Embed Size (px)
Citation preview

Journal ofNeurology, Neurosurgery, and Psychiatry, 1977, 40, 1182-1189
Bilateral occlusion of basilar artery branchesC. MILLER FISHER
From the Neurology Service of the Massachusetts General Hospital and the Department ofNeurology, Harvard Medical School, Boston, Massachusetts, USA
SUMMARY In a case in which the patient became totally paralysed except for blinking andvertical eye movements, microscopic serial sections of the pons showed bilateral infarcts whichwere due to occlusion of two small basilar branch arteries, one on each side. One basilar branchwas occluded by an atheroma lying at its junction with the basilar artery and the other by an
intramural dissection within the wall of the basilar artery. This case provides the clinico-pathological correlation for two further basilar branch infarcts. An unusual finding was thatone of the branch arteries supplied the basis pontis and medulla bilaterally.
The acute onset of total paralysis of the body withpreservation of alertness, blinking, and verticaleye movements generally indicates brainstemischaemia resulting from thrombosis of the basilarartery or the vertebral arteries. It was surprising,therefore, on pathological examination of such acase to find that, although the right vertebralartery was occluded, the basilar and left vertebralarteries were fully patent. Sections of the brain-stem disclosed infarcts in the lower pons bilater-ally which on microscopic examination proved tobe the result of occlusion of two small arterialbranches arising from the lower part of the basilarartery.
Investigation of the vascular anatomy in casesof basilar branch occlusion requires special prep-aration since routine horizontal sectioning of thebrainstem results in disruption of small arterialbranches of the basilar artery. This makes it im-possible to trace in continuity the involved vesselfrom the infarct to its origin from the basilarartery and to identify the nature of the vascularobstruction. Passing a string beneath the basilarartery in order to suspend the brain in formalin isalso contraindicated. We have used the techniqueof sectioning the brainstem frontally, beginningposteriorly in the region of the fourth ventricleand moving forward in thin sections until the in-farct is found. The rest of the brainstem withattached vessels is then embedded as a block inparaffin and serially sectioned. In two previouscases (Fisher and Caplan, 1971) it was possibleusing this method to identify the site and natureof the occlusions. Since it is rarely feasible to com-
This study was supported in part by NINCDS, Grant NS05152.Accepted 16 August 1977
bine in one case a good neurological study and thenecessary special neuropathological investigation,the present single case is reported here.
Clinical details
The patient, a mildly diabetic man aged 71 years,had severe hypertension for 15 to 20 years. Sevenyears before his final admission to hospital, he hadsuccessfully undergone surgery for a dissectingthoracic aneurysm. Two months before, he suf-fered a minor stroke which began with falling andswaying to the right, intermittent diplopia, and aninability to control his feet. Next day his rightarm was numb and slightly weak, and the next dayspeech became dysarthric. On examination at thattime there was weakness of the right side of theface, moderate dysarthria, slight weakness and acerebellar-like ataxia or clumsiness of the rightupper extremity, slight weakness of the right leg,brisker tendon reflexes on the right, a right Bab-inski sign, and listing to the right on walking andon the Romberg test. The blood pressure was200/100 mmHg. All abnormalities except slightdysarthria disappeared in about 10 days.On the day of final admission, the patient
vomited four times and noted dysarthria andweakness of both legs. During the next four hoursthere was tingling in the left arm and toes,choking on liquids and heavy sweating. He hadbeen receiving methyldopa 250 mg three timesdaily and triamterene 100 mg daily. Examinationshowed weakness of the left side of the face,slight weakness of the left arm and leg, moderatedysarthria, and bilateral Babinski signs. On tryingto walk he fell to the left. The blood pressure was
1182
guest. Protected by copyright.
