Embed Size (px)
Citation preview
Anticipated impact on HPV infection from HPV vaccination programs – cause for optimism
Dr Paddy Horner
Genital human papillomavirus infection
• The most common STI worldwide – Spread by skin to skin contact
• Sexually active women <25 years old have the highest rate of human papillomavirus (HPV) infection– Majority no visible lesions– Resolve infection after 1-3 yrs – no immunity other types
• 1% of sexually active adults (aged 15–49 years) develop genital warts
• ~10% fail to clear infection and at increased complications
Koutsky L. Am J Med 1997; 102 (5A): 3–8Koutsky L et al. Epidemiol Rev 1988; 10: 122–63

Prevalence of genital HPV infection
• It is estimated the majority of people will have been exposed to a genital HPV type in their lifetime – Only 1% of a population will have visible at a
given time
Koutsky L et al. Epidemiol Rev 1988; 10: 122–163
Genital HPV infection
• Associated– Smoking– Multiple sexual partners
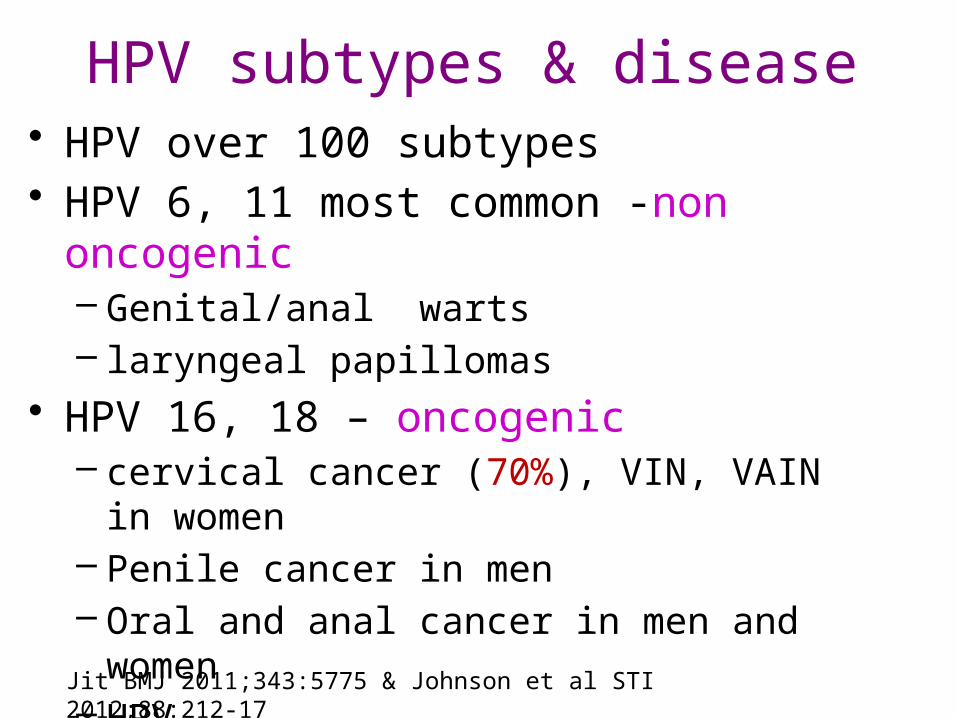
