Embed Size (px)
Citation preview

91D.C. Sigg et al. (eds.), Cardiac Electrophysiology Methods and Models, DOI 10.1007/978-1-4419-6658-2_5, © Springer Science + Business Media, LLC 2010
Abstract Normal pacemaker cell and conduction system function is fundamentally important in maintaining cardiac mechanical performance. Cardiac arrhythmias consist of a group of electrical disturbances in the heart, including pacemaker cell firing and/or conduction abnormalities. The resultant fast, slow, or irregular heart rhythm can cause significant hemodynamic compromise and discomforts, and/or death. Importantly, a thorough understanding of cardiac electrophysiology is essential for management of any cardiac patient. The electrocardiogram, as recorded from electrodes placed on the surface of the chest and extremities, is a simple, yet important diagnostic technique for identification of cardiac arrhythmias. Nevertheless, it can also be useful in diag-noses of electrolyte abnormalities, medication toxicity, ischemic heart disease, and/or enlargement of cardiac chambers.
List of Abbreviations
AF atrial fibrillationAPC atrial premature complexAV atrioventricularAVNRT atrioventricular nodal reentry tachycardiaECG electrocardiogramICD implantable cardioverter defibrillatorIHR intrinsic heart ratePSVT paroxysmal supraventricular tachycardiaSA sinoatrialSVT supraventricular tachycardiaTdP Torsades de PointesVPC ventricular premature complexVT ventricular tachycardia
F. Lü () Department of Medicine, Cardiovascular Division, University of Minnesota, Minneapolis, MN, USA e-mail: [email protected]
Chapter 5The Electrocardiogram and Clinical Cardiac Electrophysiology
John T. Nguyen, Xiaohuan Li, and Fei Lü

92 J.T. Nguyen et al.
5.1 Introduction
Despite the invaluable usefulness of the surface electrocardiogram (ECG), it remains, in a broad sense, a tool only to describe electrical depolarization and repolarization of the atrial and ventricular tissue over time. Conclusions pertaining to the precise origins of impulse formation as well as conduction pathways from the atria to the ventricles can be inferred based on the relationship of their respec-tive deflections on the ECG. In other words, invasive electrophysiologic study must be implemented by direct measurement of the electrical signals using small flexible electrode catheters placed into the heart via a transvenous approach, to provide the ability to interrogate the complex electrical system of the heart in more detail. Yet, surface ECGs and electrophysiologic studies together provide the essential tools in cardiac electrophysiology, i.e., in the science of describing, diagnosing, and treating electrical abnormalities of the heart. This chapter will focus on the basics of electrocardiography and cardiac electrophysiology.
5.2 The Specialized Cardiac Conduction System
Normally, electrical activation of the heart is initiated by a group of specialized pacemaker cells, termed the sinoatrial (SA) node, located on the epicardial surface of the heart at the junction of the right atrium and the superior vena cava. The intrinsic firing rate (automaticity) of these cells determines the rate and regularity of SA node activity and can be modulated by extrinsic factors such as autonomic neural tone, electrolytes, and medications. The normal resting sinus rate is variable, but is usually between 50 and 90 beats/min. However, rates as low as 40 beats/min are not uncommon in well-conditioned (athletic) individuals. Once generated by the sinus node cells, the cardiac electrical impulse traverses the atria by means of preferential conduction routes (determined by intra-atrial muscle band geography) to the atrioventricular (AV) node, located in the low interatrial septum near the tricuspid valve. The AV node is often considered to represent the beginning of the true anatomic specialized conduction system of the heart. Normally, impulses transit through the AV node at relatively slower rates than the remaining conduction system. Importantly, this delay allows time for mechanical transfer of blood from the atria to the ventricles prior to initiation of ventricular activation. Similar to the SA node, conduction through the AV node is influenced by sympathetic and parasympathetic neural tone, medications, and electrolytes. Once through the AV node, however, the electrical impulses travel more rapidly through the infranodal specialized conducting system comprised of the bundle of His, left and right bundle branches, and penetrating Purkinje fiber network. This concert of electrical activity ultimately results in coordinated mechanical contrac-tions of both atria followed by the ventricles. (For more details on the conduction system, see Chap. 4.).

935 The Electrocardiogram and Clinical Cardiac Electrophysiology
5.3 Electrocardiogram
The ECG is one representation of the electrical events of the cardiac cycle. Each event has associated waveforms, and careful analyses of these wave morphologies and their relationships to one another can provide insights on the electrophysiologic state of the heart. An ECG machine records atrial and ventricular depolarization and repolarization by inscribing deflections on a grid consisting of 1 mm squares. The width of these squares corresponds to duration, with standard values equal to 40 ms; the height of the squares denotes voltage amplitude of the deflection, usually representing 1 mV each centimeter.
5.3.1 ECG Leads
The ECG itself is recorded via electrodes (leads) placed on the body surface to measure the difference in electrical potential during impulse propagation. In general, when an impulse travels in the same direction as a lead (toward the posi-tive electrode), it will result in a positive deflection on the ECG; conversely, an electrical impulse traveling in the opposite direction of a lead (away from the positive electrode) will be inscribed as a negative deflection.
There are two types of lead configurations: (1) bipolar leads measure electrical potential difference between two points on the body; and (2) unipolar leads compare a point on the body with a virtual reference located in the center of the chest. In general, a series of body surface electrodes can be placed at specific points on the arms, legs, and chest wall in order to record the electrical activity of the heart. Typically, there are six limb lead configurations that are used to view the heart in the frontal plane, three of which are standard bipolar (lead I, II, and III), while the remaining three limb leads are augmented unipolar leads (aVR, aVL, and aVF). The limb leads are created in the following manner:
I: positive – left arm; negative – right armII: positive – left leg; negative – right armIII: positive – left leg; negative – left armaVR: positive – right arm; negative – left arm and legaVL: positive – left arm; negative – right arm and left legaVF: positive – left leg; negative – right and left arms
Together, these form Einthoven’s triangle to determine an electrical axis in the frontal plane (Fig. 5.1a, b).
The precordial chest leads are used in a unipolar configuration and examine the heart in the horizontal plane, including leads V1, V2, V3, V4, V5, and V6 (Fig. 5.1c, d). The location of these leads is as follows:
V1: fourth intercostal space, right border of the sternumV2: fourth intercostal space, left border of the sternum

