-
Full Terms & Conditions of access and use can be found
athttps://www.tandfonline.com/action/journalInformation?journalCode=ypch20
Paediatrics and International Child Health
ISSN: 2046-9047 (Print) 2046-9055 (Online) Journal homepage:
https://www.tandfonline.com/loi/ypch20
Bubble CPAP devices for infants and children inresource-limited
settings: review of the literature
Alice Won, Daniela Suarez-Rebling, Arianne L. Baker, Thomas F.
Burke &Brett D. Nelson
To cite this article: Alice Won, Daniela Suarez-Rebling, Arianne
L. Baker, Thomas F. Burke& Brett D. Nelson (2019) Bubble CPAP
devices for infants and children in resource-limitedsettings:
review of the literature, Paediatrics and International Child
Health, 39:3, 168-176, DOI:10.1080/20469047.2018.1534389
To link to this article:
https://doi.org/10.1080/20469047.2018.1534389
Published online: 30 Oct 2018.
Submit your article to this journal
Article views: 110
View Crossmark data
Citing articles: 1 View citing articles
https://www.tandfonline.com/action/journalInformation?journalCode=ypch20https://www.tandfonline.com/loi/ypch20https://www.tandfonline.com/action/showCitFormats?doi=10.1080/20469047.2018.1534389https://doi.org/10.1080/20469047.2018.1534389https://www.tandfonline.com/action/authorSubmission?journalCode=ypch20&show=instructionshttps://www.tandfonline.com/action/authorSubmission?journalCode=ypch20&show=instructionshttp://crossmark.crossref.org/dialog/?doi=10.1080/20469047.2018.1534389&domain=pdf&date_stamp=2018-10-30http://crossmark.crossref.org/dialog/?doi=10.1080/20469047.2018.1534389&domain=pdf&date_stamp=2018-10-30https://www.tandfonline.com/doi/citedby/10.1080/20469047.2018.1534389#tabModulehttps://www.tandfonline.com/doi/citedby/10.1080/20469047.2018.1534389#tabModule
-
Bubble CPAP devices for infants and children in resource-limited
settings:review of the literatureAlice Wona, Daniela
Suarez-Reblinga, Arianne L. Bakerb,c, Thomas F. Burkea,b and Brett
D. Nelson b,d
aDivision of Global Health and Human Rights, Department of
Emergency Medicine, Massachusetts General Hospital, Boston, MA,
USA;bDepartment of Pediatrics, Harvard Medical School, Boston, USA;
cDepartment of Emergency Medicine, Harvard Medical School,
Boston,MA, USA; dDivision of Global Health, Department of
Pediatrics, Massachusetts General Hospital, Boston, USA
ABSTRACTBackground: Early management of respiratory distress is
critical to reducing mortality ininfants and children in
resource-limited settings. Bubble continuous positive airway
pressure(bCPAP) can offer effective and affordable non-invasive
respiratory support.Objective: To determine the best physical
components of bubble CPAP circuits for respira-tory support of
children in low-resource settings. Methods: Using PubMed, CINAHL
andLILACS, studies of any design in any language published before
June 2017 which examinedthe physical components of bCPAP circuits
were identified and reviewed.Results: After screening, the review
included 45 articles: 17 clinical trials, 11 literature reviews,10
technical assessments of bCPAP components, three reports of
real-world implementationin low-resource settings, three cost
analyses and one case report. There is no ideal bCPAPcircuit for
all settings and patients, but some choices are generally better
than others indesigning a circuit for low-resource settings. Oxygen
concentrators are usually the bestsource of oxygen. As yet, there
is no affordable and accurate oxygen blender. Nasal prongsare the
simplest patient interface to use with the fewest complications but
are not thecheapest option. Expiratory limbs should be at least 1
cm in diameter. Home-made pressuregenerators are effective, safe
and affordable.Conclusion: This narrative review found many studies
which evaluated the real clinicaloutcomes with bCPAP in the target
population as well as technical comparison of bCPAPcomponents.
However, many studies were not blinded or randomised and there was
sig-nificant heterogeneity in design and outcome measures.
Abbreviations: bCPAP, bubble continuous positive airway
pressure; CPAP, continuous posi-tive airway pressure; FiO2,
fractional oxygen concentration; HFNC, high-flow nasal cannula;HIC,
high-income countries; LMIC, low- and middle-income countries; NP,
nasopharyngeal;O2, oxygen; PEEP, positive end-expiratory pressure;
PICO, Population, Intervention,Comparison and Outcome
ARTICLE HISTORYReceived 30 April 2018Accepted 7 October 2018
KEYWORDSBubble CPAP; respiratorysupport; respiratory
illness;newborns; infants; low-resource setting
Introduction
Nearly three million newborns die each year in thefirst month of
life, most of them in low- and middle-income countries (LMIC). The
main causes are prema-turity, complications during labour and birth
andinfections [1,2], all of which can lead to severe respira-tory
distress. In LMIC, as many as 20% of infants withsevere respiratory
distress die [3].
Continuous positive airway pressure (CPAP) is widelyused in
high-income countries (HIC) and has reducedneonatal morbidity
andmortality as well as the need formechanical ventilation and
surfactant [4–6]. All forms ofCPAP require the patient to exhale
against a constantopening pressure, which produces positive
end-expira-tory pressure (PEEP). CPAP, therefore, delivers
continu-ous positive pressure into the airways that distends
thelungs, prevents alveolar and lung collapse, improvesoxygenation
and ventilation and reduces respiratory
fatigue [3,6]. CPAP is typically delivered via
mechanicalventilators or commercial pressure drivers in
high-resource hospitals; however, it can also be deliveredvia
high-flow nasal cannula (HFNC) therapy as well asbubble CPAP
(bCPAP) [3].
