Embed Size (px)
Citation preview
Cardiothoracic Critical Care:Cardiothoracic Critical Care:
The Ongoing EvolutionThe Ongoing Evolution
AATS / STS AATS / STS
CARDIOTHORACIC CRITICAL CARE SYMPOSIUM CARDIOTHORACIC CRITICAL CARE SYMPOSIUM
Sunday April 29, 2012Sunday April 29, 2012Sunday April 29, 2012Sunday April 29, 2012
San Francisco, CASan Francisco, CA
NevinNevin M. Katz, M.D.M. Katz, M.D.
Johns Hopkins UniversityJohns Hopkins University
Foundation for the Advancement of CTS CareFoundation for the Advancement of CTS Care
(FACTS(FACTS--Care)Care)

DisclosuresDisclosures
•• No disclosures relevant to this presentation. No disclosures relevant to this presentation.
•• Opinions are my own, based on 30 + years in the field of CVT Opinions are my own, based on 30 + years in the field of CVT
surgery and critical care and my interpretation of the surgery and critical care and my interpretation of the
literature.literature.
PerspectivePerspective
CT Surgeon CT Surgeon -- Georgetown University 20 yearsGeorgetown University 20 years
•• Heart Transplantation Program DirectorHeart Transplantation Program Director
Cardiothoracic Surgical Critical Care Cardiothoracic Surgical Critical Care
•• George Washington University Medical CenterGeorge Washington University Medical Center
•• Johns Hopkins University Johns Hopkins University –– Cardiac Surgery ICUCardiac Surgery ICU
Development and Direction of the Annual ConferencesDevelopment and Direction of the Annual ConferencesDevelopment and Direction of the Annual ConferencesDevelopment and Direction of the Annual Conferences
•• Cardiothoracic Surgical (CTS) Critical Care 2004 Cardiothoracic Surgical (CTS) Critical Care 2004 -- 20082008
•• CardiovascularCardiovascular--Thoracic (CVT) Critical Care 2009 Thoracic (CVT) Critical Care 2009 -- 20112011
Creation & Development of NonCreation & Development of Non--Profit Educational Profit Educational Found’nFound’n: FACTS: FACTS--Care Care
CoCo--Director AATS/STS Postgraduate CT Critical Care Course Director AATS/STS Postgraduate CT Critical Care Course 2010, 20112010, 2011
CoCo--Director STS CT Critical Care Symposium Director STS CT Critical Care Symposium 2011, 20122011, 2012
Setting the Stage for theSetting the Stage for the
“AATS/STS“AATS/STS
Cardiothoracic Critical Care Cardiothoracic Critical Care Cardiothoracic Critical Care Cardiothoracic Critical Care
Symposium”Symposium”

Driving the “The Ongoing Evolution”Driving the “The Ongoing Evolution”
•• Increased Severity of Clinical States Increased Severity of Clinical States
•• Advances in Supportive Technology & Advances in Supportive Technology &
PharmacologyPharmacology
•• The Changing CT Critical Care TeamThe Changing CT Critical Care Team
•• New Information TechnologyNew Information Technology
•• Quality Improvement InitiativesQuality Improvement Initiatives
Increased Severity Increased Severity
of of of of
Clinical StatesClinical States
More Complex Critical Care SituationsMore Complex Critical Care Situations
Maximally Support TechnologyMaximally Support Technology
•• Now creates possibility of survival, when Now creates possibility of survival, when
previously there was none!previously there was none!previously there was none!previously there was none!
•• New Protocols, SideNew Protocols, Side--effects & Risks effects & Risks
New Surgical / Interventional ProceduresNew Surgical / Interventional Procedures
•• Some suitable for highSome suitable for high--risk patients, previously risk patients, previously
considered “inoperable” considered “inoperable”
High Acuity Clinical IssuesHigh Acuity Clinical Issues
•• LV / RV Failure +/LV / RV Failure +/-- Requiring Mechanical SupportRequiring Mechanical Support
