Embed Size (px)
DESCRIPTION
An excellent ENT lecture from a professor of medicine in the university of Iasi, Romania.
Citation preview

ENT Course for English Module
bull Conf UnivDrIon ANGHEL MD PhDbull Head of the ENT Clinic bdquoColteardquoHospitalbull University of Medicine bdquoCarol Davilardquobull Bucharest-Romania
ENT as a subject and career
bull ENT is a fantastic specialty that is every bit as exciting in practice as it is in theory
bull It is difficult to conceive of any specialty which can provide such diversity in medical practice
bullENT conditions make up 25-50 of all general practice consultations
bullENT conditions affect people of all ages from neonates to the elderly
bullSurgical skills are broad from microsurgery on the smallest bones in the body to major head and neck reconstructive surgerybullENT is an expanding surgical specialty that is taking over traditional general surgical areas such as salivary gland surgery and thyroid surgery
bullCosmetic surgery is undertaken by ENT in the form of facial plasticsbullSurgery is also performed on the skull base and pituitary glandbullENT offers enormous research potential from nasal polyps to congenital hearing lossbullThere are cutting edge developments occurring in ENT such as cochlear implantation
We hope that your experiences in ENT will fill you with enthusiasm for this specialty
ENT learning aims and objectives for clinical medical students
AimsTo acquire sufficient knowledge of ENT conditions to be able to
recognize common problems and when and what to referTo understand that ENT conditions are extremely common and form
a large part of the workload of a general practitionerTo learn the skills required to examine patients with ear nose and
throat diseases and to make a presumptive diagnosisTo learn how to prioritize and manage different ENT conditionsTo become stimulated and interested in the specialty of ENT
Objectives To learn the signs and symptoms of common ENT conditions To learn the techniques of ear nasal and neck examination To demonstrate an understanding of the basic anatomy and physiology of the ear
and upper aero-digestive tract and relate this knowledge to the signs and symptoms of ENT disease
To understand the medical and surgical treatment of common ENT conditions To be familiar with the commonly used medications for treating ENT problems and
their side effects To understand the risks and complications of surgery To recognise the different ways in which head and neck malignancy can present
and to understand that early diagnosis of head and neck cancer leads to improved survival
To learn the ways in which ENT related communication difficulties can arise and be overcome
To appreciate and be sensitive to the impact of ENT conditions on patients and their families
Student ENT curriculum
Practical skillsUse of the auriscope to examine the external auditory meatus and tympanic membraneBasic examination of the noseExamination of the oral cavity and oropharynxExamination of the neckHow to manage a nosebleedHow to deal with a tracheostomy
Earbull Basic anatomy and physiology of the earbull Presentation and management of common ear disease eg otitis externa
otitis media glue ear chronic suppurative otitis media with or without cholesteatoma vertigo and facial palsy
bull Examination of the ear including the pinna ear canal and otoscopybull Testing hearing with tuning fork testsbull The advantages of the microscope and the fibreoptic otoscopebull Basic interpretation of play audiometry pure tone audiograms and
tympanogramsbull The principles of grommet insertion mastoid surgery and the treatment of
Menieres diseasebull Identifying postoperative problems following ear surgery ie sensorineural
hearing loss facial nerve palsy and vestibular dysfunctionbull Understanding the differential diagnosis of facial nerve palsy and its
treatment
Nosebull Anatomy and physiology of the nosebull Symptoms and signs of common sinonasal disease eg
rhinitis sinusitis nasal polypsbull Examination of the nose including an assessment of the
appearance the septum the turbinates and the mucosabull The endoscopic evaluation of the nosebull Management of a fractured nose and the timing of
interventionbull Management of epistaxis from minor nosebleeds to
torrential haemorrhagebull The principles of common nasal operations including septal
surgery functional endoscopic sinus surgery and rhinoplasty
Head and neckmdashbenign and malignant disease
bull The basic anatomy and physiology of the oral cavity salivary glands pharynx larynx oesophagus and lymph node drainage
bull The presentation of head and neck cancerbull The presentation and management of salivary gland diseasebull Examining the oral cavity larynx and pharynx including the use of the nasendoscopebull Examining the neck with reference to the lymph nodesbull The role of fine needle aspiration cytology (FNAC)bull The principles and limitations of radiological investigation of the head and neck regionbull Management of neck lumps in particular the malignant lymph node with an unknown
primarybull The management of the airway in patients with a tracheostomy or end tracheostomy after
laryngectomybull A basic knowledge of the principles of operative surgery in particular the principles of
reconstructive surgery and the surgery for salivary gland disease eg parotidectomybull The postoperative management of a patient who has undergone major head and neck surgerybull The role of the multidisciplinary team in head and neck cancer and voice disorders
Supplementary knowledgebull The role of otoacoustic emissions and evoked auditory potentials in managing
hearing lossbull The use of speech audiometrybull The surgery for otosclerosisbull Bone-anchored hearing aids for conductive hearing lossbull Cochlear implantation and the reactions of the deaf community to this
interventionbull The use of sign languagebull Neuro-otology in particular the presentation and management of acoustic
neuromasbull Craniofacial surgery and the interplay between ENT plastic surgery and
neurosurgerybull The management of cleft palate and the increased risk of glue earbull Advanced endoscopic sinus surgery for the mangement of sinonasal malignancy
pituitary tumours and skull base tumoursbull Microlaryngeal surgery and surgical voice restorationbull The use of chemotherapy and radiotherapy in head and neck malignancy
Working in ENT
bull Working in ENT should be a very enjoyable experience whether it is a temporary attachment or a long-term career plan
bull It is helpful if you have an understanding of what others expect of you
bull It is also important for you to think about your own career development
Your duties
bull Patient care and continuitybull Professional developmentbull Research
The ENT Examination
EquipmentA fully equipped ENT department will have all the necessary instruments for performing a full ENT examination
Basic equipment
bull A light sourcemdasha portable headlight that runs off batteries is ideal
bull Wooden tongue depressorsbull Thudicum nasal speculumbull An otoscope with several speculaebull Pneumatic attachment for the otoscopebull Tuning fork 512Hzbull Pen and paperbull Gloves
Advanced equipment
bull Co-phenylcaine spraybull A flexible nasendoscope with light sourcebull Alcohol wipe to act as demist for the scopebull Aqueous lubricating gel for the scope
Emergency equipment
bull Large nasal tampons (you can always cut 10cm ones to size)
bull Silver nitrate sticksbull Foley catheters
Basic Anatomy of the Nose
bull The structural anatomy of the nose is important
bull for both aesthetic and functional reasons since the
bull nose as the gateway to the respiratory tract performs
bull a variety of physiologic functions
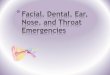
External NoseThe shape of the external nose is defined by the nasalbones a pair of rectangular bones in the upper nasaldorsum and by lateral cartilages (uppernasal cartilages) and alar cartilages (major alar cartilages)in the central and lower portions of the noseThe lateral portions of the nasal alae alsocontain several small accessory cartilages called theminor alar cartilages which are embedded in the lateralsoft tissues of the noseThe shape and stability of the alar cartilages each ofwhich consists of a medial and lateral crus
External Nose
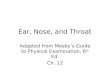
Anatomy of the nasal base
bull Besides thebull medial crura the
inferior septal margin and the connective-
bull tissue septum (columella) are also responsible
bull for stabilizing the base of the nose
Anatomy of the nasal base
Anatomy of the nasal base
bull The nasal septum is subluxed toward the left side partially
bull obstructing the nasal airway
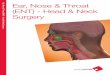
Nasal CavitiesThe nasal cavities begin anteriorly at the nasal vestibulewhich is bordered posteriorly by the internal nasalvalve (limen nasi) located between the posteriorborder of the alar cartilage and the anterior border ofthe lateral cartilage This valve area is the narrowestportion of the upper respiratory tract
Nasal Cavities
The interior ofthe nose behind the nasal valve is divided by the nasalseptum into two main cavities
Nasal CavitiesThe nasal septum iscomposed of an anterior cartilaginous part and twoposterior bony parts Abnormalities in the shape ofthe nasal septum which may consist of a deviated septum tensionseptum spurs or ridges are a frequent cause ofnasal airway obstructionThe choanae are the paired posterior openingsthrough which the nasal cavities communicate withthe nasopharynx
Nasal CavitiesThe nasal cavity is bounded laterally by the lateral nasalwalls which are formed by the ethmoid bone andmaxilla and posteriorly by the palatine bone and thepterygoid process of the sphenoid bone Several functionallyimportant structures are located on the lateralnasal wall the nasal turbinates and their associatedpassages (meati) sinus ostia and the orifice ofthe nasolacrimal duct (Fig 15)
The inferior turbinate consists of a separate bone thatis attached to the medial wall of the maxillary sinusThe opening of the nasolacrimal duct is located in thecorresponding inferior meatus The middle andsuperior turbinates are part of the ethmoid bone In rare cases a rudimentary ldquosupreme turbinaterdquo is alsopresent above the superior turbinate
The middle turbinate has by far the greatest functionalimportance because most of the drainage tracts fromthe surrounding paranasal sinuses open into the middlemeatus The nasal cavity is bounded superiorly by the cribriformplate of the ethmoid bone This thin bony platehas numerous openings for the passage of the fila olfactoriaand also forms the boundary of the anteriorcranial fossa
Nasal Cavities
The floor of the nasal cavity is formedmostly by the hard palate which is formed in turn bythe two palatine processes of the maxilla and the horizontallaminae of the palatine bone
Structure of the lateral nasal wall
Inferior meatus
Paranasal Sinuses
The paranasal sinuses are air-filled cavities that communicatewith the nasal cavities
-The maxillary sinus frontalsinus and anterior ethmoid cells drain into the nasalcavity through the middle meatusmdashie below themiddle turbinate -The posterior ethmoidcells drain into the nasal cavity through the superiormeatus The ostium of the sphenoid sinus is locatedin the anterior wall directly above the choanae- The anatomical connections between the nasal cavity andparanasal sinuses are functionally important and playa key role in the pathogenesis of many rhinologic diseasesthat involve the paranasal sinuses
Vascular SupplyThe external nose derives most of its blood supply
from the facial artery which arises from the external
carotid artery and from the ophthalmic artery which
springs from the internal carotid artery
Vascular Supply
The internalnose receives blood from the territories of the externaland internal carotid arteries- the terminalbranches of the sphenopalatine artery which arisesfrom the maxillary artery - the anterior and posteriorethmoid arteries which arise from the ophthalmicartery-internal carotid arterie
venous drainage
The venous drainageof the facial region is handled by -the facial vein -retromandibular vein -internal jugular vein
lymphatic drainage
The regional lymphatic drainage of the face and externalnose is handled mainly by- the submandibularlymph nodes while the nasal cavity is additionallydrained by -the retropharyngeal and deep - -cervical lymph nodes
Morphology of the Nasal Mucosa
Besides the anatomical structure of the external noseand nasal cavity the nasal mucosa plays an essentialrole in numerous functions of the nose in the respiratory tract
Morphology of the Nasal Mucosa
The anterior part of the nasal cavity (the nasal vestibule)like the external nose is covered by skin composedof a multilayer keratinizing squamous epithelium and finally a ciliated respiratory epithelium A small areaon the upper nasal septum superior turbinate andpart of the middle turbinate located adjacent to thecribriform plate is covered by olfactory mucosa and iscalled the olfactory region
Nerve SupplyThe facial skin receives its sensory innervation fromterminal branches of the trigeminal nerve that enterthe facial region through the supraorbital infraorbitaland mental foramina Thefacial muscles are classified as mimetic or mastica- tory each of these groups receiving different motorinnervationbythe facial nerve
History and Clinical Examination of the Nose
Historybull The main symptomsbull nasal obstruction (ldquostuffy
noserdquo)bull nasal dischargebull Headachesbull Olfactory
dysfunction
Palpationbony discontinuitiesNeuralgias to check
over- the supraorbital -infraorbital -mental foramina
Anterior Rhinoscopy
bull The rhinologic examination itself begins with anterior
bull rhinoscopy to evaluate the nasal vestibule and the anterior
bull portions of the nasal cavity
Nasal Endoscopy Nasal endoscopy has become the most important andrewarding clinical examination method in rhinologic diagnosis
- rigid endoscopes which are available in 4-mm and 28- mm diameters and assorted viewing angles (eg 01048576 301048576 1201048576) -flexible endoscopes are also available for inspecting the nose and nasopharynx and exploring all of the pharynx and larynx in one sitting
Nasal endoscopy
Nasal Endoscopy
Nasal Endoscopy
Imaging of the Nose and Paranasal Sinuses
Conventional RadiographsStandard paranasal sinus radiographs in the occipitomental
projection ( Water projection) and
occipitofrontal projection Caldwell projection) in cases of acute inflammation
They are also obtained to evaluate midfacial fractures
Computed Tomography (CT) the main indicationsfor CT scanning of the
nose and paranasal sinuses
are- chronic sinusitis - -trauma (especially
frontobasal -fractures)
-and tumors
The occipitofrontal projection is better for evaluating theethmoid cells and frontal sinus
occipitomental projection demonstrates the maxillarysinus and gives a limited view of the sphenoid sinus
Computed tomography of the paranasal sinuses
Four representative coronal CT scans are shown
Four representative coronal CT scans are shown
Magnetic Resonance Imaging
Magnetic maging
Magnetic resonance imaging (MRI) has fewer indicationsthan CT in patients with paranasal sinus diseaseThis is primarily because MRI is markedly inferior toCT in defining the bony boundaries of the sinusesThe strength of MRI lies in its superior soft-tissue discriminationMRI is indicated in diseases that involve the paranasal sinuses in addition to thecranial cavity or orbit (eg tumors and congenitalmalformations such as encephaloceles)
MRI of the paranasal sinuses
The Nose and Sinuses
Structure The structure of the nose is made up of
four partsbull The surface anatomybull The nasal skeletonmdashcomposed of the
two nasal bones the paired upper lateral and lower lateral cartilages and the nasal septum covered in subcutaneous tissue and skin
bull The internal anatomymdashincludes the septum of the nose which forms the medial wall of the nasal cavity The turbinates on the lateral wall are also called conchae
bull The osteomeatal complexmdasha key functional area of the nose
Function The nose is the main route for inspired
air and its structure is related to this function As the air passes over the large surface area of the turbinates
The inspired gases are warmed and humidified Mucus on the mucosa of the nose removes large dust particles from the air as it is breathed in
The voice resonates in the sinuses and nose and this provides character to the speech
Pneumatization of the sinusesmdashthey are air filled spacesmdashreduces the weight of the skull
Diseases of thDiseases of the Outer and Inner Nosee Outer and
Inner Nose Erysipelas Definition of the disease ndash Erysipela is a skin infection that affects the superficial dermis and is caused by Streptococcus pyogenes (group A) It usually develops in the extremities and the face and less commonly on the scalp and genitals bull Epidemiologyaetiology ndash Erysipelas are more often seen in elderly infants and children patients with compromised immunology and diabetes -Predisposing factors are alcoholism skin ulceration puncture wounds fungal infections malnutrition and burns
Erysipelas
bull Symptomsbull ndash It usually presents of fever general fatigue bull -The skin lesion is a redindurated and elevated plaque
with borders that expand rapidly bull It is painful warm and accompanied by variable oedemabull -On the second or third day a flaccid bulla may develop
and desquamationbull bull Presence of regional lymph nodes is common
Erysipelas
bull Complicationsndash The most common complication is recurrencewhich is seen in 18ndash30 of the cases even afterproper antibiotic therapy Recurrence is seen moreoften in females than in malesA skin infection with S pyogenes could lead toglomerulonephritis
Erysipelas
bull Complicationsbull ndash The most common complication is recurrencebull which is seen in 18ndash30 of the cases even afterbull proper antibiotic therapy bull -Recurrence is seen morebull often in females than in males bull -A skin infection with S pyogenes could lead tobull glomerulonephritis
Erysipelas
bull bull Diagnosisbull ndash Diagnosis is based on the patientrsquos personal
historybull and physical examination particularly on inspectionbull of the skin
bull Blood cultures are positive in less thanbull 5 of cases
ErysipelasTherapyndash Conservative therapybull The preferred antibiotic is penicillin In mildcases with minor systemic symptoms penicillinV 500 mg orally every 6 h for 10 days or penicillinG benzathine 12 mil U intramuscularlyonceOther possibilities are amoxicillin 500 mgorally twice a day for 10 days or cephalexin 500mg orally every 6 h for 10 days
ErysipelasIn moderate and severe cases with significantsystemic symptoms hospitalization and intravenoustreatment is required penicillin G 2ndash4mil U intravenously every 4ndash6 h Cefazolin05ndash15 gm intravenously every 8 h cefotaxime1ndash2 gm intravenously every 8 h or ceftriaxone1ndash2 gm intravenously once a day should be administeredIn patients with a penicillin allergyclindamycin 600 mg intravenously every 8 h orvancomycin 15 mgkg intravenously twice a daymay be given
ErysipelaAdditional useful therapeutic optionsbull Prednisone 30 mg over 8 days might be consideredas well as elevation of the affected siteMoist heat compresses may be usefulbull Surgeryndash Debridement and drainage are indicated when bullaeabscesses or necroses are presentbull Differential diagnosisndash Contact dermatitisndash Asteatotic eczemandash Herpes zosterndash Angioneurotic oedemandash Osteomyelitis
Furuncle
bull Definition of the diseasebull ndash A furuncle is an infection that beginsbull at the hair follicle and spreads deeper into thebull dermis and subcutaneous tissue forming abull nodule After several days it developsbull into an abscess - red painful and fluctuantbull bull bull Epidemiologyaetiologybull ndash The aetiologic agent is Staphylococcus aureus
FuruncleSymptomsndashsymptoms are local and limited to thesite of infection Furuncles usually are wherehair follicles are present bull Complicationndash One complication is furunculosis multiple draining furunclesDiagnosisndash The diagnosis is based on clinical inspection - Cultures are not necessary when there is no systemic involvement but should beconsidered if systemic therapy (in case of feversignificant cellulitis or hospitalization) or whenmethicillin-resistant Staphylococcusaureus (MRSA) is considered
FuruncleTherapyndash When the furuncle is small application of moist heat compress to promote drainage -Larger furuncles should be drained by surgical incision-After drainage the area should be cleaned with anantiseptic (with chlorhexidinebetadine) should be applied twice
a dayndash If no systemic symptoms or extensive cellulitis arepresent simple topical care is usually curative andoral antibiotics are not necessary Otherwise systemictreatment is indicated and should cover anypossible MRSA
Furuncle
bull -Recommended antibiotics are trimethoprim-sulfamethoxazole
bull 1ndash2 tablets orally twice daily doxycyclinebull 100 mg orally twice dailybull or clindamycin 300ndash450 mg orally every 8 hbull - In severe cases vancomycin 15 mgkg
intravenouslybull every 12 h or clindamycin 600 mg intravenouslybull every 8 h
Midline Granulomabull A midline granuloma is an angiocentricbull lymphoma it was referred to as polymorphicbull reticulosis lethal midline granuloma and midline
malignant reticulosisbull bull Definition of the diseasebull ndash This rare disease is a lymphoma of extranodal
presentationall cases are positive for the Epstein-Barr virus
bull -This lymphoma most commonly appears in the midface region
Midline GranulomaEpidemiologyaetiologyndash This form of lymphoma is rare in Europe and theUnited States with a higher prevalence in Asia and PeruSymptomsndash The most common presentation is nasal obstruction with a destructive mass occupying the nosesinuses and palate
-Fever night sweatsand weight loss seen usually in Hodgkinrsquos lymphomaand other non-Hodgkinrsquos lymphomas (knownas ldquoB symptomsrdquo) are uncommon
Midline GranulomaDiagnosisndash The diagnosis is based on anatomopathologicalstudy The malignancy of the tumour manifested byextensive necrosis makes the histological diagnosisdifficult and often more biopsies are required forconfirmationbull Therapyndash Therapy consists of radiotherapy with or withoutchemotherapy
Midline Granuloma
bull Prognosisbull ndash Depending on the stage long-term remission or
experience a worseningbull prognosis with relapses which may include otherbull extranodal sites bull Involvement of extranodal sitesbull including the upper airway gastrointestinal tractbull skin
Wegenerrsquos Granulomatosis
bull Definition of the diseasebull ndash Wegenerrsquos granulomatosis is a systemic chronicbull vasculitis of small- and medium-sized blood vesselsbull with an autoimmune component It affectsbull particular organs with variable predilectionbull Epidemiologyaetiologybull ndash Wegenerrsquos granulomatosis is a rare disease It affects
about 1 in 20000ndash30000 people It is more prevalentbull in middle-aged Caucasian patients
Wegenerrsquos Granulomatosis
Symptomsndash The disease may present pulmonary upper
respiratory tract or renal In the disseminated form-The localised form ndash confinedto the upper respiratory region ndash is present in 25of the patients- It consists of nonspecific manifestationssuch as nasal obstruction crusting purulentor bloody rhinorrhea and painful or painless ulcers in oral or nasal cavities which are unresponsive tostandard medical treatment
Wegenerrsquos Granulomatosis
bull In some patients the nasal septum is perforatedbull which leads to saddle-nose deformity Less
commonbull symptoms are hoarseness stridor due to
subglotticbull stenosis otalgia otorrhea and conductivebull and sensorineural hearing loss Also ocular
symptomsbull such as scleritis conjunctivitis uveitis andbull episcleritis may be present
Wegenerrsquos Granulomatosis
bull ndash In the disseminated form pulmonary involvementbull is manifested by cough dyspnoea haemoptysisbull (due to an alveolar capillaritis necrotic lesions orbull endobronchial disease) and pleuritic painndashbull -Ninety per cent of patients have nasal symptomsbull and these symptoms are usually the first
manifestationof the diseasebull -Most patients have also renal involvementbull even if it is subclinical
Wegenerrsquos Granulomatosis
Diagnosis ndash Diagnosis of Wegenerrsquos granulomatosis is based on clinical findings that demonstrate lung (chest x-ray) kidney (urine analysis) or upper respiratory tract
involvement (oral or nasal ulcers or discharge) - positive blood analysis for cytoplasmic-staining antineutrophil
cytoplasmic antibodies (c-ANCA) and confirming proteinase 3 (PR3) ANCA or myeloperoxidase (MPO) ANCA ndash Biopsy is essential for diagnosis nonspecific chronic inflammation
and necrosis -Bacterial and fungal infections
Wegenerrsquos Granulomatosis
Therapyndash Conservative therapybull In the induction of disease remission highdosesteroids (e g prednisone 1 mgkgday) for1 month with tapering over several months aregiven In addition cyclophosphamide (2 mgkgday) should be administered for 6ndash12 monthsuntil symptoms disappear In the maintenanceof remission cyclophosphamide should be
Wegenerrsquos Granulomatosis
Antibiotics mainly trimethoprim-sulfamethoxazoleare given for prophylaxis againstPneumocystis jiroveci (formerly Pneumocystiscarinii) pneumonia (PCP) which may developduring immunosuppression and have a role inpreventing recurrencesbull Sinonasal manifestations may be treated with topical nasal steroids and nasal irrigations lowdosesystemic steroids and antibiotics when bacterial infection (typically Staphylococcus species) is suspected
Wegenerrsquos Granulomatosis
bull Prognosisbull ndash Most of the patients respond well to treatmentbull achieving symptom-free intervals of 5ndash20 yearsbull or more bull -Anatomical problems (sinusitis trachealbull stenosis) may require surgery bull Relapses can be long and troublesomebull Long-term complications are chronicbull renal failure hearing loss and deafness
Nasal Fractures Definition ndash A nasal fracture is a disruption of the nasal bone structure due to trauma It is the most frequently fractured facial bone Epidemiologyaetiology ndash Sports falls and assaults are the usual mechanisms of fracture -Males are affected twice as often as are females -Paediatric populations with a incidences during the second and third decades of life -Variables such as force impact direction nature of the striking object age and other will influence the pattern of injury to the components of the nose
Nasal Fractures
bull Symptomsbull ndash Deformity swelling epistaxis and periorbital
ecchymosis are signs that are suggestive of nasal fracture
bull bony crepitus and nasal segment mobilitybull ndash Epiphora bull Severe bilateral injuries to the lachrymal bones
arebull associated with depressed nasal fractures
Nasal Fractures Complications ndash Septal haematoma is one of the most severe early complications of nasal trauma and without drainage it results in abscess formation 6ndash7 days after trauma producing necrosis of the septal cartilage -Long-term problems such as saddle-nose deformity perforation columellar retraction and nasalbase
Septal infection could lead to osteomyelitis orbital and intracranial abscesses meningitis and cavernous sinus thrombosis -Cerebrospinal fluid leakage is a common complication of severe
nasal and frontal fractures
Nasal Fractures
bull Diagnostic proceduresbull ndash Inspectionbull bull Changes of appearance such as deviation andbull asymmetry bleeding watery drainage changesbull in nasal breathing and smell It is useful to comparebull the current presentation with old photographsbull (up to 40 of normal individuals havebull significant nose malformations)
Nasal Fractures Physical examination bull The diagnosis of a nasal fracture is made primarily by physical examination epistaxis nasal swelling and periorbital ecchymosis Nasal shape in the lateral and frontal inspection should be assessed Grasping the dorsum between two fingers and rocking the pyramid back and forth aids in assessing the mobility of nasal bones Internal structures should be evaluated by using a headlight and nasal speculum Clotted blood is removed by suction and assessment of haematoma mucosal tears and active bleeding is performed Bimanual palpation of the septum helps to differentiate septal swelling from haematoma ndash
Nasal FracturesRadiographybull There is no clear evidence of the role of radiographyin the management of nasal fracturesPlain films have up to a 66 false-positive rateas a result of misinterpretation of normal suturelines In addition old fractures are difficult todistinguishbull Three-dimensional CT is recommended for extensiveinjuries involving the nasal-orbital-ethmoidalcomplexndash
Nasal Fractures
bull Additionaluseful diagnostic proceduresbull bull Using a 0 or 30deg 4-mm endoscope is helpful inbull the assessment of posterior abnormalities If thebull patient is heavily sedated Brown-Gruss
provocationbull manoeuvres may be performed to determinebull deformities in upper middle or lower segmentsbull by compressing each compartment
Nasal FracturesConservative treatmentndash Treatment of bleedingbull For localised bleeding anterior sources may becauterised by silver nitrate or sealed with topicalmaterials such as thrombin combined withgelatin foam fibrin glue FloSealreg or other procoagulantmaterials If conservative measuresfail a formal anterior packing is placedbull Bleeding from branches of sphenopalatine orethmoid vessels requires anterior-posteriorpacking
Nasal Fractures
bull bull Surgical methods such as direct endoscopic vessel
bull cauterization or ligation have been shown tobull offer better haemostasis and patient comfortbull Angiography with embolization can also be
consideredbull in cases refractory to more conservativebull approaches
Nasal Fractures
bull Type of reductionbull bull Nondisplaced fractures should be treated withbull observation alone Closed nasal reduction is thebull best choice for simple injuries (isolated unilateralbull with medial displacement)bull bull An open approach should be considered in
severebull trauma (bilateral depressed fractures)
Nasal Fracturesbull Surgical principlesbull ndash Topical anaesthesia with cotton pledgets soakedbull with 4 cocaine or 005 oxymethazoline combinedbull with 4 topical lidocaine should be appliedbull for 5ndash10 min Local anaesthesia should also be injectedbull (1 lidocaine and 1100000 epinephrine)bull along the septum lateral walls and floor of the nasalbull cavitybull bull
Nasal FracturesClosed reductionndashndash The nasal bones are grasped between two fingersand pressure is applied laterally in theopposite direction of the deviation A bluntelevator may be used from within the nose incases of significant medial collapse Walshamforceps can be of help Reduction of the septumshould be performed with the use ofAsch forceps
Nasal Fractures
bull To prevent collapse of the postreductionbull framework nasal packing should be placedbull for 3ndash5 days Septum splints are recommendedbull in comminuted septal fractures withbull severe mucosal lesions External nasal splintingbull for 10 days (Aquaplastreg Thermoplastreg)bull provides nasal protection Nasal saline spraysbull prevent crusting and oral antibiotics should
Nasal Fractures
bull Open reductionbull ndashndash Immediate repair of fractures by using
widebull surgical exposure reduction fixation and
reconstructionbull ndashndash The second option is delayed correctionbull (6 months or more) of persistent deformitiesbull using standard techniques of rhinoplasty
Deviated Nasal Septum
bull Definition of the diseasebull ndash Deviation of the nasal septum is a common causebull of unilateral nasal airway obstruction in which thebull nasal septum is displacedbull bull Epidemiologyaetiologybull ndash Developmental septal abnormalities Septal cartilage
damage in the neonatal period andbull during birth can cause severe septal deviation inbull the absence of a history of nasal trauma
Deviated Nasal Septum
bull Symptomsbull ndash Patients may present with a history of sinusitis
allergicbull rhinitis obstructive sleep apnoea previousbull nasal surgery or recent nasal trauma Unilateral or
bilateral nasal airway obstruction that is unrelievedbull with decongestants or nasal steroid sprays is oftenbull seenbull bull
Deviated Nasal SeptumDiagnosisndashExamination external dorsal deviation or the columella and caudal septummay be deflected off the midline (caudal subluxation)ndash Inspections of the nasal cavity and anterior-posteriorrhinoscopy are helpful in diagnosing the locationtype and severity of septal deformityThe endoscope is also useful in identifying polypsthe severity and extent of posterior septaldeviations and bony spurs and locating areas ofseptal perforation or mucosal injury
Deviated Nasal Septum
bull Therapybull ndash Septoplasty is a procedurebull The areabull of deviation is corrected or resected in order tobull leave behind as much cartilage and bone as
possiblebull Cartilage resection is minimised and can be
repositioned reshaped or recontoured using a variety of methods
Deviated Nasal Septum
bull ndash Indications of septoplasty before the growth period
bull of the nose is finished should be very limited bull -In these cases surgery must preserve all the
cartilagebull in order to prevent external changes of the
shape ofbull the nose
Deviated Nasal Septum
bull Complicationsbull ndash Frequent complications include haematoma andbull infection Cerebrospinal fluid leak is a rare but
potentiallybull serious complicationbull It is usually the resultbull of avulsion or damage to the cribriform plate whenbull handling the perpendicular plate of the ethmoidbull ndash Other complications include epistaxis nasal
Deviated Nasal Septum
bull Other complications include epistaxis nasal obstruction
bull due to residual deviation synechiae returnbull of the cartilaginous deviation septal perforationbull anosmia and cosmetic nasal deformities suchbull as widened alar rim margins drooping nasal tipbull columella retraction and a sunken dorsum with abull supratip saddle formation
Septal perforation with minor crusting View from provide closure of the
incision
Septal Haematoma
bull A septal haematoma is a blood collection under the perichondrium
bull of the septum and cartilagebull bull bull Epidemiologyaetiologybull ndash A septal haematoma is one of the most
severe complications of nasal trauma
Septal Haematoma
bull Diagnosisbull ndash Signs and symptoms include intense pain
swellingbull haematoma of the upper lip and philtrum
area andbull complete nasal airway obstruction
Septal HaematomaTherapyndash Management consists of drainage through a mucoperichondrial incision Immediate treatment isnecessary to prevent long-term problems such asa saddle-nose deformity perforation columellarretraction and nasal-base widening In childrenseptal destruction can lead to devastating nasal andmidfacial growth abnormalitiesbull Surgeryndash Incision and evacuation of the collection is performedDrainage of a septal haematoma should
Septal HaematomaSurgeryndash Incision and evacuation of the collection is performedDrainage of a septal haematoma should provide closure of the incision
Splints or transseptal sutures are placed to obliterate thepotential space and prevent collectionInfection involving the septal cartilage Reconstruction with autologouscartilage is then performed in a second stage Oral antibiotics should be given
Nasal DeformitySaddle-nose deformityndash A saddle-nose deformity is characterised by a loss ofnasal dorsal height and compromised nasal supportstructures -Other case observed are depressionof the middle vault and dorsum loss of nasal tipsupport and definition shortened (vertical) nasal length over rotation of the nasal tip and retrusion ofthe nasal spine and caudal septum It is also knownas a ldquoPug noserdquo or ldquoboxerrsquos noserdquo both of which referto various degrees of nasal dorsal depressionbull
Nasal DeformityEpidemiologyaetiologyndash Prevalence is higher in population groups prone to facial trauma (ie boxers athletes) those with historiesof intranasal cocaine use nasal surgery (e g radical submucosal septal resection reductive rhinoplasty)ndash A saddle-nose deformity can be congenital or acquired It can be noticed as a part of individual familialsyndromic and ethnic characteristics - Most deformities are due to traumatic and iatrogeniccauses Medical causes are Wegenerrsquosgranulomatosis relapsing polychondritis leprosy (Hansenrsquos disease) syphilis ectodermal dysplasiaand intranasal cocaine use
Nasal Deformity
bull Therapybull ndash Nasal reconstruction indications depend on patientbull selection surgeon experience and aetiology of thebull deformity bull Indications for surgery can be functionalbull aesthetic or most commonly both In individuals
with a compromised nasal airway a nasoseptalbull reconstruction is indicated
Nasal Deformity
bull Contraindications bull include patients with malignantbull chronic or autoimmune disease conditions drugbull abuse poor perioperative risk profile and unrealisticbull expectationsbull ndash Multiple previous rhinoplasties and certain
professionsbull (mixed martial artists boxers and other contactbull sports) are relative contraindications
Nasal DeformitySeptoplastyndash Septoplasty is performed to correct nasal obstructioncaused by septal deformityndash Usually septoplasty is performed under general anaesthesiawith the patient in the supine position with the head elevated by approximately 30 (Righthandedsurgeons approach from the right side)ndash Local vasoconstrictive anaesthesia is applied notonly to reduce postoperative pain but also more importantly to achieve vasoconstriction of themucosa and less intraoperative haemorrhage Lidocainewith adrenaline or epinephrine is usedalthough in patients with cardiac hypersensitivityoxymetazoline might be preferred
Nasal Deformity
bull Septoplasty begins with the incision of septal mucosabull Most operative techniques utilise a hemitransfixionbull incision at the caudal end of septum so thatbull deviation at this point might be reached as wellbull as a transfixion incision that is easily obtained ifbull needed (Right-handed surgeons normally choosebull the left side but that may vary when deviation isbull convex towards the right)
Nasal DeformityA columella retractor is placed over the columellaand by pulling it laterally the caudal border of theseptum is exposed Ala can be protected by an alaprotector A vertical incision with a no 15 bladeover the caudal end of septum is performed untilreaching the plane of the septal cartilage It is essentialto correctly identify the perichondrium and byusing the Cottle elevator dissect and lift it creatinga flap As the dissection proceeds along the septalcartilage a longer speculum (no 5) is introduced sothat elevation of the mucoperichondrium is doneunder constant visual controlndash The next step is to dissect the mucoperiostium
Nasal DeformityDissecting over the bony-cartilaginous junctionwhen joining both tunnels might be difficult and is
especially prone to membrane perforationndash If needed the same tunnels are to be created on the
other side of the septum Then deviated parts of
septum are identified and removed either with a
knife or a Freer chisel
Nasal Deformitybull septum from the maxillary crest the septum mustbull be separated from the perpendicular plate trimmedbull along the inferior border placed back onto the crestbull and sutured to the periosteum If the deformity involvesbull the vomer an osteotome is used Care mustbull be taken not to break the cribriform plate becausebull it could cause a cerebrospinal fistula
Nasal Deformity
bull Once the septal deviation is corrected the flapsbull and hemitransfixion incision are mattressed
withbull absorbable sutures Nasal packing to prevent
synechiaebull and postoperative septal haematoma mightbull be advised but should be removed within 72 h

ENT as a subject and career
bull ENT is a fantastic specialty that is every bit as exciting in practice as it is in theory
bull It is difficult to conceive of any specialty which can provide such diversity in medical practice
bullENT conditions make up 25-50 of all general practice consultations
bullENT conditions affect people of all ages from neonates to the elderly
bullSurgical skills are broad from microsurgery on the smallest bones in the body to major head and neck reconstructive surgerybullENT is an expanding surgical specialty that is taking over traditional general surgical areas such as salivary gland surgery and thyroid surgery
bullCosmetic surgery is undertaken by ENT in the form of facial plasticsbullSurgery is also performed on the skull base and pituitary glandbullENT offers enormous research potential from nasal polyps to congenital hearing lossbullThere are cutting edge developments occurring in ENT such as cochlear implantation
We hope that your experiences in ENT will fill you with enthusiasm for this specialty
ENT learning aims and objectives for clinical medical students
AimsTo acquire sufficient knowledge of ENT conditions to be able to
recognize common problems and when and what to referTo understand that ENT conditions are extremely common and form
a large part of the workload of a general practitionerTo learn the skills required to examine patients with ear nose and
throat diseases and to make a presumptive diagnosisTo learn how to prioritize and manage different ENT conditionsTo become stimulated and interested in the specialty of ENT
Objectives To learn the signs and symptoms of common ENT conditions To learn the techniques of ear nasal and neck examination To demonstrate an understanding of the basic anatomy and physiology of the ear
and upper aero-digestive tract and relate this knowledge to the signs and symptoms of ENT disease
To understand the medical and surgical treatment of common ENT conditions To be familiar with the commonly used medications for treating ENT problems and
their side effects To understand the risks and complications of surgery To recognise the different ways in which head and neck malignancy can present
and to understand that early diagnosis of head and neck cancer leads to improved survival
To learn the ways in which ENT related communication difficulties can arise and be overcome
To appreciate and be sensitive to the impact of ENT conditions on patients and their families
Student ENT curriculum
Practical skillsUse of the auriscope to examine the external auditory meatus and tympanic membraneBasic examination of the noseExamination of the oral cavity and oropharynxExamination of the neckHow to manage a nosebleedHow to deal with a tracheostomy
Earbull Basic anatomy and physiology of the earbull Presentation and management of common ear disease eg otitis externa
otitis media glue ear chronic suppurative otitis media with or without cholesteatoma vertigo and facial palsy
bull Examination of the ear including the pinna ear canal and otoscopybull Testing hearing with tuning fork testsbull The advantages of the microscope and the fibreoptic otoscopebull Basic interpretation of play audiometry pure tone audiograms and
tympanogramsbull The principles of grommet insertion mastoid surgery and the treatment of
Menieres diseasebull Identifying postoperative problems following ear surgery ie sensorineural
hearing loss facial nerve palsy and vestibular dysfunctionbull Understanding the differential diagnosis of facial nerve palsy and its
treatment
Nosebull Anatomy and physiology of the nosebull Symptoms and signs of common sinonasal disease eg
rhinitis sinusitis nasal polypsbull Examination of the nose including an assessment of the
appearance the septum the turbinates and the mucosabull The endoscopic evaluation of the nosebull Management of a fractured nose and the timing of
interventionbull Management of epistaxis from minor nosebleeds to
torrential haemorrhagebull The principles of common nasal operations including septal
surgery functional endoscopic sinus surgery and rhinoplasty
Head and neckmdashbenign and malignant disease
bull The basic anatomy and physiology of the oral cavity salivary glands pharynx larynx oesophagus and lymph node drainage
bull The presentation of head and neck cancerbull The presentation and management of salivary gland diseasebull Examining the oral cavity larynx and pharynx including the use of the nasendoscopebull Examining the neck with reference to the lymph nodesbull The role of fine needle aspiration cytology (FNAC)bull The principles and limitations of radiological investigation of the head and neck regionbull Management of neck lumps in particular the malignant lymph node with an unknown
primarybull The management of the airway in patients with a tracheostomy or end tracheostomy after
laryngectomybull A basic knowledge of the principles of operative surgery in particular the principles of
reconstructive surgery and the surgery for salivary gland disease eg parotidectomybull The postoperative management of a patient who has undergone major head and neck surgerybull The role of the multidisciplinary team in head and neck cancer and voice disorders
Supplementary knowledgebull The role of otoacoustic emissions and evoked auditory potentials in managing
hearing lossbull The use of speech audiometrybull The surgery for otosclerosisbull Bone-anchored hearing aids for conductive hearing lossbull Cochlear implantation and the reactions of the deaf community to this
interventionbull The use of sign languagebull Neuro-otology in particular the presentation and management of acoustic
neuromasbull Craniofacial surgery and the interplay between ENT plastic surgery and
neurosurgerybull The management of cleft palate and the increased risk of glue earbull Advanced endoscopic sinus surgery for the mangement of sinonasal malignancy
pituitary tumours and skull base tumoursbull Microlaryngeal surgery and surgical voice restorationbull The use of chemotherapy and radiotherapy in head and neck malignancy
Working in ENT
bull Working in ENT should be a very enjoyable experience whether it is a temporary attachment or a long-term career plan
bull It is helpful if you have an understanding of what others expect of you
bull It is also important for you to think about your own career development
Your duties
bull Patient care and continuitybull Professional developmentbull Research
The ENT Examination
EquipmentA fully equipped ENT department will have all the necessary instruments for performing a full ENT examination
Basic equipment
bull A light sourcemdasha portable headlight that runs off batteries is ideal
bull Wooden tongue depressorsbull Thudicum nasal speculumbull An otoscope with several speculaebull Pneumatic attachment for the otoscopebull Tuning fork 512Hzbull Pen and paperbull Gloves
Advanced equipment
bull Co-phenylcaine spraybull A flexible nasendoscope with light sourcebull Alcohol wipe to act as demist for the scopebull Aqueous lubricating gel for the scope
Emergency equipment
bull Large nasal tampons (you can always cut 10cm ones to size)
bull Silver nitrate sticksbull Foley catheters
Basic Anatomy of the Nose
bull The structural anatomy of the nose is important
bull for both aesthetic and functional reasons since the
bull nose as the gateway to the respiratory tract performs
bull a variety of physiologic functions
External NoseThe shape of the external nose is defined by the nasalbones a pair of rectangular bones in the upper nasaldorsum and by lateral cartilages (uppernasal cartilages) and alar cartilages (major alar cartilages)in the central and lower portions of the noseThe lateral portions of the nasal alae alsocontain several small accessory cartilages called theminor alar cartilages which are embedded in the lateralsoft tissues of the noseThe shape and stability of the alar cartilages each ofwhich consists of a medial and lateral crus
External Nose
Anatomy of the nasal base
bull Besides thebull medial crura the
inferior septal margin and the connective-
bull tissue septum (columella) are also responsible
bull for stabilizing the base of the nose
Anatomy of the nasal base
Anatomy of the nasal base
bull The nasal septum is subluxed toward the left side partially
bull obstructing the nasal airway
Nasal CavitiesThe nasal cavities begin anteriorly at the nasal vestibulewhich is bordered posteriorly by the internal nasalvalve (limen nasi) located between the posteriorborder of the alar cartilage and the anterior border ofthe lateral cartilage This valve area is the narrowestportion of the upper respiratory tract
Nasal Cavities
The interior ofthe nose behind the nasal valve is divided by the nasalseptum into two main cavities
Nasal CavitiesThe nasal septum iscomposed of an anterior cartilaginous part and twoposterior bony parts Abnormalities in the shape ofthe nasal septum which may consist of a deviated septum tensionseptum spurs or ridges are a frequent cause ofnasal airway obstructionThe choanae are the paired posterior openingsthrough which the nasal cavities communicate withthe nasopharynx
Nasal CavitiesThe nasal cavity is bounded laterally by the lateral nasalwalls which are formed by the ethmoid bone andmaxilla and posteriorly by the palatine bone and thepterygoid process of the sphenoid bone Several functionallyimportant structures are located on the lateralnasal wall the nasal turbinates and their associatedpassages (meati) sinus ostia and the orifice ofthe nasolacrimal duct (Fig 15)
The inferior turbinate consists of a separate bone thatis attached to the medial wall of the maxillary sinusThe opening of the nasolacrimal duct is located in thecorresponding inferior meatus The middle andsuperior turbinates are part of the ethmoid bone In rare cases a rudimentary ldquosupreme turbinaterdquo is alsopresent above the superior turbinate
The middle turbinate has by far the greatest functionalimportance because most of the drainage tracts fromthe surrounding paranasal sinuses open into the middlemeatus The nasal cavity is bounded superiorly by the cribriformplate of the ethmoid bone This thin bony platehas numerous openings for the passage of the fila olfactoriaand also forms the boundary of the anteriorcranial fossa
Nasal Cavities
The floor of the nasal cavity is formedmostly by the hard palate which is formed in turn bythe two palatine processes of the maxilla and the horizontallaminae of the palatine bone
Structure of the lateral nasal wall
Inferior meatus
Paranasal Sinuses
The paranasal sinuses are air-filled cavities that communicatewith the nasal cavities
-The maxillary sinus frontalsinus and anterior ethmoid cells drain into the nasalcavity through the middle meatusmdashie below themiddle turbinate -The posterior ethmoidcells drain into the nasal cavity through the superiormeatus The ostium of the sphenoid sinus is locatedin the anterior wall directly above the choanae- The anatomical connections between the nasal cavity andparanasal sinuses are functionally important and playa key role in the pathogenesis of many rhinologic diseasesthat involve the paranasal sinuses
Vascular SupplyThe external nose derives most of its blood supply
from the facial artery which arises from the external
carotid artery and from the ophthalmic artery which
springs from the internal carotid artery
Vascular Supply
The internalnose receives blood from the territories of the externaland internal carotid arteries- the terminalbranches of the sphenopalatine artery which arisesfrom the maxillary artery - the anterior and posteriorethmoid arteries which arise from the ophthalmicartery-internal carotid arterie
venous drainage
The venous drainageof the facial region is handled by -the facial vein -retromandibular vein -internal jugular vein
lymphatic drainage
The regional lymphatic drainage of the face and externalnose is handled mainly by- the submandibularlymph nodes while the nasal cavity is additionallydrained by -the retropharyngeal and deep - -cervical lymph nodes
Morphology of the Nasal Mucosa
Besides the anatomical structure of the external noseand nasal cavity the nasal mucosa plays an essentialrole in numerous functions of the nose in the respiratory tract
Morphology of the Nasal Mucosa
The anterior part of the nasal cavity (the nasal vestibule)like the external nose is covered by skin composedof a multilayer keratinizing squamous epithelium and finally a ciliated respiratory epithelium A small areaon the upper nasal septum superior turbinate andpart of the middle turbinate located adjacent to thecribriform plate is covered by olfactory mucosa and iscalled the olfactory region
Nerve SupplyThe facial skin receives its sensory innervation fromterminal branches of the trigeminal nerve that enterthe facial region through the supraorbital infraorbitaland mental foramina Thefacial muscles are classified as mimetic or mastica- tory each of these groups receiving different motorinnervationbythe facial nerve
History and Clinical Examination of the Nose
Historybull The main symptomsbull nasal obstruction (ldquostuffy
noserdquo)bull nasal dischargebull Headachesbull Olfactory
dysfunction
Palpationbony discontinuitiesNeuralgias to check
over- the supraorbital -infraorbital -mental foramina
Anterior Rhinoscopy
bull The rhinologic examination itself begins with anterior
bull rhinoscopy to evaluate the nasal vestibule and the anterior
bull portions of the nasal cavity
Nasal Endoscopy Nasal endoscopy has become the most important andrewarding clinical examination method in rhinologic diagnosis
- rigid endoscopes which are available in 4-mm and 28- mm diameters and assorted viewing angles (eg 01048576 301048576 1201048576) -flexible endoscopes are also available for inspecting the nose and nasopharynx and exploring all of the pharynx and larynx in one sitting
Nasal endoscopy
Nasal Endoscopy
Nasal Endoscopy
Imaging of the Nose and Paranasal Sinuses
Conventional RadiographsStandard paranasal sinus radiographs in the occipitomental
projection ( Water projection) and
occipitofrontal projection Caldwell projection) in cases of acute inflammation
They are also obtained to evaluate midfacial fractures
Computed Tomography (CT) the main indicationsfor CT scanning of the
nose and paranasal sinuses
are- chronic sinusitis - -trauma (especially
frontobasal -fractures)
-and tumors
The occipitofrontal projection is better for evaluating theethmoid cells and frontal sinus
occipitomental projection demonstrates the maxillarysinus and gives a limited view of the sphenoid sinus
Computed tomography of the paranasal sinuses
Four representative coronal CT scans are shown
Four representative coronal CT scans are shown
Magnetic Resonance Imaging
Magnetic maging
Magnetic resonance imaging (MRI) has fewer indicationsthan CT in patients with paranasal sinus diseaseThis is primarily because MRI is markedly inferior toCT in defining the bony boundaries of the sinusesThe strength of MRI lies in its superior soft-tissue discriminationMRI is indicated in diseases that involve the paranasal sinuses in addition to thecranial cavity or orbit (eg tumors and congenitalmalformations such as encephaloceles)
MRI of the paranasal sinuses
The Nose and Sinuses
Structure The structure of the nose is made up of
four partsbull The surface anatomybull The nasal skeletonmdashcomposed of the
two nasal bones the paired upper lateral and lower lateral cartilages and the nasal septum covered in subcutaneous tissue and skin
bull The internal anatomymdashincludes the septum of the nose which forms the medial wall of the nasal cavity The turbinates on the lateral wall are also called conchae
bull The osteomeatal complexmdasha key functional area of the nose
Function The nose is the main route for inspired
air and its structure is related to this function As the air passes over the large surface area of the turbinates
The inspired gases are warmed and humidified Mucus on the mucosa of the nose removes large dust particles from the air as it is breathed in
The voice resonates in the sinuses and nose and this provides character to the speech
Pneumatization of the sinusesmdashthey are air filled spacesmdashreduces the weight of the skull
Diseases of thDiseases of the Outer and Inner Nosee Outer and
Inner Nose Erysipelas Definition of the disease ndash Erysipela is a skin infection that affects the superficial dermis and is caused by Streptococcus pyogenes (group A) It usually develops in the extremities and the face and less commonly on the scalp and genitals bull Epidemiologyaetiology ndash Erysipelas are more often seen in elderly infants and children patients with compromised immunology and diabetes -Predisposing factors are alcoholism skin ulceration puncture wounds fungal infections malnutrition and burns
Erysipelas
bull Symptomsbull ndash It usually presents of fever general fatigue bull -The skin lesion is a redindurated and elevated plaque
with borders that expand rapidly bull It is painful warm and accompanied by variable oedemabull -On the second or third day a flaccid bulla may develop
and desquamationbull bull Presence of regional lymph nodes is common
Erysipelas
bull Complicationsndash The most common complication is recurrencewhich is seen in 18ndash30 of the cases even afterproper antibiotic therapy Recurrence is seen moreoften in females than in malesA skin infection with S pyogenes could lead toglomerulonephritis
Erysipelas
bull Complicationsbull ndash The most common complication is recurrencebull which is seen in 18ndash30 of the cases even afterbull proper antibiotic therapy bull -Recurrence is seen morebull often in females than in males bull -A skin infection with S pyogenes could lead tobull glomerulonephritis
Erysipelas
bull bull Diagnosisbull ndash Diagnosis is based on the patientrsquos personal
historybull and physical examination particularly on inspectionbull of the skin
bull Blood cultures are positive in less thanbull 5 of cases
ErysipelasTherapyndash Conservative therapybull The preferred antibiotic is penicillin In mildcases with minor systemic symptoms penicillinV 500 mg orally every 6 h for 10 days or penicillinG benzathine 12 mil U intramuscularlyonceOther possibilities are amoxicillin 500 mgorally twice a day for 10 days or cephalexin 500mg orally every 6 h for 10 days
ErysipelasIn moderate and severe cases with significantsystemic symptoms hospitalization and intravenoustreatment is required penicillin G 2ndash4mil U intravenously every 4ndash6 h Cefazolin05ndash15 gm intravenously every 8 h cefotaxime1ndash2 gm intravenously every 8 h or ceftriaxone1ndash2 gm intravenously once a day should be administeredIn patients with a penicillin allergyclindamycin 600 mg intravenously every 8 h orvancomycin 15 mgkg intravenously twice a daymay be given
ErysipelaAdditional useful therapeutic optionsbull Prednisone 30 mg over 8 days might be consideredas well as elevation of the affected siteMoist heat compresses may be usefulbull Surgeryndash Debridement and drainage are indicated when bullaeabscesses or necroses are presentbull Differential diagnosisndash Contact dermatitisndash Asteatotic eczemandash Herpes zosterndash Angioneurotic oedemandash Osteomyelitis
Furuncle
bull Definition of the diseasebull ndash A furuncle is an infection that beginsbull at the hair follicle and spreads deeper into thebull dermis and subcutaneous tissue forming abull nodule After several days it developsbull into an abscess - red painful and fluctuantbull bull bull Epidemiologyaetiologybull ndash The aetiologic agent is Staphylococcus aureus
FuruncleSymptomsndashsymptoms are local and limited to thesite of infection Furuncles usually are wherehair follicles are present bull Complicationndash One complication is furunculosis multiple draining furunclesDiagnosisndash The diagnosis is based on clinical inspection - Cultures are not necessary when there is no systemic involvement but should beconsidered if systemic therapy (in case of feversignificant cellulitis or hospitalization) or whenmethicillin-resistant Staphylococcusaureus (MRSA) is considered
FuruncleTherapyndash When the furuncle is small application of moist heat compress to promote drainage -Larger furuncles should be drained by surgical incision-After drainage the area should be cleaned with anantiseptic (with chlorhexidinebetadine) should be applied twice
a dayndash If no systemic symptoms or extensive cellulitis arepresent simple topical care is usually curative andoral antibiotics are not necessary Otherwise systemictreatment is indicated and should cover anypossible MRSA
Furuncle
bull -Recommended antibiotics are trimethoprim-sulfamethoxazole
bull 1ndash2 tablets orally twice daily doxycyclinebull 100 mg orally twice dailybull or clindamycin 300ndash450 mg orally every 8 hbull - In severe cases vancomycin 15 mgkg
intravenouslybull every 12 h or clindamycin 600 mg intravenouslybull every 8 h
Midline Granulomabull A midline granuloma is an angiocentricbull lymphoma it was referred to as polymorphicbull reticulosis lethal midline granuloma and midline
malignant reticulosisbull bull Definition of the diseasebull ndash This rare disease is a lymphoma of extranodal
presentationall cases are positive for the Epstein-Barr virus
bull -This lymphoma most commonly appears in the midface region
Midline GranulomaEpidemiologyaetiologyndash This form of lymphoma is rare in Europe and theUnited States with a higher prevalence in Asia and PeruSymptomsndash The most common presentation is nasal obstruction with a destructive mass occupying the nosesinuses and palate
-Fever night sweatsand weight loss seen usually in Hodgkinrsquos lymphomaand other non-Hodgkinrsquos lymphomas (knownas ldquoB symptomsrdquo) are uncommon
Midline GranulomaDiagnosisndash The diagnosis is based on anatomopathologicalstudy The malignancy of the tumour manifested byextensive necrosis makes the histological diagnosisdifficult and often more biopsies are required forconfirmationbull Therapyndash Therapy consists of radiotherapy with or withoutchemotherapy
Midline Granuloma
bull Prognosisbull ndash Depending on the stage long-term remission or
experience a worseningbull prognosis with relapses which may include otherbull extranodal sites bull Involvement of extranodal sitesbull including the upper airway gastrointestinal tractbull skin
Wegenerrsquos Granulomatosis
bull Definition of the diseasebull ndash Wegenerrsquos granulomatosis is a systemic chronicbull vasculitis of small- and medium-sized blood vesselsbull with an autoimmune component It affectsbull particular organs with variable predilectionbull Epidemiologyaetiologybull ndash Wegenerrsquos granulomatosis is a rare disease It affects
about 1 in 20000ndash30000 people It is more prevalentbull in middle-aged Caucasian patients
Wegenerrsquos Granulomatosis
Symptomsndash The disease may present pulmonary upper
respiratory tract or renal In the disseminated form-The localised form ndash confinedto the upper respiratory region ndash is present in 25of the patients- It consists of nonspecific manifestationssuch as nasal obstruction crusting purulentor bloody rhinorrhea and painful or painless ulcers in oral or nasal cavities which are unresponsive tostandard medical treatment
Wegenerrsquos Granulomatosis
bull In some patients the nasal septum is perforatedbull which leads to saddle-nose deformity Less
commonbull symptoms are hoarseness stridor due to
subglotticbull stenosis otalgia otorrhea and conductivebull and sensorineural hearing loss Also ocular
symptomsbull such as scleritis conjunctivitis uveitis andbull episcleritis may be present
Wegenerrsquos Granulomatosis
bull ndash In the disseminated form pulmonary involvementbull is manifested by cough dyspnoea haemoptysisbull (due to an alveolar capillaritis necrotic lesions orbull endobronchial disease) and pleuritic painndashbull -Ninety per cent of patients have nasal symptomsbull and these symptoms are usually the first
manifestationof the diseasebull -Most patients have also renal involvementbull even if it is subclinical
Wegenerrsquos Granulomatosis
Diagnosis ndash Diagnosis of Wegenerrsquos granulomatosis is based on clinical findings that demonstrate lung (chest x-ray) kidney (urine analysis) or upper respiratory tract
involvement (oral or nasal ulcers or discharge) - positive blood analysis for cytoplasmic-staining antineutrophil
cytoplasmic antibodies (c-ANCA) and confirming proteinase 3 (PR3) ANCA or myeloperoxidase (MPO) ANCA ndash Biopsy is essential for diagnosis nonspecific chronic inflammation
and necrosis -Bacterial and fungal infections
Wegenerrsquos Granulomatosis
Therapyndash Conservative therapybull In the induction of disease remission highdosesteroids (e g prednisone 1 mgkgday) for1 month with tapering over several months aregiven In addition cyclophosphamide (2 mgkgday) should be administered for 6ndash12 monthsuntil symptoms disappear In the maintenanceof remission cyclophosphamide should be
Wegenerrsquos Granulomatosis
Antibiotics mainly trimethoprim-sulfamethoxazoleare given for prophylaxis againstPneumocystis jiroveci (formerly Pneumocystiscarinii) pneumonia (PCP) which may developduring immunosuppression and have a role inpreventing recurrencesbull Sinonasal manifestations may be treated with topical nasal steroids and nasal irrigations lowdosesystemic steroids and antibiotics when bacterial infection (typically Staphylococcus species) is suspected
Wegenerrsquos Granulomatosis
bull Prognosisbull ndash Most of the patients respond well to treatmentbull achieving symptom-free intervals of 5ndash20 yearsbull or more bull -Anatomical problems (sinusitis trachealbull stenosis) may require surgery bull Relapses can be long and troublesomebull Long-term complications are chronicbull renal failure hearing loss and deafness
Nasal Fractures Definition ndash A nasal fracture is a disruption of the nasal bone structure due to trauma It is the most frequently fractured facial bone Epidemiologyaetiology ndash Sports falls and assaults are the usual mechanisms of fracture -Males are affected twice as often as are females -Paediatric populations with a incidences during the second and third decades of life -Variables such as force impact direction nature of the striking object age and other will influence the pattern of injury to the components of the nose
Nasal Fractures
bull Symptomsbull ndash Deformity swelling epistaxis and periorbital
ecchymosis are signs that are suggestive of nasal fracture
bull bony crepitus and nasal segment mobilitybull ndash Epiphora bull Severe bilateral injuries to the lachrymal bones
arebull associated with depressed nasal fractures
Nasal Fractures Complications ndash Septal haematoma is one of the most severe early complications of nasal trauma and without drainage it results in abscess formation 6ndash7 days after trauma producing necrosis of the septal cartilage -Long-term problems such as saddle-nose deformity perforation columellar retraction and nasalbase
Septal infection could lead to osteomyelitis orbital and intracranial abscesses meningitis and cavernous sinus thrombosis -Cerebrospinal fluid leakage is a common complication of severe
nasal and frontal fractures
Nasal Fractures
bull Diagnostic proceduresbull ndash Inspectionbull bull Changes of appearance such as deviation andbull asymmetry bleeding watery drainage changesbull in nasal breathing and smell It is useful to comparebull the current presentation with old photographsbull (up to 40 of normal individuals havebull significant nose malformations)
Nasal Fractures Physical examination bull The diagnosis of a nasal fracture is made primarily by physical examination epistaxis nasal swelling and periorbital ecchymosis Nasal shape in the lateral and frontal inspection should be assessed Grasping the dorsum between two fingers and rocking the pyramid back and forth aids in assessing the mobility of nasal bones Internal structures should be evaluated by using a headlight and nasal speculum Clotted blood is removed by suction and assessment of haematoma mucosal tears and active bleeding is performed Bimanual palpation of the septum helps to differentiate septal swelling from haematoma ndash
Nasal FracturesRadiographybull There is no clear evidence of the role of radiographyin the management of nasal fracturesPlain films have up to a 66 false-positive rateas a result of misinterpretation of normal suturelines In addition old fractures are difficult todistinguishbull Three-dimensional CT is recommended for extensiveinjuries involving the nasal-orbital-ethmoidalcomplexndash
Nasal Fractures
bull Additionaluseful diagnostic proceduresbull bull Using a 0 or 30deg 4-mm endoscope is helpful inbull the assessment of posterior abnormalities If thebull patient is heavily sedated Brown-Gruss
provocationbull manoeuvres may be performed to determinebull deformities in upper middle or lower segmentsbull by compressing each compartment
Nasal FracturesConservative treatmentndash Treatment of bleedingbull For localised bleeding anterior sources may becauterised by silver nitrate or sealed with topicalmaterials such as thrombin combined withgelatin foam fibrin glue FloSealreg or other procoagulantmaterials If conservative measuresfail a formal anterior packing is placedbull Bleeding from branches of sphenopalatine orethmoid vessels requires anterior-posteriorpacking
Nasal Fractures
bull bull Surgical methods such as direct endoscopic vessel
bull cauterization or ligation have been shown tobull offer better haemostasis and patient comfortbull Angiography with embolization can also be
consideredbull in cases refractory to more conservativebull approaches
Nasal Fractures
bull Type of reductionbull bull Nondisplaced fractures should be treated withbull observation alone Closed nasal reduction is thebull best choice for simple injuries (isolated unilateralbull with medial displacement)bull bull An open approach should be considered in
severebull trauma (bilateral depressed fractures)
Nasal Fracturesbull Surgical principlesbull ndash Topical anaesthesia with cotton pledgets soakedbull with 4 cocaine or 005 oxymethazoline combinedbull with 4 topical lidocaine should be appliedbull for 5ndash10 min Local anaesthesia should also be injectedbull (1 lidocaine and 1100000 epinephrine)bull along the septum lateral walls and floor of the nasalbull cavitybull bull
Nasal FracturesClosed reductionndashndash The nasal bones are grasped between two fingersand pressure is applied laterally in theopposite direction of the deviation A bluntelevator may be used from within the nose incases of significant medial collapse Walshamforceps can be of help Reduction of the septumshould be performed with the use ofAsch forceps
Nasal Fractures
bull To prevent collapse of the postreductionbull framework nasal packing should be placedbull for 3ndash5 days Septum splints are recommendedbull in comminuted septal fractures withbull severe mucosal lesions External nasal splintingbull for 10 days (Aquaplastreg Thermoplastreg)bull provides nasal protection Nasal saline spraysbull prevent crusting and oral antibiotics should
Nasal Fractures
bull Open reductionbull ndashndash Immediate repair of fractures by using
widebull surgical exposure reduction fixation and
reconstructionbull ndashndash The second option is delayed correctionbull (6 months or more) of persistent deformitiesbull using standard techniques of rhinoplasty
Deviated Nasal Septum
bull Definition of the diseasebull ndash Deviation of the nasal septum is a common causebull of unilateral nasal airway obstruction in which thebull nasal septum is displacedbull bull Epidemiologyaetiologybull ndash Developmental septal abnormalities Septal cartilage
damage in the neonatal period andbull during birth can cause severe septal deviation inbull the absence of a history of nasal trauma
Deviated Nasal Septum
bull Symptomsbull ndash Patients may present with a history of sinusitis
allergicbull rhinitis obstructive sleep apnoea previousbull nasal surgery or recent nasal trauma Unilateral or
bilateral nasal airway obstruction that is unrelievedbull with decongestants or nasal steroid sprays is oftenbull seenbull bull
Deviated Nasal SeptumDiagnosisndashExamination external dorsal deviation or the columella and caudal septummay be deflected off the midline (caudal subluxation)ndash Inspections of the nasal cavity and anterior-posteriorrhinoscopy are helpful in diagnosing the locationtype and severity of septal deformityThe endoscope is also useful in identifying polypsthe severity and extent of posterior septaldeviations and bony spurs and locating areas ofseptal perforation or mucosal injury
Deviated Nasal Septum
bull Therapybull ndash Septoplasty is a procedurebull The areabull of deviation is corrected or resected in order tobull leave behind as much cartilage and bone as
possiblebull Cartilage resection is minimised and can be
repositioned reshaped or recontoured using a variety of methods
Deviated Nasal Septum
bull ndash Indications of septoplasty before the growth period
bull of the nose is finished should be very limited bull -In these cases surgery must preserve all the
cartilagebull in order to prevent external changes of the
shape ofbull the nose
Deviated Nasal Septum
bull Complicationsbull ndash Frequent complications include haematoma andbull infection Cerebrospinal fluid leak is a rare but
potentiallybull serious complicationbull It is usually the resultbull of avulsion or damage to the cribriform plate whenbull handling the perpendicular plate of the ethmoidbull ndash Other complications include epistaxis nasal
Deviated Nasal Septum
bull Other complications include epistaxis nasal obstruction
bull due to residual deviation synechiae returnbull of the cartilaginous deviation septal perforationbull anosmia and cosmetic nasal deformities suchbull as widened alar rim margins drooping nasal tipbull columella retraction and a sunken dorsum with abull supratip saddle formation
Septal perforation with minor crusting View from provide closure of the
incision
Septal Haematoma
bull A septal haematoma is a blood collection under the perichondrium
bull of the septum and cartilagebull bull bull Epidemiologyaetiologybull ndash A septal haematoma is one of the most
severe complications of nasal trauma
Septal Haematoma
bull Diagnosisbull ndash Signs and symptoms include intense pain
swellingbull haematoma of the upper lip and philtrum
area andbull complete nasal airway obstruction
Septal HaematomaTherapyndash Management consists of drainage through a mucoperichondrial incision Immediate treatment isnecessary to prevent long-term problems such asa saddle-nose deformity perforation columellarretraction and nasal-base widening In childrenseptal destruction can lead to devastating nasal andmidfacial growth abnormalitiesbull Surgeryndash Incision and evacuation of the collection is performedDrainage of a septal haematoma should
Septal HaematomaSurgeryndash Incision and evacuation of the collection is performedDrainage of a septal haematoma should provide closure of the incision
Splints or transseptal sutures are placed to obliterate thepotential space and prevent collectionInfection involving the septal cartilage Reconstruction with autologouscartilage is then performed in a second stage Oral antibiotics should be given
Nasal DeformitySaddle-nose deformityndash A saddle-nose deformity is characterised by a loss ofnasal dorsal height and compromised nasal supportstructures -Other case observed are depressionof the middle vault and dorsum loss of nasal tipsupport and definition shortened (vertical) nasal length over rotation of the nasal tip and retrusion ofthe nasal spine and caudal septum It is also knownas a ldquoPug noserdquo or ldquoboxerrsquos noserdquo both of which referto various degrees of nasal dorsal depressionbull
Nasal DeformityEpidemiologyaetiologyndash Prevalence is higher in population groups prone to facial trauma (ie boxers athletes) those with historiesof intranasal cocaine use nasal surgery (e g radical submucosal septal resection reductive rhinoplasty)ndash A saddle-nose deformity can be congenital or acquired It can be noticed as a part of individual familialsyndromic and ethnic characteristics - Most deformities are due to traumatic and iatrogeniccauses Medical causes are Wegenerrsquosgranulomatosis relapsing polychondritis leprosy (Hansenrsquos disease) syphilis ectodermal dysplasiaand intranasal cocaine use
Nasal Deformity
bull Therapybull ndash Nasal reconstruction indications depend on patientbull selection surgeon experience and aetiology of thebull deformity bull Indications for surgery can be functionalbull aesthetic or most commonly both In individuals
with a compromised nasal airway a nasoseptalbull reconstruction is indicated
Nasal Deformity
bull Contraindications bull include patients with malignantbull chronic or autoimmune disease conditions drugbull abuse poor perioperative risk profile and unrealisticbull expectationsbull ndash Multiple previous rhinoplasties and certain
professionsbull (mixed martial artists boxers and other contactbull sports) are relative contraindications
Nasal DeformitySeptoplastyndash Septoplasty is performed to correct nasal obstructioncaused by septal deformityndash Usually septoplasty is performed under general anaesthesiawith the patient in the supine position with the head elevated by approximately 30 (Righthandedsurgeons approach from the right side)ndash Local vasoconstrictive anaesthesia is applied notonly to reduce postoperative pain but also more importantly to achieve vasoconstriction of themucosa and less intraoperative haemorrhage Lidocainewith adrenaline or epinephrine is usedalthough in patients with cardiac hypersensitivityoxymetazoline might be preferred
Nasal Deformity
bull Septoplasty begins with the incision of septal mucosabull Most operative techniques utilise a hemitransfixionbull incision at the caudal end of septum so thatbull deviation at this point might be reached as wellbull as a transfixion incision that is easily obtained ifbull needed (Right-handed surgeons normally choosebull the left side but that may vary when deviation isbull convex towards the right)
Nasal DeformityA columella retractor is placed over the columellaand by pulling it laterally the caudal border of theseptum is exposed Ala can be protected by an alaprotector A vertical incision with a no 15 bladeover the caudal end of septum is performed untilreaching the plane of the septal cartilage It is essentialto correctly identify the perichondrium and byusing the Cottle elevator dissect and lift it creatinga flap As the dissection proceeds along the septalcartilage a longer speculum (no 5) is introduced sothat elevation of the mucoperichondrium is doneunder constant visual controlndash The next step is to dissect the mucoperiostium
Nasal DeformityDissecting over the bony-cartilaginous junctionwhen joining both tunnels might be difficult and is
especially prone to membrane perforationndash If needed the same tunnels are to be created on the
other side of the septum Then deviated parts of
septum are identified and removed either with a
knife or a Freer chisel
Nasal Deformitybull septum from the maxillary crest the septum mustbull be separated from the perpendicular plate trimmedbull along the inferior border placed back onto the crestbull and sutured to the periosteum If the deformity involvesbull the vomer an osteotome is used Care mustbull be taken not to break the cribriform plate becausebull it could cause a cerebrospinal fistula
Nasal Deformity
bull Once the septal deviation is corrected the flapsbull and hemitransfixion incision are mattressed
withbull absorbable sutures Nasal packing to prevent
synechiaebull and postoperative septal haematoma mightbull be advised but should be removed within 72 h

bullENT conditions make up 25-50 of all general practice consultations
bullENT conditions affect people of all ages from neonates to the elderly
bullSurgical skills are broad from microsurgery on the smallest bones in the body to major head and neck reconstructive surgerybullENT is an expanding surgical specialty that is taking over traditional general surgical areas such as salivary gland surgery and thyroid surgery
bullCosmetic surgery is undertaken by ENT in the form of facial plasticsbullSurgery is also performed on the skull base and pituitary glandbullENT offers enormous research potential from nasal polyps to congenital hearing lossbullThere are cutting edge developments occurring in ENT such as cochlear implantation
We hope that your experiences in ENT will fill you with enthusiasm for this specialty
ENT learning aims and objectives for clinical medical students
AimsTo acquire sufficient knowledge of ENT conditions to be able to
recognize common problems and when and what to referTo understand that ENT conditions are extremely common and form
a large part of the workload of a general practitionerTo learn the skills required to examine patients with ear nose and
throat diseases and to make a presumptive diagnosisTo learn how to prioritize and manage different ENT conditionsTo become stimulated and interested in the specialty of ENT
Objectives To learn the signs and symptoms of common ENT conditions To learn the techniques of ear nasal and neck examination To demonstrate an understanding of the basic anatomy and physiology of the ear
and upper aero-digestive tract and relate this knowledge to the signs and symptoms of ENT disease
To understand the medical and surgical treatment of common ENT conditions To be familiar with the commonly used medications for treating ENT problems and
their side effects To understand the risks and complications of surgery To recognise the different ways in which head and neck malignancy can present
and to understand that early diagnosis of head and neck cancer leads to improved survival
To learn the ways in which ENT related communication difficulties can arise and be overcome
To appreciate and be sensitive to the impact of ENT conditions on patients and their families
Student ENT curriculum
Practical skillsUse of the auriscope to examine the external auditory meatus and tympanic membraneBasic examination of the noseExamination of the oral cavity and oropharynxExamination of the neckHow to manage a nosebleedHow to deal with a tracheostomy
Earbull Basic anatomy and physiology of the earbull Presentation and management of common ear disease eg otitis externa
otitis media glue ear chronic suppurative otitis media with or without cholesteatoma vertigo and facial palsy
bull Examination of the ear including the pinna ear canal and otoscopybull Testing hearing with tuning fork testsbull The advantages of the microscope and the fibreoptic otoscopebull Basic interpretation of play audiometry pure tone audiograms and
tympanogramsbull The principles of grommet insertion mastoid surgery and the treatment of
Menieres diseasebull Identifying postoperative problems following ear surgery ie sensorineural
hearing loss facial nerve palsy and vestibular dysfunctionbull Understanding the differential diagnosis of facial nerve palsy and its
treatment
Nosebull Anatomy and physiology of the nosebull Symptoms and signs of common sinonasal disease eg
rhinitis sinusitis nasal polypsbull Examination of the nose including an assessment of the
appearance the septum the turbinates and the mucosabull The endoscopic evaluation of the nosebull Management of a fractured nose and the timing of
interventionbull Management of epistaxis from minor nosebleeds to
torrential haemorrhagebull The principles of common nasal operations including septal
surgery functional endoscopic sinus surgery and rhinoplasty
Head and neckmdashbenign and malignant disease
bull The basic anatomy and physiology of the oral cavity salivary glands pharynx larynx oesophagus and lymph node drainage
bull The presentation of head and neck cancerbull The presentation and management of salivary gland diseasebull Examining the oral cavity larynx and pharynx including the use of the nasendoscopebull Examining the neck with reference to the lymph nodesbull The role of fine needle aspiration cytology (FNAC)bull The principles and limitations of radiological investigation of the head and neck regionbull Management of neck lumps in particular the malignant lymph node with an unknown
primarybull The management of the airway in patients with a tracheostomy or end tracheostomy after
laryngectomybull A basic knowledge of the principles of operative surgery in particular the principles of
reconstructive surgery and the surgery for salivary gland disease eg parotidectomybull The postoperative management of a patient who has undergone major head and neck surgerybull The role of the multidisciplinary team in head and neck cancer and voice disorders
Supplementary knowledgebull The role of otoacoustic emissions and evoked auditory potentials in managing
hearing lossbull The use of speech audiometrybull The surgery for otosclerosisbull Bone-anchored hearing aids for conductive hearing lossbull Cochlear implantation and the reactions of the deaf community to this
interventionbull The use of sign languagebull Neuro-otology in particular the presentation and management of acoustic
neuromasbull Craniofacial surgery and the interplay between ENT plastic surgery and
neurosurgerybull The management of cleft palate and the increased risk of glue earbull Advanced endoscopic sinus surgery for the mangement of sinonasal malignancy
pituitary tumours and skull base tumoursbull Microlaryngeal surgery and surgical voice restorationbull The use of chemotherapy and radiotherapy in head and neck malignancy
Working in ENT
bull Working in ENT should be a very enjoyable experience whether it is a temporary attachment or a long-term career plan
bull It is helpful if you have an understanding of what others expect of you
bull It is also important for you to think about your own career development
Your duties
bull Patient care and continuitybull Professional developmentbull Research
The ENT Examination
EquipmentA fully equipped ENT department will have all the necessary instruments for performing a full ENT examination
Basic equipment
bull A light sourcemdasha portable headlight that runs off batteries is ideal
bull Wooden tongue depressorsbull Thudicum nasal speculumbull An otoscope with several speculaebull Pneumatic attachment for the otoscopebull Tuning fork 512Hzbull Pen and paperbull Gloves
Advanced equipment
bull Co-phenylcaine spraybull A flexible nasendoscope with light sourcebull Alcohol wipe to act as demist for the scopebull Aqueous lubricating gel for the scope
Emergency equipment
bull Large nasal tampons (you can always cut 10cm ones to size)
bull Silver nitrate sticksbull Foley catheters
Basic Anatomy of the Nose
bull The structural anatomy of the nose is important
bull for both aesthetic and functional reasons since the
bull nose as the gateway to the respiratory tract performs
bull a variety of physiologic functions
External NoseThe shape of the external nose is defined by the nasalbones a pair of rectangular bones in the upper nasaldorsum and by lateral cartilages (uppernasal cartilages) and alar cartilages (major alar cartilages)in the central and lower portions of the noseThe lateral portions of the nasal alae alsocontain several small accessory cartilages called theminor alar cartilages which are embedded in the lateralsoft tissues of the noseThe shape and stability of the alar cartilages each ofwhich consists of a medial and lateral crus
External Nose
Anatomy of the nasal base
bull Besides thebull medial crura the
inferior septal margin and the connective-
bull tissue septum (columella) are also responsible
bull for stabilizing the base of the nose
Anatomy of the nasal base
Anatomy of the nasal base
bull The nasal septum is subluxed toward the left side partially
bull obstructing the nasal airway
Nasal CavitiesThe nasal cavities begin anteriorly at the nasal vestibulewhich is bordered posteriorly by the internal nasalvalve (limen nasi) located between the posteriorborder of the alar cartilage and the anterior border ofthe lateral cartilage This valve area is the narrowestportion of the upper respiratory tract
Nasal Cavities
The interior ofthe nose behind the nasal valve is divided by the nasalseptum into two main cavities
Nasal CavitiesThe nasal septum iscomposed of an anterior cartilaginous part and twoposterior bony parts Abnormalities in the shape ofthe nasal septum which may consist of a deviated septum tensionseptum spurs or ridges are a frequent cause ofnasal airway obstructionThe choanae are the paired posterior openingsthrough which the nasal cavities communicate withthe nasopharynx
Nasal CavitiesThe nasal cavity is bounded laterally by the lateral nasalwalls which are formed by the ethmoid bone andmaxilla and posteriorly by the palatine bone and thepterygoid process of the sphenoid bone Several functionallyimportant structures are located on the lateralnasal wall the nasal turbinates and their associatedpassages (meati) sinus ostia and the orifice ofthe nasolacrimal duct (Fig 15)
The inferior turbinate consists of a separate bone thatis attached to the medial wall of the maxillary sinusThe opening of the nasolacrimal duct is located in thecorresponding inferior meatus The middle andsuperior turbinates are part of the ethmoid bone In rare cases a rudimentary ldquosupreme turbinaterdquo is alsopresent above the superior turbinate
The middle turbinate has by far the greatest functionalimportance because most of the drainage tracts fromthe surrounding paranasal sinuses open into the middlemeatus The nasal cavity is bounded superiorly by the cribriformplate of the ethmoid bone This thin bony platehas numerous openings for the passage of the fila olfactoriaand also forms the boundary of the anteriorcranial fossa
Nasal Cavities
The floor of the nasal cavity is formedmostly by the hard palate which is formed in turn bythe two palatine processes of the maxilla and the horizontallaminae of the palatine bone
Structure of the lateral nasal wall
Inferior meatus
Paranasal Sinuses
The paranasal sinuses are air-filled cavities that communicatewith the nasal cavities
-The maxillary sinus frontalsinus and anterior ethmoid cells drain into the nasalcavity through the middle meatusmdashie below themiddle turbinate -The posterior ethmoidcells drain into the nasal cavity through the superiormeatus The ostium of the sphenoid sinus is locatedin the anterior wall directly above the choanae- The anatomical connections between the nasal cavity andparanasal sinuses are functionally important and playa key role in the pathogenesis of many rhinologic diseasesthat involve the paranasal sinuses
Vascular SupplyThe external nose derives most of its blood supply
from the facial artery which arises from the external
carotid artery and from the ophthalmic artery which
springs from the internal carotid artery
Vascular Supply
The internalnose receives blood from the territories of the externaland internal carotid arteries- the terminalbranches of the sphenopalatine artery which arisesfrom the maxillary artery - the anterior and posteriorethmoid arteries which arise from the ophthalmicartery-internal carotid arterie
venous drainage
The venous drainageof the facial region is handled by -the facial vein -retromandibular vein -internal jugular vein
lymphatic drainage
The regional lymphatic drainage of the face and externalnose is handled mainly by- the submandibularlymph nodes while the nasal cavity is additionallydrained by -the retropharyngeal and deep - -cervical lymph nodes
Morphology of the Nasal Mucosa
Besides the anatomical structure of the external noseand nasal cavity the nasal mucosa plays an essentialrole in numerous functions of the nose in the respiratory tract
Morphology of the Nasal Mucosa
The anterior part of the nasal cavity (the nasal vestibule)like the external nose is covered by skin composedof a multilayer keratinizing squamous epithelium and finally a ciliated respiratory epithelium A small areaon the upper nasal septum superior turbinate andpart of the middle turbinate located adjacent to thecribriform plate is covered by olfactory mucosa and iscalled the olfactory region
Nerve SupplyThe facial skin receives its sensory innervation fromterminal branches of the trigeminal nerve that enterthe facial region through the supraorbital infraorbitaland mental foramina Thefacial muscles are classified as mimetic or mastica- tory each of these groups receiving different motorinnervationbythe facial nerve
History and Clinical Examination of the Nose
Historybull The main symptomsbull nasal obstruction (ldquostuffy
noserdquo)bull nasal dischargebull Headachesbull Olfactory
dysfunction
Palpationbony discontinuitiesNeuralgias to check
over- the supraorbital -infraorbital -mental foramina
Anterior Rhinoscopy
bull The rhinologic examination itself begins with anterior
bull rhinoscopy to evaluate the nasal vestibule and the anterior
bull portions of the nasal cavity
Nasal Endoscopy Nasal endoscopy has become the most important andrewarding clinical examination method in rhinologic diagnosis
- rigid endoscopes which are available in 4-mm and 28- mm diameters and assorted viewing angles (eg 01048576 301048576 1201048576) -flexible endoscopes are also available for inspecting the nose and nasopharynx and exploring all of the pharynx and larynx in one sitting
Nasal endoscopy
Nasal Endoscopy
Nasal Endoscopy
Imaging of the Nose and Paranasal Sinuses
Conventional RadiographsStandard paranasal sinus radiographs in the occipitomental
projection ( Water projection) and
occipitofrontal projection Caldwell projection) in cases of acute inflammation
They are also obtained to evaluate midfacial fractures
Computed Tomography (CT) the main indicationsfor CT scanning of the
nose and paranasal sinuses
are- chronic sinusitis - -trauma (especially
frontobasal -fractures)
-and tumors
The occipitofrontal projection is better for evaluating theethmoid cells and frontal sinus
occipitomental projection demonstrates the maxillarysinus and gives a limited view of the sphenoid sinus
Computed tomography of the paranasal sinuses
Four representative coronal CT scans are shown
Four representative coronal CT scans are shown
Magnetic Resonance Imaging
Magnetic maging
Magnetic resonance imaging (MRI) has fewer indicationsthan CT in patients with paranasal sinus diseaseThis is primarily because MRI is markedly inferior toCT in defining the bony boundaries of the sinusesThe strength of MRI lies in its superior soft-tissue discriminationMRI is indicated in diseases that involve the paranasal sinuses in addition to thecranial cavity or orbit (eg tumors and congenitalmalformations such as encephaloceles)
MRI of the paranasal sinuses
The Nose and Sinuses
Structure The structure of the nose is made up of
four partsbull The surface anatomybull The nasal skeletonmdashcomposed of the
two nasal bones the paired upper lateral and lower lateral cartilages and the nasal septum covered in subcutaneous tissue and skin
bull The internal anatomymdashincludes the septum of the nose which forms the medial wall of the nasal cavity The turbinates on the lateral wall are also called conchae
bull The osteomeatal complexmdasha key functional area of the nose
Function The nose is the main route for inspired
air and its structure is related to this function As the air passes over the large surface area of the turbinates
The inspired gases are warmed and humidified Mucus on the mucosa of the nose removes large dust particles from the air as it is breathed in
The voice resonates in the sinuses and nose and this provides character to the speech
Pneumatization of the sinusesmdashthey are air filled spacesmdashreduces the weight of the skull
Diseases of thDiseases of the Outer and Inner Nosee Outer and
Inner Nose Erysipelas Definition of the disease ndash Erysipela is a skin infection that affects the superficial dermis and is caused by Streptococcus pyogenes (group A) It usually develops in the extremities and the face and less commonly on the scalp and genitals bull Epidemiologyaetiology ndash Erysipelas are more often seen in elderly infants and children patients with compromised immunology and diabetes -Predisposing factors are alcoholism skin ulceration puncture wounds fungal infections malnutrition and burns
Erysipelas
bull Symptomsbull ndash It usually presents of fever general fatigue bull -The skin lesion is a redindurated and elevated plaque
with borders that expand rapidly bull It is painful warm and accompanied by variable oedemabull -On the second or third day a flaccid bulla may develop
and desquamationbull bull Presence of regional lymph nodes is common
Erysipelas
bull Complicationsndash The most common complication is recurrencewhich is seen in 18ndash30 of the cases even afterproper antibiotic therapy Recurrence is seen moreoften in females than in malesA skin infection with S pyogenes could lead toglomerulonephritis
Erysipelas
bull Complicationsbull ndash The most common complication is recurrencebull which is seen in 18ndash30 of the cases even afterbull proper antibiotic therapy bull -Recurrence is seen morebull often in females than in males bull -A skin infection with S pyogenes could lead tobull glomerulonephritis
Erysipelas
bull bull Diagnosisbull ndash Diagnosis is based on the patientrsquos personal
historybull and physical examination particularly on inspectionbull of the skin
bull Blood cultures are positive in less thanbull 5 of cases
ErysipelasTherapyndash Conservative therapybull The preferred antibiotic is penicillin In mildcases with minor systemic symptoms penicillinV 500 mg orally every 6 h for 10 days or penicillinG benzathine 12 mil U intramuscularlyonceOther possibilities are amoxicillin 500 mgorally twice a day for 10 days or cephalexin 500mg orally every 6 h for 10 days
ErysipelasIn moderate and severe cases with significantsystemic symptoms hospitalization and intravenoustreatment is required penicillin G 2ndash4mil U intravenously every 4ndash6 h Cefazolin05ndash15 gm intravenously every 8 h cefotaxime1ndash2 gm intravenously every 8 h or ceftriaxone1ndash2 gm intravenously once a day should be administeredIn patients with a penicillin allergyclindamycin 600 mg intravenously every 8 h orvancomycin 15 mgkg intravenously twice a daymay be given
ErysipelaAdditional useful therapeutic optionsbull Prednisone 30 mg over 8 days might be consideredas well as elevation of the affected siteMoist heat compresses may be usefulbull Surgeryndash Debridement and drainage are indicated when bullaeabscesses or necroses are presentbull Differential diagnosisndash Contact dermatitisndash Asteatotic eczemandash Herpes zosterndash Angioneurotic oedemandash Osteomyelitis
Furuncle
bull Definition of the diseasebull ndash A furuncle is an infection that beginsbull at the hair follicle and spreads deeper into thebull dermis and subcutaneous tissue forming abull nodule After several days it developsbull into an abscess - red painful and fluctuantbull bull bull Epidemiologyaetiologybull ndash The aetiologic agent is Staphylococcus aureus
FuruncleSymptomsndashsymptoms are local and limited to thesite of infection Furuncles usually are wherehair follicles are present bull Complicationndash One complication is furunculosis multiple draining furunclesDiagnosisndash The diagnosis is based on clinical inspection - Cultures are not necessary when there is no systemic involvement but should beconsidered if systemic therapy (in case of feversignificant cellulitis or hospitalization) or whenmethicillin-resistant Staphylococcusaureus (MRSA) is considered
FuruncleTherapyndash When the furuncle is small application of moist heat compress to promote drainage -Larger furuncles should be drained by surgical incision-After drainage the area should be cleaned with anantiseptic (with chlorhexidinebetadine) should be applied twice
a dayndash If no systemic symptoms or extensive cellulitis arepresent simple topical care is usually curative andoral antibiotics are not necessary Otherwise systemictreatment is indicated and should cover anypossible MRSA
Furuncle
bull -Recommended antibiotics are trimethoprim-sulfamethoxazole
bull 1ndash2 tablets orally twice daily doxycyclinebull 100 mg orally twice dailybull or clindamycin 300ndash450 mg orally every 8 hbull - In severe cases vancomycin 15 mgkg
intravenouslybull every 12 h or clindamycin 600 mg intravenouslybull every 8 h
Midline Granulomabull A midline granuloma is an angiocentricbull lymphoma it was referred to as polymorphicbull reticulosis lethal midline granuloma and midline
malignant reticulosisbull bull Definition of the diseasebull ndash This rare disease is a lymphoma of extranodal
presentationall cases are positive for the Epstein-Barr virus
bull -This lymphoma most commonly appears in the midface region
Midline GranulomaEpidemiologyaetiologyndash This form of lymphoma is rare in Europe and theUnited States with a higher prevalence in Asia and PeruSymptomsndash The most common presentation is nasal obstruction with a destructive mass occupying the nosesinuses and palate
-Fever night sweatsand weight loss seen usually in Hodgkinrsquos lymphomaand other non-Hodgkinrsquos lymphomas (knownas ldquoB symptomsrdquo) are uncommon
Midline GranulomaDiagnosisndash The diagnosis is based on anatomopathologicalstudy The malignancy of the tumour manifested byextensive necrosis makes the histological diagnosisdifficult and often more biopsies are required forconfirmationbull Therapyndash Therapy consists of radiotherapy with or withoutchemotherapy
Midline Granuloma
bull Prognosisbull ndash Depending on the stage long-term remission or
experience a worseningbull prognosis with relapses which may include otherbull extranodal sites bull Involvement of extranodal sitesbull including the upper airway gastrointestinal tractbull skin
Wegenerrsquos Granulomatosis
bull Definition of the diseasebull ndash Wegenerrsquos granulomatosis is a systemic chronicbull vasculitis of small- and medium-sized blood vesselsbull with an autoimmune component It affectsbull particular organs with variable predilectionbull Epidemiologyaetiologybull ndash Wegenerrsquos granulomatosis is a rare disease It affects
about 1 in 20000ndash30000 people It is more prevalentbull in middle-aged Caucasian patients
Wegenerrsquos Granulomatosis
Symptomsndash The disease may present pulmonary upper
respiratory tract or renal In the disseminated form-The localised form ndash confinedto the upper respiratory region ndash is present in 25of the patients- It consists of nonspecific manifestationssuch as nasal obstruction crusting purulentor bloody rhinorrhea and painful or painless ulcers in oral or nasal cavities which are unresponsive tostandard medical treatment
Wegenerrsquos Granulomatosis
bull In some patients the nasal septum is perforatedbull which leads to saddle-nose deformity Less
commonbull symptoms are hoarseness stridor due to
subglotticbull stenosis otalgia otorrhea and conductivebull and sensorineural hearing loss Also ocular
symptomsbull such as scleritis conjunctivitis uveitis andbull episcleritis may be present
Wegenerrsquos Granulomatosis
bull ndash In the disseminated form pulmonary involvementbull is manifested by cough dyspnoea haemoptysisbull (due to an alveolar capillaritis necrotic lesions orbull endobronchial disease) and pleuritic painndashbull -Ninety per cent of patients have nasal symptomsbull and these symptoms are usually the first
manifestationof the diseasebull -Most patients have also renal involvementbull even if it is subclinical
Wegenerrsquos Granulomatosis
Diagnosis ndash Diagnosis of Wegenerrsquos granulomatosis is based on clinical findings that demonstrate lung (chest x-ray) kidney (urine analysis) or upper respiratory tract
involvement (oral or nasal ulcers or discharge) - positive blood analysis for cytoplasmic-staining antineutrophil
cytoplasmic antibodies (c-ANCA) and confirming proteinase 3 (PR3) ANCA or myeloperoxidase (MPO) ANCA ndash Biopsy is essential for diagnosis nonspecific chronic inflammation
and necrosis -Bacterial and fungal infections
Wegenerrsquos Granulomatosis
Therapyndash Conservative therapybull In the induction of disease remission highdosesteroids (e g prednisone 1 mgkgday) for1 month with tapering over several months aregiven In addition cyclophosphamide (2 mgkgday) should be administered for 6ndash12 monthsuntil symptoms disappear In the maintenanceof remission cyclophosphamide should be
Wegenerrsquos Granulomatosis
Antibiotics mainly trimethoprim-sulfamethoxazoleare given for prophylaxis againstPneumocystis jiroveci (formerly Pneumocystiscarinii) pneumonia (PCP) which may developduring immunosuppression and have a role inpreventing recurrencesbull Sinonasal manifestations may be treated with topical nasal steroids and nasal irrigations lowdosesystemic steroids and antibiotics when bacterial infection (typically Staphylococcus species) is suspected
Wegenerrsquos Granulomatosis
bull Prognosisbull ndash Most of the patients respond well to treatmentbull achieving symptom-free intervals of 5ndash20 yearsbull or more bull -Anatomical problems (sinusitis trachealbull stenosis) may require surgery bull Relapses can be long and troublesomebull Long-term complications are chronicbull renal failure hearing loss and deafness
Nasal Fractures Definition ndash A nasal fracture is a disruption of the nasal bone structure due to trauma It is the most frequently fractured facial bone Epidemiologyaetiology ndash Sports falls and assaults are the usual mechanisms of fracture -Males are affected twice as often as are females -Paediatric populations with a incidences during the second and third decades of life -Variables such as force impact direction nature of the striking object age and other will influence the pattern of injury to the components of the nose
Nasal Fractures
bull Symptomsbull ndash Deformity swelling epistaxis and periorbital
ecchymosis are signs that are suggestive of nasal fracture
bull bony crepitus and nasal segment mobilitybull ndash Epiphora bull Severe bilateral injuries to the lachrymal bones
arebull associated with depressed nasal fractures
Nasal Fractures Complications ndash Septal haematoma is one of the most severe early complications of nasal trauma and without drainage it results in abscess formation 6ndash7 days after trauma producing necrosis of the septal cartilage -Long-term problems such as saddle-nose deformity perforation columellar retraction and nasalbase
Septal infection could lead to osteomyelitis orbital and intracranial abscesses meningitis and cavernous sinus thrombosis -Cerebrospinal fluid leakage is a common complication of severe
nasal and frontal fractures
Nasal Fractures
bull Diagnostic proceduresbull ndash Inspectionbull bull Changes of appearance such as deviation andbull asymmetry bleeding watery drainage changesbull in nasal breathing and smell It is useful to comparebull the current presentation with old photographsbull (up to 40 of normal individuals havebull significant nose malformations)
Nasal Fractures Physical examination bull The diagnosis of a nasal fracture is made primarily by physical examination epistaxis nasal swelling and periorbital ecchymosis Nasal shape in the lateral and frontal inspection should be assessed Grasping the dorsum between two fingers and rocking the pyramid back and forth aids in assessing the mobility of nasal bones Internal structures should be evaluated by using a headlight and nasal speculum Clotted blood is removed by suction and assessment of haematoma mucosal tears and active bleeding is performed Bimanual palpation of the septum helps to differentiate septal swelling from haematoma ndash
Nasal FracturesRadiographybull There is no clear evidence of the role of radiographyin the management of nasal fracturesPlain films have up to a 66 false-positive rateas a result of misinterpretation of normal suturelines In addition old fractures are difficult todistinguishbull Three-dimensional CT is recommended for extensiveinjuries involving the nasal-orbital-ethmoidalcomplexndash
Nasal Fractures
bull Additionaluseful diagnostic proceduresbull bull Using a 0 or 30deg 4-mm endoscope is helpful inbull the assessment of posterior abnormalities If thebull patient is heavily sedated Brown-Gruss
provocationbull manoeuvres may be performed to determinebull deformities in upper middle or lower segmentsbull by compressing each compartment
Nasal FracturesConservative treatmentndash Treatment of bleedingbull For localised bleeding anterior sources may becauterised by silver nitrate or sealed with topicalmaterials such as thrombin combined withgelatin foam fibrin glue FloSealreg or other procoagulantmaterials If conservative measuresfail a formal anterior packing is placedbull Bleeding from branches of sphenopalatine orethmoid vessels requires anterior-posteriorpacking
Nasal Fractures
bull bull Surgical methods such as direct endoscopic vessel
bull cauterization or ligation have been shown tobull offer better haemostasis and patient comfortbull Angiography with embolization can also be
consideredbull in cases refractory to more conservativebull approaches
Nasal Fractures
bull Type of reductionbull bull Nondisplaced fractures should be treated withbull observation alone Closed nasal reduction is thebull best choice for simple injuries (isolated unilateralbull with medial displacement)bull bull An open approach should be considered in
severebull trauma (bilateral depressed fractures)
Nasal Fracturesbull Surgical principlesbull ndash Topical anaesthesia with cotton pledgets soakedbull with 4 cocaine or 005 oxymethazoline combinedbull with 4 topical lidocaine should be appliedbull for 5ndash10 min Local anaesthesia should also be injectedbull (1 lidocaine and 1100000 epinephrine)bull along the septum lateral walls and floor of the nasalbull cavitybull bull
Nasal FracturesClosed reductionndashndash The nasal bones are grasped between two fingersand pressure is applied laterally in theopposite direction of the deviation A bluntelevator may be used from within the nose incases of significant medial collapse Walshamforceps can be of help Reduction of the septumshould be performed with the use ofAsch forceps
Nasal Fractures
bull To prevent collapse of the postreductionbull framework nasal packing should be placedbull for 3ndash5 days Septum splints are recommendedbull in comminuted septal fractures withbull severe mucosal lesions External nasal splintingbull for 10 days (Aquaplastreg Thermoplastreg)bull provides nasal protection Nasal saline spraysbull prevent crusting and oral antibiotics should
Nasal Fractures
bull Open reductionbull ndashndash Immediate repair of fractures by using
widebull surgical exposure reduction fixation and
reconstructionbull ndashndash The second option is delayed correctionbull (6 months or more) of persistent deformitiesbull using standard techniques of rhinoplasty
Deviated Nasal Septum
bull Definition of the diseasebull ndash Deviation of the nasal septum is a common causebull of unilateral nasal airway obstruction in which thebull nasal septum is displacedbull bull Epidemiologyaetiologybull ndash Developmental septal abnormalities Septal cartilage
damage in the neonatal period andbull during birth can cause severe septal deviation inbull the absence of a history of nasal trauma
Deviated Nasal Septum
bull Symptomsbull ndash Patients may present with a history of sinusitis
allergicbull rhinitis obstructive sleep apnoea previousbull nasal surgery or recent nasal trauma Unilateral or
bilateral nasal airway obstruction that is unrelievedbull with decongestants or nasal steroid sprays is oftenbull seenbull bull
Deviated Nasal SeptumDiagnosisndashExamination external dorsal deviation or the columella and caudal septummay be deflected off the midline (caudal subluxation)ndash Inspections of the nasal cavity and anterior-posteriorrhinoscopy are helpful in diagnosing the locationtype and severity of septal deformityThe endoscope is also useful in identifying polypsthe severity and extent of posterior septaldeviations and bony spurs and locating areas ofseptal perforation or mucosal injury
Deviated Nasal Septum
bull Therapybull ndash Septoplasty is a procedurebull The areabull of deviation is corrected or resected in order tobull leave behind as much cartilage and bone as
possiblebull Cartilage resection is minimised and can be
repositioned reshaped or recontoured using a variety of methods
Deviated Nasal Septum
bull ndash Indications of septoplasty before the growth period
bull of the nose is finished should be very limited bull -In these cases surgery must preserve all the
cartilagebull in order to prevent external changes of the
shape ofbull the nose
Deviated Nasal Septum
bull Complicationsbull ndash Frequent complications include haematoma andbull infection Cerebrospinal fluid leak is a rare but
potentiallybull serious complicationbull It is usually the resultbull of avulsion or damage to the cribriform plate whenbull handling the perpendicular plate of the ethmoidbull ndash Other complications include epistaxis nasal
Deviated Nasal Septum
bull Other complications include epistaxis nasal obstruction
bull due to residual deviation synechiae returnbull of the cartilaginous deviation septal perforationbull anosmia and cosmetic nasal deformities suchbull as widened alar rim margins drooping nasal tipbull columella retraction and a sunken dorsum with abull supratip saddle formation
Septal perforation with minor crusting View from provide closure of the
incision
Septal Haematoma
bull A septal haematoma is a blood collection under the perichondrium
bull of the septum and cartilagebull bull bull Epidemiologyaetiologybull ndash A septal haematoma is one of the most
severe complications of nasal trauma
Septal Haematoma
bull Diagnosisbull ndash Signs and symptoms include intense pain
swellingbull haematoma of the upper lip and philtrum
area andbull complete nasal airway obstruction
Septal HaematomaTherapyndash Management consists of drainage through a mucoperichondrial incision Immediate treatment isnecessary to prevent long-term problems such asa saddle-nose deformity perforation columellarretraction and nasal-base widening In childrenseptal destruction can lead to devastating nasal andmidfacial growth abnormalitiesbull Surgeryndash Incision and evacuation of the collection is performedDrainage of a septal haematoma should
Septal HaematomaSurgeryndash Incision and evacuation of the collection is performedDrainage of a septal haematoma should provide closure of the incision
Splints or transseptal sutures are placed to obliterate thepotential space and prevent collectionInfection involving the septal cartilage Reconstruction with autologouscartilage is then performed in a second stage Oral antibiotics should be given
Nasal DeformitySaddle-nose deformityndash A saddle-nose deformity is characterised by a loss ofnasal dorsal height and compromised nasal supportstructures -Other case observed are depressionof the middle vault and dorsum loss of nasal tipsupport and definition shortened (vertical) nasal length over rotation of the nasal tip and retrusion ofthe nasal spine and caudal septum It is also knownas a ldquoPug noserdquo or ldquoboxerrsquos noserdquo both of which referto various degrees of nasal dorsal depressionbull
Nasal DeformityEpidemiologyaetiologyndash Prevalence is higher in population groups prone to facial trauma (ie boxers athletes) those with historiesof intranasal cocaine use nasal surgery (e g radical submucosal septal resection reductive rhinoplasty)ndash A saddle-nose deformity can be congenital or acquired It can be noticed as a part of individual familialsyndromic and ethnic characteristics - Most deformities are due to traumatic and iatrogeniccauses Medical causes are Wegenerrsquosgranulomatosis relapsing polychondritis leprosy (Hansenrsquos disease) syphilis ectodermal dysplasiaand intranasal cocaine use
Nasal Deformity
bull Therapybull ndash Nasal reconstruction indications depend on patientbull selection surgeon experience and aetiology of thebull deformity bull Indications for surgery can be functionalbull aesthetic or most commonly both In individuals
with a compromised nasal airway a nasoseptalbull reconstruction is indicated
Nasal Deformity
bull Contraindications bull include patients with malignantbull chronic or autoimmune disease conditions drugbull abuse poor perioperative risk profile and unrealisticbull expectationsbull ndash Multiple previous rhinoplasties and certain
professionsbull (mixed martial artists boxers and other contactbull sports) are relative contraindications
Nasal DeformitySeptoplastyndash Septoplasty is performed to correct nasal obstructioncaused by septal deformityndash Usually septoplasty is performed under general anaesthesiawith the patient in the supine position with the head elevated by approximately 30 (Righthandedsurgeons approach from the right side)ndash Local vasoconstrictive anaesthesia is applied notonly to reduce postoperative pain but also more importantly to achieve vasoconstriction of themucosa and less intraoperative haemorrhage Lidocainewith adrenaline or epinephrine is usedalthough in patients with cardiac hypersensitivityoxymetazoline might be preferred
Nasal Deformity
bull Septoplasty begins with the incision of septal mucosabull Most operative techniques utilise a hemitransfixionbull incision at the caudal end of septum so thatbull deviation at this point might be reached as wellbull as a transfixion incision that is easily obtained ifbull needed (Right-handed surgeons normally choosebull the left side but that may vary when deviation isbull convex towards the right)
Nasal DeformityA columella retractor is placed over the columellaand by pulling it laterally the caudal border of theseptum is exposed Ala can be protected by an alaprotector A vertical incision with a no 15 bladeover the caudal end of septum is performed untilreaching the plane of the septal cartilage It is essentialto correctly identify the perichondrium and byusing the Cottle elevator dissect and lift it creatinga flap As the dissection proceeds along the septalcartilage a longer speculum (no 5) is introduced sothat elevation of the mucoperichondrium is doneunder constant visual controlndash The next step is to dissect the mucoperiostium
Nasal DeformityDissecting over the bony-cartilaginous junctionwhen joining both tunnels might be difficult and is
especially prone to membrane perforationndash If needed the same tunnels are to be created on the
other side of the septum Then deviated parts of
septum are identified and removed either with a
knife or a Freer chisel
Nasal Deformitybull septum from the maxillary crest the septum mustbull be separated from the perpendicular plate trimmedbull along the inferior border placed back onto the crestbull and sutured to the periosteum If the deformity involvesbull the vomer an osteotome is used Care mustbull be taken not to break the cribriform plate becausebull it could cause a cerebrospinal fistula
Nasal Deformity
bull Once the septal deviation is corrected the flapsbull and hemitransfixion incision are mattressed
withbull absorbable sutures Nasal packing to prevent
synechiaebull and postoperative septal haematoma mightbull be advised but should be removed within 72 h

ENT learning aims and objectives for clinical medical students
AimsTo acquire sufficient knowledge of ENT conditions to be able to
recognize common problems and when and what to referTo understand that ENT conditions are extremely common and form
a large part of the workload of a general practitionerTo learn the skills required to examine patients with ear nose and
throat diseases and to make a presumptive diagnosisTo learn how to prioritize and manage different ENT conditionsTo become stimulated and interested in the specialty of ENT
Objectives To learn the signs and symptoms of common ENT conditions To learn the techniques of ear nasal and neck examination To demonstrate an understanding of the basic anatomy and physiology of the ear
and upper aero-digestive tract and relate this knowledge to the signs and symptoms of ENT disease
To understand the medical and surgical treatment of common ENT conditions To be familiar with the commonly used medications for treating ENT problems and
their side effects To understand the risks and complications of surgery To recognise the different ways in which head and neck malignancy can present
and to understand that early diagnosis of head and neck cancer leads to improved survival
To learn the ways in which ENT related communication difficulties can arise and be overcome
To appreciate and be sensitive to the impact of ENT conditions on patients and their families
Student ENT curriculum
Practical skillsUse of the auriscope to examine the external auditory meatus and tympanic membraneBasic examination of the noseExamination of the oral cavity and oropharynxExamination of the neckHow to manage a nosebleedHow to deal with a tracheostomy
Earbull Basic anatomy and physiology of the earbull Presentation and management of common ear disease eg otitis externa
otitis media glue ear chronic suppurative otitis media with or without cholesteatoma vertigo and facial palsy
bull Examination of the ear including the pinna ear canal and otoscopybull Testing hearing with tuning fork testsbull The advantages of the microscope and the fibreoptic otoscopebull Basic interpretation of play audiometry pure tone audiograms and
tympanogramsbull The principles of grommet insertion mastoid surgery and the treatment of
Menieres diseasebull Identifying postoperative problems following ear surgery ie sensorineural
hearing loss facial nerve palsy and vestibular dysfunctionbull Understanding the differential diagnosis of facial nerve palsy and its
treatment
Nosebull Anatomy and physiology of the nosebull Symptoms and signs of common sinonasal disease eg
rhinitis sinusitis nasal polypsbull Examination of the nose including an assessment of the
appearance the septum the turbinates and the mucosabull The endoscopic evaluation of the nosebull Management of a fractured nose and the timing of
interventionbull Management of epistaxis from minor nosebleeds to
torrential haemorrhagebull The principles of common nasal operations including septal
surgery functional endoscopic sinus surgery and rhinoplasty
Head and neckmdashbenign and malignant disease
bull The basic anatomy and physiology of the oral cavity salivary glands pharynx larynx oesophagus and lymph node drainage
bull The presentation of head and neck cancerbull The presentation and management of salivary gland diseasebull Examining the oral cavity larynx and pharynx including the use of the nasendoscopebull Examining the neck with reference to the lymph nodesbull The role of fine needle aspiration cytology (FNAC)bull The principles and limitations of radiological investigation of the head and neck regionbull Management of neck lumps in particular the malignant lymph node with an unknown
primarybull The management of the airway in patients with a tracheostomy or end tracheostomy after
laryngectomybull A basic knowledge of the principles of operative surgery in particular the principles of
reconstructive surgery and the surgery for salivary gland disease eg parotidectomybull The postoperative management of a patient who has undergone major head and neck surgerybull The role of the multidisciplinary team in head and neck cancer and voice disorders
Supplementary knowledgebull The role of otoacoustic emissions and evoked auditory potentials in managing
hearing lossbull The use of speech audiometrybull The surgery for otosclerosisbull Bone-anchored hearing aids for conductive hearing lossbull Cochlear implantation and the reactions of the deaf community to this
interventionbull The use of sign languagebull Neuro-otology in particular the presentation and management of acoustic
neuromasbull Craniofacial surgery and the interplay between ENT plastic surgery and
neurosurgerybull The management of cleft palate and the increased risk of glue earbull Advanced endoscopic sinus surgery for the mangement of sinonasal malignancy
pituitary tumours and skull base tumoursbull Microlaryngeal surgery and surgical voice restorationbull The use of chemotherapy and radiotherapy in head and neck malignancy
Working in ENT
bull Working in ENT should be a very enjoyable experience whether it is a temporary attachment or a long-term career plan
bull It is helpful if you have an understanding of what others expect of you
bull It is also important for you to think about your own career development
Your duties
bull Patient care and continuitybull Professional developmentbull Research
The ENT Examination
EquipmentA fully equipped ENT department will have all the necessary instruments for performing a full ENT examination
Basic equipment
bull A light sourcemdasha portable headlight that runs off batteries is ideal
bull Wooden tongue depressorsbull Thudicum nasal speculumbull An otoscope with several speculaebull Pneumatic attachment for the otoscopebull Tuning fork 512Hzbull Pen and paperbull Gloves
Advanced equipment
bull Co-phenylcaine spraybull A flexible nasendoscope with light sourcebull Alcohol wipe to act as demist for the scopebull Aqueous lubricating gel for the scope
Emergency equipment
bull Large nasal tampons (you can always cut 10cm ones to size)
bull Silver nitrate sticksbull Foley catheters
Basic Anatomy of the Nose
bull The structural anatomy of the nose is important
bull for both aesthetic and functional reasons since the
bull nose as the gateway to the respiratory tract performs
bull a variety of physiologic functions
External NoseThe shape of the external nose is defined by the nasalbones a pair of rectangular bones in the upper nasaldorsum and by lateral cartilages (uppernasal cartilages) and alar cartilages (major alar cartilages)in the central and lower portions of the noseThe lateral portions of the nasal alae alsocontain several small accessory cartilages called theminor alar cartilages which are embedded in the lateralsoft tissues of the noseThe shape and stability of the alar cartilages each ofwhich consists of a medial and lateral crus
External Nose
Anatomy of the nasal base
bull Besides thebull medial crura the
inferior septal margin and the connective-
bull tissue septum (columella) are also responsible
bull for stabilizing the base of the nose
Anatomy of the nasal base
Anatomy of the nasal base
bull The nasal septum is subluxed toward the left side partially
bull obstructing the nasal airway
Nasal CavitiesThe nasal cavities begin anteriorly at the nasal vestibulewhich is bordered posteriorly by the internal nasalvalve (limen nasi) located between the posteriorborder of the alar cartilage and the anterior border ofthe lateral cartilage This valve area is the narrowestportion of the upper respiratory tract
Nasal Cavities
The interior ofthe nose behind the nasal valve is divided by the nasalseptum into two main cavities
Nasal CavitiesThe nasal septum iscomposed of an anterior cartilaginous part and twoposterior bony parts Abnormalities in the shape ofthe nasal septum which may consist of a deviated septum tensionseptum spurs or ridges are a frequent cause ofnasal airway obstructionThe choanae are the paired posterior openingsthrough which the nasal cavities communicate withthe nasopharynx
Nasal CavitiesThe nasal cavity is bounded laterally by the lateral nasalwalls which are formed by the ethmoid bone andmaxilla and posteriorly by the palatine bone and thepterygoid process of the sphenoid bone Several functionallyimportant structures are located on the lateralnasal wall the nasal turbinates and their associatedpassages (meati) sinus ostia and the orifice ofthe nasolacrimal duct (Fig 15)
The inferior turbinate consists of a separate bone thatis attached to the medial wall of the maxillary sinusThe opening of the nasolacrimal duct is located in thecorresponding inferior meatus The middle andsuperior turbinates are part of the ethmoid bone In rare cases a rudimentary ldquosupreme turbinaterdquo is alsopresent above the superior turbinate
The middle turbinate has by far the greatest functionalimportance because most of the drainage tracts fromthe surrounding paranasal sinuses open into the middlemeatus The nasal cavity is bounded superiorly by the cribriformplate of the ethmoid bone This thin bony platehas numerous openings for the passage of the fila olfactoriaand also forms the boundary of the anteriorcranial fossa
Nasal Cavities
The floor of the nasal cavity is formedmostly by the hard palate which is formed in turn bythe two palatine processes of the maxilla and the horizontallaminae of the palatine bone
Structure of the lateral nasal wall
Inferior meatus
Paranasal Sinuses
The paranasal sinuses are air-filled cavities that communicatewith the nasal cavities
-The maxillary sinus frontalsinus and anterior ethmoid cells drain into the nasalcavity through the middle meatusmdashie below themiddle turbinate -The posterior ethmoidcells drain into the nasal cavity through the superiormeatus The ostium of the sphenoid sinus is locatedin the anterior wall directly above the choanae- The anatomical connections between the nasal cavity andparanasal sinuses are functionally important and playa key role in the pathogenesis of many rhinologic diseasesthat involve the paranasal sinuses
Vascular SupplyThe external nose derives most of its blood supply
from the facial artery which arises from the external
carotid artery and from the ophthalmic artery which
springs from the internal carotid artery
Vascular Supply
The internalnose receives blood from the territories of the externaland internal carotid arteries- the terminalbranches of the sphenopalatine artery which arisesfrom the maxillary artery - the anterior and posteriorethmoid arteries which arise from the ophthalmicartery-internal carotid arterie
venous drainage
The venous drainageof the facial region is handled by -the facial vein -retromandibular vein -internal jugular vein
lymphatic drainage
The regional lymphatic drainage of the face and externalnose is handled mainly by- the submandibularlymph nodes while the nasal cavity is additionallydrained by -the retropharyngeal and deep - -cervical lymph nodes
Morphology of the Nasal Mucosa
Besides the anatomical structure of the external noseand nasal cavity the nasal mucosa plays an essentialrole in numerous functions of the nose in the respiratory tract
Morphology of the Nasal Mucosa
The anterior part of the nasal cavity (the nasal vestibule)like the external nose is covered by skin composedof a multilayer keratinizing squamous epithelium and finally a ciliated respiratory epithelium A small areaon the upper nasal septum superior turbinate andpart of the middle turbinate located adjacent to thecribriform plate is covered by olfactory mucosa and iscalled the olfactory region
Nerve SupplyThe facial skin receives its sensory innervation fromterminal branches of the trigeminal nerve that enterthe facial region through the supraorbital infraorbitaland mental foramina Thefacial muscles are classified as mimetic or mastica- tory each of these groups receiving different motorinnervationbythe facial nerve
History and Clinical Examination of the Nose
Historybull The main symptomsbull nasal obstruction (ldquostuffy
noserdquo)bull nasal dischargebull Headachesbull Olfactory
dysfunction
Palpationbony discontinuitiesNeuralgias to check
over- the supraorbital -infraorbital -mental foramina
Anterior Rhinoscopy
bull The rhinologic examination itself begins with anterior
bull rhinoscopy to evaluate the nasal vestibule and the anterior
bull portions of the nasal cavity
Nasal Endoscopy Nasal endoscopy has become the most important andrewarding clinical examination method in rhinologic diagnosis
- rigid endoscopes which are available in 4-mm and 28- mm diameters and assorted viewing angles (eg 01048576 301048576 1201048576) -flexible endoscopes are also available for inspecting the nose and nasopharynx and exploring all of the pharynx and larynx in one sitting
Nasal endoscopy
Nasal Endoscopy
Nasal Endoscopy
Imaging of the Nose and Paranasal Sinuses
Conventional RadiographsStandard paranasal sinus radiographs in the occipitomental
projection ( Water projection) and
occipitofrontal projection Caldwell projection) in cases of acute inflammation
They are also obtained to evaluate midfacial fractures
Computed Tomography (CT) the main indicationsfor CT scanning of the
nose and paranasal sinuses
are- chronic sinusitis - -trauma (especially
frontobasal -fractures)
-and tumors
The occipitofrontal projection is better for evaluating theethmoid cells and frontal sinus
occipitomental projection demonstrates the maxillarysinus and gives a limited view of the sphenoid sinus
Computed tomography of the paranasal sinuses
Four representative coronal CT scans are shown
Four representative coronal CT scans are shown
Magnetic Resonance Imaging
Magnetic maging
Magnetic resonance imaging (MRI) has fewer indicationsthan CT in patients with paranasal sinus diseaseThis is primarily because MRI is markedly inferior toCT in defining the bony boundaries of the sinusesThe strength of MRI lies in its superior soft-tissue discriminationMRI is indicated in diseases that involve the paranasal sinuses in addition to thecranial cavity or orbit (eg tumors and congenitalmalformations such as encephaloceles)
MRI of the paranasal sinuses
The Nose and Sinuses
Structure The structure of the nose is made up of
four partsbull The surface anatomybull The nasal skeletonmdashcomposed of the
two nasal bones the paired upper lateral and lower lateral cartilages and the nasal septum covered in subcutaneous tissue and skin
bull The internal anatomymdashincludes the septum of the nose which forms the medial wall of the nasal cavity The turbinates on the lateral wall are also called conchae
bull The osteomeatal complexmdasha key functional area of the nose
Function The nose is the main route for inspired
air and its structure is related to this function As the air passes over the large surface area of the turbinates
The inspired gases are warmed and humidified Mucus on the mucosa of the nose removes large dust particles from the air as it is breathed in
The voice resonates in the sinuses and nose and this provides character to the speech
Pneumatization of the sinusesmdashthey are air filled spacesmdashreduces the weight of the skull
Diseases of thDiseases of the Outer and Inner Nosee Outer and
Inner Nose Erysipelas Definition of the disease ndash Erysipela is a skin infection that affects the superficial dermis and is caused by Streptococcus pyogenes (group A) It usually develops in the extremities and the face and less commonly on the scalp and genitals bull Epidemiologyaetiology ndash Erysipelas are more often seen in elderly infants and children patients with compromised immunology and diabetes -Predisposing factors are alcoholism skin ulceration puncture wounds fungal infections malnutrition and burns
Erysipelas
bull Symptomsbull ndash It usually presents of fever general fatigue bull -The skin lesion is a redindurated and elevated plaque
with borders that expand rapidly bull It is painful warm and accompanied by variable oedemabull -On the second or third day a flaccid bulla may develop
and desquamationbull bull Presence of regional lymph nodes is common
Erysipelas
bull Complicationsndash The most common complication is recurrencewhich is seen in 18ndash30 of the cases even afterproper antibiotic therapy Recurrence is seen moreoften in females than in malesA skin infection with S pyogenes could lead toglomerulonephritis
Erysipelas
bull Complicationsbull ndash The most common complication is recurrencebull which is seen in 18ndash30 of the cases even afterbull proper antibiotic therapy bull -Recurrence is seen morebull often in females than in males bull -A skin infection with S pyogenes could lead tobull glomerulonephritis
Erysipelas
bull bull Diagnosisbull ndash Diagnosis is based on the patientrsquos personal
historybull and physical examination particularly on inspectionbull of the skin
bull Blood cultures are positive in less thanbull 5 of cases
ErysipelasTherapyndash Conservative therapybull The preferred antibiotic is penicillin In mildcases with minor systemic symptoms penicillinV 500 mg orally every 6 h for 10 days or penicillinG benzathine 12 mil U intramuscularlyonceOther possibilities are amoxicillin 500 mgorally twice a day for 10 days or cephalexin 500mg orally every 6 h for 10 days
ErysipelasIn moderate and severe cases with significantsystemic symptoms hospitalization and intravenoustreatment is required penicillin G 2ndash4mil U intravenously every 4ndash6 h Cefazolin05ndash15 gm intravenously every 8 h cefotaxime1ndash2 gm intravenously every 8 h or ceftriaxone1ndash2 gm intravenously once a day should be administeredIn patients with a penicillin allergyclindamycin 600 mg intravenously every 8 h orvancomycin 15 mgkg intravenously twice a daymay be given
ErysipelaAdditional useful therapeutic optionsbull Prednisone 30 mg over 8 days might be consideredas well as elevation of the affected siteMoist heat compresses may be usefulbull Surgeryndash Debridement and drainage are indicated when bullaeabscesses or necroses are presentbull Differential diagnosisndash Contact dermatitisndash Asteatotic eczemandash Herpes zosterndash Angioneurotic oedemandash Osteomyelitis
Furuncle
bull Definition of the diseasebull ndash A furuncle is an infection that beginsbull at the hair follicle and spreads deeper into thebull dermis and subcutaneous tissue forming abull nodule After several days it developsbull into an abscess - red painful and fluctuantbull bull bull Epidemiologyaetiologybull ndash The aetiologic agent is Staphylococcus aureus
FuruncleSymptomsndashsymptoms are local and limited to thesite of infection Furuncles usually are wherehair follicles are present bull Complicationndash One complication is furunculosis multiple draining furunclesDiagnosisndash The diagnosis is based on clinical inspection - Cultures are not necessary when there is no systemic involvement but should beconsidered if systemic therapy (in case of feversignificant cellulitis or hospitalization) or whenmethicillin-resistant Staphylococcusaureus (MRSA) is considered
FuruncleTherapyndash When the furuncle is small application of moist heat compress to promote drainage -Larger furuncles should be drained by surgical incision-After drainage the area should be cleaned with anantiseptic (with chlorhexidinebetadine) should be applied twice
a dayndash If no systemic symptoms or extensive cellulitis arepresent simple topical care is usually curative andoral antibiotics are not necessary Otherwise systemictreatment is indicated and should cover anypossible MRSA
Furuncle
bull -Recommended antibiotics are trimethoprim-sulfamethoxazole
bull 1ndash2 tablets orally twice daily doxycyclinebull 100 mg orally twice dailybull or clindamycin 300ndash450 mg orally every 8 hbull - In severe cases vancomycin 15 mgkg
intravenouslybull every 12 h or clindamycin 600 mg intravenouslybull every 8 h
Midline Granulomabull A midline granuloma is an angiocentricbull lymphoma it was referred to as polymorphicbull reticulosis lethal midline granuloma and midline
malignant reticulosisbull bull Definition of the diseasebull ndash This rare disease is a lymphoma of extranodal
presentationall cases are positive for the Epstein-Barr virus
bull -This lymphoma most commonly appears in the midface region
Midline GranulomaEpidemiologyaetiologyndash This form of lymphoma is rare in Europe and theUnited States with a higher prevalence in Asia and PeruSymptomsndash The most common presentation is nasal obstruction with a destructive mass occupying the nosesinuses and palate
-Fever night sweatsand weight loss seen usually in Hodgkinrsquos lymphomaand other non-Hodgkinrsquos lymphomas (knownas ldquoB symptomsrdquo) are uncommon
Midline GranulomaDiagnosisndash The diagnosis is based on anatomopathologicalstudy The malignancy of the tumour manifested byextensive necrosis makes the histological diagnosisdifficult and often more biopsies are required forconfirmationbull Therapyndash Therapy consists of radiotherapy with or withoutchemotherapy
Midline Granuloma
bull Prognosisbull ndash Depending on the stage long-term remission or
experience a worseningbull prognosis with relapses which may include otherbull extranodal sites bull Involvement of extranodal sitesbull including the upper airway gastrointestinal tractbull skin
Wegenerrsquos Granulomatosis
bull Definition of the diseasebull ndash Wegenerrsquos granulomatosis is a systemic chronicbull vasculitis of small- and medium-sized blood vesselsbull with an autoimmune component It affectsbull particular organs with variable predilectionbull Epidemiologyaetiologybull ndash Wegenerrsquos granulomatosis is a rare disease It affects
about 1 in 20000ndash30000 people It is more prevalentbull in middle-aged Caucasian patients
Wegenerrsquos Granulomatosis
Symptomsndash The disease may present pulmonary upper
respiratory tract or renal In the disseminated form-The localised form ndash confinedto the upper respiratory region ndash is present in 25of the patients- It consists of nonspecific manifestationssuch as nasal obstruction crusting purulentor bloody rhinorrhea and painful or painless ulcers in oral or nasal cavities which are unresponsive tostandard medical treatment
Wegenerrsquos Granulomatosis
bull In some patients the nasal septum is perforatedbull which leads to saddle-nose deformity Less
commonbull symptoms are hoarseness stridor due to
subglotticbull stenosis otalgia otorrhea and conductivebull and sensorineural hearing loss Also ocular
symptomsbull such as scleritis conjunctivitis uveitis andbull episcleritis may be present
Wegenerrsquos Granulomatosis
bull ndash In the disseminated form pulmonary involvementbull is manifested by cough dyspnoea haemoptysisbull (due to an alveolar capillaritis necrotic lesions orbull endobronchial disease) and pleuritic painndashbull -Ninety per cent of patients have nasal symptomsbull and these symptoms are usually the first
manifestationof the diseasebull -Most patients have also renal involvementbull even if it is subclinical
Wegenerrsquos Granulomatosis
Diagnosis ndash Diagnosis of Wegenerrsquos granulomatosis is based on clinical findings that demonstrate lung (chest x-ray) kidney (urine analysis) or upper respiratory tract
involvement (oral or nasal ulcers or discharge) - positive blood analysis for cytoplasmic-staining antineutrophil
cytoplasmic antibodies (c-ANCA) and confirming proteinase 3 (PR3) ANCA or myeloperoxidase (MPO) ANCA ndash Biopsy is essential for diagnosis nonspecific chronic inflammation
and necrosis -Bacterial and fungal infections
Wegenerrsquos Granulomatosis
Therapyndash Conservative therapybull In the induction of disease remission highdosesteroids (e g prednisone 1 mgkgday) for1 month with tapering over several months aregiven In addition cyclophosphamide (2 mgkgday) should be administered for 6ndash12 monthsuntil symptoms disappear In the maintenanceof remission cyclophosphamide should be
Wegenerrsquos Granulomatosis
Antibiotics mainly trimethoprim-sulfamethoxazoleare given for prophylaxis againstPneumocystis jiroveci (formerly Pneumocystiscarinii) pneumonia (PCP) which may developduring immunosuppression and have a role inpreventing recurrencesbull Sinonasal manifestations may be treated with topical nasal steroids and nasal irrigations lowdosesystemic steroids and antibiotics when bacterial infection (typically Staphylococcus species) is suspected
Wegenerrsquos Granulomatosis
bull Prognosisbull ndash Most of the patients respond well to treatmentbull achieving symptom-free intervals of 5ndash20 yearsbull or more bull -Anatomical problems (sinusitis trachealbull stenosis) may require surgery bull Relapses can be long and troublesomebull Long-term complications are chronicbull renal failure hearing loss and deafness
Nasal Fractures Definition ndash A nasal fracture is a disruption of the nasal bone structure due to trauma It is the most frequently fractured facial bone Epidemiologyaetiology ndash Sports falls and assaults are the usual mechanisms of fracture -Males are affected twice as often as are females -Paediatric populations with a incidences during the second and third decades of life -Variables such as force impact direction nature of the striking object age and other will influence the pattern of injury to the components of the nose
Nasal Fractures
bull Symptomsbull ndash Deformity swelling epistaxis and periorbital
ecchymosis are signs that are suggestive of nasal fracture
bull bony crepitus and nasal segment mobilitybull ndash Epiphora bull Severe bilateral injuries to the lachrymal bones
arebull associated with depressed nasal fractures
Nasal Fractures Complications ndash Septal haematoma is one of the most severe early complications of nasal trauma and without drainage it results in abscess formation 6ndash7 days after trauma producing necrosis of the septal cartilage -Long-term problems such as saddle-nose deformity perforation columellar retraction and nasalbase
Septal infection could lead to osteomyelitis orbital and intracranial abscesses meningitis and cavernous sinus thrombosis -Cerebrospinal fluid leakage is a common complication of severe
nasal and frontal fractures
Nasal Fractures
bull Diagnostic proceduresbull ndash Inspectionbull bull Changes of appearance such as deviation andbull asymmetry bleeding watery drainage changesbull in nasal breathing and smell It is useful to comparebull the current presentation with old photographsbull (up to 40 of normal individuals havebull significant nose malformations)
Nasal Fractures Physical examination bull The diagnosis of a nasal fracture is made primarily by physical examination epistaxis nasal swelling and periorbital ecchymosis Nasal shape in the lateral and frontal inspection should be assessed Grasping the dorsum between two fingers and rocking the pyramid back and forth aids in assessing the mobility of nasal bones Internal structures should be evaluated by using a headlight and nasal speculum Clotted blood is removed by suction and assessment of haematoma mucosal tears and active bleeding is performed Bimanual palpation of the septum helps to differentiate septal swelling from haematoma ndash
Nasal FracturesRadiographybull There is no clear evidence of the role of radiographyin the management of nasal fracturesPlain films have up to a 66 false-positive rateas a result of misinterpretation of normal suturelines In addition old fractures are difficult todistinguishbull Three-dimensional CT is recommended for extensiveinjuries involving the nasal-orbital-ethmoidalcomplexndash
Nasal Fractures
bull Additionaluseful diagnostic proceduresbull bull Using a 0 or 30deg 4-mm endoscope is helpful inbull the assessment of posterior abnormalities If thebull patient is heavily sedated Brown-Gruss
provocationbull manoeuvres may be performed to determinebull deformities in upper middle or lower segmentsbull by compressing each compartment
Nasal FracturesConservative treatmentndash Treatment of bleedingbull For localised bleeding anterior sources may becauterised by silver nitrate or sealed with topicalmaterials such as thrombin combined withgelatin foam fibrin glue FloSealreg or other procoagulantmaterials If conservative measuresfail a formal anterior packing is placedbull Bleeding from branches of sphenopalatine orethmoid vessels requires anterior-posteriorpacking
Nasal Fractures
bull bull Surgical methods such as direct endoscopic vessel
bull cauterization or ligation have been shown tobull offer better haemostasis and patient comfortbull Angiography with embolization can also be
consideredbull in cases refractory to more conservativebull approaches
Nasal Fractures
bull Type of reductionbull bull Nondisplaced fractures should be treated withbull observation alone Closed nasal reduction is thebull best choice for simple injuries (isolated unilateralbull with medial displacement)bull bull An open approach should be considered in
severebull trauma (bilateral depressed fractures)
Nasal Fracturesbull Surgical principlesbull ndash Topical anaesthesia with cotton pledgets soakedbull with 4 cocaine or 005 oxymethazoline combinedbull with 4 topical lidocaine should be appliedbull for 5ndash10 min Local anaesthesia should also be injectedbull (1 lidocaine and 1100000 epinephrine)bull along the septum lateral walls and floor of the nasalbull cavitybull bull
Nasal FracturesClosed reductionndashndash The nasal bones are grasped between two fingersand pressure is applied laterally in theopposite direction of the deviation A bluntelevator may be used from within the nose incases of significant medial collapse Walshamforceps can be of help Reduction of the septumshould be performed with the use ofAsch forceps
Nasal Fractures
bull To prevent collapse of the postreductionbull framework nasal packing should be placedbull for 3ndash5 days Septum splints are recommendedbull in comminuted septal fractures withbull severe mucosal lesions External nasal splintingbull for 10 days (Aquaplastreg Thermoplastreg)bull provides nasal protection Nasal saline spraysbull prevent crusting and oral antibiotics should
Nasal Fractures
bull Open reductionbull ndashndash Immediate repair of fractures by using
widebull surgical exposure reduction fixation and
reconstructionbull ndashndash The second option is delayed correctionbull (6 months or more) of persistent deformitiesbull using standard techniques of rhinoplasty
Deviated Nasal Septum
bull Definition of the diseasebull ndash Deviation of the nasal septum is a common causebull of unilateral nasal airway obstruction in which thebull nasal septum is displacedbull bull Epidemiologyaetiologybull ndash Developmental septal abnormalities Septal cartilage
damage in the neonatal period andbull during birth can cause severe septal deviation inbull the absence of a history of nasal trauma
Deviated Nasal Septum
bull Symptomsbull ndash Patients may present with a history of sinusitis
allergicbull rhinitis obstructive sleep apnoea previousbull nasal surgery or recent nasal trauma Unilateral or
bilateral nasal airway obstruction that is unrelievedbull with decongestants or nasal steroid sprays is oftenbull seenbull bull
Deviated Nasal SeptumDiagnosisndashExamination external dorsal deviation or the columella and caudal septummay be deflected off the midline (caudal subluxation)ndash Inspections of the nasal cavity and anterior-posteriorrhinoscopy are helpful in diagnosing the locationtype and severity of septal deformityThe endoscope is also useful in identifying polypsthe severity and extent of posterior septaldeviations and bony spurs and locating areas ofseptal perforation or mucosal injury
Deviated Nasal Septum
bull Therapybull ndash Septoplasty is a procedurebull The areabull of deviation is corrected or resected in order tobull leave behind as much cartilage and bone as
possiblebull Cartilage resection is minimised and can be
repositioned reshaped or recontoured using a variety of methods
Deviated Nasal Septum
bull ndash Indications of septoplasty before the growth period
bull of the nose is finished should be very limited bull -In these cases surgery must preserve all the
cartilagebull in order to prevent external changes of the
shape ofbull the nose
Deviated Nasal Septum
bull Complicationsbull ndash Frequent complications include haematoma andbull infection Cerebrospinal fluid leak is a rare but
potentiallybull serious complicationbull It is usually the resultbull of avulsion or damage to the cribriform plate whenbull handling the perpendicular plate of the ethmoidbull ndash Other complications include epistaxis nasal
Deviated Nasal Septum
bull Other complications include epistaxis nasal obstruction
bull due to residual deviation synechiae returnbull of the cartilaginous deviation septal perforationbull anosmia and cosmetic nasal deformities suchbull as widened alar rim margins drooping nasal tipbull columella retraction and a sunken dorsum with abull supratip saddle formation
Septal perforation with minor crusting View from provide closure of the
incision
Septal Haematoma
bull A septal haematoma is a blood collection under the perichondrium
bull of the septum and cartilagebull bull bull Epidemiologyaetiologybull ndash A septal haematoma is one of the most
severe complications of nasal trauma
Septal Haematoma
bull Diagnosisbull ndash Signs and symptoms include intense pain
swellingbull haematoma of the upper lip and philtrum
area andbull complete nasal airway obstruction
Septal HaematomaTherapyndash Management consists of drainage through a mucoperichondrial incision Immediate treatment isnecessary to prevent long-term problems such asa saddle-nose deformity perforation columellarretraction and nasal-base widening In childrenseptal destruction can lead to devastating nasal andmidfacial growth abnormalitiesbull Surgeryndash Incision and evacuation of the collection is performedDrainage of a septal haematoma should
Septal HaematomaSurgeryndash Incision and evacuation of the collection is performedDrainage of a septal haematoma should provide closure of the incision
Splints or transseptal sutures are placed to obliterate thepotential space and prevent collectionInfection involving the septal cartilage Reconstruction with autologouscartilage is then performed in a second stage Oral antibiotics should be given
Nasal DeformitySaddle-nose deformityndash A saddle-nose deformity is characterised by a loss ofnasal dorsal height and compromised nasal supportstructures -Other case observed are depressionof the middle vault and dorsum loss of nasal tipsupport and definition shortened (vertical) nasal length over rotation of the nasal tip and retrusion ofthe nasal spine and caudal septum It is also knownas a ldquoPug noserdquo or ldquoboxerrsquos noserdquo both of which referto various degrees of nasal dorsal depressionbull
Nasal DeformityEpidemiologyaetiologyndash Prevalence is higher in population groups prone to facial trauma (ie boxers athletes) those with historiesof intranasal cocaine use nasal surgery (e g radical submucosal septal resection reductive rhinoplasty)ndash A saddle-nose deformity can be congenital or acquired It can be noticed as a part of individual familialsyndromic and ethnic characteristics - Most deformities are due to traumatic and iatrogeniccauses Medical causes are Wegenerrsquosgranulomatosis relapsing polychondritis leprosy (Hansenrsquos disease) syphilis ectodermal dysplasiaand intranasal cocaine use
Nasal Deformity
bull Therapybull ndash Nasal reconstruction indications depend on patientbull selection surgeon experience and aetiology of thebull deformity bull Indications for surgery can be functionalbull aesthetic or most commonly both In individuals
with a compromised nasal airway a nasoseptalbull reconstruction is indicated
Nasal Deformity
bull Contraindications bull include patients with malignantbull chronic or autoimmune disease conditions drugbull abuse poor perioperative risk profile and unrealisticbull expectationsbull ndash Multiple previous rhinoplasties and certain
professionsbull (mixed martial artists boxers and other contactbull sports) are relative contraindications
Nasal DeformitySeptoplastyndash Septoplasty is performed to correct nasal obstructioncaused by septal deformityndash Usually septoplasty is performed under general anaesthesiawith the patient in the supine position with the head elevated by approximately 30 (Righthandedsurgeons approach from the right side)ndash Local vasoconstrictive anaesthesia is applied notonly to reduce postoperative pain but also more importantly to achieve vasoconstriction of themucosa and less intraoperative haemorrhage Lidocainewith adrenaline or epinephrine is usedalthough in patients with cardiac hypersensitivityoxymetazoline might be preferred
Nasal Deformity
bull Septoplasty begins with the incision of septal mucosabull Most operative techniques utilise a hemitransfixionbull incision at the caudal end of septum so thatbull deviation at this point might be reached as wellbull as a transfixion incision that is easily obtained ifbull needed (Right-handed surgeons normally choosebull the left side but that may vary when deviation isbull convex towards the right)
Nasal DeformityA columella retractor is placed over the columellaand by pulling it laterally the caudal border of theseptum is exposed Ala can be protected by an alaprotector A vertical incision with a no 15 bladeover the caudal end of septum is performed untilreaching the plane of the septal cartilage It is essentialto correctly identify the perichondrium and byusing the Cottle elevator dissect and lift it creatinga flap As the dissection proceeds along the septalcartilage a longer speculum (no 5) is introduced sothat elevation of the mucoperichondrium is doneunder constant visual controlndash The next step is to dissect the mucoperiostium
Nasal DeformityDissecting over the bony-cartilaginous junctionwhen joining both tunnels might be difficult and is
especially prone to membrane perforationndash If needed the same tunnels are to be created on the
other side of the septum Then deviated parts of
septum are identified and removed either with a
knife or a Freer chisel
Nasal Deformitybull septum from the maxillary crest the septum mustbull be separated from the perpendicular plate trimmedbull along the inferior border placed back onto the crestbull and sutured to the periosteum If the deformity involvesbull the vomer an osteotome is used Care mustbull be taken not to break the cribriform plate becausebull it could cause a cerebrospinal fistula
Nasal Deformity
bull Once the septal deviation is corrected the flapsbull and hemitransfixion incision are mattressed
withbull absorbable sutures Nasal packing to prevent
synechiaebull and postoperative septal haematoma mightbull be advised but should be removed within 72 h

Objectives To learn the signs and symptoms of common ENT conditions To learn the techniques of ear nasal and neck examination To demonstrate an understanding of the basic anatomy and physiology of the ear
and upper aero-digestive tract and relate this knowledge to the signs and symptoms of ENT disease
To understand the medical and surgical treatment of common ENT conditions To be familiar with the commonly used medications for treating ENT problems and
their side effects To understand the risks and complications of surgery To recognise the different ways in which head and neck malignancy can present
and to understand that early diagnosis of head and neck cancer leads to improved survival
To learn the ways in which ENT related communication difficulties can arise and be overcome
To appreciate and be sensitive to the impact of ENT conditions on patients and their families
Student ENT curriculum
Practical skillsUse of the auriscope to examine the external auditory meatus and tympanic membraneBasic examination of the noseExamination of the oral cavity and oropharynxExamination of the neckHow to manage a nosebleedHow to deal with a tracheostomy
Earbull Basic anatomy and physiology of the earbull Presentation and management of common ear disease eg otitis externa
otitis media glue ear chronic suppurative otitis media with or without cholesteatoma vertigo and facial palsy
bull Examination of the ear including the pinna ear canal and otoscopybull Testing hearing with tuning fork testsbull The advantages of the microscope and the fibreoptic otoscopebull Basic interpretation of play audiometry pure tone audiograms and
tympanogramsbull The principles of grommet insertion mastoid surgery and the treatment of
Menieres diseasebull Identifying postoperative problems following ear surgery ie sensorineural
hearing loss facial nerve palsy and vestibular dysfunctionbull Understanding the differential diagnosis of facial nerve palsy and its
treatment
Nosebull Anatomy and physiology of the nosebull Symptoms and signs of common sinonasal disease eg
rhinitis sinusitis nasal polypsbull Examination of the nose including an assessment of the
appearance the septum the turbinates and the mucosabull The endoscopic evaluation of the nosebull Management of a fractured nose and the timing of
interventionbull Management of epistaxis from minor nosebleeds to
torrential haemorrhagebull The principles of common nasal operations including septal
surgery functional endoscopic sinus surgery and rhinoplasty
Head and neckmdashbenign and malignant disease
bull The basic anatomy and physiology of the oral cavity salivary glands pharynx larynx oesophagus and lymph node drainage
bull The presentation of head and neck cancerbull The presentation and management of salivary gland diseasebull Examining the oral cavity larynx and pharynx including the use of the nasendoscopebull Examining the neck with reference to the lymph nodesbull The role of fine needle aspiration cytology (FNAC)bull The principles and limitations of radiological investigation of the head and neck regionbull Management of neck lumps in particular the malignant lymph node with an unknown
primarybull The management of the airway in patients with a tracheostomy or end tracheostomy after
laryngectomybull A basic knowledge of the principles of operative surgery in particular the principles of
reconstructive surgery and the surgery for salivary gland disease eg parotidectomybull The postoperative management of a patient who has undergone major head and neck surgerybull The role of the multidisciplinary team in head and neck cancer and voice disorders
Supplementary knowledgebull The role of otoacoustic emissions and evoked auditory potentials in managing
hearing lossbull The use of speech audiometrybull The surgery for otosclerosisbull Bone-anchored hearing aids for conductive hearing lossbull Cochlear implantation and the reactions of the deaf community to this
interventionbull The use of sign languagebull Neuro-otology in particular the presentation and management of acoustic
neuromasbull Craniofacial surgery and the interplay between ENT plastic surgery and
neurosurgerybull The management of cleft palate and the increased risk of glue earbull Advanced endoscopic sinus surgery for the mangement of sinonasal malignancy
pituitary tumours and skull base tumoursbull Microlaryngeal surgery and surgical voice restorationbull The use of chemotherapy and radiotherapy in head and neck malignancy
Working in ENT
bull Working in ENT should be a very enjoyable experience whether it is a temporary attachment or a long-term career plan
bull It is helpful if you have an understanding of what others expect of you
bull It is also important for you to think about your own career development
Your duties
bull Patient care and continuitybull Professional developmentbull Research
The ENT Examination
EquipmentA fully equipped ENT department will have all the necessary instruments for performing a full ENT examination
Basic equipment
bull A light sourcemdasha portable headlight that runs off batteries is ideal
bull Wooden tongue depressorsbull Thudicum nasal speculumbull An otoscope with several speculaebull Pneumatic attachment for the otoscopebull Tuning fork 512Hzbull Pen and paperbull Gloves
Advanced equipment
bull Co-phenylcaine spraybull A flexible nasendoscope with light sourcebull Alcohol wipe to act as demist for the scopebull Aqueous lubricating gel for the scope
Emergency equipment
bull Large nasal tampons (you can always cut 10cm ones to size)
bull Silver nitrate sticksbull Foley catheters
Basic Anatomy of the Nose
bull The structural anatomy of the nose is important
bull for both aesthetic and functional reasons since the
bull nose as the gateway to the respiratory tract performs
bull a variety of physiologic functions
External NoseThe shape of the external nose is defined by the nasalbones a pair of rectangular bones in the upper nasaldorsum and by lateral cartilages (uppernasal cartilages) and alar cartilages (major alar cartilages)in the central and lower portions of the noseThe lateral portions of the nasal alae alsocontain several small accessory cartilages called theminor alar cartilages which are embedded in the lateralsoft tissues of the noseThe shape and stability of the alar cartilages each ofwhich consists of a medial and lateral crus
External Nose
Anatomy of the nasal base
bull Besides thebull medial crura the
inferior septal margin and the connective-
bull tissue septum (columella) are also responsible
bull for stabilizing the base of the nose
Anatomy of the nasal base
Anatomy of the nasal base
bull The nasal septum is subluxed toward the left side partially
bull obstructing the nasal airway
Nasal CavitiesThe nasal cavities begin anteriorly at the nasal vestibulewhich is bordered posteriorly by the internal nasalvalve (limen nasi) located between the posteriorborder of the alar cartilage and the anterior border ofthe lateral cartilage This valve area is the narrowestportion of the upper respiratory tract
Nasal Cavities
The interior ofthe nose behind the nasal valve is divided by the nasalseptum into two main cavities
Nasal CavitiesThe nasal septum iscomposed of an anterior cartilaginous part and twoposterior bony parts Abnormalities in the shape ofthe nasal septum which may consist of a deviated septum tensionseptum spurs or ridges are a frequent cause ofnasal airway obstructionThe choanae are the paired posterior openingsthrough which the nasal cavities communicate withthe nasopharynx
Nasal CavitiesThe nasal cavity is bounded laterally by the lateral nasalwalls which are formed by the ethmoid bone andmaxilla and posteriorly by the palatine bone and thepterygoid process of the sphenoid bone Several functionallyimportant structures are located on the lateralnasal wall the nasal turbinates and their associatedpassages (meati) sinus ostia and the orifice ofthe nasolacrimal duct (Fig 15)
The inferior turbinate consists of a separate bone thatis attached to the medial wall of the maxillary sinusThe opening of the nasolacrimal duct is located in thecorresponding inferior meatus The middle andsuperior turbinates are part of the ethmoid bone In rare cases a rudimentary ldquosupreme turbinaterdquo is alsopresent above the superior turbinate
The middle turbinate has by far the greatest functionalimportance because most of the drainage tracts fromthe surrounding paranasal sinuses open into the middlemeatus The nasal cavity is bounded superiorly by the cribriformplate of the ethmoid bone This thin bony platehas numerous openings for the passage of the fila olfactoriaand also forms the boundary of the anteriorcranial fossa
Nasal Cavities
The floor of the nasal cavity is formedmostly by the hard palate which is formed in turn bythe two palatine processes of the maxilla and the horizontallaminae of the palatine bone
Structure of the lateral nasal wall
Inferior meatus
Paranasal Sinuses
The paranasal sinuses are air-filled cavities that communicatewith the nasal cavities
-The maxillary sinus frontalsinus and anterior ethmoid cells drain into the nasalcavity through the middle meatusmdashie below themiddle turbinate -The posterior ethmoidcells drain into the nasal cavity through the superiormeatus The ostium of the sphenoid sinus is locatedin the anterior wall directly above the choanae- The anatomical connections between the nasal cavity andparanasal sinuses are functionally important and playa key role in the pathogenesis of many rhinologic diseasesthat involve the paranasal sinuses
Vascular SupplyThe external nose derives most of its blood supply
from the facial artery which arises from the external
carotid artery and from the ophthalmic artery which
springs from the internal carotid artery
Vascular Supply
The internalnose receives blood from the territories of the externaland internal carotid arteries- the terminalbranches of the sphenopalatine artery which arisesfrom the maxillary artery - the anterior and posteriorethmoid arteries which arise from the ophthalmicartery-internal carotid arterie
venous drainage
The venous drainageof the facial region is handled by -the facial vein -retromandibular vein -internal jugular vein
lymphatic drainage
The regional lymphatic drainage of the face and externalnose is handled mainly by- the submandibularlymph nodes while the nasal cavity is additionallydrained by -the retropharyngeal and deep - -cervical lymph nodes
Morphology of the Nasal Mucosa
Besides the anatomical structure of the external noseand nasal cavity the nasal mucosa plays an essentialrole in numerous functions of the nose in the respiratory tract
Morphology of the Nasal Mucosa
The anterior part of the nasal cavity (the nasal vestibule)like the external nose is covered by skin composedof a multilayer keratinizing squamous epithelium and finally a ciliated respiratory epithelium A small areaon the upper nasal septum superior turbinate andpart of the middle turbinate located adjacent to thecribriform plate is covered by olfactory mucosa and iscalled the olfactory region
Nerve SupplyThe facial skin receives its sensory innervation fromterminal branches of the trigeminal nerve that enterthe facial region through the supraorbital infraorbitaland mental foramina Thefacial muscles are classified as mimetic or mastica- tory each of these groups receiving different motorinnervationbythe facial nerve
History and Clinical Examination of the Nose
Historybull The main symptomsbull nasal obstruction (ldquostuffy
noserdquo)bull nasal dischargebull Headachesbull Olfactory
dysfunction
Palpationbony discontinuitiesNeuralgias to check
over- the supraorbital -infraorbital -mental foramina
Anterior Rhinoscopy
bull The rhinologic examination itself begins with anterior
bull rhinoscopy to evaluate the nasal vestibule and the anterior
bull portions of the nasal cavity
Nasal Endoscopy Nasal endoscopy has become the most important andrewarding clinical examination method in rhinologic diagnosis
- rigid endoscopes which are available in 4-mm and 28- mm diameters and assorted viewing angles (eg 01048576 301048576 1201048576) -flexible endoscopes are also available for inspecting the nose and nasopharynx and exploring all of the pharynx and larynx in one sitting
Nasal endoscopy
Nasal Endoscopy
Nasal Endoscopy
Imaging of the Nose and Paranasal Sinuses
Conventional RadiographsStandard paranasal sinus radiographs in the occipitomental
projection ( Water projection) and
occipitofrontal projection Caldwell projection) in cases of acute inflammation
They are also obtained to evaluate midfacial fractures
Computed Tomography (CT) the main indicationsfor CT scanning of the
nose and paranasal sinuses
are- chronic sinusitis - -trauma (especially
frontobasal -fractures)
-and tumors
The occipitofrontal projection is better for evaluating theethmoid cells and frontal sinus
occipitomental projection demonstrates the maxillarysinus and gives a limited view of the sphenoid sinus
Computed tomography of the paranasal sinuses
Four representative coronal CT scans are shown
Four representative coronal CT scans are shown
Magnetic Resonance Imaging
Magnetic maging
Magnetic resonance imaging (MRI) has fewer indicationsthan CT in patients with paranasal sinus diseaseThis is primarily because MRI is markedly inferior toCT in defining the bony boundaries of the sinusesThe strength of MRI lies in its superior soft-tissue discriminationMRI is indicated in diseases that involve the paranasal sinuses in addition to thecranial cavity or orbit (eg tumors and congenitalmalformations such as encephaloceles)
MRI of the paranasal sinuses
The Nose and Sinuses
Structure The structure of the nose is made up of
four partsbull The surface anatomybull The nasal skeletonmdashcomposed of the
two nasal bones the paired upper lateral and lower lateral cartilages and the nasal septum covered in subcutaneous tissue and skin
bull The internal anatomymdashincludes the septum of the nose which forms the medial wall of the nasal cavity The turbinates on the lateral wall are also called conchae
bull The osteomeatal complexmdasha key functional area of the nose
Function The nose is the main route for inspired
air and its structure is related to this function As the air passes over the large surface area of the turbinates
The inspired gases are warmed and humidified Mucus on the mucosa of the nose removes large dust particles from the air as it is breathed in
The voice resonates in the sinuses and nose and this provides character to the speech
Pneumatization of the sinusesmdashthey are air filled spacesmdashreduces the weight of the skull
Diseases of thDiseases of the Outer and Inner Nosee Outer and
Inner Nose Erysipelas Definition of the disease ndash Erysipela is a skin infection that affects the superficial dermis and is caused by Streptococcus pyogenes (group A) It usually develops in the extremities and the face and less commonly on the scalp and genitals bull Epidemiologyaetiology ndash Erysipelas are more often seen in elderly infants and children patients with compromised immunology and diabetes -Predisposing factors are alcoholism skin ulceration puncture wounds fungal infections malnutrition and burns
Erysipelas
bull Symptomsbull ndash It usually presents of fever general fatigue bull -The skin lesion is a redindurated and elevated plaque
with borders that expand rapidly bull It is painful warm and accompanied by variable oedemabull -On the second or third day a flaccid bulla may develop
and desquamationbull bull Presence of regional lymph nodes is common
Erysipelas
bull Complicationsndash The most common complication is recurrencewhich is seen in 18ndash30 of the cases even afterproper antibiotic therapy Recurrence is seen moreoften in females than in malesA skin infection with S pyogenes could lead toglomerulonephritis
Erysipelas
bull Complicationsbull ndash The most common complication is recurrencebull which is seen in 18ndash30 of the cases even afterbull proper antibiotic therapy bull -Recurrence is seen morebull often in females than in males bull -A skin infection with S pyogenes could lead tobull glomerulonephritis
Erysipelas
bull bull Diagnosisbull ndash Diagnosis is based on the patientrsquos personal
historybull and physical examination particularly on inspectionbull of the skin
bull Blood cultures are positive in less thanbull 5 of cases
ErysipelasTherapyndash Conservative therapybull The preferred antibiotic is penicillin In mildcases with minor systemic symptoms penicillinV 500 mg orally every 6 h for 10 days or penicillinG benzathine 12 mil U intramuscularlyonceOther possibilities are amoxicillin 500 mgorally twice a day for 10 days or cephalexin 500mg orally every 6 h for 10 days
ErysipelasIn moderate and severe cases with significantsystemic symptoms hospitalization and intravenoustreatment is required penicillin G 2ndash4mil U intravenously every 4ndash6 h Cefazolin05ndash15 gm intravenously every 8 h cefotaxime1ndash2 gm intravenously every 8 h or ceftriaxone1ndash2 gm intravenously once a day should be administeredIn patients with a penicillin allergyclindamycin 600 mg intravenously every 8 h orvancomycin 15 mgkg intravenously twice a daymay be given
ErysipelaAdditional useful therapeutic optionsbull Prednisone 30 mg over 8 days might be consideredas well as elevation of the affected siteMoist heat compresses may be usefulbull Surgeryndash Debridement and drainage are indicated when bullaeabscesses or necroses are presentbull Differential diagnosisndash Contact dermatitisndash Asteatotic eczemandash Herpes zosterndash Angioneurotic oedemandash Osteomyelitis
Furuncle
bull Definition of the diseasebull ndash A furuncle is an infection that beginsbull at the hair follicle and spreads deeper into thebull dermis and subcutaneous tissue forming abull nodule After several days it developsbull into an abscess - red painful and fluctuantbull bull bull Epidemiologyaetiologybull ndash The aetiologic agent is Staphylococcus aureus
FuruncleSymptomsndashsymptoms are local and limited to thesite of infection Furuncles usually are wherehair follicles are present bull Complicationndash One complication is furunculosis multiple draining furunclesDiagnosisndash The diagnosis is based on clinical inspection - Cultures are not necessary when there is no systemic involvement but should beconsidered if systemic therapy (in case of feversignificant cellulitis or hospitalization) or whenmethicillin-resistant Staphylococcusaureus (MRSA) is considered
FuruncleTherapyndash When the furuncle is small application of moist heat compress to promote drainage -Larger furuncles should be drained by surgical incision-After drainage the area should be cleaned with anantiseptic (with chlorhexidinebetadine) should be applied twice
a dayndash If no systemic symptoms or extensive cellulitis arepresent simple topical care is usually curative andoral antibiotics are not necessary Otherwise systemictreatment is indicated and should cover anypossible MRSA
Furuncle
bull -Recommended antibiotics are trimethoprim-sulfamethoxazole
bull 1ndash2 tablets orally twice daily doxycyclinebull 100 mg orally twice dailybull or clindamycin 300ndash450 mg orally every 8 hbull - In severe cases vancomycin 15 mgkg
intravenouslybull every 12 h or clindamycin 600 mg intravenouslybull every 8 h
Midline Granulomabull A midline granuloma is an angiocentricbull lymphoma it was referred to as polymorphicbull reticulosis lethal midline granuloma and midline
malignant reticulosisbull bull Definition of the diseasebull ndash This rare disease is a lymphoma of extranodal
presentationall cases are positive for the Epstein-Barr virus
bull -This lymphoma most commonly appears in the midface region
Midline GranulomaEpidemiologyaetiologyndash This form of lymphoma is rare in Europe and theUnited States with a higher prevalence in Asia and PeruSymptomsndash The most common presentation is nasal obstruction with a destructive mass occupying the nosesinuses and palate
-Fever night sweatsand weight loss seen usually in Hodgkinrsquos lymphomaand other non-Hodgkinrsquos lymphomas (knownas ldquoB symptomsrdquo) are uncommon
Midline GranulomaDiagnosisndash The diagnosis is based on anatomopathologicalstudy The malignancy of the tumour manifested byextensive necrosis makes the histological diagnosisdifficult and often more biopsies are required forconfirmationbull Therapyndash Therapy consists of radiotherapy with or withoutchemotherapy
Midline Granuloma
bull Prognosisbull ndash Depending on the stage long-term remission or
experience a worseningbull prognosis with relapses which may include otherbull extranodal sites bull Involvement of extranodal sitesbull including the upper airway gastrointestinal tractbull skin
Wegenerrsquos Granulomatosis
bull Definition of the diseasebull ndash Wegenerrsquos granulomatosis is a systemic chronicbull vasculitis of small- and medium-sized blood vesselsbull with an autoimmune component It affectsbull particular organs with variable predilectionbull Epidemiologyaetiologybull ndash Wegenerrsquos granulomatosis is a rare disease It affects
about 1 in 20000ndash30000 people It is more prevalentbull in middle-aged Caucasian patients
Wegenerrsquos Granulomatosis
Symptomsndash The disease may present pulmonary upper
respiratory tract or renal In the disseminated form-The localised form ndash confinedto the upper respiratory region ndash is present in 25of the patients- It consists of nonspecific manifestationssuch as nasal obstruction crusting purulentor bloody rhinorrhea and painful or painless ulcers in oral or nasal cavities which are unresponsive tostandard medical treatment
Wegenerrsquos Granulomatosis
bull In some patients the nasal septum is perforatedbull which leads to saddle-nose deformity Less
commonbull symptoms are hoarseness stridor due to
subglotticbull stenosis otalgia otorrhea and conductivebull and sensorineural hearing loss Also ocular
symptomsbull such as scleritis conjunctivitis uveitis andbull episcleritis may be present
Wegenerrsquos Granulomatosis
bull ndash In the disseminated form pulmonary involvementbull is manifested by cough dyspnoea haemoptysisbull (due to an alveolar capillaritis necrotic lesions orbull endobronchial disease) and pleuritic painndashbull -Ninety per cent of patients have nasal symptomsbull and these symptoms are usually the first
manifestationof the diseasebull -Most patients have also renal involvementbull even if it is subclinical
Wegenerrsquos Granulomatosis
Diagnosis ndash Diagnosis of Wegenerrsquos granulomatosis is based on clinical findings that demonstrate lung (chest x-ray) kidney (urine analysis) or upper respiratory tract
involvement (oral or nasal ulcers or discharge) - positive blood analysis for cytoplasmic-staining antineutrophil
cytoplasmic antibodies (c-ANCA) and confirming proteinase 3 (PR3) ANCA or myeloperoxidase (MPO) ANCA ndash Biopsy is essential for diagnosis nonspecific chronic inflammation
and necrosis -Bacterial and fungal infections
Wegenerrsquos Granulomatosis
Therapyndash Conservative therapybull In the induction of disease remission highdosesteroids (e g prednisone 1 mgkgday) for1 month with tapering over several months aregiven In addition cyclophosphamide (2 mgkgday) should be administered for 6ndash12 monthsuntil symptoms disappear In the maintenanceof remission cyclophosphamide should be
Wegenerrsquos Granulomatosis
Antibiotics mainly trimethoprim-sulfamethoxazoleare given for prophylaxis againstPneumocystis jiroveci (formerly Pneumocystiscarinii) pneumonia (PCP) which may developduring immunosuppression and have a role inpreventing recurrencesbull Sinonasal manifestations may be treated with topical nasal steroids and nasal irrigations lowdosesystemic steroids and antibiotics when bacterial infection (typically Staphylococcus species) is suspected
Wegenerrsquos Granulomatosis
bull Prognosisbull ndash Most of the patients respond well to treatmentbull achieving symptom-free intervals of 5ndash20 yearsbull or more bull -Anatomical problems (sinusitis trachealbull stenosis) may require surgery bull Relapses can be long and troublesomebull Long-term complications are chronicbull renal failure hearing loss and deafness
Nasal Fractures Definition ndash A nasal fracture is a disruption of the nasal bone structure due to trauma It is the most frequently fractured facial bone Epidemiologyaetiology ndash Sports falls and assaults are the usual mechanisms of fracture -Males are affected twice as often as are females -Paediatric populations with a incidences during the second and third decades of life -Variables such as force impact direction nature of the striking object age and other will influence the pattern of injury to the components of the nose
Nasal Fractures
bull Symptomsbull ndash Deformity swelling epistaxis and periorbital
ecchymosis are signs that are suggestive of nasal fracture
bull bony crepitus and nasal segment mobilitybull ndash Epiphora bull Severe bilateral injuries to the lachrymal bones
arebull associated with depressed nasal fractures
Nasal Fractures Complications ndash Septal haematoma is one of the most severe early complications of nasal trauma and without drainage it results in abscess formation 6ndash7 days after trauma producing necrosis of the septal cartilage -Long-term problems such as saddle-nose deformity perforation columellar retraction and nasalbase
Septal infection could lead to osteomyelitis orbital and intracranial abscesses meningitis and cavernous sinus thrombosis -Cerebrospinal fluid leakage is a common complication of severe
nasal and frontal fractures
Nasal Fractures
bull Diagnostic proceduresbull ndash Inspectionbull bull Changes of appearance such as deviation andbull asymmetry bleeding watery drainage changesbull in nasal breathing and smell It is useful to comparebull the current presentation with old photographsbull (up to 40 of normal individuals havebull significant nose malformations)
Nasal Fractures Physical examination bull The diagnosis of a nasal fracture is made primarily by physical examination epistaxis nasal swelling and periorbital ecchymosis Nasal shape in the lateral and frontal inspection should be assessed Grasping the dorsum between two fingers and rocking the pyramid back and forth aids in assessing the mobility of nasal bones Internal structures should be evaluated by using a headlight and nasal speculum Clotted blood is removed by suction and assessment of haematoma mucosal tears and active bleeding is performed Bimanual palpation of the septum helps to differentiate septal swelling from haematoma ndash
Nasal FracturesRadiographybull There is no clear evidence of the role of radiographyin the management of nasal fracturesPlain films have up to a 66 false-positive rateas a result of misinterpretation of normal suturelines In addition old fractures are difficult todistinguishbull Three-dimensional CT is recommended for extensiveinjuries involving the nasal-orbital-ethmoidalcomplexndash
Nasal Fractures
bull Additionaluseful diagnostic proceduresbull bull Using a 0 or 30deg 4-mm endoscope is helpful inbull the assessment of posterior abnormalities If thebull patient is heavily sedated Brown-Gruss
provocationbull manoeuvres may be performed to determinebull deformities in upper middle or lower segmentsbull by compressing each compartment
Nasal FracturesConservative treatmentndash Treatment of bleedingbull For localised bleeding anterior sources may becauterised by silver nitrate or sealed with topicalmaterials such as thrombin combined withgelatin foam fibrin glue FloSealreg or other procoagulantmaterials If conservative measuresfail a formal anterior packing is placedbull Bleeding from branches of sphenopalatine orethmoid vessels requires anterior-posteriorpacking
Nasal Fractures
bull bull Surgical methods such as direct endoscopic vessel
bull cauterization or ligation have been shown tobull offer better haemostasis and patient comfortbull Angiography with embolization can also be
consideredbull in cases refractory to more conservativebull approaches
Nasal Fractures
bull Type of reductionbull bull Nondisplaced fractures should be treated withbull observation alone Closed nasal reduction is thebull best choice for simple injuries (isolated unilateralbull with medial displacement)bull bull An open approach should be considered in
severebull trauma (bilateral depressed fractures)
Nasal Fracturesbull Surgical principlesbull ndash Topical anaesthesia with cotton pledgets soakedbull with 4 cocaine or 005 oxymethazoline combinedbull with 4 topical lidocaine should be appliedbull for 5ndash10 min Local anaesthesia should also be injectedbull (1 lidocaine and 1100000 epinephrine)bull along the septum lateral walls and floor of the nasalbull cavitybull bull
Nasal FracturesClosed reductionndashndash The nasal bones are grasped between two fingersand pressure is applied laterally in theopposite direction of the deviation A bluntelevator may be used from within the nose incases of significant medial collapse Walshamforceps can be of help Reduction of the septumshould be performed with the use ofAsch forceps
Nasal Fractures
bull To prevent collapse of the postreductionbull framework nasal packing should be placedbull for 3ndash5 days Septum splints are recommendedbull in comminuted septal fractures withbull severe mucosal lesions External nasal splintingbull for 10 days (Aquaplastreg Thermoplastreg)bull provides nasal protection Nasal saline spraysbull prevent crusting and oral antibiotics should
Nasal Fractures
bull Open reductionbull ndashndash Immediate repair of fractures by using
widebull surgical exposure reduction fixation and
reconstructionbull ndashndash The second option is delayed correctionbull (6 months or more) of persistent deformitiesbull using standard techniques of rhinoplasty
Deviated Nasal Septum
bull Definition of the diseasebull ndash Deviation of the nasal septum is a common causebull of unilateral nasal airway obstruction in which thebull nasal septum is displacedbull bull Epidemiologyaetiologybull ndash Developmental septal abnormalities Septal cartilage
damage in the neonatal period andbull during birth can cause severe septal deviation inbull the absence of a history of nasal trauma
Deviated Nasal Septum
bull Symptomsbull ndash Patients may present with a history of sinusitis
allergicbull rhinitis obstructive sleep apnoea previousbull nasal surgery or recent nasal trauma Unilateral or
bilateral nasal airway obstruction that is unrelievedbull with decongestants or nasal steroid sprays is oftenbull seenbull bull
Deviated Nasal SeptumDiagnosisndashExamination external dorsal deviation or the columella and caudal septummay be deflected off the midline (caudal subluxation)ndash Inspections of the nasal cavity and anterior-posteriorrhinoscopy are helpful in diagnosing the locationtype and severity of septal deformityThe endoscope is also useful in identifying polypsthe severity and extent of posterior septaldeviations and bony spurs and locating areas ofseptal perforation or mucosal injury
Deviated Nasal Septum
bull Therapybull ndash Septoplasty is a procedurebull The areabull of deviation is corrected or resected in order tobull leave behind as much cartilage and bone as
possiblebull Cartilage resection is minimised and can be
repositioned reshaped or recontoured using a variety of methods
Deviated Nasal Septum
bull ndash Indications of septoplasty before the growth period
bull of the nose is finished should be very limited bull -In these cases surgery must preserve all the
cartilagebull in order to prevent external changes of the
shape ofbull the nose
Deviated Nasal Septum
bull Complicationsbull ndash Frequent complications include haematoma andbull infection Cerebrospinal fluid leak is a rare but
potentiallybull serious complicationbull It is usually the resultbull of avulsion or damage to the cribriform plate whenbull handling the perpendicular plate of the ethmoidbull ndash Other complications include epistaxis nasal
Deviated Nasal Septum
bull Other complications include epistaxis nasal obstruction
bull due to residual deviation synechiae returnbull of the cartilaginous deviation septal perforationbull anosmia and cosmetic nasal deformities suchbull as widened alar rim margins drooping nasal tipbull columella retraction and a sunken dorsum with abull supratip saddle formation
Septal perforation with minor crusting View from provide closure of the
incision
Septal Haematoma
bull A septal haematoma is a blood collection under the perichondrium
bull of the septum and cartilagebull bull bull Epidemiologyaetiologybull ndash A septal haematoma is one of the most
severe complications of nasal trauma
Septal Haematoma
bull Diagnosisbull ndash Signs and symptoms include intense pain
swellingbull haematoma of the upper lip and philtrum
area andbull complete nasal airway obstruction
Septal HaematomaTherapyndash Management consists of drainage through a mucoperichondrial incision Immediate treatment isnecessary to prevent long-term problems such asa saddle-nose deformity perforation columellarretraction and nasal-base widening In childrenseptal destruction can lead to devastating nasal andmidfacial growth abnormalitiesbull Surgeryndash Incision and evacuation of the collection is performedDrainage of a septal haematoma should
Septal HaematomaSurgeryndash Incision and evacuation of the collection is performedDrainage of a septal haematoma should provide closure of the incision
Splints or transseptal sutures are placed to obliterate thepotential space and prevent collectionInfection involving the septal cartilage Reconstruction with autologouscartilage is then performed in a second stage Oral antibiotics should be given
Nasal DeformitySaddle-nose deformityndash A saddle-nose deformity is characterised by a loss ofnasal dorsal height and compromised nasal supportstructures -Other case observed are depressionof the middle vault and dorsum loss of nasal tipsupport and definition shortened (vertical) nasal length over rotation of the nasal tip and retrusion ofthe nasal spine and caudal septum It is also knownas a ldquoPug noserdquo or ldquoboxerrsquos noserdquo both of which referto various degrees of nasal dorsal depressionbull
Nasal DeformityEpidemiologyaetiologyndash Prevalence is higher in population groups prone to facial trauma (ie boxers athletes) those with historiesof intranasal cocaine use nasal surgery (e g radical submucosal septal resection reductive rhinoplasty)ndash A saddle-nose deformity can be congenital or acquired It can be noticed as a part of individual familialsyndromic and ethnic characteristics - Most deformities are due to traumatic and iatrogeniccauses Medical causes are Wegenerrsquosgranulomatosis relapsing polychondritis leprosy (Hansenrsquos disease) syphilis ectodermal dysplasiaand intranasal cocaine use
Nasal Deformity
bull Therapybull ndash Nasal reconstruction indications depend on patientbull selection surgeon experience and aetiology of thebull deformity bull Indications for surgery can be functionalbull aesthetic or most commonly both In individuals
with a compromised nasal airway a nasoseptalbull reconstruction is indicated
Nasal Deformity
bull Contraindications bull include patients with malignantbull chronic or autoimmune disease conditions drugbull abuse poor perioperative risk profile and unrealisticbull expectationsbull ndash Multiple previous rhinoplasties and certain
professionsbull (mixed martial artists boxers and other contactbull sports) are relative contraindications
Nasal DeformitySeptoplastyndash Septoplasty is performed to correct nasal obstructioncaused by septal deformityndash Usually septoplasty is performed under general anaesthesiawith the patient in the supine position with the head elevated by approximately 30 (Righthandedsurgeons approach from the right side)ndash Local vasoconstrictive anaesthesia is applied notonly to reduce postoperative pain but also more importantly to achieve vasoconstriction of themucosa and less intraoperative haemorrhage Lidocainewith adrenaline or epinephrine is usedalthough in patients with cardiac hypersensitivityoxymetazoline might be preferred
Nasal Deformity
bull Septoplasty begins with the incision of septal mucosabull Most operative techniques utilise a hemitransfixionbull incision at the caudal end of septum so thatbull deviation at this point might be reached as wellbull as a transfixion incision that is easily obtained ifbull needed (Right-handed surgeons normally choosebull the left side but that may vary when deviation isbull convex towards the right)
Nasal DeformityA columella retractor is placed over the columellaand by pulling it laterally the caudal border of theseptum is exposed Ala can be protected by an alaprotector A vertical incision with a no 15 bladeover the caudal end of septum is performed untilreaching the plane of the septal cartilage It is essentialto correctly identify the perichondrium and byusing the Cottle elevator dissect and lift it creatinga flap As the dissection proceeds along the septalcartilage a longer speculum (no 5) is introduced sothat elevation of the mucoperichondrium is doneunder constant visual controlndash The next step is to dissect the mucoperiostium
Nasal DeformityDissecting over the bony-cartilaginous junctionwhen joining both tunnels might be difficult and is
especially prone to membrane perforationndash If needed the same tunnels are to be created on the
other side of the septum Then deviated parts of
septum are identified and removed either with a
knife or a Freer chisel
Nasal Deformitybull septum from the maxillary crest the septum mustbull be separated from the perpendicular plate trimmedbull along the inferior border placed back onto the crestbull and sutured to the periosteum If the deformity involvesbull the vomer an osteotome is used Care mustbull be taken not to break the cribriform plate becausebull it could cause a cerebrospinal fistula
Nasal Deformity
bull Once the septal deviation is corrected the flapsbull and hemitransfixion incision are mattressed
withbull absorbable sutures Nasal packing to prevent
synechiaebull and postoperative septal haematoma mightbull be advised but should be removed within 72 h

Student ENT curriculum
Practical skillsUse of the auriscope to examine the external auditory meatus and tympanic membraneBasic examination of the noseExamination of the oral cavity and oropharynxExamination of the neckHow to manage a nosebleedHow to deal with a tracheostomy
Earbull Basic anatomy and physiology of the earbull Presentation and management of common ear disease eg otitis externa
otitis media glue ear chronic suppurative otitis media with or without cholesteatoma vertigo and facial palsy
bull Examination of the ear including the pinna ear canal and otoscopybull Testing hearing with tuning fork testsbull The advantages of the microscope and the fibreoptic otoscopebull Basic interpretation of play audiometry pure tone audiograms and
tympanogramsbull The principles of grommet insertion mastoid surgery and the treatment of
Menieres diseasebull Identifying postoperative problems following ear surgery ie sensorineural
hearing loss facial nerve palsy and vestibular dysfunctionbull Understanding the differential diagnosis of facial nerve palsy and its
treatment
Nosebull Anatomy and physiology of the nosebull Symptoms and signs of common sinonasal disease eg
rhinitis sinusitis nasal polypsbull Examination of the nose including an assessment of the
appearance the septum the turbinates and the mucosabull The endoscopic evaluation of the nosebull Management of a fractured nose and the timing of
interventionbull Management of epistaxis from minor nosebleeds to
torrential haemorrhagebull The principles of common nasal operations including septal
surgery functional endoscopic sinus surgery and rhinoplasty
Head and neckmdashbenign and malignant disease
bull The basic anatomy and physiology of the oral cavity salivary glands pharynx larynx oesophagus and lymph node drainage
bull The presentation of head and neck cancerbull The presentation and management of salivary gland diseasebull Examining the oral cavity larynx and pharynx including the use of the nasendoscopebull Examining the neck with reference to the lymph nodesbull The role of fine needle aspiration cytology (FNAC)bull The principles and limitations of radiological investigation of the head and neck regionbull Management of neck lumps in particular the malignant lymph node with an unknown
primarybull The management of the airway in patients with a tracheostomy or end tracheostomy after
laryngectomybull A basic knowledge of the principles of operative surgery in particular the principles of
reconstructive surgery and the surgery for salivary gland disease eg parotidectomybull The postoperative management of a patient who has undergone major head and neck surgerybull The role of the multidisciplinary team in head and neck cancer and voice disorders
Supplementary knowledgebull The role of otoacoustic emissions and evoked auditory potentials in managing
hearing lossbull The use of speech audiometrybull The surgery for otosclerosisbull Bone-anchored hearing aids for conductive hearing lossbull Cochlear implantation and the reactions of the deaf community to this
interventionbull The use of sign languagebull Neuro-otology in particular the presentation and management of acoustic
neuromasbull Craniofacial surgery and the interplay between ENT plastic surgery and
neurosurgerybull The management of cleft palate and the increased risk of glue earbull Advanced endoscopic sinus surgery for the mangement of sinonasal malignancy
pituitary tumours and skull base tumoursbull Microlaryngeal surgery and surgical voice restorationbull The use of chemotherapy and radiotherapy in head and neck malignancy
Working in ENT
bull Working in ENT should be a very enjoyable experience whether it is a temporary attachment or a long-term career plan
bull It is helpful if you have an understanding of what others expect of you
bull It is also important for you to think about your own career development
Your duties
bull Patient care and continuitybull Professional developmentbull Research
The ENT Examination
EquipmentA fully equipped ENT department will have all the necessary instruments for performing a full ENT examination
Basic equipment
bull A light sourcemdasha portable headlight that runs off batteries is ideal
bull Wooden tongue depressorsbull Thudicum nasal speculumbull An otoscope with several speculaebull Pneumatic attachment for the otoscopebull Tuning fork 512Hzbull Pen and paperbull Gloves
Advanced equipment
bull Co-phenylcaine spraybull A flexible nasendoscope with light sourcebull Alcohol wipe to act as demist for the scopebull Aqueous lubricating gel for the scope
Emergency equipment
bull Large nasal tampons (you can always cut 10cm ones to size)
bull Silver nitrate sticksbull Foley catheters
Basic Anatomy of the Nose
bull The structural anatomy of the nose is important
bull for both aesthetic and functional reasons since the
bull nose as the gateway to the respiratory tract performs
bull a variety of physiologic functions
External NoseThe shape of the external nose is defined by the nasalbones a pair of rectangular bones in the upper nasaldorsum and by lateral cartilages (uppernasal cartilages) and alar cartilages (major alar cartilages)in the central and lower portions of the noseThe lateral portions of the nasal alae alsocontain several small accessory cartilages called theminor alar cartilages which are embedded in the lateralsoft tissues of the noseThe shape and stability of the alar cartilages each ofwhich consists of a medial and lateral crus
External Nose
Anatomy of the nasal base
bull Besides thebull medial crura the
inferior septal margin and the connective-
bull tissue septum (columella) are also responsible
bull for stabilizing the base of the nose
Anatomy of the nasal base
Anatomy of the nasal base
bull The nasal septum is subluxed toward the left side partially
bull obstructing the nasal airway
Nasal CavitiesThe nasal cavities begin anteriorly at the nasal vestibulewhich is bordered posteriorly by the internal nasalvalve (limen nasi) located between the posteriorborder of the alar cartilage and the anterior border ofthe lateral cartilage This valve area is the narrowestportion of the upper respiratory tract
Nasal Cavities
The interior ofthe nose behind the nasal valve is divided by the nasalseptum into two main cavities
Nasal CavitiesThe nasal septum iscomposed of an anterior cartilaginous part and twoposterior bony parts Abnormalities in the shape ofthe nasal septum which may consist of a deviated septum tensionseptum spurs or ridges are a frequent cause ofnasal airway obstructionThe choanae are the paired posterior openingsthrough which the nasal cavities communicate withthe nasopharynx
Nasal CavitiesThe nasal cavity is bounded laterally by the lateral nasalwalls which are formed by the ethmoid bone andmaxilla and posteriorly by the palatine bone and thepterygoid process of the sphenoid bone Several functionallyimportant structures are located on the lateralnasal wall the nasal turbinates and their associatedpassages (meati) sinus ostia and the orifice ofthe nasolacrimal duct (Fig 15)
The inferior turbinate consists of a separate bone thatis attached to the medial wall of the maxillary sinusThe opening of the nasolacrimal duct is located in thecorresponding inferior meatus The middle andsuperior turbinates are part of the ethmoid bone In rare cases a rudimentary ldquosupreme turbinaterdquo is alsopresent above the superior turbinate
The middle turbinate has by far the greatest functionalimportance because most of the drainage tracts fromthe surrounding paranasal sinuses open into the middlemeatus The nasal cavity is bounded superiorly by the cribriformplate of the ethmoid bone This thin bony platehas numerous openings for the passage of the fila olfactoriaand also forms the boundary of the anteriorcranial fossa
Nasal Cavities
The floor of the nasal cavity is formedmostly by the hard palate which is formed in turn bythe two palatine processes of the maxilla and the horizontallaminae of the palatine bone
Structure of the lateral nasal wall
Inferior meatus
Paranasal Sinuses
The paranasal sinuses are air-filled cavities that communicatewith the nasal cavities
-The maxillary sinus frontalsinus and anterior ethmoid cells drain into the nasalcavity through the middle meatusmdashie below themiddle turbinate -The posterior ethmoidcells drain into the nasal cavity through the superiormeatus The ostium of the sphenoid sinus is locatedin the anterior wall directly above the choanae- The anatomical connections between the nasal cavity andparanasal sinuses are functionally important and playa key role in the pathogenesis of many rhinologic diseasesthat involve the paranasal sinuses
Vascular SupplyThe external nose derives most of its blood supply
from the facial artery which arises from the external
carotid artery and from the ophthalmic artery which
springs from the internal carotid artery
Vascular Supply
The internalnose receives blood from the territories of the externaland internal carotid arteries- the terminalbranches of the sphenopalatine artery which arisesfrom the maxillary artery - the anterior and posteriorethmoid arteries which arise from the ophthalmicartery-internal carotid arterie
venous drainage
The venous drainageof the facial region is handled by -the facial vein -retromandibular vein -internal jugular vein
lymphatic drainage
The regional lymphatic drainage of the face and externalnose is handled mainly by- the submandibularlymph nodes while the nasal cavity is additionallydrained by -the retropharyngeal and deep - -cervical lymph nodes
Morphology of the Nasal Mucosa
Besides the anatomical structure of the external noseand nasal cavity the nasal mucosa plays an essentialrole in numerous functions of the nose in the respiratory tract
Morphology of the Nasal Mucosa
The anterior part of the nasal cavity (the nasal vestibule)like the external nose is covered by skin composedof a multilayer keratinizing squamous epithelium and finally a ciliated respiratory epithelium A small areaon the upper nasal septum superior turbinate andpart of the middle turbinate located adjacent to thecribriform plate is covered by olfactory mucosa and iscalled the olfactory region
Nerve SupplyThe facial skin receives its sensory innervation fromterminal branches of the trigeminal nerve that enterthe facial region through the supraorbital infraorbitaland mental foramina Thefacial muscles are classified as mimetic or mastica- tory each of these groups receiving different motorinnervationbythe facial nerve
History and Clinical Examination of the Nose
Historybull The main symptomsbull nasal obstruction (ldquostuffy
noserdquo)bull nasal dischargebull Headachesbull Olfactory
dysfunction
Palpationbony discontinuitiesNeuralgias to check
over- the supraorbital -infraorbital -mental foramina
Anterior Rhinoscopy
bull The rhinologic examination itself begins with anterior
bull rhinoscopy to evaluate the nasal vestibule and the anterior
bull portions of the nasal cavity
Nasal Endoscopy Nasal endoscopy has become the most important andrewarding clinical examination method in rhinologic diagnosis
- rigid endoscopes which are available in 4-mm and 28- mm diameters and assorted viewing angles (eg 01048576 301048576 1201048576) -flexible endoscopes are also available for inspecting the nose and nasopharynx and exploring all of the pharynx and larynx in one sitting
Nasal endoscopy
Nasal Endoscopy
Nasal Endoscopy
Imaging of the Nose and Paranasal Sinuses
Conventional RadiographsStandard paranasal sinus radiographs in the occipitomental
projection ( Water projection) and
occipitofrontal projection Caldwell projection) in cases of acute inflammation
They are also obtained to evaluate midfacial fractures
Computed Tomography (CT) the main indicationsfor CT scanning of the
nose and paranasal sinuses
are- chronic sinusitis - -trauma (especially
frontobasal -fractures)
-and tumors
The occipitofrontal projection is better for evaluating theethmoid cells and frontal sinus
occipitomental projection demonstrates the maxillarysinus and gives a limited view of the sphenoid sinus
Computed tomography of the paranasal sinuses
Four representative coronal CT scans are shown
Four representative coronal CT scans are shown
Magnetic Resonance Imaging
Magnetic maging
Magnetic resonance imaging (MRI) has fewer indicationsthan CT in patients with paranasal sinus diseaseThis is primarily because MRI is markedly inferior toCT in defining the bony boundaries of the sinusesThe strength of MRI lies in its superior soft-tissue discriminationMRI is indicated in diseases that involve the paranasal sinuses in addition to thecranial cavity or orbit (eg tumors and congenitalmalformations such as encephaloceles)
MRI of the paranasal sinuses
The Nose and Sinuses
Structure The structure of the nose is made up of
four partsbull The surface anatomybull The nasal skeletonmdashcomposed of the
two nasal bones the paired upper lateral and lower lateral cartilages and the nasal septum covered in subcutaneous tissue and skin
bull The internal anatomymdashincludes the septum of the nose which forms the medial wall of the nasal cavity The turbinates on the lateral wall are also called conchae
bull The osteomeatal complexmdasha key functional area of the nose
Function The nose is the main route for inspired
air and its structure is related to this function As the air passes over the large surface area of the turbinates
The inspired gases are warmed and humidified Mucus on the mucosa of the nose removes large dust particles from the air as it is breathed in
The voice resonates in the sinuses and nose and this provides character to the speech
Pneumatization of the sinusesmdashthey are air filled spacesmdashreduces the weight of the skull
Diseases of thDiseases of the Outer and Inner Nosee Outer and
Inner Nose Erysipelas Definition of the disease ndash Erysipela is a skin infection that affects the superficial dermis and is caused by Streptococcus pyogenes (group A) It usually develops in the extremities and the face and less commonly on the scalp and genitals bull Epidemiologyaetiology ndash Erysipelas are more often seen in elderly infants and children patients with compromised immunology and diabetes -Predisposing factors are alcoholism skin ulceration puncture wounds fungal infections malnutrition and burns
Erysipelas
bull Symptomsbull ndash It usually presents of fever general fatigue bull -The skin lesion is a redindurated and elevated plaque
with borders that expand rapidly bull It is painful warm and accompanied by variable oedemabull -On the second or third day a flaccid bulla may develop
and desquamationbull bull Presence of regional lymph nodes is common
Erysipelas
bull Complicationsndash The most common complication is recurrencewhich is seen in 18ndash30 of the cases even afterproper antibiotic therapy Recurrence is seen moreoften in females than in malesA skin infection with S pyogenes could lead toglomerulonephritis
Erysipelas
bull Complicationsbull ndash The most common complication is recurrencebull which is seen in 18ndash30 of the cases even afterbull proper antibiotic therapy bull -Recurrence is seen morebull often in females than in males bull -A skin infection with S pyogenes could lead tobull glomerulonephritis
Erysipelas
bull bull Diagnosisbull ndash Diagnosis is based on the patientrsquos personal
historybull and physical examination particularly on inspectionbull of the skin
bull Blood cultures are positive in less thanbull 5 of cases
ErysipelasTherapyndash Conservative therapybull The preferred antibiotic is penicillin In mildcases with minor systemic symptoms penicillinV 500 mg orally every 6 h for 10 days or penicillinG benzathine 12 mil U intramuscularlyonceOther possibilities are amoxicillin 500 mgorally twice a day for 10 days or cephalexin 500mg orally every 6 h for 10 days
ErysipelasIn moderate and severe cases with significantsystemic symptoms hospitalization and intravenoustreatment is required penicillin G 2ndash4mil U intravenously every 4ndash6 h Cefazolin05ndash15 gm intravenously every 8 h cefotaxime1ndash2 gm intravenously every 8 h or ceftriaxone1ndash2 gm intravenously once a day should be administeredIn patients with a penicillin allergyclindamycin 600 mg intravenously every 8 h orvancomycin 15 mgkg intravenously twice a daymay be given
ErysipelaAdditional useful therapeutic optionsbull Prednisone 30 mg over 8 days might be consideredas well as elevation of the affected siteMoist heat compresses may be usefulbull Surgeryndash Debridement and drainage are indicated when bullaeabscesses or necroses are presentbull Differential diagnosisndash Contact dermatitisndash Asteatotic eczemandash Herpes zosterndash Angioneurotic oedemandash Osteomyelitis
Furuncle
bull Definition of the diseasebull ndash A furuncle is an infection that beginsbull at the hair follicle and spreads deeper into thebull dermis and subcutaneous tissue forming abull nodule After several days it developsbull into an abscess - red painful and fluctuantbull bull bull Epidemiologyaetiologybull ndash The aetiologic agent is Staphylococcus aureus
FuruncleSymptomsndashsymptoms are local and limited to thesite of infection Furuncles usually are wherehair follicles are present bull Complicationndash One complication is furunculosis multiple draining furunclesDiagnosisndash The diagnosis is based on clinical inspection - Cultures are not necessary when there is no systemic involvement but should beconsidered if systemic therapy (in case of feversignificant cellulitis or hospitalization) or whenmethicillin-resistant Staphylococcusaureus (MRSA) is considered
FuruncleTherapyndash When the furuncle is small application of moist heat compress to promote drainage -Larger furuncles should be drained by surgical incision-After drainage the area should be cleaned with anantiseptic (with chlorhexidinebetadine) should be applied twice
a dayndash If no systemic symptoms or extensive cellulitis arepresent simple topical care is usually curative andoral antibiotics are not necessary Otherwise systemictreatment is indicated and should cover anypossible MRSA
Furuncle
bull -Recommended antibiotics are trimethoprim-sulfamethoxazole
bull 1ndash2 tablets orally twice daily doxycyclinebull 100 mg orally twice dailybull or clindamycin 300ndash450 mg orally every 8 hbull - In severe cases vancomycin 15 mgkg
intravenouslybull every 12 h or clindamycin 600 mg intravenouslybull every 8 h
Midline Granulomabull A midline granuloma is an angiocentricbull lymphoma it was referred to as polymorphicbull reticulosis lethal midline granuloma and midline
malignant reticulosisbull bull Definition of the diseasebull ndash This rare disease is a lymphoma of extranodal
presentationall cases are positive for the Epstein-Barr virus
bull -This lymphoma most commonly appears in the midface region
Midline GranulomaEpidemiologyaetiologyndash This form of lymphoma is rare in Europe and theUnited States with a higher prevalence in Asia and PeruSymptomsndash The most common presentation is nasal obstruction with a destructive mass occupying the nosesinuses and palate
-Fever night sweatsand weight loss seen usually in Hodgkinrsquos lymphomaand other non-Hodgkinrsquos lymphomas (knownas ldquoB symptomsrdquo) are uncommon
Midline GranulomaDiagnosisndash The diagnosis is based on anatomopathologicalstudy The malignancy of the tumour manifested byextensive necrosis makes the histological diagnosisdifficult and often more biopsies are required forconfirmationbull Therapyndash Therapy consists of radiotherapy with or withoutchemotherapy
Midline Granuloma
bull Prognosisbull ndash Depending on the stage long-term remission or
experience a worseningbull prognosis with relapses which may include otherbull extranodal sites bull Involvement of extranodal sitesbull including the upper airway gastrointestinal tractbull skin
Wegenerrsquos Granulomatosis
bull Definition of the diseasebull ndash Wegenerrsquos granulomatosis is a systemic chronicbull vasculitis of small- and medium-sized blood vesselsbull with an autoimmune component It affectsbull particular organs with variable predilectionbull Epidemiologyaetiologybull ndash Wegenerrsquos granulomatosis is a rare disease It affects
about 1 in 20000ndash30000 people It is more prevalentbull in middle-aged Caucasian patients
Wegenerrsquos Granulomatosis
Symptomsndash The disease may present pulmonary upper
respiratory tract or renal In the disseminated form-The localised form ndash confinedto the upper respiratory region ndash is present in 25of the patients- It consists of nonspecific manifestationssuch as nasal obstruction crusting purulentor bloody rhinorrhea and painful or painless ulcers in oral or nasal cavities which are unresponsive tostandard medical treatment
Wegenerrsquos Granulomatosis
bull In some patients the nasal septum is perforatedbull which leads to saddle-nose deformity Less
commonbull symptoms are hoarseness stridor due to
subglotticbull stenosis otalgia otorrhea and conductivebull and sensorineural hearing loss Also ocular
symptomsbull such as scleritis conjunctivitis uveitis andbull episcleritis may be present
Wegenerrsquos Granulomatosis
bull ndash In the disseminated form pulmonary involvementbull is manifested by cough dyspnoea haemoptysisbull (due to an alveolar capillaritis necrotic lesions orbull endobronchial disease) and pleuritic painndashbull -Ninety per cent of patients have nasal symptomsbull and these symptoms are usually the first
manifestationof the diseasebull -Most patients have also renal involvementbull even if it is subclinical
Wegenerrsquos Granulomatosis
Diagnosis ndash Diagnosis of Wegenerrsquos granulomatosis is based on clinical findings that demonstrate lung (chest x-ray) kidney (urine analysis) or upper respiratory tract
involvement (oral or nasal ulcers or discharge) - positive blood analysis for cytoplasmic-staining antineutrophil
cytoplasmic antibodies (c-ANCA) and confirming proteinase 3 (PR3) ANCA or myeloperoxidase (MPO) ANCA ndash Biopsy is essential for diagnosis nonspecific chronic inflammation
and necrosis -Bacterial and fungal infections
Wegenerrsquos Granulomatosis
Therapyndash Conservative therapybull In the induction of disease remission highdosesteroids (e g prednisone 1 mgkgday) for1 month with tapering over several months aregiven In addition cyclophosphamide (2 mgkgday) should be administered for 6ndash12 monthsuntil symptoms disappear In the maintenanceof remission cyclophosphamide should be
Wegenerrsquos Granulomatosis
Antibiotics mainly trimethoprim-sulfamethoxazoleare given for prophylaxis againstPneumocystis jiroveci (formerly Pneumocystiscarinii) pneumonia (PCP) which may developduring immunosuppression and have a role inpreventing recurrencesbull Sinonasal manifestations may be treated with topical nasal steroids and nasal irrigations lowdosesystemic steroids and antibiotics when bacterial infection (typically Staphylococcus species) is suspected
Wegenerrsquos Granulomatosis
bull Prognosisbull ndash Most of the patients respond well to treatmentbull achieving symptom-free intervals of 5ndash20 yearsbull or more bull -Anatomical problems (sinusitis trachealbull stenosis) may require surgery bull Relapses can be long and troublesomebull Long-term complications are chronicbull renal failure hearing loss and deafness
Nasal Fractures Definition ndash A nasal fracture is a disruption of the nasal bone structure due to trauma It is the most frequently fractured facial bone Epidemiologyaetiology ndash Sports falls and assaults are the usual mechanisms of fracture -Males are affected twice as often as are females -Paediatric populations with a incidences during the second and third decades of life -Variables such as force impact direction nature of the striking object age and other will influence the pattern of injury to the components of the nose
Nasal Fractures
bull Symptomsbull ndash Deformity swelling epistaxis and periorbital
ecchymosis are signs that are suggestive of nasal fracture
bull bony crepitus and nasal segment mobilitybull ndash Epiphora bull Severe bilateral injuries to the lachrymal bones
arebull associated with depressed nasal fractures
Nasal Fractures Complications ndash Septal haematoma is one of the most severe early complications of nasal trauma and without drainage it results in abscess formation 6ndash7 days after trauma producing necrosis of the septal cartilage -Long-term problems such as saddle-nose deformity perforation columellar retraction and nasalbase
Septal infection could lead to osteomyelitis orbital and intracranial abscesses meningitis and cavernous sinus thrombosis -Cerebrospinal fluid leakage is a common complication of severe
nasal and frontal fractures
Nasal Fractures
bull Diagnostic proceduresbull ndash Inspectionbull bull Changes of appearance such as deviation andbull asymmetry bleeding watery drainage changesbull in nasal breathing and smell It is useful to comparebull the current presentation with old photographsbull (up to 40 of normal individuals havebull significant nose malformations)
Nasal Fractures Physical examination bull The diagnosis of a nasal fracture is made primarily by physical examination epistaxis nasal swelling and periorbital ecchymosis Nasal shape in the lateral and frontal inspection should be assessed Grasping the dorsum between two fingers and rocking the pyramid back and forth aids in assessing the mobility of nasal bones Internal structures should be evaluated by using a headlight and nasal speculum Clotted blood is removed by suction and assessment of haematoma mucosal tears and active bleeding is performed Bimanual palpation of the septum helps to differentiate septal swelling from haematoma ndash
Nasal FracturesRadiographybull There is no clear evidence of the role of radiographyin the management of nasal fracturesPlain films have up to a 66 false-positive rateas a result of misinterpretation of normal suturelines In addition old fractures are difficult todistinguishbull Three-dimensional CT is recommended for extensiveinjuries involving the nasal-orbital-ethmoidalcomplexndash
Nasal Fractures
bull Additionaluseful diagnostic proceduresbull bull Using a 0 or 30deg 4-mm endoscope is helpful inbull the assessment of posterior abnormalities If thebull patient is heavily sedated Brown-Gruss
provocationbull manoeuvres may be performed to determinebull deformities in upper middle or lower segmentsbull by compressing each compartment
Nasal FracturesConservative treatmentndash Treatment of bleedingbull For localised bleeding anterior sources may becauterised by silver nitrate or sealed with topicalmaterials such as thrombin combined withgelatin foam fibrin glue FloSealreg or other procoagulantmaterials If conservative measuresfail a formal anterior packing is placedbull Bleeding from branches of sphenopalatine orethmoid vessels requires anterior-posteriorpacking
Nasal Fractures
bull bull Surgical methods such as direct endoscopic vessel
bull cauterization or ligation have been shown tobull offer better haemostasis and patient comfortbull Angiography with embolization can also be
consideredbull in cases refractory to more conservativebull approaches
Nasal Fractures
bull Type of reductionbull bull Nondisplaced fractures should be treated withbull observation alone Closed nasal reduction is thebull best choice for simple injuries (isolated unilateralbull with medial displacement)bull bull An open approach should be considered in
severebull trauma (bilateral depressed fractures)
Nasal Fracturesbull Surgical principlesbull ndash Topical anaesthesia with cotton pledgets soakedbull with 4 cocaine or 005 oxymethazoline combinedbull with 4 topical lidocaine should be appliedbull for 5ndash10 min Local anaesthesia should also be injectedbull (1 lidocaine and 1100000 epinephrine)bull along the septum lateral walls and floor of the nasalbull cavitybull bull
Nasal FracturesClosed reductionndashndash The nasal bones are grasped between two fingersand pressure is applied laterally in theopposite direction of the deviation A bluntelevator may be used from within the nose incases of significant medial collapse Walshamforceps can be of help Reduction of the septumshould be performed with the use ofAsch forceps
Nasal Fractures
bull To prevent collapse of the postreductionbull framework nasal packing should be placedbull for 3ndash5 days Septum splints are recommendedbull in comminuted septal fractures withbull severe mucosal lesions External nasal splintingbull for 10 days (Aquaplastreg Thermoplastreg)bull provides nasal protection Nasal saline spraysbull prevent crusting and oral antibiotics should
Nasal Fractures
bull Open reductionbull ndashndash Immediate repair of fractures by using
widebull surgical exposure reduction fixation and
reconstructionbull ndashndash The second option is delayed correctionbull (6 months or more) of persistent deformitiesbull using standard techniques of rhinoplasty
Deviated Nasal Septum
bull Definition of the diseasebull ndash Deviation of the nasal septum is a common causebull of unilateral nasal airway obstruction in which thebull nasal septum is displacedbull bull Epidemiologyaetiologybull ndash Developmental septal abnormalities Septal cartilage
damage in the neonatal period andbull during birth can cause severe septal deviation inbull the absence of a history of nasal trauma
Deviated Nasal Septum
bull Symptomsbull ndash Patients may present with a history of sinusitis
allergicbull rhinitis obstructive sleep apnoea previousbull nasal surgery or recent nasal trauma Unilateral or
bilateral nasal airway obstruction that is unrelievedbull with decongestants or nasal steroid sprays is oftenbull seenbull bull
Deviated Nasal SeptumDiagnosisndashExamination external dorsal deviation or the columella and caudal septummay be deflected off the midline (caudal subluxation)ndash Inspections of the nasal cavity and anterior-posteriorrhinoscopy are helpful in diagnosing the locationtype and severity of septal deformityThe endoscope is also useful in identifying polypsthe severity and extent of posterior septaldeviations and bony spurs and locating areas ofseptal perforation or mucosal injury
Deviated Nasal Septum
bull Therapybull ndash Septoplasty is a procedurebull The areabull of deviation is corrected or resected in order tobull leave behind as much cartilage and bone as
possiblebull Cartilage resection is minimised and can be
repositioned reshaped or recontoured using a variety of methods
Deviated Nasal Septum
bull ndash Indications of septoplasty before the growth period
bull of the nose is finished should be very limited bull -In these cases surgery must preserve all the
cartilagebull in order to prevent external changes of the
shape ofbull the nose
Deviated Nasal Septum
bull Complicationsbull ndash Frequent complications include haematoma andbull infection Cerebrospinal fluid leak is a rare but
potentiallybull serious complicationbull It is usually the resultbull of avulsion or damage to the cribriform plate whenbull handling the perpendicular plate of the ethmoidbull ndash Other complications include epistaxis nasal
Deviated Nasal Septum
bull Other complications include epistaxis nasal obstruction
bull due to residual deviation synechiae returnbull of the cartilaginous deviation septal perforationbull anosmia and cosmetic nasal deformities suchbull as widened alar rim margins drooping nasal tipbull columella retraction and a sunken dorsum with abull supratip saddle formation
Septal perforation with minor crusting View from provide closure of the
incision
Septal Haematoma
bull A septal haematoma is a blood collection under the perichondrium
bull of the septum and cartilagebull bull bull Epidemiologyaetiologybull ndash A septal haematoma is one of the most
severe complications of nasal trauma
Septal Haematoma
bull Diagnosisbull ndash Signs and symptoms include intense pain
swellingbull haematoma of the upper lip and philtrum
area andbull complete nasal airway obstruction
Septal HaematomaTherapyndash Management consists of drainage through a mucoperichondrial incision Immediate treatment isnecessary to prevent long-term problems such asa saddle-nose deformity perforation columellarretraction and nasal-base widening In childrenseptal destruction can lead to devastating nasal andmidfacial growth abnormalitiesbull Surgeryndash Incision and evacuation of the collection is performedDrainage of a septal haematoma should
Septal HaematomaSurgeryndash Incision and evacuation of the collection is performedDrainage of a septal haematoma should provide closure of the incision
Splints or transseptal sutures are placed to obliterate thepotential space and prevent collectionInfection involving the septal cartilage Reconstruction with autologouscartilage is then performed in a second stage Oral antibiotics should be given
Nasal DeformitySaddle-nose deformityndash A saddle-nose deformity is characterised by a loss ofnasal dorsal height and compromised nasal supportstructures -Other case observed are depressionof the middle vault and dorsum loss of nasal tipsupport and definition shortened (vertical) nasal length over rotation of the nasal tip and retrusion ofthe nasal spine and caudal septum It is also knownas a ldquoPug noserdquo or ldquoboxerrsquos noserdquo both of which referto various degrees of nasal dorsal depressionbull
Nasal DeformityEpidemiologyaetiologyndash Prevalence is higher in population groups prone to facial trauma (ie boxers athletes) those with historiesof intranasal cocaine use nasal surgery (e g radical submucosal septal resection reductive rhinoplasty)ndash A saddle-nose deformity can be congenital or acquired It can be noticed as a part of individual familialsyndromic and ethnic characteristics - Most deformities are due to traumatic and iatrogeniccauses Medical causes are Wegenerrsquosgranulomatosis relapsing polychondritis leprosy (Hansenrsquos disease) syphilis ectodermal dysplasiaand intranasal cocaine use
Nasal Deformity
bull Therapybull ndash Nasal reconstruction indications depend on patientbull selection surgeon experience and aetiology of thebull deformity bull Indications for surgery can be functionalbull aesthetic or most commonly both In individuals
with a compromised nasal airway a nasoseptalbull reconstruction is indicated
Nasal Deformity
bull Contraindications bull include patients with malignantbull chronic or autoimmune disease conditions drugbull abuse poor perioperative risk profile and unrealisticbull expectationsbull ndash Multiple previous rhinoplasties and certain
professionsbull (mixed martial artists boxers and other contactbull sports) are relative contraindications
Nasal DeformitySeptoplastyndash Septoplasty is performed to correct nasal obstructioncaused by septal deformityndash Usually septoplasty is performed under general anaesthesiawith the patient in the supine position with the head elevated by approximately 30 (Righthandedsurgeons approach from the right side)ndash Local vasoconstrictive anaesthesia is applied notonly to reduce postoperative pain but also more importantly to achieve vasoconstriction of themucosa and less intraoperative haemorrhage Lidocainewith adrenaline or epinephrine is usedalthough in patients with cardiac hypersensitivityoxymetazoline might be preferred
Nasal Deformity
bull Septoplasty begins with the incision of septal mucosabull Most operative techniques utilise a hemitransfixionbull incision at the caudal end of septum so thatbull deviation at this point might be reached as wellbull as a transfixion incision that is easily obtained ifbull needed (Right-handed surgeons normally choosebull the left side but that may vary when deviation isbull convex towards the right)
Nasal DeformityA columella retractor is placed over the columellaand by pulling it laterally the caudal border of theseptum is exposed Ala can be protected by an alaprotector A vertical incision with a no 15 bladeover the caudal end of septum is performed untilreaching the plane of the septal cartilage It is essentialto correctly identify the perichondrium and byusing the Cottle elevator dissect and lift it creatinga flap As the dissection proceeds along the septalcartilage a longer speculum (no 5) is introduced sothat elevation of the mucoperichondrium is doneunder constant visual controlndash The next step is to dissect the mucoperiostium
Nasal DeformityDissecting over the bony-cartilaginous junctionwhen joining both tunnels might be difficult and is
especially prone to membrane perforationndash If needed the same tunnels are to be created on the
other side of the septum Then deviated parts of
septum are identified and removed either with a
knife or a Freer chisel
Nasal Deformitybull septum from the maxillary crest the septum mustbull be separated from the perpendicular plate trimmedbull along the inferior border placed back onto the crestbull and sutured to the periosteum If the deformity involvesbull the vomer an osteotome is used Care mustbull be taken not to break the cribriform plate becausebull it could cause a cerebrospinal fistula
Nasal Deformity
bull Once the septal deviation is corrected the flapsbull and hemitransfixion incision are mattressed
withbull absorbable sutures Nasal packing to prevent
synechiaebull and postoperative septal haematoma mightbull be advised but should be removed within 72 h

Earbull Basic anatomy and physiology of the earbull Presentation and management of common ear disease eg otitis externa
otitis media glue ear chronic suppurative otitis media with or without cholesteatoma vertigo and facial palsy
bull Examination of the ear including the pinna ear canal and otoscopybull Testing hearing with tuning fork testsbull The advantages of the microscope and the fibreoptic otoscopebull Basic interpretation of play audiometry pure tone audiograms and
tympanogramsbull The principles of grommet insertion mastoid surgery and the treatment of
Menieres diseasebull Identifying postoperative problems following ear surgery ie sensorineural
hearing loss facial nerve palsy and vestibular dysfunctionbull Understanding the differential diagnosis of facial nerve palsy and its
treatment
Nosebull Anatomy and physiology of the nosebull Symptoms and signs of common sinonasal disease eg
rhinitis sinusitis nasal polypsbull Examination of the nose including an assessment of the
appearance the septum the turbinates and the mucosabull The endoscopic evaluation of the nosebull Management of a fractured nose and the timing of
interventionbull Management of epistaxis from minor nosebleeds to
torrential haemorrhagebull The principles of common nasal operations including septal
surgery functional endoscopic sinus surgery and rhinoplasty
Head and neckmdashbenign and malignant disease
bull The basic anatomy and physiology of the oral cavity salivary glands pharynx larynx oesophagus and lymph node drainage
bull The presentation of head and neck cancerbull The presentation and management of salivary gland diseasebull Examining the oral cavity larynx and pharynx including the use of the nasendoscopebull Examining the neck with reference to the lymph nodesbull The role of fine needle aspiration cytology (FNAC)bull The principles and limitations of radiological investigation of the head and neck regionbull Management of neck lumps in particular the malignant lymph node with an unknown
primarybull The management of the airway in patients with a tracheostomy or end tracheostomy after
laryngectomybull A basic knowledge of the principles of operative surgery in particular the principles of
reconstructive surgery and the surgery for salivary gland disease eg parotidectomybull The postoperative management of a patient who has undergone major head and neck surgerybull The role of the multidisciplinary team in head and neck cancer and voice disorders
Supplementary knowledgebull The role of otoacoustic emissions and evoked auditory potentials in managing
hearing lossbull The use of speech audiometrybull The surgery for otosclerosisbull Bone-anchored hearing aids for conductive hearing lossbull Cochlear implantation and the reactions of the deaf community to this
interventionbull The use of sign languagebull Neuro-otology in particular the presentation and management of acoustic
neuromasbull Craniofacial surgery and the interplay between ENT plastic surgery and
neurosurgerybull The management of cleft palate and the increased risk of glue earbull Advanced endoscopic sinus surgery for the mangement of sinonasal malignancy
pituitary tumours and skull base tumoursbull Microlaryngeal surgery and surgical voice restorationbull The use of chemotherapy and radiotherapy in head and neck malignancy
Working in ENT
bull Working in ENT should be a very enjoyable experience whether it is a temporary attachment or a long-term career plan
bull It is helpful if you have an understanding of what others expect of you
bull It is also important for you to think about your own career development
Your duties
bull Patient care and continuitybull Professional developmentbull Research
The ENT Examination
EquipmentA fully equipped ENT department will have all the necessary instruments for performing a full ENT examination
Basic equipment
bull A light sourcemdasha portable headlight that runs off batteries is ideal
bull Wooden tongue depressorsbull Thudicum nasal speculumbull An otoscope with several speculaebull Pneumatic attachment for the otoscopebull Tuning fork 512Hzbull Pen and paperbull Gloves
Advanced equipment
bull Co-phenylcaine spraybull A flexible nasendoscope with light sourcebull Alcohol wipe to act as demist for the scopebull Aqueous lubricating gel for the scope
Emergency equipment
bull Large nasal tampons (you can always cut 10cm ones to size)
bull Silver nitrate sticksbull Foley catheters
Basic Anatomy of the Nose
bull The structural anatomy of the nose is important
bull for both aesthetic and functional reasons since the
bull nose as the gateway to the respiratory tract performs
bull a variety of physiologic functions
External NoseThe shape of the external nose is defined by the nasalbones a pair of rectangular bones in the upper nasaldorsum and by lateral cartilages (uppernasal cartilages) and alar cartilages (major alar cartilages)in the central and lower portions of the noseThe lateral portions of the nasal alae alsocontain several small accessory cartilages called theminor alar cartilages which are embedded in the lateralsoft tissues of the noseThe shape and stability of the alar cartilages each ofwhich consists of a medial and lateral crus
External Nose
Anatomy of the nasal base
bull Besides thebull medial crura the
inferior septal margin and the connective-
bull tissue septum (columella) are also responsible
bull for stabilizing the base of the nose
Anatomy of the nasal base
Anatomy of the nasal base
bull The nasal septum is subluxed toward the left side partially
bull obstructing the nasal airway
Nasal CavitiesThe nasal cavities begin anteriorly at the nasal vestibulewhich is bordered posteriorly by the internal nasalvalve (limen nasi) located between the posteriorborder of the alar cartilage and the anterior border ofthe lateral cartilage This valve area is the narrowestportion of the upper respiratory tract
Nasal Cavities
The interior ofthe nose behind the nasal valve is divided by the nasalseptum into two main cavities
Nasal CavitiesThe nasal septum iscomposed of an anterior cartilaginous part and twoposterior bony parts Abnormalities in the shape ofthe nasal septum which may consist of a deviated septum tensionseptum spurs or ridges are a frequent cause ofnasal airway obstructionThe choanae are the paired posterior openingsthrough which the nasal cavities communicate withthe nasopharynx
Nasal CavitiesThe nasal cavity is bounded laterally by the lateral nasalwalls which are formed by the ethmoid bone andmaxilla and posteriorly by the palatine bone and thepterygoid process of the sphenoid bone Several functionallyimportant structures are located on the lateralnasal wall the nasal turbinates and their associatedpassages (meati) sinus ostia and the orifice ofthe nasolacrimal duct (Fig 15)
The inferior turbinate consists of a separate bone thatis attached to the medial wall of the maxillary sinusThe opening of the nasolacrimal duct is located in thecorresponding inferior meatus The middle andsuperior turbinates are part of the ethmoid bone In rare cases a rudimentary ldquosupreme turbinaterdquo is alsopresent above the superior turbinate
The middle turbinate has by far the greatest functionalimportance because most of the drainage tracts fromthe surrounding paranasal sinuses open into the middlemeatus The nasal cavity is bounded superiorly by the cribriformplate of the ethmoid bone This thin bony platehas numerous openings for the passage of the fila olfactoriaand also forms the boundary of the anteriorcranial fossa
Nasal Cavities
The floor of the nasal cavity is formedmostly by the hard palate which is formed in turn bythe two palatine processes of the maxilla and the horizontallaminae of the palatine bone
Structure of the lateral nasal wall
Inferior meatus
Paranasal Sinuses
The paranasal sinuses are air-filled cavities that communicatewith the nasal cavities
-The maxillary sinus frontalsinus and anterior ethmoid cells drain into the nasalcavity through the middle meatusmdashie below themiddle turbinate -The posterior ethmoidcells drain into the nasal cavity through the superiormeatus The ostium of the sphenoid sinus is locatedin the anterior wall directly above the choanae- The anatomical connections between the nasal cavity andparanasal sinuses are functionally important and playa key role in the pathogenesis of many rhinologic diseasesthat involve the paranasal sinuses
Vascular SupplyThe external nose derives most of its blood supply
from the facial artery which arises from the external
carotid artery and from the ophthalmic artery which
springs from the internal carotid artery
Vascular Supply
The internalnose receives blood from the territories of the externaland internal carotid arteries- the terminalbranches of the sphenopalatine artery which arisesfrom the maxillary artery - the anterior and posteriorethmoid arteries which arise from the ophthalmicartery-internal carotid arterie
venous drainage
The venous drainageof the facial region is handled by -the facial vein -retromandibular vein -internal jugular vein
lymphatic drainage
The regional lymphatic drainage of the face and externalnose is handled mainly by- the submandibularlymph nodes while the nasal cavity is additionallydrained by -the retropharyngeal and deep - -cervical lymph nodes
Morphology of the Nasal Mucosa
Besides the anatomical structure of the external noseand nasal cavity the nasal mucosa plays an essentialrole in numerous functions of the nose in the respiratory tract
Morphology of the Nasal Mucosa
The anterior part of the nasal cavity (the nasal vestibule)like the external nose is covered by skin composedof a multilayer keratinizing squamous epithelium and finally a ciliated respiratory epithelium A small areaon the upper nasal septum superior turbinate andpart of the middle turbinate located adjacent to thecribriform plate is covered by olfactory mucosa and iscalled the olfactory region
Nerve SupplyThe facial skin receives its sensory innervation fromterminal branches of the trigeminal nerve that enterthe facial region through the supraorbital infraorbitaland mental foramina Thefacial muscles are classified as mimetic or mastica- tory each of these groups receiving different motorinnervationbythe facial nerve
History and Clinical Examination of the Nose
Historybull The main symptomsbull nasal obstruction (ldquostuffy
noserdquo)bull nasal dischargebull Headachesbull Olfactory
dysfunction
Palpationbony discontinuitiesNeuralgias to check
over- the supraorbital -infraorbital -mental foramina
Anterior Rhinoscopy
bull The rhinologic examination itself begins with anterior
bull rhinoscopy to evaluate the nasal vestibule and the anterior
bull portions of the nasal cavity
Nasal Endoscopy Nasal endoscopy has become the most important andrewarding clinical examination method in rhinologic diagnosis
- rigid endoscopes which are available in 4-mm and 28- mm diameters and assorted viewing angles (eg 01048576 301048576 1201048576) -flexible endoscopes are also available for inspecting the nose and nasopharynx and exploring all of the pharynx and larynx in one sitting
Nasal endoscopy
Nasal Endoscopy
Nasal Endoscopy
Imaging of the Nose and Paranasal Sinuses
Conventional RadiographsStandard paranasal sinus radiographs in the occipitomental
projection ( Water projection) and
occipitofrontal projection Caldwell projection) in cases of acute inflammation
They are also obtained to evaluate midfacial fractures
Computed Tomography (CT) the main indicationsfor CT scanning of the
nose and paranasal sinuses
are- chronic sinusitis - -trauma (especially
frontobasal -fractures)
-and tumors
The occipitofrontal projection is better for evaluating theethmoid cells and frontal sinus
occipitomental projection demonstrates the maxillarysinus and gives a limited view of the sphenoid sinus
Computed tomography of the paranasal sinuses
Four representative coronal CT scans are shown
Four representative coronal CT scans are shown
Magnetic Resonance Imaging
Magnetic maging
Magnetic resonance imaging (MRI) has fewer indicationsthan CT in patients with paranasal sinus diseaseThis is primarily because MRI is markedly inferior toCT in defining the bony boundaries of the sinusesThe strength of MRI lies in its superior soft-tissue discriminationMRI is indicated in diseases that involve the paranasal sinuses in addition to thecranial cavity or orbit (eg tumors and congenitalmalformations such as encephaloceles)
MRI of the paranasal sinuses
The Nose and Sinuses
Structure The structure of the nose is made up of
four partsbull The surface anatomybull The nasal skeletonmdashcomposed of the
two nasal bones the paired upper lateral and lower lateral cartilages and the nasal septum covered in subcutaneous tissue and skin
bull The internal anatomymdashincludes the septum of the nose which forms the medial wall of the nasal cavity The turbinates on the lateral wall are also called conchae
bull The osteomeatal complexmdasha key functional area of the nose
Function The nose is the main route for inspired
air and its structure is related to this function As the air passes over the large surface area of the turbinates
The inspired gases are warmed and humidified Mucus on the mucosa of the nose removes large dust particles from the air as it is breathed in
The voice resonates in the sinuses and nose and this provides character to the speech
Pneumatization of the sinusesmdashthey are air filled spacesmdashreduces the weight of the skull
Diseases of thDiseases of the Outer and Inner Nosee Outer and
Inner Nose Erysipelas Definition of the disease ndash Erysipela is a skin infection that affects the superficial dermis and is caused by Streptococcus pyogenes (group A) It usually develops in the extremities and the face and less commonly on the scalp and genitals bull Epidemiologyaetiology ndash Erysipelas are more often seen in elderly infants and children patients with compromised immunology and diabetes -Predisposing factors are alcoholism skin ulceration puncture wounds fungal infections malnutrition and burns
Erysipelas
bull Symptomsbull ndash It usually presents of fever general fatigue bull -The skin lesion is a redindurated and elevated plaque
with borders that expand rapidly bull It is painful warm and accompanied by variable oedemabull -On the second or third day a flaccid bulla may develop
and desquamationbull bull Presence of regional lymph nodes is common
Erysipelas
bull Complicationsndash The most common complication is recurrencewhich is seen in 18ndash30 of the cases even afterproper antibiotic therapy Recurrence is seen moreoften in females than in malesA skin infection with S pyogenes could lead toglomerulonephritis
Erysipelas
bull Complicationsbull ndash The most common complication is recurrencebull which is seen in 18ndash30 of the cases even afterbull proper antibiotic therapy bull -Recurrence is seen morebull often in females than in males bull -A skin infection with S pyogenes could lead tobull glomerulonephritis
Erysipelas
bull bull Diagnosisbull ndash Diagnosis is based on the patientrsquos personal
historybull and physical examination particularly on inspectionbull of the skin
bull Blood cultures are positive in less thanbull 5 of cases
ErysipelasTherapyndash Conservative therapybull The preferred antibiotic is penicillin In mildcases with minor systemic symptoms penicillinV 500 mg orally every 6 h for 10 days or penicillinG benzathine 12 mil U intramuscularlyonceOther possibilities are amoxicillin 500 mgorally twice a day for 10 days or cephalexin 500mg orally every 6 h for 10 days
ErysipelasIn moderate and severe cases with significantsystemic symptoms hospitalization and intravenoustreatment is required penicillin G 2ndash4mil U intravenously every 4ndash6 h Cefazolin05ndash15 gm intravenously every 8 h cefotaxime1ndash2 gm intravenously every 8 h or ceftriaxone1ndash2 gm intravenously once a day should be administeredIn patients with a penicillin allergyclindamycin 600 mg intravenously every 8 h orvancomycin 15 mgkg intravenously twice a daymay be given
ErysipelaAdditional useful therapeutic optionsbull Prednisone 30 mg over 8 days might be consideredas well as elevation of the affected siteMoist heat compresses may be usefulbull Surgeryndash Debridement and drainage are indicated when bullaeabscesses or necroses are presentbull Differential diagnosisndash Contact dermatitisndash Asteatotic eczemandash Herpes zosterndash Angioneurotic oedemandash Osteomyelitis
Furuncle
bull Definition of the diseasebull ndash A furuncle is an infection that beginsbull at the hair follicle and spreads deeper into thebull dermis and subcutaneous tissue forming abull nodule After several days it developsbull into an abscess - red painful and fluctuantbull bull bull Epidemiologyaetiologybull ndash The aetiologic agent is Staphylococcus aureus
FuruncleSymptomsndashsymptoms are local and limited to thesite of infection Furuncles usually are wherehair follicles are present bull Complicationndash One complication is furunculosis multiple draining furunclesDiagnosisndash The diagnosis is based on clinical inspection - Cultures are not necessary when there is no systemic involvement but should beconsidered if systemic therapy (in case of feversignificant cellulitis or hospitalization) or whenmethicillin-resistant Staphylococcusaureus (MRSA) is considered
FuruncleTherapyndash When the furuncle is small application of moist heat compress to promote drainage -Larger furuncles should be drained by surgical incision-After drainage the area should be cleaned with anantiseptic (with chlorhexidinebetadine) should be applied twice
a dayndash If no systemic symptoms or extensive cellulitis arepresent simple topical care is usually curative andoral antibiotics are not necessary Otherwise systemictreatment is indicated and should cover anypossible MRSA
Furuncle
bull -Recommended antibiotics are trimethoprim-sulfamethoxazole
bull 1ndash2 tablets orally twice daily doxycyclinebull 100 mg orally twice dailybull or clindamycin 300ndash450 mg orally every 8 hbull - In severe cases vancomycin 15 mgkg
intravenouslybull every 12 h or clindamycin 600 mg intravenouslybull every 8 h
Midline Granulomabull A midline granuloma is an angiocentricbull lymphoma it was referred to as polymorphicbull reticulosis lethal midline granuloma and midline
malignant reticulosisbull bull Definition of the diseasebull ndash This rare disease is a lymphoma of extranodal
presentationall cases are positive for the Epstein-Barr virus
bull -This lymphoma most commonly appears in the midface region
Midline GranulomaEpidemiologyaetiologyndash This form of lymphoma is rare in Europe and theUnited States with a higher prevalence in Asia and PeruSymptomsndash The most common presentation is nasal obstruction with a destructive mass occupying the nosesinuses and palate
-Fever night sweatsand weight loss seen usually in Hodgkinrsquos lymphomaand other non-Hodgkinrsquos lymphomas (knownas ldquoB symptomsrdquo) are uncommon
Midline GranulomaDiagnosisndash The diagnosis is based on anatomopathologicalstudy The malignancy of the tumour manifested byextensive necrosis makes the histological diagnosisdifficult and often more biopsies are required forconfirmationbull Therapyndash Therapy consists of radiotherapy with or withoutchemotherapy
Midline Granuloma
bull Prognosisbull ndash Depending on the stage long-term remission or
experience a worseningbull prognosis with relapses which may include otherbull extranodal sites bull Involvement of extranodal sitesbull including the upper airway gastrointestinal tractbull skin
Wegenerrsquos Granulomatosis
bull Definition of the diseasebull ndash Wegenerrsquos granulomatosis is a systemic chronicbull vasculitis of small- and medium-sized blood vesselsbull with an autoimmune component It affectsbull particular organs with variable predilectionbull Epidemiologyaetiologybull ndash Wegenerrsquos granulomatosis is a rare disease It affects
about 1 in 20000ndash30000 people It is more prevalentbull in middle-aged Caucasian patients
Wegenerrsquos Granulomatosis
Symptomsndash The disease may present pulmonary upper
respiratory tract or renal In the disseminated form-The localised form ndash confinedto the upper respiratory region ndash is present in 25of the patients- It consists of nonspecific manifestationssuch as nasal obstruction crusting purulentor bloody rhinorrhea and painful or painless ulcers in oral or nasal cavities which are unresponsive tostandard medical treatment
Wegenerrsquos Granulomatosis
bull In some patients the nasal septum is perforatedbull which leads to saddle-nose deformity Less
commonbull symptoms are hoarseness stridor due to
subglotticbull stenosis otalgia otorrhea and conductivebull and sensorineural hearing loss Also ocular
symptomsbull such as scleritis conjunctivitis uveitis andbull episcleritis may be present
Wegenerrsquos Granulomatosis
bull ndash In the disseminated form pulmonary involvementbull is manifested by cough dyspnoea haemoptysisbull (due to an alveolar capillaritis necrotic lesions orbull endobronchial disease) and pleuritic painndashbull -Ninety per cent of patients have nasal symptomsbull and these symptoms are usually the first
manifestationof the diseasebull -Most patients have also renal involvementbull even if it is subclinical
Wegenerrsquos Granulomatosis
Diagnosis ndash Diagnosis of Wegenerrsquos granulomatosis is based on clinical findings that demonstrate lung (chest x-ray) kidney (urine analysis) or upper respiratory tract
involvement (oral or nasal ulcers or discharge) - positive blood analysis for cytoplasmic-staining antineutrophil
cytoplasmic antibodies (c-ANCA) and confirming proteinase 3 (PR3) ANCA or myeloperoxidase (MPO) ANCA ndash Biopsy is essential for diagnosis nonspecific chronic inflammation
and necrosis -Bacterial and fungal infections
Wegenerrsquos Granulomatosis
Therapyndash Conservative therapybull In the induction of disease remission highdosesteroids (e g prednisone 1 mgkgday) for1 month with tapering over several months aregiven In addition cyclophosphamide (2 mgkgday) should be administered for 6ndash12 monthsuntil symptoms disappear In the maintenanceof remission cyclophosphamide should be
Wegenerrsquos Granulomatosis
Antibiotics mainly trimethoprim-sulfamethoxazoleare given for prophylaxis againstPneumocystis jiroveci (formerly Pneumocystiscarinii) pneumonia (PCP) which may developduring immunosuppression and have a role inpreventing recurrencesbull Sinonasal manifestations may be treated with topical nasal steroids and nasal irrigations lowdosesystemic steroids and antibiotics when bacterial infection (typically Staphylococcus species) is suspected
Wegenerrsquos Granulomatosis
bull Prognosisbull ndash Most of the patients respond well to treatmentbull achieving symptom-free intervals of 5ndash20 yearsbull or more bull -Anatomical problems (sinusitis trachealbull stenosis) may require surgery bull Relapses can be long and troublesomebull Long-term complications are chronicbull renal failure hearing loss and deafness
Nasal Fractures Definition ndash A nasal fracture is a disruption of the nasal bone structure due to trauma It is the most frequently fractured facial bone Epidemiologyaetiology ndash Sports falls and assaults are the usual mechanisms of fracture -Males are affected twice as often as are females -Paediatric populations with a incidences during the second and third decades of life -Variables such as force impact direction nature of the striking object age and other will influence the pattern of injury to the components of the nose
Nasal Fractures
bull Symptomsbull ndash Deformity swelling epistaxis and periorbital
ecchymosis are signs that are suggestive of nasal fracture
bull bony crepitus and nasal segment mobilitybull ndash Epiphora bull Severe bilateral injuries to the lachrymal bones
arebull associated with depressed nasal fractures
Nasal Fractures Complications ndash Septal haematoma is one of the most severe early complications of nasal trauma and without drainage it results in abscess formation 6ndash7 days after trauma producing necrosis of the septal cartilage -Long-term problems such as saddle-nose deformity perforation columellar retraction and nasalbase
Septal infection could lead to osteomyelitis orbital and intracranial abscesses meningitis and cavernous sinus thrombosis -Cerebrospinal fluid leakage is a common complication of severe
nasal and frontal fractures
Nasal Fractures
bull Diagnostic proceduresbull ndash Inspectionbull bull Changes of appearance such as deviation andbull asymmetry bleeding watery drainage changesbull in nasal breathing and smell It is useful to comparebull the current presentation with old photographsbull (up to 40 of normal individuals havebull significant nose malformations)
Nasal Fractures Physical examination bull The diagnosis of a nasal fracture is made primarily by physical examination epistaxis nasal swelling and periorbital ecchymosis Nasal shape in the lateral and frontal inspection should be assessed Grasping the dorsum between two fingers and rocking the pyramid back and forth aids in assessing the mobility of nasal bones Internal structures should be evaluated by using a headlight and nasal speculum Clotted blood is removed by suction and assessment of haematoma mucosal tears and active bleeding is performed Bimanual palpation of the septum helps to differentiate septal swelling from haematoma ndash
Nasal FracturesRadiographybull There is no clear evidence of the role of radiographyin the management of nasal fracturesPlain films have up to a 66 false-positive rateas a result of misinterpretation of normal suturelines In addition old fractures are difficult todistinguishbull Three-dimensional CT is recommended for extensiveinjuries involving the nasal-orbital-ethmoidalcomplexndash
Nasal Fractures
bull Additionaluseful diagnostic proceduresbull bull Using a 0 or 30deg 4-mm endoscope is helpful inbull the assessment of posterior abnormalities If thebull patient is heavily sedated Brown-Gruss
provocationbull manoeuvres may be performed to determinebull deformities in upper middle or lower segmentsbull by compressing each compartment
Nasal FracturesConservative treatmentndash Treatment of bleedingbull For localised bleeding anterior sources may becauterised by silver nitrate or sealed with topicalmaterials such as thrombin combined withgelatin foam fibrin glue FloSealreg or other procoagulantmaterials If conservative measuresfail a formal anterior packing is placedbull Bleeding from branches of sphenopalatine orethmoid vessels requires anterior-posteriorpacking
Nasal Fractures
bull bull Surgical methods such as direct endoscopic vessel
bull cauterization or ligation have been shown tobull offer better haemostasis and patient comfortbull Angiography with embolization can also be
consideredbull in cases refractory to more conservativebull approaches
Nasal Fractures
bull Type of reductionbull bull Nondisplaced fractures should be treated withbull observation alone Closed nasal reduction is thebull best choice for simple injuries (isolated unilateralbull with medial displacement)bull bull An open approach should be considered in
severebull trauma (bilateral depressed fractures)
Nasal Fracturesbull Surgical principlesbull ndash Topical anaesthesia with cotton pledgets soakedbull with 4 cocaine or 005 oxymethazoline combinedbull with 4 topical lidocaine should be appliedbull for 5ndash10 min Local anaesthesia should also be injectedbull (1 lidocaine and 1100000 epinephrine)bull along the septum lateral walls and floor of the nasalbull cavitybull bull
Nasal FracturesClosed reductionndashndash The nasal bones are grasped between two fingersand pressure is applied laterally in theopposite direction of the deviation A bluntelevator may be used from within the nose incases of significant medial collapse Walshamforceps can be of help Reduction of the septumshould be performed with the use ofAsch forceps
Nasal Fractures
bull To prevent collapse of the postreductionbull framework nasal packing should be placedbull for 3ndash5 days Septum splints are recommendedbull in comminuted septal fractures withbull severe mucosal lesions External nasal splintingbull for 10 days (Aquaplastreg Thermoplastreg)bull provides nasal protection Nasal saline spraysbull prevent crusting and oral antibiotics should
Nasal Fractures
bull Open reductionbull ndashndash Immediate repair of fractures by using
widebull surgical exposure reduction fixation and
reconstructionbull ndashndash The second option is delayed correctionbull (6 months or more) of persistent deformitiesbull using standard techniques of rhinoplasty
Deviated Nasal Septum
bull Definition of the diseasebull ndash Deviation of the nasal septum is a common causebull of unilateral nasal airway obstruction in which thebull nasal septum is displacedbull bull Epidemiologyaetiologybull ndash Developmental septal abnormalities Septal cartilage
damage in the neonatal period andbull during birth can cause severe septal deviation inbull the absence of a history of nasal trauma
Deviated Nasal Septum
bull Symptomsbull ndash Patients may present with a history of sinusitis
allergicbull rhinitis obstructive sleep apnoea previousbull nasal surgery or recent nasal trauma Unilateral or
bilateral nasal airway obstruction that is unrelievedbull with decongestants or nasal steroid sprays is oftenbull seenbull bull
Deviated Nasal SeptumDiagnosisndashExamination external dorsal deviation or the columella and caudal septummay be deflected off the midline (caudal subluxation)ndash Inspections of the nasal cavity and anterior-posteriorrhinoscopy are helpful in diagnosing the locationtype and severity of septal deformityThe endoscope is also useful in identifying polypsthe severity and extent of posterior septaldeviations and bony spurs and locating areas ofseptal perforation or mucosal injury
Deviated Nasal Septum
bull Therapybull ndash Septoplasty is a procedurebull The areabull of deviation is corrected or resected in order tobull leave behind as much cartilage and bone as
possiblebull Cartilage resection is minimised and can be
repositioned reshaped or recontoured using a variety of methods
Deviated Nasal Septum
bull ndash Indications of septoplasty before the growth period
bull of the nose is finished should be very limited bull -In these cases surgery must preserve all the
cartilagebull in order to prevent external changes of the
shape ofbull the nose
Deviated Nasal Septum
bull Complicationsbull ndash Frequent complications include haematoma andbull infection Cerebrospinal fluid leak is a rare but
potentiallybull serious complicationbull It is usually the resultbull of avulsion or damage to the cribriform plate whenbull handling the perpendicular plate of the ethmoidbull ndash Other complications include epistaxis nasal
Deviated Nasal Septum
bull Other complications include epistaxis nasal obstruction
bull due to residual deviation synechiae returnbull of the cartilaginous deviation septal perforationbull anosmia and cosmetic nasal deformities suchbull as widened alar rim margins drooping nasal tipbull columella retraction and a sunken dorsum with abull supratip saddle formation
Septal perforation with minor crusting View from provide closure of the
incision
Septal Haematoma
bull A septal haematoma is a blood collection under the perichondrium
bull of the septum and cartilagebull bull bull Epidemiologyaetiologybull ndash A septal haematoma is one of the most
severe complications of nasal trauma
Septal Haematoma
bull Diagnosisbull ndash Signs and symptoms include intense pain
swellingbull haematoma of the upper lip and philtrum
area andbull complete nasal airway obstruction
Septal HaematomaTherapyndash Management consists of drainage through a mucoperichondrial incision Immediate treatment isnecessary to prevent long-term problems such asa saddle-nose deformity perforation columellarretraction and nasal-base widening In childrenseptal destruction can lead to devastating nasal andmidfacial growth abnormalitiesbull Surgeryndash Incision and evacuation of the collection is performedDrainage of a septal haematoma should
Septal HaematomaSurgeryndash Incision and evacuation of the collection is performedDrainage of a septal haematoma should provide closure of the incision
Splints or transseptal sutures are placed to obliterate thepotential space and prevent collectionInfection involving the septal cartilage Reconstruction with autologouscartilage is then performed in a second stage Oral antibiotics should be given
Nasal DeformitySaddle-nose deformityndash A saddle-nose deformity is characterised by a loss ofnasal dorsal height and compromised nasal supportstructures -Other case observed are depressionof the middle vault and dorsum loss of nasal tipsupport and definition shortened (vertical) nasal length over rotation of the nasal tip and retrusion ofthe nasal spine and caudal septum It is also knownas a ldquoPug noserdquo or ldquoboxerrsquos noserdquo both of which referto various degrees of nasal dorsal depressionbull
Nasal DeformityEpidemiologyaetiologyndash Prevalence is higher in population groups prone to facial trauma (ie boxers athletes) those with historiesof intranasal cocaine use nasal surgery (e g radical submucosal septal resection reductive rhinoplasty)ndash A saddle-nose deformity can be congenital or acquired It can be noticed as a part of individual familialsyndromic and ethnic characteristics - Most deformities are due to traumatic and iatrogeniccauses Medical causes are Wegenerrsquosgranulomatosis relapsing polychondritis leprosy (Hansenrsquos disease) syphilis ectodermal dysplasiaand intranasal cocaine use
Nasal Deformity
bull Therapybull ndash Nasal reconstruction indications depend on patientbull selection surgeon experience and aetiology of thebull deformity bull Indications for surgery can be functionalbull aesthetic or most commonly both In individuals
with a compromised nasal airway a nasoseptalbull reconstruction is indicated
Nasal Deformity
bull Contraindications bull include patients with malignantbull chronic or autoimmune disease conditions drugbull abuse poor perioperative risk profile and unrealisticbull expectationsbull ndash Multiple previous rhinoplasties and certain
professionsbull (mixed martial artists boxers and other contactbull sports) are relative contraindications
Nasal DeformitySeptoplastyndash Septoplasty is performed to correct nasal obstructioncaused by septal deformityndash Usually septoplasty is performed under general anaesthesiawith the patient in the supine position with the head elevated by approximately 30 (Righthandedsurgeons approach from the right side)ndash Local vasoconstrictive anaesthesia is applied notonly to reduce postoperative pain but also more importantly to achieve vasoconstriction of themucosa and less intraoperative haemorrhage Lidocainewith adrenaline or epinephrine is usedalthough in patients with cardiac hypersensitivityoxymetazoline might be preferred
Nasal Deformity
bull Septoplasty begins with the incision of septal mucosabull Most operative techniques utilise a hemitransfixionbull incision at the caudal end of septum so thatbull deviation at this point might be reached as wellbull as a transfixion incision that is easily obtained ifbull needed (Right-handed surgeons normally choosebull the left side but that may vary when deviation isbull convex towards the right)
Nasal DeformityA columella retractor is placed over the columellaand by pulling it laterally the caudal border of theseptum is exposed Ala can be protected by an alaprotector A vertical incision with a no 15 bladeover the caudal end of septum is performed untilreaching the plane of the septal cartilage It is essentialto correctly identify the perichondrium and byusing the Cottle elevator dissect and lift it creatinga flap As the dissection proceeds along the septalcartilage a longer speculum (no 5) is introduced sothat elevation of the mucoperichondrium is doneunder constant visual controlndash The next step is to dissect the mucoperiostium
Nasal DeformityDissecting over the bony-cartilaginous junctionwhen joining both tunnels might be difficult and is
especially prone to membrane perforationndash If needed the same tunnels are to be created on the
other side of the septum Then deviated parts of
septum are identified and removed either with a
knife or a Freer chisel
Nasal Deformitybull septum from the maxillary crest the septum mustbull be separated from the perpendicular plate trimmedbull along the inferior border placed back onto the crestbull and sutured to the periosteum If the deformity involvesbull the vomer an osteotome is used Care mustbull be taken not to break the cribriform plate becausebull it could cause a cerebrospinal fistula
Nasal Deformity
bull Once the septal deviation is corrected the flapsbull and hemitransfixion incision are mattressed
withbull absorbable sutures Nasal packing to prevent
synechiaebull and postoperative septal haematoma mightbull be advised but should be removed within 72 h

Nosebull Anatomy and physiology of the nosebull Symptoms and signs of common sinonasal disease eg
rhinitis sinusitis nasal polypsbull Examination of the nose including an assessment of the
appearance the septum the turbinates and the mucosabull The endoscopic evaluation of the nosebull Management of a fractured nose and the timing of
interventionbull Management of epistaxis from minor nosebleeds to
torrential haemorrhagebull The principles of common nasal operations including septal
surgery functional endoscopic sinus surgery and rhinoplasty
Head and neckmdashbenign and malignant disease
bull The basic anatomy and physiology of the oral cavity salivary glands pharynx larynx oesophagus and lymph node drainage
bull The presentation of head and neck cancerbull The presentation and management of salivary gland diseasebull Examining the oral cavity larynx and pharynx including the use of the nasendoscopebull Examining the neck with reference to the lymph nodesbull The role of fine needle aspiration cytology (FNAC)bull The principles and limitations of radiological investigation of the head and neck regionbull Management of neck lumps in particular the malignant lymph node with an unknown
primarybull The management of the airway in patients with a tracheostomy or end tracheostomy after
laryngectomybull A basic knowledge of the principles of operative surgery in particular the principles of
reconstructive surgery and the surgery for salivary gland disease eg parotidectomybull The postoperative management of a patient who has undergone major head and neck surgerybull The role of the multidisciplinary team in head and neck cancer and voice disorders
Supplementary knowledgebull The role of otoacoustic emissions and evoked auditory potentials in managing
hearing lossbull The use of speech audiometrybull The surgery for otosclerosisbull Bone-anchored hearing aids for conductive hearing lossbull Cochlear implantation and the reactions of the deaf community to this
interventionbull The use of sign languagebull Neuro-otology in particular the presentation and management of acoustic
neuromasbull Craniofacial surgery and the interplay between ENT plastic surgery and
neurosurgerybull The management of cleft palate and the increased risk of glue earbull Advanced endoscopic sinus surgery for the mangement of sinonasal malignancy
pituitary tumours and skull base tumoursbull Microlaryngeal surgery and surgical voice restorationbull The use of chemotherapy and radiotherapy in head and neck malignancy
Working in ENT
bull Working in ENT should be a very enjoyable experience whether it is a temporary attachment or a long-term career plan
bull It is helpful if you have an understanding of what others expect of you
bull It is also important for you to think about your own career development
Your duties
bull Patient care and continuitybull Professional developmentbull Research
The ENT Examination
EquipmentA fully equipped ENT department will have all the necessary instruments for performing a full ENT examination
Basic equipment
bull A light sourcemdasha portable headlight that runs off batteries is ideal
bull Wooden tongue depressorsbull Thudicum nasal speculumbull An otoscope with several speculaebull Pneumatic attachment for the otoscopebull Tuning fork 512Hzbull Pen and paperbull Gloves
Advanced equipment
bull Co-phenylcaine spraybull A flexible nasendoscope with light sourcebull Alcohol wipe to act as demist for the scopebull Aqueous lubricating gel for the scope
Emergency equipment
bull Large nasal tampons (you can always cut 10cm ones to size)
bull Silver nitrate sticksbull Foley catheters
Basic Anatomy of the Nose
bull The structural anatomy of the nose is important
bull for both aesthetic and functional reasons since the
bull nose as the gateway to the respiratory tract performs
bull a variety of physiologic functions
External NoseThe shape of the external nose is defined by the nasalbones a pair of rectangular bones in the upper nasaldorsum and by lateral cartilages (uppernasal cartilages) and alar cartilages (major alar cartilages)in the central and lower portions of the noseThe lateral portions of the nasal alae alsocontain several small accessory cartilages called theminor alar cartilages which are embedded in the lateralsoft tissues of the noseThe shape and stability of the alar cartilages each ofwhich consists of a medial and lateral crus
External Nose
Anatomy of the nasal base
bull Besides thebull medial crura the
inferior septal margin and the connective-
bull tissue septum (columella) are also responsible
bull for stabilizing the base of the nose
Anatomy of the nasal base
Anatomy of the nasal base
bull The nasal septum is subluxed toward the left side partially
bull obstructing the nasal airway
Nasal CavitiesThe nasal cavities begin anteriorly at the nasal vestibulewhich is bordered posteriorly by the internal nasalvalve (limen nasi) located between the posteriorborder of the alar cartilage and the anterior border ofthe lateral cartilage This valve area is the narrowestportion of the upper respiratory tract
Nasal Cavities
The interior ofthe nose behind the nasal valve is divided by the nasalseptum into two main cavities
Nasal CavitiesThe nasal septum iscomposed of an anterior cartilaginous part and twoposterior bony parts Abnormalities in the shape ofthe nasal septum which may consist of a deviated septum tensionseptum spurs or ridges are a frequent cause ofnasal airway obstructionThe choanae are the paired posterior openingsthrough which the nasal cavities communicate withthe nasopharynx
Nasal CavitiesThe nasal cavity is bounded laterally by the lateral nasalwalls which are formed by the ethmoid bone andmaxilla and posteriorly by the palatine bone and thepterygoid process of the sphenoid bone Several functionallyimportant structures are located on the lateralnasal wall the nasal turbinates and their associatedpassages (meati) sinus ostia and the orifice ofthe nasolacrimal duct (Fig 15)
The inferior turbinate consists of a separate bone thatis attached to the medial wall of the maxillary sinusThe opening of the nasolacrimal duct is located in thecorresponding inferior meatus The middle andsuperior turbinates are part of the ethmoid bone In rare cases a rudimentary ldquosupreme turbinaterdquo is alsopresent above the superior turbinate
The middle turbinate has by far the greatest functionalimportance because most of the drainage tracts fromthe surrounding paranasal sinuses open into the middlemeatus The nasal cavity is bounded superiorly by the cribriformplate of the ethmoid bone This thin bony platehas numerous openings for the passage of the fila olfactoriaand also forms the boundary of the anteriorcranial fossa
Nasal Cavities
The floor of the nasal cavity is formedmostly by the hard palate which is formed in turn bythe two palatine processes of the maxilla and the horizontallaminae of the palatine bone
Structure of the lateral nasal wall
Inferior meatus
Paranasal Sinuses
The paranasal sinuses are air-filled cavities that communicatewith the nasal cavities
-The maxillary sinus frontalsinus and anterior ethmoid cells drain into the nasalcavity through the middle meatusmdashie below themiddle turbinate -The posterior ethmoidcells drain into the nasal cavity through the superiormeatus The ostium of the sphenoid sinus is locatedin the anterior wall directly above the choanae- The anatomical connections between the nasal cavity andparanasal sinuses are functionally important and playa key role in the pathogenesis of many rhinologic diseasesthat involve the paranasal sinuses
Vascular SupplyThe external nose derives most of its blood supply
from the facial artery which arises from the external
carotid artery and from the ophthalmic artery which
springs from the internal carotid artery
Vascular Supply
The internalnose receives blood from the territories of the externaland internal carotid arteries- the terminalbranches of the sphenopalatine artery which arisesfrom the maxillary artery - the anterior and posteriorethmoid arteries which arise from the ophthalmicartery-internal carotid arterie
venous drainage
The venous drainageof the facial region is handled by -the facial vein -retromandibular vein -internal jugular vein
lymphatic drainage
The regional lymphatic drainage of the face and externalnose is handled mainly by- the submandibularlymph nodes while the nasal cavity is additionallydrained by -the retropharyngeal and deep - -cervical lymph nodes
Morphology of the Nasal Mucosa
Besides the anatomical structure of the external noseand nasal cavity the nasal mucosa plays an essentialrole in numerous functions of the nose in the respiratory tract
Morphology of the Nasal Mucosa
The anterior part of the nasal cavity (the nasal vestibule)like the external nose is covered by skin composedof a multilayer keratinizing squamous epithelium and finally a ciliated respiratory epithelium A small areaon the upper nasal septum superior turbinate andpart of the middle turbinate located adjacent to thecribriform plate is covered by olfactory mucosa and iscalled the olfactory region
Nerve SupplyThe facial skin receives its sensory innervation fromterminal branches of the trigeminal nerve that enterthe facial region through the supraorbital infraorbitaland mental foramina Thefacial muscles are classified as mimetic or mastica- tory each of these groups receiving different motorinnervationbythe facial nerve
History and Clinical Examination of the Nose
Historybull The main symptomsbull nasal obstruction (ldquostuffy
noserdquo)bull nasal dischargebull Headachesbull Olfactory
dysfunction
Palpationbony discontinuitiesNeuralgias to check
over- the supraorbital -infraorbital -mental foramina
Anterior Rhinoscopy
bull The rhinologic examination itself begins with anterior
bull rhinoscopy to evaluate the nasal vestibule and the anterior
bull portions of the nasal cavity
Nasal Endoscopy Nasal endoscopy has become the most important andrewarding clinical examination method in rhinologic diagnosis
- rigid endoscopes which are available in 4-mm and 28- mm diameters and assorted viewing angles (eg 01048576 301048576 1201048576) -flexible endoscopes are also available for inspecting the nose and nasopharynx and exploring all of the pharynx and larynx in one sitting
Nasal endoscopy
Nasal Endoscopy
Nasal Endoscopy
Imaging of the Nose and Paranasal Sinuses
Conventional RadiographsStandard paranasal sinus radiographs in the occipitomental
projection ( Water projection) and
occipitofrontal projection Caldwell projection) in cases of acute inflammation
They are also obtained to evaluate midfacial fractures
Computed Tomography (CT) the main indicationsfor CT scanning of the
nose and paranasal sinuses
are- chronic sinusitis - -trauma (especially
frontobasal -fractures)
-and tumors
The occipitofrontal projection is better for evaluating theethmoid cells and frontal sinus
occipitomental projection demonstrates the maxillarysinus and gives a limited view of the sphenoid sinus
Computed tomography of the paranasal sinuses
Four representative coronal CT scans are shown
Four representative coronal CT scans are shown
Magnetic Resonance Imaging
Magnetic maging
Magnetic resonance imaging (MRI) has fewer indicationsthan CT in patients with paranasal sinus diseaseThis is primarily because MRI is markedly inferior toCT in defining the bony boundaries of the sinusesThe strength of MRI lies in its superior soft-tissue discriminationMRI is indicated in diseases that involve the paranasal sinuses in addition to thecranial cavity or orbit (eg tumors and congenitalmalformations such as encephaloceles)
MRI of the paranasal sinuses
The Nose and Sinuses
Structure The structure of the nose is made up of
four partsbull The surface anatomybull The nasal skeletonmdashcomposed of the
two nasal bones the paired upper lateral and lower lateral cartilages and the nasal septum covered in subcutaneous tissue and skin
bull The internal anatomymdashincludes the septum of the nose which forms the medial wall of the nasal cavity The turbinates on the lateral wall are also called conchae
bull The osteomeatal complexmdasha key functional area of the nose
Function The nose is the main route for inspired
air and its structure is related to this function As the air passes over the large surface area of the turbinates
The inspired gases are warmed and humidified Mucus on the mucosa of the nose removes large dust particles from the air as it is breathed in
The voice resonates in the sinuses and nose and this provides character to the speech
Pneumatization of the sinusesmdashthey are air filled spacesmdashreduces the weight of the skull
Diseases of thDiseases of the Outer and Inner Nosee Outer and
Inner Nose Erysipelas Definition of the disease ndash Erysipela is a skin infection that affects the superficial dermis and is caused by Streptococcus pyogenes (group A) It usually develops in the extremities and the face and less commonly on the scalp and genitals bull Epidemiologyaetiology ndash Erysipelas are more often seen in elderly infants and children patients with compromised immunology and diabetes -Predisposing factors are alcoholism skin ulceration puncture wounds fungal infections malnutrition and burns
Erysipelas
bull Symptomsbull ndash It usually presents of fever general fatigue bull -The skin lesion is a redindurated and elevated plaque
with borders that expand rapidly bull It is painful warm and accompanied by variable oedemabull -On the second or third day a flaccid bulla may develop
and desquamationbull bull Presence of regional lymph nodes is common
Erysipelas
bull Complicationsndash The most common complication is recurrencewhich is seen in 18ndash30 of the cases even afterproper antibiotic therapy Recurrence is seen moreoften in females than in malesA skin infection with S pyogenes could lead toglomerulonephritis
Erysipelas
bull Complicationsbull ndash The most common complication is recurrencebull which is seen in 18ndash30 of the cases even afterbull proper antibiotic therapy bull -Recurrence is seen morebull often in females than in males bull -A skin infection with S pyogenes could lead tobull glomerulonephritis
Erysipelas
bull bull Diagnosisbull ndash Diagnosis is based on the patientrsquos personal
historybull and physical examination particularly on inspectionbull of the skin
bull Blood cultures are positive in less thanbull 5 of cases
ErysipelasTherapyndash Conservative therapybull The preferred antibiotic is penicillin In mildcases with minor systemic symptoms penicillinV 500 mg orally every 6 h for 10 days or penicillinG benzathine 12 mil U intramuscularlyonceOther possibilities are amoxicillin 500 mgorally twice a day for 10 days or cephalexin 500mg orally every 6 h for 10 days
ErysipelasIn moderate and severe cases with significantsystemic symptoms hospitalization and intravenoustreatment is required penicillin G 2ndash4mil U intravenously every 4ndash6 h Cefazolin05ndash15 gm intravenously every 8 h cefotaxime1ndash2 gm intravenously every 8 h or ceftriaxone1ndash2 gm intravenously once a day should be administeredIn patients with a penicillin allergyclindamycin 600 mg intravenously every 8 h orvancomycin 15 mgkg intravenously twice a daymay be given
ErysipelaAdditional useful therapeutic optionsbull Prednisone 30 mg over 8 days might be consideredas well as elevation of the affected siteMoist heat compresses may be usefulbull Surgeryndash Debridement and drainage are indicated when bullaeabscesses or necroses are presentbull Differential diagnosisndash Contact dermatitisndash Asteatotic eczemandash Herpes zosterndash Angioneurotic oedemandash Osteomyelitis
Furuncle
bull Definition of the diseasebull ndash A furuncle is an infection that beginsbull at the hair follicle and spreads deeper into thebull dermis and subcutaneous tissue forming abull nodule After several days it developsbull into an abscess - red painful and fluctuantbull bull bull Epidemiologyaetiologybull ndash The aetiologic agent is Staphylococcus aureus
FuruncleSymptomsndashsymptoms are local and limited to thesite of infection Furuncles usually are wherehair follicles are present bull Complicationndash One complication is furunculosis multiple draining furunclesDiagnosisndash The diagnosis is based on clinical inspection - Cultures are not necessary when there is no systemic involvement but should beconsidered if systemic therapy (in case of feversignificant cellulitis or hospitalization) or whenmethicillin-resistant Staphylococcusaureus (MRSA) is considered
FuruncleTherapyndash When the furuncle is small application of moist heat compress to promote drainage -Larger furuncles should be drained by surgical incision-After drainage the area should be cleaned with anantiseptic (with chlorhexidinebetadine) should be applied twice
a dayndash If no systemic symptoms or extensive cellulitis arepresent simple topical care is usually curative andoral antibiotics are not necessary Otherwise systemictreatment is indicated and should cover anypossible MRSA
Furuncle
bull -Recommended antibiotics are trimethoprim-sulfamethoxazole
bull 1ndash2 tablets orally twice daily doxycyclinebull 100 mg orally twice dailybull or clindamycin 300ndash450 mg orally every 8 hbull - In severe cases vancomycin 15 mgkg
intravenouslybull every 12 h or clindamycin 600 mg intravenouslybull every 8 h
Midline Granulomabull A midline granuloma is an angiocentricbull lymphoma it was referred to as polymorphicbull reticulosis lethal midline granuloma and midline
malignant reticulosisbull bull Definition of the diseasebull ndash This rare disease is a lymphoma of extranodal
presentationall cases are positive for the Epstein-Barr virus
bull -This lymphoma most commonly appears in the midface region
Midline GranulomaEpidemiologyaetiologyndash This form of lymphoma is rare in Europe and theUnited States with a higher prevalence in Asia and PeruSymptomsndash The most common presentation is nasal obstruction with a destructive mass occupying the nosesinuses and palate
-Fever night sweatsand weight loss seen usually in Hodgkinrsquos lymphomaand other non-Hodgkinrsquos lymphomas (knownas ldquoB symptomsrdquo) are uncommon
Midline GranulomaDiagnosisndash The diagnosis is based on anatomopathologicalstudy The malignancy of the tumour manifested byextensive necrosis makes the histological diagnosisdifficult and often more biopsies are required forconfirmationbull Therapyndash Therapy consists of radiotherapy with or withoutchemotherapy
Midline Granuloma
bull Prognosisbull ndash Depending on the stage long-term remission or
experience a worseningbull prognosis with relapses which may include otherbull extranodal sites bull Involvement of extranodal sitesbull including the upper airway gastrointestinal tractbull skin
Wegenerrsquos Granulomatosis
bull Definition of the diseasebull ndash Wegenerrsquos granulomatosis is a systemic chronicbull vasculitis of small- and medium-sized blood vesselsbull with an autoimmune component It affectsbull particular organs with variable predilectionbull Epidemiologyaetiologybull ndash Wegenerrsquos granulomatosis is a rare disease It affects
about 1 in 20000ndash30000 people It is more prevalentbull in middle-aged Caucasian patients
Wegenerrsquos Granulomatosis
Symptomsndash The disease may present pulmonary upper
respiratory tract or renal In the disseminated form-The localised form ndash confinedto the upper respiratory region ndash is present in 25of the patients- It consists of nonspecific manifestationssuch as nasal obstruction crusting purulentor bloody rhinorrhea and painful or painless ulcers in oral or nasal cavities which are unresponsive tostandard medical treatment
Wegenerrsquos Granulomatosis
bull In some patients the nasal septum is perforatedbull which leads to saddle-nose deformity Less
commonbull symptoms are hoarseness stridor due to
subglotticbull stenosis otalgia otorrhea and conductivebull and sensorineural hearing loss Also ocular
symptomsbull such as scleritis conjunctivitis uveitis andbull episcleritis may be present
Wegenerrsquos Granulomatosis
bull ndash In the disseminated form pulmonary involvementbull is manifested by cough dyspnoea haemoptysisbull (due to an alveolar capillaritis necrotic lesions orbull endobronchial disease) and pleuritic painndashbull -Ninety per cent of patients have nasal symptomsbull and these symptoms are usually the first
manifestationof the diseasebull -Most patients have also renal involvementbull even if it is subclinical
Wegenerrsquos Granulomatosis
Diagnosis ndash Diagnosis of Wegenerrsquos granulomatosis is based on clinical findings that demonstrate lung (chest x-ray) kidney (urine analysis) or upper respiratory tract
involvement (oral or nasal ulcers or discharge) - positive blood analysis for cytoplasmic-staining antineutrophil
cytoplasmic antibodies (c-ANCA) and confirming proteinase 3 (PR3) ANCA or myeloperoxidase (MPO) ANCA ndash Biopsy is essential for diagnosis nonspecific chronic inflammation
and necrosis -Bacterial and fungal infections
Wegenerrsquos Granulomatosis
Therapyndash Conservative therapybull In the induction of disease remission highdosesteroids (e g prednisone 1 mgkgday) for1 month with tapering over several months aregiven In addition cyclophosphamide (2 mgkgday) should be administered for 6ndash12 monthsuntil symptoms disappear In the maintenanceof remission cyclophosphamide should be
Wegenerrsquos Granulomatosis
Antibiotics mainly trimethoprim-sulfamethoxazoleare given for prophylaxis againstPneumocystis jiroveci (formerly Pneumocystiscarinii) pneumonia (PCP) which may developduring immunosuppression and have a role inpreventing recurrencesbull Sinonasal manifestations may be treated with topical nasal steroids and nasal irrigations lowdosesystemic steroids and antibiotics when bacterial infection (typically Staphylococcus species) is suspected
Wegenerrsquos Granulomatosis
bull Prognosisbull ndash Most of the patients respond well to treatmentbull achieving symptom-free intervals of 5ndash20 yearsbull or more bull -Anatomical problems (sinusitis trachealbull stenosis) may require surgery bull Relapses can be long and troublesomebull Long-term complications are chronicbull renal failure hearing loss and deafness
Nasal Fractures Definition ndash A nasal fracture is a disruption of the nasal bone structure due to trauma It is the most frequently fractured facial bone Epidemiologyaetiology ndash Sports falls and assaults are the usual mechanisms of fracture -Males are affected twice as often as are females -Paediatric populations with a incidences during the second and third decades of life -Variables such as force impact direction nature of the striking object age and other will influence the pattern of injury to the components of the nose
Nasal Fractures
bull Symptomsbull ndash Deformity swelling epistaxis and periorbital
ecchymosis are signs that are suggestive of nasal fracture
bull bony crepitus and nasal segment mobilitybull ndash Epiphora bull Severe bilateral injuries to the lachrymal bones
arebull associated with depressed nasal fractures
Nasal Fractures Complications ndash Septal haematoma is one of the most severe early complications of nasal trauma and without drainage it results in abscess formation 6ndash7 days after trauma producing necrosis of the septal cartilage -Long-term problems such as saddle-nose deformity perforation columellar retraction and nasalbase
Septal infection could lead to osteomyelitis orbital and intracranial abscesses meningitis and cavernous sinus thrombosis -Cerebrospinal fluid leakage is a common complication of severe
nasal and frontal fractures
Nasal Fractures
bull Diagnostic proceduresbull ndash Inspectionbull bull Changes of appearance such as deviation andbull asymmetry bleeding watery drainage changesbull in nasal breathing and smell It is useful to comparebull the current presentation with old photographsbull (up to 40 of normal individuals havebull significant nose malformations)
Nasal Fractures Physical examination bull The diagnosis of a nasal fracture is made primarily by physical examination epistaxis nasal swelling and periorbital ecchymosis Nasal shape in the lateral and frontal inspection should be assessed Grasping the dorsum between two fingers and rocking the pyramid back and forth aids in assessing the mobility of nasal bones Internal structures should be evaluated by using a headlight and nasal speculum Clotted blood is removed by suction and assessment of haematoma mucosal tears and active bleeding is performed Bimanual palpation of the septum helps to differentiate septal swelling from haematoma ndash
Nasal FracturesRadiographybull There is no clear evidence of the role of radiographyin the management of nasal fracturesPlain films have up to a 66 false-positive rateas a result of misinterpretation of normal suturelines In addition old fractures are difficult todistinguishbull Three-dimensional CT is recommended for extensiveinjuries involving the nasal-orbital-ethmoidalcomplexndash
Nasal Fractures
bull Additionaluseful diagnostic proceduresbull bull Using a 0 or 30deg 4-mm endoscope is helpful inbull the assessment of posterior abnormalities If thebull patient is heavily sedated Brown-Gruss
provocationbull manoeuvres may be performed to determinebull deformities in upper middle or lower segmentsbull by compressing each compartment
Nasal FracturesConservative treatmentndash Treatment of bleedingbull For localised bleeding anterior sources may becauterised by silver nitrate or sealed with topicalmaterials such as thrombin combined withgelatin foam fibrin glue FloSealreg or other procoagulantmaterials If conservative measuresfail a formal anterior packing is placedbull Bleeding from branches of sphenopalatine orethmoid vessels requires anterior-posteriorpacking
Nasal Fractures
bull bull Surgical methods such as direct endoscopic vessel
bull cauterization or ligation have been shown tobull offer better haemostasis and patient comfortbull Angiography with embolization can also be
consideredbull in cases refractory to more conservativebull approaches
Nasal Fractures
bull Type of reductionbull bull Nondisplaced fractures should be treated withbull observation alone Closed nasal reduction is thebull best choice for simple injuries (isolated unilateralbull with medial displacement)bull bull An open approach should be considered in
severebull trauma (bilateral depressed fractures)
Nasal Fracturesbull Surgical principlesbull ndash Topical anaesthesia with cotton pledgets soakedbull with 4 cocaine or 005 oxymethazoline combinedbull with 4 topical lidocaine should be appliedbull for 5ndash10 min Local anaesthesia should also be injectedbull (1 lidocaine and 1100000 epinephrine)bull along the septum lateral walls and floor of the nasalbull cavitybull bull
Nasal FracturesClosed reductionndashndash The nasal bones are grasped between two fingersand pressure is applied laterally in theopposite direction of the deviation A bluntelevator may be used from within the nose incases of significant medial collapse Walshamforceps can be of help Reduction of the septumshould be performed with the use ofAsch forceps
Nasal Fractures
bull To prevent collapse of the postreductionbull framework nasal packing should be placedbull for 3ndash5 days Septum splints are recommendedbull in comminuted septal fractures withbull severe mucosal lesions External nasal splintingbull for 10 days (Aquaplastreg Thermoplastreg)bull provides nasal protection Nasal saline spraysbull prevent crusting and oral antibiotics should
Nasal Fractures
bull Open reductionbull ndashndash Immediate repair of fractures by using
widebull surgical exposure reduction fixation and
reconstructionbull ndashndash The second option is delayed correctionbull (6 months or more) of persistent deformitiesbull using standard techniques of rhinoplasty
Deviated Nasal Septum
bull Definition of the diseasebull ndash Deviation of the nasal septum is a common causebull of unilateral nasal airway obstruction in which thebull nasal septum is displacedbull bull Epidemiologyaetiologybull ndash Developmental septal abnormalities Septal cartilage
damage in the neonatal period andbull during birth can cause severe septal deviation inbull the absence of a history of nasal trauma
Deviated Nasal Septum
bull Symptomsbull ndash Patients may present with a history of sinusitis
allergicbull rhinitis obstructive sleep apnoea previousbull nasal surgery or recent nasal trauma Unilateral or
bilateral nasal airway obstruction that is unrelievedbull with decongestants or nasal steroid sprays is oftenbull seenbull bull
Deviated Nasal SeptumDiagnosisndashExamination external dorsal deviation or the columella and caudal septummay be deflected off the midline (caudal subluxation)ndash Inspections of the nasal cavity and anterior-posteriorrhinoscopy are helpful in diagnosing the locationtype and severity of septal deformityThe endoscope is also useful in identifying polypsthe severity and extent of posterior septaldeviations and bony spurs and locating areas ofseptal perforation or mucosal injury
Deviated Nasal Septum
bull Therapybull ndash Septoplasty is a procedurebull The areabull of deviation is corrected or resected in order tobull leave behind as much cartilage and bone as
possiblebull Cartilage resection is minimised and can be
repositioned reshaped or recontoured using a variety of methods
Deviated Nasal Septum
bull ndash Indications of septoplasty before the growth period
bull of the nose is finished should be very limited bull -In these cases surgery must preserve all the
cartilagebull in order to prevent external changes of the
shape ofbull the nose
Deviated Nasal Septum
bull Complicationsbull ndash Frequent complications include haematoma andbull infection Cerebrospinal fluid leak is a rare but
potentiallybull serious complicationbull It is usually the resultbull of avulsion or damage to the cribriform plate whenbull handling the perpendicular plate of the ethmoidbull ndash Other complications include epistaxis nasal
Deviated Nasal Septum
bull Other complications include epistaxis nasal obstruction
bull due to residual deviation synechiae returnbull of the cartilaginous deviation septal perforationbull anosmia and cosmetic nasal deformities suchbull as widened alar rim margins drooping nasal tipbull columella retraction and a sunken dorsum with abull supratip saddle formation
Septal perforation with minor crusting View from provide closure of the
incision
Septal Haematoma
bull A septal haematoma is a blood collection under the perichondrium
bull of the septum and cartilagebull bull bull Epidemiologyaetiologybull ndash A septal haematoma is one of the most
severe complications of nasal trauma
Septal Haematoma
bull Diagnosisbull ndash Signs and symptoms include intense pain
swellingbull haematoma of the upper lip and philtrum
area andbull complete nasal airway obstruction
Septal HaematomaTherapyndash Management consists of drainage through a mucoperichondrial incision Immediate treatment isnecessary to prevent long-term problems such asa saddle-nose deformity perforation columellarretraction and nasal-base widening In childrenseptal destruction can lead to devastating nasal andmidfacial growth abnormalitiesbull Surgeryndash Incision and evacuation of the collection is performedDrainage of a septal haematoma should
Septal HaematomaSurgeryndash Incision and evacuation of the collection is performedDrainage of a septal haematoma should provide closure of the incision
Splints or transseptal sutures are placed to obliterate thepotential space and prevent collectionInfection involving the septal cartilage Reconstruction with autologouscartilage is then performed in a second stage Oral antibiotics should be given
Nasal DeformitySaddle-nose deformityndash A saddle-nose deformity is characterised by a loss ofnasal dorsal height and compromised nasal supportstructures -Other case observed are depressionof the middle vault and dorsum loss of nasal tipsupport and definition shortened (vertical) nasal length over rotation of the nasal tip and retrusion ofthe nasal spine and caudal septum It is also knownas a ldquoPug noserdquo or ldquoboxerrsquos noserdquo both of which referto various degrees of nasal dorsal depressionbull
Nasal DeformityEpidemiologyaetiologyndash Prevalence is higher in population groups prone to facial trauma (ie boxers athletes) those with historiesof intranasal cocaine use nasal surgery (e g radical submucosal septal resection reductive rhinoplasty)ndash A saddle-nose deformity can be congenital or acquired It can be noticed as a part of individual familialsyndromic and ethnic characteristics - Most deformities are due to traumatic and iatrogeniccauses Medical causes are Wegenerrsquosgranulomatosis relapsing polychondritis leprosy (Hansenrsquos disease) syphilis ectodermal dysplasiaand intranasal cocaine use
Nasal Deformity
bull Therapybull ndash Nasal reconstruction indications depend on patientbull selection surgeon experience and aetiology of thebull deformity bull Indications for surgery can be functionalbull aesthetic or most commonly both In individuals
with a compromised nasal airway a nasoseptalbull reconstruction is indicated
Nasal Deformity
bull Contraindications bull include patients with malignantbull chronic or autoimmune disease conditions drugbull abuse poor perioperative risk profile and unrealisticbull expectationsbull ndash Multiple previous rhinoplasties and certain
professionsbull (mixed martial artists boxers and other contactbull sports) are relative contraindications
Nasal DeformitySeptoplastyndash Septoplasty is performed to correct nasal obstructioncaused by septal deformityndash Usually septoplasty is performed under general anaesthesiawith the patient in the supine position with the head elevated by approximately 30 (Righthandedsurgeons approach from the right side)ndash Local vasoconstrictive anaesthesia is applied notonly to reduce postoperative pain but also more importantly to achieve vasoconstriction of themucosa and less intraoperative haemorrhage Lidocainewith adrenaline or epinephrine is usedalthough in patients with cardiac hypersensitivityoxymetazoline might be preferred
Nasal Deformity
bull Septoplasty begins with the incision of septal mucosabull Most operative techniques utilise a hemitransfixionbull incision at the caudal end of septum so thatbull deviation at this point might be reached as wellbull as a transfixion incision that is easily obtained ifbull needed (Right-handed surgeons normally choosebull the left side but that may vary when deviation isbull convex towards the right)
Nasal DeformityA columella retractor is placed over the columellaand by pulling it laterally the caudal border of theseptum is exposed Ala can be protected by an alaprotector A vertical incision with a no 15 bladeover the caudal end of septum is performed untilreaching the plane of the septal cartilage It is essentialto correctly identify the perichondrium and byusing the Cottle elevator dissect and lift it creatinga flap As the dissection proceeds along the septalcartilage a longer speculum (no 5) is introduced sothat elevation of the mucoperichondrium is doneunder constant visual controlndash The next step is to dissect the mucoperiostium
Nasal DeformityDissecting over the bony-cartilaginous junctionwhen joining both tunnels might be difficult and is
especially prone to membrane perforationndash If needed the same tunnels are to be created on the
other side of the septum Then deviated parts of
septum are identified and removed either with a
knife or a Freer chisel
Nasal Deformitybull septum from the maxillary crest the septum mustbull be separated from the perpendicular plate trimmedbull along the inferior border placed back onto the crestbull and sutured to the periosteum If the deformity involvesbull the vomer an osteotome is used Care mustbull be taken not to break the cribriform plate becausebull it could cause a cerebrospinal fistula
Nasal Deformity
bull Once the septal deviation is corrected the flapsbull and hemitransfixion incision are mattressed
withbull absorbable sutures Nasal packing to prevent
synechiaebull and postoperative septal haematoma mightbull be advised but should be removed within 72 h

