Embed Size (px)
Citation preview
Bronchopulmonary Dysplasia (BPD)
Developed by - Lisa Fikac, MSN, RNC-NIC
Expiration Date - 7/7/17
This continuing education activity is provided by Cape Fear Valley Health System, Training and Development Department, which is an approved provider of Continuing Nursing Education by the North Carolina Nurses Association, an accredited approver by the American Nurses Credentialing Center’s Commission on Accreditation.
2.3 Contact hours will be awarded upon completion of the following criteria:
• Completion of the entire activity • Submission of a completed evaluation form • Completion a post-test with a grade of at least 85%.
The planning committee members and content experts have declared no financial relationships which would influence the planning of this activity.
Microsoft Office Clip Art and Creative Memories are the sources for all graphics unless otherwise noted.
The author would like to thank Stacey Cashwell for her work as original author.
• Discuss the etiology, risk factors, and pathophysiology of bronchopulmonary dysplasia.
• Describe the clinical presentation of bronchopulmonary dysplasia. • Discuss the prevention, management, complications and outcomes of
bronchopulmonary dysplasia.
Bronchopulmonary dysplasia (BPD) was first described by Northway and Rosan who reported x-ray changes in the lungs of infants who survived hyaline membrane disease (HLD).
• With current changes in neonatal respiratory management, BPD definitions have evolved from the initial stages described in 1967.
• Compared to original findings, infants with BPD today are much more premature, smaller, and lack many of the cystic lung disease changes that were so evident on early X-rays in the 1960s.
o The confounding factor is that the cycle of chronic lung injury and repair may prolong the need for oxygen and mechanical ventilation.
Older definitions of BPD classified it as a disorder that is characterized by respiratory distress and impaired gas exchange.
• In this version of BPD, the pathology is related to chronic recurring lung injury - o Created by mechanical ventilation and oxygen therapy o With ongoing repair and healing of the injury
The current definition of BPD includes infants who have a supplemental oxygen requirement at 28-30 days of life or at 36 weeks post-menstrual age (PMA).
• Grading of severity is based on oxygen requirement and the need for continuous positive airway pressure (CPAP) or mechanical ventilation.
o Mild - FiO2 0.21 o Moderate - FiO2 0.22-0.29 o Severe - FiO2 > 0.30 or requirement of CPAP or mechanical ventilation
The "new" BPD is characterized by an alteration in alveolarization and vascularization that is caused by an interruption in lung development.
• Alveolar development is interrupted causing a loss in the structural complexity of the lung.
o Fewer, larger alveoli o Reduction in the overall surface available for gas exchange
Suggested etiologies for BPD have included -
• Pulmonary immaturity • Oxygen toxicity from high concentrations of oxygen • Barotrauma and volutrauma from mechanical ventilation used for respiratory
support o Lung inflammation increases the chance of volutrauma and oxidant-
induced lung injury. • Fluid overload - particularly in those neonates who develop symptoms of fluid
overload within the first initial days of life o Patent ductus arteriosus (PDA) -
• Nutrition - inadequate nutrition may contribute by altering the growth of immature lungs.
• Failed antioxidant protection o Oxidant injuries continue to be investigated.
• Genetic predisposition o Those infants with a strong family history of asthma may be at greater
risk.
Who Is At Risk?
Infants who experience surfactant deficiency
• Respiratory distress syndrome (RDS) - primarily preterm infants • Especially the extremely premature infant
Infants who experience conditions that interfere with surfactant metabolism -
• Infants of diabetic mothers (IDM) of classes A, B, and C • Infants with erythroblastosis fetalis • The smaller infant in a set of twins • Infants whose mothers experience prenatal complications that lead to hypoxia or
ischemia at the level of the placenta. Such complications include - o Cardiorespiratory disease o Hypoxia o Hemorrhage
o Shock o Hypotension or hypertension
Neonatal conditions that increase the risk of respiratory disease -
• Congenital heart disease • Congenital diaphragmatic hernia • Hypoplastic lungs • Respiratory tract anomalies
o Choanal atresia o Tracheoesophageal fistula
• Meconium aspiration
Caucasian male infants also seem more prone to developing BPD.
What Happens?
