-
End-of-life care in the pediatric intensive care
unit: research review and recommendations
Jeffrey P. Burns, MD, MPHa,*,Cynda Hylton Rushton, DNSc, RN,
FAANb
aMedical-Surgical Intensive Care Unit, Childrens Hospital
Boston, 300 Longwood Avenue,
Boston, MA 02115, USAbPhoebe Berman Bioethics Institute, Harriet
Lane Compassionate Care Program School of Nursing,
525 N. Wolfe Street, Box 420, Baltimore, MD 21205-2110, USA
In the United States, most children die in hospitals, typically
in a critical care
setting [1,2] About 55,000 children die each year in America,
more than half
of them in the first year of life [1]. Beyond infancy,
unintentional injuries,
congenital anomalies, malignant neoplasms, and intentional
injuries are the
leading causes of death. Although this distribution of the
underlying causes for
pediatric deaths has remained relatively stable over the last 20
years, what is
changing, are the events leading to the death of a child. The
success of critical
care medicine in the last 25 years has meant that the
progression of many
disorders can be forestalled but not permanently reversed. In
many instances
families and clinicians must weigh the benefits and burdens of
ongoing life-
sustaining treatments. Indeed, the most recent observational
studies of death in
the pediatric intensive care unit (PICU) reveals that 40% to 60%
of all deaths
occur following a decision to limit life-sustaining therapies
[3,4]. End-of-life care
is receiving increased scrutiny from all aspects of our society
and profession [5].
The recent Institute of Medicine report calls for sweeping
improvements to
address current gaps in care [1]. To address these gaps, several
national initiatives
are addressing various aspects of pediatric palliative care. The
Initiative for
Pediatric Palliative Care (IPPC) has conducted research,
provided technical
assistance to childrens hospitals developing new quality
improvement initiatives,
Crit Care Clin 20 (2004) 467485and completed a comprehensive,
interdisciplinary curriculum [6].
The National Hospice and Palliative Care Organization has also
developed
educational materials targeted to hospices [7]. In addition, a
curriculum specifi-
0749-0704/04/$ see front matter D 2004 Elsevier Inc. All rights
reserved.
doi:10.1016/j.ccc.2004.03.004
* Corresponding author.
E-mail address: [email protected] (J.P. Burns).
-
agreed or strongly agreed that withholding and withdrawing are
ethically the
same (P < 0.001). Physicians were more likely than nurses to
report that familiesare well informed about the advantages and
limitations of further therapy (99%
versus 89%, P < 0.003); that ethical issues are discussed
well within the team
(92% versus 59%, P < 0.0003), and that ethical issues are
discussed well with
the family (91% versus 79%, P < 0.0002). On multivariable
analyses, this study
found that fewer of years of practice in pediatric critical care
was the only
clinician characteristic associated with attitudes on
end-of-life care dissimilar to
the consensus positions reached by national medical and nursing
organizations on
these issues. The investigators found no association between
clinician character-
istics such as their political or religious affiliation,
practice related variables such
as the size of their intensive care unit (ICU) or the presence
of residents and
fellows, and particular attitudes about end-of-life care.
One notable finding of this national survey was that the
attitudes and reportedcally targeted to pediatric nurses has been
developed as part of the End-of-Life
Nursing Education Consortium project [8] and Childrens Hospice
International
is working with the Center for Medicaid and Medicare Services to
encourage
more coordination of care for children and families across the
continuum of care.
Taken together, these efforts reflect burgeoning clinical and
behavioral research
leading to organizational and educational initiatives to improve
the quality of care
in this area [9,10]. Indeed, increased accountability for the
quality of end-of-life
care provided demands that actual practice in this important
area of pediatric
critical care medicine receive more rigorous examination than in
years past [11].
Our goal here is to review the empirical data that exists on
end-of-life care in the
PICU and to address some of the practical aspects of providing
this care.
The literature on end-of-life care in the pediatric intensive
care unit
Attitudes of pediatric critical care physicians and nurses on
end-of-life care
Several studies have examined attitudes of critical care
clinicians and provide
insights into the current quality of end-of-life care in
pediatric intensive care
units. One of the largest studies on end-of-life care in the
Pediatric intensive care
unit was a three-part investigation recently reported as a
series of special articles
in the journal Critical Care Medicine [3,12,13]. The first part
was a survey of the
attitudes and practices of pediatric critical care clinicians on
end-of-life care from
a random sample of clinicians at 31 pediatric hospitals in the
United States [12].
The survey was completed by 110 of 130 (85%) pediatric critical
care attending
physicians and 92 of 130 (71%) pediatric critical care nurses.
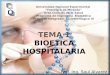
As seen in Tables 1
and 2, no physician or nurse agreed with the statement that
withholding and
withdrawing life support is unethical. More physicians (78%),
than nurses (57%)
J.P. Burns, C.H. Rushton / Crit Care Clin 20 (2004)
467485468practices of these pediatric critical care practitioners
were in alignment with the
existing theory on how clinicians should behave. Two thirds of
pediatric critical
care physicians and nurses reported attitudes about end-of-life
practice in strong
-
Table 1
Clinicians attitudes toward end-of-life care
Physicians, % Nurses, % P-value
Percentage of respondents who agreed or strongly agreed with the
statement:
J.P. Burns, C.H. Rushton / Crit Care Clin 20 (2004) 467485
469agreement with the ethical and legal consensus that has evolved
in these areas.
Further, over 90% of physicians and nurses cited
patient-centered variables as the
most important determinants of decision making about
life-sustaining treatments,
and the majority rated as less important nonpatient-centered
variables such as
financial costs to society or ICU bed availability. Both
physicians and nurses
were far more likely to rate as important in decision-making
quality-of-life
considerations from the perspective of the patient and family
rather than the
(On a scale where 1 = strongly disagree, 2 = disagree, 3 =
neutral, 4 = agree, 5 = strongly agree)
Withholding or withdrawing
life support is unethical.
0 (1.15 0.39) 0 (1.24 0.43) 0.09
Withholding is more
ethical than withdrawing.
5 (1.67 0.89) 18 (2.45 0.99) 0.0001
Withdrawing is more ethical
than withholding.
7 (1.77 0.99) 9 (2.51 0.87) 0.0001
Withholding and withdrawing
are ethically the same.
78 (4.16 1.06) 57 (3.43 1.13) 0.0001
Percentage of respondents, in answering the question How
important are the following factors in
influencing your decision on the extent of life support therapy
to provide a patient? who rated the
following variables as important or very important (On a scale
where 1 = not important, 2 = less
important, 3 = neutral, 4 = important, 5 = very important)
Quality of life as viewed by the patient 99 (4.60 0.64) 99 (4.77
0.42) 0.05
Quality of life as viewed by the family 95 (4.39 0.72) 96 (4.49
0.69) 0.24
Patient unlikely to survive 94 (4.08 0.96) 91 (4.07 1.00)
0.98
Potential for neurologically intact survival 81 (4.12 0.85) 77
(4.33 0.79) 0.06
Quality of life with a chronic disorder 61 (3.50 0.99) 73 (3.85
1.09) 0.009
Fear of litigation or breaking the law 23 (2.46 1.12) 32 (2.91
1.10) 0.002
Financial costs to society 13 (2.19 1.00) 33 (2.82 1.18)
0.0002
ICU bed availability 3 (1.32 0.71) 4 (1.50 0.85) 0.05
Percentage of respondents, in answering the question If the
circumstances for withdrawing life
support are indicated, do you think the following medications
should be added or increased in the
patients regimen as life support is discontinued? who responded
frequently or always to the
following variables.