on July 28, 2021 byhttp://jnnp.bm
j.com/
J Neurol N
eurosurg Psychiatry: first published as 10.1136/jnnp.40.12.1182 on 1 D
ecember 1977. D
ownloaded from

Bilateral occlusion of basilar artery branches
240/140 mmHg. Next day dysarthria was severe,the left arm was extremely weak, and the left legdid not move at all. The blood pressure was 190/130 mmHg. Hydralazine 35 mg was given intra-venously and four hours later the blood pressurehad fallen to 120/80 mmHg. The left side wastotally paralysed, and paralysis of conjugate lateralgaze to the right was noted. Atrial fibrillationappeared. Heparin intravenously was begun. Eighthours later, the blood pressure having remainedabout 140/80 mmHg, all limbs were paralysed, andthe patient was mute. Horizontal eye movementswere absent except for abduction of the left eye.
Secretions pooled in the throat. The patientopened and closed his eyes on command. Pinchingeither arm evoked an extensor posture. Bothplantar responses were extensor. The blood pres-sure had risen to 170/80 mmHg. The patient diedon the ninth day.
Neuropathological findings
Gross examination of the brain showed moderateatherosclerosis of the vessels at the base and oc-clusion of the right vertebral artery 5 mm fromthe basilar artery. The basilar artery was patent.
Fig. 1 Recent infarct on rightside of pons. Superficial (A),and deep (B). PTAH X3X.
1183
0M-M-W.. w
. *.:...
40..i
guest. Protected by copyright.
on July 28, 2021 byhttp://jnnp.bm
j.com/
J Neurol N
eurosurg Psychiatry: first published as 10.1136/jnnp.40.12.1182 on 1 D
ecember 1977. D
ownloaded from

C. Miller Fisher
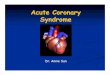
Fig. 2 Diagram of (1) location of infarcts andarrangement of vessels, and (2, 3) occlusions of basilarartery branches. A =recent infarct on right side,B=recent infarct on left, C=older infarct on left,Oc=occlusion of right vertebral artery; (2) branchocclusion of right side, D=dissection, MT=mixtureof fatty macrophages and thrombus; (3) branchocclusion of left side, A T=plaque of atheroma,T= thrombus.
The cerebral hemispheres contained three smalllesions-two petechial haemorrhages, one in theright occipital cortex and one in the posteriorparietal cortex, and a 6X6 mm lacune in the leftparietal white matter. On the assumption that thestrokes were the result of small artery disease ofthe brainstem, the pons and upper medulla weresectioned frontally moving posteroanteriorly asalready described until a softening appeared in thelower pons. The block was then embedded inparaffin and sectioned in a frontal plane. Allsections were stained with phosphotungstic acidhaematoxylin.A small old infarct in the lower basis pontis on
the left side probably accounted for the minorright sided stroke about two months before death.Recent extensive bilateral infarction of the basispontis explained the final illness. This large recentsoftening consisted of two separate parts, one oneach side of the lower pons. The recent infarct onthe left side was in the same vascular territoryas the old infarct of which it appeared to be anextension. This combined old and recent infarc-tion resulted from occlusion of a small branch ofthe lower basilar artery. The recent infarct onthe right side was due to occlusion of a small
median branch of the basilar artery at its bifurca-tion. It was noteworthy that this infarct extendedacross the midline to involve several millimetresof tissue of the opposite side-that is, a singlebranch artery supplied a segment of the lowerbrainstem bilaterally.
