Embed Size (px)
Citation preview

BRIEF REPORT
ATHEROEMBOLIC ARTERITIS
John Sheehan and Eamon Sweeney
School of Pathology, Trinity College, Dublin 2.
Summary Atheroembolism accurring spontaneously in an
elderly male without an abdominal aortic aneur- ysm is described. Arteritis was present at the sites of impaction of the emboli. The aetiology, diagnosis and clinical presentation of this unusual form of arteritis are discussed.
Introduction Autopsy studies suggest that atheroembolism is
a rare phenomenon and in most cases is asso- ciated with trauma (surgical or otherwise) to an a',heromatous aortic aneurysm (Flory, 1945; Hand- ler, 1956; Thurlbeck and Castleman, 1957; Gore and Collins, 1960; Schornagel, 1961; Maurizi et al, 1968; Kealy, 1978). Usually such embolisation excites only a mild inflammatory response in the wall of the affected vessel but cases have been documented in which a necrotizing vasculitis developed locally (Zak and Elias, 1949; Fisher et al, 1960; Anderson, 1965; Anderson and, MacDon- nell Richards, 1968). This unorthodox vascular response may be related to the composition of the embolus (Otken, 1959) or its duration (Kealy, 1978; Zak and Elias, 1949), but whatever its pathogenesis the distinction of atheroembolic arteritis from other arteritides, particularly poly- arteritis nodosa (PAN) is of great clinical im- portance.
Case Report A 72 year old male with a 10 year history of
hypertension and controlled atrial fibrillation was admitted in acute congestive cardiac failure. There was no evidence of myocardial infarction. Biochemical profile was normal apart from a urea of 89 mg/dl, creatinine of 6.7 mg/d l and SGOT of 300 units/ml. Haemoglobin and white cell count were normal. Urinalysis revealed haema- turia and albuminuria. The patient remained oligurio in spite of diuretic therapy.
Delayed excretion of contrast medium on in- travenous pyelography suggested renal parenchy- mal damage. During the first 24 hours the serum potassium rose to 7.0 mEq/I and the blood urea to 145 mg/dl. Peritoneal dialysis was instituted with rapid resolution of the cardiac failure and gradual resumption of renal function and partial correction of the biochemical abnormalities. The haemoglobin at this stage was 10.3 g/d l , the
white cell count slightly elevated at 12.9 x 109/L and the .ESR was 130 mm in one hour. A rapidly developing petechial rash was then noticed: on the dorsa of both feet and subsequently skin ulceration developed: on 2 toes on the left. The peripheral pulses were normal. A clinical diag- nosis of cholesterol/platelet embolism was made and the patient was treated' with oral dipyrida- mole. This was followed by healing of the toe ulcers and disappearance of the rash. The pat- ient was then discharged from hospital.
Three months later he was re-admitted for investigation of anaemia. The haemoglobin was now 9.6 g/d l and the WCC 23 x IO~/L (neutr~- phils 87%, lymphocytes 7%, monocytes 3%, eosinophils 2% and myelocytes 1%). The red blood' cells were normochromic, anisocytic and there was slight rouleaux formation on blood film. The pJatelet count was 478,000 per mm ~. Bone marrow aspirate was normal. The ESR remained at 130 mm in one hour.
Blood urea and r were still slightly elevated but other biochemical parameters were normal. Serum immunoglobulins were normal and hepatitis B antigen screen was negative. Twelve days after admission the patient died of severe progressive cardiac failure of acute onset.
Autopsy Findings There was gross generalised atheroma. The
lower thoracic and abdominal aorta were of nor- mal bore but exhibited large soft plaques of atheroma many of which were ulcerated. The heart was enlarged (710 gm) and showed biven- tricular hypertrophy, thrombosis of the left atrial appendage, recent thrombosis of the right coron- ary artery and extensixe fresh posterior wall infarction. The pleural cavities contained large effusions and the lungs showed oedema and patchy bronchopneumonia. The kidneys (90 and 115 gms) had a coarsely granular capsular sur- face and an averarge cortical thickness of 3 ram. Atheromatous narrowing of both renal artery ostia was present. The liver was of normal size but the cut surface exhibited several ill-defined; yellow zones of necrosis measuring up to 2 cm diameter. Multiple small gastric erosions were present with a small amount of altered blood in the proximal small bowel.
