Embed Size (px)
Citation preview
CARBOHYDRATE METABOLISM
There are six parts: 1. INTRODUCTION 2. DIGESTION, ABSORPTION AND TRANSPORT OF THE MAJOR DIETARY
CARBOHYDRATES a description of the enzymes that digest the major dietary carbohydrates to monosaccharides and the transporters of monosaccharide between intestine and blood, kidney and blood and cells and blood
3. METABOLIC ENERGY
a summary of small molecules commonly used in metabolism for the production and utilization of energy by cells
4. HORMONE REGULATION OF METABOLISM
a description of the hormones the regulate blood glucose homeostasis and their signaling pathways
5. PATHWAYS OF GLUCOSE METABOLISM
a chart showing the five metabolic pathways with numbered reactions (glycolysis # 1 - 11, tricarboxylic acid cycle #12 - 20, pentose phosphate shunt #21 - 28, gluconeogenesis # 29, 30, 9, 8, 7, 6, 5, 4, 31, 32, glycogen metabolism #33 - 39 - Important features of each reaction are described.),
6. IRREVERSIBLE AND REGULATED STEPS OF GLUCOSE METABOLISM
a review of the regulated steps in glucose metabolism
NOTE: You are NOT required to learn the chemical structures. They are included merely as a
reference.
- 1 -
INTRODUCTION
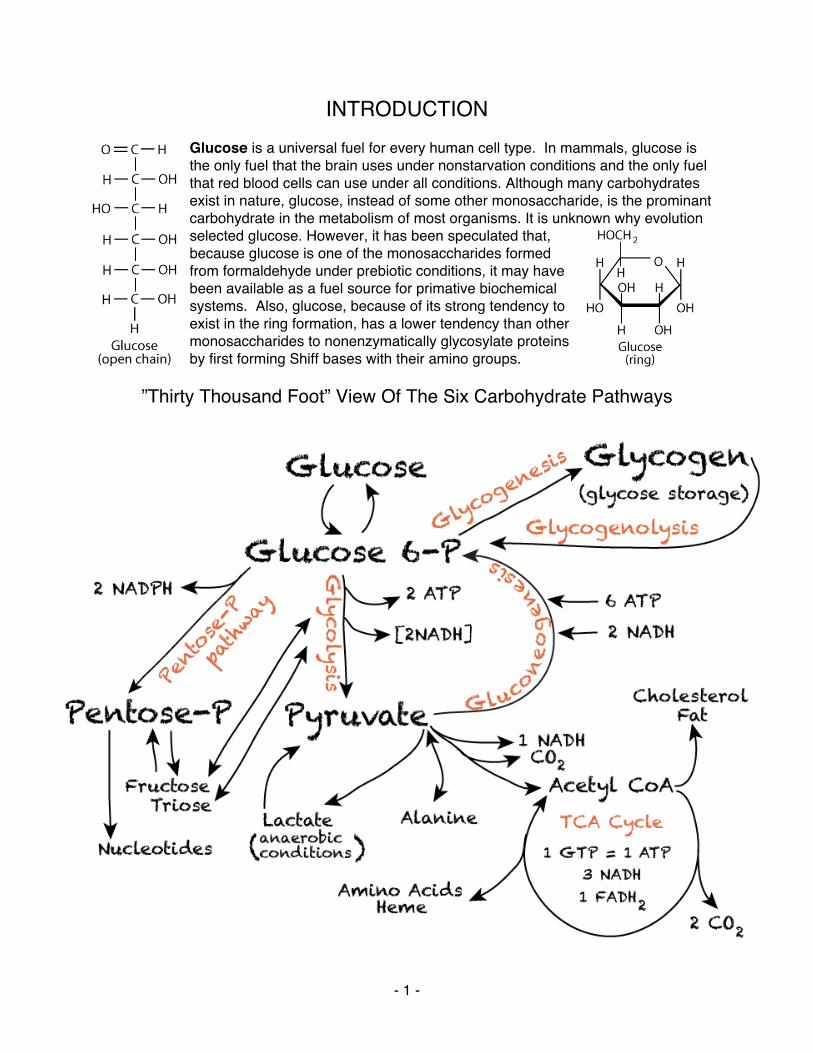
Glucose is a universal fuel for every human cell type. In mammals, glucose is the only fuel that the brain uses under nonstarvation conditions and the only fuel that red blood cells can use under all conditions. Although many carbohydrates exist in nature, glucose, instead of some other monosaccharide, is the prominant carbohydrate in the metabolism of most organisms. It is unknown why evolution selected glucose. However, it has been speculated that, because glucose is one of the monosaccharides formed from formaldehyde under prebiotic conditions, it may have been available as a fuel source for primative biochemical systems. Also, glucose, because of its strong tendency to exist in the ring formation, has a lower tendency than other monosaccharides to nonenzymatically glycosylate proteins by first forming Shiff bases with their amino groups.
”Thirty Thousand Foot” View Of The Six Carbohydrate Pathways
- 2 -
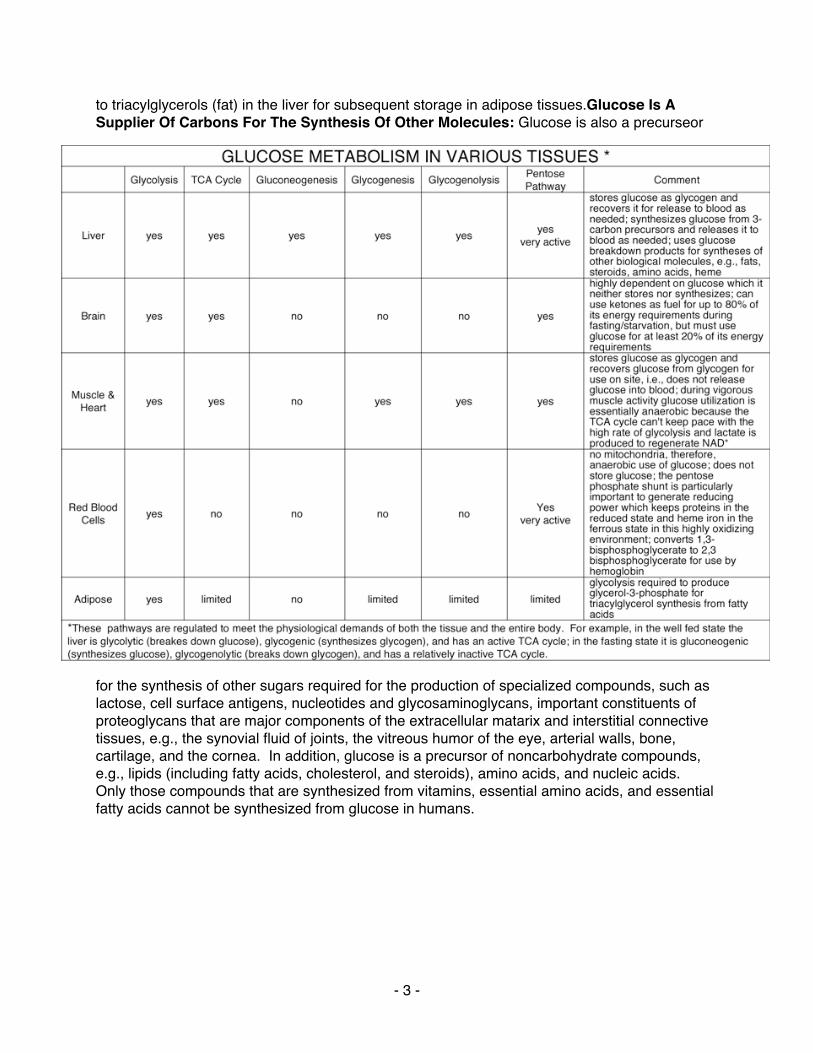
Energy From Glucose: As for all fuel molecules, glucose is a reduced compound from which electrons are harvested by oxidation reactions. Electrons are captured by electron carriers and, when mitochondria and sufficient oxygen is available, transferred to the electron transport chain, where they are ultimately donated to molecular oxygen with the formation of water and a relatively large amount of ATP. The complete oxidation of glucose is acheived by the process of glycolysis, which yields a relatively small amount of ATP and a small number of electrons, and the reactions of the tricarboxylic acid (TCA) cycle, which yield a small amount of ATP and a relatively larger number of electrons. All of the glucose carbons are oxidized to carbon dioxide, which is ultimately released into the environment. When mitochondria are absent or oxygen is limiting, glucose is partially oxidized and the captured electrons are transferred to pyruvate, the end-product of glycolysis, to form lactate (fermentation), with a net yield of only a relatively small amount of ATP. Neither water nor carbon dioxide is produced. Reducing Power And Pentose Sugars From Glucose: A second pathway, the pentose phosphate pathway, partially oxides glucose to obtain electrons that are used for reductive biosynthetic reactions and to prevent or reverse oxidative damage to cells. In this pathway glucose is oxidatively decarboxylated to yield five-carbon sugars (pentoses) that may be used for nucleotide synthesis or returned, after a series of inteconrversions, to the glycolytic pathway. Glucose homeostasis ensures that blood glucose concentration is maintained within a normal physiological range to supply glucose for the continued function of tissues that require it as an energy source, in particular, red blood cells, brain and renal medulla. Glucose Synthesis From Non-Carbohydrate Compounds: In the post-absorbtive state (after food has been absorbed from the gut) gluconeogenesis, the synthesis of glucose from non-carbohydrate compounds, contributes glucose to maintain blood glucose homeostasis during a fast. After a long fast (longer than 24 hours - starvation) it is the only process that contributes glucose to maintain blood glucose homeostasis. The liver and renal cortex are the only tissues that synthesize glucose. The liver synthesizes the most glucose, the renal cortex synthesizes considerably less glucose, much of which is used by the renal medulla, a tissue with relative few mitochondria, and therefore reduced capacity to use other biological fuels. Glucose Storage As Glycogen And Subsequent Release: After a meal, when glucose is abundant, much of it is converted to glycocen − glycogenesis − for storage, predominantly in the liver and muscles. The liver is capable of storing up to 10% of its volume in glycogen, or approximately 100 –120 grams in an adult, in contrast to the 1% storage by volume in skeletal muscles, which, because of their larger total mass in the body are capable of storing approximately 350 – 400 grams. Glucose generated from the degredation of glycogen −glycogenolysis − has different purposes in muscle and liver. Glucose generated from muscle glycogen is used to generate ATP during muscle contraction. Glucose generated from liver glycogen is used to maintain blood glucose homeostasis during fasting or during periods of enhanced need. Liver glycogen is depleted after a fast of more than 24 hours, when gluconeogenesis becomes the sole source of glucose to maintain blood glucose homeostasis. Just as too low a blood glucose concentration is detrimental, too high a blood glucose concentration is also detrimental. High blood glucose concentration is prevented both by the conversion to glucose to glycogen, predominantly in the liver and muscles, and by its conversion
- 3 -
to triacylglycerols (fat) in the liver for subsequent storage in adipose tissues.Glucose Is A Supplier Of Carbons For The Synthesis Of Other Molecules: Glucose is also a precurseor
for the synthesis of other sugars required for the production of specialized compounds, such as lactose, cell surface antigens, nucleotides and glycosaminoglycans, important constituents of proteoglycans that are major components of the extracellular matarix and interstitial connective tissues, e.g., the synovial fluid of joints, the vitreous humor of the eye, arterial walls, bone, cartilage, and the cornea. In addition, glucose is a precursor of noncarbohydrate compounds, e.g., lipids (including fatty acids, cholesterol, and steroids), amino acids, and nucleic acids. Only those compounds that are synthesized from vitamins, essential amino acids, and essential fatty acids cannot be synthesized from glucose in humans.
- 4 -
DIGESTION, ABSORPTION AND TRANSPORT OF THE MAJOR DIETARY CARBOHYDRATES
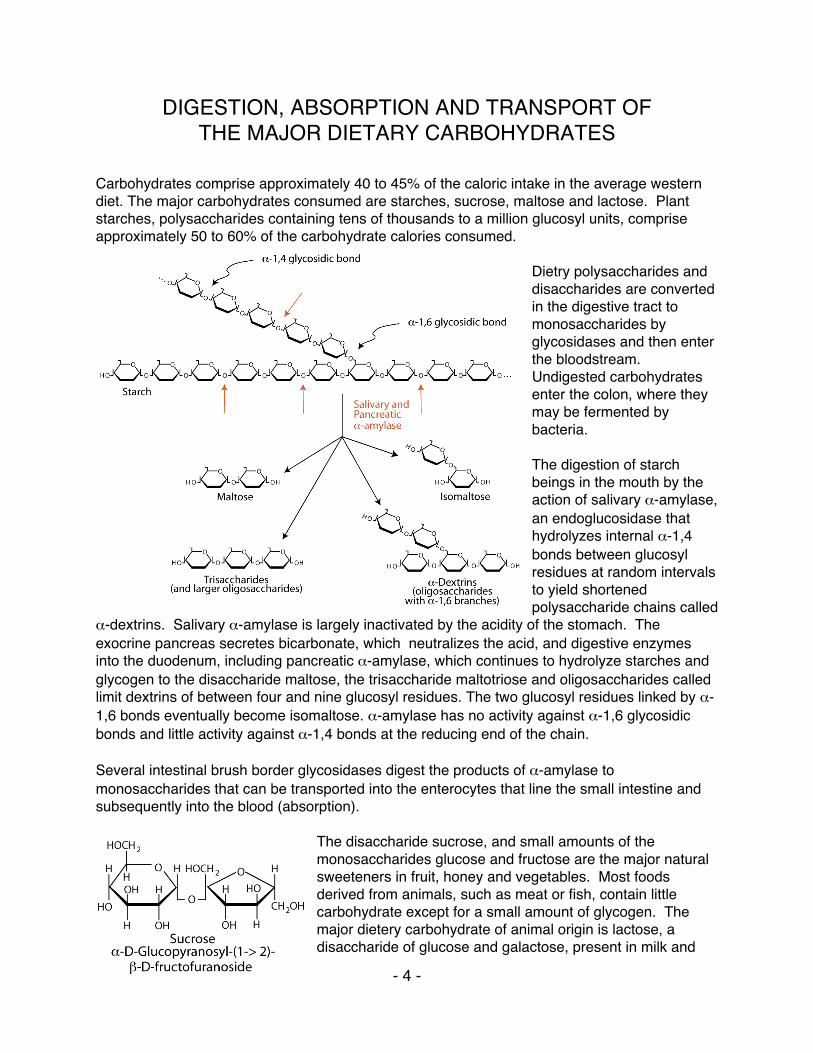
Carbohydrates comprise approximately 40 to 45% of the caloric intake in the average western diet. The major carbohydrates consumed are starches, sucrose, maltose and lactose. Plant starches, polysaccharides containing tens of thousands to a million glucosyl units, comprise approximately 50 to 60% of the carbohydrate calories consumed.
Dietry polysaccharides and disaccharides are converted in the digestive tract to monosaccharides by glycosidases and then enter the bloodstream. Undigested carbohydrates enter the colon, where they may be fermented by bacteria. The digestion of starch beings in the mouth by the action of salivary α-amylase, an endoglucosidase that hydrolyzes internal α-1,4 bonds between glucosyl residues at random intervals to yield shortened polysaccharide chains called
α-dextrins. Salivary α-amylase is largely inactivated by the acidity of the stomach. The exocrine pancreas secretes bicarbonate, which neutralizes the acid, and digestive enzymes into the duodenum, including pancreatic α-amylase, which continues to hydrolyze starches and glycogen to the disaccharide maltose, the trisaccharide maltotriose and oligosaccharides called limit dextrins of between four and nine glucosyl residues. The two glucosyl residues linked by α-1,6 bonds eventually become isomaltose. α-amylase has no activity against α-1,6 glycosidic bonds and little activity against α-1,4 bonds at the reducing end of the chain. Several intestinal brush border glycosidases digest the products of α-amylase to monosaccharides that can be transported into the enterocytes that line the small intestine and subsequently into the blood (absorption).
The disaccharide sucrose, and small amounts of the monosaccharides glucose and fructose are the major natural sweeteners in fruit, honey and vegetables. Most foods derived from animals, such as meat or fish, contain little carbohydrate except for a small amount of glycogen. The major dietery carbohydrate of animal origin is lactose, a disaccharide of glucose and galactose, present in milk and
- 5 -
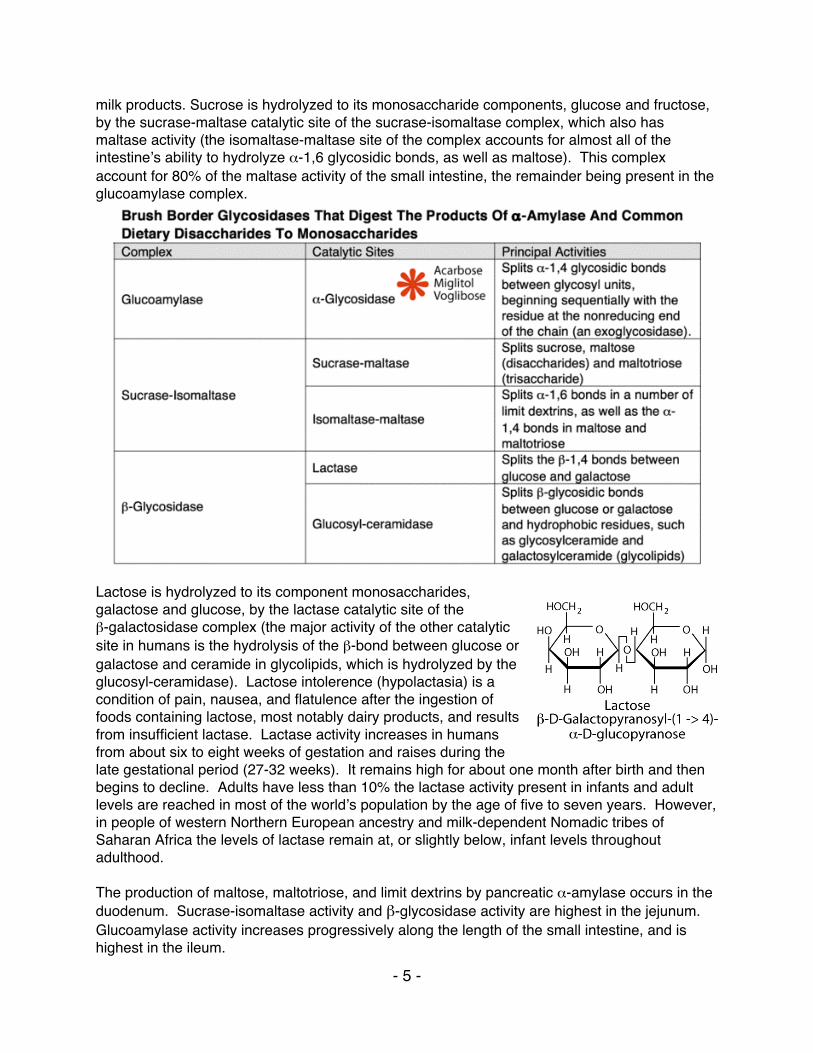
milk products. Sucrose is hydrolyzed to its monosaccharide components, glucose and fructose, by the sucrase-maltase catalytic site of the sucrase-isomaltase complex, which also has maltase activity (the isomaltase-maltase site of the complex accounts for almost all of the intestineʼs ability to hydrolyze α-1,6 glycosidic bonds, as well as maltose). This complex account for 80% of the maltase activity of the small intestine, the remainder being present in the glucoamylase complex.
Lactose is hydrolyzed to its component monosaccharides, galactose and glucose, by the lactase catalytic site of the β-galactosidase complex (the major activity of the other catalytic site in humans is the hydrolysis of the β-bond between glucose or galactose and ceramide in glycolipids, which is hydrolyzed by the glucosyl-ceramidase). Lactose intolerence (hypolactasia) is a condition of pain, nausea, and flatulence after the ingestion of foods containing lactose, most notably dairy products, and results from insufficient lactase. Lactase activity increases in humans from about six to eight weeks of gestation and raises during the late gestational period (27-32 weeks). It remains high for about one month after birth and then begins to decline. Adults have less than 10% the lactase activity present in infants and adult levels are reached in most of the worldʼs population by the age of five to seven years. However, in people of western Northern European ancestry and milk-dependent Nomadic tribes of Saharan Africa the levels of lactase remain at, or slightly below, infant levels throughout adulthood. The production of maltose, maltotriose, and limit dextrins by pancreatic α-amylase occurs in the duodenum. Sucrase-isomaltase activity and β-glycosidase activity are highest in the jejunum. Glucoamylase activity increases progressively along the length of the small intestine, and is highest in the ileum.
- 6 -
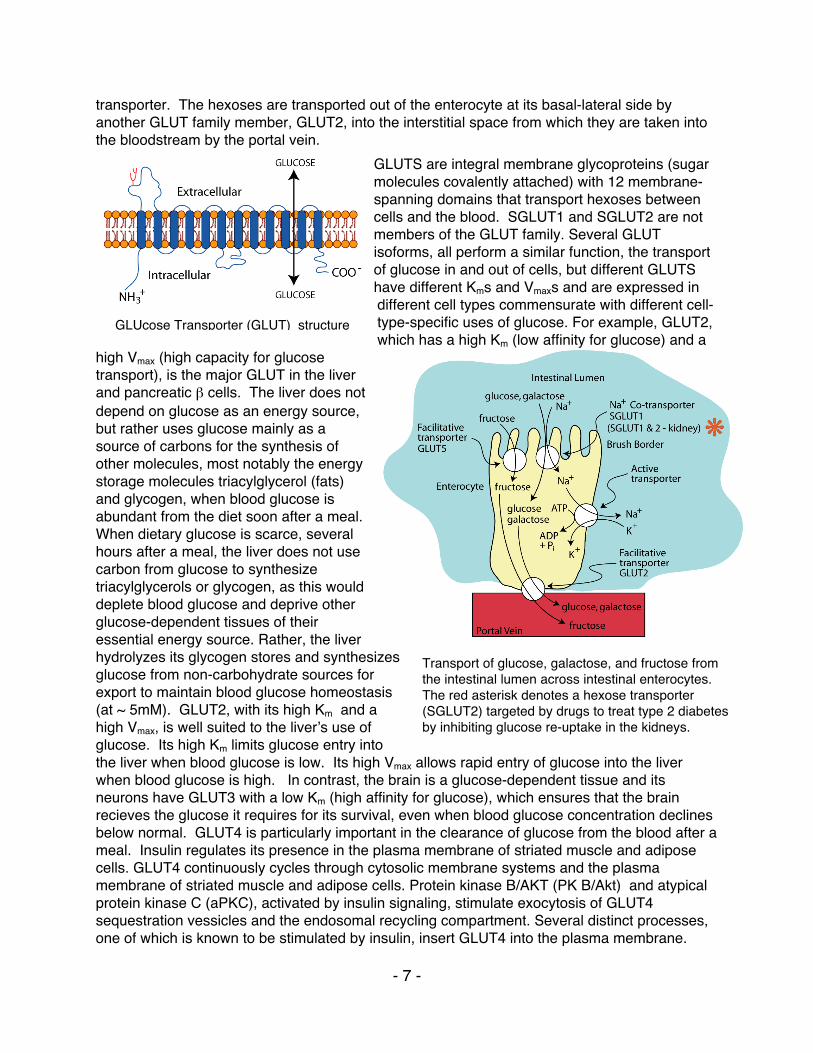
Some starchs, particularly those high in amylose or less well hydrated (e.g., starch in dried beans), are not well digested and enter the colon where colonic bacteria metabolize them, producing gases, short-chain fatty acids, and lactate. The major short chain fatty acids are acetic acid ( two carbons), propionic acid (three carbons) and butyric acid (four carbons). They are absorbed by the colonic mucosal cells where they can provide a substantial energy source. Some of these fatty acids may travel to the liver through the hepatic portal vein. The hexoses, glucose, galactose and fructose, are polar molecules that require transporter proteins for entry into and exit from cells. Two distinct groups of hexose transporters have been identified and classified based on their dependence on cellular energy: GLUTs, facilitative GLUcose Transporters, transport hexoses down a concentration gradient and do not require an input of energy. SGLUT1, a Sodium GLUcose co-Transporter located at the apical side of the enterocyte and on absorptive cells of the kidney, and SGLUT2, located on the absorptive cells of the kidney, transport glucose and galactose against a concentration gradient. This transport
requires an energy-dependent electrochemical gradient of sodium. Two sodium ions are co-transported with each hexose molecule. Sodium ions are pumped out of the cell by a membrane ATP-dependent ion pump (active transporter), which maintains the sodium gradient by exchanging three sodium ions for two potassium ions − the ”sodium-potassium ATPase”. The energy expended by this ATPase allows the enterocyte to transport glucose and galactose against a concentration gradient (lower concentration in the intestinal lumen, higher concentration in the enterocyte). Fructose is transported across the apical enterocyte membrane by GLUT5, which was initially classified as a glucose tansporter because of its amino acid sequence similarity to known GLUTS, but was subsequently identified functionally as a fructose
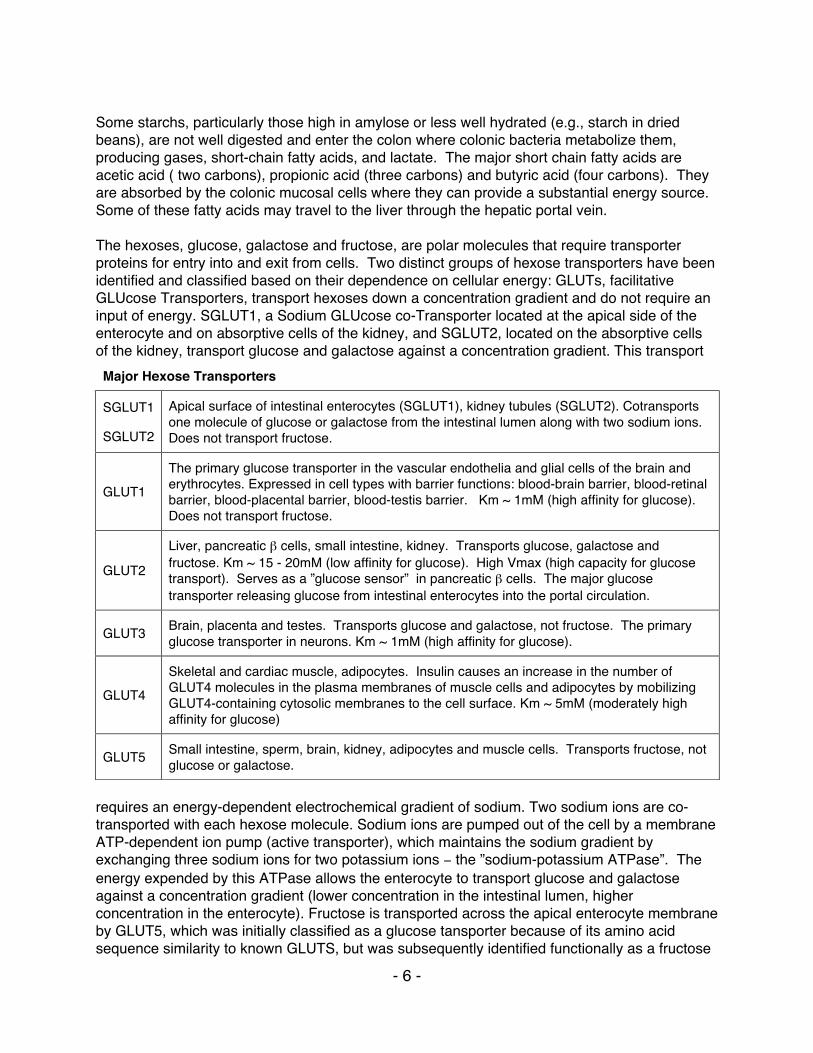
Major Hexose Transporters
SGLUT1
SGLUT2
Apical surface of intestinal enterocytes (SGLUT1), kidney tubules (SGLUT2). Cotransports one molecule of glucose or galactose from the intestinal lumen along with two sodium ions. Does not transport fructose.
