Embed Size (px)
Citation preview

Györgyi Műzes
Semmelweis University, 2nd Dept. of Medicine
Approach to patient with
musculoskeletal disease

Musculoskeletal disorders
common problems affecting (mainly) the elderly
with age, musculoskeletal tissues show
increased bone fragility
loss of cartilage resilience
reduced ligament elasticity
loss of muscular strength
fat redistribution
decreasing the ability of the tissues to provide
their normal functions

MSDs: assessment
health history
chief complaints
onset of problems
precipitating events, e.g., trauma

MSDs: assessment
pain (recurrent – constant)
location
duration
radiation
character (sharp/ dull)
swelling
stiffness
aggravating, or alleviating factors
fever, fatigue, weight changes, rash

MSDs: diagnostic tests
blood tests
X-rays
bone density
ultrasound
CT
MRI
bone scan
arthrocentesis

Osteoarthritis
Definition – degenerative joint process
arising from the biochemical breakdown of articular (hyaline) cartilage in the synovial joints;
characterized by focal loss of cartilage, new bone formation (spurring)
Consequences: subsequent pain + loss of function
Most common type of joint diseases
> half of affected individuals are > 55 ys with
radiographic evidence (up to 90% at age > 70 !)
Female predominance (3:1)


OA: risk factors Age, Gender, Obesity ,Trauma
Genetics (significant family history)
Reduced levels of sex hormones
Muscle weakness
Repetitive use (ie, heavy jobs)
Infection
Crystal deposition
Previous inflammatory arthritis (eg, burn-out RA)
Endocrine abnormalities (eg, acromegaly)
Heritable metabolic causes (eg, alkaptonuria, hemochromatosis, Wilson disease)
Hemoglobinopathies (eg, sickle cell disease, thalassemia)
Neuropathic disorders leading to a Charcot join
(eg, syringomyelia, tabes dorsalis, and diabetes)

OA: stages
Stage 1 – Proteolytic breakdown of the cartilage matrix
Stage 2 – Fibrillation and erosion of the cartilage
surface, with subsequent release of proteoglycan and
collagen fragments into the synovial fluid
Stage 3 – Breakdown products of cartilage induce a
chronic inflammatory response in the synovium, which
contributes to further cartilage breakdown

OA
predominantly involves the weight-bearing joints
involves not only the articular cartilage but also the
entire joint organ, including the subchondral bone and synovium
caused largely by excessive wear and tear, with
dominant contributions of abnormal mechanics and inflammation
OA: symtomps
deep, achy joint pain (primary symptom !)
exacerbated by extensive use
decreased with rest
progression with aging
reduced range of motion
crepitus (cracking or grinding noise with joint
movement)
bony swelling (effusion)
stiffness during rest (may develop with morning joint
stiffness usually lasting for < 30 min)
joint deformity

History: gradual onset of symptoms
lack of inflammation
sometimes history of prior injury or other
secondary triggers
Physical exam: crepitus, hypertrophic changes, lack of erythema or warmth, usually no much tenderness
X-ray: asymmetric joint space narrowing, sclerosis near to the joint line, and spurring
OA: diagnosis

OA:
affected joints

very common
with obesity !
bilateral disease manifestation
OA: hip and knee



Heberden’s nodes – DIP-joint (bony nodules)
Bouchard’s nodes – PIP-joint (bony nodules)
Both “nodes” (= palpable osteophytes): diagnostic
for hand OA
(10x more common in women than men, with a strong
genetic component)
Base of thumb (1st CMC joint): comonly affected, more likely due to wear-and-tear than nodes
OA: hands