319

320 IRISH JOURNAL OF MEDICAL SCIENCE
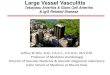
Microscopy Multiple atheromatous emboli were present in
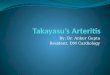
the arcuate and interlobular arteries of both kid- neys, many of the vessels exhibiting fibrinoid nec- rosis of the wall, disruption of the internal elastic lamina and intense acute inflammation with eosinophils (Figs. 1 and 2). Ischaernia distal to
Fig 1--Arcuate artery containing atheroembolus.
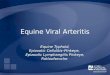
the obstruction was evidenced by Iocalised tub- ular atrophy, interstitial inflammation and fibrosis. The glomeruli and arterioles appeared' normal. Similar emboli with arteritis were present in the stomach, jejunum, pancreas, spleen, adrenal, prostate and liver. In the latter site, large areas of hepatocyte necrosis were present in the mid zonal and periportal areas related to emboli in
Fig. 2 ~ a m e artery proximal to embolus showing necrotising arteritis.
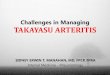
the hepatic artery radicles (Fig. 3). The central parts of the liver Iobules showed evidence of acute on chronic hypoperfusion (Fig. 4). No cholesterol emboli were detected above the diaphragm even in the markedly arteriosclerotic and thrornbosed coronary vessels.
Discussion The true incidence of atheroembolism is un-
known but in a number of autopsy studies the phenomenon has been recorded in from less than 1% to more than 12% of cases (Flory, 1945; Handler, 1956; Thurlbeck and Castleman, 1957; Gore and Collins, 1960; Schornagel, 1961; Maurizi eta/ , 1968; Kealy, 1978). Most of the authors of these studies agree that the post-mortem incid- ence varies with the extent of tissue sampling but it is recognised that atheroembolism occurs with greater frequency in subjects with more advanced aortic disease. In patients who develop mural thrombus or an aneurysm in the diseased aorta atheroembolism is common whilst in those cases where surgical correction of an atheromatous aneurysm is undertaken it is virtually the rule (Thurlbeck and Castleman, 1957). Atheroembol- ism is commonest in males over 60 years of age and may affect any organ in the body (Gore and Collins, 1960). The kidneys are the most frequent site of embolisation and in most, if not all such cases there is concomitant involvement of lower limb vessels (Maurizi et al, 1968). MOst athero- emboli are incidental findings at autopsy but they can cause death most commonly by myocardial infarction, encephalomalacia or renal failure (Gore and Collins, 1960). Flory (1945) documen- ted the microscopic appearances most commonly found in atheroembolism - - hyperplastic intima and occasional giant cells surrounding choles- terol clefts--but in only one experimental animal injected with scrapings from an atheromatous plaque was a vasculitis noted. Since that time periarteritis resulting from atheroembolism has been confirmed ir~ experimental animals (Otken, 1959) and the association has been observed sporadically in humans (Zak and Elias, 1949; Fisher et af, 1960; Anderson, 1965; Anderson and MacDonnell Richards, 1968). )On the basis of experimental evidence, Otken (1959) postulated that the vessel response depended on the com- position of the embolus - - mixed atheromatous elements exciting a vasculitic response rather than the bland foreign body reaction associated with the impaction of cholesterol crystals. Other authors (Flory, 1945; Handler, 1956; Thurlbeck and Castleman, 1957; Gore and Collins, 1960; Schornagel, 1961; Maurizi et at, 1968; Kealy, 1978; Zak and Elias, 1949) have suggested that the duration of impactJon of the embolus is of importance in the development of the arteritic response and fibrinoid degeneration in the vessel wall has been attributed to prolonged vasospasm ( Fisher et "al, 1960).

Fig. 3
ATHEROEMBO,LIC ARTERITIS
Fig. 4
321
Atheroembolus in hepatic artery radicle, with adjacent acute hepatocyte necrosis and evidence of chronic hypoperfusion.
