Embed Size (px)
Citation preview

ARTERIAL DISAESE

Carotid Artery Dissection• Dissection of the carotid artery accounts for approximately 20% of• strokes in patients younger than 45 years of age The etiology and• Pathogenesis of spontaneous carotid artery dissection remains incompletely• understood. Arterial dissection involves hemorrhage• within the media, which can extend into the subadventitial and• Subintimal layers.When the dissection extends into the subadventitial• space,there is an increased risk of aneurysm formation. Subintimal• dissections can lead to intramural clot or thrombosis• Traumatic dissection is typically a result of hyperextension of the• neck during blunt trauma, neck manipulation, strangulation, or• penetrating injuries to the neck. Even in supposedly spontaneous• Cases a history of preceding unrecognized minor neck trauma is not• uncommon. Connective disorders such as Ehlers-Danlos syndrome,• Marfan syndrome, alphar-antitrypsin deficiency, or FMD• may predispose to carotid artery dissection. Iatrogenic dissections• also can occur due to catheter manipulation or balloon angioplasty

• Typical clinical features of carotid artery dissection include• unilateral neck pain, headache and ipsilateral Horner's syndrome• in up to 50% of patients,followed b y manifestations of the cerebral• or ocular ischemia and cranial nerve palsies .Neurologic deficits can• result either because of hemodynamic failure (caused by luminal• stenosis)or by an artery to artery thromboembolism.• The ischemia may cause TIAs or infarctions, or both Catheter• angiography has been the method of choice to diagnose arterial• Dissections but with the advent of duplex ultrasonography• MRI/MRA' and CTA, most dissections can now be diagnosed using• noninvasive imaging modalitie.




Carotid Artery Aneurysms• Carotid artery aneurysms are rare,encountered in less than 1%o
f• all carotid operations . The true carotid artery aneurysm• Generally is due to atherosclerosis or medial degeneration • The F MD and spontaneousd issection of the• carotid artery can lead to the formation of true aneurysms or• Pseudoaneurysms.Whereas conventional surgery has been the • Primary treatmenti n the past,c arotid aneurysms are currently• Being treated more commonly using endovascular approaches.




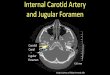
Carotid Body Tumor• The carotid body originates from the third branchial arch and from• neuroectodermal-derivede nural crest lineage.• 'T he normal carotid body is located in the adventitia or• periadventitial tissue at the bifuication of the CCA .• The gland is innerwated by the glossopharyngeale nerve. Its blood• supply is derived predominantly• From external carotid artery, but also can come from the• vertebral artery. Carotid body tumor is a rare lesion of the• neuroendocrine system.• Other glands of neural crest origin are seen in the• neck, parapharyngeasl paces mediastinum,r etroperitoneum‘ and• adrenal medulla. Tumors involving these structures have been• referred to as paraganglioma, glomus tumor, or chemodectoma

• Approximately 5 to 7% of carotid body tumors are malignant.• Although chronic hypoxemia has been invoked as a stimulus for• Hyperplasia of carotid body, approximately 35% of carotid body• tumors are hereditary.The risk of malignancy is greatest in young• patients with familial tumors. Symptoms related to the endocrine• products of the carotid body• tumor are rare. • Patients usually present between the fifth and• Seventh decade of life with an asymptomatic lateral neck mass.The• diagnosis of carotid body tumor requires confirmation on imaging• studies. Carotid duplex scan can localize the tumor to the carotid• bifurcation, but CT or MR imaging usually is required to further• delineate the relationship of the tumor to the adjacent structures





Carotid Trauma• Blunt or penetrating trauma to the neck can cause injury to the• carotid artery Notwithstanding the massive bleeding from carotid• artery transection, injury to the carotid artery can result in carotid• Dissection thrombosis,or pseudoaneurysm formation. Carotid duplex• ultrasound can be useful to locate the site of injury in the• cervical segment of the carotid artery. Spiral CTA has become the• modality of choice to detect extracranial carotid artery injury.• Confirmation of carotid injury by contrast cerebral angiography• remains the gold standard diagnostic test. Injuries to the cervical• segment of the common and internal carotid arteries can be repaired• surgically. Acute carotid artery thrombosis usually is treated• medically with anticoagulation if the patient is asymptomatic.• Revascularization should be considered for patients presenting with• ongoing cerebral ischemia related to carotid artery thrombosis.