Square thumb


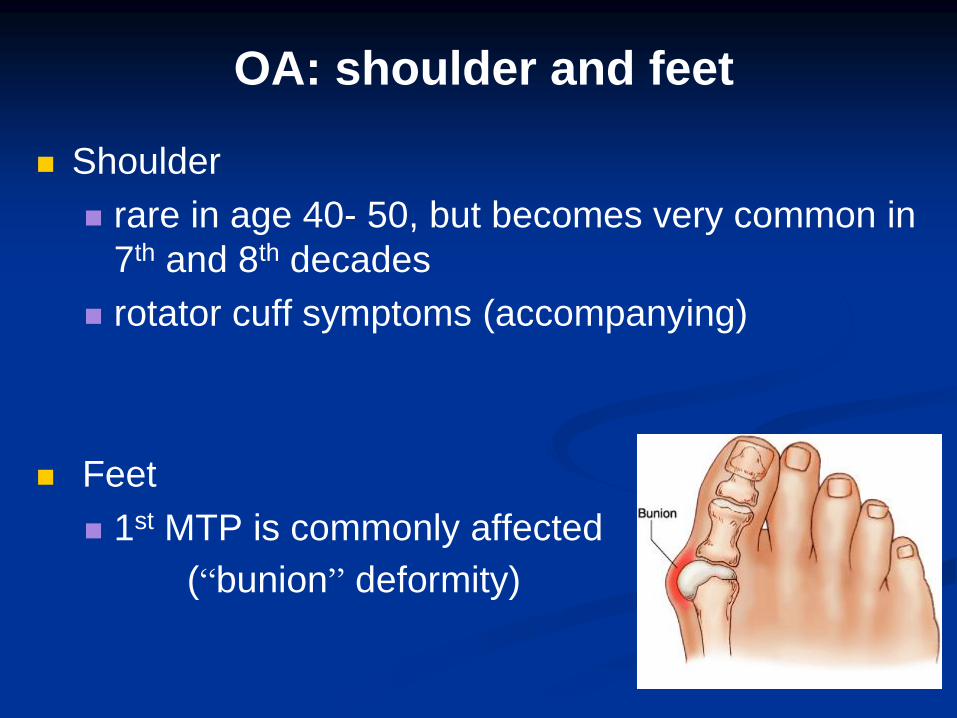
Shoulder
rare in age 40- 50, but becomes very common in
7th and 8th decades
rotator cuff symptoms (accompanying)
Feet
1st MTP is commonly affected
(“bunion” deformity)
OA: shoulder and feet
(unless injury / secondary causes):
MCPs
wrist
elbow
ankle
above localisations: think on inflammation !
OA: joints typically not affected


Rheumatoid arthritis: seropositive
symmetric inflammatory joint condition characterized by pannus formation, joint erosion, and chronic systemic inflammation
systemic autoimmune disease
common inflammatory arthritis, 1-3 % of the population, 2-3:1 female to male ratio, peak incidence between ages 40 to 60





persistent symmetric polyarthritis (synovitis) of
hands and feet
progressive articular deterioration
extraarticular involvement
difficulty performing activities of daily living
constitutional symptoms (fatigue, weight loss)
RA: signs and symptoms

RA: joints
stiffness
tenderness
pain on motion
swelling
deformity
limitation of motion
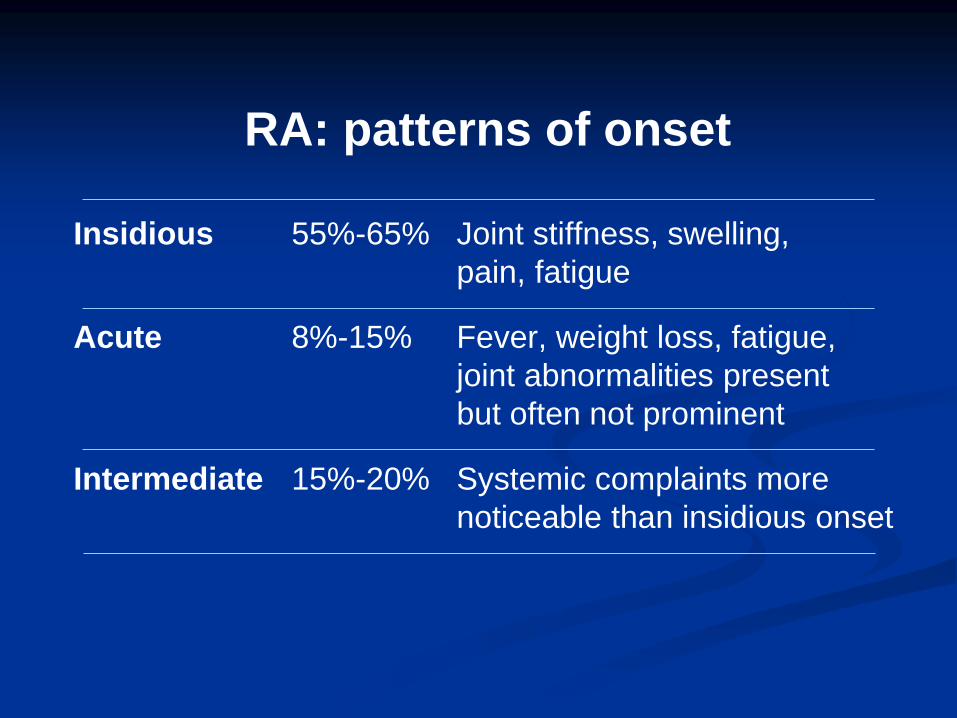
RA: patterns of onset
Insidious 55%-65% Joint stiffness, swelling,
pain, fatigue
Acute 8%-15% Fever, weight loss, fatigue,
joint abnormalities present
but often not prominent
Intermediate 15%-20% Systemic complaints more
noticeable than insidious onset