•• ALI / ARDS / TRALIALI / ARDS / TRALI
•• Acute Renal Failure Acute Renal Failure –– CSA CSA -- AKIAKI
•• Mesenteric IschemiaMesenteric Ischemia•• Mesenteric IschemiaMesenteric Ischemia
•• Cerebral Dysfunction / Edema / InfarctionCerebral Dysfunction / Edema / Infarction
•• Endocrine Insufficiencies Endocrine Insufficiencies –– Hyperglycemia, Adrenal, Hyperglycemia, Adrenal,
ThyroidThyroid
•• Coagulopathies / Blood Product TransfusionsCoagulopathies / Blood Product Transfusions
•• Systemic & Local InfectionsSystemic & Local Infections
•• MultiMulti--System Organ FailureSystem Organ Failure
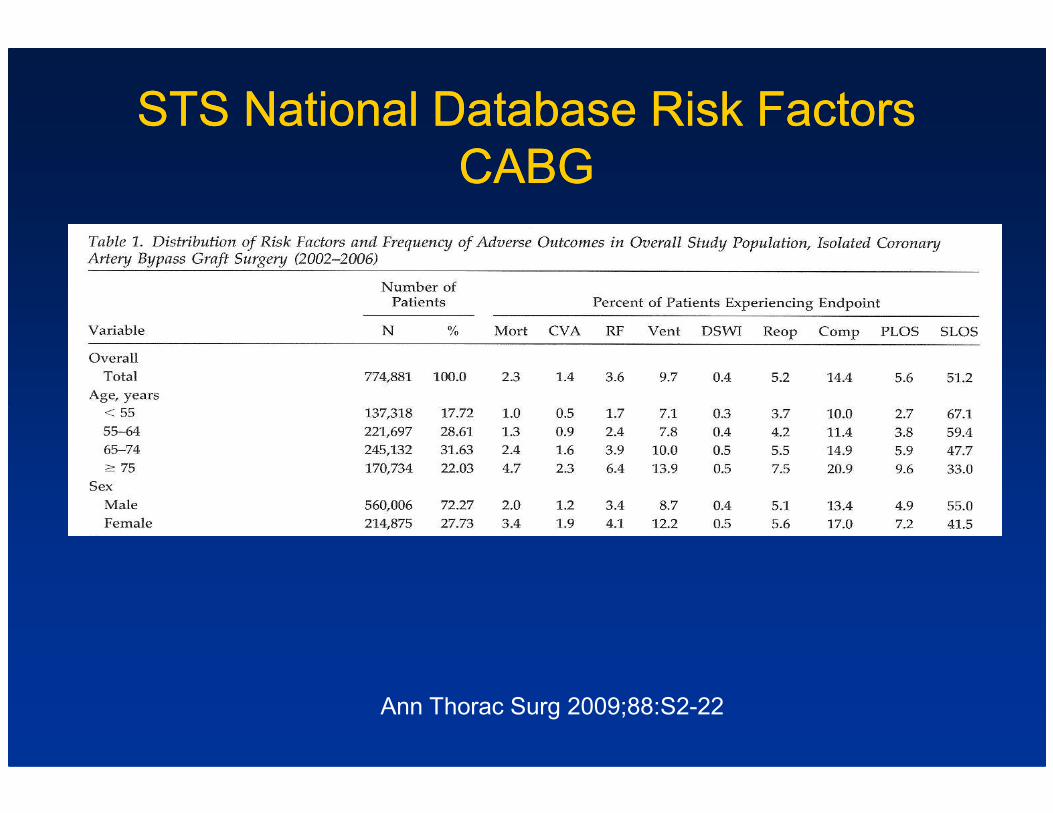
STS National Database Risk Factors STS National Database Risk Factors
CABGCABG
Ann Thorac Surg 2009;88:S2-22
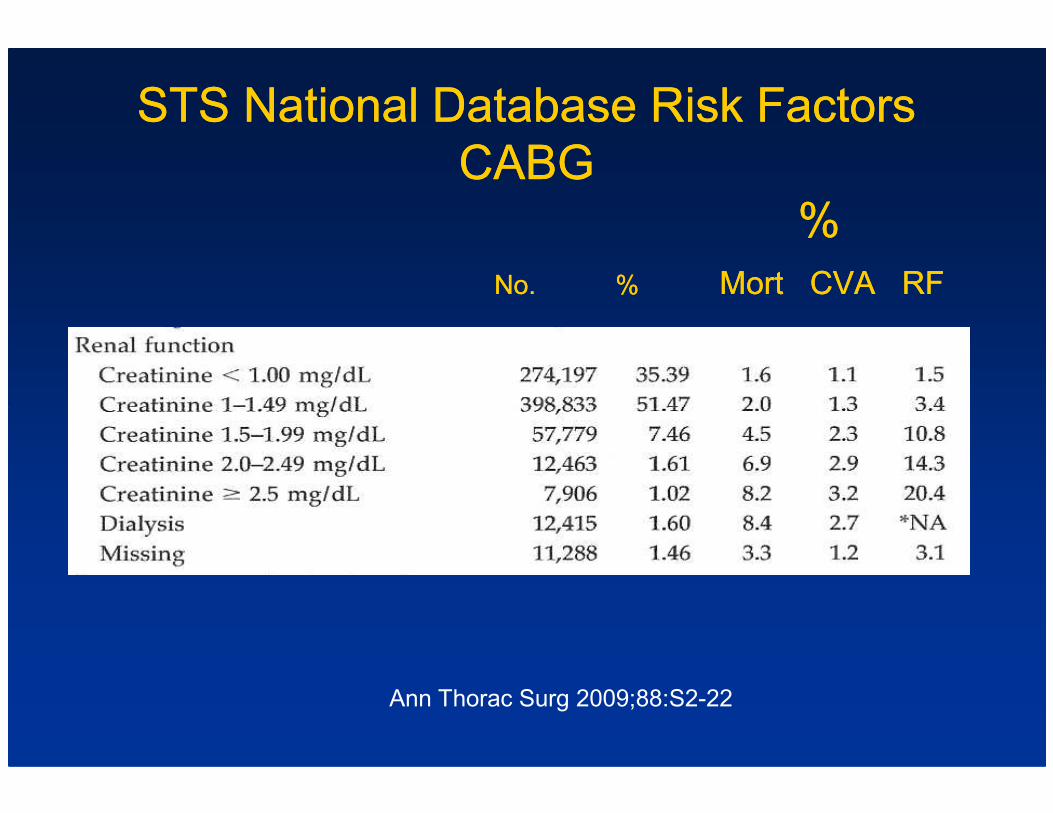
STS National Database Risk Factors STS National Database Risk Factors
CABGCABG
%%
No.No. % % Mort CVA RFMort CVA RF
Ann Thorac Surg 2009;88:S2-22
Acute Renal FailureAcute Renal Failure
Clinical Issues in Cardiac Surgery PatientsClinical Issues in Cardiac Surgery Patients
•• Volume Overload ConsequencesVolume Overload Consequences•• Volume Overload ConsequencesVolume Overload Consequences
•• Increase Risk of InfectionsIncrease Risk of Infections
High Acuity Case ExampleHigh Acuity Case Example
•• 65 65 yoyo man, S/P AVR (Tissue) 5 years previouslyman, S/P AVR (Tissue) 5 years previously
•• Developed Developed CoagCoag negative Staph negative Staph BioprostheticBioprosthetic Valve Valve
EndocarditisEndocarditis with an Aortic Root Abscesswith an Aortic Root Abscess
Underwent Underwent ReRe--operative Median operative Median SternotomySternotomy, Removal of , Removal of •• Underwent Underwent ReRe--operative Median operative Median SternotomySternotomy, Removal of , Removal of
AVR, Debridement of Abscess Cavity, Reconstruction of AVR, Debridement of Abscess Cavity, Reconstruction of
Aortic Root with HomograftAortic Root with Homograft
•• Extensive adhesionsExtensive adhesions
•• TBT 195’ TBT 195’
•• Major Coagulopathy Major Coagulopathy –– Packing to ControlPacking to Control
“Open Chest Protocol”“Open Chest Protocol”
Used in Extreme Situations:Used in Extreme Situations:
•• Continued bleeding / Continued bleeding / CoagulopathyCoagulopathy requiring requiring mediastinalmediastinal
packingpacking
•• Marked Marked MediastinalMediastinal & Pulmonary & Pulmonary EdmaEdma
•• Prolonged CPB timeProlonged CPB time
•• Preoperative shock state Preoperative shock state –– MI, CP ArrestMI, CP Arrest
•• Emergency ECMO / Temporary VAD Emergency ECMO / Temporary VAD
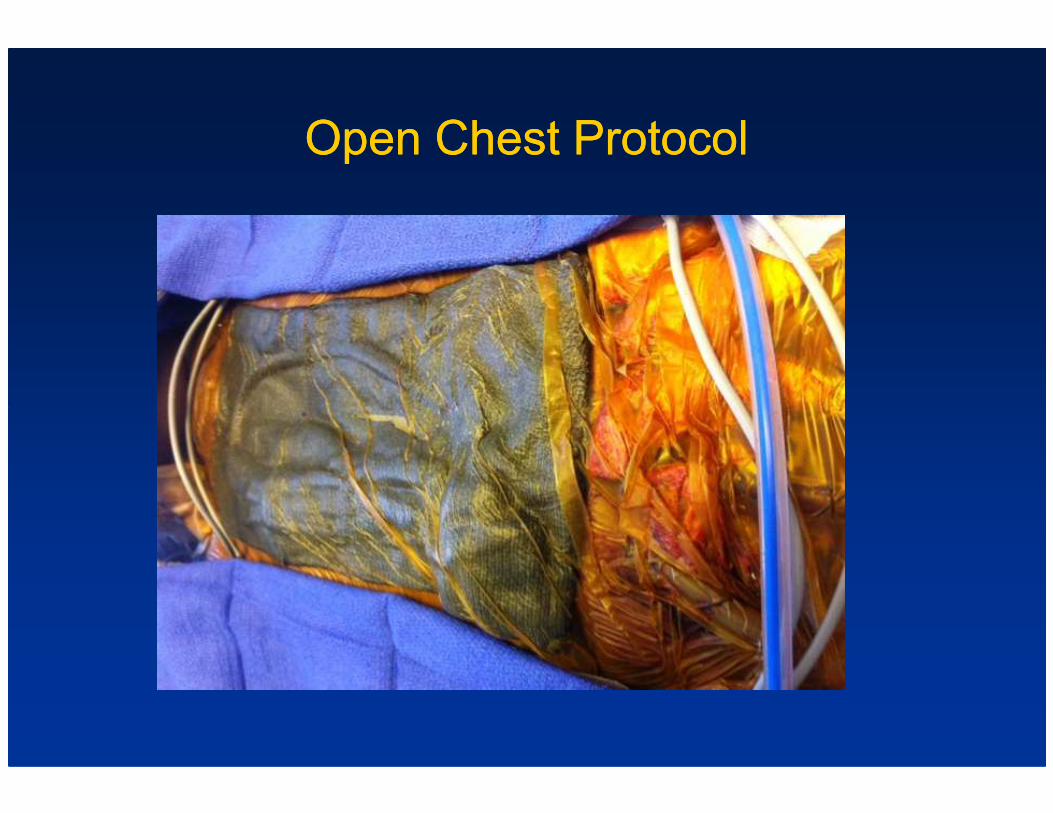
Open Chest ProtocolOpen Chest Protocol
ICU “Open Chest Protocol”ICU “Open Chest Protocol”
•• Full Full VentilatoryVentilatory Support Support –– SIMV with PS & PEEPSIMV with PS & PEEP
•• Compromised Respiratory MechanicsCompromised Respiratory Mechanics
•• Transfusion Associated Acute Lung Injury (TRALI) Transfusion Associated Acute Lung Injury (TRALI)
•• Hemodynamic Monitoring Hemodynamic Monitoring inclincl Mixed Venous O2 Mixed Venous O2 SatsSats
•• Optimizing Optimizing Hemodynamics & Hemodynamics & Perfusion Perfusion
•• Potential Mechanical Assist / ECMOPotential Mechanical Assist / ECMO
ICU “Open Chest Protocol”ICU “Open Chest Protocol”
•• Acute Renal Insufficiency Acute Renal Insufficiency
•• Optimal Renal PerfusionOptimal Renal Perfusion
•• Management of Volume Management of Volume OverloadOverload
DiureticsDiuretics•• DiureticsDiuretics
•• Hemofiltration / CVVHDHemofiltration / CVVHD
•• ContCont IV Sedation & Analgesia IV Sedation & Analgesia
•• Periodic Periodic NeuroNeuro AssessmentAssessment
•• Optimal Cerebral Perfusion Optimal Cerebral Perfusion
