG1 Psoriasis Novartis 2015 (US) 2015 (EU)Nivolumab Anti PD-1 human IgG4 Melanoma BMS Not approvedKeytruda pembrolizuumab Anti-PD-1 humanized
IgG4Melanoma Merck 2014 (US)
aAntibodies approved but later withdrawnbCLL chronic lymphocytic leukemia
8 HEY
FIGURE 1 (Left panel) Model of antibody structure exemplified by IgG On top the antigen-binding sitesin orange each contain one variable light and variable heavy domain with the three complementaritydetermining regions (CDRs) that are responsible for the specific binding of the antibody to its target Foreach arm of the antibody an additional set of variable heavy and light domains together with the CDR-containing domains represent the two fragment antigen binding (Fab) regions The two Fabs are heldtogether via two disulfide bridges Below the Fabs is the Fc region which contains four constant heavydomains On the upper pair of these domains are binding sites for oligosaccharides which have majorimportance for the ability of the antibody Fc part to trigger effector functions when the Fc portion isbound to Fc gamma receptors on natural killer cells neutrophil granulocytes monocytesmacrophagesdendritic cells and B cells (Right panel) Examples of some of the antibody-derived alternative formatsused to exploit the specific features of the CDRs the Fabs and the Fc parts of the antibodies ScFv Thesingle chain fragment variable consists of the variable domains of the heavy and light chains heldtogether by a flexible linker This can also be used as a carrier of a cytotoxic drug in a so-called antibodydrug complex (ADC) where the specificity of the ScFv is used to target the cytotoxic drug to eg atumor Bite (bi-specific T cell engager) Fusion proteins consisting of two ScFvs one directed against thetarget on a tumor cell and the other against the T cell receptor (CD3) Diabody ScFv dimers where shortlinker peptides (five amino acids) ensure dimerization and not folding of the ScFvs Fab and F(ab)2fragments Single Fab fragments or fragments containing two Fabs linked via disulfide bridges This isused where effector functions related to the Fc part of the antibody are unwanted and where a smallersize is desired to obtain better tissue penetration in eg tumors Due to the lack of the FcRn binding viathe Fc part Fab and F(ab)2 fragments have much shorter half-lives (hours or days) than full-sizeantibodies (weeks) These can also be used as carriers of cytotoxic payloads or cytotoxic radioactiveisotopes and for the F(ab)2 fragments can be constructed as bi-specifics which can cross-link immunecells and target cells Fc fusion protein Fusion protein containing the Fc domain of an immunoglobulinbound to a peptide The peptide can be a ligand for a specific receptor on a target cell or a blockingpeptide for a soluble ligand The Fc part provides a longer half-life to the construct and the potential tobind to and engage effector functions in the killing of eg tumor cells or infected cells ADCsRIAs andbi-specifics Full-size IgG antibodies carrying either a cytotoxic chemical or radioactive payload whichmay also carry different CDRs enabling cross-linking of effector and target cells for increased killingdoi101128microbiolspecAID-0026-2014f1
CHAPTER 1 bull History and Practice Antibodies in Infectious Diseases 9
contain special hyper-variable segments calledcomplementarity-determining regions (CDRs)which allow the B cells via genetic recom-bination to generate antibodies to all thedifferent antigens specific to amino acid se-quences or three-dimensional structuralmotifs(polysaccharides DNA and RNA) found onpathogens
Based on the structure of their heavy chainconstant regions antibodies or immuno-globulins are separated into five classesmdashIgM IgG IgE IgD and IgA Differences inthe sequences of the constant regions providedistinct characteristics to these different clas-ses These characteristics include the numberof heavy chain constant segments the numberand location of interconnecting disulfidebridges the length of the hinge region andthe number and location of oligosaccharidemoieties For IgG four heavy chain versionsexist creating IgG1 2 3 and 4 isotypes eachwith different characteristics in their serumhalf-lives and ability to trigger different effec-tor functions Because of the combined ad-vantage from ability to trigger effectormechanisms long [21 days] half-life theirability to be transported over the placentaand their stability in the production processantibodies of the IgG class and of the IgG1isotype are preferred as the basis for newantibody-based therapies The effector func-tions are triggered by the Fc part of an antibodywhen the variable parts of the antibody arebound directly to an infectious agent or toproteins from an infectious agent expressed onan infected cell This binding leaves the Fc partfree to interactwithFc receptors onphagocyticcells and neutrophils eosinophils and naturalkiller cells capable of inducing phagocytosis orlysis of infectious agents or infected cellsThese effector functions include (i) the abilityto activate the complement system for lysis(complement-dependent cellular cytotoxicity)(ii) triggering of uptake and destruction byphagocytic cells such as macrophages andneutrophils via interaction with Fc receptorson these cells (iii) activation of macrophageseosinophils neutrophils and natural killer
cells to kill infected cells via binding to Fcreceptors on these cells and antibody-depen-dent cellular cytotoxicity and (iv) neutraliza-tion of bacterial toxins and blocking of bindingand uptake of bacteria or viruses to target cells(see Fig 2) (9)
The Fcpart of IgG antibodies also contains aregion that interacts with the neonatal Fcreceptor (FcRn) expressed on most immuno-competent cells and inmany other cells such asendothelial cells in kidney liver placenta lungand breast (10) which protects antibodies fromdegradation by phagocytoticexocytotic cy-cling into FcRn-expressing cells thereby pro-longing their half-life This results in half-livesof 20 to 21 days for most IgG1 2 and 4antibodies whereas half-lives are 10 6 and 2days respectively for IgM IgA and IgE Thehighly specific binding sites on the variableregions of the upper arms of the antibody allowfor several important features of antibodiesndashbinding to and neutralization of eg bacterialtoxins binding to pathogens and blocking theirbinding to or interaction with target cells (egcyncytia formation of CMV-infected cells) orblocking of binding and interactions of infec-tious agents with target cells via blockingreceptors on the target cells
METHODS AND PLATFORMS FORGENERATING ANTIBODIES
As described above the early use of passiveantibody transfer as a therapy in infectiousdiseases involved the use of immune serumfrom immunized sheep and horses These pre-parations were crude and contained a broadmixture of neutralizing and non-neutralizingantibodies and both the foreign nature of theantibodies and the numerous host serumproteins This resulted in less specific andthus less efficient therapies due to a highvariability in efficacy between batches derivedfrom different animals immunized with dif-ferent strains of bacteria in different labor-atories and resulted in multiple unwantedside effects related to hypersensitivity and
