Embed Size (px)
Citation preview

Cancer Therapy: PreclinicalSee related commentary by Maus and June, p. 1917
B-cell Maturation Antigen Is a Promising Target for AdoptiveT-cell Therapy of Multiple Myeloma
Robert O. Carpenter1, Moses O. Evbuomwan2, Stefania Pittaluga2, Jeremy J. Rose1, Mark Raffeld2,Shicheng Yang3, Ronald E. Gress1, Frances T. Hakim1, and James N. Kochenderfer1
AbstractPurpose:Multiplemyeloma is a usually incurablemalignancy of plasma cells. New therapies are urgently
needed for multiple myeloma. Adoptive transfer of chimeric antigen receptor (CAR)–expressing T cells is a
promising new therapy for hematologic malignancies, but an ideal target antigen for CAR-expressing T-cell
therapies for multiple myeloma has not been identified. B-cell maturation antigen (BCMA) is a protein that
has been reported to be selectively expressed by B-lineage cells including multiple myeloma cells. Our goal
was to determine if BCMA is a suitable target for CAR-expressing T cells.
Experimental Design:We conducted an assessment of BCMA expression in normal human tissues and
multiplemyeloma cells by flow cytometry, quantitative PCR, and immunohistochemistry.We designed and
tested novel anti-BCMA CARs.
Results: BCMA had a restricted RNA expression pattern. Except for expression in plasma cells, BCMA
protein was not detected in normal human tissues. BCMA was not detected on primary human CD34þ
hematopoietic cells.We detected uniformBCMA cell-surface expression on primarymultiplemyeloma cells
from five of five patients. We designed the first anti-BCMA CARs to be reported and we transduced T cells
with lentiviral vectors encoding these CARs. TheCARs gave T cells the ability to specifically recognize BCMA.
The anti-BCMA-CAR–transduced T cells exhibited BCMA-specific functions including cytokine production,
proliferation, cytotoxicity, and in vivo tumor eradication. Importantly, anti-BCMA-CAR–transduced T cells
recognized and killed primary multiple myeloma cells.
Conclusions: BCMA is a suitable target for CAR-expressing T cells, and adoptive transfer of anti-
BCMA-CAR–expressing T cells is a promising new strategy for treating multiple myeloma. Clin Cancer
Res; 19(8); 2048–60. �2013 AACR.
IntroductionMultiple myeloma is a malignancy characterized by an
accumulation of clonal plasma cells (1–3). Current thera-pies for multiple myeloma often cause remissions, butnearly all patients eventually relapse and die (1, 2). Thereis substantial evidence of an immune-mediated eliminationof myeloma cells in the setting of allogeneic hematopoieticstem cell transplantation; however, the toxicity of thisapproach is high, and few patients are cured (1, 4).Although some monoclonal antibodies have shown prom-ise for treating multiple myeloma in preclinical studies and
early clinical trials, consistent clinical efficacy of anymono-clonal antibody therapy formultiplemyelomahas not beenconclusively shown (5–7). There is clearly a great need fornew immunotherapies for multiple myeloma, and devel-oping an effective antigen-specific adoptive T-cell therapyfor this disease would be a major advance.
Adoptive transfer of T cells genetically modified to recog-nizemalignancy-associated antigens is a promisingapproachfor cancer therapy (8, 9). T cells can be genetically modifiedtoexpress chimeric antigen receptors (CAR),whichare fusionproteins that include an antigen recognition moiety andT-cell activationdomains (9, 10). ForB-lineagemalignancies,substantial progress has been made recently in developingadoptive T-cell approaches that use anti-CD19 CARs(11–18). Anti-CD19-CAR–transduced T cells have curedleukemia and lymphoma in mice (19, 20). Several patientsobtained remissions in early clinical trials of adoptivelytransferred anti-CD19-CAR–transduced T cells, and T cellstransduced with anti-CD19 CARs also eradicated normal Bcells (12, 13, 17, 21).Unfortunately,CD19 is rarely expressedin the malignant plasma cells of multiple myeloma, sotreating multiple myeloma with CAR-expressing T cells willrequire identifying other antigens to target (22, 23).
Authors' Affiliations: 1Experimental Transplantation and ImmunologyBranch; 2Laboratory of Pathology, National Cancer Institute, Bethesda,Maryland; and 3Division of Neurosurgery, Department of Surgery, DukeUniversity School of Medicine, Durham, North Carolina
Note: Supplementary data for this article are available at Clinical CancerResearch Online (http://clincancerres.aacrjournals.org/).
Corresponding Author: James N. Kochenderfer, National Cancer Insti-tute, NIH, 10 Center Drive CRC, Room 3-3330, Bethesda, MD 20892.Phone: 301-594-5340; Fax: 301-480-8146; E-mail: [email protected]
doi: 10.1158/1078-0432.CCR-12-2422
�2013 American Association for Cancer Research.
ClinicalCancer
Research
Clin Cancer Res; 19(8) April 15, 20132048
on July 10, 2020. © 2013 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst January 23, 2013; DOI: 10.1158/1078-0432.CCR-12-2422

One candidate antigen of immunotherapies for multiplemyeloma is B-cell maturation antigen (BCMA, CD269;refs. 24, 25). BCMA RNA was detected universally in mul-tiplemyeloma cells, and BCMA protein was detected on thesurface of plasma cells from patients with multiple myelo-ma by several investigators (26–29). BCMA is a member ofthe TNF receptor superfamily (30, 31). BCMA binds B-cellactivating factor (BAFF) and a proliferation-inducing ligand(APRIL; refs. 31–33). Among nonmalignant cells, BCMAhas been reported to be expressed mostly by plasma cellsand subsets of mature B cells (24, 25, 32, 34, 35). Micedeficient in BCMA were healthy and had a normal physicalappearance (36, 37). BCMA-deficient mice had normalnumbers of B cells, but survival of long-lived plasma cellswas impaired (34, 36).We reasoned that BCMA would be an appropriate target
antigen for treatingmultiplemyelomawithCAR-expressingT cells. Except for expression in plasma cells, we found thatBCMA is not expressed in the cells of major human organs.We designed lentiviral vectors that encoded BCMA-specificCARs. T cells transduced with these vectors performedBCMA-specific functions including cytokine production,proliferation, and cytotoxicity.
Materials and MethodsCell lines and primary cellsH929, U266, and RPMI-8226 are all BCMAþ multiple
myeloma cell lines that were obtained from American TypeCulture Collection (ATCC). A549 is a BCMA-negative lungcancer cell line (ATCC). TC71 is a BCMA-negative sarcomacell line. CCRF-CEM is a BCMA-negative T-cell line (ATCC).BCMA-K562 are K562 cells (ATCC) transduced with the
gene for full-length BCMA in our laboratory. NGFR-K562are K562 cells transduced with the gene for low-affinitynerve growth factor in our laboratory (38). The samegammaretroviral vector and methods were used to trans-duce BCMA-K562 andNGFR-K562.We used tissue samplesor peripheral blood mononuclear cells (PBMC) from6 patients with multiple myeloma designated myelomapatients 1 to 6. We used PBMC from 3 subjects with mela-noma: donor A, B, and C. We obtained primary CD34þ
hematopoietic cells from 3 healthy normal donors. All ofthe human samples mentioned earlier were obtained frompatients enrolled on Institutional Review Board (IRB)–approved clinical trials at the National Cancer Institute(Bethesda, MD).
Real-time qPCR to quantitate BCMA transcript copiesWe quantitated BCMA cDNA copies in samples of cDNA
from human tissues included in the Human Major TissueqPCR panel II (Origene) by conducting quantitative PCR(qPCR) with a BCMA-specific primer and probe set(Applied Biosystems, catalog number 4331182). As a pos-itive control, we quantitated BCMA cDNA copies in cDNAofmultiplemyeloma cells fromaplasmacytomaof a patientwith advanced multiple myeloma. RNA was extracted fromthe plasmacytoma cells with an RNeasy mini kit (Qiagen),and cDNA was synthesized with standard methods. Astandard curve for the BCMA qPCR was created by ampli-fying dilutions of a plasmid that encoded the full-lengthcDNA of BCMA (Origene). The qPCR accurately detectedcopy numbers from102 to 109 copies of BCMAper reaction.We also quantitated the number of b-actin cDNA copies inthe same tissueswith a TaqManb-actin primer andprobe kit(Applied Biosystems). A b-actin standard curve was createdby amplifying serial dilutions of a b-actin plasmid. All qPCRreactions were carried out on a Roche LightCycler480machine.
