Embed Size (px)
Citation preview

Unit 464 November 2010
Bipolar disorders
www.racgp.org.au/check
Unit 469 April 2011
Ear nose and throat
Independent learning program for GPs
Independent learning program for GPs

RACGP member $130 Nonmember $190 Medical student/registrar/AMC $90 Overseas nonmember $175 Overseas member $125 Overseas medical student/registrar/AMC $85
CD/USB price per program
RACGP member $161 Nonmember $202 Medical student/registrar/AMC $86 Overseas nonmember $214 Overseas member $176 Overseas medical student/registrar/AMC $109
Print price per program
The check Program is a monthly quality improvement and continuing professional development (QI&CPD) activity and independent learning program developed by the RACGP. The 2008 and 2009 check Programs are available in both CD and print format. The 2010 program is available in print, as well as a handy, interactive USB format.
Independent learning program for GPs
Independent learning program for GPs
2008–2010 triennium
• Hypertension• Polycystic ovary syndrome• Evidence based medicine• Imaging• Influenza
• Patient initiated violence• Psychosis• Endocrinology and the skin• Haematology• Patient safety in general practice
2008 topics Print CD
•Male reproductive health•Chronic disease management•Chronic obstructive
pulmonary disease• Fatigue•Sexually transmissible infections
• Type 2 diabetes•Palliative care•Gastroenterology•Motivational interviewing•Cardiovascular emergencies•Sport medicine
2009 topics Print CD
•Stroke•Challenging consultations•Anxiety disorders•Office based procedures• Juvenile idiopathic arthritis and
rheumatoid arthritis
•Ophthalmology •Wound management• Thyroid•Rashes •Osteoarthritis•Child and adolescent behaviour
2010 topics Print USB
Post, fax, phone or email your order to:The RACGP, 1 Palmerston Crescent, South Melbourne, Victoria 3205, AustraliaFax 03 8699 0400 Tel 03 8699 0495 Email [email protected] 000 223 807 ABN 34 000 223 807
FOR OFFICE USE ONLY RAGGP NO. (Bill to) _______________________________ BATCH NO. _____________________ ORDER NO. _____________________ INVOICE NO. ___________________
Delivery details (please print clearly and retain a copy for your records)
Date Name RACGP no.
/ / Student/AMC no. University
Street address Suburb
State Postcode Country Telephone
Payment detailsPayment type
Amex Visa MasterCard Cheque (make payable to the RACGP)
Card number Expiry date Total amount
/ $
Cardholder name (please print clearly) Cardholder signature
Please allow up to 14 days for delivery of goods. The College must be notified of missing or incorrect orders within 28 days of placing the order. Orders returned must be received within 28 days of receipt in order to obtain refund or replacement. Prices include GST, postage and handling. Overseas prices exclude GST.
check 2008–2010 order form ad.indd 1 11/03/11 2:33 PM

From the editor 2
Case 1 Chris’ concern 3
Case 2 Dorothy is experiencing pain in her groin 6
Case 3 Jill’s knee pain 9
Case 4 Angela presents with painful and stiff joints 12
Case 5 Jan has ongoing knee pain 16
References 21
Resources 22
Category 2 QI&CPD activity 24
Unit 464 November 2010
Bipolar disorders
The five domains of general practice Communication skills and the patient-doctor relationship
Applied professional knowledge and skills Population health and the context of general practice
Professional and ethical role Organisational and legal dimensions
Independent learning program for GPs
Independent learning program for GPs
Medical Editor Catherine Dodgshun
Editor Nicole Kouros
Production Coordinator Morgan Liotta
Senior Graphic Designer Jason Farrugia
Graphic Designer Beverly Jongue
Authors June Choo Michael Dobson Ana Teresa Licup Mark Paine Elizabeth Rose Philip Michael Carmel Crock
Reviewer Tracy Cheffins
Subscriptions Call the Subscription Coordinator for all enquiries on 03 8699 0495 or email [email protected].
Published by
The Royal Australian College of General Practitioners College House, 1 Palmerston Crescent South Melbourne, Victoria 3205, Australia Telephone 03 8699 0414 Facsimile 03 8699 0400 www.racgp.org.au
ACN 000 223 807 ABN 34 000 223 807 ISSN 0812-9630
© The Royal Australian College of General Practitioners 2011. All rights reserved.
The opinions expressed in check are not necessarily those of the RACGP.
Please address all letters concerning the content to the medical editor.
Printed by
Printgraphics Pty Ltd, 14 Hardner Road, Mount Waverley, Victoria 3149 Telephone 03 9562 9600.
From the editor 2
Case 1 Adriana has a hoarse voice 3
Case 2 Jean’s sudden loss of hearing 6
Case 3 Robbie’s ongoing ear problems 9
Case 4 Nigel is experiencing vertigo and nausea 16
Case 5 John’s nosebleed 21
Case 6 Claire’s onging allergies 25
Case 7 Julie’s had a runny nose and feels congested 28
Case 8 Jim has painful blocked ears 31
Resources and References 34
Category 2 QI&CPD activity 35
Unit 469 April 2011
Ear nose and throat
The five domains of general practice Communication skills and the patient-doctor relationship
Applied professional knowledge and skills Population health and the context of general practice
Professional and ethical role Organisational and legal dimensions
RACGP member $130 Nonmember $190 Medical student/registrar/AMC $90 Overseas nonmember $175 Overseas member $125 Overseas medical student/registrar/AMC $85
CD/USB price per program
RACGP member $161 Nonmember $202 Medical student/registrar/AMC $86 Overseas nonmember $214 Overseas member $176 Overseas medical student/registrar/AMC $109
Print price per program
The check Program is a monthly quality improvement and continuing professional development (QI&CPD) activity and independent learning program developed by the RACGP. The 2008 and 2009 check Programs are available in both CD and print format. The 2010 program is available in print, as well as a handy, interactive USB format.
Independent learning program for GPs
Independent learning program for GPs
2008–2010 triennium
• Hypertension• Polycystic ovary syndrome• Evidence based medicine• Imaging• Influenza
• Patient initiated violence• Psychosis• Endocrinology and the skin• Haematology• Patient safety in general practice
2008 topics Print CD
•Male reproductive health•Chronic disease management•Chronic obstructive
pulmonary disease• Fatigue•Sexually transmissible infections
• Type 2 diabetes•Palliative care•Gastroenterology•Motivational interviewing•Cardiovascular emergencies•Sport medicine
2009 topics Print CD
•Stroke•Challenging consultations•Anxiety disorders•Office based procedures• Juvenile idiopathic arthritis and
rheumatoid arthritis
•Ophthalmology •Wound management• Thyroid•Rashes •Osteoarthritis•Child and adolescent behaviour
2010 topics Print USB
Post, fax, phone or email your order to:The RACGP, 1 Palmerston Crescent, South Melbourne, Victoria 3205, AustraliaFax 03 8699 0400 Tel 03 8699 0495 Email [email protected] 000 223 807 ABN 34 000 223 807
FOR OFFICE USE ONLY RAGGP NO. (Bill to) _______________________________ BATCH NO. _____________________ ORDER NO. _____________________ INVOICE NO. ___________________
Delivery details (please print clearly and retain a copy for your records)
Date Name RACGP no.
/ / Student/AMC no. University
Street address Suburb
State Postcode Country Telephone
Payment detailsPayment type
Amex Visa MasterCard Cheque (make payable to the RACGP)
Card number Expiry date Total amount
/ $
Cardholder name (please print clearly) Cardholder signature
Please allow up to 14 days for delivery of goods. The College must be notified of missing or incorrect orders within 28 days of placing the order. Orders returned must be received within 28 days of receipt in order to obtain refund or replacement. Prices include GST, postage and handling. Overseas prices exclude GST.
check 2008–2010 order form ad.indd 1 11/03/11 2:33 PM
Independent learning program for GPs
Independent learning program for GPs

check Ear nose and throatfrom the editor
2
This unit of check looks at a variety of clinical scenarios relating to ear nose and throat (ENT) problems which are commonly seen in general practice. It is important that general practitioners are competent in their assessment of these problems. History and examination should aim to determine the diagnosis, exclude serious differential diagnoses, and identify indications for referral to ENT surgeons and other specialists such as neurologists and allergists, depending on the clinical situation. Management should be evidence based as far as possible.
The authors bring a wealth of clinical, research and teaching experience in the area of ENT surgery, otolaryngology, rhinology and neuro-ophthamology.
The authors of this unit are:
June Choo MBBS, FRACS, otolaryngologist, head and neck surgeon, Royal Victorian Eye and Ear Hospital and The Alfred, Victoria. Her special interests include voice disorders and surgery for snoring and obstructive sleep apnoea
Michael Dobson MBBS, FRACS, general otorhinolaryngologist, Royal Victorian Eye and Ear Hospital, and specialist in otology and general ENT, and head and neck surgeon at Box Hill Hospital, Victoria. He has over 25 years experience in otology and paediatric ear disease and he has experience with indigenous ear disease in Alice Springs and South East Asia. His clinical and research interests are middle ear surgery and surgery for deafness
Ana Teresa Licup MD, DPBO-HNS, Senior House Medical Officer for ENT, Royal Victorian Eye and Ear Hospital, Victoria. Her special interest is paediatric otolaryngology
Mark Paine MBBS, FRACP, Head of Vestibular Investigation Unit, Head of Neuro-ophthalmology Clinic, Royal Victorian Eye and Ear Hospital, Head of Neuroimmunology Unit, St Vincent’s Hospital, Victoria. His special interests include neuro-ophthalmology, neuro-otology and multiple sclerosis
Elizabeth Rose MBBS, FRACS, otolaryngologist, Royal Children’s Hospital and Royal Victorian Eye and Ear Hospital, and Senior Lecturer, University of Melbourne. Her area of interest and expertise is paediatric otolaryngology, especially hearing loss
Philip Michael MBBS, DLO, FRCSED (ORL-HNS), Rhinology Fellow, Royal Victorian Eye and Ear Hospital Melbourne. His special interests include endoscopic sinus surgery, functional rhinoplasty and medical education
Carmel Crock MBBS, FACEM, BLitt, Director, Emergency Department, Royal Victorian Eye and Ear Hospital, Victoria. Her interests are in patient safety and medical error. She is involved in medical education, including undergraduate, emergency medicine and GP education in eye and ENT emergencies.
The learning objectives of this unit are to:
• display increased confidence in the assessment and management of patients who present with otitis media, otitis externa, vertigo, hoarseness of the voice, sudden hearing loss, allergic rhinitis, chronic sinusitis and epistaxis
• recognise the importance of urgent referral in conditions such as stroke presenting as vertigo, certain cases of epistaxis, idiopathic sudden sensorineural hearing loss and malignant otitis externa, and recognise the importance of prompt referral in cases of suspected carcinoma of the pharynx, larynx and nasal passages
• display increased confidence in performing certain aspects of examination of a patient, such as the head impulse test, Hallpike manoeuvre and Weber test
• display increased confidence in interpreting signs on otoscopic examination of common conditions such as otitis media and otitis externa
• recognise the importance of certain procedures such as the use of tissue spears in otitis media with perforation, ear canal debridement in otitis externa and nasal packing in epistaxis in the management of these problems in general practice.
This issue of check heralds a change in the medical editor. We thank Dr Kath O’Connor as the outgoing medical editor of the check Program for all her work over the years and for her contribution in helping to make this publication successful. I would like to introduce myself as the new medical editor. I look forward to the privilege of working with you in the months to come.
I hope this unit will assist you to manage ear nose and throat problems in general practice.
Kind regards
Catherine Dodgshun
Medical Editor

Case 1
3
Case 1Chris has a hoarse voiCe
Chris is 58 years of age, he is a builder who has come for his annual cardiovascular and prostate health check. You find he is overweight with a body mass index (BMI) of 29 kg/m2. At the close of your physical exam and testing he mentions that he has been getting pain on and off in his right knee and that it is interfering with work, particularly climbing up and down ladders and carrying heavy timber loads. The knee has been swollen after some busy days at work. He reports playing a lot of sport in his youth with previous knee injuries but no prior surgery. He is worried about his future as a builder.
You quickly ascertain that the knee is not currently swollen and has full range of movement and you schedule another appointment to focus on diagnosis and management of his knee pain.
check Ear nose and throat
QuesTion 3
How would you manage her hoarseness at this stage? Would you prescribe medication such as antibiotics or corticosteroids?
QuesTion 4
Could Adriana’s intake of ibuprofen be related to her voice hoarseness?
QuesTion 5
What are the main risk factors for ‘throat cancer’? What symptoms or signs would arouse suspicion of cancer?
QuesTion 6
If Adriana had woken up after an operation with hoarseness of the voice, could it be related to the operation? Explain your answer.
QuesTion 1
What is the most likely cause for Adriana’s symptoms?
QuesTion 2
What other diagnoses should be considered? What other features in the history would you be interested in?
Case 1adriana has a hoarse voiCe
Adriana is 50 years of age and is a receptionist at an accounting firm. She developed a hoarse voice 6 weeks ago and has not been able to take any time off work as the firm is experiencing a busy period. She finds that as the day progresses, the hoarseness worsens, her stress levels increase and she also experiences a tightness in her throat. When Adriana originally presented 1 week after the onset of her symptoms, she was treated for laryngitis with two courses of oral antibiotics but does not feel that her voice is improving. She would like to try a ‘stronger’ antibiotic.
Adriana is mindful of her family history of ‘throat cancer’, which her father developed in his 60s and is concerned about her risk. You note from Adriana’s medical record that she has a past history of osteoarthritis of the lumbar spine, for which she says she has been taking ibuprofen on a regular basis.