(On a scale where 1 = never, 2 = infrequently, 3 = sometimes, 4
= frequently, 5 = always)
Narcotics 74 (3.96 0.75) 86 (4.26 0.69) 0.005
Benzodiazepines 62 (3.70 0.72) 66 (3.84 0.94) 0.15
Barbiturates 24 (2.70 1.03) 27 (2.97 0.97) 0.07
Neuromuscular blocking agents
(ex. Pavulon)
2 (1.28 0.68) 2 (1.53 0.81) 0.10
Percentages represent respondents who answered with scores of 4
or 5, on a five-point scale shown.
Numbers in parentheses are group mean scores SD. P-values are
for the comparison between
physician and nurse responses by Wilcoxon rank sums.
Data from Burns JP, Mitchell C, Griffith JL, Truog RD.
End-of-life care in the pediatric intensive care
unit: attitudes and practices of pediatric critical care
physicians and nurses. Crit Care Med 2001;29(3):
65864.
-
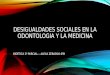
Table 2
Clinicians reports of actual end-of-life practices in their
ICU
Physicians, % Nurses, % P-Value
In your experience, who usually initiates the discussion to
limit life-sustaining treatment?
(On a scale where 1 = never, 2 = infrequently, 3 = sometimes, 4
= frequently, 5 = always)
Physicians 96 (4.05 0.40) 86 (4.00 0.53) 0.35
Nurses 28 (2.95 0.78) 55 (3.41 0.74) 0.0001
Family 4 (2.56 0.56) 4 (2.61 0.57) 0.56
Other (clergy, consultants) 1 (1.75 0.61) 1 (1.79 0.71) 0.86
Who else, if anyone, do you consult when making decisions about
limitations of life support on
patients in your PICU?
(On a scale where 1 = never, 2 = infrequently, 3 = sometimes, 4
= frequently, 5 = always)
Hospital legal representatives 6 (1.89 0.80) 4 (2.08 0.77)
0.05
Hospital ethics committee 8 (2.28 0.85) 7 (2.46 0.77) 0.20
Other clinicians from within the unit 66 (3.78 0.91) 57 (3.54
1.02) 0.09
Clinicians outside the unit 8 (2.27 0.98) 9 (2.14 0.93) 0.44
At the time that withholding and withdrawing life support is
discussed, how would you rate the
following areas as it is practiced in your unit?
(On a scale where 1 = strongly disagree, 2 = disagree, 3 =
neutral, 4 = agree, 5 = strongly agree)
Families are well informed about prognosis 100 (4.86 0.34) 97
(4.67 0.61) 0.01
Families are well informed about the advantages
and limitations of further therapy
99 (4.77 0.48) 89 (4.47 0.80) 0.003
The ethical issues for each patient are
well discussed within the care team
92 (4.39 0.69) 59 (3.80 1.14) 0.0003
The ethical issues for each patient are well
discussed between the care team and family
91 (4.40 0.76) 79 (3.98 0.91) 0.0002
If the family insists on continuing life support, even if the
care team concludes that further
therapy is futile, what is the usual response as it is practiced
in your unit?
(On a scale where 1 = never, 2 = infrequently, 3 = sometimes, 4
= frequently, 5 = always)
We continue for a short time for them to reconsider,
but then we terminate life support unilaterally
1 (1.21 0.51) 3 (1.74 0.87) 0.01
We continue for a short time for them to reconsider,
but then we transfer care to another institution
1 (1.55 0.70) 3 (1.56 0.79) 0.79
We withdraw life support without the
agreement of the family, after consultation
with the hospital ethics or legal representatives
1 (1.21 0.58) 0 (1.37 0.55) 0.40
We continue to provide life support for as long as
requested, and usually, through ongoing
discussions, a consensus between the family
and care team is reached
93 (4.17 0.65) 88 (4.08 0.68) 0.27
When life support is withdrawn, how involved is the physician in
the actual process at the bedside?
(On a scale where 1 = never, 2 = infrequently, 3 = sometimes, 4
= frequently, 5 = always)
100 (4.87 0.34) 84 (4.35 0.77) 0.0001
Percentages represent respondents who answered with scores of 4
or 5, on a five-point scale shown.
Numbers in parentheses are group mean scores SD. P-values are
for the comparison between
physician and nurse responses by Wilcoxon rank sums.
Data from Burns JP, Mitchell C, Griffith JL, Truog RD.
End-of-life care in the pediatric intensive care
unit: attitudes and practices of pediatric critical care
physicians and nurses. Crit Care Med 2001;
29(3):65864.
J.P. Burns, C.H. Rushton / Crit Care Clin 20 (2004)
467485470
-
statement quality of life with a chronic disorder. In accordance
with published
consensus recommendations, quality-of-life determinations,
especially when con-
sidered as a factor in the decision to forego life-sustaining
treatment, should
only be judged from the patients perspective, and not by health
care workers
personal assessments. Finally, over two thirds of physicians and
nurses were
willing to add or increase analgesia and sedation to a patients
regimen as life-
sustaining treatment is discontinued, a position also consistent
with a series of
recent recommendations from national medical organizations [12].
A large
majority of physicians and nurses did not agree with the
addition of neuromus-
cular blocking agents, medications devoid of any sedative or
analgesic proper-
ties, as life-sustaining treatment is discontinued, a view again
in keeping with
recent recommendations on this issue put forth by the Society of
Critical Care
Medicine [14].
However, this national survey study also found that pediatric
critical care
clinicians with fewer years of experience espoused attitudes and
practices that are
divergent with consensus recommendations on these issues. For
example, this
study found an association between fewer years of experience as
practitioners of
pediatric critical care and a greater reluctance to withdraw
life-sustaining
treatment and a greater reluctance to administer analgesics or
sedatives as life-
sustaining treatment is withdrawn [12]. Previous studies have
also found that less
experienced clinicians are less willing to forgo life-sustaining
treatment. Cook
et al reported that, among ICU attending staff, house staff and
nurses in 37
Canadian university-affiliated hospitals, the longer the
duration since graduation,
the less likely clinicians were to offer aggressive care in
response to 12 different
clinical scenarios [15].
