Embed Size (px)
Citation preview
Thorax (1972), 27, 657.
Benign and malignant mixed tumours of the lungP. W. DAVIS, J. C. BRIGGS, R. M. E. SEAL, and
F. K. STORRING
Llandough and Sully Hospitals, Cardiff, and Frenchay Hospital, Bristol
Ten patients are presented with tumours complying with the criteria established by the WorldHealth Organization for 'mixed tumours of the lung'.A slowly growing intrabronchial neoplasm indistinguishable from a pleomorphic adenoma
(mixed salivary tumour) and a peripheral circumscribed tumour with most of the features of achondromatous hamartoma were considered benign.Of eight malignant neoplasms two were regarded as 'pulmonary blastomas', one with a
benign epithelial tubular component and the other with cytological evidence of malignancy inthe tubular epithelium; in both, the stroma was 'embryonic' and pleomorphic. Three tumourswere considered carcinosarcomas with a mainly epidermoid epithelial component and a pleo-morphic spindle-cell connective tissue component. In the remaining three tumours the malignantepithelial component showed mixed, viz., epidermoid, tubular, and a variety of undifferentiatedappearances, while the 'stroma' exhibited features seen in both blastomas and carcinosarcomas.These three neoplasms were considered 'transitional'.The spectrum of appearances encountered constitutes, in our opinion, a serious objection
to the thesis that peripheral pulmonary blastomas and carcinosarcomas are distinct entitieswith a separate histogenesis. Exceptions were found to 'blastomas' being peripheral andcarcinosarcomas being central growths. A case is made for reclassification of the benign andmalignant neoplasms included in the WHO group IX 'mixed tumours of the lung'.
The most authoritative classification of lungtumours is that by the World Health Organization,namely the International Histological Classifica-tion of Tumours: No. 1. Histological Typing ofLung Tumours (Kreyberg, 1967). Many tumourswhich may be regarded as mixed are included.A mixed epithelial malignancy, the combinationof epidermoid and adenocarcinoma (V), and themucoepidermoid tumours (VII2) are classifiedseparately and are clearly defined. Teratomaswhich occur in the lung rarely are not listedseparately.There remains an ill-defined group of tumours
(IX), headed 'mixed' tumours and carcino-sarcomas. The general description of this groupstates that tumours with a structure resemblingmixed salivary tumours are tentatively groupedwith other tumours in which elements resemblingepithelium are mixed with cells resembling thoseof connective tissue. Three subdivisions are listedin this group, viz.:
1. 'mixed' tumours2. carcinosarcomas of embryonal type('blastomas')3. other carcinosarcomas.
It is not apparent which benign tumours areincluded in the group under subdivision 1. Clearly,from the general description, which mentionstumours with a structure resembling mixed salivarytumours, the rare pleomorphic adenoma of thebronchus is included. However, it is not clearwhether the benign common 'chondromatoushamartoma' warrants inclusion and whether acytologically 'benign' form of blastoma is intendedto fall into this category.A review of the literature also reveals some
confusion regarding terminology and interrela-tionships of the benign tumours of the group.Willis (1962), for example, refers to the 'chondro-matous hamartoma' as a benign mixed tumour ofthe bronchus, while Spencer (1968) prefers theterm 'local pulmonary hamartoma' and describestwo varieties, both peripheral in location, the firstbeing the common variety with cartilage as aconstant component (chondromatous hamartoma),and the rarer second variety without cartilage,consisting of tubular structures within undiffer-entiated mesenchymal tissue. The latter he con-siders to be closely related to pulmonary blastomas.Spencer (1968), accepting Waddell's (1949)
theory of the development of the lung, which
657
on 23 June 2018 by guest. Protected by copyright.
http://thorax.bmj.com
/T
horax: first published as 10.1136/thx.27.6.657 on 1 Novem
ber 1972. Dow
nloaded from
P. W. Davis, J. C. Briggs, R. M. E. Seal, and F. K. Storring
postulates that major bronchi develop from theentodermal bud and peripheral airways and airsacs from mesoderm, designates the commoncartilage-containing tumour as 'central', and therarer non-cartilagenous neoplasm with anembryonic stroma as 'peripheral'. These terms areclearly used in a histogenetic sense.The term 'pulmonary blastoma' was used by
Spencer (1961) when presenting three examples ofa neoplasm consisting of tubular epithelial-linedstructures in a polymorphic and spindle-cellstroma. In this report he included a fourth casepreviously reported by Barnard (1952) as an'embryoma' of the lung. Two of these tumourswere malignant in that either blood or lymphaticmetastasis occurred. The WHO description for thecomparable tumour, 'carcinosarcoma of embryonaltype' (blastoma), is 'masses of polygonal or stellatecells in a very loose stroma that resemblesembryonic mesenchyme and in which irregularacinar tissue is frequently embedded and some-times masses of squamous epithelium. Musclefibres are sometimes present'.
Carcinosarcomas of the lung, although rare,have been reported in the literature for manyyears. Since the first well-documented case reportsby Saltykow (1914) and Frank (1915) over 30cases of carcinosarcoma of the lung have beenpublished. This figure includes a series of casesderived from a review by Stackhouse, Harrison,and Ellis (1969). Opinion is divided concerning theconnective tissue origin of the sarcoma-like com-ponent in these tumours. Saphir and Vass (1938)and Willis (1962), for example, consider that inthe majority the sarcoma-like areas are derivedfrom the epithelial component. Among others,Drury and Stirland (1959) make a strong case forthe acceptance of a true sarcomatous componentin these rare tumours.The WHO description of this type of carcino-
sarcoma is that of poorly differentiated cells havingcharacteristics of sarcoma of soft tissue togetherwith well-differentiated epithelium of the typesoccurring in carcinoma of the bronchus. A sub-type mentioned is a polypoid intrabronchialtumour with mucus-producing cells in severallayers lining large acini with a stroma of pro-liferating spindle-shaped cells.Bergmann, Ackerman, and Kemler (1951),
Taylor and Rae (1952), and Drury and Stirland(1959) have suggested that carcinosarcomas havea more favourable prognosis than carcinoma ofthe lung. A similar claim has been made for pul-monary blastomas by Spencer (1961), Souza,Peasley, and Takaro (1965), and Barson, Jones,and Lodge (1968).
We describe 10 patients with lung tumours ful-filling the criteria of histopathological type IX(Kreyberg, 1967). These tumours illustrate theinadequacy of the present criteria: they show awide spectrum of histological patterns with a con-siderable overlap between the individual tumours.Modifications to the classification are suggested.
CLINICAL MATERIAL
Our material has been drawn from two regionalthoracic centres (Sully/Llandough Hospitals, Cardiff,and Frenchay Hospital, Bristol), covering a period ofsix years, with the exception of our first case, a raremixed salivary tumour (pleomorphic adenoma) of thebronchus, which had been resected 24 years ago. Theother benign tumour presented (case 2) was one of 36peripheral circumscribed hamartomas containingcartilage and was one of a few consisting entirely ofembryonic stroma and tubular epithelium at its grow-ing margin. It was selected to illustrate this feature.The malignant tumours represent all the neoplasmsof this type recognized in both centres during thisperiod.
METHODS
Appropriate blocks were taken from the material afterformol saline inflation of the lungs, and the stainsused were phosphotungstic acid haematoxylin(PTAH), periodic acid Schiff (PAS), alcian blue(Lison's), and reticulin stain (Gordon and Sweet) inaddition to haematoxylin and eosin (H and E) and vanGieson's stain.
CASE REPORTS
CASE 1 M.S., a woman, aged 52 years, wasadmitted in 1948 with respiratory symptoms follow-ing an attack of pneumonia four years previously. Achest radiograph showed a homogeneous irregularopacity in the right upper lobe. At bronchoscopy awhite jelly-like growth was seen protruding from theright upper lobe bronchus. A bronchial biopsy speci-men at the time was reported as being indistinguish-able from a 'mixed salivary tumour'. At operation aright pneumonectomy was performed. The patient diedin the postoperative period and no necropsy was per-formed.
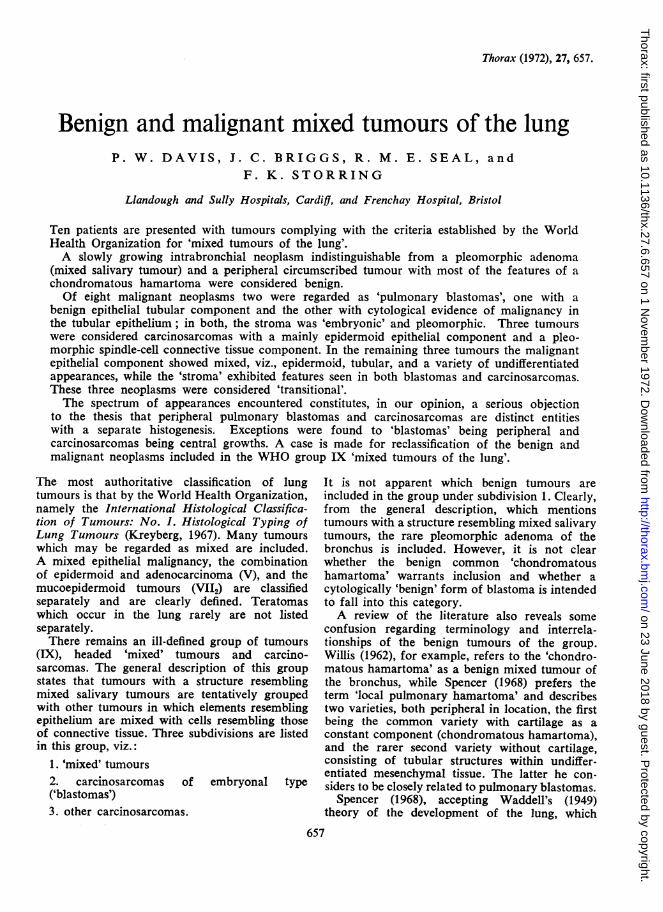
Surgical specimen The macroscopic appearanceswere those of a right pneumonectomy specimen show-ing a white glistening mucoid tumour, approximately45 x 25 x 25 mm, in the upper lobe bronchus. Thetumour grew distally to distend a segmental bronchuswith marked associated bronchiectasis and chronicpneumonitis of the apical and posterior segments(Fig. 1).
Microscopic appearances The epithelial elementsof the tumour were arranged in strands and occa-sional clumps were dispersed throughout a somewhat
658
on 23 June 2018 by guest. Protected by copyright.
http://thorax.bmj.com
/T
horax: first published as 10.1136/thx.27.6.657 on 1 Novem
ber 1972. Dow
nloaded from
Benign and malignant mixed tumours of the lung
4w.