Head and neckmdashbenign and malignant disease
bull The basic anatomy and physiology of the oral cavity salivary glands pharynx larynx oesophagus and lymph node drainage
bull The presentation of head and neck cancerbull The presentation and management of salivary gland diseasebull Examining the oral cavity larynx and pharynx including the use of the nasendoscopebull Examining the neck with reference to the lymph nodesbull The role of fine needle aspiration cytology (FNAC)bull The principles and limitations of radiological investigation of the head and neck regionbull Management of neck lumps in particular the malignant lymph node with an unknown
primarybull The management of the airway in patients with a tracheostomy or end tracheostomy after
laryngectomybull A basic knowledge of the principles of operative surgery in particular the principles of
reconstructive surgery and the surgery for salivary gland disease eg parotidectomybull The postoperative management of a patient who has undergone major head and neck surgerybull The role of the multidisciplinary team in head and neck cancer and voice disorders
Supplementary knowledgebull The role of otoacoustic emissions and evoked auditory potentials in managing
hearing lossbull The use of speech audiometrybull The surgery for otosclerosisbull Bone-anchored hearing aids for conductive hearing lossbull Cochlear implantation and the reactions of the deaf community to this
interventionbull The use of sign languagebull Neuro-otology in particular the presentation and management of acoustic
neuromasbull Craniofacial surgery and the interplay between ENT plastic surgery and
neurosurgerybull The management of cleft palate and the increased risk of glue earbull Advanced endoscopic sinus surgery for the mangement of sinonasal malignancy
pituitary tumours and skull base tumoursbull Microlaryngeal surgery and surgical voice restorationbull The use of chemotherapy and radiotherapy in head and neck malignancy
Working in ENT
bull Working in ENT should be a very enjoyable experience whether it is a temporary attachment or a long-term career plan
bull It is helpful if you have an understanding of what others expect of you
bull It is also important for you to think about your own career development
Your duties
bull Patient care and continuitybull Professional developmentbull Research
The ENT Examination
EquipmentA fully equipped ENT department will have all the necessary instruments for performing a full ENT examination
Basic equipment
bull A light sourcemdasha portable headlight that runs off batteries is ideal
bull Wooden tongue depressorsbull Thudicum nasal speculumbull An otoscope with several speculaebull Pneumatic attachment for the otoscopebull Tuning fork 512Hzbull Pen and paperbull Gloves
Advanced equipment
bull Co-phenylcaine spraybull A flexible nasendoscope with light sourcebull Alcohol wipe to act as demist for the scopebull Aqueous lubricating gel for the scope
Emergency equipment
bull Large nasal tampons (you can always cut 10cm ones to size)
bull Silver nitrate sticksbull Foley catheters
Basic Anatomy of the Nose
bull The structural anatomy of the nose is important
bull for both aesthetic and functional reasons since the
bull nose as the gateway to the respiratory tract performs
bull a variety of physiologic functions
External NoseThe shape of the external nose is defined by the nasalbones a pair of rectangular bones in the upper nasaldorsum and by lateral cartilages (uppernasal cartilages) and alar cartilages (major alar cartilages)in the central and lower portions of the noseThe lateral portions of the nasal alae alsocontain several small accessory cartilages called theminor alar cartilages which are embedded in the lateralsoft tissues of the noseThe shape and stability of the alar cartilages each ofwhich consists of a medial and lateral crus
External Nose
Anatomy of the nasal base
bull Besides thebull medial crura the
inferior septal margin and the connective-
bull tissue septum (columella) are also responsible
bull for stabilizing the base of the nose
Anatomy of the nasal base
Anatomy of the nasal base
bull The nasal septum is subluxed toward the left side partially
bull obstructing the nasal airway
Nasal CavitiesThe nasal cavities begin anteriorly at the nasal vestibulewhich is bordered posteriorly by the internal nasalvalve (limen nasi) located between the posteriorborder of the alar cartilage and the anterior border ofthe lateral cartilage This valve area is the narrowestportion of the upper respiratory tract
Nasal Cavities
The interior ofthe nose behind the nasal valve is divided by the nasalseptum into two main cavities
Nasal CavitiesThe nasal septum iscomposed of an anterior cartilaginous part and twoposterior bony parts Abnormalities in the shape ofthe nasal septum which may consist of a deviated septum tensionseptum spurs or ridges are a frequent cause ofnasal airway obstructionThe choanae are the paired posterior openingsthrough which the nasal cavities communicate withthe nasopharynx
Nasal CavitiesThe nasal cavity is bounded laterally by the lateral nasalwalls which are formed by the ethmoid bone andmaxilla and posteriorly by the palatine bone and thepterygoid process of the sphenoid bone Several functionallyimportant structures are located on the lateralnasal wall the nasal turbinates and their associatedpassages (meati) sinus ostia and the orifice ofthe nasolacrimal duct (Fig 15)
The inferior turbinate consists of a separate bone thatis attached to the medial wall of the maxillary sinusThe opening of the nasolacrimal duct is located in thecorresponding inferior meatus The middle andsuperior turbinates are part of the ethmoid bone In rare cases a rudimentary ldquosupreme turbinaterdquo is alsopresent above the superior turbinate
The middle turbinate has by far the greatest functionalimportance because most of the drainage tracts fromthe surrounding paranasal sinuses open into the middlemeatus The nasal cavity is bounded superiorly by the cribriformplate of the ethmoid bone This thin bony platehas numerous openings for the passage of the fila olfactoriaand also forms the boundary of the anteriorcranial fossa
Nasal Cavities
The floor of the nasal cavity is formedmostly by the hard palate which is formed in turn bythe two palatine processes of the maxilla and the horizontallaminae of the palatine bone
Structure of the lateral nasal wall
Inferior meatus
Paranasal Sinuses
The paranasal sinuses are air-filled cavities that communicatewith the nasal cavities
-The maxillary sinus frontalsinus and anterior ethmoid cells drain into the nasalcavity through the middle meatusmdashie below themiddle turbinate -The posterior ethmoidcells drain into the nasal cavity through the superiormeatus The ostium of the sphenoid sinus is locatedin the anterior wall directly above the choanae- The anatomical connections between the nasal cavity andparanasal sinuses are functionally important and playa key role in the pathogenesis of many rhinologic diseasesthat involve the paranasal sinuses
Vascular SupplyThe external nose derives most of its blood supply
from the facial artery which arises from the external
carotid artery and from the ophthalmic artery which
springs from the internal carotid artery
Vascular Supply
The internalnose receives blood from the territories of the externaland internal carotid arteries- the terminalbranches of the sphenopalatine artery which arisesfrom the maxillary artery - the anterior and posteriorethmoid arteries which arise from the ophthalmicartery-internal carotid arterie
venous drainage
The venous drainageof the facial region is handled by -the facial vein -retromandibular vein -internal jugular vein
lymphatic drainage
The regional lymphatic drainage of the face and externalnose is handled mainly by- the submandibularlymph nodes while the nasal cavity is additionallydrained by -the retropharyngeal and deep - -cervical lymph nodes
Morphology of the Nasal Mucosa
Besides the anatomical structure of the external noseand nasal cavity the nasal mucosa plays an essentialrole in numerous functions of the nose in the respiratory tract
Morphology of the Nasal Mucosa
The anterior part of the nasal cavity (the nasal vestibule)like the external nose is covered by skin composedof a multilayer keratinizing squamous epithelium and finally a ciliated respiratory epithelium A small areaon the upper nasal septum superior turbinate andpart of the middle turbinate located adjacent to thecribriform plate is covered by olfactory mucosa and iscalled the olfactory region
Nerve SupplyThe facial skin receives its sensory innervation fromterminal branches of the trigeminal nerve that enterthe facial region through the supraorbital infraorbitaland mental foramina Thefacial muscles are classified as mimetic or mastica- tory each of these groups receiving different motorinnervationbythe facial nerve
History and Clinical Examination of the Nose
Historybull The main symptomsbull nasal obstruction (ldquostuffy
noserdquo)bull nasal dischargebull Headachesbull Olfactory
dysfunction
Palpationbony discontinuitiesNeuralgias to check
over- the supraorbital -infraorbital -mental foramina
Anterior Rhinoscopy
bull The rhinologic examination itself begins with anterior
bull rhinoscopy to evaluate the nasal vestibule and the anterior
bull portions of the nasal cavity
Nasal Endoscopy Nasal endoscopy has become the most important andrewarding clinical examination method in rhinologic diagnosis
- rigid endoscopes which are available in 4-mm and 28- mm diameters and assorted viewing angles (eg 01048576 301048576 1201048576) -flexible endoscopes are also available for inspecting the nose and nasopharynx and exploring all of the pharynx and larynx in one sitting
Nasal endoscopy
Nasal Endoscopy
Nasal Endoscopy
Imaging of the Nose and Paranasal Sinuses
Conventional RadiographsStandard paranasal sinus radiographs in the occipitomental
projection ( Water projection) and
occipitofrontal projection Caldwell projection) in cases of acute inflammation
They are also obtained to evaluate midfacial fractures
Computed Tomography (CT) the main indicationsfor CT scanning of the
nose and paranasal sinuses
are- chronic sinusitis - -trauma (especially
frontobasal -fractures)
-and tumors
The occipitofrontal projection is better for evaluating theethmoid cells and frontal sinus
occipitomental projection demonstrates the maxillarysinus and gives a limited view of the sphenoid sinus
Computed tomography of the paranasal sinuses
Four representative coronal CT scans are shown
Four representative coronal CT scans are shown
Magnetic Resonance Imaging
Magnetic maging
Magnetic resonance imaging (MRI) has fewer indicationsthan CT in patients with paranasal sinus diseaseThis is primarily because MRI is markedly inferior toCT in defining the bony boundaries of the sinusesThe strength of MRI lies in its superior soft-tissue discriminationMRI is indicated in diseases that involve the paranasal sinuses in addition to thecranial cavity or orbit (eg tumors and congenitalmalformations such as encephaloceles)
MRI of the paranasal sinuses
The Nose and Sinuses
Structure The structure of the nose is made up of
four partsbull The surface anatomybull The nasal skeletonmdashcomposed of the
two nasal bones the paired upper lateral and lower lateral cartilages and the nasal septum covered in subcutaneous tissue and skin
bull The internal anatomymdashincludes the septum of the nose which forms the medial wall of the nasal cavity The turbinates on the lateral wall are also called conchae
bull The osteomeatal complexmdasha key functional area of the nose
Function The nose is the main route for inspired
air and its structure is related to this function As the air passes over the large surface area of the turbinates
The inspired gases are warmed and humidified Mucus on the mucosa of the nose removes large dust particles from the air as it is breathed in
The voice resonates in the sinuses and nose and this provides character to the speech
Pneumatization of the sinusesmdashthey are air filled spacesmdashreduces the weight of the skull
Diseases of thDiseases of the Outer and Inner Nosee Outer and
Inner Nose Erysipelas Definition of the disease ndash Erysipela is a skin infection that affects the superficial dermis and is caused by Streptococcus pyogenes (group A) It usually develops in the extremities and the face and less commonly on the scalp and genitals bull Epidemiologyaetiology ndash Erysipelas are more often seen in elderly infants and children patients with compromised immunology and diabetes -Predisposing factors are alcoholism skin ulceration puncture wounds fungal infections malnutrition and burns
Erysipelas
bull Symptomsbull ndash It usually presents of fever general fatigue bull -The skin lesion is a redindurated and elevated plaque
with borders that expand rapidly bull It is painful warm and accompanied by variable oedemabull -On the second or third day a flaccid bulla may develop
and desquamationbull bull Presence of regional lymph nodes is common
Erysipelas
bull Complicationsndash The most common complication is recurrencewhich is seen in 18ndash30 of the cases even afterproper antibiotic therapy Recurrence is seen moreoften in females than in malesA skin infection with S pyogenes could lead toglomerulonephritis
Erysipelas
bull Complicationsbull ndash The most common complication is recurrencebull which is seen in 18ndash30 of the cases even afterbull proper antibiotic therapy bull -Recurrence is seen morebull often in females than in males bull -A skin infection with S pyogenes could lead tobull glomerulonephritis
Erysipelas
bull bull Diagnosisbull ndash Diagnosis is based on the patientrsquos personal
historybull and physical examination particularly on inspectionbull of the skin
bull Blood cultures are positive in less thanbull 5 of cases
ErysipelasTherapyndash Conservative therapybull The preferred antibiotic is penicillin In mildcases with minor systemic symptoms penicillinV 500 mg orally every 6 h for 10 days or penicillinG benzathine 12 mil U intramuscularlyonceOther possibilities are amoxicillin 500 mgorally twice a day for 10 days or cephalexin 500mg orally every 6 h for 10 days
ErysipelasIn moderate and severe cases with significantsystemic symptoms hospitalization and intravenoustreatment is required penicillin G 2ndash4mil U intravenously every 4ndash6 h Cefazolin05ndash15 gm intravenously every 8 h cefotaxime1ndash2 gm intravenously every 8 h or ceftriaxone1ndash2 gm intravenously once a day should be administeredIn patients with a penicillin allergyclindamycin 600 mg intravenously every 8 h orvancomycin 15 mgkg intravenously twice a daymay be given
ErysipelaAdditional useful therapeutic optionsbull Prednisone 30 mg over 8 days might be consideredas well as elevation of the affected siteMoist heat compresses may be usefulbull Surgeryndash Debridement and drainage are indicated when bullaeabscesses or necroses are presentbull Differential diagnosisndash Contact dermatitisndash Asteatotic eczemandash Herpes zosterndash Angioneurotic oedemandash Osteomyelitis
Furuncle
bull Definition of the diseasebull ndash A furuncle is an infection that beginsbull at the hair follicle and spreads deeper into thebull dermis and subcutaneous tissue forming abull nodule After several days it developsbull into an abscess - red painful and fluctuantbull bull bull Epidemiologyaetiologybull ndash The aetiologic agent is Staphylococcus aureus
FuruncleSymptomsndashsymptoms are local and limited to thesite of infection Furuncles usually are wherehair follicles are present bull Complicationndash One complication is furunculosis multiple draining furunclesDiagnosisndash The diagnosis is based on clinical inspection - Cultures are not necessary when there is no systemic involvement but should beconsidered if systemic therapy (in case of feversignificant cellulitis or hospitalization) or whenmethicillin-resistant Staphylococcusaureus (MRSA) is considered
FuruncleTherapyndash When the furuncle is small application of moist heat compress to promote drainage -Larger furuncles should be drained by surgical incision-After drainage the area should be cleaned with anantiseptic (with chlorhexidinebetadine) should be applied twice
a dayndash If no systemic symptoms or extensive cellulitis arepresent simple topical care is usually curative andoral antibiotics are not necessary Otherwise systemictreatment is indicated and should cover anypossible MRSA
Furuncle
bull -Recommended antibiotics are trimethoprim-sulfamethoxazole
bull 1ndash2 tablets orally twice daily doxycyclinebull 100 mg orally twice dailybull or clindamycin 300ndash450 mg orally every 8 hbull - In severe cases vancomycin 15 mgkg
intravenouslybull every 12 h or clindamycin 600 mg intravenouslybull every 8 h
Midline Granulomabull A midline granuloma is an angiocentricbull lymphoma it was referred to as polymorphicbull reticulosis lethal midline granuloma and midline
malignant reticulosisbull bull Definition of the diseasebull ndash This rare disease is a lymphoma of extranodal
presentationall cases are positive for the Epstein-Barr virus
bull -This lymphoma most commonly appears in the midface region
Midline GranulomaEpidemiologyaetiologyndash This form of lymphoma is rare in Europe and theUnited States with a higher prevalence in Asia and PeruSymptomsndash The most common presentation is nasal obstruction with a destructive mass occupying the nosesinuses and palate
-Fever night sweatsand weight loss seen usually in Hodgkinrsquos lymphomaand other non-Hodgkinrsquos lymphomas (knownas ldquoB symptomsrdquo) are uncommon
Midline GranulomaDiagnosisndash The diagnosis is based on anatomopathologicalstudy The malignancy of the tumour manifested byextensive necrosis makes the histological diagnosisdifficult and often more biopsies are required forconfirmationbull Therapyndash Therapy consists of radiotherapy with or withoutchemotherapy
Midline Granuloma
bull Prognosisbull ndash Depending on the stage long-term remission or
experience a worseningbull prognosis with relapses which may include otherbull extranodal sites bull Involvement of extranodal sitesbull including the upper airway gastrointestinal tractbull skin
Wegenerrsquos Granulomatosis
bull Definition of the diseasebull ndash Wegenerrsquos granulomatosis is a systemic chronicbull vasculitis of small- and medium-sized blood vesselsbull with an autoimmune component It affectsbull particular organs with variable predilectionbull Epidemiologyaetiologybull ndash Wegenerrsquos granulomatosis is a rare disease It affects
about 1 in 20000ndash30000 people It is more prevalentbull in middle-aged Caucasian patients
Wegenerrsquos Granulomatosis
Symptomsndash The disease may present pulmonary upper
respiratory tract or renal In the disseminated form-The localised form ndash confinedto the upper respiratory region ndash is present in 25of the patients- It consists of nonspecific manifestationssuch as nasal obstruction crusting purulentor bloody rhinorrhea and painful or painless ulcers in oral or nasal cavities which are unresponsive tostandard medical treatment
Wegenerrsquos Granulomatosis
bull In some patients the nasal septum is perforatedbull which leads to saddle-nose deformity Less
commonbull symptoms are hoarseness stridor due to
subglotticbull stenosis otalgia otorrhea and conductivebull and sensorineural hearing loss Also ocular
symptomsbull such as scleritis conjunctivitis uveitis andbull episcleritis may be present
Wegenerrsquos Granulomatosis
bull ndash In the disseminated form pulmonary involvementbull is manifested by cough dyspnoea haemoptysisbull (due to an alveolar capillaritis necrotic lesions orbull endobronchial disease) and pleuritic painndashbull -Ninety per cent of patients have nasal symptomsbull and these symptoms are usually the first
manifestationof the diseasebull -Most patients have also renal involvementbull even if it is subclinical
Wegenerrsquos Granulomatosis
Diagnosis ndash Diagnosis of Wegenerrsquos granulomatosis is based on clinical findings that demonstrate lung (chest x-ray) kidney (urine analysis) or upper respiratory tract
involvement (oral or nasal ulcers or discharge) - positive blood analysis for cytoplasmic-staining antineutrophil
cytoplasmic antibodies (c-ANCA) and confirming proteinase 3 (PR3) ANCA or myeloperoxidase (MPO) ANCA ndash Biopsy is essential for diagnosis nonspecific chronic inflammation
and necrosis -Bacterial and fungal infections
Wegenerrsquos Granulomatosis
Therapyndash Conservative therapybull In the induction of disease remission highdosesteroids (e g prednisone 1 mgkgday) for1 month with tapering over several months aregiven In addition cyclophosphamide (2 mgkgday) should be administered for 6ndash12 monthsuntil symptoms disappear In the maintenanceof remission cyclophosphamide should be
Wegenerrsquos Granulomatosis
Antibiotics mainly trimethoprim-sulfamethoxazoleare given for prophylaxis againstPneumocystis jiroveci (formerly Pneumocystiscarinii) pneumonia (PCP) which may developduring immunosuppression and have a role inpreventing recurrencesbull Sinonasal manifestations may be treated with topical nasal steroids and nasal irrigations lowdosesystemic steroids and antibiotics when bacterial infection (typically Staphylococcus species) is suspected
Wegenerrsquos Granulomatosis
bull Prognosisbull ndash Most of the patients respond well to treatmentbull achieving symptom-free intervals of 5ndash20 yearsbull or more bull -Anatomical problems (sinusitis trachealbull stenosis) may require surgery bull Relapses can be long and troublesomebull Long-term complications are chronicbull renal failure hearing loss and deafness
Nasal Fractures Definition ndash A nasal fracture is a disruption of the nasal bone structure due to trauma It is the most frequently fractured facial bone Epidemiologyaetiology ndash Sports falls and assaults are the usual mechanisms of fracture -Males are affected twice as often as are females -Paediatric populations with a incidences during the second and third decades of life -Variables such as force impact direction nature of the striking object age and other will influence the pattern of injury to the components of the nose
Nasal Fractures
bull Symptomsbull ndash Deformity swelling epistaxis and periorbital
ecchymosis are signs that are suggestive of nasal fracture
bull bony crepitus and nasal segment mobilitybull ndash Epiphora bull Severe bilateral injuries to the lachrymal bones
arebull associated with depressed nasal fractures
Nasal Fractures Complications ndash Septal haematoma is one of the most severe early complications of nasal trauma and without drainage it results in abscess formation 6ndash7 days after trauma producing necrosis of the septal cartilage -Long-term problems such as saddle-nose deformity perforation columellar retraction and nasalbase
Septal infection could lead to osteomyelitis orbital and intracranial abscesses meningitis and cavernous sinus thrombosis -Cerebrospinal fluid leakage is a common complication of severe
nasal and frontal fractures
Nasal Fractures
bull Diagnostic proceduresbull ndash Inspectionbull bull Changes of appearance such as deviation andbull asymmetry bleeding watery drainage changesbull in nasal breathing and smell It is useful to comparebull the current presentation with old photographsbull (up to 40 of normal individuals havebull significant nose malformations)
Nasal Fractures Physical examination bull The diagnosis of a nasal fracture is made primarily by physical examination epistaxis nasal swelling and periorbital ecchymosis Nasal shape in the lateral and frontal inspection should be assessed Grasping the dorsum between two fingers and rocking the pyramid back and forth aids in assessing the mobility of nasal bones Internal structures should be evaluated by using a headlight and nasal speculum Clotted blood is removed by suction and assessment of haematoma mucosal tears and active bleeding is performed Bimanual palpation of the septum helps to differentiate septal swelling from haematoma ndash
Nasal FracturesRadiographybull There is no clear evidence of the role of radiographyin the management of nasal fracturesPlain films have up to a 66 false-positive rateas a result of misinterpretation of normal suturelines In addition old fractures are difficult todistinguishbull Three-dimensional CT is recommended for extensiveinjuries involving the nasal-orbital-ethmoidalcomplexndash
Nasal Fractures
bull Additionaluseful diagnostic proceduresbull bull Using a 0 or 30deg 4-mm endoscope is helpful inbull the assessment of posterior abnormalities If thebull patient is heavily sedated Brown-Gruss
provocationbull manoeuvres may be performed to determinebull deformities in upper middle or lower segmentsbull by compressing each compartment
Nasal FracturesConservative treatmentndash Treatment of bleedingbull For localised bleeding anterior sources may becauterised by silver nitrate or sealed with topicalmaterials such as thrombin combined withgelatin foam fibrin glue FloSealreg or other procoagulantmaterials If conservative measuresfail a formal anterior packing is placedbull Bleeding from branches of sphenopalatine orethmoid vessels requires anterior-posteriorpacking
Nasal Fractures
bull bull Surgical methods such as direct endoscopic vessel
bull cauterization or ligation have been shown tobull offer better haemostasis and patient comfortbull Angiography with embolization can also be
consideredbull in cases refractory to more conservativebull approaches
Nasal Fractures
bull Type of reductionbull bull Nondisplaced fractures should be treated withbull observation alone Closed nasal reduction is thebull best choice for simple injuries (isolated unilateralbull with medial displacement)bull bull An open approach should be considered in
severebull trauma (bilateral depressed fractures)
Nasal Fracturesbull Surgical principlesbull ndash Topical anaesthesia with cotton pledgets soakedbull with 4 cocaine or 005 oxymethazoline combinedbull with 4 topical lidocaine should be appliedbull for 5ndash10 min Local anaesthesia should also be injectedbull (1 lidocaine and 1100000 epinephrine)bull along the septum lateral walls and floor of the nasalbull cavitybull bull
Nasal FracturesClosed reductionndashndash The nasal bones are grasped between two fingersand pressure is applied laterally in theopposite direction of the deviation A bluntelevator may be used from within the nose incases of significant medial collapse Walshamforceps can be of help Reduction of the septumshould be performed with the use ofAsch forceps
Nasal Fractures
bull To prevent collapse of the postreductionbull framework nasal packing should be placedbull for 3ndash5 days Septum splints are recommendedbull in comminuted septal fractures withbull severe mucosal lesions External nasal splintingbull for 10 days (Aquaplastreg Thermoplastreg)bull provides nasal protection Nasal saline spraysbull prevent crusting and oral antibiotics should
Nasal Fractures
bull Open reductionbull ndashndash Immediate repair of fractures by using
widebull surgical exposure reduction fixation and
reconstructionbull ndashndash The second option is delayed correctionbull (6 months or more) of persistent deformitiesbull using standard techniques of rhinoplasty
Deviated Nasal Septum
bull Definition of the diseasebull ndash Deviation of the nasal septum is a common causebull of unilateral nasal airway obstruction in which thebull nasal septum is displacedbull bull Epidemiologyaetiologybull ndash Developmental septal abnormalities Septal cartilage
damage in the neonatal period andbull during birth can cause severe septal deviation inbull the absence of a history of nasal trauma
Deviated Nasal Septum
bull Symptomsbull ndash Patients may present with a history of sinusitis
allergicbull rhinitis obstructive sleep apnoea previousbull nasal surgery or recent nasal trauma Unilateral or
bilateral nasal airway obstruction that is unrelievedbull with decongestants or nasal steroid sprays is oftenbull seenbull bull
Deviated Nasal SeptumDiagnosisndashExamination external dorsal deviation or the columella and caudal septummay be deflected off the midline (caudal subluxation)ndash Inspections of the nasal cavity and anterior-posteriorrhinoscopy are helpful in diagnosing the locationtype and severity of septal deformityThe endoscope is also useful in identifying polypsthe severity and extent of posterior septaldeviations and bony spurs and locating areas ofseptal perforation or mucosal injury
Deviated Nasal Septum
bull Therapybull ndash Septoplasty is a procedurebull The areabull of deviation is corrected or resected in order tobull leave behind as much cartilage and bone as
possiblebull Cartilage resection is minimised and can be
repositioned reshaped or recontoured using a variety of methods
Deviated Nasal Septum
bull ndash Indications of septoplasty before the growth period
bull of the nose is finished should be very limited bull -In these cases surgery must preserve all the
cartilagebull in order to prevent external changes of the
shape ofbull the nose
Deviated Nasal Septum
bull Complicationsbull ndash Frequent complications include haematoma andbull infection Cerebrospinal fluid leak is a rare but
potentiallybull serious complicationbull It is usually the resultbull of avulsion or damage to the cribriform plate whenbull handling the perpendicular plate of the ethmoidbull ndash Other complications include epistaxis nasal
Deviated Nasal Septum
bull Other complications include epistaxis nasal obstruction
bull due to residual deviation synechiae returnbull of the cartilaginous deviation septal perforationbull anosmia and cosmetic nasal deformities suchbull as widened alar rim margins drooping nasal tipbull columella retraction and a sunken dorsum with abull supratip saddle formation
Septal perforation with minor crusting View from provide closure of the
incision
Septal Haematoma
bull A septal haematoma is a blood collection under the perichondrium
bull of the septum and cartilagebull bull bull Epidemiologyaetiologybull ndash A septal haematoma is one of the most
severe complications of nasal trauma
Septal Haematoma
bull Diagnosisbull ndash Signs and symptoms include intense pain
swellingbull haematoma of the upper lip and philtrum
area andbull complete nasal airway obstruction
Septal HaematomaTherapyndash Management consists of drainage through a mucoperichondrial incision Immediate treatment isnecessary to prevent long-term problems such asa saddle-nose deformity perforation columellarretraction and nasal-base widening In childrenseptal destruction can lead to devastating nasal andmidfacial growth abnormalitiesbull Surgeryndash Incision and evacuation of the collection is performedDrainage of a septal haematoma should
Septal HaematomaSurgeryndash Incision and evacuation of the collection is performedDrainage of a septal haematoma should provide closure of the incision
Splints or transseptal sutures are placed to obliterate thepotential space and prevent collectionInfection involving the septal cartilage Reconstruction with autologouscartilage is then performed in a second stage Oral antibiotics should be given
Nasal DeformitySaddle-nose deformityndash A saddle-nose deformity is characterised by a loss ofnasal dorsal height and compromised nasal supportstructures -Other case observed are depressionof the middle vault and dorsum loss of nasal tipsupport and definition shortened (vertical) nasal length over rotation of the nasal tip and retrusion ofthe nasal spine and caudal septum It is also knownas a ldquoPug noserdquo or ldquoboxerrsquos noserdquo both of which referto various degrees of nasal dorsal depressionbull
Nasal DeformityEpidemiologyaetiologyndash Prevalence is higher in population groups prone to facial trauma (ie boxers athletes) those with historiesof intranasal cocaine use nasal surgery (e g radical submucosal septal resection reductive rhinoplasty)ndash A saddle-nose deformity can be congenital or acquired It can be noticed as a part of individual familialsyndromic and ethnic characteristics - Most deformities are due to traumatic and iatrogeniccauses Medical causes are Wegenerrsquosgranulomatosis relapsing polychondritis leprosy (Hansenrsquos disease) syphilis ectodermal dysplasiaand intranasal cocaine use
Nasal Deformity
bull Therapybull ndash Nasal reconstruction indications depend on patientbull selection surgeon experience and aetiology of thebull deformity bull Indications for surgery can be functionalbull aesthetic or most commonly both In individuals
with a compromised nasal airway a nasoseptalbull reconstruction is indicated
Nasal Deformity
bull Contraindications bull include patients with malignantbull chronic or autoimmune disease conditions drugbull abuse poor perioperative risk profile and unrealisticbull expectationsbull ndash Multiple previous rhinoplasties and certain
professionsbull (mixed martial artists boxers and other contactbull sports) are relative contraindications
Nasal DeformitySeptoplastyndash Septoplasty is performed to correct nasal obstructioncaused by septal deformityndash Usually septoplasty is performed under general anaesthesiawith the patient in the supine position with the head elevated by approximately 30 (Righthandedsurgeons approach from the right side)ndash Local vasoconstrictive anaesthesia is applied notonly to reduce postoperative pain but also more importantly to achieve vasoconstriction of themucosa and less intraoperative haemorrhage Lidocainewith adrenaline or epinephrine is usedalthough in patients with cardiac hypersensitivityoxymetazoline might be preferred
Nasal Deformity
bull Septoplasty begins with the incision of septal mucosabull Most operative techniques utilise a hemitransfixionbull incision at the caudal end of septum so thatbull deviation at this point might be reached as wellbull as a transfixion incision that is easily obtained ifbull needed (Right-handed surgeons normally choosebull the left side but that may vary when deviation isbull convex towards the right)
Nasal DeformityA columella retractor is placed over the columellaand by pulling it laterally the caudal border of theseptum is exposed Ala can be protected by an alaprotector A vertical incision with a no 15 bladeover the caudal end of septum is performed untilreaching the plane of the septal cartilage It is essentialto correctly identify the perichondrium and byusing the Cottle elevator dissect and lift it creatinga flap As the dissection proceeds along the septalcartilage a longer speculum (no 5) is introduced sothat elevation of the mucoperichondrium is doneunder constant visual controlndash The next step is to dissect the mucoperiostium
Nasal DeformityDissecting over the bony-cartilaginous junctionwhen joining both tunnels might be difficult and is
especially prone to membrane perforationndash If needed the same tunnels are to be created on the
other side of the septum Then deviated parts of
septum are identified and removed either with a
knife or a Freer chisel
Nasal Deformitybull septum from the maxillary crest the septum mustbull be separated from the perpendicular plate trimmedbull along the inferior border placed back onto the crestbull and sutured to the periosteum If the deformity involvesbull the vomer an osteotome is used Care mustbull be taken not to break the cribriform plate becausebull it could cause a cerebrospinal fistula
Nasal Deformity
bull Once the septal deviation is corrected the flapsbull and hemitransfixion incision are mattressed
withbull absorbable sutures Nasal packing to prevent
synechiaebull and postoperative septal haematoma mightbull be advised but should be removed within 72 h

Supplementary knowledgebull The role of otoacoustic emissions and evoked auditory potentials in managing
hearing lossbull The use of speech audiometrybull The surgery for otosclerosisbull Bone-anchored hearing aids for conductive hearing lossbull Cochlear implantation and the reactions of the deaf community to this
interventionbull The use of sign languagebull Neuro-otology in particular the presentation and management of acoustic
neuromasbull Craniofacial surgery and the interplay between ENT plastic surgery and
neurosurgerybull The management of cleft palate and the increased risk of glue earbull Advanced endoscopic sinus surgery for the mangement of sinonasal malignancy
pituitary tumours and skull base tumoursbull Microlaryngeal surgery and surgical voice restorationbull The use of chemotherapy and radiotherapy in head and neck malignancy
Working in ENT
bull Working in ENT should be a very enjoyable experience whether it is a temporary attachment or a long-term career plan
bull It is helpful if you have an understanding of what others expect of you
bull It is also important for you to think about your own career development
Your duties
bull Patient care and continuitybull Professional developmentbull Research
The ENT Examination
EquipmentA fully equipped ENT department will have all the necessary instruments for performing a full ENT examination
Basic equipment
bull A light sourcemdasha portable headlight that runs off batteries is ideal
bull Wooden tongue depressorsbull Thudicum nasal speculumbull An otoscope with several speculaebull Pneumatic attachment for the otoscopebull Tuning fork 512Hzbull Pen and paperbull Gloves
Advanced equipment
bull Co-phenylcaine spraybull A flexible nasendoscope with light sourcebull Alcohol wipe to act as demist for the scopebull Aqueous lubricating gel for the scope
Emergency equipment
bull Large nasal tampons (you can always cut 10cm ones to size)
bull Silver nitrate sticksbull Foley catheters
Basic Anatomy of the Nose
bull The structural anatomy of the nose is important
bull for both aesthetic and functional reasons since the
bull nose as the gateway to the respiratory tract performs
bull a variety of physiologic functions
External NoseThe shape of the external nose is defined by the nasalbones a pair of rectangular bones in the upper nasaldorsum and by lateral cartilages (uppernasal cartilages) and alar cartilages (major alar cartilages)in the central and lower portions of the noseThe lateral portions of the nasal alae alsocontain several small accessory cartilages called theminor alar cartilages which are embedded in the lateralsoft tissues of the noseThe shape and stability of the alar cartilages each ofwhich consists of a medial and lateral crus
External Nose
Anatomy of the nasal base
bull Besides thebull medial crura the
inferior septal margin and the connective-
bull tissue septum (columella) are also responsible
bull for stabilizing the base of the nose
Anatomy of the nasal base
Anatomy of the nasal base
bull The nasal septum is subluxed toward the left side partially
bull obstructing the nasal airway
Nasal CavitiesThe nasal cavities begin anteriorly at the nasal vestibulewhich is bordered posteriorly by the internal nasalvalve (limen nasi) located between the posteriorborder of the alar cartilage and the anterior border ofthe lateral cartilage This valve area is the narrowestportion of the upper respiratory tract
Nasal Cavities
The interior ofthe nose behind the nasal valve is divided by the nasalseptum into two main cavities
Nasal CavitiesThe nasal septum iscomposed of an anterior cartilaginous part and twoposterior bony parts Abnormalities in the shape ofthe nasal septum which may consist of a deviated septum tensionseptum spurs or ridges are a frequent cause ofnasal airway obstructionThe choanae are the paired posterior openingsthrough which the nasal cavities communicate withthe nasopharynx
Nasal CavitiesThe nasal cavity is bounded laterally by the lateral nasalwalls which are formed by the ethmoid bone andmaxilla and posteriorly by the palatine bone and thepterygoid process of the sphenoid bone Several functionallyimportant structures are located on the lateralnasal wall the nasal turbinates and their associatedpassages (meati) sinus ostia and the orifice ofthe nasolacrimal duct (Fig 15)
The inferior turbinate consists of a separate bone thatis attached to the medial wall of the maxillary sinusThe opening of the nasolacrimal duct is located in thecorresponding inferior meatus The middle andsuperior turbinates are part of the ethmoid bone In rare cases a rudimentary ldquosupreme turbinaterdquo is alsopresent above the superior turbinate
The middle turbinate has by far the greatest functionalimportance because most of the drainage tracts fromthe surrounding paranasal sinuses open into the middlemeatus The nasal cavity is bounded superiorly by the cribriformplate of the ethmoid bone This thin bony platehas numerous openings for the passage of the fila olfactoriaand also forms the boundary of the anteriorcranial fossa
Nasal Cavities
The floor of the nasal cavity is formedmostly by the hard palate which is formed in turn bythe two palatine processes of the maxilla and the horizontallaminae of the palatine bone
Structure of the lateral nasal wall
Inferior meatus
Paranasal Sinuses
The paranasal sinuses are air-filled cavities that communicatewith the nasal cavities
-The maxillary sinus frontalsinus and anterior ethmoid cells drain into the nasalcavity through the middle meatusmdashie below themiddle turbinate -The posterior ethmoidcells drain into the nasal cavity through the superiormeatus The ostium of the sphenoid sinus is locatedin the anterior wall directly above the choanae- The anatomical connections between the nasal cavity andparanasal sinuses are functionally important and playa key role in the pathogenesis of many rhinologic diseasesthat involve the paranasal sinuses
Vascular SupplyThe external nose derives most of its blood supply
from the facial artery which arises from the external
carotid artery and from the ophthalmic artery which
springs from the internal carotid artery
Vascular Supply
The internalnose receives blood from the territories of the externaland internal carotid arteries- the terminalbranches of the sphenopalatine artery which arisesfrom the maxillary artery - the anterior and posteriorethmoid arteries which arise from the ophthalmicartery-internal carotid arterie
venous drainage
The venous drainageof the facial region is handled by -the facial vein -retromandibular vein -internal jugular vein
lymphatic drainage
The regional lymphatic drainage of the face and externalnose is handled mainly by- the submandibularlymph nodes while the nasal cavity is additionallydrained by -the retropharyngeal and deep - -cervical lymph nodes
Morphology of the Nasal Mucosa
Besides the anatomical structure of the external noseand nasal cavity the nasal mucosa plays an essentialrole in numerous functions of the nose in the respiratory tract
Morphology of the Nasal Mucosa
The anterior part of the nasal cavity (the nasal vestibule)like the external nose is covered by skin composedof a multilayer keratinizing squamous epithelium and finally a ciliated respiratory epithelium A small areaon the upper nasal septum superior turbinate andpart of the middle turbinate located adjacent to thecribriform plate is covered by olfactory mucosa and iscalled the olfactory region
Nerve SupplyThe facial skin receives its sensory innervation fromterminal branches of the trigeminal nerve that enterthe facial region through the supraorbital infraorbitaland mental foramina Thefacial muscles are classified as mimetic or mastica- tory each of these groups receiving different motorinnervationbythe facial nerve
History and Clinical Examination of the Nose
Historybull The main symptomsbull nasal obstruction (ldquostuffy
noserdquo)bull nasal dischargebull Headachesbull Olfactory
dysfunction
Palpationbony discontinuitiesNeuralgias to check
over- the supraorbital -infraorbital -mental foramina
Anterior Rhinoscopy
bull The rhinologic examination itself begins with anterior
bull rhinoscopy to evaluate the nasal vestibule and the anterior
bull portions of the nasal cavity
Nasal Endoscopy Nasal endoscopy has become the most important andrewarding clinical examination method in rhinologic diagnosis
- rigid endoscopes which are available in 4-mm and 28- mm diameters and assorted viewing angles (eg 01048576 301048576 1201048576) -flexible endoscopes are also available for inspecting the nose and nasopharynx and exploring all of the pharynx and larynx in one sitting
Nasal endoscopy
Nasal Endoscopy
Nasal Endoscopy
Imaging of the Nose and Paranasal Sinuses
Conventional RadiographsStandard paranasal sinus radiographs in the occipitomental
projection ( Water projection) and
occipitofrontal projection Caldwell projection) in cases of acute inflammation
They are also obtained to evaluate midfacial fractures
Computed Tomography (CT) the main indicationsfor CT scanning of the
nose and paranasal sinuses
are- chronic sinusitis - -trauma (especially
frontobasal -fractures)
-and tumors
The occipitofrontal projection is better for evaluating theethmoid cells and frontal sinus
occipitomental projection demonstrates the maxillarysinus and gives a limited view of the sphenoid sinus
Computed tomography of the paranasal sinuses
Four representative coronal CT scans are shown
Four representative coronal CT scans are shown
Magnetic Resonance Imaging
Magnetic maging
Magnetic resonance imaging (MRI) has fewer indicationsthan CT in patients with paranasal sinus diseaseThis is primarily because MRI is markedly inferior toCT in defining the bony boundaries of the sinusesThe strength of MRI lies in its superior soft-tissue discriminationMRI is indicated in diseases that involve the paranasal sinuses in addition to thecranial cavity or orbit (eg tumors and congenitalmalformations such as encephaloceles)
MRI of the paranasal sinuses
The Nose and Sinuses
Structure The structure of the nose is made up of
four partsbull The surface anatomybull The nasal skeletonmdashcomposed of the
two nasal bones the paired upper lateral and lower lateral cartilages and the nasal septum covered in subcutaneous tissue and skin
bull The internal anatomymdashincludes the septum of the nose which forms the medial wall of the nasal cavity The turbinates on the lateral wall are also called conchae
bull The osteomeatal complexmdasha key functional area of the nose
Function The nose is the main route for inspired
air and its structure is related to this function As the air passes over the large surface area of the turbinates
The inspired gases are warmed and humidified Mucus on the mucosa of the nose removes large dust particles from the air as it is breathed in
The voice resonates in the sinuses and nose and this provides character to the speech
Pneumatization of the sinusesmdashthey are air filled spacesmdashreduces the weight of the skull
Diseases of thDiseases of the Outer and Inner Nosee Outer and
Inner Nose Erysipelas Definition of the disease ndash Erysipela is a skin infection that affects the superficial dermis and is caused by Streptococcus pyogenes (group A) It usually develops in the extremities and the face and less commonly on the scalp and genitals bull Epidemiologyaetiology ndash Erysipelas are more often seen in elderly infants and children patients with compromised immunology and diabetes -Predisposing factors are alcoholism skin ulceration puncture wounds fungal infections malnutrition and burns
Erysipelas
bull Symptomsbull ndash It usually presents of fever general fatigue bull -The skin lesion is a redindurated and elevated plaque
with borders that expand rapidly bull It is painful warm and accompanied by variable oedemabull -On the second or third day a flaccid bulla may develop
and desquamationbull bull Presence of regional lymph nodes is common
Erysipelas
bull Complicationsndash The most common complication is recurrencewhich is seen in 18ndash30 of the cases even afterproper antibiotic therapy Recurrence is seen moreoften in females than in malesA skin infection with S pyogenes could lead toglomerulonephritis
Erysipelas
bull Complicationsbull ndash The most common complication is recurrencebull which is seen in 18ndash30 of the cases even afterbull proper antibiotic therapy bull -Recurrence is seen morebull often in females than in males bull -A skin infection with S pyogenes could lead tobull glomerulonephritis
Erysipelas
bull bull Diagnosisbull ndash Diagnosis is based on the patientrsquos personal
historybull and physical examination particularly on inspectionbull of the skin
bull Blood cultures are positive in less thanbull 5 of cases
ErysipelasTherapyndash Conservative therapybull The preferred antibiotic is penicillin In mildcases with minor systemic symptoms penicillinV 500 mg orally every 6 h for 10 days or penicillinG benzathine 12 mil U intramuscularlyonceOther possibilities are amoxicillin 500 mgorally twice a day for 10 days or cephalexin 500mg orally every 6 h for 10 days
ErysipelasIn moderate and severe cases with significantsystemic symptoms hospitalization and intravenoustreatment is required penicillin G 2ndash4mil U intravenously every 4ndash6 h Cefazolin05ndash15 gm intravenously every 8 h cefotaxime1ndash2 gm intravenously every 8 h or ceftriaxone1ndash2 gm intravenously once a day should be administeredIn patients with a penicillin allergyclindamycin 600 mg intravenously every 8 h orvancomycin 15 mgkg intravenously twice a daymay be given
ErysipelaAdditional useful therapeutic optionsbull Prednisone 30 mg over 8 days might be consideredas well as elevation of the affected siteMoist heat compresses may be usefulbull Surgeryndash Debridement and drainage are indicated when bullaeabscesses or necroses are presentbull Differential diagnosisndash Contact dermatitisndash Asteatotic eczemandash Herpes zosterndash Angioneurotic oedemandash Osteomyelitis
Furuncle
bull Definition of the diseasebull ndash A furuncle is an infection that beginsbull at the hair follicle and spreads deeper into thebull dermis and subcutaneous tissue forming abull nodule After several days it developsbull into an abscess - red painful and fluctuantbull bull bull Epidemiologyaetiologybull ndash The aetiologic agent is Staphylococcus aureus
FuruncleSymptomsndashsymptoms are local and limited to thesite of infection Furuncles usually are wherehair follicles are present bull Complicationndash One complication is furunculosis multiple draining furunclesDiagnosisndash The diagnosis is based on clinical inspection - Cultures are not necessary when there is no systemic involvement but should beconsidered if systemic therapy (in case of feversignificant cellulitis or hospitalization) or whenmethicillin-resistant Staphylococcusaureus (MRSA) is considered
FuruncleTherapyndash When the furuncle is small application of moist heat compress to promote drainage -Larger furuncles should be drained by surgical incision-After drainage the area should be cleaned with anantiseptic (with chlorhexidinebetadine) should be applied twice
a dayndash If no systemic symptoms or extensive cellulitis arepresent simple topical care is usually curative andoral antibiotics are not necessary Otherwise systemictreatment is indicated and should cover anypossible MRSA
Furuncle
bull -Recommended antibiotics are trimethoprim-sulfamethoxazole
bull 1ndash2 tablets orally twice daily doxycyclinebull 100 mg orally twice dailybull or clindamycin 300ndash450 mg orally every 8 hbull - In severe cases vancomycin 15 mgkg
intravenouslybull every 12 h or clindamycin 600 mg intravenouslybull every 8 h
Midline Granulomabull A midline granuloma is an angiocentricbull lymphoma it was referred to as polymorphicbull reticulosis lethal midline granuloma and midline
malignant reticulosisbull bull Definition of the diseasebull ndash This rare disease is a lymphoma of extranodal
presentationall cases are positive for the Epstein-Barr virus
bull -This lymphoma most commonly appears in the midface region
Midline GranulomaEpidemiologyaetiologyndash This form of lymphoma is rare in Europe and theUnited States with a higher prevalence in Asia and PeruSymptomsndash The most common presentation is nasal obstruction with a destructive mass occupying the nosesinuses and palate
-Fever night sweatsand weight loss seen usually in Hodgkinrsquos lymphomaand other non-Hodgkinrsquos lymphomas (knownas ldquoB symptomsrdquo) are uncommon
Midline GranulomaDiagnosisndash The diagnosis is based on anatomopathologicalstudy The malignancy of the tumour manifested byextensive necrosis makes the histological diagnosisdifficult and often more biopsies are required forconfirmationbull Therapyndash Therapy consists of radiotherapy with or withoutchemotherapy
Midline Granuloma
bull Prognosisbull ndash Depending on the stage long-term remission or
experience a worseningbull prognosis with relapses which may include otherbull extranodal sites bull Involvement of extranodal sitesbull including the upper airway gastrointestinal tractbull skin
Wegenerrsquos Granulomatosis
bull Definition of the diseasebull ndash Wegenerrsquos granulomatosis is a systemic chronicbull vasculitis of small- and medium-sized blood vesselsbull with an autoimmune component It affectsbull particular organs with variable predilectionbull Epidemiologyaetiologybull ndash Wegenerrsquos granulomatosis is a rare disease It affects
about 1 in 20000ndash30000 people It is more prevalentbull in middle-aged Caucasian patients
Wegenerrsquos Granulomatosis
Symptomsndash The disease may present pulmonary upper
respiratory tract or renal In the disseminated form-The localised form ndash confinedto the upper respiratory region ndash is present in 25of the patients- It consists of nonspecific manifestationssuch as nasal obstruction crusting purulentor bloody rhinorrhea and painful or painless ulcers in oral or nasal cavities which are unresponsive tostandard medical treatment
Wegenerrsquos Granulomatosis
bull In some patients the nasal septum is perforatedbull which leads to saddle-nose deformity Less
commonbull symptoms are hoarseness stridor due to
subglotticbull stenosis otalgia otorrhea and conductivebull and sensorineural hearing loss Also ocular
symptomsbull such as scleritis conjunctivitis uveitis andbull episcleritis may be present
Wegenerrsquos Granulomatosis
bull ndash In the disseminated form pulmonary involvementbull is manifested by cough dyspnoea haemoptysisbull (due to an alveolar capillaritis necrotic lesions orbull endobronchial disease) and pleuritic painndashbull -Ninety per cent of patients have nasal symptomsbull and these symptoms are usually the first
manifestationof the diseasebull -Most patients have also renal involvementbull even if it is subclinical
Wegenerrsquos Granulomatosis
Diagnosis ndash Diagnosis of Wegenerrsquos granulomatosis is based on clinical findings that demonstrate lung (chest x-ray) kidney (urine analysis) or upper respiratory tract
involvement (oral or nasal ulcers or discharge) - positive blood analysis for cytoplasmic-staining antineutrophil
cytoplasmic antibodies (c-ANCA) and confirming proteinase 3 (PR3) ANCA or myeloperoxidase (MPO) ANCA ndash Biopsy is essential for diagnosis nonspecific chronic inflammation
and necrosis -Bacterial and fungal infections
Wegenerrsquos Granulomatosis
Therapyndash Conservative therapybull In the induction of disease remission highdosesteroids (e g prednisone 1 mgkgday) for1 month with tapering over several months aregiven In addition cyclophosphamide (2 mgkgday) should be administered for 6ndash12 monthsuntil symptoms disappear In the maintenanceof remission cyclophosphamide should be
Wegenerrsquos Granulomatosis
Antibiotics mainly trimethoprim-sulfamethoxazoleare given for prophylaxis againstPneumocystis jiroveci (formerly Pneumocystiscarinii) pneumonia (PCP) which may developduring immunosuppression and have a role inpreventing recurrencesbull Sinonasal manifestations may be treated with topical nasal steroids and nasal irrigations lowdosesystemic steroids and antibiotics when bacterial infection (typically Staphylococcus species) is suspected
Wegenerrsquos Granulomatosis
bull Prognosisbull ndash Most of the patients respond well to treatmentbull achieving symptom-free intervals of 5ndash20 yearsbull or more bull -Anatomical problems (sinusitis trachealbull stenosis) may require surgery bull Relapses can be long and troublesomebull Long-term complications are chronicbull renal failure hearing loss and deafness
Nasal Fractures Definition ndash A nasal fracture is a disruption of the nasal bone structure due to trauma It is the most frequently fractured facial bone Epidemiologyaetiology ndash Sports falls and assaults are the usual mechanisms of fracture -Males are affected twice as often as are females -Paediatric populations with a incidences during the second and third decades of life -Variables such as force impact direction nature of the striking object age and other will influence the pattern of injury to the components of the nose
Nasal Fractures
bull Symptomsbull ndash Deformity swelling epistaxis and periorbital
ecchymosis are signs that are suggestive of nasal fracture
bull bony crepitus and nasal segment mobilitybull ndash Epiphora bull Severe bilateral injuries to the lachrymal bones
arebull associated with depressed nasal fractures
Nasal Fractures Complications ndash Septal haematoma is one of the most severe early complications of nasal trauma and without drainage it results in abscess formation 6ndash7 days after trauma producing necrosis of the septal cartilage -Long-term problems such as saddle-nose deformity perforation columellar retraction and nasalbase
Septal infection could lead to osteomyelitis orbital and intracranial abscesses meningitis and cavernous sinus thrombosis -Cerebrospinal fluid leakage is a common complication of severe
nasal and frontal fractures
Nasal Fractures
bull Diagnostic proceduresbull ndash Inspectionbull bull Changes of appearance such as deviation andbull asymmetry bleeding watery drainage changesbull in nasal breathing and smell It is useful to comparebull the current presentation with old photographsbull (up to 40 of normal individuals havebull significant nose malformations)
Nasal Fractures Physical examination bull The diagnosis of a nasal fracture is made primarily by physical examination epistaxis nasal swelling and periorbital ecchymosis Nasal shape in the lateral and frontal inspection should be assessed Grasping the dorsum between two fingers and rocking the pyramid back and forth aids in assessing the mobility of nasal bones Internal structures should be evaluated by using a headlight and nasal speculum Clotted blood is removed by suction and assessment of haematoma mucosal tears and active bleeding is performed Bimanual palpation of the septum helps to differentiate septal swelling from haematoma ndash
Nasal FracturesRadiographybull There is no clear evidence of the role of radiographyin the management of nasal fracturesPlain films have up to a 66 false-positive rateas a result of misinterpretation of normal suturelines In addition old fractures are difficult todistinguishbull Three-dimensional CT is recommended for extensiveinjuries involving the nasal-orbital-ethmoidalcomplexndash
Nasal Fractures
bull Additionaluseful diagnostic proceduresbull bull Using a 0 or 30deg 4-mm endoscope is helpful inbull the assessment of posterior abnormalities If thebull patient is heavily sedated Brown-Gruss
provocationbull manoeuvres may be performed to determinebull deformities in upper middle or lower segmentsbull by compressing each compartment
Nasal FracturesConservative treatmentndash Treatment of bleedingbull For localised bleeding anterior sources may becauterised by silver nitrate or sealed with topicalmaterials such as thrombin combined withgelatin foam fibrin glue FloSealreg or other procoagulantmaterials If conservative measuresfail a formal anterior packing is placedbull Bleeding from branches of sphenopalatine orethmoid vessels requires anterior-posteriorpacking
Nasal Fractures
bull bull Surgical methods such as direct endoscopic vessel
bull cauterization or ligation have been shown tobull offer better haemostasis and patient comfortbull Angiography with embolization can also be
consideredbull in cases refractory to more conservativebull approaches
Nasal Fractures
bull Type of reductionbull bull Nondisplaced fractures should be treated withbull observation alone Closed nasal reduction is thebull best choice for simple injuries (isolated unilateralbull with medial displacement)bull bull An open approach should be considered in
severebull trauma (bilateral depressed fractures)
Nasal Fracturesbull Surgical principlesbull ndash Topical anaesthesia with cotton pledgets soakedbull with 4 cocaine or 005 oxymethazoline combinedbull with 4 topical lidocaine should be appliedbull for 5ndash10 min Local anaesthesia should also be injectedbull (1 lidocaine and 1100000 epinephrine)bull along the septum lateral walls and floor of the nasalbull cavitybull bull
Nasal FracturesClosed reductionndashndash The nasal bones are grasped between two fingersand pressure is applied laterally in theopposite direction of the deviation A bluntelevator may be used from within the nose incases of significant medial collapse Walshamforceps can be of help Reduction of the septumshould be performed with the use ofAsch forceps
Nasal Fractures
bull To prevent collapse of the postreductionbull framework nasal packing should be placedbull for 3ndash5 days Septum splints are recommendedbull in comminuted septal fractures withbull severe mucosal lesions External nasal splintingbull for 10 days (Aquaplastreg Thermoplastreg)bull provides nasal protection Nasal saline spraysbull prevent crusting and oral antibiotics should
Nasal Fractures
bull Open reductionbull ndashndash Immediate repair of fractures by using
widebull surgical exposure reduction fixation and
reconstructionbull ndashndash The second option is delayed correctionbull (6 months or more) of persistent deformitiesbull using standard techniques of rhinoplasty
Deviated Nasal Septum
bull Definition of the diseasebull ndash Deviation of the nasal septum is a common causebull of unilateral nasal airway obstruction in which thebull nasal septum is displacedbull bull Epidemiologyaetiologybull ndash Developmental septal abnormalities Septal cartilage
damage in the neonatal period andbull during birth can cause severe septal deviation inbull the absence of a history of nasal trauma
Deviated Nasal Septum
bull Symptomsbull ndash Patients may present with a history of sinusitis
allergicbull rhinitis obstructive sleep apnoea previousbull nasal surgery or recent nasal trauma Unilateral or
bilateral nasal airway obstruction that is unrelievedbull with decongestants or nasal steroid sprays is oftenbull seenbull bull
Deviated Nasal SeptumDiagnosisndashExamination external dorsal deviation or the columella and caudal septummay be deflected off the midline (caudal subluxation)ndash Inspections of the nasal cavity and anterior-posteriorrhinoscopy are helpful in diagnosing the locationtype and severity of septal deformityThe endoscope is also useful in identifying polypsthe severity and extent of posterior septaldeviations and bony spurs and locating areas ofseptal perforation or mucosal injury
Deviated Nasal Septum
bull Therapybull ndash Septoplasty is a procedurebull The areabull of deviation is corrected or resected in order tobull leave behind as much cartilage and bone as
possiblebull Cartilage resection is minimised and can be
repositioned reshaped or recontoured using a variety of methods
Deviated Nasal Septum
bull ndash Indications of septoplasty before the growth period
bull of the nose is finished should be very limited bull -In these cases surgery must preserve all the
cartilagebull in order to prevent external changes of the
shape ofbull the nose
Deviated Nasal Septum
bull Complicationsbull ndash Frequent complications include haematoma andbull infection Cerebrospinal fluid leak is a rare but
potentiallybull serious complicationbull It is usually the resultbull of avulsion or damage to the cribriform plate whenbull handling the perpendicular plate of the ethmoidbull ndash Other complications include epistaxis nasal
Deviated Nasal Septum
bull Other complications include epistaxis nasal obstruction
bull due to residual deviation synechiae returnbull of the cartilaginous deviation septal perforationbull anosmia and cosmetic nasal deformities suchbull as widened alar rim margins drooping nasal tipbull columella retraction and a sunken dorsum with abull supratip saddle formation
Septal perforation with minor crusting View from provide closure of the
incision
Septal Haematoma
bull A septal haematoma is a blood collection under the perichondrium
bull of the septum and cartilagebull bull bull Epidemiologyaetiologybull ndash A septal haematoma is one of the most
severe complications of nasal trauma
Septal Haematoma
bull Diagnosisbull ndash Signs and symptoms include intense pain
swellingbull haematoma of the upper lip and philtrum
area andbull complete nasal airway obstruction
Septal HaematomaTherapyndash Management consists of drainage through a mucoperichondrial incision Immediate treatment isnecessary to prevent long-term problems such asa saddle-nose deformity perforation columellarretraction and nasal-base widening In childrenseptal destruction can lead to devastating nasal andmidfacial growth abnormalitiesbull Surgeryndash Incision and evacuation of the collection is performedDrainage of a septal haematoma should
Septal HaematomaSurgeryndash Incision and evacuation of the collection is performedDrainage of a septal haematoma should provide closure of the incision
Splints or transseptal sutures are placed to obliterate thepotential space and prevent collectionInfection involving the septal cartilage Reconstruction with autologouscartilage is then performed in a second stage Oral antibiotics should be given
Nasal DeformitySaddle-nose deformityndash A saddle-nose deformity is characterised by a loss ofnasal dorsal height and compromised nasal supportstructures -Other case observed are depressionof the middle vault and dorsum loss of nasal tipsupport and definition shortened (vertical) nasal length over rotation of the nasal tip and retrusion ofthe nasal spine and caudal septum It is also knownas a ldquoPug noserdquo or ldquoboxerrsquos noserdquo both of which referto various degrees of nasal dorsal depressionbull
Nasal DeformityEpidemiologyaetiologyndash Prevalence is higher in population groups prone to facial trauma (ie boxers athletes) those with historiesof intranasal cocaine use nasal surgery (e g radical submucosal septal resection reductive rhinoplasty)ndash A saddle-nose deformity can be congenital or acquired It can be noticed as a part of individual familialsyndromic and ethnic characteristics - Most deformities are due to traumatic and iatrogeniccauses Medical causes are Wegenerrsquosgranulomatosis relapsing polychondritis leprosy (Hansenrsquos disease) syphilis ectodermal dysplasiaand intranasal cocaine use
Nasal Deformity
bull Therapybull ndash Nasal reconstruction indications depend on patientbull selection surgeon experience and aetiology of thebull deformity bull Indications for surgery can be functionalbull aesthetic or most commonly both In individuals
with a compromised nasal airway a nasoseptalbull reconstruction is indicated
Nasal Deformity
bull Contraindications bull include patients with malignantbull chronic or autoimmune disease conditions drugbull abuse poor perioperative risk profile and unrealisticbull expectationsbull ndash Multiple previous rhinoplasties and certain
professionsbull (mixed martial artists boxers and other contactbull sports) are relative contraindications
Nasal DeformitySeptoplastyndash Septoplasty is performed to correct nasal obstructioncaused by septal deformityndash Usually septoplasty is performed under general anaesthesiawith the patient in the supine position with the head elevated by approximately 30 (Righthandedsurgeons approach from the right side)ndash Local vasoconstrictive anaesthesia is applied notonly to reduce postoperative pain but also more importantly to achieve vasoconstriction of themucosa and less intraoperative haemorrhage Lidocainewith adrenaline or epinephrine is usedalthough in patients with cardiac hypersensitivityoxymetazoline might be preferred
Nasal Deformity
bull Septoplasty begins with the incision of septal mucosabull Most operative techniques utilise a hemitransfixionbull incision at the caudal end of septum so thatbull deviation at this point might be reached as wellbull as a transfixion incision that is easily obtained ifbull needed (Right-handed surgeons normally choosebull the left side but that may vary when deviation isbull convex towards the right)
Nasal DeformityA columella retractor is placed over the columellaand by pulling it laterally the caudal border of theseptum is exposed Ala can be protected by an alaprotector A vertical incision with a no 15 bladeover the caudal end of septum is performed untilreaching the plane of the septal cartilage It is essentialto correctly identify the perichondrium and byusing the Cottle elevator dissect and lift it creatinga flap As the dissection proceeds along the septalcartilage a longer speculum (no 5) is introduced sothat elevation of the mucoperichondrium is doneunder constant visual controlndash The next step is to dissect the mucoperiostium
Nasal DeformityDissecting over the bony-cartilaginous junctionwhen joining both tunnels might be difficult and is
especially prone to membrane perforationndash If needed the same tunnels are to be created on the
other side of the septum Then deviated parts of
septum are identified and removed either with a
knife or a Freer chisel
Nasal Deformitybull septum from the maxillary crest the septum mustbull be separated from the perpendicular plate trimmedbull along the inferior border placed back onto the crestbull and sutured to the periosteum If the deformity involvesbull the vomer an osteotome is used Care mustbull be taken not to break the cribriform plate becausebull it could cause a cerebrospinal fistula
Nasal Deformity
bull Once the septal deviation is corrected the flapsbull and hemitransfixion incision are mattressed
withbull absorbable sutures Nasal packing to prevent
synechiaebull and postoperative septal haematoma mightbull be advised but should be removed within 72 h

Working in ENT
bull Working in ENT should be a very enjoyable experience whether it is a temporary attachment or a long-term career plan
bull It is helpful if you have an understanding of what others expect of you
bull It is also important for you to think about your own career development
Your duties
bull Patient care and continuitybull Professional developmentbull Research
The ENT Examination
EquipmentA fully equipped ENT department will have all the necessary instruments for performing a full ENT examination
Basic equipment
bull A light sourcemdasha portable headlight that runs off batteries is ideal
bull Wooden tongue depressorsbull Thudicum nasal speculumbull An otoscope with several speculaebull Pneumatic attachment for the otoscopebull Tuning fork 512Hzbull Pen and paperbull Gloves
Advanced equipment
bull Co-phenylcaine spraybull A flexible nasendoscope with light sourcebull Alcohol wipe to act as demist for the scopebull Aqueous lubricating gel for the scope
Emergency equipment
bull Large nasal tampons (you can always cut 10cm ones to size)
bull Silver nitrate sticksbull Foley catheters
Basic Anatomy of the Nose
bull The structural anatomy of the nose is important
bull for both aesthetic and functional reasons since the
bull nose as the gateway to the respiratory tract performs
bull a variety of physiologic functions
External NoseThe shape of the external nose is defined by the nasalbones a pair of rectangular bones in the upper nasaldorsum and by lateral cartilages (uppernasal cartilages) and alar cartilages (major alar cartilages)in the central and lower portions of the noseThe lateral portions of the nasal alae alsocontain several small accessory cartilages called theminor alar cartilages which are embedded in the lateralsoft tissues of the noseThe shape and stability of the alar cartilages each ofwhich consists of a medial and lateral crus
External Nose
Anatomy of the nasal base
bull Besides thebull medial crura the
inferior septal margin and the connective-
bull tissue septum (columella) are also responsible
bull for stabilizing the base of the nose
Anatomy of the nasal base
Anatomy of the nasal base
bull The nasal septum is subluxed toward the left side partially
bull obstructing the nasal airway
Nasal CavitiesThe nasal cavities begin anteriorly at the nasal vestibulewhich is bordered posteriorly by the internal nasalvalve (limen nasi) located between the posteriorborder of the alar cartilage and the anterior border ofthe lateral cartilage This valve area is the narrowestportion of the upper respiratory tract
Nasal Cavities
The interior ofthe nose behind the nasal valve is divided by the nasalseptum into two main cavities
Nasal CavitiesThe nasal septum iscomposed of an anterior cartilaginous part and twoposterior bony parts Abnormalities in the shape ofthe nasal septum which may consist of a deviated septum tensionseptum spurs or ridges are a frequent cause ofnasal airway obstructionThe choanae are the paired posterior openingsthrough which the nasal cavities communicate withthe nasopharynx
Nasal CavitiesThe nasal cavity is bounded laterally by the lateral nasalwalls which are formed by the ethmoid bone andmaxilla and posteriorly by the palatine bone and thepterygoid process of the sphenoid bone Several functionallyimportant structures are located on the lateralnasal wall the nasal turbinates and their associatedpassages (meati) sinus ostia and the orifice ofthe nasolacrimal duct (Fig 15)
The inferior turbinate consists of a separate bone thatis attached to the medial wall of the maxillary sinusThe opening of the nasolacrimal duct is located in thecorresponding inferior meatus The middle andsuperior turbinates are part of the ethmoid bone In rare cases a rudimentary ldquosupreme turbinaterdquo is alsopresent above the superior turbinate
The middle turbinate has by far the greatest functionalimportance because most of the drainage tracts fromthe surrounding paranasal sinuses open into the middlemeatus The nasal cavity is bounded superiorly by the cribriformplate of the ethmoid bone This thin bony platehas numerous openings for the passage of the fila olfactoriaand also forms the boundary of the anteriorcranial fossa
Nasal Cavities
The floor of the nasal cavity is formedmostly by the hard palate which is formed in turn bythe two palatine processes of the maxilla and the horizontallaminae of the palatine bone
Structure of the lateral nasal wall
Inferior meatus
Paranasal Sinuses
The paranasal sinuses are air-filled cavities that communicatewith the nasal cavities
-The maxillary sinus frontalsinus and anterior ethmoid cells drain into the nasalcavity through the middle meatusmdashie below themiddle turbinate -The posterior ethmoidcells drain into the nasal cavity through the superiormeatus The ostium of the sphenoid sinus is locatedin the anterior wall directly above the choanae- The anatomical connections between the nasal cavity andparanasal sinuses are functionally important and playa key role in the pathogenesis of many rhinologic diseasesthat involve the paranasal sinuses
Vascular SupplyThe external nose derives most of its blood supply
from the facial artery which arises from the external
carotid artery and from the ophthalmic artery which
springs from the internal carotid artery
Vascular Supply
The internalnose receives blood from the territories of the externaland internal carotid arteries- the terminalbranches of the sphenopalatine artery which arisesfrom the maxillary artery - the anterior and posteriorethmoid arteries which arise from the ophthalmicartery-internal carotid arterie
venous drainage
The venous drainageof the facial region is handled by -the facial vein -retromandibular vein -internal jugular vein
lymphatic drainage
The regional lymphatic drainage of the face and externalnose is handled mainly by- the submandibularlymph nodes while the nasal cavity is additionallydrained by -the retropharyngeal and deep - -cervical lymph nodes
Morphology of the Nasal Mucosa
Besides the anatomical structure of the external noseand nasal cavity the nasal mucosa plays an essentialrole in numerous functions of the nose in the respiratory tract
Morphology of the Nasal Mucosa
The anterior part of the nasal cavity (the nasal vestibule)like the external nose is covered by skin composedof a multilayer keratinizing squamous epithelium and finally a ciliated respiratory epithelium A small areaon the upper nasal septum superior turbinate andpart of the middle turbinate located adjacent to thecribriform plate is covered by olfactory mucosa and iscalled the olfactory region
Nerve SupplyThe facial skin receives its sensory innervation fromterminal branches of the trigeminal nerve that enterthe facial region through the supraorbital infraorbitaland mental foramina Thefacial muscles are classified as mimetic or mastica- tory each of these groups receiving different motorinnervationbythe facial nerve
History and Clinical Examination of the Nose
Historybull The main symptomsbull nasal obstruction (ldquostuffy
noserdquo)bull nasal dischargebull Headachesbull Olfactory
dysfunction
Palpationbony discontinuitiesNeuralgias to check
over- the supraorbital -infraorbital -mental foramina
Anterior Rhinoscopy
bull The rhinologic examination itself begins with anterior
bull rhinoscopy to evaluate the nasal vestibule and the anterior
bull portions of the nasal cavity
Nasal Endoscopy Nasal endoscopy has become the most important andrewarding clinical examination method in rhinologic diagnosis
- rigid endoscopes which are available in 4-mm and 28- mm diameters and assorted viewing angles (eg 01048576 301048576 1201048576) -flexible endoscopes are also available for inspecting the nose and nasopharynx and exploring all of the pharynx and larynx in one sitting
Nasal endoscopy
Nasal Endoscopy
Nasal Endoscopy
Imaging of the Nose and Paranasal Sinuses
Conventional RadiographsStandard paranasal sinus radiographs in the occipitomental
projection ( Water projection) and
occipitofrontal projection Caldwell projection) in cases of acute inflammation
They are also obtained to evaluate midfacial fractures
Computed Tomography (CT) the main indicationsfor CT scanning of the
nose and paranasal sinuses
are- chronic sinusitis - -trauma (especially
frontobasal -fractures)
-and tumors
The occipitofrontal projection is better for evaluating theethmoid cells and frontal sinus
occipitomental projection demonstrates the maxillarysinus and gives a limited view of the sphenoid sinus
Computed tomography of the paranasal sinuses
Four representative coronal CT scans are shown
Four representative coronal CT scans are shown
Magnetic Resonance Imaging
Magnetic maging
Magnetic resonance imaging (MRI) has fewer indicationsthan CT in patients with paranasal sinus diseaseThis is primarily because MRI is markedly inferior toCT in defining the bony boundaries of the sinusesThe strength of MRI lies in its superior soft-tissue discriminationMRI is indicated in diseases that involve the paranasal sinuses in addition to thecranial cavity or orbit (eg tumors and congenitalmalformations such as encephaloceles)
MRI of the paranasal sinuses
The Nose and Sinuses
Structure The structure of the nose is made up of
four partsbull The surface anatomybull The nasal skeletonmdashcomposed of the
two nasal bones the paired upper lateral and lower lateral cartilages and the nasal septum covered in subcutaneous tissue and skin
bull The internal anatomymdashincludes the septum of the nose which forms the medial wall of the nasal cavity The turbinates on the lateral wall are also called conchae
bull The osteomeatal complexmdasha key functional area of the nose
Function The nose is the main route for inspired
air and its structure is related to this function As the air passes over the large surface area of the turbinates
The inspired gases are warmed and humidified Mucus on the mucosa of the nose removes large dust particles from the air as it is breathed in
The voice resonates in the sinuses and nose and this provides character to the speech
Pneumatization of the sinusesmdashthey are air filled spacesmdashreduces the weight of the skull
Diseases of thDiseases of the Outer and Inner Nosee Outer and
Inner Nose Erysipelas Definition of the disease ndash Erysipela is a skin infection that affects the superficial dermis and is caused by Streptococcus pyogenes (group A) It usually develops in the extremities and the face and less commonly on the scalp and genitals bull Epidemiologyaetiology ndash Erysipelas are more often seen in elderly infants and children patients with compromised immunology and diabetes -Predisposing factors are alcoholism skin ulceration puncture wounds fungal infections malnutrition and burns
Erysipelas
bull Symptomsbull ndash It usually presents of fever general fatigue bull -The skin lesion is a redindurated and elevated plaque
with borders that expand rapidly bull It is painful warm and accompanied by variable oedemabull -On the second or third day a flaccid bulla may develop
and desquamationbull bull Presence of regional lymph nodes is common
Erysipelas
bull Complicationsndash The most common complication is recurrencewhich is seen in 18ndash30 of the cases even afterproper antibiotic therapy Recurrence is seen moreoften in females than in malesA skin infection with S pyogenes could lead toglomerulonephritis
Erysipelas
bull Complicationsbull ndash The most common complication is recurrencebull which is seen in 18ndash30 of the cases even afterbull proper antibiotic therapy bull -Recurrence is seen morebull often in females than in males bull -A skin infection with S pyogenes could lead tobull glomerulonephritis
Erysipelas
bull bull Diagnosisbull ndash Diagnosis is based on the patientrsquos personal
historybull and physical examination particularly on inspectionbull of the skin
bull Blood cultures are positive in less thanbull 5 of cases
ErysipelasTherapyndash Conservative therapybull The preferred antibiotic is penicillin In mildcases with minor systemic symptoms penicillinV 500 mg orally every 6 h for 10 days or penicillinG benzathine 12 mil U intramuscularlyonceOther possibilities are amoxicillin 500 mgorally twice a day for 10 days or cephalexin 500mg orally every 6 h for 10 days
ErysipelasIn moderate and severe cases with significantsystemic symptoms hospitalization and intravenoustreatment is required penicillin G 2ndash4mil U intravenously every 4ndash6 h Cefazolin05ndash15 gm intravenously every 8 h cefotaxime1ndash2 gm intravenously every 8 h or ceftriaxone1ndash2 gm intravenously once a day should be administeredIn patients with a penicillin allergyclindamycin 600 mg intravenously every 8 h orvancomycin 15 mgkg intravenously twice a daymay be given
ErysipelaAdditional useful therapeutic optionsbull Prednisone 30 mg over 8 days might be consideredas well as elevation of the affected siteMoist heat compresses may be usefulbull Surgeryndash Debridement and drainage are indicated when bullaeabscesses or necroses are presentbull Differential diagnosisndash Contact dermatitisndash Asteatotic eczemandash Herpes zosterndash Angioneurotic oedemandash Osteomyelitis
Furuncle
bull Definition of the diseasebull ndash A furuncle is an infection that beginsbull at the hair follicle and spreads deeper into thebull dermis and subcutaneous tissue forming abull nodule After several days it developsbull into an abscess - red painful and fluctuantbull bull bull Epidemiologyaetiologybull ndash The aetiologic agent is Staphylococcus aureus
FuruncleSymptomsndashsymptoms are local and limited to thesite of infection Furuncles usually are wherehair follicles are present bull Complicationndash One complication is furunculosis multiple draining furunclesDiagnosisndash The diagnosis is based on clinical inspection - Cultures are not necessary when there is no systemic involvement but should beconsidered if systemic therapy (in case of feversignificant cellulitis or hospitalization) or whenmethicillin-resistant Staphylococcusaureus (MRSA) is considered
FuruncleTherapyndash When the furuncle is small application of moist heat compress to promote drainage -Larger furuncles should be drained by surgical incision-After drainage the area should be cleaned with anantiseptic (with chlorhexidinebetadine) should be applied twice
a dayndash If no systemic symptoms or extensive cellulitis arepresent simple topical care is usually curative andoral antibiotics are not necessary Otherwise systemictreatment is indicated and should cover anypossible MRSA
Furuncle
bull -Recommended antibiotics are trimethoprim-sulfamethoxazole
bull 1ndash2 tablets orally twice daily doxycyclinebull 100 mg orally twice dailybull or clindamycin 300ndash450 mg orally every 8 hbull - In severe cases vancomycin 15 mgkg
intravenouslybull every 12 h or clindamycin 600 mg intravenouslybull every 8 h
Midline Granulomabull A midline granuloma is an angiocentricbull lymphoma it was referred to as polymorphicbull reticulosis lethal midline granuloma and midline
malignant reticulosisbull bull Definition of the diseasebull ndash This rare disease is a lymphoma of extranodal
presentationall cases are positive for the Epstein-Barr virus
bull -This lymphoma most commonly appears in the midface region
Midline GranulomaEpidemiologyaetiologyndash This form of lymphoma is rare in Europe and theUnited States with a higher prevalence in Asia and PeruSymptomsndash The most common presentation is nasal obstruction with a destructive mass occupying the nosesinuses and palate
-Fever night sweatsand weight loss seen usually in Hodgkinrsquos lymphomaand other non-Hodgkinrsquos lymphomas (knownas ldquoB symptomsrdquo) are uncommon
Midline GranulomaDiagnosisndash The diagnosis is based on anatomopathologicalstudy The malignancy of the tumour manifested byextensive necrosis makes the histological diagnosisdifficult and often more biopsies are required forconfirmationbull Therapyndash Therapy consists of radiotherapy with or withoutchemotherapy
Midline Granuloma
bull Prognosisbull ndash Depending on the stage long-term remission or
experience a worseningbull prognosis with relapses which may include otherbull extranodal sites bull Involvement of extranodal sitesbull including the upper airway gastrointestinal tractbull skin
Wegenerrsquos Granulomatosis
bull Definition of the diseasebull ndash Wegenerrsquos granulomatosis is a systemic chronicbull vasculitis of small- and medium-sized blood vesselsbull with an autoimmune component It affectsbull particular organs with variable predilectionbull Epidemiologyaetiologybull ndash Wegenerrsquos granulomatosis is a rare disease It affects
about 1 in 20000ndash30000 people It is more prevalentbull in middle-aged Caucasian patients
Wegenerrsquos Granulomatosis
Symptomsndash The disease may present pulmonary upper
respiratory tract or renal In the disseminated form-The localised form ndash confinedto the upper respiratory region ndash is present in 25of the patients- It consists of nonspecific manifestationssuch as nasal obstruction crusting purulentor bloody rhinorrhea and painful or painless ulcers in oral or nasal cavities which are unresponsive tostandard medical treatment
Wegenerrsquos Granulomatosis
bull In some patients the nasal septum is perforatedbull which leads to saddle-nose deformity Less
commonbull symptoms are hoarseness stridor due to
subglotticbull stenosis otalgia otorrhea and conductivebull and sensorineural hearing loss Also ocular
symptomsbull such as scleritis conjunctivitis uveitis andbull episcleritis may be present
Wegenerrsquos Granulomatosis
bull ndash In the disseminated form pulmonary involvementbull is manifested by cough dyspnoea haemoptysisbull (due to an alveolar capillaritis necrotic lesions orbull endobronchial disease) and pleuritic painndashbull -Ninety per cent of patients have nasal symptomsbull and these symptoms are usually the first
manifestationof the diseasebull -Most patients have also renal involvementbull even if it is subclinical
Wegenerrsquos Granulomatosis
Diagnosis ndash Diagnosis of Wegenerrsquos granulomatosis is based on clinical findings that demonstrate lung (chest x-ray) kidney (urine analysis) or upper respiratory tract
involvement (oral or nasal ulcers or discharge) - positive blood analysis for cytoplasmic-staining antineutrophil
cytoplasmic antibodies (c-ANCA) and confirming proteinase 3 (PR3) ANCA or myeloperoxidase (MPO) ANCA ndash Biopsy is essential for diagnosis nonspecific chronic inflammation
and necrosis -Bacterial and fungal infections
Wegenerrsquos Granulomatosis
Therapyndash Conservative therapybull In the induction of disease remission highdosesteroids (e g prednisone 1 mgkgday) for1 month with tapering over several months aregiven In addition cyclophosphamide (2 mgkgday) should be administered for 6ndash12 monthsuntil symptoms disappear In the maintenanceof remission cyclophosphamide should be
Wegenerrsquos Granulomatosis
Antibiotics mainly trimethoprim-sulfamethoxazoleare given for prophylaxis againstPneumocystis jiroveci (formerly Pneumocystiscarinii) pneumonia (PCP) which may developduring immunosuppression and have a role inpreventing recurrencesbull Sinonasal manifestations may be treated with topical nasal steroids and nasal irrigations lowdosesystemic steroids and antibiotics when bacterial infection (typically Staphylococcus species) is suspected
Wegenerrsquos Granulomatosis
bull Prognosisbull ndash Most of the patients respond well to treatmentbull achieving symptom-free intervals of 5ndash20 yearsbull or more bull -Anatomical problems (sinusitis trachealbull stenosis) may require surgery bull Relapses can be long and troublesomebull Long-term complications are chronicbull renal failure hearing loss and deafness
Nasal Fractures Definition ndash A nasal fracture is a disruption of the nasal bone structure due to trauma It is the most frequently fractured facial bone Epidemiologyaetiology ndash Sports falls and assaults are the usual mechanisms of fracture -Males are affected twice as often as are females -Paediatric populations with a incidences during the second and third decades of life -Variables such as force impact direction nature of the striking object age and other will influence the pattern of injury to the components of the nose
Nasal Fractures
bull Symptomsbull ndash Deformity swelling epistaxis and periorbital
ecchymosis are signs that are suggestive of nasal fracture
bull bony crepitus and nasal segment mobilitybull ndash Epiphora bull Severe bilateral injuries to the lachrymal bones
arebull associated with depressed nasal fractures
Nasal Fractures Complications ndash Septal haematoma is one of the most severe early complications of nasal trauma and without drainage it results in abscess formation 6ndash7 days after trauma producing necrosis of the septal cartilage -Long-term problems such as saddle-nose deformity perforation columellar retraction and nasalbase
Septal infection could lead to osteomyelitis orbital and intracranial abscesses meningitis and cavernous sinus thrombosis -Cerebrospinal fluid leakage is a common complication of severe
nasal and frontal fractures
Nasal Fractures
bull Diagnostic proceduresbull ndash Inspectionbull bull Changes of appearance such as deviation andbull asymmetry bleeding watery drainage changesbull in nasal breathing and smell It is useful to comparebull the current presentation with old photographsbull (up to 40 of normal individuals havebull significant nose malformations)
Nasal Fractures Physical examination bull The diagnosis of a nasal fracture is made primarily by physical examination epistaxis nasal swelling and periorbital ecchymosis Nasal shape in the lateral and frontal inspection should be assessed Grasping the dorsum between two fingers and rocking the pyramid back and forth aids in assessing the mobility of nasal bones Internal structures should be evaluated by using a headlight and nasal speculum Clotted blood is removed by suction and assessment of haematoma mucosal tears and active bleeding is performed Bimanual palpation of the septum helps to differentiate septal swelling from haematoma ndash
Nasal FracturesRadiographybull There is no clear evidence of the role of radiographyin the management of nasal fracturesPlain films have up to a 66 false-positive rateas a result of misinterpretation of normal suturelines In addition old fractures are difficult todistinguishbull Three-dimensional CT is recommended for extensiveinjuries involving the nasal-orbital-ethmoidalcomplexndash
Nasal Fractures
bull Additionaluseful diagnostic proceduresbull bull Using a 0 or 30deg 4-mm endoscope is helpful inbull the assessment of posterior abnormalities If thebull patient is heavily sedated Brown-Gruss
provocationbull manoeuvres may be performed to determinebull deformities in upper middle or lower segmentsbull by compressing each compartment
Nasal FracturesConservative treatmentndash Treatment of bleedingbull For localised bleeding anterior sources may becauterised by silver nitrate or sealed with topicalmaterials such as thrombin combined withgelatin foam fibrin glue FloSealreg or other procoagulantmaterials If conservative measuresfail a formal anterior packing is placedbull Bleeding from branches of sphenopalatine orethmoid vessels requires anterior-posteriorpacking
Nasal Fractures
bull bull Surgical methods such as direct endoscopic vessel
bull cauterization or ligation have been shown tobull offer better haemostasis and patient comfortbull Angiography with embolization can also be
consideredbull in cases refractory to more conservativebull approaches
Nasal Fractures
bull Type of reductionbull bull Nondisplaced fractures should be treated withbull observation alone Closed nasal reduction is thebull best choice for simple injuries (isolated unilateralbull with medial displacement)bull bull An open approach should be considered in
severebull trauma (bilateral depressed fractures)
Nasal Fracturesbull Surgical principlesbull ndash Topical anaesthesia with cotton pledgets soakedbull with 4 cocaine or 005 oxymethazoline combinedbull with 4 topical lidocaine should be appliedbull for 5ndash10 min Local anaesthesia should also be injectedbull (1 lidocaine and 1100000 epinephrine)bull along the septum lateral walls and floor of the nasalbull cavitybull bull
Nasal FracturesClosed reductionndashndash The nasal bones are grasped between two fingersand pressure is applied laterally in theopposite direction of the deviation A bluntelevator may be used from within the nose incases of significant medial collapse Walshamforceps can be of help Reduction of the septumshould be performed with the use ofAsch forceps
Nasal Fractures
bull To prevent collapse of the postreductionbull framework nasal packing should be placedbull for 3ndash5 days Septum splints are recommendedbull in comminuted septal fractures withbull severe mucosal lesions External nasal splintingbull for 10 days (Aquaplastreg Thermoplastreg)bull provides nasal protection Nasal saline spraysbull prevent crusting and oral antibiotics should
Nasal Fractures
bull Open reductionbull ndashndash Immediate repair of fractures by using
widebull surgical exposure reduction fixation and
reconstructionbull ndashndash The second option is delayed correctionbull (6 months or more) of persistent deformitiesbull using standard techniques of rhinoplasty
Deviated Nasal Septum
bull Definition of the diseasebull ndash Deviation of the nasal septum is a common causebull of unilateral nasal airway obstruction in which thebull nasal septum is displacedbull bull Epidemiologyaetiologybull ndash Developmental septal abnormalities Septal cartilage
damage in the neonatal period andbull during birth can cause severe septal deviation inbull the absence of a history of nasal trauma
Deviated Nasal Septum
bull Symptomsbull ndash Patients may present with a history of sinusitis
allergicbull rhinitis obstructive sleep apnoea previousbull nasal surgery or recent nasal trauma Unilateral or
bilateral nasal airway obstruction that is unrelievedbull with decongestants or nasal steroid sprays is oftenbull seenbull bull
Deviated Nasal SeptumDiagnosisndashExamination external dorsal deviation or the columella and caudal septummay be deflected off the midline (caudal subluxation)ndash Inspections of the nasal cavity and anterior-posteriorrhinoscopy are helpful in diagnosing the locationtype and severity of septal deformityThe endoscope is also useful in identifying polypsthe severity and extent of posterior septaldeviations and bony spurs and locating areas ofseptal perforation or mucosal injury
Deviated Nasal Septum
bull Therapybull ndash Septoplasty is a procedurebull The areabull of deviation is corrected or resected in order tobull leave behind as much cartilage and bone as
possiblebull Cartilage resection is minimised and can be
repositioned reshaped or recontoured using a variety of methods
Deviated Nasal Septum
bull ndash Indications of septoplasty before the growth period
bull of the nose is finished should be very limited bull -In these cases surgery must preserve all the
cartilagebull in order to prevent external changes of the
shape ofbull the nose
Deviated Nasal Septum
bull Complicationsbull ndash Frequent complications include haematoma andbull infection Cerebrospinal fluid leak is a rare but
potentiallybull serious complicationbull It is usually the resultbull of avulsion or damage to the cribriform plate whenbull handling the perpendicular plate of the ethmoidbull ndash Other complications include epistaxis nasal
Deviated Nasal Septum
bull Other complications include epistaxis nasal obstruction
bull due to residual deviation synechiae returnbull of the cartilaginous deviation septal perforationbull anosmia and cosmetic nasal deformities suchbull as widened alar rim margins drooping nasal tipbull columella retraction and a sunken dorsum with abull supratip saddle formation
Septal perforation with minor crusting View from provide closure of the
incision
Septal Haematoma
bull A septal haematoma is a blood collection under the perichondrium
bull of the septum and cartilagebull bull bull Epidemiologyaetiologybull ndash A septal haematoma is one of the most
severe complications of nasal trauma
Septal Haematoma
bull Diagnosisbull ndash Signs and symptoms include intense pain
swellingbull haematoma of the upper lip and philtrum
area andbull complete nasal airway obstruction
Septal HaematomaTherapyndash Management consists of drainage through a mucoperichondrial incision Immediate treatment isnecessary to prevent long-term problems such asa saddle-nose deformity perforation columellarretraction and nasal-base widening In childrenseptal destruction can lead to devastating nasal andmidfacial growth abnormalitiesbull Surgeryndash Incision and evacuation of the collection is performedDrainage of a septal haematoma should
Septal HaematomaSurgeryndash Incision and evacuation of the collection is performedDrainage of a septal haematoma should provide closure of the incision
Splints or transseptal sutures are placed to obliterate thepotential space and prevent collectionInfection involving the septal cartilage Reconstruction with autologouscartilage is then performed in a second stage Oral antibiotics should be given
Nasal DeformitySaddle-nose deformityndash A saddle-nose deformity is characterised by a loss ofnasal dorsal height and compromised nasal supportstructures -Other case observed are depressionof the middle vault and dorsum loss of nasal tipsupport and definition shortened (vertical) nasal length over rotation of the nasal tip and retrusion ofthe nasal spine and caudal septum It is also knownas a ldquoPug noserdquo or ldquoboxerrsquos noserdquo both of which referto various degrees of nasal dorsal depressionbull
Nasal DeformityEpidemiologyaetiologyndash Prevalence is higher in population groups prone to facial trauma (ie boxers athletes) those with historiesof intranasal cocaine use nasal surgery (e g radical submucosal septal resection reductive rhinoplasty)ndash A saddle-nose deformity can be congenital or acquired It can be noticed as a part of individual familialsyndromic and ethnic characteristics - Most deformities are due to traumatic and iatrogeniccauses Medical causes are Wegenerrsquosgranulomatosis relapsing polychondritis leprosy (Hansenrsquos disease) syphilis ectodermal dysplasiaand intranasal cocaine use
Nasal Deformity
bull Therapybull ndash Nasal reconstruction indications depend on patientbull selection surgeon experience and aetiology of thebull deformity bull Indications for surgery can be functionalbull aesthetic or most commonly both In individuals
with a compromised nasal airway a nasoseptalbull reconstruction is indicated
Nasal Deformity
bull Contraindications bull include patients with malignantbull chronic or autoimmune disease conditions drugbull abuse poor perioperative risk profile and unrealisticbull expectationsbull ndash Multiple previous rhinoplasties and certain
professionsbull (mixed martial artists boxers and other contactbull sports) are relative contraindications
Nasal DeformitySeptoplastyndash Septoplasty is performed to correct nasal obstructioncaused by septal deformityndash Usually septoplasty is performed under general anaesthesiawith the patient in the supine position with the head elevated by approximately 30 (Righthandedsurgeons approach from the right side)ndash Local vasoconstrictive anaesthesia is applied notonly to reduce postoperative pain but also more importantly to achieve vasoconstriction of themucosa and less intraoperative haemorrhage Lidocainewith adrenaline or epinephrine is usedalthough in patients with cardiac hypersensitivityoxymetazoline might be preferred
Nasal Deformity
bull Septoplasty begins with the incision of septal mucosabull Most operative techniques utilise a hemitransfixionbull incision at the caudal end of septum so thatbull deviation at this point might be reached as wellbull as a transfixion incision that is easily obtained ifbull needed (Right-handed surgeons normally choosebull the left side but that may vary when deviation isbull convex towards the right)
Nasal DeformityA columella retractor is placed over the columellaand by pulling it laterally the caudal border of theseptum is exposed Ala can be protected by an alaprotector A vertical incision with a no 15 bladeover the caudal end of septum is performed untilreaching the plane of the septal cartilage It is essentialto correctly identify the perichondrium and byusing the Cottle elevator dissect and lift it creatinga flap As the dissection proceeds along the septalcartilage a longer speculum (no 5) is introduced sothat elevation of the mucoperichondrium is doneunder constant visual controlndash The next step is to dissect the mucoperiostium
Nasal DeformityDissecting over the bony-cartilaginous junctionwhen joining both tunnels might be difficult and is
especially prone to membrane perforationndash If needed the same tunnels are to be created on the
other side of the septum Then deviated parts of
septum are identified and removed either with a
knife or a Freer chisel
Nasal Deformitybull septum from the maxillary crest the septum mustbull be separated from the perpendicular plate trimmedbull along the inferior border placed back onto the crestbull and sutured to the periosteum If the deformity involvesbull the vomer an osteotome is used Care mustbull be taken not to break the cribriform plate becausebull it could cause a cerebrospinal fistula
Nasal Deformity
bull Once the septal deviation is corrected the flapsbull and hemitransfixion incision are mattressed
withbull absorbable sutures Nasal packing to prevent
synechiaebull and postoperative septal haematoma mightbull be advised but should be removed within 72 h

Your duties
bull Patient care and continuitybull Professional developmentbull Research
The ENT Examination
EquipmentA fully equipped ENT department will have all the necessary instruments for performing a full ENT examination
Basic equipment
bull A light sourcemdasha portable headlight that runs off batteries is ideal
bull Wooden tongue depressorsbull Thudicum nasal speculumbull An otoscope with several speculaebull Pneumatic attachment for the otoscopebull Tuning fork 512Hzbull Pen and paperbull Gloves
Advanced equipment
bull Co-phenylcaine spraybull A flexible nasendoscope with light sourcebull Alcohol wipe to act as demist for the scopebull Aqueous lubricating gel for the scope
Emergency equipment
bull Large nasal tampons (you can always cut 10cm ones to size)
bull Silver nitrate sticksbull Foley catheters
Basic Anatomy of the Nose
bull The structural anatomy of the nose is important
bull for both aesthetic and functional reasons since the
bull nose as the gateway to the respiratory tract performs
bull a variety of physiologic functions
External NoseThe shape of the external nose is defined by the nasalbones a pair of rectangular bones in the upper nasaldorsum and by lateral cartilages (uppernasal cartilages) and alar cartilages (major alar cartilages)in the central and lower portions of the noseThe lateral portions of the nasal alae alsocontain several small accessory cartilages called theminor alar cartilages which are embedded in the lateralsoft tissues of the noseThe shape and stability of the alar cartilages each ofwhich consists of a medial and lateral crus
External Nose
Anatomy of the nasal base
bull Besides thebull medial crura the
inferior septal margin and the connective-
bull tissue septum (columella) are also responsible
bull for stabilizing the base of the nose
Anatomy of the nasal base
Anatomy of the nasal base
bull The nasal septum is subluxed toward the left side partially
bull obstructing the nasal airway
Nasal CavitiesThe nasal cavities begin anteriorly at the nasal vestibulewhich is bordered posteriorly by the internal nasalvalve (limen nasi) located between the posteriorborder of the alar cartilage and the anterior border ofthe lateral cartilage This valve area is the narrowestportion of the upper respiratory tract
Nasal Cavities
The interior ofthe nose behind the nasal valve is divided by the nasalseptum into two main cavities
Nasal CavitiesThe nasal septum iscomposed of an anterior cartilaginous part and twoposterior bony parts Abnormalities in the shape ofthe nasal septum which may consist of a deviated septum tensionseptum spurs or ridges are a frequent cause ofnasal airway obstructionThe choanae are the paired posterior openingsthrough which the nasal cavities communicate withthe nasopharynx
Nasal CavitiesThe nasal cavity is bounded laterally by the lateral nasalwalls which are formed by the ethmoid bone andmaxilla and posteriorly by the palatine bone and thepterygoid process of the sphenoid bone Several functionallyimportant structures are located on the lateralnasal wall the nasal turbinates and their associatedpassages (meati) sinus ostia and the orifice ofthe nasolacrimal duct (Fig 15)
The inferior turbinate consists of a separate bone thatis attached to the medial wall of the maxillary sinusThe opening of the nasolacrimal duct is located in thecorresponding inferior meatus The middle andsuperior turbinates are part of the ethmoid bone In rare cases a rudimentary ldquosupreme turbinaterdquo is alsopresent above the superior turbinate
The middle turbinate has by far the greatest functionalimportance because most of the drainage tracts fromthe surrounding paranasal sinuses open into the middlemeatus The nasal cavity is bounded superiorly by the cribriformplate of the ethmoid bone This thin bony platehas numerous openings for the passage of the fila olfactoriaand also forms the boundary of the anteriorcranial fossa
Nasal Cavities
The floor of the nasal cavity is formedmostly by the hard palate which is formed in turn bythe two palatine processes of the maxilla and the horizontallaminae of the palatine bone
Structure of the lateral nasal wall
Inferior meatus
Paranasal Sinuses
The paranasal sinuses are air-filled cavities that communicatewith the nasal cavities
-The maxillary sinus frontalsinus and anterior ethmoid cells drain into the nasalcavity through the middle meatusmdashie below themiddle turbinate -The posterior ethmoidcells drain into the nasal cavity through the superiormeatus The ostium of the sphenoid sinus is locatedin the anterior wall directly above the choanae- The anatomical connections between the nasal cavity andparanasal sinuses are functionally important and playa key role in the pathogenesis of many rhinologic diseasesthat involve the paranasal sinuses
Vascular SupplyThe external nose derives most of its blood supply
from the facial artery which arises from the external
carotid artery and from the ophthalmic artery which
springs from the internal carotid artery
Vascular Supply
The internalnose receives blood from the territories of the externaland internal carotid arteries- the terminalbranches of the sphenopalatine artery which arisesfrom the maxillary artery - the anterior and posteriorethmoid arteries which arise from the ophthalmicartery-internal carotid arterie
venous drainage
The venous drainageof the facial region is handled by -the facial vein -retromandibular vein -internal jugular vein
lymphatic drainage
The regional lymphatic drainage of the face and externalnose is handled mainly by- the submandibularlymph nodes while the nasal cavity is additionallydrained by -the retropharyngeal and deep - -cervical lymph nodes
Morphology of the Nasal Mucosa
Besides the anatomical structure of the external noseand nasal cavity the nasal mucosa plays an essentialrole in numerous functions of the nose in the respiratory tract
Morphology of the Nasal Mucosa
The anterior part of the nasal cavity (the nasal vestibule)like the external nose is covered by skin composedof a multilayer keratinizing squamous epithelium and finally a ciliated respiratory epithelium A small areaon the upper nasal septum superior turbinate andpart of the middle turbinate located adjacent to thecribriform plate is covered by olfactory mucosa and iscalled the olfactory region
Nerve SupplyThe facial skin receives its sensory innervation fromterminal branches of the trigeminal nerve that enterthe facial region through the supraorbital infraorbitaland mental foramina Thefacial muscles are classified as mimetic or mastica- tory each of these groups receiving different motorinnervationbythe facial nerve
History and Clinical Examination of the Nose
Historybull The main symptomsbull nasal obstruction (ldquostuffy
noserdquo)bull nasal dischargebull Headachesbull Olfactory
dysfunction
Palpationbony discontinuitiesNeuralgias to check
over- the supraorbital -infraorbital -mental foramina
Anterior Rhinoscopy
bull The rhinologic examination itself begins with anterior
bull rhinoscopy to evaluate the nasal vestibule and the anterior
bull portions of the nasal cavity
Nasal Endoscopy Nasal endoscopy has become the most important andrewarding clinical examination method in rhinologic diagnosis
- rigid endoscopes which are available in 4-mm and 28- mm diameters and assorted viewing angles (eg 01048576 301048576 1201048576) -flexible endoscopes are also available for inspecting the nose and nasopharynx and exploring all of the pharynx and larynx in one sitting
Nasal endoscopy
Nasal Endoscopy
Nasal Endoscopy
Imaging of the Nose and Paranasal Sinuses
Conventional RadiographsStandard paranasal sinus radiographs in the occipitomental
projection ( Water projection) and
occipitofrontal projection Caldwell projection) in cases of acute inflammation
They are also obtained to evaluate midfacial fractures
Computed Tomography (CT) the main indicationsfor CT scanning of the
nose and paranasal sinuses
are- chronic sinusitis - -trauma (especially
frontobasal -fractures)
-and tumors
The occipitofrontal projection is better for evaluating theethmoid cells and frontal sinus
occipitomental projection demonstrates the maxillarysinus and gives a limited view of the sphenoid sinus
Computed tomography of the paranasal sinuses
Four representative coronal CT scans are shown
Four representative coronal CT scans are shown
Magnetic Resonance Imaging
Magnetic maging
Magnetic resonance imaging (MRI) has fewer indicationsthan CT in patients with paranasal sinus diseaseThis is primarily because MRI is markedly inferior toCT in defining the bony boundaries of the sinusesThe strength of MRI lies in its superior soft-tissue discriminationMRI is indicated in diseases that involve the paranasal sinuses in addition to thecranial cavity or orbit (eg tumors and congenitalmalformations such as encephaloceles)
MRI of the paranasal sinuses
The Nose and Sinuses
Structure The structure of the nose is made up of
four partsbull The surface anatomybull The nasal skeletonmdashcomposed of the
two nasal bones the paired upper lateral and lower lateral cartilages and the nasal septum covered in subcutaneous tissue and skin
bull The internal anatomymdashincludes the septum of the nose which forms the medial wall of the nasal cavity The turbinates on the lateral wall are also called conchae
bull The osteomeatal complexmdasha key functional area of the nose
Function The nose is the main route for inspired
air and its structure is related to this function As the air passes over the large surface area of the turbinates
The inspired gases are warmed and humidified Mucus on the mucosa of the nose removes large dust particles from the air as it is breathed in
The voice resonates in the sinuses and nose and this provides character to the speech
Pneumatization of the sinusesmdashthey are air filled spacesmdashreduces the weight of the skull
Diseases of thDiseases of the Outer and Inner Nosee Outer and
Inner Nose Erysipelas Definition of the disease ndash Erysipela is a skin infection that affects the superficial dermis and is caused by Streptococcus pyogenes (group A) It usually develops in the extremities and the face and less commonly on the scalp and genitals bull Epidemiologyaetiology ndash Erysipelas are more often seen in elderly infants and children patients with compromised immunology and diabetes -Predisposing factors are alcoholism skin ulceration puncture wounds fungal infections malnutrition and burns
Erysipelas
bull Symptomsbull ndash It usually presents of fever general fatigue bull -The skin lesion is a redindurated and elevated plaque
with borders that expand rapidly bull It is painful warm and accompanied by variable oedemabull -On the second or third day a flaccid bulla may develop
and desquamationbull bull Presence of regional lymph nodes is common
Erysipelas
bull Complicationsndash The most common complication is recurrencewhich is seen in 18ndash30 of the cases even afterproper antibiotic therapy Recurrence is seen moreoften in females than in malesA skin infection with S pyogenes could lead toglomerulonephritis
Erysipelas
bull Complicationsbull ndash The most common complication is recurrencebull which is seen in 18ndash30 of the cases even afterbull proper antibiotic therapy bull -Recurrence is seen morebull often in females than in males bull -A skin infection with S pyogenes could lead tobull glomerulonephritis
Erysipelas
bull bull Diagnosisbull ndash Diagnosis is based on the patientrsquos personal
historybull and physical examination particularly on inspectionbull of the skin
bull Blood cultures are positive in less thanbull 5 of cases
ErysipelasTherapyndash Conservative therapybull The preferred antibiotic is penicillin In mildcases with minor systemic symptoms penicillinV 500 mg orally every 6 h for 10 days or penicillinG benzathine 12 mil U intramuscularlyonceOther possibilities are amoxicillin 500 mgorally twice a day for 10 days or cephalexin 500mg orally every 6 h for 10 days
ErysipelasIn moderate and severe cases with significantsystemic symptoms hospitalization and intravenoustreatment is required penicillin G 2ndash4mil U intravenously every 4ndash6 h Cefazolin05ndash15 gm intravenously every 8 h cefotaxime1ndash2 gm intravenously every 8 h or ceftriaxone1ndash2 gm intravenously once a day should be administeredIn patients with a penicillin allergyclindamycin 600 mg intravenously every 8 h orvancomycin 15 mgkg intravenously twice a daymay be given
ErysipelaAdditional useful therapeutic optionsbull Prednisone 30 mg over 8 days might be consideredas well as elevation of the affected siteMoist heat compresses may be usefulbull Surgeryndash Debridement and drainage are indicated when bullaeabscesses or necroses are presentbull Differential diagnosisndash Contact dermatitisndash Asteatotic eczemandash Herpes zosterndash Angioneurotic oedemandash Osteomyelitis
Furuncle
bull Definition of the diseasebull ndash A furuncle is an infection that beginsbull at the hair follicle and spreads deeper into thebull dermis and subcutaneous tissue forming abull nodule After several days it developsbull into an abscess - red painful and fluctuantbull bull bull Epidemiologyaetiologybull ndash The aetiologic agent is Staphylococcus aureus
FuruncleSymptomsndashsymptoms are local and limited to thesite of infection Furuncles usually are wherehair follicles are present bull Complicationndash One complication is furunculosis multiple draining furunclesDiagnosisndash The diagnosis is based on clinical inspection - Cultures are not necessary when there is no systemic involvement but should beconsidered if systemic therapy (in case of feversignificant cellulitis or hospitalization) or whenmethicillin-resistant Staphylococcusaureus (MRSA) is considered
FuruncleTherapyndash When the furuncle is small application of moist heat compress to promote drainage -Larger furuncles should be drained by surgical incision-After drainage the area should be cleaned with anantiseptic (with chlorhexidinebetadine) should be applied twice
a dayndash If no systemic symptoms or extensive cellulitis arepresent simple topical care is usually curative andoral antibiotics are not necessary Otherwise systemictreatment is indicated and should cover anypossible MRSA
Furuncle
bull -Recommended antibiotics are trimethoprim-sulfamethoxazole
bull 1ndash2 tablets orally twice daily doxycyclinebull 100 mg orally twice dailybull or clindamycin 300ndash450 mg orally every 8 hbull - In severe cases vancomycin 15 mgkg
intravenouslybull every 12 h or clindamycin 600 mg intravenouslybull every 8 h
Midline Granulomabull A midline granuloma is an angiocentricbull lymphoma it was referred to as polymorphicbull reticulosis lethal midline granuloma and midline
malignant reticulosisbull bull Definition of the diseasebull ndash This rare disease is a lymphoma of extranodal
presentationall cases are positive for the Epstein-Barr virus
bull -This lymphoma most commonly appears in the midface region
Midline GranulomaEpidemiologyaetiologyndash This form of lymphoma is rare in Europe and theUnited States with a higher prevalence in Asia and PeruSymptomsndash The most common presentation is nasal obstruction with a destructive mass occupying the nosesinuses and palate
-Fever night sweatsand weight loss seen usually in Hodgkinrsquos lymphomaand other non-Hodgkinrsquos lymphomas (knownas ldquoB symptomsrdquo) are uncommon
Midline GranulomaDiagnosisndash The diagnosis is based on anatomopathologicalstudy The malignancy of the tumour manifested byextensive necrosis makes the histological diagnosisdifficult and often more biopsies are required forconfirmationbull Therapyndash Therapy consists of radiotherapy with or withoutchemotherapy
Midline Granuloma
bull Prognosisbull ndash Depending on the stage long-term remission or
experience a worseningbull prognosis with relapses which may include otherbull extranodal sites bull Involvement of extranodal sitesbull including the upper airway gastrointestinal tractbull skin
Wegenerrsquos Granulomatosis
bull Definition of the diseasebull ndash Wegenerrsquos granulomatosis is a systemic chronicbull vasculitis of small- and medium-sized blood vesselsbull with an autoimmune component It affectsbull particular organs with variable predilectionbull Epidemiologyaetiologybull ndash Wegenerrsquos granulomatosis is a rare disease It affects
about 1 in 20000ndash30000 people It is more prevalentbull in middle-aged Caucasian patients
Wegenerrsquos Granulomatosis
Symptomsndash The disease may present pulmonary upper
respiratory tract or renal In the disseminated form-The localised form ndash confinedto the upper respiratory region ndash is present in 25of the patients- It consists of nonspecific manifestationssuch as nasal obstruction crusting purulentor bloody rhinorrhea and painful or painless ulcers in oral or nasal cavities which are unresponsive tostandard medical treatment
Wegenerrsquos Granulomatosis
bull In some patients the nasal septum is perforatedbull which leads to saddle-nose deformity Less
commonbull symptoms are hoarseness stridor due to
subglotticbull stenosis otalgia otorrhea and conductivebull and sensorineural hearing loss Also ocular
symptomsbull such as scleritis conjunctivitis uveitis andbull episcleritis may be present
Wegenerrsquos Granulomatosis
bull ndash In the disseminated form pulmonary involvementbull is manifested by cough dyspnoea haemoptysisbull (due to an alveolar capillaritis necrotic lesions orbull endobronchial disease) and pleuritic painndashbull -Ninety per cent of patients have nasal symptomsbull and these symptoms are usually the first
manifestationof the diseasebull -Most patients have also renal involvementbull even if it is subclinical
Wegenerrsquos Granulomatosis
Diagnosis ndash Diagnosis of Wegenerrsquos granulomatosis is based on clinical findings that demonstrate lung (chest x-ray) kidney (urine analysis) or upper respiratory tract
involvement (oral or nasal ulcers or discharge) - positive blood analysis for cytoplasmic-staining antineutrophil
cytoplasmic antibodies (c-ANCA) and confirming proteinase 3 (PR3) ANCA or myeloperoxidase (MPO) ANCA ndash Biopsy is essential for diagnosis nonspecific chronic inflammation
and necrosis -Bacterial and fungal infections
Wegenerrsquos Granulomatosis
Therapyndash Conservative therapybull In the induction of disease remission highdosesteroids (e g prednisone 1 mgkgday) for1 month with tapering over several months aregiven In addition cyclophosphamide (2 mgkgday) should be administered for 6ndash12 monthsuntil symptoms disappear In the maintenanceof remission cyclophosphamide should be
Wegenerrsquos Granulomatosis
Antibiotics mainly trimethoprim-sulfamethoxazoleare given for prophylaxis againstPneumocystis jiroveci (formerly Pneumocystiscarinii) pneumonia (PCP) which may developduring immunosuppression and have a role inpreventing recurrencesbull Sinonasal manifestations may be treated with topical nasal steroids and nasal irrigations lowdosesystemic steroids and antibiotics when bacterial infection (typically Staphylococcus species) is suspected
Wegenerrsquos Granulomatosis
bull Prognosisbull ndash Most of the patients respond well to treatmentbull achieving symptom-free intervals of 5ndash20 yearsbull or more bull -Anatomical problems (sinusitis trachealbull stenosis) may require surgery bull Relapses can be long and troublesomebull Long-term complications are chronicbull renal failure hearing loss and deafness
Nasal Fractures Definition ndash A nasal fracture is a disruption of the nasal bone structure due to trauma It is the most frequently fractured facial bone Epidemiologyaetiology ndash Sports falls and assaults are the usual mechanisms of fracture -Males are affected twice as often as are females -Paediatric populations with a incidences during the second and third decades of life -Variables such as force impact direction nature of the striking object age and other will influence the pattern of injury to the components of the nose
Nasal Fractures
bull Symptomsbull ndash Deformity swelling epistaxis and periorbital
ecchymosis are signs that are suggestive of nasal fracture
bull bony crepitus and nasal segment mobilitybull ndash Epiphora bull Severe bilateral injuries to the lachrymal bones
arebull associated with depressed nasal fractures
Nasal Fractures Complications ndash Septal haematoma is one of the most severe early complications of nasal trauma and without drainage it results in abscess formation 6ndash7 days after trauma producing necrosis of the septal cartilage -Long-term problems such as saddle-nose deformity perforation columellar retraction and nasalbase
Septal infection could lead to osteomyelitis orbital and intracranial abscesses meningitis and cavernous sinus thrombosis -Cerebrospinal fluid leakage is a common complication of severe
nasal and frontal fractures
Nasal Fractures
bull Diagnostic proceduresbull ndash Inspectionbull bull Changes of appearance such as deviation andbull asymmetry bleeding watery drainage changesbull in nasal breathing and smell It is useful to comparebull the current presentation with old photographsbull (up to 40 of normal individuals havebull significant nose malformations)
Nasal Fractures Physical examination bull The diagnosis of a nasal fracture is made primarily by physical examination epistaxis nasal swelling and periorbital ecchymosis Nasal shape in the lateral and frontal inspection should be assessed Grasping the dorsum between two fingers and rocking the pyramid back and forth aids in assessing the mobility of nasal bones Internal structures should be evaluated by using a headlight and nasal speculum Clotted blood is removed by suction and assessment of haematoma mucosal tears and active bleeding is performed Bimanual palpation of the septum helps to differentiate septal swelling from haematoma ndash
Nasal FracturesRadiographybull There is no clear evidence of the role of radiographyin the management of nasal fracturesPlain films have up to a 66 false-positive rateas a result of misinterpretation of normal suturelines In addition old fractures are difficult todistinguishbull Three-dimensional CT is recommended for extensiveinjuries involving the nasal-orbital-ethmoidalcomplexndash
Nasal Fractures
bull Additionaluseful diagnostic proceduresbull bull Using a 0 or 30deg 4-mm endoscope is helpful inbull the assessment of posterior abnormalities If thebull patient is heavily sedated Brown-Gruss
provocationbull manoeuvres may be performed to determinebull deformities in upper middle or lower segmentsbull by compressing each compartment
Nasal FracturesConservative treatmentndash Treatment of bleedingbull For localised bleeding anterior sources may becauterised by silver nitrate or sealed with topicalmaterials such as thrombin combined withgelatin foam fibrin glue FloSealreg or other procoagulantmaterials If conservative measuresfail a formal anterior packing is placedbull Bleeding from branches of sphenopalatine orethmoid vessels requires anterior-posteriorpacking
Nasal Fractures
bull bull Surgical methods such as direct endoscopic vessel
bull cauterization or ligation have been shown tobull offer better haemostasis and patient comfortbull Angiography with embolization can also be
consideredbull in cases refractory to more conservativebull approaches
Nasal Fractures
bull Type of reductionbull bull Nondisplaced fractures should be treated withbull observation alone Closed nasal reduction is thebull best choice for simple injuries (isolated unilateralbull with medial displacement)bull bull An open approach should be considered in
severebull trauma (bilateral depressed fractures)
Nasal Fracturesbull Surgical principlesbull ndash Topical anaesthesia with cotton pledgets soakedbull with 4 cocaine or 005 oxymethazoline combinedbull with 4 topical lidocaine should be appliedbull for 5ndash10 min Local anaesthesia should also be injectedbull (1 lidocaine and 1100000 epinephrine)bull along the septum lateral walls and floor of the nasalbull cavitybull bull
Nasal FracturesClosed reductionndashndash The nasal bones are grasped between two fingersand pressure is applied laterally in theopposite direction of the deviation A bluntelevator may be used from within the nose incases of significant medial collapse Walshamforceps can be of help Reduction of the septumshould be performed with the use ofAsch forceps
Nasal Fractures
bull To prevent collapse of the postreductionbull framework nasal packing should be placedbull for 3ndash5 days Septum splints are recommendedbull in comminuted septal fractures withbull severe mucosal lesions External nasal splintingbull for 10 days (Aquaplastreg Thermoplastreg)bull provides nasal protection Nasal saline spraysbull prevent crusting and oral antibiotics should
Nasal Fractures
bull Open reductionbull ndashndash Immediate repair of fractures by using
widebull surgical exposure reduction fixation and
reconstructionbull ndashndash The second option is delayed correctionbull (6 months or more) of persistent deformitiesbull using standard techniques of rhinoplasty
Deviated Nasal Septum
bull Definition of the diseasebull ndash Deviation of the nasal septum is a common causebull of unilateral nasal airway obstruction in which thebull nasal septum is displacedbull bull Epidemiologyaetiologybull ndash Developmental septal abnormalities Septal cartilage
damage in the neonatal period andbull during birth can cause severe septal deviation inbull the absence of a history of nasal trauma
Deviated Nasal Septum
bull Symptomsbull ndash Patients may present with a history of sinusitis
allergicbull rhinitis obstructive sleep apnoea previousbull nasal surgery or recent nasal trauma Unilateral or
bilateral nasal airway obstruction that is unrelievedbull with decongestants or nasal steroid sprays is oftenbull seenbull bull
Deviated Nasal SeptumDiagnosisndashExamination external dorsal deviation or the columella and caudal septummay be deflected off the midline (caudal subluxation)ndash Inspections of the nasal cavity and anterior-posteriorrhinoscopy are helpful in diagnosing the locationtype and severity of septal deformityThe endoscope is also useful in identifying polypsthe severity and extent of posterior septaldeviations and bony spurs and locating areas ofseptal perforation or mucosal injury
Deviated Nasal Septum
bull Therapybull ndash Septoplasty is a procedurebull The areabull of deviation is corrected or resected in order tobull leave behind as much cartilage and bone as
possiblebull Cartilage resection is minimised and can be
repositioned reshaped or recontoured using a variety of methods
Deviated Nasal Septum
bull ndash Indications of septoplasty before the growth period
bull of the nose is finished should be very limited bull -In these cases surgery must preserve all the
cartilagebull in order to prevent external changes of the
shape ofbull the nose
Deviated Nasal Septum
bull Complicationsbull ndash Frequent complications include haematoma andbull infection Cerebrospinal fluid leak is a rare but
potentiallybull serious complicationbull It is usually the resultbull of avulsion or damage to the cribriform plate whenbull handling the perpendicular plate of the ethmoidbull ndash Other complications include epistaxis nasal
Deviated Nasal Septum
bull Other complications include epistaxis nasal obstruction
bull due to residual deviation synechiae returnbull of the cartilaginous deviation septal perforationbull anosmia and cosmetic nasal deformities suchbull as widened alar rim margins drooping nasal tipbull columella retraction and a sunken dorsum with abull supratip saddle formation
Septal perforation with minor crusting View from provide closure of the
incision
Septal Haematoma
bull A septal haematoma is a blood collection under the perichondrium
bull of the septum and cartilagebull bull bull Epidemiologyaetiologybull ndash A septal haematoma is one of the most
severe complications of nasal trauma
Septal Haematoma
bull Diagnosisbull ndash Signs and symptoms include intense pain
swellingbull haematoma of the upper lip and philtrum
area andbull complete nasal airway obstruction
Septal HaematomaTherapyndash Management consists of drainage through a mucoperichondrial incision Immediate treatment isnecessary to prevent long-term problems such asa saddle-nose deformity perforation columellarretraction and nasal-base widening In childrenseptal destruction can lead to devastating nasal andmidfacial growth abnormalitiesbull Surgeryndash Incision and evacuation of the collection is performedDrainage of a septal haematoma should
Septal HaematomaSurgeryndash Incision and evacuation of the collection is performedDrainage of a septal haematoma should provide closure of the incision
Splints or transseptal sutures are placed to obliterate thepotential space and prevent collectionInfection involving the septal cartilage Reconstruction with autologouscartilage is then performed in a second stage Oral antibiotics should be given
Nasal DeformitySaddle-nose deformityndash A saddle-nose deformity is characterised by a loss ofnasal dorsal height and compromised nasal supportstructures -Other case observed are depressionof the middle vault and dorsum loss of nasal tipsupport and definition shortened (vertical) nasal length over rotation of the nasal tip and retrusion ofthe nasal spine and caudal septum It is also knownas a ldquoPug noserdquo or ldquoboxerrsquos noserdquo both of which referto various degrees of nasal dorsal depressionbull
Nasal DeformityEpidemiologyaetiologyndash Prevalence is higher in population groups prone to facial trauma (ie boxers athletes) those with historiesof intranasal cocaine use nasal surgery (e g radical submucosal septal resection reductive rhinoplasty)ndash A saddle-nose deformity can be congenital or acquired It can be noticed as a part of individual familialsyndromic and ethnic characteristics - Most deformities are due to traumatic and iatrogeniccauses Medical causes are Wegenerrsquosgranulomatosis relapsing polychondritis leprosy (Hansenrsquos disease) syphilis ectodermal dysplasiaand intranasal cocaine use
Nasal Deformity
bull Therapybull ndash Nasal reconstruction indications depend on patientbull selection surgeon experience and aetiology of thebull deformity bull Indications for surgery can be functionalbull aesthetic or most commonly both In individuals
with a compromised nasal airway a nasoseptalbull reconstruction is indicated
Nasal Deformity
bull Contraindications bull include patients with malignantbull chronic or autoimmune disease conditions drugbull abuse poor perioperative risk profile and unrealisticbull expectationsbull ndash Multiple previous rhinoplasties and certain
professionsbull (mixed martial artists boxers and other contactbull sports) are relative contraindications
Nasal DeformitySeptoplastyndash Septoplasty is performed to correct nasal obstructioncaused by septal deformityndash Usually septoplasty is performed under general anaesthesiawith the patient in the supine position with the head elevated by approximately 30 (Righthandedsurgeons approach from the right side)ndash Local vasoconstrictive anaesthesia is applied notonly to reduce postoperative pain but also more importantly to achieve vasoconstriction of themucosa and less intraoperative haemorrhage Lidocainewith adrenaline or epinephrine is usedalthough in patients with cardiac hypersensitivityoxymetazoline might be preferred
Nasal Deformity
bull Septoplasty begins with the incision of septal mucosabull Most operative techniques utilise a hemitransfixionbull incision at the caudal end of septum so thatbull deviation at this point might be reached as wellbull as a transfixion incision that is easily obtained ifbull needed (Right-handed surgeons normally choosebull the left side but that may vary when deviation isbull convex towards the right)
Nasal DeformityA columella retractor is placed over the columellaand by pulling it laterally the caudal border of theseptum is exposed Ala can be protected by an alaprotector A vertical incision with a no 15 bladeover the caudal end of septum is performed untilreaching the plane of the septal cartilage It is essentialto correctly identify the perichondrium and byusing the Cottle elevator dissect and lift it creatinga flap As the dissection proceeds along the septalcartilage a longer speculum (no 5) is introduced sothat elevation of the mucoperichondrium is doneunder constant visual controlndash The next step is to dissect the mucoperiostium
Nasal DeformityDissecting over the bony-cartilaginous junctionwhen joining both tunnels might be difficult and is
especially prone to membrane perforationndash If needed the same tunnels are to be created on the
other side of the septum Then deviated parts of
septum are identified and removed either with a
knife or a Freer chisel
Nasal Deformitybull septum from the maxillary crest the septum mustbull be separated from the perpendicular plate trimmedbull along the inferior border placed back onto the crestbull and sutured to the periosteum If the deformity involvesbull the vomer an osteotome is used Care mustbull be taken not to break the cribriform plate becausebull it could cause a cerebrospinal fistula
Nasal Deformity
bull Once the septal deviation is corrected the flapsbull and hemitransfixion incision are mattressed
withbull absorbable sutures Nasal packing to prevent
synechiaebull and postoperative septal haematoma mightbull be advised but should be removed within 72 h

The ENT Examination
EquipmentA fully equipped ENT department will have all the necessary instruments for performing a full ENT examination
Basic equipment
bull A light sourcemdasha portable headlight that runs off batteries is ideal
bull Wooden tongue depressorsbull Thudicum nasal speculumbull An otoscope with several speculaebull Pneumatic attachment for the otoscopebull Tuning fork 512Hzbull Pen and paperbull Gloves
Advanced equipment
bull Co-phenylcaine spraybull A flexible nasendoscope with light sourcebull Alcohol wipe to act as demist for the scopebull Aqueous lubricating gel for the scope
Emergency equipment
bull Large nasal tampons (you can always cut 10cm ones to size)
bull Silver nitrate sticksbull Foley catheters
Basic Anatomy of the Nose
bull The structural anatomy of the nose is important
bull for both aesthetic and functional reasons since the
bull nose as the gateway to the respiratory tract performs
bull a variety of physiologic functions
External NoseThe shape of the external nose is defined by the nasalbones a pair of rectangular bones in the upper nasaldorsum and by lateral cartilages (uppernasal cartilages) and alar cartilages (major alar cartilages)in the central and lower portions of the noseThe lateral portions of the nasal alae alsocontain several small accessory cartilages called theminor alar cartilages which are embedded in the lateralsoft tissues of the noseThe shape and stability of the alar cartilages each ofwhich consists of a medial and lateral crus
External Nose
Anatomy of the nasal base
bull Besides thebull medial crura the
inferior septal margin and the connective-
bull tissue septum (columella) are also responsible
bull for stabilizing the base of the nose
Anatomy of the nasal base
Anatomy of the nasal base
bull The nasal septum is subluxed toward the left side partially
bull obstructing the nasal airway
Nasal CavitiesThe nasal cavities begin anteriorly at the nasal vestibulewhich is bordered posteriorly by the internal nasalvalve (limen nasi) located between the posteriorborder of the alar cartilage and the anterior border ofthe lateral cartilage This valve area is the narrowestportion of the upper respiratory tract
Nasal Cavities
The interior ofthe nose behind the nasal valve is divided by the nasalseptum into two main cavities
Nasal CavitiesThe nasal septum iscomposed of an anterior cartilaginous part and twoposterior bony parts Abnormalities in the shape ofthe nasal septum which may consist of a deviated septum tensionseptum spurs or ridges are a frequent cause ofnasal airway obstructionThe choanae are the paired posterior openingsthrough which the nasal cavities communicate withthe nasopharynx
Nasal CavitiesThe nasal cavity is bounded laterally by the lateral nasalwalls which are formed by the ethmoid bone andmaxilla and posteriorly by the palatine bone and thepterygoid process of the sphenoid bone Several functionallyimportant structures are located on the lateralnasal wall the nasal turbinates and their associatedpassages (meati) sinus ostia and the orifice ofthe nasolacrimal duct (Fig 15)
The inferior turbinate consists of a separate bone thatis attached to the medial wall of the maxillary sinusThe opening of the nasolacrimal duct is located in thecorresponding inferior meatus The middle andsuperior turbinates are part of the ethmoid bone In rare cases a rudimentary ldquosupreme turbinaterdquo is alsopresent above the superior turbinate
The middle turbinate has by far the greatest functionalimportance because most of the drainage tracts fromthe surrounding paranasal sinuses open into the middlemeatus The nasal cavity is bounded superiorly by the cribriformplate of the ethmoid bone This thin bony platehas numerous openings for the passage of the fila olfactoriaand also forms the boundary of the anteriorcranial fossa
Nasal Cavities
The floor of the nasal cavity is formedmostly by the hard palate which is formed in turn bythe two palatine processes of the maxilla and the horizontallaminae of the palatine bone
Structure of the lateral nasal wall
Inferior meatus
Paranasal Sinuses
The paranasal sinuses are air-filled cavities that communicatewith the nasal cavities
-The maxillary sinus frontalsinus and anterior ethmoid cells drain into the nasalcavity through the middle meatusmdashie below themiddle turbinate -The posterior ethmoidcells drain into the nasal cavity through the superiormeatus The ostium of the sphenoid sinus is locatedin the anterior wall directly above the choanae- The anatomical connections between the nasal cavity andparanasal sinuses are functionally important and playa key role in the pathogenesis of many rhinologic diseasesthat involve the paranasal sinuses
Vascular SupplyThe external nose derives most of its blood supply
from the facial artery which arises from the external
carotid artery and from the ophthalmic artery which
springs from the internal carotid artery
Vascular Supply
The internalnose receives blood from the territories of the externaland internal carotid arteries- the terminalbranches of the sphenopalatine artery which arisesfrom the maxillary artery - the anterior and posteriorethmoid arteries which arise from the ophthalmicartery-internal carotid arterie
venous drainage
The venous drainageof the facial region is handled by -the facial vein -retromandibular vein -internal jugular vein
lymphatic drainage
The regional lymphatic drainage of the face and externalnose is handled mainly by- the submandibularlymph nodes while the nasal cavity is additionallydrained by -the retropharyngeal and deep - -cervical lymph nodes
Morphology of the Nasal Mucosa
Besides the anatomical structure of the external noseand nasal cavity the nasal mucosa plays an essentialrole in numerous functions of the nose in the respiratory tract
Morphology of the Nasal Mucosa
The anterior part of the nasal cavity (the nasal vestibule)like the external nose is covered by skin composedof a multilayer keratinizing squamous epithelium and finally a ciliated respiratory epithelium A small areaon the upper nasal septum superior turbinate andpart of the middle turbinate located adjacent to thecribriform plate is covered by olfactory mucosa and iscalled the olfactory region
Nerve SupplyThe facial skin receives its sensory innervation fromterminal branches of the trigeminal nerve that enterthe facial region through the supraorbital infraorbitaland mental foramina Thefacial muscles are classified as mimetic or mastica- tory each of these groups receiving different motorinnervationbythe facial nerve
History and Clinical Examination of the Nose
Historybull The main symptomsbull nasal obstruction (ldquostuffy
noserdquo)bull nasal dischargebull Headachesbull Olfactory
dysfunction
Palpationbony discontinuitiesNeuralgias to check
over- the supraorbital -infraorbital -mental foramina
Anterior Rhinoscopy
bull The rhinologic examination itself begins with anterior
bull rhinoscopy to evaluate the nasal vestibule and the anterior
bull portions of the nasal cavity
Nasal Endoscopy Nasal endoscopy has become the most important andrewarding clinical examination method in rhinologic diagnosis
- rigid endoscopes which are available in 4-mm and 28- mm diameters and assorted viewing angles (eg 01048576 301048576 1201048576) -flexible endoscopes are also available for inspecting the nose and nasopharynx and exploring all of the pharynx and larynx in one sitting
Nasal endoscopy
Nasal Endoscopy
Nasal Endoscopy
Imaging of the Nose and Paranasal Sinuses
Conventional RadiographsStandard paranasal sinus radiographs in the occipitomental
projection ( Water projection) and
occipitofrontal projection Caldwell projection) in cases of acute inflammation
They are also obtained to evaluate midfacial fractures
Computed Tomography (CT) the main indicationsfor CT scanning of the
nose and paranasal sinuses
are- chronic sinusitis - -trauma (especially
frontobasal -fractures)
-and tumors
The occipitofrontal projection is better for evaluating theethmoid cells and frontal sinus
occipitomental projection demonstrates the maxillarysinus and gives a limited view of the sphenoid sinus
Computed tomography of the paranasal sinuses
Four representative coronal CT scans are shown
Four representative coronal CT scans are shown
Magnetic Resonance Imaging
Magnetic maging
Magnetic resonance imaging (MRI) has fewer indicationsthan CT in patients with paranasal sinus diseaseThis is primarily because MRI is markedly inferior toCT in defining the bony boundaries of the sinusesThe strength of MRI lies in its superior soft-tissue discriminationMRI is indicated in diseases that involve the paranasal sinuses in addition to thecranial cavity or orbit (eg tumors and congenitalmalformations such as encephaloceles)
MRI of the paranasal sinuses
The Nose and Sinuses
Structure The structure of the nose is made up of
four partsbull The surface anatomybull The nasal skeletonmdashcomposed of the
two nasal bones the paired upper lateral and lower lateral cartilages and the nasal septum covered in subcutaneous tissue and skin
bull The internal anatomymdashincludes the septum of the nose which forms the medial wall of the nasal cavity The turbinates on the lateral wall are also called conchae
bull The osteomeatal complexmdasha key functional area of the nose
Function The nose is the main route for inspired
air and its structure is related to this function As the air passes over the large surface area of the turbinates
The inspired gases are warmed and humidified Mucus on the mucosa of the nose removes large dust particles from the air as it is breathed in
The voice resonates in the sinuses and nose and this provides character to the speech
Pneumatization of the sinusesmdashthey are air filled spacesmdashreduces the weight of the skull
Diseases of thDiseases of the Outer and Inner Nosee Outer and
Inner Nose Erysipelas Definition of the disease ndash Erysipela is a skin infection that affects the superficial dermis and is caused by Streptococcus pyogenes (group A) It usually develops in the extremities and the face and less commonly on the scalp and genitals bull Epidemiologyaetiology ndash Erysipelas are more often seen in elderly infants and children patients with compromised immunology and diabetes -Predisposing factors are alcoholism skin ulceration puncture wounds fungal infections malnutrition and burns
Erysipelas
bull Symptomsbull ndash It usually presents of fever general fatigue bull -The skin lesion is a redindurated and elevated plaque
with borders that expand rapidly bull It is painful warm and accompanied by variable oedemabull -On the second or third day a flaccid bulla may develop
and desquamationbull bull Presence of regional lymph nodes is common
Erysipelas
bull Complicationsndash The most common complication is recurrencewhich is seen in 18ndash30 of the cases even afterproper antibiotic therapy Recurrence is seen moreoften in females than in malesA skin infection with S pyogenes could lead toglomerulonephritis
Erysipelas
bull Complicationsbull ndash The most common complication is recurrencebull which is seen in 18ndash30 of the cases even afterbull proper antibiotic therapy bull -Recurrence is seen morebull often in females than in males bull -A skin infection with S pyogenes could lead tobull glomerulonephritis
Erysipelas
bull bull Diagnosisbull ndash Diagnosis is based on the patientrsquos personal
historybull and physical examination particularly on inspectionbull of the skin
bull Blood cultures are positive in less thanbull 5 of cases
ErysipelasTherapyndash Conservative therapybull The preferred antibiotic is penicillin In mildcases with minor systemic symptoms penicillinV 500 mg orally every 6 h for 10 days or penicillinG benzathine 12 mil U intramuscularlyonceOther possibilities are amoxicillin 500 mgorally twice a day for 10 days or cephalexin 500mg orally every 6 h for 10 days
ErysipelasIn moderate and severe cases with significantsystemic symptoms hospitalization and intravenoustreatment is required penicillin G 2ndash4mil U intravenously every 4ndash6 h Cefazolin05ndash15 gm intravenously every 8 h cefotaxime1ndash2 gm intravenously every 8 h or ceftriaxone1ndash2 gm intravenously once a day should be administeredIn patients with a penicillin allergyclindamycin 600 mg intravenously every 8 h orvancomycin 15 mgkg intravenously twice a daymay be given
ErysipelaAdditional useful therapeutic optionsbull Prednisone 30 mg over 8 days might be consideredas well as elevation of the affected siteMoist heat compresses may be usefulbull Surgeryndash Debridement and drainage are indicated when bullaeabscesses or necroses are presentbull Differential diagnosisndash Contact dermatitisndash Asteatotic eczemandash Herpes zosterndash Angioneurotic oedemandash Osteomyelitis
Furuncle
bull Definition of the diseasebull ndash A furuncle is an infection that beginsbull at the hair follicle and spreads deeper into thebull dermis and subcutaneous tissue forming abull nodule After several days it developsbull into an abscess - red painful and fluctuantbull bull bull Epidemiologyaetiologybull ndash The aetiologic agent is Staphylococcus aureus
FuruncleSymptomsndashsymptoms are local and limited to thesite of infection Furuncles usually are wherehair follicles are present bull Complicationndash One complication is furunculosis multiple draining furunclesDiagnosisndash The diagnosis is based on clinical inspection - Cultures are not necessary when there is no systemic involvement but should beconsidered if systemic therapy (in case of feversignificant cellulitis or hospitalization) or whenmethicillin-resistant Staphylococcusaureus (MRSA) is considered
FuruncleTherapyndash When the furuncle is small application of moist heat compress to promote drainage -Larger furuncles should be drained by surgical incision-After drainage the area should be cleaned with anantiseptic (with chlorhexidinebetadine) should be applied twice
a dayndash If no systemic symptoms or extensive cellulitis arepresent simple topical care is usually curative andoral antibiotics are not necessary Otherwise systemictreatment is indicated and should cover anypossible MRSA
Furuncle
bull -Recommended antibiotics are trimethoprim-sulfamethoxazole
bull 1ndash2 tablets orally twice daily doxycyclinebull 100 mg orally twice dailybull or clindamycin 300ndash450 mg orally every 8 hbull - In severe cases vancomycin 15 mgkg
intravenouslybull every 12 h or clindamycin 600 mg intravenouslybull every 8 h
Midline Granulomabull A midline granuloma is an angiocentricbull lymphoma it was referred to as polymorphicbull reticulosis lethal midline granuloma and midline
malignant reticulosisbull bull Definition of the diseasebull ndash This rare disease is a lymphoma of extranodal
presentationall cases are positive for the Epstein-Barr virus
bull -This lymphoma most commonly appears in the midface region
Midline GranulomaEpidemiologyaetiologyndash This form of lymphoma is rare in Europe and theUnited States with a higher prevalence in Asia and PeruSymptomsndash The most common presentation is nasal obstruction with a destructive mass occupying the nosesinuses and palate
-Fever night sweatsand weight loss seen usually in Hodgkinrsquos lymphomaand other non-Hodgkinrsquos lymphomas (knownas ldquoB symptomsrdquo) are uncommon
Midline GranulomaDiagnosisndash The diagnosis is based on anatomopathologicalstudy The malignancy of the tumour manifested byextensive necrosis makes the histological diagnosisdifficult and often more biopsies are required forconfirmationbull Therapyndash Therapy consists of radiotherapy with or withoutchemotherapy
Midline Granuloma
bull Prognosisbull ndash Depending on the stage long-term remission or
experience a worseningbull prognosis with relapses which may include otherbull extranodal sites bull Involvement of extranodal sitesbull including the upper airway gastrointestinal tractbull skin
Wegenerrsquos Granulomatosis
bull Definition of the diseasebull ndash Wegenerrsquos granulomatosis is a systemic chronicbull vasculitis of small- and medium-sized blood vesselsbull with an autoimmune component It affectsbull particular organs with variable predilectionbull Epidemiologyaetiologybull ndash Wegenerrsquos granulomatosis is a rare disease It affects
about 1 in 20000ndash30000 people It is more prevalentbull in middle-aged Caucasian patients
Wegenerrsquos Granulomatosis
Symptomsndash The disease may present pulmonary upper
respiratory tract or renal In the disseminated form-The localised form ndash confinedto the upper respiratory region ndash is present in 25of the patients- It consists of nonspecific manifestationssuch as nasal obstruction crusting purulentor bloody rhinorrhea and painful or painless ulcers in oral or nasal cavities which are unresponsive tostandard medical treatment
Wegenerrsquos Granulomatosis
bull In some patients the nasal septum is perforatedbull which leads to saddle-nose deformity Less
commonbull symptoms are hoarseness stridor due to
subglotticbull stenosis otalgia otorrhea and conductivebull and sensorineural hearing loss Also ocular
symptomsbull such as scleritis conjunctivitis uveitis andbull episcleritis may be present
Wegenerrsquos Granulomatosis
bull ndash In the disseminated form pulmonary involvementbull is manifested by cough dyspnoea haemoptysisbull (due to an alveolar capillaritis necrotic lesions orbull endobronchial disease) and pleuritic painndashbull -Ninety per cent of patients have nasal symptomsbull and these symptoms are usually the first
manifestationof the diseasebull -Most patients have also renal involvementbull even if it is subclinical
Wegenerrsquos Granulomatosis
Diagnosis ndash Diagnosis of Wegenerrsquos granulomatosis is based on clinical findings that demonstrate lung (chest x-ray) kidney (urine analysis) or upper respiratory tract
involvement (oral or nasal ulcers or discharge) - positive blood analysis for cytoplasmic-staining antineutrophil
cytoplasmic antibodies (c-ANCA) and confirming proteinase 3 (PR3) ANCA or myeloperoxidase (MPO) ANCA ndash Biopsy is essential for diagnosis nonspecific chronic inflammation
and necrosis -Bacterial and fungal infections
Wegenerrsquos Granulomatosis
Therapyndash Conservative therapybull In the induction of disease remission highdosesteroids (e g prednisone 1 mgkgday) for1 month with tapering over several months aregiven In addition cyclophosphamide (2 mgkgday) should be administered for 6ndash12 monthsuntil symptoms disappear In the maintenanceof remission cyclophosphamide should be
Wegenerrsquos Granulomatosis
Antibiotics mainly trimethoprim-sulfamethoxazoleare given for prophylaxis againstPneumocystis jiroveci (formerly Pneumocystiscarinii) pneumonia (PCP) which may developduring immunosuppression and have a role inpreventing recurrencesbull Sinonasal manifestations may be treated with topical nasal steroids and nasal irrigations lowdosesystemic steroids and antibiotics when bacterial infection (typically Staphylococcus species) is suspected
Wegenerrsquos Granulomatosis
bull Prognosisbull ndash Most of the patients respond well to treatmentbull achieving symptom-free intervals of 5ndash20 yearsbull or more bull -Anatomical problems (sinusitis trachealbull stenosis) may require surgery bull Relapses can be long and troublesomebull Long-term complications are chronicbull renal failure hearing loss and deafness
Nasal Fractures Definition ndash A nasal fracture is a disruption of the nasal bone structure due to trauma It is the most frequently fractured facial bone Epidemiologyaetiology ndash Sports falls and assaults are the usual mechanisms of fracture -Males are affected twice as often as are females -Paediatric populations with a incidences during the second and third decades of life -Variables such as force impact direction nature of the striking object age and other will influence the pattern of injury to the components of the nose
Nasal Fractures
bull Symptomsbull ndash Deformity swelling epistaxis and periorbital
ecchymosis are signs that are suggestive of nasal fracture
bull bony crepitus and nasal segment mobilitybull ndash Epiphora bull Severe bilateral injuries to the lachrymal bones
arebull associated with depressed nasal fractures
Nasal Fractures Complications ndash Septal haematoma is one of the most severe early complications of nasal trauma and without drainage it results in abscess formation 6ndash7 days after trauma producing necrosis of the septal cartilage -Long-term problems such as saddle-nose deformity perforation columellar retraction and nasalbase
Septal infection could lead to osteomyelitis orbital and intracranial abscesses meningitis and cavernous sinus thrombosis -Cerebrospinal fluid leakage is a common complication of severe
nasal and frontal fractures
Nasal Fractures
bull Diagnostic proceduresbull ndash Inspectionbull bull Changes of appearance such as deviation andbull asymmetry bleeding watery drainage changesbull in nasal breathing and smell It is useful to comparebull the current presentation with old photographsbull (up to 40 of normal individuals havebull significant nose malformations)
Nasal Fractures Physical examination bull The diagnosis of a nasal fracture is made primarily by physical examination epistaxis nasal swelling and periorbital ecchymosis Nasal shape in the lateral and frontal inspection should be assessed Grasping the dorsum between two fingers and rocking the pyramid back and forth aids in assessing the mobility of nasal bones Internal structures should be evaluated by using a headlight and nasal speculum Clotted blood is removed by suction and assessment of haematoma mucosal tears and active bleeding is performed Bimanual palpation of the septum helps to differentiate septal swelling from haematoma ndash
Nasal FracturesRadiographybull There is no clear evidence of the role of radiographyin the management of nasal fracturesPlain films have up to a 66 false-positive rateas a result of misinterpretation of normal suturelines In addition old fractures are difficult todistinguishbull Three-dimensional CT is recommended for extensiveinjuries involving the nasal-orbital-ethmoidalcomplexndash
Nasal Fractures
bull Additionaluseful diagnostic proceduresbull bull Using a 0 or 30deg 4-mm endoscope is helpful inbull the assessment of posterior abnormalities If thebull patient is heavily sedated Brown-Gruss
provocationbull manoeuvres may be performed to determinebull deformities in upper middle or lower segmentsbull by compressing each compartment
Nasal FracturesConservative treatmentndash Treatment of bleedingbull For localised bleeding anterior sources may becauterised by silver nitrate or sealed with topicalmaterials such as thrombin combined withgelatin foam fibrin glue FloSealreg or other procoagulantmaterials If conservative measuresfail a formal anterior packing is placedbull Bleeding from branches of sphenopalatine orethmoid vessels requires anterior-posteriorpacking
Nasal Fractures
bull bull Surgical methods such as direct endoscopic vessel
bull cauterization or ligation have been shown tobull offer better haemostasis and patient comfortbull Angiography with embolization can also be
consideredbull in cases refractory to more conservativebull approaches
Nasal Fractures
bull Type of reductionbull bull Nondisplaced fractures should be treated withbull observation alone Closed nasal reduction is thebull best choice for simple injuries (isolated unilateralbull with medial displacement)bull bull An open approach should be considered in
severebull trauma (bilateral depressed fractures)
Nasal Fracturesbull Surgical principlesbull ndash Topical anaesthesia with cotton pledgets soakedbull with 4 cocaine or 005 oxymethazoline combinedbull with 4 topical lidocaine should be appliedbull for 5ndash10 min Local anaesthesia should also be injectedbull (1 lidocaine and 1100000 epinephrine)bull along the septum lateral walls and floor of the nasalbull cavitybull bull
Nasal FracturesClosed reductionndashndash The nasal bones are grasped between two fingersand pressure is applied laterally in theopposite direction of the deviation A bluntelevator may be used from within the nose incases of significant medial collapse Walshamforceps can be of help Reduction of the septumshould be performed with the use ofAsch forceps
Nasal Fractures
bull To prevent collapse of the postreductionbull framework nasal packing should be placedbull for 3ndash5 days Septum splints are recommendedbull in comminuted septal fractures withbull severe mucosal lesions External nasal splintingbull for 10 days (Aquaplastreg Thermoplastreg)bull provides nasal protection Nasal saline spraysbull prevent crusting and oral antibiotics should
Nasal Fractures
bull Open reductionbull ndashndash Immediate repair of fractures by using
widebull surgical exposure reduction fixation and
reconstructionbull ndashndash The second option is delayed correctionbull (6 months or more) of persistent deformitiesbull using standard techniques of rhinoplasty
Deviated Nasal Septum
bull Definition of the diseasebull ndash Deviation of the nasal septum is a common causebull of unilateral nasal airway obstruction in which thebull nasal septum is displacedbull bull Epidemiologyaetiologybull ndash Developmental septal abnormalities Septal cartilage
damage in the neonatal period andbull during birth can cause severe septal deviation inbull the absence of a history of nasal trauma
Deviated Nasal Septum
bull Symptomsbull ndash Patients may present with a history of sinusitis
allergicbull rhinitis obstructive sleep apnoea previousbull nasal surgery or recent nasal trauma Unilateral or
bilateral nasal airway obstruction that is unrelievedbull with decongestants or nasal steroid sprays is oftenbull seenbull bull
Deviated Nasal SeptumDiagnosisndashExamination external dorsal deviation or the columella and caudal septummay be deflected off the midline (caudal subluxation)ndash Inspections of the nasal cavity and anterior-posteriorrhinoscopy are helpful in diagnosing the locationtype and severity of septal deformityThe endoscope is also useful in identifying polypsthe severity and extent of posterior septaldeviations and bony spurs and locating areas ofseptal perforation or mucosal injury
Deviated Nasal Septum
bull Therapybull ndash Septoplasty is a procedurebull The areabull of deviation is corrected or resected in order tobull leave behind as much cartilage and bone as
possiblebull Cartilage resection is minimised and can be
repositioned reshaped or recontoured using a variety of methods
Deviated Nasal Septum
bull ndash Indications of septoplasty before the growth period
bull of the nose is finished should be very limited bull -In these cases surgery must preserve all the
cartilagebull in order to prevent external changes of the
shape ofbull the nose
Deviated Nasal Septum
bull Complicationsbull ndash Frequent complications include haematoma andbull infection Cerebrospinal fluid leak is a rare but
potentiallybull serious complicationbull It is usually the resultbull of avulsion or damage to the cribriform plate whenbull handling the perpendicular plate of the ethmoidbull ndash Other complications include epistaxis nasal
Deviated Nasal Septum
bull Other complications include epistaxis nasal obstruction
bull due to residual deviation synechiae returnbull of the cartilaginous deviation septal perforationbull anosmia and cosmetic nasal deformities suchbull as widened alar rim margins drooping nasal tipbull columella retraction and a sunken dorsum with abull supratip saddle formation
Septal perforation with minor crusting View from provide closure of the
incision
Septal Haematoma
bull A septal haematoma is a blood collection under the perichondrium
bull of the septum and cartilagebull bull bull Epidemiologyaetiologybull ndash A septal haematoma is one of the most
severe complications of nasal trauma
Septal Haematoma
bull Diagnosisbull ndash Signs and symptoms include intense pain
swellingbull haematoma of the upper lip and philtrum
area andbull complete nasal airway obstruction
Septal HaematomaTherapyndash Management consists of drainage through a mucoperichondrial incision Immediate treatment isnecessary to prevent long-term problems such asa saddle-nose deformity perforation columellarretraction and nasal-base widening In childrenseptal destruction can lead to devastating nasal andmidfacial growth abnormalitiesbull Surgeryndash Incision and evacuation of the collection is performedDrainage of a septal haematoma should
Septal HaematomaSurgeryndash Incision and evacuation of the collection is performedDrainage of a septal haematoma should provide closure of the incision
Splints or transseptal sutures are placed to obliterate thepotential space and prevent collectionInfection involving the septal cartilage Reconstruction with autologouscartilage is then performed in a second stage Oral antibiotics should be given
Nasal DeformitySaddle-nose deformityndash A saddle-nose deformity is characterised by a loss ofnasal dorsal height and compromised nasal supportstructures -Other case observed are depressionof the middle vault and dorsum loss of nasal tipsupport and definition shortened (vertical) nasal length over rotation of the nasal tip and retrusion ofthe nasal spine and caudal septum It is also knownas a ldquoPug noserdquo or ldquoboxerrsquos noserdquo both of which referto various degrees of nasal dorsal depressionbull
Nasal DeformityEpidemiologyaetiologyndash Prevalence is higher in population groups prone to facial trauma (ie boxers athletes) those with historiesof intranasal cocaine use nasal surgery (e g radical submucosal septal resection reductive rhinoplasty)ndash A saddle-nose deformity can be congenital or acquired It can be noticed as a part of individual familialsyndromic and ethnic characteristics - Most deformities are due to traumatic and iatrogeniccauses Medical causes are Wegenerrsquosgranulomatosis relapsing polychondritis leprosy (Hansenrsquos disease) syphilis ectodermal dysplasiaand intranasal cocaine use
Nasal Deformity
bull Therapybull ndash Nasal reconstruction indications depend on patientbull selection surgeon experience and aetiology of thebull deformity bull Indications for surgery can be functionalbull aesthetic or most commonly both In individuals
with a compromised nasal airway a nasoseptalbull reconstruction is indicated
Nasal Deformity
bull Contraindications bull include patients with malignantbull chronic or autoimmune disease conditions drugbull abuse poor perioperative risk profile and unrealisticbull expectationsbull ndash Multiple previous rhinoplasties and certain
professionsbull (mixed martial artists boxers and other contactbull sports) are relative contraindications
Nasal DeformitySeptoplastyndash Septoplasty is performed to correct nasal obstructioncaused by septal deformityndash Usually septoplasty is performed under general anaesthesiawith the patient in the supine position with the head elevated by approximately 30 (Righthandedsurgeons approach from the right side)ndash Local vasoconstrictive anaesthesia is applied notonly to reduce postoperative pain but also more importantly to achieve vasoconstriction of themucosa and less intraoperative haemorrhage Lidocainewith adrenaline or epinephrine is usedalthough in patients with cardiac hypersensitivityoxymetazoline might be preferred
Nasal Deformity
bull Septoplasty begins with the incision of septal mucosabull Most operative techniques utilise a hemitransfixionbull incision at the caudal end of septum so thatbull deviation at this point might be reached as wellbull as a transfixion incision that is easily obtained ifbull needed (Right-handed surgeons normally choosebull the left side but that may vary when deviation isbull convex towards the right)
Nasal DeformityA columella retractor is placed over the columellaand by pulling it laterally the caudal border of theseptum is exposed Ala can be protected by an alaprotector A vertical incision with a no 15 bladeover the caudal end of septum is performed untilreaching the plane of the septal cartilage It is essentialto correctly identify the perichondrium and byusing the Cottle elevator dissect and lift it creatinga flap As the dissection proceeds along the septalcartilage a longer speculum (no 5) is introduced sothat elevation of the mucoperichondrium is doneunder constant visual controlndash The next step is to dissect the mucoperiostium
Nasal DeformityDissecting over the bony-cartilaginous junctionwhen joining both tunnels might be difficult and is
especially prone to membrane perforationndash If needed the same tunnels are to be created on the
other side of the septum Then deviated parts of
septum are identified and removed either with a
knife or a Freer chisel
Nasal Deformitybull septum from the maxillary crest the septum mustbull be separated from the perpendicular plate trimmedbull along the inferior border placed back onto the crestbull and sutured to the periosteum If the deformity involvesbull the vomer an osteotome is used Care mustbull be taken not to break the cribriform plate becausebull it could cause a cerebrospinal fistula
Nasal Deformity
bull Once the septal deviation is corrected the flapsbull and hemitransfixion incision are mattressed
withbull absorbable sutures Nasal packing to prevent
synechiaebull and postoperative septal haematoma mightbull be advised but should be removed within 72 h

Basic equipment
bull A light sourcemdasha portable headlight that runs off batteries is ideal
bull Wooden tongue depressorsbull Thudicum nasal speculumbull An otoscope with several speculaebull Pneumatic attachment for the otoscopebull Tuning fork 512Hzbull Pen and paperbull Gloves
Advanced equipment
bull Co-phenylcaine spraybull A flexible nasendoscope with light sourcebull Alcohol wipe to act as demist for the scopebull Aqueous lubricating gel for the scope
Emergency equipment
bull Large nasal tampons (you can always cut 10cm ones to size)
bull Silver nitrate sticksbull Foley catheters
Basic Anatomy of the Nose
bull The structural anatomy of the nose is important
bull for both aesthetic and functional reasons since the
bull nose as the gateway to the respiratory tract performs
bull a variety of physiologic functions
External NoseThe shape of the external nose is defined by the nasalbones a pair of rectangular bones in the upper nasaldorsum and by lateral cartilages (uppernasal cartilages) and alar cartilages (major alar cartilages)in the central and lower portions of the noseThe lateral portions of the nasal alae alsocontain several small accessory cartilages called theminor alar cartilages which are embedded in the lateralsoft tissues of the noseThe shape and stability of the alar cartilages each ofwhich consists of a medial and lateral crus
External Nose
Anatomy of the nasal base
bull Besides thebull medial crura the
inferior septal margin and the connective-
bull tissue septum (columella) are also responsible
bull for stabilizing the base of the nose
Anatomy of the nasal base
Anatomy of the nasal base
bull The nasal septum is subluxed toward the left side partially
bull obstructing the nasal airway
Nasal CavitiesThe nasal cavities begin anteriorly at the nasal vestibulewhich is bordered posteriorly by the internal nasalvalve (limen nasi) located between the posteriorborder of the alar cartilage and the anterior border ofthe lateral cartilage This valve area is the narrowestportion of the upper respiratory tract
Nasal Cavities
The interior ofthe nose behind the nasal valve is divided by the nasalseptum into two main cavities
Nasal CavitiesThe nasal septum iscomposed of an anterior cartilaginous part and twoposterior bony parts Abnormalities in the shape ofthe nasal septum which may consist of a deviated septum tensionseptum spurs or ridges are a frequent cause ofnasal airway obstructionThe choanae are the paired posterior openingsthrough which the nasal cavities communicate withthe nasopharynx
Nasal CavitiesThe nasal cavity is bounded laterally by the lateral nasalwalls which are formed by the ethmoid bone andmaxilla and posteriorly by the palatine bone and thepterygoid process of the sphenoid bone Several functionallyimportant structures are located on the lateralnasal wall the nasal turbinates and their associatedpassages (meati) sinus ostia and the orifice ofthe nasolacrimal duct (Fig 15)
The inferior turbinate consists of a separate bone thatis attached to the medial wall of the maxillary sinusThe opening of the nasolacrimal duct is located in thecorresponding inferior meatus The middle andsuperior turbinates are part of the ethmoid bone In rare cases a rudimentary ldquosupreme turbinaterdquo is alsopresent above the superior turbinate
The middle turbinate has by far the greatest functionalimportance because most of the drainage tracts fromthe surrounding paranasal sinuses open into the middlemeatus The nasal cavity is bounded superiorly by the cribriformplate of the ethmoid bone This thin bony platehas numerous openings for the passage of the fila olfactoriaand also forms the boundary of the anteriorcranial fossa
Nasal Cavities
The floor of the nasal cavity is formedmostly by the hard palate which is formed in turn bythe two palatine processes of the maxilla and the horizontallaminae of the palatine bone
Structure of the lateral nasal wall
Inferior meatus
Paranasal Sinuses
The paranasal sinuses are air-filled cavities that communicatewith the nasal cavities
-The maxillary sinus frontalsinus and anterior ethmoid cells drain into the nasalcavity through the middle meatusmdashie below themiddle turbinate -The posterior ethmoidcells drain into the nasal cavity through the superiormeatus The ostium of the sphenoid sinus is locatedin the anterior wall directly above the choanae- The anatomical connections between the nasal cavity andparanasal sinuses are functionally important and playa key role in the pathogenesis of many rhinologic diseasesthat involve the paranasal sinuses
Vascular SupplyThe external nose derives most of its blood supply
from the facial artery which arises from the external
carotid artery and from the ophthalmic artery which
springs from the internal carotid artery
Vascular Supply
The internalnose receives blood from the territories of the externaland internal carotid arteries- the terminalbranches of the sphenopalatine artery which arisesfrom the maxillary artery - the anterior and posteriorethmoid arteries which arise from the ophthalmicartery-internal carotid arterie
venous drainage
The venous drainageof the facial region is handled by -the facial vein -retromandibular vein -internal jugular vein
lymphatic drainage
The regional lymphatic drainage of the face and externalnose is handled mainly by- the submandibularlymph nodes while the nasal cavity is additionallydrained by -the retropharyngeal and deep - -cervical lymph nodes
Morphology of the Nasal Mucosa
Besides the anatomical structure of the external noseand nasal cavity the nasal mucosa plays an essentialrole in numerous functions of the nose in the respiratory tract
Morphology of the Nasal Mucosa
The anterior part of the nasal cavity (the nasal vestibule)like the external nose is covered by skin composedof a multilayer keratinizing squamous epithelium and finally a ciliated respiratory epithelium A small areaon the upper nasal septum superior turbinate andpart of the middle turbinate located adjacent to thecribriform plate is covered by olfactory mucosa and iscalled the olfactory region
Nerve SupplyThe facial skin receives its sensory innervation fromterminal branches of the trigeminal nerve that enterthe facial region through the supraorbital infraorbitaland mental foramina Thefacial muscles are classified as mimetic or mastica- tory each of these groups receiving different motorinnervationbythe facial nerve
History and Clinical Examination of the Nose
Historybull The main symptomsbull nasal obstruction (ldquostuffy
noserdquo)bull nasal dischargebull Headachesbull Olfactory
dysfunction
Palpationbony discontinuitiesNeuralgias to check
over- the supraorbital -infraorbital -mental foramina
Anterior Rhinoscopy
bull The rhinologic examination itself begins with anterior
bull rhinoscopy to evaluate the nasal vestibule and the anterior
bull portions of the nasal cavity
Nasal Endoscopy Nasal endoscopy has become the most important andrewarding clinical examination method in rhinologic diagnosis
- rigid endoscopes which are available in 4-mm and 28- mm diameters and assorted viewing angles (eg 01048576 301048576 1201048576) -flexible endoscopes are also available for inspecting the nose and nasopharynx and exploring all of the pharynx and larynx in one sitting
Nasal endoscopy
Nasal Endoscopy
Nasal Endoscopy
Imaging of the Nose and Paranasal Sinuses
Conventional RadiographsStandard paranasal sinus radiographs in the occipitomental
projection ( Water projection) and
occipitofrontal projection Caldwell projection) in cases of acute inflammation
They are also obtained to evaluate midfacial fractures
Computed Tomography (CT) the main indicationsfor CT scanning of the
nose and paranasal sinuses
are- chronic sinusitis - -trauma (especially
frontobasal -fractures)
-and tumors
The occipitofrontal projection is better for evaluating theethmoid cells and frontal sinus
occipitomental projection demonstrates the maxillarysinus and gives a limited view of the sphenoid sinus
Computed tomography of the paranasal sinuses
Four representative coronal CT scans are shown
Four representative coronal CT scans are shown
Magnetic Resonance Imaging
Magnetic maging
Magnetic resonance imaging (MRI) has fewer indicationsthan CT in patients with paranasal sinus diseaseThis is primarily because MRI is markedly inferior toCT in defining the bony boundaries of the sinusesThe strength of MRI lies in its superior soft-tissue discriminationMRI is indicated in diseases that involve the paranasal sinuses in addition to thecranial cavity or orbit (eg tumors and congenitalmalformations such as encephaloceles)
MRI of the paranasal sinuses
The Nose and Sinuses
Structure The structure of the nose is made up of
four partsbull The surface anatomybull The nasal skeletonmdashcomposed of the
two nasal bones the paired upper lateral and lower lateral cartilages and the nasal septum covered in subcutaneous tissue and skin
bull The internal anatomymdashincludes the septum of the nose which forms the medial wall of the nasal cavity The turbinates on the lateral wall are also called conchae
bull The osteomeatal complexmdasha key functional area of the nose
Function The nose is the main route for inspired
air and its structure is related to this function As the air passes over the large surface area of the turbinates
The inspired gases are warmed and humidified Mucus on the mucosa of the nose removes large dust particles from the air as it is breathed in
The voice resonates in the sinuses and nose and this provides character to the speech
Pneumatization of the sinusesmdashthey are air filled spacesmdashreduces the weight of the skull
Diseases of thDiseases of the Outer and Inner Nosee Outer and
Inner Nose Erysipelas Definition of the disease ndash Erysipela is a skin infection that affects the superficial dermis and is caused by Streptococcus pyogenes (group A) It usually develops in the extremities and the face and less commonly on the scalp and genitals bull Epidemiologyaetiology ndash Erysipelas are more often seen in elderly infants and children patients with compromised immunology and diabetes -Predisposing factors are alcoholism skin ulceration puncture wounds fungal infections malnutrition and burns
Erysipelas
bull Symptomsbull ndash It usually presents of fever general fatigue bull -The skin lesion is a redindurated and elevated plaque
with borders that expand rapidly bull It is painful warm and accompanied by variable oedemabull -On the second or third day a flaccid bulla may develop
and desquamationbull bull Presence of regional lymph nodes is common
Erysipelas
bull Complicationsndash The most common complication is recurrencewhich is seen in 18ndash30 of the cases even afterproper antibiotic therapy Recurrence is seen moreoften in females than in malesA skin infection with S pyogenes could lead toglomerulonephritis
Erysipelas
bull Complicationsbull ndash The most common complication is recurrencebull which is seen in 18ndash30 of the cases even afterbull proper antibiotic therapy bull -Recurrence is seen morebull often in females than in males bull -A skin infection with S pyogenes could lead tobull glomerulonephritis
Erysipelas
bull bull Diagnosisbull ndash Diagnosis is based on the patientrsquos personal
historybull and physical examination particularly on inspectionbull of the skin
bull Blood cultures are positive in less thanbull 5 of cases
ErysipelasTherapyndash Conservative therapybull The preferred antibiotic is penicillin In mildcases with minor systemic symptoms penicillinV 500 mg orally every 6 h for 10 days or penicillinG benzathine 12 mil U intramuscularlyonceOther possibilities are amoxicillin 500 mgorally twice a day for 10 days or cephalexin 500mg orally every 6 h for 10 days
ErysipelasIn moderate and severe cases with significantsystemic symptoms hospitalization and intravenoustreatment is required penicillin G 2ndash4mil U intravenously every 4ndash6 h Cefazolin05ndash15 gm intravenously every 8 h cefotaxime1ndash2 gm intravenously every 8 h or ceftriaxone1ndash2 gm intravenously once a day should be administeredIn patients with a penicillin allergyclindamycin 600 mg intravenously every 8 h orvancomycin 15 mgkg intravenously twice a daymay be given
ErysipelaAdditional useful therapeutic optionsbull Prednisone 30 mg over 8 days might be consideredas well as elevation of the affected siteMoist heat compresses may be usefulbull Surgeryndash Debridement and drainage are indicated when bullaeabscesses or necroses are presentbull Differential diagnosisndash Contact dermatitisndash Asteatotic eczemandash Herpes zosterndash Angioneurotic oedemandash Osteomyelitis
Furuncle
bull Definition of the diseasebull ndash A furuncle is an infection that beginsbull at the hair follicle and spreads deeper into thebull dermis and subcutaneous tissue forming abull nodule After several days it developsbull into an abscess - red painful and fluctuantbull bull bull Epidemiologyaetiologybull ndash The aetiologic agent is Staphylococcus aureus
FuruncleSymptomsndashsymptoms are local and limited to thesite of infection Furuncles usually are wherehair follicles are present bull Complicationndash One complication is furunculosis multiple draining furunclesDiagnosisndash The diagnosis is based on clinical inspection - Cultures are not necessary when there is no systemic involvement but should beconsidered if systemic therapy (in case of feversignificant cellulitis or hospitalization) or whenmethicillin-resistant Staphylococcusaureus (MRSA) is considered
FuruncleTherapyndash When the furuncle is small application of moist heat compress to promote drainage -Larger furuncles should be drained by surgical incision-After drainage the area should be cleaned with anantiseptic (with chlorhexidinebetadine) should be applied twice
a dayndash If no systemic symptoms or extensive cellulitis arepresent simple topical care is usually curative andoral antibiotics are not necessary Otherwise systemictreatment is indicated and should cover anypossible MRSA
Furuncle
bull -Recommended antibiotics are trimethoprim-sulfamethoxazole
bull 1ndash2 tablets orally twice daily doxycyclinebull 100 mg orally twice dailybull or clindamycin 300ndash450 mg orally every 8 hbull - In severe cases vancomycin 15 mgkg
intravenouslybull every 12 h or clindamycin 600 mg intravenouslybull every 8 h
Midline Granulomabull A midline granuloma is an angiocentricbull lymphoma it was referred to as polymorphicbull reticulosis lethal midline granuloma and midline
malignant reticulosisbull bull Definition of the diseasebull ndash This rare disease is a lymphoma of extranodal
presentationall cases are positive for the Epstein-Barr virus
bull -This lymphoma most commonly appears in the midface region
Midline GranulomaEpidemiologyaetiologyndash This form of lymphoma is rare in Europe and theUnited States with a higher prevalence in Asia and PeruSymptomsndash The most common presentation is nasal obstruction with a destructive mass occupying the nosesinuses and palate
-Fever night sweatsand weight loss seen usually in Hodgkinrsquos lymphomaand other non-Hodgkinrsquos lymphomas (knownas ldquoB symptomsrdquo) are uncommon
Midline GranulomaDiagnosisndash The diagnosis is based on anatomopathologicalstudy The malignancy of the tumour manifested byextensive necrosis makes the histological diagnosisdifficult and often more biopsies are required forconfirmationbull Therapyndash Therapy consists of radiotherapy with or withoutchemotherapy
Midline Granuloma
bull Prognosisbull ndash Depending on the stage long-term remission or
experience a worseningbull prognosis with relapses which may include otherbull extranodal sites bull Involvement of extranodal sitesbull including the upper airway gastrointestinal tractbull skin
Wegenerrsquos Granulomatosis
bull Definition of the diseasebull ndash Wegenerrsquos granulomatosis is a systemic chronicbull vasculitis of small- and medium-sized blood vesselsbull with an autoimmune component It affectsbull particular organs with variable predilectionbull Epidemiologyaetiologybull ndash Wegenerrsquos granulomatosis is a rare disease It affects
about 1 in 20000ndash30000 people It is more prevalentbull in middle-aged Caucasian patients
Wegenerrsquos Granulomatosis
Symptomsndash The disease may present pulmonary upper
respiratory tract or renal In the disseminated form-The localised form ndash confinedto the upper respiratory region ndash is present in 25of the patients- It consists of nonspecific manifestationssuch as nasal obstruction crusting purulentor bloody rhinorrhea and painful or painless ulcers in oral or nasal cavities which are unresponsive tostandard medical treatment
Wegenerrsquos Granulomatosis
bull In some patients the nasal septum is perforatedbull which leads to saddle-nose deformity Less
commonbull symptoms are hoarseness stridor due to
subglotticbull stenosis otalgia otorrhea and conductivebull and sensorineural hearing loss Also ocular
symptomsbull such as scleritis conjunctivitis uveitis andbull episcleritis may be present
Wegenerrsquos Granulomatosis
bull ndash In the disseminated form pulmonary involvementbull is manifested by cough dyspnoea haemoptysisbull (due to an alveolar capillaritis necrotic lesions orbull endobronchial disease) and pleuritic painndashbull -Ninety per cent of patients have nasal symptomsbull and these symptoms are usually the first
manifestationof the diseasebull -Most patients have also renal involvementbull even if it is subclinical
Wegenerrsquos Granulomatosis
Diagnosis ndash Diagnosis of Wegenerrsquos granulomatosis is based on clinical findings that demonstrate lung (chest x-ray) kidney (urine analysis) or upper respiratory tract
involvement (oral or nasal ulcers or discharge) - positive blood analysis for cytoplasmic-staining antineutrophil
cytoplasmic antibodies (c-ANCA) and confirming proteinase 3 (PR3) ANCA or myeloperoxidase (MPO) ANCA ndash Biopsy is essential for diagnosis nonspecific chronic inflammation
and necrosis -Bacterial and fungal infections
Wegenerrsquos Granulomatosis
Therapyndash Conservative therapybull In the induction of disease remission highdosesteroids (e g prednisone 1 mgkgday) for1 month with tapering over several months aregiven In addition cyclophosphamide (2 mgkgday) should be administered for 6ndash12 monthsuntil symptoms disappear In the maintenanceof remission cyclophosphamide should be
Wegenerrsquos Granulomatosis
Antibiotics mainly trimethoprim-sulfamethoxazoleare given for prophylaxis againstPneumocystis jiroveci (formerly Pneumocystiscarinii) pneumonia (PCP) which may developduring immunosuppression and have a role inpreventing recurrencesbull Sinonasal manifestations may be treated with topical nasal steroids and nasal irrigations lowdosesystemic steroids and antibiotics when bacterial infection (typically Staphylococcus species) is suspected
Wegenerrsquos Granulomatosis
bull Prognosisbull ndash Most of the patients respond well to treatmentbull achieving symptom-free intervals of 5ndash20 yearsbull or more bull -Anatomical problems (sinusitis trachealbull stenosis) may require surgery bull Relapses can be long and troublesomebull Long-term complications are chronicbull renal failure hearing loss and deafness
Nasal Fractures Definition ndash A nasal fracture is a disruption of the nasal bone structure due to trauma It is the most frequently fractured facial bone Epidemiologyaetiology ndash Sports falls and assaults are the usual mechanisms of fracture -Males are affected twice as often as are females -Paediatric populations with a incidences during the second and third decades of life -Variables such as force impact direction nature of the striking object age and other will influence the pattern of injury to the components of the nose
Nasal Fractures
bull Symptomsbull ndash Deformity swelling epistaxis and periorbital
ecchymosis are signs that are suggestive of nasal fracture
bull bony crepitus and nasal segment mobilitybull ndash Epiphora bull Severe bilateral injuries to the lachrymal bones
arebull associated with depressed nasal fractures
Nasal Fractures Complications ndash Septal haematoma is one of the most severe early complications of nasal trauma and without drainage it results in abscess formation 6ndash7 days after trauma producing necrosis of the septal cartilage -Long-term problems such as saddle-nose deformity perforation columellar retraction and nasalbase
Septal infection could lead to osteomyelitis orbital and intracranial abscesses meningitis and cavernous sinus thrombosis -Cerebrospinal fluid leakage is a common complication of severe
nasal and frontal fractures
Nasal Fractures
bull Diagnostic proceduresbull ndash Inspectionbull bull Changes of appearance such as deviation andbull asymmetry bleeding watery drainage changesbull in nasal breathing and smell It is useful to comparebull the current presentation with old photographsbull (up to 40 of normal individuals havebull significant nose malformations)
Nasal Fractures Physical examination bull The diagnosis of a nasal fracture is made primarily by physical examination epistaxis nasal swelling and periorbital ecchymosis Nasal shape in the lateral and frontal inspection should be assessed Grasping the dorsum between two fingers and rocking the pyramid back and forth aids in assessing the mobility of nasal bones Internal structures should be evaluated by using a headlight and nasal speculum Clotted blood is removed by suction and assessment of haematoma mucosal tears and active bleeding is performed Bimanual palpation of the septum helps to differentiate septal swelling from haematoma ndash
Nasal FracturesRadiographybull There is no clear evidence of the role of radiographyin the management of nasal fracturesPlain films have up to a 66 false-positive rateas a result of misinterpretation of normal suturelines In addition old fractures are difficult todistinguishbull Three-dimensional CT is recommended for extensiveinjuries involving the nasal-orbital-ethmoidalcomplexndash
Nasal Fractures
bull Additionaluseful diagnostic proceduresbull bull Using a 0 or 30deg 4-mm endoscope is helpful inbull the assessment of posterior abnormalities If thebull patient is heavily sedated Brown-Gruss
provocationbull manoeuvres may be performed to determinebull deformities in upper middle or lower segmentsbull by compressing each compartment
Nasal FracturesConservative treatmentndash Treatment of bleedingbull For localised bleeding anterior sources may becauterised by silver nitrate or sealed with topicalmaterials such as thrombin combined withgelatin foam fibrin glue FloSealreg or other procoagulantmaterials If conservative measuresfail a formal anterior packing is placedbull Bleeding from branches of sphenopalatine orethmoid vessels requires anterior-posteriorpacking
Nasal Fractures
bull bull Surgical methods such as direct endoscopic vessel
bull cauterization or ligation have been shown tobull offer better haemostasis and patient comfortbull Angiography with embolization can also be
consideredbull in cases refractory to more conservativebull approaches
Nasal Fractures
bull Type of reductionbull bull Nondisplaced fractures should be treated withbull observation alone Closed nasal reduction is thebull best choice for simple injuries (isolated unilateralbull with medial displacement)bull bull An open approach should be considered in
severebull trauma (bilateral depressed fractures)
Nasal Fracturesbull Surgical principlesbull ndash Topical anaesthesia with cotton pledgets soakedbull with 4 cocaine or 005 oxymethazoline combinedbull with 4 topical lidocaine should be appliedbull for 5ndash10 min Local anaesthesia should also be injectedbull (1 lidocaine and 1100000 epinephrine)bull along the septum lateral walls and floor of the nasalbull cavitybull bull
Nasal FracturesClosed reductionndashndash The nasal bones are grasped between two fingersand pressure is applied laterally in theopposite direction of the deviation A bluntelevator may be used from within the nose incases of significant medial collapse Walshamforceps can be of help Reduction of the septumshould be performed with the use ofAsch forceps
Nasal Fractures
bull To prevent collapse of the postreductionbull framework nasal packing should be placedbull for 3ndash5 days Septum splints are recommendedbull in comminuted septal fractures withbull severe mucosal lesions External nasal splintingbull for 10 days (Aquaplastreg Thermoplastreg)bull provides nasal protection Nasal saline spraysbull prevent crusting and oral antibiotics should
Nasal Fractures
bull Open reductionbull ndashndash Immediate repair of fractures by using
widebull surgical exposure reduction fixation and
reconstructionbull ndashndash The second option is delayed correctionbull (6 months or more) of persistent deformitiesbull using standard techniques of rhinoplasty
Deviated Nasal Septum
bull Definition of the diseasebull ndash Deviation of the nasal septum is a common causebull of unilateral nasal airway obstruction in which thebull nasal septum is displacedbull bull Epidemiologyaetiologybull ndash Developmental septal abnormalities Septal cartilage
damage in the neonatal period andbull during birth can cause severe septal deviation inbull the absence of a history of nasal trauma
Deviated Nasal Septum
bull Symptomsbull ndash Patients may present with a history of sinusitis
allergicbull rhinitis obstructive sleep apnoea previousbull nasal surgery or recent nasal trauma Unilateral or
bilateral nasal airway obstruction that is unrelievedbull with decongestants or nasal steroid sprays is oftenbull seenbull bull
Deviated Nasal SeptumDiagnosisndashExamination external dorsal deviation or the columella and caudal septummay be deflected off the midline (caudal subluxation)ndash Inspections of the nasal cavity and anterior-posteriorrhinoscopy are helpful in diagnosing the locationtype and severity of septal deformityThe endoscope is also useful in identifying polypsthe severity and extent of posterior septaldeviations and bony spurs and locating areas ofseptal perforation or mucosal injury
Deviated Nasal Septum
bull Therapybull ndash Septoplasty is a procedurebull The areabull of deviation is corrected or resected in order tobull leave behind as much cartilage and bone as
possiblebull Cartilage resection is minimised and can be
repositioned reshaped or recontoured using a variety of methods
Deviated Nasal Septum
bull ndash Indications of septoplasty before the growth period
bull of the nose is finished should be very limited bull -In these cases surgery must preserve all the
cartilagebull in order to prevent external changes of the
shape ofbull the nose
Deviated Nasal Septum
bull Complicationsbull ndash Frequent complications include haematoma andbull infection Cerebrospinal fluid leak is a rare but
potentiallybull serious complicationbull It is usually the resultbull of avulsion or damage to the cribriform plate whenbull handling the perpendicular plate of the ethmoidbull ndash Other complications include epistaxis nasal
Deviated Nasal Septum
bull Other complications include epistaxis nasal obstruction
bull due to residual deviation synechiae returnbull of the cartilaginous deviation septal perforationbull anosmia and cosmetic nasal deformities suchbull as widened alar rim margins drooping nasal tipbull columella retraction and a sunken dorsum with abull supratip saddle formation
Septal perforation with minor crusting View from provide closure of the
incision
Septal Haematoma
bull A septal haematoma is a blood collection under the perichondrium
bull of the septum and cartilagebull bull bull Epidemiologyaetiologybull ndash A septal haematoma is one of the most
severe complications of nasal trauma
Septal Haematoma
bull Diagnosisbull ndash Signs and symptoms include intense pain
swellingbull haematoma of the upper lip and philtrum
area andbull complete nasal airway obstruction
Septal HaematomaTherapyndash Management consists of drainage through a mucoperichondrial incision Immediate treatment isnecessary to prevent long-term problems such asa saddle-nose deformity perforation columellarretraction and nasal-base widening In childrenseptal destruction can lead to devastating nasal andmidfacial growth abnormalitiesbull Surgeryndash Incision and evacuation of the collection is performedDrainage of a septal haematoma should
Septal HaematomaSurgeryndash Incision and evacuation of the collection is performedDrainage of a septal haematoma should provide closure of the incision
Splints or transseptal sutures are placed to obliterate thepotential space and prevent collectionInfection involving the septal cartilage Reconstruction with autologouscartilage is then performed in a second stage Oral antibiotics should be given
Nasal DeformitySaddle-nose deformityndash A saddle-nose deformity is characterised by a loss ofnasal dorsal height and compromised nasal supportstructures -Other case observed are depressionof the middle vault and dorsum loss of nasal tipsupport and definition shortened (vertical) nasal length over rotation of the nasal tip and retrusion ofthe nasal spine and caudal septum It is also knownas a ldquoPug noserdquo or ldquoboxerrsquos noserdquo both of which referto various degrees of nasal dorsal depressionbull
Nasal DeformityEpidemiologyaetiologyndash Prevalence is higher in population groups prone to facial trauma (ie boxers athletes) those with historiesof intranasal cocaine use nasal surgery (e g radical submucosal septal resection reductive rhinoplasty)ndash A saddle-nose deformity can be congenital or acquired It can be noticed as a part of individual familialsyndromic and ethnic characteristics - Most deformities are due to traumatic and iatrogeniccauses Medical causes are Wegenerrsquosgranulomatosis relapsing polychondritis leprosy (Hansenrsquos disease) syphilis ectodermal dysplasiaand intranasal cocaine use
Nasal Deformity
bull Therapybull ndash Nasal reconstruction indications depend on patientbull selection surgeon experience and aetiology of thebull deformity bull Indications for surgery can be functionalbull aesthetic or most commonly both In individuals
with a compromised nasal airway a nasoseptalbull reconstruction is indicated
Nasal Deformity
bull Contraindications bull include patients with malignantbull chronic or autoimmune disease conditions drugbull abuse poor perioperative risk profile and unrealisticbull expectationsbull ndash Multiple previous rhinoplasties and certain
professionsbull (mixed martial artists boxers and other contactbull sports) are relative contraindications
Nasal DeformitySeptoplastyndash Septoplasty is performed to correct nasal obstructioncaused by septal deformityndash Usually septoplasty is performed under general anaesthesiawith the patient in the supine position with the head elevated by approximately 30 (Righthandedsurgeons approach from the right side)ndash Local vasoconstrictive anaesthesia is applied notonly to reduce postoperative pain but also more importantly to achieve vasoconstriction of themucosa and less intraoperative haemorrhage Lidocainewith adrenaline or epinephrine is usedalthough in patients with cardiac hypersensitivityoxymetazoline might be preferred
Nasal Deformity
bull Septoplasty begins with the incision of septal mucosabull Most operative techniques utilise a hemitransfixionbull incision at the caudal end of septum so thatbull deviation at this point might be reached as wellbull as a transfixion incision that is easily obtained ifbull needed (Right-handed surgeons normally choosebull the left side but that may vary when deviation isbull convex towards the right)
Nasal DeformityA columella retractor is placed over the columellaand by pulling it laterally the caudal border of theseptum is exposed Ala can be protected by an alaprotector A vertical incision with a no 15 bladeover the caudal end of septum is performed untilreaching the plane of the septal cartilage It is essentialto correctly identify the perichondrium and byusing the Cottle elevator dissect and lift it creatinga flap As the dissection proceeds along the septalcartilage a longer speculum (no 5) is introduced sothat elevation of the mucoperichondrium is doneunder constant visual controlndash The next step is to dissect the mucoperiostium
Nasal DeformityDissecting over the bony-cartilaginous junctionwhen joining both tunnels might be difficult and is
especially prone to membrane perforationndash If needed the same tunnels are to be created on the
other side of the septum Then deviated parts of
septum are identified and removed either with a
knife or a Freer chisel
Nasal Deformitybull septum from the maxillary crest the septum mustbull be separated from the perpendicular plate trimmedbull along the inferior border placed back onto the crestbull and sutured to the periosteum If the deformity involvesbull the vomer an osteotome is used Care mustbull be taken not to break the cribriform plate becausebull it could cause a cerebrospinal fistula
Nasal Deformity
bull Once the septal deviation is corrected the flapsbull and hemitransfixion incision are mattressed
withbull absorbable sutures Nasal packing to prevent
synechiaebull and postoperative septal haematoma mightbull be advised but should be removed within 72 h

Advanced equipment
bull Co-phenylcaine spraybull A flexible nasendoscope with light sourcebull Alcohol wipe to act as demist for the scopebull Aqueous lubricating gel for the scope
Emergency equipment
bull Large nasal tampons (you can always cut 10cm ones to size)
bull Silver nitrate sticksbull Foley catheters
Basic Anatomy of the Nose
bull The structural anatomy of the nose is important
bull for both aesthetic and functional reasons since the
bull nose as the gateway to the respiratory tract performs
bull a variety of physiologic functions
External NoseThe shape of the external nose is defined by the nasalbones a pair of rectangular bones in the upper nasaldorsum and by lateral cartilages (uppernasal cartilages) and alar cartilages (major alar cartilages)in the central and lower portions of the noseThe lateral portions of the nasal alae alsocontain several small accessory cartilages called theminor alar cartilages which are embedded in the lateralsoft tissues of the noseThe shape and stability of the alar cartilages each ofwhich consists of a medial and lateral crus
External Nose
Anatomy of the nasal base
bull Besides thebull medial crura the
inferior septal margin and the connective-
bull tissue septum (columella) are also responsible
bull for stabilizing the base of the nose
Anatomy of the nasal base
Anatomy of the nasal base
bull The nasal septum is subluxed toward the left side partially
bull obstructing the nasal airway
Nasal CavitiesThe nasal cavities begin anteriorly at the nasal vestibulewhich is bordered posteriorly by the internal nasalvalve (limen nasi) located between the posteriorborder of the alar cartilage and the anterior border ofthe lateral cartilage This valve area is the narrowestportion of the upper respiratory tract
Nasal Cavities
The interior ofthe nose behind the nasal valve is divided by the nasalseptum into two main cavities
Nasal CavitiesThe nasal septum iscomposed of an anterior cartilaginous part and twoposterior bony parts Abnormalities in the shape ofthe nasal septum which may consist of a deviated septum tensionseptum spurs or ridges are a frequent cause ofnasal airway obstructionThe choanae are the paired posterior openingsthrough which the nasal cavities communicate withthe nasopharynx
Nasal CavitiesThe nasal cavity is bounded laterally by the lateral nasalwalls which are formed by the ethmoid bone andmaxilla and posteriorly by the palatine bone and thepterygoid process of the sphenoid bone Several functionallyimportant structures are located on the lateralnasal wall the nasal turbinates and their associatedpassages (meati) sinus ostia and the orifice ofthe nasolacrimal duct (Fig 15)
The inferior turbinate consists of a separate bone thatis attached to the medial wall of the maxillary sinusThe opening of the nasolacrimal duct is located in thecorresponding inferior meatus The middle andsuperior turbinates are part of the ethmoid bone In rare cases a rudimentary ldquosupreme turbinaterdquo is alsopresent above the superior turbinate
The middle turbinate has by far the greatest functionalimportance because most of the drainage tracts fromthe surrounding paranasal sinuses open into the middlemeatus The nasal cavity is bounded superiorly by the cribriformplate of the ethmoid bone This thin bony platehas numerous openings for the passage of the fila olfactoriaand also forms the boundary of the anteriorcranial fossa
Nasal Cavities
The floor of the nasal cavity is formedmostly by the hard palate which is formed in turn bythe two palatine processes of the maxilla and the horizontallaminae of the palatine bone
Structure of the lateral nasal wall
Inferior meatus
Paranasal Sinuses
The paranasal sinuses are air-filled cavities that communicatewith the nasal cavities
-The maxillary sinus frontalsinus and anterior ethmoid cells drain into the nasalcavity through the middle meatusmdashie below themiddle turbinate -The posterior ethmoidcells drain into the nasal cavity through the superiormeatus The ostium of the sphenoid sinus is locatedin the anterior wall directly above the choanae- The anatomical connections between the nasal cavity andparanasal sinuses are functionally important and playa key role in the pathogenesis of many rhinologic diseasesthat involve the paranasal sinuses
Vascular SupplyThe external nose derives most of its blood supply
from the facial artery which arises from the external
carotid artery and from the ophthalmic artery which
springs from the internal carotid artery
Vascular Supply
The internalnose receives blood from the territories of the externaland internal carotid arteries- the terminalbranches of the sphenopalatine artery which arisesfrom the maxillary artery - the anterior and posteriorethmoid arteries which arise from the ophthalmicartery-internal carotid arterie
venous drainage
The venous drainageof the facial region is handled by -the facial vein -retromandibular vein -internal jugular vein
lymphatic drainage
The regional lymphatic drainage of the face and externalnose is handled mainly by- the submandibularlymph nodes while the nasal cavity is additionallydrained by -the retropharyngeal and deep - -cervical lymph nodes
Morphology of the Nasal Mucosa
Besides the anatomical structure of the external noseand nasal cavity the nasal mucosa plays an essentialrole in numerous functions of the nose in the respiratory tract
Morphology of the Nasal Mucosa
The anterior part of the nasal cavity (the nasal vestibule)like the external nose is covered by skin composedof a multilayer keratinizing squamous epithelium and finally a ciliated respiratory epithelium A small areaon the upper nasal septum superior turbinate andpart of the middle turbinate located adjacent to thecribriform plate is covered by olfactory mucosa and iscalled the olfactory region
Nerve SupplyThe facial skin receives its sensory innervation fromterminal branches of the trigeminal nerve that enterthe facial region through the supraorbital infraorbitaland mental foramina Thefacial muscles are classified as mimetic or mastica- tory each of these groups receiving different motorinnervationbythe facial nerve
History and Clinical Examination of the Nose
Historybull The main symptomsbull nasal obstruction (ldquostuffy
noserdquo)bull nasal dischargebull Headachesbull Olfactory
dysfunction
Palpationbony discontinuitiesNeuralgias to check
over- the supraorbital -infraorbital -mental foramina
Anterior Rhinoscopy
bull The rhinologic examination itself begins with anterior
bull rhinoscopy to evaluate the nasal vestibule and the anterior
bull portions of the nasal cavity
Nasal Endoscopy Nasal endoscopy has become the most important andrewarding clinical examination method in rhinologic diagnosis
- rigid endoscopes which are available in 4-mm and 28- mm diameters and assorted viewing angles (eg 01048576 301048576 1201048576) -flexible endoscopes are also available for inspecting the nose and nasopharynx and exploring all of the pharynx and larynx in one sitting
Nasal endoscopy
Nasal Endoscopy
Nasal Endoscopy
Imaging of the Nose and Paranasal Sinuses
Conventional RadiographsStandard paranasal sinus radiographs in the occipitomental
projection ( Water projection) and
occipitofrontal projection Caldwell projection) in cases of acute inflammation
They are also obtained to evaluate midfacial fractures
Computed Tomography (CT) the main indicationsfor CT scanning of the
nose and paranasal sinuses
are- chronic sinusitis - -trauma (especially
frontobasal -fractures)
-and tumors
The occipitofrontal projection is better for evaluating theethmoid cells and frontal sinus
occipitomental projection demonstrates the maxillarysinus and gives a limited view of the sphenoid sinus
Computed tomography of the paranasal sinuses
Four representative coronal CT scans are shown
Four representative coronal CT scans are shown
Magnetic Resonance Imaging
Magnetic maging
Magnetic resonance imaging (MRI) has fewer indicationsthan CT in patients with paranasal sinus diseaseThis is primarily because MRI is markedly inferior toCT in defining the bony boundaries of the sinusesThe strength of MRI lies in its superior soft-tissue discriminationMRI is indicated in diseases that involve the paranasal sinuses in addition to thecranial cavity or orbit (eg tumors and congenitalmalformations such as encephaloceles)
MRI of the paranasal sinuses
The Nose and Sinuses
Structure The structure of the nose is made up of
four partsbull The surface anatomybull The nasal skeletonmdashcomposed of the
two nasal bones the paired upper lateral and lower lateral cartilages and the nasal septum covered in subcutaneous tissue and skin
bull The internal anatomymdashincludes the septum of the nose which forms the medial wall of the nasal cavity The turbinates on the lateral wall are also called conchae
bull The osteomeatal complexmdasha key functional area of the nose
Function The nose is the main route for inspired
air and its structure is related to this function As the air passes over the large surface area of the turbinates
The inspired gases are warmed and humidified Mucus on the mucosa of the nose removes large dust particles from the air as it is breathed in
The voice resonates in the sinuses and nose and this provides character to the speech
Pneumatization of the sinusesmdashthey are air filled spacesmdashreduces the weight of the skull
Diseases of thDiseases of the Outer and Inner Nosee Outer and
Inner Nose Erysipelas Definition of the disease ndash Erysipela is a skin infection that affects the superficial dermis and is caused by Streptococcus pyogenes (group A) It usually develops in the extremities and the face and less commonly on the scalp and genitals bull Epidemiologyaetiology ndash Erysipelas are more often seen in elderly infants and children patients with compromised immunology and diabetes -Predisposing factors are alcoholism skin ulceration puncture wounds fungal infections malnutrition and burns
Erysipelas
bull Symptomsbull ndash It usually presents of fever general fatigue bull -The skin lesion is a redindurated and elevated plaque
with borders that expand rapidly bull It is painful warm and accompanied by variable oedemabull -On the second or third day a flaccid bulla may develop
and desquamationbull bull Presence of regional lymph nodes is common
Erysipelas
bull Complicationsndash The most common complication is recurrencewhich is seen in 18ndash30 of the cases even afterproper antibiotic therapy Recurrence is seen moreoften in females than in malesA skin infection with S pyogenes could lead toglomerulonephritis
Erysipelas
bull Complicationsbull ndash The most common complication is recurrencebull which is seen in 18ndash30 of the cases even afterbull proper antibiotic therapy bull -Recurrence is seen morebull often in females than in males bull -A skin infection with S pyogenes could lead tobull glomerulonephritis
Erysipelas
bull bull Diagnosisbull ndash Diagnosis is based on the patientrsquos personal
historybull and physical examination particularly on inspectionbull of the skin
bull Blood cultures are positive in less thanbull 5 of cases
ErysipelasTherapyndash Conservative therapybull The preferred antibiotic is penicillin In mildcases with minor systemic symptoms penicillinV 500 mg orally every 6 h for 10 days or penicillinG benzathine 12 mil U intramuscularlyonceOther possibilities are amoxicillin 500 mgorally twice a day for 10 days or cephalexin 500mg orally every 6 h for 10 days
ErysipelasIn moderate and severe cases with significantsystemic symptoms hospitalization and intravenoustreatment is required penicillin G 2ndash4mil U intravenously every 4ndash6 h Cefazolin05ndash15 gm intravenously every 8 h cefotaxime1ndash2 gm intravenously every 8 h or ceftriaxone1ndash2 gm intravenously once a day should be administeredIn patients with a penicillin allergyclindamycin 600 mg intravenously every 8 h orvancomycin 15 mgkg intravenously twice a daymay be given
ErysipelaAdditional useful therapeutic optionsbull Prednisone 30 mg over 8 days might be consideredas well as elevation of the affected siteMoist heat compresses may be usefulbull Surgeryndash Debridement and drainage are indicated when bullaeabscesses or necroses are presentbull Differential diagnosisndash Contact dermatitisndash Asteatotic eczemandash Herpes zosterndash Angioneurotic oedemandash Osteomyelitis
Furuncle
bull Definition of the diseasebull ndash A furuncle is an infection that beginsbull at the hair follicle and spreads deeper into thebull dermis and subcutaneous tissue forming abull nodule After several days it developsbull into an abscess - red painful and fluctuantbull bull bull Epidemiologyaetiologybull ndash The aetiologic agent is Staphylococcus aureus
FuruncleSymptomsndashsymptoms are local and limited to thesite of infection Furuncles usually are wherehair follicles are present bull Complicationndash One complication is furunculosis multiple draining furunclesDiagnosisndash The diagnosis is based on clinical inspection - Cultures are not necessary when there is no systemic involvement but should beconsidered if systemic therapy (in case of feversignificant cellulitis or hospitalization) or whenmethicillin-resistant Staphylococcusaureus (MRSA) is considered
FuruncleTherapyndash When the furuncle is small application of moist heat compress to promote drainage -Larger furuncles should be drained by surgical incision-After drainage the area should be cleaned with anantiseptic (with chlorhexidinebetadine) should be applied twice
a dayndash If no systemic symptoms or extensive cellulitis arepresent simple topical care is usually curative andoral antibiotics are not necessary Otherwise systemictreatment is indicated and should cover anypossible MRSA
Furuncle
bull -Recommended antibiotics are trimethoprim-sulfamethoxazole
bull 1ndash2 tablets orally twice daily doxycyclinebull 100 mg orally twice dailybull or clindamycin 300ndash450 mg orally every 8 hbull - In severe cases vancomycin 15 mgkg
intravenouslybull every 12 h or clindamycin 600 mg intravenouslybull every 8 h
Midline Granulomabull A midline granuloma is an angiocentricbull lymphoma it was referred to as polymorphicbull reticulosis lethal midline granuloma and midline
malignant reticulosisbull bull Definition of the diseasebull ndash This rare disease is a lymphoma of extranodal
presentationall cases are positive for the Epstein-Barr virus
bull -This lymphoma most commonly appears in the midface region
Midline GranulomaEpidemiologyaetiologyndash This form of lymphoma is rare in Europe and theUnited States with a higher prevalence in Asia and PeruSymptomsndash The most common presentation is nasal obstruction with a destructive mass occupying the nosesinuses and palate
-Fever night sweatsand weight loss seen usually in Hodgkinrsquos lymphomaand other non-Hodgkinrsquos lymphomas (knownas ldquoB symptomsrdquo) are uncommon
Midline GranulomaDiagnosisndash The diagnosis is based on anatomopathologicalstudy The malignancy of the tumour manifested byextensive necrosis makes the histological diagnosisdifficult and often more biopsies are required forconfirmationbull Therapyndash Therapy consists of radiotherapy with or withoutchemotherapy
Midline Granuloma
bull Prognosisbull ndash Depending on the stage long-term remission or
experience a worseningbull prognosis with relapses which may include otherbull extranodal sites bull Involvement of extranodal sitesbull including the upper airway gastrointestinal tractbull skin
Wegenerrsquos Granulomatosis
bull Definition of the diseasebull ndash Wegenerrsquos granulomatosis is a systemic chronicbull vasculitis of small- and medium-sized blood vesselsbull with an autoimmune component It affectsbull particular organs with variable predilectionbull Epidemiologyaetiologybull ndash Wegenerrsquos granulomatosis is a rare disease It affects
about 1 in 20000ndash30000 people It is more prevalentbull in middle-aged Caucasian patients
Wegenerrsquos Granulomatosis
Symptomsndash The disease may present pulmonary upper
respiratory tract or renal In the disseminated form-The localised form ndash confinedto the upper respiratory region ndash is present in 25of the patients- It consists of nonspecific manifestationssuch as nasal obstruction crusting purulentor bloody rhinorrhea and painful or painless ulcers in oral or nasal cavities which are unresponsive tostandard medical treatment
Wegenerrsquos Granulomatosis
bull In some patients the nasal septum is perforatedbull which leads to saddle-nose deformity Less
commonbull symptoms are hoarseness stridor due to
subglotticbull stenosis otalgia otorrhea and conductivebull and sensorineural hearing loss Also ocular
symptomsbull such as scleritis conjunctivitis uveitis andbull episcleritis may be present
Wegenerrsquos Granulomatosis
bull ndash In the disseminated form pulmonary involvementbull is manifested by cough dyspnoea haemoptysisbull (due to an alveolar capillaritis necrotic lesions orbull endobronchial disease) and pleuritic painndashbull -Ninety per cent of patients have nasal symptomsbull and these symptoms are usually the first
manifestationof the diseasebull -Most patients have also renal involvementbull even if it is subclinical
Wegenerrsquos Granulomatosis
Diagnosis ndash Diagnosis of Wegenerrsquos granulomatosis is based on clinical findings that demonstrate lung (chest x-ray) kidney (urine analysis) or upper respiratory tract
involvement (oral or nasal ulcers or discharge) - positive blood analysis for cytoplasmic-staining antineutrophil
cytoplasmic antibodies (c-ANCA) and confirming proteinase 3 (PR3) ANCA or myeloperoxidase (MPO) ANCA ndash Biopsy is essential for diagnosis nonspecific chronic inflammation
and necrosis -Bacterial and fungal infections
Wegenerrsquos Granulomatosis
Therapyndash Conservative therapybull In the induction of disease remission highdosesteroids (e g prednisone 1 mgkgday) for1 month with tapering over several months aregiven In addition cyclophosphamide (2 mgkgday) should be administered for 6ndash12 monthsuntil symptoms disappear In the maintenanceof remission cyclophosphamide should be
Wegenerrsquos Granulomatosis
Antibiotics mainly trimethoprim-sulfamethoxazoleare given for prophylaxis againstPneumocystis jiroveci (formerly Pneumocystiscarinii) pneumonia (PCP) which may developduring immunosuppression and have a role inpreventing recurrencesbull Sinonasal manifestations may be treated with topical nasal steroids and nasal irrigations lowdosesystemic steroids and antibiotics when bacterial infection (typically Staphylococcus species) is suspected
Wegenerrsquos Granulomatosis
bull Prognosisbull ndash Most of the patients respond well to treatmentbull achieving symptom-free intervals of 5ndash20 yearsbull or more bull -Anatomical problems (sinusitis trachealbull stenosis) may require surgery bull Relapses can be long and troublesomebull Long-term complications are chronicbull renal failure hearing loss and deafness
Nasal Fractures Definition ndash A nasal fracture is a disruption of the nasal bone structure due to trauma It is the most frequently fractured facial bone Epidemiologyaetiology ndash Sports falls and assaults are the usual mechanisms of fracture -Males are affected twice as often as are females -Paediatric populations with a incidences during the second and third decades of life -Variables such as force impact direction nature of the striking object age and other will influence the pattern of injury to the components of the nose
Nasal Fractures
bull Symptomsbull ndash Deformity swelling epistaxis and periorbital
ecchymosis are signs that are suggestive of nasal fracture
bull bony crepitus and nasal segment mobilitybull ndash Epiphora bull Severe bilateral injuries to the lachrymal bones
arebull associated with depressed nasal fractures
Nasal Fractures Complications ndash Septal haematoma is one of the most severe early complications of nasal trauma and without drainage it results in abscess formation 6ndash7 days after trauma producing necrosis of the septal cartilage -Long-term problems such as saddle-nose deformity perforation columellar retraction and nasalbase
Septal infection could lead to osteomyelitis orbital and intracranial abscesses meningitis and cavernous sinus thrombosis -Cerebrospinal fluid leakage is a common complication of severe
nasal and frontal fractures
Nasal Fractures
bull Diagnostic proceduresbull ndash Inspectionbull bull Changes of appearance such as deviation andbull asymmetry bleeding watery drainage changesbull in nasal breathing and smell It is useful to comparebull the current presentation with old photographsbull (up to 40 of normal individuals havebull significant nose malformations)
Nasal Fractures Physical examination bull The diagnosis of a nasal fracture is made primarily by physical examination epistaxis nasal swelling and periorbital ecchymosis Nasal shape in the lateral and frontal inspection should be assessed Grasping the dorsum between two fingers and rocking the pyramid back and forth aids in assessing the mobility of nasal bones Internal structures should be evaluated by using a headlight and nasal speculum Clotted blood is removed by suction and assessment of haematoma mucosal tears and active bleeding is performed Bimanual palpation of the septum helps to differentiate septal swelling from haematoma ndash
Nasal FracturesRadiographybull There is no clear evidence of the role of radiographyin the management of nasal fracturesPlain films have up to a 66 false-positive rateas a result of misinterpretation of normal suturelines In addition old fractures are difficult todistinguishbull Three-dimensional CT is recommended for extensiveinjuries involving the nasal-orbital-ethmoidalcomplexndash
Nasal Fractures
bull Additionaluseful diagnostic proceduresbull bull Using a 0 or 30deg 4-mm endoscope is helpful inbull the assessment of posterior abnormalities If thebull patient is heavily sedated Brown-Gruss
provocationbull manoeuvres may be performed to determinebull deformities in upper middle or lower segmentsbull by compressing each compartment
Nasal FracturesConservative treatmentndash Treatment of bleedingbull For localised bleeding anterior sources may becauterised by silver nitrate or sealed with topicalmaterials such as thrombin combined withgelatin foam fibrin glue FloSealreg or other procoagulantmaterials If conservative measuresfail a formal anterior packing is placedbull Bleeding from branches of sphenopalatine orethmoid vessels requires anterior-posteriorpacking
Nasal Fractures
bull bull Surgical methods such as direct endoscopic vessel
bull cauterization or ligation have been shown tobull offer better haemostasis and patient comfortbull Angiography with embolization can also be
consideredbull in cases refractory to more conservativebull approaches
Nasal Fractures
bull Type of reductionbull bull Nondisplaced fractures should be treated withbull observation alone Closed nasal reduction is thebull best choice for simple injuries (isolated unilateralbull with medial displacement)bull bull An open approach should be considered in
severebull trauma (bilateral depressed fractures)
Nasal Fracturesbull Surgical principlesbull ndash Topical anaesthesia with cotton pledgets soakedbull with 4 cocaine or 005 oxymethazoline combinedbull with 4 topical lidocaine should be appliedbull for 5ndash10 min Local anaesthesia should also be injectedbull (1 lidocaine and 1100000 epinephrine)bull along the septum lateral walls and floor of the nasalbull cavitybull bull
Nasal FracturesClosed reductionndashndash The nasal bones are grasped between two fingersand pressure is applied laterally in theopposite direction of the deviation A bluntelevator may be used from within the nose incases of significant medial collapse Walshamforceps can be of help Reduction of the septumshould be performed with the use ofAsch forceps
Nasal Fractures
bull To prevent collapse of the postreductionbull framework nasal packing should be placedbull for 3ndash5 days Septum splints are recommendedbull in comminuted septal fractures withbull severe mucosal lesions External nasal splintingbull for 10 days (Aquaplastreg Thermoplastreg)bull provides nasal protection Nasal saline spraysbull prevent crusting and oral antibiotics should
Nasal Fractures
bull Open reductionbull ndashndash Immediate repair of fractures by using
widebull surgical exposure reduction fixation and
reconstructionbull ndashndash The second option is delayed correctionbull (6 months or more) of persistent deformitiesbull using standard techniques of rhinoplasty
Deviated Nasal Septum
bull Definition of the diseasebull ndash Deviation of the nasal septum is a common causebull of unilateral nasal airway obstruction in which thebull nasal septum is displacedbull bull Epidemiologyaetiologybull ndash Developmental septal abnormalities Septal cartilage
damage in the neonatal period andbull during birth can cause severe septal deviation inbull the absence of a history of nasal trauma
Deviated Nasal Septum
bull Symptomsbull ndash Patients may present with a history of sinusitis
allergicbull rhinitis obstructive sleep apnoea previousbull nasal surgery or recent nasal trauma Unilateral or
bilateral nasal airway obstruction that is unrelievedbull with decongestants or nasal steroid sprays is oftenbull seenbull bull
Deviated Nasal SeptumDiagnosisndashExamination external dorsal deviation or the columella and caudal septummay be deflected off the midline (caudal subluxation)ndash Inspections of the nasal cavity and anterior-posteriorrhinoscopy are helpful in diagnosing the locationtype and severity of septal deformityThe endoscope is also useful in identifying polypsthe severity and extent of posterior septaldeviations and bony spurs and locating areas ofseptal perforation or mucosal injury
Deviated Nasal Septum
bull Therapybull ndash Septoplasty is a procedurebull The areabull of deviation is corrected or resected in order tobull leave behind as much cartilage and bone as
possiblebull Cartilage resection is minimised and can be
repositioned reshaped or recontoured using a variety of methods
Deviated Nasal Septum
bull ndash Indications of septoplasty before the growth period
bull of the nose is finished should be very limited bull -In these cases surgery must preserve all the
cartilagebull in order to prevent external changes of the
shape ofbull the nose
Deviated Nasal Septum
bull Complicationsbull ndash Frequent complications include haematoma andbull infection Cerebrospinal fluid leak is a rare but
potentiallybull serious complicationbull It is usually the resultbull of avulsion or damage to the cribriform plate whenbull handling the perpendicular plate of the ethmoidbull ndash Other complications include epistaxis nasal
Deviated Nasal Septum
bull Other complications include epistaxis nasal obstruction
bull due to residual deviation synechiae returnbull of the cartilaginous deviation septal perforationbull anosmia and cosmetic nasal deformities suchbull as widened alar rim margins drooping nasal tipbull columella retraction and a sunken dorsum with abull supratip saddle formation
Septal perforation with minor crusting View from provide closure of the
incision
Septal Haematoma
bull A septal haematoma is a blood collection under the perichondrium
bull of the septum and cartilagebull bull bull Epidemiologyaetiologybull ndash A septal haematoma is one of the most
severe complications of nasal trauma
Septal Haematoma
bull Diagnosisbull ndash Signs and symptoms include intense pain
swellingbull haematoma of the upper lip and philtrum
area andbull complete nasal airway obstruction
Septal HaematomaTherapyndash Management consists of drainage through a mucoperichondrial incision Immediate treatment isnecessary to prevent long-term problems such asa saddle-nose deformity perforation columellarretraction and nasal-base widening In childrenseptal destruction can lead to devastating nasal andmidfacial growth abnormalitiesbull Surgeryndash Incision and evacuation of the collection is performedDrainage of a septal haematoma should
Septal HaematomaSurgeryndash Incision and evacuation of the collection is performedDrainage of a septal haematoma should provide closure of the incision
Splints or transseptal sutures are placed to obliterate thepotential space and prevent collectionInfection involving the septal cartilage Reconstruction with autologouscartilage is then performed in a second stage Oral antibiotics should be given
Nasal DeformitySaddle-nose deformityndash A saddle-nose deformity is characterised by a loss ofnasal dorsal height and compromised nasal supportstructures -Other case observed are depressionof the middle vault and dorsum loss of nasal tipsupport and definition shortened (vertical) nasal length over rotation of the nasal tip and retrusion ofthe nasal spine and caudal septum It is also knownas a ldquoPug noserdquo or ldquoboxerrsquos noserdquo both of which referto various degrees of nasal dorsal depressionbull
Nasal DeformityEpidemiologyaetiologyndash Prevalence is higher in population groups prone to facial trauma (ie boxers athletes) those with historiesof intranasal cocaine use nasal surgery (e g radical submucosal septal resection reductive rhinoplasty)ndash A saddle-nose deformity can be congenital or acquired It can be noticed as a part of individual familialsyndromic and ethnic characteristics - Most deformities are due to traumatic and iatrogeniccauses Medical causes are Wegenerrsquosgranulomatosis relapsing polychondritis leprosy (Hansenrsquos disease) syphilis ectodermal dysplasiaand intranasal cocaine use
Nasal Deformity
bull Therapybull ndash Nasal reconstruction indications depend on patientbull selection surgeon experience and aetiology of thebull deformity bull Indications for surgery can be functionalbull aesthetic or most commonly both In individuals
with a compromised nasal airway a nasoseptalbull reconstruction is indicated
Nasal Deformity
bull Contraindications bull include patients with malignantbull chronic or autoimmune disease conditions drugbull abuse poor perioperative risk profile and unrealisticbull expectationsbull ndash Multiple previous rhinoplasties and certain
professionsbull (mixed martial artists boxers and other contactbull sports) are relative contraindications
Nasal DeformitySeptoplastyndash Septoplasty is performed to correct nasal obstructioncaused by septal deformityndash Usually septoplasty is performed under general anaesthesiawith the patient in the supine position with the head elevated by approximately 30 (Righthandedsurgeons approach from the right side)ndash Local vasoconstrictive anaesthesia is applied notonly to reduce postoperative pain but also more importantly to achieve vasoconstriction of themucosa and less intraoperative haemorrhage Lidocainewith adrenaline or epinephrine is usedalthough in patients with cardiac hypersensitivityoxymetazoline might be preferred
Nasal Deformity
bull Septoplasty begins with the incision of septal mucosabull Most operative techniques utilise a hemitransfixionbull incision at the caudal end of septum so thatbull deviation at this point might be reached as wellbull as a transfixion incision that is easily obtained ifbull needed (Right-handed surgeons normally choosebull the left side but that may vary when deviation isbull convex towards the right)
Nasal DeformityA columella retractor is placed over the columellaand by pulling it laterally the caudal border of theseptum is exposed Ala can be protected by an alaprotector A vertical incision with a no 15 bladeover the caudal end of septum is performed untilreaching the plane of the septal cartilage It is essentialto correctly identify the perichondrium and byusing the Cottle elevator dissect and lift it creatinga flap As the dissection proceeds along the septalcartilage a longer speculum (no 5) is introduced sothat elevation of the mucoperichondrium is doneunder constant visual controlndash The next step is to dissect the mucoperiostium
Nasal DeformityDissecting over the bony-cartilaginous junctionwhen joining both tunnels might be difficult and is
especially prone to membrane perforationndash If needed the same tunnels are to be created on the
other side of the septum Then deviated parts of
septum are identified and removed either with a
knife or a Freer chisel
Nasal Deformitybull septum from the maxillary crest the septum mustbull be separated from the perpendicular plate trimmedbull along the inferior border placed back onto the crestbull and sutured to the periosteum If the deformity involvesbull the vomer an osteotome is used Care mustbull be taken not to break the cribriform plate becausebull it could cause a cerebrospinal fistula
Nasal Deformity
bull Once the septal deviation is corrected the flapsbull and hemitransfixion incision are mattressed
withbull absorbable sutures Nasal packing to prevent
synechiaebull and postoperative septal haematoma mightbull be advised but should be removed within 72 h

Emergency equipment
bull Large nasal tampons (you can always cut 10cm ones to size)
bull Silver nitrate sticksbull Foley catheters
Basic Anatomy of the Nose
bull The structural anatomy of the nose is important
bull for both aesthetic and functional reasons since the
bull nose as the gateway to the respiratory tract performs
bull a variety of physiologic functions
External NoseThe shape of the external nose is defined by the nasalbones a pair of rectangular bones in the upper nasaldorsum and by lateral cartilages (uppernasal cartilages) and alar cartilages (major alar cartilages)in the central and lower portions of the noseThe lateral portions of the nasal alae alsocontain several small accessory cartilages called theminor alar cartilages which are embedded in the lateralsoft tissues of the noseThe shape and stability of the alar cartilages each ofwhich consists of a medial and lateral crus
External Nose
Anatomy of the nasal base
bull Besides thebull medial crura the
inferior septal margin and the connective-
bull tissue septum (columella) are also responsible
bull for stabilizing the base of the nose
Anatomy of the nasal base
Anatomy of the nasal base
bull The nasal septum is subluxed toward the left side partially
bull obstructing the nasal airway
Nasal CavitiesThe nasal cavities begin anteriorly at the nasal vestibulewhich is bordered posteriorly by the internal nasalvalve (limen nasi) located between the posteriorborder of the alar cartilage and the anterior border ofthe lateral cartilage This valve area is the narrowestportion of the upper respiratory tract
Nasal Cavities
The interior ofthe nose behind the nasal valve is divided by the nasalseptum into two main cavities
Nasal CavitiesThe nasal septum iscomposed of an anterior cartilaginous part and twoposterior bony parts Abnormalities in the shape ofthe nasal septum which may consist of a deviated septum tensionseptum spurs or ridges are a frequent cause ofnasal airway obstructionThe choanae are the paired posterior openingsthrough which the nasal cavities communicate withthe nasopharynx
Nasal CavitiesThe nasal cavity is bounded laterally by the lateral nasalwalls which are formed by the ethmoid bone andmaxilla and posteriorly by the palatine bone and thepterygoid process of the sphenoid bone Several functionallyimportant structures are located on the lateralnasal wall the nasal turbinates and their associatedpassages (meati) sinus ostia and the orifice ofthe nasolacrimal duct (Fig 15)
The inferior turbinate consists of a separate bone thatis attached to the medial wall of the maxillary sinusThe opening of the nasolacrimal duct is located in thecorresponding inferior meatus The middle andsuperior turbinates are part of the ethmoid bone In rare cases a rudimentary ldquosupreme turbinaterdquo is alsopresent above the superior turbinate
The middle turbinate has by far the greatest functionalimportance because most of the drainage tracts fromthe surrounding paranasal sinuses open into the middlemeatus The nasal cavity is bounded superiorly by the cribriformplate of the ethmoid bone This thin bony platehas numerous openings for the passage of the fila olfactoriaand also forms the boundary of the anteriorcranial fossa
Nasal Cavities
The floor of the nasal cavity is formedmostly by the hard palate which is formed in turn bythe two palatine processes of the maxilla and the horizontallaminae of the palatine bone
Structure of the lateral nasal wall
Inferior meatus
Paranasal Sinuses
The paranasal sinuses are air-filled cavities that communicatewith the nasal cavities
-The maxillary sinus frontalsinus and anterior ethmoid cells drain into the nasalcavity through the middle meatusmdashie below themiddle turbinate -The posterior ethmoidcells drain into the nasal cavity through the superiormeatus The ostium of the sphenoid sinus is locatedin the anterior wall directly above the choanae- The anatomical connections between the nasal cavity andparanasal sinuses are functionally important and playa key role in the pathogenesis of many rhinologic diseasesthat involve the paranasal sinuses
Vascular SupplyThe external nose derives most of its blood supply
from the facial artery which arises from the external
carotid artery and from the ophthalmic artery which
springs from the internal carotid artery
Vascular Supply
The internalnose receives blood from the territories of the externaland internal carotid arteries- the terminalbranches of the sphenopalatine artery which arisesfrom the maxillary artery - the anterior and posteriorethmoid arteries which arise from the ophthalmicartery-internal carotid arterie
venous drainage
The venous drainageof the facial region is handled by -the facial vein -retromandibular vein -internal jugular vein
lymphatic drainage
The regional lymphatic drainage of the face and externalnose is handled mainly by- the submandibularlymph nodes while the nasal cavity is additionallydrained by -the retropharyngeal and deep - -cervical lymph nodes
Morphology of the Nasal Mucosa
Besides the anatomical structure of the external noseand nasal cavity the nasal mucosa plays an essentialrole in numerous functions of the nose in the respiratory tract
Morphology of the Nasal Mucosa
The anterior part of the nasal cavity (the nasal vestibule)like the external nose is covered by skin composedof a multilayer keratinizing squamous epithelium and finally a ciliated respiratory epithelium A small areaon the upper nasal septum superior turbinate andpart of the middle turbinate located adjacent to thecribriform plate is covered by olfactory mucosa and iscalled the olfactory region
Nerve SupplyThe facial skin receives its sensory innervation fromterminal branches of the trigeminal nerve that enterthe facial region through the supraorbital infraorbitaland mental foramina Thefacial muscles are classified as mimetic or mastica- tory each of these groups receiving different motorinnervationbythe facial nerve
History and Clinical Examination of the Nose
Historybull The main symptomsbull nasal obstruction (ldquostuffy
noserdquo)bull nasal dischargebull Headachesbull Olfactory
dysfunction
Palpationbony discontinuitiesNeuralgias to check
over- the supraorbital -infraorbital -mental foramina
Anterior Rhinoscopy
bull The rhinologic examination itself begins with anterior
bull rhinoscopy to evaluate the nasal vestibule and the anterior
bull portions of the nasal cavity
Nasal Endoscopy Nasal endoscopy has become the most important andrewarding clinical examination method in rhinologic diagnosis
- rigid endoscopes which are available in 4-mm and 28- mm diameters and assorted viewing angles (eg 01048576 301048576 1201048576) -flexible endoscopes are also available for inspecting the nose and nasopharynx and exploring all of the pharynx and larynx in one sitting
Nasal endoscopy
Nasal Endoscopy
Nasal Endoscopy
Imaging of the Nose and Paranasal Sinuses
Conventional RadiographsStandard paranasal sinus radiographs in the occipitomental
projection ( Water projection) and
occipitofrontal projection Caldwell projection) in cases of acute inflammation
They are also obtained to evaluate midfacial fractures
Computed Tomography (CT) the main indicationsfor CT scanning of the
nose and paranasal sinuses
are- chronic sinusitis - -trauma (especially
frontobasal -fractures)
-and tumors
The occipitofrontal projection is better for evaluating theethmoid cells and frontal sinus
occipitomental projection demonstrates the maxillarysinus and gives a limited view of the sphenoid sinus
Computed tomography of the paranasal sinuses
Four representative coronal CT scans are shown
Four representative coronal CT scans are shown
Magnetic Resonance Imaging
Magnetic maging
Magnetic resonance imaging (MRI) has fewer indicationsthan CT in patients with paranasal sinus diseaseThis is primarily because MRI is markedly inferior toCT in defining the bony boundaries of the sinusesThe strength of MRI lies in its superior soft-tissue discriminationMRI is indicated in diseases that involve the paranasal sinuses in addition to thecranial cavity or orbit (eg tumors and congenitalmalformations such as encephaloceles)
MRI of the paranasal sinuses
The Nose and Sinuses
Structure The structure of the nose is made up of
four partsbull The surface anatomybull The nasal skeletonmdashcomposed of the
two nasal bones the paired upper lateral and lower lateral cartilages and the nasal septum covered in subcutaneous tissue and skin
bull The internal anatomymdashincludes the septum of the nose which forms the medial wall of the nasal cavity The turbinates on the lateral wall are also called conchae
bull The osteomeatal complexmdasha key functional area of the nose
Function The nose is the main route for inspired
air and its structure is related to this function As the air passes over the large surface area of the turbinates
The inspired gases are warmed and humidified Mucus on the mucosa of the nose removes large dust particles from the air as it is breathed in
The voice resonates in the sinuses and nose and this provides character to the speech
Pneumatization of the sinusesmdashthey are air filled spacesmdashreduces the weight of the skull
Diseases of thDiseases of the Outer and Inner Nosee Outer and
Inner Nose Erysipelas Definition of the disease ndash Erysipela is a skin infection that affects the superficial dermis and is caused by Streptococcus pyogenes (group A) It usually develops in the extremities and the face and less commonly on the scalp and genitals bull Epidemiologyaetiology ndash Erysipelas are more often seen in elderly infants and children patients with compromised immunology and diabetes -Predisposing factors are alcoholism skin ulceration puncture wounds fungal infections malnutrition and burns
Erysipelas
bull Symptomsbull ndash It usually presents of fever general fatigue bull -The skin lesion is a redindurated and elevated plaque
with borders that expand rapidly bull It is painful warm and accompanied by variable oedemabull -On the second or third day a flaccid bulla may develop
and desquamationbull bull Presence of regional lymph nodes is common
Erysipelas
bull Complicationsndash The most common complication is recurrencewhich is seen in 18ndash30 of the cases even afterproper antibiotic therapy Recurrence is seen moreoften in females than in malesA skin infection with S pyogenes could lead toglomerulonephritis
Erysipelas
bull Complicationsbull ndash The most common complication is recurrencebull which is seen in 18ndash30 of the cases even afterbull proper antibiotic therapy bull -Recurrence is seen morebull often in females than in males bull -A skin infection with S pyogenes could lead tobull glomerulonephritis
Erysipelas
bull bull Diagnosisbull ndash Diagnosis is based on the patientrsquos personal
historybull and physical examination particularly on inspectionbull of the skin
bull Blood cultures are positive in less thanbull 5 of cases
ErysipelasTherapyndash Conservative therapybull The preferred antibiotic is penicillin In mildcases with minor systemic symptoms penicillinV 500 mg orally every 6 h for 10 days or penicillinG benzathine 12 mil U intramuscularlyonceOther possibilities are amoxicillin 500 mgorally twice a day for 10 days or cephalexin 500mg orally every 6 h for 10 days
ErysipelasIn moderate and severe cases with significantsystemic symptoms hospitalization and intravenoustreatment is required penicillin G 2ndash4mil U intravenously every 4ndash6 h Cefazolin05ndash15 gm intravenously every 8 h cefotaxime1ndash2 gm intravenously every 8 h or ceftriaxone1ndash2 gm intravenously once a day should be administeredIn patients with a penicillin allergyclindamycin 600 mg intravenously every 8 h orvancomycin 15 mgkg intravenously twice a daymay be given
ErysipelaAdditional useful therapeutic optionsbull Prednisone 30 mg over 8 days might be consideredas well as elevation of the affected siteMoist heat compresses may be usefulbull Surgeryndash Debridement and drainage are indicated when bullaeabscesses or necroses are presentbull Differential diagnosisndash Contact dermatitisndash Asteatotic eczemandash Herpes zosterndash Angioneurotic oedemandash Osteomyelitis
Furuncle
bull Definition of the diseasebull ndash A furuncle is an infection that beginsbull at the hair follicle and spreads deeper into thebull dermis and subcutaneous tissue forming abull nodule After several days it developsbull into an abscess - red painful and fluctuantbull bull bull Epidemiologyaetiologybull ndash The aetiologic agent is Staphylococcus aureus
FuruncleSymptomsndashsymptoms are local and limited to thesite of infection Furuncles usually are wherehair follicles are present bull Complicationndash One complication is furunculosis multiple draining furunclesDiagnosisndash The diagnosis is based on clinical inspection - Cultures are not necessary when there is no systemic involvement but should beconsidered if systemic therapy (in case of feversignificant cellulitis or hospitalization) or whenmethicillin-resistant Staphylococcusaureus (MRSA) is considered
FuruncleTherapyndash When the furuncle is small application of moist heat compress to promote drainage -Larger furuncles should be drained by surgical incision-After drainage the area should be cleaned with anantiseptic (with chlorhexidinebetadine) should be applied twice
a dayndash If no systemic symptoms or extensive cellulitis arepresent simple topical care is usually curative andoral antibiotics are not necessary Otherwise systemictreatment is indicated and should cover anypossible MRSA
Furuncle
bull -Recommended antibiotics are trimethoprim-sulfamethoxazole
bull 1ndash2 tablets orally twice daily doxycyclinebull 100 mg orally twice dailybull or clindamycin 300ndash450 mg orally every 8 hbull - In severe cases vancomycin 15 mgkg
intravenouslybull every 12 h or clindamycin 600 mg intravenouslybull every 8 h
Midline Granulomabull A midline granuloma is an angiocentricbull lymphoma it was referred to as polymorphicbull reticulosis lethal midline granuloma and midline
malignant reticulosisbull bull Definition of the diseasebull ndash This rare disease is a lymphoma of extranodal
presentationall cases are positive for the Epstein-Barr virus
bull -This lymphoma most commonly appears in the midface region
Midline GranulomaEpidemiologyaetiologyndash This form of lymphoma is rare in Europe and theUnited States with a higher prevalence in Asia and PeruSymptomsndash The most common presentation is nasal obstruction with a destructive mass occupying the nosesinuses and palate
-Fever night sweatsand weight loss seen usually in Hodgkinrsquos lymphomaand other non-Hodgkinrsquos lymphomas (knownas ldquoB symptomsrdquo) are uncommon
Midline GranulomaDiagnosisndash The diagnosis is based on anatomopathologicalstudy The malignancy of the tumour manifested byextensive necrosis makes the histological diagnosisdifficult and often more biopsies are required forconfirmationbull Therapyndash Therapy consists of radiotherapy with or withoutchemotherapy
Midline Granuloma
bull Prognosisbull ndash Depending on the stage long-term remission or
experience a worseningbull prognosis with relapses which may include otherbull extranodal sites bull Involvement of extranodal sitesbull including the upper airway gastrointestinal tractbull skin
Wegenerrsquos Granulomatosis
bull Definition of the diseasebull ndash Wegenerrsquos granulomatosis is a systemic chronicbull vasculitis of small- and medium-sized blood vesselsbull with an autoimmune component It affectsbull particular organs with variable predilectionbull Epidemiologyaetiologybull ndash Wegenerrsquos granulomatosis is a rare disease It affects
about 1 in 20000ndash30000 people It is more prevalentbull in middle-aged Caucasian patients
Wegenerrsquos Granulomatosis
Symptomsndash The disease may present pulmonary upper
respiratory tract or renal In the disseminated form-The localised form ndash confinedto the upper respiratory region ndash is present in 25of the patients- It consists of nonspecific manifestationssuch as nasal obstruction crusting purulentor bloody rhinorrhea and painful or painless ulcers in oral or nasal cavities which are unresponsive tostandard medical treatment
Wegenerrsquos Granulomatosis
bull In some patients the nasal septum is perforatedbull which leads to saddle-nose deformity Less
commonbull symptoms are hoarseness stridor due to
subglotticbull stenosis otalgia otorrhea and conductivebull and sensorineural hearing loss Also ocular
symptomsbull such as scleritis conjunctivitis uveitis andbull episcleritis may be present
Wegenerrsquos Granulomatosis
bull ndash In the disseminated form pulmonary involvementbull is manifested by cough dyspnoea haemoptysisbull (due to an alveolar capillaritis necrotic lesions orbull endobronchial disease) and pleuritic painndashbull -Ninety per cent of patients have nasal symptomsbull and these symptoms are usually the first
manifestationof the diseasebull -Most patients have also renal involvementbull even if it is subclinical
Wegenerrsquos Granulomatosis
Diagnosis ndash Diagnosis of Wegenerrsquos granulomatosis is based on clinical findings that demonstrate lung (chest x-ray) kidney (urine analysis) or upper respiratory tract
involvement (oral or nasal ulcers or discharge) - positive blood analysis for cytoplasmic-staining antineutrophil
cytoplasmic antibodies (c-ANCA) and confirming proteinase 3 (PR3) ANCA or myeloperoxidase (MPO) ANCA ndash Biopsy is essential for diagnosis nonspecific chronic inflammation
and necrosis -Bacterial and fungal infections
Wegenerrsquos Granulomatosis
Therapyndash Conservative therapybull In the induction of disease remission highdosesteroids (e g prednisone 1 mgkgday) for1 month with tapering over several months aregiven In addition cyclophosphamide (2 mgkgday) should be administered for 6ndash12 monthsuntil symptoms disappear In the maintenanceof remission cyclophosphamide should be
Wegenerrsquos Granulomatosis
Antibiotics mainly trimethoprim-sulfamethoxazoleare given for prophylaxis againstPneumocystis jiroveci (formerly Pneumocystiscarinii) pneumonia (PCP) which may developduring immunosuppression and have a role inpreventing recurrencesbull Sinonasal manifestations may be treated with topical nasal steroids and nasal irrigations lowdosesystemic steroids and antibiotics when bacterial infection (typically Staphylococcus species) is suspected
Wegenerrsquos Granulomatosis
bull Prognosisbull ndash Most of the patients respond well to treatmentbull achieving symptom-free intervals of 5ndash20 yearsbull or more bull -Anatomical problems (sinusitis trachealbull stenosis) may require surgery bull Relapses can be long and troublesomebull Long-term complications are chronicbull renal failure hearing loss and deafness
Nasal Fractures Definition ndash A nasal fracture is a disruption of the nasal bone structure due to trauma It is the most frequently fractured facial bone Epidemiologyaetiology ndash Sports falls and assaults are the usual mechanisms of fracture -Males are affected twice as often as are females -Paediatric populations with a incidences during the second and third decades of life -Variables such as force impact direction nature of the striking object age and other will influence the pattern of injury to the components of the nose
Nasal Fractures
bull Symptomsbull ndash Deformity swelling epistaxis and periorbital
ecchymosis are signs that are suggestive of nasal fracture
bull bony crepitus and nasal segment mobilitybull ndash Epiphora bull Severe bilateral injuries to the lachrymal bones
arebull associated with depressed nasal fractures
Nasal Fractures Complications ndash Septal haematoma is one of the most severe early complications of nasal trauma and without drainage it results in abscess formation 6ndash7 days after trauma producing necrosis of the septal cartilage -Long-term problems such as saddle-nose deformity perforation columellar retraction and nasalbase
Septal infection could lead to osteomyelitis orbital and intracranial abscesses meningitis and cavernous sinus thrombosis -Cerebrospinal fluid leakage is a common complication of severe
nasal and frontal fractures
Nasal Fractures
bull Diagnostic proceduresbull ndash Inspectionbull bull Changes of appearance such as deviation andbull asymmetry bleeding watery drainage changesbull in nasal breathing and smell It is useful to comparebull the current presentation with old photographsbull (up to 40 of normal individuals havebull significant nose malformations)
Nasal Fractures Physical examination bull The diagnosis of a nasal fracture is made primarily by physical examination epistaxis nasal swelling and periorbital ecchymosis Nasal shape in the lateral and frontal inspection should be assessed Grasping the dorsum between two fingers and rocking the pyramid back and forth aids in assessing the mobility of nasal bones Internal structures should be evaluated by using a headlight and nasal speculum Clotted blood is removed by suction and assessment of haematoma mucosal tears and active bleeding is performed Bimanual palpation of the septum helps to differentiate septal swelling from haematoma ndash
Nasal FracturesRadiographybull There is no clear evidence of the role of radiographyin the management of nasal fracturesPlain films have up to a 66 false-positive rateas a result of misinterpretation of normal suturelines In addition old fractures are difficult todistinguishbull Three-dimensional CT is recommended for extensiveinjuries involving the nasal-orbital-ethmoidalcomplexndash
Nasal Fractures
bull Additionaluseful diagnostic proceduresbull bull Using a 0 or 30deg 4-mm endoscope is helpful inbull the assessment of posterior abnormalities If thebull patient is heavily sedated Brown-Gruss
provocationbull manoeuvres may be performed to determinebull deformities in upper middle or lower segmentsbull by compressing each compartment
Nasal FracturesConservative treatmentndash Treatment of bleedingbull For localised bleeding anterior sources may becauterised by silver nitrate or sealed with topicalmaterials such as thrombin combined withgelatin foam fibrin glue FloSealreg or other procoagulantmaterials If conservative measuresfail a formal anterior packing is placedbull Bleeding from branches of sphenopalatine orethmoid vessels requires anterior-posteriorpacking
Nasal Fractures
bull bull Surgical methods such as direct endoscopic vessel
bull cauterization or ligation have been shown tobull offer better haemostasis and patient comfortbull Angiography with embolization can also be
consideredbull in cases refractory to more conservativebull approaches
Nasal Fractures
bull Type of reductionbull bull Nondisplaced fractures should be treated withbull observation alone Closed nasal reduction is thebull best choice for simple injuries (isolated unilateralbull with medial displacement)bull bull An open approach should be considered in
severebull trauma (bilateral depressed fractures)
Nasal Fracturesbull Surgical principlesbull ndash Topical anaesthesia with cotton pledgets soakedbull with 4 cocaine or 005 oxymethazoline combinedbull with 4 topical lidocaine should be appliedbull for 5ndash10 min Local anaesthesia should also be injectedbull (1 lidocaine and 1100000 epinephrine)bull along the septum lateral walls and floor of the nasalbull cavitybull bull
Nasal FracturesClosed reductionndashndash The nasal bones are grasped between two fingersand pressure is applied laterally in theopposite direction of the deviation A bluntelevator may be used from within the nose incases of significant medial collapse Walshamforceps can be of help Reduction of the septumshould be performed with the use ofAsch forceps
Nasal Fractures
bull To prevent collapse of the postreductionbull framework nasal packing should be placedbull for 3ndash5 days Septum splints are recommendedbull in comminuted septal fractures withbull severe mucosal lesions External nasal splintingbull for 10 days (Aquaplastreg Thermoplastreg)bull provides nasal protection Nasal saline spraysbull prevent crusting and oral antibiotics should
Nasal Fractures
bull Open reductionbull ndashndash Immediate repair of fractures by using
widebull surgical exposure reduction fixation and
reconstructionbull ndashndash The second option is delayed correctionbull (6 months or more) of persistent deformitiesbull using standard techniques of rhinoplasty
Deviated Nasal Septum
bull Definition of the diseasebull ndash Deviation of the nasal septum is a common causebull of unilateral nasal airway obstruction in which thebull nasal septum is displacedbull bull Epidemiologyaetiologybull ndash Developmental septal abnormalities Septal cartilage
damage in the neonatal period andbull during birth can cause severe septal deviation inbull the absence of a history of nasal trauma
Deviated Nasal Septum
bull Symptomsbull ndash Patients may present with a history of sinusitis
allergicbull rhinitis obstructive sleep apnoea previousbull nasal surgery or recent nasal trauma Unilateral or
bilateral nasal airway obstruction that is unrelievedbull with decongestants or nasal steroid sprays is oftenbull seenbull bull
Deviated Nasal SeptumDiagnosisndashExamination external dorsal deviation or the columella and caudal septummay be deflected off the midline (caudal subluxation)ndash Inspections of the nasal cavity and anterior-posteriorrhinoscopy are helpful in diagnosing the locationtype and severity of septal deformityThe endoscope is also useful in identifying polypsthe severity and extent of posterior septaldeviations and bony spurs and locating areas ofseptal perforation or mucosal injury
Deviated Nasal Septum
bull Therapybull ndash Septoplasty is a procedurebull The areabull of deviation is corrected or resected in order tobull leave behind as much cartilage and bone as
possiblebull Cartilage resection is minimised and can be
repositioned reshaped or recontoured using a variety of methods
Deviated Nasal Septum
bull ndash Indications of septoplasty before the growth period
bull of the nose is finished should be very limited bull -In these cases surgery must preserve all the
cartilagebull in order to prevent external changes of the
shape ofbull the nose
Deviated Nasal Septum
bull Complicationsbull ndash Frequent complications include haematoma andbull infection Cerebrospinal fluid leak is a rare but
potentiallybull serious complicationbull It is usually the resultbull of avulsion or damage to the cribriform plate whenbull handling the perpendicular plate of the ethmoidbull ndash Other complications include epistaxis nasal
Deviated Nasal Septum
bull Other complications include epistaxis nasal obstruction
bull due to residual deviation synechiae returnbull of the cartilaginous deviation septal perforationbull anosmia and cosmetic nasal deformities suchbull as widened alar rim margins drooping nasal tipbull columella retraction and a sunken dorsum with abull supratip saddle formation
Septal perforation with minor crusting View from provide closure of the
incision
Septal Haematoma
bull A septal haematoma is a blood collection under the perichondrium
bull of the septum and cartilagebull bull bull Epidemiologyaetiologybull ndash A septal haematoma is one of the most
severe complications of nasal trauma
Septal Haematoma
bull Diagnosisbull ndash Signs and symptoms include intense pain
swellingbull haematoma of the upper lip and philtrum
area andbull complete nasal airway obstruction
Septal HaematomaTherapyndash Management consists of drainage through a mucoperichondrial incision Immediate treatment isnecessary to prevent long-term problems such asa saddle-nose deformity perforation columellarretraction and nasal-base widening In childrenseptal destruction can lead to devastating nasal andmidfacial growth abnormalitiesbull Surgeryndash Incision and evacuation of the collection is performedDrainage of a septal haematoma should
Septal HaematomaSurgeryndash Incision and evacuation of the collection is performedDrainage of a septal haematoma should provide closure of the incision
Splints or transseptal sutures are placed to obliterate thepotential space and prevent collectionInfection involving the septal cartilage Reconstruction with autologouscartilage is then performed in a second stage Oral antibiotics should be given
Nasal DeformitySaddle-nose deformityndash A saddle-nose deformity is characterised by a loss ofnasal dorsal height and compromised nasal supportstructures -Other case observed are depressionof the middle vault and dorsum loss of nasal tipsupport and definition shortened (vertical) nasal length over rotation of the nasal tip and retrusion ofthe nasal spine and caudal septum It is also knownas a ldquoPug noserdquo or ldquoboxerrsquos noserdquo both of which referto various degrees of nasal dorsal depressionbull
Nasal DeformityEpidemiologyaetiologyndash Prevalence is higher in population groups prone to facial trauma (ie boxers athletes) those with historiesof intranasal cocaine use nasal surgery (e g radical submucosal septal resection reductive rhinoplasty)ndash A saddle-nose deformity can be congenital or acquired It can be noticed as a part of individual familialsyndromic and ethnic characteristics - Most deformities are due to traumatic and iatrogeniccauses Medical causes are Wegenerrsquosgranulomatosis relapsing polychondritis leprosy (Hansenrsquos disease) syphilis ectodermal dysplasiaand intranasal cocaine use
Nasal Deformity
bull Therapybull ndash Nasal reconstruction indications depend on patientbull selection surgeon experience and aetiology of thebull deformity bull Indications for surgery can be functionalbull aesthetic or most commonly both In individuals
with a compromised nasal airway a nasoseptalbull reconstruction is indicated
Nasal Deformity
bull Contraindications bull include patients with malignantbull chronic or autoimmune disease conditions drugbull abuse poor perioperative risk profile and unrealisticbull expectationsbull ndash Multiple previous rhinoplasties and certain
professionsbull (mixed martial artists boxers and other contactbull sports) are relative contraindications
Nasal DeformitySeptoplastyndash Septoplasty is performed to correct nasal obstructioncaused by septal deformityndash Usually septoplasty is performed under general anaesthesiawith the patient in the supine position with the head elevated by approximately 30 (Righthandedsurgeons approach from the right side)ndash Local vasoconstrictive anaesthesia is applied notonly to reduce postoperative pain but also more importantly to achieve vasoconstriction of themucosa and less intraoperative haemorrhage Lidocainewith adrenaline or epinephrine is usedalthough in patients with cardiac hypersensitivityoxymetazoline might be preferred
Nasal Deformity
bull Septoplasty begins with the incision of septal mucosabull Most operative techniques utilise a hemitransfixionbull incision at the caudal end of septum so thatbull deviation at this point might be reached as wellbull as a transfixion incision that is easily obtained ifbull needed (Right-handed surgeons normally choosebull the left side but that may vary when deviation isbull convex towards the right)
Nasal DeformityA columella retractor is placed over the columellaand by pulling it laterally the caudal border of theseptum is exposed Ala can be protected by an alaprotector A vertical incision with a no 15 bladeover the caudal end of septum is performed untilreaching the plane of the septal cartilage It is essentialto correctly identify the perichondrium and byusing the Cottle elevator dissect and lift it creatinga flap As the dissection proceeds along the septalcartilage a longer speculum (no 5) is introduced sothat elevation of the mucoperichondrium is doneunder constant visual controlndash The next step is to dissect the mucoperiostium
Nasal DeformityDissecting over the bony-cartilaginous junctionwhen joining both tunnels might be difficult and is
especially prone to membrane perforationndash If needed the same tunnels are to be created on the
other side of the septum Then deviated parts of
septum are identified and removed either with a
knife or a Freer chisel
Nasal Deformitybull septum from the maxillary crest the septum mustbull be separated from the perpendicular plate trimmedbull along the inferior border placed back onto the crestbull and sutured to the periosteum If the deformity involvesbull the vomer an osteotome is used Care mustbull be taken not to break the cribriform plate becausebull it could cause a cerebrospinal fistula
Nasal Deformity
bull Once the septal deviation is corrected the flapsbull and hemitransfixion incision are mattressed
withbull absorbable sutures Nasal packing to prevent
synechiaebull and postoperative septal haematoma mightbull be advised but should be removed within 72 h