94 J.T. Nguyen et al.
V3: right between leads V2 and V4V4: fifth intercostal space in the midclavicular lineV5: lateral to V4 in the anterior axillary lineV6: lateral to V4 and V5 in the midaxillary line
5.3.2 Waves and Intervals
The basic ECG signal during a normal cardiac cycle consists of a P-wave, QRS complex, and T-wave (Fig. 5.2). Sometimes, the T-wave is followed by a small deflection called the U-wave, often associated with after-depolarizations in the ventricles. The baseline voltage of the ECG is referred to as the isoelectric line.
5.3.2.1 P-wave
The P-wave is the result of atrial depolarization. Normally, a sinus impulse initiates in the SA node (located in the high right atrium) and travels leftward and inferiorly,
Fig. 5.1 Twelve ECG recording leads. The Einthoven’s triangle (a) and the hexaxial reference system (b) depicting frontal plane ECG leads are shown at the top. Direction of chest lead axis (c) with cor-responding recording sites on the chest (d) is shown at the bottom (Source: Dupre A, Vincent S, Iaizzo PA. Basic ECG theory, recordings, and interpretation. In: Iaizzo PA, editor. Handbook of Cardiac Anatomy, Physiology, and Devices. Totowa, NJ: Humana Press, 2005:191–201)

955 The Electrocardiogram and Clinical Cardiac Electrophysiology
thus the P-wave on the ECG during normal sinus rhythm is upright in II and aVF, and inverted in aVR. Normal P-wave duration is usually <100 ms with an amplitude between 2 and 3 mV.
5.3.2.2 PR Interval
The PR interval is the interval measured from the beginning of the P-wave to the beginning of the QRS complex. Normal PR intervals range between 120 and 200 ms. A prolonged PR interval suggests a “first-degree AV block,” whereas a shorter PR interval is typically seen in ventricular pre-excitation such as Wolff–Parkinson–White syndrome.
5.3.2.3 QRS Complex
The deflection complex following the PR interval is the QRS complex, representing primarily ventricular depolarization. It is comprised of the Q (first downward deflec-tion after the P-wave), R (the first positive deflection after the P-wave), and S waves
Fig. 5.2 ECG waves and intervals (modified from: Cecil RL, Goldman L, Bennett JC, editors. Cecil Textbook of Medicine, 21st edition. Philadelphia: W.B. Saunders, 2000)

96 J.T. Nguyen et al.
(the first downward deflection after the R-wave). In the normal heart, its total duration is <110 ms. A prolonged QRS complex duration may suggest the presence of either left or right bundle branch block or some other pathology. Q-waves wider than 40 ms or deeper than 25% of the QRS complex will typically signify a prior myocardial infarction. Normally, the R-wave is small in lead V1, and gradually becomes larger across the precordial leads with maximum R-wave amplitude around lead V5. Poor R-wave progression often suggests a prior anterior myocardial infarction. Note that the R-wave height should normally not exceed 25 mm in leads V5 and V6, or 12 mm in lead aVL, otherwise disease such as left ventricular hypertrophy may be underlying.
5.3.2.4 ST Segment
This ST segment begins with the J-point (the point in which the ST segment takes off from the QRS) and terminates with initiation of the T-wave. This segment is usually isoelectric; a ST segment elevation may represent (1) myocardial injury if the pattern is consistent with a coronary distribution pattern; (2) pericarditis if the elevation is diffusely distributed among all the ECG leads; or (3) the presence of a ventricular aneurysm if persistent after an acute myocardial infarction.
5.3.2.5 T-wave
The T-wave is associated with ventricular repolarization. Atypically, it may be “peaked” with large pointed amplitude in the setting of hyperkalemia; a peaked T-wave can also be one of the earliest signs of an acute infarction.
5.3.2.6 QT Interval
QT interval is measured from the Q-wave to the end of the T-wave. It varies with gender and age, e.g., in adolescence, males and females have similar QT intervals, however, this value shortens in males as maturity is reached. It is important to note that the QT interval is heart rate dependent and is usually corrected by the square root of the preced-ing RR interval (QTc=QT/√RR). In adults, a corrected QT interval of >460 ms in females and >440 ms for males is considered prolonged. Additionally, common causes of prolonged QT durations include congenital channelopathies (long QT syndromes), medications, and electrolyte disturbances (such as hypokalemia and hypocalcemia).
5.4 Mechanisms of Arrhythmias
The term “arrhythmia” is mainly used to refer to disturbances of the normal heart rhythm, and is generally categorized as either bradycardia or tachycardia. Bradycardia is generally defined as a heart rate <60 beats/min, whereas tachycardia

975 The Electrocardiogram and Clinical Cardiac Electrophysiology
refers to heart rates >100 beats/min. Yet, bradycardia may be “physiologic” in some individuals, e.g., the endurance athlete. In an individual eliciting a disease state with an associated bradycardia, the typical cause is either in the SA node (sinus node dysfunction) or AV node (AV block). Most commonly, either of these condi-tions can be caused by intrinsic disease in the pacemaker cells or conduction system, or extrinsic factors such as medications or autonomic system disturbances.
The mechanisms underlying tachycardias are typically more numerous and complex than those causing bradycardias. Nevertheless, different tachycardias can generally be classified as being due to abnormal impulse initiation, abnormal impulse conduction, or a combination of both (Table 5.1). Importantly, intracardiac recordings can greatly facilitate interpretation of arrhythmias (Fig. 5.3).
5.5 Clinical Presentation and Diagnosis
Some arrhythmias can and often do occur in apparently healthy individuals with normal hearts, but they are more commonly associated with structural heart disease. Myocardial ischemia is the most important substrate for serious arrhythmias. However, other forms of cardiac dysfunction such as cardiomyopathies, valvular heart disease, and certain genetically determined disorders (e.g., long QT syndrome, Brugada syndrome) are also associated with arrhythmias in some patients.
In general, the clinical presentation of cardiac arrhythmias may range from completely asymptomatic or mild symptoms (palpitations and anxiety) to syncope (fainting) to even sudden cardiac death; the symptoms are largely dependent on the degree of arrhythmia-induced hemodynamic changes. The electrophysiologic and hemodynamic consequences of a particular arrhythmia are primarily determined by the rates, durations, and/or chambers of origin (atrial versus ventricular). Importantly,
Table 5.1 Mechanisms of tachycardias
• Abnormalimpulseinitiation• Automaticity
• Enhancednormalautomaticity:seenininappropriatesinustachycardia,someidiopathic ventricular tachycardias (VT)
• Abnormalautomaticity:presumedtobethecaseinectopicatrialtachycardia,accelerated junctional rhythm, and possibly certain idiopathic VTs
• Triggeredactivity• Earlyafter-depolarization:presumedtobethecaseintorsadesdepointes• Delayedafter-depolarization:seenindigitalis-inducedarrhythmiasor
presumed to occur in certain exercise-induced arrhythmias• Abnormalimpulseconduction
• Ectopicescapeafterblock:suchasjunctionalescape• Unidirectionalblockandreentry
• Orderlyreentry:macro-reentryinatrialflutterandmicro-reentryinatrialorVT• Randomreentry:asseeninatrialfibrillation
• Otherconcepts(reflection,phase2reentry,andanisotropicreentry)

