Embed Size (px)
Citation preview

Published by DiscoverSys | Bali Journal of Ophthalmology 2019; 3(1): 10-13 | doi:10.15562/bjo.v3i1.4210
CASE REPORTBali Journal of Ophthalmology (BJO) 2019, Volume 3, Number 1: 10-13P-ISSN. 2581-1258, E-ISSN.2581-1266
Right lower lid entropion in a 79-year-old female: a case-report
A.A.A. Putri Prematura Sri Anasary1*, I Gusti Ngurah Made Sugiana1
1Sanjiwani General Hospital, Gianyar- Bali
ABSTRACT
Introduction: Entropion is a condition in which eyelid margin turns inward. Four types of entropion including spastic, cicatricial, congenital, and involutional. Involutional entropion prevalence has been reported to be 2.1% and increases with advancing age. Case: A 79-year-old female complained of foreign body sensation with tearing in the right eye for the last one year. She had a history of cataract surgery on both eyes. Ophthalmology examination
revealed right lower lid entropion and bilateral pseudophakia. Surgical correction was done to tighten the orbicularis oculi muscle, along with appropriate postoperative treatment adjuncts such as analgesics and antibiotics. Surgical approach was chosen in favor of its lower recurrence rate.Conclusion: After surgical procedure and four days followup, the patient was released with good prognosis prediction.
Keywords: entropion, involutional, eye, palpebra disease, ophtalmologyCite This Article: Anasary, A.A.A.P.P.S., Sugiana, I.G.N.M. 2019. Right lower lid entropion in a 79-year-old female: a case-report. Bali Journal of Ophthalmology 3(1): 10-13. DOI: 10.15562/bjo.v3i1.42
*Coresponding to:A.A.A. Putri Prematura Sri Anasary; Sanjiwani General Hospital, Gianyar- Bali;[email protected]
Received : 2019-04-12Accepted : 2019-05-21Published: 2019-06-01
Open access: http://balijournalophth.org10
INTRODUCTIONEntropion is an inward rotation of the eyelid margin.1 Etiological classification of entropion comprising spastic due to inflammation, cicatricial with a posttrauma scar, congenital in children, and involutional affecting majority elderly aged over 60 years.1 Involutional entropion is found in 2.1% of 25,000 patients aged above 60 years and there is an inclining trend with advancing age. Bilateral manifestation is three times more likely than unilateral. The higher prevalence in females (2.4%) than males (1,9%) reflects gender predilection of entropion. Upper lid involvement is predominantly cicatricial etiology, while lower lid involvement is related to involutional type.1,2
Involutional entropion is closely related to aging. Tissue atrophy and weakening of capsulopalpebral fascia or eyelid muscle retractor mainly contribute to the disease mechanism. Once losing its elasticity, the tarsal plate hence in turn together with the lid margin.3-5 Consequently, this leads to posteriorly directing eyelashes towards the globe. Continuous friction results in conjunctival inflammation and abrasion. The patient may complain of foreign body sensation, redness, tearing, and discharge. Conjunctival hyperemia and eyelid laxity constitute supporting physical findings.3,6,7
CASE REPORTWe report a case from Rumah Sakit Sanjiwani,
Gianyar in November 2019. A 79-year-old female presented to eye policlinic with foreign body sensation in the right eye that had been going for a year. She would often blink and rub her eyes from the discomfort. In the past 2 and 3 months prior to the visit she underwent cataract surgical treatment for the left and right eye, respectively. Despite the excellent outcome on her visual acuity, she found the grittiness in both of her eyes unbearable. She denied any history of wearing spectacles and ocular trauma. There was not any notable past medication use other than postoperative medication for cataracts. History of other systemic diseases such as hypertension and diabetes was denied.
