Embed Size (px)
Citation preview

This article appeared in a journal published by Elsevier. The attachedcopy is furnished to the author for internal non-commercial researchand education use, including for instruction at the authors institution
and sharing with colleagues.
Other uses, including reproduction and distribution, or selling orlicensing copies, or posting to personal, institutional or third party
websites are prohibited.
In most cases authors are permitted to post their version of thearticle (e.g. in Word or Tex form) to their personal website orinstitutional repository. Authors requiring further information
regarding Elsevier’s archiving and manuscript policies areencouraged to visit:
http://www.elsevier.com/authorsrights

Author's personal copy
Review
Closed-loop cortical neuromodulation in Parkinson’s disease: Analternative to deep brain stimulation?
Anne Beuter a,⇑, Jean-Pascal Lefaucheur b,c,⇑, Julien Modolo d,e
a Institut Polytechnique de Bordeaux, Talence, Franceb Université Paris Est Créteil, Faculté de Médecine, EA 4391, Créteil, Francec Assistance Publique – Hôpitaux de Paris, Hôpital Henri Mondor, Service de Physiologie – Explorations Fonctionnelles, Créteil, Franced Lawson Health Research Institute, Human Threshold Research Group, London, ON, Canadae Western University, Departments of Medical Biophysics and Medical Imaging, London, ON, Canada
a r t i c l e i n f o
Article history:Accepted 14 January 2014Available online 18 January 2014
Keywords:Closed-loopCortexDeep brain stimulationFunctional neurosurgeryNeuromodulationParkinson’s diseaseTreatment
h i g h l i g h t s
� Current neuromodulation therapy for Parkinson’s disease consists of deep brain stimulation usingopen-loop technique.
� In contrast to open-loop approach, closed-loop stimulation is modulated online by the feedback ofneuronal activity recording.
� This review presents the evidences for the application of closed-loop technique to cortical stimulationfor the treatment of Parkinson’s disease.
a b s t r a c t
Deep brain stimulation (DBS) is usually performed to treat advanced Parkinson’s disease (PD) patientswith electrodes permanently implanted in basal ganglia while the stimulator delivers electrical impulsescontinuously and independently of any feedback (open-loop stimulation). Conversely, in closed-loopstimulation, electrical stimulation is delivered as a function of neuronal activities recorded and analyzedonline. There is an emerging development of closed-loop DBS in the treatment of PD and a growing dis-cussion about proposing cortical stimulation rather than DBS for this purpose. Why does it make sense to‘‘close the loop’’ to treat parkinsonian symptoms? Could closed-loop stimulation applied to the cortexbecome a valuable therapeutic strategy for PD? Can mathematical modeling contribute to the develop-ment of this technique? We review the various evidences in favor of the use of closed-loop cortical stim-ulation for the treatment of advanced PD, as an emerging technique which might offer substantial clinicalbenefits for PD patients.� 2014 International Federation of Clinical Neurophysiology. Published by Elsevier Ireland Ltd. All rights
reserved
Contents
1. Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 8752. Parkinson’s disease and brain stimulation . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 875
2.1. Parkinson’s disease . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 8752.2. Deep brain stimulation (DBS) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 8752.3. Motor cortex stimulation (MCS). . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 876
http://dx.doi.org/10.1016/j.clinph.2014.01.0061388-2457/$36.00 � 2014 International Federation of Clinical Neurophysiology. Published by Elsevier Ireland Ltd. All rights reserved
⇑ Corresponding authors. Addresses: Institut Polytechnique de Bordeaux, 1 avenue du Dr Albert Schweitzer, 33402 Talence, France. Tel.: +33 6 8030 7940 (A. Beuter). ServicePhysiologie, Explorations Fonctionnelles, Hôpital Henri Mondor, 51 avenue de Lattre de Tassigny, 94010 Créteil cedex, France. Tel.: +33 1 4981 2694; fax: +33 1 4981 4660(J.-P. Lefaucheur).
E-mail addresses: [email protected] (A. Beuter), [email protected] (J.-P. Lefaucheur).
Clinical Neurophysiology 125 (2014) 874–885
Contents lists available at ScienceDirect
Clinical Neurophysiology
journal homepage: www.elsevier .com/locate /c l inph
Author's personal copy
3. ‘‘Open-loop’’ versus ‘‘closed-loop’’ stimulation. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 8784. Pathological brain rhythms in PD . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 8795. Specificities of cortical stimulation . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 8806. Translating closed-loop cortical stimulation from bench to bedside . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 880
6.1. Checklist of objectives. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 8806.2. Engineering closed-loop cortical stimulation using biomathematical modeling . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 881
7. Concluding remarks . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 881Acknowledgement . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 882References . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 882
1. Introduction
Therapeutic neuromodulation for Parkinson’s disease (PD) usu-ally consists of an open-loop stimulation of deep brain structures,such as the subthalamic nucleus (STN) or the internal part of theglobus pallidus (GPi) (Bronstein et al., 2011). On the other hand,the therapeutic efficacy of stimulation delivered to superficialcortical regions remains to be proved (Lefaucheur, 2009b). Actu-ally, PD pathophysiology relies on the existence of pathologicalrhythms in neural networks between cortical and deep brain (basalganglia) structures (Brown, 2006). Therefore, techniques of closed-loop brain stimulation with online modulation according to feed-back information provided neuronal activity recording, could bevaluable in this context (Eusebio et al., 2012). The purpose of thisreview is to give evidences for the application of a closed-loop ap-proach to cortical stimulation for the treatment of PD. First, we willbriefly present the disease and the principles and results of itstreatment by deep brain stimulation (DBS) and motor cortex stim-ulation (MCS).
2. Parkinson’s disease and brain stimulation
2.1. Parkinson’s disease
Parkinson’s disease (PD), the second most common neurode-generative disease of the central nervous system after Alzheimer’sdisease, affecting more than 6 million people worldwide and 1.2million in Europe (Dorsey et al., 2007). It represents about 1% ofthe global population over 65 years of age, and 5% above 85 yearsof age (de Rijk et al., 1997). The clinical picture of this diseaseconsists of a wide variety of motor manifestations, including resttremor, abnormal posture and gait, stiffness and rigidity, bradyki-nesia, and voice changes (Fahn, 2003; Jankovic, 2008). Non-motormanifestations include psychiatric and cognitive symptoms, hallu-cinations, dysautonomia, sleep and sensory disturbances (Chaudh-uri and Schapira, 2009; Park and Stacy, 2009). When clinicalmanifestations are noticed, about 70–80% of the dopaminergicneurons have already degenerated in the substantia nigra parscompacta located in the midbrain (Riederer and Wuketich, 1976).The neurophysiological hallmark of PD pathophysiology is anexcessive synchronous activity in cortical–basal ganglia networks(Brown, 2003, 2006). This can be considered as the theoretical ba-sis for the therapeutic efficacy of neuromodulation techniques,which are increasingly indicated in case of resistance to drug treat-ment (Bronstein et al., 2011).
2.2. Deep brain stimulation (DBS)
DBS is a therapeutic strategy proposed in PD, based on contin-uous electrical stimulation of subcortical structures at a frequency>100 Hz using chronically implanted electrodes. It is a highly effec-tive and reversible surgical procedure, with marked benefits andminimal morbidity (Wojtecki et al., 2012). The rationale of DBS
was largely based on past surgical experience with ablation of deepbrain structures such as the ventrointermediate nucleus of thethalamus (Vim), later replaced by Vim stimulation (Benabidet al., 1987).
A battery-operated, subcutaneously implanted pulse generator(IPG) in pectoral or abdominal region (Fig. 1) delivers electricalstimuli at high frequency to the targeted structure via an insolatedpolyurethane extension connected to one (unilateral) or two (bilat-eral) platinum iridium electrodes (or leads). The most commonDBS targets used to treat motor symptoms of PD patients are theSTN and the GPi. Stimulation parameters (electrode polarity, pulseamplitude and duration, and stimulus frequency) are empiricallyadjusted by the clinician to minimize side effects while optimizingtherapeutic efficacy (Volkmann et al., 2006).
On average, DBS reduces by 50% the motor scores of UPDRS(Unified Parkinson’s Disease Rating Scale) and the daily dose ofL-Dopa, while patients’ quality of life significantly increases. The ef-fects of DBS are observed within seconds (Fig. 2), and its efficacy isnow recognized worldwide: over 80,000 PD patients benefit fromit, including patients with early motor complications (Schuepbachet al., 2013). DBS has been also investigated as a therapeutic optionin a variety of disabling drug-resistant pathological conditionsother than PD, including dystonia, essential tremor, chronic pain,obsessive compulsive disorders, Tourette’s syndrome, and depres-sion. These applications are based on various stimulation sites andparameters and they are validated in varying degrees as a thera-peutic option. However, DBS has several drawbacks: it is expensiveand invasive, including risk of surgical complications (hemorrhage:1–2%; infection: 3–5%) and hardware dysfunction (lead breaking orbattery failure) (Schuepbach et al., 2013). Furthermore, in the con-text of PD treatment, clinical side effects such as postural instabil-ity, depression, speech difficulties, gain of weight, or cognitivedecline are not uncommon (Guehl et al., 2007).
Neurostimulation therapy for PD aims at modulating neuronalactivity in cortical–basal ganglia networks. Therefore, effectivesites of electrode implantation can be theoretically located at anypoint of these networks. Recent studies converge on the fact thatexcessive synchrony propagating and amplifying around these net-works can be explained by a resonance phenomenon (sensitivity ofneurons to afferences having frequencies close to their intrinsicfrequency). However, the mechanisms of action of DBS in PD re-main unclear, even if a large catalogue of hypotheses has been pro-posed in an abundant literature on this topic (McIntyre et al., 2004;Chang et al., 2008; Hammond et al., 2008; Johnson et al., 2008;Modolo et al., 2008; Montgomery and Gale, 2008; Vitek, 2008;Modolo and Beuter, 2009a,b; McIntyre and Hahn, 2010). DBS ef-fects likely result from a combination of local changes and modu-lation of distant structures in cortical–basal ganglia–thalamicloops, possibly involving activation of afferent and efferent axons,with both antidromic and orthodromic spike propagation (Hanaj-ima et al., 2004; Santaniello et al., 2012). Thus, DBS could modulateabnormal synchronous oscillatory activity between the basalganglia and various cortical regions, including the primary motorcortex (M1) (Brown, 2003, 2006; Wingeier et al., 2006; Walker
A. Beuter et al. / Clinical Neurophysiology 125 (2014) 874–885 875

Author's personal copy
et al., 2009; Whitmer et al., 2012). At various sites, this rhythmicactivity can be recorded with macroelectrodes as oscillatory localfield potentials (LFPs), which are extracellular voltage fluctuationsin membrane potential of a local neuronal population (Fig. 3)(Brown and Williams, 2005).