GLUT1
The primary glucose transporter in the vascular endothelia and glial cells of the brain and erythrocytes. Expressed in cell types with barrier functions: blood-brain barrier, blood-retinal barrier, blood-placental barrier, blood-testis barrier. Km ~ 1mM (high affinity for glucose). Does not transport fructose.
GLUT2
Liver, pancreatic β cells, small intestine, kidney. Transports glucose, galactose and fructose. Km ~ 15 - 20mM (low affinity for glucose). High Vmax (high capacity for glucose transport). Serves as a ”glucose sensor” in pancreatic β cells. The major glucose transporter releasing glucose from intestinal enterocytes into the portal circulation.
GLUT3 Brain, placenta and testes. Transports glucose and galactose, not fructose. The primary glucose transporter in neurons. Km ~ 1mM (high affinity for glucose).
GLUT4
Skeletal and cardiac muscle, adipocytes. Insulin causes an increase in the number of GLUT4 molecules in the plasma membranes of muscle cells and adipocytes by mobilizing GLUT4-containing cytosolic membranes to the cell surface. Km ~ 5mM (moderately high affinity for glucose)
GLUT5 Small intestine, sperm, brain, kidney, adipocytes and muscle cells. Transports fructose, not glucose or galactose.
- 7 -
transporter. The hexoses are transported out of the enterocyte at its basal-lateral side by another GLUT family member, GLUT2, into the interstitial space from which they are taken into the bloodstream by the portal vein.
GLUTS are integral membrane glycoproteins (sugar molecules covalently attached) with 12 membrane-spanning domains that transport hexoses between cells and the blood. SGLUT1 and SGLUT2 are not members of the GLUT family. Several GLUT isoforms, all perform a similar function, the transport of glucose in and out of cells, but different GLUTS have different Kms and Vmaxs and are expressed in different cell types commensurate with different cell-type-specific uses of glucose. For example, GLUT2, which has a high Km (low affinity for glucose) and a
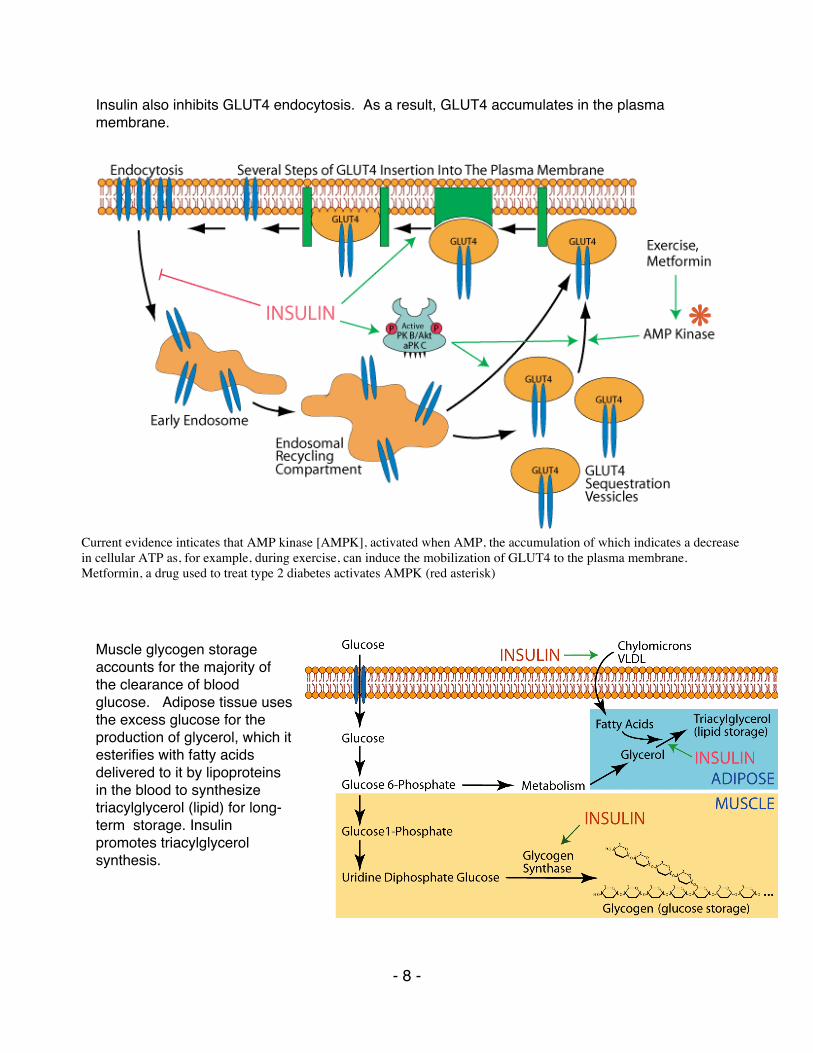
high Vmax (high capacity for glucose transport), is the major GLUT in the liver and pancreatic β cells. The liver does not depend on glucose as an energy source, but rather uses glucose mainly as a source of carbons for the synthesis of other molecules, most notably the energy storage molecules triacylglycerol (fats) and glycogen, when blood glucose is abundant from the diet soon after a meal. When dietary glucose is scarce, several hours after a meal, the liver does not use carbon from glucose to synthesize triacylglycerols or glycogen, as this would deplete blood glucose and deprive other glucose-dependent tissues of their essential energy source. Rather, the liver hydrolyzes its glycogen stores and synthesizes glucose from non-carbohydrate sources for export to maintain blood glucose homeostasis (at ~ 5mM). GLUT2, with its high Km and a high Vmax, is well suited to the liverʼs use of glucose. Its high Km limits glucose entry into the liver when blood glucose is low. Its high Vmax allows rapid entry of glucose into the liver when blood glucose is high. In contrast, the brain is a glucose-dependent tissue and its neurons have GLUT3 with a low Km (high affinity for glucose), which ensures that the brain recieves the glucose it requires for its survival, even when blood glucose concentration declines below normal. GLUT4 is particularly important in the clearance of glucose from the blood after a meal. Insulin regulates its presence in the plasma membrane of striated muscle and adipose cells. GLUT4 continuously cycles through cytosolic membrane systems and the plasma membrane of striated muscle and adipose cells. Protein kinase B/AKT (PK B/Akt) and atypical protein kinase C (aPKC), activated by insulin signaling, stimulate exocytosis of GLUT4 sequestration vessicles and the endosomal recycling compartment. Several distinct processes, one of which is known to be stimulated by insulin, insert GLUT4 into the plasma membrane.
Transport of glucose, galactose, and fructose from the intestinal lumen across intestinal enterocytes. The red asterisk denotes a hexose transporter (SGLUT2) targeted by drugs to treat type 2 diabetes by inhibiting glucose re-uptake in the kidneys.
GLUcose Transporter (GLUT) structure
- 8 -
Insulin also inhibits GLUT4 endocytosis. As a result, GLUT4 accumulates in the plasma membrane.
Muscle glycogen storage accounts for the majority of the clearance of blood glucose." Adipose tissue uses the excess glucose for the production of glycerol, which it esterifies with fatty acids delivered to it by lipoproteins in the blood to synthesize triacylglycerol (lipid) for long-term storage. Insulin promotes triacylglycerol synthesis.
Current evidence inticates that AMP kinase [AMPK], activated when AMP, the accumulation of which indicates a decrease in cellular ATP as, for example, during exercise, can induce the mobilization of GLUT4 to the plasma membrane. Metformin, a drug used to treat type 2 diabetes activates AMPK (red asterisk)
- 9 -
METABOLIC ENERGY
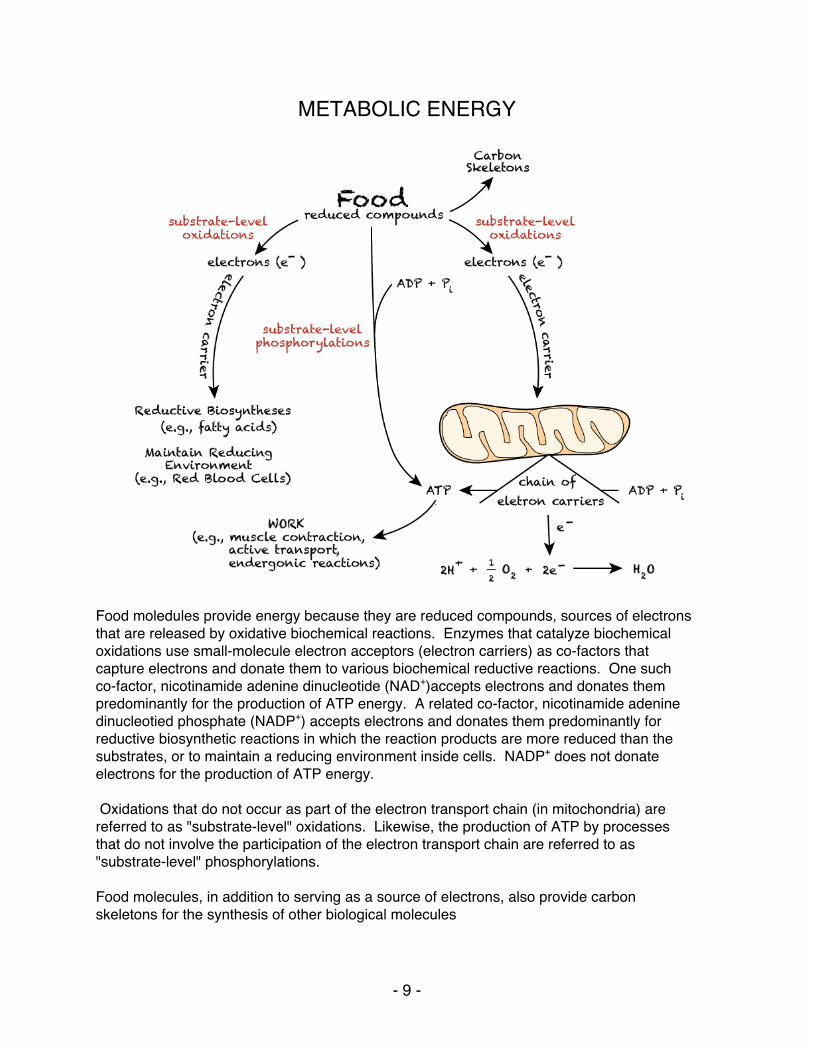
Food moledules provide energy because they are reduced compounds, sources of electrons that are released by oxidative biochemical reactions. Enzymes that catalyze biochemical oxidations use small-molecule electron acceptors (electron carriers) as co-factors that capture electrons and donate them to various biochemical reductive reactions. One such co-factor, nicotinamide adenine dinucleotide (NAD+)accepts electrons and donates them predominantly for the production of ATP energy. A related co-factor, nicotinamide adenine dinucleotied phosphate (NADP+) accepts electrons and donates them predominantly for reductive biosynthetic reactions in which the reaction products are more reduced than the substrates, or to maintain a reducing environment inside cells. NADP+ does not donate electrons for the production of ATP energy. Oxidations that do not occur as part of the electron transport chain (in mitochondria) are referred to as "substrate-level" oxidations. Likewise, the production of ATP by processes that do not involve the participation of the electron transport chain are referred to as "substrate-level" phosphorylations. Food molecules, in addition to serving as a source of electrons, also provide carbon skeletons for the synthesis of other biological molecules
- 10 -
A. All living organisms require a continual input of energy to maintain the multitude of
metabolic reactions in a state far from equilibrium (equilibrium = death). Three major purposes for energy in biological organisms: • Mechanical Work - e.g., muscle contraction • Active Transport - to maintain chemical balance, e.g., cells need to continually
pump out Na+ ions, which are taken in as part of transport mechanisms for other molecules - achieved by the Na+/K+ ATPase, which uses energy to pump Na+ against a concentration gradient. Active transport accounts for about 10% - 30% of the energy needs of an organism.
• Synthesis of essential biological molecules
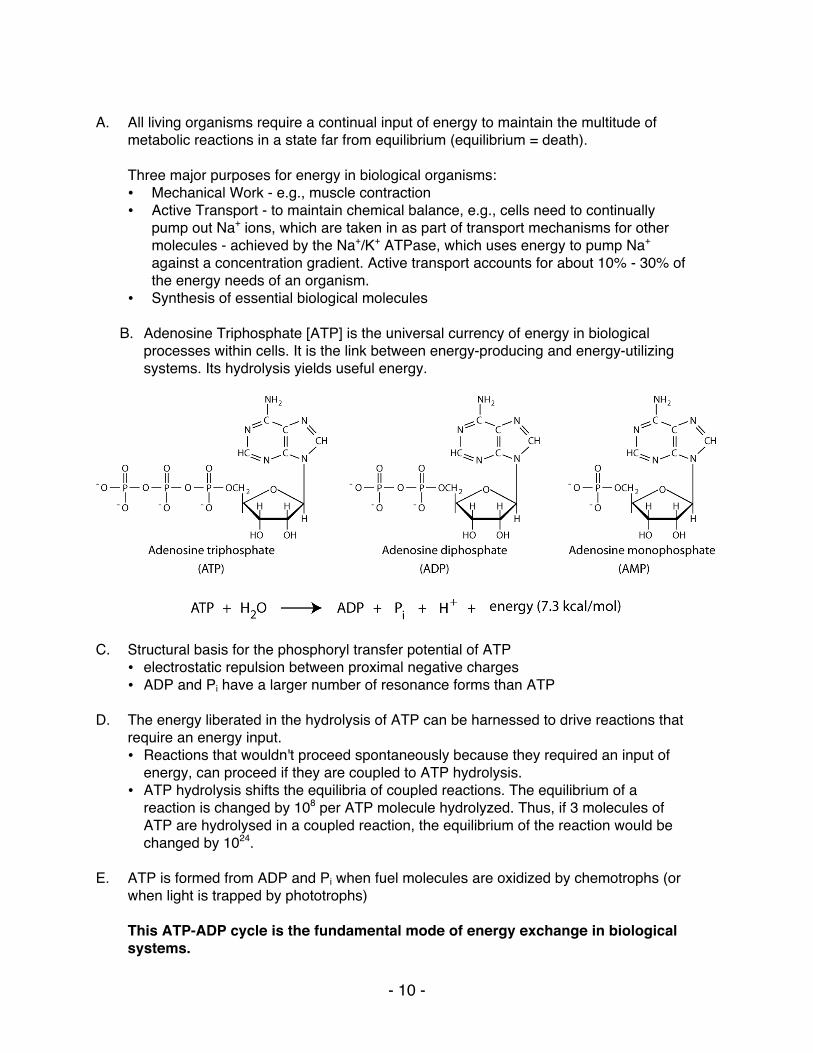
B. Adenosine Triphosphate [ATP] is the universal currency of energy in biological processes within cells. It is the link between energy-producing and energy-utilizing systems. Its hydrolysis yields useful energy.
C. Structural basis for the phosphoryl transfer potential of ATP
• electrostatic repulsion between proximal negative charges • ADP and Pi have a larger number of resonance forms than ATP
D. The energy liberated in the hydrolysis of ATP can be harnessed to drive reactions that
require an energy input. • Reactions that wouldn't proceed spontaneously because they required an input of
energy, can proceed if they are coupled to ATP hydrolysis. • ATP hydrolysis shifts the equilibria of coupled reactions. The equilibrium of a
reaction is changed by 108 per ATP molecule hydrolyzed. Thus, if 3 molecules of ATP are hydrolysed in a coupled reaction, the equilibrium of the reaction would be changed by 1024.
E. ATP is formed from ADP and Pi when fuel molecules are oxidized by chemotrophs (or
when light is trapped by phototrophs)
This ATP-ADP cycle is the fundamental mode of energy exchange in biological systems.
- 11 -
• ATP turnover is high. The half-life of an ATP molecule in many tissues is approximately one minute.
• A resting human uses approximately 40 kg of ATP in 24 hours = approximately 1000 tons in a lifetime. During strenuous exertion ATP use can be as high as 0.5 kg / min.
F. NADH and FADH2 are the major electron carriers in the oxidation (dehydrogenation) of fuel
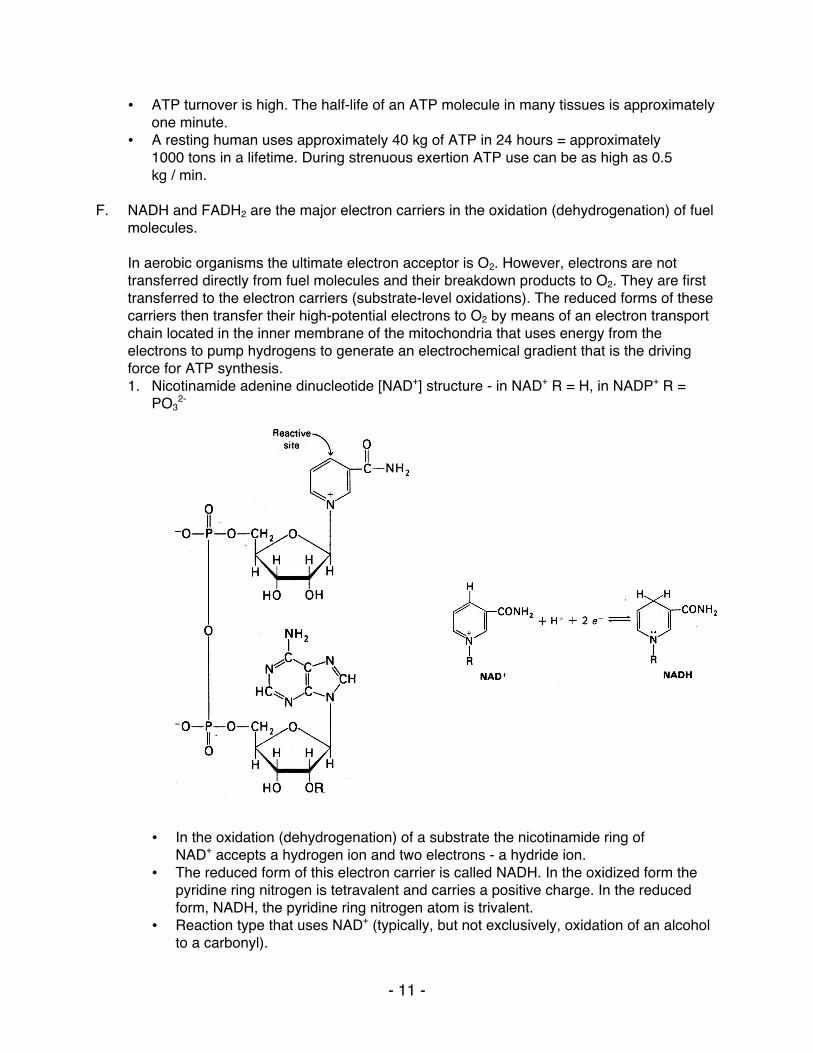
molecules. In aerobic organisms the ultimate electron acceptor is O2. However, electrons are not transferred directly from fuel molecules and their breakdown products to O2. They are first transferred to the electron carriers (substrate-level oxidations). The reduced forms of these carriers then transfer their high-potential electrons to O2 by means of an electron transport chain located in the inner membrane of the mitochondria that uses energy from the electrons to pump hydrogens to generate an electrochemical gradient that is the driving force for ATP synthesis. 1. Nicotinamide adenine dinucleotide [NAD+] structure - in NAD+ R = H, in NADP+ R =
PO32-
• In the oxidation (dehydrogenation) of a substrate the nicotinamide ring of
NAD+ accepts a hydrogen ion and two electrons - a hydride ion. • The reduced form of this electron carrier is called NADH. In the oxidized form the
pyridine ring nitrogen is tetravalent and carries a positive charge. In the reduced form, NADH, the pyridine ring nitrogen atom is trivalent.
• Reaction type that uses NAD+ (typically, but not exclusively, oxidation of an alcohol to a carbonyl).
- 12 -
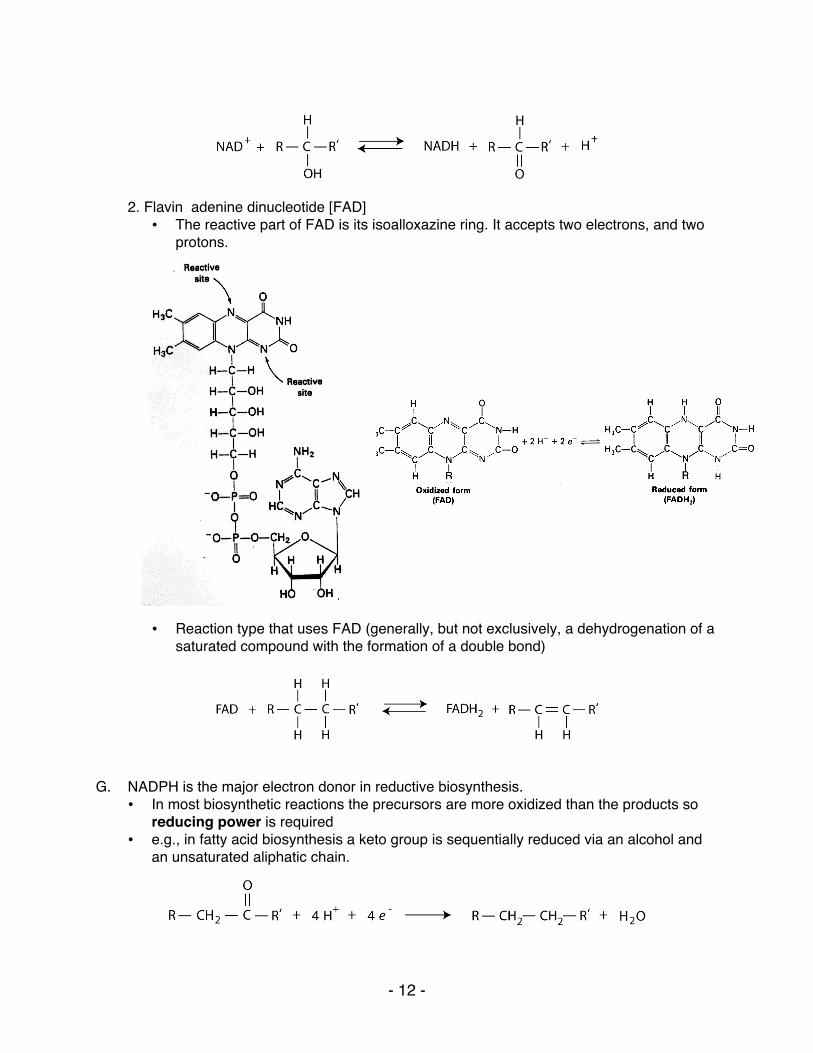
2. Flavin adenine dinucleotide [FAD] • The reactive part of FAD is its isoalloxazine ring. It accepts two electrons, and two
protons.
• • • • • • • • • • • • • • • • • •
• Reaction type that uses FAD (generally, but not exclusively, a dehydrogenation of a
saturated compound with the formation of a double bond)
G. NADPH is the major electron donor in reductive biosynthesis.
• In most biosynthetic reactions the precursors are more oxidized than the products so reducing power is required
• e.g., in fatty acid biosynthesis a keto group is sequentially reduced via an alcohol and an unsaturated aliphatic chain.

- 13 -
• NADPH differs from NADH in that the 2'-OH of its adenosine moiety is esterified with phosphate. This extra phosphate is a tag that directs this reducing agent to discerning biosynthetic enzymes.
• NADPH carries electrons in the same way as NADH. • Electrons carried by NADPH are used almost exclusively for reductive
biosynthesis, whereas electrons carried by NADH are used primarily for the generation of ATP.
H. Why have both NADP+ and NAD+ ?
• The cellular ratio of NADP+/NADPH = 0.014 • The cellular ratio of NAD+/NADH = 700 • The cell can thus maintain a high level of reducing equivalents for biosynthetic
reactions while simultaneously maintaining high capacity for substrate-level oxidations so that energy can be generated.
I. Coenzyme A (A for acetylation ) is a universal carrier and donor of acyl groups,
• The terminal sulfhydryl group is the reactive site, which forms thioesters with acyl (not only acetyl) groups.