Both HFNC and bCPAP may be useful in resource-limited settings
[7]. The amount of distending pres-sure delivered via HFNC varies
and is difficult to mea-sure, whereas in bCPAP, the end of the
expiratorylimb of the respiratory circuit is immersed to a depthof
water in centimetres that indicates the deliveredCPAP pressure [6].
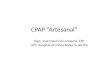
Furthermore, bubbling generatedby exhalation against the column of
water producesnoisy pressure oscillations superimposed over
pres-sure fluctuations (stochastic resonance effect) whichpromotes
further alveolar recruitment aiding oxyge-nation (Figure 1)
[8].
bCPAP can be a low-tech, safe and easy-to-usealternative to
conventional CPAP, making it an ideal
CONTACT Alice Won [email protected]; [email protected];
[email protected]
PAEDIATRICS AND INTERNATIONAL CHILD HEALTH2019, VOL. 39, NO. 3,
168–176https://doi.org/10.1080/20469047.2018.1534389
© 2018 Informa UK Limited, trading as Taylor & Francis
Group
http://orcid.org/0000-0002-5049-1798http://www.tandfonline.comhttp://crossmark.crossref.org/dialog/?doi=10.1080/20469047.2018.1534389&domain=pdf
-
choice in LMIC. Current commercially available bCPAPcan be
relatively affordable at 15% of the cost of amechanical ventilator
[9]. However, most bCPAP mod-els remain prohibitively expensive for
resource-limitedsettings at prices ranging from approximately
US$800to US$6000 [10]. Non-commercial, locally improvisedbCPAP
devices assembled from materials found inlocal hospital and
community settings may cost aslittle as US$3–5 per single unit
[11,12]. Such non-commercial devices, however, may have
importantdesign limitations such as the absence of a blenderor a
pressure regulator [6,13]. Furthermore, theseprices do not include
the cost of oxygen (O2).
While the effectiveness and safety of bCPAP arewell documented
[14,15], including in randomisedcontrolled trials in
resource-limited settings [16–18],no comprehensive literature
review has evaluated theindividual components of bCPAP for
feasibility andclinical outcomes in LMIC. This review sought
toexamine the evidence and determine the best physi-cal components
of bCPAP circuits in LMIC.
Methods
A review protocol was employed that searchedPubMed, CINAHL and
LILACS databases using thesearch terms outlined in Table 1. The
grey literaturewas also searched using the British Library
andGoogle advanced search engine using similar terms.The reference
lists of all identified articles were alsosearched and reviewed.
The search strategy was
based on the Population, Intervention, Comparisonand Outcome
(PICO) format (Table 1).
The literature was searched up to June 2017 withno limits
applied to year of publication. The greyliterature was searched up
to December 2017. Tomaximize the search sensitivity, search terms
pertain-ing to population age and specific outcome cate-gories were
not used to generate search results.
Studies that examined various components of abCPAP circuit and
described how they affected theO2 delivery to infants and children
were included forsystematic review. bCPAP circuit components
identifiedfor review throughout various sources were O2
source,inspiratory and expiratory limbs, patient interface
andpressure generator (e.g. water reservoir). In addition,
rele-vant device parameters such as flow andO2 concentration were
also examined as a part of circuitcomponents. Studies that examined
the mentioned cir-cuit components in conjunction with non-invasive
venti-latory support other than bCPAP were also reviewed.
AW and DS independently reviewed the titles,abstracts and full
texts using Covidence (Melbourne,Victoria, Australia) as the main
citation managing tool.Each conducted a preliminary screening of
titles toexclude studies clearly unrelated to the topic.
Theremaining abstracts were screened for appropriate-ness and
relevance, followed by perusal of the fulltext for further
exclusion of irrelevant papers. Duringeach step of the title,
abstract and full-text screening,the two reviewers resolved
conflicts by holding dis-cussions and reaching consensus in
consultation withthe other authors. Studies not relating to infants
or
Figure 1. bCPAP circuit example. A bCPAP circuit includes an
oxygen source with humidification canister (A), inspiratory (B)
andexpiratory (D) limbs, a patient interface (C) and a pressure
generator/water reservoir (E). The depth at which the expiratory
limbof the bCPAP circuit is placed underwater determines the amount
of pressure generated.
PAEDIATRICS AND INTERNATIONAL CHILD HEALTH 169
-
children were excluded. No studies were excluded onthe basis of
language or design.
Various causes of respiratory distress were considered,including
respiratory distress syndrome, pneumonia, sep-sis and transient
tachypnoea of the newborn, but studiesaddressing congenital
anomalies and structural patholo-gies were excluded. Studies
exclusively involving HIC andthose examining the efficacy of
commercial devices with-out adding to the originally published data
regardingtheir individual components were also excluded. A sum-mary
of the findings from the included studies was com-piled in
Microsoft Excel (Redmond, WA, USA).
Results
After screening, the review included 45 articles: 17clinical
trials, 11 literature reviews, 10 technical assess-ments of bCPAP
component, three reports of real-world implementation in
low-resource settings, threecost analyses and one case report
(Figure 2).