98 J.T. Nguyen et al.
both underlying comorbidities and the patients’ relative cardiovascular status also play large roles in clinical presentations.
A standard 12-lead ECG can be employed to readily diagnose some types of arrhythmias, however, it is limited by providing only a brief glance at rhythm abnor-malities that are often short lived. Consequently, other techniques are frequently required in order to establish more accurate diagnoses: (1) prolonged ambulatory ECG monitoring (event monitor, Holter monitor, mobile outpatient cardiac telemetry from CardioNet®, Conshohocken, PA); (2) implantable loop recorders (Reveal®, Medtronic Inc., Minneapolis, MN; Confirm®, St Jude Medical Inc., St. Paul, MN; and Sleuth®, Transoma Medical Inc., St. Paul, MN); and/or (3) electrophysiologic testing. In selected cases, exercise stress testing or signal-averaged ECG recording may also be used for additional assessment regarding the precise nature of an arrhythmia or even the relative susceptibility of the patient to an arrhythmia. Other techniques such as analysis of heart rate variability, baroreflex sensitivity, assessment of QT dispersion, T-wave alternans, and body surface potential mapping have also
I
II
V1
V5
CS p
CS 7,8
CS 5,6
CS 3,4
CS d
His p
A H
His d
RVa
Stim
P V
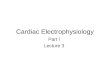
Fig. 5.3 Measurements in the His bundle electrogram. These measurements are important for evaluation of atrioventricular (AV) conduction. AH interval, measured from the earliest reproducible rapid deflection of the atrial electrogram in the His recording to the onset of the His deflection, represents conduction time from the low right atrium at the interatrial septum through the AV node to the His bundle (AV node function). The HV interval, measured from the beginning of the His deflection to the earliest onset of ventricular activation (surface leads or intracardiac recordings), represents conduction time from the proximal His bundle to the ventricular myocardium (infra-His conduction function). I = surface ECG lead I; II = surface ECG lead II; III = surface ECG lead III; V1 = surface ECG lead V1; V5 = surface ECG lead V5; CS d = distal coronary sinus; CS p = proximal coronary sinus; His d = distal His bundle; His p = proximal His bundle; RVa = right ventricular apex; Stim = stimulation; P = onset of P-wave; A = onset of atrial activation; H = onset of His activation; V = onset of ventricular activation

995 The Electrocardiogram and Clinical Cardiac Electrophysiology
been used to provide useful research information, but their value in daily practice remains to be fully defined at this time.
5.6 Treatment Considerations
The goals for treatment of arrhythmias are twofold: (1) to alleviate symptoms and improve quality of life; and (2) to prolong survival. Pharmacologic treatment has been the mainstay for management of most cardiac arrhythmias, although implant-able devices and transcatheter ablation have become increasingly important in recent years. With regard to antiarrhythmic drugs, many clinicians find it conve-nient to group them according to the widely used Vaughn–Williams classification. This classification is simple and offers a means to keep the principal pharmacologic effects of drugs in mind (Table 5.2). A more comprehensive classification of antiarrhythmic drugs, termed the Sicilian Gambit, was introduced in 1991. Regardless, the selection of antiarrhythmic drugs for a given patient should be individualized based on the arrhythmia being treated, the nature and severity of any underlying heart disease, the proposed drug’s antiarrhythmic and proarrhythmic actions, and/or its potential side effects.
In patients with tachycardias associated with ischemia or left ventricular dysfunction, class I antiarrhythmic agents should be avoided due to their potential
Table 5.2 Vaughn – Williams classification
• Class I: sodium channel blockers• ClassIa:drugsthatreduceVmax(phase0upstrokeofactionpotential)andprolongaction
potential duration, such as quinidine, procainamide, and disopyramide• ClassIb:drugsthatdonotreduceV
max and shorten action potential duration, such as
lidocaine, mexiletine, and phenytoin• ClassIc:drugsthatpredominantlyslowconduction,moderatelyreduceV
max, and
minimally prolong refractoriness, such as flecainide, propafenone, and moricizine
• ClassII:b-adrenergic receptor blockers• b-blockers may be cardio- or b
1-selective (atenolol, esmolol, and metoprolol) or
noncardioselective (carvedilol, pindolol, and propranolol)• Someexertintrinsicsympathomimeticactivity(acebutolol,bucindolol,andpindolol)• Somehavequinidine-likemembranestabilizingactivity(acebutolol,carvedilol,and
propranolol)• d-sotalol has a strong class III effect and has been regarded as a class III agent in many
conditions
• ClassIII:potassiumchannelblockersthatprolongrefractoriness,suchasamiodarone,bretylium, dofetilide, ibutilide, and sotalol; amiodarone has all the four class effects
• ClassIV:calciumchannelblockers• Dihydropyridine(amlodipineandnefedipine)• Nondihydropyridinedrugs(diltiazemandverapamil)
As discussed in the text, the utility of this classification in terms of selection of therapy is limited, but the grouping permits important toxicity issues to be more readily kept in mind, an important factor in choosing drugs for individual patients