J. Acetyl CoA is a common intermediate in different catabolic pathways.
• glycolysis, beta-oxidation of fatty acids and amino acid degradation all supply the cellular pool of acetyl CoA
- 14 -
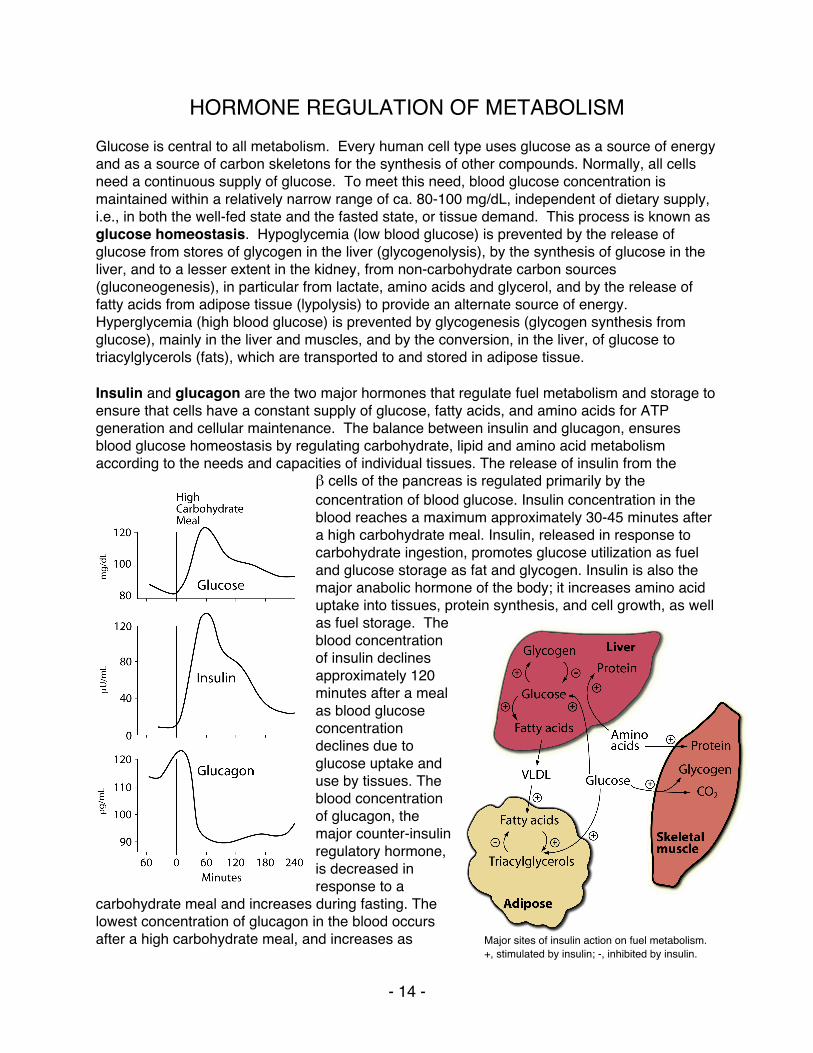
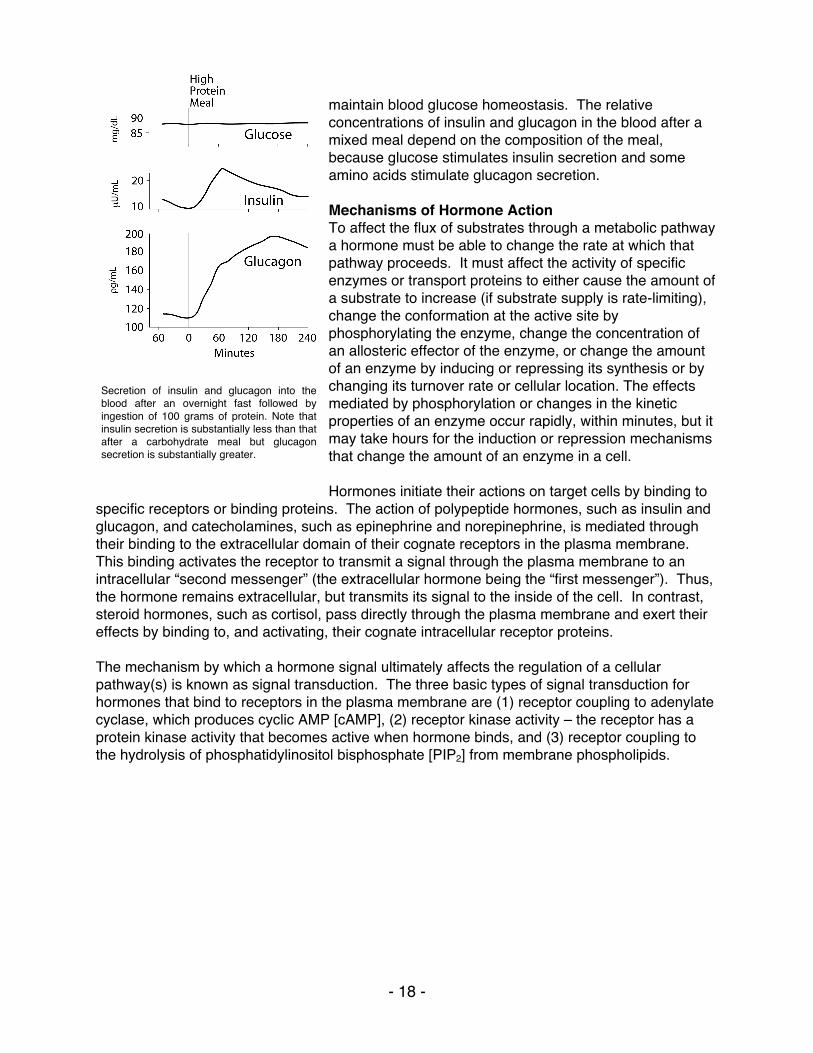
HORMONE REGULATION OF METABOLISM Glucose is central to all metabolism. Every human cell type uses glucose as a source of energy and as a source of carbon skeletons for the synthesis of other compounds. Normally, all cells need a continuous supply of glucose. To meet this need, blood glucose concentration is maintained within a relatively narrow range of ca. 80-100 mg/dL, independent of dietary supply, i.e., in both the well-fed state and the fasted state, or tissue demand. This process is known as glucose homeostasis. Hypoglycemia (low blood glucose) is prevented by the release of glucose from stores of glycogen in the liver (glycogenolysis), by the synthesis of glucose in the liver, and to a lesser extent in the kidney, from non-carbohydrate carbon sources (gluconeogenesis), in particular from lactate, amino acids and glycerol, and by the release of fatty acids from adipose tissue (lypolysis) to provide an alternate source of energy. Hyperglycemia (high blood glucose) is prevented by glycogenesis (glycogen synthesis from glucose), mainly in the liver and muscles, and by the conversion, in the liver, of glucose to triacylglycerols (fats), which are transported to and stored in adipose tissue. Insulin and glucagon are the two major hormones that regulate fuel metabolism and storage to ensure that cells have a constant supply of glucose, fatty acids, and amino acids for ATP generation and cellular maintenance. The balance between insulin and glucagon, ensures blood glucose homeostasis by regulating carbohydrate, lipid and amino acid metabolism according to the needs and capacities of individual tissues. The release of insulin from the
β cells of the pancreas is regulated primarily by the concentration of blood glucose. Insulin concentration in the blood reaches a maximum approximately 30-45 minutes after a high carbohydrate meal. Insulin, released in response to carbohydrate ingestion, promotes glucose utilization as fuel and glucose storage as fat and glycogen. Insulin is also the major anabolic hormone of the body; it increases amino acid uptake into tissues, protein synthesis, and cell growth, as well as fuel storage. The blood concentration of insulin declines approximately 120 minutes after a meal as blood glucose concentration declines due to glucose uptake and use by tissues. The blood concentration of glucagon, the major counter-insulin regulatory hormone, is decreased in response to a
carbohydrate meal and increases during fasting. The lowest concentration of glucagon in the blood occurs after a high carbohydrate meal, and increases as Major sites of insulin action on fuel metabolism.
+, stimulated by insulin; -, inhibited by insulin.

- 15 -
blood glucose concentration decreases. Glucagon functions to maintain fuel availability in the absence of dietary glucose by promoting glycogenolysis and gluconeogenesis. The release of glucagon from the α cells of the pancreas is controlled primarily through suppression by glucose and insulin. Decreased blood insulin, at times when blood glucagon is increased, stimulates the mobilization of fatty acids from adipose tissue stores of triacylglycerols. Because the effects of glucagon are opposed by insulin, the simultaneous secretion of insulin and suppression of glucagon secretion by a high carbohydrate meal provides integrated control of the metabolism
of carbohydrate, fat and protein. Epinephrine, the acute stress, or “fight or flight” hormone and cortisol, a glucocorticoid (steroid hormone), are synthesized in the adrenal gland and released, respectively, in response to acute or chronic stress. They are counter-insulin regulatory hormones that have effects on fuel metabolism opposite to those of insulin. They function to increase fuel availability so the body can respond to a variety of different stressful conditions. Fuels taken in the diet in excess of immediate needs are stored and the appropriate fuel is mobilized when demand occurs. These processes maintain metabolic homeostasis so that tissues have a constant source of fuels from which to synthesize ATP for the maintenance of normal cell function and growth. For example, if dietary glucose is not available in sufficient quantities that all tissues can use, fatty acids are mobilized and can be used by muscle and other tissues, and the liver can convert fatty acids to ketone bodies,
which the brain and other tissues can use for their energy needs. The brain can use ketone bodies for ca. 80% of its energy needs, but cannot use fatty acids, and must always have glucose for ca. 20% of its energy needs. The use of fatty acids for energy spares glucose for use by the brain and other glucose-dependent tissues (such as red blood cells). Insulin and glucagon are synthesized in the endocrine pancreas and secreted into the hepatic portal vein; insulin is synthesized in the β cells, and glucagon is synthesized in the α cells of the islets of Lengerhans. Active insulin, a polypeptide hormone, is composed of two polypeptide chains, the A-chain and the B-chain, covalently linked by two interchain disulfide bonds. The A-chain has one additional intrachain disulfide bond. Insulin is synthesized as a preprohormone that is converted to proinsulin in the rough endoplasmic reticulum (RER). The “pre” sequence at the N–terminal end is cleaved as it enters the lumen of the RER. Proinsulin folds into its proper conformation and disulfide bonds are formed between the specific cysteine residues. It is transported in membrane-bound vesicles to the Golgi complex, from which it leaves in storage vesicles, where it is cleaved by a protease to release the C-peptide fragment and a few small remnants, which have no hormonal activity. Cleavage of the C-peptide decreases the solubility of the insulin, which co-precipitates with zinc ions that are also present in the storage vesicles.
Major sites of glucagon action on fuel metabolism. +, stimulated by glucagon; -, inhibited by glucagon. NOTE that in Adipocytes low insulin, not increased glucagon, is the regulator of fatty acid generation from triacylglycerols for export to the blood. Also, muscle does not respond to glucagon – it has no glucagon receptors.
- 16 -
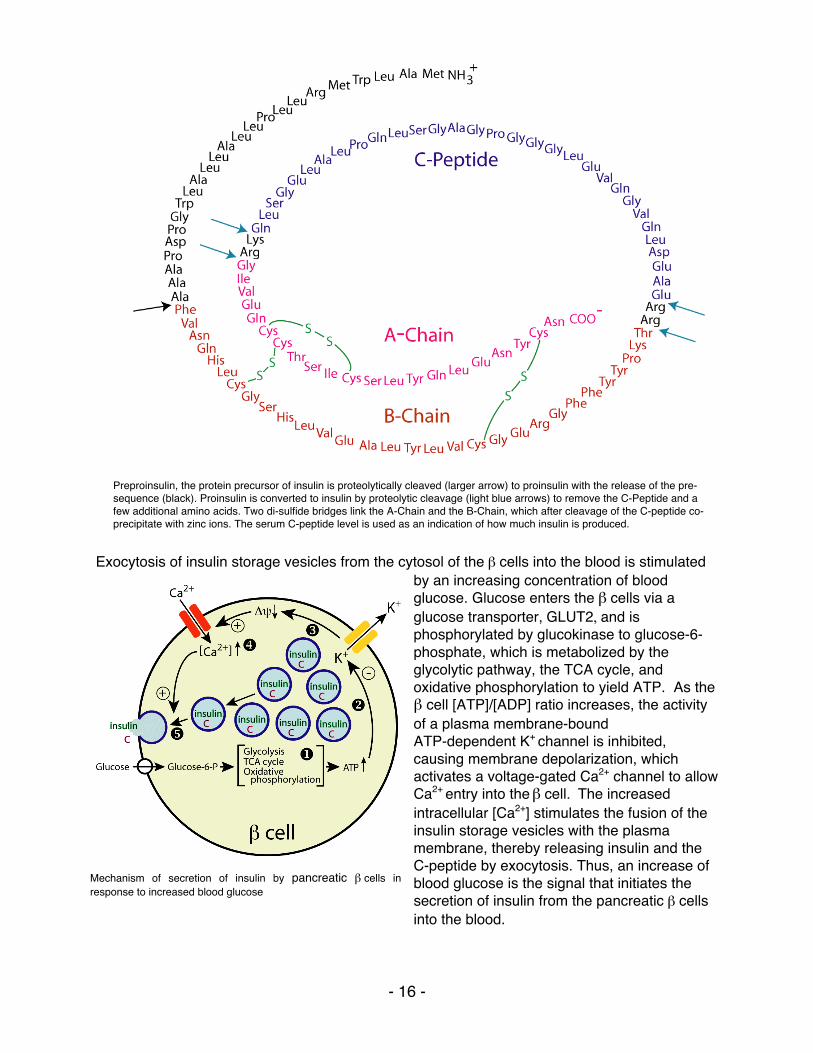
Exocytosis of insulin storage vesicles from the cytosol of the β cells into the blood is stimulated
by an increasing concentration of blood glucose. Glucose enters the β cells via a glucose transporter, GLUT2, and is phosphorylated by glucokinase to glucose-6-phosphate, which is metabolized by the glycolytic pathway, the TCA cycle, and oxidative phosphorylation to yield ATP. As the β cell [ATP]/[ADP] ratio increases, the activity of a plasma membrane-bound ATP-dependent K+ channel is inhibited, causing membrane depolarization, which activates a voltage-gated Ca2+ channel to allow Ca2+ entry into the β cell. The increased intracellular [Ca2+] stimulates the fusion of the insulin storage vesicles with the plasma membrane, thereby releasing insulin and the C-peptide by exocytosis. Thus, an increase of blood glucose is the signal that initiates the secretion of insulin from the pancreatic β cells into the blood.
Preproinsulin, the protein precursor of insulin is proteolytically cleaved (larger arrow) to proinsulin with the release of the pre-sequence (black). Proinsulin is converted to insulin by proteolytic cleavage (light blue arrows) to remove the C-Peptide and a few additional amino acids. Two di-sulfide bridges link the A-Chain and the B-Chain, which after cleavage of the C-peptide co-precipitate with zinc ions. The serum C-peptide level is used as an indication of how much insulin is produced.
Mechanism of secretion of insulin by pancreatic β cells in response to increased blood glucose
- 17 -
Factors other than blood glucose concentration also modulate insulin release. The pancreatic islets are innervated by the autonomic nervous system, including a branch of the vagus nerve. Neural signals help to coordinate insulin release with the secretory signals initiated by the ingestion of fuels, but signals from the central nervous system are not required for insulin secretion in response to fuel ingestion. Some amino acids can also stimulate insulin secretion, although the amount of insulin released in response to the ingestion of a high-protein meal is very much lower than that released in response to the ingestion of a high-carbohydrate meal.
Gastric inhibitory polypeptide (GIP), also called glucose-dependent insulinotropic peptide and glucagon-like peptide-1 (GLP-1), two gut hormones (incretins) released after the ingestion of food, also aid in the onset of insulin release. Epinephrine, which is secreted in response to fasting, stress, trauma and vigorous exercise, decreases the release of insulin, thereby promoting the mobilization of stored fuels for the generation of the energy required to respond to these physiological conditions, rather than fuel storage, as promoted by increased insulin.
Glucagon, a 29 amino acid polypeptide hormone, is synthesized in the α cells of the pancreas by cleavage from a larger preproglucagon protein. Like insulin, it is synthesized in RER and converted to proglucagon as it enters the lumen of the RER. Proteolytic cleavage generates the mature 29-amino acid glucagon and larger glucagon-containing fragments, glucagon-like polypeptides 1 and 2. Glucagon secretion is regulated principally by the blood glucose concentration and insulin. Increasing concentrations of each inhibit glucagon secretion. The direction of blood flow in the islets of the pancreas carries insulin from the β cells at the center of the islets to the peripheral α cells, where it suppresses glucagon secretion. Some hormones stimulate glucagon secretion, particularly, catecholamines (including epinephrine), cortisol, and some gastrointestional hormones. In addition, some amino acids stimulate glucagon secretion. Thus, the increased concentration of glucagon that would be expected in the fasted state does not decrease after a high-protein, low glucose meal, and the increased glucagon stimulates gluconeogenesis to
Regulators of Insulin Secretion From Pancreatic β Cells Major Regulators Effect Glucose + Minor Regulators Some Amino acids + Neural Input + Gut hormones + Epinephrine - Effect: +, stimulates; -, inhibits
Regulators of Glucagon Secretion From Pancreatic α Cells Major Regulators Effect Glucose - Insulin - Some Amino Acids + Minor Regulators Cortisol + Neural Input (stress) + Epinephrine + Gut hormones + Effect: +, stimulates; -, inhibits
- 18 -
maintain blood glucose homeostasis. The relative concentrations of insulin and glucagon in the blood after a mixed meal depend on the composition of the meal, because glucose stimulates insulin secretion and some amino acids stimulate glucagon secretion. Mechanisms of Hormone Action To affect the flux of substrates through a metabolic pathway a hormone must be able to change the rate at which that pathway proceeds. It must affect the activity of specific enzymes or transport proteins to either cause the amount of a substrate to increase (if substrate supply is rate-limiting), change the conformation at the active site by phosphorylating the enzyme, change the concentration of an allosteric effector of the enzyme, or change the amount of an enzyme by inducing or repressing its synthesis or by changing its turnover rate or cellular location. The effects mediated by phosphorylation or changes in the kinetic properties of an enzyme occur rapidly, within minutes, but it may take hours for the induction or repression mechanisms that change the amount of an enzyme in a cell. Hormones initiate their actions on target cells by binding to
specific receptors or binding proteins. The action of polypeptide hormones, such as insulin and glucagon, and catecholamines, such as epinephrine and norepinephrine, is mediated through their binding to the extracellular domain of their cognate receptors in the plasma membrane. This binding activates the receptor to transmit a signal through the plasma membrane to an intracellular “second messenger” (the extracellular hormone being the “first messenger”). Thus, the hormone remains extracellular, but transmits its signal to the inside of the cell. In contrast, steroid hormones, such as cortisol, pass directly through the plasma membrane and exert their effects by binding to, and activating, their cognate intracellular receptor proteins. The mechanism by which a hormone signal ultimately affects the regulation of a cellular pathway(s) is known as signal transduction. The three basic types of signal transduction for hormones that bind to receptors in the plasma membrane are (1) receptor coupling to adenylate cyclase, which produces cyclic AMP [cAMP], (2) receptor kinase activity – the receptor has a protein kinase activity that becomes active when hormone binds, and (3) receptor coupling to the hydrolysis of phosphatidylinositol bisphosphate [PIP2] from membrane phospholipids.
Secretion of insulin and glucagon into the blood after an overnight fast followed by ingestion of 100 grams of protein. Note that insulin secretion is substantially less than that after a carbohydrate meal but glucagon secretion is substantially greater.
- 19 -
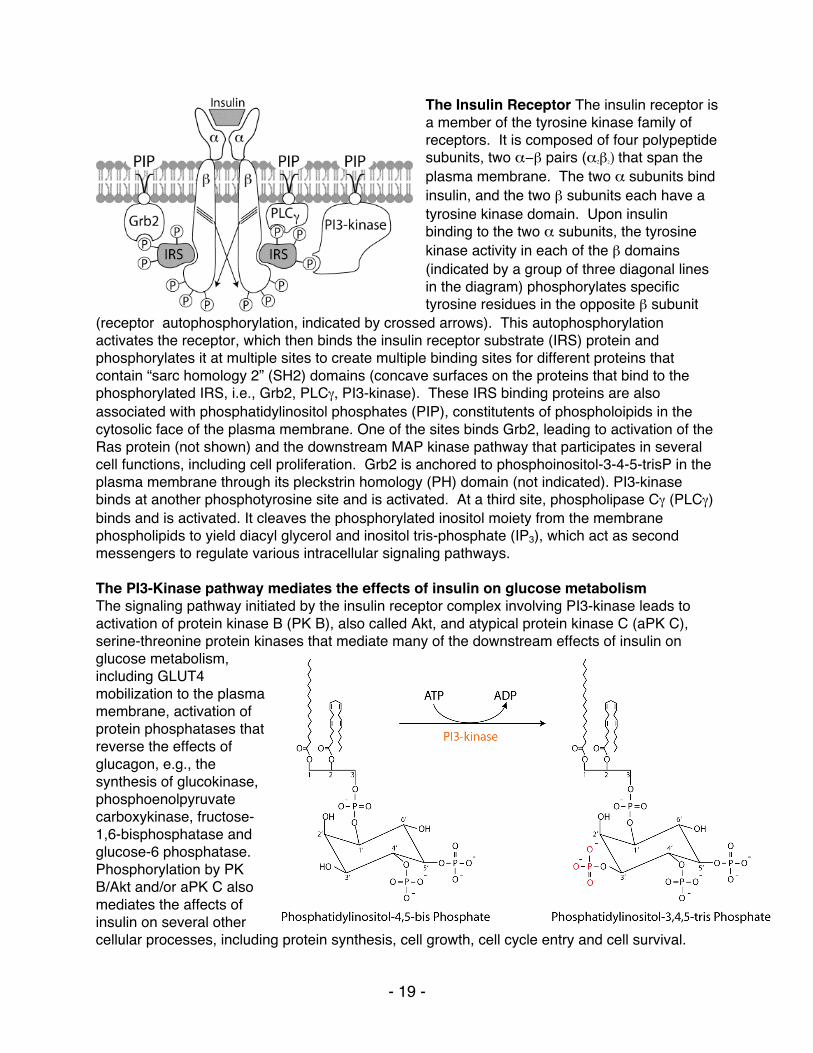
The Insulin Receptor The insulin receptor is a member of the tyrosine kinase family of receptors. It is composed of four polypeptide subunits, two α−β pairs (α2β2) that span the plasma membrane. The two α subunits bind insulin, and the two β subunits each have a tyrosine kinase domain. Upon insulin binding to the two α subunits, the tyrosine kinase activity in each of the β domains (indicated by a group of three diagonal lines in the diagram) phosphorylates specific tyrosine residues in the opposite β subunit
(receptor autophosphorylation, indicated by crossed arrows). This autophosphorylation activates the receptor, which then binds the insulin receptor substrate (IRS) protein and phosphorylates it at multiple sites to create multiple binding sites for different proteins that contain “sarc homology 2” (SH2) domains (concave surfaces on the proteins that bind to the phosphorylated IRS, i.e., Grb2, PLCγ, PI3-kinase). These IRS binding proteins are also associated with phosphatidylinositol phosphates (PIP), constitutents of phospholoipids in the cytosolic face of the plasma membrane. One of the sites binds Grb2, leading to activation of the Ras protein (not shown) and the downstream MAP kinase pathway that participates in several cell functions, including cell proliferation. Grb2 is anchored to phosphoinositol-3-4-5-trisP in the plasma membrane through its pleckstrin homology (PH) domain (not indicated). PI3-kinase binds at another phosphotyrosine site and is activated. At a third site, phospholipase Cγ (PLCγ) binds and is activated. It cleaves the phosphorylated inositol moiety from the membrane phospholipids to yield diacyl glycerol and inositol tris-phosphate (IP3), which act as second messengers to regulate various intracellular signaling pathways. The PI3-Kinase pathway mediates the effects of insulin on glucose metabolism The signaling pathway initiated by the insulin receptor complex involving PI3-kinase leads to activation of protein kinase B (PK B), also called Akt, and atypical protein kinase C (aPK C), serine-threonine protein kinases that mediate many of the downstream effects of insulin on glucose metabolism, including GLUT4 mobilization to the plasma membrane, activation of protein phosphatases that reverse the effects of glucagon, e.g., the synthesis of glucokinase, phosphoenolpyruvate carboxykinase, fructose-1,6-bisphosphatase and glucose-6 phosphatase. Phosphorylation by PK B/Akt and/or aPK C also mediates the affects of insulin on several other cellular processes, including protein synthesis, cell growth, cell cycle entry and cell survival.
- 20 -
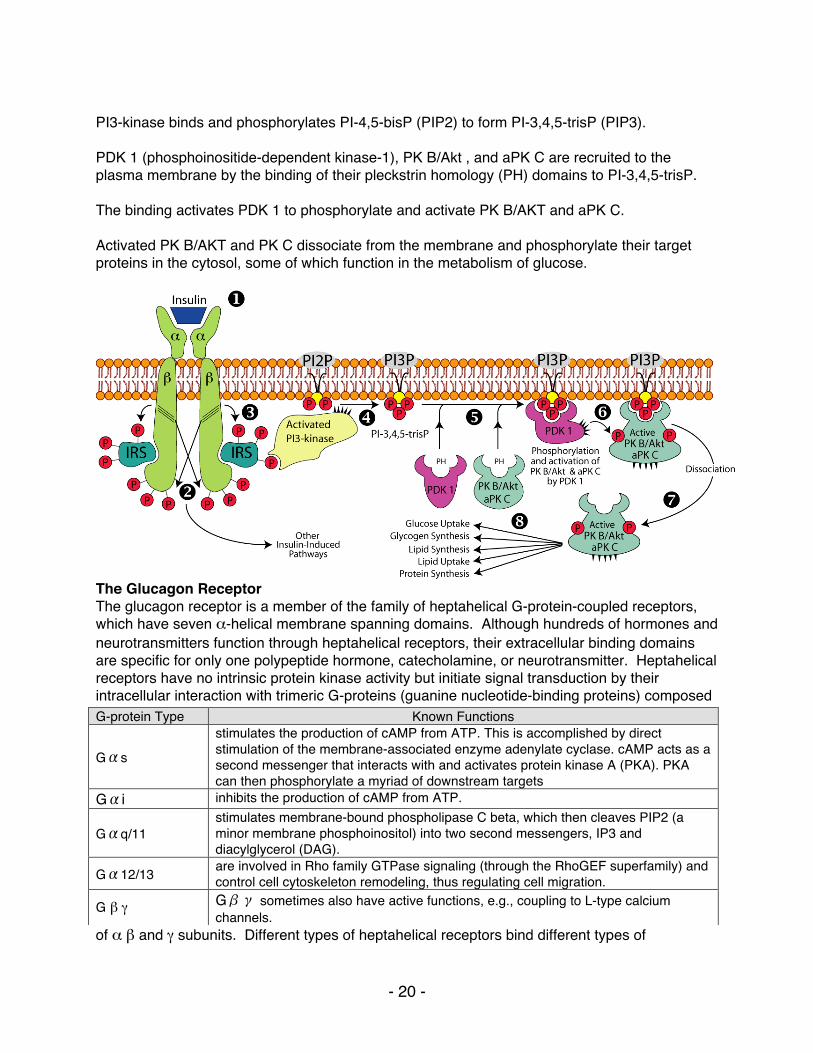
PI3-kinase binds and phosphorylates PI-4,5-bisP (PIP2) to form PI-3,4,5-trisP (PIP3). PDK 1 (phosphoinositide-dependent kinase-1), PK B/Akt , and aPK C are recruited to the plasma membrane by the binding of their pleckstrin homology (PH) domains to PI-3,4,5-trisP. The binding activates PDK 1 to phosphorylate and activate PK B/AKT and aPK C. Activated PK B/AKT and PK C dissociate from the membrane and phosphorylate their target proteins in the cytosol, some of which function in the metabolism of glucose.
The Glucagon Receptor The glucagon receptor is a member of the family of heptahelical G-protein-coupled receptors, which have seven α-helical membrane spanning domains. Although hundreds of hormones and neurotransmitters function through heptahelical receptors, their extracellular binding domains are specific for only one polypeptide hormone, catecholamine, or neurotransmitter. Heptahelical receptors have no intrinsic protein kinase activity but initiate signal transduction by their intracellular interaction with trimeric G-proteins (guanine nucleotide-binding proteins) composed
of α β and γ subunits. Different types of heptahelical receptors bind different types of
G-protein Type Known Functions
Gαs stimulates the production of cAMP from ATP. This is accomplished by direct stimulation of the membrane-associated enzyme adenylate cyclase. cAMP acts as a second messenger that interacts with and activates protein kinase A (PKA). PKA can then phosphorylate a myriad of downstream targets
Gαi inhibits the production of cAMP from ATP.
Gαq/11 stimulates membrane-bound phospholipase C beta, which then cleaves PIP2 (a minor membrane phosphoinositol) into two second messengers, IP3 and diacylglycerol (DAG).
Gα12/13 are involved in Rho family GTPase signaling (through the RhoGEF superfamily) and control cell cytoskeleton remodeling, thus regulating cell migration.
G β γ Gβγ sometimes also have active functions, e.g., coupling to L-type calcium channels.