Oxygen source
The two common sources of O2 for bCPAP areO2 cylinders and O2
concentrators. O2 cylinders con-tain liquid O2 that is distilled at
very low temperaturesand high pressures in a special facility and,
therefore,must be transported back and forth from the hospitalfor
regular refilling. O2 concentrators are suitcase-sized electrically
powered machines which draw inambient air and extract nitrogen,
leaving 90–95%pure O2 for use [19]. A simple comparison is
sum-marised in Table 2.
Field studies of O2 concentrators implemented inlarge-scale
programmes in low-resource settings found
that the majority remained in use years afterwards [20–22].
However, these studies were typically using stan-dard-flow oxygen
delivery and not the higher flow ratestypically required in bCPAP.
Under the demands ofbCPAP, many concentrators fall short of the
requisiterobustness. One study evaluated seven
commerciallyavailable concentrators and found that only one
per-formed acceptably well in the conditions specified byWHO for
low-resource settings, although the study didnot specifically
assess performance at the higher flowrates used in bCPAP [13]. In a
randomised clinical trial ofbCPAP in Bangladesh, the study’s
specific concentratormodel failed 21% of the time during bCPAP,
requiringback-up O2 supplies to continue patient treatment
[16].
The main challenge with O2 concentrators is theneed for constant
electricity [23] and solar power isemerging as a potential solution
[24,25]. Anothersolution reported is an O2 reservoir which consists
ofa non-elastic balloon connected to an O2 concentratorwhich fills
the reservoir and can be used in the eventof power failure
[26].
O2 flow meter and flow splitter
Flow rates in bCPAP circuits affect the delivered pressure.Flow
can be regulated either by controlling the amountof O2 from an O2
source or at the point of blending airand O2 [27]. The literature
review did not find any directcomparison of different flowmeters,
although the major-ity of reports of bCPAP included flow meters
that coulddeliver child-appropriate flow rates.
Flow through a bCPAP circuit is influenced by thecircuit’s
diameter, length and integrity, including thedegree of seal at the
nasal interface. The approximateflow can be visually assessed by
observing the rate of
Table 1. PICO search strategy used for literature search.a
PICO terms Description Search terms
Population Newborns and infants with respiratory distress in
low- and middle-income countries
Childb, childrenb, infant(s)b, infancyb, paediatricb,
paediatricb,neonate(s)b, neonatalb, newbornb, developing
country,developing countries, underdeveloped country,
underdevelopedcountries, low income country, low income countries,
middleincome country, middle income countries, resource
poor,resource limited, low resource
Intervention Bubble CPAP Bubble CPAP, bubbling CPAP, bCPAP,
bubble continuous positiveairway pressure
Comparison Other forms of non-invasive oxygen therapy, including
nasal CPAPand standard oxygen via nasal cannula
Continuous positive airway pressure, positive-pressure
respiration,positive airway pressure device, nCPAP, nasal
continuouspositive airway pressure, oxygen therapy, respiratory
supportdevice, nasal cannula, nasal cannulae, non-invasive
respiratorysupport, non-invasive ventilation
Outcome Treatment failure, treatment complications, improvement
inrespiratory parameters (e.g. respiratory rate), rate of
intubation,rate of invasive/mechanical ventilation, severity of
respiratorydistress, mortality/survival to discharge
Outcome-based search termsb were not applied in the
searchprocess
Question For newborns and infants with respiratory distress
treated inresource-limited settings, what are the best components
of abubble CPAP circuit and other related non-invasive
ventilationmethods that contribute to improved outcomes?
aSimilar search terms were used for other databases with
adaptations as needed. bAge-specific search terms and outcome-based
search terms were notapplied in the search process to maximize the
search sensitivity.
170 A. WON ET AL.
-
bubbling in the circuit. While strategies for choosingflow rates
were beyond the scope of this review, onestudy reported that using
a fixed flow delivered accu-rate pressures to patients as opposed
to titrating flowto produce bubbling [27].
Managing O2 flow is also important for conservingO2 supplies
[28]. If multiple children can tolerate thesame flow rate, a flow
splitter device can be used tomaximize O2 supplies and decrease the
overall cost of
O2 [22,29,30]. CPAP usually requires O2 flow rates of2–10 L/min,
whereas a concentrator can usually pro-vide only up to 5–8 L/min
and, when split, will have aproportionally lower flow. For example,
one groupmeasured actual flow rates for each identical limb ofa
four-way flow-splitter and found that a concentratorset at 4 L/min
would deliver 0.5 L/min to each limb[22]. One innovative system
used an O2 concentratorfor CPAP by adding an air compressor via a
Y-piece to
Table 2. Comparison of oxygen delivery systems.Requirements
Cylinders Concentrator References
Infrastructure Reliable transportation to/from central
processing centres Continuous electrical supply
20,22,23,30,50Additionalequipment
Pressure regulator (~US$200/cylinder), flow meter (~US$400),
humidifier
None 20,22
Cost ~US$1500 for 1 million L oxygen; cost of cylinder may
behigher in LMICOngoing costs of transportation for frequent
refilling;standard cylinders lasting 2–3 days with continuous useA
2-year operational cost of ~US$168,500a (largeprovincial hospital)
and ~US$102,000a (small districthospitalb) in Papua New
Guinea~2.5–15× more expensive overall
~US$1500 per machine which can produce ~1 million Loxygen in 6
mthsModerate up-front costs of procuring initial equipmentand
installation, but small ongoing costs (electricity,maintenance)A
2-year operational cost of ~US$68,300a (largeprovincial hospital)
and ~US$10,100a (small districthospitalb) in Papua New Guinea
20,22,23,50
Maintenance Minimal; in central facility where oxygen is
compressed athigh pressure and low temperature
Local maintenance and repair, spare parts 20,21,22
aApproximated by conversion from values in Papua New Guinea’s
currency, Kina (PGK).bOperational cost in a small district hospital
not including the cost of an anaesthetic machine required for major
surgery.