2.3. Motor cortex stimulation (MCS)
Excision of premotor or motor cortical regions was historicallyused to treat movement disorders, often with limited success
(Horsley, 1890; Bucy and Buchanan, 1932; Bucy and Case, 1939;Klemme, 1940, 1942). Regarding electrical stimulation of the mo-tor cortex, this technique goes back to the work of Aldini (1803),who applied noninvasive cortical stimulation in patients withmental illness for the first time. Much later on, Alberts (1972)showed that cortical stimulation at 60 Hz near the Rolandic fissurebetween motor and sensory cortices could evoke or increase tre-mor in PD patients. More relevant to current clinical applications,Woolsey et al. (1979) observed that M1 stimulation, at asubthreshold intensity for the elicitation of movement, resulted
Fig. 1. Implanted motor cortex stimulation. Two Resume II electrodes (Medtronic, Inc., Minneapolis, MN) implanted on the primary motor cortices are connected to two ItrelIII pulse generators (Medtronic) implanted in the pectoral region (with permission from Tani and Saitoh, 2011).
Fig. 2. Deep brain stimulation (DBS) of the globus pallidus internal part (GPi, top), ventrointermediate nucleus of the thalamus (Vim, middle) or subthalamic nucleus (STN,bottom) in three patients with tremor. Data recorded using a velocity laser pointed at patient’s finger after 5 min of continuous DBS and illustrating the transitions occurringduring the sequence EOEIOI with E = effective stimulation (frequency ranging between 135 and 185 Hz), O = no stimulation, I = ineffective stimulation (effective stimulationfrequency divided by 2) (with permission from Beuter and Titcombe, 2003).
876 A. Beuter et al. / Clinical Neurophysiology 125 (2014) 874–885

Author's personal copy
in disappearance of tremor and rigidity for a short period beyondthe time of stimulation in a patient with severe PD.
Nowadays, chronic MCS via epidurally implanted electrodes(EMCS) is used with undeniable success to treat various chronicrefractory pain conditions such as trigeminal neuralgia, post-strokepain, and other neuropathic pain syndromes related to peripheralor central nervous system injury (Nguyen et al., 2011; Nizardet al., 2012). EMCS was found to concomitantly alleviate motor dis-orders (mainly tremor) associated with pain (Nguyen et al., 1998;Franzini et al., 2000; Katayama et al., 2002). Flat electrodes are im-planted and placed extradurally over M1 via a small craniotomy,and then connected to an IPG. In general, few surgical complica-tions or adverse events are reported in this type of intervention.Compared to DBS, EMCS is a less invasive and safer surgical proce-dure that can be proposed in older patients without contraindica-tions (Canavero, 2011).
In PD patients, positive effects of EMCS have been first reportedby Canavero and Paolotti (2000) and Canavero et al. (2002, 2003),but clinical benefits are variable. Actually, no conclusive resultshave been reached so far and improvement of PD patients treatedby EMCS is usually limited (review in Canavero and Bonicalzi,2007; Cioni, 2007; Priori and Lefaucheur, 2007; Gutiérrez et al.,2009; Lefaucheur, 2009b; Tani and Saitoh, 2011). Recent results re-ported by Bentivoglio et al. (2012) showed moderate effects, espe-cially on axial symptoms and quality of life, following unilateralEMCS at a frequency of 80 Hz in 9 PD patients over a 12-monthperiod. Clinical effects were bilateral, likely due to bihemisphericconnections between cortical and deep brain structures. Nochanges in cognitive functions or behavior, and no seizures orother epileptic features were reported.
It is difficult to compare the various EMCS studies performed inPD patients because of marked differences in selection criteria,surgical procedures, stimulation settings, and methods to assessmotor improvement (Pagni et al., 2005a,b, 2008; Benvenuti et al.,2006; Cilia et al., 2007, 2008; Cioni, 2007; Arle et al., 2008;Gutiérrez et al., 2009). For example, clinical features were evalu-ated using UPDRS, while more specific scales could be requiredto highlight the effects of EMCS (Bentivoglio et al., 2012). More
importantly, there are significant variations between studies inthe frequency of stimulation, ranging from 10 to 130 Hz and ad-justed empirically. This reveals the lack of knowledge regardingthe biological mechanisms involved. Overall, higher stimulationfrequencies (80–130 Hz) tend to provide better results than lowerstimulation frequencies (10–60 Hz). Finally, it is likely that the flatelectrode paddle leads currently used for EMCS have not an opti-mal design, especially because they include a small number ofwidely spaced contacts. Taken together, these elements contributeto explain why EMCS results are less than compelling and nevergained wider acceptance in the treatment of PD.
Regarding the mechanisms of action, EMCS can reactivate somehypoactive brain structures and/or inhibit some hyperactive ones(Tani et al., 2007; Cilia et al., 2008). We know from neuroimagingand neurophysiological studies (review in Grafton, 2004; Lefauc-heur, 2005) that PD is associated with functional disturbance invarious motor cortical areas, mainly hypoactivation of the supple-mentary motor area and hyperactivation of both M1 and premotorcortex. Transcranial magnetic stimulation studies using paired-pulse paradigms showed reduced inhibition in M1, partiallyrelated to increased synaptic facilitation (Bares et al., 2003, 2007;Lefaucheur et al., 2004; MacKinnon et al., 2005; Kojovic et al.,2012; Kacar et al., 2013; Leon-Sarmiento et al., 2013; Ni et al.,2013). These processes may reveal an alteration of motor corticalcontrol associated with a compensatory or maladaptive corticalplasticity (review in Lindenbach and Bishop, 2013; Rothwell andEdwards, 2013). The relationships between such changes and clin-ical features of PD are not clear. Moreover, this does not necessarilyimply the interest of a target located at the cortical level. Indeed,intracortical excitability parameters can be improved in PDpatients by a DBS approach (Cunic et al., 2002; Däuper et al.,2002; Fraix et al., 2008). Actually, antiparkinsonian effects of STNstimulation may result from selective neuronal activations in layerV of M1 due to the excitation of STN-M1 pathways (Gradinaruet al., 2009). On the other hand, EMCS was found to normalizethe mean firing rate of GPi and STN neurons in monkeys renderedparkinsonian by MPTP (1-methyl-4-phenyl-1,2,3,6-tetrahydropyri-dine) intoxication: EMCS could reduce synchronized oscillatory
Fig. 3. Concomitant recordings of electrocorticographic activity (ECoG) of the frontal cortex and local field potentials (LFPs) in the basal ganglia during slow-wave activity andglobal activation. The ECoG was dominated by a slow oscillation (�1 Hz) of large amplitude during spontaneous slow-wave activity. LFPs simultaneously recorded in thesubthalamic nucleus (STN), globus pallidus (GP) and substantia nigra pars reticulata (SNr) displayed similar oscillatory phenomena, but with reversed polarities compared toECoG. Note that LFPs in GP did not reflect the cortical slow oscillation as did LFPs in STN and SNr (see epoch under open bar). Global activation of the forebrain following pinchonset (arrow) was exemplified by a loss of slow-wave oscillations in the ECoG, and a shift to oscillatory activity of smaller amplitude and higher frequency. Local fieldpotentials in GP, STN and SNr displayed similar shifts in oscillatory phenomena. Calibration bars apply to all panels (with permission from Sharott et al., 2005).
A. Beuter et al. / Clinical Neurophysiology 125 (2014) 874–885 877
Author's personal copy
activities in both nuclei (Drouot et al., 2004) similar to what is pro-duced by STN stimulation (Meissner et al., 2005).
Taken together, these results support the concept that neurosti-mulation preferentially modulates remote structures than localcells, since fibers of passage are more excitable than local cellbodies at the site of stimulation (Ranck, 1975; Nowak and Bullier,1998; McIntyre and Grill, 2002). These results also support theconcept that either by stimulating deep brain structures or the mo-tor cortex, the therapeutic efficacy of neuromodulation in PD couldconsist primarily of changes in brain rhythms in cortical–basalganglia networks, secondarily resulting in a modulation of neuro-nal activity at the cortical level. Thus, these data form the rationalefor developing original strategies of neuromodulation of these net-works based on a closed-loop approach in the treatment of PD.
3. ‘‘Open-loop’’ versus ‘‘closed-loop’’ stimulation
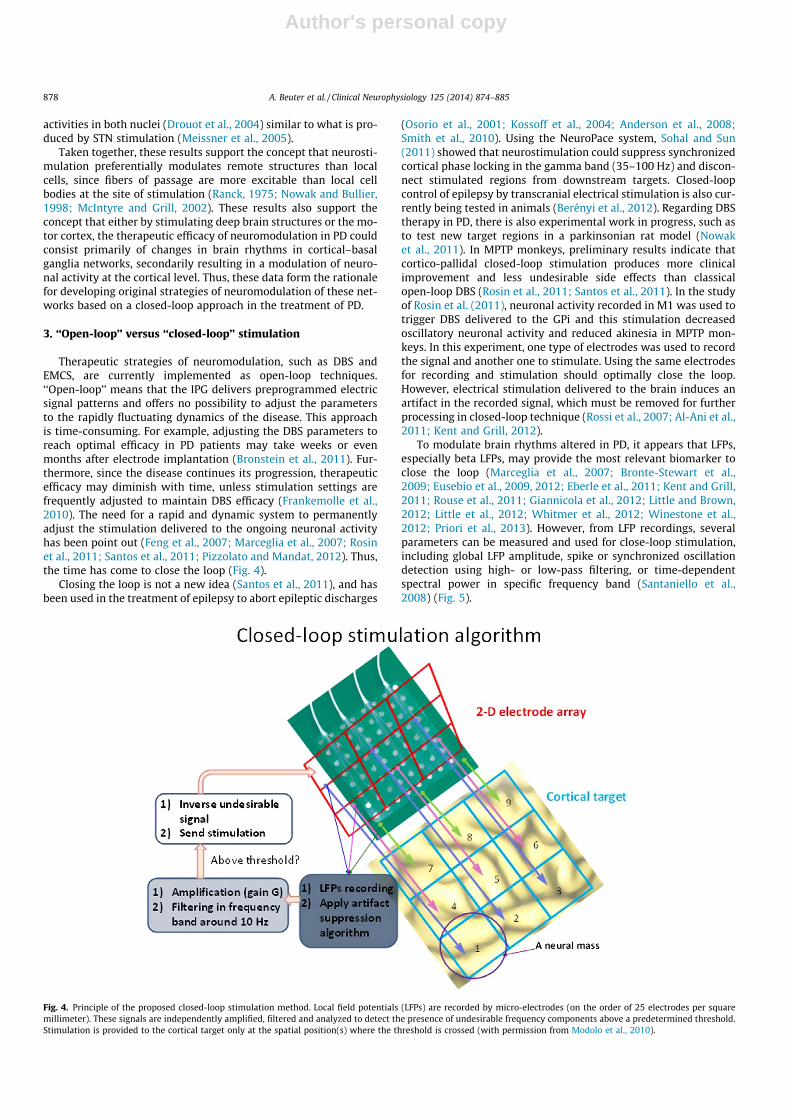
Therapeutic strategies of neuromodulation, such as DBS andEMCS, are currently implemented as open-loop techniques.‘‘Open-loop’’ means that the IPG delivers preprogrammed electricsignal patterns and offers no possibility to adjust the parametersto the rapidly fluctuating dynamics of the disease. This approachis time-consuming. For example, adjusting the DBS parameters toreach optimal efficacy in PD patients may take weeks or evenmonths after electrode implantation (Bronstein et al., 2011). Fur-thermore, since the disease continues its progression, therapeuticefficacy may diminish with time, unless stimulation settings arefrequently adjusted to maintain DBS efficacy (Frankemolle et al.,2010). The need for a rapid and dynamic system to permanentlyadjust the stimulation delivered to the ongoing neuronal activityhas been point out (Feng et al., 2007; Marceglia et al., 2007; Rosinet al., 2011; Santos et al., 2011; Pizzolato and Mandat, 2012). Thus,the time has come to close the loop (Fig. 4).