Premature infants have immature lungs that are unable to support effective carbon dioxide and oxygen exchange.
• Immature lungs have insufficient alveolar surface area and blood vessels that are needed to allow -
o Oxygen from the air to travel into the blood stream. o Carbon dioxide to travel from the blood stream across
the lung surface into the air.
After birth, oxygen and ventilation support are initiated.
• The high pressures of mechanical ventilation and high concentrations of oxygen needed to inflate the immature lungs cause -
o Stretching of the alveoli which damages the lungs o Potential slowing of lung growth

As the lungs become irritated and inflamed, the following occurs -
• Inflammation leads to scarring of lungs • Gas exchange becomes more difficult
In response to the damage, oxygen and ventilation support are increased to support and maintain the infant, and this causes additional –
• Irritation, inflammation and scarring to worsen • Gas exchange continues to diminish
The end result is the development of BPD!
Why Does it Happen?
Since the development of BPD has multifactorial causes, it is difficult to understand why infants with similar backgrounds do not have similar outcomes.
The development of BPD for each individual infant depends on -
• Antenatal exposures such as - o Prenatal steroids o Maternal infection, such as chorioamnionitis o Intrauterine growth restriction
• Infant lung development • Postnatal exposure
o Ventilator-induced barotrauma o Oxidative injury o Infections o Steroid use o Pulmonary fluid overload
o Nutritional deficits o Extrauterine environment
Other contributory factors might include the following conditions -
• Pulmonary Interstitial Emphysema (PIE) • Patent ductus arteriosus (PDA)
The infant who develops BPD typically has an initial history that reflects a combination of the following -
• Moderate to severe respiratory distress due to one of the following -