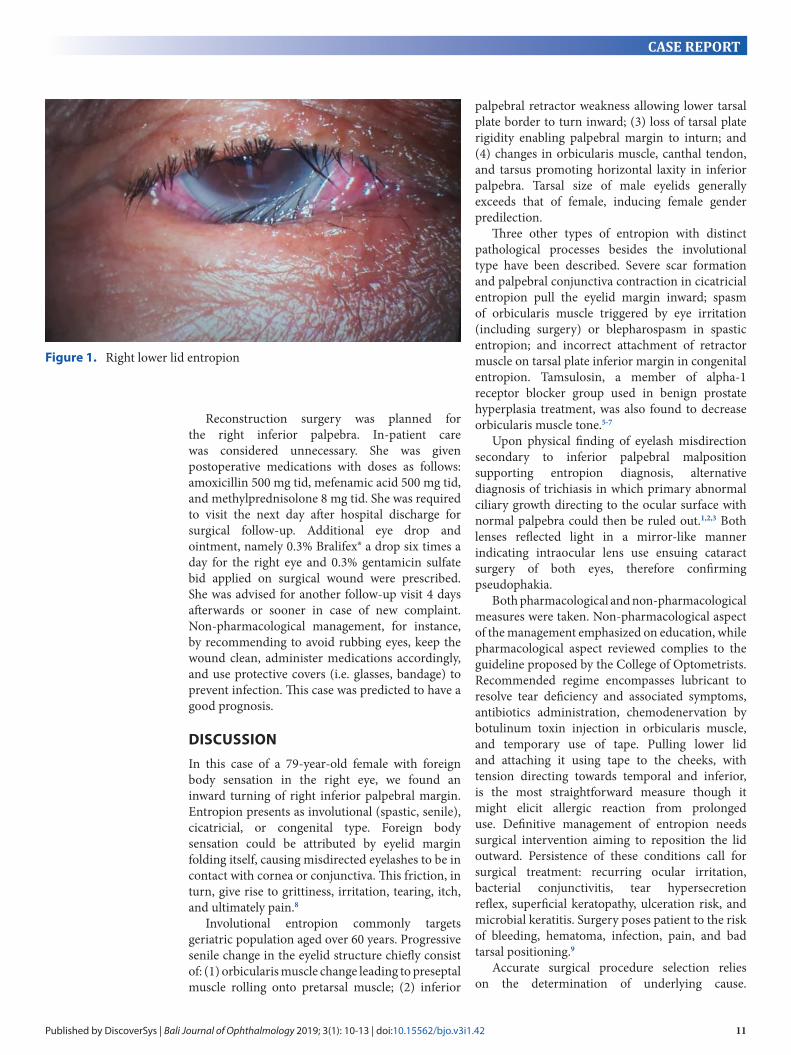
Patient was fully alert and otherwise well general appearance with vital signs as follows: blood pressure 120/70 millimeters of mercury, pulse 78 beats per minute, respiration rate16 breaths per minute, and temperature 36.2oC. General physical examination of head, neck, thorax, abdomen, and extremity was within normal limit. Ophthalmologic examination revealed right and left visual acuity of 6/9.5 and 6/12, respectively. There was tearing in both eyes without conjunctival injection, clear cornea, round pupil measuring 3 mm in diameter, isocoria, bilateral positive pupillary light reflex, implanted intraocular lens, and intraocular pressure 17.3 millimeters of mercury in both eyes. Right lower lid entropion (Figure 1) resulted in positive snapback test. We assessed her with ODS pseudophakia with OD inferior entropion.
Published by DiscoverSys | Bali Journal of Ophthalmology 2019; 3(1): 10-13 | doi:10.15562/bjo.v3i1.42 11
CASE REPORT
palpebral retractor weakness allowing lower tarsal plate border to turn inward; (3) loss of tarsal plate rigidity enabling palpebral margin to inturn; and (4) changes in orbicularis muscle, canthal tendon, and tarsus promoting horizontal laxity in inferior palpebra. Tarsal size of male eyelids generally exceeds that of female, inducing female gender predilection.
Three other types of entropion with distinct pathological processes besides the involutional type have been described. Severe scar formation and palpebral conjunctiva contraction in cicatricial entropion pull the eyelid margin inward; spasm of orbicularis muscle triggered by eye irritation (including surgery) or blepharospasm in spastic entropion; and incorrect attachment of retractor muscle on tarsal plate inferior margin in congenital entropion. Tamsulosin, a member of alpha-1 receptor blocker group used in benign prostate hyperplasia treatment, was also found to decrease orbicularis muscle tone.5-7
Upon physical finding of eyelash misdirection secondary to inferior palpebral malposition supporting entropion diagnosis, alternative diagnosis of trichiasis in which primary abnormal ciliary growth directing to the ocular surface with normal palpebra could then be ruled out.1,2,3 Both lenses reflected light in a mirror-like manner indicating intraocular lens use ensuing cataract surgery of both eyes, therefore confirming pseudophakia.