Case 1
4
check Ear nose and throat
It is important to take a history relating to:
• the onset of hoarseness
• whether hoarseness is constant (which tends to occur in structural lesions and traumatic injury) or intermittent (which tends to occur in muscle tension dysphonia, gastro-oesphageal reflux and postnasal drip)
• aggravating and relieving factors
• associated symptoms such as cough (as can occur in gastro-oesphageal reflux, allergies and as an effect of chronic laryngitis)
• risk factors for ‘throat cancer’ (see Answer 4)
• determining each of the causes of hoarseness in Answer 2 above:
– voice abuse
– symptoms such as heartburn and waterbrash
– symptoms such as postnasal drip
– symptoms associated with throat cancer (see Answer 4)
– history of neck trauma
– recent surgery
– general state of health
• excluding each of the causes of throat tightness in Answer 2 above.
answer 3
Adriana’s hoarseness should be managed by referral to an ear, nose and throat (ENT) consultant for consideration of laryngoscopy.
Antibiotics are unlikely to be helpful for Adriana’s hoarseness and, in general, are not helpful in most cases of hoarseness.
There is no evidence that empirical use of corticosteroids is helpful for voice hoarseness.3 Corticosteroids could be helpful in previously diagnosed autoimmune conditions affecting the larynx, such as systemic lupus erythematosus, sarcoidosis and Wegener granulomatosis.
Corticosteriods should be considered in airway inflammation and oedema, as can occur in emergency situations, as should transfer by ambulance to an appropriate hospital emergency department.
answer 4
It is possible that ibuprofen could exacerbate gastro-oesophageal reflux into the laryngopharynx or contribute to the formation of a haemorrhagic polyp, therefore contributing to voice hoarseness.
answer 5
‘Throat cancer’ is a nonspecific term and can mean cancer of the pharynx or larynx. The most common malignancy in the pharynx and larynx is squamous cell carcinoma and the main risk factors are smoking and heavy alcohol intake. Other less common risk factors include immunosuppression, exposure to asbestos and previous radiotherapy.
Case 1 answers
answer 1
The most likely cause for Adriana’s symptoms is ‘muscle tension dysphonia’, which is a common functional disorder of the larynx. Muscle tension dysphonia is a clinical diagnosis with pointers in the history as well as findings on laryngoscopy. Laryngoscopy is performed both to exclude other pathology and to demonstrate muscle tension dysphonia. Muscle tension dysphonia usually responds well to voice therapy.1
FeedbaCk
The majority of hoarseness in the community is due to viral laryngitis. Hoarseness from viral laryngitis typically lasts up to 3 weeks.2 If hoarseness persists beyond 3 weeks, referral for laryngoscopy should be considered to exclude other causes.
answer 2
Other diagnoses to consider as a cause for Adriana’s hoarseness include:
• structural lesions which can either be benign (eg. nodules, polyps and papillomas) or malignant (eg. carcinoma of the larynx)
• gastro-oesophageal reflux
• postnasal drip
• irritation from inhaled corticosteroids used to treat asthma
• irritation from fumes, dust or cigarette smoke
• autoimmune disease (eg. systemic lupus erythematosus, sarcoidosis and Wegener granulomatosis)
• infection (eg. Candida, or with Staphylococcus aureus)
• allergy
• traumatic injury.
The other important symptom which Adriana describes is throat tightness. Possible causes for Adriana’s throat tightness include:
• ischaemic heart disease – throat tightness may be atypical pain which could indicate underlying ischaemic heart disease. It is important to exclude ischaemic heart disease by appropriate investigations if this diagnosis is considered
• allergy – while allergy is a possible cause for Adriana’s throat tightness, in the absence of perioral swelling or rash, allergy is not likely
• asthma – asthma can present as throat tightness, though there are likely to be other symptoms such as cough, shortness of breath or wheeze present
• globus pharyngis – globus pharyngis is another condition which causes throat tightness but it usually presents with a sensation of a lump in the throat in the absence of signs.

Case 1
5
check Ear nose and throat
Some patients with squamous cell carcinoma of the head and neck region do not have the common risk factors. Symptoms and signs of concern include:
• dysphagia
• odynophagia
• loss of appetite or weight
• otalgia
• stridor or a neck mass.
If a patient has a persistently hoarse voice and risk factors for malignancy, or symptoms or signs of concern, an urgent referral to an ENT consultant should be made.
answer 6
Yes, hoarseness of the voice could be related to the operation. Voice hoarseness is not uncommon following surgery where an endotracheal tube or laryngeal mask has been used. The hoarseness is usually due to laryngeal oedema and resolves spontaneously over a period of up to 6 weeks. Hoarseness can also be from a vocal cord granuloma3 or dislocation of the arytenoid cartilage resulting in an immobile vocal fold. It is important that the patient be referred to an ENT specialist for investigation with flexible laryngoscopy.
Voice hoarseness after surgery can also be due to trauma to the recurrent laryngeal nerve. Some surgical procedures are more likely to be associated with trauma to the recurrent laryngeal nerve. These include:
• cervical laminectomy via the anterior approach
• thyroid surgery
• carotid endarterectomy
• cardiac surgery
• surgery for oesophageal cancer.
Recurrent laryngeal nerve palsy could resolve and while awaiting recovery, voice therapy could improve function. Treatment of vocal cord granuloma usually includes a combination of voice therapy, acid suppression and surgical excision.

6
check Ear nose and throatCase 2
FurTher inFormaTion
Jean’s Weber test lateralises to the left ear. Your otoscopic examination reveals a nonobstructed ear canal and a normal tympanic membrane.
QuesTion 4
What is the likely diagnosis? What is your next step in management?
QuesTion 5
If Jean’s Weber test had lateralised to the right ear, what would this indicate?
QuesTion 1
What would be your first step on examination?
QuesTion 2
Describe how you would perform this office test.
QuesTion 3
What should you do if you do not have a tuning fork?
Case 2Jean’s sudden loss oF hearing
Jean, a busy housewife of 41 years of age, presents to you in the afternoon after having woken up with a blocked feeling in her right ear. She had tried to ring her husband at work and thought that the phone was dead. Before ringing the telephone company she got her son to check the phone and her son said that the phone was working fine. Jean then put the handpiece to her left ear and she was able to hear with her left ear. She tells you that 1 week ago she had a minor upper respiratory sniffle which resolved without any treatment.

7
check Ear nose and throat Case 2
• There is consensus that immediate steroid treatment increases the chance of recovery. Prednisolone is used at a starting dose of 1 mg/kg and continued for 10 days; the dose is tapered after 3 days of maximum dose4
• Antiviral medications have been advocated but there is no hard evidence that there is any significant benefit
• Between 20–30% of cases will improve spontaneously.
Figure 1 shows a normal tympanic membrane.
Case 2 answers
answer 1
The first step on examination is to perform a Weber tuning fork test. This simple office test will quickly differentiate between conductive deafness and sensorineural deafness. An otoscopic examination should also be performed.
answer 2
The Weber test is performed using a tuning fork of 512 Hertz (middle C).
Strike the tuning fork and then place the stem firmly on the midpoint of the patient’s forehead. Ask the patient which ear the sound of the fork is louder in. The test is interpreted as follows:
• normal hearing – the sound is heard in the midline
• conductive deafness – the sound is heard in the deaf ear
• sensorineural deafness – the sound is heard in the nondeaf ear.
answer 3
Ask the patient to hum. Ask in which ear they hear the hum. The same interpretation principles of the Weber test apply.
answer 4
If the Weber test lateralises to the nondeaf ear, this suggests sensorineural hearing loss. In Jean’s case, as the hearing loss has been sudden, the most likely diagnosis is idiopathic sudden sensorineural hearing loss (ISSHL). The next step would be to obtain immediate advice from an ENT surgeon either by phone or by a referral that day. Further information on ISSHL is presented below.
• Incidence – this varies between 5–20/100 000 per annum
• Aetiology – there is ongoing debate about the cause. A viral theory is plausible, however, a microvascular event involving the cochlear-vestibular circulation may explain a proportion of presentations
• About 40% of cases report associated balance disturbance
• Approximately 10% of acoustic neuromata present with sudden sensorineural deafness therefore part of the diagnostic workup will involve a magnetic resonance imaging (MRI) scan
• ISSHL is an emergency needing immediate treatment
Figure 1. A normal tympanic membrane. Reproduced with permission from hawkelibrary.com
Figure 2. Ear obstructed with wax. Reproduced with permission from hawkelibrary.com

8
check Ear nose and throat
answer 5
If the Weber test lateralises to the right, this indicates that there is a conductive deafness which can be caused by obstruction of the external ear canal (Figure 2) or by pathology in the middle ear (Figure 3).
If pathology in the middle ear was the cause, Jean’s tympanic membrane would look abnormal due to the presence of middle ear fluid reflecting eustachian tube blockage secondary to upper respiratory inflammation.
If this is the case, treatment should be with nasal decongestants, either topical or systemic. If otalgia was present, this might represent otitis media.
FeedbaCk
Another possible cause of sensorineural deafness is shown in Figure 4. This is an early herpes zoster vesicle on the ear drum. The patient presented with the onset of severe otalgia and a sensorineural deafness before proceeding to develop a facial nerve palsy (Ramsay Hunt syndrome). In this instance antiviral medication and steroids together are the first line treatments.
Case 2
Figure 3. Otitis media with effusion. Reproduced with permission from hawkelibrary.com
Figure 4. Early herpes zoster vesicle on the ear drum. Author’s image

9
check Ear nose and throat Case 3
QuesTion 1
What is your diagnosis?
QuesTion 2
What is meant by the term recurrent acute otitis media (AOM)?
Case 3robbie’s ongoing ear problems
Robbie, 5 years of age, is brought to see you with a discharge coming from his left ear (otorrhoea). He has a cold this week and cried with earache during the night, but went back to sleep after taking paracetamol. You check his medical record and note that he has had about 2–3 episodes of acute otitis media (AOM) every winter for the last 2 years, and has been treated with antibiotics for each of these episodes. He started school this year and has had several colds as well as gastroenteritis since then. It is May and this is his third ear infection since February. His mother is alarmed as he has never had otorrhoea before. Robbie is alert and interactive with a temperature of 37.8°C. His cervical nodes are slightly enlarged, throat examination is normal and chest is clear. Otoscopic findings are shown in Figure 5 and 6.
Figure 6. Robbie’s left ear. Reproduced with permission from hawkelibrary.com
Figure 5. Robbie’s right ear. Reproduced with permission from hawkelibrary.com