o Surfactant deficiency (RDS) o Conditions that interfere with surfactant metabolism o Hypoxia or ischemia at the level of the placenta o A neonatal condition that increases the risk of
respiratory disease • Positive pressure ventilation with supplemental oxygen during the first week of
life
Signs and symptoms of BPD include -
• Tachypnea with shallow breathing • Exercise intolerance with feeding and handling • Oxygen dependence • Respiratory distress
o Audible râles, rhonchi, and/or wheezing Wheezing may be more common in the older infant with BPD and
may indicate significant airway obstruction. o Retractions o Nasal flaring o See-saw breathing
The chest and abdomen move in the opposite direction with each breath.
• Increasing respiratory support OR the inability to wean from mechanical ventilation
o Especially after reaching 36 weeks post-conceptual age • Respiratory acidosis with hypercapnia • Fluid intolerance despite little or no change in fluid intake
o Edema o Weight gain, not attributed to caloric intake o Decreased urine output
• Increased secretions, occasionally • Bronchospasms • Color changes
Infants with more severe BPD may exhibit the following -
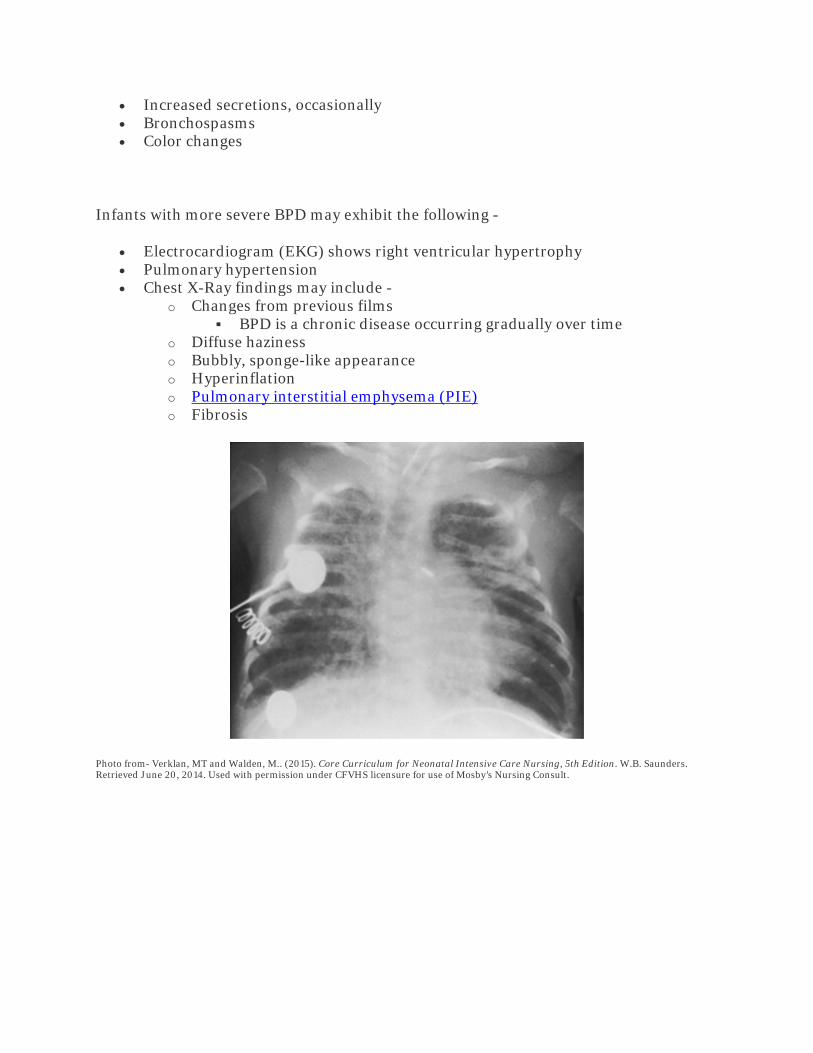
• Electrocardiogram (EKG) shows right ventricular hypertrophy • Pulmonary hypertension • Chest X-Ray findings may include -
o Changes from previous films BPD is a chronic disease occurring gradually over time
o Diffuse haziness o Bubbly, sponge-like appearance o Hyperinflation o Pulmonary interstitial emphysema (PIE) o Fibrosis
Photo from- Verklan, MT and Walden, M.. (2015). Core Curriculum for Neonatal Intensive Care Nursing, 5th Edition. W.B. Saunders. Retrieved June 20, 2014. Used with permission under CFVHS licensure for use of Mosby’s Nursing Consult.
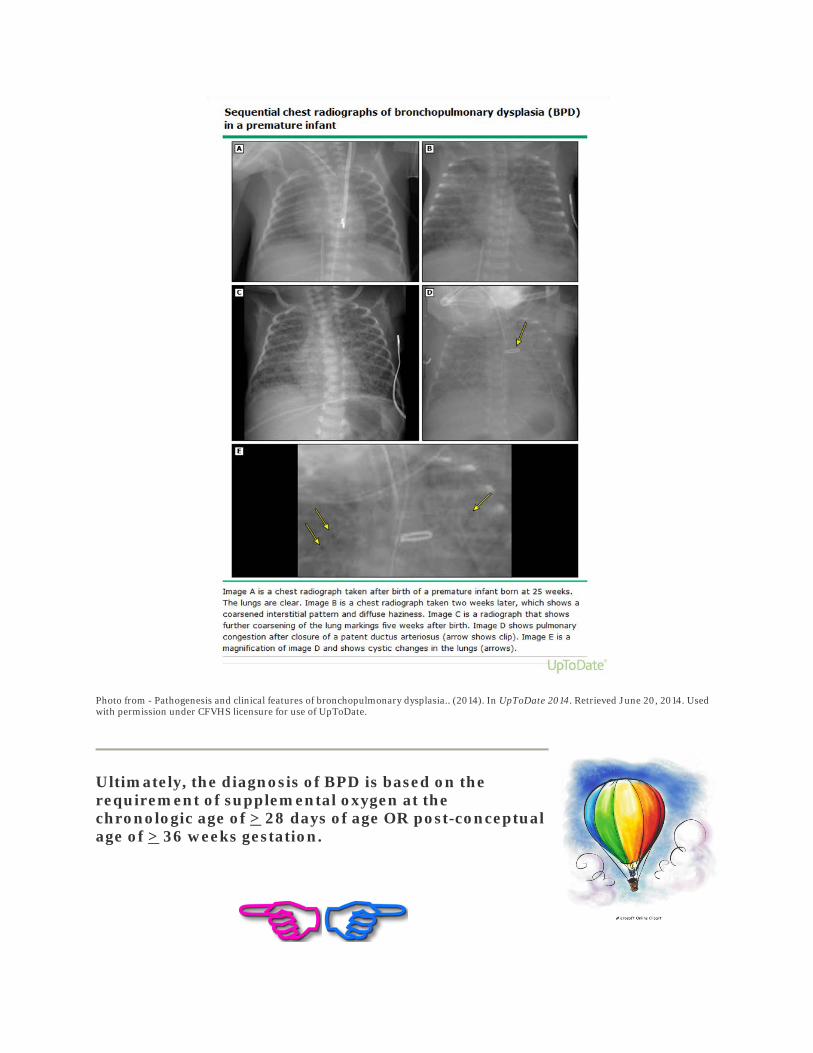
Photo from - Pathogenesis and clinical features of bronchopulmonary dysplasia.. (2014). In UpToDate 2014. Retrieved June 20, 2014. Used with permission under CFVHS licensure for use of UpToDate.