ICU “Open Chest Protocol”ICU “Open Chest Protocol”
•• Correction of CoagulopathyCorrection of Coagulopathy
•• Preoperative AntiPreoperative Anti--Platelet TherapyPlatelet Therapy
•• AprotininAprotinin ControversyControversy
•• Increasingly Increasingly RecogizedRecogized Risks of Blood TransfusionRisks of Blood Transfusion•• Increasingly Increasingly RecogizedRecogized Risks of Blood TransfusionRisks of Blood Transfusion
•• Return to OR for Removal of Pack, Reassessment, & ClosureReturn to OR for Removal of Pack, Reassessment, & Closure
•• Prevention of InfectionPrevention of Infection
•• Antibiotics until 24 hrs after Chest ClosureAntibiotics until 24 hrs after Chest Closure
Advances in Supportive Advances in Supportive
Technology & PharmacologyTechnology & PharmacologyTechnology & PharmacologyTechnology & Pharmacology
New & Recurrent New & Recurrent
IssuesIssues & & ControversiesControversies
Support of the CirculationSupport of the Circulation
•• Optimal Combinations of Pharmacologic AgentsOptimal Combinations of Pharmacologic Agents
•• When to Use Mechanical Support & What SystemWhen to Use Mechanical Support & What System•• When to Use Mechanical Support & What SystemWhen to Use Mechanical Support & What System
Management of Pulmonary Hypertension
• Latest Strategies
New & Recurrent New & Recurrent
IssuesIssues & & ControversiesControversies
Respiratory FailureRespiratory Failure
•• Optimal Ventilator Mode & Protocol to Wean Complex Optimal Ventilator Mode & Protocol to Wean Complex
Patients from the VentilatorPatients from the Ventilator
ALI / ARDS ALI / ARDS –– Optimal Optimal VentilatoryVentilatory SupportSupport•• ALI / ARDS ALI / ARDS –– Optimal Optimal VentilatoryVentilatory SupportSupport
ECMOECMO
•• IndicationsIndications
•• TechnologyTechnology
•• VenoVeno--Venous vs. Venous vs. VenoVeno--ArterialArterial
New & Recurrent New & Recurrent
IssuesIssues & & ControversiesControversies cont’dcont’d
Renal Insufficiency / Renal FailureRenal Insufficiency / Renal Failure
•• Management of Volume OverloadManagement of Volume Overload
•• Renal Replacement TherapyRenal Replacement Therapy•• Renal Replacement TherapyRenal Replacement Therapy
•• When to StartWhen to Start
•• What System & What Dose What System & What Dose
Advances in PharmacologyAdvances in Pharmacology
•• Vasoactive AgentsVasoactive Agents
•• Anticoagulants & Antiplatelet AgentsAnticoagulants & Antiplatelet Agents
•• AntiarrhythmicsAntiarrhythmics
•• AntimicrobialsAntimicrobials•• AntimicrobialsAntimicrobials
•• DiureticsDiuretics
•• Sedatives/AnalgesicsSedatives/Analgesics
Complex Supportive Complex Supportive TechnolgyTechnolgy
•• Advanced Ventilator SystemsAdvanced Ventilator Systems
•• Ventricular Assist DevicesVentricular Assist Devices
•• ECMO SystemsECMO Systems
•• Renal ReplacementRenal Replacement
Advances in Supportive Advances in Supportive TechnolgyTechnolgy
•• Invasive & NonInvasive & Non--Invasive Monitoring SystemsInvasive Monitoring Systems
•• Point of Care Laboratory SystemsPoint of Care Laboratory Systems
•• ICU Monitoring & Alert SystemsICU Monitoring & Alert Systems
InvitationInvitation -- Visit “The ICU of the Future”Visit “The ICU of the Future”
The Changing MultiThe Changing Multi--Disciplinary Disciplinary The Changing MultiThe Changing Multi--Disciplinary Disciplinary
CT Critical CT Critical CareTeamCareTeam
Earlier Model of CT Critical CareEarlier Model of CT Critical Care
•• CT Surgeon directs the Critical Care.CT Surgeon directs the Critical Care.
•• CT Surgeon, CT Surgeon, His/HerHis/Her House Staff, PA’s and Critical House Staff, PA’s and Critical
Care Nurses perform most of the care.Care Nurses perform most of the care.