• Traumatic carotid artery dissection can cause cerebral ischemia due• to thromboembolization, decreased flow, or thrombosis.• Commonly, the dissection involves the distal Portion of the• cervical and petrous segment of the ICA, Medical management• With antiplatelet or anticoagulation usually is adequate for• uncomplicated traumatic carotid dissection.• In patients with pseudoaneurysms Of the carotid• artery that are located in a segment that is out of surgical reach, the• Use of selective coil embolization of the pseudoaneurysm o r• exclusion of the pseudoaneurysm by a covered stent graft has been• reported. Bare metal stent has been used with success in the• treatment of traumatic carotid artery dissection.

ABDOMINAL AORTIC ANEURYSM• The incidence appears to be increasing, and this is due in• part to improvements in diagnostic imaging and, more importantly,• is a result of a growing elderly population. With early diagnosis and• timely intervention, aneurysm rupture-related death is largely preventable.• Conventional treatment of an AAA involves replacing the• aneurysmal segment of the aorta with a prosthetic graft, with the• operation performed through a large abdominal incision. Techniques• for this open abdominal surgery have been refined, adapted,• and extensively studied by vascular surgeons over the past four• Decades.Despitea well-documented,low perioperative mortality rate• of 2 to 3%In large academic institutions, the thought of undergoing• an open abdominal aortic operation often provokes a sense of anxiety• in many patients due in part to the postoperative pain associated with• the large abdominal incision as well as the long recovery time needed• before the patient can return to normal physical activity.



• The most common location of aortic aneurysms is the infrarenal• aorta. Endovascular stent graft placement represents a revolutionary• and minimally invasive treatment for infrarenal AAAs that only• requires 1 to 2 days of hospitalization, and the patient can return to• normal physical activity within I week.
• The concept of using an• endoluminal device in the management of vascular disease was first• Proposed by Dotter and colleagues who successfully treated a patient• with iliac occlusion using transluminal angioplasty in 1964.Nearly• three decades later, Parodi and colleagues reported the first successful• Endovascular repair of AAA using a stent graft device• The rapid innovation of this new treatment modality has• undoubtedly captured the attention of patients with aortic aneurysms• as well as physicians who practice endovascular therapy

Natural History of Aortic Aneurysm• The natural history of an AAA is to expand and rupture. Therefore, although an• individual pattern of growth cannot be predicted, average aggregate• growth is approximately 3 to 4 mm/y. There is some evidence to• suggest that larger aneurysms may expand faster than smaller• one, but there is significant overlap between the ranges of• growth rates at each strata of size.• Rupture risk appears to be directly related to aneurysm size as• predicied by Laplace's law. Although more sophisticated methods• of assessing rupture risk based on finite element analysis of wall
• stress is under active investigation, maximum transverse diameter• remains the standard method of risk assessment for aneurysm• rupture.
• In the past, AAA rupture risk has been overestimated'• More recently, two landmark studies have served to better define• the natural history of AAA.


• The rupture risk is• quite low for aneurysms <5'5 cm and begins to rise exponentially• thereafter. This size can serve as an appropriate threshold for• recommending elective repair provided one's surgical mortality is• below 5%. For each size strata, however, women appear to be at• higher risk for rupture than men, and a lower threshold of 4.5 to 5'0• Cm may be reasonable in good-risk patients. Although data are less• compelling, a pattern of rapid expansion of >0.5 cm within 6
• months can be considered a relative indication for elective repair'• Aneurysms that fall below these indications may safely be followed• with CT or ultrasound at 6-month intervals, with long-term • Outcomes equivalent to earlier surgical repair. Interestingly, in the• ADAM study, 80% of all patients with AAA who were followed in• this manner eventually came to repair within 5 years.

Clinical Manifestations• Most AAAs are asymptomatic, and they are usually found incidentally• during work-up for chronic back pain or kidney stones' physical examination is • neither sensitive nor specific except in thin patients.• Large aneurysms may be missed in the obese, while normal aortic• pulsations may be mistaken for an aneurysm in thin individuais.• Rarely, patients present with back pain and/or abdominal pain with a• tender pulsatile mass. Patients with these symptoms must be treated• as if they had a rupture until proven othrerwise. If the patient is• hemodlnamically stable and the aneurysm is intact on a CT scan, the• patient is admitted for BP control with IV antihyrertensive agents• and repaired usually within 12 to 24 hours or at least during the same• hospitalization. In contrast, patients who are hemodynamically unstable• with a history of aute back pain and/or syncope and a known• unrepaired AAA or a pulsatile abdominal mass should be immediately• taken to the OR with a presumed diagnosis of a ruptured AAA.