10 HEY
anaphylactic reactions to foreign proteinsThese days antibodies being developed fortreatment of diseases in humans are highlypurified and are mostly fully human mono-clonal antibodies The term monoclonal anti-body refers to that cell cultures used forgenerating these antibodies each originatesfrom a single cell and thus produces onlyone specific antibody Development of fullyhuman monoclonal antibodies happened instages over a time span of more than 15 yearsFirst stage in this process was generation ofmonoclonalmurine IgG antibodies (eg OKT3[muronomab-CD3 Johnson and Johnson] ap-proved in 1986) Next stage was generation ofso called chimeric antibodies consisting ofhuman heavy and light chain constant sec-tions but with murine variable sections (eg
Rituxan [rituximab Genentech]) Next stagewas then the humanized antibodies wherethe only remaining murine part of the anti-body is the antigen-binding CDR (eg Xolair[omalizumab NovartisGenentech]) Both thefirst chimeric and humanized antibodies wereapproved in the late 1990s Then finally 16years later the first fully human antibodyHumira (adalimumab Abbott) was approvedin 2002 Since the time of the crude and low-scale manufacturing of the original antibodyserum products much has changed andtherapeutic antibodies are now produced byfermentation in 5000 liter scale using highlycontrolled and documented yeast or mamma-lian cell lines that are genetically engineered toexpress a single specific antibody This hasresulted in a pure and highly specific antibody
FIGURE 2 Effector functions of antibodies (a) Antibodies bind to pathogen-derived or endogenousantigens expressed on the surface of an infected cell which triggers binding to Fc receptors on naturalkiller cells and lysis of the infected cell by antibody-dependent cellular cytotoxicity (b) Antibodies bindto pathogen-derived or endogenous antigens expressed on the surface of infected cells which triggersactivation of complement through binding of complement factor C1q (c) Neutralization Top Bacterialtoxin neutralized by bound antigen Bottom Antibody bound to either receptor for the virus or to thevirus itself which blocks virus binding and entry into the cell (d) Antibody bound to viral surfaceproteins binds to Fc receptors on phagocytic cells eg macrophages and triggers endocytosis anddestruction of virus in endolysosome doi101128microbiolspecAID-0026-2014f2
CHAPTER 1 bull History and Practice Antibodies in Infectious Diseases 11

TABLE 1 Approved and pending antibody-based therapies
Name antibody Target antibody type Indication Company Approval date
OKT3a Muronomab-CD3 CD3 murine IgG2a Autoimmune Johnson ampJohnson
1986 (US)
ReoPro abciximab PIIbIIIa chimeric IgG1Fab
Homeostasis Johnson ampJohnson
1984 (US)
Rituxan rituximab CD20 chimeric IgG1 Cancer Genentech 1997 (US) 1998 (EU)Zenapaxa daclizumab CD25 humanized IgG1 Autoimmune Roche 1997 (US) 1999 (EU)Simulect basiliximab CD25 chimeric IgG1 Autoimmune Novartis 1998 (US EU)Synagis palivizumab RSV humanized IgG1 Infections MedImmune 1998 (US) 1999 (EU)Remicade infliximab TNFα chimeric IgG1 Autoimmune Johnson amp
Johnson1998 (US) 1999 (EU)
Herceptin trastuzumab HER2 humanized IgG1 Cancer GenentechRoche
1998 (US) 2000 (EU)
Mylotarga gemtuzumabozogamicin
CD33 humanized IgG4immunotoxin
Cancer WyethPfizer 2000 (US)
Campath alemtuzumab CD52 humanized IgG1 Cancer Genzyme 2001 (US) 2001 (EU)Zevalin ibritumomabtiuxetan
CD20 murine IgG1radiolabeled (yttrium 90)
Cancer Biogen Idec 2002 (US) 2004 (EU)
Humira adalimumab TNFα human IgG1 Autoimmune Abbott 2002 (US) 2003 (EU)Xolair omalizumab IgE humanized IgG1 Autoimmune Genentech
Roche2003 (US)
Bexxar tositumomab-I-131 CD20 murine IgG2aradiolabeled (iodine131)
Cancer CorixaGSK 2003 (US)
Raptivaa falizumab CD11a humanized IgG1 Autoimmune GenentechRoche
2003 (US) 2004 (EU)
Erbitux cetuximab EGFR chimeric IgG1 Cancer ImcloneLilly 2004 (US) 2004 (EU)Avastin bevacizumab VEGF humanized IgG1 Cancer Genentech
Roche2004 (US) 2005 (EU)
Tysabri natalizumab α4-Intergrin humanizedIgG4
Autoimmune Biogen Idec 2004 (US)
Actemra tocilizumab Anti-IL-6R humanizedIgG1
Autoimmune ChugaiRoche
2005 (Japan) 2010 (US)
Vectibix panitumumab EGFR human IgG2 Cancer Amgen 2006 (US)Lucentis ranibizumab VEGF humanized IgG1
FabMaculardegeneration
GenentechRoche
2006 (US)
Soliris eculizumab C5 humanized IgG24 Blood disorders Alexion 2007 (US)Cimzia certolizumab pegol TNFα humanized
pegylated FabAutoimmune UCB 2008 (US)
Simponi golimumab TNFα human IgG1 Autoimmune Johnson ampJohnson
2009 (US EU Canada)
Ilaris canakinumab IL1b human IgG1 Infalmmatory Novartis 2009 (US EU)Stelara ustekinumab IL-1223 human IgG1 Autoimmune Johnson amp
Johnson2008 (EU) 2009 (US)
Arzerra ofatumumab CD20 human IgG1 Cancer Genmab 2009 (EU)Prolia denosumab RANK ligand human
IgG2Bone loss Amgen 2010 (US)
Numax motavizumab RSV humanized IgG1 Anti-infective MedImmune PendingABthrax Raxibacumab B anthrasis PA human
IgG1Anti-infection GSK 2012 (US)
Benlysta belimumab BLyS human IgG1 Autoimmune HGS 2011 (US)Yervoy ipilimumab CTLA-4 human IgG1 Cancer BMS 2011 (US)Adcetris brentuximabvedotin
CD30 chimeric IgG1drug- conjugate
Cancer SeattleGenetics
2011 (US)
(Continued on next page)
CHAPTER 1 bull History and Practice Antibodies in Infectious Diseases 7
INTRODUCTION TO ANTIBODIES
Antibodies also called immunoglobulins basedon their combined structure and function inimmune responses are produced by B cells ofthe immune system They are part of theadaptive immune response and are speciallydesigned for neutralizing and eliminating theinfectious agents and toxins produced by theseAntibodies are present in blood plasma andextracellular fluids and since these fluids wereformerly known as humors they were said tobe part of the humoral immune responseAntibodies are Y-shaped structures consistingof two main parts the upper arms of the Ywhich contain two identical variable-regionantigen binding sites and the lower regioncalled the constant regionwhich is responsiblefor the initiation of effector functions that leadto the removal and destruction of the pathogenor cells harboring the pathogen (see Fig 1) Theantigen-binding sites on an antibody can bythemselves bind to and neutralize bacterialtoxins and viruses thereby preventing themfrom binding to their target cells or receptorscausing toxic effects or spread of the infection