Ultimately, the diagnosis of BPD is based on the requirement of supplemental oxygen at the chronologic age of > 28 days of age OR post-conceptual age of > 36 weeks gestation.
The best defense is a good offense...
It makes sense that prevention of BPD should be part of the plan of treatment.
Treatment strategies that may potentially reduce the incidence of BPD include -
• Early use of CPAP to prevent lung injury o In the delivery room AND o After surfactant treatment with immediate extubation
• Timely surfactant replacement therapy aimed at - o Decreasing atelectasis o Sustaining lung recruitment o Achieving and maintaining optimal lung inflation
• Careful ventilation strategies with increased use of permissive hypercapnia • Use of lower target oxygen saturations
o This requires commitment and diligence of staff to wean oxygen. o Provision of blended oxygen for use in the delivery room and during transport is
also essential since this minimizes exposure to unnecessary high levels of oxygen. • Use of a t-piece resuscitator (e.g. Neopuff®, Neotee®) rather than manual positive
pressure ventilation devices reduces potential overinflation of the lungs with the administration of manual breaths.
• Early PDA management • Use of the antioxidant, vitamin A
However, BPD is not always preventable...
In the event that BPD is unavoidable, treatment goals include -
• Reducing factors that re-injure lungs • Letting the lungs heal so that normal lung function can occur
There are no specific treatments, techniques, therapies, etc. for BPD......treatment is more a regimen of support and time.
• Time for the normal repair processes within the lungs to improve lung functioning • Time for the infant to grow and thrive
Therapies that support the infant as the lungs grow and repair include -
• Maintaining adequate oxygenation and ventilation • Providing adequate nutrition and fluid restriction • Providing early treatment to close the PDA • Providing pharmacologic therapies
....so SUPPORT may include
Maintaining adequate oxygenation and ventilation
Despite their implication in the disease process, both supplemental oxygen and respiratory support are continued until the infant is able to breathe on his own and maintain acceptable saturation levels in room air
• Adequate amount of pressure to prevent atelectasis must be used while providing the lowest FiO2 possible to maintain adequate oxygenation.
• Early use of CPAP, as soon as possible, is encouraged.
One strategy to maximize oxygen carrying capacity is maintaining an adequate hematocrit between 30-40%.
The infant may remain hospitalized until the he is able to breathe without supplemental respiratory support.
• Hospital stay may extend over weeks to months--the average length of stay for infants with moderate to severe BPD is reported to be about 120 days.
• The infant may be discharged on nasal cannula O2--but rarely on ventilator or CPAP support.
The need for a tracheostomy is rare, but may be considered if -
• Repeated intubations are necessary due to endotracheal tube displacement
OR
• Long-term ventilation is expected
• A tracheostomy may reduce airway complications such as tracheomalacia and/or bronchomalacia.
• In the event that a tracheostomy is needed, be prepared to manage the usual surgical concerns such as post-op bleeding, infection, etc.
Providing adequate nutrition and fluid restriction
Infants with BPD have a higher metabolic rate at rest.
Chronic lung disease also places strain on the heart. This increases the potential for fluid overload.
• Closely monitor fluid intake and restrict, as needed to minimize the possibility of pulmonary edema and right-sided heart failure.