Both pharmacological and non-pharmacological measures were taken. Non-pharmacological aspect of the management emphasized on education, while pharmacological aspect reviewed complies to the guideline proposed by the College of Optometrists. Recommended regime encompasses lubricant to resolve tear deficiency and associated symptoms, antibiotics administration, chemodenervation by botulinum toxin injection in orbicularis muscle, and temporary use of tape. Pulling lower lid and attaching it using tape to the cheeks, with tension directing towards temporal and inferior, is the most straightforward measure though it might elicit allergic reaction from prolonged use. Definitive management of entropion needs surgical intervention aiming to reposition the lid outward. Persistence of these conditions call for surgical treatment: recurring ocular irritation, bacterial conjunctivitis, tear hypersecretion reflex, superficial keratopathy, ulceration risk, and microbial keratitis. Surgery poses patient to the risk of bleeding, hematoma, infection, pain, and bad tarsal positioning.9
Accurate surgical procedure selection relies on the determination of underlying cause.
Figure 1. Right lower lid entropion
Reconstruction surgery was planned for the right inferior palpebra. In-patient care was considered unnecessary. She was given postoperative medications with doses as follows: amoxicillin 500 mg tid, mefenamic acid 500 mg tid, and methylprednisolone 8 mg tid. She was required to visit the next day after hospital discharge for surgical follow-up. Additional eye drop and ointment, namely 0.3% Bralifex® a drop six times a day for the right eye and 0.3% gentamicin sulfate bid applied on surgical wound were prescribed. She was advised for another follow-up visit 4 days afterwards or sooner in case of new complaint. Non-pharmacological management, for instance, by recommending to avoid rubbing eyes, keep the wound clean, administer medications accordingly, and use protective covers (i.e. glasses, bandage) to prevent infection. This case was predicted to have a good prognosis.
DISCUSSIONIn this case of a 79-year-old female with foreign body sensation in the right eye, we found an inward turning of right inferior palpebral margin. Entropion presents as involutional (spastic, senile), cicatricial, or congenital type. Foreign body sensation could be attributed by eyelid margin folding itself, causing misdirected eyelashes to be in contact with cornea or conjunctiva. This friction, in turn, give rise to grittiness, irritation, tearing, itch, and ultimately pain.8
Involutional entropion commonly targets geriatric population aged over 60 years. Progressive senile change in the eyelid structure chiefly consist of: (1) orbicularis muscle change leading to preseptal muscle rolling onto pretarsal muscle; (2) inferior
Published by DiscoverSys | Bali Journal of Ophthalmology 2019; 3(1): 10-13 | doi:10.15562/bjo.v3i1.4212
CASE REPORT