Closing the loop is not a new idea (Santos et al., 2011), and hasbeen used in the treatment of epilepsy to abort epileptic discharges
(Osorio et al., 2001; Kossoff et al., 2004; Anderson et al., 2008;Smith et al., 2010). Using the NeuroPace system, Sohal and Sun(2011) showed that neurostimulation could suppress synchronizedcortical phase locking in the gamma band (35–100 Hz) and discon-nect stimulated regions from downstream targets. Closed-loopcontrol of epilepsy by transcranial electrical stimulation is also cur-rently being tested in animals (Berényi et al., 2012). Regarding DBStherapy in PD, there is also experimental work in progress, such asto test new target regions in a parkinsonian rat model (Nowaket al., 2011). In MPTP monkeys, preliminary results indicate thatcortico-pallidal closed-loop stimulation produces more clinicalimprovement and less undesirable side effects than classicalopen-loop DBS (Rosin et al., 2011; Santos et al., 2011). In the studyof Rosin et al. (2011), neuronal activity recorded in M1 was used totrigger DBS delivered to the GPi and this stimulation decreasedoscillatory neuronal activity and reduced akinesia in MPTP mon-keys. In this experiment, one type of electrodes was used to recordthe signal and another one to stimulate. Using the same electrodesfor recording and stimulation should optimally close the loop.However, electrical stimulation delivered to the brain induces anartifact in the recorded signal, which must be removed for furtherprocessing in closed-loop technique (Rossi et al., 2007; Al-Ani et al.,2011; Kent and Grill, 2012).
To modulate brain rhythms altered in PD, it appears that LFPs,especially beta LFPs, may provide the most relevant biomarker toclose the loop (Marceglia et al., 2007; Bronte-Stewart et al.,2009; Eusebio et al., 2009, 2012; Eberle et al., 2011; Kent and Grill,2011; Rouse et al., 2011; Giannicola et al., 2012; Little and Brown,2012; Little et al., 2012; Whitmer et al., 2012; Winestone et al.,2012; Priori et al., 2013). However, from LFP recordings, severalparameters can be measured and used for close-loop stimulation,including global LFP amplitude, spike or synchronized oscillationdetection using high- or low-pass filtering, or time-dependentspectral power in specific frequency band (Santaniello et al.,2008) (Fig. 5).
Fig. 4. Principle of the proposed closed-loop stimulation method. Local field potentials (LFPs) are recorded by micro-electrodes (on the order of 25 electrodes per squaremillimeter). These signals are independently amplified, filtered and analyzed to detect the presence of undesirable frequency components above a predetermined threshold.Stimulation is provided to the cortical target only at the spatial position(s) where the threshold is crossed (with permission from Modolo et al., 2010).
878 A. Beuter et al. / Clinical Neurophysiology 125 (2014) 874–885

Author's personal copy
4. Pathological brain rhythms in PD
In PD, two pathological brain rhythms have been mainly associ-ated with motor symptoms (Timmermann and Fink, 2011): theseverity of motor impairment in PD patients appears to relate toan increased activity in the 8–12 Hz frequency range (alpharhythm, termed more specifically mu rhythm in the motor region)and more importantly in the 13–30 Hz frequency range (betarhythm), as shown by LFPs recorded through DBS electrodes im-planted in the STN or GPi (Brown et al., 2001, 2004; Cassidyet al., 2002; Williams et al., 2002; Priori et al., 2004; Silbersteinet al., 2005; Ray et al., 2008; Rossi et al., 2008). Alteration in thebeta band was associated with bradykinesia and rigidity (Brownet al., 2001; Kühn et al., 2004, 2006, 2008), while alteration inthe alpha/mu band was associated with tremor (Volkmann,1998; Timmermann et al., 2003; Reck et al., 2009, 2010). Thisexcessive oscillatory activity is reduced and even returns to normalfollowing L-Dopa intake or by switching ‘‘on’’ DBS (Brown et al.,2001; Foffani et al., 2005; Weinberger et al., 2006; Kühn et al.,2008; Giannicola et al., 2010; Jenkinson and Brown, 2011; Rosaet al., 2011; Litvak et al., 2012). Conversely, L-Dopa therapy andDBS increase high-frequency LFPs (200–350 Hz), theta (3–7 Hz)and especially gamma (60–90 Hz) rhythms that are reduced in PD.
These oscillatory activities are modulated before and duringmovement, according to the motor task undertaken (Williamset al., 2003; Kühn et al., 2004, 2006; Androulidakis et al., 2008;Marceglia et al., 2009). Finally, there remains some uncertaintyregarding which brain areas underlie the generation of theserhythms. Hirschmann et al. (2011) showed that oscillations werecoherent between the STN and either the ipsilateral temporal cor-tex in the alpha band or the ipsilateral sensorimotor and premotorcortices (precentral gyrus, postcentral gyrus, medial frontal gyrus)in the beta band. In another study based on spectral and spatialcluster analysis combined with causality analysis, Litvak et al.(2011) identified two temporospatially different networks: one inthe 10 Hz range involving temporoparietal-brainstem areas andanother in the 20 Hz range being a predominantly frontal network.
Smirnov et al. (2008) investigated the relationship betweenLFPs recorded in the STN and tremor using phase models andconcluded that the relationship between brain activity and tre-mor-related activity was bidirectional. To study this bidirectional
relationship, studies have combined electroencephalography(EEG) or magnetoencephalography (MEG) with electromyography(EMG). Timmermann et al. (2003) have identified significant corti-comuscular coherence at twice the tremor frequency (10 Hz) inM1, while Raethjen et al. (2009) found both the presence of tremorfrequency and its first harmonic in M1. These studies have beeninformative to identify brain rhythms reflecting the presence oftremor, however the methods used were not able to identify thecausality between signals (cortical activity driving tremor, or viceversa). To address this issue, advanced signal processing tech-niques, such as Granger causality and its generalization such asPartial Directed Coherence (Granger, 1969) could be used. In brief,the Granger causality principle states that, if two signals A and Bhave some form of causality between them, then the knowledgeof one signal to the statistical model of the other should improvemodel predictions. The application of these signal-processingtechniques showed that M1 was, at least to some extent, activelyinvolved in the generation of PD tremor (Timmermann et al.,2007; Raethjen et al., 2009). Proprioceptive feedback from theperiphery appears also to play a role, suggesting a bi-directionalnetwork between the brain and peripheral muscles. Taken to-gether, these results clearly point out at the possibility of modulat-ing tremor-related brain rhythms in order to decrease neuronalactivity at the tremor frequency (and possibly its first harmonic).
As stated in the introduction, PD involves complex multi-sys-tem dysfunction, including motor and non-motor signs. It is likelythat pathological oscillations may underlie both motor and non-motor manifestations, including cognitive dysfunctions (reviewin Uhlhaas and Singer, 2006). Indeed, oscillations in various basalganglia–cortical networks were found to be neurophysiologicalmarkers of cognitive and behavioral impairment in PD (review inMarceglia et al., 2011). Specifically, studies based on intracerebralrecordings of brain rhythms or LFPs (Kühn et al., 2005; Cavanaghet al., 2011; Fumagalli et al., 2011; Wojtecki et al., 2011; Brittainet al., 2012; Eitan et al., 2013; Oswal et al., 2013) or event-relatedpotentials (Baláz et al., 2008, 2010; Rektor et al., 2009, 2010; Bock-ová et al., 2011) through DBS electrodes implanted in basal gangliaof PD patients provided evidence for an involvement of thesestructures in emotional, attentional, decisional, or executivedysfunctions, which are all common in PD. Pathological oscillationsinvolved in motor and non-motor manifestations of PD could occur
Fig. 5. Raw electrophysiological data and local field potential (LFP) autospectra recorded in globus pallidus (GP) of a patient with Parkinson’s disease (PD) in ‘‘off’’ (A–C) and‘‘on’’ (D–F) condition of levodopa intake. Autospectra are expressed as a percentage of total power up to 100 Hz (with permission from Silberstein et al., 2003).
A. Beuter et al. / Clinical Neurophysiology 125 (2014) 874–885 879

Author's personal copy
in the same frequency ranges and the same brain regions, but maybe also task-specific. As described above, there are increasingly evi-dences that a closed-loop system could tune abnormal oscillationsassociated with tremor or rigidity, but it remains to determine howthis approach can be use to treat non-motor signs. If applied toEMCS rather than DBS, anatomical peculiarities must be taken intoaccount, as shown in the following chapter.