10
check Ear nose and throatCase 3
QuesTion 6
How will you treat Robbie’s current episode?
FurTher inFormaTion
Robbie has a new sister, Alice, age 4 months. Their mother has been on maternity leave, but plans to return to work next month. She would like to know whether it is likely that Alice will have a lot of problems with her ears as well, and if there is anything she can do to prevent this.
QuesTion 7
What will you tell Robbie and Alice’s mother?
QuesTion 8
When would you ask Robbie to come back for review?
QuesTion 3
What are the organisms that commonly cause AOM?
QuesTion 4
What else would you like to know before deciding on a treatment plan?
QuesTion 5
How would you clean his left ear?
11
check Ear nose and throat Case 3
QuesTion 9
Describe the otoscopic findings and what your advice is now.
FurTher inFormaTion
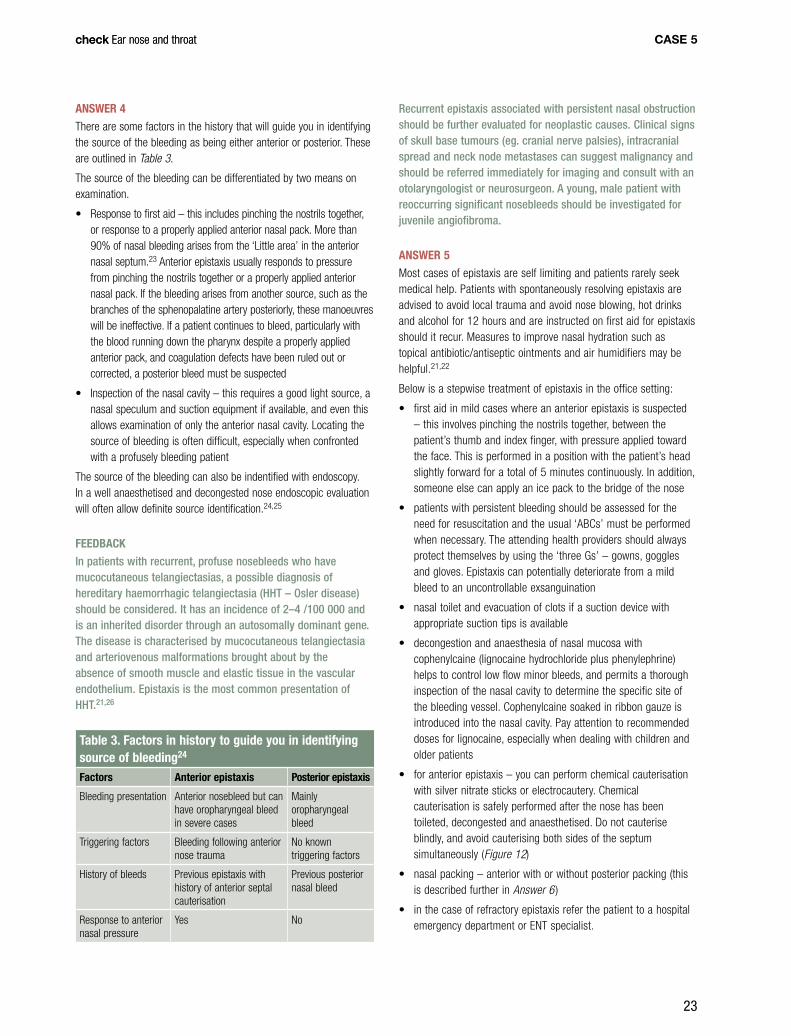
Robbie returns 5 weeks later. The night before Robbie had a bad night and is still in pain. His mother has been for his parent-teacher interview, and the teacher has concerns that Robbie is not paying attention, and he is not learning his spelling as well as he was earlier in the year. His mother reports that he often seems grumpy and does not do as he is told, especially if he is watching television. He has a constantly runny nose and wipes it but cannot blow it efficiently. He often comes into his parents’ bed at night, which he has not done since he was a toddler. They note that he snores and mouth breathes but does not appear to stop breathing. Otoscopic findings are shown in Figure 9 and 10.
FurTher inFormaTion
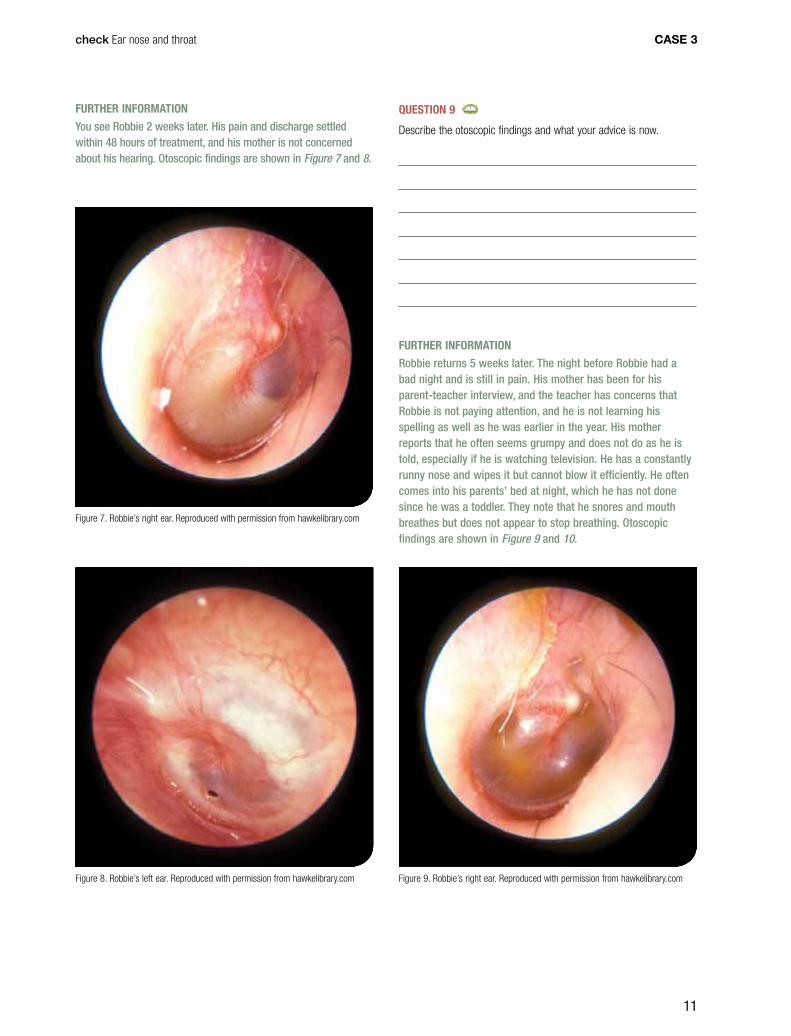
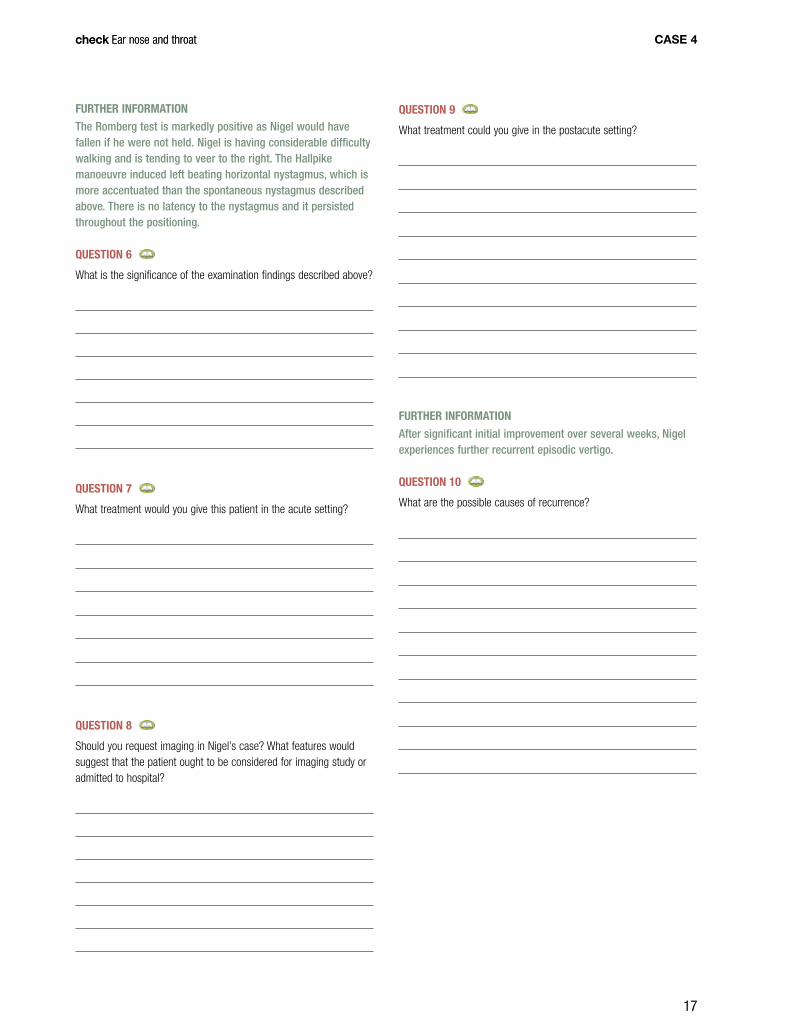
You see Robbie 2 weeks later. His pain and discharge settled within 48 hours of treatment, and his mother is not concerned about his hearing. Otoscopic findings are shown in Figure 7 and 8.
Figure 7. Robbie’s right ear. Reproduced with permission from hawkelibrary.com
Figure 9. Robbie’s right ear. Reproduced with permission from hawkelibrary.comFigure 8. Robbie’s left ear. Reproduced with permission from hawkelibrary.com

12
check Ear nose and throatcheck Ear nose and throatCase 3
QuesTion 12
What are the indications for insertion of middle ear ventilation tubes?
QuesTion 13
What is the efficacy of prophylactic antibiotics for the prevention of otitis media in young children?
QuesTion 14
What is the efficacy of adenoidectomy for a child with middle ear disease?
QuesTion 10
What is your diagnosis for each ear?
QuesTion 11
What is your management for Robbie now?
Figure 10. Robbie’s left ear. Reproduced with permission from hawkelibrary.com

13
check Ear nose and throatcheck Ear nose and throat Case 3
answer 5
This can be done with suction if available, or with mopping with tissue spears. His mother can continue with use of tissue spears at home as well (Figure 11).
answer 6
Treatment of AOM involves the following.
adequate analgesia
Usually with an oral agent such as paracetamol. Topical anaesthetic drops such as amethocaine, benzocaine or lidocaine have some efficacy at 30 minutes after administration, but not more than paracetamol once they have been absorbed.8 Topical anaesthetic drops should not be administered when there is a perforation as they may enter the inner ear and cause vertigo.
antibiotic therapy
The current recommendations are that children older than 2 years who are not very ill (ie. no systemic features such as significant fever or vomiting) can be treated with observation only; the parents can be given a prescription to be filled if the child is still in pain after 48 hours.9 However, there are groups of children who should be treated. These include:
• children 2 years of age or younger, because:
– they are not able to describe their symptoms
– they are more likely to have suppurative complications such as meningitis and mastoiditis
– they are less likely to improve spontaneously
Case 3 answers
answer 1
The diagnosis pertaining to the right ear is AOM. The tympanic membrane is red and injected, and there is loss of the prominence of the anterior process of the malleus, consistent with pus under pressure.
The diagnosis pertaining to the left ear is likely to be AOM with perforation. The ear needs to be cleaned to assess the tympanic membrane (the process by which this is performed is described in Answer 5 ).
The diagnosis of AOM may be difficult to make, especially in children younger than 3 years who have small external auditory canals, may not be cooperative and/or have wax obscuring the view. In a comparison of doctors it was found that the accuracy in diagnosing whether or not there is middle ear fluid was: ENT surgeons – 74%; paediatricians – 51%; GPs – 46%.5
Using pneumatic otoscopy or a tympanogram can improve the diagnostic accuracy.
answer 2
Recurrent AOM is defined as three or more episodes in 6 months, or four or more in 12 months.6 This is an indication that a child is having more infections than would usually be expected.
answer 3
The organisms that commonly cause AOM are Streptococcus pneumoniae, Haemophilus influenzae – nontypeable, and Moraxella catarrhalis.5
answer 4
Further questions to ask include the following.
• Is this Robbie’s first year of having a lot of contact with other children? (If he has not had previous exposure to infections through childcare then he is likely to continue having colds and ear infections)
• Does Robbie have a past history of other infections, such as pneumonia, suggestive of an immune deficiency?
• Does he swim regularly in a swimming pool? (Although there is evidence that for Aboriginal children in remote communities in Western Australia, swimming in pools can reduce ear infections, this mainly relates to children with perforated tympanic membranes and chronic otorrhoea. Although swimming on the surface of the water is not usually associated with eustachian tube and middle ear problems, swimming more than 60 cm below the surface is sufficient to insufflate infected nasopharyngeal secretions into the middle ear during an upper respiratory infection.7 If Robbie is having regular swimming lessons his parents could try keeping him out of the pool for winter)
• Are there concerns about his hearing either at home or in school?
Figure 11. Tissue spears. Author’s image

14
check Ear nose and throatcheck Ear nose and throat
• vaccination with the polyvalent pneumococcal vaccine reduces the incidence of AOM by 8%.
answer 8
Robbie should be reviewed in 2 days if he is no better. At that stage, if the AOM has not resolved, institute change to an antibiotic such as amoxycillin/clavulanate.
Robbie should also be reviewed at the 2 week mark to ensure that the perforation of the tympanic membrane has healed. Note that at 2 weeks following an episode of AOM, 70% of children will still have a middle ear effusion but most perforations will have healed.
answer 9
The infection in his right ear is resolving, and there is some air in the middle ear, indicating that the eustachian tube is starting to open and function again.
In his left ear, there is still a perforation of the tympanic membrane, but it is small and may close. There is also a patch of tympanosclerosis in the tympanic membrane, consistent with previous infection.
Your advice to Robbie’s mother should be to keep the left ear dry and return in about 3 months to check the perforation and the fluid.
answer 10
In his right ear, there is a middle ear effusion. It is opaque and the anterior process of the malleus is prominent. The tympanic membrane is retracted, especially posterosuperiorly.
In his left ear, the perforation has healed and there is AOM; the tympanic membrane may perforate again.
answer 11
Robbie has had a further ear infection and has an ongoing middle ear effusion. These factors are likely to be affecting his hearing and school work.
Management could involve:
• use of amoxycillin/clavulanate in case Robbie had a resistant Pneumococcus as he has had a recent infection treated with amoxycillin
• referral for audiology
• treating his nose – saline sprays help to clear the mucus, and steroid sprays help to reduce the size of the adenoids, but there is no evidence that either will improve the eustachian tube function and clear fluid from the middle ear.11
answer 12
The guidelines published in the American Academy of Family Physicians, American Academy of Otolaryngology-Head and Neck Surgery and American Academy of Pediatrics Subcommittee on Otitis Media With Effusion propose that indications for insertion of middle ear ventilation tubes include:12
• children with severe illness with pain, or a tympanic membrane perforation (these imply a more virulent organism)
• a child with known immunodeficiency
• indigenous children, including Aboriginal, Torres Strait Islander and Maori and other Pacific Islander children
• children with a cochlear implant.
The usual antibiotic recommended is amoxycillin, 15 mg/kg up to 500 mg three times per day for 5 days. If the child has an allergy to penicillin (excluding immediate hypersensitivity), the alternative medication is cefuroxime in a dose of 10 mg/kg up to 500 mg twice per day for 5 days, or ceflacor in a dose of 10 mg/kg up to 250 mg three times per day for 5 days.10 The efficacy of ceflacor is thought to be similar to that of amoxycillin but it may be less as it penetrates middle ear mucosa less efficiently.6
With a perforation of the eardrum, topical antibiotic drops are useful both to treat the middle ear and also to treat secondary otitis externa if present. The recommended antibiotics are quinolones such as ciprofloxacin with or without steroid, which are not ototoxic when there is a tympanic membrane perforation.6 If the tympanic membrane is intact there is no advantage in treating with topical antibiotics.
As Robbie has a perforation this ear should be kept dry. As there is infection and fluid in both his ears Robbie may not be hearing well. His mother should be warned of this and asked to notify the teachers at school to report concerns about his hearing or behavioural changes which could suggest hearing difficulties.
answer 7
Alice’s risk of recurrent otitis media depends on the presence of recognised risk factors for otitis media. These are:6
• age – especially 6–11 months
• race – eg. Indigenous Australian children. There are differences in the eustachian tube and immunological response, but socioeconomic factors are also important
• craniofacial abnormalities – including cleft palate and those caused by Down syndrome
• genetic – both anatomical and immunological
• birth order – children with older siblings are more likely to have infections than the first born.
There are recognised environmental factors, and Alice’s mother can help control these by implementing the following:
• reduce contact with people with upper respiratory infections, especially large group childcare centres
• avoid tobacco smoke both during and after pregnancy. Children exposed to passive smoking are more likely to have recurrent otitis media and have middle ear effusions that persist for longer
• breastfeed for at least 6 months, preferably 12 months. If bottle fed, prop the baby up as milk can reflux into the ear if lying flat, causing inflammation
• avoid pacifiers/dummies – this possibly increases the risk of AOM by inadvertent sharing in childcare centres
Case 3