FIG. 1. Cut surface of right upper lobe to show tumour andparenchymal damage.
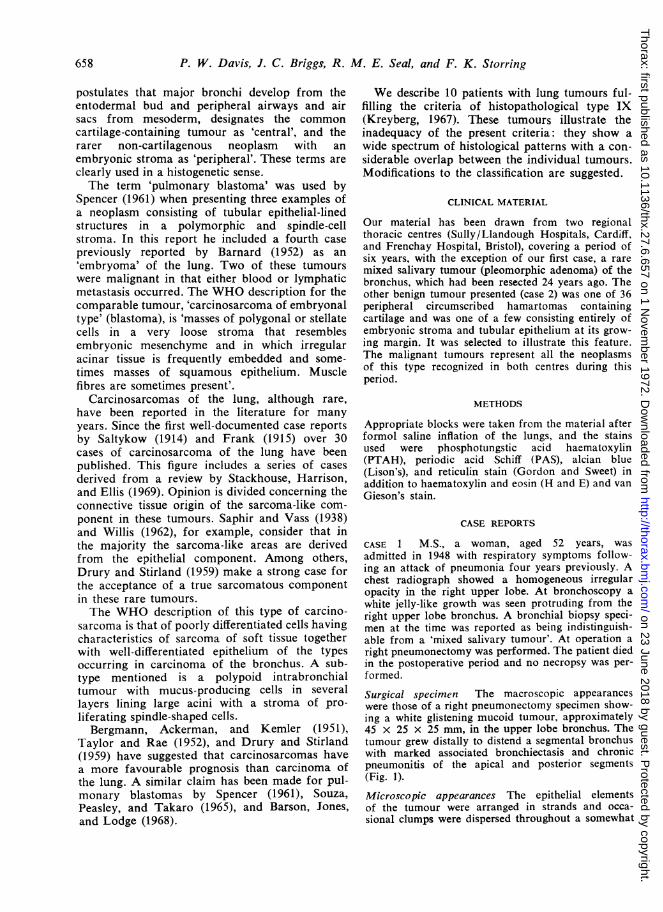
hyaline stroma. There was no differentiation intotubules or squamous epithelium. The cells, for themost part, were regular and no mitoses could be seen.The 'stromal' component of the tumour was basicallystructureless but there were areas of fibril formation.Alcian blue staining revealed the presence of largeamounts of connective tissue mucin (Fig. 2).Commlent The overall features of this tumour arethose of a pleomorphic adenoma arising almostcertainly from the bronchial submucous glands.CASE 2 I.T.B., a man aged 68 years, was admittedon 4 February 1971 with myocardial infarction.He gave a recent history of dyspepsia and haema-temesis. He died on the day of admission. Necropsyconfirmed myocardial infarction as the immediatecause of death; also found were a neoplasm of thestomach (adenocarcinoma) and a tumour in the leftlung.
Surgical specimen The macroscopic appearanceswere those of a circumscribed glistening peripheralwhite, slightly lobulated tumour, 25 mm in diameter,in the left lower lobe.
Microscopic appearances This was a benign tumourwith several components. The central area had thetypical appearance of a chondromatous hamartoma,
3C
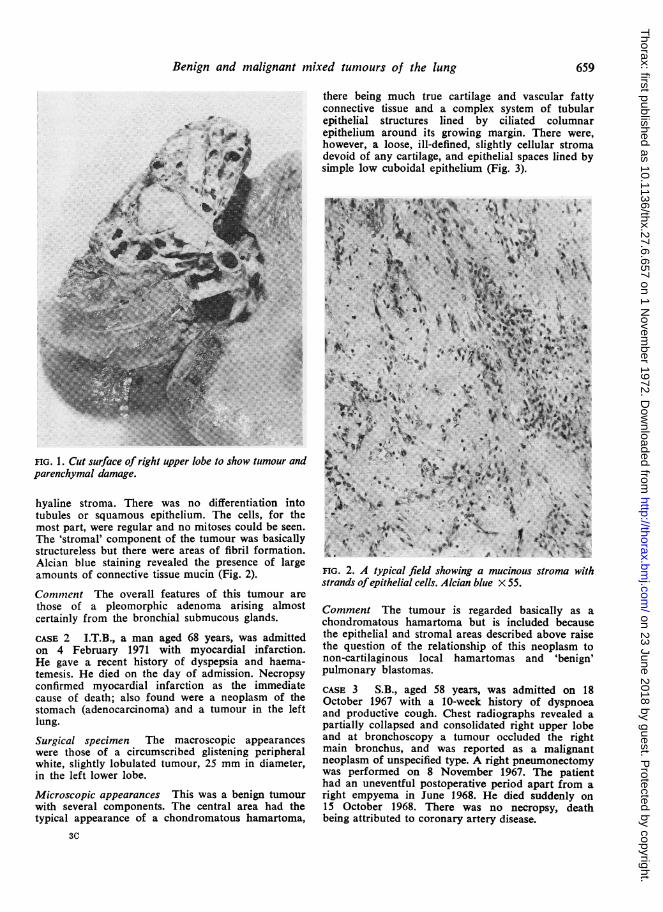
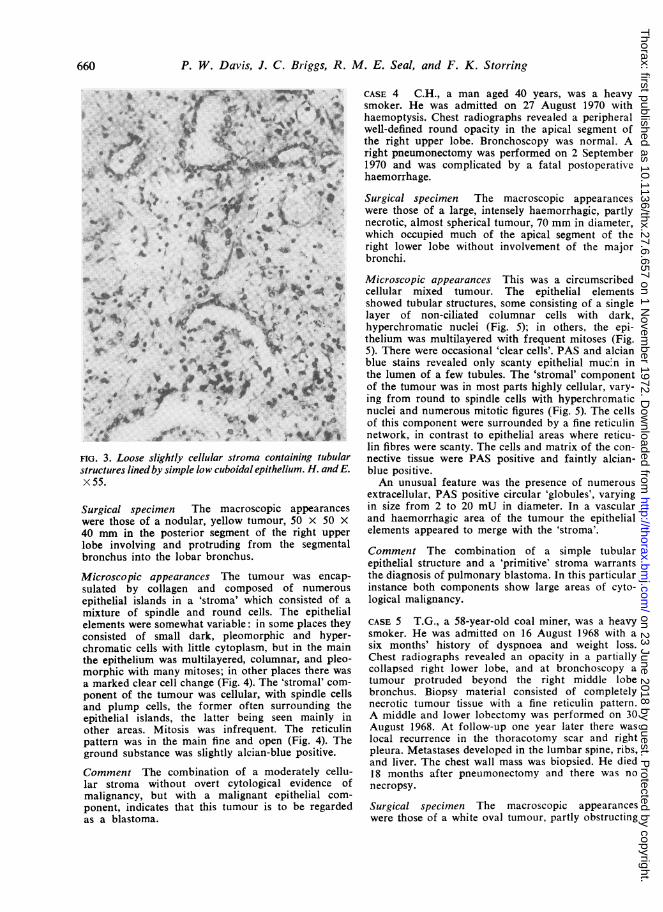
there being much true cartilage and vascular fattyconnective tissue and a complex system of tubularepithelial structures lined by ciliated columnarepithelium around its growing margin. There were,however, a loose, ill-defined, slightly cellular stromadevoid of any cartilage, and epithelial spaces lined bysimple low cuboidal epithelium (Fig. 3).
, 4Me-v w Xt t
IO44 I
.j.
.. w.
'9iPf
v s0, \ 8
9S;^e s.
:X: s.4fs.w. 8,e. a * ' + % s
FIG. 2. A typical field showing a mucinous stroma withstrands ofepithelial cells. Alcian blue X 55.
Comment The tumour is regarded basically as achondromatous hamartoma but is included becausethe epithelial and stromal areas described above raisethe question of the relationship of this neoplasm tonon-cartilaginous local hamartomas and 'benign'pulmonary blastomas.
CASE 3 S.B., aged 58 years, was admitted on 18October 1967 with a 10-week history of dyspnoeaand productive cough. Chest radiographs revealed apartially collapsed and consolidated right upper lobeand at bronchoscopy a tumour occluded the rightmain bronchus, and was reported as a malignantneoplasm of unspecified type. A right pneumonectomywas performed on 8 November 1967. The patienthad an uneventful postoperative period apart from aright empyema in June 1968. He died suddenly on15 October 1968. There was no necropsy, deathbeing attributed to coronary artery disease.
659
on 23 June 2018 by guest. Protected by copyright.
http://thorax.bmj.com
/T
horax: first published as 10.1136/thx.27.6.657 on 1 Novem
ber 1972. Dow
nloaded from
P. W. Davis, J. C. Briggs, R. M. E. Seal, and F. K. Storring
* y ^i ''
4b ~ N
*
.. to9¢.. ;:t'
A..%
a a4 g5,ri s .bfM o .9is
V 0~~:
FIG. 3. Loose slightly cellular stroma containing tubularstructures lined by simple low cuboidalepithelium. H. andE.X55.
Surgical specimen The macroscopic appearanceswere those of a nodular, yellow tumour, 50 x 50 X40 mm in the posterior segment of the right upperlobe involving and protruding from the segmentalbronchus into the lobar bronchus.
Microscopic appearanccs The tumour was encap-sulated by collagen and composed of numerousepithelial islands in a 'stroma' which consisted of amixture of spindle and round cells. The epithelialelements were somewhat variable: in some places theyconsisted of small dark, pleomorphic and hyper-chromatic cells with little cytoplasm, but in the mainthe epithelium was multilayered, columnar, and pleo-morphic with many mitoses; in other places there wasa marked clear cell change (Fig. 4). The 'stromal' com-ponent of the tumour was cellular, with spindle cellsand plump cells, the former often surrounding theepithelial islands, the latter being seen mainly inother areas. Mitosis was infrequent. The reticulinpattern was in the main fine and open (Fig. 4). Theground substance was slightly alcian-blue positive.
Comment The combination of a moderately cellu-lar stroma without overt cytological evidence ofmalignancy, but with a malignant epithelial com-ponent, indicates that this tumour is to be regardedas a blastoma.
CASE 4 C.H., a man aged 40 years, was a heavysmoker. He was admitted on 27 August 1970 withhaemoptysis. Chest radiographs revealed a peripheralwell-defined round opacity in the apical segment ofthe right upper lobe. Bronchoscopy was normal. Aright pneumonectomy was performed on 2 September1970 and was complicated by a fatal postoperativehaemorrhage.
