Embed Size (px)
Citation preview

Bulletin of the NYU Hospital for Joint Diseases 2009;67(1):6-146
Gruson KI, Kwon YW. Atraumatic osteonecrosis of the humberal head. Bull NYU Hosp Jt Dis. 2009;67(1):6-14.
Abstract
While much literature has focused on the management of osteonecrosis of the femoral head, far less information is available regarding the treatment and outcomes of this disease in the proximal humerus. To a great extent, man-agement of humeral head osteonecrosis has been inferred from studies involving the femoral head. The etiologies for this disease can be categorized most usefully as traumatic versus atraumatic. Regardless of the underlying etiology, the common pathway involves disruption of the arterial inflow or the venous outflow of the bone, with resultant osseous cell death. The general treatment strategies for humeral head osteonecrosis include nonoperative modalities for symp-tomatic early disease, with surgical intervention reserved for more advanced disease or those with recalcitrant pain.
The humeral head remains the second most common site of osteonecrosis following the femoral head.1 De-spite this fact, there is a paucity of literature regarding
osteonecrosis of the proximal humerus. While similarities in the etiology and the pathogenesis of this disorder exist between these anatomic sites, significant differences war-rant considering humeral head osteonecrosis as a distinct
separate entity.1,2 The glenohumeral joint is not exposed to the same weightbearing forces as the hip joint. Furthermore, less constraint within the glenohumeral joint allows for ac-commodation of significant deformity in advanced disease. An increase in scapulothoracic motion may compensate for restricted motion at the glenohumeral articulation. Finally, the proximal humerus has been shown in multiple dissec-tion studies to have an extensive anastomotic arterial supply, mitigating the effect of a loss of any single arterial inflow.3,4 For these reasons, surgeons should be cautioned against blindly applying the treatment protocols for the femoral head to cases of humeral head osteonecrosis.
Vascular AnatomySeveral cadaveric dissection studies have defined the vas-cular supply to the proximal humerus. These findings have significant implications with regard to the potential devel-opment of osteonecrosis of the humeral head following a vascular insult. Meyer and colleagues3 studied the arterial supply of six fresh frozen proximal humeri and found that the epiphysis received contributions from both the anterior and posterior circumflex humeral arteries. The anterior circumflex artery, arising from the axillary artery, courses laterally under the tendon of the long head of the biceps and terminates with smaller branches in the greater tuberosity. The arcuate artery arises from the anterolateral branch of the anterior circumflex and ascends proximally into the humeral head, acting as its major intraosseous supply. The lesser tuberosity receives blood from the anterolateral branch as well. The contribution from the posterior circumflex artery was more variable, though a group of vessels was consistently found penetrating the bone-cartilage interface medially. Cadaveric selective injection studies performed by Gerber and associates4 demonstrated that the posterior circumflex artery supplies only a small posteroinferior por-tion of the humeral epiphysis (Fig. 1). After injury to the
Atraumatic Osteonecrosis of the Humeral Head
Konrad I. Gruson, M.D., and Young W. Kwon, M.D., Ph.D.
Konrad I. Gruson, M.D., was an Administrative Chief Resident in the Department of Orthopaedic Surgery, NYU Hospital for Joint Diseases and is currently Assistant Professor of Orthopaedic Sur-gery, Department of Orthopaedic Surgery, Albert Einstein College of Medicine, Bronx, New York. Young W. Kwon, M.D., Ph.D., is Assistant Professor of Orthopaedic Surgery, New York University School of Medicine, and an Attending in the Division of Shoulder and Elbow Surgery, Department of Orthopaedic Surgery, NYU Hospital for Joint Diseases, NYU Langone Medical Center, New York, New York. Correspondence: Young W. Kwon, M.D., Department of Ortho-paedic Surgery, NYU Hospital for Joint Diseases, 301 East 17th Street, New York, New York 10003; [email protected].

7Bulletin of the NYU Hospital for Joint Diseases 2009;67(1):6-14
anterior circumflex artery, the posterior circumflex artery is believed to provide additional blood flow to the humeral head, though the exact extent to which this artery increases its inflow capacity is unknown.