HPV subtypes & disease• HPV over 100 subtypes• HPV 6, 11 most common -non oncogenic
– Genital/anal warts– laryngeal papillomas
• HPV 16, 18 – oncogenic – cervical cancer (70%), VIN, VAIN in women – Penile cancer in men– Oral and anal cancer in men and women– HPV 31,33,35,39,45,51,52,56,58,59,68
Jit BMJ 2011;343:5775 & Johnson et al STI 2012;88:212-17
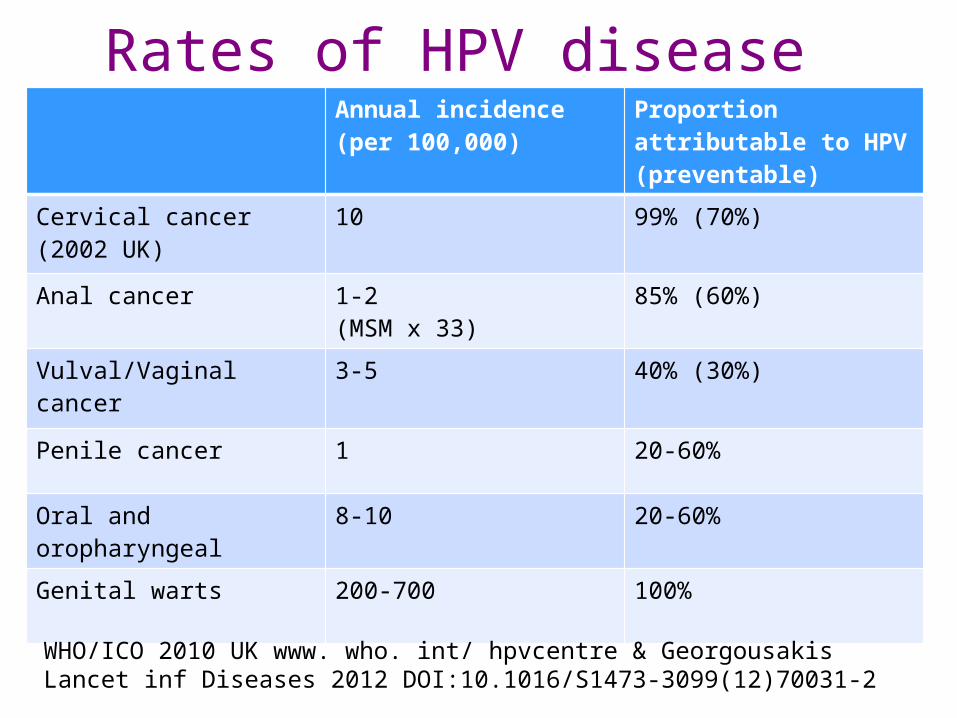
Rates of HPV disease Annual incidence (per 100,000)
Proportion attributable to HPV (preventable)
Cervical cancer (2002 UK)
10 99% (70%)
Anal cancer 1-2(MSM x 33)
85% (60%)
Vulval/Vaginal cancer 3-5 40% (30%)
Penile cancer 1 20-60%
Oral and oropharyngeal 8-10 20-60%
Genital warts 200-700 100%
WHO/ICO 2010 UK www. who. int/ hpvcentre & Georgousakis Lancet inf Diseases 2012 DOI:10.1016/S1473-3099(12)70031-2
HPV vaccination• Vaccines -
• Gardasil – Merck• Quadrivalent 16, 18, 6, 11 (includes genital warts)
• Cervarix – GSK• Bivavlent 16, 18
• Prevent HPV infection & pre cancerous lesions• Gardasil more cost effective - warts• Cervarix better cross protection other HPV types