• Overall mortality of AAA rupture is 7l to 77%,whtch
• in cludes all out-of-hospital and inhospital deaths,as
• Compared to 2 to 6% for elective open surgical• repair.as Nearly one half of all patients with• ruptured AAA will die before reaching the
hospital.

Relevant Anatomy• An AAA is defined as a pathologic focal dilation of the aorta that is• >30 mm or 1.5 times the adjacent diameter of the normal aorta .• Male aortas tend to be larger than female, and there is• Generalized growth of the aortic diameter with each decade of life.• Ninety percent of AAA are infrarenal in location and have a• fusiform morphology. There is a higher predilection for juxtarenal• and suprarenal AAA in women as compared to men. Concomitant• common iliac and/or hypogastric artery aneurysms can be found in• 20 to 25% of patients.Although the etiology of most aortic aneurysms• is atherosclerotic clinically significant peripheral occlusive• Disease is unusual and present in less than l0% of all cases.
• Although extravascular anatomy is important for open surgical• repair of AAA, intravascular anatomy and aortoiliac morphology• are important for endovascular repair.

Diagnostic Evaluation• Preoperative evaluation should include routine history and physical• examination with particular attention to (a) any symptoms referable• to the aneurysm, which may impact the timing of repair, (b) a• history of pelvic surgery or radiation, in the event retroperitoneal• exposure is required or interruption of hypogastric circulation is• planned, (c) claudication suggestive of significant iliac occlusive• disease(d ) LE bypass or other femoral reconstructive procedures,• and (e) chronic renal insufficiency or contrast allergy.• Cross-sectional imaging is required for definitive evaluation of• AAA. Although ultrasound is safe, widely available, relatively accurate,• and inexpensive, and, therefore, is the screening modality of
• choice, the CT scan remains the gold standard for determination of• anatomic eligibility for endovascular repair.
• Size of AAA may differ• up to I cm between CT and ultrasound, and, during longitudinal• follow-up, comparisons should be made between identical modalities.• With modern multirow detector scanners, a timed-bolus IV• contrast enhanced, 2.5 to 3.0-mm slice spiral CT of the chest,• abdomen, and pelvis can be performed in <30 seconds with a single• breath hold.• The only major drawback to CT is the risk of contrast nephropathy in• diabetics and in patients with renal insufiiciency..





Surgical Repair of Abdominal AorticAneurysm
• General anesthesia is necessary when performing a conventional• open AAA repair. Although a retroperitoneal incision is a well accepted• Surgical approach,a midline transabdominal incision remains• the more common approach for open aortic aneurysm operation.• Because the abdominal incision can lead to significant pain and• discomfort, an epidural catheter can be placed before the operation• for postoperative analgesic infusion to provide pain control. Once• the abdominal cavity is opened, the small intestines and transverse• colon are retracted to expose the retroperitoneum overlying the• AAA. The retroperitoneum is next divided,followed by isolation of• both proximal and distal segments of the AAA. IV heparin( 100I U/• kg) is given, followed by clamping of the proximal and distal• Segments of the aneurysm The aneurysm sac is opened next, and a• Prosthetic graft is used to reconstruc the aorta.

Endovascular Repair of Abdominal Aortic Aneurysm
• The principle of endovascular repair of AAA involves the implantation• of an aortic stent graft that is fixed proximally and• distally to the nonaneurysmal aortoiliac segment, and thereby• endoluminally excludes the aneurysm from the aortic circulation
• Unlike open surgical repair, endovascular treatment• does not remove or eliminate the aneurysm sac, which therefore is• subjected to potential aneurysm expanston or even rupture as• persistent aneurysm sac pressurization may occur following en_• dograft implantation. Importantly, aortic branches such as lumbar• arteries or the inferior mesenteric artery (IMA) are ligated, which• can lead to persistent aneurysm pressurization and aneurysm expansion.• Currently, five devices are available for elective repair of• intact infrarenal AAA





MESENTERIC ARTERY DISEASE• Vascular occlusive disease of the mesenteric vessels is a relatively• uncommon but potentially devastating condition that generally pre_• sents in patients more than 60 years of age, is three times more• frequent in women, and has been recognized as an entity since1936.• The incidence of such a disease is low and represents 2 % of• the revascularization operations for atheromatous lesions. The most• common cause of mesenteric ischemia is atherosclerotic vascular• Disease. Autopsy studies have demonstrated splanchnic atherosclerosis• in 35 to 70% of cases.Other etiology is exist and include FMD,• Pan arteritis nodosa, arteritis, and celiac artery (CA) compression• from a median arcuate ligament, but they are unusual and have an• incidence of one in nine compared to that of atherosclerosis

