Embed Size (px)
Citation preview

J Phys Fitness Sports Med, 1(2): 281-286 (2012)
JPFSM: Review Article
Blood flow in non-muscle tissues and organs during exercise:Nature of splanchnic and ocular circulation
1 Institute of Health Science, Kyushu University, 6-1 Kasuga-koen, Kasuga, Fukuoka 816-8580, Japan2 Department of Health Science, Prefectural University of Hiroshima, 1-1-71 Ujina-higashi, Minami-ku, Hiroshima 734-8558, Japan
3 Graduate School of Life Science and Systems Engineering, Kyushu Institute of Technology, 2-4 Hibikino, Wakamatsu-ku, Kitakyushu, Fukuoka 808-0196, Japan
Received: May 10, 2012 / Accepted: June 22, 2012
Abstract In response to increased vascular conductance associated with vasodilation in ex-ercising muscles, many non-exercising organs suppress their blood flow by vasoconstriction, thus helping to maintain blood pressure. This vasoconstriction in non-exercising organs con-tributes to ensuring a favorable distribution of the blood flow. However, a consequent excessive decrease of blood flow in non-exercising organs should be avoided so that they can maintain appropriate functioning during and/or after exercise. There is now evidence of a decrease in splanchnic blood flow with vasoconstriction during dynamic exercise, which indirectly con-tributes to an increase in flow in exercising muscles. Hypoperfusion in the splanchnic area, induced by such vasoconstriction, may result in gastrointestinal symptoms. On the other hand, such vasoconstriction is suppressed when exercise is performed after food intake, which may be associated with the maintenance of digestive and absorptive functions in the gastrointesti-nal tract. In contrast to organs that decrease their blood flow, the choroidal flow, which forms part of the ocular blood flow, increases with exercise intensity, but without vasodilation. The relevance of this phenomenon to visual function and the nature of ocular circulation remain un-clear. Competition in blood flow between exercising muscles and non-exercising organs should be examined from the viewpoint of the functions of non-exercising organs and exercising con-dition, such as the postprandial condition.Keywords : gastrointestinal tract, portal vein, blood flow, ocular flow
Introduction
The aerobic capacity of exercising muscles could be improved if exercising muscles were able to capture all of the increased cardiac output that occurs during dynamic exercise. Shutting down the blood flow to non-exercising organs is impossible, in part, as a result of myogenic autoregulation. The blood flow in non-exercising organs decreases to maintain the blood pressure against the in-creased vascular conductance that results from vasodila-tion in vast vessels in exercising muscles. Renal flow de-creases proportionally with increasing exercise intensity via vasoconstriction1-3), while cardiac output increases up to fivefold of the resting value in exercising humans3). Even light-intensity exercise decreased renal flow by 20% within 30 s of exercise onset4). In addition, during exer-cise the blood flow increases in organs other than exer-cising muscles. The most well known, but still generally unexplained, example is cerebral blood flow, which was
originally believed to be stable during exercise, but recent studies have revealed actually increases5). It is important to be able to increase the blood flow into exercising muscles to enable them to adequately perform a given physical activity. Conversely, it is also important to prevent an excessive reduction in blood flow into non-exercising organs to allow them to maintain their func-tions both during and after exercise. The question arises, then, as to which of the non-exercising organs allow an exercise-induced reduction in blood flow, which would consequently suppress their function. Evidence is accu-mulating regarding the actions of the splanchnic and ocu-lar circulations during exercise. The nature of the blood flow of these two circulatory systems is herein discussed, and focus is particularly given to the relationship between the nature and function of each system in the gastrointes-tinal tract and eyes in humans.