Antibodies consist of two pairs of heavy andlight chainswhich as described above are heldtogether in a Y-shaped arrangement Each ofthe heavy and light chains in these pairs isseparated into constant and variable chainsThe upper armsof theY each contain a variableand a constant sectionof the light and theheavychain where the upper variable parts of theheavy and light chains contain the antigen-binding site and the constant parts areconnected via disulfide bonds The lower partof theYcalled theconstantpart consistsof twoor three constant segments (immunoglobulindomains) from each of the two heavy chainsinteracting and also linked via disulfide bondsThe sectionsof theheavy chains connecting theconstant part of the upper arms to the constantparts of the constant region contain specialhinge regions that provide flexibility to thedifferent sections of the antibody to bind toantigens and effector cells The constant re-gions of the heavy chain also contain attachedoligosaccharide moieties which provide func-tional specialization to the antibodies (8)
The variable domains of the heavy and lightchains form the antigen-binding sites and
TABLE 1 Approved and pending antibody-based therapies (Continued)
Name antibody Target antibody type Indication Company Approval date
Perjeta pertuzumab Her2 humanized IgG1 Cancer GenentechRoche
2012 (US)
Kadcyla ado-trastuzumabemtansine
Her2 humanized IgG1Drug-conjugate
Cancer GenentechRoche
2013 (US)
Raxibacumab Anti-B anthrasis PAhuman IgG1
Anthraxinfection
Notapproved
2012
Entyvio vedolizumab Integrin α4β7humanized IgG1
Crohnrsquos diseaseulcerative colitis
Takeda 2014 (US)
Cyramza ramuciruumab Anti-VEGFR2Human IgG1
Gastric cancer Lilly 2014 (US)
Gazyva obinutuzumab Anti-CD20 humanizedIgG1 glucoengineered
CancerCLLb GenentechRoche
2014 (US)
Sylvant situximab Anti IL-6 chimeric IgG1 Castlemandisease
Janssen 2014 (US) 2014 (EU)
Cosentyx sekukinumab Anti IL-17a human IgG1 Psoriasis Novartis 2015 (US) 2015 (EU)Nivolumab Anti PD-1 human IgG4 Melanoma BMS Not approvedKeytruda pembrolizuumab Anti-PD-1 humanized
IgG4Melanoma Merck 2014 (US)
aAntibodies approved but later withdrawnbCLL chronic lymphocytic leukemia
8 HEY
FIGURE 1 (Left panel) Model of antibody structure exemplified by IgG On top the antigen-binding sitesin orange each contain one variable light and variable heavy domain with the three complementaritydetermining regions (CDRs) that are responsible for the specific binding of the antibody to its target Foreach arm of the antibody an additional set of variable heavy and light domains together with the CDR-containing domains represent the two fragment antigen binding (Fab) regions The two Fabs are heldtogether via two disulfide bridges Below the Fabs is the Fc region which contains four constant heavydomains On the upper pair of these domains are binding sites for oligosaccharides which have majorimportance for the ability of the antibody Fc part to trigger effector functions when the Fc portion isbound to Fc gamma receptors on natural killer cells neutrophil granulocytes monocytesmacrophagesdendritic cells and B cells (Right panel) Examples of some of the antibody-derived alternative formatsused to exploit the specific features of the CDRs the Fabs and the Fc parts of the antibodies ScFv Thesingle chain fragment variable consists of the variable domains of the heavy and light chains heldtogether by a flexible linker This can also be used as a carrier of a cytotoxic drug in a so-called antibodydrug complex (ADC) where the specificity of the ScFv is used to target the cytotoxic drug to eg atumor Bite (bi-specific T cell engager) Fusion proteins consisting of two ScFvs one directed against thetarget on a tumor cell and the other against the T cell receptor (CD3) Diabody ScFv dimers where shortlinker peptides (five amino acids) ensure dimerization and not folding of the ScFvs Fab and F(ab)2fragments Single Fab fragments or fragments containing two Fabs linked via disulfide bridges This isused where effector functions related to the Fc part of the antibody are unwanted and where a smallersize is desired to obtain better tissue penetration in eg tumors Due to the lack of the FcRn binding viathe Fc part Fab and F(ab)2 fragments have much shorter half-lives (hours or days) than full-sizeantibodies (weeks) These can also be used as carriers of cytotoxic payloads or cytotoxic radioactiveisotopes and for the F(ab)2 fragments can be constructed as bi-specifics which can cross-link immunecells and target cells Fc fusion protein Fusion protein containing the Fc domain of an immunoglobulinbound to a peptide The peptide can be a ligand for a specific receptor on a target cell or a blockingpeptide for a soluble ligand The Fc part provides a longer half-life to the construct and the potential tobind to and engage effector functions in the killing of eg tumor cells or infected cells ADCsRIAs andbi-specifics Full-size IgG antibodies carrying either a cytotoxic chemical or radioactive payload whichmay also carry different CDRs enabling cross-linking of effector and target cells for increased killingdoi101128microbiolspecAID-0026-2014f1
CHAPTER 1 bull History and Practice Antibodies in Infectious Diseases 9
contain special hyper-variable segments calledcomplementarity-determining regions (CDRs)which allow the B cells via genetic recom-bination to generate antibodies to all thedifferent antigens specific to amino acid se-quences or three-dimensional structuralmotifs(polysaccharides DNA and RNA) found onpathogens
Based on the structure of their heavy chainconstant regions antibodies or immuno-globulins are separated into five classesmdashIgM IgG IgE IgD and IgA Differences inthe sequences of the constant regions providedistinct characteristics to these different clas-ses These characteristics include the numberof heavy chain constant segments the numberand location of interconnecting disulfidebridges the length of the hinge region andthe number and location of oligosaccharidemoieties For IgG four heavy chain versionsexist creating IgG1 2 3 and 4 isotypes eachwith different characteristics in their serumhalf-lives and ability to trigger different effec-tor functions Because of the combined ad-vantage from ability to trigger effectormechanisms long [21 days] half-life theirability to be transported over the placentaand their stability in the production processantibodies of the IgG class and of the IgG1isotype are preferred as the basis for newantibody-based therapies The effector func-tions are triggered by the Fc part of an antibodywhen the variable parts of the antibody arebound directly to an infectious agent or toproteins from an infectious agent expressed onan infected cell This binding leaves the Fc partfree to interactwithFc receptors onphagocyticcells and neutrophils eosinophils and naturalkiller cells capable of inducing phagocytosis orlysis of infectious agents or infected cellsThese effector functions include (i) the abilityto activate the complement system for lysis(complement-dependent cellular cytotoxicity)(ii) triggering of uptake and destruction byphagocytic cells such as macrophages andneutrophils via interaction with Fc receptorson these cells (iii) activation of macrophageseosinophils neutrophils and natural killer
cells to kill infected cells via binding to Fcreceptors on these cells and antibody-depen-dent cellular cytotoxicity and (iv) neutraliza-tion of bacterial toxins and blocking of bindingand uptake of bacteria or viruses to target cells(see Fig 2) (9)