• Chronic mesenteric ischemia is related to a lack of blood supply• in the splanchnic region and is caused by disease in one or more• visceral arteries: the celiac trunk, the SMA, and the IMA. Mesenteric• ischemia is thought to occur when two of the three visceral• vessels are affected with severe stenosis or occlusion; however' in as• many as 9% of cases, only a single vessel is involved [superior• Mesenteric artery (SMA) in 5% and celiac trunk in 4% of cases• This disease process may evolve in a chronic fashion,as in the case• of progressive luminal obliteration due to atherosclerosis • On the other hand, mesenteric ischemia can occur suddenly,as in the
case• of thromboembolism. Despite recent Progress in perioperative• management and better understanding in pathophysiology, mesenteric• Ischemia is considered one of the most catastrophic vascular• disorders,w ith mortality rates ranging from 50 to 75% Delay in• diagnosis and treatment are the main contributing factors in its• high mortality.

• The prevalence is rising due in part to the• increased awareness of this disease,• the advanced age of the population, and the• significant comorbidity of these elderly patients.• Early recognition and prompt treatment• before the onset of irreversible intestinal• ischemia are essential to improve the outcome.

Anatomy and Pathophysiology• Mesenteric arterial circulation is remarkable for its rich collateral• network. Three main mesenteric arteries provide the arterial perfusion• to the GI system:the CA, SMA, and IMA. In general,the CA• provides arterial circulation to the foregut (distal esophagus to• duodenum), hepatobiliary system, and spleen; the SMA supplies the• midgut (jejunum to midcolon); and the IMA supplies the hindgut• (midcolon to rectum). The CA and SMA arise from the ventral• surface of the infradiaphragmatic suprarenal abdominal aorta, while• the IMA originates from the left lateral portion of the infrarenal• aorta. These anatomic origins in relation to the aorta are important• when a mesenteric angiogram is performed to determine the luminal• patency. To fully visualize the origins of the CA and SMA, it is• Necessary to perform both an anteroposterior and a lateral projection• Of the aorta because most arterial occlusive lesions occur in the• proximal segments of these mesenteric trunks.





• Because of the abundant collateral flow between these mesenteric• arteries, progressive diminution of flow in one or even two of• the main mesenteric trunks is usually tolerated, provided that• uninvolved mesenteric branches can enlarge over time to provide• Sufficient compensatory collateral flow. In contrast,acute occlusion• of a main mesenteric trunk may result in profound ischemia due to• lack of sufficient collateral flow. Collateral network between the CA• and the SMA exist primarily through the superior and inferior• pancreaticoduodenal arteries. The IMA may provide collateral• arterial flow to the SMA through the marginal artery of Drummond,• the arc of Rioland,and other unnamed retroperitoneal collateral• vessels termed meandering mesenteric arteries (Fig. 23-36).• Lastly,collateral visceral vessels may provide imPortant arterial flow• to the IMA and the hindgut through the hypogastric arteries and• the hemorrhoidal arterial network.




Types of Mesenteric Artery Occlusive Disease
• There are three major mechanisms of visceral ischemia involving the• mesenteric arteries, which include: (a) acute mesenteric ischemia'• which can be either embolic or thrombotic in origin; (b) chronic• mesenteric ischemia; and (c) nonocclusive mesenteric ischemia'• Despite the variability of these syndromes, a common anatomic• pathology is involved in these Processes. The SMA is the most• commonly involved vessel in acute mesenteric ischemia' Acute• thrombosis occurs in patients with underlying mesenteric atheroschlrosis. • F. urthermore,a cute visceral ischemia may develop in aortic• dissectiont hat invoives the mesenteric arteries,or after coarctation• repair.Finally,other unusual causes of ischemia include mesenteric• arteritis,radiation arteritis,and cholesterol emboli.

