Embed Size (px)
Citation preview

Research Article
Urinary Leukotriene E4 and 2,3-DinorThromboxane B2 Are Biomarkers of PotentialHarm in Short-Term Tobacco Switching StudiesPatrudu Makena1, Gang Liu1, Peter Chen1, Charles R. Yates2, and G.L. Prasad1
Abstract
Background: Modified risk tobacco products (MRTP) canreduce harm by decreasing exposure to combustion-relatedtoxicants. In the absence of epidemiologic data, biomarkers ofpotential harm (BoPH) are useful to evaluate the harm-reducing potential of MRTPs. This study evaluated whetherarachidonic acid (AA)-derivedmetabolites serve as short-termBoPH for predicting harm reduction in tobacco product–switching studies.
Methods:Weused 24-hour urine samples fromparticipantsin a series of short-term studies in which smokers switchedfrom combustible to noncombustible tobacco products [oralsmokeless tobacco products or electronic nicotine deliverysystem (ENDS)] or abstinence. Pre- and postswitching sam-ples were analyzed by LC/MS-MS for alterations in select AAmetabolites, including prostaglandins, isoprostanes, throm-boxanes, and leukotrienes.
Results: Switching to abstinence, dual use of combustibleand noncombustible products, or exclusive use of noncom-
bustible products resulted in reduced 2,3-d-TXB2 levels.Moreover, switching smokers to either abstinence or exclu-sive use of oral tobacco products resulted in reduced LTE4,but dual use of combustible and oral tobacco products orENDS did not. A two-biomarker classification model com-prising 2,3-d-TXB2 and LTE4 demonstrated the highestperformance in distinguishing smokers switched to eitherabstinence or to ENDS and oral smokeless tobacco pro-ducts.
Conclusions: Urinary 2,3-d-TXB2 and LTE4 can discrim-inate between combustible tobacco users and combustibletobacco users switched to either abstinence or noncombus-tible products for 5 days.
Impact: 2,3-d-TXB2 and LTE4, which are linked to plateletactivation and inflammation, represent BoPH in short-termtobacco product–switching studies. Thus, from a regulatoryperspective, 2,3-d-TXB2 and LTE4 may aid in assessing theharm reduction potential of MRTPs.
IntroductionCigarette smoking is an independent risk factor for lung cancer,
chronic obstructive pulmonary disease (COPD), and cardiovas-cular disease (1–4). Cigarette smoke is a dynamic aerosol contain-ing several thousand chemicals, including various toxicants,which are generated during the combustion process. Many of thetoxicants cause long-term adverse health outcomes includingcancer due to chronic smoking (5). Ninety-three of the toxicantshave been designated as harmful and potentially harmful con-stituents by the FDA (6). Smoking abstinence is the best option toreduce harm from cigarette smoking (7).
Epidemiologic outcomes require the availability of potentiallyreduced harm products in the marketplace and sustained exclu-sive use of these products over many years. Hence, interimmeasures, such as short-term biomarkers, are useful to evaluate
the effect of alternate, novel, potentially reduced harm tobaccoproducts on consumers. In the context of tobacco products, suchbiomarkers have been described as biomarkers of potential harm(BoPH; ref. 8). Several BoPH have been suggested and extensivelyinvestigated in smokers (9–11). These markers serve as earlyindicators of physiologic changes due to product use, whichcould potentially inform of perturbations in biological processesleading to smoking-related diseases.
Smoking-induced oxidative stress and inflammation areimportant drivers of underlying disease mechanisms. However,there are fewwell-established and validated functional BoPH thatserve as predictive biomarkers of smoking-related diseases. Forexample, forced expiratory volume 1 (FEV1) is the most widelyused BoPH of respiratory function and is used as a quantitativemeasure to characterize COPD. Two potential BoPH related tothese mechanisms that have consistently distinguished smokersfrom nonsmokers include F2 isoprostane iP2FaIII and whiteblood cell counts (12–14).
Combustion-related toxicants drive the adverse health effectsassociated with cigarette smoking (5, 8, 15). In addition tocigarettes, noncombustible tobacco products including smoke-less tobacco products (e.g., chewing tobacco, moist snuff, snus),electronic nicotine delivery systems (ENDS), and tobacco heatingproducts (THP), which do not generate combustion-related tox-icants, exist in the current marketplace (16, 17). Although, thereare differences in the product constituents and consumer popu-lation (18), existing U.S. and Swedish epidemiologic data dem-onstrate that both products may present less risk than cigarette
1RAI Services Company, Winston-Salem, North Carolina. 2Quinn Pharms, Inc.,Knoxville, Tennessee.
Note: Supplementary data for this article are available at Cancer Epidemiology,Biomarkers & Prevention Online (http://cebp.aacrjournals.org/).
Corresponding Author: Patrudu Makena, RAI Services Company, PO Box 1487,Winston-Salem, NC 27102. Phone: 901-438-1990; Fax: 336-728-4923; E-mail:[email protected]
Cancer Epidemiol Biomarkers Prev 2019;28:2095–105
doi: 10.1158/1055-9965.EPI-19-0342
�2019 American Association for Cancer Research.
CancerEpidemiology,Biomarkers& Prevention
www.aacrjournals.org 2095
on July 29, 2021. © 2019 American Association for Cancer Research. cebp.aacrjournals.org Downloaded from
Published OnlineFirst September 26, 2019; DOI: 10.1158/1055-9965.EPI-19-0342

smoking (19). For example, the risks of lung cancer are muchlower for U.S. (11.7-fold) and Swedish (12.8-fold) smokelesstobacco users as well as for switchers from cigarettes to smokelesstobacco than for cigarette smokers (19, 20). Therefore, smokelesstobacco products may serve as an alternative for those smokerswho cannot or are unwilling to quit tobacco product use (19, 21).However, there is limited information on the effects of the use ofother noncombustible tobacco products (i.e., ENDS and THPs),which produce an aerosol that is chemically far less complex thancigarette smoke.
To better understand the biological and pathophysiologiceffects of combustible and noncombustible tobacco products,several cross-sectional biomarker discovery studies, which includ-ed cigarette smokers (SMK), moist snuff consumers (MSC), andnontobacco consumers (NTC) have been conducted to identifyBoPH for product evaluation (22, 23). Furthermore, SMK exhibitenhanced arachidonic acid (AA)metabolism comparedwithMSCand NTC, as evidenced by increased AA production (22). In thisstudy, increased production of AA metabolites, isoprostanes andleukotriene E4 (LTE4), which are markers of oxidative stress andinflammation, were observed. Thus, cigarette smoking evokes aproinflammatory phenotype, highlighted by increased synthesisof AA and its metabolites that include prostaglandins, prostacy-clins, thromboxanes, leukotrienes, and hydroxyeicosatetraenoicacids (12, 13, 24).