Figure 2. Flow chart of literature search results.
PAEDIATRICS AND INTERNATIONAL CHILD HEALTH 171
-
increase the total flow rate, making it suitable forCPAP [29].
No studies comparing use of a flow splitterwith not using a flow
splitter were identified.
O2 blender
In low-resource settings, air–O2 blenders that incorpo-rate
ambient room air and pure O2 to supply preciselymixed FiO2 are not
usually available [11,12,28,29,31,32].Without an O2 blender,
several authors reported noability to regulate FiO2 or difficulty
in maintainingtarget FiO2 as well as differences between
predictedand measured FiO2 [11,28,31–33]. Some
commerciallyavailable bCPAP systems do include an air–O2
blender,which allows for use with premature newborns, buthomemade
bCPAP usually does not [6]. Air–O2 blenders also require a high
pressure O2 sourcebeyond the capability of most O2
concentrators,which produce low-pressure O2 [33].
For patients such as premature newborns who areat particularly
high risk of O2 toxicity and retinopathyof prematurity, WHO
recommends blended O2 withFiO2 of 0.3 or room air (0.21 FiO2)
[34,35]. However,data show that excessive use of oxygen in adults
isalso associated with excess mortality [12,36].
Several authors reported innovative systems toadjust the
concentration of O2 without a blender. AY-tubing set-up delivers a
mixture of air and O2 fromtwo separate supplies with independent
flow metersand can be used to change the relative concentrationof
O2 [29,33]. Kaur et al. tested calculatedO2 concentrations of
19–95% using such a Y-tubingsystem and found actual O2
concentrations of 21–98%with variable accuracy [33]. Alternatively,
an air pumpcan add O2 from a concentrator to air, with separateflow
control for pure O2 to control the FiO2 [27,37].
Another option is an entrainment device whichuses a small jet of
O2 and draws in ambient airthrough an adjustable inlet hole, thus
mixing theO2 and air to achieve a set concentration. However,one
common entrainment device designed for adultsdid not deliver an
appropriate O2 concentration orflow when used with nasal
cannula-like tubing at achild-appropriate flow rate [28].
Patient interface
Four patient interface devices for bCPAP were identi-fied: nasal
prongs/cannulas, nasal catheters, nasophar-yngeal (NP) catheters
and nasal/face mask [3,7]. Acomparison of their basic
characteristics is shown inTable 3. In this review, the most common
patientinterface used for bCPAP was nasal prongs. Nasaland NP
catheters may also be used for CPAP,although they require more
nursing intervention andare more prone to complications
[33,38,39].
When used to deliver low-flow O2, nasal cannulason average
require higher O2 flow rates than NPcatheters to achieve the same
partial pressure ofO2 [12]. At equal flow rates, NP catheters
deliver thehighest FiO2 compared with nasal catheters andprongs
[38].
NP catheters produce increased PEEP with lowerO2 flow rates than
nasal prongs [40]. Larger NP cathe-ters were found to produce PEEP
in infants; for exam-ple, size 8 Fr catheters produce PEEP (6.3 cm
at 1 L/min, 10.6 at 2 L/min) while size 6 Fr do not [12,40].
Nasal prongs are the easiest to use with the leastserious
complications that can occur with catheterssuch as displacement
into the airway and gastric dis-tension [38,41]. High-flow air
through nasal prongsdoes require a humidification device, however,
as do
Table 3. Comparison of patient interface devices for bCPAP.Nasal
prong/
cannula Nasal catheter Nasopharyngeal catheter Face mask
References
O2 flowrequired*
1.26× ~1× 1× Higher flow requirements 12,41
Cost per device ~US$2–5 ~US$0.10 ~US$0.10 Higher cost
38Humidificationrequired
Yes Yes Yes No 12,51
Risk of airwayobstructionby mucus
Low/Slight High High Low 38,41
Complications Dislodgement;tube breakage
Nasal bleeding; small risk ofdisplacement and
gastricdistension
Displacement and gastricdistention; airwayperforation
Carbon dioxide accumulation 12,38
Limitations Not easy todetermineprecise FiO2
Higher nursing demand Highest nursing demand;highest
complicationrate
Special ordering required – notgenerally available;
incompatiblewith feeding tube
38,40,41
Other Reservoir prongscan conserveoxygen
Nasogastric tube required Nasogastric tuberequired
45
*O2 flow required compared with nasopharyngeal catheter.
172 A. WON ET AL.
-
nasal and NP catheters since they bypass the nasalpassages which
typically provide humidification.Studies of bCPAP have included
humidified O2 foruse with all three interfaces [3,6,33].
Several comparisons of different types of nasalprongs were
identified. Short binasal prongs aremore effective in CPAP than
single prongs, with lessresistance to flow, and they are more
effective atpreventing re-intubation [7,42,43]. Commercially
avail-able prongs are equally effective for reaching targetPEEP and
O2 saturation [43]. When tested on a lungmodel, standard infant- or
newborn-sized nasalprongs delivered consistently higher mean
CPAPthan thinner-walled prongs [44].