Basic Anatomy of the Nose
bull The structural anatomy of the nose is important
bull for both aesthetic and functional reasons since the
bull nose as the gateway to the respiratory tract performs
bull a variety of physiologic functions
External NoseThe shape of the external nose is defined by the nasalbones a pair of rectangular bones in the upper nasaldorsum and by lateral cartilages (uppernasal cartilages) and alar cartilages (major alar cartilages)in the central and lower portions of the noseThe lateral portions of the nasal alae alsocontain several small accessory cartilages called theminor alar cartilages which are embedded in the lateralsoft tissues of the noseThe shape and stability of the alar cartilages each ofwhich consists of a medial and lateral crus
External Nose
Anatomy of the nasal base
bull Besides thebull medial crura the
inferior septal margin and the connective-
bull tissue septum (columella) are also responsible
bull for stabilizing the base of the nose
Anatomy of the nasal base
Anatomy of the nasal base
bull The nasal septum is subluxed toward the left side partially
bull obstructing the nasal airway
Nasal CavitiesThe nasal cavities begin anteriorly at the nasal vestibulewhich is bordered posteriorly by the internal nasalvalve (limen nasi) located between the posteriorborder of the alar cartilage and the anterior border ofthe lateral cartilage This valve area is the narrowestportion of the upper respiratory tract
Nasal Cavities
The interior ofthe nose behind the nasal valve is divided by the nasalseptum into two main cavities
Nasal CavitiesThe nasal septum iscomposed of an anterior cartilaginous part and twoposterior bony parts Abnormalities in the shape ofthe nasal septum which may consist of a deviated septum tensionseptum spurs or ridges are a frequent cause ofnasal airway obstructionThe choanae are the paired posterior openingsthrough which the nasal cavities communicate withthe nasopharynx
Nasal CavitiesThe nasal cavity is bounded laterally by the lateral nasalwalls which are formed by the ethmoid bone andmaxilla and posteriorly by the palatine bone and thepterygoid process of the sphenoid bone Several functionallyimportant structures are located on the lateralnasal wall the nasal turbinates and their associatedpassages (meati) sinus ostia and the orifice ofthe nasolacrimal duct (Fig 15)
The inferior turbinate consists of a separate bone thatis attached to the medial wall of the maxillary sinusThe opening of the nasolacrimal duct is located in thecorresponding inferior meatus The middle andsuperior turbinates are part of the ethmoid bone In rare cases a rudimentary ldquosupreme turbinaterdquo is alsopresent above the superior turbinate
The middle turbinate has by far the greatest functionalimportance because most of the drainage tracts fromthe surrounding paranasal sinuses open into the middlemeatus The nasal cavity is bounded superiorly by the cribriformplate of the ethmoid bone This thin bony platehas numerous openings for the passage of the fila olfactoriaand also forms the boundary of the anteriorcranial fossa
Nasal Cavities
The floor of the nasal cavity is formedmostly by the hard palate which is formed in turn bythe two palatine processes of the maxilla and the horizontallaminae of the palatine bone
Structure of the lateral nasal wall
Inferior meatus
Paranasal Sinuses
The paranasal sinuses are air-filled cavities that communicatewith the nasal cavities
-The maxillary sinus frontalsinus and anterior ethmoid cells drain into the nasalcavity through the middle meatusmdashie below themiddle turbinate -The posterior ethmoidcells drain into the nasal cavity through the superiormeatus The ostium of the sphenoid sinus is locatedin the anterior wall directly above the choanae- The anatomical connections between the nasal cavity andparanasal sinuses are functionally important and playa key role in the pathogenesis of many rhinologic diseasesthat involve the paranasal sinuses
Vascular SupplyThe external nose derives most of its blood supply
from the facial artery which arises from the external
carotid artery and from the ophthalmic artery which
springs from the internal carotid artery
Vascular Supply
The internalnose receives blood from the territories of the externaland internal carotid arteries- the terminalbranches of the sphenopalatine artery which arisesfrom the maxillary artery - the anterior and posteriorethmoid arteries which arise from the ophthalmicartery-internal carotid arterie
venous drainage
The venous drainageof the facial region is handled by -the facial vein -retromandibular vein -internal jugular vein
lymphatic drainage
The regional lymphatic drainage of the face and externalnose is handled mainly by- the submandibularlymph nodes while the nasal cavity is additionallydrained by -the retropharyngeal and deep - -cervical lymph nodes
Morphology of the Nasal Mucosa
Besides the anatomical structure of the external noseand nasal cavity the nasal mucosa plays an essentialrole in numerous functions of the nose in the respiratory tract
Morphology of the Nasal Mucosa
The anterior part of the nasal cavity (the nasal vestibule)like the external nose is covered by skin composedof a multilayer keratinizing squamous epithelium and finally a ciliated respiratory epithelium A small areaon the upper nasal septum superior turbinate andpart of the middle turbinate located adjacent to thecribriform plate is covered by olfactory mucosa and iscalled the olfactory region
Nerve SupplyThe facial skin receives its sensory innervation fromterminal branches of the trigeminal nerve that enterthe facial region through the supraorbital infraorbitaland mental foramina Thefacial muscles are classified as mimetic or mastica- tory each of these groups receiving different motorinnervationbythe facial nerve
History and Clinical Examination of the Nose
Historybull The main symptomsbull nasal obstruction (ldquostuffy
noserdquo)bull nasal dischargebull Headachesbull Olfactory
dysfunction
Palpationbony discontinuitiesNeuralgias to check
over- the supraorbital -infraorbital -mental foramina
Anterior Rhinoscopy
bull The rhinologic examination itself begins with anterior
bull rhinoscopy to evaluate the nasal vestibule and the anterior
bull portions of the nasal cavity
Nasal Endoscopy Nasal endoscopy has become the most important andrewarding clinical examination method in rhinologic diagnosis
- rigid endoscopes which are available in 4-mm and 28- mm diameters and assorted viewing angles (eg 01048576 301048576 1201048576) -flexible endoscopes are also available for inspecting the nose and nasopharynx and exploring all of the pharynx and larynx in one sitting
Nasal endoscopy
Nasal Endoscopy
Nasal Endoscopy
Imaging of the Nose and Paranasal Sinuses
Conventional RadiographsStandard paranasal sinus radiographs in the occipitomental
projection ( Water projection) and
occipitofrontal projection Caldwell projection) in cases of acute inflammation
They are also obtained to evaluate midfacial fractures
Computed Tomography (CT) the main indicationsfor CT scanning of the
nose and paranasal sinuses
are- chronic sinusitis - -trauma (especially
frontobasal -fractures)
-and tumors
The occipitofrontal projection is better for evaluating theethmoid cells and frontal sinus
occipitomental projection demonstrates the maxillarysinus and gives a limited view of the sphenoid sinus
Computed tomography of the paranasal sinuses
Four representative coronal CT scans are shown
Four representative coronal CT scans are shown
Magnetic Resonance Imaging
Magnetic maging
Magnetic resonance imaging (MRI) has fewer indicationsthan CT in patients with paranasal sinus diseaseThis is primarily because MRI is markedly inferior toCT in defining the bony boundaries of the sinusesThe strength of MRI lies in its superior soft-tissue discriminationMRI is indicated in diseases that involve the paranasal sinuses in addition to thecranial cavity or orbit (eg tumors and congenitalmalformations such as encephaloceles)
MRI of the paranasal sinuses
The Nose and Sinuses
Structure The structure of the nose is made up of
four partsbull The surface anatomybull The nasal skeletonmdashcomposed of the
two nasal bones the paired upper lateral and lower lateral cartilages and the nasal septum covered in subcutaneous tissue and skin
bull The internal anatomymdashincludes the septum of the nose which forms the medial wall of the nasal cavity The turbinates on the lateral wall are also called conchae
bull The osteomeatal complexmdasha key functional area of the nose
Function The nose is the main route for inspired
air and its structure is related to this function As the air passes over the large surface area of the turbinates
The inspired gases are warmed and humidified Mucus on the mucosa of the nose removes large dust particles from the air as it is breathed in
The voice resonates in the sinuses and nose and this provides character to the speech
Pneumatization of the sinusesmdashthey are air filled spacesmdashreduces the weight of the skull
Diseases of thDiseases of the Outer and Inner Nosee Outer and
Inner Nose Erysipelas Definition of the disease ndash Erysipela is a skin infection that affects the superficial dermis and is caused by Streptococcus pyogenes (group A) It usually develops in the extremities and the face and less commonly on the scalp and genitals bull Epidemiologyaetiology ndash Erysipelas are more often seen in elderly infants and children patients with compromised immunology and diabetes -Predisposing factors are alcoholism skin ulceration puncture wounds fungal infections malnutrition and burns
Erysipelas
bull Symptomsbull ndash It usually presents of fever general fatigue bull -The skin lesion is a redindurated and elevated plaque
with borders that expand rapidly bull It is painful warm and accompanied by variable oedemabull -On the second or third day a flaccid bulla may develop
and desquamationbull bull Presence of regional lymph nodes is common
Erysipelas
bull Complicationsndash The most common complication is recurrencewhich is seen in 18ndash30 of the cases even afterproper antibiotic therapy Recurrence is seen moreoften in females than in malesA skin infection with S pyogenes could lead toglomerulonephritis
Erysipelas
bull Complicationsbull ndash The most common complication is recurrencebull which is seen in 18ndash30 of the cases even afterbull proper antibiotic therapy bull -Recurrence is seen morebull often in females than in males bull -A skin infection with S pyogenes could lead tobull glomerulonephritis
Erysipelas
bull bull Diagnosisbull ndash Diagnosis is based on the patientrsquos personal
historybull and physical examination particularly on inspectionbull of the skin
bull Blood cultures are positive in less thanbull 5 of cases
ErysipelasTherapyndash Conservative therapybull The preferred antibiotic is penicillin In mildcases with minor systemic symptoms penicillinV 500 mg orally every 6 h for 10 days or penicillinG benzathine 12 mil U intramuscularlyonceOther possibilities are amoxicillin 500 mgorally twice a day for 10 days or cephalexin 500mg orally every 6 h for 10 days
ErysipelasIn moderate and severe cases with significantsystemic symptoms hospitalization and intravenoustreatment is required penicillin G 2ndash4mil U intravenously every 4ndash6 h Cefazolin05ndash15 gm intravenously every 8 h cefotaxime1ndash2 gm intravenously every 8 h or ceftriaxone1ndash2 gm intravenously once a day should be administeredIn patients with a penicillin allergyclindamycin 600 mg intravenously every 8 h orvancomycin 15 mgkg intravenously twice a daymay be given
ErysipelaAdditional useful therapeutic optionsbull Prednisone 30 mg over 8 days might be consideredas well as elevation of the affected siteMoist heat compresses may be usefulbull Surgeryndash Debridement and drainage are indicated when bullaeabscesses or necroses are presentbull Differential diagnosisndash Contact dermatitisndash Asteatotic eczemandash Herpes zosterndash Angioneurotic oedemandash Osteomyelitis
Furuncle
bull Definition of the diseasebull ndash A furuncle is an infection that beginsbull at the hair follicle and spreads deeper into thebull dermis and subcutaneous tissue forming abull nodule After several days it developsbull into an abscess - red painful and fluctuantbull bull bull Epidemiologyaetiologybull ndash The aetiologic agent is Staphylococcus aureus
FuruncleSymptomsndashsymptoms are local and limited to thesite of infection Furuncles usually are wherehair follicles are present bull Complicationndash One complication is furunculosis multiple draining furunclesDiagnosisndash The diagnosis is based on clinical inspection - Cultures are not necessary when there is no systemic involvement but should beconsidered if systemic therapy (in case of feversignificant cellulitis or hospitalization) or whenmethicillin-resistant Staphylococcusaureus (MRSA) is considered
FuruncleTherapyndash When the furuncle is small application of moist heat compress to promote drainage -Larger furuncles should be drained by surgical incision-After drainage the area should be cleaned with anantiseptic (with chlorhexidinebetadine) should be applied twice
a dayndash If no systemic symptoms or extensive cellulitis arepresent simple topical care is usually curative andoral antibiotics are not necessary Otherwise systemictreatment is indicated and should cover anypossible MRSA
Furuncle
bull -Recommended antibiotics are trimethoprim-sulfamethoxazole
bull 1ndash2 tablets orally twice daily doxycyclinebull 100 mg orally twice dailybull or clindamycin 300ndash450 mg orally every 8 hbull - In severe cases vancomycin 15 mgkg
intravenouslybull every 12 h or clindamycin 600 mg intravenouslybull every 8 h
Midline Granulomabull A midline granuloma is an angiocentricbull lymphoma it was referred to as polymorphicbull reticulosis lethal midline granuloma and midline
malignant reticulosisbull bull Definition of the diseasebull ndash This rare disease is a lymphoma of extranodal
presentationall cases are positive for the Epstein-Barr virus
bull -This lymphoma most commonly appears in the midface region
Midline GranulomaEpidemiologyaetiologyndash This form of lymphoma is rare in Europe and theUnited States with a higher prevalence in Asia and PeruSymptomsndash The most common presentation is nasal obstruction with a destructive mass occupying the nosesinuses and palate
-Fever night sweatsand weight loss seen usually in Hodgkinrsquos lymphomaand other non-Hodgkinrsquos lymphomas (knownas ldquoB symptomsrdquo) are uncommon
Midline GranulomaDiagnosisndash The diagnosis is based on anatomopathologicalstudy The malignancy of the tumour manifested byextensive necrosis makes the histological diagnosisdifficult and often more biopsies are required forconfirmationbull Therapyndash Therapy consists of radiotherapy with or withoutchemotherapy
Midline Granuloma
bull Prognosisbull ndash Depending on the stage long-term remission or
experience a worseningbull prognosis with relapses which may include otherbull extranodal sites bull Involvement of extranodal sitesbull including the upper airway gastrointestinal tractbull skin
Wegenerrsquos Granulomatosis
bull Definition of the diseasebull ndash Wegenerrsquos granulomatosis is a systemic chronicbull vasculitis of small- and medium-sized blood vesselsbull with an autoimmune component It affectsbull particular organs with variable predilectionbull Epidemiologyaetiologybull ndash Wegenerrsquos granulomatosis is a rare disease It affects
about 1 in 20000ndash30000 people It is more prevalentbull in middle-aged Caucasian patients
Wegenerrsquos Granulomatosis
Symptomsndash The disease may present pulmonary upper
respiratory tract or renal In the disseminated form-The localised form ndash confinedto the upper respiratory region ndash is present in 25of the patients- It consists of nonspecific manifestationssuch as nasal obstruction crusting purulentor bloody rhinorrhea and painful or painless ulcers in oral or nasal cavities which are unresponsive tostandard medical treatment
Wegenerrsquos Granulomatosis
bull In some patients the nasal septum is perforatedbull which leads to saddle-nose deformity Less
commonbull symptoms are hoarseness stridor due to
subglotticbull stenosis otalgia otorrhea and conductivebull and sensorineural hearing loss Also ocular
symptomsbull such as scleritis conjunctivitis uveitis andbull episcleritis may be present
Wegenerrsquos Granulomatosis
bull ndash In the disseminated form pulmonary involvementbull is manifested by cough dyspnoea haemoptysisbull (due to an alveolar capillaritis necrotic lesions orbull endobronchial disease) and pleuritic painndashbull -Ninety per cent of patients have nasal symptomsbull and these symptoms are usually the first
manifestationof the diseasebull -Most patients have also renal involvementbull even if it is subclinical
Wegenerrsquos Granulomatosis
Diagnosis ndash Diagnosis of Wegenerrsquos granulomatosis is based on clinical findings that demonstrate lung (chest x-ray) kidney (urine analysis) or upper respiratory tract
involvement (oral or nasal ulcers or discharge) - positive blood analysis for cytoplasmic-staining antineutrophil
cytoplasmic antibodies (c-ANCA) and confirming proteinase 3 (PR3) ANCA or myeloperoxidase (MPO) ANCA ndash Biopsy is essential for diagnosis nonspecific chronic inflammation
and necrosis -Bacterial and fungal infections
Wegenerrsquos Granulomatosis
Therapyndash Conservative therapybull In the induction of disease remission highdosesteroids (e g prednisone 1 mgkgday) for1 month with tapering over several months aregiven In addition cyclophosphamide (2 mgkgday) should be administered for 6ndash12 monthsuntil symptoms disappear In the maintenanceof remission cyclophosphamide should be
Wegenerrsquos Granulomatosis
Antibiotics mainly trimethoprim-sulfamethoxazoleare given for prophylaxis againstPneumocystis jiroveci (formerly Pneumocystiscarinii) pneumonia (PCP) which may developduring immunosuppression and have a role inpreventing recurrencesbull Sinonasal manifestations may be treated with topical nasal steroids and nasal irrigations lowdosesystemic steroids and antibiotics when bacterial infection (typically Staphylococcus species) is suspected
Wegenerrsquos Granulomatosis
bull Prognosisbull ndash Most of the patients respond well to treatmentbull achieving symptom-free intervals of 5ndash20 yearsbull or more bull -Anatomical problems (sinusitis trachealbull stenosis) may require surgery bull Relapses can be long and troublesomebull Long-term complications are chronicbull renal failure hearing loss and deafness
Nasal Fractures Definition ndash A nasal fracture is a disruption of the nasal bone structure due to trauma It is the most frequently fractured facial bone Epidemiologyaetiology ndash Sports falls and assaults are the usual mechanisms of fracture -Males are affected twice as often as are females -Paediatric populations with a incidences during the second and third decades of life -Variables such as force impact direction nature of the striking object age and other will influence the pattern of injury to the components of the nose
Nasal Fractures
bull Symptomsbull ndash Deformity swelling epistaxis and periorbital
ecchymosis are signs that are suggestive of nasal fracture
bull bony crepitus and nasal segment mobilitybull ndash Epiphora bull Severe bilateral injuries to the lachrymal bones
arebull associated with depressed nasal fractures
Nasal Fractures Complications ndash Septal haematoma is one of the most severe early complications of nasal trauma and without drainage it results in abscess formation 6ndash7 days after trauma producing necrosis of the septal cartilage -Long-term problems such as saddle-nose deformity perforation columellar retraction and nasalbase
Septal infection could lead to osteomyelitis orbital and intracranial abscesses meningitis and cavernous sinus thrombosis -Cerebrospinal fluid leakage is a common complication of severe
nasal and frontal fractures
Nasal Fractures
bull Diagnostic proceduresbull ndash Inspectionbull bull Changes of appearance such as deviation andbull asymmetry bleeding watery drainage changesbull in nasal breathing and smell It is useful to comparebull the current presentation with old photographsbull (up to 40 of normal individuals havebull significant nose malformations)
Nasal Fractures Physical examination bull The diagnosis of a nasal fracture is made primarily by physical examination epistaxis nasal swelling and periorbital ecchymosis Nasal shape in the lateral and frontal inspection should be assessed Grasping the dorsum between two fingers and rocking the pyramid back and forth aids in assessing the mobility of nasal bones Internal structures should be evaluated by using a headlight and nasal speculum Clotted blood is removed by suction and assessment of haematoma mucosal tears and active bleeding is performed Bimanual palpation of the septum helps to differentiate septal swelling from haematoma ndash
Nasal FracturesRadiographybull There is no clear evidence of the role of radiographyin the management of nasal fracturesPlain films have up to a 66 false-positive rateas a result of misinterpretation of normal suturelines In addition old fractures are difficult todistinguishbull Three-dimensional CT is recommended for extensiveinjuries involving the nasal-orbital-ethmoidalcomplexndash
Nasal Fractures
bull Additionaluseful diagnostic proceduresbull bull Using a 0 or 30deg 4-mm endoscope is helpful inbull the assessment of posterior abnormalities If thebull patient is heavily sedated Brown-Gruss
provocationbull manoeuvres may be performed to determinebull deformities in upper middle or lower segmentsbull by compressing each compartment
Nasal FracturesConservative treatmentndash Treatment of bleedingbull For localised bleeding anterior sources may becauterised by silver nitrate or sealed with topicalmaterials such as thrombin combined withgelatin foam fibrin glue FloSealreg or other procoagulantmaterials If conservative measuresfail a formal anterior packing is placedbull Bleeding from branches of sphenopalatine orethmoid vessels requires anterior-posteriorpacking
Nasal Fractures
bull bull Surgical methods such as direct endoscopic vessel
bull cauterization or ligation have been shown tobull offer better haemostasis and patient comfortbull Angiography with embolization can also be
consideredbull in cases refractory to more conservativebull approaches
Nasal Fractures
bull Type of reductionbull bull Nondisplaced fractures should be treated withbull observation alone Closed nasal reduction is thebull best choice for simple injuries (isolated unilateralbull with medial displacement)bull bull An open approach should be considered in
severebull trauma (bilateral depressed fractures)
Nasal Fracturesbull Surgical principlesbull ndash Topical anaesthesia with cotton pledgets soakedbull with 4 cocaine or 005 oxymethazoline combinedbull with 4 topical lidocaine should be appliedbull for 5ndash10 min Local anaesthesia should also be injectedbull (1 lidocaine and 1100000 epinephrine)bull along the septum lateral walls and floor of the nasalbull cavitybull bull
Nasal FracturesClosed reductionndashndash The nasal bones are grasped between two fingersand pressure is applied laterally in theopposite direction of the deviation A bluntelevator may be used from within the nose incases of significant medial collapse Walshamforceps can be of help Reduction of the septumshould be performed with the use ofAsch forceps
Nasal Fractures
bull To prevent collapse of the postreductionbull framework nasal packing should be placedbull for 3ndash5 days Septum splints are recommendedbull in comminuted septal fractures withbull severe mucosal lesions External nasal splintingbull for 10 days (Aquaplastreg Thermoplastreg)bull provides nasal protection Nasal saline spraysbull prevent crusting and oral antibiotics should
Nasal Fractures
bull Open reductionbull ndashndash Immediate repair of fractures by using
widebull surgical exposure reduction fixation and
reconstructionbull ndashndash The second option is delayed correctionbull (6 months or more) of persistent deformitiesbull using standard techniques of rhinoplasty
Deviated Nasal Septum
bull Definition of the diseasebull ndash Deviation of the nasal septum is a common causebull of unilateral nasal airway obstruction in which thebull nasal septum is displacedbull bull Epidemiologyaetiologybull ndash Developmental septal abnormalities Septal cartilage
damage in the neonatal period andbull during birth can cause severe septal deviation inbull the absence of a history of nasal trauma
Deviated Nasal Septum
bull Symptomsbull ndash Patients may present with a history of sinusitis
allergicbull rhinitis obstructive sleep apnoea previousbull nasal surgery or recent nasal trauma Unilateral or
bilateral nasal airway obstruction that is unrelievedbull with decongestants or nasal steroid sprays is oftenbull seenbull bull
Deviated Nasal SeptumDiagnosisndashExamination external dorsal deviation or the columella and caudal septummay be deflected off the midline (caudal subluxation)ndash Inspections of the nasal cavity and anterior-posteriorrhinoscopy are helpful in diagnosing the locationtype and severity of septal deformityThe endoscope is also useful in identifying polypsthe severity and extent of posterior septaldeviations and bony spurs and locating areas ofseptal perforation or mucosal injury
Deviated Nasal Septum
bull Therapybull ndash Septoplasty is a procedurebull The areabull of deviation is corrected or resected in order tobull leave behind as much cartilage and bone as
possiblebull Cartilage resection is minimised and can be
repositioned reshaped or recontoured using a variety of methods
Deviated Nasal Septum
bull ndash Indications of septoplasty before the growth period
bull of the nose is finished should be very limited bull -In these cases surgery must preserve all the
cartilagebull in order to prevent external changes of the
shape ofbull the nose
Deviated Nasal Septum
bull Complicationsbull ndash Frequent complications include haematoma andbull infection Cerebrospinal fluid leak is a rare but
potentiallybull serious complicationbull It is usually the resultbull of avulsion or damage to the cribriform plate whenbull handling the perpendicular plate of the ethmoidbull ndash Other complications include epistaxis nasal
Deviated Nasal Septum
bull Other complications include epistaxis nasal obstruction
bull due to residual deviation synechiae returnbull of the cartilaginous deviation septal perforationbull anosmia and cosmetic nasal deformities suchbull as widened alar rim margins drooping nasal tipbull columella retraction and a sunken dorsum with abull supratip saddle formation
Septal perforation with minor crusting View from provide closure of the
incision
Septal Haematoma
bull A septal haematoma is a blood collection under the perichondrium
bull of the septum and cartilagebull bull bull Epidemiologyaetiologybull ndash A septal haematoma is one of the most
severe complications of nasal trauma
Septal Haematoma
bull Diagnosisbull ndash Signs and symptoms include intense pain
swellingbull haematoma of the upper lip and philtrum
area andbull complete nasal airway obstruction
Septal HaematomaTherapyndash Management consists of drainage through a mucoperichondrial incision Immediate treatment isnecessary to prevent long-term problems such asa saddle-nose deformity perforation columellarretraction and nasal-base widening In childrenseptal destruction can lead to devastating nasal andmidfacial growth abnormalitiesbull Surgeryndash Incision and evacuation of the collection is performedDrainage of a septal haematoma should
Septal HaematomaSurgeryndash Incision and evacuation of the collection is performedDrainage of a septal haematoma should provide closure of the incision
Splints or transseptal sutures are placed to obliterate thepotential space and prevent collectionInfection involving the septal cartilage Reconstruction with autologouscartilage is then performed in a second stage Oral antibiotics should be given
Nasal DeformitySaddle-nose deformityndash A saddle-nose deformity is characterised by a loss ofnasal dorsal height and compromised nasal supportstructures -Other case observed are depressionof the middle vault and dorsum loss of nasal tipsupport and definition shortened (vertical) nasal length over rotation of the nasal tip and retrusion ofthe nasal spine and caudal septum It is also knownas a ldquoPug noserdquo or ldquoboxerrsquos noserdquo both of which referto various degrees of nasal dorsal depressionbull
Nasal DeformityEpidemiologyaetiologyndash Prevalence is higher in population groups prone to facial trauma (ie boxers athletes) those with historiesof intranasal cocaine use nasal surgery (e g radical submucosal septal resection reductive rhinoplasty)ndash A saddle-nose deformity can be congenital or acquired It can be noticed as a part of individual familialsyndromic and ethnic characteristics - Most deformities are due to traumatic and iatrogeniccauses Medical causes are Wegenerrsquosgranulomatosis relapsing polychondritis leprosy (Hansenrsquos disease) syphilis ectodermal dysplasiaand intranasal cocaine use
Nasal Deformity
bull Therapybull ndash Nasal reconstruction indications depend on patientbull selection surgeon experience and aetiology of thebull deformity bull Indications for surgery can be functionalbull aesthetic or most commonly both In individuals
with a compromised nasal airway a nasoseptalbull reconstruction is indicated
Nasal Deformity
bull Contraindications bull include patients with malignantbull chronic or autoimmune disease conditions drugbull abuse poor perioperative risk profile and unrealisticbull expectationsbull ndash Multiple previous rhinoplasties and certain
professionsbull (mixed martial artists boxers and other contactbull sports) are relative contraindications
Nasal DeformitySeptoplastyndash Septoplasty is performed to correct nasal obstructioncaused by septal deformityndash Usually septoplasty is performed under general anaesthesiawith the patient in the supine position with the head elevated by approximately 30 (Righthandedsurgeons approach from the right side)ndash Local vasoconstrictive anaesthesia is applied notonly to reduce postoperative pain but also more importantly to achieve vasoconstriction of themucosa and less intraoperative haemorrhage Lidocainewith adrenaline or epinephrine is usedalthough in patients with cardiac hypersensitivityoxymetazoline might be preferred
Nasal Deformity
bull Septoplasty begins with the incision of septal mucosabull Most operative techniques utilise a hemitransfixionbull incision at the caudal end of septum so thatbull deviation at this point might be reached as wellbull as a transfixion incision that is easily obtained ifbull needed (Right-handed surgeons normally choosebull the left side but that may vary when deviation isbull convex towards the right)
Nasal DeformityA columella retractor is placed over the columellaand by pulling it laterally the caudal border of theseptum is exposed Ala can be protected by an alaprotector A vertical incision with a no 15 bladeover the caudal end of septum is performed untilreaching the plane of the septal cartilage It is essentialto correctly identify the perichondrium and byusing the Cottle elevator dissect and lift it creatinga flap As the dissection proceeds along the septalcartilage a longer speculum (no 5) is introduced sothat elevation of the mucoperichondrium is doneunder constant visual controlndash The next step is to dissect the mucoperiostium
Nasal DeformityDissecting over the bony-cartilaginous junctionwhen joining both tunnels might be difficult and is
especially prone to membrane perforationndash If needed the same tunnels are to be created on the
other side of the septum Then deviated parts of
septum are identified and removed either with a
knife or a Freer chisel
Nasal Deformitybull septum from the maxillary crest the septum mustbull be separated from the perpendicular plate trimmedbull along the inferior border placed back onto the crestbull and sutured to the periosteum If the deformity involvesbull the vomer an osteotome is used Care mustbull be taken not to break the cribriform plate becausebull it could cause a cerebrospinal fistula
Nasal Deformity
bull Once the septal deviation is corrected the flapsbull and hemitransfixion incision are mattressed
withbull absorbable sutures Nasal packing to prevent
synechiaebull and postoperative septal haematoma mightbull be advised but should be removed within 72 h

External NoseThe shape of the external nose is defined by the nasalbones a pair of rectangular bones in the upper nasaldorsum and by lateral cartilages (uppernasal cartilages) and alar cartilages (major alar cartilages)in the central and lower portions of the noseThe lateral portions of the nasal alae alsocontain several small accessory cartilages called theminor alar cartilages which are embedded in the lateralsoft tissues of the noseThe shape and stability of the alar cartilages each ofwhich consists of a medial and lateral crus
External Nose
Anatomy of the nasal base
bull Besides thebull medial crura the
inferior septal margin and the connective-
bull tissue septum (columella) are also responsible
bull for stabilizing the base of the nose
Anatomy of the nasal base
Anatomy of the nasal base
bull The nasal septum is subluxed toward the left side partially
bull obstructing the nasal airway
Nasal CavitiesThe nasal cavities begin anteriorly at the nasal vestibulewhich is bordered posteriorly by the internal nasalvalve (limen nasi) located between the posteriorborder of the alar cartilage and the anterior border ofthe lateral cartilage This valve area is the narrowestportion of the upper respiratory tract
Nasal Cavities
The interior ofthe nose behind the nasal valve is divided by the nasalseptum into two main cavities
Nasal CavitiesThe nasal septum iscomposed of an anterior cartilaginous part and twoposterior bony parts Abnormalities in the shape ofthe nasal septum which may consist of a deviated septum tensionseptum spurs or ridges are a frequent cause ofnasal airway obstructionThe choanae are the paired posterior openingsthrough which the nasal cavities communicate withthe nasopharynx
Nasal CavitiesThe nasal cavity is bounded laterally by the lateral nasalwalls which are formed by the ethmoid bone andmaxilla and posteriorly by the palatine bone and thepterygoid process of the sphenoid bone Several functionallyimportant structures are located on the lateralnasal wall the nasal turbinates and their associatedpassages (meati) sinus ostia and the orifice ofthe nasolacrimal duct (Fig 15)
The inferior turbinate consists of a separate bone thatis attached to the medial wall of the maxillary sinusThe opening of the nasolacrimal duct is located in thecorresponding inferior meatus The middle andsuperior turbinates are part of the ethmoid bone In rare cases a rudimentary ldquosupreme turbinaterdquo is alsopresent above the superior turbinate
The middle turbinate has by far the greatest functionalimportance because most of the drainage tracts fromthe surrounding paranasal sinuses open into the middlemeatus The nasal cavity is bounded superiorly by the cribriformplate of the ethmoid bone This thin bony platehas numerous openings for the passage of the fila olfactoriaand also forms the boundary of the anteriorcranial fossa
Nasal Cavities
The floor of the nasal cavity is formedmostly by the hard palate which is formed in turn bythe two palatine processes of the maxilla and the horizontallaminae of the palatine bone
Structure of the lateral nasal wall
Inferior meatus
Paranasal Sinuses
The paranasal sinuses are air-filled cavities that communicatewith the nasal cavities
-The maxillary sinus frontalsinus and anterior ethmoid cells drain into the nasalcavity through the middle meatusmdashie below themiddle turbinate -The posterior ethmoidcells drain into the nasal cavity through the superiormeatus The ostium of the sphenoid sinus is locatedin the anterior wall directly above the choanae- The anatomical connections between the nasal cavity andparanasal sinuses are functionally important and playa key role in the pathogenesis of many rhinologic diseasesthat involve the paranasal sinuses
Vascular SupplyThe external nose derives most of its blood supply
from the facial artery which arises from the external
carotid artery and from the ophthalmic artery which
springs from the internal carotid artery
Vascular Supply
The internalnose receives blood from the territories of the externaland internal carotid arteries- the terminalbranches of the sphenopalatine artery which arisesfrom the maxillary artery - the anterior and posteriorethmoid arteries which arise from the ophthalmicartery-internal carotid arterie
venous drainage
The venous drainageof the facial region is handled by -the facial vein -retromandibular vein -internal jugular vein
lymphatic drainage
The regional lymphatic drainage of the face and externalnose is handled mainly by- the submandibularlymph nodes while the nasal cavity is additionallydrained by -the retropharyngeal and deep - -cervical lymph nodes
Morphology of the Nasal Mucosa
Besides the anatomical structure of the external noseand nasal cavity the nasal mucosa plays an essentialrole in numerous functions of the nose in the respiratory tract
Morphology of the Nasal Mucosa
The anterior part of the nasal cavity (the nasal vestibule)like the external nose is covered by skin composedof a multilayer keratinizing squamous epithelium and finally a ciliated respiratory epithelium A small areaon the upper nasal septum superior turbinate andpart of the middle turbinate located adjacent to thecribriform plate is covered by olfactory mucosa and iscalled the olfactory region
Nerve SupplyThe facial skin receives its sensory innervation fromterminal branches of the trigeminal nerve that enterthe facial region through the supraorbital infraorbitaland mental foramina Thefacial muscles are classified as mimetic or mastica- tory each of these groups receiving different motorinnervationbythe facial nerve
History and Clinical Examination of the Nose
Historybull The main symptomsbull nasal obstruction (ldquostuffy
noserdquo)bull nasal dischargebull Headachesbull Olfactory
dysfunction
Palpationbony discontinuitiesNeuralgias to check
over- the supraorbital -infraorbital -mental foramina
Anterior Rhinoscopy
bull The rhinologic examination itself begins with anterior
bull rhinoscopy to evaluate the nasal vestibule and the anterior
bull portions of the nasal cavity
Nasal Endoscopy Nasal endoscopy has become the most important andrewarding clinical examination method in rhinologic diagnosis
- rigid endoscopes which are available in 4-mm and 28- mm diameters and assorted viewing angles (eg 01048576 301048576 1201048576) -flexible endoscopes are also available for inspecting the nose and nasopharynx and exploring all of the pharynx and larynx in one sitting
Nasal endoscopy
Nasal Endoscopy
Nasal Endoscopy
Imaging of the Nose and Paranasal Sinuses
Conventional RadiographsStandard paranasal sinus radiographs in the occipitomental
projection ( Water projection) and
occipitofrontal projection Caldwell projection) in cases of acute inflammation
They are also obtained to evaluate midfacial fractures
Computed Tomography (CT) the main indicationsfor CT scanning of the
nose and paranasal sinuses
are- chronic sinusitis - -trauma (especially
frontobasal -fractures)
-and tumors
The occipitofrontal projection is better for evaluating theethmoid cells and frontal sinus
occipitomental projection demonstrates the maxillarysinus and gives a limited view of the sphenoid sinus
Computed tomography of the paranasal sinuses
Four representative coronal CT scans are shown
Four representative coronal CT scans are shown
Magnetic Resonance Imaging
Magnetic maging
Magnetic resonance imaging (MRI) has fewer indicationsthan CT in patients with paranasal sinus diseaseThis is primarily because MRI is markedly inferior toCT in defining the bony boundaries of the sinusesThe strength of MRI lies in its superior soft-tissue discriminationMRI is indicated in diseases that involve the paranasal sinuses in addition to thecranial cavity or orbit (eg tumors and congenitalmalformations such as encephaloceles)
MRI of the paranasal sinuses
The Nose and Sinuses
Structure The structure of the nose is made up of
four partsbull The surface anatomybull The nasal skeletonmdashcomposed of the
two nasal bones the paired upper lateral and lower lateral cartilages and the nasal septum covered in subcutaneous tissue and skin
bull The internal anatomymdashincludes the septum of the nose which forms the medial wall of the nasal cavity The turbinates on the lateral wall are also called conchae
bull The osteomeatal complexmdasha key functional area of the nose
Function The nose is the main route for inspired
air and its structure is related to this function As the air passes over the large surface area of the turbinates
The inspired gases are warmed and humidified Mucus on the mucosa of the nose removes large dust particles from the air as it is breathed in
The voice resonates in the sinuses and nose and this provides character to the speech
Pneumatization of the sinusesmdashthey are air filled spacesmdashreduces the weight of the skull
Diseases of thDiseases of the Outer and Inner Nosee Outer and
Inner Nose Erysipelas Definition of the disease ndash Erysipela is a skin infection that affects the superficial dermis and is caused by Streptococcus pyogenes (group A) It usually develops in the extremities and the face and less commonly on the scalp and genitals bull Epidemiologyaetiology ndash Erysipelas are more often seen in elderly infants and children patients with compromised immunology and diabetes -Predisposing factors are alcoholism skin ulceration puncture wounds fungal infections malnutrition and burns
Erysipelas
bull Symptomsbull ndash It usually presents of fever general fatigue bull -The skin lesion is a redindurated and elevated plaque
with borders that expand rapidly bull It is painful warm and accompanied by variable oedemabull -On the second or third day a flaccid bulla may develop
and desquamationbull bull Presence of regional lymph nodes is common
Erysipelas
bull Complicationsndash The most common complication is recurrencewhich is seen in 18ndash30 of the cases even afterproper antibiotic therapy Recurrence is seen moreoften in females than in malesA skin infection with S pyogenes could lead toglomerulonephritis
Erysipelas
bull Complicationsbull ndash The most common complication is recurrencebull which is seen in 18ndash30 of the cases even afterbull proper antibiotic therapy bull -Recurrence is seen morebull often in females than in males bull -A skin infection with S pyogenes could lead tobull glomerulonephritis
Erysipelas
bull bull Diagnosisbull ndash Diagnosis is based on the patientrsquos personal
historybull and physical examination particularly on inspectionbull of the skin
bull Blood cultures are positive in less thanbull 5 of cases
ErysipelasTherapyndash Conservative therapybull The preferred antibiotic is penicillin In mildcases with minor systemic symptoms penicillinV 500 mg orally every 6 h for 10 days or penicillinG benzathine 12 mil U intramuscularlyonceOther possibilities are amoxicillin 500 mgorally twice a day for 10 days or cephalexin 500mg orally every 6 h for 10 days
ErysipelasIn moderate and severe cases with significantsystemic symptoms hospitalization and intravenoustreatment is required penicillin G 2ndash4mil U intravenously every 4ndash6 h Cefazolin05ndash15 gm intravenously every 8 h cefotaxime1ndash2 gm intravenously every 8 h or ceftriaxone1ndash2 gm intravenously once a day should be administeredIn patients with a penicillin allergyclindamycin 600 mg intravenously every 8 h orvancomycin 15 mgkg intravenously twice a daymay be given
ErysipelaAdditional useful therapeutic optionsbull Prednisone 30 mg over 8 days might be consideredas well as elevation of the affected siteMoist heat compresses may be usefulbull Surgeryndash Debridement and drainage are indicated when bullaeabscesses or necroses are presentbull Differential diagnosisndash Contact dermatitisndash Asteatotic eczemandash Herpes zosterndash Angioneurotic oedemandash Osteomyelitis
Furuncle
bull Definition of the diseasebull ndash A furuncle is an infection that beginsbull at the hair follicle and spreads deeper into thebull dermis and subcutaneous tissue forming abull nodule After several days it developsbull into an abscess - red painful and fluctuantbull bull bull Epidemiologyaetiologybull ndash The aetiologic agent is Staphylococcus aureus
FuruncleSymptomsndashsymptoms are local and limited to thesite of infection Furuncles usually are wherehair follicles are present bull Complicationndash One complication is furunculosis multiple draining furunclesDiagnosisndash The diagnosis is based on clinical inspection - Cultures are not necessary when there is no systemic involvement but should beconsidered if systemic therapy (in case of feversignificant cellulitis or hospitalization) or whenmethicillin-resistant Staphylococcusaureus (MRSA) is considered
FuruncleTherapyndash When the furuncle is small application of moist heat compress to promote drainage -Larger furuncles should be drained by surgical incision-After drainage the area should be cleaned with anantiseptic (with chlorhexidinebetadine) should be applied twice
a dayndash If no systemic symptoms or extensive cellulitis arepresent simple topical care is usually curative andoral antibiotics are not necessary Otherwise systemictreatment is indicated and should cover anypossible MRSA
Furuncle
bull -Recommended antibiotics are trimethoprim-sulfamethoxazole
bull 1ndash2 tablets orally twice daily doxycyclinebull 100 mg orally twice dailybull or clindamycin 300ndash450 mg orally every 8 hbull - In severe cases vancomycin 15 mgkg
intravenouslybull every 12 h or clindamycin 600 mg intravenouslybull every 8 h
Midline Granulomabull A midline granuloma is an angiocentricbull lymphoma it was referred to as polymorphicbull reticulosis lethal midline granuloma and midline
malignant reticulosisbull bull Definition of the diseasebull ndash This rare disease is a lymphoma of extranodal
presentationall cases are positive for the Epstein-Barr virus
bull -This lymphoma most commonly appears in the midface region
Midline GranulomaEpidemiologyaetiologyndash This form of lymphoma is rare in Europe and theUnited States with a higher prevalence in Asia and PeruSymptomsndash The most common presentation is nasal obstruction with a destructive mass occupying the nosesinuses and palate
-Fever night sweatsand weight loss seen usually in Hodgkinrsquos lymphomaand other non-Hodgkinrsquos lymphomas (knownas ldquoB symptomsrdquo) are uncommon
Midline GranulomaDiagnosisndash The diagnosis is based on anatomopathologicalstudy The malignancy of the tumour manifested byextensive necrosis makes the histological diagnosisdifficult and often more biopsies are required forconfirmationbull Therapyndash Therapy consists of radiotherapy with or withoutchemotherapy
Midline Granuloma
bull Prognosisbull ndash Depending on the stage long-term remission or
experience a worseningbull prognosis with relapses which may include otherbull extranodal sites bull Involvement of extranodal sitesbull including the upper airway gastrointestinal tractbull skin
Wegenerrsquos Granulomatosis
bull Definition of the diseasebull ndash Wegenerrsquos granulomatosis is a systemic chronicbull vasculitis of small- and medium-sized blood vesselsbull with an autoimmune component It affectsbull particular organs with variable predilectionbull Epidemiologyaetiologybull ndash Wegenerrsquos granulomatosis is a rare disease It affects
about 1 in 20000ndash30000 people It is more prevalentbull in middle-aged Caucasian patients
Wegenerrsquos Granulomatosis
Symptomsndash The disease may present pulmonary upper
respiratory tract or renal In the disseminated form-The localised form ndash confinedto the upper respiratory region ndash is present in 25of the patients- It consists of nonspecific manifestationssuch as nasal obstruction crusting purulentor bloody rhinorrhea and painful or painless ulcers in oral or nasal cavities which are unresponsive tostandard medical treatment
Wegenerrsquos Granulomatosis
bull In some patients the nasal septum is perforatedbull which leads to saddle-nose deformity Less
commonbull symptoms are hoarseness stridor due to
subglotticbull stenosis otalgia otorrhea and conductivebull and sensorineural hearing loss Also ocular
symptomsbull such as scleritis conjunctivitis uveitis andbull episcleritis may be present
Wegenerrsquos Granulomatosis
bull ndash In the disseminated form pulmonary involvementbull is manifested by cough dyspnoea haemoptysisbull (due to an alveolar capillaritis necrotic lesions orbull endobronchial disease) and pleuritic painndashbull -Ninety per cent of patients have nasal symptomsbull and these symptoms are usually the first
manifestationof the diseasebull -Most patients have also renal involvementbull even if it is subclinical
Wegenerrsquos Granulomatosis
Diagnosis ndash Diagnosis of Wegenerrsquos granulomatosis is based on clinical findings that demonstrate lung (chest x-ray) kidney (urine analysis) or upper respiratory tract
involvement (oral or nasal ulcers or discharge) - positive blood analysis for cytoplasmic-staining antineutrophil
cytoplasmic antibodies (c-ANCA) and confirming proteinase 3 (PR3) ANCA or myeloperoxidase (MPO) ANCA ndash Biopsy is essential for diagnosis nonspecific chronic inflammation
and necrosis -Bacterial and fungal infections
Wegenerrsquos Granulomatosis
Therapyndash Conservative therapybull In the induction of disease remission highdosesteroids (e g prednisone 1 mgkgday) for1 month with tapering over several months aregiven In addition cyclophosphamide (2 mgkgday) should be administered for 6ndash12 monthsuntil symptoms disappear In the maintenanceof remission cyclophosphamide should be
Wegenerrsquos Granulomatosis
Antibiotics mainly trimethoprim-sulfamethoxazoleare given for prophylaxis againstPneumocystis jiroveci (formerly Pneumocystiscarinii) pneumonia (PCP) which may developduring immunosuppression and have a role inpreventing recurrencesbull Sinonasal manifestations may be treated with topical nasal steroids and nasal irrigations lowdosesystemic steroids and antibiotics when bacterial infection (typically Staphylococcus species) is suspected
Wegenerrsquos Granulomatosis
bull Prognosisbull ndash Most of the patients respond well to treatmentbull achieving symptom-free intervals of 5ndash20 yearsbull or more bull -Anatomical problems (sinusitis trachealbull stenosis) may require surgery bull Relapses can be long and troublesomebull Long-term complications are chronicbull renal failure hearing loss and deafness
Nasal Fractures Definition ndash A nasal fracture is a disruption of the nasal bone structure due to trauma It is the most frequently fractured facial bone Epidemiologyaetiology ndash Sports falls and assaults are the usual mechanisms of fracture -Males are affected twice as often as are females -Paediatric populations with a incidences during the second and third decades of life -Variables such as force impact direction nature of the striking object age and other will influence the pattern of injury to the components of the nose
Nasal Fractures
bull Symptomsbull ndash Deformity swelling epistaxis and periorbital
ecchymosis are signs that are suggestive of nasal fracture
bull bony crepitus and nasal segment mobilitybull ndash Epiphora bull Severe bilateral injuries to the lachrymal bones
arebull associated with depressed nasal fractures
Nasal Fractures Complications ndash Septal haematoma is one of the most severe early complications of nasal trauma and without drainage it results in abscess formation 6ndash7 days after trauma producing necrosis of the septal cartilage -Long-term problems such as saddle-nose deformity perforation columellar retraction and nasalbase
Septal infection could lead to osteomyelitis orbital and intracranial abscesses meningitis and cavernous sinus thrombosis -Cerebrospinal fluid leakage is a common complication of severe
nasal and frontal fractures
Nasal Fractures
bull Diagnostic proceduresbull ndash Inspectionbull bull Changes of appearance such as deviation andbull asymmetry bleeding watery drainage changesbull in nasal breathing and smell It is useful to comparebull the current presentation with old photographsbull (up to 40 of normal individuals havebull significant nose malformations)
Nasal Fractures Physical examination bull The diagnosis of a nasal fracture is made primarily by physical examination epistaxis nasal swelling and periorbital ecchymosis Nasal shape in the lateral and frontal inspection should be assessed Grasping the dorsum between two fingers and rocking the pyramid back and forth aids in assessing the mobility of nasal bones Internal structures should be evaluated by using a headlight and nasal speculum Clotted blood is removed by suction and assessment of haematoma mucosal tears and active bleeding is performed Bimanual palpation of the septum helps to differentiate septal swelling from haematoma ndash
Nasal FracturesRadiographybull There is no clear evidence of the role of radiographyin the management of nasal fracturesPlain films have up to a 66 false-positive rateas a result of misinterpretation of normal suturelines In addition old fractures are difficult todistinguishbull Three-dimensional CT is recommended for extensiveinjuries involving the nasal-orbital-ethmoidalcomplexndash
Nasal Fractures
bull Additionaluseful diagnostic proceduresbull bull Using a 0 or 30deg 4-mm endoscope is helpful inbull the assessment of posterior abnormalities If thebull patient is heavily sedated Brown-Gruss
provocationbull manoeuvres may be performed to determinebull deformities in upper middle or lower segmentsbull by compressing each compartment
Nasal FracturesConservative treatmentndash Treatment of bleedingbull For localised bleeding anterior sources may becauterised by silver nitrate or sealed with topicalmaterials such as thrombin combined withgelatin foam fibrin glue FloSealreg or other procoagulantmaterials If conservative measuresfail a formal anterior packing is placedbull Bleeding from branches of sphenopalatine orethmoid vessels requires anterior-posteriorpacking
Nasal Fractures
bull bull Surgical methods such as direct endoscopic vessel
bull cauterization or ligation have been shown tobull offer better haemostasis and patient comfortbull Angiography with embolization can also be
consideredbull in cases refractory to more conservativebull approaches
Nasal Fractures
bull Type of reductionbull bull Nondisplaced fractures should be treated withbull observation alone Closed nasal reduction is thebull best choice for simple injuries (isolated unilateralbull with medial displacement)bull bull An open approach should be considered in
severebull trauma (bilateral depressed fractures)
Nasal Fracturesbull Surgical principlesbull ndash Topical anaesthesia with cotton pledgets soakedbull with 4 cocaine or 005 oxymethazoline combinedbull with 4 topical lidocaine should be appliedbull for 5ndash10 min Local anaesthesia should also be injectedbull (1 lidocaine and 1100000 epinephrine)bull along the septum lateral walls and floor of the nasalbull cavitybull bull
Nasal FracturesClosed reductionndashndash The nasal bones are grasped between two fingersand pressure is applied laterally in theopposite direction of the deviation A bluntelevator may be used from within the nose incases of significant medial collapse Walshamforceps can be of help Reduction of the septumshould be performed with the use ofAsch forceps
Nasal Fractures
bull To prevent collapse of the postreductionbull framework nasal packing should be placedbull for 3ndash5 days Septum splints are recommendedbull in comminuted septal fractures withbull severe mucosal lesions External nasal splintingbull for 10 days (Aquaplastreg Thermoplastreg)bull provides nasal protection Nasal saline spraysbull prevent crusting and oral antibiotics should
Nasal Fractures
bull Open reductionbull ndashndash Immediate repair of fractures by using
widebull surgical exposure reduction fixation and
reconstructionbull ndashndash The second option is delayed correctionbull (6 months or more) of persistent deformitiesbull using standard techniques of rhinoplasty
Deviated Nasal Septum
bull Definition of the diseasebull ndash Deviation of the nasal septum is a common causebull of unilateral nasal airway obstruction in which thebull nasal septum is displacedbull bull Epidemiologyaetiologybull ndash Developmental septal abnormalities Septal cartilage
damage in the neonatal period andbull during birth can cause severe septal deviation inbull the absence of a history of nasal trauma
Deviated Nasal Septum
bull Symptomsbull ndash Patients may present with a history of sinusitis
allergicbull rhinitis obstructive sleep apnoea previousbull nasal surgery or recent nasal trauma Unilateral or
bilateral nasal airway obstruction that is unrelievedbull with decongestants or nasal steroid sprays is oftenbull seenbull bull
Deviated Nasal SeptumDiagnosisndashExamination external dorsal deviation or the columella and caudal septummay be deflected off the midline (caudal subluxation)ndash Inspections of the nasal cavity and anterior-posteriorrhinoscopy are helpful in diagnosing the locationtype and severity of septal deformityThe endoscope is also useful in identifying polypsthe severity and extent of posterior septaldeviations and bony spurs and locating areas ofseptal perforation or mucosal injury
Deviated Nasal Septum
bull Therapybull ndash Septoplasty is a procedurebull The areabull of deviation is corrected or resected in order tobull leave behind as much cartilage and bone as
possiblebull Cartilage resection is minimised and can be
repositioned reshaped or recontoured using a variety of methods
Deviated Nasal Septum
bull ndash Indications of septoplasty before the growth period
bull of the nose is finished should be very limited bull -In these cases surgery must preserve all the
cartilagebull in order to prevent external changes of the
shape ofbull the nose
Deviated Nasal Septum
bull Complicationsbull ndash Frequent complications include haematoma andbull infection Cerebrospinal fluid leak is a rare but
potentiallybull serious complicationbull It is usually the resultbull of avulsion or damage to the cribriform plate whenbull handling the perpendicular plate of the ethmoidbull ndash Other complications include epistaxis nasal
Deviated Nasal Septum
bull Other complications include epistaxis nasal obstruction
bull due to residual deviation synechiae returnbull of the cartilaginous deviation septal perforationbull anosmia and cosmetic nasal deformities suchbull as widened alar rim margins drooping nasal tipbull columella retraction and a sunken dorsum with abull supratip saddle formation
Septal perforation with minor crusting View from provide closure of the
incision
Septal Haematoma
bull A septal haematoma is a blood collection under the perichondrium
bull of the septum and cartilagebull bull bull Epidemiologyaetiologybull ndash A septal haematoma is one of the most
severe complications of nasal trauma
Septal Haematoma
bull Diagnosisbull ndash Signs and symptoms include intense pain
swellingbull haematoma of the upper lip and philtrum
area andbull complete nasal airway obstruction
Septal HaematomaTherapyndash Management consists of drainage through a mucoperichondrial incision Immediate treatment isnecessary to prevent long-term problems such asa saddle-nose deformity perforation columellarretraction and nasal-base widening In childrenseptal destruction can lead to devastating nasal andmidfacial growth abnormalitiesbull Surgeryndash Incision and evacuation of the collection is performedDrainage of a septal haematoma should
Septal HaematomaSurgeryndash Incision and evacuation of the collection is performedDrainage of a septal haematoma should provide closure of the incision
Splints or transseptal sutures are placed to obliterate thepotential space and prevent collectionInfection involving the septal cartilage Reconstruction with autologouscartilage is then performed in a second stage Oral antibiotics should be given
Nasal DeformitySaddle-nose deformityndash A saddle-nose deformity is characterised by a loss ofnasal dorsal height and compromised nasal supportstructures -Other case observed are depressionof the middle vault and dorsum loss of nasal tipsupport and definition shortened (vertical) nasal length over rotation of the nasal tip and retrusion ofthe nasal spine and caudal septum It is also knownas a ldquoPug noserdquo or ldquoboxerrsquos noserdquo both of which referto various degrees of nasal dorsal depressionbull
Nasal DeformityEpidemiologyaetiologyndash Prevalence is higher in population groups prone to facial trauma (ie boxers athletes) those with historiesof intranasal cocaine use nasal surgery (e g radical submucosal septal resection reductive rhinoplasty)ndash A saddle-nose deformity can be congenital or acquired It can be noticed as a part of individual familialsyndromic and ethnic characteristics - Most deformities are due to traumatic and iatrogeniccauses Medical causes are Wegenerrsquosgranulomatosis relapsing polychondritis leprosy (Hansenrsquos disease) syphilis ectodermal dysplasiaand intranasal cocaine use
Nasal Deformity
bull Therapybull ndash Nasal reconstruction indications depend on patientbull selection surgeon experience and aetiology of thebull deformity bull Indications for surgery can be functionalbull aesthetic or most commonly both In individuals
with a compromised nasal airway a nasoseptalbull reconstruction is indicated
Nasal Deformity
bull Contraindications bull include patients with malignantbull chronic or autoimmune disease conditions drugbull abuse poor perioperative risk profile and unrealisticbull expectationsbull ndash Multiple previous rhinoplasties and certain
professionsbull (mixed martial artists boxers and other contactbull sports) are relative contraindications
Nasal DeformitySeptoplastyndash Septoplasty is performed to correct nasal obstructioncaused by septal deformityndash Usually septoplasty is performed under general anaesthesiawith the patient in the supine position with the head elevated by approximately 30 (Righthandedsurgeons approach from the right side)ndash Local vasoconstrictive anaesthesia is applied notonly to reduce postoperative pain but also more importantly to achieve vasoconstriction of themucosa and less intraoperative haemorrhage Lidocainewith adrenaline or epinephrine is usedalthough in patients with cardiac hypersensitivityoxymetazoline might be preferred
Nasal Deformity
bull Septoplasty begins with the incision of septal mucosabull Most operative techniques utilise a hemitransfixionbull incision at the caudal end of septum so thatbull deviation at this point might be reached as wellbull as a transfixion incision that is easily obtained ifbull needed (Right-handed surgeons normally choosebull the left side but that may vary when deviation isbull convex towards the right)
Nasal DeformityA columella retractor is placed over the columellaand by pulling it laterally the caudal border of theseptum is exposed Ala can be protected by an alaprotector A vertical incision with a no 15 bladeover the caudal end of septum is performed untilreaching the plane of the septal cartilage It is essentialto correctly identify the perichondrium and byusing the Cottle elevator dissect and lift it creatinga flap As the dissection proceeds along the septalcartilage a longer speculum (no 5) is introduced sothat elevation of the mucoperichondrium is doneunder constant visual controlndash The next step is to dissect the mucoperiostium
Nasal DeformityDissecting over the bony-cartilaginous junctionwhen joining both tunnels might be difficult and is
especially prone to membrane perforationndash If needed the same tunnels are to be created on the
other side of the septum Then deviated parts of
septum are identified and removed either with a
knife or a Freer chisel
Nasal Deformitybull septum from the maxillary crest the septum mustbull be separated from the perpendicular plate trimmedbull along the inferior border placed back onto the crestbull and sutured to the periosteum If the deformity involvesbull the vomer an osteotome is used Care mustbull be taken not to break the cribriform plate becausebull it could cause a cerebrospinal fistula
Nasal Deformity
bull Once the septal deviation is corrected the flapsbull and hemitransfixion incision are mattressed
withbull absorbable sutures Nasal packing to prevent
synechiaebull and postoperative septal haematoma mightbull be advised but should be removed within 72 h

External Nose
Anatomy of the nasal base
bull Besides thebull medial crura the
inferior septal margin and the connective-
bull tissue septum (columella) are also responsible
bull for stabilizing the base of the nose
Anatomy of the nasal base
Anatomy of the nasal base
bull The nasal septum is subluxed toward the left side partially
bull obstructing the nasal airway
Nasal CavitiesThe nasal cavities begin anteriorly at the nasal vestibulewhich is bordered posteriorly by the internal nasalvalve (limen nasi) located between the posteriorborder of the alar cartilage and the anterior border ofthe lateral cartilage This valve area is the narrowestportion of the upper respiratory tract
Nasal Cavities
The interior ofthe nose behind the nasal valve is divided by the nasalseptum into two main cavities
Nasal CavitiesThe nasal septum iscomposed of an anterior cartilaginous part and twoposterior bony parts Abnormalities in the shape ofthe nasal septum which may consist of a deviated septum tensionseptum spurs or ridges are a frequent cause ofnasal airway obstructionThe choanae are the paired posterior openingsthrough which the nasal cavities communicate withthe nasopharynx
Nasal CavitiesThe nasal cavity is bounded laterally by the lateral nasalwalls which are formed by the ethmoid bone andmaxilla and posteriorly by the palatine bone and thepterygoid process of the sphenoid bone Several functionallyimportant structures are located on the lateralnasal wall the nasal turbinates and their associatedpassages (meati) sinus ostia and the orifice ofthe nasolacrimal duct (Fig 15)
The inferior turbinate consists of a separate bone thatis attached to the medial wall of the maxillary sinusThe opening of the nasolacrimal duct is located in thecorresponding inferior meatus The middle andsuperior turbinates are part of the ethmoid bone In rare cases a rudimentary ldquosupreme turbinaterdquo is alsopresent above the superior turbinate
The middle turbinate has by far the greatest functionalimportance because most of the drainage tracts fromthe surrounding paranasal sinuses open into the middlemeatus The nasal cavity is bounded superiorly by the cribriformplate of the ethmoid bone This thin bony platehas numerous openings for the passage of the fila olfactoriaand also forms the boundary of the anteriorcranial fossa
Nasal Cavities
The floor of the nasal cavity is formedmostly by the hard palate which is formed in turn bythe two palatine processes of the maxilla and the horizontallaminae of the palatine bone
Structure of the lateral nasal wall
Inferior meatus
Paranasal Sinuses
The paranasal sinuses are air-filled cavities that communicatewith the nasal cavities
-The maxillary sinus frontalsinus and anterior ethmoid cells drain into the nasalcavity through the middle meatusmdashie below themiddle turbinate -The posterior ethmoidcells drain into the nasal cavity through the superiormeatus The ostium of the sphenoid sinus is locatedin the anterior wall directly above the choanae- The anatomical connections between the nasal cavity andparanasal sinuses are functionally important and playa key role in the pathogenesis of many rhinologic diseasesthat involve the paranasal sinuses
Vascular SupplyThe external nose derives most of its blood supply
from the facial artery which arises from the external
carotid artery and from the ophthalmic artery which
springs from the internal carotid artery
Vascular Supply
The internalnose receives blood from the territories of the externaland internal carotid arteries- the terminalbranches of the sphenopalatine artery which arisesfrom the maxillary artery - the anterior and posteriorethmoid arteries which arise from the ophthalmicartery-internal carotid arterie
venous drainage
The venous drainageof the facial region is handled by -the facial vein -retromandibular vein -internal jugular vein
lymphatic drainage
The regional lymphatic drainage of the face and externalnose is handled mainly by- the submandibularlymph nodes while the nasal cavity is additionallydrained by -the retropharyngeal and deep - -cervical lymph nodes
Morphology of the Nasal Mucosa
Besides the anatomical structure of the external noseand nasal cavity the nasal mucosa plays an essentialrole in numerous functions of the nose in the respiratory tract
Morphology of the Nasal Mucosa
The anterior part of the nasal cavity (the nasal vestibule)like the external nose is covered by skin composedof a multilayer keratinizing squamous epithelium and finally a ciliated respiratory epithelium A small areaon the upper nasal septum superior turbinate andpart of the middle turbinate located adjacent to thecribriform plate is covered by olfactory mucosa and iscalled the olfactory region
Nerve SupplyThe facial skin receives its sensory innervation fromterminal branches of the trigeminal nerve that enterthe facial region through the supraorbital infraorbitaland mental foramina Thefacial muscles are classified as mimetic or mastica- tory each of these groups receiving different motorinnervationbythe facial nerve
History and Clinical Examination of the Nose
Historybull The main symptomsbull nasal obstruction (ldquostuffy
noserdquo)bull nasal dischargebull Headachesbull Olfactory
dysfunction
Palpationbony discontinuitiesNeuralgias to check
over- the supraorbital -infraorbital -mental foramina
Anterior Rhinoscopy
bull The rhinologic examination itself begins with anterior
bull rhinoscopy to evaluate the nasal vestibule and the anterior
bull portions of the nasal cavity
Nasal Endoscopy Nasal endoscopy has become the most important andrewarding clinical examination method in rhinologic diagnosis
- rigid endoscopes which are available in 4-mm and 28- mm diameters and assorted viewing angles (eg 01048576 301048576 1201048576) -flexible endoscopes are also available for inspecting the nose and nasopharynx and exploring all of the pharynx and larynx in one sitting
Nasal endoscopy
Nasal Endoscopy
Nasal Endoscopy
Imaging of the Nose and Paranasal Sinuses
Conventional RadiographsStandard paranasal sinus radiographs in the occipitomental
projection ( Water projection) and
occipitofrontal projection Caldwell projection) in cases of acute inflammation
They are also obtained to evaluate midfacial fractures
Computed Tomography (CT) the main indicationsfor CT scanning of the
nose and paranasal sinuses
are- chronic sinusitis - -trauma (especially
frontobasal -fractures)
-and tumors
The occipitofrontal projection is better for evaluating theethmoid cells and frontal sinus
occipitomental projection demonstrates the maxillarysinus and gives a limited view of the sphenoid sinus
Computed tomography of the paranasal sinuses
Four representative coronal CT scans are shown
Four representative coronal CT scans are shown
Magnetic Resonance Imaging
Magnetic maging
Magnetic resonance imaging (MRI) has fewer indicationsthan CT in patients with paranasal sinus diseaseThis is primarily because MRI is markedly inferior toCT in defining the bony boundaries of the sinusesThe strength of MRI lies in its superior soft-tissue discriminationMRI is indicated in diseases that involve the paranasal sinuses in addition to thecranial cavity or orbit (eg tumors and congenitalmalformations such as encephaloceles)
MRI of the paranasal sinuses
The Nose and Sinuses
Structure The structure of the nose is made up of
four partsbull The surface anatomybull The nasal skeletonmdashcomposed of the
two nasal bones the paired upper lateral and lower lateral cartilages and the nasal septum covered in subcutaneous tissue and skin
bull The internal anatomymdashincludes the septum of the nose which forms the medial wall of the nasal cavity The turbinates on the lateral wall are also called conchae
bull The osteomeatal complexmdasha key functional area of the nose
Function The nose is the main route for inspired
air and its structure is related to this function As the air passes over the large surface area of the turbinates
The inspired gases are warmed and humidified Mucus on the mucosa of the nose removes large dust particles from the air as it is breathed in
The voice resonates in the sinuses and nose and this provides character to the speech
Pneumatization of the sinusesmdashthey are air filled spacesmdashreduces the weight of the skull
Diseases of thDiseases of the Outer and Inner Nosee Outer and
Inner Nose Erysipelas Definition of the disease ndash Erysipela is a skin infection that affects the superficial dermis and is caused by Streptococcus pyogenes (group A) It usually develops in the extremities and the face and less commonly on the scalp and genitals bull Epidemiologyaetiology ndash Erysipelas are more often seen in elderly infants and children patients with compromised immunology and diabetes -Predisposing factors are alcoholism skin ulceration puncture wounds fungal infections malnutrition and burns
Erysipelas
bull Symptomsbull ndash It usually presents of fever general fatigue bull -The skin lesion is a redindurated and elevated plaque
with borders that expand rapidly bull It is painful warm and accompanied by variable oedemabull -On the second or third day a flaccid bulla may develop
and desquamationbull bull Presence of regional lymph nodes is common
Erysipelas
bull Complicationsndash The most common complication is recurrencewhich is seen in 18ndash30 of the cases even afterproper antibiotic therapy Recurrence is seen moreoften in females than in malesA skin infection with S pyogenes could lead toglomerulonephritis
Erysipelas
bull Complicationsbull ndash The most common complication is recurrencebull which is seen in 18ndash30 of the cases even afterbull proper antibiotic therapy bull -Recurrence is seen morebull often in females than in males bull -A skin infection with S pyogenes could lead tobull glomerulonephritis
Erysipelas
bull bull Diagnosisbull ndash Diagnosis is based on the patientrsquos personal
historybull and physical examination particularly on inspectionbull of the skin
bull Blood cultures are positive in less thanbull 5 of cases
ErysipelasTherapyndash Conservative therapybull The preferred antibiotic is penicillin In mildcases with minor systemic symptoms penicillinV 500 mg orally every 6 h for 10 days or penicillinG benzathine 12 mil U intramuscularlyonceOther possibilities are amoxicillin 500 mgorally twice a day for 10 days or cephalexin 500mg orally every 6 h for 10 days
ErysipelasIn moderate and severe cases with significantsystemic symptoms hospitalization and intravenoustreatment is required penicillin G 2ndash4mil U intravenously every 4ndash6 h Cefazolin05ndash15 gm intravenously every 8 h cefotaxime1ndash2 gm intravenously every 8 h or ceftriaxone1ndash2 gm intravenously once a day should be administeredIn patients with a penicillin allergyclindamycin 600 mg intravenously every 8 h orvancomycin 15 mgkg intravenously twice a daymay be given
ErysipelaAdditional useful therapeutic optionsbull Prednisone 30 mg over 8 days might be consideredas well as elevation of the affected siteMoist heat compresses may be usefulbull Surgeryndash Debridement and drainage are indicated when bullaeabscesses or necroses are presentbull Differential diagnosisndash Contact dermatitisndash Asteatotic eczemandash Herpes zosterndash Angioneurotic oedemandash Osteomyelitis
Furuncle
bull Definition of the diseasebull ndash A furuncle is an infection that beginsbull at the hair follicle and spreads deeper into thebull dermis and subcutaneous tissue forming abull nodule After several days it developsbull into an abscess - red painful and fluctuantbull bull bull Epidemiologyaetiologybull ndash The aetiologic agent is Staphylococcus aureus
FuruncleSymptomsndashsymptoms are local and limited to thesite of infection Furuncles usually are wherehair follicles are present bull Complicationndash One complication is furunculosis multiple draining furunclesDiagnosisndash The diagnosis is based on clinical inspection - Cultures are not necessary when there is no systemic involvement but should beconsidered if systemic therapy (in case of feversignificant cellulitis or hospitalization) or whenmethicillin-resistant Staphylococcusaureus (MRSA) is considered
FuruncleTherapyndash When the furuncle is small application of moist heat compress to promote drainage -Larger furuncles should be drained by surgical incision-After drainage the area should be cleaned with anantiseptic (with chlorhexidinebetadine) should be applied twice
a dayndash If no systemic symptoms or extensive cellulitis arepresent simple topical care is usually curative andoral antibiotics are not necessary Otherwise systemictreatment is indicated and should cover anypossible MRSA
Furuncle
bull -Recommended antibiotics are trimethoprim-sulfamethoxazole
bull 1ndash2 tablets orally twice daily doxycyclinebull 100 mg orally twice dailybull or clindamycin 300ndash450 mg orally every 8 hbull - In severe cases vancomycin 15 mgkg
intravenouslybull every 12 h or clindamycin 600 mg intravenouslybull every 8 h
Midline Granulomabull A midline granuloma is an angiocentricbull lymphoma it was referred to as polymorphicbull reticulosis lethal midline granuloma and midline
malignant reticulosisbull bull Definition of the diseasebull ndash This rare disease is a lymphoma of extranodal
presentationall cases are positive for the Epstein-Barr virus
bull -This lymphoma most commonly appears in the midface region
Midline GranulomaEpidemiologyaetiologyndash This form of lymphoma is rare in Europe and theUnited States with a higher prevalence in Asia and PeruSymptomsndash The most common presentation is nasal obstruction with a destructive mass occupying the nosesinuses and palate
-Fever night sweatsand weight loss seen usually in Hodgkinrsquos lymphomaand other non-Hodgkinrsquos lymphomas (knownas ldquoB symptomsrdquo) are uncommon
Midline GranulomaDiagnosisndash The diagnosis is based on anatomopathologicalstudy The malignancy of the tumour manifested byextensive necrosis makes the histological diagnosisdifficult and often more biopsies are required forconfirmationbull Therapyndash Therapy consists of radiotherapy with or withoutchemotherapy
Midline Granuloma
bull Prognosisbull ndash Depending on the stage long-term remission or
experience a worseningbull prognosis with relapses which may include otherbull extranodal sites bull Involvement of extranodal sitesbull including the upper airway gastrointestinal tractbull skin
Wegenerrsquos Granulomatosis
bull Definition of the diseasebull ndash Wegenerrsquos granulomatosis is a systemic chronicbull vasculitis of small- and medium-sized blood vesselsbull with an autoimmune component It affectsbull particular organs with variable predilectionbull Epidemiologyaetiologybull ndash Wegenerrsquos granulomatosis is a rare disease It affects
about 1 in 20000ndash30000 people It is more prevalentbull in middle-aged Caucasian patients
Wegenerrsquos Granulomatosis
Symptomsndash The disease may present pulmonary upper
respiratory tract or renal In the disseminated form-The localised form ndash confinedto the upper respiratory region ndash is present in 25of the patients- It consists of nonspecific manifestationssuch as nasal obstruction crusting purulentor bloody rhinorrhea and painful or painless ulcers in oral or nasal cavities which are unresponsive tostandard medical treatment
Wegenerrsquos Granulomatosis
bull In some patients the nasal septum is perforatedbull which leads to saddle-nose deformity Less
commonbull symptoms are hoarseness stridor due to
subglotticbull stenosis otalgia otorrhea and conductivebull and sensorineural hearing loss Also ocular
symptomsbull such as scleritis conjunctivitis uveitis andbull episcleritis may be present
Wegenerrsquos Granulomatosis
bull ndash In the disseminated form pulmonary involvementbull is manifested by cough dyspnoea haemoptysisbull (due to an alveolar capillaritis necrotic lesions orbull endobronchial disease) and pleuritic painndashbull -Ninety per cent of patients have nasal symptomsbull and these symptoms are usually the first
manifestationof the diseasebull -Most patients have also renal involvementbull even if it is subclinical
Wegenerrsquos Granulomatosis
Diagnosis ndash Diagnosis of Wegenerrsquos granulomatosis is based on clinical findings that demonstrate lung (chest x-ray) kidney (urine analysis) or upper respiratory tract
involvement (oral or nasal ulcers or discharge) - positive blood analysis for cytoplasmic-staining antineutrophil
cytoplasmic antibodies (c-ANCA) and confirming proteinase 3 (PR3) ANCA or myeloperoxidase (MPO) ANCA ndash Biopsy is essential for diagnosis nonspecific chronic inflammation
and necrosis -Bacterial and fungal infections
Wegenerrsquos Granulomatosis
Therapyndash Conservative therapybull In the induction of disease remission highdosesteroids (e g prednisone 1 mgkgday) for1 month with tapering over several months aregiven In addition cyclophosphamide (2 mgkgday) should be administered for 6ndash12 monthsuntil symptoms disappear In the maintenanceof remission cyclophosphamide should be
Wegenerrsquos Granulomatosis
Antibiotics mainly trimethoprim-sulfamethoxazoleare given for prophylaxis againstPneumocystis jiroveci (formerly Pneumocystiscarinii) pneumonia (PCP) which may developduring immunosuppression and have a role inpreventing recurrencesbull Sinonasal manifestations may be treated with topical nasal steroids and nasal irrigations lowdosesystemic steroids and antibiotics when bacterial infection (typically Staphylococcus species) is suspected
Wegenerrsquos Granulomatosis
bull Prognosisbull ndash Most of the patients respond well to treatmentbull achieving symptom-free intervals of 5ndash20 yearsbull or more bull -Anatomical problems (sinusitis trachealbull stenosis) may require surgery bull Relapses can be long and troublesomebull Long-term complications are chronicbull renal failure hearing loss and deafness
Nasal Fractures Definition ndash A nasal fracture is a disruption of the nasal bone structure due to trauma It is the most frequently fractured facial bone Epidemiologyaetiology ndash Sports falls and assaults are the usual mechanisms of fracture -Males are affected twice as often as are females -Paediatric populations with a incidences during the second and third decades of life -Variables such as force impact direction nature of the striking object age and other will influence the pattern of injury to the components of the nose
Nasal Fractures
bull Symptomsbull ndash Deformity swelling epistaxis and periorbital
ecchymosis are signs that are suggestive of nasal fracture
bull bony crepitus and nasal segment mobilitybull ndash Epiphora bull Severe bilateral injuries to the lachrymal bones
arebull associated with depressed nasal fractures
Nasal Fractures Complications ndash Septal haematoma is one of the most severe early complications of nasal trauma and without drainage it results in abscess formation 6ndash7 days after trauma producing necrosis of the septal cartilage -Long-term problems such as saddle-nose deformity perforation columellar retraction and nasalbase
Septal infection could lead to osteomyelitis orbital and intracranial abscesses meningitis and cavernous sinus thrombosis -Cerebrospinal fluid leakage is a common complication of severe
nasal and frontal fractures
Nasal Fractures
bull Diagnostic proceduresbull ndash Inspectionbull bull Changes of appearance such as deviation andbull asymmetry bleeding watery drainage changesbull in nasal breathing and smell It is useful to comparebull the current presentation with old photographsbull (up to 40 of normal individuals havebull significant nose malformations)
Nasal Fractures Physical examination bull The diagnosis of a nasal fracture is made primarily by physical examination epistaxis nasal swelling and periorbital ecchymosis Nasal shape in the lateral and frontal inspection should be assessed Grasping the dorsum between two fingers and rocking the pyramid back and forth aids in assessing the mobility of nasal bones Internal structures should be evaluated by using a headlight and nasal speculum Clotted blood is removed by suction and assessment of haematoma mucosal tears and active bleeding is performed Bimanual palpation of the septum helps to differentiate septal swelling from haematoma ndash
Nasal FracturesRadiographybull There is no clear evidence of the role of radiographyin the management of nasal fracturesPlain films have up to a 66 false-positive rateas a result of misinterpretation of normal suturelines In addition old fractures are difficult todistinguishbull Three-dimensional CT is recommended for extensiveinjuries involving the nasal-orbital-ethmoidalcomplexndash
Nasal Fractures
bull Additionaluseful diagnostic proceduresbull bull Using a 0 or 30deg 4-mm endoscope is helpful inbull the assessment of posterior abnormalities If thebull patient is heavily sedated Brown-Gruss
provocationbull manoeuvres may be performed to determinebull deformities in upper middle or lower segmentsbull by compressing each compartment
Nasal FracturesConservative treatmentndash Treatment of bleedingbull For localised bleeding anterior sources may becauterised by silver nitrate or sealed with topicalmaterials such as thrombin combined withgelatin foam fibrin glue FloSealreg or other procoagulantmaterials If conservative measuresfail a formal anterior packing is placedbull Bleeding from branches of sphenopalatine orethmoid vessels requires anterior-posteriorpacking
Nasal Fractures
bull bull Surgical methods such as direct endoscopic vessel
bull cauterization or ligation have been shown tobull offer better haemostasis and patient comfortbull Angiography with embolization can also be
consideredbull in cases refractory to more conservativebull approaches
Nasal Fractures
bull Type of reductionbull bull Nondisplaced fractures should be treated withbull observation alone Closed nasal reduction is thebull best choice for simple injuries (isolated unilateralbull with medial displacement)bull bull An open approach should be considered in
severebull trauma (bilateral depressed fractures)
Nasal Fracturesbull Surgical principlesbull ndash Topical anaesthesia with cotton pledgets soakedbull with 4 cocaine or 005 oxymethazoline combinedbull with 4 topical lidocaine should be appliedbull for 5ndash10 min Local anaesthesia should also be injectedbull (1 lidocaine and 1100000 epinephrine)bull along the septum lateral walls and floor of the nasalbull cavitybull bull
Nasal FracturesClosed reductionndashndash The nasal bones are grasped between two fingersand pressure is applied laterally in theopposite direction of the deviation A bluntelevator may be used from within the nose incases of significant medial collapse Walshamforceps can be of help Reduction of the septumshould be performed with the use ofAsch forceps
Nasal Fractures
bull To prevent collapse of the postreductionbull framework nasal packing should be placedbull for 3ndash5 days Septum splints are recommendedbull in comminuted septal fractures withbull severe mucosal lesions External nasal splintingbull for 10 days (Aquaplastreg Thermoplastreg)bull provides nasal protection Nasal saline spraysbull prevent crusting and oral antibiotics should
Nasal Fractures
bull Open reductionbull ndashndash Immediate repair of fractures by using
widebull surgical exposure reduction fixation and
reconstructionbull ndashndash The second option is delayed correctionbull (6 months or more) of persistent deformitiesbull using standard techniques of rhinoplasty
Deviated Nasal Septum
bull Definition of the diseasebull ndash Deviation of the nasal septum is a common causebull of unilateral nasal airway obstruction in which thebull nasal septum is displacedbull bull Epidemiologyaetiologybull ndash Developmental septal abnormalities Septal cartilage
damage in the neonatal period andbull during birth can cause severe septal deviation inbull the absence of a history of nasal trauma
Deviated Nasal Septum
bull Symptomsbull ndash Patients may present with a history of sinusitis
allergicbull rhinitis obstructive sleep apnoea previousbull nasal surgery or recent nasal trauma Unilateral or
bilateral nasal airway obstruction that is unrelievedbull with decongestants or nasal steroid sprays is oftenbull seenbull bull
Deviated Nasal SeptumDiagnosisndashExamination external dorsal deviation or the columella and caudal septummay be deflected off the midline (caudal subluxation)ndash Inspections of the nasal cavity and anterior-posteriorrhinoscopy are helpful in diagnosing the locationtype and severity of septal deformityThe endoscope is also useful in identifying polypsthe severity and extent of posterior septaldeviations and bony spurs and locating areas ofseptal perforation or mucosal injury
Deviated Nasal Septum
bull Therapybull ndash Septoplasty is a procedurebull The areabull of deviation is corrected or resected in order tobull leave behind as much cartilage and bone as
possiblebull Cartilage resection is minimised and can be
repositioned reshaped or recontoured using a variety of methods
Deviated Nasal Septum
bull ndash Indications of septoplasty before the growth period
bull of the nose is finished should be very limited bull -In these cases surgery must preserve all the
cartilagebull in order to prevent external changes of the
shape ofbull the nose
Deviated Nasal Septum
bull Complicationsbull ndash Frequent complications include haematoma andbull infection Cerebrospinal fluid leak is a rare but
potentiallybull serious complicationbull It is usually the resultbull of avulsion or damage to the cribriform plate whenbull handling the perpendicular plate of the ethmoidbull ndash Other complications include epistaxis nasal
Deviated Nasal Septum
bull Other complications include epistaxis nasal obstruction
bull due to residual deviation synechiae returnbull of the cartilaginous deviation septal perforationbull anosmia and cosmetic nasal deformities suchbull as widened alar rim margins drooping nasal tipbull columella retraction and a sunken dorsum with abull supratip saddle formation
Septal perforation with minor crusting View from provide closure of the
incision
Septal Haematoma
bull A septal haematoma is a blood collection under the perichondrium
bull of the septum and cartilagebull bull bull Epidemiologyaetiologybull ndash A septal haematoma is one of the most
severe complications of nasal trauma
Septal Haematoma
bull Diagnosisbull ndash Signs and symptoms include intense pain
swellingbull haematoma of the upper lip and philtrum
area andbull complete nasal airway obstruction
Septal HaematomaTherapyndash Management consists of drainage through a mucoperichondrial incision Immediate treatment isnecessary to prevent long-term problems such asa saddle-nose deformity perforation columellarretraction and nasal-base widening In childrenseptal destruction can lead to devastating nasal andmidfacial growth abnormalitiesbull Surgeryndash Incision and evacuation of the collection is performedDrainage of a septal haematoma should
Septal HaematomaSurgeryndash Incision and evacuation of the collection is performedDrainage of a septal haematoma should provide closure of the incision
Splints or transseptal sutures are placed to obliterate thepotential space and prevent collectionInfection involving the septal cartilage Reconstruction with autologouscartilage is then performed in a second stage Oral antibiotics should be given
Nasal DeformitySaddle-nose deformityndash A saddle-nose deformity is characterised by a loss ofnasal dorsal height and compromised nasal supportstructures -Other case observed are depressionof the middle vault and dorsum loss of nasal tipsupport and definition shortened (vertical) nasal length over rotation of the nasal tip and retrusion ofthe nasal spine and caudal septum It is also knownas a ldquoPug noserdquo or ldquoboxerrsquos noserdquo both of which referto various degrees of nasal dorsal depressionbull
Nasal DeformityEpidemiologyaetiologyndash Prevalence is higher in population groups prone to facial trauma (ie boxers athletes) those with historiesof intranasal cocaine use nasal surgery (e g radical submucosal septal resection reductive rhinoplasty)ndash A saddle-nose deformity can be congenital or acquired It can be noticed as a part of individual familialsyndromic and ethnic characteristics - Most deformities are due to traumatic and iatrogeniccauses Medical causes are Wegenerrsquosgranulomatosis relapsing polychondritis leprosy (Hansenrsquos disease) syphilis ectodermal dysplasiaand intranasal cocaine use
Nasal Deformity
bull Therapybull ndash Nasal reconstruction indications depend on patientbull selection surgeon experience and aetiology of thebull deformity bull Indications for surgery can be functionalbull aesthetic or most commonly both In individuals
with a compromised nasal airway a nasoseptalbull reconstruction is indicated
Nasal Deformity
bull Contraindications bull include patients with malignantbull chronic or autoimmune disease conditions drugbull abuse poor perioperative risk profile and unrealisticbull expectationsbull ndash Multiple previous rhinoplasties and certain
professionsbull (mixed martial artists boxers and other contactbull sports) are relative contraindications
Nasal DeformitySeptoplastyndash Septoplasty is performed to correct nasal obstructioncaused by septal deformityndash Usually septoplasty is performed under general anaesthesiawith the patient in the supine position with the head elevated by approximately 30 (Righthandedsurgeons approach from the right side)ndash Local vasoconstrictive anaesthesia is applied notonly to reduce postoperative pain but also more importantly to achieve vasoconstriction of themucosa and less intraoperative haemorrhage Lidocainewith adrenaline or epinephrine is usedalthough in patients with cardiac hypersensitivityoxymetazoline might be preferred
Nasal Deformity
bull Septoplasty begins with the incision of septal mucosabull Most operative techniques utilise a hemitransfixionbull incision at the caudal end of septum so thatbull deviation at this point might be reached as wellbull as a transfixion incision that is easily obtained ifbull needed (Right-handed surgeons normally choosebull the left side but that may vary when deviation isbull convex towards the right)
Nasal DeformityA columella retractor is placed over the columellaand by pulling it laterally the caudal border of theseptum is exposed Ala can be protected by an alaprotector A vertical incision with a no 15 bladeover the caudal end of septum is performed untilreaching the plane of the septal cartilage It is essentialto correctly identify the perichondrium and byusing the Cottle elevator dissect and lift it creatinga flap As the dissection proceeds along the septalcartilage a longer speculum (no 5) is introduced sothat elevation of the mucoperichondrium is doneunder constant visual controlndash The next step is to dissect the mucoperiostium
Nasal DeformityDissecting over the bony-cartilaginous junctionwhen joining both tunnels might be difficult and is
especially prone to membrane perforationndash If needed the same tunnels are to be created on the
other side of the septum Then deviated parts of
septum are identified and removed either with a
knife or a Freer chisel
Nasal Deformitybull septum from the maxillary crest the septum mustbull be separated from the perpendicular plate trimmedbull along the inferior border placed back onto the crestbull and sutured to the periosteum If the deformity involvesbull the vomer an osteotome is used Care mustbull be taken not to break the cribriform plate becausebull it could cause a cerebrospinal fistula
Nasal Deformity
bull Once the septal deviation is corrected the flapsbull and hemitransfixion incision are mattressed
withbull absorbable sutures Nasal packing to prevent
synechiaebull and postoperative septal haematoma mightbull be advised but should be removed within 72 h

Anatomy of the nasal base
bull Besides thebull medial crura the
inferior septal margin and the connective-
bull tissue septum (columella) are also responsible
bull for stabilizing the base of the nose
Anatomy of the nasal base
Anatomy of the nasal base
bull The nasal septum is subluxed toward the left side partially
bull obstructing the nasal airway
Nasal CavitiesThe nasal cavities begin anteriorly at the nasal vestibulewhich is bordered posteriorly by the internal nasalvalve (limen nasi) located between the posteriorborder of the alar cartilage and the anterior border ofthe lateral cartilage This valve area is the narrowestportion of the upper respiratory tract
Nasal Cavities
The interior ofthe nose behind the nasal valve is divided by the nasalseptum into two main cavities
Nasal CavitiesThe nasal septum iscomposed of an anterior cartilaginous part and twoposterior bony parts Abnormalities in the shape ofthe nasal septum which may consist of a deviated septum tensionseptum spurs or ridges are a frequent cause ofnasal airway obstructionThe choanae are the paired posterior openingsthrough which the nasal cavities communicate withthe nasopharynx
Nasal CavitiesThe nasal cavity is bounded laterally by the lateral nasalwalls which are formed by the ethmoid bone andmaxilla and posteriorly by the palatine bone and thepterygoid process of the sphenoid bone Several functionallyimportant structures are located on the lateralnasal wall the nasal turbinates and their associatedpassages (meati) sinus ostia and the orifice ofthe nasolacrimal duct (Fig 15)
The inferior turbinate consists of a separate bone thatis attached to the medial wall of the maxillary sinusThe opening of the nasolacrimal duct is located in thecorresponding inferior meatus The middle andsuperior turbinates are part of the ethmoid bone In rare cases a rudimentary ldquosupreme turbinaterdquo is alsopresent above the superior turbinate
The middle turbinate has by far the greatest functionalimportance because most of the drainage tracts fromthe surrounding paranasal sinuses open into the middlemeatus The nasal cavity is bounded superiorly by the cribriformplate of the ethmoid bone This thin bony platehas numerous openings for the passage of the fila olfactoriaand also forms the boundary of the anteriorcranial fossa
Nasal Cavities
The floor of the nasal cavity is formedmostly by the hard palate which is formed in turn bythe two palatine processes of the maxilla and the horizontallaminae of the palatine bone
Structure of the lateral nasal wall
Inferior meatus
Paranasal Sinuses
The paranasal sinuses are air-filled cavities that communicatewith the nasal cavities
-The maxillary sinus frontalsinus and anterior ethmoid cells drain into the nasalcavity through the middle meatusmdashie below themiddle turbinate -The posterior ethmoidcells drain into the nasal cavity through the superiormeatus The ostium of the sphenoid sinus is locatedin the anterior wall directly above the choanae- The anatomical connections between the nasal cavity andparanasal sinuses are functionally important and playa key role in the pathogenesis of many rhinologic diseasesthat involve the paranasal sinuses
Vascular SupplyThe external nose derives most of its blood supply
from the facial artery which arises from the external
carotid artery and from the ophthalmic artery which
springs from the internal carotid artery
Vascular Supply
The internalnose receives blood from the territories of the externaland internal carotid arteries- the terminalbranches of the sphenopalatine artery which arisesfrom the maxillary artery - the anterior and posteriorethmoid arteries which arise from the ophthalmicartery-internal carotid arterie
venous drainage
The venous drainageof the facial region is handled by -the facial vein -retromandibular vein -internal jugular vein
lymphatic drainage
The regional lymphatic drainage of the face and externalnose is handled mainly by- the submandibularlymph nodes while the nasal cavity is additionallydrained by -the retropharyngeal and deep - -cervical lymph nodes
Morphology of the Nasal Mucosa
Besides the anatomical structure of the external noseand nasal cavity the nasal mucosa plays an essentialrole in numerous functions of the nose in the respiratory tract
Morphology of the Nasal Mucosa
The anterior part of the nasal cavity (the nasal vestibule)like the external nose is covered by skin composedof a multilayer keratinizing squamous epithelium and finally a ciliated respiratory epithelium A small areaon the upper nasal septum superior turbinate andpart of the middle turbinate located adjacent to thecribriform plate is covered by olfactory mucosa and iscalled the olfactory region
Nerve SupplyThe facial skin receives its sensory innervation fromterminal branches of the trigeminal nerve that enterthe facial region through the supraorbital infraorbitaland mental foramina Thefacial muscles are classified as mimetic or mastica- tory each of these groups receiving different motorinnervationbythe facial nerve
History and Clinical Examination of the Nose
Historybull The main symptomsbull nasal obstruction (ldquostuffy
noserdquo)bull nasal dischargebull Headachesbull Olfactory
dysfunction
Palpationbony discontinuitiesNeuralgias to check
over- the supraorbital -infraorbital -mental foramina
Anterior Rhinoscopy
bull The rhinologic examination itself begins with anterior
bull rhinoscopy to evaluate the nasal vestibule and the anterior
bull portions of the nasal cavity
Nasal Endoscopy Nasal endoscopy has become the most important andrewarding clinical examination method in rhinologic diagnosis
- rigid endoscopes which are available in 4-mm and 28- mm diameters and assorted viewing angles (eg 01048576 301048576 1201048576) -flexible endoscopes are also available for inspecting the nose and nasopharynx and exploring all of the pharynx and larynx in one sitting
Nasal endoscopy
Nasal Endoscopy
Nasal Endoscopy
Imaging of the Nose and Paranasal Sinuses
Conventional RadiographsStandard paranasal sinus radiographs in the occipitomental
projection ( Water projection) and
occipitofrontal projection Caldwell projection) in cases of acute inflammation
They are also obtained to evaluate midfacial fractures
Computed Tomography (CT) the main indicationsfor CT scanning of the
nose and paranasal sinuses
are- chronic sinusitis - -trauma (especially
frontobasal -fractures)
-and tumors
The occipitofrontal projection is better for evaluating theethmoid cells and frontal sinus
occipitomental projection demonstrates the maxillarysinus and gives a limited view of the sphenoid sinus
Computed tomography of the paranasal sinuses
Four representative coronal CT scans are shown
Four representative coronal CT scans are shown
Magnetic Resonance Imaging
Magnetic maging
Magnetic resonance imaging (MRI) has fewer indicationsthan CT in patients with paranasal sinus diseaseThis is primarily because MRI is markedly inferior toCT in defining the bony boundaries of the sinusesThe strength of MRI lies in its superior soft-tissue discriminationMRI is indicated in diseases that involve the paranasal sinuses in addition to thecranial cavity or orbit (eg tumors and congenitalmalformations such as encephaloceles)
MRI of the paranasal sinuses
The Nose and Sinuses
Structure The structure of the nose is made up of
four partsbull The surface anatomybull The nasal skeletonmdashcomposed of the
two nasal bones the paired upper lateral and lower lateral cartilages and the nasal septum covered in subcutaneous tissue and skin
bull The internal anatomymdashincludes the septum of the nose which forms the medial wall of the nasal cavity The turbinates on the lateral wall are also called conchae
bull The osteomeatal complexmdasha key functional area of the nose
Function The nose is the main route for inspired
air and its structure is related to this function As the air passes over the large surface area of the turbinates
The inspired gases are warmed and humidified Mucus on the mucosa of the nose removes large dust particles from the air as it is breathed in
The voice resonates in the sinuses and nose and this provides character to the speech
Pneumatization of the sinusesmdashthey are air filled spacesmdashreduces the weight of the skull
Diseases of thDiseases of the Outer and Inner Nosee Outer and
Inner Nose Erysipelas Definition of the disease ndash Erysipela is a skin infection that affects the superficial dermis and is caused by Streptococcus pyogenes (group A) It usually develops in the extremities and the face and less commonly on the scalp and genitals bull Epidemiologyaetiology ndash Erysipelas are more often seen in elderly infants and children patients with compromised immunology and diabetes -Predisposing factors are alcoholism skin ulceration puncture wounds fungal infections malnutrition and burns
Erysipelas
bull Symptomsbull ndash It usually presents of fever general fatigue bull -The skin lesion is a redindurated and elevated plaque
with borders that expand rapidly bull It is painful warm and accompanied by variable oedemabull -On the second or third day a flaccid bulla may develop
and desquamationbull bull Presence of regional lymph nodes is common
Erysipelas
bull Complicationsndash The most common complication is recurrencewhich is seen in 18ndash30 of the cases even afterproper antibiotic therapy Recurrence is seen moreoften in females than in malesA skin infection with S pyogenes could lead toglomerulonephritis
Erysipelas
bull Complicationsbull ndash The most common complication is recurrencebull which is seen in 18ndash30 of the cases even afterbull proper antibiotic therapy bull -Recurrence is seen morebull often in females than in males bull -A skin infection with S pyogenes could lead tobull glomerulonephritis
Erysipelas
bull bull Diagnosisbull ndash Diagnosis is based on the patientrsquos personal
historybull and physical examination particularly on inspectionbull of the skin
bull Blood cultures are positive in less thanbull 5 of cases
ErysipelasTherapyndash Conservative therapybull The preferred antibiotic is penicillin In mildcases with minor systemic symptoms penicillinV 500 mg orally every 6 h for 10 days or penicillinG benzathine 12 mil U intramuscularlyonceOther possibilities are amoxicillin 500 mgorally twice a day for 10 days or cephalexin 500mg orally every 6 h for 10 days
ErysipelasIn moderate and severe cases with significantsystemic symptoms hospitalization and intravenoustreatment is required penicillin G 2ndash4mil U intravenously every 4ndash6 h Cefazolin05ndash15 gm intravenously every 8 h cefotaxime1ndash2 gm intravenously every 8 h or ceftriaxone1ndash2 gm intravenously once a day should be administeredIn patients with a penicillin allergyclindamycin 600 mg intravenously every 8 h orvancomycin 15 mgkg intravenously twice a daymay be given
ErysipelaAdditional useful therapeutic optionsbull Prednisone 30 mg over 8 days might be consideredas well as elevation of the affected siteMoist heat compresses may be usefulbull Surgeryndash Debridement and drainage are indicated when bullaeabscesses or necroses are presentbull Differential diagnosisndash Contact dermatitisndash Asteatotic eczemandash Herpes zosterndash Angioneurotic oedemandash Osteomyelitis
Furuncle
bull Definition of the diseasebull ndash A furuncle is an infection that beginsbull at the hair follicle and spreads deeper into thebull dermis and subcutaneous tissue forming abull nodule After several days it developsbull into an abscess - red painful and fluctuantbull bull bull Epidemiologyaetiologybull ndash The aetiologic agent is Staphylococcus aureus
FuruncleSymptomsndashsymptoms are local and limited to thesite of infection Furuncles usually are wherehair follicles are present bull Complicationndash One complication is furunculosis multiple draining furunclesDiagnosisndash The diagnosis is based on clinical inspection - Cultures are not necessary when there is no systemic involvement but should beconsidered if systemic therapy (in case of feversignificant cellulitis or hospitalization) or whenmethicillin-resistant Staphylococcusaureus (MRSA) is considered
FuruncleTherapyndash When the furuncle is small application of moist heat compress to promote drainage -Larger furuncles should be drained by surgical incision-After drainage the area should be cleaned with anantiseptic (with chlorhexidinebetadine) should be applied twice
a dayndash If no systemic symptoms or extensive cellulitis arepresent simple topical care is usually curative andoral antibiotics are not necessary Otherwise systemictreatment is indicated and should cover anypossible MRSA
Furuncle
bull -Recommended antibiotics are trimethoprim-sulfamethoxazole
bull 1ndash2 tablets orally twice daily doxycyclinebull 100 mg orally twice dailybull or clindamycin 300ndash450 mg orally every 8 hbull - In severe cases vancomycin 15 mgkg
intravenouslybull every 12 h or clindamycin 600 mg intravenouslybull every 8 h
Midline Granulomabull A midline granuloma is an angiocentricbull lymphoma it was referred to as polymorphicbull reticulosis lethal midline granuloma and midline
malignant reticulosisbull bull Definition of the diseasebull ndash This rare disease is a lymphoma of extranodal
presentationall cases are positive for the Epstein-Barr virus
bull -This lymphoma most commonly appears in the midface region
Midline GranulomaEpidemiologyaetiologyndash This form of lymphoma is rare in Europe and theUnited States with a higher prevalence in Asia and PeruSymptomsndash The most common presentation is nasal obstruction with a destructive mass occupying the nosesinuses and palate
-Fever night sweatsand weight loss seen usually in Hodgkinrsquos lymphomaand other non-Hodgkinrsquos lymphomas (knownas ldquoB symptomsrdquo) are uncommon
Midline GranulomaDiagnosisndash The diagnosis is based on anatomopathologicalstudy The malignancy of the tumour manifested byextensive necrosis makes the histological diagnosisdifficult and often more biopsies are required forconfirmationbull Therapyndash Therapy consists of radiotherapy with or withoutchemotherapy
Midline Granuloma
bull Prognosisbull ndash Depending on the stage long-term remission or
experience a worseningbull prognosis with relapses which may include otherbull extranodal sites bull Involvement of extranodal sitesbull including the upper airway gastrointestinal tractbull skin
Wegenerrsquos Granulomatosis
bull Definition of the diseasebull ndash Wegenerrsquos granulomatosis is a systemic chronicbull vasculitis of small- and medium-sized blood vesselsbull with an autoimmune component It affectsbull particular organs with variable predilectionbull Epidemiologyaetiologybull ndash Wegenerrsquos granulomatosis is a rare disease It affects
about 1 in 20000ndash30000 people It is more prevalentbull in middle-aged Caucasian patients
Wegenerrsquos Granulomatosis
Symptomsndash The disease may present pulmonary upper
respiratory tract or renal In the disseminated form-The localised form ndash confinedto the upper respiratory region ndash is present in 25of the patients- It consists of nonspecific manifestationssuch as nasal obstruction crusting purulentor bloody rhinorrhea and painful or painless ulcers in oral or nasal cavities which are unresponsive tostandard medical treatment
Wegenerrsquos Granulomatosis
bull In some patients the nasal septum is perforatedbull which leads to saddle-nose deformity Less
commonbull symptoms are hoarseness stridor due to
subglotticbull stenosis otalgia otorrhea and conductivebull and sensorineural hearing loss Also ocular
symptomsbull such as scleritis conjunctivitis uveitis andbull episcleritis may be present
Wegenerrsquos Granulomatosis
bull ndash In the disseminated form pulmonary involvementbull is manifested by cough dyspnoea haemoptysisbull (due to an alveolar capillaritis necrotic lesions orbull endobronchial disease) and pleuritic painndashbull -Ninety per cent of patients have nasal symptomsbull and these symptoms are usually the first
manifestationof the diseasebull -Most patients have also renal involvementbull even if it is subclinical
Wegenerrsquos Granulomatosis
Diagnosis ndash Diagnosis of Wegenerrsquos granulomatosis is based on clinical findings that demonstrate lung (chest x-ray) kidney (urine analysis) or upper respiratory tract
involvement (oral or nasal ulcers or discharge) - positive blood analysis for cytoplasmic-staining antineutrophil
cytoplasmic antibodies (c-ANCA) and confirming proteinase 3 (PR3) ANCA or myeloperoxidase (MPO) ANCA ndash Biopsy is essential for diagnosis nonspecific chronic inflammation
and necrosis -Bacterial and fungal infections
Wegenerrsquos Granulomatosis
Therapyndash Conservative therapybull In the induction of disease remission highdosesteroids (e g prednisone 1 mgkgday) for1 month with tapering over several months aregiven In addition cyclophosphamide (2 mgkgday) should be administered for 6ndash12 monthsuntil symptoms disappear In the maintenanceof remission cyclophosphamide should be
Wegenerrsquos Granulomatosis
Antibiotics mainly trimethoprim-sulfamethoxazoleare given for prophylaxis againstPneumocystis jiroveci (formerly Pneumocystiscarinii) pneumonia (PCP) which may developduring immunosuppression and have a role inpreventing recurrencesbull Sinonasal manifestations may be treated with topical nasal steroids and nasal irrigations lowdosesystemic steroids and antibiotics when bacterial infection (typically Staphylococcus species) is suspected
Wegenerrsquos Granulomatosis
bull Prognosisbull ndash Most of the patients respond well to treatmentbull achieving symptom-free intervals of 5ndash20 yearsbull or more bull -Anatomical problems (sinusitis trachealbull stenosis) may require surgery bull Relapses can be long and troublesomebull Long-term complications are chronicbull renal failure hearing loss and deafness
Nasal Fractures Definition ndash A nasal fracture is a disruption of the nasal bone structure due to trauma It is the most frequently fractured facial bone Epidemiologyaetiology ndash Sports falls and assaults are the usual mechanisms of fracture -Males are affected twice as often as are females -Paediatric populations with a incidences during the second and third decades of life -Variables such as force impact direction nature of the striking object age and other will influence the pattern of injury to the components of the nose
Nasal Fractures
bull Symptomsbull ndash Deformity swelling epistaxis and periorbital
ecchymosis are signs that are suggestive of nasal fracture
bull bony crepitus and nasal segment mobilitybull ndash Epiphora bull Severe bilateral injuries to the lachrymal bones
arebull associated with depressed nasal fractures
Nasal Fractures Complications ndash Septal haematoma is one of the most severe early complications of nasal trauma and without drainage it results in abscess formation 6ndash7 days after trauma producing necrosis of the septal cartilage -Long-term problems such as saddle-nose deformity perforation columellar retraction and nasalbase
Septal infection could lead to osteomyelitis orbital and intracranial abscesses meningitis and cavernous sinus thrombosis -Cerebrospinal fluid leakage is a common complication of severe
nasal and frontal fractures
Nasal Fractures
bull Diagnostic proceduresbull ndash Inspectionbull bull Changes of appearance such as deviation andbull asymmetry bleeding watery drainage changesbull in nasal breathing and smell It is useful to comparebull the current presentation with old photographsbull (up to 40 of normal individuals havebull significant nose malformations)
Nasal Fractures Physical examination bull The diagnosis of a nasal fracture is made primarily by physical examination epistaxis nasal swelling and periorbital ecchymosis Nasal shape in the lateral and frontal inspection should be assessed Grasping the dorsum between two fingers and rocking the pyramid back and forth aids in assessing the mobility of nasal bones Internal structures should be evaluated by using a headlight and nasal speculum Clotted blood is removed by suction and assessment of haematoma mucosal tears and active bleeding is performed Bimanual palpation of the septum helps to differentiate septal swelling from haematoma ndash
Nasal FracturesRadiographybull There is no clear evidence of the role of radiographyin the management of nasal fracturesPlain films have up to a 66 false-positive rateas a result of misinterpretation of normal suturelines In addition old fractures are difficult todistinguishbull Three-dimensional CT is recommended for extensiveinjuries involving the nasal-orbital-ethmoidalcomplexndash
Nasal Fractures
bull Additionaluseful diagnostic proceduresbull bull Using a 0 or 30deg 4-mm endoscope is helpful inbull the assessment of posterior abnormalities If thebull patient is heavily sedated Brown-Gruss
provocationbull manoeuvres may be performed to determinebull deformities in upper middle or lower segmentsbull by compressing each compartment
Nasal FracturesConservative treatmentndash Treatment of bleedingbull For localised bleeding anterior sources may becauterised by silver nitrate or sealed with topicalmaterials such as thrombin combined withgelatin foam fibrin glue FloSealreg or other procoagulantmaterials If conservative measuresfail a formal anterior packing is placedbull Bleeding from branches of sphenopalatine orethmoid vessels requires anterior-posteriorpacking
Nasal Fractures
bull bull Surgical methods such as direct endoscopic vessel
bull cauterization or ligation have been shown tobull offer better haemostasis and patient comfortbull Angiography with embolization can also be
consideredbull in cases refractory to more conservativebull approaches
Nasal Fractures
bull Type of reductionbull bull Nondisplaced fractures should be treated withbull observation alone Closed nasal reduction is thebull best choice for simple injuries (isolated unilateralbull with medial displacement)bull bull An open approach should be considered in
severebull trauma (bilateral depressed fractures)
Nasal Fracturesbull Surgical principlesbull ndash Topical anaesthesia with cotton pledgets soakedbull with 4 cocaine or 005 oxymethazoline combinedbull with 4 topical lidocaine should be appliedbull for 5ndash10 min Local anaesthesia should also be injectedbull (1 lidocaine and 1100000 epinephrine)bull along the septum lateral walls and floor of the nasalbull cavitybull bull
Nasal FracturesClosed reductionndashndash The nasal bones are grasped between two fingersand pressure is applied laterally in theopposite direction of the deviation A bluntelevator may be used from within the nose incases of significant medial collapse Walshamforceps can be of help Reduction of the septumshould be performed with the use ofAsch forceps
Nasal Fractures
bull To prevent collapse of the postreductionbull framework nasal packing should be placedbull for 3ndash5 days Septum splints are recommendedbull in comminuted septal fractures withbull severe mucosal lesions External nasal splintingbull for 10 days (Aquaplastreg Thermoplastreg)bull provides nasal protection Nasal saline spraysbull prevent crusting and oral antibiotics should
Nasal Fractures
bull Open reductionbull ndashndash Immediate repair of fractures by using
widebull surgical exposure reduction fixation and
reconstructionbull ndashndash The second option is delayed correctionbull (6 months or more) of persistent deformitiesbull using standard techniques of rhinoplasty
Deviated Nasal Septum
bull Definition of the diseasebull ndash Deviation of the nasal septum is a common causebull of unilateral nasal airway obstruction in which thebull nasal septum is displacedbull bull Epidemiologyaetiologybull ndash Developmental septal abnormalities Septal cartilage
damage in the neonatal period andbull during birth can cause severe septal deviation inbull the absence of a history of nasal trauma
Deviated Nasal Septum
bull Symptomsbull ndash Patients may present with a history of sinusitis
allergicbull rhinitis obstructive sleep apnoea previousbull nasal surgery or recent nasal trauma Unilateral or
bilateral nasal airway obstruction that is unrelievedbull with decongestants or nasal steroid sprays is oftenbull seenbull bull
Deviated Nasal SeptumDiagnosisndashExamination external dorsal deviation or the columella and caudal septummay be deflected off the midline (caudal subluxation)ndash Inspections of the nasal cavity and anterior-posteriorrhinoscopy are helpful in diagnosing the locationtype and severity of septal deformityThe endoscope is also useful in identifying polypsthe severity and extent of posterior septaldeviations and bony spurs and locating areas ofseptal perforation or mucosal injury
Deviated Nasal Septum
bull Therapybull ndash Septoplasty is a procedurebull The areabull of deviation is corrected or resected in order tobull leave behind as much cartilage and bone as
possiblebull Cartilage resection is minimised and can be
repositioned reshaped or recontoured using a variety of methods
Deviated Nasal Septum
bull ndash Indications of septoplasty before the growth period
bull of the nose is finished should be very limited bull -In these cases surgery must preserve all the
cartilagebull in order to prevent external changes of the
shape ofbull the nose
Deviated Nasal Septum
bull Complicationsbull ndash Frequent complications include haematoma andbull infection Cerebrospinal fluid leak is a rare but
potentiallybull serious complicationbull It is usually the resultbull of avulsion or damage to the cribriform plate whenbull handling the perpendicular plate of the ethmoidbull ndash Other complications include epistaxis nasal
Deviated Nasal Septum
bull Other complications include epistaxis nasal obstruction
bull due to residual deviation synechiae returnbull of the cartilaginous deviation septal perforationbull anosmia and cosmetic nasal deformities suchbull as widened alar rim margins drooping nasal tipbull columella retraction and a sunken dorsum with abull supratip saddle formation
Septal perforation with minor crusting View from provide closure of the
incision
Septal Haematoma
bull A septal haematoma is a blood collection under the perichondrium
bull of the septum and cartilagebull bull bull Epidemiologyaetiologybull ndash A septal haematoma is one of the most
severe complications of nasal trauma
Septal Haematoma
bull Diagnosisbull ndash Signs and symptoms include intense pain
swellingbull haematoma of the upper lip and philtrum
area andbull complete nasal airway obstruction
Septal HaematomaTherapyndash Management consists of drainage through a mucoperichondrial incision Immediate treatment isnecessary to prevent long-term problems such asa saddle-nose deformity perforation columellarretraction and nasal-base widening In childrenseptal destruction can lead to devastating nasal andmidfacial growth abnormalitiesbull Surgeryndash Incision and evacuation of the collection is performedDrainage of a septal haematoma should
Septal HaematomaSurgeryndash Incision and evacuation of the collection is performedDrainage of a septal haematoma should provide closure of the incision
Splints or transseptal sutures are placed to obliterate thepotential space and prevent collectionInfection involving the septal cartilage Reconstruction with autologouscartilage is then performed in a second stage Oral antibiotics should be given
Nasal DeformitySaddle-nose deformityndash A saddle-nose deformity is characterised by a loss ofnasal dorsal height and compromised nasal supportstructures -Other case observed are depressionof the middle vault and dorsum loss of nasal tipsupport and definition shortened (vertical) nasal length over rotation of the nasal tip and retrusion ofthe nasal spine and caudal septum It is also knownas a ldquoPug noserdquo or ldquoboxerrsquos noserdquo both of which referto various degrees of nasal dorsal depressionbull
Nasal DeformityEpidemiologyaetiologyndash Prevalence is higher in population groups prone to facial trauma (ie boxers athletes) those with historiesof intranasal cocaine use nasal surgery (e g radical submucosal septal resection reductive rhinoplasty)ndash A saddle-nose deformity can be congenital or acquired It can be noticed as a part of individual familialsyndromic and ethnic characteristics - Most deformities are due to traumatic and iatrogeniccauses Medical causes are Wegenerrsquosgranulomatosis relapsing polychondritis leprosy (Hansenrsquos disease) syphilis ectodermal dysplasiaand intranasal cocaine use
Nasal Deformity
bull Therapybull ndash Nasal reconstruction indications depend on patientbull selection surgeon experience and aetiology of thebull deformity bull Indications for surgery can be functionalbull aesthetic or most commonly both In individuals
with a compromised nasal airway a nasoseptalbull reconstruction is indicated
Nasal Deformity
bull Contraindications bull include patients with malignantbull chronic or autoimmune disease conditions drugbull abuse poor perioperative risk profile and unrealisticbull expectationsbull ndash Multiple previous rhinoplasties and certain
professionsbull (mixed martial artists boxers and other contactbull sports) are relative contraindications
Nasal DeformitySeptoplastyndash Septoplasty is performed to correct nasal obstructioncaused by septal deformityndash Usually septoplasty is performed under general anaesthesiawith the patient in the supine position with the head elevated by approximately 30 (Righthandedsurgeons approach from the right side)ndash Local vasoconstrictive anaesthesia is applied notonly to reduce postoperative pain but also more importantly to achieve vasoconstriction of themucosa and less intraoperative haemorrhage Lidocainewith adrenaline or epinephrine is usedalthough in patients with cardiac hypersensitivityoxymetazoline might be preferred
Nasal Deformity
bull Septoplasty begins with the incision of septal mucosabull Most operative techniques utilise a hemitransfixionbull incision at the caudal end of septum so thatbull deviation at this point might be reached as wellbull as a transfixion incision that is easily obtained ifbull needed (Right-handed surgeons normally choosebull the left side but that may vary when deviation isbull convex towards the right)
Nasal DeformityA columella retractor is placed over the columellaand by pulling it laterally the caudal border of theseptum is exposed Ala can be protected by an alaprotector A vertical incision with a no 15 bladeover the caudal end of septum is performed untilreaching the plane of the septal cartilage It is essentialto correctly identify the perichondrium and byusing the Cottle elevator dissect and lift it creatinga flap As the dissection proceeds along the septalcartilage a longer speculum (no 5) is introduced sothat elevation of the mucoperichondrium is doneunder constant visual controlndash The next step is to dissect the mucoperiostium
Nasal DeformityDissecting over the bony-cartilaginous junctionwhen joining both tunnels might be difficult and is
especially prone to membrane perforationndash If needed the same tunnels are to be created on the
other side of the septum Then deviated parts of
septum are identified and removed either with a
knife or a Freer chisel
Nasal Deformitybull septum from the maxillary crest the septum mustbull be separated from the perpendicular plate trimmedbull along the inferior border placed back onto the crestbull and sutured to the periosteum If the deformity involvesbull the vomer an osteotome is used Care mustbull be taken not to break the cribriform plate becausebull it could cause a cerebrospinal fistula
Nasal Deformity
bull Once the septal deviation is corrected the flapsbull and hemitransfixion incision are mattressed
withbull absorbable sutures Nasal packing to prevent
synechiaebull and postoperative septal haematoma mightbull be advised but should be removed within 72 h

Anatomy of the nasal base
bull The nasal septum is subluxed toward the left side partially
bull obstructing the nasal airway
Nasal CavitiesThe nasal cavities begin anteriorly at the nasal vestibulewhich is bordered posteriorly by the internal nasalvalve (limen nasi) located between the posteriorborder of the alar cartilage and the anterior border ofthe lateral cartilage This valve area is the narrowestportion of the upper respiratory tract
Nasal Cavities
The interior ofthe nose behind the nasal valve is divided by the nasalseptum into two main cavities
Nasal CavitiesThe nasal septum iscomposed of an anterior cartilaginous part and twoposterior bony parts Abnormalities in the shape ofthe nasal septum which may consist of a deviated septum tensionseptum spurs or ridges are a frequent cause ofnasal airway obstructionThe choanae are the paired posterior openingsthrough which the nasal cavities communicate withthe nasopharynx
Nasal CavitiesThe nasal cavity is bounded laterally by the lateral nasalwalls which are formed by the ethmoid bone andmaxilla and posteriorly by the palatine bone and thepterygoid process of the sphenoid bone Several functionallyimportant structures are located on the lateralnasal wall the nasal turbinates and their associatedpassages (meati) sinus ostia and the orifice ofthe nasolacrimal duct (Fig 15)
The inferior turbinate consists of a separate bone thatis attached to the medial wall of the maxillary sinusThe opening of the nasolacrimal duct is located in thecorresponding inferior meatus The middle andsuperior turbinates are part of the ethmoid bone In rare cases a rudimentary ldquosupreme turbinaterdquo is alsopresent above the superior turbinate
The middle turbinate has by far the greatest functionalimportance because most of the drainage tracts fromthe surrounding paranasal sinuses open into the middlemeatus The nasal cavity is bounded superiorly by the cribriformplate of the ethmoid bone This thin bony platehas numerous openings for the passage of the fila olfactoriaand also forms the boundary of the anteriorcranial fossa
Nasal Cavities
The floor of the nasal cavity is formedmostly by the hard palate which is formed in turn bythe two palatine processes of the maxilla and the horizontallaminae of the palatine bone
Structure of the lateral nasal wall
Inferior meatus
Paranasal Sinuses
The paranasal sinuses are air-filled cavities that communicatewith the nasal cavities
-The maxillary sinus frontalsinus and anterior ethmoid cells drain into the nasalcavity through the middle meatusmdashie below themiddle turbinate -The posterior ethmoidcells drain into the nasal cavity through the superiormeatus The ostium of the sphenoid sinus is locatedin the anterior wall directly above the choanae- The anatomical connections between the nasal cavity andparanasal sinuses are functionally important and playa key role in the pathogenesis of many rhinologic diseasesthat involve the paranasal sinuses
Vascular SupplyThe external nose derives most of its blood supply
from the facial artery which arises from the external
carotid artery and from the ophthalmic artery which
springs from the internal carotid artery
Vascular Supply
The internalnose receives blood from the territories of the externaland internal carotid arteries- the terminalbranches of the sphenopalatine artery which arisesfrom the maxillary artery - the anterior and posteriorethmoid arteries which arise from the ophthalmicartery-internal carotid arterie
venous drainage
The venous drainageof the facial region is handled by -the facial vein -retromandibular vein -internal jugular vein
lymphatic drainage
The regional lymphatic drainage of the face and externalnose is handled mainly by- the submandibularlymph nodes while the nasal cavity is additionallydrained by -the retropharyngeal and deep - -cervical lymph nodes
Morphology of the Nasal Mucosa
Besides the anatomical structure of the external noseand nasal cavity the nasal mucosa plays an essentialrole in numerous functions of the nose in the respiratory tract
Morphology of the Nasal Mucosa
The anterior part of the nasal cavity (the nasal vestibule)like the external nose is covered by skin composedof a multilayer keratinizing squamous epithelium and finally a ciliated respiratory epithelium A small areaon the upper nasal septum superior turbinate andpart of the middle turbinate located adjacent to thecribriform plate is covered by olfactory mucosa and iscalled the olfactory region
Nerve SupplyThe facial skin receives its sensory innervation fromterminal branches of the trigeminal nerve that enterthe facial region through the supraorbital infraorbitaland mental foramina Thefacial muscles are classified as mimetic or mastica- tory each of these groups receiving different motorinnervationbythe facial nerve
History and Clinical Examination of the Nose
Historybull The main symptomsbull nasal obstruction (ldquostuffy
noserdquo)bull nasal dischargebull Headachesbull Olfactory
dysfunction
Palpationbony discontinuitiesNeuralgias to check
over- the supraorbital -infraorbital -mental foramina
Anterior Rhinoscopy
bull The rhinologic examination itself begins with anterior
bull rhinoscopy to evaluate the nasal vestibule and the anterior
bull portions of the nasal cavity
Nasal Endoscopy Nasal endoscopy has become the most important andrewarding clinical examination method in rhinologic diagnosis
- rigid endoscopes which are available in 4-mm and 28- mm diameters and assorted viewing angles (eg 01048576 301048576 1201048576) -flexible endoscopes are also available for inspecting the nose and nasopharynx and exploring all of the pharynx and larynx in one sitting
Nasal endoscopy
Nasal Endoscopy
Nasal Endoscopy
Imaging of the Nose and Paranasal Sinuses
Conventional RadiographsStandard paranasal sinus radiographs in the occipitomental
projection ( Water projection) and
occipitofrontal projection Caldwell projection) in cases of acute inflammation
They are also obtained to evaluate midfacial fractures
Computed Tomography (CT) the main indicationsfor CT scanning of the
nose and paranasal sinuses
are- chronic sinusitis - -trauma (especially
frontobasal -fractures)
-and tumors
The occipitofrontal projection is better for evaluating theethmoid cells and frontal sinus
occipitomental projection demonstrates the maxillarysinus and gives a limited view of the sphenoid sinus
Computed tomography of the paranasal sinuses
Four representative coronal CT scans are shown
Four representative coronal CT scans are shown
Magnetic Resonance Imaging
Magnetic maging
Magnetic resonance imaging (MRI) has fewer indicationsthan CT in patients with paranasal sinus diseaseThis is primarily because MRI is markedly inferior toCT in defining the bony boundaries of the sinusesThe strength of MRI lies in its superior soft-tissue discriminationMRI is indicated in diseases that involve the paranasal sinuses in addition to thecranial cavity or orbit (eg tumors and congenitalmalformations such as encephaloceles)
MRI of the paranasal sinuses
The Nose and Sinuses
Structure The structure of the nose is made up of
four partsbull The surface anatomybull The nasal skeletonmdashcomposed of the
two nasal bones the paired upper lateral and lower lateral cartilages and the nasal septum covered in subcutaneous tissue and skin
bull The internal anatomymdashincludes the septum of the nose which forms the medial wall of the nasal cavity The turbinates on the lateral wall are also called conchae
bull The osteomeatal complexmdasha key functional area of the nose
Function The nose is the main route for inspired
air and its structure is related to this function As the air passes over the large surface area of the turbinates
The inspired gases are warmed and humidified Mucus on the mucosa of the nose removes large dust particles from the air as it is breathed in
The voice resonates in the sinuses and nose and this provides character to the speech
Pneumatization of the sinusesmdashthey are air filled spacesmdashreduces the weight of the skull
Diseases of thDiseases of the Outer and Inner Nosee Outer and
Inner Nose Erysipelas Definition of the disease ndash Erysipela is a skin infection that affects the superficial dermis and is caused by Streptococcus pyogenes (group A) It usually develops in the extremities and the face and less commonly on the scalp and genitals bull Epidemiologyaetiology ndash Erysipelas are more often seen in elderly infants and children patients with compromised immunology and diabetes -Predisposing factors are alcoholism skin ulceration puncture wounds fungal infections malnutrition and burns
Erysipelas
bull Symptomsbull ndash It usually presents of fever general fatigue bull -The skin lesion is a redindurated and elevated plaque
with borders that expand rapidly bull It is painful warm and accompanied by variable oedemabull -On the second or third day a flaccid bulla may develop
and desquamationbull bull Presence of regional lymph nodes is common
Erysipelas
bull Complicationsndash The most common complication is recurrencewhich is seen in 18ndash30 of the cases even afterproper antibiotic therapy Recurrence is seen moreoften in females than in malesA skin infection with S pyogenes could lead toglomerulonephritis
Erysipelas
bull Complicationsbull ndash The most common complication is recurrencebull which is seen in 18ndash30 of the cases even afterbull proper antibiotic therapy bull -Recurrence is seen morebull often in females than in males bull -A skin infection with S pyogenes could lead tobull glomerulonephritis
Erysipelas
bull bull Diagnosisbull ndash Diagnosis is based on the patientrsquos personal
historybull and physical examination particularly on inspectionbull of the skin
bull Blood cultures are positive in less thanbull 5 of cases
ErysipelasTherapyndash Conservative therapybull The preferred antibiotic is penicillin In mildcases with minor systemic symptoms penicillinV 500 mg orally every 6 h for 10 days or penicillinG benzathine 12 mil U intramuscularlyonceOther possibilities are amoxicillin 500 mgorally twice a day for 10 days or cephalexin 500mg orally every 6 h for 10 days
ErysipelasIn moderate and severe cases with significantsystemic symptoms hospitalization and intravenoustreatment is required penicillin G 2ndash4mil U intravenously every 4ndash6 h Cefazolin05ndash15 gm intravenously every 8 h cefotaxime1ndash2 gm intravenously every 8 h or ceftriaxone1ndash2 gm intravenously once a day should be administeredIn patients with a penicillin allergyclindamycin 600 mg intravenously every 8 h orvancomycin 15 mgkg intravenously twice a daymay be given
ErysipelaAdditional useful therapeutic optionsbull Prednisone 30 mg over 8 days might be consideredas well as elevation of the affected siteMoist heat compresses may be usefulbull Surgeryndash Debridement and drainage are indicated when bullaeabscesses or necroses are presentbull Differential diagnosisndash Contact dermatitisndash Asteatotic eczemandash Herpes zosterndash Angioneurotic oedemandash Osteomyelitis
Furuncle
bull Definition of the diseasebull ndash A furuncle is an infection that beginsbull at the hair follicle and spreads deeper into thebull dermis and subcutaneous tissue forming abull nodule After several days it developsbull into an abscess - red painful and fluctuantbull bull bull Epidemiologyaetiologybull ndash The aetiologic agent is Staphylococcus aureus
FuruncleSymptomsndashsymptoms are local and limited to thesite of infection Furuncles usually are wherehair follicles are present bull Complicationndash One complication is furunculosis multiple draining furunclesDiagnosisndash The diagnosis is based on clinical inspection - Cultures are not necessary when there is no systemic involvement but should beconsidered if systemic therapy (in case of feversignificant cellulitis or hospitalization) or whenmethicillin-resistant Staphylococcusaureus (MRSA) is considered
FuruncleTherapyndash When the furuncle is small application of moist heat compress to promote drainage -Larger furuncles should be drained by surgical incision-After drainage the area should be cleaned with anantiseptic (with chlorhexidinebetadine) should be applied twice
a dayndash If no systemic symptoms or extensive cellulitis arepresent simple topical care is usually curative andoral antibiotics are not necessary Otherwise systemictreatment is indicated and should cover anypossible MRSA
Furuncle
bull -Recommended antibiotics are trimethoprim-sulfamethoxazole
bull 1ndash2 tablets orally twice daily doxycyclinebull 100 mg orally twice dailybull or clindamycin 300ndash450 mg orally every 8 hbull - In severe cases vancomycin 15 mgkg
intravenouslybull every 12 h or clindamycin 600 mg intravenouslybull every 8 h
Midline Granulomabull A midline granuloma is an angiocentricbull lymphoma it was referred to as polymorphicbull reticulosis lethal midline granuloma and midline
malignant reticulosisbull bull Definition of the diseasebull ndash This rare disease is a lymphoma of extranodal
presentationall cases are positive for the Epstein-Barr virus
bull -This lymphoma most commonly appears in the midface region
Midline GranulomaEpidemiologyaetiologyndash This form of lymphoma is rare in Europe and theUnited States with a higher prevalence in Asia and PeruSymptomsndash The most common presentation is nasal obstruction with a destructive mass occupying the nosesinuses and palate
-Fever night sweatsand weight loss seen usually in Hodgkinrsquos lymphomaand other non-Hodgkinrsquos lymphomas (knownas ldquoB symptomsrdquo) are uncommon
Midline GranulomaDiagnosisndash The diagnosis is based on anatomopathologicalstudy The malignancy of the tumour manifested byextensive necrosis makes the histological diagnosisdifficult and often more biopsies are required forconfirmationbull Therapyndash Therapy consists of radiotherapy with or withoutchemotherapy
Midline Granuloma
bull Prognosisbull ndash Depending on the stage long-term remission or
experience a worseningbull prognosis with relapses which may include otherbull extranodal sites bull Involvement of extranodal sitesbull including the upper airway gastrointestinal tractbull skin
Wegenerrsquos Granulomatosis
bull Definition of the diseasebull ndash Wegenerrsquos granulomatosis is a systemic chronicbull vasculitis of small- and medium-sized blood vesselsbull with an autoimmune component It affectsbull particular organs with variable predilectionbull Epidemiologyaetiologybull ndash Wegenerrsquos granulomatosis is a rare disease It affects
about 1 in 20000ndash30000 people It is more prevalentbull in middle-aged Caucasian patients
Wegenerrsquos Granulomatosis
Symptomsndash The disease may present pulmonary upper
respiratory tract or renal In the disseminated form-The localised form ndash confinedto the upper respiratory region ndash is present in 25of the patients- It consists of nonspecific manifestationssuch as nasal obstruction crusting purulentor bloody rhinorrhea and painful or painless ulcers in oral or nasal cavities which are unresponsive tostandard medical treatment
Wegenerrsquos Granulomatosis
bull In some patients the nasal septum is perforatedbull which leads to saddle-nose deformity Less
commonbull symptoms are hoarseness stridor due to
subglotticbull stenosis otalgia otorrhea and conductivebull and sensorineural hearing loss Also ocular
symptomsbull such as scleritis conjunctivitis uveitis andbull episcleritis may be present
Wegenerrsquos Granulomatosis
bull ndash In the disseminated form pulmonary involvementbull is manifested by cough dyspnoea haemoptysisbull (due to an alveolar capillaritis necrotic lesions orbull endobronchial disease) and pleuritic painndashbull -Ninety per cent of patients have nasal symptomsbull and these symptoms are usually the first
manifestationof the diseasebull -Most patients have also renal involvementbull even if it is subclinical
Wegenerrsquos Granulomatosis
Diagnosis ndash Diagnosis of Wegenerrsquos granulomatosis is based on clinical findings that demonstrate lung (chest x-ray) kidney (urine analysis) or upper respiratory tract
involvement (oral or nasal ulcers or discharge) - positive blood analysis for cytoplasmic-staining antineutrophil
cytoplasmic antibodies (c-ANCA) and confirming proteinase 3 (PR3) ANCA or myeloperoxidase (MPO) ANCA ndash Biopsy is essential for diagnosis nonspecific chronic inflammation
and necrosis -Bacterial and fungal infections
Wegenerrsquos Granulomatosis
Therapyndash Conservative therapybull In the induction of disease remission highdosesteroids (e g prednisone 1 mgkgday) for1 month with tapering over several months aregiven In addition cyclophosphamide (2 mgkgday) should be administered for 6ndash12 monthsuntil symptoms disappear In the maintenanceof remission cyclophosphamide should be
Wegenerrsquos Granulomatosis
Antibiotics mainly trimethoprim-sulfamethoxazoleare given for prophylaxis againstPneumocystis jiroveci (formerly Pneumocystiscarinii) pneumonia (PCP) which may developduring immunosuppression and have a role inpreventing recurrencesbull Sinonasal manifestations may be treated with topical nasal steroids and nasal irrigations lowdosesystemic steroids and antibiotics when bacterial infection (typically Staphylococcus species) is suspected
Wegenerrsquos Granulomatosis
bull Prognosisbull ndash Most of the patients respond well to treatmentbull achieving symptom-free intervals of 5ndash20 yearsbull or more bull -Anatomical problems (sinusitis trachealbull stenosis) may require surgery bull Relapses can be long and troublesomebull Long-term complications are chronicbull renal failure hearing loss and deafness
Nasal Fractures Definition ndash A nasal fracture is a disruption of the nasal bone structure due to trauma It is the most frequently fractured facial bone Epidemiologyaetiology ndash Sports falls and assaults are the usual mechanisms of fracture -Males are affected twice as often as are females -Paediatric populations with a incidences during the second and third decades of life -Variables such as force impact direction nature of the striking object age and other will influence the pattern of injury to the components of the nose
Nasal Fractures
bull Symptomsbull ndash Deformity swelling epistaxis and periorbital
ecchymosis are signs that are suggestive of nasal fracture
bull bony crepitus and nasal segment mobilitybull ndash Epiphora bull Severe bilateral injuries to the lachrymal bones
arebull associated with depressed nasal fractures
Nasal Fractures Complications ndash Septal haematoma is one of the most severe early complications of nasal trauma and without drainage it results in abscess formation 6ndash7 days after trauma producing necrosis of the septal cartilage -Long-term problems such as saddle-nose deformity perforation columellar retraction and nasalbase
Septal infection could lead to osteomyelitis orbital and intracranial abscesses meningitis and cavernous sinus thrombosis -Cerebrospinal fluid leakage is a common complication of severe
nasal and frontal fractures
Nasal Fractures
bull Diagnostic proceduresbull ndash Inspectionbull bull Changes of appearance such as deviation andbull asymmetry bleeding watery drainage changesbull in nasal breathing and smell It is useful to comparebull the current presentation with old photographsbull (up to 40 of normal individuals havebull significant nose malformations)
Nasal Fractures Physical examination bull The diagnosis of a nasal fracture is made primarily by physical examination epistaxis nasal swelling and periorbital ecchymosis Nasal shape in the lateral and frontal inspection should be assessed Grasping the dorsum between two fingers and rocking the pyramid back and forth aids in assessing the mobility of nasal bones Internal structures should be evaluated by using a headlight and nasal speculum Clotted blood is removed by suction and assessment of haematoma mucosal tears and active bleeding is performed Bimanual palpation of the septum helps to differentiate septal swelling from haematoma ndash
Nasal FracturesRadiographybull There is no clear evidence of the role of radiographyin the management of nasal fracturesPlain films have up to a 66 false-positive rateas a result of misinterpretation of normal suturelines In addition old fractures are difficult todistinguishbull Three-dimensional CT is recommended for extensiveinjuries involving the nasal-orbital-ethmoidalcomplexndash
Nasal Fractures
bull Additionaluseful diagnostic proceduresbull bull Using a 0 or 30deg 4-mm endoscope is helpful inbull the assessment of posterior abnormalities If thebull patient is heavily sedated Brown-Gruss
provocationbull manoeuvres may be performed to determinebull deformities in upper middle or lower segmentsbull by compressing each compartment
Nasal FracturesConservative treatmentndash Treatment of bleedingbull For localised bleeding anterior sources may becauterised by silver nitrate or sealed with topicalmaterials such as thrombin combined withgelatin foam fibrin glue FloSealreg or other procoagulantmaterials If conservative measuresfail a formal anterior packing is placedbull Bleeding from branches of sphenopalatine orethmoid vessels requires anterior-posteriorpacking
Nasal Fractures
bull bull Surgical methods such as direct endoscopic vessel
bull cauterization or ligation have been shown tobull offer better haemostasis and patient comfortbull Angiography with embolization can also be
consideredbull in cases refractory to more conservativebull approaches
Nasal Fractures
bull Type of reductionbull bull Nondisplaced fractures should be treated withbull observation alone Closed nasal reduction is thebull best choice for simple injuries (isolated unilateralbull with medial displacement)bull bull An open approach should be considered in
severebull trauma (bilateral depressed fractures)
Nasal Fracturesbull Surgical principlesbull ndash Topical anaesthesia with cotton pledgets soakedbull with 4 cocaine or 005 oxymethazoline combinedbull with 4 topical lidocaine should be appliedbull for 5ndash10 min Local anaesthesia should also be injectedbull (1 lidocaine and 1100000 epinephrine)bull along the septum lateral walls and floor of the nasalbull cavitybull bull
Nasal FracturesClosed reductionndashndash The nasal bones are grasped between two fingersand pressure is applied laterally in theopposite direction of the deviation A bluntelevator may be used from within the nose incases of significant medial collapse Walshamforceps can be of help Reduction of the septumshould be performed with the use ofAsch forceps
Nasal Fractures
bull To prevent collapse of the postreductionbull framework nasal packing should be placedbull for 3ndash5 days Septum splints are recommendedbull in comminuted septal fractures withbull severe mucosal lesions External nasal splintingbull for 10 days (Aquaplastreg Thermoplastreg)bull provides nasal protection Nasal saline spraysbull prevent crusting and oral antibiotics should
Nasal Fractures
bull Open reductionbull ndashndash Immediate repair of fractures by using
widebull surgical exposure reduction fixation and
reconstructionbull ndashndash The second option is delayed correctionbull (6 months or more) of persistent deformitiesbull using standard techniques of rhinoplasty
Deviated Nasal Septum
bull Definition of the diseasebull ndash Deviation of the nasal septum is a common causebull of unilateral nasal airway obstruction in which thebull nasal septum is displacedbull bull Epidemiologyaetiologybull ndash Developmental septal abnormalities Septal cartilage
damage in the neonatal period andbull during birth can cause severe septal deviation inbull the absence of a history of nasal trauma
Deviated Nasal Septum
bull Symptomsbull ndash Patients may present with a history of sinusitis
allergicbull rhinitis obstructive sleep apnoea previousbull nasal surgery or recent nasal trauma Unilateral or
bilateral nasal airway obstruction that is unrelievedbull with decongestants or nasal steroid sprays is oftenbull seenbull bull
Deviated Nasal SeptumDiagnosisndashExamination external dorsal deviation or the columella and caudal septummay be deflected off the midline (caudal subluxation)ndash Inspections of the nasal cavity and anterior-posteriorrhinoscopy are helpful in diagnosing the locationtype and severity of septal deformityThe endoscope is also useful in identifying polypsthe severity and extent of posterior septaldeviations and bony spurs and locating areas ofseptal perforation or mucosal injury
Deviated Nasal Septum
bull Therapybull ndash Septoplasty is a procedurebull The areabull of deviation is corrected or resected in order tobull leave behind as much cartilage and bone as
possiblebull Cartilage resection is minimised and can be
repositioned reshaped or recontoured using a variety of methods
Deviated Nasal Septum
bull ndash Indications of septoplasty before the growth period
bull of the nose is finished should be very limited bull -In these cases surgery must preserve all the
cartilagebull in order to prevent external changes of the
shape ofbull the nose
Deviated Nasal Septum
bull Complicationsbull ndash Frequent complications include haematoma andbull infection Cerebrospinal fluid leak is a rare but
potentiallybull serious complicationbull It is usually the resultbull of avulsion or damage to the cribriform plate whenbull handling the perpendicular plate of the ethmoidbull ndash Other complications include epistaxis nasal
Deviated Nasal Septum
bull Other complications include epistaxis nasal obstruction
bull due to residual deviation synechiae returnbull of the cartilaginous deviation septal perforationbull anosmia and cosmetic nasal deformities suchbull as widened alar rim margins drooping nasal tipbull columella retraction and a sunken dorsum with abull supratip saddle formation
Septal perforation with minor crusting View from provide closure of the
incision
Septal Haematoma
bull A septal haematoma is a blood collection under the perichondrium
bull of the septum and cartilagebull bull bull Epidemiologyaetiologybull ndash A septal haematoma is one of the most
severe complications of nasal trauma
Septal Haematoma
bull Diagnosisbull ndash Signs and symptoms include intense pain
swellingbull haematoma of the upper lip and philtrum
area andbull complete nasal airway obstruction
Septal HaematomaTherapyndash Management consists of drainage through a mucoperichondrial incision Immediate treatment isnecessary to prevent long-term problems such asa saddle-nose deformity perforation columellarretraction and nasal-base widening In childrenseptal destruction can lead to devastating nasal andmidfacial growth abnormalitiesbull Surgeryndash Incision and evacuation of the collection is performedDrainage of a septal haematoma should
Septal HaematomaSurgeryndash Incision and evacuation of the collection is performedDrainage of a septal haematoma should provide closure of the incision
Splints or transseptal sutures are placed to obliterate thepotential space and prevent collectionInfection involving the septal cartilage Reconstruction with autologouscartilage is then performed in a second stage Oral antibiotics should be given
Nasal DeformitySaddle-nose deformityndash A saddle-nose deformity is characterised by a loss ofnasal dorsal height and compromised nasal supportstructures -Other case observed are depressionof the middle vault and dorsum loss of nasal tipsupport and definition shortened (vertical) nasal length over rotation of the nasal tip and retrusion ofthe nasal spine and caudal septum It is also knownas a ldquoPug noserdquo or ldquoboxerrsquos noserdquo both of which referto various degrees of nasal dorsal depressionbull
Nasal DeformityEpidemiologyaetiologyndash Prevalence is higher in population groups prone to facial trauma (ie boxers athletes) those with historiesof intranasal cocaine use nasal surgery (e g radical submucosal septal resection reductive rhinoplasty)ndash A saddle-nose deformity can be congenital or acquired It can be noticed as a part of individual familialsyndromic and ethnic characteristics - Most deformities are due to traumatic and iatrogeniccauses Medical causes are Wegenerrsquosgranulomatosis relapsing polychondritis leprosy (Hansenrsquos disease) syphilis ectodermal dysplasiaand intranasal cocaine use
Nasal Deformity
bull Therapybull ndash Nasal reconstruction indications depend on patientbull selection surgeon experience and aetiology of thebull deformity bull Indications for surgery can be functionalbull aesthetic or most commonly both In individuals
with a compromised nasal airway a nasoseptalbull reconstruction is indicated
Nasal Deformity
bull Contraindications bull include patients with malignantbull chronic or autoimmune disease conditions drugbull abuse poor perioperative risk profile and unrealisticbull expectationsbull ndash Multiple previous rhinoplasties and certain
professionsbull (mixed martial artists boxers and other contactbull sports) are relative contraindications
Nasal DeformitySeptoplastyndash Septoplasty is performed to correct nasal obstructioncaused by septal deformityndash Usually septoplasty is performed under general anaesthesiawith the patient in the supine position with the head elevated by approximately 30 (Righthandedsurgeons approach from the right side)ndash Local vasoconstrictive anaesthesia is applied notonly to reduce postoperative pain but also more importantly to achieve vasoconstriction of themucosa and less intraoperative haemorrhage Lidocainewith adrenaline or epinephrine is usedalthough in patients with cardiac hypersensitivityoxymetazoline might be preferred
Nasal Deformity
bull Septoplasty begins with the incision of septal mucosabull Most operative techniques utilise a hemitransfixionbull incision at the caudal end of septum so thatbull deviation at this point might be reached as wellbull as a transfixion incision that is easily obtained ifbull needed (Right-handed surgeons normally choosebull the left side but that may vary when deviation isbull convex towards the right)
Nasal DeformityA columella retractor is placed over the columellaand by pulling it laterally the caudal border of theseptum is exposed Ala can be protected by an alaprotector A vertical incision with a no 15 bladeover the caudal end of septum is performed untilreaching the plane of the septal cartilage It is essentialto correctly identify the perichondrium and byusing the Cottle elevator dissect and lift it creatinga flap As the dissection proceeds along the septalcartilage a longer speculum (no 5) is introduced sothat elevation of the mucoperichondrium is doneunder constant visual controlndash The next step is to dissect the mucoperiostium
Nasal DeformityDissecting over the bony-cartilaginous junctionwhen joining both tunnels might be difficult and is
especially prone to membrane perforationndash If needed the same tunnels are to be created on the
other side of the septum Then deviated parts of
septum are identified and removed either with a
knife or a Freer chisel
Nasal Deformitybull septum from the maxillary crest the septum mustbull be separated from the perpendicular plate trimmedbull along the inferior border placed back onto the crestbull and sutured to the periosteum If the deformity involvesbull the vomer an osteotome is used Care mustbull be taken not to break the cribriform plate becausebull it could cause a cerebrospinal fistula
Nasal Deformity
bull Once the septal deviation is corrected the flapsbull and hemitransfixion incision are mattressed
withbull absorbable sutures Nasal packing to prevent
synechiaebull and postoperative septal haematoma mightbull be advised but should be removed within 72 h

Nasal CavitiesThe nasal cavities begin anteriorly at the nasal vestibulewhich is bordered posteriorly by the internal nasalvalve (limen nasi) located between the posteriorborder of the alar cartilage and the anterior border ofthe lateral cartilage This valve area is the narrowestportion of the upper respiratory tract
Nasal Cavities
The interior ofthe nose behind the nasal valve is divided by the nasalseptum into two main cavities
Nasal CavitiesThe nasal septum iscomposed of an anterior cartilaginous part and twoposterior bony parts Abnormalities in the shape ofthe nasal septum which may consist of a deviated septum tensionseptum spurs or ridges are a frequent cause ofnasal airway obstructionThe choanae are the paired posterior openingsthrough which the nasal cavities communicate withthe nasopharynx
Nasal CavitiesThe nasal cavity is bounded laterally by the lateral nasalwalls which are formed by the ethmoid bone andmaxilla and posteriorly by the palatine bone and thepterygoid process of the sphenoid bone Several functionallyimportant structures are located on the lateralnasal wall the nasal turbinates and their associatedpassages (meati) sinus ostia and the orifice ofthe nasolacrimal duct (Fig 15)
The inferior turbinate consists of a separate bone thatis attached to the medial wall of the maxillary sinusThe opening of the nasolacrimal duct is located in thecorresponding inferior meatus The middle andsuperior turbinates are part of the ethmoid bone In rare cases a rudimentary ldquosupreme turbinaterdquo is alsopresent above the superior turbinate
The middle turbinate has by far the greatest functionalimportance because most of the drainage tracts fromthe surrounding paranasal sinuses open into the middlemeatus The nasal cavity is bounded superiorly by the cribriformplate of the ethmoid bone This thin bony platehas numerous openings for the passage of the fila olfactoriaand also forms the boundary of the anteriorcranial fossa
Nasal Cavities
The floor of the nasal cavity is formedmostly by the hard palate which is formed in turn bythe two palatine processes of the maxilla and the horizontallaminae of the palatine bone
Structure of the lateral nasal wall
Inferior meatus
Paranasal Sinuses
The paranasal sinuses are air-filled cavities that communicatewith the nasal cavities
-The maxillary sinus frontalsinus and anterior ethmoid cells drain into the nasalcavity through the middle meatusmdashie below themiddle turbinate -The posterior ethmoidcells drain into the nasal cavity through the superiormeatus The ostium of the sphenoid sinus is locatedin the anterior wall directly above the choanae- The anatomical connections between the nasal cavity andparanasal sinuses are functionally important and playa key role in the pathogenesis of many rhinologic diseasesthat involve the paranasal sinuses
Vascular SupplyThe external nose derives most of its blood supply
from the facial artery which arises from the external
carotid artery and from the ophthalmic artery which
springs from the internal carotid artery
Vascular Supply
The internalnose receives blood from the territories of the externaland internal carotid arteries- the terminalbranches of the sphenopalatine artery which arisesfrom the maxillary artery - the anterior and posteriorethmoid arteries which arise from the ophthalmicartery-internal carotid arterie
venous drainage
The venous drainageof the facial region is handled by -the facial vein -retromandibular vein -internal jugular vein
lymphatic drainage
The regional lymphatic drainage of the face and externalnose is handled mainly by- the submandibularlymph nodes while the nasal cavity is additionallydrained by -the retropharyngeal and deep - -cervical lymph nodes
Morphology of the Nasal Mucosa
Besides the anatomical structure of the external noseand nasal cavity the nasal mucosa plays an essentialrole in numerous functions of the nose in the respiratory tract
Morphology of the Nasal Mucosa
The anterior part of the nasal cavity (the nasal vestibule)like the external nose is covered by skin composedof a multilayer keratinizing squamous epithelium and finally a ciliated respiratory epithelium A small areaon the upper nasal septum superior turbinate andpart of the middle turbinate located adjacent to thecribriform plate is covered by olfactory mucosa and iscalled the olfactory region
Nerve SupplyThe facial skin receives its sensory innervation fromterminal branches of the trigeminal nerve that enterthe facial region through the supraorbital infraorbitaland mental foramina Thefacial muscles are classified as mimetic or mastica- tory each of these groups receiving different motorinnervationbythe facial nerve
History and Clinical Examination of the Nose
Historybull The main symptomsbull nasal obstruction (ldquostuffy
noserdquo)bull nasal dischargebull Headachesbull Olfactory
dysfunction
Palpationbony discontinuitiesNeuralgias to check
over- the supraorbital -infraorbital -mental foramina
Anterior Rhinoscopy
bull The rhinologic examination itself begins with anterior
bull rhinoscopy to evaluate the nasal vestibule and the anterior
bull portions of the nasal cavity
Nasal Endoscopy Nasal endoscopy has become the most important andrewarding clinical examination method in rhinologic diagnosis
- rigid endoscopes which are available in 4-mm and 28- mm diameters and assorted viewing angles (eg 01048576 301048576 1201048576) -flexible endoscopes are also available for inspecting the nose and nasopharynx and exploring all of the pharynx and larynx in one sitting
Nasal endoscopy
Nasal Endoscopy
Nasal Endoscopy
Imaging of the Nose and Paranasal Sinuses
Conventional RadiographsStandard paranasal sinus radiographs in the occipitomental
projection ( Water projection) and
occipitofrontal projection Caldwell projection) in cases of acute inflammation
They are also obtained to evaluate midfacial fractures
Computed Tomography (CT) the main indicationsfor CT scanning of the
nose and paranasal sinuses
are- chronic sinusitis - -trauma (especially
frontobasal -fractures)
-and tumors
The occipitofrontal projection is better for evaluating theethmoid cells and frontal sinus
occipitomental projection demonstrates the maxillarysinus and gives a limited view of the sphenoid sinus
Computed tomography of the paranasal sinuses
Four representative coronal CT scans are shown
Four representative coronal CT scans are shown
Magnetic Resonance Imaging
Magnetic maging
Magnetic resonance imaging (MRI) has fewer indicationsthan CT in patients with paranasal sinus diseaseThis is primarily because MRI is markedly inferior toCT in defining the bony boundaries of the sinusesThe strength of MRI lies in its superior soft-tissue discriminationMRI is indicated in diseases that involve the paranasal sinuses in addition to thecranial cavity or orbit (eg tumors and congenitalmalformations such as encephaloceles)
MRI of the paranasal sinuses
The Nose and Sinuses
Structure The structure of the nose is made up of
four partsbull The surface anatomybull The nasal skeletonmdashcomposed of the
two nasal bones the paired upper lateral and lower lateral cartilages and the nasal septum covered in subcutaneous tissue and skin
bull The internal anatomymdashincludes the septum of the nose which forms the medial wall of the nasal cavity The turbinates on the lateral wall are also called conchae
bull The osteomeatal complexmdasha key functional area of the nose
Function The nose is the main route for inspired
air and its structure is related to this function As the air passes over the large surface area of the turbinates
The inspired gases are warmed and humidified Mucus on the mucosa of the nose removes large dust particles from the air as it is breathed in
The voice resonates in the sinuses and nose and this provides character to the speech
Pneumatization of the sinusesmdashthey are air filled spacesmdashreduces the weight of the skull
Diseases of thDiseases of the Outer and Inner Nosee Outer and
Inner Nose Erysipelas Definition of the disease ndash Erysipela is a skin infection that affects the superficial dermis and is caused by Streptococcus pyogenes (group A) It usually develops in the extremities and the face and less commonly on the scalp and genitals bull Epidemiologyaetiology ndash Erysipelas are more often seen in elderly infants and children patients with compromised immunology and diabetes -Predisposing factors are alcoholism skin ulceration puncture wounds fungal infections malnutrition and burns
Erysipelas
bull Symptomsbull ndash It usually presents of fever general fatigue bull -The skin lesion is a redindurated and elevated plaque
with borders that expand rapidly bull It is painful warm and accompanied by variable oedemabull -On the second or third day a flaccid bulla may develop
and desquamationbull bull Presence of regional lymph nodes is common
Erysipelas
bull Complicationsndash The most common complication is recurrencewhich is seen in 18ndash30 of the cases even afterproper antibiotic therapy Recurrence is seen moreoften in females than in malesA skin infection with S pyogenes could lead toglomerulonephritis
Erysipelas
bull Complicationsbull ndash The most common complication is recurrencebull which is seen in 18ndash30 of the cases even afterbull proper antibiotic therapy bull -Recurrence is seen morebull often in females than in males bull -A skin infection with S pyogenes could lead tobull glomerulonephritis
Erysipelas
bull bull Diagnosisbull ndash Diagnosis is based on the patientrsquos personal
historybull and physical examination particularly on inspectionbull of the skin
bull Blood cultures are positive in less thanbull 5 of cases
ErysipelasTherapyndash Conservative therapybull The preferred antibiotic is penicillin In mildcases with minor systemic symptoms penicillinV 500 mg orally every 6 h for 10 days or penicillinG benzathine 12 mil U intramuscularlyonceOther possibilities are amoxicillin 500 mgorally twice a day for 10 days or cephalexin 500mg orally every 6 h for 10 days
ErysipelasIn moderate and severe cases with significantsystemic symptoms hospitalization and intravenoustreatment is required penicillin G 2ndash4mil U intravenously every 4ndash6 h Cefazolin05ndash15 gm intravenously every 8 h cefotaxime1ndash2 gm intravenously every 8 h or ceftriaxone1ndash2 gm intravenously once a day should be administeredIn patients with a penicillin allergyclindamycin 600 mg intravenously every 8 h orvancomycin 15 mgkg intravenously twice a daymay be given
ErysipelaAdditional useful therapeutic optionsbull Prednisone 30 mg over 8 days might be consideredas well as elevation of the affected siteMoist heat compresses may be usefulbull Surgeryndash Debridement and drainage are indicated when bullaeabscesses or necroses are presentbull Differential diagnosisndash Contact dermatitisndash Asteatotic eczemandash Herpes zosterndash Angioneurotic oedemandash Osteomyelitis
Furuncle
bull Definition of the diseasebull ndash A furuncle is an infection that beginsbull at the hair follicle and spreads deeper into thebull dermis and subcutaneous tissue forming abull nodule After several days it developsbull into an abscess - red painful and fluctuantbull bull bull Epidemiologyaetiologybull ndash The aetiologic agent is Staphylococcus aureus
FuruncleSymptomsndashsymptoms are local and limited to thesite of infection Furuncles usually are wherehair follicles are present bull Complicationndash One complication is furunculosis multiple draining furunclesDiagnosisndash The diagnosis is based on clinical inspection - Cultures are not necessary when there is no systemic involvement but should beconsidered if systemic therapy (in case of feversignificant cellulitis or hospitalization) or whenmethicillin-resistant Staphylococcusaureus (MRSA) is considered
FuruncleTherapyndash When the furuncle is small application of moist heat compress to promote drainage -Larger furuncles should be drained by surgical incision-After drainage the area should be cleaned with anantiseptic (with chlorhexidinebetadine) should be applied twice
a dayndash If no systemic symptoms or extensive cellulitis arepresent simple topical care is usually curative andoral antibiotics are not necessary Otherwise systemictreatment is indicated and should cover anypossible MRSA
Furuncle
bull -Recommended antibiotics are trimethoprim-sulfamethoxazole
bull 1ndash2 tablets orally twice daily doxycyclinebull 100 mg orally twice dailybull or clindamycin 300ndash450 mg orally every 8 hbull - In severe cases vancomycin 15 mgkg
intravenouslybull every 12 h or clindamycin 600 mg intravenouslybull every 8 h
Midline Granulomabull A midline granuloma is an angiocentricbull lymphoma it was referred to as polymorphicbull reticulosis lethal midline granuloma and midline
malignant reticulosisbull bull Definition of the diseasebull ndash This rare disease is a lymphoma of extranodal
presentationall cases are positive for the Epstein-Barr virus
bull -This lymphoma most commonly appears in the midface region
Midline GranulomaEpidemiologyaetiologyndash This form of lymphoma is rare in Europe and theUnited States with a higher prevalence in Asia and PeruSymptomsndash The most common presentation is nasal obstruction with a destructive mass occupying the nosesinuses and palate
-Fever night sweatsand weight loss seen usually in Hodgkinrsquos lymphomaand other non-Hodgkinrsquos lymphomas (knownas ldquoB symptomsrdquo) are uncommon
Midline GranulomaDiagnosisndash The diagnosis is based on anatomopathologicalstudy The malignancy of the tumour manifested byextensive necrosis makes the histological diagnosisdifficult and often more biopsies are required forconfirmationbull Therapyndash Therapy consists of radiotherapy with or withoutchemotherapy
Midline Granuloma
bull Prognosisbull ndash Depending on the stage long-term remission or
experience a worseningbull prognosis with relapses which may include otherbull extranodal sites bull Involvement of extranodal sitesbull including the upper airway gastrointestinal tractbull skin
Wegenerrsquos Granulomatosis
bull Definition of the diseasebull ndash Wegenerrsquos granulomatosis is a systemic chronicbull vasculitis of small- and medium-sized blood vesselsbull with an autoimmune component It affectsbull particular organs with variable predilectionbull Epidemiologyaetiologybull ndash Wegenerrsquos granulomatosis is a rare disease It affects
about 1 in 20000ndash30000 people It is more prevalentbull in middle-aged Caucasian patients
Wegenerrsquos Granulomatosis
Symptomsndash The disease may present pulmonary upper
respiratory tract or renal In the disseminated form-The localised form ndash confinedto the upper respiratory region ndash is present in 25of the patients- It consists of nonspecific manifestationssuch as nasal obstruction crusting purulentor bloody rhinorrhea and painful or painless ulcers in oral or nasal cavities which are unresponsive tostandard medical treatment
Wegenerrsquos Granulomatosis
bull In some patients the nasal septum is perforatedbull which leads to saddle-nose deformity Less
commonbull symptoms are hoarseness stridor due to
subglotticbull stenosis otalgia otorrhea and conductivebull and sensorineural hearing loss Also ocular
symptomsbull such as scleritis conjunctivitis uveitis andbull episcleritis may be present
Wegenerrsquos Granulomatosis
bull ndash In the disseminated form pulmonary involvementbull is manifested by cough dyspnoea haemoptysisbull (due to an alveolar capillaritis necrotic lesions orbull endobronchial disease) and pleuritic painndashbull -Ninety per cent of patients have nasal symptomsbull and these symptoms are usually the first
manifestationof the diseasebull -Most patients have also renal involvementbull even if it is subclinical
Wegenerrsquos Granulomatosis
Diagnosis ndash Diagnosis of Wegenerrsquos granulomatosis is based on clinical findings that demonstrate lung (chest x-ray) kidney (urine analysis) or upper respiratory tract
involvement (oral or nasal ulcers or discharge) - positive blood analysis for cytoplasmic-staining antineutrophil
cytoplasmic antibodies (c-ANCA) and confirming proteinase 3 (PR3) ANCA or myeloperoxidase (MPO) ANCA ndash Biopsy is essential for diagnosis nonspecific chronic inflammation
and necrosis -Bacterial and fungal infections
Wegenerrsquos Granulomatosis
Therapyndash Conservative therapybull In the induction of disease remission highdosesteroids (e g prednisone 1 mgkgday) for1 month with tapering over several months aregiven In addition cyclophosphamide (2 mgkgday) should be administered for 6ndash12 monthsuntil symptoms disappear In the maintenanceof remission cyclophosphamide should be
Wegenerrsquos Granulomatosis
Antibiotics mainly trimethoprim-sulfamethoxazoleare given for prophylaxis againstPneumocystis jiroveci (formerly Pneumocystiscarinii) pneumonia (PCP) which may developduring immunosuppression and have a role inpreventing recurrencesbull Sinonasal manifestations may be treated with topical nasal steroids and nasal irrigations lowdosesystemic steroids and antibiotics when bacterial infection (typically Staphylococcus species) is suspected
Wegenerrsquos Granulomatosis
bull Prognosisbull ndash Most of the patients respond well to treatmentbull achieving symptom-free intervals of 5ndash20 yearsbull or more bull -Anatomical problems (sinusitis trachealbull stenosis) may require surgery bull Relapses can be long and troublesomebull Long-term complications are chronicbull renal failure hearing loss and deafness
Nasal Fractures Definition ndash A nasal fracture is a disruption of the nasal bone structure due to trauma It is the most frequently fractured facial bone Epidemiologyaetiology ndash Sports falls and assaults are the usual mechanisms of fracture -Males are affected twice as often as are females -Paediatric populations with a incidences during the second and third decades of life -Variables such as force impact direction nature of the striking object age and other will influence the pattern of injury to the components of the nose
Nasal Fractures
bull Symptomsbull ndash Deformity swelling epistaxis and periorbital
ecchymosis are signs that are suggestive of nasal fracture
bull bony crepitus and nasal segment mobilitybull ndash Epiphora bull Severe bilateral injuries to the lachrymal bones
arebull associated with depressed nasal fractures
Nasal Fractures Complications ndash Septal haematoma is one of the most severe early complications of nasal trauma and without drainage it results in abscess formation 6ndash7 days after trauma producing necrosis of the septal cartilage -Long-term problems such as saddle-nose deformity perforation columellar retraction and nasalbase
Septal infection could lead to osteomyelitis orbital and intracranial abscesses meningitis and cavernous sinus thrombosis -Cerebrospinal fluid leakage is a common complication of severe
nasal and frontal fractures
Nasal Fractures
bull Diagnostic proceduresbull ndash Inspectionbull bull Changes of appearance such as deviation andbull asymmetry bleeding watery drainage changesbull in nasal breathing and smell It is useful to comparebull the current presentation with old photographsbull (up to 40 of normal individuals havebull significant nose malformations)
Nasal Fractures Physical examination bull The diagnosis of a nasal fracture is made primarily by physical examination epistaxis nasal swelling and periorbital ecchymosis Nasal shape in the lateral and frontal inspection should be assessed Grasping the dorsum between two fingers and rocking the pyramid back and forth aids in assessing the mobility of nasal bones Internal structures should be evaluated by using a headlight and nasal speculum Clotted blood is removed by suction and assessment of haematoma mucosal tears and active bleeding is performed Bimanual palpation of the septum helps to differentiate septal swelling from haematoma ndash
Nasal FracturesRadiographybull There is no clear evidence of the role of radiographyin the management of nasal fracturesPlain films have up to a 66 false-positive rateas a result of misinterpretation of normal suturelines In addition old fractures are difficult todistinguishbull Three-dimensional CT is recommended for extensiveinjuries involving the nasal-orbital-ethmoidalcomplexndash
Nasal Fractures
bull Additionaluseful diagnostic proceduresbull bull Using a 0 or 30deg 4-mm endoscope is helpful inbull the assessment of posterior abnormalities If thebull patient is heavily sedated Brown-Gruss
provocationbull manoeuvres may be performed to determinebull deformities in upper middle or lower segmentsbull by compressing each compartment
Nasal FracturesConservative treatmentndash Treatment of bleedingbull For localised bleeding anterior sources may becauterised by silver nitrate or sealed with topicalmaterials such as thrombin combined withgelatin foam fibrin glue FloSealreg or other procoagulantmaterials If conservative measuresfail a formal anterior packing is placedbull Bleeding from branches of sphenopalatine orethmoid vessels requires anterior-posteriorpacking
Nasal Fractures
bull bull Surgical methods such as direct endoscopic vessel
bull cauterization or ligation have been shown tobull offer better haemostasis and patient comfortbull Angiography with embolization can also be
consideredbull in cases refractory to more conservativebull approaches
Nasal Fractures
bull Type of reductionbull bull Nondisplaced fractures should be treated withbull observation alone Closed nasal reduction is thebull best choice for simple injuries (isolated unilateralbull with medial displacement)bull bull An open approach should be considered in
severebull trauma (bilateral depressed fractures)
Nasal Fracturesbull Surgical principlesbull ndash Topical anaesthesia with cotton pledgets soakedbull with 4 cocaine or 005 oxymethazoline combinedbull with 4 topical lidocaine should be appliedbull for 5ndash10 min Local anaesthesia should also be injectedbull (1 lidocaine and 1100000 epinephrine)bull along the septum lateral walls and floor of the nasalbull cavitybull bull
Nasal FracturesClosed reductionndashndash The nasal bones are grasped between two fingersand pressure is applied laterally in theopposite direction of the deviation A bluntelevator may be used from within the nose incases of significant medial collapse Walshamforceps can be of help Reduction of the septumshould be performed with the use ofAsch forceps
Nasal Fractures
bull To prevent collapse of the postreductionbull framework nasal packing should be placedbull for 3ndash5 days Septum splints are recommendedbull in comminuted septal fractures withbull severe mucosal lesions External nasal splintingbull for 10 days (Aquaplastreg Thermoplastreg)bull provides nasal protection Nasal saline spraysbull prevent crusting and oral antibiotics should
Nasal Fractures
bull Open reductionbull ndashndash Immediate repair of fractures by using
widebull surgical exposure reduction fixation and
reconstructionbull ndashndash The second option is delayed correctionbull (6 months or more) of persistent deformitiesbull using standard techniques of rhinoplasty
Deviated Nasal Septum
bull Definition of the diseasebull ndash Deviation of the nasal septum is a common causebull of unilateral nasal airway obstruction in which thebull nasal septum is displacedbull bull Epidemiologyaetiologybull ndash Developmental septal abnormalities Septal cartilage
damage in the neonatal period andbull during birth can cause severe septal deviation inbull the absence of a history of nasal trauma
Deviated Nasal Septum
bull Symptomsbull ndash Patients may present with a history of sinusitis
allergicbull rhinitis obstructive sleep apnoea previousbull nasal surgery or recent nasal trauma Unilateral or
bilateral nasal airway obstruction that is unrelievedbull with decongestants or nasal steroid sprays is oftenbull seenbull bull
Deviated Nasal SeptumDiagnosisndashExamination external dorsal deviation or the columella and caudal septummay be deflected off the midline (caudal subluxation)ndash Inspections of the nasal cavity and anterior-posteriorrhinoscopy are helpful in diagnosing the locationtype and severity of septal deformityThe endoscope is also useful in identifying polypsthe severity and extent of posterior septaldeviations and bony spurs and locating areas ofseptal perforation or mucosal injury
Deviated Nasal Septum
bull Therapybull ndash Septoplasty is a procedurebull The areabull of deviation is corrected or resected in order tobull leave behind as much cartilage and bone as
possiblebull Cartilage resection is minimised and can be
repositioned reshaped or recontoured using a variety of methods
Deviated Nasal Septum
bull ndash Indications of septoplasty before the growth period
bull of the nose is finished should be very limited bull -In these cases surgery must preserve all the
cartilagebull in order to prevent external changes of the
shape ofbull the nose
Deviated Nasal Septum
bull Complicationsbull ndash Frequent complications include haematoma andbull infection Cerebrospinal fluid leak is a rare but
potentiallybull serious complicationbull It is usually the resultbull of avulsion or damage to the cribriform plate whenbull handling the perpendicular plate of the ethmoidbull ndash Other complications include epistaxis nasal
Deviated Nasal Septum
bull Other complications include epistaxis nasal obstruction
bull due to residual deviation synechiae returnbull of the cartilaginous deviation septal perforationbull anosmia and cosmetic nasal deformities suchbull as widened alar rim margins drooping nasal tipbull columella retraction and a sunken dorsum with abull supratip saddle formation
Septal perforation with minor crusting View from provide closure of the
incision
Septal Haematoma
bull A septal haematoma is a blood collection under the perichondrium
bull of the septum and cartilagebull bull bull Epidemiologyaetiologybull ndash A septal haematoma is one of the most
severe complications of nasal trauma
Septal Haematoma
bull Diagnosisbull ndash Signs and symptoms include intense pain
swellingbull haematoma of the upper lip and philtrum
area andbull complete nasal airway obstruction
Septal HaematomaTherapyndash Management consists of drainage through a mucoperichondrial incision Immediate treatment isnecessary to prevent long-term problems such asa saddle-nose deformity perforation columellarretraction and nasal-base widening In childrenseptal destruction can lead to devastating nasal andmidfacial growth abnormalitiesbull Surgeryndash Incision and evacuation of the collection is performedDrainage of a septal haematoma should
Septal HaematomaSurgeryndash Incision and evacuation of the collection is performedDrainage of a septal haematoma should provide closure of the incision
Splints or transseptal sutures are placed to obliterate thepotential space and prevent collectionInfection involving the septal cartilage Reconstruction with autologouscartilage is then performed in a second stage Oral antibiotics should be given
Nasal DeformitySaddle-nose deformityndash A saddle-nose deformity is characterised by a loss ofnasal dorsal height and compromised nasal supportstructures -Other case observed are depressionof the middle vault and dorsum loss of nasal tipsupport and definition shortened (vertical) nasal length over rotation of the nasal tip and retrusion ofthe nasal spine and caudal septum It is also knownas a ldquoPug noserdquo or ldquoboxerrsquos noserdquo both of which referto various degrees of nasal dorsal depressionbull
Nasal DeformityEpidemiologyaetiologyndash Prevalence is higher in population groups prone to facial trauma (ie boxers athletes) those with historiesof intranasal cocaine use nasal surgery (e g radical submucosal septal resection reductive rhinoplasty)ndash A saddle-nose deformity can be congenital or acquired It can be noticed as a part of individual familialsyndromic and ethnic characteristics - Most deformities are due to traumatic and iatrogeniccauses Medical causes are Wegenerrsquosgranulomatosis relapsing polychondritis leprosy (Hansenrsquos disease) syphilis ectodermal dysplasiaand intranasal cocaine use
Nasal Deformity
bull Therapybull ndash Nasal reconstruction indications depend on patientbull selection surgeon experience and aetiology of thebull deformity bull Indications for surgery can be functionalbull aesthetic or most commonly both In individuals
with a compromised nasal airway a nasoseptalbull reconstruction is indicated
Nasal Deformity
bull Contraindications bull include patients with malignantbull chronic or autoimmune disease conditions drugbull abuse poor perioperative risk profile and unrealisticbull expectationsbull ndash Multiple previous rhinoplasties and certain
professionsbull (mixed martial artists boxers and other contactbull sports) are relative contraindications
Nasal DeformitySeptoplastyndash Septoplasty is performed to correct nasal obstructioncaused by septal deformityndash Usually septoplasty is performed under general anaesthesiawith the patient in the supine position with the head elevated by approximately 30 (Righthandedsurgeons approach from the right side)ndash Local vasoconstrictive anaesthesia is applied notonly to reduce postoperative pain but also more importantly to achieve vasoconstriction of themucosa and less intraoperative haemorrhage Lidocainewith adrenaline or epinephrine is usedalthough in patients with cardiac hypersensitivityoxymetazoline might be preferred
Nasal Deformity
bull Septoplasty begins with the incision of septal mucosabull Most operative techniques utilise a hemitransfixionbull incision at the caudal end of septum so thatbull deviation at this point might be reached as wellbull as a transfixion incision that is easily obtained ifbull needed (Right-handed surgeons normally choosebull the left side but that may vary when deviation isbull convex towards the right)
Nasal DeformityA columella retractor is placed over the columellaand by pulling it laterally the caudal border of theseptum is exposed Ala can be protected by an alaprotector A vertical incision with a no 15 bladeover the caudal end of septum is performed untilreaching the plane of the septal cartilage It is essentialto correctly identify the perichondrium and byusing the Cottle elevator dissect and lift it creatinga flap As the dissection proceeds along the septalcartilage a longer speculum (no 5) is introduced sothat elevation of the mucoperichondrium is doneunder constant visual controlndash The next step is to dissect the mucoperiostium
Nasal DeformityDissecting over the bony-cartilaginous junctionwhen joining both tunnels might be difficult and is
especially prone to membrane perforationndash If needed the same tunnels are to be created on the
other side of the septum Then deviated parts of
septum are identified and removed either with a
knife or a Freer chisel
Nasal Deformitybull septum from the maxillary crest the septum mustbull be separated from the perpendicular plate trimmedbull along the inferior border placed back onto the crestbull and sutured to the periosteum If the deformity involvesbull the vomer an osteotome is used Care mustbull be taken not to break the cribriform plate becausebull it could cause a cerebrospinal fistula
Nasal Deformity
bull Once the septal deviation is corrected the flapsbull and hemitransfixion incision are mattressed
withbull absorbable sutures Nasal packing to prevent
synechiaebull and postoperative septal haematoma mightbull be advised but should be removed within 72 h

Nasal Cavities
The interior ofthe nose behind the nasal valve is divided by the nasalseptum into two main cavities
Nasal CavitiesThe nasal septum iscomposed of an anterior cartilaginous part and twoposterior bony parts Abnormalities in the shape ofthe nasal septum which may consist of a deviated septum tensionseptum spurs or ridges are a frequent cause ofnasal airway obstructionThe choanae are the paired posterior openingsthrough which the nasal cavities communicate withthe nasopharynx
Nasal CavitiesThe nasal cavity is bounded laterally by the lateral nasalwalls which are formed by the ethmoid bone andmaxilla and posteriorly by the palatine bone and thepterygoid process of the sphenoid bone Several functionallyimportant structures are located on the lateralnasal wall the nasal turbinates and their associatedpassages (meati) sinus ostia and the orifice ofthe nasolacrimal duct (Fig 15)
The inferior turbinate consists of a separate bone thatis attached to the medial wall of the maxillary sinusThe opening of the nasolacrimal duct is located in thecorresponding inferior meatus The middle andsuperior turbinates are part of the ethmoid bone In rare cases a rudimentary ldquosupreme turbinaterdquo is alsopresent above the superior turbinate
The middle turbinate has by far the greatest functionalimportance because most of the drainage tracts fromthe surrounding paranasal sinuses open into the middlemeatus The nasal cavity is bounded superiorly by the cribriformplate of the ethmoid bone This thin bony platehas numerous openings for the passage of the fila olfactoriaand also forms the boundary of the anteriorcranial fossa
Nasal Cavities
The floor of the nasal cavity is formedmostly by the hard palate which is formed in turn bythe two palatine processes of the maxilla and the horizontallaminae of the palatine bone
Structure of the lateral nasal wall
Inferior meatus
Paranasal Sinuses
The paranasal sinuses are air-filled cavities that communicatewith the nasal cavities
-The maxillary sinus frontalsinus and anterior ethmoid cells drain into the nasalcavity through the middle meatusmdashie below themiddle turbinate -The posterior ethmoidcells drain into the nasal cavity through the superiormeatus The ostium of the sphenoid sinus is locatedin the anterior wall directly above the choanae- The anatomical connections between the nasal cavity andparanasal sinuses are functionally important and playa key role in the pathogenesis of many rhinologic diseasesthat involve the paranasal sinuses
Vascular SupplyThe external nose derives most of its blood supply
from the facial artery which arises from the external
carotid artery and from the ophthalmic artery which
springs from the internal carotid artery
Vascular Supply
The internalnose receives blood from the territories of the externaland internal carotid arteries- the terminalbranches of the sphenopalatine artery which arisesfrom the maxillary artery - the anterior and posteriorethmoid arteries which arise from the ophthalmicartery-internal carotid arterie
venous drainage
The venous drainageof the facial region is handled by -the facial vein -retromandibular vein -internal jugular vein
lymphatic drainage
The regional lymphatic drainage of the face and externalnose is handled mainly by- the submandibularlymph nodes while the nasal cavity is additionallydrained by -the retropharyngeal and deep - -cervical lymph nodes
Morphology of the Nasal Mucosa
Besides the anatomical structure of the external noseand nasal cavity the nasal mucosa plays an essentialrole in numerous functions of the nose in the respiratory tract
Morphology of the Nasal Mucosa
The anterior part of the nasal cavity (the nasal vestibule)like the external nose is covered by skin composedof a multilayer keratinizing squamous epithelium and finally a ciliated respiratory epithelium A small areaon the upper nasal septum superior turbinate andpart of the middle turbinate located adjacent to thecribriform plate is covered by olfactory mucosa and iscalled the olfactory region
Nerve SupplyThe facial skin receives its sensory innervation fromterminal branches of the trigeminal nerve that enterthe facial region through the supraorbital infraorbitaland mental foramina Thefacial muscles are classified as mimetic or mastica- tory each of these groups receiving different motorinnervationbythe facial nerve
History and Clinical Examination of the Nose
Historybull The main symptomsbull nasal obstruction (ldquostuffy
noserdquo)bull nasal dischargebull Headachesbull Olfactory
dysfunction
Palpationbony discontinuitiesNeuralgias to check
over- the supraorbital -infraorbital -mental foramina
Anterior Rhinoscopy
bull The rhinologic examination itself begins with anterior
bull rhinoscopy to evaluate the nasal vestibule and the anterior
bull portions of the nasal cavity
Nasal Endoscopy Nasal endoscopy has become the most important andrewarding clinical examination method in rhinologic diagnosis
- rigid endoscopes which are available in 4-mm and 28- mm diameters and assorted viewing angles (eg 01048576 301048576 1201048576) -flexible endoscopes are also available for inspecting the nose and nasopharynx and exploring all of the pharynx and larynx in one sitting
Nasal endoscopy
Nasal Endoscopy
Nasal Endoscopy
Imaging of the Nose and Paranasal Sinuses
Conventional RadiographsStandard paranasal sinus radiographs in the occipitomental
projection ( Water projection) and
occipitofrontal projection Caldwell projection) in cases of acute inflammation
They are also obtained to evaluate midfacial fractures
Computed Tomography (CT) the main indicationsfor CT scanning of the
nose and paranasal sinuses
are- chronic sinusitis - -trauma (especially
frontobasal -fractures)
-and tumors
The occipitofrontal projection is better for evaluating theethmoid cells and frontal sinus
occipitomental projection demonstrates the maxillarysinus and gives a limited view of the sphenoid sinus
Computed tomography of the paranasal sinuses
Four representative coronal CT scans are shown
Four representative coronal CT scans are shown
Magnetic Resonance Imaging
Magnetic maging
Magnetic resonance imaging (MRI) has fewer indicationsthan CT in patients with paranasal sinus diseaseThis is primarily because MRI is markedly inferior toCT in defining the bony boundaries of the sinusesThe strength of MRI lies in its superior soft-tissue discriminationMRI is indicated in diseases that involve the paranasal sinuses in addition to thecranial cavity or orbit (eg tumors and congenitalmalformations such as encephaloceles)
MRI of the paranasal sinuses
The Nose and Sinuses
Structure The structure of the nose is made up of
four partsbull The surface anatomybull The nasal skeletonmdashcomposed of the
two nasal bones the paired upper lateral and lower lateral cartilages and the nasal septum covered in subcutaneous tissue and skin
bull The internal anatomymdashincludes the septum of the nose which forms the medial wall of the nasal cavity The turbinates on the lateral wall are also called conchae
bull The osteomeatal complexmdasha key functional area of the nose
Function The nose is the main route for inspired
air and its structure is related to this function As the air passes over the large surface area of the turbinates
The inspired gases are warmed and humidified Mucus on the mucosa of the nose removes large dust particles from the air as it is breathed in
The voice resonates in the sinuses and nose and this provides character to the speech
Pneumatization of the sinusesmdashthey are air filled spacesmdashreduces the weight of the skull
Diseases of thDiseases of the Outer and Inner Nosee Outer and
Inner Nose Erysipelas Definition of the disease ndash Erysipela is a skin infection that affects the superficial dermis and is caused by Streptococcus pyogenes (group A) It usually develops in the extremities and the face and less commonly on the scalp and genitals bull Epidemiologyaetiology ndash Erysipelas are more often seen in elderly infants and children patients with compromised immunology and diabetes -Predisposing factors are alcoholism skin ulceration puncture wounds fungal infections malnutrition and burns
Erysipelas
bull Symptomsbull ndash It usually presents of fever general fatigue bull -The skin lesion is a redindurated and elevated plaque
with borders that expand rapidly bull It is painful warm and accompanied by variable oedemabull -On the second or third day a flaccid bulla may develop
and desquamationbull bull Presence of regional lymph nodes is common
Erysipelas
bull Complicationsndash The most common complication is recurrencewhich is seen in 18ndash30 of the cases even afterproper antibiotic therapy Recurrence is seen moreoften in females than in malesA skin infection with S pyogenes could lead toglomerulonephritis
Erysipelas
bull Complicationsbull ndash The most common complication is recurrencebull which is seen in 18ndash30 of the cases even afterbull proper antibiotic therapy bull -Recurrence is seen morebull often in females than in males bull -A skin infection with S pyogenes could lead tobull glomerulonephritis
Erysipelas
bull bull Diagnosisbull ndash Diagnosis is based on the patientrsquos personal
historybull and physical examination particularly on inspectionbull of the skin
bull Blood cultures are positive in less thanbull 5 of cases
ErysipelasTherapyndash Conservative therapybull The preferred antibiotic is penicillin In mildcases with minor systemic symptoms penicillinV 500 mg orally every 6 h for 10 days or penicillinG benzathine 12 mil U intramuscularlyonceOther possibilities are amoxicillin 500 mgorally twice a day for 10 days or cephalexin 500mg orally every 6 h for 10 days
ErysipelasIn moderate and severe cases with significantsystemic symptoms hospitalization and intravenoustreatment is required penicillin G 2ndash4mil U intravenously every 4ndash6 h Cefazolin05ndash15 gm intravenously every 8 h cefotaxime1ndash2 gm intravenously every 8 h or ceftriaxone1ndash2 gm intravenously once a day should be administeredIn patients with a penicillin allergyclindamycin 600 mg intravenously every 8 h orvancomycin 15 mgkg intravenously twice a daymay be given
ErysipelaAdditional useful therapeutic optionsbull Prednisone 30 mg over 8 days might be consideredas well as elevation of the affected siteMoist heat compresses may be usefulbull Surgeryndash Debridement and drainage are indicated when bullaeabscesses or necroses are presentbull Differential diagnosisndash Contact dermatitisndash Asteatotic eczemandash Herpes zosterndash Angioneurotic oedemandash Osteomyelitis
Furuncle
bull Definition of the diseasebull ndash A furuncle is an infection that beginsbull at the hair follicle and spreads deeper into thebull dermis and subcutaneous tissue forming abull nodule After several days it developsbull into an abscess - red painful and fluctuantbull bull bull Epidemiologyaetiologybull ndash The aetiologic agent is Staphylococcus aureus
FuruncleSymptomsndashsymptoms are local and limited to thesite of infection Furuncles usually are wherehair follicles are present bull Complicationndash One complication is furunculosis multiple draining furunclesDiagnosisndash The diagnosis is based on clinical inspection - Cultures are not necessary when there is no systemic involvement but should beconsidered if systemic therapy (in case of feversignificant cellulitis or hospitalization) or whenmethicillin-resistant Staphylococcusaureus (MRSA) is considered
FuruncleTherapyndash When the furuncle is small application of moist heat compress to promote drainage -Larger furuncles should be drained by surgical incision-After drainage the area should be cleaned with anantiseptic (with chlorhexidinebetadine) should be applied twice
a dayndash If no systemic symptoms or extensive cellulitis arepresent simple topical care is usually curative andoral antibiotics are not necessary Otherwise systemictreatment is indicated and should cover anypossible MRSA
Furuncle
bull -Recommended antibiotics are trimethoprim-sulfamethoxazole
bull 1ndash2 tablets orally twice daily doxycyclinebull 100 mg orally twice dailybull or clindamycin 300ndash450 mg orally every 8 hbull - In severe cases vancomycin 15 mgkg
intravenouslybull every 12 h or clindamycin 600 mg intravenouslybull every 8 h
Midline Granulomabull A midline granuloma is an angiocentricbull lymphoma it was referred to as polymorphicbull reticulosis lethal midline granuloma and midline
malignant reticulosisbull bull Definition of the diseasebull ndash This rare disease is a lymphoma of extranodal
presentationall cases are positive for the Epstein-Barr virus
bull -This lymphoma most commonly appears in the midface region
Midline GranulomaEpidemiologyaetiologyndash This form of lymphoma is rare in Europe and theUnited States with a higher prevalence in Asia and PeruSymptomsndash The most common presentation is nasal obstruction with a destructive mass occupying the nosesinuses and palate
-Fever night sweatsand weight loss seen usually in Hodgkinrsquos lymphomaand other non-Hodgkinrsquos lymphomas (knownas ldquoB symptomsrdquo) are uncommon
Midline GranulomaDiagnosisndash The diagnosis is based on anatomopathologicalstudy The malignancy of the tumour manifested byextensive necrosis makes the histological diagnosisdifficult and often more biopsies are required forconfirmationbull Therapyndash Therapy consists of radiotherapy with or withoutchemotherapy
Midline Granuloma
bull Prognosisbull ndash Depending on the stage long-term remission or
experience a worseningbull prognosis with relapses which may include otherbull extranodal sites bull Involvement of extranodal sitesbull including the upper airway gastrointestinal tractbull skin
Wegenerrsquos Granulomatosis
bull Definition of the diseasebull ndash Wegenerrsquos granulomatosis is a systemic chronicbull vasculitis of small- and medium-sized blood vesselsbull with an autoimmune component It affectsbull particular organs with variable predilectionbull Epidemiologyaetiologybull ndash Wegenerrsquos granulomatosis is a rare disease It affects
about 1 in 20000ndash30000 people It is more prevalentbull in middle-aged Caucasian patients
Wegenerrsquos Granulomatosis
Symptomsndash The disease may present pulmonary upper
respiratory tract or renal In the disseminated form-The localised form ndash confinedto the upper respiratory region ndash is present in 25of the patients- It consists of nonspecific manifestationssuch as nasal obstruction crusting purulentor bloody rhinorrhea and painful or painless ulcers in oral or nasal cavities which are unresponsive tostandard medical treatment
Wegenerrsquos Granulomatosis
bull In some patients the nasal septum is perforatedbull which leads to saddle-nose deformity Less
commonbull symptoms are hoarseness stridor due to
subglotticbull stenosis otalgia otorrhea and conductivebull and sensorineural hearing loss Also ocular
symptomsbull such as scleritis conjunctivitis uveitis andbull episcleritis may be present
Wegenerrsquos Granulomatosis
bull ndash In the disseminated form pulmonary involvementbull is manifested by cough dyspnoea haemoptysisbull (due to an alveolar capillaritis necrotic lesions orbull endobronchial disease) and pleuritic painndashbull -Ninety per cent of patients have nasal symptomsbull and these symptoms are usually the first
manifestationof the diseasebull -Most patients have also renal involvementbull even if it is subclinical
Wegenerrsquos Granulomatosis
Diagnosis ndash Diagnosis of Wegenerrsquos granulomatosis is based on clinical findings that demonstrate lung (chest x-ray) kidney (urine analysis) or upper respiratory tract
involvement (oral or nasal ulcers or discharge) - positive blood analysis for cytoplasmic-staining antineutrophil
cytoplasmic antibodies (c-ANCA) and confirming proteinase 3 (PR3) ANCA or myeloperoxidase (MPO) ANCA ndash Biopsy is essential for diagnosis nonspecific chronic inflammation
and necrosis -Bacterial and fungal infections
Wegenerrsquos Granulomatosis
Therapyndash Conservative therapybull In the induction of disease remission highdosesteroids (e g prednisone 1 mgkgday) for1 month with tapering over several months aregiven In addition cyclophosphamide (2 mgkgday) should be administered for 6ndash12 monthsuntil symptoms disappear In the maintenanceof remission cyclophosphamide should be
Wegenerrsquos Granulomatosis
Antibiotics mainly trimethoprim-sulfamethoxazoleare given for prophylaxis againstPneumocystis jiroveci (formerly Pneumocystiscarinii) pneumonia (PCP) which may developduring immunosuppression and have a role inpreventing recurrencesbull Sinonasal manifestations may be treated with topical nasal steroids and nasal irrigations lowdosesystemic steroids and antibiotics when bacterial infection (typically Staphylococcus species) is suspected
Wegenerrsquos Granulomatosis
bull Prognosisbull ndash Most of the patients respond well to treatmentbull achieving symptom-free intervals of 5ndash20 yearsbull or more bull -Anatomical problems (sinusitis trachealbull stenosis) may require surgery bull Relapses can be long and troublesomebull Long-term complications are chronicbull renal failure hearing loss and deafness
Nasal Fractures Definition ndash A nasal fracture is a disruption of the nasal bone structure due to trauma It is the most frequently fractured facial bone Epidemiologyaetiology ndash Sports falls and assaults are the usual mechanisms of fracture -Males are affected twice as often as are females -Paediatric populations with a incidences during the second and third decades of life -Variables such as force impact direction nature of the striking object age and other will influence the pattern of injury to the components of the nose
Nasal Fractures
bull Symptomsbull ndash Deformity swelling epistaxis and periorbital
ecchymosis are signs that are suggestive of nasal fracture
bull bony crepitus and nasal segment mobilitybull ndash Epiphora bull Severe bilateral injuries to the lachrymal bones
arebull associated with depressed nasal fractures
Nasal Fractures Complications ndash Septal haematoma is one of the most severe early complications of nasal trauma and without drainage it results in abscess formation 6ndash7 days after trauma producing necrosis of the septal cartilage -Long-term problems such as saddle-nose deformity perforation columellar retraction and nasalbase
Septal infection could lead to osteomyelitis orbital and intracranial abscesses meningitis and cavernous sinus thrombosis -Cerebrospinal fluid leakage is a common complication of severe
nasal and frontal fractures
Nasal Fractures
bull Diagnostic proceduresbull ndash Inspectionbull bull Changes of appearance such as deviation andbull asymmetry bleeding watery drainage changesbull in nasal breathing and smell It is useful to comparebull the current presentation with old photographsbull (up to 40 of normal individuals havebull significant nose malformations)
Nasal Fractures Physical examination bull The diagnosis of a nasal fracture is made primarily by physical examination epistaxis nasal swelling and periorbital ecchymosis Nasal shape in the lateral and frontal inspection should be assessed Grasping the dorsum between two fingers and rocking the pyramid back and forth aids in assessing the mobility of nasal bones Internal structures should be evaluated by using a headlight and nasal speculum Clotted blood is removed by suction and assessment of haematoma mucosal tears and active bleeding is performed Bimanual palpation of the septum helps to differentiate septal swelling from haematoma ndash
Nasal FracturesRadiographybull There is no clear evidence of the role of radiographyin the management of nasal fracturesPlain films have up to a 66 false-positive rateas a result of misinterpretation of normal suturelines In addition old fractures are difficult todistinguishbull Three-dimensional CT is recommended for extensiveinjuries involving the nasal-orbital-ethmoidalcomplexndash
Nasal Fractures
bull Additionaluseful diagnostic proceduresbull bull Using a 0 or 30deg 4-mm endoscope is helpful inbull the assessment of posterior abnormalities If thebull patient is heavily sedated Brown-Gruss
provocationbull manoeuvres may be performed to determinebull deformities in upper middle or lower segmentsbull by compressing each compartment
Nasal FracturesConservative treatmentndash Treatment of bleedingbull For localised bleeding anterior sources may becauterised by silver nitrate or sealed with topicalmaterials such as thrombin combined withgelatin foam fibrin glue FloSealreg or other procoagulantmaterials If conservative measuresfail a formal anterior packing is placedbull Bleeding from branches of sphenopalatine orethmoid vessels requires anterior-posteriorpacking
Nasal Fractures
bull bull Surgical methods such as direct endoscopic vessel
bull cauterization or ligation have been shown tobull offer better haemostasis and patient comfortbull Angiography with embolization can also be
consideredbull in cases refractory to more conservativebull approaches
Nasal Fractures
bull Type of reductionbull bull Nondisplaced fractures should be treated withbull observation alone Closed nasal reduction is thebull best choice for simple injuries (isolated unilateralbull with medial displacement)bull bull An open approach should be considered in
severebull trauma (bilateral depressed fractures)
Nasal Fracturesbull Surgical principlesbull ndash Topical anaesthesia with cotton pledgets soakedbull with 4 cocaine or 005 oxymethazoline combinedbull with 4 topical lidocaine should be appliedbull for 5ndash10 min Local anaesthesia should also be injectedbull (1 lidocaine and 1100000 epinephrine)bull along the septum lateral walls and floor of the nasalbull cavitybull bull
Nasal FracturesClosed reductionndashndash The nasal bones are grasped between two fingersand pressure is applied laterally in theopposite direction of the deviation A bluntelevator may be used from within the nose incases of significant medial collapse Walshamforceps can be of help Reduction of the septumshould be performed with the use ofAsch forceps
Nasal Fractures
bull To prevent collapse of the postreductionbull framework nasal packing should be placedbull for 3ndash5 days Septum splints are recommendedbull in comminuted septal fractures withbull severe mucosal lesions External nasal splintingbull for 10 days (Aquaplastreg Thermoplastreg)bull provides nasal protection Nasal saline spraysbull prevent crusting and oral antibiotics should
Nasal Fractures
bull Open reductionbull ndashndash Immediate repair of fractures by using
widebull surgical exposure reduction fixation and
reconstructionbull ndashndash The second option is delayed correctionbull (6 months or more) of persistent deformitiesbull using standard techniques of rhinoplasty
Deviated Nasal Septum
bull Definition of the diseasebull ndash Deviation of the nasal septum is a common causebull of unilateral nasal airway obstruction in which thebull nasal septum is displacedbull bull Epidemiologyaetiologybull ndash Developmental septal abnormalities Septal cartilage
damage in the neonatal period andbull during birth can cause severe septal deviation inbull the absence of a history of nasal trauma
Deviated Nasal Septum
bull Symptomsbull ndash Patients may present with a history of sinusitis
allergicbull rhinitis obstructive sleep apnoea previousbull nasal surgery or recent nasal trauma Unilateral or
bilateral nasal airway obstruction that is unrelievedbull with decongestants or nasal steroid sprays is oftenbull seenbull bull
Deviated Nasal SeptumDiagnosisndashExamination external dorsal deviation or the columella and caudal septummay be deflected off the midline (caudal subluxation)ndash Inspections of the nasal cavity and anterior-posteriorrhinoscopy are helpful in diagnosing the locationtype and severity of septal deformityThe endoscope is also useful in identifying polypsthe severity and extent of posterior septaldeviations and bony spurs and locating areas ofseptal perforation or mucosal injury
Deviated Nasal Septum
bull Therapybull ndash Septoplasty is a procedurebull The areabull of deviation is corrected or resected in order tobull leave behind as much cartilage and bone as
possiblebull Cartilage resection is minimised and can be
repositioned reshaped or recontoured using a variety of methods
Deviated Nasal Septum
bull ndash Indications of septoplasty before the growth period
bull of the nose is finished should be very limited bull -In these cases surgery must preserve all the
cartilagebull in order to prevent external changes of the
shape ofbull the nose
Deviated Nasal Septum
bull Complicationsbull ndash Frequent complications include haematoma andbull infection Cerebrospinal fluid leak is a rare but
potentiallybull serious complicationbull It is usually the resultbull of avulsion or damage to the cribriform plate whenbull handling the perpendicular plate of the ethmoidbull ndash Other complications include epistaxis nasal
Deviated Nasal Septum
bull Other complications include epistaxis nasal obstruction
bull due to residual deviation synechiae returnbull of the cartilaginous deviation septal perforationbull anosmia and cosmetic nasal deformities suchbull as widened alar rim margins drooping nasal tipbull columella retraction and a sunken dorsum with abull supratip saddle formation
Septal perforation with minor crusting View from provide closure of the
incision
Septal Haematoma
bull A septal haematoma is a blood collection under the perichondrium
bull of the septum and cartilagebull bull bull Epidemiologyaetiologybull ndash A septal haematoma is one of the most
severe complications of nasal trauma
Septal Haematoma
bull Diagnosisbull ndash Signs and symptoms include intense pain
swellingbull haematoma of the upper lip and philtrum
area andbull complete nasal airway obstruction
Septal HaematomaTherapyndash Management consists of drainage through a mucoperichondrial incision Immediate treatment isnecessary to prevent long-term problems such asa saddle-nose deformity perforation columellarretraction and nasal-base widening In childrenseptal destruction can lead to devastating nasal andmidfacial growth abnormalitiesbull Surgeryndash Incision and evacuation of the collection is performedDrainage of a septal haematoma should
Septal HaematomaSurgeryndash Incision and evacuation of the collection is performedDrainage of a septal haematoma should provide closure of the incision
Splints or transseptal sutures are placed to obliterate thepotential space and prevent collectionInfection involving the septal cartilage Reconstruction with autologouscartilage is then performed in a second stage Oral antibiotics should be given
Nasal DeformitySaddle-nose deformityndash A saddle-nose deformity is characterised by a loss ofnasal dorsal height and compromised nasal supportstructures -Other case observed are depressionof the middle vault and dorsum loss of nasal tipsupport and definition shortened (vertical) nasal length over rotation of the nasal tip and retrusion ofthe nasal spine and caudal septum It is also knownas a ldquoPug noserdquo or ldquoboxerrsquos noserdquo both of which referto various degrees of nasal dorsal depressionbull
Nasal DeformityEpidemiologyaetiologyndash Prevalence is higher in population groups prone to facial trauma (ie boxers athletes) those with historiesof intranasal cocaine use nasal surgery (e g radical submucosal septal resection reductive rhinoplasty)ndash A saddle-nose deformity can be congenital or acquired It can be noticed as a part of individual familialsyndromic and ethnic characteristics - Most deformities are due to traumatic and iatrogeniccauses Medical causes are Wegenerrsquosgranulomatosis relapsing polychondritis leprosy (Hansenrsquos disease) syphilis ectodermal dysplasiaand intranasal cocaine use
Nasal Deformity
bull Therapybull ndash Nasal reconstruction indications depend on patientbull selection surgeon experience and aetiology of thebull deformity bull Indications for surgery can be functionalbull aesthetic or most commonly both In individuals
with a compromised nasal airway a nasoseptalbull reconstruction is indicated
Nasal Deformity
bull Contraindications bull include patients with malignantbull chronic or autoimmune disease conditions drugbull abuse poor perioperative risk profile and unrealisticbull expectationsbull ndash Multiple previous rhinoplasties and certain
professionsbull (mixed martial artists boxers and other contactbull sports) are relative contraindications
Nasal DeformitySeptoplastyndash Septoplasty is performed to correct nasal obstructioncaused by septal deformityndash Usually septoplasty is performed under general anaesthesiawith the patient in the supine position with the head elevated by approximately 30 (Righthandedsurgeons approach from the right side)ndash Local vasoconstrictive anaesthesia is applied notonly to reduce postoperative pain but also more importantly to achieve vasoconstriction of themucosa and less intraoperative haemorrhage Lidocainewith adrenaline or epinephrine is usedalthough in patients with cardiac hypersensitivityoxymetazoline might be preferred
Nasal Deformity
bull Septoplasty begins with the incision of septal mucosabull Most operative techniques utilise a hemitransfixionbull incision at the caudal end of septum so thatbull deviation at this point might be reached as wellbull as a transfixion incision that is easily obtained ifbull needed (Right-handed surgeons normally choosebull the left side but that may vary when deviation isbull convex towards the right)
Nasal DeformityA columella retractor is placed over the columellaand by pulling it laterally the caudal border of theseptum is exposed Ala can be protected by an alaprotector A vertical incision with a no 15 bladeover the caudal end of septum is performed untilreaching the plane of the septal cartilage It is essentialto correctly identify the perichondrium and byusing the Cottle elevator dissect and lift it creatinga flap As the dissection proceeds along the septalcartilage a longer speculum (no 5) is introduced sothat elevation of the mucoperichondrium is doneunder constant visual controlndash The next step is to dissect the mucoperiostium
Nasal DeformityDissecting over the bony-cartilaginous junctionwhen joining both tunnels might be difficult and is
especially prone to membrane perforationndash If needed the same tunnels are to be created on the
other side of the septum Then deviated parts of
septum are identified and removed either with a
knife or a Freer chisel
Nasal Deformitybull septum from the maxillary crest the septum mustbull be separated from the perpendicular plate trimmedbull along the inferior border placed back onto the crestbull and sutured to the periosteum If the deformity involvesbull the vomer an osteotome is used Care mustbull be taken not to break the cribriform plate becausebull it could cause a cerebrospinal fistula
Nasal Deformity
bull Once the septal deviation is corrected the flapsbull and hemitransfixion incision are mattressed
withbull absorbable sutures Nasal packing to prevent
synechiaebull and postoperative septal haematoma mightbull be advised but should be removed within 72 h

Nasal CavitiesThe nasal septum iscomposed of an anterior cartilaginous part and twoposterior bony parts Abnormalities in the shape ofthe nasal septum which may consist of a deviated septum tensionseptum spurs or ridges are a frequent cause ofnasal airway obstructionThe choanae are the paired posterior openingsthrough which the nasal cavities communicate withthe nasopharynx
Nasal CavitiesThe nasal cavity is bounded laterally by the lateral nasalwalls which are formed by the ethmoid bone andmaxilla and posteriorly by the palatine bone and thepterygoid process of the sphenoid bone Several functionallyimportant structures are located on the lateralnasal wall the nasal turbinates and their associatedpassages (meati) sinus ostia and the orifice ofthe nasolacrimal duct (Fig 15)
The inferior turbinate consists of a separate bone thatis attached to the medial wall of the maxillary sinusThe opening of the nasolacrimal duct is located in thecorresponding inferior meatus The middle andsuperior turbinates are part of the ethmoid bone In rare cases a rudimentary ldquosupreme turbinaterdquo is alsopresent above the superior turbinate
The middle turbinate has by far the greatest functionalimportance because most of the drainage tracts fromthe surrounding paranasal sinuses open into the middlemeatus The nasal cavity is bounded superiorly by the cribriformplate of the ethmoid bone This thin bony platehas numerous openings for the passage of the fila olfactoriaand also forms the boundary of the anteriorcranial fossa
Nasal Cavities
The floor of the nasal cavity is formedmostly by the hard palate which is formed in turn bythe two palatine processes of the maxilla and the horizontallaminae of the palatine bone
Structure of the lateral nasal wall
Inferior meatus
Paranasal Sinuses
The paranasal sinuses are air-filled cavities that communicatewith the nasal cavities
-The maxillary sinus frontalsinus and anterior ethmoid cells drain into the nasalcavity through the middle meatusmdashie below themiddle turbinate -The posterior ethmoidcells drain into the nasal cavity through the superiormeatus The ostium of the sphenoid sinus is locatedin the anterior wall directly above the choanae- The anatomical connections between the nasal cavity andparanasal sinuses are functionally important and playa key role in the pathogenesis of many rhinologic diseasesthat involve the paranasal sinuses
Vascular SupplyThe external nose derives most of its blood supply
from the facial artery which arises from the external
carotid artery and from the ophthalmic artery which
springs from the internal carotid artery
Vascular Supply
The internalnose receives blood from the territories of the externaland internal carotid arteries- the terminalbranches of the sphenopalatine artery which arisesfrom the maxillary artery - the anterior and posteriorethmoid arteries which arise from the ophthalmicartery-internal carotid arterie
venous drainage
The venous drainageof the facial region is handled by -the facial vein -retromandibular vein -internal jugular vein
lymphatic drainage
The regional lymphatic drainage of the face and externalnose is handled mainly by- the submandibularlymph nodes while the nasal cavity is additionallydrained by -the retropharyngeal and deep - -cervical lymph nodes
Morphology of the Nasal Mucosa
Besides the anatomical structure of the external noseand nasal cavity the nasal mucosa plays an essentialrole in numerous functions of the nose in the respiratory tract
Morphology of the Nasal Mucosa
The anterior part of the nasal cavity (the nasal vestibule)like the external nose is covered by skin composedof a multilayer keratinizing squamous epithelium and finally a ciliated respiratory epithelium A small areaon the upper nasal septum superior turbinate andpart of the middle turbinate located adjacent to thecribriform plate is covered by olfactory mucosa and iscalled the olfactory region
Nerve SupplyThe facial skin receives its sensory innervation fromterminal branches of the trigeminal nerve that enterthe facial region through the supraorbital infraorbitaland mental foramina Thefacial muscles are classified as mimetic or mastica- tory each of these groups receiving different motorinnervationbythe facial nerve
History and Clinical Examination of the Nose
Historybull The main symptomsbull nasal obstruction (ldquostuffy
noserdquo)bull nasal dischargebull Headachesbull Olfactory
dysfunction
Palpationbony discontinuitiesNeuralgias to check
over- the supraorbital -infraorbital -mental foramina
Anterior Rhinoscopy
bull The rhinologic examination itself begins with anterior
bull rhinoscopy to evaluate the nasal vestibule and the anterior
bull portions of the nasal cavity
Nasal Endoscopy Nasal endoscopy has become the most important andrewarding clinical examination method in rhinologic diagnosis
- rigid endoscopes which are available in 4-mm and 28- mm diameters and assorted viewing angles (eg 01048576 301048576 1201048576) -flexible endoscopes are also available for inspecting the nose and nasopharynx and exploring all of the pharynx and larynx in one sitting
Nasal endoscopy
Nasal Endoscopy
Nasal Endoscopy
Imaging of the Nose and Paranasal Sinuses
Conventional RadiographsStandard paranasal sinus radiographs in the occipitomental
projection ( Water projection) and
occipitofrontal projection Caldwell projection) in cases of acute inflammation
They are also obtained to evaluate midfacial fractures
Computed Tomography (CT) the main indicationsfor CT scanning of the
nose and paranasal sinuses
are- chronic sinusitis - -trauma (especially
frontobasal -fractures)
-and tumors
The occipitofrontal projection is better for evaluating theethmoid cells and frontal sinus
occipitomental projection demonstrates the maxillarysinus and gives a limited view of the sphenoid sinus
Computed tomography of the paranasal sinuses
Four representative coronal CT scans are shown
Four representative coronal CT scans are shown
Magnetic Resonance Imaging
Magnetic maging
Magnetic resonance imaging (MRI) has fewer indicationsthan CT in patients with paranasal sinus diseaseThis is primarily because MRI is markedly inferior toCT in defining the bony boundaries of the sinusesThe strength of MRI lies in its superior soft-tissue discriminationMRI is indicated in diseases that involve the paranasal sinuses in addition to thecranial cavity or orbit (eg tumors and congenitalmalformations such as encephaloceles)
MRI of the paranasal sinuses
The Nose and Sinuses
Structure The structure of the nose is made up of
four partsbull The surface anatomybull The nasal skeletonmdashcomposed of the
two nasal bones the paired upper lateral and lower lateral cartilages and the nasal septum covered in subcutaneous tissue and skin
bull The internal anatomymdashincludes the septum of the nose which forms the medial wall of the nasal cavity The turbinates on the lateral wall are also called conchae
bull The osteomeatal complexmdasha key functional area of the nose
Function The nose is the main route for inspired
air and its structure is related to this function As the air passes over the large surface area of the turbinates
The inspired gases are warmed and humidified Mucus on the mucosa of the nose removes large dust particles from the air as it is breathed in
The voice resonates in the sinuses and nose and this provides character to the speech
Pneumatization of the sinusesmdashthey are air filled spacesmdashreduces the weight of the skull
Diseases of thDiseases of the Outer and Inner Nosee Outer and
Inner Nose Erysipelas Definition of the disease ndash Erysipela is a skin infection that affects the superficial dermis and is caused by Streptococcus pyogenes (group A) It usually develops in the extremities and the face and less commonly on the scalp and genitals bull Epidemiologyaetiology ndash Erysipelas are more often seen in elderly infants and children patients with compromised immunology and diabetes -Predisposing factors are alcoholism skin ulceration puncture wounds fungal infections malnutrition and burns
Erysipelas
bull Symptomsbull ndash It usually presents of fever general fatigue bull -The skin lesion is a redindurated and elevated plaque
with borders that expand rapidly bull It is painful warm and accompanied by variable oedemabull -On the second or third day a flaccid bulla may develop
and desquamationbull bull Presence of regional lymph nodes is common
Erysipelas
bull Complicationsndash The most common complication is recurrencewhich is seen in 18ndash30 of the cases even afterproper antibiotic therapy Recurrence is seen moreoften in females than in malesA skin infection with S pyogenes could lead toglomerulonephritis
Erysipelas
bull Complicationsbull ndash The most common complication is recurrencebull which is seen in 18ndash30 of the cases even afterbull proper antibiotic therapy bull -Recurrence is seen morebull often in females than in males bull -A skin infection with S pyogenes could lead tobull glomerulonephritis
Erysipelas
bull bull Diagnosisbull ndash Diagnosis is based on the patientrsquos personal
historybull and physical examination particularly on inspectionbull of the skin
bull Blood cultures are positive in less thanbull 5 of cases
ErysipelasTherapyndash Conservative therapybull The preferred antibiotic is penicillin In mildcases with minor systemic symptoms penicillinV 500 mg orally every 6 h for 10 days or penicillinG benzathine 12 mil U intramuscularlyonceOther possibilities are amoxicillin 500 mgorally twice a day for 10 days or cephalexin 500mg orally every 6 h for 10 days
ErysipelasIn moderate and severe cases with significantsystemic symptoms hospitalization and intravenoustreatment is required penicillin G 2ndash4mil U intravenously every 4ndash6 h Cefazolin05ndash15 gm intravenously every 8 h cefotaxime1ndash2 gm intravenously every 8 h or ceftriaxone1ndash2 gm intravenously once a day should be administeredIn patients with a penicillin allergyclindamycin 600 mg intravenously every 8 h orvancomycin 15 mgkg intravenously twice a daymay be given
ErysipelaAdditional useful therapeutic optionsbull Prednisone 30 mg over 8 days might be consideredas well as elevation of the affected siteMoist heat compresses may be usefulbull Surgeryndash Debridement and drainage are indicated when bullaeabscesses or necroses are presentbull Differential diagnosisndash Contact dermatitisndash Asteatotic eczemandash Herpes zosterndash Angioneurotic oedemandash Osteomyelitis
Furuncle
bull Definition of the diseasebull ndash A furuncle is an infection that beginsbull at the hair follicle and spreads deeper into thebull dermis and subcutaneous tissue forming abull nodule After several days it developsbull into an abscess - red painful and fluctuantbull bull bull Epidemiologyaetiologybull ndash The aetiologic agent is Staphylococcus aureus
FuruncleSymptomsndashsymptoms are local and limited to thesite of infection Furuncles usually are wherehair follicles are present bull Complicationndash One complication is furunculosis multiple draining furunclesDiagnosisndash The diagnosis is based on clinical inspection - Cultures are not necessary when there is no systemic involvement but should beconsidered if systemic therapy (in case of feversignificant cellulitis or hospitalization) or whenmethicillin-resistant Staphylococcusaureus (MRSA) is considered
FuruncleTherapyndash When the furuncle is small application of moist heat compress to promote drainage -Larger furuncles should be drained by surgical incision-After drainage the area should be cleaned with anantiseptic (with chlorhexidinebetadine) should be applied twice
a dayndash If no systemic symptoms or extensive cellulitis arepresent simple topical care is usually curative andoral antibiotics are not necessary Otherwise systemictreatment is indicated and should cover anypossible MRSA
Furuncle
bull -Recommended antibiotics are trimethoprim-sulfamethoxazole
bull 1ndash2 tablets orally twice daily doxycyclinebull 100 mg orally twice dailybull or clindamycin 300ndash450 mg orally every 8 hbull - In severe cases vancomycin 15 mgkg
intravenouslybull every 12 h or clindamycin 600 mg intravenouslybull every 8 h
Midline Granulomabull A midline granuloma is an angiocentricbull lymphoma it was referred to as polymorphicbull reticulosis lethal midline granuloma and midline
malignant reticulosisbull bull Definition of the diseasebull ndash This rare disease is a lymphoma of extranodal
presentationall cases are positive for the Epstein-Barr virus
bull -This lymphoma most commonly appears in the midface region
Midline GranulomaEpidemiologyaetiologyndash This form of lymphoma is rare in Europe and theUnited States with a higher prevalence in Asia and PeruSymptomsndash The most common presentation is nasal obstruction with a destructive mass occupying the nosesinuses and palate
-Fever night sweatsand weight loss seen usually in Hodgkinrsquos lymphomaand other non-Hodgkinrsquos lymphomas (knownas ldquoB symptomsrdquo) are uncommon
Midline GranulomaDiagnosisndash The diagnosis is based on anatomopathologicalstudy The malignancy of the tumour manifested byextensive necrosis makes the histological diagnosisdifficult and often more biopsies are required forconfirmationbull Therapyndash Therapy consists of radiotherapy with or withoutchemotherapy
Midline Granuloma
bull Prognosisbull ndash Depending on the stage long-term remission or
experience a worseningbull prognosis with relapses which may include otherbull extranodal sites bull Involvement of extranodal sitesbull including the upper airway gastrointestinal tractbull skin
Wegenerrsquos Granulomatosis
bull Definition of the diseasebull ndash Wegenerrsquos granulomatosis is a systemic chronicbull vasculitis of small- and medium-sized blood vesselsbull with an autoimmune component It affectsbull particular organs with variable predilectionbull Epidemiologyaetiologybull ndash Wegenerrsquos granulomatosis is a rare disease It affects
about 1 in 20000ndash30000 people It is more prevalentbull in middle-aged Caucasian patients
Wegenerrsquos Granulomatosis
Symptomsndash The disease may present pulmonary upper
respiratory tract or renal In the disseminated form-The localised form ndash confinedto the upper respiratory region ndash is present in 25of the patients- It consists of nonspecific manifestationssuch as nasal obstruction crusting purulentor bloody rhinorrhea and painful or painless ulcers in oral or nasal cavities which are unresponsive tostandard medical treatment
Wegenerrsquos Granulomatosis
bull In some patients the nasal septum is perforatedbull which leads to saddle-nose deformity Less
commonbull symptoms are hoarseness stridor due to
subglotticbull stenosis otalgia otorrhea and conductivebull and sensorineural hearing loss Also ocular
symptomsbull such as scleritis conjunctivitis uveitis andbull episcleritis may be present
Wegenerrsquos Granulomatosis
bull ndash In the disseminated form pulmonary involvementbull is manifested by cough dyspnoea haemoptysisbull (due to an alveolar capillaritis necrotic lesions orbull endobronchial disease) and pleuritic painndashbull -Ninety per cent of patients have nasal symptomsbull and these symptoms are usually the first
manifestationof the diseasebull -Most patients have also renal involvementbull even if it is subclinical
Wegenerrsquos Granulomatosis
Diagnosis ndash Diagnosis of Wegenerrsquos granulomatosis is based on clinical findings that demonstrate lung (chest x-ray) kidney (urine analysis) or upper respiratory tract
involvement (oral or nasal ulcers or discharge) - positive blood analysis for cytoplasmic-staining antineutrophil
cytoplasmic antibodies (c-ANCA) and confirming proteinase 3 (PR3) ANCA or myeloperoxidase (MPO) ANCA ndash Biopsy is essential for diagnosis nonspecific chronic inflammation
and necrosis -Bacterial and fungal infections
Wegenerrsquos Granulomatosis
Therapyndash Conservative therapybull In the induction of disease remission highdosesteroids (e g prednisone 1 mgkgday) for1 month with tapering over several months aregiven In addition cyclophosphamide (2 mgkgday) should be administered for 6ndash12 monthsuntil symptoms disappear In the maintenanceof remission cyclophosphamide should be
Wegenerrsquos Granulomatosis
Antibiotics mainly trimethoprim-sulfamethoxazoleare given for prophylaxis againstPneumocystis jiroveci (formerly Pneumocystiscarinii) pneumonia (PCP) which may developduring immunosuppression and have a role inpreventing recurrencesbull Sinonasal manifestations may be treated with topical nasal steroids and nasal irrigations lowdosesystemic steroids and antibiotics when bacterial infection (typically Staphylococcus species) is suspected
Wegenerrsquos Granulomatosis
bull Prognosisbull ndash Most of the patients respond well to treatmentbull achieving symptom-free intervals of 5ndash20 yearsbull or more bull -Anatomical problems (sinusitis trachealbull stenosis) may require surgery bull Relapses can be long and troublesomebull Long-term complications are chronicbull renal failure hearing loss and deafness
Nasal Fractures Definition ndash A nasal fracture is a disruption of the nasal bone structure due to trauma It is the most frequently fractured facial bone Epidemiologyaetiology ndash Sports falls and assaults are the usual mechanisms of fracture -Males are affected twice as often as are females -Paediatric populations with a incidences during the second and third decades of life -Variables such as force impact direction nature of the striking object age and other will influence the pattern of injury to the components of the nose
Nasal Fractures
bull Symptomsbull ndash Deformity swelling epistaxis and periorbital
ecchymosis are signs that are suggestive of nasal fracture
bull bony crepitus and nasal segment mobilitybull ndash Epiphora bull Severe bilateral injuries to the lachrymal bones
arebull associated with depressed nasal fractures
Nasal Fractures Complications ndash Septal haematoma is one of the most severe early complications of nasal trauma and without drainage it results in abscess formation 6ndash7 days after trauma producing necrosis of the septal cartilage -Long-term problems such as saddle-nose deformity perforation columellar retraction and nasalbase
Septal infection could lead to osteomyelitis orbital and intracranial abscesses meningitis and cavernous sinus thrombosis -Cerebrospinal fluid leakage is a common complication of severe
nasal and frontal fractures
Nasal Fractures
bull Diagnostic proceduresbull ndash Inspectionbull bull Changes of appearance such as deviation andbull asymmetry bleeding watery drainage changesbull in nasal breathing and smell It is useful to comparebull the current presentation with old photographsbull (up to 40 of normal individuals havebull significant nose malformations)
Nasal Fractures Physical examination bull The diagnosis of a nasal fracture is made primarily by physical examination epistaxis nasal swelling and periorbital ecchymosis Nasal shape in the lateral and frontal inspection should be assessed Grasping the dorsum between two fingers and rocking the pyramid back and forth aids in assessing the mobility of nasal bones Internal structures should be evaluated by using a headlight and nasal speculum Clotted blood is removed by suction and assessment of haematoma mucosal tears and active bleeding is performed Bimanual palpation of the septum helps to differentiate septal swelling from haematoma ndash
Nasal FracturesRadiographybull There is no clear evidence of the role of radiographyin the management of nasal fracturesPlain films have up to a 66 false-positive rateas a result of misinterpretation of normal suturelines In addition old fractures are difficult todistinguishbull Three-dimensional CT is recommended for extensiveinjuries involving the nasal-orbital-ethmoidalcomplexndash
Nasal Fractures
bull Additionaluseful diagnostic proceduresbull bull Using a 0 or 30deg 4-mm endoscope is helpful inbull the assessment of posterior abnormalities If thebull patient is heavily sedated Brown-Gruss
provocationbull manoeuvres may be performed to determinebull deformities in upper middle or lower segmentsbull by compressing each compartment
Nasal FracturesConservative treatmentndash Treatment of bleedingbull For localised bleeding anterior sources may becauterised by silver nitrate or sealed with topicalmaterials such as thrombin combined withgelatin foam fibrin glue FloSealreg or other procoagulantmaterials If conservative measuresfail a formal anterior packing is placedbull Bleeding from branches of sphenopalatine orethmoid vessels requires anterior-posteriorpacking
Nasal Fractures
bull bull Surgical methods such as direct endoscopic vessel
bull cauterization or ligation have been shown tobull offer better haemostasis and patient comfortbull Angiography with embolization can also be
consideredbull in cases refractory to more conservativebull approaches
Nasal Fractures
bull Type of reductionbull bull Nondisplaced fractures should be treated withbull observation alone Closed nasal reduction is thebull best choice for simple injuries (isolated unilateralbull with medial displacement)bull bull An open approach should be considered in
severebull trauma (bilateral depressed fractures)
Nasal Fracturesbull Surgical principlesbull ndash Topical anaesthesia with cotton pledgets soakedbull with 4 cocaine or 005 oxymethazoline combinedbull with 4 topical lidocaine should be appliedbull for 5ndash10 min Local anaesthesia should also be injectedbull (1 lidocaine and 1100000 epinephrine)bull along the septum lateral walls and floor of the nasalbull cavitybull bull
Nasal FracturesClosed reductionndashndash The nasal bones are grasped between two fingersand pressure is applied laterally in theopposite direction of the deviation A bluntelevator may be used from within the nose incases of significant medial collapse Walshamforceps can be of help Reduction of the septumshould be performed with the use ofAsch forceps
Nasal Fractures
bull To prevent collapse of the postreductionbull framework nasal packing should be placedbull for 3ndash5 days Septum splints are recommendedbull in comminuted septal fractures withbull severe mucosal lesions External nasal splintingbull for 10 days (Aquaplastreg Thermoplastreg)bull provides nasal protection Nasal saline spraysbull prevent crusting and oral antibiotics should
Nasal Fractures
bull Open reductionbull ndashndash Immediate repair of fractures by using
widebull surgical exposure reduction fixation and
reconstructionbull ndashndash The second option is delayed correctionbull (6 months or more) of persistent deformitiesbull using standard techniques of rhinoplasty
Deviated Nasal Septum
bull Definition of the diseasebull ndash Deviation of the nasal septum is a common causebull of unilateral nasal airway obstruction in which thebull nasal septum is displacedbull bull Epidemiologyaetiologybull ndash Developmental septal abnormalities Septal cartilage
damage in the neonatal period andbull during birth can cause severe septal deviation inbull the absence of a history of nasal trauma
Deviated Nasal Septum
bull Symptomsbull ndash Patients may present with a history of sinusitis
allergicbull rhinitis obstructive sleep apnoea previousbull nasal surgery or recent nasal trauma Unilateral or
bilateral nasal airway obstruction that is unrelievedbull with decongestants or nasal steroid sprays is oftenbull seenbull bull
Deviated Nasal SeptumDiagnosisndashExamination external dorsal deviation or the columella and caudal septummay be deflected off the midline (caudal subluxation)ndash Inspections of the nasal cavity and anterior-posteriorrhinoscopy are helpful in diagnosing the locationtype and severity of septal deformityThe endoscope is also useful in identifying polypsthe severity and extent of posterior septaldeviations and bony spurs and locating areas ofseptal perforation or mucosal injury
Deviated Nasal Septum
bull Therapybull ndash Septoplasty is a procedurebull The areabull of deviation is corrected or resected in order tobull leave behind as much cartilage and bone as
possiblebull Cartilage resection is minimised and can be
repositioned reshaped or recontoured using a variety of methods
Deviated Nasal Septum
bull ndash Indications of septoplasty before the growth period
bull of the nose is finished should be very limited bull -In these cases surgery must preserve all the
cartilagebull in order to prevent external changes of the
shape ofbull the nose
Deviated Nasal Septum
bull Complicationsbull ndash Frequent complications include haematoma andbull infection Cerebrospinal fluid leak is a rare but
potentiallybull serious complicationbull It is usually the resultbull of avulsion or damage to the cribriform plate whenbull handling the perpendicular plate of the ethmoidbull ndash Other complications include epistaxis nasal
Deviated Nasal Septum
bull Other complications include epistaxis nasal obstruction
bull due to residual deviation synechiae returnbull of the cartilaginous deviation septal perforationbull anosmia and cosmetic nasal deformities suchbull as widened alar rim margins drooping nasal tipbull columella retraction and a sunken dorsum with abull supratip saddle formation
Septal perforation with minor crusting View from provide closure of the
incision
Septal Haematoma
bull A septal haematoma is a blood collection under the perichondrium
bull of the septum and cartilagebull bull bull Epidemiologyaetiologybull ndash A septal haematoma is one of the most
severe complications of nasal trauma
Septal Haematoma
bull Diagnosisbull ndash Signs and symptoms include intense pain
swellingbull haematoma of the upper lip and philtrum
area andbull complete nasal airway obstruction
Septal HaematomaTherapyndash Management consists of drainage through a mucoperichondrial incision Immediate treatment isnecessary to prevent long-term problems such asa saddle-nose deformity perforation columellarretraction and nasal-base widening In childrenseptal destruction can lead to devastating nasal andmidfacial growth abnormalitiesbull Surgeryndash Incision and evacuation of the collection is performedDrainage of a septal haematoma should
Septal HaematomaSurgeryndash Incision and evacuation of the collection is performedDrainage of a septal haematoma should provide closure of the incision
Splints or transseptal sutures are placed to obliterate thepotential space and prevent collectionInfection involving the septal cartilage Reconstruction with autologouscartilage is then performed in a second stage Oral antibiotics should be given
Nasal DeformitySaddle-nose deformityndash A saddle-nose deformity is characterised by a loss ofnasal dorsal height and compromised nasal supportstructures -Other case observed are depressionof the middle vault and dorsum loss of nasal tipsupport and definition shortened (vertical) nasal length over rotation of the nasal tip and retrusion ofthe nasal spine and caudal septum It is also knownas a ldquoPug noserdquo or ldquoboxerrsquos noserdquo both of which referto various degrees of nasal dorsal depressionbull
Nasal DeformityEpidemiologyaetiologyndash Prevalence is higher in population groups prone to facial trauma (ie boxers athletes) those with historiesof intranasal cocaine use nasal surgery (e g radical submucosal septal resection reductive rhinoplasty)ndash A saddle-nose deformity can be congenital or acquired It can be noticed as a part of individual familialsyndromic and ethnic characteristics - Most deformities are due to traumatic and iatrogeniccauses Medical causes are Wegenerrsquosgranulomatosis relapsing polychondritis leprosy (Hansenrsquos disease) syphilis ectodermal dysplasiaand intranasal cocaine use
Nasal Deformity
bull Therapybull ndash Nasal reconstruction indications depend on patientbull selection surgeon experience and aetiology of thebull deformity bull Indications for surgery can be functionalbull aesthetic or most commonly both In individuals
with a compromised nasal airway a nasoseptalbull reconstruction is indicated
Nasal Deformity
bull Contraindications bull include patients with malignantbull chronic or autoimmune disease conditions drugbull abuse poor perioperative risk profile and unrealisticbull expectationsbull ndash Multiple previous rhinoplasties and certain
professionsbull (mixed martial artists boxers and other contactbull sports) are relative contraindications
Nasal DeformitySeptoplastyndash Septoplasty is performed to correct nasal obstructioncaused by septal deformityndash Usually septoplasty is performed under general anaesthesiawith the patient in the supine position with the head elevated by approximately 30 (Righthandedsurgeons approach from the right side)ndash Local vasoconstrictive anaesthesia is applied notonly to reduce postoperative pain but also more importantly to achieve vasoconstriction of themucosa and less intraoperative haemorrhage Lidocainewith adrenaline or epinephrine is usedalthough in patients with cardiac hypersensitivityoxymetazoline might be preferred
Nasal Deformity
bull Septoplasty begins with the incision of septal mucosabull Most operative techniques utilise a hemitransfixionbull incision at the caudal end of septum so thatbull deviation at this point might be reached as wellbull as a transfixion incision that is easily obtained ifbull needed (Right-handed surgeons normally choosebull the left side but that may vary when deviation isbull convex towards the right)
Nasal DeformityA columella retractor is placed over the columellaand by pulling it laterally the caudal border of theseptum is exposed Ala can be protected by an alaprotector A vertical incision with a no 15 bladeover the caudal end of septum is performed untilreaching the plane of the septal cartilage It is essentialto correctly identify the perichondrium and byusing the Cottle elevator dissect and lift it creatinga flap As the dissection proceeds along the septalcartilage a longer speculum (no 5) is introduced sothat elevation of the mucoperichondrium is doneunder constant visual controlndash The next step is to dissect the mucoperiostium
Nasal DeformityDissecting over the bony-cartilaginous junctionwhen joining both tunnels might be difficult and is
especially prone to membrane perforationndash If needed the same tunnels are to be created on the
other side of the septum Then deviated parts of
septum are identified and removed either with a
knife or a Freer chisel
Nasal Deformitybull septum from the maxillary crest the septum mustbull be separated from the perpendicular plate trimmedbull along the inferior border placed back onto the crestbull and sutured to the periosteum If the deformity involvesbull the vomer an osteotome is used Care mustbull be taken not to break the cribriform plate becausebull it could cause a cerebrospinal fistula
Nasal Deformity
bull Once the septal deviation is corrected the flapsbull and hemitransfixion incision are mattressed
withbull absorbable sutures Nasal packing to prevent
synechiaebull and postoperative septal haematoma mightbull be advised but should be removed within 72 h

Nasal CavitiesThe nasal cavity is bounded laterally by the lateral nasalwalls which are formed by the ethmoid bone andmaxilla and posteriorly by the palatine bone and thepterygoid process of the sphenoid bone Several functionallyimportant structures are located on the lateralnasal wall the nasal turbinates and their associatedpassages (meati) sinus ostia and the orifice ofthe nasolacrimal duct (Fig 15)
The inferior turbinate consists of a separate bone thatis attached to the medial wall of the maxillary sinusThe opening of the nasolacrimal duct is located in thecorresponding inferior meatus The middle andsuperior turbinates are part of the ethmoid bone In rare cases a rudimentary ldquosupreme turbinaterdquo is alsopresent above the superior turbinate
The middle turbinate has by far the greatest functionalimportance because most of the drainage tracts fromthe surrounding paranasal sinuses open into the middlemeatus The nasal cavity is bounded superiorly by the cribriformplate of the ethmoid bone This thin bony platehas numerous openings for the passage of the fila olfactoriaand also forms the boundary of the anteriorcranial fossa
Nasal Cavities
The floor of the nasal cavity is formedmostly by the hard palate which is formed in turn bythe two palatine processes of the maxilla and the horizontallaminae of the palatine bone
Structure of the lateral nasal wall
Inferior meatus
Paranasal Sinuses
The paranasal sinuses are air-filled cavities that communicatewith the nasal cavities
-The maxillary sinus frontalsinus and anterior ethmoid cells drain into the nasalcavity through the middle meatusmdashie below themiddle turbinate -The posterior ethmoidcells drain into the nasal cavity through the superiormeatus The ostium of the sphenoid sinus is locatedin the anterior wall directly above the choanae- The anatomical connections between the nasal cavity andparanasal sinuses are functionally important and playa key role in the pathogenesis of many rhinologic diseasesthat involve the paranasal sinuses
Vascular SupplyThe external nose derives most of its blood supply
from the facial artery which arises from the external
carotid artery and from the ophthalmic artery which
springs from the internal carotid artery
Vascular Supply
The internalnose receives blood from the territories of the externaland internal carotid arteries- the terminalbranches of the sphenopalatine artery which arisesfrom the maxillary artery - the anterior and posteriorethmoid arteries which arise from the ophthalmicartery-internal carotid arterie
venous drainage
The venous drainageof the facial region is handled by -the facial vein -retromandibular vein -internal jugular vein
lymphatic drainage
The regional lymphatic drainage of the face and externalnose is handled mainly by- the submandibularlymph nodes while the nasal cavity is additionallydrained by -the retropharyngeal and deep - -cervical lymph nodes
Morphology of the Nasal Mucosa
Besides the anatomical structure of the external noseand nasal cavity the nasal mucosa plays an essentialrole in numerous functions of the nose in the respiratory tract
Morphology of the Nasal Mucosa
The anterior part of the nasal cavity (the nasal vestibule)like the external nose is covered by skin composedof a multilayer keratinizing squamous epithelium and finally a ciliated respiratory epithelium A small areaon the upper nasal septum superior turbinate andpart of the middle turbinate located adjacent to thecribriform plate is covered by olfactory mucosa and iscalled the olfactory region
Nerve SupplyThe facial skin receives its sensory innervation fromterminal branches of the trigeminal nerve that enterthe facial region through the supraorbital infraorbitaland mental foramina Thefacial muscles are classified as mimetic or mastica- tory each of these groups receiving different motorinnervationbythe facial nerve
History and Clinical Examination of the Nose
Historybull The main symptomsbull nasal obstruction (ldquostuffy
noserdquo)bull nasal dischargebull Headachesbull Olfactory
dysfunction
Palpationbony discontinuitiesNeuralgias to check
over- the supraorbital -infraorbital -mental foramina
Anterior Rhinoscopy
bull The rhinologic examination itself begins with anterior
bull rhinoscopy to evaluate the nasal vestibule and the anterior
bull portions of the nasal cavity
Nasal Endoscopy Nasal endoscopy has become the most important andrewarding clinical examination method in rhinologic diagnosis
- rigid endoscopes which are available in 4-mm and 28- mm diameters and assorted viewing angles (eg 01048576 301048576 1201048576) -flexible endoscopes are also available for inspecting the nose and nasopharynx and exploring all of the pharynx and larynx in one sitting
Nasal endoscopy
Nasal Endoscopy
Nasal Endoscopy
Imaging of the Nose and Paranasal Sinuses
Conventional RadiographsStandard paranasal sinus radiographs in the occipitomental
projection ( Water projection) and
occipitofrontal projection Caldwell projection) in cases of acute inflammation
They are also obtained to evaluate midfacial fractures
Computed Tomography (CT) the main indicationsfor CT scanning of the
nose and paranasal sinuses
are- chronic sinusitis - -trauma (especially
frontobasal -fractures)
-and tumors
The occipitofrontal projection is better for evaluating theethmoid cells and frontal sinus
occipitomental projection demonstrates the maxillarysinus and gives a limited view of the sphenoid sinus
Computed tomography of the paranasal sinuses
Four representative coronal CT scans are shown
Four representative coronal CT scans are shown
Magnetic Resonance Imaging
Magnetic maging
Magnetic resonance imaging (MRI) has fewer indicationsthan CT in patients with paranasal sinus diseaseThis is primarily because MRI is markedly inferior toCT in defining the bony boundaries of the sinusesThe strength of MRI lies in its superior soft-tissue discriminationMRI is indicated in diseases that involve the paranasal sinuses in addition to thecranial cavity or orbit (eg tumors and congenitalmalformations such as encephaloceles)
MRI of the paranasal sinuses
The Nose and Sinuses
Structure The structure of the nose is made up of
four partsbull The surface anatomybull The nasal skeletonmdashcomposed of the
two nasal bones the paired upper lateral and lower lateral cartilages and the nasal septum covered in subcutaneous tissue and skin
bull The internal anatomymdashincludes the septum of the nose which forms the medial wall of the nasal cavity The turbinates on the lateral wall are also called conchae
bull The osteomeatal complexmdasha key functional area of the nose
Function The nose is the main route for inspired
air and its structure is related to this function As the air passes over the large surface area of the turbinates
The inspired gases are warmed and humidified Mucus on the mucosa of the nose removes large dust particles from the air as it is breathed in
The voice resonates in the sinuses and nose and this provides character to the speech
Pneumatization of the sinusesmdashthey are air filled spacesmdashreduces the weight of the skull
Diseases of thDiseases of the Outer and Inner Nosee Outer and
Inner Nose Erysipelas Definition of the disease ndash Erysipela is a skin infection that affects the superficial dermis and is caused by Streptococcus pyogenes (group A) It usually develops in the extremities and the face and less commonly on the scalp and genitals bull Epidemiologyaetiology ndash Erysipelas are more often seen in elderly infants and children patients with compromised immunology and diabetes -Predisposing factors are alcoholism skin ulceration puncture wounds fungal infections malnutrition and burns
Erysipelas
bull Symptomsbull ndash It usually presents of fever general fatigue bull -The skin lesion is a redindurated and elevated plaque
with borders that expand rapidly bull It is painful warm and accompanied by variable oedemabull -On the second or third day a flaccid bulla may develop
and desquamationbull bull Presence of regional lymph nodes is common
Erysipelas
bull Complicationsndash The most common complication is recurrencewhich is seen in 18ndash30 of the cases even afterproper antibiotic therapy Recurrence is seen moreoften in females than in malesA skin infection with S pyogenes could lead toglomerulonephritis
Erysipelas
bull Complicationsbull ndash The most common complication is recurrencebull which is seen in 18ndash30 of the cases even afterbull proper antibiotic therapy bull -Recurrence is seen morebull often in females than in males bull -A skin infection with S pyogenes could lead tobull glomerulonephritis
Erysipelas
bull bull Diagnosisbull ndash Diagnosis is based on the patientrsquos personal
historybull and physical examination particularly on inspectionbull of the skin
bull Blood cultures are positive in less thanbull 5 of cases
ErysipelasTherapyndash Conservative therapybull The preferred antibiotic is penicillin In mildcases with minor systemic symptoms penicillinV 500 mg orally every 6 h for 10 days or penicillinG benzathine 12 mil U intramuscularlyonceOther possibilities are amoxicillin 500 mgorally twice a day for 10 days or cephalexin 500mg orally every 6 h for 10 days
ErysipelasIn moderate and severe cases with significantsystemic symptoms hospitalization and intravenoustreatment is required penicillin G 2ndash4mil U intravenously every 4ndash6 h Cefazolin05ndash15 gm intravenously every 8 h cefotaxime1ndash2 gm intravenously every 8 h or ceftriaxone1ndash2 gm intravenously once a day should be administeredIn patients with a penicillin allergyclindamycin 600 mg intravenously every 8 h orvancomycin 15 mgkg intravenously twice a daymay be given
ErysipelaAdditional useful therapeutic optionsbull Prednisone 30 mg over 8 days might be consideredas well as elevation of the affected siteMoist heat compresses may be usefulbull Surgeryndash Debridement and drainage are indicated when bullaeabscesses or necroses are presentbull Differential diagnosisndash Contact dermatitisndash Asteatotic eczemandash Herpes zosterndash Angioneurotic oedemandash Osteomyelitis
Furuncle
bull Definition of the diseasebull ndash A furuncle is an infection that beginsbull at the hair follicle and spreads deeper into thebull dermis and subcutaneous tissue forming abull nodule After several days it developsbull into an abscess - red painful and fluctuantbull bull bull Epidemiologyaetiologybull ndash The aetiologic agent is Staphylococcus aureus
FuruncleSymptomsndashsymptoms are local and limited to thesite of infection Furuncles usually are wherehair follicles are present bull Complicationndash One complication is furunculosis multiple draining furunclesDiagnosisndash The diagnosis is based on clinical inspection - Cultures are not necessary when there is no systemic involvement but should beconsidered if systemic therapy (in case of feversignificant cellulitis or hospitalization) or whenmethicillin-resistant Staphylococcusaureus (MRSA) is considered
FuruncleTherapyndash When the furuncle is small application of moist heat compress to promote drainage -Larger furuncles should be drained by surgical incision-After drainage the area should be cleaned with anantiseptic (with chlorhexidinebetadine) should be applied twice
a dayndash If no systemic symptoms or extensive cellulitis arepresent simple topical care is usually curative andoral antibiotics are not necessary Otherwise systemictreatment is indicated and should cover anypossible MRSA
Furuncle
bull -Recommended antibiotics are trimethoprim-sulfamethoxazole
bull 1ndash2 tablets orally twice daily doxycyclinebull 100 mg orally twice dailybull or clindamycin 300ndash450 mg orally every 8 hbull - In severe cases vancomycin 15 mgkg
intravenouslybull every 12 h or clindamycin 600 mg intravenouslybull every 8 h
Midline Granulomabull A midline granuloma is an angiocentricbull lymphoma it was referred to as polymorphicbull reticulosis lethal midline granuloma and midline
malignant reticulosisbull bull Definition of the diseasebull ndash This rare disease is a lymphoma of extranodal
presentationall cases are positive for the Epstein-Barr virus
bull -This lymphoma most commonly appears in the midface region
Midline GranulomaEpidemiologyaetiologyndash This form of lymphoma is rare in Europe and theUnited States with a higher prevalence in Asia and PeruSymptomsndash The most common presentation is nasal obstruction with a destructive mass occupying the nosesinuses and palate
-Fever night sweatsand weight loss seen usually in Hodgkinrsquos lymphomaand other non-Hodgkinrsquos lymphomas (knownas ldquoB symptomsrdquo) are uncommon
Midline GranulomaDiagnosisndash The diagnosis is based on anatomopathologicalstudy The malignancy of the tumour manifested byextensive necrosis makes the histological diagnosisdifficult and often more biopsies are required forconfirmationbull Therapyndash Therapy consists of radiotherapy with or withoutchemotherapy
Midline Granuloma
bull Prognosisbull ndash Depending on the stage long-term remission or
experience a worseningbull prognosis with relapses which may include otherbull extranodal sites bull Involvement of extranodal sitesbull including the upper airway gastrointestinal tractbull skin
Wegenerrsquos Granulomatosis
bull Definition of the diseasebull ndash Wegenerrsquos granulomatosis is a systemic chronicbull vasculitis of small- and medium-sized blood vesselsbull with an autoimmune component It affectsbull particular organs with variable predilectionbull Epidemiologyaetiologybull ndash Wegenerrsquos granulomatosis is a rare disease It affects
about 1 in 20000ndash30000 people It is more prevalentbull in middle-aged Caucasian patients
Wegenerrsquos Granulomatosis
Symptomsndash The disease may present pulmonary upper
respiratory tract or renal In the disseminated form-The localised form ndash confinedto the upper respiratory region ndash is present in 25of the patients- It consists of nonspecific manifestationssuch as nasal obstruction crusting purulentor bloody rhinorrhea and painful or painless ulcers in oral or nasal cavities which are unresponsive tostandard medical treatment
Wegenerrsquos Granulomatosis
bull In some patients the nasal septum is perforatedbull which leads to saddle-nose deformity Less
commonbull symptoms are hoarseness stridor due to
subglotticbull stenosis otalgia otorrhea and conductivebull and sensorineural hearing loss Also ocular
symptomsbull such as scleritis conjunctivitis uveitis andbull episcleritis may be present
Wegenerrsquos Granulomatosis
bull ndash In the disseminated form pulmonary involvementbull is manifested by cough dyspnoea haemoptysisbull (due to an alveolar capillaritis necrotic lesions orbull endobronchial disease) and pleuritic painndashbull -Ninety per cent of patients have nasal symptomsbull and these symptoms are usually the first
manifestationof the diseasebull -Most patients have also renal involvementbull even if it is subclinical
Wegenerrsquos Granulomatosis
Diagnosis ndash Diagnosis of Wegenerrsquos granulomatosis is based on clinical findings that demonstrate lung (chest x-ray) kidney (urine analysis) or upper respiratory tract
involvement (oral or nasal ulcers or discharge) - positive blood analysis for cytoplasmic-staining antineutrophil
cytoplasmic antibodies (c-ANCA) and confirming proteinase 3 (PR3) ANCA or myeloperoxidase (MPO) ANCA ndash Biopsy is essential for diagnosis nonspecific chronic inflammation
and necrosis -Bacterial and fungal infections
Wegenerrsquos Granulomatosis
Therapyndash Conservative therapybull In the induction of disease remission highdosesteroids (e g prednisone 1 mgkgday) for1 month with tapering over several months aregiven In addition cyclophosphamide (2 mgkgday) should be administered for 6ndash12 monthsuntil symptoms disappear In the maintenanceof remission cyclophosphamide should be
Wegenerrsquos Granulomatosis
Antibiotics mainly trimethoprim-sulfamethoxazoleare given for prophylaxis againstPneumocystis jiroveci (formerly Pneumocystiscarinii) pneumonia (PCP) which may developduring immunosuppression and have a role inpreventing recurrencesbull Sinonasal manifestations may be treated with topical nasal steroids and nasal irrigations lowdosesystemic steroids and antibiotics when bacterial infection (typically Staphylococcus species) is suspected
Wegenerrsquos Granulomatosis
bull Prognosisbull ndash Most of the patients respond well to treatmentbull achieving symptom-free intervals of 5ndash20 yearsbull or more bull -Anatomical problems (sinusitis trachealbull stenosis) may require surgery bull Relapses can be long and troublesomebull Long-term complications are chronicbull renal failure hearing loss and deafness
Nasal Fractures Definition ndash A nasal fracture is a disruption of the nasal bone structure due to trauma It is the most frequently fractured facial bone Epidemiologyaetiology ndash Sports falls and assaults are the usual mechanisms of fracture -Males are affected twice as often as are females -Paediatric populations with a incidences during the second and third decades of life -Variables such as force impact direction nature of the striking object age and other will influence the pattern of injury to the components of the nose
Nasal Fractures
bull Symptomsbull ndash Deformity swelling epistaxis and periorbital
ecchymosis are signs that are suggestive of nasal fracture
bull bony crepitus and nasal segment mobilitybull ndash Epiphora bull Severe bilateral injuries to the lachrymal bones
arebull associated with depressed nasal fractures
Nasal Fractures Complications ndash Septal haematoma is one of the most severe early complications of nasal trauma and without drainage it results in abscess formation 6ndash7 days after trauma producing necrosis of the septal cartilage -Long-term problems such as saddle-nose deformity perforation columellar retraction and nasalbase
Septal infection could lead to osteomyelitis orbital and intracranial abscesses meningitis and cavernous sinus thrombosis -Cerebrospinal fluid leakage is a common complication of severe
nasal and frontal fractures
Nasal Fractures
bull Diagnostic proceduresbull ndash Inspectionbull bull Changes of appearance such as deviation andbull asymmetry bleeding watery drainage changesbull in nasal breathing and smell It is useful to comparebull the current presentation with old photographsbull (up to 40 of normal individuals havebull significant nose malformations)
Nasal Fractures Physical examination bull The diagnosis of a nasal fracture is made primarily by physical examination epistaxis nasal swelling and periorbital ecchymosis Nasal shape in the lateral and frontal inspection should be assessed Grasping the dorsum between two fingers and rocking the pyramid back and forth aids in assessing the mobility of nasal bones Internal structures should be evaluated by using a headlight and nasal speculum Clotted blood is removed by suction and assessment of haematoma mucosal tears and active bleeding is performed Bimanual palpation of the septum helps to differentiate septal swelling from haematoma ndash
Nasal FracturesRadiographybull There is no clear evidence of the role of radiographyin the management of nasal fracturesPlain films have up to a 66 false-positive rateas a result of misinterpretation of normal suturelines In addition old fractures are difficult todistinguishbull Three-dimensional CT is recommended for extensiveinjuries involving the nasal-orbital-ethmoidalcomplexndash
Nasal Fractures
bull Additionaluseful diagnostic proceduresbull bull Using a 0 or 30deg 4-mm endoscope is helpful inbull the assessment of posterior abnormalities If thebull patient is heavily sedated Brown-Gruss
provocationbull manoeuvres may be performed to determinebull deformities in upper middle or lower segmentsbull by compressing each compartment
Nasal FracturesConservative treatmentndash Treatment of bleedingbull For localised bleeding anterior sources may becauterised by silver nitrate or sealed with topicalmaterials such as thrombin combined withgelatin foam fibrin glue FloSealreg or other procoagulantmaterials If conservative measuresfail a formal anterior packing is placedbull Bleeding from branches of sphenopalatine orethmoid vessels requires anterior-posteriorpacking
Nasal Fractures
bull bull Surgical methods such as direct endoscopic vessel
bull cauterization or ligation have been shown tobull offer better haemostasis and patient comfortbull Angiography with embolization can also be
consideredbull in cases refractory to more conservativebull approaches
Nasal Fractures
bull Type of reductionbull bull Nondisplaced fractures should be treated withbull observation alone Closed nasal reduction is thebull best choice for simple injuries (isolated unilateralbull with medial displacement)bull bull An open approach should be considered in
severebull trauma (bilateral depressed fractures)
Nasal Fracturesbull Surgical principlesbull ndash Topical anaesthesia with cotton pledgets soakedbull with 4 cocaine or 005 oxymethazoline combinedbull with 4 topical lidocaine should be appliedbull for 5ndash10 min Local anaesthesia should also be injectedbull (1 lidocaine and 1100000 epinephrine)bull along the septum lateral walls and floor of the nasalbull cavitybull bull
Nasal FracturesClosed reductionndashndash The nasal bones are grasped between two fingersand pressure is applied laterally in theopposite direction of the deviation A bluntelevator may be used from within the nose incases of significant medial collapse Walshamforceps can be of help Reduction of the septumshould be performed with the use ofAsch forceps
Nasal Fractures
bull To prevent collapse of the postreductionbull framework nasal packing should be placedbull for 3ndash5 days Septum splints are recommendedbull in comminuted septal fractures withbull severe mucosal lesions External nasal splintingbull for 10 days (Aquaplastreg Thermoplastreg)bull provides nasal protection Nasal saline spraysbull prevent crusting and oral antibiotics should
Nasal Fractures
bull Open reductionbull ndashndash Immediate repair of fractures by using
widebull surgical exposure reduction fixation and
reconstructionbull ndashndash The second option is delayed correctionbull (6 months or more) of persistent deformitiesbull using standard techniques of rhinoplasty
Deviated Nasal Septum
bull Definition of the diseasebull ndash Deviation of the nasal septum is a common causebull of unilateral nasal airway obstruction in which thebull nasal septum is displacedbull bull Epidemiologyaetiologybull ndash Developmental septal abnormalities Septal cartilage
damage in the neonatal period andbull during birth can cause severe septal deviation inbull the absence of a history of nasal trauma
Deviated Nasal Septum
bull Symptomsbull ndash Patients may present with a history of sinusitis
allergicbull rhinitis obstructive sleep apnoea previousbull nasal surgery or recent nasal trauma Unilateral or
bilateral nasal airway obstruction that is unrelievedbull with decongestants or nasal steroid sprays is oftenbull seenbull bull
Deviated Nasal SeptumDiagnosisndashExamination external dorsal deviation or the columella and caudal septummay be deflected off the midline (caudal subluxation)ndash Inspections of the nasal cavity and anterior-posteriorrhinoscopy are helpful in diagnosing the locationtype and severity of septal deformityThe endoscope is also useful in identifying polypsthe severity and extent of posterior septaldeviations and bony spurs and locating areas ofseptal perforation or mucosal injury
Deviated Nasal Septum
bull Therapybull ndash Septoplasty is a procedurebull The areabull of deviation is corrected or resected in order tobull leave behind as much cartilage and bone as
possiblebull Cartilage resection is minimised and can be
repositioned reshaped or recontoured using a variety of methods
Deviated Nasal Septum
bull ndash Indications of septoplasty before the growth period
bull of the nose is finished should be very limited bull -In these cases surgery must preserve all the
cartilagebull in order to prevent external changes of the
shape ofbull the nose
Deviated Nasal Septum
bull Complicationsbull ndash Frequent complications include haematoma andbull infection Cerebrospinal fluid leak is a rare but
potentiallybull serious complicationbull It is usually the resultbull of avulsion or damage to the cribriform plate whenbull handling the perpendicular plate of the ethmoidbull ndash Other complications include epistaxis nasal
Deviated Nasal Septum
bull Other complications include epistaxis nasal obstruction
bull due to residual deviation synechiae returnbull of the cartilaginous deviation septal perforationbull anosmia and cosmetic nasal deformities suchbull as widened alar rim margins drooping nasal tipbull columella retraction and a sunken dorsum with abull supratip saddle formation
Septal perforation with minor crusting View from provide closure of the
incision
Septal Haematoma
bull A septal haematoma is a blood collection under the perichondrium
bull of the septum and cartilagebull bull bull Epidemiologyaetiologybull ndash A septal haematoma is one of the most
severe complications of nasal trauma
Septal Haematoma
bull Diagnosisbull ndash Signs and symptoms include intense pain
swellingbull haematoma of the upper lip and philtrum
area andbull complete nasal airway obstruction
Septal HaematomaTherapyndash Management consists of drainage through a mucoperichondrial incision Immediate treatment isnecessary to prevent long-term problems such asa saddle-nose deformity perforation columellarretraction and nasal-base widening In childrenseptal destruction can lead to devastating nasal andmidfacial growth abnormalitiesbull Surgeryndash Incision and evacuation of the collection is performedDrainage of a septal haematoma should
Septal HaematomaSurgeryndash Incision and evacuation of the collection is performedDrainage of a septal haematoma should provide closure of the incision
Splints or transseptal sutures are placed to obliterate thepotential space and prevent collectionInfection involving the septal cartilage Reconstruction with autologouscartilage is then performed in a second stage Oral antibiotics should be given
Nasal DeformitySaddle-nose deformityndash A saddle-nose deformity is characterised by a loss ofnasal dorsal height and compromised nasal supportstructures -Other case observed are depressionof the middle vault and dorsum loss of nasal tipsupport and definition shortened (vertical) nasal length over rotation of the nasal tip and retrusion ofthe nasal spine and caudal septum It is also knownas a ldquoPug noserdquo or ldquoboxerrsquos noserdquo both of which referto various degrees of nasal dorsal depressionbull
Nasal DeformityEpidemiologyaetiologyndash Prevalence is higher in population groups prone to facial trauma (ie boxers athletes) those with historiesof intranasal cocaine use nasal surgery (e g radical submucosal septal resection reductive rhinoplasty)ndash A saddle-nose deformity can be congenital or acquired It can be noticed as a part of individual familialsyndromic and ethnic characteristics - Most deformities are due to traumatic and iatrogeniccauses Medical causes are Wegenerrsquosgranulomatosis relapsing polychondritis leprosy (Hansenrsquos disease) syphilis ectodermal dysplasiaand intranasal cocaine use
Nasal Deformity
bull Therapybull ndash Nasal reconstruction indications depend on patientbull selection surgeon experience and aetiology of thebull deformity bull Indications for surgery can be functionalbull aesthetic or most commonly both In individuals
with a compromised nasal airway a nasoseptalbull reconstruction is indicated
Nasal Deformity
bull Contraindications bull include patients with malignantbull chronic or autoimmune disease conditions drugbull abuse poor perioperative risk profile and unrealisticbull expectationsbull ndash Multiple previous rhinoplasties and certain
professionsbull (mixed martial artists boxers and other contactbull sports) are relative contraindications
Nasal DeformitySeptoplastyndash Septoplasty is performed to correct nasal obstructioncaused by septal deformityndash Usually septoplasty is performed under general anaesthesiawith the patient in the supine position with the head elevated by approximately 30 (Righthandedsurgeons approach from the right side)ndash Local vasoconstrictive anaesthesia is applied notonly to reduce postoperative pain but also more importantly to achieve vasoconstriction of themucosa and less intraoperative haemorrhage Lidocainewith adrenaline or epinephrine is usedalthough in patients with cardiac hypersensitivityoxymetazoline might be preferred
Nasal Deformity
bull Septoplasty begins with the incision of septal mucosabull Most operative techniques utilise a hemitransfixionbull incision at the caudal end of septum so thatbull deviation at this point might be reached as wellbull as a transfixion incision that is easily obtained ifbull needed (Right-handed surgeons normally choosebull the left side but that may vary when deviation isbull convex towards the right)
Nasal DeformityA columella retractor is placed over the columellaand by pulling it laterally the caudal border of theseptum is exposed Ala can be protected by an alaprotector A vertical incision with a no 15 bladeover the caudal end of septum is performed untilreaching the plane of the septal cartilage It is essentialto correctly identify the perichondrium and byusing the Cottle elevator dissect and lift it creatinga flap As the dissection proceeds along the septalcartilage a longer speculum (no 5) is introduced sothat elevation of the mucoperichondrium is doneunder constant visual controlndash The next step is to dissect the mucoperiostium
Nasal DeformityDissecting over the bony-cartilaginous junctionwhen joining both tunnels might be difficult and is
especially prone to membrane perforationndash If needed the same tunnels are to be created on the
other side of the septum Then deviated parts of
septum are identified and removed either with a
knife or a Freer chisel
Nasal Deformitybull septum from the maxillary crest the septum mustbull be separated from the perpendicular plate trimmedbull along the inferior border placed back onto the crestbull and sutured to the periosteum If the deformity involvesbull the vomer an osteotome is used Care mustbull be taken not to break the cribriform plate becausebull it could cause a cerebrospinal fistula
Nasal Deformity
bull Once the septal deviation is corrected the flapsbull and hemitransfixion incision are mattressed
withbull absorbable sutures Nasal packing to prevent
synechiaebull and postoperative septal haematoma mightbull be advised but should be removed within 72 h