ImmunohistochemistryBCMA stains were conducted on formalin-fixed paraffin-
embedded tissue sections and on a commercial normalhuman tissue array (Pantomics Inc., catalog numberMN0661). NGFR-K562 cells (BCMA-negative), BCMA-K562 cells (BCMA-positive), and sections from reactivetonsils were used as controls. Sections were deparaffinizedin xylene, rehydrated in graded-alcohol, placed in 1� lowpH antigen retrieval solution (Dako, catalog numberS1699), and steamed for 30minutes. Sections were blockedwith Dako protein block serum-free (catalog numberX0909) for 30minutes, and blocked with 5% bovine serumalbumin (Sigma-Aldrich) for another 30 minutes. The sec-tions were then incubated for 60 minutes at room temper-ature with either 1 mg/mL anti-BCMA goat polyclonalantibody (R&D Systems, catalog number AF193) or withan isotype control of 1 mg/mL normal purified goat immu-noglobulin G (IgG). Biotinylated rabbit anti-goat IgG wasused as the secondary antibody (Vector Lab, catalognumberBA-5000; 7.5 mg/mL, 30-minute incubation, room temper-ature). Vectastain ABC Kit (Vector Lab, catalog number
Translational RelevanceOne way to improve outcomes of patients with mul-
tiple myeloma might be to develop effective immu-notherapies targeting antigens expressed by multiplemyeloma cells. T cells expressing chimeric antigen recep-tors (CAR) that target the B-cell antigen CD19 havepotent in vivo activity. Unfortunately, a suitable targetfor CAR-expressing T-cell therapy for multiple myelomahas not beenpreviously identified becausemost proteinsexpressed in multiple myeloma cells are also expressedin essential normal cells. We assessed B-cell maturationantigen (BCMA) as a possible target for CAR-expressingT cells. Our results show that BCMA is expressed uni-formly on the malignant plasma cells of many patientswith multiple myeloma. BCMA expression was notdetected on essential normal cells. We designed the firstanti-BCMA CARs to be reported. T cells expressing theseCARs could recognize and destroy primary human mul-tiple myeloma cells. These findings are the first stepstoward clinical trials of anti-BCMA CAR-expressingT cells.
Anti-BCMA Chimeric Antigen Receptor
www.aacrjournals.org Clin Cancer Res; 19(8) April 15, 2013 2049
on July 10, 2020. © 2013 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst January 23, 2013; DOI: 10.1158/1078-0432.CCR-12-2422

PK4005; 30-minute incubation, room temperature) andDABþChromogen (Dako, catalog number K4011; 5-min-ute incubation, room temperature) were used for detection.For BCMA andmultiple myeloma 1 (MUM1) double stain-ing, BCMA stained sections were re-retrieved in hot Dako1� low pH antigen retrieval solution andmicrowaved for 6minutes. Sections were blocked with Dako protein blockserum-free for 30 minutes, incubated with MUM1 mousemonoclonal antibody (Dako, M7259; 1:100 dilution, 120-minute incubation, room temperature) and detected withVentana BenchMark XT with Ventana ultraView universalalkaline phosphatase red detection kit (AZ, 760-501).Images were taken with an Olympus Bx41 microscope:objective UPlanFI 100�/1.30 oil, adaptor U-TV0.5�C, dig-ital camera Q-imaging Micropublisher 5.0 RTV. The imageswere captured with "Q-Capture Version 3.1" and importedto Adobe Photoshop 7.0.
Construction of anti-BCMA CARsSequences of 2 mouse anti-human BCMA antibodies
were obtained from a patent (39). The specific antibodiesused were designated in the patent as C12A3.2 andC11D5.3. The heavy chain and light chain variable-regionsequences of these antibodies were used to design singlechain variable fragments (scFv) with the following pattern:light chain variable region-linker-heavy chain variableregion. The linker had the following amino acid sequence:GSTSGSGKPGSGEGSTKG (15). CARs incorporating vari-able regions from C12A3.2 and C11D5.3 were designatedanti-bcma1 and anti-bcma2, respectively. DNA sequencesencoding these CARs were designed. The sequence of eachCAR followed this pattern from the 50-end to the 30-end: theCD8a signal sequence, scFv, hinge and transmembraneregions of the human CD8a molecule, the cytoplasmicportion of theCD28molecule, and the cytoplasmic portionof the CD3z molecule. The sequences used for CD8a,CD28, and CD3z were obtained from the National Centerfor Biotechnology Information (Bethesda, MD) website(www.ncbi.nlm.nih.gov/). Guidance about the portions ofeach molecule to include in the CARs was obtained fromprior work (38). DNA encoding the CARs was codon-optimized and synthesized by GeneArt AGwith appropriaterestriction sites. The CAR sequences were ligated into alentiviral vector plasmid designated pRRLSIN.cPPT.MSCV.coDMF5.oPRE (40). The coDMF5 portion of this vectorwas replaced with the CAR sequences by using standardmethods. Two anti-BCMA–encoding CAR vectors wereconstructed: pRRLSIN.cPPT.MSCV.anti-bcma1.oPRE andpRRLSIN.cPPT.MSCV.anti-bcma2.oPRE. A negative-controlCAR that contained the SP6 scFv, which recognized thehapten 2,4,6-trinitrophenyl, was also constructed (10). ThisCARwas referred to as SP6. The SP6CARwas cloned into thesame lentiviral vector as the anti-BCMACARs and containedthe same signaling domains as the anti-BCMA CARs.
Lentiviral supernatant productionSupernatant that contained lentiviruses encoding each
CAR was produced by following a previously published
protocol (40). To produce the supernatant, 293T-17 cells(ATCC) were transfected with the following plasmids asdetailed previously: pMDG (encoding the vesicular stoma-titis virus envelope), pMDLg/pRRE (encoding gag and pol),pRSV-Rev (encoding Rev), and the appropriate CAR-encod-ing plasmid (40).
T-cell transductionsT cells were cultured as described previously (38). In brief,
PBMC were stimulated with the anti-CD3 monoclonal anti-bodyOKT3 (Ortho) in AIMVmedium (Invitrogen) contain-ing5%humanblood typeABserum(ValleyBiomedical) and300 international units (IU)/mL of interleukin-2 (IL-2;Chiron). Thirty-six hours after the cultures were started, theactivated PBMC were suspended in lentiviral supernatantwith protamine sulfate and 300 IU/mL IL-2. The cells werecentrifuged for 1 hour at 1,200 � g. The cells were thencultured for 3 hours at 37�C. Next, the supernatant wasdiluted 1:1 with RPMI (Mediatech)þ10% FBS (Invitrogen)and IL-2. The cells were cultured in the diluted supernatantovernight and then they were returned to culture in AIM Vmedium plus 5% human AB serum with IL-2.
CAR detection on transduced T cells by anti-Fabantibody staining
T cells were stained with biotin-labeled polyclonal goatanti-mouse-F(ab)2 antibodies (anti-Fab; Jackson Immunor-esearch) to detect the anti-BCMA CARs as described previ-ously (38).
Flow cytometryFor anti-BCMA staining, cells were stainedwith polyclon-
al biotin-labeled goat anti-human BCMA antibodies (R&D,catalog number BAF 193) followed by streptavidin (BDBiosciences). Bonemarrow cells were also stainedwith anti-CD38 (eBioscience) and anti-CD56 (BD Biosciences). Flowcytometry analysis for all experiments was carried out byusing FlowJo (Tree Star, Inc.).
ELISA, CD107a, intracellular cytokine staining, andproliferation assays
These assays were conducted by using standardmethods,as previously published (17, 38). Details of themethods forthese techniques are in the Supplementary Methods.
Cytotoxicity assayCytotoxicity assays were conducted as previously describ-
ed (38). Cytotoxicitywasmeasured by comparing survival ofBCMAþ target cells relative to the survival of negative-controlCCRF-CEM cells. Both of these cell types were combined inthe same tubes with CAR-transduced T cells. CCRF-CEM–negative control cellswere labeledwith the fluorescent dye 5-(and-6)-(((4-chloromethyl)benzoyl)amino) tetramethylr-hodamine (CMTMR; Invitrogen), and BCMAþ target cellswere labeledwith carboxyfluorescein diacetate succinimidylester (CFSE). Cocultures were set up in sterile 5mL test tubes(BD Biosciences) in duplicate at multiple T cell to target cellratios. The target cells contained in the tubes were 50,000
Carpenter et al.