Splanchnic blood-flow response to exercise
The alimentary tract governs digestion and absorption *Correspondence: [email protected]
Naoyuki Hayashi1*, Masako Yamaoka-Endo2, Nami Someya3 and Yoshiyuki Fukuba2

JPFSM : Hayashi N, et al.282
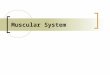
from the mouth to the anus. Blood flow within the organs from the stomach to the large intestine—including the liver, pancreas, and spleen—is considered a part of the splanchnic circulatory system in the present review. The splanchnic circulatory system accounts for about 25% of cardiac output at rest3), and is supplied from three major arteries that branch off from the abdominal aorta: the ce-liac artery (CA), superior mesenteric artery (SMA), and inferior mesenteric artery (IMA). The CA supplies blood to the stomach, liver, and spleen, and its flow at rest is reported to be 460~1080 ml/min6,7); the SMA supplies the duodenum, jejunum, ileum, ascending colon, transverse colon, and pancreas, and its flow at rest is 220~540 ml/min7,8); while the IMA supplies the descending colon, sigmoid colon, and upper rectum, and its flow at rest is 80~130 ml/min9,10). Blood in these three arteries flows through the liver via the portal vein. Splanchnic blood flow decreases during long-duration exercise. Pulsed-Doppler ultrasonography has revealed the nature of this change in human subjects. Cycling at 40–75% of maximum oxygen consumption (V・O2max) for 15 and 120 min was found to decrease the blood flow in the CA and SMA by roughly 30% and 50%, respective-ly11-13). However, lower-intensity exercise at 40 watts for 4 min did not affect the blood flow in the SMA as shown in Fig. 14). The portal vein receives blood from the gastrointestinal tract, and its flow at rest is 500–800 ml/min14-16). This vein is formed by the confluence of the superior mesenteric and splenic veins, and it also receives blood from the inferior mesenteric, gastric, and cystic veins. Thus it is
natural that blood flow in the portal vein would decrease during exercise, reflecting a reduced blood flow to the major intestinal organs. Blood flow in the portal vein was reported to decrease by 35% during 25 min of arm cranking at an exercise in-tensity of 50% of V・O2max
16), and by 26% and 50% during 20 and 60 min of cycling at 70% of V・O2max, respective-ly15,17). Furthermore, after 10 min of treadmill walking at 14 metabolic equivalents (METs), portal vein blood flow was 32% lower than the resting value14). The duration of exercise therefore appears to affect blood-flow response in the portal vein. Portal-vein flow was observed to de-crease, during 60 min of exercise at 70% V・O2max, relative to the elapsed time15). Blood flow response in the proper hepatic artery to dy-namic exercise has yet to be reported, probably due to the technical difficulty of measuring the flow therein. Blood is supplied to the liver by the proper hepatic artery and the portal vein. Blood flow in the proper hepatic artery is reported to be about 250 ml/min at rest (as assessed using a noninvasive technique)18,19). This corresponds to 20% of the total hepatic blood flow. Up to 70% of the blood flow to the liver is thus supplied by the portal vein3). The role of sympathetic activation, in vasoconstric-tion in non-exercising organs, has been demonstrated by comparing blood flow response in the portal vein and femoral artery during arm cranking between normal sub-jects and subjects with a spinal cord lesion (SCL)16). The portal-vein flow decreased in normal and low-level SCL patients, but not in high-level SCL patients. Similarly, SMA blood flow and resistance changed in response to isometric exercise, cold pressor testing, and tilting, but not in response to pure autonomic failure or in subjects with multiple system atrophy20). The splanchnic blood-flow response to dynamic ex-ercise may be non-uniform among splanchnic regions, although very few studies have examined this. One study found that the blood flow decreased by 30% in the SMA, whereas it decreased by 50% in the CA during dynamic exercise at 75% V・O2max
12). In another study, the blood flow decreased by 30% in the spleen, but not in the SMA, during light-intensity exercise4). It appears reasonable to assume that non-uniform responses in the splanchnic blood flow are controlled multifactorially by the autonomic, humoral, and local organ-specific regulatory systems. The human splanchnic artery and vein are innervated by the sympathetic nervous system, and sympathetic vasoconstriction occurs during exercise. There is a well-documented close relationship between splanchnic blood flow and serum norepinephrine concentration at different work rates21). Some authors consider that the renin-angiotensin system—and in particular angiotensin II (not vasopres-sion)—plays a role in the vasoconstriction that occurs in the visceral regions during exercise, similar to the sys-temic effect of the other vessels22), while others take the
16
Figure 1
Fig. 1 Splanchnic blood flow response to cycling exercise is shown. The blood velocity of the renal artery (RA) and splenic artery (SA) decreased by ~27% from resting values at the end of exercise. In contrast, the blood ve-locity of the superior mesenteric artery (SMA) remained constant. The circles, triangles and squares represent data for RA, SMA and SA, respectively. Modified from Endo et al.4).