Unlike previous research that has demonstrated that physicians
caring for adult
patients frequently make treatment decisions based on their own
personal values
rather than patient-centered factors, this study of pediatric
critical care practi-
tioners found no evidence that decision making is significantly
influenced by the
clinicians religious beliefs, religiosity, specialty, age, or
practice locale. Burns
et al speculated that although it is possible that the
less-experienced physicians
and nurses are aware of recommendations and consensus statements
regarding
life-sustaining treatments and simply disagree with them, it is
more likely that
they are unfamiliar or uncomfortable with these issues [12]. In
support of this,
other data from the medical literature demonstrates that both
physicians and
nurses are often not well trained in end-of-life patient
management. A study of
115 medical residents at three teaching hospitals found that one
third of them
reported that they had never been supervised discussing
do-not-resuscitate
discussions with patients [16]. These deficiencies have also
been noted in the
education of nurses. The American Association of Colleges of
Nursing consensus
group concluded that there were major deficiencies, or complete
neglect, of end-
of-life content in nursing curricula [17]. More than half of 300
nurses at an acute
J.P. Burns, C.H. Rushton / Crit Care Clin 20 (2004) 467485
471care teaching hospital for adult patients reported that they did
not have a good
understanding of advance directives [18]. In addition, there are
special issues that
should receive particular attention. For example, a survey
conducted by Solomon
-
et al found that 37% of pediatric specialists and 44% of nurses
caring for
critically ill or dying children believed that Even if life
supports such as
mechanical ventilation and dialysis are stopped, medically
supplied food and
water should always be continued [9]. These beliefs are contrary
to published
guidelines permitting the forgoing of artificial nutrition and
hydration in pediatric
end-of-life care [19,20].
The data revealing inadequate training of clinicians in ethical
concerns as-
sumes even greater importance because the pediatric critical
care clinicians in
the national survey reported a relatively insulated process of
decision making
[12]. Respondents stated that discussions to limit
life-sustaining treatment are
typically initiated by the pediatric critical care clinicians.
Further, in less than
10% of cases are clinicians outside of the ICU, hospital
ethicists, or legal rep-
resentatives consulted for advice on these matters; yet a
majority of respondents
stated that they do consult with other clinicians within the ICU
for advice on
these issues. It could not be determined from this study whether
the less-
experienced pediatric critical care clinicians seek advice for
these pivotal de-
cisions from their more senior colleagues.
The national survey of pediatric critical care physicians and
nurses also found
that significant perceptual differences exist between physicians
and nurses on the
quality of end-of-life care as it is actually practiced [12].
Compared with
physicians, nurses were significantly less likely to report that
ethical issues are
well discussed within the care team, between the care team and
family, or that
families are well informed about the advantages and limitations
of further
therapy. For example, 92% of physicians reported that ethical
issues for each
patient were well discussed with the care team, while only 59%
of nurses thought
so. In addition, nearly one out of five pediatric critical care
nurses reported
that physicians are not always or frequently at the bedside as
life-support
is withdrawn.
Other studies that have reported nurses feeling disenfranchised
in the decision-
making process and dissatisfied with the level of support for
families facing end-
of-life decisions for their childrendespite, or perhaps because
of the fact that
nurses bear major responsibility for implementing end-of-life
decisions, provid-
ing terminal care and helping families through their childs
death. Using
qualitative methods, Oberle and Hughes identified and compared
Canadian
doctors and nurses perceptions of ethical problems related to
their work in
adult oncology [21]. They concluded that the most pressing
ethical problem at the
end of life was witnessing and responding to the suffering of
others, and that it
created significant moral burden for each group. These
investigators postulated
that differences in responses of each discipline were a function
of their pro-
fessional role rather than differences in ethical reasoning or
moral orientation.
The primary differences were because doctors are responsible for
making
decisions and nurses must live with and carry out the decisions.
In response to
J.P. Burns, C.H. Rushton / Crit Care Clin 20 (2004)
467485472moral quandaries and the associated distress, each group
approached the issues
through a lens of competing values, hierarchical processes,
scarce resources, and
communication patterns [21].
-
Observational studies of clinical practice regarding death in
the pediatric
intensive care unit
A common concern with surveys of attitudes is that the responses
may reflect
only what the clinicians believe, or want to believe, but not
actually how they
behave. Yet, there is emerging data on how clinicians actually
provide care in this
context. In the past 5 years several studies have examined the
actual practices of
critical care physicians and nurses in providing end-of-life
care in the pediatric
intensive care unit. For example, Part II of the Boston study
was an observational
study of 53 consecutive patients who died following the
withdrawal of life-
sustaining treatment in the PICU at three teaching hospitals
[3]. Data on the
reasons why medications were given were obtained from a
self-administered,
anonymous questionnaire completed by the critical care physician
and nurse for
J.P. Burns, C.H. Rushton / Crit Care Clin 20 (2004) 467485
473each case. Data on what medications were given were obtained
from a review of
the medical record.
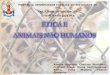
As seen in Table 3, the investigators found that sedatives or
analgesics were
administered to 47 (89%) patients who died following the
withdrawal of life-
sustaining treatment. Patients who were comatose were less
likely to receive
these medications. Physicians and nurses cited treatment of
pain, anxiety, and air
hunger as the most common reasons, and hastening death as the
least common
reason, for administration of these medications, as seen in
Table 4. The mean
dose of sedatives and analgesics administered nearly doubled as
life support was
withdrawn, and the degree of escalation in dose did not
correlate with clinicians
views on hastening death. These investigators concluded that the
clinicians in this
study frequently escalate the dose of sedatives or analgesics to
dying patients as
life-sustaining treatment is withdrawn, citing patient-centered
reasons as their
principle justification, and were satisfied with the care
provided.
Hastening death was viewed by the pediatric critical clinicians
in this study
as an unintended consequence of appropriate care. This line of
reasoning is fre-
Table 3
Mean dose of benzodiazepines and opiates administered to
patients around the withdrawal of life-
sustaining treatment
24 hours before
withdrawal
4 hours before
withdrawal
4 hours after
withdrawal
24 hours after
withdrawal
Benzodiazepine dose:
mg/kg/ha0.54 0.59 0.98 1.4
(diazepam equivalents) n = 44 n = 44 n = 44 n = 6
Opiate dose: mg/kg/ha 0.54 0.55 1.00 1.80
(morphine equivalents) n = 41 n = 44 n = 46 n = 4
a Comparison of doses 4 hours prior to withdrawal of
life-sustaining treatment with doses 4 hours
after withdrawal of life-sustaining treatment, P < 0.0001 by
Wilcoxon matched-pairs signed-ranks test.Data from Burns JP,
Mitchell C, Outwater KM, Geller M, Griffith JL, Todres ID, et al.
End-of-life care
in the pediatric intensive cave unit after the forgoing of
life-sustaining treatment. Crit Care Med
2000;28(8):30606.