Nasal prongs are 20–50 times more expensive thancatheters at an
estimated cost of US$2–5 per set ofprongs compared with US$0.10 for
a paediatric naso-gastric tube or suction tube which can be used as
acatheter [38]. If O2 conservation is a priority, reservoircannulas
include an inline compliant reservoir thatcaptures exhaled O2
between breaths and delivers itduring inhalation, which can further
conserveO2 supplies [45].
Expiratory limb
The expiratory limb for bCPAP is a tube of non-col-lapsible
plastic leading from the patient interface tothe pressure generator
where it is immersed in water.
When different diameters of the expiratory limbwere compared in
a lung model, a larger expiratorylimb (>10 mm) with greater
depth caused greateroscillations in pressure and volume, especially
ininfants with low lung compliance, which shouldimprove gas
exchange [46].
The expiratory limb should be emptied at least every2–3 h since
condensation collecting in the limbincreased the delivered pressure
beyond set levels [47].
Water reservoir or pressure generator
The water reservoir used to generate pressure may behome-made or
commercially produced. Home-madewater reservoirs consist of a
water-filled bottle (e.g.intravenous solution bottle, shampoo
bottle or glassgraduated cylinder). The expiratory limb is
submergedand stabilised in the bottle, and the water columnheight
within the limb determines the pressure.Several field studies have
reported the feasibility,affordability and effectiveness of
home-made pres-sure generators in LMIC [6,11,16,27,29,32,48].
Commercial models have different mechanisms forcontrolling the
pressure generated by the water col-umn [49]. Fisher and Paykel’s
system has a rigid tubemoulded to fit inside the reservoir which
generatespressure. Babi Plus has a rotation mechanism insidethe
expiratory limb that changes the depth and
controls pressure. WaterPAP uses a water bottle witha corrugated
tube with a plastic lid that holds thecorrugated tubing in
place.
Home-made water reservoirs tested in low-resourcesettings
accurately delivered pressures within 1 cmacross a range of pre-set
pressures [32]. In one studycomparing home-made systems with
commercial ones,a home-made pressure generator had more
variableairway pressure and volume oscillations with the
leastincrease in pressure at increasing flows but the home-made
system is not as foolproof [49].
One lung model using different home-made pres-sure generators
found that a smaller bottle such as a500-ml graduated cylinder
should be used to increasepressure and volume oscillations
[46].
Discussion
The ideal bCPAP device for low-resource settingswould be safe,
effective, affordable, reusable, readilyavailable and simple to
use. On reviewing the indivi-dual components of bCPAP in LMIC, the
evidencepoints to several superior choices while highlightingareas
for further studies with potential for innovationand
development.
O2 concentrators are safe and cost-efficient, poten-tially
making them the best choice as a source of O2 inmost low-resource
settings. They do not require layersof widescale infrastructure,
whereas for O2 cylinders,there is a chain of infrastructure from
the financing ofhigh-energy production of liquid oxygen at an
oxygenplant to reliable road and transportation systems[20,30,50].
The need for an uninterrupted power sup-ply, however, can be a
limiting factor in LMIC. Solarpower or O2 reservoirs may allow
concentrator useeven without reliable electricity. Furthermore,
whilethe initial cost of installing a solar-powered system ishigh,
operational costs tend to be low with only airand sun being
required [24]. It is essential, however,to ensure the purchase and
implementation ofO2 concentrators that meet the performance
stan-dards outlined by the WHO guideline for
technicalspecifications for O2 concentrators in
low-resourcesettings [34]. It is also essential to thoroughly
assessa facility’s O2 requirements, conduct local training
inmaintenance and repair and ensure the presence ofback-up power or
O2 supply.
Traditional commercially available O2 blenders aretoo expensive
for low-resource settings and home-made blending systems have
limited precision andaccuracy. Low-resource settings need an
affordableand reliable O2 blender in order to expand the safeuse of
bCPAP, especially for premature infants whoare vulnerable to
retinopathy of prematurity owing toO2 toxicity. O2 concentrators
with built-in blenders arecurrently the best choice for premature
infants.
PAEDIATRICS AND INTERNATIONAL CHILD HEALTH 173
-
However, an air entrainment device designed on thebasis of the
Venturi effect – a pressure differentialgenerated by a simple
manipulation of oxygen inletand outlet orifices that can lead to
variable air–oxy-gen blending capacities – is a potentially
powerfuland revolutionary tool [28]. Future studies shouldoptimise
the design and application of such entrain-ment devices with
attention to cost-efficiency as wellas reported limitations.
For the patient interface, nasal prongs are the sim-plest to use
with the fewest serious complications.The most common complications
of nasal prongsare dislodgement and nasal irritation, whereas
com-plications associated with catheters include displace-ment into
the lower airways with the risk of airwayperforation and gastric
distension. However, nasalprongs do require more O2 flow, and they
are muchmore expensive than nasal and NP catheters. Anotherpossible
limitation with narrow, high-resistance nasalprongs is a
pseudo-CPAP bubbling effect. Our reviewrevealed a lack of data that
specifically analyses thebubbling effect of bCPAP with variables
that deter-mine the resistance of the circuit.
Home-made pressure generators are reliable, accu-rate and
affordable and in some respects (such as increating oscillation in
pressure and volume whichencourages gas exchange) may be superior
to com-mercially available devices. The diameter should benarrow,
approximately 5–6 cm, to increase pressureand volume oscillation.
Lastly, the expiratory limbshould be at least 1 cm in diameter for
increasedpressure and volume oscillations to facilitate gasexchange
in the lung.
