Embed Size (px)
Citation preview
The Ins and Outs of EMTALA – EmergencyEMTALA Emergency Medical Treatment and Labor Actand Labor ActDoran StampsDirector of Risk Management and ComplianceBaptist Health System
Denise Cicchella, CIA, CFE, CCA,
Baptist Health System
PMPExecutive director
AuspiciumAuspicium
1AHIA 31st Annual Conference – August 26‐29, 2012 – Philadelphia PA
www.ahia.org
Also known as….Also known as….
• COBRA• COBRA
• Patient dumping law
• Patient anti‐Patient antidumping act
2
HistoryHistory
• As part of the Consolidated Omnibus Budget p gReconciliation Act (COBRA), Congress enacted in 1986 the Emergency Medical Treatment and Labor Act (EMTALA) to:and Labor Act (EMTALA) to:
• insure public access to emergency services regardless of ability to payservices regardless of ability to pay.
3
HistoryHistory
S ti 1867 f th S i l S it A t i• Section 1867 of the Social Security Act imposes specific obligations on Medicare participating hospitals that offer emergency services to provide:
• a medical screening examination (MSE) when a request is made for an emergency medical condition (EMC).
• Hospitals are then required to provide stabilizing treatment for patients with EMC’s.
• If the hospital is unable to stabilize a patient within its capability, or if the patient requests, an appropriate transfer should be implementedappropriate transfer should be implemented.
4
Hospital ObligationsHospital Obligations
• For any person who comes to a hospital emergency department,department,
• "the hospital must provide for an appropriate• the hospital must provide for an appropriate medical screening examination . . . to determine whether or not an emergency medical condition g y(EMC) exists“
5
Definition of an “emergency d ”department”
• Specifically licensed by the state as an emergency departmentemergency department
• Held out to the public as providing emergency care without requiring anemergency care without requiring an appointment
• Has provided during a calendar yearHas provided, during a calendar year, emergency services for at least one third of its outpatient visits p
6
“Comes” to the emergency d l ddepartment includes:
• Patients presenting to hospital property includingPatients presenting to hospital property, including parking lots, sidewalks, driveways, and includes "Anyone whom a layperson would believe, based y yp ,on the individual's appearance and behavior, that the individual needs examination or treatment.“
• Does not include non hospital entities such asDoes not include non hospital entities such as doctor’s offices, that are adjacent to the hospital but not owned or operated by the hospital. p y p
7
Requirements under the lawRequirements under the law
• Medical screening exam‐ to determine if theMedical screening exam to determine if the individual has an emergency condition, or is in active labor
• If so, the hospital must provide stabilizing treatment within the capabilities and services it offers
• If transferred, the pt. must be stabilized, or the transfer must be certified; ie. the transfer is appropriate and meets certain conditions.
8
Medical Screening ExamMedical Screening Exam• Generally, should be done by a physician
• Triage is not a medical screening exam
• Hospital bylaws rules and regs or policies should indicate who is qualified• Hospital bylaws, rules and regs, or policies should indicate who is qualified to perform a medical screening exam
• The MSE is an ongoing process utilizing capabilities of the hospital, g g p g p p ,(including necessary testing, use of ancillary services, on call services) in order to reach an exclusion of a legally defined emergency medical condition
• Once admitted, obligations under EMTALA have generally been satisfied
• MSE CANNOT be delayed to obtain financial information or to obtain pre‐y f f pauthorization for treatment
9
Emergency Medical ConditionEmergency Medical Condition
Emergency Medical Condition (EMC) means:
A medical condition manifesting itself by acute symptoms of sufficient severity (including severe pain, psychiatric y ( g p p ydisturbances and/or symptoms of substance abuse) such that the absence of immediate medical attention could reasonably be expected to result in:
• Placing the health of the individual (or with respect to a pregnant woman, the health of the woman or her unborn hild) i i j dchild) in serious jeopardy;
• Serious impairment to bodily functions, or• Serious dysfunction to any bodily organ or part
10
EMC, cont.EMC, cont.