5. Specificities of cortical stimulation
The human neocortex comprises six layers and at least 52 cyto-architectonically distinct areas having specific connections andplaying different functional roles (Castro-Alamancos, 2013). Itssurface is estimated to be around 2500 cm2 and its estimated num-ber of neurons is between 10 and 20 billions. Each cortical areacontains an unknown number of networks of interconnected neu-rons, and especially in M1, there is a complex integration of multi-ple information originating from both hemispheres. Propagatingwaves of electrical activity mediate specific information at specificrhythms in different cortical regions (Patten et al., 2012). Forexample, propagation of beta oscillations conveys motor informa-tion from M1 in animals (Rubino et al., 2006) and humans (Takah-ashi et al., 2011). The interaction of the current delivered duringcortical stimulation with such propagating waves carrying physio-logical or pathological information between cortical regions shouldbe taken under consideration in the stimulation paradigm.
Another factor to take into account in the design of corticalstimulation is that neural fibers are curved, bent, and oriented invarious directions in the cerebral cortex. The three-dimensionalstructure of the cortex with sulci and gyri results in a marked het-erogeneity of neural fiber orientation. The lowest activationthreshold is reached at fiber ending or at bending points, especiallyat the interface between the grey and white matters. This zone isespecially sensitive, presumably because of the gradient of electricconductivity (Manola et al., 2005). Biophysical models can be usedto identify the most relevant brain tissue parameters that deter-mine the diffusion of current induced by cortical stimulation tech-niques. For example, Radman et al. (2009) have investigated howthe morphology and type of cortical neurons affect the responseto DC cortical stimulation in rats. They characterized the processof linear polarization of axonal membrane as a function of theintensity of the DC electric field and of the angle between axonsand the electrical field vector. Thus, brain stimulation techniquestaking into account neural fiber orientation in the stimulation area,as well as endogenous rhythms in the targeted circuits, couldachieve desirable biological effect while minimizing currentspreading into the brain tissue.
The major part of M1 is located in the anterior wall of the cen-tral sulcus, far from the cortical surface, which may be one factorexplaining why clinical results of EMCS for PD have been inconclu-sive so far. Conversely, the premotor cortex, which extends overthe convexity of the precentral gyrus and contains pyramidal cellsand descending projections to the spinal cord, is a more reachabletarget for epidural stimulation. The intensity of stimulation, as wellas the thickness of the cerebrospinal fluid layer between the duramater and the underlying cortex, influence the distribution of theelectric field induced into the brain through epidural stimulation,because the cerebrospinal fluid layer has a 6–7-fold higher conduc-tivity than the grey matter (Manola et al., 2005). However, even ap-plied epidurally, cortical stimulation is able to activate fiberslocated superficially in a gyrus but projecting at a distance andthus modulate neuronal activities in the depth of a sulcus, as wellas in deeper brain structures.
In fact, stimulation of a deep nucleus differs from superficialcortical stimulation, even if the both structures belong to the samenetwork, because neural networks are outspread onto the cortical
surface and much more concentrated in the depth of the brain.According to this ‘‘fanning-out’’ distribution of neuronal projec-tions, the modulation of a given brain network requires a largerarea of stimulation at the cortical level than at deeper sites. In con-trast, more focal currents need to be delivered in deep structures toobtain efficacy without producing adverse events.
The wide spacing between contacts of the EMCS leads generallyused in therapeutics does not increase cortical activation volumeas initially suggested (Kleiner-Fisman et al., 2003), but results inactivating more distinct neural fibers according to a ‘‘bifocal’’ dis-tribution of monopolar stimuli (Manola et al., 2005). Therefore,specific matrices of electrodes (with more contacts of smaller areaand less widely spaced) should be designed for cortical stimula-tion. In addition, activation threshold depends on the orientationof fibers with respect to electrode polarity and the resultingelectric field geometry (Wongsarnpigoon and Grill, 2011, 2012).An epidural electrode selected as cathode excites preferentiallythe fibers that run horizontally under it (tangential component),whereas an anode excites the fibers that are perpendicular to it(radial component) (Gorman, 1966; Rosenthal et al., 1967; Hols-heimer et al., 2007; Manola et al., 2007).
Thus, cortical stimulation involves a number of specific chal-lenges that need to be addressed in terms of neural engineering.One of the most significant issues is the complexity of the corticalarchitecture (highly complex nonhomogeneous folded structurecomposed of interconnected areas) and the identification ofrhythms related to specific physiological and pathological func-tions. However, one advantage of stimulating a superficial corticalarea is to entrain the whole network of interconnected structureswith a relatively minimally invasive procedure compared to DBS(Canavero, 2011).
Another advantage of cortical targeting is to authorize noninva-sive approach through transcranial stimulation (review in Lefauc-heur, 2008, 2009a, 2012). In a recent pilot study, Brittain et al.(2013) showed that transcranial stimulation might be used in aclosed-loop system for controlling tremor in PD patients. Transcra-nial alternating current stimulation was delivered over M1 at tre-mor frequency and phase-locked to tremor signal to induce phasecancellation of the tremor rhythm. The optimal suppressive phasealignment produced 50% average reduction in resting tremor. It isunclear whether tremor attenuation was due to a modulation of cor-tical inputs or efferent drive, but this work was a pioneering appli-cation of noninvasive closed-loop stimulation in humans to treatsymptoms caused by synchronized oscillations, such as tremor. Fur-ther developments are expected in this domain (Hess, 2013).
Such a closed-loop approach based on accelerometric measure-ment of tremor in the limbs of PD patients was also proposed as amodeling and automatic feedback control to adapt stimulationparameters of DBS (frequency, amplitude, and pulse width) (Rehanand Hong, 2013). However, our proposal is rather to use brainrhythms recorded at the cortical level to provide feedback informa-tion for closing the loop. This strategy should be more efficient,both regarding PD pathophysiology and device engineering, sinceonly one set of implanted electrodes is sufficient. The developmentof this type of device for therapeutic use in humans must respondto different objectives and also may benefit from mathematicalmodeling, as described in the next chapter.
6. Translating closed-loop cortical stimulation from bench tobedside
6.1. Checklist of objectives
We identified in Table 1 the objectives that should allow to suc-cessfully move from bench/model to bedside/clinic and to propose
880 A. Beuter et al. / Clinical Neurophysiology 125 (2014) 874–885

Author's personal copy
a novel closed-loop cortical stimulation therapy for PD. Let us men-tion that the development of closed-loop stimulation techniquesfor the treatment of PD patients is now taken very seriously bymajor companies. For example, investigators from one of thesecompanies (Afshar et al., 2013) proposed an investigational plat-form including: (i) an implanted sensing and stimulation deviceto collect data and run automated closed-loop algorithms; (ii) anexternal tool to prototype classifier and control policy algorithms(biomarkers); and (iii) a real-time telemetry to update the im-planted firmware and monitor its state. This initiative relates tothe development of new mechanistic models implemented in auto-mated closed-loop systems suitable for the treatment of PD.
6.2. Engineering closed-loop cortical stimulation usingbiomathematical modeling
As mentioned previously, designing an optimal method ofclosed-loop cortical stimulation is an extraordinarily difficult taskdue to the anatomical and functional complexity of the cortexand the multiple potential interactions with the current deliveredto the brain. However, a line of research to help engineering thenext generation of neurostimulators is to use computational mod-els of brain activity. This approach has indeed gained prominencein recent years. For this purpose, a number of constraints need tobe taken into account.
First, the model must describe the dynamics of biomarkers,such as LFPs, to enable comparisons with experimental and clinicaldata. Closed-loop stimulation should allow these biomarkers to re-turn to their ‘physiological’ values, according to the concept ofdynamical disease, in which control parameters are outside theirphysiological range (Mackey and Glass, 1997). Beuter and Vasilakos(1995) have argued that biomathematical models describing thedynamics of neural tissue to ends of controlling neuronal activitywith electrical stimulation seems relevant in PD, which is indeeda dynamical disease. One example of model-guided closed-loopstimulation method was proposed by Modolo et al. (2010, 2011)with a modulation of cortical rhythms based on a validatedbiomathematical modeling of brain tissue including time delays(Wilson and Cowan, 1973; Amari, 1977; Ermentrout and Cowan,1979; Bressloff et al., 2001; Huang et al., 2004; Rubino et al.,2006; Kerr et al., 2013). Modolo et al. (2010, 2011) presented atwo-dimensional electrode array that could be used both for corti-cal activity recording and stimulation, using a stimulation signaladaptive in space and time. Global oscillations were modulated
by a closed-loop stimulation triggered as a function of local meanmembrane potential.
Another example of neural engineering of closed-loop stimula-tion guided by modeling is the work of Tass et al. (Tass, 2001; Tasset al., 2009). These authors proposed multi-site stimulation tech-niques, based on principles of statistical physics and networks ofphase oscillators. For example, the Coordinated Reset (CR) methodof neuromodulation, able to produce lasting desynchronization ofrhythmic neuronal activity, was recently shown to provide benefi-cial motor effects when used to control DBS in MPTP monkeys(Tass et al., 2012). These promising results further illustrate howbiomathematical modeling approach dealing with the complexityand non-linearity of brain dynamics may play an important rolein the development of future neurostimulation therapies.
7. Concluding remarks
For now, DBS is the neuromodulation procedure of choice totreat PD symptoms but the strategic inflection point of this technol-ogy is estimated to occur around 2030 (Fitz Coy et al., 2011). A newgeneration of neurostimulators must be developed without delayand may include closed-loop cortical neuromodulation. Using guid-ance from biomathematical models, it is reasonable to expect thepossibility, in the near future, that novel neurostimulators couldcontrol pathological brain rhythms by adjusting stimulationparameters automatically in real-time. This will maximize the ther-apeutic efficacy, while minimizing the amount of stimulation (spar-ing the batteries) and the need for empirical adjustment ofstimulation settings (saving time). The same location of the record-ing and stimulating electrodes should be used to improve surgicalimplantability (Rouse et al., 2011). The main argument for the supe-riority of cortical stimulation is that it is less invasive than DBS andthus it can be proposed more widely as a therapeutic option withless contraindications (Canavero, 2011). However, this goal re-quires the development of new electrodes, specifically adapted tothe anatomy of the superficial neural networks of the cortex.
One final element to consider is the economic burden of PD,evaluated in 2011 to 13.9 billion € for about 1,200,000 patientsin Europe, partly due to the significant cost of DBS stimulatorsand associated surgical interventions. A switch from open-loopDBS to closed-loop EMCS would represent a significant financialinvestment in research and development at first. Therefore, a proofof concept is legitimately necessary to verify that closed-loopcortical stimulation is feasible and effective in treating PD symp-toms, and beyond, other movement disorders.