Etiology and PathogenesisOsteonecrosis results from disruption of the osseous arterial inflow or the venous outflow. Common atraumatic etiologies are listed in Table 1. In comparison, three- and four-part frac-tures of the proximal humerus have been associated with an osteonecrosis rate ranging from 15% to 30%. Paradoxically, this rate has been previously shown to increase following open reduction and internal fixation (ORIF), presumably due to iatrogenic disruption of the remaining blood supply to the humeral head.5
Corticosteroid UseLong-standing corticosteroid use represents the most com-monly reported atraumatic cause for osteonecrosis. Although no consensus has been reached on the definitive pathogen-esis, some have proposed an increase in the intraosseous pressure secondary to adipocyte hypertrophy, with resultant local ischemia.6,7 Another theory suggests an embolic phe-nomenon involving hyperlipidemia induced by steroid use.8 As supportive evidence, the increase in circulating serum lipids has been shown to embolize to the subchondral arteri-oles, with radio-labeled adipocytes localizing to subchondral bone of both the hip and shoulder. The incidence of steroid-induced osteonecrosis has de-clined because of increased awareness of this association and the resultant decrease in the drug use. Typically, osteo-necrosis follows the chronic administration of high-dose steroids. However, many investigators have demonstrated the difficulty in predicting which patients will ultimately develop the disease. A recent retrospective review of spinal cord injured patients, who received short-term megadoses of methylprednisolone, demonstrated no case of avascular necrosis of either the humeral or femoral heads by mag-netic resonance imaging (MRI), with a minimum 6-month follow-up.9 In contrast, others have reported the develop-ment of osteonecrosis in patients who were treated with high-dose corticosteroid, even for a short period of time.10-12 Interestingly, several cases of multifocal osteonecrosis fol-lowing intra-articular long-acting corticosteroid injections have been reported.13 The interval between corticosteroid administration and onset of symptoms has been reported to be between 6 and 18 months.14
Alcohol UseWhile chronic alcohol abuse is clearly associated with the development of osteonecrosis, the actual incidence is still debated. Estimates in the literature range from 6% to 39% of nontraumatic cases.7 The pathophysiology of osteonecrosis following alcohol use has been proposed to be similar to that for corticosteroids. Therefore, it is believed that changes in the bone marrow following fat embolization to the sub-chondral vasculature leads to venous stasis and a cycle of progressive ischemia. Regular alcohol consumption has been found to result in an 8-fold increased risk for femoral head
Table 1 Etiologies and Pathogenesis for Atraumatic OsteonecrosisRisk Factor Proposed Pathogenesis
Corticosteroid use 1. Ischemia from lipocyte hypertrophy2. Fat embolism
Hemoglobinopathy EmbolismAlcohol use Fat embolismGaucher’s disease 1. Ischemia from lipid-laden cells
2. Vascular spasmDysbarism EmbolismConnective tissue disorders 1. Corticosteroid use(i.e., rheumatoid arthritis, systemic lupus erythematosus) 2. Vascular inflammation
Figure 1 Vascular supply of the humeral head: 1. axillary artery; 2. posterior circumflex artery; 3. anterior circumflex artery; 4. antero-lateral branch of anterior circumflex artery; 5. greater tuberosity; 6. lesser tuberosity. (Reproduced from Gerber C, Schneeberger AG, Vinh TV (1990).4 © The Journal of Bone and Joint Surgery, Inc. With permission.)

Bulletin of the NYU Hospital for Joint Diseases 2009;67(1):6-148
osteonecrosis.15 A dose-related effect was demonstrated, with a 3.3-fold risk increase with less than 400 mL/week consumption and a 17.9-fold risk increase with more than 1 L/week consumption.
Sickle Cell HemoglobinopathiesOcclusion of the arterial blood supply to the subchondral bone from deformed blood cells initiating microinfarcts has been the proposed mechanism of the sickle cell hemoglobin-opathies, of which sickle cell disease is the most common.2,16 Other investigators have proposed that marrow hyperplasia, as a response to chronic anemia, may cause increased in-tramedullary pressure and compression of the vasculature. Higher hematocrit levels among certain genotype patients may further precipitate humeral head osteonecrosis, second-ary to relative vascular stasis and increased blood viscosity.16 Milner and coworkers17 presented one of the largest epidemiologic series of sickle cell patients and found a prevalence of osteonecrosis of 5.6%. The incidence of osteonecrosis, when adjusted for patient age, was highest among sickle cell disease with concurrent α-thalassemia and HbS/β0-thalassemia. In patients older than 35 years, the incidence of osteonecrosis was highest amongst those with HbS/β+-thalassemia. The patients with HbSS/α-thalassemia had a higher hematocrit level, which may have contributed to the higher incidence of osteonecrosis. Interestingly, the vast majority of new cases were initially asymptomatic. The increased prevalence of periarticular osteonecrosis among sickle cell patients has been confirmed, with later disease correlated with worsening function.16 The investigators also noted that the highest incidence of osteonecrosis was among those patients with HbS/β+-thalassemia.
Dysbarism (Caisson Disease)Dysbarism affects deep-sea divers and those exposed to environments of increased air pressure. The pathogenesis appears to be related to gas embolism following a rapid decrease in surrounding atmospheric pressure. These gas emboli are believed to occlude the smaller vessels and induce ischemia.1,2 Additionally, extravascular gas bubbles may compress surrounding vasculature and disrupt arterial inflow or venous outflow. Miyanishi and colleagues studied 56 div-ers for the presence of dysbaric osteonecrosis and found that an elevated level of plasminogen activator inhibitor was an independent predictor of osteonecrosis.18 The investigators believe that this hypercoagulability was the cause of the variable incidence of dysbaric osteonecrosis among divers who had previously experienced decompression sickness.
Gaucher’s DiseaseGaucher’s disease is an autosomal recessive lysosomal stor-age disorder, characterized by an accumulation of the lipid glucosylceramide in various tissues, including the bone mar-row.19 It remains an important cause of osteonecrosis among the Ashkenazi Jewish population. Male gender and a high
platelet count were correlated with humeral osteonecrosis in a series of patients with known type 1 Gaucher’s disease.20 Lipid-laden macrophages are thought to act via mass ef-fect, effectively compressing the intraosseous vasculature. Additionally, vasoactive substances released from these cells are thought to induce vasospasm.2 These effects then act cumulatively to cause local ischemia and osteonecrosis.