Reconstruction for involutional entropion can be done through repairing capsulopalpebral fascia, Quickert sutures, modified Quickert sutures with lateral tarsal strip, and tightening of orbicularis oculi muscle. Congenital entropion is managed by proper attachment of capsulopalpebral fascia, epiblepharon correction if keratopathy co-occurs, and fish-tail resection. Although spontaneous resolution is possible, spastic entropion would otherwise benefit from combined surgical techniques as in horizontal eyelid shortening or pretarsal and orbicularis muscle fibers lifting, and vertical skin reduction. Wies procedure, hammock flap method, modified tarsotomy method, superior palpebral margin rotation method through palpebral fold incision with anterior internal lamellar traction, tarsotomy, and tarsal overlap without external suture, among others, provide surgical technique alternatives for cicatricial entropion.9-13
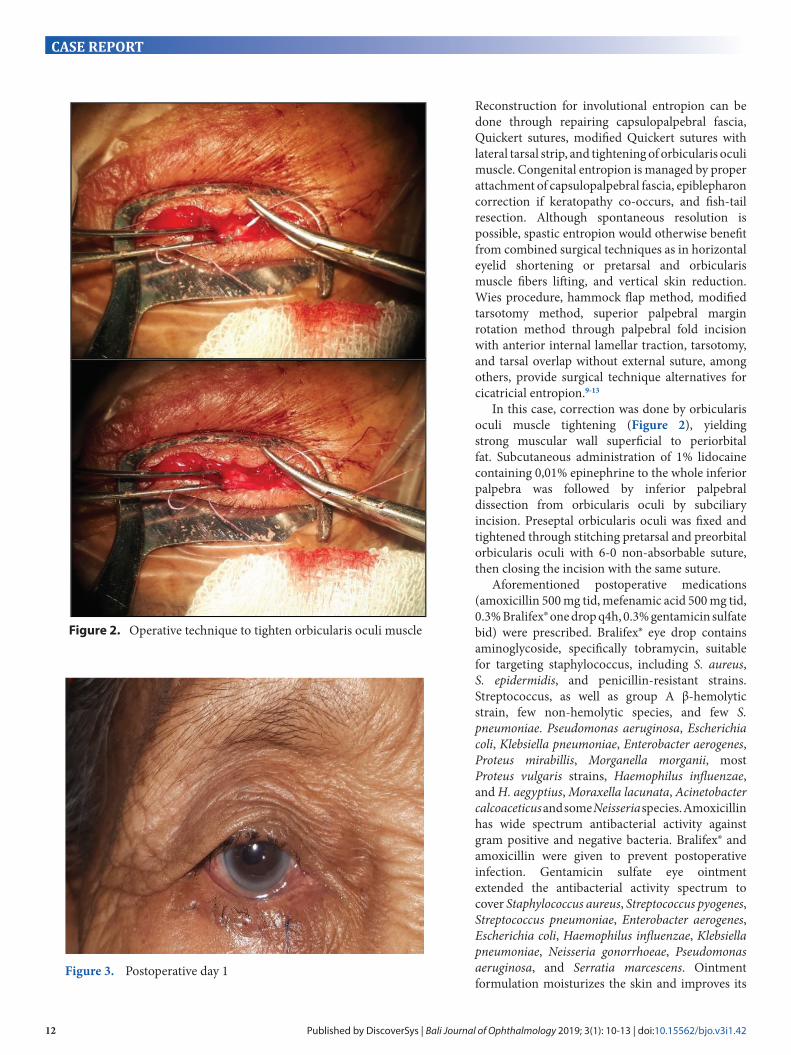
In this case, correction was done by orbicularis oculi muscle tightening (Figure 2), yielding strong muscular wall superficial to periorbital fat. Subcutaneous administration of 1% lidocaine containing 0,01% epinephrine to the whole inferior palpebra was followed by inferior palpebral dissection from orbicularis oculi by subciliary incision. Preseptal orbicularis oculi was fixed and tightened through stitching pretarsal and preorbital orbicularis oculi with 6-0 non-absorbable suture, then closing the incision with the same suture.
Aforementioned postoperative medications (amoxicillin 500 mg tid, mefenamic acid 500 mg tid, 0.3% Bralifex® one drop q4h, 0.3% gentamicin sulfate bid) were prescribed. Bralifex® eye drop contains aminoglycoside, specifically tobramycin, suitable for targeting staphylococcus, including S. aureus, S. epidermidis, and penicillin-resistant strains. Streptococcus, as well as group A β-hemolytic strain, few non-hemolytic species, and few S. pneumoniae. Pseudomonas aeruginosa, Escherichia coli, Klebsiella pneumoniae, Enterobacter aerogenes, Proteus mirabillis, Morganella morganii, most Proteus vulgaris strains, Haemophilus influenzae, and H. aegyptius, Moraxella lacunata, Acinetobacter calcoaceticus and some Neisseria species. Amoxicillin has wide spectrum antibacterial activity against gram positive and negative bacteria. Bralifex® and amoxicillin were given to prevent postoperative infection. Gentamicin sulfate eye ointment extended the antibacterial activity spectrum to cover Staphylococcus aureus, Streptococcus pyogenes, Streptococcus pneumoniae, Enterobacter aerogenes, Escherichia coli, Haemophilus influenzae, Klebsiella pneumoniae, Neisseria gonorrhoeae, Pseudomonas aeruginosa, and Serratia marcescens. Ointment formulation moisturizes the skin and improves its
Figure 2. Operative technique to tighten orbicularis oculi muscle
Figure 3. Postoperative day 1

Published by DiscoverSys | Bali Journal of Ophthalmology 2019; 3(1): 10-13 | doi:10.15562/bjo.v3i1.42 13
CASE REPORT
recovery rate. Postoperative pain was addressed with mefenamic acid.14,15
Majority of entropion cases have good prognosis. Management efficacy is determined by underlying cause and degree of disease severity. Despite low surgical recurrence rate reported by evidence, future follow-up visits warrant prompt recognition of recurrence.16
CONCLUSIONEntropion is defined as inward turning of palpebral margin, which could result in misdirected cilia towards the ocular surface. Development of conjunctivitis, keratitis, and corneal ulcer as its complication could be prevented with appropriate treatment. Given that there are various surgical and non-surgical treatment choices, consideration of underlying cause and any existing surgical indication is essential for making treatment decision.