- 21 -
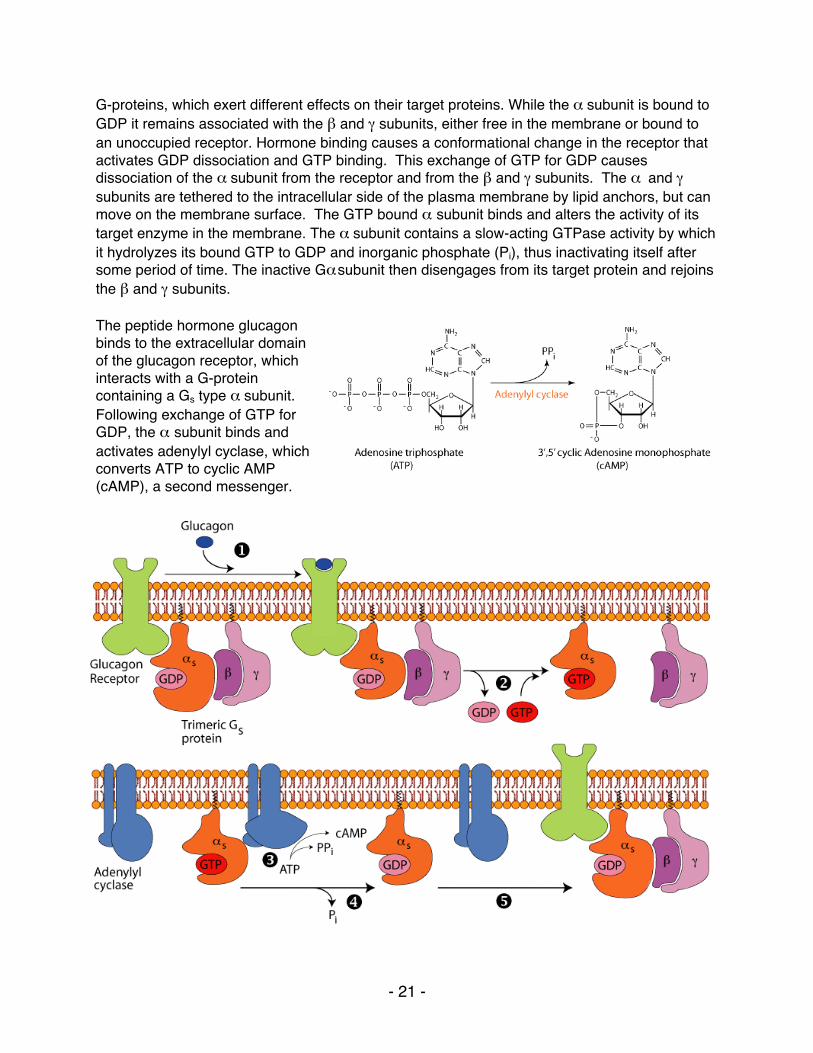
G-proteins, which exert different effects on their target proteins. While the α subunit is bound to GDP it remains associated with the β and γ subunits, either free in the membrane or bound to an unoccupied receptor. Hormone binding causes a conformational change in the receptor that activates GDP dissociation and GTP binding. This exchange of GTP for GDP causes dissociation of the α subunit from the receptor and from the β and γ subunits. The α and γ subunits are tethered to the intracellular side of the plasma membrane by lipid anchors, but can move on the membrane surface. The GTP bound α subunit binds and alters the activity of its target enzyme in the membrane. The α subunit contains a slow-acting GTPase activity by which it hydrolyzes its bound GTP to GDP and inorganic phosphate (Pi), thus inactivating itself after some period of time. The inactive Gα subunit then disengages from its target protein and rejoins the β and γ subunits. The peptide hormone glucagon binds to the extracellular domain of the glucagon receptor, which interacts with a G-protein containing a Gs type α subunit. Following exchange of GTP for GDP, the α subunit binds and activates adenylyl cyclase, which converts ATP to cyclic AMP (cAMP), a second messenger.
- 22 -
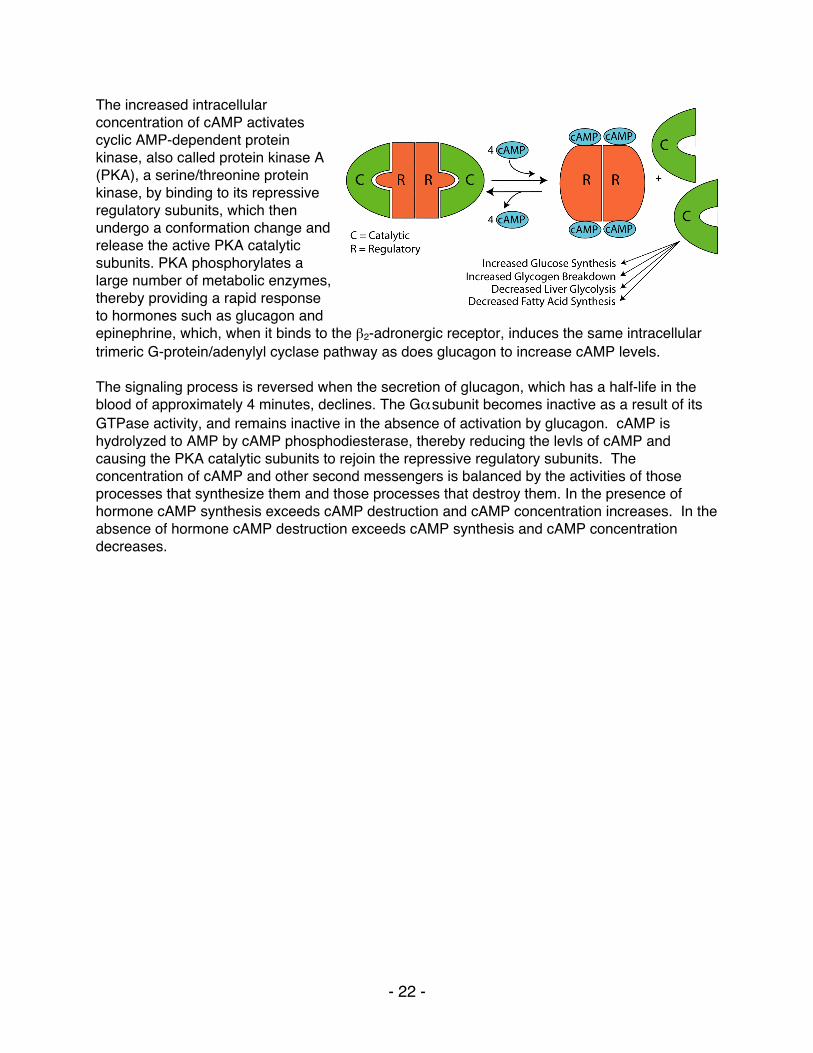
The increased intracellular concentration of cAMP activates cyclic AMP-dependent protein kinase, also called protein kinase A (PKA), a serine/threonine protein kinase, by binding to its repressive regulatory subunits, which then undergo a conformation change and release the active PKA catalytic subunits. PKA phosphorylates a large number of metabolic enzymes, thereby providing a rapid response to hormones such as glucagon and epinephrine, which, when it binds to the β2-adronergic receptor, induces the same intracellular trimeric G-protein/adenylyl cyclase pathway as does glucagon to increase cAMP levels. The signaling process is reversed when the secretion of glucagon, which has a half-life in the blood of approximately 4 minutes, declines. The Gα subunit becomes inactive as a result of its GTPase activity, and remains inactive in the absence of activation by glucagon. cAMP is hydrolyzed to AMP by cAMP phosphodiesterase, thereby reducing the levls of cAMP and causing the PKA catalytic subunits to rejoin the repressive regulatory subunits. The concentration of cAMP and other second messengers is balanced by the activities of those processes that synthesize them and those processes that destroy them. In the presence of hormone cAMP synthesis exceeds cAMP destruction and cAMP concentration increases. In the absence of hormone cAMP destruction exceeds cAMP synthesis and cAMP concentration decreases.
- 23 -
PATHWAYS OF GLUCOSE METABOLISM I. The intracellular form of glucose is glucose-6-phosphate, which is the starting
substrate for all the pathways of glucose metabolism.
1. Phosphorylation of glucose to form glucose-6-phosphate by hexokinase: • irreversible, regulated step • ATP is expended • feedback inhibited by glucose-6-phosphate, the product of the reaction • relatively low Km for glucose (about 0.1 mM) • Glucose-6-phosphate, unlike glucose, is negatively charged, which prevents its exit
from cells. • The liver and pancreatic β cells have a different hexokinase isoform called
Glucokinase. o In the liver the synthesis of Glucokinase is stimulated by insulin in response to
high blood glucose levels. It has a high Km (about 10 mM) and high Vmax for glucose, and is not product-inhibited. The liver does not require glucose as a fuel. Rather, it uses the carbons of glucose for the synthesis of triacylglycerols (fats), which are stored in adipose tissue, and it stores glucose as glycogen when blood glucose levels are high (e.g., after a meal), and recovers glucose from the stored glycogen for release into the blood when blood glucose is low (e.g., during fasting). The high Km , high Vmax , and inducibility of glucokinase allow the liver to capture glucose for storage as glycogen and to synthesize triacylglycerols when blood glucose levels are high, and to reduce the capture of glucose, thereby conserving it for other tissues that use it as a primary fuel (e.g., brain, heart, white muscle), when blood glucose levels are low. The non-product-inhibition of glucokinase allows the liver to capture glucose even when its intracellular levels of glucose-6-phosphate are high. Glucokinase gene transcription is repressed by glucagon, a hormone secreted by the pancreatic alpha cells in response to low blood glucose levels. When glucose levels are limited (low blood glucose) existing glucokinase is bound by the Glucokinase Regulatory Protein [GKRP], which inactivates and sequesters it in the cell nucleus, thereby preventing the glucose produced by gluconeogenesis and glycogenolysis from being rephosphorylated and trapped in the liver. Glucokinase gene transcription is stimulated by insulin, a hormone secreted by the pancreatic β cells in response to high blood glucose levels.
o In the pancreatic β cells, glucokinase is thought to be a key component of the glucose-sensing mechanism, and several different mutations of the human glucokinase gene have been shown to be associated with Maturity-Onset Diabetes of the Young (MODY)
II. Glycolysis occurs in the cytosol, yielding 2 ATP, 2 pyruvate and 2 (NADH + H+) from
each glucose molecule The glycolytic pathway is present in all cells and has a central role in generating ATP with and without oxygen. One mole of glucose is converted to two moles of pyruvate and two moles of
- 24 -
NADH. The pathway uses energy from the oxidation of glucose to generate ATP by substrate-level phosphorylation (transfer of phosphate from a high-energy intermediate to ADP).
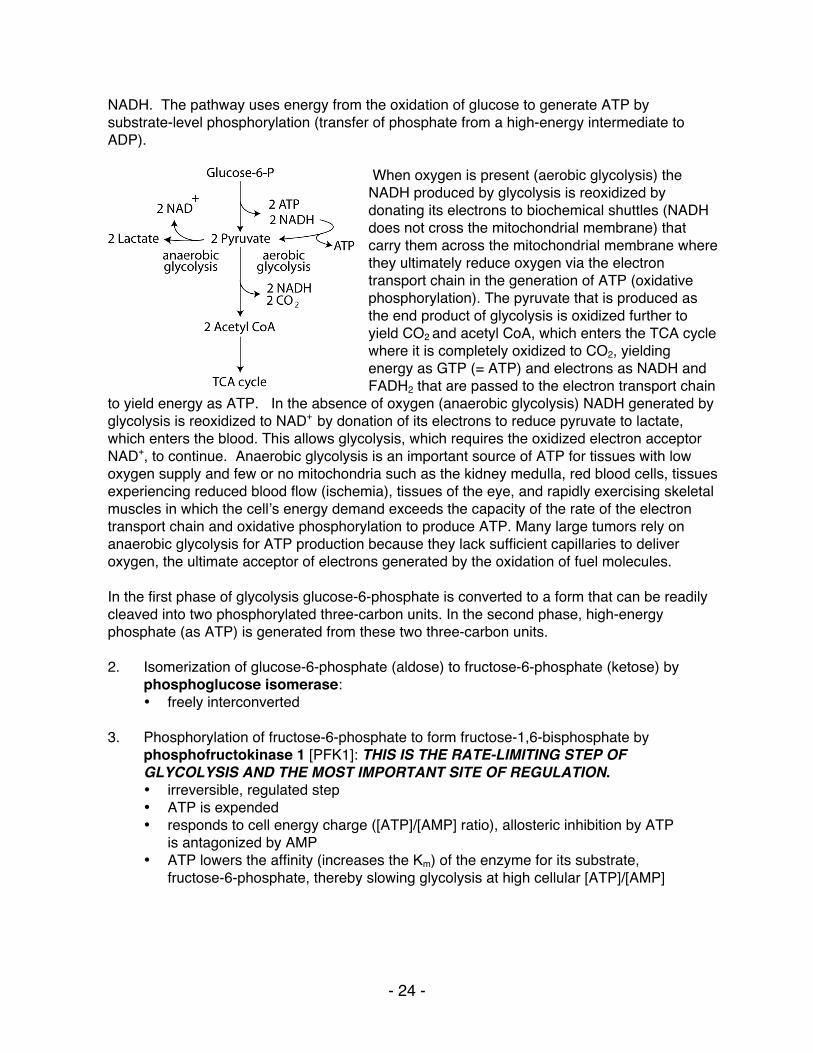
When oxygen is present (aerobic glycolysis) the NADH produced by glycolysis is reoxidized by donating its electrons to biochemical shuttles (NADH does not cross the mitochondrial membrane) that carry them across the mitochondrial membrane where they ultimately reduce oxygen via the electron transport chain in the generation of ATP (oxidative phosphorylation). The pyruvate that is produced as the end product of glycolysis is oxidized further to yield CO2 and acetyl CoA, which enters the TCA cycle where it is completely oxidized to CO2, yielding energy as GTP (= ATP) and electrons as NADH and FADH2 that are passed to the electron transport chain
to yield energy as ATP. In the absence of oxygen (anaerobic glycolysis) NADH generated by glycolysis is reoxidized to NAD+ by donation of its electrons to reduce pyruvate to lactate, which enters the blood. This allows glycolysis, which requires the oxidized electron acceptor NAD+, to continue. Anaerobic glycolysis is an important source of ATP for tissues with low oxygen supply and few or no mitochondria such as the kidney medulla, red blood cells, tissues experiencing reduced blood flow (ischemia), tissues of the eye, and rapidly exercising skeletal muscles in which the cellʼs energy demand exceeds the capacity of the rate of the electron transport chain and oxidative phosphorylation to produce ATP. Many large tumors rely on anaerobic glycolysis for ATP production because they lack sufficient capillaries to deliver oxygen, the ultimate acceptor of electrons generated by the oxidation of fuel molecules. In the first phase of glycolysis glucose-6-phosphate is converted to a form that can be readily cleaved into two phosphorylated three-carbon units. In the second phase, high-energy phosphate (as ATP) is generated from these two three-carbon units. 2. Isomerization of glucose-6-phosphate (aldose) to fructose-6-phosphate (ketose) by
phosphoglucose isomerase: • freely interconverted
3. Phosphorylation of fructose-6-phosphate to form fructose-1,6-bisphosphate by
phosphofructokinase 1 [PFK1]: THIS IS THE RATE-LIMITING STEP OF GLYCOLYSIS AND THE MOST IMPORTANT SITE OF REGULATION. • irreversible, regulated step • ATP is expended • responds to cell energy charge ([ATP]/[AMP] ratio), allosteric inhibition by ATP
is antagonized by AMP • ATP lowers the affinity (increases the Km) of the enzyme for its substrate,
fructose-6-phosphate, thereby slowing glycolysis at high cellular [ATP]/[AMP]
- 25 -
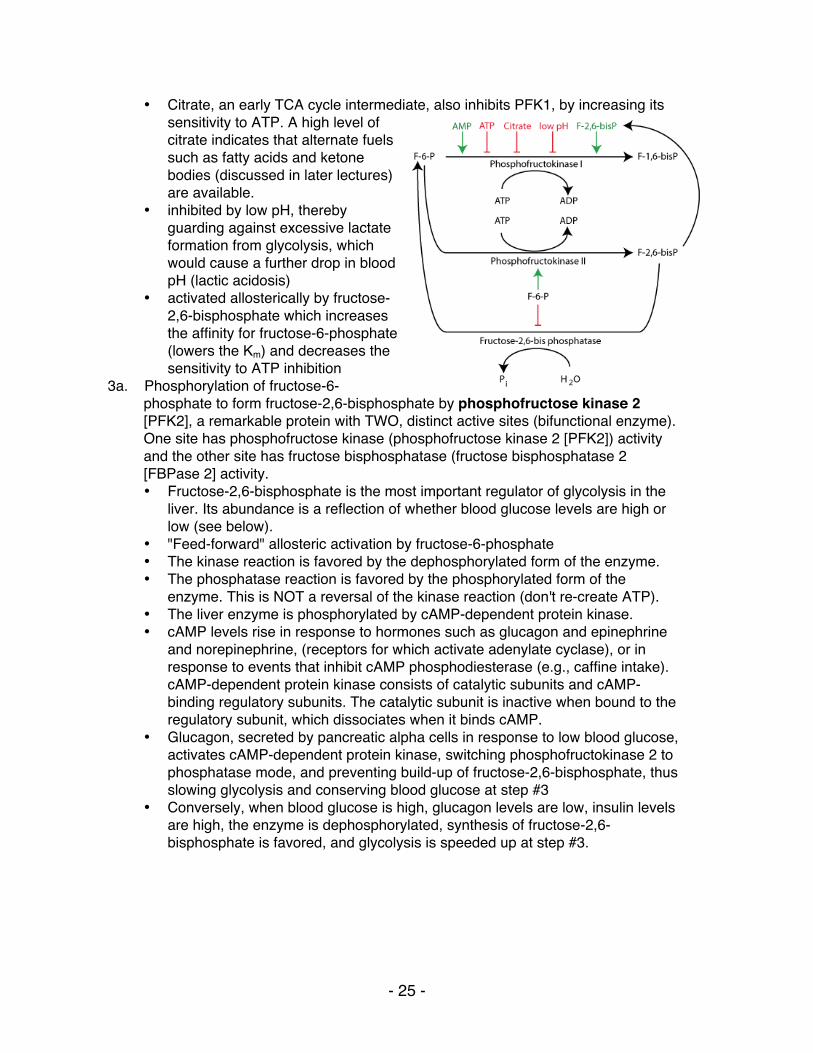
• Citrate, an early TCA cycle intermediate, also inhibits PFK1, by increasing its sensitivity to ATP. A high level of citrate indicates that alternate fuels such as fatty acids and ketone bodies (discussed in later lectures) are available.
• inhibited by low pH, thereby guarding against excessive lactate formation from glycolysis, which would cause a further drop in blood pH (lactic acidosis)
• activated allosterically by fructose-2,6-bisphosphate which increases the affinity for fructose-6-phosphate (lowers the Km) and decreases the sensitivity to ATP inhibition
3a. Phosphorylation of fructose-6-phosphate to form fructose-2,6-bisphosphate by phosphofructose kinase 2 [PFK2], a remarkable protein with TWO, distinct active sites (bifunctional enzyme). One site has phosphofructose kinase (phosphofructose kinase 2 [PFK2]) activity and the other site has fructose bisphosphatase (fructose bisphosphatase 2 [FBPase 2] activity. • Fructose-2,6-bisphosphate is the most important regulator of glycolysis in the
liver. Its abundance is a reflection of whether blood glucose levels are high or low (see below).
• "Feed-forward" allosteric activation by fructose-6-phosphate • The kinase reaction is favored by the dephosphorylated form of the enzyme. • The phosphatase reaction is favored by the phosphorylated form of the
enzyme. This is NOT a reversal of the kinase reaction (don't re-create ATP). • The liver enzyme is phosphorylated by cAMP-dependent protein kinase. • cAMP levels rise in response to hormones such as glucagon and epinephrine
and norepinephrine, (receptors for which activate adenylate cyclase), or in response to events that inhibit cAMP phosphodiesterase (e.g., caffine intake). cAMP-dependent protein kinase consists of catalytic subunits and cAMP-binding regulatory subunits. The catalytic subunit is inactive when bound to the regulatory subunit, which dissociates when it binds cAMP.
• Glucagon, secreted by pancreatic alpha cells in response to low blood glucose, activates cAMP-dependent protein kinase, switching phosphofructokinase 2 to phosphatase mode, and preventing build-up of fructose-2,6-bisphosphate, thus slowing glycolysis and conserving blood glucose at step #3
• Conversely, when blood glucose is high, glucagon levels are low, insulin levels are high, the enzyme is dephosphorylated, synthesis of fructose-2,6-bisphosphate is favored, and glycolysis is speeded up at step #3.
- 26 -
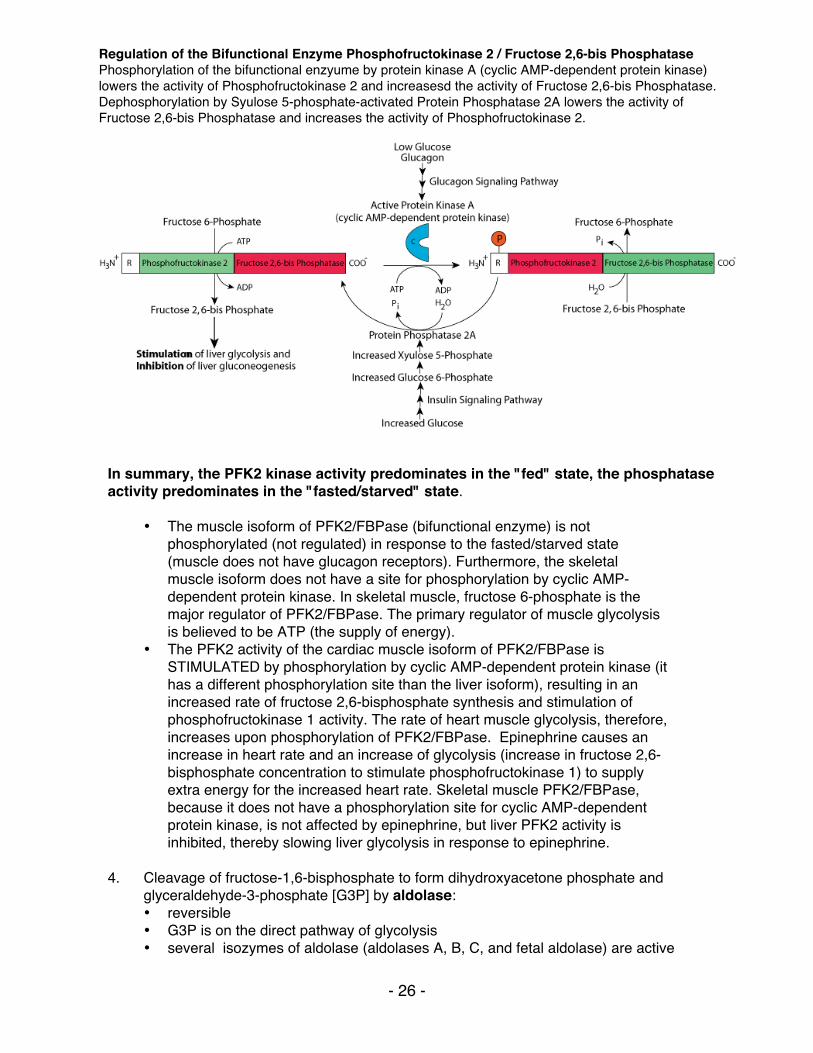
In summary, the PFK2 kinase activity predominates in the "fed" state, the phosphatase activity predominates in the "fasted/starved" state.
• The muscle isoform of PFK2/FBPase (bifunctional enzyme) is not phosphorylated (not regulated) in response to the fasted/starved state (muscle does not have glucagon receptors). Furthermore, the skeletal muscle isoform does not have a site for phosphorylation by cyclic AMP-dependent protein kinase. In skeletal muscle, fructose 6-phosphate is the major regulator of PFK2/FBPase. The primary regulator of muscle glycolysis is believed to be ATP (the supply of energy).
• The PFK2 activity of the cardiac muscle isoform of PFK2/FBPase is STIMULATED by phosphorylation by cyclic AMP-dependent protein kinase (it has a different phosphorylation site than the liver isoform), resulting in an increased rate of fructose 2,6-bisphosphate synthesis and stimulation of phosphofructokinase 1 activity. The rate of heart muscle glycolysis, therefore, increases upon phosphorylation of PFK2/FBPase. Epinephrine causes an increase in heart rate and an increase of glycolysis (increase in fructose 2,6-bisphosphate concentration to stimulate phosphofructokinase 1) to supply extra energy for the increased heart rate. Skeletal muscle PFK2/FBPase, because it does not have a phosphorylation site for cyclic AMP-dependent protein kinase, is not affected by epinephrine, but liver PFK2 activity is inhibited, thereby slowing liver glycolysis in response to epinephrine.
4. Cleavage of fructose-1,6-bisphosphate to form dihydroxyacetone phosphate and glyceraldehyde-3-phosphate [G3P] by aldolase: • reversible • G3P is on the direct pathway of glycolysis • several isozymes of aldolase (aldolases A, B, C, and fetal aldolase) are active
Regulation of the Bifunctional Enzyme Phosphofructokinase 2 / Fructose 2,6-bis Phosphatase Phosphorylation of the bifunctional enzyume by protein kinase A (cyclic AMP-dependent protein kinase) lowers the activity of Phosphofructokinase 2 and increasesd the activity of Fructose 2,6-bis Phosphatase. Dephosphorylation by Syulose 5-phosphate-activated Protein Phosphatase 2A lowers the activity of Fructose 2,6-bis Phosphatase and increases the activity of Phosphofructokinase 2.
- 27 -
against fructose-1-6-bisphosphate • dihydroxyacetone phosphate is the substrate for the synthesis of the glycerol
phosphate required by adipose tissue for the synthesis of stored triacylglycerols (fat) - adipose tissues rely on glucose (glycolysis) for its production
5. Interconversion of dihydroxyacetone phosphate and glyceraldehyde-3-phosphate by triose phosphate isomerase: • reversible
6. Oxidation of glyceraldehyde-3-phosphate to form 1,3-bisphosphoglycerate [1,3-BPG], a high-potential phosphorylated compound, by glyceraldehyde-3-
phosphate dehydrogenase: • reversible • ATP NOT expended − part of the energy obtained in the oxidation of G3P is
harvested as an electron pair donated to NAD+ − under anaerobic conditions the resulting NADH will be recycled back to NAD+ by donating its electrons to pyruvate at reaction #11, under aerobic conditions it will donate its electrons to oxygen in the production of ATP by oxidative phosphorylation, becoming reoxidized back to NAD+
• Carbon 1 of 1,3-BFG is at the oxidation level of a carboxylic acid. The phosphoryl group of this mixed anhydride has high transfer potential.
• 1,3-bisphosphoglycerate is converted to form large amounts of 2,3-bisphosphoglycerate in red blood cells by bisphosphoglycerate mutase. 2,3-bisphosphoglycerate regulates the hemoglobin/O2 dissociation curve − deficiency of glycolytic enzymes can cause hemolytic anemia. (Red blood cells, whose primary function is to supply oxygen to tissues, are themselves restricted to anaerobic metabolism, since they lack mitochondria.)