15
check Ear nose and throatcheck Ear nose and throat
• chronic otitis media with effusion for 4 months or longer with conductive hearing loss. The level of hearing that is significant is not known, and probably differs for each child
• significant hearing loss
• known language delay
• learning/intellectual problems
• visual impairment in addition to hearing loss from chronic otitis media with effusion
• damage to the tympanic membrane with retraction pockets to prevent permanent ossicular erosion.
Middle ear ventilation tubes are also effective in preventing recurrent acute otitis media, and for the treatment of complications of acute otitis media such as facial nerve paresis and meningitis.6
answer 13
Treatment with prophylactic antibiotics (usually a single daily dose of amoxycillin 20 mg/kg) has some efficacy, however, due to concerns about antibiotic resistance, prophylactic antibiotics are reserved for children under special circumstances.13 This includes children who are a poor risk for general anaesthesia, or those who have had tubes inserted and have persistent infections.
answer 14
It is usually recommended that adenoidectomy be performed if the child needs a second set of ventilation tubes, unless there is significant nasal obstruction, in which case it may be performed earlier. Adenoidectomy has not been shown to be effective in preventing recurrent AOM.6
Case 3

16
check Ear nose and throatcheck Ear nose and throatCase 4
QuesTion 3
What ‘red flags’ suggest stroke syndrome?
QuesTion 4
You perform a head impulse test on Nigel to add weight to your suspected diagnosis. Describe how to perform a head impulse test.
QuesTion 5
What further examination could you perform to help identify the cause of Nigel’s vertigo?
QuesTion 1
What is the most likely clinical diagnosis on the basis of the information presented so far?
QuesTion 2
What is the differential diagnosis?
Case 4nigel is experienCing verTigo and nausea
Nigel is 52 years of age with a background history of hypertension, hypercholesterolaemia, impaired glucose tolerance and migraine, and a long history of heavy cigarette use. He presents to your clinic after the onset of severe vertigo and vomiting. The vertigo came on over a 20 minute period 5 hours earlier in the day. There is no history of previous vertiginous episodes even with his previous migraines. On examination, you note that Nigel is pale and sweaty with normal vital signs. You note that he has a left beating nystagmus which is enhanced on left gaze. The head impulse test is abnormal to the right with an abnormal corrective refixation movement. There were no other neurological signs evident. Hearing is clinically normal and otoscopy is clear.
17
check Ear nose and throatcheck Ear nose and throat Case 4
QuesTion 9
What treatment could you give in the postacute setting?
FurTher inFormaTion
After significant initial improvement over several weeks, Nigel experiences further recurrent episodic vertigo.
QuesTion 10
What are the possible causes of recurrence?
FurTher inFormaTion
The Romberg test is markedly positive as Nigel would have fallen if he were not held. Nigel is having considerable difficulty walking and is tending to veer to the right. The Hallpike manoeuvre induced left beating horizontal nystagmus, which is more accentuated than the spontaneous nystagmus described above. There is no latency to the nystagmus and it persisted throughout the positioning.
QuesTion 6
What is the significance of the examination findings described above?
QuesTion 7
What treatment would you give this patient in the acute setting?
QuesTion 8
Should you request imaging in Nigel’s case? What features would suggest that the patient ought to be considered for imaging study or admitted to hospital?

18
check Ear nose and throatcheck Ear nose and throat
Case 4 answers
answer 1
The most likely clinical diagnosis is acute vestibular syndrome. Acute vestibular syndrome is a description of a clinical syndrome which usually implies an acute peripheral vestibulopathy, however, occasionally a central disturbance can mimic this syndrome. The presumptive cause of acute vestibular syndrome is vestibular neuritis, otherwise known as vestibular neuronitis or viral neurolabyrinthitis. This clinical syndrome is commonly thought to be related to reactivation of herpes simplex virus infection of vestibular nerve ganglion (also known as Scarpa ganglion).
answer 2
The differential diagnoses are outlined below.
stroke
The vestibular pseudoneuritis syndrome can appear very similar to vestibular neuritis. Vestibular pseudoneuritis is due to brainstem/cerebellar ischaemia (ie. ischaemia in the posterior inferior cerebellar artery or anterior inferior cerebellar artery territories). Stroke should be considered when there are vascular risk factors, the presence of any one of the red flags or abnormal signs on examination of the cranial nerves. A careful ocular motor examination can help distinguish central vestibular pseudoneuritis and vestibular neuritis.14 The clinical signs in this case synopsis do not suggest a stroke syndrome. There are a number of red flags to consider in patients presenting with vertigo and nausea that are not present in Nigel’s case – these are outlined in Answer 3.
meniere disease
While Meniere disease, which is frequently overdiagnosed, can cause acute vertigo, it is not the likely cause in this case because:
• usually the vertigo of acute Meniere disease attacks would not last as long as 5 hours, though the after effects of nausea, disequilibrium and ear symptoms may last hours to days
• recurrent episodes are required to make the diagnosis
• associated ear symptoms (eg. fluctuating low frequency sensorineural hearing loss, aural fullness and tinnitus) while not invariably, are often present15 – Table 1 outlines the diagnostic criteria for Meniere disease.
benign paroxysmal positional vertigo
Episodes of vertigo in benign paroxysmal positional vertigo (BPPV) are usually:
• provoked by a change in position of the head or change in posture
• brief and not accompanied by vomiting and not associated with spontaneous nystagmus before provocation.
Case 4
Table 1. meniere diseaseThe american academy of otolaryngology-head and neck surgery Criteria for diagnosis of meniere disease16
• Recurrentspontaneousandepisodicvertigo–adefinitivespellofvertigo lasting at least 20 minutes, often prostrating, accompanied by disequilibrium than can last several days; usually nausea or vomiting, or both; no loss of consciousness. Horizontal rotatory nystagmus is always present
• Hearingloss(notnecessarilyfluctuating)
• Eithertinnitusorauralfullness,orboth
Certain Meniere disease Definite disease with histopathological confirmation
Definite Meniere disease Two or more definitive episodes of vertigo with hearing loss, plus tinnitus, aural fullness or both
Probable Meniere disease Only one definitive episode of vertigo and the other symptoms and signs
Possible Meniere disease Definitive vertigo with no hearing loss, or hearing loss with nondefinitive disequilibrium
Table 2. vestibular migraine
neuhauser criteria for diagnosing migrainous vertigo17
definite – all of the following features
probable – all of the following features
Episodic vestibular symptoms of moderate severity, such as:
•vertigo (spinning)
•positional vertigo
•head motion intolerance
Episodic vestibular symptoms of moderate severity, such as:
•vertigo (spinning)
•positional vertigo
•head motion intolerance
Migraine according to International Headache Society criteria*
One or more of the following features:
•migrainous headache
•migrainous symptoms during vertigo
•migraine specific triggers of vertigo (eg. specific foods, lack of sleep)
• response to antimigraine therapy
One or more of the following features during at least two vertiginous attacks:
•migrainous headache
•photophobia
•phonophobia
•migraine aura
Other diagnoses excluded by appropriate tests
Other diagnoses excluded by appropriate tests
* Headache Classification Committee of the International Headache Society. Classification and diagnostic criteria for headache disorders, cranial neuralgias and facial pain. Cephalalgia 1998;8(Suppl 7):1–96.

19
check Ear nose and throatcheck Ear nose and throat
to the opposite side. The test may then be repeated to assess for fatigability of the response (see Resources).
A positive Hallpike test has the following characteristics and suggests a diagnosis of BPPV:
• brief latency – in BPPV, there is usually a brief latency of several seconds before the onset of nystagmus and it usually lasts 10–20 seconds
• nystagmus – usually torsional (rotational around the anteroposterior axis of the eye globe) but may be horizontal. In BPPV, on performing the Hallpike manoeuvre, there is usually upbeating, torsional nystagmus arising from otolithic debris in the ipsilateral posterior semicircular canal. Horizontal nystagmus on positioning suggests that the lateral canal is affected. Downbeating, torsional nystagmus which occurs on positioning indicates that the ipsilateral anterior semicircular canal is affected
• reversal – upon sitting after a positive manoeuvre, the direction of nystagmus is reversed for a brief period of time
• fatigability – repetition of the test will result in less nystagmus each time.
answer 6
The presence of a positive Romberg test (a Romberg sign) indicates loss of proprioceptive or vestibular input, which, in the context of Nigel’s presentation, is supportive of a diagnosis of vestibular neuritis. On the other hand, when a central lesion is present where the cerebellum is affected, such as in the case of a stroke, while the patient is also unstable at rest, they are not made more unstable when performing a Romberg test (this constitutes a negative Romberg test).
In cases of acute vestibular syndrome such as Nigel’s, there is spontaneous horizontal nystagmus before performing the Hallpike manoeuvre, which suggests a peripheral cause of vertigo other than BPPV. In acute vestibular syndrome caused by vestibular neuritis, nystagmus is often noted while performing the Hallpike manoeuvre as well as it being present before performing the maneouvre. In these cases the Hallpike manoeuvre will not result in latency, reversal and fatigability in vestibular neuritis as it tends to in cases of BPPV.
In cerebrovascular causes of vertigo, spontaneous nystagmus can occur and it will usually be vertical or direction changing. On performing the Hallpike manoeuvre, there is upbeating, downbeating or direction changing nystagmus but no latency, reversibility or fatigability.
answer 7
Once a diagnosis of acute vestibular neuritis is made, treatment could consist of the following:
• symptomatic treatment with antiemetics and fluids for rehydration if necessary
• benzodiazepines may be useful in reducing the intensity of vertigo for the first 24–48 hours but should be used sparingly after this time period
• steroids – a course of steroids similar to that given for Bell palsy should be considered18,19
migraine
Migraine can cause acute vertigo, however, usually there are no clinical signs and there is usually, but not invariably, significant headache present. Consider a diagnosis of migraine where there is a past or family history of migraine. Like Meniere disease, recurrent episodes are required before a diagnosis of vestibular migraine can be made. The criteria for diagnosing migrainous vertigo are listed in Table 2.
answer 3
Any one of the following red flags suggests the possibility of a stroke or other central lesion:
•acuteunaccustomedheadache
•inabilitytostandorwalk
•thepresenceofspontaneousdirectionchangingnystagmus
•spontaneousverticalnystagmus
•anormalheadimpulse
•thepresenceofadditionalfocalneurologicalsigns.
answer 4
The head impulse test is performed by rapidly rotating the patient’s head while the patient is instructed to fixate on a central object such as the examiner’s nose. When the vestibulo-ocular reflex is intact, an equal and opposite eye movement keeps the eyes stationary in space. An abnormal result is indicated by failure to maintain fixation. In this case, movement of the eyes occurs then the patient will suddenly perform corrective refixation back to focus on the central object. An abnormal test suggests an acute vestibular syndrome due to vestibular neuritis and a normal test usually suggests the symptoms are due to a central lesion such as stroke, though this is not always the case and must be interpreted in context (see Resources).
answer 5
Further examination could consist of the following:
• Romberg test – to perform this test, the patient stands erect with their feet close together and eyes closed and is observed for 1 minute. Romberg sign is said to be positive if the patient becomes unsteady in this position
• bedside assessment of hearing
• assessment of gait and preponderance to veer to one or other side
• Hallpike manoeuvre – take care with the manoeuvre in patients who have neck disease and avoid performing the manoeuvre in patients with major cervical spine instability. After explaining to the patient what you are going to do, the patient sits upright with the head rotated 30–45 degrees laterally. The patient is then rapidly moved into a supine position on the examination couch with the head hanging over the end of the couch or a pillow placed behind the shoulders. The patient’s head is supported either by the examiner or by the couch if a pillow is placed behind the shoulders. The examiner then observes the patient for nystagmus and asks about vertigo. Then the test is repeated with the patient’s head turned
Case 4