• 47% vs 23%
• Not a treatment for established infection• Administered sexually naive young adolescents
Jit BMJ 2011;343:5775
HPV vaccination
• Duration immunity probably > 10 yrs• Antibody mediated capsular protein
• Type specific• Some protection other HPV serotypes
• Phylogenetically related
Joura et al BMJ 2012;344:1401
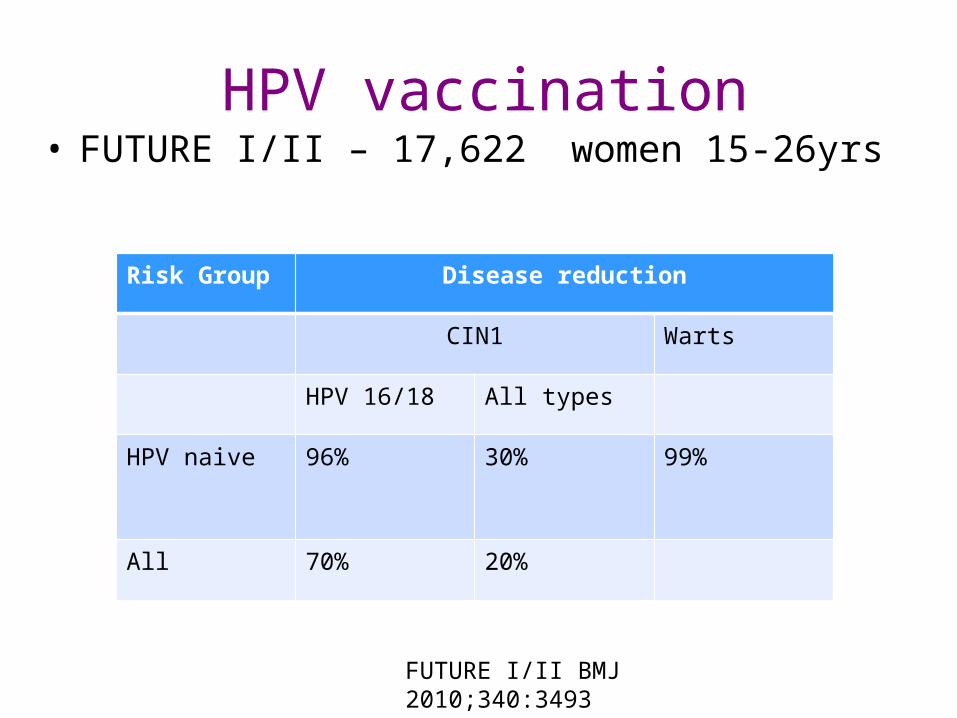
HPV vaccination• FUTURE I/II – 17,622 women 15-26yrs
Risk Group Disease reduction
CIN1 Warts
HPV 16/18 All types
HPV naive 96% 30% 99%
All 70% 20%
FUTURE I/II BMJ 2010;340:3493
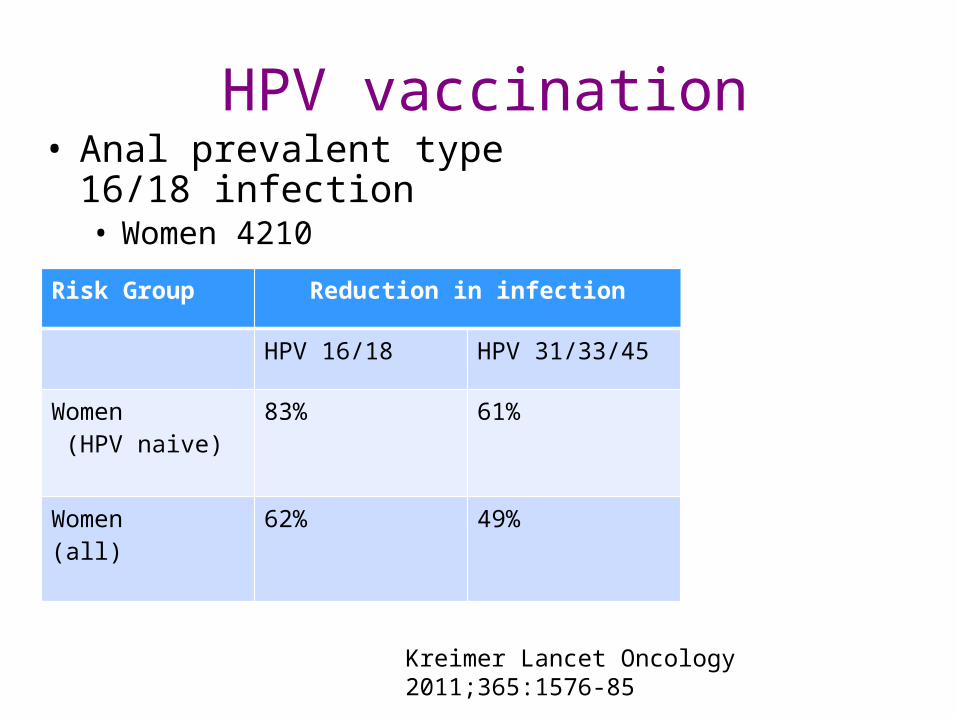
HPV vaccination• Anal prevalent type 16/18
infection• Women 4210
Risk Group Reduction in infection
HPV 16/18 HPV 31/33/45
Women (HPV naive)
83% 61%
Women (all)
62% 49%
Kreimer Lancet Oncology 2011;365:1576-85
HPV vaccination
• Men• 4065 boys and men• 90% reduction PIN (inc Warts)• 85% reduction persistent infection
Giuliano NEJM 2011;364:401Palefsky N Engl J Med 2011;365:1576-85.