The Fcpart of IgG antibodies also contains aregion that interacts with the neonatal Fcreceptor (FcRn) expressed on most immuno-competent cells and inmany other cells such asendothelial cells in kidney liver placenta lungand breast (10) which protects antibodies fromdegradation by phagocytoticexocytotic cy-cling into FcRn-expressing cells thereby pro-longing their half-life This results in half-livesof 20 to 21 days for most IgG1 2 and 4antibodies whereas half-lives are 10 6 and 2days respectively for IgM IgA and IgE Thehighly specific binding sites on the variableregions of the upper arms of the antibody allowfor several important features of antibodiesndashbinding to and neutralization of eg bacterialtoxins binding to pathogens and blocking theirbinding to or interaction with target cells (egcyncytia formation of CMV-infected cells) orblocking of binding and interactions of infec-tious agents with target cells via blockingreceptors on the target cells
METHODS AND PLATFORMS FORGENERATING ANTIBODIES
As described above the early use of passiveantibody transfer as a therapy in infectiousdiseases involved the use of immune serumfrom immunized sheep and horses These pre-parations were crude and contained a broadmixture of neutralizing and non-neutralizingantibodies and both the foreign nature of theantibodies and the numerous host serumproteins This resulted in less specific andthus less efficient therapies due to a highvariability in efficacy between batches derivedfrom different animals immunized with dif-ferent strains of bacteria in different labor-atories and resulted in multiple unwantedside effects related to hypersensitivity and
10 HEY
anaphylactic reactions to foreign proteinsThese days antibodies being developed fortreatment of diseases in humans are highlypurified and are mostly fully human mono-clonal antibodies The term monoclonal anti-body refers to that cell cultures used forgenerating these antibodies each originatesfrom a single cell and thus produces onlyone specific antibody Development of fullyhuman monoclonal antibodies happened instages over a time span of more than 15 yearsFirst stage in this process was generation ofmonoclonalmurine IgG antibodies (eg OKT3[muronomab-CD3 Johnson and Johnson] ap-proved in 1986) Next stage was generation ofso called chimeric antibodies consisting ofhuman heavy and light chain constant sec-tions but with murine variable sections (eg
Rituxan [rituximab Genentech]) Next stagewas then the humanized antibodies wherethe only remaining murine part of the anti-body is the antigen-binding CDR (eg Xolair[omalizumab NovartisGenentech]) Both thefirst chimeric and humanized antibodies wereapproved in the late 1990s Then finally 16years later the first fully human antibodyHumira (adalimumab Abbott) was approvedin 2002 Since the time of the crude and low-scale manufacturing of the original antibodyserum products much has changed andtherapeutic antibodies are now produced byfermentation in 5000 liter scale using highlycontrolled and documented yeast or mamma-lian cell lines that are genetically engineered toexpress a single specific antibody This hasresulted in a pure and highly specific antibody
FIGURE 2 Effector functions of antibodies (a) Antibodies bind to pathogen-derived or endogenousantigens expressed on the surface of an infected cell which triggers binding to Fc receptors on naturalkiller cells and lysis of the infected cell by antibody-dependent cellular cytotoxicity (b) Antibodies bindto pathogen-derived or endogenous antigens expressed on the surface of infected cells which triggersactivation of complement through binding of complement factor C1q (c) Neutralization Top Bacterialtoxin neutralized by bound antigen Bottom Antibody bound to either receptor for the virus or to thevirus itself which blocks virus binding and entry into the cell (d) Antibody bound to viral surfaceproteins binds to Fc receptors on phagocytic cells eg macrophages and triggers endocytosis anddestruction of virus in endolysosome doi101128microbiolspecAID-0026-2014f2
CHAPTER 1 bull History and Practice Antibodies in Infectious Diseases 11

INTRODUCTION TO ANTIBODIES
Antibodies also called immunoglobulins basedon their combined structure and function inimmune responses are produced by B cells ofthe immune system They are part of theadaptive immune response and are speciallydesigned for neutralizing and eliminating theinfectious agents and toxins produced by theseAntibodies are present in blood plasma andextracellular fluids and since these fluids wereformerly known as humors they were said tobe part of the humoral immune responseAntibodies are Y-shaped structures consistingof two main parts the upper arms of the Ywhich contain two identical variable-regionantigen binding sites and the lower regioncalled the constant regionwhich is responsiblefor the initiation of effector functions that leadto the removal and destruction of the pathogenor cells harboring the pathogen (see Fig 1) Theantigen-binding sites on an antibody can bythemselves bind to and neutralize bacterialtoxins and viruses thereby preventing themfrom binding to their target cells or receptorscausing toxic effects or spread of the infection
Antibodies consist of two pairs of heavy andlight chainswhich as described above are heldtogether in a Y-shaped arrangement Each ofthe heavy and light chains in these pairs isseparated into constant and variable chainsThe upper armsof theY each contain a variableand a constant sectionof the light and theheavychain where the upper variable parts of theheavy and light chains contain the antigen-binding site and the constant parts areconnected via disulfide bonds The lower partof theYcalled theconstantpart consistsof twoor three constant segments (immunoglobulindomains) from each of the two heavy chainsinteracting and also linked via disulfide bondsThe sectionsof theheavy chains connecting theconstant part of the upper arms to the constantparts of the constant region contain specialhinge regions that provide flexibility to thedifferent sections of the antibody to bind toantigens and effector cells The constant re-gions of the heavy chain also contain attachedoligosaccharide moieties which provide func-tional specialization to the antibodies (8)
The variable domains of the heavy and lightchains form the antigen-binding sites and
TABLE 1 Approved and pending antibody-based therapies (Continued)
Name antibody Target antibody type Indication Company Approval date
Perjeta pertuzumab Her2 humanized IgG1 Cancer GenentechRoche
2012 (US)
Kadcyla ado-trastuzumabemtansine
Her2 humanized IgG1Drug-conjugate
Cancer GenentechRoche
2013 (US)
Raxibacumab Anti-B anthrasis PAhuman IgG1
Anthraxinfection
Notapproved
2012
Entyvio vedolizumab Integrin α4β7humanized IgG1
Crohnrsquos diseaseulcerative colitis
Takeda 2014 (US)
Cyramza ramuciruumab Anti-VEGFR2Human IgG1
Gastric cancer Lilly 2014 (US)
Gazyva obinutuzumab Anti-CD20 humanizedIgG1 glucoengineered
CancerCLLb GenentechRoche
2014 (US)
Sylvant situximab Anti IL-6 chimeric IgG1 Castlemandisease