The inferior turbinate consists of a separate bone thatis attached to the medial wall of the maxillary sinusThe opening of the nasolacrimal duct is located in thecorresponding inferior meatus The middle andsuperior turbinates are part of the ethmoid bone In rare cases a rudimentary ldquosupreme turbinaterdquo is alsopresent above the superior turbinate
The middle turbinate has by far the greatest functionalimportance because most of the drainage tracts fromthe surrounding paranasal sinuses open into the middlemeatus The nasal cavity is bounded superiorly by the cribriformplate of the ethmoid bone This thin bony platehas numerous openings for the passage of the fila olfactoriaand also forms the boundary of the anteriorcranial fossa
Nasal Cavities
The floor of the nasal cavity is formedmostly by the hard palate which is formed in turn bythe two palatine processes of the maxilla and the horizontallaminae of the palatine bone
Structure of the lateral nasal wall
Inferior meatus
Paranasal Sinuses
The paranasal sinuses are air-filled cavities that communicatewith the nasal cavities
-The maxillary sinus frontalsinus and anterior ethmoid cells drain into the nasalcavity through the middle meatusmdashie below themiddle turbinate -The posterior ethmoidcells drain into the nasal cavity through the superiormeatus The ostium of the sphenoid sinus is locatedin the anterior wall directly above the choanae- The anatomical connections between the nasal cavity andparanasal sinuses are functionally important and playa key role in the pathogenesis of many rhinologic diseasesthat involve the paranasal sinuses
Vascular SupplyThe external nose derives most of its blood supply
from the facial artery which arises from the external
carotid artery and from the ophthalmic artery which
springs from the internal carotid artery
Vascular Supply
The internalnose receives blood from the territories of the externaland internal carotid arteries- the terminalbranches of the sphenopalatine artery which arisesfrom the maxillary artery - the anterior and posteriorethmoid arteries which arise from the ophthalmicartery-internal carotid arterie
venous drainage
The venous drainageof the facial region is handled by -the facial vein -retromandibular vein -internal jugular vein
lymphatic drainage
The regional lymphatic drainage of the face and externalnose is handled mainly by- the submandibularlymph nodes while the nasal cavity is additionallydrained by -the retropharyngeal and deep - -cervical lymph nodes
Morphology of the Nasal Mucosa
Besides the anatomical structure of the external noseand nasal cavity the nasal mucosa plays an essentialrole in numerous functions of the nose in the respiratory tract
Morphology of the Nasal Mucosa
The anterior part of the nasal cavity (the nasal vestibule)like the external nose is covered by skin composedof a multilayer keratinizing squamous epithelium and finally a ciliated respiratory epithelium A small areaon the upper nasal septum superior turbinate andpart of the middle turbinate located adjacent to thecribriform plate is covered by olfactory mucosa and iscalled the olfactory region
Nerve SupplyThe facial skin receives its sensory innervation fromterminal branches of the trigeminal nerve that enterthe facial region through the supraorbital infraorbitaland mental foramina Thefacial muscles are classified as mimetic or mastica- tory each of these groups receiving different motorinnervationbythe facial nerve
History and Clinical Examination of the Nose
Historybull The main symptomsbull nasal obstruction (ldquostuffy
noserdquo)bull nasal dischargebull Headachesbull Olfactory
dysfunction
Palpationbony discontinuitiesNeuralgias to check
over- the supraorbital -infraorbital -mental foramina
Anterior Rhinoscopy
bull The rhinologic examination itself begins with anterior
bull rhinoscopy to evaluate the nasal vestibule and the anterior
bull portions of the nasal cavity
Nasal Endoscopy Nasal endoscopy has become the most important andrewarding clinical examination method in rhinologic diagnosis
- rigid endoscopes which are available in 4-mm and 28- mm diameters and assorted viewing angles (eg 01048576 301048576 1201048576) -flexible endoscopes are also available for inspecting the nose and nasopharynx and exploring all of the pharynx and larynx in one sitting
Nasal endoscopy
Nasal Endoscopy
Nasal Endoscopy
Imaging of the Nose and Paranasal Sinuses
Conventional RadiographsStandard paranasal sinus radiographs in the occipitomental
projection ( Water projection) and
occipitofrontal projection Caldwell projection) in cases of acute inflammation
They are also obtained to evaluate midfacial fractures
Computed Tomography (CT) the main indicationsfor CT scanning of the
nose and paranasal sinuses
are- chronic sinusitis - -trauma (especially
frontobasal -fractures)
-and tumors
The occipitofrontal projection is better for evaluating theethmoid cells and frontal sinus
occipitomental projection demonstrates the maxillarysinus and gives a limited view of the sphenoid sinus
Computed tomography of the paranasal sinuses
Four representative coronal CT scans are shown
Four representative coronal CT scans are shown
Magnetic Resonance Imaging
Magnetic maging
Magnetic resonance imaging (MRI) has fewer indicationsthan CT in patients with paranasal sinus diseaseThis is primarily because MRI is markedly inferior toCT in defining the bony boundaries of the sinusesThe strength of MRI lies in its superior soft-tissue discriminationMRI is indicated in diseases that involve the paranasal sinuses in addition to thecranial cavity or orbit (eg tumors and congenitalmalformations such as encephaloceles)
MRI of the paranasal sinuses
The Nose and Sinuses
Structure The structure of the nose is made up of
four partsbull The surface anatomybull The nasal skeletonmdashcomposed of the
two nasal bones the paired upper lateral and lower lateral cartilages and the nasal septum covered in subcutaneous tissue and skin
bull The internal anatomymdashincludes the septum of the nose which forms the medial wall of the nasal cavity The turbinates on the lateral wall are also called conchae
bull The osteomeatal complexmdasha key functional area of the nose
Function The nose is the main route for inspired
air and its structure is related to this function As the air passes over the large surface area of the turbinates
The inspired gases are warmed and humidified Mucus on the mucosa of the nose removes large dust particles from the air as it is breathed in
The voice resonates in the sinuses and nose and this provides character to the speech
Pneumatization of the sinusesmdashthey are air filled spacesmdashreduces the weight of the skull
Diseases of thDiseases of the Outer and Inner Nosee Outer and
Inner Nose Erysipelas Definition of the disease ndash Erysipela is a skin infection that affects the superficial dermis and is caused by Streptococcus pyogenes (group A) It usually develops in the extremities and the face and less commonly on the scalp and genitals bull Epidemiologyaetiology ndash Erysipelas are more often seen in elderly infants and children patients with compromised immunology and diabetes -Predisposing factors are alcoholism skin ulceration puncture wounds fungal infections malnutrition and burns
Erysipelas
bull Symptomsbull ndash It usually presents of fever general fatigue bull -The skin lesion is a redindurated and elevated plaque
with borders that expand rapidly bull It is painful warm and accompanied by variable oedemabull -On the second or third day a flaccid bulla may develop
and desquamationbull bull Presence of regional lymph nodes is common
Erysipelas
bull Complicationsndash The most common complication is recurrencewhich is seen in 18ndash30 of the cases even afterproper antibiotic therapy Recurrence is seen moreoften in females than in malesA skin infection with S pyogenes could lead toglomerulonephritis
Erysipelas
bull Complicationsbull ndash The most common complication is recurrencebull which is seen in 18ndash30 of the cases even afterbull proper antibiotic therapy bull -Recurrence is seen morebull often in females than in males bull -A skin infection with S pyogenes could lead tobull glomerulonephritis
Erysipelas
bull bull Diagnosisbull ndash Diagnosis is based on the patientrsquos personal
historybull and physical examination particularly on inspectionbull of the skin
bull Blood cultures are positive in less thanbull 5 of cases
ErysipelasTherapyndash Conservative therapybull The preferred antibiotic is penicillin In mildcases with minor systemic symptoms penicillinV 500 mg orally every 6 h for 10 days or penicillinG benzathine 12 mil U intramuscularlyonceOther possibilities are amoxicillin 500 mgorally twice a day for 10 days or cephalexin 500mg orally every 6 h for 10 days
ErysipelasIn moderate and severe cases with significantsystemic symptoms hospitalization and intravenoustreatment is required penicillin G 2ndash4mil U intravenously every 4ndash6 h Cefazolin05ndash15 gm intravenously every 8 h cefotaxime1ndash2 gm intravenously every 8 h or ceftriaxone1ndash2 gm intravenously once a day should be administeredIn patients with a penicillin allergyclindamycin 600 mg intravenously every 8 h orvancomycin 15 mgkg intravenously twice a daymay be given
ErysipelaAdditional useful therapeutic optionsbull Prednisone 30 mg over 8 days might be consideredas well as elevation of the affected siteMoist heat compresses may be usefulbull Surgeryndash Debridement and drainage are indicated when bullaeabscesses or necroses are presentbull Differential diagnosisndash Contact dermatitisndash Asteatotic eczemandash Herpes zosterndash Angioneurotic oedemandash Osteomyelitis
Furuncle
bull Definition of the diseasebull ndash A furuncle is an infection that beginsbull at the hair follicle and spreads deeper into thebull dermis and subcutaneous tissue forming abull nodule After several days it developsbull into an abscess - red painful and fluctuantbull bull bull Epidemiologyaetiologybull ndash The aetiologic agent is Staphylococcus aureus
FuruncleSymptomsndashsymptoms are local and limited to thesite of infection Furuncles usually are wherehair follicles are present bull Complicationndash One complication is furunculosis multiple draining furunclesDiagnosisndash The diagnosis is based on clinical inspection - Cultures are not necessary when there is no systemic involvement but should beconsidered if systemic therapy (in case of feversignificant cellulitis or hospitalization) or whenmethicillin-resistant Staphylococcusaureus (MRSA) is considered
FuruncleTherapyndash When the furuncle is small application of moist heat compress to promote drainage -Larger furuncles should be drained by surgical incision-After drainage the area should be cleaned with anantiseptic (with chlorhexidinebetadine) should be applied twice
a dayndash If no systemic symptoms or extensive cellulitis arepresent simple topical care is usually curative andoral antibiotics are not necessary Otherwise systemictreatment is indicated and should cover anypossible MRSA
Furuncle
bull -Recommended antibiotics are trimethoprim-sulfamethoxazole
bull 1ndash2 tablets orally twice daily doxycyclinebull 100 mg orally twice dailybull or clindamycin 300ndash450 mg orally every 8 hbull - In severe cases vancomycin 15 mgkg
intravenouslybull every 12 h or clindamycin 600 mg intravenouslybull every 8 h
Midline Granulomabull A midline granuloma is an angiocentricbull lymphoma it was referred to as polymorphicbull reticulosis lethal midline granuloma and midline
malignant reticulosisbull bull Definition of the diseasebull ndash This rare disease is a lymphoma of extranodal
presentationall cases are positive for the Epstein-Barr virus
bull -This lymphoma most commonly appears in the midface region
Midline GranulomaEpidemiologyaetiologyndash This form of lymphoma is rare in Europe and theUnited States with a higher prevalence in Asia and PeruSymptomsndash The most common presentation is nasal obstruction with a destructive mass occupying the nosesinuses and palate
-Fever night sweatsand weight loss seen usually in Hodgkinrsquos lymphomaand other non-Hodgkinrsquos lymphomas (knownas ldquoB symptomsrdquo) are uncommon
Midline GranulomaDiagnosisndash The diagnosis is based on anatomopathologicalstudy The malignancy of the tumour manifested byextensive necrosis makes the histological diagnosisdifficult and often more biopsies are required forconfirmationbull Therapyndash Therapy consists of radiotherapy with or withoutchemotherapy
Midline Granuloma
bull Prognosisbull ndash Depending on the stage long-term remission or
experience a worseningbull prognosis with relapses which may include otherbull extranodal sites bull Involvement of extranodal sitesbull including the upper airway gastrointestinal tractbull skin
Wegenerrsquos Granulomatosis
bull Definition of the diseasebull ndash Wegenerrsquos granulomatosis is a systemic chronicbull vasculitis of small- and medium-sized blood vesselsbull with an autoimmune component It affectsbull particular organs with variable predilectionbull Epidemiologyaetiologybull ndash Wegenerrsquos granulomatosis is a rare disease It affects
about 1 in 20000ndash30000 people It is more prevalentbull in middle-aged Caucasian patients
Wegenerrsquos Granulomatosis
Symptomsndash The disease may present pulmonary upper
respiratory tract or renal In the disseminated form-The localised form ndash confinedto the upper respiratory region ndash is present in 25of the patients- It consists of nonspecific manifestationssuch as nasal obstruction crusting purulentor bloody rhinorrhea and painful or painless ulcers in oral or nasal cavities which are unresponsive tostandard medical treatment
Wegenerrsquos Granulomatosis
bull In some patients the nasal septum is perforatedbull which leads to saddle-nose deformity Less
commonbull symptoms are hoarseness stridor due to
subglotticbull stenosis otalgia otorrhea and conductivebull and sensorineural hearing loss Also ocular
symptomsbull such as scleritis conjunctivitis uveitis andbull episcleritis may be present
Wegenerrsquos Granulomatosis
bull ndash In the disseminated form pulmonary involvementbull is manifested by cough dyspnoea haemoptysisbull (due to an alveolar capillaritis necrotic lesions orbull endobronchial disease) and pleuritic painndashbull -Ninety per cent of patients have nasal symptomsbull and these symptoms are usually the first
manifestationof the diseasebull -Most patients have also renal involvementbull even if it is subclinical
Wegenerrsquos Granulomatosis
Diagnosis ndash Diagnosis of Wegenerrsquos granulomatosis is based on clinical findings that demonstrate lung (chest x-ray) kidney (urine analysis) or upper respiratory tract
involvement (oral or nasal ulcers or discharge) - positive blood analysis for cytoplasmic-staining antineutrophil
cytoplasmic antibodies (c-ANCA) and confirming proteinase 3 (PR3) ANCA or myeloperoxidase (MPO) ANCA ndash Biopsy is essential for diagnosis nonspecific chronic inflammation
and necrosis -Bacterial and fungal infections
Wegenerrsquos Granulomatosis
Therapyndash Conservative therapybull In the induction of disease remission highdosesteroids (e g prednisone 1 mgkgday) for1 month with tapering over several months aregiven In addition cyclophosphamide (2 mgkgday) should be administered for 6ndash12 monthsuntil symptoms disappear In the maintenanceof remission cyclophosphamide should be
Wegenerrsquos Granulomatosis
Antibiotics mainly trimethoprim-sulfamethoxazoleare given for prophylaxis againstPneumocystis jiroveci (formerly Pneumocystiscarinii) pneumonia (PCP) which may developduring immunosuppression and have a role inpreventing recurrencesbull Sinonasal manifestations may be treated with topical nasal steroids and nasal irrigations lowdosesystemic steroids and antibiotics when bacterial infection (typically Staphylococcus species) is suspected
Wegenerrsquos Granulomatosis
bull Prognosisbull ndash Most of the patients respond well to treatmentbull achieving symptom-free intervals of 5ndash20 yearsbull or more bull -Anatomical problems (sinusitis trachealbull stenosis) may require surgery bull Relapses can be long and troublesomebull Long-term complications are chronicbull renal failure hearing loss and deafness
Nasal Fractures Definition ndash A nasal fracture is a disruption of the nasal bone structure due to trauma It is the most frequently fractured facial bone Epidemiologyaetiology ndash Sports falls and assaults are the usual mechanisms of fracture -Males are affected twice as often as are females -Paediatric populations with a incidences during the second and third decades of life -Variables such as force impact direction nature of the striking object age and other will influence the pattern of injury to the components of the nose
Nasal Fractures
bull Symptomsbull ndash Deformity swelling epistaxis and periorbital
ecchymosis are signs that are suggestive of nasal fracture
bull bony crepitus and nasal segment mobilitybull ndash Epiphora bull Severe bilateral injuries to the lachrymal bones
arebull associated with depressed nasal fractures
Nasal Fractures Complications ndash Septal haematoma is one of the most severe early complications of nasal trauma and without drainage it results in abscess formation 6ndash7 days after trauma producing necrosis of the septal cartilage -Long-term problems such as saddle-nose deformity perforation columellar retraction and nasalbase
Septal infection could lead to osteomyelitis orbital and intracranial abscesses meningitis and cavernous sinus thrombosis -Cerebrospinal fluid leakage is a common complication of severe
nasal and frontal fractures
Nasal Fractures
bull Diagnostic proceduresbull ndash Inspectionbull bull Changes of appearance such as deviation andbull asymmetry bleeding watery drainage changesbull in nasal breathing and smell It is useful to comparebull the current presentation with old photographsbull (up to 40 of normal individuals havebull significant nose malformations)
Nasal Fractures Physical examination bull The diagnosis of a nasal fracture is made primarily by physical examination epistaxis nasal swelling and periorbital ecchymosis Nasal shape in the lateral and frontal inspection should be assessed Grasping the dorsum between two fingers and rocking the pyramid back and forth aids in assessing the mobility of nasal bones Internal structures should be evaluated by using a headlight and nasal speculum Clotted blood is removed by suction and assessment of haematoma mucosal tears and active bleeding is performed Bimanual palpation of the septum helps to differentiate septal swelling from haematoma ndash
Nasal FracturesRadiographybull There is no clear evidence of the role of radiographyin the management of nasal fracturesPlain films have up to a 66 false-positive rateas a result of misinterpretation of normal suturelines In addition old fractures are difficult todistinguishbull Three-dimensional CT is recommended for extensiveinjuries involving the nasal-orbital-ethmoidalcomplexndash
Nasal Fractures
bull Additionaluseful diagnostic proceduresbull bull Using a 0 or 30deg 4-mm endoscope is helpful inbull the assessment of posterior abnormalities If thebull patient is heavily sedated Brown-Gruss
provocationbull manoeuvres may be performed to determinebull deformities in upper middle or lower segmentsbull by compressing each compartment
Nasal FracturesConservative treatmentndash Treatment of bleedingbull For localised bleeding anterior sources may becauterised by silver nitrate or sealed with topicalmaterials such as thrombin combined withgelatin foam fibrin glue FloSealreg or other procoagulantmaterials If conservative measuresfail a formal anterior packing is placedbull Bleeding from branches of sphenopalatine orethmoid vessels requires anterior-posteriorpacking
Nasal Fractures
bull bull Surgical methods such as direct endoscopic vessel
bull cauterization or ligation have been shown tobull offer better haemostasis and patient comfortbull Angiography with embolization can also be
consideredbull in cases refractory to more conservativebull approaches
Nasal Fractures
bull Type of reductionbull bull Nondisplaced fractures should be treated withbull observation alone Closed nasal reduction is thebull best choice for simple injuries (isolated unilateralbull with medial displacement)bull bull An open approach should be considered in
severebull trauma (bilateral depressed fractures)
Nasal Fracturesbull Surgical principlesbull ndash Topical anaesthesia with cotton pledgets soakedbull with 4 cocaine or 005 oxymethazoline combinedbull with 4 topical lidocaine should be appliedbull for 5ndash10 min Local anaesthesia should also be injectedbull (1 lidocaine and 1100000 epinephrine)bull along the septum lateral walls and floor of the nasalbull cavitybull bull
Nasal FracturesClosed reductionndashndash The nasal bones are grasped between two fingersand pressure is applied laterally in theopposite direction of the deviation A bluntelevator may be used from within the nose incases of significant medial collapse Walshamforceps can be of help Reduction of the septumshould be performed with the use ofAsch forceps
Nasal Fractures
bull To prevent collapse of the postreductionbull framework nasal packing should be placedbull for 3ndash5 days Septum splints are recommendedbull in comminuted septal fractures withbull severe mucosal lesions External nasal splintingbull for 10 days (Aquaplastreg Thermoplastreg)bull provides nasal protection Nasal saline spraysbull prevent crusting and oral antibiotics should
Nasal Fractures
bull Open reductionbull ndashndash Immediate repair of fractures by using
widebull surgical exposure reduction fixation and
reconstructionbull ndashndash The second option is delayed correctionbull (6 months or more) of persistent deformitiesbull using standard techniques of rhinoplasty
Deviated Nasal Septum
bull Definition of the diseasebull ndash Deviation of the nasal septum is a common causebull of unilateral nasal airway obstruction in which thebull nasal septum is displacedbull bull Epidemiologyaetiologybull ndash Developmental septal abnormalities Septal cartilage
damage in the neonatal period andbull during birth can cause severe septal deviation inbull the absence of a history of nasal trauma
Deviated Nasal Septum
bull Symptomsbull ndash Patients may present with a history of sinusitis
allergicbull rhinitis obstructive sleep apnoea previousbull nasal surgery or recent nasal trauma Unilateral or
bilateral nasal airway obstruction that is unrelievedbull with decongestants or nasal steroid sprays is oftenbull seenbull bull
Deviated Nasal SeptumDiagnosisndashExamination external dorsal deviation or the columella and caudal septummay be deflected off the midline (caudal subluxation)ndash Inspections of the nasal cavity and anterior-posteriorrhinoscopy are helpful in diagnosing the locationtype and severity of septal deformityThe endoscope is also useful in identifying polypsthe severity and extent of posterior septaldeviations and bony spurs and locating areas ofseptal perforation or mucosal injury
Deviated Nasal Septum
bull Therapybull ndash Septoplasty is a procedurebull The areabull of deviation is corrected or resected in order tobull leave behind as much cartilage and bone as
possiblebull Cartilage resection is minimised and can be
repositioned reshaped or recontoured using a variety of methods
Deviated Nasal Septum
bull ndash Indications of septoplasty before the growth period
bull of the nose is finished should be very limited bull -In these cases surgery must preserve all the
cartilagebull in order to prevent external changes of the
shape ofbull the nose
Deviated Nasal Septum
bull Complicationsbull ndash Frequent complications include haematoma andbull infection Cerebrospinal fluid leak is a rare but
potentiallybull serious complicationbull It is usually the resultbull of avulsion or damage to the cribriform plate whenbull handling the perpendicular plate of the ethmoidbull ndash Other complications include epistaxis nasal
Deviated Nasal Septum
bull Other complications include epistaxis nasal obstruction
bull due to residual deviation synechiae returnbull of the cartilaginous deviation septal perforationbull anosmia and cosmetic nasal deformities suchbull as widened alar rim margins drooping nasal tipbull columella retraction and a sunken dorsum with abull supratip saddle formation
Septal perforation with minor crusting View from provide closure of the
incision
Septal Haematoma
bull A septal haematoma is a blood collection under the perichondrium
bull of the septum and cartilagebull bull bull Epidemiologyaetiologybull ndash A septal haematoma is one of the most
severe complications of nasal trauma
Septal Haematoma
bull Diagnosisbull ndash Signs and symptoms include intense pain
swellingbull haematoma of the upper lip and philtrum
area andbull complete nasal airway obstruction
Septal HaematomaTherapyndash Management consists of drainage through a mucoperichondrial incision Immediate treatment isnecessary to prevent long-term problems such asa saddle-nose deformity perforation columellarretraction and nasal-base widening In childrenseptal destruction can lead to devastating nasal andmidfacial growth abnormalitiesbull Surgeryndash Incision and evacuation of the collection is performedDrainage of a septal haematoma should
Septal HaematomaSurgeryndash Incision and evacuation of the collection is performedDrainage of a septal haematoma should provide closure of the incision
Splints or transseptal sutures are placed to obliterate thepotential space and prevent collectionInfection involving the septal cartilage Reconstruction with autologouscartilage is then performed in a second stage Oral antibiotics should be given
Nasal DeformitySaddle-nose deformityndash A saddle-nose deformity is characterised by a loss ofnasal dorsal height and compromised nasal supportstructures -Other case observed are depressionof the middle vault and dorsum loss of nasal tipsupport and definition shortened (vertical) nasal length over rotation of the nasal tip and retrusion ofthe nasal spine and caudal septum It is also knownas a ldquoPug noserdquo or ldquoboxerrsquos noserdquo both of which referto various degrees of nasal dorsal depressionbull
Nasal DeformityEpidemiologyaetiologyndash Prevalence is higher in population groups prone to facial trauma (ie boxers athletes) those with historiesof intranasal cocaine use nasal surgery (e g radical submucosal septal resection reductive rhinoplasty)ndash A saddle-nose deformity can be congenital or acquired It can be noticed as a part of individual familialsyndromic and ethnic characteristics - Most deformities are due to traumatic and iatrogeniccauses Medical causes are Wegenerrsquosgranulomatosis relapsing polychondritis leprosy (Hansenrsquos disease) syphilis ectodermal dysplasiaand intranasal cocaine use
Nasal Deformity
bull Therapybull ndash Nasal reconstruction indications depend on patientbull selection surgeon experience and aetiology of thebull deformity bull Indications for surgery can be functionalbull aesthetic or most commonly both In individuals
with a compromised nasal airway a nasoseptalbull reconstruction is indicated
Nasal Deformity
bull Contraindications bull include patients with malignantbull chronic or autoimmune disease conditions drugbull abuse poor perioperative risk profile and unrealisticbull expectationsbull ndash Multiple previous rhinoplasties and certain
professionsbull (mixed martial artists boxers and other contactbull sports) are relative contraindications
Nasal DeformitySeptoplastyndash Septoplasty is performed to correct nasal obstructioncaused by septal deformityndash Usually septoplasty is performed under general anaesthesiawith the patient in the supine position with the head elevated by approximately 30 (Righthandedsurgeons approach from the right side)ndash Local vasoconstrictive anaesthesia is applied notonly to reduce postoperative pain but also more importantly to achieve vasoconstriction of themucosa and less intraoperative haemorrhage Lidocainewith adrenaline or epinephrine is usedalthough in patients with cardiac hypersensitivityoxymetazoline might be preferred
Nasal Deformity
bull Septoplasty begins with the incision of septal mucosabull Most operative techniques utilise a hemitransfixionbull incision at the caudal end of septum so thatbull deviation at this point might be reached as wellbull as a transfixion incision that is easily obtained ifbull needed (Right-handed surgeons normally choosebull the left side but that may vary when deviation isbull convex towards the right)
Nasal DeformityA columella retractor is placed over the columellaand by pulling it laterally the caudal border of theseptum is exposed Ala can be protected by an alaprotector A vertical incision with a no 15 bladeover the caudal end of septum is performed untilreaching the plane of the septal cartilage It is essentialto correctly identify the perichondrium and byusing the Cottle elevator dissect and lift it creatinga flap As the dissection proceeds along the septalcartilage a longer speculum (no 5) is introduced sothat elevation of the mucoperichondrium is doneunder constant visual controlndash The next step is to dissect the mucoperiostium
Nasal DeformityDissecting over the bony-cartilaginous junctionwhen joining both tunnels might be difficult and is
especially prone to membrane perforationndash If needed the same tunnels are to be created on the
other side of the septum Then deviated parts of
septum are identified and removed either with a
knife or a Freer chisel
Nasal Deformitybull septum from the maxillary crest the septum mustbull be separated from the perpendicular plate trimmedbull along the inferior border placed back onto the crestbull and sutured to the periosteum If the deformity involvesbull the vomer an osteotome is used Care mustbull be taken not to break the cribriform plate becausebull it could cause a cerebrospinal fistula
Nasal Deformity
bull Once the septal deviation is corrected the flapsbull and hemitransfixion incision are mattressed
withbull absorbable sutures Nasal packing to prevent
synechiaebull and postoperative septal haematoma mightbull be advised but should be removed within 72 h

The middle turbinate has by far the greatest functionalimportance because most of the drainage tracts fromthe surrounding paranasal sinuses open into the middlemeatus The nasal cavity is bounded superiorly by the cribriformplate of the ethmoid bone This thin bony platehas numerous openings for the passage of the fila olfactoriaand also forms the boundary of the anteriorcranial fossa
Nasal Cavities
The floor of the nasal cavity is formedmostly by the hard palate which is formed in turn bythe two palatine processes of the maxilla and the horizontallaminae of the palatine bone
Structure of the lateral nasal wall
Inferior meatus
Paranasal Sinuses
The paranasal sinuses are air-filled cavities that communicatewith the nasal cavities
-The maxillary sinus frontalsinus and anterior ethmoid cells drain into the nasalcavity through the middle meatusmdashie below themiddle turbinate -The posterior ethmoidcells drain into the nasal cavity through the superiormeatus The ostium of the sphenoid sinus is locatedin the anterior wall directly above the choanae- The anatomical connections between the nasal cavity andparanasal sinuses are functionally important and playa key role in the pathogenesis of many rhinologic diseasesthat involve the paranasal sinuses
Vascular SupplyThe external nose derives most of its blood supply
from the facial artery which arises from the external
carotid artery and from the ophthalmic artery which
springs from the internal carotid artery
Vascular Supply
The internalnose receives blood from the territories of the externaland internal carotid arteries- the terminalbranches of the sphenopalatine artery which arisesfrom the maxillary artery - the anterior and posteriorethmoid arteries which arise from the ophthalmicartery-internal carotid arterie
venous drainage
The venous drainageof the facial region is handled by -the facial vein -retromandibular vein -internal jugular vein
lymphatic drainage
The regional lymphatic drainage of the face and externalnose is handled mainly by- the submandibularlymph nodes while the nasal cavity is additionallydrained by -the retropharyngeal and deep - -cervical lymph nodes
Morphology of the Nasal Mucosa
Besides the anatomical structure of the external noseand nasal cavity the nasal mucosa plays an essentialrole in numerous functions of the nose in the respiratory tract
Morphology of the Nasal Mucosa
The anterior part of the nasal cavity (the nasal vestibule)like the external nose is covered by skin composedof a multilayer keratinizing squamous epithelium and finally a ciliated respiratory epithelium A small areaon the upper nasal septum superior turbinate andpart of the middle turbinate located adjacent to thecribriform plate is covered by olfactory mucosa and iscalled the olfactory region
Nerve SupplyThe facial skin receives its sensory innervation fromterminal branches of the trigeminal nerve that enterthe facial region through the supraorbital infraorbitaland mental foramina Thefacial muscles are classified as mimetic or mastica- tory each of these groups receiving different motorinnervationbythe facial nerve
History and Clinical Examination of the Nose
Historybull The main symptomsbull nasal obstruction (ldquostuffy
noserdquo)bull nasal dischargebull Headachesbull Olfactory
dysfunction
Palpationbony discontinuitiesNeuralgias to check
over- the supraorbital -infraorbital -mental foramina
Anterior Rhinoscopy
bull The rhinologic examination itself begins with anterior
bull rhinoscopy to evaluate the nasal vestibule and the anterior
bull portions of the nasal cavity
Nasal Endoscopy Nasal endoscopy has become the most important andrewarding clinical examination method in rhinologic diagnosis
- rigid endoscopes which are available in 4-mm and 28- mm diameters and assorted viewing angles (eg 01048576 301048576 1201048576) -flexible endoscopes are also available for inspecting the nose and nasopharynx and exploring all of the pharynx and larynx in one sitting
Nasal endoscopy
Nasal Endoscopy
Nasal Endoscopy
Imaging of the Nose and Paranasal Sinuses
Conventional RadiographsStandard paranasal sinus radiographs in the occipitomental
projection ( Water projection) and
occipitofrontal projection Caldwell projection) in cases of acute inflammation
They are also obtained to evaluate midfacial fractures
Computed Tomography (CT) the main indicationsfor CT scanning of the
nose and paranasal sinuses
are- chronic sinusitis - -trauma (especially
frontobasal -fractures)
-and tumors
The occipitofrontal projection is better for evaluating theethmoid cells and frontal sinus
occipitomental projection demonstrates the maxillarysinus and gives a limited view of the sphenoid sinus
Computed tomography of the paranasal sinuses
Four representative coronal CT scans are shown
Four representative coronal CT scans are shown
Magnetic Resonance Imaging
Magnetic maging
Magnetic resonance imaging (MRI) has fewer indicationsthan CT in patients with paranasal sinus diseaseThis is primarily because MRI is markedly inferior toCT in defining the bony boundaries of the sinusesThe strength of MRI lies in its superior soft-tissue discriminationMRI is indicated in diseases that involve the paranasal sinuses in addition to thecranial cavity or orbit (eg tumors and congenitalmalformations such as encephaloceles)
MRI of the paranasal sinuses
The Nose and Sinuses
Structure The structure of the nose is made up of
four partsbull The surface anatomybull The nasal skeletonmdashcomposed of the
two nasal bones the paired upper lateral and lower lateral cartilages and the nasal septum covered in subcutaneous tissue and skin
bull The internal anatomymdashincludes the septum of the nose which forms the medial wall of the nasal cavity The turbinates on the lateral wall are also called conchae
bull The osteomeatal complexmdasha key functional area of the nose
Function The nose is the main route for inspired
air and its structure is related to this function As the air passes over the large surface area of the turbinates
The inspired gases are warmed and humidified Mucus on the mucosa of the nose removes large dust particles from the air as it is breathed in
The voice resonates in the sinuses and nose and this provides character to the speech
Pneumatization of the sinusesmdashthey are air filled spacesmdashreduces the weight of the skull
Diseases of thDiseases of the Outer and Inner Nosee Outer and
Inner Nose Erysipelas Definition of the disease ndash Erysipela is a skin infection that affects the superficial dermis and is caused by Streptococcus pyogenes (group A) It usually develops in the extremities and the face and less commonly on the scalp and genitals bull Epidemiologyaetiology ndash Erysipelas are more often seen in elderly infants and children patients with compromised immunology and diabetes -Predisposing factors are alcoholism skin ulceration puncture wounds fungal infections malnutrition and burns
Erysipelas
bull Symptomsbull ndash It usually presents of fever general fatigue bull -The skin lesion is a redindurated and elevated plaque
with borders that expand rapidly bull It is painful warm and accompanied by variable oedemabull -On the second or third day a flaccid bulla may develop
and desquamationbull bull Presence of regional lymph nodes is common
Erysipelas
bull Complicationsndash The most common complication is recurrencewhich is seen in 18ndash30 of the cases even afterproper antibiotic therapy Recurrence is seen moreoften in females than in malesA skin infection with S pyogenes could lead toglomerulonephritis
Erysipelas
bull Complicationsbull ndash The most common complication is recurrencebull which is seen in 18ndash30 of the cases even afterbull proper antibiotic therapy bull -Recurrence is seen morebull often in females than in males bull -A skin infection with S pyogenes could lead tobull glomerulonephritis
Erysipelas
bull bull Diagnosisbull ndash Diagnosis is based on the patientrsquos personal
historybull and physical examination particularly on inspectionbull of the skin
bull Blood cultures are positive in less thanbull 5 of cases
ErysipelasTherapyndash Conservative therapybull The preferred antibiotic is penicillin In mildcases with minor systemic symptoms penicillinV 500 mg orally every 6 h for 10 days or penicillinG benzathine 12 mil U intramuscularlyonceOther possibilities are amoxicillin 500 mgorally twice a day for 10 days or cephalexin 500mg orally every 6 h for 10 days
ErysipelasIn moderate and severe cases with significantsystemic symptoms hospitalization and intravenoustreatment is required penicillin G 2ndash4mil U intravenously every 4ndash6 h Cefazolin05ndash15 gm intravenously every 8 h cefotaxime1ndash2 gm intravenously every 8 h or ceftriaxone1ndash2 gm intravenously once a day should be administeredIn patients with a penicillin allergyclindamycin 600 mg intravenously every 8 h orvancomycin 15 mgkg intravenously twice a daymay be given
ErysipelaAdditional useful therapeutic optionsbull Prednisone 30 mg over 8 days might be consideredas well as elevation of the affected siteMoist heat compresses may be usefulbull Surgeryndash Debridement and drainage are indicated when bullaeabscesses or necroses are presentbull Differential diagnosisndash Contact dermatitisndash Asteatotic eczemandash Herpes zosterndash Angioneurotic oedemandash Osteomyelitis
Furuncle
bull Definition of the diseasebull ndash A furuncle is an infection that beginsbull at the hair follicle and spreads deeper into thebull dermis and subcutaneous tissue forming abull nodule After several days it developsbull into an abscess - red painful and fluctuantbull bull bull Epidemiologyaetiologybull ndash The aetiologic agent is Staphylococcus aureus
FuruncleSymptomsndashsymptoms are local and limited to thesite of infection Furuncles usually are wherehair follicles are present bull Complicationndash One complication is furunculosis multiple draining furunclesDiagnosisndash The diagnosis is based on clinical inspection - Cultures are not necessary when there is no systemic involvement but should beconsidered if systemic therapy (in case of feversignificant cellulitis or hospitalization) or whenmethicillin-resistant Staphylococcusaureus (MRSA) is considered
FuruncleTherapyndash When the furuncle is small application of moist heat compress to promote drainage -Larger furuncles should be drained by surgical incision-After drainage the area should be cleaned with anantiseptic (with chlorhexidinebetadine) should be applied twice
a dayndash If no systemic symptoms or extensive cellulitis arepresent simple topical care is usually curative andoral antibiotics are not necessary Otherwise systemictreatment is indicated and should cover anypossible MRSA
Furuncle
bull -Recommended antibiotics are trimethoprim-sulfamethoxazole
bull 1ndash2 tablets orally twice daily doxycyclinebull 100 mg orally twice dailybull or clindamycin 300ndash450 mg orally every 8 hbull - In severe cases vancomycin 15 mgkg
intravenouslybull every 12 h or clindamycin 600 mg intravenouslybull every 8 h
Midline Granulomabull A midline granuloma is an angiocentricbull lymphoma it was referred to as polymorphicbull reticulosis lethal midline granuloma and midline
malignant reticulosisbull bull Definition of the diseasebull ndash This rare disease is a lymphoma of extranodal
presentationall cases are positive for the Epstein-Barr virus
bull -This lymphoma most commonly appears in the midface region
Midline GranulomaEpidemiologyaetiologyndash This form of lymphoma is rare in Europe and theUnited States with a higher prevalence in Asia and PeruSymptomsndash The most common presentation is nasal obstruction with a destructive mass occupying the nosesinuses and palate
-Fever night sweatsand weight loss seen usually in Hodgkinrsquos lymphomaand other non-Hodgkinrsquos lymphomas (knownas ldquoB symptomsrdquo) are uncommon
Midline GranulomaDiagnosisndash The diagnosis is based on anatomopathologicalstudy The malignancy of the tumour manifested byextensive necrosis makes the histological diagnosisdifficult and often more biopsies are required forconfirmationbull Therapyndash Therapy consists of radiotherapy with or withoutchemotherapy
Midline Granuloma
bull Prognosisbull ndash Depending on the stage long-term remission or
experience a worseningbull prognosis with relapses which may include otherbull extranodal sites bull Involvement of extranodal sitesbull including the upper airway gastrointestinal tractbull skin
Wegenerrsquos Granulomatosis
bull Definition of the diseasebull ndash Wegenerrsquos granulomatosis is a systemic chronicbull vasculitis of small- and medium-sized blood vesselsbull with an autoimmune component It affectsbull particular organs with variable predilectionbull Epidemiologyaetiologybull ndash Wegenerrsquos granulomatosis is a rare disease It affects
about 1 in 20000ndash30000 people It is more prevalentbull in middle-aged Caucasian patients
Wegenerrsquos Granulomatosis
Symptomsndash The disease may present pulmonary upper
respiratory tract or renal In the disseminated form-The localised form ndash confinedto the upper respiratory region ndash is present in 25of the patients- It consists of nonspecific manifestationssuch as nasal obstruction crusting purulentor bloody rhinorrhea and painful or painless ulcers in oral or nasal cavities which are unresponsive tostandard medical treatment
Wegenerrsquos Granulomatosis
bull In some patients the nasal septum is perforatedbull which leads to saddle-nose deformity Less
commonbull symptoms are hoarseness stridor due to
subglotticbull stenosis otalgia otorrhea and conductivebull and sensorineural hearing loss Also ocular
symptomsbull such as scleritis conjunctivitis uveitis andbull episcleritis may be present
Wegenerrsquos Granulomatosis
bull ndash In the disseminated form pulmonary involvementbull is manifested by cough dyspnoea haemoptysisbull (due to an alveolar capillaritis necrotic lesions orbull endobronchial disease) and pleuritic painndashbull -Ninety per cent of patients have nasal symptomsbull and these symptoms are usually the first
manifestationof the diseasebull -Most patients have also renal involvementbull even if it is subclinical
Wegenerrsquos Granulomatosis
Diagnosis ndash Diagnosis of Wegenerrsquos granulomatosis is based on clinical findings that demonstrate lung (chest x-ray) kidney (urine analysis) or upper respiratory tract
involvement (oral or nasal ulcers or discharge) - positive blood analysis for cytoplasmic-staining antineutrophil
cytoplasmic antibodies (c-ANCA) and confirming proteinase 3 (PR3) ANCA or myeloperoxidase (MPO) ANCA ndash Biopsy is essential for diagnosis nonspecific chronic inflammation
and necrosis -Bacterial and fungal infections
Wegenerrsquos Granulomatosis
Therapyndash Conservative therapybull In the induction of disease remission highdosesteroids (e g prednisone 1 mgkgday) for1 month with tapering over several months aregiven In addition cyclophosphamide (2 mgkgday) should be administered for 6ndash12 monthsuntil symptoms disappear In the maintenanceof remission cyclophosphamide should be
Wegenerrsquos Granulomatosis
Antibiotics mainly trimethoprim-sulfamethoxazoleare given for prophylaxis againstPneumocystis jiroveci (formerly Pneumocystiscarinii) pneumonia (PCP) which may developduring immunosuppression and have a role inpreventing recurrencesbull Sinonasal manifestations may be treated with topical nasal steroids and nasal irrigations lowdosesystemic steroids and antibiotics when bacterial infection (typically Staphylococcus species) is suspected
Wegenerrsquos Granulomatosis
bull Prognosisbull ndash Most of the patients respond well to treatmentbull achieving symptom-free intervals of 5ndash20 yearsbull or more bull -Anatomical problems (sinusitis trachealbull stenosis) may require surgery bull Relapses can be long and troublesomebull Long-term complications are chronicbull renal failure hearing loss and deafness
Nasal Fractures Definition ndash A nasal fracture is a disruption of the nasal bone structure due to trauma It is the most frequently fractured facial bone Epidemiologyaetiology ndash Sports falls and assaults are the usual mechanisms of fracture -Males are affected twice as often as are females -Paediatric populations with a incidences during the second and third decades of life -Variables such as force impact direction nature of the striking object age and other will influence the pattern of injury to the components of the nose
Nasal Fractures
bull Symptomsbull ndash Deformity swelling epistaxis and periorbital
ecchymosis are signs that are suggestive of nasal fracture
bull bony crepitus and nasal segment mobilitybull ndash Epiphora bull Severe bilateral injuries to the lachrymal bones
arebull associated with depressed nasal fractures
Nasal Fractures Complications ndash Septal haematoma is one of the most severe early complications of nasal trauma and without drainage it results in abscess formation 6ndash7 days after trauma producing necrosis of the septal cartilage -Long-term problems such as saddle-nose deformity perforation columellar retraction and nasalbase
Septal infection could lead to osteomyelitis orbital and intracranial abscesses meningitis and cavernous sinus thrombosis -Cerebrospinal fluid leakage is a common complication of severe
nasal and frontal fractures
Nasal Fractures
bull Diagnostic proceduresbull ndash Inspectionbull bull Changes of appearance such as deviation andbull asymmetry bleeding watery drainage changesbull in nasal breathing and smell It is useful to comparebull the current presentation with old photographsbull (up to 40 of normal individuals havebull significant nose malformations)
Nasal Fractures Physical examination bull The diagnosis of a nasal fracture is made primarily by physical examination epistaxis nasal swelling and periorbital ecchymosis Nasal shape in the lateral and frontal inspection should be assessed Grasping the dorsum between two fingers and rocking the pyramid back and forth aids in assessing the mobility of nasal bones Internal structures should be evaluated by using a headlight and nasal speculum Clotted blood is removed by suction and assessment of haematoma mucosal tears and active bleeding is performed Bimanual palpation of the septum helps to differentiate septal swelling from haematoma ndash
Nasal FracturesRadiographybull There is no clear evidence of the role of radiographyin the management of nasal fracturesPlain films have up to a 66 false-positive rateas a result of misinterpretation of normal suturelines In addition old fractures are difficult todistinguishbull Three-dimensional CT is recommended for extensiveinjuries involving the nasal-orbital-ethmoidalcomplexndash
Nasal Fractures
bull Additionaluseful diagnostic proceduresbull bull Using a 0 or 30deg 4-mm endoscope is helpful inbull the assessment of posterior abnormalities If thebull patient is heavily sedated Brown-Gruss
provocationbull manoeuvres may be performed to determinebull deformities in upper middle or lower segmentsbull by compressing each compartment
Nasal FracturesConservative treatmentndash Treatment of bleedingbull For localised bleeding anterior sources may becauterised by silver nitrate or sealed with topicalmaterials such as thrombin combined withgelatin foam fibrin glue FloSealreg or other procoagulantmaterials If conservative measuresfail a formal anterior packing is placedbull Bleeding from branches of sphenopalatine orethmoid vessels requires anterior-posteriorpacking
Nasal Fractures
bull bull Surgical methods such as direct endoscopic vessel
bull cauterization or ligation have been shown tobull offer better haemostasis and patient comfortbull Angiography with embolization can also be
consideredbull in cases refractory to more conservativebull approaches
Nasal Fractures
bull Type of reductionbull bull Nondisplaced fractures should be treated withbull observation alone Closed nasal reduction is thebull best choice for simple injuries (isolated unilateralbull with medial displacement)bull bull An open approach should be considered in
severebull trauma (bilateral depressed fractures)
Nasal Fracturesbull Surgical principlesbull ndash Topical anaesthesia with cotton pledgets soakedbull with 4 cocaine or 005 oxymethazoline combinedbull with 4 topical lidocaine should be appliedbull for 5ndash10 min Local anaesthesia should also be injectedbull (1 lidocaine and 1100000 epinephrine)bull along the septum lateral walls and floor of the nasalbull cavitybull bull
Nasal FracturesClosed reductionndashndash The nasal bones are grasped between two fingersand pressure is applied laterally in theopposite direction of the deviation A bluntelevator may be used from within the nose incases of significant medial collapse Walshamforceps can be of help Reduction of the septumshould be performed with the use ofAsch forceps
Nasal Fractures
bull To prevent collapse of the postreductionbull framework nasal packing should be placedbull for 3ndash5 days Septum splints are recommendedbull in comminuted septal fractures withbull severe mucosal lesions External nasal splintingbull for 10 days (Aquaplastreg Thermoplastreg)bull provides nasal protection Nasal saline spraysbull prevent crusting and oral antibiotics should
Nasal Fractures
bull Open reductionbull ndashndash Immediate repair of fractures by using
widebull surgical exposure reduction fixation and
reconstructionbull ndashndash The second option is delayed correctionbull (6 months or more) of persistent deformitiesbull using standard techniques of rhinoplasty
Deviated Nasal Septum
bull Definition of the diseasebull ndash Deviation of the nasal septum is a common causebull of unilateral nasal airway obstruction in which thebull nasal septum is displacedbull bull Epidemiologyaetiologybull ndash Developmental septal abnormalities Septal cartilage
damage in the neonatal period andbull during birth can cause severe septal deviation inbull the absence of a history of nasal trauma
Deviated Nasal Septum
bull Symptomsbull ndash Patients may present with a history of sinusitis
allergicbull rhinitis obstructive sleep apnoea previousbull nasal surgery or recent nasal trauma Unilateral or
bilateral nasal airway obstruction that is unrelievedbull with decongestants or nasal steroid sprays is oftenbull seenbull bull
Deviated Nasal SeptumDiagnosisndashExamination external dorsal deviation or the columella and caudal septummay be deflected off the midline (caudal subluxation)ndash Inspections of the nasal cavity and anterior-posteriorrhinoscopy are helpful in diagnosing the locationtype and severity of septal deformityThe endoscope is also useful in identifying polypsthe severity and extent of posterior septaldeviations and bony spurs and locating areas ofseptal perforation or mucosal injury
Deviated Nasal Septum
bull Therapybull ndash Septoplasty is a procedurebull The areabull of deviation is corrected or resected in order tobull leave behind as much cartilage and bone as
possiblebull Cartilage resection is minimised and can be
repositioned reshaped or recontoured using a variety of methods
Deviated Nasal Septum
bull ndash Indications of septoplasty before the growth period
bull of the nose is finished should be very limited bull -In these cases surgery must preserve all the
cartilagebull in order to prevent external changes of the
shape ofbull the nose
Deviated Nasal Septum
bull Complicationsbull ndash Frequent complications include haematoma andbull infection Cerebrospinal fluid leak is a rare but
potentiallybull serious complicationbull It is usually the resultbull of avulsion or damage to the cribriform plate whenbull handling the perpendicular plate of the ethmoidbull ndash Other complications include epistaxis nasal
Deviated Nasal Septum
bull Other complications include epistaxis nasal obstruction
bull due to residual deviation synechiae returnbull of the cartilaginous deviation septal perforationbull anosmia and cosmetic nasal deformities suchbull as widened alar rim margins drooping nasal tipbull columella retraction and a sunken dorsum with abull supratip saddle formation
Septal perforation with minor crusting View from provide closure of the
incision
Septal Haematoma
bull A septal haematoma is a blood collection under the perichondrium
bull of the septum and cartilagebull bull bull Epidemiologyaetiologybull ndash A septal haematoma is one of the most
severe complications of nasal trauma
Septal Haematoma
bull Diagnosisbull ndash Signs and symptoms include intense pain
swellingbull haematoma of the upper lip and philtrum
area andbull complete nasal airway obstruction
Septal HaematomaTherapyndash Management consists of drainage through a mucoperichondrial incision Immediate treatment isnecessary to prevent long-term problems such asa saddle-nose deformity perforation columellarretraction and nasal-base widening In childrenseptal destruction can lead to devastating nasal andmidfacial growth abnormalitiesbull Surgeryndash Incision and evacuation of the collection is performedDrainage of a septal haematoma should
Septal HaematomaSurgeryndash Incision and evacuation of the collection is performedDrainage of a septal haematoma should provide closure of the incision
Splints or transseptal sutures are placed to obliterate thepotential space and prevent collectionInfection involving the septal cartilage Reconstruction with autologouscartilage is then performed in a second stage Oral antibiotics should be given
Nasal DeformitySaddle-nose deformityndash A saddle-nose deformity is characterised by a loss ofnasal dorsal height and compromised nasal supportstructures -Other case observed are depressionof the middle vault and dorsum loss of nasal tipsupport and definition shortened (vertical) nasal length over rotation of the nasal tip and retrusion ofthe nasal spine and caudal septum It is also knownas a ldquoPug noserdquo or ldquoboxerrsquos noserdquo both of which referto various degrees of nasal dorsal depressionbull
Nasal DeformityEpidemiologyaetiologyndash Prevalence is higher in population groups prone to facial trauma (ie boxers athletes) those with historiesof intranasal cocaine use nasal surgery (e g radical submucosal septal resection reductive rhinoplasty)ndash A saddle-nose deformity can be congenital or acquired It can be noticed as a part of individual familialsyndromic and ethnic characteristics - Most deformities are due to traumatic and iatrogeniccauses Medical causes are Wegenerrsquosgranulomatosis relapsing polychondritis leprosy (Hansenrsquos disease) syphilis ectodermal dysplasiaand intranasal cocaine use
Nasal Deformity
bull Therapybull ndash Nasal reconstruction indications depend on patientbull selection surgeon experience and aetiology of thebull deformity bull Indications for surgery can be functionalbull aesthetic or most commonly both In individuals
with a compromised nasal airway a nasoseptalbull reconstruction is indicated
Nasal Deformity
bull Contraindications bull include patients with malignantbull chronic or autoimmune disease conditions drugbull abuse poor perioperative risk profile and unrealisticbull expectationsbull ndash Multiple previous rhinoplasties and certain
professionsbull (mixed martial artists boxers and other contactbull sports) are relative contraindications
Nasal DeformitySeptoplastyndash Septoplasty is performed to correct nasal obstructioncaused by septal deformityndash Usually septoplasty is performed under general anaesthesiawith the patient in the supine position with the head elevated by approximately 30 (Righthandedsurgeons approach from the right side)ndash Local vasoconstrictive anaesthesia is applied notonly to reduce postoperative pain but also more importantly to achieve vasoconstriction of themucosa and less intraoperative haemorrhage Lidocainewith adrenaline or epinephrine is usedalthough in patients with cardiac hypersensitivityoxymetazoline might be preferred
Nasal Deformity
bull Septoplasty begins with the incision of septal mucosabull Most operative techniques utilise a hemitransfixionbull incision at the caudal end of septum so thatbull deviation at this point might be reached as wellbull as a transfixion incision that is easily obtained ifbull needed (Right-handed surgeons normally choosebull the left side but that may vary when deviation isbull convex towards the right)
Nasal DeformityA columella retractor is placed over the columellaand by pulling it laterally the caudal border of theseptum is exposed Ala can be protected by an alaprotector A vertical incision with a no 15 bladeover the caudal end of septum is performed untilreaching the plane of the septal cartilage It is essentialto correctly identify the perichondrium and byusing the Cottle elevator dissect and lift it creatinga flap As the dissection proceeds along the septalcartilage a longer speculum (no 5) is introduced sothat elevation of the mucoperichondrium is doneunder constant visual controlndash The next step is to dissect the mucoperiostium
Nasal DeformityDissecting over the bony-cartilaginous junctionwhen joining both tunnels might be difficult and is
especially prone to membrane perforationndash If needed the same tunnels are to be created on the
other side of the septum Then deviated parts of
septum are identified and removed either with a
knife or a Freer chisel
Nasal Deformitybull septum from the maxillary crest the septum mustbull be separated from the perpendicular plate trimmedbull along the inferior border placed back onto the crestbull and sutured to the periosteum If the deformity involvesbull the vomer an osteotome is used Care mustbull be taken not to break the cribriform plate becausebull it could cause a cerebrospinal fistula
Nasal Deformity
bull Once the septal deviation is corrected the flapsbull and hemitransfixion incision are mattressed
withbull absorbable sutures Nasal packing to prevent
synechiaebull and postoperative septal haematoma mightbull be advised but should be removed within 72 h

Nasal Cavities
The floor of the nasal cavity is formedmostly by the hard palate which is formed in turn bythe two palatine processes of the maxilla and the horizontallaminae of the palatine bone
Structure of the lateral nasal wall
Inferior meatus
Paranasal Sinuses
The paranasal sinuses are air-filled cavities that communicatewith the nasal cavities
-The maxillary sinus frontalsinus and anterior ethmoid cells drain into the nasalcavity through the middle meatusmdashie below themiddle turbinate -The posterior ethmoidcells drain into the nasal cavity through the superiormeatus The ostium of the sphenoid sinus is locatedin the anterior wall directly above the choanae- The anatomical connections between the nasal cavity andparanasal sinuses are functionally important and playa key role in the pathogenesis of many rhinologic diseasesthat involve the paranasal sinuses
Vascular SupplyThe external nose derives most of its blood supply
from the facial artery which arises from the external
carotid artery and from the ophthalmic artery which
springs from the internal carotid artery
Vascular Supply
The internalnose receives blood from the territories of the externaland internal carotid arteries- the terminalbranches of the sphenopalatine artery which arisesfrom the maxillary artery - the anterior and posteriorethmoid arteries which arise from the ophthalmicartery-internal carotid arterie
venous drainage
The venous drainageof the facial region is handled by -the facial vein -retromandibular vein -internal jugular vein
lymphatic drainage
The regional lymphatic drainage of the face and externalnose is handled mainly by- the submandibularlymph nodes while the nasal cavity is additionallydrained by -the retropharyngeal and deep - -cervical lymph nodes
Morphology of the Nasal Mucosa
Besides the anatomical structure of the external noseand nasal cavity the nasal mucosa plays an essentialrole in numerous functions of the nose in the respiratory tract
Morphology of the Nasal Mucosa
The anterior part of the nasal cavity (the nasal vestibule)like the external nose is covered by skin composedof a multilayer keratinizing squamous epithelium and finally a ciliated respiratory epithelium A small areaon the upper nasal septum superior turbinate andpart of the middle turbinate located adjacent to thecribriform plate is covered by olfactory mucosa and iscalled the olfactory region
Nerve SupplyThe facial skin receives its sensory innervation fromterminal branches of the trigeminal nerve that enterthe facial region through the supraorbital infraorbitaland mental foramina Thefacial muscles are classified as mimetic or mastica- tory each of these groups receiving different motorinnervationbythe facial nerve
History and Clinical Examination of the Nose
Historybull The main symptomsbull nasal obstruction (ldquostuffy
noserdquo)bull nasal dischargebull Headachesbull Olfactory
dysfunction
Palpationbony discontinuitiesNeuralgias to check
over- the supraorbital -infraorbital -mental foramina
Anterior Rhinoscopy
bull The rhinologic examination itself begins with anterior
bull rhinoscopy to evaluate the nasal vestibule and the anterior
bull portions of the nasal cavity
Nasal Endoscopy Nasal endoscopy has become the most important andrewarding clinical examination method in rhinologic diagnosis
- rigid endoscopes which are available in 4-mm and 28- mm diameters and assorted viewing angles (eg 01048576 301048576 1201048576) -flexible endoscopes are also available for inspecting the nose and nasopharynx and exploring all of the pharynx and larynx in one sitting
Nasal endoscopy
Nasal Endoscopy
Nasal Endoscopy
Imaging of the Nose and Paranasal Sinuses
Conventional RadiographsStandard paranasal sinus radiographs in the occipitomental
projection ( Water projection) and
occipitofrontal projection Caldwell projection) in cases of acute inflammation
They are also obtained to evaluate midfacial fractures
Computed Tomography (CT) the main indicationsfor CT scanning of the
nose and paranasal sinuses
are- chronic sinusitis - -trauma (especially
frontobasal -fractures)
-and tumors
The occipitofrontal projection is better for evaluating theethmoid cells and frontal sinus
occipitomental projection demonstrates the maxillarysinus and gives a limited view of the sphenoid sinus
Computed tomography of the paranasal sinuses
Four representative coronal CT scans are shown
Four representative coronal CT scans are shown
Magnetic Resonance Imaging
Magnetic maging
Magnetic resonance imaging (MRI) has fewer indicationsthan CT in patients with paranasal sinus diseaseThis is primarily because MRI is markedly inferior toCT in defining the bony boundaries of the sinusesThe strength of MRI lies in its superior soft-tissue discriminationMRI is indicated in diseases that involve the paranasal sinuses in addition to thecranial cavity or orbit (eg tumors and congenitalmalformations such as encephaloceles)
MRI of the paranasal sinuses
The Nose and Sinuses
Structure The structure of the nose is made up of
four partsbull The surface anatomybull The nasal skeletonmdashcomposed of the
two nasal bones the paired upper lateral and lower lateral cartilages and the nasal septum covered in subcutaneous tissue and skin
bull The internal anatomymdashincludes the septum of the nose which forms the medial wall of the nasal cavity The turbinates on the lateral wall are also called conchae
bull The osteomeatal complexmdasha key functional area of the nose
Function The nose is the main route for inspired
air and its structure is related to this function As the air passes over the large surface area of the turbinates
The inspired gases are warmed and humidified Mucus on the mucosa of the nose removes large dust particles from the air as it is breathed in
The voice resonates in the sinuses and nose and this provides character to the speech
Pneumatization of the sinusesmdashthey are air filled spacesmdashreduces the weight of the skull
Diseases of thDiseases of the Outer and Inner Nosee Outer and
Inner Nose Erysipelas Definition of the disease ndash Erysipela is a skin infection that affects the superficial dermis and is caused by Streptococcus pyogenes (group A) It usually develops in the extremities and the face and less commonly on the scalp and genitals bull Epidemiologyaetiology ndash Erysipelas are more often seen in elderly infants and children patients with compromised immunology and diabetes -Predisposing factors are alcoholism skin ulceration puncture wounds fungal infections malnutrition and burns
Erysipelas
bull Symptomsbull ndash It usually presents of fever general fatigue bull -The skin lesion is a redindurated and elevated plaque
with borders that expand rapidly bull It is painful warm and accompanied by variable oedemabull -On the second or third day a flaccid bulla may develop
and desquamationbull bull Presence of regional lymph nodes is common
Erysipelas
bull Complicationsndash The most common complication is recurrencewhich is seen in 18ndash30 of the cases even afterproper antibiotic therapy Recurrence is seen moreoften in females than in malesA skin infection with S pyogenes could lead toglomerulonephritis
Erysipelas
bull Complicationsbull ndash The most common complication is recurrencebull which is seen in 18ndash30 of the cases even afterbull proper antibiotic therapy bull -Recurrence is seen morebull often in females than in males bull -A skin infection with S pyogenes could lead tobull glomerulonephritis
Erysipelas
bull bull Diagnosisbull ndash Diagnosis is based on the patientrsquos personal
historybull and physical examination particularly on inspectionbull of the skin
bull Blood cultures are positive in less thanbull 5 of cases
ErysipelasTherapyndash Conservative therapybull The preferred antibiotic is penicillin In mildcases with minor systemic symptoms penicillinV 500 mg orally every 6 h for 10 days or penicillinG benzathine 12 mil U intramuscularlyonceOther possibilities are amoxicillin 500 mgorally twice a day for 10 days or cephalexin 500mg orally every 6 h for 10 days
ErysipelasIn moderate and severe cases with significantsystemic symptoms hospitalization and intravenoustreatment is required penicillin G 2ndash4mil U intravenously every 4ndash6 h Cefazolin05ndash15 gm intravenously every 8 h cefotaxime1ndash2 gm intravenously every 8 h or ceftriaxone1ndash2 gm intravenously once a day should be administeredIn patients with a penicillin allergyclindamycin 600 mg intravenously every 8 h orvancomycin 15 mgkg intravenously twice a daymay be given
ErysipelaAdditional useful therapeutic optionsbull Prednisone 30 mg over 8 days might be consideredas well as elevation of the affected siteMoist heat compresses may be usefulbull Surgeryndash Debridement and drainage are indicated when bullaeabscesses or necroses are presentbull Differential diagnosisndash Contact dermatitisndash Asteatotic eczemandash Herpes zosterndash Angioneurotic oedemandash Osteomyelitis
Furuncle
bull Definition of the diseasebull ndash A furuncle is an infection that beginsbull at the hair follicle and spreads deeper into thebull dermis and subcutaneous tissue forming abull nodule After several days it developsbull into an abscess - red painful and fluctuantbull bull bull Epidemiologyaetiologybull ndash The aetiologic agent is Staphylococcus aureus
FuruncleSymptomsndashsymptoms are local and limited to thesite of infection Furuncles usually are wherehair follicles are present bull Complicationndash One complication is furunculosis multiple draining furunclesDiagnosisndash The diagnosis is based on clinical inspection - Cultures are not necessary when there is no systemic involvement but should beconsidered if systemic therapy (in case of feversignificant cellulitis or hospitalization) or whenmethicillin-resistant Staphylococcusaureus (MRSA) is considered
FuruncleTherapyndash When the furuncle is small application of moist heat compress to promote drainage -Larger furuncles should be drained by surgical incision-After drainage the area should be cleaned with anantiseptic (with chlorhexidinebetadine) should be applied twice
a dayndash If no systemic symptoms or extensive cellulitis arepresent simple topical care is usually curative andoral antibiotics are not necessary Otherwise systemictreatment is indicated and should cover anypossible MRSA
Furuncle
bull -Recommended antibiotics are trimethoprim-sulfamethoxazole
bull 1ndash2 tablets orally twice daily doxycyclinebull 100 mg orally twice dailybull or clindamycin 300ndash450 mg orally every 8 hbull - In severe cases vancomycin 15 mgkg
intravenouslybull every 12 h or clindamycin 600 mg intravenouslybull every 8 h
Midline Granulomabull A midline granuloma is an angiocentricbull lymphoma it was referred to as polymorphicbull reticulosis lethal midline granuloma and midline
malignant reticulosisbull bull Definition of the diseasebull ndash This rare disease is a lymphoma of extranodal
presentationall cases are positive for the Epstein-Barr virus
bull -This lymphoma most commonly appears in the midface region
Midline GranulomaEpidemiologyaetiologyndash This form of lymphoma is rare in Europe and theUnited States with a higher prevalence in Asia and PeruSymptomsndash The most common presentation is nasal obstruction with a destructive mass occupying the nosesinuses and palate
-Fever night sweatsand weight loss seen usually in Hodgkinrsquos lymphomaand other non-Hodgkinrsquos lymphomas (knownas ldquoB symptomsrdquo) are uncommon
Midline GranulomaDiagnosisndash The diagnosis is based on anatomopathologicalstudy The malignancy of the tumour manifested byextensive necrosis makes the histological diagnosisdifficult and often more biopsies are required forconfirmationbull Therapyndash Therapy consists of radiotherapy with or withoutchemotherapy
Midline Granuloma
bull Prognosisbull ndash Depending on the stage long-term remission or
experience a worseningbull prognosis with relapses which may include otherbull extranodal sites bull Involvement of extranodal sitesbull including the upper airway gastrointestinal tractbull skin
Wegenerrsquos Granulomatosis
bull Definition of the diseasebull ndash Wegenerrsquos granulomatosis is a systemic chronicbull vasculitis of small- and medium-sized blood vesselsbull with an autoimmune component It affectsbull particular organs with variable predilectionbull Epidemiologyaetiologybull ndash Wegenerrsquos granulomatosis is a rare disease It affects
about 1 in 20000ndash30000 people It is more prevalentbull in middle-aged Caucasian patients
Wegenerrsquos Granulomatosis
Symptomsndash The disease may present pulmonary upper
respiratory tract or renal In the disseminated form-The localised form ndash confinedto the upper respiratory region ndash is present in 25of the patients- It consists of nonspecific manifestationssuch as nasal obstruction crusting purulentor bloody rhinorrhea and painful or painless ulcers in oral or nasal cavities which are unresponsive tostandard medical treatment
Wegenerrsquos Granulomatosis
bull In some patients the nasal septum is perforatedbull which leads to saddle-nose deformity Less
commonbull symptoms are hoarseness stridor due to
subglotticbull stenosis otalgia otorrhea and conductivebull and sensorineural hearing loss Also ocular
symptomsbull such as scleritis conjunctivitis uveitis andbull episcleritis may be present
Wegenerrsquos Granulomatosis
bull ndash In the disseminated form pulmonary involvementbull is manifested by cough dyspnoea haemoptysisbull (due to an alveolar capillaritis necrotic lesions orbull endobronchial disease) and pleuritic painndashbull -Ninety per cent of patients have nasal symptomsbull and these symptoms are usually the first
manifestationof the diseasebull -Most patients have also renal involvementbull even if it is subclinical
Wegenerrsquos Granulomatosis
Diagnosis ndash Diagnosis of Wegenerrsquos granulomatosis is based on clinical findings that demonstrate lung (chest x-ray) kidney (urine analysis) or upper respiratory tract
involvement (oral or nasal ulcers or discharge) - positive blood analysis for cytoplasmic-staining antineutrophil
cytoplasmic antibodies (c-ANCA) and confirming proteinase 3 (PR3) ANCA or myeloperoxidase (MPO) ANCA ndash Biopsy is essential for diagnosis nonspecific chronic inflammation
and necrosis -Bacterial and fungal infections
Wegenerrsquos Granulomatosis
Therapyndash Conservative therapybull In the induction of disease remission highdosesteroids (e g prednisone 1 mgkgday) for1 month with tapering over several months aregiven In addition cyclophosphamide (2 mgkgday) should be administered for 6ndash12 monthsuntil symptoms disappear In the maintenanceof remission cyclophosphamide should be
Wegenerrsquos Granulomatosis
Antibiotics mainly trimethoprim-sulfamethoxazoleare given for prophylaxis againstPneumocystis jiroveci (formerly Pneumocystiscarinii) pneumonia (PCP) which may developduring immunosuppression and have a role inpreventing recurrencesbull Sinonasal manifestations may be treated with topical nasal steroids and nasal irrigations lowdosesystemic steroids and antibiotics when bacterial infection (typically Staphylococcus species) is suspected
Wegenerrsquos Granulomatosis
bull Prognosisbull ndash Most of the patients respond well to treatmentbull achieving symptom-free intervals of 5ndash20 yearsbull or more bull -Anatomical problems (sinusitis trachealbull stenosis) may require surgery bull Relapses can be long and troublesomebull Long-term complications are chronicbull renal failure hearing loss and deafness
Nasal Fractures Definition ndash A nasal fracture is a disruption of the nasal bone structure due to trauma It is the most frequently fractured facial bone Epidemiologyaetiology ndash Sports falls and assaults are the usual mechanisms of fracture -Males are affected twice as often as are females -Paediatric populations with a incidences during the second and third decades of life -Variables such as force impact direction nature of the striking object age and other will influence the pattern of injury to the components of the nose
Nasal Fractures
bull Symptomsbull ndash Deformity swelling epistaxis and periorbital
ecchymosis are signs that are suggestive of nasal fracture
bull bony crepitus and nasal segment mobilitybull ndash Epiphora bull Severe bilateral injuries to the lachrymal bones
arebull associated with depressed nasal fractures
Nasal Fractures Complications ndash Septal haematoma is one of the most severe early complications of nasal trauma and without drainage it results in abscess formation 6ndash7 days after trauma producing necrosis of the septal cartilage -Long-term problems such as saddle-nose deformity perforation columellar retraction and nasalbase
Septal infection could lead to osteomyelitis orbital and intracranial abscesses meningitis and cavernous sinus thrombosis -Cerebrospinal fluid leakage is a common complication of severe
nasal and frontal fractures
Nasal Fractures
bull Diagnostic proceduresbull ndash Inspectionbull bull Changes of appearance such as deviation andbull asymmetry bleeding watery drainage changesbull in nasal breathing and smell It is useful to comparebull the current presentation with old photographsbull (up to 40 of normal individuals havebull significant nose malformations)
Nasal Fractures Physical examination bull The diagnosis of a nasal fracture is made primarily by physical examination epistaxis nasal swelling and periorbital ecchymosis Nasal shape in the lateral and frontal inspection should be assessed Grasping the dorsum between two fingers and rocking the pyramid back and forth aids in assessing the mobility of nasal bones Internal structures should be evaluated by using a headlight and nasal speculum Clotted blood is removed by suction and assessment of haematoma mucosal tears and active bleeding is performed Bimanual palpation of the septum helps to differentiate septal swelling from haematoma ndash
Nasal FracturesRadiographybull There is no clear evidence of the role of radiographyin the management of nasal fracturesPlain films have up to a 66 false-positive rateas a result of misinterpretation of normal suturelines In addition old fractures are difficult todistinguishbull Three-dimensional CT is recommended for extensiveinjuries involving the nasal-orbital-ethmoidalcomplexndash
Nasal Fractures
bull Additionaluseful diagnostic proceduresbull bull Using a 0 or 30deg 4-mm endoscope is helpful inbull the assessment of posterior abnormalities If thebull patient is heavily sedated Brown-Gruss
provocationbull manoeuvres may be performed to determinebull deformities in upper middle or lower segmentsbull by compressing each compartment
Nasal FracturesConservative treatmentndash Treatment of bleedingbull For localised bleeding anterior sources may becauterised by silver nitrate or sealed with topicalmaterials such as thrombin combined withgelatin foam fibrin glue FloSealreg or other procoagulantmaterials If conservative measuresfail a formal anterior packing is placedbull Bleeding from branches of sphenopalatine orethmoid vessels requires anterior-posteriorpacking
Nasal Fractures
bull bull Surgical methods such as direct endoscopic vessel
bull cauterization or ligation have been shown tobull offer better haemostasis and patient comfortbull Angiography with embolization can also be
consideredbull in cases refractory to more conservativebull approaches
Nasal Fractures
bull Type of reductionbull bull Nondisplaced fractures should be treated withbull observation alone Closed nasal reduction is thebull best choice for simple injuries (isolated unilateralbull with medial displacement)bull bull An open approach should be considered in
severebull trauma (bilateral depressed fractures)
Nasal Fracturesbull Surgical principlesbull ndash Topical anaesthesia with cotton pledgets soakedbull with 4 cocaine or 005 oxymethazoline combinedbull with 4 topical lidocaine should be appliedbull for 5ndash10 min Local anaesthesia should also be injectedbull (1 lidocaine and 1100000 epinephrine)bull along the septum lateral walls and floor of the nasalbull cavitybull bull
Nasal FracturesClosed reductionndashndash The nasal bones are grasped between two fingersand pressure is applied laterally in theopposite direction of the deviation A bluntelevator may be used from within the nose incases of significant medial collapse Walshamforceps can be of help Reduction of the septumshould be performed with the use ofAsch forceps
Nasal Fractures
bull To prevent collapse of the postreductionbull framework nasal packing should be placedbull for 3ndash5 days Septum splints are recommendedbull in comminuted septal fractures withbull severe mucosal lesions External nasal splintingbull for 10 days (Aquaplastreg Thermoplastreg)bull provides nasal protection Nasal saline spraysbull prevent crusting and oral antibiotics should
Nasal Fractures
bull Open reductionbull ndashndash Immediate repair of fractures by using
widebull surgical exposure reduction fixation and
reconstructionbull ndashndash The second option is delayed correctionbull (6 months or more) of persistent deformitiesbull using standard techniques of rhinoplasty
Deviated Nasal Septum
bull Definition of the diseasebull ndash Deviation of the nasal septum is a common causebull of unilateral nasal airway obstruction in which thebull nasal septum is displacedbull bull Epidemiologyaetiologybull ndash Developmental septal abnormalities Septal cartilage
damage in the neonatal period andbull during birth can cause severe septal deviation inbull the absence of a history of nasal trauma
Deviated Nasal Septum
bull Symptomsbull ndash Patients may present with a history of sinusitis
allergicbull rhinitis obstructive sleep apnoea previousbull nasal surgery or recent nasal trauma Unilateral or
bilateral nasal airway obstruction that is unrelievedbull with decongestants or nasal steroid sprays is oftenbull seenbull bull
Deviated Nasal SeptumDiagnosisndashExamination external dorsal deviation or the columella and caudal septummay be deflected off the midline (caudal subluxation)ndash Inspections of the nasal cavity and anterior-posteriorrhinoscopy are helpful in diagnosing the locationtype and severity of septal deformityThe endoscope is also useful in identifying polypsthe severity and extent of posterior septaldeviations and bony spurs and locating areas ofseptal perforation or mucosal injury
Deviated Nasal Septum
bull Therapybull ndash Septoplasty is a procedurebull The areabull of deviation is corrected or resected in order tobull leave behind as much cartilage and bone as
possiblebull Cartilage resection is minimised and can be
repositioned reshaped or recontoured using a variety of methods
Deviated Nasal Septum
bull ndash Indications of septoplasty before the growth period
bull of the nose is finished should be very limited bull -In these cases surgery must preserve all the
cartilagebull in order to prevent external changes of the
shape ofbull the nose
Deviated Nasal Septum
bull Complicationsbull ndash Frequent complications include haematoma andbull infection Cerebrospinal fluid leak is a rare but
potentiallybull serious complicationbull It is usually the resultbull of avulsion or damage to the cribriform plate whenbull handling the perpendicular plate of the ethmoidbull ndash Other complications include epistaxis nasal
Deviated Nasal Septum
bull Other complications include epistaxis nasal obstruction
bull due to residual deviation synechiae returnbull of the cartilaginous deviation septal perforationbull anosmia and cosmetic nasal deformities suchbull as widened alar rim margins drooping nasal tipbull columella retraction and a sunken dorsum with abull supratip saddle formation
Septal perforation with minor crusting View from provide closure of the
incision
Septal Haematoma
bull A septal haematoma is a blood collection under the perichondrium
bull of the septum and cartilagebull bull bull Epidemiologyaetiologybull ndash A septal haematoma is one of the most
severe complications of nasal trauma
Septal Haematoma
bull Diagnosisbull ndash Signs and symptoms include intense pain
swellingbull haematoma of the upper lip and philtrum
area andbull complete nasal airway obstruction
Septal HaematomaTherapyndash Management consists of drainage through a mucoperichondrial incision Immediate treatment isnecessary to prevent long-term problems such asa saddle-nose deformity perforation columellarretraction and nasal-base widening In childrenseptal destruction can lead to devastating nasal andmidfacial growth abnormalitiesbull Surgeryndash Incision and evacuation of the collection is performedDrainage of a septal haematoma should
Septal HaematomaSurgeryndash Incision and evacuation of the collection is performedDrainage of a septal haematoma should provide closure of the incision
Splints or transseptal sutures are placed to obliterate thepotential space and prevent collectionInfection involving the septal cartilage Reconstruction with autologouscartilage is then performed in a second stage Oral antibiotics should be given
Nasal DeformitySaddle-nose deformityndash A saddle-nose deformity is characterised by a loss ofnasal dorsal height and compromised nasal supportstructures -Other case observed are depressionof the middle vault and dorsum loss of nasal tipsupport and definition shortened (vertical) nasal length over rotation of the nasal tip and retrusion ofthe nasal spine and caudal septum It is also knownas a ldquoPug noserdquo or ldquoboxerrsquos noserdquo both of which referto various degrees of nasal dorsal depressionbull
Nasal DeformityEpidemiologyaetiologyndash Prevalence is higher in population groups prone to facial trauma (ie boxers athletes) those with historiesof intranasal cocaine use nasal surgery (e g radical submucosal septal resection reductive rhinoplasty)ndash A saddle-nose deformity can be congenital or acquired It can be noticed as a part of individual familialsyndromic and ethnic characteristics - Most deformities are due to traumatic and iatrogeniccauses Medical causes are Wegenerrsquosgranulomatosis relapsing polychondritis leprosy (Hansenrsquos disease) syphilis ectodermal dysplasiaand intranasal cocaine use
Nasal Deformity
bull Therapybull ndash Nasal reconstruction indications depend on patientbull selection surgeon experience and aetiology of thebull deformity bull Indications for surgery can be functionalbull aesthetic or most commonly both In individuals
with a compromised nasal airway a nasoseptalbull reconstruction is indicated
Nasal Deformity
bull Contraindications bull include patients with malignantbull chronic or autoimmune disease conditions drugbull abuse poor perioperative risk profile and unrealisticbull expectationsbull ndash Multiple previous rhinoplasties and certain
professionsbull (mixed martial artists boxers and other contactbull sports) are relative contraindications
Nasal DeformitySeptoplastyndash Septoplasty is performed to correct nasal obstructioncaused by septal deformityndash Usually septoplasty is performed under general anaesthesiawith the patient in the supine position with the head elevated by approximately 30 (Righthandedsurgeons approach from the right side)ndash Local vasoconstrictive anaesthesia is applied notonly to reduce postoperative pain but also more importantly to achieve vasoconstriction of themucosa and less intraoperative haemorrhage Lidocainewith adrenaline or epinephrine is usedalthough in patients with cardiac hypersensitivityoxymetazoline might be preferred
Nasal Deformity
bull Septoplasty begins with the incision of septal mucosabull Most operative techniques utilise a hemitransfixionbull incision at the caudal end of septum so thatbull deviation at this point might be reached as wellbull as a transfixion incision that is easily obtained ifbull needed (Right-handed surgeons normally choosebull the left side but that may vary when deviation isbull convex towards the right)
Nasal DeformityA columella retractor is placed over the columellaand by pulling it laterally the caudal border of theseptum is exposed Ala can be protected by an alaprotector A vertical incision with a no 15 bladeover the caudal end of septum is performed untilreaching the plane of the septal cartilage It is essentialto correctly identify the perichondrium and byusing the Cottle elevator dissect and lift it creatinga flap As the dissection proceeds along the septalcartilage a longer speculum (no 5) is introduced sothat elevation of the mucoperichondrium is doneunder constant visual controlndash The next step is to dissect the mucoperiostium
Nasal DeformityDissecting over the bony-cartilaginous junctionwhen joining both tunnels might be difficult and is
especially prone to membrane perforationndash If needed the same tunnels are to be created on the
other side of the septum Then deviated parts of
septum are identified and removed either with a
knife or a Freer chisel
Nasal Deformitybull septum from the maxillary crest the septum mustbull be separated from the perpendicular plate trimmedbull along the inferior border placed back onto the crestbull and sutured to the periosteum If the deformity involvesbull the vomer an osteotome is used Care mustbull be taken not to break the cribriform plate becausebull it could cause a cerebrospinal fistula
Nasal Deformity
bull Once the septal deviation is corrected the flapsbull and hemitransfixion incision are mattressed
withbull absorbable sutures Nasal packing to prevent
synechiaebull and postoperative septal haematoma mightbull be advised but should be removed within 72 h

Structure of the lateral nasal wall
Inferior meatus
Paranasal Sinuses
The paranasal sinuses are air-filled cavities that communicatewith the nasal cavities
-The maxillary sinus frontalsinus and anterior ethmoid cells drain into the nasalcavity through the middle meatusmdashie below themiddle turbinate -The posterior ethmoidcells drain into the nasal cavity through the superiormeatus The ostium of the sphenoid sinus is locatedin the anterior wall directly above the choanae- The anatomical connections between the nasal cavity andparanasal sinuses are functionally important and playa key role in the pathogenesis of many rhinologic diseasesthat involve the paranasal sinuses
Vascular SupplyThe external nose derives most of its blood supply
from the facial artery which arises from the external
carotid artery and from the ophthalmic artery which
springs from the internal carotid artery
Vascular Supply
The internalnose receives blood from the territories of the externaland internal carotid arteries- the terminalbranches of the sphenopalatine artery which arisesfrom the maxillary artery - the anterior and posteriorethmoid arteries which arise from the ophthalmicartery-internal carotid arterie
venous drainage
The venous drainageof the facial region is handled by -the facial vein -retromandibular vein -internal jugular vein
lymphatic drainage
The regional lymphatic drainage of the face and externalnose is handled mainly by- the submandibularlymph nodes while the nasal cavity is additionallydrained by -the retropharyngeal and deep - -cervical lymph nodes
Morphology of the Nasal Mucosa
Besides the anatomical structure of the external noseand nasal cavity the nasal mucosa plays an essentialrole in numerous functions of the nose in the respiratory tract
Morphology of the Nasal Mucosa
The anterior part of the nasal cavity (the nasal vestibule)like the external nose is covered by skin composedof a multilayer keratinizing squamous epithelium and finally a ciliated respiratory epithelium A small areaon the upper nasal septum superior turbinate andpart of the middle turbinate located adjacent to thecribriform plate is covered by olfactory mucosa and iscalled the olfactory region
Nerve SupplyThe facial skin receives its sensory innervation fromterminal branches of the trigeminal nerve that enterthe facial region through the supraorbital infraorbitaland mental foramina Thefacial muscles are classified as mimetic or mastica- tory each of these groups receiving different motorinnervationbythe facial nerve
History and Clinical Examination of the Nose
Historybull The main symptomsbull nasal obstruction (ldquostuffy
noserdquo)bull nasal dischargebull Headachesbull Olfactory
dysfunction
Palpationbony discontinuitiesNeuralgias to check
over- the supraorbital -infraorbital -mental foramina
Anterior Rhinoscopy
bull The rhinologic examination itself begins with anterior
bull rhinoscopy to evaluate the nasal vestibule and the anterior
bull portions of the nasal cavity
Nasal Endoscopy Nasal endoscopy has become the most important andrewarding clinical examination method in rhinologic diagnosis
- rigid endoscopes which are available in 4-mm and 28- mm diameters and assorted viewing angles (eg 01048576 301048576 1201048576) -flexible endoscopes are also available for inspecting the nose and nasopharynx and exploring all of the pharynx and larynx in one sitting
Nasal endoscopy
Nasal Endoscopy
Nasal Endoscopy
Imaging of the Nose and Paranasal Sinuses
Conventional RadiographsStandard paranasal sinus radiographs in the occipitomental
projection ( Water projection) and
occipitofrontal projection Caldwell projection) in cases of acute inflammation
They are also obtained to evaluate midfacial fractures
Computed Tomography (CT) the main indicationsfor CT scanning of the
nose and paranasal sinuses
are- chronic sinusitis - -trauma (especially
frontobasal -fractures)
-and tumors
The occipitofrontal projection is better for evaluating theethmoid cells and frontal sinus
occipitomental projection demonstrates the maxillarysinus and gives a limited view of the sphenoid sinus
Computed tomography of the paranasal sinuses
Four representative coronal CT scans are shown
Four representative coronal CT scans are shown
Magnetic Resonance Imaging
Magnetic maging
Magnetic resonance imaging (MRI) has fewer indicationsthan CT in patients with paranasal sinus diseaseThis is primarily because MRI is markedly inferior toCT in defining the bony boundaries of the sinusesThe strength of MRI lies in its superior soft-tissue discriminationMRI is indicated in diseases that involve the paranasal sinuses in addition to thecranial cavity or orbit (eg tumors and congenitalmalformations such as encephaloceles)
MRI of the paranasal sinuses
The Nose and Sinuses
Structure The structure of the nose is made up of
four partsbull The surface anatomybull The nasal skeletonmdashcomposed of the
two nasal bones the paired upper lateral and lower lateral cartilages and the nasal septum covered in subcutaneous tissue and skin
bull The internal anatomymdashincludes the septum of the nose which forms the medial wall of the nasal cavity The turbinates on the lateral wall are also called conchae
bull The osteomeatal complexmdasha key functional area of the nose
Function The nose is the main route for inspired
air and its structure is related to this function As the air passes over the large surface area of the turbinates
The inspired gases are warmed and humidified Mucus on the mucosa of the nose removes large dust particles from the air as it is breathed in
The voice resonates in the sinuses and nose and this provides character to the speech
Pneumatization of the sinusesmdashthey are air filled spacesmdashreduces the weight of the skull
Diseases of thDiseases of the Outer and Inner Nosee Outer and
Inner Nose Erysipelas Definition of the disease ndash Erysipela is a skin infection that affects the superficial dermis and is caused by Streptococcus pyogenes (group A) It usually develops in the extremities and the face and less commonly on the scalp and genitals bull Epidemiologyaetiology ndash Erysipelas are more often seen in elderly infants and children patients with compromised immunology and diabetes -Predisposing factors are alcoholism skin ulceration puncture wounds fungal infections malnutrition and burns
Erysipelas
bull Symptomsbull ndash It usually presents of fever general fatigue bull -The skin lesion is a redindurated and elevated plaque
with borders that expand rapidly bull It is painful warm and accompanied by variable oedemabull -On the second or third day a flaccid bulla may develop
and desquamationbull bull Presence of regional lymph nodes is common
Erysipelas
bull Complicationsndash The most common complication is recurrencewhich is seen in 18ndash30 of the cases even afterproper antibiotic therapy Recurrence is seen moreoften in females than in malesA skin infection with S pyogenes could lead toglomerulonephritis
Erysipelas
bull Complicationsbull ndash The most common complication is recurrencebull which is seen in 18ndash30 of the cases even afterbull proper antibiotic therapy bull -Recurrence is seen morebull often in females than in males bull -A skin infection with S pyogenes could lead tobull glomerulonephritis
Erysipelas
bull bull Diagnosisbull ndash Diagnosis is based on the patientrsquos personal
historybull and physical examination particularly on inspectionbull of the skin
bull Blood cultures are positive in less thanbull 5 of cases
ErysipelasTherapyndash Conservative therapybull The preferred antibiotic is penicillin In mildcases with minor systemic symptoms penicillinV 500 mg orally every 6 h for 10 days or penicillinG benzathine 12 mil U intramuscularlyonceOther possibilities are amoxicillin 500 mgorally twice a day for 10 days or cephalexin 500mg orally every 6 h for 10 days
ErysipelasIn moderate and severe cases with significantsystemic symptoms hospitalization and intravenoustreatment is required penicillin G 2ndash4mil U intravenously every 4ndash6 h Cefazolin05ndash15 gm intravenously every 8 h cefotaxime1ndash2 gm intravenously every 8 h or ceftriaxone1ndash2 gm intravenously once a day should be administeredIn patients with a penicillin allergyclindamycin 600 mg intravenously every 8 h orvancomycin 15 mgkg intravenously twice a daymay be given
ErysipelaAdditional useful therapeutic optionsbull Prednisone 30 mg over 8 days might be consideredas well as elevation of the affected siteMoist heat compresses may be usefulbull Surgeryndash Debridement and drainage are indicated when bullaeabscesses or necroses are presentbull Differential diagnosisndash Contact dermatitisndash Asteatotic eczemandash Herpes zosterndash Angioneurotic oedemandash Osteomyelitis
Furuncle
bull Definition of the diseasebull ndash A furuncle is an infection that beginsbull at the hair follicle and spreads deeper into thebull dermis and subcutaneous tissue forming abull nodule After several days it developsbull into an abscess - red painful and fluctuantbull bull bull Epidemiologyaetiologybull ndash The aetiologic agent is Staphylococcus aureus
FuruncleSymptomsndashsymptoms are local and limited to thesite of infection Furuncles usually are wherehair follicles are present bull Complicationndash One complication is furunculosis multiple draining furunclesDiagnosisndash The diagnosis is based on clinical inspection - Cultures are not necessary when there is no systemic involvement but should beconsidered if systemic therapy (in case of feversignificant cellulitis or hospitalization) or whenmethicillin-resistant Staphylococcusaureus (MRSA) is considered
FuruncleTherapyndash When the furuncle is small application of moist heat compress to promote drainage -Larger furuncles should be drained by surgical incision-After drainage the area should be cleaned with anantiseptic (with chlorhexidinebetadine) should be applied twice
a dayndash If no systemic symptoms or extensive cellulitis arepresent simple topical care is usually curative andoral antibiotics are not necessary Otherwise systemictreatment is indicated and should cover anypossible MRSA
Furuncle
bull -Recommended antibiotics are trimethoprim-sulfamethoxazole
bull 1ndash2 tablets orally twice daily doxycyclinebull 100 mg orally twice dailybull or clindamycin 300ndash450 mg orally every 8 hbull - In severe cases vancomycin 15 mgkg
intravenouslybull every 12 h or clindamycin 600 mg intravenouslybull every 8 h
Midline Granulomabull A midline granuloma is an angiocentricbull lymphoma it was referred to as polymorphicbull reticulosis lethal midline granuloma and midline
malignant reticulosisbull bull Definition of the diseasebull ndash This rare disease is a lymphoma of extranodal
presentationall cases are positive for the Epstein-Barr virus
bull -This lymphoma most commonly appears in the midface region
Midline GranulomaEpidemiologyaetiologyndash This form of lymphoma is rare in Europe and theUnited States with a higher prevalence in Asia and PeruSymptomsndash The most common presentation is nasal obstruction with a destructive mass occupying the nosesinuses and palate
-Fever night sweatsand weight loss seen usually in Hodgkinrsquos lymphomaand other non-Hodgkinrsquos lymphomas (knownas ldquoB symptomsrdquo) are uncommon
Midline GranulomaDiagnosisndash The diagnosis is based on anatomopathologicalstudy The malignancy of the tumour manifested byextensive necrosis makes the histological diagnosisdifficult and often more biopsies are required forconfirmationbull Therapyndash Therapy consists of radiotherapy with or withoutchemotherapy
Midline Granuloma
bull Prognosisbull ndash Depending on the stage long-term remission or
experience a worseningbull prognosis with relapses which may include otherbull extranodal sites bull Involvement of extranodal sitesbull including the upper airway gastrointestinal tractbull skin
Wegenerrsquos Granulomatosis
bull Definition of the diseasebull ndash Wegenerrsquos granulomatosis is a systemic chronicbull vasculitis of small- and medium-sized blood vesselsbull with an autoimmune component It affectsbull particular organs with variable predilectionbull Epidemiologyaetiologybull ndash Wegenerrsquos granulomatosis is a rare disease It affects
about 1 in 20000ndash30000 people It is more prevalentbull in middle-aged Caucasian patients
Wegenerrsquos Granulomatosis
Symptomsndash The disease may present pulmonary upper
respiratory tract or renal In the disseminated form-The localised form ndash confinedto the upper respiratory region ndash is present in 25of the patients- It consists of nonspecific manifestationssuch as nasal obstruction crusting purulentor bloody rhinorrhea and painful or painless ulcers in oral or nasal cavities which are unresponsive tostandard medical treatment
Wegenerrsquos Granulomatosis
bull In some patients the nasal septum is perforatedbull which leads to saddle-nose deformity Less
commonbull symptoms are hoarseness stridor due to
subglotticbull stenosis otalgia otorrhea and conductivebull and sensorineural hearing loss Also ocular
symptomsbull such as scleritis conjunctivitis uveitis andbull episcleritis may be present
Wegenerrsquos Granulomatosis
bull ndash In the disseminated form pulmonary involvementbull is manifested by cough dyspnoea haemoptysisbull (due to an alveolar capillaritis necrotic lesions orbull endobronchial disease) and pleuritic painndashbull -Ninety per cent of patients have nasal symptomsbull and these symptoms are usually the first
manifestationof the diseasebull -Most patients have also renal involvementbull even if it is subclinical
Wegenerrsquos Granulomatosis
Diagnosis ndash Diagnosis of Wegenerrsquos granulomatosis is based on clinical findings that demonstrate lung (chest x-ray) kidney (urine analysis) or upper respiratory tract
involvement (oral or nasal ulcers or discharge) - positive blood analysis for cytoplasmic-staining antineutrophil
cytoplasmic antibodies (c-ANCA) and confirming proteinase 3 (PR3) ANCA or myeloperoxidase (MPO) ANCA ndash Biopsy is essential for diagnosis nonspecific chronic inflammation
and necrosis -Bacterial and fungal infections
Wegenerrsquos Granulomatosis
Therapyndash Conservative therapybull In the induction of disease remission highdosesteroids (e g prednisone 1 mgkgday) for1 month with tapering over several months aregiven In addition cyclophosphamide (2 mgkgday) should be administered for 6ndash12 monthsuntil symptoms disappear In the maintenanceof remission cyclophosphamide should be
Wegenerrsquos Granulomatosis
Antibiotics mainly trimethoprim-sulfamethoxazoleare given for prophylaxis againstPneumocystis jiroveci (formerly Pneumocystiscarinii) pneumonia (PCP) which may developduring immunosuppression and have a role inpreventing recurrencesbull Sinonasal manifestations may be treated with topical nasal steroids and nasal irrigations lowdosesystemic steroids and antibiotics when bacterial infection (typically Staphylococcus species) is suspected
Wegenerrsquos Granulomatosis
bull Prognosisbull ndash Most of the patients respond well to treatmentbull achieving symptom-free intervals of 5ndash20 yearsbull or more bull -Anatomical problems (sinusitis trachealbull stenosis) may require surgery bull Relapses can be long and troublesomebull Long-term complications are chronicbull renal failure hearing loss and deafness
Nasal Fractures Definition ndash A nasal fracture is a disruption of the nasal bone structure due to trauma It is the most frequently fractured facial bone Epidemiologyaetiology ndash Sports falls and assaults are the usual mechanisms of fracture -Males are affected twice as often as are females -Paediatric populations with a incidences during the second and third decades of life -Variables such as force impact direction nature of the striking object age and other will influence the pattern of injury to the components of the nose
Nasal Fractures
bull Symptomsbull ndash Deformity swelling epistaxis and periorbital
ecchymosis are signs that are suggestive of nasal fracture
bull bony crepitus and nasal segment mobilitybull ndash Epiphora bull Severe bilateral injuries to the lachrymal bones
arebull associated with depressed nasal fractures
Nasal Fractures Complications ndash Septal haematoma is one of the most severe early complications of nasal trauma and without drainage it results in abscess formation 6ndash7 days after trauma producing necrosis of the septal cartilage -Long-term problems such as saddle-nose deformity perforation columellar retraction and nasalbase
Septal infection could lead to osteomyelitis orbital and intracranial abscesses meningitis and cavernous sinus thrombosis -Cerebrospinal fluid leakage is a common complication of severe
nasal and frontal fractures
Nasal Fractures
bull Diagnostic proceduresbull ndash Inspectionbull bull Changes of appearance such as deviation andbull asymmetry bleeding watery drainage changesbull in nasal breathing and smell It is useful to comparebull the current presentation with old photographsbull (up to 40 of normal individuals havebull significant nose malformations)
Nasal Fractures Physical examination bull The diagnosis of a nasal fracture is made primarily by physical examination epistaxis nasal swelling and periorbital ecchymosis Nasal shape in the lateral and frontal inspection should be assessed Grasping the dorsum between two fingers and rocking the pyramid back and forth aids in assessing the mobility of nasal bones Internal structures should be evaluated by using a headlight and nasal speculum Clotted blood is removed by suction and assessment of haematoma mucosal tears and active bleeding is performed Bimanual palpation of the septum helps to differentiate septal swelling from haematoma ndash
Nasal FracturesRadiographybull There is no clear evidence of the role of radiographyin the management of nasal fracturesPlain films have up to a 66 false-positive rateas a result of misinterpretation of normal suturelines In addition old fractures are difficult todistinguishbull Three-dimensional CT is recommended for extensiveinjuries involving the nasal-orbital-ethmoidalcomplexndash
Nasal Fractures
bull Additionaluseful diagnostic proceduresbull bull Using a 0 or 30deg 4-mm endoscope is helpful inbull the assessment of posterior abnormalities If thebull patient is heavily sedated Brown-Gruss
provocationbull manoeuvres may be performed to determinebull deformities in upper middle or lower segmentsbull by compressing each compartment
Nasal FracturesConservative treatmentndash Treatment of bleedingbull For localised bleeding anterior sources may becauterised by silver nitrate or sealed with topicalmaterials such as thrombin combined withgelatin foam fibrin glue FloSealreg or other procoagulantmaterials If conservative measuresfail a formal anterior packing is placedbull Bleeding from branches of sphenopalatine orethmoid vessels requires anterior-posteriorpacking
Nasal Fractures
bull bull Surgical methods such as direct endoscopic vessel
bull cauterization or ligation have been shown tobull offer better haemostasis and patient comfortbull Angiography with embolization can also be
consideredbull in cases refractory to more conservativebull approaches
Nasal Fractures
bull Type of reductionbull bull Nondisplaced fractures should be treated withbull observation alone Closed nasal reduction is thebull best choice for simple injuries (isolated unilateralbull with medial displacement)bull bull An open approach should be considered in
severebull trauma (bilateral depressed fractures)
Nasal Fracturesbull Surgical principlesbull ndash Topical anaesthesia with cotton pledgets soakedbull with 4 cocaine or 005 oxymethazoline combinedbull with 4 topical lidocaine should be appliedbull for 5ndash10 min Local anaesthesia should also be injectedbull (1 lidocaine and 1100000 epinephrine)bull along the septum lateral walls and floor of the nasalbull cavitybull bull
Nasal FracturesClosed reductionndashndash The nasal bones are grasped between two fingersand pressure is applied laterally in theopposite direction of the deviation A bluntelevator may be used from within the nose incases of significant medial collapse Walshamforceps can be of help Reduction of the septumshould be performed with the use ofAsch forceps
Nasal Fractures
bull To prevent collapse of the postreductionbull framework nasal packing should be placedbull for 3ndash5 days Septum splints are recommendedbull in comminuted septal fractures withbull severe mucosal lesions External nasal splintingbull for 10 days (Aquaplastreg Thermoplastreg)bull provides nasal protection Nasal saline spraysbull prevent crusting and oral antibiotics should
Nasal Fractures
bull Open reductionbull ndashndash Immediate repair of fractures by using
widebull surgical exposure reduction fixation and
reconstructionbull ndashndash The second option is delayed correctionbull (6 months or more) of persistent deformitiesbull using standard techniques of rhinoplasty
Deviated Nasal Septum
bull Definition of the diseasebull ndash Deviation of the nasal septum is a common causebull of unilateral nasal airway obstruction in which thebull nasal septum is displacedbull bull Epidemiologyaetiologybull ndash Developmental septal abnormalities Septal cartilage
damage in the neonatal period andbull during birth can cause severe septal deviation inbull the absence of a history of nasal trauma
Deviated Nasal Septum
bull Symptomsbull ndash Patients may present with a history of sinusitis
allergicbull rhinitis obstructive sleep apnoea previousbull nasal surgery or recent nasal trauma Unilateral or
bilateral nasal airway obstruction that is unrelievedbull with decongestants or nasal steroid sprays is oftenbull seenbull bull
Deviated Nasal SeptumDiagnosisndashExamination external dorsal deviation or the columella and caudal septummay be deflected off the midline (caudal subluxation)ndash Inspections of the nasal cavity and anterior-posteriorrhinoscopy are helpful in diagnosing the locationtype and severity of septal deformityThe endoscope is also useful in identifying polypsthe severity and extent of posterior septaldeviations and bony spurs and locating areas ofseptal perforation or mucosal injury
Deviated Nasal Septum
bull Therapybull ndash Septoplasty is a procedurebull The areabull of deviation is corrected or resected in order tobull leave behind as much cartilage and bone as
possiblebull Cartilage resection is minimised and can be
repositioned reshaped or recontoured using a variety of methods
Deviated Nasal Septum
bull ndash Indications of septoplasty before the growth period
bull of the nose is finished should be very limited bull -In these cases surgery must preserve all the
cartilagebull in order to prevent external changes of the
shape ofbull the nose
Deviated Nasal Septum
bull Complicationsbull ndash Frequent complications include haematoma andbull infection Cerebrospinal fluid leak is a rare but
potentiallybull serious complicationbull It is usually the resultbull of avulsion or damage to the cribriform plate whenbull handling the perpendicular plate of the ethmoidbull ndash Other complications include epistaxis nasal
Deviated Nasal Septum
bull Other complications include epistaxis nasal obstruction
bull due to residual deviation synechiae returnbull of the cartilaginous deviation septal perforationbull anosmia and cosmetic nasal deformities suchbull as widened alar rim margins drooping nasal tipbull columella retraction and a sunken dorsum with abull supratip saddle formation
Septal perforation with minor crusting View from provide closure of the
incision
Septal Haematoma
bull A septal haematoma is a blood collection under the perichondrium
bull of the septum and cartilagebull bull bull Epidemiologyaetiologybull ndash A septal haematoma is one of the most
severe complications of nasal trauma
Septal Haematoma
bull Diagnosisbull ndash Signs and symptoms include intense pain
swellingbull haematoma of the upper lip and philtrum
area andbull complete nasal airway obstruction
Septal HaematomaTherapyndash Management consists of drainage through a mucoperichondrial incision Immediate treatment isnecessary to prevent long-term problems such asa saddle-nose deformity perforation columellarretraction and nasal-base widening In childrenseptal destruction can lead to devastating nasal andmidfacial growth abnormalitiesbull Surgeryndash Incision and evacuation of the collection is performedDrainage of a septal haematoma should
Septal HaematomaSurgeryndash Incision and evacuation of the collection is performedDrainage of a septal haematoma should provide closure of the incision
Splints or transseptal sutures are placed to obliterate thepotential space and prevent collectionInfection involving the septal cartilage Reconstruction with autologouscartilage is then performed in a second stage Oral antibiotics should be given
Nasal DeformitySaddle-nose deformityndash A saddle-nose deformity is characterised by a loss ofnasal dorsal height and compromised nasal supportstructures -Other case observed are depressionof the middle vault and dorsum loss of nasal tipsupport and definition shortened (vertical) nasal length over rotation of the nasal tip and retrusion ofthe nasal spine and caudal septum It is also knownas a ldquoPug noserdquo or ldquoboxerrsquos noserdquo both of which referto various degrees of nasal dorsal depressionbull
Nasal DeformityEpidemiologyaetiologyndash Prevalence is higher in population groups prone to facial trauma (ie boxers athletes) those with historiesof intranasal cocaine use nasal surgery (e g radical submucosal septal resection reductive rhinoplasty)ndash A saddle-nose deformity can be congenital or acquired It can be noticed as a part of individual familialsyndromic and ethnic characteristics - Most deformities are due to traumatic and iatrogeniccauses Medical causes are Wegenerrsquosgranulomatosis relapsing polychondritis leprosy (Hansenrsquos disease) syphilis ectodermal dysplasiaand intranasal cocaine use
Nasal Deformity
bull Therapybull ndash Nasal reconstruction indications depend on patientbull selection surgeon experience and aetiology of thebull deformity bull Indications for surgery can be functionalbull aesthetic or most commonly both In individuals
with a compromised nasal airway a nasoseptalbull reconstruction is indicated
Nasal Deformity
bull Contraindications bull include patients with malignantbull chronic or autoimmune disease conditions drugbull abuse poor perioperative risk profile and unrealisticbull expectationsbull ndash Multiple previous rhinoplasties and certain
professionsbull (mixed martial artists boxers and other contactbull sports) are relative contraindications
Nasal DeformitySeptoplastyndash Septoplasty is performed to correct nasal obstructioncaused by septal deformityndash Usually septoplasty is performed under general anaesthesiawith the patient in the supine position with the head elevated by approximately 30 (Righthandedsurgeons approach from the right side)ndash Local vasoconstrictive anaesthesia is applied notonly to reduce postoperative pain but also more importantly to achieve vasoconstriction of themucosa and less intraoperative haemorrhage Lidocainewith adrenaline or epinephrine is usedalthough in patients with cardiac hypersensitivityoxymetazoline might be preferred
Nasal Deformity
bull Septoplasty begins with the incision of septal mucosabull Most operative techniques utilise a hemitransfixionbull incision at the caudal end of septum so thatbull deviation at this point might be reached as wellbull as a transfixion incision that is easily obtained ifbull needed (Right-handed surgeons normally choosebull the left side but that may vary when deviation isbull convex towards the right)
Nasal DeformityA columella retractor is placed over the columellaand by pulling it laterally the caudal border of theseptum is exposed Ala can be protected by an alaprotector A vertical incision with a no 15 bladeover the caudal end of septum is performed untilreaching the plane of the septal cartilage It is essentialto correctly identify the perichondrium and byusing the Cottle elevator dissect and lift it creatinga flap As the dissection proceeds along the septalcartilage a longer speculum (no 5) is introduced sothat elevation of the mucoperichondrium is doneunder constant visual controlndash The next step is to dissect the mucoperiostium
Nasal DeformityDissecting over the bony-cartilaginous junctionwhen joining both tunnels might be difficult and is
especially prone to membrane perforationndash If needed the same tunnels are to be created on the
other side of the septum Then deviated parts of
septum are identified and removed either with a
knife or a Freer chisel
Nasal Deformitybull septum from the maxillary crest the septum mustbull be separated from the perpendicular plate trimmedbull along the inferior border placed back onto the crestbull and sutured to the periosteum If the deformity involvesbull the vomer an osteotome is used Care mustbull be taken not to break the cribriform plate becausebull it could cause a cerebrospinal fistula
Nasal Deformity
bull Once the septal deviation is corrected the flapsbull and hemitransfixion incision are mattressed
withbull absorbable sutures Nasal packing to prevent
synechiaebull and postoperative septal haematoma mightbull be advised but should be removed within 72 h

Paranasal Sinuses
The paranasal sinuses are air-filled cavities that communicatewith the nasal cavities
-The maxillary sinus frontalsinus and anterior ethmoid cells drain into the nasalcavity through the middle meatusmdashie below themiddle turbinate -The posterior ethmoidcells drain into the nasal cavity through the superiormeatus The ostium of the sphenoid sinus is locatedin the anterior wall directly above the choanae- The anatomical connections between the nasal cavity andparanasal sinuses are functionally important and playa key role in the pathogenesis of many rhinologic diseasesthat involve the paranasal sinuses
Vascular SupplyThe external nose derives most of its blood supply
from the facial artery which arises from the external
carotid artery and from the ophthalmic artery which
springs from the internal carotid artery
Vascular Supply
The internalnose receives blood from the territories of the externaland internal carotid arteries- the terminalbranches of the sphenopalatine artery which arisesfrom the maxillary artery - the anterior and posteriorethmoid arteries which arise from the ophthalmicartery-internal carotid arterie
venous drainage
The venous drainageof the facial region is handled by -the facial vein -retromandibular vein -internal jugular vein
lymphatic drainage
The regional lymphatic drainage of the face and externalnose is handled mainly by- the submandibularlymph nodes while the nasal cavity is additionallydrained by -the retropharyngeal and deep - -cervical lymph nodes
Morphology of the Nasal Mucosa
Besides the anatomical structure of the external noseand nasal cavity the nasal mucosa plays an essentialrole in numerous functions of the nose in the respiratory tract
Morphology of the Nasal Mucosa
The anterior part of the nasal cavity (the nasal vestibule)like the external nose is covered by skin composedof a multilayer keratinizing squamous epithelium and finally a ciliated respiratory epithelium A small areaon the upper nasal septum superior turbinate andpart of the middle turbinate located adjacent to thecribriform plate is covered by olfactory mucosa and iscalled the olfactory region
Nerve SupplyThe facial skin receives its sensory innervation fromterminal branches of the trigeminal nerve that enterthe facial region through the supraorbital infraorbitaland mental foramina Thefacial muscles are classified as mimetic or mastica- tory each of these groups receiving different motorinnervationbythe facial nerve
History and Clinical Examination of the Nose
Historybull The main symptomsbull nasal obstruction (ldquostuffy
noserdquo)bull nasal dischargebull Headachesbull Olfactory
dysfunction
Palpationbony discontinuitiesNeuralgias to check
over- the supraorbital -infraorbital -mental foramina
Anterior Rhinoscopy
bull The rhinologic examination itself begins with anterior
bull rhinoscopy to evaluate the nasal vestibule and the anterior
bull portions of the nasal cavity
Nasal Endoscopy Nasal endoscopy has become the most important andrewarding clinical examination method in rhinologic diagnosis
- rigid endoscopes which are available in 4-mm and 28- mm diameters and assorted viewing angles (eg 01048576 301048576 1201048576) -flexible endoscopes are also available for inspecting the nose and nasopharynx and exploring all of the pharynx and larynx in one sitting
Nasal endoscopy
Nasal Endoscopy
Nasal Endoscopy
Imaging of the Nose and Paranasal Sinuses
Conventional RadiographsStandard paranasal sinus radiographs in the occipitomental
projection ( Water projection) and
occipitofrontal projection Caldwell projection) in cases of acute inflammation
They are also obtained to evaluate midfacial fractures
Computed Tomography (CT) the main indicationsfor CT scanning of the
nose and paranasal sinuses
are- chronic sinusitis - -trauma (especially
frontobasal -fractures)
-and tumors
The occipitofrontal projection is better for evaluating theethmoid cells and frontal sinus
occipitomental projection demonstrates the maxillarysinus and gives a limited view of the sphenoid sinus
Computed tomography of the paranasal sinuses
Four representative coronal CT scans are shown
Four representative coronal CT scans are shown
Magnetic Resonance Imaging
Magnetic maging
Magnetic resonance imaging (MRI) has fewer indicationsthan CT in patients with paranasal sinus diseaseThis is primarily because MRI is markedly inferior toCT in defining the bony boundaries of the sinusesThe strength of MRI lies in its superior soft-tissue discriminationMRI is indicated in diseases that involve the paranasal sinuses in addition to thecranial cavity or orbit (eg tumors and congenitalmalformations such as encephaloceles)
MRI of the paranasal sinuses
The Nose and Sinuses
Structure The structure of the nose is made up of
four partsbull The surface anatomybull The nasal skeletonmdashcomposed of the
two nasal bones the paired upper lateral and lower lateral cartilages and the nasal septum covered in subcutaneous tissue and skin
bull The internal anatomymdashincludes the septum of the nose which forms the medial wall of the nasal cavity The turbinates on the lateral wall are also called conchae
bull The osteomeatal complexmdasha key functional area of the nose
Function The nose is the main route for inspired
air and its structure is related to this function As the air passes over the large surface area of the turbinates
The inspired gases are warmed and humidified Mucus on the mucosa of the nose removes large dust particles from the air as it is breathed in
The voice resonates in the sinuses and nose and this provides character to the speech
Pneumatization of the sinusesmdashthey are air filled spacesmdashreduces the weight of the skull
Diseases of thDiseases of the Outer and Inner Nosee Outer and
Inner Nose Erysipelas Definition of the disease ndash Erysipela is a skin infection that affects the superficial dermis and is caused by Streptococcus pyogenes (group A) It usually develops in the extremities and the face and less commonly on the scalp and genitals bull Epidemiologyaetiology ndash Erysipelas are more often seen in elderly infants and children patients with compromised immunology and diabetes -Predisposing factors are alcoholism skin ulceration puncture wounds fungal infections malnutrition and burns
Erysipelas
bull Symptomsbull ndash It usually presents of fever general fatigue bull -The skin lesion is a redindurated and elevated plaque
with borders that expand rapidly bull It is painful warm and accompanied by variable oedemabull -On the second or third day a flaccid bulla may develop
and desquamationbull bull Presence of regional lymph nodes is common
Erysipelas
bull Complicationsndash The most common complication is recurrencewhich is seen in 18ndash30 of the cases even afterproper antibiotic therapy Recurrence is seen moreoften in females than in malesA skin infection with S pyogenes could lead toglomerulonephritis
Erysipelas
bull Complicationsbull ndash The most common complication is recurrencebull which is seen in 18ndash30 of the cases even afterbull proper antibiotic therapy bull -Recurrence is seen morebull often in females than in males bull -A skin infection with S pyogenes could lead tobull glomerulonephritis
Erysipelas
bull bull Diagnosisbull ndash Diagnosis is based on the patientrsquos personal
historybull and physical examination particularly on inspectionbull of the skin
bull Blood cultures are positive in less thanbull 5 of cases
ErysipelasTherapyndash Conservative therapybull The preferred antibiotic is penicillin In mildcases with minor systemic symptoms penicillinV 500 mg orally every 6 h for 10 days or penicillinG benzathine 12 mil U intramuscularlyonceOther possibilities are amoxicillin 500 mgorally twice a day for 10 days or cephalexin 500mg orally every 6 h for 10 days
ErysipelasIn moderate and severe cases with significantsystemic symptoms hospitalization and intravenoustreatment is required penicillin G 2ndash4mil U intravenously every 4ndash6 h Cefazolin05ndash15 gm intravenously every 8 h cefotaxime1ndash2 gm intravenously every 8 h or ceftriaxone1ndash2 gm intravenously once a day should be administeredIn patients with a penicillin allergyclindamycin 600 mg intravenously every 8 h orvancomycin 15 mgkg intravenously twice a daymay be given
ErysipelaAdditional useful therapeutic optionsbull Prednisone 30 mg over 8 days might be consideredas well as elevation of the affected siteMoist heat compresses may be usefulbull Surgeryndash Debridement and drainage are indicated when bullaeabscesses or necroses are presentbull Differential diagnosisndash Contact dermatitisndash Asteatotic eczemandash Herpes zosterndash Angioneurotic oedemandash Osteomyelitis
Furuncle
bull Definition of the diseasebull ndash A furuncle is an infection that beginsbull at the hair follicle and spreads deeper into thebull dermis and subcutaneous tissue forming abull nodule After several days it developsbull into an abscess - red painful and fluctuantbull bull bull Epidemiologyaetiologybull ndash The aetiologic agent is Staphylococcus aureus
FuruncleSymptomsndashsymptoms are local and limited to thesite of infection Furuncles usually are wherehair follicles are present bull Complicationndash One complication is furunculosis multiple draining furunclesDiagnosisndash The diagnosis is based on clinical inspection - Cultures are not necessary when there is no systemic involvement but should beconsidered if systemic therapy (in case of feversignificant cellulitis or hospitalization) or whenmethicillin-resistant Staphylococcusaureus (MRSA) is considered
FuruncleTherapyndash When the furuncle is small application of moist heat compress to promote drainage -Larger furuncles should be drained by surgical incision-After drainage the area should be cleaned with anantiseptic (with chlorhexidinebetadine) should be applied twice
a dayndash If no systemic symptoms or extensive cellulitis arepresent simple topical care is usually curative andoral antibiotics are not necessary Otherwise systemictreatment is indicated and should cover anypossible MRSA
Furuncle
bull -Recommended antibiotics are trimethoprim-sulfamethoxazole
bull 1ndash2 tablets orally twice daily doxycyclinebull 100 mg orally twice dailybull or clindamycin 300ndash450 mg orally every 8 hbull - In severe cases vancomycin 15 mgkg
intravenouslybull every 12 h or clindamycin 600 mg intravenouslybull every 8 h
Midline Granulomabull A midline granuloma is an angiocentricbull lymphoma it was referred to as polymorphicbull reticulosis lethal midline granuloma and midline
malignant reticulosisbull bull Definition of the diseasebull ndash This rare disease is a lymphoma of extranodal
presentationall cases are positive for the Epstein-Barr virus
bull -This lymphoma most commonly appears in the midface region
Midline GranulomaEpidemiologyaetiologyndash This form of lymphoma is rare in Europe and theUnited States with a higher prevalence in Asia and PeruSymptomsndash The most common presentation is nasal obstruction with a destructive mass occupying the nosesinuses and palate
-Fever night sweatsand weight loss seen usually in Hodgkinrsquos lymphomaand other non-Hodgkinrsquos lymphomas (knownas ldquoB symptomsrdquo) are uncommon
Midline GranulomaDiagnosisndash The diagnosis is based on anatomopathologicalstudy The malignancy of the tumour manifested byextensive necrosis makes the histological diagnosisdifficult and often more biopsies are required forconfirmationbull Therapyndash Therapy consists of radiotherapy with or withoutchemotherapy
Midline Granuloma
bull Prognosisbull ndash Depending on the stage long-term remission or
experience a worseningbull prognosis with relapses which may include otherbull extranodal sites bull Involvement of extranodal sitesbull including the upper airway gastrointestinal tractbull skin
Wegenerrsquos Granulomatosis
bull Definition of the diseasebull ndash Wegenerrsquos granulomatosis is a systemic chronicbull vasculitis of small- and medium-sized blood vesselsbull with an autoimmune component It affectsbull particular organs with variable predilectionbull Epidemiologyaetiologybull ndash Wegenerrsquos granulomatosis is a rare disease It affects
about 1 in 20000ndash30000 people It is more prevalentbull in middle-aged Caucasian patients
Wegenerrsquos Granulomatosis
Symptomsndash The disease may present pulmonary upper
respiratory tract or renal In the disseminated form-The localised form ndash confinedto the upper respiratory region ndash is present in 25of the patients- It consists of nonspecific manifestationssuch as nasal obstruction crusting purulentor bloody rhinorrhea and painful or painless ulcers in oral or nasal cavities which are unresponsive tostandard medical treatment
Wegenerrsquos Granulomatosis
bull In some patients the nasal septum is perforatedbull which leads to saddle-nose deformity Less
commonbull symptoms are hoarseness stridor due to
subglotticbull stenosis otalgia otorrhea and conductivebull and sensorineural hearing loss Also ocular
symptomsbull such as scleritis conjunctivitis uveitis andbull episcleritis may be present
Wegenerrsquos Granulomatosis
bull ndash In the disseminated form pulmonary involvementbull is manifested by cough dyspnoea haemoptysisbull (due to an alveolar capillaritis necrotic lesions orbull endobronchial disease) and pleuritic painndashbull -Ninety per cent of patients have nasal symptomsbull and these symptoms are usually the first
manifestationof the diseasebull -Most patients have also renal involvementbull even if it is subclinical
Wegenerrsquos Granulomatosis
Diagnosis ndash Diagnosis of Wegenerrsquos granulomatosis is based on clinical findings that demonstrate lung (chest x-ray) kidney (urine analysis) or upper respiratory tract
involvement (oral or nasal ulcers or discharge) - positive blood analysis for cytoplasmic-staining antineutrophil
cytoplasmic antibodies (c-ANCA) and confirming proteinase 3 (PR3) ANCA or myeloperoxidase (MPO) ANCA ndash Biopsy is essential for diagnosis nonspecific chronic inflammation
and necrosis -Bacterial and fungal infections
Wegenerrsquos Granulomatosis
Therapyndash Conservative therapybull In the induction of disease remission highdosesteroids (e g prednisone 1 mgkgday) for1 month with tapering over several months aregiven In addition cyclophosphamide (2 mgkgday) should be administered for 6ndash12 monthsuntil symptoms disappear In the maintenanceof remission cyclophosphamide should be
Wegenerrsquos Granulomatosis
Antibiotics mainly trimethoprim-sulfamethoxazoleare given for prophylaxis againstPneumocystis jiroveci (formerly Pneumocystiscarinii) pneumonia (PCP) which may developduring immunosuppression and have a role inpreventing recurrencesbull Sinonasal manifestations may be treated with topical nasal steroids and nasal irrigations lowdosesystemic steroids and antibiotics when bacterial infection (typically Staphylococcus species) is suspected
Wegenerrsquos Granulomatosis
bull Prognosisbull ndash Most of the patients respond well to treatmentbull achieving symptom-free intervals of 5ndash20 yearsbull or more bull -Anatomical problems (sinusitis trachealbull stenosis) may require surgery bull Relapses can be long and troublesomebull Long-term complications are chronicbull renal failure hearing loss and deafness
Nasal Fractures Definition ndash A nasal fracture is a disruption of the nasal bone structure due to trauma It is the most frequently fractured facial bone Epidemiologyaetiology ndash Sports falls and assaults are the usual mechanisms of fracture -Males are affected twice as often as are females -Paediatric populations with a incidences during the second and third decades of life -Variables such as force impact direction nature of the striking object age and other will influence the pattern of injury to the components of the nose
Nasal Fractures
bull Symptomsbull ndash Deformity swelling epistaxis and periorbital
ecchymosis are signs that are suggestive of nasal fracture
bull bony crepitus and nasal segment mobilitybull ndash Epiphora bull Severe bilateral injuries to the lachrymal bones
arebull associated with depressed nasal fractures
Nasal Fractures Complications ndash Septal haematoma is one of the most severe early complications of nasal trauma and without drainage it results in abscess formation 6ndash7 days after trauma producing necrosis of the septal cartilage -Long-term problems such as saddle-nose deformity perforation columellar retraction and nasalbase
Septal infection could lead to osteomyelitis orbital and intracranial abscesses meningitis and cavernous sinus thrombosis -Cerebrospinal fluid leakage is a common complication of severe
nasal and frontal fractures
Nasal Fractures
bull Diagnostic proceduresbull ndash Inspectionbull bull Changes of appearance such as deviation andbull asymmetry bleeding watery drainage changesbull in nasal breathing and smell It is useful to comparebull the current presentation with old photographsbull (up to 40 of normal individuals havebull significant nose malformations)
Nasal Fractures Physical examination bull The diagnosis of a nasal fracture is made primarily by physical examination epistaxis nasal swelling and periorbital ecchymosis Nasal shape in the lateral and frontal inspection should be assessed Grasping the dorsum between two fingers and rocking the pyramid back and forth aids in assessing the mobility of nasal bones Internal structures should be evaluated by using a headlight and nasal speculum Clotted blood is removed by suction and assessment of haematoma mucosal tears and active bleeding is performed Bimanual palpation of the septum helps to differentiate septal swelling from haematoma ndash
Nasal FracturesRadiographybull There is no clear evidence of the role of radiographyin the management of nasal fracturesPlain films have up to a 66 false-positive rateas a result of misinterpretation of normal suturelines In addition old fractures are difficult todistinguishbull Three-dimensional CT is recommended for extensiveinjuries involving the nasal-orbital-ethmoidalcomplexndash
Nasal Fractures
bull Additionaluseful diagnostic proceduresbull bull Using a 0 or 30deg 4-mm endoscope is helpful inbull the assessment of posterior abnormalities If thebull patient is heavily sedated Brown-Gruss
provocationbull manoeuvres may be performed to determinebull deformities in upper middle or lower segmentsbull by compressing each compartment
Nasal FracturesConservative treatmentndash Treatment of bleedingbull For localised bleeding anterior sources may becauterised by silver nitrate or sealed with topicalmaterials such as thrombin combined withgelatin foam fibrin glue FloSealreg or other procoagulantmaterials If conservative measuresfail a formal anterior packing is placedbull Bleeding from branches of sphenopalatine orethmoid vessels requires anterior-posteriorpacking
Nasal Fractures
bull bull Surgical methods such as direct endoscopic vessel
bull cauterization or ligation have been shown tobull offer better haemostasis and patient comfortbull Angiography with embolization can also be
consideredbull in cases refractory to more conservativebull approaches
Nasal Fractures
bull Type of reductionbull bull Nondisplaced fractures should be treated withbull observation alone Closed nasal reduction is thebull best choice for simple injuries (isolated unilateralbull with medial displacement)bull bull An open approach should be considered in
severebull trauma (bilateral depressed fractures)
Nasal Fracturesbull Surgical principlesbull ndash Topical anaesthesia with cotton pledgets soakedbull with 4 cocaine or 005 oxymethazoline combinedbull with 4 topical lidocaine should be appliedbull for 5ndash10 min Local anaesthesia should also be injectedbull (1 lidocaine and 1100000 epinephrine)bull along the septum lateral walls and floor of the nasalbull cavitybull bull
Nasal FracturesClosed reductionndashndash The nasal bones are grasped between two fingersand pressure is applied laterally in theopposite direction of the deviation A bluntelevator may be used from within the nose incases of significant medial collapse Walshamforceps can be of help Reduction of the septumshould be performed with the use ofAsch forceps
Nasal Fractures
bull To prevent collapse of the postreductionbull framework nasal packing should be placedbull for 3ndash5 days Septum splints are recommendedbull in comminuted septal fractures withbull severe mucosal lesions External nasal splintingbull for 10 days (Aquaplastreg Thermoplastreg)bull provides nasal protection Nasal saline spraysbull prevent crusting and oral antibiotics should
Nasal Fractures
bull Open reductionbull ndashndash Immediate repair of fractures by using
widebull surgical exposure reduction fixation and
reconstructionbull ndashndash The second option is delayed correctionbull (6 months or more) of persistent deformitiesbull using standard techniques of rhinoplasty
Deviated Nasal Septum
bull Definition of the diseasebull ndash Deviation of the nasal septum is a common causebull of unilateral nasal airway obstruction in which thebull nasal septum is displacedbull bull Epidemiologyaetiologybull ndash Developmental septal abnormalities Septal cartilage
damage in the neonatal period andbull during birth can cause severe septal deviation inbull the absence of a history of nasal trauma
Deviated Nasal Septum
bull Symptomsbull ndash Patients may present with a history of sinusitis
allergicbull rhinitis obstructive sleep apnoea previousbull nasal surgery or recent nasal trauma Unilateral or
bilateral nasal airway obstruction that is unrelievedbull with decongestants or nasal steroid sprays is oftenbull seenbull bull
Deviated Nasal SeptumDiagnosisndashExamination external dorsal deviation or the columella and caudal septummay be deflected off the midline (caudal subluxation)ndash Inspections of the nasal cavity and anterior-posteriorrhinoscopy are helpful in diagnosing the locationtype and severity of septal deformityThe endoscope is also useful in identifying polypsthe severity and extent of posterior septaldeviations and bony spurs and locating areas ofseptal perforation or mucosal injury
Deviated Nasal Septum
bull Therapybull ndash Septoplasty is a procedurebull The areabull of deviation is corrected or resected in order tobull leave behind as much cartilage and bone as
possiblebull Cartilage resection is minimised and can be
repositioned reshaped or recontoured using a variety of methods
Deviated Nasal Septum
bull ndash Indications of septoplasty before the growth period
bull of the nose is finished should be very limited bull -In these cases surgery must preserve all the
cartilagebull in order to prevent external changes of the
shape ofbull the nose
Deviated Nasal Septum
bull Complicationsbull ndash Frequent complications include haematoma andbull infection Cerebrospinal fluid leak is a rare but
potentiallybull serious complicationbull It is usually the resultbull of avulsion or damage to the cribriform plate whenbull handling the perpendicular plate of the ethmoidbull ndash Other complications include epistaxis nasal
Deviated Nasal Septum
bull Other complications include epistaxis nasal obstruction
bull due to residual deviation synechiae returnbull of the cartilaginous deviation septal perforationbull anosmia and cosmetic nasal deformities suchbull as widened alar rim margins drooping nasal tipbull columella retraction and a sunken dorsum with abull supratip saddle formation
Septal perforation with minor crusting View from provide closure of the
incision
Septal Haematoma
bull A septal haematoma is a blood collection under the perichondrium
bull of the septum and cartilagebull bull bull Epidemiologyaetiologybull ndash A septal haematoma is one of the most
severe complications of nasal trauma
Septal Haematoma
bull Diagnosisbull ndash Signs and symptoms include intense pain
swellingbull haematoma of the upper lip and philtrum
area andbull complete nasal airway obstruction
Septal HaematomaTherapyndash Management consists of drainage through a mucoperichondrial incision Immediate treatment isnecessary to prevent long-term problems such asa saddle-nose deformity perforation columellarretraction and nasal-base widening In childrenseptal destruction can lead to devastating nasal andmidfacial growth abnormalitiesbull Surgeryndash Incision and evacuation of the collection is performedDrainage of a septal haematoma should
Septal HaematomaSurgeryndash Incision and evacuation of the collection is performedDrainage of a septal haematoma should provide closure of the incision
Splints or transseptal sutures are placed to obliterate thepotential space and prevent collectionInfection involving the septal cartilage Reconstruction with autologouscartilage is then performed in a second stage Oral antibiotics should be given
Nasal DeformitySaddle-nose deformityndash A saddle-nose deformity is characterised by a loss ofnasal dorsal height and compromised nasal supportstructures -Other case observed are depressionof the middle vault and dorsum loss of nasal tipsupport and definition shortened (vertical) nasal length over rotation of the nasal tip and retrusion ofthe nasal spine and caudal septum It is also knownas a ldquoPug noserdquo or ldquoboxerrsquos noserdquo both of which referto various degrees of nasal dorsal depressionbull
Nasal DeformityEpidemiologyaetiologyndash Prevalence is higher in population groups prone to facial trauma (ie boxers athletes) those with historiesof intranasal cocaine use nasal surgery (e g radical submucosal septal resection reductive rhinoplasty)ndash A saddle-nose deformity can be congenital or acquired It can be noticed as a part of individual familialsyndromic and ethnic characteristics - Most deformities are due to traumatic and iatrogeniccauses Medical causes are Wegenerrsquosgranulomatosis relapsing polychondritis leprosy (Hansenrsquos disease) syphilis ectodermal dysplasiaand intranasal cocaine use
Nasal Deformity
bull Therapybull ndash Nasal reconstruction indications depend on patientbull selection surgeon experience and aetiology of thebull deformity bull Indications for surgery can be functionalbull aesthetic or most commonly both In individuals
with a compromised nasal airway a nasoseptalbull reconstruction is indicated
Nasal Deformity
bull Contraindications bull include patients with malignantbull chronic or autoimmune disease conditions drugbull abuse poor perioperative risk profile and unrealisticbull expectationsbull ndash Multiple previous rhinoplasties and certain
professionsbull (mixed martial artists boxers and other contactbull sports) are relative contraindications
Nasal DeformitySeptoplastyndash Septoplasty is performed to correct nasal obstructioncaused by septal deformityndash Usually septoplasty is performed under general anaesthesiawith the patient in the supine position with the head elevated by approximately 30 (Righthandedsurgeons approach from the right side)ndash Local vasoconstrictive anaesthesia is applied notonly to reduce postoperative pain but also more importantly to achieve vasoconstriction of themucosa and less intraoperative haemorrhage Lidocainewith adrenaline or epinephrine is usedalthough in patients with cardiac hypersensitivityoxymetazoline might be preferred
Nasal Deformity
bull Septoplasty begins with the incision of septal mucosabull Most operative techniques utilise a hemitransfixionbull incision at the caudal end of septum so thatbull deviation at this point might be reached as wellbull as a transfixion incision that is easily obtained ifbull needed (Right-handed surgeons normally choosebull the left side but that may vary when deviation isbull convex towards the right)
Nasal DeformityA columella retractor is placed over the columellaand by pulling it laterally the caudal border of theseptum is exposed Ala can be protected by an alaprotector A vertical incision with a no 15 bladeover the caudal end of septum is performed untilreaching the plane of the septal cartilage It is essentialto correctly identify the perichondrium and byusing the Cottle elevator dissect and lift it creatinga flap As the dissection proceeds along the septalcartilage a longer speculum (no 5) is introduced sothat elevation of the mucoperichondrium is doneunder constant visual controlndash The next step is to dissect the mucoperiostium
Nasal DeformityDissecting over the bony-cartilaginous junctionwhen joining both tunnels might be difficult and is
especially prone to membrane perforationndash If needed the same tunnels are to be created on the
other side of the septum Then deviated parts of
septum are identified and removed either with a
knife or a Freer chisel
Nasal Deformitybull septum from the maxillary crest the septum mustbull be separated from the perpendicular plate trimmedbull along the inferior border placed back onto the crestbull and sutured to the periosteum If the deformity involvesbull the vomer an osteotome is used Care mustbull be taken not to break the cribriform plate becausebull it could cause a cerebrospinal fistula
Nasal Deformity
bull Once the septal deviation is corrected the flapsbull and hemitransfixion incision are mattressed
withbull absorbable sutures Nasal packing to prevent
synechiaebull and postoperative septal haematoma mightbull be advised but should be removed within 72 h

-The maxillary sinus frontalsinus and anterior ethmoid cells drain into the nasalcavity through the middle meatusmdashie below themiddle turbinate -The posterior ethmoidcells drain into the nasal cavity through the superiormeatus The ostium of the sphenoid sinus is locatedin the anterior wall directly above the choanae- The anatomical connections between the nasal cavity andparanasal sinuses are functionally important and playa key role in the pathogenesis of many rhinologic diseasesthat involve the paranasal sinuses
Vascular SupplyThe external nose derives most of its blood supply
from the facial artery which arises from the external
carotid artery and from the ophthalmic artery which
springs from the internal carotid artery
Vascular Supply
The internalnose receives blood from the territories of the externaland internal carotid arteries- the terminalbranches of the sphenopalatine artery which arisesfrom the maxillary artery - the anterior and posteriorethmoid arteries which arise from the ophthalmicartery-internal carotid arterie
venous drainage
The venous drainageof the facial region is handled by -the facial vein -retromandibular vein -internal jugular vein
lymphatic drainage
The regional lymphatic drainage of the face and externalnose is handled mainly by- the submandibularlymph nodes while the nasal cavity is additionallydrained by -the retropharyngeal and deep - -cervical lymph nodes
Morphology of the Nasal Mucosa
Besides the anatomical structure of the external noseand nasal cavity the nasal mucosa plays an essentialrole in numerous functions of the nose in the respiratory tract
Morphology of the Nasal Mucosa
The anterior part of the nasal cavity (the nasal vestibule)like the external nose is covered by skin composedof a multilayer keratinizing squamous epithelium and finally a ciliated respiratory epithelium A small areaon the upper nasal septum superior turbinate andpart of the middle turbinate located adjacent to thecribriform plate is covered by olfactory mucosa and iscalled the olfactory region
Nerve SupplyThe facial skin receives its sensory innervation fromterminal branches of the trigeminal nerve that enterthe facial region through the supraorbital infraorbitaland mental foramina Thefacial muscles are classified as mimetic or mastica- tory each of these groups receiving different motorinnervationbythe facial nerve
History and Clinical Examination of the Nose
Historybull The main symptomsbull nasal obstruction (ldquostuffy
noserdquo)bull nasal dischargebull Headachesbull Olfactory
dysfunction
Palpationbony discontinuitiesNeuralgias to check
over- the supraorbital -infraorbital -mental foramina
Anterior Rhinoscopy
bull The rhinologic examination itself begins with anterior
bull rhinoscopy to evaluate the nasal vestibule and the anterior
bull portions of the nasal cavity
Nasal Endoscopy Nasal endoscopy has become the most important andrewarding clinical examination method in rhinologic diagnosis
- rigid endoscopes which are available in 4-mm and 28- mm diameters and assorted viewing angles (eg 01048576 301048576 1201048576) -flexible endoscopes are also available for inspecting the nose and nasopharynx and exploring all of the pharynx and larynx in one sitting
Nasal endoscopy
Nasal Endoscopy
Nasal Endoscopy
Imaging of the Nose and Paranasal Sinuses
Conventional RadiographsStandard paranasal sinus radiographs in the occipitomental
projection ( Water projection) and
occipitofrontal projection Caldwell projection) in cases of acute inflammation
They are also obtained to evaluate midfacial fractures
Computed Tomography (CT) the main indicationsfor CT scanning of the
nose and paranasal sinuses
are- chronic sinusitis - -trauma (especially
frontobasal -fractures)
-and tumors
The occipitofrontal projection is better for evaluating theethmoid cells and frontal sinus
occipitomental projection demonstrates the maxillarysinus and gives a limited view of the sphenoid sinus
Computed tomography of the paranasal sinuses
Four representative coronal CT scans are shown
Four representative coronal CT scans are shown
Magnetic Resonance Imaging
Magnetic maging
Magnetic resonance imaging (MRI) has fewer indicationsthan CT in patients with paranasal sinus diseaseThis is primarily because MRI is markedly inferior toCT in defining the bony boundaries of the sinusesThe strength of MRI lies in its superior soft-tissue discriminationMRI is indicated in diseases that involve the paranasal sinuses in addition to thecranial cavity or orbit (eg tumors and congenitalmalformations such as encephaloceles)
MRI of the paranasal sinuses
The Nose and Sinuses
Structure The structure of the nose is made up of
four partsbull The surface anatomybull The nasal skeletonmdashcomposed of the
two nasal bones the paired upper lateral and lower lateral cartilages and the nasal septum covered in subcutaneous tissue and skin
bull The internal anatomymdashincludes the septum of the nose which forms the medial wall of the nasal cavity The turbinates on the lateral wall are also called conchae
bull The osteomeatal complexmdasha key functional area of the nose
Function The nose is the main route for inspired
air and its structure is related to this function As the air passes over the large surface area of the turbinates
The inspired gases are warmed and humidified Mucus on the mucosa of the nose removes large dust particles from the air as it is breathed in
The voice resonates in the sinuses and nose and this provides character to the speech
Pneumatization of the sinusesmdashthey are air filled spacesmdashreduces the weight of the skull
Diseases of thDiseases of the Outer and Inner Nosee Outer and
Inner Nose Erysipelas Definition of the disease ndash Erysipela is a skin infection that affects the superficial dermis and is caused by Streptococcus pyogenes (group A) It usually develops in the extremities and the face and less commonly on the scalp and genitals bull Epidemiologyaetiology ndash Erysipelas are more often seen in elderly infants and children patients with compromised immunology and diabetes -Predisposing factors are alcoholism skin ulceration puncture wounds fungal infections malnutrition and burns
Erysipelas
bull Symptomsbull ndash It usually presents of fever general fatigue bull -The skin lesion is a redindurated and elevated plaque
with borders that expand rapidly bull It is painful warm and accompanied by variable oedemabull -On the second or third day a flaccid bulla may develop
and desquamationbull bull Presence of regional lymph nodes is common
Erysipelas
bull Complicationsndash The most common complication is recurrencewhich is seen in 18ndash30 of the cases even afterproper antibiotic therapy Recurrence is seen moreoften in females than in malesA skin infection with S pyogenes could lead toglomerulonephritis
Erysipelas
bull Complicationsbull ndash The most common complication is recurrencebull which is seen in 18ndash30 of the cases even afterbull proper antibiotic therapy bull -Recurrence is seen morebull often in females than in males bull -A skin infection with S pyogenes could lead tobull glomerulonephritis
Erysipelas
bull bull Diagnosisbull ndash Diagnosis is based on the patientrsquos personal
historybull and physical examination particularly on inspectionbull of the skin
bull Blood cultures are positive in less thanbull 5 of cases
ErysipelasTherapyndash Conservative therapybull The preferred antibiotic is penicillin In mildcases with minor systemic symptoms penicillinV 500 mg orally every 6 h for 10 days or penicillinG benzathine 12 mil U intramuscularlyonceOther possibilities are amoxicillin 500 mgorally twice a day for 10 days or cephalexin 500mg orally every 6 h for 10 days
ErysipelasIn moderate and severe cases with significantsystemic symptoms hospitalization and intravenoustreatment is required penicillin G 2ndash4mil U intravenously every 4ndash6 h Cefazolin05ndash15 gm intravenously every 8 h cefotaxime1ndash2 gm intravenously every 8 h or ceftriaxone1ndash2 gm intravenously once a day should be administeredIn patients with a penicillin allergyclindamycin 600 mg intravenously every 8 h orvancomycin 15 mgkg intravenously twice a daymay be given
ErysipelaAdditional useful therapeutic optionsbull Prednisone 30 mg over 8 days might be consideredas well as elevation of the affected siteMoist heat compresses may be usefulbull Surgeryndash Debridement and drainage are indicated when bullaeabscesses or necroses are presentbull Differential diagnosisndash Contact dermatitisndash Asteatotic eczemandash Herpes zosterndash Angioneurotic oedemandash Osteomyelitis
Furuncle
bull Definition of the diseasebull ndash A furuncle is an infection that beginsbull at the hair follicle and spreads deeper into thebull dermis and subcutaneous tissue forming abull nodule After several days it developsbull into an abscess - red painful and fluctuantbull bull bull Epidemiologyaetiologybull ndash The aetiologic agent is Staphylococcus aureus
FuruncleSymptomsndashsymptoms are local and limited to thesite of infection Furuncles usually are wherehair follicles are present bull Complicationndash One complication is furunculosis multiple draining furunclesDiagnosisndash The diagnosis is based on clinical inspection - Cultures are not necessary when there is no systemic involvement but should beconsidered if systemic therapy (in case of feversignificant cellulitis or hospitalization) or whenmethicillin-resistant Staphylococcusaureus (MRSA) is considered
FuruncleTherapyndash When the furuncle is small application of moist heat compress to promote drainage -Larger furuncles should be drained by surgical incision-After drainage the area should be cleaned with anantiseptic (with chlorhexidinebetadine) should be applied twice
a dayndash If no systemic symptoms or extensive cellulitis arepresent simple topical care is usually curative andoral antibiotics are not necessary Otherwise systemictreatment is indicated and should cover anypossible MRSA
Furuncle
bull -Recommended antibiotics are trimethoprim-sulfamethoxazole
bull 1ndash2 tablets orally twice daily doxycyclinebull 100 mg orally twice dailybull or clindamycin 300ndash450 mg orally every 8 hbull - In severe cases vancomycin 15 mgkg
intravenouslybull every 12 h or clindamycin 600 mg intravenouslybull every 8 h
Midline Granulomabull A midline granuloma is an angiocentricbull lymphoma it was referred to as polymorphicbull reticulosis lethal midline granuloma and midline
malignant reticulosisbull bull Definition of the diseasebull ndash This rare disease is a lymphoma of extranodal
presentationall cases are positive for the Epstein-Barr virus
bull -This lymphoma most commonly appears in the midface region
Midline GranulomaEpidemiologyaetiologyndash This form of lymphoma is rare in Europe and theUnited States with a higher prevalence in Asia and PeruSymptomsndash The most common presentation is nasal obstruction with a destructive mass occupying the nosesinuses and palate
-Fever night sweatsand weight loss seen usually in Hodgkinrsquos lymphomaand other non-Hodgkinrsquos lymphomas (knownas ldquoB symptomsrdquo) are uncommon
Midline GranulomaDiagnosisndash The diagnosis is based on anatomopathologicalstudy The malignancy of the tumour manifested byextensive necrosis makes the histological diagnosisdifficult and often more biopsies are required forconfirmationbull Therapyndash Therapy consists of radiotherapy with or withoutchemotherapy
Midline Granuloma
bull Prognosisbull ndash Depending on the stage long-term remission or
experience a worseningbull prognosis with relapses which may include otherbull extranodal sites bull Involvement of extranodal sitesbull including the upper airway gastrointestinal tractbull skin
Wegenerrsquos Granulomatosis
bull Definition of the diseasebull ndash Wegenerrsquos granulomatosis is a systemic chronicbull vasculitis of small- and medium-sized blood vesselsbull with an autoimmune component It affectsbull particular organs with variable predilectionbull Epidemiologyaetiologybull ndash Wegenerrsquos granulomatosis is a rare disease It affects
about 1 in 20000ndash30000 people It is more prevalentbull in middle-aged Caucasian patients
Wegenerrsquos Granulomatosis
Symptomsndash The disease may present pulmonary upper
respiratory tract or renal In the disseminated form-The localised form ndash confinedto the upper respiratory region ndash is present in 25of the patients- It consists of nonspecific manifestationssuch as nasal obstruction crusting purulentor bloody rhinorrhea and painful or painless ulcers in oral or nasal cavities which are unresponsive tostandard medical treatment
Wegenerrsquos Granulomatosis
bull In some patients the nasal septum is perforatedbull which leads to saddle-nose deformity Less
commonbull symptoms are hoarseness stridor due to
subglotticbull stenosis otalgia otorrhea and conductivebull and sensorineural hearing loss Also ocular
symptomsbull such as scleritis conjunctivitis uveitis andbull episcleritis may be present
Wegenerrsquos Granulomatosis
bull ndash In the disseminated form pulmonary involvementbull is manifested by cough dyspnoea haemoptysisbull (due to an alveolar capillaritis necrotic lesions orbull endobronchial disease) and pleuritic painndashbull -Ninety per cent of patients have nasal symptomsbull and these symptoms are usually the first
manifestationof the diseasebull -Most patients have also renal involvementbull even if it is subclinical
Wegenerrsquos Granulomatosis
Diagnosis ndash Diagnosis of Wegenerrsquos granulomatosis is based on clinical findings that demonstrate lung (chest x-ray) kidney (urine analysis) or upper respiratory tract
involvement (oral or nasal ulcers or discharge) - positive blood analysis for cytoplasmic-staining antineutrophil
cytoplasmic antibodies (c-ANCA) and confirming proteinase 3 (PR3) ANCA or myeloperoxidase (MPO) ANCA ndash Biopsy is essential for diagnosis nonspecific chronic inflammation
and necrosis -Bacterial and fungal infections
Wegenerrsquos Granulomatosis
Therapyndash Conservative therapybull In the induction of disease remission highdosesteroids (e g prednisone 1 mgkgday) for1 month with tapering over several months aregiven In addition cyclophosphamide (2 mgkgday) should be administered for 6ndash12 monthsuntil symptoms disappear In the maintenanceof remission cyclophosphamide should be
Wegenerrsquos Granulomatosis
Antibiotics mainly trimethoprim-sulfamethoxazoleare given for prophylaxis againstPneumocystis jiroveci (formerly Pneumocystiscarinii) pneumonia (PCP) which may developduring immunosuppression and have a role inpreventing recurrencesbull Sinonasal manifestations may be treated with topical nasal steroids and nasal irrigations lowdosesystemic steroids and antibiotics when bacterial infection (typically Staphylococcus species) is suspected
Wegenerrsquos Granulomatosis
bull Prognosisbull ndash Most of the patients respond well to treatmentbull achieving symptom-free intervals of 5ndash20 yearsbull or more bull -Anatomical problems (sinusitis trachealbull stenosis) may require surgery bull Relapses can be long and troublesomebull Long-term complications are chronicbull renal failure hearing loss and deafness
Nasal Fractures Definition ndash A nasal fracture is a disruption of the nasal bone structure due to trauma It is the most frequently fractured facial bone Epidemiologyaetiology ndash Sports falls and assaults are the usual mechanisms of fracture -Males are affected twice as often as are females -Paediatric populations with a incidences during the second and third decades of life -Variables such as force impact direction nature of the striking object age and other will influence the pattern of injury to the components of the nose
Nasal Fractures
bull Symptomsbull ndash Deformity swelling epistaxis and periorbital
ecchymosis are signs that are suggestive of nasal fracture
bull bony crepitus and nasal segment mobilitybull ndash Epiphora bull Severe bilateral injuries to the lachrymal bones
arebull associated with depressed nasal fractures
Nasal Fractures Complications ndash Septal haematoma is one of the most severe early complications of nasal trauma and without drainage it results in abscess formation 6ndash7 days after trauma producing necrosis of the septal cartilage -Long-term problems such as saddle-nose deformity perforation columellar retraction and nasalbase
Septal infection could lead to osteomyelitis orbital and intracranial abscesses meningitis and cavernous sinus thrombosis -Cerebrospinal fluid leakage is a common complication of severe
nasal and frontal fractures
Nasal Fractures
bull Diagnostic proceduresbull ndash Inspectionbull bull Changes of appearance such as deviation andbull asymmetry bleeding watery drainage changesbull in nasal breathing and smell It is useful to comparebull the current presentation with old photographsbull (up to 40 of normal individuals havebull significant nose malformations)
Nasal Fractures Physical examination bull The diagnosis of a nasal fracture is made primarily by physical examination epistaxis nasal swelling and periorbital ecchymosis Nasal shape in the lateral and frontal inspection should be assessed Grasping the dorsum between two fingers and rocking the pyramid back and forth aids in assessing the mobility of nasal bones Internal structures should be evaluated by using a headlight and nasal speculum Clotted blood is removed by suction and assessment of haematoma mucosal tears and active bleeding is performed Bimanual palpation of the septum helps to differentiate septal swelling from haematoma ndash
Nasal FracturesRadiographybull There is no clear evidence of the role of radiographyin the management of nasal fracturesPlain films have up to a 66 false-positive rateas a result of misinterpretation of normal suturelines In addition old fractures are difficult todistinguishbull Three-dimensional CT is recommended for extensiveinjuries involving the nasal-orbital-ethmoidalcomplexndash
Nasal Fractures
bull Additionaluseful diagnostic proceduresbull bull Using a 0 or 30deg 4-mm endoscope is helpful inbull the assessment of posterior abnormalities If thebull patient is heavily sedated Brown-Gruss
provocationbull manoeuvres may be performed to determinebull deformities in upper middle or lower segmentsbull by compressing each compartment
Nasal FracturesConservative treatmentndash Treatment of bleedingbull For localised bleeding anterior sources may becauterised by silver nitrate or sealed with topicalmaterials such as thrombin combined withgelatin foam fibrin glue FloSealreg or other procoagulantmaterials If conservative measuresfail a formal anterior packing is placedbull Bleeding from branches of sphenopalatine orethmoid vessels requires anterior-posteriorpacking
Nasal Fractures
bull bull Surgical methods such as direct endoscopic vessel
bull cauterization or ligation have been shown tobull offer better haemostasis and patient comfortbull Angiography with embolization can also be
consideredbull in cases refractory to more conservativebull approaches
Nasal Fractures
bull Type of reductionbull bull Nondisplaced fractures should be treated withbull observation alone Closed nasal reduction is thebull best choice for simple injuries (isolated unilateralbull with medial displacement)bull bull An open approach should be considered in
severebull trauma (bilateral depressed fractures)
Nasal Fracturesbull Surgical principlesbull ndash Topical anaesthesia with cotton pledgets soakedbull with 4 cocaine or 005 oxymethazoline combinedbull with 4 topical lidocaine should be appliedbull for 5ndash10 min Local anaesthesia should also be injectedbull (1 lidocaine and 1100000 epinephrine)bull along the septum lateral walls and floor of the nasalbull cavitybull bull
Nasal FracturesClosed reductionndashndash The nasal bones are grasped between two fingersand pressure is applied laterally in theopposite direction of the deviation A bluntelevator may be used from within the nose incases of significant medial collapse Walshamforceps can be of help Reduction of the septumshould be performed with the use ofAsch forceps
Nasal Fractures
bull To prevent collapse of the postreductionbull framework nasal packing should be placedbull for 3ndash5 days Septum splints are recommendedbull in comminuted septal fractures withbull severe mucosal lesions External nasal splintingbull for 10 days (Aquaplastreg Thermoplastreg)bull provides nasal protection Nasal saline spraysbull prevent crusting and oral antibiotics should
Nasal Fractures
bull Open reductionbull ndashndash Immediate repair of fractures by using
widebull surgical exposure reduction fixation and
reconstructionbull ndashndash The second option is delayed correctionbull (6 months or more) of persistent deformitiesbull using standard techniques of rhinoplasty
Deviated Nasal Septum
bull Definition of the diseasebull ndash Deviation of the nasal septum is a common causebull of unilateral nasal airway obstruction in which thebull nasal septum is displacedbull bull Epidemiologyaetiologybull ndash Developmental septal abnormalities Septal cartilage
damage in the neonatal period andbull during birth can cause severe septal deviation inbull the absence of a history of nasal trauma
Deviated Nasal Septum
bull Symptomsbull ndash Patients may present with a history of sinusitis
allergicbull rhinitis obstructive sleep apnoea previousbull nasal surgery or recent nasal trauma Unilateral or
bilateral nasal airway obstruction that is unrelievedbull with decongestants or nasal steroid sprays is oftenbull seenbull bull
Deviated Nasal SeptumDiagnosisndashExamination external dorsal deviation or the columella and caudal septummay be deflected off the midline (caudal subluxation)ndash Inspections of the nasal cavity and anterior-posteriorrhinoscopy are helpful in diagnosing the locationtype and severity of septal deformityThe endoscope is also useful in identifying polypsthe severity and extent of posterior septaldeviations and bony spurs and locating areas ofseptal perforation or mucosal injury
Deviated Nasal Septum
bull Therapybull ndash Septoplasty is a procedurebull The areabull of deviation is corrected or resected in order tobull leave behind as much cartilage and bone as
possiblebull Cartilage resection is minimised and can be
repositioned reshaped or recontoured using a variety of methods
Deviated Nasal Septum
bull ndash Indications of septoplasty before the growth period
bull of the nose is finished should be very limited bull -In these cases surgery must preserve all the
cartilagebull in order to prevent external changes of the
shape ofbull the nose
Deviated Nasal Septum
bull Complicationsbull ndash Frequent complications include haematoma andbull infection Cerebrospinal fluid leak is a rare but
potentiallybull serious complicationbull It is usually the resultbull of avulsion or damage to the cribriform plate whenbull handling the perpendicular plate of the ethmoidbull ndash Other complications include epistaxis nasal
Deviated Nasal Septum
bull Other complications include epistaxis nasal obstruction
bull due to residual deviation synechiae returnbull of the cartilaginous deviation septal perforationbull anosmia and cosmetic nasal deformities suchbull as widened alar rim margins drooping nasal tipbull columella retraction and a sunken dorsum with abull supratip saddle formation
Septal perforation with minor crusting View from provide closure of the
incision
Septal Haematoma
bull A septal haematoma is a blood collection under the perichondrium
bull of the septum and cartilagebull bull bull Epidemiologyaetiologybull ndash A septal haematoma is one of the most
severe complications of nasal trauma
Septal Haematoma
bull Diagnosisbull ndash Signs and symptoms include intense pain
swellingbull haematoma of the upper lip and philtrum
area andbull complete nasal airway obstruction
Septal HaematomaTherapyndash Management consists of drainage through a mucoperichondrial incision Immediate treatment isnecessary to prevent long-term problems such asa saddle-nose deformity perforation columellarretraction and nasal-base widening In childrenseptal destruction can lead to devastating nasal andmidfacial growth abnormalitiesbull Surgeryndash Incision and evacuation of the collection is performedDrainage of a septal haematoma should
Septal HaematomaSurgeryndash Incision and evacuation of the collection is performedDrainage of a septal haematoma should provide closure of the incision
Splints or transseptal sutures are placed to obliterate thepotential space and prevent collectionInfection involving the septal cartilage Reconstruction with autologouscartilage is then performed in a second stage Oral antibiotics should be given
Nasal DeformitySaddle-nose deformityndash A saddle-nose deformity is characterised by a loss ofnasal dorsal height and compromised nasal supportstructures -Other case observed are depressionof the middle vault and dorsum loss of nasal tipsupport and definition shortened (vertical) nasal length over rotation of the nasal tip and retrusion ofthe nasal spine and caudal septum It is also knownas a ldquoPug noserdquo or ldquoboxerrsquos noserdquo both of which referto various degrees of nasal dorsal depressionbull
Nasal DeformityEpidemiologyaetiologyndash Prevalence is higher in population groups prone to facial trauma (ie boxers athletes) those with historiesof intranasal cocaine use nasal surgery (e g radical submucosal septal resection reductive rhinoplasty)ndash A saddle-nose deformity can be congenital or acquired It can be noticed as a part of individual familialsyndromic and ethnic characteristics - Most deformities are due to traumatic and iatrogeniccauses Medical causes are Wegenerrsquosgranulomatosis relapsing polychondritis leprosy (Hansenrsquos disease) syphilis ectodermal dysplasiaand intranasal cocaine use
Nasal Deformity
bull Therapybull ndash Nasal reconstruction indications depend on patientbull selection surgeon experience and aetiology of thebull deformity bull Indications for surgery can be functionalbull aesthetic or most commonly both In individuals
with a compromised nasal airway a nasoseptalbull reconstruction is indicated
Nasal Deformity
bull Contraindications bull include patients with malignantbull chronic or autoimmune disease conditions drugbull abuse poor perioperative risk profile and unrealisticbull expectationsbull ndash Multiple previous rhinoplasties and certain
professionsbull (mixed martial artists boxers and other contactbull sports) are relative contraindications
Nasal DeformitySeptoplastyndash Septoplasty is performed to correct nasal obstructioncaused by septal deformityndash Usually septoplasty is performed under general anaesthesiawith the patient in the supine position with the head elevated by approximately 30 (Righthandedsurgeons approach from the right side)ndash Local vasoconstrictive anaesthesia is applied notonly to reduce postoperative pain but also more importantly to achieve vasoconstriction of themucosa and less intraoperative haemorrhage Lidocainewith adrenaline or epinephrine is usedalthough in patients with cardiac hypersensitivityoxymetazoline might be preferred
Nasal Deformity
bull Septoplasty begins with the incision of septal mucosabull Most operative techniques utilise a hemitransfixionbull incision at the caudal end of septum so thatbull deviation at this point might be reached as wellbull as a transfixion incision that is easily obtained ifbull needed (Right-handed surgeons normally choosebull the left side but that may vary when deviation isbull convex towards the right)
Nasal DeformityA columella retractor is placed over the columellaand by pulling it laterally the caudal border of theseptum is exposed Ala can be protected by an alaprotector A vertical incision with a no 15 bladeover the caudal end of septum is performed untilreaching the plane of the septal cartilage It is essentialto correctly identify the perichondrium and byusing the Cottle elevator dissect and lift it creatinga flap As the dissection proceeds along the septalcartilage a longer speculum (no 5) is introduced sothat elevation of the mucoperichondrium is doneunder constant visual controlndash The next step is to dissect the mucoperiostium
Nasal DeformityDissecting over the bony-cartilaginous junctionwhen joining both tunnels might be difficult and is
especially prone to membrane perforationndash If needed the same tunnels are to be created on the
other side of the septum Then deviated parts of
septum are identified and removed either with a
knife or a Freer chisel
Nasal Deformitybull septum from the maxillary crest the septum mustbull be separated from the perpendicular plate trimmedbull along the inferior border placed back onto the crestbull and sutured to the periosteum If the deformity involvesbull the vomer an osteotome is used Care mustbull be taken not to break the cribriform plate becausebull it could cause a cerebrospinal fistula
Nasal Deformity
bull Once the septal deviation is corrected the flapsbull and hemitransfixion incision are mattressed
withbull absorbable sutures Nasal packing to prevent
synechiaebull and postoperative septal haematoma mightbull be advised but should be removed within 72 h

Vascular SupplyThe external nose derives most of its blood supply
from the facial artery which arises from the external
carotid artery and from the ophthalmic artery which
springs from the internal carotid artery
Vascular Supply
The internalnose receives blood from the territories of the externaland internal carotid arteries- the terminalbranches of the sphenopalatine artery which arisesfrom the maxillary artery - the anterior and posteriorethmoid arteries which arise from the ophthalmicartery-internal carotid arterie
venous drainage
The venous drainageof the facial region is handled by -the facial vein -retromandibular vein -internal jugular vein
lymphatic drainage
The regional lymphatic drainage of the face and externalnose is handled mainly by- the submandibularlymph nodes while the nasal cavity is additionallydrained by -the retropharyngeal and deep - -cervical lymph nodes
Morphology of the Nasal Mucosa
Besides the anatomical structure of the external noseand nasal cavity the nasal mucosa plays an essentialrole in numerous functions of the nose in the respiratory tract
Morphology of the Nasal Mucosa
The anterior part of the nasal cavity (the nasal vestibule)like the external nose is covered by skin composedof a multilayer keratinizing squamous epithelium and finally a ciliated respiratory epithelium A small areaon the upper nasal septum superior turbinate andpart of the middle turbinate located adjacent to thecribriform plate is covered by olfactory mucosa and iscalled the olfactory region
Nerve SupplyThe facial skin receives its sensory innervation fromterminal branches of the trigeminal nerve that enterthe facial region through the supraorbital infraorbitaland mental foramina Thefacial muscles are classified as mimetic or mastica- tory each of these groups receiving different motorinnervationbythe facial nerve
History and Clinical Examination of the Nose
Historybull The main symptomsbull nasal obstruction (ldquostuffy
noserdquo)bull nasal dischargebull Headachesbull Olfactory
dysfunction
Palpationbony discontinuitiesNeuralgias to check
over- the supraorbital -infraorbital -mental foramina
Anterior Rhinoscopy
bull The rhinologic examination itself begins with anterior
bull rhinoscopy to evaluate the nasal vestibule and the anterior
bull portions of the nasal cavity
Nasal Endoscopy Nasal endoscopy has become the most important andrewarding clinical examination method in rhinologic diagnosis
- rigid endoscopes which are available in 4-mm and 28- mm diameters and assorted viewing angles (eg 01048576 301048576 1201048576) -flexible endoscopes are also available for inspecting the nose and nasopharynx and exploring all of the pharynx and larynx in one sitting
Nasal endoscopy
Nasal Endoscopy
Nasal Endoscopy
Imaging of the Nose and Paranasal Sinuses
Conventional RadiographsStandard paranasal sinus radiographs in the occipitomental
projection ( Water projection) and
occipitofrontal projection Caldwell projection) in cases of acute inflammation
They are also obtained to evaluate midfacial fractures
Computed Tomography (CT) the main indicationsfor CT scanning of the
nose and paranasal sinuses
are- chronic sinusitis - -trauma (especially
frontobasal -fractures)
-and tumors
The occipitofrontal projection is better for evaluating theethmoid cells and frontal sinus
occipitomental projection demonstrates the maxillarysinus and gives a limited view of the sphenoid sinus
Computed tomography of the paranasal sinuses
Four representative coronal CT scans are shown
Four representative coronal CT scans are shown
Magnetic Resonance Imaging
Magnetic maging
Magnetic resonance imaging (MRI) has fewer indicationsthan CT in patients with paranasal sinus diseaseThis is primarily because MRI is markedly inferior toCT in defining the bony boundaries of the sinusesThe strength of MRI lies in its superior soft-tissue discriminationMRI is indicated in diseases that involve the paranasal sinuses in addition to thecranial cavity or orbit (eg tumors and congenitalmalformations such as encephaloceles)
MRI of the paranasal sinuses
The Nose and Sinuses
Structure The structure of the nose is made up of
four partsbull The surface anatomybull The nasal skeletonmdashcomposed of the
two nasal bones the paired upper lateral and lower lateral cartilages and the nasal septum covered in subcutaneous tissue and skin
bull The internal anatomymdashincludes the septum of the nose which forms the medial wall of the nasal cavity The turbinates on the lateral wall are also called conchae
bull The osteomeatal complexmdasha key functional area of the nose
Function The nose is the main route for inspired
air and its structure is related to this function As the air passes over the large surface area of the turbinates
The inspired gases are warmed and humidified Mucus on the mucosa of the nose removes large dust particles from the air as it is breathed in
The voice resonates in the sinuses and nose and this provides character to the speech
Pneumatization of the sinusesmdashthey are air filled spacesmdashreduces the weight of the skull
Diseases of thDiseases of the Outer and Inner Nosee Outer and
Inner Nose Erysipelas Definition of the disease ndash Erysipela is a skin infection that affects the superficial dermis and is caused by Streptococcus pyogenes (group A) It usually develops in the extremities and the face and less commonly on the scalp and genitals bull Epidemiologyaetiology ndash Erysipelas are more often seen in elderly infants and children patients with compromised immunology and diabetes -Predisposing factors are alcoholism skin ulceration puncture wounds fungal infections malnutrition and burns
Erysipelas
bull Symptomsbull ndash It usually presents of fever general fatigue bull -The skin lesion is a redindurated and elevated plaque
with borders that expand rapidly bull It is painful warm and accompanied by variable oedemabull -On the second or third day a flaccid bulla may develop
and desquamationbull bull Presence of regional lymph nodes is common
Erysipelas
bull Complicationsndash The most common complication is recurrencewhich is seen in 18ndash30 of the cases even afterproper antibiotic therapy Recurrence is seen moreoften in females than in malesA skin infection with S pyogenes could lead toglomerulonephritis
Erysipelas
bull Complicationsbull ndash The most common complication is recurrencebull which is seen in 18ndash30 of the cases even afterbull proper antibiotic therapy bull -Recurrence is seen morebull often in females than in males bull -A skin infection with S pyogenes could lead tobull glomerulonephritis
Erysipelas
bull bull Diagnosisbull ndash Diagnosis is based on the patientrsquos personal
historybull and physical examination particularly on inspectionbull of the skin
bull Blood cultures are positive in less thanbull 5 of cases
ErysipelasTherapyndash Conservative therapybull The preferred antibiotic is penicillin In mildcases with minor systemic symptoms penicillinV 500 mg orally every 6 h for 10 days or penicillinG benzathine 12 mil U intramuscularlyonceOther possibilities are amoxicillin 500 mgorally twice a day for 10 days or cephalexin 500mg orally every 6 h for 10 days
ErysipelasIn moderate and severe cases with significantsystemic symptoms hospitalization and intravenoustreatment is required penicillin G 2ndash4mil U intravenously every 4ndash6 h Cefazolin05ndash15 gm intravenously every 8 h cefotaxime1ndash2 gm intravenously every 8 h or ceftriaxone1ndash2 gm intravenously once a day should be administeredIn patients with a penicillin allergyclindamycin 600 mg intravenously every 8 h orvancomycin 15 mgkg intravenously twice a daymay be given
ErysipelaAdditional useful therapeutic optionsbull Prednisone 30 mg over 8 days might be consideredas well as elevation of the affected siteMoist heat compresses may be usefulbull Surgeryndash Debridement and drainage are indicated when bullaeabscesses or necroses are presentbull Differential diagnosisndash Contact dermatitisndash Asteatotic eczemandash Herpes zosterndash Angioneurotic oedemandash Osteomyelitis
Furuncle
bull Definition of the diseasebull ndash A furuncle is an infection that beginsbull at the hair follicle and spreads deeper into thebull dermis and subcutaneous tissue forming abull nodule After several days it developsbull into an abscess - red painful and fluctuantbull bull bull Epidemiologyaetiologybull ndash The aetiologic agent is Staphylococcus aureus
FuruncleSymptomsndashsymptoms are local and limited to thesite of infection Furuncles usually are wherehair follicles are present bull Complicationndash One complication is furunculosis multiple draining furunclesDiagnosisndash The diagnosis is based on clinical inspection - Cultures are not necessary when there is no systemic involvement but should beconsidered if systemic therapy (in case of feversignificant cellulitis or hospitalization) or whenmethicillin-resistant Staphylococcusaureus (MRSA) is considered
FuruncleTherapyndash When the furuncle is small application of moist heat compress to promote drainage -Larger furuncles should be drained by surgical incision-After drainage the area should be cleaned with anantiseptic (with chlorhexidinebetadine) should be applied twice
a dayndash If no systemic symptoms or extensive cellulitis arepresent simple topical care is usually curative andoral antibiotics are not necessary Otherwise systemictreatment is indicated and should cover anypossible MRSA
Furuncle
bull -Recommended antibiotics are trimethoprim-sulfamethoxazole
bull 1ndash2 tablets orally twice daily doxycyclinebull 100 mg orally twice dailybull or clindamycin 300ndash450 mg orally every 8 hbull - In severe cases vancomycin 15 mgkg
intravenouslybull every 12 h or clindamycin 600 mg intravenouslybull every 8 h
Midline Granulomabull A midline granuloma is an angiocentricbull lymphoma it was referred to as polymorphicbull reticulosis lethal midline granuloma and midline
malignant reticulosisbull bull Definition of the diseasebull ndash This rare disease is a lymphoma of extranodal
presentationall cases are positive for the Epstein-Barr virus
bull -This lymphoma most commonly appears in the midface region
Midline GranulomaEpidemiologyaetiologyndash This form of lymphoma is rare in Europe and theUnited States with a higher prevalence in Asia and PeruSymptomsndash The most common presentation is nasal obstruction with a destructive mass occupying the nosesinuses and palate
-Fever night sweatsand weight loss seen usually in Hodgkinrsquos lymphomaand other non-Hodgkinrsquos lymphomas (knownas ldquoB symptomsrdquo) are uncommon
Midline GranulomaDiagnosisndash The diagnosis is based on anatomopathologicalstudy The malignancy of the tumour manifested byextensive necrosis makes the histological diagnosisdifficult and often more biopsies are required forconfirmationbull Therapyndash Therapy consists of radiotherapy with or withoutchemotherapy
Midline Granuloma
bull Prognosisbull ndash Depending on the stage long-term remission or
experience a worseningbull prognosis with relapses which may include otherbull extranodal sites bull Involvement of extranodal sitesbull including the upper airway gastrointestinal tractbull skin
Wegenerrsquos Granulomatosis
bull Definition of the diseasebull ndash Wegenerrsquos granulomatosis is a systemic chronicbull vasculitis of small- and medium-sized blood vesselsbull with an autoimmune component It affectsbull particular organs with variable predilectionbull Epidemiologyaetiologybull ndash Wegenerrsquos granulomatosis is a rare disease It affects
about 1 in 20000ndash30000 people It is more prevalentbull in middle-aged Caucasian patients
Wegenerrsquos Granulomatosis
Symptomsndash The disease may present pulmonary upper
respiratory tract or renal In the disseminated form-The localised form ndash confinedto the upper respiratory region ndash is present in 25of the patients- It consists of nonspecific manifestationssuch as nasal obstruction crusting purulentor bloody rhinorrhea and painful or painless ulcers in oral or nasal cavities which are unresponsive tostandard medical treatment
Wegenerrsquos Granulomatosis
bull In some patients the nasal septum is perforatedbull which leads to saddle-nose deformity Less
commonbull symptoms are hoarseness stridor due to
subglotticbull stenosis otalgia otorrhea and conductivebull and sensorineural hearing loss Also ocular
symptomsbull such as scleritis conjunctivitis uveitis andbull episcleritis may be present
Wegenerrsquos Granulomatosis
bull ndash In the disseminated form pulmonary involvementbull is manifested by cough dyspnoea haemoptysisbull (due to an alveolar capillaritis necrotic lesions orbull endobronchial disease) and pleuritic painndashbull -Ninety per cent of patients have nasal symptomsbull and these symptoms are usually the first
manifestationof the diseasebull -Most patients have also renal involvementbull even if it is subclinical
Wegenerrsquos Granulomatosis
Diagnosis ndash Diagnosis of Wegenerrsquos granulomatosis is based on clinical findings that demonstrate lung (chest x-ray) kidney (urine analysis) or upper respiratory tract
involvement (oral or nasal ulcers or discharge) - positive blood analysis for cytoplasmic-staining antineutrophil
cytoplasmic antibodies (c-ANCA) and confirming proteinase 3 (PR3) ANCA or myeloperoxidase (MPO) ANCA ndash Biopsy is essential for diagnosis nonspecific chronic inflammation
and necrosis -Bacterial and fungal infections
Wegenerrsquos Granulomatosis
Therapyndash Conservative therapybull In the induction of disease remission highdosesteroids (e g prednisone 1 mgkgday) for1 month with tapering over several months aregiven In addition cyclophosphamide (2 mgkgday) should be administered for 6ndash12 monthsuntil symptoms disappear In the maintenanceof remission cyclophosphamide should be
Wegenerrsquos Granulomatosis
Antibiotics mainly trimethoprim-sulfamethoxazoleare given for prophylaxis againstPneumocystis jiroveci (formerly Pneumocystiscarinii) pneumonia (PCP) which may developduring immunosuppression and have a role inpreventing recurrencesbull Sinonasal manifestations may be treated with topical nasal steroids and nasal irrigations lowdosesystemic steroids and antibiotics when bacterial infection (typically Staphylococcus species) is suspected
Wegenerrsquos Granulomatosis
bull Prognosisbull ndash Most of the patients respond well to treatmentbull achieving symptom-free intervals of 5ndash20 yearsbull or more bull -Anatomical problems (sinusitis trachealbull stenosis) may require surgery bull Relapses can be long and troublesomebull Long-term complications are chronicbull renal failure hearing loss and deafness
Nasal Fractures Definition ndash A nasal fracture is a disruption of the nasal bone structure due to trauma It is the most frequently fractured facial bone Epidemiologyaetiology ndash Sports falls and assaults are the usual mechanisms of fracture -Males are affected twice as often as are females -Paediatric populations with a incidences during the second and third decades of life -Variables such as force impact direction nature of the striking object age and other will influence the pattern of injury to the components of the nose
Nasal Fractures
bull Symptomsbull ndash Deformity swelling epistaxis and periorbital
ecchymosis are signs that are suggestive of nasal fracture
bull bony crepitus and nasal segment mobilitybull ndash Epiphora bull Severe bilateral injuries to the lachrymal bones
arebull associated with depressed nasal fractures
Nasal Fractures Complications ndash Septal haematoma is one of the most severe early complications of nasal trauma and without drainage it results in abscess formation 6ndash7 days after trauma producing necrosis of the septal cartilage -Long-term problems such as saddle-nose deformity perforation columellar retraction and nasalbase
Septal infection could lead to osteomyelitis orbital and intracranial abscesses meningitis and cavernous sinus thrombosis -Cerebrospinal fluid leakage is a common complication of severe
nasal and frontal fractures
Nasal Fractures
bull Diagnostic proceduresbull ndash Inspectionbull bull Changes of appearance such as deviation andbull asymmetry bleeding watery drainage changesbull in nasal breathing and smell It is useful to comparebull the current presentation with old photographsbull (up to 40 of normal individuals havebull significant nose malformations)
Nasal Fractures Physical examination bull The diagnosis of a nasal fracture is made primarily by physical examination epistaxis nasal swelling and periorbital ecchymosis Nasal shape in the lateral and frontal inspection should be assessed Grasping the dorsum between two fingers and rocking the pyramid back and forth aids in assessing the mobility of nasal bones Internal structures should be evaluated by using a headlight and nasal speculum Clotted blood is removed by suction and assessment of haematoma mucosal tears and active bleeding is performed Bimanual palpation of the septum helps to differentiate septal swelling from haematoma ndash
Nasal FracturesRadiographybull There is no clear evidence of the role of radiographyin the management of nasal fracturesPlain films have up to a 66 false-positive rateas a result of misinterpretation of normal suturelines In addition old fractures are difficult todistinguishbull Three-dimensional CT is recommended for extensiveinjuries involving the nasal-orbital-ethmoidalcomplexndash
Nasal Fractures
bull Additionaluseful diagnostic proceduresbull bull Using a 0 or 30deg 4-mm endoscope is helpful inbull the assessment of posterior abnormalities If thebull patient is heavily sedated Brown-Gruss
provocationbull manoeuvres may be performed to determinebull deformities in upper middle or lower segmentsbull by compressing each compartment
Nasal FracturesConservative treatmentndash Treatment of bleedingbull For localised bleeding anterior sources may becauterised by silver nitrate or sealed with topicalmaterials such as thrombin combined withgelatin foam fibrin glue FloSealreg or other procoagulantmaterials If conservative measuresfail a formal anterior packing is placedbull Bleeding from branches of sphenopalatine orethmoid vessels requires anterior-posteriorpacking
Nasal Fractures
bull bull Surgical methods such as direct endoscopic vessel
bull cauterization or ligation have been shown tobull offer better haemostasis and patient comfortbull Angiography with embolization can also be
consideredbull in cases refractory to more conservativebull approaches
Nasal Fractures
bull Type of reductionbull bull Nondisplaced fractures should be treated withbull observation alone Closed nasal reduction is thebull best choice for simple injuries (isolated unilateralbull with medial displacement)bull bull An open approach should be considered in
severebull trauma (bilateral depressed fractures)
Nasal Fracturesbull Surgical principlesbull ndash Topical anaesthesia with cotton pledgets soakedbull with 4 cocaine or 005 oxymethazoline combinedbull with 4 topical lidocaine should be appliedbull for 5ndash10 min Local anaesthesia should also be injectedbull (1 lidocaine and 1100000 epinephrine)bull along the septum lateral walls and floor of the nasalbull cavitybull bull
Nasal FracturesClosed reductionndashndash The nasal bones are grasped between two fingersand pressure is applied laterally in theopposite direction of the deviation A bluntelevator may be used from within the nose incases of significant medial collapse Walshamforceps can be of help Reduction of the septumshould be performed with the use ofAsch forceps
Nasal Fractures
bull To prevent collapse of the postreductionbull framework nasal packing should be placedbull for 3ndash5 days Septum splints are recommendedbull in comminuted septal fractures withbull severe mucosal lesions External nasal splintingbull for 10 days (Aquaplastreg Thermoplastreg)bull provides nasal protection Nasal saline spraysbull prevent crusting and oral antibiotics should
Nasal Fractures
bull Open reductionbull ndashndash Immediate repair of fractures by using
widebull surgical exposure reduction fixation and
reconstructionbull ndashndash The second option is delayed correctionbull (6 months or more) of persistent deformitiesbull using standard techniques of rhinoplasty
Deviated Nasal Septum
bull Definition of the diseasebull ndash Deviation of the nasal septum is a common causebull of unilateral nasal airway obstruction in which thebull nasal septum is displacedbull bull Epidemiologyaetiologybull ndash Developmental septal abnormalities Septal cartilage
damage in the neonatal period andbull during birth can cause severe septal deviation inbull the absence of a history of nasal trauma
Deviated Nasal Septum
bull Symptomsbull ndash Patients may present with a history of sinusitis
allergicbull rhinitis obstructive sleep apnoea previousbull nasal surgery or recent nasal trauma Unilateral or
bilateral nasal airway obstruction that is unrelievedbull with decongestants or nasal steroid sprays is oftenbull seenbull bull
Deviated Nasal SeptumDiagnosisndashExamination external dorsal deviation or the columella and caudal septummay be deflected off the midline (caudal subluxation)ndash Inspections of the nasal cavity and anterior-posteriorrhinoscopy are helpful in diagnosing the locationtype and severity of septal deformityThe endoscope is also useful in identifying polypsthe severity and extent of posterior septaldeviations and bony spurs and locating areas ofseptal perforation or mucosal injury
Deviated Nasal Septum
bull Therapybull ndash Septoplasty is a procedurebull The areabull of deviation is corrected or resected in order tobull leave behind as much cartilage and bone as
possiblebull Cartilage resection is minimised and can be
repositioned reshaped or recontoured using a variety of methods
Deviated Nasal Septum
bull ndash Indications of septoplasty before the growth period
bull of the nose is finished should be very limited bull -In these cases surgery must preserve all the
cartilagebull in order to prevent external changes of the
shape ofbull the nose
Deviated Nasal Septum
bull Complicationsbull ndash Frequent complications include haematoma andbull infection Cerebrospinal fluid leak is a rare but
potentiallybull serious complicationbull It is usually the resultbull of avulsion or damage to the cribriform plate whenbull handling the perpendicular plate of the ethmoidbull ndash Other complications include epistaxis nasal
Deviated Nasal Septum
bull Other complications include epistaxis nasal obstruction
bull due to residual deviation synechiae returnbull of the cartilaginous deviation septal perforationbull anosmia and cosmetic nasal deformities suchbull as widened alar rim margins drooping nasal tipbull columella retraction and a sunken dorsum with abull supratip saddle formation
Septal perforation with minor crusting View from provide closure of the
incision
Septal Haematoma
bull A septal haematoma is a blood collection under the perichondrium
bull of the septum and cartilagebull bull bull Epidemiologyaetiologybull ndash A septal haematoma is one of the most
severe complications of nasal trauma
Septal Haematoma
bull Diagnosisbull ndash Signs and symptoms include intense pain
swellingbull haematoma of the upper lip and philtrum
area andbull complete nasal airway obstruction
Septal HaematomaTherapyndash Management consists of drainage through a mucoperichondrial incision Immediate treatment isnecessary to prevent long-term problems such asa saddle-nose deformity perforation columellarretraction and nasal-base widening In childrenseptal destruction can lead to devastating nasal andmidfacial growth abnormalitiesbull Surgeryndash Incision and evacuation of the collection is performedDrainage of a septal haematoma should
Septal HaematomaSurgeryndash Incision and evacuation of the collection is performedDrainage of a septal haematoma should provide closure of the incision
Splints or transseptal sutures are placed to obliterate thepotential space and prevent collectionInfection involving the septal cartilage Reconstruction with autologouscartilage is then performed in a second stage Oral antibiotics should be given
Nasal DeformitySaddle-nose deformityndash A saddle-nose deformity is characterised by a loss ofnasal dorsal height and compromised nasal supportstructures -Other case observed are depressionof the middle vault and dorsum loss of nasal tipsupport and definition shortened (vertical) nasal length over rotation of the nasal tip and retrusion ofthe nasal spine and caudal septum It is also knownas a ldquoPug noserdquo or ldquoboxerrsquos noserdquo both of which referto various degrees of nasal dorsal depressionbull
Nasal DeformityEpidemiologyaetiologyndash Prevalence is higher in population groups prone to facial trauma (ie boxers athletes) those with historiesof intranasal cocaine use nasal surgery (e g radical submucosal septal resection reductive rhinoplasty)ndash A saddle-nose deformity can be congenital or acquired It can be noticed as a part of individual familialsyndromic and ethnic characteristics - Most deformities are due to traumatic and iatrogeniccauses Medical causes are Wegenerrsquosgranulomatosis relapsing polychondritis leprosy (Hansenrsquos disease) syphilis ectodermal dysplasiaand intranasal cocaine use
Nasal Deformity
bull Therapybull ndash Nasal reconstruction indications depend on patientbull selection surgeon experience and aetiology of thebull deformity bull Indications for surgery can be functionalbull aesthetic or most commonly both In individuals
with a compromised nasal airway a nasoseptalbull reconstruction is indicated
Nasal Deformity
bull Contraindications bull include patients with malignantbull chronic or autoimmune disease conditions drugbull abuse poor perioperative risk profile and unrealisticbull expectationsbull ndash Multiple previous rhinoplasties and certain
professionsbull (mixed martial artists boxers and other contactbull sports) are relative contraindications
Nasal DeformitySeptoplastyndash Septoplasty is performed to correct nasal obstructioncaused by septal deformityndash Usually septoplasty is performed under general anaesthesiawith the patient in the supine position with the head elevated by approximately 30 (Righthandedsurgeons approach from the right side)ndash Local vasoconstrictive anaesthesia is applied notonly to reduce postoperative pain but also more importantly to achieve vasoconstriction of themucosa and less intraoperative haemorrhage Lidocainewith adrenaline or epinephrine is usedalthough in patients with cardiac hypersensitivityoxymetazoline might be preferred
Nasal Deformity
bull Septoplasty begins with the incision of septal mucosabull Most operative techniques utilise a hemitransfixionbull incision at the caudal end of septum so thatbull deviation at this point might be reached as wellbull as a transfixion incision that is easily obtained ifbull needed (Right-handed surgeons normally choosebull the left side but that may vary when deviation isbull convex towards the right)
Nasal DeformityA columella retractor is placed over the columellaand by pulling it laterally the caudal border of theseptum is exposed Ala can be protected by an alaprotector A vertical incision with a no 15 bladeover the caudal end of septum is performed untilreaching the plane of the septal cartilage It is essentialto correctly identify the perichondrium and byusing the Cottle elevator dissect and lift it creatinga flap As the dissection proceeds along the septalcartilage a longer speculum (no 5) is introduced sothat elevation of the mucoperichondrium is doneunder constant visual controlndash The next step is to dissect the mucoperiostium
Nasal DeformityDissecting over the bony-cartilaginous junctionwhen joining both tunnels might be difficult and is
especially prone to membrane perforationndash If needed the same tunnels are to be created on the
other side of the septum Then deviated parts of
septum are identified and removed either with a
knife or a Freer chisel
Nasal Deformitybull septum from the maxillary crest the septum mustbull be separated from the perpendicular plate trimmedbull along the inferior border placed back onto the crestbull and sutured to the periosteum If the deformity involvesbull the vomer an osteotome is used Care mustbull be taken not to break the cribriform plate becausebull it could cause a cerebrospinal fistula
Nasal Deformity
bull Once the septal deviation is corrected the flapsbull and hemitransfixion incision are mattressed
withbull absorbable sutures Nasal packing to prevent
synechiaebull and postoperative septal haematoma mightbull be advised but should be removed within 72 h

Vascular Supply
The internalnose receives blood from the territories of the externaland internal carotid arteries- the terminalbranches of the sphenopalatine artery which arisesfrom the maxillary artery - the anterior and posteriorethmoid arteries which arise from the ophthalmicartery-internal carotid arterie
venous drainage
The venous drainageof the facial region is handled by -the facial vein -retromandibular vein -internal jugular vein
lymphatic drainage
The regional lymphatic drainage of the face and externalnose is handled mainly by- the submandibularlymph nodes while the nasal cavity is additionallydrained by -the retropharyngeal and deep - -cervical lymph nodes
Morphology of the Nasal Mucosa
Besides the anatomical structure of the external noseand nasal cavity the nasal mucosa plays an essentialrole in numerous functions of the nose in the respiratory tract
Morphology of the Nasal Mucosa
The anterior part of the nasal cavity (the nasal vestibule)like the external nose is covered by skin composedof a multilayer keratinizing squamous epithelium and finally a ciliated respiratory epithelium A small areaon the upper nasal septum superior turbinate andpart of the middle turbinate located adjacent to thecribriform plate is covered by olfactory mucosa and iscalled the olfactory region
Nerve SupplyThe facial skin receives its sensory innervation fromterminal branches of the trigeminal nerve that enterthe facial region through the supraorbital infraorbitaland mental foramina Thefacial muscles are classified as mimetic or mastica- tory each of these groups receiving different motorinnervationbythe facial nerve
History and Clinical Examination of the Nose
Historybull The main symptomsbull nasal obstruction (ldquostuffy
noserdquo)bull nasal dischargebull Headachesbull Olfactory
dysfunction
Palpationbony discontinuitiesNeuralgias to check
over- the supraorbital -infraorbital -mental foramina
Anterior Rhinoscopy
bull The rhinologic examination itself begins with anterior
bull rhinoscopy to evaluate the nasal vestibule and the anterior
bull portions of the nasal cavity
Nasal Endoscopy Nasal endoscopy has become the most important andrewarding clinical examination method in rhinologic diagnosis
- rigid endoscopes which are available in 4-mm and 28- mm diameters and assorted viewing angles (eg 01048576 301048576 1201048576) -flexible endoscopes are also available for inspecting the nose and nasopharynx and exploring all of the pharynx and larynx in one sitting
Nasal endoscopy
Nasal Endoscopy
Nasal Endoscopy
Imaging of the Nose and Paranasal Sinuses
Conventional RadiographsStandard paranasal sinus radiographs in the occipitomental
projection ( Water projection) and
occipitofrontal projection Caldwell projection) in cases of acute inflammation
They are also obtained to evaluate midfacial fractures
Computed Tomography (CT) the main indicationsfor CT scanning of the
nose and paranasal sinuses
are- chronic sinusitis - -trauma (especially
frontobasal -fractures)
-and tumors
The occipitofrontal projection is better for evaluating theethmoid cells and frontal sinus
occipitomental projection demonstrates the maxillarysinus and gives a limited view of the sphenoid sinus
Computed tomography of the paranasal sinuses
Four representative coronal CT scans are shown
Four representative coronal CT scans are shown
Magnetic Resonance Imaging
Magnetic maging
Magnetic resonance imaging (MRI) has fewer indicationsthan CT in patients with paranasal sinus diseaseThis is primarily because MRI is markedly inferior toCT in defining the bony boundaries of the sinusesThe strength of MRI lies in its superior soft-tissue discriminationMRI is indicated in diseases that involve the paranasal sinuses in addition to thecranial cavity or orbit (eg tumors and congenitalmalformations such as encephaloceles)
MRI of the paranasal sinuses
The Nose and Sinuses
Structure The structure of the nose is made up of
four partsbull The surface anatomybull The nasal skeletonmdashcomposed of the
two nasal bones the paired upper lateral and lower lateral cartilages and the nasal septum covered in subcutaneous tissue and skin
bull The internal anatomymdashincludes the septum of the nose which forms the medial wall of the nasal cavity The turbinates on the lateral wall are also called conchae
bull The osteomeatal complexmdasha key functional area of the nose
Function The nose is the main route for inspired
air and its structure is related to this function As the air passes over the large surface area of the turbinates
The inspired gases are warmed and humidified Mucus on the mucosa of the nose removes large dust particles from the air as it is breathed in
The voice resonates in the sinuses and nose and this provides character to the speech
Pneumatization of the sinusesmdashthey are air filled spacesmdashreduces the weight of the skull
Diseases of thDiseases of the Outer and Inner Nosee Outer and
Inner Nose Erysipelas Definition of the disease ndash Erysipela is a skin infection that affects the superficial dermis and is caused by Streptococcus pyogenes (group A) It usually develops in the extremities and the face and less commonly on the scalp and genitals bull Epidemiologyaetiology ndash Erysipelas are more often seen in elderly infants and children patients with compromised immunology and diabetes -Predisposing factors are alcoholism skin ulceration puncture wounds fungal infections malnutrition and burns
Erysipelas
bull Symptomsbull ndash It usually presents of fever general fatigue bull -The skin lesion is a redindurated and elevated plaque
with borders that expand rapidly bull It is painful warm and accompanied by variable oedemabull -On the second or third day a flaccid bulla may develop
and desquamationbull bull Presence of regional lymph nodes is common
Erysipelas
bull Complicationsndash The most common complication is recurrencewhich is seen in 18ndash30 of the cases even afterproper antibiotic therapy Recurrence is seen moreoften in females than in malesA skin infection with S pyogenes could lead toglomerulonephritis
Erysipelas
bull Complicationsbull ndash The most common complication is recurrencebull which is seen in 18ndash30 of the cases even afterbull proper antibiotic therapy bull -Recurrence is seen morebull often in females than in males bull -A skin infection with S pyogenes could lead tobull glomerulonephritis
Erysipelas
bull bull Diagnosisbull ndash Diagnosis is based on the patientrsquos personal
historybull and physical examination particularly on inspectionbull of the skin
bull Blood cultures are positive in less thanbull 5 of cases
ErysipelasTherapyndash Conservative therapybull The preferred antibiotic is penicillin In mildcases with minor systemic symptoms penicillinV 500 mg orally every 6 h for 10 days or penicillinG benzathine 12 mil U intramuscularlyonceOther possibilities are amoxicillin 500 mgorally twice a day for 10 days or cephalexin 500mg orally every 6 h for 10 days
ErysipelasIn moderate and severe cases with significantsystemic symptoms hospitalization and intravenoustreatment is required penicillin G 2ndash4mil U intravenously every 4ndash6 h Cefazolin05ndash15 gm intravenously every 8 h cefotaxime1ndash2 gm intravenously every 8 h or ceftriaxone1ndash2 gm intravenously once a day should be administeredIn patients with a penicillin allergyclindamycin 600 mg intravenously every 8 h orvancomycin 15 mgkg intravenously twice a daymay be given
ErysipelaAdditional useful therapeutic optionsbull Prednisone 30 mg over 8 days might be consideredas well as elevation of the affected siteMoist heat compresses may be usefulbull Surgeryndash Debridement and drainage are indicated when bullaeabscesses or necroses are presentbull Differential diagnosisndash Contact dermatitisndash Asteatotic eczemandash Herpes zosterndash Angioneurotic oedemandash Osteomyelitis
Furuncle
bull Definition of the diseasebull ndash A furuncle is an infection that beginsbull at the hair follicle and spreads deeper into thebull dermis and subcutaneous tissue forming abull nodule After several days it developsbull into an abscess - red painful and fluctuantbull bull bull Epidemiologyaetiologybull ndash The aetiologic agent is Staphylococcus aureus
FuruncleSymptomsndashsymptoms are local and limited to thesite of infection Furuncles usually are wherehair follicles are present bull Complicationndash One complication is furunculosis multiple draining furunclesDiagnosisndash The diagnosis is based on clinical inspection - Cultures are not necessary when there is no systemic involvement but should beconsidered if systemic therapy (in case of feversignificant cellulitis or hospitalization) or whenmethicillin-resistant Staphylococcusaureus (MRSA) is considered
FuruncleTherapyndash When the furuncle is small application of moist heat compress to promote drainage -Larger furuncles should be drained by surgical incision-After drainage the area should be cleaned with anantiseptic (with chlorhexidinebetadine) should be applied twice
a dayndash If no systemic symptoms or extensive cellulitis arepresent simple topical care is usually curative andoral antibiotics are not necessary Otherwise systemictreatment is indicated and should cover anypossible MRSA
Furuncle
bull -Recommended antibiotics are trimethoprim-sulfamethoxazole
bull 1ndash2 tablets orally twice daily doxycyclinebull 100 mg orally twice dailybull or clindamycin 300ndash450 mg orally every 8 hbull - In severe cases vancomycin 15 mgkg
intravenouslybull every 12 h or clindamycin 600 mg intravenouslybull every 8 h
Midline Granulomabull A midline granuloma is an angiocentricbull lymphoma it was referred to as polymorphicbull reticulosis lethal midline granuloma and midline
malignant reticulosisbull bull Definition of the diseasebull ndash This rare disease is a lymphoma of extranodal
presentationall cases are positive for the Epstein-Barr virus
bull -This lymphoma most commonly appears in the midface region
Midline GranulomaEpidemiologyaetiologyndash This form of lymphoma is rare in Europe and theUnited States with a higher prevalence in Asia and PeruSymptomsndash The most common presentation is nasal obstruction with a destructive mass occupying the nosesinuses and palate
-Fever night sweatsand weight loss seen usually in Hodgkinrsquos lymphomaand other non-Hodgkinrsquos lymphomas (knownas ldquoB symptomsrdquo) are uncommon
Midline GranulomaDiagnosisndash The diagnosis is based on anatomopathologicalstudy The malignancy of the tumour manifested byextensive necrosis makes the histological diagnosisdifficult and often more biopsies are required forconfirmationbull Therapyndash Therapy consists of radiotherapy with or withoutchemotherapy
Midline Granuloma
bull Prognosisbull ndash Depending on the stage long-term remission or
experience a worseningbull prognosis with relapses which may include otherbull extranodal sites bull Involvement of extranodal sitesbull including the upper airway gastrointestinal tractbull skin
Wegenerrsquos Granulomatosis
bull Definition of the diseasebull ndash Wegenerrsquos granulomatosis is a systemic chronicbull vasculitis of small- and medium-sized blood vesselsbull with an autoimmune component It affectsbull particular organs with variable predilectionbull Epidemiologyaetiologybull ndash Wegenerrsquos granulomatosis is a rare disease It affects
about 1 in 20000ndash30000 people It is more prevalentbull in middle-aged Caucasian patients
Wegenerrsquos Granulomatosis
Symptomsndash The disease may present pulmonary upper
respiratory tract or renal In the disseminated form-The localised form ndash confinedto the upper respiratory region ndash is present in 25of the patients- It consists of nonspecific manifestationssuch as nasal obstruction crusting purulentor bloody rhinorrhea and painful or painless ulcers in oral or nasal cavities which are unresponsive tostandard medical treatment
Wegenerrsquos Granulomatosis
bull In some patients the nasal septum is perforatedbull which leads to saddle-nose deformity Less
commonbull symptoms are hoarseness stridor due to
subglotticbull stenosis otalgia otorrhea and conductivebull and sensorineural hearing loss Also ocular
symptomsbull such as scleritis conjunctivitis uveitis andbull episcleritis may be present
Wegenerrsquos Granulomatosis
bull ndash In the disseminated form pulmonary involvementbull is manifested by cough dyspnoea haemoptysisbull (due to an alveolar capillaritis necrotic lesions orbull endobronchial disease) and pleuritic painndashbull -Ninety per cent of patients have nasal symptomsbull and these symptoms are usually the first
manifestationof the diseasebull -Most patients have also renal involvementbull even if it is subclinical
Wegenerrsquos Granulomatosis
Diagnosis ndash Diagnosis of Wegenerrsquos granulomatosis is based on clinical findings that demonstrate lung (chest x-ray) kidney (urine analysis) or upper respiratory tract
involvement (oral or nasal ulcers or discharge) - positive blood analysis for cytoplasmic-staining antineutrophil
cytoplasmic antibodies (c-ANCA) and confirming proteinase 3 (PR3) ANCA or myeloperoxidase (MPO) ANCA ndash Biopsy is essential for diagnosis nonspecific chronic inflammation
and necrosis -Bacterial and fungal infections
Wegenerrsquos Granulomatosis
Therapyndash Conservative therapybull In the induction of disease remission highdosesteroids (e g prednisone 1 mgkgday) for1 month with tapering over several months aregiven In addition cyclophosphamide (2 mgkgday) should be administered for 6ndash12 monthsuntil symptoms disappear In the maintenanceof remission cyclophosphamide should be
Wegenerrsquos Granulomatosis
Antibiotics mainly trimethoprim-sulfamethoxazoleare given for prophylaxis againstPneumocystis jiroveci (formerly Pneumocystiscarinii) pneumonia (PCP) which may developduring immunosuppression and have a role inpreventing recurrencesbull Sinonasal manifestations may be treated with topical nasal steroids and nasal irrigations lowdosesystemic steroids and antibiotics when bacterial infection (typically Staphylococcus species) is suspected
Wegenerrsquos Granulomatosis
bull Prognosisbull ndash Most of the patients respond well to treatmentbull achieving symptom-free intervals of 5ndash20 yearsbull or more bull -Anatomical problems (sinusitis trachealbull stenosis) may require surgery bull Relapses can be long and troublesomebull Long-term complications are chronicbull renal failure hearing loss and deafness
Nasal Fractures Definition ndash A nasal fracture is a disruption of the nasal bone structure due to trauma It is the most frequently fractured facial bone Epidemiologyaetiology ndash Sports falls and assaults are the usual mechanisms of fracture -Males are affected twice as often as are females -Paediatric populations with a incidences during the second and third decades of life -Variables such as force impact direction nature of the striking object age and other will influence the pattern of injury to the components of the nose
Nasal Fractures
bull Symptomsbull ndash Deformity swelling epistaxis and periorbital
ecchymosis are signs that are suggestive of nasal fracture
bull bony crepitus and nasal segment mobilitybull ndash Epiphora bull Severe bilateral injuries to the lachrymal bones
arebull associated with depressed nasal fractures
Nasal Fractures Complications ndash Septal haematoma is one of the most severe early complications of nasal trauma and without drainage it results in abscess formation 6ndash7 days after trauma producing necrosis of the septal cartilage -Long-term problems such as saddle-nose deformity perforation columellar retraction and nasalbase
Septal infection could lead to osteomyelitis orbital and intracranial abscesses meningitis and cavernous sinus thrombosis -Cerebrospinal fluid leakage is a common complication of severe
nasal and frontal fractures
Nasal Fractures
bull Diagnostic proceduresbull ndash Inspectionbull bull Changes of appearance such as deviation andbull asymmetry bleeding watery drainage changesbull in nasal breathing and smell It is useful to comparebull the current presentation with old photographsbull (up to 40 of normal individuals havebull significant nose malformations)
Nasal Fractures Physical examination bull The diagnosis of a nasal fracture is made primarily by physical examination epistaxis nasal swelling and periorbital ecchymosis Nasal shape in the lateral and frontal inspection should be assessed Grasping the dorsum between two fingers and rocking the pyramid back and forth aids in assessing the mobility of nasal bones Internal structures should be evaluated by using a headlight and nasal speculum Clotted blood is removed by suction and assessment of haematoma mucosal tears and active bleeding is performed Bimanual palpation of the septum helps to differentiate septal swelling from haematoma ndash
Nasal FracturesRadiographybull There is no clear evidence of the role of radiographyin the management of nasal fracturesPlain films have up to a 66 false-positive rateas a result of misinterpretation of normal suturelines In addition old fractures are difficult todistinguishbull Three-dimensional CT is recommended for extensiveinjuries involving the nasal-orbital-ethmoidalcomplexndash
Nasal Fractures
bull Additionaluseful diagnostic proceduresbull bull Using a 0 or 30deg 4-mm endoscope is helpful inbull the assessment of posterior abnormalities If thebull patient is heavily sedated Brown-Gruss
provocationbull manoeuvres may be performed to determinebull deformities in upper middle or lower segmentsbull by compressing each compartment
Nasal FracturesConservative treatmentndash Treatment of bleedingbull For localised bleeding anterior sources may becauterised by silver nitrate or sealed with topicalmaterials such as thrombin combined withgelatin foam fibrin glue FloSealreg or other procoagulantmaterials If conservative measuresfail a formal anterior packing is placedbull Bleeding from branches of sphenopalatine orethmoid vessels requires anterior-posteriorpacking
Nasal Fractures
bull bull Surgical methods such as direct endoscopic vessel
bull cauterization or ligation have been shown tobull offer better haemostasis and patient comfortbull Angiography with embolization can also be
consideredbull in cases refractory to more conservativebull approaches
Nasal Fractures
bull Type of reductionbull bull Nondisplaced fractures should be treated withbull observation alone Closed nasal reduction is thebull best choice for simple injuries (isolated unilateralbull with medial displacement)bull bull An open approach should be considered in
severebull trauma (bilateral depressed fractures)
Nasal Fracturesbull Surgical principlesbull ndash Topical anaesthesia with cotton pledgets soakedbull with 4 cocaine or 005 oxymethazoline combinedbull with 4 topical lidocaine should be appliedbull for 5ndash10 min Local anaesthesia should also be injectedbull (1 lidocaine and 1100000 epinephrine)bull along the septum lateral walls and floor of the nasalbull cavitybull bull
Nasal FracturesClosed reductionndashndash The nasal bones are grasped between two fingersand pressure is applied laterally in theopposite direction of the deviation A bluntelevator may be used from within the nose incases of significant medial collapse Walshamforceps can be of help Reduction of the septumshould be performed with the use ofAsch forceps
Nasal Fractures
bull To prevent collapse of the postreductionbull framework nasal packing should be placedbull for 3ndash5 days Septum splints are recommendedbull in comminuted septal fractures withbull severe mucosal lesions External nasal splintingbull for 10 days (Aquaplastreg Thermoplastreg)bull provides nasal protection Nasal saline spraysbull prevent crusting and oral antibiotics should
Nasal Fractures
bull Open reductionbull ndashndash Immediate repair of fractures by using
widebull surgical exposure reduction fixation and
reconstructionbull ndashndash The second option is delayed correctionbull (6 months or more) of persistent deformitiesbull using standard techniques of rhinoplasty
Deviated Nasal Septum
bull Definition of the diseasebull ndash Deviation of the nasal septum is a common causebull of unilateral nasal airway obstruction in which thebull nasal septum is displacedbull bull Epidemiologyaetiologybull ndash Developmental septal abnormalities Septal cartilage
damage in the neonatal period andbull during birth can cause severe septal deviation inbull the absence of a history of nasal trauma
Deviated Nasal Septum
bull Symptomsbull ndash Patients may present with a history of sinusitis
allergicbull rhinitis obstructive sleep apnoea previousbull nasal surgery or recent nasal trauma Unilateral or
bilateral nasal airway obstruction that is unrelievedbull with decongestants or nasal steroid sprays is oftenbull seenbull bull
Deviated Nasal SeptumDiagnosisndashExamination external dorsal deviation or the columella and caudal septummay be deflected off the midline (caudal subluxation)ndash Inspections of the nasal cavity and anterior-posteriorrhinoscopy are helpful in diagnosing the locationtype and severity of septal deformityThe endoscope is also useful in identifying polypsthe severity and extent of posterior septaldeviations and bony spurs and locating areas ofseptal perforation or mucosal injury
Deviated Nasal Septum
bull Therapybull ndash Septoplasty is a procedurebull The areabull of deviation is corrected or resected in order tobull leave behind as much cartilage and bone as
possiblebull Cartilage resection is minimised and can be
repositioned reshaped or recontoured using a variety of methods
Deviated Nasal Septum
bull ndash Indications of septoplasty before the growth period
bull of the nose is finished should be very limited bull -In these cases surgery must preserve all the
cartilagebull in order to prevent external changes of the
shape ofbull the nose
Deviated Nasal Septum
bull Complicationsbull ndash Frequent complications include haematoma andbull infection Cerebrospinal fluid leak is a rare but
potentiallybull serious complicationbull It is usually the resultbull of avulsion or damage to the cribriform plate whenbull handling the perpendicular plate of the ethmoidbull ndash Other complications include epistaxis nasal
Deviated Nasal Septum
bull Other complications include epistaxis nasal obstruction
bull due to residual deviation synechiae returnbull of the cartilaginous deviation septal perforationbull anosmia and cosmetic nasal deformities suchbull as widened alar rim margins drooping nasal tipbull columella retraction and a sunken dorsum with abull supratip saddle formation
Septal perforation with minor crusting View from provide closure of the
incision
Septal Haematoma
bull A septal haematoma is a blood collection under the perichondrium
bull of the septum and cartilagebull bull bull Epidemiologyaetiologybull ndash A septal haematoma is one of the most
severe complications of nasal trauma
Septal Haematoma
bull Diagnosisbull ndash Signs and symptoms include intense pain
swellingbull haematoma of the upper lip and philtrum
area andbull complete nasal airway obstruction
Septal HaematomaTherapyndash Management consists of drainage through a mucoperichondrial incision Immediate treatment isnecessary to prevent long-term problems such asa saddle-nose deformity perforation columellarretraction and nasal-base widening In childrenseptal destruction can lead to devastating nasal andmidfacial growth abnormalitiesbull Surgeryndash Incision and evacuation of the collection is performedDrainage of a septal haematoma should
Septal HaematomaSurgeryndash Incision and evacuation of the collection is performedDrainage of a septal haematoma should provide closure of the incision
Splints or transseptal sutures are placed to obliterate thepotential space and prevent collectionInfection involving the septal cartilage Reconstruction with autologouscartilage is then performed in a second stage Oral antibiotics should be given
Nasal DeformitySaddle-nose deformityndash A saddle-nose deformity is characterised by a loss ofnasal dorsal height and compromised nasal supportstructures -Other case observed are depressionof the middle vault and dorsum loss of nasal tipsupport and definition shortened (vertical) nasal length over rotation of the nasal tip and retrusion ofthe nasal spine and caudal septum It is also knownas a ldquoPug noserdquo or ldquoboxerrsquos noserdquo both of which referto various degrees of nasal dorsal depressionbull
Nasal DeformityEpidemiologyaetiologyndash Prevalence is higher in population groups prone to facial trauma (ie boxers athletes) those with historiesof intranasal cocaine use nasal surgery (e g radical submucosal septal resection reductive rhinoplasty)ndash A saddle-nose deformity can be congenital or acquired It can be noticed as a part of individual familialsyndromic and ethnic characteristics - Most deformities are due to traumatic and iatrogeniccauses Medical causes are Wegenerrsquosgranulomatosis relapsing polychondritis leprosy (Hansenrsquos disease) syphilis ectodermal dysplasiaand intranasal cocaine use
Nasal Deformity
bull Therapybull ndash Nasal reconstruction indications depend on patientbull selection surgeon experience and aetiology of thebull deformity bull Indications for surgery can be functionalbull aesthetic or most commonly both In individuals
with a compromised nasal airway a nasoseptalbull reconstruction is indicated
Nasal Deformity
bull Contraindications bull include patients with malignantbull chronic or autoimmune disease conditions drugbull abuse poor perioperative risk profile and unrealisticbull expectationsbull ndash Multiple previous rhinoplasties and certain
professionsbull (mixed martial artists boxers and other contactbull sports) are relative contraindications
Nasal DeformitySeptoplastyndash Septoplasty is performed to correct nasal obstructioncaused by septal deformityndash Usually septoplasty is performed under general anaesthesiawith the patient in the supine position with the head elevated by approximately 30 (Righthandedsurgeons approach from the right side)ndash Local vasoconstrictive anaesthesia is applied notonly to reduce postoperative pain but also more importantly to achieve vasoconstriction of themucosa and less intraoperative haemorrhage Lidocainewith adrenaline or epinephrine is usedalthough in patients with cardiac hypersensitivityoxymetazoline might be preferred
Nasal Deformity
bull Septoplasty begins with the incision of septal mucosabull Most operative techniques utilise a hemitransfixionbull incision at the caudal end of septum so thatbull deviation at this point might be reached as wellbull as a transfixion incision that is easily obtained ifbull needed (Right-handed surgeons normally choosebull the left side but that may vary when deviation isbull convex towards the right)
Nasal DeformityA columella retractor is placed over the columellaand by pulling it laterally the caudal border of theseptum is exposed Ala can be protected by an alaprotector A vertical incision with a no 15 bladeover the caudal end of septum is performed untilreaching the plane of the septal cartilage It is essentialto correctly identify the perichondrium and byusing the Cottle elevator dissect and lift it creatinga flap As the dissection proceeds along the septalcartilage a longer speculum (no 5) is introduced sothat elevation of the mucoperichondrium is doneunder constant visual controlndash The next step is to dissect the mucoperiostium
Nasal DeformityDissecting over the bony-cartilaginous junctionwhen joining both tunnels might be difficult and is
especially prone to membrane perforationndash If needed the same tunnels are to be created on the
other side of the septum Then deviated parts of
septum are identified and removed either with a
knife or a Freer chisel
Nasal Deformitybull septum from the maxillary crest the septum mustbull be separated from the perpendicular plate trimmedbull along the inferior border placed back onto the crestbull and sutured to the periosteum If the deformity involvesbull the vomer an osteotome is used Care mustbull be taken not to break the cribriform plate becausebull it could cause a cerebrospinal fistula
Nasal Deformity
bull Once the septal deviation is corrected the flapsbull and hemitransfixion incision are mattressed
withbull absorbable sutures Nasal packing to prevent
synechiaebull and postoperative septal haematoma mightbull be advised but should be removed within 72 h

venous drainage
The venous drainageof the facial region is handled by -the facial vein -retromandibular vein -internal jugular vein
lymphatic drainage
The regional lymphatic drainage of the face and externalnose is handled mainly by- the submandibularlymph nodes while the nasal cavity is additionallydrained by -the retropharyngeal and deep - -cervical lymph nodes
Morphology of the Nasal Mucosa
Besides the anatomical structure of the external noseand nasal cavity the nasal mucosa plays an essentialrole in numerous functions of the nose in the respiratory tract
Morphology of the Nasal Mucosa
The anterior part of the nasal cavity (the nasal vestibule)like the external nose is covered by skin composedof a multilayer keratinizing squamous epithelium and finally a ciliated respiratory epithelium A small areaon the upper nasal septum superior turbinate andpart of the middle turbinate located adjacent to thecribriform plate is covered by olfactory mucosa and iscalled the olfactory region
Nerve SupplyThe facial skin receives its sensory innervation fromterminal branches of the trigeminal nerve that enterthe facial region through the supraorbital infraorbitaland mental foramina Thefacial muscles are classified as mimetic or mastica- tory each of these groups receiving different motorinnervationbythe facial nerve
History and Clinical Examination of the Nose
Historybull The main symptomsbull nasal obstruction (ldquostuffy
noserdquo)bull nasal dischargebull Headachesbull Olfactory
dysfunction
Palpationbony discontinuitiesNeuralgias to check
over- the supraorbital -infraorbital -mental foramina
Anterior Rhinoscopy
bull The rhinologic examination itself begins with anterior
bull rhinoscopy to evaluate the nasal vestibule and the anterior
bull portions of the nasal cavity
Nasal Endoscopy Nasal endoscopy has become the most important andrewarding clinical examination method in rhinologic diagnosis
- rigid endoscopes which are available in 4-mm and 28- mm diameters and assorted viewing angles (eg 01048576 301048576 1201048576) -flexible endoscopes are also available for inspecting the nose and nasopharynx and exploring all of the pharynx and larynx in one sitting
Nasal endoscopy
Nasal Endoscopy
Nasal Endoscopy
Imaging of the Nose and Paranasal Sinuses
Conventional RadiographsStandard paranasal sinus radiographs in the occipitomental
projection ( Water projection) and
occipitofrontal projection Caldwell projection) in cases of acute inflammation
They are also obtained to evaluate midfacial fractures
Computed Tomography (CT) the main indicationsfor CT scanning of the
nose and paranasal sinuses
are- chronic sinusitis - -trauma (especially
frontobasal -fractures)
-and tumors
The occipitofrontal projection is better for evaluating theethmoid cells and frontal sinus
occipitomental projection demonstrates the maxillarysinus and gives a limited view of the sphenoid sinus
Computed tomography of the paranasal sinuses
Four representative coronal CT scans are shown
Four representative coronal CT scans are shown
Magnetic Resonance Imaging
Magnetic maging
Magnetic resonance imaging (MRI) has fewer indicationsthan CT in patients with paranasal sinus diseaseThis is primarily because MRI is markedly inferior toCT in defining the bony boundaries of the sinusesThe strength of MRI lies in its superior soft-tissue discriminationMRI is indicated in diseases that involve the paranasal sinuses in addition to thecranial cavity or orbit (eg tumors and congenitalmalformations such as encephaloceles)
MRI of the paranasal sinuses
The Nose and Sinuses
Structure The structure of the nose is made up of
four partsbull The surface anatomybull The nasal skeletonmdashcomposed of the
two nasal bones the paired upper lateral and lower lateral cartilages and the nasal septum covered in subcutaneous tissue and skin
bull The internal anatomymdashincludes the septum of the nose which forms the medial wall of the nasal cavity The turbinates on the lateral wall are also called conchae
bull The osteomeatal complexmdasha key functional area of the nose
Function The nose is the main route for inspired
air and its structure is related to this function As the air passes over the large surface area of the turbinates
The inspired gases are warmed and humidified Mucus on the mucosa of the nose removes large dust particles from the air as it is breathed in
The voice resonates in the sinuses and nose and this provides character to the speech
Pneumatization of the sinusesmdashthey are air filled spacesmdashreduces the weight of the skull
Diseases of thDiseases of the Outer and Inner Nosee Outer and
Inner Nose Erysipelas Definition of the disease ndash Erysipela is a skin infection that affects the superficial dermis and is caused by Streptococcus pyogenes (group A) It usually develops in the extremities and the face and less commonly on the scalp and genitals bull Epidemiologyaetiology ndash Erysipelas are more often seen in elderly infants and children patients with compromised immunology and diabetes -Predisposing factors are alcoholism skin ulceration puncture wounds fungal infections malnutrition and burns
Erysipelas
bull Symptomsbull ndash It usually presents of fever general fatigue bull -The skin lesion is a redindurated and elevated plaque
with borders that expand rapidly bull It is painful warm and accompanied by variable oedemabull -On the second or third day a flaccid bulla may develop
and desquamationbull bull Presence of regional lymph nodes is common
Erysipelas
bull Complicationsndash The most common complication is recurrencewhich is seen in 18ndash30 of the cases even afterproper antibiotic therapy Recurrence is seen moreoften in females than in malesA skin infection with S pyogenes could lead toglomerulonephritis
Erysipelas
bull Complicationsbull ndash The most common complication is recurrencebull which is seen in 18ndash30 of the cases even afterbull proper antibiotic therapy bull -Recurrence is seen morebull often in females than in males bull -A skin infection with S pyogenes could lead tobull glomerulonephritis
Erysipelas
bull bull Diagnosisbull ndash Diagnosis is based on the patientrsquos personal
historybull and physical examination particularly on inspectionbull of the skin
bull Blood cultures are positive in less thanbull 5 of cases
ErysipelasTherapyndash Conservative therapybull The preferred antibiotic is penicillin In mildcases with minor systemic symptoms penicillinV 500 mg orally every 6 h for 10 days or penicillinG benzathine 12 mil U intramuscularlyonceOther possibilities are amoxicillin 500 mgorally twice a day for 10 days or cephalexin 500mg orally every 6 h for 10 days
ErysipelasIn moderate and severe cases with significantsystemic symptoms hospitalization and intravenoustreatment is required penicillin G 2ndash4mil U intravenously every 4ndash6 h Cefazolin05ndash15 gm intravenously every 8 h cefotaxime1ndash2 gm intravenously every 8 h or ceftriaxone1ndash2 gm intravenously once a day should be administeredIn patients with a penicillin allergyclindamycin 600 mg intravenously every 8 h orvancomycin 15 mgkg intravenously twice a daymay be given
ErysipelaAdditional useful therapeutic optionsbull Prednisone 30 mg over 8 days might be consideredas well as elevation of the affected siteMoist heat compresses may be usefulbull Surgeryndash Debridement and drainage are indicated when bullaeabscesses or necroses are presentbull Differential diagnosisndash Contact dermatitisndash Asteatotic eczemandash Herpes zosterndash Angioneurotic oedemandash Osteomyelitis
Furuncle
bull Definition of the diseasebull ndash A furuncle is an infection that beginsbull at the hair follicle and spreads deeper into thebull dermis and subcutaneous tissue forming abull nodule After several days it developsbull into an abscess - red painful and fluctuantbull bull bull Epidemiologyaetiologybull ndash The aetiologic agent is Staphylococcus aureus
FuruncleSymptomsndashsymptoms are local and limited to thesite of infection Furuncles usually are wherehair follicles are present bull Complicationndash One complication is furunculosis multiple draining furunclesDiagnosisndash The diagnosis is based on clinical inspection - Cultures are not necessary when there is no systemic involvement but should beconsidered if systemic therapy (in case of feversignificant cellulitis or hospitalization) or whenmethicillin-resistant Staphylococcusaureus (MRSA) is considered
FuruncleTherapyndash When the furuncle is small application of moist heat compress to promote drainage -Larger furuncles should be drained by surgical incision-After drainage the area should be cleaned with anantiseptic (with chlorhexidinebetadine) should be applied twice
a dayndash If no systemic symptoms or extensive cellulitis arepresent simple topical care is usually curative andoral antibiotics are not necessary Otherwise systemictreatment is indicated and should cover anypossible MRSA
Furuncle
bull -Recommended antibiotics are trimethoprim-sulfamethoxazole
bull 1ndash2 tablets orally twice daily doxycyclinebull 100 mg orally twice dailybull or clindamycin 300ndash450 mg orally every 8 hbull - In severe cases vancomycin 15 mgkg
intravenouslybull every 12 h or clindamycin 600 mg intravenouslybull every 8 h
Midline Granulomabull A midline granuloma is an angiocentricbull lymphoma it was referred to as polymorphicbull reticulosis lethal midline granuloma and midline
malignant reticulosisbull bull Definition of the diseasebull ndash This rare disease is a lymphoma of extranodal
presentationall cases are positive for the Epstein-Barr virus
bull -This lymphoma most commonly appears in the midface region
Midline GranulomaEpidemiologyaetiologyndash This form of lymphoma is rare in Europe and theUnited States with a higher prevalence in Asia and PeruSymptomsndash The most common presentation is nasal obstruction with a destructive mass occupying the nosesinuses and palate
-Fever night sweatsand weight loss seen usually in Hodgkinrsquos lymphomaand other non-Hodgkinrsquos lymphomas (knownas ldquoB symptomsrdquo) are uncommon
Midline GranulomaDiagnosisndash The diagnosis is based on anatomopathologicalstudy The malignancy of the tumour manifested byextensive necrosis makes the histological diagnosisdifficult and often more biopsies are required forconfirmationbull Therapyndash Therapy consists of radiotherapy with or withoutchemotherapy
Midline Granuloma
bull Prognosisbull ndash Depending on the stage long-term remission or
experience a worseningbull prognosis with relapses which may include otherbull extranodal sites bull Involvement of extranodal sitesbull including the upper airway gastrointestinal tractbull skin
Wegenerrsquos Granulomatosis
bull Definition of the diseasebull ndash Wegenerrsquos granulomatosis is a systemic chronicbull vasculitis of small- and medium-sized blood vesselsbull with an autoimmune component It affectsbull particular organs with variable predilectionbull Epidemiologyaetiologybull ndash Wegenerrsquos granulomatosis is a rare disease It affects
about 1 in 20000ndash30000 people It is more prevalentbull in middle-aged Caucasian patients
Wegenerrsquos Granulomatosis
Symptomsndash The disease may present pulmonary upper
respiratory tract or renal In the disseminated form-The localised form ndash confinedto the upper respiratory region ndash is present in 25of the patients- It consists of nonspecific manifestationssuch as nasal obstruction crusting purulentor bloody rhinorrhea and painful or painless ulcers in oral or nasal cavities which are unresponsive tostandard medical treatment
Wegenerrsquos Granulomatosis
bull In some patients the nasal septum is perforatedbull which leads to saddle-nose deformity Less
commonbull symptoms are hoarseness stridor due to
subglotticbull stenosis otalgia otorrhea and conductivebull and sensorineural hearing loss Also ocular
symptomsbull such as scleritis conjunctivitis uveitis andbull episcleritis may be present
Wegenerrsquos Granulomatosis
bull ndash In the disseminated form pulmonary involvementbull is manifested by cough dyspnoea haemoptysisbull (due to an alveolar capillaritis necrotic lesions orbull endobronchial disease) and pleuritic painndashbull -Ninety per cent of patients have nasal symptomsbull and these symptoms are usually the first
manifestationof the diseasebull -Most patients have also renal involvementbull even if it is subclinical
Wegenerrsquos Granulomatosis
Diagnosis ndash Diagnosis of Wegenerrsquos granulomatosis is based on clinical findings that demonstrate lung (chest x-ray) kidney (urine analysis) or upper respiratory tract
involvement (oral or nasal ulcers or discharge) - positive blood analysis for cytoplasmic-staining antineutrophil
cytoplasmic antibodies (c-ANCA) and confirming proteinase 3 (PR3) ANCA or myeloperoxidase (MPO) ANCA ndash Biopsy is essential for diagnosis nonspecific chronic inflammation
and necrosis -Bacterial and fungal infections
Wegenerrsquos Granulomatosis
Therapyndash Conservative therapybull In the induction of disease remission highdosesteroids (e g prednisone 1 mgkgday) for1 month with tapering over several months aregiven In addition cyclophosphamide (2 mgkgday) should be administered for 6ndash12 monthsuntil symptoms disappear In the maintenanceof remission cyclophosphamide should be
Wegenerrsquos Granulomatosis
Antibiotics mainly trimethoprim-sulfamethoxazoleare given for prophylaxis againstPneumocystis jiroveci (formerly Pneumocystiscarinii) pneumonia (PCP) which may developduring immunosuppression and have a role inpreventing recurrencesbull Sinonasal manifestations may be treated with topical nasal steroids and nasal irrigations lowdosesystemic steroids and antibiotics when bacterial infection (typically Staphylococcus species) is suspected
Wegenerrsquos Granulomatosis
bull Prognosisbull ndash Most of the patients respond well to treatmentbull achieving symptom-free intervals of 5ndash20 yearsbull or more bull -Anatomical problems (sinusitis trachealbull stenosis) may require surgery bull Relapses can be long and troublesomebull Long-term complications are chronicbull renal failure hearing loss and deafness
Nasal Fractures Definition ndash A nasal fracture is a disruption of the nasal bone structure due to trauma It is the most frequently fractured facial bone Epidemiologyaetiology ndash Sports falls and assaults are the usual mechanisms of fracture -Males are affected twice as often as are females -Paediatric populations with a incidences during the second and third decades of life -Variables such as force impact direction nature of the striking object age and other will influence the pattern of injury to the components of the nose
Nasal Fractures
bull Symptomsbull ndash Deformity swelling epistaxis and periorbital
ecchymosis are signs that are suggestive of nasal fracture
bull bony crepitus and nasal segment mobilitybull ndash Epiphora bull Severe bilateral injuries to the lachrymal bones
arebull associated with depressed nasal fractures
Nasal Fractures Complications ndash Septal haematoma is one of the most severe early complications of nasal trauma and without drainage it results in abscess formation 6ndash7 days after trauma producing necrosis of the septal cartilage -Long-term problems such as saddle-nose deformity perforation columellar retraction and nasalbase
Septal infection could lead to osteomyelitis orbital and intracranial abscesses meningitis and cavernous sinus thrombosis -Cerebrospinal fluid leakage is a common complication of severe
nasal and frontal fractures
Nasal Fractures
bull Diagnostic proceduresbull ndash Inspectionbull bull Changes of appearance such as deviation andbull asymmetry bleeding watery drainage changesbull in nasal breathing and smell It is useful to comparebull the current presentation with old photographsbull (up to 40 of normal individuals havebull significant nose malformations)
Nasal Fractures Physical examination bull The diagnosis of a nasal fracture is made primarily by physical examination epistaxis nasal swelling and periorbital ecchymosis Nasal shape in the lateral and frontal inspection should be assessed Grasping the dorsum between two fingers and rocking the pyramid back and forth aids in assessing the mobility of nasal bones Internal structures should be evaluated by using a headlight and nasal speculum Clotted blood is removed by suction and assessment of haematoma mucosal tears and active bleeding is performed Bimanual palpation of the septum helps to differentiate septal swelling from haematoma ndash
Nasal FracturesRadiographybull There is no clear evidence of the role of radiographyin the management of nasal fracturesPlain films have up to a 66 false-positive rateas a result of misinterpretation of normal suturelines In addition old fractures are difficult todistinguishbull Three-dimensional CT is recommended for extensiveinjuries involving the nasal-orbital-ethmoidalcomplexndash
Nasal Fractures
bull Additionaluseful diagnostic proceduresbull bull Using a 0 or 30deg 4-mm endoscope is helpful inbull the assessment of posterior abnormalities If thebull patient is heavily sedated Brown-Gruss
provocationbull manoeuvres may be performed to determinebull deformities in upper middle or lower segmentsbull by compressing each compartment
Nasal FracturesConservative treatmentndash Treatment of bleedingbull For localised bleeding anterior sources may becauterised by silver nitrate or sealed with topicalmaterials such as thrombin combined withgelatin foam fibrin glue FloSealreg or other procoagulantmaterials If conservative measuresfail a formal anterior packing is placedbull Bleeding from branches of sphenopalatine orethmoid vessels requires anterior-posteriorpacking
Nasal Fractures
bull bull Surgical methods such as direct endoscopic vessel
bull cauterization or ligation have been shown tobull offer better haemostasis and patient comfortbull Angiography with embolization can also be
consideredbull in cases refractory to more conservativebull approaches
Nasal Fractures
bull Type of reductionbull bull Nondisplaced fractures should be treated withbull observation alone Closed nasal reduction is thebull best choice for simple injuries (isolated unilateralbull with medial displacement)bull bull An open approach should be considered in
severebull trauma (bilateral depressed fractures)
Nasal Fracturesbull Surgical principlesbull ndash Topical anaesthesia with cotton pledgets soakedbull with 4 cocaine or 005 oxymethazoline combinedbull with 4 topical lidocaine should be appliedbull for 5ndash10 min Local anaesthesia should also be injectedbull (1 lidocaine and 1100000 epinephrine)bull along the septum lateral walls and floor of the nasalbull cavitybull bull
Nasal FracturesClosed reductionndashndash The nasal bones are grasped between two fingersand pressure is applied laterally in theopposite direction of the deviation A bluntelevator may be used from within the nose incases of significant medial collapse Walshamforceps can be of help Reduction of the septumshould be performed with the use ofAsch forceps
Nasal Fractures
bull To prevent collapse of the postreductionbull framework nasal packing should be placedbull for 3ndash5 days Septum splints are recommendedbull in comminuted septal fractures withbull severe mucosal lesions External nasal splintingbull for 10 days (Aquaplastreg Thermoplastreg)bull provides nasal protection Nasal saline spraysbull prevent crusting and oral antibiotics should
Nasal Fractures
bull Open reductionbull ndashndash Immediate repair of fractures by using
widebull surgical exposure reduction fixation and
reconstructionbull ndashndash The second option is delayed correctionbull (6 months or more) of persistent deformitiesbull using standard techniques of rhinoplasty
Deviated Nasal Septum
bull Definition of the diseasebull ndash Deviation of the nasal septum is a common causebull of unilateral nasal airway obstruction in which thebull nasal septum is displacedbull bull Epidemiologyaetiologybull ndash Developmental septal abnormalities Septal cartilage
damage in the neonatal period andbull during birth can cause severe septal deviation inbull the absence of a history of nasal trauma
Deviated Nasal Septum
bull Symptomsbull ndash Patients may present with a history of sinusitis
allergicbull rhinitis obstructive sleep apnoea previousbull nasal surgery or recent nasal trauma Unilateral or
bilateral nasal airway obstruction that is unrelievedbull with decongestants or nasal steroid sprays is oftenbull seenbull bull
Deviated Nasal SeptumDiagnosisndashExamination external dorsal deviation or the columella and caudal septummay be deflected off the midline (caudal subluxation)ndash Inspections of the nasal cavity and anterior-posteriorrhinoscopy are helpful in diagnosing the locationtype and severity of septal deformityThe endoscope is also useful in identifying polypsthe severity and extent of posterior septaldeviations and bony spurs and locating areas ofseptal perforation or mucosal injury
Deviated Nasal Septum
bull Therapybull ndash Septoplasty is a procedurebull The areabull of deviation is corrected or resected in order tobull leave behind as much cartilage and bone as
possiblebull Cartilage resection is minimised and can be
repositioned reshaped or recontoured using a variety of methods
Deviated Nasal Septum
bull ndash Indications of septoplasty before the growth period
bull of the nose is finished should be very limited bull -In these cases surgery must preserve all the
cartilagebull in order to prevent external changes of the
shape ofbull the nose
Deviated Nasal Septum
bull Complicationsbull ndash Frequent complications include haematoma andbull infection Cerebrospinal fluid leak is a rare but
potentiallybull serious complicationbull It is usually the resultbull of avulsion or damage to the cribriform plate whenbull handling the perpendicular plate of the ethmoidbull ndash Other complications include epistaxis nasal
Deviated Nasal Septum
bull Other complications include epistaxis nasal obstruction
bull due to residual deviation synechiae returnbull of the cartilaginous deviation septal perforationbull anosmia and cosmetic nasal deformities suchbull as widened alar rim margins drooping nasal tipbull columella retraction and a sunken dorsum with abull supratip saddle formation
Septal perforation with minor crusting View from provide closure of the
incision
Septal Haematoma
bull A septal haematoma is a blood collection under the perichondrium
bull of the septum and cartilagebull bull bull Epidemiologyaetiologybull ndash A septal haematoma is one of the most
severe complications of nasal trauma
Septal Haematoma
bull Diagnosisbull ndash Signs and symptoms include intense pain
swellingbull haematoma of the upper lip and philtrum
area andbull complete nasal airway obstruction
Septal HaematomaTherapyndash Management consists of drainage through a mucoperichondrial incision Immediate treatment isnecessary to prevent long-term problems such asa saddle-nose deformity perforation columellarretraction and nasal-base widening In childrenseptal destruction can lead to devastating nasal andmidfacial growth abnormalitiesbull Surgeryndash Incision and evacuation of the collection is performedDrainage of a septal haematoma should
Septal HaematomaSurgeryndash Incision and evacuation of the collection is performedDrainage of a septal haematoma should provide closure of the incision
Splints or transseptal sutures are placed to obliterate thepotential space and prevent collectionInfection involving the septal cartilage Reconstruction with autologouscartilage is then performed in a second stage Oral antibiotics should be given
Nasal DeformitySaddle-nose deformityndash A saddle-nose deformity is characterised by a loss ofnasal dorsal height and compromised nasal supportstructures -Other case observed are depressionof the middle vault and dorsum loss of nasal tipsupport and definition shortened (vertical) nasal length over rotation of the nasal tip and retrusion ofthe nasal spine and caudal septum It is also knownas a ldquoPug noserdquo or ldquoboxerrsquos noserdquo both of which referto various degrees of nasal dorsal depressionbull
Nasal DeformityEpidemiologyaetiologyndash Prevalence is higher in population groups prone to facial trauma (ie boxers athletes) those with historiesof intranasal cocaine use nasal surgery (e g radical submucosal septal resection reductive rhinoplasty)ndash A saddle-nose deformity can be congenital or acquired It can be noticed as a part of individual familialsyndromic and ethnic characteristics - Most deformities are due to traumatic and iatrogeniccauses Medical causes are Wegenerrsquosgranulomatosis relapsing polychondritis leprosy (Hansenrsquos disease) syphilis ectodermal dysplasiaand intranasal cocaine use
Nasal Deformity
bull Therapybull ndash Nasal reconstruction indications depend on patientbull selection surgeon experience and aetiology of thebull deformity bull Indications for surgery can be functionalbull aesthetic or most commonly both In individuals
with a compromised nasal airway a nasoseptalbull reconstruction is indicated
Nasal Deformity
bull Contraindications bull include patients with malignantbull chronic or autoimmune disease conditions drugbull abuse poor perioperative risk profile and unrealisticbull expectationsbull ndash Multiple previous rhinoplasties and certain
professionsbull (mixed martial artists boxers and other contactbull sports) are relative contraindications
Nasal DeformitySeptoplastyndash Septoplasty is performed to correct nasal obstructioncaused by septal deformityndash Usually septoplasty is performed under general anaesthesiawith the patient in the supine position with the head elevated by approximately 30 (Righthandedsurgeons approach from the right side)ndash Local vasoconstrictive anaesthesia is applied notonly to reduce postoperative pain but also more importantly to achieve vasoconstriction of themucosa and less intraoperative haemorrhage Lidocainewith adrenaline or epinephrine is usedalthough in patients with cardiac hypersensitivityoxymetazoline might be preferred
Nasal Deformity
bull Septoplasty begins with the incision of septal mucosabull Most operative techniques utilise a hemitransfixionbull incision at the caudal end of septum so thatbull deviation at this point might be reached as wellbull as a transfixion incision that is easily obtained ifbull needed (Right-handed surgeons normally choosebull the left side but that may vary when deviation isbull convex towards the right)
Nasal DeformityA columella retractor is placed over the columellaand by pulling it laterally the caudal border of theseptum is exposed Ala can be protected by an alaprotector A vertical incision with a no 15 bladeover the caudal end of septum is performed untilreaching the plane of the septal cartilage It is essentialto correctly identify the perichondrium and byusing the Cottle elevator dissect and lift it creatinga flap As the dissection proceeds along the septalcartilage a longer speculum (no 5) is introduced sothat elevation of the mucoperichondrium is doneunder constant visual controlndash The next step is to dissect the mucoperiostium
Nasal DeformityDissecting over the bony-cartilaginous junctionwhen joining both tunnels might be difficult and is
especially prone to membrane perforationndash If needed the same tunnels are to be created on the
other side of the septum Then deviated parts of
septum are identified and removed either with a
knife or a Freer chisel
Nasal Deformitybull septum from the maxillary crest the septum mustbull be separated from the perpendicular plate trimmedbull along the inferior border placed back onto the crestbull and sutured to the periosteum If the deformity involvesbull the vomer an osteotome is used Care mustbull be taken not to break the cribriform plate becausebull it could cause a cerebrospinal fistula
Nasal Deformity
bull Once the septal deviation is corrected the flapsbull and hemitransfixion incision are mattressed
withbull absorbable sutures Nasal packing to prevent
synechiaebull and postoperative septal haematoma mightbull be advised but should be removed within 72 h

lymphatic drainage
The regional lymphatic drainage of the face and externalnose is handled mainly by- the submandibularlymph nodes while the nasal cavity is additionallydrained by -the retropharyngeal and deep - -cervical lymph nodes
Morphology of the Nasal Mucosa
Besides the anatomical structure of the external noseand nasal cavity the nasal mucosa plays an essentialrole in numerous functions of the nose in the respiratory tract
Morphology of the Nasal Mucosa
The anterior part of the nasal cavity (the nasal vestibule)like the external nose is covered by skin composedof a multilayer keratinizing squamous epithelium and finally a ciliated respiratory epithelium A small areaon the upper nasal septum superior turbinate andpart of the middle turbinate located adjacent to thecribriform plate is covered by olfactory mucosa and iscalled the olfactory region
Nerve SupplyThe facial skin receives its sensory innervation fromterminal branches of the trigeminal nerve that enterthe facial region through the supraorbital infraorbitaland mental foramina Thefacial muscles are classified as mimetic or mastica- tory each of these groups receiving different motorinnervationbythe facial nerve
History and Clinical Examination of the Nose
Historybull The main symptomsbull nasal obstruction (ldquostuffy
noserdquo)bull nasal dischargebull Headachesbull Olfactory
dysfunction
Palpationbony discontinuitiesNeuralgias to check
over- the supraorbital -infraorbital -mental foramina
Anterior Rhinoscopy
bull The rhinologic examination itself begins with anterior
bull rhinoscopy to evaluate the nasal vestibule and the anterior
bull portions of the nasal cavity
Nasal Endoscopy Nasal endoscopy has become the most important andrewarding clinical examination method in rhinologic diagnosis
- rigid endoscopes which are available in 4-mm and 28- mm diameters and assorted viewing angles (eg 01048576 301048576 1201048576) -flexible endoscopes are also available for inspecting the nose and nasopharynx and exploring all of the pharynx and larynx in one sitting
Nasal endoscopy
Nasal Endoscopy
Nasal Endoscopy
Imaging of the Nose and Paranasal Sinuses
Conventional RadiographsStandard paranasal sinus radiographs in the occipitomental
projection ( Water projection) and
occipitofrontal projection Caldwell projection) in cases of acute inflammation
They are also obtained to evaluate midfacial fractures
Computed Tomography (CT) the main indicationsfor CT scanning of the
nose and paranasal sinuses
are- chronic sinusitis - -trauma (especially
frontobasal -fractures)
-and tumors
The occipitofrontal projection is better for evaluating theethmoid cells and frontal sinus
occipitomental projection demonstrates the maxillarysinus and gives a limited view of the sphenoid sinus
Computed tomography of the paranasal sinuses
Four representative coronal CT scans are shown
Four representative coronal CT scans are shown
Magnetic Resonance Imaging
Magnetic maging
Magnetic resonance imaging (MRI) has fewer indicationsthan CT in patients with paranasal sinus diseaseThis is primarily because MRI is markedly inferior toCT in defining the bony boundaries of the sinusesThe strength of MRI lies in its superior soft-tissue discriminationMRI is indicated in diseases that involve the paranasal sinuses in addition to thecranial cavity or orbit (eg tumors and congenitalmalformations such as encephaloceles)
MRI of the paranasal sinuses
The Nose and Sinuses
Structure The structure of the nose is made up of
four partsbull The surface anatomybull The nasal skeletonmdashcomposed of the
two nasal bones the paired upper lateral and lower lateral cartilages and the nasal septum covered in subcutaneous tissue and skin
bull The internal anatomymdashincludes the septum of the nose which forms the medial wall of the nasal cavity The turbinates on the lateral wall are also called conchae
bull The osteomeatal complexmdasha key functional area of the nose
Function The nose is the main route for inspired
air and its structure is related to this function As the air passes over the large surface area of the turbinates
The inspired gases are warmed and humidified Mucus on the mucosa of the nose removes large dust particles from the air as it is breathed in
The voice resonates in the sinuses and nose and this provides character to the speech
Pneumatization of the sinusesmdashthey are air filled spacesmdashreduces the weight of the skull
Diseases of thDiseases of the Outer and Inner Nosee Outer and
Inner Nose Erysipelas Definition of the disease ndash Erysipela is a skin infection that affects the superficial dermis and is caused by Streptococcus pyogenes (group A) It usually develops in the extremities and the face and less commonly on the scalp and genitals bull Epidemiologyaetiology ndash Erysipelas are more often seen in elderly infants and children patients with compromised immunology and diabetes -Predisposing factors are alcoholism skin ulceration puncture wounds fungal infections malnutrition and burns
Erysipelas
bull Symptomsbull ndash It usually presents of fever general fatigue bull -The skin lesion is a redindurated and elevated plaque
with borders that expand rapidly bull It is painful warm and accompanied by variable oedemabull -On the second or third day a flaccid bulla may develop
and desquamationbull bull Presence of regional lymph nodes is common
Erysipelas
bull Complicationsndash The most common complication is recurrencewhich is seen in 18ndash30 of the cases even afterproper antibiotic therapy Recurrence is seen moreoften in females than in malesA skin infection with S pyogenes could lead toglomerulonephritis
Erysipelas
bull Complicationsbull ndash The most common complication is recurrencebull which is seen in 18ndash30 of the cases even afterbull proper antibiotic therapy bull -Recurrence is seen morebull often in females than in males bull -A skin infection with S pyogenes could lead tobull glomerulonephritis
Erysipelas
bull bull Diagnosisbull ndash Diagnosis is based on the patientrsquos personal
historybull and physical examination particularly on inspectionbull of the skin
bull Blood cultures are positive in less thanbull 5 of cases
ErysipelasTherapyndash Conservative therapybull The preferred antibiotic is penicillin In mildcases with minor systemic symptoms penicillinV 500 mg orally every 6 h for 10 days or penicillinG benzathine 12 mil U intramuscularlyonceOther possibilities are amoxicillin 500 mgorally twice a day for 10 days or cephalexin 500mg orally every 6 h for 10 days
ErysipelasIn moderate and severe cases with significantsystemic symptoms hospitalization and intravenoustreatment is required penicillin G 2ndash4mil U intravenously every 4ndash6 h Cefazolin05ndash15 gm intravenously every 8 h cefotaxime1ndash2 gm intravenously every 8 h or ceftriaxone1ndash2 gm intravenously once a day should be administeredIn patients with a penicillin allergyclindamycin 600 mg intravenously every 8 h orvancomycin 15 mgkg intravenously twice a daymay be given
ErysipelaAdditional useful therapeutic optionsbull Prednisone 30 mg over 8 days might be consideredas well as elevation of the affected siteMoist heat compresses may be usefulbull Surgeryndash Debridement and drainage are indicated when bullaeabscesses or necroses are presentbull Differential diagnosisndash Contact dermatitisndash Asteatotic eczemandash Herpes zosterndash Angioneurotic oedemandash Osteomyelitis
Furuncle
bull Definition of the diseasebull ndash A furuncle is an infection that beginsbull at the hair follicle and spreads deeper into thebull dermis and subcutaneous tissue forming abull nodule After several days it developsbull into an abscess - red painful and fluctuantbull bull bull Epidemiologyaetiologybull ndash The aetiologic agent is Staphylococcus aureus
FuruncleSymptomsndashsymptoms are local and limited to thesite of infection Furuncles usually are wherehair follicles are present bull Complicationndash One complication is furunculosis multiple draining furunclesDiagnosisndash The diagnosis is based on clinical inspection - Cultures are not necessary when there is no systemic involvement but should beconsidered if systemic therapy (in case of feversignificant cellulitis or hospitalization) or whenmethicillin-resistant Staphylococcusaureus (MRSA) is considered
FuruncleTherapyndash When the furuncle is small application of moist heat compress to promote drainage -Larger furuncles should be drained by surgical incision-After drainage the area should be cleaned with anantiseptic (with chlorhexidinebetadine) should be applied twice
a dayndash If no systemic symptoms or extensive cellulitis arepresent simple topical care is usually curative andoral antibiotics are not necessary Otherwise systemictreatment is indicated and should cover anypossible MRSA
Furuncle
bull -Recommended antibiotics are trimethoprim-sulfamethoxazole
bull 1ndash2 tablets orally twice daily doxycyclinebull 100 mg orally twice dailybull or clindamycin 300ndash450 mg orally every 8 hbull - In severe cases vancomycin 15 mgkg
intravenouslybull every 12 h or clindamycin 600 mg intravenouslybull every 8 h
Midline Granulomabull A midline granuloma is an angiocentricbull lymphoma it was referred to as polymorphicbull reticulosis lethal midline granuloma and midline
malignant reticulosisbull bull Definition of the diseasebull ndash This rare disease is a lymphoma of extranodal
presentationall cases are positive for the Epstein-Barr virus
bull -This lymphoma most commonly appears in the midface region
Midline GranulomaEpidemiologyaetiologyndash This form of lymphoma is rare in Europe and theUnited States with a higher prevalence in Asia and PeruSymptomsndash The most common presentation is nasal obstruction with a destructive mass occupying the nosesinuses and palate
-Fever night sweatsand weight loss seen usually in Hodgkinrsquos lymphomaand other non-Hodgkinrsquos lymphomas (knownas ldquoB symptomsrdquo) are uncommon
Midline GranulomaDiagnosisndash The diagnosis is based on anatomopathologicalstudy The malignancy of the tumour manifested byextensive necrosis makes the histological diagnosisdifficult and often more biopsies are required forconfirmationbull Therapyndash Therapy consists of radiotherapy with or withoutchemotherapy
Midline Granuloma
bull Prognosisbull ndash Depending on the stage long-term remission or
experience a worseningbull prognosis with relapses which may include otherbull extranodal sites bull Involvement of extranodal sitesbull including the upper airway gastrointestinal tractbull skin
Wegenerrsquos Granulomatosis
bull Definition of the diseasebull ndash Wegenerrsquos granulomatosis is a systemic chronicbull vasculitis of small- and medium-sized blood vesselsbull with an autoimmune component It affectsbull particular organs with variable predilectionbull Epidemiologyaetiologybull ndash Wegenerrsquos granulomatosis is a rare disease It affects
about 1 in 20000ndash30000 people It is more prevalentbull in middle-aged Caucasian patients
Wegenerrsquos Granulomatosis
Symptomsndash The disease may present pulmonary upper
respiratory tract or renal In the disseminated form-The localised form ndash confinedto the upper respiratory region ndash is present in 25of the patients- It consists of nonspecific manifestationssuch as nasal obstruction crusting purulentor bloody rhinorrhea and painful or painless ulcers in oral or nasal cavities which are unresponsive tostandard medical treatment
Wegenerrsquos Granulomatosis
bull In some patients the nasal septum is perforatedbull which leads to saddle-nose deformity Less
commonbull symptoms are hoarseness stridor due to
subglotticbull stenosis otalgia otorrhea and conductivebull and sensorineural hearing loss Also ocular
symptomsbull such as scleritis conjunctivitis uveitis andbull episcleritis may be present
Wegenerrsquos Granulomatosis
bull ndash In the disseminated form pulmonary involvementbull is manifested by cough dyspnoea haemoptysisbull (due to an alveolar capillaritis necrotic lesions orbull endobronchial disease) and pleuritic painndashbull -Ninety per cent of patients have nasal symptomsbull and these symptoms are usually the first
manifestationof the diseasebull -Most patients have also renal involvementbull even if it is subclinical
Wegenerrsquos Granulomatosis
Diagnosis ndash Diagnosis of Wegenerrsquos granulomatosis is based on clinical findings that demonstrate lung (chest x-ray) kidney (urine analysis) or upper respiratory tract
involvement (oral or nasal ulcers or discharge) - positive blood analysis for cytoplasmic-staining antineutrophil
cytoplasmic antibodies (c-ANCA) and confirming proteinase 3 (PR3) ANCA or myeloperoxidase (MPO) ANCA ndash Biopsy is essential for diagnosis nonspecific chronic inflammation
and necrosis -Bacterial and fungal infections
Wegenerrsquos Granulomatosis
Therapyndash Conservative therapybull In the induction of disease remission highdosesteroids (e g prednisone 1 mgkgday) for1 month with tapering over several months aregiven In addition cyclophosphamide (2 mgkgday) should be administered for 6ndash12 monthsuntil symptoms disappear In the maintenanceof remission cyclophosphamide should be
Wegenerrsquos Granulomatosis
Antibiotics mainly trimethoprim-sulfamethoxazoleare given for prophylaxis againstPneumocystis jiroveci (formerly Pneumocystiscarinii) pneumonia (PCP) which may developduring immunosuppression and have a role inpreventing recurrencesbull Sinonasal manifestations may be treated with topical nasal steroids and nasal irrigations lowdosesystemic steroids and antibiotics when bacterial infection (typically Staphylococcus species) is suspected
Wegenerrsquos Granulomatosis
bull Prognosisbull ndash Most of the patients respond well to treatmentbull achieving symptom-free intervals of 5ndash20 yearsbull or more bull -Anatomical problems (sinusitis trachealbull stenosis) may require surgery bull Relapses can be long and troublesomebull Long-term complications are chronicbull renal failure hearing loss and deafness
Nasal Fractures Definition ndash A nasal fracture is a disruption of the nasal bone structure due to trauma It is the most frequently fractured facial bone Epidemiologyaetiology ndash Sports falls and assaults are the usual mechanisms of fracture -Males are affected twice as often as are females -Paediatric populations with a incidences during the second and third decades of life -Variables such as force impact direction nature of the striking object age and other will influence the pattern of injury to the components of the nose
Nasal Fractures
bull Symptomsbull ndash Deformity swelling epistaxis and periorbital
ecchymosis are signs that are suggestive of nasal fracture
bull bony crepitus and nasal segment mobilitybull ndash Epiphora bull Severe bilateral injuries to the lachrymal bones
arebull associated with depressed nasal fractures
Nasal Fractures Complications ndash Septal haematoma is one of the most severe early complications of nasal trauma and without drainage it results in abscess formation 6ndash7 days after trauma producing necrosis of the septal cartilage -Long-term problems such as saddle-nose deformity perforation columellar retraction and nasalbase
Septal infection could lead to osteomyelitis orbital and intracranial abscesses meningitis and cavernous sinus thrombosis -Cerebrospinal fluid leakage is a common complication of severe
nasal and frontal fractures
Nasal Fractures
bull Diagnostic proceduresbull ndash Inspectionbull bull Changes of appearance such as deviation andbull asymmetry bleeding watery drainage changesbull in nasal breathing and smell It is useful to comparebull the current presentation with old photographsbull (up to 40 of normal individuals havebull significant nose malformations)
Nasal Fractures Physical examination bull The diagnosis of a nasal fracture is made primarily by physical examination epistaxis nasal swelling and periorbital ecchymosis Nasal shape in the lateral and frontal inspection should be assessed Grasping the dorsum between two fingers and rocking the pyramid back and forth aids in assessing the mobility of nasal bones Internal structures should be evaluated by using a headlight and nasal speculum Clotted blood is removed by suction and assessment of haematoma mucosal tears and active bleeding is performed Bimanual palpation of the septum helps to differentiate septal swelling from haematoma ndash
Nasal FracturesRadiographybull There is no clear evidence of the role of radiographyin the management of nasal fracturesPlain films have up to a 66 false-positive rateas a result of misinterpretation of normal suturelines In addition old fractures are difficult todistinguishbull Three-dimensional CT is recommended for extensiveinjuries involving the nasal-orbital-ethmoidalcomplexndash
Nasal Fractures
bull Additionaluseful diagnostic proceduresbull bull Using a 0 or 30deg 4-mm endoscope is helpful inbull the assessment of posterior abnormalities If thebull patient is heavily sedated Brown-Gruss
provocationbull manoeuvres may be performed to determinebull deformities in upper middle or lower segmentsbull by compressing each compartment
Nasal FracturesConservative treatmentndash Treatment of bleedingbull For localised bleeding anterior sources may becauterised by silver nitrate or sealed with topicalmaterials such as thrombin combined withgelatin foam fibrin glue FloSealreg or other procoagulantmaterials If conservative measuresfail a formal anterior packing is placedbull Bleeding from branches of sphenopalatine orethmoid vessels requires anterior-posteriorpacking
Nasal Fractures
bull bull Surgical methods such as direct endoscopic vessel
bull cauterization or ligation have been shown tobull offer better haemostasis and patient comfortbull Angiography with embolization can also be
consideredbull in cases refractory to more conservativebull approaches
Nasal Fractures
bull Type of reductionbull bull Nondisplaced fractures should be treated withbull observation alone Closed nasal reduction is thebull best choice for simple injuries (isolated unilateralbull with medial displacement)bull bull An open approach should be considered in
severebull trauma (bilateral depressed fractures)
Nasal Fracturesbull Surgical principlesbull ndash Topical anaesthesia with cotton pledgets soakedbull with 4 cocaine or 005 oxymethazoline combinedbull with 4 topical lidocaine should be appliedbull for 5ndash10 min Local anaesthesia should also be injectedbull (1 lidocaine and 1100000 epinephrine)bull along the septum lateral walls and floor of the nasalbull cavitybull bull
Nasal FracturesClosed reductionndashndash The nasal bones are grasped between two fingersand pressure is applied laterally in theopposite direction of the deviation A bluntelevator may be used from within the nose incases of significant medial collapse Walshamforceps can be of help Reduction of the septumshould be performed with the use ofAsch forceps
Nasal Fractures
bull To prevent collapse of the postreductionbull framework nasal packing should be placedbull for 3ndash5 days Septum splints are recommendedbull in comminuted septal fractures withbull severe mucosal lesions External nasal splintingbull for 10 days (Aquaplastreg Thermoplastreg)bull provides nasal protection Nasal saline spraysbull prevent crusting and oral antibiotics should
Nasal Fractures
bull Open reductionbull ndashndash Immediate repair of fractures by using
widebull surgical exposure reduction fixation and
reconstructionbull ndashndash The second option is delayed correctionbull (6 months or more) of persistent deformitiesbull using standard techniques of rhinoplasty
Deviated Nasal Septum
bull Definition of the diseasebull ndash Deviation of the nasal septum is a common causebull of unilateral nasal airway obstruction in which thebull nasal septum is displacedbull bull Epidemiologyaetiologybull ndash Developmental septal abnormalities Septal cartilage
damage in the neonatal period andbull during birth can cause severe septal deviation inbull the absence of a history of nasal trauma
Deviated Nasal Septum
bull Symptomsbull ndash Patients may present with a history of sinusitis
allergicbull rhinitis obstructive sleep apnoea previousbull nasal surgery or recent nasal trauma Unilateral or
bilateral nasal airway obstruction that is unrelievedbull with decongestants or nasal steroid sprays is oftenbull seenbull bull
Deviated Nasal SeptumDiagnosisndashExamination external dorsal deviation or the columella and caudal septummay be deflected off the midline (caudal subluxation)ndash Inspections of the nasal cavity and anterior-posteriorrhinoscopy are helpful in diagnosing the locationtype and severity of septal deformityThe endoscope is also useful in identifying polypsthe severity and extent of posterior septaldeviations and bony spurs and locating areas ofseptal perforation or mucosal injury
Deviated Nasal Septum
bull Therapybull ndash Septoplasty is a procedurebull The areabull of deviation is corrected or resected in order tobull leave behind as much cartilage and bone as
possiblebull Cartilage resection is minimised and can be
repositioned reshaped or recontoured using a variety of methods
Deviated Nasal Septum
bull ndash Indications of septoplasty before the growth period
bull of the nose is finished should be very limited bull -In these cases surgery must preserve all the
cartilagebull in order to prevent external changes of the
shape ofbull the nose
Deviated Nasal Septum
bull Complicationsbull ndash Frequent complications include haematoma andbull infection Cerebrospinal fluid leak is a rare but
potentiallybull serious complicationbull It is usually the resultbull of avulsion or damage to the cribriform plate whenbull handling the perpendicular plate of the ethmoidbull ndash Other complications include epistaxis nasal
Deviated Nasal Septum
bull Other complications include epistaxis nasal obstruction
bull due to residual deviation synechiae returnbull of the cartilaginous deviation septal perforationbull anosmia and cosmetic nasal deformities suchbull as widened alar rim margins drooping nasal tipbull columella retraction and a sunken dorsum with abull supratip saddle formation
Septal perforation with minor crusting View from provide closure of the
incision
Septal Haematoma
bull A septal haematoma is a blood collection under the perichondrium
bull of the septum and cartilagebull bull bull Epidemiologyaetiologybull ndash A septal haematoma is one of the most
severe complications of nasal trauma
Septal Haematoma
bull Diagnosisbull ndash Signs and symptoms include intense pain
swellingbull haematoma of the upper lip and philtrum
area andbull complete nasal airway obstruction
Septal HaematomaTherapyndash Management consists of drainage through a mucoperichondrial incision Immediate treatment isnecessary to prevent long-term problems such asa saddle-nose deformity perforation columellarretraction and nasal-base widening In childrenseptal destruction can lead to devastating nasal andmidfacial growth abnormalitiesbull Surgeryndash Incision and evacuation of the collection is performedDrainage of a septal haematoma should
Septal HaematomaSurgeryndash Incision and evacuation of the collection is performedDrainage of a septal haematoma should provide closure of the incision
Splints or transseptal sutures are placed to obliterate thepotential space and prevent collectionInfection involving the septal cartilage Reconstruction with autologouscartilage is then performed in a second stage Oral antibiotics should be given
Nasal DeformitySaddle-nose deformityndash A saddle-nose deformity is characterised by a loss ofnasal dorsal height and compromised nasal supportstructures -Other case observed are depressionof the middle vault and dorsum loss of nasal tipsupport and definition shortened (vertical) nasal length over rotation of the nasal tip and retrusion ofthe nasal spine and caudal septum It is also knownas a ldquoPug noserdquo or ldquoboxerrsquos noserdquo both of which referto various degrees of nasal dorsal depressionbull
Nasal DeformityEpidemiologyaetiologyndash Prevalence is higher in population groups prone to facial trauma (ie boxers athletes) those with historiesof intranasal cocaine use nasal surgery (e g radical submucosal septal resection reductive rhinoplasty)ndash A saddle-nose deformity can be congenital or acquired It can be noticed as a part of individual familialsyndromic and ethnic characteristics - Most deformities are due to traumatic and iatrogeniccauses Medical causes are Wegenerrsquosgranulomatosis relapsing polychondritis leprosy (Hansenrsquos disease) syphilis ectodermal dysplasiaand intranasal cocaine use
Nasal Deformity
bull Therapybull ndash Nasal reconstruction indications depend on patientbull selection surgeon experience and aetiology of thebull deformity bull Indications for surgery can be functionalbull aesthetic or most commonly both In individuals
with a compromised nasal airway a nasoseptalbull reconstruction is indicated
Nasal Deformity
bull Contraindications bull include patients with malignantbull chronic or autoimmune disease conditions drugbull abuse poor perioperative risk profile and unrealisticbull expectationsbull ndash Multiple previous rhinoplasties and certain
professionsbull (mixed martial artists boxers and other contactbull sports) are relative contraindications
Nasal DeformitySeptoplastyndash Septoplasty is performed to correct nasal obstructioncaused by septal deformityndash Usually septoplasty is performed under general anaesthesiawith the patient in the supine position with the head elevated by approximately 30 (Righthandedsurgeons approach from the right side)ndash Local vasoconstrictive anaesthesia is applied notonly to reduce postoperative pain but also more importantly to achieve vasoconstriction of themucosa and less intraoperative haemorrhage Lidocainewith adrenaline or epinephrine is usedalthough in patients with cardiac hypersensitivityoxymetazoline might be preferred
Nasal Deformity
bull Septoplasty begins with the incision of septal mucosabull Most operative techniques utilise a hemitransfixionbull incision at the caudal end of septum so thatbull deviation at this point might be reached as wellbull as a transfixion incision that is easily obtained ifbull needed (Right-handed surgeons normally choosebull the left side but that may vary when deviation isbull convex towards the right)
Nasal DeformityA columella retractor is placed over the columellaand by pulling it laterally the caudal border of theseptum is exposed Ala can be protected by an alaprotector A vertical incision with a no 15 bladeover the caudal end of septum is performed untilreaching the plane of the septal cartilage It is essentialto correctly identify the perichondrium and byusing the Cottle elevator dissect and lift it creatinga flap As the dissection proceeds along the septalcartilage a longer speculum (no 5) is introduced sothat elevation of the mucoperichondrium is doneunder constant visual controlndash The next step is to dissect the mucoperiostium
Nasal DeformityDissecting over the bony-cartilaginous junctionwhen joining both tunnels might be difficult and is
especially prone to membrane perforationndash If needed the same tunnels are to be created on the
other side of the septum Then deviated parts of
septum are identified and removed either with a
knife or a Freer chisel
Nasal Deformitybull septum from the maxillary crest the septum mustbull be separated from the perpendicular plate trimmedbull along the inferior border placed back onto the crestbull and sutured to the periosteum If the deformity involvesbull the vomer an osteotome is used Care mustbull be taken not to break the cribriform plate becausebull it could cause a cerebrospinal fistula
Nasal Deformity
bull Once the septal deviation is corrected the flapsbull and hemitransfixion incision are mattressed
withbull absorbable sutures Nasal packing to prevent
synechiaebull and postoperative septal haematoma mightbull be advised but should be removed within 72 h