JPFSM : Blood flow in splanchnic and ocular vessels during exercise 283
opposite view11). The mechanism underlying the regional differences in blood flow among the splanchnic vessels remains to be established. While there is no clear evi-dence that the sympathetic nerves, supplying the different vascular beds in the splanchnic organs, are not equally activated during exercise, the differential responses of the sympathetic nerves, and/or their sensitivities, appear to result in a non-uniform redistribution of blood flows to the splanchnic organs. The decrement in total splanchnic blood flow ap-pears to be mainly due to a decreased inflow to the liver and spleen, rather than to the intestinal tract; although evidence is still accumulating with regard to the local distribution of the blood flow of the supplying vessels among the different splanchnic organs in response to dy-namic exercise. Details of the regional differences in the splanchnic circulation during and after exercise need to be resolved.
Effect of food ingestion on the gastrointestinal tract at rest and during exercise
Several researchers have investigated another aspect of human blood distribution during exercise: the prioritiza-tion of blood flow to exercising muscles over the gas-trointestinal organs in the postprandial condition. This is important from the viewpoint of human behavior, since exercise was originally related to eating behaviors such as hunting and gathering. It is also particularly important for long-duration exercise such as marathon running and cycle road racing, since appropriate supplementation of foods and water is essential during these races. In addition to the provision of appropriate or optimum food intake during exercise, it is clinically important to protect the gastrointestinal organs from unnecessary stress induced by hypoperfusion; although the gastrointestinal organs are less vulnerable to hypoperfusion than other regions—only long-lasting hypoperfusion increases its permeability23). Exercise exerts both positive and negative effects on the splanchnic organs. It has been well established from large-population studies and meta-analyses that there is an inverse relationship between physical activity and the incidences of colorectal carcinoma, cancer, and diver-ticulitis24,25). Conversely, gastrointestinal symptoms are a well-known downside of exercise. A mailed questionnaire survey found that 40–70% of endurance athletes experi-enced gastrointestinal symptoms during acute exercise, and 11% of runners suffered from serious gastrointestinal complaints when running26-28). Exercise-induced splanch-nic hypoperfusion is assumed to result in gut dysfunc-tion27-29), with the symptoms found to be related to food intake28). It can be readily assumed that food intake induces an unusual competition for blood flow between the alimen-tary tract and exercising muscles. Food intake increases splanchnic blood flow, contrary to the effect of exercise;
food intake instantly increases the flow in the CA and SMA. According to research, the flow in the CA rapidly peaked at a 38–60% increase from resting levels6,30), while that in the SMA increased 1.5- to 3.5-fold at 5–60 min af-ter food ingestion6,31-34). The effect was greatly affected by the content of the ingested food, such that a richer energy content produced a greater peak34), and either protein or fat intake delayed the peak but increased its value32,33). No increase was observed in the IMA after food intake35). These increases in blood flow in the splanchnic circula-tion are affected by the nervous and humoral systems. Cholinergic nerves play a role in postprandial hyper-emia36), and beta adrenoreceptors form part of a humoral mechanism37). The effects of these nervous activities on vasodilation in the gastrointestinal tract are relatively small. Several of the gastrointestinal hormones—such as cholecystokinin, secretin, gastrin 17, and glucagon—are candidate mechanisms, although their involvement in postprandial splanchnic hyperemia is not clear38). This is partly because these hormones also activate the nervous system39). Moreover, metabolic products also regulate the splanchnic circulation40). Food intake could modify blood flow distribution dur-ing exercise. Blood flow in the gastrointestinal tract is