Embed Size (px)
Citation preview

Fluid & Electrolytes : Balance and disturbance Pre –adult
1
Fluid & Electrolytes : Balance & Disturbance
*Nurses need to understand the physiology of fluid and electrolyte balance to
anticipate ,identify and respond to possible imbalances.
سيولوجية توازن السوائل والشوارد )الأيونات ( لحتى نعرف يا ممرضين المستقبل احنا بحاجة لفهم ف. كيف نتعامل مع الحالة الغير طبيعية التي من الممكن أن تحصل )عدم التوازن(
*Amount and composition of body fluids:
Approximately 60% of typical adults weight consist of fluid ( water&electrolyte).
*Intracellular fluid (2/3) [skeletal muscle mass]
* Extracellular fluid (1/3) [transports electrolytes; carries other substances, such as enzymes and hormones].
*Intravascular (plasma) [3L of the average 6 L
of blood volume is made up of plasma] The remaining 3L is erythrocytes, leukocytes, and thrombocytes].
* Interstitial السوائل المحيطة بالخلية(fluid surround the cells 11-12L)
*Transcellular (1L) [contained within epithelial lined spaces] (eg. cerebrospinal, pericardial, synovial, intraocular, and pleural fluids).
*Factors that influence the amount of body fluids are :
1.Age 2.gender 3.Body fats
*Electrolyte concentrations differ in fluid
compartments for example: the major electrolytes in the ICF are potassium and phosphate. The
ECF has a low concentration of potassium and can tolerate only small changes in
potassium.
تركيز الشوارد أي الأيونات داخل الخلية أو خارجها بيختلف مثال على ذلك أيونات البوتاسيوم والفوسفات
حيث أنه تركيز البوتاسيوم داخل الخلية أعلى من خارجها .
أطلق العنان لروحك القطاعة في البداية وركز لسا احنا

Fluid & Electrolytes : Balance and disturbance Pre –adult
2
*Active chemicals that carry:
• Positive(+) electrical charges (cations),_ Major cations: sodium, potassium, calcium, magnesium, hydrogen ions .
• Negative(-) electrical charges (anions) (mEq/L) _Major anions: chloride, bicarbonate, phosphate, sulfate,
and proteinate ions.
Normal movement and direction of fluids through the capillary wall into the tissues depend on differences of
Hydrostatic pressure ( the pressure exerted by the fluid on the walls of the blood vessel )
Osmotic pressure ( exerted by protein of plasma )
*Regulation of body fluid compartments :
√Osmosis : the diffusion of water solutions caused by a fluid concentration gradient ( area
of Low solute concentration to area of high solute concentration )
Three other terms are associated with osmosis
√Osmotic pressure : is the amount of hydrostatic pressure needed to stop the flow of
water by osmosis .
√Oncotic pressure: is the osmotic pressure exerted by proteins e.g (albumin )
√Osmotic diuresis: is increase in urine output caused by the excretion of substance ,such as an
glucose.
√Diffusion (الانتشار): solutes move from area of higher concentration to one of lower concentration.
√Filtration: movement of water, solutes occurs from area of high hydrostatic pressure to area of low
hydrostatic pressure.
√ Active transport : physiologic pump that moves fluid from area of lower concentration of one
of higher concentration • Movement against concentration gradient • Sodium-potassium pump: maintains
higher concentration of extracellular sodium, intracellular potassium • Requires adenosine (ATP) for
energy.
*Systemic Routs of Gain and losses:
➢ Gain: drinking and eating ,daily average I&O of water water are approximately
equal , parenteral fluid . ➢ Loss: 1-kidney :urine output.
2-Skin loss : sensible ,insensible losses