Rheumatoid factor (RF)
antibody against the Fc fragment of Ig
not specific
~ 80% of RA patients
RF+ patients:
more severe disease
extraarticular manifestations
Anti-cyclic citrullinated peptide
(anti-CCP)
- specificity: 90%
- sensitivity: 50-80%

RA: subsets based on ACPA

RA: classification criteria, ACR 1987

2010

RA - pannus



periarticular osteopenia
symmetric joint space
narrowing/ loss
marginal erosions

Atlantoaxial instability

Popliteal cyst

RA: extraarticular features
rheumatoid nodules (15%)
central necrosis surrounded by palisading fibroblasts and lymphocytes
subcutaneous, bursal, tendon sheaths
extensor surfaces / pressure points
forearms
Achilles
ischial area
MTP’s
flexor surface of fingers


RA: affected
organs

RA: extraarticular manifestations
pulmonary
pleural effusions
interstitial lung disease
nodules
cardiac
pericarditis
myocarditis
atherosclerosis – 3x increased risk of CAD
renal: interstitial nephritis

RA: fibrosis RA: rheumatoid nodules

RA: extraarticular manifestations
Vasculitis
leukocytoclastic vasculitis
palpable purpura
vasculitic lesions on fingers
mononeuritis multiplex
visceral involvement


RA: hematologic
anemia of chronic disease
low Fe, low/N TIBC, ferritin: high
Felty’s syndrome
triad
RA
splenomegaly
neutropenia
frequent infections / leg ulcers
iron deficiency anemia (sec. to NSAIDs !)
We, CRP: high

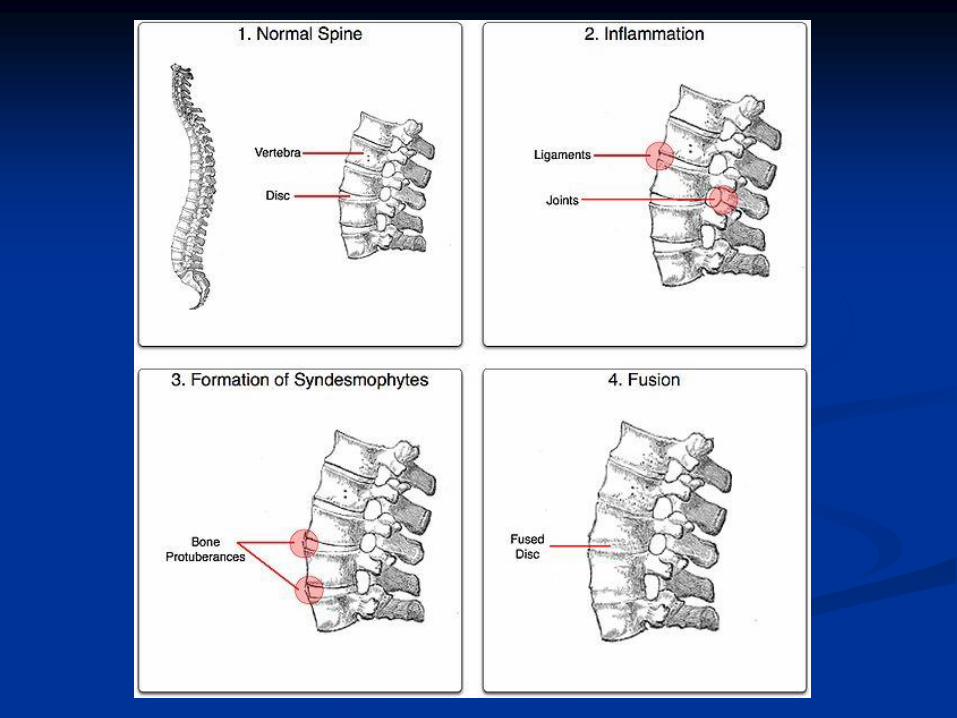
Spondyloarthropathies
Group of inflammatory conditions affecting the axial skeleton (spine, pelvis), and also demonstrating asymmetric migratory oligoarthritis
Types:
Ankylosing spondylitis
Reactive / postinfectious arthritis
Arthritis associated with inflammatory bowel disease (IBD)
Psoriatic spondyloarthritis
Undifferentiated spondyloarthopathy
Juvenile enthesitis-related arthropathy