100 J.T. Nguyen et al.
proarrhythmic risks and marked negative inotropic effects. Class III drugs, on the other hand (i.e., amiodarone, sotalol, dofetilide), appear to have neutral effects on survival in these patients and fewer negative inotropic concerns. b-blockers (Class II) have been proven to prolong survival in patients with structural heart disease, but in terms of use for suppression of symptomatic arrhythmias, they are mainly useful for the prevention of AV node-dependent reentrant supraventricular tachycardias (SVT) and/or catecholamine-sensitive arrhythmias. It is noteworthy that nonpharmacologic interventions, such as catheter ablation for SVTs and implantable cardioverter defibrillators (ICD) for primary and secondary prevention of sudden cardiac death, are currently considered as the treatments of choice in these clinical settings.
5.7 Bradyarrhythmias
As discussed earlier, bradycardia may result from either sinus node dysfunction or AV conduction block. Acute treatment options for symptomatic bradycardia include atropine, isoproterenol, and/or temporary pacing. When the underlying cause is reversible, such as in the case of drug toxicity (e.g., excess digitalis or b-blocker), temporary pacing and elimination of the offending agent is usually sufficient. However, if the cause is not reversible, a permanent electronic pacemaker is usually warranted.
5.7.1 Sinus Node Dysfunction
Sinus node dysfunction can be related to impaired impulse formation within the SA node (also often referred to as sick sinus syndrome), or due to impaired impulse conduction from the node into the atrium (termed SA block). The electrocardio-graphic manifestation may be excessive sinus bradycardia, or alternating periods of bradycardia and atrial tachycardia/fibrillation (tachy-brady syndrome). Patients with such symptoms often deteriorate further with age and/or age-related disease states. Additionally, the sinus node may simply become less responsive to physical exertion over time in terms of generating an appropriate heart rate (i.e., the patient will present with chronotropic incompetence).
In such patients, the typical resultant symptoms include fatigue, dizziness, confusion, exertional intolerance, diminished mental acuity, syncope, and/or congestive heart failure. Sinus node dysfunction may also present as various forms of SA exit block which may be classified into three general categories: (1) first-degree blocks; (2) second-degree type I and II blocks; and (3) third-degree blocks. Only the second-degree SA blocks can be recognized on the surface ECG.

1015 The Electrocardiogram and Clinical Cardiac Electrophysiology
Since sinus rate can be slowed by increased vagal tone, the intrinsic heart rate (IHR) after complete autonomic blockage is often used to assess integrity of sinus node function. Complete autonomic blockade can be achieved after the intravenous administration of propranolol (0.2 mg/kg) and atropine (0.04 mg/kg). Normal IHR is equal to 118.1 - (0.57 × age); an IHR < 80 beats/min in the elderly is usually suggestive of sinus node dysfunction. More specifically, sinus node recovery times (normal value <1,500 ms), corrected sinus node recovery times (normal value <550 ms), and less frequently, SA conduction times (normal value <125 ms) can be assessed within the electrophysiology laboratory to more precisely evaluate SA node function, i.e., when clinical diagnosis is uncertain.
5.7.2 AV Block
The term first-degree AV block is used to characterize a PR interval >0.20 s without loss of a QRS complex following each P-wave (Fig. 5.4a). Second-degree AV block is defined as when some atrial impulses fail to conduct to the ventricles. Mobitz type I second-degree AV block (Fig. 5.4b) is characterized by progressive PR inter-val prolongation until an atrial impulse is blocked (Wenckebach phenomenon). After an incomplete compensatory pause, the Wenckebach cycle starts again with a shorter PR interval compared with the last PR interval prior to block. Mobitz type I block is almost always located within the AV node and, importantly, the risk of developing complete AV block is low. In contrast, in Mobitz type II second-degree AV block (Fig. 5.4c), AV conduction fails suddenly without a change in the
Fig. 5.4 AV block. The figures show (a) first-degree, (b) Mobitz type I second-degree, (c) Mobitz type II second-degree, and (d) third-degree AV block. See text for discussion

102 J.T. Nguyen et al.
preceding PR interval. This type of block is usually due to His-Purkinje disease and is associated with a higher risk of progressing to complete AV block, with a slow and unreliable escape rhythm. When two or more consecutive atrial impulses fail to conduct, high-degree AV block is present and pacemaker implantation is often necessary. Third-degree AV block (complete AV block; Fig. 5.4d) occurs when no atrial impulses can conduct to the ventricles, resulting in no relationship between P-waves and QRS complexes on ECG.
The clinical significance of AV block depends on the (1) site of block; (2) risk of progression to complete block; and (3) subsidiary escape rate. When complete AV block occurs above the His bundle, the ventricular escape rhythm is believed to originate from the His bundle (40–60 beats/min); this is usually termed as a junctional escape rhythm and results in a narrow QRS complex. When AV block occurs below the His bundle, the escape is generated in the distal His-Purkinje fibers and the escape rhythm is much slower and less reliable (25–45 beats/min); this is referred to as a ventricular escape rhythm with a wide QRS complex. A permanent pacemaker is usually required in the third-degree AV block. In this regard, dual-chamber pacing (i.e., pacing both the atrium and ventricle) has become widely accepted as the approach of choice.
5.8 Tachyarrhythmias
5.8.1 Premature Complexes
Ectopic premature beats may originate from the atria, the AV junction, or the ventricles. Treatment of premature complexes is usually not necessary, however, if symptomatic, precipitating factors (such as alcohol, tobacco, and caffeine) should be identified and eliminated. Although anxiolytic agents and b-blockers may be tried therapeutically, they often produce more adverse side-effects than clinical benefits. Antiarrhythmic drugs may be used depending on the severity of symptoms and underlying cardiac disease. Further, catheter ablation may sometimes be used to eliminate symptomatic premature complexes.
5.8.1.1 Atrial Premature Complexes
Atrial premature complexes (APC) can typically be recognized on the ECG as early P-waves with a different morphology from that of sinus origin (Fig. 5.5a). The APCs may conduct to the ventricles with (1) a normal PR interval if they occur during the period when the AV junction is not refractory; (2) prolonged PR interval when they fall within the relative refractory period; or (3) they may be blocked entirely when the AV junction is in its effective refractory period. The appearance of bundle branch aberrancy may become evident if APCs occur when either bundle branch is refrac-tory. APCs almost always enter the sinus node and reset the sinus cycle length,