Fluid & Electrolytes : Balance and disturbance Pre –adult
3
3- Lungs
4- GI tract
*Laboratory Tests for evaluating fluid status:
✓ Osmolality is the concentration of fluid that affects the movement of water
between fluid compartments by osmosis.
Serum osmolality primarily reflects the concentration of sodium, blood urea
nitrogen (BUN) and glucose.
– Urine osmolality is determined by urea, creatinine, and uric acid.
– serum osmolality is 280 to 300 mOsm/kg, and normal urine osmolality is 200 to
800 mOsm/kg.
– Urine specific gravity measures the kidneys’ ability to excrete or conserve
water (1.010 to 1.025).
✓ BUN( Blood urine Nitrogen): is made up of urea, which is an end product of the
metabolism of protein by the liver. (10 to 20 mg/dL) ✓ Creatinine is the end product of muscle metabolism. (0.7 to 1.4 mg/dL).
( ا الفحص بنعتمد عليه في تحديد إذا الكلية فيها خلل ماهذ ) ✓ Hematocrit :measures the volume percentage of red blood cells (erythrocytes) in whole
blood and normally ranges from 42% to 52% for males and 35% to 47% for females. هذا المصطلح بيعني قياس نسبة كريات الدم الحمراء في الدم ككل ) بتتذكروا الفسيولوجي يا أبطال ؟؟
ليه بيهمنا لأنه زيادة نسبة هذا النوع من خلايا الدم عن النسبة الطبيعية بيسبب وجود خلل و هو تجلط الدم وعادة بيكونوا المدخنين بيعانوا من هذا الشيء لذلك بننصح مدخنين الكلية يعملوا اشي صالح
فترة بدماتهم . ويتبرعوا كل *Regulation of water balance :
✓ Homeostasis: maintenance of a constant internal equilibrium (involves positive and negative
feedback mechanisms)
هي عملية الحفاظ على التوازن داخل الجسم ثابت من خلال
-ORGANS INVOLVED IN HEMEOSTATIC :
❖ Renal regulation : (kidney) are primary organs for regulating fluid &electrolyte
balance Selective reabsorption of water and electrolytes, Excretion of electrolytes occurs, Renal tubules are sites of action of ADH and aldosterone.
هي كل هادي الأرقاااام ضروري أحفظها ؟؟ نعم يااا
ممرض المستقبل بكرا لما يجيك مريضك بنتيجة
المختبر مهم يكون عندك فكرة .

Fluid & Electrolytes : Balance and disturbance Pre –adult
4
❖ Cardiac regulation : ( Heart & blood vessel) Atrial natriuretic factor
(ANF) is released by the cardiac atria in response to increased atrial pressure ANF causes vasodilation and increased urinary excretion of sodium & H2O.
❖ Adrenal Cortical Regulation(غدة فوق كلوية) Adrenal cortex releases
hormones to regulate both water and electrolytes 1. Glucocorticoids 2. Mineralcorticoids Aldosterone is a mineralocorticoid with
potent sodium-retaining and potassium excreting capability.
❖ Pituitary regulation :
Under control of hypothalamus, posterior pituitary releases ADH • Stress, nausea, nicotine, and morphine also stimulate ADH release
❖ Hypothalmic regulation(؛)منطقة تحت المهاد : Osmoreceptors in hypothalamus sense
fluid deficit or increase in plasma osmolality Stimulates thirst and antidiuretic hormone (ADH) release, Result in increased free water and decreased plasma osmolarity.
❖ Gastrointestinal regulation : Gastrointestinal tract accounts for most of the water
intake Small amounts of water are eliminated by GI tract in feces. ❖ Insensible Water Loss: Invisible vaporization from lungs and skin Approximately
900 ml per day is lost. No electrolytes are lost with insensible water loss. • Excessive sweating, not insensible loss, leads to loss of water and electrolytes. *Fluid volume deficit (FVD):
✓ Hypovolemia: occurs wen loss of ECF volume exceeds the intake of fluid.It
occurs when water and electrolytes are lost in the same proportion as they exist in
normal body fluids. الداخلية بالخلية مقارنة يحدث انخفاض حجم الدم بسبب فقدان في السوائل
نسبة فقدان كل من وخلينا نفهم الأمر بكل تركيز وهي بأنه سوائل التي يتم إدخالها إلى الجسم لبامتساوية. الماء الشوارد و
✓ Dehydration: loss of water along with increased serum sodium level.
. هي فقدان الماء مع ازدياد في مستوى الصوديوم
➢ Causes: (المسببات) ▪ Vomiting ( القيء) ,Diarrhea(الإسهال ) , GI Suctioning,sweating(e.g NG tube),
decreased intake, inability to gain access to fluid. ➢ Risk factors (العوامل التي تسبب في نقص حجم السوائل في الدم) ▪ Diabetes insipidus( فيها مع مرض السكري الكاذب يعني أعراضه بيشترك
(السكري