20
check Ear nose and throatcheck Ear nose and throatCase 4
decompensation
After initial improvement from vestibular neuritis, decompensation can occur and the reasons are often not clear. Formal vestibular investigations and vestibular physiotherapy may be useful in clarifying this clinical scenario.
If the original bout of acute vertigo lasts less than 24 hours, and the Hallpike manoeuvre is repeatedly negative, then other possible diagnoses such as vestibular migraine, Meniere disease or even ‘recurrent vestibulopathy’ (a term used for recurrent unexplained vertigo) may explain recurrent symptoms.
migraine
With migraine, vertigo may occur with or without headache.
meniere disease
Additional clinical features such as those outlined in Table 1 and 2 should sort out whether migraine or Meniere disease is most likely.
recurrent vestibulopathy
A term used for recurrent unexplained vertigo.
recurrent vestibular neuritis
Recurrent vestibular neuritis may occur but is uncommon.
vascular vertigo
In Nigel’s case, vascular vertigo (vertigo due to cerebrovascular disease) might be suspected with the occurrence of recurrent vertigo, particularly in the presence of vascular risk factors. Usually the recurrent symptoms would be brief, lasting seconds to minutes, and would not ordinarily continue beyond 6–8 weeks without other transient ischaemic attack manifestations or permanent posterior circulation territory infarction.
perilymph fistula or autoimmune inner ear disease
Perilymph fistula and autoimmune inner ear disease would be other much less common causes of recurrent vertigo and would usually be associated with hearing loss.
• antiviral therapy – there is controversy over the use of antiviral therapy in this situation, although the existing evidence does not support its routine use.19
answer 8
In Nigel’s case, computed tomography (CT) or MRI brain would not be considered absolutely necessary. Nigel could be referred to hospital for imaging to look for evidence of stroke if there is in any doubt about the diagnosis, or for rehydration if his vomiting is severe.
If there is significant suspicion of a stroke, then the patient ought to be admitted for observation and investigation. The presence of any one of the red flags described in Answer 3 with the presence of vascular risk factors suggest a possible stroke, in which case a neuroimaging study, preferably MRI, needs to be ordered. Frequently a CT brain is ordered in this situation, however, a CT scan is not sufficient to rule out a stroke in the posterior fossa. A CT brain scan may reveal a large cerebellar hemisphere infarct or a posterior fossa haemorrhage. Usually the CT brain in the clinical scenario described above is normal. Certainly if there is no, or limited, access to MRI, then it would be reasonable to get a CT brain and consider transfer to another institution with MRI access. If there is doubt about the diagnosis, admission for observation would be wise.
answer 9
Following a bout of vestibular neuritis, recovery usually begins after a few days, although the patient may be rendered bedbound or housebound for up to 1 week.
As the patient recovers from the acute disturbance, vestibular adaptation exercises or even formal vestibular physiotherapy should be considered to aid further recovery over the ensuing weeks or months.
answer 10
Possible causes of recurrent vertigo include the following.
postvestibular neuritis benign positional vertigo
The recurrence of vertigo after a few weeks in Nigel most likely indicates postvestibular neuritis benign positional vertigo. Vestibular neuritis frequently involves the superior division of the vestibular nerve resulting in damage/dysfunction to the afferents from the superior and lateral semicircular canals and sparing the posterior semicircular canal afferents. Therefore any otolithic debris dislodged by the acute vestibular insult may accumulate in the posterior semicircular canal and give rise to benign positional vertigo.
This diagnosis may be confirmed by performing a Hallpike manoeuvre, which will be positive. It is treated satisfactorily with a particle repositioning manoeuvre such as the Epley (see Resources) or Semont manoeuvre.19,20

21
check Ear nose and throatcheck Ear nose and throat Case 5
QuesTion 3
What features would you be interested in on examination?
QuesTion 4
How would you differentiate an anterior and posterior nasal bleed?
QuesTion 5
What are the steps in treating epistaxis?
QuesTion 1
What are the predisposing factors for epistaxis? Which of these are you concerned about in John?
QuesTion 2
What other features would you be interested in when taking further history from John?
Case 5John’s nosebleed
John is 65 years of age and presents to your clinic with a sudden onset of a right sided nosebleed. He has had no significant nasal or sinus problems in the past. He has a past history of mild hypertension and coronary heart disease and takes aspirin 100 mg/day, atorvastatin 10 mg/day and ramipril 10 mg/day.

22
check Ear nose and throatcheck Ear nose and throatCase 5
Case 5 answers
answer 1
There are various local and systemic conditions which can predispose to epistaxis. These include:
• local conditions – conditions such as trauma, structural abnormalities (eg. septal deviation/perforation); inflammatory diseases (eg. infection, allergy, granulomatous disorders); tumours and vascular malformations21
• environmental conditions – the decrease in ambient humidity during winter causes a drying effect of the nasal mucosa that impairs wound healing and enhances crust formation.22 This encourages local digital trauma, and a vicious cycle of trauma and inflammation ensues
• medications – such as intranasal steroids used for allergic rhinitis, aspirin, anti-inflammatories, clopidogrel and warfarin, and drugs such as cocaine used on a long term basis, may predispose to epistaxis
• systemic factors – such as deficiencies in coagulation, vascular diseases and cardiac/pulmonary diseases (the latter, as a result of the combination of increased intravascular pressure and medically-induced coagulopathy) have been associated with more severe epistaxis (as well as higher risk for posterior nasal bleeds).21 Investigation for coagulation disorders should be considered in recurrent and multifocal bleeds.
John has one important predisposing factor for epistaxis, which is his use of aspirin. While John has hypertension, the association between hypertension and severe epistaxis is still debateable.21
answer 2
It is important to ask John about the initial laterality, duration and amount of blood loss and whether he has had nose bleeds before. It is also important to ask him questions directed at establishing the cause of his nosebleed, such as a recent common cold, nasal blockage, discharge or crusts, local digital trauma, use of medications, intake of alcohol and drugs, past history of allergic rhinitis and systemic disease and whether he has had any bleeding elsewhere. It is also important to ask him questions directed at identifying the source of bleeding, namely whether it is from an anterior nasal source or posterior nasal source. To elicit this, ask where the bulk of the bleeding seems to be presenting (into the throat or out through the nose), as well as about triggers and response to any first aid applied.
answer 3
Important features on examination include assessment of haemodynamic status and examination of John’s nose to identify the source of the bleeding. The rest of the examination depends on features elicited in the history. In cases of significant bleeding, history, examination and treatment will proceed concurrently.
FurTher hisTory
You advise John to pinch the soft part of his nose with pressure exerted toward his face with his head tilted slighty forward for a period of 5 minutes but John continues to bleed through his mouth. On examination, there is blood oozing from both nostrils but more profuse on the right side. There is difficulty visualising the nasal cavity because of continuous bleeding and you decide to pack the nose blindly with nasal tampons. Despite this intervention, John continues to bleed into the oropharynx.
QuesTion 6
What packing materials can you use to stop John’s bleeding?
QuesTion 7
What situations would prompt you to send a patient with epistaxis to a hospital emergency department?
23
check Ear nose and throatcheck Ear nose and throat Case 5
Recurrent epistaxis associated with persistent nasal obstruction should be further evaluated for neoplastic causes. Clinical signs of skull base tumours (eg. cranial nerve palsies), intracranial spread and neck node metastases can suggest malignancy and should be referred immediately for imaging and consult with an otolaryngologist or neurosurgeon. A young, male patient with reoccurring significant nosebleeds should be investigated for juvenile angiofibroma.
answer 5
Most cases of epistaxis are self limiting and patients rarely seek medical help. Patients with spontaneously resolving epistaxis are advised to avoid local trauma and avoid nose blowing, hot drinks and alcohol for 12 hours and are instructed on first aid for epistaxis should it recur. Measures to improve nasal hydration such as topical antibiotic/antiseptic ointments and air humidifiers may be helpful.21,22
Below is a stepwise treatment of epistaxis in the office setting:
• first aid in mild cases where an anterior epistaxis is suspected – this involves pinching the nostrils together, between the patient’s thumb and index finger, with pressure applied toward the face. This is performed in a position with the patient’s head slightly forward for a total of 5 minutes continuously. In addition, someone else can apply an ice pack to the bridge of the nose
• patients with persistent bleeding should be assessed for the need for resuscitation and the usual ‘ABCs’ must be performed when necessary. The attending health providers should always protect themselves by using the ‘three Gs’ – gowns, goggles and gloves. Epistaxis can potentially deteriorate from a mild bleed to an uncontrollable exsanguination
• nasal toilet and evacuation of clots if a suction device with appropriate suction tips is available
• decongestion and anaesthesia of nasal mucosa with cophenylcaine (lignocaine hydrochloride plus phenylephrine) helps to control low flow minor bleeds, and permits a thorough inspection of the nasal cavity to determine the specific site of the bleeding vessel. Cophenylcaine soaked in ribbon gauze is introduced into the nasal cavity. Pay attention to recommended doses for lignocaine, especially when dealing with children and older patients
• for anterior epistaxis – you can perform chemical cauterisation with silver nitrate sticks or electrocautery. Chemical cauterisation is safely performed after the nose has been toileted, decongested and anaesthetised. Do not cauterise blindly, and avoid cauterising both sides of the septum simultaneously (Figure 12)
• nasal packing – anterior with or without posterior packing (this is described further in Answer 6 )
• in the case of refractory epistaxis refer the patient to a hospital emergency department or ENT specialist.
answer 4
There are some factors in the history that will guide you in identifying the source of the bleeding as being either anterior or posterior. These are outlined in Table 3.
The source of the bleeding can be differentiated by two means on examination.
• Response to first aid – this includes pinching the nostrils together, or response to a properly applied anterior nasal pack. More than 90% of nasal bleeding arises from the ‘Little area’ in the anterior nasal septum.23 Anterior epistaxis usually responds to pressure from pinching the nostrils together or a properly applied anterior nasal pack. If the bleeding arises from another source, such as the branches of the sphenopalatine artery posteriorly, these manoeuvres will be ineffective. If a patient continues to bleed, particularly with the blood running down the pharynx despite a properly applied anterior pack, and coagulation defects have been ruled out or corrected, a posterior bleed must be suspected
• Inspection of the nasal cavity – this requires a good light source, a nasal speculum and suction equipment if available, and even this allows examination of only the anterior nasal cavity. Locating the source of bleeding is often difficult, especially when confronted with a profusely bleeding patient
The source of the bleeding can also be indentified with endoscopy. In a well anaesthetised and decongested nose endoscopic evaluation will often allow definite source identification.24,25
FeedbaCk
In patients with recurrent, profuse nosebleeds who have mucocutaneous telangiectasias, a possible diagnosis of hereditary haemorrhagic telangiectasia (HHT – Osler disease) should be considered. It has an incidence of 2–4 /100 000 and is an inherited disorder through an autosomally dominant gene. The disease is characterised by mucocutaneous telangiectasia and arteriovenous malformations brought about by the absence of smooth muscle and elastic tissue in the vascular endothelium. Epistaxis is the most common presentation of HHT.21,26
Table 3. Factors in history to guide you in identifying source of bleeding24
Factors anterior epistaxis posterior epistaxis
Bleeding presentation Anterior nosebleed but can have oropharyngeal bleed in severe cases
Mainly oropharyngeal bleed
Triggering factors Bleeding following anterior nose trauma
No known triggering factors
History of bleeds Previous epistaxis with history of anterior septal cauterisation
Previous posterior nasal bleed
Response to anterior nasal pressure
Yes No

24
check Ear nose and throatcheck Ear nose and throatCase 5
answer 6
Packing materials include absorbable or nonabsorbable types.
Absorbable materials include oxidised regenerated cellulose (Surgicel®) and gelatin foams (Gelfoam®). The mechanism of action is not well described but oxidised regenerated cellulose is believed to form a scaffold for platelets to attach to. The effect of gelatin foams on the other hand is thought to be physical rather than an alteration of clotting mechanism.
Nonabsorbable packs include polyvinyl acetyl sponge (Merocel®), impregnated ribbon gauze (BIPP Gauze®), calcium alginate (Kaltostat®) or inflatable balloon catheters (Rapid Rhino®, Foley Catheter®). Once the nose has been adequately decongested and anaesthetised with cophenylcaine (lignocaine hydrochloride plus phenylephrine), most of these packs are easy to introduce with forceps. Packs are generally left in situ for 1–5 days depending on the patient’s risk factors, coagulation state and severity of bleed.27
Consider antibiotic cover for S. aureus to minimise the risk for toxic shock syndrome.
answer 7
Situations that would prompt you to send a patient with epistaxis to a hospital emergency department include:
• signs of haemodynamic shock (eg. pallor, tachycardia, hypotension, tachypnoea, vasovagal reflex)
• persistent bleeding despite adequate first aid measures
• suspicion of posterior nasal bleed
• recurrent anterior epistaxis not responding to cauterisation
• patients with medical comorbidities requiring close observation
• epistaxis secondary to severe coagulation deficits requiring reversal or blood transfusion
• bleeding from a suspected nasal mass or vascular malformation
• significant bleeding after nasal, sinus or anterior skull base surgery. Brand names are for example only and no particular
brand is recommended or endorsed either by the editors or publishers.
Figure 12. A) Arrow pointing to source of right anterior epistaxis after the nose has been decongested; B) Right anterior epistaxis after being cauterised with silver nitrate; C) Cauterised area covered with oxidised regenerated cellulose (Surgicel®). IT = inferior turbinate. Author’s image
iT iT
septum septum
a b C

25
check Ear nose and throatcheck Ear nose and throat Case 6
QuesTion 3
What features would you be interested in on examination?
QuesTion 4
What investigations would you request to confirm your working diagnosis?
QuesTion 1
What is the likely diagnosis?
QuesTion 2
What features suggest this diagnosis in Claire? What other questions would you ask Claire in relation to contributory/exacerbating factors and associated conditions?
Case 6Claire’s ongoing allergies
Claire is a cleaner who is 32 years of age and presents with symptoms of clear nasal discharge (rhinorrhoea) and nasal irritation that have been present for the last few years but are worsening. Symptoms occur on most days but she finds them to be worse at certain times of the year, especially during the spring and summer months. Over the last 6 weeks the symptoms have been present every week. She remains otherwise well, with no drug allergies, but reports that her daughter who is 7 years of age has had similar symptoms.