ClinicaMl anifestations• Abdominal pain out of proportion to physical findings is the classic• Presentation in patients with acute mesenteric ischemia and
occurs• following an embolic or thrombotic ischemic event of the SMA.• Other manifestations include sudden onset of abdominal cramps
in • patients with underlying cardiac or atherosclerotic disease,often• Associated with bloody diarrhea,as a result of mucosal sloughing• secondary to ischemia. Fever, nausea, vomiting, and abdominal• distention are some common but nonspecific minifestations.• Diffuse abdominal tenderness rebound,and rigidity are late signs• And usually indicate bowel infarction and necrosis

• Clinical manifestations of chronic mesenteric ischemia are more• subtle owing to the extensive collateral development. However,• when intestinal blood flow is unable to meet the physiologic GI• demands, mesenteric insufficiency ensues. The classic symptoms• include postprandial abdominal pain, "food fear," and weight loss.• Persistent nausea and occasionally diarrhea,may coexist.Diagnosis• remains challenging, and most of the patients will undergo an• extensive and expensive GI tract work-up for the above symptoms• before referral to a vascular service.

• The typical patients who develop nonocclusive mesenteric ischemia• are elderly patients.Comorbidities include congestive heart• failure, acute myocardial infarction with cardiogenic shock, hypovolemic• or hemorrhagics hock,sepsis pancreatitis and administration• of digitalis or vasoconstrictor agents such as epinephrine.• Abdominal pain is only present in approximately 70% of these• patients. When present, the pain is usually severe bur may vary in• location, character and intensity.In the absence of abdominal pain,• Progressive abdominal distention with acidosis may be an early sign• of ischemia and impending bowel infarction.• Abdominal pain due to narrowing of the origin of the CA may• occur as a result of extrinsic compression or impingement by the
• median arcuate ligament. This condition is known as• celiac artery compression syndrome or median arcuate ligament• Syndrome. Angiographically therei s CA compression that augments• with deep expiration,and poststenotic dilatation.The CA compression• syndrome has been implicated in some variants of chronic• mesenteric ischemia. Most patients are young females between 20• and 40 years of age. Abdominal symptom is nonspeciic.

DiagnosticE valuation• Plain abdominal radiographs may provide helpful information• to exclude other causes of abdominal pain such as intestinal ob_• struction, perforation, or volvulus, which may exhibit symptoms• mimicking intestinal ischemia. Pneumoperitoneum, pneumatosis• intestinalis,and gas in the portal vein may indicate infarcted
bowel.• In contrast,radiographic appearance of an adynamic ileus with a• Gasless abdomen is the most common finding in patients with• acute mesenterici schemia.• Definitive diagnosis is made with arteriography.





• Upper endoscopy colonoscopy or barium radiography does not• provide any useful information when evaluating acute mesenteric• ischemia.Moreover,barium enema is contraindicated if the• diagnosis of mesenteric ischemia is being considered' The• intraluminal barium can obscure accurate visualization• Of mesenteric circulation during angiography.In addition,• intraperitoneal leakage of barium can occur in the setting of intestinal perforation, which can lead
to• Added therapeutic challenges during mesenteric revascularization

• Diagnosis of chronic mesenteric ischemia can be more challenging.• Usually, before the evaluation by a vascular service, the patients• have undergone an extensive work-up for the symptoms of chronic• abdominal pain, weight loss, and anorexia. Rarely, the vascular• surgeon is the first to encounter a patient with the above symptoms• In this situation, it is advisable to keep in mind that mesenteric• ischemia is a rare entity, and that a full diagnostic work-up that• should include CT scan of the abdomen and evaluation by a• Gastroenterologist should be performed.Mesenteric occlusive disease• may coexist with malignancy, and symptoms of mesenteric• vessesle stenosis may be the result of extrinsic compression by a tumor.• Duplex ultrasonography is a valuable noninvasive means of• assessintgh e patency of the mesenteric vessele.

• Mesenteric arteriography also can play a therapeutic role. Once• the diagnosis of nonocclusive mesenteric ischemia is made on the• arteriogram, an infusion catheter can be placed at the SMA orifice• and vasodilating agents such as papaverine can be administered• intra arterially.T he papaverine infusion may be continued postop• Eratively to treat persistent vasospasm a, common occurrence fol_• lowing mesenteric reperfusion.