1035 The Electrocardiogram and Clinical Cardiac Electrophysiology
resulting in an incomplete compensatory pause (i.e., the sum of pre- and post-APC intervals is less than that of two normal sinus PP intervals).
5.8.1.2 Multifocal Atrial Tachycardia
Multifocal atrial tachycardia is a relatively uncommon arrhythmia characterized by atrial rates between 100 and 130 beats/min, with marked variations in P-wave morphology (arbitrarily defined as at least three different P-wave contours). In such patients, multifocal atrial tachycardia often manifests as a short burst of tachycardia (Fig. 5.5d), and typically occurs in older individuals with moderate to severe cardio-pulmonary disease (especially during an exacerbation).
Fig. 5.5 Premature complexes. (a) atrial, (b) junctional, (c) ventricular, (d) multifocal atrial tachycardia

104 J.T. Nguyen et al.
5.8.1.3 AV Junctional Premature Complexes
These complexes are recognized on the ECG as normal QRS complexes without a preceding P-wave (Fig. 5.5b); retrograde P-waves (inverted in II, III, and aVF) may be seen after the QRS complexes, further supporting the diagnosis. Atrioventricular junc-tional complexes are less common than APCs and are often associated with drug intoxi-cation and cardiac diseases. Most junctional beats have an incomplete compensatory sinus pause (like an APC) because the atrium is activated retrogradely, i.e., resetting the sinus node in the process. On rare occasions, a junctional premature beat may fail to conduct to either the atria or ventricles (concealed junctional beat), but results in refrac-toriness in the AV junction and blocks subsequent supraventricular beats.
5.8.1.4 Ventricular Premature Complexes
Ventricular premature complexes (VPCs) are recognized as wide bizarre QRS com-plexes not preceded by P-waves (Fig. 5.5c). They often fail to conduct retrograde to the atria and thus do not typically reset the sinus node; this results in a full com-pensatory pause (the sum of pre- and post-APC intervals equals that of two normal sinus PP intervals). An interpolated VPC does not influence the following sinus beats (i.e., its occurrence is timed so as not to impair the next sinus beat from tra-versing the AV node and reaching the ventricles at the expected moment). The VPCs may occur as a single event, but may also occur in patterns of bigeminy (repeating pattern of sinus beat followed by a VPC) and trigeminy (two sinus beats coupled with a VPC). Couplets or pairs (two consecutive VPCs) and nonsustained ventricular tachycardia (VT, arbitrarily defined as three or more consecutive VPCs at a rate of >100 beats/min) are also relatively common observations during moni-toring of patients with heart disease. The morphology may be monomorphic (uni-form) or polymorphic (multiform).
The VPCs often bear a fixed coupling interval, i.e., a given period between the onset of VPC and the onset of its preceding sinus QRS complex. When there is a protected ventricular ectopic focus, the focus is constantly firing without being reset by sinus beats; this is clinically referred to as ventricular parasystole and is characterized by varying coupling intervals with relatively fixed inter-VPC inter-vals (i.e., variation <120 ms). Currently, pharmacologic treatment of VPCs is aimed at alleviating symptoms rather than prolongation of survival.
5.8.2 Sinus Tachycardias
5.8.2.1 Physiological Sinus Tachycardia
Physiologic sinus tachycardia represents a normal response to a variety of physi-ologic (anxiety and exercise) and/or pathologic stresses (fever, hypotension,

1055 The Electrocardiogram and Clinical Cardiac Electrophysiology
thyrotoxicosis, hypoxemia, and congestive heart failure). Sinus tachycardia rarely exceeds 200 beats/min and, by itself, should not be the target of treatment; in other words, therapy should be directed towards the underlying etiology if warranted (e.g., fever, anemia, hyperthyroidism, sepsis).
5.8.2.2 Inappropriate Sinus Tachycardia
Inappropriate sinus tachycardia is characterized by an increased resting heart rate (often >100 beats/min) and an exaggerated heart rate response to minimal stress. The ECG for this arrhythmia is indistinguishable from physiologic sinus tachycardia, presenting with normal P-wave morphology. b-blockers and calcium channel blockers can be used for symptomatic treatment, although with imperfect results. Subsequently, radiofrequency therapeutic modifications of the sinus node can be considered if drug therapy fails, as is often the case.
5.8.3 Paroxysmal Supraventricular Tachycardias
Paroxysmal supraventricular tachycardias (PSVTs) are a group of SVTs with sudden onset and termination. They are usually recurrent and often occur in otherwise seemingly healthy individuals.
5.8.3.1 Sinus Node Reentry Tachycardia
Sinus node reentry tachycardias are relatively rare, accounting for approximately 3% of all PSVTs. The average heart rate ranges between 130 and 140 beats/min, yet it can be quite labile, suggesting autonomic influences may be at play. Sinus node reentry tachycardias should be suspected in “anxiety-related sinus tachycardia.” b-blockers and/or calcium channel blockers (e.g., verapamil, dilti-azem) as well as ablation are common treatment options.
5.8.3.2 Atrial Tachycardias
Atrial tachycardias refer to those tachyarrhythmias that arise in atrial tissues due to abnormal automaticities or reentries. Typical atrial tachycardias have atrial rates between 150 and 200 beats/min, with P-wave morphologies that are usually different from those of P-waves with sinus node origins. Atrial tachycardias account for 5–10% of all PSVTs. Since atrial tachycardias arise within and are sustained by atrial tissues alone, AV block may develop without interrupting the tachycardia. The atrial rates often gradually accelerate after initiation until stabilizing between