Systemic DiseasesVarious systemic diseases, including rheumatoid arthritis (RA), systemic lupus erythematosus (SLE), and Cushing’s syndrome have also been associated with the development of osteonecrosis.7,21,22 The independent impact of these diseases on inducing osteonecrosis is difficult to estimate, as many patients are often taking steroids concurrently as part of their treatment. In addition, with SLE there may be a separate contribution from systemic vasculitis that induces osteonecrosis.
EpidemiologyConcomitant involvement of other joints, particularly the femoral head, in the presence of proximal humeral osteo-necrosis has been reported sporadically in the literature. L’Insalata and associates found that three-quarters of patients had multifocal involvement when humeral head osteone-crosis was identified.23 Specific to corticosteroid-induced humeral head osteonecrosis, the rate of other joint involve-ment has reached 90%.14,23 Finally, others have reported that approximately 75% of sickle cell and HbS/C patients with humeral head osteonecrosis also had femoral head disease.17 In a study of patients with Gaucher’s disease, 29% (15/51) of patients had at least one site of osteonecrosis; eight shoulders in seven patients were involved.20 Patients with humeral osteonecrosis were 13 times more likely to have concomitant femoral involvement. Conversely, it is estimated that only 20% of patients with femoral head osteonecrosis have humeral disease.
ClassificationThe anatomy and the function of the glenohumeral joint is vastly different than the hip joint and, consequently, result in delayed presentation and diagnosis of proximal humeral osteonecrosis. The shoulder, for example, rarely acts as a weightbearing joint. Additionally, the glenohumeral articu-lation is less conforming than the hip joint, and restricted shoulder motion can be compensated by surrounding joints. This allows for maintenance of shoulder function even with advanced disease. Thus, upon presentation, many patients with humeral head osteonecrosis may already exhibit advanced degenerative changes, precluding nonoperative management. The superior central portion of the humeral head is most often affected by the early disease process and is, therefore, often the region of collapse and flattening.19 A retrospective MRI review of 13 patients with humeral head osteonecro-

9Bulletin of the NYU Hospital for Joint Diseases 2009;67(1):6-14
sis verified that the superior humeral head was most often involved.24 The majority of patients had greater than 75% articular involvement. The superior head region contacts the glenoid at 60° of abduction or 90° of forward flexion.19 Patients with documented humeral head osteonecrosis are discouraged from performing repetitive overhead activities to limit contact between the affected portion of the humeral head and the glenoid. The original radiographic classification of femoral head osteonecrosis by Ficat and Arlet25 was adapted to the proximal humerus by Cruess in 1978.14 It remains the most commonly used classification system for humeral head osteonecrosis and is based on radiographic findings (Fig. 2). This classification system allows for appropriate disease staging, meaningful comparison of study results, and guide-lines for treatment. Additional imaging modalities may be used for improved visualization and characterization of the disease involvement.
Stage 1 The initial stage is represented by absent radiographic find-ings, with marrow signal changes detectable only with MRI or bone scan. Underlying histopathology is present despite the benign appearance of plain radiographs.
Stage 2 This stage is marked by sclerosis, typically, in the superior portion of the humeral head. The sclerosis, which may be focal or diffuse, results from subchondral microfracture without articular collapse (Figs. 3 and 4). Histologically, there is evidence of cell death without significant resorp-tion and healing.