While the microscopic discrimination between atheroembolic arteritis and polyarteritis nodosa at post-mortem is of some academic interest, it is in the clinical setting that the distinction between the two diseases assumes critical impor- tance because different treatments are required. As in this case multifocal atheroembolism may present clinically with a low grade fever, leuco- cytosis with absolute eosinophilia and high ESR combined with unstable hypertension, ischaemic heart disease and rapidly deteriorating renal funct ion--a complex of symptoms and signs in- distinguishable from polyarteritis nodosa (PAN). Abrupt onset of lower limb signs weighs in favour of atheroembolism and further support for the diagnosis can be obtained by arteriographic de- monstration of discrete ulcerative atheroma in the relevant vessel~ (Wagner and Martin, 1973). Ran- dom lower extremity muscle biopsy in clinically suspected cases of atheroembolism has proved diagnostically successful (Anderson and MacDon- nell Richards, 1968) and in most instances classical bland atheroembolic occlusion of vessels has been found. Difficulties in diagnosis arise when the arteritic form of atheroembolism occurs.
Although Anderson (1968) suggests that there are subtle histological changes which serve to differentiate this from PAN, we feel that the only reliable feature is the presence of cholesterol clefts in the embolus and' it is apparent that these may be missed in small biopsies if an inadequate number of sections is examined. A spurious diag- nosis of PAN in such an instance and treatment with steroids could prove disastrous in a disease
where surgery, salicylates and possibly anticoag- ulants are more appropriate.
The suggestion that the vascular lesion in the case described here might have resulted from the fortuitous impaction of atheroemboli in arter- ies narrowed by concurrent PAN is untenable. Every arteritic lesion in this case exhibited cholesterol clefts at some point on step section- ing, an unlikely event if the above postulate were true, and no evidence of arteritis was found above the diaphragm, an extraordinary geographic limitation, if the primary disease were PAN. The absence of glomerular lesions and hepatitis B antigen which is detected in 25-40% of cases of polyarteritis nodosa (Gocke et af, 1970) is further strong evidence against PAN in this patient.
Rafarences
Anderson, W. R. 1965. Necrotising angiitis asso- ciated with embolisation of cholesterol. Am. J. Clin. Path. 43, 65-71.
Anderson, W. R. and MacDonell, Richards, A. 1968. Evaluation of lower extremity muscle biopsies in the diagnosis of atheroembolism. Arch Path. 86, 535.
Fisher, E. R., Hellstrom, H. R. and Myers, J. D. 1960. Disseminated atheromatous emboli. Am. J. Med. 29, 176.
Flory, C. M. 1945. Arterial occlusions produced by emboli from eroded aortic atheromatous plaques. Am. J. Path. 21, 549.

322 IRISH JOURNAL OF MEDICAL SCIENCE
Gocke, D. J., Hsu, K., Morgan, C. 1970. Associa- tion between polyarteritis and Australia antigen. Lancet ii, 1149.
Gore, I. and Collins, D. P. 1960. Spontaneous atheromatous embolisation. Am. J. Clin. Path. 33, 416.
Handler, F. P. 1956. Clinical and pathologic sig- nificance of atheromatous embolisation, with emphasis on an etio.logy of renal hypertension. Am. J. Med. 20, 366.
Kealy, W. F. 1978. Atheroembolism. J. Clin. Path. 31, 984.
Kwaan, J. H. M., Molen, R. V., Stemmer, E. A. 1975. Peripheral embolism resulting from un- suspected atheromatous aortic plaques. Surgery 78, 583.
Maurizi, C. P., Barker, A. E., Trueheart, R. E. 1968. Atheromatous emboli. Arch. Path. 86, 528.
Otken, L B. 1959. Experimental production of atheromatous embolisation. Arch. Path. 68, 685.
Schornagel, H. E. 1961. Emboli of cholesterol crystals. J. Path. Bact. 81, 119.
Thurlbeck, W. M. and Castleman, B. 1957. Athero- matous emboli to the kidneys after aortic surg- ery. New England J. Med. 257, 442.
Wagner, R. B. and Martin, A. S. 1973. Peripheral atheroembolism : confirmation of a clinical con- cept, with a case report and review of the literature. Surgery 73, 353.
Zak, F, G. and Elias, K. 1949. Embolisation with material from atheromata. Am. J. Med. Sc. 218, 510.