Morphology of the Nasal Mucosa
Besides the anatomical structure of the external noseand nasal cavity the nasal mucosa plays an essentialrole in numerous functions of the nose in the respiratory tract
Morphology of the Nasal Mucosa
The anterior part of the nasal cavity (the nasal vestibule)like the external nose is covered by skin composedof a multilayer keratinizing squamous epithelium and finally a ciliated respiratory epithelium A small areaon the upper nasal septum superior turbinate andpart of the middle turbinate located adjacent to thecribriform plate is covered by olfactory mucosa and iscalled the olfactory region
Nerve SupplyThe facial skin receives its sensory innervation fromterminal branches of the trigeminal nerve that enterthe facial region through the supraorbital infraorbitaland mental foramina Thefacial muscles are classified as mimetic or mastica- tory each of these groups receiving different motorinnervationbythe facial nerve
History and Clinical Examination of the Nose
Historybull The main symptomsbull nasal obstruction (ldquostuffy
noserdquo)bull nasal dischargebull Headachesbull Olfactory
dysfunction
Palpationbony discontinuitiesNeuralgias to check
over- the supraorbital -infraorbital -mental foramina
Anterior Rhinoscopy
bull The rhinologic examination itself begins with anterior
bull rhinoscopy to evaluate the nasal vestibule and the anterior
bull portions of the nasal cavity
Nasal Endoscopy Nasal endoscopy has become the most important andrewarding clinical examination method in rhinologic diagnosis
- rigid endoscopes which are available in 4-mm and 28- mm diameters and assorted viewing angles (eg 01048576 301048576 1201048576) -flexible endoscopes are also available for inspecting the nose and nasopharynx and exploring all of the pharynx and larynx in one sitting
Nasal endoscopy
Nasal Endoscopy
Nasal Endoscopy
Imaging of the Nose and Paranasal Sinuses
Conventional RadiographsStandard paranasal sinus radiographs in the occipitomental
projection ( Water projection) and
occipitofrontal projection Caldwell projection) in cases of acute inflammation
They are also obtained to evaluate midfacial fractures
Computed Tomography (CT) the main indicationsfor CT scanning of the
nose and paranasal sinuses
are- chronic sinusitis - -trauma (especially
frontobasal -fractures)
-and tumors
The occipitofrontal projection is better for evaluating theethmoid cells and frontal sinus
occipitomental projection demonstrates the maxillarysinus and gives a limited view of the sphenoid sinus
Computed tomography of the paranasal sinuses
Four representative coronal CT scans are shown
Four representative coronal CT scans are shown
Magnetic Resonance Imaging
Magnetic maging
Magnetic resonance imaging (MRI) has fewer indicationsthan CT in patients with paranasal sinus diseaseThis is primarily because MRI is markedly inferior toCT in defining the bony boundaries of the sinusesThe strength of MRI lies in its superior soft-tissue discriminationMRI is indicated in diseases that involve the paranasal sinuses in addition to thecranial cavity or orbit (eg tumors and congenitalmalformations such as encephaloceles)
MRI of the paranasal sinuses
The Nose and Sinuses
Structure The structure of the nose is made up of
four partsbull The surface anatomybull The nasal skeletonmdashcomposed of the
two nasal bones the paired upper lateral and lower lateral cartilages and the nasal septum covered in subcutaneous tissue and skin
bull The internal anatomymdashincludes the septum of the nose which forms the medial wall of the nasal cavity The turbinates on the lateral wall are also called conchae
bull The osteomeatal complexmdasha key functional area of the nose
Function The nose is the main route for inspired
air and its structure is related to this function As the air passes over the large surface area of the turbinates
The inspired gases are warmed and humidified Mucus on the mucosa of the nose removes large dust particles from the air as it is breathed in
The voice resonates in the sinuses and nose and this provides character to the speech
Pneumatization of the sinusesmdashthey are air filled spacesmdashreduces the weight of the skull
Diseases of thDiseases of the Outer and Inner Nosee Outer and
Inner Nose Erysipelas Definition of the disease ndash Erysipela is a skin infection that affects the superficial dermis and is caused by Streptococcus pyogenes (group A) It usually develops in the extremities and the face and less commonly on the scalp and genitals bull Epidemiologyaetiology ndash Erysipelas are more often seen in elderly infants and children patients with compromised immunology and diabetes -Predisposing factors are alcoholism skin ulceration puncture wounds fungal infections malnutrition and burns
Erysipelas
bull Symptomsbull ndash It usually presents of fever general fatigue bull -The skin lesion is a redindurated and elevated plaque
with borders that expand rapidly bull It is painful warm and accompanied by variable oedemabull -On the second or third day a flaccid bulla may develop
and desquamationbull bull Presence of regional lymph nodes is common
Erysipelas
bull Complicationsndash The most common complication is recurrencewhich is seen in 18ndash30 of the cases even afterproper antibiotic therapy Recurrence is seen moreoften in females than in malesA skin infection with S pyogenes could lead toglomerulonephritis
Erysipelas
bull Complicationsbull ndash The most common complication is recurrencebull which is seen in 18ndash30 of the cases even afterbull proper antibiotic therapy bull -Recurrence is seen morebull often in females than in males bull -A skin infection with S pyogenes could lead tobull glomerulonephritis
Erysipelas
bull bull Diagnosisbull ndash Diagnosis is based on the patientrsquos personal
historybull and physical examination particularly on inspectionbull of the skin
bull Blood cultures are positive in less thanbull 5 of cases
ErysipelasTherapyndash Conservative therapybull The preferred antibiotic is penicillin In mildcases with minor systemic symptoms penicillinV 500 mg orally every 6 h for 10 days or penicillinG benzathine 12 mil U intramuscularlyonceOther possibilities are amoxicillin 500 mgorally twice a day for 10 days or cephalexin 500mg orally every 6 h for 10 days
ErysipelasIn moderate and severe cases with significantsystemic symptoms hospitalization and intravenoustreatment is required penicillin G 2ndash4mil U intravenously every 4ndash6 h Cefazolin05ndash15 gm intravenously every 8 h cefotaxime1ndash2 gm intravenously every 8 h or ceftriaxone1ndash2 gm intravenously once a day should be administeredIn patients with a penicillin allergyclindamycin 600 mg intravenously every 8 h orvancomycin 15 mgkg intravenously twice a daymay be given
ErysipelaAdditional useful therapeutic optionsbull Prednisone 30 mg over 8 days might be consideredas well as elevation of the affected siteMoist heat compresses may be usefulbull Surgeryndash Debridement and drainage are indicated when bullaeabscesses or necroses are presentbull Differential diagnosisndash Contact dermatitisndash Asteatotic eczemandash Herpes zosterndash Angioneurotic oedemandash Osteomyelitis
Furuncle
bull Definition of the diseasebull ndash A furuncle is an infection that beginsbull at the hair follicle and spreads deeper into thebull dermis and subcutaneous tissue forming abull nodule After several days it developsbull into an abscess - red painful and fluctuantbull bull bull Epidemiologyaetiologybull ndash The aetiologic agent is Staphylococcus aureus
FuruncleSymptomsndashsymptoms are local and limited to thesite of infection Furuncles usually are wherehair follicles are present bull Complicationndash One complication is furunculosis multiple draining furunclesDiagnosisndash The diagnosis is based on clinical inspection - Cultures are not necessary when there is no systemic involvement but should beconsidered if systemic therapy (in case of feversignificant cellulitis or hospitalization) or whenmethicillin-resistant Staphylococcusaureus (MRSA) is considered
FuruncleTherapyndash When the furuncle is small application of moist heat compress to promote drainage -Larger furuncles should be drained by surgical incision-After drainage the area should be cleaned with anantiseptic (with chlorhexidinebetadine) should be applied twice
a dayndash If no systemic symptoms or extensive cellulitis arepresent simple topical care is usually curative andoral antibiotics are not necessary Otherwise systemictreatment is indicated and should cover anypossible MRSA
Furuncle
bull -Recommended antibiotics are trimethoprim-sulfamethoxazole
bull 1ndash2 tablets orally twice daily doxycyclinebull 100 mg orally twice dailybull or clindamycin 300ndash450 mg orally every 8 hbull - In severe cases vancomycin 15 mgkg
intravenouslybull every 12 h or clindamycin 600 mg intravenouslybull every 8 h
Midline Granulomabull A midline granuloma is an angiocentricbull lymphoma it was referred to as polymorphicbull reticulosis lethal midline granuloma and midline
malignant reticulosisbull bull Definition of the diseasebull ndash This rare disease is a lymphoma of extranodal
presentationall cases are positive for the Epstein-Barr virus
bull -This lymphoma most commonly appears in the midface region
Midline GranulomaEpidemiologyaetiologyndash This form of lymphoma is rare in Europe and theUnited States with a higher prevalence in Asia and PeruSymptomsndash The most common presentation is nasal obstruction with a destructive mass occupying the nosesinuses and palate
-Fever night sweatsand weight loss seen usually in Hodgkinrsquos lymphomaand other non-Hodgkinrsquos lymphomas (knownas ldquoB symptomsrdquo) are uncommon
Midline GranulomaDiagnosisndash The diagnosis is based on anatomopathologicalstudy The malignancy of the tumour manifested byextensive necrosis makes the histological diagnosisdifficult and often more biopsies are required forconfirmationbull Therapyndash Therapy consists of radiotherapy with or withoutchemotherapy
Midline Granuloma
bull Prognosisbull ndash Depending on the stage long-term remission or
experience a worseningbull prognosis with relapses which may include otherbull extranodal sites bull Involvement of extranodal sitesbull including the upper airway gastrointestinal tractbull skin
Wegenerrsquos Granulomatosis
bull Definition of the diseasebull ndash Wegenerrsquos granulomatosis is a systemic chronicbull vasculitis of small- and medium-sized blood vesselsbull with an autoimmune component It affectsbull particular organs with variable predilectionbull Epidemiologyaetiologybull ndash Wegenerrsquos granulomatosis is a rare disease It affects
about 1 in 20000ndash30000 people It is more prevalentbull in middle-aged Caucasian patients
Wegenerrsquos Granulomatosis
Symptomsndash The disease may present pulmonary upper
respiratory tract or renal In the disseminated form-The localised form ndash confinedto the upper respiratory region ndash is present in 25of the patients- It consists of nonspecific manifestationssuch as nasal obstruction crusting purulentor bloody rhinorrhea and painful or painless ulcers in oral or nasal cavities which are unresponsive tostandard medical treatment
Wegenerrsquos Granulomatosis
bull In some patients the nasal septum is perforatedbull which leads to saddle-nose deformity Less
commonbull symptoms are hoarseness stridor due to
subglotticbull stenosis otalgia otorrhea and conductivebull and sensorineural hearing loss Also ocular
symptomsbull such as scleritis conjunctivitis uveitis andbull episcleritis may be present
Wegenerrsquos Granulomatosis
bull ndash In the disseminated form pulmonary involvementbull is manifested by cough dyspnoea haemoptysisbull (due to an alveolar capillaritis necrotic lesions orbull endobronchial disease) and pleuritic painndashbull -Ninety per cent of patients have nasal symptomsbull and these symptoms are usually the first
manifestationof the diseasebull -Most patients have also renal involvementbull even if it is subclinical
Wegenerrsquos Granulomatosis
Diagnosis ndash Diagnosis of Wegenerrsquos granulomatosis is based on clinical findings that demonstrate lung (chest x-ray) kidney (urine analysis) or upper respiratory tract
involvement (oral or nasal ulcers or discharge) - positive blood analysis for cytoplasmic-staining antineutrophil
cytoplasmic antibodies (c-ANCA) and confirming proteinase 3 (PR3) ANCA or myeloperoxidase (MPO) ANCA ndash Biopsy is essential for diagnosis nonspecific chronic inflammation
and necrosis -Bacterial and fungal infections
Wegenerrsquos Granulomatosis
Therapyndash Conservative therapybull In the induction of disease remission highdosesteroids (e g prednisone 1 mgkgday) for1 month with tapering over several months aregiven In addition cyclophosphamide (2 mgkgday) should be administered for 6ndash12 monthsuntil symptoms disappear In the maintenanceof remission cyclophosphamide should be
Wegenerrsquos Granulomatosis
Antibiotics mainly trimethoprim-sulfamethoxazoleare given for prophylaxis againstPneumocystis jiroveci (formerly Pneumocystiscarinii) pneumonia (PCP) which may developduring immunosuppression and have a role inpreventing recurrencesbull Sinonasal manifestations may be treated with topical nasal steroids and nasal irrigations lowdosesystemic steroids and antibiotics when bacterial infection (typically Staphylococcus species) is suspected
Wegenerrsquos Granulomatosis
bull Prognosisbull ndash Most of the patients respond well to treatmentbull achieving symptom-free intervals of 5ndash20 yearsbull or more bull -Anatomical problems (sinusitis trachealbull stenosis) may require surgery bull Relapses can be long and troublesomebull Long-term complications are chronicbull renal failure hearing loss and deafness
Nasal Fractures Definition ndash A nasal fracture is a disruption of the nasal bone structure due to trauma It is the most frequently fractured facial bone Epidemiologyaetiology ndash Sports falls and assaults are the usual mechanisms of fracture -Males are affected twice as often as are females -Paediatric populations with a incidences during the second and third decades of life -Variables such as force impact direction nature of the striking object age and other will influence the pattern of injury to the components of the nose
Nasal Fractures
bull Symptomsbull ndash Deformity swelling epistaxis and periorbital
ecchymosis are signs that are suggestive of nasal fracture
bull bony crepitus and nasal segment mobilitybull ndash Epiphora bull Severe bilateral injuries to the lachrymal bones
arebull associated with depressed nasal fractures
Nasal Fractures Complications ndash Septal haematoma is one of the most severe early complications of nasal trauma and without drainage it results in abscess formation 6ndash7 days after trauma producing necrosis of the septal cartilage -Long-term problems such as saddle-nose deformity perforation columellar retraction and nasalbase
Septal infection could lead to osteomyelitis orbital and intracranial abscesses meningitis and cavernous sinus thrombosis -Cerebrospinal fluid leakage is a common complication of severe
nasal and frontal fractures
Nasal Fractures
bull Diagnostic proceduresbull ndash Inspectionbull bull Changes of appearance such as deviation andbull asymmetry bleeding watery drainage changesbull in nasal breathing and smell It is useful to comparebull the current presentation with old photographsbull (up to 40 of normal individuals havebull significant nose malformations)
Nasal Fractures Physical examination bull The diagnosis of a nasal fracture is made primarily by physical examination epistaxis nasal swelling and periorbital ecchymosis Nasal shape in the lateral and frontal inspection should be assessed Grasping the dorsum between two fingers and rocking the pyramid back and forth aids in assessing the mobility of nasal bones Internal structures should be evaluated by using a headlight and nasal speculum Clotted blood is removed by suction and assessment of haematoma mucosal tears and active bleeding is performed Bimanual palpation of the septum helps to differentiate septal swelling from haematoma ndash
Nasal FracturesRadiographybull There is no clear evidence of the role of radiographyin the management of nasal fracturesPlain films have up to a 66 false-positive rateas a result of misinterpretation of normal suturelines In addition old fractures are difficult todistinguishbull Three-dimensional CT is recommended for extensiveinjuries involving the nasal-orbital-ethmoidalcomplexndash
Nasal Fractures
bull Additionaluseful diagnostic proceduresbull bull Using a 0 or 30deg 4-mm endoscope is helpful inbull the assessment of posterior abnormalities If thebull patient is heavily sedated Brown-Gruss
provocationbull manoeuvres may be performed to determinebull deformities in upper middle or lower segmentsbull by compressing each compartment
Nasal FracturesConservative treatmentndash Treatment of bleedingbull For localised bleeding anterior sources may becauterised by silver nitrate or sealed with topicalmaterials such as thrombin combined withgelatin foam fibrin glue FloSealreg or other procoagulantmaterials If conservative measuresfail a formal anterior packing is placedbull Bleeding from branches of sphenopalatine orethmoid vessels requires anterior-posteriorpacking
Nasal Fractures
bull bull Surgical methods such as direct endoscopic vessel
bull cauterization or ligation have been shown tobull offer better haemostasis and patient comfortbull Angiography with embolization can also be
consideredbull in cases refractory to more conservativebull approaches
Nasal Fractures
bull Type of reductionbull bull Nondisplaced fractures should be treated withbull observation alone Closed nasal reduction is thebull best choice for simple injuries (isolated unilateralbull with medial displacement)bull bull An open approach should be considered in
severebull trauma (bilateral depressed fractures)
Nasal Fracturesbull Surgical principlesbull ndash Topical anaesthesia with cotton pledgets soakedbull with 4 cocaine or 005 oxymethazoline combinedbull with 4 topical lidocaine should be appliedbull for 5ndash10 min Local anaesthesia should also be injectedbull (1 lidocaine and 1100000 epinephrine)bull along the septum lateral walls and floor of the nasalbull cavitybull bull
Nasal FracturesClosed reductionndashndash The nasal bones are grasped between two fingersand pressure is applied laterally in theopposite direction of the deviation A bluntelevator may be used from within the nose incases of significant medial collapse Walshamforceps can be of help Reduction of the septumshould be performed with the use ofAsch forceps
Nasal Fractures
bull To prevent collapse of the postreductionbull framework nasal packing should be placedbull for 3ndash5 days Septum splints are recommendedbull in comminuted septal fractures withbull severe mucosal lesions External nasal splintingbull for 10 days (Aquaplastreg Thermoplastreg)bull provides nasal protection Nasal saline spraysbull prevent crusting and oral antibiotics should
Nasal Fractures
bull Open reductionbull ndashndash Immediate repair of fractures by using
widebull surgical exposure reduction fixation and
reconstructionbull ndashndash The second option is delayed correctionbull (6 months or more) of persistent deformitiesbull using standard techniques of rhinoplasty
Deviated Nasal Septum
bull Definition of the diseasebull ndash Deviation of the nasal septum is a common causebull of unilateral nasal airway obstruction in which thebull nasal septum is displacedbull bull Epidemiologyaetiologybull ndash Developmental septal abnormalities Septal cartilage
damage in the neonatal period andbull during birth can cause severe septal deviation inbull the absence of a history of nasal trauma
Deviated Nasal Septum
bull Symptomsbull ndash Patients may present with a history of sinusitis
allergicbull rhinitis obstructive sleep apnoea previousbull nasal surgery or recent nasal trauma Unilateral or
bilateral nasal airway obstruction that is unrelievedbull with decongestants or nasal steroid sprays is oftenbull seenbull bull
Deviated Nasal SeptumDiagnosisndashExamination external dorsal deviation or the columella and caudal septummay be deflected off the midline (caudal subluxation)ndash Inspections of the nasal cavity and anterior-posteriorrhinoscopy are helpful in diagnosing the locationtype and severity of septal deformityThe endoscope is also useful in identifying polypsthe severity and extent of posterior septaldeviations and bony spurs and locating areas ofseptal perforation or mucosal injury
Deviated Nasal Septum
bull Therapybull ndash Septoplasty is a procedurebull The areabull of deviation is corrected or resected in order tobull leave behind as much cartilage and bone as
possiblebull Cartilage resection is minimised and can be
repositioned reshaped or recontoured using a variety of methods
Deviated Nasal Septum
bull ndash Indications of septoplasty before the growth period
bull of the nose is finished should be very limited bull -In these cases surgery must preserve all the
cartilagebull in order to prevent external changes of the
shape ofbull the nose
Deviated Nasal Septum
bull Complicationsbull ndash Frequent complications include haematoma andbull infection Cerebrospinal fluid leak is a rare but
potentiallybull serious complicationbull It is usually the resultbull of avulsion or damage to the cribriform plate whenbull handling the perpendicular plate of the ethmoidbull ndash Other complications include epistaxis nasal
Deviated Nasal Septum
bull Other complications include epistaxis nasal obstruction
bull due to residual deviation synechiae returnbull of the cartilaginous deviation septal perforationbull anosmia and cosmetic nasal deformities suchbull as widened alar rim margins drooping nasal tipbull columella retraction and a sunken dorsum with abull supratip saddle formation
Septal perforation with minor crusting View from provide closure of the
incision
Septal Haematoma
bull A septal haematoma is a blood collection under the perichondrium
bull of the septum and cartilagebull bull bull Epidemiologyaetiologybull ndash A septal haematoma is one of the most
severe complications of nasal trauma
Septal Haematoma
bull Diagnosisbull ndash Signs and symptoms include intense pain
swellingbull haematoma of the upper lip and philtrum
area andbull complete nasal airway obstruction
Septal HaematomaTherapyndash Management consists of drainage through a mucoperichondrial incision Immediate treatment isnecessary to prevent long-term problems such asa saddle-nose deformity perforation columellarretraction and nasal-base widening In childrenseptal destruction can lead to devastating nasal andmidfacial growth abnormalitiesbull Surgeryndash Incision and evacuation of the collection is performedDrainage of a septal haematoma should
Septal HaematomaSurgeryndash Incision and evacuation of the collection is performedDrainage of a septal haematoma should provide closure of the incision
Splints or transseptal sutures are placed to obliterate thepotential space and prevent collectionInfection involving the septal cartilage Reconstruction with autologouscartilage is then performed in a second stage Oral antibiotics should be given
Nasal DeformitySaddle-nose deformityndash A saddle-nose deformity is characterised by a loss ofnasal dorsal height and compromised nasal supportstructures -Other case observed are depressionof the middle vault and dorsum loss of nasal tipsupport and definition shortened (vertical) nasal length over rotation of the nasal tip and retrusion ofthe nasal spine and caudal septum It is also knownas a ldquoPug noserdquo or ldquoboxerrsquos noserdquo both of which referto various degrees of nasal dorsal depressionbull
Nasal DeformityEpidemiologyaetiologyndash Prevalence is higher in population groups prone to facial trauma (ie boxers athletes) those with historiesof intranasal cocaine use nasal surgery (e g radical submucosal septal resection reductive rhinoplasty)ndash A saddle-nose deformity can be congenital or acquired It can be noticed as a part of individual familialsyndromic and ethnic characteristics - Most deformities are due to traumatic and iatrogeniccauses Medical causes are Wegenerrsquosgranulomatosis relapsing polychondritis leprosy (Hansenrsquos disease) syphilis ectodermal dysplasiaand intranasal cocaine use
Nasal Deformity
bull Therapybull ndash Nasal reconstruction indications depend on patientbull selection surgeon experience and aetiology of thebull deformity bull Indications for surgery can be functionalbull aesthetic or most commonly both In individuals
with a compromised nasal airway a nasoseptalbull reconstruction is indicated
Nasal Deformity
bull Contraindications bull include patients with malignantbull chronic or autoimmune disease conditions drugbull abuse poor perioperative risk profile and unrealisticbull expectationsbull ndash Multiple previous rhinoplasties and certain
professionsbull (mixed martial artists boxers and other contactbull sports) are relative contraindications
Nasal DeformitySeptoplastyndash Septoplasty is performed to correct nasal obstructioncaused by septal deformityndash Usually septoplasty is performed under general anaesthesiawith the patient in the supine position with the head elevated by approximately 30 (Righthandedsurgeons approach from the right side)ndash Local vasoconstrictive anaesthesia is applied notonly to reduce postoperative pain but also more importantly to achieve vasoconstriction of themucosa and less intraoperative haemorrhage Lidocainewith adrenaline or epinephrine is usedalthough in patients with cardiac hypersensitivityoxymetazoline might be preferred
Nasal Deformity
bull Septoplasty begins with the incision of septal mucosabull Most operative techniques utilise a hemitransfixionbull incision at the caudal end of septum so thatbull deviation at this point might be reached as wellbull as a transfixion incision that is easily obtained ifbull needed (Right-handed surgeons normally choosebull the left side but that may vary when deviation isbull convex towards the right)
Nasal DeformityA columella retractor is placed over the columellaand by pulling it laterally the caudal border of theseptum is exposed Ala can be protected by an alaprotector A vertical incision with a no 15 bladeover the caudal end of septum is performed untilreaching the plane of the septal cartilage It is essentialto correctly identify the perichondrium and byusing the Cottle elevator dissect and lift it creatinga flap As the dissection proceeds along the septalcartilage a longer speculum (no 5) is introduced sothat elevation of the mucoperichondrium is doneunder constant visual controlndash The next step is to dissect the mucoperiostium
Nasal DeformityDissecting over the bony-cartilaginous junctionwhen joining both tunnels might be difficult and is
especially prone to membrane perforationndash If needed the same tunnels are to be created on the
other side of the septum Then deviated parts of
septum are identified and removed either with a
knife or a Freer chisel
Nasal Deformitybull septum from the maxillary crest the septum mustbull be separated from the perpendicular plate trimmedbull along the inferior border placed back onto the crestbull and sutured to the periosteum If the deformity involvesbull the vomer an osteotome is used Care mustbull be taken not to break the cribriform plate becausebull it could cause a cerebrospinal fistula
Nasal Deformity
bull Once the septal deviation is corrected the flapsbull and hemitransfixion incision are mattressed
withbull absorbable sutures Nasal packing to prevent
synechiaebull and postoperative septal haematoma mightbull be advised but should be removed within 72 h

Morphology of the Nasal Mucosa
The anterior part of the nasal cavity (the nasal vestibule)like the external nose is covered by skin composedof a multilayer keratinizing squamous epithelium and finally a ciliated respiratory epithelium A small areaon the upper nasal septum superior turbinate andpart of the middle turbinate located adjacent to thecribriform plate is covered by olfactory mucosa and iscalled the olfactory region
Nerve SupplyThe facial skin receives its sensory innervation fromterminal branches of the trigeminal nerve that enterthe facial region through the supraorbital infraorbitaland mental foramina Thefacial muscles are classified as mimetic or mastica- tory each of these groups receiving different motorinnervationbythe facial nerve
History and Clinical Examination of the Nose
Historybull The main symptomsbull nasal obstruction (ldquostuffy
noserdquo)bull nasal dischargebull Headachesbull Olfactory
dysfunction
Palpationbony discontinuitiesNeuralgias to check
over- the supraorbital -infraorbital -mental foramina
Anterior Rhinoscopy
bull The rhinologic examination itself begins with anterior
bull rhinoscopy to evaluate the nasal vestibule and the anterior
bull portions of the nasal cavity
Nasal Endoscopy Nasal endoscopy has become the most important andrewarding clinical examination method in rhinologic diagnosis
- rigid endoscopes which are available in 4-mm and 28- mm diameters and assorted viewing angles (eg 01048576 301048576 1201048576) -flexible endoscopes are also available for inspecting the nose and nasopharynx and exploring all of the pharynx and larynx in one sitting
Nasal endoscopy
Nasal Endoscopy
Nasal Endoscopy
Imaging of the Nose and Paranasal Sinuses
Conventional RadiographsStandard paranasal sinus radiographs in the occipitomental
projection ( Water projection) and
occipitofrontal projection Caldwell projection) in cases of acute inflammation
They are also obtained to evaluate midfacial fractures
Computed Tomography (CT) the main indicationsfor CT scanning of the
nose and paranasal sinuses
are- chronic sinusitis - -trauma (especially
frontobasal -fractures)
-and tumors
The occipitofrontal projection is better for evaluating theethmoid cells and frontal sinus
occipitomental projection demonstrates the maxillarysinus and gives a limited view of the sphenoid sinus
Computed tomography of the paranasal sinuses
Four representative coronal CT scans are shown
Four representative coronal CT scans are shown
Magnetic Resonance Imaging
Magnetic maging
Magnetic resonance imaging (MRI) has fewer indicationsthan CT in patients with paranasal sinus diseaseThis is primarily because MRI is markedly inferior toCT in defining the bony boundaries of the sinusesThe strength of MRI lies in its superior soft-tissue discriminationMRI is indicated in diseases that involve the paranasal sinuses in addition to thecranial cavity or orbit (eg tumors and congenitalmalformations such as encephaloceles)
MRI of the paranasal sinuses
The Nose and Sinuses
Structure The structure of the nose is made up of
four partsbull The surface anatomybull The nasal skeletonmdashcomposed of the
two nasal bones the paired upper lateral and lower lateral cartilages and the nasal septum covered in subcutaneous tissue and skin
bull The internal anatomymdashincludes the septum of the nose which forms the medial wall of the nasal cavity The turbinates on the lateral wall are also called conchae
bull The osteomeatal complexmdasha key functional area of the nose
Function The nose is the main route for inspired
air and its structure is related to this function As the air passes over the large surface area of the turbinates
The inspired gases are warmed and humidified Mucus on the mucosa of the nose removes large dust particles from the air as it is breathed in
The voice resonates in the sinuses and nose and this provides character to the speech
Pneumatization of the sinusesmdashthey are air filled spacesmdashreduces the weight of the skull
Diseases of thDiseases of the Outer and Inner Nosee Outer and
Inner Nose Erysipelas Definition of the disease ndash Erysipela is a skin infection that affects the superficial dermis and is caused by Streptococcus pyogenes (group A) It usually develops in the extremities and the face and less commonly on the scalp and genitals bull Epidemiologyaetiology ndash Erysipelas are more often seen in elderly infants and children patients with compromised immunology and diabetes -Predisposing factors are alcoholism skin ulceration puncture wounds fungal infections malnutrition and burns
Erysipelas
bull Symptomsbull ndash It usually presents of fever general fatigue bull -The skin lesion is a redindurated and elevated plaque
with borders that expand rapidly bull It is painful warm and accompanied by variable oedemabull -On the second or third day a flaccid bulla may develop
and desquamationbull bull Presence of regional lymph nodes is common
Erysipelas
bull Complicationsndash The most common complication is recurrencewhich is seen in 18ndash30 of the cases even afterproper antibiotic therapy Recurrence is seen moreoften in females than in malesA skin infection with S pyogenes could lead toglomerulonephritis
Erysipelas
bull Complicationsbull ndash The most common complication is recurrencebull which is seen in 18ndash30 of the cases even afterbull proper antibiotic therapy bull -Recurrence is seen morebull often in females than in males bull -A skin infection with S pyogenes could lead tobull glomerulonephritis
Erysipelas
bull bull Diagnosisbull ndash Diagnosis is based on the patientrsquos personal
historybull and physical examination particularly on inspectionbull of the skin
bull Blood cultures are positive in less thanbull 5 of cases
ErysipelasTherapyndash Conservative therapybull The preferred antibiotic is penicillin In mildcases with minor systemic symptoms penicillinV 500 mg orally every 6 h for 10 days or penicillinG benzathine 12 mil U intramuscularlyonceOther possibilities are amoxicillin 500 mgorally twice a day for 10 days or cephalexin 500mg orally every 6 h for 10 days
ErysipelasIn moderate and severe cases with significantsystemic symptoms hospitalization and intravenoustreatment is required penicillin G 2ndash4mil U intravenously every 4ndash6 h Cefazolin05ndash15 gm intravenously every 8 h cefotaxime1ndash2 gm intravenously every 8 h or ceftriaxone1ndash2 gm intravenously once a day should be administeredIn patients with a penicillin allergyclindamycin 600 mg intravenously every 8 h orvancomycin 15 mgkg intravenously twice a daymay be given
ErysipelaAdditional useful therapeutic optionsbull Prednisone 30 mg over 8 days might be consideredas well as elevation of the affected siteMoist heat compresses may be usefulbull Surgeryndash Debridement and drainage are indicated when bullaeabscesses or necroses are presentbull Differential diagnosisndash Contact dermatitisndash Asteatotic eczemandash Herpes zosterndash Angioneurotic oedemandash Osteomyelitis
Furuncle
bull Definition of the diseasebull ndash A furuncle is an infection that beginsbull at the hair follicle and spreads deeper into thebull dermis and subcutaneous tissue forming abull nodule After several days it developsbull into an abscess - red painful and fluctuantbull bull bull Epidemiologyaetiologybull ndash The aetiologic agent is Staphylococcus aureus
FuruncleSymptomsndashsymptoms are local and limited to thesite of infection Furuncles usually are wherehair follicles are present bull Complicationndash One complication is furunculosis multiple draining furunclesDiagnosisndash The diagnosis is based on clinical inspection - Cultures are not necessary when there is no systemic involvement but should beconsidered if systemic therapy (in case of feversignificant cellulitis or hospitalization) or whenmethicillin-resistant Staphylococcusaureus (MRSA) is considered
FuruncleTherapyndash When the furuncle is small application of moist heat compress to promote drainage -Larger furuncles should be drained by surgical incision-After drainage the area should be cleaned with anantiseptic (with chlorhexidinebetadine) should be applied twice
a dayndash If no systemic symptoms or extensive cellulitis arepresent simple topical care is usually curative andoral antibiotics are not necessary Otherwise systemictreatment is indicated and should cover anypossible MRSA
Furuncle
bull -Recommended antibiotics are trimethoprim-sulfamethoxazole
bull 1ndash2 tablets orally twice daily doxycyclinebull 100 mg orally twice dailybull or clindamycin 300ndash450 mg orally every 8 hbull - In severe cases vancomycin 15 mgkg
intravenouslybull every 12 h or clindamycin 600 mg intravenouslybull every 8 h
Midline Granulomabull A midline granuloma is an angiocentricbull lymphoma it was referred to as polymorphicbull reticulosis lethal midline granuloma and midline
malignant reticulosisbull bull Definition of the diseasebull ndash This rare disease is a lymphoma of extranodal
presentationall cases are positive for the Epstein-Barr virus
bull -This lymphoma most commonly appears in the midface region
Midline GranulomaEpidemiologyaetiologyndash This form of lymphoma is rare in Europe and theUnited States with a higher prevalence in Asia and PeruSymptomsndash The most common presentation is nasal obstruction with a destructive mass occupying the nosesinuses and palate
-Fever night sweatsand weight loss seen usually in Hodgkinrsquos lymphomaand other non-Hodgkinrsquos lymphomas (knownas ldquoB symptomsrdquo) are uncommon
Midline GranulomaDiagnosisndash The diagnosis is based on anatomopathologicalstudy The malignancy of the tumour manifested byextensive necrosis makes the histological diagnosisdifficult and often more biopsies are required forconfirmationbull Therapyndash Therapy consists of radiotherapy with or withoutchemotherapy
Midline Granuloma
bull Prognosisbull ndash Depending on the stage long-term remission or
experience a worseningbull prognosis with relapses which may include otherbull extranodal sites bull Involvement of extranodal sitesbull including the upper airway gastrointestinal tractbull skin
Wegenerrsquos Granulomatosis
bull Definition of the diseasebull ndash Wegenerrsquos granulomatosis is a systemic chronicbull vasculitis of small- and medium-sized blood vesselsbull with an autoimmune component It affectsbull particular organs with variable predilectionbull Epidemiologyaetiologybull ndash Wegenerrsquos granulomatosis is a rare disease It affects
about 1 in 20000ndash30000 people It is more prevalentbull in middle-aged Caucasian patients
Wegenerrsquos Granulomatosis
Symptomsndash The disease may present pulmonary upper
respiratory tract or renal In the disseminated form-The localised form ndash confinedto the upper respiratory region ndash is present in 25of the patients- It consists of nonspecific manifestationssuch as nasal obstruction crusting purulentor bloody rhinorrhea and painful or painless ulcers in oral or nasal cavities which are unresponsive tostandard medical treatment
Wegenerrsquos Granulomatosis
bull In some patients the nasal septum is perforatedbull which leads to saddle-nose deformity Less
commonbull symptoms are hoarseness stridor due to
subglotticbull stenosis otalgia otorrhea and conductivebull and sensorineural hearing loss Also ocular
symptomsbull such as scleritis conjunctivitis uveitis andbull episcleritis may be present
Wegenerrsquos Granulomatosis
bull ndash In the disseminated form pulmonary involvementbull is manifested by cough dyspnoea haemoptysisbull (due to an alveolar capillaritis necrotic lesions orbull endobronchial disease) and pleuritic painndashbull -Ninety per cent of patients have nasal symptomsbull and these symptoms are usually the first
manifestationof the diseasebull -Most patients have also renal involvementbull even if it is subclinical
Wegenerrsquos Granulomatosis
Diagnosis ndash Diagnosis of Wegenerrsquos granulomatosis is based on clinical findings that demonstrate lung (chest x-ray) kidney (urine analysis) or upper respiratory tract
involvement (oral or nasal ulcers or discharge) - positive blood analysis for cytoplasmic-staining antineutrophil
cytoplasmic antibodies (c-ANCA) and confirming proteinase 3 (PR3) ANCA or myeloperoxidase (MPO) ANCA ndash Biopsy is essential for diagnosis nonspecific chronic inflammation
and necrosis -Bacterial and fungal infections
Wegenerrsquos Granulomatosis
Therapyndash Conservative therapybull In the induction of disease remission highdosesteroids (e g prednisone 1 mgkgday) for1 month with tapering over several months aregiven In addition cyclophosphamide (2 mgkgday) should be administered for 6ndash12 monthsuntil symptoms disappear In the maintenanceof remission cyclophosphamide should be
Wegenerrsquos Granulomatosis
Antibiotics mainly trimethoprim-sulfamethoxazoleare given for prophylaxis againstPneumocystis jiroveci (formerly Pneumocystiscarinii) pneumonia (PCP) which may developduring immunosuppression and have a role inpreventing recurrencesbull Sinonasal manifestations may be treated with topical nasal steroids and nasal irrigations lowdosesystemic steroids and antibiotics when bacterial infection (typically Staphylococcus species) is suspected
Wegenerrsquos Granulomatosis
bull Prognosisbull ndash Most of the patients respond well to treatmentbull achieving symptom-free intervals of 5ndash20 yearsbull or more bull -Anatomical problems (sinusitis trachealbull stenosis) may require surgery bull Relapses can be long and troublesomebull Long-term complications are chronicbull renal failure hearing loss and deafness
Nasal Fractures Definition ndash A nasal fracture is a disruption of the nasal bone structure due to trauma It is the most frequently fractured facial bone Epidemiologyaetiology ndash Sports falls and assaults are the usual mechanisms of fracture -Males are affected twice as often as are females -Paediatric populations with a incidences during the second and third decades of life -Variables such as force impact direction nature of the striking object age and other will influence the pattern of injury to the components of the nose
Nasal Fractures
bull Symptomsbull ndash Deformity swelling epistaxis and periorbital
ecchymosis are signs that are suggestive of nasal fracture
bull bony crepitus and nasal segment mobilitybull ndash Epiphora bull Severe bilateral injuries to the lachrymal bones
arebull associated with depressed nasal fractures
Nasal Fractures Complications ndash Septal haematoma is one of the most severe early complications of nasal trauma and without drainage it results in abscess formation 6ndash7 days after trauma producing necrosis of the septal cartilage -Long-term problems such as saddle-nose deformity perforation columellar retraction and nasalbase
Septal infection could lead to osteomyelitis orbital and intracranial abscesses meningitis and cavernous sinus thrombosis -Cerebrospinal fluid leakage is a common complication of severe
nasal and frontal fractures
Nasal Fractures
bull Diagnostic proceduresbull ndash Inspectionbull bull Changes of appearance such as deviation andbull asymmetry bleeding watery drainage changesbull in nasal breathing and smell It is useful to comparebull the current presentation with old photographsbull (up to 40 of normal individuals havebull significant nose malformations)
Nasal Fractures Physical examination bull The diagnosis of a nasal fracture is made primarily by physical examination epistaxis nasal swelling and periorbital ecchymosis Nasal shape in the lateral and frontal inspection should be assessed Grasping the dorsum between two fingers and rocking the pyramid back and forth aids in assessing the mobility of nasal bones Internal structures should be evaluated by using a headlight and nasal speculum Clotted blood is removed by suction and assessment of haematoma mucosal tears and active bleeding is performed Bimanual palpation of the septum helps to differentiate septal swelling from haematoma ndash
Nasal FracturesRadiographybull There is no clear evidence of the role of radiographyin the management of nasal fracturesPlain films have up to a 66 false-positive rateas a result of misinterpretation of normal suturelines In addition old fractures are difficult todistinguishbull Three-dimensional CT is recommended for extensiveinjuries involving the nasal-orbital-ethmoidalcomplexndash
Nasal Fractures
bull Additionaluseful diagnostic proceduresbull bull Using a 0 or 30deg 4-mm endoscope is helpful inbull the assessment of posterior abnormalities If thebull patient is heavily sedated Brown-Gruss
provocationbull manoeuvres may be performed to determinebull deformities in upper middle or lower segmentsbull by compressing each compartment
Nasal FracturesConservative treatmentndash Treatment of bleedingbull For localised bleeding anterior sources may becauterised by silver nitrate or sealed with topicalmaterials such as thrombin combined withgelatin foam fibrin glue FloSealreg or other procoagulantmaterials If conservative measuresfail a formal anterior packing is placedbull Bleeding from branches of sphenopalatine orethmoid vessels requires anterior-posteriorpacking
Nasal Fractures
bull bull Surgical methods such as direct endoscopic vessel
bull cauterization or ligation have been shown tobull offer better haemostasis and patient comfortbull Angiography with embolization can also be
consideredbull in cases refractory to more conservativebull approaches
Nasal Fractures
bull Type of reductionbull bull Nondisplaced fractures should be treated withbull observation alone Closed nasal reduction is thebull best choice for simple injuries (isolated unilateralbull with medial displacement)bull bull An open approach should be considered in
severebull trauma (bilateral depressed fractures)
Nasal Fracturesbull Surgical principlesbull ndash Topical anaesthesia with cotton pledgets soakedbull with 4 cocaine or 005 oxymethazoline combinedbull with 4 topical lidocaine should be appliedbull for 5ndash10 min Local anaesthesia should also be injectedbull (1 lidocaine and 1100000 epinephrine)bull along the septum lateral walls and floor of the nasalbull cavitybull bull
Nasal FracturesClosed reductionndashndash The nasal bones are grasped between two fingersand pressure is applied laterally in theopposite direction of the deviation A bluntelevator may be used from within the nose incases of significant medial collapse Walshamforceps can be of help Reduction of the septumshould be performed with the use ofAsch forceps
Nasal Fractures
bull To prevent collapse of the postreductionbull framework nasal packing should be placedbull for 3ndash5 days Septum splints are recommendedbull in comminuted septal fractures withbull severe mucosal lesions External nasal splintingbull for 10 days (Aquaplastreg Thermoplastreg)bull provides nasal protection Nasal saline spraysbull prevent crusting and oral antibiotics should
Nasal Fractures
bull Open reductionbull ndashndash Immediate repair of fractures by using
widebull surgical exposure reduction fixation and
reconstructionbull ndashndash The second option is delayed correctionbull (6 months or more) of persistent deformitiesbull using standard techniques of rhinoplasty
Deviated Nasal Septum
bull Definition of the diseasebull ndash Deviation of the nasal septum is a common causebull of unilateral nasal airway obstruction in which thebull nasal septum is displacedbull bull Epidemiologyaetiologybull ndash Developmental septal abnormalities Septal cartilage
damage in the neonatal period andbull during birth can cause severe septal deviation inbull the absence of a history of nasal trauma
Deviated Nasal Septum
bull Symptomsbull ndash Patients may present with a history of sinusitis
allergicbull rhinitis obstructive sleep apnoea previousbull nasal surgery or recent nasal trauma Unilateral or
bilateral nasal airway obstruction that is unrelievedbull with decongestants or nasal steroid sprays is oftenbull seenbull bull
Deviated Nasal SeptumDiagnosisndashExamination external dorsal deviation or the columella and caudal septummay be deflected off the midline (caudal subluxation)ndash Inspections of the nasal cavity and anterior-posteriorrhinoscopy are helpful in diagnosing the locationtype and severity of septal deformityThe endoscope is also useful in identifying polypsthe severity and extent of posterior septaldeviations and bony spurs and locating areas ofseptal perforation or mucosal injury
Deviated Nasal Septum
bull Therapybull ndash Septoplasty is a procedurebull The areabull of deviation is corrected or resected in order tobull leave behind as much cartilage and bone as
possiblebull Cartilage resection is minimised and can be
repositioned reshaped or recontoured using a variety of methods
Deviated Nasal Septum
bull ndash Indications of septoplasty before the growth period
bull of the nose is finished should be very limited bull -In these cases surgery must preserve all the
cartilagebull in order to prevent external changes of the
shape ofbull the nose
Deviated Nasal Septum
bull Complicationsbull ndash Frequent complications include haematoma andbull infection Cerebrospinal fluid leak is a rare but
potentiallybull serious complicationbull It is usually the resultbull of avulsion or damage to the cribriform plate whenbull handling the perpendicular plate of the ethmoidbull ndash Other complications include epistaxis nasal
Deviated Nasal Septum
bull Other complications include epistaxis nasal obstruction
bull due to residual deviation synechiae returnbull of the cartilaginous deviation septal perforationbull anosmia and cosmetic nasal deformities suchbull as widened alar rim margins drooping nasal tipbull columella retraction and a sunken dorsum with abull supratip saddle formation
Septal perforation with minor crusting View from provide closure of the
incision
Septal Haematoma
bull A septal haematoma is a blood collection under the perichondrium
bull of the septum and cartilagebull bull bull Epidemiologyaetiologybull ndash A septal haematoma is one of the most
severe complications of nasal trauma
Septal Haematoma
bull Diagnosisbull ndash Signs and symptoms include intense pain
swellingbull haematoma of the upper lip and philtrum
area andbull complete nasal airway obstruction
Septal HaematomaTherapyndash Management consists of drainage through a mucoperichondrial incision Immediate treatment isnecessary to prevent long-term problems such asa saddle-nose deformity perforation columellarretraction and nasal-base widening In childrenseptal destruction can lead to devastating nasal andmidfacial growth abnormalitiesbull Surgeryndash Incision and evacuation of the collection is performedDrainage of a septal haematoma should
Septal HaematomaSurgeryndash Incision and evacuation of the collection is performedDrainage of a septal haematoma should provide closure of the incision
Splints or transseptal sutures are placed to obliterate thepotential space and prevent collectionInfection involving the septal cartilage Reconstruction with autologouscartilage is then performed in a second stage Oral antibiotics should be given
Nasal DeformitySaddle-nose deformityndash A saddle-nose deformity is characterised by a loss ofnasal dorsal height and compromised nasal supportstructures -Other case observed are depressionof the middle vault and dorsum loss of nasal tipsupport and definition shortened (vertical) nasal length over rotation of the nasal tip and retrusion ofthe nasal spine and caudal septum It is also knownas a ldquoPug noserdquo or ldquoboxerrsquos noserdquo both of which referto various degrees of nasal dorsal depressionbull
Nasal DeformityEpidemiologyaetiologyndash Prevalence is higher in population groups prone to facial trauma (ie boxers athletes) those with historiesof intranasal cocaine use nasal surgery (e g radical submucosal septal resection reductive rhinoplasty)ndash A saddle-nose deformity can be congenital or acquired It can be noticed as a part of individual familialsyndromic and ethnic characteristics - Most deformities are due to traumatic and iatrogeniccauses Medical causes are Wegenerrsquosgranulomatosis relapsing polychondritis leprosy (Hansenrsquos disease) syphilis ectodermal dysplasiaand intranasal cocaine use
Nasal Deformity
bull Therapybull ndash Nasal reconstruction indications depend on patientbull selection surgeon experience and aetiology of thebull deformity bull Indications for surgery can be functionalbull aesthetic or most commonly both In individuals
with a compromised nasal airway a nasoseptalbull reconstruction is indicated
Nasal Deformity
bull Contraindications bull include patients with malignantbull chronic or autoimmune disease conditions drugbull abuse poor perioperative risk profile and unrealisticbull expectationsbull ndash Multiple previous rhinoplasties and certain
professionsbull (mixed martial artists boxers and other contactbull sports) are relative contraindications
Nasal DeformitySeptoplastyndash Septoplasty is performed to correct nasal obstructioncaused by septal deformityndash Usually septoplasty is performed under general anaesthesiawith the patient in the supine position with the head elevated by approximately 30 (Righthandedsurgeons approach from the right side)ndash Local vasoconstrictive anaesthesia is applied notonly to reduce postoperative pain but also more importantly to achieve vasoconstriction of themucosa and less intraoperative haemorrhage Lidocainewith adrenaline or epinephrine is usedalthough in patients with cardiac hypersensitivityoxymetazoline might be preferred
Nasal Deformity
bull Septoplasty begins with the incision of septal mucosabull Most operative techniques utilise a hemitransfixionbull incision at the caudal end of septum so thatbull deviation at this point might be reached as wellbull as a transfixion incision that is easily obtained ifbull needed (Right-handed surgeons normally choosebull the left side but that may vary when deviation isbull convex towards the right)
Nasal DeformityA columella retractor is placed over the columellaand by pulling it laterally the caudal border of theseptum is exposed Ala can be protected by an alaprotector A vertical incision with a no 15 bladeover the caudal end of septum is performed untilreaching the plane of the septal cartilage It is essentialto correctly identify the perichondrium and byusing the Cottle elevator dissect and lift it creatinga flap As the dissection proceeds along the septalcartilage a longer speculum (no 5) is introduced sothat elevation of the mucoperichondrium is doneunder constant visual controlndash The next step is to dissect the mucoperiostium
Nasal DeformityDissecting over the bony-cartilaginous junctionwhen joining both tunnels might be difficult and is
especially prone to membrane perforationndash If needed the same tunnels are to be created on the
other side of the septum Then deviated parts of
septum are identified and removed either with a
knife or a Freer chisel
Nasal Deformitybull septum from the maxillary crest the septum mustbull be separated from the perpendicular plate trimmedbull along the inferior border placed back onto the crestbull and sutured to the periosteum If the deformity involvesbull the vomer an osteotome is used Care mustbull be taken not to break the cribriform plate becausebull it could cause a cerebrospinal fistula
Nasal Deformity
bull Once the septal deviation is corrected the flapsbull and hemitransfixion incision are mattressed
withbull absorbable sutures Nasal packing to prevent
synechiaebull and postoperative septal haematoma mightbull be advised but should be removed within 72 h

Nerve SupplyThe facial skin receives its sensory innervation fromterminal branches of the trigeminal nerve that enterthe facial region through the supraorbital infraorbitaland mental foramina Thefacial muscles are classified as mimetic or mastica- tory each of these groups receiving different motorinnervationbythe facial nerve
History and Clinical Examination of the Nose
Historybull The main symptomsbull nasal obstruction (ldquostuffy
noserdquo)bull nasal dischargebull Headachesbull Olfactory
dysfunction
Palpationbony discontinuitiesNeuralgias to check
over- the supraorbital -infraorbital -mental foramina
Anterior Rhinoscopy
bull The rhinologic examination itself begins with anterior
bull rhinoscopy to evaluate the nasal vestibule and the anterior
bull portions of the nasal cavity
Nasal Endoscopy Nasal endoscopy has become the most important andrewarding clinical examination method in rhinologic diagnosis
- rigid endoscopes which are available in 4-mm and 28- mm diameters and assorted viewing angles (eg 01048576 301048576 1201048576) -flexible endoscopes are also available for inspecting the nose and nasopharynx and exploring all of the pharynx and larynx in one sitting
Nasal endoscopy
Nasal Endoscopy
Nasal Endoscopy
Imaging of the Nose and Paranasal Sinuses
Conventional RadiographsStandard paranasal sinus radiographs in the occipitomental
projection ( Water projection) and
occipitofrontal projection Caldwell projection) in cases of acute inflammation
They are also obtained to evaluate midfacial fractures
Computed Tomography (CT) the main indicationsfor CT scanning of the
nose and paranasal sinuses
are- chronic sinusitis - -trauma (especially
frontobasal -fractures)
-and tumors
The occipitofrontal projection is better for evaluating theethmoid cells and frontal sinus
occipitomental projection demonstrates the maxillarysinus and gives a limited view of the sphenoid sinus
Computed tomography of the paranasal sinuses
Four representative coronal CT scans are shown
Four representative coronal CT scans are shown
Magnetic Resonance Imaging
Magnetic maging
Magnetic resonance imaging (MRI) has fewer indicationsthan CT in patients with paranasal sinus diseaseThis is primarily because MRI is markedly inferior toCT in defining the bony boundaries of the sinusesThe strength of MRI lies in its superior soft-tissue discriminationMRI is indicated in diseases that involve the paranasal sinuses in addition to thecranial cavity or orbit (eg tumors and congenitalmalformations such as encephaloceles)
MRI of the paranasal sinuses
The Nose and Sinuses
Structure The structure of the nose is made up of
four partsbull The surface anatomybull The nasal skeletonmdashcomposed of the
two nasal bones the paired upper lateral and lower lateral cartilages and the nasal septum covered in subcutaneous tissue and skin
bull The internal anatomymdashincludes the septum of the nose which forms the medial wall of the nasal cavity The turbinates on the lateral wall are also called conchae
bull The osteomeatal complexmdasha key functional area of the nose
Function The nose is the main route for inspired
air and its structure is related to this function As the air passes over the large surface area of the turbinates
The inspired gases are warmed and humidified Mucus on the mucosa of the nose removes large dust particles from the air as it is breathed in
The voice resonates in the sinuses and nose and this provides character to the speech
Pneumatization of the sinusesmdashthey are air filled spacesmdashreduces the weight of the skull
Diseases of thDiseases of the Outer and Inner Nosee Outer and
Inner Nose Erysipelas Definition of the disease ndash Erysipela is a skin infection that affects the superficial dermis and is caused by Streptococcus pyogenes (group A) It usually develops in the extremities and the face and less commonly on the scalp and genitals bull Epidemiologyaetiology ndash Erysipelas are more often seen in elderly infants and children patients with compromised immunology and diabetes -Predisposing factors are alcoholism skin ulceration puncture wounds fungal infections malnutrition and burns
Erysipelas
bull Symptomsbull ndash It usually presents of fever general fatigue bull -The skin lesion is a redindurated and elevated plaque
with borders that expand rapidly bull It is painful warm and accompanied by variable oedemabull -On the second or third day a flaccid bulla may develop
and desquamationbull bull Presence of regional lymph nodes is common
Erysipelas
bull Complicationsndash The most common complication is recurrencewhich is seen in 18ndash30 of the cases even afterproper antibiotic therapy Recurrence is seen moreoften in females than in malesA skin infection with S pyogenes could lead toglomerulonephritis
Erysipelas
bull Complicationsbull ndash The most common complication is recurrencebull which is seen in 18ndash30 of the cases even afterbull proper antibiotic therapy bull -Recurrence is seen morebull often in females than in males bull -A skin infection with S pyogenes could lead tobull glomerulonephritis
Erysipelas
bull bull Diagnosisbull ndash Diagnosis is based on the patientrsquos personal
historybull and physical examination particularly on inspectionbull of the skin
bull Blood cultures are positive in less thanbull 5 of cases
ErysipelasTherapyndash Conservative therapybull The preferred antibiotic is penicillin In mildcases with minor systemic symptoms penicillinV 500 mg orally every 6 h for 10 days or penicillinG benzathine 12 mil U intramuscularlyonceOther possibilities are amoxicillin 500 mgorally twice a day for 10 days or cephalexin 500mg orally every 6 h for 10 days
ErysipelasIn moderate and severe cases with significantsystemic symptoms hospitalization and intravenoustreatment is required penicillin G 2ndash4mil U intravenously every 4ndash6 h Cefazolin05ndash15 gm intravenously every 8 h cefotaxime1ndash2 gm intravenously every 8 h or ceftriaxone1ndash2 gm intravenously once a day should be administeredIn patients with a penicillin allergyclindamycin 600 mg intravenously every 8 h orvancomycin 15 mgkg intravenously twice a daymay be given
ErysipelaAdditional useful therapeutic optionsbull Prednisone 30 mg over 8 days might be consideredas well as elevation of the affected siteMoist heat compresses may be usefulbull Surgeryndash Debridement and drainage are indicated when bullaeabscesses or necroses are presentbull Differential diagnosisndash Contact dermatitisndash Asteatotic eczemandash Herpes zosterndash Angioneurotic oedemandash Osteomyelitis
Furuncle
bull Definition of the diseasebull ndash A furuncle is an infection that beginsbull at the hair follicle and spreads deeper into thebull dermis and subcutaneous tissue forming abull nodule After several days it developsbull into an abscess - red painful and fluctuantbull bull bull Epidemiologyaetiologybull ndash The aetiologic agent is Staphylococcus aureus
FuruncleSymptomsndashsymptoms are local and limited to thesite of infection Furuncles usually are wherehair follicles are present bull Complicationndash One complication is furunculosis multiple draining furunclesDiagnosisndash The diagnosis is based on clinical inspection - Cultures are not necessary when there is no systemic involvement but should beconsidered if systemic therapy (in case of feversignificant cellulitis or hospitalization) or whenmethicillin-resistant Staphylococcusaureus (MRSA) is considered
FuruncleTherapyndash When the furuncle is small application of moist heat compress to promote drainage -Larger furuncles should be drained by surgical incision-After drainage the area should be cleaned with anantiseptic (with chlorhexidinebetadine) should be applied twice
a dayndash If no systemic symptoms or extensive cellulitis arepresent simple topical care is usually curative andoral antibiotics are not necessary Otherwise systemictreatment is indicated and should cover anypossible MRSA
Furuncle
bull -Recommended antibiotics are trimethoprim-sulfamethoxazole
bull 1ndash2 tablets orally twice daily doxycyclinebull 100 mg orally twice dailybull or clindamycin 300ndash450 mg orally every 8 hbull - In severe cases vancomycin 15 mgkg
intravenouslybull every 12 h or clindamycin 600 mg intravenouslybull every 8 h
Midline Granulomabull A midline granuloma is an angiocentricbull lymphoma it was referred to as polymorphicbull reticulosis lethal midline granuloma and midline
malignant reticulosisbull bull Definition of the diseasebull ndash This rare disease is a lymphoma of extranodal
presentationall cases are positive for the Epstein-Barr virus
bull -This lymphoma most commonly appears in the midface region
Midline GranulomaEpidemiologyaetiologyndash This form of lymphoma is rare in Europe and theUnited States with a higher prevalence in Asia and PeruSymptomsndash The most common presentation is nasal obstruction with a destructive mass occupying the nosesinuses and palate
-Fever night sweatsand weight loss seen usually in Hodgkinrsquos lymphomaand other non-Hodgkinrsquos lymphomas (knownas ldquoB symptomsrdquo) are uncommon
Midline GranulomaDiagnosisndash The diagnosis is based on anatomopathologicalstudy The malignancy of the tumour manifested byextensive necrosis makes the histological diagnosisdifficult and often more biopsies are required forconfirmationbull Therapyndash Therapy consists of radiotherapy with or withoutchemotherapy
Midline Granuloma
bull Prognosisbull ndash Depending on the stage long-term remission or
experience a worseningbull prognosis with relapses which may include otherbull extranodal sites bull Involvement of extranodal sitesbull including the upper airway gastrointestinal tractbull skin
Wegenerrsquos Granulomatosis
bull Definition of the diseasebull ndash Wegenerrsquos granulomatosis is a systemic chronicbull vasculitis of small- and medium-sized blood vesselsbull with an autoimmune component It affectsbull particular organs with variable predilectionbull Epidemiologyaetiologybull ndash Wegenerrsquos granulomatosis is a rare disease It affects
about 1 in 20000ndash30000 people It is more prevalentbull in middle-aged Caucasian patients
Wegenerrsquos Granulomatosis
Symptomsndash The disease may present pulmonary upper
respiratory tract or renal In the disseminated form-The localised form ndash confinedto the upper respiratory region ndash is present in 25of the patients- It consists of nonspecific manifestationssuch as nasal obstruction crusting purulentor bloody rhinorrhea and painful or painless ulcers in oral or nasal cavities which are unresponsive tostandard medical treatment
Wegenerrsquos Granulomatosis
bull In some patients the nasal septum is perforatedbull which leads to saddle-nose deformity Less
commonbull symptoms are hoarseness stridor due to
subglotticbull stenosis otalgia otorrhea and conductivebull and sensorineural hearing loss Also ocular
symptomsbull such as scleritis conjunctivitis uveitis andbull episcleritis may be present
Wegenerrsquos Granulomatosis
bull ndash In the disseminated form pulmonary involvementbull is manifested by cough dyspnoea haemoptysisbull (due to an alveolar capillaritis necrotic lesions orbull endobronchial disease) and pleuritic painndashbull -Ninety per cent of patients have nasal symptomsbull and these symptoms are usually the first
manifestationof the diseasebull -Most patients have also renal involvementbull even if it is subclinical
Wegenerrsquos Granulomatosis
Diagnosis ndash Diagnosis of Wegenerrsquos granulomatosis is based on clinical findings that demonstrate lung (chest x-ray) kidney (urine analysis) or upper respiratory tract
involvement (oral or nasal ulcers or discharge) - positive blood analysis for cytoplasmic-staining antineutrophil
cytoplasmic antibodies (c-ANCA) and confirming proteinase 3 (PR3) ANCA or myeloperoxidase (MPO) ANCA ndash Biopsy is essential for diagnosis nonspecific chronic inflammation
and necrosis -Bacterial and fungal infections
Wegenerrsquos Granulomatosis
Therapyndash Conservative therapybull In the induction of disease remission highdosesteroids (e g prednisone 1 mgkgday) for1 month with tapering over several months aregiven In addition cyclophosphamide (2 mgkgday) should be administered for 6ndash12 monthsuntil symptoms disappear In the maintenanceof remission cyclophosphamide should be
Wegenerrsquos Granulomatosis
Antibiotics mainly trimethoprim-sulfamethoxazoleare given for prophylaxis againstPneumocystis jiroveci (formerly Pneumocystiscarinii) pneumonia (PCP) which may developduring immunosuppression and have a role inpreventing recurrencesbull Sinonasal manifestations may be treated with topical nasal steroids and nasal irrigations lowdosesystemic steroids and antibiotics when bacterial infection (typically Staphylococcus species) is suspected
Wegenerrsquos Granulomatosis
bull Prognosisbull ndash Most of the patients respond well to treatmentbull achieving symptom-free intervals of 5ndash20 yearsbull or more bull -Anatomical problems (sinusitis trachealbull stenosis) may require surgery bull Relapses can be long and troublesomebull Long-term complications are chronicbull renal failure hearing loss and deafness
Nasal Fractures Definition ndash A nasal fracture is a disruption of the nasal bone structure due to trauma It is the most frequently fractured facial bone Epidemiologyaetiology ndash Sports falls and assaults are the usual mechanisms of fracture -Males are affected twice as often as are females -Paediatric populations with a incidences during the second and third decades of life -Variables such as force impact direction nature of the striking object age and other will influence the pattern of injury to the components of the nose
Nasal Fractures
bull Symptomsbull ndash Deformity swelling epistaxis and periorbital
ecchymosis are signs that are suggestive of nasal fracture
bull bony crepitus and nasal segment mobilitybull ndash Epiphora bull Severe bilateral injuries to the lachrymal bones
arebull associated with depressed nasal fractures
Nasal Fractures Complications ndash Septal haematoma is one of the most severe early complications of nasal trauma and without drainage it results in abscess formation 6ndash7 days after trauma producing necrosis of the septal cartilage -Long-term problems such as saddle-nose deformity perforation columellar retraction and nasalbase
Septal infection could lead to osteomyelitis orbital and intracranial abscesses meningitis and cavernous sinus thrombosis -Cerebrospinal fluid leakage is a common complication of severe
nasal and frontal fractures
Nasal Fractures
bull Diagnostic proceduresbull ndash Inspectionbull bull Changes of appearance such as deviation andbull asymmetry bleeding watery drainage changesbull in nasal breathing and smell It is useful to comparebull the current presentation with old photographsbull (up to 40 of normal individuals havebull significant nose malformations)
Nasal Fractures Physical examination bull The diagnosis of a nasal fracture is made primarily by physical examination epistaxis nasal swelling and periorbital ecchymosis Nasal shape in the lateral and frontal inspection should be assessed Grasping the dorsum between two fingers and rocking the pyramid back and forth aids in assessing the mobility of nasal bones Internal structures should be evaluated by using a headlight and nasal speculum Clotted blood is removed by suction and assessment of haematoma mucosal tears and active bleeding is performed Bimanual palpation of the septum helps to differentiate septal swelling from haematoma ndash
Nasal FracturesRadiographybull There is no clear evidence of the role of radiographyin the management of nasal fracturesPlain films have up to a 66 false-positive rateas a result of misinterpretation of normal suturelines In addition old fractures are difficult todistinguishbull Three-dimensional CT is recommended for extensiveinjuries involving the nasal-orbital-ethmoidalcomplexndash
Nasal Fractures
bull Additionaluseful diagnostic proceduresbull bull Using a 0 or 30deg 4-mm endoscope is helpful inbull the assessment of posterior abnormalities If thebull patient is heavily sedated Brown-Gruss
provocationbull manoeuvres may be performed to determinebull deformities in upper middle or lower segmentsbull by compressing each compartment
Nasal FracturesConservative treatmentndash Treatment of bleedingbull For localised bleeding anterior sources may becauterised by silver nitrate or sealed with topicalmaterials such as thrombin combined withgelatin foam fibrin glue FloSealreg or other procoagulantmaterials If conservative measuresfail a formal anterior packing is placedbull Bleeding from branches of sphenopalatine orethmoid vessels requires anterior-posteriorpacking
Nasal Fractures
bull bull Surgical methods such as direct endoscopic vessel
bull cauterization or ligation have been shown tobull offer better haemostasis and patient comfortbull Angiography with embolization can also be
consideredbull in cases refractory to more conservativebull approaches
Nasal Fractures
bull Type of reductionbull bull Nondisplaced fractures should be treated withbull observation alone Closed nasal reduction is thebull best choice for simple injuries (isolated unilateralbull with medial displacement)bull bull An open approach should be considered in
severebull trauma (bilateral depressed fractures)
Nasal Fracturesbull Surgical principlesbull ndash Topical anaesthesia with cotton pledgets soakedbull with 4 cocaine or 005 oxymethazoline combinedbull with 4 topical lidocaine should be appliedbull for 5ndash10 min Local anaesthesia should also be injectedbull (1 lidocaine and 1100000 epinephrine)bull along the septum lateral walls and floor of the nasalbull cavitybull bull
Nasal FracturesClosed reductionndashndash The nasal bones are grasped between two fingersand pressure is applied laterally in theopposite direction of the deviation A bluntelevator may be used from within the nose incases of significant medial collapse Walshamforceps can be of help Reduction of the septumshould be performed with the use ofAsch forceps
Nasal Fractures
bull To prevent collapse of the postreductionbull framework nasal packing should be placedbull for 3ndash5 days Septum splints are recommendedbull in comminuted septal fractures withbull severe mucosal lesions External nasal splintingbull for 10 days (Aquaplastreg Thermoplastreg)bull provides nasal protection Nasal saline spraysbull prevent crusting and oral antibiotics should
Nasal Fractures
bull Open reductionbull ndashndash Immediate repair of fractures by using
widebull surgical exposure reduction fixation and
reconstructionbull ndashndash The second option is delayed correctionbull (6 months or more) of persistent deformitiesbull using standard techniques of rhinoplasty
Deviated Nasal Septum
bull Definition of the diseasebull ndash Deviation of the nasal septum is a common causebull of unilateral nasal airway obstruction in which thebull nasal septum is displacedbull bull Epidemiologyaetiologybull ndash Developmental septal abnormalities Septal cartilage
damage in the neonatal period andbull during birth can cause severe septal deviation inbull the absence of a history of nasal trauma
Deviated Nasal Septum
bull Symptomsbull ndash Patients may present with a history of sinusitis
allergicbull rhinitis obstructive sleep apnoea previousbull nasal surgery or recent nasal trauma Unilateral or
bilateral nasal airway obstruction that is unrelievedbull with decongestants or nasal steroid sprays is oftenbull seenbull bull
Deviated Nasal SeptumDiagnosisndashExamination external dorsal deviation or the columella and caudal septummay be deflected off the midline (caudal subluxation)ndash Inspections of the nasal cavity and anterior-posteriorrhinoscopy are helpful in diagnosing the locationtype and severity of septal deformityThe endoscope is also useful in identifying polypsthe severity and extent of posterior septaldeviations and bony spurs and locating areas ofseptal perforation or mucosal injury
Deviated Nasal Septum
bull Therapybull ndash Septoplasty is a procedurebull The areabull of deviation is corrected or resected in order tobull leave behind as much cartilage and bone as
possiblebull Cartilage resection is minimised and can be
repositioned reshaped or recontoured using a variety of methods
Deviated Nasal Septum
bull ndash Indications of septoplasty before the growth period
bull of the nose is finished should be very limited bull -In these cases surgery must preserve all the
cartilagebull in order to prevent external changes of the
shape ofbull the nose
Deviated Nasal Septum
bull Complicationsbull ndash Frequent complications include haematoma andbull infection Cerebrospinal fluid leak is a rare but
potentiallybull serious complicationbull It is usually the resultbull of avulsion or damage to the cribriform plate whenbull handling the perpendicular plate of the ethmoidbull ndash Other complications include epistaxis nasal
Deviated Nasal Septum
bull Other complications include epistaxis nasal obstruction
bull due to residual deviation synechiae returnbull of the cartilaginous deviation septal perforationbull anosmia and cosmetic nasal deformities suchbull as widened alar rim margins drooping nasal tipbull columella retraction and a sunken dorsum with abull supratip saddle formation
Septal perforation with minor crusting View from provide closure of the
incision
Septal Haematoma
bull A septal haematoma is a blood collection under the perichondrium
bull of the septum and cartilagebull bull bull Epidemiologyaetiologybull ndash A septal haematoma is one of the most
severe complications of nasal trauma
Septal Haematoma
bull Diagnosisbull ndash Signs and symptoms include intense pain
swellingbull haematoma of the upper lip and philtrum
area andbull complete nasal airway obstruction
Septal HaematomaTherapyndash Management consists of drainage through a mucoperichondrial incision Immediate treatment isnecessary to prevent long-term problems such asa saddle-nose deformity perforation columellarretraction and nasal-base widening In childrenseptal destruction can lead to devastating nasal andmidfacial growth abnormalitiesbull Surgeryndash Incision and evacuation of the collection is performedDrainage of a septal haematoma should
Septal HaematomaSurgeryndash Incision and evacuation of the collection is performedDrainage of a septal haematoma should provide closure of the incision
Splints or transseptal sutures are placed to obliterate thepotential space and prevent collectionInfection involving the septal cartilage Reconstruction with autologouscartilage is then performed in a second stage Oral antibiotics should be given
Nasal DeformitySaddle-nose deformityndash A saddle-nose deformity is characterised by a loss ofnasal dorsal height and compromised nasal supportstructures -Other case observed are depressionof the middle vault and dorsum loss of nasal tipsupport and definition shortened (vertical) nasal length over rotation of the nasal tip and retrusion ofthe nasal spine and caudal septum It is also knownas a ldquoPug noserdquo or ldquoboxerrsquos noserdquo both of which referto various degrees of nasal dorsal depressionbull
Nasal DeformityEpidemiologyaetiologyndash Prevalence is higher in population groups prone to facial trauma (ie boxers athletes) those with historiesof intranasal cocaine use nasal surgery (e g radical submucosal septal resection reductive rhinoplasty)ndash A saddle-nose deformity can be congenital or acquired It can be noticed as a part of individual familialsyndromic and ethnic characteristics - Most deformities are due to traumatic and iatrogeniccauses Medical causes are Wegenerrsquosgranulomatosis relapsing polychondritis leprosy (Hansenrsquos disease) syphilis ectodermal dysplasiaand intranasal cocaine use
Nasal Deformity
bull Therapybull ndash Nasal reconstruction indications depend on patientbull selection surgeon experience and aetiology of thebull deformity bull Indications for surgery can be functionalbull aesthetic or most commonly both In individuals
with a compromised nasal airway a nasoseptalbull reconstruction is indicated
Nasal Deformity
bull Contraindications bull include patients with malignantbull chronic or autoimmune disease conditions drugbull abuse poor perioperative risk profile and unrealisticbull expectationsbull ndash Multiple previous rhinoplasties and certain
professionsbull (mixed martial artists boxers and other contactbull sports) are relative contraindications
Nasal DeformitySeptoplastyndash Septoplasty is performed to correct nasal obstructioncaused by septal deformityndash Usually septoplasty is performed under general anaesthesiawith the patient in the supine position with the head elevated by approximately 30 (Righthandedsurgeons approach from the right side)ndash Local vasoconstrictive anaesthesia is applied notonly to reduce postoperative pain but also more importantly to achieve vasoconstriction of themucosa and less intraoperative haemorrhage Lidocainewith adrenaline or epinephrine is usedalthough in patients with cardiac hypersensitivityoxymetazoline might be preferred
Nasal Deformity
bull Septoplasty begins with the incision of septal mucosabull Most operative techniques utilise a hemitransfixionbull incision at the caudal end of septum so thatbull deviation at this point might be reached as wellbull as a transfixion incision that is easily obtained ifbull needed (Right-handed surgeons normally choosebull the left side but that may vary when deviation isbull convex towards the right)
Nasal DeformityA columella retractor is placed over the columellaand by pulling it laterally the caudal border of theseptum is exposed Ala can be protected by an alaprotector A vertical incision with a no 15 bladeover the caudal end of septum is performed untilreaching the plane of the septal cartilage It is essentialto correctly identify the perichondrium and byusing the Cottle elevator dissect and lift it creatinga flap As the dissection proceeds along the septalcartilage a longer speculum (no 5) is introduced sothat elevation of the mucoperichondrium is doneunder constant visual controlndash The next step is to dissect the mucoperiostium
Nasal DeformityDissecting over the bony-cartilaginous junctionwhen joining both tunnels might be difficult and is
especially prone to membrane perforationndash If needed the same tunnels are to be created on the
other side of the septum Then deviated parts of
septum are identified and removed either with a
knife or a Freer chisel
Nasal Deformitybull septum from the maxillary crest the septum mustbull be separated from the perpendicular plate trimmedbull along the inferior border placed back onto the crestbull and sutured to the periosteum If the deformity involvesbull the vomer an osteotome is used Care mustbull be taken not to break the cribriform plate becausebull it could cause a cerebrospinal fistula
Nasal Deformity
bull Once the septal deviation is corrected the flapsbull and hemitransfixion incision are mattressed
withbull absorbable sutures Nasal packing to prevent
synechiaebull and postoperative septal haematoma mightbull be advised but should be removed within 72 h

History and Clinical Examination of the Nose
Historybull The main symptomsbull nasal obstruction (ldquostuffy
noserdquo)bull nasal dischargebull Headachesbull Olfactory
dysfunction
Palpationbony discontinuitiesNeuralgias to check
over- the supraorbital -infraorbital -mental foramina
Anterior Rhinoscopy
bull The rhinologic examination itself begins with anterior
bull rhinoscopy to evaluate the nasal vestibule and the anterior
bull portions of the nasal cavity
Nasal Endoscopy Nasal endoscopy has become the most important andrewarding clinical examination method in rhinologic diagnosis
- rigid endoscopes which are available in 4-mm and 28- mm diameters and assorted viewing angles (eg 01048576 301048576 1201048576) -flexible endoscopes are also available for inspecting the nose and nasopharynx and exploring all of the pharynx and larynx in one sitting
Nasal endoscopy
Nasal Endoscopy
Nasal Endoscopy
Imaging of the Nose and Paranasal Sinuses
Conventional RadiographsStandard paranasal sinus radiographs in the occipitomental
projection ( Water projection) and
occipitofrontal projection Caldwell projection) in cases of acute inflammation
They are also obtained to evaluate midfacial fractures
Computed Tomography (CT) the main indicationsfor CT scanning of the
nose and paranasal sinuses
are- chronic sinusitis - -trauma (especially
frontobasal -fractures)
-and tumors
The occipitofrontal projection is better for evaluating theethmoid cells and frontal sinus
occipitomental projection demonstrates the maxillarysinus and gives a limited view of the sphenoid sinus
Computed tomography of the paranasal sinuses
Four representative coronal CT scans are shown
Four representative coronal CT scans are shown
Magnetic Resonance Imaging
Magnetic maging
Magnetic resonance imaging (MRI) has fewer indicationsthan CT in patients with paranasal sinus diseaseThis is primarily because MRI is markedly inferior toCT in defining the bony boundaries of the sinusesThe strength of MRI lies in its superior soft-tissue discriminationMRI is indicated in diseases that involve the paranasal sinuses in addition to thecranial cavity or orbit (eg tumors and congenitalmalformations such as encephaloceles)
MRI of the paranasal sinuses
The Nose and Sinuses
Structure The structure of the nose is made up of
four partsbull The surface anatomybull The nasal skeletonmdashcomposed of the
two nasal bones the paired upper lateral and lower lateral cartilages and the nasal septum covered in subcutaneous tissue and skin
bull The internal anatomymdashincludes the septum of the nose which forms the medial wall of the nasal cavity The turbinates on the lateral wall are also called conchae
bull The osteomeatal complexmdasha key functional area of the nose
Function The nose is the main route for inspired
air and its structure is related to this function As the air passes over the large surface area of the turbinates
The inspired gases are warmed and humidified Mucus on the mucosa of the nose removes large dust particles from the air as it is breathed in
The voice resonates in the sinuses and nose and this provides character to the speech
Pneumatization of the sinusesmdashthey are air filled spacesmdashreduces the weight of the skull
Diseases of thDiseases of the Outer and Inner Nosee Outer and
Inner Nose Erysipelas Definition of the disease ndash Erysipela is a skin infection that affects the superficial dermis and is caused by Streptococcus pyogenes (group A) It usually develops in the extremities and the face and less commonly on the scalp and genitals bull Epidemiologyaetiology ndash Erysipelas are more often seen in elderly infants and children patients with compromised immunology and diabetes -Predisposing factors are alcoholism skin ulceration puncture wounds fungal infections malnutrition and burns
Erysipelas
bull Symptomsbull ndash It usually presents of fever general fatigue bull -The skin lesion is a redindurated and elevated plaque
with borders that expand rapidly bull It is painful warm and accompanied by variable oedemabull -On the second or third day a flaccid bulla may develop
and desquamationbull bull Presence of regional lymph nodes is common
Erysipelas
bull Complicationsndash The most common complication is recurrencewhich is seen in 18ndash30 of the cases even afterproper antibiotic therapy Recurrence is seen moreoften in females than in malesA skin infection with S pyogenes could lead toglomerulonephritis
Erysipelas
bull Complicationsbull ndash The most common complication is recurrencebull which is seen in 18ndash30 of the cases even afterbull proper antibiotic therapy bull -Recurrence is seen morebull often in females than in males bull -A skin infection with S pyogenes could lead tobull glomerulonephritis
Erysipelas
bull bull Diagnosisbull ndash Diagnosis is based on the patientrsquos personal
historybull and physical examination particularly on inspectionbull of the skin
bull Blood cultures are positive in less thanbull 5 of cases
ErysipelasTherapyndash Conservative therapybull The preferred antibiotic is penicillin In mildcases with minor systemic symptoms penicillinV 500 mg orally every 6 h for 10 days or penicillinG benzathine 12 mil U intramuscularlyonceOther possibilities are amoxicillin 500 mgorally twice a day for 10 days or cephalexin 500mg orally every 6 h for 10 days
ErysipelasIn moderate and severe cases with significantsystemic symptoms hospitalization and intravenoustreatment is required penicillin G 2ndash4mil U intravenously every 4ndash6 h Cefazolin05ndash15 gm intravenously every 8 h cefotaxime1ndash2 gm intravenously every 8 h or ceftriaxone1ndash2 gm intravenously once a day should be administeredIn patients with a penicillin allergyclindamycin 600 mg intravenously every 8 h orvancomycin 15 mgkg intravenously twice a daymay be given
ErysipelaAdditional useful therapeutic optionsbull Prednisone 30 mg over 8 days might be consideredas well as elevation of the affected siteMoist heat compresses may be usefulbull Surgeryndash Debridement and drainage are indicated when bullaeabscesses or necroses are presentbull Differential diagnosisndash Contact dermatitisndash Asteatotic eczemandash Herpes zosterndash Angioneurotic oedemandash Osteomyelitis
Furuncle
bull Definition of the diseasebull ndash A furuncle is an infection that beginsbull at the hair follicle and spreads deeper into thebull dermis and subcutaneous tissue forming abull nodule After several days it developsbull into an abscess - red painful and fluctuantbull bull bull Epidemiologyaetiologybull ndash The aetiologic agent is Staphylococcus aureus
FuruncleSymptomsndashsymptoms are local and limited to thesite of infection Furuncles usually are wherehair follicles are present bull Complicationndash One complication is furunculosis multiple draining furunclesDiagnosisndash The diagnosis is based on clinical inspection - Cultures are not necessary when there is no systemic involvement but should beconsidered if systemic therapy (in case of feversignificant cellulitis or hospitalization) or whenmethicillin-resistant Staphylococcusaureus (MRSA) is considered
FuruncleTherapyndash When the furuncle is small application of moist heat compress to promote drainage -Larger furuncles should be drained by surgical incision-After drainage the area should be cleaned with anantiseptic (with chlorhexidinebetadine) should be applied twice
a dayndash If no systemic symptoms or extensive cellulitis arepresent simple topical care is usually curative andoral antibiotics are not necessary Otherwise systemictreatment is indicated and should cover anypossible MRSA
Furuncle
bull -Recommended antibiotics are trimethoprim-sulfamethoxazole
bull 1ndash2 tablets orally twice daily doxycyclinebull 100 mg orally twice dailybull or clindamycin 300ndash450 mg orally every 8 hbull - In severe cases vancomycin 15 mgkg
intravenouslybull every 12 h or clindamycin 600 mg intravenouslybull every 8 h
Midline Granulomabull A midline granuloma is an angiocentricbull lymphoma it was referred to as polymorphicbull reticulosis lethal midline granuloma and midline
malignant reticulosisbull bull Definition of the diseasebull ndash This rare disease is a lymphoma of extranodal
presentationall cases are positive for the Epstein-Barr virus
bull -This lymphoma most commonly appears in the midface region
Midline GranulomaEpidemiologyaetiologyndash This form of lymphoma is rare in Europe and theUnited States with a higher prevalence in Asia and PeruSymptomsndash The most common presentation is nasal obstruction with a destructive mass occupying the nosesinuses and palate
-Fever night sweatsand weight loss seen usually in Hodgkinrsquos lymphomaand other non-Hodgkinrsquos lymphomas (knownas ldquoB symptomsrdquo) are uncommon
Midline GranulomaDiagnosisndash The diagnosis is based on anatomopathologicalstudy The malignancy of the tumour manifested byextensive necrosis makes the histological diagnosisdifficult and often more biopsies are required forconfirmationbull Therapyndash Therapy consists of radiotherapy with or withoutchemotherapy
Midline Granuloma
bull Prognosisbull ndash Depending on the stage long-term remission or
experience a worseningbull prognosis with relapses which may include otherbull extranodal sites bull Involvement of extranodal sitesbull including the upper airway gastrointestinal tractbull skin
Wegenerrsquos Granulomatosis
bull Definition of the diseasebull ndash Wegenerrsquos granulomatosis is a systemic chronicbull vasculitis of small- and medium-sized blood vesselsbull with an autoimmune component It affectsbull particular organs with variable predilectionbull Epidemiologyaetiologybull ndash Wegenerrsquos granulomatosis is a rare disease It affects
about 1 in 20000ndash30000 people It is more prevalentbull in middle-aged Caucasian patients
Wegenerrsquos Granulomatosis
Symptomsndash The disease may present pulmonary upper
respiratory tract or renal In the disseminated form-The localised form ndash confinedto the upper respiratory region ndash is present in 25of the patients- It consists of nonspecific manifestationssuch as nasal obstruction crusting purulentor bloody rhinorrhea and painful or painless ulcers in oral or nasal cavities which are unresponsive tostandard medical treatment
Wegenerrsquos Granulomatosis
bull In some patients the nasal septum is perforatedbull which leads to saddle-nose deformity Less
commonbull symptoms are hoarseness stridor due to
subglotticbull stenosis otalgia otorrhea and conductivebull and sensorineural hearing loss Also ocular
symptomsbull such as scleritis conjunctivitis uveitis andbull episcleritis may be present
Wegenerrsquos Granulomatosis
bull ndash In the disseminated form pulmonary involvementbull is manifested by cough dyspnoea haemoptysisbull (due to an alveolar capillaritis necrotic lesions orbull endobronchial disease) and pleuritic painndashbull -Ninety per cent of patients have nasal symptomsbull and these symptoms are usually the first
manifestationof the diseasebull -Most patients have also renal involvementbull even if it is subclinical
Wegenerrsquos Granulomatosis
Diagnosis ndash Diagnosis of Wegenerrsquos granulomatosis is based on clinical findings that demonstrate lung (chest x-ray) kidney (urine analysis) or upper respiratory tract
involvement (oral or nasal ulcers or discharge) - positive blood analysis for cytoplasmic-staining antineutrophil
cytoplasmic antibodies (c-ANCA) and confirming proteinase 3 (PR3) ANCA or myeloperoxidase (MPO) ANCA ndash Biopsy is essential for diagnosis nonspecific chronic inflammation
and necrosis -Bacterial and fungal infections
Wegenerrsquos Granulomatosis
Therapyndash Conservative therapybull In the induction of disease remission highdosesteroids (e g prednisone 1 mgkgday) for1 month with tapering over several months aregiven In addition cyclophosphamide (2 mgkgday) should be administered for 6ndash12 monthsuntil symptoms disappear In the maintenanceof remission cyclophosphamide should be
Wegenerrsquos Granulomatosis
Antibiotics mainly trimethoprim-sulfamethoxazoleare given for prophylaxis againstPneumocystis jiroveci (formerly Pneumocystiscarinii) pneumonia (PCP) which may developduring immunosuppression and have a role inpreventing recurrencesbull Sinonasal manifestations may be treated with topical nasal steroids and nasal irrigations lowdosesystemic steroids and antibiotics when bacterial infection (typically Staphylococcus species) is suspected
Wegenerrsquos Granulomatosis
bull Prognosisbull ndash Most of the patients respond well to treatmentbull achieving symptom-free intervals of 5ndash20 yearsbull or more bull -Anatomical problems (sinusitis trachealbull stenosis) may require surgery bull Relapses can be long and troublesomebull Long-term complications are chronicbull renal failure hearing loss and deafness
Nasal Fractures Definition ndash A nasal fracture is a disruption of the nasal bone structure due to trauma It is the most frequently fractured facial bone Epidemiologyaetiology ndash Sports falls and assaults are the usual mechanisms of fracture -Males are affected twice as often as are females -Paediatric populations with a incidences during the second and third decades of life -Variables such as force impact direction nature of the striking object age and other will influence the pattern of injury to the components of the nose
Nasal Fractures
bull Symptomsbull ndash Deformity swelling epistaxis and periorbital
ecchymosis are signs that are suggestive of nasal fracture
bull bony crepitus and nasal segment mobilitybull ndash Epiphora bull Severe bilateral injuries to the lachrymal bones
arebull associated with depressed nasal fractures
Nasal Fractures Complications ndash Septal haematoma is one of the most severe early complications of nasal trauma and without drainage it results in abscess formation 6ndash7 days after trauma producing necrosis of the septal cartilage -Long-term problems such as saddle-nose deformity perforation columellar retraction and nasalbase
Septal infection could lead to osteomyelitis orbital and intracranial abscesses meningitis and cavernous sinus thrombosis -Cerebrospinal fluid leakage is a common complication of severe
nasal and frontal fractures
Nasal Fractures
bull Diagnostic proceduresbull ndash Inspectionbull bull Changes of appearance such as deviation andbull asymmetry bleeding watery drainage changesbull in nasal breathing and smell It is useful to comparebull the current presentation with old photographsbull (up to 40 of normal individuals havebull significant nose malformations)
Nasal Fractures Physical examination bull The diagnosis of a nasal fracture is made primarily by physical examination epistaxis nasal swelling and periorbital ecchymosis Nasal shape in the lateral and frontal inspection should be assessed Grasping the dorsum between two fingers and rocking the pyramid back and forth aids in assessing the mobility of nasal bones Internal structures should be evaluated by using a headlight and nasal speculum Clotted blood is removed by suction and assessment of haematoma mucosal tears and active bleeding is performed Bimanual palpation of the septum helps to differentiate septal swelling from haematoma ndash
Nasal FracturesRadiographybull There is no clear evidence of the role of radiographyin the management of nasal fracturesPlain films have up to a 66 false-positive rateas a result of misinterpretation of normal suturelines In addition old fractures are difficult todistinguishbull Three-dimensional CT is recommended for extensiveinjuries involving the nasal-orbital-ethmoidalcomplexndash
Nasal Fractures
bull Additionaluseful diagnostic proceduresbull bull Using a 0 or 30deg 4-mm endoscope is helpful inbull the assessment of posterior abnormalities If thebull patient is heavily sedated Brown-Gruss
provocationbull manoeuvres may be performed to determinebull deformities in upper middle or lower segmentsbull by compressing each compartment
Nasal FracturesConservative treatmentndash Treatment of bleedingbull For localised bleeding anterior sources may becauterised by silver nitrate or sealed with topicalmaterials such as thrombin combined withgelatin foam fibrin glue FloSealreg or other procoagulantmaterials If conservative measuresfail a formal anterior packing is placedbull Bleeding from branches of sphenopalatine orethmoid vessels requires anterior-posteriorpacking
Nasal Fractures
bull bull Surgical methods such as direct endoscopic vessel
bull cauterization or ligation have been shown tobull offer better haemostasis and patient comfortbull Angiography with embolization can also be
consideredbull in cases refractory to more conservativebull approaches
Nasal Fractures
bull Type of reductionbull bull Nondisplaced fractures should be treated withbull observation alone Closed nasal reduction is thebull best choice for simple injuries (isolated unilateralbull with medial displacement)bull bull An open approach should be considered in
severebull trauma (bilateral depressed fractures)
Nasal Fracturesbull Surgical principlesbull ndash Topical anaesthesia with cotton pledgets soakedbull with 4 cocaine or 005 oxymethazoline combinedbull with 4 topical lidocaine should be appliedbull for 5ndash10 min Local anaesthesia should also be injectedbull (1 lidocaine and 1100000 epinephrine)bull along the septum lateral walls and floor of the nasalbull cavitybull bull
Nasal FracturesClosed reductionndashndash The nasal bones are grasped between two fingersand pressure is applied laterally in theopposite direction of the deviation A bluntelevator may be used from within the nose incases of significant medial collapse Walshamforceps can be of help Reduction of the septumshould be performed with the use ofAsch forceps
Nasal Fractures
bull To prevent collapse of the postreductionbull framework nasal packing should be placedbull for 3ndash5 days Septum splints are recommendedbull in comminuted septal fractures withbull severe mucosal lesions External nasal splintingbull for 10 days (Aquaplastreg Thermoplastreg)bull provides nasal protection Nasal saline spraysbull prevent crusting and oral antibiotics should
Nasal Fractures
bull Open reductionbull ndashndash Immediate repair of fractures by using
widebull surgical exposure reduction fixation and
reconstructionbull ndashndash The second option is delayed correctionbull (6 months or more) of persistent deformitiesbull using standard techniques of rhinoplasty
Deviated Nasal Septum
bull Definition of the diseasebull ndash Deviation of the nasal septum is a common causebull of unilateral nasal airway obstruction in which thebull nasal septum is displacedbull bull Epidemiologyaetiologybull ndash Developmental septal abnormalities Septal cartilage
damage in the neonatal period andbull during birth can cause severe septal deviation inbull the absence of a history of nasal trauma
Deviated Nasal Septum
bull Symptomsbull ndash Patients may present with a history of sinusitis
allergicbull rhinitis obstructive sleep apnoea previousbull nasal surgery or recent nasal trauma Unilateral or
bilateral nasal airway obstruction that is unrelievedbull with decongestants or nasal steroid sprays is oftenbull seenbull bull
Deviated Nasal SeptumDiagnosisndashExamination external dorsal deviation or the columella and caudal septummay be deflected off the midline (caudal subluxation)ndash Inspections of the nasal cavity and anterior-posteriorrhinoscopy are helpful in diagnosing the locationtype and severity of septal deformityThe endoscope is also useful in identifying polypsthe severity and extent of posterior septaldeviations and bony spurs and locating areas ofseptal perforation or mucosal injury
Deviated Nasal Septum
bull Therapybull ndash Septoplasty is a procedurebull The areabull of deviation is corrected or resected in order tobull leave behind as much cartilage and bone as
possiblebull Cartilage resection is minimised and can be
repositioned reshaped or recontoured using a variety of methods
Deviated Nasal Septum
bull ndash Indications of septoplasty before the growth period
bull of the nose is finished should be very limited bull -In these cases surgery must preserve all the
cartilagebull in order to prevent external changes of the
shape ofbull the nose
Deviated Nasal Septum
bull Complicationsbull ndash Frequent complications include haematoma andbull infection Cerebrospinal fluid leak is a rare but
potentiallybull serious complicationbull It is usually the resultbull of avulsion or damage to the cribriform plate whenbull handling the perpendicular plate of the ethmoidbull ndash Other complications include epistaxis nasal
Deviated Nasal Septum
bull Other complications include epistaxis nasal obstruction
bull due to residual deviation synechiae returnbull of the cartilaginous deviation septal perforationbull anosmia and cosmetic nasal deformities suchbull as widened alar rim margins drooping nasal tipbull columella retraction and a sunken dorsum with abull supratip saddle formation
Septal perforation with minor crusting View from provide closure of the
incision
Septal Haematoma
bull A septal haematoma is a blood collection under the perichondrium
bull of the septum and cartilagebull bull bull Epidemiologyaetiologybull ndash A septal haematoma is one of the most
severe complications of nasal trauma
Septal Haematoma
bull Diagnosisbull ndash Signs and symptoms include intense pain
swellingbull haematoma of the upper lip and philtrum
area andbull complete nasal airway obstruction
Septal HaematomaTherapyndash Management consists of drainage through a mucoperichondrial incision Immediate treatment isnecessary to prevent long-term problems such asa saddle-nose deformity perforation columellarretraction and nasal-base widening In childrenseptal destruction can lead to devastating nasal andmidfacial growth abnormalitiesbull Surgeryndash Incision and evacuation of the collection is performedDrainage of a septal haematoma should
Septal HaematomaSurgeryndash Incision and evacuation of the collection is performedDrainage of a septal haematoma should provide closure of the incision
Splints or transseptal sutures are placed to obliterate thepotential space and prevent collectionInfection involving the septal cartilage Reconstruction with autologouscartilage is then performed in a second stage Oral antibiotics should be given
Nasal DeformitySaddle-nose deformityndash A saddle-nose deformity is characterised by a loss ofnasal dorsal height and compromised nasal supportstructures -Other case observed are depressionof the middle vault and dorsum loss of nasal tipsupport and definition shortened (vertical) nasal length over rotation of the nasal tip and retrusion ofthe nasal spine and caudal septum It is also knownas a ldquoPug noserdquo or ldquoboxerrsquos noserdquo both of which referto various degrees of nasal dorsal depressionbull
Nasal DeformityEpidemiologyaetiologyndash Prevalence is higher in population groups prone to facial trauma (ie boxers athletes) those with historiesof intranasal cocaine use nasal surgery (e g radical submucosal septal resection reductive rhinoplasty)ndash A saddle-nose deformity can be congenital or acquired It can be noticed as a part of individual familialsyndromic and ethnic characteristics - Most deformities are due to traumatic and iatrogeniccauses Medical causes are Wegenerrsquosgranulomatosis relapsing polychondritis leprosy (Hansenrsquos disease) syphilis ectodermal dysplasiaand intranasal cocaine use
Nasal Deformity
bull Therapybull ndash Nasal reconstruction indications depend on patientbull selection surgeon experience and aetiology of thebull deformity bull Indications for surgery can be functionalbull aesthetic or most commonly both In individuals
with a compromised nasal airway a nasoseptalbull reconstruction is indicated
Nasal Deformity
bull Contraindications bull include patients with malignantbull chronic or autoimmune disease conditions drugbull abuse poor perioperative risk profile and unrealisticbull expectationsbull ndash Multiple previous rhinoplasties and certain
professionsbull (mixed martial artists boxers and other contactbull sports) are relative contraindications
Nasal DeformitySeptoplastyndash Septoplasty is performed to correct nasal obstructioncaused by septal deformityndash Usually septoplasty is performed under general anaesthesiawith the patient in the supine position with the head elevated by approximately 30 (Righthandedsurgeons approach from the right side)ndash Local vasoconstrictive anaesthesia is applied notonly to reduce postoperative pain but also more importantly to achieve vasoconstriction of themucosa and less intraoperative haemorrhage Lidocainewith adrenaline or epinephrine is usedalthough in patients with cardiac hypersensitivityoxymetazoline might be preferred
Nasal Deformity
bull Septoplasty begins with the incision of septal mucosabull Most operative techniques utilise a hemitransfixionbull incision at the caudal end of septum so thatbull deviation at this point might be reached as wellbull as a transfixion incision that is easily obtained ifbull needed (Right-handed surgeons normally choosebull the left side but that may vary when deviation isbull convex towards the right)
Nasal DeformityA columella retractor is placed over the columellaand by pulling it laterally the caudal border of theseptum is exposed Ala can be protected by an alaprotector A vertical incision with a no 15 bladeover the caudal end of septum is performed untilreaching the plane of the septal cartilage It is essentialto correctly identify the perichondrium and byusing the Cottle elevator dissect and lift it creatinga flap As the dissection proceeds along the septalcartilage a longer speculum (no 5) is introduced sothat elevation of the mucoperichondrium is doneunder constant visual controlndash The next step is to dissect the mucoperiostium
Nasal DeformityDissecting over the bony-cartilaginous junctionwhen joining both tunnels might be difficult and is
especially prone to membrane perforationndash If needed the same tunnels are to be created on the
other side of the septum Then deviated parts of
septum are identified and removed either with a
knife or a Freer chisel
Nasal Deformitybull septum from the maxillary crest the septum mustbull be separated from the perpendicular plate trimmedbull along the inferior border placed back onto the crestbull and sutured to the periosteum If the deformity involvesbull the vomer an osteotome is used Care mustbull be taken not to break the cribriform plate becausebull it could cause a cerebrospinal fistula
Nasal Deformity
bull Once the septal deviation is corrected the flapsbull and hemitransfixion incision are mattressed
withbull absorbable sutures Nasal packing to prevent
synechiaebull and postoperative septal haematoma mightbull be advised but should be removed within 72 h

Anterior Rhinoscopy
bull The rhinologic examination itself begins with anterior
bull rhinoscopy to evaluate the nasal vestibule and the anterior
bull portions of the nasal cavity
Nasal Endoscopy Nasal endoscopy has become the most important andrewarding clinical examination method in rhinologic diagnosis
- rigid endoscopes which are available in 4-mm and 28- mm diameters and assorted viewing angles (eg 01048576 301048576 1201048576) -flexible endoscopes are also available for inspecting the nose and nasopharynx and exploring all of the pharynx and larynx in one sitting
Nasal endoscopy
Nasal Endoscopy
Nasal Endoscopy
Imaging of the Nose and Paranasal Sinuses
Conventional RadiographsStandard paranasal sinus radiographs in the occipitomental
projection ( Water projection) and
occipitofrontal projection Caldwell projection) in cases of acute inflammation
They are also obtained to evaluate midfacial fractures
Computed Tomography (CT) the main indicationsfor CT scanning of the
nose and paranasal sinuses
are- chronic sinusitis - -trauma (especially
frontobasal -fractures)
-and tumors
The occipitofrontal projection is better for evaluating theethmoid cells and frontal sinus
occipitomental projection demonstrates the maxillarysinus and gives a limited view of the sphenoid sinus
Computed tomography of the paranasal sinuses
Four representative coronal CT scans are shown
Four representative coronal CT scans are shown
Magnetic Resonance Imaging
Magnetic maging
Magnetic resonance imaging (MRI) has fewer indicationsthan CT in patients with paranasal sinus diseaseThis is primarily because MRI is markedly inferior toCT in defining the bony boundaries of the sinusesThe strength of MRI lies in its superior soft-tissue discriminationMRI is indicated in diseases that involve the paranasal sinuses in addition to thecranial cavity or orbit (eg tumors and congenitalmalformations such as encephaloceles)
MRI of the paranasal sinuses
The Nose and Sinuses
Structure The structure of the nose is made up of
four partsbull The surface anatomybull The nasal skeletonmdashcomposed of the
two nasal bones the paired upper lateral and lower lateral cartilages and the nasal septum covered in subcutaneous tissue and skin
bull The internal anatomymdashincludes the septum of the nose which forms the medial wall of the nasal cavity The turbinates on the lateral wall are also called conchae
bull The osteomeatal complexmdasha key functional area of the nose
Function The nose is the main route for inspired
air and its structure is related to this function As the air passes over the large surface area of the turbinates
The inspired gases are warmed and humidified Mucus on the mucosa of the nose removes large dust particles from the air as it is breathed in
The voice resonates in the sinuses and nose and this provides character to the speech
Pneumatization of the sinusesmdashthey are air filled spacesmdashreduces the weight of the skull
Diseases of thDiseases of the Outer and Inner Nosee Outer and
Inner Nose Erysipelas Definition of the disease ndash Erysipela is a skin infection that affects the superficial dermis and is caused by Streptococcus pyogenes (group A) It usually develops in the extremities and the face and less commonly on the scalp and genitals bull Epidemiologyaetiology ndash Erysipelas are more often seen in elderly infants and children patients with compromised immunology and diabetes -Predisposing factors are alcoholism skin ulceration puncture wounds fungal infections malnutrition and burns
Erysipelas
bull Symptomsbull ndash It usually presents of fever general fatigue bull -The skin lesion is a redindurated and elevated plaque
with borders that expand rapidly bull It is painful warm and accompanied by variable oedemabull -On the second or third day a flaccid bulla may develop
and desquamationbull bull Presence of regional lymph nodes is common
Erysipelas
bull Complicationsndash The most common complication is recurrencewhich is seen in 18ndash30 of the cases even afterproper antibiotic therapy Recurrence is seen moreoften in females than in malesA skin infection with S pyogenes could lead toglomerulonephritis
Erysipelas
bull Complicationsbull ndash The most common complication is recurrencebull which is seen in 18ndash30 of the cases even afterbull proper antibiotic therapy bull -Recurrence is seen morebull often in females than in males bull -A skin infection with S pyogenes could lead tobull glomerulonephritis
Erysipelas
bull bull Diagnosisbull ndash Diagnosis is based on the patientrsquos personal
historybull and physical examination particularly on inspectionbull of the skin
bull Blood cultures are positive in less thanbull 5 of cases
ErysipelasTherapyndash Conservative therapybull The preferred antibiotic is penicillin In mildcases with minor systemic symptoms penicillinV 500 mg orally every 6 h for 10 days or penicillinG benzathine 12 mil U intramuscularlyonceOther possibilities are amoxicillin 500 mgorally twice a day for 10 days or cephalexin 500mg orally every 6 h for 10 days
ErysipelasIn moderate and severe cases with significantsystemic symptoms hospitalization and intravenoustreatment is required penicillin G 2ndash4mil U intravenously every 4ndash6 h Cefazolin05ndash15 gm intravenously every 8 h cefotaxime1ndash2 gm intravenously every 8 h or ceftriaxone1ndash2 gm intravenously once a day should be administeredIn patients with a penicillin allergyclindamycin 600 mg intravenously every 8 h orvancomycin 15 mgkg intravenously twice a daymay be given
ErysipelaAdditional useful therapeutic optionsbull Prednisone 30 mg over 8 days might be consideredas well as elevation of the affected siteMoist heat compresses may be usefulbull Surgeryndash Debridement and drainage are indicated when bullaeabscesses or necroses are presentbull Differential diagnosisndash Contact dermatitisndash Asteatotic eczemandash Herpes zosterndash Angioneurotic oedemandash Osteomyelitis
Furuncle
bull Definition of the diseasebull ndash A furuncle is an infection that beginsbull at the hair follicle and spreads deeper into thebull dermis and subcutaneous tissue forming abull nodule After several days it developsbull into an abscess - red painful and fluctuantbull bull bull Epidemiologyaetiologybull ndash The aetiologic agent is Staphylococcus aureus
FuruncleSymptomsndashsymptoms are local and limited to thesite of infection Furuncles usually are wherehair follicles are present bull Complicationndash One complication is furunculosis multiple draining furunclesDiagnosisndash The diagnosis is based on clinical inspection - Cultures are not necessary when there is no systemic involvement but should beconsidered if systemic therapy (in case of feversignificant cellulitis or hospitalization) or whenmethicillin-resistant Staphylococcusaureus (MRSA) is considered
FuruncleTherapyndash When the furuncle is small application of moist heat compress to promote drainage -Larger furuncles should be drained by surgical incision-After drainage the area should be cleaned with anantiseptic (with chlorhexidinebetadine) should be applied twice
a dayndash If no systemic symptoms or extensive cellulitis arepresent simple topical care is usually curative andoral antibiotics are not necessary Otherwise systemictreatment is indicated and should cover anypossible MRSA
Furuncle
bull -Recommended antibiotics are trimethoprim-sulfamethoxazole
bull 1ndash2 tablets orally twice daily doxycyclinebull 100 mg orally twice dailybull or clindamycin 300ndash450 mg orally every 8 hbull - In severe cases vancomycin 15 mgkg
intravenouslybull every 12 h or clindamycin 600 mg intravenouslybull every 8 h
Midline Granulomabull A midline granuloma is an angiocentricbull lymphoma it was referred to as polymorphicbull reticulosis lethal midline granuloma and midline
malignant reticulosisbull bull Definition of the diseasebull ndash This rare disease is a lymphoma of extranodal
presentationall cases are positive for the Epstein-Barr virus
bull -This lymphoma most commonly appears in the midface region
Midline GranulomaEpidemiologyaetiologyndash This form of lymphoma is rare in Europe and theUnited States with a higher prevalence in Asia and PeruSymptomsndash The most common presentation is nasal obstruction with a destructive mass occupying the nosesinuses and palate
-Fever night sweatsand weight loss seen usually in Hodgkinrsquos lymphomaand other non-Hodgkinrsquos lymphomas (knownas ldquoB symptomsrdquo) are uncommon
Midline GranulomaDiagnosisndash The diagnosis is based on anatomopathologicalstudy The malignancy of the tumour manifested byextensive necrosis makes the histological diagnosisdifficult and often more biopsies are required forconfirmationbull Therapyndash Therapy consists of radiotherapy with or withoutchemotherapy
Midline Granuloma
bull Prognosisbull ndash Depending on the stage long-term remission or
experience a worseningbull prognosis with relapses which may include otherbull extranodal sites bull Involvement of extranodal sitesbull including the upper airway gastrointestinal tractbull skin
Wegenerrsquos Granulomatosis
bull Definition of the diseasebull ndash Wegenerrsquos granulomatosis is a systemic chronicbull vasculitis of small- and medium-sized blood vesselsbull with an autoimmune component It affectsbull particular organs with variable predilectionbull Epidemiologyaetiologybull ndash Wegenerrsquos granulomatosis is a rare disease It affects
about 1 in 20000ndash30000 people It is more prevalentbull in middle-aged Caucasian patients
Wegenerrsquos Granulomatosis
Symptomsndash The disease may present pulmonary upper
respiratory tract or renal In the disseminated form-The localised form ndash confinedto the upper respiratory region ndash is present in 25of the patients- It consists of nonspecific manifestationssuch as nasal obstruction crusting purulentor bloody rhinorrhea and painful or painless ulcers in oral or nasal cavities which are unresponsive tostandard medical treatment
Wegenerrsquos Granulomatosis
bull In some patients the nasal septum is perforatedbull which leads to saddle-nose deformity Less
commonbull symptoms are hoarseness stridor due to
subglotticbull stenosis otalgia otorrhea and conductivebull and sensorineural hearing loss Also ocular
symptomsbull such as scleritis conjunctivitis uveitis andbull episcleritis may be present
Wegenerrsquos Granulomatosis
bull ndash In the disseminated form pulmonary involvementbull is manifested by cough dyspnoea haemoptysisbull (due to an alveolar capillaritis necrotic lesions orbull endobronchial disease) and pleuritic painndashbull -Ninety per cent of patients have nasal symptomsbull and these symptoms are usually the first
manifestationof the diseasebull -Most patients have also renal involvementbull even if it is subclinical
Wegenerrsquos Granulomatosis
Diagnosis ndash Diagnosis of Wegenerrsquos granulomatosis is based on clinical findings that demonstrate lung (chest x-ray) kidney (urine analysis) or upper respiratory tract
involvement (oral or nasal ulcers or discharge) - positive blood analysis for cytoplasmic-staining antineutrophil
cytoplasmic antibodies (c-ANCA) and confirming proteinase 3 (PR3) ANCA or myeloperoxidase (MPO) ANCA ndash Biopsy is essential for diagnosis nonspecific chronic inflammation
and necrosis -Bacterial and fungal infections
Wegenerrsquos Granulomatosis
Therapyndash Conservative therapybull In the induction of disease remission highdosesteroids (e g prednisone 1 mgkgday) for1 month with tapering over several months aregiven In addition cyclophosphamide (2 mgkgday) should be administered for 6ndash12 monthsuntil symptoms disappear In the maintenanceof remission cyclophosphamide should be
Wegenerrsquos Granulomatosis
Antibiotics mainly trimethoprim-sulfamethoxazoleare given for prophylaxis againstPneumocystis jiroveci (formerly Pneumocystiscarinii) pneumonia (PCP) which may developduring immunosuppression and have a role inpreventing recurrencesbull Sinonasal manifestations may be treated with topical nasal steroids and nasal irrigations lowdosesystemic steroids and antibiotics when bacterial infection (typically Staphylococcus species) is suspected
Wegenerrsquos Granulomatosis
bull Prognosisbull ndash Most of the patients respond well to treatmentbull achieving symptom-free intervals of 5ndash20 yearsbull or more bull -Anatomical problems (sinusitis trachealbull stenosis) may require surgery bull Relapses can be long and troublesomebull Long-term complications are chronicbull renal failure hearing loss and deafness
Nasal Fractures Definition ndash A nasal fracture is a disruption of the nasal bone structure due to trauma It is the most frequently fractured facial bone Epidemiologyaetiology ndash Sports falls and assaults are the usual mechanisms of fracture -Males are affected twice as often as are females -Paediatric populations with a incidences during the second and third decades of life -Variables such as force impact direction nature of the striking object age and other will influence the pattern of injury to the components of the nose
Nasal Fractures
bull Symptomsbull ndash Deformity swelling epistaxis and periorbital
ecchymosis are signs that are suggestive of nasal fracture
bull bony crepitus and nasal segment mobilitybull ndash Epiphora bull Severe bilateral injuries to the lachrymal bones
arebull associated with depressed nasal fractures
Nasal Fractures Complications ndash Septal haematoma is one of the most severe early complications of nasal trauma and without drainage it results in abscess formation 6ndash7 days after trauma producing necrosis of the septal cartilage -Long-term problems such as saddle-nose deformity perforation columellar retraction and nasalbase
Septal infection could lead to osteomyelitis orbital and intracranial abscesses meningitis and cavernous sinus thrombosis -Cerebrospinal fluid leakage is a common complication of severe
nasal and frontal fractures
Nasal Fractures
bull Diagnostic proceduresbull ndash Inspectionbull bull Changes of appearance such as deviation andbull asymmetry bleeding watery drainage changesbull in nasal breathing and smell It is useful to comparebull the current presentation with old photographsbull (up to 40 of normal individuals havebull significant nose malformations)
Nasal Fractures Physical examination bull The diagnosis of a nasal fracture is made primarily by physical examination epistaxis nasal swelling and periorbital ecchymosis Nasal shape in the lateral and frontal inspection should be assessed Grasping the dorsum between two fingers and rocking the pyramid back and forth aids in assessing the mobility of nasal bones Internal structures should be evaluated by using a headlight and nasal speculum Clotted blood is removed by suction and assessment of haematoma mucosal tears and active bleeding is performed Bimanual palpation of the septum helps to differentiate septal swelling from haematoma ndash
Nasal FracturesRadiographybull There is no clear evidence of the role of radiographyin the management of nasal fracturesPlain films have up to a 66 false-positive rateas a result of misinterpretation of normal suturelines In addition old fractures are difficult todistinguishbull Three-dimensional CT is recommended for extensiveinjuries involving the nasal-orbital-ethmoidalcomplexndash
Nasal Fractures
bull Additionaluseful diagnostic proceduresbull bull Using a 0 or 30deg 4-mm endoscope is helpful inbull the assessment of posterior abnormalities If thebull patient is heavily sedated Brown-Gruss
provocationbull manoeuvres may be performed to determinebull deformities in upper middle or lower segmentsbull by compressing each compartment
Nasal FracturesConservative treatmentndash Treatment of bleedingbull For localised bleeding anterior sources may becauterised by silver nitrate or sealed with topicalmaterials such as thrombin combined withgelatin foam fibrin glue FloSealreg or other procoagulantmaterials If conservative measuresfail a formal anterior packing is placedbull Bleeding from branches of sphenopalatine orethmoid vessels requires anterior-posteriorpacking
Nasal Fractures
bull bull Surgical methods such as direct endoscopic vessel
bull cauterization or ligation have been shown tobull offer better haemostasis and patient comfortbull Angiography with embolization can also be
consideredbull in cases refractory to more conservativebull approaches
Nasal Fractures
bull Type of reductionbull bull Nondisplaced fractures should be treated withbull observation alone Closed nasal reduction is thebull best choice for simple injuries (isolated unilateralbull with medial displacement)bull bull An open approach should be considered in
severebull trauma (bilateral depressed fractures)
Nasal Fracturesbull Surgical principlesbull ndash Topical anaesthesia with cotton pledgets soakedbull with 4 cocaine or 005 oxymethazoline combinedbull with 4 topical lidocaine should be appliedbull for 5ndash10 min Local anaesthesia should also be injectedbull (1 lidocaine and 1100000 epinephrine)bull along the septum lateral walls and floor of the nasalbull cavitybull bull
Nasal FracturesClosed reductionndashndash The nasal bones are grasped between two fingersand pressure is applied laterally in theopposite direction of the deviation A bluntelevator may be used from within the nose incases of significant medial collapse Walshamforceps can be of help Reduction of the septumshould be performed with the use ofAsch forceps
Nasal Fractures
bull To prevent collapse of the postreductionbull framework nasal packing should be placedbull for 3ndash5 days Septum splints are recommendedbull in comminuted septal fractures withbull severe mucosal lesions External nasal splintingbull for 10 days (Aquaplastreg Thermoplastreg)bull provides nasal protection Nasal saline spraysbull prevent crusting and oral antibiotics should
Nasal Fractures
bull Open reductionbull ndashndash Immediate repair of fractures by using
widebull surgical exposure reduction fixation and
reconstructionbull ndashndash The second option is delayed correctionbull (6 months or more) of persistent deformitiesbull using standard techniques of rhinoplasty
Deviated Nasal Septum
bull Definition of the diseasebull ndash Deviation of the nasal septum is a common causebull of unilateral nasal airway obstruction in which thebull nasal septum is displacedbull bull Epidemiologyaetiologybull ndash Developmental septal abnormalities Septal cartilage
damage in the neonatal period andbull during birth can cause severe septal deviation inbull the absence of a history of nasal trauma
Deviated Nasal Septum
bull Symptomsbull ndash Patients may present with a history of sinusitis
allergicbull rhinitis obstructive sleep apnoea previousbull nasal surgery or recent nasal trauma Unilateral or
bilateral nasal airway obstruction that is unrelievedbull with decongestants or nasal steroid sprays is oftenbull seenbull bull
Deviated Nasal SeptumDiagnosisndashExamination external dorsal deviation or the columella and caudal septummay be deflected off the midline (caudal subluxation)ndash Inspections of the nasal cavity and anterior-posteriorrhinoscopy are helpful in diagnosing the locationtype and severity of septal deformityThe endoscope is also useful in identifying polypsthe severity and extent of posterior septaldeviations and bony spurs and locating areas ofseptal perforation or mucosal injury
Deviated Nasal Septum
bull Therapybull ndash Septoplasty is a procedurebull The areabull of deviation is corrected or resected in order tobull leave behind as much cartilage and bone as
possiblebull Cartilage resection is minimised and can be
repositioned reshaped or recontoured using a variety of methods
Deviated Nasal Septum
bull ndash Indications of septoplasty before the growth period
bull of the nose is finished should be very limited bull -In these cases surgery must preserve all the
cartilagebull in order to prevent external changes of the
shape ofbull the nose
Deviated Nasal Septum
bull Complicationsbull ndash Frequent complications include haematoma andbull infection Cerebrospinal fluid leak is a rare but
potentiallybull serious complicationbull It is usually the resultbull of avulsion or damage to the cribriform plate whenbull handling the perpendicular plate of the ethmoidbull ndash Other complications include epistaxis nasal
Deviated Nasal Septum
bull Other complications include epistaxis nasal obstruction
bull due to residual deviation synechiae returnbull of the cartilaginous deviation septal perforationbull anosmia and cosmetic nasal deformities suchbull as widened alar rim margins drooping nasal tipbull columella retraction and a sunken dorsum with abull supratip saddle formation
Septal perforation with minor crusting View from provide closure of the
incision
Septal Haematoma
bull A septal haematoma is a blood collection under the perichondrium
bull of the septum and cartilagebull bull bull Epidemiologyaetiologybull ndash A septal haematoma is one of the most
severe complications of nasal trauma
Septal Haematoma
bull Diagnosisbull ndash Signs and symptoms include intense pain
swellingbull haematoma of the upper lip and philtrum
area andbull complete nasal airway obstruction
Septal HaematomaTherapyndash Management consists of drainage through a mucoperichondrial incision Immediate treatment isnecessary to prevent long-term problems such asa saddle-nose deformity perforation columellarretraction and nasal-base widening In childrenseptal destruction can lead to devastating nasal andmidfacial growth abnormalitiesbull Surgeryndash Incision and evacuation of the collection is performedDrainage of a septal haematoma should
Septal HaematomaSurgeryndash Incision and evacuation of the collection is performedDrainage of a septal haematoma should provide closure of the incision
Splints or transseptal sutures are placed to obliterate thepotential space and prevent collectionInfection involving the septal cartilage Reconstruction with autologouscartilage is then performed in a second stage Oral antibiotics should be given
Nasal DeformitySaddle-nose deformityndash A saddle-nose deformity is characterised by a loss ofnasal dorsal height and compromised nasal supportstructures -Other case observed are depressionof the middle vault and dorsum loss of nasal tipsupport and definition shortened (vertical) nasal length over rotation of the nasal tip and retrusion ofthe nasal spine and caudal septum It is also knownas a ldquoPug noserdquo or ldquoboxerrsquos noserdquo both of which referto various degrees of nasal dorsal depressionbull
Nasal DeformityEpidemiologyaetiologyndash Prevalence is higher in population groups prone to facial trauma (ie boxers athletes) those with historiesof intranasal cocaine use nasal surgery (e g radical submucosal septal resection reductive rhinoplasty)ndash A saddle-nose deformity can be congenital or acquired It can be noticed as a part of individual familialsyndromic and ethnic characteristics - Most deformities are due to traumatic and iatrogeniccauses Medical causes are Wegenerrsquosgranulomatosis relapsing polychondritis leprosy (Hansenrsquos disease) syphilis ectodermal dysplasiaand intranasal cocaine use
Nasal Deformity
bull Therapybull ndash Nasal reconstruction indications depend on patientbull selection surgeon experience and aetiology of thebull deformity bull Indications for surgery can be functionalbull aesthetic or most commonly both In individuals
with a compromised nasal airway a nasoseptalbull reconstruction is indicated
Nasal Deformity
bull Contraindications bull include patients with malignantbull chronic or autoimmune disease conditions drugbull abuse poor perioperative risk profile and unrealisticbull expectationsbull ndash Multiple previous rhinoplasties and certain
professionsbull (mixed martial artists boxers and other contactbull sports) are relative contraindications
Nasal DeformitySeptoplastyndash Septoplasty is performed to correct nasal obstructioncaused by septal deformityndash Usually septoplasty is performed under general anaesthesiawith the patient in the supine position with the head elevated by approximately 30 (Righthandedsurgeons approach from the right side)ndash Local vasoconstrictive anaesthesia is applied notonly to reduce postoperative pain but also more importantly to achieve vasoconstriction of themucosa and less intraoperative haemorrhage Lidocainewith adrenaline or epinephrine is usedalthough in patients with cardiac hypersensitivityoxymetazoline might be preferred
Nasal Deformity
bull Septoplasty begins with the incision of septal mucosabull Most operative techniques utilise a hemitransfixionbull incision at the caudal end of septum so thatbull deviation at this point might be reached as wellbull as a transfixion incision that is easily obtained ifbull needed (Right-handed surgeons normally choosebull the left side but that may vary when deviation isbull convex towards the right)
Nasal DeformityA columella retractor is placed over the columellaand by pulling it laterally the caudal border of theseptum is exposed Ala can be protected by an alaprotector A vertical incision with a no 15 bladeover the caudal end of septum is performed untilreaching the plane of the septal cartilage It is essentialto correctly identify the perichondrium and byusing the Cottle elevator dissect and lift it creatinga flap As the dissection proceeds along the septalcartilage a longer speculum (no 5) is introduced sothat elevation of the mucoperichondrium is doneunder constant visual controlndash The next step is to dissect the mucoperiostium
Nasal DeformityDissecting over the bony-cartilaginous junctionwhen joining both tunnels might be difficult and is
especially prone to membrane perforationndash If needed the same tunnels are to be created on the
other side of the septum Then deviated parts of
septum are identified and removed either with a
knife or a Freer chisel
Nasal Deformitybull septum from the maxillary crest the septum mustbull be separated from the perpendicular plate trimmedbull along the inferior border placed back onto the crestbull and sutured to the periosteum If the deformity involvesbull the vomer an osteotome is used Care mustbull be taken not to break the cribriform plate becausebull it could cause a cerebrospinal fistula
Nasal Deformity
bull Once the septal deviation is corrected the flapsbull and hemitransfixion incision are mattressed
withbull absorbable sutures Nasal packing to prevent
synechiaebull and postoperative septal haematoma mightbull be advised but should be removed within 72 h

Nasal Endoscopy Nasal endoscopy has become the most important andrewarding clinical examination method in rhinologic diagnosis
- rigid endoscopes which are available in 4-mm and 28- mm diameters and assorted viewing angles (eg 01048576 301048576 1201048576) -flexible endoscopes are also available for inspecting the nose and nasopharynx and exploring all of the pharynx and larynx in one sitting
Nasal endoscopy
Nasal Endoscopy
Nasal Endoscopy
Imaging of the Nose and Paranasal Sinuses
Conventional RadiographsStandard paranasal sinus radiographs in the occipitomental
projection ( Water projection) and
occipitofrontal projection Caldwell projection) in cases of acute inflammation
They are also obtained to evaluate midfacial fractures
Computed Tomography (CT) the main indicationsfor CT scanning of the
nose and paranasal sinuses
are- chronic sinusitis - -trauma (especially
frontobasal -fractures)
-and tumors
The occipitofrontal projection is better for evaluating theethmoid cells and frontal sinus
occipitomental projection demonstrates the maxillarysinus and gives a limited view of the sphenoid sinus
Computed tomography of the paranasal sinuses
Four representative coronal CT scans are shown
Four representative coronal CT scans are shown
Magnetic Resonance Imaging
Magnetic maging
Magnetic resonance imaging (MRI) has fewer indicationsthan CT in patients with paranasal sinus diseaseThis is primarily because MRI is markedly inferior toCT in defining the bony boundaries of the sinusesThe strength of MRI lies in its superior soft-tissue discriminationMRI is indicated in diseases that involve the paranasal sinuses in addition to thecranial cavity or orbit (eg tumors and congenitalmalformations such as encephaloceles)
MRI of the paranasal sinuses
The Nose and Sinuses
Structure The structure of the nose is made up of
four partsbull The surface anatomybull The nasal skeletonmdashcomposed of the
two nasal bones the paired upper lateral and lower lateral cartilages and the nasal septum covered in subcutaneous tissue and skin
bull The internal anatomymdashincludes the septum of the nose which forms the medial wall of the nasal cavity The turbinates on the lateral wall are also called conchae
bull The osteomeatal complexmdasha key functional area of the nose
Function The nose is the main route for inspired
air and its structure is related to this function As the air passes over the large surface area of the turbinates
The inspired gases are warmed and humidified Mucus on the mucosa of the nose removes large dust particles from the air as it is breathed in
The voice resonates in the sinuses and nose and this provides character to the speech
Pneumatization of the sinusesmdashthey are air filled spacesmdashreduces the weight of the skull
Diseases of thDiseases of the Outer and Inner Nosee Outer and
Inner Nose Erysipelas Definition of the disease ndash Erysipela is a skin infection that affects the superficial dermis and is caused by Streptococcus pyogenes (group A) It usually develops in the extremities and the face and less commonly on the scalp and genitals bull Epidemiologyaetiology ndash Erysipelas are more often seen in elderly infants and children patients with compromised immunology and diabetes -Predisposing factors are alcoholism skin ulceration puncture wounds fungal infections malnutrition and burns
Erysipelas
bull Symptomsbull ndash It usually presents of fever general fatigue bull -The skin lesion is a redindurated and elevated plaque
with borders that expand rapidly bull It is painful warm and accompanied by variable oedemabull -On the second or third day a flaccid bulla may develop
and desquamationbull bull Presence of regional lymph nodes is common
Erysipelas
bull Complicationsndash The most common complication is recurrencewhich is seen in 18ndash30 of the cases even afterproper antibiotic therapy Recurrence is seen moreoften in females than in malesA skin infection with S pyogenes could lead toglomerulonephritis
Erysipelas
bull Complicationsbull ndash The most common complication is recurrencebull which is seen in 18ndash30 of the cases even afterbull proper antibiotic therapy bull -Recurrence is seen morebull often in females than in males bull -A skin infection with S pyogenes could lead tobull glomerulonephritis
Erysipelas
bull bull Diagnosisbull ndash Diagnosis is based on the patientrsquos personal
historybull and physical examination particularly on inspectionbull of the skin
bull Blood cultures are positive in less thanbull 5 of cases
ErysipelasTherapyndash Conservative therapybull The preferred antibiotic is penicillin In mildcases with minor systemic symptoms penicillinV 500 mg orally every 6 h for 10 days or penicillinG benzathine 12 mil U intramuscularlyonceOther possibilities are amoxicillin 500 mgorally twice a day for 10 days or cephalexin 500mg orally every 6 h for 10 days
ErysipelasIn moderate and severe cases with significantsystemic symptoms hospitalization and intravenoustreatment is required penicillin G 2ndash4mil U intravenously every 4ndash6 h Cefazolin05ndash15 gm intravenously every 8 h cefotaxime1ndash2 gm intravenously every 8 h or ceftriaxone1ndash2 gm intravenously once a day should be administeredIn patients with a penicillin allergyclindamycin 600 mg intravenously every 8 h orvancomycin 15 mgkg intravenously twice a daymay be given
ErysipelaAdditional useful therapeutic optionsbull Prednisone 30 mg over 8 days might be consideredas well as elevation of the affected siteMoist heat compresses may be usefulbull Surgeryndash Debridement and drainage are indicated when bullaeabscesses or necroses are presentbull Differential diagnosisndash Contact dermatitisndash Asteatotic eczemandash Herpes zosterndash Angioneurotic oedemandash Osteomyelitis
Furuncle
bull Definition of the diseasebull ndash A furuncle is an infection that beginsbull at the hair follicle and spreads deeper into thebull dermis and subcutaneous tissue forming abull nodule After several days it developsbull into an abscess - red painful and fluctuantbull bull bull Epidemiologyaetiologybull ndash The aetiologic agent is Staphylococcus aureus
FuruncleSymptomsndashsymptoms are local and limited to thesite of infection Furuncles usually are wherehair follicles are present bull Complicationndash One complication is furunculosis multiple draining furunclesDiagnosisndash The diagnosis is based on clinical inspection - Cultures are not necessary when there is no systemic involvement but should beconsidered if systemic therapy (in case of feversignificant cellulitis or hospitalization) or whenmethicillin-resistant Staphylococcusaureus (MRSA) is considered
FuruncleTherapyndash When the furuncle is small application of moist heat compress to promote drainage -Larger furuncles should be drained by surgical incision-After drainage the area should be cleaned with anantiseptic (with chlorhexidinebetadine) should be applied twice
a dayndash If no systemic symptoms or extensive cellulitis arepresent simple topical care is usually curative andoral antibiotics are not necessary Otherwise systemictreatment is indicated and should cover anypossible MRSA
Furuncle
bull -Recommended antibiotics are trimethoprim-sulfamethoxazole
bull 1ndash2 tablets orally twice daily doxycyclinebull 100 mg orally twice dailybull or clindamycin 300ndash450 mg orally every 8 hbull - In severe cases vancomycin 15 mgkg
intravenouslybull every 12 h or clindamycin 600 mg intravenouslybull every 8 h
Midline Granulomabull A midline granuloma is an angiocentricbull lymphoma it was referred to as polymorphicbull reticulosis lethal midline granuloma and midline
malignant reticulosisbull bull Definition of the diseasebull ndash This rare disease is a lymphoma of extranodal
presentationall cases are positive for the Epstein-Barr virus
bull -This lymphoma most commonly appears in the midface region
Midline GranulomaEpidemiologyaetiologyndash This form of lymphoma is rare in Europe and theUnited States with a higher prevalence in Asia and PeruSymptomsndash The most common presentation is nasal obstruction with a destructive mass occupying the nosesinuses and palate
-Fever night sweatsand weight loss seen usually in Hodgkinrsquos lymphomaand other non-Hodgkinrsquos lymphomas (knownas ldquoB symptomsrdquo) are uncommon
Midline GranulomaDiagnosisndash The diagnosis is based on anatomopathologicalstudy The malignancy of the tumour manifested byextensive necrosis makes the histological diagnosisdifficult and often more biopsies are required forconfirmationbull Therapyndash Therapy consists of radiotherapy with or withoutchemotherapy
Midline Granuloma
bull Prognosisbull ndash Depending on the stage long-term remission or
experience a worseningbull prognosis with relapses which may include otherbull extranodal sites bull Involvement of extranodal sitesbull including the upper airway gastrointestinal tractbull skin
Wegenerrsquos Granulomatosis
bull Definition of the diseasebull ndash Wegenerrsquos granulomatosis is a systemic chronicbull vasculitis of small- and medium-sized blood vesselsbull with an autoimmune component It affectsbull particular organs with variable predilectionbull Epidemiologyaetiologybull ndash Wegenerrsquos granulomatosis is a rare disease It affects
about 1 in 20000ndash30000 people It is more prevalentbull in middle-aged Caucasian patients
Wegenerrsquos Granulomatosis
Symptomsndash The disease may present pulmonary upper
respiratory tract or renal In the disseminated form-The localised form ndash confinedto the upper respiratory region ndash is present in 25of the patients- It consists of nonspecific manifestationssuch as nasal obstruction crusting purulentor bloody rhinorrhea and painful or painless ulcers in oral or nasal cavities which are unresponsive tostandard medical treatment
Wegenerrsquos Granulomatosis
bull In some patients the nasal septum is perforatedbull which leads to saddle-nose deformity Less
commonbull symptoms are hoarseness stridor due to
subglotticbull stenosis otalgia otorrhea and conductivebull and sensorineural hearing loss Also ocular
symptomsbull such as scleritis conjunctivitis uveitis andbull episcleritis may be present
Wegenerrsquos Granulomatosis
bull ndash In the disseminated form pulmonary involvementbull is manifested by cough dyspnoea haemoptysisbull (due to an alveolar capillaritis necrotic lesions orbull endobronchial disease) and pleuritic painndashbull -Ninety per cent of patients have nasal symptomsbull and these symptoms are usually the first
manifestationof the diseasebull -Most patients have also renal involvementbull even if it is subclinical
Wegenerrsquos Granulomatosis
Diagnosis ndash Diagnosis of Wegenerrsquos granulomatosis is based on clinical findings that demonstrate lung (chest x-ray) kidney (urine analysis) or upper respiratory tract
involvement (oral or nasal ulcers or discharge) - positive blood analysis for cytoplasmic-staining antineutrophil
cytoplasmic antibodies (c-ANCA) and confirming proteinase 3 (PR3) ANCA or myeloperoxidase (MPO) ANCA ndash Biopsy is essential for diagnosis nonspecific chronic inflammation
and necrosis -Bacterial and fungal infections
Wegenerrsquos Granulomatosis
Therapyndash Conservative therapybull In the induction of disease remission highdosesteroids (e g prednisone 1 mgkgday) for1 month with tapering over several months aregiven In addition cyclophosphamide (2 mgkgday) should be administered for 6ndash12 monthsuntil symptoms disappear In the maintenanceof remission cyclophosphamide should be
Wegenerrsquos Granulomatosis
Antibiotics mainly trimethoprim-sulfamethoxazoleare given for prophylaxis againstPneumocystis jiroveci (formerly Pneumocystiscarinii) pneumonia (PCP) which may developduring immunosuppression and have a role inpreventing recurrencesbull Sinonasal manifestations may be treated with topical nasal steroids and nasal irrigations lowdosesystemic steroids and antibiotics when bacterial infection (typically Staphylococcus species) is suspected
Wegenerrsquos Granulomatosis
bull Prognosisbull ndash Most of the patients respond well to treatmentbull achieving symptom-free intervals of 5ndash20 yearsbull or more bull -Anatomical problems (sinusitis trachealbull stenosis) may require surgery bull Relapses can be long and troublesomebull Long-term complications are chronicbull renal failure hearing loss and deafness
Nasal Fractures Definition ndash A nasal fracture is a disruption of the nasal bone structure due to trauma It is the most frequently fractured facial bone Epidemiologyaetiology ndash Sports falls and assaults are the usual mechanisms of fracture -Males are affected twice as often as are females -Paediatric populations with a incidences during the second and third decades of life -Variables such as force impact direction nature of the striking object age and other will influence the pattern of injury to the components of the nose
Nasal Fractures
bull Symptomsbull ndash Deformity swelling epistaxis and periorbital
ecchymosis are signs that are suggestive of nasal fracture
bull bony crepitus and nasal segment mobilitybull ndash Epiphora bull Severe bilateral injuries to the lachrymal bones
arebull associated with depressed nasal fractures
Nasal Fractures Complications ndash Septal haematoma is one of the most severe early complications of nasal trauma and without drainage it results in abscess formation 6ndash7 days after trauma producing necrosis of the septal cartilage -Long-term problems such as saddle-nose deformity perforation columellar retraction and nasalbase
Septal infection could lead to osteomyelitis orbital and intracranial abscesses meningitis and cavernous sinus thrombosis -Cerebrospinal fluid leakage is a common complication of severe
nasal and frontal fractures
Nasal Fractures
bull Diagnostic proceduresbull ndash Inspectionbull bull Changes of appearance such as deviation andbull asymmetry bleeding watery drainage changesbull in nasal breathing and smell It is useful to comparebull the current presentation with old photographsbull (up to 40 of normal individuals havebull significant nose malformations)
Nasal Fractures Physical examination bull The diagnosis of a nasal fracture is made primarily by physical examination epistaxis nasal swelling and periorbital ecchymosis Nasal shape in the lateral and frontal inspection should be assessed Grasping the dorsum between two fingers and rocking the pyramid back and forth aids in assessing the mobility of nasal bones Internal structures should be evaluated by using a headlight and nasal speculum Clotted blood is removed by suction and assessment of haematoma mucosal tears and active bleeding is performed Bimanual palpation of the septum helps to differentiate septal swelling from haematoma ndash
Nasal FracturesRadiographybull There is no clear evidence of the role of radiographyin the management of nasal fracturesPlain films have up to a 66 false-positive rateas a result of misinterpretation of normal suturelines In addition old fractures are difficult todistinguishbull Three-dimensional CT is recommended for extensiveinjuries involving the nasal-orbital-ethmoidalcomplexndash
Nasal Fractures
bull Additionaluseful diagnostic proceduresbull bull Using a 0 or 30deg 4-mm endoscope is helpful inbull the assessment of posterior abnormalities If thebull patient is heavily sedated Brown-Gruss
provocationbull manoeuvres may be performed to determinebull deformities in upper middle or lower segmentsbull by compressing each compartment
Nasal FracturesConservative treatmentndash Treatment of bleedingbull For localised bleeding anterior sources may becauterised by silver nitrate or sealed with topicalmaterials such as thrombin combined withgelatin foam fibrin glue FloSealreg or other procoagulantmaterials If conservative measuresfail a formal anterior packing is placedbull Bleeding from branches of sphenopalatine orethmoid vessels requires anterior-posteriorpacking
Nasal Fractures
bull bull Surgical methods such as direct endoscopic vessel
bull cauterization or ligation have been shown tobull offer better haemostasis and patient comfortbull Angiography with embolization can also be
consideredbull in cases refractory to more conservativebull approaches
Nasal Fractures
bull Type of reductionbull bull Nondisplaced fractures should be treated withbull observation alone Closed nasal reduction is thebull best choice for simple injuries (isolated unilateralbull with medial displacement)bull bull An open approach should be considered in
severebull trauma (bilateral depressed fractures)
Nasal Fracturesbull Surgical principlesbull ndash Topical anaesthesia with cotton pledgets soakedbull with 4 cocaine or 005 oxymethazoline combinedbull with 4 topical lidocaine should be appliedbull for 5ndash10 min Local anaesthesia should also be injectedbull (1 lidocaine and 1100000 epinephrine)bull along the septum lateral walls and floor of the nasalbull cavitybull bull
Nasal FracturesClosed reductionndashndash The nasal bones are grasped between two fingersand pressure is applied laterally in theopposite direction of the deviation A bluntelevator may be used from within the nose incases of significant medial collapse Walshamforceps can be of help Reduction of the septumshould be performed with the use ofAsch forceps
Nasal Fractures
bull To prevent collapse of the postreductionbull framework nasal packing should be placedbull for 3ndash5 days Septum splints are recommendedbull in comminuted septal fractures withbull severe mucosal lesions External nasal splintingbull for 10 days (Aquaplastreg Thermoplastreg)bull provides nasal protection Nasal saline spraysbull prevent crusting and oral antibiotics should
Nasal Fractures
bull Open reductionbull ndashndash Immediate repair of fractures by using
widebull surgical exposure reduction fixation and
reconstructionbull ndashndash The second option is delayed correctionbull (6 months or more) of persistent deformitiesbull using standard techniques of rhinoplasty
Deviated Nasal Septum
bull Definition of the diseasebull ndash Deviation of the nasal septum is a common causebull of unilateral nasal airway obstruction in which thebull nasal septum is displacedbull bull Epidemiologyaetiologybull ndash Developmental septal abnormalities Septal cartilage
damage in the neonatal period andbull during birth can cause severe septal deviation inbull the absence of a history of nasal trauma
Deviated Nasal Septum
bull Symptomsbull ndash Patients may present with a history of sinusitis
allergicbull rhinitis obstructive sleep apnoea previousbull nasal surgery or recent nasal trauma Unilateral or
bilateral nasal airway obstruction that is unrelievedbull with decongestants or nasal steroid sprays is oftenbull seenbull bull
Deviated Nasal SeptumDiagnosisndashExamination external dorsal deviation or the columella and caudal septummay be deflected off the midline (caudal subluxation)ndash Inspections of the nasal cavity and anterior-posteriorrhinoscopy are helpful in diagnosing the locationtype and severity of septal deformityThe endoscope is also useful in identifying polypsthe severity and extent of posterior septaldeviations and bony spurs and locating areas ofseptal perforation or mucosal injury
Deviated Nasal Septum
bull Therapybull ndash Septoplasty is a procedurebull The areabull of deviation is corrected or resected in order tobull leave behind as much cartilage and bone as
possiblebull Cartilage resection is minimised and can be
repositioned reshaped or recontoured using a variety of methods
Deviated Nasal Septum
bull ndash Indications of septoplasty before the growth period
bull of the nose is finished should be very limited bull -In these cases surgery must preserve all the
cartilagebull in order to prevent external changes of the
shape ofbull the nose
Deviated Nasal Septum
bull Complicationsbull ndash Frequent complications include haematoma andbull infection Cerebrospinal fluid leak is a rare but
potentiallybull serious complicationbull It is usually the resultbull of avulsion or damage to the cribriform plate whenbull handling the perpendicular plate of the ethmoidbull ndash Other complications include epistaxis nasal
Deviated Nasal Septum
bull Other complications include epistaxis nasal obstruction
bull due to residual deviation synechiae returnbull of the cartilaginous deviation septal perforationbull anosmia and cosmetic nasal deformities suchbull as widened alar rim margins drooping nasal tipbull columella retraction and a sunken dorsum with abull supratip saddle formation
Septal perforation with minor crusting View from provide closure of the
incision
Septal Haematoma
bull A septal haematoma is a blood collection under the perichondrium
bull of the septum and cartilagebull bull bull Epidemiologyaetiologybull ndash A septal haematoma is one of the most
severe complications of nasal trauma
Septal Haematoma
bull Diagnosisbull ndash Signs and symptoms include intense pain
swellingbull haematoma of the upper lip and philtrum
area andbull complete nasal airway obstruction
Septal HaematomaTherapyndash Management consists of drainage through a mucoperichondrial incision Immediate treatment isnecessary to prevent long-term problems such asa saddle-nose deformity perforation columellarretraction and nasal-base widening In childrenseptal destruction can lead to devastating nasal andmidfacial growth abnormalitiesbull Surgeryndash Incision and evacuation of the collection is performedDrainage of a septal haematoma should
Septal HaematomaSurgeryndash Incision and evacuation of the collection is performedDrainage of a septal haematoma should provide closure of the incision
Splints or transseptal sutures are placed to obliterate thepotential space and prevent collectionInfection involving the septal cartilage Reconstruction with autologouscartilage is then performed in a second stage Oral antibiotics should be given
Nasal DeformitySaddle-nose deformityndash A saddle-nose deformity is characterised by a loss ofnasal dorsal height and compromised nasal supportstructures -Other case observed are depressionof the middle vault and dorsum loss of nasal tipsupport and definition shortened (vertical) nasal length over rotation of the nasal tip and retrusion ofthe nasal spine and caudal septum It is also knownas a ldquoPug noserdquo or ldquoboxerrsquos noserdquo both of which referto various degrees of nasal dorsal depressionbull
Nasal DeformityEpidemiologyaetiologyndash Prevalence is higher in population groups prone to facial trauma (ie boxers athletes) those with historiesof intranasal cocaine use nasal surgery (e g radical submucosal septal resection reductive rhinoplasty)ndash A saddle-nose deformity can be congenital or acquired It can be noticed as a part of individual familialsyndromic and ethnic characteristics - Most deformities are due to traumatic and iatrogeniccauses Medical causes are Wegenerrsquosgranulomatosis relapsing polychondritis leprosy (Hansenrsquos disease) syphilis ectodermal dysplasiaand intranasal cocaine use
Nasal Deformity
bull Therapybull ndash Nasal reconstruction indications depend on patientbull selection surgeon experience and aetiology of thebull deformity bull Indications for surgery can be functionalbull aesthetic or most commonly both In individuals
with a compromised nasal airway a nasoseptalbull reconstruction is indicated
Nasal Deformity
bull Contraindications bull include patients with malignantbull chronic or autoimmune disease conditions drugbull abuse poor perioperative risk profile and unrealisticbull expectationsbull ndash Multiple previous rhinoplasties and certain
professionsbull (mixed martial artists boxers and other contactbull sports) are relative contraindications
Nasal DeformitySeptoplastyndash Septoplasty is performed to correct nasal obstructioncaused by septal deformityndash Usually septoplasty is performed under general anaesthesiawith the patient in the supine position with the head elevated by approximately 30 (Righthandedsurgeons approach from the right side)ndash Local vasoconstrictive anaesthesia is applied notonly to reduce postoperative pain but also more importantly to achieve vasoconstriction of themucosa and less intraoperative haemorrhage Lidocainewith adrenaline or epinephrine is usedalthough in patients with cardiac hypersensitivityoxymetazoline might be preferred
Nasal Deformity
bull Septoplasty begins with the incision of septal mucosabull Most operative techniques utilise a hemitransfixionbull incision at the caudal end of septum so thatbull deviation at this point might be reached as wellbull as a transfixion incision that is easily obtained ifbull needed (Right-handed surgeons normally choosebull the left side but that may vary when deviation isbull convex towards the right)
Nasal DeformityA columella retractor is placed over the columellaand by pulling it laterally the caudal border of theseptum is exposed Ala can be protected by an alaprotector A vertical incision with a no 15 bladeover the caudal end of septum is performed untilreaching the plane of the septal cartilage It is essentialto correctly identify the perichondrium and byusing the Cottle elevator dissect and lift it creatinga flap As the dissection proceeds along the septalcartilage a longer speculum (no 5) is introduced sothat elevation of the mucoperichondrium is doneunder constant visual controlndash The next step is to dissect the mucoperiostium
Nasal DeformityDissecting over the bony-cartilaginous junctionwhen joining both tunnels might be difficult and is
especially prone to membrane perforationndash If needed the same tunnels are to be created on the
other side of the septum Then deviated parts of
septum are identified and removed either with a
knife or a Freer chisel
Nasal Deformitybull septum from the maxillary crest the septum mustbull be separated from the perpendicular plate trimmedbull along the inferior border placed back onto the crestbull and sutured to the periosteum If the deformity involvesbull the vomer an osteotome is used Care mustbull be taken not to break the cribriform plate becausebull it could cause a cerebrospinal fistula
Nasal Deformity
bull Once the septal deviation is corrected the flapsbull and hemitransfixion incision are mattressed
withbull absorbable sutures Nasal packing to prevent
synechiaebull and postoperative septal haematoma mightbull be advised but should be removed within 72 h

Nasal endoscopy
Nasal Endoscopy
Nasal Endoscopy
Imaging of the Nose and Paranasal Sinuses
Conventional RadiographsStandard paranasal sinus radiographs in the occipitomental
projection ( Water projection) and
occipitofrontal projection Caldwell projection) in cases of acute inflammation
They are also obtained to evaluate midfacial fractures
Computed Tomography (CT) the main indicationsfor CT scanning of the
nose and paranasal sinuses
are- chronic sinusitis - -trauma (especially
frontobasal -fractures)
-and tumors
The occipitofrontal projection is better for evaluating theethmoid cells and frontal sinus
occipitomental projection demonstrates the maxillarysinus and gives a limited view of the sphenoid sinus
Computed tomography of the paranasal sinuses
Four representative coronal CT scans are shown
Four representative coronal CT scans are shown
Magnetic Resonance Imaging
Magnetic maging
Magnetic resonance imaging (MRI) has fewer indicationsthan CT in patients with paranasal sinus diseaseThis is primarily because MRI is markedly inferior toCT in defining the bony boundaries of the sinusesThe strength of MRI lies in its superior soft-tissue discriminationMRI is indicated in diseases that involve the paranasal sinuses in addition to thecranial cavity or orbit (eg tumors and congenitalmalformations such as encephaloceles)
MRI of the paranasal sinuses
The Nose and Sinuses
Structure The structure of the nose is made up of
four partsbull The surface anatomybull The nasal skeletonmdashcomposed of the
two nasal bones the paired upper lateral and lower lateral cartilages and the nasal septum covered in subcutaneous tissue and skin
bull The internal anatomymdashincludes the septum of the nose which forms the medial wall of the nasal cavity The turbinates on the lateral wall are also called conchae
bull The osteomeatal complexmdasha key functional area of the nose
Function The nose is the main route for inspired
air and its structure is related to this function As the air passes over the large surface area of the turbinates
The inspired gases are warmed and humidified Mucus on the mucosa of the nose removes large dust particles from the air as it is breathed in
The voice resonates in the sinuses and nose and this provides character to the speech
Pneumatization of the sinusesmdashthey are air filled spacesmdashreduces the weight of the skull
Diseases of thDiseases of the Outer and Inner Nosee Outer and
Inner Nose Erysipelas Definition of the disease ndash Erysipela is a skin infection that affects the superficial dermis and is caused by Streptococcus pyogenes (group A) It usually develops in the extremities and the face and less commonly on the scalp and genitals bull Epidemiologyaetiology ndash Erysipelas are more often seen in elderly infants and children patients with compromised immunology and diabetes -Predisposing factors are alcoholism skin ulceration puncture wounds fungal infections malnutrition and burns
Erysipelas
bull Symptomsbull ndash It usually presents of fever general fatigue bull -The skin lesion is a redindurated and elevated plaque
with borders that expand rapidly bull It is painful warm and accompanied by variable oedemabull -On the second or third day a flaccid bulla may develop
and desquamationbull bull Presence of regional lymph nodes is common
Erysipelas
bull Complicationsndash The most common complication is recurrencewhich is seen in 18ndash30 of the cases even afterproper antibiotic therapy Recurrence is seen moreoften in females than in malesA skin infection with S pyogenes could lead toglomerulonephritis
Erysipelas
bull Complicationsbull ndash The most common complication is recurrencebull which is seen in 18ndash30 of the cases even afterbull proper antibiotic therapy bull -Recurrence is seen morebull often in females than in males bull -A skin infection with S pyogenes could lead tobull glomerulonephritis
Erysipelas
bull bull Diagnosisbull ndash Diagnosis is based on the patientrsquos personal
historybull and physical examination particularly on inspectionbull of the skin
bull Blood cultures are positive in less thanbull 5 of cases
ErysipelasTherapyndash Conservative therapybull The preferred antibiotic is penicillin In mildcases with minor systemic symptoms penicillinV 500 mg orally every 6 h for 10 days or penicillinG benzathine 12 mil U intramuscularlyonceOther possibilities are amoxicillin 500 mgorally twice a day for 10 days or cephalexin 500mg orally every 6 h for 10 days
ErysipelasIn moderate and severe cases with significantsystemic symptoms hospitalization and intravenoustreatment is required penicillin G 2ndash4mil U intravenously every 4ndash6 h Cefazolin05ndash15 gm intravenously every 8 h cefotaxime1ndash2 gm intravenously every 8 h or ceftriaxone1ndash2 gm intravenously once a day should be administeredIn patients with a penicillin allergyclindamycin 600 mg intravenously every 8 h orvancomycin 15 mgkg intravenously twice a daymay be given
ErysipelaAdditional useful therapeutic optionsbull Prednisone 30 mg over 8 days might be consideredas well as elevation of the affected siteMoist heat compresses may be usefulbull Surgeryndash Debridement and drainage are indicated when bullaeabscesses or necroses are presentbull Differential diagnosisndash Contact dermatitisndash Asteatotic eczemandash Herpes zosterndash Angioneurotic oedemandash Osteomyelitis
Furuncle
bull Definition of the diseasebull ndash A furuncle is an infection that beginsbull at the hair follicle and spreads deeper into thebull dermis and subcutaneous tissue forming abull nodule After several days it developsbull into an abscess - red painful and fluctuantbull bull bull Epidemiologyaetiologybull ndash The aetiologic agent is Staphylococcus aureus
FuruncleSymptomsndashsymptoms are local and limited to thesite of infection Furuncles usually are wherehair follicles are present bull Complicationndash One complication is furunculosis multiple draining furunclesDiagnosisndash The diagnosis is based on clinical inspection - Cultures are not necessary when there is no systemic involvement but should beconsidered if systemic therapy (in case of feversignificant cellulitis or hospitalization) or whenmethicillin-resistant Staphylococcusaureus (MRSA) is considered
FuruncleTherapyndash When the furuncle is small application of moist heat compress to promote drainage -Larger furuncles should be drained by surgical incision-After drainage the area should be cleaned with anantiseptic (with chlorhexidinebetadine) should be applied twice
a dayndash If no systemic symptoms or extensive cellulitis arepresent simple topical care is usually curative andoral antibiotics are not necessary Otherwise systemictreatment is indicated and should cover anypossible MRSA
Furuncle
bull -Recommended antibiotics are trimethoprim-sulfamethoxazole
bull 1ndash2 tablets orally twice daily doxycyclinebull 100 mg orally twice dailybull or clindamycin 300ndash450 mg orally every 8 hbull - In severe cases vancomycin 15 mgkg
intravenouslybull every 12 h or clindamycin 600 mg intravenouslybull every 8 h
Midline Granulomabull A midline granuloma is an angiocentricbull lymphoma it was referred to as polymorphicbull reticulosis lethal midline granuloma and midline
malignant reticulosisbull bull Definition of the diseasebull ndash This rare disease is a lymphoma of extranodal
presentationall cases are positive for the Epstein-Barr virus
bull -This lymphoma most commonly appears in the midface region
Midline GranulomaEpidemiologyaetiologyndash This form of lymphoma is rare in Europe and theUnited States with a higher prevalence in Asia and PeruSymptomsndash The most common presentation is nasal obstruction with a destructive mass occupying the nosesinuses and palate
-Fever night sweatsand weight loss seen usually in Hodgkinrsquos lymphomaand other non-Hodgkinrsquos lymphomas (knownas ldquoB symptomsrdquo) are uncommon
Midline GranulomaDiagnosisndash The diagnosis is based on anatomopathologicalstudy The malignancy of the tumour manifested byextensive necrosis makes the histological diagnosisdifficult and often more biopsies are required forconfirmationbull Therapyndash Therapy consists of radiotherapy with or withoutchemotherapy
Midline Granuloma
bull Prognosisbull ndash Depending on the stage long-term remission or
experience a worseningbull prognosis with relapses which may include otherbull extranodal sites bull Involvement of extranodal sitesbull including the upper airway gastrointestinal tractbull skin
Wegenerrsquos Granulomatosis
bull Definition of the diseasebull ndash Wegenerrsquos granulomatosis is a systemic chronicbull vasculitis of small- and medium-sized blood vesselsbull with an autoimmune component It affectsbull particular organs with variable predilectionbull Epidemiologyaetiologybull ndash Wegenerrsquos granulomatosis is a rare disease It affects
about 1 in 20000ndash30000 people It is more prevalentbull in middle-aged Caucasian patients
Wegenerrsquos Granulomatosis
Symptomsndash The disease may present pulmonary upper
respiratory tract or renal In the disseminated form-The localised form ndash confinedto the upper respiratory region ndash is present in 25of the patients- It consists of nonspecific manifestationssuch as nasal obstruction crusting purulentor bloody rhinorrhea and painful or painless ulcers in oral or nasal cavities which are unresponsive tostandard medical treatment
Wegenerrsquos Granulomatosis
bull In some patients the nasal septum is perforatedbull which leads to saddle-nose deformity Less
commonbull symptoms are hoarseness stridor due to
subglotticbull stenosis otalgia otorrhea and conductivebull and sensorineural hearing loss Also ocular
symptomsbull such as scleritis conjunctivitis uveitis andbull episcleritis may be present
Wegenerrsquos Granulomatosis
bull ndash In the disseminated form pulmonary involvementbull is manifested by cough dyspnoea haemoptysisbull (due to an alveolar capillaritis necrotic lesions orbull endobronchial disease) and pleuritic painndashbull -Ninety per cent of patients have nasal symptomsbull and these symptoms are usually the first
manifestationof the diseasebull -Most patients have also renal involvementbull even if it is subclinical
Wegenerrsquos Granulomatosis
Diagnosis ndash Diagnosis of Wegenerrsquos granulomatosis is based on clinical findings that demonstrate lung (chest x-ray) kidney (urine analysis) or upper respiratory tract
involvement (oral or nasal ulcers or discharge) - positive blood analysis for cytoplasmic-staining antineutrophil
cytoplasmic antibodies (c-ANCA) and confirming proteinase 3 (PR3) ANCA or myeloperoxidase (MPO) ANCA ndash Biopsy is essential for diagnosis nonspecific chronic inflammation
and necrosis -Bacterial and fungal infections
Wegenerrsquos Granulomatosis
Therapyndash Conservative therapybull In the induction of disease remission highdosesteroids (e g prednisone 1 mgkgday) for1 month with tapering over several months aregiven In addition cyclophosphamide (2 mgkgday) should be administered for 6ndash12 monthsuntil symptoms disappear In the maintenanceof remission cyclophosphamide should be
Wegenerrsquos Granulomatosis
Antibiotics mainly trimethoprim-sulfamethoxazoleare given for prophylaxis againstPneumocystis jiroveci (formerly Pneumocystiscarinii) pneumonia (PCP) which may developduring immunosuppression and have a role inpreventing recurrencesbull Sinonasal manifestations may be treated with topical nasal steroids and nasal irrigations lowdosesystemic steroids and antibiotics when bacterial infection (typically Staphylococcus species) is suspected
Wegenerrsquos Granulomatosis
bull Prognosisbull ndash Most of the patients respond well to treatmentbull achieving symptom-free intervals of 5ndash20 yearsbull or more bull -Anatomical problems (sinusitis trachealbull stenosis) may require surgery bull Relapses can be long and troublesomebull Long-term complications are chronicbull renal failure hearing loss and deafness
Nasal Fractures Definition ndash A nasal fracture is a disruption of the nasal bone structure due to trauma It is the most frequently fractured facial bone Epidemiologyaetiology ndash Sports falls and assaults are the usual mechanisms of fracture -Males are affected twice as often as are females -Paediatric populations with a incidences during the second and third decades of life -Variables such as force impact direction nature of the striking object age and other will influence the pattern of injury to the components of the nose
Nasal Fractures
bull Symptomsbull ndash Deformity swelling epistaxis and periorbital
ecchymosis are signs that are suggestive of nasal fracture
bull bony crepitus and nasal segment mobilitybull ndash Epiphora bull Severe bilateral injuries to the lachrymal bones
arebull associated with depressed nasal fractures
Nasal Fractures Complications ndash Septal haematoma is one of the most severe early complications of nasal trauma and without drainage it results in abscess formation 6ndash7 days after trauma producing necrosis of the septal cartilage -Long-term problems such as saddle-nose deformity perforation columellar retraction and nasalbase
Septal infection could lead to osteomyelitis orbital and intracranial abscesses meningitis and cavernous sinus thrombosis -Cerebrospinal fluid leakage is a common complication of severe
nasal and frontal fractures
Nasal Fractures
bull Diagnostic proceduresbull ndash Inspectionbull bull Changes of appearance such as deviation andbull asymmetry bleeding watery drainage changesbull in nasal breathing and smell It is useful to comparebull the current presentation with old photographsbull (up to 40 of normal individuals havebull significant nose malformations)
Nasal Fractures Physical examination bull The diagnosis of a nasal fracture is made primarily by physical examination epistaxis nasal swelling and periorbital ecchymosis Nasal shape in the lateral and frontal inspection should be assessed Grasping the dorsum between two fingers and rocking the pyramid back and forth aids in assessing the mobility of nasal bones Internal structures should be evaluated by using a headlight and nasal speculum Clotted blood is removed by suction and assessment of haematoma mucosal tears and active bleeding is performed Bimanual palpation of the septum helps to differentiate septal swelling from haematoma ndash
Nasal FracturesRadiographybull There is no clear evidence of the role of radiographyin the management of nasal fracturesPlain films have up to a 66 false-positive rateas a result of misinterpretation of normal suturelines In addition old fractures are difficult todistinguishbull Three-dimensional CT is recommended for extensiveinjuries involving the nasal-orbital-ethmoidalcomplexndash
Nasal Fractures
bull Additionaluseful diagnostic proceduresbull bull Using a 0 or 30deg 4-mm endoscope is helpful inbull the assessment of posterior abnormalities If thebull patient is heavily sedated Brown-Gruss
provocationbull manoeuvres may be performed to determinebull deformities in upper middle or lower segmentsbull by compressing each compartment
Nasal FracturesConservative treatmentndash Treatment of bleedingbull For localised bleeding anterior sources may becauterised by silver nitrate or sealed with topicalmaterials such as thrombin combined withgelatin foam fibrin glue FloSealreg or other procoagulantmaterials If conservative measuresfail a formal anterior packing is placedbull Bleeding from branches of sphenopalatine orethmoid vessels requires anterior-posteriorpacking
Nasal Fractures
bull bull Surgical methods such as direct endoscopic vessel
bull cauterization or ligation have been shown tobull offer better haemostasis and patient comfortbull Angiography with embolization can also be
consideredbull in cases refractory to more conservativebull approaches
Nasal Fractures
bull Type of reductionbull bull Nondisplaced fractures should be treated withbull observation alone Closed nasal reduction is thebull best choice for simple injuries (isolated unilateralbull with medial displacement)bull bull An open approach should be considered in
severebull trauma (bilateral depressed fractures)
Nasal Fracturesbull Surgical principlesbull ndash Topical anaesthesia with cotton pledgets soakedbull with 4 cocaine or 005 oxymethazoline combinedbull with 4 topical lidocaine should be appliedbull for 5ndash10 min Local anaesthesia should also be injectedbull (1 lidocaine and 1100000 epinephrine)bull along the septum lateral walls and floor of the nasalbull cavitybull bull
Nasal FracturesClosed reductionndashndash The nasal bones are grasped between two fingersand pressure is applied laterally in theopposite direction of the deviation A bluntelevator may be used from within the nose incases of significant medial collapse Walshamforceps can be of help Reduction of the septumshould be performed with the use ofAsch forceps
Nasal Fractures
bull To prevent collapse of the postreductionbull framework nasal packing should be placedbull for 3ndash5 days Septum splints are recommendedbull in comminuted septal fractures withbull severe mucosal lesions External nasal splintingbull for 10 days (Aquaplastreg Thermoplastreg)bull provides nasal protection Nasal saline spraysbull prevent crusting and oral antibiotics should
Nasal Fractures
bull Open reductionbull ndashndash Immediate repair of fractures by using
widebull surgical exposure reduction fixation and
reconstructionbull ndashndash The second option is delayed correctionbull (6 months or more) of persistent deformitiesbull using standard techniques of rhinoplasty
Deviated Nasal Septum
bull Definition of the diseasebull ndash Deviation of the nasal septum is a common causebull of unilateral nasal airway obstruction in which thebull nasal septum is displacedbull bull Epidemiologyaetiologybull ndash Developmental septal abnormalities Septal cartilage
damage in the neonatal period andbull during birth can cause severe septal deviation inbull the absence of a history of nasal trauma
Deviated Nasal Septum
bull Symptomsbull ndash Patients may present with a history of sinusitis
allergicbull rhinitis obstructive sleep apnoea previousbull nasal surgery or recent nasal trauma Unilateral or
bilateral nasal airway obstruction that is unrelievedbull with decongestants or nasal steroid sprays is oftenbull seenbull bull
Deviated Nasal SeptumDiagnosisndashExamination external dorsal deviation or the columella and caudal septummay be deflected off the midline (caudal subluxation)ndash Inspections of the nasal cavity and anterior-posteriorrhinoscopy are helpful in diagnosing the locationtype and severity of septal deformityThe endoscope is also useful in identifying polypsthe severity and extent of posterior septaldeviations and bony spurs and locating areas ofseptal perforation or mucosal injury
Deviated Nasal Septum
bull Therapybull ndash Septoplasty is a procedurebull The areabull of deviation is corrected or resected in order tobull leave behind as much cartilage and bone as
possiblebull Cartilage resection is minimised and can be
repositioned reshaped or recontoured using a variety of methods
Deviated Nasal Septum
bull ndash Indications of septoplasty before the growth period
bull of the nose is finished should be very limited bull -In these cases surgery must preserve all the
cartilagebull in order to prevent external changes of the
shape ofbull the nose
Deviated Nasal Septum
bull Complicationsbull ndash Frequent complications include haematoma andbull infection Cerebrospinal fluid leak is a rare but
potentiallybull serious complicationbull It is usually the resultbull of avulsion or damage to the cribriform plate whenbull handling the perpendicular plate of the ethmoidbull ndash Other complications include epistaxis nasal
Deviated Nasal Septum
bull Other complications include epistaxis nasal obstruction
bull due to residual deviation synechiae returnbull of the cartilaginous deviation septal perforationbull anosmia and cosmetic nasal deformities suchbull as widened alar rim margins drooping nasal tipbull columella retraction and a sunken dorsum with abull supratip saddle formation
Septal perforation with minor crusting View from provide closure of the
incision
Septal Haematoma
bull A septal haematoma is a blood collection under the perichondrium
bull of the septum and cartilagebull bull bull Epidemiologyaetiologybull ndash A septal haematoma is one of the most
severe complications of nasal trauma
Septal Haematoma
bull Diagnosisbull ndash Signs and symptoms include intense pain
swellingbull haematoma of the upper lip and philtrum
area andbull complete nasal airway obstruction
Septal HaematomaTherapyndash Management consists of drainage through a mucoperichondrial incision Immediate treatment isnecessary to prevent long-term problems such asa saddle-nose deformity perforation columellarretraction and nasal-base widening In childrenseptal destruction can lead to devastating nasal andmidfacial growth abnormalitiesbull Surgeryndash Incision and evacuation of the collection is performedDrainage of a septal haematoma should
Septal HaematomaSurgeryndash Incision and evacuation of the collection is performedDrainage of a septal haematoma should provide closure of the incision
Splints or transseptal sutures are placed to obliterate thepotential space and prevent collectionInfection involving the septal cartilage Reconstruction with autologouscartilage is then performed in a second stage Oral antibiotics should be given
Nasal DeformitySaddle-nose deformityndash A saddle-nose deformity is characterised by a loss ofnasal dorsal height and compromised nasal supportstructures -Other case observed are depressionof the middle vault and dorsum loss of nasal tipsupport and definition shortened (vertical) nasal length over rotation of the nasal tip and retrusion ofthe nasal spine and caudal septum It is also knownas a ldquoPug noserdquo or ldquoboxerrsquos noserdquo both of which referto various degrees of nasal dorsal depressionbull
Nasal DeformityEpidemiologyaetiologyndash Prevalence is higher in population groups prone to facial trauma (ie boxers athletes) those with historiesof intranasal cocaine use nasal surgery (e g radical submucosal septal resection reductive rhinoplasty)ndash A saddle-nose deformity can be congenital or acquired It can be noticed as a part of individual familialsyndromic and ethnic characteristics - Most deformities are due to traumatic and iatrogeniccauses Medical causes are Wegenerrsquosgranulomatosis relapsing polychondritis leprosy (Hansenrsquos disease) syphilis ectodermal dysplasiaand intranasal cocaine use
Nasal Deformity
bull Therapybull ndash Nasal reconstruction indications depend on patientbull selection surgeon experience and aetiology of thebull deformity bull Indications for surgery can be functionalbull aesthetic or most commonly both In individuals
with a compromised nasal airway a nasoseptalbull reconstruction is indicated
Nasal Deformity
bull Contraindications bull include patients with malignantbull chronic or autoimmune disease conditions drugbull abuse poor perioperative risk profile and unrealisticbull expectationsbull ndash Multiple previous rhinoplasties and certain
professionsbull (mixed martial artists boxers and other contactbull sports) are relative contraindications
Nasal DeformitySeptoplastyndash Septoplasty is performed to correct nasal obstructioncaused by septal deformityndash Usually septoplasty is performed under general anaesthesiawith the patient in the supine position with the head elevated by approximately 30 (Righthandedsurgeons approach from the right side)ndash Local vasoconstrictive anaesthesia is applied notonly to reduce postoperative pain but also more importantly to achieve vasoconstriction of themucosa and less intraoperative haemorrhage Lidocainewith adrenaline or epinephrine is usedalthough in patients with cardiac hypersensitivityoxymetazoline might be preferred
Nasal Deformity
bull Septoplasty begins with the incision of septal mucosabull Most operative techniques utilise a hemitransfixionbull incision at the caudal end of septum so thatbull deviation at this point might be reached as wellbull as a transfixion incision that is easily obtained ifbull needed (Right-handed surgeons normally choosebull the left side but that may vary when deviation isbull convex towards the right)
Nasal DeformityA columella retractor is placed over the columellaand by pulling it laterally the caudal border of theseptum is exposed Ala can be protected by an alaprotector A vertical incision with a no 15 bladeover the caudal end of septum is performed untilreaching the plane of the septal cartilage It is essentialto correctly identify the perichondrium and byusing the Cottle elevator dissect and lift it creatinga flap As the dissection proceeds along the septalcartilage a longer speculum (no 5) is introduced sothat elevation of the mucoperichondrium is doneunder constant visual controlndash The next step is to dissect the mucoperiostium
Nasal DeformityDissecting over the bony-cartilaginous junctionwhen joining both tunnels might be difficult and is
especially prone to membrane perforationndash If needed the same tunnels are to be created on the
other side of the septum Then deviated parts of
septum are identified and removed either with a
knife or a Freer chisel
Nasal Deformitybull septum from the maxillary crest the septum mustbull be separated from the perpendicular plate trimmedbull along the inferior border placed back onto the crestbull and sutured to the periosteum If the deformity involvesbull the vomer an osteotome is used Care mustbull be taken not to break the cribriform plate becausebull it could cause a cerebrospinal fistula
Nasal Deformity
bull Once the septal deviation is corrected the flapsbull and hemitransfixion incision are mattressed
withbull absorbable sutures Nasal packing to prevent
synechiaebull and postoperative septal haematoma mightbull be advised but should be removed within 72 h

Nasal Endoscopy
Nasal Endoscopy
Imaging of the Nose and Paranasal Sinuses
Conventional RadiographsStandard paranasal sinus radiographs in the occipitomental
projection ( Water projection) and
occipitofrontal projection Caldwell projection) in cases of acute inflammation
They are also obtained to evaluate midfacial fractures
Computed Tomography (CT) the main indicationsfor CT scanning of the
nose and paranasal sinuses
are- chronic sinusitis - -trauma (especially
frontobasal -fractures)
-and tumors
The occipitofrontal projection is better for evaluating theethmoid cells and frontal sinus
occipitomental projection demonstrates the maxillarysinus and gives a limited view of the sphenoid sinus
Computed tomography of the paranasal sinuses
Four representative coronal CT scans are shown
Four representative coronal CT scans are shown
Magnetic Resonance Imaging
Magnetic maging
Magnetic resonance imaging (MRI) has fewer indicationsthan CT in patients with paranasal sinus diseaseThis is primarily because MRI is markedly inferior toCT in defining the bony boundaries of the sinusesThe strength of MRI lies in its superior soft-tissue discriminationMRI is indicated in diseases that involve the paranasal sinuses in addition to thecranial cavity or orbit (eg tumors and congenitalmalformations such as encephaloceles)
MRI of the paranasal sinuses
The Nose and Sinuses
Structure The structure of the nose is made up of
four partsbull The surface anatomybull The nasal skeletonmdashcomposed of the
two nasal bones the paired upper lateral and lower lateral cartilages and the nasal septum covered in subcutaneous tissue and skin
bull The internal anatomymdashincludes the septum of the nose which forms the medial wall of the nasal cavity The turbinates on the lateral wall are also called conchae
bull The osteomeatal complexmdasha key functional area of the nose
Function The nose is the main route for inspired
air and its structure is related to this function As the air passes over the large surface area of the turbinates
The inspired gases are warmed and humidified Mucus on the mucosa of the nose removes large dust particles from the air as it is breathed in
The voice resonates in the sinuses and nose and this provides character to the speech
Pneumatization of the sinusesmdashthey are air filled spacesmdashreduces the weight of the skull
Diseases of thDiseases of the Outer and Inner Nosee Outer and
Inner Nose Erysipelas Definition of the disease ndash Erysipela is a skin infection that affects the superficial dermis and is caused by Streptococcus pyogenes (group A) It usually develops in the extremities and the face and less commonly on the scalp and genitals bull Epidemiologyaetiology ndash Erysipelas are more often seen in elderly infants and children patients with compromised immunology and diabetes -Predisposing factors are alcoholism skin ulceration puncture wounds fungal infections malnutrition and burns
Erysipelas
bull Symptomsbull ndash It usually presents of fever general fatigue bull -The skin lesion is a redindurated and elevated plaque
with borders that expand rapidly bull It is painful warm and accompanied by variable oedemabull -On the second or third day a flaccid bulla may develop
and desquamationbull bull Presence of regional lymph nodes is common
Erysipelas
bull Complicationsndash The most common complication is recurrencewhich is seen in 18ndash30 of the cases even afterproper antibiotic therapy Recurrence is seen moreoften in females than in malesA skin infection with S pyogenes could lead toglomerulonephritis
Erysipelas
bull Complicationsbull ndash The most common complication is recurrencebull which is seen in 18ndash30 of the cases even afterbull proper antibiotic therapy bull -Recurrence is seen morebull often in females than in males bull -A skin infection with S pyogenes could lead tobull glomerulonephritis
Erysipelas
bull bull Diagnosisbull ndash Diagnosis is based on the patientrsquos personal
historybull and physical examination particularly on inspectionbull of the skin
bull Blood cultures are positive in less thanbull 5 of cases
ErysipelasTherapyndash Conservative therapybull The preferred antibiotic is penicillin In mildcases with minor systemic symptoms penicillinV 500 mg orally every 6 h for 10 days or penicillinG benzathine 12 mil U intramuscularlyonceOther possibilities are amoxicillin 500 mgorally twice a day for 10 days or cephalexin 500mg orally every 6 h for 10 days
ErysipelasIn moderate and severe cases with significantsystemic symptoms hospitalization and intravenoustreatment is required penicillin G 2ndash4mil U intravenously every 4ndash6 h Cefazolin05ndash15 gm intravenously every 8 h cefotaxime1ndash2 gm intravenously every 8 h or ceftriaxone1ndash2 gm intravenously once a day should be administeredIn patients with a penicillin allergyclindamycin 600 mg intravenously every 8 h orvancomycin 15 mgkg intravenously twice a daymay be given
ErysipelaAdditional useful therapeutic optionsbull Prednisone 30 mg over 8 days might be consideredas well as elevation of the affected siteMoist heat compresses may be usefulbull Surgeryndash Debridement and drainage are indicated when bullaeabscesses or necroses are presentbull Differential diagnosisndash Contact dermatitisndash Asteatotic eczemandash Herpes zosterndash Angioneurotic oedemandash Osteomyelitis
Furuncle
bull Definition of the diseasebull ndash A furuncle is an infection that beginsbull at the hair follicle and spreads deeper into thebull dermis and subcutaneous tissue forming abull nodule After several days it developsbull into an abscess - red painful and fluctuantbull bull bull Epidemiologyaetiologybull ndash The aetiologic agent is Staphylococcus aureus
FuruncleSymptomsndashsymptoms are local and limited to thesite of infection Furuncles usually are wherehair follicles are present bull Complicationndash One complication is furunculosis multiple draining furunclesDiagnosisndash The diagnosis is based on clinical inspection - Cultures are not necessary when there is no systemic involvement but should beconsidered if systemic therapy (in case of feversignificant cellulitis or hospitalization) or whenmethicillin-resistant Staphylococcusaureus (MRSA) is considered
FuruncleTherapyndash When the furuncle is small application of moist heat compress to promote drainage -Larger furuncles should be drained by surgical incision-After drainage the area should be cleaned with anantiseptic (with chlorhexidinebetadine) should be applied twice
a dayndash If no systemic symptoms or extensive cellulitis arepresent simple topical care is usually curative andoral antibiotics are not necessary Otherwise systemictreatment is indicated and should cover anypossible MRSA
Furuncle
bull -Recommended antibiotics are trimethoprim-sulfamethoxazole
bull 1ndash2 tablets orally twice daily doxycyclinebull 100 mg orally twice dailybull or clindamycin 300ndash450 mg orally every 8 hbull - In severe cases vancomycin 15 mgkg
intravenouslybull every 12 h or clindamycin 600 mg intravenouslybull every 8 h
Midline Granulomabull A midline granuloma is an angiocentricbull lymphoma it was referred to as polymorphicbull reticulosis lethal midline granuloma and midline
malignant reticulosisbull bull Definition of the diseasebull ndash This rare disease is a lymphoma of extranodal
presentationall cases are positive for the Epstein-Barr virus
bull -This lymphoma most commonly appears in the midface region
Midline GranulomaEpidemiologyaetiologyndash This form of lymphoma is rare in Europe and theUnited States with a higher prevalence in Asia and PeruSymptomsndash The most common presentation is nasal obstruction with a destructive mass occupying the nosesinuses and palate
-Fever night sweatsand weight loss seen usually in Hodgkinrsquos lymphomaand other non-Hodgkinrsquos lymphomas (knownas ldquoB symptomsrdquo) are uncommon
Midline GranulomaDiagnosisndash The diagnosis is based on anatomopathologicalstudy The malignancy of the tumour manifested byextensive necrosis makes the histological diagnosisdifficult and often more biopsies are required forconfirmationbull Therapyndash Therapy consists of radiotherapy with or withoutchemotherapy
Midline Granuloma
bull Prognosisbull ndash Depending on the stage long-term remission or
experience a worseningbull prognosis with relapses which may include otherbull extranodal sites bull Involvement of extranodal sitesbull including the upper airway gastrointestinal tractbull skin
Wegenerrsquos Granulomatosis
bull Definition of the diseasebull ndash Wegenerrsquos granulomatosis is a systemic chronicbull vasculitis of small- and medium-sized blood vesselsbull with an autoimmune component It affectsbull particular organs with variable predilectionbull Epidemiologyaetiologybull ndash Wegenerrsquos granulomatosis is a rare disease It affects
about 1 in 20000ndash30000 people It is more prevalentbull in middle-aged Caucasian patients
Wegenerrsquos Granulomatosis
Symptomsndash The disease may present pulmonary upper
respiratory tract or renal In the disseminated form-The localised form ndash confinedto the upper respiratory region ndash is present in 25of the patients- It consists of nonspecific manifestationssuch as nasal obstruction crusting purulentor bloody rhinorrhea and painful or painless ulcers in oral or nasal cavities which are unresponsive tostandard medical treatment
Wegenerrsquos Granulomatosis
bull In some patients the nasal septum is perforatedbull which leads to saddle-nose deformity Less
commonbull symptoms are hoarseness stridor due to
subglotticbull stenosis otalgia otorrhea and conductivebull and sensorineural hearing loss Also ocular
symptomsbull such as scleritis conjunctivitis uveitis andbull episcleritis may be present
Wegenerrsquos Granulomatosis
bull ndash In the disseminated form pulmonary involvementbull is manifested by cough dyspnoea haemoptysisbull (due to an alveolar capillaritis necrotic lesions orbull endobronchial disease) and pleuritic painndashbull -Ninety per cent of patients have nasal symptomsbull and these symptoms are usually the first
manifestationof the diseasebull -Most patients have also renal involvementbull even if it is subclinical
Wegenerrsquos Granulomatosis
Diagnosis ndash Diagnosis of Wegenerrsquos granulomatosis is based on clinical findings that demonstrate lung (chest x-ray) kidney (urine analysis) or upper respiratory tract
involvement (oral or nasal ulcers or discharge) - positive blood analysis for cytoplasmic-staining antineutrophil
cytoplasmic antibodies (c-ANCA) and confirming proteinase 3 (PR3) ANCA or myeloperoxidase (MPO) ANCA ndash Biopsy is essential for diagnosis nonspecific chronic inflammation
and necrosis -Bacterial and fungal infections
Wegenerrsquos Granulomatosis
Therapyndash Conservative therapybull In the induction of disease remission highdosesteroids (e g prednisone 1 mgkgday) for1 month with tapering over several months aregiven In addition cyclophosphamide (2 mgkgday) should be administered for 6ndash12 monthsuntil symptoms disappear In the maintenanceof remission cyclophosphamide should be
Wegenerrsquos Granulomatosis
Antibiotics mainly trimethoprim-sulfamethoxazoleare given for prophylaxis againstPneumocystis jiroveci (formerly Pneumocystiscarinii) pneumonia (PCP) which may developduring immunosuppression and have a role inpreventing recurrencesbull Sinonasal manifestations may be treated with topical nasal steroids and nasal irrigations lowdosesystemic steroids and antibiotics when bacterial infection (typically Staphylococcus species) is suspected
Wegenerrsquos Granulomatosis
bull Prognosisbull ndash Most of the patients respond well to treatmentbull achieving symptom-free intervals of 5ndash20 yearsbull or more bull -Anatomical problems (sinusitis trachealbull stenosis) may require surgery bull Relapses can be long and troublesomebull Long-term complications are chronicbull renal failure hearing loss and deafness
Nasal Fractures Definition ndash A nasal fracture is a disruption of the nasal bone structure due to trauma It is the most frequently fractured facial bone Epidemiologyaetiology ndash Sports falls and assaults are the usual mechanisms of fracture -Males are affected twice as often as are females -Paediatric populations with a incidences during the second and third decades of life -Variables such as force impact direction nature of the striking object age and other will influence the pattern of injury to the components of the nose
Nasal Fractures
bull Symptomsbull ndash Deformity swelling epistaxis and periorbital
ecchymosis are signs that are suggestive of nasal fracture
bull bony crepitus and nasal segment mobilitybull ndash Epiphora bull Severe bilateral injuries to the lachrymal bones
arebull associated with depressed nasal fractures
Nasal Fractures Complications ndash Septal haematoma is one of the most severe early complications of nasal trauma and without drainage it results in abscess formation 6ndash7 days after trauma producing necrosis of the septal cartilage -Long-term problems such as saddle-nose deformity perforation columellar retraction and nasalbase
Septal infection could lead to osteomyelitis orbital and intracranial abscesses meningitis and cavernous sinus thrombosis -Cerebrospinal fluid leakage is a common complication of severe
nasal and frontal fractures
Nasal Fractures
bull Diagnostic proceduresbull ndash Inspectionbull bull Changes of appearance such as deviation andbull asymmetry bleeding watery drainage changesbull in nasal breathing and smell It is useful to comparebull the current presentation with old photographsbull (up to 40 of normal individuals havebull significant nose malformations)
Nasal Fractures Physical examination bull The diagnosis of a nasal fracture is made primarily by physical examination epistaxis nasal swelling and periorbital ecchymosis Nasal shape in the lateral and frontal inspection should be assessed Grasping the dorsum between two fingers and rocking the pyramid back and forth aids in assessing the mobility of nasal bones Internal structures should be evaluated by using a headlight and nasal speculum Clotted blood is removed by suction and assessment of haematoma mucosal tears and active bleeding is performed Bimanual palpation of the septum helps to differentiate septal swelling from haematoma ndash
Nasal FracturesRadiographybull There is no clear evidence of the role of radiographyin the management of nasal fracturesPlain films have up to a 66 false-positive rateas a result of misinterpretation of normal suturelines In addition old fractures are difficult todistinguishbull Three-dimensional CT is recommended for extensiveinjuries involving the nasal-orbital-ethmoidalcomplexndash
Nasal Fractures
bull Additionaluseful diagnostic proceduresbull bull Using a 0 or 30deg 4-mm endoscope is helpful inbull the assessment of posterior abnormalities If thebull patient is heavily sedated Brown-Gruss
provocationbull manoeuvres may be performed to determinebull deformities in upper middle or lower segmentsbull by compressing each compartment
Nasal FracturesConservative treatmentndash Treatment of bleedingbull For localised bleeding anterior sources may becauterised by silver nitrate or sealed with topicalmaterials such as thrombin combined withgelatin foam fibrin glue FloSealreg or other procoagulantmaterials If conservative measuresfail a formal anterior packing is placedbull Bleeding from branches of sphenopalatine orethmoid vessels requires anterior-posteriorpacking
Nasal Fractures
bull bull Surgical methods such as direct endoscopic vessel
bull cauterization or ligation have been shown tobull offer better haemostasis and patient comfortbull Angiography with embolization can also be
consideredbull in cases refractory to more conservativebull approaches
Nasal Fractures
bull Type of reductionbull bull Nondisplaced fractures should be treated withbull observation alone Closed nasal reduction is thebull best choice for simple injuries (isolated unilateralbull with medial displacement)bull bull An open approach should be considered in
severebull trauma (bilateral depressed fractures)
Nasal Fracturesbull Surgical principlesbull ndash Topical anaesthesia with cotton pledgets soakedbull with 4 cocaine or 005 oxymethazoline combinedbull with 4 topical lidocaine should be appliedbull for 5ndash10 min Local anaesthesia should also be injectedbull (1 lidocaine and 1100000 epinephrine)bull along the septum lateral walls and floor of the nasalbull cavitybull bull
Nasal FracturesClosed reductionndashndash The nasal bones are grasped between two fingersand pressure is applied laterally in theopposite direction of the deviation A bluntelevator may be used from within the nose incases of significant medial collapse Walshamforceps can be of help Reduction of the septumshould be performed with the use ofAsch forceps
Nasal Fractures
bull To prevent collapse of the postreductionbull framework nasal packing should be placedbull for 3ndash5 days Septum splints are recommendedbull in comminuted septal fractures withbull severe mucosal lesions External nasal splintingbull for 10 days (Aquaplastreg Thermoplastreg)bull provides nasal protection Nasal saline spraysbull prevent crusting and oral antibiotics should
Nasal Fractures
bull Open reductionbull ndashndash Immediate repair of fractures by using
widebull surgical exposure reduction fixation and
reconstructionbull ndashndash The second option is delayed correctionbull (6 months or more) of persistent deformitiesbull using standard techniques of rhinoplasty
Deviated Nasal Septum
bull Definition of the diseasebull ndash Deviation of the nasal septum is a common causebull of unilateral nasal airway obstruction in which thebull nasal septum is displacedbull bull Epidemiologyaetiologybull ndash Developmental septal abnormalities Septal cartilage
damage in the neonatal period andbull during birth can cause severe septal deviation inbull the absence of a history of nasal trauma
Deviated Nasal Septum
bull Symptomsbull ndash Patients may present with a history of sinusitis
allergicbull rhinitis obstructive sleep apnoea previousbull nasal surgery or recent nasal trauma Unilateral or
bilateral nasal airway obstruction that is unrelievedbull with decongestants or nasal steroid sprays is oftenbull seenbull bull
Deviated Nasal SeptumDiagnosisndashExamination external dorsal deviation or the columella and caudal septummay be deflected off the midline (caudal subluxation)ndash Inspections of the nasal cavity and anterior-posteriorrhinoscopy are helpful in diagnosing the locationtype and severity of septal deformityThe endoscope is also useful in identifying polypsthe severity and extent of posterior septaldeviations and bony spurs and locating areas ofseptal perforation or mucosal injury
Deviated Nasal Septum
bull Therapybull ndash Septoplasty is a procedurebull The areabull of deviation is corrected or resected in order tobull leave behind as much cartilage and bone as
possiblebull Cartilage resection is minimised and can be
repositioned reshaped or recontoured using a variety of methods
Deviated Nasal Septum
bull ndash Indications of septoplasty before the growth period
bull of the nose is finished should be very limited bull -In these cases surgery must preserve all the
cartilagebull in order to prevent external changes of the
shape ofbull the nose
Deviated Nasal Septum
bull Complicationsbull ndash Frequent complications include haematoma andbull infection Cerebrospinal fluid leak is a rare but
potentiallybull serious complicationbull It is usually the resultbull of avulsion or damage to the cribriform plate whenbull handling the perpendicular plate of the ethmoidbull ndash Other complications include epistaxis nasal
Deviated Nasal Septum
bull Other complications include epistaxis nasal obstruction
bull due to residual deviation synechiae returnbull of the cartilaginous deviation septal perforationbull anosmia and cosmetic nasal deformities suchbull as widened alar rim margins drooping nasal tipbull columella retraction and a sunken dorsum with abull supratip saddle formation
Septal perforation with minor crusting View from provide closure of the
incision
Septal Haematoma
bull A septal haematoma is a blood collection under the perichondrium
bull of the septum and cartilagebull bull bull Epidemiologyaetiologybull ndash A septal haematoma is one of the most
severe complications of nasal trauma
Septal Haematoma
bull Diagnosisbull ndash Signs and symptoms include intense pain
swellingbull haematoma of the upper lip and philtrum
area andbull complete nasal airway obstruction
Septal HaematomaTherapyndash Management consists of drainage through a mucoperichondrial incision Immediate treatment isnecessary to prevent long-term problems such asa saddle-nose deformity perforation columellarretraction and nasal-base widening In childrenseptal destruction can lead to devastating nasal andmidfacial growth abnormalitiesbull Surgeryndash Incision and evacuation of the collection is performedDrainage of a septal haematoma should
Septal HaematomaSurgeryndash Incision and evacuation of the collection is performedDrainage of a septal haematoma should provide closure of the incision
Splints or transseptal sutures are placed to obliterate thepotential space and prevent collectionInfection involving the septal cartilage Reconstruction with autologouscartilage is then performed in a second stage Oral antibiotics should be given
Nasal DeformitySaddle-nose deformityndash A saddle-nose deformity is characterised by a loss ofnasal dorsal height and compromised nasal supportstructures -Other case observed are depressionof the middle vault and dorsum loss of nasal tipsupport and definition shortened (vertical) nasal length over rotation of the nasal tip and retrusion ofthe nasal spine and caudal septum It is also knownas a ldquoPug noserdquo or ldquoboxerrsquos noserdquo both of which referto various degrees of nasal dorsal depressionbull
Nasal DeformityEpidemiologyaetiologyndash Prevalence is higher in population groups prone to facial trauma (ie boxers athletes) those with historiesof intranasal cocaine use nasal surgery (e g radical submucosal septal resection reductive rhinoplasty)ndash A saddle-nose deformity can be congenital or acquired It can be noticed as a part of individual familialsyndromic and ethnic characteristics - Most deformities are due to traumatic and iatrogeniccauses Medical causes are Wegenerrsquosgranulomatosis relapsing polychondritis leprosy (Hansenrsquos disease) syphilis ectodermal dysplasiaand intranasal cocaine use
Nasal Deformity
bull Therapybull ndash Nasal reconstruction indications depend on patientbull selection surgeon experience and aetiology of thebull deformity bull Indications for surgery can be functionalbull aesthetic or most commonly both In individuals
with a compromised nasal airway a nasoseptalbull reconstruction is indicated
Nasal Deformity
bull Contraindications bull include patients with malignantbull chronic or autoimmune disease conditions drugbull abuse poor perioperative risk profile and unrealisticbull expectationsbull ndash Multiple previous rhinoplasties and certain
professionsbull (mixed martial artists boxers and other contactbull sports) are relative contraindications
Nasal DeformitySeptoplastyndash Septoplasty is performed to correct nasal obstructioncaused by septal deformityndash Usually septoplasty is performed under general anaesthesiawith the patient in the supine position with the head elevated by approximately 30 (Righthandedsurgeons approach from the right side)ndash Local vasoconstrictive anaesthesia is applied notonly to reduce postoperative pain but also more importantly to achieve vasoconstriction of themucosa and less intraoperative haemorrhage Lidocainewith adrenaline or epinephrine is usedalthough in patients with cardiac hypersensitivityoxymetazoline might be preferred
Nasal Deformity
bull Septoplasty begins with the incision of septal mucosabull Most operative techniques utilise a hemitransfixionbull incision at the caudal end of septum so thatbull deviation at this point might be reached as wellbull as a transfixion incision that is easily obtained ifbull needed (Right-handed surgeons normally choosebull the left side but that may vary when deviation isbull convex towards the right)
Nasal DeformityA columella retractor is placed over the columellaand by pulling it laterally the caudal border of theseptum is exposed Ala can be protected by an alaprotector A vertical incision with a no 15 bladeover the caudal end of septum is performed untilreaching the plane of the septal cartilage It is essentialto correctly identify the perichondrium and byusing the Cottle elevator dissect and lift it creatinga flap As the dissection proceeds along the septalcartilage a longer speculum (no 5) is introduced sothat elevation of the mucoperichondrium is doneunder constant visual controlndash The next step is to dissect the mucoperiostium
Nasal DeformityDissecting over the bony-cartilaginous junctionwhen joining both tunnels might be difficult and is
especially prone to membrane perforationndash If needed the same tunnels are to be created on the
other side of the septum Then deviated parts of
septum are identified and removed either with a
knife or a Freer chisel
Nasal Deformitybull septum from the maxillary crest the septum mustbull be separated from the perpendicular plate trimmedbull along the inferior border placed back onto the crestbull and sutured to the periosteum If the deformity involvesbull the vomer an osteotome is used Care mustbull be taken not to break the cribriform plate becausebull it could cause a cerebrospinal fistula
Nasal Deformity
bull Once the septal deviation is corrected the flapsbull and hemitransfixion incision are mattressed
withbull absorbable sutures Nasal packing to prevent
synechiaebull and postoperative septal haematoma mightbull be advised but should be removed within 72 h

Nasal Endoscopy
Imaging of the Nose and Paranasal Sinuses
Conventional RadiographsStandard paranasal sinus radiographs in the occipitomental
projection ( Water projection) and
occipitofrontal projection Caldwell projection) in cases of acute inflammation
They are also obtained to evaluate midfacial fractures
Computed Tomography (CT) the main indicationsfor CT scanning of the
nose and paranasal sinuses
are- chronic sinusitis - -trauma (especially
frontobasal -fractures)
-and tumors
The occipitofrontal projection is better for evaluating theethmoid cells and frontal sinus
occipitomental projection demonstrates the maxillarysinus and gives a limited view of the sphenoid sinus
Computed tomography of the paranasal sinuses
Four representative coronal CT scans are shown
Four representative coronal CT scans are shown
Magnetic Resonance Imaging
Magnetic maging
Magnetic resonance imaging (MRI) has fewer indicationsthan CT in patients with paranasal sinus diseaseThis is primarily because MRI is markedly inferior toCT in defining the bony boundaries of the sinusesThe strength of MRI lies in its superior soft-tissue discriminationMRI is indicated in diseases that involve the paranasal sinuses in addition to thecranial cavity or orbit (eg tumors and congenitalmalformations such as encephaloceles)
MRI of the paranasal sinuses
The Nose and Sinuses
Structure The structure of the nose is made up of
four partsbull The surface anatomybull The nasal skeletonmdashcomposed of the
two nasal bones the paired upper lateral and lower lateral cartilages and the nasal septum covered in subcutaneous tissue and skin
bull The internal anatomymdashincludes the septum of the nose which forms the medial wall of the nasal cavity The turbinates on the lateral wall are also called conchae
bull The osteomeatal complexmdasha key functional area of the nose
Function The nose is the main route for inspired
air and its structure is related to this function As the air passes over the large surface area of the turbinates
The inspired gases are warmed and humidified Mucus on the mucosa of the nose removes large dust particles from the air as it is breathed in
The voice resonates in the sinuses and nose and this provides character to the speech
Pneumatization of the sinusesmdashthey are air filled spacesmdashreduces the weight of the skull
Diseases of thDiseases of the Outer and Inner Nosee Outer and
Inner Nose Erysipelas Definition of the disease ndash Erysipela is a skin infection that affects the superficial dermis and is caused by Streptococcus pyogenes (group A) It usually develops in the extremities and the face and less commonly on the scalp and genitals bull Epidemiologyaetiology ndash Erysipelas are more often seen in elderly infants and children patients with compromised immunology and diabetes -Predisposing factors are alcoholism skin ulceration puncture wounds fungal infections malnutrition and burns
Erysipelas
bull Symptomsbull ndash It usually presents of fever general fatigue bull -The skin lesion is a redindurated and elevated plaque
with borders that expand rapidly bull It is painful warm and accompanied by variable oedemabull -On the second or third day a flaccid bulla may develop
and desquamationbull bull Presence of regional lymph nodes is common
Erysipelas
bull Complicationsndash The most common complication is recurrencewhich is seen in 18ndash30 of the cases even afterproper antibiotic therapy Recurrence is seen moreoften in females than in malesA skin infection with S pyogenes could lead toglomerulonephritis
Erysipelas
bull Complicationsbull ndash The most common complication is recurrencebull which is seen in 18ndash30 of the cases even afterbull proper antibiotic therapy bull -Recurrence is seen morebull often in females than in males bull -A skin infection with S pyogenes could lead tobull glomerulonephritis
Erysipelas
bull bull Diagnosisbull ndash Diagnosis is based on the patientrsquos personal
historybull and physical examination particularly on inspectionbull of the skin
bull Blood cultures are positive in less thanbull 5 of cases
ErysipelasTherapyndash Conservative therapybull The preferred antibiotic is penicillin In mildcases with minor systemic symptoms penicillinV 500 mg orally every 6 h for 10 days or penicillinG benzathine 12 mil U intramuscularlyonceOther possibilities are amoxicillin 500 mgorally twice a day for 10 days or cephalexin 500mg orally every 6 h for 10 days
ErysipelasIn moderate and severe cases with significantsystemic symptoms hospitalization and intravenoustreatment is required penicillin G 2ndash4mil U intravenously every 4ndash6 h Cefazolin05ndash15 gm intravenously every 8 h cefotaxime1ndash2 gm intravenously every 8 h or ceftriaxone1ndash2 gm intravenously once a day should be administeredIn patients with a penicillin allergyclindamycin 600 mg intravenously every 8 h orvancomycin 15 mgkg intravenously twice a daymay be given
ErysipelaAdditional useful therapeutic optionsbull Prednisone 30 mg over 8 days might be consideredas well as elevation of the affected siteMoist heat compresses may be usefulbull Surgeryndash Debridement and drainage are indicated when bullaeabscesses or necroses are presentbull Differential diagnosisndash Contact dermatitisndash Asteatotic eczemandash Herpes zosterndash Angioneurotic oedemandash Osteomyelitis
Furuncle
bull Definition of the diseasebull ndash A furuncle is an infection that beginsbull at the hair follicle and spreads deeper into thebull dermis and subcutaneous tissue forming abull nodule After several days it developsbull into an abscess - red painful and fluctuantbull bull bull Epidemiologyaetiologybull ndash The aetiologic agent is Staphylococcus aureus
FuruncleSymptomsndashsymptoms are local and limited to thesite of infection Furuncles usually are wherehair follicles are present bull Complicationndash One complication is furunculosis multiple draining furunclesDiagnosisndash The diagnosis is based on clinical inspection - Cultures are not necessary when there is no systemic involvement but should beconsidered if systemic therapy (in case of feversignificant cellulitis or hospitalization) or whenmethicillin-resistant Staphylococcusaureus (MRSA) is considered
FuruncleTherapyndash When the furuncle is small application of moist heat compress to promote drainage -Larger furuncles should be drained by surgical incision-After drainage the area should be cleaned with anantiseptic (with chlorhexidinebetadine) should be applied twice
a dayndash If no systemic symptoms or extensive cellulitis arepresent simple topical care is usually curative andoral antibiotics are not necessary Otherwise systemictreatment is indicated and should cover anypossible MRSA
Furuncle
bull -Recommended antibiotics are trimethoprim-sulfamethoxazole
bull 1ndash2 tablets orally twice daily doxycyclinebull 100 mg orally twice dailybull or clindamycin 300ndash450 mg orally every 8 hbull - In severe cases vancomycin 15 mgkg
intravenouslybull every 12 h or clindamycin 600 mg intravenouslybull every 8 h
Midline Granulomabull A midline granuloma is an angiocentricbull lymphoma it was referred to as polymorphicbull reticulosis lethal midline granuloma and midline
malignant reticulosisbull bull Definition of the diseasebull ndash This rare disease is a lymphoma of extranodal
presentationall cases are positive for the Epstein-Barr virus
bull -This lymphoma most commonly appears in the midface region
Midline GranulomaEpidemiologyaetiologyndash This form of lymphoma is rare in Europe and theUnited States with a higher prevalence in Asia and PeruSymptomsndash The most common presentation is nasal obstruction with a destructive mass occupying the nosesinuses and palate
-Fever night sweatsand weight loss seen usually in Hodgkinrsquos lymphomaand other non-Hodgkinrsquos lymphomas (knownas ldquoB symptomsrdquo) are uncommon
Midline GranulomaDiagnosisndash The diagnosis is based on anatomopathologicalstudy The malignancy of the tumour manifested byextensive necrosis makes the histological diagnosisdifficult and often more biopsies are required forconfirmationbull Therapyndash Therapy consists of radiotherapy with or withoutchemotherapy
Midline Granuloma
bull Prognosisbull ndash Depending on the stage long-term remission or
experience a worseningbull prognosis with relapses which may include otherbull extranodal sites bull Involvement of extranodal sitesbull including the upper airway gastrointestinal tractbull skin
Wegenerrsquos Granulomatosis
bull Definition of the diseasebull ndash Wegenerrsquos granulomatosis is a systemic chronicbull vasculitis of small- and medium-sized blood vesselsbull with an autoimmune component It affectsbull particular organs with variable predilectionbull Epidemiologyaetiologybull ndash Wegenerrsquos granulomatosis is a rare disease It affects
about 1 in 20000ndash30000 people It is more prevalentbull in middle-aged Caucasian patients
Wegenerrsquos Granulomatosis
Symptomsndash The disease may present pulmonary upper
respiratory tract or renal In the disseminated form-The localised form ndash confinedto the upper respiratory region ndash is present in 25of the patients- It consists of nonspecific manifestationssuch as nasal obstruction crusting purulentor bloody rhinorrhea and painful or painless ulcers in oral or nasal cavities which are unresponsive tostandard medical treatment
Wegenerrsquos Granulomatosis
bull In some patients the nasal septum is perforatedbull which leads to saddle-nose deformity Less
commonbull symptoms are hoarseness stridor due to
subglotticbull stenosis otalgia otorrhea and conductivebull and sensorineural hearing loss Also ocular
symptomsbull such as scleritis conjunctivitis uveitis andbull episcleritis may be present
Wegenerrsquos Granulomatosis
bull ndash In the disseminated form pulmonary involvementbull is manifested by cough dyspnoea haemoptysisbull (due to an alveolar capillaritis necrotic lesions orbull endobronchial disease) and pleuritic painndashbull -Ninety per cent of patients have nasal symptomsbull and these symptoms are usually the first
manifestationof the diseasebull -Most patients have also renal involvementbull even if it is subclinical
Wegenerrsquos Granulomatosis
Diagnosis ndash Diagnosis of Wegenerrsquos granulomatosis is based on clinical findings that demonstrate lung (chest x-ray) kidney (urine analysis) or upper respiratory tract
involvement (oral or nasal ulcers or discharge) - positive blood analysis for cytoplasmic-staining antineutrophil
cytoplasmic antibodies (c-ANCA) and confirming proteinase 3 (PR3) ANCA or myeloperoxidase (MPO) ANCA ndash Biopsy is essential for diagnosis nonspecific chronic inflammation
and necrosis -Bacterial and fungal infections
Wegenerrsquos Granulomatosis
Therapyndash Conservative therapybull In the induction of disease remission highdosesteroids (e g prednisone 1 mgkgday) for1 month with tapering over several months aregiven In addition cyclophosphamide (2 mgkgday) should be administered for 6ndash12 monthsuntil symptoms disappear In the maintenanceof remission cyclophosphamide should be
Wegenerrsquos Granulomatosis
Antibiotics mainly trimethoprim-sulfamethoxazoleare given for prophylaxis againstPneumocystis jiroveci (formerly Pneumocystiscarinii) pneumonia (PCP) which may developduring immunosuppression and have a role inpreventing recurrencesbull Sinonasal manifestations may be treated with topical nasal steroids and nasal irrigations lowdosesystemic steroids and antibiotics when bacterial infection (typically Staphylococcus species) is suspected
Wegenerrsquos Granulomatosis
bull Prognosisbull ndash Most of the patients respond well to treatmentbull achieving symptom-free intervals of 5ndash20 yearsbull or more bull -Anatomical problems (sinusitis trachealbull stenosis) may require surgery bull Relapses can be long and troublesomebull Long-term complications are chronicbull renal failure hearing loss and deafness
Nasal Fractures Definition ndash A nasal fracture is a disruption of the nasal bone structure due to trauma It is the most frequently fractured facial bone Epidemiologyaetiology ndash Sports falls and assaults are the usual mechanisms of fracture -Males are affected twice as often as are females -Paediatric populations with a incidences during the second and third decades of life -Variables such as force impact direction nature of the striking object age and other will influence the pattern of injury to the components of the nose
Nasal Fractures
bull Symptomsbull ndash Deformity swelling epistaxis and periorbital
ecchymosis are signs that are suggestive of nasal fracture
bull bony crepitus and nasal segment mobilitybull ndash Epiphora bull Severe bilateral injuries to the lachrymal bones
arebull associated with depressed nasal fractures
Nasal Fractures Complications ndash Septal haematoma is one of the most severe early complications of nasal trauma and without drainage it results in abscess formation 6ndash7 days after trauma producing necrosis of the septal cartilage -Long-term problems such as saddle-nose deformity perforation columellar retraction and nasalbase
Septal infection could lead to osteomyelitis orbital and intracranial abscesses meningitis and cavernous sinus thrombosis -Cerebrospinal fluid leakage is a common complication of severe
nasal and frontal fractures
Nasal Fractures
bull Diagnostic proceduresbull ndash Inspectionbull bull Changes of appearance such as deviation andbull asymmetry bleeding watery drainage changesbull in nasal breathing and smell It is useful to comparebull the current presentation with old photographsbull (up to 40 of normal individuals havebull significant nose malformations)
Nasal Fractures Physical examination bull The diagnosis of a nasal fracture is made primarily by physical examination epistaxis nasal swelling and periorbital ecchymosis Nasal shape in the lateral and frontal inspection should be assessed Grasping the dorsum between two fingers and rocking the pyramid back and forth aids in assessing the mobility of nasal bones Internal structures should be evaluated by using a headlight and nasal speculum Clotted blood is removed by suction and assessment of haematoma mucosal tears and active bleeding is performed Bimanual palpation of the septum helps to differentiate septal swelling from haematoma ndash
Nasal FracturesRadiographybull There is no clear evidence of the role of radiographyin the management of nasal fracturesPlain films have up to a 66 false-positive rateas a result of misinterpretation of normal suturelines In addition old fractures are difficult todistinguishbull Three-dimensional CT is recommended for extensiveinjuries involving the nasal-orbital-ethmoidalcomplexndash
Nasal Fractures
bull Additionaluseful diagnostic proceduresbull bull Using a 0 or 30deg 4-mm endoscope is helpful inbull the assessment of posterior abnormalities If thebull patient is heavily sedated Brown-Gruss
provocationbull manoeuvres may be performed to determinebull deformities in upper middle or lower segmentsbull by compressing each compartment
Nasal FracturesConservative treatmentndash Treatment of bleedingbull For localised bleeding anterior sources may becauterised by silver nitrate or sealed with topicalmaterials such as thrombin combined withgelatin foam fibrin glue FloSealreg or other procoagulantmaterials If conservative measuresfail a formal anterior packing is placedbull Bleeding from branches of sphenopalatine orethmoid vessels requires anterior-posteriorpacking
Nasal Fractures
bull bull Surgical methods such as direct endoscopic vessel
bull cauterization or ligation have been shown tobull offer better haemostasis and patient comfortbull Angiography with embolization can also be
consideredbull in cases refractory to more conservativebull approaches
Nasal Fractures
bull Type of reductionbull bull Nondisplaced fractures should be treated withbull observation alone Closed nasal reduction is thebull best choice for simple injuries (isolated unilateralbull with medial displacement)bull bull An open approach should be considered in
severebull trauma (bilateral depressed fractures)
Nasal Fracturesbull Surgical principlesbull ndash Topical anaesthesia with cotton pledgets soakedbull with 4 cocaine or 005 oxymethazoline combinedbull with 4 topical lidocaine should be appliedbull for 5ndash10 min Local anaesthesia should also be injectedbull (1 lidocaine and 1100000 epinephrine)bull along the septum lateral walls and floor of the nasalbull cavitybull bull
Nasal FracturesClosed reductionndashndash The nasal bones are grasped between two fingersand pressure is applied laterally in theopposite direction of the deviation A bluntelevator may be used from within the nose incases of significant medial collapse Walshamforceps can be of help Reduction of the septumshould be performed with the use ofAsch forceps
Nasal Fractures
bull To prevent collapse of the postreductionbull framework nasal packing should be placedbull for 3ndash5 days Septum splints are recommendedbull in comminuted septal fractures withbull severe mucosal lesions External nasal splintingbull for 10 days (Aquaplastreg Thermoplastreg)bull provides nasal protection Nasal saline spraysbull prevent crusting and oral antibiotics should
Nasal Fractures
bull Open reductionbull ndashndash Immediate repair of fractures by using
widebull surgical exposure reduction fixation and
reconstructionbull ndashndash The second option is delayed correctionbull (6 months or more) of persistent deformitiesbull using standard techniques of rhinoplasty
Deviated Nasal Septum
bull Definition of the diseasebull ndash Deviation of the nasal septum is a common causebull of unilateral nasal airway obstruction in which thebull nasal septum is displacedbull bull Epidemiologyaetiologybull ndash Developmental septal abnormalities Septal cartilage
damage in the neonatal period andbull during birth can cause severe septal deviation inbull the absence of a history of nasal trauma
Deviated Nasal Septum
bull Symptomsbull ndash Patients may present with a history of sinusitis
allergicbull rhinitis obstructive sleep apnoea previousbull nasal surgery or recent nasal trauma Unilateral or
bilateral nasal airway obstruction that is unrelievedbull with decongestants or nasal steroid sprays is oftenbull seenbull bull
Deviated Nasal SeptumDiagnosisndashExamination external dorsal deviation or the columella and caudal septummay be deflected off the midline (caudal subluxation)ndash Inspections of the nasal cavity and anterior-posteriorrhinoscopy are helpful in diagnosing the locationtype and severity of septal deformityThe endoscope is also useful in identifying polypsthe severity and extent of posterior septaldeviations and bony spurs and locating areas ofseptal perforation or mucosal injury
Deviated Nasal Septum
bull Therapybull ndash Septoplasty is a procedurebull The areabull of deviation is corrected or resected in order tobull leave behind as much cartilage and bone as
possiblebull Cartilage resection is minimised and can be
repositioned reshaped or recontoured using a variety of methods
Deviated Nasal Septum
bull ndash Indications of septoplasty before the growth period
bull of the nose is finished should be very limited bull -In these cases surgery must preserve all the
cartilagebull in order to prevent external changes of the
shape ofbull the nose
Deviated Nasal Septum
bull Complicationsbull ndash Frequent complications include haematoma andbull infection Cerebrospinal fluid leak is a rare but
potentiallybull serious complicationbull It is usually the resultbull of avulsion or damage to the cribriform plate whenbull handling the perpendicular plate of the ethmoidbull ndash Other complications include epistaxis nasal
Deviated Nasal Septum
bull Other complications include epistaxis nasal obstruction
bull due to residual deviation synechiae returnbull of the cartilaginous deviation septal perforationbull anosmia and cosmetic nasal deformities suchbull as widened alar rim margins drooping nasal tipbull columella retraction and a sunken dorsum with abull supratip saddle formation
Septal perforation with minor crusting View from provide closure of the
incision
Septal Haematoma
bull A septal haematoma is a blood collection under the perichondrium
bull of the septum and cartilagebull bull bull Epidemiologyaetiologybull ndash A septal haematoma is one of the most
severe complications of nasal trauma
Septal Haematoma
bull Diagnosisbull ndash Signs and symptoms include intense pain
swellingbull haematoma of the upper lip and philtrum
area andbull complete nasal airway obstruction
Septal HaematomaTherapyndash Management consists of drainage through a mucoperichondrial incision Immediate treatment isnecessary to prevent long-term problems such asa saddle-nose deformity perforation columellarretraction and nasal-base widening In childrenseptal destruction can lead to devastating nasal andmidfacial growth abnormalitiesbull Surgeryndash Incision and evacuation of the collection is performedDrainage of a septal haematoma should
Septal HaematomaSurgeryndash Incision and evacuation of the collection is performedDrainage of a septal haematoma should provide closure of the incision
Splints or transseptal sutures are placed to obliterate thepotential space and prevent collectionInfection involving the septal cartilage Reconstruction with autologouscartilage is then performed in a second stage Oral antibiotics should be given
Nasal DeformitySaddle-nose deformityndash A saddle-nose deformity is characterised by a loss ofnasal dorsal height and compromised nasal supportstructures -Other case observed are depressionof the middle vault and dorsum loss of nasal tipsupport and definition shortened (vertical) nasal length over rotation of the nasal tip and retrusion ofthe nasal spine and caudal septum It is also knownas a ldquoPug noserdquo or ldquoboxerrsquos noserdquo both of which referto various degrees of nasal dorsal depressionbull
Nasal DeformityEpidemiologyaetiologyndash Prevalence is higher in population groups prone to facial trauma (ie boxers athletes) those with historiesof intranasal cocaine use nasal surgery (e g radical submucosal septal resection reductive rhinoplasty)ndash A saddle-nose deformity can be congenital or acquired It can be noticed as a part of individual familialsyndromic and ethnic characteristics - Most deformities are due to traumatic and iatrogeniccauses Medical causes are Wegenerrsquosgranulomatosis relapsing polychondritis leprosy (Hansenrsquos disease) syphilis ectodermal dysplasiaand intranasal cocaine use
Nasal Deformity
bull Therapybull ndash Nasal reconstruction indications depend on patientbull selection surgeon experience and aetiology of thebull deformity bull Indications for surgery can be functionalbull aesthetic or most commonly both In individuals
with a compromised nasal airway a nasoseptalbull reconstruction is indicated
Nasal Deformity
bull Contraindications bull include patients with malignantbull chronic or autoimmune disease conditions drugbull abuse poor perioperative risk profile and unrealisticbull expectationsbull ndash Multiple previous rhinoplasties and certain
professionsbull (mixed martial artists boxers and other contactbull sports) are relative contraindications
Nasal DeformitySeptoplastyndash Septoplasty is performed to correct nasal obstructioncaused by septal deformityndash Usually septoplasty is performed under general anaesthesiawith the patient in the supine position with the head elevated by approximately 30 (Righthandedsurgeons approach from the right side)ndash Local vasoconstrictive anaesthesia is applied notonly to reduce postoperative pain but also more importantly to achieve vasoconstriction of themucosa and less intraoperative haemorrhage Lidocainewith adrenaline or epinephrine is usedalthough in patients with cardiac hypersensitivityoxymetazoline might be preferred
Nasal Deformity
bull Septoplasty begins with the incision of septal mucosabull Most operative techniques utilise a hemitransfixionbull incision at the caudal end of septum so thatbull deviation at this point might be reached as wellbull as a transfixion incision that is easily obtained ifbull needed (Right-handed surgeons normally choosebull the left side but that may vary when deviation isbull convex towards the right)
Nasal DeformityA columella retractor is placed over the columellaand by pulling it laterally the caudal border of theseptum is exposed Ala can be protected by an alaprotector A vertical incision with a no 15 bladeover the caudal end of septum is performed untilreaching the plane of the septal cartilage It is essentialto correctly identify the perichondrium and byusing the Cottle elevator dissect and lift it creatinga flap As the dissection proceeds along the septalcartilage a longer speculum (no 5) is introduced sothat elevation of the mucoperichondrium is doneunder constant visual controlndash The next step is to dissect the mucoperiostium
Nasal DeformityDissecting over the bony-cartilaginous junctionwhen joining both tunnels might be difficult and is
especially prone to membrane perforationndash If needed the same tunnels are to be created on the
other side of the septum Then deviated parts of
septum are identified and removed either with a
knife or a Freer chisel
Nasal Deformitybull septum from the maxillary crest the septum mustbull be separated from the perpendicular plate trimmedbull along the inferior border placed back onto the crestbull and sutured to the periosteum If the deformity involvesbull the vomer an osteotome is used Care mustbull be taken not to break the cribriform plate becausebull it could cause a cerebrospinal fistula
Nasal Deformity
bull Once the septal deviation is corrected the flapsbull and hemitransfixion incision are mattressed
withbull absorbable sutures Nasal packing to prevent
synechiaebull and postoperative septal haematoma mightbull be advised but should be removed within 72 h

Imaging of the Nose and Paranasal Sinuses
Conventional RadiographsStandard paranasal sinus radiographs in the occipitomental
projection ( Water projection) and
occipitofrontal projection Caldwell projection) in cases of acute inflammation
They are also obtained to evaluate midfacial fractures
Computed Tomography (CT) the main indicationsfor CT scanning of the
nose and paranasal sinuses
are- chronic sinusitis - -trauma (especially
frontobasal -fractures)
-and tumors
The occipitofrontal projection is better for evaluating theethmoid cells and frontal sinus
occipitomental projection demonstrates the maxillarysinus and gives a limited view of the sphenoid sinus
Computed tomography of the paranasal sinuses
Four representative coronal CT scans are shown
Four representative coronal CT scans are shown
Magnetic Resonance Imaging
Magnetic maging
Magnetic resonance imaging (MRI) has fewer indicationsthan CT in patients with paranasal sinus diseaseThis is primarily because MRI is markedly inferior toCT in defining the bony boundaries of the sinusesThe strength of MRI lies in its superior soft-tissue discriminationMRI is indicated in diseases that involve the paranasal sinuses in addition to thecranial cavity or orbit (eg tumors and congenitalmalformations such as encephaloceles)
MRI of the paranasal sinuses
The Nose and Sinuses
Structure The structure of the nose is made up of
four partsbull The surface anatomybull The nasal skeletonmdashcomposed of the
two nasal bones the paired upper lateral and lower lateral cartilages and the nasal septum covered in subcutaneous tissue and skin
bull The internal anatomymdashincludes the septum of the nose which forms the medial wall of the nasal cavity The turbinates on the lateral wall are also called conchae
bull The osteomeatal complexmdasha key functional area of the nose
Function The nose is the main route for inspired
air and its structure is related to this function As the air passes over the large surface area of the turbinates
The inspired gases are warmed and humidified Mucus on the mucosa of the nose removes large dust particles from the air as it is breathed in
The voice resonates in the sinuses and nose and this provides character to the speech
Pneumatization of the sinusesmdashthey are air filled spacesmdashreduces the weight of the skull
Diseases of thDiseases of the Outer and Inner Nosee Outer and
Inner Nose Erysipelas Definition of the disease ndash Erysipela is a skin infection that affects the superficial dermis and is caused by Streptococcus pyogenes (group A) It usually develops in the extremities and the face and less commonly on the scalp and genitals bull Epidemiologyaetiology ndash Erysipelas are more often seen in elderly infants and children patients with compromised immunology and diabetes -Predisposing factors are alcoholism skin ulceration puncture wounds fungal infections malnutrition and burns
Erysipelas
bull Symptomsbull ndash It usually presents of fever general fatigue bull -The skin lesion is a redindurated and elevated plaque
with borders that expand rapidly bull It is painful warm and accompanied by variable oedemabull -On the second or third day a flaccid bulla may develop
and desquamationbull bull Presence of regional lymph nodes is common
Erysipelas
bull Complicationsndash The most common complication is recurrencewhich is seen in 18ndash30 of the cases even afterproper antibiotic therapy Recurrence is seen moreoften in females than in malesA skin infection with S pyogenes could lead toglomerulonephritis
Erysipelas
bull Complicationsbull ndash The most common complication is recurrencebull which is seen in 18ndash30 of the cases even afterbull proper antibiotic therapy bull -Recurrence is seen morebull often in females than in males bull -A skin infection with S pyogenes could lead tobull glomerulonephritis
Erysipelas
bull bull Diagnosisbull ndash Diagnosis is based on the patientrsquos personal
historybull and physical examination particularly on inspectionbull of the skin
bull Blood cultures are positive in less thanbull 5 of cases
ErysipelasTherapyndash Conservative therapybull The preferred antibiotic is penicillin In mildcases with minor systemic symptoms penicillinV 500 mg orally every 6 h for 10 days or penicillinG benzathine 12 mil U intramuscularlyonceOther possibilities are amoxicillin 500 mgorally twice a day for 10 days or cephalexin 500mg orally every 6 h for 10 days
ErysipelasIn moderate and severe cases with significantsystemic symptoms hospitalization and intravenoustreatment is required penicillin G 2ndash4mil U intravenously every 4ndash6 h Cefazolin05ndash15 gm intravenously every 8 h cefotaxime1ndash2 gm intravenously every 8 h or ceftriaxone1ndash2 gm intravenously once a day should be administeredIn patients with a penicillin allergyclindamycin 600 mg intravenously every 8 h orvancomycin 15 mgkg intravenously twice a daymay be given
ErysipelaAdditional useful therapeutic optionsbull Prednisone 30 mg over 8 days might be consideredas well as elevation of the affected siteMoist heat compresses may be usefulbull Surgeryndash Debridement and drainage are indicated when bullaeabscesses or necroses are presentbull Differential diagnosisndash Contact dermatitisndash Asteatotic eczemandash Herpes zosterndash Angioneurotic oedemandash Osteomyelitis
Furuncle
bull Definition of the diseasebull ndash A furuncle is an infection that beginsbull at the hair follicle and spreads deeper into thebull dermis and subcutaneous tissue forming abull nodule After several days it developsbull into an abscess - red painful and fluctuantbull bull bull Epidemiologyaetiologybull ndash The aetiologic agent is Staphylococcus aureus
FuruncleSymptomsndashsymptoms are local and limited to thesite of infection Furuncles usually are wherehair follicles are present bull Complicationndash One complication is furunculosis multiple draining furunclesDiagnosisndash The diagnosis is based on clinical inspection - Cultures are not necessary when there is no systemic involvement but should beconsidered if systemic therapy (in case of feversignificant cellulitis or hospitalization) or whenmethicillin-resistant Staphylococcusaureus (MRSA) is considered
FuruncleTherapyndash When the furuncle is small application of moist heat compress to promote drainage -Larger furuncles should be drained by surgical incision-After drainage the area should be cleaned with anantiseptic (with chlorhexidinebetadine) should be applied twice
a dayndash If no systemic symptoms or extensive cellulitis arepresent simple topical care is usually curative andoral antibiotics are not necessary Otherwise systemictreatment is indicated and should cover anypossible MRSA
Furuncle
bull -Recommended antibiotics are trimethoprim-sulfamethoxazole
bull 1ndash2 tablets orally twice daily doxycyclinebull 100 mg orally twice dailybull or clindamycin 300ndash450 mg orally every 8 hbull - In severe cases vancomycin 15 mgkg
intravenouslybull every 12 h or clindamycin 600 mg intravenouslybull every 8 h
Midline Granulomabull A midline granuloma is an angiocentricbull lymphoma it was referred to as polymorphicbull reticulosis lethal midline granuloma and midline
malignant reticulosisbull bull Definition of the diseasebull ndash This rare disease is a lymphoma of extranodal
presentationall cases are positive for the Epstein-Barr virus
bull -This lymphoma most commonly appears in the midface region
Midline GranulomaEpidemiologyaetiologyndash This form of lymphoma is rare in Europe and theUnited States with a higher prevalence in Asia and PeruSymptomsndash The most common presentation is nasal obstruction with a destructive mass occupying the nosesinuses and palate
-Fever night sweatsand weight loss seen usually in Hodgkinrsquos lymphomaand other non-Hodgkinrsquos lymphomas (knownas ldquoB symptomsrdquo) are uncommon
Midline GranulomaDiagnosisndash The diagnosis is based on anatomopathologicalstudy The malignancy of the tumour manifested byextensive necrosis makes the histological diagnosisdifficult and often more biopsies are required forconfirmationbull Therapyndash Therapy consists of radiotherapy with or withoutchemotherapy
Midline Granuloma
bull Prognosisbull ndash Depending on the stage long-term remission or
experience a worseningbull prognosis with relapses which may include otherbull extranodal sites bull Involvement of extranodal sitesbull including the upper airway gastrointestinal tractbull skin
Wegenerrsquos Granulomatosis
bull Definition of the diseasebull ndash Wegenerrsquos granulomatosis is a systemic chronicbull vasculitis of small- and medium-sized blood vesselsbull with an autoimmune component It affectsbull particular organs with variable predilectionbull Epidemiologyaetiologybull ndash Wegenerrsquos granulomatosis is a rare disease It affects
about 1 in 20000ndash30000 people It is more prevalentbull in middle-aged Caucasian patients
Wegenerrsquos Granulomatosis
Symptomsndash The disease may present pulmonary upper
respiratory tract or renal In the disseminated form-The localised form ndash confinedto the upper respiratory region ndash is present in 25of the patients- It consists of nonspecific manifestationssuch as nasal obstruction crusting purulentor bloody rhinorrhea and painful or painless ulcers in oral or nasal cavities which are unresponsive tostandard medical treatment
Wegenerrsquos Granulomatosis
bull In some patients the nasal septum is perforatedbull which leads to saddle-nose deformity Less
commonbull symptoms are hoarseness stridor due to
subglotticbull stenosis otalgia otorrhea and conductivebull and sensorineural hearing loss Also ocular
symptomsbull such as scleritis conjunctivitis uveitis andbull episcleritis may be present
Wegenerrsquos Granulomatosis
bull ndash In the disseminated form pulmonary involvementbull is manifested by cough dyspnoea haemoptysisbull (due to an alveolar capillaritis necrotic lesions orbull endobronchial disease) and pleuritic painndashbull -Ninety per cent of patients have nasal symptomsbull and these symptoms are usually the first
manifestationof the diseasebull -Most patients have also renal involvementbull even if it is subclinical
Wegenerrsquos Granulomatosis
Diagnosis ndash Diagnosis of Wegenerrsquos granulomatosis is based on clinical findings that demonstrate lung (chest x-ray) kidney (urine analysis) or upper respiratory tract
involvement (oral or nasal ulcers or discharge) - positive blood analysis for cytoplasmic-staining antineutrophil
cytoplasmic antibodies (c-ANCA) and confirming proteinase 3 (PR3) ANCA or myeloperoxidase (MPO) ANCA ndash Biopsy is essential for diagnosis nonspecific chronic inflammation
and necrosis -Bacterial and fungal infections
Wegenerrsquos Granulomatosis
Therapyndash Conservative therapybull In the induction of disease remission highdosesteroids (e g prednisone 1 mgkgday) for1 month with tapering over several months aregiven In addition cyclophosphamide (2 mgkgday) should be administered for 6ndash12 monthsuntil symptoms disappear In the maintenanceof remission cyclophosphamide should be
Wegenerrsquos Granulomatosis
Antibiotics mainly trimethoprim-sulfamethoxazoleare given for prophylaxis againstPneumocystis jiroveci (formerly Pneumocystiscarinii) pneumonia (PCP) which may developduring immunosuppression and have a role inpreventing recurrencesbull Sinonasal manifestations may be treated with topical nasal steroids and nasal irrigations lowdosesystemic steroids and antibiotics when bacterial infection (typically Staphylococcus species) is suspected
Wegenerrsquos Granulomatosis
bull Prognosisbull ndash Most of the patients respond well to treatmentbull achieving symptom-free intervals of 5ndash20 yearsbull or more bull -Anatomical problems (sinusitis trachealbull stenosis) may require surgery bull Relapses can be long and troublesomebull Long-term complications are chronicbull renal failure hearing loss and deafness
Nasal Fractures Definition ndash A nasal fracture is a disruption of the nasal bone structure due to trauma It is the most frequently fractured facial bone Epidemiologyaetiology ndash Sports falls and assaults are the usual mechanisms of fracture -Males are affected twice as often as are females -Paediatric populations with a incidences during the second and third decades of life -Variables such as force impact direction nature of the striking object age and other will influence the pattern of injury to the components of the nose
Nasal Fractures
bull Symptomsbull ndash Deformity swelling epistaxis and periorbital
ecchymosis are signs that are suggestive of nasal fracture
bull bony crepitus and nasal segment mobilitybull ndash Epiphora bull Severe bilateral injuries to the lachrymal bones
arebull associated with depressed nasal fractures
Nasal Fractures Complications ndash Septal haematoma is one of the most severe early complications of nasal trauma and without drainage it results in abscess formation 6ndash7 days after trauma producing necrosis of the septal cartilage -Long-term problems such as saddle-nose deformity perforation columellar retraction and nasalbase
Septal infection could lead to osteomyelitis orbital and intracranial abscesses meningitis and cavernous sinus thrombosis -Cerebrospinal fluid leakage is a common complication of severe
nasal and frontal fractures
Nasal Fractures
bull Diagnostic proceduresbull ndash Inspectionbull bull Changes of appearance such as deviation andbull asymmetry bleeding watery drainage changesbull in nasal breathing and smell It is useful to comparebull the current presentation with old photographsbull (up to 40 of normal individuals havebull significant nose malformations)
Nasal Fractures Physical examination bull The diagnosis of a nasal fracture is made primarily by physical examination epistaxis nasal swelling and periorbital ecchymosis Nasal shape in the lateral and frontal inspection should be assessed Grasping the dorsum between two fingers and rocking the pyramid back and forth aids in assessing the mobility of nasal bones Internal structures should be evaluated by using a headlight and nasal speculum Clotted blood is removed by suction and assessment of haematoma mucosal tears and active bleeding is performed Bimanual palpation of the septum helps to differentiate septal swelling from haematoma ndash
Nasal FracturesRadiographybull There is no clear evidence of the role of radiographyin the management of nasal fracturesPlain films have up to a 66 false-positive rateas a result of misinterpretation of normal suturelines In addition old fractures are difficult todistinguishbull Three-dimensional CT is recommended for extensiveinjuries involving the nasal-orbital-ethmoidalcomplexndash
Nasal Fractures
bull Additionaluseful diagnostic proceduresbull bull Using a 0 or 30deg 4-mm endoscope is helpful inbull the assessment of posterior abnormalities If thebull patient is heavily sedated Brown-Gruss
provocationbull manoeuvres may be performed to determinebull deformities in upper middle or lower segmentsbull by compressing each compartment
Nasal FracturesConservative treatmentndash Treatment of bleedingbull For localised bleeding anterior sources may becauterised by silver nitrate or sealed with topicalmaterials such as thrombin combined withgelatin foam fibrin glue FloSealreg or other procoagulantmaterials If conservative measuresfail a formal anterior packing is placedbull Bleeding from branches of sphenopalatine orethmoid vessels requires anterior-posteriorpacking
Nasal Fractures
bull bull Surgical methods such as direct endoscopic vessel
bull cauterization or ligation have been shown tobull offer better haemostasis and patient comfortbull Angiography with embolization can also be
consideredbull in cases refractory to more conservativebull approaches
Nasal Fractures
bull Type of reductionbull bull Nondisplaced fractures should be treated withbull observation alone Closed nasal reduction is thebull best choice for simple injuries (isolated unilateralbull with medial displacement)bull bull An open approach should be considered in
severebull trauma (bilateral depressed fractures)
Nasal Fracturesbull Surgical principlesbull ndash Topical anaesthesia with cotton pledgets soakedbull with 4 cocaine or 005 oxymethazoline combinedbull with 4 topical lidocaine should be appliedbull for 5ndash10 min Local anaesthesia should also be injectedbull (1 lidocaine and 1100000 epinephrine)bull along the septum lateral walls and floor of the nasalbull cavitybull bull
Nasal FracturesClosed reductionndashndash The nasal bones are grasped between two fingersand pressure is applied laterally in theopposite direction of the deviation A bluntelevator may be used from within the nose incases of significant medial collapse Walshamforceps can be of help Reduction of the septumshould be performed with the use ofAsch forceps
Nasal Fractures
bull To prevent collapse of the postreductionbull framework nasal packing should be placedbull for 3ndash5 days Septum splints are recommendedbull in comminuted septal fractures withbull severe mucosal lesions External nasal splintingbull for 10 days (Aquaplastreg Thermoplastreg)bull provides nasal protection Nasal saline spraysbull prevent crusting and oral antibiotics should
Nasal Fractures
bull Open reductionbull ndashndash Immediate repair of fractures by using
widebull surgical exposure reduction fixation and
reconstructionbull ndashndash The second option is delayed correctionbull (6 months or more) of persistent deformitiesbull using standard techniques of rhinoplasty
Deviated Nasal Septum
bull Definition of the diseasebull ndash Deviation of the nasal septum is a common causebull of unilateral nasal airway obstruction in which thebull nasal septum is displacedbull bull Epidemiologyaetiologybull ndash Developmental septal abnormalities Septal cartilage
damage in the neonatal period andbull during birth can cause severe septal deviation inbull the absence of a history of nasal trauma
Deviated Nasal Septum
bull Symptomsbull ndash Patients may present with a history of sinusitis
allergicbull rhinitis obstructive sleep apnoea previousbull nasal surgery or recent nasal trauma Unilateral or
bilateral nasal airway obstruction that is unrelievedbull with decongestants or nasal steroid sprays is oftenbull seenbull bull
Deviated Nasal SeptumDiagnosisndashExamination external dorsal deviation or the columella and caudal septummay be deflected off the midline (caudal subluxation)ndash Inspections of the nasal cavity and anterior-posteriorrhinoscopy are helpful in diagnosing the locationtype and severity of septal deformityThe endoscope is also useful in identifying polypsthe severity and extent of posterior septaldeviations and bony spurs and locating areas ofseptal perforation or mucosal injury
Deviated Nasal Septum
bull Therapybull ndash Septoplasty is a procedurebull The areabull of deviation is corrected or resected in order tobull leave behind as much cartilage and bone as
possiblebull Cartilage resection is minimised and can be
repositioned reshaped or recontoured using a variety of methods
Deviated Nasal Septum
bull ndash Indications of septoplasty before the growth period
bull of the nose is finished should be very limited bull -In these cases surgery must preserve all the
cartilagebull in order to prevent external changes of the
shape ofbull the nose
Deviated Nasal Septum
bull Complicationsbull ndash Frequent complications include haematoma andbull infection Cerebrospinal fluid leak is a rare but
potentiallybull serious complicationbull It is usually the resultbull of avulsion or damage to the cribriform plate whenbull handling the perpendicular plate of the ethmoidbull ndash Other complications include epistaxis nasal
Deviated Nasal Septum
bull Other complications include epistaxis nasal obstruction
bull due to residual deviation synechiae returnbull of the cartilaginous deviation septal perforationbull anosmia and cosmetic nasal deformities suchbull as widened alar rim margins drooping nasal tipbull columella retraction and a sunken dorsum with abull supratip saddle formation
Septal perforation with minor crusting View from provide closure of the
incision
Septal Haematoma
bull A septal haematoma is a blood collection under the perichondrium
bull of the septum and cartilagebull bull bull Epidemiologyaetiologybull ndash A septal haematoma is one of the most
severe complications of nasal trauma
Septal Haematoma
bull Diagnosisbull ndash Signs and symptoms include intense pain
swellingbull haematoma of the upper lip and philtrum
area andbull complete nasal airway obstruction
Septal HaematomaTherapyndash Management consists of drainage through a mucoperichondrial incision Immediate treatment isnecessary to prevent long-term problems such asa saddle-nose deformity perforation columellarretraction and nasal-base widening In childrenseptal destruction can lead to devastating nasal andmidfacial growth abnormalitiesbull Surgeryndash Incision and evacuation of the collection is performedDrainage of a septal haematoma should
Septal HaematomaSurgeryndash Incision and evacuation of the collection is performedDrainage of a septal haematoma should provide closure of the incision
Splints or transseptal sutures are placed to obliterate thepotential space and prevent collectionInfection involving the septal cartilage Reconstruction with autologouscartilage is then performed in a second stage Oral antibiotics should be given
Nasal DeformitySaddle-nose deformityndash A saddle-nose deformity is characterised by a loss ofnasal dorsal height and compromised nasal supportstructures -Other case observed are depressionof the middle vault and dorsum loss of nasal tipsupport and definition shortened (vertical) nasal length over rotation of the nasal tip and retrusion ofthe nasal spine and caudal septum It is also knownas a ldquoPug noserdquo or ldquoboxerrsquos noserdquo both of which referto various degrees of nasal dorsal depressionbull
Nasal DeformityEpidemiologyaetiologyndash Prevalence is higher in population groups prone to facial trauma (ie boxers athletes) those with historiesof intranasal cocaine use nasal surgery (e g radical submucosal septal resection reductive rhinoplasty)ndash A saddle-nose deformity can be congenital or acquired It can be noticed as a part of individual familialsyndromic and ethnic characteristics - Most deformities are due to traumatic and iatrogeniccauses Medical causes are Wegenerrsquosgranulomatosis relapsing polychondritis leprosy (Hansenrsquos disease) syphilis ectodermal dysplasiaand intranasal cocaine use
Nasal Deformity
bull Therapybull ndash Nasal reconstruction indications depend on patientbull selection surgeon experience and aetiology of thebull deformity bull Indications for surgery can be functionalbull aesthetic or most commonly both In individuals
with a compromised nasal airway a nasoseptalbull reconstruction is indicated
Nasal Deformity
bull Contraindications bull include patients with malignantbull chronic or autoimmune disease conditions drugbull abuse poor perioperative risk profile and unrealisticbull expectationsbull ndash Multiple previous rhinoplasties and certain
professionsbull (mixed martial artists boxers and other contactbull sports) are relative contraindications
Nasal DeformitySeptoplastyndash Septoplasty is performed to correct nasal obstructioncaused by septal deformityndash Usually septoplasty is performed under general anaesthesiawith the patient in the supine position with the head elevated by approximately 30 (Righthandedsurgeons approach from the right side)ndash Local vasoconstrictive anaesthesia is applied notonly to reduce postoperative pain but also more importantly to achieve vasoconstriction of themucosa and less intraoperative haemorrhage Lidocainewith adrenaline or epinephrine is usedalthough in patients with cardiac hypersensitivityoxymetazoline might be preferred
Nasal Deformity
bull Septoplasty begins with the incision of septal mucosabull Most operative techniques utilise a hemitransfixionbull incision at the caudal end of septum so thatbull deviation at this point might be reached as wellbull as a transfixion incision that is easily obtained ifbull needed (Right-handed surgeons normally choosebull the left side but that may vary when deviation isbull convex towards the right)
Nasal DeformityA columella retractor is placed over the columellaand by pulling it laterally the caudal border of theseptum is exposed Ala can be protected by an alaprotector A vertical incision with a no 15 bladeover the caudal end of septum is performed untilreaching the plane of the septal cartilage It is essentialto correctly identify the perichondrium and byusing the Cottle elevator dissect and lift it creatinga flap As the dissection proceeds along the septalcartilage a longer speculum (no 5) is introduced sothat elevation of the mucoperichondrium is doneunder constant visual controlndash The next step is to dissect the mucoperiostium
Nasal DeformityDissecting over the bony-cartilaginous junctionwhen joining both tunnels might be difficult and is
especially prone to membrane perforationndash If needed the same tunnels are to be created on the
other side of the septum Then deviated parts of
septum are identified and removed either with a
knife or a Freer chisel
Nasal Deformitybull septum from the maxillary crest the septum mustbull be separated from the perpendicular plate trimmedbull along the inferior border placed back onto the crestbull and sutured to the periosteum If the deformity involvesbull the vomer an osteotome is used Care mustbull be taken not to break the cribriform plate becausebull it could cause a cerebrospinal fistula
Nasal Deformity
bull Once the septal deviation is corrected the flapsbull and hemitransfixion incision are mattressed
withbull absorbable sutures Nasal packing to prevent
synechiaebull and postoperative septal haematoma mightbull be advised but should be removed within 72 h

The occipitofrontal projection is better for evaluating theethmoid cells and frontal sinus
occipitomental projection demonstrates the maxillarysinus and gives a limited view of the sphenoid sinus
Computed tomography of the paranasal sinuses
Four representative coronal CT scans are shown
Four representative coronal CT scans are shown
Magnetic Resonance Imaging
Magnetic maging
Magnetic resonance imaging (MRI) has fewer indicationsthan CT in patients with paranasal sinus diseaseThis is primarily because MRI is markedly inferior toCT in defining the bony boundaries of the sinusesThe strength of MRI lies in its superior soft-tissue discriminationMRI is indicated in diseases that involve the paranasal sinuses in addition to thecranial cavity or orbit (eg tumors and congenitalmalformations such as encephaloceles)
MRI of the paranasal sinuses
The Nose and Sinuses
Structure The structure of the nose is made up of
four partsbull The surface anatomybull The nasal skeletonmdashcomposed of the
two nasal bones the paired upper lateral and lower lateral cartilages and the nasal septum covered in subcutaneous tissue and skin
bull The internal anatomymdashincludes the septum of the nose which forms the medial wall of the nasal cavity The turbinates on the lateral wall are also called conchae
bull The osteomeatal complexmdasha key functional area of the nose
Function The nose is the main route for inspired
air and its structure is related to this function As the air passes over the large surface area of the turbinates
The inspired gases are warmed and humidified Mucus on the mucosa of the nose removes large dust particles from the air as it is breathed in
The voice resonates in the sinuses and nose and this provides character to the speech
Pneumatization of the sinusesmdashthey are air filled spacesmdashreduces the weight of the skull
Diseases of thDiseases of the Outer and Inner Nosee Outer and
Inner Nose Erysipelas Definition of the disease ndash Erysipela is a skin infection that affects the superficial dermis and is caused by Streptococcus pyogenes (group A) It usually develops in the extremities and the face and less commonly on the scalp and genitals bull Epidemiologyaetiology ndash Erysipelas are more often seen in elderly infants and children patients with compromised immunology and diabetes -Predisposing factors are alcoholism skin ulceration puncture wounds fungal infections malnutrition and burns
Erysipelas
bull Symptomsbull ndash It usually presents of fever general fatigue bull -The skin lesion is a redindurated and elevated plaque
with borders that expand rapidly bull It is painful warm and accompanied by variable oedemabull -On the second or third day a flaccid bulla may develop
and desquamationbull bull Presence of regional lymph nodes is common
Erysipelas
bull Complicationsndash The most common complication is recurrencewhich is seen in 18ndash30 of the cases even afterproper antibiotic therapy Recurrence is seen moreoften in females than in malesA skin infection with S pyogenes could lead toglomerulonephritis
Erysipelas
bull Complicationsbull ndash The most common complication is recurrencebull which is seen in 18ndash30 of the cases even afterbull proper antibiotic therapy bull -Recurrence is seen morebull often in females than in males bull -A skin infection with S pyogenes could lead tobull glomerulonephritis
Erysipelas
bull bull Diagnosisbull ndash Diagnosis is based on the patientrsquos personal
historybull and physical examination particularly on inspectionbull of the skin
bull Blood cultures are positive in less thanbull 5 of cases
ErysipelasTherapyndash Conservative therapybull The preferred antibiotic is penicillin In mildcases with minor systemic symptoms penicillinV 500 mg orally every 6 h for 10 days or penicillinG benzathine 12 mil U intramuscularlyonceOther possibilities are amoxicillin 500 mgorally twice a day for 10 days or cephalexin 500mg orally every 6 h for 10 days
ErysipelasIn moderate and severe cases with significantsystemic symptoms hospitalization and intravenoustreatment is required penicillin G 2ndash4mil U intravenously every 4ndash6 h Cefazolin05ndash15 gm intravenously every 8 h cefotaxime1ndash2 gm intravenously every 8 h or ceftriaxone1ndash2 gm intravenously once a day should be administeredIn patients with a penicillin allergyclindamycin 600 mg intravenously every 8 h orvancomycin 15 mgkg intravenously twice a daymay be given
ErysipelaAdditional useful therapeutic optionsbull Prednisone 30 mg over 8 days might be consideredas well as elevation of the affected siteMoist heat compresses may be usefulbull Surgeryndash Debridement and drainage are indicated when bullaeabscesses or necroses are presentbull Differential diagnosisndash Contact dermatitisndash Asteatotic eczemandash Herpes zosterndash Angioneurotic oedemandash Osteomyelitis
Furuncle
bull Definition of the diseasebull ndash A furuncle is an infection that beginsbull at the hair follicle and spreads deeper into thebull dermis and subcutaneous tissue forming abull nodule After several days it developsbull into an abscess - red painful and fluctuantbull bull bull Epidemiologyaetiologybull ndash The aetiologic agent is Staphylococcus aureus
FuruncleSymptomsndashsymptoms are local and limited to thesite of infection Furuncles usually are wherehair follicles are present bull Complicationndash One complication is furunculosis multiple draining furunclesDiagnosisndash The diagnosis is based on clinical inspection - Cultures are not necessary when there is no systemic involvement but should beconsidered if systemic therapy (in case of feversignificant cellulitis or hospitalization) or whenmethicillin-resistant Staphylococcusaureus (MRSA) is considered
FuruncleTherapyndash When the furuncle is small application of moist heat compress to promote drainage -Larger furuncles should be drained by surgical incision-After drainage the area should be cleaned with anantiseptic (with chlorhexidinebetadine) should be applied twice
a dayndash If no systemic symptoms or extensive cellulitis arepresent simple topical care is usually curative andoral antibiotics are not necessary Otherwise systemictreatment is indicated and should cover anypossible MRSA
Furuncle
bull -Recommended antibiotics are trimethoprim-sulfamethoxazole
bull 1ndash2 tablets orally twice daily doxycyclinebull 100 mg orally twice dailybull or clindamycin 300ndash450 mg orally every 8 hbull - In severe cases vancomycin 15 mgkg
intravenouslybull every 12 h or clindamycin 600 mg intravenouslybull every 8 h
Midline Granulomabull A midline granuloma is an angiocentricbull lymphoma it was referred to as polymorphicbull reticulosis lethal midline granuloma and midline
malignant reticulosisbull bull Definition of the diseasebull ndash This rare disease is a lymphoma of extranodal
presentationall cases are positive for the Epstein-Barr virus
bull -This lymphoma most commonly appears in the midface region
Midline GranulomaEpidemiologyaetiologyndash This form of lymphoma is rare in Europe and theUnited States with a higher prevalence in Asia and PeruSymptomsndash The most common presentation is nasal obstruction with a destructive mass occupying the nosesinuses and palate
-Fever night sweatsand weight loss seen usually in Hodgkinrsquos lymphomaand other non-Hodgkinrsquos lymphomas (knownas ldquoB symptomsrdquo) are uncommon
Midline GranulomaDiagnosisndash The diagnosis is based on anatomopathologicalstudy The malignancy of the tumour manifested byextensive necrosis makes the histological diagnosisdifficult and often more biopsies are required forconfirmationbull Therapyndash Therapy consists of radiotherapy with or withoutchemotherapy
Midline Granuloma
bull Prognosisbull ndash Depending on the stage long-term remission or
experience a worseningbull prognosis with relapses which may include otherbull extranodal sites bull Involvement of extranodal sitesbull including the upper airway gastrointestinal tractbull skin
Wegenerrsquos Granulomatosis
bull Definition of the diseasebull ndash Wegenerrsquos granulomatosis is a systemic chronicbull vasculitis of small- and medium-sized blood vesselsbull with an autoimmune component It affectsbull particular organs with variable predilectionbull Epidemiologyaetiologybull ndash Wegenerrsquos granulomatosis is a rare disease It affects
about 1 in 20000ndash30000 people It is more prevalentbull in middle-aged Caucasian patients
Wegenerrsquos Granulomatosis
Symptomsndash The disease may present pulmonary upper
respiratory tract or renal In the disseminated form-The localised form ndash confinedto the upper respiratory region ndash is present in 25of the patients- It consists of nonspecific manifestationssuch as nasal obstruction crusting purulentor bloody rhinorrhea and painful or painless ulcers in oral or nasal cavities which are unresponsive tostandard medical treatment
Wegenerrsquos Granulomatosis
bull In some patients the nasal septum is perforatedbull which leads to saddle-nose deformity Less
commonbull symptoms are hoarseness stridor due to
subglotticbull stenosis otalgia otorrhea and conductivebull and sensorineural hearing loss Also ocular
symptomsbull such as scleritis conjunctivitis uveitis andbull episcleritis may be present
Wegenerrsquos Granulomatosis
bull ndash In the disseminated form pulmonary involvementbull is manifested by cough dyspnoea haemoptysisbull (due to an alveolar capillaritis necrotic lesions orbull endobronchial disease) and pleuritic painndashbull -Ninety per cent of patients have nasal symptomsbull and these symptoms are usually the first
manifestationof the diseasebull -Most patients have also renal involvementbull even if it is subclinical
Wegenerrsquos Granulomatosis
Diagnosis ndash Diagnosis of Wegenerrsquos granulomatosis is based on clinical findings that demonstrate lung (chest x-ray) kidney (urine analysis) or upper respiratory tract
involvement (oral or nasal ulcers or discharge) - positive blood analysis for cytoplasmic-staining antineutrophil
cytoplasmic antibodies (c-ANCA) and confirming proteinase 3 (PR3) ANCA or myeloperoxidase (MPO) ANCA ndash Biopsy is essential for diagnosis nonspecific chronic inflammation
and necrosis -Bacterial and fungal infections
Wegenerrsquos Granulomatosis
Therapyndash Conservative therapybull In the induction of disease remission highdosesteroids (e g prednisone 1 mgkgday) for1 month with tapering over several months aregiven In addition cyclophosphamide (2 mgkgday) should be administered for 6ndash12 monthsuntil symptoms disappear In the maintenanceof remission cyclophosphamide should be
Wegenerrsquos Granulomatosis
Antibiotics mainly trimethoprim-sulfamethoxazoleare given for prophylaxis againstPneumocystis jiroveci (formerly Pneumocystiscarinii) pneumonia (PCP) which may developduring immunosuppression and have a role inpreventing recurrencesbull Sinonasal manifestations may be treated with topical nasal steroids and nasal irrigations lowdosesystemic steroids and antibiotics when bacterial infection (typically Staphylococcus species) is suspected
Wegenerrsquos Granulomatosis
bull Prognosisbull ndash Most of the patients respond well to treatmentbull achieving symptom-free intervals of 5ndash20 yearsbull or more bull -Anatomical problems (sinusitis trachealbull stenosis) may require surgery bull Relapses can be long and troublesomebull Long-term complications are chronicbull renal failure hearing loss and deafness
Nasal Fractures Definition ndash A nasal fracture is a disruption of the nasal bone structure due to trauma It is the most frequently fractured facial bone Epidemiologyaetiology ndash Sports falls and assaults are the usual mechanisms of fracture -Males are affected twice as often as are females -Paediatric populations with a incidences during the second and third decades of life -Variables such as force impact direction nature of the striking object age and other will influence the pattern of injury to the components of the nose
Nasal Fractures
bull Symptomsbull ndash Deformity swelling epistaxis and periorbital
ecchymosis are signs that are suggestive of nasal fracture
bull bony crepitus and nasal segment mobilitybull ndash Epiphora bull Severe bilateral injuries to the lachrymal bones
arebull associated with depressed nasal fractures
Nasal Fractures Complications ndash Septal haematoma is one of the most severe early complications of nasal trauma and without drainage it results in abscess formation 6ndash7 days after trauma producing necrosis of the septal cartilage -Long-term problems such as saddle-nose deformity perforation columellar retraction and nasalbase
Septal infection could lead to osteomyelitis orbital and intracranial abscesses meningitis and cavernous sinus thrombosis -Cerebrospinal fluid leakage is a common complication of severe
nasal and frontal fractures
Nasal Fractures
bull Diagnostic proceduresbull ndash Inspectionbull bull Changes of appearance such as deviation andbull asymmetry bleeding watery drainage changesbull in nasal breathing and smell It is useful to comparebull the current presentation with old photographsbull (up to 40 of normal individuals havebull significant nose malformations)
Nasal Fractures Physical examination bull The diagnosis of a nasal fracture is made primarily by physical examination epistaxis nasal swelling and periorbital ecchymosis Nasal shape in the lateral and frontal inspection should be assessed Grasping the dorsum between two fingers and rocking the pyramid back and forth aids in assessing the mobility of nasal bones Internal structures should be evaluated by using a headlight and nasal speculum Clotted blood is removed by suction and assessment of haematoma mucosal tears and active bleeding is performed Bimanual palpation of the septum helps to differentiate septal swelling from haematoma ndash
Nasal FracturesRadiographybull There is no clear evidence of the role of radiographyin the management of nasal fracturesPlain films have up to a 66 false-positive rateas a result of misinterpretation of normal suturelines In addition old fractures are difficult todistinguishbull Three-dimensional CT is recommended for extensiveinjuries involving the nasal-orbital-ethmoidalcomplexndash
Nasal Fractures
bull Additionaluseful diagnostic proceduresbull bull Using a 0 or 30deg 4-mm endoscope is helpful inbull the assessment of posterior abnormalities If thebull patient is heavily sedated Brown-Gruss
provocationbull manoeuvres may be performed to determinebull deformities in upper middle or lower segmentsbull by compressing each compartment
Nasal FracturesConservative treatmentndash Treatment of bleedingbull For localised bleeding anterior sources may becauterised by silver nitrate or sealed with topicalmaterials such as thrombin combined withgelatin foam fibrin glue FloSealreg or other procoagulantmaterials If conservative measuresfail a formal anterior packing is placedbull Bleeding from branches of sphenopalatine orethmoid vessels requires anterior-posteriorpacking
Nasal Fractures
bull bull Surgical methods such as direct endoscopic vessel
bull cauterization or ligation have been shown tobull offer better haemostasis and patient comfortbull Angiography with embolization can also be
consideredbull in cases refractory to more conservativebull approaches
Nasal Fractures
bull Type of reductionbull bull Nondisplaced fractures should be treated withbull observation alone Closed nasal reduction is thebull best choice for simple injuries (isolated unilateralbull with medial displacement)bull bull An open approach should be considered in
severebull trauma (bilateral depressed fractures)
Nasal Fracturesbull Surgical principlesbull ndash Topical anaesthesia with cotton pledgets soakedbull with 4 cocaine or 005 oxymethazoline combinedbull with 4 topical lidocaine should be appliedbull for 5ndash10 min Local anaesthesia should also be injectedbull (1 lidocaine and 1100000 epinephrine)bull along the septum lateral walls and floor of the nasalbull cavitybull bull
Nasal FracturesClosed reductionndashndash The nasal bones are grasped between two fingersand pressure is applied laterally in theopposite direction of the deviation A bluntelevator may be used from within the nose incases of significant medial collapse Walshamforceps can be of help Reduction of the septumshould be performed with the use ofAsch forceps
Nasal Fractures
bull To prevent collapse of the postreductionbull framework nasal packing should be placedbull for 3ndash5 days Septum splints are recommendedbull in comminuted septal fractures withbull severe mucosal lesions External nasal splintingbull for 10 days (Aquaplastreg Thermoplastreg)bull provides nasal protection Nasal saline spraysbull prevent crusting and oral antibiotics should
Nasal Fractures
bull Open reductionbull ndashndash Immediate repair of fractures by using
widebull surgical exposure reduction fixation and
reconstructionbull ndashndash The second option is delayed correctionbull (6 months or more) of persistent deformitiesbull using standard techniques of rhinoplasty
Deviated Nasal Septum
bull Definition of the diseasebull ndash Deviation of the nasal septum is a common causebull of unilateral nasal airway obstruction in which thebull nasal septum is displacedbull bull Epidemiologyaetiologybull ndash Developmental septal abnormalities Septal cartilage
damage in the neonatal period andbull during birth can cause severe septal deviation inbull the absence of a history of nasal trauma
Deviated Nasal Septum
bull Symptomsbull ndash Patients may present with a history of sinusitis
allergicbull rhinitis obstructive sleep apnoea previousbull nasal surgery or recent nasal trauma Unilateral or
bilateral nasal airway obstruction that is unrelievedbull with decongestants or nasal steroid sprays is oftenbull seenbull bull
Deviated Nasal SeptumDiagnosisndashExamination external dorsal deviation or the columella and caudal septummay be deflected off the midline (caudal subluxation)ndash Inspections of the nasal cavity and anterior-posteriorrhinoscopy are helpful in diagnosing the locationtype and severity of septal deformityThe endoscope is also useful in identifying polypsthe severity and extent of posterior septaldeviations and bony spurs and locating areas ofseptal perforation or mucosal injury
Deviated Nasal Septum
bull Therapybull ndash Septoplasty is a procedurebull The areabull of deviation is corrected or resected in order tobull leave behind as much cartilage and bone as
possiblebull Cartilage resection is minimised and can be
repositioned reshaped or recontoured using a variety of methods
Deviated Nasal Septum
bull ndash Indications of septoplasty before the growth period
bull of the nose is finished should be very limited bull -In these cases surgery must preserve all the
cartilagebull in order to prevent external changes of the
shape ofbull the nose
Deviated Nasal Septum
bull Complicationsbull ndash Frequent complications include haematoma andbull infection Cerebrospinal fluid leak is a rare but
potentiallybull serious complicationbull It is usually the resultbull of avulsion or damage to the cribriform plate whenbull handling the perpendicular plate of the ethmoidbull ndash Other complications include epistaxis nasal
Deviated Nasal Septum
bull Other complications include epistaxis nasal obstruction
bull due to residual deviation synechiae returnbull of the cartilaginous deviation septal perforationbull anosmia and cosmetic nasal deformities suchbull as widened alar rim margins drooping nasal tipbull columella retraction and a sunken dorsum with abull supratip saddle formation
Septal perforation with minor crusting View from provide closure of the
incision
Septal Haematoma
bull A septal haematoma is a blood collection under the perichondrium
bull of the septum and cartilagebull bull bull Epidemiologyaetiologybull ndash A septal haematoma is one of the most
severe complications of nasal trauma
Septal Haematoma
bull Diagnosisbull ndash Signs and symptoms include intense pain
swellingbull haematoma of the upper lip and philtrum
area andbull complete nasal airway obstruction
Septal HaematomaTherapyndash Management consists of drainage through a mucoperichondrial incision Immediate treatment isnecessary to prevent long-term problems such asa saddle-nose deformity perforation columellarretraction and nasal-base widening In childrenseptal destruction can lead to devastating nasal andmidfacial growth abnormalitiesbull Surgeryndash Incision and evacuation of the collection is performedDrainage of a septal haematoma should
Septal HaematomaSurgeryndash Incision and evacuation of the collection is performedDrainage of a septal haematoma should provide closure of the incision
Splints or transseptal sutures are placed to obliterate thepotential space and prevent collectionInfection involving the septal cartilage Reconstruction with autologouscartilage is then performed in a second stage Oral antibiotics should be given
Nasal DeformitySaddle-nose deformityndash A saddle-nose deformity is characterised by a loss ofnasal dorsal height and compromised nasal supportstructures -Other case observed are depressionof the middle vault and dorsum loss of nasal tipsupport and definition shortened (vertical) nasal length over rotation of the nasal tip and retrusion ofthe nasal spine and caudal septum It is also knownas a ldquoPug noserdquo or ldquoboxerrsquos noserdquo both of which referto various degrees of nasal dorsal depressionbull
Nasal DeformityEpidemiologyaetiologyndash Prevalence is higher in population groups prone to facial trauma (ie boxers athletes) those with historiesof intranasal cocaine use nasal surgery (e g radical submucosal septal resection reductive rhinoplasty)ndash A saddle-nose deformity can be congenital or acquired It can be noticed as a part of individual familialsyndromic and ethnic characteristics - Most deformities are due to traumatic and iatrogeniccauses Medical causes are Wegenerrsquosgranulomatosis relapsing polychondritis leprosy (Hansenrsquos disease) syphilis ectodermal dysplasiaand intranasal cocaine use
Nasal Deformity
bull Therapybull ndash Nasal reconstruction indications depend on patientbull selection surgeon experience and aetiology of thebull deformity bull Indications for surgery can be functionalbull aesthetic or most commonly both In individuals
with a compromised nasal airway a nasoseptalbull reconstruction is indicated
Nasal Deformity
bull Contraindications bull include patients with malignantbull chronic or autoimmune disease conditions drugbull abuse poor perioperative risk profile and unrealisticbull expectationsbull ndash Multiple previous rhinoplasties and certain
professionsbull (mixed martial artists boxers and other contactbull sports) are relative contraindications
Nasal DeformitySeptoplastyndash Septoplasty is performed to correct nasal obstructioncaused by septal deformityndash Usually septoplasty is performed under general anaesthesiawith the patient in the supine position with the head elevated by approximately 30 (Righthandedsurgeons approach from the right side)ndash Local vasoconstrictive anaesthesia is applied notonly to reduce postoperative pain but also more importantly to achieve vasoconstriction of themucosa and less intraoperative haemorrhage Lidocainewith adrenaline or epinephrine is usedalthough in patients with cardiac hypersensitivityoxymetazoline might be preferred
Nasal Deformity
bull Septoplasty begins with the incision of septal mucosabull Most operative techniques utilise a hemitransfixionbull incision at the caudal end of septum so thatbull deviation at this point might be reached as wellbull as a transfixion incision that is easily obtained ifbull needed (Right-handed surgeons normally choosebull the left side but that may vary when deviation isbull convex towards the right)
Nasal DeformityA columella retractor is placed over the columellaand by pulling it laterally the caudal border of theseptum is exposed Ala can be protected by an alaprotector A vertical incision with a no 15 bladeover the caudal end of septum is performed untilreaching the plane of the septal cartilage It is essentialto correctly identify the perichondrium and byusing the Cottle elevator dissect and lift it creatinga flap As the dissection proceeds along the septalcartilage a longer speculum (no 5) is introduced sothat elevation of the mucoperichondrium is doneunder constant visual controlndash The next step is to dissect the mucoperiostium
Nasal DeformityDissecting over the bony-cartilaginous junctionwhen joining both tunnels might be difficult and is
especially prone to membrane perforationndash If needed the same tunnels are to be created on the
other side of the septum Then deviated parts of
septum are identified and removed either with a
knife or a Freer chisel
Nasal Deformitybull septum from the maxillary crest the septum mustbull be separated from the perpendicular plate trimmedbull along the inferior border placed back onto the crestbull and sutured to the periosteum If the deformity involvesbull the vomer an osteotome is used Care mustbull be taken not to break the cribriform plate becausebull it could cause a cerebrospinal fistula
Nasal Deformity
bull Once the septal deviation is corrected the flapsbull and hemitransfixion incision are mattressed
withbull absorbable sutures Nasal packing to prevent
synechiaebull and postoperative septal haematoma mightbull be advised but should be removed within 72 h

occipitomental projection demonstrates the maxillarysinus and gives a limited view of the sphenoid sinus
Computed tomography of the paranasal sinuses
Four representative coronal CT scans are shown
Four representative coronal CT scans are shown
Magnetic Resonance Imaging
Magnetic maging
Magnetic resonance imaging (MRI) has fewer indicationsthan CT in patients with paranasal sinus diseaseThis is primarily because MRI is markedly inferior toCT in defining the bony boundaries of the sinusesThe strength of MRI lies in its superior soft-tissue discriminationMRI is indicated in diseases that involve the paranasal sinuses in addition to thecranial cavity or orbit (eg tumors and congenitalmalformations such as encephaloceles)
MRI of the paranasal sinuses
The Nose and Sinuses
Structure The structure of the nose is made up of
four partsbull The surface anatomybull The nasal skeletonmdashcomposed of the
two nasal bones the paired upper lateral and lower lateral cartilages and the nasal septum covered in subcutaneous tissue and skin
bull The internal anatomymdashincludes the septum of the nose which forms the medial wall of the nasal cavity The turbinates on the lateral wall are also called conchae
bull The osteomeatal complexmdasha key functional area of the nose
Function The nose is the main route for inspired
air and its structure is related to this function As the air passes over the large surface area of the turbinates
The inspired gases are warmed and humidified Mucus on the mucosa of the nose removes large dust particles from the air as it is breathed in
The voice resonates in the sinuses and nose and this provides character to the speech
Pneumatization of the sinusesmdashthey are air filled spacesmdashreduces the weight of the skull
Diseases of thDiseases of the Outer and Inner Nosee Outer and
Inner Nose Erysipelas Definition of the disease ndash Erysipela is a skin infection that affects the superficial dermis and is caused by Streptococcus pyogenes (group A) It usually develops in the extremities and the face and less commonly on the scalp and genitals bull Epidemiologyaetiology ndash Erysipelas are more often seen in elderly infants and children patients with compromised immunology and diabetes -Predisposing factors are alcoholism skin ulceration puncture wounds fungal infections malnutrition and burns
Erysipelas
bull Symptomsbull ndash It usually presents of fever general fatigue bull -The skin lesion is a redindurated and elevated plaque
with borders that expand rapidly bull It is painful warm and accompanied by variable oedemabull -On the second or third day a flaccid bulla may develop
and desquamationbull bull Presence of regional lymph nodes is common
Erysipelas
bull Complicationsndash The most common complication is recurrencewhich is seen in 18ndash30 of the cases even afterproper antibiotic therapy Recurrence is seen moreoften in females than in malesA skin infection with S pyogenes could lead toglomerulonephritis
Erysipelas
bull Complicationsbull ndash The most common complication is recurrencebull which is seen in 18ndash30 of the cases even afterbull proper antibiotic therapy bull -Recurrence is seen morebull often in females than in males bull -A skin infection with S pyogenes could lead tobull glomerulonephritis
Erysipelas
bull bull Diagnosisbull ndash Diagnosis is based on the patientrsquos personal
historybull and physical examination particularly on inspectionbull of the skin
bull Blood cultures are positive in less thanbull 5 of cases
ErysipelasTherapyndash Conservative therapybull The preferred antibiotic is penicillin In mildcases with minor systemic symptoms penicillinV 500 mg orally every 6 h for 10 days or penicillinG benzathine 12 mil U intramuscularlyonceOther possibilities are amoxicillin 500 mgorally twice a day for 10 days or cephalexin 500mg orally every 6 h for 10 days
ErysipelasIn moderate and severe cases with significantsystemic symptoms hospitalization and intravenoustreatment is required penicillin G 2ndash4mil U intravenously every 4ndash6 h Cefazolin05ndash15 gm intravenously every 8 h cefotaxime1ndash2 gm intravenously every 8 h or ceftriaxone1ndash2 gm intravenously once a day should be administeredIn patients with a penicillin allergyclindamycin 600 mg intravenously every 8 h orvancomycin 15 mgkg intravenously twice a daymay be given
ErysipelaAdditional useful therapeutic optionsbull Prednisone 30 mg over 8 days might be consideredas well as elevation of the affected siteMoist heat compresses may be usefulbull Surgeryndash Debridement and drainage are indicated when bullaeabscesses or necroses are presentbull Differential diagnosisndash Contact dermatitisndash Asteatotic eczemandash Herpes zosterndash Angioneurotic oedemandash Osteomyelitis
Furuncle
bull Definition of the diseasebull ndash A furuncle is an infection that beginsbull at the hair follicle and spreads deeper into thebull dermis and subcutaneous tissue forming abull nodule After several days it developsbull into an abscess - red painful and fluctuantbull bull bull Epidemiologyaetiologybull ndash The aetiologic agent is Staphylococcus aureus
FuruncleSymptomsndashsymptoms are local and limited to thesite of infection Furuncles usually are wherehair follicles are present bull Complicationndash One complication is furunculosis multiple draining furunclesDiagnosisndash The diagnosis is based on clinical inspection - Cultures are not necessary when there is no systemic involvement but should beconsidered if systemic therapy (in case of feversignificant cellulitis or hospitalization) or whenmethicillin-resistant Staphylococcusaureus (MRSA) is considered
FuruncleTherapyndash When the furuncle is small application of moist heat compress to promote drainage -Larger furuncles should be drained by surgical incision-After drainage the area should be cleaned with anantiseptic (with chlorhexidinebetadine) should be applied twice
a dayndash If no systemic symptoms or extensive cellulitis arepresent simple topical care is usually curative andoral antibiotics are not necessary Otherwise systemictreatment is indicated and should cover anypossible MRSA
Furuncle
bull -Recommended antibiotics are trimethoprim-sulfamethoxazole
bull 1ndash2 tablets orally twice daily doxycyclinebull 100 mg orally twice dailybull or clindamycin 300ndash450 mg orally every 8 hbull - In severe cases vancomycin 15 mgkg
intravenouslybull every 12 h or clindamycin 600 mg intravenouslybull every 8 h
Midline Granulomabull A midline granuloma is an angiocentricbull lymphoma it was referred to as polymorphicbull reticulosis lethal midline granuloma and midline
malignant reticulosisbull bull Definition of the diseasebull ndash This rare disease is a lymphoma of extranodal
presentationall cases are positive for the Epstein-Barr virus
bull -This lymphoma most commonly appears in the midface region
Midline GranulomaEpidemiologyaetiologyndash This form of lymphoma is rare in Europe and theUnited States with a higher prevalence in Asia and PeruSymptomsndash The most common presentation is nasal obstruction with a destructive mass occupying the nosesinuses and palate
-Fever night sweatsand weight loss seen usually in Hodgkinrsquos lymphomaand other non-Hodgkinrsquos lymphomas (knownas ldquoB symptomsrdquo) are uncommon
Midline GranulomaDiagnosisndash The diagnosis is based on anatomopathologicalstudy The malignancy of the tumour manifested byextensive necrosis makes the histological diagnosisdifficult and often more biopsies are required forconfirmationbull Therapyndash Therapy consists of radiotherapy with or withoutchemotherapy
Midline Granuloma
bull Prognosisbull ndash Depending on the stage long-term remission or
experience a worseningbull prognosis with relapses which may include otherbull extranodal sites bull Involvement of extranodal sitesbull including the upper airway gastrointestinal tractbull skin
Wegenerrsquos Granulomatosis
bull Definition of the diseasebull ndash Wegenerrsquos granulomatosis is a systemic chronicbull vasculitis of small- and medium-sized blood vesselsbull with an autoimmune component It affectsbull particular organs with variable predilectionbull Epidemiologyaetiologybull ndash Wegenerrsquos granulomatosis is a rare disease It affects
about 1 in 20000ndash30000 people It is more prevalentbull in middle-aged Caucasian patients
Wegenerrsquos Granulomatosis
Symptomsndash The disease may present pulmonary upper
respiratory tract or renal In the disseminated form-The localised form ndash confinedto the upper respiratory region ndash is present in 25of the patients- It consists of nonspecific manifestationssuch as nasal obstruction crusting purulentor bloody rhinorrhea and painful or painless ulcers in oral or nasal cavities which are unresponsive tostandard medical treatment
Wegenerrsquos Granulomatosis
bull In some patients the nasal septum is perforatedbull which leads to saddle-nose deformity Less
commonbull symptoms are hoarseness stridor due to
subglotticbull stenosis otalgia otorrhea and conductivebull and sensorineural hearing loss Also ocular
symptomsbull such as scleritis conjunctivitis uveitis andbull episcleritis may be present
Wegenerrsquos Granulomatosis
bull ndash In the disseminated form pulmonary involvementbull is manifested by cough dyspnoea haemoptysisbull (due to an alveolar capillaritis necrotic lesions orbull endobronchial disease) and pleuritic painndashbull -Ninety per cent of patients have nasal symptomsbull and these symptoms are usually the first
manifestationof the diseasebull -Most patients have also renal involvementbull even if it is subclinical
Wegenerrsquos Granulomatosis
Diagnosis ndash Diagnosis of Wegenerrsquos granulomatosis is based on clinical findings that demonstrate lung (chest x-ray) kidney (urine analysis) or upper respiratory tract
involvement (oral or nasal ulcers or discharge) - positive blood analysis for cytoplasmic-staining antineutrophil
cytoplasmic antibodies (c-ANCA) and confirming proteinase 3 (PR3) ANCA or myeloperoxidase (MPO) ANCA ndash Biopsy is essential for diagnosis nonspecific chronic inflammation
and necrosis -Bacterial and fungal infections
Wegenerrsquos Granulomatosis
Therapyndash Conservative therapybull In the induction of disease remission highdosesteroids (e g prednisone 1 mgkgday) for1 month with tapering over several months aregiven In addition cyclophosphamide (2 mgkgday) should be administered for 6ndash12 monthsuntil symptoms disappear In the maintenanceof remission cyclophosphamide should be
Wegenerrsquos Granulomatosis
Antibiotics mainly trimethoprim-sulfamethoxazoleare given for prophylaxis againstPneumocystis jiroveci (formerly Pneumocystiscarinii) pneumonia (PCP) which may developduring immunosuppression and have a role inpreventing recurrencesbull Sinonasal manifestations may be treated with topical nasal steroids and nasal irrigations lowdosesystemic steroids and antibiotics when bacterial infection (typically Staphylococcus species) is suspected
Wegenerrsquos Granulomatosis
bull Prognosisbull ndash Most of the patients respond well to treatmentbull achieving symptom-free intervals of 5ndash20 yearsbull or more bull -Anatomical problems (sinusitis trachealbull stenosis) may require surgery bull Relapses can be long and troublesomebull Long-term complications are chronicbull renal failure hearing loss and deafness
Nasal Fractures Definition ndash A nasal fracture is a disruption of the nasal bone structure due to trauma It is the most frequently fractured facial bone Epidemiologyaetiology ndash Sports falls and assaults are the usual mechanisms of fracture -Males are affected twice as often as are females -Paediatric populations with a incidences during the second and third decades of life -Variables such as force impact direction nature of the striking object age and other will influence the pattern of injury to the components of the nose
Nasal Fractures
bull Symptomsbull ndash Deformity swelling epistaxis and periorbital
ecchymosis are signs that are suggestive of nasal fracture
bull bony crepitus and nasal segment mobilitybull ndash Epiphora bull Severe bilateral injuries to the lachrymal bones
arebull associated with depressed nasal fractures
Nasal Fractures Complications ndash Septal haematoma is one of the most severe early complications of nasal trauma and without drainage it results in abscess formation 6ndash7 days after trauma producing necrosis of the septal cartilage -Long-term problems such as saddle-nose deformity perforation columellar retraction and nasalbase
Septal infection could lead to osteomyelitis orbital and intracranial abscesses meningitis and cavernous sinus thrombosis -Cerebrospinal fluid leakage is a common complication of severe
nasal and frontal fractures
Nasal Fractures
bull Diagnostic proceduresbull ndash Inspectionbull bull Changes of appearance such as deviation andbull asymmetry bleeding watery drainage changesbull in nasal breathing and smell It is useful to comparebull the current presentation with old photographsbull (up to 40 of normal individuals havebull significant nose malformations)
Nasal Fractures Physical examination bull The diagnosis of a nasal fracture is made primarily by physical examination epistaxis nasal swelling and periorbital ecchymosis Nasal shape in the lateral and frontal inspection should be assessed Grasping the dorsum between two fingers and rocking the pyramid back and forth aids in assessing the mobility of nasal bones Internal structures should be evaluated by using a headlight and nasal speculum Clotted blood is removed by suction and assessment of haematoma mucosal tears and active bleeding is performed Bimanual palpation of the septum helps to differentiate septal swelling from haematoma ndash
Nasal FracturesRadiographybull There is no clear evidence of the role of radiographyin the management of nasal fracturesPlain films have up to a 66 false-positive rateas a result of misinterpretation of normal suturelines In addition old fractures are difficult todistinguishbull Three-dimensional CT is recommended for extensiveinjuries involving the nasal-orbital-ethmoidalcomplexndash
Nasal Fractures
bull Additionaluseful diagnostic proceduresbull bull Using a 0 or 30deg 4-mm endoscope is helpful inbull the assessment of posterior abnormalities If thebull patient is heavily sedated Brown-Gruss
provocationbull manoeuvres may be performed to determinebull deformities in upper middle or lower segmentsbull by compressing each compartment
Nasal FracturesConservative treatmentndash Treatment of bleedingbull For localised bleeding anterior sources may becauterised by silver nitrate or sealed with topicalmaterials such as thrombin combined withgelatin foam fibrin glue FloSealreg or other procoagulantmaterials If conservative measuresfail a formal anterior packing is placedbull Bleeding from branches of sphenopalatine orethmoid vessels requires anterior-posteriorpacking
Nasal Fractures
bull bull Surgical methods such as direct endoscopic vessel
bull cauterization or ligation have been shown tobull offer better haemostasis and patient comfortbull Angiography with embolization can also be
consideredbull in cases refractory to more conservativebull approaches
Nasal Fractures
bull Type of reductionbull bull Nondisplaced fractures should be treated withbull observation alone Closed nasal reduction is thebull best choice for simple injuries (isolated unilateralbull with medial displacement)bull bull An open approach should be considered in
severebull trauma (bilateral depressed fractures)
Nasal Fracturesbull Surgical principlesbull ndash Topical anaesthesia with cotton pledgets soakedbull with 4 cocaine or 005 oxymethazoline combinedbull with 4 topical lidocaine should be appliedbull for 5ndash10 min Local anaesthesia should also be injectedbull (1 lidocaine and 1100000 epinephrine)bull along the septum lateral walls and floor of the nasalbull cavitybull bull
Nasal FracturesClosed reductionndashndash The nasal bones are grasped between two fingersand pressure is applied laterally in theopposite direction of the deviation A bluntelevator may be used from within the nose incases of significant medial collapse Walshamforceps can be of help Reduction of the septumshould be performed with the use ofAsch forceps
Nasal Fractures
bull To prevent collapse of the postreductionbull framework nasal packing should be placedbull for 3ndash5 days Septum splints are recommendedbull in comminuted septal fractures withbull severe mucosal lesions External nasal splintingbull for 10 days (Aquaplastreg Thermoplastreg)bull provides nasal protection Nasal saline spraysbull prevent crusting and oral antibiotics should
Nasal Fractures
bull Open reductionbull ndashndash Immediate repair of fractures by using
widebull surgical exposure reduction fixation and
reconstructionbull ndashndash The second option is delayed correctionbull (6 months or more) of persistent deformitiesbull using standard techniques of rhinoplasty
Deviated Nasal Septum
bull Definition of the diseasebull ndash Deviation of the nasal septum is a common causebull of unilateral nasal airway obstruction in which thebull nasal septum is displacedbull bull Epidemiologyaetiologybull ndash Developmental septal abnormalities Septal cartilage
damage in the neonatal period andbull during birth can cause severe septal deviation inbull the absence of a history of nasal trauma
Deviated Nasal Septum
bull Symptomsbull ndash Patients may present with a history of sinusitis
allergicbull rhinitis obstructive sleep apnoea previousbull nasal surgery or recent nasal trauma Unilateral or
bilateral nasal airway obstruction that is unrelievedbull with decongestants or nasal steroid sprays is oftenbull seenbull bull
Deviated Nasal SeptumDiagnosisndashExamination external dorsal deviation or the columella and caudal septummay be deflected off the midline (caudal subluxation)ndash Inspections of the nasal cavity and anterior-posteriorrhinoscopy are helpful in diagnosing the locationtype and severity of septal deformityThe endoscope is also useful in identifying polypsthe severity and extent of posterior septaldeviations and bony spurs and locating areas ofseptal perforation or mucosal injury
Deviated Nasal Septum
bull Therapybull ndash Septoplasty is a procedurebull The areabull of deviation is corrected or resected in order tobull leave behind as much cartilage and bone as
possiblebull Cartilage resection is minimised and can be
repositioned reshaped or recontoured using a variety of methods
Deviated Nasal Septum
bull ndash Indications of septoplasty before the growth period
bull of the nose is finished should be very limited bull -In these cases surgery must preserve all the
cartilagebull in order to prevent external changes of the
shape ofbull the nose
Deviated Nasal Septum
bull Complicationsbull ndash Frequent complications include haematoma andbull infection Cerebrospinal fluid leak is a rare but
potentiallybull serious complicationbull It is usually the resultbull of avulsion or damage to the cribriform plate whenbull handling the perpendicular plate of the ethmoidbull ndash Other complications include epistaxis nasal
Deviated Nasal Septum
bull Other complications include epistaxis nasal obstruction
bull due to residual deviation synechiae returnbull of the cartilaginous deviation septal perforationbull anosmia and cosmetic nasal deformities suchbull as widened alar rim margins drooping nasal tipbull columella retraction and a sunken dorsum with abull supratip saddle formation
Septal perforation with minor crusting View from provide closure of the
incision
Septal Haematoma
bull A septal haematoma is a blood collection under the perichondrium
bull of the septum and cartilagebull bull bull Epidemiologyaetiologybull ndash A septal haematoma is one of the most
severe complications of nasal trauma
Septal Haematoma
bull Diagnosisbull ndash Signs and symptoms include intense pain
swellingbull haematoma of the upper lip and philtrum
area andbull complete nasal airway obstruction
Septal HaematomaTherapyndash Management consists of drainage through a mucoperichondrial incision Immediate treatment isnecessary to prevent long-term problems such asa saddle-nose deformity perforation columellarretraction and nasal-base widening In childrenseptal destruction can lead to devastating nasal andmidfacial growth abnormalitiesbull Surgeryndash Incision and evacuation of the collection is performedDrainage of a septal haematoma should
Septal HaematomaSurgeryndash Incision and evacuation of the collection is performedDrainage of a septal haematoma should provide closure of the incision
Splints or transseptal sutures are placed to obliterate thepotential space and prevent collectionInfection involving the septal cartilage Reconstruction with autologouscartilage is then performed in a second stage Oral antibiotics should be given
Nasal DeformitySaddle-nose deformityndash A saddle-nose deformity is characterised by a loss ofnasal dorsal height and compromised nasal supportstructures -Other case observed are depressionof the middle vault and dorsum loss of nasal tipsupport and definition shortened (vertical) nasal length over rotation of the nasal tip and retrusion ofthe nasal spine and caudal septum It is also knownas a ldquoPug noserdquo or ldquoboxerrsquos noserdquo both of which referto various degrees of nasal dorsal depressionbull
Nasal DeformityEpidemiologyaetiologyndash Prevalence is higher in population groups prone to facial trauma (ie boxers athletes) those with historiesof intranasal cocaine use nasal surgery (e g radical submucosal septal resection reductive rhinoplasty)ndash A saddle-nose deformity can be congenital or acquired It can be noticed as a part of individual familialsyndromic and ethnic characteristics - Most deformities are due to traumatic and iatrogeniccauses Medical causes are Wegenerrsquosgranulomatosis relapsing polychondritis leprosy (Hansenrsquos disease) syphilis ectodermal dysplasiaand intranasal cocaine use
Nasal Deformity
bull Therapybull ndash Nasal reconstruction indications depend on patientbull selection surgeon experience and aetiology of thebull deformity bull Indications for surgery can be functionalbull aesthetic or most commonly both In individuals
with a compromised nasal airway a nasoseptalbull reconstruction is indicated
Nasal Deformity
bull Contraindications bull include patients with malignantbull chronic or autoimmune disease conditions drugbull abuse poor perioperative risk profile and unrealisticbull expectationsbull ndash Multiple previous rhinoplasties and certain
professionsbull (mixed martial artists boxers and other contactbull sports) are relative contraindications
Nasal DeformitySeptoplastyndash Septoplasty is performed to correct nasal obstructioncaused by septal deformityndash Usually septoplasty is performed under general anaesthesiawith the patient in the supine position with the head elevated by approximately 30 (Righthandedsurgeons approach from the right side)ndash Local vasoconstrictive anaesthesia is applied notonly to reduce postoperative pain but also more importantly to achieve vasoconstriction of themucosa and less intraoperative haemorrhage Lidocainewith adrenaline or epinephrine is usedalthough in patients with cardiac hypersensitivityoxymetazoline might be preferred
Nasal Deformity
bull Septoplasty begins with the incision of septal mucosabull Most operative techniques utilise a hemitransfixionbull incision at the caudal end of septum so thatbull deviation at this point might be reached as wellbull as a transfixion incision that is easily obtained ifbull needed (Right-handed surgeons normally choosebull the left side but that may vary when deviation isbull convex towards the right)
Nasal DeformityA columella retractor is placed over the columellaand by pulling it laterally the caudal border of theseptum is exposed Ala can be protected by an alaprotector A vertical incision with a no 15 bladeover the caudal end of septum is performed untilreaching the plane of the septal cartilage It is essentialto correctly identify the perichondrium and byusing the Cottle elevator dissect and lift it creatinga flap As the dissection proceeds along the septalcartilage a longer speculum (no 5) is introduced sothat elevation of the mucoperichondrium is doneunder constant visual controlndash The next step is to dissect the mucoperiostium
Nasal DeformityDissecting over the bony-cartilaginous junctionwhen joining both tunnels might be difficult and is
especially prone to membrane perforationndash If needed the same tunnels are to be created on the
other side of the septum Then deviated parts of
septum are identified and removed either with a
knife or a Freer chisel
Nasal Deformitybull septum from the maxillary crest the septum mustbull be separated from the perpendicular plate trimmedbull along the inferior border placed back onto the crestbull and sutured to the periosteum If the deformity involvesbull the vomer an osteotome is used Care mustbull be taken not to break the cribriform plate becausebull it could cause a cerebrospinal fistula
Nasal Deformity
bull Once the septal deviation is corrected the flapsbull and hemitransfixion incision are mattressed
withbull absorbable sutures Nasal packing to prevent
synechiaebull and postoperative septal haematoma mightbull be advised but should be removed within 72 h