• With respect to a pregnant woman who is having p p g gcontractions:
• That there is inadequate time to effect a safe transfer to th h it l b f d lianother hospital before delivery; or
• That transfer may pose a threat to the health or safety of the woman or the unborn child
• Obstetric patients with contractions are generally considered unstable until delivery of baby and placenta, and EMTALA h i i d bili i f bthen requires screening and stabilization of newborn
11
What happens if a patient refuses f ”treatment or transfer”
• DOCUMENT
• Use AMA , Refusal of Treatment, or Transfer to other Institution forms to carefully document the circumstances of the patient refusal
12
Appropriate transferAppropriate transfer
A transfer to another facility will be appropriate only in those f f y pp p ycases which:
The transferring hospital provides medical treatment within its it th t i i i th i k t th i di id l’ h lthcapacity that minimizes the risks to the individual’s health
and, in the case of a woman in labor, the health of the unborn child;
The receiving facility:
• Has available space and qualified personnel for the treatment f h i di id l dof the individual; and
• Has agreed to accept transfer of the individual and to provide appropriate medical treatmentappropriate medical treatment
13
Recipient hospital responsibilitiesRecipient hospital responsibilities
• A participating hospital that has specializedA participating hospital that has specialized capabilities or facilities may not refuse to accept from a referring hospital within theaccept from a referring hospital within the boundaries of the United States, an appropriate transfer of an individual whoappropriate transfer of an individual who requires such specialized capabilities or facilities if the receiving hospital has thefacilities if the receiving hospital has the capacity to treat the individual
14