suppressed during postprandial exercise. Treadmill run-ning for 15 min was reported to reduce the SMA flow by 43%, whereas food intake increased it by 60%. Combin-ing exercise and food increased the flow by 40%, dem-onstrating the counterbalancing effects of vasodilation by food intake and vasoconstriction by exercise31). Similarly, food ingestion modulates blood-flow response in the por-tal vein to exercise. Carbohydrate ingestion affected por-tal vein blood flow during exercise, as well as resulted in a carbohydrate-induced increase at rest. Portal vein flow also decreased after 60 min of cycling at 70% V・O2max, whereas the decrease tended to be smaller when carbohy-drates were consumed before and during the exercise17). A positive correlation has also been observed between glucagon level and blood flow. This suggests that eating before and during exercise modulates blood flow in the gastrointestinal tract. On the other hand, no difference in blood flow and conductance was observed in exercising limbs and the splanchnic circulation between the normal and postprandial conditions41). Exercise in the postprandi-al condition was shown to increase cardiac output, super-imposing its increase on the blood flow into the SMA42). The question regarding competition in the blood flow between the splanchnic circulation and exercising muscle remains to be resolved.
Ocular flow during exercise
A continuous supply of blood to the retina is essential for eye function, since it has a high oxygen demand and oxygen is not stored in the retina or surrounding tissues43). Furthermore, it is also necessary to keep the flow stable

284 JPFSM : Hayashi N, et al.
so as to maintain visual function. The ocular circulation comprises the retinal and choroi-dal circulations. The retinal circulation exists in the in-ner part of the retina and is characterized by a low blood supply, whereas the choroidal circulation exists on the outside of the retina, and has a very high blood supply - 85% of total ocular flow44). The anatomical characteristics of the eye mean that increases in retinal circulation may interfere with light reaching the retina. It has been shown that submaximal dynamic exercise resulting in a heart rate of 100–140 bpm increases the choroidal flow by up to 30% of the resting baseline, de-pending upon the intensity, but does not alter retinal flow as shown in Fig. 245,46). However, the increase in choroidal flow is not associated with an increase in the conductance index, indicating an association with the pressor response to exercise. At dynamic-exercise-induced exhaustion with hypocapnia, findings showed the choroidal flow did not change from the resting baseline value, and the retinal flow decreased by 13%46). The conductance index in both the choroidal and retinal flows decreased from the resting baseline, suggesting that ocular blood flow is suppressed by the hypocapnia associated with exhaustion. Animal studies have led to a general acceptance that autoregulation exists in the retina, but not (or, if so, at a very weak level) in the choroidal circulation47). How-ever, whether autoregulation exists in the human retina has yet to be established. One study found no change in the retinal circulation during either the cold pressor test or handgrip exercise, indirectly suggesting the existence of autoregulation48). Consistent with the presence of au-toregulation, choroidal flow did not change during sub-maximal dynamic exercise even where there was a pres-sor response45,46). The choroidal flow increased in these studies, and hence autoregulation seems to be present in the retinal circulation, but not in the choroidal circulation. Nevertheless, autoregulation against short-term fluctua-
tions in arterial pressure has not been observed. Measure-ment of blood flow in the ophthalmic artery by Doppler ultrasound during an acute fall in systemic pressure induced by thigh cuff deflation did not reveal evidence of autoregulation49). The autoregulatory effect on blood flow might have been weakened by choroidal flow, since the ophthalmic artery is upstream of both the choroidal and retinal flows. This matter is difficult to clarify since continuous observation of the ocular flow is impossible simply because subjects can not keep their eyes open for long periods.