Computed tomography of the paranasal sinuses
Four representative coronal CT scans are shown
Four representative coronal CT scans are shown
Magnetic Resonance Imaging
Magnetic maging
Magnetic resonance imaging (MRI) has fewer indicationsthan CT in patients with paranasal sinus diseaseThis is primarily because MRI is markedly inferior toCT in defining the bony boundaries of the sinusesThe strength of MRI lies in its superior soft-tissue discriminationMRI is indicated in diseases that involve the paranasal sinuses in addition to thecranial cavity or orbit (eg tumors and congenitalmalformations such as encephaloceles)
MRI of the paranasal sinuses
The Nose and Sinuses
Structure The structure of the nose is made up of
four partsbull The surface anatomybull The nasal skeletonmdashcomposed of the
two nasal bones the paired upper lateral and lower lateral cartilages and the nasal septum covered in subcutaneous tissue and skin
bull The internal anatomymdashincludes the septum of the nose which forms the medial wall of the nasal cavity The turbinates on the lateral wall are also called conchae
bull The osteomeatal complexmdasha key functional area of the nose
Function The nose is the main route for inspired
air and its structure is related to this function As the air passes over the large surface area of the turbinates
The inspired gases are warmed and humidified Mucus on the mucosa of the nose removes large dust particles from the air as it is breathed in
The voice resonates in the sinuses and nose and this provides character to the speech
Pneumatization of the sinusesmdashthey are air filled spacesmdashreduces the weight of the skull
Diseases of thDiseases of the Outer and Inner Nosee Outer and
Inner Nose Erysipelas Definition of the disease ndash Erysipela is a skin infection that affects the superficial dermis and is caused by Streptococcus pyogenes (group A) It usually develops in the extremities and the face and less commonly on the scalp and genitals bull Epidemiologyaetiology ndash Erysipelas are more often seen in elderly infants and children patients with compromised immunology and diabetes -Predisposing factors are alcoholism skin ulceration puncture wounds fungal infections malnutrition and burns
Erysipelas
bull Symptomsbull ndash It usually presents of fever general fatigue bull -The skin lesion is a redindurated and elevated plaque
with borders that expand rapidly bull It is painful warm and accompanied by variable oedemabull -On the second or third day a flaccid bulla may develop
and desquamationbull bull Presence of regional lymph nodes is common
Erysipelas
bull Complicationsndash The most common complication is recurrencewhich is seen in 18ndash30 of the cases even afterproper antibiotic therapy Recurrence is seen moreoften in females than in malesA skin infection with S pyogenes could lead toglomerulonephritis
Erysipelas
bull Complicationsbull ndash The most common complication is recurrencebull which is seen in 18ndash30 of the cases even afterbull proper antibiotic therapy bull -Recurrence is seen morebull often in females than in males bull -A skin infection with S pyogenes could lead tobull glomerulonephritis
Erysipelas
bull bull Diagnosisbull ndash Diagnosis is based on the patientrsquos personal
historybull and physical examination particularly on inspectionbull of the skin
bull Blood cultures are positive in less thanbull 5 of cases
ErysipelasTherapyndash Conservative therapybull The preferred antibiotic is penicillin In mildcases with minor systemic symptoms penicillinV 500 mg orally every 6 h for 10 days or penicillinG benzathine 12 mil U intramuscularlyonceOther possibilities are amoxicillin 500 mgorally twice a day for 10 days or cephalexin 500mg orally every 6 h for 10 days
ErysipelasIn moderate and severe cases with significantsystemic symptoms hospitalization and intravenoustreatment is required penicillin G 2ndash4mil U intravenously every 4ndash6 h Cefazolin05ndash15 gm intravenously every 8 h cefotaxime1ndash2 gm intravenously every 8 h or ceftriaxone1ndash2 gm intravenously once a day should be administeredIn patients with a penicillin allergyclindamycin 600 mg intravenously every 8 h orvancomycin 15 mgkg intravenously twice a daymay be given
ErysipelaAdditional useful therapeutic optionsbull Prednisone 30 mg over 8 days might be consideredas well as elevation of the affected siteMoist heat compresses may be usefulbull Surgeryndash Debridement and drainage are indicated when bullaeabscesses or necroses are presentbull Differential diagnosisndash Contact dermatitisndash Asteatotic eczemandash Herpes zosterndash Angioneurotic oedemandash Osteomyelitis
Furuncle
bull Definition of the diseasebull ndash A furuncle is an infection that beginsbull at the hair follicle and spreads deeper into thebull dermis and subcutaneous tissue forming abull nodule After several days it developsbull into an abscess - red painful and fluctuantbull bull bull Epidemiologyaetiologybull ndash The aetiologic agent is Staphylococcus aureus
FuruncleSymptomsndashsymptoms are local and limited to thesite of infection Furuncles usually are wherehair follicles are present bull Complicationndash One complication is furunculosis multiple draining furunclesDiagnosisndash The diagnosis is based on clinical inspection - Cultures are not necessary when there is no systemic involvement but should beconsidered if systemic therapy (in case of feversignificant cellulitis or hospitalization) or whenmethicillin-resistant Staphylococcusaureus (MRSA) is considered
FuruncleTherapyndash When the furuncle is small application of moist heat compress to promote drainage -Larger furuncles should be drained by surgical incision-After drainage the area should be cleaned with anantiseptic (with chlorhexidinebetadine) should be applied twice
a dayndash If no systemic symptoms or extensive cellulitis arepresent simple topical care is usually curative andoral antibiotics are not necessary Otherwise systemictreatment is indicated and should cover anypossible MRSA
Furuncle
bull -Recommended antibiotics are trimethoprim-sulfamethoxazole
bull 1ndash2 tablets orally twice daily doxycyclinebull 100 mg orally twice dailybull or clindamycin 300ndash450 mg orally every 8 hbull - In severe cases vancomycin 15 mgkg
intravenouslybull every 12 h or clindamycin 600 mg intravenouslybull every 8 h
Midline Granulomabull A midline granuloma is an angiocentricbull lymphoma it was referred to as polymorphicbull reticulosis lethal midline granuloma and midline
malignant reticulosisbull bull Definition of the diseasebull ndash This rare disease is a lymphoma of extranodal
presentationall cases are positive for the Epstein-Barr virus
bull -This lymphoma most commonly appears in the midface region
Midline GranulomaEpidemiologyaetiologyndash This form of lymphoma is rare in Europe and theUnited States with a higher prevalence in Asia and PeruSymptomsndash The most common presentation is nasal obstruction with a destructive mass occupying the nosesinuses and palate
-Fever night sweatsand weight loss seen usually in Hodgkinrsquos lymphomaand other non-Hodgkinrsquos lymphomas (knownas ldquoB symptomsrdquo) are uncommon
Midline GranulomaDiagnosisndash The diagnosis is based on anatomopathologicalstudy The malignancy of the tumour manifested byextensive necrosis makes the histological diagnosisdifficult and often more biopsies are required forconfirmationbull Therapyndash Therapy consists of radiotherapy with or withoutchemotherapy
Midline Granuloma
bull Prognosisbull ndash Depending on the stage long-term remission or
experience a worseningbull prognosis with relapses which may include otherbull extranodal sites bull Involvement of extranodal sitesbull including the upper airway gastrointestinal tractbull skin
Wegenerrsquos Granulomatosis
bull Definition of the diseasebull ndash Wegenerrsquos granulomatosis is a systemic chronicbull vasculitis of small- and medium-sized blood vesselsbull with an autoimmune component It affectsbull particular organs with variable predilectionbull Epidemiologyaetiologybull ndash Wegenerrsquos granulomatosis is a rare disease It affects
about 1 in 20000ndash30000 people It is more prevalentbull in middle-aged Caucasian patients
Wegenerrsquos Granulomatosis
Symptomsndash The disease may present pulmonary upper
respiratory tract or renal In the disseminated form-The localised form ndash confinedto the upper respiratory region ndash is present in 25of the patients- It consists of nonspecific manifestationssuch as nasal obstruction crusting purulentor bloody rhinorrhea and painful or painless ulcers in oral or nasal cavities which are unresponsive tostandard medical treatment
Wegenerrsquos Granulomatosis
bull In some patients the nasal septum is perforatedbull which leads to saddle-nose deformity Less
commonbull symptoms are hoarseness stridor due to
subglotticbull stenosis otalgia otorrhea and conductivebull and sensorineural hearing loss Also ocular
symptomsbull such as scleritis conjunctivitis uveitis andbull episcleritis may be present
Wegenerrsquos Granulomatosis
bull ndash In the disseminated form pulmonary involvementbull is manifested by cough dyspnoea haemoptysisbull (due to an alveolar capillaritis necrotic lesions orbull endobronchial disease) and pleuritic painndashbull -Ninety per cent of patients have nasal symptomsbull and these symptoms are usually the first
manifestationof the diseasebull -Most patients have also renal involvementbull even if it is subclinical
Wegenerrsquos Granulomatosis
Diagnosis ndash Diagnosis of Wegenerrsquos granulomatosis is based on clinical findings that demonstrate lung (chest x-ray) kidney (urine analysis) or upper respiratory tract
involvement (oral or nasal ulcers or discharge) - positive blood analysis for cytoplasmic-staining antineutrophil
cytoplasmic antibodies (c-ANCA) and confirming proteinase 3 (PR3) ANCA or myeloperoxidase (MPO) ANCA ndash Biopsy is essential for diagnosis nonspecific chronic inflammation
and necrosis -Bacterial and fungal infections
Wegenerrsquos Granulomatosis
Therapyndash Conservative therapybull In the induction of disease remission highdosesteroids (e g prednisone 1 mgkgday) for1 month with tapering over several months aregiven In addition cyclophosphamide (2 mgkgday) should be administered for 6ndash12 monthsuntil symptoms disappear In the maintenanceof remission cyclophosphamide should be
Wegenerrsquos Granulomatosis
Antibiotics mainly trimethoprim-sulfamethoxazoleare given for prophylaxis againstPneumocystis jiroveci (formerly Pneumocystiscarinii) pneumonia (PCP) which may developduring immunosuppression and have a role inpreventing recurrencesbull Sinonasal manifestations may be treated with topical nasal steroids and nasal irrigations lowdosesystemic steroids and antibiotics when bacterial infection (typically Staphylococcus species) is suspected
Wegenerrsquos Granulomatosis
bull Prognosisbull ndash Most of the patients respond well to treatmentbull achieving symptom-free intervals of 5ndash20 yearsbull or more bull -Anatomical problems (sinusitis trachealbull stenosis) may require surgery bull Relapses can be long and troublesomebull Long-term complications are chronicbull renal failure hearing loss and deafness
Nasal Fractures Definition ndash A nasal fracture is a disruption of the nasal bone structure due to trauma It is the most frequently fractured facial bone Epidemiologyaetiology ndash Sports falls and assaults are the usual mechanisms of fracture -Males are affected twice as often as are females -Paediatric populations with a incidences during the second and third decades of life -Variables such as force impact direction nature of the striking object age and other will influence the pattern of injury to the components of the nose
Nasal Fractures
bull Symptomsbull ndash Deformity swelling epistaxis and periorbital
ecchymosis are signs that are suggestive of nasal fracture
bull bony crepitus and nasal segment mobilitybull ndash Epiphora bull Severe bilateral injuries to the lachrymal bones
arebull associated with depressed nasal fractures
Nasal Fractures Complications ndash Septal haematoma is one of the most severe early complications of nasal trauma and without drainage it results in abscess formation 6ndash7 days after trauma producing necrosis of the septal cartilage -Long-term problems such as saddle-nose deformity perforation columellar retraction and nasalbase
Septal infection could lead to osteomyelitis orbital and intracranial abscesses meningitis and cavernous sinus thrombosis -Cerebrospinal fluid leakage is a common complication of severe
nasal and frontal fractures
Nasal Fractures
bull Diagnostic proceduresbull ndash Inspectionbull bull Changes of appearance such as deviation andbull asymmetry bleeding watery drainage changesbull in nasal breathing and smell It is useful to comparebull the current presentation with old photographsbull (up to 40 of normal individuals havebull significant nose malformations)
Nasal Fractures Physical examination bull The diagnosis of a nasal fracture is made primarily by physical examination epistaxis nasal swelling and periorbital ecchymosis Nasal shape in the lateral and frontal inspection should be assessed Grasping the dorsum between two fingers and rocking the pyramid back and forth aids in assessing the mobility of nasal bones Internal structures should be evaluated by using a headlight and nasal speculum Clotted blood is removed by suction and assessment of haematoma mucosal tears and active bleeding is performed Bimanual palpation of the septum helps to differentiate septal swelling from haematoma ndash
Nasal FracturesRadiographybull There is no clear evidence of the role of radiographyin the management of nasal fracturesPlain films have up to a 66 false-positive rateas a result of misinterpretation of normal suturelines In addition old fractures are difficult todistinguishbull Three-dimensional CT is recommended for extensiveinjuries involving the nasal-orbital-ethmoidalcomplexndash
Nasal Fractures
bull Additionaluseful diagnostic proceduresbull bull Using a 0 or 30deg 4-mm endoscope is helpful inbull the assessment of posterior abnormalities If thebull patient is heavily sedated Brown-Gruss
provocationbull manoeuvres may be performed to determinebull deformities in upper middle or lower segmentsbull by compressing each compartment
Nasal FracturesConservative treatmentndash Treatment of bleedingbull For localised bleeding anterior sources may becauterised by silver nitrate or sealed with topicalmaterials such as thrombin combined withgelatin foam fibrin glue FloSealreg or other procoagulantmaterials If conservative measuresfail a formal anterior packing is placedbull Bleeding from branches of sphenopalatine orethmoid vessels requires anterior-posteriorpacking
Nasal Fractures
bull bull Surgical methods such as direct endoscopic vessel
bull cauterization or ligation have been shown tobull offer better haemostasis and patient comfortbull Angiography with embolization can also be
consideredbull in cases refractory to more conservativebull approaches
Nasal Fractures
bull Type of reductionbull bull Nondisplaced fractures should be treated withbull observation alone Closed nasal reduction is thebull best choice for simple injuries (isolated unilateralbull with medial displacement)bull bull An open approach should be considered in
severebull trauma (bilateral depressed fractures)
Nasal Fracturesbull Surgical principlesbull ndash Topical anaesthesia with cotton pledgets soakedbull with 4 cocaine or 005 oxymethazoline combinedbull with 4 topical lidocaine should be appliedbull for 5ndash10 min Local anaesthesia should also be injectedbull (1 lidocaine and 1100000 epinephrine)bull along the septum lateral walls and floor of the nasalbull cavitybull bull
Nasal FracturesClosed reductionndashndash The nasal bones are grasped between two fingersand pressure is applied laterally in theopposite direction of the deviation A bluntelevator may be used from within the nose incases of significant medial collapse Walshamforceps can be of help Reduction of the septumshould be performed with the use ofAsch forceps
Nasal Fractures
bull To prevent collapse of the postreductionbull framework nasal packing should be placedbull for 3ndash5 days Septum splints are recommendedbull in comminuted septal fractures withbull severe mucosal lesions External nasal splintingbull for 10 days (Aquaplastreg Thermoplastreg)bull provides nasal protection Nasal saline spraysbull prevent crusting and oral antibiotics should
Nasal Fractures
bull Open reductionbull ndashndash Immediate repair of fractures by using
widebull surgical exposure reduction fixation and
reconstructionbull ndashndash The second option is delayed correctionbull (6 months or more) of persistent deformitiesbull using standard techniques of rhinoplasty
Deviated Nasal Septum
bull Definition of the diseasebull ndash Deviation of the nasal septum is a common causebull of unilateral nasal airway obstruction in which thebull nasal septum is displacedbull bull Epidemiologyaetiologybull ndash Developmental septal abnormalities Septal cartilage
damage in the neonatal period andbull during birth can cause severe septal deviation inbull the absence of a history of nasal trauma
Deviated Nasal Septum
bull Symptomsbull ndash Patients may present with a history of sinusitis
allergicbull rhinitis obstructive sleep apnoea previousbull nasal surgery or recent nasal trauma Unilateral or
bilateral nasal airway obstruction that is unrelievedbull with decongestants or nasal steroid sprays is oftenbull seenbull bull
Deviated Nasal SeptumDiagnosisndashExamination external dorsal deviation or the columella and caudal septummay be deflected off the midline (caudal subluxation)ndash Inspections of the nasal cavity and anterior-posteriorrhinoscopy are helpful in diagnosing the locationtype and severity of septal deformityThe endoscope is also useful in identifying polypsthe severity and extent of posterior septaldeviations and bony spurs and locating areas ofseptal perforation or mucosal injury
Deviated Nasal Septum
bull Therapybull ndash Septoplasty is a procedurebull The areabull of deviation is corrected or resected in order tobull leave behind as much cartilage and bone as
possiblebull Cartilage resection is minimised and can be
repositioned reshaped or recontoured using a variety of methods
Deviated Nasal Septum
bull ndash Indications of septoplasty before the growth period
bull of the nose is finished should be very limited bull -In these cases surgery must preserve all the
cartilagebull in order to prevent external changes of the
shape ofbull the nose
Deviated Nasal Septum
bull Complicationsbull ndash Frequent complications include haematoma andbull infection Cerebrospinal fluid leak is a rare but
potentiallybull serious complicationbull It is usually the resultbull of avulsion or damage to the cribriform plate whenbull handling the perpendicular plate of the ethmoidbull ndash Other complications include epistaxis nasal
Deviated Nasal Septum
bull Other complications include epistaxis nasal obstruction
bull due to residual deviation synechiae returnbull of the cartilaginous deviation septal perforationbull anosmia and cosmetic nasal deformities suchbull as widened alar rim margins drooping nasal tipbull columella retraction and a sunken dorsum with abull supratip saddle formation
Septal perforation with minor crusting View from provide closure of the
incision
Septal Haematoma
bull A septal haematoma is a blood collection under the perichondrium
bull of the septum and cartilagebull bull bull Epidemiologyaetiologybull ndash A septal haematoma is one of the most
severe complications of nasal trauma
Septal Haematoma
bull Diagnosisbull ndash Signs and symptoms include intense pain
swellingbull haematoma of the upper lip and philtrum
area andbull complete nasal airway obstruction
Septal HaematomaTherapyndash Management consists of drainage through a mucoperichondrial incision Immediate treatment isnecessary to prevent long-term problems such asa saddle-nose deformity perforation columellarretraction and nasal-base widening In childrenseptal destruction can lead to devastating nasal andmidfacial growth abnormalitiesbull Surgeryndash Incision and evacuation of the collection is performedDrainage of a septal haematoma should
Septal HaematomaSurgeryndash Incision and evacuation of the collection is performedDrainage of a septal haematoma should provide closure of the incision
Splints or transseptal sutures are placed to obliterate thepotential space and prevent collectionInfection involving the septal cartilage Reconstruction with autologouscartilage is then performed in a second stage Oral antibiotics should be given
Nasal DeformitySaddle-nose deformityndash A saddle-nose deformity is characterised by a loss ofnasal dorsal height and compromised nasal supportstructures -Other case observed are depressionof the middle vault and dorsum loss of nasal tipsupport and definition shortened (vertical) nasal length over rotation of the nasal tip and retrusion ofthe nasal spine and caudal septum It is also knownas a ldquoPug noserdquo or ldquoboxerrsquos noserdquo both of which referto various degrees of nasal dorsal depressionbull
Nasal DeformityEpidemiologyaetiologyndash Prevalence is higher in population groups prone to facial trauma (ie boxers athletes) those with historiesof intranasal cocaine use nasal surgery (e g radical submucosal septal resection reductive rhinoplasty)ndash A saddle-nose deformity can be congenital or acquired It can be noticed as a part of individual familialsyndromic and ethnic characteristics - Most deformities are due to traumatic and iatrogeniccauses Medical causes are Wegenerrsquosgranulomatosis relapsing polychondritis leprosy (Hansenrsquos disease) syphilis ectodermal dysplasiaand intranasal cocaine use
Nasal Deformity
bull Therapybull ndash Nasal reconstruction indications depend on patientbull selection surgeon experience and aetiology of thebull deformity bull Indications for surgery can be functionalbull aesthetic or most commonly both In individuals
with a compromised nasal airway a nasoseptalbull reconstruction is indicated
Nasal Deformity
bull Contraindications bull include patients with malignantbull chronic or autoimmune disease conditions drugbull abuse poor perioperative risk profile and unrealisticbull expectationsbull ndash Multiple previous rhinoplasties and certain
professionsbull (mixed martial artists boxers and other contactbull sports) are relative contraindications
Nasal DeformitySeptoplastyndash Septoplasty is performed to correct nasal obstructioncaused by septal deformityndash Usually septoplasty is performed under general anaesthesiawith the patient in the supine position with the head elevated by approximately 30 (Righthandedsurgeons approach from the right side)ndash Local vasoconstrictive anaesthesia is applied notonly to reduce postoperative pain but also more importantly to achieve vasoconstriction of themucosa and less intraoperative haemorrhage Lidocainewith adrenaline or epinephrine is usedalthough in patients with cardiac hypersensitivityoxymetazoline might be preferred
Nasal Deformity
bull Septoplasty begins with the incision of septal mucosabull Most operative techniques utilise a hemitransfixionbull incision at the caudal end of septum so thatbull deviation at this point might be reached as wellbull as a transfixion incision that is easily obtained ifbull needed (Right-handed surgeons normally choosebull the left side but that may vary when deviation isbull convex towards the right)
Nasal DeformityA columella retractor is placed over the columellaand by pulling it laterally the caudal border of theseptum is exposed Ala can be protected by an alaprotector A vertical incision with a no 15 bladeover the caudal end of septum is performed untilreaching the plane of the septal cartilage It is essentialto correctly identify the perichondrium and byusing the Cottle elevator dissect and lift it creatinga flap As the dissection proceeds along the septalcartilage a longer speculum (no 5) is introduced sothat elevation of the mucoperichondrium is doneunder constant visual controlndash The next step is to dissect the mucoperiostium
Nasal DeformityDissecting over the bony-cartilaginous junctionwhen joining both tunnels might be difficult and is
especially prone to membrane perforationndash If needed the same tunnels are to be created on the
other side of the septum Then deviated parts of
septum are identified and removed either with a
knife or a Freer chisel
Nasal Deformitybull septum from the maxillary crest the septum mustbull be separated from the perpendicular plate trimmedbull along the inferior border placed back onto the crestbull and sutured to the periosteum If the deformity involvesbull the vomer an osteotome is used Care mustbull be taken not to break the cribriform plate becausebull it could cause a cerebrospinal fistula
Nasal Deformity
bull Once the septal deviation is corrected the flapsbull and hemitransfixion incision are mattressed
withbull absorbable sutures Nasal packing to prevent
synechiaebull and postoperative septal haematoma mightbull be advised but should be removed within 72 h

Four representative coronal CT scans are shown
Four representative coronal CT scans are shown
Magnetic Resonance Imaging
Magnetic maging
Magnetic resonance imaging (MRI) has fewer indicationsthan CT in patients with paranasal sinus diseaseThis is primarily because MRI is markedly inferior toCT in defining the bony boundaries of the sinusesThe strength of MRI lies in its superior soft-tissue discriminationMRI is indicated in diseases that involve the paranasal sinuses in addition to thecranial cavity or orbit (eg tumors and congenitalmalformations such as encephaloceles)
MRI of the paranasal sinuses
The Nose and Sinuses
Structure The structure of the nose is made up of
four partsbull The surface anatomybull The nasal skeletonmdashcomposed of the
two nasal bones the paired upper lateral and lower lateral cartilages and the nasal septum covered in subcutaneous tissue and skin
bull The internal anatomymdashincludes the septum of the nose which forms the medial wall of the nasal cavity The turbinates on the lateral wall are also called conchae
bull The osteomeatal complexmdasha key functional area of the nose
Function The nose is the main route for inspired
air and its structure is related to this function As the air passes over the large surface area of the turbinates
The inspired gases are warmed and humidified Mucus on the mucosa of the nose removes large dust particles from the air as it is breathed in
The voice resonates in the sinuses and nose and this provides character to the speech
Pneumatization of the sinusesmdashthey are air filled spacesmdashreduces the weight of the skull
Diseases of thDiseases of the Outer and Inner Nosee Outer and
Inner Nose Erysipelas Definition of the disease ndash Erysipela is a skin infection that affects the superficial dermis and is caused by Streptococcus pyogenes (group A) It usually develops in the extremities and the face and less commonly on the scalp and genitals bull Epidemiologyaetiology ndash Erysipelas are more often seen in elderly infants and children patients with compromised immunology and diabetes -Predisposing factors are alcoholism skin ulceration puncture wounds fungal infections malnutrition and burns
Erysipelas
bull Symptomsbull ndash It usually presents of fever general fatigue bull -The skin lesion is a redindurated and elevated plaque
with borders that expand rapidly bull It is painful warm and accompanied by variable oedemabull -On the second or third day a flaccid bulla may develop
and desquamationbull bull Presence of regional lymph nodes is common
Erysipelas
bull Complicationsndash The most common complication is recurrencewhich is seen in 18ndash30 of the cases even afterproper antibiotic therapy Recurrence is seen moreoften in females than in malesA skin infection with S pyogenes could lead toglomerulonephritis
Erysipelas
bull Complicationsbull ndash The most common complication is recurrencebull which is seen in 18ndash30 of the cases even afterbull proper antibiotic therapy bull -Recurrence is seen morebull often in females than in males bull -A skin infection with S pyogenes could lead tobull glomerulonephritis
Erysipelas
bull bull Diagnosisbull ndash Diagnosis is based on the patientrsquos personal
historybull and physical examination particularly on inspectionbull of the skin
bull Blood cultures are positive in less thanbull 5 of cases
ErysipelasTherapyndash Conservative therapybull The preferred antibiotic is penicillin In mildcases with minor systemic symptoms penicillinV 500 mg orally every 6 h for 10 days or penicillinG benzathine 12 mil U intramuscularlyonceOther possibilities are amoxicillin 500 mgorally twice a day for 10 days or cephalexin 500mg orally every 6 h for 10 days
ErysipelasIn moderate and severe cases with significantsystemic symptoms hospitalization and intravenoustreatment is required penicillin G 2ndash4mil U intravenously every 4ndash6 h Cefazolin05ndash15 gm intravenously every 8 h cefotaxime1ndash2 gm intravenously every 8 h or ceftriaxone1ndash2 gm intravenously once a day should be administeredIn patients with a penicillin allergyclindamycin 600 mg intravenously every 8 h orvancomycin 15 mgkg intravenously twice a daymay be given
ErysipelaAdditional useful therapeutic optionsbull Prednisone 30 mg over 8 days might be consideredas well as elevation of the affected siteMoist heat compresses may be usefulbull Surgeryndash Debridement and drainage are indicated when bullaeabscesses or necroses are presentbull Differential diagnosisndash Contact dermatitisndash Asteatotic eczemandash Herpes zosterndash Angioneurotic oedemandash Osteomyelitis
Furuncle
bull Definition of the diseasebull ndash A furuncle is an infection that beginsbull at the hair follicle and spreads deeper into thebull dermis and subcutaneous tissue forming abull nodule After several days it developsbull into an abscess - red painful and fluctuantbull bull bull Epidemiologyaetiologybull ndash The aetiologic agent is Staphylococcus aureus
FuruncleSymptomsndashsymptoms are local and limited to thesite of infection Furuncles usually are wherehair follicles are present bull Complicationndash One complication is furunculosis multiple draining furunclesDiagnosisndash The diagnosis is based on clinical inspection - Cultures are not necessary when there is no systemic involvement but should beconsidered if systemic therapy (in case of feversignificant cellulitis or hospitalization) or whenmethicillin-resistant Staphylococcusaureus (MRSA) is considered
FuruncleTherapyndash When the furuncle is small application of moist heat compress to promote drainage -Larger furuncles should be drained by surgical incision-After drainage the area should be cleaned with anantiseptic (with chlorhexidinebetadine) should be applied twice
a dayndash If no systemic symptoms or extensive cellulitis arepresent simple topical care is usually curative andoral antibiotics are not necessary Otherwise systemictreatment is indicated and should cover anypossible MRSA
Furuncle
bull -Recommended antibiotics are trimethoprim-sulfamethoxazole
bull 1ndash2 tablets orally twice daily doxycyclinebull 100 mg orally twice dailybull or clindamycin 300ndash450 mg orally every 8 hbull - In severe cases vancomycin 15 mgkg
intravenouslybull every 12 h or clindamycin 600 mg intravenouslybull every 8 h
Midline Granulomabull A midline granuloma is an angiocentricbull lymphoma it was referred to as polymorphicbull reticulosis lethal midline granuloma and midline
malignant reticulosisbull bull Definition of the diseasebull ndash This rare disease is a lymphoma of extranodal
presentationall cases are positive for the Epstein-Barr virus
bull -This lymphoma most commonly appears in the midface region
Midline GranulomaEpidemiologyaetiologyndash This form of lymphoma is rare in Europe and theUnited States with a higher prevalence in Asia and PeruSymptomsndash The most common presentation is nasal obstruction with a destructive mass occupying the nosesinuses and palate
-Fever night sweatsand weight loss seen usually in Hodgkinrsquos lymphomaand other non-Hodgkinrsquos lymphomas (knownas ldquoB symptomsrdquo) are uncommon
Midline GranulomaDiagnosisndash The diagnosis is based on anatomopathologicalstudy The malignancy of the tumour manifested byextensive necrosis makes the histological diagnosisdifficult and often more biopsies are required forconfirmationbull Therapyndash Therapy consists of radiotherapy with or withoutchemotherapy
Midline Granuloma
bull Prognosisbull ndash Depending on the stage long-term remission or
experience a worseningbull prognosis with relapses which may include otherbull extranodal sites bull Involvement of extranodal sitesbull including the upper airway gastrointestinal tractbull skin
Wegenerrsquos Granulomatosis
bull Definition of the diseasebull ndash Wegenerrsquos granulomatosis is a systemic chronicbull vasculitis of small- and medium-sized blood vesselsbull with an autoimmune component It affectsbull particular organs with variable predilectionbull Epidemiologyaetiologybull ndash Wegenerrsquos granulomatosis is a rare disease It affects
about 1 in 20000ndash30000 people It is more prevalentbull in middle-aged Caucasian patients
Wegenerrsquos Granulomatosis
Symptomsndash The disease may present pulmonary upper
respiratory tract or renal In the disseminated form-The localised form ndash confinedto the upper respiratory region ndash is present in 25of the patients- It consists of nonspecific manifestationssuch as nasal obstruction crusting purulentor bloody rhinorrhea and painful or painless ulcers in oral or nasal cavities which are unresponsive tostandard medical treatment
Wegenerrsquos Granulomatosis
bull In some patients the nasal septum is perforatedbull which leads to saddle-nose deformity Less
commonbull symptoms are hoarseness stridor due to
subglotticbull stenosis otalgia otorrhea and conductivebull and sensorineural hearing loss Also ocular
symptomsbull such as scleritis conjunctivitis uveitis andbull episcleritis may be present
Wegenerrsquos Granulomatosis
bull ndash In the disseminated form pulmonary involvementbull is manifested by cough dyspnoea haemoptysisbull (due to an alveolar capillaritis necrotic lesions orbull endobronchial disease) and pleuritic painndashbull -Ninety per cent of patients have nasal symptomsbull and these symptoms are usually the first
manifestationof the diseasebull -Most patients have also renal involvementbull even if it is subclinical
Wegenerrsquos Granulomatosis
Diagnosis ndash Diagnosis of Wegenerrsquos granulomatosis is based on clinical findings that demonstrate lung (chest x-ray) kidney (urine analysis) or upper respiratory tract
involvement (oral or nasal ulcers or discharge) - positive blood analysis for cytoplasmic-staining antineutrophil
cytoplasmic antibodies (c-ANCA) and confirming proteinase 3 (PR3) ANCA or myeloperoxidase (MPO) ANCA ndash Biopsy is essential for diagnosis nonspecific chronic inflammation
and necrosis -Bacterial and fungal infections
Wegenerrsquos Granulomatosis
Therapyndash Conservative therapybull In the induction of disease remission highdosesteroids (e g prednisone 1 mgkgday) for1 month with tapering over several months aregiven In addition cyclophosphamide (2 mgkgday) should be administered for 6ndash12 monthsuntil symptoms disappear In the maintenanceof remission cyclophosphamide should be
Wegenerrsquos Granulomatosis
Antibiotics mainly trimethoprim-sulfamethoxazoleare given for prophylaxis againstPneumocystis jiroveci (formerly Pneumocystiscarinii) pneumonia (PCP) which may developduring immunosuppression and have a role inpreventing recurrencesbull Sinonasal manifestations may be treated with topical nasal steroids and nasal irrigations lowdosesystemic steroids and antibiotics when bacterial infection (typically Staphylococcus species) is suspected
Wegenerrsquos Granulomatosis
bull Prognosisbull ndash Most of the patients respond well to treatmentbull achieving symptom-free intervals of 5ndash20 yearsbull or more bull -Anatomical problems (sinusitis trachealbull stenosis) may require surgery bull Relapses can be long and troublesomebull Long-term complications are chronicbull renal failure hearing loss and deafness
Nasal Fractures Definition ndash A nasal fracture is a disruption of the nasal bone structure due to trauma It is the most frequently fractured facial bone Epidemiologyaetiology ndash Sports falls and assaults are the usual mechanisms of fracture -Males are affected twice as often as are females -Paediatric populations with a incidences during the second and third decades of life -Variables such as force impact direction nature of the striking object age and other will influence the pattern of injury to the components of the nose
Nasal Fractures
bull Symptomsbull ndash Deformity swelling epistaxis and periorbital
ecchymosis are signs that are suggestive of nasal fracture
bull bony crepitus and nasal segment mobilitybull ndash Epiphora bull Severe bilateral injuries to the lachrymal bones
arebull associated with depressed nasal fractures
Nasal Fractures Complications ndash Septal haematoma is one of the most severe early complications of nasal trauma and without drainage it results in abscess formation 6ndash7 days after trauma producing necrosis of the septal cartilage -Long-term problems such as saddle-nose deformity perforation columellar retraction and nasalbase
Septal infection could lead to osteomyelitis orbital and intracranial abscesses meningitis and cavernous sinus thrombosis -Cerebrospinal fluid leakage is a common complication of severe
nasal and frontal fractures
Nasal Fractures
bull Diagnostic proceduresbull ndash Inspectionbull bull Changes of appearance such as deviation andbull asymmetry bleeding watery drainage changesbull in nasal breathing and smell It is useful to comparebull the current presentation with old photographsbull (up to 40 of normal individuals havebull significant nose malformations)
Nasal Fractures Physical examination bull The diagnosis of a nasal fracture is made primarily by physical examination epistaxis nasal swelling and periorbital ecchymosis Nasal shape in the lateral and frontal inspection should be assessed Grasping the dorsum between two fingers and rocking the pyramid back and forth aids in assessing the mobility of nasal bones Internal structures should be evaluated by using a headlight and nasal speculum Clotted blood is removed by suction and assessment of haematoma mucosal tears and active bleeding is performed Bimanual palpation of the septum helps to differentiate septal swelling from haematoma ndash
Nasal FracturesRadiographybull There is no clear evidence of the role of radiographyin the management of nasal fracturesPlain films have up to a 66 false-positive rateas a result of misinterpretation of normal suturelines In addition old fractures are difficult todistinguishbull Three-dimensional CT is recommended for extensiveinjuries involving the nasal-orbital-ethmoidalcomplexndash
Nasal Fractures
bull Additionaluseful diagnostic proceduresbull bull Using a 0 or 30deg 4-mm endoscope is helpful inbull the assessment of posterior abnormalities If thebull patient is heavily sedated Brown-Gruss
provocationbull manoeuvres may be performed to determinebull deformities in upper middle or lower segmentsbull by compressing each compartment
Nasal FracturesConservative treatmentndash Treatment of bleedingbull For localised bleeding anterior sources may becauterised by silver nitrate or sealed with topicalmaterials such as thrombin combined withgelatin foam fibrin glue FloSealreg or other procoagulantmaterials If conservative measuresfail a formal anterior packing is placedbull Bleeding from branches of sphenopalatine orethmoid vessels requires anterior-posteriorpacking
Nasal Fractures
bull bull Surgical methods such as direct endoscopic vessel
bull cauterization or ligation have been shown tobull offer better haemostasis and patient comfortbull Angiography with embolization can also be
consideredbull in cases refractory to more conservativebull approaches
Nasal Fractures
bull Type of reductionbull bull Nondisplaced fractures should be treated withbull observation alone Closed nasal reduction is thebull best choice for simple injuries (isolated unilateralbull with medial displacement)bull bull An open approach should be considered in
severebull trauma (bilateral depressed fractures)
Nasal Fracturesbull Surgical principlesbull ndash Topical anaesthesia with cotton pledgets soakedbull with 4 cocaine or 005 oxymethazoline combinedbull with 4 topical lidocaine should be appliedbull for 5ndash10 min Local anaesthesia should also be injectedbull (1 lidocaine and 1100000 epinephrine)bull along the septum lateral walls and floor of the nasalbull cavitybull bull
Nasal FracturesClosed reductionndashndash The nasal bones are grasped between two fingersand pressure is applied laterally in theopposite direction of the deviation A bluntelevator may be used from within the nose incases of significant medial collapse Walshamforceps can be of help Reduction of the septumshould be performed with the use ofAsch forceps
Nasal Fractures
bull To prevent collapse of the postreductionbull framework nasal packing should be placedbull for 3ndash5 days Septum splints are recommendedbull in comminuted septal fractures withbull severe mucosal lesions External nasal splintingbull for 10 days (Aquaplastreg Thermoplastreg)bull provides nasal protection Nasal saline spraysbull prevent crusting and oral antibiotics should
Nasal Fractures
bull Open reductionbull ndashndash Immediate repair of fractures by using
widebull surgical exposure reduction fixation and
reconstructionbull ndashndash The second option is delayed correctionbull (6 months or more) of persistent deformitiesbull using standard techniques of rhinoplasty
Deviated Nasal Septum
bull Definition of the diseasebull ndash Deviation of the nasal septum is a common causebull of unilateral nasal airway obstruction in which thebull nasal septum is displacedbull bull Epidemiologyaetiologybull ndash Developmental septal abnormalities Septal cartilage
damage in the neonatal period andbull during birth can cause severe septal deviation inbull the absence of a history of nasal trauma
Deviated Nasal Septum
bull Symptomsbull ndash Patients may present with a history of sinusitis
allergicbull rhinitis obstructive sleep apnoea previousbull nasal surgery or recent nasal trauma Unilateral or
bilateral nasal airway obstruction that is unrelievedbull with decongestants or nasal steroid sprays is oftenbull seenbull bull
Deviated Nasal SeptumDiagnosisndashExamination external dorsal deviation or the columella and caudal septummay be deflected off the midline (caudal subluxation)ndash Inspections of the nasal cavity and anterior-posteriorrhinoscopy are helpful in diagnosing the locationtype and severity of septal deformityThe endoscope is also useful in identifying polypsthe severity and extent of posterior septaldeviations and bony spurs and locating areas ofseptal perforation or mucosal injury
Deviated Nasal Septum
bull Therapybull ndash Septoplasty is a procedurebull The areabull of deviation is corrected or resected in order tobull leave behind as much cartilage and bone as
possiblebull Cartilage resection is minimised and can be
repositioned reshaped or recontoured using a variety of methods
Deviated Nasal Septum
bull ndash Indications of septoplasty before the growth period
bull of the nose is finished should be very limited bull -In these cases surgery must preserve all the
cartilagebull in order to prevent external changes of the
shape ofbull the nose
Deviated Nasal Septum
bull Complicationsbull ndash Frequent complications include haematoma andbull infection Cerebrospinal fluid leak is a rare but
potentiallybull serious complicationbull It is usually the resultbull of avulsion or damage to the cribriform plate whenbull handling the perpendicular plate of the ethmoidbull ndash Other complications include epistaxis nasal
Deviated Nasal Septum
bull Other complications include epistaxis nasal obstruction
bull due to residual deviation synechiae returnbull of the cartilaginous deviation septal perforationbull anosmia and cosmetic nasal deformities suchbull as widened alar rim margins drooping nasal tipbull columella retraction and a sunken dorsum with abull supratip saddle formation
Septal perforation with minor crusting View from provide closure of the
incision
Septal Haematoma
bull A septal haematoma is a blood collection under the perichondrium
bull of the septum and cartilagebull bull bull Epidemiologyaetiologybull ndash A septal haematoma is one of the most
severe complications of nasal trauma
Septal Haematoma
bull Diagnosisbull ndash Signs and symptoms include intense pain
swellingbull haematoma of the upper lip and philtrum
area andbull complete nasal airway obstruction
Septal HaematomaTherapyndash Management consists of drainage through a mucoperichondrial incision Immediate treatment isnecessary to prevent long-term problems such asa saddle-nose deformity perforation columellarretraction and nasal-base widening In childrenseptal destruction can lead to devastating nasal andmidfacial growth abnormalitiesbull Surgeryndash Incision and evacuation of the collection is performedDrainage of a septal haematoma should
Septal HaematomaSurgeryndash Incision and evacuation of the collection is performedDrainage of a septal haematoma should provide closure of the incision
Splints or transseptal sutures are placed to obliterate thepotential space and prevent collectionInfection involving the septal cartilage Reconstruction with autologouscartilage is then performed in a second stage Oral antibiotics should be given
Nasal DeformitySaddle-nose deformityndash A saddle-nose deformity is characterised by a loss ofnasal dorsal height and compromised nasal supportstructures -Other case observed are depressionof the middle vault and dorsum loss of nasal tipsupport and definition shortened (vertical) nasal length over rotation of the nasal tip and retrusion ofthe nasal spine and caudal septum It is also knownas a ldquoPug noserdquo or ldquoboxerrsquos noserdquo both of which referto various degrees of nasal dorsal depressionbull
Nasal DeformityEpidemiologyaetiologyndash Prevalence is higher in population groups prone to facial trauma (ie boxers athletes) those with historiesof intranasal cocaine use nasal surgery (e g radical submucosal septal resection reductive rhinoplasty)ndash A saddle-nose deformity can be congenital or acquired It can be noticed as a part of individual familialsyndromic and ethnic characteristics - Most deformities are due to traumatic and iatrogeniccauses Medical causes are Wegenerrsquosgranulomatosis relapsing polychondritis leprosy (Hansenrsquos disease) syphilis ectodermal dysplasiaand intranasal cocaine use
Nasal Deformity
bull Therapybull ndash Nasal reconstruction indications depend on patientbull selection surgeon experience and aetiology of thebull deformity bull Indications for surgery can be functionalbull aesthetic or most commonly both In individuals
with a compromised nasal airway a nasoseptalbull reconstruction is indicated
Nasal Deformity
bull Contraindications bull include patients with malignantbull chronic or autoimmune disease conditions drugbull abuse poor perioperative risk profile and unrealisticbull expectationsbull ndash Multiple previous rhinoplasties and certain
professionsbull (mixed martial artists boxers and other contactbull sports) are relative contraindications
Nasal DeformitySeptoplastyndash Septoplasty is performed to correct nasal obstructioncaused by septal deformityndash Usually septoplasty is performed under general anaesthesiawith the patient in the supine position with the head elevated by approximately 30 (Righthandedsurgeons approach from the right side)ndash Local vasoconstrictive anaesthesia is applied notonly to reduce postoperative pain but also more importantly to achieve vasoconstriction of themucosa and less intraoperative haemorrhage Lidocainewith adrenaline or epinephrine is usedalthough in patients with cardiac hypersensitivityoxymetazoline might be preferred
Nasal Deformity
bull Septoplasty begins with the incision of septal mucosabull Most operative techniques utilise a hemitransfixionbull incision at the caudal end of septum so thatbull deviation at this point might be reached as wellbull as a transfixion incision that is easily obtained ifbull needed (Right-handed surgeons normally choosebull the left side but that may vary when deviation isbull convex towards the right)
Nasal DeformityA columella retractor is placed over the columellaand by pulling it laterally the caudal border of theseptum is exposed Ala can be protected by an alaprotector A vertical incision with a no 15 bladeover the caudal end of septum is performed untilreaching the plane of the septal cartilage It is essentialto correctly identify the perichondrium and byusing the Cottle elevator dissect and lift it creatinga flap As the dissection proceeds along the septalcartilage a longer speculum (no 5) is introduced sothat elevation of the mucoperichondrium is doneunder constant visual controlndash The next step is to dissect the mucoperiostium
Nasal DeformityDissecting over the bony-cartilaginous junctionwhen joining both tunnels might be difficult and is
especially prone to membrane perforationndash If needed the same tunnels are to be created on the
other side of the septum Then deviated parts of
septum are identified and removed either with a
knife or a Freer chisel
Nasal Deformitybull septum from the maxillary crest the septum mustbull be separated from the perpendicular plate trimmedbull along the inferior border placed back onto the crestbull and sutured to the periosteum If the deformity involvesbull the vomer an osteotome is used Care mustbull be taken not to break the cribriform plate becausebull it could cause a cerebrospinal fistula
Nasal Deformity
bull Once the septal deviation is corrected the flapsbull and hemitransfixion incision are mattressed
withbull absorbable sutures Nasal packing to prevent
synechiaebull and postoperative septal haematoma mightbull be advised but should be removed within 72 h

Four representative coronal CT scans are shown
Magnetic Resonance Imaging
Magnetic maging
Magnetic resonance imaging (MRI) has fewer indicationsthan CT in patients with paranasal sinus diseaseThis is primarily because MRI is markedly inferior toCT in defining the bony boundaries of the sinusesThe strength of MRI lies in its superior soft-tissue discriminationMRI is indicated in diseases that involve the paranasal sinuses in addition to thecranial cavity or orbit (eg tumors and congenitalmalformations such as encephaloceles)
MRI of the paranasal sinuses
The Nose and Sinuses
Structure The structure of the nose is made up of
four partsbull The surface anatomybull The nasal skeletonmdashcomposed of the
two nasal bones the paired upper lateral and lower lateral cartilages and the nasal septum covered in subcutaneous tissue and skin
bull The internal anatomymdashincludes the septum of the nose which forms the medial wall of the nasal cavity The turbinates on the lateral wall are also called conchae
bull The osteomeatal complexmdasha key functional area of the nose
Function The nose is the main route for inspired
air and its structure is related to this function As the air passes over the large surface area of the turbinates
The inspired gases are warmed and humidified Mucus on the mucosa of the nose removes large dust particles from the air as it is breathed in
The voice resonates in the sinuses and nose and this provides character to the speech
Pneumatization of the sinusesmdashthey are air filled spacesmdashreduces the weight of the skull
Diseases of thDiseases of the Outer and Inner Nosee Outer and
Inner Nose Erysipelas Definition of the disease ndash Erysipela is a skin infection that affects the superficial dermis and is caused by Streptococcus pyogenes (group A) It usually develops in the extremities and the face and less commonly on the scalp and genitals bull Epidemiologyaetiology ndash Erysipelas are more often seen in elderly infants and children patients with compromised immunology and diabetes -Predisposing factors are alcoholism skin ulceration puncture wounds fungal infections malnutrition and burns
Erysipelas
bull Symptomsbull ndash It usually presents of fever general fatigue bull -The skin lesion is a redindurated and elevated plaque
with borders that expand rapidly bull It is painful warm and accompanied by variable oedemabull -On the second or third day a flaccid bulla may develop
and desquamationbull bull Presence of regional lymph nodes is common
Erysipelas
bull Complicationsndash The most common complication is recurrencewhich is seen in 18ndash30 of the cases even afterproper antibiotic therapy Recurrence is seen moreoften in females than in malesA skin infection with S pyogenes could lead toglomerulonephritis
Erysipelas
bull Complicationsbull ndash The most common complication is recurrencebull which is seen in 18ndash30 of the cases even afterbull proper antibiotic therapy bull -Recurrence is seen morebull often in females than in males bull -A skin infection with S pyogenes could lead tobull glomerulonephritis
Erysipelas
bull bull Diagnosisbull ndash Diagnosis is based on the patientrsquos personal
historybull and physical examination particularly on inspectionbull of the skin
bull Blood cultures are positive in less thanbull 5 of cases
ErysipelasTherapyndash Conservative therapybull The preferred antibiotic is penicillin In mildcases with minor systemic symptoms penicillinV 500 mg orally every 6 h for 10 days or penicillinG benzathine 12 mil U intramuscularlyonceOther possibilities are amoxicillin 500 mgorally twice a day for 10 days or cephalexin 500mg orally every 6 h for 10 days
ErysipelasIn moderate and severe cases with significantsystemic symptoms hospitalization and intravenoustreatment is required penicillin G 2ndash4mil U intravenously every 4ndash6 h Cefazolin05ndash15 gm intravenously every 8 h cefotaxime1ndash2 gm intravenously every 8 h or ceftriaxone1ndash2 gm intravenously once a day should be administeredIn patients with a penicillin allergyclindamycin 600 mg intravenously every 8 h orvancomycin 15 mgkg intravenously twice a daymay be given
ErysipelaAdditional useful therapeutic optionsbull Prednisone 30 mg over 8 days might be consideredas well as elevation of the affected siteMoist heat compresses may be usefulbull Surgeryndash Debridement and drainage are indicated when bullaeabscesses or necroses are presentbull Differential diagnosisndash Contact dermatitisndash Asteatotic eczemandash Herpes zosterndash Angioneurotic oedemandash Osteomyelitis
Furuncle
bull Definition of the diseasebull ndash A furuncle is an infection that beginsbull at the hair follicle and spreads deeper into thebull dermis and subcutaneous tissue forming abull nodule After several days it developsbull into an abscess - red painful and fluctuantbull bull bull Epidemiologyaetiologybull ndash The aetiologic agent is Staphylococcus aureus
FuruncleSymptomsndashsymptoms are local and limited to thesite of infection Furuncles usually are wherehair follicles are present bull Complicationndash One complication is furunculosis multiple draining furunclesDiagnosisndash The diagnosis is based on clinical inspection - Cultures are not necessary when there is no systemic involvement but should beconsidered if systemic therapy (in case of feversignificant cellulitis or hospitalization) or whenmethicillin-resistant Staphylococcusaureus (MRSA) is considered
FuruncleTherapyndash When the furuncle is small application of moist heat compress to promote drainage -Larger furuncles should be drained by surgical incision-After drainage the area should be cleaned with anantiseptic (with chlorhexidinebetadine) should be applied twice
a dayndash If no systemic symptoms or extensive cellulitis arepresent simple topical care is usually curative andoral antibiotics are not necessary Otherwise systemictreatment is indicated and should cover anypossible MRSA
Furuncle
bull -Recommended antibiotics are trimethoprim-sulfamethoxazole
bull 1ndash2 tablets orally twice daily doxycyclinebull 100 mg orally twice dailybull or clindamycin 300ndash450 mg orally every 8 hbull - In severe cases vancomycin 15 mgkg
intravenouslybull every 12 h or clindamycin 600 mg intravenouslybull every 8 h
Midline Granulomabull A midline granuloma is an angiocentricbull lymphoma it was referred to as polymorphicbull reticulosis lethal midline granuloma and midline
malignant reticulosisbull bull Definition of the diseasebull ndash This rare disease is a lymphoma of extranodal
presentationall cases are positive for the Epstein-Barr virus
bull -This lymphoma most commonly appears in the midface region
Midline GranulomaEpidemiologyaetiologyndash This form of lymphoma is rare in Europe and theUnited States with a higher prevalence in Asia and PeruSymptomsndash The most common presentation is nasal obstruction with a destructive mass occupying the nosesinuses and palate
-Fever night sweatsand weight loss seen usually in Hodgkinrsquos lymphomaand other non-Hodgkinrsquos lymphomas (knownas ldquoB symptomsrdquo) are uncommon
Midline GranulomaDiagnosisndash The diagnosis is based on anatomopathologicalstudy The malignancy of the tumour manifested byextensive necrosis makes the histological diagnosisdifficult and often more biopsies are required forconfirmationbull Therapyndash Therapy consists of radiotherapy with or withoutchemotherapy
Midline Granuloma
bull Prognosisbull ndash Depending on the stage long-term remission or
experience a worseningbull prognosis with relapses which may include otherbull extranodal sites bull Involvement of extranodal sitesbull including the upper airway gastrointestinal tractbull skin
Wegenerrsquos Granulomatosis
bull Definition of the diseasebull ndash Wegenerrsquos granulomatosis is a systemic chronicbull vasculitis of small- and medium-sized blood vesselsbull with an autoimmune component It affectsbull particular organs with variable predilectionbull Epidemiologyaetiologybull ndash Wegenerrsquos granulomatosis is a rare disease It affects
about 1 in 20000ndash30000 people It is more prevalentbull in middle-aged Caucasian patients
Wegenerrsquos Granulomatosis
Symptomsndash The disease may present pulmonary upper
respiratory tract or renal In the disseminated form-The localised form ndash confinedto the upper respiratory region ndash is present in 25of the patients- It consists of nonspecific manifestationssuch as nasal obstruction crusting purulentor bloody rhinorrhea and painful or painless ulcers in oral or nasal cavities which are unresponsive tostandard medical treatment
Wegenerrsquos Granulomatosis
bull In some patients the nasal septum is perforatedbull which leads to saddle-nose deformity Less
commonbull symptoms are hoarseness stridor due to
subglotticbull stenosis otalgia otorrhea and conductivebull and sensorineural hearing loss Also ocular
symptomsbull such as scleritis conjunctivitis uveitis andbull episcleritis may be present
Wegenerrsquos Granulomatosis
bull ndash In the disseminated form pulmonary involvementbull is manifested by cough dyspnoea haemoptysisbull (due to an alveolar capillaritis necrotic lesions orbull endobronchial disease) and pleuritic painndashbull -Ninety per cent of patients have nasal symptomsbull and these symptoms are usually the first
manifestationof the diseasebull -Most patients have also renal involvementbull even if it is subclinical
Wegenerrsquos Granulomatosis
Diagnosis ndash Diagnosis of Wegenerrsquos granulomatosis is based on clinical findings that demonstrate lung (chest x-ray) kidney (urine analysis) or upper respiratory tract
involvement (oral or nasal ulcers or discharge) - positive blood analysis for cytoplasmic-staining antineutrophil
cytoplasmic antibodies (c-ANCA) and confirming proteinase 3 (PR3) ANCA or myeloperoxidase (MPO) ANCA ndash Biopsy is essential for diagnosis nonspecific chronic inflammation
and necrosis -Bacterial and fungal infections
Wegenerrsquos Granulomatosis
Therapyndash Conservative therapybull In the induction of disease remission highdosesteroids (e g prednisone 1 mgkgday) for1 month with tapering over several months aregiven In addition cyclophosphamide (2 mgkgday) should be administered for 6ndash12 monthsuntil symptoms disappear In the maintenanceof remission cyclophosphamide should be
Wegenerrsquos Granulomatosis
Antibiotics mainly trimethoprim-sulfamethoxazoleare given for prophylaxis againstPneumocystis jiroveci (formerly Pneumocystiscarinii) pneumonia (PCP) which may developduring immunosuppression and have a role inpreventing recurrencesbull Sinonasal manifestations may be treated with topical nasal steroids and nasal irrigations lowdosesystemic steroids and antibiotics when bacterial infection (typically Staphylococcus species) is suspected
Wegenerrsquos Granulomatosis
bull Prognosisbull ndash Most of the patients respond well to treatmentbull achieving symptom-free intervals of 5ndash20 yearsbull or more bull -Anatomical problems (sinusitis trachealbull stenosis) may require surgery bull Relapses can be long and troublesomebull Long-term complications are chronicbull renal failure hearing loss and deafness
Nasal Fractures Definition ndash A nasal fracture is a disruption of the nasal bone structure due to trauma It is the most frequently fractured facial bone Epidemiologyaetiology ndash Sports falls and assaults are the usual mechanisms of fracture -Males are affected twice as often as are females -Paediatric populations with a incidences during the second and third decades of life -Variables such as force impact direction nature of the striking object age and other will influence the pattern of injury to the components of the nose
Nasal Fractures
bull Symptomsbull ndash Deformity swelling epistaxis and periorbital
ecchymosis are signs that are suggestive of nasal fracture
bull bony crepitus and nasal segment mobilitybull ndash Epiphora bull Severe bilateral injuries to the lachrymal bones
arebull associated with depressed nasal fractures
Nasal Fractures Complications ndash Septal haematoma is one of the most severe early complications of nasal trauma and without drainage it results in abscess formation 6ndash7 days after trauma producing necrosis of the septal cartilage -Long-term problems such as saddle-nose deformity perforation columellar retraction and nasalbase
Septal infection could lead to osteomyelitis orbital and intracranial abscesses meningitis and cavernous sinus thrombosis -Cerebrospinal fluid leakage is a common complication of severe
nasal and frontal fractures
Nasal Fractures
bull Diagnostic proceduresbull ndash Inspectionbull bull Changes of appearance such as deviation andbull asymmetry bleeding watery drainage changesbull in nasal breathing and smell It is useful to comparebull the current presentation with old photographsbull (up to 40 of normal individuals havebull significant nose malformations)
Nasal Fractures Physical examination bull The diagnosis of a nasal fracture is made primarily by physical examination epistaxis nasal swelling and periorbital ecchymosis Nasal shape in the lateral and frontal inspection should be assessed Grasping the dorsum between two fingers and rocking the pyramid back and forth aids in assessing the mobility of nasal bones Internal structures should be evaluated by using a headlight and nasal speculum Clotted blood is removed by suction and assessment of haematoma mucosal tears and active bleeding is performed Bimanual palpation of the septum helps to differentiate septal swelling from haematoma ndash
Nasal FracturesRadiographybull There is no clear evidence of the role of radiographyin the management of nasal fracturesPlain films have up to a 66 false-positive rateas a result of misinterpretation of normal suturelines In addition old fractures are difficult todistinguishbull Three-dimensional CT is recommended for extensiveinjuries involving the nasal-orbital-ethmoidalcomplexndash
Nasal Fractures
bull Additionaluseful diagnostic proceduresbull bull Using a 0 or 30deg 4-mm endoscope is helpful inbull the assessment of posterior abnormalities If thebull patient is heavily sedated Brown-Gruss
provocationbull manoeuvres may be performed to determinebull deformities in upper middle or lower segmentsbull by compressing each compartment
Nasal FracturesConservative treatmentndash Treatment of bleedingbull For localised bleeding anterior sources may becauterised by silver nitrate or sealed with topicalmaterials such as thrombin combined withgelatin foam fibrin glue FloSealreg or other procoagulantmaterials If conservative measuresfail a formal anterior packing is placedbull Bleeding from branches of sphenopalatine orethmoid vessels requires anterior-posteriorpacking
Nasal Fractures
bull bull Surgical methods such as direct endoscopic vessel
bull cauterization or ligation have been shown tobull offer better haemostasis and patient comfortbull Angiography with embolization can also be
consideredbull in cases refractory to more conservativebull approaches
Nasal Fractures
bull Type of reductionbull bull Nondisplaced fractures should be treated withbull observation alone Closed nasal reduction is thebull best choice for simple injuries (isolated unilateralbull with medial displacement)bull bull An open approach should be considered in
severebull trauma (bilateral depressed fractures)
Nasal Fracturesbull Surgical principlesbull ndash Topical anaesthesia with cotton pledgets soakedbull with 4 cocaine or 005 oxymethazoline combinedbull with 4 topical lidocaine should be appliedbull for 5ndash10 min Local anaesthesia should also be injectedbull (1 lidocaine and 1100000 epinephrine)bull along the septum lateral walls and floor of the nasalbull cavitybull bull
Nasal FracturesClosed reductionndashndash The nasal bones are grasped between two fingersand pressure is applied laterally in theopposite direction of the deviation A bluntelevator may be used from within the nose incases of significant medial collapse Walshamforceps can be of help Reduction of the septumshould be performed with the use ofAsch forceps
Nasal Fractures
bull To prevent collapse of the postreductionbull framework nasal packing should be placedbull for 3ndash5 days Septum splints are recommendedbull in comminuted septal fractures withbull severe mucosal lesions External nasal splintingbull for 10 days (Aquaplastreg Thermoplastreg)bull provides nasal protection Nasal saline spraysbull prevent crusting and oral antibiotics should
Nasal Fractures
bull Open reductionbull ndashndash Immediate repair of fractures by using
widebull surgical exposure reduction fixation and
reconstructionbull ndashndash The second option is delayed correctionbull (6 months or more) of persistent deformitiesbull using standard techniques of rhinoplasty
Deviated Nasal Septum
bull Definition of the diseasebull ndash Deviation of the nasal septum is a common causebull of unilateral nasal airway obstruction in which thebull nasal septum is displacedbull bull Epidemiologyaetiologybull ndash Developmental septal abnormalities Septal cartilage
damage in the neonatal period andbull during birth can cause severe septal deviation inbull the absence of a history of nasal trauma
Deviated Nasal Septum
bull Symptomsbull ndash Patients may present with a history of sinusitis
allergicbull rhinitis obstructive sleep apnoea previousbull nasal surgery or recent nasal trauma Unilateral or
bilateral nasal airway obstruction that is unrelievedbull with decongestants or nasal steroid sprays is oftenbull seenbull bull
Deviated Nasal SeptumDiagnosisndashExamination external dorsal deviation or the columella and caudal septummay be deflected off the midline (caudal subluxation)ndash Inspections of the nasal cavity and anterior-posteriorrhinoscopy are helpful in diagnosing the locationtype and severity of septal deformityThe endoscope is also useful in identifying polypsthe severity and extent of posterior septaldeviations and bony spurs and locating areas ofseptal perforation or mucosal injury
Deviated Nasal Septum
bull Therapybull ndash Septoplasty is a procedurebull The areabull of deviation is corrected or resected in order tobull leave behind as much cartilage and bone as
possiblebull Cartilage resection is minimised and can be
repositioned reshaped or recontoured using a variety of methods
Deviated Nasal Septum
bull ndash Indications of septoplasty before the growth period
bull of the nose is finished should be very limited bull -In these cases surgery must preserve all the
cartilagebull in order to prevent external changes of the
shape ofbull the nose
Deviated Nasal Septum
bull Complicationsbull ndash Frequent complications include haematoma andbull infection Cerebrospinal fluid leak is a rare but
potentiallybull serious complicationbull It is usually the resultbull of avulsion or damage to the cribriform plate whenbull handling the perpendicular plate of the ethmoidbull ndash Other complications include epistaxis nasal
Deviated Nasal Septum
bull Other complications include epistaxis nasal obstruction
bull due to residual deviation synechiae returnbull of the cartilaginous deviation septal perforationbull anosmia and cosmetic nasal deformities suchbull as widened alar rim margins drooping nasal tipbull columella retraction and a sunken dorsum with abull supratip saddle formation
Septal perforation with minor crusting View from provide closure of the
incision
Septal Haematoma
bull A septal haematoma is a blood collection under the perichondrium
bull of the septum and cartilagebull bull bull Epidemiologyaetiologybull ndash A septal haematoma is one of the most
severe complications of nasal trauma
Septal Haematoma
bull Diagnosisbull ndash Signs and symptoms include intense pain
swellingbull haematoma of the upper lip and philtrum
area andbull complete nasal airway obstruction
Septal HaematomaTherapyndash Management consists of drainage through a mucoperichondrial incision Immediate treatment isnecessary to prevent long-term problems such asa saddle-nose deformity perforation columellarretraction and nasal-base widening In childrenseptal destruction can lead to devastating nasal andmidfacial growth abnormalitiesbull Surgeryndash Incision and evacuation of the collection is performedDrainage of a septal haematoma should
Septal HaematomaSurgeryndash Incision and evacuation of the collection is performedDrainage of a septal haematoma should provide closure of the incision
Splints or transseptal sutures are placed to obliterate thepotential space and prevent collectionInfection involving the septal cartilage Reconstruction with autologouscartilage is then performed in a second stage Oral antibiotics should be given
Nasal DeformitySaddle-nose deformityndash A saddle-nose deformity is characterised by a loss ofnasal dorsal height and compromised nasal supportstructures -Other case observed are depressionof the middle vault and dorsum loss of nasal tipsupport and definition shortened (vertical) nasal length over rotation of the nasal tip and retrusion ofthe nasal spine and caudal septum It is also knownas a ldquoPug noserdquo or ldquoboxerrsquos noserdquo both of which referto various degrees of nasal dorsal depressionbull
Nasal DeformityEpidemiologyaetiologyndash Prevalence is higher in population groups prone to facial trauma (ie boxers athletes) those with historiesof intranasal cocaine use nasal surgery (e g radical submucosal septal resection reductive rhinoplasty)ndash A saddle-nose deformity can be congenital or acquired It can be noticed as a part of individual familialsyndromic and ethnic characteristics - Most deformities are due to traumatic and iatrogeniccauses Medical causes are Wegenerrsquosgranulomatosis relapsing polychondritis leprosy (Hansenrsquos disease) syphilis ectodermal dysplasiaand intranasal cocaine use
Nasal Deformity
bull Therapybull ndash Nasal reconstruction indications depend on patientbull selection surgeon experience and aetiology of thebull deformity bull Indications for surgery can be functionalbull aesthetic or most commonly both In individuals
with a compromised nasal airway a nasoseptalbull reconstruction is indicated
Nasal Deformity
bull Contraindications bull include patients with malignantbull chronic or autoimmune disease conditions drugbull abuse poor perioperative risk profile and unrealisticbull expectationsbull ndash Multiple previous rhinoplasties and certain
professionsbull (mixed martial artists boxers and other contactbull sports) are relative contraindications
Nasal DeformitySeptoplastyndash Septoplasty is performed to correct nasal obstructioncaused by septal deformityndash Usually septoplasty is performed under general anaesthesiawith the patient in the supine position with the head elevated by approximately 30 (Righthandedsurgeons approach from the right side)ndash Local vasoconstrictive anaesthesia is applied notonly to reduce postoperative pain but also more importantly to achieve vasoconstriction of themucosa and less intraoperative haemorrhage Lidocainewith adrenaline or epinephrine is usedalthough in patients with cardiac hypersensitivityoxymetazoline might be preferred
Nasal Deformity
bull Septoplasty begins with the incision of septal mucosabull Most operative techniques utilise a hemitransfixionbull incision at the caudal end of septum so thatbull deviation at this point might be reached as wellbull as a transfixion incision that is easily obtained ifbull needed (Right-handed surgeons normally choosebull the left side but that may vary when deviation isbull convex towards the right)
Nasal DeformityA columella retractor is placed over the columellaand by pulling it laterally the caudal border of theseptum is exposed Ala can be protected by an alaprotector A vertical incision with a no 15 bladeover the caudal end of septum is performed untilreaching the plane of the septal cartilage It is essentialto correctly identify the perichondrium and byusing the Cottle elevator dissect and lift it creatinga flap As the dissection proceeds along the septalcartilage a longer speculum (no 5) is introduced sothat elevation of the mucoperichondrium is doneunder constant visual controlndash The next step is to dissect the mucoperiostium
Nasal DeformityDissecting over the bony-cartilaginous junctionwhen joining both tunnels might be difficult and is
especially prone to membrane perforationndash If needed the same tunnels are to be created on the
other side of the septum Then deviated parts of
septum are identified and removed either with a
knife or a Freer chisel
Nasal Deformitybull septum from the maxillary crest the septum mustbull be separated from the perpendicular plate trimmedbull along the inferior border placed back onto the crestbull and sutured to the periosteum If the deformity involvesbull the vomer an osteotome is used Care mustbull be taken not to break the cribriform plate becausebull it could cause a cerebrospinal fistula
Nasal Deformity
bull Once the septal deviation is corrected the flapsbull and hemitransfixion incision are mattressed
withbull absorbable sutures Nasal packing to prevent
synechiaebull and postoperative septal haematoma mightbull be advised but should be removed within 72 h

Magnetic Resonance Imaging
Magnetic maging
Magnetic resonance imaging (MRI) has fewer indicationsthan CT in patients with paranasal sinus diseaseThis is primarily because MRI is markedly inferior toCT in defining the bony boundaries of the sinusesThe strength of MRI lies in its superior soft-tissue discriminationMRI is indicated in diseases that involve the paranasal sinuses in addition to thecranial cavity or orbit (eg tumors and congenitalmalformations such as encephaloceles)
MRI of the paranasal sinuses
The Nose and Sinuses
Structure The structure of the nose is made up of
four partsbull The surface anatomybull The nasal skeletonmdashcomposed of the
two nasal bones the paired upper lateral and lower lateral cartilages and the nasal septum covered in subcutaneous tissue and skin
bull The internal anatomymdashincludes the septum of the nose which forms the medial wall of the nasal cavity The turbinates on the lateral wall are also called conchae
bull The osteomeatal complexmdasha key functional area of the nose
Function The nose is the main route for inspired
air and its structure is related to this function As the air passes over the large surface area of the turbinates
The inspired gases are warmed and humidified Mucus on the mucosa of the nose removes large dust particles from the air as it is breathed in
The voice resonates in the sinuses and nose and this provides character to the speech
Pneumatization of the sinusesmdashthey are air filled spacesmdashreduces the weight of the skull
Diseases of thDiseases of the Outer and Inner Nosee Outer and
Inner Nose Erysipelas Definition of the disease ndash Erysipela is a skin infection that affects the superficial dermis and is caused by Streptococcus pyogenes (group A) It usually develops in the extremities and the face and less commonly on the scalp and genitals bull Epidemiologyaetiology ndash Erysipelas are more often seen in elderly infants and children patients with compromised immunology and diabetes -Predisposing factors are alcoholism skin ulceration puncture wounds fungal infections malnutrition and burns
Erysipelas
bull Symptomsbull ndash It usually presents of fever general fatigue bull -The skin lesion is a redindurated and elevated plaque
with borders that expand rapidly bull It is painful warm and accompanied by variable oedemabull -On the second or third day a flaccid bulla may develop
and desquamationbull bull Presence of regional lymph nodes is common
Erysipelas
bull Complicationsndash The most common complication is recurrencewhich is seen in 18ndash30 of the cases even afterproper antibiotic therapy Recurrence is seen moreoften in females than in malesA skin infection with S pyogenes could lead toglomerulonephritis
Erysipelas
bull Complicationsbull ndash The most common complication is recurrencebull which is seen in 18ndash30 of the cases even afterbull proper antibiotic therapy bull -Recurrence is seen morebull often in females than in males bull -A skin infection with S pyogenes could lead tobull glomerulonephritis
Erysipelas
bull bull Diagnosisbull ndash Diagnosis is based on the patientrsquos personal
historybull and physical examination particularly on inspectionbull of the skin
bull Blood cultures are positive in less thanbull 5 of cases
ErysipelasTherapyndash Conservative therapybull The preferred antibiotic is penicillin In mildcases with minor systemic symptoms penicillinV 500 mg orally every 6 h for 10 days or penicillinG benzathine 12 mil U intramuscularlyonceOther possibilities are amoxicillin 500 mgorally twice a day for 10 days or cephalexin 500mg orally every 6 h for 10 days
ErysipelasIn moderate and severe cases with significantsystemic symptoms hospitalization and intravenoustreatment is required penicillin G 2ndash4mil U intravenously every 4ndash6 h Cefazolin05ndash15 gm intravenously every 8 h cefotaxime1ndash2 gm intravenously every 8 h or ceftriaxone1ndash2 gm intravenously once a day should be administeredIn patients with a penicillin allergyclindamycin 600 mg intravenously every 8 h orvancomycin 15 mgkg intravenously twice a daymay be given
ErysipelaAdditional useful therapeutic optionsbull Prednisone 30 mg over 8 days might be consideredas well as elevation of the affected siteMoist heat compresses may be usefulbull Surgeryndash Debridement and drainage are indicated when bullaeabscesses or necroses are presentbull Differential diagnosisndash Contact dermatitisndash Asteatotic eczemandash Herpes zosterndash Angioneurotic oedemandash Osteomyelitis
Furuncle
bull Definition of the diseasebull ndash A furuncle is an infection that beginsbull at the hair follicle and spreads deeper into thebull dermis and subcutaneous tissue forming abull nodule After several days it developsbull into an abscess - red painful and fluctuantbull bull bull Epidemiologyaetiologybull ndash The aetiologic agent is Staphylococcus aureus
FuruncleSymptomsndashsymptoms are local and limited to thesite of infection Furuncles usually are wherehair follicles are present bull Complicationndash One complication is furunculosis multiple draining furunclesDiagnosisndash The diagnosis is based on clinical inspection - Cultures are not necessary when there is no systemic involvement but should beconsidered if systemic therapy (in case of feversignificant cellulitis or hospitalization) or whenmethicillin-resistant Staphylococcusaureus (MRSA) is considered
FuruncleTherapyndash When the furuncle is small application of moist heat compress to promote drainage -Larger furuncles should be drained by surgical incision-After drainage the area should be cleaned with anantiseptic (with chlorhexidinebetadine) should be applied twice
a dayndash If no systemic symptoms or extensive cellulitis arepresent simple topical care is usually curative andoral antibiotics are not necessary Otherwise systemictreatment is indicated and should cover anypossible MRSA
Furuncle
bull -Recommended antibiotics are trimethoprim-sulfamethoxazole
bull 1ndash2 tablets orally twice daily doxycyclinebull 100 mg orally twice dailybull or clindamycin 300ndash450 mg orally every 8 hbull - In severe cases vancomycin 15 mgkg
intravenouslybull every 12 h or clindamycin 600 mg intravenouslybull every 8 h
Midline Granulomabull A midline granuloma is an angiocentricbull lymphoma it was referred to as polymorphicbull reticulosis lethal midline granuloma and midline
malignant reticulosisbull bull Definition of the diseasebull ndash This rare disease is a lymphoma of extranodal
presentationall cases are positive for the Epstein-Barr virus
bull -This lymphoma most commonly appears in the midface region
Midline GranulomaEpidemiologyaetiologyndash This form of lymphoma is rare in Europe and theUnited States with a higher prevalence in Asia and PeruSymptomsndash The most common presentation is nasal obstruction with a destructive mass occupying the nosesinuses and palate
-Fever night sweatsand weight loss seen usually in Hodgkinrsquos lymphomaand other non-Hodgkinrsquos lymphomas (knownas ldquoB symptomsrdquo) are uncommon
Midline GranulomaDiagnosisndash The diagnosis is based on anatomopathologicalstudy The malignancy of the tumour manifested byextensive necrosis makes the histological diagnosisdifficult and often more biopsies are required forconfirmationbull Therapyndash Therapy consists of radiotherapy with or withoutchemotherapy
Midline Granuloma
bull Prognosisbull ndash Depending on the stage long-term remission or
experience a worseningbull prognosis with relapses which may include otherbull extranodal sites bull Involvement of extranodal sitesbull including the upper airway gastrointestinal tractbull skin
Wegenerrsquos Granulomatosis
bull Definition of the diseasebull ndash Wegenerrsquos granulomatosis is a systemic chronicbull vasculitis of small- and medium-sized blood vesselsbull with an autoimmune component It affectsbull particular organs with variable predilectionbull Epidemiologyaetiologybull ndash Wegenerrsquos granulomatosis is a rare disease It affects
about 1 in 20000ndash30000 people It is more prevalentbull in middle-aged Caucasian patients
Wegenerrsquos Granulomatosis
Symptomsndash The disease may present pulmonary upper
respiratory tract or renal In the disseminated form-The localised form ndash confinedto the upper respiratory region ndash is present in 25of the patients- It consists of nonspecific manifestationssuch as nasal obstruction crusting purulentor bloody rhinorrhea and painful or painless ulcers in oral or nasal cavities which are unresponsive tostandard medical treatment
Wegenerrsquos Granulomatosis
bull In some patients the nasal septum is perforatedbull which leads to saddle-nose deformity Less
commonbull symptoms are hoarseness stridor due to
subglotticbull stenosis otalgia otorrhea and conductivebull and sensorineural hearing loss Also ocular
symptomsbull such as scleritis conjunctivitis uveitis andbull episcleritis may be present
Wegenerrsquos Granulomatosis
bull ndash In the disseminated form pulmonary involvementbull is manifested by cough dyspnoea haemoptysisbull (due to an alveolar capillaritis necrotic lesions orbull endobronchial disease) and pleuritic painndashbull -Ninety per cent of patients have nasal symptomsbull and these symptoms are usually the first
manifestationof the diseasebull -Most patients have also renal involvementbull even if it is subclinical
Wegenerrsquos Granulomatosis
Diagnosis ndash Diagnosis of Wegenerrsquos granulomatosis is based on clinical findings that demonstrate lung (chest x-ray) kidney (urine analysis) or upper respiratory tract
involvement (oral or nasal ulcers or discharge) - positive blood analysis for cytoplasmic-staining antineutrophil
cytoplasmic antibodies (c-ANCA) and confirming proteinase 3 (PR3) ANCA or myeloperoxidase (MPO) ANCA ndash Biopsy is essential for diagnosis nonspecific chronic inflammation
and necrosis -Bacterial and fungal infections
Wegenerrsquos Granulomatosis
Therapyndash Conservative therapybull In the induction of disease remission highdosesteroids (e g prednisone 1 mgkgday) for1 month with tapering over several months aregiven In addition cyclophosphamide (2 mgkgday) should be administered for 6ndash12 monthsuntil symptoms disappear In the maintenanceof remission cyclophosphamide should be
Wegenerrsquos Granulomatosis
Antibiotics mainly trimethoprim-sulfamethoxazoleare given for prophylaxis againstPneumocystis jiroveci (formerly Pneumocystiscarinii) pneumonia (PCP) which may developduring immunosuppression and have a role inpreventing recurrencesbull Sinonasal manifestations may be treated with topical nasal steroids and nasal irrigations lowdosesystemic steroids and antibiotics when bacterial infection (typically Staphylococcus species) is suspected
Wegenerrsquos Granulomatosis
bull Prognosisbull ndash Most of the patients respond well to treatmentbull achieving symptom-free intervals of 5ndash20 yearsbull or more bull -Anatomical problems (sinusitis trachealbull stenosis) may require surgery bull Relapses can be long and troublesomebull Long-term complications are chronicbull renal failure hearing loss and deafness
Nasal Fractures Definition ndash A nasal fracture is a disruption of the nasal bone structure due to trauma It is the most frequently fractured facial bone Epidemiologyaetiology ndash Sports falls and assaults are the usual mechanisms of fracture -Males are affected twice as often as are females -Paediatric populations with a incidences during the second and third decades of life -Variables such as force impact direction nature of the striking object age and other will influence the pattern of injury to the components of the nose
Nasal Fractures
bull Symptomsbull ndash Deformity swelling epistaxis and periorbital
ecchymosis are signs that are suggestive of nasal fracture
bull bony crepitus and nasal segment mobilitybull ndash Epiphora bull Severe bilateral injuries to the lachrymal bones
arebull associated with depressed nasal fractures
Nasal Fractures Complications ndash Septal haematoma is one of the most severe early complications of nasal trauma and without drainage it results in abscess formation 6ndash7 days after trauma producing necrosis of the septal cartilage -Long-term problems such as saddle-nose deformity perforation columellar retraction and nasalbase
Septal infection could lead to osteomyelitis orbital and intracranial abscesses meningitis and cavernous sinus thrombosis -Cerebrospinal fluid leakage is a common complication of severe
nasal and frontal fractures
Nasal Fractures
bull Diagnostic proceduresbull ndash Inspectionbull bull Changes of appearance such as deviation andbull asymmetry bleeding watery drainage changesbull in nasal breathing and smell It is useful to comparebull the current presentation with old photographsbull (up to 40 of normal individuals havebull significant nose malformations)
Nasal Fractures Physical examination bull The diagnosis of a nasal fracture is made primarily by physical examination epistaxis nasal swelling and periorbital ecchymosis Nasal shape in the lateral and frontal inspection should be assessed Grasping the dorsum between two fingers and rocking the pyramid back and forth aids in assessing the mobility of nasal bones Internal structures should be evaluated by using a headlight and nasal speculum Clotted blood is removed by suction and assessment of haematoma mucosal tears and active bleeding is performed Bimanual palpation of the septum helps to differentiate septal swelling from haematoma ndash
Nasal FracturesRadiographybull There is no clear evidence of the role of radiographyin the management of nasal fracturesPlain films have up to a 66 false-positive rateas a result of misinterpretation of normal suturelines In addition old fractures are difficult todistinguishbull Three-dimensional CT is recommended for extensiveinjuries involving the nasal-orbital-ethmoidalcomplexndash
Nasal Fractures
bull Additionaluseful diagnostic proceduresbull bull Using a 0 or 30deg 4-mm endoscope is helpful inbull the assessment of posterior abnormalities If thebull patient is heavily sedated Brown-Gruss
provocationbull manoeuvres may be performed to determinebull deformities in upper middle or lower segmentsbull by compressing each compartment
Nasal FracturesConservative treatmentndash Treatment of bleedingbull For localised bleeding anterior sources may becauterised by silver nitrate or sealed with topicalmaterials such as thrombin combined withgelatin foam fibrin glue FloSealreg or other procoagulantmaterials If conservative measuresfail a formal anterior packing is placedbull Bleeding from branches of sphenopalatine orethmoid vessels requires anterior-posteriorpacking
Nasal Fractures
bull bull Surgical methods such as direct endoscopic vessel
bull cauterization or ligation have been shown tobull offer better haemostasis and patient comfortbull Angiography with embolization can also be
consideredbull in cases refractory to more conservativebull approaches
Nasal Fractures
bull Type of reductionbull bull Nondisplaced fractures should be treated withbull observation alone Closed nasal reduction is thebull best choice for simple injuries (isolated unilateralbull with medial displacement)bull bull An open approach should be considered in
severebull trauma (bilateral depressed fractures)
Nasal Fracturesbull Surgical principlesbull ndash Topical anaesthesia with cotton pledgets soakedbull with 4 cocaine or 005 oxymethazoline combinedbull with 4 topical lidocaine should be appliedbull for 5ndash10 min Local anaesthesia should also be injectedbull (1 lidocaine and 1100000 epinephrine)bull along the septum lateral walls and floor of the nasalbull cavitybull bull
Nasal FracturesClosed reductionndashndash The nasal bones are grasped between two fingersand pressure is applied laterally in theopposite direction of the deviation A bluntelevator may be used from within the nose incases of significant medial collapse Walshamforceps can be of help Reduction of the septumshould be performed with the use ofAsch forceps
Nasal Fractures
bull To prevent collapse of the postreductionbull framework nasal packing should be placedbull for 3ndash5 days Septum splints are recommendedbull in comminuted septal fractures withbull severe mucosal lesions External nasal splintingbull for 10 days (Aquaplastreg Thermoplastreg)bull provides nasal protection Nasal saline spraysbull prevent crusting and oral antibiotics should
Nasal Fractures
bull Open reductionbull ndashndash Immediate repair of fractures by using
widebull surgical exposure reduction fixation and
reconstructionbull ndashndash The second option is delayed correctionbull (6 months or more) of persistent deformitiesbull using standard techniques of rhinoplasty
Deviated Nasal Septum
bull Definition of the diseasebull ndash Deviation of the nasal septum is a common causebull of unilateral nasal airway obstruction in which thebull nasal septum is displacedbull bull Epidemiologyaetiologybull ndash Developmental septal abnormalities Septal cartilage
damage in the neonatal period andbull during birth can cause severe septal deviation inbull the absence of a history of nasal trauma
Deviated Nasal Septum
bull Symptomsbull ndash Patients may present with a history of sinusitis
allergicbull rhinitis obstructive sleep apnoea previousbull nasal surgery or recent nasal trauma Unilateral or
bilateral nasal airway obstruction that is unrelievedbull with decongestants or nasal steroid sprays is oftenbull seenbull bull
Deviated Nasal SeptumDiagnosisndashExamination external dorsal deviation or the columella and caudal septummay be deflected off the midline (caudal subluxation)ndash Inspections of the nasal cavity and anterior-posteriorrhinoscopy are helpful in diagnosing the locationtype and severity of septal deformityThe endoscope is also useful in identifying polypsthe severity and extent of posterior septaldeviations and bony spurs and locating areas ofseptal perforation or mucosal injury
Deviated Nasal Septum
bull Therapybull ndash Septoplasty is a procedurebull The areabull of deviation is corrected or resected in order tobull leave behind as much cartilage and bone as
possiblebull Cartilage resection is minimised and can be
repositioned reshaped or recontoured using a variety of methods
Deviated Nasal Septum
bull ndash Indications of septoplasty before the growth period
bull of the nose is finished should be very limited bull -In these cases surgery must preserve all the
cartilagebull in order to prevent external changes of the
shape ofbull the nose
Deviated Nasal Septum
bull Complicationsbull ndash Frequent complications include haematoma andbull infection Cerebrospinal fluid leak is a rare but
potentiallybull serious complicationbull It is usually the resultbull of avulsion or damage to the cribriform plate whenbull handling the perpendicular plate of the ethmoidbull ndash Other complications include epistaxis nasal
Deviated Nasal Septum
bull Other complications include epistaxis nasal obstruction
bull due to residual deviation synechiae returnbull of the cartilaginous deviation septal perforationbull anosmia and cosmetic nasal deformities suchbull as widened alar rim margins drooping nasal tipbull columella retraction and a sunken dorsum with abull supratip saddle formation
Septal perforation with minor crusting View from provide closure of the
incision
Septal Haematoma
bull A septal haematoma is a blood collection under the perichondrium
bull of the septum and cartilagebull bull bull Epidemiologyaetiologybull ndash A septal haematoma is one of the most
severe complications of nasal trauma
Septal Haematoma
bull Diagnosisbull ndash Signs and symptoms include intense pain
swellingbull haematoma of the upper lip and philtrum
area andbull complete nasal airway obstruction
Septal HaematomaTherapyndash Management consists of drainage through a mucoperichondrial incision Immediate treatment isnecessary to prevent long-term problems such asa saddle-nose deformity perforation columellarretraction and nasal-base widening In childrenseptal destruction can lead to devastating nasal andmidfacial growth abnormalitiesbull Surgeryndash Incision and evacuation of the collection is performedDrainage of a septal haematoma should
Septal HaematomaSurgeryndash Incision and evacuation of the collection is performedDrainage of a septal haematoma should provide closure of the incision
Splints or transseptal sutures are placed to obliterate thepotential space and prevent collectionInfection involving the septal cartilage Reconstruction with autologouscartilage is then performed in a second stage Oral antibiotics should be given
Nasal DeformitySaddle-nose deformityndash A saddle-nose deformity is characterised by a loss ofnasal dorsal height and compromised nasal supportstructures -Other case observed are depressionof the middle vault and dorsum loss of nasal tipsupport and definition shortened (vertical) nasal length over rotation of the nasal tip and retrusion ofthe nasal spine and caudal septum It is also knownas a ldquoPug noserdquo or ldquoboxerrsquos noserdquo both of which referto various degrees of nasal dorsal depressionbull
Nasal DeformityEpidemiologyaetiologyndash Prevalence is higher in population groups prone to facial trauma (ie boxers athletes) those with historiesof intranasal cocaine use nasal surgery (e g radical submucosal septal resection reductive rhinoplasty)ndash A saddle-nose deformity can be congenital or acquired It can be noticed as a part of individual familialsyndromic and ethnic characteristics - Most deformities are due to traumatic and iatrogeniccauses Medical causes are Wegenerrsquosgranulomatosis relapsing polychondritis leprosy (Hansenrsquos disease) syphilis ectodermal dysplasiaand intranasal cocaine use
Nasal Deformity
bull Therapybull ndash Nasal reconstruction indications depend on patientbull selection surgeon experience and aetiology of thebull deformity bull Indications for surgery can be functionalbull aesthetic or most commonly both In individuals
with a compromised nasal airway a nasoseptalbull reconstruction is indicated
Nasal Deformity
bull Contraindications bull include patients with malignantbull chronic or autoimmune disease conditions drugbull abuse poor perioperative risk profile and unrealisticbull expectationsbull ndash Multiple previous rhinoplasties and certain
professionsbull (mixed martial artists boxers and other contactbull sports) are relative contraindications
Nasal DeformitySeptoplastyndash Septoplasty is performed to correct nasal obstructioncaused by septal deformityndash Usually septoplasty is performed under general anaesthesiawith the patient in the supine position with the head elevated by approximately 30 (Righthandedsurgeons approach from the right side)ndash Local vasoconstrictive anaesthesia is applied notonly to reduce postoperative pain but also more importantly to achieve vasoconstriction of themucosa and less intraoperative haemorrhage Lidocainewith adrenaline or epinephrine is usedalthough in patients with cardiac hypersensitivityoxymetazoline might be preferred
Nasal Deformity
bull Septoplasty begins with the incision of septal mucosabull Most operative techniques utilise a hemitransfixionbull incision at the caudal end of septum so thatbull deviation at this point might be reached as wellbull as a transfixion incision that is easily obtained ifbull needed (Right-handed surgeons normally choosebull the left side but that may vary when deviation isbull convex towards the right)
Nasal DeformityA columella retractor is placed over the columellaand by pulling it laterally the caudal border of theseptum is exposed Ala can be protected by an alaprotector A vertical incision with a no 15 bladeover the caudal end of septum is performed untilreaching the plane of the septal cartilage It is essentialto correctly identify the perichondrium and byusing the Cottle elevator dissect and lift it creatinga flap As the dissection proceeds along the septalcartilage a longer speculum (no 5) is introduced sothat elevation of the mucoperichondrium is doneunder constant visual controlndash The next step is to dissect the mucoperiostium
Nasal DeformityDissecting over the bony-cartilaginous junctionwhen joining both tunnels might be difficult and is
especially prone to membrane perforationndash If needed the same tunnels are to be created on the
other side of the septum Then deviated parts of
septum are identified and removed either with a
knife or a Freer chisel
Nasal Deformitybull septum from the maxillary crest the septum mustbull be separated from the perpendicular plate trimmedbull along the inferior border placed back onto the crestbull and sutured to the periosteum If the deformity involvesbull the vomer an osteotome is used Care mustbull be taken not to break the cribriform plate becausebull it could cause a cerebrospinal fistula
Nasal Deformity
bull Once the septal deviation is corrected the flapsbull and hemitransfixion incision are mattressed
withbull absorbable sutures Nasal packing to prevent
synechiaebull and postoperative septal haematoma mightbull be advised but should be removed within 72 h

MRI of the paranasal sinuses
The Nose and Sinuses
Structure The structure of the nose is made up of
four partsbull The surface anatomybull The nasal skeletonmdashcomposed of the
two nasal bones the paired upper lateral and lower lateral cartilages and the nasal septum covered in subcutaneous tissue and skin
bull The internal anatomymdashincludes the septum of the nose which forms the medial wall of the nasal cavity The turbinates on the lateral wall are also called conchae
bull The osteomeatal complexmdasha key functional area of the nose
Function The nose is the main route for inspired
air and its structure is related to this function As the air passes over the large surface area of the turbinates
The inspired gases are warmed and humidified Mucus on the mucosa of the nose removes large dust particles from the air as it is breathed in
The voice resonates in the sinuses and nose and this provides character to the speech
Pneumatization of the sinusesmdashthey are air filled spacesmdashreduces the weight of the skull
Diseases of thDiseases of the Outer and Inner Nosee Outer and
Inner Nose Erysipelas Definition of the disease ndash Erysipela is a skin infection that affects the superficial dermis and is caused by Streptococcus pyogenes (group A) It usually develops in the extremities and the face and less commonly on the scalp and genitals bull Epidemiologyaetiology ndash Erysipelas are more often seen in elderly infants and children patients with compromised immunology and diabetes -Predisposing factors are alcoholism skin ulceration puncture wounds fungal infections malnutrition and burns
Erysipelas
bull Symptomsbull ndash It usually presents of fever general fatigue bull -The skin lesion is a redindurated and elevated plaque
with borders that expand rapidly bull It is painful warm and accompanied by variable oedemabull -On the second or third day a flaccid bulla may develop
and desquamationbull bull Presence of regional lymph nodes is common
Erysipelas
bull Complicationsndash The most common complication is recurrencewhich is seen in 18ndash30 of the cases even afterproper antibiotic therapy Recurrence is seen moreoften in females than in malesA skin infection with S pyogenes could lead toglomerulonephritis
Erysipelas
bull Complicationsbull ndash The most common complication is recurrencebull which is seen in 18ndash30 of the cases even afterbull proper antibiotic therapy bull -Recurrence is seen morebull often in females than in males bull -A skin infection with S pyogenes could lead tobull glomerulonephritis
Erysipelas
bull bull Diagnosisbull ndash Diagnosis is based on the patientrsquos personal
historybull and physical examination particularly on inspectionbull of the skin
bull Blood cultures are positive in less thanbull 5 of cases
ErysipelasTherapyndash Conservative therapybull The preferred antibiotic is penicillin In mildcases with minor systemic symptoms penicillinV 500 mg orally every 6 h for 10 days or penicillinG benzathine 12 mil U intramuscularlyonceOther possibilities are amoxicillin 500 mgorally twice a day for 10 days or cephalexin 500mg orally every 6 h for 10 days
ErysipelasIn moderate and severe cases with significantsystemic symptoms hospitalization and intravenoustreatment is required penicillin G 2ndash4mil U intravenously every 4ndash6 h Cefazolin05ndash15 gm intravenously every 8 h cefotaxime1ndash2 gm intravenously every 8 h or ceftriaxone1ndash2 gm intravenously once a day should be administeredIn patients with a penicillin allergyclindamycin 600 mg intravenously every 8 h orvancomycin 15 mgkg intravenously twice a daymay be given
ErysipelaAdditional useful therapeutic optionsbull Prednisone 30 mg over 8 days might be consideredas well as elevation of the affected siteMoist heat compresses may be usefulbull Surgeryndash Debridement and drainage are indicated when bullaeabscesses or necroses are presentbull Differential diagnosisndash Contact dermatitisndash Asteatotic eczemandash Herpes zosterndash Angioneurotic oedemandash Osteomyelitis
Furuncle
bull Definition of the diseasebull ndash A furuncle is an infection that beginsbull at the hair follicle and spreads deeper into thebull dermis and subcutaneous tissue forming abull nodule After several days it developsbull into an abscess - red painful and fluctuantbull bull bull Epidemiologyaetiologybull ndash The aetiologic agent is Staphylococcus aureus
FuruncleSymptomsndashsymptoms are local and limited to thesite of infection Furuncles usually are wherehair follicles are present bull Complicationndash One complication is furunculosis multiple draining furunclesDiagnosisndash The diagnosis is based on clinical inspection - Cultures are not necessary when there is no systemic involvement but should beconsidered if systemic therapy (in case of feversignificant cellulitis or hospitalization) or whenmethicillin-resistant Staphylococcusaureus (MRSA) is considered
FuruncleTherapyndash When the furuncle is small application of moist heat compress to promote drainage -Larger furuncles should be drained by surgical incision-After drainage the area should be cleaned with anantiseptic (with chlorhexidinebetadine) should be applied twice
a dayndash If no systemic symptoms or extensive cellulitis arepresent simple topical care is usually curative andoral antibiotics are not necessary Otherwise systemictreatment is indicated and should cover anypossible MRSA
Furuncle
bull -Recommended antibiotics are trimethoprim-sulfamethoxazole
bull 1ndash2 tablets orally twice daily doxycyclinebull 100 mg orally twice dailybull or clindamycin 300ndash450 mg orally every 8 hbull - In severe cases vancomycin 15 mgkg
intravenouslybull every 12 h or clindamycin 600 mg intravenouslybull every 8 h
Midline Granulomabull A midline granuloma is an angiocentricbull lymphoma it was referred to as polymorphicbull reticulosis lethal midline granuloma and midline
malignant reticulosisbull bull Definition of the diseasebull ndash This rare disease is a lymphoma of extranodal
presentationall cases are positive for the Epstein-Barr virus
bull -This lymphoma most commonly appears in the midface region
Midline GranulomaEpidemiologyaetiologyndash This form of lymphoma is rare in Europe and theUnited States with a higher prevalence in Asia and PeruSymptomsndash The most common presentation is nasal obstruction with a destructive mass occupying the nosesinuses and palate
-Fever night sweatsand weight loss seen usually in Hodgkinrsquos lymphomaand other non-Hodgkinrsquos lymphomas (knownas ldquoB symptomsrdquo) are uncommon
Midline GranulomaDiagnosisndash The diagnosis is based on anatomopathologicalstudy The malignancy of the tumour manifested byextensive necrosis makes the histological diagnosisdifficult and often more biopsies are required forconfirmationbull Therapyndash Therapy consists of radiotherapy with or withoutchemotherapy
Midline Granuloma
bull Prognosisbull ndash Depending on the stage long-term remission or
experience a worseningbull prognosis with relapses which may include otherbull extranodal sites bull Involvement of extranodal sitesbull including the upper airway gastrointestinal tractbull skin
Wegenerrsquos Granulomatosis
bull Definition of the diseasebull ndash Wegenerrsquos granulomatosis is a systemic chronicbull vasculitis of small- and medium-sized blood vesselsbull with an autoimmune component It affectsbull particular organs with variable predilectionbull Epidemiologyaetiologybull ndash Wegenerrsquos granulomatosis is a rare disease It affects
about 1 in 20000ndash30000 people It is more prevalentbull in middle-aged Caucasian patients
Wegenerrsquos Granulomatosis
Symptomsndash The disease may present pulmonary upper
respiratory tract or renal In the disseminated form-The localised form ndash confinedto the upper respiratory region ndash is present in 25of the patients- It consists of nonspecific manifestationssuch as nasal obstruction crusting purulentor bloody rhinorrhea and painful or painless ulcers in oral or nasal cavities which are unresponsive tostandard medical treatment
Wegenerrsquos Granulomatosis
bull In some patients the nasal septum is perforatedbull which leads to saddle-nose deformity Less
commonbull symptoms are hoarseness stridor due to
subglotticbull stenosis otalgia otorrhea and conductivebull and sensorineural hearing loss Also ocular
symptomsbull such as scleritis conjunctivitis uveitis andbull episcleritis may be present
Wegenerrsquos Granulomatosis
bull ndash In the disseminated form pulmonary involvementbull is manifested by cough dyspnoea haemoptysisbull (due to an alveolar capillaritis necrotic lesions orbull endobronchial disease) and pleuritic painndashbull -Ninety per cent of patients have nasal symptomsbull and these symptoms are usually the first
manifestationof the diseasebull -Most patients have also renal involvementbull even if it is subclinical
Wegenerrsquos Granulomatosis
Diagnosis ndash Diagnosis of Wegenerrsquos granulomatosis is based on clinical findings that demonstrate lung (chest x-ray) kidney (urine analysis) or upper respiratory tract
involvement (oral or nasal ulcers or discharge) - positive blood analysis for cytoplasmic-staining antineutrophil
cytoplasmic antibodies (c-ANCA) and confirming proteinase 3 (PR3) ANCA or myeloperoxidase (MPO) ANCA ndash Biopsy is essential for diagnosis nonspecific chronic inflammation
and necrosis -Bacterial and fungal infections
Wegenerrsquos Granulomatosis
Therapyndash Conservative therapybull In the induction of disease remission highdosesteroids (e g prednisone 1 mgkgday) for1 month with tapering over several months aregiven In addition cyclophosphamide (2 mgkgday) should be administered for 6ndash12 monthsuntil symptoms disappear In the maintenanceof remission cyclophosphamide should be
Wegenerrsquos Granulomatosis
Antibiotics mainly trimethoprim-sulfamethoxazoleare given for prophylaxis againstPneumocystis jiroveci (formerly Pneumocystiscarinii) pneumonia (PCP) which may developduring immunosuppression and have a role inpreventing recurrencesbull Sinonasal manifestations may be treated with topical nasal steroids and nasal irrigations lowdosesystemic steroids and antibiotics when bacterial infection (typically Staphylococcus species) is suspected
Wegenerrsquos Granulomatosis
bull Prognosisbull ndash Most of the patients respond well to treatmentbull achieving symptom-free intervals of 5ndash20 yearsbull or more bull -Anatomical problems (sinusitis trachealbull stenosis) may require surgery bull Relapses can be long and troublesomebull Long-term complications are chronicbull renal failure hearing loss and deafness
Nasal Fractures Definition ndash A nasal fracture is a disruption of the nasal bone structure due to trauma It is the most frequently fractured facial bone Epidemiologyaetiology ndash Sports falls and assaults are the usual mechanisms of fracture -Males are affected twice as often as are females -Paediatric populations with a incidences during the second and third decades of life -Variables such as force impact direction nature of the striking object age and other will influence the pattern of injury to the components of the nose
Nasal Fractures
bull Symptomsbull ndash Deformity swelling epistaxis and periorbital
ecchymosis are signs that are suggestive of nasal fracture
bull bony crepitus and nasal segment mobilitybull ndash Epiphora bull Severe bilateral injuries to the lachrymal bones
arebull associated with depressed nasal fractures
Nasal Fractures Complications ndash Septal haematoma is one of the most severe early complications of nasal trauma and without drainage it results in abscess formation 6ndash7 days after trauma producing necrosis of the septal cartilage -Long-term problems such as saddle-nose deformity perforation columellar retraction and nasalbase
Septal infection could lead to osteomyelitis orbital and intracranial abscesses meningitis and cavernous sinus thrombosis -Cerebrospinal fluid leakage is a common complication of severe
nasal and frontal fractures
Nasal Fractures
bull Diagnostic proceduresbull ndash Inspectionbull bull Changes of appearance such as deviation andbull asymmetry bleeding watery drainage changesbull in nasal breathing and smell It is useful to comparebull the current presentation with old photographsbull (up to 40 of normal individuals havebull significant nose malformations)
Nasal Fractures Physical examination bull The diagnosis of a nasal fracture is made primarily by physical examination epistaxis nasal swelling and periorbital ecchymosis Nasal shape in the lateral and frontal inspection should be assessed Grasping the dorsum between two fingers and rocking the pyramid back and forth aids in assessing the mobility of nasal bones Internal structures should be evaluated by using a headlight and nasal speculum Clotted blood is removed by suction and assessment of haematoma mucosal tears and active bleeding is performed Bimanual palpation of the septum helps to differentiate septal swelling from haematoma ndash
Nasal FracturesRadiographybull There is no clear evidence of the role of radiographyin the management of nasal fracturesPlain films have up to a 66 false-positive rateas a result of misinterpretation of normal suturelines In addition old fractures are difficult todistinguishbull Three-dimensional CT is recommended for extensiveinjuries involving the nasal-orbital-ethmoidalcomplexndash
Nasal Fractures
bull Additionaluseful diagnostic proceduresbull bull Using a 0 or 30deg 4-mm endoscope is helpful inbull the assessment of posterior abnormalities If thebull patient is heavily sedated Brown-Gruss
provocationbull manoeuvres may be performed to determinebull deformities in upper middle or lower segmentsbull by compressing each compartment
Nasal FracturesConservative treatmentndash Treatment of bleedingbull For localised bleeding anterior sources may becauterised by silver nitrate or sealed with topicalmaterials such as thrombin combined withgelatin foam fibrin glue FloSealreg or other procoagulantmaterials If conservative measuresfail a formal anterior packing is placedbull Bleeding from branches of sphenopalatine orethmoid vessels requires anterior-posteriorpacking
Nasal Fractures
bull bull Surgical methods such as direct endoscopic vessel
bull cauterization or ligation have been shown tobull offer better haemostasis and patient comfortbull Angiography with embolization can also be
consideredbull in cases refractory to more conservativebull approaches
Nasal Fractures
bull Type of reductionbull bull Nondisplaced fractures should be treated withbull observation alone Closed nasal reduction is thebull best choice for simple injuries (isolated unilateralbull with medial displacement)bull bull An open approach should be considered in
severebull trauma (bilateral depressed fractures)
Nasal Fracturesbull Surgical principlesbull ndash Topical anaesthesia with cotton pledgets soakedbull with 4 cocaine or 005 oxymethazoline combinedbull with 4 topical lidocaine should be appliedbull for 5ndash10 min Local anaesthesia should also be injectedbull (1 lidocaine and 1100000 epinephrine)bull along the septum lateral walls and floor of the nasalbull cavitybull bull
Nasal FracturesClosed reductionndashndash The nasal bones are grasped between two fingersand pressure is applied laterally in theopposite direction of the deviation A bluntelevator may be used from within the nose incases of significant medial collapse Walshamforceps can be of help Reduction of the septumshould be performed with the use ofAsch forceps
Nasal Fractures
bull To prevent collapse of the postreductionbull framework nasal packing should be placedbull for 3ndash5 days Septum splints are recommendedbull in comminuted septal fractures withbull severe mucosal lesions External nasal splintingbull for 10 days (Aquaplastreg Thermoplastreg)bull provides nasal protection Nasal saline spraysbull prevent crusting and oral antibiotics should
Nasal Fractures
bull Open reductionbull ndashndash Immediate repair of fractures by using
widebull surgical exposure reduction fixation and
reconstructionbull ndashndash The second option is delayed correctionbull (6 months or more) of persistent deformitiesbull using standard techniques of rhinoplasty
Deviated Nasal Septum
bull Definition of the diseasebull ndash Deviation of the nasal septum is a common causebull of unilateral nasal airway obstruction in which thebull nasal septum is displacedbull bull Epidemiologyaetiologybull ndash Developmental septal abnormalities Septal cartilage
damage in the neonatal period andbull during birth can cause severe septal deviation inbull the absence of a history of nasal trauma
Deviated Nasal Septum
bull Symptomsbull ndash Patients may present with a history of sinusitis
allergicbull rhinitis obstructive sleep apnoea previousbull nasal surgery or recent nasal trauma Unilateral or
bilateral nasal airway obstruction that is unrelievedbull with decongestants or nasal steroid sprays is oftenbull seenbull bull
Deviated Nasal SeptumDiagnosisndashExamination external dorsal deviation or the columella and caudal septummay be deflected off the midline (caudal subluxation)ndash Inspections of the nasal cavity and anterior-posteriorrhinoscopy are helpful in diagnosing the locationtype and severity of septal deformityThe endoscope is also useful in identifying polypsthe severity and extent of posterior septaldeviations and bony spurs and locating areas ofseptal perforation or mucosal injury
Deviated Nasal Septum
bull Therapybull ndash Septoplasty is a procedurebull The areabull of deviation is corrected or resected in order tobull leave behind as much cartilage and bone as
possiblebull Cartilage resection is minimised and can be
repositioned reshaped or recontoured using a variety of methods
Deviated Nasal Septum
bull ndash Indications of septoplasty before the growth period
bull of the nose is finished should be very limited bull -In these cases surgery must preserve all the
cartilagebull in order to prevent external changes of the
shape ofbull the nose
Deviated Nasal Septum
bull Complicationsbull ndash Frequent complications include haematoma andbull infection Cerebrospinal fluid leak is a rare but
potentiallybull serious complicationbull It is usually the resultbull of avulsion or damage to the cribriform plate whenbull handling the perpendicular plate of the ethmoidbull ndash Other complications include epistaxis nasal
Deviated Nasal Septum
bull Other complications include epistaxis nasal obstruction
bull due to residual deviation synechiae returnbull of the cartilaginous deviation septal perforationbull anosmia and cosmetic nasal deformities suchbull as widened alar rim margins drooping nasal tipbull columella retraction and a sunken dorsum with abull supratip saddle formation
Septal perforation with minor crusting View from provide closure of the
incision
Septal Haematoma
bull A septal haematoma is a blood collection under the perichondrium
bull of the septum and cartilagebull bull bull Epidemiologyaetiologybull ndash A septal haematoma is one of the most
severe complications of nasal trauma
Septal Haematoma
bull Diagnosisbull ndash Signs and symptoms include intense pain
swellingbull haematoma of the upper lip and philtrum
area andbull complete nasal airway obstruction
Septal HaematomaTherapyndash Management consists of drainage through a mucoperichondrial incision Immediate treatment isnecessary to prevent long-term problems such asa saddle-nose deformity perforation columellarretraction and nasal-base widening In childrenseptal destruction can lead to devastating nasal andmidfacial growth abnormalitiesbull Surgeryndash Incision and evacuation of the collection is performedDrainage of a septal haematoma should
Septal HaematomaSurgeryndash Incision and evacuation of the collection is performedDrainage of a septal haematoma should provide closure of the incision
Splints or transseptal sutures are placed to obliterate thepotential space and prevent collectionInfection involving the septal cartilage Reconstruction with autologouscartilage is then performed in a second stage Oral antibiotics should be given
Nasal DeformitySaddle-nose deformityndash A saddle-nose deformity is characterised by a loss ofnasal dorsal height and compromised nasal supportstructures -Other case observed are depressionof the middle vault and dorsum loss of nasal tipsupport and definition shortened (vertical) nasal length over rotation of the nasal tip and retrusion ofthe nasal spine and caudal septum It is also knownas a ldquoPug noserdquo or ldquoboxerrsquos noserdquo both of which referto various degrees of nasal dorsal depressionbull
Nasal DeformityEpidemiologyaetiologyndash Prevalence is higher in population groups prone to facial trauma (ie boxers athletes) those with historiesof intranasal cocaine use nasal surgery (e g radical submucosal septal resection reductive rhinoplasty)ndash A saddle-nose deformity can be congenital or acquired It can be noticed as a part of individual familialsyndromic and ethnic characteristics - Most deformities are due to traumatic and iatrogeniccauses Medical causes are Wegenerrsquosgranulomatosis relapsing polychondritis leprosy (Hansenrsquos disease) syphilis ectodermal dysplasiaand intranasal cocaine use
Nasal Deformity
bull Therapybull ndash Nasal reconstruction indications depend on patientbull selection surgeon experience and aetiology of thebull deformity bull Indications for surgery can be functionalbull aesthetic or most commonly both In individuals
with a compromised nasal airway a nasoseptalbull reconstruction is indicated
Nasal Deformity
bull Contraindications bull include patients with malignantbull chronic or autoimmune disease conditions drugbull abuse poor perioperative risk profile and unrealisticbull expectationsbull ndash Multiple previous rhinoplasties and certain
professionsbull (mixed martial artists boxers and other contactbull sports) are relative contraindications
Nasal DeformitySeptoplastyndash Septoplasty is performed to correct nasal obstructioncaused by septal deformityndash Usually septoplasty is performed under general anaesthesiawith the patient in the supine position with the head elevated by approximately 30 (Righthandedsurgeons approach from the right side)ndash Local vasoconstrictive anaesthesia is applied notonly to reduce postoperative pain but also more importantly to achieve vasoconstriction of themucosa and less intraoperative haemorrhage Lidocainewith adrenaline or epinephrine is usedalthough in patients with cardiac hypersensitivityoxymetazoline might be preferred
Nasal Deformity
bull Septoplasty begins with the incision of septal mucosabull Most operative techniques utilise a hemitransfixionbull incision at the caudal end of septum so thatbull deviation at this point might be reached as wellbull as a transfixion incision that is easily obtained ifbull needed (Right-handed surgeons normally choosebull the left side but that may vary when deviation isbull convex towards the right)
Nasal DeformityA columella retractor is placed over the columellaand by pulling it laterally the caudal border of theseptum is exposed Ala can be protected by an alaprotector A vertical incision with a no 15 bladeover the caudal end of septum is performed untilreaching the plane of the septal cartilage It is essentialto correctly identify the perichondrium and byusing the Cottle elevator dissect and lift it creatinga flap As the dissection proceeds along the septalcartilage a longer speculum (no 5) is introduced sothat elevation of the mucoperichondrium is doneunder constant visual controlndash The next step is to dissect the mucoperiostium
Nasal DeformityDissecting over the bony-cartilaginous junctionwhen joining both tunnels might be difficult and is
especially prone to membrane perforationndash If needed the same tunnels are to be created on the
other side of the septum Then deviated parts of
septum are identified and removed either with a
knife or a Freer chisel
Nasal Deformitybull septum from the maxillary crest the septum mustbull be separated from the perpendicular plate trimmedbull along the inferior border placed back onto the crestbull and sutured to the periosteum If the deformity involvesbull the vomer an osteotome is used Care mustbull be taken not to break the cribriform plate becausebull it could cause a cerebrospinal fistula
Nasal Deformity
bull Once the septal deviation is corrected the flapsbull and hemitransfixion incision are mattressed
withbull absorbable sutures Nasal packing to prevent
synechiaebull and postoperative septal haematoma mightbull be advised but should be removed within 72 h

The Nose and Sinuses
Structure The structure of the nose is made up of
four partsbull The surface anatomybull The nasal skeletonmdashcomposed of the
two nasal bones the paired upper lateral and lower lateral cartilages and the nasal septum covered in subcutaneous tissue and skin
bull The internal anatomymdashincludes the septum of the nose which forms the medial wall of the nasal cavity The turbinates on the lateral wall are also called conchae
bull The osteomeatal complexmdasha key functional area of the nose
Function The nose is the main route for inspired
air and its structure is related to this function As the air passes over the large surface area of the turbinates
The inspired gases are warmed and humidified Mucus on the mucosa of the nose removes large dust particles from the air as it is breathed in
The voice resonates in the sinuses and nose and this provides character to the speech
Pneumatization of the sinusesmdashthey are air filled spacesmdashreduces the weight of the skull
Diseases of thDiseases of the Outer and Inner Nosee Outer and
Inner Nose Erysipelas Definition of the disease ndash Erysipela is a skin infection that affects the superficial dermis and is caused by Streptococcus pyogenes (group A) It usually develops in the extremities and the face and less commonly on the scalp and genitals bull Epidemiologyaetiology ndash Erysipelas are more often seen in elderly infants and children patients with compromised immunology and diabetes -Predisposing factors are alcoholism skin ulceration puncture wounds fungal infections malnutrition and burns
Erysipelas
bull Symptomsbull ndash It usually presents of fever general fatigue bull -The skin lesion is a redindurated and elevated plaque
with borders that expand rapidly bull It is painful warm and accompanied by variable oedemabull -On the second or third day a flaccid bulla may develop
and desquamationbull bull Presence of regional lymph nodes is common
Erysipelas
bull Complicationsndash The most common complication is recurrencewhich is seen in 18ndash30 of the cases even afterproper antibiotic therapy Recurrence is seen moreoften in females than in malesA skin infection with S pyogenes could lead toglomerulonephritis
Erysipelas
bull Complicationsbull ndash The most common complication is recurrencebull which is seen in 18ndash30 of the cases even afterbull proper antibiotic therapy bull -Recurrence is seen morebull often in females than in males bull -A skin infection with S pyogenes could lead tobull glomerulonephritis
Erysipelas
bull bull Diagnosisbull ndash Diagnosis is based on the patientrsquos personal
historybull and physical examination particularly on inspectionbull of the skin
bull Blood cultures are positive in less thanbull 5 of cases
ErysipelasTherapyndash Conservative therapybull The preferred antibiotic is penicillin In mildcases with minor systemic symptoms penicillinV 500 mg orally every 6 h for 10 days or penicillinG benzathine 12 mil U intramuscularlyonceOther possibilities are amoxicillin 500 mgorally twice a day for 10 days or cephalexin 500mg orally every 6 h for 10 days
ErysipelasIn moderate and severe cases with significantsystemic symptoms hospitalization and intravenoustreatment is required penicillin G 2ndash4mil U intravenously every 4ndash6 h Cefazolin05ndash15 gm intravenously every 8 h cefotaxime1ndash2 gm intravenously every 8 h or ceftriaxone1ndash2 gm intravenously once a day should be administeredIn patients with a penicillin allergyclindamycin 600 mg intravenously every 8 h orvancomycin 15 mgkg intravenously twice a daymay be given
ErysipelaAdditional useful therapeutic optionsbull Prednisone 30 mg over 8 days might be consideredas well as elevation of the affected siteMoist heat compresses may be usefulbull Surgeryndash Debridement and drainage are indicated when bullaeabscesses or necroses are presentbull Differential diagnosisndash Contact dermatitisndash Asteatotic eczemandash Herpes zosterndash Angioneurotic oedemandash Osteomyelitis
Furuncle
bull Definition of the diseasebull ndash A furuncle is an infection that beginsbull at the hair follicle and spreads deeper into thebull dermis and subcutaneous tissue forming abull nodule After several days it developsbull into an abscess - red painful and fluctuantbull bull bull Epidemiologyaetiologybull ndash The aetiologic agent is Staphylococcus aureus
FuruncleSymptomsndashsymptoms are local and limited to thesite of infection Furuncles usually are wherehair follicles are present bull Complicationndash One complication is furunculosis multiple draining furunclesDiagnosisndash The diagnosis is based on clinical inspection - Cultures are not necessary when there is no systemic involvement but should beconsidered if systemic therapy (in case of feversignificant cellulitis or hospitalization) or whenmethicillin-resistant Staphylococcusaureus (MRSA) is considered
FuruncleTherapyndash When the furuncle is small application of moist heat compress to promote drainage -Larger furuncles should be drained by surgical incision-After drainage the area should be cleaned with anantiseptic (with chlorhexidinebetadine) should be applied twice
a dayndash If no systemic symptoms or extensive cellulitis arepresent simple topical care is usually curative andoral antibiotics are not necessary Otherwise systemictreatment is indicated and should cover anypossible MRSA
Furuncle
bull -Recommended antibiotics are trimethoprim-sulfamethoxazole
bull 1ndash2 tablets orally twice daily doxycyclinebull 100 mg orally twice dailybull or clindamycin 300ndash450 mg orally every 8 hbull - In severe cases vancomycin 15 mgkg
intravenouslybull every 12 h or clindamycin 600 mg intravenouslybull every 8 h
Midline Granulomabull A midline granuloma is an angiocentricbull lymphoma it was referred to as polymorphicbull reticulosis lethal midline granuloma and midline
malignant reticulosisbull bull Definition of the diseasebull ndash This rare disease is a lymphoma of extranodal
presentationall cases are positive for the Epstein-Barr virus
bull -This lymphoma most commonly appears in the midface region
Midline GranulomaEpidemiologyaetiologyndash This form of lymphoma is rare in Europe and theUnited States with a higher prevalence in Asia and PeruSymptomsndash The most common presentation is nasal obstruction with a destructive mass occupying the nosesinuses and palate
-Fever night sweatsand weight loss seen usually in Hodgkinrsquos lymphomaand other non-Hodgkinrsquos lymphomas (knownas ldquoB symptomsrdquo) are uncommon
Midline GranulomaDiagnosisndash The diagnosis is based on anatomopathologicalstudy The malignancy of the tumour manifested byextensive necrosis makes the histological diagnosisdifficult and often more biopsies are required forconfirmationbull Therapyndash Therapy consists of radiotherapy with or withoutchemotherapy
Midline Granuloma
bull Prognosisbull ndash Depending on the stage long-term remission or
experience a worseningbull prognosis with relapses which may include otherbull extranodal sites bull Involvement of extranodal sitesbull including the upper airway gastrointestinal tractbull skin
Wegenerrsquos Granulomatosis
bull Definition of the diseasebull ndash Wegenerrsquos granulomatosis is a systemic chronicbull vasculitis of small- and medium-sized blood vesselsbull with an autoimmune component It affectsbull particular organs with variable predilectionbull Epidemiologyaetiologybull ndash Wegenerrsquos granulomatosis is a rare disease It affects
about 1 in 20000ndash30000 people It is more prevalentbull in middle-aged Caucasian patients
Wegenerrsquos Granulomatosis
Symptomsndash The disease may present pulmonary upper
respiratory tract or renal In the disseminated form-The localised form ndash confinedto the upper respiratory region ndash is present in 25of the patients- It consists of nonspecific manifestationssuch as nasal obstruction crusting purulentor bloody rhinorrhea and painful or painless ulcers in oral or nasal cavities which are unresponsive tostandard medical treatment
Wegenerrsquos Granulomatosis
bull In some patients the nasal septum is perforatedbull which leads to saddle-nose deformity Less
commonbull symptoms are hoarseness stridor due to
subglotticbull stenosis otalgia otorrhea and conductivebull and sensorineural hearing loss Also ocular
symptomsbull such as scleritis conjunctivitis uveitis andbull episcleritis may be present
Wegenerrsquos Granulomatosis
bull ndash In the disseminated form pulmonary involvementbull is manifested by cough dyspnoea haemoptysisbull (due to an alveolar capillaritis necrotic lesions orbull endobronchial disease) and pleuritic painndashbull -Ninety per cent of patients have nasal symptomsbull and these symptoms are usually the first
manifestationof the diseasebull -Most patients have also renal involvementbull even if it is subclinical
Wegenerrsquos Granulomatosis
Diagnosis ndash Diagnosis of Wegenerrsquos granulomatosis is based on clinical findings that demonstrate lung (chest x-ray) kidney (urine analysis) or upper respiratory tract
involvement (oral or nasal ulcers or discharge) - positive blood analysis for cytoplasmic-staining antineutrophil
cytoplasmic antibodies (c-ANCA) and confirming proteinase 3 (PR3) ANCA or myeloperoxidase (MPO) ANCA ndash Biopsy is essential for diagnosis nonspecific chronic inflammation
and necrosis -Bacterial and fungal infections
Wegenerrsquos Granulomatosis
Therapyndash Conservative therapybull In the induction of disease remission highdosesteroids (e g prednisone 1 mgkgday) for1 month with tapering over several months aregiven In addition cyclophosphamide (2 mgkgday) should be administered for 6ndash12 monthsuntil symptoms disappear In the maintenanceof remission cyclophosphamide should be
Wegenerrsquos Granulomatosis
Antibiotics mainly trimethoprim-sulfamethoxazoleare given for prophylaxis againstPneumocystis jiroveci (formerly Pneumocystiscarinii) pneumonia (PCP) which may developduring immunosuppression and have a role inpreventing recurrencesbull Sinonasal manifestations may be treated with topical nasal steroids and nasal irrigations lowdosesystemic steroids and antibiotics when bacterial infection (typically Staphylococcus species) is suspected
Wegenerrsquos Granulomatosis
bull Prognosisbull ndash Most of the patients respond well to treatmentbull achieving symptom-free intervals of 5ndash20 yearsbull or more bull -Anatomical problems (sinusitis trachealbull stenosis) may require surgery bull Relapses can be long and troublesomebull Long-term complications are chronicbull renal failure hearing loss and deafness
Nasal Fractures Definition ndash A nasal fracture is a disruption of the nasal bone structure due to trauma It is the most frequently fractured facial bone Epidemiologyaetiology ndash Sports falls and assaults are the usual mechanisms of fracture -Males are affected twice as often as are females -Paediatric populations with a incidences during the second and third decades of life -Variables such as force impact direction nature of the striking object age and other will influence the pattern of injury to the components of the nose
Nasal Fractures
bull Symptomsbull ndash Deformity swelling epistaxis and periorbital
ecchymosis are signs that are suggestive of nasal fracture
bull bony crepitus and nasal segment mobilitybull ndash Epiphora bull Severe bilateral injuries to the lachrymal bones
arebull associated with depressed nasal fractures
Nasal Fractures Complications ndash Septal haematoma is one of the most severe early complications of nasal trauma and without drainage it results in abscess formation 6ndash7 days after trauma producing necrosis of the septal cartilage -Long-term problems such as saddle-nose deformity perforation columellar retraction and nasalbase
Septal infection could lead to osteomyelitis orbital and intracranial abscesses meningitis and cavernous sinus thrombosis -Cerebrospinal fluid leakage is a common complication of severe
nasal and frontal fractures
Nasal Fractures
bull Diagnostic proceduresbull ndash Inspectionbull bull Changes of appearance such as deviation andbull asymmetry bleeding watery drainage changesbull in nasal breathing and smell It is useful to comparebull the current presentation with old photographsbull (up to 40 of normal individuals havebull significant nose malformations)
Nasal Fractures Physical examination bull The diagnosis of a nasal fracture is made primarily by physical examination epistaxis nasal swelling and periorbital ecchymosis Nasal shape in the lateral and frontal inspection should be assessed Grasping the dorsum between two fingers and rocking the pyramid back and forth aids in assessing the mobility of nasal bones Internal structures should be evaluated by using a headlight and nasal speculum Clotted blood is removed by suction and assessment of haematoma mucosal tears and active bleeding is performed Bimanual palpation of the septum helps to differentiate septal swelling from haematoma ndash
Nasal FracturesRadiographybull There is no clear evidence of the role of radiographyin the management of nasal fracturesPlain films have up to a 66 false-positive rateas a result of misinterpretation of normal suturelines In addition old fractures are difficult todistinguishbull Three-dimensional CT is recommended for extensiveinjuries involving the nasal-orbital-ethmoidalcomplexndash
Nasal Fractures
bull Additionaluseful diagnostic proceduresbull bull Using a 0 or 30deg 4-mm endoscope is helpful inbull the assessment of posterior abnormalities If thebull patient is heavily sedated Brown-Gruss
provocationbull manoeuvres may be performed to determinebull deformities in upper middle or lower segmentsbull by compressing each compartment
Nasal FracturesConservative treatmentndash Treatment of bleedingbull For localised bleeding anterior sources may becauterised by silver nitrate or sealed with topicalmaterials such as thrombin combined withgelatin foam fibrin glue FloSealreg or other procoagulantmaterials If conservative measuresfail a formal anterior packing is placedbull Bleeding from branches of sphenopalatine orethmoid vessels requires anterior-posteriorpacking
Nasal Fractures
bull bull Surgical methods such as direct endoscopic vessel
bull cauterization or ligation have been shown tobull offer better haemostasis and patient comfortbull Angiography with embolization can also be
consideredbull in cases refractory to more conservativebull approaches
Nasal Fractures
bull Type of reductionbull bull Nondisplaced fractures should be treated withbull observation alone Closed nasal reduction is thebull best choice for simple injuries (isolated unilateralbull with medial displacement)bull bull An open approach should be considered in
severebull trauma (bilateral depressed fractures)
Nasal Fracturesbull Surgical principlesbull ndash Topical anaesthesia with cotton pledgets soakedbull with 4 cocaine or 005 oxymethazoline combinedbull with 4 topical lidocaine should be appliedbull for 5ndash10 min Local anaesthesia should also be injectedbull (1 lidocaine and 1100000 epinephrine)bull along the septum lateral walls and floor of the nasalbull cavitybull bull
Nasal FracturesClosed reductionndashndash The nasal bones are grasped between two fingersand pressure is applied laterally in theopposite direction of the deviation A bluntelevator may be used from within the nose incases of significant medial collapse Walshamforceps can be of help Reduction of the septumshould be performed with the use ofAsch forceps
Nasal Fractures
bull To prevent collapse of the postreductionbull framework nasal packing should be placedbull for 3ndash5 days Septum splints are recommendedbull in comminuted septal fractures withbull severe mucosal lesions External nasal splintingbull for 10 days (Aquaplastreg Thermoplastreg)bull provides nasal protection Nasal saline spraysbull prevent crusting and oral antibiotics should
Nasal Fractures
bull Open reductionbull ndashndash Immediate repair of fractures by using
widebull surgical exposure reduction fixation and
reconstructionbull ndashndash The second option is delayed correctionbull (6 months or more) of persistent deformitiesbull using standard techniques of rhinoplasty
Deviated Nasal Septum
bull Definition of the diseasebull ndash Deviation of the nasal septum is a common causebull of unilateral nasal airway obstruction in which thebull nasal septum is displacedbull bull Epidemiologyaetiologybull ndash Developmental septal abnormalities Septal cartilage
damage in the neonatal period andbull during birth can cause severe septal deviation inbull the absence of a history of nasal trauma
Deviated Nasal Septum
bull Symptomsbull ndash Patients may present with a history of sinusitis
allergicbull rhinitis obstructive sleep apnoea previousbull nasal surgery or recent nasal trauma Unilateral or
bilateral nasal airway obstruction that is unrelievedbull with decongestants or nasal steroid sprays is oftenbull seenbull bull
Deviated Nasal SeptumDiagnosisndashExamination external dorsal deviation or the columella and caudal septummay be deflected off the midline (caudal subluxation)ndash Inspections of the nasal cavity and anterior-posteriorrhinoscopy are helpful in diagnosing the locationtype and severity of septal deformityThe endoscope is also useful in identifying polypsthe severity and extent of posterior septaldeviations and bony spurs and locating areas ofseptal perforation or mucosal injury
Deviated Nasal Septum
bull Therapybull ndash Septoplasty is a procedurebull The areabull of deviation is corrected or resected in order tobull leave behind as much cartilage and bone as
possiblebull Cartilage resection is minimised and can be
repositioned reshaped or recontoured using a variety of methods
Deviated Nasal Septum
bull ndash Indications of septoplasty before the growth period
bull of the nose is finished should be very limited bull -In these cases surgery must preserve all the
cartilagebull in order to prevent external changes of the
shape ofbull the nose
Deviated Nasal Septum
bull Complicationsbull ndash Frequent complications include haematoma andbull infection Cerebrospinal fluid leak is a rare but
potentiallybull serious complicationbull It is usually the resultbull of avulsion or damage to the cribriform plate whenbull handling the perpendicular plate of the ethmoidbull ndash Other complications include epistaxis nasal
Deviated Nasal Septum
bull Other complications include epistaxis nasal obstruction
bull due to residual deviation synechiae returnbull of the cartilaginous deviation septal perforationbull anosmia and cosmetic nasal deformities suchbull as widened alar rim margins drooping nasal tipbull columella retraction and a sunken dorsum with abull supratip saddle formation
Septal perforation with minor crusting View from provide closure of the
incision
Septal Haematoma
bull A septal haematoma is a blood collection under the perichondrium
bull of the septum and cartilagebull bull bull Epidemiologyaetiologybull ndash A septal haematoma is one of the most
severe complications of nasal trauma
Septal Haematoma
bull Diagnosisbull ndash Signs and symptoms include intense pain
swellingbull haematoma of the upper lip and philtrum
area andbull complete nasal airway obstruction
Septal HaematomaTherapyndash Management consists of drainage through a mucoperichondrial incision Immediate treatment isnecessary to prevent long-term problems such asa saddle-nose deformity perforation columellarretraction and nasal-base widening In childrenseptal destruction can lead to devastating nasal andmidfacial growth abnormalitiesbull Surgeryndash Incision and evacuation of the collection is performedDrainage of a septal haematoma should
Septal HaematomaSurgeryndash Incision and evacuation of the collection is performedDrainage of a septal haematoma should provide closure of the incision
Splints or transseptal sutures are placed to obliterate thepotential space and prevent collectionInfection involving the septal cartilage Reconstruction with autologouscartilage is then performed in a second stage Oral antibiotics should be given
Nasal DeformitySaddle-nose deformityndash A saddle-nose deformity is characterised by a loss ofnasal dorsal height and compromised nasal supportstructures -Other case observed are depressionof the middle vault and dorsum loss of nasal tipsupport and definition shortened (vertical) nasal length over rotation of the nasal tip and retrusion ofthe nasal spine and caudal septum It is also knownas a ldquoPug noserdquo or ldquoboxerrsquos noserdquo both of which referto various degrees of nasal dorsal depressionbull
Nasal DeformityEpidemiologyaetiologyndash Prevalence is higher in population groups prone to facial trauma (ie boxers athletes) those with historiesof intranasal cocaine use nasal surgery (e g radical submucosal septal resection reductive rhinoplasty)ndash A saddle-nose deformity can be congenital or acquired It can be noticed as a part of individual familialsyndromic and ethnic characteristics - Most deformities are due to traumatic and iatrogeniccauses Medical causes are Wegenerrsquosgranulomatosis relapsing polychondritis leprosy (Hansenrsquos disease) syphilis ectodermal dysplasiaand intranasal cocaine use
Nasal Deformity
bull Therapybull ndash Nasal reconstruction indications depend on patientbull selection surgeon experience and aetiology of thebull deformity bull Indications for surgery can be functionalbull aesthetic or most commonly both In individuals
with a compromised nasal airway a nasoseptalbull reconstruction is indicated
Nasal Deformity
bull Contraindications bull include patients with malignantbull chronic or autoimmune disease conditions drugbull abuse poor perioperative risk profile and unrealisticbull expectationsbull ndash Multiple previous rhinoplasties and certain
professionsbull (mixed martial artists boxers and other contactbull sports) are relative contraindications
Nasal DeformitySeptoplastyndash Septoplasty is performed to correct nasal obstructioncaused by septal deformityndash Usually septoplasty is performed under general anaesthesiawith the patient in the supine position with the head elevated by approximately 30 (Righthandedsurgeons approach from the right side)ndash Local vasoconstrictive anaesthesia is applied notonly to reduce postoperative pain but also more importantly to achieve vasoconstriction of themucosa and less intraoperative haemorrhage Lidocainewith adrenaline or epinephrine is usedalthough in patients with cardiac hypersensitivityoxymetazoline might be preferred
Nasal Deformity
bull Septoplasty begins with the incision of septal mucosabull Most operative techniques utilise a hemitransfixionbull incision at the caudal end of septum so thatbull deviation at this point might be reached as wellbull as a transfixion incision that is easily obtained ifbull needed (Right-handed surgeons normally choosebull the left side but that may vary when deviation isbull convex towards the right)
Nasal DeformityA columella retractor is placed over the columellaand by pulling it laterally the caudal border of theseptum is exposed Ala can be protected by an alaprotector A vertical incision with a no 15 bladeover the caudal end of septum is performed untilreaching the plane of the septal cartilage It is essentialto correctly identify the perichondrium and byusing the Cottle elevator dissect and lift it creatinga flap As the dissection proceeds along the septalcartilage a longer speculum (no 5) is introduced sothat elevation of the mucoperichondrium is doneunder constant visual controlndash The next step is to dissect the mucoperiostium
Nasal DeformityDissecting over the bony-cartilaginous junctionwhen joining both tunnels might be difficult and is
especially prone to membrane perforationndash If needed the same tunnels are to be created on the
other side of the septum Then deviated parts of
septum are identified and removed either with a
knife or a Freer chisel
Nasal Deformitybull septum from the maxillary crest the septum mustbull be separated from the perpendicular plate trimmedbull along the inferior border placed back onto the crestbull and sutured to the periosteum If the deformity involvesbull the vomer an osteotome is used Care mustbull be taken not to break the cribriform plate becausebull it could cause a cerebrospinal fistula
Nasal Deformity
bull Once the septal deviation is corrected the flapsbull and hemitransfixion incision are mattressed
withbull absorbable sutures Nasal packing to prevent
synechiaebull and postoperative septal haematoma mightbull be advised but should be removed within 72 h

Diseases of thDiseases of the Outer and Inner Nosee Outer and
Inner Nose Erysipelas Definition of the disease ndash Erysipela is a skin infection that affects the superficial dermis and is caused by Streptococcus pyogenes (group A) It usually develops in the extremities and the face and less commonly on the scalp and genitals bull Epidemiologyaetiology ndash Erysipelas are more often seen in elderly infants and children patients with compromised immunology and diabetes -Predisposing factors are alcoholism skin ulceration puncture wounds fungal infections malnutrition and burns
Erysipelas
bull Symptomsbull ndash It usually presents of fever general fatigue bull -The skin lesion is a redindurated and elevated plaque
with borders that expand rapidly bull It is painful warm and accompanied by variable oedemabull -On the second or third day a flaccid bulla may develop
and desquamationbull bull Presence of regional lymph nodes is common
Erysipelas
bull Complicationsndash The most common complication is recurrencewhich is seen in 18ndash30 of the cases even afterproper antibiotic therapy Recurrence is seen moreoften in females than in malesA skin infection with S pyogenes could lead toglomerulonephritis
Erysipelas
bull Complicationsbull ndash The most common complication is recurrencebull which is seen in 18ndash30 of the cases even afterbull proper antibiotic therapy bull -Recurrence is seen morebull often in females than in males bull -A skin infection with S pyogenes could lead tobull glomerulonephritis
Erysipelas
bull bull Diagnosisbull ndash Diagnosis is based on the patientrsquos personal
historybull and physical examination particularly on inspectionbull of the skin
bull Blood cultures are positive in less thanbull 5 of cases
ErysipelasTherapyndash Conservative therapybull The preferred antibiotic is penicillin In mildcases with minor systemic symptoms penicillinV 500 mg orally every 6 h for 10 days or penicillinG benzathine 12 mil U intramuscularlyonceOther possibilities are amoxicillin 500 mgorally twice a day for 10 days or cephalexin 500mg orally every 6 h for 10 days
ErysipelasIn moderate and severe cases with significantsystemic symptoms hospitalization and intravenoustreatment is required penicillin G 2ndash4mil U intravenously every 4ndash6 h Cefazolin05ndash15 gm intravenously every 8 h cefotaxime1ndash2 gm intravenously every 8 h or ceftriaxone1ndash2 gm intravenously once a day should be administeredIn patients with a penicillin allergyclindamycin 600 mg intravenously every 8 h orvancomycin 15 mgkg intravenously twice a daymay be given
ErysipelaAdditional useful therapeutic optionsbull Prednisone 30 mg over 8 days might be consideredas well as elevation of the affected siteMoist heat compresses may be usefulbull Surgeryndash Debridement and drainage are indicated when bullaeabscesses or necroses are presentbull Differential diagnosisndash Contact dermatitisndash Asteatotic eczemandash Herpes zosterndash Angioneurotic oedemandash Osteomyelitis
Furuncle
bull Definition of the diseasebull ndash A furuncle is an infection that beginsbull at the hair follicle and spreads deeper into thebull dermis and subcutaneous tissue forming abull nodule After several days it developsbull into an abscess - red painful and fluctuantbull bull bull Epidemiologyaetiologybull ndash The aetiologic agent is Staphylococcus aureus
FuruncleSymptomsndashsymptoms are local and limited to thesite of infection Furuncles usually are wherehair follicles are present bull Complicationndash One complication is furunculosis multiple draining furunclesDiagnosisndash The diagnosis is based on clinical inspection - Cultures are not necessary when there is no systemic involvement but should beconsidered if systemic therapy (in case of feversignificant cellulitis or hospitalization) or whenmethicillin-resistant Staphylococcusaureus (MRSA) is considered
FuruncleTherapyndash When the furuncle is small application of moist heat compress to promote drainage -Larger furuncles should be drained by surgical incision-After drainage the area should be cleaned with anantiseptic (with chlorhexidinebetadine) should be applied twice
a dayndash If no systemic symptoms or extensive cellulitis arepresent simple topical care is usually curative andoral antibiotics are not necessary Otherwise systemictreatment is indicated and should cover anypossible MRSA
Furuncle
bull -Recommended antibiotics are trimethoprim-sulfamethoxazole
bull 1ndash2 tablets orally twice daily doxycyclinebull 100 mg orally twice dailybull or clindamycin 300ndash450 mg orally every 8 hbull - In severe cases vancomycin 15 mgkg
intravenouslybull every 12 h or clindamycin 600 mg intravenouslybull every 8 h
Midline Granulomabull A midline granuloma is an angiocentricbull lymphoma it was referred to as polymorphicbull reticulosis lethal midline granuloma and midline
malignant reticulosisbull bull Definition of the diseasebull ndash This rare disease is a lymphoma of extranodal
presentationall cases are positive for the Epstein-Barr virus
bull -This lymphoma most commonly appears in the midface region
Midline GranulomaEpidemiologyaetiologyndash This form of lymphoma is rare in Europe and theUnited States with a higher prevalence in Asia and PeruSymptomsndash The most common presentation is nasal obstruction with a destructive mass occupying the nosesinuses and palate
-Fever night sweatsand weight loss seen usually in Hodgkinrsquos lymphomaand other non-Hodgkinrsquos lymphomas (knownas ldquoB symptomsrdquo) are uncommon
Midline GranulomaDiagnosisndash The diagnosis is based on anatomopathologicalstudy The malignancy of the tumour manifested byextensive necrosis makes the histological diagnosisdifficult and often more biopsies are required forconfirmationbull Therapyndash Therapy consists of radiotherapy with or withoutchemotherapy
Midline Granuloma
bull Prognosisbull ndash Depending on the stage long-term remission or
experience a worseningbull prognosis with relapses which may include otherbull extranodal sites bull Involvement of extranodal sitesbull including the upper airway gastrointestinal tractbull skin
Wegenerrsquos Granulomatosis
bull Definition of the diseasebull ndash Wegenerrsquos granulomatosis is a systemic chronicbull vasculitis of small- and medium-sized blood vesselsbull with an autoimmune component It affectsbull particular organs with variable predilectionbull Epidemiologyaetiologybull ndash Wegenerrsquos granulomatosis is a rare disease It affects
about 1 in 20000ndash30000 people It is more prevalentbull in middle-aged Caucasian patients
Wegenerrsquos Granulomatosis
Symptomsndash The disease may present pulmonary upper
respiratory tract or renal In the disseminated form-The localised form ndash confinedto the upper respiratory region ndash is present in 25of the patients- It consists of nonspecific manifestationssuch as nasal obstruction crusting purulentor bloody rhinorrhea and painful or painless ulcers in oral or nasal cavities which are unresponsive tostandard medical treatment
Wegenerrsquos Granulomatosis
bull In some patients the nasal septum is perforatedbull which leads to saddle-nose deformity Less
commonbull symptoms are hoarseness stridor due to
subglotticbull stenosis otalgia otorrhea and conductivebull and sensorineural hearing loss Also ocular
symptomsbull such as scleritis conjunctivitis uveitis andbull episcleritis may be present
Wegenerrsquos Granulomatosis
bull ndash In the disseminated form pulmonary involvementbull is manifested by cough dyspnoea haemoptysisbull (due to an alveolar capillaritis necrotic lesions orbull endobronchial disease) and pleuritic painndashbull -Ninety per cent of patients have nasal symptomsbull and these symptoms are usually the first
manifestationof the diseasebull -Most patients have also renal involvementbull even if it is subclinical
Wegenerrsquos Granulomatosis
Diagnosis ndash Diagnosis of Wegenerrsquos granulomatosis is based on clinical findings that demonstrate lung (chest x-ray) kidney (urine analysis) or upper respiratory tract
involvement (oral or nasal ulcers or discharge) - positive blood analysis for cytoplasmic-staining antineutrophil
cytoplasmic antibodies (c-ANCA) and confirming proteinase 3 (PR3) ANCA or myeloperoxidase (MPO) ANCA ndash Biopsy is essential for diagnosis nonspecific chronic inflammation
and necrosis -Bacterial and fungal infections
Wegenerrsquos Granulomatosis
Therapyndash Conservative therapybull In the induction of disease remission highdosesteroids (e g prednisone 1 mgkgday) for1 month with tapering over several months aregiven In addition cyclophosphamide (2 mgkgday) should be administered for 6ndash12 monthsuntil symptoms disappear In the maintenanceof remission cyclophosphamide should be
Wegenerrsquos Granulomatosis
Antibiotics mainly trimethoprim-sulfamethoxazoleare given for prophylaxis againstPneumocystis jiroveci (formerly Pneumocystiscarinii) pneumonia (PCP) which may developduring immunosuppression and have a role inpreventing recurrencesbull Sinonasal manifestations may be treated with topical nasal steroids and nasal irrigations lowdosesystemic steroids and antibiotics when bacterial infection (typically Staphylococcus species) is suspected
Wegenerrsquos Granulomatosis
bull Prognosisbull ndash Most of the patients respond well to treatmentbull achieving symptom-free intervals of 5ndash20 yearsbull or more bull -Anatomical problems (sinusitis trachealbull stenosis) may require surgery bull Relapses can be long and troublesomebull Long-term complications are chronicbull renal failure hearing loss and deafness
Nasal Fractures Definition ndash A nasal fracture is a disruption of the nasal bone structure due to trauma It is the most frequently fractured facial bone Epidemiologyaetiology ndash Sports falls and assaults are the usual mechanisms of fracture -Males are affected twice as often as are females -Paediatric populations with a incidences during the second and third decades of life -Variables such as force impact direction nature of the striking object age and other will influence the pattern of injury to the components of the nose
Nasal Fractures
bull Symptomsbull ndash Deformity swelling epistaxis and periorbital
ecchymosis are signs that are suggestive of nasal fracture
bull bony crepitus and nasal segment mobilitybull ndash Epiphora bull Severe bilateral injuries to the lachrymal bones
arebull associated with depressed nasal fractures
Nasal Fractures Complications ndash Septal haematoma is one of the most severe early complications of nasal trauma and without drainage it results in abscess formation 6ndash7 days after trauma producing necrosis of the septal cartilage -Long-term problems such as saddle-nose deformity perforation columellar retraction and nasalbase
Septal infection could lead to osteomyelitis orbital and intracranial abscesses meningitis and cavernous sinus thrombosis -Cerebrospinal fluid leakage is a common complication of severe
nasal and frontal fractures
Nasal Fractures
bull Diagnostic proceduresbull ndash Inspectionbull bull Changes of appearance such as deviation andbull asymmetry bleeding watery drainage changesbull in nasal breathing and smell It is useful to comparebull the current presentation with old photographsbull (up to 40 of normal individuals havebull significant nose malformations)
Nasal Fractures Physical examination bull The diagnosis of a nasal fracture is made primarily by physical examination epistaxis nasal swelling and periorbital ecchymosis Nasal shape in the lateral and frontal inspection should be assessed Grasping the dorsum between two fingers and rocking the pyramid back and forth aids in assessing the mobility of nasal bones Internal structures should be evaluated by using a headlight and nasal speculum Clotted blood is removed by suction and assessment of haematoma mucosal tears and active bleeding is performed Bimanual palpation of the septum helps to differentiate septal swelling from haematoma ndash
Nasal FracturesRadiographybull There is no clear evidence of the role of radiographyin the management of nasal fracturesPlain films have up to a 66 false-positive rateas a result of misinterpretation of normal suturelines In addition old fractures are difficult todistinguishbull Three-dimensional CT is recommended for extensiveinjuries involving the nasal-orbital-ethmoidalcomplexndash
Nasal Fractures
bull Additionaluseful diagnostic proceduresbull bull Using a 0 or 30deg 4-mm endoscope is helpful inbull the assessment of posterior abnormalities If thebull patient is heavily sedated Brown-Gruss
provocationbull manoeuvres may be performed to determinebull deformities in upper middle or lower segmentsbull by compressing each compartment
Nasal FracturesConservative treatmentndash Treatment of bleedingbull For localised bleeding anterior sources may becauterised by silver nitrate or sealed with topicalmaterials such as thrombin combined withgelatin foam fibrin glue FloSealreg or other procoagulantmaterials If conservative measuresfail a formal anterior packing is placedbull Bleeding from branches of sphenopalatine orethmoid vessels requires anterior-posteriorpacking
Nasal Fractures
bull bull Surgical methods such as direct endoscopic vessel
bull cauterization or ligation have been shown tobull offer better haemostasis and patient comfortbull Angiography with embolization can also be
consideredbull in cases refractory to more conservativebull approaches
Nasal Fractures
bull Type of reductionbull bull Nondisplaced fractures should be treated withbull observation alone Closed nasal reduction is thebull best choice for simple injuries (isolated unilateralbull with medial displacement)bull bull An open approach should be considered in
severebull trauma (bilateral depressed fractures)
Nasal Fracturesbull Surgical principlesbull ndash Topical anaesthesia with cotton pledgets soakedbull with 4 cocaine or 005 oxymethazoline combinedbull with 4 topical lidocaine should be appliedbull for 5ndash10 min Local anaesthesia should also be injectedbull (1 lidocaine and 1100000 epinephrine)bull along the septum lateral walls and floor of the nasalbull cavitybull bull
Nasal FracturesClosed reductionndashndash The nasal bones are grasped between two fingersand pressure is applied laterally in theopposite direction of the deviation A bluntelevator may be used from within the nose incases of significant medial collapse Walshamforceps can be of help Reduction of the septumshould be performed with the use ofAsch forceps
Nasal Fractures
bull To prevent collapse of the postreductionbull framework nasal packing should be placedbull for 3ndash5 days Septum splints are recommendedbull in comminuted septal fractures withbull severe mucosal lesions External nasal splintingbull for 10 days (Aquaplastreg Thermoplastreg)bull provides nasal protection Nasal saline spraysbull prevent crusting and oral antibiotics should
Nasal Fractures
bull Open reductionbull ndashndash Immediate repair of fractures by using
widebull surgical exposure reduction fixation and
reconstructionbull ndashndash The second option is delayed correctionbull (6 months or more) of persistent deformitiesbull using standard techniques of rhinoplasty
Deviated Nasal Septum
bull Definition of the diseasebull ndash Deviation of the nasal septum is a common causebull of unilateral nasal airway obstruction in which thebull nasal septum is displacedbull bull Epidemiologyaetiologybull ndash Developmental septal abnormalities Septal cartilage
damage in the neonatal period andbull during birth can cause severe septal deviation inbull the absence of a history of nasal trauma
Deviated Nasal Septum
bull Symptomsbull ndash Patients may present with a history of sinusitis
allergicbull rhinitis obstructive sleep apnoea previousbull nasal surgery or recent nasal trauma Unilateral or
bilateral nasal airway obstruction that is unrelievedbull with decongestants or nasal steroid sprays is oftenbull seenbull bull
Deviated Nasal SeptumDiagnosisndashExamination external dorsal deviation or the columella and caudal septummay be deflected off the midline (caudal subluxation)ndash Inspections of the nasal cavity and anterior-posteriorrhinoscopy are helpful in diagnosing the locationtype and severity of septal deformityThe endoscope is also useful in identifying polypsthe severity and extent of posterior septaldeviations and bony spurs and locating areas ofseptal perforation or mucosal injury
Deviated Nasal Septum
bull Therapybull ndash Septoplasty is a procedurebull The areabull of deviation is corrected or resected in order tobull leave behind as much cartilage and bone as
possiblebull Cartilage resection is minimised and can be
repositioned reshaped or recontoured using a variety of methods
Deviated Nasal Septum
bull ndash Indications of septoplasty before the growth period
bull of the nose is finished should be very limited bull -In these cases surgery must preserve all the
cartilagebull in order to prevent external changes of the
shape ofbull the nose
Deviated Nasal Septum
bull Complicationsbull ndash Frequent complications include haematoma andbull infection Cerebrospinal fluid leak is a rare but
potentiallybull serious complicationbull It is usually the resultbull of avulsion or damage to the cribriform plate whenbull handling the perpendicular plate of the ethmoidbull ndash Other complications include epistaxis nasal
Deviated Nasal Septum
bull Other complications include epistaxis nasal obstruction
bull due to residual deviation synechiae returnbull of the cartilaginous deviation septal perforationbull anosmia and cosmetic nasal deformities suchbull as widened alar rim margins drooping nasal tipbull columella retraction and a sunken dorsum with abull supratip saddle formation
Septal perforation with minor crusting View from provide closure of the
incision
Septal Haematoma
bull A septal haematoma is a blood collection under the perichondrium
bull of the septum and cartilagebull bull bull Epidemiologyaetiologybull ndash A septal haematoma is one of the most
severe complications of nasal trauma
Septal Haematoma
bull Diagnosisbull ndash Signs and symptoms include intense pain
swellingbull haematoma of the upper lip and philtrum
area andbull complete nasal airway obstruction
Septal HaematomaTherapyndash Management consists of drainage through a mucoperichondrial incision Immediate treatment isnecessary to prevent long-term problems such asa saddle-nose deformity perforation columellarretraction and nasal-base widening In childrenseptal destruction can lead to devastating nasal andmidfacial growth abnormalitiesbull Surgeryndash Incision and evacuation of the collection is performedDrainage of a septal haematoma should
Septal HaematomaSurgeryndash Incision and evacuation of the collection is performedDrainage of a septal haematoma should provide closure of the incision
Splints or transseptal sutures are placed to obliterate thepotential space and prevent collectionInfection involving the septal cartilage Reconstruction with autologouscartilage is then performed in a second stage Oral antibiotics should be given
Nasal DeformitySaddle-nose deformityndash A saddle-nose deformity is characterised by a loss ofnasal dorsal height and compromised nasal supportstructures -Other case observed are depressionof the middle vault and dorsum loss of nasal tipsupport and definition shortened (vertical) nasal length over rotation of the nasal tip and retrusion ofthe nasal spine and caudal septum It is also knownas a ldquoPug noserdquo or ldquoboxerrsquos noserdquo both of which referto various degrees of nasal dorsal depressionbull
Nasal DeformityEpidemiologyaetiologyndash Prevalence is higher in population groups prone to facial trauma (ie boxers athletes) those with historiesof intranasal cocaine use nasal surgery (e g radical submucosal septal resection reductive rhinoplasty)ndash A saddle-nose deformity can be congenital or acquired It can be noticed as a part of individual familialsyndromic and ethnic characteristics - Most deformities are due to traumatic and iatrogeniccauses Medical causes are Wegenerrsquosgranulomatosis relapsing polychondritis leprosy (Hansenrsquos disease) syphilis ectodermal dysplasiaand intranasal cocaine use
Nasal Deformity
bull Therapybull ndash Nasal reconstruction indications depend on patientbull selection surgeon experience and aetiology of thebull deformity bull Indications for surgery can be functionalbull aesthetic or most commonly both In individuals
with a compromised nasal airway a nasoseptalbull reconstruction is indicated
Nasal Deformity
bull Contraindications bull include patients with malignantbull chronic or autoimmune disease conditions drugbull abuse poor perioperative risk profile and unrealisticbull expectationsbull ndash Multiple previous rhinoplasties and certain
professionsbull (mixed martial artists boxers and other contactbull sports) are relative contraindications
Nasal DeformitySeptoplastyndash Septoplasty is performed to correct nasal obstructioncaused by septal deformityndash Usually septoplasty is performed under general anaesthesiawith the patient in the supine position with the head elevated by approximately 30 (Righthandedsurgeons approach from the right side)ndash Local vasoconstrictive anaesthesia is applied notonly to reduce postoperative pain but also more importantly to achieve vasoconstriction of themucosa and less intraoperative haemorrhage Lidocainewith adrenaline or epinephrine is usedalthough in patients with cardiac hypersensitivityoxymetazoline might be preferred
Nasal Deformity
bull Septoplasty begins with the incision of septal mucosabull Most operative techniques utilise a hemitransfixionbull incision at the caudal end of septum so thatbull deviation at this point might be reached as wellbull as a transfixion incision that is easily obtained ifbull needed (Right-handed surgeons normally choosebull the left side but that may vary when deviation isbull convex towards the right)
Nasal DeformityA columella retractor is placed over the columellaand by pulling it laterally the caudal border of theseptum is exposed Ala can be protected by an alaprotector A vertical incision with a no 15 bladeover the caudal end of septum is performed untilreaching the plane of the septal cartilage It is essentialto correctly identify the perichondrium and byusing the Cottle elevator dissect and lift it creatinga flap As the dissection proceeds along the septalcartilage a longer speculum (no 5) is introduced sothat elevation of the mucoperichondrium is doneunder constant visual controlndash The next step is to dissect the mucoperiostium
Nasal DeformityDissecting over the bony-cartilaginous junctionwhen joining both tunnels might be difficult and is
especially prone to membrane perforationndash If needed the same tunnels are to be created on the
other side of the septum Then deviated parts of
septum are identified and removed either with a
knife or a Freer chisel
Nasal Deformitybull septum from the maxillary crest the septum mustbull be separated from the perpendicular plate trimmedbull along the inferior border placed back onto the crestbull and sutured to the periosteum If the deformity involvesbull the vomer an osteotome is used Care mustbull be taken not to break the cribriform plate becausebull it could cause a cerebrospinal fistula
Nasal Deformity
bull Once the septal deviation is corrected the flapsbull and hemitransfixion incision are mattressed
withbull absorbable sutures Nasal packing to prevent
synechiaebull and postoperative septal haematoma mightbull be advised but should be removed within 72 h

Erysipelas
bull Symptomsbull ndash It usually presents of fever general fatigue bull -The skin lesion is a redindurated and elevated plaque
with borders that expand rapidly bull It is painful warm and accompanied by variable oedemabull -On the second or third day a flaccid bulla may develop
and desquamationbull bull Presence of regional lymph nodes is common
Erysipelas
bull Complicationsndash The most common complication is recurrencewhich is seen in 18ndash30 of the cases even afterproper antibiotic therapy Recurrence is seen moreoften in females than in malesA skin infection with S pyogenes could lead toglomerulonephritis
Erysipelas
bull Complicationsbull ndash The most common complication is recurrencebull which is seen in 18ndash30 of the cases even afterbull proper antibiotic therapy bull -Recurrence is seen morebull often in females than in males bull -A skin infection with S pyogenes could lead tobull glomerulonephritis
Erysipelas
bull bull Diagnosisbull ndash Diagnosis is based on the patientrsquos personal
historybull and physical examination particularly on inspectionbull of the skin
bull Blood cultures are positive in less thanbull 5 of cases
ErysipelasTherapyndash Conservative therapybull The preferred antibiotic is penicillin In mildcases with minor systemic symptoms penicillinV 500 mg orally every 6 h for 10 days or penicillinG benzathine 12 mil U intramuscularlyonceOther possibilities are amoxicillin 500 mgorally twice a day for 10 days or cephalexin 500mg orally every 6 h for 10 days
ErysipelasIn moderate and severe cases with significantsystemic symptoms hospitalization and intravenoustreatment is required penicillin G 2ndash4mil U intravenously every 4ndash6 h Cefazolin05ndash15 gm intravenously every 8 h cefotaxime1ndash2 gm intravenously every 8 h or ceftriaxone1ndash2 gm intravenously once a day should be administeredIn patients with a penicillin allergyclindamycin 600 mg intravenously every 8 h orvancomycin 15 mgkg intravenously twice a daymay be given
ErysipelaAdditional useful therapeutic optionsbull Prednisone 30 mg over 8 days might be consideredas well as elevation of the affected siteMoist heat compresses may be usefulbull Surgeryndash Debridement and drainage are indicated when bullaeabscesses or necroses are presentbull Differential diagnosisndash Contact dermatitisndash Asteatotic eczemandash Herpes zosterndash Angioneurotic oedemandash Osteomyelitis
Furuncle
bull Definition of the diseasebull ndash A furuncle is an infection that beginsbull at the hair follicle and spreads deeper into thebull dermis and subcutaneous tissue forming abull nodule After several days it developsbull into an abscess - red painful and fluctuantbull bull bull Epidemiologyaetiologybull ndash The aetiologic agent is Staphylococcus aureus
FuruncleSymptomsndashsymptoms are local and limited to thesite of infection Furuncles usually are wherehair follicles are present bull Complicationndash One complication is furunculosis multiple draining furunclesDiagnosisndash The diagnosis is based on clinical inspection - Cultures are not necessary when there is no systemic involvement but should beconsidered if systemic therapy (in case of feversignificant cellulitis or hospitalization) or whenmethicillin-resistant Staphylococcusaureus (MRSA) is considered
FuruncleTherapyndash When the furuncle is small application of moist heat compress to promote drainage -Larger furuncles should be drained by surgical incision-After drainage the area should be cleaned with anantiseptic (with chlorhexidinebetadine) should be applied twice
a dayndash If no systemic symptoms or extensive cellulitis arepresent simple topical care is usually curative andoral antibiotics are not necessary Otherwise systemictreatment is indicated and should cover anypossible MRSA
Furuncle
bull -Recommended antibiotics are trimethoprim-sulfamethoxazole
bull 1ndash2 tablets orally twice daily doxycyclinebull 100 mg orally twice dailybull or clindamycin 300ndash450 mg orally every 8 hbull - In severe cases vancomycin 15 mgkg
intravenouslybull every 12 h or clindamycin 600 mg intravenouslybull every 8 h
Midline Granulomabull A midline granuloma is an angiocentricbull lymphoma it was referred to as polymorphicbull reticulosis lethal midline granuloma and midline
malignant reticulosisbull bull Definition of the diseasebull ndash This rare disease is a lymphoma of extranodal
presentationall cases are positive for the Epstein-Barr virus
bull -This lymphoma most commonly appears in the midface region
Midline GranulomaEpidemiologyaetiologyndash This form of lymphoma is rare in Europe and theUnited States with a higher prevalence in Asia and PeruSymptomsndash The most common presentation is nasal obstruction with a destructive mass occupying the nosesinuses and palate
-Fever night sweatsand weight loss seen usually in Hodgkinrsquos lymphomaand other non-Hodgkinrsquos lymphomas (knownas ldquoB symptomsrdquo) are uncommon
Midline GranulomaDiagnosisndash The diagnosis is based on anatomopathologicalstudy The malignancy of the tumour manifested byextensive necrosis makes the histological diagnosisdifficult and often more biopsies are required forconfirmationbull Therapyndash Therapy consists of radiotherapy with or withoutchemotherapy
Midline Granuloma
bull Prognosisbull ndash Depending on the stage long-term remission or
experience a worseningbull prognosis with relapses which may include otherbull extranodal sites bull Involvement of extranodal sitesbull including the upper airway gastrointestinal tractbull skin
Wegenerrsquos Granulomatosis
bull Definition of the diseasebull ndash Wegenerrsquos granulomatosis is a systemic chronicbull vasculitis of small- and medium-sized blood vesselsbull with an autoimmune component It affectsbull particular organs with variable predilectionbull Epidemiologyaetiologybull ndash Wegenerrsquos granulomatosis is a rare disease It affects
about 1 in 20000ndash30000 people It is more prevalentbull in middle-aged Caucasian patients
Wegenerrsquos Granulomatosis
Symptomsndash The disease may present pulmonary upper
respiratory tract or renal In the disseminated form-The localised form ndash confinedto the upper respiratory region ndash is present in 25of the patients- It consists of nonspecific manifestationssuch as nasal obstruction crusting purulentor bloody rhinorrhea and painful or painless ulcers in oral or nasal cavities which are unresponsive tostandard medical treatment
Wegenerrsquos Granulomatosis
bull In some patients the nasal septum is perforatedbull which leads to saddle-nose deformity Less
commonbull symptoms are hoarseness stridor due to
subglotticbull stenosis otalgia otorrhea and conductivebull and sensorineural hearing loss Also ocular
symptomsbull such as scleritis conjunctivitis uveitis andbull episcleritis may be present
Wegenerrsquos Granulomatosis
bull ndash In the disseminated form pulmonary involvementbull is manifested by cough dyspnoea haemoptysisbull (due to an alveolar capillaritis necrotic lesions orbull endobronchial disease) and pleuritic painndashbull -Ninety per cent of patients have nasal symptomsbull and these symptoms are usually the first
manifestationof the diseasebull -Most patients have also renal involvementbull even if it is subclinical
Wegenerrsquos Granulomatosis
Diagnosis ndash Diagnosis of Wegenerrsquos granulomatosis is based on clinical findings that demonstrate lung (chest x-ray) kidney (urine analysis) or upper respiratory tract
involvement (oral or nasal ulcers or discharge) - positive blood analysis for cytoplasmic-staining antineutrophil
cytoplasmic antibodies (c-ANCA) and confirming proteinase 3 (PR3) ANCA or myeloperoxidase (MPO) ANCA ndash Biopsy is essential for diagnosis nonspecific chronic inflammation
and necrosis -Bacterial and fungal infections
Wegenerrsquos Granulomatosis
Therapyndash Conservative therapybull In the induction of disease remission highdosesteroids (e g prednisone 1 mgkgday) for1 month with tapering over several months aregiven In addition cyclophosphamide (2 mgkgday) should be administered for 6ndash12 monthsuntil symptoms disappear In the maintenanceof remission cyclophosphamide should be
Wegenerrsquos Granulomatosis
Antibiotics mainly trimethoprim-sulfamethoxazoleare given for prophylaxis againstPneumocystis jiroveci (formerly Pneumocystiscarinii) pneumonia (PCP) which may developduring immunosuppression and have a role inpreventing recurrencesbull Sinonasal manifestations may be treated with topical nasal steroids and nasal irrigations lowdosesystemic steroids and antibiotics when bacterial infection (typically Staphylococcus species) is suspected
Wegenerrsquos Granulomatosis
bull Prognosisbull ndash Most of the patients respond well to treatmentbull achieving symptom-free intervals of 5ndash20 yearsbull or more bull -Anatomical problems (sinusitis trachealbull stenosis) may require surgery bull Relapses can be long and troublesomebull Long-term complications are chronicbull renal failure hearing loss and deafness
Nasal Fractures Definition ndash A nasal fracture is a disruption of the nasal bone structure due to trauma It is the most frequently fractured facial bone Epidemiologyaetiology ndash Sports falls and assaults are the usual mechanisms of fracture -Males are affected twice as often as are females -Paediatric populations with a incidences during the second and third decades of life -Variables such as force impact direction nature of the striking object age and other will influence the pattern of injury to the components of the nose
Nasal Fractures
bull Symptomsbull ndash Deformity swelling epistaxis and periorbital
ecchymosis are signs that are suggestive of nasal fracture
bull bony crepitus and nasal segment mobilitybull ndash Epiphora bull Severe bilateral injuries to the lachrymal bones
arebull associated with depressed nasal fractures
Nasal Fractures Complications ndash Septal haematoma is one of the most severe early complications of nasal trauma and without drainage it results in abscess formation 6ndash7 days after trauma producing necrosis of the septal cartilage -Long-term problems such as saddle-nose deformity perforation columellar retraction and nasalbase
Septal infection could lead to osteomyelitis orbital and intracranial abscesses meningitis and cavernous sinus thrombosis -Cerebrospinal fluid leakage is a common complication of severe
nasal and frontal fractures
Nasal Fractures
bull Diagnostic proceduresbull ndash Inspectionbull bull Changes of appearance such as deviation andbull asymmetry bleeding watery drainage changesbull in nasal breathing and smell It is useful to comparebull the current presentation with old photographsbull (up to 40 of normal individuals havebull significant nose malformations)
Nasal Fractures Physical examination bull The diagnosis of a nasal fracture is made primarily by physical examination epistaxis nasal swelling and periorbital ecchymosis Nasal shape in the lateral and frontal inspection should be assessed Grasping the dorsum between two fingers and rocking the pyramid back and forth aids in assessing the mobility of nasal bones Internal structures should be evaluated by using a headlight and nasal speculum Clotted blood is removed by suction and assessment of haematoma mucosal tears and active bleeding is performed Bimanual palpation of the septum helps to differentiate septal swelling from haematoma ndash
Nasal FracturesRadiographybull There is no clear evidence of the role of radiographyin the management of nasal fracturesPlain films have up to a 66 false-positive rateas a result of misinterpretation of normal suturelines In addition old fractures are difficult todistinguishbull Three-dimensional CT is recommended for extensiveinjuries involving the nasal-orbital-ethmoidalcomplexndash
Nasal Fractures
bull Additionaluseful diagnostic proceduresbull bull Using a 0 or 30deg 4-mm endoscope is helpful inbull the assessment of posterior abnormalities If thebull patient is heavily sedated Brown-Gruss
provocationbull manoeuvres may be performed to determinebull deformities in upper middle or lower segmentsbull by compressing each compartment
Nasal FracturesConservative treatmentndash Treatment of bleedingbull For localised bleeding anterior sources may becauterised by silver nitrate or sealed with topicalmaterials such as thrombin combined withgelatin foam fibrin glue FloSealreg or other procoagulantmaterials If conservative measuresfail a formal anterior packing is placedbull Bleeding from branches of sphenopalatine orethmoid vessels requires anterior-posteriorpacking
Nasal Fractures
bull bull Surgical methods such as direct endoscopic vessel
bull cauterization or ligation have been shown tobull offer better haemostasis and patient comfortbull Angiography with embolization can also be
consideredbull in cases refractory to more conservativebull approaches
Nasal Fractures
bull Type of reductionbull bull Nondisplaced fractures should be treated withbull observation alone Closed nasal reduction is thebull best choice for simple injuries (isolated unilateralbull with medial displacement)bull bull An open approach should be considered in
severebull trauma (bilateral depressed fractures)
Nasal Fracturesbull Surgical principlesbull ndash Topical anaesthesia with cotton pledgets soakedbull with 4 cocaine or 005 oxymethazoline combinedbull with 4 topical lidocaine should be appliedbull for 5ndash10 min Local anaesthesia should also be injectedbull (1 lidocaine and 1100000 epinephrine)bull along the septum lateral walls and floor of the nasalbull cavitybull bull
Nasal FracturesClosed reductionndashndash The nasal bones are grasped between two fingersand pressure is applied laterally in theopposite direction of the deviation A bluntelevator may be used from within the nose incases of significant medial collapse Walshamforceps can be of help Reduction of the septumshould be performed with the use ofAsch forceps
Nasal Fractures
bull To prevent collapse of the postreductionbull framework nasal packing should be placedbull for 3ndash5 days Septum splints are recommendedbull in comminuted septal fractures withbull severe mucosal lesions External nasal splintingbull for 10 days (Aquaplastreg Thermoplastreg)bull provides nasal protection Nasal saline spraysbull prevent crusting and oral antibiotics should
Nasal Fractures
bull Open reductionbull ndashndash Immediate repair of fractures by using
widebull surgical exposure reduction fixation and
reconstructionbull ndashndash The second option is delayed correctionbull (6 months or more) of persistent deformitiesbull using standard techniques of rhinoplasty
Deviated Nasal Septum
bull Definition of the diseasebull ndash Deviation of the nasal septum is a common causebull of unilateral nasal airway obstruction in which thebull nasal septum is displacedbull bull Epidemiologyaetiologybull ndash Developmental septal abnormalities Septal cartilage
damage in the neonatal period andbull during birth can cause severe septal deviation inbull the absence of a history of nasal trauma
Deviated Nasal Septum
bull Symptomsbull ndash Patients may present with a history of sinusitis
allergicbull rhinitis obstructive sleep apnoea previousbull nasal surgery or recent nasal trauma Unilateral or
bilateral nasal airway obstruction that is unrelievedbull with decongestants or nasal steroid sprays is oftenbull seenbull bull
Deviated Nasal SeptumDiagnosisndashExamination external dorsal deviation or the columella and caudal septummay be deflected off the midline (caudal subluxation)ndash Inspections of the nasal cavity and anterior-posteriorrhinoscopy are helpful in diagnosing the locationtype and severity of septal deformityThe endoscope is also useful in identifying polypsthe severity and extent of posterior septaldeviations and bony spurs and locating areas ofseptal perforation or mucosal injury
Deviated Nasal Septum
bull Therapybull ndash Septoplasty is a procedurebull The areabull of deviation is corrected or resected in order tobull leave behind as much cartilage and bone as
possiblebull Cartilage resection is minimised and can be
repositioned reshaped or recontoured using a variety of methods
Deviated Nasal Septum
bull ndash Indications of septoplasty before the growth period
bull of the nose is finished should be very limited bull -In these cases surgery must preserve all the
cartilagebull in order to prevent external changes of the
shape ofbull the nose
Deviated Nasal Septum
bull Complicationsbull ndash Frequent complications include haematoma andbull infection Cerebrospinal fluid leak is a rare but
potentiallybull serious complicationbull It is usually the resultbull of avulsion or damage to the cribriform plate whenbull handling the perpendicular plate of the ethmoidbull ndash Other complications include epistaxis nasal
Deviated Nasal Septum
bull Other complications include epistaxis nasal obstruction
bull due to residual deviation synechiae returnbull of the cartilaginous deviation septal perforationbull anosmia and cosmetic nasal deformities suchbull as widened alar rim margins drooping nasal tipbull columella retraction and a sunken dorsum with abull supratip saddle formation
Septal perforation with minor crusting View from provide closure of the
incision
Septal Haematoma
bull A septal haematoma is a blood collection under the perichondrium
bull of the septum and cartilagebull bull bull Epidemiologyaetiologybull ndash A septal haematoma is one of the most
severe complications of nasal trauma
Septal Haematoma
bull Diagnosisbull ndash Signs and symptoms include intense pain
swellingbull haematoma of the upper lip and philtrum
area andbull complete nasal airway obstruction
Septal HaematomaTherapyndash Management consists of drainage through a mucoperichondrial incision Immediate treatment isnecessary to prevent long-term problems such asa saddle-nose deformity perforation columellarretraction and nasal-base widening In childrenseptal destruction can lead to devastating nasal andmidfacial growth abnormalitiesbull Surgeryndash Incision and evacuation of the collection is performedDrainage of a septal haematoma should
Septal HaematomaSurgeryndash Incision and evacuation of the collection is performedDrainage of a septal haematoma should provide closure of the incision
Splints or transseptal sutures are placed to obliterate thepotential space and prevent collectionInfection involving the septal cartilage Reconstruction with autologouscartilage is then performed in a second stage Oral antibiotics should be given
Nasal DeformitySaddle-nose deformityndash A saddle-nose deformity is characterised by a loss ofnasal dorsal height and compromised nasal supportstructures -Other case observed are depressionof the middle vault and dorsum loss of nasal tipsupport and definition shortened (vertical) nasal length over rotation of the nasal tip and retrusion ofthe nasal spine and caudal septum It is also knownas a ldquoPug noserdquo or ldquoboxerrsquos noserdquo both of which referto various degrees of nasal dorsal depressionbull
Nasal DeformityEpidemiologyaetiologyndash Prevalence is higher in population groups prone to facial trauma (ie boxers athletes) those with historiesof intranasal cocaine use nasal surgery (e g radical submucosal septal resection reductive rhinoplasty)ndash A saddle-nose deformity can be congenital or acquired It can be noticed as a part of individual familialsyndromic and ethnic characteristics - Most deformities are due to traumatic and iatrogeniccauses Medical causes are Wegenerrsquosgranulomatosis relapsing polychondritis leprosy (Hansenrsquos disease) syphilis ectodermal dysplasiaand intranasal cocaine use
Nasal Deformity
bull Therapybull ndash Nasal reconstruction indications depend on patientbull selection surgeon experience and aetiology of thebull deformity bull Indications for surgery can be functionalbull aesthetic or most commonly both In individuals
with a compromised nasal airway a nasoseptalbull reconstruction is indicated
Nasal Deformity
bull Contraindications bull include patients with malignantbull chronic or autoimmune disease conditions drugbull abuse poor perioperative risk profile and unrealisticbull expectationsbull ndash Multiple previous rhinoplasties and certain
professionsbull (mixed martial artists boxers and other contactbull sports) are relative contraindications
Nasal DeformitySeptoplastyndash Septoplasty is performed to correct nasal obstructioncaused by septal deformityndash Usually septoplasty is performed under general anaesthesiawith the patient in the supine position with the head elevated by approximately 30 (Righthandedsurgeons approach from the right side)ndash Local vasoconstrictive anaesthesia is applied notonly to reduce postoperative pain but also more importantly to achieve vasoconstriction of themucosa and less intraoperative haemorrhage Lidocainewith adrenaline or epinephrine is usedalthough in patients with cardiac hypersensitivityoxymetazoline might be preferred
Nasal Deformity
bull Septoplasty begins with the incision of septal mucosabull Most operative techniques utilise a hemitransfixionbull incision at the caudal end of septum so thatbull deviation at this point might be reached as wellbull as a transfixion incision that is easily obtained ifbull needed (Right-handed surgeons normally choosebull the left side but that may vary when deviation isbull convex towards the right)
Nasal DeformityA columella retractor is placed over the columellaand by pulling it laterally the caudal border of theseptum is exposed Ala can be protected by an alaprotector A vertical incision with a no 15 bladeover the caudal end of septum is performed untilreaching the plane of the septal cartilage It is essentialto correctly identify the perichondrium and byusing the Cottle elevator dissect and lift it creatinga flap As the dissection proceeds along the septalcartilage a longer speculum (no 5) is introduced sothat elevation of the mucoperichondrium is doneunder constant visual controlndash The next step is to dissect the mucoperiostium
Nasal DeformityDissecting over the bony-cartilaginous junctionwhen joining both tunnels might be difficult and is
especially prone to membrane perforationndash If needed the same tunnels are to be created on the
other side of the septum Then deviated parts of
septum are identified and removed either with a
knife or a Freer chisel
Nasal Deformitybull septum from the maxillary crest the septum mustbull be separated from the perpendicular plate trimmedbull along the inferior border placed back onto the crestbull and sutured to the periosteum If the deformity involvesbull the vomer an osteotome is used Care mustbull be taken not to break the cribriform plate becausebull it could cause a cerebrospinal fistula
Nasal Deformity
bull Once the septal deviation is corrected the flapsbull and hemitransfixion incision are mattressed
withbull absorbable sutures Nasal packing to prevent
synechiaebull and postoperative septal haematoma mightbull be advised but should be removed within 72 h

Erysipelas
bull Complicationsndash The most common complication is recurrencewhich is seen in 18ndash30 of the cases even afterproper antibiotic therapy Recurrence is seen moreoften in females than in malesA skin infection with S pyogenes could lead toglomerulonephritis
Erysipelas
bull Complicationsbull ndash The most common complication is recurrencebull which is seen in 18ndash30 of the cases even afterbull proper antibiotic therapy bull -Recurrence is seen morebull often in females than in males bull -A skin infection with S pyogenes could lead tobull glomerulonephritis
Erysipelas
bull bull Diagnosisbull ndash Diagnosis is based on the patientrsquos personal
historybull and physical examination particularly on inspectionbull of the skin
bull Blood cultures are positive in less thanbull 5 of cases
ErysipelasTherapyndash Conservative therapybull The preferred antibiotic is penicillin In mildcases with minor systemic symptoms penicillinV 500 mg orally every 6 h for 10 days or penicillinG benzathine 12 mil U intramuscularlyonceOther possibilities are amoxicillin 500 mgorally twice a day for 10 days or cephalexin 500mg orally every 6 h for 10 days
ErysipelasIn moderate and severe cases with significantsystemic symptoms hospitalization and intravenoustreatment is required penicillin G 2ndash4mil U intravenously every 4ndash6 h Cefazolin05ndash15 gm intravenously every 8 h cefotaxime1ndash2 gm intravenously every 8 h or ceftriaxone1ndash2 gm intravenously once a day should be administeredIn patients with a penicillin allergyclindamycin 600 mg intravenously every 8 h orvancomycin 15 mgkg intravenously twice a daymay be given
ErysipelaAdditional useful therapeutic optionsbull Prednisone 30 mg over 8 days might be consideredas well as elevation of the affected siteMoist heat compresses may be usefulbull Surgeryndash Debridement and drainage are indicated when bullaeabscesses or necroses are presentbull Differential diagnosisndash Contact dermatitisndash Asteatotic eczemandash Herpes zosterndash Angioneurotic oedemandash Osteomyelitis
Furuncle
bull Definition of the diseasebull ndash A furuncle is an infection that beginsbull at the hair follicle and spreads deeper into thebull dermis and subcutaneous tissue forming abull nodule After several days it developsbull into an abscess - red painful and fluctuantbull bull bull Epidemiologyaetiologybull ndash The aetiologic agent is Staphylococcus aureus
FuruncleSymptomsndashsymptoms are local and limited to thesite of infection Furuncles usually are wherehair follicles are present bull Complicationndash One complication is furunculosis multiple draining furunclesDiagnosisndash The diagnosis is based on clinical inspection - Cultures are not necessary when there is no systemic involvement but should beconsidered if systemic therapy (in case of feversignificant cellulitis or hospitalization) or whenmethicillin-resistant Staphylococcusaureus (MRSA) is considered
FuruncleTherapyndash When the furuncle is small application of moist heat compress to promote drainage -Larger furuncles should be drained by surgical incision-After drainage the area should be cleaned with anantiseptic (with chlorhexidinebetadine) should be applied twice
a dayndash If no systemic symptoms or extensive cellulitis arepresent simple topical care is usually curative andoral antibiotics are not necessary Otherwise systemictreatment is indicated and should cover anypossible MRSA
Furuncle
bull -Recommended antibiotics are trimethoprim-sulfamethoxazole
bull 1ndash2 tablets orally twice daily doxycyclinebull 100 mg orally twice dailybull or clindamycin 300ndash450 mg orally every 8 hbull - In severe cases vancomycin 15 mgkg
intravenouslybull every 12 h or clindamycin 600 mg intravenouslybull every 8 h
Midline Granulomabull A midline granuloma is an angiocentricbull lymphoma it was referred to as polymorphicbull reticulosis lethal midline granuloma and midline
malignant reticulosisbull bull Definition of the diseasebull ndash This rare disease is a lymphoma of extranodal
presentationall cases are positive for the Epstein-Barr virus
bull -This lymphoma most commonly appears in the midface region
Midline GranulomaEpidemiologyaetiologyndash This form of lymphoma is rare in Europe and theUnited States with a higher prevalence in Asia and PeruSymptomsndash The most common presentation is nasal obstruction with a destructive mass occupying the nosesinuses and palate
-Fever night sweatsand weight loss seen usually in Hodgkinrsquos lymphomaand other non-Hodgkinrsquos lymphomas (knownas ldquoB symptomsrdquo) are uncommon
Midline GranulomaDiagnosisndash The diagnosis is based on anatomopathologicalstudy The malignancy of the tumour manifested byextensive necrosis makes the histological diagnosisdifficult and often more biopsies are required forconfirmationbull Therapyndash Therapy consists of radiotherapy with or withoutchemotherapy
Midline Granuloma
bull Prognosisbull ndash Depending on the stage long-term remission or
experience a worseningbull prognosis with relapses which may include otherbull extranodal sites bull Involvement of extranodal sitesbull including the upper airway gastrointestinal tractbull skin
Wegenerrsquos Granulomatosis
bull Definition of the diseasebull ndash Wegenerrsquos granulomatosis is a systemic chronicbull vasculitis of small- and medium-sized blood vesselsbull with an autoimmune component It affectsbull particular organs with variable predilectionbull Epidemiologyaetiologybull ndash Wegenerrsquos granulomatosis is a rare disease It affects
about 1 in 20000ndash30000 people It is more prevalentbull in middle-aged Caucasian patients
Wegenerrsquos Granulomatosis
Symptomsndash The disease may present pulmonary upper
respiratory tract or renal In the disseminated form-The localised form ndash confinedto the upper respiratory region ndash is present in 25of the patients- It consists of nonspecific manifestationssuch as nasal obstruction crusting purulentor bloody rhinorrhea and painful or painless ulcers in oral or nasal cavities which are unresponsive tostandard medical treatment
Wegenerrsquos Granulomatosis
bull In some patients the nasal septum is perforatedbull which leads to saddle-nose deformity Less
commonbull symptoms are hoarseness stridor due to
subglotticbull stenosis otalgia otorrhea and conductivebull and sensorineural hearing loss Also ocular
symptomsbull such as scleritis conjunctivitis uveitis andbull episcleritis may be present
Wegenerrsquos Granulomatosis
bull ndash In the disseminated form pulmonary involvementbull is manifested by cough dyspnoea haemoptysisbull (due to an alveolar capillaritis necrotic lesions orbull endobronchial disease) and pleuritic painndashbull -Ninety per cent of patients have nasal symptomsbull and these symptoms are usually the first
manifestationof the diseasebull -Most patients have also renal involvementbull even if it is subclinical
Wegenerrsquos Granulomatosis
Diagnosis ndash Diagnosis of Wegenerrsquos granulomatosis is based on clinical findings that demonstrate lung (chest x-ray) kidney (urine analysis) or upper respiratory tract
involvement (oral or nasal ulcers or discharge) - positive blood analysis for cytoplasmic-staining antineutrophil
cytoplasmic antibodies (c-ANCA) and confirming proteinase 3 (PR3) ANCA or myeloperoxidase (MPO) ANCA ndash Biopsy is essential for diagnosis nonspecific chronic inflammation
and necrosis -Bacterial and fungal infections
Wegenerrsquos Granulomatosis
Therapyndash Conservative therapybull In the induction of disease remission highdosesteroids (e g prednisone 1 mgkgday) for1 month with tapering over several months aregiven In addition cyclophosphamide (2 mgkgday) should be administered for 6ndash12 monthsuntil symptoms disappear In the maintenanceof remission cyclophosphamide should be
Wegenerrsquos Granulomatosis
Antibiotics mainly trimethoprim-sulfamethoxazoleare given for prophylaxis againstPneumocystis jiroveci (formerly Pneumocystiscarinii) pneumonia (PCP) which may developduring immunosuppression and have a role inpreventing recurrencesbull Sinonasal manifestations may be treated with topical nasal steroids and nasal irrigations lowdosesystemic steroids and antibiotics when bacterial infection (typically Staphylococcus species) is suspected
Wegenerrsquos Granulomatosis
bull Prognosisbull ndash Most of the patients respond well to treatmentbull achieving symptom-free intervals of 5ndash20 yearsbull or more bull -Anatomical problems (sinusitis trachealbull stenosis) may require surgery bull Relapses can be long and troublesomebull Long-term complications are chronicbull renal failure hearing loss and deafness
Nasal Fractures Definition ndash A nasal fracture is a disruption of the nasal bone structure due to trauma It is the most frequently fractured facial bone Epidemiologyaetiology ndash Sports falls and assaults are the usual mechanisms of fracture -Males are affected twice as often as are females -Paediatric populations with a incidences during the second and third decades of life -Variables such as force impact direction nature of the striking object age and other will influence the pattern of injury to the components of the nose
Nasal Fractures
bull Symptomsbull ndash Deformity swelling epistaxis and periorbital
ecchymosis are signs that are suggestive of nasal fracture
bull bony crepitus and nasal segment mobilitybull ndash Epiphora bull Severe bilateral injuries to the lachrymal bones
arebull associated with depressed nasal fractures
Nasal Fractures Complications ndash Septal haematoma is one of the most severe early complications of nasal trauma and without drainage it results in abscess formation 6ndash7 days after trauma producing necrosis of the septal cartilage -Long-term problems such as saddle-nose deformity perforation columellar retraction and nasalbase
Septal infection could lead to osteomyelitis orbital and intracranial abscesses meningitis and cavernous sinus thrombosis -Cerebrospinal fluid leakage is a common complication of severe
nasal and frontal fractures
Nasal Fractures
bull Diagnostic proceduresbull ndash Inspectionbull bull Changes of appearance such as deviation andbull asymmetry bleeding watery drainage changesbull in nasal breathing and smell It is useful to comparebull the current presentation with old photographsbull (up to 40 of normal individuals havebull significant nose malformations)
Nasal Fractures Physical examination bull The diagnosis of a nasal fracture is made primarily by physical examination epistaxis nasal swelling and periorbital ecchymosis Nasal shape in the lateral and frontal inspection should be assessed Grasping the dorsum between two fingers and rocking the pyramid back and forth aids in assessing the mobility of nasal bones Internal structures should be evaluated by using a headlight and nasal speculum Clotted blood is removed by suction and assessment of haematoma mucosal tears and active bleeding is performed Bimanual palpation of the septum helps to differentiate septal swelling from haematoma ndash
Nasal FracturesRadiographybull There is no clear evidence of the role of radiographyin the management of nasal fracturesPlain films have up to a 66 false-positive rateas a result of misinterpretation of normal suturelines In addition old fractures are difficult todistinguishbull Three-dimensional CT is recommended for extensiveinjuries involving the nasal-orbital-ethmoidalcomplexndash
Nasal Fractures
bull Additionaluseful diagnostic proceduresbull bull Using a 0 or 30deg 4-mm endoscope is helpful inbull the assessment of posterior abnormalities If thebull patient is heavily sedated Brown-Gruss
provocationbull manoeuvres may be performed to determinebull deformities in upper middle or lower segmentsbull by compressing each compartment
Nasal FracturesConservative treatmentndash Treatment of bleedingbull For localised bleeding anterior sources may becauterised by silver nitrate or sealed with topicalmaterials such as thrombin combined withgelatin foam fibrin glue FloSealreg or other procoagulantmaterials If conservative measuresfail a formal anterior packing is placedbull Bleeding from branches of sphenopalatine orethmoid vessels requires anterior-posteriorpacking
Nasal Fractures
bull bull Surgical methods such as direct endoscopic vessel
bull cauterization or ligation have been shown tobull offer better haemostasis and patient comfortbull Angiography with embolization can also be
consideredbull in cases refractory to more conservativebull approaches
Nasal Fractures
bull Type of reductionbull bull Nondisplaced fractures should be treated withbull observation alone Closed nasal reduction is thebull best choice for simple injuries (isolated unilateralbull with medial displacement)bull bull An open approach should be considered in
severebull trauma (bilateral depressed fractures)
Nasal Fracturesbull Surgical principlesbull ndash Topical anaesthesia with cotton pledgets soakedbull with 4 cocaine or 005 oxymethazoline combinedbull with 4 topical lidocaine should be appliedbull for 5ndash10 min Local anaesthesia should also be injectedbull (1 lidocaine and 1100000 epinephrine)bull along the septum lateral walls and floor of the nasalbull cavitybull bull
Nasal FracturesClosed reductionndashndash The nasal bones are grasped between two fingersand pressure is applied laterally in theopposite direction of the deviation A bluntelevator may be used from within the nose incases of significant medial collapse Walshamforceps can be of help Reduction of the septumshould be performed with the use ofAsch forceps
Nasal Fractures
bull To prevent collapse of the postreductionbull framework nasal packing should be placedbull for 3ndash5 days Septum splints are recommendedbull in comminuted septal fractures withbull severe mucosal lesions External nasal splintingbull for 10 days (Aquaplastreg Thermoplastreg)bull provides nasal protection Nasal saline spraysbull prevent crusting and oral antibiotics should
Nasal Fractures
bull Open reductionbull ndashndash Immediate repair of fractures by using
widebull surgical exposure reduction fixation and
reconstructionbull ndashndash The second option is delayed correctionbull (6 months or more) of persistent deformitiesbull using standard techniques of rhinoplasty
Deviated Nasal Septum
bull Definition of the diseasebull ndash Deviation of the nasal septum is a common causebull of unilateral nasal airway obstruction in which thebull nasal septum is displacedbull bull Epidemiologyaetiologybull ndash Developmental septal abnormalities Septal cartilage
damage in the neonatal period andbull during birth can cause severe septal deviation inbull the absence of a history of nasal trauma
Deviated Nasal Septum
bull Symptomsbull ndash Patients may present with a history of sinusitis
allergicbull rhinitis obstructive sleep apnoea previousbull nasal surgery or recent nasal trauma Unilateral or
bilateral nasal airway obstruction that is unrelievedbull with decongestants or nasal steroid sprays is oftenbull seenbull bull
Deviated Nasal SeptumDiagnosisndashExamination external dorsal deviation or the columella and caudal septummay be deflected off the midline (caudal subluxation)ndash Inspections of the nasal cavity and anterior-posteriorrhinoscopy are helpful in diagnosing the locationtype and severity of septal deformityThe endoscope is also useful in identifying polypsthe severity and extent of posterior septaldeviations and bony spurs and locating areas ofseptal perforation or mucosal injury
Deviated Nasal Septum
bull Therapybull ndash Septoplasty is a procedurebull The areabull of deviation is corrected or resected in order tobull leave behind as much cartilage and bone as
possiblebull Cartilage resection is minimised and can be
repositioned reshaped or recontoured using a variety of methods
Deviated Nasal Septum
bull ndash Indications of septoplasty before the growth period
bull of the nose is finished should be very limited bull -In these cases surgery must preserve all the
cartilagebull in order to prevent external changes of the
shape ofbull the nose
Deviated Nasal Septum
bull Complicationsbull ndash Frequent complications include haematoma andbull infection Cerebrospinal fluid leak is a rare but
potentiallybull serious complicationbull It is usually the resultbull of avulsion or damage to the cribriform plate whenbull handling the perpendicular plate of the ethmoidbull ndash Other complications include epistaxis nasal
Deviated Nasal Septum
bull Other complications include epistaxis nasal obstruction
bull due to residual deviation synechiae returnbull of the cartilaginous deviation septal perforationbull anosmia and cosmetic nasal deformities suchbull as widened alar rim margins drooping nasal tipbull columella retraction and a sunken dorsum with abull supratip saddle formation
Septal perforation with minor crusting View from provide closure of the
incision
Septal Haematoma
bull A septal haematoma is a blood collection under the perichondrium
bull of the septum and cartilagebull bull bull Epidemiologyaetiologybull ndash A septal haematoma is one of the most
severe complications of nasal trauma
Septal Haematoma
bull Diagnosisbull ndash Signs and symptoms include intense pain
swellingbull haematoma of the upper lip and philtrum
area andbull complete nasal airway obstruction
Septal HaematomaTherapyndash Management consists of drainage through a mucoperichondrial incision Immediate treatment isnecessary to prevent long-term problems such asa saddle-nose deformity perforation columellarretraction and nasal-base widening In childrenseptal destruction can lead to devastating nasal andmidfacial growth abnormalitiesbull Surgeryndash Incision and evacuation of the collection is performedDrainage of a septal haematoma should
Septal HaematomaSurgeryndash Incision and evacuation of the collection is performedDrainage of a septal haematoma should provide closure of the incision
Splints or transseptal sutures are placed to obliterate thepotential space and prevent collectionInfection involving the septal cartilage Reconstruction with autologouscartilage is then performed in a second stage Oral antibiotics should be given
Nasal DeformitySaddle-nose deformityndash A saddle-nose deformity is characterised by a loss ofnasal dorsal height and compromised nasal supportstructures -Other case observed are depressionof the middle vault and dorsum loss of nasal tipsupport and definition shortened (vertical) nasal length over rotation of the nasal tip and retrusion ofthe nasal spine and caudal septum It is also knownas a ldquoPug noserdquo or ldquoboxerrsquos noserdquo both of which referto various degrees of nasal dorsal depressionbull
Nasal DeformityEpidemiologyaetiologyndash Prevalence is higher in population groups prone to facial trauma (ie boxers athletes) those with historiesof intranasal cocaine use nasal surgery (e g radical submucosal septal resection reductive rhinoplasty)ndash A saddle-nose deformity can be congenital or acquired It can be noticed as a part of individual familialsyndromic and ethnic characteristics - Most deformities are due to traumatic and iatrogeniccauses Medical causes are Wegenerrsquosgranulomatosis relapsing polychondritis leprosy (Hansenrsquos disease) syphilis ectodermal dysplasiaand intranasal cocaine use
Nasal Deformity
bull Therapybull ndash Nasal reconstruction indications depend on patientbull selection surgeon experience and aetiology of thebull deformity bull Indications for surgery can be functionalbull aesthetic or most commonly both In individuals
with a compromised nasal airway a nasoseptalbull reconstruction is indicated
Nasal Deformity
bull Contraindications bull include patients with malignantbull chronic or autoimmune disease conditions drugbull abuse poor perioperative risk profile and unrealisticbull expectationsbull ndash Multiple previous rhinoplasties and certain
professionsbull (mixed martial artists boxers and other contactbull sports) are relative contraindications
Nasal DeformitySeptoplastyndash Septoplasty is performed to correct nasal obstructioncaused by septal deformityndash Usually septoplasty is performed under general anaesthesiawith the patient in the supine position with the head elevated by approximately 30 (Righthandedsurgeons approach from the right side)ndash Local vasoconstrictive anaesthesia is applied notonly to reduce postoperative pain but also more importantly to achieve vasoconstriction of themucosa and less intraoperative haemorrhage Lidocainewith adrenaline or epinephrine is usedalthough in patients with cardiac hypersensitivityoxymetazoline might be preferred
Nasal Deformity
bull Septoplasty begins with the incision of septal mucosabull Most operative techniques utilise a hemitransfixionbull incision at the caudal end of septum so thatbull deviation at this point might be reached as wellbull as a transfixion incision that is easily obtained ifbull needed (Right-handed surgeons normally choosebull the left side but that may vary when deviation isbull convex towards the right)
Nasal DeformityA columella retractor is placed over the columellaand by pulling it laterally the caudal border of theseptum is exposed Ala can be protected by an alaprotector A vertical incision with a no 15 bladeover the caudal end of septum is performed untilreaching the plane of the septal cartilage It is essentialto correctly identify the perichondrium and byusing the Cottle elevator dissect and lift it creatinga flap As the dissection proceeds along the septalcartilage a longer speculum (no 5) is introduced sothat elevation of the mucoperichondrium is doneunder constant visual controlndash The next step is to dissect the mucoperiostium
Nasal DeformityDissecting over the bony-cartilaginous junctionwhen joining both tunnels might be difficult and is
especially prone to membrane perforationndash If needed the same tunnels are to be created on the
other side of the septum Then deviated parts of
septum are identified and removed either with a
knife or a Freer chisel
Nasal Deformitybull septum from the maxillary crest the septum mustbull be separated from the perpendicular plate trimmedbull along the inferior border placed back onto the crestbull and sutured to the periosteum If the deformity involvesbull the vomer an osteotome is used Care mustbull be taken not to break the cribriform plate becausebull it could cause a cerebrospinal fistula
Nasal Deformity
bull Once the septal deviation is corrected the flapsbull and hemitransfixion incision are mattressed
withbull absorbable sutures Nasal packing to prevent
synechiaebull and postoperative septal haematoma mightbull be advised but should be removed within 72 h

Erysipelas
bull Complicationsbull ndash The most common complication is recurrencebull which is seen in 18ndash30 of the cases even afterbull proper antibiotic therapy bull -Recurrence is seen morebull often in females than in males bull -A skin infection with S pyogenes could lead tobull glomerulonephritis
Erysipelas
bull bull Diagnosisbull ndash Diagnosis is based on the patientrsquos personal
historybull and physical examination particularly on inspectionbull of the skin
bull Blood cultures are positive in less thanbull 5 of cases
ErysipelasTherapyndash Conservative therapybull The preferred antibiotic is penicillin In mildcases with minor systemic symptoms penicillinV 500 mg orally every 6 h for 10 days or penicillinG benzathine 12 mil U intramuscularlyonceOther possibilities are amoxicillin 500 mgorally twice a day for 10 days or cephalexin 500mg orally every 6 h for 10 days
ErysipelasIn moderate and severe cases with significantsystemic symptoms hospitalization and intravenoustreatment is required penicillin G 2ndash4mil U intravenously every 4ndash6 h Cefazolin05ndash15 gm intravenously every 8 h cefotaxime1ndash2 gm intravenously every 8 h or ceftriaxone1ndash2 gm intravenously once a day should be administeredIn patients with a penicillin allergyclindamycin 600 mg intravenously every 8 h orvancomycin 15 mgkg intravenously twice a daymay be given
ErysipelaAdditional useful therapeutic optionsbull Prednisone 30 mg over 8 days might be consideredas well as elevation of the affected siteMoist heat compresses may be usefulbull Surgeryndash Debridement and drainage are indicated when bullaeabscesses or necroses are presentbull Differential diagnosisndash Contact dermatitisndash Asteatotic eczemandash Herpes zosterndash Angioneurotic oedemandash Osteomyelitis
Furuncle
bull Definition of the diseasebull ndash A furuncle is an infection that beginsbull at the hair follicle and spreads deeper into thebull dermis and subcutaneous tissue forming abull nodule After several days it developsbull into an abscess - red painful and fluctuantbull bull bull Epidemiologyaetiologybull ndash The aetiologic agent is Staphylococcus aureus
FuruncleSymptomsndashsymptoms are local and limited to thesite of infection Furuncles usually are wherehair follicles are present bull Complicationndash One complication is furunculosis multiple draining furunclesDiagnosisndash The diagnosis is based on clinical inspection - Cultures are not necessary when there is no systemic involvement but should beconsidered if systemic therapy (in case of feversignificant cellulitis or hospitalization) or whenmethicillin-resistant Staphylococcusaureus (MRSA) is considered
FuruncleTherapyndash When the furuncle is small application of moist heat compress to promote drainage -Larger furuncles should be drained by surgical incision-After drainage the area should be cleaned with anantiseptic (with chlorhexidinebetadine) should be applied twice
a dayndash If no systemic symptoms or extensive cellulitis arepresent simple topical care is usually curative andoral antibiotics are not necessary Otherwise systemictreatment is indicated and should cover anypossible MRSA
Furuncle
bull -Recommended antibiotics are trimethoprim-sulfamethoxazole
bull 1ndash2 tablets orally twice daily doxycyclinebull 100 mg orally twice dailybull or clindamycin 300ndash450 mg orally every 8 hbull - In severe cases vancomycin 15 mgkg
intravenouslybull every 12 h or clindamycin 600 mg intravenouslybull every 8 h
Midline Granulomabull A midline granuloma is an angiocentricbull lymphoma it was referred to as polymorphicbull reticulosis lethal midline granuloma and midline
malignant reticulosisbull bull Definition of the diseasebull ndash This rare disease is a lymphoma of extranodal
presentationall cases are positive for the Epstein-Barr virus
bull -This lymphoma most commonly appears in the midface region
Midline GranulomaEpidemiologyaetiologyndash This form of lymphoma is rare in Europe and theUnited States with a higher prevalence in Asia and PeruSymptomsndash The most common presentation is nasal obstruction with a destructive mass occupying the nosesinuses and palate
-Fever night sweatsand weight loss seen usually in Hodgkinrsquos lymphomaand other non-Hodgkinrsquos lymphomas (knownas ldquoB symptomsrdquo) are uncommon
Midline GranulomaDiagnosisndash The diagnosis is based on anatomopathologicalstudy The malignancy of the tumour manifested byextensive necrosis makes the histological diagnosisdifficult and often more biopsies are required forconfirmationbull Therapyndash Therapy consists of radiotherapy with or withoutchemotherapy
Midline Granuloma
bull Prognosisbull ndash Depending on the stage long-term remission or
experience a worseningbull prognosis with relapses which may include otherbull extranodal sites bull Involvement of extranodal sitesbull including the upper airway gastrointestinal tractbull skin
Wegenerrsquos Granulomatosis
bull Definition of the diseasebull ndash Wegenerrsquos granulomatosis is a systemic chronicbull vasculitis of small- and medium-sized blood vesselsbull with an autoimmune component It affectsbull particular organs with variable predilectionbull Epidemiologyaetiologybull ndash Wegenerrsquos granulomatosis is a rare disease It affects
about 1 in 20000ndash30000 people It is more prevalentbull in middle-aged Caucasian patients
Wegenerrsquos Granulomatosis
Symptomsndash The disease may present pulmonary upper
respiratory tract or renal In the disseminated form-The localised form ndash confinedto the upper respiratory region ndash is present in 25of the patients- It consists of nonspecific manifestationssuch as nasal obstruction crusting purulentor bloody rhinorrhea and painful or painless ulcers in oral or nasal cavities which are unresponsive tostandard medical treatment
Wegenerrsquos Granulomatosis
bull In some patients the nasal septum is perforatedbull which leads to saddle-nose deformity Less
commonbull symptoms are hoarseness stridor due to
subglotticbull stenosis otalgia otorrhea and conductivebull and sensorineural hearing loss Also ocular
symptomsbull such as scleritis conjunctivitis uveitis andbull episcleritis may be present
Wegenerrsquos Granulomatosis
bull ndash In the disseminated form pulmonary involvementbull is manifested by cough dyspnoea haemoptysisbull (due to an alveolar capillaritis necrotic lesions orbull endobronchial disease) and pleuritic painndashbull -Ninety per cent of patients have nasal symptomsbull and these symptoms are usually the first
manifestationof the diseasebull -Most patients have also renal involvementbull even if it is subclinical
Wegenerrsquos Granulomatosis
Diagnosis ndash Diagnosis of Wegenerrsquos granulomatosis is based on clinical findings that demonstrate lung (chest x-ray) kidney (urine analysis) or upper respiratory tract
involvement (oral or nasal ulcers or discharge) - positive blood analysis for cytoplasmic-staining antineutrophil
cytoplasmic antibodies (c-ANCA) and confirming proteinase 3 (PR3) ANCA or myeloperoxidase (MPO) ANCA ndash Biopsy is essential for diagnosis nonspecific chronic inflammation
and necrosis -Bacterial and fungal infections
Wegenerrsquos Granulomatosis
Therapyndash Conservative therapybull In the induction of disease remission highdosesteroids (e g prednisone 1 mgkgday) for1 month with tapering over several months aregiven In addition cyclophosphamide (2 mgkgday) should be administered for 6ndash12 monthsuntil symptoms disappear In the maintenanceof remission cyclophosphamide should be
Wegenerrsquos Granulomatosis
Antibiotics mainly trimethoprim-sulfamethoxazoleare given for prophylaxis againstPneumocystis jiroveci (formerly Pneumocystiscarinii) pneumonia (PCP) which may developduring immunosuppression and have a role inpreventing recurrencesbull Sinonasal manifestations may be treated with topical nasal steroids and nasal irrigations lowdosesystemic steroids and antibiotics when bacterial infection (typically Staphylococcus species) is suspected
Wegenerrsquos Granulomatosis
bull Prognosisbull ndash Most of the patients respond well to treatmentbull achieving symptom-free intervals of 5ndash20 yearsbull or more bull -Anatomical problems (sinusitis trachealbull stenosis) may require surgery bull Relapses can be long and troublesomebull Long-term complications are chronicbull renal failure hearing loss and deafness
Nasal Fractures Definition ndash A nasal fracture is a disruption of the nasal bone structure due to trauma It is the most frequently fractured facial bone Epidemiologyaetiology ndash Sports falls and assaults are the usual mechanisms of fracture -Males are affected twice as often as are females -Paediatric populations with a incidences during the second and third decades of life -Variables such as force impact direction nature of the striking object age and other will influence the pattern of injury to the components of the nose
Nasal Fractures
bull Symptomsbull ndash Deformity swelling epistaxis and periorbital
ecchymosis are signs that are suggestive of nasal fracture
bull bony crepitus and nasal segment mobilitybull ndash Epiphora bull Severe bilateral injuries to the lachrymal bones
arebull associated with depressed nasal fractures
Nasal Fractures Complications ndash Septal haematoma is one of the most severe early complications of nasal trauma and without drainage it results in abscess formation 6ndash7 days after trauma producing necrosis of the septal cartilage -Long-term problems such as saddle-nose deformity perforation columellar retraction and nasalbase
Septal infection could lead to osteomyelitis orbital and intracranial abscesses meningitis and cavernous sinus thrombosis -Cerebrospinal fluid leakage is a common complication of severe
nasal and frontal fractures
Nasal Fractures
bull Diagnostic proceduresbull ndash Inspectionbull bull Changes of appearance such as deviation andbull asymmetry bleeding watery drainage changesbull in nasal breathing and smell It is useful to comparebull the current presentation with old photographsbull (up to 40 of normal individuals havebull significant nose malformations)
Nasal Fractures Physical examination bull The diagnosis of a nasal fracture is made primarily by physical examination epistaxis nasal swelling and periorbital ecchymosis Nasal shape in the lateral and frontal inspection should be assessed Grasping the dorsum between two fingers and rocking the pyramid back and forth aids in assessing the mobility of nasal bones Internal structures should be evaluated by using a headlight and nasal speculum Clotted blood is removed by suction and assessment of haematoma mucosal tears and active bleeding is performed Bimanual palpation of the septum helps to differentiate septal swelling from haematoma ndash
Nasal FracturesRadiographybull There is no clear evidence of the role of radiographyin the management of nasal fracturesPlain films have up to a 66 false-positive rateas a result of misinterpretation of normal suturelines In addition old fractures are difficult todistinguishbull Three-dimensional CT is recommended for extensiveinjuries involving the nasal-orbital-ethmoidalcomplexndash
Nasal Fractures
bull Additionaluseful diagnostic proceduresbull bull Using a 0 or 30deg 4-mm endoscope is helpful inbull the assessment of posterior abnormalities If thebull patient is heavily sedated Brown-Gruss
provocationbull manoeuvres may be performed to determinebull deformities in upper middle or lower segmentsbull by compressing each compartment
Nasal FracturesConservative treatmentndash Treatment of bleedingbull For localised bleeding anterior sources may becauterised by silver nitrate or sealed with topicalmaterials such as thrombin combined withgelatin foam fibrin glue FloSealreg or other procoagulantmaterials If conservative measuresfail a formal anterior packing is placedbull Bleeding from branches of sphenopalatine orethmoid vessels requires anterior-posteriorpacking
Nasal Fractures
bull bull Surgical methods such as direct endoscopic vessel
bull cauterization or ligation have been shown tobull offer better haemostasis and patient comfortbull Angiography with embolization can also be
consideredbull in cases refractory to more conservativebull approaches
Nasal Fractures
bull Type of reductionbull bull Nondisplaced fractures should be treated withbull observation alone Closed nasal reduction is thebull best choice for simple injuries (isolated unilateralbull with medial displacement)bull bull An open approach should be considered in
severebull trauma (bilateral depressed fractures)
Nasal Fracturesbull Surgical principlesbull ndash Topical anaesthesia with cotton pledgets soakedbull with 4 cocaine or 005 oxymethazoline combinedbull with 4 topical lidocaine should be appliedbull for 5ndash10 min Local anaesthesia should also be injectedbull (1 lidocaine and 1100000 epinephrine)bull along the septum lateral walls and floor of the nasalbull cavitybull bull
Nasal FracturesClosed reductionndashndash The nasal bones are grasped between two fingersand pressure is applied laterally in theopposite direction of the deviation A bluntelevator may be used from within the nose incases of significant medial collapse Walshamforceps can be of help Reduction of the septumshould be performed with the use ofAsch forceps
Nasal Fractures
bull To prevent collapse of the postreductionbull framework nasal packing should be placedbull for 3ndash5 days Septum splints are recommendedbull in comminuted septal fractures withbull severe mucosal lesions External nasal splintingbull for 10 days (Aquaplastreg Thermoplastreg)bull provides nasal protection Nasal saline spraysbull prevent crusting and oral antibiotics should
Nasal Fractures
bull Open reductionbull ndashndash Immediate repair of fractures by using
widebull surgical exposure reduction fixation and
reconstructionbull ndashndash The second option is delayed correctionbull (6 months or more) of persistent deformitiesbull using standard techniques of rhinoplasty
Deviated Nasal Septum
bull Definition of the diseasebull ndash Deviation of the nasal septum is a common causebull of unilateral nasal airway obstruction in which thebull nasal septum is displacedbull bull Epidemiologyaetiologybull ndash Developmental septal abnormalities Septal cartilage
damage in the neonatal period andbull during birth can cause severe septal deviation inbull the absence of a history of nasal trauma
Deviated Nasal Septum
bull Symptomsbull ndash Patients may present with a history of sinusitis
allergicbull rhinitis obstructive sleep apnoea previousbull nasal surgery or recent nasal trauma Unilateral or
bilateral nasal airway obstruction that is unrelievedbull with decongestants or nasal steroid sprays is oftenbull seenbull bull
Deviated Nasal SeptumDiagnosisndashExamination external dorsal deviation or the columella and caudal septummay be deflected off the midline (caudal subluxation)ndash Inspections of the nasal cavity and anterior-posteriorrhinoscopy are helpful in diagnosing the locationtype and severity of septal deformityThe endoscope is also useful in identifying polypsthe severity and extent of posterior septaldeviations and bony spurs and locating areas ofseptal perforation or mucosal injury
Deviated Nasal Septum
bull Therapybull ndash Septoplasty is a procedurebull The areabull of deviation is corrected or resected in order tobull leave behind as much cartilage and bone as
possiblebull Cartilage resection is minimised and can be
repositioned reshaped or recontoured using a variety of methods
Deviated Nasal Septum
bull ndash Indications of septoplasty before the growth period
bull of the nose is finished should be very limited bull -In these cases surgery must preserve all the
cartilagebull in order to prevent external changes of the
shape ofbull the nose
Deviated Nasal Septum
bull Complicationsbull ndash Frequent complications include haematoma andbull infection Cerebrospinal fluid leak is a rare but
potentiallybull serious complicationbull It is usually the resultbull of avulsion or damage to the cribriform plate whenbull handling the perpendicular plate of the ethmoidbull ndash Other complications include epistaxis nasal
Deviated Nasal Septum
bull Other complications include epistaxis nasal obstruction
bull due to residual deviation synechiae returnbull of the cartilaginous deviation septal perforationbull anosmia and cosmetic nasal deformities suchbull as widened alar rim margins drooping nasal tipbull columella retraction and a sunken dorsum with abull supratip saddle formation
Septal perforation with minor crusting View from provide closure of the
incision
Septal Haematoma
bull A septal haematoma is a blood collection under the perichondrium
bull of the septum and cartilagebull bull bull Epidemiologyaetiologybull ndash A septal haematoma is one of the most
severe complications of nasal trauma
Septal Haematoma
bull Diagnosisbull ndash Signs and symptoms include intense pain
swellingbull haematoma of the upper lip and philtrum
area andbull complete nasal airway obstruction
Septal HaematomaTherapyndash Management consists of drainage through a mucoperichondrial incision Immediate treatment isnecessary to prevent long-term problems such asa saddle-nose deformity perforation columellarretraction and nasal-base widening In childrenseptal destruction can lead to devastating nasal andmidfacial growth abnormalitiesbull Surgeryndash Incision and evacuation of the collection is performedDrainage of a septal haematoma should
Septal HaematomaSurgeryndash Incision and evacuation of the collection is performedDrainage of a septal haematoma should provide closure of the incision
Splints or transseptal sutures are placed to obliterate thepotential space and prevent collectionInfection involving the septal cartilage Reconstruction with autologouscartilage is then performed in a second stage Oral antibiotics should be given
Nasal DeformitySaddle-nose deformityndash A saddle-nose deformity is characterised by a loss ofnasal dorsal height and compromised nasal supportstructures -Other case observed are depressionof the middle vault and dorsum loss of nasal tipsupport and definition shortened (vertical) nasal length over rotation of the nasal tip and retrusion ofthe nasal spine and caudal septum It is also knownas a ldquoPug noserdquo or ldquoboxerrsquos noserdquo both of which referto various degrees of nasal dorsal depressionbull
Nasal DeformityEpidemiologyaetiologyndash Prevalence is higher in population groups prone to facial trauma (ie boxers athletes) those with historiesof intranasal cocaine use nasal surgery (e g radical submucosal septal resection reductive rhinoplasty)ndash A saddle-nose deformity can be congenital or acquired It can be noticed as a part of individual familialsyndromic and ethnic characteristics - Most deformities are due to traumatic and iatrogeniccauses Medical causes are Wegenerrsquosgranulomatosis relapsing polychondritis leprosy (Hansenrsquos disease) syphilis ectodermal dysplasiaand intranasal cocaine use
Nasal Deformity
bull Therapybull ndash Nasal reconstruction indications depend on patientbull selection surgeon experience and aetiology of thebull deformity bull Indications for surgery can be functionalbull aesthetic or most commonly both In individuals
with a compromised nasal airway a nasoseptalbull reconstruction is indicated
Nasal Deformity
bull Contraindications bull include patients with malignantbull chronic or autoimmune disease conditions drugbull abuse poor perioperative risk profile and unrealisticbull expectationsbull ndash Multiple previous rhinoplasties and certain
professionsbull (mixed martial artists boxers and other contactbull sports) are relative contraindications
Nasal DeformitySeptoplastyndash Septoplasty is performed to correct nasal obstructioncaused by septal deformityndash Usually septoplasty is performed under general anaesthesiawith the patient in the supine position with the head elevated by approximately 30 (Righthandedsurgeons approach from the right side)ndash Local vasoconstrictive anaesthesia is applied notonly to reduce postoperative pain but also more importantly to achieve vasoconstriction of themucosa and less intraoperative haemorrhage Lidocainewith adrenaline or epinephrine is usedalthough in patients with cardiac hypersensitivityoxymetazoline might be preferred
Nasal Deformity
bull Septoplasty begins with the incision of septal mucosabull Most operative techniques utilise a hemitransfixionbull incision at the caudal end of septum so thatbull deviation at this point might be reached as wellbull as a transfixion incision that is easily obtained ifbull needed (Right-handed surgeons normally choosebull the left side but that may vary when deviation isbull convex towards the right)
Nasal DeformityA columella retractor is placed over the columellaand by pulling it laterally the caudal border of theseptum is exposed Ala can be protected by an alaprotector A vertical incision with a no 15 bladeover the caudal end of septum is performed untilreaching the plane of the septal cartilage It is essentialto correctly identify the perichondrium and byusing the Cottle elevator dissect and lift it creatinga flap As the dissection proceeds along the septalcartilage a longer speculum (no 5) is introduced sothat elevation of the mucoperichondrium is doneunder constant visual controlndash The next step is to dissect the mucoperiostium
Nasal DeformityDissecting over the bony-cartilaginous junctionwhen joining both tunnels might be difficult and is
especially prone to membrane perforationndash If needed the same tunnels are to be created on the
other side of the septum Then deviated parts of
septum are identified and removed either with a
knife or a Freer chisel
Nasal Deformitybull septum from the maxillary crest the septum mustbull be separated from the perpendicular plate trimmedbull along the inferior border placed back onto the crestbull and sutured to the periosteum If the deformity involvesbull the vomer an osteotome is used Care mustbull be taken not to break the cribriform plate becausebull it could cause a cerebrospinal fistula
Nasal Deformity
bull Once the septal deviation is corrected the flapsbull and hemitransfixion incision are mattressed
withbull absorbable sutures Nasal packing to prevent
synechiaebull and postoperative septal haematoma mightbull be advised but should be removed within 72 h

Erysipelas
bull bull Diagnosisbull ndash Diagnosis is based on the patientrsquos personal
historybull and physical examination particularly on inspectionbull of the skin
bull Blood cultures are positive in less thanbull 5 of cases
ErysipelasTherapyndash Conservative therapybull The preferred antibiotic is penicillin In mildcases with minor systemic symptoms penicillinV 500 mg orally every 6 h for 10 days or penicillinG benzathine 12 mil U intramuscularlyonceOther possibilities are amoxicillin 500 mgorally twice a day for 10 days or cephalexin 500mg orally every 6 h for 10 days
ErysipelasIn moderate and severe cases with significantsystemic symptoms hospitalization and intravenoustreatment is required penicillin G 2ndash4mil U intravenously every 4ndash6 h Cefazolin05ndash15 gm intravenously every 8 h cefotaxime1ndash2 gm intravenously every 8 h or ceftriaxone1ndash2 gm intravenously once a day should be administeredIn patients with a penicillin allergyclindamycin 600 mg intravenously every 8 h orvancomycin 15 mgkg intravenously twice a daymay be given
ErysipelaAdditional useful therapeutic optionsbull Prednisone 30 mg over 8 days might be consideredas well as elevation of the affected siteMoist heat compresses may be usefulbull Surgeryndash Debridement and drainage are indicated when bullaeabscesses or necroses are presentbull Differential diagnosisndash Contact dermatitisndash Asteatotic eczemandash Herpes zosterndash Angioneurotic oedemandash Osteomyelitis
Furuncle
bull Definition of the diseasebull ndash A furuncle is an infection that beginsbull at the hair follicle and spreads deeper into thebull dermis and subcutaneous tissue forming abull nodule After several days it developsbull into an abscess - red painful and fluctuantbull bull bull Epidemiologyaetiologybull ndash The aetiologic agent is Staphylococcus aureus
FuruncleSymptomsndashsymptoms are local and limited to thesite of infection Furuncles usually are wherehair follicles are present bull Complicationndash One complication is furunculosis multiple draining furunclesDiagnosisndash The diagnosis is based on clinical inspection - Cultures are not necessary when there is no systemic involvement but should beconsidered if systemic therapy (in case of feversignificant cellulitis or hospitalization) or whenmethicillin-resistant Staphylococcusaureus (MRSA) is considered
FuruncleTherapyndash When the furuncle is small application of moist heat compress to promote drainage -Larger furuncles should be drained by surgical incision-After drainage the area should be cleaned with anantiseptic (with chlorhexidinebetadine) should be applied twice
a dayndash If no systemic symptoms or extensive cellulitis arepresent simple topical care is usually curative andoral antibiotics are not necessary Otherwise systemictreatment is indicated and should cover anypossible MRSA
Furuncle
bull -Recommended antibiotics are trimethoprim-sulfamethoxazole
bull 1ndash2 tablets orally twice daily doxycyclinebull 100 mg orally twice dailybull or clindamycin 300ndash450 mg orally every 8 hbull - In severe cases vancomycin 15 mgkg
intravenouslybull every 12 h or clindamycin 600 mg intravenouslybull every 8 h
Midline Granulomabull A midline granuloma is an angiocentricbull lymphoma it was referred to as polymorphicbull reticulosis lethal midline granuloma and midline
malignant reticulosisbull bull Definition of the diseasebull ndash This rare disease is a lymphoma of extranodal
presentationall cases are positive for the Epstein-Barr virus
bull -This lymphoma most commonly appears in the midface region
Midline GranulomaEpidemiologyaetiologyndash This form of lymphoma is rare in Europe and theUnited States with a higher prevalence in Asia and PeruSymptomsndash The most common presentation is nasal obstruction with a destructive mass occupying the nosesinuses and palate
-Fever night sweatsand weight loss seen usually in Hodgkinrsquos lymphomaand other non-Hodgkinrsquos lymphomas (knownas ldquoB symptomsrdquo) are uncommon
Midline GranulomaDiagnosisndash The diagnosis is based on anatomopathologicalstudy The malignancy of the tumour manifested byextensive necrosis makes the histological diagnosisdifficult and often more biopsies are required forconfirmationbull Therapyndash Therapy consists of radiotherapy with or withoutchemotherapy
Midline Granuloma
bull Prognosisbull ndash Depending on the stage long-term remission or
experience a worseningbull prognosis with relapses which may include otherbull extranodal sites bull Involvement of extranodal sitesbull including the upper airway gastrointestinal tractbull skin
Wegenerrsquos Granulomatosis
bull Definition of the diseasebull ndash Wegenerrsquos granulomatosis is a systemic chronicbull vasculitis of small- and medium-sized blood vesselsbull with an autoimmune component It affectsbull particular organs with variable predilectionbull Epidemiologyaetiologybull ndash Wegenerrsquos granulomatosis is a rare disease It affects
about 1 in 20000ndash30000 people It is more prevalentbull in middle-aged Caucasian patients
Wegenerrsquos Granulomatosis
Symptomsndash The disease may present pulmonary upper
respiratory tract or renal In the disseminated form-The localised form ndash confinedto the upper respiratory region ndash is present in 25of the patients- It consists of nonspecific manifestationssuch as nasal obstruction crusting purulentor bloody rhinorrhea and painful or painless ulcers in oral or nasal cavities which are unresponsive tostandard medical treatment
Wegenerrsquos Granulomatosis
bull In some patients the nasal septum is perforatedbull which leads to saddle-nose deformity Less
commonbull symptoms are hoarseness stridor due to
subglotticbull stenosis otalgia otorrhea and conductivebull and sensorineural hearing loss Also ocular
symptomsbull such as scleritis conjunctivitis uveitis andbull episcleritis may be present
Wegenerrsquos Granulomatosis
bull ndash In the disseminated form pulmonary involvementbull is manifested by cough dyspnoea haemoptysisbull (due to an alveolar capillaritis necrotic lesions orbull endobronchial disease) and pleuritic painndashbull -Ninety per cent of patients have nasal symptomsbull and these symptoms are usually the first
manifestationof the diseasebull -Most patients have also renal involvementbull even if it is subclinical
Wegenerrsquos Granulomatosis
Diagnosis ndash Diagnosis of Wegenerrsquos granulomatosis is based on clinical findings that demonstrate lung (chest x-ray) kidney (urine analysis) or upper respiratory tract
involvement (oral or nasal ulcers or discharge) - positive blood analysis for cytoplasmic-staining antineutrophil
cytoplasmic antibodies (c-ANCA) and confirming proteinase 3 (PR3) ANCA or myeloperoxidase (MPO) ANCA ndash Biopsy is essential for diagnosis nonspecific chronic inflammation
and necrosis -Bacterial and fungal infections
Wegenerrsquos Granulomatosis
Therapyndash Conservative therapybull In the induction of disease remission highdosesteroids (e g prednisone 1 mgkgday) for1 month with tapering over several months aregiven In addition cyclophosphamide (2 mgkgday) should be administered for 6ndash12 monthsuntil symptoms disappear In the maintenanceof remission cyclophosphamide should be
Wegenerrsquos Granulomatosis
Antibiotics mainly trimethoprim-sulfamethoxazoleare given for prophylaxis againstPneumocystis jiroveci (formerly Pneumocystiscarinii) pneumonia (PCP) which may developduring immunosuppression and have a role inpreventing recurrencesbull Sinonasal manifestations may be treated with topical nasal steroids and nasal irrigations lowdosesystemic steroids and antibiotics when bacterial infection (typically Staphylococcus species) is suspected
Wegenerrsquos Granulomatosis
bull Prognosisbull ndash Most of the patients respond well to treatmentbull achieving symptom-free intervals of 5ndash20 yearsbull or more bull -Anatomical problems (sinusitis trachealbull stenosis) may require surgery bull Relapses can be long and troublesomebull Long-term complications are chronicbull renal failure hearing loss and deafness
Nasal Fractures Definition ndash A nasal fracture is a disruption of the nasal bone structure due to trauma It is the most frequently fractured facial bone Epidemiologyaetiology ndash Sports falls and assaults are the usual mechanisms of fracture -Males are affected twice as often as are females -Paediatric populations with a incidences during the second and third decades of life -Variables such as force impact direction nature of the striking object age and other will influence the pattern of injury to the components of the nose
Nasal Fractures
bull Symptomsbull ndash Deformity swelling epistaxis and periorbital
ecchymosis are signs that are suggestive of nasal fracture
bull bony crepitus and nasal segment mobilitybull ndash Epiphora bull Severe bilateral injuries to the lachrymal bones
arebull associated with depressed nasal fractures
Nasal Fractures Complications ndash Septal haematoma is one of the most severe early complications of nasal trauma and without drainage it results in abscess formation 6ndash7 days after trauma producing necrosis of the septal cartilage -Long-term problems such as saddle-nose deformity perforation columellar retraction and nasalbase
Septal infection could lead to osteomyelitis orbital and intracranial abscesses meningitis and cavernous sinus thrombosis -Cerebrospinal fluid leakage is a common complication of severe
nasal and frontal fractures
Nasal Fractures
bull Diagnostic proceduresbull ndash Inspectionbull bull Changes of appearance such as deviation andbull asymmetry bleeding watery drainage changesbull in nasal breathing and smell It is useful to comparebull the current presentation with old photographsbull (up to 40 of normal individuals havebull significant nose malformations)
Nasal Fractures Physical examination bull The diagnosis of a nasal fracture is made primarily by physical examination epistaxis nasal swelling and periorbital ecchymosis Nasal shape in the lateral and frontal inspection should be assessed Grasping the dorsum between two fingers and rocking the pyramid back and forth aids in assessing the mobility of nasal bones Internal structures should be evaluated by using a headlight and nasal speculum Clotted blood is removed by suction and assessment of haematoma mucosal tears and active bleeding is performed Bimanual palpation of the septum helps to differentiate septal swelling from haematoma ndash
Nasal FracturesRadiographybull There is no clear evidence of the role of radiographyin the management of nasal fracturesPlain films have up to a 66 false-positive rateas a result of misinterpretation of normal suturelines In addition old fractures are difficult todistinguishbull Three-dimensional CT is recommended for extensiveinjuries involving the nasal-orbital-ethmoidalcomplexndash
Nasal Fractures
bull Additionaluseful diagnostic proceduresbull bull Using a 0 or 30deg 4-mm endoscope is helpful inbull the assessment of posterior abnormalities If thebull patient is heavily sedated Brown-Gruss
provocationbull manoeuvres may be performed to determinebull deformities in upper middle or lower segmentsbull by compressing each compartment
Nasal FracturesConservative treatmentndash Treatment of bleedingbull For localised bleeding anterior sources may becauterised by silver nitrate or sealed with topicalmaterials such as thrombin combined withgelatin foam fibrin glue FloSealreg or other procoagulantmaterials If conservative measuresfail a formal anterior packing is placedbull Bleeding from branches of sphenopalatine orethmoid vessels requires anterior-posteriorpacking
Nasal Fractures
bull bull Surgical methods such as direct endoscopic vessel
bull cauterization or ligation have been shown tobull offer better haemostasis and patient comfortbull Angiography with embolization can also be
consideredbull in cases refractory to more conservativebull approaches
Nasal Fractures
bull Type of reductionbull bull Nondisplaced fractures should be treated withbull observation alone Closed nasal reduction is thebull best choice for simple injuries (isolated unilateralbull with medial displacement)bull bull An open approach should be considered in
severebull trauma (bilateral depressed fractures)
Nasal Fracturesbull Surgical principlesbull ndash Topical anaesthesia with cotton pledgets soakedbull with 4 cocaine or 005 oxymethazoline combinedbull with 4 topical lidocaine should be appliedbull for 5ndash10 min Local anaesthesia should also be injectedbull (1 lidocaine and 1100000 epinephrine)bull along the septum lateral walls and floor of the nasalbull cavitybull bull
Nasal FracturesClosed reductionndashndash The nasal bones are grasped between two fingersand pressure is applied laterally in theopposite direction of the deviation A bluntelevator may be used from within the nose incases of significant medial collapse Walshamforceps can be of help Reduction of the septumshould be performed with the use ofAsch forceps
Nasal Fractures
bull To prevent collapse of the postreductionbull framework nasal packing should be placedbull for 3ndash5 days Septum splints are recommendedbull in comminuted septal fractures withbull severe mucosal lesions External nasal splintingbull for 10 days (Aquaplastreg Thermoplastreg)bull provides nasal protection Nasal saline spraysbull prevent crusting and oral antibiotics should
Nasal Fractures
bull Open reductionbull ndashndash Immediate repair of fractures by using
widebull surgical exposure reduction fixation and
reconstructionbull ndashndash The second option is delayed correctionbull (6 months or more) of persistent deformitiesbull using standard techniques of rhinoplasty
Deviated Nasal Septum
bull Definition of the diseasebull ndash Deviation of the nasal septum is a common causebull of unilateral nasal airway obstruction in which thebull nasal septum is displacedbull bull Epidemiologyaetiologybull ndash Developmental septal abnormalities Septal cartilage
damage in the neonatal period andbull during birth can cause severe septal deviation inbull the absence of a history of nasal trauma
Deviated Nasal Septum
bull Symptomsbull ndash Patients may present with a history of sinusitis
allergicbull rhinitis obstructive sleep apnoea previousbull nasal surgery or recent nasal trauma Unilateral or
bilateral nasal airway obstruction that is unrelievedbull with decongestants or nasal steroid sprays is oftenbull seenbull bull
Deviated Nasal SeptumDiagnosisndashExamination external dorsal deviation or the columella and caudal septummay be deflected off the midline (caudal subluxation)ndash Inspections of the nasal cavity and anterior-posteriorrhinoscopy are helpful in diagnosing the locationtype and severity of septal deformityThe endoscope is also useful in identifying polypsthe severity and extent of posterior septaldeviations and bony spurs and locating areas ofseptal perforation or mucosal injury
Deviated Nasal Septum
bull Therapybull ndash Septoplasty is a procedurebull The areabull of deviation is corrected or resected in order tobull leave behind as much cartilage and bone as
possiblebull Cartilage resection is minimised and can be
repositioned reshaped or recontoured using a variety of methods
Deviated Nasal Septum
bull ndash Indications of septoplasty before the growth period
bull of the nose is finished should be very limited bull -In these cases surgery must preserve all the
cartilagebull in order to prevent external changes of the
shape ofbull the nose
Deviated Nasal Septum
bull Complicationsbull ndash Frequent complications include haematoma andbull infection Cerebrospinal fluid leak is a rare but
potentiallybull serious complicationbull It is usually the resultbull of avulsion or damage to the cribriform plate whenbull handling the perpendicular plate of the ethmoidbull ndash Other complications include epistaxis nasal
Deviated Nasal Septum
bull Other complications include epistaxis nasal obstruction
bull due to residual deviation synechiae returnbull of the cartilaginous deviation septal perforationbull anosmia and cosmetic nasal deformities suchbull as widened alar rim margins drooping nasal tipbull columella retraction and a sunken dorsum with abull supratip saddle formation
Septal perforation with minor crusting View from provide closure of the
incision
Septal Haematoma
bull A septal haematoma is a blood collection under the perichondrium
bull of the septum and cartilagebull bull bull Epidemiologyaetiologybull ndash A septal haematoma is one of the most
severe complications of nasal trauma
Septal Haematoma
bull Diagnosisbull ndash Signs and symptoms include intense pain
swellingbull haematoma of the upper lip and philtrum
area andbull complete nasal airway obstruction
Septal HaematomaTherapyndash Management consists of drainage through a mucoperichondrial incision Immediate treatment isnecessary to prevent long-term problems such asa saddle-nose deformity perforation columellarretraction and nasal-base widening In childrenseptal destruction can lead to devastating nasal andmidfacial growth abnormalitiesbull Surgeryndash Incision and evacuation of the collection is performedDrainage of a septal haematoma should
Septal HaematomaSurgeryndash Incision and evacuation of the collection is performedDrainage of a septal haematoma should provide closure of the incision
Splints or transseptal sutures are placed to obliterate thepotential space and prevent collectionInfection involving the septal cartilage Reconstruction with autologouscartilage is then performed in a second stage Oral antibiotics should be given
Nasal DeformitySaddle-nose deformityndash A saddle-nose deformity is characterised by a loss ofnasal dorsal height and compromised nasal supportstructures -Other case observed are depressionof the middle vault and dorsum loss of nasal tipsupport and definition shortened (vertical) nasal length over rotation of the nasal tip and retrusion ofthe nasal spine and caudal septum It is also knownas a ldquoPug noserdquo or ldquoboxerrsquos noserdquo both of which referto various degrees of nasal dorsal depressionbull
Nasal DeformityEpidemiologyaetiologyndash Prevalence is higher in population groups prone to facial trauma (ie boxers athletes) those with historiesof intranasal cocaine use nasal surgery (e g radical submucosal septal resection reductive rhinoplasty)ndash A saddle-nose deformity can be congenital or acquired It can be noticed as a part of individual familialsyndromic and ethnic characteristics - Most deformities are due to traumatic and iatrogeniccauses Medical causes are Wegenerrsquosgranulomatosis relapsing polychondritis leprosy (Hansenrsquos disease) syphilis ectodermal dysplasiaand intranasal cocaine use
Nasal Deformity
bull Therapybull ndash Nasal reconstruction indications depend on patientbull selection surgeon experience and aetiology of thebull deformity bull Indications for surgery can be functionalbull aesthetic or most commonly both In individuals
with a compromised nasal airway a nasoseptalbull reconstruction is indicated
Nasal Deformity
bull Contraindications bull include patients with malignantbull chronic or autoimmune disease conditions drugbull abuse poor perioperative risk profile and unrealisticbull expectationsbull ndash Multiple previous rhinoplasties and certain
professionsbull (mixed martial artists boxers and other contactbull sports) are relative contraindications
Nasal DeformitySeptoplastyndash Septoplasty is performed to correct nasal obstructioncaused by septal deformityndash Usually septoplasty is performed under general anaesthesiawith the patient in the supine position with the head elevated by approximately 30 (Righthandedsurgeons approach from the right side)ndash Local vasoconstrictive anaesthesia is applied notonly to reduce postoperative pain but also more importantly to achieve vasoconstriction of themucosa and less intraoperative haemorrhage Lidocainewith adrenaline or epinephrine is usedalthough in patients with cardiac hypersensitivityoxymetazoline might be preferred
Nasal Deformity
bull Septoplasty begins with the incision of septal mucosabull Most operative techniques utilise a hemitransfixionbull incision at the caudal end of septum so thatbull deviation at this point might be reached as wellbull as a transfixion incision that is easily obtained ifbull needed (Right-handed surgeons normally choosebull the left side but that may vary when deviation isbull convex towards the right)
Nasal DeformityA columella retractor is placed over the columellaand by pulling it laterally the caudal border of theseptum is exposed Ala can be protected by an alaprotector A vertical incision with a no 15 bladeover the caudal end of septum is performed untilreaching the plane of the septal cartilage It is essentialto correctly identify the perichondrium and byusing the Cottle elevator dissect and lift it creatinga flap As the dissection proceeds along the septalcartilage a longer speculum (no 5) is introduced sothat elevation of the mucoperichondrium is doneunder constant visual controlndash The next step is to dissect the mucoperiostium
Nasal DeformityDissecting over the bony-cartilaginous junctionwhen joining both tunnels might be difficult and is
especially prone to membrane perforationndash If needed the same tunnels are to be created on the
other side of the septum Then deviated parts of
septum are identified and removed either with a
knife or a Freer chisel
Nasal Deformitybull septum from the maxillary crest the septum mustbull be separated from the perpendicular plate trimmedbull along the inferior border placed back onto the crestbull and sutured to the periosteum If the deformity involvesbull the vomer an osteotome is used Care mustbull be taken not to break the cribriform plate becausebull it could cause a cerebrospinal fistula
Nasal Deformity
bull Once the septal deviation is corrected the flapsbull and hemitransfixion incision are mattressed
withbull absorbable sutures Nasal packing to prevent
synechiaebull and postoperative septal haematoma mightbull be advised but should be removed within 72 h

ErysipelasTherapyndash Conservative therapybull The preferred antibiotic is penicillin In mildcases with minor systemic symptoms penicillinV 500 mg orally every 6 h for 10 days or penicillinG benzathine 12 mil U intramuscularlyonceOther possibilities are amoxicillin 500 mgorally twice a day for 10 days or cephalexin 500mg orally every 6 h for 10 days
ErysipelasIn moderate and severe cases with significantsystemic symptoms hospitalization and intravenoustreatment is required penicillin G 2ndash4mil U intravenously every 4ndash6 h Cefazolin05ndash15 gm intravenously every 8 h cefotaxime1ndash2 gm intravenously every 8 h or ceftriaxone1ndash2 gm intravenously once a day should be administeredIn patients with a penicillin allergyclindamycin 600 mg intravenously every 8 h orvancomycin 15 mgkg intravenously twice a daymay be given
ErysipelaAdditional useful therapeutic optionsbull Prednisone 30 mg over 8 days might be consideredas well as elevation of the affected siteMoist heat compresses may be usefulbull Surgeryndash Debridement and drainage are indicated when bullaeabscesses or necroses are presentbull Differential diagnosisndash Contact dermatitisndash Asteatotic eczemandash Herpes zosterndash Angioneurotic oedemandash Osteomyelitis
Furuncle
bull Definition of the diseasebull ndash A furuncle is an infection that beginsbull at the hair follicle and spreads deeper into thebull dermis and subcutaneous tissue forming abull nodule After several days it developsbull into an abscess - red painful and fluctuantbull bull bull Epidemiologyaetiologybull ndash The aetiologic agent is Staphylococcus aureus
FuruncleSymptomsndashsymptoms are local and limited to thesite of infection Furuncles usually are wherehair follicles are present bull Complicationndash One complication is furunculosis multiple draining furunclesDiagnosisndash The diagnosis is based on clinical inspection - Cultures are not necessary when there is no systemic involvement but should beconsidered if systemic therapy (in case of feversignificant cellulitis or hospitalization) or whenmethicillin-resistant Staphylococcusaureus (MRSA) is considered
FuruncleTherapyndash When the furuncle is small application of moist heat compress to promote drainage -Larger furuncles should be drained by surgical incision-After drainage the area should be cleaned with anantiseptic (with chlorhexidinebetadine) should be applied twice
a dayndash If no systemic symptoms or extensive cellulitis arepresent simple topical care is usually curative andoral antibiotics are not necessary Otherwise systemictreatment is indicated and should cover anypossible MRSA
Furuncle
bull -Recommended antibiotics are trimethoprim-sulfamethoxazole
bull 1ndash2 tablets orally twice daily doxycyclinebull 100 mg orally twice dailybull or clindamycin 300ndash450 mg orally every 8 hbull - In severe cases vancomycin 15 mgkg
intravenouslybull every 12 h or clindamycin 600 mg intravenouslybull every 8 h
Midline Granulomabull A midline granuloma is an angiocentricbull lymphoma it was referred to as polymorphicbull reticulosis lethal midline granuloma and midline
malignant reticulosisbull bull Definition of the diseasebull ndash This rare disease is a lymphoma of extranodal
presentationall cases are positive for the Epstein-Barr virus
bull -This lymphoma most commonly appears in the midface region
Midline GranulomaEpidemiologyaetiologyndash This form of lymphoma is rare in Europe and theUnited States with a higher prevalence in Asia and PeruSymptomsndash The most common presentation is nasal obstruction with a destructive mass occupying the nosesinuses and palate
-Fever night sweatsand weight loss seen usually in Hodgkinrsquos lymphomaand other non-Hodgkinrsquos lymphomas (knownas ldquoB symptomsrdquo) are uncommon
Midline GranulomaDiagnosisndash The diagnosis is based on anatomopathologicalstudy The malignancy of the tumour manifested byextensive necrosis makes the histological diagnosisdifficult and often more biopsies are required forconfirmationbull Therapyndash Therapy consists of radiotherapy with or withoutchemotherapy
Midline Granuloma
bull Prognosisbull ndash Depending on the stage long-term remission or
experience a worseningbull prognosis with relapses which may include otherbull extranodal sites bull Involvement of extranodal sitesbull including the upper airway gastrointestinal tractbull skin
Wegenerrsquos Granulomatosis
bull Definition of the diseasebull ndash Wegenerrsquos granulomatosis is a systemic chronicbull vasculitis of small- and medium-sized blood vesselsbull with an autoimmune component It affectsbull particular organs with variable predilectionbull Epidemiologyaetiologybull ndash Wegenerrsquos granulomatosis is a rare disease It affects
about 1 in 20000ndash30000 people It is more prevalentbull in middle-aged Caucasian patients
Wegenerrsquos Granulomatosis
Symptomsndash The disease may present pulmonary upper
respiratory tract or renal In the disseminated form-The localised form ndash confinedto the upper respiratory region ndash is present in 25of the patients- It consists of nonspecific manifestationssuch as nasal obstruction crusting purulentor bloody rhinorrhea and painful or painless ulcers in oral or nasal cavities which are unresponsive tostandard medical treatment
Wegenerrsquos Granulomatosis
bull In some patients the nasal septum is perforatedbull which leads to saddle-nose deformity Less
commonbull symptoms are hoarseness stridor due to
subglotticbull stenosis otalgia otorrhea and conductivebull and sensorineural hearing loss Also ocular
symptomsbull such as scleritis conjunctivitis uveitis andbull episcleritis may be present
Wegenerrsquos Granulomatosis
bull ndash In the disseminated form pulmonary involvementbull is manifested by cough dyspnoea haemoptysisbull (due to an alveolar capillaritis necrotic lesions orbull endobronchial disease) and pleuritic painndashbull -Ninety per cent of patients have nasal symptomsbull and these symptoms are usually the first
manifestationof the diseasebull -Most patients have also renal involvementbull even if it is subclinical
Wegenerrsquos Granulomatosis
Diagnosis ndash Diagnosis of Wegenerrsquos granulomatosis is based on clinical findings that demonstrate lung (chest x-ray) kidney (urine analysis) or upper respiratory tract
involvement (oral or nasal ulcers or discharge) - positive blood analysis for cytoplasmic-staining antineutrophil
cytoplasmic antibodies (c-ANCA) and confirming proteinase 3 (PR3) ANCA or myeloperoxidase (MPO) ANCA ndash Biopsy is essential for diagnosis nonspecific chronic inflammation
and necrosis -Bacterial and fungal infections
Wegenerrsquos Granulomatosis
Therapyndash Conservative therapybull In the induction of disease remission highdosesteroids (e g prednisone 1 mgkgday) for1 month with tapering over several months aregiven In addition cyclophosphamide (2 mgkgday) should be administered for 6ndash12 monthsuntil symptoms disappear In the maintenanceof remission cyclophosphamide should be
Wegenerrsquos Granulomatosis
Antibiotics mainly trimethoprim-sulfamethoxazoleare given for prophylaxis againstPneumocystis jiroveci (formerly Pneumocystiscarinii) pneumonia (PCP) which may developduring immunosuppression and have a role inpreventing recurrencesbull Sinonasal manifestations may be treated with topical nasal steroids and nasal irrigations lowdosesystemic steroids and antibiotics when bacterial infection (typically Staphylococcus species) is suspected
Wegenerrsquos Granulomatosis
bull Prognosisbull ndash Most of the patients respond well to treatmentbull achieving symptom-free intervals of 5ndash20 yearsbull or more bull -Anatomical problems (sinusitis trachealbull stenosis) may require surgery bull Relapses can be long and troublesomebull Long-term complications are chronicbull renal failure hearing loss and deafness
Nasal Fractures Definition ndash A nasal fracture is a disruption of the nasal bone structure due to trauma It is the most frequently fractured facial bone Epidemiologyaetiology ndash Sports falls and assaults are the usual mechanisms of fracture -Males are affected twice as often as are females -Paediatric populations with a incidences during the second and third decades of life -Variables such as force impact direction nature of the striking object age and other will influence the pattern of injury to the components of the nose
Nasal Fractures
bull Symptomsbull ndash Deformity swelling epistaxis and periorbital
ecchymosis are signs that are suggestive of nasal fracture
bull bony crepitus and nasal segment mobilitybull ndash Epiphora bull Severe bilateral injuries to the lachrymal bones
arebull associated with depressed nasal fractures
Nasal Fractures Complications ndash Septal haematoma is one of the most severe early complications of nasal trauma and without drainage it results in abscess formation 6ndash7 days after trauma producing necrosis of the septal cartilage -Long-term problems such as saddle-nose deformity perforation columellar retraction and nasalbase
Septal infection could lead to osteomyelitis orbital and intracranial abscesses meningitis and cavernous sinus thrombosis -Cerebrospinal fluid leakage is a common complication of severe
nasal and frontal fractures
Nasal Fractures
bull Diagnostic proceduresbull ndash Inspectionbull bull Changes of appearance such as deviation andbull asymmetry bleeding watery drainage changesbull in nasal breathing and smell It is useful to comparebull the current presentation with old photographsbull (up to 40 of normal individuals havebull significant nose malformations)
Nasal Fractures Physical examination bull The diagnosis of a nasal fracture is made primarily by physical examination epistaxis nasal swelling and periorbital ecchymosis Nasal shape in the lateral and frontal inspection should be assessed Grasping the dorsum between two fingers and rocking the pyramid back and forth aids in assessing the mobility of nasal bones Internal structures should be evaluated by using a headlight and nasal speculum Clotted blood is removed by suction and assessment of haematoma mucosal tears and active bleeding is performed Bimanual palpation of the septum helps to differentiate septal swelling from haematoma ndash
Nasal FracturesRadiographybull There is no clear evidence of the role of radiographyin the management of nasal fracturesPlain films have up to a 66 false-positive rateas a result of misinterpretation of normal suturelines In addition old fractures are difficult todistinguishbull Three-dimensional CT is recommended for extensiveinjuries involving the nasal-orbital-ethmoidalcomplexndash
Nasal Fractures
bull Additionaluseful diagnostic proceduresbull bull Using a 0 or 30deg 4-mm endoscope is helpful inbull the assessment of posterior abnormalities If thebull patient is heavily sedated Brown-Gruss
provocationbull manoeuvres may be performed to determinebull deformities in upper middle or lower segmentsbull by compressing each compartment
Nasal FracturesConservative treatmentndash Treatment of bleedingbull For localised bleeding anterior sources may becauterised by silver nitrate or sealed with topicalmaterials such as thrombin combined withgelatin foam fibrin glue FloSealreg or other procoagulantmaterials If conservative measuresfail a formal anterior packing is placedbull Bleeding from branches of sphenopalatine orethmoid vessels requires anterior-posteriorpacking
Nasal Fractures
bull bull Surgical methods such as direct endoscopic vessel
bull cauterization or ligation have been shown tobull offer better haemostasis and patient comfortbull Angiography with embolization can also be
consideredbull in cases refractory to more conservativebull approaches
Nasal Fractures
bull Type of reductionbull bull Nondisplaced fractures should be treated withbull observation alone Closed nasal reduction is thebull best choice for simple injuries (isolated unilateralbull with medial displacement)bull bull An open approach should be considered in
severebull trauma (bilateral depressed fractures)
Nasal Fracturesbull Surgical principlesbull ndash Topical anaesthesia with cotton pledgets soakedbull with 4 cocaine or 005 oxymethazoline combinedbull with 4 topical lidocaine should be appliedbull for 5ndash10 min Local anaesthesia should also be injectedbull (1 lidocaine and 1100000 epinephrine)bull along the septum lateral walls and floor of the nasalbull cavitybull bull
Nasal FracturesClosed reductionndashndash The nasal bones are grasped between two fingersand pressure is applied laterally in theopposite direction of the deviation A bluntelevator may be used from within the nose incases of significant medial collapse Walshamforceps can be of help Reduction of the septumshould be performed with the use ofAsch forceps
Nasal Fractures
bull To prevent collapse of the postreductionbull framework nasal packing should be placedbull for 3ndash5 days Septum splints are recommendedbull in comminuted septal fractures withbull severe mucosal lesions External nasal splintingbull for 10 days (Aquaplastreg Thermoplastreg)bull provides nasal protection Nasal saline spraysbull prevent crusting and oral antibiotics should
Nasal Fractures
bull Open reductionbull ndashndash Immediate repair of fractures by using
widebull surgical exposure reduction fixation and
reconstructionbull ndashndash The second option is delayed correctionbull (6 months or more) of persistent deformitiesbull using standard techniques of rhinoplasty
Deviated Nasal Septum
bull Definition of the diseasebull ndash Deviation of the nasal septum is a common causebull of unilateral nasal airway obstruction in which thebull nasal septum is displacedbull bull Epidemiologyaetiologybull ndash Developmental septal abnormalities Septal cartilage
damage in the neonatal period andbull during birth can cause severe septal deviation inbull the absence of a history of nasal trauma
Deviated Nasal Septum
bull Symptomsbull ndash Patients may present with a history of sinusitis
allergicbull rhinitis obstructive sleep apnoea previousbull nasal surgery or recent nasal trauma Unilateral or
bilateral nasal airway obstruction that is unrelievedbull with decongestants or nasal steroid sprays is oftenbull seenbull bull
Deviated Nasal SeptumDiagnosisndashExamination external dorsal deviation or the columella and caudal septummay be deflected off the midline (caudal subluxation)ndash Inspections of the nasal cavity and anterior-posteriorrhinoscopy are helpful in diagnosing the locationtype and severity of septal deformityThe endoscope is also useful in identifying polypsthe severity and extent of posterior septaldeviations and bony spurs and locating areas ofseptal perforation or mucosal injury
Deviated Nasal Septum
bull Therapybull ndash Septoplasty is a procedurebull The areabull of deviation is corrected or resected in order tobull leave behind as much cartilage and bone as
possiblebull Cartilage resection is minimised and can be
repositioned reshaped or recontoured using a variety of methods
Deviated Nasal Septum
bull ndash Indications of septoplasty before the growth period
bull of the nose is finished should be very limited bull -In these cases surgery must preserve all the
cartilagebull in order to prevent external changes of the
shape ofbull the nose
Deviated Nasal Septum
bull Complicationsbull ndash Frequent complications include haematoma andbull infection Cerebrospinal fluid leak is a rare but
potentiallybull serious complicationbull It is usually the resultbull of avulsion or damage to the cribriform plate whenbull handling the perpendicular plate of the ethmoidbull ndash Other complications include epistaxis nasal
Deviated Nasal Septum
bull Other complications include epistaxis nasal obstruction
bull due to residual deviation synechiae returnbull of the cartilaginous deviation septal perforationbull anosmia and cosmetic nasal deformities suchbull as widened alar rim margins drooping nasal tipbull columella retraction and a sunken dorsum with abull supratip saddle formation
Septal perforation with minor crusting View from provide closure of the
incision
Septal Haematoma
bull A septal haematoma is a blood collection under the perichondrium
bull of the septum and cartilagebull bull bull Epidemiologyaetiologybull ndash A septal haematoma is one of the most
severe complications of nasal trauma
Septal Haematoma
bull Diagnosisbull ndash Signs and symptoms include intense pain
swellingbull haematoma of the upper lip and philtrum
area andbull complete nasal airway obstruction
Septal HaematomaTherapyndash Management consists of drainage through a mucoperichondrial incision Immediate treatment isnecessary to prevent long-term problems such asa saddle-nose deformity perforation columellarretraction and nasal-base widening In childrenseptal destruction can lead to devastating nasal andmidfacial growth abnormalitiesbull Surgeryndash Incision and evacuation of the collection is performedDrainage of a septal haematoma should
Septal HaematomaSurgeryndash Incision and evacuation of the collection is performedDrainage of a septal haematoma should provide closure of the incision
Splints or transseptal sutures are placed to obliterate thepotential space and prevent collectionInfection involving the septal cartilage Reconstruction with autologouscartilage is then performed in a second stage Oral antibiotics should be given
Nasal DeformitySaddle-nose deformityndash A saddle-nose deformity is characterised by a loss ofnasal dorsal height and compromised nasal supportstructures -Other case observed are depressionof the middle vault and dorsum loss of nasal tipsupport and definition shortened (vertical) nasal length over rotation of the nasal tip and retrusion ofthe nasal spine and caudal septum It is also knownas a ldquoPug noserdquo or ldquoboxerrsquos noserdquo both of which referto various degrees of nasal dorsal depressionbull
Nasal DeformityEpidemiologyaetiologyndash Prevalence is higher in population groups prone to facial trauma (ie boxers athletes) those with historiesof intranasal cocaine use nasal surgery (e g radical submucosal septal resection reductive rhinoplasty)ndash A saddle-nose deformity can be congenital or acquired It can be noticed as a part of individual familialsyndromic and ethnic characteristics - Most deformities are due to traumatic and iatrogeniccauses Medical causes are Wegenerrsquosgranulomatosis relapsing polychondritis leprosy (Hansenrsquos disease) syphilis ectodermal dysplasiaand intranasal cocaine use
Nasal Deformity
bull Therapybull ndash Nasal reconstruction indications depend on patientbull selection surgeon experience and aetiology of thebull deformity bull Indications for surgery can be functionalbull aesthetic or most commonly both In individuals
with a compromised nasal airway a nasoseptalbull reconstruction is indicated
Nasal Deformity
bull Contraindications bull include patients with malignantbull chronic or autoimmune disease conditions drugbull abuse poor perioperative risk profile and unrealisticbull expectationsbull ndash Multiple previous rhinoplasties and certain
professionsbull (mixed martial artists boxers and other contactbull sports) are relative contraindications
Nasal DeformitySeptoplastyndash Septoplasty is performed to correct nasal obstructioncaused by septal deformityndash Usually septoplasty is performed under general anaesthesiawith the patient in the supine position with the head elevated by approximately 30 (Righthandedsurgeons approach from the right side)ndash Local vasoconstrictive anaesthesia is applied notonly to reduce postoperative pain but also more importantly to achieve vasoconstriction of themucosa and less intraoperative haemorrhage Lidocainewith adrenaline or epinephrine is usedalthough in patients with cardiac hypersensitivityoxymetazoline might be preferred
Nasal Deformity
bull Septoplasty begins with the incision of septal mucosabull Most operative techniques utilise a hemitransfixionbull incision at the caudal end of septum so thatbull deviation at this point might be reached as wellbull as a transfixion incision that is easily obtained ifbull needed (Right-handed surgeons normally choosebull the left side but that may vary when deviation isbull convex towards the right)
Nasal DeformityA columella retractor is placed over the columellaand by pulling it laterally the caudal border of theseptum is exposed Ala can be protected by an alaprotector A vertical incision with a no 15 bladeover the caudal end of septum is performed untilreaching the plane of the septal cartilage It is essentialto correctly identify the perichondrium and byusing the Cottle elevator dissect and lift it creatinga flap As the dissection proceeds along the septalcartilage a longer speculum (no 5) is introduced sothat elevation of the mucoperichondrium is doneunder constant visual controlndash The next step is to dissect the mucoperiostium
Nasal DeformityDissecting over the bony-cartilaginous junctionwhen joining both tunnels might be difficult and is
especially prone to membrane perforationndash If needed the same tunnels are to be created on the
other side of the septum Then deviated parts of
septum are identified and removed either with a
knife or a Freer chisel
Nasal Deformitybull septum from the maxillary crest the septum mustbull be separated from the perpendicular plate trimmedbull along the inferior border placed back onto the crestbull and sutured to the periosteum If the deformity involvesbull the vomer an osteotome is used Care mustbull be taken not to break the cribriform plate becausebull it could cause a cerebrospinal fistula
Nasal Deformity
bull Once the septal deviation is corrected the flapsbull and hemitransfixion incision are mattressed
withbull absorbable sutures Nasal packing to prevent
synechiaebull and postoperative septal haematoma mightbull be advised but should be removed within 72 h