The biological effects of smoking have been known to persistfor a long time after complete cessation, and the evaluation ofcertain effects of switching to modified risk tobacco products(MRTP) also could require several months. For example, 6 ormore months of smoking abstinence is necessary to detectchanges in WBC levels (25, 26). A significant change in FEV1 isdetectablemore than6–12months after smokingabstinence (27),suggesting that FEV1 is a long-term biomarker of lung function.Therefore, evaluation of the health effects of potential MRTPs inclinical trials becomes challenging, as confining study volunteersfor extended periods to ensure study compliance in residentialsettings is not practical. Hence, we sought to identify BoPH thatrapidly change after a few days of smoking abstinence and/orswitching to alternate tobacco products. On the basis of previousstudies, which reported that select AAmetabolites rapidly changeupon smoking abstinence (28), and their established role asmarkers of oxidative stress and inflammation, we set out todetermine whether the AA metabolites would serve as short-term reversible BoPH.
In this study, we assessed the levels of a panel of urinaryAA-derived metabolites, including prostaglandins, isoprostanes,thromboxanes, and leukotrienes, as BoPH in smokers who eitherabstained from smoking or switched to an alternate tobaccoproduct for five days in a residential setting. Urine samples wereobtained from three separate short-term product switching stud-ies in which SMK were switched from their usual brand (UB)combustible cigarette to noncombustible products (i.e., oralsmokeless tobacco products or ENDS products) or abstinence.
Materials and MethodsEthical conduct of clinical studies
Clinical studies were performed in accordance with the USCode of Federal Regulations (CFR) governing Protection ofHuman Subjects (21 CFR Part 50), Financial Disclosure byClinical Investigators (21 CFR Part 54), and Institutional Review
Board (IRB; 21 CFR Part 56). In addition to these federal regula-tions, these studies followed the 1996 guidelines of the Interna-tional Conference on Harmonization, commonly known asGood Clinical Practice (GCP), which are consistent with theDeclaration of Helsinki as adopted in 2008.
Study designA brief description of three sponsored clinical studies [from RJ
Reynolds Tobacco Company (RJRT) and RJR Vapor (RJRV)company] in which smokers who completely switched to eitherabstinence or to test products in a confinement setting for a periodof 5 days is provided (Supplementary Fig. S1). The demographicsof enrolled subjects in the three studies are summarized inTable 1.The three studies included generally healthy adult male andfemale smokers whowere primarily Caucasian and African Amer-ican. The mean subject age ranged from 38 to 43 years. Therepresentation of Hispanics was very limited in the study groups.
Study I [Cigarette Per Day Reduction (CPDR) study] was asingle-center, randomized, controlled, open-label, parallel groupstudy, designed to evaluate the dose–effect relationships betweencigarette per day reduction and biomarkers of exposure (BoE;ref. 29). For the current analysis, 24-hour urine samples fromsmokers switched from 20 cigarettes per day (CPD) to abstinence(0 CPD cohort) were used to evaluate AA metabolites.
Study II [Modern Smokeless Tobacco Product (STP) study]was a multicenter, open-label, randomized, forced-switching,parallel cohort study designed to evaluate changes in tobaccoproduct use behavior and levels of selected BoE (30). Smokerswere randomized into one of six different test product groups:Group 1: dual use of UB cigarettes and Camel Snus; Group 2:exclusive Camel Snus use; Group 3: exclusive Camel Sticks use;Group 4: exclusive Camel Strips use; Group 5: exclusive CamelOrbs use; and Group 6: tobacco product abstinence. In thistrial, two Snus variants were available for participant selection:frost (mint) or Mellow (non-mint). The Sticks, Strips, and Orbstested were generally similar in composition, consisting offinely milled tobacco and other food-grade ingredients, andcontained a total alkaloid content of approximately 3.2, 1.0,and 1.1 mg, respectively. These products are used orally andallowed to dissolve in the mouth.
Study III (ENDS exposure study) was a single-center, random-ized, controlled, switching, open-label, parallel cohort study (31).Smokers were enrolled and randomized to one of two cohortsswitching to either Vuse (VS) Original or Menthol variant, for 5days after baseline ad libitum smoking of their UB cigarettes.Smoking status at enrollment was defined as self-reported smok-ing of at least 10CPD for at least 6months with an expired carbonmonoxide (ECO) level of >15 ppm.
The VS products are composed of a battery, heating element,microchip, sensor, and a cartridge containing propylene glycol,glycerin, nicotine, flavorings, and water. Drawing on the mouth-piece causes the heating element to aerosolize the liquid in thecartridge and delivers a puff of aerosol to the user.
Urine biomarker measurementTwenty-four–hour urine samples were collected beginning on
study days �3 and 4 (29–31). LC/MS-MS was used to measureurinary AA metabolites including PGF2a, 8-i-PGF2a, 2,3-d-8-i-PGF2a, t-PGDM, t-PGEM, 2,3-d-TXB2, 11-d-TXB2, LTE4, and 12(S)-HETE at Analytisch-Biologisches Forschungslabor GmbH(ABF GmbH; ref. 32).
Makena et al.
Cancer Epidemiol Biomarkers Prev; 28(12) December 2019 Cancer Epidemiology, Biomarkers & Prevention2096
on July 29, 2021. © 2019 American Association for Cancer Research. cebp.aacrjournals.org Downloaded from
Published OnlineFirst September 26, 2019; DOI: 10.1158/1055-9965.EPI-19-0342

Classification modelsA biomarker-based gradient boosting model was constructed
to classify smoker status (i.e., pre- and postswitching). Themodelperformance, defined as the classifier's ability to identify thetobacco use groups correctly, was computed as the AUC fromthe receiver operator characteristic (ROC) curve. The ROC curvewas plotted as a true positive rate (sensitivity) as a functionof falsepositive rate (1�specificity). To build biomarker-based classifiersfor evaluation of VS products, the datasets from Study III (i.e., VSOriginal and VS Menthol; 75 subjects and 2 time points) wereused to build, train, and cross-validate the model. During modelfitting, the datasets were randomly split into five folds, four ofwhichwere used to train themodel and one ofwhichwas used forcross-validation. This process (five-fold cross-validation) wasrepeated 10 times and the average of the model performancemetrics were computed.
After model cross-validation, the datasets from Study I (0CPD cohort) and Study II (Group 6: abstinence cohort) wereused as inputs to test the model's accuracy in distinguishingbetween smokers pre- and postabstinence. The performance ofthe classification model in the smokeless tobacco product–switching studies was evaluated using the datasets from Groups2–5 (snus, Sticks, Strips, and Orbs, respectively) in Study II. The"caret" package written in R (http://topepo.github.io/caret/index.html) was used for model training, cross-validation, andprediction.
Statistical analysesThe BoPH levels are presented as total mass (ng/24 hours).
Mean and SD of the biomarkers were calculated for baseline andpostswitching in each tobacco use group. To compare the differ-ences between baseline and postswitching in each group, a pairedt test was conducted to determine statistical significance(P < 0.05). JMP 10 (SAS Institute) was used for data analysis.