Surgical RepairAcute Embolic Mesenteric lschemia
• InitIal management of patients with acute mesenteric ischemia• Includes fluid resuscitation and systemic anticoagulation with heparin• to prevent further thrombus propagation.Significant metabolic aci_• Dosis not responding to fluid resuscitation should be corrected with• sodium bicarbonate.A central venous catheter,peripheral arterial• catheter, and a Foley catheter should be placed For hemodynamic• status monitoring. Appropriate antibiotics are given before surgical• Exploration.The operative management of acute mesenteric ischemia• is dictated by the cause of the occlusion. It is helpful to obtain a• Preoperative mesenteric arteriogram to confirm the diagnosis and to• plan appropriate treatment options.However,the diagnosis of mes_• enteric ischemia frequently cannot be established before surgical• exploration; and therefore, patients in a moribund condition with• acute abdominal symptoms should undergo immediate surgical ex_• ploration, avoiding the delay required to perform an arteriogram

• The primary goal of surgical treatment in embolic mesenteric• Ischemia is to restore arterial perfusion with removal of the • embolusfrom the vessel. The abdomen is explored through a • Midline incision,which often reveals variable degrees of intesiinal• ischemia from the midjejunum to the ascending colon. The• transverse colon is lifted superiorly, and the small intestine is• reflected toward the right upper quadrant. The SMA is approached• at the root of the small bowel.
. Once the proximal SMA is identified and controlled with• vascular clamps, a transverse arteriotomy is made to extract the• embolus, using standard balloon embolectomy catheters

Chronic Mesenteric ischemia• The therapeutic goal in patients with chronic mesenteric ischemia• is to revascularize mesenteric circulation and prevent the development• of bowel infarction. Mesenteric occlusive disease can be• Treated successfully by either transaortic endarterectomy or mesenteric• artery bypass. Transaortic endarterectomy is indicated for• ostial lesions of patent CA and SMA. A left medial rotation is• performed,a nd the aorta and the mesenteric branchesa re exposed.• A lateral aortotomy is performed,e ncompassing both the CA and• SMA orifices.The visceral arteries must be adequately mobilizeds o• that the termination site of endarterectomy can be visualized.• Otherwise, an intimal flap may develop, which can lead to early• thrombosis or distal embolization

Ceilac Artery Compressoin Syndrome
• The decision to intervene in patients with CA compression syndrome• should be based on both an appropriate symptom complex and the• finding of CA compression in the absence of other findings to explain• the symptoms. The treatment goal is to release the ligamentous• structure that compresses the proximal CA and to correct any• persistent stricture by bypass grafting. The patient should be cautioned• that relief of the celiac compression cannot be guaranteed to• relieve the synptoms. In a number of reports on endovascular• management of chronic mesenteric ischemia, the presence of CA• compression syndrome has been identified as a major factor of• technical failure and recurrence. Therefore, angioplasty and stenting• should not be undertaken if extrinsic compression of the CA by the• median arcuate ligament is suspected based on Preoperative imaging• studies. Open surgical treatment should be performed instead.




RENAL ARTERY DISEASE• Obstructive lesions of the renal artery can produce hypertension,• resulting in a condition known as renovascular hypertension, which• is the most common form of hypertension amenable to therapeutic• intervention,and affects 5 to 10% of all hypertensive patients in the• United States.Patients with renovascular hypertensron are at an• increased risk for irreversible end-organ dysfunction, including• permanent kidney damage, if inadequate pharmacologic therapies• are used to control the BP. The majority of patients with renal artery• obstructive disease have vascular lesions of either atherosclerotic• disease or fibrodysplasia involving the renal arteries. The proximal portion of the• renal artery represents the most common location for• the development of atherosclerotic d iseaseI.
The decision for intervention is complex, and needs to take into consideration• a variety of anatomic, physiologic, and clinical features,• unique for the individual patient

Etiology• Approximately 8 % of all renal artery occlusive lesions are caused by• Atherosclerosis which typically involves a short segment of the renal• artery ostia, • Atherosclerotic lesions are bilateral in• two thirds of patients. Individuals with this disease commonly• present during the slxth decade of life. Men are affected twice as• frequently as women. Atherosclerotic lesions in other territories• such as the coronary, mesenteric,c erebrovascular and peripheral• arterial circulation are common. When a unilateral lesion is present,• the disease process equally affects the right and left renal artery.• The second most common cause of renal artery stenosisis FMD,• which accounst for 20o/of cases and is most frequently encountered• in young, often multiparous women. FMD of the renal artery• Represents aheterogeneous group of lesions that can produce histopathologic• changes in the intima, media, or adventitia.

ClinicaMl anifestations
• Renovascular hypertension is the most common sequelae of renal
• artery occlusive disease.Its prevalence varies• from 2% in patients• with diastolic BP >100 mmHg, to almost 30%• in those with diastolic BP over 125 mmHg.

DiagnosticE valuation
• The diagnostic requisites for renovascular hypertension include
• both hypertension and renal artery stenosis. Impairment of the
• renal function may coexist, although the occurrence of renal
• insufficiency before the development of hypertension is
• uncommon.