Embed Size (px)
Citation preview

Intr
od
ucti
on
4
Approach to Clinical Presentation
IntroductionPatients with thoracic disease may present with a variety ofcomplaints and are typically initially imaged with radiography.Presenting symptoms may include chest pain, cough, dyspnea,wheezing, and stridor. Patients may also present forassessment of minor or major thoracic trauma. In someinstances, thoracic imaging is ordered in asymptomaticpatients, including those undergoing routine physicalexamination or elective extrathoracic surgery. Patients withextrathoracic complaints may also undergo chest imaging aspart of their evaluation. While imaging of such asymptomaticpatients is generally discouraged, this practice is common andmany such imaging studies demonstrate no abnormalities.However, chest imaging of asymptomatic patients may revealincidental abnormalities that require additional assessmentand definitive management.
Clinical PresentationChest PainChest pain is a common presenting complaint both in theEmergency Department and in the outpatient setting.Because it may occur as a symptom of both life-threateningand relatively benign conditions, it often poses a diagnosticchallenge for the clinician. Chest pain may be due tonumerous etiologies. Important life-threatening conditionsthat manifest with chest pain include myocardial ischemia andinfarction, pulmonary thromboembolism, acute aorticsyndrome, heart failure, and pneumothorax. In some cases,the clinical history provides helpful clues to the etiology ofchest pain. For example, patients with pulmonarythromboembolism may have well-known risk factors orcomplain of lower extremity symptoms of deep venousthrombosis. Patients with acute aortic syndrome are typicallyin the seventh decade of life, present with acute chest pain,and exhibit systemic hypertension. Patients with sickle cellanemia may present with chest pain from acute chestsyndrome.
Several non-life-threatening conditions may initially manifestwith chest pain and include pneumonia, chronic obstructivepulmonary disease, asthma, and pulmonary hypertension.Patients with pulmonary &/or cardiac sarcoidosis may alsopresent with chest pain, often in association with dyspnea andcough. Some patients with thoracic malignancy may initiallypresent with chest pain. While chest pain is typically associatedwith cardiopulmonary disease, other conditions may alsoproduce this symptom, including esophageal and othergastrointestinal disorders and diseases of the thoracicmusculoskeletal system.
Chest radiography allows rapid identification of pulmonaryconsolidation, pleural effusion, and pneumothorax. In manycases, chest CT follows and is usually tailored to the clinicalpresentation, with specific techniques including CT pulmonaryangiography, CT aortography, and cardiac CT. MR is oftenreserved for patients in whom iodinated contrastadministration is contraindicated and those with suspectedcardiac disease.
CoughCough is a very common complaint in the outpatient settingand is classified based on its duration as acute (< 3 weeks),subacute (3-8 weeks), or chronic (> 8 weeks). Acute cough isoften due to pulmonary infection, but other conditions mayalso cause it, including pulmonary embolism and exacerbationof chronic lung disease. Subacute and chronic cough may be
related to upper airway cough syndrome, which is associatedwith postnasal drip and characteristically affects women.Additional etiologies include asthma, gastroesophageal refluxdisease, and viral, mycoplasma, and chlamydia infections.Bordetella pertussis is associated with subacute or chronicpersistent cough. Important etiologies of chronic coughinclude bronchitis (cough and sputum production for at least 3months in the absence of another explanation) andbronchiectasis. Lung cancer may also manifest with cough,particularly when the neoplasm involves the central airways.
Acute cough is typically evaluated with chest radiography, thepreferred imaging modality for diagnosing pneumonia, whichmay manifest with sublobar, lobar, &/or multifocalconsolidations. In cases in which the radiograph is normal ornearly normal, chest CT may demonstrate acinar opacities&/or cellular bronchiolitis, which allows the radiologist tosuggest pulmonary infection. Patients with pulmonaryinfection should be stratified as immunocompetent orimmunocompromised, as the latter may be affected byatypical infections &/or neoplastic disorders.
Patients with subacute or chronic cough may have normal ornearly normal chest radiographs. In such cases, chest CT isoften performed to exclude morphologic airwayabnormalities that include bronchiectasis and bronchial wallthickening characteristic of bronchitis.
DyspneaDyspnea refers to subjective breathing discomfort and may beacute (hours to days) or chronic (> 4-8 weeks). It may becaused by both cardiovascular and respiratory disorders.Cardiovascular disorders that produce dyspnea include heartfailure, anemia, and deconditioning. Respiratory causes ofdyspnea include chronic obstructive pulmonary disease thatmay manifest with emphysema and restrictive disease relatedto pulmonary fibrosis. Neuromuscular disorders such asmyasthenia gravis and Guillain-Barré syndrome may alsomanifest with dyspnea. Evaluation of affected patients usuallyincludes both chest radiography and CT. In patients withsuspected chronic fibrosing interstitial lung disease, chest CTand high-resolution CT are invaluable imaging tools fordetermining the distribution of pulmonary fibrosis,formulating a differential diagnosis, and assessing diseaseprogression.
WheezingPatients who present with wheezing are often suspected ofhaving either asthma or chronic obstructive pulmonarydisease. However, "all that wheezes is not asthma," and otherentities must be considered in the differential diagnosis.These include anaphylaxis, upper airway stenosis, cervical ormediastinal mass (including vascular rings), upper airwayneoplasms, tracheomalacia/tracheobronchomalacia,constrictive bronchiolitis, and diffuse idiopathic pulmonaryneuroendocrine cell hyperplasia, among many others.
StridorStridor refers to a high-pitched, monophonic sound madeduring inspiration or expiration. It typically signifies largeairway obstruction located in supraglottic, glottic, subglottic,or intrathoracic regions. Stridor often suggests foreign bodyaspiration but may also be secondary to centrally obstructiveinflammatory or neoplastic conditions. While radiography isusually initially performed, CT allows optimal assessment ofcentral airway obstructive lesions.

Introd
uction
5
Approach to Clinical Presentation
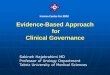
(Left) Composite image withaxial NECT (left) and CECT(right) of a 68-year-old manwith chest pain andhypertension shows anascending aortic intramuralhematoma and adescending aortic dissection. (Right) Composite imagewith axial NECT (left) andCECT (right) of a patient withsuspected acute aorticsyndrome shows a saddlepulmonary embolus thatexhibits high attenuation onNECT. CT angiography tailoredto the clinical history isvaluable for evaluatingpatients with acute chest pain.
Acute Aortic Syndrome Pulmonary Thromboembolism
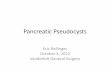
(Left) PA chest radiograph of a45-year-old woman whopresented with productivecough and fever showsairspace consolidation in theright lung base , consistentwith pneumonia. Note obliqueorientation of the anterior ribs characteristic of pectusexcavatum deformity. (Right)Lateral chest radiograph ofthe same patient confirmsboth pectus excavatumdeformity and a right lowerlobe pneumonia thatproduces the spine sign. Chestradiography is the study ofchoice for the diagnosis ofpneumonia.
Pneumonia Pneumonia
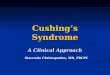
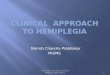
(Left) PA chest radiograph of a48-year-old man whopresented with dyspnea showssevere bilateral upper and midlung zone-predominantbullous emphysema. (Right)Axial HRCT of a 58-year-oldwoman with scleroderma anddyspnea shows basilarpredominant fibrosinginterstitial lung disease,consistent with usualinterstitial pneumonia (UIP)pattern. Imaging is very usefulin the assessment of patientswith chronic dyspnea andoften allows evaluation andassessment of obstructive andrestrictive lung diseases.
Emphysema Usual Interstitial Pneumonia