Janssen 2014 (US) 2014 (EU)
Cosentyx sekukinumab Anti IL-17a human IgG1 Psoriasis Novartis 2015 (US) 2015 (EU)Nivolumab Anti PD-1 human IgG4 Melanoma BMS Not approvedKeytruda pembrolizuumab Anti-PD-1 humanized
IgG4Melanoma Merck 2014 (US)
aAntibodies approved but later withdrawnbCLL chronic lymphocytic leukemia
8 HEY
FIGURE 1 (Left panel) Model of antibody structure exemplified by IgG On top the antigen-binding sitesin orange each contain one variable light and variable heavy domain with the three complementaritydetermining regions (CDRs) that are responsible for the specific binding of the antibody to its target Foreach arm of the antibody an additional set of variable heavy and light domains together with the CDR-containing domains represent the two fragment antigen binding (Fab) regions The two Fabs are heldtogether via two disulfide bridges Below the Fabs is the Fc region which contains four constant heavydomains On the upper pair of these domains are binding sites for oligosaccharides which have majorimportance for the ability of the antibody Fc part to trigger effector functions when the Fc portion isbound to Fc gamma receptors on natural killer cells neutrophil granulocytes monocytesmacrophagesdendritic cells and B cells (Right panel) Examples of some of the antibody-derived alternative formatsused to exploit the specific features of the CDRs the Fabs and the Fc parts of the antibodies ScFv Thesingle chain fragment variable consists of the variable domains of the heavy and light chains heldtogether by a flexible linker This can also be used as a carrier of a cytotoxic drug in a so-called antibodydrug complex (ADC) where the specificity of the ScFv is used to target the cytotoxic drug to eg atumor Bite (bi-specific T cell engager) Fusion proteins consisting of two ScFvs one directed against thetarget on a tumor cell and the other against the T cell receptor (CD3) Diabody ScFv dimers where shortlinker peptides (five amino acids) ensure dimerization and not folding of the ScFvs Fab and F(ab)2fragments Single Fab fragments or fragments containing two Fabs linked via disulfide bridges This isused where effector functions related to the Fc part of the antibody are unwanted and where a smallersize is desired to obtain better tissue penetration in eg tumors Due to the lack of the FcRn binding viathe Fc part Fab and F(ab)2 fragments have much shorter half-lives (hours or days) than full-sizeantibodies (weeks) These can also be used as carriers of cytotoxic payloads or cytotoxic radioactiveisotopes and for the F(ab)2 fragments can be constructed as bi-specifics which can cross-link immunecells and target cells Fc fusion protein Fusion protein containing the Fc domain of an immunoglobulinbound to a peptide The peptide can be a ligand for a specific receptor on a target cell or a blockingpeptide for a soluble ligand The Fc part provides a longer half-life to the construct and the potential tobind to and engage effector functions in the killing of eg tumor cells or infected cells ADCsRIAs andbi-specifics Full-size IgG antibodies carrying either a cytotoxic chemical or radioactive payload whichmay also carry different CDRs enabling cross-linking of effector and target cells for increased killingdoi101128microbiolspecAID-0026-2014f1
CHAPTER 1 bull History and Practice Antibodies in Infectious Diseases 9
contain special hyper-variable segments calledcomplementarity-determining regions (CDRs)which allow the B cells via genetic recom-bination to generate antibodies to all thedifferent antigens specific to amino acid se-quences or three-dimensional structuralmotifs(polysaccharides DNA and RNA) found onpathogens
Based on the structure of their heavy chainconstant regions antibodies or immuno-globulins are separated into five classesmdashIgM IgG IgE IgD and IgA Differences inthe sequences of the constant regions providedistinct characteristics to these different clas-ses These characteristics include the numberof heavy chain constant segments the numberand location of interconnecting disulfidebridges the length of the hinge region andthe number and location of oligosaccharidemoieties For IgG four heavy chain versionsexist creating IgG1 2 3 and 4 isotypes eachwith different characteristics in their serumhalf-lives and ability to trigger different effec-tor functions Because of the combined ad-vantage from ability to trigger effectormechanisms long [21 days] half-life theirability to be transported over the placentaand their stability in the production processantibodies of the IgG class and of the IgG1isotype are preferred as the basis for newantibody-based therapies The effector func-tions are triggered by the Fc part of an antibodywhen the variable parts of the antibody arebound directly to an infectious agent or toproteins from an infectious agent expressed onan infected cell This binding leaves the Fc partfree to interactwithFc receptors onphagocyticcells and neutrophils eosinophils and naturalkiller cells capable of inducing phagocytosis orlysis of infectious agents or infected cellsThese effector functions include (i) the abilityto activate the complement system for lysis(complement-dependent cellular cytotoxicity)(ii) triggering of uptake and destruction byphagocytic cells such as macrophages andneutrophils via interaction with Fc receptorson these cells (iii) activation of macrophageseosinophils neutrophils and natural killer
cells to kill infected cells via binding to Fcreceptors on these cells and antibody-depen-dent cellular cytotoxicity and (iv) neutraliza-tion of bacterial toxins and blocking of bindingand uptake of bacteria or viruses to target cells(see Fig 2) (9)
The Fcpart of IgG antibodies also contains aregion that interacts with the neonatal Fcreceptor (FcRn) expressed on most immuno-competent cells and inmany other cells such asendothelial cells in kidney liver placenta lungand breast (10) which protects antibodies fromdegradation by phagocytoticexocytotic cy-cling into FcRn-expressing cells thereby pro-longing their half-life This results in half-livesof 20 to 21 days for most IgG1 2 and 4antibodies whereas half-lives are 10 6 and 2days respectively for IgM IgA and IgE Thehighly specific binding sites on the variableregions of the upper arms of the antibody allowfor several important features of antibodiesndashbinding to and neutralization of eg bacterialtoxins binding to pathogens and blocking theirbinding to or interaction with target cells (egcyncytia formation of CMV-infected cells) orblocking of binding and interactions of infec-tious agents with target cells via blockingreceptors on the target cells
METHODS AND PLATFORMS FORGENERATING ANTIBODIES
As described above the early use of passiveantibody transfer as a therapy in infectiousdiseases involved the use of immune serumfrom immunized sheep and horses These pre-parations were crude and contained a broadmixture of neutralizing and non-neutralizingantibodies and both the foreign nature of theantibodies and the numerous host serumproteins This resulted in less specific andthus less efficient therapies due to a highvariability in efficacy between batches derivedfrom different animals immunized with dif-ferent strains of bacteria in different labor-atories and resulted in multiple unwantedside effects related to hypersensitivity and