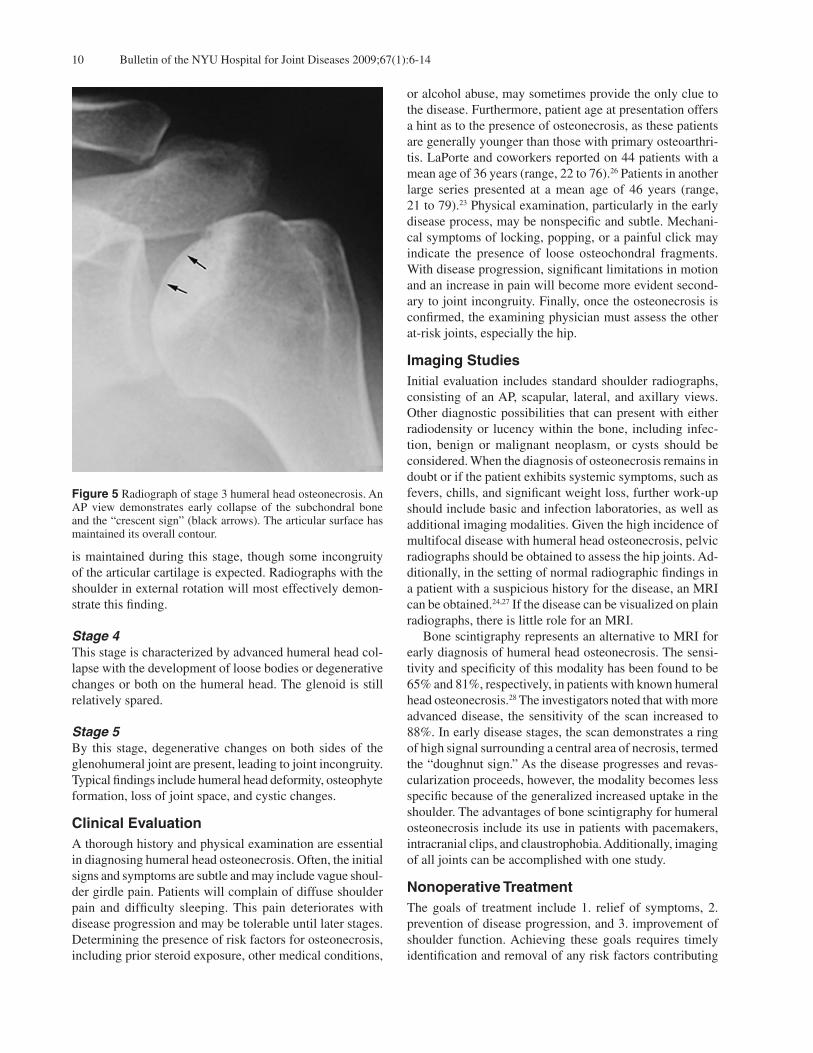
Stage 3 The radiographic hallmark of this stage is the “crescent sign,” which represents subchondral bone collapse (Fig. 5). Typically, the general sphericity of the humeral head
Figure 4 MRI of stage 2 disease. Note the characteristic involve-ment of a significant portion of the superior articular surface, as well as the clear demarcation between the relatively normal distal bone and the ischemic subchondral bone.
Figure 3 Radiographs of late stage 2, humeral head osteonecrosis. AP views in (A) external and (B) internal rotation demonstrate areas of sclerosis involving a major portion of the humeral head.
Figure 2 Stages of humeral head osteonecrosis.
Bulletin of the NYU Hospital for Joint Diseases 2009;67(1):6-1410
is maintained during this stage, though some incongruity of the articular cartilage is expected. Radiographs with the shoulder in external rotation will most effectively demon-strate this finding.
Stage 4 This stage is characterized by advanced humeral head col-lapse with the development of loose bodies or degenerative changes or both on the humeral head. The glenoid is still relatively spared.
Stage 5 By this stage, degenerative changes on both sides of the glenohumeral joint are present, leading to joint incongruity. Typical findings include humeral head deformity, osteophyte formation, loss of joint space, and cystic changes.
Clinical EvaluationA thorough history and physical examination are essential in diagnosing humeral head osteonecrosis. Often, the initial signs and symptoms are subtle and may include vague shoul-der girdle pain. Patients will complain of diffuse shoulder pain and difficulty sleeping. This pain deteriorates with disease progression and may be tolerable until later stages. Determining the presence of risk factors for osteonecrosis, including prior steroid exposure, other medical conditions,
or alcohol abuse, may sometimes provide the only clue to the disease. Furthermore, patient age at presentation offers a hint as to the presence of osteonecrosis, as these patients are generally younger than those with primary osteoarthri-tis. LaPorte and coworkers reported on 44 patients with a mean age of 36 years (range, 22 to 76).26 Patients in another large series presented at a mean age of 46 years (range, 21 to 79).23 Physical examination, particularly in the early disease process, may be nonspecific and subtle. Mechani-cal symptoms of locking, popping, or a painful click may indicate the presence of loose osteochondral fragments. With disease progression, significant limitations in motion and an increase in pain will become more evident second-ary to joint incongruity. Finally, once the osteonecrosis is confirmed, the examining physician must assess the other at-risk joints, especially the hip.
Imaging StudiesInitial evaluation includes standard shoulder radiographs, consisting of an AP, scapular, lateral, and axillary views. Other diagnostic possibilities that can present with either radiodensity or lucency within the bone, including infec-tion, benign or malignant neoplasm, or cysts should be considered. When the diagnosis of osteonecrosis remains in doubt or if the patient exhibits systemic symptoms, such as fevers, chills, and significant weight loss, further work-up should include basic and infection laboratories, as well as additional imaging modalities. Given the high incidence of multifocal disease with humeral head osteonecrosis, pelvic radiographs should be obtained to assess the hip joints. Ad-ditionally, in the setting of normal radiographic findings in a patient with a suspicious history for the disease, an MRI can be obtained.24,27 If the disease can be visualized on plain radiographs, there is little role for an MRI. Bone scintigraphy represents an alternative to MRI for early diagnosis of humeral head osteonecrosis. The sensi-tivity and specificity of this modality has been found to be 65% and 81%, respectively, in patients with known humeral head osteonecrosis.28 The investigators noted that with more advanced disease, the sensitivity of the scan increased to 88%. In early disease stages, the scan demonstrates a ring of high signal surrounding a central area of necrosis, termed the “doughnut sign.” As the disease progresses and revas-cularization proceeds, however, the modality becomes less specific because of the generalized increased uptake in the shoulder. The advantages of bone scintigraphy for humeral osteonecrosis include its use in patients with pacemakers, intracranial clips, and claustrophobia. Additionally, imaging of all joints can be accomplished with one study.