•• Critical Care is learned during Residency and in Critical Care is learned during Residency and in
Clinical PracticeClinical Practice
The CT Surgeon as The CT Surgeon as
Critical Care PhysicianCritical Care Physician
•• Critical Care is inherent to the specialty of CT surgery.Critical Care is inherent to the specialty of CT surgery.
•• CT Surgeons from the beginning of Training take care of CT Surgeons from the beginning of Training take care of many of their patients in ICU’smany of their patients in ICU’smany of their patients in ICU’smany of their patients in ICU’s
•• Surgeons have the best understanding of the procedures Surgeons have the best understanding of the procedures performed and the potential complications for a particular performed and the potential complications for a particular patient.patient.
•• The Patient “places his/her life in the surgeon’s hands.”The Patient “places his/her life in the surgeon’s hands.”
Definition of Thoracic Surgery by Definition of Thoracic Surgery by
American Board of Thoracic SurgeryAmerican Board of Thoracic Surgery
• THORACIC SURGERY ENCOMPASSES THE OPERATIVE,
PERIOPERATIVE, AND SURGICAL CRITICAL CARE OF
PATIENTS WITH ACQUIRED AND CONGENITAL PATIENTS WITH ACQUIRED AND CONGENITAL
PATHOLOGIC CONDITIONS WITHIN THE
CHEST. INCLUDED ARE N
Changing Role of CT SurgeonsChanging Role of CT Surgeons
ICU ICU AttendingsAttendings
•• CT Surgeons CT Surgeons
•• NonNon--Surgeon Surgeon IntensivistsIntensivists
•• Certification Certification •• Certification Certification
CT Surgical Residents & FellowsCT Surgical Residents & Fellows
•• Operative Operative vsvs Critical Care ExperienceCritical Care Experience
•• Training Training
•• Balance of Responsibility & CommunicationBalance of Responsibility & Communication
The MultiThe Multi--Disciplinary TeamDisciplinary Team
• Increasingly Recognized as the Optimal Approach
• Specialized Knowledge & Experience
The CT Surgeon continues to have a Leadership Role on the • The CT Surgeon continues to have a Leadership Role on the
team
• Even if not directing minute to minute care.
•• Important ChallengesImportant Challenges
•• CommunicationCommunication
•• PowerPower--SharingSharing
Critical Care Certification for CT SurgeonsCritical Care Certification for CT Surgeons
American Board of Surgery American Board of Surgery
•• One of the Subspecialty Certifications: One of the Subspecialty Certifications:
Surgical Critical CareSurgical Critical Care
•• Requires a 1Requires a 1--Year FellowshipYear Fellowship
American Board of Thoracic SurgeryAmerican Board of Thoracic Surgery
•• Only Subspecialty Certification: Only Subspecialty Certification:
Congenital Cardiac SurgeryCongenital Cardiac Surgery
•• Potential Certification in the Subspecialty of CT Critical Potential Certification in the Subspecialty of CT Critical
CareCare
Certification in the Subspecialty of Certification in the Subspecialty of
CT Critical CareCT Critical Care
Potential Criteria for CertificationPotential Criteria for Certification
Clinical Experience DocumentationClinical Experience Documentation•• Clinical Experience DocumentationClinical Experience Documentation
•• CME RequirementCME Requirement
•• Examination in CT Critical CareExamination in CT Critical Care
Political Issues Political Issues
Development of Development of CT CT Critical Critical CareCare
as a Specialty fromas a Specialty from
Within CT SurgeryWithin CT Surgery
•• FACTSFACTS--Care MultiCare Multi--DisciplinaryDisciplinary
“CVT “CVT Critical Critical Care” Care” ConferencesConferences::
20042004, 2005, , 2005, 2006, 2007, 2008, 2009, 2010, 2011,20122006, 2007, 2008, 2009, 2010, 2011,2012
•• AATS Postgraduate CT Critical Care Courses:AATS Postgraduate CT Critical Care Courses:
2010, 2011, 20122010, 2011, 2012
•• STS CT Critical Care SymposiaSTS CT Critical Care Symposia
2011, 2012 2011, 2012
Heightened Role of Heightened Role of
Advance Practice ProvidersAdvance Practice Providers
NonNon--Physician Providers: Physician Providers:
•• Nurse PractitionersNurse Practitioners
•• Physician AssistantsPhysician Assistants
Factors :Factors :
•• Increased Staffing Needs with Increased Patient AcuityIncreased Staffing Needs with Increased Patient Acuity
•• Mandated Restriction of Resident Work HoursMandated Restriction of Resident Work Hours
•• Need for Surgical Residents to Maximize their Operative Need for Surgical Residents to Maximize their Operative
ExperienceExperience
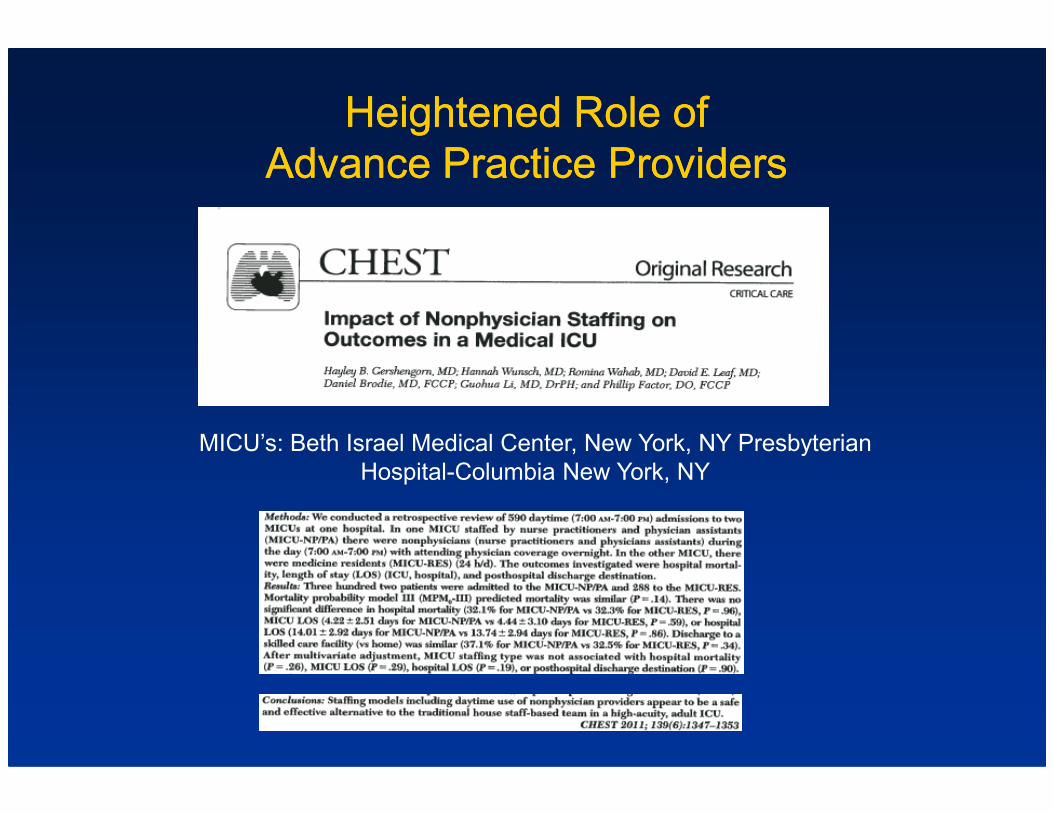
Heightened Role of Heightened Role of