Fluid & Electrolytes : Balance and disturbance Pre –adult
5
▪ Adrenal insufficiency , osmotic dieresis ( مدرات البول(,hemorrhage(فقدان الدم
),coma( غيبوبة) ➢ Manifestation (الأعراض المصاحبة):
▪ rapid weight loss(نقص سريع بالوزن( decreased skin turgor(سلامة الجلد تقل(, cool clammy skin due to vasoconstriction oliguria(نقص إخراج البولي(, concentrated urine( بول مركز يعني نسبة الأملاح عالية(
▪ postural hypotension( flattened ( انخفاض في الضغط مع تغير في وضعية الجسم
neck veins()تسطح بأوعية الرقبة rapid weak pulse, increased temperature,
thirst, nausea, muscle weakness, cramps( تشنجات( ➢ Laboratory Data: elevated BUN in relation to serum creatinine, increased
hematocrit; Serum electrolyte changes may occur. ➢ Medical manegemnt: provide fluids to meet body needs Oral & IV. ➢ Nursing manegment:
▪ I&O, VS (vital sign) ▪ Monitor for symptoms: skin and tongue turgor, mucosa, UO(urine out put), ▪ mental status ▪ Measures to minimize fluid loss ▪ Oral care ▪ Administration of oral fluids ▪ Administration of parenteral fluids.
*Fluid Volume Excess (Hypervolemia) – FVE
➢ When sodium increases in the body -> water increases which leads to FVE
*لما معدل الصوديوم او الاملاح بشكل عام يزيد في الجسم بجذب اله الماء بسبب الخاصية
فبزيد معاه حجم الماء. الاسموزية
➢ FVE: Isotonic Expansion of the extracellular fluid (ECF) due to abnormal
retention of water and sodium in the same proportions.
*زيادة حجم الدم : حالة زيادة في حجم السوائل خارج الخلايا بسبب احتباس الماء والصوديوم
بنِسب متساوية في هاي المنطقة. يعني الجسم للأسباب الي رح نذكرها للأمام بحتفظ بالماء بين
. الخلايا بمعدل غير طبيعي بجانب زيادة معدل الأملاح

Fluid & Electrolytes : Balance and disturbance Pre –adult
6
➢ Causes of FVE:
• Fluid overload: high fluids intake
• Diminished Homeostasis Mechanisms -regulates fluid balance
*أسباب زيادة حجم الدم: زيادة السوائل الي داخلة الجسم أولاً, وثانياً خلل في توازن العمليات
. الحيوية الي في الجسم الي من دورها تحقق توازن سوائل الجسم
➢ Risk Factors | عوامل الخطر:
• Heart Failure | سكتة قلبية
• Kidney Failure | فشل كلوي
• Cirrhosis of the liver | تشمع الكبد
➢ Contributing Factors | عوامل مساعدة على تفاقم المشكلة :
• Consumption excessive amount of Na or salt.
• Excessive administration of sodium-containing solutions
الأملاح أو محاليل بتحتوي على نسب عالية من الصوديوم استهلاك كميات عالية من *
Manifestation:هيئة او وصف الحالة ومن شو بعانوا المصابين • Edeme (peripheral) || تجمع السوائل في الأطراف العلوية أو السفلية
• Distended neck veins (Jagular Veins) || انتفاخ الأوردة في منطقة العنق
• Crackles (Abnormal lung sound) || صوت خشخشة عند التنفس
• Wight gain || زيادة الوزن
• High central venous pressure (CVP) || ارتفاع ضغط الدم في الأوردة
• Breath shortness || ضيق النفس
• High blood pressure || ارتفاع ضغط الدم
• Full and bounding pulse || ة جداً النبضة بتكون كاملة وقوي
• High respiratory rate || ارتفاع معدل التنفس
• High urinary output || ارتفاع معدل البول
• Low hemoglobin || انخفاض نسبة الهيموغلوبين بالدم
• Low hematocrit || انخفاض كريات الدم الحمراء
• Low osmolality || انخفاض الاسموزية
• Low urine sodium || ديوم في البول انخفاض نسبة الصو