Nonoperative TreatmentThe goals of treatment include 1. relief of symptoms, 2. prevention of disease progression, and 3. improvement of shoulder function. Achieving these goals requires timely identification and removal of any risk factors contributing
Figure 5 Radiograph of stage 3 humeral head osteonecrosis. An AP view demonstrates early collapse of the subchondral bone and the “crescent sign” (black arrows). The articular surface has maintained its overall contour.

11Bulletin of the NYU Hospital for Joint Diseases 2009;67(1):6-14
to disease development. For example, use of alternative medications and discontinuing steroids may reduce the risk of osteonecrosis to other, uninvolved joints and may slow the disease progression in the proximal humerus. In addition to risk assessment, patients should be placed in a formal therapy program encouraging maintenance of mo-tion and strengthening of the surrounding shoulder girdle musculature. Therapy to prevent disuse-associated adhesive capsulitis has been advocated.2 Adequate pain medication may allow for more effective participation with therapy. Ac-tivity modification should be emphasized to avoid shoulder positions that increase joint reactive forces. Generally, stage 1 and 2 disease respond well to nonoperative modalities and these patients tend to heal with minimal deformity. In the setting of intractable pain or disease progression, surgical intervention should be considered. The natural history of humeral head osteonecrosis has been difficult to define because of the many variables that affect the disease process. The disease course has generally been thought to be slow, explaining the advanced changes at initial presentation. Identifying patients who are likely to develop severe, disabling arthritis would be an important part of any treatment algorithm. Most published series have regarded the need for arthroplasty as a poor or unsatisfactory result.23,29-31 The existing literature has demonstrated that earlier disease stages, when treated appropriately, result in good long-term clinical and radiographic outcomes, with fewer patients progressing to arthroplasty.14,29,30 Hattrup and Cofield, using survivorship analysis, demonstrated that 42% of stage 2, 29% of stage 3, 55% of stage 4, and 79% of stage 5 patients required arthroplasty within 3 years after initial presentation.30 The extent of head involvement at presenta-tion significantly affected the need for shoulder replacement. Interestingly, traumatic osteonecrosis cases had a higher need for arthroplasty than their atraumatic counterparts (78% vs 47%). Patients with minimal presenting symptoms and, thus, treated without surgical intervention remained mostly pain-free at follow-up and were able to carry out their basic activities of daily living. In contrast to the above findings, L’Insalata and colleagues found less favorable long-term results in their series of 65 shoulders.23 Thirteen shoulders were treated early on with shoulder arthroplasty because of severe pain and disability, with another 22 shoulders undergoing arthroplasty during the study period. Of the remaining 30 shoulders treated nonoperatively, half reported poor functional outcomes. The investigators noted that all shoulders with radiographic progression, and those at stage 3 or worse upon presenta-tion, had poor outcomes. Corticosteroid-induced disease has been correlated with better overall clinical outcomes.23,32 It is certainly feasible that the nonsteroid-induced patients have multiple other medical issues that hold more subjective pre-cedence over their shoulder disease. Similarly, others have found that corticosteroid-induced osteonecrosis results in fewer shoulder arthroplasties at medium-term follow-up than
traumatic osteonecrosis cases (44% vs 78%).32 Interestingly, patients whose humeral head osteonecrosis was secondary to sickle cell disease tended not to progress to shoulder arthroplasty.16,17
ArthroscopyIn later stages of osteonecrosis, arthroscopy may be used for synovectomy, debridement of chondral flaps, and removal of loose bodies. Hayes reported on loose body removal in an elderly male with late-stage steroid-induced necrosis, with resolution of mechanical symptoms and pain relief at 20 months.33 More recently, Hardy and associates described ar-throscopic debridement and loose body removal for bilateral avascular necrosis in a patient with chronic renal failure and steroid use.34 While both shoulders demonstrated advanced disease, improvement in motion and variable pain relief was achieved. The investigators recommended arthroscopy as an acceptable modality for dealing with mechanical symptoms.