10 HEY
anaphylactic reactions to foreign proteinsThese days antibodies being developed fortreatment of diseases in humans are highlypurified and are mostly fully human mono-clonal antibodies The term monoclonal anti-body refers to that cell cultures used forgenerating these antibodies each originatesfrom a single cell and thus produces onlyone specific antibody Development of fullyhuman monoclonal antibodies happened instages over a time span of more than 15 yearsFirst stage in this process was generation ofmonoclonalmurine IgG antibodies (eg OKT3[muronomab-CD3 Johnson and Johnson] ap-proved in 1986) Next stage was generation ofso called chimeric antibodies consisting ofhuman heavy and light chain constant sec-tions but with murine variable sections (eg
Rituxan [rituximab Genentech]) Next stagewas then the humanized antibodies wherethe only remaining murine part of the anti-body is the antigen-binding CDR (eg Xolair[omalizumab NovartisGenentech]) Both thefirst chimeric and humanized antibodies wereapproved in the late 1990s Then finally 16years later the first fully human antibodyHumira (adalimumab Abbott) was approvedin 2002 Since the time of the crude and low-scale manufacturing of the original antibodyserum products much has changed andtherapeutic antibodies are now produced byfermentation in 5000 liter scale using highlycontrolled and documented yeast or mamma-lian cell lines that are genetically engineered toexpress a single specific antibody This hasresulted in a pure and highly specific antibody
FIGURE 2 Effector functions of antibodies (a) Antibodies bind to pathogen-derived or endogenousantigens expressed on the surface of an infected cell which triggers binding to Fc receptors on naturalkiller cells and lysis of the infected cell by antibody-dependent cellular cytotoxicity (b) Antibodies bindto pathogen-derived or endogenous antigens expressed on the surface of infected cells which triggersactivation of complement through binding of complement factor C1q (c) Neutralization Top Bacterialtoxin neutralized by bound antigen Bottom Antibody bound to either receptor for the virus or to thevirus itself which blocks virus binding and entry into the cell (d) Antibody bound to viral surfaceproteins binds to Fc receptors on phagocytic cells eg macrophages and triggers endocytosis anddestruction of virus in endolysosome doi101128microbiolspecAID-0026-2014f2
CHAPTER 1 bull History and Practice Antibodies in Infectious Diseases 11

FIGURE 1 (Left panel) Model of antibody structure exemplified by IgG On top the antigen-binding sitesin orange each contain one variable light and variable heavy domain with the three complementaritydetermining regions (CDRs) that are responsible for the specific binding of the antibody to its target Foreach arm of the antibody an additional set of variable heavy and light domains together with the CDR-containing domains represent the two fragment antigen binding (Fab) regions The two Fabs are heldtogether via two disulfide bridges Below the Fabs is the Fc region which contains four constant heavydomains On the upper pair of these domains are binding sites for oligosaccharides which have majorimportance for the ability of the antibody Fc part to trigger effector functions when the Fc portion isbound to Fc gamma receptors on natural killer cells neutrophil granulocytes monocytesmacrophagesdendritic cells and B cells (Right panel) Examples of some of the antibody-derived alternative formatsused to exploit the specific features of the CDRs the Fabs and the Fc parts of the antibodies ScFv Thesingle chain fragment variable consists of the variable domains of the heavy and light chains heldtogether by a flexible linker This can also be used as a carrier of a cytotoxic drug in a so-called antibodydrug complex (ADC) where the specificity of the ScFv is used to target the cytotoxic drug to eg atumor Bite (bi-specific T cell engager) Fusion proteins consisting of two ScFvs one directed against thetarget on a tumor cell and the other against the T cell receptor (CD3) Diabody ScFv dimers where shortlinker peptides (five amino acids) ensure dimerization and not folding of the ScFvs Fab and F(ab)2fragments Single Fab fragments or fragments containing two Fabs linked via disulfide bridges This isused where effector functions related to the Fc part of the antibody are unwanted and where a smallersize is desired to obtain better tissue penetration in eg tumors Due to the lack of the FcRn binding viathe Fc part Fab and F(ab)2 fragments have much shorter half-lives (hours or days) than full-sizeantibodies (weeks) These can also be used as carriers of cytotoxic payloads or cytotoxic radioactiveisotopes and for the F(ab)2 fragments can be constructed as bi-specifics which can cross-link immunecells and target cells Fc fusion protein Fusion protein containing the Fc domain of an immunoglobulinbound to a peptide The peptide can be a ligand for a specific receptor on a target cell or a blockingpeptide for a soluble ligand The Fc part provides a longer half-life to the construct and the potential tobind to and engage effector functions in the killing of eg tumor cells or infected cells ADCsRIAs andbi-specifics Full-size IgG antibodies carrying either a cytotoxic chemical or radioactive payload whichmay also carry different CDRs enabling cross-linking of effector and target cells for increased killingdoi101128microbiolspecAID-0026-2014f1
CHAPTER 1 bull History and Practice Antibodies in Infectious Diseases 9
contain special hyper-variable segments calledcomplementarity-determining regions (CDRs)which allow the B cells via genetic recom-bination to generate antibodies to all thedifferent antigens specific to amino acid se-quences or three-dimensional structuralmotifs(polysaccharides DNA and RNA) found onpathogens
Based on the structure of their heavy chainconstant regions antibodies or immuno-globulins are separated into five classesmdashIgM IgG IgE IgD and IgA Differences inthe sequences of the constant regions providedistinct characteristics to these different clas-ses These characteristics include the numberof heavy chain constant segments the numberand location of interconnecting disulfidebridges the length of the hinge region andthe number and location of oligosaccharidemoieties For IgG four heavy chain versionsexist creating IgG1 2 3 and 4 isotypes eachwith different characteristics in their serumhalf-lives and ability to trigger different effec-tor functions Because of the combined ad-vantage from ability to trigger effectormechanisms long [21 days] half-life theirability to be transported over the placentaand their stability in the production processantibodies of the IgG class and of the IgG1isotype are preferred as the basis for newantibody-based therapies The effector func-tions are triggered by the Fc part of an antibodywhen the variable parts of the antibody arebound directly to an infectious agent or toproteins from an infectious agent expressed onan infected cell This binding leaves the Fc partfree to interactwithFc receptors onphagocyticcells and neutrophils eosinophils and naturalkiller cells capable of inducing phagocytosis orlysis of infectious agents or infected cellsThese effector functions include (i) the abilityto activate the complement system for lysis(complement-dependent cellular cytotoxicity)(ii) triggering of uptake and destruction byphagocytic cells such as macrophages andneutrophils via interaction with Fc receptorson these cells (iii) activation of macrophageseosinophils neutrophils and natural killer