• TPN may be used to provide essential nutrients for growth. • Lipids may be used to provide maximum calories with minimal fluid. • Enteral feedings may require fortification to provide high caloric formula/breastmilk for
growth with minimal fluid intake.
Providing early treatment to close PDA
A thorough physical assessment of cardiac status should be performed daily to rule out the presence of a patent ductus arteriosus (PDA) and the need to treat.
An echocardiogram may be performed to rule out or document the presence of -
• PDA • Right ventricular hypertrophy - Cor Pulmonale • Increased pulmonary vascular resistance
• Left ventricular hypertrophy
An electrocardiogram (EKG) may be helpful to rule out or document right ventricular hypertrophy.
Pharmacologic Support
Diuretics may be used - furosemide (Lasix®), chlorothiazide (Diuril®), hydrochlorothiazide (HydroDiuril®), spiranolactone(Aldactone®).
• Diuretics lower the circulating blood volume which helps eliminate extra fluid from the lungs and decreases the possibility of pulmonary edema......However, use with caution.
• Diuretic usage can reduce cardiac output and renal perfusion. • Diuretic usage may also cause metabolic disturbances. Therefore, healthcare providers
must monitor for hypokalemia (K+), chloride depletion (Cl-) [hypochloremia], and metabolic alkalosis.
• Monitor intake and output.
Bronchodilators such as albuterol (Proventil®) may be necessary for some infants because they dilate the air passages and improve the flow of air in and out of the lungs.
Inhaled or systemic steroids such as dexamethasone (Decadron®) may be used.
• Steroids reduce the swelling and inflammation of the lungs and airway but should be used with great caution.
• Significant side effects of steroid use includes - o Slower head growth which leads to a reduction in brain size and volume of gray
matter o Interference with pulmonary alveolarization and vascularization o Increased rates of cerebral palsy (CP) o Increased incidence of learning disabilities o Increased severity of retinopathy of prematurity (ROP) o Steroids also contribute to long-term issues such as -
Cardiovascular disease Immune disorders Renal calcifications Neurologic and behavioral deficits
Methylxanthines such as caffeine citrate may be used to reduce pulmonary resistance and promote weaning from respiratory support. Other positive effects include -
• Improvement in lung compliance • Improvement in diaphragmatic contractility • There is a diuretic effect • Side effects are rare
Antibiotics are used exclusively to treat infections.
• Due to an immature immune system and the lack of protective maternal antibodies, premature infants with BPD are more prone to bacterial infections than term infants.
For the extremely unstable infant who becomes agitated or irritable, sedation may be needed to prevent hypoxemia and facilitate effective ventilation.
Vitamin A supplementation provides antioxidant protection for the lungs.
• This helps to protect the lungs from oxidative damage from administration of supplemental oxygen.
• Preterm infants are born with smaller vitamin A stores which could potentially place them at risk for developing BPD.
• There are no current recommendations for dosage nor administration route to achieve therapeutic plasma levels .
o 5000 International Units, intramuscularly 3 times weekly is thought to be necessary.
• Supplementation may be successful in preventing BPD. • Since no current recommendations regarding dosage, administration, or need for
universal supplementation, many facilities/physicians do not provide supplementation. o Additional well-controlled studies are recommended.
*Please note that Vitamin A remains on national back order*
Palivizumab (Synagis®), a humanized monoclonal antibody, can be used as prophylaxis against infection with respiratory syncytial virus (RSV).
• Palivizumab is administered as a monthly injection to at risk infants during RSV season, typically September until April.

Family Involvement
Parents should be encouraged to spend as much time as possible with their baby since this contact promotes bonding and helps to facilitate normal infant development through tactile and auditory stimulation.
Parents should also be encouraged to become involved in the care of their infant as much as possible because this -
• Further promotes bonding and the development of the parental role. • Enhances parental confidence in their ability to care for their child. • Provides parents with a tangible sense of control in relation to the care of their child.
Promotion of frequent communication between parents and the medical team and participation in care decisions helps to facilitate informed decision-making regarding their infant's care.
The level of severity of BPD can range from mild to severe.