Surgical specimen The macroscopic appearanceswere those of a large, intensely haemorrhagic, partlynecrotic, almost spherical tumour, 70 mm in diameter,which occupied much of the apical segment of theright lower lobe without involvement of the majorbronchi.
Microscopic appearances This was a circumscribedcellular mixed tumour. The epithelial elementsshowed tubular structures, some consisting of a singlelayer of non-ciliated columnar cells with dark,hyperchromatic nuclei (Fig. 5); in others, the epi-thelium was multilayered with frequent mitoses (Fig.5). There were occasional 'clear cells'. PAS and alcianblue stains revealed only scanty epithelial muc.n inthe lumen of a few tubules. The 'stromal' componentof the tumour was in most parts highly cellular, vary-ing from round to spindle cells with hyperchromaticnuclei and numerous mitotic figures (Fig. 5). The cellsof this component were surrounded by a fine reticulinnetwork, in contrast to epithelial areas where reticu-lin fibres were scanty. The cells and matrix of the con-nective tissue were PAS positive and faintly alcian-blue positive.An unusual feature was the presence of numerous
extracellular, PAS positive circular 'globules', varyingin size from 2 to 20 mU in diameter. In a vascularand haemorrhagic area of the tumour the epithelialelements appeared to merge with the 'stroma'.
Comment The combination of a simple tubularepithelial structure and a 'primitive' stroma warrantsthe diagnosis of pulmonary blastoma. In this particularinstance both components show large areas of cyto-logical malignancy.
CASE 5 T.G., a 58-year-old coal miner, was a heavysmoker. He was admitted on 16 August 1968 with asix months' history of dyspnoea and weight loss.Chest radiographs revealed an opacity in a partiallycollapsed right lower lobe, and at bronchoscopy atumour protruded beyond the right middle lobebronchus. Biopsy material consisted of completelynecrotic tumour tissue with a fine reticulin pattern.A middle and lower lobectomy was performed on 30August 1968. At follow-up one year later there waslocal recurrence in the thoracotomy scar and rightpleura. Metastases developed in the lumbar spine, ribs,and liver. The chest wall mass was biopsied. He died18 months after pneumonectomy and there was nonecropsy.
Surgical specinen The macroscopic appearanceswere those of a white oval tumour, partly obstructing
660
on 23 June 2018 by guest. Protected by copyright.
http://thorax.bmj.com
/T
horax: first published as 10.1136/thx.27.6.657 on 1 Novem
ber 1972. Dow
nloaded from

.V . .-
. 6,*a.w
Ik4a,.. -t..
4'k~~~~A, 4, i4
V.~~~~~~~ ~ ~ ~ 9b~~~~~~iK:~~~~~~~0
4AP*~ ~ ~ ~ ~ -iFIG4(ef) helage eitelalisan miny ler ellwih hapl dmacaedcetrl ecoss.Smllr slndcotiigdr!kmrhcclsi6;arl pnl-elsrm.H n .x3. Rgt iertclnpteni hconc Ivetsu opnn urudn apteililn-ihcnrl erss eiui ti 5
4~~~~~~~~~~~~~4
~~~~~~%t~~~~~~~~~~~~o
FbG5. 4-v M ~i~ rFIG. 5. (Left) Tubular epithelial structures in a slightly cellular stroma. H. and E. x 55. (Right) Multilayered epithelialstructures (bottom right) in a cellular stroma withfrequent mitoticfigures in both components ofthe tumour. H. andE. x 70.
on 23 June 2018 by guest. Protected by copyright.
http://thorax.bmj.com
/T
horax: first published as 10.1136/thx.27.6.657 on 1 Novem
ber 1972. Dow
nloaded from
't xi .-w i &4 + ^ffi<&-l0
FS&$>v^9z$ tS f~* )<>\; :554 ti
9 S t **mi 'tt' - K
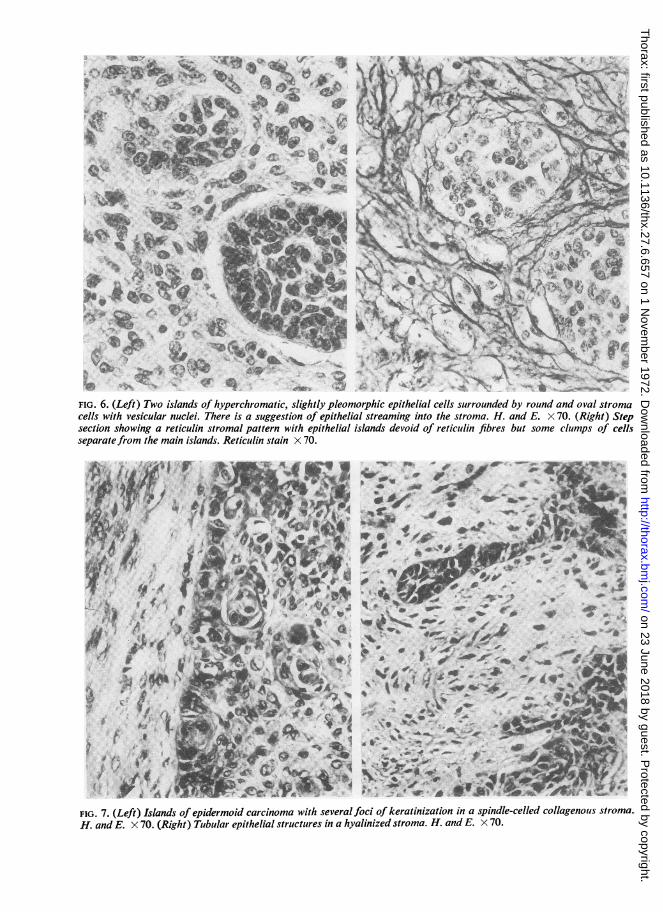
FIG. 6. (Left) Two islands of hyperchromatic, slightly pleomorphic epithelial cells surrounded by round and oval stromacells with vesicular nuclei. There is a suggestion of epithelial streaming into the stroma. H. and E. X 70. (Right) Stepsection showing a reticulin stromal pattern with epithelial islands devoid of reticulin fibres but some clumps of cellsseparate from the main islands. Reticulin stain X 70.
Io# , ,1r!..
.'IS*I
t
:
* . .,4 -*
:1'. K*.~+ i
4;E JF7.VV;..Y7
:. .$ "h
FIG. 7. (Left) Islands of epidermoid carcinoma with several foci of keratinization in a spindle-celled collagenous stroma.
H. and E. X 70. (Right) Tubular epithelial structures in a hyalinized stroma. H. and E. X 70.
..e\
.K ':s9p
We 't '*.l*f >,.
*:n,* #,. .A
X ss AcE ;a
> 'Me.<. v ,... ..
,. w
I.- V.71:1.,"I.. ..
rff"W
0"` 0%.1I
11 1) lrA'AI.A.),
*e
on 23 June 2018 by guest. Protected by copyright.
http://thorax.bmj.com
/T
horax: first published as 10.1136/thx.27.6.657 on 1 Novem
ber 1972. Dow
nloaded from
Benign and malignant mixed tiumours of the lung
the lower lobe bronchus and involving the adjacentpulmonary parenchyma, producing a firm mass 50 x20 x 20 mm. There was distal obstructive pneumonitis.
Microscopic appearances The tumour was composedof epithelial and 'stromal' components with a widevariation within each. The epithelial elements near thesurface of the intrabronchial portion of the tumourshowed islands of small hyperchromatic, slightlypleomorphic epithelial cells (Fig. 6). In other partsof the tumour the islands of epithelium were overtlyepidermoid with cell nests (Fig. 7). In yet other partsthere were tubular epithelial structures in a lesscellular hyalinized stroma, many fields being reminis-cent of a mixed salivary tumour (Fig. 7). The 'stromal'component in the intrabronchial portion of the tumourconsisted in places of loose 'embryonic' tissue. Therewere round and spindle cells with marked pleo-morphism, and occasional elongated non-striatedtumour giant cells. Mitoses were numerous. Therewere fine fibrillary structures in a lightly eosinophilic,PAS positive matrix. As in the bronchoscopic biopsy,the 'embryonic' stromal areas contained a uniformfine reticulin pattern: elsewhere the reticulin patternwas somewhat coarser, surrounding small groups ofcells near the epithelial islands, suggesting the possi-bility of epithelial streaming into the stroma (Fig. 6).
Microscopic appearances of recurrence in scar Thisshowed a pleomorphic, spindle-cell tumour with muchcollagen in some fasciculi, and occasional gianttumour cells as seen in the stroma of the originaltumour. The appearances suggested a metastasis ofthe sarcomatous component.
Comment The simple forms of 'stroma' and epi-thelium seen in some places in this tumour are similarto those of a pulmonary blastoma. Elsewhere thestromal and epithelial differentiation is more suggestiveof a carcinosarcoma. This tumour is considered to bea 'transitional' form between blastoma and carcino-sarcoma.
CASE 6. W.T., a 65-year-old man, was a heavysmoker with a chronic productive cough. He wasadmitted on 22 February 1970 with a two-monthhistory of haemoptysis. Chest radiographs revealedcollapse consolidation of the left lower lobe. Furtherradiographs showed progressive atelectasis proceedingto total collapse of the left lung. At bronchoscopy theleft main bronchus was found to be almost completelyobstructed by a fungating neoplasm, a biopsy beingreported as a malignant neoplasm, possibly asquamous carcinoma. On 29 March 1970 a left pneu-monectomy was performed followed by artificialventilation for respiratory failure. Subsequent deathwas due to hypoxic cerebral damage.
Surgical specimen The macroscopic appearanceswere those of a polypoid tumour, 30 mm in greatestdiameter, growing from the upper lobe bronchus,occluding the main bronchus, and extending into thelumen of the anterior segmental bronchus of the upper
lobe. The tumour was attached to the wall of theupper lobe bronchus but did not appear to infiltratethe lung tissue.