Ocular flow and visual function
While the relationships between the ocular circulation and visual function are readily apparent, changes in ocu-lar flow and the effects on visual function have not been elucidated (with the exception of pathological conditions). The chronic loss of ocular blood flow associated with pathological conditions such as diabetes and glaucoma is associated with impaired visual function43,47,50,51). In Japan, the prevalence of primary open-angle glaucoma is esti-mated to be 2% in patients aged in their 40s, and 10% of those older than 70 years52). Thus, the correct functioning of the ocular circulation is important, and the administra-tion of certain drugs that alter ocular flow can improve visual function in these patients. However, the effect of regular exercise on ocular circulation remains unclear. Some researchers have observed acute changes in visual function induced by ocular blood flow in healthy humans. Increases in ocular blood flow induced by either inhala-tion of high concentrations of CO2 or administration of sildenafil was shown to improve static visual acuity and contrast sensitivity53,54). In addition, an increase in the retrobulbar circulation - which supplies blood to the ocu-lar circulation - by CO2 inhalation, was associated with improved contrast sensitivity55). Nevertheless, the effects of acute changes in ocular blood flow on visual function have yet to be established, in part because these changes in ocular flow are also associated with changes in cerebral blood flow, which is strongly related to brain function, including visual information processing53). Changes in visual function during exercise have been reported. An important aim of visual information process-ing is to judge the speed and distance of objects, which makes it important to be able to maintain visual function during exercise. Visual field and contrast sensitivities were reported to increase after jogging in many subjects, but to decrease after exercise in others56-58). Unclear changes in visual function may be due to the complicated mechanisms underlying the maintenance of eye function, not just in the eyes themselves, where there are several such mechanisms (including pupil diameter regulation), but also in the brain, where major processing of the infor-mation from the eyes occurs. Thus, eye functionality is too complex for it to be studied during exercise, although
Figure 2Fig. 2 Relative changes in blood flow in the retinal and cho-
roidal vessels (RCV, mainly reflecting choroidal flow), inferior and superior and inferior temporal retinal arte-rioles (ITRA and STRA, respectively, reflecting retinal flow) are shown compared to heart rate during cycling exercise. Hayashi et al.45)

285JPFSM : Blood flow in splanchnic and ocular vessels during exercise
some researchers have attempted to characterize neuro-vascular coupling during dynamic exercise59). Research into eye function during exercise has really only just be-gun from the viewpoint of circulatory changes.
Summary and perspective
Blood flow in the splanchnic circulation is reduced dur-ing exercise, as in other organs such as the kidney. This decrease is suppressed by food intake, possibly due to efforts by the body to maintain digestive and absorptive functions in the gastrointestinal tract. Conversely, choroi-dal blood flow increases during submaximal exercise. The relevance of this is unclear. However, retinal blood flow remains unchanged during exercise, presumably so that it does not interfere with light reaching the retina. Competition in the blood flow between exercising muscles and non-exercising organs should be examined from the viewpoint of the functions of the non-exercising organs and the particular exercising condition (e.g., post-prandial). Before recommending regular exercise train-ing to patients or the elderly, it is necessary to determine blood-flow responses to exercise and the significance of such responses regarding the functions of various organs.
meals in young subjects. Am J Physiol 261: H1430-H1436. 9) Siğirci A, Senol M, Aydin E, Kutlu R, Alkan A, Altinok MT,
Yoloğlu S, Baysal T, Saraç K. 2003. Doppler waveforms and blood flow parameters of the superior and inferior mesenter-ic arteries in patients having Behçet disease with and without gastrointestinal symptoms: preliminary data. J Ultrasound Med 22: 449-457.
10) Mirk P, Palazzoni G, Gimondo P. 1999. Doppler sonography of hemodynamic changes of the inferior mesenteric artery in inflammatory bowel disease: preliminary data. Am J Roent-genol 173: 381-387.
11) Bergeron R, Kjaer M, Simonsen L, Bülow J, Skovgaard D, Howlett K, Galbo H. 2001. Splanchnic blood flow and hepatic glucose production in exercising humans: role of renin-angiotensin system. Am J Physiol Regul Integr Comp Physiol 281: R1854-R1861.