The limitations of this review include its limitedscope. Best
practices for system-wide implementationof bCPAP and training of
clinical staff were notdirectly part of the search strategy,
although theauthors discussed the importance of good trainingin its
use as well as maintenance and repair. Oneelement of safe bCPAP
implementation, as with anyuse of supplemental O2, is monitoring
with pulseoximetry. WHO guidelines support this recommenda-tion
[34,51,52]. This review also included a limitedgrey literature
search and there is probably a wealthof information from innovative
providers not widelypublished and not seen in this review. Finally,
this wasa narrative review that aimed to assess all of therelevant
data published but it did not include sys-tematic evaluation of the
quality of the literatureincluded.
CPAP is a safe and effective method of treatinginfants and young
children with life-threateningrespiratory distress and can be
successfully adaptedfor use in resource-limited settings. This
literature
review found that the most feasible, safe and cost-effective
bCPAP system in LMIC would be anO2 concentrator connected to short
binasal prongswith an attached humidifier, with a
large-diameterexpiratory limb submerged into a
small-diameterhome-made pressure generator such as a
graduatedcylinder. There is a need for an affordable O2-blending
device to expand the use of bCPAP to pre-mature infants and others.
Successful bCPAP imple-mentation will depend on the establishment
ofreliable infrastructure such as electricity, strong clin-ical
training and local training in device maintenanceand repair.
Disclosure statement
No potential conflict of interest was reported by
theauthors.
Notes on contributors
Alice Won is a fourth-year medical student at TuftsUniversity
School of Medicine and spent a research concen-tration year at
Massachusetts General Hospital's Division ofGlobal Health and Human
Rights. She is interested in opera-tional research utilizing
existing healthcare resources andsystems to address gaps in access
to quality care in com-munities at home and abroad.
Daniela Suarez-Rebling is a program coordinator at
theMassachusetts General Hospital Division of Global Healthand
Human Rights. She is interested in public healthresearch,
specifically identifying how to scale innovationsto impact
vulnerable populations and to address healthdisparities in
populations.
Arianne L. Baker is a resident in Pediatrics at theMassachusetts
General Hospital and Harvard MedicalSchool. Her research work
focuses on leadership develop-ment and medical education. She has
also worked on qual-ity improvement for mothers and their infants
in a Boston-area pediatric primary care community health center.
Herclinical interests include pediatric acute care.
Thomas F. Burke is Chief of the Division of Global Healthand
Human Rights in the Department of EmergencyMedicine at the
Massachusetts General Hospital. He is asenior emergency physician
and an Associate Professor atHarvard Medical School. He has
extensive experience instrategic planning and development of
service and researchcapacity for global health interventions, most
notably forcommunity-based maternal and infant health delivery.
Hehas been a leader in the nonprofit sector directing
overseashealth interventions since 1994.
Brett D. Nelson is Associate Professor and global
healthpediatrician at Massachusetts General Hospital andHarvard
Medical School. He has been involved in clinicalcare and program
management in dozens of low- and mid-dle-income countries. His
research interests are healthcareprovision, development, research,
and advocacy for
174 A. WON ET AL.
-
vulnerable populations, particularly newborns and childrenin
settings affected by poverty, conflict, or disaster. Hedirects
Harvard Medical School’s course on global healthand serves as
editor of a textbook on clinical global health.
ORCID
Brett D. Nelson http://orcid.org/0000-0002-5049-1798
References
[1] UNICEF, WHO, World Bank Group and United Nations.Levels and
trends in child mortality report 2017.Accessed October 18, 2018.
https://www.unicef.org/publications/index_101071.html. Updated
2017.
[2] Lawn JE, Blencowe H, Oza S, et al. Every newborn:progress,
priorities, and potential beyond survival.Lancet.
2014;384:189–205.
[3] Duke T. CPAP: a guide for clinicians in developingcountries.
Paediatr Int Child Health. 2014;34:3–11.
[4] Jensen EA, Chaudhary A, Bhutta ZA, et al. Non-inva-sive
respiratory support for infants in low- and mid-dle-income
countries. Semin Fetal Neonatal Med.2016;21:181–188.
[5] Ho JJ, Subramaniam P, Davis PG. Continuous distend-ing
pressure for respiratory distress in preterminfants. Cochrane
Database Syst Rev. 2015;7:CD002271.
[6] Dewez JE, van den Broek N. Continuous positive air-way
pressure (CPAP) to treat respiratory distress innewborns in low-
and middle-income countries. TropDoct. 2017;47:19–22.
[7] Gupta N, Saini SS, Murki S, et al. Continuous positiveairway
pressure in preterm neonates: an update ofcurrent evidence and
implications for developingcountries. Indian Pediatr.
2015;52:319–328.
[8] Pillow JJ, Hillman N, Moss TJ, et al. Bubble
continuouspositive airway pressure enhances lung volume andgas
exchange in preterm lambs. Am J Respir Crit CareMed.
2007;176:63–69.
[9] Wyatt J. Appropriate medical technology for perinatalcare in
low-resource settings. Ann Trop Paediatr.2008;28:243–251.
[10] PATH, USAID. Continuous positive airway pressure(CPAP) –
Guide to selection, 2014 Accessed October18, 2018.
https://www.path.org/publications/files/DT_guide_to_select_cpap.pdf
[11] Daga S, Mhatre S, Borhade A, et al. Home-made con-tinuous
positive airways pressure device may reducemortality in neonates
with respiratory distress in low-resource setting. J Trop Pediatr.
2014;60:343–347.
[12] Frey B, Shann F. Oxygen administration in infants.Arch Dis
Child Fetal Neonatal Ed. 2003;88:84.