Spondylarthropathies: common
features
familial clustering
association with HLA-B27
axial joint involvement
sacroiliitis with / without spondylitis
asymmetrical peripheral joint involvement
enthesitis (inflammation of tendon insertions to bone)
dactylitis
extraarticular signs
negative rheumatoid factor

Spondylarthropathies:
leading symptoms
insidious onset of low back pain, that
worses in the morning or with inactivity
improvement of symptoms with exercise
stiffness of the spine and kyphosis
peripheral enthesitis and arthritis
constitutional and organ-specific extra-articular
manifestations


Radiography
bony erosions and osteitis (“whiskering”)
squaring of the vertebral bodies
syndesmophytes
bridging syndesmophytes
bamboo spine
sacroiliitis

Imaging
Magnetic resonance imaging (MRI)
demonstrates early stages of sacroiliitis
Computed tomography (CT)
for the detection of bone changes, such as
erosions, and ankylosis, CT can be superior
to MRI imaging

Bamboo spine





Lumbar flexion (Schober)
A mark is placed between the anterior and posterior iliac spines,
a further mark 10 cm above, the patient bends forward as far as
possible, the difference is recorded
Result: 0.5 cm (normal > 4 cm)


Tragus to wall distance
Patient stands, heels and buttocks against the wall, the head
is placed back as far as possible, keeping the chin horizontal


Ankylosing spondylitis:
extraskeletal manifestations
Eye: iritis
Cardiac
conduction disturbances
aortic valve insuff.
Pulmonary
fibrosis
Neurologic
spinal fracture, instability, compression, or inflam.
atlantoaxial subluxation
myelopathy ; Cauda equina syndrome
Renal: IgA nephropathy; microscopic hematuria


Reactive arthritis
classic triad: urethritis, arthritis, conjunctivitis
occurs 2-4 weeks after the infection
responsible organisms have an affinity for mucous membranes
secondary immune reaction, in susceptible individuals, to primary infective agents: Yersinia
Campylobacter
Shigella
Salmonella
Chlamydia
Ureaplasma

Myopathies
definition
neuromuscular disorders in which the
primary symptom is muscle weakness due to
dysfunction of muscle fiber *
* by the National Institute of Neurological Disorders and Stroke

Neuromuscular disorders
plexopathies
mononeuropathies
polyneuropathies
radiculopathies
motoneuron diseases
disorders of the neuromuscular junction
myopathies

Patient with a suspected myopathy
Main goals:
to determine the exact site/s of the lesion
to determine the cause of myopathy
to determine what kind of specific treatment is available

Myopathy: symptoms
weakness
fatigue
excercise intolerance
myalgia
muscle cramps
muscle atrophy
contractures

muscle weakness
proximal > distal muscles
fatigue
difficulty rising from a chair
difficulty with stairs
difficulty with overhead tasks
respiratory muscles !
bulbar weakness - speech, swallowing
oculomotor, facial

pain
mostly with inflammatory and metabolic origin
high serum CK
aching, dull, cramping
patients often say: like “sore”, “ache”, “spasm”
no numbness or paresthesias !