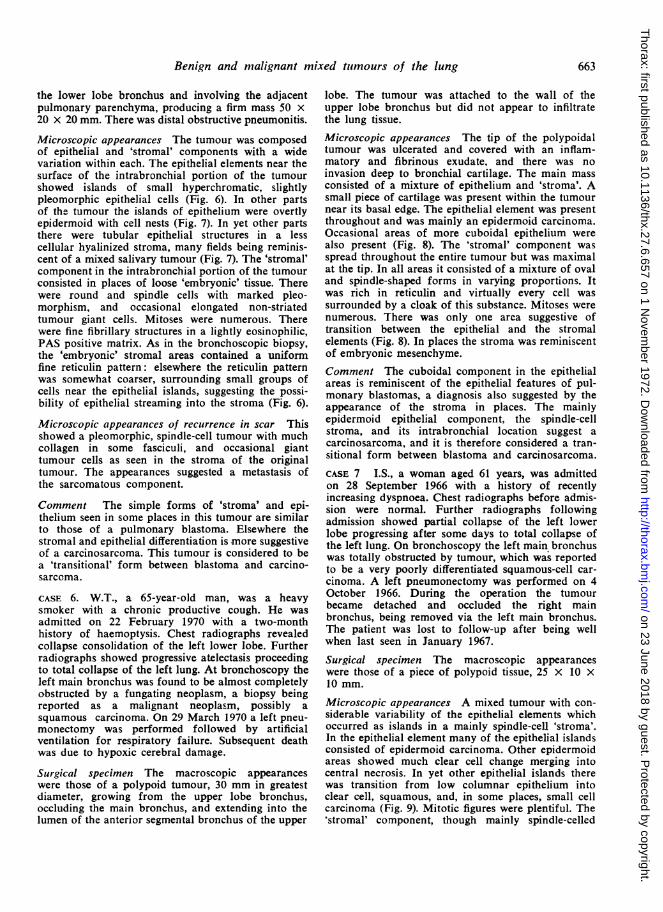
Microscopic appearances The tip of the polypoidaltumour was ulcerated and covered with an inflam-matory and fibrinous exudate, and there was noinvasion deep to bronchial cartilage. The main massconsisted of a mixture of epithelium and 'stroma'. Asmall piece of cartilage was present within the tumournear its basal edge. The epithelial element was presentthroughout and was mainly an epidermoid carcinoma.Occasional areas of more cuboidal epithelium werealso present (Fig. 8). The 'stromal' component wasspread throughout the entire tumour but was maximalat the tip. In all areas it consisted of a mixture of ovaland spindle-shaped forms in varying proportions. Itwas rich in reticulin and virtually every cell wassurrounded by a cloak of this substance. Mitoses werenumerous. There was only one area suggestive oftransition between the epithelial and the stromalelements (Fig. 8). In places the stroma was reminiscentof embryonic mesenchyme.Comment The cuboidal component in the epithelialareas is reminiscent of the epithelial features of pul-monary blastomas, a diagnosis also suggested by theappearance of the stroma in places. The mainlyepidermoid epithelial component, the spindle-cellstroma, and its intrabronchial location suggest acarcinosarcoma, and it is therefore considered a tran-sitional form between blastoma and carcinosarcoma.CASE 7 I.S., a woman aged 61 years, was admittedon 28 September 1966 with a history of recentlyincreasing dyspnoea. Chest radiographs before admis-sion were normal. Further radiographs followingadmission showed partial collapse of the left lowerlobe progressing after some days to total collapse ofthe left lung. On bronchoscopy the left main bronchuswas totally obstructed by tumour, which was reportedto be a very poorly differentiated squamous-cell car-cinoma. A left pneumonectomy was performed on 4October 1966. During the operation the tumourbecame detached and occluded the right mainbronchus, being removed via the left main bronchus.The patient was lost to follow-up after being wellwhen last seen in January 1967.
Surgical specimen The macroscopic appearanceswere those of a piece of polypoid tissue, 25 x 10 X10 mm.
Microscopic appearances A mixed tumour with con-siderable variability of the epithelial elements whichoccurred as islands in a mainly spindle-cell 'stroma'.In the epithelial element many of the epithelial islandsconsisted of epidermoid carcinoma. Other epidermoidareas showed much clear cell change merging intocentral necrosis. In yet other epithelial islands therewas transition from low columnar epithelium intoclear cell, squamous, and, in some places, small cellcarcinoma (Fig. 9). Mitotic figures were plentiful. The'stromal' component, though mainly spindle-celled
663
on 23 June 2018 by guest. Protected by copyright.
http://thorax.bmj.com
/T
horax: first published as 10.1136/thx.27.6.657 on 1 Novem
ber 1972. Dow
nloaded from

itt' ¢F' | |
I £~~~~~~~~~~~~~~~~~~~~~- *
.(Left) Obvious epidermoid areas with oval and spindle-cell stroma, with an area which sugg{ium into the stroma. H. and E. x 75. (Right) The epithelial component shows epidermoid carcidal epithelium producing tubular appearances. H. and E. x 75.
o ', 2.t ^,S;w; V1 *AS
''"''t%
:~~~~~~~~~ff,,6 bbe ?. /* \4e \wS --.h;
.~~~~~~~~~~~~~~~~.
*~~~~~~~r ~ r
A~~~
Ik4 ~ ~*%.,~~~~~~~~~ Af
.W. ....
A.
plmh---
"N -
*- v
...:
ests megn ofthoma meringit
FIG. 9. Marked variability ofepithelial component and more cellular pleomorphic area of connective tissue component oftumour. H. and E. x 55. (Inset) Epidermoid areas with some keratinization. H. and E. x 70.
'4.
FIG. 8.epithelcuboid
on 23 June 2018 by guest. Protected by copyright.
http://thorax.bmj.com
/T
horax: first published as 10.1136/thx.27.6.657 on 1 Novem
ber 1972. Dow
nloaded from
P. W. Davis, J. C. Briggs, R. M. E. Seal, and F. K. Storring
and containing reticulin and collagen fibrils, was insome places more cellular and pleomorphic (Fig. 9).In yet other places there was marked hyalinization.Only in one area near the surface was a less cellular,oedematous, 'embryonic' type of stroma noted.
Comment The predominance of pleomorphic spindlecells with epithelial malignancy suggests a carcino-sarcoma. The 'embryonic' stromal area and the con-siderable variability of the epithelial componentrecalls features shared in common with cases 3 and 4(blastomas).
CASE 8 I.B., a 49-year-old woman and a known caseof dextrocardia, presented with a non-resolving pneu-monia in February 1968. Chest radiographs suggesteda peripheral neoplasm in the left lower lobe withenlargement of the hilar lymph nodes. At operationon 10 April 1968 inversion of the lungs was noted.The lower lobe and hilar nodes on the left side wereremoved. At follow-up in July 1968, she presentedwith subacute small bowel obstruction with melaena.Radiographic examination revealed recurrence of thepulmonary neoplasm and a filling defect in the thirdpart of the duodenum and complete situs inversus. Atlaparotomy on 18 August 1968 a firm nodular, oval
rrS= = _ A.,.. itFRLAAsB/A j P J
.~N%IV41d-I~
lk*
-- -..
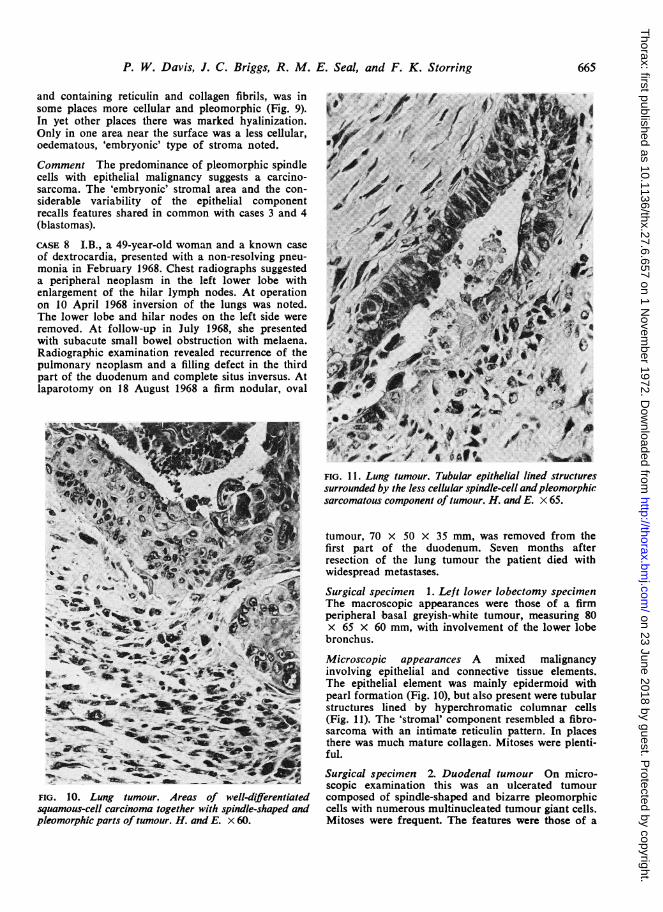
FIG. 10. Lung tumour. Areas of well-differentiated
squamous-cell carcinoma together with spindle-shaped andpleomorphic parts of tumour. H. and E. x 60.
FIG. 11. Lung tumour. Tubular epithelial lined structuressurrounded by the less cellular spindle-cell andpleomorphicsarcomatous component of tumour. H. and E. x 65.
tumour, 70 x 50 x 35 mm, was removed from thefirst part of the duodenum. Seven months afterresection of the lung tumour the patient died withwidespread metastases.
Surgical specimen 1. Left lower lobectomy specimenThe macroscopic appearances were those of a firmperipheral basal greyish-white tumour, measuring 80x 65 x 60 mm, with involvement of the lower lobebronchus.
Microscopic appearances A mixed malignancyinvolving epithelial and connective tissue elements.The epithelial element was mainly epidermoid withpearl formation (Fig. 10), but also present were tubularstructures lined by hyperchromatic columnar cells(Fig. 11). The 'stromal' component resembled a fibro-sarcoma with an intimate reticulin pattern. In placesthere was much mature collagen. Mitoses were plenti-ful.