Advance Practice ProvidersAdvance Practice Providers
MICU’s: Beth Israel Medical Center, New York, NY Presbyterian
Hospital-Columbia New York, NY
MultiMulti--Disciplinary Team Dedicated Disciplinary Team Dedicated to the to the Critical Critical
Care Care of of CT PatientsCT Patients
•• CT SurgeonsCT Surgeons
•• Anesthesiologists & Anesthesiologists & IntensivistsIntensivists
•• Cardiologists & RadiologistsCardiologists & Radiologists•• Cardiologists & RadiologistsCardiologists & Radiologists
•• Nurse PractitionersNurse Practitioners
•• Physician AssistantsPhysician Assistants
•• Bedside Critical Care Nurses Bedside Critical Care Nurses
•• PerfusionistsPerfusionists
•• Respiratory TherapistsRespiratory Therapists
IntensivistsIntensivists, Critical Care Nurses, NP’s,, Critical Care Nurses, NP’s,
PA’s, Residents & FellowsPA’s, Residents & Fellows
CT SurgeonsCT Surgeons

PerfusionistsPerfusionists
Respiratory TherapistsRespiratory Therapists
Respiratory TherapistsRespiratory Therapists
Members of the Members of the
Expanded MultiExpanded Multi--Disciplinary Team Disciplinary Team
•• PharmacistsPharmacists
•• Speech Language Pathologists (SLPs)Speech Language Pathologists (SLPs)
•• Physical Therapists & Occupational TherapistsPhysical Therapists & Occupational Therapists•• Physical Therapists & Occupational TherapistsPhysical Therapists & Occupational Therapists
•• NutritionistsNutritionists
•• Social WorkersSocial Workers
•• Patient Service RepresentativesPatient Service Representatives
•• Pastoral Care StaffPastoral Care Staff
PharmacistsPharmacists
CV Pharmacists CV Pharmacists
Cardiovascular Cardiovascular PharacotherapyPharacotherapy
•• Newly Recognized SpecialtyNewly Recognized Specialty
Pioneer in Developing the Specialty:Pioneer in Developing the Specialty:Pioneer in Developing the Specialty:Pioneer in Developing the Specialty:
•• Dr. Joseph Dr. Joseph DastaDasta
•• Ohio State UniversityOhio State University
Cardiovascular PharmacologyCardiovascular Pharmacology
•• Variety of Pharmaceuticals Used in the CT ICUVariety of Pharmaceuticals Used in the CT ICU
•• Vasopressors / InotropesVasopressors / Inotropes
•• Vasodilators / Vasodilators / AntihypertensivesAntihypertensives / Beta Blockers/ Beta Blockers•• Vasodilators / Vasodilators / AntihypertensivesAntihypertensives / Beta Blockers/ Beta Blockers
•• DiureticsDiuretics
•• Anticoagulants / Antiplatelet AgentsAnticoagulants / Antiplatelet Agents
•• Lipid Lowering AgentsLipid Lowering Agents
•• Antibiotics/ Antifungal AgentsAntibiotics/ Antifungal Agents
•• Immunosuppressive AgentsImmunosuppressive Agents
Cardiovascular PharmacologyCardiovascular Pharmacology
•• IssuesIssues
•• Effects of Hepatic & Renal InsufficiencyEffects of Hepatic & Renal Insufficiency
•• Drug InteractionsDrug Interactions
•• Determination of EffectivenessDetermination of Effectiveness•• Determination of EffectivenessDetermination of Effectiveness
•• Dose & DurationDose & Duration

Speech PathologistsSpeech Pathologists
Common Types of Cases When Consulted:Common Types of Cases When Consulted:
•• Prolonged Intubation or Hoarseness after Prolonged Intubation or Hoarseness after ExtubationExtubation
•• Signs of Aspiration after Signs of Aspiration after ExtubationExtubation•• Signs of Aspiration after Signs of Aspiration after ExtubationExtubation
•• Neurologic ComplicationsNeurologic Complications
•• Aortic Reconstructive SurgeryAortic Reconstructive Surgery
•• Lung TransplantationLung Transplantation
•• TracheostomyTracheostomy
•• Esophageal ReconstructionEsophageal Reconstruction
•• Oral Communication for Oral Communication for TrachTrach/Vent Patients (speaking /Vent Patients (speaking
valves)valves)

Speech PathologistsSpeech Pathologists
Diagnosis and management of: Diagnosis and management of:
•• DysphagiaDysphagia
•• Aphasia and cognitive disorders Aphasia and cognitive disorders
•• Voice disordersVoice disorders
Oral communication for Oral communication for TrachTrach/Vent patients (speaking /Vent patients (speaking •• Oral communication for Oral communication for TrachTrach/Vent patients (speaking /Vent patients (speaking
valves)valves)
Education and training for: Education and training for:
•• Patients Patients
•• Family membersFamily members
Speech Pathology EvaluationSpeech Pathology Evaluation
•• Bedside Swallow EvaluationBedside Swallow Evaluation
•• Video Fluoroscopic Swallow StudyVideo Fluoroscopic Swallow Study
Physical TherapistsPhysical Therapists
NutritionistsNutritionists
Formulations for Enteric FeedingFormulations for Enteric Feeding