26
check Ear nose and throatcheck Ear nose and throatCase 6
Case 6 answers
answer 1
Claire presents with symptoms of rhinitis. As these are occurring on most days of the week (more than 4) and for more than 4 consecutive weeks, they are termed persistent. Previously, terminology classified rhinitis as seasonal or perennial. However, the terms intermittent and persistent are now favoured. Claire’s rhinitic symptoms may then be also subclassified as allergic or nonallergic and as mild, moderate or severe.28 From the history given, it is likely that Claire has persistent allergic rhinitis.
answer 2
Features of Claire’s history supportive of a diagnosis of allergic rhinitis include:
• the fact that her symptoms are seasonal
• the fact that her daughter also has symptoms, suggesting a possible genetic predisposition
• her profession as a cleaner, and therefore exposure to chemicals in cleaning products.
Taking further history should aim to help establish the initial diagnosis of allergic rhinitis and rule out alternative contributory factors such as medications. Further history should include enquiries about:
• atopy – personal history of atopy including the presence of eczema and asthma and precipitation or exacerbation of symptoms with the presence of pets at home
• family history of rhinitis – the fact that her daughter has similar symptoms is relevant because genetic factors within the human leukocyte antigen system have been identified in allergic rhinitic patients.29 However, the causes for allergic rhinitis are multifactorial and environmental factors play a significant part
• asthma – symptoms suggestive of asthma. Take a full respiratory history and, if possible, assess airway function before and after bronchodilator use, owing to the potential of individuals with persistent rhinitis to have undiagnosed asthma or bronchial hyper-reactivity. Additionally, rhinitic patients with asthma have been shown to experience more hospital admissions and visits to GPs,30 which supports the idea of the unified airway and that rhinitis and asthma represent a continuum of disease at differing locales along the respiratory tract
• occupational – Claire’s profession may also be a source of her symptoms either through exposure to an increased allergen load while cleaning or due to sensitivity to cleaning chemicals
• medications – a wide range of medications including nonsteroidal anti-inflammatory drugs (NSAIDs), angiotensin coverting enzyme (commonly known as ACE) inhibitors, beta-blockers and oral contraceptives can generate nasal
QuesTion 5
What would your next management step be and what therapeutic options are available?
QuesTion 6
What recourse would you undertake if Claire’s symptoms were persistent?

27
check Ear nose and throatcheck Ear nose and throat Case 6
• Antihistamines – the previous generation of sedating H1-blockers has given way to the second generation of nonsedating antihistamines which can provide excellent symptom control
• Intranasal corticosteroids – intranasal corticosteroids are also excellent at controlling nasal symptoms but do not have an immediate onset of action. Their method of delivery and low dose results in minimal risks owing to low systemic absorption but can cause dryness, bleeding and nasal irritation/stinging. While effective for nasal symptoms, the presence of ocular symptoms may require additional therapy directed at the eye
• Intranasal anticholinergics – these can be very effective in the control of rhinorrhoea and while not being a first line choice in allergic rhinitis, can be helpful in vasomotor rhinitis in the elderly
• Cromone – again, while effective at symptom control in a subgroup of people, their regimen requires frequent and continued administration that can affect compliance
• Leukotriene antagonists – these have been found to be beneficial in treating symptoms of allergic rhinitis on par with H1-blockers but inferior to corticosteroids.35
When symptoms are mild, any of the above groups may be used in symptom control but when moderate or severe, intranasal corticosteroids would be preferred.
answer 6
If symptoms persisted despite treatment, referral to a specialist should be considered. At that stage, associated anatomical abnormalities would be assessed and perhaps a short course of oral steroids trialled. Failure of medical therapy to control symptoms may then prompt consideration of surgical intervention in the form of inferior turbinoplasties to improve symptoms of nasal congestion/obstruction. However, such intervention would be an adjunctive therapeutic modality as the underlying allergic aetiology would not have been dealt with. Alternatively, referral to an immunologist for consideration of immunotherapy may be considered. However, while current regimens can provide excellent rates of control, patients should be counselled regarding prolonged therapeutic times, the potential for anaphylaxis and failure of treatment.
symptoms. In particular, intranasal vasoconstrictors may cause rebound rhinitic symptoms following extended use, a condition termed ‘rhinitis medicamentosa’.31
answer 3
Examination is secondary in the diagnostic process in this condition. Examination should aim to exclude alternate pathology such as septal deflection (septal deviation) or nasal polyposis. However, features such as hypertrophied inferior turbinates and the ‘allergic salute’ which results in a crease on the nose due to the patient repeatedly rubbing the nose upwards, would further lend weight to a rhinitic aetiology.
answer 4
A number of modalities exist to investigate allergic aetiologies. However, skin prick testing (SPT) has been shown to provide favourable sensitivity32 when performed by trained practitioners in patients who have been correctly counselled before testing, ie. to avoid medications that would suppress the wheal and flare response before testing. Blood tests in the form of immunoglobulin E specific, radioallergosorbent (RAST) tests provide lower sensitivity but higher specificity and do not expose the patient to the risk of anaphylaxis. However, the relationship between allergen identified on testing and symptoms is less certain with RAST testing than with SPT.
A common allergy test battery would assess sensitivity to house dust mites (the most common being dermatophagoides pteronyssinus and farinae), grasses, pollens, fungi, cats and dogs.
answer 5
Your next management step in Claire could include advice on the following conservative measures and discussion about various initial medical therapeutic options.
Conservative advice
If SPT was positive to specific allergens, allergen avoidance advice would be appropriate. Measures to combat dust mites include the reduction of soft furnishings, regular cleaning with a vacuum cleaner which has a high efficiency particulate air filter (commonly known as HEPA filter) and the use of protective bedding. Dust mites thrive in areas of high humidity (>80%) and high temperature (>20°C). Therefore, closed environments using central heating may contribute to their proliferation. Humidity levels <50% cause dust mite death.33 A Cochrane Review34 has suggested that measures to reduce dust mites result in some minimal improvement in symptoms but the studies were generally small and of poor methodological stature.
Broadly speaking, initial medical therapeutic options fall into the drug categories outlined below.
• Decongestants – these are generally alpha-agonists and achieve symptom control through vasoconstrictive mechanisms. They should not be used for more than 3 days in a row owing to the risk of leading to rhinitis medicamentosa described in Answer 2

28
check Ear nose and throatcheck Ear nose and throat
QuesTion 3
Would you arrange any investigations at this stage?
QuesTion 4
What treatment options could you offer Julie at this stage?
QuesTion 5
What management would you consider if Julie’s symptoms failed to resolve? At what stage would you consider this?
QuesTion 6
You see Julie at the 1 month mark and her symptoms are well controlled. What will you do now?
QuesTion 1
State the most likely diagnosis and other features within the history that you would enquire about in relation to this.
QuesTion 2
What would be your next step in the consultation?
FurTher inFormaTion
Examination of the nose reveals a reddened, swollen mucosa with no focal lesions. Julie’s sinuses are nontender. Examination of the throat and ears is normal. There are no cervical lymph nodes palpable.
Case 7
Case 7Julie’s had a runny nose and Feels CongesTed
Julie is 42 years of age, has a past history of asthma and is a smoker. She attends your practice with a 4 month history of postnasal drip and bilateral nasal congestion. She is otherwise well but reports being allergic to aspirin and NSAIDs.

29
check Ear nose and throatcheck Ear nose and throat
Case 7 answers
answer 1
Julie presents with symptoms that suggest chronic rhinosinusitis (CRS). Symptoms suggestive of this diagnosis that you would enquire about include nasal congestion/blockage/obstruction, anterior nasal discharge and postnasal drip. Symptoms such as halitosis and mouth breathing may occur secondary to either nasal obstruction or nasal discharge. Additionally, symptoms of facial pressure or pain or reduction or loss of sense of smell may be present. When these symptoms are present for more than 12 weeks in 1 year, they are termed chronic (persistent) rhinosinusitis and acute (intermittent) when they occur for fewer than 12 weeks in 1 year.36 The history should be completed with enquiries into the presence of nasal bleeding, crusting, cacosmia (perception of a foul odour when none exists), and unilateral symptoms. The presence of nasal bleeding, cacosmia or unilateral symptoms or the presence of neurological, visual or systemic symptoms would merit urgent referral to an ENT specialist.
answer 2
The next step would be to examine Julie. Examination of the anterior portion of the nasal cavity (anterior rhinoscopy) involves inspection with the naked eye and then inspection with a headlight, nasal speculum or otoscope to identify the presence of any signs of infection such as mucopus or obstructive lesions such as a septal deflection, nasal polyposis or turbinate hypertrophy.
answer 3
Investigations such as X-ray and CT scanning are not helpful at this presentation. X-ray and CT scans are not usually necessary when managing uncomplicated sinonasal disease in general practice Plain radiograph correlation with CRS is poor although CT can be useful in surgical planning to identify anatomical features.37 Magnetic resonance imaging is not indicated for the diagnosis or management of CRS but may be useful in combination with CT for the differentiation of fungal and neoplastic disease.
If the history and/or examination suggested sinister pathology, investigations targeted towards the suspected pathology should be considered.
answer 4
If your history and examination led to the diagnosis proposed in Question 1, then treatment with a topical steroid spray together with nasal douching is appropriate. Nasal douching has potential beneficial effects through mechanical cleansing of nasal mucous and also improvement in mucociliary transport. Nasal douching can be administered using commercial preparations or may be made up by adding 1 teaspoon of salt (non-iodised with no caking ingredients) and 1 teaspoon of baking soda to a pint of water that has been boiled and cooled. This can then be sniffed in from a cupped hand to the
QuesTion 7
If Julie had left sided (instead of bilateral) nasal obstruction and anterior rhinoscopy revealed a polypoid lesion in her left nasal cavity, what diagnoses would you consider and what would be your next management step?
QuesTion 8
Are there any other features in Julie’s history that prompt special consideration?
QuesTion 9
What red flag symptoms are important to ascertain in cases of sinus pathology?
Case 7

30
check Ear nose and throatcheck Ear nose and throatCase 7
answer 8
Three features in Julie’s history prompt special consideration.
• First, her smoking is important. Smoking and other atmospheric pollutants have been shown to affect nasal mucosa in vitro, however, population based data has not supported this40
• Second, Julie’s asthma is important. In patients with asthma in coexistence with nasal polyposis, the literature presents evidence that control of nasal polyposis through surgical measures may have beneficial effects on pulmonary function41
• Third, her aspirin sensitivity is important when combined with nasal polyposis and asthma. This symptom complex has been termed Samter triad. Patients with Samter triad are notoriously difficult to manage owing to their recalcitrant disease process despite medical and surgical therapy and may require frequent courses of oral steroids and nasal polypectomy procedures. Consequently, a multidisciplinary approach including a chest physician, ENT surgeon, endocrinologist and immunologist may be appropriate.
answer 9
Red flag symptoms that are important to ask about include:
• unilateral nasal obstruction or discharge – the differential diagnoses of unilateral symptoms have been discussed in Answer 7
• symptoms due to extension of pathology into the nearby orbit – these symptoms include epiphoria (watery eyes), particularly if it is unilateral, diplopia and reduced vision. Owing to the proximity of the orbit to the nose and paranasal sinuses, pathologies within the latter region may cause obstruction of the nasolacrimal duct resulting in tearing. Expansion may result in globe displacement with invasion, possibly causing ophthalmoplegia and/or visual loss. The coexistence of such findings would merit urgent specialist referral
• symptoms which may indicate serious underlying pathologies. These include:
– blood in the saliva or in the nasal discharge. This could suggest neoplasm
– constitutional symptoms such as weight loss and anorexia could suggest neoplasm or an inflammatory disorder
– respiratory symptoms such as cough and shortness of breath or recurrent respiratory infections could suggest cystic fibrosis or Kartagener syndrome in the paediatric population.
postnasal space and then spat out. The side effect profile for topical steroid sprays is minimal and mainly includes initial stinging sensation, nasal dryness and epistaxis. The initial stinging sensation usually settles after a few days of use but may be reduced through the use of aqueous based intranasal corticosteroid preparations.
The side effect of dryness may be helped through douching, and epistaxis helped through instilling the nasal spray such that it is not always directed medially toward the nasal septum. Systemic absorption and influence upon the hypothalamic pituitary axis38 are minimal owing to the relatively low concentration dose and local nature of application and should therefore not discourage prescription of topical nasal steroids.
answer 5
If symptoms are not controlled after 1 month of the above treatment, referral to an ENT specialist is advised. An ENT specialist will often investigate infective components and comorbidities, including allergies, and consider further trials with topical and oral steroids. Additionally, a 3 month trial of macrolide therapy may also be prescribed. The use of macrolides in this manner is related to their anti-inflammatory properties and has been shown to have good efficacy.39 A desensitisation injection regimen may be appropriate where a specific allergy has been identified on skin prick testing. Surgery may be considered in specific cases if medical therapy fails.
answer 6
If Julie’s symptoms are controlled at the 1 month mark, the treatment regimen with intranasal steroids and nasal douching should be continued to the 3 month mark followed by a period of cessation with recommencement should symptoms recur.
answer 7
The most likely diagnosis if this were the clinical scenario is a benign inflammatory polyp. A benign inflammatory polyp is the most common cause of persistent unilateral obstruction if anatomical deformities such as septal deflection are excluded. A benign inflammatory polyp can appear as a uniform, slightly translucent swelling usually arising from beneath the middle turbinate. If large, a polyp may occlude the entire nasal passage and even present at the nares (nostrils).
Hypertrophy of the inferior turbinate may appear similar to a nasal polyp and be misinterpreted as such. However, hypertrophied inferior turbinates appear more opaque, arise from the lateral wall and are very sensitive if touched by a probe. Further, application of a decongestant spray can reduce the turbinates to clarify their nature but will not alter the size of true nasal polyps.
However, as the history in Julie’s case suggests unilateral symptoms, it is important to consider the possibility of an antrochoanal polyp, inverted papilloma, or other sinonasal inflammatory or neoplastic aetiologies.
The initial presentation of unilateral signs and symptoms should always prompt caution and consequently the next management step would be to refer to a specialist to exclude sinister pathologies. A specialist is likely to perform formal nasendoscopy to assess for sinister pathologies and identify the presence of further polyps on the contralateral side.