Surgical specimen 2. Duodenal tumour On micro-scopic examination this was an ulcerated tumourcomposed of spindle-shaped and bizarre pleomorphiccells with numerous multinucleated tumour giant cells.Mitoses were frequent The features were those of a
665
on 23 June 2018 by guest. Protected by copyright.
http://thorax.bmj.com
/T
horax: first published as 10.1136/thx.27.6.657 on 1 Novem
ber 1972. Dow
nloaded from
P. W. Davis, J. C. Briggs, R. M. E. Seal, and F. K. Storring
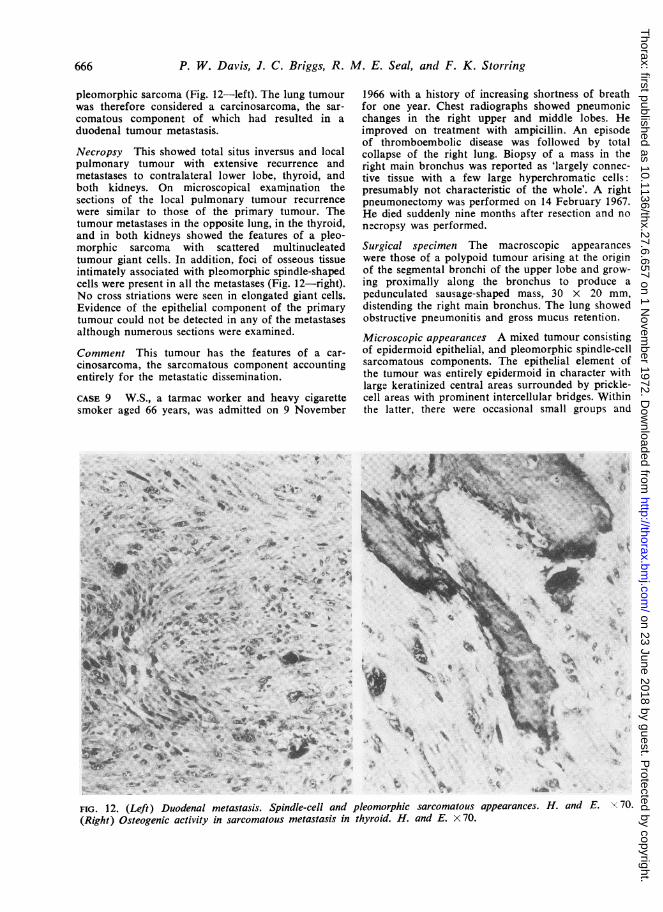
pleomorphic sarcoma (Fig. 12-left). The lung tumourwas therefore considered a carcinosarcoma, the sar-comatous component of which had resulted in aduodenal tumour metastasis.
Necropsy This showed total situs inversus and localpulmonary tumour with extensive recurrence andmetastases to contralateral lower lobe, thyroid, andboth kidneys. On microscopical examination thesections of the local pulmonary tumour recurrencewere similar to those of the primary tumour. Thetumour metastases in the opposite lung, in the thyroid,and in both kidneys showed the features of a pleo-morphic sarcoma with scattered multinucleatedtumour giant cells. In addition, foci of osseous tissueintimately associated with pleomorphic spindle-shapedcells were present in all the metastases (Fig. 12-right).No cross striations were seen in elongated giant cells.Evidence of the epithelial component of the primarytumour could not be detected in any of the metastasesalthough numerous sections were examined.
Comment This tumour has the features of a car-cinosarcoma, the sarcomatous component accountingentirely for the metastatic dissemination.
CASE 9 W.S., a tarmac worker and heavy cigarettesmoker aged 66 years, was admitted on 9 November
s. 4 -F ., -4 A
Rt.w.o7 .@ + k.
AixESk t V Jx v +
4.' A. f. N
_-_~ , x A *1i _
v *t A V % Lc s .^ .tt. w49~~~~~~~Ai... X . . w s~~~~~~~.,
1966 with a history of increasing shortness of breathfor one year. Chest radiographs showed pneumonicchanges in the right upper and middle lobes. Heimproved on treatment with ampicillin. An episodeof thromboembolic disease was followed by totalcollapse of the right lung. Biopsy of a mass in theright main bronchus was reported as 'largely connec-tive tissue with a few large hyperchromatic cells:presumably not characteristic of the whole'. A rightpneumonectomy was performed on 14 February 1967.He died suddenly nine months after resection and nonecropsy was performed.
Surgical specimen The macroscopic appearanceswere those of a polypoid tumour arising at the originof the segmental bronchi of the upper lobe and grow-ing proximally along the bronchus to produce apedunculated sausage-shaped mass, 30 x 20 mm,distending the right main bronchus. The lung showedobstructive pneumonitis and gross mucus retention.
Microscopic appearances A mixed tumour consistingof epidermoid epithelial, and pleomorphic spindle-cellsarcomatous components. The epithelial element ofthe tumour was entirely epidermoid in character withlarge keratinized central areas surrounded by prickle-cell areas with prominent intercellular bridges. Withinthe latter, there were occasional small groups and
Pt
A.I* e%
FIG. 12. (Left) Duodenal metastasis. Spindle-cell and pleomorphic sarcomatous appearances. H. and E. x 70.(Right) Osteogenic activity in sarcomatous metastasis in thyroid. H. and E. x 70.
666
"I. A.
-A,.Ab
on 23 June 2018 by guest. Protected by copyright.
http://thorax.bmj.com
/T
horax: first published as 10.1136/thx.27.6.657 on 1 Novem
ber 1972. Dow
nloaded from
Benign and malignant mixed tumours of the lung
0-~~~~~~~~~-
~~.~~~~.*~~~~~~m~~~~4~~~V -~40rA~~~~~~~.~ ~~~~~~A
~~~~~;j,*4~~~~~- I V~~~
~~~~ -~~;-t
Al.~~~~~~~~~~~~~~~-~~ ~ ~ ~ M
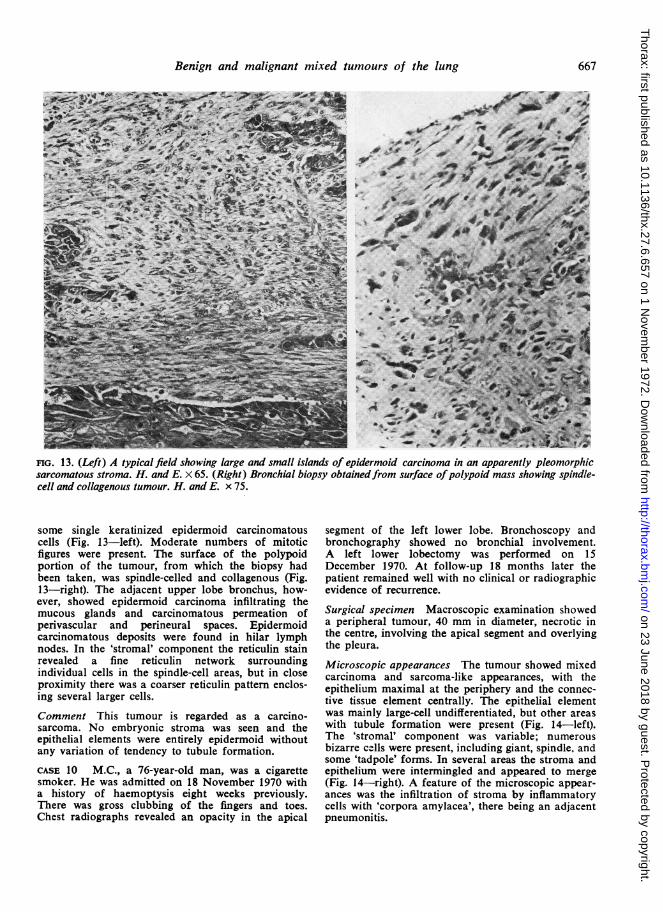
nG. 13. (Left) A typical field showing large and small islands of epidermoid carcinoma in an apparently pleomorphicsarcomatous stroma. H. and E. X 65. (Right) Bronchial biopsy obtainedfrom surface ofpolypoid mass showing spindle-cell and collagenous tumour. H. and E. x 75.
some single keratinized epidermoid carcinomatouscells (Fig. 13-left). Moderate numbers of mitoticfigures were present. The surface of the polypoidportion of the tumour, from which the biopsy hadbeen taken, was spindle-celled and collagenous (Fig.13-right). The adjacent upper lobe bronchus, how-ever, showed epidermoid carcinoma infiltrating themucous glands and carcinomatous permeation ofperivascular and perineural spaces. Epidermoidcarcinomatous deposits were found in hilar lymphnodes. In the 'stromal' component the reticulin stainrevealed a fine reticulin network surroundingindividual cells in the spindle-cell areas, but in closeproximity there was a coarser reticulin pattern enclos-ing several larger cells.
Comment This tumour is regarded as a carcino-sarcoma. No embryonic stroma was seen and theepithelial elements were entirely epidermoid withoutany variation of tendency to tubule formation.
CASE 10 M.C., a 76-year-old man, was a cigarettesmoker. He was admitted on 18 November 1970 witha history of haemoptysis eight weeks previously.There was gross clubbing of the fingers and toes.Chest radiographs revealed an opacity in the apical
segment of the left lower lobe. Bronchoscopy andbronchography showed no bronchial involvement.A left lower lobectomy was performed on 15December 1970. At follow-up 18 months later thepatient remained well with no clinical or radiographicevidence of recurrence.
Surgical specimen Macroscopic examination showeda peripheral tumour, 40 mm in diameter, necrotic inthe centre, involving the apical segment and overlyingthe pleura.
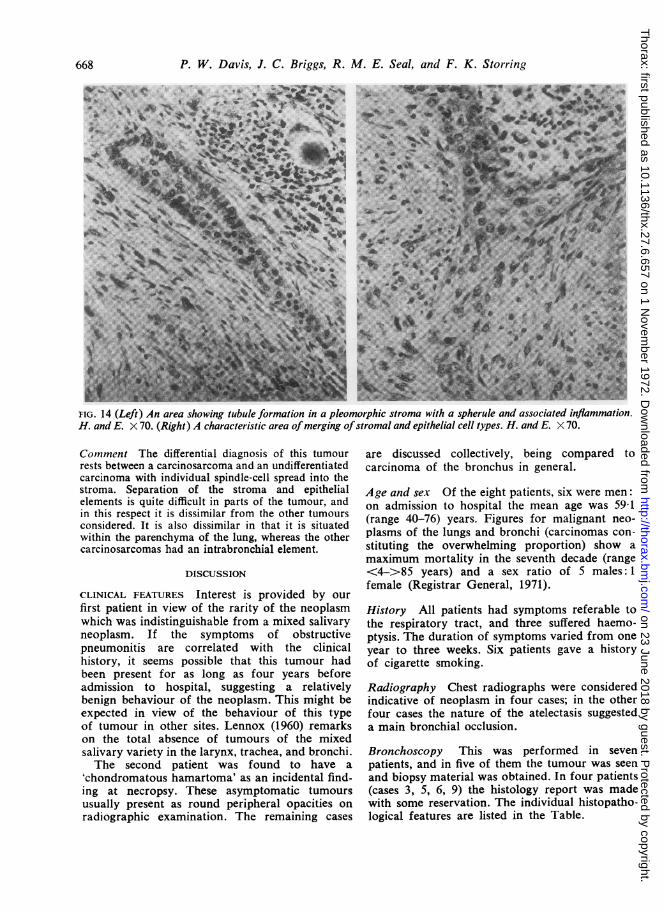
Microscopic appearances The tumour showed mixedcarcinoma and sarcoma-like appearances, with theepithelium maximal at the periphery and the connec-tive tissue element centrally. The epithelial elementwas mainly large-cell undifferentiated, but other areaswith tubule formation were present (Fig. 14-left).The 'stromal' component was variable; numerousbizarre cells were present, including giant, spindle, andsome 'tadpole' forms. In several areas the stroma andepithelium were intermingled and appeared to merge(Fig. 14-right). A feature of the microscopic appear-ances was the infiltration of stroma by inflammatorycells with 'corpora amylacea', there being an adjacentpneumonitis.