myalgia
• episodic (metabolic myopathies)
• constant (inflammatory muscle disorders)
• more likely to be due to orthopedic or
rheumatological disorders

Myopathic disorders
inflammatory myopathies
polymyositis
dermatomyositis
inclusion body myositis
viral
muscular dystrophies
X-linked
limb-girdle(ar/d)
congenital
fasioscapulohumeral (ad)
scapuloperoneal (ad)
distal (Welander) (ad/r)
myotonic syndromes
myotonic dystrophy (ad)
inherited
Schwarz-Jampel
congenital myopathies
central core disease
nemaline myopathy
myotubular
fiber-type disproportion
metabolic myopathies
glycogenoses
mitochondrial
periodic paralysis
endocrine myopathies
thyroid
parathyroid
adrenal / steroid
pituitary
drug-induced / toxic

Diagnosis of myopathy
Serum enzymes
- ALT, AST, LDH, aldolase : found in skeletal muscles & liver
- CK (CK-MM): preferred enzyme / isoenzyme
Electrodiagnostic studies
- ENG: repetitive nerve stimulation : neuropathies
- EMG: myopathies
myopathic EMG: low amplitude, short duration, polyphasic MUPs
inflammatory myopathies: increased spontaneous activity,
irritability

Inflammatory myopathy

DNA analysis
- for definite diagnosis of certain muscle disorders
associated with gene defects (deletions or mutations)
Muscle biopsy
- safe ! (for final diagnosis of a suspected myopathy)
- different techniques of microscopic evaluation !
- site: muscle selected w/ mild to moderate weakness
common muscles used for biopsy
proximal – biceps, triceps, quadriceps
distal – extensor carpi radialis, anterior tibialis
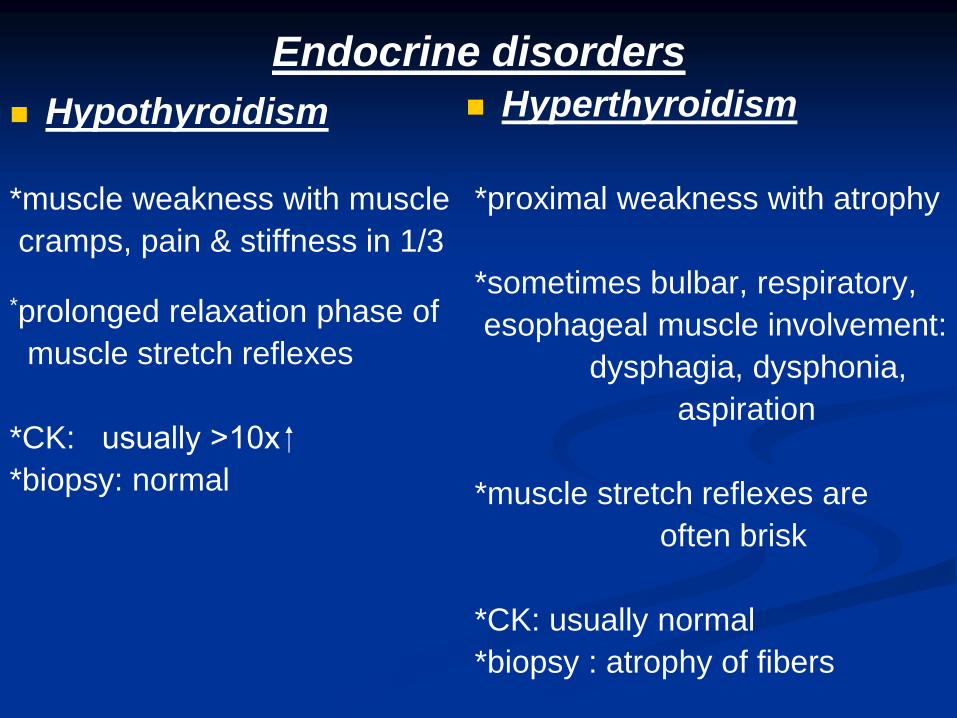
Endocrine disorders
Hypothyroidism
*muscle weakness with muscle
cramps, pain & stiffness in 1/3
*prolonged relaxation phase of
muscle stretch reflexes
*CK: usually >10x
*biopsy: normal
Hyperthyroidism
*proximal weakness with atrophy
*sometimes bulbar, respiratory,
esophageal muscle involvement:
dysphagia, dysphonia,
aspiration
*muscle stretch reflexes are
often brisk
*CK: usually normal
*biopsy : atrophy of fibers