Clin Cancer Res; 19(8) April 15, 2013 Clinical Cancer Research2050
on July 10, 2020. © 2013 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst January 23, 2013; DOI: 10.1158/1078-0432.CCR-12-2422

BCMAþ target cells along with 50,000 CCRF-CEM–negativecontrol cells. The cultures were incubated for 4 hours at37�C. Immediately after the incubation, 7-AAD (7-amino-actinomycin D; BD Biosciences) was added and flow cyto-metry acquisition was conducted. For each T cell plus target-cell culture, the percentage survival of BCMAþ target cellswas determined by dividing the percentage live BCMAþ cellsby thepercentage liveCCRF-CEM–negative control cells. Thecorrected percentage survival of BCMAþ target cells wascalculated by dividing the percentage survival of BCMAþ
target cells in each T cell plus target cell culture by the ratio ofthe percentage live BCMAþ target cells to percentage liveCCRF-CEM–negative control cells in tubes containing onlyBCMAþ target cells and CCRF-CEM cells without effector Tcells. This correction was necessary to account for variationin the starting cell numbers and for spontaneous target celldeath. Cytotoxicity was calculated as follows: the percentagecytotoxicity of BCMAþ target cells ¼ 100 � corrected per-centage survival of BCMAþ target cells.
In vivo treatment model murine experimentsNSG mice (NOD.Cg-Prkdcscid Il2rgtm1Wjl/SzJ) from The
Jackson Laboratory were used. Mice received intradermalinjectionsof RPMI-8226 cells. Tumorswere allowed to growfor 17 to 19 days, and then the mice received intravenousinfusions of 8 � 106 human T cells that were transducedwith either anti-bcma2 or SP6. Tumors were measured withcalipers every 3 days. The longest length and the lengthperpendicular to the longest length were multiplied toobtain the tumor size (area) in mm2. When the longestlength reached 15mm,mice were sacrificed. Animal studieswere approved by the National Cancer Institute AnimalCare and Use Committee.
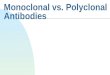
ResultsBCMAwas expressed inmultiplemyeloma cell lines butnot in several other types of cell linesWe used flow cytometry to characterize the expression of
BCMA on the cell surfaces of a variety of cells (Fig. 1A). Asexpected, K562 cells transduced with the gene for BCMAexpressed cell-surface BCMA. The multiple myeloma celllines H929, U266, and RPMI-8226 also expressed cell-surface BCMA. In contrast, NGFR-K562 cells, the sarcomacell line TC71, the T-cell leukemia line CCRF-CEM, and thekidney cell line 293T-17 did not express cell-surface BCMA.Importantly, primary CD34þ hematopoietic cells lackedcell-surface BCMA expression.
BCMA had a restricted mRNA expression patternA critical factor for any antigen being considered as a
target for immunotherapies is the antigen’s expressionpattern in normal tissues. BCMA has been reported to beexpressed on plasma cells and on some B cells but to other-wise have limited expression (24–26, 35). To morecompletely assess the expression pattern of BCMA, weconducted qPCR on a panel of cDNA samples from awide range of normal tissues (Fig. 1B). As a positive control,
we conducted qPCR on cDNA from cells of a plasmacytomathat was resected from myeloma patient 1, a patient withadvanced multiple myeloma. Ninety-three percent of thecells from the plasmacytoma sample were plasma cells asdetermined by flow cytometry. The BCMA expression of theplasmacytoma sample was dramatically higher than theBCMA expression of any other tissue. Not surprisingly,BCMA cDNA copies were detected in several hematologictissues, such as blood leukocytes, bone marrow, spleen,lymph node, and tonsil. Low levels of BCMA cDNA copieswere detected in the samples of testis and trachea. Inaddition, low levels of BCMA cDNA copies were detectedinmost gastrointestinal organs, such as duodenum, rectum,and stomach. One possible explanation for BCMA expres-sion in gastrointestinal organs and the trachea was theknown presence of plasma cells and B cells in tissues suchas lamina propria and Peyer’s Patches (41, 42).
BCMA protein was expressed by multiple myelomacells. Except for plasma cells, BCMAprotein expressionwas not detected in normal human organs
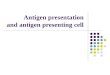
After showing a very restricted expression pattern ofBCMA RNA, we carried out an assessment of BCMA proteinexpression by immunohistochemistry (IHC). As expected,our anti-BCMA immunohistochemical staining procedureyielded strong staining of BCMA-K562 cells and a lack ofstaining with NGFR-K562–negative control cells (Fig. 2Aand B).Wewent on to evaluate BCMAprotein expression innormal human organs. Except for plasma cells, we did notdetect BCMA protein expression by the cells of any of theorgans that we stained. We detected plasma cells expressingcell-surface BCMA in gastrointestinal organs. Examples ofBCMA-expressing plasma cells that were detected in thestomach and rectumare shown in Fig. 2C andD.MUM1 is aprotein that is expressed by many malignant and benignlymphocytes and by plasma cells (43). Except for lympho-cytes and plasma cells, MUM1 is not expressed by normalgastrointestinal tissues (43). We conducted immunohisto-chemical double staining of colon and duodenum withanti-BCMA and anti-MUM1 and found that BCMA wasexpressed only by lymphoid cells and plasma cells (Fig.2E). BCMA expression by plasma cells probably accountsfor the low levels of BCMA RNA detected in these organsbecause we did not detect BCMA expression by any of theother cells in these organs. We detected BCMA-expressingplasma cells in the tonsil (data not shown). The organsassessed by IHC and found to lack BCMA expression exceptfor plasma cells included the following: adrenal, bladder,bone, eye, breast, cerebellum, cerebral cortex, fallopiantube, esophagus, stomach, small intestine, colon, rectum,heart, kidney, liver, lung, ovary, pancreas, parathyroid,pituitary, placenta, prostate, skin, spinal cord, spleen, skel-etal muscle, testis, thymus, thyroid, trachea, cervix, anduterine endometrium.
For a protein to be an appropriate target for CAR-expres-sing T cells aimed atmultiplemyeloma, the proteinmust beexpressed on the surface of multiple myeloma cells. Toassess BCMA expression by multiple myeloma cells, we
Anti-BCMA Chimeric Antigen Receptor
www.aacrjournals.org Clin Cancer Res; 19(8) April 15, 2013 2051
on July 10, 2020. © 2013 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst January 23, 2013; DOI: 10.1158/1078-0432.CCR-12-2422

Figure 1. BCMA had a restrictedpattern of expression. A, cell-surface BCMA was detected onmultiple myeloma cell lines, butBCMA was not detected in othercell lines. For all plots, the solid linerepresents staining with anti-BCMA antibodies, and the dashedline represents staining withisotype-matched controlantibodies. BCMA was expressedby BCMA-K562 cells but not byNGFR-K562 cells. Flow cytometrystaining revealed BCMA on the cellsurface of the multiple myelomacell lines H929, U266, and RPMI-8226. BCMA was not detected inthe sarcoma cell line TC71, in the Tcell leukemia line CCRF-CEM, or inthe kidney cell line 293T-17.Primary CD34þ hematopoieticcells lacked cell-surface BCMAexpression. All plots are gated onlive cells. The primary CD34þ cellsplot is also gated on CD34þ cells.B, BCMA cDNA copies weremeasured in samples of theindicated normal tissues by qPCR.In addition, qPCR was conductedon cDNA from cells of aplasmacytoma from myelomapatient 1 as a positive control.Neoplastic plasma cells made up93%of the total cells in the sample.Actin copies were also measuredby qPCR in all of the samples, andthe results were expressed as thenumber of BCMA cDNA copies per105 actin cDNA copies.
Carpenter et al.
Clin Cancer Res; 19(8) April 15, 2013 Clinical Cancer Research2052
on July 10, 2020. © 2013 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst January 23, 2013; DOI: 10.1158/1078-0432.CCR-12-2422

stained tissue sections from 3 different patients with mul-tiplemyeloma (Fig. 2F–H). These sections are shown in Fig.2. In all 3 of the samples, the neoplastic plasma cellsexpressed cell-surface BCMA.