ErysipelasIn moderate and severe cases with significantsystemic symptoms hospitalization and intravenoustreatment is required penicillin G 2ndash4mil U intravenously every 4ndash6 h Cefazolin05ndash15 gm intravenously every 8 h cefotaxime1ndash2 gm intravenously every 8 h or ceftriaxone1ndash2 gm intravenously once a day should be administeredIn patients with a penicillin allergyclindamycin 600 mg intravenously every 8 h orvancomycin 15 mgkg intravenously twice a daymay be given
ErysipelaAdditional useful therapeutic optionsbull Prednisone 30 mg over 8 days might be consideredas well as elevation of the affected siteMoist heat compresses may be usefulbull Surgeryndash Debridement and drainage are indicated when bullaeabscesses or necroses are presentbull Differential diagnosisndash Contact dermatitisndash Asteatotic eczemandash Herpes zosterndash Angioneurotic oedemandash Osteomyelitis
Furuncle
bull Definition of the diseasebull ndash A furuncle is an infection that beginsbull at the hair follicle and spreads deeper into thebull dermis and subcutaneous tissue forming abull nodule After several days it developsbull into an abscess - red painful and fluctuantbull bull bull Epidemiologyaetiologybull ndash The aetiologic agent is Staphylococcus aureus
FuruncleSymptomsndashsymptoms are local and limited to thesite of infection Furuncles usually are wherehair follicles are present bull Complicationndash One complication is furunculosis multiple draining furunclesDiagnosisndash The diagnosis is based on clinical inspection - Cultures are not necessary when there is no systemic involvement but should beconsidered if systemic therapy (in case of feversignificant cellulitis or hospitalization) or whenmethicillin-resistant Staphylococcusaureus (MRSA) is considered
FuruncleTherapyndash When the furuncle is small application of moist heat compress to promote drainage -Larger furuncles should be drained by surgical incision-After drainage the area should be cleaned with anantiseptic (with chlorhexidinebetadine) should be applied twice
a dayndash If no systemic symptoms or extensive cellulitis arepresent simple topical care is usually curative andoral antibiotics are not necessary Otherwise systemictreatment is indicated and should cover anypossible MRSA
Furuncle
bull -Recommended antibiotics are trimethoprim-sulfamethoxazole
bull 1ndash2 tablets orally twice daily doxycyclinebull 100 mg orally twice dailybull or clindamycin 300ndash450 mg orally every 8 hbull - In severe cases vancomycin 15 mgkg
intravenouslybull every 12 h or clindamycin 600 mg intravenouslybull every 8 h
Midline Granulomabull A midline granuloma is an angiocentricbull lymphoma it was referred to as polymorphicbull reticulosis lethal midline granuloma and midline
malignant reticulosisbull bull Definition of the diseasebull ndash This rare disease is a lymphoma of extranodal
presentationall cases are positive for the Epstein-Barr virus
bull -This lymphoma most commonly appears in the midface region
Midline GranulomaEpidemiologyaetiologyndash This form of lymphoma is rare in Europe and theUnited States with a higher prevalence in Asia and PeruSymptomsndash The most common presentation is nasal obstruction with a destructive mass occupying the nosesinuses and palate
-Fever night sweatsand weight loss seen usually in Hodgkinrsquos lymphomaand other non-Hodgkinrsquos lymphomas (knownas ldquoB symptomsrdquo) are uncommon
Midline GranulomaDiagnosisndash The diagnosis is based on anatomopathologicalstudy The malignancy of the tumour manifested byextensive necrosis makes the histological diagnosisdifficult and often more biopsies are required forconfirmationbull Therapyndash Therapy consists of radiotherapy with or withoutchemotherapy
Midline Granuloma
bull Prognosisbull ndash Depending on the stage long-term remission or
experience a worseningbull prognosis with relapses which may include otherbull extranodal sites bull Involvement of extranodal sitesbull including the upper airway gastrointestinal tractbull skin
Wegenerrsquos Granulomatosis
bull Definition of the diseasebull ndash Wegenerrsquos granulomatosis is a systemic chronicbull vasculitis of small- and medium-sized blood vesselsbull with an autoimmune component It affectsbull particular organs with variable predilectionbull Epidemiologyaetiologybull ndash Wegenerrsquos granulomatosis is a rare disease It affects
about 1 in 20000ndash30000 people It is more prevalentbull in middle-aged Caucasian patients
Wegenerrsquos Granulomatosis
Symptomsndash The disease may present pulmonary upper
respiratory tract or renal In the disseminated form-The localised form ndash confinedto the upper respiratory region ndash is present in 25of the patients- It consists of nonspecific manifestationssuch as nasal obstruction crusting purulentor bloody rhinorrhea and painful or painless ulcers in oral or nasal cavities which are unresponsive tostandard medical treatment
Wegenerrsquos Granulomatosis
bull In some patients the nasal septum is perforatedbull which leads to saddle-nose deformity Less
commonbull symptoms are hoarseness stridor due to
subglotticbull stenosis otalgia otorrhea and conductivebull and sensorineural hearing loss Also ocular
symptomsbull such as scleritis conjunctivitis uveitis andbull episcleritis may be present
Wegenerrsquos Granulomatosis
bull ndash In the disseminated form pulmonary involvementbull is manifested by cough dyspnoea haemoptysisbull (due to an alveolar capillaritis necrotic lesions orbull endobronchial disease) and pleuritic painndashbull -Ninety per cent of patients have nasal symptomsbull and these symptoms are usually the first
manifestationof the diseasebull -Most patients have also renal involvementbull even if it is subclinical
Wegenerrsquos Granulomatosis
Diagnosis ndash Diagnosis of Wegenerrsquos granulomatosis is based on clinical findings that demonstrate lung (chest x-ray) kidney (urine analysis) or upper respiratory tract
involvement (oral or nasal ulcers or discharge) - positive blood analysis for cytoplasmic-staining antineutrophil
cytoplasmic antibodies (c-ANCA) and confirming proteinase 3 (PR3) ANCA or myeloperoxidase (MPO) ANCA ndash Biopsy is essential for diagnosis nonspecific chronic inflammation
and necrosis -Bacterial and fungal infections
Wegenerrsquos Granulomatosis
Therapyndash Conservative therapybull In the induction of disease remission highdosesteroids (e g prednisone 1 mgkgday) for1 month with tapering over several months aregiven In addition cyclophosphamide (2 mgkgday) should be administered for 6ndash12 monthsuntil symptoms disappear In the maintenanceof remission cyclophosphamide should be
Wegenerrsquos Granulomatosis
Antibiotics mainly trimethoprim-sulfamethoxazoleare given for prophylaxis againstPneumocystis jiroveci (formerly Pneumocystiscarinii) pneumonia (PCP) which may developduring immunosuppression and have a role inpreventing recurrencesbull Sinonasal manifestations may be treated with topical nasal steroids and nasal irrigations lowdosesystemic steroids and antibiotics when bacterial infection (typically Staphylococcus species) is suspected
Wegenerrsquos Granulomatosis
bull Prognosisbull ndash Most of the patients respond well to treatmentbull achieving symptom-free intervals of 5ndash20 yearsbull or more bull -Anatomical problems (sinusitis trachealbull stenosis) may require surgery bull Relapses can be long and troublesomebull Long-term complications are chronicbull renal failure hearing loss and deafness
Nasal Fractures Definition ndash A nasal fracture is a disruption of the nasal bone structure due to trauma It is the most frequently fractured facial bone Epidemiologyaetiology ndash Sports falls and assaults are the usual mechanisms of fracture -Males are affected twice as often as are females -Paediatric populations with a incidences during the second and third decades of life -Variables such as force impact direction nature of the striking object age and other will influence the pattern of injury to the components of the nose
Nasal Fractures
bull Symptomsbull ndash Deformity swelling epistaxis and periorbital
ecchymosis are signs that are suggestive of nasal fracture
bull bony crepitus and nasal segment mobilitybull ndash Epiphora bull Severe bilateral injuries to the lachrymal bones
arebull associated with depressed nasal fractures
Nasal Fractures Complications ndash Septal haematoma is one of the most severe early complications of nasal trauma and without drainage it results in abscess formation 6ndash7 days after trauma producing necrosis of the septal cartilage -Long-term problems such as saddle-nose deformity perforation columellar retraction and nasalbase
Septal infection could lead to osteomyelitis orbital and intracranial abscesses meningitis and cavernous sinus thrombosis -Cerebrospinal fluid leakage is a common complication of severe
nasal and frontal fractures
Nasal Fractures
bull Diagnostic proceduresbull ndash Inspectionbull bull Changes of appearance such as deviation andbull asymmetry bleeding watery drainage changesbull in nasal breathing and smell It is useful to comparebull the current presentation with old photographsbull (up to 40 of normal individuals havebull significant nose malformations)
Nasal Fractures Physical examination bull The diagnosis of a nasal fracture is made primarily by physical examination epistaxis nasal swelling and periorbital ecchymosis Nasal shape in the lateral and frontal inspection should be assessed Grasping the dorsum between two fingers and rocking the pyramid back and forth aids in assessing the mobility of nasal bones Internal structures should be evaluated by using a headlight and nasal speculum Clotted blood is removed by suction and assessment of haematoma mucosal tears and active bleeding is performed Bimanual palpation of the septum helps to differentiate septal swelling from haematoma ndash
Nasal FracturesRadiographybull There is no clear evidence of the role of radiographyin the management of nasal fracturesPlain films have up to a 66 false-positive rateas a result of misinterpretation of normal suturelines In addition old fractures are difficult todistinguishbull Three-dimensional CT is recommended for extensiveinjuries involving the nasal-orbital-ethmoidalcomplexndash
Nasal Fractures
bull Additionaluseful diagnostic proceduresbull bull Using a 0 or 30deg 4-mm endoscope is helpful inbull the assessment of posterior abnormalities If thebull patient is heavily sedated Brown-Gruss
provocationbull manoeuvres may be performed to determinebull deformities in upper middle or lower segmentsbull by compressing each compartment
Nasal FracturesConservative treatmentndash Treatment of bleedingbull For localised bleeding anterior sources may becauterised by silver nitrate or sealed with topicalmaterials such as thrombin combined withgelatin foam fibrin glue FloSealreg or other procoagulantmaterials If conservative measuresfail a formal anterior packing is placedbull Bleeding from branches of sphenopalatine orethmoid vessels requires anterior-posteriorpacking
Nasal Fractures
bull bull Surgical methods such as direct endoscopic vessel
bull cauterization or ligation have been shown tobull offer better haemostasis and patient comfortbull Angiography with embolization can also be
consideredbull in cases refractory to more conservativebull approaches
Nasal Fractures
bull Type of reductionbull bull Nondisplaced fractures should be treated withbull observation alone Closed nasal reduction is thebull best choice for simple injuries (isolated unilateralbull with medial displacement)bull bull An open approach should be considered in
severebull trauma (bilateral depressed fractures)
Nasal Fracturesbull Surgical principlesbull ndash Topical anaesthesia with cotton pledgets soakedbull with 4 cocaine or 005 oxymethazoline combinedbull with 4 topical lidocaine should be appliedbull for 5ndash10 min Local anaesthesia should also be injectedbull (1 lidocaine and 1100000 epinephrine)bull along the septum lateral walls and floor of the nasalbull cavitybull bull
Nasal FracturesClosed reductionndashndash The nasal bones are grasped between two fingersand pressure is applied laterally in theopposite direction of the deviation A bluntelevator may be used from within the nose incases of significant medial collapse Walshamforceps can be of help Reduction of the septumshould be performed with the use ofAsch forceps
Nasal Fractures
bull To prevent collapse of the postreductionbull framework nasal packing should be placedbull for 3ndash5 days Septum splints are recommendedbull in comminuted septal fractures withbull severe mucosal lesions External nasal splintingbull for 10 days (Aquaplastreg Thermoplastreg)bull provides nasal protection Nasal saline spraysbull prevent crusting and oral antibiotics should
Nasal Fractures
bull Open reductionbull ndashndash Immediate repair of fractures by using
widebull surgical exposure reduction fixation and
reconstructionbull ndashndash The second option is delayed correctionbull (6 months or more) of persistent deformitiesbull using standard techniques of rhinoplasty
Deviated Nasal Septum
bull Definition of the diseasebull ndash Deviation of the nasal septum is a common causebull of unilateral nasal airway obstruction in which thebull nasal septum is displacedbull bull Epidemiologyaetiologybull ndash Developmental septal abnormalities Septal cartilage
damage in the neonatal period andbull during birth can cause severe septal deviation inbull the absence of a history of nasal trauma
Deviated Nasal Septum
bull Symptomsbull ndash Patients may present with a history of sinusitis
allergicbull rhinitis obstructive sleep apnoea previousbull nasal surgery or recent nasal trauma Unilateral or
bilateral nasal airway obstruction that is unrelievedbull with decongestants or nasal steroid sprays is oftenbull seenbull bull
Deviated Nasal SeptumDiagnosisndashExamination external dorsal deviation or the columella and caudal septummay be deflected off the midline (caudal subluxation)ndash Inspections of the nasal cavity and anterior-posteriorrhinoscopy are helpful in diagnosing the locationtype and severity of septal deformityThe endoscope is also useful in identifying polypsthe severity and extent of posterior septaldeviations and bony spurs and locating areas ofseptal perforation or mucosal injury
Deviated Nasal Septum
bull Therapybull ndash Septoplasty is a procedurebull The areabull of deviation is corrected or resected in order tobull leave behind as much cartilage and bone as
possiblebull Cartilage resection is minimised and can be
repositioned reshaped or recontoured using a variety of methods
Deviated Nasal Septum
bull ndash Indications of septoplasty before the growth period
bull of the nose is finished should be very limited bull -In these cases surgery must preserve all the
cartilagebull in order to prevent external changes of the
shape ofbull the nose
Deviated Nasal Septum
bull Complicationsbull ndash Frequent complications include haematoma andbull infection Cerebrospinal fluid leak is a rare but
potentiallybull serious complicationbull It is usually the resultbull of avulsion or damage to the cribriform plate whenbull handling the perpendicular plate of the ethmoidbull ndash Other complications include epistaxis nasal
Deviated Nasal Septum
bull Other complications include epistaxis nasal obstruction
bull due to residual deviation synechiae returnbull of the cartilaginous deviation septal perforationbull anosmia and cosmetic nasal deformities suchbull as widened alar rim margins drooping nasal tipbull columella retraction and a sunken dorsum with abull supratip saddle formation
Septal perforation with minor crusting View from provide closure of the
incision
Septal Haematoma
bull A septal haematoma is a blood collection under the perichondrium
bull of the septum and cartilagebull bull bull Epidemiologyaetiologybull ndash A septal haematoma is one of the most
severe complications of nasal trauma
Septal Haematoma
bull Diagnosisbull ndash Signs and symptoms include intense pain
swellingbull haematoma of the upper lip and philtrum
area andbull complete nasal airway obstruction
Septal HaematomaTherapyndash Management consists of drainage through a mucoperichondrial incision Immediate treatment isnecessary to prevent long-term problems such asa saddle-nose deformity perforation columellarretraction and nasal-base widening In childrenseptal destruction can lead to devastating nasal andmidfacial growth abnormalitiesbull Surgeryndash Incision and evacuation of the collection is performedDrainage of a septal haematoma should
Septal HaematomaSurgeryndash Incision and evacuation of the collection is performedDrainage of a septal haematoma should provide closure of the incision
Splints or transseptal sutures are placed to obliterate thepotential space and prevent collectionInfection involving the septal cartilage Reconstruction with autologouscartilage is then performed in a second stage Oral antibiotics should be given
Nasal DeformitySaddle-nose deformityndash A saddle-nose deformity is characterised by a loss ofnasal dorsal height and compromised nasal supportstructures -Other case observed are depressionof the middle vault and dorsum loss of nasal tipsupport and definition shortened (vertical) nasal length over rotation of the nasal tip and retrusion ofthe nasal spine and caudal septum It is also knownas a ldquoPug noserdquo or ldquoboxerrsquos noserdquo both of which referto various degrees of nasal dorsal depressionbull
Nasal DeformityEpidemiologyaetiologyndash Prevalence is higher in population groups prone to facial trauma (ie boxers athletes) those with historiesof intranasal cocaine use nasal surgery (e g radical submucosal septal resection reductive rhinoplasty)ndash A saddle-nose deformity can be congenital or acquired It can be noticed as a part of individual familialsyndromic and ethnic characteristics - Most deformities are due to traumatic and iatrogeniccauses Medical causes are Wegenerrsquosgranulomatosis relapsing polychondritis leprosy (Hansenrsquos disease) syphilis ectodermal dysplasiaand intranasal cocaine use
Nasal Deformity
bull Therapybull ndash Nasal reconstruction indications depend on patientbull selection surgeon experience and aetiology of thebull deformity bull Indications for surgery can be functionalbull aesthetic or most commonly both In individuals
with a compromised nasal airway a nasoseptalbull reconstruction is indicated
Nasal Deformity
bull Contraindications bull include patients with malignantbull chronic or autoimmune disease conditions drugbull abuse poor perioperative risk profile and unrealisticbull expectationsbull ndash Multiple previous rhinoplasties and certain
professionsbull (mixed martial artists boxers and other contactbull sports) are relative contraindications
Nasal DeformitySeptoplastyndash Septoplasty is performed to correct nasal obstructioncaused by septal deformityndash Usually septoplasty is performed under general anaesthesiawith the patient in the supine position with the head elevated by approximately 30 (Righthandedsurgeons approach from the right side)ndash Local vasoconstrictive anaesthesia is applied notonly to reduce postoperative pain but also more importantly to achieve vasoconstriction of themucosa and less intraoperative haemorrhage Lidocainewith adrenaline or epinephrine is usedalthough in patients with cardiac hypersensitivityoxymetazoline might be preferred
Nasal Deformity
bull Septoplasty begins with the incision of septal mucosabull Most operative techniques utilise a hemitransfixionbull incision at the caudal end of septum so thatbull deviation at this point might be reached as wellbull as a transfixion incision that is easily obtained ifbull needed (Right-handed surgeons normally choosebull the left side but that may vary when deviation isbull convex towards the right)
Nasal DeformityA columella retractor is placed over the columellaand by pulling it laterally the caudal border of theseptum is exposed Ala can be protected by an alaprotector A vertical incision with a no 15 bladeover the caudal end of septum is performed untilreaching the plane of the septal cartilage It is essentialto correctly identify the perichondrium and byusing the Cottle elevator dissect and lift it creatinga flap As the dissection proceeds along the septalcartilage a longer speculum (no 5) is introduced sothat elevation of the mucoperichondrium is doneunder constant visual controlndash The next step is to dissect the mucoperiostium
Nasal DeformityDissecting over the bony-cartilaginous junctionwhen joining both tunnels might be difficult and is
especially prone to membrane perforationndash If needed the same tunnels are to be created on the
other side of the septum Then deviated parts of
septum are identified and removed either with a
knife or a Freer chisel
Nasal Deformitybull septum from the maxillary crest the septum mustbull be separated from the perpendicular plate trimmedbull along the inferior border placed back onto the crestbull and sutured to the periosteum If the deformity involvesbull the vomer an osteotome is used Care mustbull be taken not to break the cribriform plate becausebull it could cause a cerebrospinal fistula
Nasal Deformity
bull Once the septal deviation is corrected the flapsbull and hemitransfixion incision are mattressed
withbull absorbable sutures Nasal packing to prevent
synechiaebull and postoperative septal haematoma mightbull be advised but should be removed within 72 h

ErysipelaAdditional useful therapeutic optionsbull Prednisone 30 mg over 8 days might be consideredas well as elevation of the affected siteMoist heat compresses may be usefulbull Surgeryndash Debridement and drainage are indicated when bullaeabscesses or necroses are presentbull Differential diagnosisndash Contact dermatitisndash Asteatotic eczemandash Herpes zosterndash Angioneurotic oedemandash Osteomyelitis
Furuncle
bull Definition of the diseasebull ndash A furuncle is an infection that beginsbull at the hair follicle and spreads deeper into thebull dermis and subcutaneous tissue forming abull nodule After several days it developsbull into an abscess - red painful and fluctuantbull bull bull Epidemiologyaetiologybull ndash The aetiologic agent is Staphylococcus aureus
FuruncleSymptomsndashsymptoms are local and limited to thesite of infection Furuncles usually are wherehair follicles are present bull Complicationndash One complication is furunculosis multiple draining furunclesDiagnosisndash The diagnosis is based on clinical inspection - Cultures are not necessary when there is no systemic involvement but should beconsidered if systemic therapy (in case of feversignificant cellulitis or hospitalization) or whenmethicillin-resistant Staphylococcusaureus (MRSA) is considered
FuruncleTherapyndash When the furuncle is small application of moist heat compress to promote drainage -Larger furuncles should be drained by surgical incision-After drainage the area should be cleaned with anantiseptic (with chlorhexidinebetadine) should be applied twice
a dayndash If no systemic symptoms or extensive cellulitis arepresent simple topical care is usually curative andoral antibiotics are not necessary Otherwise systemictreatment is indicated and should cover anypossible MRSA
Furuncle
bull -Recommended antibiotics are trimethoprim-sulfamethoxazole
bull 1ndash2 tablets orally twice daily doxycyclinebull 100 mg orally twice dailybull or clindamycin 300ndash450 mg orally every 8 hbull - In severe cases vancomycin 15 mgkg
intravenouslybull every 12 h or clindamycin 600 mg intravenouslybull every 8 h
Midline Granulomabull A midline granuloma is an angiocentricbull lymphoma it was referred to as polymorphicbull reticulosis lethal midline granuloma and midline
malignant reticulosisbull bull Definition of the diseasebull ndash This rare disease is a lymphoma of extranodal
presentationall cases are positive for the Epstein-Barr virus
bull -This lymphoma most commonly appears in the midface region
Midline GranulomaEpidemiologyaetiologyndash This form of lymphoma is rare in Europe and theUnited States with a higher prevalence in Asia and PeruSymptomsndash The most common presentation is nasal obstruction with a destructive mass occupying the nosesinuses and palate
-Fever night sweatsand weight loss seen usually in Hodgkinrsquos lymphomaand other non-Hodgkinrsquos lymphomas (knownas ldquoB symptomsrdquo) are uncommon
Midline GranulomaDiagnosisndash The diagnosis is based on anatomopathologicalstudy The malignancy of the tumour manifested byextensive necrosis makes the histological diagnosisdifficult and often more biopsies are required forconfirmationbull Therapyndash Therapy consists of radiotherapy with or withoutchemotherapy
Midline Granuloma
bull Prognosisbull ndash Depending on the stage long-term remission or
experience a worseningbull prognosis with relapses which may include otherbull extranodal sites bull Involvement of extranodal sitesbull including the upper airway gastrointestinal tractbull skin
Wegenerrsquos Granulomatosis
bull Definition of the diseasebull ndash Wegenerrsquos granulomatosis is a systemic chronicbull vasculitis of small- and medium-sized blood vesselsbull with an autoimmune component It affectsbull particular organs with variable predilectionbull Epidemiologyaetiologybull ndash Wegenerrsquos granulomatosis is a rare disease It affects
about 1 in 20000ndash30000 people It is more prevalentbull in middle-aged Caucasian patients
Wegenerrsquos Granulomatosis
Symptomsndash The disease may present pulmonary upper
respiratory tract or renal In the disseminated form-The localised form ndash confinedto the upper respiratory region ndash is present in 25of the patients- It consists of nonspecific manifestationssuch as nasal obstruction crusting purulentor bloody rhinorrhea and painful or painless ulcers in oral or nasal cavities which are unresponsive tostandard medical treatment
Wegenerrsquos Granulomatosis
bull In some patients the nasal septum is perforatedbull which leads to saddle-nose deformity Less
commonbull symptoms are hoarseness stridor due to
subglotticbull stenosis otalgia otorrhea and conductivebull and sensorineural hearing loss Also ocular
symptomsbull such as scleritis conjunctivitis uveitis andbull episcleritis may be present
Wegenerrsquos Granulomatosis
bull ndash In the disseminated form pulmonary involvementbull is manifested by cough dyspnoea haemoptysisbull (due to an alveolar capillaritis necrotic lesions orbull endobronchial disease) and pleuritic painndashbull -Ninety per cent of patients have nasal symptomsbull and these symptoms are usually the first
manifestationof the diseasebull -Most patients have also renal involvementbull even if it is subclinical
Wegenerrsquos Granulomatosis
Diagnosis ndash Diagnosis of Wegenerrsquos granulomatosis is based on clinical findings that demonstrate lung (chest x-ray) kidney (urine analysis) or upper respiratory tract
involvement (oral or nasal ulcers or discharge) - positive blood analysis for cytoplasmic-staining antineutrophil
cytoplasmic antibodies (c-ANCA) and confirming proteinase 3 (PR3) ANCA or myeloperoxidase (MPO) ANCA ndash Biopsy is essential for diagnosis nonspecific chronic inflammation
and necrosis -Bacterial and fungal infections
Wegenerrsquos Granulomatosis
Therapyndash Conservative therapybull In the induction of disease remission highdosesteroids (e g prednisone 1 mgkgday) for1 month with tapering over several months aregiven In addition cyclophosphamide (2 mgkgday) should be administered for 6ndash12 monthsuntil symptoms disappear In the maintenanceof remission cyclophosphamide should be
Wegenerrsquos Granulomatosis
Antibiotics mainly trimethoprim-sulfamethoxazoleare given for prophylaxis againstPneumocystis jiroveci (formerly Pneumocystiscarinii) pneumonia (PCP) which may developduring immunosuppression and have a role inpreventing recurrencesbull Sinonasal manifestations may be treated with topical nasal steroids and nasal irrigations lowdosesystemic steroids and antibiotics when bacterial infection (typically Staphylococcus species) is suspected
Wegenerrsquos Granulomatosis
bull Prognosisbull ndash Most of the patients respond well to treatmentbull achieving symptom-free intervals of 5ndash20 yearsbull or more bull -Anatomical problems (sinusitis trachealbull stenosis) may require surgery bull Relapses can be long and troublesomebull Long-term complications are chronicbull renal failure hearing loss and deafness
Nasal Fractures Definition ndash A nasal fracture is a disruption of the nasal bone structure due to trauma It is the most frequently fractured facial bone Epidemiologyaetiology ndash Sports falls and assaults are the usual mechanisms of fracture -Males are affected twice as often as are females -Paediatric populations with a incidences during the second and third decades of life -Variables such as force impact direction nature of the striking object age and other will influence the pattern of injury to the components of the nose
Nasal Fractures
bull Symptomsbull ndash Deformity swelling epistaxis and periorbital
ecchymosis are signs that are suggestive of nasal fracture
bull bony crepitus and nasal segment mobilitybull ndash Epiphora bull Severe bilateral injuries to the lachrymal bones
arebull associated with depressed nasal fractures
Nasal Fractures Complications ndash Septal haematoma is one of the most severe early complications of nasal trauma and without drainage it results in abscess formation 6ndash7 days after trauma producing necrosis of the septal cartilage -Long-term problems such as saddle-nose deformity perforation columellar retraction and nasalbase
Septal infection could lead to osteomyelitis orbital and intracranial abscesses meningitis and cavernous sinus thrombosis -Cerebrospinal fluid leakage is a common complication of severe
nasal and frontal fractures
Nasal Fractures
bull Diagnostic proceduresbull ndash Inspectionbull bull Changes of appearance such as deviation andbull asymmetry bleeding watery drainage changesbull in nasal breathing and smell It is useful to comparebull the current presentation with old photographsbull (up to 40 of normal individuals havebull significant nose malformations)
Nasal Fractures Physical examination bull The diagnosis of a nasal fracture is made primarily by physical examination epistaxis nasal swelling and periorbital ecchymosis Nasal shape in the lateral and frontal inspection should be assessed Grasping the dorsum between two fingers and rocking the pyramid back and forth aids in assessing the mobility of nasal bones Internal structures should be evaluated by using a headlight and nasal speculum Clotted blood is removed by suction and assessment of haematoma mucosal tears and active bleeding is performed Bimanual palpation of the septum helps to differentiate septal swelling from haematoma ndash
Nasal FracturesRadiographybull There is no clear evidence of the role of radiographyin the management of nasal fracturesPlain films have up to a 66 false-positive rateas a result of misinterpretation of normal suturelines In addition old fractures are difficult todistinguishbull Three-dimensional CT is recommended for extensiveinjuries involving the nasal-orbital-ethmoidalcomplexndash
Nasal Fractures
bull Additionaluseful diagnostic proceduresbull bull Using a 0 or 30deg 4-mm endoscope is helpful inbull the assessment of posterior abnormalities If thebull patient is heavily sedated Brown-Gruss
provocationbull manoeuvres may be performed to determinebull deformities in upper middle or lower segmentsbull by compressing each compartment
Nasal FracturesConservative treatmentndash Treatment of bleedingbull For localised bleeding anterior sources may becauterised by silver nitrate or sealed with topicalmaterials such as thrombin combined withgelatin foam fibrin glue FloSealreg or other procoagulantmaterials If conservative measuresfail a formal anterior packing is placedbull Bleeding from branches of sphenopalatine orethmoid vessels requires anterior-posteriorpacking
Nasal Fractures
bull bull Surgical methods such as direct endoscopic vessel
bull cauterization or ligation have been shown tobull offer better haemostasis and patient comfortbull Angiography with embolization can also be
consideredbull in cases refractory to more conservativebull approaches
Nasal Fractures
bull Type of reductionbull bull Nondisplaced fractures should be treated withbull observation alone Closed nasal reduction is thebull best choice for simple injuries (isolated unilateralbull with medial displacement)bull bull An open approach should be considered in
severebull trauma (bilateral depressed fractures)
Nasal Fracturesbull Surgical principlesbull ndash Topical anaesthesia with cotton pledgets soakedbull with 4 cocaine or 005 oxymethazoline combinedbull with 4 topical lidocaine should be appliedbull for 5ndash10 min Local anaesthesia should also be injectedbull (1 lidocaine and 1100000 epinephrine)bull along the septum lateral walls and floor of the nasalbull cavitybull bull
Nasal FracturesClosed reductionndashndash The nasal bones are grasped between two fingersand pressure is applied laterally in theopposite direction of the deviation A bluntelevator may be used from within the nose incases of significant medial collapse Walshamforceps can be of help Reduction of the septumshould be performed with the use ofAsch forceps
Nasal Fractures
bull To prevent collapse of the postreductionbull framework nasal packing should be placedbull for 3ndash5 days Septum splints are recommendedbull in comminuted septal fractures withbull severe mucosal lesions External nasal splintingbull for 10 days (Aquaplastreg Thermoplastreg)bull provides nasal protection Nasal saline spraysbull prevent crusting and oral antibiotics should
Nasal Fractures
bull Open reductionbull ndashndash Immediate repair of fractures by using
widebull surgical exposure reduction fixation and
reconstructionbull ndashndash The second option is delayed correctionbull (6 months or more) of persistent deformitiesbull using standard techniques of rhinoplasty
Deviated Nasal Septum
bull Definition of the diseasebull ndash Deviation of the nasal septum is a common causebull of unilateral nasal airway obstruction in which thebull nasal septum is displacedbull bull Epidemiologyaetiologybull ndash Developmental septal abnormalities Septal cartilage
damage in the neonatal period andbull during birth can cause severe septal deviation inbull the absence of a history of nasal trauma
Deviated Nasal Septum
bull Symptomsbull ndash Patients may present with a history of sinusitis
allergicbull rhinitis obstructive sleep apnoea previousbull nasal surgery or recent nasal trauma Unilateral or
bilateral nasal airway obstruction that is unrelievedbull with decongestants or nasal steroid sprays is oftenbull seenbull bull
Deviated Nasal SeptumDiagnosisndashExamination external dorsal deviation or the columella and caudal septummay be deflected off the midline (caudal subluxation)ndash Inspections of the nasal cavity and anterior-posteriorrhinoscopy are helpful in diagnosing the locationtype and severity of septal deformityThe endoscope is also useful in identifying polypsthe severity and extent of posterior septaldeviations and bony spurs and locating areas ofseptal perforation or mucosal injury
Deviated Nasal Septum
bull Therapybull ndash Septoplasty is a procedurebull The areabull of deviation is corrected or resected in order tobull leave behind as much cartilage and bone as
possiblebull Cartilage resection is minimised and can be
repositioned reshaped or recontoured using a variety of methods
Deviated Nasal Septum
bull ndash Indications of septoplasty before the growth period
bull of the nose is finished should be very limited bull -In these cases surgery must preserve all the
cartilagebull in order to prevent external changes of the
shape ofbull the nose
Deviated Nasal Septum
bull Complicationsbull ndash Frequent complications include haematoma andbull infection Cerebrospinal fluid leak is a rare but
potentiallybull serious complicationbull It is usually the resultbull of avulsion or damage to the cribriform plate whenbull handling the perpendicular plate of the ethmoidbull ndash Other complications include epistaxis nasal
Deviated Nasal Septum
bull Other complications include epistaxis nasal obstruction
bull due to residual deviation synechiae returnbull of the cartilaginous deviation septal perforationbull anosmia and cosmetic nasal deformities suchbull as widened alar rim margins drooping nasal tipbull columella retraction and a sunken dorsum with abull supratip saddle formation
Septal perforation with minor crusting View from provide closure of the
incision
Septal Haematoma
bull A septal haematoma is a blood collection under the perichondrium
bull of the septum and cartilagebull bull bull Epidemiologyaetiologybull ndash A septal haematoma is one of the most
severe complications of nasal trauma
Septal Haematoma
bull Diagnosisbull ndash Signs and symptoms include intense pain
swellingbull haematoma of the upper lip and philtrum
area andbull complete nasal airway obstruction
Septal HaematomaTherapyndash Management consists of drainage through a mucoperichondrial incision Immediate treatment isnecessary to prevent long-term problems such asa saddle-nose deformity perforation columellarretraction and nasal-base widening In childrenseptal destruction can lead to devastating nasal andmidfacial growth abnormalitiesbull Surgeryndash Incision and evacuation of the collection is performedDrainage of a septal haematoma should
Septal HaematomaSurgeryndash Incision and evacuation of the collection is performedDrainage of a septal haematoma should provide closure of the incision
Splints or transseptal sutures are placed to obliterate thepotential space and prevent collectionInfection involving the septal cartilage Reconstruction with autologouscartilage is then performed in a second stage Oral antibiotics should be given
Nasal DeformitySaddle-nose deformityndash A saddle-nose deformity is characterised by a loss ofnasal dorsal height and compromised nasal supportstructures -Other case observed are depressionof the middle vault and dorsum loss of nasal tipsupport and definition shortened (vertical) nasal length over rotation of the nasal tip and retrusion ofthe nasal spine and caudal septum It is also knownas a ldquoPug noserdquo or ldquoboxerrsquos noserdquo both of which referto various degrees of nasal dorsal depressionbull
Nasal DeformityEpidemiologyaetiologyndash Prevalence is higher in population groups prone to facial trauma (ie boxers athletes) those with historiesof intranasal cocaine use nasal surgery (e g radical submucosal septal resection reductive rhinoplasty)ndash A saddle-nose deformity can be congenital or acquired It can be noticed as a part of individual familialsyndromic and ethnic characteristics - Most deformities are due to traumatic and iatrogeniccauses Medical causes are Wegenerrsquosgranulomatosis relapsing polychondritis leprosy (Hansenrsquos disease) syphilis ectodermal dysplasiaand intranasal cocaine use
Nasal Deformity
bull Therapybull ndash Nasal reconstruction indications depend on patientbull selection surgeon experience and aetiology of thebull deformity bull Indications for surgery can be functionalbull aesthetic or most commonly both In individuals
with a compromised nasal airway a nasoseptalbull reconstruction is indicated
Nasal Deformity
bull Contraindications bull include patients with malignantbull chronic or autoimmune disease conditions drugbull abuse poor perioperative risk profile and unrealisticbull expectationsbull ndash Multiple previous rhinoplasties and certain
professionsbull (mixed martial artists boxers and other contactbull sports) are relative contraindications
Nasal DeformitySeptoplastyndash Septoplasty is performed to correct nasal obstructioncaused by septal deformityndash Usually septoplasty is performed under general anaesthesiawith the patient in the supine position with the head elevated by approximately 30 (Righthandedsurgeons approach from the right side)ndash Local vasoconstrictive anaesthesia is applied notonly to reduce postoperative pain but also more importantly to achieve vasoconstriction of themucosa and less intraoperative haemorrhage Lidocainewith adrenaline or epinephrine is usedalthough in patients with cardiac hypersensitivityoxymetazoline might be preferred
Nasal Deformity
bull Septoplasty begins with the incision of septal mucosabull Most operative techniques utilise a hemitransfixionbull incision at the caudal end of septum so thatbull deviation at this point might be reached as wellbull as a transfixion incision that is easily obtained ifbull needed (Right-handed surgeons normally choosebull the left side but that may vary when deviation isbull convex towards the right)
Nasal DeformityA columella retractor is placed over the columellaand by pulling it laterally the caudal border of theseptum is exposed Ala can be protected by an alaprotector A vertical incision with a no 15 bladeover the caudal end of septum is performed untilreaching the plane of the septal cartilage It is essentialto correctly identify the perichondrium and byusing the Cottle elevator dissect and lift it creatinga flap As the dissection proceeds along the septalcartilage a longer speculum (no 5) is introduced sothat elevation of the mucoperichondrium is doneunder constant visual controlndash The next step is to dissect the mucoperiostium
Nasal DeformityDissecting over the bony-cartilaginous junctionwhen joining both tunnels might be difficult and is
especially prone to membrane perforationndash If needed the same tunnels are to be created on the
other side of the septum Then deviated parts of
septum are identified and removed either with a
knife or a Freer chisel
Nasal Deformitybull septum from the maxillary crest the septum mustbull be separated from the perpendicular plate trimmedbull along the inferior border placed back onto the crestbull and sutured to the periosteum If the deformity involvesbull the vomer an osteotome is used Care mustbull be taken not to break the cribriform plate becausebull it could cause a cerebrospinal fistula
Nasal Deformity
bull Once the septal deviation is corrected the flapsbull and hemitransfixion incision are mattressed
withbull absorbable sutures Nasal packing to prevent
synechiaebull and postoperative septal haematoma mightbull be advised but should be removed within 72 h

Furuncle
bull Definition of the diseasebull ndash A furuncle is an infection that beginsbull at the hair follicle and spreads deeper into thebull dermis and subcutaneous tissue forming abull nodule After several days it developsbull into an abscess - red painful and fluctuantbull bull bull Epidemiologyaetiologybull ndash The aetiologic agent is Staphylococcus aureus
FuruncleSymptomsndashsymptoms are local and limited to thesite of infection Furuncles usually are wherehair follicles are present bull Complicationndash One complication is furunculosis multiple draining furunclesDiagnosisndash The diagnosis is based on clinical inspection - Cultures are not necessary when there is no systemic involvement but should beconsidered if systemic therapy (in case of feversignificant cellulitis or hospitalization) or whenmethicillin-resistant Staphylococcusaureus (MRSA) is considered
FuruncleTherapyndash When the furuncle is small application of moist heat compress to promote drainage -Larger furuncles should be drained by surgical incision-After drainage the area should be cleaned with anantiseptic (with chlorhexidinebetadine) should be applied twice
a dayndash If no systemic symptoms or extensive cellulitis arepresent simple topical care is usually curative andoral antibiotics are not necessary Otherwise systemictreatment is indicated and should cover anypossible MRSA
Furuncle
bull -Recommended antibiotics are trimethoprim-sulfamethoxazole
bull 1ndash2 tablets orally twice daily doxycyclinebull 100 mg orally twice dailybull or clindamycin 300ndash450 mg orally every 8 hbull - In severe cases vancomycin 15 mgkg
intravenouslybull every 12 h or clindamycin 600 mg intravenouslybull every 8 h
Midline Granulomabull A midline granuloma is an angiocentricbull lymphoma it was referred to as polymorphicbull reticulosis lethal midline granuloma and midline
malignant reticulosisbull bull Definition of the diseasebull ndash This rare disease is a lymphoma of extranodal
presentationall cases are positive for the Epstein-Barr virus
bull -This lymphoma most commonly appears in the midface region
Midline GranulomaEpidemiologyaetiologyndash This form of lymphoma is rare in Europe and theUnited States with a higher prevalence in Asia and PeruSymptomsndash The most common presentation is nasal obstruction with a destructive mass occupying the nosesinuses and palate
-Fever night sweatsand weight loss seen usually in Hodgkinrsquos lymphomaand other non-Hodgkinrsquos lymphomas (knownas ldquoB symptomsrdquo) are uncommon
Midline GranulomaDiagnosisndash The diagnosis is based on anatomopathologicalstudy The malignancy of the tumour manifested byextensive necrosis makes the histological diagnosisdifficult and often more biopsies are required forconfirmationbull Therapyndash Therapy consists of radiotherapy with or withoutchemotherapy
Midline Granuloma
bull Prognosisbull ndash Depending on the stage long-term remission or
experience a worseningbull prognosis with relapses which may include otherbull extranodal sites bull Involvement of extranodal sitesbull including the upper airway gastrointestinal tractbull skin
Wegenerrsquos Granulomatosis
bull Definition of the diseasebull ndash Wegenerrsquos granulomatosis is a systemic chronicbull vasculitis of small- and medium-sized blood vesselsbull with an autoimmune component It affectsbull particular organs with variable predilectionbull Epidemiologyaetiologybull ndash Wegenerrsquos granulomatosis is a rare disease It affects
about 1 in 20000ndash30000 people It is more prevalentbull in middle-aged Caucasian patients
Wegenerrsquos Granulomatosis
Symptomsndash The disease may present pulmonary upper
respiratory tract or renal In the disseminated form-The localised form ndash confinedto the upper respiratory region ndash is present in 25of the patients- It consists of nonspecific manifestationssuch as nasal obstruction crusting purulentor bloody rhinorrhea and painful or painless ulcers in oral or nasal cavities which are unresponsive tostandard medical treatment
Wegenerrsquos Granulomatosis
bull In some patients the nasal septum is perforatedbull which leads to saddle-nose deformity Less
commonbull symptoms are hoarseness stridor due to
subglotticbull stenosis otalgia otorrhea and conductivebull and sensorineural hearing loss Also ocular
symptomsbull such as scleritis conjunctivitis uveitis andbull episcleritis may be present
Wegenerrsquos Granulomatosis
bull ndash In the disseminated form pulmonary involvementbull is manifested by cough dyspnoea haemoptysisbull (due to an alveolar capillaritis necrotic lesions orbull endobronchial disease) and pleuritic painndashbull -Ninety per cent of patients have nasal symptomsbull and these symptoms are usually the first
manifestationof the diseasebull -Most patients have also renal involvementbull even if it is subclinical
Wegenerrsquos Granulomatosis
Diagnosis ndash Diagnosis of Wegenerrsquos granulomatosis is based on clinical findings that demonstrate lung (chest x-ray) kidney (urine analysis) or upper respiratory tract
involvement (oral or nasal ulcers or discharge) - positive blood analysis for cytoplasmic-staining antineutrophil
cytoplasmic antibodies (c-ANCA) and confirming proteinase 3 (PR3) ANCA or myeloperoxidase (MPO) ANCA ndash Biopsy is essential for diagnosis nonspecific chronic inflammation
and necrosis -Bacterial and fungal infections
Wegenerrsquos Granulomatosis
Therapyndash Conservative therapybull In the induction of disease remission highdosesteroids (e g prednisone 1 mgkgday) for1 month with tapering over several months aregiven In addition cyclophosphamide (2 mgkgday) should be administered for 6ndash12 monthsuntil symptoms disappear In the maintenanceof remission cyclophosphamide should be
Wegenerrsquos Granulomatosis
Antibiotics mainly trimethoprim-sulfamethoxazoleare given for prophylaxis againstPneumocystis jiroveci (formerly Pneumocystiscarinii) pneumonia (PCP) which may developduring immunosuppression and have a role inpreventing recurrencesbull Sinonasal manifestations may be treated with topical nasal steroids and nasal irrigations lowdosesystemic steroids and antibiotics when bacterial infection (typically Staphylococcus species) is suspected
Wegenerrsquos Granulomatosis
bull Prognosisbull ndash Most of the patients respond well to treatmentbull achieving symptom-free intervals of 5ndash20 yearsbull or more bull -Anatomical problems (sinusitis trachealbull stenosis) may require surgery bull Relapses can be long and troublesomebull Long-term complications are chronicbull renal failure hearing loss and deafness
Nasal Fractures Definition ndash A nasal fracture is a disruption of the nasal bone structure due to trauma It is the most frequently fractured facial bone Epidemiologyaetiology ndash Sports falls and assaults are the usual mechanisms of fracture -Males are affected twice as often as are females -Paediatric populations with a incidences during the second and third decades of life -Variables such as force impact direction nature of the striking object age and other will influence the pattern of injury to the components of the nose
Nasal Fractures
bull Symptomsbull ndash Deformity swelling epistaxis and periorbital
ecchymosis are signs that are suggestive of nasal fracture
bull bony crepitus and nasal segment mobilitybull ndash Epiphora bull Severe bilateral injuries to the lachrymal bones
arebull associated with depressed nasal fractures
Nasal Fractures Complications ndash Septal haematoma is one of the most severe early complications of nasal trauma and without drainage it results in abscess formation 6ndash7 days after trauma producing necrosis of the septal cartilage -Long-term problems such as saddle-nose deformity perforation columellar retraction and nasalbase
Septal infection could lead to osteomyelitis orbital and intracranial abscesses meningitis and cavernous sinus thrombosis -Cerebrospinal fluid leakage is a common complication of severe
nasal and frontal fractures
Nasal Fractures
bull Diagnostic proceduresbull ndash Inspectionbull bull Changes of appearance such as deviation andbull asymmetry bleeding watery drainage changesbull in nasal breathing and smell It is useful to comparebull the current presentation with old photographsbull (up to 40 of normal individuals havebull significant nose malformations)
Nasal Fractures Physical examination bull The diagnosis of a nasal fracture is made primarily by physical examination epistaxis nasal swelling and periorbital ecchymosis Nasal shape in the lateral and frontal inspection should be assessed Grasping the dorsum between two fingers and rocking the pyramid back and forth aids in assessing the mobility of nasal bones Internal structures should be evaluated by using a headlight and nasal speculum Clotted blood is removed by suction and assessment of haematoma mucosal tears and active bleeding is performed Bimanual palpation of the septum helps to differentiate septal swelling from haematoma ndash
Nasal FracturesRadiographybull There is no clear evidence of the role of radiographyin the management of nasal fracturesPlain films have up to a 66 false-positive rateas a result of misinterpretation of normal suturelines In addition old fractures are difficult todistinguishbull Three-dimensional CT is recommended for extensiveinjuries involving the nasal-orbital-ethmoidalcomplexndash
Nasal Fractures
bull Additionaluseful diagnostic proceduresbull bull Using a 0 or 30deg 4-mm endoscope is helpful inbull the assessment of posterior abnormalities If thebull patient is heavily sedated Brown-Gruss
provocationbull manoeuvres may be performed to determinebull deformities in upper middle or lower segmentsbull by compressing each compartment
Nasal FracturesConservative treatmentndash Treatment of bleedingbull For localised bleeding anterior sources may becauterised by silver nitrate or sealed with topicalmaterials such as thrombin combined withgelatin foam fibrin glue FloSealreg or other procoagulantmaterials If conservative measuresfail a formal anterior packing is placedbull Bleeding from branches of sphenopalatine orethmoid vessels requires anterior-posteriorpacking
Nasal Fractures
bull bull Surgical methods such as direct endoscopic vessel
bull cauterization or ligation have been shown tobull offer better haemostasis and patient comfortbull Angiography with embolization can also be
consideredbull in cases refractory to more conservativebull approaches
Nasal Fractures
bull Type of reductionbull bull Nondisplaced fractures should be treated withbull observation alone Closed nasal reduction is thebull best choice for simple injuries (isolated unilateralbull with medial displacement)bull bull An open approach should be considered in
severebull trauma (bilateral depressed fractures)
Nasal Fracturesbull Surgical principlesbull ndash Topical anaesthesia with cotton pledgets soakedbull with 4 cocaine or 005 oxymethazoline combinedbull with 4 topical lidocaine should be appliedbull for 5ndash10 min Local anaesthesia should also be injectedbull (1 lidocaine and 1100000 epinephrine)bull along the septum lateral walls and floor of the nasalbull cavitybull bull
Nasal FracturesClosed reductionndashndash The nasal bones are grasped between two fingersand pressure is applied laterally in theopposite direction of the deviation A bluntelevator may be used from within the nose incases of significant medial collapse Walshamforceps can be of help Reduction of the septumshould be performed with the use ofAsch forceps
Nasal Fractures
bull To prevent collapse of the postreductionbull framework nasal packing should be placedbull for 3ndash5 days Septum splints are recommendedbull in comminuted septal fractures withbull severe mucosal lesions External nasal splintingbull for 10 days (Aquaplastreg Thermoplastreg)bull provides nasal protection Nasal saline spraysbull prevent crusting and oral antibiotics should
Nasal Fractures
bull Open reductionbull ndashndash Immediate repair of fractures by using
widebull surgical exposure reduction fixation and
reconstructionbull ndashndash The second option is delayed correctionbull (6 months or more) of persistent deformitiesbull using standard techniques of rhinoplasty
Deviated Nasal Septum
bull Definition of the diseasebull ndash Deviation of the nasal septum is a common causebull of unilateral nasal airway obstruction in which thebull nasal septum is displacedbull bull Epidemiologyaetiologybull ndash Developmental septal abnormalities Septal cartilage
damage in the neonatal period andbull during birth can cause severe septal deviation inbull the absence of a history of nasal trauma
Deviated Nasal Septum
bull Symptomsbull ndash Patients may present with a history of sinusitis
allergicbull rhinitis obstructive sleep apnoea previousbull nasal surgery or recent nasal trauma Unilateral or
bilateral nasal airway obstruction that is unrelievedbull with decongestants or nasal steroid sprays is oftenbull seenbull bull
Deviated Nasal SeptumDiagnosisndashExamination external dorsal deviation or the columella and caudal septummay be deflected off the midline (caudal subluxation)ndash Inspections of the nasal cavity and anterior-posteriorrhinoscopy are helpful in diagnosing the locationtype and severity of septal deformityThe endoscope is also useful in identifying polypsthe severity and extent of posterior septaldeviations and bony spurs and locating areas ofseptal perforation or mucosal injury
Deviated Nasal Septum
bull Therapybull ndash Septoplasty is a procedurebull The areabull of deviation is corrected or resected in order tobull leave behind as much cartilage and bone as
possiblebull Cartilage resection is minimised and can be
repositioned reshaped or recontoured using a variety of methods
Deviated Nasal Septum
bull ndash Indications of septoplasty before the growth period
bull of the nose is finished should be very limited bull -In these cases surgery must preserve all the
cartilagebull in order to prevent external changes of the
shape ofbull the nose
Deviated Nasal Septum
bull Complicationsbull ndash Frequent complications include haematoma andbull infection Cerebrospinal fluid leak is a rare but
potentiallybull serious complicationbull It is usually the resultbull of avulsion or damage to the cribriform plate whenbull handling the perpendicular plate of the ethmoidbull ndash Other complications include epistaxis nasal
Deviated Nasal Septum
bull Other complications include epistaxis nasal obstruction
bull due to residual deviation synechiae returnbull of the cartilaginous deviation septal perforationbull anosmia and cosmetic nasal deformities suchbull as widened alar rim margins drooping nasal tipbull columella retraction and a sunken dorsum with abull supratip saddle formation
Septal perforation with minor crusting View from provide closure of the
incision
Septal Haematoma
bull A septal haematoma is a blood collection under the perichondrium
bull of the septum and cartilagebull bull bull Epidemiologyaetiologybull ndash A septal haematoma is one of the most
severe complications of nasal trauma
Septal Haematoma
bull Diagnosisbull ndash Signs and symptoms include intense pain
swellingbull haematoma of the upper lip and philtrum
area andbull complete nasal airway obstruction
Septal HaematomaTherapyndash Management consists of drainage through a mucoperichondrial incision Immediate treatment isnecessary to prevent long-term problems such asa saddle-nose deformity perforation columellarretraction and nasal-base widening In childrenseptal destruction can lead to devastating nasal andmidfacial growth abnormalitiesbull Surgeryndash Incision and evacuation of the collection is performedDrainage of a septal haematoma should
Septal HaematomaSurgeryndash Incision and evacuation of the collection is performedDrainage of a septal haematoma should provide closure of the incision
Splints or transseptal sutures are placed to obliterate thepotential space and prevent collectionInfection involving the septal cartilage Reconstruction with autologouscartilage is then performed in a second stage Oral antibiotics should be given
Nasal DeformitySaddle-nose deformityndash A saddle-nose deformity is characterised by a loss ofnasal dorsal height and compromised nasal supportstructures -Other case observed are depressionof the middle vault and dorsum loss of nasal tipsupport and definition shortened (vertical) nasal length over rotation of the nasal tip and retrusion ofthe nasal spine and caudal septum It is also knownas a ldquoPug noserdquo or ldquoboxerrsquos noserdquo both of which referto various degrees of nasal dorsal depressionbull
Nasal DeformityEpidemiologyaetiologyndash Prevalence is higher in population groups prone to facial trauma (ie boxers athletes) those with historiesof intranasal cocaine use nasal surgery (e g radical submucosal septal resection reductive rhinoplasty)ndash A saddle-nose deformity can be congenital or acquired It can be noticed as a part of individual familialsyndromic and ethnic characteristics - Most deformities are due to traumatic and iatrogeniccauses Medical causes are Wegenerrsquosgranulomatosis relapsing polychondritis leprosy (Hansenrsquos disease) syphilis ectodermal dysplasiaand intranasal cocaine use
Nasal Deformity
bull Therapybull ndash Nasal reconstruction indications depend on patientbull selection surgeon experience and aetiology of thebull deformity bull Indications for surgery can be functionalbull aesthetic or most commonly both In individuals
with a compromised nasal airway a nasoseptalbull reconstruction is indicated
Nasal Deformity
bull Contraindications bull include patients with malignantbull chronic or autoimmune disease conditions drugbull abuse poor perioperative risk profile and unrealisticbull expectationsbull ndash Multiple previous rhinoplasties and certain
professionsbull (mixed martial artists boxers and other contactbull sports) are relative contraindications
Nasal DeformitySeptoplastyndash Septoplasty is performed to correct nasal obstructioncaused by septal deformityndash Usually septoplasty is performed under general anaesthesiawith the patient in the supine position with the head elevated by approximately 30 (Righthandedsurgeons approach from the right side)ndash Local vasoconstrictive anaesthesia is applied notonly to reduce postoperative pain but also more importantly to achieve vasoconstriction of themucosa and less intraoperative haemorrhage Lidocainewith adrenaline or epinephrine is usedalthough in patients with cardiac hypersensitivityoxymetazoline might be preferred
Nasal Deformity
bull Septoplasty begins with the incision of septal mucosabull Most operative techniques utilise a hemitransfixionbull incision at the caudal end of septum so thatbull deviation at this point might be reached as wellbull as a transfixion incision that is easily obtained ifbull needed (Right-handed surgeons normally choosebull the left side but that may vary when deviation isbull convex towards the right)
Nasal DeformityA columella retractor is placed over the columellaand by pulling it laterally the caudal border of theseptum is exposed Ala can be protected by an alaprotector A vertical incision with a no 15 bladeover the caudal end of septum is performed untilreaching the plane of the septal cartilage It is essentialto correctly identify the perichondrium and byusing the Cottle elevator dissect and lift it creatinga flap As the dissection proceeds along the septalcartilage a longer speculum (no 5) is introduced sothat elevation of the mucoperichondrium is doneunder constant visual controlndash The next step is to dissect the mucoperiostium
Nasal DeformityDissecting over the bony-cartilaginous junctionwhen joining both tunnels might be difficult and is
especially prone to membrane perforationndash If needed the same tunnels are to be created on the
other side of the septum Then deviated parts of
septum are identified and removed either with a
knife or a Freer chisel
Nasal Deformitybull septum from the maxillary crest the septum mustbull be separated from the perpendicular plate trimmedbull along the inferior border placed back onto the crestbull and sutured to the periosteum If the deformity involvesbull the vomer an osteotome is used Care mustbull be taken not to break the cribriform plate becausebull it could cause a cerebrospinal fistula
Nasal Deformity
bull Once the septal deviation is corrected the flapsbull and hemitransfixion incision are mattressed
withbull absorbable sutures Nasal packing to prevent
synechiaebull and postoperative septal haematoma mightbull be advised but should be removed within 72 h

FuruncleSymptomsndashsymptoms are local and limited to thesite of infection Furuncles usually are wherehair follicles are present bull Complicationndash One complication is furunculosis multiple draining furunclesDiagnosisndash The diagnosis is based on clinical inspection - Cultures are not necessary when there is no systemic involvement but should beconsidered if systemic therapy (in case of feversignificant cellulitis or hospitalization) or whenmethicillin-resistant Staphylococcusaureus (MRSA) is considered
FuruncleTherapyndash When the furuncle is small application of moist heat compress to promote drainage -Larger furuncles should be drained by surgical incision-After drainage the area should be cleaned with anantiseptic (with chlorhexidinebetadine) should be applied twice
a dayndash If no systemic symptoms or extensive cellulitis arepresent simple topical care is usually curative andoral antibiotics are not necessary Otherwise systemictreatment is indicated and should cover anypossible MRSA
Furuncle
bull -Recommended antibiotics are trimethoprim-sulfamethoxazole
bull 1ndash2 tablets orally twice daily doxycyclinebull 100 mg orally twice dailybull or clindamycin 300ndash450 mg orally every 8 hbull - In severe cases vancomycin 15 mgkg
intravenouslybull every 12 h or clindamycin 600 mg intravenouslybull every 8 h
Midline Granulomabull A midline granuloma is an angiocentricbull lymphoma it was referred to as polymorphicbull reticulosis lethal midline granuloma and midline
malignant reticulosisbull bull Definition of the diseasebull ndash This rare disease is a lymphoma of extranodal
presentationall cases are positive for the Epstein-Barr virus
bull -This lymphoma most commonly appears in the midface region
Midline GranulomaEpidemiologyaetiologyndash This form of lymphoma is rare in Europe and theUnited States with a higher prevalence in Asia and PeruSymptomsndash The most common presentation is nasal obstruction with a destructive mass occupying the nosesinuses and palate
-Fever night sweatsand weight loss seen usually in Hodgkinrsquos lymphomaand other non-Hodgkinrsquos lymphomas (knownas ldquoB symptomsrdquo) are uncommon
Midline GranulomaDiagnosisndash The diagnosis is based on anatomopathologicalstudy The malignancy of the tumour manifested byextensive necrosis makes the histological diagnosisdifficult and often more biopsies are required forconfirmationbull Therapyndash Therapy consists of radiotherapy with or withoutchemotherapy
Midline Granuloma
bull Prognosisbull ndash Depending on the stage long-term remission or
experience a worseningbull prognosis with relapses which may include otherbull extranodal sites bull Involvement of extranodal sitesbull including the upper airway gastrointestinal tractbull skin
Wegenerrsquos Granulomatosis
bull Definition of the diseasebull ndash Wegenerrsquos granulomatosis is a systemic chronicbull vasculitis of small- and medium-sized blood vesselsbull with an autoimmune component It affectsbull particular organs with variable predilectionbull Epidemiologyaetiologybull ndash Wegenerrsquos granulomatosis is a rare disease It affects
about 1 in 20000ndash30000 people It is more prevalentbull in middle-aged Caucasian patients
Wegenerrsquos Granulomatosis
Symptomsndash The disease may present pulmonary upper
respiratory tract or renal In the disseminated form-The localised form ndash confinedto the upper respiratory region ndash is present in 25of the patients- It consists of nonspecific manifestationssuch as nasal obstruction crusting purulentor bloody rhinorrhea and painful or painless ulcers in oral or nasal cavities which are unresponsive tostandard medical treatment
Wegenerrsquos Granulomatosis
bull In some patients the nasal septum is perforatedbull which leads to saddle-nose deformity Less
commonbull symptoms are hoarseness stridor due to
subglotticbull stenosis otalgia otorrhea and conductivebull and sensorineural hearing loss Also ocular
symptomsbull such as scleritis conjunctivitis uveitis andbull episcleritis may be present
Wegenerrsquos Granulomatosis
bull ndash In the disseminated form pulmonary involvementbull is manifested by cough dyspnoea haemoptysisbull (due to an alveolar capillaritis necrotic lesions orbull endobronchial disease) and pleuritic painndashbull -Ninety per cent of patients have nasal symptomsbull and these symptoms are usually the first
manifestationof the diseasebull -Most patients have also renal involvementbull even if it is subclinical
Wegenerrsquos Granulomatosis
Diagnosis ndash Diagnosis of Wegenerrsquos granulomatosis is based on clinical findings that demonstrate lung (chest x-ray) kidney (urine analysis) or upper respiratory tract
involvement (oral or nasal ulcers or discharge) - positive blood analysis for cytoplasmic-staining antineutrophil
cytoplasmic antibodies (c-ANCA) and confirming proteinase 3 (PR3) ANCA or myeloperoxidase (MPO) ANCA ndash Biopsy is essential for diagnosis nonspecific chronic inflammation
and necrosis -Bacterial and fungal infections
Wegenerrsquos Granulomatosis
Therapyndash Conservative therapybull In the induction of disease remission highdosesteroids (e g prednisone 1 mgkgday) for1 month with tapering over several months aregiven In addition cyclophosphamide (2 mgkgday) should be administered for 6ndash12 monthsuntil symptoms disappear In the maintenanceof remission cyclophosphamide should be
Wegenerrsquos Granulomatosis
Antibiotics mainly trimethoprim-sulfamethoxazoleare given for prophylaxis againstPneumocystis jiroveci (formerly Pneumocystiscarinii) pneumonia (PCP) which may developduring immunosuppression and have a role inpreventing recurrencesbull Sinonasal manifestations may be treated with topical nasal steroids and nasal irrigations lowdosesystemic steroids and antibiotics when bacterial infection (typically Staphylococcus species) is suspected
Wegenerrsquos Granulomatosis
bull Prognosisbull ndash Most of the patients respond well to treatmentbull achieving symptom-free intervals of 5ndash20 yearsbull or more bull -Anatomical problems (sinusitis trachealbull stenosis) may require surgery bull Relapses can be long and troublesomebull Long-term complications are chronicbull renal failure hearing loss and deafness
Nasal Fractures Definition ndash A nasal fracture is a disruption of the nasal bone structure due to trauma It is the most frequently fractured facial bone Epidemiologyaetiology ndash Sports falls and assaults are the usual mechanisms of fracture -Males are affected twice as often as are females -Paediatric populations with a incidences during the second and third decades of life -Variables such as force impact direction nature of the striking object age and other will influence the pattern of injury to the components of the nose
Nasal Fractures
bull Symptomsbull ndash Deformity swelling epistaxis and periorbital
ecchymosis are signs that are suggestive of nasal fracture
bull bony crepitus and nasal segment mobilitybull ndash Epiphora bull Severe bilateral injuries to the lachrymal bones
arebull associated with depressed nasal fractures
Nasal Fractures Complications ndash Septal haematoma is one of the most severe early complications of nasal trauma and without drainage it results in abscess formation 6ndash7 days after trauma producing necrosis of the septal cartilage -Long-term problems such as saddle-nose deformity perforation columellar retraction and nasalbase
Septal infection could lead to osteomyelitis orbital and intracranial abscesses meningitis and cavernous sinus thrombosis -Cerebrospinal fluid leakage is a common complication of severe
nasal and frontal fractures
Nasal Fractures
bull Diagnostic proceduresbull ndash Inspectionbull bull Changes of appearance such as deviation andbull asymmetry bleeding watery drainage changesbull in nasal breathing and smell It is useful to comparebull the current presentation with old photographsbull (up to 40 of normal individuals havebull significant nose malformations)
Nasal Fractures Physical examination bull The diagnosis of a nasal fracture is made primarily by physical examination epistaxis nasal swelling and periorbital ecchymosis Nasal shape in the lateral and frontal inspection should be assessed Grasping the dorsum between two fingers and rocking the pyramid back and forth aids in assessing the mobility of nasal bones Internal structures should be evaluated by using a headlight and nasal speculum Clotted blood is removed by suction and assessment of haematoma mucosal tears and active bleeding is performed Bimanual palpation of the septum helps to differentiate septal swelling from haematoma ndash
Nasal FracturesRadiographybull There is no clear evidence of the role of radiographyin the management of nasal fracturesPlain films have up to a 66 false-positive rateas a result of misinterpretation of normal suturelines In addition old fractures are difficult todistinguishbull Three-dimensional CT is recommended for extensiveinjuries involving the nasal-orbital-ethmoidalcomplexndash
Nasal Fractures
bull Additionaluseful diagnostic proceduresbull bull Using a 0 or 30deg 4-mm endoscope is helpful inbull the assessment of posterior abnormalities If thebull patient is heavily sedated Brown-Gruss
provocationbull manoeuvres may be performed to determinebull deformities in upper middle or lower segmentsbull by compressing each compartment
Nasal FracturesConservative treatmentndash Treatment of bleedingbull For localised bleeding anterior sources may becauterised by silver nitrate or sealed with topicalmaterials such as thrombin combined withgelatin foam fibrin glue FloSealreg or other procoagulantmaterials If conservative measuresfail a formal anterior packing is placedbull Bleeding from branches of sphenopalatine orethmoid vessels requires anterior-posteriorpacking
Nasal Fractures
bull bull Surgical methods such as direct endoscopic vessel
bull cauterization or ligation have been shown tobull offer better haemostasis and patient comfortbull Angiography with embolization can also be
consideredbull in cases refractory to more conservativebull approaches
Nasal Fractures
bull Type of reductionbull bull Nondisplaced fractures should be treated withbull observation alone Closed nasal reduction is thebull best choice for simple injuries (isolated unilateralbull with medial displacement)bull bull An open approach should be considered in
severebull trauma (bilateral depressed fractures)
Nasal Fracturesbull Surgical principlesbull ndash Topical anaesthesia with cotton pledgets soakedbull with 4 cocaine or 005 oxymethazoline combinedbull with 4 topical lidocaine should be appliedbull for 5ndash10 min Local anaesthesia should also be injectedbull (1 lidocaine and 1100000 epinephrine)bull along the septum lateral walls and floor of the nasalbull cavitybull bull
Nasal FracturesClosed reductionndashndash The nasal bones are grasped between two fingersand pressure is applied laterally in theopposite direction of the deviation A bluntelevator may be used from within the nose incases of significant medial collapse Walshamforceps can be of help Reduction of the septumshould be performed with the use ofAsch forceps
Nasal Fractures
bull To prevent collapse of the postreductionbull framework nasal packing should be placedbull for 3ndash5 days Septum splints are recommendedbull in comminuted septal fractures withbull severe mucosal lesions External nasal splintingbull for 10 days (Aquaplastreg Thermoplastreg)bull provides nasal protection Nasal saline spraysbull prevent crusting and oral antibiotics should
Nasal Fractures
bull Open reductionbull ndashndash Immediate repair of fractures by using
widebull surgical exposure reduction fixation and
reconstructionbull ndashndash The second option is delayed correctionbull (6 months or more) of persistent deformitiesbull using standard techniques of rhinoplasty
Deviated Nasal Septum
bull Definition of the diseasebull ndash Deviation of the nasal septum is a common causebull of unilateral nasal airway obstruction in which thebull nasal septum is displacedbull bull Epidemiologyaetiologybull ndash Developmental septal abnormalities Septal cartilage
damage in the neonatal period andbull during birth can cause severe septal deviation inbull the absence of a history of nasal trauma
Deviated Nasal Septum
bull Symptomsbull ndash Patients may present with a history of sinusitis
allergicbull rhinitis obstructive sleep apnoea previousbull nasal surgery or recent nasal trauma Unilateral or
bilateral nasal airway obstruction that is unrelievedbull with decongestants or nasal steroid sprays is oftenbull seenbull bull
Deviated Nasal SeptumDiagnosisndashExamination external dorsal deviation or the columella and caudal septummay be deflected off the midline (caudal subluxation)ndash Inspections of the nasal cavity and anterior-posteriorrhinoscopy are helpful in diagnosing the locationtype and severity of septal deformityThe endoscope is also useful in identifying polypsthe severity and extent of posterior septaldeviations and bony spurs and locating areas ofseptal perforation or mucosal injury
Deviated Nasal Septum
bull Therapybull ndash Septoplasty is a procedurebull The areabull of deviation is corrected or resected in order tobull leave behind as much cartilage and bone as
possiblebull Cartilage resection is minimised and can be
repositioned reshaped or recontoured using a variety of methods
Deviated Nasal Septum
bull ndash Indications of septoplasty before the growth period
bull of the nose is finished should be very limited bull -In these cases surgery must preserve all the
cartilagebull in order to prevent external changes of the
shape ofbull the nose
Deviated Nasal Septum
bull Complicationsbull ndash Frequent complications include haematoma andbull infection Cerebrospinal fluid leak is a rare but
potentiallybull serious complicationbull It is usually the resultbull of avulsion or damage to the cribriform plate whenbull handling the perpendicular plate of the ethmoidbull ndash Other complications include epistaxis nasal
Deviated Nasal Septum
bull Other complications include epistaxis nasal obstruction
bull due to residual deviation synechiae returnbull of the cartilaginous deviation septal perforationbull anosmia and cosmetic nasal deformities suchbull as widened alar rim margins drooping nasal tipbull columella retraction and a sunken dorsum with abull supratip saddle formation
Septal perforation with minor crusting View from provide closure of the
incision
Septal Haematoma
bull A septal haematoma is a blood collection under the perichondrium
bull of the septum and cartilagebull bull bull Epidemiologyaetiologybull ndash A septal haematoma is one of the most
severe complications of nasal trauma
Septal Haematoma
bull Diagnosisbull ndash Signs and symptoms include intense pain
swellingbull haematoma of the upper lip and philtrum
area andbull complete nasal airway obstruction
Septal HaematomaTherapyndash Management consists of drainage through a mucoperichondrial incision Immediate treatment isnecessary to prevent long-term problems such asa saddle-nose deformity perforation columellarretraction and nasal-base widening In childrenseptal destruction can lead to devastating nasal andmidfacial growth abnormalitiesbull Surgeryndash Incision and evacuation of the collection is performedDrainage of a septal haematoma should
Septal HaematomaSurgeryndash Incision and evacuation of the collection is performedDrainage of a septal haematoma should provide closure of the incision
Splints or transseptal sutures are placed to obliterate thepotential space and prevent collectionInfection involving the septal cartilage Reconstruction with autologouscartilage is then performed in a second stage Oral antibiotics should be given
Nasal DeformitySaddle-nose deformityndash A saddle-nose deformity is characterised by a loss ofnasal dorsal height and compromised nasal supportstructures -Other case observed are depressionof the middle vault and dorsum loss of nasal tipsupport and definition shortened (vertical) nasal length over rotation of the nasal tip and retrusion ofthe nasal spine and caudal septum It is also knownas a ldquoPug noserdquo or ldquoboxerrsquos noserdquo both of which referto various degrees of nasal dorsal depressionbull
Nasal DeformityEpidemiologyaetiologyndash Prevalence is higher in population groups prone to facial trauma (ie boxers athletes) those with historiesof intranasal cocaine use nasal surgery (e g radical submucosal septal resection reductive rhinoplasty)ndash A saddle-nose deformity can be congenital or acquired It can be noticed as a part of individual familialsyndromic and ethnic characteristics - Most deformities are due to traumatic and iatrogeniccauses Medical causes are Wegenerrsquosgranulomatosis relapsing polychondritis leprosy (Hansenrsquos disease) syphilis ectodermal dysplasiaand intranasal cocaine use
Nasal Deformity
bull Therapybull ndash Nasal reconstruction indications depend on patientbull selection surgeon experience and aetiology of thebull deformity bull Indications for surgery can be functionalbull aesthetic or most commonly both In individuals
with a compromised nasal airway a nasoseptalbull reconstruction is indicated
Nasal Deformity
bull Contraindications bull include patients with malignantbull chronic or autoimmune disease conditions drugbull abuse poor perioperative risk profile and unrealisticbull expectationsbull ndash Multiple previous rhinoplasties and certain
professionsbull (mixed martial artists boxers and other contactbull sports) are relative contraindications
Nasal DeformitySeptoplastyndash Septoplasty is performed to correct nasal obstructioncaused by septal deformityndash Usually septoplasty is performed under general anaesthesiawith the patient in the supine position with the head elevated by approximately 30 (Righthandedsurgeons approach from the right side)ndash Local vasoconstrictive anaesthesia is applied notonly to reduce postoperative pain but also more importantly to achieve vasoconstriction of themucosa and less intraoperative haemorrhage Lidocainewith adrenaline or epinephrine is usedalthough in patients with cardiac hypersensitivityoxymetazoline might be preferred
Nasal Deformity
bull Septoplasty begins with the incision of septal mucosabull Most operative techniques utilise a hemitransfixionbull incision at the caudal end of septum so thatbull deviation at this point might be reached as wellbull as a transfixion incision that is easily obtained ifbull needed (Right-handed surgeons normally choosebull the left side but that may vary when deviation isbull convex towards the right)
Nasal DeformityA columella retractor is placed over the columellaand by pulling it laterally the caudal border of theseptum is exposed Ala can be protected by an alaprotector A vertical incision with a no 15 bladeover the caudal end of septum is performed untilreaching the plane of the septal cartilage It is essentialto correctly identify the perichondrium and byusing the Cottle elevator dissect and lift it creatinga flap As the dissection proceeds along the septalcartilage a longer speculum (no 5) is introduced sothat elevation of the mucoperichondrium is doneunder constant visual controlndash The next step is to dissect the mucoperiostium
Nasal DeformityDissecting over the bony-cartilaginous junctionwhen joining both tunnels might be difficult and is
especially prone to membrane perforationndash If needed the same tunnels are to be created on the
other side of the septum Then deviated parts of
septum are identified and removed either with a
knife or a Freer chisel
Nasal Deformitybull septum from the maxillary crest the septum mustbull be separated from the perpendicular plate trimmedbull along the inferior border placed back onto the crestbull and sutured to the periosteum If the deformity involvesbull the vomer an osteotome is used Care mustbull be taken not to break the cribriform plate becausebull it could cause a cerebrospinal fistula
Nasal Deformity
bull Once the septal deviation is corrected the flapsbull and hemitransfixion incision are mattressed
withbull absorbable sutures Nasal packing to prevent
synechiaebull and postoperative septal haematoma mightbull be advised but should be removed within 72 h

FuruncleTherapyndash When the furuncle is small application of moist heat compress to promote drainage -Larger furuncles should be drained by surgical incision-After drainage the area should be cleaned with anantiseptic (with chlorhexidinebetadine) should be applied twice
a dayndash If no systemic symptoms or extensive cellulitis arepresent simple topical care is usually curative andoral antibiotics are not necessary Otherwise systemictreatment is indicated and should cover anypossible MRSA
Furuncle
bull -Recommended antibiotics are trimethoprim-sulfamethoxazole
bull 1ndash2 tablets orally twice daily doxycyclinebull 100 mg orally twice dailybull or clindamycin 300ndash450 mg orally every 8 hbull - In severe cases vancomycin 15 mgkg
intravenouslybull every 12 h or clindamycin 600 mg intravenouslybull every 8 h
Midline Granulomabull A midline granuloma is an angiocentricbull lymphoma it was referred to as polymorphicbull reticulosis lethal midline granuloma and midline
malignant reticulosisbull bull Definition of the diseasebull ndash This rare disease is a lymphoma of extranodal
presentationall cases are positive for the Epstein-Barr virus
bull -This lymphoma most commonly appears in the midface region
Midline GranulomaEpidemiologyaetiologyndash This form of lymphoma is rare in Europe and theUnited States with a higher prevalence in Asia and PeruSymptomsndash The most common presentation is nasal obstruction with a destructive mass occupying the nosesinuses and palate
-Fever night sweatsand weight loss seen usually in Hodgkinrsquos lymphomaand other non-Hodgkinrsquos lymphomas (knownas ldquoB symptomsrdquo) are uncommon
Midline GranulomaDiagnosisndash The diagnosis is based on anatomopathologicalstudy The malignancy of the tumour manifested byextensive necrosis makes the histological diagnosisdifficult and often more biopsies are required forconfirmationbull Therapyndash Therapy consists of radiotherapy with or withoutchemotherapy
Midline Granuloma
bull Prognosisbull ndash Depending on the stage long-term remission or
experience a worseningbull prognosis with relapses which may include otherbull extranodal sites bull Involvement of extranodal sitesbull including the upper airway gastrointestinal tractbull skin
Wegenerrsquos Granulomatosis
bull Definition of the diseasebull ndash Wegenerrsquos granulomatosis is a systemic chronicbull vasculitis of small- and medium-sized blood vesselsbull with an autoimmune component It affectsbull particular organs with variable predilectionbull Epidemiologyaetiologybull ndash Wegenerrsquos granulomatosis is a rare disease It affects
about 1 in 20000ndash30000 people It is more prevalentbull in middle-aged Caucasian patients
Wegenerrsquos Granulomatosis
Symptomsndash The disease may present pulmonary upper
respiratory tract or renal In the disseminated form-The localised form ndash confinedto the upper respiratory region ndash is present in 25of the patients- It consists of nonspecific manifestationssuch as nasal obstruction crusting purulentor bloody rhinorrhea and painful or painless ulcers in oral or nasal cavities which are unresponsive tostandard medical treatment
Wegenerrsquos Granulomatosis
bull In some patients the nasal septum is perforatedbull which leads to saddle-nose deformity Less
commonbull symptoms are hoarseness stridor due to
subglotticbull stenosis otalgia otorrhea and conductivebull and sensorineural hearing loss Also ocular
symptomsbull such as scleritis conjunctivitis uveitis andbull episcleritis may be present
Wegenerrsquos Granulomatosis
bull ndash In the disseminated form pulmonary involvementbull is manifested by cough dyspnoea haemoptysisbull (due to an alveolar capillaritis necrotic lesions orbull endobronchial disease) and pleuritic painndashbull -Ninety per cent of patients have nasal symptomsbull and these symptoms are usually the first
manifestationof the diseasebull -Most patients have also renal involvementbull even if it is subclinical
Wegenerrsquos Granulomatosis
Diagnosis ndash Diagnosis of Wegenerrsquos granulomatosis is based on clinical findings that demonstrate lung (chest x-ray) kidney (urine analysis) or upper respiratory tract
involvement (oral or nasal ulcers or discharge) - positive blood analysis for cytoplasmic-staining antineutrophil
cytoplasmic antibodies (c-ANCA) and confirming proteinase 3 (PR3) ANCA or myeloperoxidase (MPO) ANCA ndash Biopsy is essential for diagnosis nonspecific chronic inflammation
and necrosis -Bacterial and fungal infections
Wegenerrsquos Granulomatosis
Therapyndash Conservative therapybull In the induction of disease remission highdosesteroids (e g prednisone 1 mgkgday) for1 month with tapering over several months aregiven In addition cyclophosphamide (2 mgkgday) should be administered for 6ndash12 monthsuntil symptoms disappear In the maintenanceof remission cyclophosphamide should be
Wegenerrsquos Granulomatosis
Antibiotics mainly trimethoprim-sulfamethoxazoleare given for prophylaxis againstPneumocystis jiroveci (formerly Pneumocystiscarinii) pneumonia (PCP) which may developduring immunosuppression and have a role inpreventing recurrencesbull Sinonasal manifestations may be treated with topical nasal steroids and nasal irrigations lowdosesystemic steroids and antibiotics when bacterial infection (typically Staphylococcus species) is suspected
Wegenerrsquos Granulomatosis
bull Prognosisbull ndash Most of the patients respond well to treatmentbull achieving symptom-free intervals of 5ndash20 yearsbull or more bull -Anatomical problems (sinusitis trachealbull stenosis) may require surgery bull Relapses can be long and troublesomebull Long-term complications are chronicbull renal failure hearing loss and deafness
Nasal Fractures Definition ndash A nasal fracture is a disruption of the nasal bone structure due to trauma It is the most frequently fractured facial bone Epidemiologyaetiology ndash Sports falls and assaults are the usual mechanisms of fracture -Males are affected twice as often as are females -Paediatric populations with a incidences during the second and third decades of life -Variables such as force impact direction nature of the striking object age and other will influence the pattern of injury to the components of the nose
Nasal Fractures
bull Symptomsbull ndash Deformity swelling epistaxis and periorbital
ecchymosis are signs that are suggestive of nasal fracture
bull bony crepitus and nasal segment mobilitybull ndash Epiphora bull Severe bilateral injuries to the lachrymal bones
arebull associated with depressed nasal fractures
Nasal Fractures Complications ndash Septal haematoma is one of the most severe early complications of nasal trauma and without drainage it results in abscess formation 6ndash7 days after trauma producing necrosis of the septal cartilage -Long-term problems such as saddle-nose deformity perforation columellar retraction and nasalbase
Septal infection could lead to osteomyelitis orbital and intracranial abscesses meningitis and cavernous sinus thrombosis -Cerebrospinal fluid leakage is a common complication of severe
nasal and frontal fractures
Nasal Fractures
bull Diagnostic proceduresbull ndash Inspectionbull bull Changes of appearance such as deviation andbull asymmetry bleeding watery drainage changesbull in nasal breathing and smell It is useful to comparebull the current presentation with old photographsbull (up to 40 of normal individuals havebull significant nose malformations)
Nasal Fractures Physical examination bull The diagnosis of a nasal fracture is made primarily by physical examination epistaxis nasal swelling and periorbital ecchymosis Nasal shape in the lateral and frontal inspection should be assessed Grasping the dorsum between two fingers and rocking the pyramid back and forth aids in assessing the mobility of nasal bones Internal structures should be evaluated by using a headlight and nasal speculum Clotted blood is removed by suction and assessment of haematoma mucosal tears and active bleeding is performed Bimanual palpation of the septum helps to differentiate septal swelling from haematoma ndash
Nasal FracturesRadiographybull There is no clear evidence of the role of radiographyin the management of nasal fracturesPlain films have up to a 66 false-positive rateas a result of misinterpretation of normal suturelines In addition old fractures are difficult todistinguishbull Three-dimensional CT is recommended for extensiveinjuries involving the nasal-orbital-ethmoidalcomplexndash
Nasal Fractures
bull Additionaluseful diagnostic proceduresbull bull Using a 0 or 30deg 4-mm endoscope is helpful inbull the assessment of posterior abnormalities If thebull patient is heavily sedated Brown-Gruss
provocationbull manoeuvres may be performed to determinebull deformities in upper middle or lower segmentsbull by compressing each compartment
Nasal FracturesConservative treatmentndash Treatment of bleedingbull For localised bleeding anterior sources may becauterised by silver nitrate or sealed with topicalmaterials such as thrombin combined withgelatin foam fibrin glue FloSealreg or other procoagulantmaterials If conservative measuresfail a formal anterior packing is placedbull Bleeding from branches of sphenopalatine orethmoid vessels requires anterior-posteriorpacking
Nasal Fractures
bull bull Surgical methods such as direct endoscopic vessel
bull cauterization or ligation have been shown tobull offer better haemostasis and patient comfortbull Angiography with embolization can also be
consideredbull in cases refractory to more conservativebull approaches
Nasal Fractures
bull Type of reductionbull bull Nondisplaced fractures should be treated withbull observation alone Closed nasal reduction is thebull best choice for simple injuries (isolated unilateralbull with medial displacement)bull bull An open approach should be considered in
severebull trauma (bilateral depressed fractures)
Nasal Fracturesbull Surgical principlesbull ndash Topical anaesthesia with cotton pledgets soakedbull with 4 cocaine or 005 oxymethazoline combinedbull with 4 topical lidocaine should be appliedbull for 5ndash10 min Local anaesthesia should also be injectedbull (1 lidocaine and 1100000 epinephrine)bull along the septum lateral walls and floor of the nasalbull cavitybull bull
Nasal FracturesClosed reductionndashndash The nasal bones are grasped between two fingersand pressure is applied laterally in theopposite direction of the deviation A bluntelevator may be used from within the nose incases of significant medial collapse Walshamforceps can be of help Reduction of the septumshould be performed with the use ofAsch forceps
Nasal Fractures
bull To prevent collapse of the postreductionbull framework nasal packing should be placedbull for 3ndash5 days Septum splints are recommendedbull in comminuted septal fractures withbull severe mucosal lesions External nasal splintingbull for 10 days (Aquaplastreg Thermoplastreg)bull provides nasal protection Nasal saline spraysbull prevent crusting and oral antibiotics should
Nasal Fractures
bull Open reductionbull ndashndash Immediate repair of fractures by using
widebull surgical exposure reduction fixation and
reconstructionbull ndashndash The second option is delayed correctionbull (6 months or more) of persistent deformitiesbull using standard techniques of rhinoplasty
Deviated Nasal Septum
bull Definition of the diseasebull ndash Deviation of the nasal septum is a common causebull of unilateral nasal airway obstruction in which thebull nasal septum is displacedbull bull Epidemiologyaetiologybull ndash Developmental septal abnormalities Septal cartilage
damage in the neonatal period andbull during birth can cause severe septal deviation inbull the absence of a history of nasal trauma
Deviated Nasal Septum
bull Symptomsbull ndash Patients may present with a history of sinusitis
allergicbull rhinitis obstructive sleep apnoea previousbull nasal surgery or recent nasal trauma Unilateral or
bilateral nasal airway obstruction that is unrelievedbull with decongestants or nasal steroid sprays is oftenbull seenbull bull
Deviated Nasal SeptumDiagnosisndashExamination external dorsal deviation or the columella and caudal septummay be deflected off the midline (caudal subluxation)ndash Inspections of the nasal cavity and anterior-posteriorrhinoscopy are helpful in diagnosing the locationtype and severity of septal deformityThe endoscope is also useful in identifying polypsthe severity and extent of posterior septaldeviations and bony spurs and locating areas ofseptal perforation or mucosal injury
Deviated Nasal Septum
bull Therapybull ndash Septoplasty is a procedurebull The areabull of deviation is corrected or resected in order tobull leave behind as much cartilage and bone as
possiblebull Cartilage resection is minimised and can be
repositioned reshaped or recontoured using a variety of methods
Deviated Nasal Septum
bull ndash Indications of septoplasty before the growth period
bull of the nose is finished should be very limited bull -In these cases surgery must preserve all the
cartilagebull in order to prevent external changes of the
shape ofbull the nose
Deviated Nasal Septum
bull Complicationsbull ndash Frequent complications include haematoma andbull infection Cerebrospinal fluid leak is a rare but
potentiallybull serious complicationbull It is usually the resultbull of avulsion or damage to the cribriform plate whenbull handling the perpendicular plate of the ethmoidbull ndash Other complications include epistaxis nasal
Deviated Nasal Septum
bull Other complications include epistaxis nasal obstruction
bull due to residual deviation synechiae returnbull of the cartilaginous deviation septal perforationbull anosmia and cosmetic nasal deformities suchbull as widened alar rim margins drooping nasal tipbull columella retraction and a sunken dorsum with abull supratip saddle formation
Septal perforation with minor crusting View from provide closure of the
incision
Septal Haematoma
bull A septal haematoma is a blood collection under the perichondrium
bull of the septum and cartilagebull bull bull Epidemiologyaetiologybull ndash A septal haematoma is one of the most
severe complications of nasal trauma
Septal Haematoma
bull Diagnosisbull ndash Signs and symptoms include intense pain
swellingbull haematoma of the upper lip and philtrum
area andbull complete nasal airway obstruction
Septal HaematomaTherapyndash Management consists of drainage through a mucoperichondrial incision Immediate treatment isnecessary to prevent long-term problems such asa saddle-nose deformity perforation columellarretraction and nasal-base widening In childrenseptal destruction can lead to devastating nasal andmidfacial growth abnormalitiesbull Surgeryndash Incision and evacuation of the collection is performedDrainage of a septal haematoma should
Septal HaematomaSurgeryndash Incision and evacuation of the collection is performedDrainage of a septal haematoma should provide closure of the incision
Splints or transseptal sutures are placed to obliterate thepotential space and prevent collectionInfection involving the septal cartilage Reconstruction with autologouscartilage is then performed in a second stage Oral antibiotics should be given
Nasal DeformitySaddle-nose deformityndash A saddle-nose deformity is characterised by a loss ofnasal dorsal height and compromised nasal supportstructures -Other case observed are depressionof the middle vault and dorsum loss of nasal tipsupport and definition shortened (vertical) nasal length over rotation of the nasal tip and retrusion ofthe nasal spine and caudal septum It is also knownas a ldquoPug noserdquo or ldquoboxerrsquos noserdquo both of which referto various degrees of nasal dorsal depressionbull
Nasal DeformityEpidemiologyaetiologyndash Prevalence is higher in population groups prone to facial trauma (ie boxers athletes) those with historiesof intranasal cocaine use nasal surgery (e g radical submucosal septal resection reductive rhinoplasty)ndash A saddle-nose deformity can be congenital or acquired It can be noticed as a part of individual familialsyndromic and ethnic characteristics - Most deformities are due to traumatic and iatrogeniccauses Medical causes are Wegenerrsquosgranulomatosis relapsing polychondritis leprosy (Hansenrsquos disease) syphilis ectodermal dysplasiaand intranasal cocaine use
Nasal Deformity
bull Therapybull ndash Nasal reconstruction indications depend on patientbull selection surgeon experience and aetiology of thebull deformity bull Indications for surgery can be functionalbull aesthetic or most commonly both In individuals
with a compromised nasal airway a nasoseptalbull reconstruction is indicated
Nasal Deformity
bull Contraindications bull include patients with malignantbull chronic or autoimmune disease conditions drugbull abuse poor perioperative risk profile and unrealisticbull expectationsbull ndash Multiple previous rhinoplasties and certain
professionsbull (mixed martial artists boxers and other contactbull sports) are relative contraindications
Nasal DeformitySeptoplastyndash Septoplasty is performed to correct nasal obstructioncaused by septal deformityndash Usually septoplasty is performed under general anaesthesiawith the patient in the supine position with the head elevated by approximately 30 (Righthandedsurgeons approach from the right side)ndash Local vasoconstrictive anaesthesia is applied notonly to reduce postoperative pain but also more importantly to achieve vasoconstriction of themucosa and less intraoperative haemorrhage Lidocainewith adrenaline or epinephrine is usedalthough in patients with cardiac hypersensitivityoxymetazoline might be preferred
Nasal Deformity
bull Septoplasty begins with the incision of septal mucosabull Most operative techniques utilise a hemitransfixionbull incision at the caudal end of septum so thatbull deviation at this point might be reached as wellbull as a transfixion incision that is easily obtained ifbull needed (Right-handed surgeons normally choosebull the left side but that may vary when deviation isbull convex towards the right)
Nasal DeformityA columella retractor is placed over the columellaand by pulling it laterally the caudal border of theseptum is exposed Ala can be protected by an alaprotector A vertical incision with a no 15 bladeover the caudal end of septum is performed untilreaching the plane of the septal cartilage It is essentialto correctly identify the perichondrium and byusing the Cottle elevator dissect and lift it creatinga flap As the dissection proceeds along the septalcartilage a longer speculum (no 5) is introduced sothat elevation of the mucoperichondrium is doneunder constant visual controlndash The next step is to dissect the mucoperiostium
Nasal DeformityDissecting over the bony-cartilaginous junctionwhen joining both tunnels might be difficult and is
especially prone to membrane perforationndash If needed the same tunnels are to be created on the
other side of the septum Then deviated parts of
septum are identified and removed either with a
knife or a Freer chisel
Nasal Deformitybull septum from the maxillary crest the septum mustbull be separated from the perpendicular plate trimmedbull along the inferior border placed back onto the crestbull and sutured to the periosteum If the deformity involvesbull the vomer an osteotome is used Care mustbull be taken not to break the cribriform plate becausebull it could cause a cerebrospinal fistula
Nasal Deformity
bull Once the septal deviation is corrected the flapsbull and hemitransfixion incision are mattressed
withbull absorbable sutures Nasal packing to prevent
synechiaebull and postoperative septal haematoma mightbull be advised but should be removed within 72 h

Furuncle
bull -Recommended antibiotics are trimethoprim-sulfamethoxazole
bull 1ndash2 tablets orally twice daily doxycyclinebull 100 mg orally twice dailybull or clindamycin 300ndash450 mg orally every 8 hbull - In severe cases vancomycin 15 mgkg
intravenouslybull every 12 h or clindamycin 600 mg intravenouslybull every 8 h
Midline Granulomabull A midline granuloma is an angiocentricbull lymphoma it was referred to as polymorphicbull reticulosis lethal midline granuloma and midline
malignant reticulosisbull bull Definition of the diseasebull ndash This rare disease is a lymphoma of extranodal
presentationall cases are positive for the Epstein-Barr virus
bull -This lymphoma most commonly appears in the midface region
Midline GranulomaEpidemiologyaetiologyndash This form of lymphoma is rare in Europe and theUnited States with a higher prevalence in Asia and PeruSymptomsndash The most common presentation is nasal obstruction with a destructive mass occupying the nosesinuses and palate
-Fever night sweatsand weight loss seen usually in Hodgkinrsquos lymphomaand other non-Hodgkinrsquos lymphomas (knownas ldquoB symptomsrdquo) are uncommon
Midline GranulomaDiagnosisndash The diagnosis is based on anatomopathologicalstudy The malignancy of the tumour manifested byextensive necrosis makes the histological diagnosisdifficult and often more biopsies are required forconfirmationbull Therapyndash Therapy consists of radiotherapy with or withoutchemotherapy
Midline Granuloma
bull Prognosisbull ndash Depending on the stage long-term remission or
experience a worseningbull prognosis with relapses which may include otherbull extranodal sites bull Involvement of extranodal sitesbull including the upper airway gastrointestinal tractbull skin
Wegenerrsquos Granulomatosis
bull Definition of the diseasebull ndash Wegenerrsquos granulomatosis is a systemic chronicbull vasculitis of small- and medium-sized blood vesselsbull with an autoimmune component It affectsbull particular organs with variable predilectionbull Epidemiologyaetiologybull ndash Wegenerrsquos granulomatosis is a rare disease It affects
about 1 in 20000ndash30000 people It is more prevalentbull in middle-aged Caucasian patients
Wegenerrsquos Granulomatosis
Symptomsndash The disease may present pulmonary upper
respiratory tract or renal In the disseminated form-The localised form ndash confinedto the upper respiratory region ndash is present in 25of the patients- It consists of nonspecific manifestationssuch as nasal obstruction crusting purulentor bloody rhinorrhea and painful or painless ulcers in oral or nasal cavities which are unresponsive tostandard medical treatment
Wegenerrsquos Granulomatosis
bull In some patients the nasal septum is perforatedbull which leads to saddle-nose deformity Less
commonbull symptoms are hoarseness stridor due to
subglotticbull stenosis otalgia otorrhea and conductivebull and sensorineural hearing loss Also ocular
symptomsbull such as scleritis conjunctivitis uveitis andbull episcleritis may be present
Wegenerrsquos Granulomatosis
bull ndash In the disseminated form pulmonary involvementbull is manifested by cough dyspnoea haemoptysisbull (due to an alveolar capillaritis necrotic lesions orbull endobronchial disease) and pleuritic painndashbull -Ninety per cent of patients have nasal symptomsbull and these symptoms are usually the first
manifestationof the diseasebull -Most patients have also renal involvementbull even if it is subclinical
Wegenerrsquos Granulomatosis
Diagnosis ndash Diagnosis of Wegenerrsquos granulomatosis is based on clinical findings that demonstrate lung (chest x-ray) kidney (urine analysis) or upper respiratory tract
involvement (oral or nasal ulcers or discharge) - positive blood analysis for cytoplasmic-staining antineutrophil
cytoplasmic antibodies (c-ANCA) and confirming proteinase 3 (PR3) ANCA or myeloperoxidase (MPO) ANCA ndash Biopsy is essential for diagnosis nonspecific chronic inflammation
and necrosis -Bacterial and fungal infections
Wegenerrsquos Granulomatosis
Therapyndash Conservative therapybull In the induction of disease remission highdosesteroids (e g prednisone 1 mgkgday) for1 month with tapering over several months aregiven In addition cyclophosphamide (2 mgkgday) should be administered for 6ndash12 monthsuntil symptoms disappear In the maintenanceof remission cyclophosphamide should be
Wegenerrsquos Granulomatosis
Antibiotics mainly trimethoprim-sulfamethoxazoleare given for prophylaxis againstPneumocystis jiroveci (formerly Pneumocystiscarinii) pneumonia (PCP) which may developduring immunosuppression and have a role inpreventing recurrencesbull Sinonasal manifestations may be treated with topical nasal steroids and nasal irrigations lowdosesystemic steroids and antibiotics when bacterial infection (typically Staphylococcus species) is suspected
Wegenerrsquos Granulomatosis
bull Prognosisbull ndash Most of the patients respond well to treatmentbull achieving symptom-free intervals of 5ndash20 yearsbull or more bull -Anatomical problems (sinusitis trachealbull stenosis) may require surgery bull Relapses can be long and troublesomebull Long-term complications are chronicbull renal failure hearing loss and deafness
Nasal Fractures Definition ndash A nasal fracture is a disruption of the nasal bone structure due to trauma It is the most frequently fractured facial bone Epidemiologyaetiology ndash Sports falls and assaults are the usual mechanisms of fracture -Males are affected twice as often as are females -Paediatric populations with a incidences during the second and third decades of life -Variables such as force impact direction nature of the striking object age and other will influence the pattern of injury to the components of the nose
Nasal Fractures
bull Symptomsbull ndash Deformity swelling epistaxis and periorbital
ecchymosis are signs that are suggestive of nasal fracture
bull bony crepitus and nasal segment mobilitybull ndash Epiphora bull Severe bilateral injuries to the lachrymal bones
arebull associated with depressed nasal fractures
Nasal Fractures Complications ndash Septal haematoma is one of the most severe early complications of nasal trauma and without drainage it results in abscess formation 6ndash7 days after trauma producing necrosis of the septal cartilage -Long-term problems such as saddle-nose deformity perforation columellar retraction and nasalbase
Septal infection could lead to osteomyelitis orbital and intracranial abscesses meningitis and cavernous sinus thrombosis -Cerebrospinal fluid leakage is a common complication of severe
nasal and frontal fractures
Nasal Fractures
bull Diagnostic proceduresbull ndash Inspectionbull bull Changes of appearance such as deviation andbull asymmetry bleeding watery drainage changesbull in nasal breathing and smell It is useful to comparebull the current presentation with old photographsbull (up to 40 of normal individuals havebull significant nose malformations)
Nasal Fractures Physical examination bull The diagnosis of a nasal fracture is made primarily by physical examination epistaxis nasal swelling and periorbital ecchymosis Nasal shape in the lateral and frontal inspection should be assessed Grasping the dorsum between two fingers and rocking the pyramid back and forth aids in assessing the mobility of nasal bones Internal structures should be evaluated by using a headlight and nasal speculum Clotted blood is removed by suction and assessment of haematoma mucosal tears and active bleeding is performed Bimanual palpation of the septum helps to differentiate septal swelling from haematoma ndash
Nasal FracturesRadiographybull There is no clear evidence of the role of radiographyin the management of nasal fracturesPlain films have up to a 66 false-positive rateas a result of misinterpretation of normal suturelines In addition old fractures are difficult todistinguishbull Three-dimensional CT is recommended for extensiveinjuries involving the nasal-orbital-ethmoidalcomplexndash
Nasal Fractures
bull Additionaluseful diagnostic proceduresbull bull Using a 0 or 30deg 4-mm endoscope is helpful inbull the assessment of posterior abnormalities If thebull patient is heavily sedated Brown-Gruss
provocationbull manoeuvres may be performed to determinebull deformities in upper middle or lower segmentsbull by compressing each compartment
Nasal FracturesConservative treatmentndash Treatment of bleedingbull For localised bleeding anterior sources may becauterised by silver nitrate or sealed with topicalmaterials such as thrombin combined withgelatin foam fibrin glue FloSealreg or other procoagulantmaterials If conservative measuresfail a formal anterior packing is placedbull Bleeding from branches of sphenopalatine orethmoid vessels requires anterior-posteriorpacking
Nasal Fractures
bull bull Surgical methods such as direct endoscopic vessel
bull cauterization or ligation have been shown tobull offer better haemostasis and patient comfortbull Angiography with embolization can also be
consideredbull in cases refractory to more conservativebull approaches
Nasal Fractures
bull Type of reductionbull bull Nondisplaced fractures should be treated withbull observation alone Closed nasal reduction is thebull best choice for simple injuries (isolated unilateralbull with medial displacement)bull bull An open approach should be considered in
severebull trauma (bilateral depressed fractures)
Nasal Fracturesbull Surgical principlesbull ndash Topical anaesthesia with cotton pledgets soakedbull with 4 cocaine or 005 oxymethazoline combinedbull with 4 topical lidocaine should be appliedbull for 5ndash10 min Local anaesthesia should also be injectedbull (1 lidocaine and 1100000 epinephrine)bull along the septum lateral walls and floor of the nasalbull cavitybull bull
Nasal FracturesClosed reductionndashndash The nasal bones are grasped between two fingersand pressure is applied laterally in theopposite direction of the deviation A bluntelevator may be used from within the nose incases of significant medial collapse Walshamforceps can be of help Reduction of the septumshould be performed with the use ofAsch forceps
Nasal Fractures
bull To prevent collapse of the postreductionbull framework nasal packing should be placedbull for 3ndash5 days Septum splints are recommendedbull in comminuted septal fractures withbull severe mucosal lesions External nasal splintingbull for 10 days (Aquaplastreg Thermoplastreg)bull provides nasal protection Nasal saline spraysbull prevent crusting and oral antibiotics should
Nasal Fractures
bull Open reductionbull ndashndash Immediate repair of fractures by using
widebull surgical exposure reduction fixation and
reconstructionbull ndashndash The second option is delayed correctionbull (6 months or more) of persistent deformitiesbull using standard techniques of rhinoplasty
Deviated Nasal Septum
bull Definition of the diseasebull ndash Deviation of the nasal septum is a common causebull of unilateral nasal airway obstruction in which thebull nasal septum is displacedbull bull Epidemiologyaetiologybull ndash Developmental septal abnormalities Septal cartilage
damage in the neonatal period andbull during birth can cause severe septal deviation inbull the absence of a history of nasal trauma
Deviated Nasal Septum
bull Symptomsbull ndash Patients may present with a history of sinusitis
allergicbull rhinitis obstructive sleep apnoea previousbull nasal surgery or recent nasal trauma Unilateral or
bilateral nasal airway obstruction that is unrelievedbull with decongestants or nasal steroid sprays is oftenbull seenbull bull
Deviated Nasal SeptumDiagnosisndashExamination external dorsal deviation or the columella and caudal septummay be deflected off the midline (caudal subluxation)ndash Inspections of the nasal cavity and anterior-posteriorrhinoscopy are helpful in diagnosing the locationtype and severity of septal deformityThe endoscope is also useful in identifying polypsthe severity and extent of posterior septaldeviations and bony spurs and locating areas ofseptal perforation or mucosal injury
Deviated Nasal Septum
bull Therapybull ndash Septoplasty is a procedurebull The areabull of deviation is corrected or resected in order tobull leave behind as much cartilage and bone as
possiblebull Cartilage resection is minimised and can be
repositioned reshaped or recontoured using a variety of methods
Deviated Nasal Septum
bull ndash Indications of septoplasty before the growth period
bull of the nose is finished should be very limited bull -In these cases surgery must preserve all the
cartilagebull in order to prevent external changes of the
shape ofbull the nose
Deviated Nasal Septum
bull Complicationsbull ndash Frequent complications include haematoma andbull infection Cerebrospinal fluid leak is a rare but
potentiallybull serious complicationbull It is usually the resultbull of avulsion or damage to the cribriform plate whenbull handling the perpendicular plate of the ethmoidbull ndash Other complications include epistaxis nasal
Deviated Nasal Septum
bull Other complications include epistaxis nasal obstruction
bull due to residual deviation synechiae returnbull of the cartilaginous deviation septal perforationbull anosmia and cosmetic nasal deformities suchbull as widened alar rim margins drooping nasal tipbull columella retraction and a sunken dorsum with abull supratip saddle formation
Septal perforation with minor crusting View from provide closure of the
incision
Septal Haematoma
bull A septal haematoma is a blood collection under the perichondrium
bull of the septum and cartilagebull bull bull Epidemiologyaetiologybull ndash A septal haematoma is one of the most
severe complications of nasal trauma
Septal Haematoma
bull Diagnosisbull ndash Signs and symptoms include intense pain
swellingbull haematoma of the upper lip and philtrum
area andbull complete nasal airway obstruction
Septal HaematomaTherapyndash Management consists of drainage through a mucoperichondrial incision Immediate treatment isnecessary to prevent long-term problems such asa saddle-nose deformity perforation columellarretraction and nasal-base widening In childrenseptal destruction can lead to devastating nasal andmidfacial growth abnormalitiesbull Surgeryndash Incision and evacuation of the collection is performedDrainage of a septal haematoma should
Septal HaematomaSurgeryndash Incision and evacuation of the collection is performedDrainage of a septal haematoma should provide closure of the incision
Splints or transseptal sutures are placed to obliterate thepotential space and prevent collectionInfection involving the septal cartilage Reconstruction with autologouscartilage is then performed in a second stage Oral antibiotics should be given
Nasal DeformitySaddle-nose deformityndash A saddle-nose deformity is characterised by a loss ofnasal dorsal height and compromised nasal supportstructures -Other case observed are depressionof the middle vault and dorsum loss of nasal tipsupport and definition shortened (vertical) nasal length over rotation of the nasal tip and retrusion ofthe nasal spine and caudal septum It is also knownas a ldquoPug noserdquo or ldquoboxerrsquos noserdquo both of which referto various degrees of nasal dorsal depressionbull
Nasal DeformityEpidemiologyaetiologyndash Prevalence is higher in population groups prone to facial trauma (ie boxers athletes) those with historiesof intranasal cocaine use nasal surgery (e g radical submucosal septal resection reductive rhinoplasty)ndash A saddle-nose deformity can be congenital or acquired It can be noticed as a part of individual familialsyndromic and ethnic characteristics - Most deformities are due to traumatic and iatrogeniccauses Medical causes are Wegenerrsquosgranulomatosis relapsing polychondritis leprosy (Hansenrsquos disease) syphilis ectodermal dysplasiaand intranasal cocaine use
Nasal Deformity
bull Therapybull ndash Nasal reconstruction indications depend on patientbull selection surgeon experience and aetiology of thebull deformity bull Indications for surgery can be functionalbull aesthetic or most commonly both In individuals
with a compromised nasal airway a nasoseptalbull reconstruction is indicated
Nasal Deformity
bull Contraindications bull include patients with malignantbull chronic or autoimmune disease conditions drugbull abuse poor perioperative risk profile and unrealisticbull expectationsbull ndash Multiple previous rhinoplasties and certain
professionsbull (mixed martial artists boxers and other contactbull sports) are relative contraindications
Nasal DeformitySeptoplastyndash Septoplasty is performed to correct nasal obstructioncaused by septal deformityndash Usually septoplasty is performed under general anaesthesiawith the patient in the supine position with the head elevated by approximately 30 (Righthandedsurgeons approach from the right side)ndash Local vasoconstrictive anaesthesia is applied notonly to reduce postoperative pain but also more importantly to achieve vasoconstriction of themucosa and less intraoperative haemorrhage Lidocainewith adrenaline or epinephrine is usedalthough in patients with cardiac hypersensitivityoxymetazoline might be preferred
Nasal Deformity
bull Septoplasty begins with the incision of septal mucosabull Most operative techniques utilise a hemitransfixionbull incision at the caudal end of septum so thatbull deviation at this point might be reached as wellbull as a transfixion incision that is easily obtained ifbull needed (Right-handed surgeons normally choosebull the left side but that may vary when deviation isbull convex towards the right)
Nasal DeformityA columella retractor is placed over the columellaand by pulling it laterally the caudal border of theseptum is exposed Ala can be protected by an alaprotector A vertical incision with a no 15 bladeover the caudal end of septum is performed untilreaching the plane of the septal cartilage It is essentialto correctly identify the perichondrium and byusing the Cottle elevator dissect and lift it creatinga flap As the dissection proceeds along the septalcartilage a longer speculum (no 5) is introduced sothat elevation of the mucoperichondrium is doneunder constant visual controlndash The next step is to dissect the mucoperiostium
Nasal DeformityDissecting over the bony-cartilaginous junctionwhen joining both tunnels might be difficult and is
especially prone to membrane perforationndash If needed the same tunnels are to be created on the
other side of the septum Then deviated parts of
septum are identified and removed either with a
knife or a Freer chisel
Nasal Deformitybull septum from the maxillary crest the septum mustbull be separated from the perpendicular plate trimmedbull along the inferior border placed back onto the crestbull and sutured to the periosteum If the deformity involvesbull the vomer an osteotome is used Care mustbull be taken not to break the cribriform plate becausebull it could cause a cerebrospinal fistula
Nasal Deformity
bull Once the septal deviation is corrected the flapsbull and hemitransfixion incision are mattressed
withbull absorbable sutures Nasal packing to prevent
synechiaebull and postoperative septal haematoma mightbull be advised but should be removed within 72 h

Midline Granulomabull A midline granuloma is an angiocentricbull lymphoma it was referred to as polymorphicbull reticulosis lethal midline granuloma and midline
malignant reticulosisbull bull Definition of the diseasebull ndash This rare disease is a lymphoma of extranodal
presentationall cases are positive for the Epstein-Barr virus
bull -This lymphoma most commonly appears in the midface region
Midline GranulomaEpidemiologyaetiologyndash This form of lymphoma is rare in Europe and theUnited States with a higher prevalence in Asia and PeruSymptomsndash The most common presentation is nasal obstruction with a destructive mass occupying the nosesinuses and palate
-Fever night sweatsand weight loss seen usually in Hodgkinrsquos lymphomaand other non-Hodgkinrsquos lymphomas (knownas ldquoB symptomsrdquo) are uncommon
Midline GranulomaDiagnosisndash The diagnosis is based on anatomopathologicalstudy The malignancy of the tumour manifested byextensive necrosis makes the histological diagnosisdifficult and often more biopsies are required forconfirmationbull Therapyndash Therapy consists of radiotherapy with or withoutchemotherapy
Midline Granuloma
bull Prognosisbull ndash Depending on the stage long-term remission or
experience a worseningbull prognosis with relapses which may include otherbull extranodal sites bull Involvement of extranodal sitesbull including the upper airway gastrointestinal tractbull skin
Wegenerrsquos Granulomatosis
bull Definition of the diseasebull ndash Wegenerrsquos granulomatosis is a systemic chronicbull vasculitis of small- and medium-sized blood vesselsbull with an autoimmune component It affectsbull particular organs with variable predilectionbull Epidemiologyaetiologybull ndash Wegenerrsquos granulomatosis is a rare disease It affects
about 1 in 20000ndash30000 people It is more prevalentbull in middle-aged Caucasian patients
Wegenerrsquos Granulomatosis
Symptomsndash The disease may present pulmonary upper
respiratory tract or renal In the disseminated form-The localised form ndash confinedto the upper respiratory region ndash is present in 25of the patients- It consists of nonspecific manifestationssuch as nasal obstruction crusting purulentor bloody rhinorrhea and painful or painless ulcers in oral or nasal cavities which are unresponsive tostandard medical treatment
Wegenerrsquos Granulomatosis
bull In some patients the nasal septum is perforatedbull which leads to saddle-nose deformity Less
commonbull symptoms are hoarseness stridor due to
subglotticbull stenosis otalgia otorrhea and conductivebull and sensorineural hearing loss Also ocular
symptomsbull such as scleritis conjunctivitis uveitis andbull episcleritis may be present
Wegenerrsquos Granulomatosis
bull ndash In the disseminated form pulmonary involvementbull is manifested by cough dyspnoea haemoptysisbull (due to an alveolar capillaritis necrotic lesions orbull endobronchial disease) and pleuritic painndashbull -Ninety per cent of patients have nasal symptomsbull and these symptoms are usually the first
manifestationof the diseasebull -Most patients have also renal involvementbull even if it is subclinical
Wegenerrsquos Granulomatosis
Diagnosis ndash Diagnosis of Wegenerrsquos granulomatosis is based on clinical findings that demonstrate lung (chest x-ray) kidney (urine analysis) or upper respiratory tract
involvement (oral or nasal ulcers or discharge) - positive blood analysis for cytoplasmic-staining antineutrophil
cytoplasmic antibodies (c-ANCA) and confirming proteinase 3 (PR3) ANCA or myeloperoxidase (MPO) ANCA ndash Biopsy is essential for diagnosis nonspecific chronic inflammation
and necrosis -Bacterial and fungal infections
Wegenerrsquos Granulomatosis
Therapyndash Conservative therapybull In the induction of disease remission highdosesteroids (e g prednisone 1 mgkgday) for1 month with tapering over several months aregiven In addition cyclophosphamide (2 mgkgday) should be administered for 6ndash12 monthsuntil symptoms disappear In the maintenanceof remission cyclophosphamide should be
Wegenerrsquos Granulomatosis
Antibiotics mainly trimethoprim-sulfamethoxazoleare given for prophylaxis againstPneumocystis jiroveci (formerly Pneumocystiscarinii) pneumonia (PCP) which may developduring immunosuppression and have a role inpreventing recurrencesbull Sinonasal manifestations may be treated with topical nasal steroids and nasal irrigations lowdosesystemic steroids and antibiotics when bacterial infection (typically Staphylococcus species) is suspected
Wegenerrsquos Granulomatosis
bull Prognosisbull ndash Most of the patients respond well to treatmentbull achieving symptom-free intervals of 5ndash20 yearsbull or more bull -Anatomical problems (sinusitis trachealbull stenosis) may require surgery bull Relapses can be long and troublesomebull Long-term complications are chronicbull renal failure hearing loss and deafness
Nasal Fractures Definition ndash A nasal fracture is a disruption of the nasal bone structure due to trauma It is the most frequently fractured facial bone Epidemiologyaetiology ndash Sports falls and assaults are the usual mechanisms of fracture -Males are affected twice as often as are females -Paediatric populations with a incidences during the second and third decades of life -Variables such as force impact direction nature of the striking object age and other will influence the pattern of injury to the components of the nose
Nasal Fractures
bull Symptomsbull ndash Deformity swelling epistaxis and periorbital
ecchymosis are signs that are suggestive of nasal fracture
bull bony crepitus and nasal segment mobilitybull ndash Epiphora bull Severe bilateral injuries to the lachrymal bones
arebull associated with depressed nasal fractures
Nasal Fractures Complications ndash Septal haematoma is one of the most severe early complications of nasal trauma and without drainage it results in abscess formation 6ndash7 days after trauma producing necrosis of the septal cartilage -Long-term problems such as saddle-nose deformity perforation columellar retraction and nasalbase
Septal infection could lead to osteomyelitis orbital and intracranial abscesses meningitis and cavernous sinus thrombosis -Cerebrospinal fluid leakage is a common complication of severe
nasal and frontal fractures
Nasal Fractures
bull Diagnostic proceduresbull ndash Inspectionbull bull Changes of appearance such as deviation andbull asymmetry bleeding watery drainage changesbull in nasal breathing and smell It is useful to comparebull the current presentation with old photographsbull (up to 40 of normal individuals havebull significant nose malformations)
Nasal Fractures Physical examination bull The diagnosis of a nasal fracture is made primarily by physical examination epistaxis nasal swelling and periorbital ecchymosis Nasal shape in the lateral and frontal inspection should be assessed Grasping the dorsum between two fingers and rocking the pyramid back and forth aids in assessing the mobility of nasal bones Internal structures should be evaluated by using a headlight and nasal speculum Clotted blood is removed by suction and assessment of haematoma mucosal tears and active bleeding is performed Bimanual palpation of the septum helps to differentiate septal swelling from haematoma ndash
Nasal FracturesRadiographybull There is no clear evidence of the role of radiographyin the management of nasal fracturesPlain films have up to a 66 false-positive rateas a result of misinterpretation of normal suturelines In addition old fractures are difficult todistinguishbull Three-dimensional CT is recommended for extensiveinjuries involving the nasal-orbital-ethmoidalcomplexndash
Nasal Fractures
bull Additionaluseful diagnostic proceduresbull bull Using a 0 or 30deg 4-mm endoscope is helpful inbull the assessment of posterior abnormalities If thebull patient is heavily sedated Brown-Gruss
provocationbull manoeuvres may be performed to determinebull deformities in upper middle or lower segmentsbull by compressing each compartment
Nasal FracturesConservative treatmentndash Treatment of bleedingbull For localised bleeding anterior sources may becauterised by silver nitrate or sealed with topicalmaterials such as thrombin combined withgelatin foam fibrin glue FloSealreg or other procoagulantmaterials If conservative measuresfail a formal anterior packing is placedbull Bleeding from branches of sphenopalatine orethmoid vessels requires anterior-posteriorpacking
Nasal Fractures
bull bull Surgical methods such as direct endoscopic vessel
bull cauterization or ligation have been shown tobull offer better haemostasis and patient comfortbull Angiography with embolization can also be
consideredbull in cases refractory to more conservativebull approaches
Nasal Fractures
bull Type of reductionbull bull Nondisplaced fractures should be treated withbull observation alone Closed nasal reduction is thebull best choice for simple injuries (isolated unilateralbull with medial displacement)bull bull An open approach should be considered in
severebull trauma (bilateral depressed fractures)
Nasal Fracturesbull Surgical principlesbull ndash Topical anaesthesia with cotton pledgets soakedbull with 4 cocaine or 005 oxymethazoline combinedbull with 4 topical lidocaine should be appliedbull for 5ndash10 min Local anaesthesia should also be injectedbull (1 lidocaine and 1100000 epinephrine)bull along the septum lateral walls and floor of the nasalbull cavitybull bull
Nasal FracturesClosed reductionndashndash The nasal bones are grasped between two fingersand pressure is applied laterally in theopposite direction of the deviation A bluntelevator may be used from within the nose incases of significant medial collapse Walshamforceps can be of help Reduction of the septumshould be performed with the use ofAsch forceps
Nasal Fractures
bull To prevent collapse of the postreductionbull framework nasal packing should be placedbull for 3ndash5 days Septum splints are recommendedbull in comminuted septal fractures withbull severe mucosal lesions External nasal splintingbull for 10 days (Aquaplastreg Thermoplastreg)bull provides nasal protection Nasal saline spraysbull prevent crusting and oral antibiotics should
Nasal Fractures
bull Open reductionbull ndashndash Immediate repair of fractures by using
widebull surgical exposure reduction fixation and
reconstructionbull ndashndash The second option is delayed correctionbull (6 months or more) of persistent deformitiesbull using standard techniques of rhinoplasty
Deviated Nasal Septum
bull Definition of the diseasebull ndash Deviation of the nasal septum is a common causebull of unilateral nasal airway obstruction in which thebull nasal septum is displacedbull bull Epidemiologyaetiologybull ndash Developmental septal abnormalities Septal cartilage
damage in the neonatal period andbull during birth can cause severe septal deviation inbull the absence of a history of nasal trauma
Deviated Nasal Septum
bull Symptomsbull ndash Patients may present with a history of sinusitis
allergicbull rhinitis obstructive sleep apnoea previousbull nasal surgery or recent nasal trauma Unilateral or
bilateral nasal airway obstruction that is unrelievedbull with decongestants or nasal steroid sprays is oftenbull seenbull bull
Deviated Nasal SeptumDiagnosisndashExamination external dorsal deviation or the columella and caudal septummay be deflected off the midline (caudal subluxation)ndash Inspections of the nasal cavity and anterior-posteriorrhinoscopy are helpful in diagnosing the locationtype and severity of septal deformityThe endoscope is also useful in identifying polypsthe severity and extent of posterior septaldeviations and bony spurs and locating areas ofseptal perforation or mucosal injury
Deviated Nasal Septum
bull Therapybull ndash Septoplasty is a procedurebull The areabull of deviation is corrected or resected in order tobull leave behind as much cartilage and bone as
possiblebull Cartilage resection is minimised and can be
repositioned reshaped or recontoured using a variety of methods
Deviated Nasal Septum
bull ndash Indications of septoplasty before the growth period
bull of the nose is finished should be very limited bull -In these cases surgery must preserve all the
cartilagebull in order to prevent external changes of the
shape ofbull the nose
Deviated Nasal Septum
bull Complicationsbull ndash Frequent complications include haematoma andbull infection Cerebrospinal fluid leak is a rare but
potentiallybull serious complicationbull It is usually the resultbull of avulsion or damage to the cribriform plate whenbull handling the perpendicular plate of the ethmoidbull ndash Other complications include epistaxis nasal
Deviated Nasal Septum
bull Other complications include epistaxis nasal obstruction
bull due to residual deviation synechiae returnbull of the cartilaginous deviation septal perforationbull anosmia and cosmetic nasal deformities suchbull as widened alar rim margins drooping nasal tipbull columella retraction and a sunken dorsum with abull supratip saddle formation
Septal perforation with minor crusting View from provide closure of the
incision
Septal Haematoma
bull A septal haematoma is a blood collection under the perichondrium
bull of the septum and cartilagebull bull bull Epidemiologyaetiologybull ndash A septal haematoma is one of the most
severe complications of nasal trauma
Septal Haematoma
bull Diagnosisbull ndash Signs and symptoms include intense pain
swellingbull haematoma of the upper lip and philtrum
area andbull complete nasal airway obstruction
Septal HaematomaTherapyndash Management consists of drainage through a mucoperichondrial incision Immediate treatment isnecessary to prevent long-term problems such asa saddle-nose deformity perforation columellarretraction and nasal-base widening In childrenseptal destruction can lead to devastating nasal andmidfacial growth abnormalitiesbull Surgeryndash Incision and evacuation of the collection is performedDrainage of a septal haematoma should
Septal HaematomaSurgeryndash Incision and evacuation of the collection is performedDrainage of a septal haematoma should provide closure of the incision
Splints or transseptal sutures are placed to obliterate thepotential space and prevent collectionInfection involving the septal cartilage Reconstruction with autologouscartilage is then performed in a second stage Oral antibiotics should be given
Nasal DeformitySaddle-nose deformityndash A saddle-nose deformity is characterised by a loss ofnasal dorsal height and compromised nasal supportstructures -Other case observed are depressionof the middle vault and dorsum loss of nasal tipsupport and definition shortened (vertical) nasal length over rotation of the nasal tip and retrusion ofthe nasal spine and caudal septum It is also knownas a ldquoPug noserdquo or ldquoboxerrsquos noserdquo both of which referto various degrees of nasal dorsal depressionbull
Nasal DeformityEpidemiologyaetiologyndash Prevalence is higher in population groups prone to facial trauma (ie boxers athletes) those with historiesof intranasal cocaine use nasal surgery (e g radical submucosal septal resection reductive rhinoplasty)ndash A saddle-nose deformity can be congenital or acquired It can be noticed as a part of individual familialsyndromic and ethnic characteristics - Most deformities are due to traumatic and iatrogeniccauses Medical causes are Wegenerrsquosgranulomatosis relapsing polychondritis leprosy (Hansenrsquos disease) syphilis ectodermal dysplasiaand intranasal cocaine use
Nasal Deformity
bull Therapybull ndash Nasal reconstruction indications depend on patientbull selection surgeon experience and aetiology of thebull deformity bull Indications for surgery can be functionalbull aesthetic or most commonly both In individuals
with a compromised nasal airway a nasoseptalbull reconstruction is indicated
Nasal Deformity
bull Contraindications bull include patients with malignantbull chronic or autoimmune disease conditions drugbull abuse poor perioperative risk profile and unrealisticbull expectationsbull ndash Multiple previous rhinoplasties and certain
professionsbull (mixed martial artists boxers and other contactbull sports) are relative contraindications
Nasal DeformitySeptoplastyndash Septoplasty is performed to correct nasal obstructioncaused by septal deformityndash Usually septoplasty is performed under general anaesthesiawith the patient in the supine position with the head elevated by approximately 30 (Righthandedsurgeons approach from the right side)ndash Local vasoconstrictive anaesthesia is applied notonly to reduce postoperative pain but also more importantly to achieve vasoconstriction of themucosa and less intraoperative haemorrhage Lidocainewith adrenaline or epinephrine is usedalthough in patients with cardiac hypersensitivityoxymetazoline might be preferred
Nasal Deformity
bull Septoplasty begins with the incision of septal mucosabull Most operative techniques utilise a hemitransfixionbull incision at the caudal end of septum so thatbull deviation at this point might be reached as wellbull as a transfixion incision that is easily obtained ifbull needed (Right-handed surgeons normally choosebull the left side but that may vary when deviation isbull convex towards the right)
Nasal DeformityA columella retractor is placed over the columellaand by pulling it laterally the caudal border of theseptum is exposed Ala can be protected by an alaprotector A vertical incision with a no 15 bladeover the caudal end of septum is performed untilreaching the plane of the septal cartilage It is essentialto correctly identify the perichondrium and byusing the Cottle elevator dissect and lift it creatinga flap As the dissection proceeds along the septalcartilage a longer speculum (no 5) is introduced sothat elevation of the mucoperichondrium is doneunder constant visual controlndash The next step is to dissect the mucoperiostium
Nasal DeformityDissecting over the bony-cartilaginous junctionwhen joining both tunnels might be difficult and is
especially prone to membrane perforationndash If needed the same tunnels are to be created on the
other side of the septum Then deviated parts of
septum are identified and removed either with a
knife or a Freer chisel
Nasal Deformitybull septum from the maxillary crest the septum mustbull be separated from the perpendicular plate trimmedbull along the inferior border placed back onto the crestbull and sutured to the periosteum If the deformity involvesbull the vomer an osteotome is used Care mustbull be taken not to break the cribriform plate becausebull it could cause a cerebrospinal fistula
Nasal Deformity
bull Once the septal deviation is corrected the flapsbull and hemitransfixion incision are mattressed
withbull absorbable sutures Nasal packing to prevent
synechiaebull and postoperative septal haematoma mightbull be advised but should be removed within 72 h

Midline GranulomaEpidemiologyaetiologyndash This form of lymphoma is rare in Europe and theUnited States with a higher prevalence in Asia and PeruSymptomsndash The most common presentation is nasal obstruction with a destructive mass occupying the nosesinuses and palate
-Fever night sweatsand weight loss seen usually in Hodgkinrsquos lymphomaand other non-Hodgkinrsquos lymphomas (knownas ldquoB symptomsrdquo) are uncommon
Midline GranulomaDiagnosisndash The diagnosis is based on anatomopathologicalstudy The malignancy of the tumour manifested byextensive necrosis makes the histological diagnosisdifficult and often more biopsies are required forconfirmationbull Therapyndash Therapy consists of radiotherapy with or withoutchemotherapy
Midline Granuloma
bull Prognosisbull ndash Depending on the stage long-term remission or
experience a worseningbull prognosis with relapses which may include otherbull extranodal sites bull Involvement of extranodal sitesbull including the upper airway gastrointestinal tractbull skin
Wegenerrsquos Granulomatosis
bull Definition of the diseasebull ndash Wegenerrsquos granulomatosis is a systemic chronicbull vasculitis of small- and medium-sized blood vesselsbull with an autoimmune component It affectsbull particular organs with variable predilectionbull Epidemiologyaetiologybull ndash Wegenerrsquos granulomatosis is a rare disease It affects
about 1 in 20000ndash30000 people It is more prevalentbull in middle-aged Caucasian patients
Wegenerrsquos Granulomatosis
Symptomsndash The disease may present pulmonary upper
respiratory tract or renal In the disseminated form-The localised form ndash confinedto the upper respiratory region ndash is present in 25of the patients- It consists of nonspecific manifestationssuch as nasal obstruction crusting purulentor bloody rhinorrhea and painful or painless ulcers in oral or nasal cavities which are unresponsive tostandard medical treatment
Wegenerrsquos Granulomatosis
bull In some patients the nasal septum is perforatedbull which leads to saddle-nose deformity Less
commonbull symptoms are hoarseness stridor due to
subglotticbull stenosis otalgia otorrhea and conductivebull and sensorineural hearing loss Also ocular
symptomsbull such as scleritis conjunctivitis uveitis andbull episcleritis may be present
Wegenerrsquos Granulomatosis
bull ndash In the disseminated form pulmonary involvementbull is manifested by cough dyspnoea haemoptysisbull (due to an alveolar capillaritis necrotic lesions orbull endobronchial disease) and pleuritic painndashbull -Ninety per cent of patients have nasal symptomsbull and these symptoms are usually the first
manifestationof the diseasebull -Most patients have also renal involvementbull even if it is subclinical
Wegenerrsquos Granulomatosis
Diagnosis ndash Diagnosis of Wegenerrsquos granulomatosis is based on clinical findings that demonstrate lung (chest x-ray) kidney (urine analysis) or upper respiratory tract
involvement (oral or nasal ulcers or discharge) - positive blood analysis for cytoplasmic-staining antineutrophil
cytoplasmic antibodies (c-ANCA) and confirming proteinase 3 (PR3) ANCA or myeloperoxidase (MPO) ANCA ndash Biopsy is essential for diagnosis nonspecific chronic inflammation
and necrosis -Bacterial and fungal infections
Wegenerrsquos Granulomatosis
Therapyndash Conservative therapybull In the induction of disease remission highdosesteroids (e g prednisone 1 mgkgday) for1 month with tapering over several months aregiven In addition cyclophosphamide (2 mgkgday) should be administered for 6ndash12 monthsuntil symptoms disappear In the maintenanceof remission cyclophosphamide should be
Wegenerrsquos Granulomatosis
Antibiotics mainly trimethoprim-sulfamethoxazoleare given for prophylaxis againstPneumocystis jiroveci (formerly Pneumocystiscarinii) pneumonia (PCP) which may developduring immunosuppression and have a role inpreventing recurrencesbull Sinonasal manifestations may be treated with topical nasal steroids and nasal irrigations lowdosesystemic steroids and antibiotics when bacterial infection (typically Staphylococcus species) is suspected
Wegenerrsquos Granulomatosis
bull Prognosisbull ndash Most of the patients respond well to treatmentbull achieving symptom-free intervals of 5ndash20 yearsbull or more bull -Anatomical problems (sinusitis trachealbull stenosis) may require surgery bull Relapses can be long and troublesomebull Long-term complications are chronicbull renal failure hearing loss and deafness
Nasal Fractures Definition ndash A nasal fracture is a disruption of the nasal bone structure due to trauma It is the most frequently fractured facial bone Epidemiologyaetiology ndash Sports falls and assaults are the usual mechanisms of fracture -Males are affected twice as often as are females -Paediatric populations with a incidences during the second and third decades of life -Variables such as force impact direction nature of the striking object age and other will influence the pattern of injury to the components of the nose
Nasal Fractures
bull Symptomsbull ndash Deformity swelling epistaxis and periorbital
ecchymosis are signs that are suggestive of nasal fracture
bull bony crepitus and nasal segment mobilitybull ndash Epiphora bull Severe bilateral injuries to the lachrymal bones
arebull associated with depressed nasal fractures
Nasal Fractures Complications ndash Septal haematoma is one of the most severe early complications of nasal trauma and without drainage it results in abscess formation 6ndash7 days after trauma producing necrosis of the septal cartilage -Long-term problems such as saddle-nose deformity perforation columellar retraction and nasalbase
Septal infection could lead to osteomyelitis orbital and intracranial abscesses meningitis and cavernous sinus thrombosis -Cerebrospinal fluid leakage is a common complication of severe
nasal and frontal fractures
Nasal Fractures
bull Diagnostic proceduresbull ndash Inspectionbull bull Changes of appearance such as deviation andbull asymmetry bleeding watery drainage changesbull in nasal breathing and smell It is useful to comparebull the current presentation with old photographsbull (up to 40 of normal individuals havebull significant nose malformations)
Nasal Fractures Physical examination bull The diagnosis of a nasal fracture is made primarily by physical examination epistaxis nasal swelling and periorbital ecchymosis Nasal shape in the lateral and frontal inspection should be assessed Grasping the dorsum between two fingers and rocking the pyramid back and forth aids in assessing the mobility of nasal bones Internal structures should be evaluated by using a headlight and nasal speculum Clotted blood is removed by suction and assessment of haematoma mucosal tears and active bleeding is performed Bimanual palpation of the septum helps to differentiate septal swelling from haematoma ndash
Nasal FracturesRadiographybull There is no clear evidence of the role of radiographyin the management of nasal fracturesPlain films have up to a 66 false-positive rateas a result of misinterpretation of normal suturelines In addition old fractures are difficult todistinguishbull Three-dimensional CT is recommended for extensiveinjuries involving the nasal-orbital-ethmoidalcomplexndash
Nasal Fractures
bull Additionaluseful diagnostic proceduresbull bull Using a 0 or 30deg 4-mm endoscope is helpful inbull the assessment of posterior abnormalities If thebull patient is heavily sedated Brown-Gruss
provocationbull manoeuvres may be performed to determinebull deformities in upper middle or lower segmentsbull by compressing each compartment
Nasal FracturesConservative treatmentndash Treatment of bleedingbull For localised bleeding anterior sources may becauterised by silver nitrate or sealed with topicalmaterials such as thrombin combined withgelatin foam fibrin glue FloSealreg or other procoagulantmaterials If conservative measuresfail a formal anterior packing is placedbull Bleeding from branches of sphenopalatine orethmoid vessels requires anterior-posteriorpacking
Nasal Fractures
bull bull Surgical methods such as direct endoscopic vessel
bull cauterization or ligation have been shown tobull offer better haemostasis and patient comfortbull Angiography with embolization can also be
consideredbull in cases refractory to more conservativebull approaches
Nasal Fractures
bull Type of reductionbull bull Nondisplaced fractures should be treated withbull observation alone Closed nasal reduction is thebull best choice for simple injuries (isolated unilateralbull with medial displacement)bull bull An open approach should be considered in
severebull trauma (bilateral depressed fractures)
Nasal Fracturesbull Surgical principlesbull ndash Topical anaesthesia with cotton pledgets soakedbull with 4 cocaine or 005 oxymethazoline combinedbull with 4 topical lidocaine should be appliedbull for 5ndash10 min Local anaesthesia should also be injectedbull (1 lidocaine and 1100000 epinephrine)bull along the septum lateral walls and floor of the nasalbull cavitybull bull
Nasal FracturesClosed reductionndashndash The nasal bones are grasped between two fingersand pressure is applied laterally in theopposite direction of the deviation A bluntelevator may be used from within the nose incases of significant medial collapse Walshamforceps can be of help Reduction of the septumshould be performed with the use ofAsch forceps
Nasal Fractures
bull To prevent collapse of the postreductionbull framework nasal packing should be placedbull for 3ndash5 days Septum splints are recommendedbull in comminuted septal fractures withbull severe mucosal lesions External nasal splintingbull for 10 days (Aquaplastreg Thermoplastreg)bull provides nasal protection Nasal saline spraysbull prevent crusting and oral antibiotics should
Nasal Fractures
bull Open reductionbull ndashndash Immediate repair of fractures by using
widebull surgical exposure reduction fixation and
reconstructionbull ndashndash The second option is delayed correctionbull (6 months or more) of persistent deformitiesbull using standard techniques of rhinoplasty
Deviated Nasal Septum
bull Definition of the diseasebull ndash Deviation of the nasal septum is a common causebull of unilateral nasal airway obstruction in which thebull nasal septum is displacedbull bull Epidemiologyaetiologybull ndash Developmental septal abnormalities Septal cartilage
damage in the neonatal period andbull during birth can cause severe septal deviation inbull the absence of a history of nasal trauma
Deviated Nasal Septum
bull Symptomsbull ndash Patients may present with a history of sinusitis
allergicbull rhinitis obstructive sleep apnoea previousbull nasal surgery or recent nasal trauma Unilateral or
bilateral nasal airway obstruction that is unrelievedbull with decongestants or nasal steroid sprays is oftenbull seenbull bull
Deviated Nasal SeptumDiagnosisndashExamination external dorsal deviation or the columella and caudal septummay be deflected off the midline (caudal subluxation)ndash Inspections of the nasal cavity and anterior-posteriorrhinoscopy are helpful in diagnosing the locationtype and severity of septal deformityThe endoscope is also useful in identifying polypsthe severity and extent of posterior septaldeviations and bony spurs and locating areas ofseptal perforation or mucosal injury
Deviated Nasal Septum
bull Therapybull ndash Septoplasty is a procedurebull The areabull of deviation is corrected or resected in order tobull leave behind as much cartilage and bone as
possiblebull Cartilage resection is minimised and can be
repositioned reshaped or recontoured using a variety of methods
Deviated Nasal Septum
bull ndash Indications of septoplasty before the growth period
bull of the nose is finished should be very limited bull -In these cases surgery must preserve all the
cartilagebull in order to prevent external changes of the
shape ofbull the nose
Deviated Nasal Septum
bull Complicationsbull ndash Frequent complications include haematoma andbull infection Cerebrospinal fluid leak is a rare but
potentiallybull serious complicationbull It is usually the resultbull of avulsion or damage to the cribriform plate whenbull handling the perpendicular plate of the ethmoidbull ndash Other complications include epistaxis nasal
Deviated Nasal Septum
bull Other complications include epistaxis nasal obstruction
bull due to residual deviation synechiae returnbull of the cartilaginous deviation septal perforationbull anosmia and cosmetic nasal deformities suchbull as widened alar rim margins drooping nasal tipbull columella retraction and a sunken dorsum with abull supratip saddle formation
Septal perforation with minor crusting View from provide closure of the
incision
Septal Haematoma
bull A septal haematoma is a blood collection under the perichondrium
bull of the septum and cartilagebull bull bull Epidemiologyaetiologybull ndash A septal haematoma is one of the most
severe complications of nasal trauma
Septal Haematoma
bull Diagnosisbull ndash Signs and symptoms include intense pain
swellingbull haematoma of the upper lip and philtrum
area andbull complete nasal airway obstruction
Septal HaematomaTherapyndash Management consists of drainage through a mucoperichondrial incision Immediate treatment isnecessary to prevent long-term problems such asa saddle-nose deformity perforation columellarretraction and nasal-base widening In childrenseptal destruction can lead to devastating nasal andmidfacial growth abnormalitiesbull Surgeryndash Incision and evacuation of the collection is performedDrainage of a septal haematoma should
Septal HaematomaSurgeryndash Incision and evacuation of the collection is performedDrainage of a septal haematoma should provide closure of the incision
Splints or transseptal sutures are placed to obliterate thepotential space and prevent collectionInfection involving the septal cartilage Reconstruction with autologouscartilage is then performed in a second stage Oral antibiotics should be given
Nasal DeformitySaddle-nose deformityndash A saddle-nose deformity is characterised by a loss ofnasal dorsal height and compromised nasal supportstructures -Other case observed are depressionof the middle vault and dorsum loss of nasal tipsupport and definition shortened (vertical) nasal length over rotation of the nasal tip and retrusion ofthe nasal spine and caudal septum It is also knownas a ldquoPug noserdquo or ldquoboxerrsquos noserdquo both of which referto various degrees of nasal dorsal depressionbull
Nasal DeformityEpidemiologyaetiologyndash Prevalence is higher in population groups prone to facial trauma (ie boxers athletes) those with historiesof intranasal cocaine use nasal surgery (e g radical submucosal septal resection reductive rhinoplasty)ndash A saddle-nose deformity can be congenital or acquired It can be noticed as a part of individual familialsyndromic and ethnic characteristics - Most deformities are due to traumatic and iatrogeniccauses Medical causes are Wegenerrsquosgranulomatosis relapsing polychondritis leprosy (Hansenrsquos disease) syphilis ectodermal dysplasiaand intranasal cocaine use
Nasal Deformity
bull Therapybull ndash Nasal reconstruction indications depend on patientbull selection surgeon experience and aetiology of thebull deformity bull Indications for surgery can be functionalbull aesthetic or most commonly both In individuals
with a compromised nasal airway a nasoseptalbull reconstruction is indicated
Nasal Deformity
bull Contraindications bull include patients with malignantbull chronic or autoimmune disease conditions drugbull abuse poor perioperative risk profile and unrealisticbull expectationsbull ndash Multiple previous rhinoplasties and certain
professionsbull (mixed martial artists boxers and other contactbull sports) are relative contraindications
Nasal DeformitySeptoplastyndash Septoplasty is performed to correct nasal obstructioncaused by septal deformityndash Usually septoplasty is performed under general anaesthesiawith the patient in the supine position with the head elevated by approximately 30 (Righthandedsurgeons approach from the right side)ndash Local vasoconstrictive anaesthesia is applied notonly to reduce postoperative pain but also more importantly to achieve vasoconstriction of themucosa and less intraoperative haemorrhage Lidocainewith adrenaline or epinephrine is usedalthough in patients with cardiac hypersensitivityoxymetazoline might be preferred
Nasal Deformity
bull Septoplasty begins with the incision of septal mucosabull Most operative techniques utilise a hemitransfixionbull incision at the caudal end of septum so thatbull deviation at this point might be reached as wellbull as a transfixion incision that is easily obtained ifbull needed (Right-handed surgeons normally choosebull the left side but that may vary when deviation isbull convex towards the right)
Nasal DeformityA columella retractor is placed over the columellaand by pulling it laterally the caudal border of theseptum is exposed Ala can be protected by an alaprotector A vertical incision with a no 15 bladeover the caudal end of septum is performed untilreaching the plane of the septal cartilage It is essentialto correctly identify the perichondrium and byusing the Cottle elevator dissect and lift it creatinga flap As the dissection proceeds along the septalcartilage a longer speculum (no 5) is introduced sothat elevation of the mucoperichondrium is doneunder constant visual controlndash The next step is to dissect the mucoperiostium
Nasal DeformityDissecting over the bony-cartilaginous junctionwhen joining both tunnels might be difficult and is
especially prone to membrane perforationndash If needed the same tunnels are to be created on the
other side of the septum Then deviated parts of
septum are identified and removed either with a
knife or a Freer chisel
Nasal Deformitybull septum from the maxillary crest the septum mustbull be separated from the perpendicular plate trimmedbull along the inferior border placed back onto the crestbull and sutured to the periosteum If the deformity involvesbull the vomer an osteotome is used Care mustbull be taken not to break the cribriform plate becausebull it could cause a cerebrospinal fistula
Nasal Deformity
bull Once the septal deviation is corrected the flapsbull and hemitransfixion incision are mattressed
withbull absorbable sutures Nasal packing to prevent
synechiaebull and postoperative septal haematoma mightbull be advised but should be removed within 72 h

Midline GranulomaDiagnosisndash The diagnosis is based on anatomopathologicalstudy The malignancy of the tumour manifested byextensive necrosis makes the histological diagnosisdifficult and often more biopsies are required forconfirmationbull Therapyndash Therapy consists of radiotherapy with or withoutchemotherapy
Midline Granuloma
bull Prognosisbull ndash Depending on the stage long-term remission or
experience a worseningbull prognosis with relapses which may include otherbull extranodal sites bull Involvement of extranodal sitesbull including the upper airway gastrointestinal tractbull skin
Wegenerrsquos Granulomatosis
bull Definition of the diseasebull ndash Wegenerrsquos granulomatosis is a systemic chronicbull vasculitis of small- and medium-sized blood vesselsbull with an autoimmune component It affectsbull particular organs with variable predilectionbull Epidemiologyaetiologybull ndash Wegenerrsquos granulomatosis is a rare disease It affects
about 1 in 20000ndash30000 people It is more prevalentbull in middle-aged Caucasian patients
Wegenerrsquos Granulomatosis
Symptomsndash The disease may present pulmonary upper
respiratory tract or renal In the disseminated form-The localised form ndash confinedto the upper respiratory region ndash is present in 25of the patients- It consists of nonspecific manifestationssuch as nasal obstruction crusting purulentor bloody rhinorrhea and painful or painless ulcers in oral or nasal cavities which are unresponsive tostandard medical treatment
Wegenerrsquos Granulomatosis
bull In some patients the nasal septum is perforatedbull which leads to saddle-nose deformity Less
commonbull symptoms are hoarseness stridor due to
subglotticbull stenosis otalgia otorrhea and conductivebull and sensorineural hearing loss Also ocular
symptomsbull such as scleritis conjunctivitis uveitis andbull episcleritis may be present
Wegenerrsquos Granulomatosis
bull ndash In the disseminated form pulmonary involvementbull is manifested by cough dyspnoea haemoptysisbull (due to an alveolar capillaritis necrotic lesions orbull endobronchial disease) and pleuritic painndashbull -Ninety per cent of patients have nasal symptomsbull and these symptoms are usually the first
manifestationof the diseasebull -Most patients have also renal involvementbull even if it is subclinical
Wegenerrsquos Granulomatosis
Diagnosis ndash Diagnosis of Wegenerrsquos granulomatosis is based on clinical findings that demonstrate lung (chest x-ray) kidney (urine analysis) or upper respiratory tract
involvement (oral or nasal ulcers or discharge) - positive blood analysis for cytoplasmic-staining antineutrophil
cytoplasmic antibodies (c-ANCA) and confirming proteinase 3 (PR3) ANCA or myeloperoxidase (MPO) ANCA ndash Biopsy is essential for diagnosis nonspecific chronic inflammation
and necrosis -Bacterial and fungal infections
Wegenerrsquos Granulomatosis
Therapyndash Conservative therapybull In the induction of disease remission highdosesteroids (e g prednisone 1 mgkgday) for1 month with tapering over several months aregiven In addition cyclophosphamide (2 mgkgday) should be administered for 6ndash12 monthsuntil symptoms disappear In the maintenanceof remission cyclophosphamide should be
Wegenerrsquos Granulomatosis
Antibiotics mainly trimethoprim-sulfamethoxazoleare given for prophylaxis againstPneumocystis jiroveci (formerly Pneumocystiscarinii) pneumonia (PCP) which may developduring immunosuppression and have a role inpreventing recurrencesbull Sinonasal manifestations may be treated with topical nasal steroids and nasal irrigations lowdosesystemic steroids and antibiotics when bacterial infection (typically Staphylococcus species) is suspected
Wegenerrsquos Granulomatosis
bull Prognosisbull ndash Most of the patients respond well to treatmentbull achieving symptom-free intervals of 5ndash20 yearsbull or more bull -Anatomical problems (sinusitis trachealbull stenosis) may require surgery bull Relapses can be long and troublesomebull Long-term complications are chronicbull renal failure hearing loss and deafness
Nasal Fractures Definition ndash A nasal fracture is a disruption of the nasal bone structure due to trauma It is the most frequently fractured facial bone Epidemiologyaetiology ndash Sports falls and assaults are the usual mechanisms of fracture -Males are affected twice as often as are females -Paediatric populations with a incidences during the second and third decades of life -Variables such as force impact direction nature of the striking object age and other will influence the pattern of injury to the components of the nose
Nasal Fractures
bull Symptomsbull ndash Deformity swelling epistaxis and periorbital
ecchymosis are signs that are suggestive of nasal fracture
bull bony crepitus and nasal segment mobilitybull ndash Epiphora bull Severe bilateral injuries to the lachrymal bones
arebull associated with depressed nasal fractures
Nasal Fractures Complications ndash Septal haematoma is one of the most severe early complications of nasal trauma and without drainage it results in abscess formation 6ndash7 days after trauma producing necrosis of the septal cartilage -Long-term problems such as saddle-nose deformity perforation columellar retraction and nasalbase
Septal infection could lead to osteomyelitis orbital and intracranial abscesses meningitis and cavernous sinus thrombosis -Cerebrospinal fluid leakage is a common complication of severe
nasal and frontal fractures
Nasal Fractures
bull Diagnostic proceduresbull ndash Inspectionbull bull Changes of appearance such as deviation andbull asymmetry bleeding watery drainage changesbull in nasal breathing and smell It is useful to comparebull the current presentation with old photographsbull (up to 40 of normal individuals havebull significant nose malformations)
Nasal Fractures Physical examination bull The diagnosis of a nasal fracture is made primarily by physical examination epistaxis nasal swelling and periorbital ecchymosis Nasal shape in the lateral and frontal inspection should be assessed Grasping the dorsum between two fingers and rocking the pyramid back and forth aids in assessing the mobility of nasal bones Internal structures should be evaluated by using a headlight and nasal speculum Clotted blood is removed by suction and assessment of haematoma mucosal tears and active bleeding is performed Bimanual palpation of the septum helps to differentiate septal swelling from haematoma ndash
Nasal FracturesRadiographybull There is no clear evidence of the role of radiographyin the management of nasal fracturesPlain films have up to a 66 false-positive rateas a result of misinterpretation of normal suturelines In addition old fractures are difficult todistinguishbull Three-dimensional CT is recommended for extensiveinjuries involving the nasal-orbital-ethmoidalcomplexndash
Nasal Fractures
bull Additionaluseful diagnostic proceduresbull bull Using a 0 or 30deg 4-mm endoscope is helpful inbull the assessment of posterior abnormalities If thebull patient is heavily sedated Brown-Gruss
provocationbull manoeuvres may be performed to determinebull deformities in upper middle or lower segmentsbull by compressing each compartment
Nasal FracturesConservative treatmentndash Treatment of bleedingbull For localised bleeding anterior sources may becauterised by silver nitrate or sealed with topicalmaterials such as thrombin combined withgelatin foam fibrin glue FloSealreg or other procoagulantmaterials If conservative measuresfail a formal anterior packing is placedbull Bleeding from branches of sphenopalatine orethmoid vessels requires anterior-posteriorpacking
Nasal Fractures
bull bull Surgical methods such as direct endoscopic vessel
bull cauterization or ligation have been shown tobull offer better haemostasis and patient comfortbull Angiography with embolization can also be
consideredbull in cases refractory to more conservativebull approaches
Nasal Fractures
bull Type of reductionbull bull Nondisplaced fractures should be treated withbull observation alone Closed nasal reduction is thebull best choice for simple injuries (isolated unilateralbull with medial displacement)bull bull An open approach should be considered in
severebull trauma (bilateral depressed fractures)
Nasal Fracturesbull Surgical principlesbull ndash Topical anaesthesia with cotton pledgets soakedbull with 4 cocaine or 005 oxymethazoline combinedbull with 4 topical lidocaine should be appliedbull for 5ndash10 min Local anaesthesia should also be injectedbull (1 lidocaine and 1100000 epinephrine)bull along the septum lateral walls and floor of the nasalbull cavitybull bull
Nasal FracturesClosed reductionndashndash The nasal bones are grasped between two fingersand pressure is applied laterally in theopposite direction of the deviation A bluntelevator may be used from within the nose incases of significant medial collapse Walshamforceps can be of help Reduction of the septumshould be performed with the use ofAsch forceps
Nasal Fractures
bull To prevent collapse of the postreductionbull framework nasal packing should be placedbull for 3ndash5 days Septum splints are recommendedbull in comminuted septal fractures withbull severe mucosal lesions External nasal splintingbull for 10 days (Aquaplastreg Thermoplastreg)bull provides nasal protection Nasal saline spraysbull prevent crusting and oral antibiotics should
Nasal Fractures
bull Open reductionbull ndashndash Immediate repair of fractures by using
widebull surgical exposure reduction fixation and
reconstructionbull ndashndash The second option is delayed correctionbull (6 months or more) of persistent deformitiesbull using standard techniques of rhinoplasty
Deviated Nasal Septum
bull Definition of the diseasebull ndash Deviation of the nasal septum is a common causebull of unilateral nasal airway obstruction in which thebull nasal septum is displacedbull bull Epidemiologyaetiologybull ndash Developmental septal abnormalities Septal cartilage
damage in the neonatal period andbull during birth can cause severe septal deviation inbull the absence of a history of nasal trauma
Deviated Nasal Septum
bull Symptomsbull ndash Patients may present with a history of sinusitis
allergicbull rhinitis obstructive sleep apnoea previousbull nasal surgery or recent nasal trauma Unilateral or
bilateral nasal airway obstruction that is unrelievedbull with decongestants or nasal steroid sprays is oftenbull seenbull bull
Deviated Nasal SeptumDiagnosisndashExamination external dorsal deviation or the columella and caudal septummay be deflected off the midline (caudal subluxation)ndash Inspections of the nasal cavity and anterior-posteriorrhinoscopy are helpful in diagnosing the locationtype and severity of septal deformityThe endoscope is also useful in identifying polypsthe severity and extent of posterior septaldeviations and bony spurs and locating areas ofseptal perforation or mucosal injury
Deviated Nasal Septum
bull Therapybull ndash Septoplasty is a procedurebull The areabull of deviation is corrected or resected in order tobull leave behind as much cartilage and bone as
possiblebull Cartilage resection is minimised and can be
repositioned reshaped or recontoured using a variety of methods
Deviated Nasal Septum
bull ndash Indications of septoplasty before the growth period
bull of the nose is finished should be very limited bull -In these cases surgery must preserve all the
cartilagebull in order to prevent external changes of the
shape ofbull the nose
Deviated Nasal Septum
bull Complicationsbull ndash Frequent complications include haematoma andbull infection Cerebrospinal fluid leak is a rare but
potentiallybull serious complicationbull It is usually the resultbull of avulsion or damage to the cribriform plate whenbull handling the perpendicular plate of the ethmoidbull ndash Other complications include epistaxis nasal
Deviated Nasal Septum
bull Other complications include epistaxis nasal obstruction
bull due to residual deviation synechiae returnbull of the cartilaginous deviation septal perforationbull anosmia and cosmetic nasal deformities suchbull as widened alar rim margins drooping nasal tipbull columella retraction and a sunken dorsum with abull supratip saddle formation
Septal perforation with minor crusting View from provide closure of the
incision
Septal Haematoma
bull A septal haematoma is a blood collection under the perichondrium
bull of the septum and cartilagebull bull bull Epidemiologyaetiologybull ndash A septal haematoma is one of the most
severe complications of nasal trauma
Septal Haematoma
bull Diagnosisbull ndash Signs and symptoms include intense pain
swellingbull haematoma of the upper lip and philtrum
area andbull complete nasal airway obstruction
Septal HaematomaTherapyndash Management consists of drainage through a mucoperichondrial incision Immediate treatment isnecessary to prevent long-term problems such asa saddle-nose deformity perforation columellarretraction and nasal-base widening In childrenseptal destruction can lead to devastating nasal andmidfacial growth abnormalitiesbull Surgeryndash Incision and evacuation of the collection is performedDrainage of a septal haematoma should
Septal HaematomaSurgeryndash Incision and evacuation of the collection is performedDrainage of a septal haematoma should provide closure of the incision
Splints or transseptal sutures are placed to obliterate thepotential space and prevent collectionInfection involving the septal cartilage Reconstruction with autologouscartilage is then performed in a second stage Oral antibiotics should be given
Nasal DeformitySaddle-nose deformityndash A saddle-nose deformity is characterised by a loss ofnasal dorsal height and compromised nasal supportstructures -Other case observed are depressionof the middle vault and dorsum loss of nasal tipsupport and definition shortened (vertical) nasal length over rotation of the nasal tip and retrusion ofthe nasal spine and caudal septum It is also knownas a ldquoPug noserdquo or ldquoboxerrsquos noserdquo both of which referto various degrees of nasal dorsal depressionbull
Nasal DeformityEpidemiologyaetiologyndash Prevalence is higher in population groups prone to facial trauma (ie boxers athletes) those with historiesof intranasal cocaine use nasal surgery (e g radical submucosal septal resection reductive rhinoplasty)ndash A saddle-nose deformity can be congenital or acquired It can be noticed as a part of individual familialsyndromic and ethnic characteristics - Most deformities are due to traumatic and iatrogeniccauses Medical causes are Wegenerrsquosgranulomatosis relapsing polychondritis leprosy (Hansenrsquos disease) syphilis ectodermal dysplasiaand intranasal cocaine use
Nasal Deformity
bull Therapybull ndash Nasal reconstruction indications depend on patientbull selection surgeon experience and aetiology of thebull deformity bull Indications for surgery can be functionalbull aesthetic or most commonly both In individuals
with a compromised nasal airway a nasoseptalbull reconstruction is indicated
Nasal Deformity
bull Contraindications bull include patients with malignantbull chronic or autoimmune disease conditions drugbull abuse poor perioperative risk profile and unrealisticbull expectationsbull ndash Multiple previous rhinoplasties and certain
professionsbull (mixed martial artists boxers and other contactbull sports) are relative contraindications
Nasal DeformitySeptoplastyndash Septoplasty is performed to correct nasal obstructioncaused by septal deformityndash Usually septoplasty is performed under general anaesthesiawith the patient in the supine position with the head elevated by approximately 30 (Righthandedsurgeons approach from the right side)ndash Local vasoconstrictive anaesthesia is applied notonly to reduce postoperative pain but also more importantly to achieve vasoconstriction of themucosa and less intraoperative haemorrhage Lidocainewith adrenaline or epinephrine is usedalthough in patients with cardiac hypersensitivityoxymetazoline might be preferred
Nasal Deformity
bull Septoplasty begins with the incision of septal mucosabull Most operative techniques utilise a hemitransfixionbull incision at the caudal end of septum so thatbull deviation at this point might be reached as wellbull as a transfixion incision that is easily obtained ifbull needed (Right-handed surgeons normally choosebull the left side but that may vary when deviation isbull convex towards the right)
Nasal DeformityA columella retractor is placed over the columellaand by pulling it laterally the caudal border of theseptum is exposed Ala can be protected by an alaprotector A vertical incision with a no 15 bladeover the caudal end of septum is performed untilreaching the plane of the septal cartilage It is essentialto correctly identify the perichondrium and byusing the Cottle elevator dissect and lift it creatinga flap As the dissection proceeds along the septalcartilage a longer speculum (no 5) is introduced sothat elevation of the mucoperichondrium is doneunder constant visual controlndash The next step is to dissect the mucoperiostium
Nasal DeformityDissecting over the bony-cartilaginous junctionwhen joining both tunnels might be difficult and is
especially prone to membrane perforationndash If needed the same tunnels are to be created on the
other side of the septum Then deviated parts of
septum are identified and removed either with a
knife or a Freer chisel
Nasal Deformitybull septum from the maxillary crest the septum mustbull be separated from the perpendicular plate trimmedbull along the inferior border placed back onto the crestbull and sutured to the periosteum If the deformity involvesbull the vomer an osteotome is used Care mustbull be taken not to break the cribriform plate becausebull it could cause a cerebrospinal fistula
Nasal Deformity
bull Once the septal deviation is corrected the flapsbull and hemitransfixion incision are mattressed
withbull absorbable sutures Nasal packing to prevent
synechiaebull and postoperative septal haematoma mightbull be advised but should be removed within 72 h

Midline Granuloma
bull Prognosisbull ndash Depending on the stage long-term remission or
experience a worseningbull prognosis with relapses which may include otherbull extranodal sites bull Involvement of extranodal sitesbull including the upper airway gastrointestinal tractbull skin
Wegenerrsquos Granulomatosis
bull Definition of the diseasebull ndash Wegenerrsquos granulomatosis is a systemic chronicbull vasculitis of small- and medium-sized blood vesselsbull with an autoimmune component It affectsbull particular organs with variable predilectionbull Epidemiologyaetiologybull ndash Wegenerrsquos granulomatosis is a rare disease It affects
about 1 in 20000ndash30000 people It is more prevalentbull in middle-aged Caucasian patients
Wegenerrsquos Granulomatosis
Symptomsndash The disease may present pulmonary upper
respiratory tract or renal In the disseminated form-The localised form ndash confinedto the upper respiratory region ndash is present in 25of the patients- It consists of nonspecific manifestationssuch as nasal obstruction crusting purulentor bloody rhinorrhea and painful or painless ulcers in oral or nasal cavities which are unresponsive tostandard medical treatment
Wegenerrsquos Granulomatosis
bull In some patients the nasal septum is perforatedbull which leads to saddle-nose deformity Less
commonbull symptoms are hoarseness stridor due to
subglotticbull stenosis otalgia otorrhea and conductivebull and sensorineural hearing loss Also ocular
symptomsbull such as scleritis conjunctivitis uveitis andbull episcleritis may be present
Wegenerrsquos Granulomatosis
bull ndash In the disseminated form pulmonary involvementbull is manifested by cough dyspnoea haemoptysisbull (due to an alveolar capillaritis necrotic lesions orbull endobronchial disease) and pleuritic painndashbull -Ninety per cent of patients have nasal symptomsbull and these symptoms are usually the first
manifestationof the diseasebull -Most patients have also renal involvementbull even if it is subclinical
Wegenerrsquos Granulomatosis
Diagnosis ndash Diagnosis of Wegenerrsquos granulomatosis is based on clinical findings that demonstrate lung (chest x-ray) kidney (urine analysis) or upper respiratory tract
involvement (oral or nasal ulcers or discharge) - positive blood analysis for cytoplasmic-staining antineutrophil
cytoplasmic antibodies (c-ANCA) and confirming proteinase 3 (PR3) ANCA or myeloperoxidase (MPO) ANCA ndash Biopsy is essential for diagnosis nonspecific chronic inflammation
and necrosis -Bacterial and fungal infections
Wegenerrsquos Granulomatosis
Therapyndash Conservative therapybull In the induction of disease remission highdosesteroids (e g prednisone 1 mgkgday) for1 month with tapering over several months aregiven In addition cyclophosphamide (2 mgkgday) should be administered for 6ndash12 monthsuntil symptoms disappear In the maintenanceof remission cyclophosphamide should be
Wegenerrsquos Granulomatosis
Antibiotics mainly trimethoprim-sulfamethoxazoleare given for prophylaxis againstPneumocystis jiroveci (formerly Pneumocystiscarinii) pneumonia (PCP) which may developduring immunosuppression and have a role inpreventing recurrencesbull Sinonasal manifestations may be treated with topical nasal steroids and nasal irrigations lowdosesystemic steroids and antibiotics when bacterial infection (typically Staphylococcus species) is suspected
Wegenerrsquos Granulomatosis
bull Prognosisbull ndash Most of the patients respond well to treatmentbull achieving symptom-free intervals of 5ndash20 yearsbull or more bull -Anatomical problems (sinusitis trachealbull stenosis) may require surgery bull Relapses can be long and troublesomebull Long-term complications are chronicbull renal failure hearing loss and deafness
Nasal Fractures Definition ndash A nasal fracture is a disruption of the nasal bone structure due to trauma It is the most frequently fractured facial bone Epidemiologyaetiology ndash Sports falls and assaults are the usual mechanisms of fracture -Males are affected twice as often as are females -Paediatric populations with a incidences during the second and third decades of life -Variables such as force impact direction nature of the striking object age and other will influence the pattern of injury to the components of the nose
Nasal Fractures
bull Symptomsbull ndash Deformity swelling epistaxis and periorbital
ecchymosis are signs that are suggestive of nasal fracture
bull bony crepitus and nasal segment mobilitybull ndash Epiphora bull Severe bilateral injuries to the lachrymal bones
arebull associated with depressed nasal fractures
Nasal Fractures Complications ndash Septal haematoma is one of the most severe early complications of nasal trauma and without drainage it results in abscess formation 6ndash7 days after trauma producing necrosis of the septal cartilage -Long-term problems such as saddle-nose deformity perforation columellar retraction and nasalbase
Septal infection could lead to osteomyelitis orbital and intracranial abscesses meningitis and cavernous sinus thrombosis -Cerebrospinal fluid leakage is a common complication of severe
nasal and frontal fractures
Nasal Fractures
bull Diagnostic proceduresbull ndash Inspectionbull bull Changes of appearance such as deviation andbull asymmetry bleeding watery drainage changesbull in nasal breathing and smell It is useful to comparebull the current presentation with old photographsbull (up to 40 of normal individuals havebull significant nose malformations)
Nasal Fractures Physical examination bull The diagnosis of a nasal fracture is made primarily by physical examination epistaxis nasal swelling and periorbital ecchymosis Nasal shape in the lateral and frontal inspection should be assessed Grasping the dorsum between two fingers and rocking the pyramid back and forth aids in assessing the mobility of nasal bones Internal structures should be evaluated by using a headlight and nasal speculum Clotted blood is removed by suction and assessment of haematoma mucosal tears and active bleeding is performed Bimanual palpation of the septum helps to differentiate septal swelling from haematoma ndash
Nasal FracturesRadiographybull There is no clear evidence of the role of radiographyin the management of nasal fracturesPlain films have up to a 66 false-positive rateas a result of misinterpretation of normal suturelines In addition old fractures are difficult todistinguishbull Three-dimensional CT is recommended for extensiveinjuries involving the nasal-orbital-ethmoidalcomplexndash
Nasal Fractures
bull Additionaluseful diagnostic proceduresbull bull Using a 0 or 30deg 4-mm endoscope is helpful inbull the assessment of posterior abnormalities If thebull patient is heavily sedated Brown-Gruss
provocationbull manoeuvres may be performed to determinebull deformities in upper middle or lower segmentsbull by compressing each compartment
Nasal FracturesConservative treatmentndash Treatment of bleedingbull For localised bleeding anterior sources may becauterised by silver nitrate or sealed with topicalmaterials such as thrombin combined withgelatin foam fibrin glue FloSealreg or other procoagulantmaterials If conservative measuresfail a formal anterior packing is placedbull Bleeding from branches of sphenopalatine orethmoid vessels requires anterior-posteriorpacking
Nasal Fractures
bull bull Surgical methods such as direct endoscopic vessel
bull cauterization or ligation have been shown tobull offer better haemostasis and patient comfortbull Angiography with embolization can also be
consideredbull in cases refractory to more conservativebull approaches
Nasal Fractures
bull Type of reductionbull bull Nondisplaced fractures should be treated withbull observation alone Closed nasal reduction is thebull best choice for simple injuries (isolated unilateralbull with medial displacement)bull bull An open approach should be considered in
severebull trauma (bilateral depressed fractures)
Nasal Fracturesbull Surgical principlesbull ndash Topical anaesthesia with cotton pledgets soakedbull with 4 cocaine or 005 oxymethazoline combinedbull with 4 topical lidocaine should be appliedbull for 5ndash10 min Local anaesthesia should also be injectedbull (1 lidocaine and 1100000 epinephrine)bull along the septum lateral walls and floor of the nasalbull cavitybull bull
Nasal FracturesClosed reductionndashndash The nasal bones are grasped between two fingersand pressure is applied laterally in theopposite direction of the deviation A bluntelevator may be used from within the nose incases of significant medial collapse Walshamforceps can be of help Reduction of the septumshould be performed with the use ofAsch forceps
Nasal Fractures
bull To prevent collapse of the postreductionbull framework nasal packing should be placedbull for 3ndash5 days Septum splints are recommendedbull in comminuted septal fractures withbull severe mucosal lesions External nasal splintingbull for 10 days (Aquaplastreg Thermoplastreg)bull provides nasal protection Nasal saline spraysbull prevent crusting and oral antibiotics should
Nasal Fractures
bull Open reductionbull ndashndash Immediate repair of fractures by using
widebull surgical exposure reduction fixation and
reconstructionbull ndashndash The second option is delayed correctionbull (6 months or more) of persistent deformitiesbull using standard techniques of rhinoplasty
Deviated Nasal Septum
bull Definition of the diseasebull ndash Deviation of the nasal septum is a common causebull of unilateral nasal airway obstruction in which thebull nasal septum is displacedbull bull Epidemiologyaetiologybull ndash Developmental septal abnormalities Septal cartilage
damage in the neonatal period andbull during birth can cause severe septal deviation inbull the absence of a history of nasal trauma
Deviated Nasal Septum
bull Symptomsbull ndash Patients may present with a history of sinusitis
allergicbull rhinitis obstructive sleep apnoea previousbull nasal surgery or recent nasal trauma Unilateral or
bilateral nasal airway obstruction that is unrelievedbull with decongestants or nasal steroid sprays is oftenbull seenbull bull
Deviated Nasal SeptumDiagnosisndashExamination external dorsal deviation or the columella and caudal septummay be deflected off the midline (caudal subluxation)ndash Inspections of the nasal cavity and anterior-posteriorrhinoscopy are helpful in diagnosing the locationtype and severity of septal deformityThe endoscope is also useful in identifying polypsthe severity and extent of posterior septaldeviations and bony spurs and locating areas ofseptal perforation or mucosal injury
Deviated Nasal Septum
bull Therapybull ndash Septoplasty is a procedurebull The areabull of deviation is corrected or resected in order tobull leave behind as much cartilage and bone as
possiblebull Cartilage resection is minimised and can be
repositioned reshaped or recontoured using a variety of methods
Deviated Nasal Septum
bull ndash Indications of septoplasty before the growth period
bull of the nose is finished should be very limited bull -In these cases surgery must preserve all the
cartilagebull in order to prevent external changes of the
shape ofbull the nose
Deviated Nasal Septum
bull Complicationsbull ndash Frequent complications include haematoma andbull infection Cerebrospinal fluid leak is a rare but
potentiallybull serious complicationbull It is usually the resultbull of avulsion or damage to the cribriform plate whenbull handling the perpendicular plate of the ethmoidbull ndash Other complications include epistaxis nasal
Deviated Nasal Septum
bull Other complications include epistaxis nasal obstruction
bull due to residual deviation synechiae returnbull of the cartilaginous deviation septal perforationbull anosmia and cosmetic nasal deformities suchbull as widened alar rim margins drooping nasal tipbull columella retraction and a sunken dorsum with abull supratip saddle formation
Septal perforation with minor crusting View from provide closure of the
incision
Septal Haematoma
bull A septal haematoma is a blood collection under the perichondrium
bull of the septum and cartilagebull bull bull Epidemiologyaetiologybull ndash A septal haematoma is one of the most
severe complications of nasal trauma
Septal Haematoma
bull Diagnosisbull ndash Signs and symptoms include intense pain
swellingbull haematoma of the upper lip and philtrum
area andbull complete nasal airway obstruction
Septal HaematomaTherapyndash Management consists of drainage through a mucoperichondrial incision Immediate treatment isnecessary to prevent long-term problems such asa saddle-nose deformity perforation columellarretraction and nasal-base widening In childrenseptal destruction can lead to devastating nasal andmidfacial growth abnormalitiesbull Surgeryndash Incision and evacuation of the collection is performedDrainage of a septal haematoma should
Septal HaematomaSurgeryndash Incision and evacuation of the collection is performedDrainage of a septal haematoma should provide closure of the incision
Splints or transseptal sutures are placed to obliterate thepotential space and prevent collectionInfection involving the septal cartilage Reconstruction with autologouscartilage is then performed in a second stage Oral antibiotics should be given
Nasal DeformitySaddle-nose deformityndash A saddle-nose deformity is characterised by a loss ofnasal dorsal height and compromised nasal supportstructures -Other case observed are depressionof the middle vault and dorsum loss of nasal tipsupport and definition shortened (vertical) nasal length over rotation of the nasal tip and retrusion ofthe nasal spine and caudal septum It is also knownas a ldquoPug noserdquo or ldquoboxerrsquos noserdquo both of which referto various degrees of nasal dorsal depressionbull
Nasal DeformityEpidemiologyaetiologyndash Prevalence is higher in population groups prone to facial trauma (ie boxers athletes) those with historiesof intranasal cocaine use nasal surgery (e g radical submucosal septal resection reductive rhinoplasty)ndash A saddle-nose deformity can be congenital or acquired It can be noticed as a part of individual familialsyndromic and ethnic characteristics - Most deformities are due to traumatic and iatrogeniccauses Medical causes are Wegenerrsquosgranulomatosis relapsing polychondritis leprosy (Hansenrsquos disease) syphilis ectodermal dysplasiaand intranasal cocaine use
Nasal Deformity
bull Therapybull ndash Nasal reconstruction indications depend on patientbull selection surgeon experience and aetiology of thebull deformity bull Indications for surgery can be functionalbull aesthetic or most commonly both In individuals
with a compromised nasal airway a nasoseptalbull reconstruction is indicated
Nasal Deformity
bull Contraindications bull include patients with malignantbull chronic or autoimmune disease conditions drugbull abuse poor perioperative risk profile and unrealisticbull expectationsbull ndash Multiple previous rhinoplasties and certain
professionsbull (mixed martial artists boxers and other contactbull sports) are relative contraindications
Nasal DeformitySeptoplastyndash Septoplasty is performed to correct nasal obstructioncaused by septal deformityndash Usually septoplasty is performed under general anaesthesiawith the patient in the supine position with the head elevated by approximately 30 (Righthandedsurgeons approach from the right side)ndash Local vasoconstrictive anaesthesia is applied notonly to reduce postoperative pain but also more importantly to achieve vasoconstriction of themucosa and less intraoperative haemorrhage Lidocainewith adrenaline or epinephrine is usedalthough in patients with cardiac hypersensitivityoxymetazoline might be preferred
Nasal Deformity
bull Septoplasty begins with the incision of septal mucosabull Most operative techniques utilise a hemitransfixionbull incision at the caudal end of septum so thatbull deviation at this point might be reached as wellbull as a transfixion incision that is easily obtained ifbull needed (Right-handed surgeons normally choosebull the left side but that may vary when deviation isbull convex towards the right)
Nasal DeformityA columella retractor is placed over the columellaand by pulling it laterally the caudal border of theseptum is exposed Ala can be protected by an alaprotector A vertical incision with a no 15 bladeover the caudal end of septum is performed untilreaching the plane of the septal cartilage It is essentialto correctly identify the perichondrium and byusing the Cottle elevator dissect and lift it creatinga flap As the dissection proceeds along the septalcartilage a longer speculum (no 5) is introduced sothat elevation of the mucoperichondrium is doneunder constant visual controlndash The next step is to dissect the mucoperiostium
Nasal DeformityDissecting over the bony-cartilaginous junctionwhen joining both tunnels might be difficult and is
especially prone to membrane perforationndash If needed the same tunnels are to be created on the
other side of the septum Then deviated parts of
septum are identified and removed either with a
knife or a Freer chisel
Nasal Deformitybull septum from the maxillary crest the septum mustbull be separated from the perpendicular plate trimmedbull along the inferior border placed back onto the crestbull and sutured to the periosteum If the deformity involvesbull the vomer an osteotome is used Care mustbull be taken not to break the cribriform plate becausebull it could cause a cerebrospinal fistula
Nasal Deformity
bull Once the septal deviation is corrected the flapsbull and hemitransfixion incision are mattressed
withbull absorbable sutures Nasal packing to prevent
synechiaebull and postoperative septal haematoma mightbull be advised but should be removed within 72 h

Wegenerrsquos Granulomatosis
bull Definition of the diseasebull ndash Wegenerrsquos granulomatosis is a systemic chronicbull vasculitis of small- and medium-sized blood vesselsbull with an autoimmune component It affectsbull particular organs with variable predilectionbull Epidemiologyaetiologybull ndash Wegenerrsquos granulomatosis is a rare disease It affects
about 1 in 20000ndash30000 people It is more prevalentbull in middle-aged Caucasian patients
Wegenerrsquos Granulomatosis
Symptomsndash The disease may present pulmonary upper
respiratory tract or renal In the disseminated form-The localised form ndash confinedto the upper respiratory region ndash is present in 25of the patients- It consists of nonspecific manifestationssuch as nasal obstruction crusting purulentor bloody rhinorrhea and painful or painless ulcers in oral or nasal cavities which are unresponsive tostandard medical treatment
Wegenerrsquos Granulomatosis
bull In some patients the nasal septum is perforatedbull which leads to saddle-nose deformity Less
commonbull symptoms are hoarseness stridor due to
subglotticbull stenosis otalgia otorrhea and conductivebull and sensorineural hearing loss Also ocular
symptomsbull such as scleritis conjunctivitis uveitis andbull episcleritis may be present
Wegenerrsquos Granulomatosis
bull ndash In the disseminated form pulmonary involvementbull is manifested by cough dyspnoea haemoptysisbull (due to an alveolar capillaritis necrotic lesions orbull endobronchial disease) and pleuritic painndashbull -Ninety per cent of patients have nasal symptomsbull and these symptoms are usually the first
manifestationof the diseasebull -Most patients have also renal involvementbull even if it is subclinical
Wegenerrsquos Granulomatosis
Diagnosis ndash Diagnosis of Wegenerrsquos granulomatosis is based on clinical findings that demonstrate lung (chest x-ray) kidney (urine analysis) or upper respiratory tract
involvement (oral or nasal ulcers or discharge) - positive blood analysis for cytoplasmic-staining antineutrophil
cytoplasmic antibodies (c-ANCA) and confirming proteinase 3 (PR3) ANCA or myeloperoxidase (MPO) ANCA ndash Biopsy is essential for diagnosis nonspecific chronic inflammation
and necrosis -Bacterial and fungal infections
Wegenerrsquos Granulomatosis
Therapyndash Conservative therapybull In the induction of disease remission highdosesteroids (e g prednisone 1 mgkgday) for1 month with tapering over several months aregiven In addition cyclophosphamide (2 mgkgday) should be administered for 6ndash12 monthsuntil symptoms disappear In the maintenanceof remission cyclophosphamide should be
Wegenerrsquos Granulomatosis
Antibiotics mainly trimethoprim-sulfamethoxazoleare given for prophylaxis againstPneumocystis jiroveci (formerly Pneumocystiscarinii) pneumonia (PCP) which may developduring immunosuppression and have a role inpreventing recurrencesbull Sinonasal manifestations may be treated with topical nasal steroids and nasal irrigations lowdosesystemic steroids and antibiotics when bacterial infection (typically Staphylococcus species) is suspected
Wegenerrsquos Granulomatosis
bull Prognosisbull ndash Most of the patients respond well to treatmentbull achieving symptom-free intervals of 5ndash20 yearsbull or more bull -Anatomical problems (sinusitis trachealbull stenosis) may require surgery bull Relapses can be long and troublesomebull Long-term complications are chronicbull renal failure hearing loss and deafness
Nasal Fractures Definition ndash A nasal fracture is a disruption of the nasal bone structure due to trauma It is the most frequently fractured facial bone Epidemiologyaetiology ndash Sports falls and assaults are the usual mechanisms of fracture -Males are affected twice as often as are females -Paediatric populations with a incidences during the second and third decades of life -Variables such as force impact direction nature of the striking object age and other will influence the pattern of injury to the components of the nose
Nasal Fractures
bull Symptomsbull ndash Deformity swelling epistaxis and periorbital
ecchymosis are signs that are suggestive of nasal fracture
bull bony crepitus and nasal segment mobilitybull ndash Epiphora bull Severe bilateral injuries to the lachrymal bones
arebull associated with depressed nasal fractures
Nasal Fractures Complications ndash Septal haematoma is one of the most severe early complications of nasal trauma and without drainage it results in abscess formation 6ndash7 days after trauma producing necrosis of the septal cartilage -Long-term problems such as saddle-nose deformity perforation columellar retraction and nasalbase
Septal infection could lead to osteomyelitis orbital and intracranial abscesses meningitis and cavernous sinus thrombosis -Cerebrospinal fluid leakage is a common complication of severe
nasal and frontal fractures
Nasal Fractures
bull Diagnostic proceduresbull ndash Inspectionbull bull Changes of appearance such as deviation andbull asymmetry bleeding watery drainage changesbull in nasal breathing and smell It is useful to comparebull the current presentation with old photographsbull (up to 40 of normal individuals havebull significant nose malformations)
Nasal Fractures Physical examination bull The diagnosis of a nasal fracture is made primarily by physical examination epistaxis nasal swelling and periorbital ecchymosis Nasal shape in the lateral and frontal inspection should be assessed Grasping the dorsum between two fingers and rocking the pyramid back and forth aids in assessing the mobility of nasal bones Internal structures should be evaluated by using a headlight and nasal speculum Clotted blood is removed by suction and assessment of haematoma mucosal tears and active bleeding is performed Bimanual palpation of the septum helps to differentiate septal swelling from haematoma ndash
Nasal FracturesRadiographybull There is no clear evidence of the role of radiographyin the management of nasal fracturesPlain films have up to a 66 false-positive rateas a result of misinterpretation of normal suturelines In addition old fractures are difficult todistinguishbull Three-dimensional CT is recommended for extensiveinjuries involving the nasal-orbital-ethmoidalcomplexndash
Nasal Fractures
bull Additionaluseful diagnostic proceduresbull bull Using a 0 or 30deg 4-mm endoscope is helpful inbull the assessment of posterior abnormalities If thebull patient is heavily sedated Brown-Gruss
provocationbull manoeuvres may be performed to determinebull deformities in upper middle or lower segmentsbull by compressing each compartment
Nasal FracturesConservative treatmentndash Treatment of bleedingbull For localised bleeding anterior sources may becauterised by silver nitrate or sealed with topicalmaterials such as thrombin combined withgelatin foam fibrin glue FloSealreg or other procoagulantmaterials If conservative measuresfail a formal anterior packing is placedbull Bleeding from branches of sphenopalatine orethmoid vessels requires anterior-posteriorpacking
Nasal Fractures
bull bull Surgical methods such as direct endoscopic vessel
bull cauterization or ligation have been shown tobull offer better haemostasis and patient comfortbull Angiography with embolization can also be
consideredbull in cases refractory to more conservativebull approaches
Nasal Fractures
bull Type of reductionbull bull Nondisplaced fractures should be treated withbull observation alone Closed nasal reduction is thebull best choice for simple injuries (isolated unilateralbull with medial displacement)bull bull An open approach should be considered in
severebull trauma (bilateral depressed fractures)
Nasal Fracturesbull Surgical principlesbull ndash Topical anaesthesia with cotton pledgets soakedbull with 4 cocaine or 005 oxymethazoline combinedbull with 4 topical lidocaine should be appliedbull for 5ndash10 min Local anaesthesia should also be injectedbull (1 lidocaine and 1100000 epinephrine)bull along the septum lateral walls and floor of the nasalbull cavitybull bull
Nasal FracturesClosed reductionndashndash The nasal bones are grasped between two fingersand pressure is applied laterally in theopposite direction of the deviation A bluntelevator may be used from within the nose incases of significant medial collapse Walshamforceps can be of help Reduction of the septumshould be performed with the use ofAsch forceps
Nasal Fractures
bull To prevent collapse of the postreductionbull framework nasal packing should be placedbull for 3ndash5 days Septum splints are recommendedbull in comminuted septal fractures withbull severe mucosal lesions External nasal splintingbull for 10 days (Aquaplastreg Thermoplastreg)bull provides nasal protection Nasal saline spraysbull prevent crusting and oral antibiotics should
Nasal Fractures
bull Open reductionbull ndashndash Immediate repair of fractures by using
widebull surgical exposure reduction fixation and
reconstructionbull ndashndash The second option is delayed correctionbull (6 months or more) of persistent deformitiesbull using standard techniques of rhinoplasty
Deviated Nasal Septum
bull Definition of the diseasebull ndash Deviation of the nasal septum is a common causebull of unilateral nasal airway obstruction in which thebull nasal septum is displacedbull bull Epidemiologyaetiologybull ndash Developmental septal abnormalities Septal cartilage
damage in the neonatal period andbull during birth can cause severe septal deviation inbull the absence of a history of nasal trauma
Deviated Nasal Septum
bull Symptomsbull ndash Patients may present with a history of sinusitis
allergicbull rhinitis obstructive sleep apnoea previousbull nasal surgery or recent nasal trauma Unilateral or
bilateral nasal airway obstruction that is unrelievedbull with decongestants or nasal steroid sprays is oftenbull seenbull bull
Deviated Nasal SeptumDiagnosisndashExamination external dorsal deviation or the columella and caudal septummay be deflected off the midline (caudal subluxation)ndash Inspections of the nasal cavity and anterior-posteriorrhinoscopy are helpful in diagnosing the locationtype and severity of septal deformityThe endoscope is also useful in identifying polypsthe severity and extent of posterior septaldeviations and bony spurs and locating areas ofseptal perforation or mucosal injury
Deviated Nasal Septum
bull Therapybull ndash Septoplasty is a procedurebull The areabull of deviation is corrected or resected in order tobull leave behind as much cartilage and bone as
possiblebull Cartilage resection is minimised and can be
repositioned reshaped or recontoured using a variety of methods
Deviated Nasal Septum
bull ndash Indications of septoplasty before the growth period
bull of the nose is finished should be very limited bull -In these cases surgery must preserve all the
cartilagebull in order to prevent external changes of the
shape ofbull the nose
Deviated Nasal Septum
bull Complicationsbull ndash Frequent complications include haematoma andbull infection Cerebrospinal fluid leak is a rare but
potentiallybull serious complicationbull It is usually the resultbull of avulsion or damage to the cribriform plate whenbull handling the perpendicular plate of the ethmoidbull ndash Other complications include epistaxis nasal
Deviated Nasal Septum
bull Other complications include epistaxis nasal obstruction
bull due to residual deviation synechiae returnbull of the cartilaginous deviation septal perforationbull anosmia and cosmetic nasal deformities suchbull as widened alar rim margins drooping nasal tipbull columella retraction and a sunken dorsum with abull supratip saddle formation
Septal perforation with minor crusting View from provide closure of the
incision
Septal Haematoma
bull A septal haematoma is a blood collection under the perichondrium
bull of the septum and cartilagebull bull bull Epidemiologyaetiologybull ndash A septal haematoma is one of the most
severe complications of nasal trauma
Septal Haematoma
bull Diagnosisbull ndash Signs and symptoms include intense pain
swellingbull haematoma of the upper lip and philtrum
area andbull complete nasal airway obstruction
Septal HaematomaTherapyndash Management consists of drainage through a mucoperichondrial incision Immediate treatment isnecessary to prevent long-term problems such asa saddle-nose deformity perforation columellarretraction and nasal-base widening In childrenseptal destruction can lead to devastating nasal andmidfacial growth abnormalitiesbull Surgeryndash Incision and evacuation of the collection is performedDrainage of a septal haematoma should
Septal HaematomaSurgeryndash Incision and evacuation of the collection is performedDrainage of a septal haematoma should provide closure of the incision
Splints or transseptal sutures are placed to obliterate thepotential space and prevent collectionInfection involving the septal cartilage Reconstruction with autologouscartilage is then performed in a second stage Oral antibiotics should be given
Nasal DeformitySaddle-nose deformityndash A saddle-nose deformity is characterised by a loss ofnasal dorsal height and compromised nasal supportstructures -Other case observed are depressionof the middle vault and dorsum loss of nasal tipsupport and definition shortened (vertical) nasal length over rotation of the nasal tip and retrusion ofthe nasal spine and caudal septum It is also knownas a ldquoPug noserdquo or ldquoboxerrsquos noserdquo both of which referto various degrees of nasal dorsal depressionbull
Nasal DeformityEpidemiologyaetiologyndash Prevalence is higher in population groups prone to facial trauma (ie boxers athletes) those with historiesof intranasal cocaine use nasal surgery (e g radical submucosal septal resection reductive rhinoplasty)ndash A saddle-nose deformity can be congenital or acquired It can be noticed as a part of individual familialsyndromic and ethnic characteristics - Most deformities are due to traumatic and iatrogeniccauses Medical causes are Wegenerrsquosgranulomatosis relapsing polychondritis leprosy (Hansenrsquos disease) syphilis ectodermal dysplasiaand intranasal cocaine use
Nasal Deformity
bull Therapybull ndash Nasal reconstruction indications depend on patientbull selection surgeon experience and aetiology of thebull deformity bull Indications for surgery can be functionalbull aesthetic or most commonly both In individuals
with a compromised nasal airway a nasoseptalbull reconstruction is indicated
Nasal Deformity
bull Contraindications bull include patients with malignantbull chronic or autoimmune disease conditions drugbull abuse poor perioperative risk profile and unrealisticbull expectationsbull ndash Multiple previous rhinoplasties and certain
professionsbull (mixed martial artists boxers and other contactbull sports) are relative contraindications
Nasal DeformitySeptoplastyndash Septoplasty is performed to correct nasal obstructioncaused by septal deformityndash Usually septoplasty is performed under general anaesthesiawith the patient in the supine position with the head elevated by approximately 30 (Righthandedsurgeons approach from the right side)ndash Local vasoconstrictive anaesthesia is applied notonly to reduce postoperative pain but also more importantly to achieve vasoconstriction of themucosa and less intraoperative haemorrhage Lidocainewith adrenaline or epinephrine is usedalthough in patients with cardiac hypersensitivityoxymetazoline might be preferred
Nasal Deformity
bull Septoplasty begins with the incision of septal mucosabull Most operative techniques utilise a hemitransfixionbull incision at the caudal end of septum so thatbull deviation at this point might be reached as wellbull as a transfixion incision that is easily obtained ifbull needed (Right-handed surgeons normally choosebull the left side but that may vary when deviation isbull convex towards the right)
Nasal DeformityA columella retractor is placed over the columellaand by pulling it laterally the caudal border of theseptum is exposed Ala can be protected by an alaprotector A vertical incision with a no 15 bladeover the caudal end of septum is performed untilreaching the plane of the septal cartilage It is essentialto correctly identify the perichondrium and byusing the Cottle elevator dissect and lift it creatinga flap As the dissection proceeds along the septalcartilage a longer speculum (no 5) is introduced sothat elevation of the mucoperichondrium is doneunder constant visual controlndash The next step is to dissect the mucoperiostium
Nasal DeformityDissecting over the bony-cartilaginous junctionwhen joining both tunnels might be difficult and is
especially prone to membrane perforationndash If needed the same tunnels are to be created on the
other side of the septum Then deviated parts of
septum are identified and removed either with a
knife or a Freer chisel
Nasal Deformitybull septum from the maxillary crest the septum mustbull be separated from the perpendicular plate trimmedbull along the inferior border placed back onto the crestbull and sutured to the periosteum If the deformity involvesbull the vomer an osteotome is used Care mustbull be taken not to break the cribriform plate becausebull it could cause a cerebrospinal fistula
Nasal Deformity
bull Once the septal deviation is corrected the flapsbull and hemitransfixion incision are mattressed
withbull absorbable sutures Nasal packing to prevent
synechiaebull and postoperative septal haematoma mightbull be advised but should be removed within 72 h

Wegenerrsquos Granulomatosis
Symptomsndash The disease may present pulmonary upper
respiratory tract or renal In the disseminated form-The localised form ndash confinedto the upper respiratory region ndash is present in 25of the patients- It consists of nonspecific manifestationssuch as nasal obstruction crusting purulentor bloody rhinorrhea and painful or painless ulcers in oral or nasal cavities which are unresponsive tostandard medical treatment
Wegenerrsquos Granulomatosis
bull In some patients the nasal septum is perforatedbull which leads to saddle-nose deformity Less
commonbull symptoms are hoarseness stridor due to
subglotticbull stenosis otalgia otorrhea and conductivebull and sensorineural hearing loss Also ocular
symptomsbull such as scleritis conjunctivitis uveitis andbull episcleritis may be present
Wegenerrsquos Granulomatosis
bull ndash In the disseminated form pulmonary involvementbull is manifested by cough dyspnoea haemoptysisbull (due to an alveolar capillaritis necrotic lesions orbull endobronchial disease) and pleuritic painndashbull -Ninety per cent of patients have nasal symptomsbull and these symptoms are usually the first
manifestationof the diseasebull -Most patients have also renal involvementbull even if it is subclinical
Wegenerrsquos Granulomatosis
Diagnosis ndash Diagnosis of Wegenerrsquos granulomatosis is based on clinical findings that demonstrate lung (chest x-ray) kidney (urine analysis) or upper respiratory tract
involvement (oral or nasal ulcers or discharge) - positive blood analysis for cytoplasmic-staining antineutrophil
cytoplasmic antibodies (c-ANCA) and confirming proteinase 3 (PR3) ANCA or myeloperoxidase (MPO) ANCA ndash Biopsy is essential for diagnosis nonspecific chronic inflammation
and necrosis -Bacterial and fungal infections
Wegenerrsquos Granulomatosis
Therapyndash Conservative therapybull In the induction of disease remission highdosesteroids (e g prednisone 1 mgkgday) for1 month with tapering over several months aregiven In addition cyclophosphamide (2 mgkgday) should be administered for 6ndash12 monthsuntil symptoms disappear In the maintenanceof remission cyclophosphamide should be
Wegenerrsquos Granulomatosis
Antibiotics mainly trimethoprim-sulfamethoxazoleare given for prophylaxis againstPneumocystis jiroveci (formerly Pneumocystiscarinii) pneumonia (PCP) which may developduring immunosuppression and have a role inpreventing recurrencesbull Sinonasal manifestations may be treated with topical nasal steroids and nasal irrigations lowdosesystemic steroids and antibiotics when bacterial infection (typically Staphylococcus species) is suspected
Wegenerrsquos Granulomatosis
bull Prognosisbull ndash Most of the patients respond well to treatmentbull achieving symptom-free intervals of 5ndash20 yearsbull or more bull -Anatomical problems (sinusitis trachealbull stenosis) may require surgery bull Relapses can be long and troublesomebull Long-term complications are chronicbull renal failure hearing loss and deafness
Nasal Fractures Definition ndash A nasal fracture is a disruption of the nasal bone structure due to trauma It is the most frequently fractured facial bone Epidemiologyaetiology ndash Sports falls and assaults are the usual mechanisms of fracture -Males are affected twice as often as are females -Paediatric populations with a incidences during the second and third decades of life -Variables such as force impact direction nature of the striking object age and other will influence the pattern of injury to the components of the nose
Nasal Fractures
bull Symptomsbull ndash Deformity swelling epistaxis and periorbital
ecchymosis are signs that are suggestive of nasal fracture
bull bony crepitus and nasal segment mobilitybull ndash Epiphora bull Severe bilateral injuries to the lachrymal bones
arebull associated with depressed nasal fractures
Nasal Fractures Complications ndash Septal haematoma is one of the most severe early complications of nasal trauma and without drainage it results in abscess formation 6ndash7 days after trauma producing necrosis of the septal cartilage -Long-term problems such as saddle-nose deformity perforation columellar retraction and nasalbase
Septal infection could lead to osteomyelitis orbital and intracranial abscesses meningitis and cavernous sinus thrombosis -Cerebrospinal fluid leakage is a common complication of severe
nasal and frontal fractures
Nasal Fractures
bull Diagnostic proceduresbull ndash Inspectionbull bull Changes of appearance such as deviation andbull asymmetry bleeding watery drainage changesbull in nasal breathing and smell It is useful to comparebull the current presentation with old photographsbull (up to 40 of normal individuals havebull significant nose malformations)
Nasal Fractures Physical examination bull The diagnosis of a nasal fracture is made primarily by physical examination epistaxis nasal swelling and periorbital ecchymosis Nasal shape in the lateral and frontal inspection should be assessed Grasping the dorsum between two fingers and rocking the pyramid back and forth aids in assessing the mobility of nasal bones Internal structures should be evaluated by using a headlight and nasal speculum Clotted blood is removed by suction and assessment of haematoma mucosal tears and active bleeding is performed Bimanual palpation of the septum helps to differentiate septal swelling from haematoma ndash
Nasal FracturesRadiographybull There is no clear evidence of the role of radiographyin the management of nasal fracturesPlain films have up to a 66 false-positive rateas a result of misinterpretation of normal suturelines In addition old fractures are difficult todistinguishbull Three-dimensional CT is recommended for extensiveinjuries involving the nasal-orbital-ethmoidalcomplexndash
Nasal Fractures
bull Additionaluseful diagnostic proceduresbull bull Using a 0 or 30deg 4-mm endoscope is helpful inbull the assessment of posterior abnormalities If thebull patient is heavily sedated Brown-Gruss
provocationbull manoeuvres may be performed to determinebull deformities in upper middle or lower segmentsbull by compressing each compartment
Nasal FracturesConservative treatmentndash Treatment of bleedingbull For localised bleeding anterior sources may becauterised by silver nitrate or sealed with topicalmaterials such as thrombin combined withgelatin foam fibrin glue FloSealreg or other procoagulantmaterials If conservative measuresfail a formal anterior packing is placedbull Bleeding from branches of sphenopalatine orethmoid vessels requires anterior-posteriorpacking
Nasal Fractures
bull bull Surgical methods such as direct endoscopic vessel
bull cauterization or ligation have been shown tobull offer better haemostasis and patient comfortbull Angiography with embolization can also be
consideredbull in cases refractory to more conservativebull approaches
Nasal Fractures
bull Type of reductionbull bull Nondisplaced fractures should be treated withbull observation alone Closed nasal reduction is thebull best choice for simple injuries (isolated unilateralbull with medial displacement)bull bull An open approach should be considered in
severebull trauma (bilateral depressed fractures)
Nasal Fracturesbull Surgical principlesbull ndash Topical anaesthesia with cotton pledgets soakedbull with 4 cocaine or 005 oxymethazoline combinedbull with 4 topical lidocaine should be appliedbull for 5ndash10 min Local anaesthesia should also be injectedbull (1 lidocaine and 1100000 epinephrine)bull along the septum lateral walls and floor of the nasalbull cavitybull bull
Nasal FracturesClosed reductionndashndash The nasal bones are grasped between two fingersand pressure is applied laterally in theopposite direction of the deviation A bluntelevator may be used from within the nose incases of significant medial collapse Walshamforceps can be of help Reduction of the septumshould be performed with the use ofAsch forceps
Nasal Fractures
bull To prevent collapse of the postreductionbull framework nasal packing should be placedbull for 3ndash5 days Septum splints are recommendedbull in comminuted septal fractures withbull severe mucosal lesions External nasal splintingbull for 10 days (Aquaplastreg Thermoplastreg)bull provides nasal protection Nasal saline spraysbull prevent crusting and oral antibiotics should
Nasal Fractures
bull Open reductionbull ndashndash Immediate repair of fractures by using
widebull surgical exposure reduction fixation and
reconstructionbull ndashndash The second option is delayed correctionbull (6 months or more) of persistent deformitiesbull using standard techniques of rhinoplasty
Deviated Nasal Septum
bull Definition of the diseasebull ndash Deviation of the nasal septum is a common causebull of unilateral nasal airway obstruction in which thebull nasal septum is displacedbull bull Epidemiologyaetiologybull ndash Developmental septal abnormalities Septal cartilage
damage in the neonatal period andbull during birth can cause severe septal deviation inbull the absence of a history of nasal trauma
Deviated Nasal Septum
bull Symptomsbull ndash Patients may present with a history of sinusitis
allergicbull rhinitis obstructive sleep apnoea previousbull nasal surgery or recent nasal trauma Unilateral or
bilateral nasal airway obstruction that is unrelievedbull with decongestants or nasal steroid sprays is oftenbull seenbull bull
Deviated Nasal SeptumDiagnosisndashExamination external dorsal deviation or the columella and caudal septummay be deflected off the midline (caudal subluxation)ndash Inspections of the nasal cavity and anterior-posteriorrhinoscopy are helpful in diagnosing the locationtype and severity of septal deformityThe endoscope is also useful in identifying polypsthe severity and extent of posterior septaldeviations and bony spurs and locating areas ofseptal perforation or mucosal injury
Deviated Nasal Septum
bull Therapybull ndash Septoplasty is a procedurebull The areabull of deviation is corrected or resected in order tobull leave behind as much cartilage and bone as
possiblebull Cartilage resection is minimised and can be
repositioned reshaped or recontoured using a variety of methods
Deviated Nasal Septum
bull ndash Indications of septoplasty before the growth period
bull of the nose is finished should be very limited bull -In these cases surgery must preserve all the
cartilagebull in order to prevent external changes of the
shape ofbull the nose
Deviated Nasal Septum
bull Complicationsbull ndash Frequent complications include haematoma andbull infection Cerebrospinal fluid leak is a rare but
potentiallybull serious complicationbull It is usually the resultbull of avulsion or damage to the cribriform plate whenbull handling the perpendicular plate of the ethmoidbull ndash Other complications include epistaxis nasal
Deviated Nasal Septum
bull Other complications include epistaxis nasal obstruction
bull due to residual deviation synechiae returnbull of the cartilaginous deviation septal perforationbull anosmia and cosmetic nasal deformities suchbull as widened alar rim margins drooping nasal tipbull columella retraction and a sunken dorsum with abull supratip saddle formation
Septal perforation with minor crusting View from provide closure of the
incision
Septal Haematoma
bull A septal haematoma is a blood collection under the perichondrium
bull of the septum and cartilagebull bull bull Epidemiologyaetiologybull ndash A septal haematoma is one of the most
severe complications of nasal trauma
Septal Haematoma
bull Diagnosisbull ndash Signs and symptoms include intense pain
swellingbull haematoma of the upper lip and philtrum
area andbull complete nasal airway obstruction
Septal HaematomaTherapyndash Management consists of drainage through a mucoperichondrial incision Immediate treatment isnecessary to prevent long-term problems such asa saddle-nose deformity perforation columellarretraction and nasal-base widening In childrenseptal destruction can lead to devastating nasal andmidfacial growth abnormalitiesbull Surgeryndash Incision and evacuation of the collection is performedDrainage of a septal haematoma should
Septal HaematomaSurgeryndash Incision and evacuation of the collection is performedDrainage of a septal haematoma should provide closure of the incision
Splints or transseptal sutures are placed to obliterate thepotential space and prevent collectionInfection involving the septal cartilage Reconstruction with autologouscartilage is then performed in a second stage Oral antibiotics should be given
Nasal DeformitySaddle-nose deformityndash A saddle-nose deformity is characterised by a loss ofnasal dorsal height and compromised nasal supportstructures -Other case observed are depressionof the middle vault and dorsum loss of nasal tipsupport and definition shortened (vertical) nasal length over rotation of the nasal tip and retrusion ofthe nasal spine and caudal septum It is also knownas a ldquoPug noserdquo or ldquoboxerrsquos noserdquo both of which referto various degrees of nasal dorsal depressionbull
Nasal DeformityEpidemiologyaetiologyndash Prevalence is higher in population groups prone to facial trauma (ie boxers athletes) those with historiesof intranasal cocaine use nasal surgery (e g radical submucosal septal resection reductive rhinoplasty)ndash A saddle-nose deformity can be congenital or acquired It can be noticed as a part of individual familialsyndromic and ethnic characteristics - Most deformities are due to traumatic and iatrogeniccauses Medical causes are Wegenerrsquosgranulomatosis relapsing polychondritis leprosy (Hansenrsquos disease) syphilis ectodermal dysplasiaand intranasal cocaine use
Nasal Deformity
bull Therapybull ndash Nasal reconstruction indications depend on patientbull selection surgeon experience and aetiology of thebull deformity bull Indications for surgery can be functionalbull aesthetic or most commonly both In individuals
with a compromised nasal airway a nasoseptalbull reconstruction is indicated
Nasal Deformity
bull Contraindications bull include patients with malignantbull chronic or autoimmune disease conditions drugbull abuse poor perioperative risk profile and unrealisticbull expectationsbull ndash Multiple previous rhinoplasties and certain
professionsbull (mixed martial artists boxers and other contactbull sports) are relative contraindications
Nasal DeformitySeptoplastyndash Septoplasty is performed to correct nasal obstructioncaused by septal deformityndash Usually septoplasty is performed under general anaesthesiawith the patient in the supine position with the head elevated by approximately 30 (Righthandedsurgeons approach from the right side)ndash Local vasoconstrictive anaesthesia is applied notonly to reduce postoperative pain but also more importantly to achieve vasoconstriction of themucosa and less intraoperative haemorrhage Lidocainewith adrenaline or epinephrine is usedalthough in patients with cardiac hypersensitivityoxymetazoline might be preferred
Nasal Deformity
bull Septoplasty begins with the incision of septal mucosabull Most operative techniques utilise a hemitransfixionbull incision at the caudal end of septum so thatbull deviation at this point might be reached as wellbull as a transfixion incision that is easily obtained ifbull needed (Right-handed surgeons normally choosebull the left side but that may vary when deviation isbull convex towards the right)
Nasal DeformityA columella retractor is placed over the columellaand by pulling it laterally the caudal border of theseptum is exposed Ala can be protected by an alaprotector A vertical incision with a no 15 bladeover the caudal end of septum is performed untilreaching the plane of the septal cartilage It is essentialto correctly identify the perichondrium and byusing the Cottle elevator dissect and lift it creatinga flap As the dissection proceeds along the septalcartilage a longer speculum (no 5) is introduced sothat elevation of the mucoperichondrium is doneunder constant visual controlndash The next step is to dissect the mucoperiostium
Nasal DeformityDissecting over the bony-cartilaginous junctionwhen joining both tunnels might be difficult and is
especially prone to membrane perforationndash If needed the same tunnels are to be created on the
other side of the septum Then deviated parts of
septum are identified and removed either with a
knife or a Freer chisel
Nasal Deformitybull septum from the maxillary crest the septum mustbull be separated from the perpendicular plate trimmedbull along the inferior border placed back onto the crestbull and sutured to the periosteum If the deformity involvesbull the vomer an osteotome is used Care mustbull be taken not to break the cribriform plate becausebull it could cause a cerebrospinal fistula
Nasal Deformity
bull Once the septal deviation is corrected the flapsbull and hemitransfixion incision are mattressed
withbull absorbable sutures Nasal packing to prevent
synechiaebull and postoperative septal haematoma mightbull be advised but should be removed within 72 h

Wegenerrsquos Granulomatosis
bull In some patients the nasal septum is perforatedbull which leads to saddle-nose deformity Less
commonbull symptoms are hoarseness stridor due to
subglotticbull stenosis otalgia otorrhea and conductivebull and sensorineural hearing loss Also ocular
symptomsbull such as scleritis conjunctivitis uveitis andbull episcleritis may be present
Wegenerrsquos Granulomatosis
bull ndash In the disseminated form pulmonary involvementbull is manifested by cough dyspnoea haemoptysisbull (due to an alveolar capillaritis necrotic lesions orbull endobronchial disease) and pleuritic painndashbull -Ninety per cent of patients have nasal symptomsbull and these symptoms are usually the first
manifestationof the diseasebull -Most patients have also renal involvementbull even if it is subclinical
Wegenerrsquos Granulomatosis
Diagnosis ndash Diagnosis of Wegenerrsquos granulomatosis is based on clinical findings that demonstrate lung (chest x-ray) kidney (urine analysis) or upper respiratory tract
involvement (oral or nasal ulcers or discharge) - positive blood analysis for cytoplasmic-staining antineutrophil
cytoplasmic antibodies (c-ANCA) and confirming proteinase 3 (PR3) ANCA or myeloperoxidase (MPO) ANCA ndash Biopsy is essential for diagnosis nonspecific chronic inflammation
and necrosis -Bacterial and fungal infections
Wegenerrsquos Granulomatosis
Therapyndash Conservative therapybull In the induction of disease remission highdosesteroids (e g prednisone 1 mgkgday) for1 month with tapering over several months aregiven In addition cyclophosphamide (2 mgkgday) should be administered for 6ndash12 monthsuntil symptoms disappear In the maintenanceof remission cyclophosphamide should be
Wegenerrsquos Granulomatosis
Antibiotics mainly trimethoprim-sulfamethoxazoleare given for prophylaxis againstPneumocystis jiroveci (formerly Pneumocystiscarinii) pneumonia (PCP) which may developduring immunosuppression and have a role inpreventing recurrencesbull Sinonasal manifestations may be treated with topical nasal steroids and nasal irrigations lowdosesystemic steroids and antibiotics when bacterial infection (typically Staphylococcus species) is suspected
Wegenerrsquos Granulomatosis
bull Prognosisbull ndash Most of the patients respond well to treatmentbull achieving symptom-free intervals of 5ndash20 yearsbull or more bull -Anatomical problems (sinusitis trachealbull stenosis) may require surgery bull Relapses can be long and troublesomebull Long-term complications are chronicbull renal failure hearing loss and deafness
Nasal Fractures Definition ndash A nasal fracture is a disruption of the nasal bone structure due to trauma It is the most frequently fractured facial bone Epidemiologyaetiology ndash Sports falls and assaults are the usual mechanisms of fracture -Males are affected twice as often as are females -Paediatric populations with a incidences during the second and third decades of life -Variables such as force impact direction nature of the striking object age and other will influence the pattern of injury to the components of the nose
Nasal Fractures
bull Symptomsbull ndash Deformity swelling epistaxis and periorbital
ecchymosis are signs that are suggestive of nasal fracture
bull bony crepitus and nasal segment mobilitybull ndash Epiphora bull Severe bilateral injuries to the lachrymal bones
arebull associated with depressed nasal fractures
Nasal Fractures Complications ndash Septal haematoma is one of the most severe early complications of nasal trauma and without drainage it results in abscess formation 6ndash7 days after trauma producing necrosis of the septal cartilage -Long-term problems such as saddle-nose deformity perforation columellar retraction and nasalbase
Septal infection could lead to osteomyelitis orbital and intracranial abscesses meningitis and cavernous sinus thrombosis -Cerebrospinal fluid leakage is a common complication of severe
nasal and frontal fractures
Nasal Fractures
bull Diagnostic proceduresbull ndash Inspectionbull bull Changes of appearance such as deviation andbull asymmetry bleeding watery drainage changesbull in nasal breathing and smell It is useful to comparebull the current presentation with old photographsbull (up to 40 of normal individuals havebull significant nose malformations)
Nasal Fractures Physical examination bull The diagnosis of a nasal fracture is made primarily by physical examination epistaxis nasal swelling and periorbital ecchymosis Nasal shape in the lateral and frontal inspection should be assessed Grasping the dorsum between two fingers and rocking the pyramid back and forth aids in assessing the mobility of nasal bones Internal structures should be evaluated by using a headlight and nasal speculum Clotted blood is removed by suction and assessment of haematoma mucosal tears and active bleeding is performed Bimanual palpation of the septum helps to differentiate septal swelling from haematoma ndash
Nasal FracturesRadiographybull There is no clear evidence of the role of radiographyin the management of nasal fracturesPlain films have up to a 66 false-positive rateas a result of misinterpretation of normal suturelines In addition old fractures are difficult todistinguishbull Three-dimensional CT is recommended for extensiveinjuries involving the nasal-orbital-ethmoidalcomplexndash
Nasal Fractures
bull Additionaluseful diagnostic proceduresbull bull Using a 0 or 30deg 4-mm endoscope is helpful inbull the assessment of posterior abnormalities If thebull patient is heavily sedated Brown-Gruss
provocationbull manoeuvres may be performed to determinebull deformities in upper middle or lower segmentsbull by compressing each compartment
Nasal FracturesConservative treatmentndash Treatment of bleedingbull For localised bleeding anterior sources may becauterised by silver nitrate or sealed with topicalmaterials such as thrombin combined withgelatin foam fibrin glue FloSealreg or other procoagulantmaterials If conservative measuresfail a formal anterior packing is placedbull Bleeding from branches of sphenopalatine orethmoid vessels requires anterior-posteriorpacking
Nasal Fractures
bull bull Surgical methods such as direct endoscopic vessel
bull cauterization or ligation have been shown tobull offer better haemostasis and patient comfortbull Angiography with embolization can also be
consideredbull in cases refractory to more conservativebull approaches
Nasal Fractures
bull Type of reductionbull bull Nondisplaced fractures should be treated withbull observation alone Closed nasal reduction is thebull best choice for simple injuries (isolated unilateralbull with medial displacement)bull bull An open approach should be considered in
severebull trauma (bilateral depressed fractures)
Nasal Fracturesbull Surgical principlesbull ndash Topical anaesthesia with cotton pledgets soakedbull with 4 cocaine or 005 oxymethazoline combinedbull with 4 topical lidocaine should be appliedbull for 5ndash10 min Local anaesthesia should also be injectedbull (1 lidocaine and 1100000 epinephrine)bull along the septum lateral walls and floor of the nasalbull cavitybull bull
Nasal FracturesClosed reductionndashndash The nasal bones are grasped between two fingersand pressure is applied laterally in theopposite direction of the deviation A bluntelevator may be used from within the nose incases of significant medial collapse Walshamforceps can be of help Reduction of the septumshould be performed with the use ofAsch forceps
Nasal Fractures
bull To prevent collapse of the postreductionbull framework nasal packing should be placedbull for 3ndash5 days Septum splints are recommendedbull in comminuted septal fractures withbull severe mucosal lesions External nasal splintingbull for 10 days (Aquaplastreg Thermoplastreg)bull provides nasal protection Nasal saline spraysbull prevent crusting and oral antibiotics should
Nasal Fractures
bull Open reductionbull ndashndash Immediate repair of fractures by using
widebull surgical exposure reduction fixation and
reconstructionbull ndashndash The second option is delayed correctionbull (6 months or more) of persistent deformitiesbull using standard techniques of rhinoplasty
Deviated Nasal Septum
bull Definition of the diseasebull ndash Deviation of the nasal septum is a common causebull of unilateral nasal airway obstruction in which thebull nasal septum is displacedbull bull Epidemiologyaetiologybull ndash Developmental septal abnormalities Septal cartilage
damage in the neonatal period andbull during birth can cause severe septal deviation inbull the absence of a history of nasal trauma
Deviated Nasal Septum
bull Symptomsbull ndash Patients may present with a history of sinusitis
allergicbull rhinitis obstructive sleep apnoea previousbull nasal surgery or recent nasal trauma Unilateral or
bilateral nasal airway obstruction that is unrelievedbull with decongestants or nasal steroid sprays is oftenbull seenbull bull
Deviated Nasal SeptumDiagnosisndashExamination external dorsal deviation or the columella and caudal septummay be deflected off the midline (caudal subluxation)ndash Inspections of the nasal cavity and anterior-posteriorrhinoscopy are helpful in diagnosing the locationtype and severity of septal deformityThe endoscope is also useful in identifying polypsthe severity and extent of posterior septaldeviations and bony spurs and locating areas ofseptal perforation or mucosal injury
Deviated Nasal Septum
bull Therapybull ndash Septoplasty is a procedurebull The areabull of deviation is corrected or resected in order tobull leave behind as much cartilage and bone as
possiblebull Cartilage resection is minimised and can be
repositioned reshaped or recontoured using a variety of methods
Deviated Nasal Septum
bull ndash Indications of septoplasty before the growth period
bull of the nose is finished should be very limited bull -In these cases surgery must preserve all the
cartilagebull in order to prevent external changes of the
shape ofbull the nose
Deviated Nasal Septum
bull Complicationsbull ndash Frequent complications include haematoma andbull infection Cerebrospinal fluid leak is a rare but
potentiallybull serious complicationbull It is usually the resultbull of avulsion or damage to the cribriform plate whenbull handling the perpendicular plate of the ethmoidbull ndash Other complications include epistaxis nasal
Deviated Nasal Septum
bull Other complications include epistaxis nasal obstruction
bull due to residual deviation synechiae returnbull of the cartilaginous deviation septal perforationbull anosmia and cosmetic nasal deformities suchbull as widened alar rim margins drooping nasal tipbull columella retraction and a sunken dorsum with abull supratip saddle formation
Septal perforation with minor crusting View from provide closure of the
incision
Septal Haematoma
bull A septal haematoma is a blood collection under the perichondrium
bull of the septum and cartilagebull bull bull Epidemiologyaetiologybull ndash A septal haematoma is one of the most
severe complications of nasal trauma
Septal Haematoma
bull Diagnosisbull ndash Signs and symptoms include intense pain
swellingbull haematoma of the upper lip and philtrum
area andbull complete nasal airway obstruction
Septal HaematomaTherapyndash Management consists of drainage through a mucoperichondrial incision Immediate treatment isnecessary to prevent long-term problems such asa saddle-nose deformity perforation columellarretraction and nasal-base widening In childrenseptal destruction can lead to devastating nasal andmidfacial growth abnormalitiesbull Surgeryndash Incision and evacuation of the collection is performedDrainage of a septal haematoma should
Septal HaematomaSurgeryndash Incision and evacuation of the collection is performedDrainage of a septal haematoma should provide closure of the incision
Splints or transseptal sutures are placed to obliterate thepotential space and prevent collectionInfection involving the septal cartilage Reconstruction with autologouscartilage is then performed in a second stage Oral antibiotics should be given
Nasal DeformitySaddle-nose deformityndash A saddle-nose deformity is characterised by a loss ofnasal dorsal height and compromised nasal supportstructures -Other case observed are depressionof the middle vault and dorsum loss of nasal tipsupport and definition shortened (vertical) nasal length over rotation of the nasal tip and retrusion ofthe nasal spine and caudal septum It is also knownas a ldquoPug noserdquo or ldquoboxerrsquos noserdquo both of which referto various degrees of nasal dorsal depressionbull
Nasal DeformityEpidemiologyaetiologyndash Prevalence is higher in population groups prone to facial trauma (ie boxers athletes) those with historiesof intranasal cocaine use nasal surgery (e g radical submucosal septal resection reductive rhinoplasty)ndash A saddle-nose deformity can be congenital or acquired It can be noticed as a part of individual familialsyndromic and ethnic characteristics - Most deformities are due to traumatic and iatrogeniccauses Medical causes are Wegenerrsquosgranulomatosis relapsing polychondritis leprosy (Hansenrsquos disease) syphilis ectodermal dysplasiaand intranasal cocaine use
Nasal Deformity
bull Therapybull ndash Nasal reconstruction indications depend on patientbull selection surgeon experience and aetiology of thebull deformity bull Indications for surgery can be functionalbull aesthetic or most commonly both In individuals
with a compromised nasal airway a nasoseptalbull reconstruction is indicated
Nasal Deformity
bull Contraindications bull include patients with malignantbull chronic or autoimmune disease conditions drugbull abuse poor perioperative risk profile and unrealisticbull expectationsbull ndash Multiple previous rhinoplasties and certain
professionsbull (mixed martial artists boxers and other contactbull sports) are relative contraindications
Nasal DeformitySeptoplastyndash Septoplasty is performed to correct nasal obstructioncaused by septal deformityndash Usually septoplasty is performed under general anaesthesiawith the patient in the supine position with the head elevated by approximately 30 (Righthandedsurgeons approach from the right side)ndash Local vasoconstrictive anaesthesia is applied notonly to reduce postoperative pain but also more importantly to achieve vasoconstriction of themucosa and less intraoperative haemorrhage Lidocainewith adrenaline or epinephrine is usedalthough in patients with cardiac hypersensitivityoxymetazoline might be preferred
Nasal Deformity
bull Septoplasty begins with the incision of septal mucosabull Most operative techniques utilise a hemitransfixionbull incision at the caudal end of septum so thatbull deviation at this point might be reached as wellbull as a transfixion incision that is easily obtained ifbull needed (Right-handed surgeons normally choosebull the left side but that may vary when deviation isbull convex towards the right)
Nasal DeformityA columella retractor is placed over the columellaand by pulling it laterally the caudal border of theseptum is exposed Ala can be protected by an alaprotector A vertical incision with a no 15 bladeover the caudal end of septum is performed untilreaching the plane of the septal cartilage It is essentialto correctly identify the perichondrium and byusing the Cottle elevator dissect and lift it creatinga flap As the dissection proceeds along the septalcartilage a longer speculum (no 5) is introduced sothat elevation of the mucoperichondrium is doneunder constant visual controlndash The next step is to dissect the mucoperiostium
Nasal DeformityDissecting over the bony-cartilaginous junctionwhen joining both tunnels might be difficult and is
especially prone to membrane perforationndash If needed the same tunnels are to be created on the
other side of the septum Then deviated parts of
septum are identified and removed either with a
knife or a Freer chisel
Nasal Deformitybull septum from the maxillary crest the septum mustbull be separated from the perpendicular plate trimmedbull along the inferior border placed back onto the crestbull and sutured to the periosteum If the deformity involvesbull the vomer an osteotome is used Care mustbull be taken not to break the cribriform plate becausebull it could cause a cerebrospinal fistula
Nasal Deformity
bull Once the septal deviation is corrected the flapsbull and hemitransfixion incision are mattressed
withbull absorbable sutures Nasal packing to prevent
synechiaebull and postoperative septal haematoma mightbull be advised but should be removed within 72 h

Wegenerrsquos Granulomatosis
bull ndash In the disseminated form pulmonary involvementbull is manifested by cough dyspnoea haemoptysisbull (due to an alveolar capillaritis necrotic lesions orbull endobronchial disease) and pleuritic painndashbull -Ninety per cent of patients have nasal symptomsbull and these symptoms are usually the first
manifestationof the diseasebull -Most patients have also renal involvementbull even if it is subclinical
Wegenerrsquos Granulomatosis
Diagnosis ndash Diagnosis of Wegenerrsquos granulomatosis is based on clinical findings that demonstrate lung (chest x-ray) kidney (urine analysis) or upper respiratory tract
involvement (oral or nasal ulcers or discharge) - positive blood analysis for cytoplasmic-staining antineutrophil
cytoplasmic antibodies (c-ANCA) and confirming proteinase 3 (PR3) ANCA or myeloperoxidase (MPO) ANCA ndash Biopsy is essential for diagnosis nonspecific chronic inflammation
and necrosis -Bacterial and fungal infections
Wegenerrsquos Granulomatosis
Therapyndash Conservative therapybull In the induction of disease remission highdosesteroids (e g prednisone 1 mgkgday) for1 month with tapering over several months aregiven In addition cyclophosphamide (2 mgkgday) should be administered for 6ndash12 monthsuntil symptoms disappear In the maintenanceof remission cyclophosphamide should be
Wegenerrsquos Granulomatosis
Antibiotics mainly trimethoprim-sulfamethoxazoleare given for prophylaxis againstPneumocystis jiroveci (formerly Pneumocystiscarinii) pneumonia (PCP) which may developduring immunosuppression and have a role inpreventing recurrencesbull Sinonasal manifestations may be treated with topical nasal steroids and nasal irrigations lowdosesystemic steroids and antibiotics when bacterial infection (typically Staphylococcus species) is suspected
Wegenerrsquos Granulomatosis
bull Prognosisbull ndash Most of the patients respond well to treatmentbull achieving symptom-free intervals of 5ndash20 yearsbull or more bull -Anatomical problems (sinusitis trachealbull stenosis) may require surgery bull Relapses can be long and troublesomebull Long-term complications are chronicbull renal failure hearing loss and deafness
Nasal Fractures Definition ndash A nasal fracture is a disruption of the nasal bone structure due to trauma It is the most frequently fractured facial bone Epidemiologyaetiology ndash Sports falls and assaults are the usual mechanisms of fracture -Males are affected twice as often as are females -Paediatric populations with a incidences during the second and third decades of life -Variables such as force impact direction nature of the striking object age and other will influence the pattern of injury to the components of the nose
Nasal Fractures
bull Symptomsbull ndash Deformity swelling epistaxis and periorbital
ecchymosis are signs that are suggestive of nasal fracture
bull bony crepitus and nasal segment mobilitybull ndash Epiphora bull Severe bilateral injuries to the lachrymal bones
arebull associated with depressed nasal fractures
Nasal Fractures Complications ndash Septal haematoma is one of the most severe early complications of nasal trauma and without drainage it results in abscess formation 6ndash7 days after trauma producing necrosis of the septal cartilage -Long-term problems such as saddle-nose deformity perforation columellar retraction and nasalbase
Septal infection could lead to osteomyelitis orbital and intracranial abscesses meningitis and cavernous sinus thrombosis -Cerebrospinal fluid leakage is a common complication of severe
nasal and frontal fractures
Nasal Fractures
bull Diagnostic proceduresbull ndash Inspectionbull bull Changes of appearance such as deviation andbull asymmetry bleeding watery drainage changesbull in nasal breathing and smell It is useful to comparebull the current presentation with old photographsbull (up to 40 of normal individuals havebull significant nose malformations)
Nasal Fractures Physical examination bull The diagnosis of a nasal fracture is made primarily by physical examination epistaxis nasal swelling and periorbital ecchymosis Nasal shape in the lateral and frontal inspection should be assessed Grasping the dorsum between two fingers and rocking the pyramid back and forth aids in assessing the mobility of nasal bones Internal structures should be evaluated by using a headlight and nasal speculum Clotted blood is removed by suction and assessment of haematoma mucosal tears and active bleeding is performed Bimanual palpation of the septum helps to differentiate septal swelling from haematoma ndash
Nasal FracturesRadiographybull There is no clear evidence of the role of radiographyin the management of nasal fracturesPlain films have up to a 66 false-positive rateas a result of misinterpretation of normal suturelines In addition old fractures are difficult todistinguishbull Three-dimensional CT is recommended for extensiveinjuries involving the nasal-orbital-ethmoidalcomplexndash
Nasal Fractures
bull Additionaluseful diagnostic proceduresbull bull Using a 0 or 30deg 4-mm endoscope is helpful inbull the assessment of posterior abnormalities If thebull patient is heavily sedated Brown-Gruss
provocationbull manoeuvres may be performed to determinebull deformities in upper middle or lower segmentsbull by compressing each compartment
Nasal FracturesConservative treatmentndash Treatment of bleedingbull For localised bleeding anterior sources may becauterised by silver nitrate or sealed with topicalmaterials such as thrombin combined withgelatin foam fibrin glue FloSealreg or other procoagulantmaterials If conservative measuresfail a formal anterior packing is placedbull Bleeding from branches of sphenopalatine orethmoid vessels requires anterior-posteriorpacking
Nasal Fractures
bull bull Surgical methods such as direct endoscopic vessel
bull cauterization or ligation have been shown tobull offer better haemostasis and patient comfortbull Angiography with embolization can also be
consideredbull in cases refractory to more conservativebull approaches
Nasal Fractures
bull Type of reductionbull bull Nondisplaced fractures should be treated withbull observation alone Closed nasal reduction is thebull best choice for simple injuries (isolated unilateralbull with medial displacement)bull bull An open approach should be considered in
severebull trauma (bilateral depressed fractures)
Nasal Fracturesbull Surgical principlesbull ndash Topical anaesthesia with cotton pledgets soakedbull with 4 cocaine or 005 oxymethazoline combinedbull with 4 topical lidocaine should be appliedbull for 5ndash10 min Local anaesthesia should also be injectedbull (1 lidocaine and 1100000 epinephrine)bull along the septum lateral walls and floor of the nasalbull cavitybull bull
Nasal FracturesClosed reductionndashndash The nasal bones are grasped between two fingersand pressure is applied laterally in theopposite direction of the deviation A bluntelevator may be used from within the nose incases of significant medial collapse Walshamforceps can be of help Reduction of the septumshould be performed with the use ofAsch forceps
Nasal Fractures
bull To prevent collapse of the postreductionbull framework nasal packing should be placedbull for 3ndash5 days Septum splints are recommendedbull in comminuted septal fractures withbull severe mucosal lesions External nasal splintingbull for 10 days (Aquaplastreg Thermoplastreg)bull provides nasal protection Nasal saline spraysbull prevent crusting and oral antibiotics should
Nasal Fractures
bull Open reductionbull ndashndash Immediate repair of fractures by using
widebull surgical exposure reduction fixation and
reconstructionbull ndashndash The second option is delayed correctionbull (6 months or more) of persistent deformitiesbull using standard techniques of rhinoplasty
Deviated Nasal Septum
bull Definition of the diseasebull ndash Deviation of the nasal septum is a common causebull of unilateral nasal airway obstruction in which thebull nasal septum is displacedbull bull Epidemiologyaetiologybull ndash Developmental septal abnormalities Septal cartilage
damage in the neonatal period andbull during birth can cause severe septal deviation inbull the absence of a history of nasal trauma
Deviated Nasal Septum
bull Symptomsbull ndash Patients may present with a history of sinusitis
allergicbull rhinitis obstructive sleep apnoea previousbull nasal surgery or recent nasal trauma Unilateral or
bilateral nasal airway obstruction that is unrelievedbull with decongestants or nasal steroid sprays is oftenbull seenbull bull
Deviated Nasal SeptumDiagnosisndashExamination external dorsal deviation or the columella and caudal septummay be deflected off the midline (caudal subluxation)ndash Inspections of the nasal cavity and anterior-posteriorrhinoscopy are helpful in diagnosing the locationtype and severity of septal deformityThe endoscope is also useful in identifying polypsthe severity and extent of posterior septaldeviations and bony spurs and locating areas ofseptal perforation or mucosal injury
Deviated Nasal Septum
bull Therapybull ndash Septoplasty is a procedurebull The areabull of deviation is corrected or resected in order tobull leave behind as much cartilage and bone as
possiblebull Cartilage resection is minimised and can be
repositioned reshaped or recontoured using a variety of methods
Deviated Nasal Septum
bull ndash Indications of septoplasty before the growth period
bull of the nose is finished should be very limited bull -In these cases surgery must preserve all the
cartilagebull in order to prevent external changes of the
shape ofbull the nose
Deviated Nasal Septum
bull Complicationsbull ndash Frequent complications include haematoma andbull infection Cerebrospinal fluid leak is a rare but
potentiallybull serious complicationbull It is usually the resultbull of avulsion or damage to the cribriform plate whenbull handling the perpendicular plate of the ethmoidbull ndash Other complications include epistaxis nasal
Deviated Nasal Septum
bull Other complications include epistaxis nasal obstruction
bull due to residual deviation synechiae returnbull of the cartilaginous deviation septal perforationbull anosmia and cosmetic nasal deformities suchbull as widened alar rim margins drooping nasal tipbull columella retraction and a sunken dorsum with abull supratip saddle formation
Septal perforation with minor crusting View from provide closure of the
incision
Septal Haematoma
bull A septal haematoma is a blood collection under the perichondrium
bull of the septum and cartilagebull bull bull Epidemiologyaetiologybull ndash A septal haematoma is one of the most
severe complications of nasal trauma
Septal Haematoma
bull Diagnosisbull ndash Signs and symptoms include intense pain
swellingbull haematoma of the upper lip and philtrum
area andbull complete nasal airway obstruction
Septal HaematomaTherapyndash Management consists of drainage through a mucoperichondrial incision Immediate treatment isnecessary to prevent long-term problems such asa saddle-nose deformity perforation columellarretraction and nasal-base widening In childrenseptal destruction can lead to devastating nasal andmidfacial growth abnormalitiesbull Surgeryndash Incision and evacuation of the collection is performedDrainage of a septal haematoma should
Septal HaematomaSurgeryndash Incision and evacuation of the collection is performedDrainage of a septal haematoma should provide closure of the incision
Splints or transseptal sutures are placed to obliterate thepotential space and prevent collectionInfection involving the septal cartilage Reconstruction with autologouscartilage is then performed in a second stage Oral antibiotics should be given
Nasal DeformitySaddle-nose deformityndash A saddle-nose deformity is characterised by a loss ofnasal dorsal height and compromised nasal supportstructures -Other case observed are depressionof the middle vault and dorsum loss of nasal tipsupport and definition shortened (vertical) nasal length over rotation of the nasal tip and retrusion ofthe nasal spine and caudal septum It is also knownas a ldquoPug noserdquo or ldquoboxerrsquos noserdquo both of which referto various degrees of nasal dorsal depressionbull
Nasal DeformityEpidemiologyaetiologyndash Prevalence is higher in population groups prone to facial trauma (ie boxers athletes) those with historiesof intranasal cocaine use nasal surgery (e g radical submucosal septal resection reductive rhinoplasty)ndash A saddle-nose deformity can be congenital or acquired It can be noticed as a part of individual familialsyndromic and ethnic characteristics - Most deformities are due to traumatic and iatrogeniccauses Medical causes are Wegenerrsquosgranulomatosis relapsing polychondritis leprosy (Hansenrsquos disease) syphilis ectodermal dysplasiaand intranasal cocaine use
Nasal Deformity
bull Therapybull ndash Nasal reconstruction indications depend on patientbull selection surgeon experience and aetiology of thebull deformity bull Indications for surgery can be functionalbull aesthetic or most commonly both In individuals
with a compromised nasal airway a nasoseptalbull reconstruction is indicated
Nasal Deformity
bull Contraindications bull include patients with malignantbull chronic or autoimmune disease conditions drugbull abuse poor perioperative risk profile and unrealisticbull expectationsbull ndash Multiple previous rhinoplasties and certain
professionsbull (mixed martial artists boxers and other contactbull sports) are relative contraindications
Nasal DeformitySeptoplastyndash Septoplasty is performed to correct nasal obstructioncaused by septal deformityndash Usually septoplasty is performed under general anaesthesiawith the patient in the supine position with the head elevated by approximately 30 (Righthandedsurgeons approach from the right side)ndash Local vasoconstrictive anaesthesia is applied notonly to reduce postoperative pain but also more importantly to achieve vasoconstriction of themucosa and less intraoperative haemorrhage Lidocainewith adrenaline or epinephrine is usedalthough in patients with cardiac hypersensitivityoxymetazoline might be preferred
Nasal Deformity
bull Septoplasty begins with the incision of septal mucosabull Most operative techniques utilise a hemitransfixionbull incision at the caudal end of septum so thatbull deviation at this point might be reached as wellbull as a transfixion incision that is easily obtained ifbull needed (Right-handed surgeons normally choosebull the left side but that may vary when deviation isbull convex towards the right)
Nasal DeformityA columella retractor is placed over the columellaand by pulling it laterally the caudal border of theseptum is exposed Ala can be protected by an alaprotector A vertical incision with a no 15 bladeover the caudal end of septum is performed untilreaching the plane of the septal cartilage It is essentialto correctly identify the perichondrium and byusing the Cottle elevator dissect and lift it creatinga flap As the dissection proceeds along the septalcartilage a longer speculum (no 5) is introduced sothat elevation of the mucoperichondrium is doneunder constant visual controlndash The next step is to dissect the mucoperiostium
Nasal DeformityDissecting over the bony-cartilaginous junctionwhen joining both tunnels might be difficult and is
especially prone to membrane perforationndash If needed the same tunnels are to be created on the
other side of the septum Then deviated parts of
septum are identified and removed either with a
knife or a Freer chisel
Nasal Deformitybull septum from the maxillary crest the septum mustbull be separated from the perpendicular plate trimmedbull along the inferior border placed back onto the crestbull and sutured to the periosteum If the deformity involvesbull the vomer an osteotome is used Care mustbull be taken not to break the cribriform plate becausebull it could cause a cerebrospinal fistula
Nasal Deformity
bull Once the septal deviation is corrected the flapsbull and hemitransfixion incision are mattressed
withbull absorbable sutures Nasal packing to prevent
synechiaebull and postoperative septal haematoma mightbull be advised but should be removed within 72 h

Wegenerrsquos Granulomatosis
Diagnosis ndash Diagnosis of Wegenerrsquos granulomatosis is based on clinical findings that demonstrate lung (chest x-ray) kidney (urine analysis) or upper respiratory tract
involvement (oral or nasal ulcers or discharge) - positive blood analysis for cytoplasmic-staining antineutrophil
cytoplasmic antibodies (c-ANCA) and confirming proteinase 3 (PR3) ANCA or myeloperoxidase (MPO) ANCA ndash Biopsy is essential for diagnosis nonspecific chronic inflammation
and necrosis -Bacterial and fungal infections
Wegenerrsquos Granulomatosis
Therapyndash Conservative therapybull In the induction of disease remission highdosesteroids (e g prednisone 1 mgkgday) for1 month with tapering over several months aregiven In addition cyclophosphamide (2 mgkgday) should be administered for 6ndash12 monthsuntil symptoms disappear In the maintenanceof remission cyclophosphamide should be
Wegenerrsquos Granulomatosis
Antibiotics mainly trimethoprim-sulfamethoxazoleare given for prophylaxis againstPneumocystis jiroveci (formerly Pneumocystiscarinii) pneumonia (PCP) which may developduring immunosuppression and have a role inpreventing recurrencesbull Sinonasal manifestations may be treated with topical nasal steroids and nasal irrigations lowdosesystemic steroids and antibiotics when bacterial infection (typically Staphylococcus species) is suspected
Wegenerrsquos Granulomatosis
bull Prognosisbull ndash Most of the patients respond well to treatmentbull achieving symptom-free intervals of 5ndash20 yearsbull or more bull -Anatomical problems (sinusitis trachealbull stenosis) may require surgery bull Relapses can be long and troublesomebull Long-term complications are chronicbull renal failure hearing loss and deafness
Nasal Fractures Definition ndash A nasal fracture is a disruption of the nasal bone structure due to trauma It is the most frequently fractured facial bone Epidemiologyaetiology ndash Sports falls and assaults are the usual mechanisms of fracture -Males are affected twice as often as are females -Paediatric populations with a incidences during the second and third decades of life -Variables such as force impact direction nature of the striking object age and other will influence the pattern of injury to the components of the nose
Nasal Fractures
bull Symptomsbull ndash Deformity swelling epistaxis and periorbital
ecchymosis are signs that are suggestive of nasal fracture
bull bony crepitus and nasal segment mobilitybull ndash Epiphora bull Severe bilateral injuries to the lachrymal bones
arebull associated with depressed nasal fractures
Nasal Fractures Complications ndash Septal haematoma is one of the most severe early complications of nasal trauma and without drainage it results in abscess formation 6ndash7 days after trauma producing necrosis of the septal cartilage -Long-term problems such as saddle-nose deformity perforation columellar retraction and nasalbase
Septal infection could lead to osteomyelitis orbital and intracranial abscesses meningitis and cavernous sinus thrombosis -Cerebrospinal fluid leakage is a common complication of severe
nasal and frontal fractures
Nasal Fractures
bull Diagnostic proceduresbull ndash Inspectionbull bull Changes of appearance such as deviation andbull asymmetry bleeding watery drainage changesbull in nasal breathing and smell It is useful to comparebull the current presentation with old photographsbull (up to 40 of normal individuals havebull significant nose malformations)
Nasal Fractures Physical examination bull The diagnosis of a nasal fracture is made primarily by physical examination epistaxis nasal swelling and periorbital ecchymosis Nasal shape in the lateral and frontal inspection should be assessed Grasping the dorsum between two fingers and rocking the pyramid back and forth aids in assessing the mobility of nasal bones Internal structures should be evaluated by using a headlight and nasal speculum Clotted blood is removed by suction and assessment of haematoma mucosal tears and active bleeding is performed Bimanual palpation of the septum helps to differentiate septal swelling from haematoma ndash
Nasal FracturesRadiographybull There is no clear evidence of the role of radiographyin the management of nasal fracturesPlain films have up to a 66 false-positive rateas a result of misinterpretation of normal suturelines In addition old fractures are difficult todistinguishbull Three-dimensional CT is recommended for extensiveinjuries involving the nasal-orbital-ethmoidalcomplexndash
Nasal Fractures
bull Additionaluseful diagnostic proceduresbull bull Using a 0 or 30deg 4-mm endoscope is helpful inbull the assessment of posterior abnormalities If thebull patient is heavily sedated Brown-Gruss
provocationbull manoeuvres may be performed to determinebull deformities in upper middle or lower segmentsbull by compressing each compartment
Nasal FracturesConservative treatmentndash Treatment of bleedingbull For localised bleeding anterior sources may becauterised by silver nitrate or sealed with topicalmaterials such as thrombin combined withgelatin foam fibrin glue FloSealreg or other procoagulantmaterials If conservative measuresfail a formal anterior packing is placedbull Bleeding from branches of sphenopalatine orethmoid vessels requires anterior-posteriorpacking
Nasal Fractures
bull bull Surgical methods such as direct endoscopic vessel
bull cauterization or ligation have been shown tobull offer better haemostasis and patient comfortbull Angiography with embolization can also be
consideredbull in cases refractory to more conservativebull approaches
Nasal Fractures
bull Type of reductionbull bull Nondisplaced fractures should be treated withbull observation alone Closed nasal reduction is thebull best choice for simple injuries (isolated unilateralbull with medial displacement)bull bull An open approach should be considered in
severebull trauma (bilateral depressed fractures)
Nasal Fracturesbull Surgical principlesbull ndash Topical anaesthesia with cotton pledgets soakedbull with 4 cocaine or 005 oxymethazoline combinedbull with 4 topical lidocaine should be appliedbull for 5ndash10 min Local anaesthesia should also be injectedbull (1 lidocaine and 1100000 epinephrine)bull along the septum lateral walls and floor of the nasalbull cavitybull bull
Nasal FracturesClosed reductionndashndash The nasal bones are grasped between two fingersand pressure is applied laterally in theopposite direction of the deviation A bluntelevator may be used from within the nose incases of significant medial collapse Walshamforceps can be of help Reduction of the septumshould be performed with the use ofAsch forceps
Nasal Fractures
bull To prevent collapse of the postreductionbull framework nasal packing should be placedbull for 3ndash5 days Septum splints are recommendedbull in comminuted septal fractures withbull severe mucosal lesions External nasal splintingbull for 10 days (Aquaplastreg Thermoplastreg)bull provides nasal protection Nasal saline spraysbull prevent crusting and oral antibiotics should
Nasal Fractures
bull Open reductionbull ndashndash Immediate repair of fractures by using
widebull surgical exposure reduction fixation and
reconstructionbull ndashndash The second option is delayed correctionbull (6 months or more) of persistent deformitiesbull using standard techniques of rhinoplasty
Deviated Nasal Septum
bull Definition of the diseasebull ndash Deviation of the nasal septum is a common causebull of unilateral nasal airway obstruction in which thebull nasal septum is displacedbull bull Epidemiologyaetiologybull ndash Developmental septal abnormalities Septal cartilage
damage in the neonatal period andbull during birth can cause severe septal deviation inbull the absence of a history of nasal trauma
Deviated Nasal Septum
bull Symptomsbull ndash Patients may present with a history of sinusitis
allergicbull rhinitis obstructive sleep apnoea previousbull nasal surgery or recent nasal trauma Unilateral or
bilateral nasal airway obstruction that is unrelievedbull with decongestants or nasal steroid sprays is oftenbull seenbull bull
Deviated Nasal SeptumDiagnosisndashExamination external dorsal deviation or the columella and caudal septummay be deflected off the midline (caudal subluxation)ndash Inspections of the nasal cavity and anterior-posteriorrhinoscopy are helpful in diagnosing the locationtype and severity of septal deformityThe endoscope is also useful in identifying polypsthe severity and extent of posterior septaldeviations and bony spurs and locating areas ofseptal perforation or mucosal injury
Deviated Nasal Septum
bull Therapybull ndash Septoplasty is a procedurebull The areabull of deviation is corrected or resected in order tobull leave behind as much cartilage and bone as
possiblebull Cartilage resection is minimised and can be
repositioned reshaped or recontoured using a variety of methods
Deviated Nasal Septum
bull ndash Indications of septoplasty before the growth period
bull of the nose is finished should be very limited bull -In these cases surgery must preserve all the
cartilagebull in order to prevent external changes of the
shape ofbull the nose
Deviated Nasal Septum
bull Complicationsbull ndash Frequent complications include haematoma andbull infection Cerebrospinal fluid leak is a rare but
potentiallybull serious complicationbull It is usually the resultbull of avulsion or damage to the cribriform plate whenbull handling the perpendicular plate of the ethmoidbull ndash Other complications include epistaxis nasal
Deviated Nasal Septum
bull Other complications include epistaxis nasal obstruction
bull due to residual deviation synechiae returnbull of the cartilaginous deviation septal perforationbull anosmia and cosmetic nasal deformities suchbull as widened alar rim margins drooping nasal tipbull columella retraction and a sunken dorsum with abull supratip saddle formation
Septal perforation with minor crusting View from provide closure of the
incision
Septal Haematoma
bull A septal haematoma is a blood collection under the perichondrium
bull of the septum and cartilagebull bull bull Epidemiologyaetiologybull ndash A septal haematoma is one of the most
severe complications of nasal trauma
Septal Haematoma
bull Diagnosisbull ndash Signs and symptoms include intense pain
swellingbull haematoma of the upper lip and philtrum
area andbull complete nasal airway obstruction
Septal HaematomaTherapyndash Management consists of drainage through a mucoperichondrial incision Immediate treatment isnecessary to prevent long-term problems such asa saddle-nose deformity perforation columellarretraction and nasal-base widening In childrenseptal destruction can lead to devastating nasal andmidfacial growth abnormalitiesbull Surgeryndash Incision and evacuation of the collection is performedDrainage of a septal haematoma should
Septal HaematomaSurgeryndash Incision and evacuation of the collection is performedDrainage of a septal haematoma should provide closure of the incision
Splints or transseptal sutures are placed to obliterate thepotential space and prevent collectionInfection involving the septal cartilage Reconstruction with autologouscartilage is then performed in a second stage Oral antibiotics should be given
Nasal DeformitySaddle-nose deformityndash A saddle-nose deformity is characterised by a loss ofnasal dorsal height and compromised nasal supportstructures -Other case observed are depressionof the middle vault and dorsum loss of nasal tipsupport and definition shortened (vertical) nasal length over rotation of the nasal tip and retrusion ofthe nasal spine and caudal septum It is also knownas a ldquoPug noserdquo or ldquoboxerrsquos noserdquo both of which referto various degrees of nasal dorsal depressionbull
Nasal DeformityEpidemiologyaetiologyndash Prevalence is higher in population groups prone to facial trauma (ie boxers athletes) those with historiesof intranasal cocaine use nasal surgery (e g radical submucosal septal resection reductive rhinoplasty)ndash A saddle-nose deformity can be congenital or acquired It can be noticed as a part of individual familialsyndromic and ethnic characteristics - Most deformities are due to traumatic and iatrogeniccauses Medical causes are Wegenerrsquosgranulomatosis relapsing polychondritis leprosy (Hansenrsquos disease) syphilis ectodermal dysplasiaand intranasal cocaine use
Nasal Deformity
bull Therapybull ndash Nasal reconstruction indications depend on patientbull selection surgeon experience and aetiology of thebull deformity bull Indications for surgery can be functionalbull aesthetic or most commonly both In individuals
with a compromised nasal airway a nasoseptalbull reconstruction is indicated
Nasal Deformity
bull Contraindications bull include patients with malignantbull chronic or autoimmune disease conditions drugbull abuse poor perioperative risk profile and unrealisticbull expectationsbull ndash Multiple previous rhinoplasties and certain
professionsbull (mixed martial artists boxers and other contactbull sports) are relative contraindications
Nasal DeformitySeptoplastyndash Septoplasty is performed to correct nasal obstructioncaused by septal deformityndash Usually septoplasty is performed under general anaesthesiawith the patient in the supine position with the head elevated by approximately 30 (Righthandedsurgeons approach from the right side)ndash Local vasoconstrictive anaesthesia is applied notonly to reduce postoperative pain but also more importantly to achieve vasoconstriction of themucosa and less intraoperative haemorrhage Lidocainewith adrenaline or epinephrine is usedalthough in patients with cardiac hypersensitivityoxymetazoline might be preferred
Nasal Deformity
bull Septoplasty begins with the incision of septal mucosabull Most operative techniques utilise a hemitransfixionbull incision at the caudal end of septum so thatbull deviation at this point might be reached as wellbull as a transfixion incision that is easily obtained ifbull needed (Right-handed surgeons normally choosebull the left side but that may vary when deviation isbull convex towards the right)
Nasal DeformityA columella retractor is placed over the columellaand by pulling it laterally the caudal border of theseptum is exposed Ala can be protected by an alaprotector A vertical incision with a no 15 bladeover the caudal end of septum is performed untilreaching the plane of the septal cartilage It is essentialto correctly identify the perichondrium and byusing the Cottle elevator dissect and lift it creatinga flap As the dissection proceeds along the septalcartilage a longer speculum (no 5) is introduced sothat elevation of the mucoperichondrium is doneunder constant visual controlndash The next step is to dissect the mucoperiostium
Nasal DeformityDissecting over the bony-cartilaginous junctionwhen joining both tunnels might be difficult and is
especially prone to membrane perforationndash If needed the same tunnels are to be created on the
other side of the septum Then deviated parts of
septum are identified and removed either with a
knife or a Freer chisel
Nasal Deformitybull septum from the maxillary crest the septum mustbull be separated from the perpendicular plate trimmedbull along the inferior border placed back onto the crestbull and sutured to the periosteum If the deformity involvesbull the vomer an osteotome is used Care mustbull be taken not to break the cribriform plate becausebull it could cause a cerebrospinal fistula
Nasal Deformity
bull Once the septal deviation is corrected the flapsbull and hemitransfixion incision are mattressed
withbull absorbable sutures Nasal packing to prevent
synechiaebull and postoperative septal haematoma mightbull be advised but should be removed within 72 h