667
on 23 June 2018 by guest. Protected by copyright.
http://thorax.bmj.com
/T
horax: first published as 10.1136/thx.27.6.657 on 1 Novem
ber 1972. Dow
nloaded from
P. W. Davis, J. C. Briggs, R. M. E. Seal, and F. K. Storring
4
W
s~~~~~~ SI /#i*; <R*ta>¢e;N>, V
1- s 7;X* Bx > tSW ; S C<+~~~~~O'.0+-0^AW i
%~~~~~~~~~~~~~~~~~~~~~~~~~~~~%
H. a E'. 70. (Right);A characteristic area of mergingof stromal and eithelia cellwetypes.H4ad E 7
.i.77
........ .>... sw 7........ ... .......w[v....:*j..............:Mh A*: : ....1. . ..... s s. e-R ,:.;ss:B ...... z:w.wK:-s .F
*.4:w"'68Fg: : ...................:::.'::: .. .. A.. ... .; . .w: ;...e, .s - .-c m | 9 ::vA ~~~~i s ..in9jj/,4 ....e..0S ...j
X .L..AS= Ze R . ................... i,5 z|y - i 9 - S # tSt B:°8,, :, 2 z ,'Ys .:w Ne '-e f.w ............................................................................................... :M Y :: j:.g,. a..=xs . -s. ra:X .x ......................................... ^.k4:' : c.: . ..............................?:_!~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~4FI.4LftAre soin tbuefomain n lemophcstom it asheul adasocaedinlmmtin
~~~~~~~~'AW
H.anE7.Rih) carcerstc ra f erig f trml ndeptelalceltyes HndE.XV0
Comt1ment The differential diagnosis of this tumourrests between a carcinosarcoma and an undifferentiatedcarcinoma with individual spindle-cell spread into thestroma. Separation of the stroma and epithelialelements is quite difficult in parts of the tumour, andin this respect it is dissimilar from the other tumoursconsidered. It is also dissimilar in that it is situatedwithin the parenchyma of the lung, whereas the othercarcinosarcomas had an intrabronchial element.
DISCUSSION
CLINICAL FEATURES Interest is provided by our
first patient in view of the rarity of the neoplasmwhich was indistinguishable from a mixed salivaryneoplasm. If the symptoms of obstructivepneumonitis are correlated with the clinicalhistory, it seems possible that this tumour hadbeen present for as long as four years beforeadmission to hospital, suggesting a relativelybenign behaviour of the neoplasm. This might beexpected in view of the behaviour of this typeof tumour in other sites. Lennox (1960) remarkson the total absence of tumours of the mixedsalivary variety in the larynx, trachea, and bronchi.The second patient was found to have a
'chondromatous hamartoma' as an incidental find-ing at necropsy. These asymptomatic tumoursusually present as round peripheral opacities onradiographic examination. The remaining cases
are discussed collectively, being compared tocarcinoma of the bronchus in general.
Age and sex Of the eight patients, six were men:on admission to hospital the mean age was 59-1(range 40-76) years. Figures for malignant neo-plasms of the lungs and bronchi (carcinomas con-stituting the overwhelming proportion) show amaximum mortality in the seventh decade (range<4->85 years) and a sex ratio of 5 males: 1female (Registrar General, 1971).
History All patients had symptoms referable tothe respiratory tract, and three suffered haemo-ptysis. The duration of symptoms varied from oneyear to three weeks. Six patients gave a historyof cigarette smoking.
Radiography Chest radiographs were consideredindicative of neoplasm in four cases; in the otherfour cases the nature of the atelectasis suggesteda main bronchial occlusion.
Bronchoscopy This was performed in sevenpatients, and in five of them the tumour was seen
and biopsy material was obtained. In four patients(cases 3, 5, 6, 9) the histology report was madewith some reservation. The individual histopatho-logical features are listed in the Table.
668
ldlb-' ', --k. 49mm. -li, w ,Ejj -a" .-. _smfA ...
on 23 June 2018 by guest. Protected by copyright.
http://thorax.bmj.com
/T
horax: first published as 10.1136/thx.27.6.657 on 1 Novem
ber 1972. Dow
nloaded from
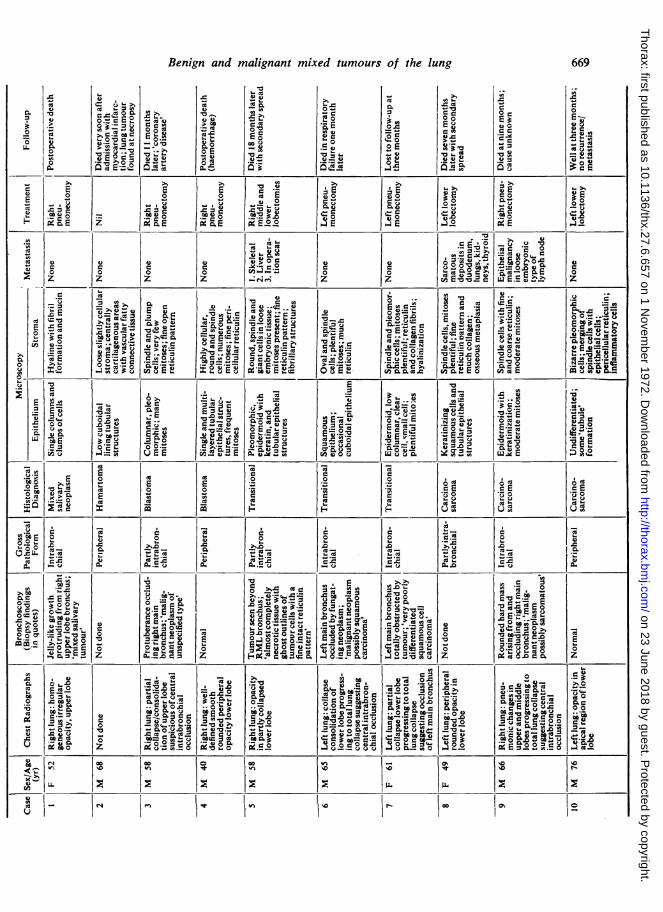
4) ; E ; E v E4) 0 0 G 0 0 C 0u 0 I...
M- .: 0u IM6
co .:.c 0 G 0 0c6E z c, cE iX E.2 0 E E 0 04 E
r. 0; . FA 0C.0 0 0 00 co .=0 0 0 0 0 a. E 0Ez z z z z z E -a -a.R N.' E z
Elu .-E C6 .9 0 Er C
.:ZV:: . E E- 5E`Cv E 0 co- Q
rn 'A&. V 0 W l;; 0 0t, W= v O 0 6..2 -6,2 N 41== E Q==
la Uz 'S.4, 8Ca E > U06 E 0 .0 0 U, C.0--.C law==== 0 la . -9.9;=t0 0 , 5 E.="= 06.2 06 0 0. C6
cn 'U"R ou U E62so, GU E uc Gav E 2= W 4 06 0 u5 E0
05E VE'U -o .9 E-3 ';to :2.2Z E! U E ='a -. . E
f.. 'a 04 v a-- - ",a rA p Ca00 2 rA E E.N'9= o E '. C E,00- E ;g E T.-
:S 0 O co C M 0 ICI-z-4 Z V,._ v E E.4'a E 0 7a -So o 0 &. = = I Et: 0:2 -..a E U.0S. C6.5 a &.i;5 C60 ao 0,0U E E 8 E 0 U U 06
to 0 E 0 .2 .2>, CA E E0 ed S. r.E c E c Eto m 0 0E U
t* E 0 0 00.2 V
0 0 co E. .26 m cocU. &. S- &. 6. L. U. 00 r. V 0 m C C C 0 S.
U
EC rA Ca 00.0 E 40
UO O C... " r. , - E=-v ii.Ll &.O= Ca
'm 0 C.- 0 E O0 E U. E ed EO co > E =4 2 >, = S. S. W G00 rA .0 , o'... U.0co O toco Go0 0 C
0'O- . 0 0 Cd ;,,-O' '-Q.= 0 US -, C E N.- 0 3 O
.0-aa v S,= O O 0 0 0 es,..2 cr oc EW.E , 0 otgO V. 0 0.00 0 a E U 0 E 0 C (AZ E Z
0 E 0 CdE 0 u 0 0
0 z crz O ;a Z
0 00 0o Z -U q.C O 0
M 0 - U 06oe M = 0cv&.0 &. 0.2 0 0 a U.0 rA G
ROA j; C E I'D.: U.-0 B.- O 0 0to 0 rA U 0 es 0 0-0 towl &O U .. O Moo.- to.0 r. ao- r. ed ' r.0, m r. r. c .0 to CC 6'te
= O 0 O O 0 0 9 '-;- Ou co =0 E 0 .0v.R O 06. C-A -0 &. 0 06 Mu Z-0 S.
W= 0 C COC 0 O &.,O, 2.0 0 jR.C 0 0 0 r. 0 &. z 0 0 u 06 0Rao z g 0 R R E Q='_0 .0. E O Cd
co 00 co tn
Benign and malignant mixed tumours of the lung 669
o_ o
C:d
r.