BCMA-specific CARs were expressed on transducedT cellsBCMA is expressed inmultiplemyeloma cells, and it has a
restricted expression pattern in normal tissues (Figs. 1and 2). Because of the expression pattern of BCMA, wereasoned that BCMA would be an appropriate target forCAR-expressing T cells. To further assess the suitability ofBCMA as a target for CAR-expressing T cells, we designed 2CARs. Each CAR contained an scFv derived from 1 of 2mouse anti-humanBCMAmonoclonal antibodies (39).We
named the 2 CARs anti-bcma1 and anti-bcma2. The CARscontained the hinge and transmembrane regions of thehuman CD8a molecule, the signaling moiety of the CD28costimulatory molecule, and the signaling domains of theCD3z molecule (Fig. 3A). We also designed a negativecontrol CAR, named SP6. The SP6 CAR contained thevariable regions of the hapten-specific SP6 monoclonalantibody (10). Except for the different variable regions, thesequence of the SP6 CAR was identical to the sequencesof anti-bcma1 and anti-bcma2. We ligated DNA encodingeach of the CARs that we designed into a self-inactivatinglentiviral vector, which has been described in detail pre-viously (40). Replication-incompetent lentiviruses en-coding the CARs were used to transduce human T cells.After transductions, we found high levels of cell-surface
××10 Duodenum ×100 Duodenum
Myeloma patient 3BCMA Isotype
Myeloma patient 1BCMA Isotype
StomachBCMA Isotype
BCMA-K562BCMA Isotype
Myeloma patient 2BCMA Isotype
RectumBCMA Isotype
NGFR-K562BCMA IsotypeA B
C D
E F
G H
Figure 2. Immunohistochemical staining revealed BCMA expression by normal plasma cells and multiple myeloma cells but not gastrointestinalepithelial cells. A and B, BCMA-K562 cells exhibited strong BCMA expression, whereas NGFR-K562 cells did not express BCMA. Isotype-matchedcontrol antibodies did not stain either cell line. Staining of sections of (C) normal stomach and (D) normal rectum showed BCMA-expressingplasma cells in the lamina propria but no BCMA expression by other cells of these organs. Immunohistochemical staining was carried out with bothanti-BCMA and isotype-matched control antibodies on consecutive sections. E, double staining of normal duodenum with anti-BCMA (surface,brown) and anti-MUM1 (nuclear, red) revealed BCMAþ plasma cells and plasmacytoid cells. BCMA was not expressed by other cells of theduodenum. The �10 and �100 views are shown. F–H, staining of myeloma tissue sections from myeloma patients 1 through 3 showed cell-surfaceBCMA expression on the majority of neoplastic plasma cells. Immunohistochemical staining was carried out with BCMA and isotype-matched controlantibodies on consecutive sections.
Anti-BCMA Chimeric Antigen Receptor
www.aacrjournals.org Clin Cancer Res; 19(8) April 15, 2013 2053
on July 10, 2020. © 2013 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst January 23, 2013; DOI: 10.1158/1078-0432.CCR-12-2422

expression of anti-bcma1, anti-bcma2, and SP6 on thetransduced T cells (Fig. 3B).
Anti-BCMA-CAR–transduced T cells degranulated andproduced cytokines specifically in response to BCMA-expressing target cells
Anti-BCMA-CAR–transduced T cells upregulated CD107aspecifically in response to stimulation with BCMA-expres-sing target cells (Fig. 3C). This indicates BCMA-specificdegranulation of the T cells, which is a requirement forperforin-mediated cytotoxicity (44).
We assessed the ability of anti-BCMA-CAR–transduced Tcells to produce cytokines in response to BCMA. T cellstransduced with either anti-bcma1 or anti-bcma2 produced
large amounts of IFN-g when they were cultured overnightwith the BCMA-expressing target cell line BCMA-K562, butthe CAR-transduced T cells only produced backgroundlevels of IFN-g when they were cultured with the nega-tive-control target cell line NGFR-K562 (Table 1). T cellstransduced with anti-BCMA CARs produced large amountsof IFN-g when they were cultured overnight with BCMA-expressingmultiplemyeloma cell lines. In contrast, the anti-BCMA CARs produced only background levels of IFN-gwhen they were cultured with a variety of BCMA-negativetarget cell lines. T cells transduced with the SP6 negativecontrol CAR produced only low levels of IFN-g whencultured with any of the cell lines. The SP6 CAR specificallyproduced IFN-g when stimulated with cells coated with its
SP6
Anti-bcma1 Anti-bcma2
CD8 CD8 CD8 CD8
CD8CD8 CD8 CD8
An
ti-f
ab
An
ti-f
ab
An
ti-f
ab
An
ti-f
ab
A
BIs
oty
pe
Iso
typ
e
Iso
typ
e
Iso
typ
e
UT
CD
107a
Anti-bcma2 SP6
BCMA-K562 NGFR-K562 BCMA-K562 NGFR-K562
CD
107a
CD
107a
CD
107a
CD8 CD8
C
CD28CD8 hinge+TM CD3ζAnti-BCMA scFv 3′ SIN LTRMSCV promoter5′ SIN LTR
Figure 3. Anti-BCMA CARs were expressed on the surface of T cells. A, a general diagram of anti-BCMA CAR fusion proteins is shown (LTR, long terminalrepeat;MSCV,mousestemcell virus; SIN, self-inactivating). From theN-terminus to theC-terminus, the anti-BCMACARsall includedananti-BCMAscFv, thehinge, and transmembrane (TM) regions of the CD8a molecule, the cytoplasmic portion of the CD28 molecule, and the cytoplasmic portion of the CD3zmolecule. B, T cells from donor B were transduced with lentiviral vectors encoding 1 of 3 CARs or left untransduced (UT). Expression of 2 anti-BCMA CARs,which were designated anti-bcma1 and anti-bcma2, was detected by flow cytometry 5 days after the transduction. Expression of the control CAR SP6was also detected. As controls, isotype-matched antibody staining was included for each cell type. The plots are gated on CD3þ lymphocytes. The numberson the plots are the percentages of cells in each quadrant. This is one of 7 experiments with similar results. C, T cells were transduced with either theanti-BCMA CAR anti-bcma2 or the negative control CAR SP6. The cells were cultured with either the BCMA-expressing cell line BCMA-K562 or theBCMA-negative cell line NGFR-K562 for 4 hours. After transduction with anti-bcma2, T cells degranulated in a BCMA-specific manner. SP6-transducedT cells from the same donors did not degranulate in a BCMA-specific manner. The plots are gated on live CD3þ lymphocytes. The numbers on the plots arethe percentages of cells in each quadrant. This is 1 of 3 experiments with similar results.
Carpenter et al.
Clin Cancer Res; 19(8) April 15, 2013 Clinical Cancer Research2054
on July 10, 2020. © 2013 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst January 23, 2013; DOI: 10.1158/1078-0432.CCR-12-2422

target, the hapten 2,4,6-trinitrophenyl (data not shown).T cells expressing either anti-bcma1 or anti-bcma2 werefunctionally similar. Compared with anti-bcma1–trans-duced T cells, anti-bcma2–transduced T cells consistentlyexhibited slightly stronger and more specific recognition ofBCMA-expressing target cells in ELISA, CD107a, and otherfunctional assays; therefore, we used anti-bcma2 in ourremaining experiments.We successfully cultured and transduced the T cells of
myeloma patient 4, a patient who had received 13 priorcycles of therapy for hermyeloma. Six days after the cultureswere initiated, anti-bcma2 was detected in 69% of the Tcells. Large populations of anti-bcma2–transduced T cellsfrommyeloma patient 4 produced IL-2, TNF, and IFN-g in aBCMA-specific manner after a 6-hour stimulation withBCMA-expressing target cells (Fig. 4A and SupplementaryFig. S1).
Anti-BCMA-CAR–transduced T cells proliferated inresponse to BCMAWe assessed anti-bcma2–transduced T cells for the ability
to proliferatewhen stimulatedwith BCMA-expressing targetcells. We cultured CFSE-labeled, anti-bcma2–transduced Tcells with either target cells that expressed BCMA or targetcells that did not express BCMA (Fig. 4B). Anti-bcma2–transduced T cells specifically proliferated when stimulatedwithBCMA-expressing target cells. As expected, therewasnoBCMA-specific proliferation when T cells transduced withthe SP6 negative control CAR were assessed. At the begin-ning of the proliferation assay reported in Fig. 4B, 0.8� 106
anti-bcma2–expressing T cells were cultured with eitherBCMA-K562 cells or NGFR-K562 cells. After 4 days ofculture, 2.7 � 106 anti-bcma2–expressing T cells werepresent in the cultures containing BCMA-K562 cells, where-as only 0.6 � 106 anti-bcma2–expressing T cells werepresent in the cultures containing NGFR-K562 cells. ThisBCMA-specific increase in the absolute number of anti-bcma2–expressing T cells confirms the results of the CFSEproliferation assay.