-
Table 4
Clinicians rationale for managing patient discomfort as
life-sustaining treatment was withdrawn
Among patients who did receive palliative medications (n =
47)
Decrease
pain
Decrease
anxiety
Decrease
air hunger
Comfort
family
Hasten
death
Ordered by physicians 89% (42) 89% (42) 85% (40) 66% (31) 4%
(2)
Administered by nurses 87% (41) 81% (38) 79% (37) 77% (36) 6%
(3)
Physician/nurse paira,b 83% (39) 77% (36) 74% (35) 49% (23) 2%
(1)
Among patients who did not receive palliative medications (n =
6)
Patient was in
vegetative state
Patient appeared
comfortable
Pain control was
unethical in this case
Physician/nurse paira 100% (6) 100% (6) 0% (0)
a Percentages of physiciannurse matched pairs that
agreed/strongly agreed with reasons for
administering medications at time of treatment withdrawal.
Numbers are in parentheses.b Among matched pairs not in agreement,
differences between physicians and nurses not sig-
nificant (P > 0.05) by McNemar chi square.
Data from Burns JP, Mitchell C, Outwater KM, Geller M, Griffith
JL, Todres ID, et al. End-of-life care
in the pediatric intensive cave unit after the forgoing of
life-sustaining treatment. Crit Care Med 2000;
28(8):30606.
J.P. Burns, C.H. Rushton / Crit Care Clin 20 (2004)
467485474quently attributed to the ethical principle of double
effect, which distinguishes
between prohibited death causing and permitted death-hastening
analgesic
administration to terminally ill patients. According to this
principle, clinicians are
permitted to give sedatives and analgesics to dying patients,
despite the foreseen
risk of possibly hastening death as a result of the medications,
provided the
intention is to relieve the patients pain and suffering and not
to cause the
patients death [22]. Wilson et al found that 75% of adult
patients from whom life
support was withheld or withdrawn at two San Francisco teaching
hospitals
received nearly a threefold increase in sedatives, analgesics,
or both during this
process [23]. Clinicians in the Wilson series justified this
practice principally to
decrease pain, anxiety, and air hunger. Similarly, the only
patients in the Wilson
series who did not receive sedatives or analgesics during
life-support withdrawal
were those judged to be deeply comatose. Wilson et al also found
a high rate
of agreement between physicians and nurses on satisfaction with
the care
provided, and the tendency of clinicians to appeal to double
effect reasoning to
justify their practice.
Part II of the Boston Study, an observational study of death in
the PICU, also
found that in 13% of cases there was dissatisfaction with the
care provided, and in
each instance it was the nurse who reported a concern that the
amount of sedation
and analgesia provided was inadequate [3]. In a similar study at
the Cleveland
Clinic, Daly found that 10% of 39 nurses caring for adult
patients following the
withdrawal of mechanical ventilation were also dissatisfied with
the level of
patient comfort achieved [24]. These data suggest that in a
significant minority
-
of cases involving dying patients in the ICU following the
forgoing of life-
sustaining treatment, nurses have very different perceptions of
the quality of
comfort care provided. Whether these data reflects variability
in clinicians
perception of suffering or systematic problems related to
untreated discomfort
remains unknown.
Parental perspectives on end-of-life care in the pediatric
intensive care unit
Bereaved parents are in a unique position to comment on current
practice in
end-of-life care. Indeed, gaining an understanding of the
perspectives of the
family on the dying process is an essential step in
understanding the quality of
care provided. Part III of the Boston study sought to identify
priorities for quality
end-of-life care from the parents perspective by surveying the
bereaved parents
of the children who died in Part II of the study [13]. In 90% of
cases, physicians
first raised withdrawal of life support, although nearly half of
parents had con-
sidered it independently. Among decision-making factors, as seen
in Table 5,
parents rated the quality of life, likelihood of improvement,
and pain as most
important. Twenty percent of parents disagreed that their
children were comfort-
able in their final days. Fifty-five percent of parents felt
that they had little to no
control during their childs final days, and nearly a quarter
reported that, if able,
J.P. Burns, C.H. Rushton / Crit Care Clin 20 (2004) 467485
475they would have made decisions differently. There were
significant differences
(P < 0.001) between the involvement of family, friends, and
staff members at the
Table 5
Factors important to parental end-of-life decision making
Factors N
% Parents who rate
as very important Mean (SD)
My childs quality of life 55 81.8% 4.75 (0.67)
My childs chance of getting better 55 78.2% 4.75 (0.52)
My childs pain or discomfort 55 76.4% 4.64 (0.78)
My child was unlikely to
survive hospitalization
53 69.8% 4.49 (0.95)
What I believe my child would
have wanted
52 53.8% 4.08 (1.22)
Information that the hospital staff provided 55 45.5% 4.22
(0.83)
My religious/spiritual beliefs 55 30.9% 3.00 (1.71)
The way my child looked or behaved 52 30.8% 3.50 (1.36)
Advice the hospital staff provided 56 28.6% 3.82 (0.99)
The attitudes of hospital staff 54 22.2% 3.07 (1.46)
Advice family and friends provided 53 5.7% 2.66 (1.25)
The financial costs 55 0% 1.22 (0.69)
Factors were rated by parents on a 15 scale (1 = not important,
5 = very important). Significantdifferences (P < 0.001) were
found on one-way weighted least squares analysis of repeated
categorical
data across all five response choices for parents who responded
to all items (n = 46).
Data from Meyer EC, Burns JP, Griffith JL, Truog RD. Parental
perspectives on end-of-life care in
the pediatric intensive care unit. Crit Care Med
2002;30(1):22631.
-
time of death, and greater agreement (P < 0.01) about the
decision to withdraw
support between parents and staff members than with other family
members.
Nearly one fifth of parents reported that their childs pain
management was not
adequate, and nearly one quarter would have made decisions
differently if they
were able to do so. One of the most striking findings of this
study of bereaved
parents was that clinicians, usually previously unknown to the
family, were
quickly drawn into the familys inner circle of support because
of their expertise,
availability, and familiarity with the hospital culture, as well
as the emotional
needs of the family. As evidence of this, nurses were considered
more involved
during the actual dying process than other family members or
friends.
The perceived inadequacies of pain management provided to
children dying
in the PICU have also been documented in others. Wolfe et al
interviewed
103 parents of children who had died of cancer between 1990 and
1997 at an
academic teaching hospital in Boston, and found that almost all
children with
cancer who died in the hospital of treatment-related
complications died in the
intensive care unit, after ventilatory support was withdrawn
[25]. These children
dying of cancer had more symptoms, less successful control of
pain and dyspnea,
and a poorer quality of life than those who died of progressive
disease. Wolfe et al
also found significant discordance between the reports of
parents and physicians
regarding the childrens symptoms, with some suggestive evidence
that this may
result in part from a lack of recognition of the problem by the
medical team.
Bereaved parents in the Wolfe study who reported that the
physician was not
actively involved in care at the end of life were more likely to
report that their
child suffered a great deal from pain. Still other studies have
found that there
remains significant concern about untreated suffering in dying
newborns despite
advances in the field of pain management and pediatric
anesthesia [26,27].
Improving end-of-life care in the pediatric intensive care unit:
whats to be
learned from the literature?