E 8sC-,_-0 4= . ,
coa
0
0-
Cd
.: 00 =0zo: 0
0 E- 0,A 20 41.4 -
o: I *> 0
cis0
v a
os s
(A vn
4) 0
EcO
X ,C
63
.C
uOc c.E.NX
'm =
=
Eo00 ;E,- = uWe.- -b
4
>"7-m) or =>-e cq:
i5 °I o o:
c X0 0
c. XX 3
9 ,,x0
11 ar. r. (
a a m
2 1- 5-Onl
1. S.^a 4>15 ,
on 23 June 2018 by guest. Protected by copyright.
http://thorax.bmj.com
/T
horax: first published as 10.1136/thx.27.6.657 on 1 Novem
ber 1972. Dow
nloaded from
P. W. Davis, J. C. Briggs, R. M. E. Seal, and F. K. Storring
Operative findings and procedure All patientswere considered operable on clinical and radio-graphic grounds. The gross findings at operation,with the exception of case 7, were consistent withmalignant growth. All operative procedures wereintended to be curative, except in case 8, in whomrespiratory function allowed lobectomy only.
Follow-up (Table) One patient remains free fromclinical recurrence 18 months after leaving hospi-tal and one patient was lost to follow-up, beingfree from recurrence when seen three months afterdischarge. Two patients died from complicationsof surgical treatment. Three patients who under-went 'curative' surgery died at 9, 11, and 18months, but only one of these (case 5) had cer-tain evidence of secondary spread at the time ofdeath. Another patient (case 8) died with localrecurrence and widespread metastases at sevenmonths. Thus, among the four patients who diedfollowing discharge from hospital, the averagesurvival time was 11-3 months.
Metastasis Three patients developed metastases.In each instance the primary tumour containedepithelium which was epidermoid. Distant meta-stases occurred in two of these (cases 5and 8), and where histological proof was possiblethese metastases were all sarcomatous in nature.In the third patient, a local lymph node showedepithelial malignancy (case 9).
Metastasis in cases of pulmonary blastoma iswell documented, and the sites quoted includeregional nodes, lungs, brain, abdominal viscera,retroperitoneal tissues, and blood vessels. It seemsrare for the epithelial component to metastasizealone: metastases described as pure sarcoma havebeen recorded infrequently (Spencer, 1961; Henryand Keal, 1966; Stackhouse et al., 1969); the mostcommon pattern of metastasis is one which in-cludes both malignant epithelial and connectivetissue components (Parker, Payne, and Woolner,1966; Spencer, 1961; Peabody, 1959; Barson et al.,1968; Stackhouse et al., 1969). The last authors,in stating that both components are usually demon-strable in the metastatic lesion, observe thatsarcoma predominates.
Metastasis has been well recognized in caseswhich have been accepted as pulmonary carcino-sarcoma, the sites quoted being regional lymphnodes, lung, skeleton, adrenals, kidneys and otherabdominal viscera, brain, and heart. A precisehistological definition of the composition of thesemetastases is often lacking and only one author(Saltykow, 1914) describes separate deposits con-taining carcinomatous, sarcomatous, and carcino-
sarcomatous tissue. Sarcomatous deposits alonehave been described by Weber (1939); carcinomaand sarcoma may occur separately in the samepatient (Motlik and Triska, 1968). Deposits con-taining a mixture of carcinoma and sarcoma havebeen described by Frank (1915) and Kakos,Williams, Assor, and Vasko (1971). The most com-mon form of metastasis is one which containscarcinoma alone (Selye, 1928; Fischer, 1938;Motlik and Triska, 1968; Razzuk et al., 1971).From the foregoing account it will be seen that
the distribution of metastases in both pulmonaryblastoma and carcinosarcoma resembles the pat-tern of distribution which has been described forcarcinoma of the lung (Hinson, 1958).
Prognosis Survival of patients with pulmonaryblastoma is variable. Bauermeister, Jennings,Beland, and Judson (1966) described a patientwho had radiological evidence of neoplasm for24 years before surgical treatment.
Spencer (1961) quotes the patient described byBarnard (1952) as being alive 15 years after sur-gical treatment. But short periods of survival fol-lowing diagnosis or treatment are recorded, e.g.,six weeks (Spencer, 1961), nine months (Barsonet al., 1968), and six and seven months (Stack-house et al., 1969) with deaths attributable tometastases.With regard to endobronchial carcinosarcoma,
some authors (Taylor and Rae, 1952; Drury andStirland, 1959) suggest that this is a relativelyfavourable lesion. However, Bergmann et al.(1951), in commenting on the six-year postopera-tive survival of one of their patients, point out thepossibility of recurrence. Reference to more recentliterature (Stackhouse et al., 1969) indicates lessersurvival times for this type of tumour. Razzuket al. (1971) report a patient who had metastasessix months after pneumonectomy and who died21 months after operation for an endobronchialpedunculated carcinosarcoma. Many cases ofcarcinosarcoma show a gross pattern of polypoidintrabronchial extension associated with paren-chymal tumour involvement, and survival periodsfollowing treatment of less than one year are notuncommon.Goldman (1965) showed that for carcinoma of
the lung survival rates were more closely associ-ated with the histological type of tumour and itsdegree of differentiation than with the method oftreatment used.Our series of patients is too small to allow us
to draw any useful conclusions concerning theprognosis of these mixed primary malignanttumours of the lungs, but whether they occur in
670
on 23 June 2018 by guest. Protected by copyright.
http://thorax.bmj.com
/T
horax: first published as 10.1136/thx.27.6.657 on 1 Novem
ber 1972. Dow
nloaded from
Benign and malignant mixed tumours of the lung
a peripheral or an intrabronchial situation, we feelthat caution is justified with regard to prognosisafter treatment.
HISTOPATHOLOGY
Benign mixed tumours Of the 10 cases presented,only cases 1 and 2 are considered benign in termsof their histopathological appearances. Case 1 isa classical example of a pleomorphic adenoma(mixed salivary tumour) growing within abronchus. This tumour complies with WHO groupIX, mixed tumours, which includes tumoursresembling mixed salivary neoplasms. However,the colour photomicrographs illustrating thisgroup, namely Figs 31 and 32, could be interpre-ted as examples of the common 'chondromatoushamartoma'. Histopathologists would not confusea pleomorphic adenoma with a chondromatoushamartoma. Pleomorphic adenomas, common neo-plasms of salivary glands but very rare in thebronchus, are well-defined entities whose cell oforigin., at least in salivary glands, is well estab-lished (Eneroth, 1964). This cell is the myoepi-thelial cell, a specialized specific cell found inlimited sites but capable of differentiation alongepithelial and mesodermal lines.The much more common chondromatous
hamartomas are composed of tubular structureslined by low cuboidal epithelium in associationwith connective tissue elements such as cartilage,and these are clearly mixed tumours in that thereis proliferation of epithelium and mesenchymaltissue. In view of this combination of fairly maturecomponents of lung, the term hamartoma hasbeen widely accepted. Willis (1962), however, doesnot regard such tumours as true hamartomas butsuggests that they are analogous to fibroadenomasof the breast. Our example of such a commontumour (case 2) is chosen for two reasons: (1) inone area the stroma contains numerous stellatecells resembling the embryonic tissue and cuboidalepitbelial-lined tubules seen in some examples ofpulmonary blastoma; (2) because such areas alsofulfil the criteria laid down by Spencer (1968) forhis second variety of non-cartilagenous local pul-monary hamartoma. Local pulmonary hamarto-mas, we feel, should find a place in any revisedclassification of lung tumours and be designatedbenign. 'The term 'benign mixed tumour ofbronchus', preferred by Willis (1962), could easilylead to confusion with the distinctive group ofmixed salivary tumours (pleomorphic adenomas)and also it might suggest an intrabronchialtumour, whereas of course they are characteristic-ally peripheral. This benign group of mixed
tumours, therefore, includes pleomorphic adeno-mas and local pulmonary hamartomas, bothcartilagenous and non-cartilagenous. The latterwould appear to correspond closely to benignpulmonary blastomas.We suggest that in a revision of the WHO
classification, type IX1 'mixed tumours' should besubdivided into 1 a pleomorphic adenomas; lblocal pulmonary hamartomas (cartilagenous); and1c local pulmonary hamartomas (non-cartilagen-ous), including histopathologically benign pul-monary blastomas. A tumour such as that ofcase 2, with some embryonic stroma and largecartilagenous areas, would be included under lb.
Malignant mixed tumours A review of the pub-lished cases of pulmonary blastomas (Spencer,1961; Souza et al., 1965; Bauermeister et al., 1966;Barson et al., 1968; Stackhouse et al., 1969) revealsthat cytological evidence of malignancy is presentin either the epithelial or the stromal component,or often in both. Carcinosarcomas reported in theliterature, as implied by their name, involve cyto-logical malignancy in both epithelial and stromalcomponents. The WHO classification of mixedtumours IX includes 'carcinosarcomas of embry-onal type' (pulmonary blastomas), in which thedistinctive criteria are the presence of stromaresembling embryonic mesenchyme and irregularacinar tissue, or squamous epithelium. The needfor histopathological evidence of malignancy isnot stressed, presumably because this is difficultto define and is somewhat subjective.
Also included with WHO IX3 are 'other carcino-sarcomas', the main distinctive feature being thepresence of 'areas characteristic of soft tissue sar-coma'. A wide range of well-differentiated epi-thelial malignancy is included within this group.Variability of the carcinomatous component,differentiated or undifferentiated, is not mentioned.The tumours which we have presented from
cases 3 to 10 inclusive are histologically malig-nant: in case 3 the epithelial elements aloneshowed malignancy but in the remainder, cases4 to 10, pleomorphism and increased mitoticactivity are present in both the epithelial and theconnective tissue components. Cases 3 and 4 ful-fil the WHO criteria for carcinosarcoma ofembryonal type and closely resemble the majorityof published examples of pulmonary blastoma.We consider cases 8, 9, and 10 to correspond toWHO IX3 ('other carcinosarcomas'). The majorityof published examples of carcinosarcoma con-sist of epidermoid carcinomatous islands in aspindle-cell sarcomatous 'stroma', as seen in thesethree cases. Cases 5, 6, and 7, however, have
671
on 23 June 2018 by guest. Protected by copyright.
http://thorax.bmj.com
/T
horax: first published as 10.1136/thx.27.6.657 on 1 Novem
ber 1972. Dow
nloaded from
P. W. Davis, J. C. Briggs, R. M. E. Seal, and F. K. Storring
features of both subgroups containing areasresembling embryonal mesenchyme. Another fea-ture common to the neoplasms in these latter threecases is the marked variability of the epithelialcomponent within each tumour. Therefore wehave termed them 'transitional'.