• As with anything, the milder the disease the quicker and more complete the recovery. • Recovery from BPD is slow and takes time.
o Some infants recover slowly while others may never fully recover. Scarred and stiffened lungs have abnormal lung functions.
o However, the lungs continue to grow for 5-7 years. o As the child grows, healthy lung tissue forms and grows, taking over much of the
lung function for the diseased portions. o Most children have normal lung functioning by the time they start school.
However, some children may still have some abnormal lung functioning even at this age.
o Some infants have long-term health issues.
....COMPLICATIONS may include
Early Complications
Pulmonary edema happens when the rate of fluid filtered from the pulmonary circulation by the pulmonary microcirculation exceeds or is faster than the rate of its removal by the lymphatics.
• The lymphatics transport interstitial fluid into the systemic venous circulation. • Fluid transport by the neonatal lymphatic system is much less efficient than adult
lymphatic system. • Impairment in lymphatic functioning, secondary to increased systemic venous pressure
from BPD, may result in accumulation of fluid in the pulmonary interstitial tissues........pulmonary edema.
Cor pulmonale or right-sided ventricular hypertrophy results from on-going increased pulmonary vascular resistance or pulmonary hypertension.
• This is a major cause of death for infants with severe BPD.
Bronchospasms may occur sporadically, and infants with BPD have a greater chance for developing asthma later in life.
Side effects from medications, diuretics in particular, may include -
• Dehydration • Low sodium, potassium and/or calcium levels • Kidney stones • Hearing problems
For infants with severe BPD, a tracheostomy may be needed.
• In the long-term, this may delay speech. • This places the infant at a greater risk for infections. • This may make home care problematic and delay discharge as parents learn to take care
of the infant.
For infants with feeding and growth issues a gastrostomy tube (G-Tube) may be needed to -
• Promote adequate caloric intake • Decrease calorie consumption from feeding • Decrease the risk of aspiration
Late Complications
Some infants may experience continued slow growth and require more calories to grow.
• Due to an increased work of breathing, this may cause consumption of more calories than child can take in 24-hours.
• Therefore, the child may lose weight quicker and to a greater degree when sick.
Potential for fractures due to rickets
Intermittent and recurrent infections such as -
• Pneumonia • Otitis media • Upper respiratory infections (URI) • Increased susceptibility to Respiratory syncytial virus (RSV) • These children are often sicker than other children and require hospitalization when they
do become sick o Some studies suggest that up to 50% of infants with BPD will require re-
hospitalization during the first year of life
There is an increased incidence of cerebral palsy
Neurological and developmental problems are also more prevalent.
• In general, premature infants are at increased risk for a variety of long-term cognitive, neurological, and behavioral problems, and BPD may exacerbate these problems.
o However, many healthcare providers attribute this to the infant's prematurity rather than the BPD.
• Problems may include - o Low average IQ o Speech and language delays o Memory and learning deficits o Visual-motor impairments o Behavioral problems
• Problems are usually global in nature rather than specific.
There is no set time frame for discharge for infants with BPD.
Discharge criteria includes -
• The ability to maintain temperature in open crib • Minimal respiratory distress, optimally • A pattern of steady weight gain • The infant is eating well and tolerating feedings
o Some infants may go home on a mixture of oral feedings and gavage feedings.
Important education for the family includes -
• Knowledge about their infant's diagnosis and plan of care • The family's skill and comfort level to provide daily care • Feeding techniques to help facilitate adequate nutrition • Medication administration • CPR training • Additional support from family and/or friends to allow
periodic respite from care • The following educational needs are based on the individual
infant - o Home oxygen management o Breathing treatments o Apnea monitor
It is also important for parents and family members to recognize any deterioration in their infant's condition so that they know when to call the doctor!