Fluid & Electrolytes : Balance and disturbance Pre –adult
7
✓ MEDICAL MANAGEMENT ❖ Directed by the causes “treat the cause”
الهدف الرئيسي للإدارة او العلاج الطبي هو التخلص من المسبب الرئيسي فبتم العمل على علاجه. *
تذكروا احنا لساتنا بنحكي عن مشكلة زيادة حجم الدم.
❖ Symptomatic treatment : administering diuretics + restricting fluids and
sodium
* أما علاج الأعراض فمن أشكالهم : اعطاء مدر للبول وتقييد نسبة السوائل والأملاح )الصوديوم(
في الجسم.
❖ To manage Hypervolemia Medically : Pharamacologic Therapy ||
Dialysis || Nutritional Therapy
حالة بيتبع الأمور هاي : العلاج بالأدوية الي هي مدرات البول , اذا ما * العلاج الطبي في هاي ال
كانت فعالة بنلجأ لغسيل الكلى , الى جانب العلاج بنظام الغذاء
Pharmacologic Therapy
➢ To inhibit Edema we use sodium dietary restriction “which means
controlling the intake of sodium” دما أو تجمع السوائل تحت طبقات الجلد, تمام .. عشان نمنع هاد اض زيادة حجم الدم الإ* من اعر
العرض او نسيطر عليه بنلجأ في البداية لنظام غذائي يقيد كمية الصوديوم الي داخلة الجسم. ➢ If this method is insufficient to reduce edema, we use diuretics.
بتكون فعالة, عشان هيك بنلجأ للأدوية المدرة بالبول. * مش دائماً الطريقة هاي
➢ Diuretics inhibits the reabsorption of Na and so inhibits the
reabsorption of water.
* الأدوية المدرة بالبول عملها بشكل عام بعتمد على إعاقة اعادة امتصاص الصوديوم والمي بتلحق
ص الماء فبتخلص منها عن طريق البول بدل ما تتخزن بالجسم.الصوديوم طبعا فبمنع اعادة امتصا
➢ The use of diuretics depends on : (الأشياء الي بنعتمد عليها خلال استخدام المدرات)
I. How sever the hypervolemia. || مدى سوء المشكلة او نسبة السوائل الزائدة
II. The degree of impairment of renal function. || درجة خلل عمل الكلية
III. Potency of diuretics. || فعالية المدر للبول الي رح نستخدمه
➢ Thiazide: diuretics that block sodium reabsorption in the distal tubule
which is only 5% - 10% of filtered sodium (Hydrochlorothiazide) ,
used for mild hypervolemia.