31
check Ear nose and throatcheck Ear nose and throat Case 8
QuesTion 2
What is the diagnosis and what organisms can cause this condition with otoscopy findings as shown in Figure 13?
QuesTion 3
What would be the diagnosis if instead of the otoscopic findings above, you had noted that there was minimal discharge, the ear canals were erythematous and tender to touch with the speculum, you were able to see the tympanic membranes and otoscopic findings were as shown in Figure 14? What organism can cause this condition with otoscopy findings as shown in Figure 14?
QuesTion 1
What is the likely diagnosis? What features are important to ascertain when taking Jim’s history?
FurTher hisTory
On otoscopic examination, you note the presence of purulent discharge and erythematous ear canals that are tender to touch with the speculum. You are unable to see the tympanic membranes. Otoscopy findings are shown in Figure 13.
Case 8Jim has painFul bloCked ears
Jim is 35 years of age and presents with a 1 week history of bilateral otalgia and blocked ears. The last 2 nights he has been unable to sleep due to pain. He has tried cleaning his ears with cotton buds and has noticed yellowish material on the tip of the cotton bud.
Figure 13. Image of Jim’s ear. Reproduced with permission from hawkelibrary.com Figure 14. Image of ear canal. Reproduced with permission from hawkelibrary.com
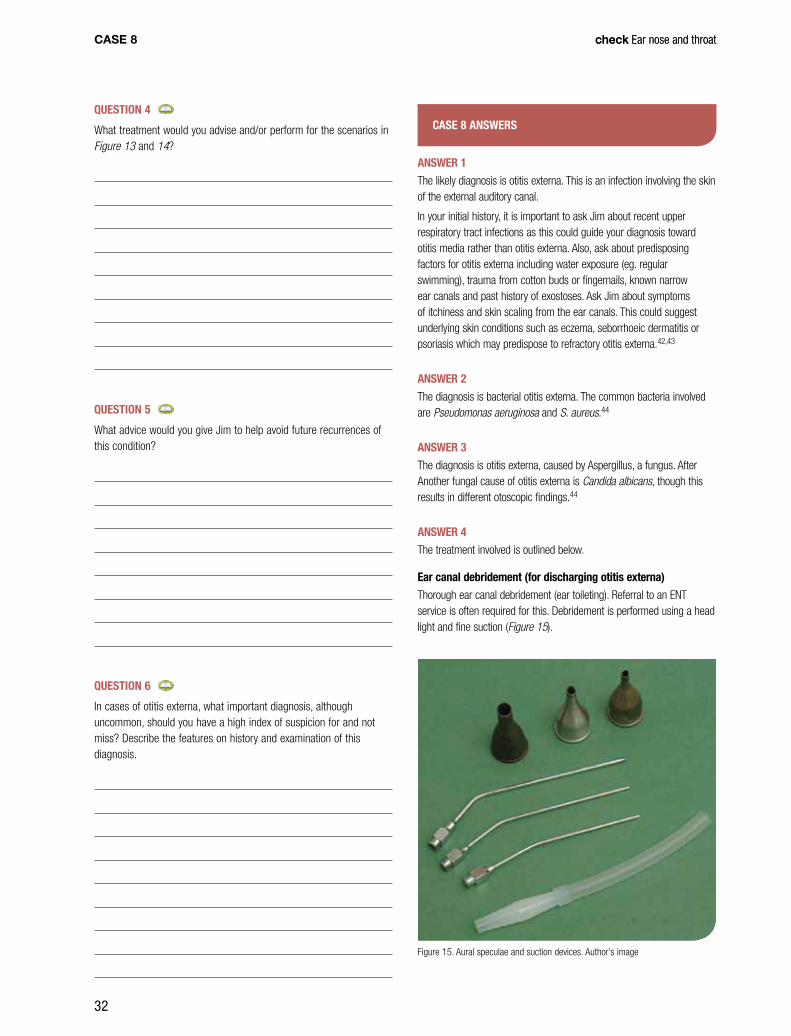
32
check Ear nose and throatcheck Ear nose and throat
Case 8 answers
answer 1
The likely diagnosis is otitis externa. This is an infection involving the skin of the external auditory canal.
In your initial history, it is important to ask Jim about recent upper respiratory tract infections as this could guide your diagnosis toward otitis media rather than otitis externa. Also, ask about predisposing factors for otitis externa including water exposure (eg. regular swimming), trauma from cotton buds or fingernails, known narrow ear canals and past history of exostoses. Ask Jim about symptoms of itchiness and skin scaling from the ear canals. This could suggest underlying skin conditions such as eczema, seborrhoeic dermatitis or psoriasis which may predispose to refractory otitis externa.42,43
answer 2
The diagnosis is bacterial otitis externa. The common bacteria involved are Pseudomonas aeruginosa and S. aureus.44
answer 3
The diagnosis is otitis externa, caused by Aspergillus, a fungus. After Another fungal cause of otitis externa is Candida albicans, though this results in different otoscopic findings.44
answer 4
The treatment involved is outlined below.
ear canal debridement (for discharging otitis externa)
Thorough ear canal debridement (ear toileting). Referral to an ENT service is often required for this. Debridement is performed using a head light and fine suction (Figure 15).
Case 8
QuesTion 4
What treatment would you advise and/or perform for the scenarios in Figure 13 and 14?
QuesTion 5
What advice would you give Jim to help avoid future recurrences of this condition?
QuesTion 6
In cases of otitis externa, what important diagnosis, although uncommon, should you have a high index of suspicion for and not miss? Describe the features on history and examination of this diagnosis.
Figure 15. Aural speculae and suction devices. Author’s image

33
check Ear nose and throatcheck Ear nose and throat
an over-the-counter preparation containing alcohol and acetic acid after swimming. Use of cotton buds should be avoided. Any underlying skin conditions should be treated.
answer 6
A diagnosis that is important not to miss is malignant otitis externa (or skull base osteitis). Malignant otitis externa is a potentially life threatening infection of the external ear and skull base. This most commonly presents in elderly patients, diabetic patients and the immunocompromised (eg. HIV-infected patients and postchemotherapy patients). It usually presents with unrelenting otalgia over several weeks. On examination there is ear discharge, with granulation tissue visible in the floor of the external ear canal. There may be facial nerve or other lower cranial nerve involvement. Investigations include:
• CT scan of the temporal bones to document the extent of disease
• bone scan to document osteomyelitis
• gallium scan to document and track active disease.
Malignant otitis externa is treated with a prolonged course of intravenous and oral antibiotics in consultation with an infectious disease unit. A high index of suspicion is needed for early diagnosis in high risk populations as the condition has a significant mortality.42 Urgent referral is indicated.
If suction is not available, a dental brooch (Figure 16) with a small piece of cotton wool wound around the tip can be used, under direct vision and with care. This procedure requires skill and training, as the ear is often exquisitely painful in otitis externa and trauma to the canal wall or tympanic membrane can occur with this technique.
Ear toileting may need to be repeated after several days to ensure the drops are effective. It is important to debride sufficiently to visualise the tympanic membrane before coming to a definitive diagnosis of otitis externa. Otitis media with a discharging perforation may mimic otitis externa.45
ear drops
Bacterial otitis externa can be treated with either framycetin sulphate/gramicidin/dexamethasone ear drops or ciproxin hydrocortisone ear drops. Treatment is usually continued for 7–10 days. If there is concern about a perforated tympanic membrane, ciproxin drops should be used without the steroid component, which may cause stinging.
An otowick is inserted (Figure 17 and 18) if there is marked canal oedema. The wick helps to reduce oedema, delivering the topical antibiotic and steroid preparation deep in the canal. It is normally removed after 48 hours and further ear toileting performed.
Fungal otitis externa may be treated with either flumethasone pivalate/cliquinol drops for 2 weeks or alternatively, the ear canal may be filled with otocomb ointment for 1 week, followed by flumethasone pivalate/cliquinol for 1 week.
oral analgesia
Moderately strong analgesia may be required for several days.
Treatment of underlying skin conditions
Underlying skin conditions, such as eczema and psoriasis, should be treated.
FeedbaCk
Oral antibiotics are not normally required unless there is associated perichondritis (in which case a course of oral ciprofloxacin is given), concurrent otitis media or systemic illness.46
Microbiologic swabs are not normally necessary to direct treatment unless the patient is not responding to the above treatments or malignant otitis externa is suspected.
answer 5
Jim should keep his ears dry for 2 weeks after this infection has resolved. When showering Jim should use cotton wool coated in petroleum jelly to prevent water entering his ears. If he is a swimmer, he could consider custom made ear plugs for swimming and the use of
Case 8
Figure 16. Dental brooch with cotton wool. Author’s image
Figure 18. An otowick inserted into ear canal. Author’s image
Figure 17. Otowicks. Author’s image

34
check Ear nose and throatresourCes and referenCes
21. Massick D, Tobin EJ. Epistaxis. In: Cummings CW, Flint PW, Haughey BH, et al, editors. Otolaryngology head and neck surgery. Philadelphia: Elsevier Mosby, 2005.
22. Calder N, Kang S, Fraser L, et al. A double-blind randomized controlled trial of management of recurrent nosebleeds in children. Otolaryngol Head Neck Surg 2009;140:670–4.
23. Douglas R, Wormald PJ. Update on epistaxis. Curr Opin Otolaryngol Head Neck Surg 2007;15:180–3.
24. Chiu TW, McGarry CW. Prospective study of bleeding sites in idiopathic adult posterior epistaxis. Otolaryngol Head and Neck Surg 2007;137:390–3.
25. Supriya M, Shakeel M, Veitch D, et al. Epistaxis: prospective evaluation of bleeding site and its impact on patient outcome. J Laryngol Otol 2010;124:744–9.
26. Gifford TO, Orlandi RR. Epistaxis. Otolaryngol Clin N Am 2008;41:525–36.
27. Daudia A, Jaiswal V, Jones NS. Guidelines for the management of idiopathic epistaxis in adults: how we do it. Clin Otolaryngol 2008;33:618–20.
28. Bousquet J, Khaltaev N, Cruz AA, et al. Allergic rhinitis and its impact on asthma (ARIA): 2008 update (in collaboration with the World Health Organization, GA(2)LEjdwdN and AllerGen). Allergy 2008;63(Suppl 86):8–160.
29. Ciprandi G, Contini P, Murdaca G, et al. Soluble HLA-G molecule in patients with perennial allergic rhinitis. Int Arch Allergy Immunol 2009;150:278–81.
30. Bousquet J, Gaugris S, Kocevar VS, et al. Increased risk of asthma attacks and emergency visits among asthma patients with allergic rhinitis: a subgroup analysis of the investigation of montelukast as a partner agent for complementary therapy [corrected]. Clin Exp Allergy 2005;35:723–7.
31. Graf P. Rhinitis medicamentosa: a review of causes and treatment. Treat Respir Med 2005;4:21–9.
32. Choi IS, Koh YI, Koh JS, et al. Sensitivity of the skin prick test and specificity of the serum-specific IgE test for airway responsiveness to house dust mites in asthma. J Asthma 2005;42:197–202.
33. Lintner TJ, Brame KA. The effects of season, climate, and air-conditioning on the prevalence of dermatophagoides mite allergens in household dust. J Allergy Clin Immunol 1993;91:862–7.
34. Sheikh A, Hurwitz B, Nurmatov U, van Schayck CP. House dust mite avoidance measures for perennial allergic rhinitis. Cochrane Database Syst Rev. 2010;7:CD001563.
35. Rodrigo GJ, Yanez A. The role of antileukotriene therapy in seasonal allergic rhinitis: a systematic review of randomized trials. Ann Allergy Asthma Immunol 2006;96:779–86.
36. Fokkens W, Lund V, Mullol J. European position paper on rhinosinusitis and nasal polyps 2007. Rhinol Suppl 2007;20:1–136.
37. Iinuma T, Hirota Y, Kase Y. Radio-opacity of the paranasal sinuses. Conventional views and CT. Rhinology 1994;32:134–6.
38. Skoner D. Update of growth effects of inhaled and intranasal corticosteroids. Curr Opin Allergy Clin Immunol 2002;2:7–10.
39. Ichimura K, Shimazaki Y, Ishibashi T, et al. Effect of new macrolide roxithromycin upon nasal polyps associated with chronic sinusitis. Auris Nasus Larynx 1996;23:48–56.
40. Bousquet PJ, Cropet C, Klossek JM, et al. Effect of smoking on symptoms of allergic rhinitis. Ann Allergy Asthma Immunol 2009;103:195–200.
41. Batra PS, Kern RC, Tripathi A, et al. Outcome analysis of endoscopic sinus surgery in patients with nasal polyps and asthma. Laryngoscope 2003;113:1703–6.
42. Lee KJ. Essential otolaryngology. 9th edn. New York: Mc Graw-Hill, 2008.
43. Ludman H, Bradley P. ABC of ear, nose and throat. 5th edn. Malden, Mass: Blackwell Publishing.
44. Brown CL, van der Straaten D, Joyce L, et al. Acute otitis externa – a local experience of clinical features and microbiology. Aust J Otolaryngology 2002;5:90–4.
45. Bull B, Clarke R. Lecture notes diseases of the ear, nose and throat. 10th edn. London: Blackwell Publishing, 2007.
46. Pasha, R. Otolaryngology head and neck surgery clinical reference guide. 2nd edn. San Diego: Plural Publishing, 2006.
resourCes
• Hawke Library of Otolaryngology. Available at www.hawkelibrary.com
• Benign paroxysmal positional vertigo (nystagmus during Dix Hallpike Manoeuvre. Available at http://video.google.com/videoplay?docid=-6201505057633350143#)
• Epley manoeuvre video. Available at www.australianprescriber.com/magazine/28/4/94/7
• Video of head impulse test in unilateral vestibular loss. Available at www.youtube.com/watch?v=P68SVfl7vAk&feature=player_detailpage#t=38s.
referenCes
1. Ruotsalainen JH, Sellman J, Lehto L, et al. Interventions for treating functional dysphonia in adults. Cochrane Database Syst Rev 2007;3:CD006373.
2. Reveiz L, Cardona AF, Ospina EG. Antibiotics for acute laryngitis in adults. Cochrane Database Syst Rev 2007;2:CD004783.
3. Schwartz SR, Dailey SH, Deutsch ES, et al. Clinical practice guideline: hoarseness (dysphonia). Otolaryngology-head and neck surgery 2009;141:S1–S31.
4. Wilson WR, Byl FM, Laird N. The efficacy of steroids in the treatment of idiopathic sudden hearing loss: a double-blind clinical study. Arch Otolaryngol 1980;106:772.
5. Pichichero ME, Poole MD. Comparison of performance by otolaryngologists, pediatricians, and general practitioners on an otoendoscopic diagnostic video examination. Int J Pediatr Otorhinolaryngol 2005;69:361–6.
6. Bluestone CD, Casselbrant ML, Dohar JE. Targeting therapies in otitis media and otitis externa. Ontario: BC Decker, 2003.
7. Bluestone CD. Eustachian tube structure, function, role in otitis media. Ontario: BC Decker, 2005.
8. Foxlee R, Johansson AC, Wejfalk J, et al. Topical analgesia for acute otitis media. Cochrane Database Syst Rev 2006;3:CD005657.
9. Sanders S, Glasziou PP, Del Mar CB, et al. Antibiotics for acute otitis media in children. Cochrane Database Syst Rev 2004;1:CD000219.
10. Antibiotics Expert Group. Therapeutic guidelines: antibiotic. Version 13. Melbourne: Therapeutic Guidelines limited, 2006.
11. Coleman C, Moore M. Decongestants and antihistamines for acute otitis media in children. Cochrane Database Syst Rev 2008;3:CD001727.
12. American Academy of Family Physicians. American Academy of Otolaryngology-Head and Neck Surgery and American Academy of Pediatrics Subcommittee on Otitis Media With Effusion. Pediatrics 2004;113:1412–1429.
13. Leach A, Morris PS. Antibiotics for the prevention of acute and chronic suppurative otitis media in children. Cochrane Database Syst Rev 2006;4:CD004401.
14. Cnyrim CD, Newman-Toker D, Karch C, et al. Bedside differentiation of vestibular neuritis from central ‘vestibular pseudoneuritis’. J Neurol Neurosurg Psychiatry 2008;79:458–60.
15. Sajjadi H, Paparella M. Meniere’s disease. Lancet 2008;372:406–14.
16. Committee on Hearing Equilibrium. Guidelines for the diagnosis and evaluation of therapy Meniere’s disease. Amer Acad Otolaryngol Head Neck Surg Foundation Inc. Otolaryngol Head Neck Surg 1995;113:176–78.
17. Neuhauser H, Leopold M, von Brevern M, et al. The interrelations of migraine, vertigo and migrainous vertigo. Neurology 2001;56:436–41.
18. Neurology Expert Group. Motion sickness and vertigo. In: Therapeutic Guidelines: neurology. Version 3. Melbourne: Therapeutic Guidelines Limited, 2007;89–101.
19. Strupp M, Carina Zingler V, Arbusow V, et al. Methylprednsiolone, valacyclovir or the combination for vestibular neuritis. New Engl J Med 2004;351:354–61.
20. Bronstein A, Lempert T. Dizziness: a practical approach to diagnosis and management (Cambridge Clinical Guides). Cambridge: Cambridge University Press, 2007.