Appropriate transfer, cont.Appropriate transfer, cont.
The transferring • test results, x‐raysf ghospital :
• Sends to receiving
• treatment notes• the name and address of
any on call physician who • Sends to receiving facility copies of all medical records l t d t th EMC
y p yhas refused or failed to appear within a reasonable time to provide necessary stabili ing treatmentrelated to the EMC
the individual presented with,
l d
stabilizing treatment• results not yet available
should be sent as soon as practical after transfer
pincluding: practical after transfer
• the transfer is effected through qualified personnel and equipment as requiredand equipment, as required
15
On‐CallOn Call• When the ED physician requests an on call physician to come in,
they must do so in a reasonable period of time
• Hospital is responsible for maintaining a workable on call system, and on call physicians must understand their on call responsibilitiesresponsibilities
• Hospital must have written policies and procedures in place to respond to situations in which a particular specialty is not
il bl th ll h i i t d b favailable or the on‐call physician cannot respond because of circumstances beyond the physician’s control;
• provide that emergency services are available to meet the p g yneeds of patients with EMC’s if it elects to permit on‐call physicians to schedule elective surgery during the time that they are on call, or to permit on‐call physicians to have simultaneous on‐call duties
16
Additional requirementsAdditional requirements
• Log‐ transfers to other institutions, transfers from g ,other institutions
• Signage• Physician on call lists with names, not initials• Protection for “whistleblowers” who refuse to authorize an inappropriate transfer or who reportauthorize an inappropriate transfer or who report a violation of the regulations
• Receiving hospitals must report suspected g p p pviolations within 72 hours when they believe the sending facility may be violating the regulations