[13] Peel D, Neighbour R, Eltringham RJ. Evaluation ofoxygen
concentrators for use in countries with lim-ited resources.
Anaesthesia. 2013;68:706–712.
[14] Martin S, Duke T, Davis P. Efficacy and safety ofbubble
CPAP in neonatal care in low and middleincome countries: a
systematic review. Arch DisChild Fetal Neonatal Ed.
2014;99:F495–F504.
[15] Thukral A, Sankar MJ, Chandrasekaran A, et al. Efficacyand
safety of CPAP in low- and middle-income coun-tries. J Perinatol.
2016;36(Suppl 1):S21–S28.
[16] Chisti MJ, Salam MA, Smith JH, et al. Bubble
continuouspositive airway pressure for children with severe
pneumonia and hypoxaemia in Bangladesh: an open,randomised
controlled trial. Lancet. 2015;386:1057–1065.
[17] Tagare A, Kadam S, Vaidya U, et al. Bubble CPAPversus
ventilator CPAP in preterm neonates withearly onset respiratory
distress: a randomized con-trolled trial. J Trop Pediatr.
2013;59:113–119.
[18] Yagui AC, Vale LA, Haddad LB, et al. Bubble CPAPversus CPAP
with variable flow in newborns withrespiratory distress: a
randomized controlled trial. JPediatr (Rio J). 2011;87:499–504.
[19] Charburn RL, Williams TJ. Performance comparison of4
portable oxygen concentrators. Respiratory
Care.2010;55:433–442.
[20] Dobson MB. Oxygen concentrators and cylinders. Int JTuberc
Lung Dis. 2001;5:520–523.
[21] La Vincente SF, Peel D, Carai S, et al. The functioningof
oxygen concentrators in resource-limited settings:a situation
assessment in two countries. Int J TubercLung Dis.
2011;15:693–699.
[22] Matai S, Peel D, Wandi F, et al. Implementing anoxygen
programme in hospitals in Papua NewGuinea. Ann Trop Paediatr.
2008;28:71–78.
[23] Mokuolu OA, Ajayi OA. Use of an oxygen concentratorin a
Nigerian neonatal unit: economic implicationsand reliability. Ann
Trop Paediatr. 2002;22:209–212.
[24] Turnbull H, Conroy A, Opoka RO, et al. Solar-poweredoxygen
delivery: proof of concept. Int J Tuberc LungDis.
2016;20:696–703.
[25] Nyende S, Conroy A, Opoka RO, et al. Solar-poweredoxygen
delivery: study protocol for a randomizedcontrolled trial. Trials.
2015;16:297.
[26] Rassool RP, Sobott BA, Peake DJ, et al. A
low-pressureoxygen storage system for oxygen supply in low-resource
settings. Respir Care. 2017;62:1582–1587.
[27] Brown J, Machen H, Kawaza K, et al. A high-value, low-cost
bubble continuous positive airway pressure systemfor low-resource
settings: technical assessment and initialcase reports. PLoS One.
2013;8:e53622.
[28] Coghill M, Ambalavanan N, Chatburn RL, et al.Accuracy of a
novel system for oxygen delivery tosmall children. Pediatrics.
2011;128:382.
[29] van den Heuvel M, Blencowe H, Mittermayer K, et
al.Introduction of bubble CPAP in a teaching hospital inMalawi. Ann
Trop Paediatr. 2011;31:59–65.
[30] Howie SRC, Hill S, Ebonyi A, et al. Meeting oxygenneeds in
Africa: an options analysis from the Gambia.Bull WHO.
2009;87:763–771.
[31] Jayashree M, KiranBabu H, Singhi S, et al. Use of
nasalbubble CPAP in children with hypoxemic clinicalpneumonia –
Report from a resource limited set-up.J Trop Pediatr.
2016;62:69–74.
[32] McAdams RM, Hedstrom AB, DiBlasi RM, et al.Implementation
of bubble CPAP in a rural Ugandanneonatal ICU. Respir Care.
2015;60:437–445.
[33] Kaur C, Sema A, Beri RS, et al. A simple circuit to
deliverbubbling CPAP. Indian Pediatr. 2008;45:312–314.
[34] World Health Organization. Technical specificationsfor
oxygen concentrators. Geneva: WHO; 2015.Accessed October 18, 2018.
http://apps.who.int/iris/bitstream/handle/10665/199326/9789241509886_eng.pdf?sequence=1
[35] World Health Organization. WHO recommendationson
interventions to improve preterm birth outcomes.Geneva: WHO; 2015.
Accessed October 18,
2018.http://apps.who.int/iris/bitstream/handle/10665/183037/9789241508988_eng.pdf?sequence=1
PAEDIATRICS AND INTERNATIONAL CHILD HEALTH 175
https://www.unicef.org/publications/index_101071.htmlhttps://www.unicef.org/publications/index_101071.htmlhttps://www.path.org/publications/files/DT_guide_to_select_cpap.pdfhttps://www.path.org/publications/files/DT_guide_to_select_cpap.pdfhttp://apps.who.int/iris/bitstream/handle/10665/199326/9789241509886_eng.pdf?sequence=1http://apps.who.int/iris/bitstream/handle/10665/199326/9789241509886_eng.pdf?sequence=1http://apps.who.int/iris/bitstream/handle/10665/199326/9789241509886_eng.pdf?sequence=1http://apps.who.int/iris/bitstream/handle/10665/183037/9789241508988_eng.pdf?sequence=1http://apps.who.int/iris/bitstream/handle/10665/183037/9789241508988_eng.pdf?sequence=1
-
[36] Chu DK, Kim LH, Young PJ, et al. Mortality and mor-bidity
in acutely ill adults treated with liberal versusconservative
oxygen therapy (IOTA): a systematicreview and meta-analysis.