Fluid & Electrolytes : Balance and disturbance Pre –adult
8
قسم من أقسام المدرات بالبول بمنع عملية اعادة امتصاص الصوديوم في الأنابيب *الثيازيد:
الملتوية البعيدة والي بتكون فيها نسبة الصوديوم قليلة, عشان هيك هاد النوع بنستخدمه لعلاج
الزيادة القليلة في حجم السوائل.
➢ Loop Diuretics: diuretics that block both sodium and water
reabsorption in the ascending limp of Henle which is 20% - 30% of
filtered sodium. (Furosemide), used for sever hypervolemia.
* أما مدرات البول الحلقية: فبتمنع اعادة امتصاص الصوديوم والماء كمان لانها بتأثر على عملية
من التواء هنلي والي بيحتوي على نسبة كبيرة اعادة الامتصاص الي بتصير في الأنبوب الصاعد
من الصوديوم. عشان هيك هاد النوع من الأدوية بنستخدمه لعلاج الزايدة العالية جدا.
➢ The side effects of Diuretics : Electrolytes Imbalances
*ضروري جدا نعرف انه مدرات البول من أعراضها اختلال توازن الأيوانات الي في
الجسم ورح نحكي عن هاي النقطة عند جزئية الإلكترولايتس
Dialysis
➢ When pharmacologic agents are not enough due to severity of
hypervolemia; we consider other modalities to remove excess
sodium and fluid from the body.
➢ Dialysis may be used to remove sodium and fluids or control
potassium and to maintain acid-base balance.
* العلاج بالأدوية والدرات ما بكون كافي للحالات الشديدة جداً فبدنا علاج اكثر فعالية في السيطرة
على هاي السوائل الزائدة في الدم.
ى نسبة البوتاسيوم * وهون بنلجأ لغسيل الكلى للتخلص من الاملاح والسوائل الزائدة ونسيطر عل
وعشان نحقق التوازن بين الحموض والقواعد.
Nutritional Therapy ❖ Dietary Restriction of sodium – the severity of this diet depends on the
needs of the patient
نسبة القيود او شدة النظام –* بنعمل نظام غذائي لتقييد كميات الصوديوم الي داخلة الجسم
هاد بعتمد على طبيعة الحالة واحتياجات المريض.
NURSING MANAGEMENT
❖ Measure I&O (Inputs and outputs) to identify excess fluid retention
*حساب السوائل الخارجة والداخلة الى الجسم عشان نحدد إذا فيه درجة عالية من احتباس السوائل

Fluid & Electrolytes : Balance and disturbance Pre –adult
9
❖ Patient must be weighed daily to note rapid weight gain. (1kg = 1L
fluids)
* لازم نقيس وزن المريض كل يوم حتى نعرف اذا في زيادة سريعة وغير طبيعية في الوزن.
لانه هاي من اعراض احتباس السوائل في الجسم.
❖ Assess breath sound || مراقبة أصوات التنفس
❖ Monitor the degree of edema in the most dependent parts of the body.
* حساب درجة الانتفاخ الناتجة عن سوائل زائدة في اكثر المناطق الي المريض عاجز عن
تحريكها او التحكم فيها.
❖ Assessing pitting edema : press one finger into the area making a pit
and evaluate it from 1+ to 4+.
ضغط على المنطقة بإصبع واحد وتقييم عمق الحفرة الي * بقيس درجة الانتفاخ عن طريق ال
+ 4+ ل 1صنعتها على سطح الجلد من
❖ Nursing Management includes : Preventing Hypervolemia || Detecting
and controlling Hypervolemia || Educating the patient about edema
Preventing Hypervolemia ➢ Sodium-restricted diets are required by most of patients
* أغلب المرضى بفضلوا اتباع نظام غذائي محدود الصوديوم او الملح➢ Instruct patients to avoid over-the-counter (OTC) medications without
checking a health provider (they may contain sodium)
ا بدون وصفة طبية لانه ممكن يكون فيه نسبة * اشير على المرضى عدم اخد دو
من الصوديوم خطيرة بالنسبة لوضعهم ➢ Consider hidden sources of sodium, such as water supply
* ممكن يكون في مصادر غير معروفة للصوديوم زي مصدر الماء الي
بشربه المريض
Detecting and Controlling Hypervolemia