12) Perko MJ, Nielsen HB, Skak C, Clemmesen JO, Schroeder TV, Secher NH. 1998. Mesenteric, coeliac and splanchnic blood flow in humans during exercise. J Physiol 513: 907-913.
13) Qamar MI, Read AE.1987. Effects of exercise on mesenteric blood flow in man. Gut 28: 583-587.
14) Iwao T, Toyonaga A, Ikegami M, Sumino M, Oho K, Sakaki M, Shigemori H, Tanikawa K, Iwao J. 1995. Effects of exer-cise-induced sympathoadrenergic activation on portal blood flow. Dig Dis Sci 40: 48-51.
15) Rehrer NJ, Smets A, Reynaert H, Goes E, De Meirleir K. 2001. Effect of exercise on portal vein blood flow in man. Med Sci Sports Exerc 33: 1533-1537.
16) Thijssen DHG, Steendijk S, Hopman MTE. 2009. Blood re-distribution during exercise in subjects with spinal cord in-jury and controls. Med Sci Sports Exerc 41: 1249-1254.
17) Rehrer NJ, Goes E, DuGardeyn C, Reynaert H, DeMeirleir K. 2005. Effect of carbohydrate on portal vein blood flow during exercise. Int J Sports Med 26: 171-176.
18) Carlisle KM, Halliwell M, Read AE, Wells PN. 1992. Esti-mation of total hepatic blood flow by duplex ultrasound. Gut 33: 92-97.
19) Yzet T, Bouzerar R, Baledent O, Renard C, Lumbala DM, Nguyen-Khac E, Regimbeau JM, Deramond H, Meyer ME. 2010. Dynamic measurements of total hepatic blood flow with Phase Contrast MRI. Eur J Radiol 73: 119-124.
20) Chaudhuri KR, Thomaides T, Mathias CJ. 1992. Abnormal-ity of superior mesenteric artery blood flow responses in hu-man sympathetic failure. J Physiol 457: 477-489.
21) Rowell LB.1984. Reflex control of regional circulations in humans. J Auton Nerv Syst 11: 101-114.
22) Symons JD, Stebbins CL. 1996. Effects of angiotensin II re-ceptor blockade during exercise: comparison of losartan and saralasin. J Cardiovasc Pharmacol 28: 223-231.
23) de Aguilar-Nascimento JE. 2005.The role of macronutrients in gastrointestinal blood flow. Curr Opin Clin Nutr Metab Care 8: 552-556.
24) Strate LL, Liu YL, Aldoori WH, Giovannucci EL. 2009. Physical activity decreases diverticular complications. Am J Gastroenterol 104: 1221-1230.
25) Wolin KY, Yan Y, Colditz GA, Lee IM. 2009. Physical activ-ity and colon cancer prevention: a meta-analysis. Br J Can-cer 100: 611-616.
26) Peters HP, Bos M, Seebregts L, Akkermans LM, van Berge Henegouwen GP, Bol E, Mosterd WL, de Vries WR. 1999.
Acknowledgement
This study was supported by Grant-in-Aid for Scientific Re-search to YF (no. 21370111).
References
1) Kenney WL, Ho CW. 1995. Age alters regional distribution of blood flow during moderate-intensity exercise. J Appl Physiol 79: 1112-1119.
2) Pricher MP, Holowatz LA, Williams JT, Lockwood JM, Hal-liwill JR. 2004. Regional hemodynamics during postexer-cise hypotension. I. Splanchnic and renal circulations. J Appl Physiol 97: 2065-2070.
3) Rowell LB. 1993. Human Cardiovascular Control. Oxford University Press, New York.
4) Endo MY, Suzuki R, Nagahata N, Hayashi N, Miura A, Koga S, Fukuba Y. 2008. Differential arterial blood flow response of splanchnic and renal organs during low-intensity cycling exercise in women. Am J Physiol Heart Circ Physiol 294: H2322-H2326.