Anti-BCMA-CAR–transduced T cells killed multiplemyeloma cell lines
T cells transduced with anti-bcma2 specifically killed theBCMA-expressing multiple myeloma cell lines H929 andRPMI-8226 in 4-hour cytotoxicity assays (Fig. 4C and D).SP6-transduced T cells exhibited much lower levels ofcytotoxicity against these cell lines.
Anti-BCMA-CAR–transduced T cells eradicate tumorsin vivo
We established RPMI-8226 human multiple myelomacell line tumors in immunodeficient mice. We allowedsizable tumors to develop over 17 to 19 days, and then wetreated the mice with a single intravenous infusion of anti-bcma2–transduced human T cells. The anti-bcma2–trans-duced T cell infusion cured 100%of themice, with dramaticregressions of all tumors occurring between day 6 and 15after the T-cell infusion (Fig. 4E and F). In contrast, tumorscontinued to increase in size in all mice receiving infusionsof T cells expressing a negative control CAR-designated SP6.The mice receiving infusions of anti-bcma2–transduced Tcells had no signs of toxicity during this experiment.
Soluble BCMA protein does not interfere with anti-BCMA CAR function
BCMA can be found in the serum of humans and serumBCMA levels are elevated inpatientswithmultiplemyeloma(45). Other investigators have previously shown that CAR-expressing T cells were not blocked from recognizing targetcells by soluble protein in vitro or in vivo (46). To determineif anti-bcma2 is blocked by soluble BCMA, we conductedELISA assays in which anti-bcma2–transduced T cells werecultured with BCMA-expressing target cells. Graded con-centrations of BCMA protein were added to the culturemedium. BCMA protein concentrations of more than10-fold higher than the median BCMA levels found in theserum of patients with multiple myeloma did not blockrecognition of BCMA target cells by anti-bcma2–transducedT cells in vitro (Supplementary Fig. S2); furthermore, we
Table 1. Anti-BCMA-CAR–transduced T cells specifically recognized BCMA
BCMA-expressing targetsb BCMA-negative targets
BCMA-K562 H929 RPMI-8226 NGFR-K562 CCRF-CEM A549 TC71 293TT cellsalone
Effector cellsa
Anti-bcma1 15,392 11,306 5,335 76 76 52 65 54 112Anti-bcma2 25,474 23,120 10,587 62 67 32 31 28 41SP6 32 60 149 27 28 21 361 73 27Untransduced T cells <12 <12 <12 <12 <12 <12 <12 12 <12Targets alone <12 <12 <12 <12 <12 <12 <12 13
aEffector cells were T cells from a patient with multiple myeloma (myeloma patient 4). The T cells were transduced with the indicatedCAR or left untransduced.bThe indicated target cells were combined with the effector cells for an overnight incubation and an IFN-g ELISA was conducted. Allunits are pg/mL IFN-g.
Anti-BCMA Chimeric Antigen Receptor
www.aacrjournals.org Clin Cancer Res; 19(8) April 15, 2013 2055
on July 10, 2020. © 2013 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst January 23, 2013; DOI: 10.1158/1078-0432.CCR-12-2422

CFSE
D
Anti-bcma2 SP6
BCMA-K562 NGFR-K562 BCMA-K562 NGFR-K562A
B
IL-2
Anti-bcma2 T cells SP6 T cells
CD8 CD8
IL-2
IL-2
IL-2
CN
orm
alize
d e
ve
nt
nu
mb
er
No
rma
lize
d e
ve
nt
nu
mb
er
E F
P < 0.0001
CFSE
Perc
en
tag
e c
yto
toxic
ity
Perc
en
tag
e c
yto
toxic
ity
Pe
rce
nta
ge
su
rviv
al
Tu
mo
r s
ize
(a
rea
) in
mm
2
Effector:target ratio
Days after T-cell infusion Days after T-cell infusion
Effector:target ratio
Figure 4. T cells expressing anti-BCMA CARs produced cytokines, proliferated, and killed in a BCMA-specific manner. Anti-BCMA CAR-transduced T cellseradicated tumors in vivo. A, T cells from myeloma patient 4 were transduced with either anti-bcma2 or the negative-control CAR SP6. Four days later, the CAR-transduced T cells were cultured for 6 hours with either the BCMA-expressing cell line BCMA-K562 or the BCMA-negative cell line NGFR-K562. Large fractions ofthe T cells transduced with anti-bcma2 produced IL-2 when cultured with BCMA-K562. Only small numbers of anti-bcma2–transduced T cells produced IL-2when they were cultured with NGFR-K562. Only small numbers of SP6-transduced T cells produced IL-2 when cultured with either BCMA-K562 or NGFR-K562.Theplots are gated onCD3þ lymphocytes. The numbers on the plots are the percentages of cells in each quadrant. This is 1 of 3 experiments with similar results. B,T cells from donor B were transduced with either anti-bcma2 or SP6. The T cells were then labeled with CFSE. The T cells were cultured with either irradiatedBCMA-K562 cells or irradiated NGFR-K562 cells. IL-2 was not included in the cultures. Four days later, the T cells were analyzed by flow cytometry. The plots aregated on CAR-expressing T cells. TheCFSE fluorescence was less intense in anti-bcma2–expressing T cells that were cultured with BCMA-K562 cells (solid) thanin anti-bcma2–expressing T cells that were cultured with NGFR-K562 cells (dashed, open). This indicates that anti-bcma2–expressing T cells proliferatedspecifically in response to BCMA. For SP6-expressing T cells, CFSE fluorescence intensity was similar for T cells cultured with either BCMA-K562 or NGFR-K562.This is 1 of 2 experiments with similar results. Anti-bcma2–transduced T cells from donor A specifically killed the multiple myeloma cell lines (C) H929 and (D)RPMI-8226 in 4-hour cytotoxicity assays at various effector:target cell ratios. T cells transduced with the negative control CAR SP6 caused much lowerlevels of cytotoxicity at all effector:target ratios. For all effector:target ratios, the cytotoxicity was determined in duplicate, and the results are displayed as themean� SEM. E, mice were injected intradermally with RPMI-8226 cells and tumors were allowed to grow for 17 to 19 days. On day 0, the mice received intravenousinfusions of 8 � 106 T cells that were transduced with either anti-bcma2 or the negative control CAR SP6. Another group of mice was left untreated. Themice all had established tumors at the timeof T-cell infusion.One-hundred percent ofmice receiving infusionsof anti-bcma2 had rapid and complete regressions oftheir tumors. In contrast, all mice receiving infusions of SP6-transduced T cells and all mice left untreated had progressive enlargement of their tumors. F,tumors did not recur inmice receiving anti-bcma2–transduced T cells for the duration of the experiment. All mice receiving anti-bcma2–transduced T cells survivedandwere healthy for the duration of the experiment. All mice receiving SP6-transduced T cells or left untreated diedwith progressive tumors. TheP < 0.0001 refersto the comparison of anti-bcma2 and SP6. E and F, combined results of 3 experiments (anti-bcma2, n ¼ 10; SP6, n ¼ 10; untreated, n ¼ 7).
Carpenter et al.
Clin Cancer Res; 19(8) April 15, 2013 Clinical Cancer Research2056
on July 10, 2020. © 2013 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst January 23, 2013; DOI: 10.1158/1078-0432.CCR-12-2422

found that RPMI-8226 cells secreted BCMA, and micebearing RPMI-8226 tumors had easily detectable serumhuman BCMA (Supplementary Fig. S3), so serum BCMAdid not preclude effective treatment of BCMAþ tumors inmice (Fig. 4E and F).