ResultsSmoking abstinence alters urinary levels of AA-derivedmetabolites
Clinical trials that evaluated the impact of reduced CPD oncigarette smoke toxicant exposure havepreviously reported reduc-
tions in tobacco-related BoE (33, 34). Usingwell-established BoE,Theophilus and colleagues expanded the tobacco exposure–response relationship by evaluatingmultiple CPDR levels, includ-ing abstinence, in a short-term (5-day) switching study (29). Inour effort to identify short-term BoPH, we determined the levelsof a panel of AA metabolites in the urine sample collected in theCPDR study.
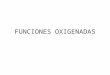
When compared with baseline, urinary LTE4 levels 5 daysafter smoking abstinence were reduced approximately 40%(154 � 128 vs. 93.1 � 49.0 ng/24 hours, P ¼ 0.004; Fig. 1).Conversely, following 5 days of abstinence in Study 1, urinarylevels of PGF2a (2,262 � 975.4 vs. 2,780 � 1186 ng/24 hours,P ¼ 0.004), 2,3-d-8-i-PGF2a (4,084 � 2,394 vs. 4,709 �1,380 ng/24 hours, P ¼ 0.02), t-PGEM (15,282 � 10,927 vs.16,043 � 7,415.0 ng/24 hours, P ¼ 0.023), and t-PGDM(3,100 � 1,274 vs. 4,565 � 1,646 ng/24 hours, P ¼ 0.0001)increased (Fig. 1). Urinary levels of 11-dehydro-TXB2, 8-i-PGF2a, and 2,3-d-TXB2 were unaltered five days after smokingabstinence.
Leukotriene and thromboxane metabolite levels were reducedafter switching from combustible cigarettes to noncombustibleoral products
To determine whether AA metabolism is altered followingshort-term switching, we measured AA-derived metabolitesin SMK switching from UB cigarettes to abstinence, tomodern smokeless tobacco products (snus, Sticks, Strips,or Orbs), or to dual use (UB cigarettes and snus) for fivedays.
Urinary LTE4 levels were reduced approximately 26%–43% inall cohorts who switched from combustible cigarettes to snus(122� 61.2 vs. 68.9� 27.9 ng/24 hours, P< 0.001), Sticks (129�101 vs. 95.1 � 72.4 ng/24 hours, P ¼ < 0.001), Strips (105 �37.4 vs. 68.7� 34.0 ng/24 hours, P < 0.001), Orbs (125� 61.4 vs.77.0� 28.7 ng/24 hours, P<0.001), or abstinence (155�96.3 vs.94.0�57.5 ng/24hours,P<0.001; Fig. 2).However, urinary LTE4levels remained unchanged in subjects switched to dual use ofcigarettes and snus (134 � 78.5 vs. 127 � 106 ng/24 hours,P > 0.05). Urinary levels of PGF-2a, 8-iPGF-2a, 2,3-d-8-iPGF-2a,t-PGEM, and t-PGDMwere unchanged by any switching or forcedabstinence.
Table 1. Summary of demographic information
Study I(CPDR) Study II (STP) Study III (ENDS)
Subjectdemographics
Smokingcessation,n ¼ 30
Tobaccoabstinence,n ¼ 24
Orbs,n ¼ 28
Snus,n ¼ 27
Sticks,n ¼ 28
Strips,n ¼ 24
Dual usage ofUB cigarettesand Snus,n ¼ 25
Vuse SoloOriginal,n ¼ 37
Vuse SoloMenthol,n ¼ 38
Age, y 42.8 � 9.17 42.83 � 11.16 39.14 � 12.90 38.03 � 11.42 41.07 � 12.29 40.16 � 11.76 42 � 12.49 41.43 � 11.31 42.71 � 11.06Gender, n (%)Male 17 (57) 14 (58) 12 (43) 16 (59) 16 (57) 14 (58) 11 (44) 11 (30) 14 (37)Female 13 (43) 10 (42) 16 (57) 11 (41) 12 (43) 10 (42) 14 (56) 26 (70) 24 (63)
Ethnicity, n (%)Hispanic or Latino 5 (17) 0 (0) 0 0 1 (4) 3 (12) 3 (12) 1 (2.6) 0Non-Hispanic orLatino
25 (83) 24 (100) 28 (100) 27 (100) 27 (96) 25 (88) 22 (88) 37 (97.4) 40 (100)
Race, n (%)Black 7 (23) 3 (13) 6 (21) 5 (19) 6 (21) 1 (4) 2 (8) 14 (38) 24 (63)White 23 (77) 20 (83) 18 (64) 22 (81) 20 (71) 21 (88) 23 (92) 20 (54) 10 (26)Other 0 1 (4) 4 (15) 0 2 (8) 2 (8) 0 3 (8) 4 (11)BMI, kg/m2 27.96 � 5.27 26.30 � 6.46 26.67 � 5.87 27.70 � 5.98 27.07 � 4.78 25.24 � 5.34 29.16 � 7.23 27.99 � 7.25 29.31 � 5.39
Abbreviation: BMI, body mass index.
LTE4 and 2,3-d-TXB2 as Biomarkers of Potential Harm
www.aacrjournals.org Cancer Epidemiol Biomarkers Prev; 28(12) December 2019 2097
on July 29, 2021. © 2019 American Association for Cancer Research. cebp.aacrjournals.org Downloaded from
Published OnlineFirst September 26, 2019; DOI: 10.1158/1055-9965.EPI-19-0342

Urinary levels of 2,3-d-TXB2were reduced approximately 24%–
48% across all cohorts randomized to short-term switching,including dual use (2,290� 1,606 vs. 1,500� 1,119 ng/24 hours,P ¼ 0.003), Orbs (1,451 � 899.7 vs. 832.6 � 439.7 ng/24 hours,P < 0.001), snus (2,120 � 2,039 vs. 1,286 � 1,125 ng/24 hours,P¼ 0.014), Sticks (1,691� 1,000 vs. 1,279� 840.9 ng/24 hours,P¼ 0.037), Strips (1,663� 913.8 vs. 923.0� 607.2 ng/24 hours,P < 0.001), and abstinence (1,834 � 921.5 vs. 947.9 � 577.2ng/24 hours, P < 0.001; Fig. 3). Urinary 11-dh-TXB2 levels werereduced in smokers who switched to snus (787 � 276 vs. 638 �207 ng/24 hours, P¼ 0.009). However, urinary 11-dh-TXB2 levelswere unaltered when subjects switched to Orbs, Sticks, Strips, orabstinence.