RECENT INFARCT ON RIGHT SIDEThis infarct (Figs. IA and IB, and Fig. 2), whichwas in a premacrophage stage of evolution, lay inthe lowermost pons and the adjacent upper 2.5mm of the medulla oblongata. It measured ap-proximately 11 mm transversely, 8 mm vertically,and 14 mm anteroposteriorly. It was irregular inshape and narrowed posteriorly. The downwardcoursing corticospinal fibres were interruptedmainly within the pons. The right medullarypyramid was extensively damaged while the leftpyramid showed a 4X3 mm softening (Fig. IB) inaddition to scattered smaller infarcts 1-2 mm inextent. Deep in the pons the infarct also crossedthe midline by about 3 mm.The small arteries running within the infarcted
tissue were traced proximally to their origin froma single small artery which coursed through thesubarachnoid space to arise from the posterioraspect of the basilar artery in the midline (Fig. 2).Measuring about 500 ,um in diameter at its origin,the branch ran upwards for a few millimetres inthe anterior median fissure of the medulla be-tween the pyramids to enter the foramen caecumin whose depths it divided into a spray of some15 or 20 small vessels which supplied all regionsof the infarct bilaterally.The arterial branch was occluded for a distance
of one millimetre from its origin from the basilarartery by a mixture of fatty macrophages, redblood cells and thrombus that was undergoingfibroblastic organisation, a process that appearedto be older than a few days (Fig. 3A). Furtherdistally the artery was normal and blood-contain-ing. Where the branch traversed the wall of thebasilar artery it entered a subintimal plaque offibrous atheroma 2 mm thick. Here the arteryappeared to be disrupted by a small mass of redblood cells that extended for 2 to 5 mm hori-zontally within the plaque, creating a crevice oflocal dissection 0.2 mm wide and approximately0.5 mm vertically (Fig. 3B). The dissection whichlay between the inner two-thirds and outer thirdof the plaque did not communicate with the lumenof the basilar artery. A small patent blood-con-taining channel which could be traced throughthe inner portion of the plaque probably was theremainder of the intramural course of the branch.It was difficult to interpret the occlusive process.
1184
guest. Protected by copyright.
on July 28, 2021 byhttp://jnnp.bm
j.com/
J Neurol N
eurosurg Psychiatry: first published as 10.1136/jnnp.40.12.1182 on 1 D
ecember 1977. D
ownloaded from

Bilateral occlusion of basilar artery branches
.*I .'...-zz.teS'6 w-
VIV7 M.-*A
.~~~~~~~~~~RA^
Fig. 3 Basilar branch corresponding to infarct in Fig. I and A in Fig. 2 occludednear its origin (A), and disrupted intramurally at site of dissection (B).BA-=basilar artery. Br-branch, D=dissection. PTAH XSO.
1185
guest. Protected by copyright.
on July 28, 2021 byhttp://jnnp.bm
j.com/
J Neurol N
eurosurg Psychiatry: first published as 10.1136/jnnp.40.12.1182 on 1 D
ecember 1977. D
ownloaded from

C. Miller Fisher
One possibility was that the vessel had becomeseverely narrowed by a lipid-macrophage atheromainto which a local haemorrhage had occurredproducing the mixture described. Or possiblytrauma had damaged the small branch in its intra-mural portion resulting in haemorrhage and localdissection. Microdissection of this type in the wallof the basilar artery has not been encounteredpreviously.Comment This recent infarct corresponded withthe first part of the final stroke, namely, a severeleft hemiplegia and right lateral gaze palsy, pre-ceded by dysarthria, vomiting, sweating, andtingling in the left arm and toes. These manifesta-tions, except for weakness and dysarthria, reflect
A
penetration of the ischaemia into the tegmentumof the pontomedullary border zone. Profuse sweat-ing is a not uncommon feature of pontine ischae-mia. The report of weakness of both legs at theonset could be the result of the bilateral pyramidallesions. When the final stroke approached itsheight, the only horizontal eye movement wasabduction of the left eye, a state which has beenreported previously as a transient occurrenceassociated with a lacunar infarct in the lower pons(Fisher, 1967).The pathological findings were of special interest
in that a single basilar branch supplied the brain-stem bilaterally although predominantly on oneside. This is probably the first time this pattern of
Fig. 4 A shows old infarct on lef tside, B recent infarct on left side. A issuperficial, B is deep. PTAH X31.
1186
guest. Protected by copyright.
on July 28, 2021 byhttp://jnnp.bm
j.com/
J Neurol N
eurosurg Psychiatry: first published as 10.1136/jnnp.40.12.1182 on 1 D
ecember 1977. D
ownloaded from

Bilateral occlusion of basilar artery branches
blood supply has been demonstrated and may ex-plain unexpected bilateral brainstem signs whenthe arteries are angiographically patent or onlyone vertebral artery is occluded.