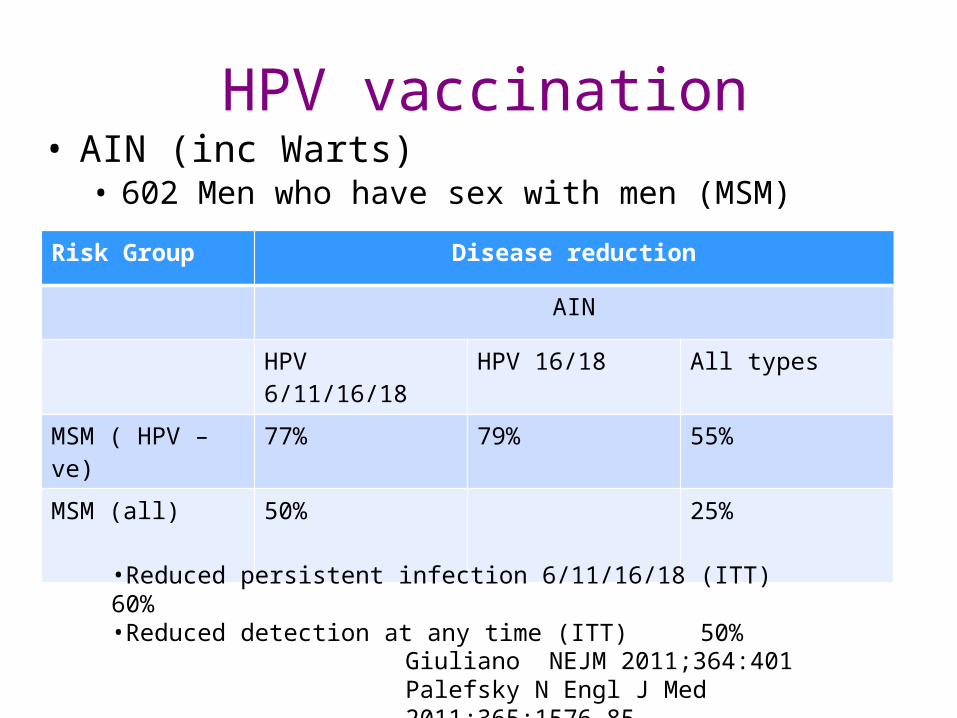
HPV vaccination• AIN (inc Warts)
• 602 Men who have sex with men (MSM)
Risk Group Disease reduction
AIN
HPV 6/11/16/18 HPV 16/18 All types
MSM ( HPV –ve) 77% 79% 55%
MSM (all) 50% 25%
Giuliano NEJM 2011;364:401Palefsky N Engl J Med 2011;365:1576-85.
•Reduced persistent infection 6/11/16/18 (ITT) 60%•Reduced detection at any time (ITT) 50%
HPV vaccination• Not a treatment for current infection/disease
• FUTURE I/II studies: • Women with treated cervical disease increased risk of
future CIN 1 or worse - 8.2%
• New infection
• Risk reduced by 48% if received vaccine (quad) - 4.3%
• Evidence that vaccine beneficial even in those with disease
Joura BMJ 2012;344:1401
HPV vaccination• Could it alter natural history of CIN/VIN/AIN?• Efficacy phase II/III treatment anogenital warts
• Is vaccine immunogen expressed in CIN/VIN/AIN?