The literature suggests that practitioners of pediatric critical
care need to invest
more effort into ensuring optimal palliative care for patients
and their families in
the PICU environment. Clinicians need to anticipate and treat
bothersome
symptoms of dying children more effectively; recognize that
family support
and contact between the dying child and family facilitate
decision making and
acceptance of death; and facilitate the coordination of care and
the development
of alternative care teams to optimize end-of-life care. Yet,
much remains
unknown as well. What are the different trajectories of death in
the PICU and
how does the quality of care vary across these different dying
trajectories? What
are the barriers and facilitators for communication among the
patient, families,
and PICU staff? How can excellent palliative care and
communication skills be
identified, measured, and taught? Finally, future efforts must
be based on
J.P. Burns, C.H. Rushton / Crit Care Clin 20 (2004)
467485476previously learned lessons. In particular, this includes
not only optimizing pal-
liative care for patients and their families, but developing
ongoing educational
initiatives and bereavement programs for PICU practitioners
themselves.
-
Practical aspects of end-of-life care
How much is too much analgesia for a child dying in the
pediatric intensive
care unit?
Can one externally validate the right amount of sedation and
analgesia that
should be given to dying child? Only the patient can truly
validate the adequacy
of the management of terminal symptoms, and in the PICU this is
typically not
possible. In the PICU context, then, the right amount of symptom
management
will always be a surrogate assessment. Yet, the constellation of
patient signs,
symptoms, or pain scores in an individual case that would meet a
universally
accepted threshold for treatment, let alone the extent of
treatment to be given
once that threshold has been reached, is not apparent.
Recently, the Society of Critical Care Medicine put forth a
comprehensive set
of guideline on this issue entitled, Recommendations for
end-of-life care in the
intensive care unit: The Ethics Committee of the Society of
Critical Care
Medicine [14]. They write, These agents should be titrated to
effect, and the
dose should not be limited solely on the basis of recommended or
suggested
maximal doses. In most cases, patients who do not respond to a
given dose of an
opioid or benzodiazepine will respond if the dose is
increasedthere is no
theoretical or practical maximal dose. Other experts have
expressed the views
of many experts on pain and symptom management: The optimal dose
of
morphine for relief of pain or dyspnea is determined by
increasing the dose until
the patient responds. Patients who have not previously received
opioids should
initially be given low doses, which should be rapidly increased
until symptoms
are relieved. For patients with particularly severe or acute
symptoms, rapid
titration requires that an experienced clinician be at the
bedside [28].
The amount of pain relief to provide to a dying patient has also
been addressed
by the United States Supreme Court [29]. In the 1997 case of
Vacco v Quill,
writing for the majority Chief Justice Rehnquist stated, It is
widely recognized
that the provision of pain medication is ethically and
professionally acceptable
even when the treatment may hasten the patients death if the
medication is
intended to alleviate pain and severe discomfort, not to cause
death. Although
this opinion does not necessarily legally sanction any dose of
sedative or
analgesic administered to dying patient, it does point to a
widely shared ethical
and legal consensus that symptom management should not be
limited by some
arbitrary level. But what is the ethical justification that
supports a practitioner of
pediatric critical care in administering sedatives and
analgesics in the PICU even
when it is foreseen that it will hasten the patients death?
Ethical justification for relieving pain and suffering
J.P. Burns, C.H. Rushton / Crit Care Clin 20 (2004) 467485
477The ethical justification most often cited for the
administration of sedatives
and analgesics to a dying patient, even when it is foreseen that
this will hasten the
patients death, is the Doctrine of Double Effect. The doctrine
states that an action
-
that has two effects, one of which is inherently good and the
other of which is
inherently bad, can be justified if certain conditions are met
[22].
Many critics argue that double effect reasoning is neither a
necessary or
sufficient determinant of morally permissible behavior by
clinicians in providing
palliative care [30,31]. First, critics assert that the
fundamental ethical justifica-
tion for care is based on the patients informed consent, not the
intentions of
clinicians. Therefore, the Doctrine of Double Effect is not
morally relevant or
logically valid, for it relies on an overly simplistic notion of
intent that is im-
possible to externally verify. Moreover, it may have the
paradoxic effect of
constraining some clinicians from providing adequate medication
for relief of
suffering because of their fear of violating the principles
absolute prohibition
against intentionally causing death. A second line of criticism
argues that those
who appeal to the moral cover of double effect reasoning are
really engaging in
disingenuous hairsplitting, a form of rationalization for a
practice that is really
surreptitious euthanasia.
Yet, some pediatric ethicists and practitioners of pediatric
critical care have
argued that double effect reasoning provides a guiding construct
for morally
permissible clinical management of children dying in the PICU.
For example,
Burns et al have written, Most terminally ill patients on
life-support, whether
pediatric or adult, lack decisional capacity; therefore,
voluntary consent is not an
option. Further, a rapid decline in patient comfort is common
when life-support is
withdrawn from the critically ill. The sedation and analgesia
adequate for a
patient receiving mechanical ventilation is usually inadequate
to treat the air
hunger experienced by imminently dying patients without severe
neurologic
injury as controlled ventilation is removed. Double effect
reasoning provides a
defensible rationale for escalating doses among practitioners
who support neither
euthanasia at one extreme nor the practice of allowing patients
to die with
untreated suffering on the other [12].
Despite the emerging theoretical understandings of the ethical
justification of
relieving pain and suffering, pediatric critical care
professional may need
additional support to implement decision they perceive may
violate important
ethical boundaries. These concerns must be anticipated and
addressed through
ongoing dialog, ethics consultation, institutional policies, and
clinical protocols.
For example, Kelly has advocated that moral decisions are shaped
by conditions
in the workplace [32]. This suggests that institutions where end
of life care is
provided have a responsibility to create support systems to
address the needs of
the caregivers who participate in and witness the suffering of
patients.
Neuromuscular blockade and end-of-life care
The presence of neuromuscular blockade at the time of
life-sustaining
treatment withdrawal, which has been reported in both adult and
pediatric pa-
J.P. Burns, C.H. Rushton / Crit Care Clin 20 (2004)
467485478tients, raises issues distinct to the practice of critical
care medicine. The relatively
high prevalence of neuromuscular blockade as part of standard
practice for the
treatment of children with poor lung compliance requiring
mechanical ventila-
-
tion, and the subsequent decision-making dilemmas produced when
life-sus-
taining treatment is withdrawn from these patients, has made
this a problem of
special concern to practitioners of pediatric critical care
[3,34]. Whether this
practice occurs with the intention of trying to assure the
appearance of patient
comfort for the benefit of the family, or because clinicians
preoccupied with all of
the concerns around the withdrawal of life-sustaining treatment
fail to consider
neuromuscular blockade, is not known. Neuromuscular blocking
agents, used
to reduce ventilator-patient asynchrony and minimize oxygen
consumption by
eliminating patient movement, have no sedative or analgesic
properties. As such,
most commentary on this issue has concluded that the initiation
of these agents
as the ventilator is being withdrawn is morally indefensible
[3,14,28,34].