5) Ogoh S, Ainslie PN. 2009. Cerebral blood flow during exer-cise: mechanisms of regulation. J Appl Physiol 107: 1370-1380.
6) Someya N, Endo MY, Fukuba Y, Hayashi N. 2008. Blood flow responses in celiac and superior mesenteric arteries in the initial phase of digestion. Am J Physiol Heart Circ Physi-ol 294: R1790-R1796.
7) Moneta GL, Taylor DC, Helton WS, Mulholland MW, Strandness DE Jr. 1988. Duplex ultrasound measurement of postprandial intestinal blood flow: effect of meal composi-tion. Gastroenterology 95: 1294-1301.
8) Sidery MB, Macdonald IA, Cowley AJ, Fullwood LJ. 1991. Cardiovascular responses to high-fat and high-carbohydrate

286 JPFSM : Hayashi N, et al.
Gastrointestinal symptoms in long-distance runners, cyclists, and triathletes: prevalence, medication, and etiology. Am J Gastroenterol 94: 1570-1581.
27) ter Steege RW, Van der Palen J, Kolkman JJ. 2008. Preva-lence of gastrointestinal complaints in runners competing in a long-distance run: an internet-based observational study in 1281 subjects. Scand J Gastroenterol 43: 1477-1482.
28) Waterman JJ, Kapur R. 2012. Upper gastrointestinal issues in athletes. Curr Sports Med Rep 11: 99-104.
29) van Wijck K, Lenaerts K, van Loon LJC, Peters WHM, Buur-man WA, Dejong CHC. 2011. Exercise-induced splanchnic hypoperfusion results in gut dysfunction in healthy men. PLoS ONE 6: e22366.
30) Qamar MI, Read AE, Skidmore R, Evans JM, Williamson RC. 1985. Transcutaneous Doppler ultrasound measurement of coeliac axis blood flow in man. Br J Surg 72: 391-393.
31) Qamar MI, Read AE. 1987. Effects of exercise on mesenteric blood flow in man. Gut 28: 583-587.
32) Qamar MI, Read AE. 1988. Effects of ingestion of carbohy-drate, fat, protein, and water on the mesenteric blood flow in man. Scand J Gastroenterol 23: 26-30.
33) Sidery MB, Macdonald IA, Cowley AJ, Fullwood LJ. 1991. Cardiovascular responses to high-fat and high-carbohydrate meals in young subjects. Am J Physiol 261: H1430-H1436.
34) Sidery MB, Macdonald IA. 1994. The effect of meal size on the cardiovascular responses to food ingestion. Br J Nutr 71: 835-848.
35) Ludwig D, Wiener S, Brüning A, Schwarting K, Jantschek G, Stange EF. 1999. Mesenteric blood flow is related to disease activity and risk of relapse in Crohn's disease: a prospective follow-up study. Am J Gastroenterol 94: 2942-2950.
36) Sieber C, Beglinger C, Jaeger K, Hildebrand P, Stalder GA. 1991. Regulation of postprandial mesenteric blood flow in humans: evidence for a cholinergic nervous reflex. Gut 32: 361-366.
37) Parker DR, Braatvedt GD, Halliwell M, Corrall RJ. 1999. Physiological control of splanchnic blood flow by adrena-line: studies during acute hypoglycaemia in man. Clin Sci 96: 623-629.
38) Chou CC, Coatney RW. 1994. Nutrient-induced changes in intestinal blood flow in the dog. Br Vet J 150: 423-437.
39) Verberne AJ, Saita M, Sartor DM. 2003. Chemical stimu-lation of vagal afferent neurons and sympathetic vasomotor tone. Brain Res Brain Res Rev 41: 288-305.
40) Matheson PJ, Wilson MA, Garrison RN. 2000. Regulation of intestinal blood flow. J Surg Res 93: 182-196.