Anti-BCMA-CAR–transduced T cells recognized andkilled primary multiple myeloma cellsWe detected BCMA expression in neoplastic plasma cells
of myeloma patients 1 through 3 by IHC (Fig. 2). We alsoassessed cell-surface BCMA expression on primary multiplemyeloma cells from myeloma patients 1, 5, and 6 by flowcytometry, and we found uniform cell-surface BCMAexpression on the plasma cells of all 3 patients. Overall,we found cell-surface BCMA expression on multiple mye-loma cells from 5 of 5 unique patients by either IHC or flowcytometry. Examples of flow cytometry staining for BCMAare shown in Fig. 5A and C.We conducted a series of experiments to show that T cells
transduced with anti-bcma2 could specifically recognizeprimarymultiplemyeloma cells. Plasma cells that uniformlyexpressed cell-surface BCMA made up 40% of the cells in abone marrow sample from myeloma patient 5 (Fig. 5A).Allogeneic anti-bcma2–transduced T cells from donor Cproduced IFN-g after coculture with the unmanipulatedmyeloma-containing bone marrrow cells of myeloma pati-ent 5 (Fig. 5B). Anti-bcma2–transduced T cells from thesame allogeneic donor producedmuch less IFN-g when theywere cultured with PBMC frommyeloma patient 5. In addi-tion, SP6-transducedT cells fromdonorCdidnot specificallyrecognize the myeloma-containing bone marrow of myelo-ma patient 5. Other investigators have previously reportedthat normal PBMC did not contain cells that expressedBCMA (35). We assessed the PBMC of myeloma patient 5for BCMA expression by flow cytometry. We found that thePBMC did not contain BCMA-expressing cells except for asmall population of CD56þCD38high cells that made upapproximately 0.75% of the PBMC. This population prob-ably consisted of circulating multiple myeloma cells.Plasma cells made up 93% of the cells from a plasmacy-
toma resected frommyeloma patient 1, and flow cytometryrevealed that these primary plasma cells uniformly express-ed BCMA (Fig. 5C). BCMA expression was also detected inthe neoplastic plasma cells of myeloma patient 1 by qPCRandby IHC (Figs. 1B and 2). Anti-bcma2–transduced T cellsfrom myeloma patient 4 produced IFN-g when culturedwith the allogeneic, unmanipulatedmultiplemyeloma cellsof myeloma patient 1 (Fig. 5D). Anti-bcma2–transduced Tcells from myeloma patient 4 did not produce significantamounts of IFN-g when culturedwithPBMC frommyelomapatient 1. SP6-transduced T cells from myeloma patient 4did not produce significant amounts of IFN-g when theywere cultured with either multiple myeloma cells or PBMCfrom myeloma patient 1. The PBMC of myeloma patient 1did not express BCMA as measured by flow cytometry (datanot shown).We successfully cultured and transduced the T cells of
myeloma patient 1, who had received 8 prior cycles of
myeloma therapy. Eight days after the cultures were initi-ated, anti-bcma2 was detected in 65% of the T cells. Theanti-bcma2–transduced T cells from myeloma patient 1produced IFN-g specifically in response to autologous mul-tiple myeloma cells (Fig. 5E). SP6-transduced T cells frommyeloma patient 1 did not recognize autologous multiplemyeloma cells. Neither anti-bcma2–transduced T cells norSP6-transduced T cells from myeloma patient 1 recognizedautologous PBMC. Anti-bcma2–transduced T cells frommyeloma patient 1 specifically killed autologous multiplemyeloma cells at low effector to target ratios; in contrast,SP6-transduced T cells from myeloma patient 1 exhibitedlow levels of cytotoxicity against autologous multiple mye-loma cells (Fig. 5F).
DiscussionBecause current therapies formultiplemyeloma are rarely
curative, new therapies for this disease are clearly needed(1, 2). In particular, there is a need for therapies to eradicateresidual malignant cells that persist in patients who obtainremissionswith current treatments.Manymonoclonal anti-bodies that could potentially be useful therapies for mul-tiple myeloma are currently being evaluated in clinicaltrials, but most of these antibodies target antigens that areexpressed in both essential normal cells and myeloma cells(5, 7). Severe toxicities have occurred after infusions ofgenetically modified T cells targeting antigens expressed bynormal epithelial tissues; therefore, when designing CAR-expressing T-cell therapies, it is prudent to avoid targetingantigens that are expressed on the cell surfaces of normalepithelial cells (47, 48). Identification of new antigens thatare expressed by multiple myeloma cells but not by normalessential cells is a critical step for development of effectiveimmunotherapies for multiple myeloma.
We chose to investigate the TNF-receptor superfamilymember BCMA as a possible target for CAR-expressing Tcells. CAR-expressing T cells recognize cell-surface antigens(9); therefore, an antigen targeted by CAR-expressing T cellsshould ideally be expressed on the cell surfaces ofmalignantcells but not on the cell surfaces of essential normal cells.BCMA has been previously detected on the cell surfaces ofmultiple myeloma cells by other investigators (26–28). Inearly studies, BCMA RNA was detected in a limited numberof normal tissues (24, 25). BCMARNAwas not expressed bynormal humanT cells ormyeloid cells (35). BCMAhas beenreported to be expressed by fibroblast-like synovial cellsfrom patients with the autoimmune disease rheumatoidarthritis, but BCMAwas not expressed by synovial cells frompatients with osteoarthritis (49). BCMA mRNA has beenpreviously detected in the gut-associated lymphoid tissues,which are known to contain B cells and plasma cells(41, 50). We measured BCMA transcript expression in awide range of normal tissues and found that BCMA mRNAexpression was quite limited (Fig. 1B). We also determinedthat BCMAwas not expressed on the cell surfaces of primaryCD34þ hematopoietic cells (Fig. 1A). Finally, we conductedan immunohistochemical analysis of BCMA protein
Anti-BCMA Chimeric Antigen Receptor
www.aacrjournals.org Clin Cancer Res; 19(8) April 15, 2013 2057
on July 10, 2020. © 2013 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst January 23, 2013; DOI: 10.1158/1078-0432.CCR-12-2422

Even
tsE
ven
ts
Fluorescence intensity
Fluorescence intensity
A B
C D
F
E
IFN
-γγ (
pg
/mL
)
IFN
-γ (
pg
/mL
)IF
N-γ
(p
g/m
L)
Effector:target ratio
Perc
en
tag
e c
yto
toxic
ity
SP6
Anti-bcma2
Figure 5. Anti-BCMA-CAR–transduced T cells specifically recognized and killed BCMA-expressing primary multiple myeloma (MM) cells. A, flowcytometry staining for BCMA (solid line) and isotype-matched control staining (dashed line) revealed BCMA expression on the surface of primarybone marrow multiple myeloma cells from myeloma patient 5. The plot is gated on CD38high CD56þ plasma cells, which made up 40% of thebone marrow cells. B, unmanipulated myeloma-containing bone marrow cells (MM) from myeloma patient 5 or PBMC from myeloma patient 5were cocultured overnight with allogeneic T cells from donor C. The T cells had been transduced with either anti-bcma2 or the negative controlCAR SP6. After the coculture, an IFN-g ELISA was conducted. C, flow cytometry for BCMA (solid line) and isotype-matched control staining(dashed line) revealed BCMA expression on the surface of multiple myeloma cells from a plasmacytoma of myeloma patient 1. The plot is gated onplasma cells, which made up 93% of the total plasmacytoma cells. D, unmanipulated myeloma cells (MM) from a plasmacytoma of myelomapatient 1 or PBMC from myeloma patient 1 were cocultured overnight with allogeneic T cells from myeloma patient 4. The T cells were transducedwith either anti-bcma2 or the negative control CAR SP6. The PBMC from myeloma patient 1 did not contain BCMAþ cells. After the coculture, anIFN-g ELISA was conducted. E, unmanipulated myeloma cells (MM) from a plasmacytoma of myeloma patient 1 or PBMC from myeloma patient1 were cultured overnight with autologous anti-bcma2–transduced T cells or autologous SP6-transduced T cells, and an IFN-g ELISA wasconducted. F, myeloma cells from a plasmacytoma of myeloma patient 1 were specifically killed by autologous anti-bcma2–transduced T cells atlow effector:target ratios, whereas autologous SP6-transduced T cells caused only a low level of cytotoxicity of the myeloma cells in a4-hour cytotoxicity assay. For all effector:target ratios, the cytotoxicity was determined in duplicate, and the results are displayed as themean � SEM.
Carpenter et al.