Is it acceptable to administer neuromuscular blockade with the
intention of
comforting the family in a context where the child clearly
cannot survive
(extreme levels of mechanical ventilation or ECMO, for example)?
Some have
argued that the desire to comfort the patients family is an
important considera-
tion, and given the certainty of the patients death following
the withdrawal of
life-sustaining treatment in some situations regardless of
muscle relaxation, these
clinicians have argued that initiating neuromuscular blockade at
the time of
withdrawal is acceptable [33]. However, others believe that the
patients well-
being always takes precedence over family interests [3,34].
Neuromuscular
blockade potentially masks symptoms of patient suffering, and
therefore inter-
feres with the clinicians primary obligation of ensuring that a
dying patient does
not experience untreated suffering. Such an action also does not
allow for the
chance that the patient may survive without mechanical
ventilation when there is
some degree of prognostic uncertainty.
What should be done when the patient is experiencing the effects
of residual
neuromuscular blockade and the family decides to withdrawal
life-sustaining
treatment such as mechanical ventilation? The Ethics Committee
of the Society of
Critical Care Medicine has taken the position in published
recommendations that
efforts should be made to allow for the restoration of
neuromuscular function
before withdrawal of mechanical ventilation from patients who
have previously
been receiving therapeutic neuromuscular blockade [14]. A
similar position has
been advocated by other experts in the field [28].
Clearly, more education about the nuances of this dimension of
clinical
practice at the end of life is needed. Forums such as ethics
rounds, team rounds,
or interdisciplinary conferences should include exploration of
the boundaries of
ethically justified practice and clinical protocols that include
procedural safe-
guards for examining the issues before implementation. These
include clear lines
of decision-making authority and avenues for raising clinical
concerns.
Family presence at resuscitation attempts
J.P. Burns, C.H. Rushton / Crit Care Clin 20 (2004) 467485
479The official position of the Guidelines 2000 for Cardiopulmonary
Resuscita-
tion and Emergency Cardiovascular Care is that family members
should be
given (the option of being present at resuscitation attempts),
but they will require
-
losses; and the death of ones self.
In the same study, Papadatou proposed a model for the common
griefreactions health care professionals experience before and
after a patients death
[36]. These included crying, thinking about the patient,
temporary withdrawal
from activities and relationships, sorrow, anger, guilt, and
despair. The length of
response varied from several hours to several days or even
months in more
extreme cases. The timing of grief also varied; some health care
professionals
experienced immediate grief responses while others postponed or
repressed their
grief with reactions occurring at unexpected times.
In a qualitative study of nurses caring for chronically ill
children who died,
Davies et al reported that nurses experienced two types of
distress when they
recognized that a childs death was inevitable [37]. The first,
grief distress,support and specific attention during the
resuscitation. This statement stems
from surveys that have found that most people would like to be
present during the
attempted resuscitation of a loved one, especially when the
resuscitation attempt
involves a child. If family members are present, this is best
done with a clinician
who is free to meet the unexpected needs of the family, a need
that may not be
possible for the limited resources of the team to fill [35].
Despite increased
attention to this issue, there may be emotional and philosophic
barriers to im-
plementing such policies. Concerted efforts to explore
institutional and profes-
sional barriers to offering families this option will be
necessary.
Grief and bereavement of health care professionals
Pediatric health care professionals face unique challenges when
caring for
dying children and their families. In a recent report, When
Children Die, the
Institute of Medicine highlighted the need to understand and
develop strategies
for supporting these caregivers so that they can provide quality
care [1].
Although research in this area has been limited to date, several
qualitative
studies have helped to describe the way health care
professionals experience and
manage grief. Their conclusions suggest that further work is
needed to develop a
new model for grief among health care professionals and new
support strategies
for them.
Papadatou identified special considerations for health care
professionals facing
the death of pediatric patients [36]. These included the level
of investment in the
relationship with the patient and family, expectations of the
health care profes-
sionals identity and roles, and personal/social constructs.
According to Papada-
tou, each death involved loss on one or more levels: loss of
relationship with the
patient; loss due to identifying with the pain of the patients
family; loss of unmet
goals and expectations of the professional self-image; loss of
beliefs and
assumptions about self, life, and death; past unresolved or
future anticipated
J.P. Burns, C.H. Rushton / Crit Care Clin 20 (2004)
467485480involved the conflict between experiencing of emotions
such as sadness and
openly expressing them, because they felt the latter
contradicted norms of
professional behavior. The second, moral distress, occurred when
nurses felt
-
obligated to implement a treatment plan in conflict with their
values about pro-
moting a dignified and peaceful death.
Davies et al identified strategies used by nurses to manage
distress [37]. These
ranged from strategies that facilitated adjustment including
open expression of
grief, creating meaning out of the childs life and death, and
peer support and
validation to constrained responses that included diminished
engagement with
others, regret, diminished energy, and withdrawal.
A small qualitative study of PICU nurses described the effects
of cumulative
exposures to death. Individualized grief response was found to
be an ongoing
experiential learning process. Similar themes in how grief was
managed emerged:
self-nurturance, termination of the relationship activities,
engaging in control-
taking activities, and self reflection [40].
In another study, Papadatou et al compared the grief responses
and experi-
ences of Greek physicians and nurses who provided care to
children dying of
cancer [39]. Both groups experienced high stress levels; for
both, common grief
reactions involved crying, sadness, withdrawal, and recurring
thoughts of the
dying process and the childs death. However, there were also
differences. The
physicians experienced withdrawal, guilt, and a search for
explanations that
would reduce their distress more often than nurses who
experienced anger but did
not withdraw. In addition, physicians experienced grief
privately and rarely
sought the support of colleagues, while nurses reported
connecting with col-
leagues as a way to manage their grief [39].
A study of interventions designed to manage grief gathered
quantitative data
from health care professionals at the Johns Hopkins Childrens
Center [38]. In
findings that mirrored the qualitative studies cited above,
health care profes-
sionals who participated in routine debriefing sessions after a
childs death cited
professional distress as the most frequent reason for initiating
a session (86%).
They identified the loss of a long-term relationship with the
patient as the most
difficult aspect of the case (81%). Other concerns ranked lower:
conflict with the
family (25%); sudden/unexpected death, inability to relieve
pain, and provision
of aggressive care (2123%).
Because the traditional model of grief may not fit the
experience of health care
professionals, attempts have been made to develop newer models
of health care
professionals grief. One type of model describes a process of
oscillation between
focusing on the loss and moving away from the loss in a dual
process model of
coping [36,41] This model of approaching/avoiding the grief
response allows the
individual nature of the griever and the social impact of
working in health care to
affect the process. The oscillation between the dual processes
and resulting fluc-
tuation allow health care professionals to accomplish several
tasks: manage their
emotional responses to the death, restore/maintain their
integrity, find meaning in
the death, and transcend the suffering to reinvest in life
[36,42]. This fluctuation in
process is thought to be a normal and adaptive response that
allows health care
J.P. Burns, C.H. Rushton / Crit Care Clin 20 (2004) 467485
481professionals to experience grief without becoming overwhelmed
by it [36].