SMALL OLD INFARCT ON LEFT SIDEThis infarct which showed numerous large macro-phages and fine fibrillar connective tissue wasseveral weeks old and correlated best with theslight right sided stroke. It lay in the lowermostpons on the left side (Fig. 4A) and measured7 mm transversely, 3 mm vertically and 3 to 6 mmanteroposteriorly, extending further posteriorly inits superior portion. The vessels supplying theterritory of this infarct were readily traced to asmall artery approximately 300 ,um in diameterwhich ran in the subarachnoid space to join an-other artery of about the same size about 5 mmbefore the resulting common trunk entered thelateral aspect of the basilar artery about 3 mmabove the lower bifurcation (Fig. 2). The 'otherartery' was the artery which supplied the territoryof the recent left sided infarct to be describednext.Comment The clinical manifestations associatedwith this old softening in the lower pons includedslight weakness of the face, arm, and leg on theright side, moderate dysarthria, transient diplopia,listing to the right, numbness of the right arm,cerebellar-like ataxia of the right upper extremity,and increased tendon reflexes and a Babinski signon the right side. The mechanism by which poweron the right side of the body is diffusely but onlyslightly reduced is not readily explained, but alimited ischaemia of the entire cross-section of thecorticospinal system may be the answer. The com-bination of ipsilateral hemiparesis and ataxia isalso of obscure origin although recognised as asign at times of unilateral involvement of thebasis pontis. Diplopia and numbness are indicativeof tegmental involvement. It is of interest that theneurological deficit disappeared despite the per-manent anatomical damage.The infarct accurately conformed to the vascu-
lar territory of one of two divisions of a basilarbranch artery which itself was occluded. Thisarrangement suggests a local embolus to thepatent branch from the parent artery but thestroke apparently evolved in two days, unlikeembolism.
LARGE RECENT INFARCT ON LEFT SIDEAs already mentioned, this infarct was in thesame region as the small old infarct describedabove, which it more or less surrounded and ex-tended. It lay in the lowermost basis pontis
anteriorly and medially, measuring 9 mm trans-versely, 6 mm vertically, and 10 mm antero-posteriorly (Fig. 4B). It did not cross the midline.Its vessel of supply which penetrated the ponsclose to the midline was traced back to its junctionwith the branch supplying the other part of thesmall old infarct.The common trunk which measured about 500
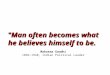
,um in diameter was traced through the subarach-noid space to its origin from the basilar artery. Atthis point and extending intramurally for a shortdistance, the branch was almost obliterated by apure lipid atheroma 1 mm in length depositedupon which was a fibrin micro-thrombus whichoccluded the remaining lumen-a typical 'junc-tional' occlusion (Figs. 5A, B).Comment This infarct obviously accounted forthe final right sided hemiplegia which when addedto the left hemiplegia resulted in complete paraly-sis of the body.The vascular lesion consisted of a bead of
atheroma with a superimposed micro-thrombus.Both old and recent infarcts lay in the territoryof supply of the basilar branch and the presenceof infarcts of different ages in the two divisions ofthe branch is puzzling. As already mentioned,local embolism may have occurred. Another possi-bility is that complete occlusion of the branch wasprecipitated by excessive lowering of the patient'sblood pressure; or collateral flow compensated forthe occlusion until the blood pressure fell abruptly.No subarachnoid anastomotic connections werepresent, and any collateral flow would have tohave been at the capillary level.
Discussion
The principal points for discussion have been in-cluded in the comments above and only a fewfurther observations remain to be made.