Hyperparathyoidism
-proximal muscle weakness,
muscle wasting, brisk stretch
reflexes
-CK : usually N
-biopsy : varying degrees of
atrophy
Hypoparathyoidism
-hypoCa resulting in sustained
tetany & muscle damage
-hypo- or areflexia
-CK : slight increase
Diabetes mellitus
-myopathy is uncommon
-rarely ischemic infarction of the
thigh muscles
-abrupt onset of pain,
tenderness
-hard & indurated area on
palpation
-biopsy: focal abnormality in
muscles
Vitamin deficiency
-myopathy is rare
-proximal muscle weakness
-vit. D / E deficiency

Cushing’s disease
- steroid excess: various degrees of muscle weakness
- proximal limb muscle weakness
- striking muscle atrophy
- cushingoid appearance
- CK: usually normal
- biopsy : atrophy of fibers
Acromegaly
- mild proximal muscle weakness without muscle atrophy
Adrenal insufficiency
- mild weakness with prominent fatigue
Conn’s syndrome
- due to persistent hypokalemia
- persistent muscle weakness
- muscle wasting if long standing
- CK : may be elevated
- biopsy : degenerating fibers

Toxic myopathies
drugs: statins, clofibrate
corticosteroids – steroid myopathy
alcohol
heroin

Direct toxicity : common !
muscle breakdown, rhabdomyolysis & myoglobinuria may
occur
(e.g. lipid-lowering drugs, glucocorticoids)
Drug induced autoimmune myopathy
e.g. D-penicillamine : features similar to polymyositis
Lipid-lowering agents
proximal weakness, myalgia, malaise, muscle tenderness
(rhabdomyolysis & myoglobinuria)
CK: elevated; EMG : myopathic; biopsy : myocyte necrosis
cessation of drugs !
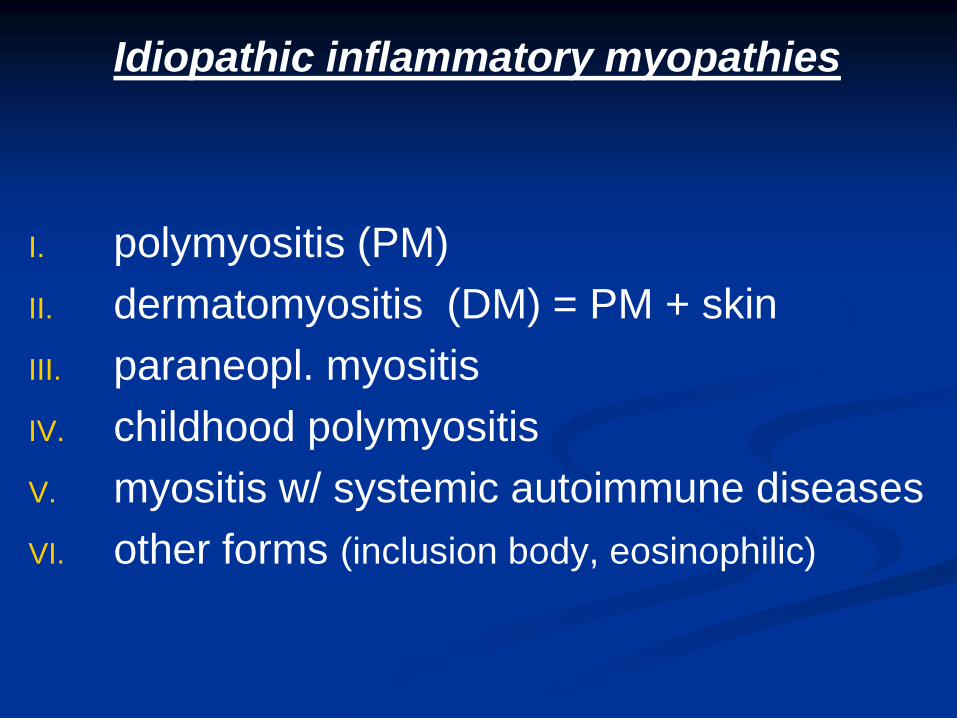
Idiopathic inflammatory myopathies
I. polymyositis (PM)
II. dermatomyositis (DM) = PM + skin
III. paraneopl. myositis
IV. childhood polymyositis
V. myositis w/ systemic autoimmune diseases
VI. other forms (inclusion body, eosinophilic)