17
Signage, EnglishSignage, English
IT’S THE LAWIF YOU HAVE A MEDICAL EMERGENCY OR ARE IN LABOR, YOU HAVE
THE RIGHT TO RECEIVE,within the capabilities of this hospital’s staff and facilities:
An appropriate medical SCREENING EXAMINATIONAn appropriate medical SCREENING EXAMINATIONNecessary STABILIZING TREATMENT
(including treatment for an unborn child) and, if necessary,
A i t TRANSFER t th f ilit if YOU CANNOT PAYAn appropriate TRANSFER to another facility, even if YOU CANNOT PAY or DO NOT HAVE MEDICAL INSURANCE
or YOU ARE NOT ENTITLED TO MEDICARE OR MEDICAIDThis hospital does participate in the Medicaid Program
18
Signage‐ Spanish
ES LA LEY
Signage Spanish
SI TIENE UNA EMERGENCIA MEDICA O SE ENCUENTRAEN PARTO, USTED TIENE EL DERECHO DE RECIBIR, dentro de la capacidad del hospital y los empleados :
Una EXAMINACION completa por un medicoUna EXAMINACION completa por un medicoESTABILIZAR TRATAMIENTO necesario (incluyendo tratamiento para el
nino que no ha nacido)Si es necesario, UNA TRANSFERENCIA apropiada para otra facilidad
AUNQUEAUNQUENO PUEDA PAGAR o NO TENGA SEGURO MEDICO
ONO ESTA CUALIFICADO PARA MEDICARE o MEDICAID
Este hospital participa en el Programa de Medicaid
19
Registration/admission/insurance evaluation processes cannotcannot
– "unduly discourage individuals fromindividuals from remaining for further evaluation”
20
UNIFORMITY‐CONSISTENCYUNIFORMITY CONSISTENCY
• All patients get the exact same screening examAll patients get the exact same screening exam (process) based on chief complaint and their medical condition whether they are a privatemedical condition, whether they are a private patient, Medicaid patient, managed‐care patient indigent illegal alien or member ofpatient, indigent, illegal alien, or member of any other protected category
21

Investigation of a complaintInvestigation of a complaint