7. Transfer of the high-energy phosphate bond from 1,3-bisphosphoglycerate to form
ATP and 3-phosphoglycerate by phosphoglycerate kinase: • reversible • substrate-level phosphorylation; ATP is produced – this and the preceding
reaction (#6) allow for a net gain of ATP from glycolysis – particularly important in tissues with no (red blood cells) or few (e.g., renal medulla) mitochondria or low oxygen
8. Interconversion of 3-phosphoglycerate and 2-phosphoglycerate by phosphoglycerate mutase: • reversible
9. Dehydration of 2-phosphoglycerate to form phosphoenolpyruvate [PEP] by
enolase: • reversible • the dehydration elevates the transfer potential of the phosphoryl group
10. Transfer of high-energy phosphate bond from phosphoenolpyruvate to form ATP
and pyruvate by pyruvate kinase:
- 28 -
• essentially irreversible, highly regulated step • substrate-level phosphorylation; ATP is produced • "feed forward" activation by fructose-1,6-bisphosphate • liver isozyme shows cooperative phosphoenolpyruvate binding, allosteric
inhibition by ATP and alanine (an amino acid synthesized from pyruvate in one metabolic step)
• inhibition by glucagon-triggered phosphorylation − this slows glycolysis in the liver when blood glucose is low, thereby conserving glucose for use by tissues that use it as a primary fuel. Recall that PFK2 (step 3) is also phosphorylated, and its kinase activity is reduced, by the same mechanism, in response to low blood glucose levels.
• muscle isozyme is NOT regulated by phosphorylation • A rare, hyperactive mutant pyruvate kinase is harmful to red blood cells
because it depletes the precursor pool, diverting substrate from the synthesis of 2,3-bisphosphoglycerate, thereby impairing hemoglobin function.
11. Regeneration of NAD+ through reduction of pyruvate (the electron acceptor) to
form lactate by lactate dehydrogenase (fermentation – the generation of ATP by a process in which both the electron donor and the electron acceptor are organic molecules): • reversible • Major option used by cells under anaerobic conditions to regenerate cytosolic
NAD+. Without O2, mitochondria can't resupply NAD+ − this step allows glycolysis to continue anaerobically by regenerating the NAD+ required in step #6. Anaerobic glycolysis is obviously necessary in red blood cells, which lack mitochondria. It is also important when the oxygen supply is limiting, e.g., in exercising muscle, or anoxia due to impaired blood supply, as in stroke.
• The microbial fermentation repertoire is vast, and includes important commercial products such as ethanol, butanol and acetone. Coelocanths, "living fossil" fish, from oxygen-poor deep-sea strata, also employ alcoholic fermentation.
Summary of aerobic glycolysis (including hexo-/glucokinase):
Glucose + 2 Pi + 2 ADP + 2 NAD+ 2 Pyruvate + 2 ATP + 2 NADH + 4 H+ + 2 H2O
Summary of anaerobic glycolysis (including hexo-/glucokinase):
Glucose + 2 Pi + 2 ADP 2 Lactate + 2 ATP + 2 H+ + 2 H2O Remember that phosphofructokinase 1 is inhibited by low pH. The lactate that is formed under anaerobic conditions contributes to lower pH. Therefore, slowing glycolysis at the committed step slows lactate production and helps prevent acidosis due to excess lactate.
- 29 -
Metabolism of galactose: Galactose occurs in many foods, especially in dairy products in which lactose is its main dietary source. It also occurs in certain pectins, gums and mucilages. Other sources include sugar beets, a large number of fruits, including apples, bananas, cherries, and grapes, and in vegetables, including broccoli, carrots, cabbage, cauliflower, tomatoes, peas, pumpkins and spinach. Dietary galactose is metabolized principally by conversion to glucose-1-phosphate. As for glucose, galactose requires phosphorylation for entry into cellular metabolism. However, unlike glucose, which is phosphorylated at carbon 6, galactose is phosphorylated at carbon 1 by the enzyme galactokinase to yield galactose-1-phosphate, Galactose + ATP Galactose-1-posphate + ADP which then receives a uridine monophosphate group from uridine-diphosphate glucose (UDP-glucose) with the release of glucose-1-phosphate in a reaction catalyzed by the enzyme galactose-1-phosphate uridyl transferase:
Galactose-1-phosphate + UDP-glucose UDP-galactose + glucose-1-phosphate
Subsequently the enzyme UDP-galactose-4-epimerase can act to regenerate UDP-glucose: UDP-galactose UDP-glucose
Summary: Galactose + ATP Glucose-1-phosphate + ADP Glucose-1-phosphate can be isomerized to glucose-6-phosphate by the enzyme phosphoglucomutase (see part VI – glycogen metabolism, below). The enzymes for the conversion of galactose to glucose-1-phosphate are present in many tissues, including the adult erythrocyte, fibroblasts and fetal tissues. The liver has a high activity of these enzymes and can convert dietary galactose to blood glucose and glycogen. The metabolism of galactose is higher in infants than in adults. Newborns ingest up to one gram of galactose (as lactose) per kilogram during feeding, but the rate of galactose metabolism is so high that the concentration in the blood remains low. Genetic deficiency of the uridyl transferase (primary galactosemia) results in inappropriate metabolism of galactose to toxic forms such as galactitol. If untreated, galactosemia may be fatal. Metabolism of fructose: Fructose is a common dietary monosaccharide. It is a component of the disaccharide sucrose, common table sugar, and a free monosaccharide in honey and in high-fructose
- 30 -
corn syrup. As for both glucose and galactose, to enter cellular metabolism fructose must be phosphorylated. Phosphorylation at carbon 1 is catalyzed by the enzyme fructokinase to yield fructose-1-phosphate, which is subsequently cleaved by the enzyme fructose-1-phosphate aldolase (aldolase B – the only one of four aldolase isozymes able to cleave fructose-1-phosphate) to dihydroxyacetone phosphate (an intermediate of glycolysis) and glyceraldehyde: Fructose-1-phosphate dihydroxyacetone phosphate + glyceraldehyde The glyceraldehyde is phosphorylated by the enzyme triose kinase to yield glyceraldehyde-3-phosphate (an intermediate of glycolysis): Glyceraldehyde + ATP Glyceraldehyde-3-phosphate + ADP Fructose-1-phosphate aldolase (aldolase B) cleavage of fructose-1-phosphate is the rate-limiting step in fructose metabolism. The enzyme has a low affinity for fructose-1-phosphate and is very slow at physiological fructose-1-phosphate concentrations. Consequently, after ingestion of a high dose of fructose, normal individuals accumulate fructose-1-phosphate in the liver. Individuals with hereditary fructose intolerance, due primarily to a deficiency of fructose-1-phosphate aldolase, accumulate much higher amounts of fructose-1-phosphate in their livers. Prolonged fructose ingestion in these infants leads ultimately to ultrastructural changes in the liver and kidney, resulting in hepatic and/or renal failure and death. Hereditary fructose intolerance is usually a disease of infancy because adults with fructose intolerance who have survived avoid eating fruits, table sugar and other sweets.
III. The Tricarboxylic Acid [TCA] Cycle occurs in mitochondria. Each turn of the cycle produces one high-energy phosphate bond in the formation of GTP (high energy phosphate transferable to ADP to form ATP) and 4 reducing equivalents (3 NADH and 1 FADH2). After the O2-dependent processes of electron transport and oxidative phosphorylation, the total number of ATP produced per cycle is 10 (2.5 ATP from each NADH oxidized, 1.5 ATP from oxidation of FADH2 and 1 GTP + ADP GDP + ATP ) Two molecules of pyruvate are generated from one molecule of glucose, fueling two turns of the TCA cycle. Gycolysis of 1 molecule of glucose (6 carbons) yields a net of two molecules of ATP, 2 molecules of NADH (= 5 ATP) and two molecules of pyruvate (3 carbons). Each of the two molecules of pyruvate generated per glucose molecule is converted to acetyl CoA (step # 12), producing one molecule of NADH (= 2 NADH, or 5 ATP per molecule of glucose). Acetyl CoA then enters the TCA cycle. Thus the complete oxidation of one molecule of glucose yields either 30 or 32 ATP, depending on which of two biochemical shuttles carries the electrons from the NADH produced by glycolysis across the mitochondrial membrane to the electron transport chain. Anaerobic glycolysis of glucose to lactate nets only 2 ATP per glucose molecule – no electrons from glucose are passed to the electron transport chain and no ATP is generated by oxidative phosphorylation.
12. Formation of acetyl CoA from pyruvate by pyruvate dehydrogenase
• pyruvate moves between cytosolic and mitochondrial compartments by carrier-
- 31 -
mediated transport. • irreversible • NADH produced, CO2 released • deactivated by phosphorylation by a protein kinase activity stimulated by high
NADH/NAD+, acetyl CoA/CoA or ATP/ADP ratios • pyruvate and ADP activate by inhibiting the kinase • dephosphorylation (by a protein phosphatase), and consequently enzymatic
activity, is stimulated by insulin. • Ca2+ activates the phosphatase in heart muscle to increase energy for rapid
contraction • acetyl CoA, NADH are competitive inhibitors • 4 vitamins are required as co-factors: thiamin (as thiamine pyrophosphate,
TPP), riboflavin (as FAD), niacin (as NAD+) and pantothenate (as Coenzyme A). Lipoate, non-essential in the diet, is also required. Alcoholism (ethanol consumption interferes with thiamine absorption), combined with poor nutrition, can deplete thiamin, thereby blocking the TCA cycle. For such malnourished individuals, glucose administration without thiamin supplementation is harmful, because its aerobic metabolism is compromised.
13. Condensation of oxaloacetate and acetyl CoA by citrate synthase to form citrate
• Irreversible • feed-back inhibited by citrate (the product of the enzymatic reaction) • ordered binding of substrates: oxaloacetate binding changes the enzyme
conformation to accept acetyl CoA • Remember, citrate is an allosteric inhibitor of reaction #3, the rate-limiting step
of glycolysis catalyzed by PFKI. • Citrate can exit the mitochomdria to the cytosol, where it is used for fatty acid
synthesis (discussed in the lectures on the metabolism of triacylglycerol).
14. Interconversion of citrate, cis-aconitate and isocitrate by aconitase • reversible
15. Conversion of isocitrate to alpha-keto-glutarate by isocitrate dehydrogenase • irreversible oxidative decarboxylation • NADH produced, C02 released • major regulation step of the cycle responsive to the energy charge of the cell • the cooperative binding of isocitrate and NAD+ is enhanced by ADP (reduced
energy) • competitively inhibited by NADH (increased reducing power for ATP
generation) • Ca2+, released from the sarcoplasmic reticulum in contracting heart muscle, and
possibly other muscle as well, lowers the Km and speeds up the velocity of the enzyme to increase energy for contraction
16. Conversion of alpha-keto-glutarate to succinyl CoA by alpha-keto-glutarate
dehydrogenase • irreversible oxidative decarboxylation • NADH produced, CO2 released • product inhibited by succinyl CoA and NADH
- 32 -
• Ca2+, released from sarcoplasmic reticulum in contracting heart muscle, and possibly other muscle as well, lowers the Km and speeds up the velocity of the enzyme to increase energy for contraction
17. Formation of succinate from succinyl CoA by succinyl CoA synthetase
(succinate thiokinase) • substrate-level phosphorylation; GTP (= ATP) produced • succinyl CoA reacts with glycine in the mitochondria to form the first
intermediate, δ-aminolevulinic acid, which exits the mitochondria to the cytosol, in the heme synthetic pathway
18. Conversion of succinate to fumarate by succinate dehydrogenase
• FADH2 produced, a C=C double bond is formed • Succinate dehydrogenase is a membrane-bound protein located on the inner
mitochondrial membrane, unlike the other enzymes of the TCA cycle, which are located in the mitochondrial matrix.
19. Conversion of fumarate to malate by fumarase
20. Oxidation of malate to form oxaloacetate by malate dehydrogenase • NADH produced
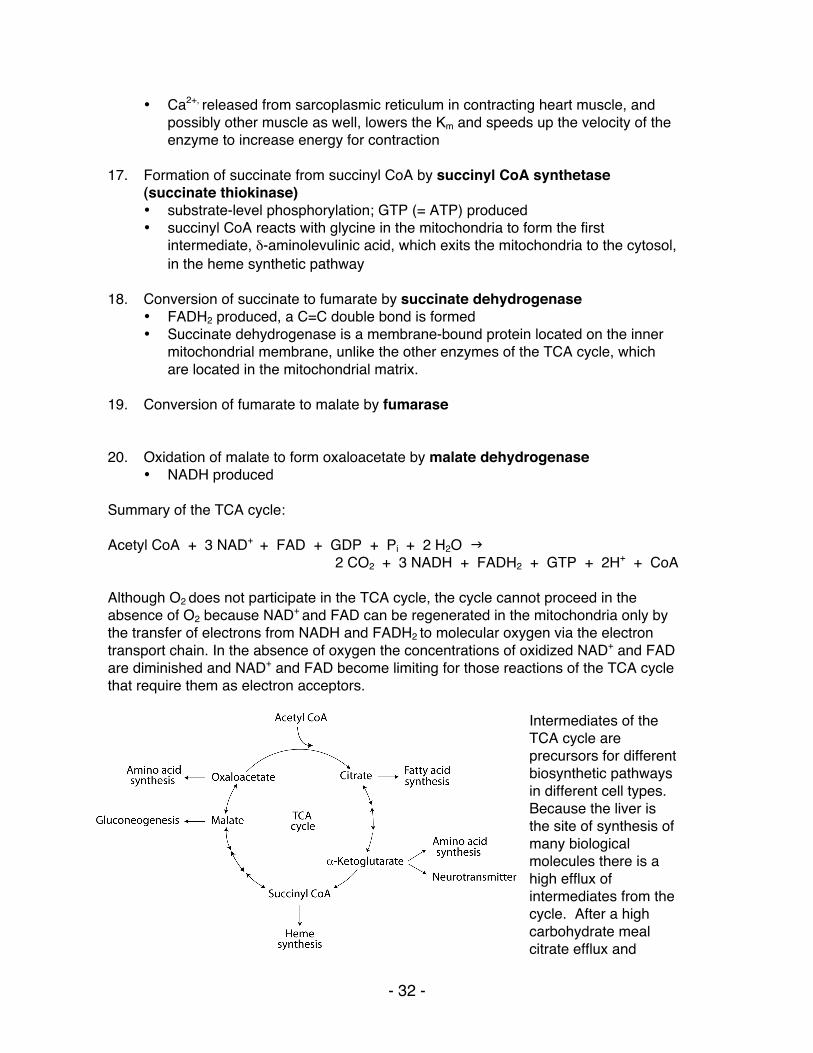
Summary of the TCA cycle: Acetyl CoA + 3 NAD+ + FAD + GDP + Pi + 2 H2O
2 CO2 + 3 NADH + FADH2 + GTP + 2H+ + CoA Although O2 does not participate in the TCA cycle, the cycle cannot proceed in the absence of O2 because NAD+ and FAD can be regenerated in the mitochondria only by the transfer of electrons from NADH and FADH2 to molecular oxygen via the electron transport chain. In the absence of oxygen the concentrations of oxidized NAD+ and FAD are diminished and NAD+ and FAD become limiting for those reactions of the TCA cycle that require them as electron acceptors.
Intermediates of the TCA cycle are precursors for different biosynthetic pathways in different cell types. Because the liver is the site of synthesis of many biological molecules there is a high efflux of intermediates from the cycle. After a high carbohydrate meal citrate efflux and
- 33 -
cleavage to acetyl CoA provides acetyl units for cytosolic fatty acid synthesis. During fasting, gluconeogenic precursors are converted to malate, which exits the mitochondria for cytosolic gluconeogenesis. The liver also uses TCA cycle intermediates to synthesize some non-essential amino acids, and succinyl CoA is used in both liver and bone marrow for the synthesis of heme. In the brain α-ketoglutarate is converted to glutamate and then to γ-aminobutyric acid (GABA), a neurotransmitter, and in skeletal muscle it is converted to glutamine, which is transported through the blood for use by other tissues. Removal of any of the TCA cycle intermediates depletes the four-carbons that regenerate oxaloacetate at each turn of the cycle, diminishing the ability of the cycle to oxidize acetyl CoA. For the TCA cycle to continue functioning, enough four-carbon intermediates must be supplied from the degradation of carbohydrates or certain other molecules to compensate for the depletion. Reactions that replenish TCA cycle intermediates are called “anaplerotic”, meaning “to fill up”. Pyruvate carboxylase (reaction #29) is a major anaplerotic enzyme, which uses ATP to catalyze the addition of CO2 to three-carbon pyruvate, forming four-carbon oxaloacetate. Many tissues contain pyruvate carboxylase as an anapleoric enzyme, but its concentration is particularly high in the liver and the kidney cortex, where gluconeogenesis withdraws four-carbon oxaloacetate and four-carbon malate from the TCA cycle for the synthesis of glucose. During the degradation of many amino acids their carbon skeletons are converted to four- and five-carbon TCA cycle intermediates that can regenerate oxaloacetate. Alanine and serine carbons can be converted to oxaloacetate by pyruvate carboxylase. Propionyl CoA, derived from the degradation of methionine, thymine and odd-chain fatty acids can be carboxylated to syccinyl CoA, a four-carbon TCA cycle intermediate.
IV. The Pentose Phosphate Shunt functions as a source of NADPH and Ribose-5-phosphate.
The pentose phosphate shunt (also known as the hexose monophosphate shunt or the 6-phosphogluconate pathway) shares the intermediates glyceraldehyde-3-phosphate and fructose-6-phosphate with the glycolytic pathway. Both pathways occur in the cytosol and, therefore, have access to one another. The pentose phosphate shunt has two phases, the oxidative phase (reactions 21 - 23), in which NADPH and pentose-5-phosphate are generated, and the non-oxidative phase (reactions 24 - 28), in which unused pentose-5-phosphate can be converted to other sugar intermediates and then returned to the glycolytic pathway as glyceraldehyde-3-phosphate and fructose-6-phosphate. Relative production of NADPH verses pentose-5-phosphate such as ribose-5-phosphate varies with metabolic demand. NADPH participates in biosynthetic reductions while NADH, which is not generated by the pentose phosphate shunt, is used primarily to donate electrons for oxidative phosphorylation to generate ATP. All cells require NADPH for reductive detoxification, and most cells require ribose-5-phosphate for nucleotide synthesis. Reactions of the Oxidative Phase:
21. Conversion of glucose-6-phosphate to 6-phosphogluconolactone by
- 34 -
glucose-6-phosphate dehydrogenase • irreversible, rate limiting step of the pathway • inhibited by NADPH which competes for NADP+ binding • NADPH produced, C=O double bond formed • Km for NAD+ is 1000-fold higher than for NADP+ (In the fed state, rat liver
NADP+/NADPH is about 0.14, while NAD+/NADH is about 700. This allows a high capacity for electron acceptor activity for oxidations, and at the same time, a high electron donor activity for reductive reactions, including the synthesis of fatty acids and sterols, and the reduction of inappropriately oxidized protein cysteine residues.)
• X-linked gene with mosaic expression in females
22. Conversion of 6-phosphogluconolactone to 6-phosphogluconate by lactonase • irreversible
23. Conversion of 6-phosphogluconate to ribulose-5-phosphate by
6-phosphogluconate dehydrogenase • irreversible • NADPH produced, CO2 released
Reactions of the Non-Oxidative Phase:
24. Interconversion of ribulose-5-phosphate and xylulose-5-phosphate by
phosphopentose epimerase (ribulose-5-phosphate epimerase) • reversible
25. Interconversion of ribulose-5-phosphate and ribose-5-phosphate by phosphopentose isomerase (ribose-5-phosphate ketoisomerase) • reversible • Ribose is a major component of nucleic acids.
26. Rearrangement of (ribose-5-phosphate + xylulose-5-phosphate) to form sedoheptulose-7-phosphate and glyceraldehyde-3-phosphate by transketolase • reversible • Glyceraldehyde-3-phosphate is a glycolysis intermediate. • requires thiamine pyrophosphate [TPP]: Measurement of red blood cell
transketolase activity is a convenient bioassay to test for TPP deficiency.
27. Rearrangement of sedoheptulose-7-phosphate and glyceraldehyde-3-phosphate to form erythrose-4-phosphate and fructose-6-phosphate by transaldolase • reversible • Fructose-6-phosphate is a glycolysis intermediate.
28. Rearrangement of xylulose-5-phosphate and erythrose-4-phosphate to form glyceraldehyde-3-phosphate and fructose-6-phosphate by transketolase • reversible • Both products are also glycolysis intermediates.
- 35 -
In summary: The oxidative branch of the pentose phosphate shunt can generate NADPH, without generating a net increase of ribose-phosphate by using the ribose-phosphate sugars formed as substrates for the non-oxidative branch, which converts them to fructose-6-phosphate and glyceraldehyde-3-phosphate, which can then enter the glycolytic or gluconeogenic pathway. 3 glucose-6-P + 6 NADP+ + 3H2O 3 CO2 + 6 NADPH + 6 H+ + 2 fructose-6-P + glyceraldehyde-3-P
Alternatively, ribose-phosphate can be generated by the non-oxidative branch, without NADPH production, from the glycolytic intermediates fructose-6-phosphate and glyceraldehyde-3-phosphate.
2 fructose-6-P + glyceraldehyde-3-P 2 xylulose-5-P + ribose-5-P
2 xylulose-5-P 2 ribulose-5-P
2 ribulose-5-P 2 ribose-5-P
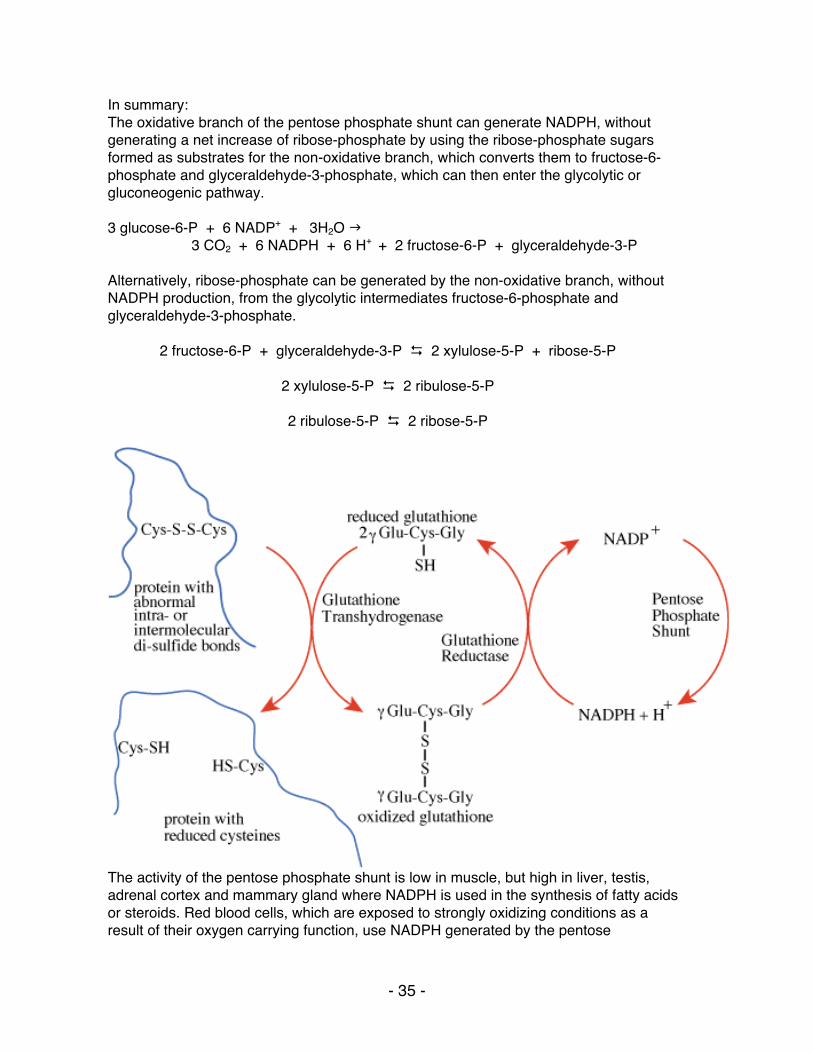
The activity of the pentose phosphate shunt is low in muscle, but high in liver, testis, adrenal cortex and mammary gland where NADPH is used in the synthesis of fatty acids or steroids. Red blood cells, which are exposed to strongly oxidizing conditions as a result of their oxygen carrying function, use NADPH generated by the pentose
- 36 -
phosphate shunt to counteract their oxidizing environment. The major role of NADPH in red blood cells is to reduce the disulfide form of glutathione (a tripeptide of sequence γ-glu-cys-gly) to the sulfhydryl form, catalyzed by glutathione reductase. The reduced glutathione serves as a "sulfhydryl buffer" to maintain the cysteine residues of hemoglobin and other red-cell proteins in the reduced state. It also serves to keep the hemoglobin iron in the ferrous state by reducing peroxides that undergo a reaction in which they extract an electron from ferrous iron, converting it to ferric iron, which impairs hemoglobin function.
V. Gluconeogenesis is NOT glycolysis run backwards.
The daily glucose requirement for a typical adult is about 160 - 190 grams, 120 - 140 grams of which are used by the brain, which depends on a continual glucose supply. Red blood cells also require glucose as a fuel (anaerobic glycolysis) because they lack mitochondria and are, therefore, unable to use other fuel molecules. The blood contains about 20 grams of glucose and approximately 190 grams are stored as glycogen, for a total reserve lasting about one day. During fasting/starvation glucose must be supplied from non-carbohydrate sources such as lactate, amino acids from muscle protein breakdown and glycerol from adipose fat breakdown. Six high energy bonds are expended to synthesize one molecule of glucose from 2 molecules of pyruvate. Synthesized glucose is usually for export from the liver into the blood during fasting. The reversible reactions of the glycolysis pathway are used for gluconeogenesis, but the irreversible reactions require other reactions to bypass them. These irreversible reactions and those that bypass them are the major sites of regulation of both pathways.
29. Carboxylation of pyruvate to form oxaloacetate by pyruvate carboxylase
• irreversible • allosteric activation by acetyl CoA • inhibited by ADP • mitochondrial localization • ATP is expended • The vitamin biotin is the required CO2 (obtained from HCO3-) carrier/donor • Oxaloacetate is transferred to the cytosol as malate, where it is regenerated by
a cytosolic malate dehydrogenase.