Core DecompressionSimilar to studies for the femoral head, core decompres-sion has been proposed to decrease intraosseous pressure during the early stages of osteonecrosis.35 Few series have reported on the results of this technique with regard to the humeral head.23,26,36-38 In general, the use of this procedure is reserved for early stages of osteonecrosis, defined as either stage 1 or 2. Some have extended the indications to stage 3 disease with minimal collapse. Core decompression can be performed open through a standard deltopectoral ap-proach, staying lateral to the bicipital groove,26,38 or with an arthroscopically-assisted technique.36,37 Mont and coworkers first described core decompression of the proximal humerus, using an open technique with a small axillary fold incision.38 A retrospective review of their results demonstrated that 14 patients with preoperative stage 1 and 2 disease had good or excellent results, while 7 of 10 patients with stage 3 disease had good or excellent results. This initial report was expanded by LaPorte and colleagues in a series that included the patients from the above men-tioned study.26 At a mean follow-up of 10 years, successful results were reported in the following: 15/16 (94%) stage 1 disease, 15/17 (88%) stage 2 disease, 16/23 (70%) stage 3 disease, and 1/7 (14%) stage 4 disease. The investigators recommended decompression only for those with disease stages 1 to 3. In contrast, a small series of patients with stage 3 disease treated with core decompression resulted in clini-cal and radiographic disease progression, with subsequent arthroplasty in all cases.23
Chapman and associates described an arthroscopic technique using an anterior cruciate ligament tibial tunnel guide.36 Arthroscopic assistance allowed the surgeon to view the glenohumeral space, limiting the amount of surgical dissection and reducing the risk of chondral penetration. A small clinical series utilizing a similar technique found good postoperative pain relief and maintenance of pre-

Bulletin of the NYU Hospital for Joint Diseases 2009;67(1):6-1412
operative shoulder motion.37 The investigators stated that arthroscopically-assisted decompression allowed for better cosmesis, decreased recovery time, and potentially lower infection rates. A novel technique for articular surface repositioning with bone grafting was described for a young patient with idiopathic stage 4 osteonecrosis.39 Following arthroscopic loose body removal, a bone tunnel was created from below the greater tuberosity to the necrotic region. Iliac crest bone graft was placed in the tunnel, and the articular surface was found to be well-positioned through a 100° arc of abduction. At 2-year follow-up, the patient remained pain free and had significant improvements in motion. This procedure was advocated for symptomatic stage 3 and 4 osteonecrosis.
Shoulder ArthroplastyProsthetic shoulder replacement has been advocated for the treatment of symptomatic osteonecrosis characterized by radiographic collapse (late stage 3 through stage 5 dis-ease).13,29,40 The decision to use hemiarthroplasty (HHA) versus total shoulder arthroplasty (TSA) has largely de-pended on surgeon preference (Fig. 6). In general, however, glenoid resurfacing has traditionally been reserved for stage 5 disease. Absolute contraindication for arthroplasty is active infection, and relative contraindications include significant brachial plexopathy and concomitant deltoid and rotator cuff insufficiency. The challenge of shoulder arthroplasty in patients with atraumatic osteonecrosis remains prosthe-sis longevity, as these patients tend to be relatively young. Sperling and colleagues evaluated the long-term results of arthroplasty in patients under 50 years of age and reported 15-year implant survival for HHA and TSA at 73% and 84%, respectively.41 Both options provided significant relief of pain, as well as improvements in shoulder motion. How-ever, a subset of five HHA patients treated for osteonecrosis yielded predominately unsatisfactory results. To preserve bone stock, the humeral stem should be press-fit, especially in younger patients.2,19,40 Cement should be used only if existing bone appears inadequate for bony ingrowth. The decision to resurface the glenoid is based on intraoperative assessment of the cartilage. Even with deteriorated cartilage,
the glenoid may not have sufficient bone to support a pros-thesis.42 A massive, irreparable rotator cuff tear precludes resurfacing the glenoid socket. Recent series focusing specifically on the outcomes of ar-throplasty for humeral head osteonecrosis have demonstrated excellent pain relief (greater than 80%) and improvement in shoulder function.43,29,32,44 Among patients undergoing HHA, progressive glenoid wear may present long-term issues. In patients treated with TSA, radiographic glenoid lucency was reported to be as high as 38%32; however, only one patient required revision surgery. Interestingly, Orfaly and coworkers found that patients undergoing arthroplasty for primary osteoarthritis had better functional gains than their osteonecrosis counterparts.44 Most studies have also demonstrated better results in arthroplasty patients with atraumatic compared to posttraumatic osteonecrosis.19,32,44
Interpositional ArthroplastyInterpositional arthroplasty has been described for osteo-arthritis in the young patient as an alternative to traditional glenoid resurfacing. The idea is to preserve bone stock in the younger, more active patient who will likely require future surgery. This technique may also be used in the revi-sion setting to allow for incorporation of bone graft with cavitary lesions. The use of interpositional arthroplasty does not preclude later conversion to a TSA or to glenohumeral arthrodesis. Burkhead and Hutton45 reported on six patients with a mean age of 48 years who underwent biological resurfacing for early glenohumeral arthritis, utilizing either anterior capsule or fascia lata autograft. With a minimum 2-year follow-up, all patients had good pain relief and signifi-cant improvement in overall motion without joint space loss. The technique for lateral meniscal allograft was described by Ball and colleagues.42 The wedge shape of the meniscus allowed for graft positioning in areas of bony defects. The investigators reported on a small patient series with good clinical and radiographic outcomes at 24 months. Meniscal allograft was proposed as a better fit for the glenoid, and no significant immune reaction against the graft has been demonstrated. The graft appears to retain its load-bearing characteristics and durability. This technique was modified to include the use of either the medial or lateral meniscus and the fashioning of an oval-shaped allograft.46 This technique may be utilized in cases of moderate posterior glenoid wear, but long-term clinical data is still lacking.42
SummaryOsteonecrosis of the humeral head remains a significant source of patient morbidity, leading to pain and shoulder dysfunction. The most successful outcomes have been demonstrated in patients whose disease is diagnosed and treated early. Vague shoulder pain in a young patient with risk factors for osteonecrosis should be evaluated thoroughly. Although plain films of the shoulder are usually sufficient to confirm the diagnosis, MRI may also be used to gain
Figure 6 Postoperative (A) AP and (B) axillary radiographs of a humeral head resurfacing in a 28-year-old female with late stage 3 steroid-induced osteonecrosis, significant pain, and functional disability. In this patient a previous core decompression failed.