PM/DM: characteristics
Symmetrical, proximal muscle weakness (insidious onset)
Muscles usually painless (myalgias: 30%)
Dysphagia (30%),aspiration: pharyngeal and esophageal muscles
Arthralgias
Difficulty kneeling, climbing or descending stairs,
stepping onto a curb, raising arms, lifting objects,
combing hair, and arising from a seated position
Weak neck extensors: difficulty holding the head up
Involvement of pelvic girdle > upper body weakness
Cardiac involvement: pericarditis or cardiomyopathy
Characteristic rash of face, trunk, and hands seen in DM


PM/DM

normal PM

Osteoporosis
Definition: metabolic bone disease
Low bone mass and microarchitectural disruption
causing weakening of bone which predisposes to
fractures



OP: risk factors
Age (increasing)
Low BMI
Ethnicity: Caucasian > Asian/Latino > African American
Family history of fracture


OP: characteristics
generally patients are asymptomatic even with
low bone densities
hip / vertebral fractures
loss of height
acute or chronic back pain secondary to
vertebral fractures
atraumatic or low impact fractures
101


Pathogenesis of osteoporotic fracture


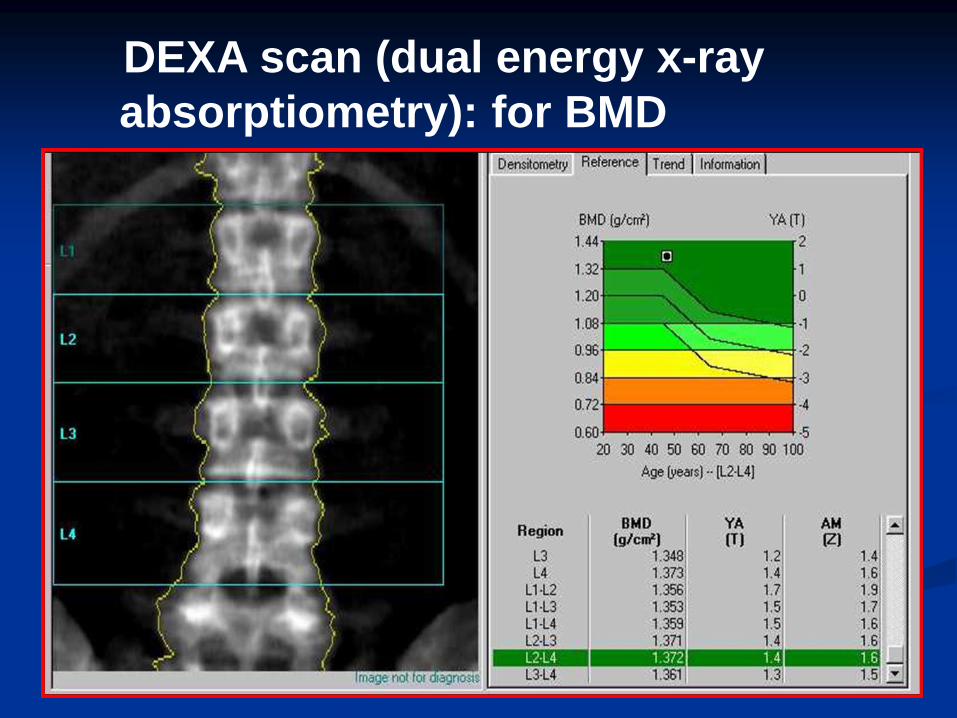
DEXA scan (dual energy x-ray
absorptiometry): for BMD

standard deviation of normal young subjects (T-score) and
age-matched (Z-score)

Thank you !