30. Transfer of a high-energy phosphate bond to oxaloacetate to form phosphoenolpyruvate by phosphoenolpyruvate carboxykinase • inhibited by ADP • GTP is expended • enzyme is transcriptionally induced by increased glucagon, decreased insulin
31. Dephosphorylation of fructose-1,6-bisphosphate to form fructose-6-phosphate by fructose-1,6-bisphosphatase • inhibited by fructose-6-phosphate, AMP and fructose-2,6-bisphosphate • stimulated by citrate • its synthesis is inhibited by insulin and stimulated by glucagon
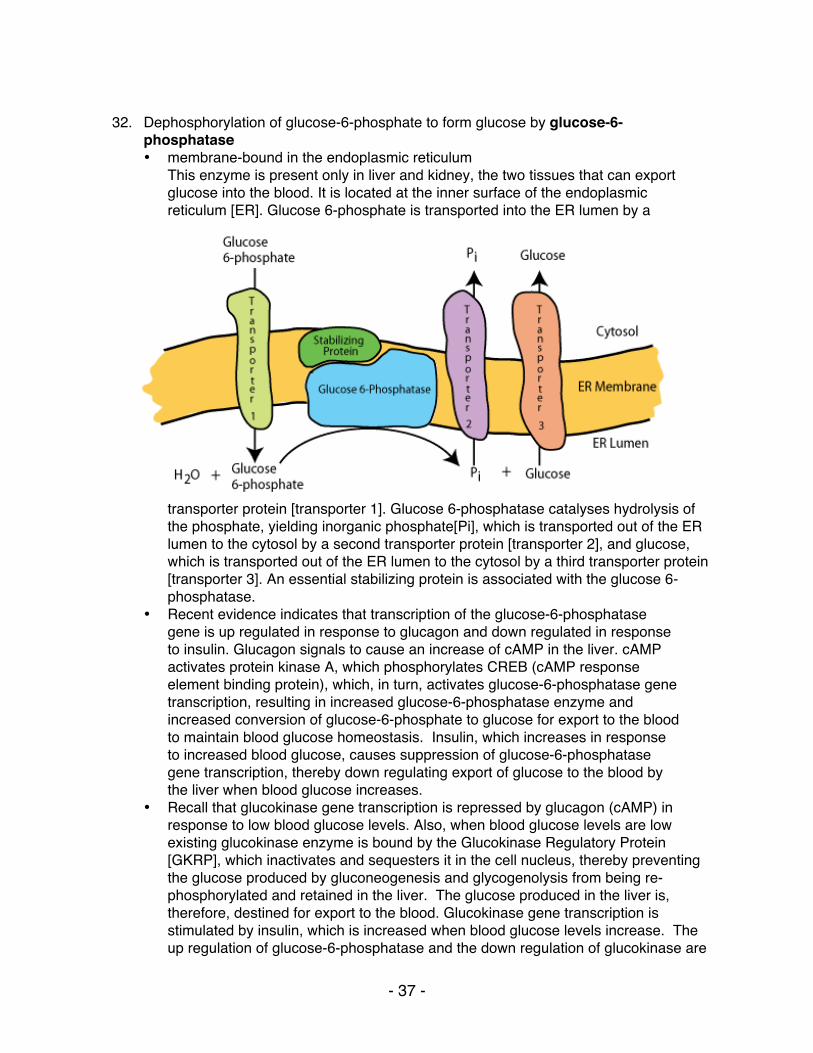
- 37 -
32. Dephosphorylation of glucose-6-phosphate to form glucose by glucose-6-
phosphatase • membrane-bound in the endoplasmic reticulum
This enzyme is present only in liver and kidney, the two tissues that can export glucose into the blood. It is located at the inner surface of the endoplasmic reticulum [ER]. Glucose 6-phosphate is transported into the ER lumen by a
transporter protein [transporter 1]. Glucose 6-phosphatase catalyses hydrolysis of the phosphate, yielding inorganic phosphate[Pi], which is transported out of the ER lumen to the cytosol by a second transporter protein [transporter 2], and glucose, which is transported out of the ER lumen to the cytosol by a third transporter protein [transporter 3]. An essential stabilizing protein is associated with the glucose 6-phosphatase.
• Recent evidence indicates that transcription of the glucose-6-phosphatase gene is up regulated in response to glucagon and down regulated in response to insulin. Glucagon signals to cause an increase of cAMP in the liver. cAMP activates protein kinase A, which phosphorylates CREB (cAMP response element binding protein), which, in turn, activates glucose-6-phosphatase gene transcription, resulting in increased glucose-6-phosphatase enzyme and increased conversion of glucose-6-phosphate to glucose for export to the blood to maintain blood glucose homeostasis. Insulin, which increases in response to increased blood glucose, causes suppression of glucose-6-phosphatase gene transcription, thereby down regulating export of glucose to the blood by the liver when blood glucose increases.
• Recall that glucokinase gene transcription is repressed by glucagon (cAMP) in response to low blood glucose levels. Also, when blood glucose levels are low existing glucokinase enzyme is bound by the Glucokinase Regulatory Protein [GKRP], which inactivates and sequesters it in the cell nucleus, thereby preventing the glucose produced by gluconeogenesis and glycogenolysis from being re-phosphorylated and retained in the liver. The glucose produced in the liver is, therefore, destined for export to the blood. Glucokinase gene transcription is stimulated by insulin, which is increased when blood glucose levels increase. The up regulation of glucose-6-phosphatase and the down regulation of glucokinase are
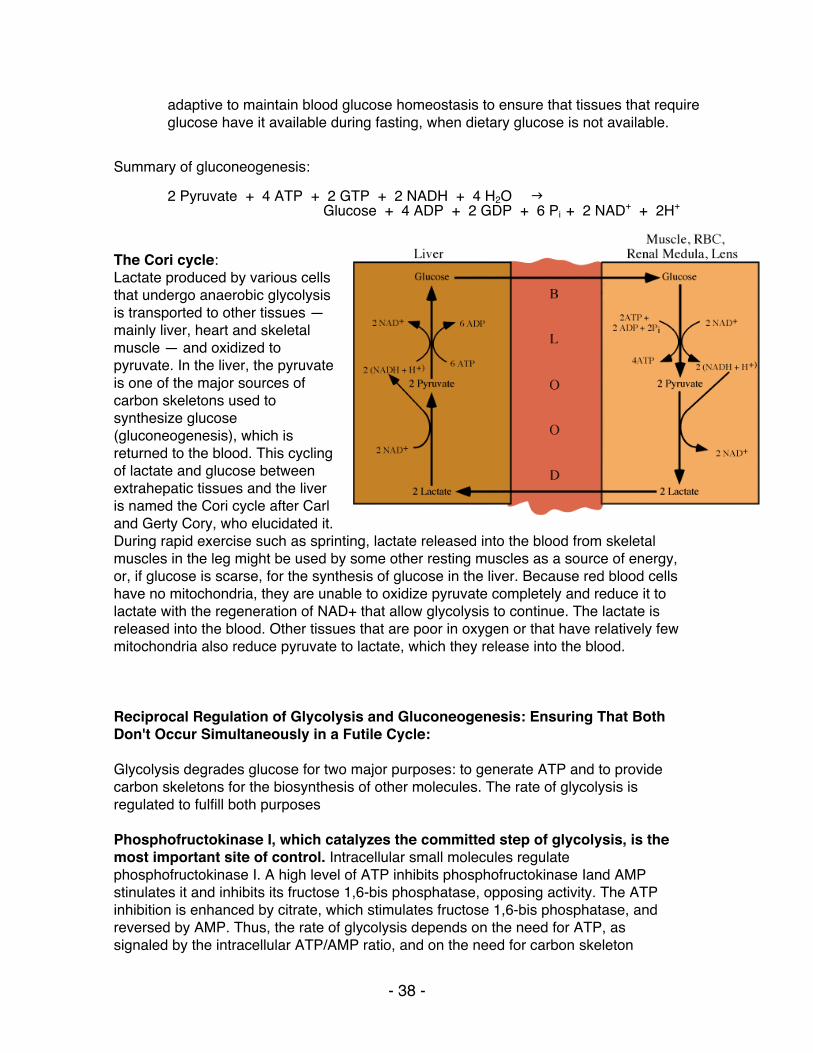
- 38 -
adaptive to maintain blood glucose homeostasis to ensure that tissues that require glucose have it available during fasting, when dietary glucose is not available.
Summary of gluconeogenesis:
2 Pyruvate + 4 ATP + 2 GTP + 2 NADH + 4 H2O
Glucose + 4 ADP + 2 GDP + 6 Pi + 2 NAD+ + 2H+
The Cori cycle: Lactate produced by various cells that undergo anaerobic glycolysis is transported to other tissues — mainly liver, heart and skeletal muscle — and oxidized to pyruvate. In the liver, the pyruvate is one of the major sources of carbon skeletons used to synthesize glucose (gluconeogenesis), which is returned to the blood. This cycling of lactate and glucose between extrahepatic tissues and the liver is named the Cori cycle after Carl and Gerty Cory, who elucidated it. During rapid exercise such as sprinting, lactate released into the blood from skeletal muscles in the leg might be used by some other resting muscles as a source of energy, or, if glucose is scarse, for the synthesis of glucose in the liver. Because red blood cells have no mitochondria, they are unable to oxidize pyruvate completely and reduce it to lactate with the regeneration of NAD+ that allow glycolysis to continue. The lactate is released into the blood. Other tissues that are poor in oxygen or that have relatively few mitochondria also reduce pyruvate to lactate, which they release into the blood.
Reciprocal Regulation of Glycolysis and Gluconeogenesis: Ensuring That Both Don't Occur Simultaneously in a Futile Cycle: Glycolysis degrades glucose for two major purposes: to generate ATP and to provide carbon skeletons for the biosynthesis of other molecules. The rate of glycolysis is regulated to fulfill both purposes Phosphofructokinase I, which catalyzes the committed step of glycolysis, is the most important site of control. Intracellular small molecules regulate phosphofructokinase I. A high level of ATP inhibits phosphofructokinase Iand AMP stinulates it and inhibits its fructose 1,6-bis phosphatase, opposing activity. The ATP inhibition is enhanced by citrate, which stimulates fructose 1,6-bis phosphatase, and reversed by AMP. Thus, the rate of glycolysis depends on the need for ATP, as signaled by the intracellular ATP/AMP ratio, and on the need for carbon skeleton
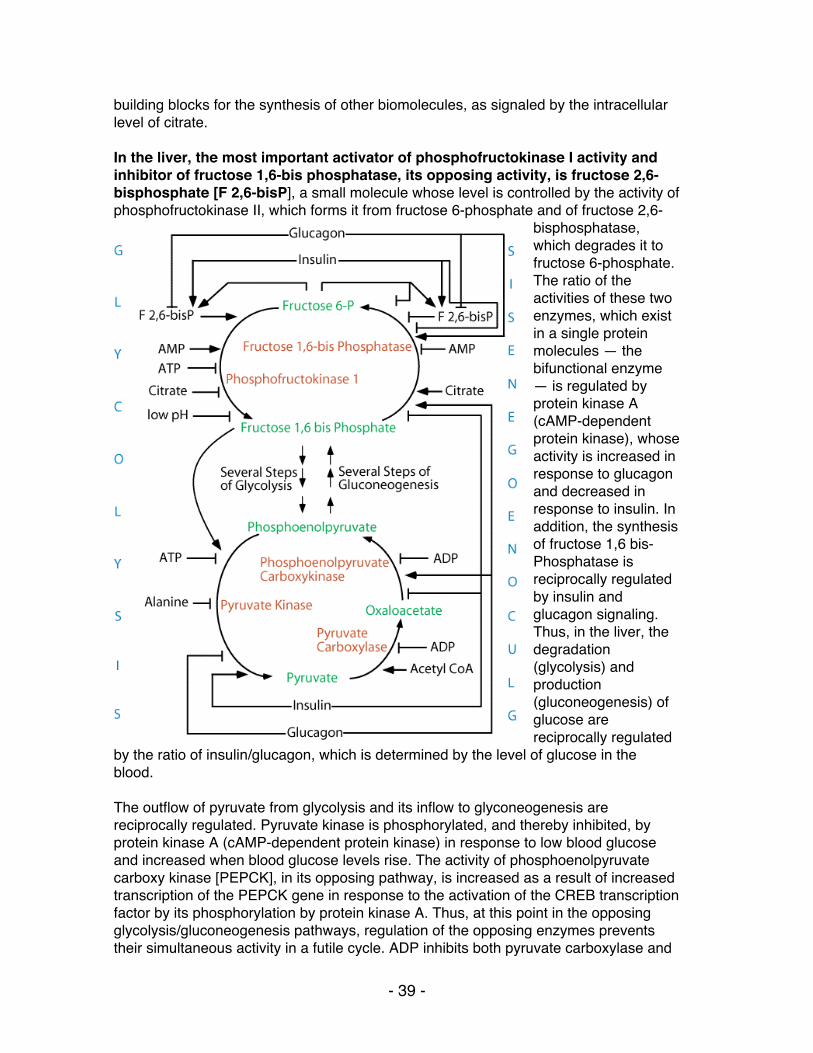
- 39 -
building blocks for the synthesis of other biomolecules, as signaled by the intracellular level of citrate. In the liver, the most important activator of phosphofructokinase I activity and inhibitor of fructose 1,6-bis phosphatase, its opposing activity, is fructose 2,6-bisphosphate [F 2,6-bisP], a small molecule whose level is controlled by the activity of phosphofructokinase II, which forms it from fructose 6-phosphate and of fructose 2,6-
bisphosphatase, which degrades it to fructose 6-phosphate. The ratio of the activities of these two enzymes, which exist in a single protein molecules — the bifunctional enzyme — is regulated by protein kinase A (cAMP-dependent protein kinase), whose activity is increased in response to glucagon and decreased in response to insulin. In addition, the synthesis of fructose 1,6 bis- Phosphatase is reciprocally regulated by insulin and glucagon signaling. Thus, in the liver, the degradation (glycolysis) and production (gluconeogenesis) of glucose are reciprocally regulated
by the ratio of insulin/glucagon, which is determined by the level of glucose in the blood. The outflow of pyruvate from glycolysis and its inflow to glyconeogenesis are reciprocally regulated. Pyruvate kinase is phosphorylated, and thereby inhibited, by protein kinase A (cAMP-dependent protein kinase) in response to low blood glucose and increased when blood glucose levels rise. The activity of phosphoenolpyruvate carboxy kinase [PEPCK], in its opposing pathway, is increased as a result of increased transcription of the PEPCK gene in response to the activation of the CREB transcription factor by its phosphorylation by protein kinase A. Thus, at this point in the opposing glycolysis/gluconeogenesis pathways, regulation of the opposing enzymes prevents their simultaneous activity in a futile cycle. ADP inhibits both pyruvate carboxylase and
- 40 -
PEPCK so that gluconeogenesis, which requires the input of ATP energy and electrons from NADH, does not proceed at the expense of the energy required to maintain hepatocyte essential functions.
VI. Glycogen Metabolism serves different purposes in muscle and liver.
The liver is a so-called "altruistic" organ, which releases glucose into the blood to meet tissue need. Glucose released from muscle glycogen stores is used on site to provide energy for muscle contraction. Like glycolysis and gluconeogenesis, glycogenolysis and glycogenesis are NOT reversals of each other.
33. Interconversion of glucose-6-phosphate and glucose-1-phosphate by phosphoglucomutase • reversible - this is the only enzyme common to both glycogen synthesis and
breakdown
34. Activation of glucose-1-phosphate to form UDP-glucose by UDPG pyrophosphorylase
35. Transfer of glucose from UDP-glucose to glycogen by glycogen synthase • does not initiate new molecules of glycogen but requires a "primer" at least 4
glucose units long • Glycogenin, a protein, autocatalyzes the synthesis of a glycogen primer,
covalently attached to itself, which glycogen synthase extends. Therefore, the number of molecules of glycogenin present determines the number of glycogen molecules synthesized.
• Glycogen synthase must always be in contact with glycogenin to be active. Therefore, the size of a glycogen molecule is limited by the physical distance between its most distal, non-reducing end and the glycogenin covalently attached to its reducing end. When this distance is longer than glycogen synthase can span elongation of the glycogen molecule halts.
• inactivated by phosphorylation via cAMP-dependent cascade • inactivation reversed by insulin, which stimulates dephosphorylation • allosteric activation of the phosphorylated form by glucose-6-phosphate
36. Transfer of (glucose)>6 from alpha-1,4 glycosidic linkage to 1,6 linkage by branching enzyme • more compact storage, more accessible free ends for synthesis and
phosphorylase (see below) • The block transferred is at least 7 residues long, must include the non-reducing
end, must come from a chain of at least 11 residues long (thereby leaving a primer of at least 4 residues as is required by glycogen synthase) and is transferred at least 4 residues away from a pre-existing branch.
Summary of glycogen synthesis:
Glucose-6-phosphate + ATP + glycogenn + H2O glycogenn+1 + ADP + 2 Pi
- 41 -
37. Phosphorolysis of alpha-1,4-glycosidic bonds of glycogen to release glucose-1-
phosphate sequentially from the non-reducing end by glycogen phosphorylase • In vivo, [Pi] is about 100-fold higher than [glucose-1-phosphate], preventing
reversal • The muscle and liver phosphorylase isoforms are distinct. • Glucagon (liver) or epinephrine (muscle and liver) triggered cAMP-dependent
phosphorylation cascade results in the phosphorylation of serine 14, switching the enzyme to the activated, "a " form. — Phosphorylation of glycogen phosphorylase requires a second protein
kinase. cAMP-dependent protein kinase (protein kinase A) phosphorylates phosphorylase kinase (the second protein kinase), converting it from the inactive "b " form to the active "a " form. Phosphorylase kinase then phosphorylates glycogen phosphorylase at serine 14, converting the inactive "b " form to the active "a " form.
• Glucose-binding causes a conformation change in the liver "a " isoform, exposing the phosphoserine to the enzymatic activity of protein phosphatase 1, which removes the activating phosphate, thereby regenerating the inactive phosphorylase "b " form. Thus, in liver, glycogen breakdown by glycogen phosphorylase is regulated by the glucose concentration, consistent with the function of the liver, to ensure that glucose is provided to other tissues.
• The muscle isoform of phosphorylase b can be activated the by binding of AMP, which is present in increased concentrations when the energy charge of the cell is low. ATP and glucose-6-phosphate reverse the activation by AMP by competing for the AMP binding site. Thus, in muscle, glycogen breakdown catalyzed by glycogen phosphorylase is regulated by the energy charge of the cell, consistent with the function of muscle glycogen, to act as an energy store to be mobilized to supply energy for muscle contraction. The liver isoform of phosphorylase b is not activated by AMP.
38. Hydrolysis of glycogen branchpoints by transferase and alpha-1,6-glucosidase
(debranching enzyme) to release glucose • two step reaction, both activities in one protein
39. Phosphorylation of glucose to form glucose-6-phosphate by hexokinase (muscle) or glucokinase (liver) and phosphoglucomutase (steps #1 and #33)
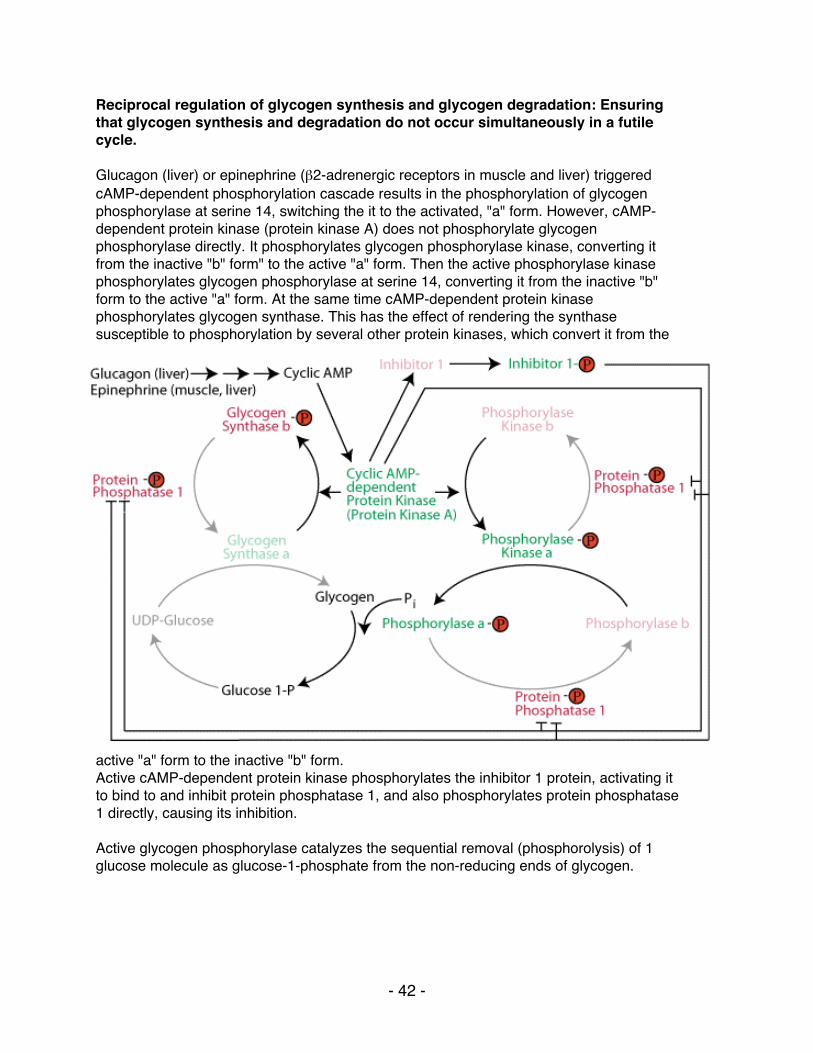
- 42 -
Reciprocal regulation of glycogen synthesis and glycogen degradation: Ensuring that glycogen synthesis and degradation do not occur simultaneously in a futile cycle. "" Glucagon (liver) or epinephrine (β2-adrenergic receptors in muscle and liver) triggered cAMP-dependent phosphorylation cascade results in the phosphorylation of glycogen phosphorylase at serine 14, switching the it to the activated, "a" form. However, cAMP- dependent protein kinase (protein kinase A) does not phosphorylate glycogen phosphorylase directly. It phosphorylates glycogen phosphorylase kinase, converting it from the inactive "b" form" to the active "a" form. Then the active phosphorylase kinase phosphorylates glycogen phosphorylase at serine 14, converting it from the inactive "b" form to the active "a" form. At the same time cAMP-dependent protein kinase phosphorylates glycogen synthase. This has the effect of rendering the synthase susceptible to phosphorylation by several other protein kinases, which convert it from the
active "a" form to the inactive "b" form. Active cAMP-dependent protein kinase phosphorylates the inhibitor 1 protein, activating it to bind to and inhibit protein phosphatase 1, and also phosphorylates protein phosphatase 1 directly, causing its inhibition. Active glycogen phosphorylase catalyzes the sequential removal (phosphorolysis) of 1 glucose molecule as glucose-1-phosphate from the non-reducing ends of glycogen.
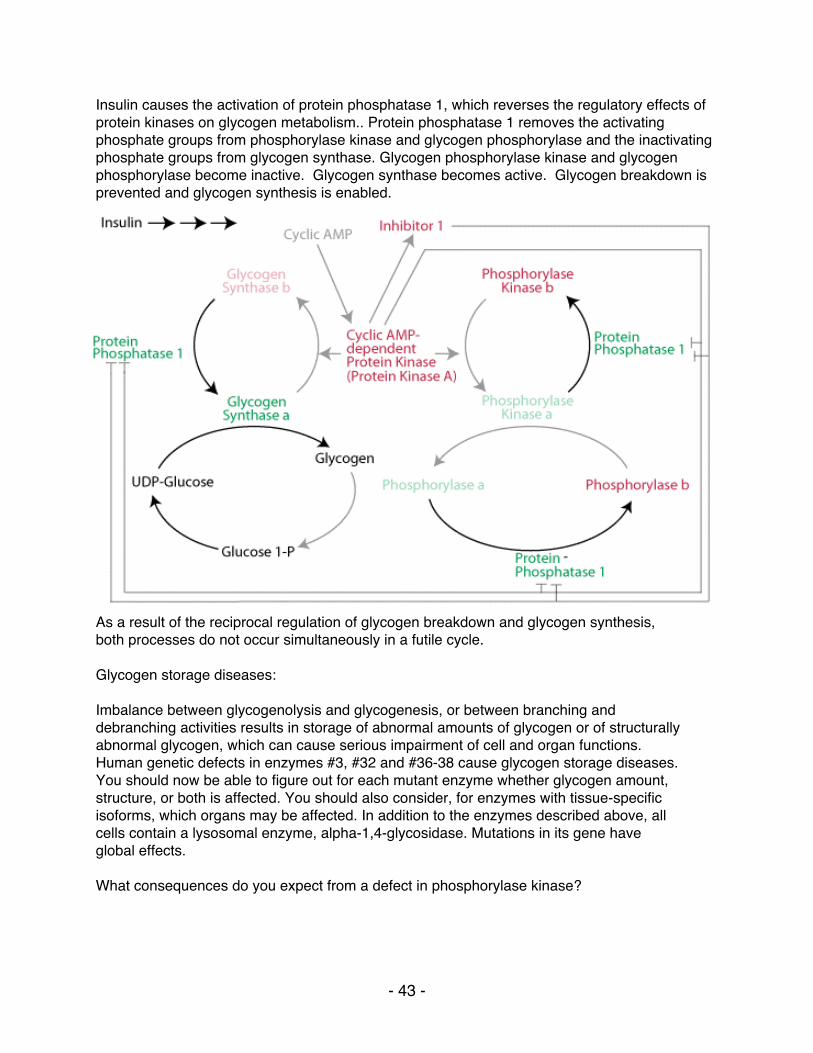
- 43 -
Insulin causes the activation of protein phosphatase 1, which reverses the regulatory effects of protein kinases on glycogen metabolism.. Protein phosphatase 1 removes the activating phosphate groups from phosphorylase kinase and glycogen phosphorylase and the inactivating phosphate groups from glycogen synthase. Glycogen phosphorylase kinase and glycogen phosphorylase become inactive. Glycogen synthase becomes active. Glycogen breakdown is prevented and glycogen synthesis is enabled.
As a result of the reciprocal regulation of glycogen breakdown and glycogen synthesis, both processes do not occur simultaneously in a futile cycle. Glycogen storage diseases: Imbalance between glycogenolysis and glycogenesis, or between branching and debranching activities results in storage of abnormal amounts of glycogen or of structurally abnormal glycogen, which can cause serious impairment of cell and organ functions. Human genetic defects in enzymes #3, #32 and #36-38 cause glycogen storage diseases. You should now be able to figure out for each mutant enzyme whether glycogen amount, structure, or both is affected. You should also consider, for enzymes with tissue-specific isoforms, which organs may be affected. In addition to the enzymes described above, all cells contain a lysosomal enzyme, alpha-1,4-glycosidase. Mutations in its gene have global effects. What consequences do you expect from a defect in phosphorylase kinase?