Leukotriene and thromboxane metabolite levels were reducedafter switching from combustible cigarettes to noncombustibleVS products
Studies have demonstrated BoE reductions in smokersswitched to ENDS (35, 36); however, to date, none of these
studies evaluated the impact of switching on candidate BoPH.Thus, we sought to identify potential urinary BoPH in smokersswitched to either VS Original or VS Menthol. Five days afterswitching to VS Menthol, urinary levels of PGF-2a (2,696 �1,293 vs. 3,185 � 1,502 ng/24 hours, P ¼ 0.0009), 8-iPGF-2a(669� 276 vs. 744� 268 ng/24 hours, P¼ 0.0205), and t-PGDM(4,243 � 2,034 vs. 4,966 � 1,956 ng/24 hours, P ¼ 0.01413)increased. 2,3-d-TXB2 urinary levels decreased in smokersswitched to either VS Menthol (3,604 � 1,917 vs. 2,011 �1,762 ng/24 hours, P < 0.001) or VS Original (2,561 � 1,618 vs.1,439 � 1,001 ng/24 hours, P < 0.001; Fig. 4). None of theremaining urinary AAmetabolites were altered upon switching toeither VS Original or VS Menthol.
Classification modelTo assess the clinical validity of the biomarkers, a two-bio-
marker-based classification model was constructed, and its per-formance quantified using the AUC from ROC (Fig. 5). In thismodel, only LTE4 and 2,3-d-TXB2 were included, because their
Figure 1.
Differentiating urinary AAmetabolites in smokers switched to abstinence. Twenty-four–hour urine samples obtained at baseline and five days postswitchingfrom smokers switched from 20 cigarettes per day to abstinence (0 cigarettes per day) were used to measure AAmetabolites by LC/MS-MS. PGF2a, 2,3-d-8-i-PGF2a, t-PGEM, and t-PGDM increased following 5 days of abstinence, while LTE4 decreased. Themetabolite measurements were presented in box plots. In eachbox plot, the top, middle, and bottom edges represent 25%, 50%, and 75% quantiles, respectively, and individual data points represent subject-levelmeasurements. � , P < 0.05, �� , P < 0.01, ���� , P < 0.0001 when comparing pre- and postswitching metabolite levels.
Makena et al.
Cancer Epidemiol Biomarkers Prev; 28(12) December 2019 Cancer Epidemiology, Biomarkers & Prevention2098
on July 29, 2021. © 2019 American Association for Cancer Research. cebp.aacrjournals.org Downloaded from
Published OnlineFirst September 26, 2019; DOI: 10.1158/1055-9965.EPI-19-0342

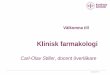
urinary levels were significantly decreased across all the variousshort-term product-switching study cohorts for at least one of themetabolites. The highest AUC was for VS Original (0.88), fol-lowed by VS Menthol (0.82) and smoking abstinence (0.72).
Furthermore, application of our model using the smokelesstobacco–switching cohorts as input data revealed AUCs of 0.76(Orbs); 0.61 (Sticks); and 0.72 (snus and Strips; SupplementaryFig. S2).
Figure 2.
Urinary LTE4 levels in smokers switched to smokeless tobacco products. Twenty-four–hour urine samples obtained at baseline and five days postswitching fromsmokers switched from usual brand (UB) cigarettes to smokeless tobacco products were used to measure AAmetabolites by LC/MS-MS. Urinary LTE4 levelswere reduced in all cohorts in which combustible tobacco products were prohibited (Orbs, snus, Sticks, Strips, and abstinence). Urinary LTE4 levels remainedunchanged in subjects switching to dual use. The metabolite measurements were presented in box plots. In each box plot, the top, middle, and bottom edgesrepresent 25%, 50%, and 75% quantiles, respectively, and individual data points represent subject-level measurements. ��� , P < 0.001, ���� , P < 0.0001 whencomparing pre- and postswitching metabolite levels. ns, not significant.
LTE4 and 2,3-d-TXB2 as Biomarkers of Potential Harm
www.aacrjournals.org Cancer Epidemiol Biomarkers Prev; 28(12) December 2019 2099
on July 29, 2021. © 2019 American Association for Cancer Research. cebp.aacrjournals.org Downloaded from
Published OnlineFirst September 26, 2019; DOI: 10.1158/1055-9965.EPI-19-0342

Figure 3.
Urinary 2,3-d-TXB2 levels in smokers switched to smokeless tobacco products. Twenty-four–hour urine samples obtained at baseline and five days postswitchingfrom smokers switched from usual brand (UB) cigarettes to smokeless tobacco products were used to measure AAmetabolites by LC/MS-MS. Urinary 2,3-d-TXB2 levels were reduced in all cohorts in which combustible tobacco products were prohibited (Orbs, snus, Sticks, Strips, and abstinence) and in smokersswitched to dual use. The metabolite measurements were presented in box plots. In each box plot, the top, middle, and bottom edges represent 25%, 50%, and75% quantiles, respectively, and individual data points represent subject-level measurements. � , P < 0.05, �� , P < 0.01, ���, P < 0.001, ���� , P < 0.0001 whencomparing pre- and postswitching metabolite levels.
Makena et al.
Cancer Epidemiol Biomarkers Prev; 28(12) December 2019 Cancer Epidemiology, Biomarkers & Prevention2100
on July 29, 2021. © 2019 American Association for Cancer Research. cebp.aacrjournals.org Downloaded from
Published OnlineFirst September 26, 2019; DOI: 10.1158/1055-9965.EPI-19-0342

Figure 4.
Urinary AA metabolites in smokers switched to VS. Twenty-four–hour urine samples obtained at baseline and five days postswitching from smokersswitched from usual brand (UB) cigarettes to VS products were used to measure AA metabolites by LC/MS-MS. Five days after switching, urinarylevels of PGF-2a, 8-iPGF-2a, and t-PGDM were increased in smokers switched to VS Menthol, while 2,3-d-TXB2 urinary levels were decreased insmokers switched to either VS Menthol or VS Original. The metabolite measurements were presented in box plots. In each box plot, the top, middle,and bottom edges represent 25%, 50%, and 75% quantiles, respectively, and individual data points represent subject-level measurements. � , P < 0.05,�� , LTE4 is statistically significant (P < 0.001) upon log transformation of the data in both cohorts (VS Menthol or VS Original), ��� , P < 0.001,���� , P < 0.0001 when comparing pre- and postswitching metabolite levels. ns, not significant.
LTE4 and 2,3-d-TXB2 as Biomarkers of Potential Harm
www.aacrjournals.org Cancer Epidemiol Biomarkers Prev; 28(12) December 2019 2101
on July 29, 2021. © 2019 American Association for Cancer Research. cebp.aacrjournals.org Downloaded from
Published OnlineFirst September 26, 2019; DOI: 10.1158/1055-9965.EPI-19-0342

DiscussionChronic smoking is associated with elevated oxidative stress
and inflammation, which are key drivers of smoking-inducedpathophysiology (13). While several potential BoPH for smok-ing-related diseases have been identified (11), it usually requiresseveral months of smoking abstinence to detect meaningfulchanges in their levels. Our goal was to identify and qualify BoPHfollowing short-term smoking abstinence or switching to poten-tial MRTPs. In this article, we investigated whether the AA meta-bolites are responsive to short-term smoking abstention andwhether they can be used as potential BoPH for potential eval-uation of tobacco products.