Lancet. 2018;391:1693–1705.
[37] Kawaza K, Machen HE, Brown J, et al. Efficacy of a low-cost
bubble CPAP system in treatment of respiratorydistress in a
neonatal ward in Malawi. PLoS One.2014;9:e86327.
[38] Muhe L, Webert M. Oxygen delivery to children
withhypoxaemia in small hospitals in developing coun-tries. Int J
Tuberc Lung Dis. 2001;5:527–532.
[39] Walk J, Dinga P, Banda C, et al. Non-invasive ventila-tion
with bubble CPAP is feasible and improvesrespiratory physiology in
hospitalised Malawian chil-dren with acute respiratory failure.
Paediatr Int ChildHealth. 2016;36:28–33.
[40] Frey B, McQuillan PJ, Shann F, et al. Nasopharyngealoxygen
therapy produces positive end-expiratorypressure in infants. Eur J
Pediatr. 2001;160:556–560.
[41] Weber MW, Palmer A, Oparaugo A, et al. Comparisonof nasal
prongs and nasopharyngeal catheter for thedelivery of oxygen in
children with hypoxemiabecause of a lower respiratory tract
infection. JPediatr. 1995;127:378–383.
[42] De Paoli AG, Davis PG, Faber B, et al. Devices andpressure
sources for administration of nasal con-tinuous positive airway
pressure (NCPAP) in pre-term neonates. Cochrane Database Syst
Rev.2008;1:CD002977.
[43] Gupta S, Donn SM. Continuous positive airway pres-sure:
physiology and comparison of devices. SeminFetal Neonatal Med.
2016;21:204–211.
[44] Bailes SA, Firestone KS, Dunn DK, et al. Evaluating
theeffect of flow and interface type on pressures
delivered with bubble CPAP in a simulated model.Respir Care.
2016;61:333–339.
[45] Wu G, Wollen A, DiBlasi RM, et al. Reservoir cannulasfor
pediatric oxygen therapy: a proof-of-conceptstudy. Int J Pediatr.
2016;2016:9214389.
[46] Wu C, Lee C, Yuh Y, et al. Influence of changing
thediameter of the bubble generator bottle and expira-tory limb on
bubble CPAP: an in vitro study. PediatrNeonatol.
2012;53:359–365.
[47] Youngquist TM, Richardson CP, Diblasi RM. Effects
ofcondensate in the exhalation limb of neonatal circuitson airway
pressure during bubble CPAP. Respir Care.2013;58:1840–1846.
[48] Myhre J, Immaculate M, Okeyo B, et al. Effect oftreatment
of premature infants with respiratory dis-tress using low-cost
bubble CPAP in a rural Africanhospital. J Trop Pediatr.
2016;62:385–389.
[49] Poli JA, Richardson CP, DiBlasi RM. Volume
oscillationsdelivered to a lung model using 4 different bubbleCPAP
systems. Respir Care. 2015;60:371–381.
[50] Duke T, Peel D, Wandi F, et al. Oxygen supplies
forhospitals in Papua New Guinea: a comparison of thefeasibility
and cost-effectiveness of methods for dif-ferent settings. PNG Med
J. 2010;53:126–138.
[51] World Health Organization. Oxygen therapy for children:a
manual for health workers. Geneva: WHO; 2016.Accessed October 18,
2018.
http://apps.who.int/iris/bitstream/handle/10665/204584/9789241549554_eng.pdf;jsessionid=33AA54C2D67C3154A1B85DCE3DDABA32?sequence=1
[52] World Health Organization. Pulse oximetry trainingmanual.
Geneva: WHO; 2011. Accessed October 18,2018.
http://www.who.int/patientsafety/safesurgery/pulse_oximetry/who_ps_pulse_oxymetry_training_manual_en.pdf
176 A. WON ET AL.
http://apps.who.int/iris/bitstream/handle/10665/204584/9789241549554_eng.pdf;jsessionid=33AA54C2D67C3154A1B85DCE3DDABA32?sequence=1http://apps.who.int/iris/bitstream/handle/10665/204584/9789241549554_eng.pdf;jsessionid=33AA54C2D67C3154A1B85DCE3DDABA32?sequence=1http://apps.who.int/iris/bitstream/handle/10665/204584/9789241549554_eng.pdf;jsessionid=33AA54C2D67C3154A1B85DCE3DDABA32?sequence=1http://apps.who.int/iris/bitstream/handle/10665/204584/9789241549554_eng.pdf;jsessionid=33AA54C2D67C3154A1B85DCE3DDABA32?sequence=1http://www.who.int/patientsafety/safesurgery/pulse_oximetry/who_ps_pulse_oxymetry_training_manual_en.pdfhttp://www.who.int/patientsafety/safesurgery/pulse_oximetry/who_ps_pulse_oxymetry_training_manual_en.pdfhttp://www.who.int/patientsafety/safesurgery/pulse_oximetry/who_ps_pulse_oxymetry_training_manual_en.pdf
AbstractIntroductionMethodsResultsOxygen sourceO2 flow meter and
flow splitterO2 blenderPatient interfaceExpiratory limbWater
reservoir or pressure generator
DiscussionDisclosure statementNotes on
contributorsORCIDReferences