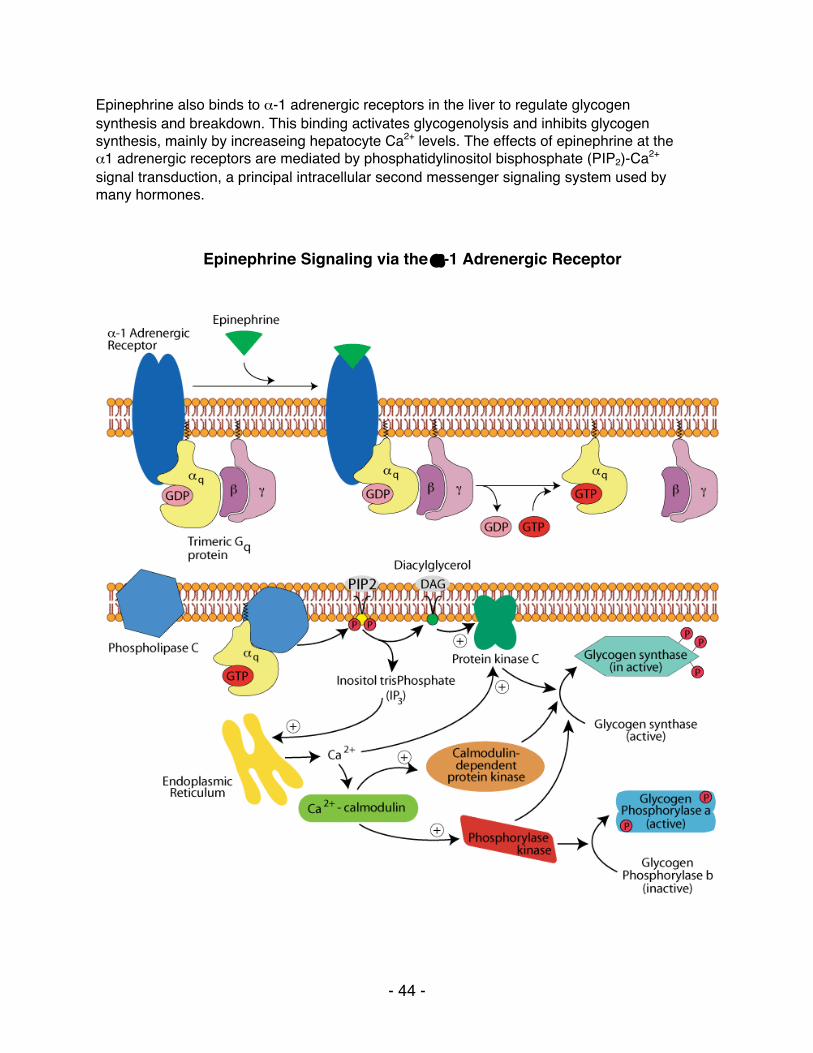
- 44 -
Epinephrine also binds to α-1 adrenergic receptors in the liver to regulate glycogen synthesis and breakdown. This binding activates glycogenolysis and inhibits glycogen synthesis, mainly by increaseing hepatocyte Ca2+ levels. The effects of epinephrine at the α1 adrenergic receptors are mediated by phosphatidylinositol bisphosphate (PIP2)-Ca2+ signal transduction, a principal intracellular second messenger signaling system used by many hormones.
Epinephrine Signaling via the α-1 Adrenergic Receptor
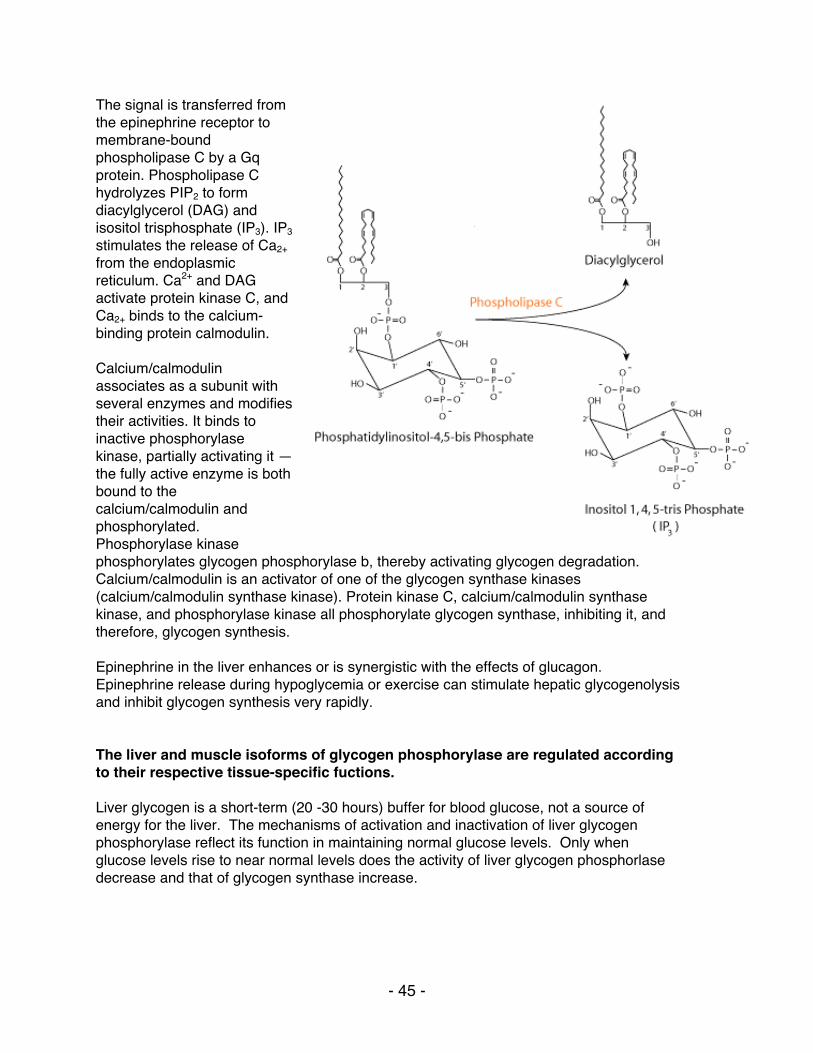
- 45 -
The signal is transferred from the epinephrine receptor to membrane-bound phospholipase C by a Gq protein. Phospholipase C hydrolyzes PIP2 to form diacylglycerol (DAG) and isositol trisphosphate (IP3). IP3 stimulates the release of Ca2+ from the endoplasmic reticulum. Ca2+ and DAG activate protein kinase C, and Ca2+ binds to the calcium-binding protein calmodulin. Calcium/calmodulin associates as a subunit with several enzymes and modifies their activities. It binds to inactive phosphorylase kinase, partially activating it — the fully active enzyme is both bound to the calcium/calmodulin and phosphorylated. Phosphorylase kinase phosphorylates glycogen phosphorylase b, thereby activating glycogen degradation. Calcium/calmodulin is an activator of one of the glycogen synthase kinases (calcium/calmodulin synthase kinase). Protein kinase C, calcium/calmodulin synthase kinase, and phosphorylase kinase all phosphorylate glycogen synthase, inhibiting it, and therefore, glycogen synthesis. Epinephrine in the liver enhances or is synergistic with the effects of glucagon. Epinephrine release during hypoglycemia or exercise can stimulate hepatic glycogenolysis and inhibit glycogen synthesis very rapidly. The liver and muscle isoforms of glycogen phosphorylase are regulated according to their respective tissue-specific fuctions. Liver glycogen is a short-term (20 -30 hours) buffer for blood glucose, not a source of energy for the liver. The mechanisms of activation and inactivation of liver glycogen phosphorylase reflect its function in maintaining normal glucose levels. Only when glucose levels rise to near normal levels does the activity of liver glycogen phosphorlase decrease and that of glycogen synthase increase.
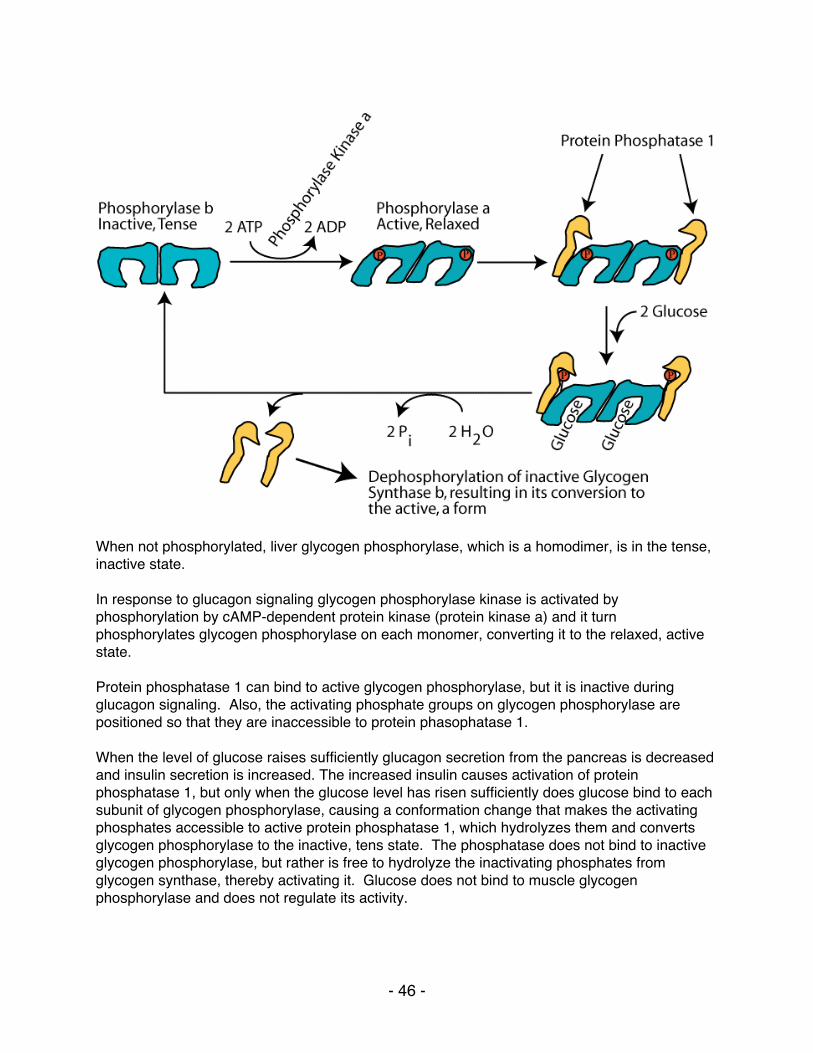
- 46 -
When not phosphorylated, liver glycogen phosphorylase, which is a homodimer, is in the tense, inactive state. In response to glucagon signaling glycogen phosphorylase kinase is activated by phosphorylation by cAMP-dependent protein kinase (protein kinase a) and it turn phosphorylates glycogen phosphorylase on each monomer, converting it to the relaxed, active state. Protein phosphatase 1 can bind to active glycogen phosphorylase, but it is inactive during glucagon signaling. Also, the activating phosphate groups on glycogen phosphorylase are positioned so that they are inaccessible to protein phasophatase 1. When the level of glucose raises sufficiently glucagon secretion from the pancreas is decreased and insulin secretion is increased. The increased insulin causes activation of protein phosphatase 1, but only when the glucose level has risen sufficiently does glucose bind to each subunit of glycogen phosphorylase, causing a conformation change that makes the activating phosphates accessible to active protein phosphatase 1, which hydrolyzes them and converts glycogen phosphorylase to the inactive, tens state. The phosphatase does not bind to inactive glycogen phosphorylase, but rather is free to hydrolyze the inactivating phosphates from glycogen synthase, thereby activating it. Glucose does not bind to muscle glycogen phosphorylase and does not regulate its activity.
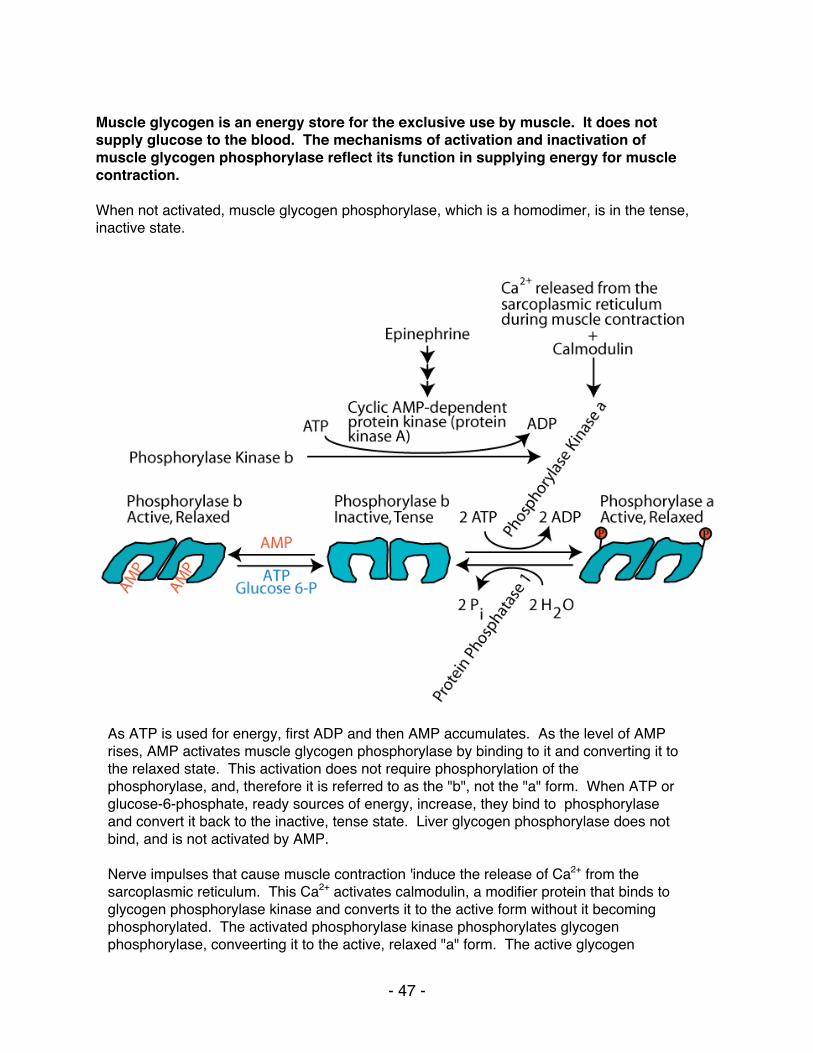
- 47 -
Muscle glycogen is an energy store for the exclusive use by muscle. It does not supply glucose to the blood. The mechanisms of activation and inactivation of muscle glycogen phosphorylase reflect its function in supplying energy for muscle contraction. When not activated, muscle glycogen phosphorylase, which is a homodimer, is in the tense, inactive state.
As ATP is used for energy, first ADP and then AMP accumulates. As the level of AMP rises, AMP activates muscle glycogen phosphorylase by binding to it and converting it to the relaxed state. This activation does not require phosphorylation of the phosphorylase, and, therefore it is referred to as the "b", not the "a" form. When ATP or glucose-6-phosphate, ready sources of energy, increase, they bind to phosphorylase and convert it back to the inactive, tense state. Liver glycogen phosphorylase does not bind, and is not activated by AMP. Nerve impulses that cause muscle contraction 'induce the release of Ca2+ from the sarcoplasmic reticulum. This Ca2+ activates calmodulin, a modifier protein that binds to glycogen phosphorylase kinase and converts it to the active form without it becoming phosphorylated. The activated phosphorylase kinase phosphorylates glycogen phosphorylase, conveerting it to the active, relaxed "a" form. The active glycogen

- 48 -
phosphorylase catalyzes the phosphorylisation of glycogen to supply glucose as a source of energy for the ensuing muscle contraction. Epinephrine, the major acute stress hormone that signals though the β 2 adrenergic receptor, a G-protein coupled receptor induces the activation of muscle cell adenylyl cyclase, which, in turn, activates cAMP-dependent protein kinase (protein kinase A), which phosphorylates and activates glycogen phosphorylase kinase. The active phosphorylase kinase then phosphorylates glycogen phosphorylase, converting it from the inactive, tense, "b" form" to the active, relaxed, "a" form. By this mechanism, epinephrine induces the breakdown of muscle glycogen to supply muscle cells with a boost of glucose as a ready source of energy to respond to the stress.
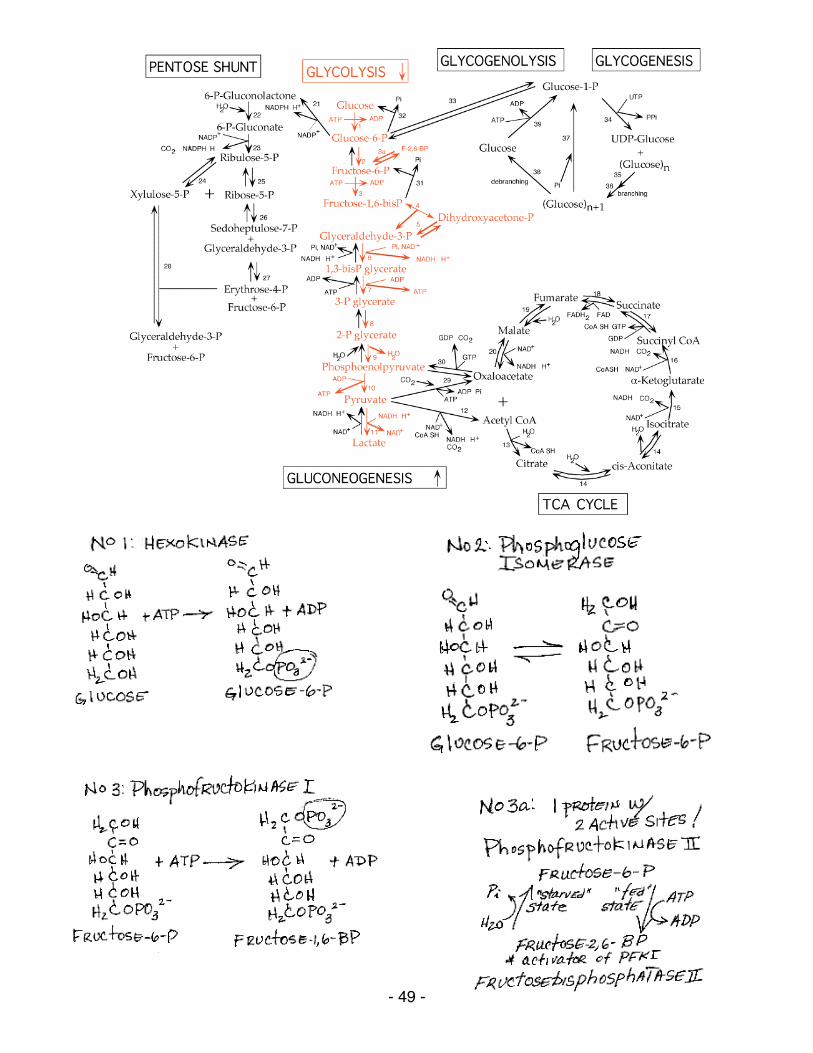
- 49 -
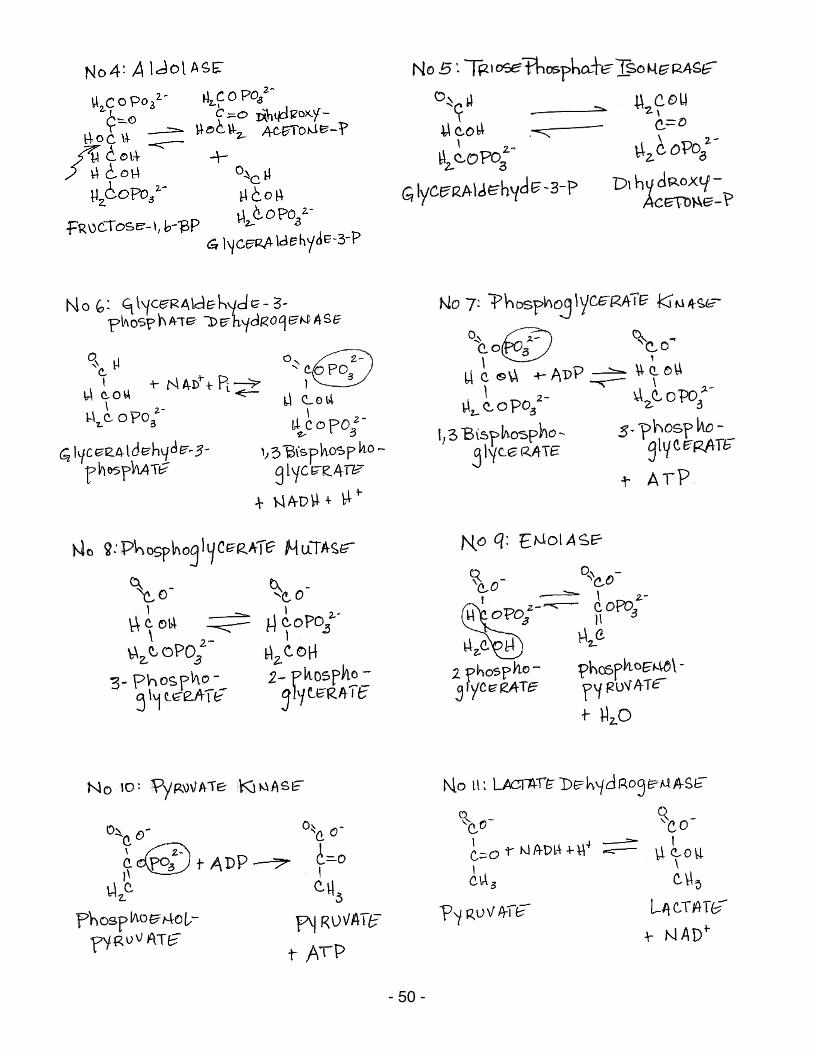
- 50 -
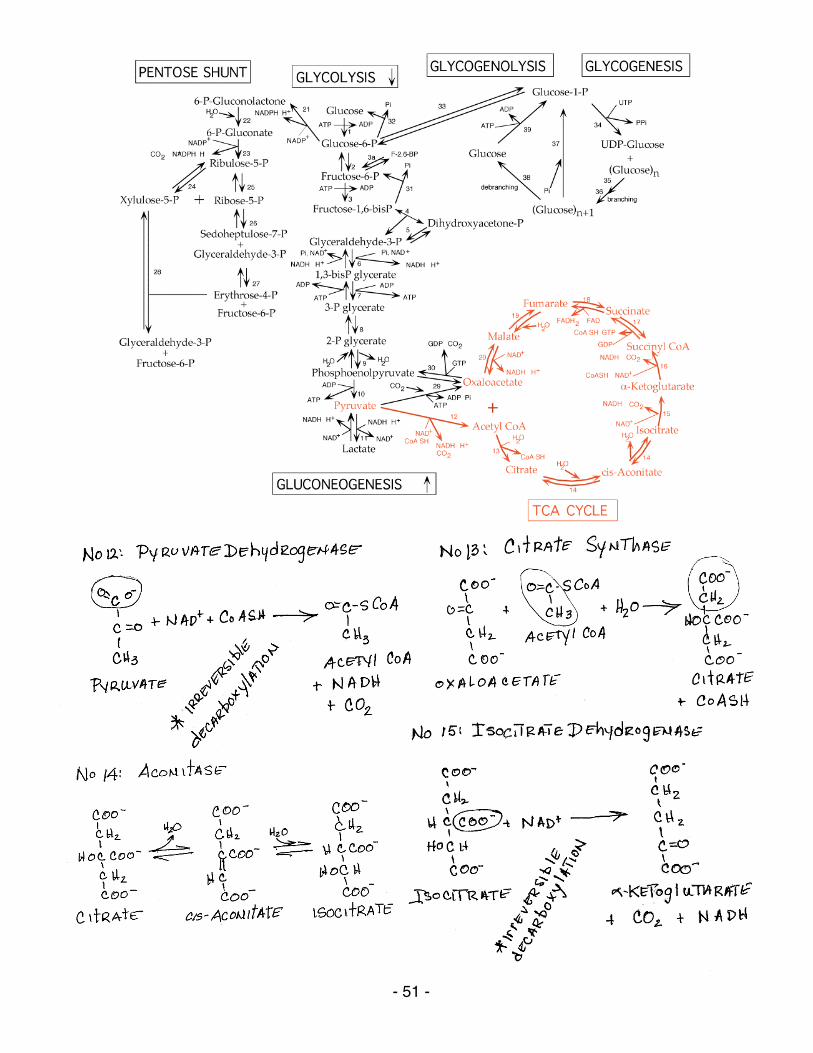
- 51 -
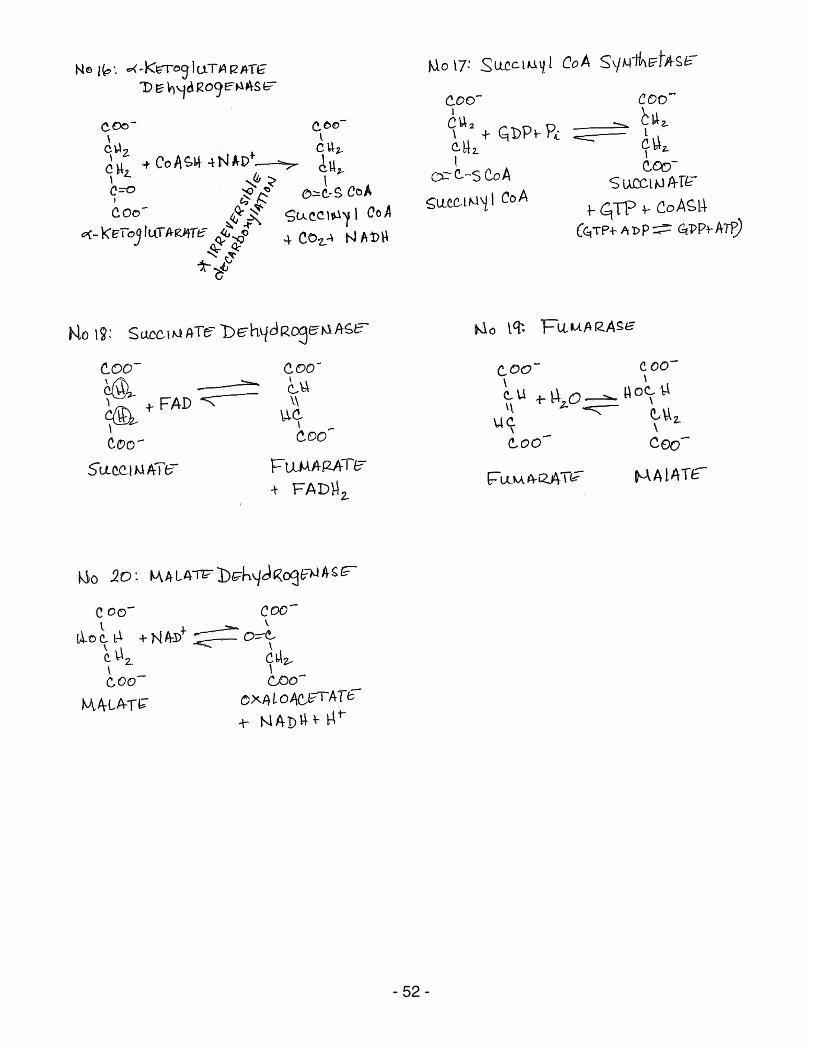
- 52 -
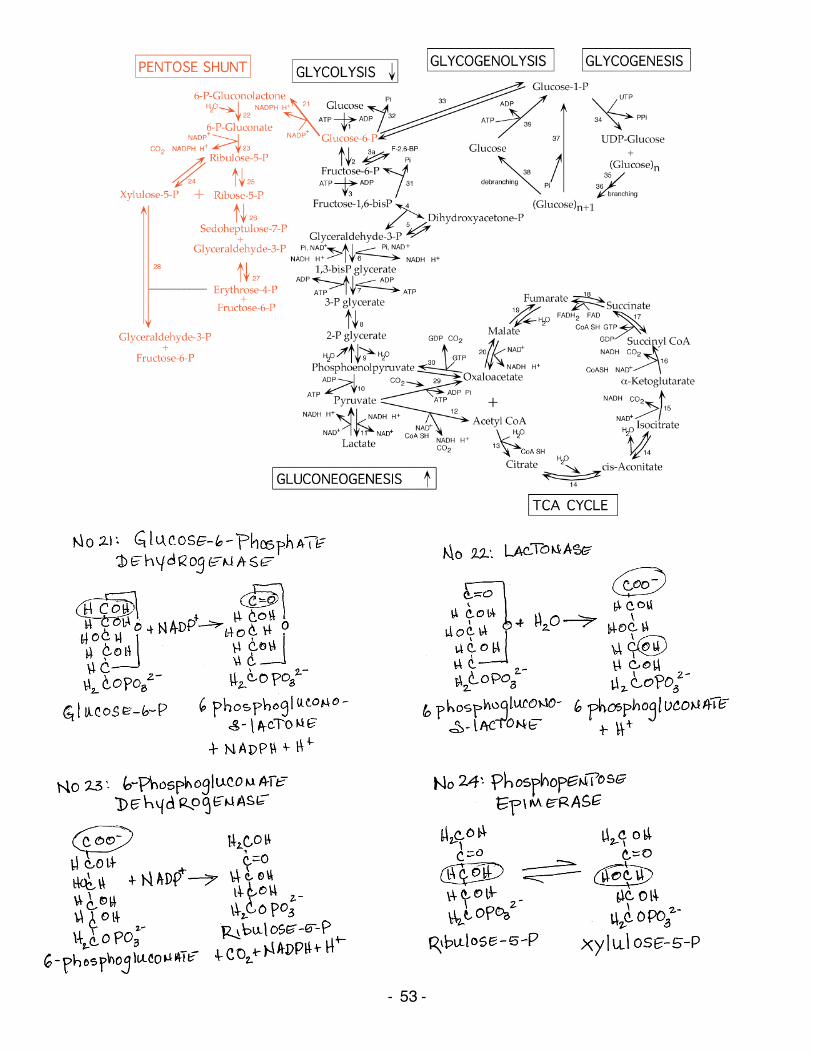
-‐ 53 -‐
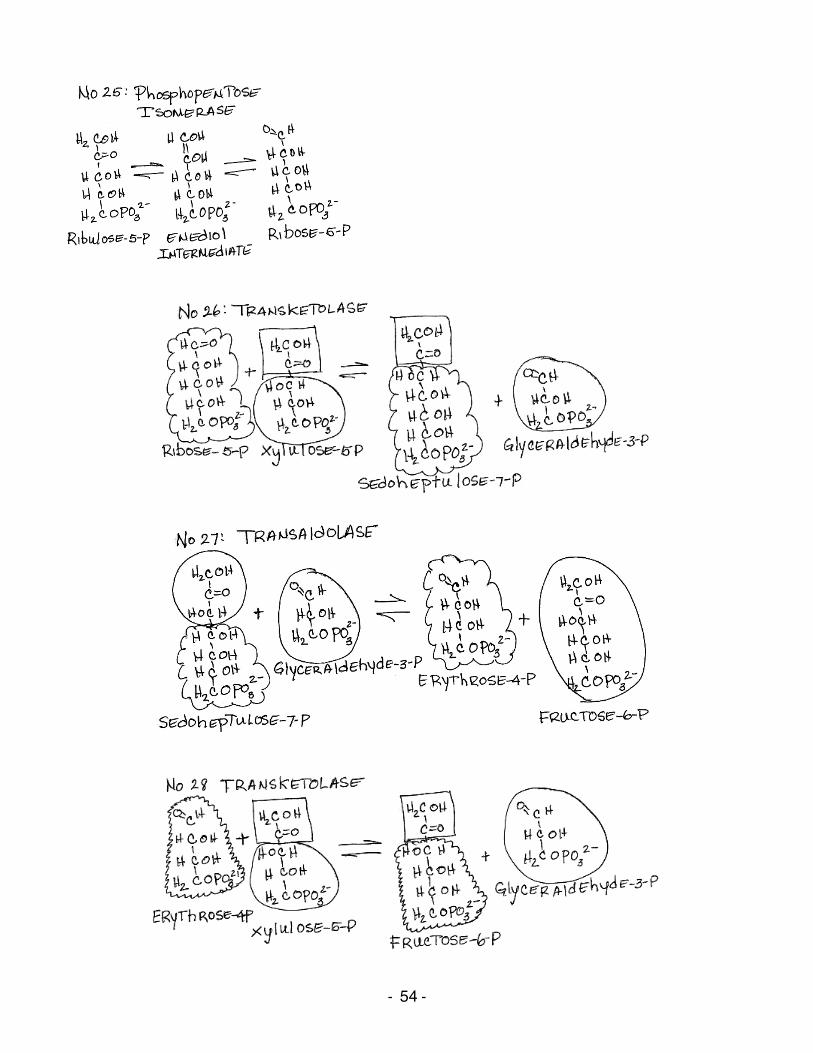
-‐ 54 -‐
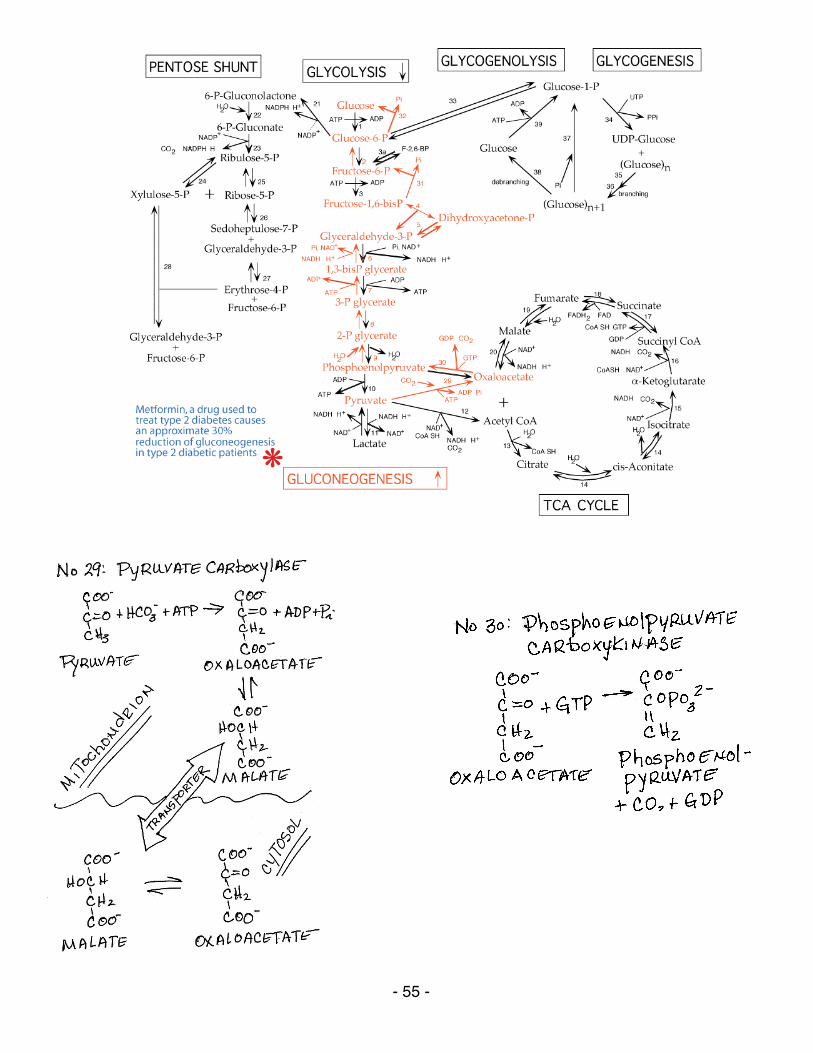
- 55 -
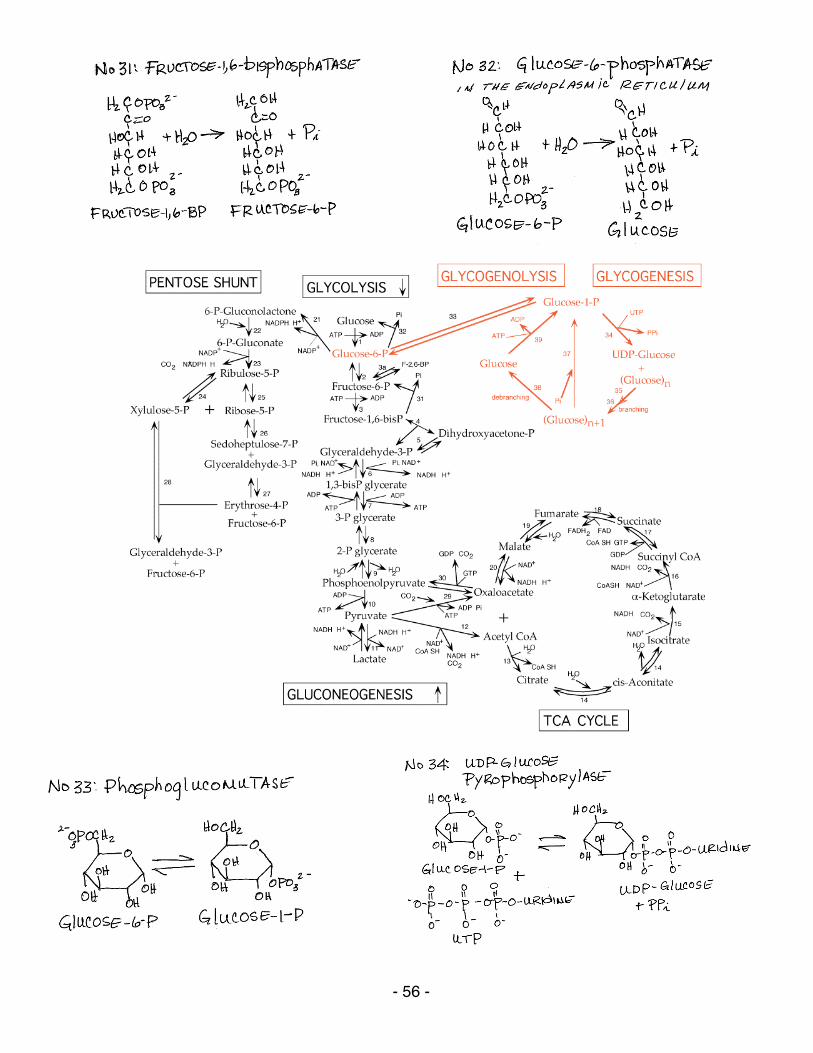
- 56 -
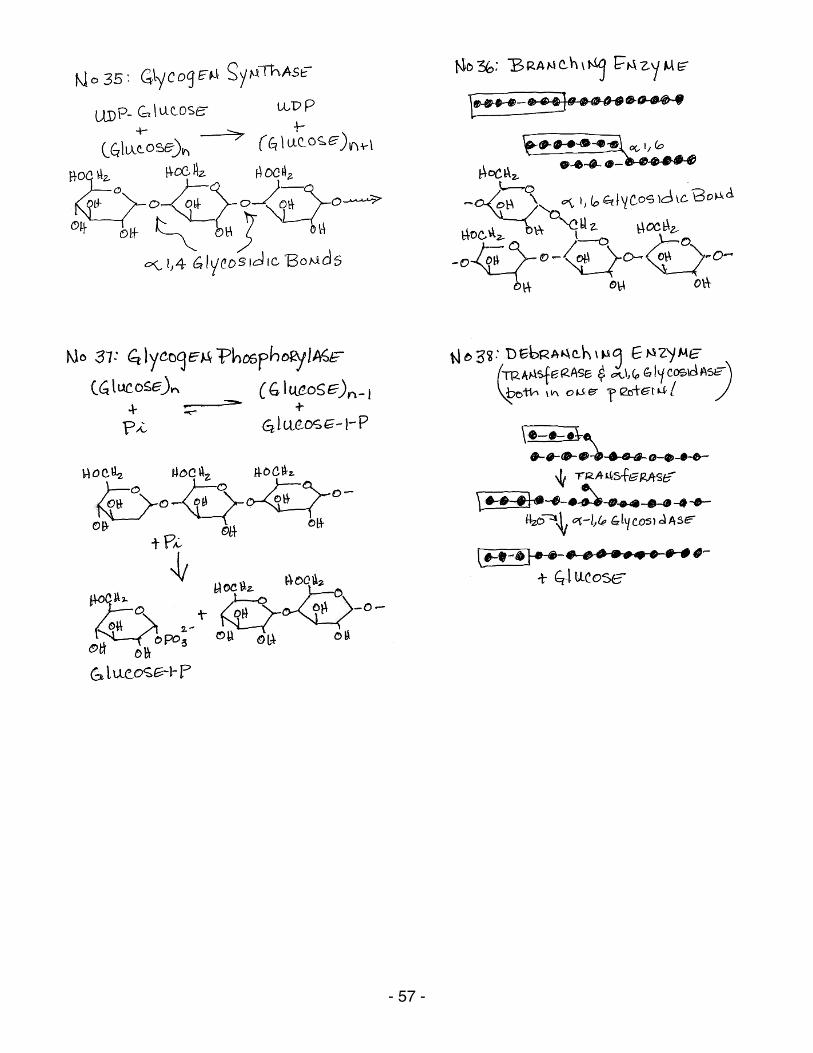
- 57 -
- 58 -
IRREVERSIBLE AND REGULATED STEPS OF GLUCOSE METABOLISM
Trapping Glucose In Cells And Release Of Glucose To Blood
Phosphorylation of Glucose to yield Glucose-6-phosphate The first step in glucose utilization is its phosphorylation, which prevents its transport out of cells due to the negative charge conferred by the phosphate group. 1. Hexokinase:
irreversible; allosterically inhibited by its product, glucose 6-phosphate; Km = 0.1 mM Glucokinase: present in liver and pancreatic beta cells; irreversible; NOT inhibited by its product, glucose 6-phosphate; Km = 10 mM; when blood glucose levels are low the enzyme level is reduced (transcription of the gene is reduced and the glucokinase protein is sequestered by the Glucokinase Regulatory Protein), thereby reducing the retention of glucose produced by glycogenolysis and gluconeogenesis in liver cells
Dephosphorylation of Glucose-6-phosphate to yield Glucose The dephosphorylation of glucose allows it to be transported out of cells. 32. Glucose-6-phosphatase:
present in liver and kidney; located in the endoplasmic reticulum; irreversible; allows liver and kidney to supply glucose, recovered from stored glycogen or synthesized from 3-carbon precursors by gluconeogenesis, to other tissues during fasting; liver is the major tissue that supplies glucose to other tissues; during severe fasting the kidney also supplies an appreciable amount of glucose. Glucose-6-phosphatase gene transcription is increased by phosphorylated CREB when blood glucose is low (signaled by glucagon)
Glycolysis and Gluconeogenesis
Phosphorylation of Fructose-6-phosphate to yield Fructose-1,6-bisphosphate This is the committed step of glycolysis, and is highly regulated. 3. Phosphofructokinase 1:
irreversible; allosterically regulated: ATP increases the Km for fructose 6-phosphate thereby slowing enzymatic activity and the rate of glycolysis; AMP reverses the inhibitory effect of ATP; inhibited by low pH; inhibited by high citrate concentration which enhances the inhibitory effect of ATP; stimulated by fructose-2,6-bisphosphate which lowers the Km for fructose-6-phosphate and decreases inhibition by ATP thereby increasing the rate of glycolysis
Dephosphorylation of Fructose-1,6-bisphosphate to yield Fructose-6-phosphate Note that the dephosphorylation of fructose-1,6-bisphosphate and the phosphorylation of fructose-6-phosphate are reciprocally regulated by AMP, fructose-2,6-bisphosphate and citrate. This prevents glycolysis and gluconeogenesis from occurring simultaneously.
- 59 -
31. Fructose-1,6-bisphosphatase: irreversible; allosterically regulated: inhibited by AMP; inhibited by fructose-2,6-bisphosphate; inhibited by fructose-6-phosphate; stimulated by citrate. Its synthesis is reciprocally regulated by insulin and glucagon.