The current work evaluated a panel of known biomarkers ofoxidative stress, inflammation, andplatelet activation in the urinesamples collected from three RJRT and RJRV sponsored studies.Keyfindings from this study are: (i) switching to either abstinence,dual use of combustible and noncombustible products, orexclusive use of noncombustible products resulted in reduced2,3-d-TXB2; and (ii) switching smokers to either abstinence ornoninhaled oral tobacco products culminated in reduced LTE4.Together, these data show 2,3-d-TXB2 and LTE4, as potentialBoPH. Furthermore, we constructed a classification model basedon these BoPH to evaluate their combined performance in dis-tinguishing smokers pre- and postswitching.
The two-biomarker-based model demonstrated the highestperformance in distinguishing smokers pre- and postswitchingto noncombustible inhaled products (i.e., VS Original and VS
Menthol). Moreover, the model performed well (AUC > 0.70) indifferentiating smokers switched to either abstinence or smoke-less oral tobacco products. Together, these data suggest that aclassificationmodel comprising bothLTE4 and2,3-d-TXB2has thepotential to categorize smokers subjected to short-term productswitching.
Smoking abstinence is the accepted "gold standard" strategy forreducing harm from cigarette smoking. Consequently, the bio-logical effects of switching to a MRTP must be considered in thecontext of both smoking and abstinence. In Study I, which wasdesigned to evaluate the dose–effect relationships between CPDRand BoE, we found that abstinence resulted in a significantdecrease in urinary LTE4 levels. Leukotrienes (LT) are lipid sig-naling mediators produced by mast cells, eosinophils, neutro-phils, basophils, and macrophages. LT synthesis is initiated byphospholipase A–mediated cleavage of AA, which then under-goes rapid conversion to LTA4 via 5-lipoxygenase (5-LO) and5-lipoxygenase-activating protein (FLAP; refs. 37, 38). LTA4 issubsequently converted to LTC4, LTD4, and LTE4, collectivelyknown as cysteinyl leukotrienes (CysLT), and LTB4 (Supplemen-tary Fig. S6). Urinary LTE4, the most stable CysLT, is frequentlyused as a marker of leukotriene synthesis (39, 40).
Urinary LTE4 levels are closely correlated with number ofcigarettes smoked (41, 42) and cotinine levels (43). In addition,adult smokers had up to 5-fold higher levels of urinary LTE4compared with nonsmokers (44). Thus, our data demonstratingincreased LTE4 levels in smokers is consistent with studies exam-ining the link between cigarette smoking and increased LTE4
Figure 5.
AAmetabolite–based classification modelpredicts short-term product switching.The tree-based binary classification modelbuilt on LTE4 and 2,3-d-TXB2 data wasevaluated using validation datasets fromVS Original (VUSE O), VS Menthol (VUSEM), and smoking abstinence cohorts. Theircorresponding ROC curves are shown inblue (VS Original), red (VS Menthol), andbrown (Smoking Abstinence from Study Iand II), respectively.
Makena et al.
Cancer Epidemiol Biomarkers Prev; 28(12) December 2019 Cancer Epidemiology, Biomarkers & Prevention2102
on July 29, 2021. © 2019 American Association for Cancer Research. cebp.aacrjournals.org Downloaded from
Published OnlineFirst September 26, 2019; DOI: 10.1158/1055-9965.EPI-19-0342

levels. Following forced abstinence or switching to smokelesstobacco products, urinary LTE4 levels declined rapidly and to asimilar degree to the decrease seen in smokers reducing thenumber of cigarettes smoked per day. Our findings align withstudies which demonstrate that urinary LTE4 levels return tobaseline within two weeks of tobacco product abstention (42).There was a similar trend toward reduction of urinary LTE4 levelsin smokers switched to either VS Original or VS Menthol; how-ever, the reductions were not statistically significant.
Thromboxane A2 (TXA2), the major product of prostaglandinendoperoxides in platelets, induces irreversible platelet aggrega-tion (45). TXA2 is rapidly converted to TXB2 followed by catab-olism to 2,3-d-TXB2 (46). 2,3-d-TXB2 is the most abundantmetabolite recovered in the urine following intravenous infusionof TXB2 to humans (47). Thromboxane urinary metabolites arefrequently used as a marker for platelet activation insmokers (13, 48–50). For example, 2,3-d-TXB2 is significantlyelevated in healthy chronic smokers when compared withnonsmokers (50). Consistent with the literature, we observedthat 2,3-d-TXB2 urinary levels were reduced following smokingabstinence. Similar results were obtained in smokers switched todual use, and in smokers switched to exclusive use of noncombus-tible products (i.e., oral tobacco products and VS products).Together, thesedata suggest diminishedTXA2 synthesis andplateletactivation when smokers switch to noncombustible products.
The lung is a major site of LT synthesis (51) and elevated LTlevels in the lung are a hallmark of airway hypersensitivity-relateddiseases such as asthma and allergic rhinitis. A decrease in LTE4levels in smokers who stop smoking or switch to smokelesstobacco products such as snus indicates a decrease in airwayhypersensitivity. In smokers who switched to VS Original or VSMenthol, LTE4 levels were lower (17% and 20%, respectively),although not statistically significant. However, a boosted tree–based classification model based on LTE4 and 2,3-d-TXB2 datafrom all three clinical studies revealed that these two BoPH clearlydifferentiate smokers who switched to noncombustible productsin several days from their baseline levels (Fig. 5). Thus, the levelsof LTE4 and 2,3-d-TXB2 decline in smokers who switch to non-combustible tobacco products, suggesting improved airwayresponsiveness and platelet function.
Few clinical studies have compared thromboxane synthesis incombustible versus noncombustible tobacco product users. Forexample, smokeless tobacco users, despite having urinary cotin-ine levels similar to that of smokers, have urinary levels of 2,3-d-TXB2 (52) and TXB2 (53) similar to those of nontobacco users.Our study examined the effect of short-term switching on AAmetabolites associated with platelet activation across a spectrumof noncombustible tobacco products includingOrbs, snus, Sticks,Strips, and VS Original and VS Menthol. Consistently, use ofnoncombustible tobacco, including vapor products, was associ-ated with reduced platelet activation, as indicated by reducedurinary excretion of 2,3-d-TXB2. Platelet activation was alsodiminished in smokers switching to either dual use or stricttobacco abstinence. It is unclear why urinary 2,3-d-TXB2 levelswere reduced in the abstinence cohort (Study II) and not insmokers abstaining from tobacco use in the CPDR study (StudyI). One possible explanation is that smokers in the CPDR studyhad 2,3-d-TXB2 levels approximately 50% lower than smokers inthe abstinence cohort (Study II).