• Anybody can report‐ EMS, other hospitals, patients,Anybody can report EMS, other hospitals, patients, families, doctors
• State Dept. of Health does the investigation for CMS, p g ,who report to OIG, OIG determines penalty
• Unannounced visit
• Rigorous and thorough!
• Doesn’t just look at the particular alleged violationj p g
• Can last 3‐5 days, may occur on a weekend
• Staff interviews are likelyStaff interviews are likely
22
PenaltiesPenalties
• Plans of correction• Revisit by State to make sure your plan of correction is in
place• Civil monetary penalties of up to $50 000 for hospital and• Civil monetary penalties of up to $50,000 for hospital and
physician per occurrence; hospitals with fewer than 100 beds, $25,000 per occurrenceP bli ti• Public notice
• Normally not covered by liability insurance• The hospital may face removal of all Medicare participatione osp ta ay ace e o a o a ed ca e pa t c pat o• The physician could lose medical license• Civil suit violation of EMTALA
23

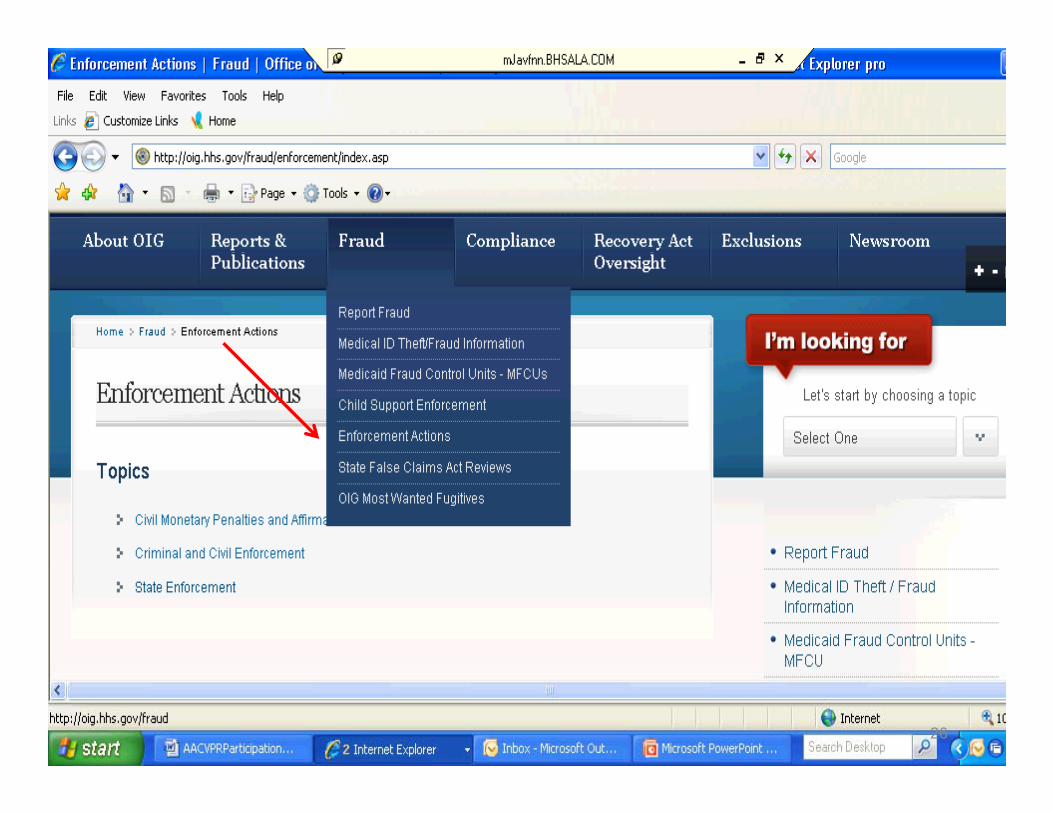
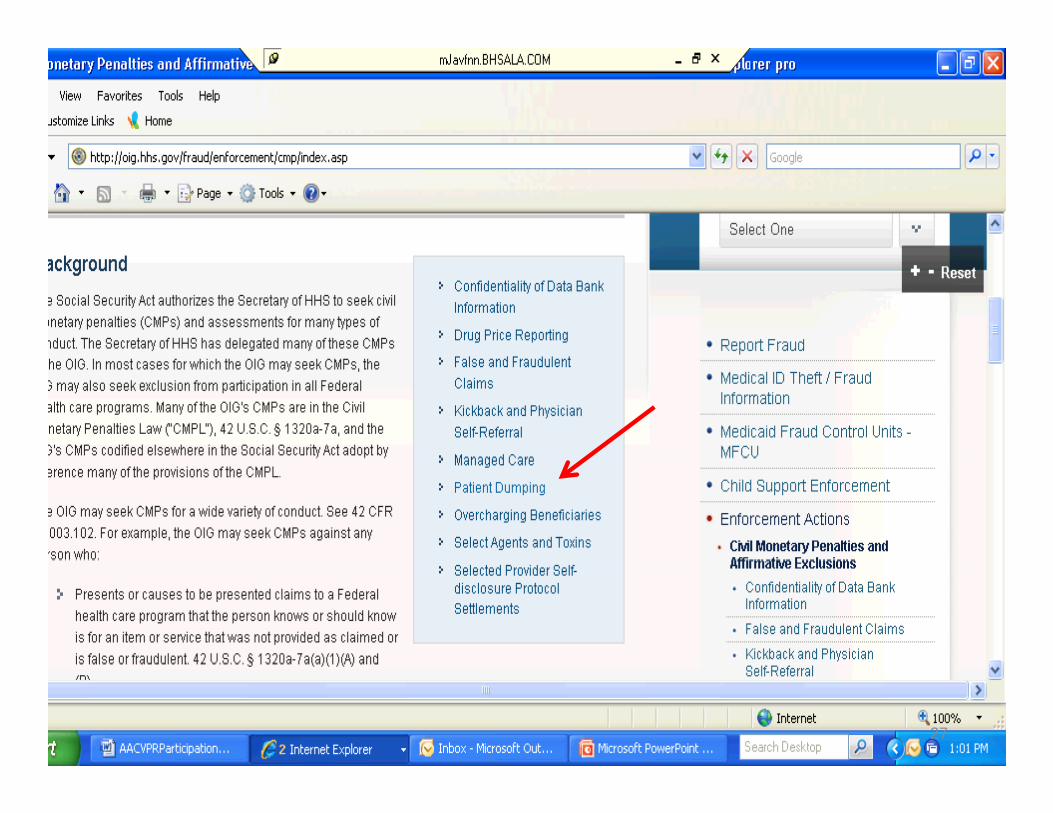
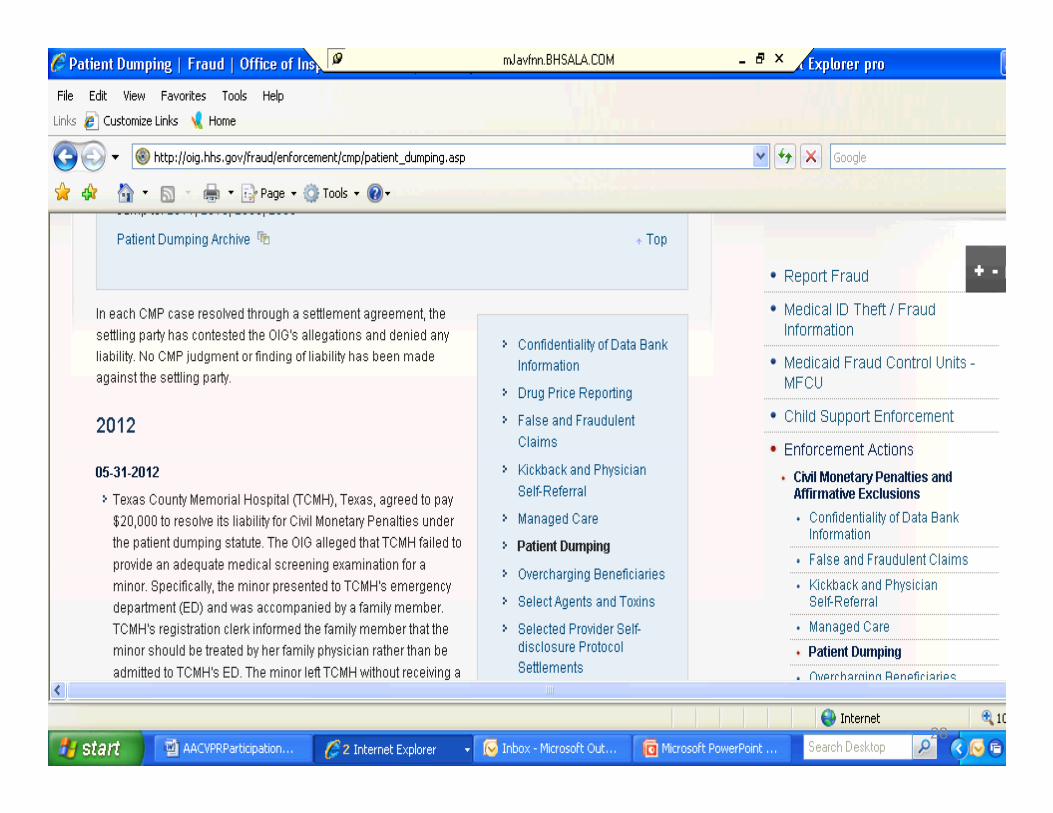
OIG Website
http://oig.hhs.gov
24
25
26
27
28
Questions?Questions?
29
ReferencesReferences
• Bitterman, RA. Providing Emergency Care Under , g g yFederal Law: EMTALA. Published by the American College of Emergency Physicians, January 2001.
• Medlaw com (Stephen Frew’s website)• Medlaw.com (Stephen Frew’s website)• CMS regulations §489‐24; and State Operations ManualManual
• OIG website• American Medical Association publication: pEMTALA Quick Reference Guide for On Call Physicians
30
Contact InformationContact Information
• Doran Stamps, Director, Risk Management and Compliance Princeton Baptist Medical CenterCompliance, Princeton Baptist Medical Center
• 205‐715‐3015
31

Save the Date: August 25‐28 2013August 25 28, 2013
32nd Annual Conference
Chi ILChicago, IL
32