Table 1Milestones to translate basic research findings into a closed-loop cortical stimulation device to treat patients with Parkinson’s disease (PD).
Preliminary knowledge To characterize spatiotemporal patterns ofpathological brain activity associated withspecific PD symptoms (to identify whatrhythms should be modulated, and thenhow, where and when)
To identify relevant biomarkers (e.g., localfield potentials, LFPs) and their optimalrecording sites in the motor regions of thecortex of PD patients
To evaluate the effect of existing andeffective therapies on these biomarkers(e.g., effects produced by dopaminergictreatment or deep brain stimulation)
Prototyping To use biomathematical models of electricalstimulation of neural tissue subject toinvestigate in silico the effect of closed-loopalgorithms on selected rhythms
To design the electrode matrix to accuratelyrecord LFPs and stimulate the corticaltarget, while paying attention to itsadaptability to cortical anatomy (sulci/gyri)and long-term implantation
To select the most suitable closed-loopcontrollersa to implement in the device
Pre-clinical testing To calibrate the stimulator and implement astimulation algorithm, so that oscillationsat specific frequency bands can beautomatically controlled in real time,tailored to patient’s needs
To determine the best stimulationparameters (frequency, amplitude, andpulse width) to produce the desired clinicaleffects
To validate a wide and standardizedbattery of measures to evaluate short-termand long-term effects of closed-loopcortical stimulation on motor and non-motor PD symptoms and the possiblyinduced side effects
a Closed-loop controllers include ‘triggered open-loop controllers’, using sensors to start and stop the stimulation; ‘continuous feedback controllers’, using regular sensingto monitor the stimulation; ‘adaptive controllers’, using feedback signals from sensors to continually adapt the stimulation parameters; and ‘learning/intelligent controllers’,outperforming all other controllers in their ability to adjust automatically and intelligently the parameters of stimulation with fine-grained feedback (Echauz et al., 2009).
A. Beuter et al. / Clinical Neurophysiology 125 (2014) 874–885 881

Author's personal copy
Acknowledgement
The authors report no conflict of interest related to this work.
References
Afshar P, Khambhati A, Stanslaski S, Carlson D, Jensen R, Linde D, et al. Atranslational platform for prototyping closed-loop neuromodulation systems.Front Neural Circuits 2013;6:117.
Al-Ani T, Cazettes F, Palfi S, Lefaucheur JP. Automatic removal of high-amplitudestimulus artifact from neuronal signal recorded in the subthalamic nucleus. JNeurosci Methods 2011;198:135–46.
Alberts WW. A simple view of parkinsonian tremor. Electrical stimulation of cortexadjacent to the rolandic fissure in awake man. Brain Res 1972;44:357–69.
Aldini J. An account of the late improvements in galvanism, with a series of curiousand interesting experiments performed before the commissioners of the Frenchnational institute, and repeated lately in the anatomical theatres ofLondon. London: Cuthell, Martin, and Murray; 1803.
Amari SI. Dynamics of pattern formation in lateral-inhibition type neural fields. BiolCybern 1977;27:77–87.
Anderson WM, Kossoff EH, Bergey GH, Jallo GI. Implantation of a responsiveneurostimulator device in patients with refractory epilepsy. Neurosurg Focus2008;25:E12.
Androulidakis AG, Brücke C, Kempf F, Kupsch A, Aziz T, Ashkan K, et al. Amplitudemodulation of oscillatory activity in the subthalamic nucleus during movement.Eur J Neurosci 2008;27:1277–84.
Arle JE, Apetauerova D, Zani J, Deletis DV, Penney DL, Hoit D, et al. Motor cortexstimulation in patients with Parkinson’s disease: 12-month follow-up in 4patients. J Neurosurg 2008;109:133–9.
Baláz M, Rektor I, Pulkrábek J. Participation of the subthalamic nucleus in executivefunctions: an intracerebral recording study. Mov Disord 2008;23:553–7.
Baláz M, Srovnalová H, Rektorová I, Rektor I. The effect of cortical repetitivetranscranial magnetic stimulation on cognitive event-related potentialsrecorded in the subthalamic nucleus. Exp Brain Res 2010;203:317–27.
Bares M, Kanovsky P, Klajblová H, Rektor I. Intracortical inhibition and facilitationare impaired in patients with early Parkinson’s disease: a paired TMS study. EurJ Neurol 2003;10:385–9.
Bares M, Kanovsky P, Rektor I. Disturbed intracortical excitability in earlyParkinson’s disease is l-DOPA dose related: a prospective 12-month pairedTMS study. Parkinsonism Relat Disord 2007;13:489–94.
Benabid AL, Pollak P, Louveau A, Henry S, de Rougemont J. Combined (thalamotomyand stimulation) stereotactic surgery of the VIM thalamic nucleus for bilateralParkinson disease. Appl Neurophysiol 1987;50:344–6.
Bentivoglio AR, Fasano A, Piano C, Soleti F, Daniele A, Zinno M, et al. Unilateralextradural motor cortex stimulation is safe and improves Parkinson’s disease at1 year. Neurosurgery 2012;71:815–25.
Benvenuti E, Cecchi F, Colombini A, Gori G. Extradural motor cortex stimulation as amethod to treat advanced Parkinson’s disease: new perspectives in geriatricmedicine. Aging Clin Exp Res 2006;18:347–8.
Berényi A, Belluscio M, Mao D, Buzsáki G. Closed-loop control of epilepsy bytranscranial electrical stimulation. Science 2012;337:735–7.
Beuter A, Titcombe M. Modulation of tremor amplitude during deep brainstimulation at different frequencies. Brain Cogn 2003;53:190–2.
Beuter A, Vasilakos K. Is Parkinsons’s disease a dynamical disease? Chaos1995;5:35–42.
Bocková M, Chládek J, Jurák P, Halámek J, Baláz M, Rektor I. Involvement of thesubthalamic nucleus and globus pallidus internus in attention. J Neural Transm2011;118:1235–45.
Bressloff PC, Cowan JD, Golubitsky M, Thomas PJ, Wiener M. Geometric visualhallucinations, Euclidean symmetry and the functional architecture of striatecortex. Philos Trans R Soc B 2001;356:299–330.
Brittain JS, Watkins KE, Joundi RA, Ray NJ, Holland P, Green AL, et al. A role for thesubthalamic nucleus in response inhibition during conflict. J Neurosci2012;32:13396–401.
Brittain JS, Probert-Smith P, Aziz TZ, Brown P. Tremor suppression by rhythmictranscranial current stimulation. Curr Biol 2013;23:436–40.
Bronstein JM, Tagliati M, Alterman RL, Lozano AM, Volkmann J, Stefani A, et al. Deepbrain stimulation for Parkinson disease: an expert consensus and review of keyissues. Arch Neurol 2011;68:165.
Bronte-Stewart H, Barberini C, Miller Koop M, Hill BC, Henderson JM, Wingeier B.The STN beta-band profile in Parkinson’s disease is stationary and showsprolonged attenuation after deep brain stimulation. Exp Neurol 2009;215:20–8.
Brown P. Oscillatory nature of human basal ganglia activity: relationship to thepathophysiology of Parkinson’s disease. Mov Disord 2003;18:357–63.
Brown P. Bad oscillations in Parkinson’s disease. J Neural Transm Suppl2006;70:27–30.
Brown P, Williams D. Basal ganglia local field potential activity: character andfunctional significance in the human. Clin Neurophysiol 2005;116:2510–9.
Brown P, Oliviero A, Mazzone P, Insola A, Tonali P, Di Lazzaro V. Dopaminedependency of oscillations between subthalamic nucleus and pallidum inParkinson’s disease. J Neurosci 2001;21:1033–8.
Brown P, Mazzone P, Oliviero A, Altibrandi MG, Pilato F, Tonali PA, et al. Effects ofstimulation of the subthalamic area on oscillatory pallidal activity inParkinson’s disease. Exp Neurol 2004;188:480–90.
Bucy PC, Buchanan DN. Athetosis. Brain 1932;55:179–92.Bucy PC, Case TJ. Tremor: physiological mechanism and abolition by surgical means.
Arch Neurol Psychiatry 1939;41:721–46.Canavero S. Cerebral-surface. In: Arle J, Shils J, editors. Essential
neuromodulation. Burlington, MA: Academic Press; 2011. p. 17–46.Canavero S, Bonicalzi V. Extradural cortical stimulation for movement disorders.
Acta Neurochir Suppl 2007;97:223–32.Canavero S, Paolotti R. Extradural motor cortex stimulation for advanced
Parkinson’s disease: case report. Mov Disord 2000;15:169–71.Canavero S, Paolotti R, Bonicalzi V, Castellano G, Greco-Crasto S, Rizzo L, et al.
Extradural motor cortex stimulation for advanced Parkinson disease: report oftwo cases. J Neurosurg 2002;97:1208–11.
Canavero S, Bonicalzi V, Paolotti R, Castellano G, Greco-Crasto S, Rizzo L, et al.Therapeutic extradural cortical stimulation for movement disorders: a review.Neurol Res 2003;25:18–22.
Cassidy M, Mazzone P, Oliviero A, Insola A, Tonali P, Di Lazzaro V, et al. Movement-related changes in synchronization in the human basal ganglia. Brain2002;125:1235–46.
Castro-Alamancos MA. The motor cortex: a network tuned to 7–14 Hz. Front NeuralCircuits 2013;7:21.
Cavanagh JF, Wiecki TV, Cohen MX, Figueroa CM, Samanta J, Sherman SJ, et al.Subthalamic nucleus stimulation reverses mediofrontal influence over decisionthreshold. Nat Neurosci 2011;14:1462–7.
Chang JY, Shi LH, Luo F, Zhang WM, Woodward DJ. Studies of the neuralmechanisms of deep brain stimulation in rodent models of Parkinson’sdisease. Neurosci Biobehav Rev 2008;32:352–66.
Chaudhuri KR, Schapira AH. Non-motor symptoms of Parkinson’s disease:dopaminergic pathophysiology and treatment. Lancet Neurol 2009;8:464–74.
Cilia R, Landi A, Vergani F, Sganzerla E, Pezzoli G, Antonini A. Extradural motorcortex stimulation in Parkinson’s disease. Mov Disord 2007;22:111–4.
Cilia R, Marotta G, Landi A, Isaias IU, Vergani F, Benti R, et al. Cerebral activitymodulation by extradural motor cortex stimulation in Parkinson’s disease: aperfusion SPECT study. Eur J Neurol 2008;15:22–8.