Platelet activation represents a well-established physiologicresponse elicited by exposure to combustible tobacco toxicants
and is known to contribute to the etiology and progression ofcardiovascular disease (54, 55). Cigarette smoke toxicants inducean inflammatory airway phenotype in which activated plateletsserve as a major cellular source of TXA2 (50). For example,acrolein, a toxicant found in cigarette smoke, potentiates plateletaggregation and TXA2 synthesis in response to thrombin byincreasing the availability of AA, a substrate for TXA2 forma-tion (56). TXA2, in turn, acts on TXA2 receptors to induce thesecond-phase response to cigarette smoke (57). Our finding thatshort-term product-switching yields reduced 2,3-d-TXB2, themost abundant urinary metabolite derived from TXA2, suggeststhat 2,3-d-TXB2 may serve as a BoPH of platelet activation.
Some limitations of this BoPH study include: (i) the relativelysmall sample sizes in all the three studies; (ii) the lack of aproportional representation of Hispanics in the studies; (iii) theneed for refinement of the classification model; and (iv) the needfor consideration of the influence of diet on AA metabolism.Enrollment of the subjects was open to all those who met theinclusion/exclusion criteria and inadequate representation ofHispanics could be due to the location of where the studies wereconducted. Although the sample sizes for each of the three clinicalstudies were relatively small, the two BoPH show consistentchanges in the direction and the magnitude. The two-biomark-er–based classificationmodel described above was built based onlimited size of biomarker data and further refinement usingindependent larger sample size of clinical datasets may be nec-essary. Because diet and genetic variation are potential determi-nants of AA metabolite levels, these factors also might requirefurther consideration (58).
In conclusion, enhanced thromboxane and leukotriene bio-synthesis are linked to platelet activation, chemotaxis, and airwayhypersensitivity, which are early pathophysiologic events in car-diovascular and pulmonary disease (Supplementary Fig. S6). 2,3-d-TXB2 and LTE4, relatively stable metabolites of TXA2 and LTA4,respectively, are used as proxies for thromboxane and leukotrienesynthesis. In this study, we demonstrated that urinary 2,3-d-TXB2and LTE4 levels are lower following reduced toxicant exposureresulting from product switching. 2,3-d-TXB2 and LTE4 can dis-criminate between smokers and smokers switched to either absti-nence or noncombustible products over a period of approximate-ly 1 week. Moreover, these two metabolites reflect altered AAmetabolism, which is linked to enhanced platelet activation,leukocyte recruitment, and inflammation. Because 2,3-d-TXB2and LTE4 possess these key attributes, they represent potentialBoPH designed to gauge the reversibility of toxicant exposureresponse in short-term tobacco product–switching studies.
Disclosure of Potential Conflicts of InterestP. Makena is a master scientist for and reports receiving a commercial
research grant from RAI Services Company. G. Liu is a senior scientist for andreports receiving a commercial research grant from RAI Services Company. P.Chen is a master scientist for and reports receiving a commercial research grantfrom RAI Services Company. C.R. Yates is a consultant for RAI ServicesCompany. G.L. Prasad is a director for and reports receiving a commercialresearch grant from RAI Services Company. No potential conflicts of interestwere disclosed by the other authors.
Authors' ContributionsConception and design: P. Makena, G.L. PrasadDevelopment of methodology: P. MakenaAcquisition of data (provided animals, acquired and managed patients,provided facilities, etc.): P. Makena, G.L. Prasad
LTE4 and 2,3-d-TXB2 as Biomarkers of Potential Harm
www.aacrjournals.org Cancer Epidemiol Biomarkers Prev; 28(12) December 2019 2103
on July 29, 2021. © 2019 American Association for Cancer Research. cebp.aacrjournals.org Downloaded from
Published OnlineFirst September 26, 2019; DOI: 10.1158/1055-9965.EPI-19-0342

Analysis and interpretation of data (e.g., statistical analysis, biostatistics,computational analysis): P. Makena, G. Liu, P. Chen, G.L. PrasadWriting, review, and/or revisionof themanuscript:P.Makena,G. Liu, P. Chen,C.R. Yates, G.L. PrasadAdministrative, technical, or material support (i.e., reporting or organizingdata, constructing databases): P. Makena, G.L. PrasadStudy supervision: P. Makena, G.L. PrasadOther (editorial communications): P. Makena
AcknowledgmentsThe studies and the manuscript preparation were funded by RAI Services
Company. RAI Services Company is a wholly owned subsidiary of ReynoldsAmerican Inc., which is a wholly owned subsidiary of British American Tobacco
plc. The authors sincerely thank Herman Krebs (RAI Services Company) forsample management and ABF GmbH for bioanalysis of this biomarker discov-ery study. In addition, the authors would like to thank Nasrin Nouri, whowas an intern of RAI Services Company, andQuynh Tran, a former employee ofRAI Services Company.
The costs of publicationof this articlewere defrayed inpart by the payment ofpage charges. This article must therefore be hereby marked advertisement inaccordance with 18 U.S.C. Section 1734 solely to indicate this fact.
Received March 28, 2019; revised August 22, 2019; accepted September 19,2019; published first September 26, 2019.
References1. Gordon T, KannelWB.Multiple risk functions for predicting coronary heart
disease: the concept, accuracy, and application. Am Heart J 1982;103:1031–9.
2. Mattson ME, Pollack ES, Cullen JW. What are the odds that smoking willkill you? Am J Public Health 1987;77:425–31.
3. Park KY, Chung CS, Lee KH, Kim GM, Kim YB, Oh K. Prevalence and riskfactors of intracranial atherosclerosis in an asymptomatic korean popula-tion. J Clin Neurol 2006;2:29–33.
4. National Center for Chronic Disease Prevention and Health Promotion(US) Office on Smoking and Health. The health consequences ofsmoking—50 years of progress: a report of the Surgeon General. Atlanta(GA): Centers for Disease Control and Prevention (US); 2014.
5. IARCWorkingGroup on the Evaluation of Carcinogenic Risks toHumans.Tobacco smoking. IARC Monogr Eval Carcinog Risks Hum 2012:83;43–211.
6. U.S. Food and Drug Administration. Food and Drug AdministrationCenter for Tobacco Products. Harmful and potentially harmful constitu-ents in tobacco products and tobacco smoke: established list; 2012. Avail-able from: https://www.fda.gov/tobacco-products/rules-regulations-and-guidance/harmful-and-potentially-harmful-constituents-tobacco-products-and-tobacco-smoke-established-list.
7. U.S. Department of Health and Human Services. The health benefits ofsmoking cessation.U.S.Department ofHealth andHuman Services, PublicHealth Service, Centers for Disease Control and Prevention, Center forChronic Disease Prevention and Health Promotion, Office on Smokingand Health. DHHS Publication No. (CDC) 90–8416; 1990. Availablefrom: https://www.cdc.gov/mmwr/preview/mmwrhtml/00001801.htm.