Collectively, cases 3 to 10 inclusive show a spec-trum from blastomas characterized by tubularepithelial structures, sometimes with keratinizedareas in an embryonic stroma, to mixed malig-nancy with acinar and epidermoid epithelial malig-nant components in a spindle-cell sarcomatousbackground, as in so-called carcinosarcomas. Wesuggest that revision of the international tumourclassification should take account of and include'transitional' forms. Further, we suggest that thecarcinosarcomas of embryonal type should bedesignated pulmonary blastomas, and thatalthough it is appreciated that it may be difficultto define histopathological malignancy in the zonebetween local pulmonary hamartoma and somepulmonary blastomas, only tumours with malig-nant features in one or both components shouldbe included.
In any revision of the classification of mixedtumours provision should also be made for therare occurrence of malignant variants of 'chondro-matous hamartoma' (Simon and Ballon, 1947;Cavin, Masters, and Moody, 1958).
The problem of apparent merging of epithelial andconnective tissue elements Illustrations of pul-monary blastomas described in various papersappear to be very similar but the authors do notcome to the same conclusions concerning theseparation or merging of the two components.Spencer (1961), in reporting four cases, concludesthat merging is a feature. This view is shared byHenry and Keal (1966) in their case report. Onthe other hand, Stackhouse et al. (1969) stress theabsence of merging of the two components intheir four cases of pulmonary blastoma. Our casematerial supports the latter view (cf. cases 3 and4), but we noted some evidence of merging incases 5 and 6 ('transitional'). The carcinosarcomas(cases 8, 9, and 10) show the presence of streamingand merging of the epithelial and stromal com-ponents. It is difficult to assess the significance ofsmall clumps of malignant cells in the stroma ofthese malignant mixed tumours. The possibilitythat these cells are epithelial in origin and accountsolely for the cytological malignancy seen in thestroma questions the validity of regarding carcino-sarcoma as a true entity. This is a point which hasbeen made by Saphir and Vass (1938) and Willis(1967). They have stressed that many examples of
carcinosarcomas represent a 'pseudo-mixed' pic-ture, an entity well accepted in some sites like thelarynx and the oesophagus. While we agree withSaphir and Vass, and Willis and others that manyexamples in the old literature with areas com-posed of spindle-cell variants may have been mis-interpreted as carcinosarcomas and that it is mostimportant to be aware of such a fallacy, we con-clude that the frequent differentiation into muscle,cartilage, and bone considered in more detailbelow leaves no doubt that carcinosarcoma is atrue entity with simultaneous malignancy of epi-thelium and connective tissue. Careful review ofour own material leaves us in some doubt onlyconcerning case 10. Several opinions were soughton this tumour and the majority favoured adiagnosis of carcinosarcoma.
Difterentiation of connective tissue componentDrury and Stirland (1959) reported a carcino-sarcoma of the lung containing areas of newbone formation in the spindle-cell areas, while theepithelial component was epidermoid, a combina-tion of appearances similar to that in our case 8,except that in the latter bone formation by thesarcomatous component was seen only in themediastinal recurrence and in metastases. Theyconsidered the production of reticulin, collagen,and bone as strong evidence that the spindle-celledareas were not epithelial variants. Similarly, Prive,Tellem, Meranze, and Chodoff (1961) regardedchondrosarcomatous areas in their case report ofa central carcinosarcoma as evidence in favourof carcinosarcoma being regarded as a true entity.Henry and Keal (1966) presented an example ofpulmonary blastoma with striated muscle inseveral areas. We did not encounter any differ-entiation of the connective tissue component intomature elements such as muscle or bone in eitherof our two pulmonary blastomas.
Histogenesis Many authors have suggested thatpulmonary blastomas, being peripheral, arederived from mesodermal tissue in accordancewith Waddell's theory of the development of thelung (Spencer, 1961; Motlik and Triska, 1968).The latter authors suggest that pulmonary blasto-mas can be regarded as 'mixed mesodermaltumours' and suggest that they may have a histo-genesis in common with peripheral chondromat-ous hamartomas. Though our example of chondro-matous hamartoma was included because of thepresence of 'embryonic stroma' at its edge, weconsider it unlikely that they have a commonorigin, because no blastoma with mature cartila-genous areas has been reported and the rare malig-
672
on 23 June 2018 by guest. Protected by copyright.
http://thorax.bmj.com
/T
horax: first published as 10.1136/thx.27.6.657 on 1 Novem
ber 1972. Dow
nloaded from
Benign and malignant mixed tumours of the lung
nant hamartomas have no resemblance to blasto-mas. If pulmonary blastomas are in any wayrelated to pulmonary hamartomas they must berelated to the non-cartilagenous ('peripheral') localpulmonary hamartoma, as suggested by Spencer(1968).
Motlik and Triska (1968) considered that cen-tral carcinosarcomas had a separate histogenesisfrom pulmonary blastoma, being derived trulyfrom central epithelium (entoderm) with simul-taneous malignancy in the epithelium and the con-nective tissue. Our material, with some malignanttumours showing transitional features and sharingthe appearances of 'centrally' and 'peripherally'derived neoplasms, makes a separate histogenesisof the tumours unlikely. In common with Stack-house et al. (1969) we consider that the histo-genesis of the entire group of mixed tumours ofthe lung remains obscure.
We are grateful to the surgeons at the Llandough,Sully, and Frenchay Hospitals for allowing us todescribe patients under their care.We are indebted to Professor E. D. Williams for
his helpful comments in the preparation of this paperand we would like to acknowledge the efforts of Mr.P. Wade, Librarian, Royal Society of Medicine, inobtaining literature from foreign journals. We areindebted to Mr. R. Boothy for the photography.
REFERENCESBarnard, W. G. (1952). Embryoma of lung. Thorax, 7, 299.Barson, A. J., Jones, A. W., and Lodge, K. V. (1968).
Pulmonary blastoma. J. clin. Path., 21, 480.Bauermeister, D. E., Jennings, E. R., Beland, A. H., and
Judson, H. A. (1966). Pulmonary blastoma, a form ofcarcinoma. Amer. J. clin. Path., 46, 322.
Bergmann, M., Ackerman, L. V., and Kemler, R. L. (1951).Carcinosarcoma of the lung. Cancer (Philad.), 4, 919.
Cavin, E., Masters, J. H., and Moody, J. (1958). Hamartomaof the lung. Report of one malignant and three benigncases. J. thorac. cardiovasc. Surg., 35, 816.
Drury, R. A. B., and Stirland, R. M. (1959). Carcino-sarcomatous tumours of the respiratory tract. J. Path.Bact., 77, 543.
Eneroth, C. M. (1964). Histological and clinical aspects ofparotid tumours. Acta oto-laryng. (Stockh.), Suppl. 191.
Fischer, W. (1938). Zur Kenntnis der Lungenkrebse. ActaUn. int. Cancr., 3, 221.
Frank, A. (1915). Ein Karzinosarkom der Lunge. SchmidtsJb. ges. Med., (Erganzungsheft), 322, p. 149.
Goldman, K. P. (1965). Histology of lung cancer in relationto prognosis. Thorax, 20, 298.
Henry, K., and Keal, E. E. (1966). Pulmonary blastoma witha striated muscle component. Brit. J. Dis. Chest, 60, 87.
Hinson, K. F. W. (1958). The spread of carcinoma of thelung. In Carcinoma of the Lung, edited by J. R. Bignall,p. 130. Livingstone, Edinburgh and London.
Kakos, G. S., Williams, T. E., Assor, D., and Vasko, J. S.(1971). Pulmonary carcinosarcoma. J. thorac. cardiovasc.Surg., 61, 777.
Kreyberg, L. (1967). International Histological Classificationof Tumours: No. 1. Histological Typing ofLung Tumours.WHO, Geneva.
Lennox, B. (1960). The pleomorphic adenomata. In RecentAdvances in Pathology, 7th ed., edited by C. V. Harrison,Ch. 1, p. 6. Churchill, London.
Motlik, K., and Triska, J. (1968). Bronchopulmonary carcino-sarcomas. Acta Univ. Carol. Med. (Praha.), 14, 3.
Parker, J. C., Payne, W. S., and Woolner, L. B. (1966).Pulmonary blastoma (embryoma). J. thorac. cardiovasc.Surg., 51, 694.
Peabody, C. N. (1959). Carcinosarcoma of lung of peripheralorigin. J. thorac. Surg., 37, 766.
Priv6, L., Tellem, M., Meranze, D. R., and Chodoff, R. D.(1961). Carcinosarcoma of the lung. Arch. Path.. 72, 351.
Razzuk, M. A., Urschel, H. C., Race, G. J., Arndt, J. H.,and Paulson, D. L. (1971). Carcinosarcoma of the lung.J. thorac. cardiovasc. Surg., 61, 541.
Registrar General (1971). Statistical Review of England andWales for the Year 1969. Part 1. Tables, Medical.H.M.S.O., London.
Saltykow, S. (1914). Beitrage zur Kenntnis des Karzino-sarkoms. Verh. dtsch. path. Ges., 17, 351.
Saphir, O., and Vass, A. (1938). Carcinosarcoma. Amer. J.Cancer, 33, 331.
Selye, H. (1928). tber zwei bemerkenswerte Falle vonKarzinosarkom. Med. Klin., 31, 1197.
Simon, M. A., and Ballon, H. C. (1947). An unusual hamar-toma (so-called chondroma of lung). J. thorac. Surg., 16,379.
Souza, R. C., Peasley, E. D., and Takaro, T. (1965). Pul-monary blastomas. A distinctive group of carcino-sarcomas of the lung. Ann. thorac. Surg., 1, 259.
Spencer, H. (1961). Pulmonary blastomas. J. Path. Bact., 82,161.(1968). Pathology of the Lung, 2nd ed. Pergamon Press,London.
Stackhouse, E. M., Harrison, E. G., and Ellis, F. H. (1969).Primary mixed malignancies of lung: carcinosarcomaand blastoma. J. thorac. cardiovasc. Surg., 57, 385.
Taylor, H. E., and Rae, M. V. (1952). Endobronchialcarcinosarcoma. J. thorac. Surg., 24, 93.
Waddell, W. R. (1949). Organoid differentiation of the fetallung. Arch. Path., 47, 227.
Weber, F. (1939). Ein Karzinosarkom der Lunge. Zbl. allg.Path. u path. Anat., 72, 113.
Willis, R. A. (1962). The Borderland of Embryology andPathology, 2nd ed., p. 386. Butterworths, London.(1967). Pathology of Tumours, 4th ed., p. 138. Butter-worths, London.
673
on 23 June 2018 by guest. Protected by copyright.
http://thorax.bmj.com
/T
horax: first published as 10.1136/thx.27.6.657 on 1 Novem
ber 1972. Dow
nloaded from