Another type of new model shifts from managing disruptive
symptoms and
sharing feelings to focus on meaning reconstruction as a way to
promote
-
Going forward several recent initiatives give promise for
significant advancesin addressing issues specific to the care of
dying children. IPPC, a project of
Educational Development Corporations Center for Applied Ethics
and Profes-
sional Practice, is a collaboration with the National
Association of Childrens
Hospitals and Related Institutions and eight childrens hospitals
[6]. The goal of
the initiative is to enhance the capacity of childrens hospitals
to provide family-
centered care in these most difficult circumstances. The IPPC
curriculum is
organized around six modules, each including videos featuring
interviews with
patients and families discussing their experiences. The six
modules are: Engaging
with Children and Families; Relieving Pain and Other Symptoms;
Sharing
Decision Making; Improving Communications and Strengthening
Relationships;
Responding to Suffering and Bereavement; and Establishing
Continuity of Care.
Another recent initiative at Childrens Hospital Boston seeks to
rectify the fact
that most clinicians learn about end-of-life care by trial and
error. The Program to
Enhance Relational and Communication Skills (PERCS) was
developed to teach
communication and relational skills through simulated Difficult
Conversations
at the End of Life between trainees and professional patient and
parent ac-
tors [45]. Structured scenarios on communicating with angry
families; handling
intrafamilial and family-staff conflict relative to the plan of
care; discussing
difficult news with families with whom there is no established
rapport; talkingrecovery [43]. Constructs such as burnout and
compassion fatigue syndrome do
not go far enough in addressing the one core issues of griefthe
process of
making meaning out of tragic circumstances. Efforts to implement
this new
model acknowledge the need to go further and develop
interventions for health
care professionals. Mount [44] suggested preventive and
restorative strategies
such as cultivating self awareness, working though past
unresolved losses, setting
limits, clarifying team roles and organizational patterns, team
support meetings,
and self-care.
A recent study by Rushton et al assessed the effectiveness of
palliative care
rounds, patient care conferences, and routine bereavement
debriefings in
enhancing health care professionals confidence and competence in
providing
palliative and end-of-life care and their ability to manage
their grief [38]. Other
activities included meaning-making rituals, such as annual and
individual
memorial services and candlelighting ceremonies. Process and
impact evaluation
data suggested that greater participation in educational, care
planning, and
bereavement activities increased health care professionals
perceptions of their
knowledge and skills in palliative and end-of-life care and
ability to manage
their grief.
Future directions
J.P. Burns, C.H. Rushton / Crit Care Clin 20 (2004)
467485482with families in times of medical uncertainty; and
understanding different cul-
tural views of end-of-life care have been created by a
multidisciplinary team of
pediatric critical care physicians, nurses, and as well as
psychologists with
-
this learning environment is that there is never only one right
answer to a
communication interaction. The IPPC and PERCS curriculum
initiatives reflect
ongoing efforts to creatively and effectively enhance quality
end-of-life care in
ment rounds will foster open discussion with all members of the
care team on
their perceptions of how well palliative care measures were
provided, identify
opportunities for improvement, and allow a forum to express the
emotional toll ofproviding such care.
References
[1] Institute of Medicine, Committee on Palliative and
End-of-Life Care for Children and Their
Families. When children die: improving palliative and
end-of-life care for children and their
families. Washington (DC): National Academy Press; 2002.
[2] McCallum DE, Byrne P, Bruera E. How children die in
hospital. J Pain Symptom Manage 2000;
20:41723.
[3] Burns JP, Mitchell C, Outwater KM, Geller M, Griffith JL,
Todres ID, et al. End-of-life care in
the pediatric intensive cave unit after the forgoing of
life-sustaining treatment. Crit Care Medthe pediatric intensive
care unit.
Summary
Although there has been a strong national movement to improve
palliative
care, data from the literature reveals that significant
perceptual differences exist
among parents, pediatric critical care physicians, and nurses on
their assessment
of the quality of end-of-life care as it is actually practiced
in the PICU. Whether
these data reflect inadequacies in care as it is actually
delivered, or gaps in
communication about that care, or some component of the two, is
not known.
Data from the literature do support several measures that can be
widely
implemented immediately. For example, more intensive
interdisciplinary collabo-
ration, through case review as well as through the
identification and support of
positive role models already on staff, can help to promote an
emphasis on
competent and compassionate end-of-life care, and assist the
bereavement
process for clinicians. Creation of regular, unit-based
multidisciplinary bereave-extensive experience in bereavement
support. Physician and nurse trainees then
go through each scenario, with the role of patients, parents,
and other family
members by actors from the Boston actors guild. The interaction
in each scenario
takes place in a simulator suite where it is videotaped, and the
scenario is
immediately debriefed, and a framework with specific
communication strategies
and skills that can be applied to the actual clinical setting is
provided by a team of
psychologists and pediatric critical care physicians. The
conceptual framework of
J.P. Burns, C.H. Rushton / Crit Care Clin 20 (2004) 467485
4832000;28(8):30606.
[4] Garros D, Rosychuk RJ, Cox PN. Circumstances surrounding end
of life in a pediatric intensive
care unit. Pediatrics 2003;112(5):e3719.
[5] Committee on Palliative and End-of-Life Care for Children
and their Families. Field MJ, Behr-
-
man RE, editors. Pediatric palliative care. In: When children
die: improving palliative and end-
of-life care for children and their families. Washington (DC):
The National Academy Press;
2003. p. 1940.
[6] Solomon MZ, Browning D, Fleischman A, Levetown M,
Riegelhaupt L, Rushton CH, et al. The
initiative for pediatric palliative care curriculum faculty
manual. Newton (MA): Education
Development Center, Inc.; 2002. Available online at
www.ippcweb.org).
[7] National Hospice and Palliative Care Organization.
(http://www.nhpco.org/templates/1/
homepage.cfm).
[8] American Association of Colleges of Nursing (AACN) and the
Los Angeles-based City of Hope
National Medical Center. The End-of-Life Nursing Education
Consortium (ELNEC) project
www.aacn.nche.edu/elnec.
[9] Solomon MZ, Sellers DE, Heller KS, Dokken D, Levetown M,
Rushton CH, et al. New research
in pediatric end-of-life care. Presented at The American Society
of Bioethics and Humanities
Annual Meeting, Salt Lake City; 2000.
[10] Danis M, Federman D, Fins JJ, Fox E, Kastenbaum B, Lanken
PN, et al. Incorporating palliative
care into critical care education: principles, challenges, and
opportunities. Crit Care Med
1999;27(9):200513.
[11] Nelson JE, Danis M. End-of-life care in the intensive care
unit: where are we now? Crit Care
Med 2001;29(2 Suppl):N29.