Nutritional Programs for:Nutritional Programs for:
•• DiabetesDiabetes•• DiabetesDiabetes
•• HypetensionHypetension
•• CHFCHF
•• Renal FailureRenal Failure
•• Pulmonary FailurePulmonary Failure
•• Hepatic FailureHepatic Failure
The MultiThe Multi--Disciplinary Critical Care Team Disciplinary Critical Care Team
ChallengesChallenges
•• Coordinating the Expertise of Multiple SpecialistsCoordinating the Expertise of Multiple Specialists
CommunicationCommunication•• CommunicationCommunication
•• “Being on the Same Page”“Being on the Same Page”

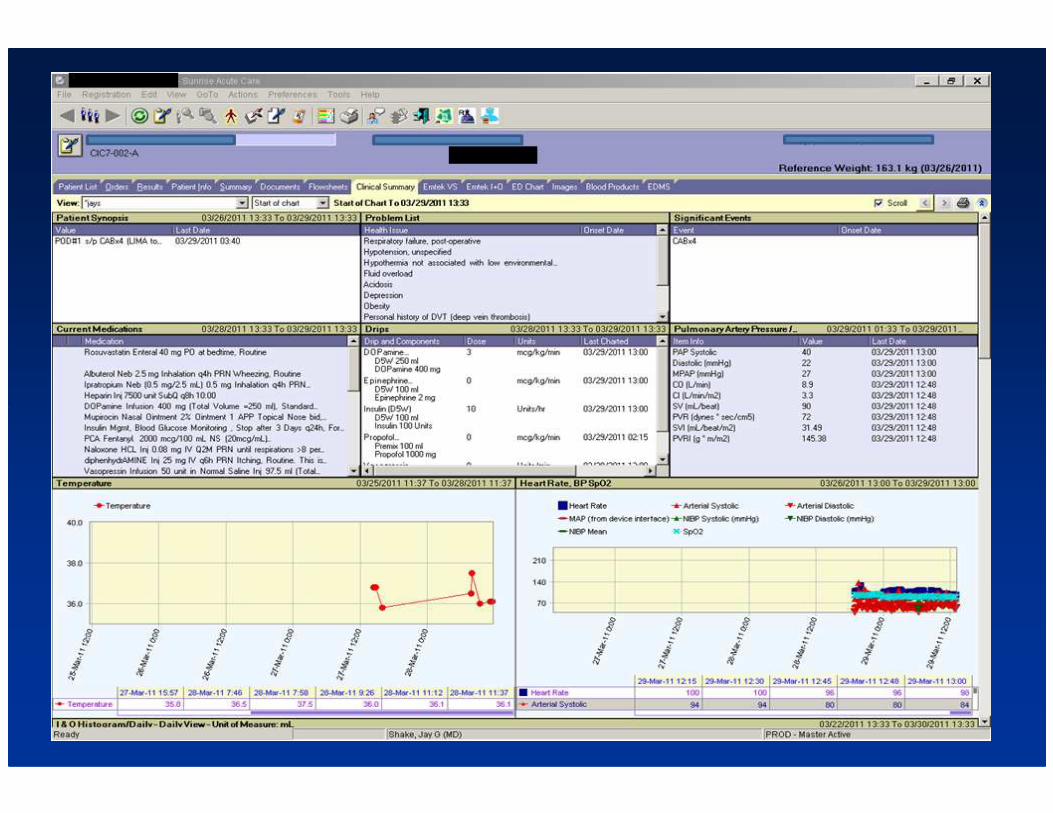
New Information TechnologyNew Information TechnologyNew Information TechnologyNew Information Technology
Challenges of New Information TechnologyChallenges of New Information Technology
•• Organization of Clinical Data to Facilitate ManagementOrganization of Clinical Data to Facilitate Management
•• Integration of Hospital Information SystemsIntegration of Hospital Information Systems
ChemistryChemistry•• ChemistryChemistry
•• HematologyHematology
•• MicrobiologyMicrobiology
•• ImagingImaging
•• Display and Analysis of Clinical TrendsDisplay and Analysis of Clinical Trends
Evolution in Information TechnologyEvolution in Information Technology
•• Electronic Medical Record Electronic Medical Record
•• Trend AnalysisTrend Analysis
•• Computerized Order EntryComputerized Order Entry
•• Wireless Technology Wireless Technology
•• Immediately AvailableImmediately Available
•• Clinical DataClinical Data
•• ImagingImaging
•• TrendsTrends
Continuing Challenges of Data DisplayContinuing Challenges of Data Display
•• Large Volume of DataLarge Volume of Data
•• Highlighting the Key IssuesHighlighting the Key Issues•• Highlighting the Key IssuesHighlighting the Key Issues
•• Organization to Guide ManagementOrganization to Guide Management
•• EfficiencyEfficiency
Presentation of Clinical DataPresentation of Clinical Data
ChallengesChallenges
•• Presentation that Guides Formulation of PlansPresentation that Guides Formulation of Plans
•• A Format that Adapts to Rapid Clinical ChangesA Format that Adapts to Rapid Clinical Changes
•• Efficiency of Implementation / Order EntryEfficiency of Implementation / Order Entry

Quality Improvement InitiativesQuality Improvement InitiativesQuality Improvement InitiativesQuality Improvement Initiatives

Drivers of Quality ImprovementDrivers of Quality Improvement
•• Pursuit of ExcellencePursuit of Excellence
•• Intrinsic to Our Health Care ProfessionsIntrinsic to Our Health Care Professions
•• Economic PressuresEconomic Pressures
•• Hospital ValueHospital Value--Based Purchasing ProgramsBased Purchasing Programs
•• Publicized Hospital DataPublicized Hospital Data

Communications / Use of ChecklistsCommunications / Use of Checklists
Concerns:Concerns:
•• Consistency of Quality CareConsistency of Quality Care
•• Safety / Avoiding ErrorsSafety / Avoiding Errors
•• Continuity of CareContinuity of Care
Completeness of CommunicationCompleteness of Communication•• Completeness of CommunicationCompleteness of Communication
Change:Change:
•• An Awareness of Communication GapsAn Awareness of Communication Gaps
•• Expanded Use of ChecklistsExpanded Use of Checklists
Communications / Use of ChecklistsCommunications / Use of Checklists
Checklists Checklists
•• To Insure Consistent, Optimal PracticeTo Insure Consistent, Optimal Practice
•• To Insure Complete Communication To Insure Complete Communication
••
Standard in the Aviation IndustryStandard in the Aviation IndustryStandard in the Aviation IndustryStandard in the Aviation Industry
Advocated by Authors:Advocated by Authors:
•• Peter Peter PronovostPronovost, MD, MD
Safe Patients, Smart Hospitals NSafe Patients, Smart Hospitals N
•• AtulAtul GawandeGawande, MD, MD
The Checklist ManifestoNThe Checklist ManifestoN
Evolution in CommunicationsEvolution in Communications
•• Rounds with the Entire Critical Care TeamRounds with the Entire Critical Care Team
•• “Handoffs” “Handoffs”
•• Within the ICUWithin the ICU
After Procedures / SurgeryAfter Procedures / Surgery•• After Procedures / SurgeryAfter Procedures / Surgery
•• “Safety Huddles”“Safety Huddles”
•• Use of Checklists to Insure CompletenessUse of Checklists to Insure Completeness
•• Better Communication to the Patient & FamilyBetter Communication to the Patient & Family
Flight 1549: All Lives Saved!Flight 1549: All Lives Saved!
Quality Improvement CommitteeQuality Improvement Committee

To Improve To Improve ––
You Need to Measure!You Need to Measure!You Need to Measure!You Need to Measure!