Fluid & Electrolytes : Balance and disturbance Pre –adult
10
➢ Promoting rest || توفير وتحسين مستوى الراحة
➢ Restricting sodium intake || تقييد نسبة الصوديوم الداخلة الجسم
➢ Monitoring parenteral fluid therapy || مراقبة كمية السوائل المعطاة بالحقن
➢ Appropriate medications || اعطاء الادوية المناسبة لتجنب اي مضاعفات خطيرة
➢ Periods of rest are important because bed rest favors diuresis of fluids
by decreasing venous pooling thus increasing effective sirculating
blood volume.
*الراحة في هاي الحلات ضرورية لأنه وضعية التمدد على السرير بتزيد من شط الدورة الدموية بسبب خفض نسبة تجمع الدم في الأوردة فبتتنادرار البول
وحركة السوائل بشكل عام وبتحسن فعالية شغل الكلية. ➢ When we administer diuretics, we should monitor the responses of the
patient.
* وفي حال اعطينا المريض مدرات لازم نراقب النتائج. ➢ If dyspnea (orthopnea) happens -which is one of the manifestations- ,
place the patient in semi-fowler position to promoy lung expansion
* ذكرنا فوق في وصف المرض انه رح يتعرض المصاب لضيق في النفس, في هاي الحالة بنحطه على الوضعية الي موضحة بالصورة حتى نحسن توسع
الرئة.
ELECTROLYTE IMBALANCE
Sodium Imbalances (Na+)
➢ Normal concentration range : 135-145 mmol/L

Fluid & Electrolytes : Balance and disturbance Pre –adult
11
➢ The most abundant electrolyte in the extracellular fluid (ECF) * وهو أكتر وفرة من بين كل الأيونات في السوائل المحيطة بالخلايا
➢ Regulated by ADH (Antidiuretic hormone), thirst and the (rennin-
angiotensin-aldosterone) system * المسؤول عن تنظيمه هرمون مانع ادرار البول والعطش ونظام رينين-انجيوتنسين-
الدوستيرون ➢ Loss and gain of sodium is related to loss and gain of water
* زيادة ونقصان الصوديوم مرتبطة بزيادة ونقصان الماء
HYPOnatremia – Sodium Deficit – Na<135
➢ Causes :
1) imbalance of water rather than sodium
( اختلال اتزان نسبة الماء مع الاملاح, يعني نسبة الصوديوم مافيها مشكلة ولكن حجم 1
السوائل اختل 2) nonrenal fluid loss (vomiting| diarrhea| sweating)
( فقدان سوائل بطرق غير البول )الاستفراغ| الاسهال| التعرق(2 3) renal salt waste (diuretics)
عنطريق البول بسبب مدرات البول ( فقدان سوائل3
4) deficiency of Aldosterone || انخفاض التستوستيرون وهم مهم لتنظيم كمية
في الدم الصوديوم
5) adrenal insufficiency || خلل في الغدة الكظرية
6) the use of certain medications || الادويةاستخدام بعض
7) SIADH (Syndrome of inappropriate Antidiuretic Hoemone
Secretion)
( حالة افراز كميات غير طبيعية من هرمون مانع ادرار البول 7 ➢ Manifestations : depends on the cause, magnitude and speed with
which the deficit occurs .
***HYPERnatremia: Serum sodium >145mEq/L
➢ Causes: excess water loss, excess sodium administration, diabetes insipidus, heat
stroke, hypertonic IV solutions.
➢ Manifestation:

Fluid & Electrolytes : Balance and disturbance Pre –adult
12
thirst; elevated temperature; dry, swollen tongue; sticky mucosa;
neurologic symptoms; restlessness; weakness ➢ Medical management: hypotonic electrolyte solution or
D5W.
➢ Nursing management: assessment and prevention, assess for OTC(over the counter) sources of
sodium, offer and encourage fluids to meet patient needs, provide
sufficient water with tube feedings ➢
HYPOkalemia :is a serum potassium <3.5 mEq/L
✓ Its life-threatening because all body system is affected.
✓ CAUSE:
▪ Actual body potassium loss{ فقدان حقيقي لأيون البوتاسيوم}
-due to excessive use of diuretics or corticosteroids{ الاستخدام الزائد لمدر
{البول
-Increased secretion of aldosterone ,such as in cushing's syndrome
{ { ارتفاع نسبة إفراز لهرمون الألدوستيرون
- Vomiting, diarrhea, Wound drainage, Prolonged nasogastric suction
-Excessive diaphoresis{ ارتفاع فقدان السوائل }
2. Inadequate potassium intake: NPO{ nothing by mouth}
3. Movement of potassium from the extracellular fluid to the intracellular fluid
a. Alkalosis b. Hyperinsulinism{زيادة إفراز هرمون الإنسولين}
4. Dilution of serum potassium (Water intoxication, IV therapy with potassiumpoor
solutions) ➢ HYPOkalemia Manifestations:
▪ Fatigue||الإجهاد

Fluid & Electrolytes : Balance and disturbance Pre –adult
13
▪ Anorexia|| فقدان الشهية
▪ Nausea || غثيان
▪ Vomiting|| التقيؤ
▪ Dysrhythmias|| عدم انتظام في ضربات القلب
▪ muscle weakness and cramps|| ضعف في العضلات وتشنج
▪ paresthesias || التخدير
▪ glucose intolerance ▪ decreased muscle strength, DTRs
*Nursing management :
▪ life-threatening, monitor ECG(electrocardiogram ) {تخطيط القلب
}and ABG(atrial blood gases)
▪ Dietary potassium nursing care related to IV potassium
administration.
▪ Oral potassium supplements may cause nausea and vomiting
and they should not be taken on an empty stomach if the client
c/o abd pain, N,V,D, or gastrointestinal bleeding,
▪ D/C (STOP)potassium
Liquid potassium (unpleasant taste and should be taken with juice )
Potassium is never administered by IV push, intramuscular, or
subcutaneous routes.
Dilute IV potassium & administered using an infusion device!
✓ HYPERkalemia: serum potassium >5 mEq\L ❖ Causes :
impaired renal function, hypoaldosteronism { ارتفاع مستوى هرمون
.tissue trauma, acidosis,{الألدوستيرون
❖ Manifestations: dysrhythmias, muscle weakness with potential respiratory impairment,
paresthesias, anxiety, GI manifestations.
❖ Medical management: monitor ECG, limit K diet, cation-exchange resin
(Kayexalate), IV sodium bicarbonate , IV calcium gluconate, regular insulin and
hypertonic dextrose -2 agonists, dialysisIV,dialysis.

Fluid & Electrolytes : Balance and disturbance Pre –adult
14
❖ Precautions with intervenously administered
potassium: الاحتياطات الواجب اتخاذها قبل تقديم جرعة تحتوي على بوتاسيوم من خلال
الوريد ▪ A dilution of no more than 1 mEq/10 mL of solution is recommended.
▪ After adding potassium to an IV solution, rotate and invert the bag
IV bag containing potassium: properly labeled.
The maximum recommended infusion rate is 5 to 10 mEq/hr, never to exceed 20
mEq/hr
If >10 mEq/hr should be placed on a cardiac monitor and infusion device.
▪ Assess the IV site frequently for signs of phlebitis or infiltration.
If either occurs, the infusion should be stopped immediately.
▪ The nurse should assess renal function before administering potassiumm and monitor
intake and output during administration.
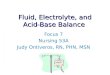
*Electrocardiograpic changes in HYPO/ERkalemia:

Fluid & Electrolytes : Balance and disturbance Pre –adult
15
*Hyperkalemia nursing management:
Assess potassium levels. قييم المسمر لمستوى البوتاسيوم لجسم المريض الت
Mix IVs containing K+ well
Monitor medication affects راقبة تأثيرات الدواءم
Restrict dietary potassium /dietary teaching for patients at risk عدم إعطاء المريض أي نوع من الأغذية بيحتوي
( : تحكيله عن الأكلات اللي بتحتوي على بوتاسيوم وتحذره من أكلها حبذا لو تقعد مع مريضك و على البوتاسيوم
Hemolysis of blood specimen or drawing of blood above IV site may result in false laboratory
result في بعض الأحيان لما تأخذ عينة دم من مريضك و يكون في تجلط ما تخضها لحتى الدم ما تتكسر الخلايا فيه لأنه من الممكن تعطيك قراءة خاطئة
شو رأيك مستر بلسم تاخدلك
شهيق وزفير فسيوووولوووجي
): !!
):

Fluid & Electrolytes : Balance and disturbance Pre –adult
16
Potassium-sparing diuretics may cause elevation of potassium بعض مدرات البول تعمل على رفع مستوى البوتاسيوم
– Should not be used in patients with renal dysfunction استخدام هذا النوع من مدرات البول للمرضى يجب عدم الذين يعانون من خلل في وظيفة الكلية
✓ HYPOCALCEMIA: Serum level less than 8.5 mg/dL, must be considered in
conjunction with serum albumin level.
➢ Causes: hypoparathyroidismقصور في الغدد الدرقية Malabsorption ( سوء الامتصاص(, pancreatitis( لتهاب البنكرياسا ), alkalosis, massive transfusion of citrated
blood, renal failure, medications, other
➢ Manifestations: Tetanyانقباض في العضلات , circumoral numbness تنمل في الأطراف, paresthesias رتخد , hyperactive DTRs, Trousseau’s sign, Chovstek's sign, seizures تشنجات, respiratory symptoms of dyspnea صعوبة في التنفس and laryngospasm تجمع البلغم في الحنجرة, abnormal clotting تخثر في الدم غير
. anxiety ,طبيعي➢ Tests for hypocalcemia: ❖ Chvostek’s sign is contraction of facial muscles in response to alight tap over the facial nerve in front
of the ear.
Trousseau’s sign is a carpal spasm induced by inflating a blood pressure cuff above the systolic pressure for a few minutes.
➢ Medical management:
IV of calcium gluconate, calcium and vitamin D supplements; diet.
➢ Nursing management: ▪ Assessment, severe hypocalcemia is life-threatening ▪ Weight-bearing exercises to decrease bone calcium loss, ▪ Patient teaching related to diet and medications
▪ Nursing care related to IV calcium administration. ▪ ECG of Hypocalcemia: Prolonged ST interval, Prolonged QT
interval.
✓ Hypercalcemia: Serum level above 10.5 mg/dL

Fluid & Electrolytes : Balance and disturbance Pre –adult
17
➢ Causes: : malignancy ورم خبيث and hyperparathyroidism نشاط بالغددالدرقية , bone loss related to
immobility خسارة العظام بسبب قلة الحركة ➢ Manifestations:
muscle weakness, incoordination عدم القدرة على التوازن, anorexia, constipation إمساك ,
nausea and vomiting, abdominal and bone pain, polyuria, thirst, ECG changes,
dysrhythmias.
➢ Medical management: treat underlying cause, fluids, furosemide, phosphates, calcitonin, biphosphonates
➢ Nursing management: ▪ Assessment, hypercalcemic crisis has high mortality ▪ Avoid foods high in calcium, Encourage ambulation ▪ fluids of 3 to 4 L/d Fiber for constipation ▪ Dialysis if medications fail to reduce the serum calcium ▪ Monitor for signs of a pathological fracture.{ مراقبة الكسور الناتجة عن مرض} ▪ Strain the urine to check for the presence of urinary stones. ▪ A client with a calcium imbalance is at risk for a pathological fracture. ▪ Move the client carefully and slowly; assist the client with ambulation
▪ ECG of Hypercalcemia : Shortened ST segment, Widened T wave
finally this work was done by NURSING LIJAN
BY STUDENTS:
ZAINA SALEH
OM-KULTHOOM AL-NAJJAR
FARAH ISMAEL