CONFLICT OF INTERESTNone.
FUNDINGAll authors responsible for financing this manuscript privately.
ETHICThis case report was already accepted by the ethic comitee of Sanjiwani General Hospital.
REFERENCES1. Ilyas S. Ilmu Penyakit Mata. Edisi ke-3. Jakarta: Fakultas
Kedokteran Universitas Indonesia; 2009.2. Cristopher L, Ioannis G. Diagnosis and management of
involutional entropion [Internet]. 2016 [cited 2020 Feb 10]. Available from: https://www.aao.org/eyenet/article/diagnosis-management-of-involutional-entropion.
3. Damasceno RW, Osaki MH, Dantas PE, Belfort R Jr. Involutional entropion and ectropion of the lower eyelid: prevalence and associated risk factors in the elderly
population. Ophthalmic Plastic and Reconstructive Surgery. 2011;27(5):317–20.
4. Tse DT. Entropion. In: Tse DT. Color Atlas of Ophthalmic Surgery: Oculoplastic Surgery. Pennsylvania: J. B. Lippincott Company. 1992;101–12.
5. Bashour M, Harvey J. Causes of involutional ectropion and entropion - age-related tarsal changes are the key. Ophthalmic Plastic and Reconstructive Surgery. 2000;16(2):131–41.
6. Deka A, Saikia SP. Lower lid entropion correction with botulinum toxin injection. Oman J Ophthalmol. 2010;3(3):158-159.
7. Michels KS, Czyz CN, Cahill KV, Foster JA, Burns JA, Everman KR. Age-matched, case-controlled comparison of clinical indicators for development of entropion and ectropion. J Ophthalmol. 2014;2014:231487.
8. Riordan-Eva P, Whitcher JP. Vaughan & Asbury Oftalmologi Umum. Edisi ke-17. Jakarta: EGC; 2008.
9. The College of Optometrists. Clinical management guidelines entropion [Internet]. 2017 [cited 2020 Feb 10]. Available from: https://www.college-optometrists.org/guidance/clinical-management-guidelines/entropion.html.
10. Sakamoto Y, Nakajima H, Imanishi N, Okumoto T, Kato T, Kishi K. A hammock flap: a modified backflip flap for the surgical correction of cicatricial entropion. J Plast Reconstr Aesthet Surg. 2015;68(5):738-40.
11. Nakauchi K, Mimura O. Fish tail resection for treating congenital entropion in Asians. Clin Ophthalmol. 2012;2012:831-6.
12. Long JA. Oculoplastic Surgery. Philadelphia: Elsevier; 2009.
13. Yaumil R. Diagnosis dan tatalaksana entropion. 2018;45(2): 151-5.
14. Drug label information of tobramycin eye drop [Internet]. 2012 [cited 2020 Feb 10]. Available from: https://www.accessdata.fda.gov/drugsatfda_docs/label/2012/050541s024lbl.pdf.
15. Drug label information of gentamicin sulfate eye ointment [Internet]. 2018 [cited 2020 Feb 10]. Available from: https://www.accessdata.fda.gov/drugsatfda_docs/label/2018/050612s021lbl.pdf.
16. Hendriati, Sherly M. Hasil Operasi Entropion Involusional di Rumah Sakit Dr. M. Djamil Padang. Jurnal Kesehatan Andalas. 2018; 7.





