Wegenerrsquos Granulomatosis
Therapyndash Conservative therapybull In the induction of disease remission highdosesteroids (e g prednisone 1 mgkgday) for1 month with tapering over several months aregiven In addition cyclophosphamide (2 mgkgday) should be administered for 6ndash12 monthsuntil symptoms disappear In the maintenanceof remission cyclophosphamide should be
Wegenerrsquos Granulomatosis
Antibiotics mainly trimethoprim-sulfamethoxazoleare given for prophylaxis againstPneumocystis jiroveci (formerly Pneumocystiscarinii) pneumonia (PCP) which may developduring immunosuppression and have a role inpreventing recurrencesbull Sinonasal manifestations may be treated with topical nasal steroids and nasal irrigations lowdosesystemic steroids and antibiotics when bacterial infection (typically Staphylococcus species) is suspected
Wegenerrsquos Granulomatosis
bull Prognosisbull ndash Most of the patients respond well to treatmentbull achieving symptom-free intervals of 5ndash20 yearsbull or more bull -Anatomical problems (sinusitis trachealbull stenosis) may require surgery bull Relapses can be long and troublesomebull Long-term complications are chronicbull renal failure hearing loss and deafness
Nasal Fractures Definition ndash A nasal fracture is a disruption of the nasal bone structure due to trauma It is the most frequently fractured facial bone Epidemiologyaetiology ndash Sports falls and assaults are the usual mechanisms of fracture -Males are affected twice as often as are females -Paediatric populations with a incidences during the second and third decades of life -Variables such as force impact direction nature of the striking object age and other will influence the pattern of injury to the components of the nose
Nasal Fractures
bull Symptomsbull ndash Deformity swelling epistaxis and periorbital
ecchymosis are signs that are suggestive of nasal fracture
bull bony crepitus and nasal segment mobilitybull ndash Epiphora bull Severe bilateral injuries to the lachrymal bones
arebull associated with depressed nasal fractures
Nasal Fractures Complications ndash Septal haematoma is one of the most severe early complications of nasal trauma and without drainage it results in abscess formation 6ndash7 days after trauma producing necrosis of the septal cartilage -Long-term problems such as saddle-nose deformity perforation columellar retraction and nasalbase
Septal infection could lead to osteomyelitis orbital and intracranial abscesses meningitis and cavernous sinus thrombosis -Cerebrospinal fluid leakage is a common complication of severe
nasal and frontal fractures
Nasal Fractures
bull Diagnostic proceduresbull ndash Inspectionbull bull Changes of appearance such as deviation andbull asymmetry bleeding watery drainage changesbull in nasal breathing and smell It is useful to comparebull the current presentation with old photographsbull (up to 40 of normal individuals havebull significant nose malformations)
Nasal Fractures Physical examination bull The diagnosis of a nasal fracture is made primarily by physical examination epistaxis nasal swelling and periorbital ecchymosis Nasal shape in the lateral and frontal inspection should be assessed Grasping the dorsum between two fingers and rocking the pyramid back and forth aids in assessing the mobility of nasal bones Internal structures should be evaluated by using a headlight and nasal speculum Clotted blood is removed by suction and assessment of haematoma mucosal tears and active bleeding is performed Bimanual palpation of the septum helps to differentiate septal swelling from haematoma ndash
Nasal FracturesRadiographybull There is no clear evidence of the role of radiographyin the management of nasal fracturesPlain films have up to a 66 false-positive rateas a result of misinterpretation of normal suturelines In addition old fractures are difficult todistinguishbull Three-dimensional CT is recommended for extensiveinjuries involving the nasal-orbital-ethmoidalcomplexndash
Nasal Fractures
bull Additionaluseful diagnostic proceduresbull bull Using a 0 or 30deg 4-mm endoscope is helpful inbull the assessment of posterior abnormalities If thebull patient is heavily sedated Brown-Gruss
provocationbull manoeuvres may be performed to determinebull deformities in upper middle or lower segmentsbull by compressing each compartment
Nasal FracturesConservative treatmentndash Treatment of bleedingbull For localised bleeding anterior sources may becauterised by silver nitrate or sealed with topicalmaterials such as thrombin combined withgelatin foam fibrin glue FloSealreg or other procoagulantmaterials If conservative measuresfail a formal anterior packing is placedbull Bleeding from branches of sphenopalatine orethmoid vessels requires anterior-posteriorpacking
Nasal Fractures
bull bull Surgical methods such as direct endoscopic vessel
bull cauterization or ligation have been shown tobull offer better haemostasis and patient comfortbull Angiography with embolization can also be
consideredbull in cases refractory to more conservativebull approaches
Nasal Fractures
bull Type of reductionbull bull Nondisplaced fractures should be treated withbull observation alone Closed nasal reduction is thebull best choice for simple injuries (isolated unilateralbull with medial displacement)bull bull An open approach should be considered in
severebull trauma (bilateral depressed fractures)
Nasal Fracturesbull Surgical principlesbull ndash Topical anaesthesia with cotton pledgets soakedbull with 4 cocaine or 005 oxymethazoline combinedbull with 4 topical lidocaine should be appliedbull for 5ndash10 min Local anaesthesia should also be injectedbull (1 lidocaine and 1100000 epinephrine)bull along the septum lateral walls and floor of the nasalbull cavitybull bull
Nasal FracturesClosed reductionndashndash The nasal bones are grasped between two fingersand pressure is applied laterally in theopposite direction of the deviation A bluntelevator may be used from within the nose incases of significant medial collapse Walshamforceps can be of help Reduction of the septumshould be performed with the use ofAsch forceps
Nasal Fractures
bull To prevent collapse of the postreductionbull framework nasal packing should be placedbull for 3ndash5 days Septum splints are recommendedbull in comminuted septal fractures withbull severe mucosal lesions External nasal splintingbull for 10 days (Aquaplastreg Thermoplastreg)bull provides nasal protection Nasal saline spraysbull prevent crusting and oral antibiotics should
Nasal Fractures
bull Open reductionbull ndashndash Immediate repair of fractures by using
widebull surgical exposure reduction fixation and
reconstructionbull ndashndash The second option is delayed correctionbull (6 months or more) of persistent deformitiesbull using standard techniques of rhinoplasty
Deviated Nasal Septum
bull Definition of the diseasebull ndash Deviation of the nasal septum is a common causebull of unilateral nasal airway obstruction in which thebull nasal septum is displacedbull bull Epidemiologyaetiologybull ndash Developmental septal abnormalities Septal cartilage
damage in the neonatal period andbull during birth can cause severe septal deviation inbull the absence of a history of nasal trauma
Deviated Nasal Septum
bull Symptomsbull ndash Patients may present with a history of sinusitis
allergicbull rhinitis obstructive sleep apnoea previousbull nasal surgery or recent nasal trauma Unilateral or
bilateral nasal airway obstruction that is unrelievedbull with decongestants or nasal steroid sprays is oftenbull seenbull bull
Deviated Nasal SeptumDiagnosisndashExamination external dorsal deviation or the columella and caudal septummay be deflected off the midline (caudal subluxation)ndash Inspections of the nasal cavity and anterior-posteriorrhinoscopy are helpful in diagnosing the locationtype and severity of septal deformityThe endoscope is also useful in identifying polypsthe severity and extent of posterior septaldeviations and bony spurs and locating areas ofseptal perforation or mucosal injury
Deviated Nasal Septum
bull Therapybull ndash Septoplasty is a procedurebull The areabull of deviation is corrected or resected in order tobull leave behind as much cartilage and bone as
possiblebull Cartilage resection is minimised and can be
repositioned reshaped or recontoured using a variety of methods
Deviated Nasal Septum
bull ndash Indications of septoplasty before the growth period
bull of the nose is finished should be very limited bull -In these cases surgery must preserve all the
cartilagebull in order to prevent external changes of the
shape ofbull the nose
Deviated Nasal Septum
bull Complicationsbull ndash Frequent complications include haematoma andbull infection Cerebrospinal fluid leak is a rare but
potentiallybull serious complicationbull It is usually the resultbull of avulsion or damage to the cribriform plate whenbull handling the perpendicular plate of the ethmoidbull ndash Other complications include epistaxis nasal
Deviated Nasal Septum
bull Other complications include epistaxis nasal obstruction
bull due to residual deviation synechiae returnbull of the cartilaginous deviation septal perforationbull anosmia and cosmetic nasal deformities suchbull as widened alar rim margins drooping nasal tipbull columella retraction and a sunken dorsum with abull supratip saddle formation
Septal perforation with minor crusting View from provide closure of the
incision
Septal Haematoma
bull A septal haematoma is a blood collection under the perichondrium
bull of the septum and cartilagebull bull bull Epidemiologyaetiologybull ndash A septal haematoma is one of the most
severe complications of nasal trauma
Septal Haematoma
bull Diagnosisbull ndash Signs and symptoms include intense pain
swellingbull haematoma of the upper lip and philtrum
area andbull complete nasal airway obstruction
Septal HaematomaTherapyndash Management consists of drainage through a mucoperichondrial incision Immediate treatment isnecessary to prevent long-term problems such asa saddle-nose deformity perforation columellarretraction and nasal-base widening In childrenseptal destruction can lead to devastating nasal andmidfacial growth abnormalitiesbull Surgeryndash Incision and evacuation of the collection is performedDrainage of a septal haematoma should
Septal HaematomaSurgeryndash Incision and evacuation of the collection is performedDrainage of a septal haematoma should provide closure of the incision
Splints or transseptal sutures are placed to obliterate thepotential space and prevent collectionInfection involving the septal cartilage Reconstruction with autologouscartilage is then performed in a second stage Oral antibiotics should be given
Nasal DeformitySaddle-nose deformityndash A saddle-nose deformity is characterised by a loss ofnasal dorsal height and compromised nasal supportstructures -Other case observed are depressionof the middle vault and dorsum loss of nasal tipsupport and definition shortened (vertical) nasal length over rotation of the nasal tip and retrusion ofthe nasal spine and caudal septum It is also knownas a ldquoPug noserdquo or ldquoboxerrsquos noserdquo both of which referto various degrees of nasal dorsal depressionbull
Nasal DeformityEpidemiologyaetiologyndash Prevalence is higher in population groups prone to facial trauma (ie boxers athletes) those with historiesof intranasal cocaine use nasal surgery (e g radical submucosal septal resection reductive rhinoplasty)ndash A saddle-nose deformity can be congenital or acquired It can be noticed as a part of individual familialsyndromic and ethnic characteristics - Most deformities are due to traumatic and iatrogeniccauses Medical causes are Wegenerrsquosgranulomatosis relapsing polychondritis leprosy (Hansenrsquos disease) syphilis ectodermal dysplasiaand intranasal cocaine use
Nasal Deformity
bull Therapybull ndash Nasal reconstruction indications depend on patientbull selection surgeon experience and aetiology of thebull deformity bull Indications for surgery can be functionalbull aesthetic or most commonly both In individuals
with a compromised nasal airway a nasoseptalbull reconstruction is indicated
Nasal Deformity
bull Contraindications bull include patients with malignantbull chronic or autoimmune disease conditions drugbull abuse poor perioperative risk profile and unrealisticbull expectationsbull ndash Multiple previous rhinoplasties and certain
professionsbull (mixed martial artists boxers and other contactbull sports) are relative contraindications
Nasal DeformitySeptoplastyndash Septoplasty is performed to correct nasal obstructioncaused by septal deformityndash Usually septoplasty is performed under general anaesthesiawith the patient in the supine position with the head elevated by approximately 30 (Righthandedsurgeons approach from the right side)ndash Local vasoconstrictive anaesthesia is applied notonly to reduce postoperative pain but also more importantly to achieve vasoconstriction of themucosa and less intraoperative haemorrhage Lidocainewith adrenaline or epinephrine is usedalthough in patients with cardiac hypersensitivityoxymetazoline might be preferred
Nasal Deformity
bull Septoplasty begins with the incision of septal mucosabull Most operative techniques utilise a hemitransfixionbull incision at the caudal end of septum so thatbull deviation at this point might be reached as wellbull as a transfixion incision that is easily obtained ifbull needed (Right-handed surgeons normally choosebull the left side but that may vary when deviation isbull convex towards the right)
Nasal DeformityA columella retractor is placed over the columellaand by pulling it laterally the caudal border of theseptum is exposed Ala can be protected by an alaprotector A vertical incision with a no 15 bladeover the caudal end of septum is performed untilreaching the plane of the septal cartilage It is essentialto correctly identify the perichondrium and byusing the Cottle elevator dissect and lift it creatinga flap As the dissection proceeds along the septalcartilage a longer speculum (no 5) is introduced sothat elevation of the mucoperichondrium is doneunder constant visual controlndash The next step is to dissect the mucoperiostium
Nasal DeformityDissecting over the bony-cartilaginous junctionwhen joining both tunnels might be difficult and is
especially prone to membrane perforationndash If needed the same tunnels are to be created on the
other side of the septum Then deviated parts of
septum are identified and removed either with a
knife or a Freer chisel
Nasal Deformitybull septum from the maxillary crest the septum mustbull be separated from the perpendicular plate trimmedbull along the inferior border placed back onto the crestbull and sutured to the periosteum If the deformity involvesbull the vomer an osteotome is used Care mustbull be taken not to break the cribriform plate becausebull it could cause a cerebrospinal fistula
Nasal Deformity
bull Once the septal deviation is corrected the flapsbull and hemitransfixion incision are mattressed
withbull absorbable sutures Nasal packing to prevent
synechiaebull and postoperative septal haematoma mightbull be advised but should be removed within 72 h

Wegenerrsquos Granulomatosis
Antibiotics mainly trimethoprim-sulfamethoxazoleare given for prophylaxis againstPneumocystis jiroveci (formerly Pneumocystiscarinii) pneumonia (PCP) which may developduring immunosuppression and have a role inpreventing recurrencesbull Sinonasal manifestations may be treated with topical nasal steroids and nasal irrigations lowdosesystemic steroids and antibiotics when bacterial infection (typically Staphylococcus species) is suspected
Wegenerrsquos Granulomatosis
bull Prognosisbull ndash Most of the patients respond well to treatmentbull achieving symptom-free intervals of 5ndash20 yearsbull or more bull -Anatomical problems (sinusitis trachealbull stenosis) may require surgery bull Relapses can be long and troublesomebull Long-term complications are chronicbull renal failure hearing loss and deafness
Nasal Fractures Definition ndash A nasal fracture is a disruption of the nasal bone structure due to trauma It is the most frequently fractured facial bone Epidemiologyaetiology ndash Sports falls and assaults are the usual mechanisms of fracture -Males are affected twice as often as are females -Paediatric populations with a incidences during the second and third decades of life -Variables such as force impact direction nature of the striking object age and other will influence the pattern of injury to the components of the nose
Nasal Fractures
bull Symptomsbull ndash Deformity swelling epistaxis and periorbital
ecchymosis are signs that are suggestive of nasal fracture
bull bony crepitus and nasal segment mobilitybull ndash Epiphora bull Severe bilateral injuries to the lachrymal bones
arebull associated with depressed nasal fractures
Nasal Fractures Complications ndash Septal haematoma is one of the most severe early complications of nasal trauma and without drainage it results in abscess formation 6ndash7 days after trauma producing necrosis of the septal cartilage -Long-term problems such as saddle-nose deformity perforation columellar retraction and nasalbase
Septal infection could lead to osteomyelitis orbital and intracranial abscesses meningitis and cavernous sinus thrombosis -Cerebrospinal fluid leakage is a common complication of severe
nasal and frontal fractures
Nasal Fractures
bull Diagnostic proceduresbull ndash Inspectionbull bull Changes of appearance such as deviation andbull asymmetry bleeding watery drainage changesbull in nasal breathing and smell It is useful to comparebull the current presentation with old photographsbull (up to 40 of normal individuals havebull significant nose malformations)
Nasal Fractures Physical examination bull The diagnosis of a nasal fracture is made primarily by physical examination epistaxis nasal swelling and periorbital ecchymosis Nasal shape in the lateral and frontal inspection should be assessed Grasping the dorsum between two fingers and rocking the pyramid back and forth aids in assessing the mobility of nasal bones Internal structures should be evaluated by using a headlight and nasal speculum Clotted blood is removed by suction and assessment of haematoma mucosal tears and active bleeding is performed Bimanual palpation of the septum helps to differentiate septal swelling from haematoma ndash
Nasal FracturesRadiographybull There is no clear evidence of the role of radiographyin the management of nasal fracturesPlain films have up to a 66 false-positive rateas a result of misinterpretation of normal suturelines In addition old fractures are difficult todistinguishbull Three-dimensional CT is recommended for extensiveinjuries involving the nasal-orbital-ethmoidalcomplexndash
Nasal Fractures
bull Additionaluseful diagnostic proceduresbull bull Using a 0 or 30deg 4-mm endoscope is helpful inbull the assessment of posterior abnormalities If thebull patient is heavily sedated Brown-Gruss
provocationbull manoeuvres may be performed to determinebull deformities in upper middle or lower segmentsbull by compressing each compartment
Nasal FracturesConservative treatmentndash Treatment of bleedingbull For localised bleeding anterior sources may becauterised by silver nitrate or sealed with topicalmaterials such as thrombin combined withgelatin foam fibrin glue FloSealreg or other procoagulantmaterials If conservative measuresfail a formal anterior packing is placedbull Bleeding from branches of sphenopalatine orethmoid vessels requires anterior-posteriorpacking
Nasal Fractures
bull bull Surgical methods such as direct endoscopic vessel
bull cauterization or ligation have been shown tobull offer better haemostasis and patient comfortbull Angiography with embolization can also be
consideredbull in cases refractory to more conservativebull approaches
Nasal Fractures
bull Type of reductionbull bull Nondisplaced fractures should be treated withbull observation alone Closed nasal reduction is thebull best choice for simple injuries (isolated unilateralbull with medial displacement)bull bull An open approach should be considered in
severebull trauma (bilateral depressed fractures)
Nasal Fracturesbull Surgical principlesbull ndash Topical anaesthesia with cotton pledgets soakedbull with 4 cocaine or 005 oxymethazoline combinedbull with 4 topical lidocaine should be appliedbull for 5ndash10 min Local anaesthesia should also be injectedbull (1 lidocaine and 1100000 epinephrine)bull along the septum lateral walls and floor of the nasalbull cavitybull bull
Nasal FracturesClosed reductionndashndash The nasal bones are grasped between two fingersand pressure is applied laterally in theopposite direction of the deviation A bluntelevator may be used from within the nose incases of significant medial collapse Walshamforceps can be of help Reduction of the septumshould be performed with the use ofAsch forceps
Nasal Fractures
bull To prevent collapse of the postreductionbull framework nasal packing should be placedbull for 3ndash5 days Septum splints are recommendedbull in comminuted septal fractures withbull severe mucosal lesions External nasal splintingbull for 10 days (Aquaplastreg Thermoplastreg)bull provides nasal protection Nasal saline spraysbull prevent crusting and oral antibiotics should
Nasal Fractures
bull Open reductionbull ndashndash Immediate repair of fractures by using
widebull surgical exposure reduction fixation and
reconstructionbull ndashndash The second option is delayed correctionbull (6 months or more) of persistent deformitiesbull using standard techniques of rhinoplasty
Deviated Nasal Septum
bull Definition of the diseasebull ndash Deviation of the nasal septum is a common causebull of unilateral nasal airway obstruction in which thebull nasal septum is displacedbull bull Epidemiologyaetiologybull ndash Developmental septal abnormalities Septal cartilage
damage in the neonatal period andbull during birth can cause severe septal deviation inbull the absence of a history of nasal trauma
Deviated Nasal Septum
bull Symptomsbull ndash Patients may present with a history of sinusitis
allergicbull rhinitis obstructive sleep apnoea previousbull nasal surgery or recent nasal trauma Unilateral or
bilateral nasal airway obstruction that is unrelievedbull with decongestants or nasal steroid sprays is oftenbull seenbull bull
Deviated Nasal SeptumDiagnosisndashExamination external dorsal deviation or the columella and caudal septummay be deflected off the midline (caudal subluxation)ndash Inspections of the nasal cavity and anterior-posteriorrhinoscopy are helpful in diagnosing the locationtype and severity of septal deformityThe endoscope is also useful in identifying polypsthe severity and extent of posterior septaldeviations and bony spurs and locating areas ofseptal perforation or mucosal injury
Deviated Nasal Septum
bull Therapybull ndash Septoplasty is a procedurebull The areabull of deviation is corrected or resected in order tobull leave behind as much cartilage and bone as
possiblebull Cartilage resection is minimised and can be
repositioned reshaped or recontoured using a variety of methods
Deviated Nasal Septum
bull ndash Indications of septoplasty before the growth period
bull of the nose is finished should be very limited bull -In these cases surgery must preserve all the
cartilagebull in order to prevent external changes of the
shape ofbull the nose
Deviated Nasal Septum
bull Complicationsbull ndash Frequent complications include haematoma andbull infection Cerebrospinal fluid leak is a rare but
potentiallybull serious complicationbull It is usually the resultbull of avulsion or damage to the cribriform plate whenbull handling the perpendicular plate of the ethmoidbull ndash Other complications include epistaxis nasal
Deviated Nasal Septum
bull Other complications include epistaxis nasal obstruction
bull due to residual deviation synechiae returnbull of the cartilaginous deviation septal perforationbull anosmia and cosmetic nasal deformities suchbull as widened alar rim margins drooping nasal tipbull columella retraction and a sunken dorsum with abull supratip saddle formation
Septal perforation with minor crusting View from provide closure of the
incision
Septal Haematoma
bull A septal haematoma is a blood collection under the perichondrium
bull of the septum and cartilagebull bull bull Epidemiologyaetiologybull ndash A septal haematoma is one of the most
severe complications of nasal trauma
Septal Haematoma
bull Diagnosisbull ndash Signs and symptoms include intense pain
swellingbull haematoma of the upper lip and philtrum
area andbull complete nasal airway obstruction
Septal HaematomaTherapyndash Management consists of drainage through a mucoperichondrial incision Immediate treatment isnecessary to prevent long-term problems such asa saddle-nose deformity perforation columellarretraction and nasal-base widening In childrenseptal destruction can lead to devastating nasal andmidfacial growth abnormalitiesbull Surgeryndash Incision and evacuation of the collection is performedDrainage of a septal haematoma should
Septal HaematomaSurgeryndash Incision and evacuation of the collection is performedDrainage of a septal haematoma should provide closure of the incision
Splints or transseptal sutures are placed to obliterate thepotential space and prevent collectionInfection involving the septal cartilage Reconstruction with autologouscartilage is then performed in a second stage Oral antibiotics should be given
Nasal DeformitySaddle-nose deformityndash A saddle-nose deformity is characterised by a loss ofnasal dorsal height and compromised nasal supportstructures -Other case observed are depressionof the middle vault and dorsum loss of nasal tipsupport and definition shortened (vertical) nasal length over rotation of the nasal tip and retrusion ofthe nasal spine and caudal septum It is also knownas a ldquoPug noserdquo or ldquoboxerrsquos noserdquo both of which referto various degrees of nasal dorsal depressionbull
Nasal DeformityEpidemiologyaetiologyndash Prevalence is higher in population groups prone to facial trauma (ie boxers athletes) those with historiesof intranasal cocaine use nasal surgery (e g radical submucosal septal resection reductive rhinoplasty)ndash A saddle-nose deformity can be congenital or acquired It can be noticed as a part of individual familialsyndromic and ethnic characteristics - Most deformities are due to traumatic and iatrogeniccauses Medical causes are Wegenerrsquosgranulomatosis relapsing polychondritis leprosy (Hansenrsquos disease) syphilis ectodermal dysplasiaand intranasal cocaine use
Nasal Deformity
bull Therapybull ndash Nasal reconstruction indications depend on patientbull selection surgeon experience and aetiology of thebull deformity bull Indications for surgery can be functionalbull aesthetic or most commonly both In individuals
with a compromised nasal airway a nasoseptalbull reconstruction is indicated
Nasal Deformity
bull Contraindications bull include patients with malignantbull chronic or autoimmune disease conditions drugbull abuse poor perioperative risk profile and unrealisticbull expectationsbull ndash Multiple previous rhinoplasties and certain
professionsbull (mixed martial artists boxers and other contactbull sports) are relative contraindications
Nasal DeformitySeptoplastyndash Septoplasty is performed to correct nasal obstructioncaused by septal deformityndash Usually septoplasty is performed under general anaesthesiawith the patient in the supine position with the head elevated by approximately 30 (Righthandedsurgeons approach from the right side)ndash Local vasoconstrictive anaesthesia is applied notonly to reduce postoperative pain but also more importantly to achieve vasoconstriction of themucosa and less intraoperative haemorrhage Lidocainewith adrenaline or epinephrine is usedalthough in patients with cardiac hypersensitivityoxymetazoline might be preferred
Nasal Deformity
bull Septoplasty begins with the incision of septal mucosabull Most operative techniques utilise a hemitransfixionbull incision at the caudal end of septum so thatbull deviation at this point might be reached as wellbull as a transfixion incision that is easily obtained ifbull needed (Right-handed surgeons normally choosebull the left side but that may vary when deviation isbull convex towards the right)
Nasal DeformityA columella retractor is placed over the columellaand by pulling it laterally the caudal border of theseptum is exposed Ala can be protected by an alaprotector A vertical incision with a no 15 bladeover the caudal end of septum is performed untilreaching the plane of the septal cartilage It is essentialto correctly identify the perichondrium and byusing the Cottle elevator dissect and lift it creatinga flap As the dissection proceeds along the septalcartilage a longer speculum (no 5) is introduced sothat elevation of the mucoperichondrium is doneunder constant visual controlndash The next step is to dissect the mucoperiostium
Nasal DeformityDissecting over the bony-cartilaginous junctionwhen joining both tunnels might be difficult and is
especially prone to membrane perforationndash If needed the same tunnels are to be created on the
other side of the septum Then deviated parts of
septum are identified and removed either with a
knife or a Freer chisel
Nasal Deformitybull septum from the maxillary crest the septum mustbull be separated from the perpendicular plate trimmedbull along the inferior border placed back onto the crestbull and sutured to the periosteum If the deformity involvesbull the vomer an osteotome is used Care mustbull be taken not to break the cribriform plate becausebull it could cause a cerebrospinal fistula
Nasal Deformity
bull Once the septal deviation is corrected the flapsbull and hemitransfixion incision are mattressed
withbull absorbable sutures Nasal packing to prevent
synechiaebull and postoperative septal haematoma mightbull be advised but should be removed within 72 h

Wegenerrsquos Granulomatosis
bull Prognosisbull ndash Most of the patients respond well to treatmentbull achieving symptom-free intervals of 5ndash20 yearsbull or more bull -Anatomical problems (sinusitis trachealbull stenosis) may require surgery bull Relapses can be long and troublesomebull Long-term complications are chronicbull renal failure hearing loss and deafness
Nasal Fractures Definition ndash A nasal fracture is a disruption of the nasal bone structure due to trauma It is the most frequently fractured facial bone Epidemiologyaetiology ndash Sports falls and assaults are the usual mechanisms of fracture -Males are affected twice as often as are females -Paediatric populations with a incidences during the second and third decades of life -Variables such as force impact direction nature of the striking object age and other will influence the pattern of injury to the components of the nose
Nasal Fractures
bull Symptomsbull ndash Deformity swelling epistaxis and periorbital
ecchymosis are signs that are suggestive of nasal fracture
bull bony crepitus and nasal segment mobilitybull ndash Epiphora bull Severe bilateral injuries to the lachrymal bones
arebull associated with depressed nasal fractures
Nasal Fractures Complications ndash Septal haematoma is one of the most severe early complications of nasal trauma and without drainage it results in abscess formation 6ndash7 days after trauma producing necrosis of the septal cartilage -Long-term problems such as saddle-nose deformity perforation columellar retraction and nasalbase
Septal infection could lead to osteomyelitis orbital and intracranial abscesses meningitis and cavernous sinus thrombosis -Cerebrospinal fluid leakage is a common complication of severe
nasal and frontal fractures
Nasal Fractures
bull Diagnostic proceduresbull ndash Inspectionbull bull Changes of appearance such as deviation andbull asymmetry bleeding watery drainage changesbull in nasal breathing and smell It is useful to comparebull the current presentation with old photographsbull (up to 40 of normal individuals havebull significant nose malformations)
Nasal Fractures Physical examination bull The diagnosis of a nasal fracture is made primarily by physical examination epistaxis nasal swelling and periorbital ecchymosis Nasal shape in the lateral and frontal inspection should be assessed Grasping the dorsum between two fingers and rocking the pyramid back and forth aids in assessing the mobility of nasal bones Internal structures should be evaluated by using a headlight and nasal speculum Clotted blood is removed by suction and assessment of haematoma mucosal tears and active bleeding is performed Bimanual palpation of the septum helps to differentiate septal swelling from haematoma ndash
Nasal FracturesRadiographybull There is no clear evidence of the role of radiographyin the management of nasal fracturesPlain films have up to a 66 false-positive rateas a result of misinterpretation of normal suturelines In addition old fractures are difficult todistinguishbull Three-dimensional CT is recommended for extensiveinjuries involving the nasal-orbital-ethmoidalcomplexndash
Nasal Fractures
bull Additionaluseful diagnostic proceduresbull bull Using a 0 or 30deg 4-mm endoscope is helpful inbull the assessment of posterior abnormalities If thebull patient is heavily sedated Brown-Gruss
provocationbull manoeuvres may be performed to determinebull deformities in upper middle or lower segmentsbull by compressing each compartment
Nasal FracturesConservative treatmentndash Treatment of bleedingbull For localised bleeding anterior sources may becauterised by silver nitrate or sealed with topicalmaterials such as thrombin combined withgelatin foam fibrin glue FloSealreg or other procoagulantmaterials If conservative measuresfail a formal anterior packing is placedbull Bleeding from branches of sphenopalatine orethmoid vessels requires anterior-posteriorpacking
Nasal Fractures
bull bull Surgical methods such as direct endoscopic vessel
bull cauterization or ligation have been shown tobull offer better haemostasis and patient comfortbull Angiography with embolization can also be
consideredbull in cases refractory to more conservativebull approaches
Nasal Fractures
bull Type of reductionbull bull Nondisplaced fractures should be treated withbull observation alone Closed nasal reduction is thebull best choice for simple injuries (isolated unilateralbull with medial displacement)bull bull An open approach should be considered in
severebull trauma (bilateral depressed fractures)
Nasal Fracturesbull Surgical principlesbull ndash Topical anaesthesia with cotton pledgets soakedbull with 4 cocaine or 005 oxymethazoline combinedbull with 4 topical lidocaine should be appliedbull for 5ndash10 min Local anaesthesia should also be injectedbull (1 lidocaine and 1100000 epinephrine)bull along the septum lateral walls and floor of the nasalbull cavitybull bull
Nasal FracturesClosed reductionndashndash The nasal bones are grasped between two fingersand pressure is applied laterally in theopposite direction of the deviation A bluntelevator may be used from within the nose incases of significant medial collapse Walshamforceps can be of help Reduction of the septumshould be performed with the use ofAsch forceps
Nasal Fractures
bull To prevent collapse of the postreductionbull framework nasal packing should be placedbull for 3ndash5 days Septum splints are recommendedbull in comminuted septal fractures withbull severe mucosal lesions External nasal splintingbull for 10 days (Aquaplastreg Thermoplastreg)bull provides nasal protection Nasal saline spraysbull prevent crusting and oral antibiotics should
Nasal Fractures
bull Open reductionbull ndashndash Immediate repair of fractures by using
widebull surgical exposure reduction fixation and
reconstructionbull ndashndash The second option is delayed correctionbull (6 months or more) of persistent deformitiesbull using standard techniques of rhinoplasty
Deviated Nasal Septum
bull Definition of the diseasebull ndash Deviation of the nasal septum is a common causebull of unilateral nasal airway obstruction in which thebull nasal septum is displacedbull bull Epidemiologyaetiologybull ndash Developmental septal abnormalities Septal cartilage
damage in the neonatal period andbull during birth can cause severe septal deviation inbull the absence of a history of nasal trauma
Deviated Nasal Septum
bull Symptomsbull ndash Patients may present with a history of sinusitis
allergicbull rhinitis obstructive sleep apnoea previousbull nasal surgery or recent nasal trauma Unilateral or
bilateral nasal airway obstruction that is unrelievedbull with decongestants or nasal steroid sprays is oftenbull seenbull bull
Deviated Nasal SeptumDiagnosisndashExamination external dorsal deviation or the columella and caudal septummay be deflected off the midline (caudal subluxation)ndash Inspections of the nasal cavity and anterior-posteriorrhinoscopy are helpful in diagnosing the locationtype and severity of septal deformityThe endoscope is also useful in identifying polypsthe severity and extent of posterior septaldeviations and bony spurs and locating areas ofseptal perforation or mucosal injury
Deviated Nasal Septum
bull Therapybull ndash Septoplasty is a procedurebull The areabull of deviation is corrected or resected in order tobull leave behind as much cartilage and bone as
possiblebull Cartilage resection is minimised and can be
repositioned reshaped or recontoured using a variety of methods
Deviated Nasal Septum
bull ndash Indications of septoplasty before the growth period
bull of the nose is finished should be very limited bull -In these cases surgery must preserve all the
cartilagebull in order to prevent external changes of the
shape ofbull the nose
Deviated Nasal Septum
bull Complicationsbull ndash Frequent complications include haematoma andbull infection Cerebrospinal fluid leak is a rare but
potentiallybull serious complicationbull It is usually the resultbull of avulsion or damage to the cribriform plate whenbull handling the perpendicular plate of the ethmoidbull ndash Other complications include epistaxis nasal
Deviated Nasal Septum
bull Other complications include epistaxis nasal obstruction
bull due to residual deviation synechiae returnbull of the cartilaginous deviation septal perforationbull anosmia and cosmetic nasal deformities suchbull as widened alar rim margins drooping nasal tipbull columella retraction and a sunken dorsum with abull supratip saddle formation
Septal perforation with minor crusting View from provide closure of the
incision
Septal Haematoma
bull A septal haematoma is a blood collection under the perichondrium
bull of the septum and cartilagebull bull bull Epidemiologyaetiologybull ndash A septal haematoma is one of the most
severe complications of nasal trauma
Septal Haematoma
bull Diagnosisbull ndash Signs and symptoms include intense pain
swellingbull haematoma of the upper lip and philtrum
area andbull complete nasal airway obstruction
Septal HaematomaTherapyndash Management consists of drainage through a mucoperichondrial incision Immediate treatment isnecessary to prevent long-term problems such asa saddle-nose deformity perforation columellarretraction and nasal-base widening In childrenseptal destruction can lead to devastating nasal andmidfacial growth abnormalitiesbull Surgeryndash Incision and evacuation of the collection is performedDrainage of a septal haematoma should
Septal HaematomaSurgeryndash Incision and evacuation of the collection is performedDrainage of a septal haematoma should provide closure of the incision
Splints or transseptal sutures are placed to obliterate thepotential space and prevent collectionInfection involving the septal cartilage Reconstruction with autologouscartilage is then performed in a second stage Oral antibiotics should be given
Nasal DeformitySaddle-nose deformityndash A saddle-nose deformity is characterised by a loss ofnasal dorsal height and compromised nasal supportstructures -Other case observed are depressionof the middle vault and dorsum loss of nasal tipsupport and definition shortened (vertical) nasal length over rotation of the nasal tip and retrusion ofthe nasal spine and caudal septum It is also knownas a ldquoPug noserdquo or ldquoboxerrsquos noserdquo both of which referto various degrees of nasal dorsal depressionbull
Nasal DeformityEpidemiologyaetiologyndash Prevalence is higher in population groups prone to facial trauma (ie boxers athletes) those with historiesof intranasal cocaine use nasal surgery (e g radical submucosal septal resection reductive rhinoplasty)ndash A saddle-nose deformity can be congenital or acquired It can be noticed as a part of individual familialsyndromic and ethnic characteristics - Most deformities are due to traumatic and iatrogeniccauses Medical causes are Wegenerrsquosgranulomatosis relapsing polychondritis leprosy (Hansenrsquos disease) syphilis ectodermal dysplasiaand intranasal cocaine use
Nasal Deformity
bull Therapybull ndash Nasal reconstruction indications depend on patientbull selection surgeon experience and aetiology of thebull deformity bull Indications for surgery can be functionalbull aesthetic or most commonly both In individuals
with a compromised nasal airway a nasoseptalbull reconstruction is indicated
Nasal Deformity
bull Contraindications bull include patients with malignantbull chronic or autoimmune disease conditions drugbull abuse poor perioperative risk profile and unrealisticbull expectationsbull ndash Multiple previous rhinoplasties and certain
professionsbull (mixed martial artists boxers and other contactbull sports) are relative contraindications
Nasal DeformitySeptoplastyndash Septoplasty is performed to correct nasal obstructioncaused by septal deformityndash Usually septoplasty is performed under general anaesthesiawith the patient in the supine position with the head elevated by approximately 30 (Righthandedsurgeons approach from the right side)ndash Local vasoconstrictive anaesthesia is applied notonly to reduce postoperative pain but also more importantly to achieve vasoconstriction of themucosa and less intraoperative haemorrhage Lidocainewith adrenaline or epinephrine is usedalthough in patients with cardiac hypersensitivityoxymetazoline might be preferred
Nasal Deformity
bull Septoplasty begins with the incision of septal mucosabull Most operative techniques utilise a hemitransfixionbull incision at the caudal end of septum so thatbull deviation at this point might be reached as wellbull as a transfixion incision that is easily obtained ifbull needed (Right-handed surgeons normally choosebull the left side but that may vary when deviation isbull convex towards the right)
Nasal DeformityA columella retractor is placed over the columellaand by pulling it laterally the caudal border of theseptum is exposed Ala can be protected by an alaprotector A vertical incision with a no 15 bladeover the caudal end of septum is performed untilreaching the plane of the septal cartilage It is essentialto correctly identify the perichondrium and byusing the Cottle elevator dissect and lift it creatinga flap As the dissection proceeds along the septalcartilage a longer speculum (no 5) is introduced sothat elevation of the mucoperichondrium is doneunder constant visual controlndash The next step is to dissect the mucoperiostium
Nasal DeformityDissecting over the bony-cartilaginous junctionwhen joining both tunnels might be difficult and is
especially prone to membrane perforationndash If needed the same tunnels are to be created on the
other side of the septum Then deviated parts of
septum are identified and removed either with a
knife or a Freer chisel
Nasal Deformitybull septum from the maxillary crest the septum mustbull be separated from the perpendicular plate trimmedbull along the inferior border placed back onto the crestbull and sutured to the periosteum If the deformity involvesbull the vomer an osteotome is used Care mustbull be taken not to break the cribriform plate becausebull it could cause a cerebrospinal fistula
Nasal Deformity
bull Once the septal deviation is corrected the flapsbull and hemitransfixion incision are mattressed
withbull absorbable sutures Nasal packing to prevent
synechiaebull and postoperative septal haematoma mightbull be advised but should be removed within 72 h

Nasal Fractures Definition ndash A nasal fracture is a disruption of the nasal bone structure due to trauma It is the most frequently fractured facial bone Epidemiologyaetiology ndash Sports falls and assaults are the usual mechanisms of fracture -Males are affected twice as often as are females -Paediatric populations with a incidences during the second and third decades of life -Variables such as force impact direction nature of the striking object age and other will influence the pattern of injury to the components of the nose
Nasal Fractures
bull Symptomsbull ndash Deformity swelling epistaxis and periorbital
ecchymosis are signs that are suggestive of nasal fracture
bull bony crepitus and nasal segment mobilitybull ndash Epiphora bull Severe bilateral injuries to the lachrymal bones
arebull associated with depressed nasal fractures
Nasal Fractures Complications ndash Septal haematoma is one of the most severe early complications of nasal trauma and without drainage it results in abscess formation 6ndash7 days after trauma producing necrosis of the septal cartilage -Long-term problems such as saddle-nose deformity perforation columellar retraction and nasalbase
Septal infection could lead to osteomyelitis orbital and intracranial abscesses meningitis and cavernous sinus thrombosis -Cerebrospinal fluid leakage is a common complication of severe
nasal and frontal fractures
Nasal Fractures
bull Diagnostic proceduresbull ndash Inspectionbull bull Changes of appearance such as deviation andbull asymmetry bleeding watery drainage changesbull in nasal breathing and smell It is useful to comparebull the current presentation with old photographsbull (up to 40 of normal individuals havebull significant nose malformations)
Nasal Fractures Physical examination bull The diagnosis of a nasal fracture is made primarily by physical examination epistaxis nasal swelling and periorbital ecchymosis Nasal shape in the lateral and frontal inspection should be assessed Grasping the dorsum between two fingers and rocking the pyramid back and forth aids in assessing the mobility of nasal bones Internal structures should be evaluated by using a headlight and nasal speculum Clotted blood is removed by suction and assessment of haematoma mucosal tears and active bleeding is performed Bimanual palpation of the septum helps to differentiate septal swelling from haematoma ndash
Nasal FracturesRadiographybull There is no clear evidence of the role of radiographyin the management of nasal fracturesPlain films have up to a 66 false-positive rateas a result of misinterpretation of normal suturelines In addition old fractures are difficult todistinguishbull Three-dimensional CT is recommended for extensiveinjuries involving the nasal-orbital-ethmoidalcomplexndash
Nasal Fractures
bull Additionaluseful diagnostic proceduresbull bull Using a 0 or 30deg 4-mm endoscope is helpful inbull the assessment of posterior abnormalities If thebull patient is heavily sedated Brown-Gruss
provocationbull manoeuvres may be performed to determinebull deformities in upper middle or lower segmentsbull by compressing each compartment
Nasal FracturesConservative treatmentndash Treatment of bleedingbull For localised bleeding anterior sources may becauterised by silver nitrate or sealed with topicalmaterials such as thrombin combined withgelatin foam fibrin glue FloSealreg or other procoagulantmaterials If conservative measuresfail a formal anterior packing is placedbull Bleeding from branches of sphenopalatine orethmoid vessels requires anterior-posteriorpacking
Nasal Fractures
bull bull Surgical methods such as direct endoscopic vessel
bull cauterization or ligation have been shown tobull offer better haemostasis and patient comfortbull Angiography with embolization can also be
consideredbull in cases refractory to more conservativebull approaches
Nasal Fractures
bull Type of reductionbull bull Nondisplaced fractures should be treated withbull observation alone Closed nasal reduction is thebull best choice for simple injuries (isolated unilateralbull with medial displacement)bull bull An open approach should be considered in
severebull trauma (bilateral depressed fractures)
Nasal Fracturesbull Surgical principlesbull ndash Topical anaesthesia with cotton pledgets soakedbull with 4 cocaine or 005 oxymethazoline combinedbull with 4 topical lidocaine should be appliedbull for 5ndash10 min Local anaesthesia should also be injectedbull (1 lidocaine and 1100000 epinephrine)bull along the septum lateral walls and floor of the nasalbull cavitybull bull
Nasal FracturesClosed reductionndashndash The nasal bones are grasped between two fingersand pressure is applied laterally in theopposite direction of the deviation A bluntelevator may be used from within the nose incases of significant medial collapse Walshamforceps can be of help Reduction of the septumshould be performed with the use ofAsch forceps
Nasal Fractures
bull To prevent collapse of the postreductionbull framework nasal packing should be placedbull for 3ndash5 days Septum splints are recommendedbull in comminuted septal fractures withbull severe mucosal lesions External nasal splintingbull for 10 days (Aquaplastreg Thermoplastreg)bull provides nasal protection Nasal saline spraysbull prevent crusting and oral antibiotics should
Nasal Fractures
bull Open reductionbull ndashndash Immediate repair of fractures by using
widebull surgical exposure reduction fixation and
reconstructionbull ndashndash The second option is delayed correctionbull (6 months or more) of persistent deformitiesbull using standard techniques of rhinoplasty
Deviated Nasal Septum
bull Definition of the diseasebull ndash Deviation of the nasal septum is a common causebull of unilateral nasal airway obstruction in which thebull nasal septum is displacedbull bull Epidemiologyaetiologybull ndash Developmental septal abnormalities Septal cartilage
damage in the neonatal period andbull during birth can cause severe septal deviation inbull the absence of a history of nasal trauma
Deviated Nasal Septum
bull Symptomsbull ndash Patients may present with a history of sinusitis
allergicbull rhinitis obstructive sleep apnoea previousbull nasal surgery or recent nasal trauma Unilateral or
bilateral nasal airway obstruction that is unrelievedbull with decongestants or nasal steroid sprays is oftenbull seenbull bull
Deviated Nasal SeptumDiagnosisndashExamination external dorsal deviation or the columella and caudal septummay be deflected off the midline (caudal subluxation)ndash Inspections of the nasal cavity and anterior-posteriorrhinoscopy are helpful in diagnosing the locationtype and severity of septal deformityThe endoscope is also useful in identifying polypsthe severity and extent of posterior septaldeviations and bony spurs and locating areas ofseptal perforation or mucosal injury
Deviated Nasal Septum
bull Therapybull ndash Septoplasty is a procedurebull The areabull of deviation is corrected or resected in order tobull leave behind as much cartilage and bone as
possiblebull Cartilage resection is minimised and can be
repositioned reshaped or recontoured using a variety of methods
Deviated Nasal Septum
bull ndash Indications of septoplasty before the growth period
bull of the nose is finished should be very limited bull -In these cases surgery must preserve all the
cartilagebull in order to prevent external changes of the
shape ofbull the nose
Deviated Nasal Septum
bull Complicationsbull ndash Frequent complications include haematoma andbull infection Cerebrospinal fluid leak is a rare but
potentiallybull serious complicationbull It is usually the resultbull of avulsion or damage to the cribriform plate whenbull handling the perpendicular plate of the ethmoidbull ndash Other complications include epistaxis nasal
Deviated Nasal Septum
bull Other complications include epistaxis nasal obstruction
bull due to residual deviation synechiae returnbull of the cartilaginous deviation septal perforationbull anosmia and cosmetic nasal deformities suchbull as widened alar rim margins drooping nasal tipbull columella retraction and a sunken dorsum with abull supratip saddle formation
Septal perforation with minor crusting View from provide closure of the
incision
Septal Haematoma
bull A septal haematoma is a blood collection under the perichondrium
bull of the septum and cartilagebull bull bull Epidemiologyaetiologybull ndash A septal haematoma is one of the most
severe complications of nasal trauma
Septal Haematoma
bull Diagnosisbull ndash Signs and symptoms include intense pain
swellingbull haematoma of the upper lip and philtrum
area andbull complete nasal airway obstruction
Septal HaematomaTherapyndash Management consists of drainage through a mucoperichondrial incision Immediate treatment isnecessary to prevent long-term problems such asa saddle-nose deformity perforation columellarretraction and nasal-base widening In childrenseptal destruction can lead to devastating nasal andmidfacial growth abnormalitiesbull Surgeryndash Incision and evacuation of the collection is performedDrainage of a septal haematoma should
Septal HaematomaSurgeryndash Incision and evacuation of the collection is performedDrainage of a septal haematoma should provide closure of the incision
Splints or transseptal sutures are placed to obliterate thepotential space and prevent collectionInfection involving the septal cartilage Reconstruction with autologouscartilage is then performed in a second stage Oral antibiotics should be given
Nasal DeformitySaddle-nose deformityndash A saddle-nose deformity is characterised by a loss ofnasal dorsal height and compromised nasal supportstructures -Other case observed are depressionof the middle vault and dorsum loss of nasal tipsupport and definition shortened (vertical) nasal length over rotation of the nasal tip and retrusion ofthe nasal spine and caudal septum It is also knownas a ldquoPug noserdquo or ldquoboxerrsquos noserdquo both of which referto various degrees of nasal dorsal depressionbull
Nasal DeformityEpidemiologyaetiologyndash Prevalence is higher in population groups prone to facial trauma (ie boxers athletes) those with historiesof intranasal cocaine use nasal surgery (e g radical submucosal septal resection reductive rhinoplasty)ndash A saddle-nose deformity can be congenital or acquired It can be noticed as a part of individual familialsyndromic and ethnic characteristics - Most deformities are due to traumatic and iatrogeniccauses Medical causes are Wegenerrsquosgranulomatosis relapsing polychondritis leprosy (Hansenrsquos disease) syphilis ectodermal dysplasiaand intranasal cocaine use
Nasal Deformity
bull Therapybull ndash Nasal reconstruction indications depend on patientbull selection surgeon experience and aetiology of thebull deformity bull Indications for surgery can be functionalbull aesthetic or most commonly both In individuals
with a compromised nasal airway a nasoseptalbull reconstruction is indicated
Nasal Deformity
bull Contraindications bull include patients with malignantbull chronic or autoimmune disease conditions drugbull abuse poor perioperative risk profile and unrealisticbull expectationsbull ndash Multiple previous rhinoplasties and certain
professionsbull (mixed martial artists boxers and other contactbull sports) are relative contraindications
Nasal DeformitySeptoplastyndash Septoplasty is performed to correct nasal obstructioncaused by septal deformityndash Usually septoplasty is performed under general anaesthesiawith the patient in the supine position with the head elevated by approximately 30 (Righthandedsurgeons approach from the right side)ndash Local vasoconstrictive anaesthesia is applied notonly to reduce postoperative pain but also more importantly to achieve vasoconstriction of themucosa and less intraoperative haemorrhage Lidocainewith adrenaline or epinephrine is usedalthough in patients with cardiac hypersensitivityoxymetazoline might be preferred
Nasal Deformity
bull Septoplasty begins with the incision of septal mucosabull Most operative techniques utilise a hemitransfixionbull incision at the caudal end of septum so thatbull deviation at this point might be reached as wellbull as a transfixion incision that is easily obtained ifbull needed (Right-handed surgeons normally choosebull the left side but that may vary when deviation isbull convex towards the right)
Nasal DeformityA columella retractor is placed over the columellaand by pulling it laterally the caudal border of theseptum is exposed Ala can be protected by an alaprotector A vertical incision with a no 15 bladeover the caudal end of septum is performed untilreaching the plane of the septal cartilage It is essentialto correctly identify the perichondrium and byusing the Cottle elevator dissect and lift it creatinga flap As the dissection proceeds along the septalcartilage a longer speculum (no 5) is introduced sothat elevation of the mucoperichondrium is doneunder constant visual controlndash The next step is to dissect the mucoperiostium
Nasal DeformityDissecting over the bony-cartilaginous junctionwhen joining both tunnels might be difficult and is
especially prone to membrane perforationndash If needed the same tunnels are to be created on the
other side of the septum Then deviated parts of
septum are identified and removed either with a
knife or a Freer chisel
Nasal Deformitybull septum from the maxillary crest the septum mustbull be separated from the perpendicular plate trimmedbull along the inferior border placed back onto the crestbull and sutured to the periosteum If the deformity involvesbull the vomer an osteotome is used Care mustbull be taken not to break the cribriform plate becausebull it could cause a cerebrospinal fistula
Nasal Deformity
bull Once the septal deviation is corrected the flapsbull and hemitransfixion incision are mattressed
withbull absorbable sutures Nasal packing to prevent
synechiaebull and postoperative septal haematoma mightbull be advised but should be removed within 72 h

Nasal Fractures
bull Symptomsbull ndash Deformity swelling epistaxis and periorbital
ecchymosis are signs that are suggestive of nasal fracture
bull bony crepitus and nasal segment mobilitybull ndash Epiphora bull Severe bilateral injuries to the lachrymal bones
arebull associated with depressed nasal fractures
Nasal Fractures Complications ndash Septal haematoma is one of the most severe early complications of nasal trauma and without drainage it results in abscess formation 6ndash7 days after trauma producing necrosis of the septal cartilage -Long-term problems such as saddle-nose deformity perforation columellar retraction and nasalbase
Septal infection could lead to osteomyelitis orbital and intracranial abscesses meningitis and cavernous sinus thrombosis -Cerebrospinal fluid leakage is a common complication of severe
nasal and frontal fractures
Nasal Fractures
bull Diagnostic proceduresbull ndash Inspectionbull bull Changes of appearance such as deviation andbull asymmetry bleeding watery drainage changesbull in nasal breathing and smell It is useful to comparebull the current presentation with old photographsbull (up to 40 of normal individuals havebull significant nose malformations)
Nasal Fractures Physical examination bull The diagnosis of a nasal fracture is made primarily by physical examination epistaxis nasal swelling and periorbital ecchymosis Nasal shape in the lateral and frontal inspection should be assessed Grasping the dorsum between two fingers and rocking the pyramid back and forth aids in assessing the mobility of nasal bones Internal structures should be evaluated by using a headlight and nasal speculum Clotted blood is removed by suction and assessment of haematoma mucosal tears and active bleeding is performed Bimanual palpation of the septum helps to differentiate septal swelling from haematoma ndash
Nasal FracturesRadiographybull There is no clear evidence of the role of radiographyin the management of nasal fracturesPlain films have up to a 66 false-positive rateas a result of misinterpretation of normal suturelines In addition old fractures are difficult todistinguishbull Three-dimensional CT is recommended for extensiveinjuries involving the nasal-orbital-ethmoidalcomplexndash
Nasal Fractures
bull Additionaluseful diagnostic proceduresbull bull Using a 0 or 30deg 4-mm endoscope is helpful inbull the assessment of posterior abnormalities If thebull patient is heavily sedated Brown-Gruss
provocationbull manoeuvres may be performed to determinebull deformities in upper middle or lower segmentsbull by compressing each compartment
Nasal FracturesConservative treatmentndash Treatment of bleedingbull For localised bleeding anterior sources may becauterised by silver nitrate or sealed with topicalmaterials such as thrombin combined withgelatin foam fibrin glue FloSealreg or other procoagulantmaterials If conservative measuresfail a formal anterior packing is placedbull Bleeding from branches of sphenopalatine orethmoid vessels requires anterior-posteriorpacking
Nasal Fractures
bull bull Surgical methods such as direct endoscopic vessel
bull cauterization or ligation have been shown tobull offer better haemostasis and patient comfortbull Angiography with embolization can also be
consideredbull in cases refractory to more conservativebull approaches
Nasal Fractures
bull Type of reductionbull bull Nondisplaced fractures should be treated withbull observation alone Closed nasal reduction is thebull best choice for simple injuries (isolated unilateralbull with medial displacement)bull bull An open approach should be considered in
severebull trauma (bilateral depressed fractures)
Nasal Fracturesbull Surgical principlesbull ndash Topical anaesthesia with cotton pledgets soakedbull with 4 cocaine or 005 oxymethazoline combinedbull with 4 topical lidocaine should be appliedbull for 5ndash10 min Local anaesthesia should also be injectedbull (1 lidocaine and 1100000 epinephrine)bull along the septum lateral walls and floor of the nasalbull cavitybull bull
Nasal FracturesClosed reductionndashndash The nasal bones are grasped between two fingersand pressure is applied laterally in theopposite direction of the deviation A bluntelevator may be used from within the nose incases of significant medial collapse Walshamforceps can be of help Reduction of the septumshould be performed with the use ofAsch forceps
Nasal Fractures
bull To prevent collapse of the postreductionbull framework nasal packing should be placedbull for 3ndash5 days Septum splints are recommendedbull in comminuted septal fractures withbull severe mucosal lesions External nasal splintingbull for 10 days (Aquaplastreg Thermoplastreg)bull provides nasal protection Nasal saline spraysbull prevent crusting and oral antibiotics should
Nasal Fractures
bull Open reductionbull ndashndash Immediate repair of fractures by using
widebull surgical exposure reduction fixation and
reconstructionbull ndashndash The second option is delayed correctionbull (6 months or more) of persistent deformitiesbull using standard techniques of rhinoplasty
Deviated Nasal Septum
bull Definition of the diseasebull ndash Deviation of the nasal septum is a common causebull of unilateral nasal airway obstruction in which thebull nasal septum is displacedbull bull Epidemiologyaetiologybull ndash Developmental septal abnormalities Septal cartilage
damage in the neonatal period andbull during birth can cause severe septal deviation inbull the absence of a history of nasal trauma
Deviated Nasal Septum
bull Symptomsbull ndash Patients may present with a history of sinusitis
allergicbull rhinitis obstructive sleep apnoea previousbull nasal surgery or recent nasal trauma Unilateral or
bilateral nasal airway obstruction that is unrelievedbull with decongestants or nasal steroid sprays is oftenbull seenbull bull
Deviated Nasal SeptumDiagnosisndashExamination external dorsal deviation or the columella and caudal septummay be deflected off the midline (caudal subluxation)ndash Inspections of the nasal cavity and anterior-posteriorrhinoscopy are helpful in diagnosing the locationtype and severity of septal deformityThe endoscope is also useful in identifying polypsthe severity and extent of posterior septaldeviations and bony spurs and locating areas ofseptal perforation or mucosal injury
Deviated Nasal Septum
bull Therapybull ndash Septoplasty is a procedurebull The areabull of deviation is corrected or resected in order tobull leave behind as much cartilage and bone as
possiblebull Cartilage resection is minimised and can be
repositioned reshaped or recontoured using a variety of methods
Deviated Nasal Septum
bull ndash Indications of septoplasty before the growth period
bull of the nose is finished should be very limited bull -In these cases surgery must preserve all the
cartilagebull in order to prevent external changes of the
shape ofbull the nose
Deviated Nasal Septum
bull Complicationsbull ndash Frequent complications include haematoma andbull infection Cerebrospinal fluid leak is a rare but
potentiallybull serious complicationbull It is usually the resultbull of avulsion or damage to the cribriform plate whenbull handling the perpendicular plate of the ethmoidbull ndash Other complications include epistaxis nasal
Deviated Nasal Septum
bull Other complications include epistaxis nasal obstruction
bull due to residual deviation synechiae returnbull of the cartilaginous deviation septal perforationbull anosmia and cosmetic nasal deformities suchbull as widened alar rim margins drooping nasal tipbull columella retraction and a sunken dorsum with abull supratip saddle formation
Septal perforation with minor crusting View from provide closure of the
incision
Septal Haematoma
bull A septal haematoma is a blood collection under the perichondrium
bull of the septum and cartilagebull bull bull Epidemiologyaetiologybull ndash A septal haematoma is one of the most
severe complications of nasal trauma
Septal Haematoma
bull Diagnosisbull ndash Signs and symptoms include intense pain
swellingbull haematoma of the upper lip and philtrum
area andbull complete nasal airway obstruction
Septal HaematomaTherapyndash Management consists of drainage through a mucoperichondrial incision Immediate treatment isnecessary to prevent long-term problems such asa saddle-nose deformity perforation columellarretraction and nasal-base widening In childrenseptal destruction can lead to devastating nasal andmidfacial growth abnormalitiesbull Surgeryndash Incision and evacuation of the collection is performedDrainage of a septal haematoma should
Septal HaematomaSurgeryndash Incision and evacuation of the collection is performedDrainage of a septal haematoma should provide closure of the incision
Splints or transseptal sutures are placed to obliterate thepotential space and prevent collectionInfection involving the septal cartilage Reconstruction with autologouscartilage is then performed in a second stage Oral antibiotics should be given
Nasal DeformitySaddle-nose deformityndash A saddle-nose deformity is characterised by a loss ofnasal dorsal height and compromised nasal supportstructures -Other case observed are depressionof the middle vault and dorsum loss of nasal tipsupport and definition shortened (vertical) nasal length over rotation of the nasal tip and retrusion ofthe nasal spine and caudal septum It is also knownas a ldquoPug noserdquo or ldquoboxerrsquos noserdquo both of which referto various degrees of nasal dorsal depressionbull
Nasal DeformityEpidemiologyaetiologyndash Prevalence is higher in population groups prone to facial trauma (ie boxers athletes) those with historiesof intranasal cocaine use nasal surgery (e g radical submucosal septal resection reductive rhinoplasty)ndash A saddle-nose deformity can be congenital or acquired It can be noticed as a part of individual familialsyndromic and ethnic characteristics - Most deformities are due to traumatic and iatrogeniccauses Medical causes are Wegenerrsquosgranulomatosis relapsing polychondritis leprosy (Hansenrsquos disease) syphilis ectodermal dysplasiaand intranasal cocaine use
Nasal Deformity
bull Therapybull ndash Nasal reconstruction indications depend on patientbull selection surgeon experience and aetiology of thebull deformity bull Indications for surgery can be functionalbull aesthetic or most commonly both In individuals
with a compromised nasal airway a nasoseptalbull reconstruction is indicated
Nasal Deformity
bull Contraindications bull include patients with malignantbull chronic or autoimmune disease conditions drugbull abuse poor perioperative risk profile and unrealisticbull expectationsbull ndash Multiple previous rhinoplasties and certain
professionsbull (mixed martial artists boxers and other contactbull sports) are relative contraindications
Nasal DeformitySeptoplastyndash Septoplasty is performed to correct nasal obstructioncaused by septal deformityndash Usually septoplasty is performed under general anaesthesiawith the patient in the supine position with the head elevated by approximately 30 (Righthandedsurgeons approach from the right side)ndash Local vasoconstrictive anaesthesia is applied notonly to reduce postoperative pain but also more importantly to achieve vasoconstriction of themucosa and less intraoperative haemorrhage Lidocainewith adrenaline or epinephrine is usedalthough in patients with cardiac hypersensitivityoxymetazoline might be preferred
Nasal Deformity
bull Septoplasty begins with the incision of septal mucosabull Most operative techniques utilise a hemitransfixionbull incision at the caudal end of septum so thatbull deviation at this point might be reached as wellbull as a transfixion incision that is easily obtained ifbull needed (Right-handed surgeons normally choosebull the left side but that may vary when deviation isbull convex towards the right)
Nasal DeformityA columella retractor is placed over the columellaand by pulling it laterally the caudal border of theseptum is exposed Ala can be protected by an alaprotector A vertical incision with a no 15 bladeover the caudal end of septum is performed untilreaching the plane of the septal cartilage It is essentialto correctly identify the perichondrium and byusing the Cottle elevator dissect and lift it creatinga flap As the dissection proceeds along the septalcartilage a longer speculum (no 5) is introduced sothat elevation of the mucoperichondrium is doneunder constant visual controlndash The next step is to dissect the mucoperiostium
Nasal DeformityDissecting over the bony-cartilaginous junctionwhen joining both tunnels might be difficult and is
especially prone to membrane perforationndash If needed the same tunnels are to be created on the
other side of the septum Then deviated parts of
septum are identified and removed either with a
knife or a Freer chisel
Nasal Deformitybull septum from the maxillary crest the septum mustbull be separated from the perpendicular plate trimmedbull along the inferior border placed back onto the crestbull and sutured to the periosteum If the deformity involvesbull the vomer an osteotome is used Care mustbull be taken not to break the cribriform plate becausebull it could cause a cerebrospinal fistula
Nasal Deformity
bull Once the septal deviation is corrected the flapsbull and hemitransfixion incision are mattressed
withbull absorbable sutures Nasal packing to prevent
synechiaebull and postoperative septal haematoma mightbull be advised but should be removed within 72 h

Nasal Fractures Complications ndash Septal haematoma is one of the most severe early complications of nasal trauma and without drainage it results in abscess formation 6ndash7 days after trauma producing necrosis of the septal cartilage -Long-term problems such as saddle-nose deformity perforation columellar retraction and nasalbase
Septal infection could lead to osteomyelitis orbital and intracranial abscesses meningitis and cavernous sinus thrombosis -Cerebrospinal fluid leakage is a common complication of severe
nasal and frontal fractures
Nasal Fractures
bull Diagnostic proceduresbull ndash Inspectionbull bull Changes of appearance such as deviation andbull asymmetry bleeding watery drainage changesbull in nasal breathing and smell It is useful to comparebull the current presentation with old photographsbull (up to 40 of normal individuals havebull significant nose malformations)
Nasal Fractures Physical examination bull The diagnosis of a nasal fracture is made primarily by physical examination epistaxis nasal swelling and periorbital ecchymosis Nasal shape in the lateral and frontal inspection should be assessed Grasping the dorsum between two fingers and rocking the pyramid back and forth aids in assessing the mobility of nasal bones Internal structures should be evaluated by using a headlight and nasal speculum Clotted blood is removed by suction and assessment of haematoma mucosal tears and active bleeding is performed Bimanual palpation of the septum helps to differentiate septal swelling from haematoma ndash
Nasal FracturesRadiographybull There is no clear evidence of the role of radiographyin the management of nasal fracturesPlain films have up to a 66 false-positive rateas a result of misinterpretation of normal suturelines In addition old fractures are difficult todistinguishbull Three-dimensional CT is recommended for extensiveinjuries involving the nasal-orbital-ethmoidalcomplexndash
Nasal Fractures
bull Additionaluseful diagnostic proceduresbull bull Using a 0 or 30deg 4-mm endoscope is helpful inbull the assessment of posterior abnormalities If thebull patient is heavily sedated Brown-Gruss
provocationbull manoeuvres may be performed to determinebull deformities in upper middle or lower segmentsbull by compressing each compartment
Nasal FracturesConservative treatmentndash Treatment of bleedingbull For localised bleeding anterior sources may becauterised by silver nitrate or sealed with topicalmaterials such as thrombin combined withgelatin foam fibrin glue FloSealreg or other procoagulantmaterials If conservative measuresfail a formal anterior packing is placedbull Bleeding from branches of sphenopalatine orethmoid vessels requires anterior-posteriorpacking
Nasal Fractures
bull bull Surgical methods such as direct endoscopic vessel
bull cauterization or ligation have been shown tobull offer better haemostasis and patient comfortbull Angiography with embolization can also be
consideredbull in cases refractory to more conservativebull approaches
Nasal Fractures
bull Type of reductionbull bull Nondisplaced fractures should be treated withbull observation alone Closed nasal reduction is thebull best choice for simple injuries (isolated unilateralbull with medial displacement)bull bull An open approach should be considered in
severebull trauma (bilateral depressed fractures)
Nasal Fracturesbull Surgical principlesbull ndash Topical anaesthesia with cotton pledgets soakedbull with 4 cocaine or 005 oxymethazoline combinedbull with 4 topical lidocaine should be appliedbull for 5ndash10 min Local anaesthesia should also be injectedbull (1 lidocaine and 1100000 epinephrine)bull along the septum lateral walls and floor of the nasalbull cavitybull bull
Nasal FracturesClosed reductionndashndash The nasal bones are grasped between two fingersand pressure is applied laterally in theopposite direction of the deviation A bluntelevator may be used from within the nose incases of significant medial collapse Walshamforceps can be of help Reduction of the septumshould be performed with the use ofAsch forceps
Nasal Fractures
bull To prevent collapse of the postreductionbull framework nasal packing should be placedbull for 3ndash5 days Septum splints are recommendedbull in comminuted septal fractures withbull severe mucosal lesions External nasal splintingbull for 10 days (Aquaplastreg Thermoplastreg)bull provides nasal protection Nasal saline spraysbull prevent crusting and oral antibiotics should
Nasal Fractures
bull Open reductionbull ndashndash Immediate repair of fractures by using
widebull surgical exposure reduction fixation and
reconstructionbull ndashndash The second option is delayed correctionbull (6 months or more) of persistent deformitiesbull using standard techniques of rhinoplasty
Deviated Nasal Septum
bull Definition of the diseasebull ndash Deviation of the nasal septum is a common causebull of unilateral nasal airway obstruction in which thebull nasal septum is displacedbull bull Epidemiologyaetiologybull ndash Developmental septal abnormalities Septal cartilage
damage in the neonatal period andbull during birth can cause severe septal deviation inbull the absence of a history of nasal trauma
Deviated Nasal Septum
bull Symptomsbull ndash Patients may present with a history of sinusitis
allergicbull rhinitis obstructive sleep apnoea previousbull nasal surgery or recent nasal trauma Unilateral or
bilateral nasal airway obstruction that is unrelievedbull with decongestants or nasal steroid sprays is oftenbull seenbull bull
Deviated Nasal SeptumDiagnosisndashExamination external dorsal deviation or the columella and caudal septummay be deflected off the midline (caudal subluxation)ndash Inspections of the nasal cavity and anterior-posteriorrhinoscopy are helpful in diagnosing the locationtype and severity of septal deformityThe endoscope is also useful in identifying polypsthe severity and extent of posterior septaldeviations and bony spurs and locating areas ofseptal perforation or mucosal injury
Deviated Nasal Septum
bull Therapybull ndash Septoplasty is a procedurebull The areabull of deviation is corrected or resected in order tobull leave behind as much cartilage and bone as
possiblebull Cartilage resection is minimised and can be
repositioned reshaped or recontoured using a variety of methods
Deviated Nasal Septum
bull ndash Indications of septoplasty before the growth period
bull of the nose is finished should be very limited bull -In these cases surgery must preserve all the
cartilagebull in order to prevent external changes of the
shape ofbull the nose
Deviated Nasal Septum
bull Complicationsbull ndash Frequent complications include haematoma andbull infection Cerebrospinal fluid leak is a rare but
potentiallybull serious complicationbull It is usually the resultbull of avulsion or damage to the cribriform plate whenbull handling the perpendicular plate of the ethmoidbull ndash Other complications include epistaxis nasal
Deviated Nasal Septum
bull Other complications include epistaxis nasal obstruction
bull due to residual deviation synechiae returnbull of the cartilaginous deviation septal perforationbull anosmia and cosmetic nasal deformities suchbull as widened alar rim margins drooping nasal tipbull columella retraction and a sunken dorsum with abull supratip saddle formation
Septal perforation with minor crusting View from provide closure of the
incision
Septal Haematoma
bull A septal haematoma is a blood collection under the perichondrium
bull of the septum and cartilagebull bull bull Epidemiologyaetiologybull ndash A septal haematoma is one of the most
severe complications of nasal trauma
Septal Haematoma
bull Diagnosisbull ndash Signs and symptoms include intense pain
swellingbull haematoma of the upper lip and philtrum
area andbull complete nasal airway obstruction
Septal HaematomaTherapyndash Management consists of drainage through a mucoperichondrial incision Immediate treatment isnecessary to prevent long-term problems such asa saddle-nose deformity perforation columellarretraction and nasal-base widening In childrenseptal destruction can lead to devastating nasal andmidfacial growth abnormalitiesbull Surgeryndash Incision and evacuation of the collection is performedDrainage of a septal haematoma should
Septal HaematomaSurgeryndash Incision and evacuation of the collection is performedDrainage of a septal haematoma should provide closure of the incision
Splints or transseptal sutures are placed to obliterate thepotential space and prevent collectionInfection involving the septal cartilage Reconstruction with autologouscartilage is then performed in a second stage Oral antibiotics should be given
Nasal DeformitySaddle-nose deformityndash A saddle-nose deformity is characterised by a loss ofnasal dorsal height and compromised nasal supportstructures -Other case observed are depressionof the middle vault and dorsum loss of nasal tipsupport and definition shortened (vertical) nasal length over rotation of the nasal tip and retrusion ofthe nasal spine and caudal septum It is also knownas a ldquoPug noserdquo or ldquoboxerrsquos noserdquo both of which referto various degrees of nasal dorsal depressionbull
Nasal DeformityEpidemiologyaetiologyndash Prevalence is higher in population groups prone to facial trauma (ie boxers athletes) those with historiesof intranasal cocaine use nasal surgery (e g radical submucosal septal resection reductive rhinoplasty)ndash A saddle-nose deformity can be congenital or acquired It can be noticed as a part of individual familialsyndromic and ethnic characteristics - Most deformities are due to traumatic and iatrogeniccauses Medical causes are Wegenerrsquosgranulomatosis relapsing polychondritis leprosy (Hansenrsquos disease) syphilis ectodermal dysplasiaand intranasal cocaine use
Nasal Deformity
bull Therapybull ndash Nasal reconstruction indications depend on patientbull selection surgeon experience and aetiology of thebull deformity bull Indications for surgery can be functionalbull aesthetic or most commonly both In individuals
with a compromised nasal airway a nasoseptalbull reconstruction is indicated
Nasal Deformity
bull Contraindications bull include patients with malignantbull chronic or autoimmune disease conditions drugbull abuse poor perioperative risk profile and unrealisticbull expectationsbull ndash Multiple previous rhinoplasties and certain
professionsbull (mixed martial artists boxers and other contactbull sports) are relative contraindications
Nasal DeformitySeptoplastyndash Septoplasty is performed to correct nasal obstructioncaused by septal deformityndash Usually septoplasty is performed under general anaesthesiawith the patient in the supine position with the head elevated by approximately 30 (Righthandedsurgeons approach from the right side)ndash Local vasoconstrictive anaesthesia is applied notonly to reduce postoperative pain but also more importantly to achieve vasoconstriction of themucosa and less intraoperative haemorrhage Lidocainewith adrenaline or epinephrine is usedalthough in patients with cardiac hypersensitivityoxymetazoline might be preferred
Nasal Deformity
bull Septoplasty begins with the incision of septal mucosabull Most operative techniques utilise a hemitransfixionbull incision at the caudal end of septum so thatbull deviation at this point might be reached as wellbull as a transfixion incision that is easily obtained ifbull needed (Right-handed surgeons normally choosebull the left side but that may vary when deviation isbull convex towards the right)
Nasal DeformityA columella retractor is placed over the columellaand by pulling it laterally the caudal border of theseptum is exposed Ala can be protected by an alaprotector A vertical incision with a no 15 bladeover the caudal end of septum is performed untilreaching the plane of the septal cartilage It is essentialto correctly identify the perichondrium and byusing the Cottle elevator dissect and lift it creatinga flap As the dissection proceeds along the septalcartilage a longer speculum (no 5) is introduced sothat elevation of the mucoperichondrium is doneunder constant visual controlndash The next step is to dissect the mucoperiostium
Nasal DeformityDissecting over the bony-cartilaginous junctionwhen joining both tunnels might be difficult and is
especially prone to membrane perforationndash If needed the same tunnels are to be created on the
other side of the septum Then deviated parts of
septum are identified and removed either with a
knife or a Freer chisel
Nasal Deformitybull septum from the maxillary crest the septum mustbull be separated from the perpendicular plate trimmedbull along the inferior border placed back onto the crestbull and sutured to the periosteum If the deformity involvesbull the vomer an osteotome is used Care mustbull be taken not to break the cribriform plate becausebull it could cause a cerebrospinal fistula
Nasal Deformity
bull Once the septal deviation is corrected the flapsbull and hemitransfixion incision are mattressed
withbull absorbable sutures Nasal packing to prevent
synechiaebull and postoperative septal haematoma mightbull be advised but should be removed within 72 h

Nasal Fractures
bull Diagnostic proceduresbull ndash Inspectionbull bull Changes of appearance such as deviation andbull asymmetry bleeding watery drainage changesbull in nasal breathing and smell It is useful to comparebull the current presentation with old photographsbull (up to 40 of normal individuals havebull significant nose malformations)
Nasal Fractures Physical examination bull The diagnosis of a nasal fracture is made primarily by physical examination epistaxis nasal swelling and periorbital ecchymosis Nasal shape in the lateral and frontal inspection should be assessed Grasping the dorsum between two fingers and rocking the pyramid back and forth aids in assessing the mobility of nasal bones Internal structures should be evaluated by using a headlight and nasal speculum Clotted blood is removed by suction and assessment of haematoma mucosal tears and active bleeding is performed Bimanual palpation of the septum helps to differentiate septal swelling from haematoma ndash
Nasal FracturesRadiographybull There is no clear evidence of the role of radiographyin the management of nasal fracturesPlain films have up to a 66 false-positive rateas a result of misinterpretation of normal suturelines In addition old fractures are difficult todistinguishbull Three-dimensional CT is recommended for extensiveinjuries involving the nasal-orbital-ethmoidalcomplexndash
Nasal Fractures
bull Additionaluseful diagnostic proceduresbull bull Using a 0 or 30deg 4-mm endoscope is helpful inbull the assessment of posterior abnormalities If thebull patient is heavily sedated Brown-Gruss
provocationbull manoeuvres may be performed to determinebull deformities in upper middle or lower segmentsbull by compressing each compartment
Nasal FracturesConservative treatmentndash Treatment of bleedingbull For localised bleeding anterior sources may becauterised by silver nitrate or sealed with topicalmaterials such as thrombin combined withgelatin foam fibrin glue FloSealreg or other procoagulantmaterials If conservative measuresfail a formal anterior packing is placedbull Bleeding from branches of sphenopalatine orethmoid vessels requires anterior-posteriorpacking
Nasal Fractures
bull bull Surgical methods such as direct endoscopic vessel
bull cauterization or ligation have been shown tobull offer better haemostasis and patient comfortbull Angiography with embolization can also be
consideredbull in cases refractory to more conservativebull approaches
Nasal Fractures
bull Type of reductionbull bull Nondisplaced fractures should be treated withbull observation alone Closed nasal reduction is thebull best choice for simple injuries (isolated unilateralbull with medial displacement)bull bull An open approach should be considered in
severebull trauma (bilateral depressed fractures)
Nasal Fracturesbull Surgical principlesbull ndash Topical anaesthesia with cotton pledgets soakedbull with 4 cocaine or 005 oxymethazoline combinedbull with 4 topical lidocaine should be appliedbull for 5ndash10 min Local anaesthesia should also be injectedbull (1 lidocaine and 1100000 epinephrine)bull along the septum lateral walls and floor of the nasalbull cavitybull bull
Nasal FracturesClosed reductionndashndash The nasal bones are grasped between two fingersand pressure is applied laterally in theopposite direction of the deviation A bluntelevator may be used from within the nose incases of significant medial collapse Walshamforceps can be of help Reduction of the septumshould be performed with the use ofAsch forceps
Nasal Fractures
bull To prevent collapse of the postreductionbull framework nasal packing should be placedbull for 3ndash5 days Septum splints are recommendedbull in comminuted septal fractures withbull severe mucosal lesions External nasal splintingbull for 10 days (Aquaplastreg Thermoplastreg)bull provides nasal protection Nasal saline spraysbull prevent crusting and oral antibiotics should
Nasal Fractures
bull Open reductionbull ndashndash Immediate repair of fractures by using
widebull surgical exposure reduction fixation and
reconstructionbull ndashndash The second option is delayed correctionbull (6 months or more) of persistent deformitiesbull using standard techniques of rhinoplasty
Deviated Nasal Septum
bull Definition of the diseasebull ndash Deviation of the nasal septum is a common causebull of unilateral nasal airway obstruction in which thebull nasal septum is displacedbull bull Epidemiologyaetiologybull ndash Developmental septal abnormalities Septal cartilage
damage in the neonatal period andbull during birth can cause severe septal deviation inbull the absence of a history of nasal trauma
Deviated Nasal Septum
bull Symptomsbull ndash Patients may present with a history of sinusitis
allergicbull rhinitis obstructive sleep apnoea previousbull nasal surgery or recent nasal trauma Unilateral or
bilateral nasal airway obstruction that is unrelievedbull with decongestants or nasal steroid sprays is oftenbull seenbull bull
Deviated Nasal SeptumDiagnosisndashExamination external dorsal deviation or the columella and caudal septummay be deflected off the midline (caudal subluxation)ndash Inspections of the nasal cavity and anterior-posteriorrhinoscopy are helpful in diagnosing the locationtype and severity of septal deformityThe endoscope is also useful in identifying polypsthe severity and extent of posterior septaldeviations and bony spurs and locating areas ofseptal perforation or mucosal injury
Deviated Nasal Septum
bull Therapybull ndash Septoplasty is a procedurebull The areabull of deviation is corrected or resected in order tobull leave behind as much cartilage and bone as
possiblebull Cartilage resection is minimised and can be
repositioned reshaped or recontoured using a variety of methods
Deviated Nasal Septum
bull ndash Indications of septoplasty before the growth period
bull of the nose is finished should be very limited bull -In these cases surgery must preserve all the
cartilagebull in order to prevent external changes of the
shape ofbull the nose
Deviated Nasal Septum
bull Complicationsbull ndash Frequent complications include haematoma andbull infection Cerebrospinal fluid leak is a rare but
potentiallybull serious complicationbull It is usually the resultbull of avulsion or damage to the cribriform plate whenbull handling the perpendicular plate of the ethmoidbull ndash Other complications include epistaxis nasal
Deviated Nasal Septum
bull Other complications include epistaxis nasal obstruction
bull due to residual deviation synechiae returnbull of the cartilaginous deviation septal perforationbull anosmia and cosmetic nasal deformities suchbull as widened alar rim margins drooping nasal tipbull columella retraction and a sunken dorsum with abull supratip saddle formation
Septal perforation with minor crusting View from provide closure of the
incision
Septal Haematoma
bull A septal haematoma is a blood collection under the perichondrium
bull of the septum and cartilagebull bull bull Epidemiologyaetiologybull ndash A septal haematoma is one of the most
severe complications of nasal trauma
Septal Haematoma
bull Diagnosisbull ndash Signs and symptoms include intense pain
swellingbull haematoma of the upper lip and philtrum
area andbull complete nasal airway obstruction
Septal HaematomaTherapyndash Management consists of drainage through a mucoperichondrial incision Immediate treatment isnecessary to prevent long-term problems such asa saddle-nose deformity perforation columellarretraction and nasal-base widening In childrenseptal destruction can lead to devastating nasal andmidfacial growth abnormalitiesbull Surgeryndash Incision and evacuation of the collection is performedDrainage of a septal haematoma should
Septal HaematomaSurgeryndash Incision and evacuation of the collection is performedDrainage of a septal haematoma should provide closure of the incision
Splints or transseptal sutures are placed to obliterate thepotential space and prevent collectionInfection involving the septal cartilage Reconstruction with autologouscartilage is then performed in a second stage Oral antibiotics should be given
Nasal DeformitySaddle-nose deformityndash A saddle-nose deformity is characterised by a loss ofnasal dorsal height and compromised nasal supportstructures -Other case observed are depressionof the middle vault and dorsum loss of nasal tipsupport and definition shortened (vertical) nasal length over rotation of the nasal tip and retrusion ofthe nasal spine and caudal septum It is also knownas a ldquoPug noserdquo or ldquoboxerrsquos noserdquo both of which referto various degrees of nasal dorsal depressionbull
Nasal DeformityEpidemiologyaetiologyndash Prevalence is higher in population groups prone to facial trauma (ie boxers athletes) those with historiesof intranasal cocaine use nasal surgery (e g radical submucosal septal resection reductive rhinoplasty)ndash A saddle-nose deformity can be congenital or acquired It can be noticed as a part of individual familialsyndromic and ethnic characteristics - Most deformities are due to traumatic and iatrogeniccauses Medical causes are Wegenerrsquosgranulomatosis relapsing polychondritis leprosy (Hansenrsquos disease) syphilis ectodermal dysplasiaand intranasal cocaine use
Nasal Deformity
bull Therapybull ndash Nasal reconstruction indications depend on patientbull selection surgeon experience and aetiology of thebull deformity bull Indications for surgery can be functionalbull aesthetic or most commonly both In individuals
with a compromised nasal airway a nasoseptalbull reconstruction is indicated
Nasal Deformity
bull Contraindications bull include patients with malignantbull chronic or autoimmune disease conditions drugbull abuse poor perioperative risk profile and unrealisticbull expectationsbull ndash Multiple previous rhinoplasties and certain
professionsbull (mixed martial artists boxers and other contactbull sports) are relative contraindications
Nasal DeformitySeptoplastyndash Septoplasty is performed to correct nasal obstructioncaused by septal deformityndash Usually septoplasty is performed under general anaesthesiawith the patient in the supine position with the head elevated by approximately 30 (Righthandedsurgeons approach from the right side)ndash Local vasoconstrictive anaesthesia is applied notonly to reduce postoperative pain but also more importantly to achieve vasoconstriction of themucosa and less intraoperative haemorrhage Lidocainewith adrenaline or epinephrine is usedalthough in patients with cardiac hypersensitivityoxymetazoline might be preferred
Nasal Deformity
bull Septoplasty begins with the incision of septal mucosabull Most operative techniques utilise a hemitransfixionbull incision at the caudal end of septum so thatbull deviation at this point might be reached as wellbull as a transfixion incision that is easily obtained ifbull needed (Right-handed surgeons normally choosebull the left side but that may vary when deviation isbull convex towards the right)
Nasal DeformityA columella retractor is placed over the columellaand by pulling it laterally the caudal border of theseptum is exposed Ala can be protected by an alaprotector A vertical incision with a no 15 bladeover the caudal end of septum is performed untilreaching the plane of the septal cartilage It is essentialto correctly identify the perichondrium and byusing the Cottle elevator dissect and lift it creatinga flap As the dissection proceeds along the septalcartilage a longer speculum (no 5) is introduced sothat elevation of the mucoperichondrium is doneunder constant visual controlndash The next step is to dissect the mucoperiostium
Nasal DeformityDissecting over the bony-cartilaginous junctionwhen joining both tunnels might be difficult and is
especially prone to membrane perforationndash If needed the same tunnels are to be created on the
other side of the septum Then deviated parts of
septum are identified and removed either with a
knife or a Freer chisel
Nasal Deformitybull septum from the maxillary crest the septum mustbull be separated from the perpendicular plate trimmedbull along the inferior border placed back onto the crestbull and sutured to the periosteum If the deformity involvesbull the vomer an osteotome is used Care mustbull be taken not to break the cribriform plate becausebull it could cause a cerebrospinal fistula
Nasal Deformity
bull Once the septal deviation is corrected the flapsbull and hemitransfixion incision are mattressed
withbull absorbable sutures Nasal packing to prevent
synechiaebull and postoperative septal haematoma mightbull be advised but should be removed within 72 h

Nasal Fractures Physical examination bull The diagnosis of a nasal fracture is made primarily by physical examination epistaxis nasal swelling and periorbital ecchymosis Nasal shape in the lateral and frontal inspection should be assessed Grasping the dorsum between two fingers and rocking the pyramid back and forth aids in assessing the mobility of nasal bones Internal structures should be evaluated by using a headlight and nasal speculum Clotted blood is removed by suction and assessment of haematoma mucosal tears and active bleeding is performed Bimanual palpation of the septum helps to differentiate septal swelling from haematoma ndash
Nasal FracturesRadiographybull There is no clear evidence of the role of radiographyin the management of nasal fracturesPlain films have up to a 66 false-positive rateas a result of misinterpretation of normal suturelines In addition old fractures are difficult todistinguishbull Three-dimensional CT is recommended for extensiveinjuries involving the nasal-orbital-ethmoidalcomplexndash
Nasal Fractures
bull Additionaluseful diagnostic proceduresbull bull Using a 0 or 30deg 4-mm endoscope is helpful inbull the assessment of posterior abnormalities If thebull patient is heavily sedated Brown-Gruss
provocationbull manoeuvres may be performed to determinebull deformities in upper middle or lower segmentsbull by compressing each compartment
Nasal FracturesConservative treatmentndash Treatment of bleedingbull For localised bleeding anterior sources may becauterised by silver nitrate or sealed with topicalmaterials such as thrombin combined withgelatin foam fibrin glue FloSealreg or other procoagulantmaterials If conservative measuresfail a formal anterior packing is placedbull Bleeding from branches of sphenopalatine orethmoid vessels requires anterior-posteriorpacking
Nasal Fractures
bull bull Surgical methods such as direct endoscopic vessel
bull cauterization or ligation have been shown tobull offer better haemostasis and patient comfortbull Angiography with embolization can also be
consideredbull in cases refractory to more conservativebull approaches
Nasal Fractures
bull Type of reductionbull bull Nondisplaced fractures should be treated withbull observation alone Closed nasal reduction is thebull best choice for simple injuries (isolated unilateralbull with medial displacement)bull bull An open approach should be considered in
severebull trauma (bilateral depressed fractures)
Nasal Fracturesbull Surgical principlesbull ndash Topical anaesthesia with cotton pledgets soakedbull with 4 cocaine or 005 oxymethazoline combinedbull with 4 topical lidocaine should be appliedbull for 5ndash10 min Local anaesthesia should also be injectedbull (1 lidocaine and 1100000 epinephrine)bull along the septum lateral walls and floor of the nasalbull cavitybull bull
Nasal FracturesClosed reductionndashndash The nasal bones are grasped between two fingersand pressure is applied laterally in theopposite direction of the deviation A bluntelevator may be used from within the nose incases of significant medial collapse Walshamforceps can be of help Reduction of the septumshould be performed with the use ofAsch forceps
Nasal Fractures
bull To prevent collapse of the postreductionbull framework nasal packing should be placedbull for 3ndash5 days Septum splints are recommendedbull in comminuted septal fractures withbull severe mucosal lesions External nasal splintingbull for 10 days (Aquaplastreg Thermoplastreg)bull provides nasal protection Nasal saline spraysbull prevent crusting and oral antibiotics should
Nasal Fractures
bull Open reductionbull ndashndash Immediate repair of fractures by using
widebull surgical exposure reduction fixation and
reconstructionbull ndashndash The second option is delayed correctionbull (6 months or more) of persistent deformitiesbull using standard techniques of rhinoplasty
Deviated Nasal Septum
bull Definition of the diseasebull ndash Deviation of the nasal septum is a common causebull of unilateral nasal airway obstruction in which thebull nasal septum is displacedbull bull Epidemiologyaetiologybull ndash Developmental septal abnormalities Septal cartilage
damage in the neonatal period andbull during birth can cause severe septal deviation inbull the absence of a history of nasal trauma
Deviated Nasal Septum
bull Symptomsbull ndash Patients may present with a history of sinusitis
allergicbull rhinitis obstructive sleep apnoea previousbull nasal surgery or recent nasal trauma Unilateral or
bilateral nasal airway obstruction that is unrelievedbull with decongestants or nasal steroid sprays is oftenbull seenbull bull
Deviated Nasal SeptumDiagnosisndashExamination external dorsal deviation or the columella and caudal septummay be deflected off the midline (caudal subluxation)ndash Inspections of the nasal cavity and anterior-posteriorrhinoscopy are helpful in diagnosing the locationtype and severity of septal deformityThe endoscope is also useful in identifying polypsthe severity and extent of posterior septaldeviations and bony spurs and locating areas ofseptal perforation or mucosal injury
Deviated Nasal Septum
bull Therapybull ndash Septoplasty is a procedurebull The areabull of deviation is corrected or resected in order tobull leave behind as much cartilage and bone as
possiblebull Cartilage resection is minimised and can be
repositioned reshaped or recontoured using a variety of methods
Deviated Nasal Septum
bull ndash Indications of septoplasty before the growth period
bull of the nose is finished should be very limited bull -In these cases surgery must preserve all the
cartilagebull in order to prevent external changes of the
shape ofbull the nose
Deviated Nasal Septum
bull Complicationsbull ndash Frequent complications include haematoma andbull infection Cerebrospinal fluid leak is a rare but
potentiallybull serious complicationbull It is usually the resultbull of avulsion or damage to the cribriform plate whenbull handling the perpendicular plate of the ethmoidbull ndash Other complications include epistaxis nasal
Deviated Nasal Septum
bull Other complications include epistaxis nasal obstruction
bull due to residual deviation synechiae returnbull of the cartilaginous deviation septal perforationbull anosmia and cosmetic nasal deformities suchbull as widened alar rim margins drooping nasal tipbull columella retraction and a sunken dorsum with abull supratip saddle formation
Septal perforation with minor crusting View from provide closure of the
incision
Septal Haematoma
bull A septal haematoma is a blood collection under the perichondrium
bull of the septum and cartilagebull bull bull Epidemiologyaetiologybull ndash A septal haematoma is one of the most
severe complications of nasal trauma
Septal Haematoma
bull Diagnosisbull ndash Signs and symptoms include intense pain
swellingbull haematoma of the upper lip and philtrum
area andbull complete nasal airway obstruction
Septal HaematomaTherapyndash Management consists of drainage through a mucoperichondrial incision Immediate treatment isnecessary to prevent long-term problems such asa saddle-nose deformity perforation columellarretraction and nasal-base widening In childrenseptal destruction can lead to devastating nasal andmidfacial growth abnormalitiesbull Surgeryndash Incision and evacuation of the collection is performedDrainage of a septal haematoma should
Septal HaematomaSurgeryndash Incision and evacuation of the collection is performedDrainage of a septal haematoma should provide closure of the incision
Splints or transseptal sutures are placed to obliterate thepotential space and prevent collectionInfection involving the septal cartilage Reconstruction with autologouscartilage is then performed in a second stage Oral antibiotics should be given
Nasal DeformitySaddle-nose deformityndash A saddle-nose deformity is characterised by a loss ofnasal dorsal height and compromised nasal supportstructures -Other case observed are depressionof the middle vault and dorsum loss of nasal tipsupport and definition shortened (vertical) nasal length over rotation of the nasal tip and retrusion ofthe nasal spine and caudal septum It is also knownas a ldquoPug noserdquo or ldquoboxerrsquos noserdquo both of which referto various degrees of nasal dorsal depressionbull
Nasal DeformityEpidemiologyaetiologyndash Prevalence is higher in population groups prone to facial trauma (ie boxers athletes) those with historiesof intranasal cocaine use nasal surgery (e g radical submucosal septal resection reductive rhinoplasty)ndash A saddle-nose deformity can be congenital or acquired It can be noticed as a part of individual familialsyndromic and ethnic characteristics - Most deformities are due to traumatic and iatrogeniccauses Medical causes are Wegenerrsquosgranulomatosis relapsing polychondritis leprosy (Hansenrsquos disease) syphilis ectodermal dysplasiaand intranasal cocaine use
Nasal Deformity
bull Therapybull ndash Nasal reconstruction indications depend on patientbull selection surgeon experience and aetiology of thebull deformity bull Indications for surgery can be functionalbull aesthetic or most commonly both In individuals
with a compromised nasal airway a nasoseptalbull reconstruction is indicated
Nasal Deformity
bull Contraindications bull include patients with malignantbull chronic or autoimmune disease conditions drugbull abuse poor perioperative risk profile and unrealisticbull expectationsbull ndash Multiple previous rhinoplasties and certain
professionsbull (mixed martial artists boxers and other contactbull sports) are relative contraindications
Nasal DeformitySeptoplastyndash Septoplasty is performed to correct nasal obstructioncaused by septal deformityndash Usually septoplasty is performed under general anaesthesiawith the patient in the supine position with the head elevated by approximately 30 (Righthandedsurgeons approach from the right side)ndash Local vasoconstrictive anaesthesia is applied notonly to reduce postoperative pain but also more importantly to achieve vasoconstriction of themucosa and less intraoperative haemorrhage Lidocainewith adrenaline or epinephrine is usedalthough in patients with cardiac hypersensitivityoxymetazoline might be preferred
Nasal Deformity
bull Septoplasty begins with the incision of septal mucosabull Most operative techniques utilise a hemitransfixionbull incision at the caudal end of septum so thatbull deviation at this point might be reached as wellbull as a transfixion incision that is easily obtained ifbull needed (Right-handed surgeons normally choosebull the left side but that may vary when deviation isbull convex towards the right)
Nasal DeformityA columella retractor is placed over the columellaand by pulling it laterally the caudal border of theseptum is exposed Ala can be protected by an alaprotector A vertical incision with a no 15 bladeover the caudal end of septum is performed untilreaching the plane of the septal cartilage It is essentialto correctly identify the perichondrium and byusing the Cottle elevator dissect and lift it creatinga flap As the dissection proceeds along the septalcartilage a longer speculum (no 5) is introduced sothat elevation of the mucoperichondrium is doneunder constant visual controlndash The next step is to dissect the mucoperiostium
Nasal DeformityDissecting over the bony-cartilaginous junctionwhen joining both tunnels might be difficult and is
especially prone to membrane perforationndash If needed the same tunnels are to be created on the
other side of the septum Then deviated parts of
septum are identified and removed either with a
knife or a Freer chisel
Nasal Deformitybull septum from the maxillary crest the septum mustbull be separated from the perpendicular plate trimmedbull along the inferior border placed back onto the crestbull and sutured to the periosteum If the deformity involvesbull the vomer an osteotome is used Care mustbull be taken not to break the cribriform plate becausebull it could cause a cerebrospinal fistula
Nasal Deformity
bull Once the septal deviation is corrected the flapsbull and hemitransfixion incision are mattressed
withbull absorbable sutures Nasal packing to prevent
synechiaebull and postoperative septal haematoma mightbull be advised but should be removed within 72 h

Nasal FracturesRadiographybull There is no clear evidence of the role of radiographyin the management of nasal fracturesPlain films have up to a 66 false-positive rateas a result of misinterpretation of normal suturelines In addition old fractures are difficult todistinguishbull Three-dimensional CT is recommended for extensiveinjuries involving the nasal-orbital-ethmoidalcomplexndash
Nasal Fractures
bull Additionaluseful diagnostic proceduresbull bull Using a 0 or 30deg 4-mm endoscope is helpful inbull the assessment of posterior abnormalities If thebull patient is heavily sedated Brown-Gruss
provocationbull manoeuvres may be performed to determinebull deformities in upper middle or lower segmentsbull by compressing each compartment
Nasal FracturesConservative treatmentndash Treatment of bleedingbull For localised bleeding anterior sources may becauterised by silver nitrate or sealed with topicalmaterials such as thrombin combined withgelatin foam fibrin glue FloSealreg or other procoagulantmaterials If conservative measuresfail a formal anterior packing is placedbull Bleeding from branches of sphenopalatine orethmoid vessels requires anterior-posteriorpacking
Nasal Fractures
bull bull Surgical methods such as direct endoscopic vessel
bull cauterization or ligation have been shown tobull offer better haemostasis and patient comfortbull Angiography with embolization can also be
consideredbull in cases refractory to more conservativebull approaches
Nasal Fractures
bull Type of reductionbull bull Nondisplaced fractures should be treated withbull observation alone Closed nasal reduction is thebull best choice for simple injuries (isolated unilateralbull with medial displacement)bull bull An open approach should be considered in
severebull trauma (bilateral depressed fractures)
Nasal Fracturesbull Surgical principlesbull ndash Topical anaesthesia with cotton pledgets soakedbull with 4 cocaine or 005 oxymethazoline combinedbull with 4 topical lidocaine should be appliedbull for 5ndash10 min Local anaesthesia should also be injectedbull (1 lidocaine and 1100000 epinephrine)bull along the septum lateral walls and floor of the nasalbull cavitybull bull
Nasal FracturesClosed reductionndashndash The nasal bones are grasped between two fingersand pressure is applied laterally in theopposite direction of the deviation A bluntelevator may be used from within the nose incases of significant medial collapse Walshamforceps can be of help Reduction of the septumshould be performed with the use ofAsch forceps
Nasal Fractures
bull To prevent collapse of the postreductionbull framework nasal packing should be placedbull for 3ndash5 days Septum splints are recommendedbull in comminuted septal fractures withbull severe mucosal lesions External nasal splintingbull for 10 days (Aquaplastreg Thermoplastreg)bull provides nasal protection Nasal saline spraysbull prevent crusting and oral antibiotics should
Nasal Fractures
bull Open reductionbull ndashndash Immediate repair of fractures by using
widebull surgical exposure reduction fixation and
reconstructionbull ndashndash The second option is delayed correctionbull (6 months or more) of persistent deformitiesbull using standard techniques of rhinoplasty
Deviated Nasal Septum
bull Definition of the diseasebull ndash Deviation of the nasal septum is a common causebull of unilateral nasal airway obstruction in which thebull nasal septum is displacedbull bull Epidemiologyaetiologybull ndash Developmental septal abnormalities Septal cartilage
damage in the neonatal period andbull during birth can cause severe septal deviation inbull the absence of a history of nasal trauma
Deviated Nasal Septum
bull Symptomsbull ndash Patients may present with a history of sinusitis
allergicbull rhinitis obstructive sleep apnoea previousbull nasal surgery or recent nasal trauma Unilateral or
bilateral nasal airway obstruction that is unrelievedbull with decongestants or nasal steroid sprays is oftenbull seenbull bull
Deviated Nasal SeptumDiagnosisndashExamination external dorsal deviation or the columella and caudal septummay be deflected off the midline (caudal subluxation)ndash Inspections of the nasal cavity and anterior-posteriorrhinoscopy are helpful in diagnosing the locationtype and severity of septal deformityThe endoscope is also useful in identifying polypsthe severity and extent of posterior septaldeviations and bony spurs and locating areas ofseptal perforation or mucosal injury
Deviated Nasal Septum
bull Therapybull ndash Septoplasty is a procedurebull The areabull of deviation is corrected or resected in order tobull leave behind as much cartilage and bone as
possiblebull Cartilage resection is minimised and can be
repositioned reshaped or recontoured using a variety of methods
Deviated Nasal Septum
bull ndash Indications of septoplasty before the growth period
bull of the nose is finished should be very limited bull -In these cases surgery must preserve all the
cartilagebull in order to prevent external changes of the
shape ofbull the nose
Deviated Nasal Septum
bull Complicationsbull ndash Frequent complications include haematoma andbull infection Cerebrospinal fluid leak is a rare but
potentiallybull serious complicationbull It is usually the resultbull of avulsion or damage to the cribriform plate whenbull handling the perpendicular plate of the ethmoidbull ndash Other complications include epistaxis nasal
Deviated Nasal Septum
bull Other complications include epistaxis nasal obstruction
bull due to residual deviation synechiae returnbull of the cartilaginous deviation septal perforationbull anosmia and cosmetic nasal deformities suchbull as widened alar rim margins drooping nasal tipbull columella retraction and a sunken dorsum with abull supratip saddle formation
Septal perforation with minor crusting View from provide closure of the
incision
Septal Haematoma
bull A septal haematoma is a blood collection under the perichondrium
bull of the septum and cartilagebull bull bull Epidemiologyaetiologybull ndash A septal haematoma is one of the most
severe complications of nasal trauma
Septal Haematoma
bull Diagnosisbull ndash Signs and symptoms include intense pain
swellingbull haematoma of the upper lip and philtrum
area andbull complete nasal airway obstruction
Septal HaematomaTherapyndash Management consists of drainage through a mucoperichondrial incision Immediate treatment isnecessary to prevent long-term problems such asa saddle-nose deformity perforation columellarretraction and nasal-base widening In childrenseptal destruction can lead to devastating nasal andmidfacial growth abnormalitiesbull Surgeryndash Incision and evacuation of the collection is performedDrainage of a septal haematoma should
Septal HaematomaSurgeryndash Incision and evacuation of the collection is performedDrainage of a septal haematoma should provide closure of the incision
Splints or transseptal sutures are placed to obliterate thepotential space and prevent collectionInfection involving the septal cartilage Reconstruction with autologouscartilage is then performed in a second stage Oral antibiotics should be given
Nasal DeformitySaddle-nose deformityndash A saddle-nose deformity is characterised by a loss ofnasal dorsal height and compromised nasal supportstructures -Other case observed are depressionof the middle vault and dorsum loss of nasal tipsupport and definition shortened (vertical) nasal length over rotation of the nasal tip and retrusion ofthe nasal spine and caudal septum It is also knownas a ldquoPug noserdquo or ldquoboxerrsquos noserdquo both of which referto various degrees of nasal dorsal depressionbull
Nasal DeformityEpidemiologyaetiologyndash Prevalence is higher in population groups prone to facial trauma (ie boxers athletes) those with historiesof intranasal cocaine use nasal surgery (e g radical submucosal septal resection reductive rhinoplasty)ndash A saddle-nose deformity can be congenital or acquired It can be noticed as a part of individual familialsyndromic and ethnic characteristics - Most deformities are due to traumatic and iatrogeniccauses Medical causes are Wegenerrsquosgranulomatosis relapsing polychondritis leprosy (Hansenrsquos disease) syphilis ectodermal dysplasiaand intranasal cocaine use
Nasal Deformity
bull Therapybull ndash Nasal reconstruction indications depend on patientbull selection surgeon experience and aetiology of thebull deformity bull Indications for surgery can be functionalbull aesthetic or most commonly both In individuals
with a compromised nasal airway a nasoseptalbull reconstruction is indicated
Nasal Deformity
bull Contraindications bull include patients with malignantbull chronic or autoimmune disease conditions drugbull abuse poor perioperative risk profile and unrealisticbull expectationsbull ndash Multiple previous rhinoplasties and certain
professionsbull (mixed martial artists boxers and other contactbull sports) are relative contraindications
Nasal DeformitySeptoplastyndash Septoplasty is performed to correct nasal obstructioncaused by septal deformityndash Usually septoplasty is performed under general anaesthesiawith the patient in the supine position with the head elevated by approximately 30 (Righthandedsurgeons approach from the right side)ndash Local vasoconstrictive anaesthesia is applied notonly to reduce postoperative pain but also more importantly to achieve vasoconstriction of themucosa and less intraoperative haemorrhage Lidocainewith adrenaline or epinephrine is usedalthough in patients with cardiac hypersensitivityoxymetazoline might be preferred
Nasal Deformity
bull Septoplasty begins with the incision of septal mucosabull Most operative techniques utilise a hemitransfixionbull incision at the caudal end of septum so thatbull deviation at this point might be reached as wellbull as a transfixion incision that is easily obtained ifbull needed (Right-handed surgeons normally choosebull the left side but that may vary when deviation isbull convex towards the right)
Nasal DeformityA columella retractor is placed over the columellaand by pulling it laterally the caudal border of theseptum is exposed Ala can be protected by an alaprotector A vertical incision with a no 15 bladeover the caudal end of septum is performed untilreaching the plane of the septal cartilage It is essentialto correctly identify the perichondrium and byusing the Cottle elevator dissect and lift it creatinga flap As the dissection proceeds along the septalcartilage a longer speculum (no 5) is introduced sothat elevation of the mucoperichondrium is doneunder constant visual controlndash The next step is to dissect the mucoperiostium
Nasal DeformityDissecting over the bony-cartilaginous junctionwhen joining both tunnels might be difficult and is
especially prone to membrane perforationndash If needed the same tunnels are to be created on the
other side of the septum Then deviated parts of
septum are identified and removed either with a
knife or a Freer chisel
Nasal Deformitybull septum from the maxillary crest the septum mustbull be separated from the perpendicular plate trimmedbull along the inferior border placed back onto the crestbull and sutured to the periosteum If the deformity involvesbull the vomer an osteotome is used Care mustbull be taken not to break the cribriform plate becausebull it could cause a cerebrospinal fistula
Nasal Deformity
bull Once the septal deviation is corrected the flapsbull and hemitransfixion incision are mattressed
withbull absorbable sutures Nasal packing to prevent
synechiaebull and postoperative septal haematoma mightbull be advised but should be removed within 72 h

Nasal Fractures
bull Additionaluseful diagnostic proceduresbull bull Using a 0 or 30deg 4-mm endoscope is helpful inbull the assessment of posterior abnormalities If thebull patient is heavily sedated Brown-Gruss
provocationbull manoeuvres may be performed to determinebull deformities in upper middle or lower segmentsbull by compressing each compartment
Nasal FracturesConservative treatmentndash Treatment of bleedingbull For localised bleeding anterior sources may becauterised by silver nitrate or sealed with topicalmaterials such as thrombin combined withgelatin foam fibrin glue FloSealreg or other procoagulantmaterials If conservative measuresfail a formal anterior packing is placedbull Bleeding from branches of sphenopalatine orethmoid vessels requires anterior-posteriorpacking
Nasal Fractures
bull bull Surgical methods such as direct endoscopic vessel
bull cauterization or ligation have been shown tobull offer better haemostasis and patient comfortbull Angiography with embolization can also be
consideredbull in cases refractory to more conservativebull approaches
Nasal Fractures
bull Type of reductionbull bull Nondisplaced fractures should be treated withbull observation alone Closed nasal reduction is thebull best choice for simple injuries (isolated unilateralbull with medial displacement)bull bull An open approach should be considered in
severebull trauma (bilateral depressed fractures)
Nasal Fracturesbull Surgical principlesbull ndash Topical anaesthesia with cotton pledgets soakedbull with 4 cocaine or 005 oxymethazoline combinedbull with 4 topical lidocaine should be appliedbull for 5ndash10 min Local anaesthesia should also be injectedbull (1 lidocaine and 1100000 epinephrine)bull along the septum lateral walls and floor of the nasalbull cavitybull bull
Nasal FracturesClosed reductionndashndash The nasal bones are grasped between two fingersand pressure is applied laterally in theopposite direction of the deviation A bluntelevator may be used from within the nose incases of significant medial collapse Walshamforceps can be of help Reduction of the septumshould be performed with the use ofAsch forceps
Nasal Fractures
bull To prevent collapse of the postreductionbull framework nasal packing should be placedbull for 3ndash5 days Septum splints are recommendedbull in comminuted septal fractures withbull severe mucosal lesions External nasal splintingbull for 10 days (Aquaplastreg Thermoplastreg)bull provides nasal protection Nasal saline spraysbull prevent crusting and oral antibiotics should
Nasal Fractures
bull Open reductionbull ndashndash Immediate repair of fractures by using
widebull surgical exposure reduction fixation and
reconstructionbull ndashndash The second option is delayed correctionbull (6 months or more) of persistent deformitiesbull using standard techniques of rhinoplasty
Deviated Nasal Septum
bull Definition of the diseasebull ndash Deviation of the nasal septum is a common causebull of unilateral nasal airway obstruction in which thebull nasal septum is displacedbull bull Epidemiologyaetiologybull ndash Developmental septal abnormalities Septal cartilage
damage in the neonatal period andbull during birth can cause severe septal deviation inbull the absence of a history of nasal trauma
Deviated Nasal Septum
bull Symptomsbull ndash Patients may present with a history of sinusitis
allergicbull rhinitis obstructive sleep apnoea previousbull nasal surgery or recent nasal trauma Unilateral or
bilateral nasal airway obstruction that is unrelievedbull with decongestants or nasal steroid sprays is oftenbull seenbull bull
Deviated Nasal SeptumDiagnosisndashExamination external dorsal deviation or the columella and caudal septummay be deflected off the midline (caudal subluxation)ndash Inspections of the nasal cavity and anterior-posteriorrhinoscopy are helpful in diagnosing the locationtype and severity of septal deformityThe endoscope is also useful in identifying polypsthe severity and extent of posterior septaldeviations and bony spurs and locating areas ofseptal perforation or mucosal injury
Deviated Nasal Septum
bull Therapybull ndash Septoplasty is a procedurebull The areabull of deviation is corrected or resected in order tobull leave behind as much cartilage and bone as
possiblebull Cartilage resection is minimised and can be
repositioned reshaped or recontoured using a variety of methods
Deviated Nasal Septum
bull ndash Indications of septoplasty before the growth period
bull of the nose is finished should be very limited bull -In these cases surgery must preserve all the
cartilagebull in order to prevent external changes of the
shape ofbull the nose
Deviated Nasal Septum
bull Complicationsbull ndash Frequent complications include haematoma andbull infection Cerebrospinal fluid leak is a rare but
potentiallybull serious complicationbull It is usually the resultbull of avulsion or damage to the cribriform plate whenbull handling the perpendicular plate of the ethmoidbull ndash Other complications include epistaxis nasal
Deviated Nasal Septum
bull Other complications include epistaxis nasal obstruction
bull due to residual deviation synechiae returnbull of the cartilaginous deviation septal perforationbull anosmia and cosmetic nasal deformities suchbull as widened alar rim margins drooping nasal tipbull columella retraction and a sunken dorsum with abull supratip saddle formation
Septal perforation with minor crusting View from provide closure of the
incision
Septal Haematoma
bull A septal haematoma is a blood collection under the perichondrium
bull of the septum and cartilagebull bull bull Epidemiologyaetiologybull ndash A septal haematoma is one of the most
severe complications of nasal trauma
Septal Haematoma
bull Diagnosisbull ndash Signs and symptoms include intense pain
swellingbull haematoma of the upper lip and philtrum
area andbull complete nasal airway obstruction
Septal HaematomaTherapyndash Management consists of drainage through a mucoperichondrial incision Immediate treatment isnecessary to prevent long-term problems such asa saddle-nose deformity perforation columellarretraction and nasal-base widening In childrenseptal destruction can lead to devastating nasal andmidfacial growth abnormalitiesbull Surgeryndash Incision and evacuation of the collection is performedDrainage of a septal haematoma should
Septal HaematomaSurgeryndash Incision and evacuation of the collection is performedDrainage of a septal haematoma should provide closure of the incision
Splints or transseptal sutures are placed to obliterate thepotential space and prevent collectionInfection involving the septal cartilage Reconstruction with autologouscartilage is then performed in a second stage Oral antibiotics should be given
Nasal DeformitySaddle-nose deformityndash A saddle-nose deformity is characterised by a loss ofnasal dorsal height and compromised nasal supportstructures -Other case observed are depressionof the middle vault and dorsum loss of nasal tipsupport and definition shortened (vertical) nasal length over rotation of the nasal tip and retrusion ofthe nasal spine and caudal septum It is also knownas a ldquoPug noserdquo or ldquoboxerrsquos noserdquo both of which referto various degrees of nasal dorsal depressionbull
Nasal DeformityEpidemiologyaetiologyndash Prevalence is higher in population groups prone to facial trauma (ie boxers athletes) those with historiesof intranasal cocaine use nasal surgery (e g radical submucosal septal resection reductive rhinoplasty)ndash A saddle-nose deformity can be congenital or acquired It can be noticed as a part of individual familialsyndromic and ethnic characteristics - Most deformities are due to traumatic and iatrogeniccauses Medical causes are Wegenerrsquosgranulomatosis relapsing polychondritis leprosy (Hansenrsquos disease) syphilis ectodermal dysplasiaand intranasal cocaine use
Nasal Deformity
bull Therapybull ndash Nasal reconstruction indications depend on patientbull selection surgeon experience and aetiology of thebull deformity bull Indications for surgery can be functionalbull aesthetic or most commonly both In individuals
with a compromised nasal airway a nasoseptalbull reconstruction is indicated
Nasal Deformity
bull Contraindications bull include patients with malignantbull chronic or autoimmune disease conditions drugbull abuse poor perioperative risk profile and unrealisticbull expectationsbull ndash Multiple previous rhinoplasties and certain
professionsbull (mixed martial artists boxers and other contactbull sports) are relative contraindications
Nasal DeformitySeptoplastyndash Septoplasty is performed to correct nasal obstructioncaused by septal deformityndash Usually septoplasty is performed under general anaesthesiawith the patient in the supine position with the head elevated by approximately 30 (Righthandedsurgeons approach from the right side)ndash Local vasoconstrictive anaesthesia is applied notonly to reduce postoperative pain but also more importantly to achieve vasoconstriction of themucosa and less intraoperative haemorrhage Lidocainewith adrenaline or epinephrine is usedalthough in patients with cardiac hypersensitivityoxymetazoline might be preferred
Nasal Deformity
bull Septoplasty begins with the incision of septal mucosabull Most operative techniques utilise a hemitransfixionbull incision at the caudal end of septum so thatbull deviation at this point might be reached as wellbull as a transfixion incision that is easily obtained ifbull needed (Right-handed surgeons normally choosebull the left side but that may vary when deviation isbull convex towards the right)
Nasal DeformityA columella retractor is placed over the columellaand by pulling it laterally the caudal border of theseptum is exposed Ala can be protected by an alaprotector A vertical incision with a no 15 bladeover the caudal end of septum is performed untilreaching the plane of the septal cartilage It is essentialto correctly identify the perichondrium and byusing the Cottle elevator dissect and lift it creatinga flap As the dissection proceeds along the septalcartilage a longer speculum (no 5) is introduced sothat elevation of the mucoperichondrium is doneunder constant visual controlndash The next step is to dissect the mucoperiostium
Nasal DeformityDissecting over the bony-cartilaginous junctionwhen joining both tunnels might be difficult and is
especially prone to membrane perforationndash If needed the same tunnels are to be created on the
other side of the septum Then deviated parts of
septum are identified and removed either with a
knife or a Freer chisel
Nasal Deformitybull septum from the maxillary crest the septum mustbull be separated from the perpendicular plate trimmedbull along the inferior border placed back onto the crestbull and sutured to the periosteum If the deformity involvesbull the vomer an osteotome is used Care mustbull be taken not to break the cribriform plate becausebull it could cause a cerebrospinal fistula
Nasal Deformity
bull Once the septal deviation is corrected the flapsbull and hemitransfixion incision are mattressed
withbull absorbable sutures Nasal packing to prevent
synechiaebull and postoperative septal haematoma mightbull be advised but should be removed within 72 h

Nasal FracturesConservative treatmentndash Treatment of bleedingbull For localised bleeding anterior sources may becauterised by silver nitrate or sealed with topicalmaterials such as thrombin combined withgelatin foam fibrin glue FloSealreg or other procoagulantmaterials If conservative measuresfail a formal anterior packing is placedbull Bleeding from branches of sphenopalatine orethmoid vessels requires anterior-posteriorpacking
Nasal Fractures
bull bull Surgical methods such as direct endoscopic vessel
bull cauterization or ligation have been shown tobull offer better haemostasis and patient comfortbull Angiography with embolization can also be
consideredbull in cases refractory to more conservativebull approaches
Nasal Fractures
bull Type of reductionbull bull Nondisplaced fractures should be treated withbull observation alone Closed nasal reduction is thebull best choice for simple injuries (isolated unilateralbull with medial displacement)bull bull An open approach should be considered in
severebull trauma (bilateral depressed fractures)
Nasal Fracturesbull Surgical principlesbull ndash Topical anaesthesia with cotton pledgets soakedbull with 4 cocaine or 005 oxymethazoline combinedbull with 4 topical lidocaine should be appliedbull for 5ndash10 min Local anaesthesia should also be injectedbull (1 lidocaine and 1100000 epinephrine)bull along the septum lateral walls and floor of the nasalbull cavitybull bull
Nasal FracturesClosed reductionndashndash The nasal bones are grasped between two fingersand pressure is applied laterally in theopposite direction of the deviation A bluntelevator may be used from within the nose incases of significant medial collapse Walshamforceps can be of help Reduction of the septumshould be performed with the use ofAsch forceps
Nasal Fractures
bull To prevent collapse of the postreductionbull framework nasal packing should be placedbull for 3ndash5 days Septum splints are recommendedbull in comminuted septal fractures withbull severe mucosal lesions External nasal splintingbull for 10 days (Aquaplastreg Thermoplastreg)bull provides nasal protection Nasal saline spraysbull prevent crusting and oral antibiotics should
Nasal Fractures
bull Open reductionbull ndashndash Immediate repair of fractures by using
widebull surgical exposure reduction fixation and
reconstructionbull ndashndash The second option is delayed correctionbull (6 months or more) of persistent deformitiesbull using standard techniques of rhinoplasty
Deviated Nasal Septum
bull Definition of the diseasebull ndash Deviation of the nasal septum is a common causebull of unilateral nasal airway obstruction in which thebull nasal septum is displacedbull bull Epidemiologyaetiologybull ndash Developmental septal abnormalities Septal cartilage
damage in the neonatal period andbull during birth can cause severe septal deviation inbull the absence of a history of nasal trauma
Deviated Nasal Septum
bull Symptomsbull ndash Patients may present with a history of sinusitis
allergicbull rhinitis obstructive sleep apnoea previousbull nasal surgery or recent nasal trauma Unilateral or
bilateral nasal airway obstruction that is unrelievedbull with decongestants or nasal steroid sprays is oftenbull seenbull bull
Deviated Nasal SeptumDiagnosisndashExamination external dorsal deviation or the columella and caudal septummay be deflected off the midline (caudal subluxation)ndash Inspections of the nasal cavity and anterior-posteriorrhinoscopy are helpful in diagnosing the locationtype and severity of septal deformityThe endoscope is also useful in identifying polypsthe severity and extent of posterior septaldeviations and bony spurs and locating areas ofseptal perforation or mucosal injury
Deviated Nasal Septum
bull Therapybull ndash Septoplasty is a procedurebull The areabull of deviation is corrected or resected in order tobull leave behind as much cartilage and bone as
possiblebull Cartilage resection is minimised and can be
repositioned reshaped or recontoured using a variety of methods
Deviated Nasal Septum
bull ndash Indications of septoplasty before the growth period
bull of the nose is finished should be very limited bull -In these cases surgery must preserve all the
cartilagebull in order to prevent external changes of the
shape ofbull the nose
Deviated Nasal Septum
bull Complicationsbull ndash Frequent complications include haematoma andbull infection Cerebrospinal fluid leak is a rare but
potentiallybull serious complicationbull It is usually the resultbull of avulsion or damage to the cribriform plate whenbull handling the perpendicular plate of the ethmoidbull ndash Other complications include epistaxis nasal
Deviated Nasal Septum
bull Other complications include epistaxis nasal obstruction
bull due to residual deviation synechiae returnbull of the cartilaginous deviation septal perforationbull anosmia and cosmetic nasal deformities suchbull as widened alar rim margins drooping nasal tipbull columella retraction and a sunken dorsum with abull supratip saddle formation
Septal perforation with minor crusting View from provide closure of the
incision
Septal Haematoma
bull A septal haematoma is a blood collection under the perichondrium
bull of the septum and cartilagebull bull bull Epidemiologyaetiologybull ndash A septal haematoma is one of the most
severe complications of nasal trauma
Septal Haematoma
bull Diagnosisbull ndash Signs and symptoms include intense pain
swellingbull haematoma of the upper lip and philtrum
area andbull complete nasal airway obstruction
Septal HaematomaTherapyndash Management consists of drainage through a mucoperichondrial incision Immediate treatment isnecessary to prevent long-term problems such asa saddle-nose deformity perforation columellarretraction and nasal-base widening In childrenseptal destruction can lead to devastating nasal andmidfacial growth abnormalitiesbull Surgeryndash Incision and evacuation of the collection is performedDrainage of a septal haematoma should
Septal HaematomaSurgeryndash Incision and evacuation of the collection is performedDrainage of a septal haematoma should provide closure of the incision
Splints or transseptal sutures are placed to obliterate thepotential space and prevent collectionInfection involving the septal cartilage Reconstruction with autologouscartilage is then performed in a second stage Oral antibiotics should be given
Nasal DeformitySaddle-nose deformityndash A saddle-nose deformity is characterised by a loss ofnasal dorsal height and compromised nasal supportstructures -Other case observed are depressionof the middle vault and dorsum loss of nasal tipsupport and definition shortened (vertical) nasal length over rotation of the nasal tip and retrusion ofthe nasal spine and caudal septum It is also knownas a ldquoPug noserdquo or ldquoboxerrsquos noserdquo both of which referto various degrees of nasal dorsal depressionbull
Nasal DeformityEpidemiologyaetiologyndash Prevalence is higher in population groups prone to facial trauma (ie boxers athletes) those with historiesof intranasal cocaine use nasal surgery (e g radical submucosal septal resection reductive rhinoplasty)ndash A saddle-nose deformity can be congenital or acquired It can be noticed as a part of individual familialsyndromic and ethnic characteristics - Most deformities are due to traumatic and iatrogeniccauses Medical causes are Wegenerrsquosgranulomatosis relapsing polychondritis leprosy (Hansenrsquos disease) syphilis ectodermal dysplasiaand intranasal cocaine use
Nasal Deformity
bull Therapybull ndash Nasal reconstruction indications depend on patientbull selection surgeon experience and aetiology of thebull deformity bull Indications for surgery can be functionalbull aesthetic or most commonly both In individuals
with a compromised nasal airway a nasoseptalbull reconstruction is indicated
Nasal Deformity
bull Contraindications bull include patients with malignantbull chronic or autoimmune disease conditions drugbull abuse poor perioperative risk profile and unrealisticbull expectationsbull ndash Multiple previous rhinoplasties and certain
professionsbull (mixed martial artists boxers and other contactbull sports) are relative contraindications
Nasal DeformitySeptoplastyndash Septoplasty is performed to correct nasal obstructioncaused by septal deformityndash Usually septoplasty is performed under general anaesthesiawith the patient in the supine position with the head elevated by approximately 30 (Righthandedsurgeons approach from the right side)ndash Local vasoconstrictive anaesthesia is applied notonly to reduce postoperative pain but also more importantly to achieve vasoconstriction of themucosa and less intraoperative haemorrhage Lidocainewith adrenaline or epinephrine is usedalthough in patients with cardiac hypersensitivityoxymetazoline might be preferred
Nasal Deformity
bull Septoplasty begins with the incision of septal mucosabull Most operative techniques utilise a hemitransfixionbull incision at the caudal end of septum so thatbull deviation at this point might be reached as wellbull as a transfixion incision that is easily obtained ifbull needed (Right-handed surgeons normally choosebull the left side but that may vary when deviation isbull convex towards the right)
Nasal DeformityA columella retractor is placed over the columellaand by pulling it laterally the caudal border of theseptum is exposed Ala can be protected by an alaprotector A vertical incision with a no 15 bladeover the caudal end of septum is performed untilreaching the plane of the septal cartilage It is essentialto correctly identify the perichondrium and byusing the Cottle elevator dissect and lift it creatinga flap As the dissection proceeds along the septalcartilage a longer speculum (no 5) is introduced sothat elevation of the mucoperichondrium is doneunder constant visual controlndash The next step is to dissect the mucoperiostium
Nasal DeformityDissecting over the bony-cartilaginous junctionwhen joining both tunnels might be difficult and is
especially prone to membrane perforationndash If needed the same tunnels are to be created on the
other side of the septum Then deviated parts of
septum are identified and removed either with a
knife or a Freer chisel
Nasal Deformitybull septum from the maxillary crest the septum mustbull be separated from the perpendicular plate trimmedbull along the inferior border placed back onto the crestbull and sutured to the periosteum If the deformity involvesbull the vomer an osteotome is used Care mustbull be taken not to break the cribriform plate becausebull it could cause a cerebrospinal fistula
Nasal Deformity
bull Once the septal deviation is corrected the flapsbull and hemitransfixion incision are mattressed
withbull absorbable sutures Nasal packing to prevent
synechiaebull and postoperative septal haematoma mightbull be advised but should be removed within 72 h

Nasal Fractures
bull bull Surgical methods such as direct endoscopic vessel
bull cauterization or ligation have been shown tobull offer better haemostasis and patient comfortbull Angiography with embolization can also be
consideredbull in cases refractory to more conservativebull approaches
Nasal Fractures
bull Type of reductionbull bull Nondisplaced fractures should be treated withbull observation alone Closed nasal reduction is thebull best choice for simple injuries (isolated unilateralbull with medial displacement)bull bull An open approach should be considered in
severebull trauma (bilateral depressed fractures)
Nasal Fracturesbull Surgical principlesbull ndash Topical anaesthesia with cotton pledgets soakedbull with 4 cocaine or 005 oxymethazoline combinedbull with 4 topical lidocaine should be appliedbull for 5ndash10 min Local anaesthesia should also be injectedbull (1 lidocaine and 1100000 epinephrine)bull along the septum lateral walls and floor of the nasalbull cavitybull bull
Nasal FracturesClosed reductionndashndash The nasal bones are grasped between two fingersand pressure is applied laterally in theopposite direction of the deviation A bluntelevator may be used from within the nose incases of significant medial collapse Walshamforceps can be of help Reduction of the septumshould be performed with the use ofAsch forceps
Nasal Fractures
bull To prevent collapse of the postreductionbull framework nasal packing should be placedbull for 3ndash5 days Septum splints are recommendedbull in comminuted septal fractures withbull severe mucosal lesions External nasal splintingbull for 10 days (Aquaplastreg Thermoplastreg)bull provides nasal protection Nasal saline spraysbull prevent crusting and oral antibiotics should
Nasal Fractures
bull Open reductionbull ndashndash Immediate repair of fractures by using
widebull surgical exposure reduction fixation and
reconstructionbull ndashndash The second option is delayed correctionbull (6 months or more) of persistent deformitiesbull using standard techniques of rhinoplasty
Deviated Nasal Septum
bull Definition of the diseasebull ndash Deviation of the nasal septum is a common causebull of unilateral nasal airway obstruction in which thebull nasal septum is displacedbull bull Epidemiologyaetiologybull ndash Developmental septal abnormalities Septal cartilage
damage in the neonatal period andbull during birth can cause severe septal deviation inbull the absence of a history of nasal trauma
Deviated Nasal Septum
bull Symptomsbull ndash Patients may present with a history of sinusitis
allergicbull rhinitis obstructive sleep apnoea previousbull nasal surgery or recent nasal trauma Unilateral or
bilateral nasal airway obstruction that is unrelievedbull with decongestants or nasal steroid sprays is oftenbull seenbull bull
Deviated Nasal SeptumDiagnosisndashExamination external dorsal deviation or the columella and caudal septummay be deflected off the midline (caudal subluxation)ndash Inspections of the nasal cavity and anterior-posteriorrhinoscopy are helpful in diagnosing the locationtype and severity of septal deformityThe endoscope is also useful in identifying polypsthe severity and extent of posterior septaldeviations and bony spurs and locating areas ofseptal perforation or mucosal injury
Deviated Nasal Septum
bull Therapybull ndash Septoplasty is a procedurebull The areabull of deviation is corrected or resected in order tobull leave behind as much cartilage and bone as
possiblebull Cartilage resection is minimised and can be
repositioned reshaped or recontoured using a variety of methods
Deviated Nasal Septum
bull ndash Indications of septoplasty before the growth period
bull of the nose is finished should be very limited bull -In these cases surgery must preserve all the
cartilagebull in order to prevent external changes of the
shape ofbull the nose
Deviated Nasal Septum
bull Complicationsbull ndash Frequent complications include haematoma andbull infection Cerebrospinal fluid leak is a rare but
potentiallybull serious complicationbull It is usually the resultbull of avulsion or damage to the cribriform plate whenbull handling the perpendicular plate of the ethmoidbull ndash Other complications include epistaxis nasal
Deviated Nasal Septum
bull Other complications include epistaxis nasal obstruction
bull due to residual deviation synechiae returnbull of the cartilaginous deviation septal perforationbull anosmia and cosmetic nasal deformities suchbull as widened alar rim margins drooping nasal tipbull columella retraction and a sunken dorsum with abull supratip saddle formation
Septal perforation with minor crusting View from provide closure of the
incision
Septal Haematoma
bull A septal haematoma is a blood collection under the perichondrium
bull of the septum and cartilagebull bull bull Epidemiologyaetiologybull ndash A septal haematoma is one of the most
severe complications of nasal trauma
Septal Haematoma
bull Diagnosisbull ndash Signs and symptoms include intense pain
swellingbull haematoma of the upper lip and philtrum
area andbull complete nasal airway obstruction
Septal HaematomaTherapyndash Management consists of drainage through a mucoperichondrial incision Immediate treatment isnecessary to prevent long-term problems such asa saddle-nose deformity perforation columellarretraction and nasal-base widening In childrenseptal destruction can lead to devastating nasal andmidfacial growth abnormalitiesbull Surgeryndash Incision and evacuation of the collection is performedDrainage of a septal haematoma should
Septal HaematomaSurgeryndash Incision and evacuation of the collection is performedDrainage of a septal haematoma should provide closure of the incision
Splints or transseptal sutures are placed to obliterate thepotential space and prevent collectionInfection involving the septal cartilage Reconstruction with autologouscartilage is then performed in a second stage Oral antibiotics should be given
Nasal DeformitySaddle-nose deformityndash A saddle-nose deformity is characterised by a loss ofnasal dorsal height and compromised nasal supportstructures -Other case observed are depressionof the middle vault and dorsum loss of nasal tipsupport and definition shortened (vertical) nasal length over rotation of the nasal tip and retrusion ofthe nasal spine and caudal septum It is also knownas a ldquoPug noserdquo or ldquoboxerrsquos noserdquo both of which referto various degrees of nasal dorsal depressionbull
Nasal DeformityEpidemiologyaetiologyndash Prevalence is higher in population groups prone to facial trauma (ie boxers athletes) those with historiesof intranasal cocaine use nasal surgery (e g radical submucosal septal resection reductive rhinoplasty)ndash A saddle-nose deformity can be congenital or acquired It can be noticed as a part of individual familialsyndromic and ethnic characteristics - Most deformities are due to traumatic and iatrogeniccauses Medical causes are Wegenerrsquosgranulomatosis relapsing polychondritis leprosy (Hansenrsquos disease) syphilis ectodermal dysplasiaand intranasal cocaine use
Nasal Deformity
bull Therapybull ndash Nasal reconstruction indications depend on patientbull selection surgeon experience and aetiology of thebull deformity bull Indications for surgery can be functionalbull aesthetic or most commonly both In individuals
with a compromised nasal airway a nasoseptalbull reconstruction is indicated
Nasal Deformity
bull Contraindications bull include patients with malignantbull chronic or autoimmune disease conditions drugbull abuse poor perioperative risk profile and unrealisticbull expectationsbull ndash Multiple previous rhinoplasties and certain
professionsbull (mixed martial artists boxers and other contactbull sports) are relative contraindications
Nasal DeformitySeptoplastyndash Septoplasty is performed to correct nasal obstructioncaused by septal deformityndash Usually septoplasty is performed under general anaesthesiawith the patient in the supine position with the head elevated by approximately 30 (Righthandedsurgeons approach from the right side)ndash Local vasoconstrictive anaesthesia is applied notonly to reduce postoperative pain but also more importantly to achieve vasoconstriction of themucosa and less intraoperative haemorrhage Lidocainewith adrenaline or epinephrine is usedalthough in patients with cardiac hypersensitivityoxymetazoline might be preferred
Nasal Deformity
bull Septoplasty begins with the incision of septal mucosabull Most operative techniques utilise a hemitransfixionbull incision at the caudal end of septum so thatbull deviation at this point might be reached as wellbull as a transfixion incision that is easily obtained ifbull needed (Right-handed surgeons normally choosebull the left side but that may vary when deviation isbull convex towards the right)
Nasal DeformityA columella retractor is placed over the columellaand by pulling it laterally the caudal border of theseptum is exposed Ala can be protected by an alaprotector A vertical incision with a no 15 bladeover the caudal end of septum is performed untilreaching the plane of the septal cartilage It is essentialto correctly identify the perichondrium and byusing the Cottle elevator dissect and lift it creatinga flap As the dissection proceeds along the septalcartilage a longer speculum (no 5) is introduced sothat elevation of the mucoperichondrium is doneunder constant visual controlndash The next step is to dissect the mucoperiostium
Nasal DeformityDissecting over the bony-cartilaginous junctionwhen joining both tunnels might be difficult and is
especially prone to membrane perforationndash If needed the same tunnels are to be created on the
other side of the septum Then deviated parts of
septum are identified and removed either with a
knife or a Freer chisel
Nasal Deformitybull septum from the maxillary crest the septum mustbull be separated from the perpendicular plate trimmedbull along the inferior border placed back onto the crestbull and sutured to the periosteum If the deformity involvesbull the vomer an osteotome is used Care mustbull be taken not to break the cribriform plate becausebull it could cause a cerebrospinal fistula
Nasal Deformity
bull Once the septal deviation is corrected the flapsbull and hemitransfixion incision are mattressed
withbull absorbable sutures Nasal packing to prevent
synechiaebull and postoperative septal haematoma mightbull be advised but should be removed within 72 h

Nasal Fractures
bull Type of reductionbull bull Nondisplaced fractures should be treated withbull observation alone Closed nasal reduction is thebull best choice for simple injuries (isolated unilateralbull with medial displacement)bull bull An open approach should be considered in
severebull trauma (bilateral depressed fractures)
Nasal Fracturesbull Surgical principlesbull ndash Topical anaesthesia with cotton pledgets soakedbull with 4 cocaine or 005 oxymethazoline combinedbull with 4 topical lidocaine should be appliedbull for 5ndash10 min Local anaesthesia should also be injectedbull (1 lidocaine and 1100000 epinephrine)bull along the septum lateral walls and floor of the nasalbull cavitybull bull
Nasal FracturesClosed reductionndashndash The nasal bones are grasped between two fingersand pressure is applied laterally in theopposite direction of the deviation A bluntelevator may be used from within the nose incases of significant medial collapse Walshamforceps can be of help Reduction of the septumshould be performed with the use ofAsch forceps
Nasal Fractures
bull To prevent collapse of the postreductionbull framework nasal packing should be placedbull for 3ndash5 days Septum splints are recommendedbull in comminuted septal fractures withbull severe mucosal lesions External nasal splintingbull for 10 days (Aquaplastreg Thermoplastreg)bull provides nasal protection Nasal saline spraysbull prevent crusting and oral antibiotics should
Nasal Fractures
bull Open reductionbull ndashndash Immediate repair of fractures by using
widebull surgical exposure reduction fixation and
reconstructionbull ndashndash The second option is delayed correctionbull (6 months or more) of persistent deformitiesbull using standard techniques of rhinoplasty
Deviated Nasal Septum
bull Definition of the diseasebull ndash Deviation of the nasal septum is a common causebull of unilateral nasal airway obstruction in which thebull nasal septum is displacedbull bull Epidemiologyaetiologybull ndash Developmental septal abnormalities Septal cartilage
damage in the neonatal period andbull during birth can cause severe septal deviation inbull the absence of a history of nasal trauma
Deviated Nasal Septum
bull Symptomsbull ndash Patients may present with a history of sinusitis
allergicbull rhinitis obstructive sleep apnoea previousbull nasal surgery or recent nasal trauma Unilateral or
bilateral nasal airway obstruction that is unrelievedbull with decongestants or nasal steroid sprays is oftenbull seenbull bull
Deviated Nasal SeptumDiagnosisndashExamination external dorsal deviation or the columella and caudal septummay be deflected off the midline (caudal subluxation)ndash Inspections of the nasal cavity and anterior-posteriorrhinoscopy are helpful in diagnosing the locationtype and severity of septal deformityThe endoscope is also useful in identifying polypsthe severity and extent of posterior septaldeviations and bony spurs and locating areas ofseptal perforation or mucosal injury
Deviated Nasal Septum
bull Therapybull ndash Septoplasty is a procedurebull The areabull of deviation is corrected or resected in order tobull leave behind as much cartilage and bone as
possiblebull Cartilage resection is minimised and can be
repositioned reshaped or recontoured using a variety of methods
Deviated Nasal Septum
bull ndash Indications of septoplasty before the growth period
bull of the nose is finished should be very limited bull -In these cases surgery must preserve all the
cartilagebull in order to prevent external changes of the
shape ofbull the nose
Deviated Nasal Septum
bull Complicationsbull ndash Frequent complications include haematoma andbull infection Cerebrospinal fluid leak is a rare but
potentiallybull serious complicationbull It is usually the resultbull of avulsion or damage to the cribriform plate whenbull handling the perpendicular plate of the ethmoidbull ndash Other complications include epistaxis nasal
Deviated Nasal Septum
bull Other complications include epistaxis nasal obstruction
bull due to residual deviation synechiae returnbull of the cartilaginous deviation septal perforationbull anosmia and cosmetic nasal deformities suchbull as widened alar rim margins drooping nasal tipbull columella retraction and a sunken dorsum with abull supratip saddle formation
Septal perforation with minor crusting View from provide closure of the
incision
Septal Haematoma
bull A septal haematoma is a blood collection under the perichondrium
bull of the septum and cartilagebull bull bull Epidemiologyaetiologybull ndash A septal haematoma is one of the most
severe complications of nasal trauma
Septal Haematoma
bull Diagnosisbull ndash Signs and symptoms include intense pain
swellingbull haematoma of the upper lip and philtrum
area andbull complete nasal airway obstruction
Septal HaematomaTherapyndash Management consists of drainage through a mucoperichondrial incision Immediate treatment isnecessary to prevent long-term problems such asa saddle-nose deformity perforation columellarretraction and nasal-base widening In childrenseptal destruction can lead to devastating nasal andmidfacial growth abnormalitiesbull Surgeryndash Incision and evacuation of the collection is performedDrainage of a septal haematoma should
Septal HaematomaSurgeryndash Incision and evacuation of the collection is performedDrainage of a septal haematoma should provide closure of the incision
Splints or transseptal sutures are placed to obliterate thepotential space and prevent collectionInfection involving the septal cartilage Reconstruction with autologouscartilage is then performed in a second stage Oral antibiotics should be given
Nasal DeformitySaddle-nose deformityndash A saddle-nose deformity is characterised by a loss ofnasal dorsal height and compromised nasal supportstructures -Other case observed are depressionof the middle vault and dorsum loss of nasal tipsupport and definition shortened (vertical) nasal length over rotation of the nasal tip and retrusion ofthe nasal spine and caudal septum It is also knownas a ldquoPug noserdquo or ldquoboxerrsquos noserdquo both of which referto various degrees of nasal dorsal depressionbull
Nasal DeformityEpidemiologyaetiologyndash Prevalence is higher in population groups prone to facial trauma (ie boxers athletes) those with historiesof intranasal cocaine use nasal surgery (e g radical submucosal septal resection reductive rhinoplasty)ndash A saddle-nose deformity can be congenital or acquired It can be noticed as a part of individual familialsyndromic and ethnic characteristics - Most deformities are due to traumatic and iatrogeniccauses Medical causes are Wegenerrsquosgranulomatosis relapsing polychondritis leprosy (Hansenrsquos disease) syphilis ectodermal dysplasiaand intranasal cocaine use
Nasal Deformity
bull Therapybull ndash Nasal reconstruction indications depend on patientbull selection surgeon experience and aetiology of thebull deformity bull Indications for surgery can be functionalbull aesthetic or most commonly both In individuals
with a compromised nasal airway a nasoseptalbull reconstruction is indicated
Nasal Deformity
bull Contraindications bull include patients with malignantbull chronic or autoimmune disease conditions drugbull abuse poor perioperative risk profile and unrealisticbull expectationsbull ndash Multiple previous rhinoplasties and certain
professionsbull (mixed martial artists boxers and other contactbull sports) are relative contraindications
Nasal DeformitySeptoplastyndash Septoplasty is performed to correct nasal obstructioncaused by septal deformityndash Usually septoplasty is performed under general anaesthesiawith the patient in the supine position with the head elevated by approximately 30 (Righthandedsurgeons approach from the right side)ndash Local vasoconstrictive anaesthesia is applied notonly to reduce postoperative pain but also more importantly to achieve vasoconstriction of themucosa and less intraoperative haemorrhage Lidocainewith adrenaline or epinephrine is usedalthough in patients with cardiac hypersensitivityoxymetazoline might be preferred
Nasal Deformity
bull Septoplasty begins with the incision of septal mucosabull Most operative techniques utilise a hemitransfixionbull incision at the caudal end of septum so thatbull deviation at this point might be reached as wellbull as a transfixion incision that is easily obtained ifbull needed (Right-handed surgeons normally choosebull the left side but that may vary when deviation isbull convex towards the right)
Nasal DeformityA columella retractor is placed over the columellaand by pulling it laterally the caudal border of theseptum is exposed Ala can be protected by an alaprotector A vertical incision with a no 15 bladeover the caudal end of septum is performed untilreaching the plane of the septal cartilage It is essentialto correctly identify the perichondrium and byusing the Cottle elevator dissect and lift it creatinga flap As the dissection proceeds along the septalcartilage a longer speculum (no 5) is introduced sothat elevation of the mucoperichondrium is doneunder constant visual controlndash The next step is to dissect the mucoperiostium
Nasal DeformityDissecting over the bony-cartilaginous junctionwhen joining both tunnels might be difficult and is
especially prone to membrane perforationndash If needed the same tunnels are to be created on the
other side of the septum Then deviated parts of
septum are identified and removed either with a
knife or a Freer chisel
Nasal Deformitybull septum from the maxillary crest the septum mustbull be separated from the perpendicular plate trimmedbull along the inferior border placed back onto the crestbull and sutured to the periosteum If the deformity involvesbull the vomer an osteotome is used Care mustbull be taken not to break the cribriform plate becausebull it could cause a cerebrospinal fistula
Nasal Deformity
bull Once the septal deviation is corrected the flapsbull and hemitransfixion incision are mattressed
withbull absorbable sutures Nasal packing to prevent
synechiaebull and postoperative septal haematoma mightbull be advised but should be removed within 72 h

Nasal Fracturesbull Surgical principlesbull ndash Topical anaesthesia with cotton pledgets soakedbull with 4 cocaine or 005 oxymethazoline combinedbull with 4 topical lidocaine should be appliedbull for 5ndash10 min Local anaesthesia should also be injectedbull (1 lidocaine and 1100000 epinephrine)bull along the septum lateral walls and floor of the nasalbull cavitybull bull
Nasal FracturesClosed reductionndashndash The nasal bones are grasped between two fingersand pressure is applied laterally in theopposite direction of the deviation A bluntelevator may be used from within the nose incases of significant medial collapse Walshamforceps can be of help Reduction of the septumshould be performed with the use ofAsch forceps
Nasal Fractures
bull To prevent collapse of the postreductionbull framework nasal packing should be placedbull for 3ndash5 days Septum splints are recommendedbull in comminuted septal fractures withbull severe mucosal lesions External nasal splintingbull for 10 days (Aquaplastreg Thermoplastreg)bull provides nasal protection Nasal saline spraysbull prevent crusting and oral antibiotics should
Nasal Fractures
bull Open reductionbull ndashndash Immediate repair of fractures by using
widebull surgical exposure reduction fixation and
reconstructionbull ndashndash The second option is delayed correctionbull (6 months or more) of persistent deformitiesbull using standard techniques of rhinoplasty
Deviated Nasal Septum
bull Definition of the diseasebull ndash Deviation of the nasal septum is a common causebull of unilateral nasal airway obstruction in which thebull nasal septum is displacedbull bull Epidemiologyaetiologybull ndash Developmental septal abnormalities Septal cartilage
damage in the neonatal period andbull during birth can cause severe septal deviation inbull the absence of a history of nasal trauma
Deviated Nasal Septum
bull Symptomsbull ndash Patients may present with a history of sinusitis
allergicbull rhinitis obstructive sleep apnoea previousbull nasal surgery or recent nasal trauma Unilateral or
bilateral nasal airway obstruction that is unrelievedbull with decongestants or nasal steroid sprays is oftenbull seenbull bull
Deviated Nasal SeptumDiagnosisndashExamination external dorsal deviation or the columella and caudal septummay be deflected off the midline (caudal subluxation)ndash Inspections of the nasal cavity and anterior-posteriorrhinoscopy are helpful in diagnosing the locationtype and severity of septal deformityThe endoscope is also useful in identifying polypsthe severity and extent of posterior septaldeviations and bony spurs and locating areas ofseptal perforation or mucosal injury
Deviated Nasal Septum
bull Therapybull ndash Septoplasty is a procedurebull The areabull of deviation is corrected or resected in order tobull leave behind as much cartilage and bone as
possiblebull Cartilage resection is minimised and can be
repositioned reshaped or recontoured using a variety of methods
Deviated Nasal Septum
bull ndash Indications of septoplasty before the growth period
bull of the nose is finished should be very limited bull -In these cases surgery must preserve all the
cartilagebull in order to prevent external changes of the
shape ofbull the nose
Deviated Nasal Septum
bull Complicationsbull ndash Frequent complications include haematoma andbull infection Cerebrospinal fluid leak is a rare but
potentiallybull serious complicationbull It is usually the resultbull of avulsion or damage to the cribriform plate whenbull handling the perpendicular plate of the ethmoidbull ndash Other complications include epistaxis nasal
Deviated Nasal Septum
bull Other complications include epistaxis nasal obstruction
bull due to residual deviation synechiae returnbull of the cartilaginous deviation septal perforationbull anosmia and cosmetic nasal deformities suchbull as widened alar rim margins drooping nasal tipbull columella retraction and a sunken dorsum with abull supratip saddle formation
Septal perforation with minor crusting View from provide closure of the
incision
Septal Haematoma
bull A septal haematoma is a blood collection under the perichondrium
bull of the septum and cartilagebull bull bull Epidemiologyaetiologybull ndash A septal haematoma is one of the most
severe complications of nasal trauma
Septal Haematoma
bull Diagnosisbull ndash Signs and symptoms include intense pain
swellingbull haematoma of the upper lip and philtrum
area andbull complete nasal airway obstruction
Septal HaematomaTherapyndash Management consists of drainage through a mucoperichondrial incision Immediate treatment isnecessary to prevent long-term problems such asa saddle-nose deformity perforation columellarretraction and nasal-base widening In childrenseptal destruction can lead to devastating nasal andmidfacial growth abnormalitiesbull Surgeryndash Incision and evacuation of the collection is performedDrainage of a septal haematoma should
Septal HaematomaSurgeryndash Incision and evacuation of the collection is performedDrainage of a septal haematoma should provide closure of the incision
Splints or transseptal sutures are placed to obliterate thepotential space and prevent collectionInfection involving the septal cartilage Reconstruction with autologouscartilage is then performed in a second stage Oral antibiotics should be given
Nasal DeformitySaddle-nose deformityndash A saddle-nose deformity is characterised by a loss ofnasal dorsal height and compromised nasal supportstructures -Other case observed are depressionof the middle vault and dorsum loss of nasal tipsupport and definition shortened (vertical) nasal length over rotation of the nasal tip and retrusion ofthe nasal spine and caudal septum It is also knownas a ldquoPug noserdquo or ldquoboxerrsquos noserdquo both of which referto various degrees of nasal dorsal depressionbull
Nasal DeformityEpidemiologyaetiologyndash Prevalence is higher in population groups prone to facial trauma (ie boxers athletes) those with historiesof intranasal cocaine use nasal surgery (e g radical submucosal septal resection reductive rhinoplasty)ndash A saddle-nose deformity can be congenital or acquired It can be noticed as a part of individual familialsyndromic and ethnic characteristics - Most deformities are due to traumatic and iatrogeniccauses Medical causes are Wegenerrsquosgranulomatosis relapsing polychondritis leprosy (Hansenrsquos disease) syphilis ectodermal dysplasiaand intranasal cocaine use
Nasal Deformity
bull Therapybull ndash Nasal reconstruction indications depend on patientbull selection surgeon experience and aetiology of thebull deformity bull Indications for surgery can be functionalbull aesthetic or most commonly both In individuals
with a compromised nasal airway a nasoseptalbull reconstruction is indicated
Nasal Deformity
bull Contraindications bull include patients with malignantbull chronic or autoimmune disease conditions drugbull abuse poor perioperative risk profile and unrealisticbull expectationsbull ndash Multiple previous rhinoplasties and certain
professionsbull (mixed martial artists boxers and other contactbull sports) are relative contraindications
Nasal DeformitySeptoplastyndash Septoplasty is performed to correct nasal obstructioncaused by septal deformityndash Usually septoplasty is performed under general anaesthesiawith the patient in the supine position with the head elevated by approximately 30 (Righthandedsurgeons approach from the right side)ndash Local vasoconstrictive anaesthesia is applied notonly to reduce postoperative pain but also more importantly to achieve vasoconstriction of themucosa and less intraoperative haemorrhage Lidocainewith adrenaline or epinephrine is usedalthough in patients with cardiac hypersensitivityoxymetazoline might be preferred
Nasal Deformity
bull Septoplasty begins with the incision of septal mucosabull Most operative techniques utilise a hemitransfixionbull incision at the caudal end of septum so thatbull deviation at this point might be reached as wellbull as a transfixion incision that is easily obtained ifbull needed (Right-handed surgeons normally choosebull the left side but that may vary when deviation isbull convex towards the right)
Nasal DeformityA columella retractor is placed over the columellaand by pulling it laterally the caudal border of theseptum is exposed Ala can be protected by an alaprotector A vertical incision with a no 15 bladeover the caudal end of septum is performed untilreaching the plane of the septal cartilage It is essentialto correctly identify the perichondrium and byusing the Cottle elevator dissect and lift it creatinga flap As the dissection proceeds along the septalcartilage a longer speculum (no 5) is introduced sothat elevation of the mucoperichondrium is doneunder constant visual controlndash The next step is to dissect the mucoperiostium
Nasal DeformityDissecting over the bony-cartilaginous junctionwhen joining both tunnels might be difficult and is
especially prone to membrane perforationndash If needed the same tunnels are to be created on the
other side of the septum Then deviated parts of
septum are identified and removed either with a
knife or a Freer chisel
Nasal Deformitybull septum from the maxillary crest the septum mustbull be separated from the perpendicular plate trimmedbull along the inferior border placed back onto the crestbull and sutured to the periosteum If the deformity involvesbull the vomer an osteotome is used Care mustbull be taken not to break the cribriform plate becausebull it could cause a cerebrospinal fistula
Nasal Deformity
bull Once the septal deviation is corrected the flapsbull and hemitransfixion incision are mattressed
withbull absorbable sutures Nasal packing to prevent
synechiaebull and postoperative septal haematoma mightbull be advised but should be removed within 72 h

Nasal FracturesClosed reductionndashndash The nasal bones are grasped between two fingersand pressure is applied laterally in theopposite direction of the deviation A bluntelevator may be used from within the nose incases of significant medial collapse Walshamforceps can be of help Reduction of the septumshould be performed with the use ofAsch forceps
Nasal Fractures
bull To prevent collapse of the postreductionbull framework nasal packing should be placedbull for 3ndash5 days Septum splints are recommendedbull in comminuted septal fractures withbull severe mucosal lesions External nasal splintingbull for 10 days (Aquaplastreg Thermoplastreg)bull provides nasal protection Nasal saline spraysbull prevent crusting and oral antibiotics should
Nasal Fractures
bull Open reductionbull ndashndash Immediate repair of fractures by using
widebull surgical exposure reduction fixation and
reconstructionbull ndashndash The second option is delayed correctionbull (6 months or more) of persistent deformitiesbull using standard techniques of rhinoplasty
Deviated Nasal Septum
bull Definition of the diseasebull ndash Deviation of the nasal septum is a common causebull of unilateral nasal airway obstruction in which thebull nasal septum is displacedbull bull Epidemiologyaetiologybull ndash Developmental septal abnormalities Septal cartilage
damage in the neonatal period andbull during birth can cause severe septal deviation inbull the absence of a history of nasal trauma
Deviated Nasal Septum
bull Symptomsbull ndash Patients may present with a history of sinusitis
allergicbull rhinitis obstructive sleep apnoea previousbull nasal surgery or recent nasal trauma Unilateral or
bilateral nasal airway obstruction that is unrelievedbull with decongestants or nasal steroid sprays is oftenbull seenbull bull
Deviated Nasal SeptumDiagnosisndashExamination external dorsal deviation or the columella and caudal septummay be deflected off the midline (caudal subluxation)ndash Inspections of the nasal cavity and anterior-posteriorrhinoscopy are helpful in diagnosing the locationtype and severity of septal deformityThe endoscope is also useful in identifying polypsthe severity and extent of posterior septaldeviations and bony spurs and locating areas ofseptal perforation or mucosal injury
Deviated Nasal Septum
bull Therapybull ndash Septoplasty is a procedurebull The areabull of deviation is corrected or resected in order tobull leave behind as much cartilage and bone as
possiblebull Cartilage resection is minimised and can be
repositioned reshaped or recontoured using a variety of methods
Deviated Nasal Septum
bull ndash Indications of septoplasty before the growth period
bull of the nose is finished should be very limited bull -In these cases surgery must preserve all the
cartilagebull in order to prevent external changes of the
shape ofbull the nose
Deviated Nasal Septum
bull Complicationsbull ndash Frequent complications include haematoma andbull infection Cerebrospinal fluid leak is a rare but
potentiallybull serious complicationbull It is usually the resultbull of avulsion or damage to the cribriform plate whenbull handling the perpendicular plate of the ethmoidbull ndash Other complications include epistaxis nasal
Deviated Nasal Septum
bull Other complications include epistaxis nasal obstruction
bull due to residual deviation synechiae returnbull of the cartilaginous deviation septal perforationbull anosmia and cosmetic nasal deformities suchbull as widened alar rim margins drooping nasal tipbull columella retraction and a sunken dorsum with abull supratip saddle formation
Septal perforation with minor crusting View from provide closure of the
incision
Septal Haematoma
bull A septal haematoma is a blood collection under the perichondrium
bull of the septum and cartilagebull bull bull Epidemiologyaetiologybull ndash A septal haematoma is one of the most
severe complications of nasal trauma
Septal Haematoma
bull Diagnosisbull ndash Signs and symptoms include intense pain
swellingbull haematoma of the upper lip and philtrum
area andbull complete nasal airway obstruction
Septal HaematomaTherapyndash Management consists of drainage through a mucoperichondrial incision Immediate treatment isnecessary to prevent long-term problems such asa saddle-nose deformity perforation columellarretraction and nasal-base widening In childrenseptal destruction can lead to devastating nasal andmidfacial growth abnormalitiesbull Surgeryndash Incision and evacuation of the collection is performedDrainage of a septal haematoma should
Septal HaematomaSurgeryndash Incision and evacuation of the collection is performedDrainage of a septal haematoma should provide closure of the incision
Splints or transseptal sutures are placed to obliterate thepotential space and prevent collectionInfection involving the septal cartilage Reconstruction with autologouscartilage is then performed in a second stage Oral antibiotics should be given
Nasal DeformitySaddle-nose deformityndash A saddle-nose deformity is characterised by a loss ofnasal dorsal height and compromised nasal supportstructures -Other case observed are depressionof the middle vault and dorsum loss of nasal tipsupport and definition shortened (vertical) nasal length over rotation of the nasal tip and retrusion ofthe nasal spine and caudal septum It is also knownas a ldquoPug noserdquo or ldquoboxerrsquos noserdquo both of which referto various degrees of nasal dorsal depressionbull
Nasal DeformityEpidemiologyaetiologyndash Prevalence is higher in population groups prone to facial trauma (ie boxers athletes) those with historiesof intranasal cocaine use nasal surgery (e g radical submucosal septal resection reductive rhinoplasty)ndash A saddle-nose deformity can be congenital or acquired It can be noticed as a part of individual familialsyndromic and ethnic characteristics - Most deformities are due to traumatic and iatrogeniccauses Medical causes are Wegenerrsquosgranulomatosis relapsing polychondritis leprosy (Hansenrsquos disease) syphilis ectodermal dysplasiaand intranasal cocaine use
Nasal Deformity
bull Therapybull ndash Nasal reconstruction indications depend on patientbull selection surgeon experience and aetiology of thebull deformity bull Indications for surgery can be functionalbull aesthetic or most commonly both In individuals
with a compromised nasal airway a nasoseptalbull reconstruction is indicated
Nasal Deformity
bull Contraindications bull include patients with malignantbull chronic or autoimmune disease conditions drugbull abuse poor perioperative risk profile and unrealisticbull expectationsbull ndash Multiple previous rhinoplasties and certain
professionsbull (mixed martial artists boxers and other contactbull sports) are relative contraindications
Nasal DeformitySeptoplastyndash Septoplasty is performed to correct nasal obstructioncaused by septal deformityndash Usually septoplasty is performed under general anaesthesiawith the patient in the supine position with the head elevated by approximately 30 (Righthandedsurgeons approach from the right side)ndash Local vasoconstrictive anaesthesia is applied notonly to reduce postoperative pain but also more importantly to achieve vasoconstriction of themucosa and less intraoperative haemorrhage Lidocainewith adrenaline or epinephrine is usedalthough in patients with cardiac hypersensitivityoxymetazoline might be preferred
Nasal Deformity
bull Septoplasty begins with the incision of septal mucosabull Most operative techniques utilise a hemitransfixionbull incision at the caudal end of septum so thatbull deviation at this point might be reached as wellbull as a transfixion incision that is easily obtained ifbull needed (Right-handed surgeons normally choosebull the left side but that may vary when deviation isbull convex towards the right)
Nasal DeformityA columella retractor is placed over the columellaand by pulling it laterally the caudal border of theseptum is exposed Ala can be protected by an alaprotector A vertical incision with a no 15 bladeover the caudal end of septum is performed untilreaching the plane of the septal cartilage It is essentialto correctly identify the perichondrium and byusing the Cottle elevator dissect and lift it creatinga flap As the dissection proceeds along the septalcartilage a longer speculum (no 5) is introduced sothat elevation of the mucoperichondrium is doneunder constant visual controlndash The next step is to dissect the mucoperiostium
Nasal DeformityDissecting over the bony-cartilaginous junctionwhen joining both tunnels might be difficult and is
especially prone to membrane perforationndash If needed the same tunnels are to be created on the
other side of the septum Then deviated parts of
septum are identified and removed either with a
knife or a Freer chisel
Nasal Deformitybull septum from the maxillary crest the septum mustbull be separated from the perpendicular plate trimmedbull along the inferior border placed back onto the crestbull and sutured to the periosteum If the deformity involvesbull the vomer an osteotome is used Care mustbull be taken not to break the cribriform plate becausebull it could cause a cerebrospinal fistula
Nasal Deformity
bull Once the septal deviation is corrected the flapsbull and hemitransfixion incision are mattressed
withbull absorbable sutures Nasal packing to prevent
synechiaebull and postoperative septal haematoma mightbull be advised but should be removed within 72 h

Nasal Fractures
bull To prevent collapse of the postreductionbull framework nasal packing should be placedbull for 3ndash5 days Septum splints are recommendedbull in comminuted septal fractures withbull severe mucosal lesions External nasal splintingbull for 10 days (Aquaplastreg Thermoplastreg)bull provides nasal protection Nasal saline spraysbull prevent crusting and oral antibiotics should
Nasal Fractures
bull Open reductionbull ndashndash Immediate repair of fractures by using
widebull surgical exposure reduction fixation and
reconstructionbull ndashndash The second option is delayed correctionbull (6 months or more) of persistent deformitiesbull using standard techniques of rhinoplasty
Deviated Nasal Septum
bull Definition of the diseasebull ndash Deviation of the nasal septum is a common causebull of unilateral nasal airway obstruction in which thebull nasal septum is displacedbull bull Epidemiologyaetiologybull ndash Developmental septal abnormalities Septal cartilage
damage in the neonatal period andbull during birth can cause severe septal deviation inbull the absence of a history of nasal trauma
Deviated Nasal Septum
bull Symptomsbull ndash Patients may present with a history of sinusitis
allergicbull rhinitis obstructive sleep apnoea previousbull nasal surgery or recent nasal trauma Unilateral or
bilateral nasal airway obstruction that is unrelievedbull with decongestants or nasal steroid sprays is oftenbull seenbull bull
Deviated Nasal SeptumDiagnosisndashExamination external dorsal deviation or the columella and caudal septummay be deflected off the midline (caudal subluxation)ndash Inspections of the nasal cavity and anterior-posteriorrhinoscopy are helpful in diagnosing the locationtype and severity of septal deformityThe endoscope is also useful in identifying polypsthe severity and extent of posterior septaldeviations and bony spurs and locating areas ofseptal perforation or mucosal injury
Deviated Nasal Septum
bull Therapybull ndash Septoplasty is a procedurebull The areabull of deviation is corrected or resected in order tobull leave behind as much cartilage and bone as
possiblebull Cartilage resection is minimised and can be
repositioned reshaped or recontoured using a variety of methods
Deviated Nasal Septum
bull ndash Indications of septoplasty before the growth period
bull of the nose is finished should be very limited bull -In these cases surgery must preserve all the
cartilagebull in order to prevent external changes of the
shape ofbull the nose
Deviated Nasal Septum
bull Complicationsbull ndash Frequent complications include haematoma andbull infection Cerebrospinal fluid leak is a rare but
potentiallybull serious complicationbull It is usually the resultbull of avulsion or damage to the cribriform plate whenbull handling the perpendicular plate of the ethmoidbull ndash Other complications include epistaxis nasal
Deviated Nasal Septum
bull Other complications include epistaxis nasal obstruction
bull due to residual deviation synechiae returnbull of the cartilaginous deviation septal perforationbull anosmia and cosmetic nasal deformities suchbull as widened alar rim margins drooping nasal tipbull columella retraction and a sunken dorsum with abull supratip saddle formation
Septal perforation with minor crusting View from provide closure of the
incision
Septal Haematoma
bull A septal haematoma is a blood collection under the perichondrium
bull of the septum and cartilagebull bull bull Epidemiologyaetiologybull ndash A septal haematoma is one of the most
severe complications of nasal trauma
Septal Haematoma
bull Diagnosisbull ndash Signs and symptoms include intense pain
swellingbull haematoma of the upper lip and philtrum
area andbull complete nasal airway obstruction
Septal HaematomaTherapyndash Management consists of drainage through a mucoperichondrial incision Immediate treatment isnecessary to prevent long-term problems such asa saddle-nose deformity perforation columellarretraction and nasal-base widening In childrenseptal destruction can lead to devastating nasal andmidfacial growth abnormalitiesbull Surgeryndash Incision and evacuation of the collection is performedDrainage of a septal haematoma should
Septal HaematomaSurgeryndash Incision and evacuation of the collection is performedDrainage of a septal haematoma should provide closure of the incision
Splints or transseptal sutures are placed to obliterate thepotential space and prevent collectionInfection involving the septal cartilage Reconstruction with autologouscartilage is then performed in a second stage Oral antibiotics should be given
Nasal DeformitySaddle-nose deformityndash A saddle-nose deformity is characterised by a loss ofnasal dorsal height and compromised nasal supportstructures -Other case observed are depressionof the middle vault and dorsum loss of nasal tipsupport and definition shortened (vertical) nasal length over rotation of the nasal tip and retrusion ofthe nasal spine and caudal septum It is also knownas a ldquoPug noserdquo or ldquoboxerrsquos noserdquo both of which referto various degrees of nasal dorsal depressionbull
Nasal DeformityEpidemiologyaetiologyndash Prevalence is higher in population groups prone to facial trauma (ie boxers athletes) those with historiesof intranasal cocaine use nasal surgery (e g radical submucosal septal resection reductive rhinoplasty)ndash A saddle-nose deformity can be congenital or acquired It can be noticed as a part of individual familialsyndromic and ethnic characteristics - Most deformities are due to traumatic and iatrogeniccauses Medical causes are Wegenerrsquosgranulomatosis relapsing polychondritis leprosy (Hansenrsquos disease) syphilis ectodermal dysplasiaand intranasal cocaine use
Nasal Deformity
bull Therapybull ndash Nasal reconstruction indications depend on patientbull selection surgeon experience and aetiology of thebull deformity bull Indications for surgery can be functionalbull aesthetic or most commonly both In individuals
with a compromised nasal airway a nasoseptalbull reconstruction is indicated
Nasal Deformity
bull Contraindications bull include patients with malignantbull chronic or autoimmune disease conditions drugbull abuse poor perioperative risk profile and unrealisticbull expectationsbull ndash Multiple previous rhinoplasties and certain
professionsbull (mixed martial artists boxers and other contactbull sports) are relative contraindications
Nasal DeformitySeptoplastyndash Septoplasty is performed to correct nasal obstructioncaused by septal deformityndash Usually septoplasty is performed under general anaesthesiawith the patient in the supine position with the head elevated by approximately 30 (Righthandedsurgeons approach from the right side)ndash Local vasoconstrictive anaesthesia is applied notonly to reduce postoperative pain but also more importantly to achieve vasoconstriction of themucosa and less intraoperative haemorrhage Lidocainewith adrenaline or epinephrine is usedalthough in patients with cardiac hypersensitivityoxymetazoline might be preferred
Nasal Deformity
bull Septoplasty begins with the incision of septal mucosabull Most operative techniques utilise a hemitransfixionbull incision at the caudal end of septum so thatbull deviation at this point might be reached as wellbull as a transfixion incision that is easily obtained ifbull needed (Right-handed surgeons normally choosebull the left side but that may vary when deviation isbull convex towards the right)
Nasal DeformityA columella retractor is placed over the columellaand by pulling it laterally the caudal border of theseptum is exposed Ala can be protected by an alaprotector A vertical incision with a no 15 bladeover the caudal end of septum is performed untilreaching the plane of the septal cartilage It is essentialto correctly identify the perichondrium and byusing the Cottle elevator dissect and lift it creatinga flap As the dissection proceeds along the septalcartilage a longer speculum (no 5) is introduced sothat elevation of the mucoperichondrium is doneunder constant visual controlndash The next step is to dissect the mucoperiostium
Nasal DeformityDissecting over the bony-cartilaginous junctionwhen joining both tunnels might be difficult and is
especially prone to membrane perforationndash If needed the same tunnels are to be created on the
other side of the septum Then deviated parts of
septum are identified and removed either with a
knife or a Freer chisel
Nasal Deformitybull septum from the maxillary crest the septum mustbull be separated from the perpendicular plate trimmedbull along the inferior border placed back onto the crestbull and sutured to the periosteum If the deformity involvesbull the vomer an osteotome is used Care mustbull be taken not to break the cribriform plate becausebull it could cause a cerebrospinal fistula
Nasal Deformity
bull Once the septal deviation is corrected the flapsbull and hemitransfixion incision are mattressed
withbull absorbable sutures Nasal packing to prevent
synechiaebull and postoperative septal haematoma mightbull be advised but should be removed within 72 h

Nasal Fractures
bull Open reductionbull ndashndash Immediate repair of fractures by using
widebull surgical exposure reduction fixation and
reconstructionbull ndashndash The second option is delayed correctionbull (6 months or more) of persistent deformitiesbull using standard techniques of rhinoplasty
Deviated Nasal Septum
bull Definition of the diseasebull ndash Deviation of the nasal septum is a common causebull of unilateral nasal airway obstruction in which thebull nasal septum is displacedbull bull Epidemiologyaetiologybull ndash Developmental septal abnormalities Septal cartilage
damage in the neonatal period andbull during birth can cause severe septal deviation inbull the absence of a history of nasal trauma
Deviated Nasal Septum
bull Symptomsbull ndash Patients may present with a history of sinusitis
allergicbull rhinitis obstructive sleep apnoea previousbull nasal surgery or recent nasal trauma Unilateral or
bilateral nasal airway obstruction that is unrelievedbull with decongestants or nasal steroid sprays is oftenbull seenbull bull
Deviated Nasal SeptumDiagnosisndashExamination external dorsal deviation or the columella and caudal septummay be deflected off the midline (caudal subluxation)ndash Inspections of the nasal cavity and anterior-posteriorrhinoscopy are helpful in diagnosing the locationtype and severity of septal deformityThe endoscope is also useful in identifying polypsthe severity and extent of posterior septaldeviations and bony spurs and locating areas ofseptal perforation or mucosal injury
Deviated Nasal Septum
bull Therapybull ndash Septoplasty is a procedurebull The areabull of deviation is corrected or resected in order tobull leave behind as much cartilage and bone as
possiblebull Cartilage resection is minimised and can be
repositioned reshaped or recontoured using a variety of methods
Deviated Nasal Septum
bull ndash Indications of septoplasty before the growth period
bull of the nose is finished should be very limited bull -In these cases surgery must preserve all the
cartilagebull in order to prevent external changes of the
shape ofbull the nose
Deviated Nasal Septum
bull Complicationsbull ndash Frequent complications include haematoma andbull infection Cerebrospinal fluid leak is a rare but
potentiallybull serious complicationbull It is usually the resultbull of avulsion or damage to the cribriform plate whenbull handling the perpendicular plate of the ethmoidbull ndash Other complications include epistaxis nasal
Deviated Nasal Septum
bull Other complications include epistaxis nasal obstruction
bull due to residual deviation synechiae returnbull of the cartilaginous deviation septal perforationbull anosmia and cosmetic nasal deformities suchbull as widened alar rim margins drooping nasal tipbull columella retraction and a sunken dorsum with abull supratip saddle formation
Septal perforation with minor crusting View from provide closure of the
incision
Septal Haematoma
bull A septal haematoma is a blood collection under the perichondrium
bull of the septum and cartilagebull bull bull Epidemiologyaetiologybull ndash A septal haematoma is one of the most
severe complications of nasal trauma
Septal Haematoma
bull Diagnosisbull ndash Signs and symptoms include intense pain
swellingbull haematoma of the upper lip and philtrum
area andbull complete nasal airway obstruction
Septal HaematomaTherapyndash Management consists of drainage through a mucoperichondrial incision Immediate treatment isnecessary to prevent long-term problems such asa saddle-nose deformity perforation columellarretraction and nasal-base widening In childrenseptal destruction can lead to devastating nasal andmidfacial growth abnormalitiesbull Surgeryndash Incision and evacuation of the collection is performedDrainage of a septal haematoma should
Septal HaematomaSurgeryndash Incision and evacuation of the collection is performedDrainage of a septal haematoma should provide closure of the incision
Splints or transseptal sutures are placed to obliterate thepotential space and prevent collectionInfection involving the septal cartilage Reconstruction with autologouscartilage is then performed in a second stage Oral antibiotics should be given
Nasal DeformitySaddle-nose deformityndash A saddle-nose deformity is characterised by a loss ofnasal dorsal height and compromised nasal supportstructures -Other case observed are depressionof the middle vault and dorsum loss of nasal tipsupport and definition shortened (vertical) nasal length over rotation of the nasal tip and retrusion ofthe nasal spine and caudal septum It is also knownas a ldquoPug noserdquo or ldquoboxerrsquos noserdquo both of which referto various degrees of nasal dorsal depressionbull
Nasal DeformityEpidemiologyaetiologyndash Prevalence is higher in population groups prone to facial trauma (ie boxers athletes) those with historiesof intranasal cocaine use nasal surgery (e g radical submucosal septal resection reductive rhinoplasty)ndash A saddle-nose deformity can be congenital or acquired It can be noticed as a part of individual familialsyndromic and ethnic characteristics - Most deformities are due to traumatic and iatrogeniccauses Medical causes are Wegenerrsquosgranulomatosis relapsing polychondritis leprosy (Hansenrsquos disease) syphilis ectodermal dysplasiaand intranasal cocaine use
Nasal Deformity
bull Therapybull ndash Nasal reconstruction indications depend on patientbull selection surgeon experience and aetiology of thebull deformity bull Indications for surgery can be functionalbull aesthetic or most commonly both In individuals
with a compromised nasal airway a nasoseptalbull reconstruction is indicated
Nasal Deformity
bull Contraindications bull include patients with malignantbull chronic or autoimmune disease conditions drugbull abuse poor perioperative risk profile and unrealisticbull expectationsbull ndash Multiple previous rhinoplasties and certain
professionsbull (mixed martial artists boxers and other contactbull sports) are relative contraindications
Nasal DeformitySeptoplastyndash Septoplasty is performed to correct nasal obstructioncaused by septal deformityndash Usually septoplasty is performed under general anaesthesiawith the patient in the supine position with the head elevated by approximately 30 (Righthandedsurgeons approach from the right side)ndash Local vasoconstrictive anaesthesia is applied notonly to reduce postoperative pain but also more importantly to achieve vasoconstriction of themucosa and less intraoperative haemorrhage Lidocainewith adrenaline or epinephrine is usedalthough in patients with cardiac hypersensitivityoxymetazoline might be preferred
Nasal Deformity
bull Septoplasty begins with the incision of septal mucosabull Most operative techniques utilise a hemitransfixionbull incision at the caudal end of septum so thatbull deviation at this point might be reached as wellbull as a transfixion incision that is easily obtained ifbull needed (Right-handed surgeons normally choosebull the left side but that may vary when deviation isbull convex towards the right)
Nasal DeformityA columella retractor is placed over the columellaand by pulling it laterally the caudal border of theseptum is exposed Ala can be protected by an alaprotector A vertical incision with a no 15 bladeover the caudal end of septum is performed untilreaching the plane of the septal cartilage It is essentialto correctly identify the perichondrium and byusing the Cottle elevator dissect and lift it creatinga flap As the dissection proceeds along the septalcartilage a longer speculum (no 5) is introduced sothat elevation of the mucoperichondrium is doneunder constant visual controlndash The next step is to dissect the mucoperiostium
Nasal DeformityDissecting over the bony-cartilaginous junctionwhen joining both tunnels might be difficult and is
especially prone to membrane perforationndash If needed the same tunnels are to be created on the
other side of the septum Then deviated parts of
septum are identified and removed either with a
knife or a Freer chisel
Nasal Deformitybull septum from the maxillary crest the septum mustbull be separated from the perpendicular plate trimmedbull along the inferior border placed back onto the crestbull and sutured to the periosteum If the deformity involvesbull the vomer an osteotome is used Care mustbull be taken not to break the cribriform plate becausebull it could cause a cerebrospinal fistula
Nasal Deformity
bull Once the septal deviation is corrected the flapsbull and hemitransfixion incision are mattressed
withbull absorbable sutures Nasal packing to prevent
synechiaebull and postoperative septal haematoma mightbull be advised but should be removed within 72 h

Deviated Nasal Septum
bull Definition of the diseasebull ndash Deviation of the nasal septum is a common causebull of unilateral nasal airway obstruction in which thebull nasal septum is displacedbull bull Epidemiologyaetiologybull ndash Developmental septal abnormalities Septal cartilage
damage in the neonatal period andbull during birth can cause severe septal deviation inbull the absence of a history of nasal trauma
Deviated Nasal Septum
bull Symptomsbull ndash Patients may present with a history of sinusitis
allergicbull rhinitis obstructive sleep apnoea previousbull nasal surgery or recent nasal trauma Unilateral or
bilateral nasal airway obstruction that is unrelievedbull with decongestants or nasal steroid sprays is oftenbull seenbull bull
Deviated Nasal SeptumDiagnosisndashExamination external dorsal deviation or the columella and caudal septummay be deflected off the midline (caudal subluxation)ndash Inspections of the nasal cavity and anterior-posteriorrhinoscopy are helpful in diagnosing the locationtype and severity of septal deformityThe endoscope is also useful in identifying polypsthe severity and extent of posterior septaldeviations and bony spurs and locating areas ofseptal perforation or mucosal injury
Deviated Nasal Septum
bull Therapybull ndash Septoplasty is a procedurebull The areabull of deviation is corrected or resected in order tobull leave behind as much cartilage and bone as
possiblebull Cartilage resection is minimised and can be
repositioned reshaped or recontoured using a variety of methods
Deviated Nasal Septum
bull ndash Indications of septoplasty before the growth period
bull of the nose is finished should be very limited bull -In these cases surgery must preserve all the
cartilagebull in order to prevent external changes of the
shape ofbull the nose
Deviated Nasal Septum
bull Complicationsbull ndash Frequent complications include haematoma andbull infection Cerebrospinal fluid leak is a rare but
potentiallybull serious complicationbull It is usually the resultbull of avulsion or damage to the cribriform plate whenbull handling the perpendicular plate of the ethmoidbull ndash Other complications include epistaxis nasal
Deviated Nasal Septum
bull Other complications include epistaxis nasal obstruction
bull due to residual deviation synechiae returnbull of the cartilaginous deviation septal perforationbull anosmia and cosmetic nasal deformities suchbull as widened alar rim margins drooping nasal tipbull columella retraction and a sunken dorsum with abull supratip saddle formation
Septal perforation with minor crusting View from provide closure of the
incision
Septal Haematoma
bull A septal haematoma is a blood collection under the perichondrium
bull of the septum and cartilagebull bull bull Epidemiologyaetiologybull ndash A septal haematoma is one of the most
severe complications of nasal trauma
Septal Haematoma
bull Diagnosisbull ndash Signs and symptoms include intense pain
swellingbull haematoma of the upper lip and philtrum
area andbull complete nasal airway obstruction
Septal HaematomaTherapyndash Management consists of drainage through a mucoperichondrial incision Immediate treatment isnecessary to prevent long-term problems such asa saddle-nose deformity perforation columellarretraction and nasal-base widening In childrenseptal destruction can lead to devastating nasal andmidfacial growth abnormalitiesbull Surgeryndash Incision and evacuation of the collection is performedDrainage of a septal haematoma should
Septal HaematomaSurgeryndash Incision and evacuation of the collection is performedDrainage of a septal haematoma should provide closure of the incision
Splints or transseptal sutures are placed to obliterate thepotential space and prevent collectionInfection involving the septal cartilage Reconstruction with autologouscartilage is then performed in a second stage Oral antibiotics should be given
Nasal DeformitySaddle-nose deformityndash A saddle-nose deformity is characterised by a loss ofnasal dorsal height and compromised nasal supportstructures -Other case observed are depressionof the middle vault and dorsum loss of nasal tipsupport and definition shortened (vertical) nasal length over rotation of the nasal tip and retrusion ofthe nasal spine and caudal septum It is also knownas a ldquoPug noserdquo or ldquoboxerrsquos noserdquo both of which referto various degrees of nasal dorsal depressionbull
Nasal DeformityEpidemiologyaetiologyndash Prevalence is higher in population groups prone to facial trauma (ie boxers athletes) those with historiesof intranasal cocaine use nasal surgery (e g radical submucosal septal resection reductive rhinoplasty)ndash A saddle-nose deformity can be congenital or acquired It can be noticed as a part of individual familialsyndromic and ethnic characteristics - Most deformities are due to traumatic and iatrogeniccauses Medical causes are Wegenerrsquosgranulomatosis relapsing polychondritis leprosy (Hansenrsquos disease) syphilis ectodermal dysplasiaand intranasal cocaine use
Nasal Deformity
bull Therapybull ndash Nasal reconstruction indications depend on patientbull selection surgeon experience and aetiology of thebull deformity bull Indications for surgery can be functionalbull aesthetic or most commonly both In individuals
with a compromised nasal airway a nasoseptalbull reconstruction is indicated
Nasal Deformity
bull Contraindications bull include patients with malignantbull chronic or autoimmune disease conditions drugbull abuse poor perioperative risk profile and unrealisticbull expectationsbull ndash Multiple previous rhinoplasties and certain
professionsbull (mixed martial artists boxers and other contactbull sports) are relative contraindications
Nasal DeformitySeptoplastyndash Septoplasty is performed to correct nasal obstructioncaused by septal deformityndash Usually septoplasty is performed under general anaesthesiawith the patient in the supine position with the head elevated by approximately 30 (Righthandedsurgeons approach from the right side)ndash Local vasoconstrictive anaesthesia is applied notonly to reduce postoperative pain but also more importantly to achieve vasoconstriction of themucosa and less intraoperative haemorrhage Lidocainewith adrenaline or epinephrine is usedalthough in patients with cardiac hypersensitivityoxymetazoline might be preferred
Nasal Deformity
bull Septoplasty begins with the incision of septal mucosabull Most operative techniques utilise a hemitransfixionbull incision at the caudal end of septum so thatbull deviation at this point might be reached as wellbull as a transfixion incision that is easily obtained ifbull needed (Right-handed surgeons normally choosebull the left side but that may vary when deviation isbull convex towards the right)
Nasal DeformityA columella retractor is placed over the columellaand by pulling it laterally the caudal border of theseptum is exposed Ala can be protected by an alaprotector A vertical incision with a no 15 bladeover the caudal end of septum is performed untilreaching the plane of the septal cartilage It is essentialto correctly identify the perichondrium and byusing the Cottle elevator dissect and lift it creatinga flap As the dissection proceeds along the septalcartilage a longer speculum (no 5) is introduced sothat elevation of the mucoperichondrium is doneunder constant visual controlndash The next step is to dissect the mucoperiostium
Nasal DeformityDissecting over the bony-cartilaginous junctionwhen joining both tunnels might be difficult and is
especially prone to membrane perforationndash If needed the same tunnels are to be created on the
other side of the septum Then deviated parts of
septum are identified and removed either with a
knife or a Freer chisel
Nasal Deformitybull septum from the maxillary crest the septum mustbull be separated from the perpendicular plate trimmedbull along the inferior border placed back onto the crestbull and sutured to the periosteum If the deformity involvesbull the vomer an osteotome is used Care mustbull be taken not to break the cribriform plate becausebull it could cause a cerebrospinal fistula
Nasal Deformity
bull Once the septal deviation is corrected the flapsbull and hemitransfixion incision are mattressed
withbull absorbable sutures Nasal packing to prevent
synechiaebull and postoperative septal haematoma mightbull be advised but should be removed within 72 h

Deviated Nasal Septum
bull Symptomsbull ndash Patients may present with a history of sinusitis
allergicbull rhinitis obstructive sleep apnoea previousbull nasal surgery or recent nasal trauma Unilateral or
bilateral nasal airway obstruction that is unrelievedbull with decongestants or nasal steroid sprays is oftenbull seenbull bull
Deviated Nasal SeptumDiagnosisndashExamination external dorsal deviation or the columella and caudal septummay be deflected off the midline (caudal subluxation)ndash Inspections of the nasal cavity and anterior-posteriorrhinoscopy are helpful in diagnosing the locationtype and severity of septal deformityThe endoscope is also useful in identifying polypsthe severity and extent of posterior septaldeviations and bony spurs and locating areas ofseptal perforation or mucosal injury
Deviated Nasal Septum
bull Therapybull ndash Septoplasty is a procedurebull The areabull of deviation is corrected or resected in order tobull leave behind as much cartilage and bone as
possiblebull Cartilage resection is minimised and can be
repositioned reshaped or recontoured using a variety of methods
Deviated Nasal Septum
bull ndash Indications of septoplasty before the growth period
bull of the nose is finished should be very limited bull -In these cases surgery must preserve all the
cartilagebull in order to prevent external changes of the
shape ofbull the nose
Deviated Nasal Septum
bull Complicationsbull ndash Frequent complications include haematoma andbull infection Cerebrospinal fluid leak is a rare but
potentiallybull serious complicationbull It is usually the resultbull of avulsion or damage to the cribriform plate whenbull handling the perpendicular plate of the ethmoidbull ndash Other complications include epistaxis nasal
Deviated Nasal Septum
bull Other complications include epistaxis nasal obstruction
bull due to residual deviation synechiae returnbull of the cartilaginous deviation septal perforationbull anosmia and cosmetic nasal deformities suchbull as widened alar rim margins drooping nasal tipbull columella retraction and a sunken dorsum with abull supratip saddle formation
Septal perforation with minor crusting View from provide closure of the
incision
Septal Haematoma
bull A septal haematoma is a blood collection under the perichondrium
bull of the septum and cartilagebull bull bull Epidemiologyaetiologybull ndash A septal haematoma is one of the most
severe complications of nasal trauma
Septal Haematoma
bull Diagnosisbull ndash Signs and symptoms include intense pain
swellingbull haematoma of the upper lip and philtrum
area andbull complete nasal airway obstruction
Septal HaematomaTherapyndash Management consists of drainage through a mucoperichondrial incision Immediate treatment isnecessary to prevent long-term problems such asa saddle-nose deformity perforation columellarretraction and nasal-base widening In childrenseptal destruction can lead to devastating nasal andmidfacial growth abnormalitiesbull Surgeryndash Incision and evacuation of the collection is performedDrainage of a septal haematoma should
Septal HaematomaSurgeryndash Incision and evacuation of the collection is performedDrainage of a septal haematoma should provide closure of the incision
Splints or transseptal sutures are placed to obliterate thepotential space and prevent collectionInfection involving the septal cartilage Reconstruction with autologouscartilage is then performed in a second stage Oral antibiotics should be given
Nasal DeformitySaddle-nose deformityndash A saddle-nose deformity is characterised by a loss ofnasal dorsal height and compromised nasal supportstructures -Other case observed are depressionof the middle vault and dorsum loss of nasal tipsupport and definition shortened (vertical) nasal length over rotation of the nasal tip and retrusion ofthe nasal spine and caudal septum It is also knownas a ldquoPug noserdquo or ldquoboxerrsquos noserdquo both of which referto various degrees of nasal dorsal depressionbull
Nasal DeformityEpidemiologyaetiologyndash Prevalence is higher in population groups prone to facial trauma (ie boxers athletes) those with historiesof intranasal cocaine use nasal surgery (e g radical submucosal septal resection reductive rhinoplasty)ndash A saddle-nose deformity can be congenital or acquired It can be noticed as a part of individual familialsyndromic and ethnic characteristics - Most deformities are due to traumatic and iatrogeniccauses Medical causes are Wegenerrsquosgranulomatosis relapsing polychondritis leprosy (Hansenrsquos disease) syphilis ectodermal dysplasiaand intranasal cocaine use
Nasal Deformity
bull Therapybull ndash Nasal reconstruction indications depend on patientbull selection surgeon experience and aetiology of thebull deformity bull Indications for surgery can be functionalbull aesthetic or most commonly both In individuals
with a compromised nasal airway a nasoseptalbull reconstruction is indicated
Nasal Deformity
bull Contraindications bull include patients with malignantbull chronic or autoimmune disease conditions drugbull abuse poor perioperative risk profile and unrealisticbull expectationsbull ndash Multiple previous rhinoplasties and certain
professionsbull (mixed martial artists boxers and other contactbull sports) are relative contraindications
Nasal DeformitySeptoplastyndash Septoplasty is performed to correct nasal obstructioncaused by septal deformityndash Usually septoplasty is performed under general anaesthesiawith the patient in the supine position with the head elevated by approximately 30 (Righthandedsurgeons approach from the right side)ndash Local vasoconstrictive anaesthesia is applied notonly to reduce postoperative pain but also more importantly to achieve vasoconstriction of themucosa and less intraoperative haemorrhage Lidocainewith adrenaline or epinephrine is usedalthough in patients with cardiac hypersensitivityoxymetazoline might be preferred
Nasal Deformity
bull Septoplasty begins with the incision of septal mucosabull Most operative techniques utilise a hemitransfixionbull incision at the caudal end of septum so thatbull deviation at this point might be reached as wellbull as a transfixion incision that is easily obtained ifbull needed (Right-handed surgeons normally choosebull the left side but that may vary when deviation isbull convex towards the right)
Nasal DeformityA columella retractor is placed over the columellaand by pulling it laterally the caudal border of theseptum is exposed Ala can be protected by an alaprotector A vertical incision with a no 15 bladeover the caudal end of septum is performed untilreaching the plane of the septal cartilage It is essentialto correctly identify the perichondrium and byusing the Cottle elevator dissect and lift it creatinga flap As the dissection proceeds along the septalcartilage a longer speculum (no 5) is introduced sothat elevation of the mucoperichondrium is doneunder constant visual controlndash The next step is to dissect the mucoperiostium
Nasal DeformityDissecting over the bony-cartilaginous junctionwhen joining both tunnels might be difficult and is
especially prone to membrane perforationndash If needed the same tunnels are to be created on the
other side of the septum Then deviated parts of
septum are identified and removed either with a
knife or a Freer chisel
Nasal Deformitybull septum from the maxillary crest the septum mustbull be separated from the perpendicular plate trimmedbull along the inferior border placed back onto the crestbull and sutured to the periosteum If the deformity involvesbull the vomer an osteotome is used Care mustbull be taken not to break the cribriform plate becausebull it could cause a cerebrospinal fistula
Nasal Deformity
bull Once the septal deviation is corrected the flapsbull and hemitransfixion incision are mattressed
withbull absorbable sutures Nasal packing to prevent
synechiaebull and postoperative septal haematoma mightbull be advised but should be removed within 72 h

Deviated Nasal SeptumDiagnosisndashExamination external dorsal deviation or the columella and caudal septummay be deflected off the midline (caudal subluxation)ndash Inspections of the nasal cavity and anterior-posteriorrhinoscopy are helpful in diagnosing the locationtype and severity of septal deformityThe endoscope is also useful in identifying polypsthe severity and extent of posterior septaldeviations and bony spurs and locating areas ofseptal perforation or mucosal injury
Deviated Nasal Septum
bull Therapybull ndash Septoplasty is a procedurebull The areabull of deviation is corrected or resected in order tobull leave behind as much cartilage and bone as
possiblebull Cartilage resection is minimised and can be
repositioned reshaped or recontoured using a variety of methods
Deviated Nasal Septum
bull ndash Indications of septoplasty before the growth period
bull of the nose is finished should be very limited bull -In these cases surgery must preserve all the
cartilagebull in order to prevent external changes of the
shape ofbull the nose
Deviated Nasal Septum
bull Complicationsbull ndash Frequent complications include haematoma andbull infection Cerebrospinal fluid leak is a rare but
potentiallybull serious complicationbull It is usually the resultbull of avulsion or damage to the cribriform plate whenbull handling the perpendicular plate of the ethmoidbull ndash Other complications include epistaxis nasal
Deviated Nasal Septum
bull Other complications include epistaxis nasal obstruction
bull due to residual deviation synechiae returnbull of the cartilaginous deviation septal perforationbull anosmia and cosmetic nasal deformities suchbull as widened alar rim margins drooping nasal tipbull columella retraction and a sunken dorsum with abull supratip saddle formation
Septal perforation with minor crusting View from provide closure of the
incision
Septal Haematoma
bull A septal haematoma is a blood collection under the perichondrium
bull of the septum and cartilagebull bull bull Epidemiologyaetiologybull ndash A septal haematoma is one of the most
severe complications of nasal trauma
Septal Haematoma
bull Diagnosisbull ndash Signs and symptoms include intense pain
swellingbull haematoma of the upper lip and philtrum
area andbull complete nasal airway obstruction
Septal HaematomaTherapyndash Management consists of drainage through a mucoperichondrial incision Immediate treatment isnecessary to prevent long-term problems such asa saddle-nose deformity perforation columellarretraction and nasal-base widening In childrenseptal destruction can lead to devastating nasal andmidfacial growth abnormalitiesbull Surgeryndash Incision and evacuation of the collection is performedDrainage of a septal haematoma should
Septal HaematomaSurgeryndash Incision and evacuation of the collection is performedDrainage of a septal haematoma should provide closure of the incision
Splints or transseptal sutures are placed to obliterate thepotential space and prevent collectionInfection involving the septal cartilage Reconstruction with autologouscartilage is then performed in a second stage Oral antibiotics should be given
Nasal DeformitySaddle-nose deformityndash A saddle-nose deformity is characterised by a loss ofnasal dorsal height and compromised nasal supportstructures -Other case observed are depressionof the middle vault and dorsum loss of nasal tipsupport and definition shortened (vertical) nasal length over rotation of the nasal tip and retrusion ofthe nasal spine and caudal septum It is also knownas a ldquoPug noserdquo or ldquoboxerrsquos noserdquo both of which referto various degrees of nasal dorsal depressionbull
Nasal DeformityEpidemiologyaetiologyndash Prevalence is higher in population groups prone to facial trauma (ie boxers athletes) those with historiesof intranasal cocaine use nasal surgery (e g radical submucosal septal resection reductive rhinoplasty)ndash A saddle-nose deformity can be congenital or acquired It can be noticed as a part of individual familialsyndromic and ethnic characteristics - Most deformities are due to traumatic and iatrogeniccauses Medical causes are Wegenerrsquosgranulomatosis relapsing polychondritis leprosy (Hansenrsquos disease) syphilis ectodermal dysplasiaand intranasal cocaine use
Nasal Deformity
bull Therapybull ndash Nasal reconstruction indications depend on patientbull selection surgeon experience and aetiology of thebull deformity bull Indications for surgery can be functionalbull aesthetic or most commonly both In individuals
with a compromised nasal airway a nasoseptalbull reconstruction is indicated
Nasal Deformity
bull Contraindications bull include patients with malignantbull chronic or autoimmune disease conditions drugbull abuse poor perioperative risk profile and unrealisticbull expectationsbull ndash Multiple previous rhinoplasties and certain
professionsbull (mixed martial artists boxers and other contactbull sports) are relative contraindications
Nasal DeformitySeptoplastyndash Septoplasty is performed to correct nasal obstructioncaused by septal deformityndash Usually septoplasty is performed under general anaesthesiawith the patient in the supine position with the head elevated by approximately 30 (Righthandedsurgeons approach from the right side)ndash Local vasoconstrictive anaesthesia is applied notonly to reduce postoperative pain but also more importantly to achieve vasoconstriction of themucosa and less intraoperative haemorrhage Lidocainewith adrenaline or epinephrine is usedalthough in patients with cardiac hypersensitivityoxymetazoline might be preferred
Nasal Deformity
bull Septoplasty begins with the incision of septal mucosabull Most operative techniques utilise a hemitransfixionbull incision at the caudal end of septum so thatbull deviation at this point might be reached as wellbull as a transfixion incision that is easily obtained ifbull needed (Right-handed surgeons normally choosebull the left side but that may vary when deviation isbull convex towards the right)
Nasal DeformityA columella retractor is placed over the columellaand by pulling it laterally the caudal border of theseptum is exposed Ala can be protected by an alaprotector A vertical incision with a no 15 bladeover the caudal end of septum is performed untilreaching the plane of the septal cartilage It is essentialto correctly identify the perichondrium and byusing the Cottle elevator dissect and lift it creatinga flap As the dissection proceeds along the septalcartilage a longer speculum (no 5) is introduced sothat elevation of the mucoperichondrium is doneunder constant visual controlndash The next step is to dissect the mucoperiostium
Nasal DeformityDissecting over the bony-cartilaginous junctionwhen joining both tunnels might be difficult and is
especially prone to membrane perforationndash If needed the same tunnels are to be created on the
other side of the septum Then deviated parts of
septum are identified and removed either with a
knife or a Freer chisel
Nasal Deformitybull septum from the maxillary crest the septum mustbull be separated from the perpendicular plate trimmedbull along the inferior border placed back onto the crestbull and sutured to the periosteum If the deformity involvesbull the vomer an osteotome is used Care mustbull be taken not to break the cribriform plate becausebull it could cause a cerebrospinal fistula
Nasal Deformity
bull Once the septal deviation is corrected the flapsbull and hemitransfixion incision are mattressed
withbull absorbable sutures Nasal packing to prevent
synechiaebull and postoperative septal haematoma mightbull be advised but should be removed within 72 h

Deviated Nasal Septum
bull Therapybull ndash Septoplasty is a procedurebull The areabull of deviation is corrected or resected in order tobull leave behind as much cartilage and bone as
possiblebull Cartilage resection is minimised and can be
repositioned reshaped or recontoured using a variety of methods
Deviated Nasal Septum
bull ndash Indications of septoplasty before the growth period
bull of the nose is finished should be very limited bull -In these cases surgery must preserve all the
cartilagebull in order to prevent external changes of the
shape ofbull the nose
Deviated Nasal Septum
bull Complicationsbull ndash Frequent complications include haematoma andbull infection Cerebrospinal fluid leak is a rare but
potentiallybull serious complicationbull It is usually the resultbull of avulsion or damage to the cribriform plate whenbull handling the perpendicular plate of the ethmoidbull ndash Other complications include epistaxis nasal
Deviated Nasal Septum
bull Other complications include epistaxis nasal obstruction
bull due to residual deviation synechiae returnbull of the cartilaginous deviation septal perforationbull anosmia and cosmetic nasal deformities suchbull as widened alar rim margins drooping nasal tipbull columella retraction and a sunken dorsum with abull supratip saddle formation
Septal perforation with minor crusting View from provide closure of the
incision
Septal Haematoma
bull A septal haematoma is a blood collection under the perichondrium
bull of the septum and cartilagebull bull bull Epidemiologyaetiologybull ndash A septal haematoma is one of the most
severe complications of nasal trauma
Septal Haematoma
bull Diagnosisbull ndash Signs and symptoms include intense pain
swellingbull haematoma of the upper lip and philtrum
area andbull complete nasal airway obstruction
Septal HaematomaTherapyndash Management consists of drainage through a mucoperichondrial incision Immediate treatment isnecessary to prevent long-term problems such asa saddle-nose deformity perforation columellarretraction and nasal-base widening In childrenseptal destruction can lead to devastating nasal andmidfacial growth abnormalitiesbull Surgeryndash Incision and evacuation of the collection is performedDrainage of a septal haematoma should
Septal HaematomaSurgeryndash Incision and evacuation of the collection is performedDrainage of a septal haematoma should provide closure of the incision
Splints or transseptal sutures are placed to obliterate thepotential space and prevent collectionInfection involving the septal cartilage Reconstruction with autologouscartilage is then performed in a second stage Oral antibiotics should be given
Nasal DeformitySaddle-nose deformityndash A saddle-nose deformity is characterised by a loss ofnasal dorsal height and compromised nasal supportstructures -Other case observed are depressionof the middle vault and dorsum loss of nasal tipsupport and definition shortened (vertical) nasal length over rotation of the nasal tip and retrusion ofthe nasal spine and caudal septum It is also knownas a ldquoPug noserdquo or ldquoboxerrsquos noserdquo both of which referto various degrees of nasal dorsal depressionbull
Nasal DeformityEpidemiologyaetiologyndash Prevalence is higher in population groups prone to facial trauma (ie boxers athletes) those with historiesof intranasal cocaine use nasal surgery (e g radical submucosal septal resection reductive rhinoplasty)ndash A saddle-nose deformity can be congenital or acquired It can be noticed as a part of individual familialsyndromic and ethnic characteristics - Most deformities are due to traumatic and iatrogeniccauses Medical causes are Wegenerrsquosgranulomatosis relapsing polychondritis leprosy (Hansenrsquos disease) syphilis ectodermal dysplasiaand intranasal cocaine use
Nasal Deformity
bull Therapybull ndash Nasal reconstruction indications depend on patientbull selection surgeon experience and aetiology of thebull deformity bull Indications for surgery can be functionalbull aesthetic or most commonly both In individuals
with a compromised nasal airway a nasoseptalbull reconstruction is indicated
Nasal Deformity
bull Contraindications bull include patients with malignantbull chronic or autoimmune disease conditions drugbull abuse poor perioperative risk profile and unrealisticbull expectationsbull ndash Multiple previous rhinoplasties and certain
professionsbull (mixed martial artists boxers and other contactbull sports) are relative contraindications
Nasal DeformitySeptoplastyndash Septoplasty is performed to correct nasal obstructioncaused by septal deformityndash Usually septoplasty is performed under general anaesthesiawith the patient in the supine position with the head elevated by approximately 30 (Righthandedsurgeons approach from the right side)ndash Local vasoconstrictive anaesthesia is applied notonly to reduce postoperative pain but also more importantly to achieve vasoconstriction of themucosa and less intraoperative haemorrhage Lidocainewith adrenaline or epinephrine is usedalthough in patients with cardiac hypersensitivityoxymetazoline might be preferred
Nasal Deformity
bull Septoplasty begins with the incision of septal mucosabull Most operative techniques utilise a hemitransfixionbull incision at the caudal end of septum so thatbull deviation at this point might be reached as wellbull as a transfixion incision that is easily obtained ifbull needed (Right-handed surgeons normally choosebull the left side but that may vary when deviation isbull convex towards the right)
Nasal DeformityA columella retractor is placed over the columellaand by pulling it laterally the caudal border of theseptum is exposed Ala can be protected by an alaprotector A vertical incision with a no 15 bladeover the caudal end of septum is performed untilreaching the plane of the septal cartilage It is essentialto correctly identify the perichondrium and byusing the Cottle elevator dissect and lift it creatinga flap As the dissection proceeds along the septalcartilage a longer speculum (no 5) is introduced sothat elevation of the mucoperichondrium is doneunder constant visual controlndash The next step is to dissect the mucoperiostium
Nasal DeformityDissecting over the bony-cartilaginous junctionwhen joining both tunnels might be difficult and is
especially prone to membrane perforationndash If needed the same tunnels are to be created on the
other side of the septum Then deviated parts of
septum are identified and removed either with a
knife or a Freer chisel
Nasal Deformitybull septum from the maxillary crest the septum mustbull be separated from the perpendicular plate trimmedbull along the inferior border placed back onto the crestbull and sutured to the periosteum If the deformity involvesbull the vomer an osteotome is used Care mustbull be taken not to break the cribriform plate becausebull it could cause a cerebrospinal fistula
Nasal Deformity
bull Once the septal deviation is corrected the flapsbull and hemitransfixion incision are mattressed
withbull absorbable sutures Nasal packing to prevent
synechiaebull and postoperative septal haematoma mightbull be advised but should be removed within 72 h

Deviated Nasal Septum
bull ndash Indications of septoplasty before the growth period
bull of the nose is finished should be very limited bull -In these cases surgery must preserve all the
cartilagebull in order to prevent external changes of the
shape ofbull the nose
Deviated Nasal Septum
bull Complicationsbull ndash Frequent complications include haematoma andbull infection Cerebrospinal fluid leak is a rare but
potentiallybull serious complicationbull It is usually the resultbull of avulsion or damage to the cribriform plate whenbull handling the perpendicular plate of the ethmoidbull ndash Other complications include epistaxis nasal
Deviated Nasal Septum
bull Other complications include epistaxis nasal obstruction
bull due to residual deviation synechiae returnbull of the cartilaginous deviation septal perforationbull anosmia and cosmetic nasal deformities suchbull as widened alar rim margins drooping nasal tipbull columella retraction and a sunken dorsum with abull supratip saddle formation
Septal perforation with minor crusting View from provide closure of the
incision
Septal Haematoma
bull A septal haematoma is a blood collection under the perichondrium
bull of the septum and cartilagebull bull bull Epidemiologyaetiologybull ndash A septal haematoma is one of the most
severe complications of nasal trauma
Septal Haematoma
bull Diagnosisbull ndash Signs and symptoms include intense pain
swellingbull haematoma of the upper lip and philtrum
area andbull complete nasal airway obstruction
Septal HaematomaTherapyndash Management consists of drainage through a mucoperichondrial incision Immediate treatment isnecessary to prevent long-term problems such asa saddle-nose deformity perforation columellarretraction and nasal-base widening In childrenseptal destruction can lead to devastating nasal andmidfacial growth abnormalitiesbull Surgeryndash Incision and evacuation of the collection is performedDrainage of a septal haematoma should
Septal HaematomaSurgeryndash Incision and evacuation of the collection is performedDrainage of a septal haematoma should provide closure of the incision
Splints or transseptal sutures are placed to obliterate thepotential space and prevent collectionInfection involving the septal cartilage Reconstruction with autologouscartilage is then performed in a second stage Oral antibiotics should be given
Nasal DeformitySaddle-nose deformityndash A saddle-nose deformity is characterised by a loss ofnasal dorsal height and compromised nasal supportstructures -Other case observed are depressionof the middle vault and dorsum loss of nasal tipsupport and definition shortened (vertical) nasal length over rotation of the nasal tip and retrusion ofthe nasal spine and caudal septum It is also knownas a ldquoPug noserdquo or ldquoboxerrsquos noserdquo both of which referto various degrees of nasal dorsal depressionbull
Nasal DeformityEpidemiologyaetiologyndash Prevalence is higher in population groups prone to facial trauma (ie boxers athletes) those with historiesof intranasal cocaine use nasal surgery (e g radical submucosal septal resection reductive rhinoplasty)ndash A saddle-nose deformity can be congenital or acquired It can be noticed as a part of individual familialsyndromic and ethnic characteristics - Most deformities are due to traumatic and iatrogeniccauses Medical causes are Wegenerrsquosgranulomatosis relapsing polychondritis leprosy (Hansenrsquos disease) syphilis ectodermal dysplasiaand intranasal cocaine use
Nasal Deformity
bull Therapybull ndash Nasal reconstruction indications depend on patientbull selection surgeon experience and aetiology of thebull deformity bull Indications for surgery can be functionalbull aesthetic or most commonly both In individuals
with a compromised nasal airway a nasoseptalbull reconstruction is indicated
Nasal Deformity
bull Contraindications bull include patients with malignantbull chronic or autoimmune disease conditions drugbull abuse poor perioperative risk profile and unrealisticbull expectationsbull ndash Multiple previous rhinoplasties and certain
professionsbull (mixed martial artists boxers and other contactbull sports) are relative contraindications
Nasal DeformitySeptoplastyndash Septoplasty is performed to correct nasal obstructioncaused by septal deformityndash Usually septoplasty is performed under general anaesthesiawith the patient in the supine position with the head elevated by approximately 30 (Righthandedsurgeons approach from the right side)ndash Local vasoconstrictive anaesthesia is applied notonly to reduce postoperative pain but also more importantly to achieve vasoconstriction of themucosa and less intraoperative haemorrhage Lidocainewith adrenaline or epinephrine is usedalthough in patients with cardiac hypersensitivityoxymetazoline might be preferred
Nasal Deformity
bull Septoplasty begins with the incision of septal mucosabull Most operative techniques utilise a hemitransfixionbull incision at the caudal end of septum so thatbull deviation at this point might be reached as wellbull as a transfixion incision that is easily obtained ifbull needed (Right-handed surgeons normally choosebull the left side but that may vary when deviation isbull convex towards the right)
Nasal DeformityA columella retractor is placed over the columellaand by pulling it laterally the caudal border of theseptum is exposed Ala can be protected by an alaprotector A vertical incision with a no 15 bladeover the caudal end of septum is performed untilreaching the plane of the septal cartilage It is essentialto correctly identify the perichondrium and byusing the Cottle elevator dissect and lift it creatinga flap As the dissection proceeds along the septalcartilage a longer speculum (no 5) is introduced sothat elevation of the mucoperichondrium is doneunder constant visual controlndash The next step is to dissect the mucoperiostium
Nasal DeformityDissecting over the bony-cartilaginous junctionwhen joining both tunnels might be difficult and is
especially prone to membrane perforationndash If needed the same tunnels are to be created on the
other side of the septum Then deviated parts of
septum are identified and removed either with a
knife or a Freer chisel
Nasal Deformitybull septum from the maxillary crest the septum mustbull be separated from the perpendicular plate trimmedbull along the inferior border placed back onto the crestbull and sutured to the periosteum If the deformity involvesbull the vomer an osteotome is used Care mustbull be taken not to break the cribriform plate becausebull it could cause a cerebrospinal fistula
Nasal Deformity
bull Once the septal deviation is corrected the flapsbull and hemitransfixion incision are mattressed
withbull absorbable sutures Nasal packing to prevent
synechiaebull and postoperative septal haematoma mightbull be advised but should be removed within 72 h

Deviated Nasal Septum
bull Complicationsbull ndash Frequent complications include haematoma andbull infection Cerebrospinal fluid leak is a rare but
potentiallybull serious complicationbull It is usually the resultbull of avulsion or damage to the cribriform plate whenbull handling the perpendicular plate of the ethmoidbull ndash Other complications include epistaxis nasal
Deviated Nasal Septum
bull Other complications include epistaxis nasal obstruction
bull due to residual deviation synechiae returnbull of the cartilaginous deviation septal perforationbull anosmia and cosmetic nasal deformities suchbull as widened alar rim margins drooping nasal tipbull columella retraction and a sunken dorsum with abull supratip saddle formation
Septal perforation with minor crusting View from provide closure of the
incision
Septal Haematoma
bull A septal haematoma is a blood collection under the perichondrium
bull of the septum and cartilagebull bull bull Epidemiologyaetiologybull ndash A septal haematoma is one of the most
severe complications of nasal trauma
Septal Haematoma
bull Diagnosisbull ndash Signs and symptoms include intense pain
swellingbull haematoma of the upper lip and philtrum
area andbull complete nasal airway obstruction
Septal HaematomaTherapyndash Management consists of drainage through a mucoperichondrial incision Immediate treatment isnecessary to prevent long-term problems such asa saddle-nose deformity perforation columellarretraction and nasal-base widening In childrenseptal destruction can lead to devastating nasal andmidfacial growth abnormalitiesbull Surgeryndash Incision and evacuation of the collection is performedDrainage of a septal haematoma should
Septal HaematomaSurgeryndash Incision and evacuation of the collection is performedDrainage of a septal haematoma should provide closure of the incision
Splints or transseptal sutures are placed to obliterate thepotential space and prevent collectionInfection involving the septal cartilage Reconstruction with autologouscartilage is then performed in a second stage Oral antibiotics should be given
Nasal DeformitySaddle-nose deformityndash A saddle-nose deformity is characterised by a loss ofnasal dorsal height and compromised nasal supportstructures -Other case observed are depressionof the middle vault and dorsum loss of nasal tipsupport and definition shortened (vertical) nasal length over rotation of the nasal tip and retrusion ofthe nasal spine and caudal septum It is also knownas a ldquoPug noserdquo or ldquoboxerrsquos noserdquo both of which referto various degrees of nasal dorsal depressionbull
Nasal DeformityEpidemiologyaetiologyndash Prevalence is higher in population groups prone to facial trauma (ie boxers athletes) those with historiesof intranasal cocaine use nasal surgery (e g radical submucosal septal resection reductive rhinoplasty)ndash A saddle-nose deformity can be congenital or acquired It can be noticed as a part of individual familialsyndromic and ethnic characteristics - Most deformities are due to traumatic and iatrogeniccauses Medical causes are Wegenerrsquosgranulomatosis relapsing polychondritis leprosy (Hansenrsquos disease) syphilis ectodermal dysplasiaand intranasal cocaine use
Nasal Deformity
bull Therapybull ndash Nasal reconstruction indications depend on patientbull selection surgeon experience and aetiology of thebull deformity bull Indications for surgery can be functionalbull aesthetic or most commonly both In individuals
with a compromised nasal airway a nasoseptalbull reconstruction is indicated
Nasal Deformity
bull Contraindications bull include patients with malignantbull chronic or autoimmune disease conditions drugbull abuse poor perioperative risk profile and unrealisticbull expectationsbull ndash Multiple previous rhinoplasties and certain
professionsbull (mixed martial artists boxers and other contactbull sports) are relative contraindications
Nasal DeformitySeptoplastyndash Septoplasty is performed to correct nasal obstructioncaused by septal deformityndash Usually septoplasty is performed under general anaesthesiawith the patient in the supine position with the head elevated by approximately 30 (Righthandedsurgeons approach from the right side)ndash Local vasoconstrictive anaesthesia is applied notonly to reduce postoperative pain but also more importantly to achieve vasoconstriction of themucosa and less intraoperative haemorrhage Lidocainewith adrenaline or epinephrine is usedalthough in patients with cardiac hypersensitivityoxymetazoline might be preferred
Nasal Deformity
bull Septoplasty begins with the incision of septal mucosabull Most operative techniques utilise a hemitransfixionbull incision at the caudal end of septum so thatbull deviation at this point might be reached as wellbull as a transfixion incision that is easily obtained ifbull needed (Right-handed surgeons normally choosebull the left side but that may vary when deviation isbull convex towards the right)
Nasal DeformityA columella retractor is placed over the columellaand by pulling it laterally the caudal border of theseptum is exposed Ala can be protected by an alaprotector A vertical incision with a no 15 bladeover the caudal end of septum is performed untilreaching the plane of the septal cartilage It is essentialto correctly identify the perichondrium and byusing the Cottle elevator dissect and lift it creatinga flap As the dissection proceeds along the septalcartilage a longer speculum (no 5) is introduced sothat elevation of the mucoperichondrium is doneunder constant visual controlndash The next step is to dissect the mucoperiostium
Nasal DeformityDissecting over the bony-cartilaginous junctionwhen joining both tunnels might be difficult and is
especially prone to membrane perforationndash If needed the same tunnels are to be created on the
other side of the septum Then deviated parts of
septum are identified and removed either with a
knife or a Freer chisel
Nasal Deformitybull septum from the maxillary crest the septum mustbull be separated from the perpendicular plate trimmedbull along the inferior border placed back onto the crestbull and sutured to the periosteum If the deformity involvesbull the vomer an osteotome is used Care mustbull be taken not to break the cribriform plate becausebull it could cause a cerebrospinal fistula
Nasal Deformity
bull Once the septal deviation is corrected the flapsbull and hemitransfixion incision are mattressed
withbull absorbable sutures Nasal packing to prevent
synechiaebull and postoperative septal haematoma mightbull be advised but should be removed within 72 h

Deviated Nasal Septum
bull Other complications include epistaxis nasal obstruction
bull due to residual deviation synechiae returnbull of the cartilaginous deviation septal perforationbull anosmia and cosmetic nasal deformities suchbull as widened alar rim margins drooping nasal tipbull columella retraction and a sunken dorsum with abull supratip saddle formation
Septal perforation with minor crusting View from provide closure of the
incision
Septal Haematoma
bull A septal haematoma is a blood collection under the perichondrium
bull of the septum and cartilagebull bull bull Epidemiologyaetiologybull ndash A septal haematoma is one of the most
severe complications of nasal trauma
Septal Haematoma
bull Diagnosisbull ndash Signs and symptoms include intense pain
swellingbull haematoma of the upper lip and philtrum
area andbull complete nasal airway obstruction
Septal HaematomaTherapyndash Management consists of drainage through a mucoperichondrial incision Immediate treatment isnecessary to prevent long-term problems such asa saddle-nose deformity perforation columellarretraction and nasal-base widening In childrenseptal destruction can lead to devastating nasal andmidfacial growth abnormalitiesbull Surgeryndash Incision and evacuation of the collection is performedDrainage of a septal haematoma should
Septal HaematomaSurgeryndash Incision and evacuation of the collection is performedDrainage of a septal haematoma should provide closure of the incision
Splints or transseptal sutures are placed to obliterate thepotential space and prevent collectionInfection involving the septal cartilage Reconstruction with autologouscartilage is then performed in a second stage Oral antibiotics should be given
Nasal DeformitySaddle-nose deformityndash A saddle-nose deformity is characterised by a loss ofnasal dorsal height and compromised nasal supportstructures -Other case observed are depressionof the middle vault and dorsum loss of nasal tipsupport and definition shortened (vertical) nasal length over rotation of the nasal tip and retrusion ofthe nasal spine and caudal septum It is also knownas a ldquoPug noserdquo or ldquoboxerrsquos noserdquo both of which referto various degrees of nasal dorsal depressionbull
Nasal DeformityEpidemiologyaetiologyndash Prevalence is higher in population groups prone to facial trauma (ie boxers athletes) those with historiesof intranasal cocaine use nasal surgery (e g radical submucosal septal resection reductive rhinoplasty)ndash A saddle-nose deformity can be congenital or acquired It can be noticed as a part of individual familialsyndromic and ethnic characteristics - Most deformities are due to traumatic and iatrogeniccauses Medical causes are Wegenerrsquosgranulomatosis relapsing polychondritis leprosy (Hansenrsquos disease) syphilis ectodermal dysplasiaand intranasal cocaine use
Nasal Deformity
bull Therapybull ndash Nasal reconstruction indications depend on patientbull selection surgeon experience and aetiology of thebull deformity bull Indications for surgery can be functionalbull aesthetic or most commonly both In individuals
with a compromised nasal airway a nasoseptalbull reconstruction is indicated
Nasal Deformity
bull Contraindications bull include patients with malignantbull chronic or autoimmune disease conditions drugbull abuse poor perioperative risk profile and unrealisticbull expectationsbull ndash Multiple previous rhinoplasties and certain
professionsbull (mixed martial artists boxers and other contactbull sports) are relative contraindications
Nasal DeformitySeptoplastyndash Septoplasty is performed to correct nasal obstructioncaused by septal deformityndash Usually septoplasty is performed under general anaesthesiawith the patient in the supine position with the head elevated by approximately 30 (Righthandedsurgeons approach from the right side)ndash Local vasoconstrictive anaesthesia is applied notonly to reduce postoperative pain but also more importantly to achieve vasoconstriction of themucosa and less intraoperative haemorrhage Lidocainewith adrenaline or epinephrine is usedalthough in patients with cardiac hypersensitivityoxymetazoline might be preferred
Nasal Deformity
bull Septoplasty begins with the incision of septal mucosabull Most operative techniques utilise a hemitransfixionbull incision at the caudal end of septum so thatbull deviation at this point might be reached as wellbull as a transfixion incision that is easily obtained ifbull needed (Right-handed surgeons normally choosebull the left side but that may vary when deviation isbull convex towards the right)
Nasal DeformityA columella retractor is placed over the columellaand by pulling it laterally the caudal border of theseptum is exposed Ala can be protected by an alaprotector A vertical incision with a no 15 bladeover the caudal end of septum is performed untilreaching the plane of the septal cartilage It is essentialto correctly identify the perichondrium and byusing the Cottle elevator dissect and lift it creatinga flap As the dissection proceeds along the septalcartilage a longer speculum (no 5) is introduced sothat elevation of the mucoperichondrium is doneunder constant visual controlndash The next step is to dissect the mucoperiostium
Nasal DeformityDissecting over the bony-cartilaginous junctionwhen joining both tunnels might be difficult and is
especially prone to membrane perforationndash If needed the same tunnels are to be created on the
other side of the septum Then deviated parts of
septum are identified and removed either with a
knife or a Freer chisel
Nasal Deformitybull septum from the maxillary crest the septum mustbull be separated from the perpendicular plate trimmedbull along the inferior border placed back onto the crestbull and sutured to the periosteum If the deformity involvesbull the vomer an osteotome is used Care mustbull be taken not to break the cribriform plate becausebull it could cause a cerebrospinal fistula
Nasal Deformity
bull Once the septal deviation is corrected the flapsbull and hemitransfixion incision are mattressed
withbull absorbable sutures Nasal packing to prevent
synechiaebull and postoperative septal haematoma mightbull be advised but should be removed within 72 h

Septal perforation with minor crusting View from provide closure of the
incision
Septal Haematoma
bull A septal haematoma is a blood collection under the perichondrium
bull of the septum and cartilagebull bull bull Epidemiologyaetiologybull ndash A septal haematoma is one of the most
severe complications of nasal trauma
Septal Haematoma
bull Diagnosisbull ndash Signs and symptoms include intense pain
swellingbull haematoma of the upper lip and philtrum
area andbull complete nasal airway obstruction
Septal HaematomaTherapyndash Management consists of drainage through a mucoperichondrial incision Immediate treatment isnecessary to prevent long-term problems such asa saddle-nose deformity perforation columellarretraction and nasal-base widening In childrenseptal destruction can lead to devastating nasal andmidfacial growth abnormalitiesbull Surgeryndash Incision and evacuation of the collection is performedDrainage of a septal haematoma should
Septal HaematomaSurgeryndash Incision and evacuation of the collection is performedDrainage of a septal haematoma should provide closure of the incision
Splints or transseptal sutures are placed to obliterate thepotential space and prevent collectionInfection involving the septal cartilage Reconstruction with autologouscartilage is then performed in a second stage Oral antibiotics should be given
Nasal DeformitySaddle-nose deformityndash A saddle-nose deformity is characterised by a loss ofnasal dorsal height and compromised nasal supportstructures -Other case observed are depressionof the middle vault and dorsum loss of nasal tipsupport and definition shortened (vertical) nasal length over rotation of the nasal tip and retrusion ofthe nasal spine and caudal septum It is also knownas a ldquoPug noserdquo or ldquoboxerrsquos noserdquo both of which referto various degrees of nasal dorsal depressionbull
Nasal DeformityEpidemiologyaetiologyndash Prevalence is higher in population groups prone to facial trauma (ie boxers athletes) those with historiesof intranasal cocaine use nasal surgery (e g radical submucosal septal resection reductive rhinoplasty)ndash A saddle-nose deformity can be congenital or acquired It can be noticed as a part of individual familialsyndromic and ethnic characteristics - Most deformities are due to traumatic and iatrogeniccauses Medical causes are Wegenerrsquosgranulomatosis relapsing polychondritis leprosy (Hansenrsquos disease) syphilis ectodermal dysplasiaand intranasal cocaine use
Nasal Deformity
bull Therapybull ndash Nasal reconstruction indications depend on patientbull selection surgeon experience and aetiology of thebull deformity bull Indications for surgery can be functionalbull aesthetic or most commonly both In individuals
with a compromised nasal airway a nasoseptalbull reconstruction is indicated
Nasal Deformity
bull Contraindications bull include patients with malignantbull chronic or autoimmune disease conditions drugbull abuse poor perioperative risk profile and unrealisticbull expectationsbull ndash Multiple previous rhinoplasties and certain
professionsbull (mixed martial artists boxers and other contactbull sports) are relative contraindications
Nasal DeformitySeptoplastyndash Septoplasty is performed to correct nasal obstructioncaused by septal deformityndash Usually septoplasty is performed under general anaesthesiawith the patient in the supine position with the head elevated by approximately 30 (Righthandedsurgeons approach from the right side)ndash Local vasoconstrictive anaesthesia is applied notonly to reduce postoperative pain but also more importantly to achieve vasoconstriction of themucosa and less intraoperative haemorrhage Lidocainewith adrenaline or epinephrine is usedalthough in patients with cardiac hypersensitivityoxymetazoline might be preferred
Nasal Deformity
bull Septoplasty begins with the incision of septal mucosabull Most operative techniques utilise a hemitransfixionbull incision at the caudal end of septum so thatbull deviation at this point might be reached as wellbull as a transfixion incision that is easily obtained ifbull needed (Right-handed surgeons normally choosebull the left side but that may vary when deviation isbull convex towards the right)
Nasal DeformityA columella retractor is placed over the columellaand by pulling it laterally the caudal border of theseptum is exposed Ala can be protected by an alaprotector A vertical incision with a no 15 bladeover the caudal end of septum is performed untilreaching the plane of the septal cartilage It is essentialto correctly identify the perichondrium and byusing the Cottle elevator dissect and lift it creatinga flap As the dissection proceeds along the septalcartilage a longer speculum (no 5) is introduced sothat elevation of the mucoperichondrium is doneunder constant visual controlndash The next step is to dissect the mucoperiostium
Nasal DeformityDissecting over the bony-cartilaginous junctionwhen joining both tunnels might be difficult and is
especially prone to membrane perforationndash If needed the same tunnels are to be created on the
other side of the septum Then deviated parts of
septum are identified and removed either with a
knife or a Freer chisel
Nasal Deformitybull septum from the maxillary crest the septum mustbull be separated from the perpendicular plate trimmedbull along the inferior border placed back onto the crestbull and sutured to the periosteum If the deformity involvesbull the vomer an osteotome is used Care mustbull be taken not to break the cribriform plate becausebull it could cause a cerebrospinal fistula
Nasal Deformity
bull Once the septal deviation is corrected the flapsbull and hemitransfixion incision are mattressed
withbull absorbable sutures Nasal packing to prevent
synechiaebull and postoperative septal haematoma mightbull be advised but should be removed within 72 h

Septal Haematoma
bull A septal haematoma is a blood collection under the perichondrium
bull of the septum and cartilagebull bull bull Epidemiologyaetiologybull ndash A septal haematoma is one of the most
severe complications of nasal trauma
Septal Haematoma
bull Diagnosisbull ndash Signs and symptoms include intense pain
swellingbull haematoma of the upper lip and philtrum
area andbull complete nasal airway obstruction
Septal HaematomaTherapyndash Management consists of drainage through a mucoperichondrial incision Immediate treatment isnecessary to prevent long-term problems such asa saddle-nose deformity perforation columellarretraction and nasal-base widening In childrenseptal destruction can lead to devastating nasal andmidfacial growth abnormalitiesbull Surgeryndash Incision and evacuation of the collection is performedDrainage of a septal haematoma should
Septal HaematomaSurgeryndash Incision and evacuation of the collection is performedDrainage of a septal haematoma should provide closure of the incision
Splints or transseptal sutures are placed to obliterate thepotential space and prevent collectionInfection involving the septal cartilage Reconstruction with autologouscartilage is then performed in a second stage Oral antibiotics should be given
Nasal DeformitySaddle-nose deformityndash A saddle-nose deformity is characterised by a loss ofnasal dorsal height and compromised nasal supportstructures -Other case observed are depressionof the middle vault and dorsum loss of nasal tipsupport and definition shortened (vertical) nasal length over rotation of the nasal tip and retrusion ofthe nasal spine and caudal septum It is also knownas a ldquoPug noserdquo or ldquoboxerrsquos noserdquo both of which referto various degrees of nasal dorsal depressionbull
Nasal DeformityEpidemiologyaetiologyndash Prevalence is higher in population groups prone to facial trauma (ie boxers athletes) those with historiesof intranasal cocaine use nasal surgery (e g radical submucosal septal resection reductive rhinoplasty)ndash A saddle-nose deformity can be congenital or acquired It can be noticed as a part of individual familialsyndromic and ethnic characteristics - Most deformities are due to traumatic and iatrogeniccauses Medical causes are Wegenerrsquosgranulomatosis relapsing polychondritis leprosy (Hansenrsquos disease) syphilis ectodermal dysplasiaand intranasal cocaine use
Nasal Deformity
bull Therapybull ndash Nasal reconstruction indications depend on patientbull selection surgeon experience and aetiology of thebull deformity bull Indications for surgery can be functionalbull aesthetic or most commonly both In individuals
with a compromised nasal airway a nasoseptalbull reconstruction is indicated
Nasal Deformity
bull Contraindications bull include patients with malignantbull chronic or autoimmune disease conditions drugbull abuse poor perioperative risk profile and unrealisticbull expectationsbull ndash Multiple previous rhinoplasties and certain
professionsbull (mixed martial artists boxers and other contactbull sports) are relative contraindications
Nasal DeformitySeptoplastyndash Septoplasty is performed to correct nasal obstructioncaused by septal deformityndash Usually septoplasty is performed under general anaesthesiawith the patient in the supine position with the head elevated by approximately 30 (Righthandedsurgeons approach from the right side)ndash Local vasoconstrictive anaesthesia is applied notonly to reduce postoperative pain but also more importantly to achieve vasoconstriction of themucosa and less intraoperative haemorrhage Lidocainewith adrenaline or epinephrine is usedalthough in patients with cardiac hypersensitivityoxymetazoline might be preferred
Nasal Deformity
bull Septoplasty begins with the incision of septal mucosabull Most operative techniques utilise a hemitransfixionbull incision at the caudal end of septum so thatbull deviation at this point might be reached as wellbull as a transfixion incision that is easily obtained ifbull needed (Right-handed surgeons normally choosebull the left side but that may vary when deviation isbull convex towards the right)
Nasal DeformityA columella retractor is placed over the columellaand by pulling it laterally the caudal border of theseptum is exposed Ala can be protected by an alaprotector A vertical incision with a no 15 bladeover the caudal end of septum is performed untilreaching the plane of the septal cartilage It is essentialto correctly identify the perichondrium and byusing the Cottle elevator dissect and lift it creatinga flap As the dissection proceeds along the septalcartilage a longer speculum (no 5) is introduced sothat elevation of the mucoperichondrium is doneunder constant visual controlndash The next step is to dissect the mucoperiostium
Nasal DeformityDissecting over the bony-cartilaginous junctionwhen joining both tunnels might be difficult and is
especially prone to membrane perforationndash If needed the same tunnels are to be created on the
other side of the septum Then deviated parts of
septum are identified and removed either with a
knife or a Freer chisel
Nasal Deformitybull septum from the maxillary crest the septum mustbull be separated from the perpendicular plate trimmedbull along the inferior border placed back onto the crestbull and sutured to the periosteum If the deformity involvesbull the vomer an osteotome is used Care mustbull be taken not to break the cribriform plate becausebull it could cause a cerebrospinal fistula
Nasal Deformity
bull Once the septal deviation is corrected the flapsbull and hemitransfixion incision are mattressed
withbull absorbable sutures Nasal packing to prevent
synechiaebull and postoperative septal haematoma mightbull be advised but should be removed within 72 h

Septal Haematoma
bull Diagnosisbull ndash Signs and symptoms include intense pain
swellingbull haematoma of the upper lip and philtrum
area andbull complete nasal airway obstruction
Septal HaematomaTherapyndash Management consists of drainage through a mucoperichondrial incision Immediate treatment isnecessary to prevent long-term problems such asa saddle-nose deformity perforation columellarretraction and nasal-base widening In childrenseptal destruction can lead to devastating nasal andmidfacial growth abnormalitiesbull Surgeryndash Incision and evacuation of the collection is performedDrainage of a septal haematoma should
Septal HaematomaSurgeryndash Incision and evacuation of the collection is performedDrainage of a septal haematoma should provide closure of the incision
Splints or transseptal sutures are placed to obliterate thepotential space and prevent collectionInfection involving the septal cartilage Reconstruction with autologouscartilage is then performed in a second stage Oral antibiotics should be given
Nasal DeformitySaddle-nose deformityndash A saddle-nose deformity is characterised by a loss ofnasal dorsal height and compromised nasal supportstructures -Other case observed are depressionof the middle vault and dorsum loss of nasal tipsupport and definition shortened (vertical) nasal length over rotation of the nasal tip and retrusion ofthe nasal spine and caudal septum It is also knownas a ldquoPug noserdquo or ldquoboxerrsquos noserdquo both of which referto various degrees of nasal dorsal depressionbull
Nasal DeformityEpidemiologyaetiologyndash Prevalence is higher in population groups prone to facial trauma (ie boxers athletes) those with historiesof intranasal cocaine use nasal surgery (e g radical submucosal septal resection reductive rhinoplasty)ndash A saddle-nose deformity can be congenital or acquired It can be noticed as a part of individual familialsyndromic and ethnic characteristics - Most deformities are due to traumatic and iatrogeniccauses Medical causes are Wegenerrsquosgranulomatosis relapsing polychondritis leprosy (Hansenrsquos disease) syphilis ectodermal dysplasiaand intranasal cocaine use
Nasal Deformity
bull Therapybull ndash Nasal reconstruction indications depend on patientbull selection surgeon experience and aetiology of thebull deformity bull Indications for surgery can be functionalbull aesthetic or most commonly both In individuals
with a compromised nasal airway a nasoseptalbull reconstruction is indicated
Nasal Deformity
bull Contraindications bull include patients with malignantbull chronic or autoimmune disease conditions drugbull abuse poor perioperative risk profile and unrealisticbull expectationsbull ndash Multiple previous rhinoplasties and certain
professionsbull (mixed martial artists boxers and other contactbull sports) are relative contraindications
Nasal DeformitySeptoplastyndash Septoplasty is performed to correct nasal obstructioncaused by septal deformityndash Usually septoplasty is performed under general anaesthesiawith the patient in the supine position with the head elevated by approximately 30 (Righthandedsurgeons approach from the right side)ndash Local vasoconstrictive anaesthesia is applied notonly to reduce postoperative pain but also more importantly to achieve vasoconstriction of themucosa and less intraoperative haemorrhage Lidocainewith adrenaline or epinephrine is usedalthough in patients with cardiac hypersensitivityoxymetazoline might be preferred
Nasal Deformity
bull Septoplasty begins with the incision of septal mucosabull Most operative techniques utilise a hemitransfixionbull incision at the caudal end of septum so thatbull deviation at this point might be reached as wellbull as a transfixion incision that is easily obtained ifbull needed (Right-handed surgeons normally choosebull the left side but that may vary when deviation isbull convex towards the right)
Nasal DeformityA columella retractor is placed over the columellaand by pulling it laterally the caudal border of theseptum is exposed Ala can be protected by an alaprotector A vertical incision with a no 15 bladeover the caudal end of septum is performed untilreaching the plane of the septal cartilage It is essentialto correctly identify the perichondrium and byusing the Cottle elevator dissect and lift it creatinga flap As the dissection proceeds along the septalcartilage a longer speculum (no 5) is introduced sothat elevation of the mucoperichondrium is doneunder constant visual controlndash The next step is to dissect the mucoperiostium
Nasal DeformityDissecting over the bony-cartilaginous junctionwhen joining both tunnels might be difficult and is
especially prone to membrane perforationndash If needed the same tunnels are to be created on the
other side of the septum Then deviated parts of
septum are identified and removed either with a
knife or a Freer chisel
Nasal Deformitybull septum from the maxillary crest the septum mustbull be separated from the perpendicular plate trimmedbull along the inferior border placed back onto the crestbull and sutured to the periosteum If the deformity involvesbull the vomer an osteotome is used Care mustbull be taken not to break the cribriform plate becausebull it could cause a cerebrospinal fistula
Nasal Deformity
bull Once the septal deviation is corrected the flapsbull and hemitransfixion incision are mattressed
withbull absorbable sutures Nasal packing to prevent
synechiaebull and postoperative septal haematoma mightbull be advised but should be removed within 72 h

Septal HaematomaTherapyndash Management consists of drainage through a mucoperichondrial incision Immediate treatment isnecessary to prevent long-term problems such asa saddle-nose deformity perforation columellarretraction and nasal-base widening In childrenseptal destruction can lead to devastating nasal andmidfacial growth abnormalitiesbull Surgeryndash Incision and evacuation of the collection is performedDrainage of a septal haematoma should
Septal HaematomaSurgeryndash Incision and evacuation of the collection is performedDrainage of a septal haematoma should provide closure of the incision
Splints or transseptal sutures are placed to obliterate thepotential space and prevent collectionInfection involving the septal cartilage Reconstruction with autologouscartilage is then performed in a second stage Oral antibiotics should be given
Nasal DeformitySaddle-nose deformityndash A saddle-nose deformity is characterised by a loss ofnasal dorsal height and compromised nasal supportstructures -Other case observed are depressionof the middle vault and dorsum loss of nasal tipsupport and definition shortened (vertical) nasal length over rotation of the nasal tip and retrusion ofthe nasal spine and caudal septum It is also knownas a ldquoPug noserdquo or ldquoboxerrsquos noserdquo both of which referto various degrees of nasal dorsal depressionbull
Nasal DeformityEpidemiologyaetiologyndash Prevalence is higher in population groups prone to facial trauma (ie boxers athletes) those with historiesof intranasal cocaine use nasal surgery (e g radical submucosal septal resection reductive rhinoplasty)ndash A saddle-nose deformity can be congenital or acquired It can be noticed as a part of individual familialsyndromic and ethnic characteristics - Most deformities are due to traumatic and iatrogeniccauses Medical causes are Wegenerrsquosgranulomatosis relapsing polychondritis leprosy (Hansenrsquos disease) syphilis ectodermal dysplasiaand intranasal cocaine use
Nasal Deformity
bull Therapybull ndash Nasal reconstruction indications depend on patientbull selection surgeon experience and aetiology of thebull deformity bull Indications for surgery can be functionalbull aesthetic or most commonly both In individuals
with a compromised nasal airway a nasoseptalbull reconstruction is indicated
Nasal Deformity
bull Contraindications bull include patients with malignantbull chronic or autoimmune disease conditions drugbull abuse poor perioperative risk profile and unrealisticbull expectationsbull ndash Multiple previous rhinoplasties and certain
professionsbull (mixed martial artists boxers and other contactbull sports) are relative contraindications
Nasal DeformitySeptoplastyndash Septoplasty is performed to correct nasal obstructioncaused by septal deformityndash Usually septoplasty is performed under general anaesthesiawith the patient in the supine position with the head elevated by approximately 30 (Righthandedsurgeons approach from the right side)ndash Local vasoconstrictive anaesthesia is applied notonly to reduce postoperative pain but also more importantly to achieve vasoconstriction of themucosa and less intraoperative haemorrhage Lidocainewith adrenaline or epinephrine is usedalthough in patients with cardiac hypersensitivityoxymetazoline might be preferred
Nasal Deformity
bull Septoplasty begins with the incision of septal mucosabull Most operative techniques utilise a hemitransfixionbull incision at the caudal end of septum so thatbull deviation at this point might be reached as wellbull as a transfixion incision that is easily obtained ifbull needed (Right-handed surgeons normally choosebull the left side but that may vary when deviation isbull convex towards the right)
Nasal DeformityA columella retractor is placed over the columellaand by pulling it laterally the caudal border of theseptum is exposed Ala can be protected by an alaprotector A vertical incision with a no 15 bladeover the caudal end of septum is performed untilreaching the plane of the septal cartilage It is essentialto correctly identify the perichondrium and byusing the Cottle elevator dissect and lift it creatinga flap As the dissection proceeds along the septalcartilage a longer speculum (no 5) is introduced sothat elevation of the mucoperichondrium is doneunder constant visual controlndash The next step is to dissect the mucoperiostium
Nasal DeformityDissecting over the bony-cartilaginous junctionwhen joining both tunnels might be difficult and is
especially prone to membrane perforationndash If needed the same tunnels are to be created on the
other side of the septum Then deviated parts of
septum are identified and removed either with a
knife or a Freer chisel
Nasal Deformitybull septum from the maxillary crest the septum mustbull be separated from the perpendicular plate trimmedbull along the inferior border placed back onto the crestbull and sutured to the periosteum If the deformity involvesbull the vomer an osteotome is used Care mustbull be taken not to break the cribriform plate becausebull it could cause a cerebrospinal fistula
Nasal Deformity
bull Once the septal deviation is corrected the flapsbull and hemitransfixion incision are mattressed
withbull absorbable sutures Nasal packing to prevent
synechiaebull and postoperative septal haematoma mightbull be advised but should be removed within 72 h

Septal HaematomaSurgeryndash Incision and evacuation of the collection is performedDrainage of a septal haematoma should provide closure of the incision
Splints or transseptal sutures are placed to obliterate thepotential space and prevent collectionInfection involving the septal cartilage Reconstruction with autologouscartilage is then performed in a second stage Oral antibiotics should be given
Nasal DeformitySaddle-nose deformityndash A saddle-nose deformity is characterised by a loss ofnasal dorsal height and compromised nasal supportstructures -Other case observed are depressionof the middle vault and dorsum loss of nasal tipsupport and definition shortened (vertical) nasal length over rotation of the nasal tip and retrusion ofthe nasal spine and caudal septum It is also knownas a ldquoPug noserdquo or ldquoboxerrsquos noserdquo both of which referto various degrees of nasal dorsal depressionbull
Nasal DeformityEpidemiologyaetiologyndash Prevalence is higher in population groups prone to facial trauma (ie boxers athletes) those with historiesof intranasal cocaine use nasal surgery (e g radical submucosal septal resection reductive rhinoplasty)ndash A saddle-nose deformity can be congenital or acquired It can be noticed as a part of individual familialsyndromic and ethnic characteristics - Most deformities are due to traumatic and iatrogeniccauses Medical causes are Wegenerrsquosgranulomatosis relapsing polychondritis leprosy (Hansenrsquos disease) syphilis ectodermal dysplasiaand intranasal cocaine use
Nasal Deformity
bull Therapybull ndash Nasal reconstruction indications depend on patientbull selection surgeon experience and aetiology of thebull deformity bull Indications for surgery can be functionalbull aesthetic or most commonly both In individuals
with a compromised nasal airway a nasoseptalbull reconstruction is indicated
Nasal Deformity
bull Contraindications bull include patients with malignantbull chronic or autoimmune disease conditions drugbull abuse poor perioperative risk profile and unrealisticbull expectationsbull ndash Multiple previous rhinoplasties and certain
professionsbull (mixed martial artists boxers and other contactbull sports) are relative contraindications
Nasal DeformitySeptoplastyndash Septoplasty is performed to correct nasal obstructioncaused by septal deformityndash Usually septoplasty is performed under general anaesthesiawith the patient in the supine position with the head elevated by approximately 30 (Righthandedsurgeons approach from the right side)ndash Local vasoconstrictive anaesthesia is applied notonly to reduce postoperative pain but also more importantly to achieve vasoconstriction of themucosa and less intraoperative haemorrhage Lidocainewith adrenaline or epinephrine is usedalthough in patients with cardiac hypersensitivityoxymetazoline might be preferred
Nasal Deformity
bull Septoplasty begins with the incision of septal mucosabull Most operative techniques utilise a hemitransfixionbull incision at the caudal end of septum so thatbull deviation at this point might be reached as wellbull as a transfixion incision that is easily obtained ifbull needed (Right-handed surgeons normally choosebull the left side but that may vary when deviation isbull convex towards the right)
Nasal DeformityA columella retractor is placed over the columellaand by pulling it laterally the caudal border of theseptum is exposed Ala can be protected by an alaprotector A vertical incision with a no 15 bladeover the caudal end of septum is performed untilreaching the plane of the septal cartilage It is essentialto correctly identify the perichondrium and byusing the Cottle elevator dissect and lift it creatinga flap As the dissection proceeds along the septalcartilage a longer speculum (no 5) is introduced sothat elevation of the mucoperichondrium is doneunder constant visual controlndash The next step is to dissect the mucoperiostium
Nasal DeformityDissecting over the bony-cartilaginous junctionwhen joining both tunnels might be difficult and is
especially prone to membrane perforationndash If needed the same tunnels are to be created on the
other side of the septum Then deviated parts of
septum are identified and removed either with a
knife or a Freer chisel
Nasal Deformitybull septum from the maxillary crest the septum mustbull be separated from the perpendicular plate trimmedbull along the inferior border placed back onto the crestbull and sutured to the periosteum If the deformity involvesbull the vomer an osteotome is used Care mustbull be taken not to break the cribriform plate becausebull it could cause a cerebrospinal fistula
Nasal Deformity
bull Once the septal deviation is corrected the flapsbull and hemitransfixion incision are mattressed
withbull absorbable sutures Nasal packing to prevent
synechiaebull and postoperative septal haematoma mightbull be advised but should be removed within 72 h

Nasal DeformitySaddle-nose deformityndash A saddle-nose deformity is characterised by a loss ofnasal dorsal height and compromised nasal supportstructures -Other case observed are depressionof the middle vault and dorsum loss of nasal tipsupport and definition shortened (vertical) nasal length over rotation of the nasal tip and retrusion ofthe nasal spine and caudal septum It is also knownas a ldquoPug noserdquo or ldquoboxerrsquos noserdquo both of which referto various degrees of nasal dorsal depressionbull
Nasal DeformityEpidemiologyaetiologyndash Prevalence is higher in population groups prone to facial trauma (ie boxers athletes) those with historiesof intranasal cocaine use nasal surgery (e g radical submucosal septal resection reductive rhinoplasty)ndash A saddle-nose deformity can be congenital or acquired It can be noticed as a part of individual familialsyndromic and ethnic characteristics - Most deformities are due to traumatic and iatrogeniccauses Medical causes are Wegenerrsquosgranulomatosis relapsing polychondritis leprosy (Hansenrsquos disease) syphilis ectodermal dysplasiaand intranasal cocaine use
Nasal Deformity
bull Therapybull ndash Nasal reconstruction indications depend on patientbull selection surgeon experience and aetiology of thebull deformity bull Indications for surgery can be functionalbull aesthetic or most commonly both In individuals
with a compromised nasal airway a nasoseptalbull reconstruction is indicated
Nasal Deformity
bull Contraindications bull include patients with malignantbull chronic or autoimmune disease conditions drugbull abuse poor perioperative risk profile and unrealisticbull expectationsbull ndash Multiple previous rhinoplasties and certain
professionsbull (mixed martial artists boxers and other contactbull sports) are relative contraindications
Nasal DeformitySeptoplastyndash Septoplasty is performed to correct nasal obstructioncaused by septal deformityndash Usually septoplasty is performed under general anaesthesiawith the patient in the supine position with the head elevated by approximately 30 (Righthandedsurgeons approach from the right side)ndash Local vasoconstrictive anaesthesia is applied notonly to reduce postoperative pain but also more importantly to achieve vasoconstriction of themucosa and less intraoperative haemorrhage Lidocainewith adrenaline or epinephrine is usedalthough in patients with cardiac hypersensitivityoxymetazoline might be preferred
Nasal Deformity
bull Septoplasty begins with the incision of septal mucosabull Most operative techniques utilise a hemitransfixionbull incision at the caudal end of septum so thatbull deviation at this point might be reached as wellbull as a transfixion incision that is easily obtained ifbull needed (Right-handed surgeons normally choosebull the left side but that may vary when deviation isbull convex towards the right)
Nasal DeformityA columella retractor is placed over the columellaand by pulling it laterally the caudal border of theseptum is exposed Ala can be protected by an alaprotector A vertical incision with a no 15 bladeover the caudal end of septum is performed untilreaching the plane of the septal cartilage It is essentialto correctly identify the perichondrium and byusing the Cottle elevator dissect and lift it creatinga flap As the dissection proceeds along the septalcartilage a longer speculum (no 5) is introduced sothat elevation of the mucoperichondrium is doneunder constant visual controlndash The next step is to dissect the mucoperiostium
Nasal DeformityDissecting over the bony-cartilaginous junctionwhen joining both tunnels might be difficult and is
especially prone to membrane perforationndash If needed the same tunnels are to be created on the
other side of the septum Then deviated parts of
septum are identified and removed either with a
knife or a Freer chisel
Nasal Deformitybull septum from the maxillary crest the septum mustbull be separated from the perpendicular plate trimmedbull along the inferior border placed back onto the crestbull and sutured to the periosteum If the deformity involvesbull the vomer an osteotome is used Care mustbull be taken not to break the cribriform plate becausebull it could cause a cerebrospinal fistula
Nasal Deformity
bull Once the septal deviation is corrected the flapsbull and hemitransfixion incision are mattressed
withbull absorbable sutures Nasal packing to prevent
synechiaebull and postoperative septal haematoma mightbull be advised but should be removed within 72 h

Nasal DeformityEpidemiologyaetiologyndash Prevalence is higher in population groups prone to facial trauma (ie boxers athletes) those with historiesof intranasal cocaine use nasal surgery (e g radical submucosal septal resection reductive rhinoplasty)ndash A saddle-nose deformity can be congenital or acquired It can be noticed as a part of individual familialsyndromic and ethnic characteristics - Most deformities are due to traumatic and iatrogeniccauses Medical causes are Wegenerrsquosgranulomatosis relapsing polychondritis leprosy (Hansenrsquos disease) syphilis ectodermal dysplasiaand intranasal cocaine use
Nasal Deformity
bull Therapybull ndash Nasal reconstruction indications depend on patientbull selection surgeon experience and aetiology of thebull deformity bull Indications for surgery can be functionalbull aesthetic or most commonly both In individuals
with a compromised nasal airway a nasoseptalbull reconstruction is indicated
Nasal Deformity
bull Contraindications bull include patients with malignantbull chronic or autoimmune disease conditions drugbull abuse poor perioperative risk profile and unrealisticbull expectationsbull ndash Multiple previous rhinoplasties and certain
professionsbull (mixed martial artists boxers and other contactbull sports) are relative contraindications
Nasal DeformitySeptoplastyndash Septoplasty is performed to correct nasal obstructioncaused by septal deformityndash Usually septoplasty is performed under general anaesthesiawith the patient in the supine position with the head elevated by approximately 30 (Righthandedsurgeons approach from the right side)ndash Local vasoconstrictive anaesthesia is applied notonly to reduce postoperative pain but also more importantly to achieve vasoconstriction of themucosa and less intraoperative haemorrhage Lidocainewith adrenaline or epinephrine is usedalthough in patients with cardiac hypersensitivityoxymetazoline might be preferred
Nasal Deformity
bull Septoplasty begins with the incision of septal mucosabull Most operative techniques utilise a hemitransfixionbull incision at the caudal end of septum so thatbull deviation at this point might be reached as wellbull as a transfixion incision that is easily obtained ifbull needed (Right-handed surgeons normally choosebull the left side but that may vary when deviation isbull convex towards the right)
Nasal DeformityA columella retractor is placed over the columellaand by pulling it laterally the caudal border of theseptum is exposed Ala can be protected by an alaprotector A vertical incision with a no 15 bladeover the caudal end of septum is performed untilreaching the plane of the septal cartilage It is essentialto correctly identify the perichondrium and byusing the Cottle elevator dissect and lift it creatinga flap As the dissection proceeds along the septalcartilage a longer speculum (no 5) is introduced sothat elevation of the mucoperichondrium is doneunder constant visual controlndash The next step is to dissect the mucoperiostium
Nasal DeformityDissecting over the bony-cartilaginous junctionwhen joining both tunnels might be difficult and is
especially prone to membrane perforationndash If needed the same tunnels are to be created on the
other side of the septum Then deviated parts of
septum are identified and removed either with a
knife or a Freer chisel
Nasal Deformitybull septum from the maxillary crest the septum mustbull be separated from the perpendicular plate trimmedbull along the inferior border placed back onto the crestbull and sutured to the periosteum If the deformity involvesbull the vomer an osteotome is used Care mustbull be taken not to break the cribriform plate becausebull it could cause a cerebrospinal fistula
Nasal Deformity
bull Once the septal deviation is corrected the flapsbull and hemitransfixion incision are mattressed
withbull absorbable sutures Nasal packing to prevent
synechiaebull and postoperative septal haematoma mightbull be advised but should be removed within 72 h

Nasal Deformity
bull Therapybull ndash Nasal reconstruction indications depend on patientbull selection surgeon experience and aetiology of thebull deformity bull Indications for surgery can be functionalbull aesthetic or most commonly both In individuals
with a compromised nasal airway a nasoseptalbull reconstruction is indicated
Nasal Deformity
bull Contraindications bull include patients with malignantbull chronic or autoimmune disease conditions drugbull abuse poor perioperative risk profile and unrealisticbull expectationsbull ndash Multiple previous rhinoplasties and certain
professionsbull (mixed martial artists boxers and other contactbull sports) are relative contraindications
Nasal DeformitySeptoplastyndash Septoplasty is performed to correct nasal obstructioncaused by septal deformityndash Usually septoplasty is performed under general anaesthesiawith the patient in the supine position with the head elevated by approximately 30 (Righthandedsurgeons approach from the right side)ndash Local vasoconstrictive anaesthesia is applied notonly to reduce postoperative pain but also more importantly to achieve vasoconstriction of themucosa and less intraoperative haemorrhage Lidocainewith adrenaline or epinephrine is usedalthough in patients with cardiac hypersensitivityoxymetazoline might be preferred
Nasal Deformity
bull Septoplasty begins with the incision of septal mucosabull Most operative techniques utilise a hemitransfixionbull incision at the caudal end of septum so thatbull deviation at this point might be reached as wellbull as a transfixion incision that is easily obtained ifbull needed (Right-handed surgeons normally choosebull the left side but that may vary when deviation isbull convex towards the right)
Nasal DeformityA columella retractor is placed over the columellaand by pulling it laterally the caudal border of theseptum is exposed Ala can be protected by an alaprotector A vertical incision with a no 15 bladeover the caudal end of septum is performed untilreaching the plane of the septal cartilage It is essentialto correctly identify the perichondrium and byusing the Cottle elevator dissect and lift it creatinga flap As the dissection proceeds along the septalcartilage a longer speculum (no 5) is introduced sothat elevation of the mucoperichondrium is doneunder constant visual controlndash The next step is to dissect the mucoperiostium
Nasal DeformityDissecting over the bony-cartilaginous junctionwhen joining both tunnels might be difficult and is
especially prone to membrane perforationndash If needed the same tunnels are to be created on the
other side of the septum Then deviated parts of
septum are identified and removed either with a
knife or a Freer chisel
Nasal Deformitybull septum from the maxillary crest the septum mustbull be separated from the perpendicular plate trimmedbull along the inferior border placed back onto the crestbull and sutured to the periosteum If the deformity involvesbull the vomer an osteotome is used Care mustbull be taken not to break the cribriform plate becausebull it could cause a cerebrospinal fistula
Nasal Deformity
bull Once the septal deviation is corrected the flapsbull and hemitransfixion incision are mattressed
withbull absorbable sutures Nasal packing to prevent
synechiaebull and postoperative septal haematoma mightbull be advised but should be removed within 72 h

Nasal Deformity
bull Contraindications bull include patients with malignantbull chronic or autoimmune disease conditions drugbull abuse poor perioperative risk profile and unrealisticbull expectationsbull ndash Multiple previous rhinoplasties and certain
professionsbull (mixed martial artists boxers and other contactbull sports) are relative contraindications
Nasal DeformitySeptoplastyndash Septoplasty is performed to correct nasal obstructioncaused by septal deformityndash Usually septoplasty is performed under general anaesthesiawith the patient in the supine position with the head elevated by approximately 30 (Righthandedsurgeons approach from the right side)ndash Local vasoconstrictive anaesthesia is applied notonly to reduce postoperative pain but also more importantly to achieve vasoconstriction of themucosa and less intraoperative haemorrhage Lidocainewith adrenaline or epinephrine is usedalthough in patients with cardiac hypersensitivityoxymetazoline might be preferred
Nasal Deformity
bull Septoplasty begins with the incision of septal mucosabull Most operative techniques utilise a hemitransfixionbull incision at the caudal end of septum so thatbull deviation at this point might be reached as wellbull as a transfixion incision that is easily obtained ifbull needed (Right-handed surgeons normally choosebull the left side but that may vary when deviation isbull convex towards the right)
Nasal DeformityA columella retractor is placed over the columellaand by pulling it laterally the caudal border of theseptum is exposed Ala can be protected by an alaprotector A vertical incision with a no 15 bladeover the caudal end of septum is performed untilreaching the plane of the septal cartilage It is essentialto correctly identify the perichondrium and byusing the Cottle elevator dissect and lift it creatinga flap As the dissection proceeds along the septalcartilage a longer speculum (no 5) is introduced sothat elevation of the mucoperichondrium is doneunder constant visual controlndash The next step is to dissect the mucoperiostium
Nasal DeformityDissecting over the bony-cartilaginous junctionwhen joining both tunnels might be difficult and is
especially prone to membrane perforationndash If needed the same tunnels are to be created on the
other side of the septum Then deviated parts of
septum are identified and removed either with a
knife or a Freer chisel
Nasal Deformitybull septum from the maxillary crest the septum mustbull be separated from the perpendicular plate trimmedbull along the inferior border placed back onto the crestbull and sutured to the periosteum If the deformity involvesbull the vomer an osteotome is used Care mustbull be taken not to break the cribriform plate becausebull it could cause a cerebrospinal fistula
Nasal Deformity
bull Once the septal deviation is corrected the flapsbull and hemitransfixion incision are mattressed
withbull absorbable sutures Nasal packing to prevent
synechiaebull and postoperative septal haematoma mightbull be advised but should be removed within 72 h

Nasal DeformitySeptoplastyndash Septoplasty is performed to correct nasal obstructioncaused by septal deformityndash Usually septoplasty is performed under general anaesthesiawith the patient in the supine position with the head elevated by approximately 30 (Righthandedsurgeons approach from the right side)ndash Local vasoconstrictive anaesthesia is applied notonly to reduce postoperative pain but also more importantly to achieve vasoconstriction of themucosa and less intraoperative haemorrhage Lidocainewith adrenaline or epinephrine is usedalthough in patients with cardiac hypersensitivityoxymetazoline might be preferred
Nasal Deformity
bull Septoplasty begins with the incision of septal mucosabull Most operative techniques utilise a hemitransfixionbull incision at the caudal end of septum so thatbull deviation at this point might be reached as wellbull as a transfixion incision that is easily obtained ifbull needed (Right-handed surgeons normally choosebull the left side but that may vary when deviation isbull convex towards the right)
Nasal DeformityA columella retractor is placed over the columellaand by pulling it laterally the caudal border of theseptum is exposed Ala can be protected by an alaprotector A vertical incision with a no 15 bladeover the caudal end of septum is performed untilreaching the plane of the septal cartilage It is essentialto correctly identify the perichondrium and byusing the Cottle elevator dissect and lift it creatinga flap As the dissection proceeds along the septalcartilage a longer speculum (no 5) is introduced sothat elevation of the mucoperichondrium is doneunder constant visual controlndash The next step is to dissect the mucoperiostium
Nasal DeformityDissecting over the bony-cartilaginous junctionwhen joining both tunnels might be difficult and is
especially prone to membrane perforationndash If needed the same tunnels are to be created on the
other side of the septum Then deviated parts of
septum are identified and removed either with a
knife or a Freer chisel
Nasal Deformitybull septum from the maxillary crest the septum mustbull be separated from the perpendicular plate trimmedbull along the inferior border placed back onto the crestbull and sutured to the periosteum If the deformity involvesbull the vomer an osteotome is used Care mustbull be taken not to break the cribriform plate becausebull it could cause a cerebrospinal fistula
Nasal Deformity
bull Once the septal deviation is corrected the flapsbull and hemitransfixion incision are mattressed
withbull absorbable sutures Nasal packing to prevent
synechiaebull and postoperative septal haematoma mightbull be advised but should be removed within 72 h

Nasal Deformity
bull Septoplasty begins with the incision of septal mucosabull Most operative techniques utilise a hemitransfixionbull incision at the caudal end of septum so thatbull deviation at this point might be reached as wellbull as a transfixion incision that is easily obtained ifbull needed (Right-handed surgeons normally choosebull the left side but that may vary when deviation isbull convex towards the right)
Nasal DeformityA columella retractor is placed over the columellaand by pulling it laterally the caudal border of theseptum is exposed Ala can be protected by an alaprotector A vertical incision with a no 15 bladeover the caudal end of septum is performed untilreaching the plane of the septal cartilage It is essentialto correctly identify the perichondrium and byusing the Cottle elevator dissect and lift it creatinga flap As the dissection proceeds along the septalcartilage a longer speculum (no 5) is introduced sothat elevation of the mucoperichondrium is doneunder constant visual controlndash The next step is to dissect the mucoperiostium
Nasal DeformityDissecting over the bony-cartilaginous junctionwhen joining both tunnels might be difficult and is
especially prone to membrane perforationndash If needed the same tunnels are to be created on the
other side of the septum Then deviated parts of
septum are identified and removed either with a
knife or a Freer chisel
Nasal Deformitybull septum from the maxillary crest the septum mustbull be separated from the perpendicular plate trimmedbull along the inferior border placed back onto the crestbull and sutured to the periosteum If the deformity involvesbull the vomer an osteotome is used Care mustbull be taken not to break the cribriform plate becausebull it could cause a cerebrospinal fistula
Nasal Deformity
bull Once the septal deviation is corrected the flapsbull and hemitransfixion incision are mattressed
withbull absorbable sutures Nasal packing to prevent
synechiaebull and postoperative septal haematoma mightbull be advised but should be removed within 72 h

Nasal DeformityA columella retractor is placed over the columellaand by pulling it laterally the caudal border of theseptum is exposed Ala can be protected by an alaprotector A vertical incision with a no 15 bladeover the caudal end of septum is performed untilreaching the plane of the septal cartilage It is essentialto correctly identify the perichondrium and byusing the Cottle elevator dissect and lift it creatinga flap As the dissection proceeds along the septalcartilage a longer speculum (no 5) is introduced sothat elevation of the mucoperichondrium is doneunder constant visual controlndash The next step is to dissect the mucoperiostium
Nasal DeformityDissecting over the bony-cartilaginous junctionwhen joining both tunnels might be difficult and is
especially prone to membrane perforationndash If needed the same tunnels are to be created on the
other side of the septum Then deviated parts of
septum are identified and removed either with a
knife or a Freer chisel
Nasal Deformitybull septum from the maxillary crest the septum mustbull be separated from the perpendicular plate trimmedbull along the inferior border placed back onto the crestbull and sutured to the periosteum If the deformity involvesbull the vomer an osteotome is used Care mustbull be taken not to break the cribriform plate becausebull it could cause a cerebrospinal fistula
Nasal Deformity
bull Once the septal deviation is corrected the flapsbull and hemitransfixion incision are mattressed
withbull absorbable sutures Nasal packing to prevent
synechiaebull and postoperative septal haematoma mightbull be advised but should be removed within 72 h

Nasal DeformityDissecting over the bony-cartilaginous junctionwhen joining both tunnels might be difficult and is
especially prone to membrane perforationndash If needed the same tunnels are to be created on the
other side of the septum Then deviated parts of
septum are identified and removed either with a
knife or a Freer chisel
Nasal Deformitybull septum from the maxillary crest the septum mustbull be separated from the perpendicular plate trimmedbull along the inferior border placed back onto the crestbull and sutured to the periosteum If the deformity involvesbull the vomer an osteotome is used Care mustbull be taken not to break the cribriform plate becausebull it could cause a cerebrospinal fistula
Nasal Deformity
bull Once the septal deviation is corrected the flapsbull and hemitransfixion incision are mattressed
withbull absorbable sutures Nasal packing to prevent
synechiaebull and postoperative septal haematoma mightbull be advised but should be removed within 72 h

Nasal Deformitybull septum from the maxillary crest the septum mustbull be separated from the perpendicular plate trimmedbull along the inferior border placed back onto the crestbull and sutured to the periosteum If the deformity involvesbull the vomer an osteotome is used Care mustbull be taken not to break the cribriform plate becausebull it could cause a cerebrospinal fistula
Nasal Deformity
bull Once the septal deviation is corrected the flapsbull and hemitransfixion incision are mattressed
withbull absorbable sutures Nasal packing to prevent
synechiaebull and postoperative septal haematoma mightbull be advised but should be removed within 72 h

Nasal Deformity
bull Once the septal deviation is corrected the flapsbull and hemitransfixion incision are mattressed
withbull absorbable sutures Nasal packing to prevent
synechiaebull and postoperative septal haematoma mightbull be advised but should be removed within 72 h