cells to kill infected cells via binding to Fcreceptors on these cells and antibody-depen-dent cellular cytotoxicity and (iv) neutraliza-tion of bacterial toxins and blocking of bindingand uptake of bacteria or viruses to target cells(see Fig 2) (9)
The Fcpart of IgG antibodies also contains aregion that interacts with the neonatal Fcreceptor (FcRn) expressed on most immuno-competent cells and inmany other cells such asendothelial cells in kidney liver placenta lungand breast (10) which protects antibodies fromdegradation by phagocytoticexocytotic cy-cling into FcRn-expressing cells thereby pro-longing their half-life This results in half-livesof 20 to 21 days for most IgG1 2 and 4antibodies whereas half-lives are 10 6 and 2days respectively for IgM IgA and IgE Thehighly specific binding sites on the variableregions of the upper arms of the antibody allowfor several important features of antibodiesndashbinding to and neutralization of eg bacterialtoxins binding to pathogens and blocking theirbinding to or interaction with target cells (egcyncytia formation of CMV-infected cells) orblocking of binding and interactions of infec-tious agents with target cells via blockingreceptors on the target cells
METHODS AND PLATFORMS FORGENERATING ANTIBODIES
As described above the early use of passiveantibody transfer as a therapy in infectiousdiseases involved the use of immune serumfrom immunized sheep and horses These pre-parations were crude and contained a broadmixture of neutralizing and non-neutralizingantibodies and both the foreign nature of theantibodies and the numerous host serumproteins This resulted in less specific andthus less efficient therapies due to a highvariability in efficacy between batches derivedfrom different animals immunized with dif-ferent strains of bacteria in different labor-atories and resulted in multiple unwantedside effects related to hypersensitivity and
10 HEY
anaphylactic reactions to foreign proteinsThese days antibodies being developed fortreatment of diseases in humans are highlypurified and are mostly fully human mono-clonal antibodies The term monoclonal anti-body refers to that cell cultures used forgenerating these antibodies each originatesfrom a single cell and thus produces onlyone specific antibody Development of fullyhuman monoclonal antibodies happened instages over a time span of more than 15 yearsFirst stage in this process was generation ofmonoclonalmurine IgG antibodies (eg OKT3[muronomab-CD3 Johnson and Johnson] ap-proved in 1986) Next stage was generation ofso called chimeric antibodies consisting ofhuman heavy and light chain constant sec-tions but with murine variable sections (eg
Rituxan [rituximab Genentech]) Next stagewas then the humanized antibodies wherethe only remaining murine part of the anti-body is the antigen-binding CDR (eg Xolair[omalizumab NovartisGenentech]) Both thefirst chimeric and humanized antibodies wereapproved in the late 1990s Then finally 16years later the first fully human antibodyHumira (adalimumab Abbott) was approvedin 2002 Since the time of the crude and low-scale manufacturing of the original antibodyserum products much has changed andtherapeutic antibodies are now produced byfermentation in 5000 liter scale using highlycontrolled and documented yeast or mamma-lian cell lines that are genetically engineered toexpress a single specific antibody This hasresulted in a pure and highly specific antibody
FIGURE 2 Effector functions of antibodies (a) Antibodies bind to pathogen-derived or endogenousantigens expressed on the surface of an infected cell which triggers binding to Fc receptors on naturalkiller cells and lysis of the infected cell by antibody-dependent cellular cytotoxicity (b) Antibodies bindto pathogen-derived or endogenous antigens expressed on the surface of infected cells which triggersactivation of complement through binding of complement factor C1q (c) Neutralization Top Bacterialtoxin neutralized by bound antigen Bottom Antibody bound to either receptor for the virus or to thevirus itself which blocks virus binding and entry into the cell (d) Antibody bound to viral surfaceproteins binds to Fc receptors on phagocytic cells eg macrophages and triggers endocytosis anddestruction of virus in endolysosome doi101128microbiolspecAID-0026-2014f2
CHAPTER 1 bull History and Practice Antibodies in Infectious Diseases 11

contain special hyper-variable segments calledcomplementarity-determining regions (CDRs)which allow the B cells via genetic recom-bination to generate antibodies to all thedifferent antigens specific to amino acid se-quences or three-dimensional structuralmotifs(polysaccharides DNA and RNA) found onpathogens
Based on the structure of their heavy chainconstant regions antibodies or immuno-globulins are separated into five classesmdashIgM IgG IgE IgD and IgA Differences inthe sequences of the constant regions providedistinct characteristics to these different clas-ses These characteristics include the numberof heavy chain constant segments the numberand location of interconnecting disulfidebridges the length of the hinge region andthe number and location of oligosaccharidemoieties For IgG four heavy chain versionsexist creating IgG1 2 3 and 4 isotypes eachwith different characteristics in their serumhalf-lives and ability to trigger different effec-tor functions Because of the combined ad-vantage from ability to trigger effectormechanisms long [21 days] half-life theirability to be transported over the placentaand their stability in the production processantibodies of the IgG class and of the IgG1isotype are preferred as the basis for newantibody-based therapies The effector func-tions are triggered by the Fc part of an antibodywhen the variable parts of the antibody arebound directly to an infectious agent or toproteins from an infectious agent expressed onan infected cell This binding leaves the Fc partfree to interactwithFc receptors onphagocyticcells and neutrophils eosinophils and naturalkiller cells capable of inducing phagocytosis orlysis of infectious agents or infected cellsThese effector functions include (i) the abilityto activate the complement system for lysis(complement-dependent cellular cytotoxicity)(ii) triggering of uptake and destruction byphagocytic cells such as macrophages andneutrophils via interaction with Fc receptorson these cells (iii) activation of macrophageseosinophils neutrophils and natural killer