Cioni B. Motor cortex stimulation for Parkinson’s disease. Acta Neurochir Suppl2007;92:233–8.
Cunic D, Roshan L, Khan FI, Lozano AM, Lang AE, Chen R. Effects of subthalamicnucleus stimulation on motor cortex excitability in Parkinson’s disease.Neurology 2002;58:1665–72.
Däuper J, Peschel T, Schrader C, Kohlmetz C, Joppich G, Nager W, et al. Effects ofsubthalamic nucleus (STN) stimulation on motor cortex excitability. Neurology2002;59:700–6.
de Rijk MC, Tzourio C, Breteler MM, Dartigues JF, Amaducci L, Lopez-Pousa S, et al.Prevalence of parkinsonism and Parkinson’s disease in Europe: theEUROPARKINSON Collaborative Study. European community concerted actionon the epidemiology of Parkinson’s disease. J Neurol Neurosurg Psychiatry1997;62:10–5.
Dorsey ER, Constantinescu R, Thompson JP, Biglan KM, Holloway RG, Kieburtz K,et al. Projected number of people with Parkinson disease in the most populousnations, 2005 through 2030. Neurology 2007;68:384–6.
Drouot X, Oshino S, Jarraya B, Besret L, Kishima H, Remy P, et al. Functional recoveryin a primate model of Parkinson’s disease following motor cortex stimulation.Neuron 2004;44:769–78.
Eberle W, Penders J, Yazicioglu RF. Closing the loop for deep brain stimulationimplants enables personalized healthcare for Parkinson’s disease patients. ConfProc IEEE Eng Med Biol Soc 2011;2011:1556–8.
Echauz J, Firpi H, Georgoulas G. Intelligent control strategies for neurostimulation. In:Valavanis KP, editor. Applications of intelligent control to engineeringsystems. Dordrecht Heidelberg: Springer Science + Business Media; 2009. p. 247–53.
Eitan R, Shamir RR, Linetsky E, Rosenbluh O, Moshel S, Ben-Hur T, et al. Asymmetricright/left encoding of emotions in the human subthalamic nucleus. Front SystNeurosci 2013;7:69.
Ermentrout GB, Cowan JD. A mathematical theory of visual hallucination patterns.Biol Cybern 1979;34:137–50.
Eusebio A, Pogosyan A, Wang S, Averbeck B, Gaynor LD, Cantiniaux S, et al.Resonance in subthalamo-cortical circuits in Parkinson’s disease. Brain2009;132:2139–50.
Eusebio A, Cagnan H, Brown P. Does suppression of oscillatory synchronisationmediate some of the therapeutic effects of DBS in patients with Parkinson’sdisease? Front Integr Neurosci 2012;6:47.
Fahn S. Description of Parkinson’s disease as a clinical syndrome. Ann N Y Acad Sci2003;991:1–14.
Feng X, Greenwald B, Rabitz H, Shea-Brown E, Kosut R. Toward closed-loopoptimization of deep brain stimulation for Parkinson’s disease: concepts andlessons from a computational model. J Neural Eng 2007;4:L14–21.
Fitz Coy A, Balaji B, Kim D, Yu X. Deep brain stimulation: a technology assessment.California Institute of Technology Report, 2011.
Foffani G, Bianchi AM, Baselli G, Priori A. Movement-related frequency modulationof beta oscillatory activity in the human subthalamic nucleus. J Physiol2005;568:699–711.
Fraix V, Pollak P, Vercueil L, Benabid AL, Mauguière F. Effects of subthalamic nucleusstimulation on motor cortex excitability in Parkinson’s disease. ClinNeurophysiol 2008;119:2513–8.
Frankemolle AMM, Wu J, Noecker AM, Voelcker-Rehage C, Ho JC, Vitek JL, et al.Reversing cognitive–motor impairments in Parkinson’s disease patients using acomputational modelling approach to deep brain stimulation programming.Brain 2010;133:746–61.
882 A. Beuter et al. / Clinical Neurophysiology 125 (2014) 874–885

Author's personal copy
Franzini A, Ferroli P, Servello D, Broggi G. Reversal of thalamic hand syndrome bylong term motor cortex stimulation. J Neurosurg 2000;93:873–5.
Fumagalli M, Giannicola G, Rosa M, Marceglia S, Lucchiari C, Mrakic-Sposta S, et al.Conflict-dependent dynamic of subthalamic nucleus oscillations during moraldecisions. Soc Neurosci 2011;6:243–56.
Giannicola G, Marceglia S, Rossi L, Mrakic-Sposta S, Rampini P, Tamma F, et al. Theeffects of levodopa and ongoing deep brain stimulation on subthalamic betaoscillations in Parkinson’s disease. Exp Neurol 2010;226:120–7.
Giannicola G, Rosa M, Servello D, Menghetti C, Carrabba G, Pacchetti C, et al.Subthalamic local field potentials after seven-year deep brain stimulation inParkinson’s disease. Exp Neurol 2012;237:312–7.
Gorman AL. Differential patterns of activation of the pyramidal system elicited bysurface anodal and cathodal cortical stimulation. J Neurophysiol1966;29:547–64.
Gradinaru V, Mogri M, Thompson KR, Henderson JM, Deisseroth K. Opticaldeconstruction of parkinsonian neural circuitry. Science 2009;324:354–9.
Grafton ST. Contributions of functional imaging to understanding parkinsoniansymptoms. Curr Opin Neurobiol 2004;14:715–9.
Granger CWJ. Investigating causal relations by econometric models and cross-spectral methods. Econometrica 1969;37:424–38.
Guehl D, Edwards R, Cuny E, Burbaud P, Rougier A, Modolo J, et al. Statisticaldetermination of optimal STN stimulation site in Parkinson’s disease. JNeurosurg 2007;106:101–10.
Gutiérrez JC, Seijo FJ, Alvarez Vega MA, Fernández González F, Lozano AM,Aragoneses B, et al. Therapeutic extradural cortical stimulation for Parkinson’sdisease: report of six cases and review of the literature. Clin Neurol Neurosurg2009;111:703–7.
Hammond C, Ammari R, Bioulac B, Garcia L. Latest view on the mechanism of actionof deep brain stimulation. Mov Disord 2008;23:2111–21.
Hanajima R, Ashby P, Lozano AM, Lang AE, Chen R. Single pulse stimulation of thehuman subthalamic nucleus facilitates the motor cortex at short intervals. JNeurophysiol 2004;92:1937–43.
Hess CW. Modulation of cortical–subcortical networks in Parkinson’s disease byapplied field effects. Front Hum Neurosci 2013;7:565.
Hirschmann J, Özkurt TE, Butz M, Homburger M, Elben S, Hartmann CJ, et al. Distinctoscillatory STN-cortical loops revealed by simultaneous MEG and local fieldpotential recordings in patients with Parkinson’s disease. NeuroImage2011;55:1159–68.
Holsheimer J, Nguyen JP, Lefaucheur JP, Manola L. Cathodal, anodal or bifocalstimulation of the motor cortex in the management of chronic pain? ActaNeurochir Suppl 2007;97:57–66.
Horsley V. Remarks on the surgery of the central nervous system. Br Med J1890;2:1286–92.
Huang X, Troy WC, Yang Q, Ma H, Laing CR, Schiff SJ, et al. Spiral waves indisinhibited mammalian neocortex. J Neurosci 2004;24:9897–902.
Jankovic J. Parkinson’s disease: clinical features and diagnosis. J Neurol NeurosurgPsychiatry 2008;79:368–76.
Jenkinson N, Brown P. New insights into the relationship between dopamine, betaoscillations and motor function. Trends Neurosci 2011;34:611–8.
Johnson MD, Miocinovic S, McIntyre CC, Vitek JL. Mechanisms and targets of deepbrain stimulation in movement disorders. Neurotherapeutics 2008;5:294–308.
Kacar A, Filipovic SR, Kresojevic N, Milanovic SD, Ljubisavljevic M, Kostic VS, et al.History of exposure to dopaminergic medication does not affect motor cortexplasticity and excitability in Parkinson’s disease. Clin Neurophysiol2013;124:697–707.
Katayama Y, Oshima H, Fukaya C, Kawamata T, Yamamoto T. Control of post-strokemovement disorders using chronic motor cortex stimulation. Acta NeurochirSuppl 2002;79:89–92.
Kent AR, Grill WM. Instrumentation to record evoked potentials for closed-loopcontrol of deep brain stimulation. Conf Proc IEEE Eng Med Biol Soc2011;2011:6777–80.
Kent AR, Grill WM. Recording evoked potentials during deep brain stimulation:development and validation of instrumentation to suppress the stimulusartefact. J Neural Eng 2012;9:036004.
Kerr CC, Van Albada SJ, Neymotin SA, Chadderdon GL, Robinson PA, Lytton WW.Cortical information flow in Parkinson’s disease: a composite network/fieldmodel. Front Comput Neurosci 2013;7:39.
Kleiner-Fisman G, Fisman DN, Kahn FI, Sime E, Lozano AM, Lang AE. Motor corticalstimulation for parkinsonism in multiple system atrophy. Arch Neurol2003;60:1554–8.
Klemme RM. Surgical treatment of dystonia, paralysis agitans and athetosis. ArchNeurol Psychiatry 1940;44:926.
Klemme RM. Surgical treatment of dystonia with report of 100 cases. Assoc ResNerv Ment Dis 1942;21:596–601.
Kojovic M, Bologna M, Kassavetis P, Murase N, Palomar FJ, Berardelli A, et al.Functional reorganization of sensorimotor cortex in early Parkinson disease.Neurology 2012;78:1441–8.
Kossoff EH, Ritzl EK, Politsky JM, Murro AM, Smith JR, Duckrow RB, et al. Effect of anexternal responsive neurostimulator on seizures and electrographic dischargesduring subdural electrode monitoring. Epilepsia 2004;45:1560–7.
Kühn AA, Williams D, Kupsch A, Limousin P, Hariz M, Schneider GH, et al. Event-related beta desynchronization in human subthalamic nucleus correlates withmotor performance. Brain 2004;127:735–46.
Kühn AA, Hariz MI, Silberstein P, Tisch S, Kupsch A, Schneider GH, et al. Activation ofthe subthalamic region during emotional processing in Parkinson disease.Neurology 2005;65:707–13.
Kühn AA, Doyle L, Pogosyan A, Yarrow K, Kupsch A, Schneider GH, et al. Modulationof beta oscillations in the subthalamic area during motor imagery in Parkinson’sdisease. Brain 2006;129:695–706.