13Bulletin of the NYU Hospital for Joint Diseases 2009;67(1):6-14
valuable information about the joint. Whenever possible, all efforts should be made to prevent the progression of disease (Fig. 7). Patients with symptomatic disease should be treated nonoperatively, with an emphasis on pain control, physical therapy for motion, and activity modification. When these modalities fail, the use of core decompression has been successful in stage 1 and 2, as well as in selective stage 3 disease. Most investigators have argued that treatment of symptomatic stage 4 and 5 disease requires arthroplasty. Although clinical experience is still limited, interpositional arthroplasty may also provide an acceptable alternative for young patients with glenohumeral arthritis and inadequate glenoid bone stock or in those who likely will require tra-ditional arthroplasty in the future.
Disclosure StatementNone of the authors have a financial or proprietary interest in the subject matter or materials discussed in the manuscript, including (but not limited to) employment, consultancies, stock ownership, honoraria, and paid expert testimony
References1. Sarris I, Weiser R, Sotereanos DG. Pathogenesis and treat-
ment of osteonecrosis of the shoulder. Orthop Clin North Am. 2004;35:397-404.
2. Cushner MA, Friedman RJ. Osteonecrosis of the humeral head. J Am Acad Orthop Surg. 1997;5:339-46.
3. Meyer C, Alt V, Hassanin H, et al. The arteries of the humeral head and their relevance in fracture treatment. Surg Radiol Anat. 2005;27:232-7.
4. Gerber C, Schneeberger AG, Vinh TV. The arterial vasculariza-
tion of the humeral head: an anatomical study. J Bone Joint Surg Am. 1990;72:1486-94.
5. Gerber C, Hersche O, Berberat C. The clinical relevance of posttraumatic avascular necrosis of the humeral head. J Shoulder Elbow Surg. 1998;7:586-90.
6. Fisher DE. The role of fat embolism in the etiology of cortico-steroid-induced avascular necrosis. Clinical and experimental results. Clin Orthop Relat Res. 1978;(130):68-80.
7. Hasan SS, Romeo AA. Nontraumatic osteonecrosis of the humeral head. J Shoulder Elbow Surg. 2002;11:281-98.
8. Moran TJ. Cortisone-induced alterations in lipid metabolism. Arch Pathol Lab Med. 1962;73:300-12.
9. Wing PC, Nance P, Connell D, Gagnon F. Risk of avascular necrosis following short term megadose methylprednisolone treatment. Spinal Cord. 1998;36:633-6.
10. O’Brien TJ, Mack GR. Multifocal osteonecrosis after short-term high-dose corticosteroid therapy: a case report. Clin Orthop Relat Res. 1992;(279):176-9.
11. Taylor LJ. Multifocal avascular necrosis after short-term high-dose steroid therapy: a report of three cases. J Bone Joint Surg Br. 1984;66:431-3.
12. Fast A, Alon M, Weiss S, Zer-Aviv FR. Avascular necrosis of the bone following short-term dexamethasone therapy for brain edema. Case report. J Neurosurg. 1984;61:983-5.
13. Laroche H, Arlet J, Mazieres B. Osteonecrosis of the femoral and humeral heads after intraarticular corticosteroid injec-tions. J Rheumatol. 1990;17:549-51.
14. Cruess RL. Experience with steroid-induced avascular necro-sis of the shoulder and etiologic considerations regarding os-teonecrosis of the hip. Clin Orthop Relat Res. 1978;(130):86-93.
15. Matsuo K, Hirohata T, Sugioka Y, et al. Influence of alcohol intake, cigarette smoking, and occupational status on idio-pathic osteonecrosis of the femoral head. Clin Orthop Relat Res. 1988;(234):115-23.
16. David HG, Bridgman SA, Davies SC, et al. The shoulder in sickle-cell disease. J Bone Joint Surg Br. 1993;75:538-45.
17. Milner PF, Kraus AP, Sebes JL, et al. Osteonecrosis of the humeral head in sickle cell disease. Clin Orthop Relat Res. 1993;(289):136-43.
18. Miyanishi K, Kamo Y, Ihara H, et al. Risk factors for dysbaric osteonecrosis. Rheumatology. 2006;45:855-8.
19. Loebenberg MI, Plate AM, Zuckerman JD. Osteonecrosis of the humeral head. Instr Course Lect. 1999;48:349-57.
20. Rodrigue SW, Rosenthal DI, Barton NW, et al. Risk factors for osteonecrosis in patients with type 1 Gaucher’s. Clin Orthop Relat Res. 1999;(362):201-7.