cells to kill infected cells via binding to Fcreceptors on these cells and antibody-depen-dent cellular cytotoxicity and (iv) neutraliza-tion of bacterial toxins and blocking of bindingand uptake of bacteria or viruses to target cells(see Fig 2) (9)
The Fcpart of IgG antibodies also contains aregion that interacts with the neonatal Fcreceptor (FcRn) expressed on most immuno-competent cells and inmany other cells such asendothelial cells in kidney liver placenta lungand breast (10) which protects antibodies fromdegradation by phagocytoticexocytotic cy-cling into FcRn-expressing cells thereby pro-longing their half-life This results in half-livesof 20 to 21 days for most IgG1 2 and 4antibodies whereas half-lives are 10 6 and 2days respectively for IgM IgA and IgE Thehighly specific binding sites on the variableregions of the upper arms of the antibody allowfor several important features of antibodiesndashbinding to and neutralization of eg bacterialtoxins binding to pathogens and blocking theirbinding to or interaction with target cells (egcyncytia formation of CMV-infected cells) orblocking of binding and interactions of infec-tious agents with target cells via blockingreceptors on the target cells
METHODS AND PLATFORMS FORGENERATING ANTIBODIES
As described above the early use of passiveantibody transfer as a therapy in infectiousdiseases involved the use of immune serumfrom immunized sheep and horses These pre-parations were crude and contained a broadmixture of neutralizing and non-neutralizingantibodies and both the foreign nature of theantibodies and the numerous host serumproteins This resulted in less specific andthus less efficient therapies due to a highvariability in efficacy between batches derivedfrom different animals immunized with dif-ferent strains of bacteria in different labor-atories and resulted in multiple unwantedside effects related to hypersensitivity and
10 HEY
anaphylactic reactions to foreign proteinsThese days antibodies being developed fortreatment of diseases in humans are highlypurified and are mostly fully human mono-clonal antibodies The term monoclonal anti-body refers to that cell cultures used forgenerating these antibodies each originatesfrom a single cell and thus produces onlyone specific antibody Development of fullyhuman monoclonal antibodies happened instages over a time span of more than 15 yearsFirst stage in this process was generation ofmonoclonalmurine IgG antibodies (eg OKT3[muronomab-CD3 Johnson and Johnson] ap-proved in 1986) Next stage was generation ofso called chimeric antibodies consisting ofhuman heavy and light chain constant sec-tions but with murine variable sections (eg
Rituxan [rituximab Genentech]) Next stagewas then the humanized antibodies wherethe only remaining murine part of the anti-body is the antigen-binding CDR (eg Xolair[omalizumab NovartisGenentech]) Both thefirst chimeric and humanized antibodies wereapproved in the late 1990s Then finally 16years later the first fully human antibodyHumira (adalimumab Abbott) was approvedin 2002 Since the time of the crude and low-scale manufacturing of the original antibodyserum products much has changed andtherapeutic antibodies are now produced byfermentation in 5000 liter scale using highlycontrolled and documented yeast or mamma-lian cell lines that are genetically engineered toexpress a single specific antibody This hasresulted in a pure and highly specific antibody
FIGURE 2 Effector functions of antibodies (a) Antibodies bind to pathogen-derived or endogenousantigens expressed on the surface of an infected cell which triggers binding to Fc receptors on naturalkiller cells and lysis of the infected cell by antibody-dependent cellular cytotoxicity (b) Antibodies bindto pathogen-derived or endogenous antigens expressed on the surface of infected cells which triggersactivation of complement through binding of complement factor C1q (c) Neutralization Top Bacterialtoxin neutralized by bound antigen Bottom Antibody bound to either receptor for the virus or to thevirus itself which blocks virus binding and entry into the cell (d) Antibody bound to viral surfaceproteins binds to Fc receptors on phagocytic cells eg macrophages and triggers endocytosis anddestruction of virus in endolysosome doi101128microbiolspecAID-0026-2014f2
CHAPTER 1 bull History and Practice Antibodies in Infectious Diseases 11

anaphylactic reactions to foreign proteinsThese days antibodies being developed fortreatment of diseases in humans are highlypurified and are mostly fully human mono-clonal antibodies The term monoclonal anti-body refers to that cell cultures used forgenerating these antibodies each originatesfrom a single cell and thus produces onlyone specific antibody Development of fullyhuman monoclonal antibodies happened instages over a time span of more than 15 yearsFirst stage in this process was generation ofmonoclonalmurine IgG antibodies (eg OKT3[muronomab-CD3 Johnson and Johnson] ap-proved in 1986) Next stage was generation ofso called chimeric antibodies consisting ofhuman heavy and light chain constant sec-tions but with murine variable sections (eg
Rituxan [rituximab Genentech]) Next stagewas then the humanized antibodies wherethe only remaining murine part of the anti-body is the antigen-binding CDR (eg Xolair[omalizumab NovartisGenentech]) Both thefirst chimeric and humanized antibodies wereapproved in the late 1990s Then finally 16years later the first fully human antibodyHumira (adalimumab Abbott) was approvedin 2002 Since the time of the crude and low-scale manufacturing of the original antibodyserum products much has changed andtherapeutic antibodies are now produced byfermentation in 5000 liter scale using highlycontrolled and documented yeast or mamma-lian cell lines that are genetically engineered toexpress a single specific antibody This hasresulted in a pure and highly specific antibody
FIGURE 2 Effector functions of antibodies (a) Antibodies bind to pathogen-derived or endogenousantigens expressed on the surface of an infected cell which triggers binding to Fc receptors on naturalkiller cells and lysis of the infected cell by antibody-dependent cellular cytotoxicity (b) Antibodies bindto pathogen-derived or endogenous antigens expressed on the surface of infected cells which triggersactivation of complement through binding of complement factor C1q (c) Neutralization Top Bacterialtoxin neutralized by bound antigen Bottom Antibody bound to either receptor for the virus or to thevirus itself which blocks virus binding and entry into the cell (d) Antibody bound to viral surfaceproteins binds to Fc receptors on phagocytic cells eg macrophages and triggers endocytosis anddestruction of virus in endolysosome doi101128microbiolspecAID-0026-2014f2
CHAPTER 1 bull History and Practice Antibodies in Infectious Diseases 11