[12] Burns JP, Mitchell C, Griffith JL, Truog RD. End-of-life
care in the pediatric intensive care
unit: attitudes and practices of pediatric critical care
physicians and nurses. Crit Care Med
2001;29(3):65864.
[13] Meyer EC, Burns JP, Griffith JL, Truog RD. Parental
perspectives on end-of-life care in the
pediatric intensive care unit. Crit Care Med
2002;30(1):22631.
[14] Truog RD, Cist AF, Bracket SE, Burns JP, Curley MA, Danis
M, et al. Recommendations for
end-of-life care in the intensive care unit: the Ethics
Committee of the Society of Critical Care
Medicine. Crit Care Med 2001;29(12):233248.
[15] Cook DJ, Guyatt GH, Jaeschke R, et al. Determinants in
Canadian health care workers of the
decision to withdraw life support from the critically ill.
Canadian Critical Care Trials Group.
JAMA 1995;273:7038.
[16] Tulsky JA, Chesney MA, Lo B. See one, do one, teach one?
House staff experience discussing
do-not-resuscitate orders. Arch Intern Med 1996;156:12859.
[17] AACN. Peaceful death: reccommended comptencies and
curricular guidelines for end of life
nursing care. (1998) [online] available at
http://www.aacn.nche.edu/Publications/deathfin.htm}.
[18] Crego PJ, Lipp EJ. Nurses knowledge of advance directives.
Am J Crit Care 1998;7:21823.
[19] Nelson L, Rushton CH, Nelson R, Cranford R, Glover J.
Foregoing medically provided hydra-
tion and nutrition in pediatric patients. J Law Med Ethics
1995;23(1):3346.
[20] American Academy of Pediatrics Committee on Bioethics.
Guidelines on foregoing life-sustain-
ing medical treatment. Pediatrics 1994;93:5326.
[21] Oberle K, Hughes D. Doctors and nurses perceptions of
ethical problems in end of life
decisions. J Adv Nurs 2001;33(6):70715.
[22] Beauchamp TL, Childress JF. Principles of biomedical
ethics. New York: Oxford University
Press; 1994.
[23] Wilson WC, Smedira NG, Fink C, et al. Ordering and
administration of sedatives and analgesics
during the withholding and withdrawal of life support from
critically ill patients. JAMA 1992;
267:94953.
[24] Daly BJ, Thomas D, Dyer MA. Procedures used in withdrawal
of mechanical ventilation. Am J
Crit Care 1996;5:3318.
[25] Wolfe J, Grier H, Klar N, Levin S, Ellenbogen J,
Salem-Schatz S, et al. Symptoms and suffering
at the end of life in children with cancer. N Engl J Med
2000;342(5):32633.
J.P. Burns, C.H. Rushton / Crit Care Clin 20 (2004)
467485484[26] Yellin PB, Levin BW, Krantz DK, Shinn M, Driscoll Jr
JM, Fleischman AR. Neonatologists
decisions about withholding and withdrawing treatments of
critically ill newborns. Pediatrics
1998;102:757.
-
[27] Abe N, Catlin A, Mihara D. End of Life in the NICU: a study
of ventilator withdrawal. MCN Am
J Mater Child Care 2001;28(3):1416.
[28] Brody H, Campbell ML, Faber-Langendoen K, et al.
Withdrawing intensive life-sustaining
treatment recommendations for compassionate clinical management.
N Engl J Med 1997;
336:6527.
[29] Vacco v. Quill 117 S. Ct 2293 (1997).
[30] Quill TE, Dresser R, Brock DW. The rule of double effecta
critique of its role in end-of-life
decision making. N Engl J Med 1997;337:176871.
[31] Brody H. Physician-assisted suicide in the courts: moral
equivalence, double effect, and clinical
practice. Minn Law Rev 1998;82(4):93963.
[32] Kelly C. Investing or discounting self: are moral decisions
shaped by conditions of the work-
J.P. Burns, C.H. Rushton / Crit Care Clin 20 (2004) 467485
485place? Adv Pract Q 1998;4(2):813.
[33] Perkin RM, Resnik DB. The agony of agonal respiration: is
the last gasp necessary? J Med
Ethics 2002;28(3):1649.
[34] Truog RD, Burns JP, Mitchell C, Johnson J, Robinson W.
Pharmacologic paralysis and with-
drawal of mechanical ventilation at the end of life. N Engl J
Med 2000;342(7):50811.
[35] Guidelines 2000 for cardiopulmonary resuscitation and
emergency cardiovascular care. Circu-
lation 2000;102(8 Suppl):I869.
[36] Papadatou D. A proposed model of health professionals
grieving process. Omega 2000;41(1):
5977.
[37] Davies B, Clarke D, Connaughty S, Cook K, MacKenzie B,
McCormick J, et al. Caring for
dying children: nurses experiences. Pediatr Nurs
1996;22(6):5007.
[38] Rushton CH, Hutton N, Reder E, Hall B, Sellers D, Commello
K. An action plan to reduce
caregiver suffering in professionals who care for dying children
(Abstract). The Initiative for
Pediatric Palliative Care National Symposium, New York; November
7, 2003.
[39] Papadatou D, Papazpglou I, Bellali T, Petraki D. Greek
nurse and physician grief as a result of
caring for children dying of cancer. Pediatr Nurs
2002;28(4):34553.
[40] Rashotte J, Fothergill-Bourbonnais & Chamberlain.
Pediatric intensive care nurses and their grief
experiences: a phenomenological study. Heart Lung
1997;September/October:37286.
[41] Strobe M, Schut H. The dual process model of coping with
bereavement: rationale and descrip-
tion. Death Stud 1999;23(3):197225.
[42] Saunders J, Valente S. Nurses grief. Cancer Nurs
1994;174(4):31825.
[43] Neimeyer RA. Lessons of loss: a guide for coping. New York:
McGraw-Hill; 1998.
[44] Mount BM. Dealing with our losses. J Clin Oncol
1986;4(7):112734.
[45] Meyer EM, Browning D, Pascucci RP, Comeau M, Stanley LJ,
Burns JP, et al. Anatomy of a
learning team: principles and guidelines to enhance debriefing
following communication simu-
lation. Presented at the 4th annual international meeting on
medical simulation, Albuquerque/
Santa Fe, NM; January 17, 2004.
End-of-life care in the pediatric intensive care unit: research
review and recommendationsThe literature on end-of-life care in the
pediatric intensive care unitAttitudes of pediatric critical care
physicians and nurses on end-of-life careObservational studies of
clinical practice regarding death in the pediatric intensive care
unitParental perspectives on end-of-life care in the pediatric
intensive care unitImproving end-of-life care in the pediatric
intensive care unit: what's to be learned from the literature?
Practical aspects of end-of-life careHow much is too much
analgesia for a child dying in the pediatric intensive care
unit?Ethical justification for relieving pain and
sufferingNeuromuscular blockade and end-of-life careFamily presence
at resuscitation attempts
Grief and bereavement of health care professionalsFuture
directionsSummaryReferences