35
CheCk Category 2 Qi&CPd aCtivitycheck Ear nose and throat
it lateralises to the left ear. Otoscopic examination of the left ear reveals a dull tympanic membrane without erythema. Which of the following is the most likely cause for his deafness?
A. Acute otitis media
B. Otitis externa
C. Idiopathic sudden sensorineural hearing loss
D. Occupational deafness
E. Otitis media with effusion (middle ear effusion).
QuesTion 3
Jan is 66 years of age with a past history of diabetes which is well controlled on metformin. She also takes simvastatin and rampiril. When she got out of bed a few days ago she noticed that she was ‘off balance’, which settled quickly, and has been recurring intermittently since, each time lasting a few minutes. She has no nausea or vomiting and no deafness or tinnitus. Her blood sugar levels have been between 6 and 8. Examination reveals a well looking lady who is afebrile, pulse rate is 76 and in sinus rhythm, blood pressure 135/80 standing and 140/75 lying. Otoscopic examination and cardiovascular examination are normal and there are no neurological deficits. The Hallpike manoeuvre is positive. Which of the following is the most likely cause for her symptoms?
A. Vestibular neuritis
B. Benign paroxysmal positional vertigo
C. Hypoglycaemia
D. Hypotension
E. Viral illness.
QuesTion 4
Susan is 59 years of age with a past history of migraine who presents to your practice at lunchtime with a fairly sudden onset of a throbbing headache, vertigo, nausea and vomiting which started earlier in the day. The headache resembles her usual migraine in character but is more severe and failed to respond to a single dose of sumatriptan as it usually does. You note that she staggers into your room and has nystagmus during history taking. Examination reveals normal otoscopic findings, an intention tremor (but no other neurological signs), a negative Romberg test and a normal head impulse test. Susan declines testing with the Hallpike manoeuvre unless it is absolutely necessary. The next most appropriate step in the management of Susan is to:
A. administer another dose of sumatriptan
B. prescribe oral prochlorperazine maleate and an oral codeine-based analgesic
C. administer a parenteral antiemetic such as intramuscular prochlorperazine maleate and a parenteral analgesic such as tramadol
D. arrange referral to hospital
E. explain the importance of performing the Hallpike manoeuvre and after obtaining consent, perform the Hallpike manoeuvre to determine the likely cause of her symptoms.
QuesTion 1
Chloe is 26 years of age, she is a physical education teacher who noticed a sore throat and runny nose 2 weeks ago and then developed a productive cough and hoarseness of voice soon after. She has had no fever and has not felt unwell. She is frustrated by her hoarseness of voice, which she notices is worse in the afternoon after coaching the school sports teams all day. The most likely cause for her hoarseness of voice is:
A. viral laryngitis
B. bacterial laryngitis
C. muscle tension dysphonia
D. postnasal drip
E. vocal nodules.
QuesTion 2
Samuel is 26 years of age and works in a factory. He presents to you having noticed deafness in his left ear when he woke up this morning, following his return the night before from an interstate holiday. He has a longstanding history of hay fever and has noticed occasional ‘popping’ of his ears. He has no ear pain and no fever. You perform a Weber test and
ear nose and throatIn order to qualify for 6 Category 2 points for the QI&CPD activity associated with this unit:
• readandcompletetheunitofcheck in hardcopy or online at the gplearning website at www.gplearning.com.au, and
• logontothegplearning website at www.gplearning.com.au and answer the following 10 multiple choice questions (MCQs) online.
• completetheonlineevaluation.
If you are not an RACGP member, please contact the gplearning helpdesk on 1800 284 789 to register in the first instance. You will be provided with a username and password that will allow you access to the test.
The expected time to complete this activity is 3 hours.
Please note:
• fromJanuary2011,therewillnolongerbeaCategory1activity (ALM) associated with check units. This decision was made due to a lack of interest in this activity. The RACGP apologises for any inconvenience caused by this change
• donotsendanswerstotheMCQsintothecheck office. This activity can only be completed online at www.gplearning.com.au.
If you have any queries or technical issues accessing the test online, please contact the gplearning helpdesk on 1800 284 789.

36
CheCk Category 2 Qi&CPd aCtivity check Ear nose and throat
C. topical antibiotic/antiseptic ointments
D. topical intranasal steriods
E. air humidifers.
QuesTion 8
Tim is 55 years of age and is an office worker who migrated to Australia 4 years ago. For each of the last 3 years he has experienced sneezing, itchiness of the nose and clear nasal discharge. The symptoms start in the spring and continue for several months and have been getting progressively worse each year. He has a past history of asthma, for which he uses occasional salbutamol. He has no other past history. He is frustrated as his nasal symptoms are getting progressively worse each year. This year he has tried intranasal corticosteroids for 6 weeks without effect. You examine him and note nasal inflammation is present. All of the following are appropriate in the management of Tim’s nasal symptoms except:
A. referral for skin prick testing
B. advice on allergen avoidance
C. use of a 2 week trial of oral antihistamines
D. use of a 2 week trial of intranasal decongestants
E. enquiry about environmental triggers.
QuesTion 9
Leanne is 40 years of age and presents for review 1 month following an episode of acute sinusitis for which you prescribed a course of amoxycillin as she had failed to respond to decongestants. Her facial pain and purulent nasal discharge settled with the course of antibiotics, but for the last 3 weeks she has been troubled by a postnasal drip and feels the need to continually clear her throat. She has had no other symptoms. Examination is normal. The next most appropriate step in her management would be:
A. referral to an ear, nose and throat (ENT) surgeon
B. request a computed tomography scan of her sinuses to check for the presence of polyps
C. advise use of an intranasal steroid spray and nasal douching
D. referral to an allergist to institute a desensitisation regimen
E. arrange for skin prick testing.
QuesTion 10
Aidan is 22 years of age and is a surfer who presents to your practice with a painful left ear of 1 week duration. He has noticed yellow discharge coming from the left ear for the last 2 days. He has also had significant ‘stuffiness’ of his nose. Otoscopic examination of his left ear is very painful and reveals copious yellow discharge but you are unable to visualise his ear drum. The most appropriate next step in management would be to:
A. prescribe benzocaine ear drops
B. prescribe sulphate/gramicidin/dexamethasone ear drops
C. prescribe ciproxin ear drops
D. advise Aidan to use cotton buds to remove the discharge
E. remove the discharge and debris if you are appropriately skilled, or arrange for an ENT specialist to do so, so that the eardrum can be visualised.
QuesTion 5
Stephanie is 4 years of age and presents the morning after the onset of a right sided earache. Stephanie and her family are well known to you and Stephanie has had an occasional episode of otitis media in the past and has no allergies. She is quieter than usual but is cooperative. Her temperature is 37.4°C per aural, and otoscopic examination of her right ear reveals an erythematous, bulging drum. Management in line with current recommendations could include:
A. advising use of paracetamol in the appropriate dose and intervals and review in 5 days
B. prescribing amoxycillin and advising her mother to fill the script straight away
C. prescribing amoxycillin and advising her mother to fill the script if Stephanie is still in pain in 48 hours
D. prescribing amoxycillin/clavulanate and advising her mother to fill the script straight away
E. prescribing amoxycillin/clavulanate and advising her mother to fill the script if Stephanie is still in pain in 48 hours.
QuesTion 6
Ella is age 15 months and presents to your practice for review following an episode of acute otitis media with perforation for which you prescribed a course of amoxycillin. Her growth and development have been normal and she is fully immunised. You ascertain that her infection has now cleared and her perforation has healed. It is her fourth episode of otitis media in the last 6 months. Her mother Tracy says she has been talking with some of the other mothers at the childcare centre that Ella has been attending for the last 6 months who have recommended that she speak with you about the possibility of Ella having ventilation tubes inserted. Which of the following is true regarding recurrent otitis media?
A. Prophylactic cefaclor is recommended to reduce the risk of further episodes of otitis media
B. Insertion of ventilation tubes reduces the risk of chronic otitis media with effusion but not the risk of recurrent otitis media
C. Audiology testing is often performed before ventilation tubes are inserted in cases where there is concern about hearing
D. An underlying significant cause such as immunodeficiency or cystic fibrosis is likely to be operating in Ella’s case
E. Reassurance that, in cases such as Ella’s, there is no need for ventilation tubes or any further follow up.
QuesTion 7
Nelson is 55 years of age and presents with a history of four nose bleeds in the last 2 weeks. Each nose bleed has lasted about 15–20 minutes. The last episode was a couple of days ago. Nelson is otherwise well with no relevant past history. He is not on any medications. You examine his nose internally and notice a clot of blood present superiorly. All of the following are appropriate in the management of Nelson except:
A. advice on first aid should his epistaxis recur
B. consideration of cauterisation

GP11THE CONFERENCE FOR GENERAL PRACTICE
Hotel Grand Chancellor Hobart 6 – 8 October 2011
www.gp11.com.au
Call for abstracts extendedThe GP11 committee invites abstract submissions for the following key themes:
• Women’s and children’s medicine
• Innovations in education
• Telemedicine
• Clinician leadership development
• Informatics / e-health
• Aboriginal and Torres Strait Islander health
• Business of medicine
• Dermatology in practice
• Emergencymedicine
Submissions close 15 April 2011
GP11_Check_ad_April_2011.indd 1 10/03/2011 11:54:52 AM

To register your interest [email protected]
THE RACGP PRESENTSA NEW LEVEL OF CLINICAL INTELLIGENCE2011New functionality available soon
Sidebar_GP_ad_275mmx355mm REVISED.indd 1 11/03/11 1:56 PM





