106 J.T. Nguyen et al.
100 and 175 beats/min, an observation termed warm-up phenomenon. Ablation is often the treatment of choice when feasible in such patients.
5.8.3.3 AV Nodal Reentry Tachycardia
AV nodal reentry tachycardias (AVNRTs) are the most common PSVTs (50–65%) and usually present with narrow QRS complexes with regular heart rates between 130 and 250 beats/min. A schematic of a typical AV nodal reentry circuit is shown in Fig. 5.6. In such patients, retrograde P-waves may not be apparent in many instances, due to being buried within the QRS complexes. P-waves may also appear as subtle distortions at the terminal portion of the QRS complexes. During electro-physiologic testing, the onset of an AVNRT is almost always associated with a prolonged AH interval, which produces sufficient conduction delay in the so-called slow pathway to ensure recovery of the fast pathway. This delay permits the fast pathway to conduct retrograde toward the atrium, thereby completing the reentry circuit. Importantly, a critical balance between conduction delay and recovery of refractoriness in the two pathways is required to sustain the tachycardia.
Acute treatments to terminate AVNRT include (1) vagal maneuvers (e.g., carotid sinus massage or Valsalva maneuver); (2) adenosine injection; (3) administration of verapamil, diltiazem, or b-blockers; and/or (4) electrical (direct current) cardiover-sion. The majority of these interventions are designed to interrupt AV nodal conductions transiently, thereby “breaking” the fragile reentry circuits. Drugs used for long-term prevention of AVNRT recurrences include digitalis (not currently recommended due to low efficacy), b-blockers, calcium channel blockers, and/or class Ia and Ic antiarrhythmic drugs. Nevertheless, the most important advance in the treatment of AVNRT is transcatheter ablation, principally of the “slow” pathway region. In experienced hands, catheter ablation of AVNRT is a safe and highly effective curative treatment (i.e., with nearly 100% success rates).
5.8.3.4 AV Reciprocating Tachycardia Using Concealed Accessory Pathway
AV reciprocating tachycardia is another common form of PSVT. In such patients, accessory conduction tissue remaining from embryonic development of the heart can create the substrate for reentry PSVT. The most common type of accessory pathway is the AV bypass tract connecting the atria to the ventricles. In many cases, accessory connections only conduct in the retrograde direction (termed “concealed” accessory connections). In these individuals, there are no apparent ECG footprints since ventricular pre-excitations do not occur. It is noteworthy that
Fig. 5.6 (continued) Since the atria and ventricles are activated near simultaneously by a circuit within the AV node, the time difference between ventricular and atrial activation is relatively short. The retrograde P-wave is often buried in QRS complex (RP interval is 0 ms), as shown in this case. Recording channels are the same as in Fig. 5.3

1075 The Electrocardiogram and Clinical Cardiac Electrophysiology
I
II
V1
V5
CS p
CS 7,8
CS 5,6
CS 3,4
CS d
His p
His d
RVaStim
Fig. 5.6 (Top) Schematic of the typical AV nodal reentry tachycardia (AVNRT). The AV node has a slow pathway with short refractoriness and a fast pathway with long refractoriness. (a) During sinus rhythm, the impulse conducts the ventricles through the fast pathway, yielding a normal PR interval. The impulse simultaneously goes down the slow pathway, but cannot conduct to the His bundle antegradely or retrogradely to the fast pathway since they are rendered refractory by the prior beat. (b) An atrial premature complex (APC) reaches the effective refractory period of the fast pathway and is blocked in the fast pathway. This APC is able to conduct slowly down to the slow pathway, yielding a prolonged PR interval. The delay in conduction over the slow pathway provides enough time for the fast pathway to recover and allow the impulse conducted from the slow pathway to continue over the fast pathway retrogradely to the atria, producing an atrial echo beat. At same time, the returned impulse tries to conduct down over the slow pathway and fails due to unrecovered refractoriness of the slow pathway. (c) A sufficient early APC occurs, producing a similar echo beat as in b. However, the returned impulse is able to conduct down the slow pathway, repeatedly producing another ven-tricular beat and atrial echo, i.e., supraventricular tachycardia or SVT (Source: Josephson ME. Clinical Cardiac Electrophysiology. Techniques and Interpretation, third edition. Philadelphia, PA: Lippincott Williams & Wilkins, 2002). (Bottom) Intracardiac recordings of typical AVNRT.

108 J.T. Nguyen et al.
this form of accessory pathway accounts for approximately 30% of all PSVTs. The electrical impulses for this type of PSVT circulate antegrade through the AV nodes and retrograde through the concealed accessory pathways (Fig. 5.7); both the atria and ventricles are necessary components of the reentry circuit in this type of arrhythmia, distinguishing it from AVNRT.
Medical treatment of AV reciprocating tachycardia is similar to that of AVNRT. Nevertheless, catheter ablation is highly effective for eliminating accessory AV connections and is often the preferred approach, especially in younger individuals.
Fig. 5.7 Typical AV reentry tachycardia. (Top) Illustration of AV reciprocating tachycardia using a left-sided concealed accessory pathway. Left bundle branch block prolongs the tachycardia cycle length by 50 ms due to the conduction delay of the tachycardia circuit in the left ventricle. (Bottom) 12-lead ECG recording of AV reentry tachycardia. Note that the retrograde P-wave is 150 ms after the onset of QRS complex (RP interval is 150 ms). AVN = atrioventricular node; HB = His bundle; LA = left atrium; LBB = left bundle branch; LV = left ventricle; RA = right atrium; RBB = right bundle branch; RV = right ventricle

1095 The Electrocardiogram and Clinical Cardiac Electrophysiology
5.9 Wolff–Parkinson–White Syndrome
When there are one or more accessory AV pathways or connections that conduct in the antegrade direction, the ventricles may become overtly pre-excited to a varying degree. This condition is referred to as Wolff–Parkinson–White syndrome, i.e., when palpitations/tachyarrhythmias occur in the setting of pre-excitation. The ECG features of a typical AV connection in Wolff–Parkinson–White syndrome are (1) shortened PR interval <120 ms during sinus rhythm; (2) widened QRS dura-tion; and (3) the presence of a delta wave (a slurred, slowly rising onset of the QRS) (Fig. 5.8). The terminal QRS portions are usually normal, and sometimes they are associated with secondary ST-T changes.
In addition to typical AV accessory pathways, other variants may exist in such patients, such as atriohisian, atriofascicular, nodofascicular, and nodoventricular fibers. More specifically, the Lown–Ganong–Levine syndrome is defined in patients with recurrent paroxysmal tachycardias or atrial fibrillation (AF) associated with short PR intervals and normal QRS complexes. Further, when present, the majority of Mahaim fibers are long right-sided atriofascicular or AV pathways between the lateral tricuspid and distal right bundle branches in the right ventricular free walls. These fibers almost represent a duplication of the AV node and are capable of only antegrade conduction with decremental conduction properties.
Fig. 5.8 ECG recording and delta wave of Wolff–Parkinson–White Syndrome. The vector of the delta waves suggests a right posterior septal accessory pathway. See text for discussion