8. Stratton K, Shetty P, Wallace R, Bondurant S. Clearing the smoke: thescience base for tobacco harm reduction—executive summary.Tob Control 2001;10:189.
9. Hatsukami DK, Joseph AM, LesageM, Jensen J, Murphy SE, Pentel PR, et al.Developing the science base for reducing tobacco harm. Nicotine Tob Res2007;9 Suppl 4:S537–53.
10. Chang CM, Cheng YC, Cho TM, Mishina EV, Del Valle-Pinero AY, vanBemmel DM, et al. Biomarkers of potential harm: summary of an FDA-sponsored public workshop. Nicotine Tob Res 2017;21:1–11.
11. HatsukamiDK, BenowitzNL, Rennard SI, Oncken C,Hecht SS. Biomarkersto assess the utility of potential reduced exposure tobacco products.Nicotine Tob Res 2006;8:600–22.
12. Higuchi T, Omata F, Tsuchihashi K, Higashioka K, Koyamada R, Okada S.Current cigarette smoking is a reversible cause of elevated white blood cellcount: cross-sectional and longitudinal studies. Prev Med Rep 2016;4:417–22.
13. Calapai G, Caputi AP, Mannucci C, Russo GA, Gregg E, Puntoni R, et al.Cardiovascular biomarkers in groups of established smokers after a decadeof smoking. Basic Clin Pharmacol Toxicol 2009;104:322–8.
14. Roest M, Voorbij HA, Van der Schouw YT, Peeters PH, Teerlink T,Scheffer PG. High levels of urinary F2-isoprostanes predict cardiovas-cular mortality in postmenopausal women. J Clin Lipidol 2008;2:298–303.
15. U.S. Department of Health and Human Services. How tobacco smokecauses disease: the biology and behavioral basis for smoking-attributabledisease: a report of the Surgeon General. Atlanta (GA): U.S. Department ofHealth and Human Services, Centers for Disease Control and Prevention,
National Center for Chronic Disease Prevention and Health Promotion,Office on Smoking and Health; 2010.
16. Benowitz NL. Emerging nicotine delivery products. Implications for publichealth. Ann Am Thorac Soc 2014;11:231–5.
17. Stepanov I, Jensen J, Hatsukami D, Hecht SS. New and traditional smoke-less tobacco: comparison of toxicant and carcinogen levels. Nicotine TobRes 2008;10:1773–82.
18. Zhu SH,Wang JB,HartmanA,ZhuangY,Gamst A,Gibson JT, et al.Quittingcigarettes completely or switching to smokeless tobacco: do US datareplicate the Swedish results? Tob Control 2009;18:82–7.
19. Henley SJ, Thun MJ, Connell C, Calle EE. Two large prospective studies ofmortality among men who use snuff or chewing tobacco (United States).Cancer Causes Control 2005;16:347–58.
20. Luo J, YeW, Zendehdel K, Adami J, Adami HO, Boffetta P, et al. Oral use ofSwedish moist snuff (snus) and risk for cancer of the mouth, lung, andpancreas inmale constructionworkers: a retrospective cohort study. Lancet2007;369:2015–20.
21. Zeller M, Hatsukami D, The Strategic Dialogue on Tobacco Harm Reduc-tion Group. The Strategic Dialogue on Tobacco Harm Reduction: a visionand blueprint for action in the US. Tob Control 2009;18:324–32.
22. Prasad GL, Jones BA, Chen P, Gregg EO. A cross-sectional study ofbiomarkers of exposure and effect in smokers and moist snuff consumers.Clin Chem Lab Med 2016;54:633–42.
23. Prasad GL, Jones BA, Schmidt E, Chen P, Kennedy AD. Global meta-bolomic profiles reveal differences in oxidative stress and inflamma-tion pathways in smokers and moist snuff consumers. J Metabol 2015;1:2.
24. Seet RC, LeeCY, LokeWM,Huang SH,HuangH, LooiWF, et al. Biomarkersof oxidative damage in cigarette smokers: which biomarkers might reflectacute versus chronic oxidative stress? Free Radical Biol Med 2011;50:1787–93.
25. King CC, Piper ME, Gepner AD, Fiore MC, Baker TB, Stein JH. Thelongitudinal impact of smoking and smoking cessation on inflammatorymarkers of cardiovascular disease risk. Arterioscler ThrombVasc Biol 2017;37:374–9.
26. Jensen EJ, Pedersen B, Frederiksen R,Dahl R. Prospective study on the effectof smoking and nicotine substitution on leucocyte blood counts andrelation between blood leucocytes and lung function. Thorax 1998;53:784–9.
27. Scanlon PD, Connett JE, Waller LA, Altose MD, Bailey WC, Buist AS, et al.Smoking cessation and lung function in mild-to-moderate chronicobstructive pulmonary disease. The Lung Health Study. Am J Respir CritCare Med 2000;161:381–90.
28. Goettel M, Niessner R, Scherer M, Scherer G, Pluym N. Analysis of urinaryeicosanoids by LC-MS/MS reveals alterations in the metabolic profile aftersmoking cessation. Chem Res Toxicol 2018;31:176–82.
29. Theophilus EH, Coggins CR, Chen P, Schmidt E, Borgerding MF. Magni-tudes of biomarker reductions in response to controlled reductions incigarettes smoked per day: a one-week clinical confinement study.Regul Toxicol Pharmacol 2015;71:225–34.
30. Krautter GR, Chen PX, Borgerding MF. Consumption patterns and bio-markers of exposure in cigarette smokers switched to Snus, various dis-solvable tobacco products, dual use, or tobacco abstinence. Regul ToxicolPharmacol 2015;71:186–97.
Makena et al.
Cancer Epidemiol Biomarkers Prev; 28(12) December 2019 Cancer Epidemiology, Biomarkers & Prevention2104
on July 29, 2021. © 2019 American Association for Cancer Research. cebp.aacrjournals.org Downloaded from
Published OnlineFirst September 26, 2019; DOI: 10.1158/1055-9965.EPI-19-0342

31. Round EK, Chen P, Taylor AK, Schmidt E. Biomarkers of tobacco exposuredecrease after smokers switch to an e-cigartette or nicotine gum.Nicotine Tob Res 2019;21:1239–47.
32. Sterz K, Scherer G, Ecker J. A simple and robust UPLC-SRM/MS method toquantify urinary eicosanoids. J Lipid Res 2012;53:1026–36.
33. Benowitz NL, Jacob PI, Kozlowski LT, Yu L. Influence of smoking fewercigarettes on exposure to tar, nicotine, and carbonmonoxide. N Engl JMed1986;315:1310–3.
34. Joseph AM, Hecht SS, Murphy SE, Carmella SG, Le CT, Zhang Y,et al. Relationships between cigarette consumption and biomarkersof tobacco toxin exposure. Cancer Epidemiol Biomarkers Prev 2005;14:2963–8.