Kühn AA, Kempf F, Brücke C, Gaynor Doyle L, Martinez-Torres I, Pogosyan A, et al.High-frequency stimulation of the subthalamic nucleus suppresses oscillatorybeta activity in patients with Parkinson’s disease in parallel with improvementin motor performance. J Neurosci 2008;28:6165–73.
Lefaucheur JP. Motor cortex dysfunction revealed by cortical excitability studies inParkinson’s disease: influence of antiparkinsonian treatment and corticalstimulation. Clin Neurophysiol 2005;116:244–53.
Lefaucheur JP. Principles of therapeutic use of transcranial and epidural corticalstimulation. Clin Neurophysiol 2008;119:2179–84.
Lefaucheur JP. Methods of therapeutic cortical stimulation. Neurophysiol Clin2009a;39:1–14.
Lefaucheur JP. Treatment of Parkinson’s disease by cortical stimulation. Expert RevNeurother 2009b;9:1755–71.
Lefaucheur JP. Neurophysiology of cortical stimulation. Int Rev Neurobiol2012;107:57–85.
Lefaucheur JP, Drouot X, Von Raison F, Ménard-Lefaucheur I, Cesaro P, Nguyen JP.Improvement of motor performance and modulation of cortical excitability byrepetitive transcranial magnetic stimulation of the motor cortex in Parkinson’sdisease. Clin Neurophysiol 2004;115:2530–41.
Leon-Sarmiento FE, Rizzo-Sierra CV, Bayona EA, Bayona-Prieto J, Doty RL, Bara-Jimenez W. Novel mechanisms underlying inhibitory and facilitatorytranscranial magnetic stimulation abnormalities in Parkinson’s disease. ArchMed Res 2013;44:221–8.
Lindenbach D, Bishop C. Critical involvement of the motor cortex in thepathophysiology and treatment of Parkinson’s disease. Neurosci Biobehav Rev2013;37:2737–50.
Little S, Brown P. What brain signals are suitable for feedback control of deep brainstimulation in Parkinson’s disease? Ann N Y Acad Sci 2012;1265:9–24.
Little S, Pogosyan A, Kuhn AA, Brown P. Beta band stability over time correlates withParkinsonian rigidity and bradykinesia. Exp Neurol 2012;236:383–8.
Litvak V, Jha A, Eusebio A, Oostenveld R, Foltynie T, Limousin P, et al. Restingoscillatory cortico-subthalamic connectivity in patients with Parkinson’sdisease. Brain 2011;134:359–74.
Litvak V, Eusebio A, Jha A, Oostenveld R, Barnes G, Foltynie T, et al. Movement-related changes in local and long-range synchronization in Parkinson’s diseaserevealed by simultaneous magnetoencephalography and intracranialrecordings. J Neurosci 2012;32:10541–53.
Mackey M, Glass L. Oscillation and chaos in physiological control systems. Science1977;197:287–9.
MacKinnon CD, Gilley EA, Weis-McNulty A, Simuni T. Pathways mediatingabnormal intracortical inhibition in Parkinson’s disease. Ann Neurol2005;58:516–24.
Manola L, Roelofsen BH, Holsheimer J, Marani E, Geelen J. Modelling motor cortexstimulation for chronic pain control: electrical potential field, activatingfunctions and responses of simple nerve fibre models. Med Biol Eng Comput2005;43:335–43.
Manola L, Holsheimer J, Veltink P, Buitenweg JR. Anodal vs cathodal stimulation ofmotor cortex: a modeling study. Clin Neurophysiol 2007;118:464–74.
Marceglia S, Rossi L, Foffani G, Bianchi AM, Cerutti S, Priori A. Basal ganglia localfield potentials: applications for the development of new deep brainstimulation devices for movement disorders. Expert Rev Med Devices2007;4:605–14.
Marceglia S, Fiorio M, Foffani G, Mrakic-Sposta S, Tiriticco M, Locatelli M, et al.Modulation of beta oscillations in the subthalamic area during actionobservation in Parkinson’s disease. Neuroscience 2009;161:1027–36.
Marceglia S, Fumagalli M, Priori A. What neurophysiological recordings tell us aboutcognitive and behavioral functions of the human subthalamic nucleus. ExpertRev Neurother 2011;11:139–49.
McIntyre CC, Grill WM. Extracellular stimulation of central neurons: influence ofstimulus waveform and frequency on neuronal output. J Neurophysiol2002;88:1592–604.
McIntyre CC, Hahn PJ. Network perspectives on the mechanisms of deep brainstimulation. Neurobiol Dis 2010;38:329–37.
McIntyre CC, Savasta M, Kerkerian-Le-Goff L, Vitek JL. Uncovering the mechanism(s)of action of deep brain stimulation: activation, inhibition or both. ClinNeurophysiol 2004;115:1239–48.
Meissner W, Leblois A, Hansel D, Bioulac B, Gross CE, Benazzouz A, et al.Subthalamic high frequency stimulation resets subthalamic firing and reducesabnormal oscillations. Brain 2005;128:2372–82.
Modolo J, Beuter A. Cortical contribution to subthalamic activity during chronicelectrical stimulation. Brain Stimul 2009a;1:300–1.
Modolo J, Beuter A. Linking brain dynamics, neural mechanisms, and deep brainstimulation in Parkinson’s disease: an integrated perspective. Med Eng Phys2009b;31:615–23.
Modolo J, Henry J, Beuter A. Dynamics of the subthalamo-pallidal complexin Parkinson’s disease during deep brain stimulation. J Biol Phys2008;34:251–66.
Modolo J, Bhattacharya B, Edwards R, Campagnaud J, Legros A, Beuter A. Using avirtual cortical module implementing a neural field model to modulate brainrhythms in Parkinson’s disease. Front Neurosci 2010;4:45.
Modolo J, Legros A, Thomas AW, Beuter A. Model-driven therapeutic treatment ofneurological disorders: reshaping brain rhythms with neuromodulation.Interface Focus 2011;1:61–74.
A. Beuter et al. / Clinical Neurophysiology 125 (2014) 874–885 883

Author's personal copy
Montgomery Jr EB, Gale JT. Mechanisms of action of deep brain stimulation (DBS).Neurosci Biobehav Rev 2008;32:388–407.
Nguyen JP, Pollin B, Feve A, Geny C, Cesaro P. Improvement of action tremor bychronic cortical stimulation. Mov Disord 1998;13:84–8.
Nguyen JP, Nizard J, Keravel Y, Lefaucheur JP. Invasive brain stimulation for thetreatment of neuropathic pain. Nat Rev Neurol 2011;7:699–709.
Ni Z, Bahl N, Gunraj CA, Mazzella F, Chen R. Increased motor cortical facilitation anddecreased inhibition in Parkinson disease. Neurology 2013;80:1746–53.
Nizard J, Raoul S, Nguyen JP, Lefaucheur JP. Invasive stimulation therapies for thetreatment of refractory pain. Discov Med 2012;14:237–46.
Nowak LG, Bullier J. Axons, but not cell bodies, are activated by electricalstimulation in cortical gray matter. I. Evidence from chronaxie measurements.Exp Brain Res 1998;118:477–88.
Nowak K, Mix E, Gimsa J, Strauss U, Sriperumbudur KK, Benecke R, et al. Optimizinga rodent model of Parkinson’s disease for exploring the effects, and mechanismsof deep brain stimulation. Parkinsons Dis 2011;2011:414682.
Osorio M, Frei G, Manly BFJ, Sunderam S, Bhavaraju NC, Wilkinson SB. Anintroduction to contingent (closed-loop) brain electrical stimulation forseizure blockage, to ultra-short-term clinical trials, and to multidimensionalstatistical analysis of therapeutic efficacy. J Clin Neurophysiol 2001;18:533–44.
Oswal A, Litvak V, Brücke C, Huebl J, Schneider GH, Kühn AA, et al. Cognitive factorsmodulate activity within the human subthalamic nucleus during voluntarymovement in Parkinson’s disease. J Neurosci 2013;33:15815–26.
Pagni CA, Cioni B, Lavano A, Mazzone P. Extradural motor cortex stimulation (EMCS)for Parkinson’s disease: history and first results by the study group of the Italianneurosurgical society. Acta Neurochir Suppl 2005a;93:113–9.
Pagni CA, Zeme S, Zenga F, Maina R. Extradural motor cortex stimulation inadvanced Parkinson’s disease. Neurosurgery 2005b;57(ONS):402.
Pagni CA, Albanese A, Bentivoglio A, Broggi G, Canavero S, Cioni B, et al. Results bymotor cortex stimulation in treatment of focal dystonia, Parkinson’s disease andpost-ictal spasticity: the experience of the Italian study group of the Italianneurosurgical society. Acta Neurochir Suppl 2008;101:13–21.
Park A, Stacy M. Non-motor symptoms in Parkinson’s disease. J Neurol2009;256(Suppl. 3):293–8.
Patten TM, Rennie CJ, Robinson PA, Gong P. Human cortical traveling waves:dynamical properties and correlations with responses. PLoS One2012;7:e38392.
Pizzolato G, Mandat T. Deep brain stimulation for movement disorders. Front IntegrNeurosci 2012;6:2.
Priori A, Lefaucheur JP. Chronic epidural motor cortical stimulation for movementdisorders. Lancet Neurol 2007;6:279–86.
Priori A, Foffani G, Pesenti A, Tamma F, Bianchi AM, Pellegrini M, et al. Rhythm-specific pharmacological modulation of subthalamic activity in Parkinson’sdisease. Exp Neurol 2004;189:369–79.
Priori A, Foffani G, Rossi L, Marceglia S. Adaptive deep brain stimulation (aDBS)controlled by local field potential oscillations. Exp Neurol 2013;245:77–86.
Radman T, Ramos RL, Brumberg JC, Bikson M. Role of cortical cell type andmorphology in subthreshold and suprathreshold uniform electric fieldstimulation in vitro. Brain Stimul 2009;2:215–28.
Raethjen J, Govindan RB, Muthuraman M, Kopper F, Volkmann J, Deuschl G. Corticalcorrelates of the basic and first harmonic frequency of Parkinsonian tremor. ClinNeurophysiol 2009;120:1866–72.
Ranck Jr JB. Which elements are excited in electrical stimulation of mammaliancentral nervous system: a review. Brain Res 1975;98:417–49.