110 J.T. Nguyen et al.
5.10 Nonparoxysmal Junctional Tachycardia
Nonparoxysmal junctional tachycardia, also called accelerated junctional rhythm, is readily recognized by a narrow QRS complex without a consistent P-wave preceding each QRS complex, at heart rates between 70 and 130 beats/min; it is usually associated with a warm-up period at the onset. Nonparoxysmal junctional tachycardia frequently results from conditions that produce enhanced automaticity or triggered activities in the AV junction, such as those associated with inferior acute myocardial infarctions, digitalis intoxications, or postvalvular surgery. Typically, treatments in such cases should be directed toward the under-lying diseases.
5.11 Atrial Flutter and Fibrillation
5.11.1 Atrial Flutter
Atrial flutter is characterized by atrial rates between 250 and 350 beats/min, usually accompanied with 2:1 AV conductions and resulting in ventricular rates of approximately 150 beats/min. Classical flutter waves (F-waves) are regular saw-tooth patterns on the ECG, most prominently detected in the inferior leads and sometimes V1 (Fig. 5.9). Although antiarrhythmic drugs may be useful to prevent recurrences of atrial flutter, they are less effective for the conversion to
Fig. 5.9 Atrial flutter. See text for discussion

1115 The Electrocardiogram and Clinical Cardiac Electrophysiology
sinus rhythm. In such patients, cardioversion (50–100 J) is oftentimes the most effective method for termination of atrial flutter. Although systemic emboliza-tion is less common in atrial flutter than in AF (discussed later), such patients should be prescribed chronic anticoagulation for stroke prophylaxes according to standardized AF guidelines.
5.11.2 Atrial Fibrillation
Atrial fibrillation (AF) is an uncoordinated atrial tachyarrhythmia characterized on ECG by (1) the absence of distinct P-waves before each QRS complex; (2) the pres-ence of rapid atrial oscillations (F-waves); and (3) irregular RR intervals (Fig. 5.10). The AF is considered recurrent when two or more episodes have occurred. Recurrent AF is designated paroxysmal if there is spontaneous termination of the arrhythmia. The term persistent is used when AF is present longer than seven days. If several attempts at cardioversion fail or are not indicated in long-standing cases (>1 year), AF is regarded as permanent. When no history is available, the term recent or new onset is often used.
The incidence of AF is highly age-dependent; other common cardiac precursors include a history of congestive heart failure, valvular heart disease, hypertension, and/or coronary artery disease. Lone AF is said to be present when this tachyar-rhythmia occurs in the absence of underlying structural heart disease or transient precipitating factors.
The mechanisms underlying AF may include multiple wavelet reentry and focal enhanced automaticity. The atrial “rates” during AF can range from 350 to 600 beats/min.
Fig. 5.10 Atrial fibrillation. See text for discussion

112 J.T. Nguyen et al.
Due to concealed AV nodal penetrations and subsequent variable degrees of AV block, the characteristic irregularly irregular ventricular rates are usually between 100 and 160 beats/min in untreated patients with normal AV conduction properties.
The major adverse clinical consequences of AF include palpitations, impaired cardiac function, and/or thromboembolism. Typical physical findings in such patients include irregularly irregular ventricular rhythms, variations in the intensity of the first heart sounds, and/or the absence of “a” waves in jugular venous pulses. If the ventricular responses are too rapid, a peripheral pulse deficit (peripheral pulse rate less than heart rate) can result from insufficient diastolic filling time. Patients with chronic rapid ventricular rates are also at risk for developing tachycardia-induced cardiomyopathies. In addition to rheumatic mitral valve disease and prosthetic valves (mechanical or tissue), major risk factors for embolization in nonvalvular AF are often assessed using a CHADS
2 scheme (Cardiac Failure,
Hypertension, Age, Diabetes, Stroke [Doubled]).The goals of therapies for AF are improvement of symptoms, reduction of
AF-associated morbidities, and improvement in prognoses. The three basic tenets of therapy for AF are (1) restoration and maintenance of sinus rhythm; (2) control of ventricular rate responses; and (3) prevention of thromboembolism.
5.12 Ventricular Tachyarrhythmias
5.12.1 Ventricular Tachycardias
Although VTs can occur in clinically normal hearts, they generally accompany some form of structural heart disease, particularly in patients with prior myocardial infarctions. A fixed substrate, such as an old infarct scar, is typically responsible for most episodes of recurrent monomorphic VT. Yet, acute ischemia may also play a more important role in the pathogenesis of polymorphic VT or ventricular fibrillation.
The VTs are characterized on ECG by a wide QRS complex and tachycardia at rates of >100 beats/min (Fig. 5.11). Like VPCs, VTs can be monomorphic (Fig. 5.11a) or polymorphic. A sustained VT is defined as a VT persisting >30 s or requiring termination due to hemodynamic compromise. A nonsustained VT is defined as lasting >3 consecutive beats but less than 30 s. Bidirectional VT refers to VT that shows an alternation in QRS amplitudes and axes. The key marker of VT on ECG is ventriculo-atrial dissociation; capture or fusion beats also strongly support the diagnosis of VT. Sustained VT is almost always symptomatic and the presentation, prognosis, and management of VT largely depend on the patient’s underlying cardiovascular state.
Procainamide and amiodarone are commonly used medications for the pharmaco-logical treatment of acute termination of VT. Yet, in patients with heart disease, sotalol, dofetilide, and amiodarone are the recommended drugs for chronic

1135 The Electrocardiogram and Clinical Cardiac Electrophysiology
suppression. An ICD, with or without supplemental dosing with amiodarone, is the most established long-term therapy for VT. Nevertheless, catheter ablation may provide cures for some forms including (1) VT in those with structurally normal hearts (idiopathic VT); (2) those with bundle-branch reentry VT; and/or (3) selected cases of scar-related VT. However, in patients with diminished left ventricular function, it may be prudent to place an ICD even after an apparently successful ablation. A complete guideline for management of ventricular arrhythmias was published in 2006.
5.12.2 Ventricular Flutter and Ventricular Fibrillation
Electrocardiographically, ventricular flutters (Fig. 5.11b) usually appear as “sine waves” with a rate between 150 and 300 beats/min; it is essentially impossible
Fig. 5.11 Ventricular tachyarrhythmias. (a) ventricular tachycardia, (b) ventricular flutter, (c) ventricular fibrillation, and (d) torsades de pointes (TdP)