21. McKee MD. Atraumatic osteonecrosis of the humeral head. J Rheumatol. 2000;27:1582-4.
22. Mont MA, Payman RK, Laporte DM, Patri M, Jones LC, Hungerford DS. Atraumatic osteonecrosis of the humeral head. J Rheumatol. 2000;27:1766-73.
23. L’Insalata JC, Pagnani MJ, Warren RF, Dines DM. Humeral head osteonecrosis: clinical course and radiographic predictors of outcome. J Shoulder Elbow Surg. 1996;5:355-61.
24. Lee JA, Farooki S, Ashman CJ, Yu JS. MR patterns of involve-ment of humeral head osteonecrosis. J Comput Assist Tomogr. 2002;26:839-42.
25. Ficat RP. Idiopathic bone necrosis of the femoral head: early diagnosis and treatment. J Bone Joint Surg Br. 1985;67:3-9.
Figure 7 Proposed treatment algorithm.

Bulletin of the NYU Hospital for Joint Diseases 2009;67(1):6-1414
26. LaPorte DM, Mont MA, Mohan V, et al. Osteonecrosis of the humeral head treated by core decompression. Clin Orthop Relat Res. 1998;(355):254-60.
27. Rao VM, Fishman M, Mitchell DG, et al. Painful sickle cell crisis: Bone marrow patterns observed with MR imaging. Radiology. 1986;165:211-15.
28. Sakai T, Sugano N, Nishii T, et al. Bone scintigraphy screen-ing for osteonecrosis of the shoulder in patients with non-traumatic osteonecrosis of the femoral head. Skeletal Radiol. 2002;31:650-5.
29. Rutherford CS, Cofield RH. Osteonecrosis of the shoulder. Orthop Trans. 1987;11:239.
30. Hattrup SJ, Cofield RH. Osteonecrosis of the humeral head: relationship of disease stage, extent and cause to natural his-tory. J Shoulder Elbow Surg. 1999;8:559-64.
31. Parsch D, Lehner B, Loew M. Shoulder arthroplasty in nontraumatic osteonecrosis of the humeral head. J Shoulder Elbow Surg. 2003;12:226-30.
32. Hattrup SJ, Cofield. Osteonecrosis of the humeral head: results of replacement. J Shoulder Elbow Surg. 2000;9:177-82.
33. Hayes JM. Arthroscopic treatment of steroid-induced osteo-necrosis of the humeral head. Arthroscopy. 1989;5:218-21.
34. Hardy P, Decrette E, Jeanrot C, et al. Arthroscopic treat-ment of bilateral humeral head osteonecrosis. Arthroscopy. 2000;16:332-5.
35. Hungerford DS, Lennox DW. The importance of increased intraosseous pressure in the development of osteonecrosis of the femoral head: implications for treatment. Orthop Clin North Am. 1985;16:635-54.
36. Chapman C, Mattern C, Levine WN. Arthroscopically as-sisted core decompression of the humeral head for avascular necrosis. Arthroscopy. 2004;20:1003-6.
37. Dines JS, Strauss EJ, Fealy S, Craig EV. Arthroscopic-as-
sisted core decompression of the humeral head. Arthroscopy. 2007;23:103e1-4.
38. Mont MA, Maar DC, Urquhart MW, et al. Avascular necrosis of the humeral head treated by core decompression. A retro-spective review. J Bone Joint Surg Br. 1993;75:785-8.
39. Nakagawa Y, Ueo T, Nakamura T. A novel surgical procedure for osteonecrosis of the humeral head: reposition of the hu-meral head and bone engraftment. Arthroscopy. 1999;15:433-8.
40. Hattrup SJ. Indications, technique, and results of shoul-der arthroplasty in osteonecrosis. Orthop Clin North Am. 1998;29:445-51.
41. Sperling JW, Cofield RH, Rowland CM. Neer hemiarthro-plasty and Neer total shoulder arthroplasty in patients fifty years old or less: long-term results. J Bone Joint Surg Am. 1998;4:464-73.
42. Ball CM, Galatz LM, Yamaguchi K. Meniscal allograft interposition arthroplasty for the arthritic shoulder: descrip-tion of a new surgical technique. Tech Shoulder Elbow Surg. 2001;2:247-54.
43. Mansat P, Huser L, Mansat M, et al. Shoulder arthroplasty for atraumatic avascular necrosis of the humeral head: nineteen shoulders followed up for a mean of seven years. J Shoulder Elbow Surg. 2005;14:114-20.
44. Orfaly RM, Rockwood CA Jr, Esenyel CZ, Wirth MA. Shoulder arthroplasty in cases with avascular necrosis of the humeral head. J Shoulder Elbow Surg. 2007;16:S27-32.
45. Burkhead WZ Jr, Hutton KS. Biologic resurfacing of the glenoid with hemiarthroplasty of the shoulder. J Shoulder Elbow Surg. 1995;4:263-70.
46. Themistocleous GS, Zalavras CG, Zachos VC, Itamura JM. Biologic resurfacing of the glenoid using a meniscal allograft. Tech Hand Up Extrem Surg. 2006; 10:145-9.