• Effect of Vaccine on CIN progression to cancer unknown• Data does not support vaccine efficacy
• Natural history AIN probably differs CIN• Longer duration before malignant transformation
• Greater similarity to VIN
• Vaccine reduces persistent infection• Could it alter the natural history of AIN?
Simpson BMJ 2011;343:d6818 doi: 10.1136/bmj.d6818
Genital warts• Australia• Using vaccine in young women since 2007• >70% uptake adolescents• Reviewed clinic data Melbourne GUM clinic
• Women < 21• Men < 21• MSM
• Marked reduction in both female and male warts• Not in MSM
Read et al STI 2011;87:544
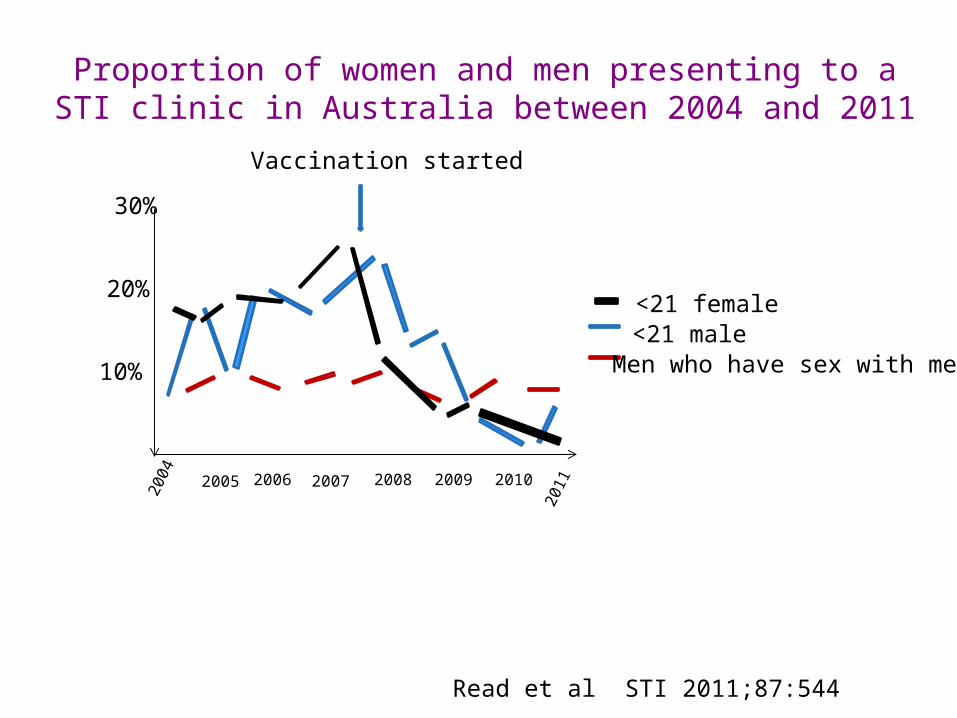
Proportion of women and men presenting to a STI clinic in Australia between 2004 and 2011
30%
10%
20%
2004 2005 2006 2007 2008 20102009
2011
<21 female<21 maleMen who have sex with men
Vaccination started
Read et al STI 2011;87:544
HPV vaccination and Men
• Heterosexual herd immunity effective for men– >70% coverage women– Not all countries have attained this– Vaccination boys recommended USA but not UK
• MSM remain at risk– Unable to identify as an adolescent– Many >20 partners by age 20
• Highly HPV exposed
– AIN much longer time course to Cancer• HIV co-factor
Pros and cons discussed Georgousakis Lancet inf Diseases 2012 DOI:10.1016/S1473-3099(12)70031-2
Cost effectiveness
• Gardasil more cost effective the Cervarix– Significant health care cost genital warts
Jit BMJ 2011;343:5775
But!
• Population based survey UK 18-44 yrs– 16% women had high risk HPV type
• Only 1/3rd were type 16/18• Suggests HPV 16 probably more oncogenic
• Condoms had some protective effect!
Johnson et al STI 2012;88:212-17