Clin Cancer Res; 19(8) April 15, 2013 Clinical Cancer Research2058
on July 10, 2020. © 2013 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst January 23, 2013; DOI: 10.1158/1078-0432.CCR-12-2422

expression in the major human organs. We did not detectBCMA protein expression by any cells except plasma cells(Fig. 2). Normal B-lineage cells are often eradicated frompatients receiving infusions of anti-CD19-CAR–expressingT cells (12, 17). Patients lacking B cells can remain freeof infections when the patients receive infusions of sup-plemental immunoglobulins (12, 17), so BCMA expres-sion in normal plasma cells and some normal B cellsdoes not preclude targeting BCMA as a therapy for multiplemyeloma.After showing that BCMA has a limited tissue expression
pattern, we designed CARs that incorporated the variableregions of anti-BCMA monoclonal antibodies (Fig. 3).T cells transduced with lentiviral vectors encoding theseCARs gained the ability to conduct a variety of in vitrofunctions in aBCMA-specificmanner and to eradicate estab-lished BCMAþ tumors in vivo (Figs. 3–5 and Table 1). BothCD4þ and CD8þ T cells exhibited BCMA-specific activation(Fig. 3C and 4A). Compared with CD8þ T cells, a higherpercentage of CD4þ T cells produced IL-2 (Fig. 4A). Theanti-BCMA-CAR–transduced T cells produced IFN-g whenstimulated with primary multiple myeloma cells and killedprimary multiple myeloma cells (Fig. 5).Evidence that BCMA might be a target for anti-myeloma
immunity in humans has been reported (28). Allogeneicstem cell transplantation (AlloSCT) is sometimes usedto treat multiple myeloma (4). In patients with relapsedor persistent multiple myeloma after AlloSCT, infusions ofunmanipulated allogeneic lymphocytes from the originaltransplant donor can sometimes induce complete remis-sions (4, 28). Two patients who obtained complete remis-sions of relapsed multiple myeloma after infusions ofallogeneic donor lymphocytes developed serumanti-BCMAantibodies only after the donor lymphocyte infusions (28).The serumof both of these patients killed BCMA-expressingtarget cells in vitro by complement-mediated lysis andantibody-dependent cellular cytotoxicity (28).
In conclusion, BCMA is a promising target for CAR-transduced T cells. We have presented evidence that BCMAis not expressed by normal essential cells, and we detecteduniform BCMA protein expression by IHC or flow cytome-try on multiple myeloma cells of 5 of 5 patients that wereassessed. We designed lentiviral vectors encoding CARs thatspecifically recognized BCMA. T cells transduced with theseCARs gained the ability to carry out BCMA-specific func-tions. Adoptive transfer of anti-BCMA-CAR–transduced Tcells could potentially be an appropriate approach to test inclinical trials enrolling patients with advanced multiplemyeloma.
Disclosure of Potential Conflicts of InterestNo potential conflicts of interest were disclosed.
Authors' ContributionsConception and design: F.T. Hakim, J.N. KochenderferDevelopment of methodology: R.O. Carpenter, M.O. Evbuomwan, S.Yang, J.N. KochenderferAcquisitionofdata (provided animals, acquired andmanagedpatients,provided facilities, etc.): R.O. Carpenter, S. Pittaluga, R.E. Gress, J.N.KochenderferAnalysis and interpretation of data (e.g., statistical analysis, biosta-tistics, computational analysis): R.O. Carpenter, S. Pittaluga, M. Raffeld,S. Yang, J.N. KochenderferWriting, review, and/or revisionof themanuscript:R.O.Carpenter,M.O.Evbuomwan, S. Pittaluga, M. Raffeld, R.E. Gress, F.T. Hakim, J.N.KochenderferAdministrative, technical, or material support (i.e., reporting or orga-nizing data, constructing databases): J.J. Rose, J.N. KochenderferStudy supervision: S. Yang, J.N. Kochenderfer
Grant SupportThis work was supported by intramural funding of the Center for Cancer
Research, National Cancer Institute, NIH.The costs of publication of this article were defrayed in part by the
payment of page charges. This article must therefore be hereby markedadvertisement in accordance with 18 U.S.C. Section 1734 solely to indicatethis fact.
Received July 19, 2012; revised January 10, 2013; accepted January 10,2013; published OnlineFirst January 23, 2013.
References1. Lonial S, Mitsiades CS, Richardson PG. Treatment options for
relapsed and refractory multiple myeloma. Clin Cancer Res 2011;17:1264–77.
2. Rajkumar SV. Treatment of multiple myeloma. Nat Rev Clin Oncol2011;8:479–91.
3. Palumbo A, Anderson K. Multiple myeloma. N Engl J Med 2011;364:1046–60.
4. Salit RB, Bishop MR. Reduced-intensity allogeneic hematopoieticstem cell transplantation for multiple myeloma: a concise review. ClinLymphoma Myeloma Leuk 2011;11:247–52.
5. Richardson PG, Lonial S, Jakubowiak AJ, Harousseau JL, AndersonKC. Monoclonal antibodies in the treatment of multiple myeloma.Br J Haemato1 2011;154:745–54.
6. Yi Q. Novel immunotherapies. Cancer J 2009;15:502–10.7. Van De Donk NWCJ, Kamps S, Mutis T, Lokhorst HM. Monoclonal
antibody-based therapy as a new treatment strategy in multiplemyeloma. Leukemia 2012;26:199–213.
8. RosenbergSA,RestifoNP, Yang JC,MorganRA,DudleyME.Adoptivecell transfer: a clinical path to effective cancer immunotherapy. NatRev Cancer 2008;8:299–308.
9. Kershaw MH, Teng MWL, Smyth MJ, Darcy PK. Supernatural T cells:genetic modification of T cells for cancer therapy. Nat Rev Immunol2005;5:928–40.
10. Eshhar Z, Waks T, Gross G, Schindler DG. Specific activation andtargeting of cytotoxic lymphocytes through chimeric single chainsconsisting of antibody-binding domains and the gamma or zeta sub-units of the immunoglobulin and T-cell receptors. Proc Nat Acad SciU S A 1993;90:720–4.
11. Jensen MC, Popplewell L, Cooper LJ, DiGiusto D, Kalos M, OstbergJR, et al. Antitransgene rejection responses contribute to attenuatedpersistence of adoptively transferred CD20/CD19-specific chimericantigen receptor redirected T cells in humans. Biol Blood MarrowTransplant 2010;16:1245–56.
12. Kochenderfer JN,WilsonWH, Janik JE, DudleyME, Stetler-StevensonM, Feldman SA, et al. Eradication of B-lineage cells and regression oflymphoma in a patient treated with autologous T cells geneticallyengineered to recognize CD19. Blood 2010;116:4099–102.
13. Porter DL, Levine BL, Kalos M, Bagg A, June CH. Chimeric antigenreceptor-modified T cells in chronic lymphoid leukemia. N Engl J Med2011;365:725–33.
Anti-BCMA Chimeric Antigen Receptor
www.aacrjournals.org Clin Cancer Res; 19(8) April 15, 2013 2059
on July 10, 2020. © 2013 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst January 23, 2013; DOI: 10.1158/1078-0432.CCR-12-2422

14. Savoldo B, Ramos CA, Liu E, Mims MP, Keating MJ, Carrum G, et al.CD28 costimulation improves expansion and persistence of chimericantigen receptor-modified T cells in lymphoma patients. J Clin Invest2011;121:1822–6.
15. Cooper LJ, ToppMS, Serrano LM, Gonzalez S, ChangWC, Naranjo A,et al. T-cell clones can be rendered specific for CD19: toward theselective augmentation of the graft-versus-B-lineage leukemia effect.Blood 2003;101:1637–44.
16. Brentjens RJ, Latouche JB, Santos E, Marti F, Gong MC, Lyddane C,et al. Eradication of systemic B-cell tumors by genetically targetedhuman T lymphocytes co-stimulated by CD80 and interleukin-15. NatMed 2003;9:279–86.
17. Kochenderfer JN, Dudley ME, Feldman SA, Wilson WH, Spaner DE,Maric I, et al. B-cell depletion and remissions of malignancy along withcytokine-associated toxicity in a clinical trial of anti-CD19 chimeric-antigen-receptor-transduced T cells. Blood 2012;119:2709–20.
18. Hoyos V, Savoldo B, Quintarelli C, Mahendravada A, ZhangM, Vera J,et al. Engineering CD19-specific T lymphocytes with interleukin-15and a suicide gene to enhance their anti-lymphoma/leukemia effectsand safety. Leukemia 2010;24:1160–70.
19. Cheadle EJ, Hawkins RE, Batha H, O'Neill AL, Dovedi SJ, Gilham DE.Natural expression of theCD19 antigen impacts the long-term engraft-ment but not antitumor activity of CD19-specific engineered T cells.J Immunol 2010;184:1885–96.
20. Kochenderfer JN, Yu Z, Frasheri D, Restifo NP, Rosenberg SA. Adop-tive transfer of syngeneic T cells transduced with a chimeric antigenreceptor that recognizes murine CD19 can eradicate lymphoma andnormal B cells. Blood 2010;116:3875–86.
21. Brentjens RJ, Rivi�ere I, Park JH, Davila ML, Wang X, Stefanski J, et al.Safety and persistence of adoptively transferred autologous CD19-targeted Tcells in patientswith relapsedor chemotherapy refractoryB-cell leukemias. Blood 2011;118:4817–28.