Phosphorylation of Fructose-6-phosphate to yield Fructose-2,6-bisphosphate and dephosphorylation of Fructose-2,6-bisphosphate to yield Fructose-6-phosphate by two different activities of a single protein, a bifunctional enzyme Fructose-2,6-bisphosphate is synthesized by phosphofructokinase 2 in small amounts and acts as a "feed-forward" activator of phosphofructokinase 1. Fructose-6-phosphate stimulates the synthesis of fructose-2,6-bisphosphate, which then stimulates phosphofructokinase 1 to synthesize fructose-1,6-bisphosphate. The bifunctional enzyme is a single protein that has both phosphofructokinase 2 and fructose-2,6-bisphosphatase activities. Its activity is regulated by protein phosphorylation/dephosphorylation. Note below the reciprocal regulation of the two opposing enzymatic activities of this single protein. 3a. Phosphofructokinase 2:
stimulated by fructose-6-phosphate; Cyclic AMP-dependent protein kinase (protein kinase A) phosphorylates and inhibits the liver enzyme in response to either glucagon, which signals low blood glucose levels, or epinephrine; heart muscle isoform is stimulated by phosphorylation in response to epinephrine, skeletal muscle isoform is not phosphorylated.
3a. Fructose-2,6-bisphosphatase:
inhibited by fructose-6-phosphate; Cyclic AMP-dependent protein kinase (protein kinase A) phosphorylates and stimulates the liver enzyme in response to either glucagon, which signals low blood glucose levels, or epinephrine.
Production of Pyruvate from Phosphoenolpyruvate This is the last step of glycolysis and is highly regulated to control the outflow of glycolytic products. 10. Pyruvate Kinase:
irreversible; ATP produced; allosterically regulated: inhibited by ATP; inhibited by alanine; "feed forward" stimulated by fructose-1,6-bisphosphate which signals a high level of glycolytic products are available; regulated by phosphorylation: cyclic AMP-dependent protein kinase (protein kinase A) phosphorylates and inactivates the liver (but not the muscle) enzyme in response to low blood glucose signalled by glucagon
Production of Phosphoenolpyruvate from Pyruvate This is a two step reaction in which oxaloacetate is first produced from pyruvate and then phosphoenolpyruvate is produced from oxaloacetate. The two steps expend more energy than is harvested when pyruvate is produced from phosphoenolpyruvate. 29. Pyruvate carboxylase:
irreversible; oxaloacetate produced; ATP expended; located in mitochondria; allosterically regulated: activated by acetyl CoA, inhibited by ADP; the oxaloacetate produced is reduced (at the expense of NADH + H+) to malate for transport from the mitochondria to the cytoplasm, where it is re-oxidized to oxaloacetate (at the expense of NAD+); Note that the stimulation of oxaloacetate production during acetyl CoA excess could help speed up the
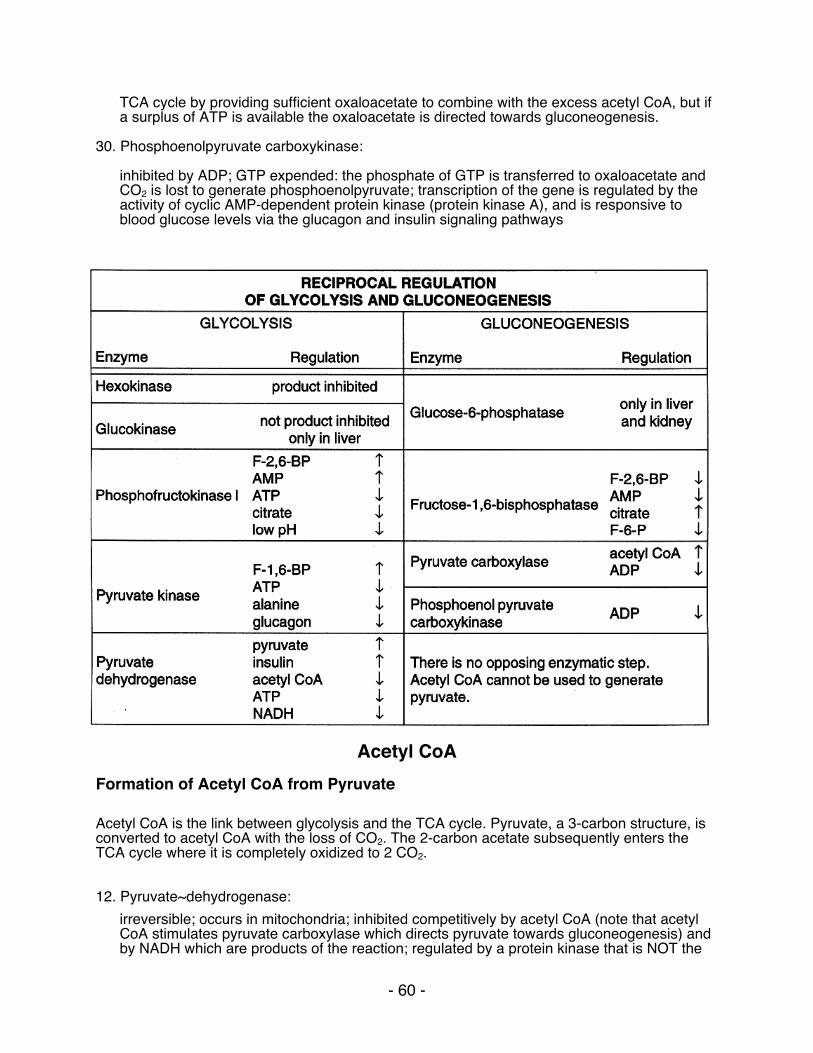
- 60 -
TCA cycle by providing sufficient oxaloacetate to combine with the excess acetyl CoA, but if a surplus of ATP is available the oxaloacetate is directed towards gluconeogenesis.
30. Phosphoenolpyruvate carboxykinase:
inhibited by ADP; GTP expended: the phosphate of GTP is transferred to oxaloacetate and CO2 is lost to generate phosphoenolpyruvate; transcription of the gene is regulated by the activity of cyclic AMP-dependent protein kinase (protein kinase A), and is responsive to blood glucose levels via the glucagon and insulin signaling pathways
Acetyl CoA
Formation of Acetyl CoA from Pyruvate Acetyl CoA is the link between glycolysis and the TCA cycle. Pyruvate, a 3-carbon structure, is converted to acetyl CoA with the loss of CO2. The 2-carbon acetate subsequently enters the TCA cycle where it is completely oxidized to 2 CO2. 12. Pyruvate~dehydrogenase:
irreversible; occurs in mitochondria; inhibited competitively by acetyl CoA (note that acetyl CoA stimulates pyruvate carboxylase which directs pyruvate towards gluconeogenesis) and by NADH which are products of the reaction; regulated by a protein kinase that is NOT the
- 61 -
cyclic AMP-dependent protein kinase: phosphorylation of pyruvate dehydrogenase, which is stimulated by high NADH/NAD+, acetyl CoA/CoA or ATP/ADP inhibits enzymatic activity; pyruvate activates by inhibiting the protein kinase; insulin stimulates by activating a phosphatase that removes the protein phosphate. Ca2+ released from the sarcoplasmic reticulum of heart muscle activates the phosphatase to increase energy for increased heart beat.
The TCA Cycle The final step in the oxidation of fuel molecules. Acetate generated from glucose (and other fuel molecules) as acetyl CoA is ultimately oxidized to 2 CO2 with the generation of 1 GTP and 4 reducing equivalents (3 NADH and 1 FADH2) from each acetate molecule that enters the cycle. These reducing equivalents are used to generate ATP via oxidative phosphorylation, where oxygen is the ultimate electron acceptor. Formation of alpha-Ketoglutarate from Isocitrate The first of four oxidation reactions of the TCA cycle and the first decarboxylation 15. Isocitrate dehydrogenase:
irreversible; NADH and CO2 produced (oxidative decarboxylation); actually a two step reaction in which oxidation of isocitrate to oxalosuccinate occurs first, followed by decarboxylation; ADP enhances the cooperative binding of NAD+ and isocitrate to the enzyme; ATP inhibits; NADH inhibits by displacing NAD+ from the enzyme. Ca2+ released from the sarcoplasmic reticulum of skeletal muscle speeds up the enzyme to supply increased energy for muscle contraction.
Formation of Succinyl CoA from alpha-Ketoglutarate and CoA The second of four oxidation reactions of the TCA cycle and the second decarboxylation 16. alpha-ketoglutarate~dehydrogenase:
irreversible; NADH and CO2 produced (oxidative decarboxylation); inhibited by NADH and succinyl CoA; the oxidation allows the formation of the energy-rich thioester bond. Ca2+ released from the sarcoplasmic reticulum of skeletal muscle speeds up the enzyme to supply increased energy for muscle contraction.
Glycogenesis and Glycogenolysis
Glycogenesis and glycogenolysis are reciprocally regulated. The two opposing, regulated enzymes are glycogen synthase (glycogenesis) and glycogen phosphorylase (glycogenolysis). Each is regulated by phosphorylation/dephosphorylation and by binding of other molecules. Phosphorylation of glycogen synthase switches it to the inactive, or "b " form. Phosphorylation of glycogen phosphorylase switches it to the active, or "a " form. The "b " forms of each enzyme can become active by binding small molecules. The differential response of the liver and muscle isoforms to different small molecules (glucose, AMP, ATP -see below) is in keeping with the different functions of liver and muscle in glucose metabolism. Muscle uses glucose as a primary fuel, on site, while the liver does not use glucose as a primary fuel, but rather acts to maintain blood glucose homeostasis. Glycogen synthase is phosphorylated directly by cyclic AMP-dependent protein kinase (protein kinase A) in response
- 62 -
to glucagon or epinephrine. Glycogen phosphorylase is phosphorylated by phosphorylase kinase, which becomes active when phosphorylated by cyclic AMP-dependent protein kinase (protein kinase A). Protein phosphatase 1, which removes protein phosphates, reverses the effect of phosphorylation. Protein phosphatase 1 is regulated by two mechanisms: (1) when phosphorylated by cyclic AMP-dependent protein kinase (protein kinase A), its G (for glycogen binding) subunit is prevented from binding to glycogen particles, (2) when phosphorylated by cyclic AMP-dependent protein kinase (protein kinase A), inhibitor 1, a small protein, inhibits protein phosphatase 1. Insulin activates protein phosphatase 1. .sp A reciprocal relationship, effected by protein phosphatase 1, exists between the activities of glycogen phosphorylase (glycogen breakdown) and glycogen synthase (glycogen synthesis). Protein phosphatase 1 binds phosphorylase " a " when glucose is low, but does not dephosphorylate phosphorylase a. When glucose levels rise, glucose binds to phosphorylase a and causes a conformational change in its structure. This allows protein phosphatase 1 to dephosphorylate phosphorylase a, converting it to phosphorylase b, which is unable to bind protein phosphatase 1. Protein phosphatase 1 is thereby freed to dephosphorylate, and activate, glycogen synthase. 35. Glycogen synthase:
cyclic AMP-dependent protein kinase (protein kinase A) phosphorylates and inactivates (switches it to the "b " form), high level of glucose-6-phosphate overcomes the inhibition; insulin activates by activating protein phosphatase 1, which removes inhibiting phosphates from the synthase, thereby switching it to the active, or "b " form; glucose activates by causing the release of protein phosphatase 1 from phosphorylase so it becomes free to dephosphorylate glycogen synthase
37. Glycogen phosphorylase:
cyclic AMP-dependent protein kinase phosphorylates phosphorylase kinase, thereby activating it to phosphorylate glycogen phosphorylase, which is thereby activated (phosphorylase a); protein phosphatase 1 dephosphorylates thereby inactivating it (phosphorylase b); the muscle "b " isoform is activated by AMP, ATP reverses the effect of AMP by competing with it for binding to the enzyme; the muscle "b " isoform is inactivated by glucose-6-phosphate; AMP has no effect on the liver isoform of phosphorylase; the liver isoform of phosphorylase is deactivated by the binding of glucose, which causes a conformational change and exposes the protein phosphate to the dephosphorylating activity of protein phosphatase 1