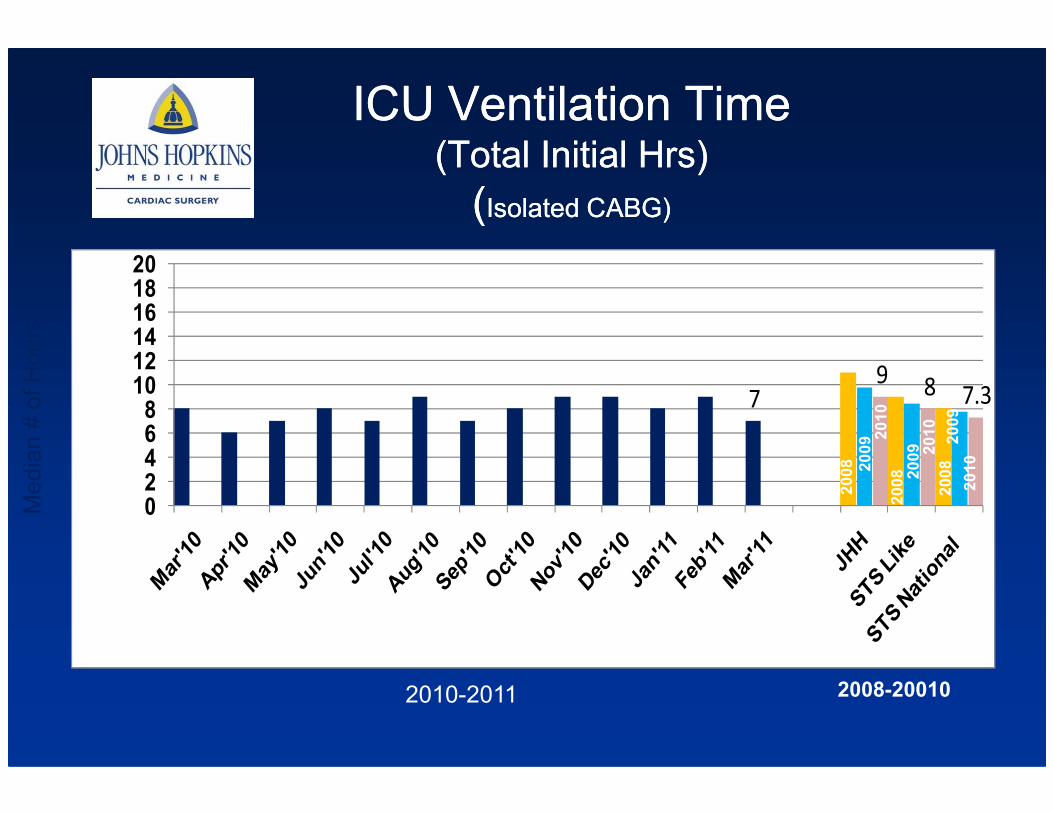
ICU Ventilation Time ICU Ventilation Time (Total Initial Hrs)(Total Initial Hrs)
((Isolated CABG)Isolated CABG)
98 7.378
101214161820
Median # of Hours
2010
7.37
02468
Median # of Hours
2010-2011 2008-20010
2008
2008
20082009 2009
2009
2010
2010
2010
“Making It Happen”“Making It Happen”“Making It Happen”“Making It Happen”
Challenges of Clinical RoundingChallenges of Clinical Rounding
•• Understanding the Issues / Problems OccurringUnderstanding the Issues / Problems Occurring
•• Arriving at an Optimal Overall PlanArriving at an Optimal Overall Plan
•• EfficiencyEfficiency•• EfficiencyEfficiency
•• Coordination of Management Coordination of Management
SystemSystem--Structured, IssueStructured, Issue--Oriented Oriented
ApproachApproach
•• Data Organization: Data Organization:
•• “System“System--Structured Profile” or “SSP”Structured Profile” or “SSP”
•• Flowchart or Computerized Display to Define the Time Flowchart or Computerized Display to Define the Time CourseCourseCourseCourse
•• Definition of the Clinical Situation:Definition of the Clinical Situation:
•• “Issues” Related to Each System“Issues” Related to Each System
•• Dx’icDx’ic and Rx Plan for Each System / Issueand Rx Plan for Each System / Issue
A Format for Clinical RoundsA Format for Clinical Rounds
•• Development of Plans / Orders Development of Plans / Orders
•• “Read Back” by the Bedside Nurse“Read Back” by the Bedside Nurse•• “Read Back” by the Bedside Nurse“Read Back” by the Bedside Nurse
•• Checklist ReviewChecklist Review
•• Orders are Transmitted on Rounds via Wireless ComputerOrders are Transmitted on Rounds via Wireless Computer
Patient Patient -- Family Centered CareFamily Centered Care