22. Gupta R, Bhaskar A, Kumar L, Sharma A, Jain P. Flow cytometricimmunophenotyping andminimal residual disease analysis in multiplemyeloma. Am J Clin Pathol 2009;132:728–32.
23. Lin P, Owens R, Tricot G, Wilson CS. Flow cytometric immunophe-notypic analysis of 306 cases of multiple myeloma. Am J Clin Pathol2004;121:482–8.
24. Laabi Y,GrasMP,Carbonnel F, Brouet JC, Berger R, LarsenCJ, et al. Anew gene, BCM, on chromosome 16 is fused to the interleukin 2 geneby a t(4;16)(q26;p13) translocation in a malignant T cell lymphoma.EMBO J 1992;11:3897–904.
25. Laabi Y, Gras MP, Brouet JC, Berger R, Larsen CJ, Tsapis A. TheBCMAgene, preferentially expressed during B lymphoidmaturation, isbidirectionally transcribed. Nucleic Acids Res 1994;22:1147–54.
26. Novak AJ, Darce JR, Arendt BK, Harder B, Henderson K, KindsvogelW, et al. Expression of BCMA, TACI, and BAFF-R inmultiple myeloma:a mechanism for growth and survival. Blood 2004;103:689–94.
27. Neri P, Kumar S, Fulciniti MT, Vallet S, Chhetri S, Mukherjee S,et al. Neutralizing B-cell-activating factor antibody improves sur-vival and inhibits osteoclastogenesis in a severe combined immu-nodeficient human multiple myeloma model. Clin Cancer Res2007;13:5903–9.
28. Bellucci R, Alyea EP, Chiaretti S, Wu CJ, Zorn E, Weller E, et al. Graft-versus-tumor response in patients with multiple myeloma is associ-ated with antibody response to BCMA, a plasma-cell membranereceptor. Blood 2005;105:3945–50.
29. Moreaux J, Legouffe E, Jourdan E,Quittet P, R�eme T, LugagneC, et al.BAFF and APRIL protect myeloma cells from apoptosis inducedby interleukin 6 deprivation and dexamethasone. Blood 2004;103:3148–57.
30. Thompson JS, Schneider P, Kalled SL, Wang L, Lefevre EA, CacheroTG, et al. BAFF binds to the tumor necrosis factor receptor-likemolecule B cell maturation antigen and is important for maintainingthe peripheral B cell population. J Exp Med 2000;192:129–35.
31. Mackay F, Schneider P, Rennert P, Browning J. BAFF and APRIL: atutorial on B cell survival. Ann Rev Immunol 2003;21:231–64.
32. Kalled SL. The role of BAFF in immune function and implications forautoimmunity. Immunol Rev 2005;204:43–54.
33. Tai YT, Li XF,Breitkreutz I, SongW,Neri P,Catley L, et al. Role ofB-cell-activating factor in adhesion and growth of human multiple myelomacells in the bone marrow microenvironment. Cancer Res 2006;66:6675–82.
34. O'Connor BP, Raman VS, Erickson LD, Cook WJ, Weaver LK, AhonenC, et al. BCMA is essential for the survival of long-lived bone marrowplasma cells. J Exp Med 2004;199:91–7.
35. Ng LG, Sutherland APR, Newton R, Qian F, Cachero TG, Scott ML,et al. B cell-activating factor belonging to the TNF family (BAFF)-R isthe principal BAFF receptor facilitating BAFF costimulation of circu-lating T and B cells. J Immunol 2004;173:807–17.
36. Xu S, Lam KP. B-cell maturation protein, which binds the tumornecrosis factor family members BAFF and APRIL, is dispensable forhumoral immune responses. Mol Cell Biol 2001;21:4067–74.
37. Schiemann B, Gommerman JL, Vora K, Cachero TG, Shutga-Mors-kaya S, Dobles M, et al. An essential role for BAFF in the normaldevelopment of B cells through a BCMA-independent pathway. Sci-ence 2001;293:2111–4.
38. Kochenderfer JN, Feldman SA, Zhao Y, Xu H, Black MA, Morgan RA,et al. Construction and preclinical evaluation of an anti-CD19 chimericantigen receptor. J Immunother 2009;32:689–702.
39. Kalled SL, Hsu Y. Anti-BCMA antibodies. World Intellectual PropertyOrganization Patent WO 2010/104949 A2. 2010 Mar 10.
40. Yang S, Dudley ME, Rosenberg SA, Morgan RA. A simplified methodfor the clinical-scale generation of central memory-like CD8þ T cellsafter transduction with lentiviral vectors encoding antitumor antigen T-cell receptors. J Immunother 2010;33:648–58.
41. Brandtzaeg P. Function of mucosa-associated lymphoid tissue inantibody formation. Immunol Invest 2010;39:303–55.
42. Soutar CA. Distribution of plasma cells and other cells containingimmunoglobulin in the respiratory tract of normal man and class ofimmunoglobulin contained therein. Thorax 1976;31:158–66.
43. Natkunam Y, Warnke RA, Montgomery K, Falini B, Van De Rijn M.Analysis of MUM1/IRF4 protein expression using tissue microarraysand immunohistochemistry. Modern Pathol 2001;14:686–94.
44. Rubio V, Stuge TB, Singh N, BettsMR,Weber JS, RoedererM, et al. Exvivo identification, isolation and analysis of tumor-cytolytic T cells. NatMed 2003;9:1377–82.
45. Sanchez E, Li M, Kitto A, Li J, Wang CS, Kirk DT, et al. Serum B-cellmaturation antigen is elevated inmultiple myeloma and correlates withdisease status and survival. Br J Haematol 2012;158:727–38.
46. Lanitis E, Poussin M, Hagemann IS, Coukos G, Sandaltzopoulos R,Scholler N, et al. Redirected antitumor activity of primary humanlymphocytes transduced with a fully human anti-mesothelin chimericreceptor. Mol Ther 2012;20:633–43.
47. MorganRA,Yang JC,KitanoM,DudleyME, LaurencotCM,RosenbergSA.Case report of a serious adverse event following the administrationof t cells transduced with a chimeric antigen receptor recognizingERBB2. Mol Ther 2010;18:843–51.
48. Parkhurst MR, Yang JC, Langan RC, Dudley ME, Nathan DAN, Feld-man SA, et al. T cells targeting carcinoembryonic antigen can mediateregression of metastatic colorectal cancer but induce severe transientcolitis. Mol Ther 2011;19:620–6.
49. Nagatani K, Itoh K, Nakajima K, Kuroki H, Katsuragawa Y, MochizukiM, et al. Rheumatoid arthritis fibroblast-like synoviocytes expressBCMA and are stimulated by APRIL. Arthritis Rheum 2007;56:3554–63.
50. Barone F, Patel P, Sanderson JD, Spencer J.Gut-associated lymphoidtissue contains the molecular machinery to support T-cell-dependentandT-cell-independent class switch recombination.Mucosal Immunol2009;2:495–503.
Carpenter et al.
Clin Cancer Res; 19(8) April 15, 2013 Clinical Cancer Research2060
on July 10, 2020. © 2013 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst January 23, 2013; DOI: 10.1158/1078-0432.CCR-12-2422

2013;19:2048-2060. Published OnlineFirst January 23, 2013.Clin Cancer Res Robert O. Carpenter, Moses O. Evbuomwan, Stefania Pittaluga, et al. Therapy of Multiple MyelomaB-cell Maturation Antigen Is a Promising Target for Adoptive T-cell
Updated version
10.1158/1078-0432.CCR-12-2422doi:
Access the most recent version of this article at:
Material
Supplementary
http://clincancerres.aacrjournals.org/content/suppl/2013/01/23/1078-0432.CCR-12-2422.DC1
Access the most recent supplemental material at:
Cited articles
http://clincancerres.aacrjournals.org/content/19/8/2048.full#ref-list-1
This article cites 49 articles, 19 of which you can access for free at:
Citing articles
http://clincancerres.aacrjournals.org/content/19/8/2048.full#related-urls
This article has been cited by 33 HighWire-hosted articles. Access the articles at:
E-mail alerts related to this article or journal.Sign up to receive free email-alerts
Subscriptions
Reprints and
To order reprints of this article or to subscribe to the journal, contact the AACR Publications Department at
Permissions
Rightslink site. Click on "Request Permissions" which will take you to the Copyright Clearance Center's (CCC)
.http://clincancerres.aacrjournals.org/content/19/8/2048To request permission to re-use all or part of this article, use this link
on July 10, 2020. © 2013 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst January 23, 2013; DOI: 10.1158/1078-0432.CCR-12-2422