Potential changes in condition that parents need to be able to recognize include -
• Signs of respiratory distress such as - o Increased respiratory rate o Decreased respiratory rate or apneic episodes o Working harder to breathe o Grunting or panting o Wheezing o Pale, dusky or cyanotic color changes to skin, circumoral area, or nail beds
• Feeding difficulties o Easily fatigued with feeding o Excessive spitting or emesis
• Signs of respiratory infection such as - o Stuffy or runny nose o Cough o Wheezing o Fever o Irritability
Post Hospital Care
After discharge, the baby will need to be followed closely. Follow-up appointments with the following are needed -
• Routine pediatric appointments to - o Monitor growth and development o Validate that the child is meeting childhood "milestones" o Administer all recommended childhood immunizations
and RSV prophylaxis o Provide care to other children in the home to make sure
they also receive all recommended childhood immunizations
• Subspecialty follow-up is very infant-specific and may include the following -
o Pulmonologist o Cardiologist o Ophthalmologist o Audiologist o Surgeon o Neurologist
• Developmental follow-up is essential for all at risk infants
Emphasize to parents the importance of keeping appointments !
Adams, J.M., Stark, A.R., Redding, G., Martin, R., and Kim, M.S. (2014). Pathogenesis and clinical features of bronchopulmonary dysplasia. In UpToDate 2014. Retrieved June 20, 2014.
Adams, J.M., Stark, A.R., Redding, G., Martin, R., and Kim, M.S. (2014). Management of bronchopulmonary dysplasia. In UpToDate 2014. Retrieved June 20, 2014.
Adams, J.M., Stark, A.R., Redding, G., Martin, R., and Kim, M.S. (2014). Outcome of infants with bronchopulmonary dysplasia. In UpToDate 2014. Retrieved June 20, 2014.
American Psychological Association. (2010). Publication Manual of the American Psychological Association, 6th Edition. Washington, DC: Author.
Anderson, P., & Doyle, L. (2006). Neurodevelopmental outcome of bronchopulmonary dysplasia. Seminars in Perinatology, 4, 227-232.
Bancalari, E. & Claure, N. (2006). Definitions and diagnostic criteria for bronchopulmonary dysplasia. Seminars in Perinatology, 30, 164-170.
Baraldi, E. & Filippone, M. (2007). Chronic lung disease after premature birth. New England Journal of Medicine, 357, 1946-1955.
Bhandari, A., & Panitch, H. (2006). Pulmonary outcomes in bronchopulmonary dysplasia. Seminars in Perinatology, 4, 219-226.
Bonner, K.M. & Mainous, R.O. (2008). The nursing care of the infant receiving bubble CPAP therapy. Advances in Neonatal Care, 8(2), 78-95.
F.A. Davis Company. (2013). Tabor’s Cyclopedic Medical Dictionary, 22nd Edition Online. http://www.tabers.com/tabersonline/ (Retrieved June 1, 2014).
Gardner, S.L., Carter, B.S., Enzman-Hines, M., & Hernandez, J.A. (2011). Merenstein & Gardner's Handbook of Neonatal Intensive Care, 7th Edition. St. Louis: Mosby-Elsevier.
Guyton, A.C. & Hall, J. (2011). Textbook of Medical Physiology, 12th Edition. Philadelphia: Elsevier-Saunders.
Miller, N.E. (2010). Techniques of early respiratory management of very low and extremely low birth weight infants. Neonatal Network, 29(3), 153-160.
Northway, W., Rosan, R., & Porter, D. (1967). Pulmonary disease following respiratory therapy for hyaline membrane disease. New England Journal of Medicine, 27, 357-368.
Nye, J. (2007). Postnatal corticosteroids in the treatment of chronic lung disease in the preterm infant: Past, present, and future. Neonatal Network,26(5), 293-299.
Palm, K., Simoneau, T., Sawicki, G. & Rhein, L. (2011). Assessment of current strategies for weaning premature infants from supplemental oxygen in the outpatient setting. Advances in Neonatal Care, 11(5), 349-356.
Peterson, S.W. (2009). Understanding the sequence of pulmonary injury in the extremely low birth weight, surfactant-deficient infant. Neonatal Network, 28(4), 221-229.
Snyder, T., Walker, W., & Clark, R.H. ( 2010). Establishing gas exchange and improving oxygenation in the delivery room management of the lung. Advances in Neonatal Care, 10(5), 256-260.
Verklan, M.T. & Walden, M. (2015). Core Curriculum for Neonatal Intensive Care Nursing, 5th Edition. St. Louis: W.B. Saunders.





