114 J.T. Nguyen et al.
to assign a specific morphology of these oscillations. Ventricular fibrillation (Fig. 5.11c) is recognized by grossly irregular undulations of varying amplitudes, contours, and rates, and is often preceded by a rapid repetitive sequence of VT. Spontaneous conversions of ventricular fibrillation to sinus rhythm are rare, and prompt electrical defibrillation is essential. Long-term prevention of sudden cardiac death in these patients predominately relies on ICDs.
5.12.3 Accelerated Idioventricular Rhythm
Accelerated idioventricular rhythm can be regarded as a type of slow VT with heart rates between 60 and 110 beats/min. These rhythms usually occur in settings such as acute myocardial infarction, particularly during reperfusion. Since these rhythms are usually transient without significant hemodynamic compromise, treatments are rarely required.
5.12.4 Torsades de Pointes
When polymorphic VT occurs in the presence of prolonged QT intervals (congenital or acquired), it is termed Torsades de Pointes (TdP). This arrhythmia is often pre-ceded by VPCs with a long-short sequence (Fig. 5.11d). Oftentimes, TdP presents with multiple nonsustained episodes causing recurrent syncope, but also has a predilection to degenerate into ventricular fibrillation. Identification of TdP has important therapeutic implications because treatments are completely different from that of non-TdP polymorphic VT. Magnesium, pacing, and/or isoprotere-nolol can be used to treat TdP if required. It should be noted that a left cervicotho-racic sympathectomy, involving resection of the lower half of the left stellate ganglion and portions of the thoracic sympathetic ganglia, has also been proposed as a form of therapy for TdP in patients with congenital long QT syndrome.
5.13 Summary
Cardiac arrhythmias encompass a wide spectrum of abnormalities in both electrical generation and conduction at all levels within the heart. These defects can manifest as either bradycardia or tachycardia. Clinical and basic laboratory research gained important insights into the mechanisms underlying these various arrhythmias (e.g., increased automaticity, triggered activity, micro- and/or macro-reentry), and has provided valuable tools for their treatment (medications, pacemakers, defibrillators, and catheter-based ablations). The clinical significance of these cardiac arrhythmias is predominantly related to hemodynamic outcomes and the risk of life-threatening consequences (e.g., ventricular fibrillation), in addition to associated symptoms.

1155 The Electrocardiogram and Clinical Cardiac Electrophysiology
Careful inspection of a patient’s ECG recordings often makes it possible to correctly diagnose many rhythm disturbances and guide clinical management. It is important to note that recent technical advancements have enabled more complex arrhythmias to be ablated, thus providing a curative treatment (Fig. 5.12).
Further Readings
Benditt DG, Lü F. Atriofascicular pathways: fuzzy nomenclature or merely wishful thinking? J Cardiovasc Electrophysiol 2006; 17:261–5.
Blomström-Lundqvist C, Scheinman MM, Aliot EM, et al. ACC/AHA/ESC guidelines for the man-agement of patients with supraventricular arrhythmias. J Am Coll Cardiol 2003; 42:1493–531.
Camm AJ, Lü F. Risk stratification after myocardial infarction. Pacing Clin Electrophysiol 1994; 17:401–16.
Fig. 5.12 TdP. Successful catheter ablation of premature ventricular ectopics in the anteroseptal wall of the right ventricular outflow tract eliminates frequent episodes of TdP (as shown on the top) that are refractory to medical management. The bottom shows an activation map using the Ensite NavX system. The red areas indicate the ablation lesions

116 J.T. Nguyen et al.
Camm AJ, Lü F. Chronotropic incompetence. Part I. Normal modulation of the heart rate. Clin Cardiol 1996; 19:424–8.
Camm AJ, Lü F. Chronotropic incompetence. Part II. Clinical significance. Clin Cardiol 1996; 19:424–8.
Epstein AE, DiMarco JP, Ellenbogen KA, et al. ACC/AHA/HRS 2008 guidelines for device-based therapy of cardiac rhythm abnormalities. J Am Coll Cardiol 2008; 51:1–62.
Lü F, Statters DJ, Hnatkova K, et al. Change of the autonomic influence on the heart immediately before the onset of spontaneous idiopathic ventricular tachycardia. J Am Coll Cardiol 1994; 24:1515–22.
Fuster V, Rydén LE, Cannom DS, et al. ACC/AHA/ESC 2006 guidelines for the management of patients with atrial fibrillation. J Am Coll Cardiol 2006; 48:854–906.
Hancock EW, Deal BJ, Mirvis DM, et al. AHA/ACCF/HRS recommendations for the standardiza-tion and interpretation of the electrocardiogram: Part V: electrocardiogram changes associated with cardiac chamber hypertrophy. J Am Coll Cardiol 2009; 53:992–1002.
Hjalmarson A, Goldstein S, Fagerberg B, et al. Effects of controlled-release metoprolol on total mortality, hospitalizations, and well-being in patients with heart failure: The metoprolol CR/XL randomized intervention trial in congestive heart failure (MERIT-HF). MERIT-HF study group. JAMA 2000; 283:1295–302.
Packer M, Bristow MR, Cohn JN, et al. The effect of carvedilol on morbidity and mortality in patients with chronic heart failure. U.S. Carvedilol Heart Failure Study Group. N Engl J Med 1996; 334:1349–55.
Preliminary report: Effect of encainide and flecainide on mortality in a randomized trial of arrhythmia suppression after myocardial infarction. The Cardiac Arrhythmia Suppression Trial (CAST) investigators. N Engl J Med 1989; 321:406–12.
Rautaharju PM, Surawicz B, Gettes LS, et al. AHA/ACCF/HRS recommendations for the standardiza-tion and interpretation of the electrocardiogram: Part IV: the ST segment, T and U waves, and the QT interval. J Am Coll Cardiol 2009; 53:982–91.
Surawicz B, Childers R, Deal BJ, et al. AHA/ACCF/HRS recommendations for the standardiza-tion and interpretation of the electrocardiogram: Part III: intraventricular conduction distur-bances J Am Coll Cardiol 2009; 53:976–81.
Wagner GS, Macfarlane P, Wellens H, et al. AHA/ACCF/HRS recommendations for the standard-ization and interpretation of the electrocardiogram: Part VI: acute ischemia/infarction. J Am Coll Cardiol 2009; 53:1003–11.
Zipes DP, Camm AJ, Borggrefe M, et al. ACC/AHA/ESC 2006 guidelines for management of patients with ventricular arrhythmias and the prevention of sudden cardiac death. J Am Coll Cardiol 2006; 48:1064–108.