Ray NJ, Jenkinson N, Wang S, Holland P, Brittain JS, Joint C, et al. Local field potentialbeta activity in the subthalamic nucleus of patients with Parkinson’s disease isassociated with improvements in bradykinesia after dopamine and deep brainstimulation. Exp Neurol 2008;213:108–13.
Reck C, Florin E, Wojtecki L, Krause H, Groiss S, Voges J, et al. Characterisation oftremor-associated local field potentials in the subthalamic nucleus inParkinson’s disease. Eur J Neurosci 2009;29:599–612.
Reck C, Himmel M, Florin E, Maarouf M, Sturm V, Wojtecki L, et al. Coherenceanalysis of local field potentials in the subthalamic nucleus: differences inparkinsonian rest and postural tremor. Eur J Neurosci 2010;32:1202–14.
Rehan M, Hong KS. Modeling and automatic feedback control of tremor: adaptiveestimation of deep brain stimulation? PLoS One 2013;8:e62888.
Rektor I, Baláz M, Bocková M. Cognitive activities in the subthalamic nucleus.Invasive studies. Parkinsonism Relat Disord 2009;15(Suppl. 3):S83–6.
Rektor I, Baláz M, Bocková M. Cognitive event-related potentials and oscillations inthe subthalamic nucleus. Neurodegener Dis 2010;7:160–2.
Riederer P, Wuketich S. Time course of nigrostriatal degeneration in parkinson’sdisease. A detailed study of influential factors in human brain amine analysis. JNeural Transm 1976;38:277–301.
Rosa M, Giannicola G, Servello D, Marceglia S, Pacchetti C, Porta M, et al.Subthalamic local field beta oscillations during ongoing deep brainstimulation in Parkinson’s disease in hyperacute and chronic phases.Neurosignals 2011;19:151–62.
Rosenthal J, Waller HJ, Amassian VE. An analysis of the activation of motor corticalneurons by surface stimulation. J Neurophysiol 1967;30:844–58.
Rosin B, Slovik M, Mitelman R, Rivlin-Etzion M, Haber SN, Israel Z, et al. Closed-loopdeep brain stimulation is superior in ameliorating parkinsonism. Neuron2011;72:370–84.
Rossi L, Foffani G, Marceglia S, Bracchi F, Barbieri S, Priori A. An electronic device forartefact suppression in human local field potential recordings during deep brainstimulation. J Neural Eng 2007;4:96–106.
Rossi L, Marceglia S, Foffani G, Cogiamanian F, Tamma F, Rampini P, et al.Subthalamic local field potential oscillations during ongoing deep brainstimulation in Parkinson’s disease. Brain Res Bull 2008;76:512–21.
Rothwell JC, Edwards MJ. Parkinson’s disease. Handb Clin Neurol 2013;116:535–42.Rouse A, Stanslaski S, Cong P, Jensen R, Afshar P, Ullestad D, et al. A chronic
generalized bi-directional brain–machine interface. J Neural Eng2011;8:036018.
Rubino D, Robbins KA, Hatsopoulos NG. Propagating waves mediate informationtransfer in the motor cortex. Nat Neurosci 2006;9:1549–57.
Santaniello S, Fiengo G, Gliemo L. Adaptive feedback control in deep brainstimulation: a simulation study. In: Proceedings of the 17th congress of theInternational Federation of Automatic, Control; 2008. p. 11624–29.
Santaniello S, Montgomery EB, Gale JT, Sarma SV. Non-stationary discharge patternsin motor cortex under subthalamic nucleus deep brain stimulation. Front IntegrNeurosci 2012;6:35.
Santos FJ, Costa RM, Tecuapetla F. Stimulation on demand: closing the loop on deepbrain stimulation. Neuron 2011;72:197–8.
Schuepbach WMM, Rau J, Knudsen K, Volkmann J, Krack P, Timmermann L, et al.Neurostimulation for Parkinson’s disease with early motor complications. NEngl J Med 2013;368:610–22.
Sharott A, Magill PJ, Bolam JP, Brown P. Directional analysis of coherent oscillatoryfield potentials in the cerebral cortex and basal ganglia in the rat. J Physiol2005;562:951–63.
Silberstein P, Kühn AA, Kupsch A, Trottenberg T, Krauss JK, Wöhrle JC, et al.Patterning of globus pallidus local field potentials differs between Parkinson’sdisease and dystonia. Brain 2003;126:2597–608.
Silberstein P, Pogosyan A, Kühn AA, Hotton G, Tisch S, Kupsch A, et al. Cortico-cortical coupling in Parkinson’s disease and its modulation by therapy. Brain2005;128:1277–91.
Smirnov DA, Barnikol UB, Barnikol TT, Bezruchko BP, Hauptmann C, Buhrle C, et al.The generation of Parkinsonian tremor as revealed by directional couplinganalysis. EPL 2008;83:20003.
Smith JR, Fountas KN, Murro AM, Park YD, Jenkins PD, Morrell M, et al. Closed-loopstimulation in the control of focal epilepsy of insular origin. Stereotact FunctNeurosurg 2010;88:281–7.
Sohal VS, Sun FT. Responsive neurostimulation suppresses synchronized corticalrhythms in patients with epilepsy. Neurosurg Clin N Am 2011;22:481–8.
Takahashi K, Saleh M, Penn RD, Hatsopoulos NG. Propagating waves in humanmotor cortex. Front Hum Neurosci 2011;5:40.
Tani N, Saitoh Y. Electrical stimulation of primary motor cortex for Parkinson’ssyndrome. In: Dushanova J, editor. Diagnostics and rehabilitation of Parkinson’sdisease. Rijeka: InTech; 2011. p. 493–508.
Tani N, Saitoh Y, Kishima H, Oshino S, Hatazawa J, Hashikawa K, et al. Motor cortexstimulation for levodopa-resistant akinesia: case report. Mov Disord2007;22:1645–9.
Tass PA. Desynchronizing double-pulse phase resetting and application to deepbrain stimulation. Biol Cybern 2001;85:343–54.
Tass PA, Silchenko AN, Hauptmann C, Barnikol UB, Speckmann EJ. Long-lastingdesynchronization in rat hippocampal slice induced by coordinated resetstimulation. Phys Rev E Stat Nonlin Soft Matter Phys 2009;80:011902.
Tass PA, Qin L, Hauptmann C, Dovero S, Bezard E, Boraud T, et al. Coordinated resethas sustained aftereffects in Parkinsonian monkeys. Ann Neurol2012;72:816–20.
Timmermann L, Fink GR. Pathological network activity in Parkinson’s disease: fromneural activity and connectivity to causality? Brain 2011;134:332–4.
Timmermann L, Gross J, Dirks M, Volkmann J, Freund HJ, Schnitzler A. The cerebraloscillatory network of parkinsonian tremor. Brain 2003;126:199–212.
Timmermann L, Florin E, Reck C. Pathological cebebral oscillatory activity inParkinson’s disease: a critical review on methods, data and hypotheses. ExpertRev Med Devices 2007;4:651–61.
Uhlhaas PJ, Singer W. Neural synchrony in brain disorders: relevance for cognitivedysfunctions and pathophysiology. Neuron 2006;52:155–68.
Vitek JL. Deep brain stimulation: how does it work? Cleve Clin J Med2008;75(S2):S59–65.
Volkmann J. Oscillations of the human sensorimotor system as revealed bymagnetoencephalography. Mov Disord 1998;13:73–6.
Volkmann J, Moro E, Pahwa R. Basic algorithms for the programming of deep brainstimulation in Parkinson’s disease. Mov Disord 2006;21(S14):S284–9.
Walker HC, Watts RL, Guthrie S, Wang D, Guthrie BL. Bilateral effects of unilateralsubthalamic deep brain stimulation on Parkinson’s disease at 1 year.Neurosurgery 2009;65:302–9.
Weinberger M, Mahant N, Hutchison WD, Lozano AM, Moro E, Hodaie M, et al. Betaoscillatory activity in the subthalamic nucleus and its relation to dopaminergicresponse in Parkinson’s disease. J Neurophysiol 2006;96:3248–56.
Whitmer D, de Solages C, Hill B, Yu H, Henderson JM, Bronte-Stewart H. Highfrequency deep brain stimulation attenuates subthalamic and cortical rhythmsin Parkinson’s disease. Front Hum Neurosci 2012;6:155.
Williams D, Tijssen M, Van Bruggen G, Bosch A, Insola A, Di Lazzaro V, et al.Dopamine-dependent changes in the functional connectivity between basalganglia and cerebral cortex in humans. Brain 2002;125:1558–69.
Williams D, Kühn A, Kupsch A, Tijssen M, van Bruggen G, Speelman H, et al.Behavioural cues are associated with modulations of synchronous oscillationsin the human subthalamic nucleus. Brain 2003;126:1975–85.
Wilson HR, Cowan JD. A mathematical theory of the functional dynamics of corticaland thalamic nervous tissue. Kybernetik 1973;13:55–80.
884 A. Beuter et al. / Clinical Neurophysiology 125 (2014) 874–885

Author's personal copy
Winestone JS, Zaidel A, Bergman H, Israel Z. The use of macroelectrodes in recordingcellular spiking activity. J Neurosci Methods 2012;206:34–9.
Wingeier B, Tcheng T, Koop MM, Hill BC, Heit G, Bronte-Stewart HM. Intra-operativeSTN DBS attenuates the prominent beta rhythm in the STN in Parkinson’sdisease. Exp Neurol 2006;197:244–51.
Wojtecki L, Elben S, Timmermann L, Reck C, Maarouf M, Jörgens S, et al. Modulationof human time processing by subthalamic deep brain stimulation. PLoS One2011;6:e24589.
Wojtecki L, Colosimo C, Fuentes R. Deep brain stimulation for movement disorders– a history of success and challenges to conquer. Front Integr Neurosci2012;6:6.
Wongsarnpigoon A, Grill WM. Effects of stimulation parameters and electrodelocation on thresholds for epidural stimulation of cat motor cortex. J Neural Eng2011;8:066016.
Wongsarnpigoon A, Grill WM. Computer-based model of epidural motor cortexstimulation: effects of electrode position and geometry on activation of corticalneurons. Clin Neurophysiol 2012;123:160–72.
Woolsey CN, Erickson TC, Gilson WE. Localization in somatic sensory and motorareas of human cerebral cortex as determined by direct recording of evokedpotentials and electrical stimulation. J Neurosurg 1979;51:476–506.
A. Beuter et al. / Clinical Neurophysiology 125 (2014) 874–885 885





