35. D'Ruiz CD, Graff DW, Robinson E. Reductions in biomarkers of exposure,impacts on smoking urge and assessment of product use and tolerability inadult smokers following partial or complete substitution of cigarettes withelectronic cigarettes. BMC Public Health 2016;16:543.
36. Goniewicz ML, Gawron M, Smith DM, Peng M, Jacob P III, Benowitz NL.Exposure to nicotine and selected toxicants in cigarette smokers whoswitched to electronic cigarettes: a longitudinal within-subjects observa-tional study. Nicotine Tob Res 2017;19:160–7.
37. Drazen JM, Israel E, O'Byrne PM. Treatment of asthma with drugs mod-ifying the leukotriene pathway. N Engl J Med 1999;340:197–206.
38. Bray MA. The pharmacology and pathophysiology of leukotriene B4.Br Med Bull 1983;39:249–54.
39. Peters-Golden M, Gleason MM, Togias A. Cysteinyl leukotrienes: multi-functional mediators in allergic rhinitis. Clin Exp Allergy 2006;36:689–703.
40. Kumlin M, Stensvad F, Larsson L, Dahl�en B, Dahl�en SE. Validation andapplication of a new simple strategy for measurements of urinary leuko-triene E4 in humans. Clin Exp Allergy 1995;25:467–79.
41. Fauler J, Frolich JC. Cigarette smoking stimulates cysteinyl leukotrieneproduction in man. Eur J Clin Invest 1997;27:43–7.
42. Saareks V, Riutta A, Alanko J, Ylitalo P, ParviainenM,Mucha I, et al. Clinicalpharmacology of eicosanoids, nicotine induced changes in man. J PhysiolPharmacol 2000;51:631–42.
43. Hern�andez-Alvídrez E, Alba-Reyes G, Mu~noz-Cedillo BC, Arreola-Ramírez
JL, Furuya MEY, Becerril-�Angeles M, et al. Passive smoking induces leu-kotriene production in children: influence of asthma. J Asthma 2013;50:347–53.
44. Saareks V, Ylitalo P, Alanko J, Mucha I, Riutta A. Effects of smokingcessation and nicotine substitution on systemic eicosanoid productionin man. Naunyn Schmiedebergs Arch Pharmacol 2001;363:556–61.
45. Hamberg M, Svensson J, Samuelsson B. Thromboxanes: a new group ofbiologically active compounds derived from prostaglandin endoperox-ides. Proc Natl Acad Sci U S A 1975;72:2994–8.
46. FitzGerald GA, Oates JA, Hawiger J, Maas RL, Roberts LJ II, Lawson JA, et al.Endogenous biosynthesis of prostacyclin and thromboxane and plateletfunction during chronic administration of aspirin in man. J Clin Invest1983;71:676–88.
47. Roberts LJ, SweetmanBJ, PayneNA,Oates JA.Metabolismof thromboxaneB2 in man. Identification of the major urinary metabolite. J Biol Chem1977;252:7415–7.
48. Barrow SE, Ward PS, Sleightholm MA, Ritter JM, Dollery CT. Cigarettesmoking: profiles of thromboxane- and prostacyclin-derived products inhuman urine. Biochim Biophys Acta 1989;993:121–7.
49. Lowe FJ, Gregg EO, McEwanM. Evaluation of biomarkers of exposure andpotential harm in smokers, former smokers andnever-smokers. ClinChemLab Med 2009;47:311–20.
50. Nowak J, Murray JJ, Oates JA, FitzGerald GA. Biochemical evidence of achronic abnormality in platelet and vascular function in healthy indivi-duals who smoke cigarettes. Circulation 1987;76:6–14.
51. Kumlin M, Dahl�en SE. Characteristics of formation and further metabo-lism of leukotrienes in the chopped human lung. Biochim Biophys Acta1990;1044:201–10.
52. WennmalmA, BenthinG,GranstromEF, Persson L, Petersson AS,Winell S.Relation between tobacco use and urinary excretion of thromboxane A2and prostacyclin metabolites in young men. Circulation 1991;83:1698–704.
53. Nordskog BK, Brown BG, Marano KM, Campell LR, Jones BA, BorgerdingMF. Study of cardiovascular disease biomarkers among tobacco consu-mers, part 2: biomarkers of biological effect. Inhal Toxicol 2015;27:157–66.
54. HuoY, Ley K. Role of platelets in the development of atherosclerosis. 2004;14:18–22.
55. GawazM, Langer H, May AE. Platelets in inflammation and atherogenesis.J Clin Invest 2005;115:3378–84.
56. Selley ML, Bartlett MR, McGuiness JA, Ardlie NG. Effects of acrolein onhuman platelet aggregation. Chem Biol Interact 1990;76:101–9.
57. Hong JL, Lee LY. Cigarette smoke-induced bronchoconstriction: causativeagents and role of thromboxane receptors. J Appl Physiol 1996;81:2053–9.
58. Mathias RA, Sergeant S, Ruczinski I, Torgerson DG, Hugenschmidt CE,Kubala M, et al. The impact of FADS genetic variants on omega6 polyun-saturated fatty acid metabolism in African Americans. BMC Genet 2011;12:50.
www.aacrjournals.org Cancer Epidemiol Biomarkers Prev; 28(12) December 2019 2105
LTE4 and 2,3-d-TXB2 as Biomarkers of Potential Harm
on July 29, 2021. © 2019 American Association for Cancer Research. cebp.aacrjournals.org Downloaded from
Published OnlineFirst September 26, 2019; DOI: 10.1158/1055-9965.EPI-19-0342

2019;28:2095-2105. Published OnlineFirst September 26, 2019.Cancer Epidemiol Biomarkers Prev Patrudu Makena, Gang Liu, Peter Chen, et al. StudiesBiomarkers of Potential Harm in Short-Term Tobacco Switching
Are2 and 2,3-Dinor Thromboxane B4Urinary Leukotriene E
Updated version
10.1158/1055-9965.EPI-19-0342doi:
Access the most recent version of this article at:
Material
Supplementary
http://cebp.aacrjournals.org/content/suppl/2019/09/26/1055-9965.EPI-19-0342.DC1
Access the most recent supplemental material at:
Cited articles
http://cebp.aacrjournals.org/content/28/12/2095.full#ref-list-1
This article cites 53 articles, 11 of which you can access for free at:
E-mail alerts related to this article or journal.Sign up to receive free email-alerts
Subscriptions
Reprints and
To order reprints of this article or to subscribe to the journal, contact the AACR Publications Department
Permissions
Rightslink site. Click on "Request Permissions" which will take you to the Copyright Clearance Center's (CCC)
.http://cebp.aacrjournals.org/content/28/12/2095To request permission to re-use all or part of this article, use this link
on July 29, 2021. © 2019 American Association for Cancer Research. cebp.aacrjournals.org Downloaded from
Published OnlineFirst September 26, 2019; DOI: 10.1158/1055-9965.EPI-19-0342