It should be emphasised that the occlusion ofthe right vertebral artery was more than 5 mmremoved from the involved basilar branches and,therefore, in all probability could not have beena factor in the infarcts.The clinical picture in this case was one which
would ordinarily have conjured up the diagnosisof a massive pontine lesion, especially of the basispontis. That two strategically placed basilarbranch infarcts could evoke a similar catastrophicparalysis is an unusual occurrence which must beadded to diagnostic considerations.The clinicopathological findings are of special
interest in that the manifestations of two furtherbrainstem or lacunar infarcts are provided to addto the two previously described (Fisher and
E
1187
guest. Protected by copyright.
on July 28, 2021 byhttp://jnnp.bm
j.com/
J Neurol N
eurosurg Psychiatry: first published as 10.1136/jnnp.40.12.1182 on 1 D
ecember 1977. D
ownloaded from

C. Miller Fisher
Br-
OCCL
NNA
-AM~ ~ ~ ~
~* ,, ~'-z "̂ < iZA
e > $ ; o 4 ; ; ... ff ffi r e31rIl
I7.V
.4.
!L.W.p ,* } - * v j .............................................................. 4' g:-..'
4 s 4s*vS'WQ"^A'*.^. 4 .........................................................................^.^:*' A , 9 £t0v@X s
S z * w ' ¢ i ~~~~~~~~~~V . t.3
Caplan, 1971). The main features have alreadybeen commented on and further discussion isunnecessary.The two vascular lesions exemplify the two
main types of branch occlusion described thus far(Fisher and Caplan, 1971), one an occludingatheroma at the junction of branch and basilarartery, and the other an interruption of thebranch within the wall of the basilar artery at thesite of an atheroscle-rotic basilar plaque. This is
Fig. 5 Basilar branch arterycorresponding to infarct inFig. 4, and B and C Fig. 2.A =occlusion near basilarartery. PTAH X45; B=highpower view of atheroma.PTAH X290.
the first time that a dissection in the basilar wallwas a factor, apparently compressing the branchas it traversed the wall. The beads of atheromawhich are deposited in basilar branch arteries inthe presence of hypertension consist almostentirely of foamy, fatty macrophages, an appear-ance which emphasises for the pathologist thefundamental role of lipid in atherosclerosis.
It is worth mentioning again that in this case itwas demonstrated that a single paramedian pene-
1188
guest. Protected by copyright.
on July 28, 2021 byhttp://jnnp.bm
j.com/
J Neurol N
eurosurg Psychiatry: first published as 10.1136/jnnp.40.12.1182 on 1 D
ecember 1977. D
ownloaded from

Bilateral occlusion of basilar artery branches
trating branch of the basilar artery straddled themidline to supply central regions of the basispontis and medulla bilaterally. It occasionallyhappens that in a minor brainstem stroke withbilateral manifestations, angiography which doesnot opacify small-calibre penetrating branchesfails to show a vascular lesion and it may besuspected on the present evidence that a branchocclusion is responsible. In the present case, one
of the branch vessels entered the 'foramencaecum', a portal of entry which allows smallarteries to reach the brainstem tegmentum directlywithout first penetrating the basis pontis or
pyramids. Adequate clinicopathological studies insuch cases are lacking.
Finally, the hazards of precipitously loweringthe blood pressure during the acute stage of a
thrombotic stroke may be illustrated in this casenot only by the disastrous clinical course but alsoby the pathological finding of an old and a recentinfarct in the territory of a single basilar arterybranch. It is our practice to avoid hypotensiveagents in ischaemic brain disease and allow theblood pressure to settle naturally.
References
Fisher, C. M. (1967). Some neuro-ophthalmologicalobservations. Journal of Neurology, Neurosurgery,and Psychiatry, 30, 383-392.
Fisher, C. M., and Caplan, L. R. (1971). Basilar arterybranch occlusion: a cause of pontine infarction.Neurology (Minneapolis), 21, 900-905.
1189
guest. Protected by copyright.
on July 28, 2021 byhttp://jnnp.bm
j.com/
J Neurol N
eurosurg Psychiatry: first published as 10.1136/jnnp.40.12.1182 on 1 D
ecember 1977. D
ownloaded from