•• Patient Patient –– Family Centered RoundsFamily Centered Rounds
•• Influence of a Variety of MediaInfluence of a Variety of Media
•• TVTV
•• InternetInternet•• InternetInternet
•• Magazines / JournalsMagazines / Journals
•• NewslettersNewsletters
•• HeightenedHeightened
•• UnderstandingUnderstanding
•• Concerns / QuestionsConcerns / Questions
ICU roundsICU rounds
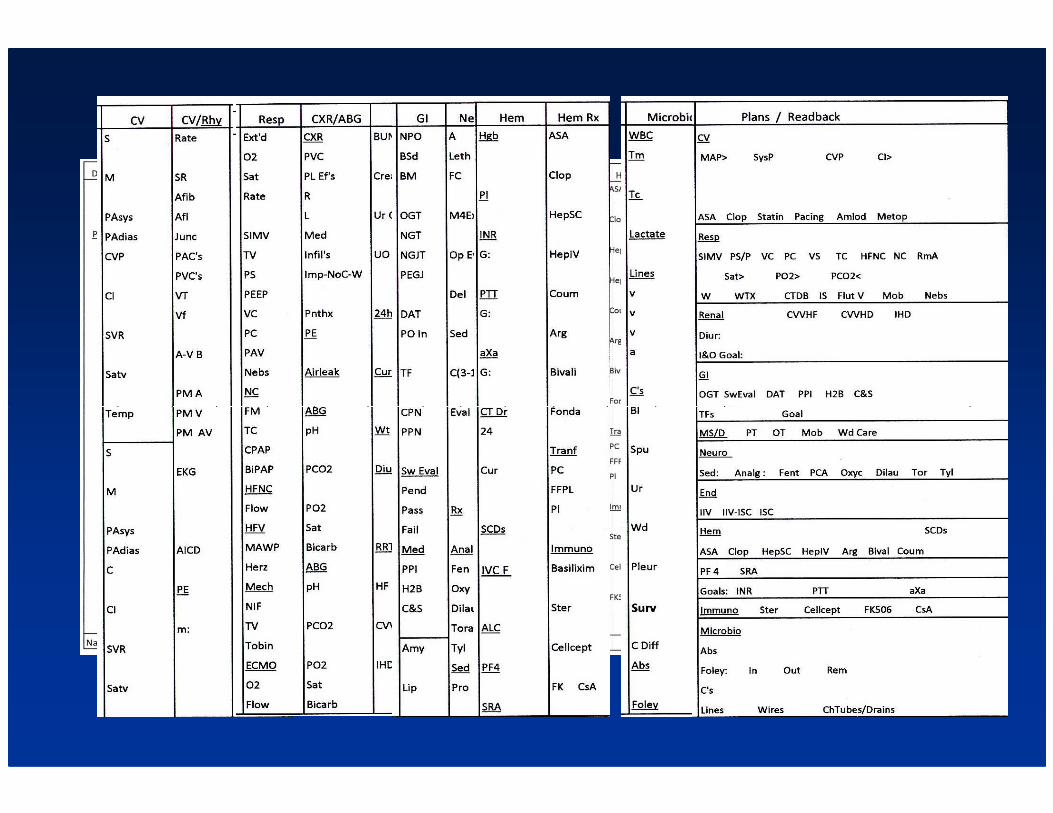
Presentation / Display of DataPresentation / Display of Data
Development of SystemDevelopment of System--Structured PlansStructured Plans
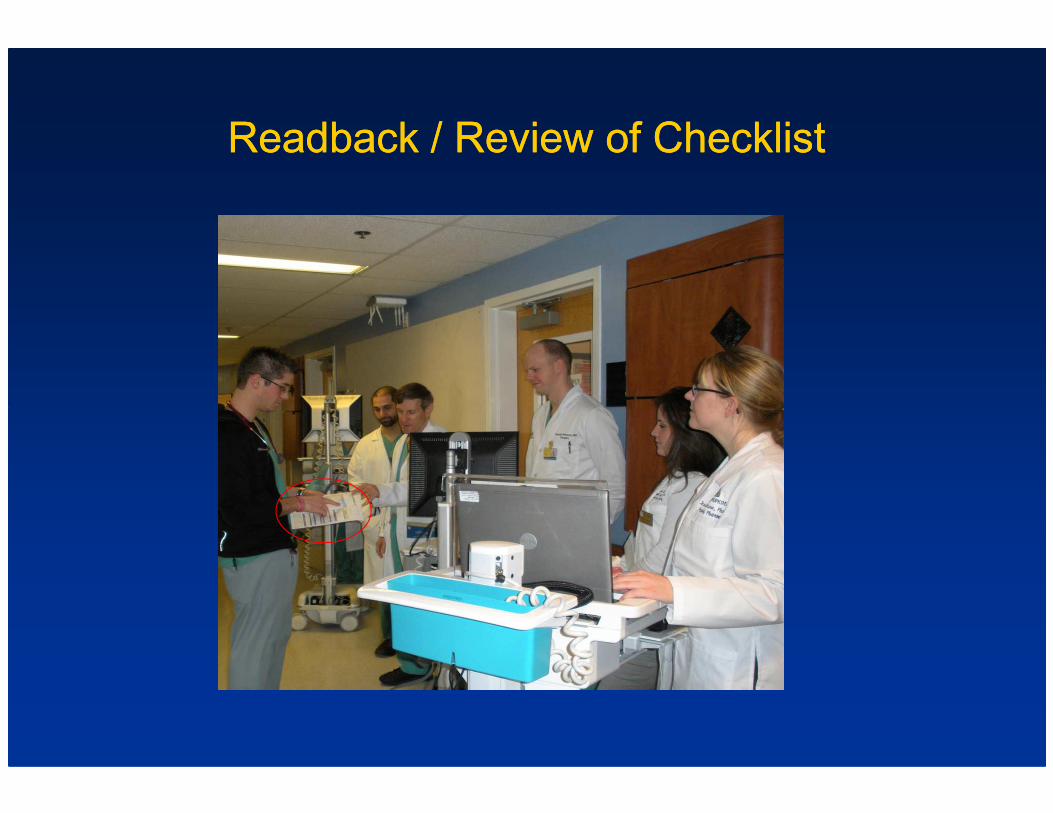
ReadbackReadback / Review of Checklist/ Review of Checklist
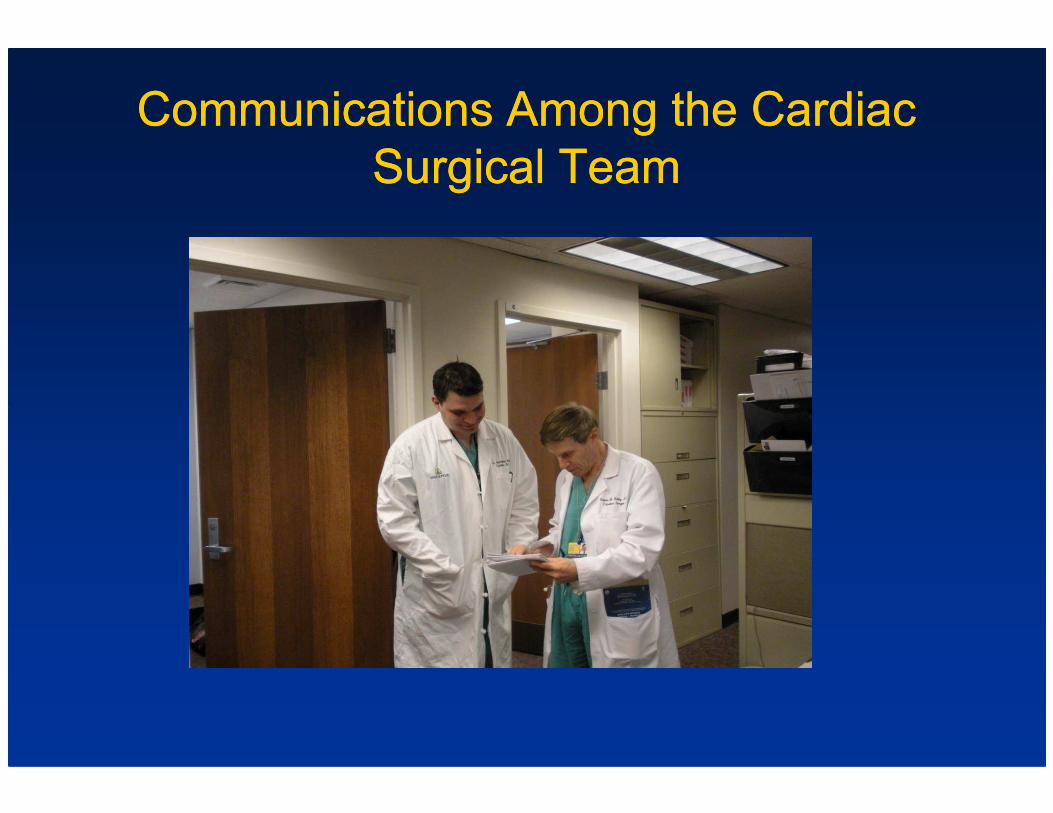
Communications Among the Cardiac Communications Among the Cardiac
Surgical Team Surgical Team
Team Building Team Building
•• Culture of Mutual RespectCulture of Mutual Respect
•• Communication Communication –– Lateral & VerticalLateral & Vertical
•• Sharing of Quality Improvement InitiativesSharing of Quality Improvement Initiatives
•• Data CollectionData Collection•• Data CollectionData Collection
•• Protocol DevelopmentProtocol Development
•• ReRe--AnalysisAnalysis
And now, And now,
to address this to address this
“Ongoing Evolution”“Ongoing Evolution”
in more detail, we continue with:in more detail, we continue with:
AATS/STS
CARDIOTHORACIC CRITICAL CARE
SYMPOSIUM
2012 2012
Welcome to All!
CardiovascularCardiovascular--Thoracic (CVT) Thoracic (CVT) Critical Care 2012Critical Care 2012Critical Care 2012Critical Care 201299thth Annual ConferenceAnnual Conference
Save the DateSave the Date
Thurs Oct 4 Thurs Oct 4 –– Sat Oct 6, 2012Sat Oct 6, 2012
Omni Shoreham HotelOmni Shoreham Hotel
Washington, DCWashington, DC
www.factswww.facts--care.orgcare.org