41) Puvi-Rajasingham S, Wijeyekoon B, Natarajan P, Mathias CJ. 1997. Systemic and regional (including superior mesen-teric) haemodynamic responses during supine exercise while fasted and fed in normal man. Clin Auton Res 7: 149-154.
42) Eriksen M, Waaler BA. 1994. Priority of blood flow to splanchnic organs in humans during pre- and post-meal ex-ercise. Acta Physiol Scand 150: 363-372.
43) Wangsa-Wirawan ND, Linsenmeier RA. 2003. Retinal oxy-
gen: fundamental and clinical aspects. Arch Ophthalmol 121: 547-557.
44) Delaey C, Van De Voorde J. 2000. Regulatory mechanisms in the retinal and choroidal circulation. Ophthalmic Res 32: 249-256
45) Hayashi N, Ikemura T, Someya N. 2011. Effects of dynamic exercise and its intensity on ocular blood flow in humans. Eur J Appl Physiol 111: 2601-2606.
46) Ikemura T, Hayashi N. 2012. Ocular circulatory responses to exhaustive exercise in humans. Eur J Appl Physiol (in press).
47) Bill A, Sperber GO. 1990. Control of retinal and choroidal blood flow. Eye (Lond) 4: 319-325.
48) Ikemura T, Someya N, Hayashi N. 2012. Autoregulation in the ocular and cerebral arteries during the cold pressor test and handgrip exercise. Eur J Appl Physiol 112: 641-646.
49) Kolodjaschna J, Berisha F, Lung S, Schima H, Polska E, Schmetterer L. 2005. Comparison of the autoregulatory mechanisms between middle cerebral artery and ophthalmic artery after thigh cuff deflation in healthy subjects. Invest Ophthalmol Vis Sci 46: 636-640.
50) Guan K, Hudson C, Wong T, Kisilevsky M, Nrusimhadevara RK, Lam WC, Mandelcorn M, Devenyi RG, Flanagan JG. 2006. Retinal hemodynamics in early diabetic macular ede-ma. Diabetes 55: 813-818.
51) Harris A, Siesky B, Zarfati D, Haine CL, Catoira Y, Sines DT, McCranor L, Garzozi HJ. 2007. Relationship of cerebral blood flow and central visual function in primary open-angle glaucoma. J Glaucoma 16: 159-163.
52) Iwase A, Suzuki Y, Araie M, Yamamoto T, Abe H, Shirato S, Kuwayama Y, Mishima HK, Shimizu H, Tomita G, Inoue Y, Kitazawa Y; Tajimi Study Group, Japan Glaucoma Society. 2004. The prevalence of primary open-angle glaucoma in Japanese: the Tajimi Study. Ophthalmology 111: 1641-1648.
53) Hayashi N, Ikemura T, Someya N. 2011. Changes in ocular flow induced by hypo- and hypercapnia relate to static visual acuity in humans. Eye Rep 1: e8.
54) Paris G, Sponsel WE, Sandoval SS, Elliott WR, Trigo Y, Sanford DK, Harison JM. 2001. Sildenafil increases ocular perfusion. Int Ophthalmol 23: 355-358.
55) Huber KK, Adams H, Remky A, Arend KO. 2006. Retrobul-bar haemodynamics and contrast sensitivity improvements after CO2 breathing. Acta Ophthalmol Scand 84: 481-487.
56) Kostela PU. 1988. Jogging and contrast sensitivity. Acta Ophthalmol 66: 725-727.
57) Kostela PU, Airaksinen PJ, Tuulonen A. 1990. The effect of jogging on visual field indices. Acta Ophthalmol (Copenh) 68: 91-93.
58) Woods RL, Thomson WD. 1995. Effects of exercise on as-pects of visual function. Ophthalmic Physiol Opt 15: 5-12.
59) Willie CK, Cowan EC, Ainslie PN, Taylor CE, Smith KJ, Sin PY, Tzeng YC. 2011. Neurovascular coupling and dis-tribution of cerebral blood flow during exercise. J Neurosci Methods 198: 270-273.